User login
What is the best surgical therapy for the secondary prevention of stroke?
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.


Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
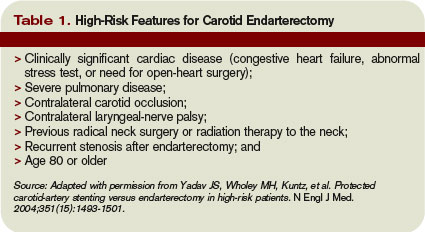
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.
Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.
Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
The Psychology of Error
What do your patient care errors have in common with financial mistakes that may compromise your retirement? Both have their underpinnings in the psychological strategies and tendencies we call heuristics.
The word derives from the Greek term “heuriskein” for discovery, but in the medical context we frequently think of these as these as mental shortcuts. Heuristics allow us to operate quickly despite the bewildering degree of complexity and uncertainty we encounter as we operate in the world but also lay the groundwork for disaster when they lead us astray. Let’s examine two mistakes and look at what they have in common: one that led to a drubbing in the stock market and the other that cost a patient his life.
A Market Misadventure
During the height of the market boom a young internist purchased shares of an exciting new biotech company poised at the forefront of tailored medical therapy based on genetic sequencing.
The stock nearly doubled, but as he rode the wild ride of the market’s fluctuations it became evident that the overall trend had changed. Almost daily monitoring of the press releases from the dynamic CEO helped reinforce his decision to hold the stock even after the dizzying drop that changed a strong gain to a significant loss. Finally after waiting months for the stock ticker to nudge back up to his entry point, he was glumly forced to face the loss.
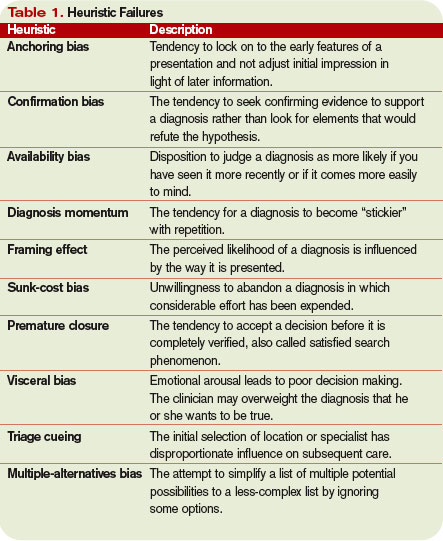
The field of behavioral finance suggests humans are subject to cognitive predispositions leading to predictable errors. The first heuristic failure demonstrated by the unfortunate internist in our example is that of anchoring (see sidebar, p. 35).
The initial impression of the value of the company or particular price at which he purchased the stock has significance to him but is completely irrelevant to the value of the company once events and profit prospects changed. Thus, when new information about the company came to light, the focus should have been exclusively on the future valuation without regard to the past. That didn’t happen in this case. Our hapless investor had become anchored to the original price and refused to sell as it plummeted in the vain hopes that it would rise again despite the absence of evidence that this was likely.
Anchoring bias affects all of us and is as true in medicine as it is in the markets. The first diagnosis, which seems likely as we hear a case described, can be surprisingly hard to shake even when the facts on the ground have changed.
A second human tendency we see leading to both financial and medical calamity is the desire to be right. A strong self-image (and many physicians have a strong one, indeed) is bolstered by seeking information that confirms prior beliefs.
Unfortunately this confirmation bias can also cause us to overvalue the positive press about a company we are invested in and discount or not read at all things that might change our minds. Back in the clinical environment, examples abound where a physician becomes fixed on a diagnosis and orders tests designed to confirm the initial impression but fails to explore alternatives. The more invested in a diagnosis we become, the more selective we tend to be in seeking and interpreting data to reinforce our convictions.
Higher Stakes
Years later and hundreds of miles away a nocturnist gets a call from the emergency department (ED) on the seventh new admission of the night.
“I’ve got another rule-out myocardial infarction (MI) for you” said the ED physician, who briefly provided the assessment that the patient was low risk, with negative enzymes, chest X-ray, and electrocardiogram.
The nocturnist noted the atypical severity of the pain, systolic blood pressure more than 200, and positive cocaine history. But this did not alter the plan as the patient was passed from the ED physician to the nocturnist and then to the hospitalist who assumed care the next morning. Unfortunately, it took the patient experiencing a severe increase in tearing pain radiating to his back during the exercise stress test to prompt the discovery of his ascending aortic dissection. The patient died on the operating room table, leaving all three physicians wondering how they could have missed the diagnosis when in retrospect it seemed so obvious.
Present the same clinical scenario at grand rounds and the third-year medical students could tell you dissection should have been considered. How did three smart experienced people all make the same fatal mistake?
This case demonstrates a number of heuristic failures. Availability bias is a form of pattern recognition and arises from our habit of perceiving the things we see often as more likely than those which we have not seen or thought about recently. Hoof beats in Kentucky, as they say, are usually not a herd of zebra. ED physicians see what at times seems like hordes of patients with low-risk chest pain, the vast majority of which lack a life-threatening etiology. Thus, we can become complacent in assuming that the next admission for chest pain reflects the same cause as the seven before.
Pattern recognition serves a vital role. Most expert physicians rely on this more than classic deductive reasoning and, much less, Bayesian analysis. Casino operators exploit this tendency to see false patterns to their profit by installing displays that show the last 10 to 20 results over the roulette table. However, just as each turn of the roulette wheel is not influenced by prior spins, each patient is unique. One must beware of the misleading power of the availability bias.
Once the initial misdiagnosis had been made, the anchoring bias and confirmation bias continued the cascade of events—turning a mistake from a temporary error to a disaster. The phrase “chest pain rule out MI” not only encourages the physician to minimize the potential severity of the symptom via the framing effect but also telegraphs the anchoring phenomenon by fixing on a single disease concern for a symptom whose etiologies are legion.
However, even accepting that the initial diagnosis by the ED doctor was influenced by the availability bias, why was this not corrected by the nocturnist or by the hospitalist on the next day? The answer lies in diagnosis momentum.
Each physician does not evaluate the patient in isolation but rather has a tendency to include the assessment of the prior clinician as part of their own decision-making process. The more people who have seen the patient and agreed with the diagnosis, the higher the mental hurdle becomes to disagree and take the work-up in a different direction.
What You Can Do
Does the mere existence of these many heuristics condemn the physician to a career of repeating these potentially fatal errors? The obvious answer is no, but the solution requires a concerted effort on the part of the physician to avoid these mistakes.
Step one is to recognize that many heuristics are essentially abbreviations of full conscious reasoning. Now take a physician who is tired, stressed, or inundated with multiple tasks. In an effort to organize the seemingly chaotic world of medicine the mind seeks a crutch. These mental shortcuts allow us to quickly process massive amounts of information and come up with a reasonable plan that will be right most of the time.
When rushed, stressed, and distracted, we are most prone to use these shortcuts. These times of pressure are exactly when it is most important to pause and consider whether we’re acting on gut feeling or on full consideration of all the evidence. Awareness of the predictable circumstances that create the set-up for heuristic failures allows for a moment of reflection to prevent falling into one of these psychological traps. This process of deliberately considering our own decision-making is referred to as meta-cognition.
An additional familiar tool available to the physician is differential diagnosis. This is essentially a form of cognitive forcing strategy designed to guard against availability and anchoring biases. By deliberately creating a list of alternative possibilities, we become less prone to anchor on a single diagnosis.
By briefly reviewing the rare possibilities we have not seen recently and bringing them to the forefront of memory, we diminish the power of the availability bias. Spending a second or two considering the differential—even in seemingly routine cases—will defuse the hold of these particular heuristics.
Hospitalists by the nature of our practice tend to have multiple transitions in patient care. At times this offers a fresh perspective to correct mistakes, but it also offers potential to compound them via diagnosis momentum.
We habitually convey diagnosis and treatment plans to our partners at handoffs. Including a level of uncertainty as part of checkout would create a cue for the accepting physician to decrease the risk of this heuristic failure. One might imagine the patient in the case above would have had a greater probability of survival if the nocturnist had conveyed a diagnosis of “chest pain of uncertain etiology” to his partner rather than “chest pain rule-out MI.”
As illustrated by the cases above, heuristics are not mistakes in and of themselves. They are the assumptions and pattern-recognition techniques that serve us well the majority of the time in and out of medicine. Recognizing when you take one of these mental shortcuts, being aware of the circumstances that predispose to error creation, and evaluating your decision-making process allows the astute physician to guard against the times when they fail. Greater self-awareness of the process of your own cognition can make for a better clinician—and perhaps even make you a better investor. TH
Drs. Cumbler and Trosterman are assistant professors in the Section of Hospital Medicine at the University of Colorado.
What do your patient care errors have in common with financial mistakes that may compromise your retirement? Both have their underpinnings in the psychological strategies and tendencies we call heuristics.
The word derives from the Greek term “heuriskein” for discovery, but in the medical context we frequently think of these as these as mental shortcuts. Heuristics allow us to operate quickly despite the bewildering degree of complexity and uncertainty we encounter as we operate in the world but also lay the groundwork for disaster when they lead us astray. Let’s examine two mistakes and look at what they have in common: one that led to a drubbing in the stock market and the other that cost a patient his life.
A Market Misadventure
During the height of the market boom a young internist purchased shares of an exciting new biotech company poised at the forefront of tailored medical therapy based on genetic sequencing.
The stock nearly doubled, but as he rode the wild ride of the market’s fluctuations it became evident that the overall trend had changed. Almost daily monitoring of the press releases from the dynamic CEO helped reinforce his decision to hold the stock even after the dizzying drop that changed a strong gain to a significant loss. Finally after waiting months for the stock ticker to nudge back up to his entry point, he was glumly forced to face the loss.
The field of behavioral finance suggests humans are subject to cognitive predispositions leading to predictable errors. The first heuristic failure demonstrated by the unfortunate internist in our example is that of anchoring (see sidebar, p. 35).
The initial impression of the value of the company or particular price at which he purchased the stock has significance to him but is completely irrelevant to the value of the company once events and profit prospects changed. Thus, when new information about the company came to light, the focus should have been exclusively on the future valuation without regard to the past. That didn’t happen in this case. Our hapless investor had become anchored to the original price and refused to sell as it plummeted in the vain hopes that it would rise again despite the absence of evidence that this was likely.
Anchoring bias affects all of us and is as true in medicine as it is in the markets. The first diagnosis, which seems likely as we hear a case described, can be surprisingly hard to shake even when the facts on the ground have changed.
A second human tendency we see leading to both financial and medical calamity is the desire to be right. A strong self-image (and many physicians have a strong one, indeed) is bolstered by seeking information that confirms prior beliefs.
Unfortunately this confirmation bias can also cause us to overvalue the positive press about a company we are invested in and discount or not read at all things that might change our minds. Back in the clinical environment, examples abound where a physician becomes fixed on a diagnosis and orders tests designed to confirm the initial impression but fails to explore alternatives. The more invested in a diagnosis we become, the more selective we tend to be in seeking and interpreting data to reinforce our convictions.
Higher Stakes
Years later and hundreds of miles away a nocturnist gets a call from the emergency department (ED) on the seventh new admission of the night.
“I’ve got another rule-out myocardial infarction (MI) for you” said the ED physician, who briefly provided the assessment that the patient was low risk, with negative enzymes, chest X-ray, and electrocardiogram.
The nocturnist noted the atypical severity of the pain, systolic blood pressure more than 200, and positive cocaine history. But this did not alter the plan as the patient was passed from the ED physician to the nocturnist and then to the hospitalist who assumed care the next morning. Unfortunately, it took the patient experiencing a severe increase in tearing pain radiating to his back during the exercise stress test to prompt the discovery of his ascending aortic dissection. The patient died on the operating room table, leaving all three physicians wondering how they could have missed the diagnosis when in retrospect it seemed so obvious.
Present the same clinical scenario at grand rounds and the third-year medical students could tell you dissection should have been considered. How did three smart experienced people all make the same fatal mistake?
This case demonstrates a number of heuristic failures. Availability bias is a form of pattern recognition and arises from our habit of perceiving the things we see often as more likely than those which we have not seen or thought about recently. Hoof beats in Kentucky, as they say, are usually not a herd of zebra. ED physicians see what at times seems like hordes of patients with low-risk chest pain, the vast majority of which lack a life-threatening etiology. Thus, we can become complacent in assuming that the next admission for chest pain reflects the same cause as the seven before.
Pattern recognition serves a vital role. Most expert physicians rely on this more than classic deductive reasoning and, much less, Bayesian analysis. Casino operators exploit this tendency to see false patterns to their profit by installing displays that show the last 10 to 20 results over the roulette table. However, just as each turn of the roulette wheel is not influenced by prior spins, each patient is unique. One must beware of the misleading power of the availability bias.
Once the initial misdiagnosis had been made, the anchoring bias and confirmation bias continued the cascade of events—turning a mistake from a temporary error to a disaster. The phrase “chest pain rule out MI” not only encourages the physician to minimize the potential severity of the symptom via the framing effect but also telegraphs the anchoring phenomenon by fixing on a single disease concern for a symptom whose etiologies are legion.
However, even accepting that the initial diagnosis by the ED doctor was influenced by the availability bias, why was this not corrected by the nocturnist or by the hospitalist on the next day? The answer lies in diagnosis momentum.
Each physician does not evaluate the patient in isolation but rather has a tendency to include the assessment of the prior clinician as part of their own decision-making process. The more people who have seen the patient and agreed with the diagnosis, the higher the mental hurdle becomes to disagree and take the work-up in a different direction.
What You Can Do
Does the mere existence of these many heuristics condemn the physician to a career of repeating these potentially fatal errors? The obvious answer is no, but the solution requires a concerted effort on the part of the physician to avoid these mistakes.
Step one is to recognize that many heuristics are essentially abbreviations of full conscious reasoning. Now take a physician who is tired, stressed, or inundated with multiple tasks. In an effort to organize the seemingly chaotic world of medicine the mind seeks a crutch. These mental shortcuts allow us to quickly process massive amounts of information and come up with a reasonable plan that will be right most of the time.
When rushed, stressed, and distracted, we are most prone to use these shortcuts. These times of pressure are exactly when it is most important to pause and consider whether we’re acting on gut feeling or on full consideration of all the evidence. Awareness of the predictable circumstances that create the set-up for heuristic failures allows for a moment of reflection to prevent falling into one of these psychological traps. This process of deliberately considering our own decision-making is referred to as meta-cognition.
An additional familiar tool available to the physician is differential diagnosis. This is essentially a form of cognitive forcing strategy designed to guard against availability and anchoring biases. By deliberately creating a list of alternative possibilities, we become less prone to anchor on a single diagnosis.
By briefly reviewing the rare possibilities we have not seen recently and bringing them to the forefront of memory, we diminish the power of the availability bias. Spending a second or two considering the differential—even in seemingly routine cases—will defuse the hold of these particular heuristics.
Hospitalists by the nature of our practice tend to have multiple transitions in patient care. At times this offers a fresh perspective to correct mistakes, but it also offers potential to compound them via diagnosis momentum.
We habitually convey diagnosis and treatment plans to our partners at handoffs. Including a level of uncertainty as part of checkout would create a cue for the accepting physician to decrease the risk of this heuristic failure. One might imagine the patient in the case above would have had a greater probability of survival if the nocturnist had conveyed a diagnosis of “chest pain of uncertain etiology” to his partner rather than “chest pain rule-out MI.”
As illustrated by the cases above, heuristics are not mistakes in and of themselves. They are the assumptions and pattern-recognition techniques that serve us well the majority of the time in and out of medicine. Recognizing when you take one of these mental shortcuts, being aware of the circumstances that predispose to error creation, and evaluating your decision-making process allows the astute physician to guard against the times when they fail. Greater self-awareness of the process of your own cognition can make for a better clinician—and perhaps even make you a better investor. TH
Drs. Cumbler and Trosterman are assistant professors in the Section of Hospital Medicine at the University of Colorado.
What do your patient care errors have in common with financial mistakes that may compromise your retirement? Both have their underpinnings in the psychological strategies and tendencies we call heuristics.
The word derives from the Greek term “heuriskein” for discovery, but in the medical context we frequently think of these as these as mental shortcuts. Heuristics allow us to operate quickly despite the bewildering degree of complexity and uncertainty we encounter as we operate in the world but also lay the groundwork for disaster when they lead us astray. Let’s examine two mistakes and look at what they have in common: one that led to a drubbing in the stock market and the other that cost a patient his life.
A Market Misadventure
During the height of the market boom a young internist purchased shares of an exciting new biotech company poised at the forefront of tailored medical therapy based on genetic sequencing.
The stock nearly doubled, but as he rode the wild ride of the market’s fluctuations it became evident that the overall trend had changed. Almost daily monitoring of the press releases from the dynamic CEO helped reinforce his decision to hold the stock even after the dizzying drop that changed a strong gain to a significant loss. Finally after waiting months for the stock ticker to nudge back up to his entry point, he was glumly forced to face the loss.
The field of behavioral finance suggests humans are subject to cognitive predispositions leading to predictable errors. The first heuristic failure demonstrated by the unfortunate internist in our example is that of anchoring (see sidebar, p. 35).
The initial impression of the value of the company or particular price at which he purchased the stock has significance to him but is completely irrelevant to the value of the company once events and profit prospects changed. Thus, when new information about the company came to light, the focus should have been exclusively on the future valuation without regard to the past. That didn’t happen in this case. Our hapless investor had become anchored to the original price and refused to sell as it plummeted in the vain hopes that it would rise again despite the absence of evidence that this was likely.
Anchoring bias affects all of us and is as true in medicine as it is in the markets. The first diagnosis, which seems likely as we hear a case described, can be surprisingly hard to shake even when the facts on the ground have changed.
A second human tendency we see leading to both financial and medical calamity is the desire to be right. A strong self-image (and many physicians have a strong one, indeed) is bolstered by seeking information that confirms prior beliefs.
Unfortunately this confirmation bias can also cause us to overvalue the positive press about a company we are invested in and discount or not read at all things that might change our minds. Back in the clinical environment, examples abound where a physician becomes fixed on a diagnosis and orders tests designed to confirm the initial impression but fails to explore alternatives. The more invested in a diagnosis we become, the more selective we tend to be in seeking and interpreting data to reinforce our convictions.
Higher Stakes
Years later and hundreds of miles away a nocturnist gets a call from the emergency department (ED) on the seventh new admission of the night.
“I’ve got another rule-out myocardial infarction (MI) for you” said the ED physician, who briefly provided the assessment that the patient was low risk, with negative enzymes, chest X-ray, and electrocardiogram.
The nocturnist noted the atypical severity of the pain, systolic blood pressure more than 200, and positive cocaine history. But this did not alter the plan as the patient was passed from the ED physician to the nocturnist and then to the hospitalist who assumed care the next morning. Unfortunately, it took the patient experiencing a severe increase in tearing pain radiating to his back during the exercise stress test to prompt the discovery of his ascending aortic dissection. The patient died on the operating room table, leaving all three physicians wondering how they could have missed the diagnosis when in retrospect it seemed so obvious.
Present the same clinical scenario at grand rounds and the third-year medical students could tell you dissection should have been considered. How did three smart experienced people all make the same fatal mistake?
This case demonstrates a number of heuristic failures. Availability bias is a form of pattern recognition and arises from our habit of perceiving the things we see often as more likely than those which we have not seen or thought about recently. Hoof beats in Kentucky, as they say, are usually not a herd of zebra. ED physicians see what at times seems like hordes of patients with low-risk chest pain, the vast majority of which lack a life-threatening etiology. Thus, we can become complacent in assuming that the next admission for chest pain reflects the same cause as the seven before.
Pattern recognition serves a vital role. Most expert physicians rely on this more than classic deductive reasoning and, much less, Bayesian analysis. Casino operators exploit this tendency to see false patterns to their profit by installing displays that show the last 10 to 20 results over the roulette table. However, just as each turn of the roulette wheel is not influenced by prior spins, each patient is unique. One must beware of the misleading power of the availability bias.
Once the initial misdiagnosis had been made, the anchoring bias and confirmation bias continued the cascade of events—turning a mistake from a temporary error to a disaster. The phrase “chest pain rule out MI” not only encourages the physician to minimize the potential severity of the symptom via the framing effect but also telegraphs the anchoring phenomenon by fixing on a single disease concern for a symptom whose etiologies are legion.
However, even accepting that the initial diagnosis by the ED doctor was influenced by the availability bias, why was this not corrected by the nocturnist or by the hospitalist on the next day? The answer lies in diagnosis momentum.
Each physician does not evaluate the patient in isolation but rather has a tendency to include the assessment of the prior clinician as part of their own decision-making process. The more people who have seen the patient and agreed with the diagnosis, the higher the mental hurdle becomes to disagree and take the work-up in a different direction.
What You Can Do
Does the mere existence of these many heuristics condemn the physician to a career of repeating these potentially fatal errors? The obvious answer is no, but the solution requires a concerted effort on the part of the physician to avoid these mistakes.
Step one is to recognize that many heuristics are essentially abbreviations of full conscious reasoning. Now take a physician who is tired, stressed, or inundated with multiple tasks. In an effort to organize the seemingly chaotic world of medicine the mind seeks a crutch. These mental shortcuts allow us to quickly process massive amounts of information and come up with a reasonable plan that will be right most of the time.
When rushed, stressed, and distracted, we are most prone to use these shortcuts. These times of pressure are exactly when it is most important to pause and consider whether we’re acting on gut feeling or on full consideration of all the evidence. Awareness of the predictable circumstances that create the set-up for heuristic failures allows for a moment of reflection to prevent falling into one of these psychological traps. This process of deliberately considering our own decision-making is referred to as meta-cognition.
An additional familiar tool available to the physician is differential diagnosis. This is essentially a form of cognitive forcing strategy designed to guard against availability and anchoring biases. By deliberately creating a list of alternative possibilities, we become less prone to anchor on a single diagnosis.
By briefly reviewing the rare possibilities we have not seen recently and bringing them to the forefront of memory, we diminish the power of the availability bias. Spending a second or two considering the differential—even in seemingly routine cases—will defuse the hold of these particular heuristics.
Hospitalists by the nature of our practice tend to have multiple transitions in patient care. At times this offers a fresh perspective to correct mistakes, but it also offers potential to compound them via diagnosis momentum.
We habitually convey diagnosis and treatment plans to our partners at handoffs. Including a level of uncertainty as part of checkout would create a cue for the accepting physician to decrease the risk of this heuristic failure. One might imagine the patient in the case above would have had a greater probability of survival if the nocturnist had conveyed a diagnosis of “chest pain of uncertain etiology” to his partner rather than “chest pain rule-out MI.”
As illustrated by the cases above, heuristics are not mistakes in and of themselves. They are the assumptions and pattern-recognition techniques that serve us well the majority of the time in and out of medicine. Recognizing when you take one of these mental shortcuts, being aware of the circumstances that predispose to error creation, and evaluating your decision-making process allows the astute physician to guard against the times when they fail. Greater self-awareness of the process of your own cognition can make for a better clinician—and perhaps even make you a better investor. TH
Drs. Cumbler and Trosterman are assistant professors in the Section of Hospital Medicine at the University of Colorado.
Close the Loop
This is the second of a two-part series examining medical errors. Part 1 addressed thought processes hospitalists use that may lead to mistaken diagnoses (October 2007, p. 36). Part 2 examines what healthcare corporations are doing to improve diagnoses and reduce errors.
Pilots taking off, Swiss cheese, low-hanging fruit. Talk to hospitalists about the issue of medical errors and the analogies come quickly.
Ever since 2000’s landmark Institute of Medicine report “To Err is Human: Building a Safer Health System” found that anywhere from 40,000 to 100,000 patients incur injury or die every year because of medical errors, debate has been constant.
Medical literature is abundant on this topic. The Joint Commission, National Center for Patient Safety, Agency for Health Care Research and Quality, and myriad other organizations and institutions, including SHM, are all helping providers and hospitals solve the problems by establishing goals, standards, guidelines, and policies.
—Evan Falchuk, president, Best Doctors Inc., Boston
Definitions and Paradigms
Best-practice recommendations for reducing errors are generally based on two essential principles: using a systems-based approach to patient safety and creating an environment that supports open dialogue about errors, their causes, and strategies for prevention.
Terminology is a key factor. The terms “error” and “mistake” carry an emotional component associated with embarrassment and shame. Healthcare providers don’t like to be associated with errors. There is an accompanying fear of litigation, and people, perhaps especially physicians, don’t want to be known as someone who was sued.
“The language we use to talk about these issues is important,” says Janet Nagamine, MD, part-time hospitalist at Kaiser Permanente Santa Clara Medical Center in Calif. and current chair of SHM’s quality and patient safety committee. In fact, because of the negativity around the terms “misdiagnosis” and “delay in diagnosis” she advocates using the term “unintended adverse event” in order to appear more neutral.
“The term error is extremely threatening and scary to any health professional because it implies a personal failure,” says Dr. Nagamine. The goal when it comes to errors is essentially to look for the how—not the who.
Reporting medical errors is one thing, but reporting misdiagnoses is another, says Lakshmi Halasyamani, MD, vice chair for the department of internal medicine at St. Joseph’s Mercy Hospital in Ann Arbor, Mich., and SHM board member. “We don’t really talk about misdiagnosis,” she says. “That’s partly because we have tended to assign more individual blame for misdiagnoses.”
Drs. Nagamine and Halasyamani agree that altering the way of viewing errors means nurturing culture change.
“We have made very little headway helping physicians understand that in the course of their careers there will be misdiagnoses and the best of physicians have misdiagnoses,” says Dr. Halasyamani. “We are not developmentally at the same stage that we are with talking about medical errors.”
She believes this is largely a professionalism issue that first means normalizing the issue of misdiagnosis. “It is kind of ludicrous to think that you will practice medicine over 40 years and not have a misdiagnosis,” she says. “But we don’t look at it from that perspective when we begin to orient trainees.”
National Efforts
To the people at the U.S. Pharmacopeia Center for the Advancement of Patient Safety (USP), the arrival of universal electronic medical records (EMR) in the coming decade will be a boon to the error-reduction effort.
“Eventually we will all have our health information stored electronically for easy retrieval,” says Rodney W. Hicks, PhD, ARNP, manager, patient safety research and practice for the USP and first author on its most recent report. The beginning of regional networks for EMR is taking hold.
“Even before the IOM report, the USP was familiar with intensivists,” says Dr. Hicks. “We recognize hospitalists as experts who bring efficiency and effectiveness to the healthcare system.”
The USP maintains perhaps the largest database of medication errors in the world.1 Each year the USP issues a report that focuses on one topic and builds its knowledge base.
This year’s report focuses exclusively on the perioperative continuum of care. Last year’s covered ICU- and radiology-related errors. Two years ago the report was a five-year data summary of errors occurring primarily in hospitals.
“The area of errors due to breakdowns in handoffs remains a huge problem for diagnosis and the continuity of care,” says Shawn C. Becker, MS, BSN, RN, director of patient safety initiatives for the USP.
Classification
In general, errors are divided into those that stem from individual factors and those that are system-related, which include environmental and organizational factors.
Environmental risks are often related to human factors. Dr. Nagamine offers an aviation analogy to demonstrate the many pulls on caregivers’ attention.
“What happens in a cockpit at take off is that you are not allowed to talk about anything other than the take-off checklist,” she says. “In medicine, we have nurses’ stations or medication carts in the middle of the hallway, so nurses are preparing meds and people are tugging on their shoulder and interrupting them during a critical task.”
Organizational factors involve culture and priorities. If your organization says it values quality and safety but doesn’t put in place policies and processes to support it, that affects diagnostics and error-free performance.
Market Drivers
“The discussion about quality is driven by medical error,” says Evan Falchuk, president of Best Doctors Inc., based in Boston. “But the issue is more interesting than simply looking for mistakes.”
Best Doctors partners with employers and health plans to help members with serious illnesses make sure they have the right diagnosis and treatment. Members can consult with specialists who assess diagnoses and can recommend treatment. The firm believes this is the best way to measure quality, and consumers around the world increasingly agree: The company serves more than 10 million people in 30 countries.
Best Doctors was founded in 1989 by two internists: Falchuk’s father, Kenneth H. Falchuk, MD, a professor of medicine at Harvard University Medical School, and Jose Halperin, MD, an associate professor of medicine at Harvard. The service they created is one in which doctors review a patient’s medical information, identify the important issues, and consult with leading experts from their peer-reviewed database. The company then has clinicians work with the patient and his or her doctor to ensure that the patient is getting appropriate care. The process has identified incorrect diagnosis or treatment in more than half of reviewed cases.
“Hospitalists should think about quality in terms of things happening outside the hospital,” says Falchuk. “The informed, demanding consumer is coming to healthcare, and their expectations are clear: to be paid attention to, to have all of their questions answered, and to be certain that their diagnosis and treatment are correct.” These sentiments affect how hospitals do business.
The increasing amount of medical information patients can find on the Internet can raise questions in their minds. “Patients want to trust their doctors,” Falchuk says. “But when the patient has lots of information and questions and finds it difficult to spend as much time as they would like with their doctor, trust is eroded—and patients start to wonder if their doctor is doing the right thing.”
The complexity of modern medicine, with new diagnoses, treatments, and testing, and ultra-specialized experts, can sometimes—ironically—lead to lesser quality.
“It is more important than ever before that doctors with differing perspectives discuss each case,” says Falchuk. “But doctors complain that the system, often because of constraints imposed by managed care, only allows for episodic interactions like that. If that kind of interaction can be made the norm, it will give patients an extraordinary amount of comfort as to the quality of their care.”
Falchuk believes the tipping point for combating errors is being reached—at least from the business point of view.
“With major employers, as many as one in 200 employees call us for help,” he says. “That is close to the incidence rate of the illnesses we commonly see: cancer, heart problems, and undiagnosed situations. When you see this flood of demand, you say, ‘Something is going on that is driving this.’ ”
These market-based factors are driving hospitals to publish and compare rates for process of care and mortality, and many medical centers are publishing report cards. With the advent of advanced technology, hospital and provider performance will be increasingly apparent and transparent. Corporations and institutions will have to be less guarded about what they share publicly as their public accountability is increased.
Interventions, Feedback
The healthcare industry has embraced British psychologist James Reason’s 1990 Swiss cheese model of error as a means of tackling the cumulative effects that cause adverse events. The model conceptualizes the factors that contributed to an error as holes in slices of Swiss cheese. Only when the holes line up does the adverse event occur; placing barriers at one or more of the holes “traps the error” from being realized.
For instance, Best Doctors notes “potholes” in the reading stage of pathology.
“We see many cases of underdiagnosis or even misdiagnosis based on one of the most difficult steps: a pathology review,” says Falchuk. “With new, specifically targeted treatments, getting that right is extremely significant.” Best Doctors experts often recommend having pathology re-reviewed. “I wouldn’t call this error, but patients view it as a question of quality,” he says.
Integrating technology with observation skills is an important way hospitals are working to improve diagnostics and reduce error.
Because the same factors contribute to a near miss as to an actual event, studying the patterns of near misses can provide a wealth of information.
“I heard some statistics that for every 19 near misses, you’re going to have one event,” says Dr. Nagamine. If on a particular day, a provider was fatigued or overtaxed and didn’t catch a contributing factor that is a risk—termed a “latent condition”—that’s when the holes line up. “An event is never just the result of one thing or one person; it is a combination of factors,” says Dr. Nagamine.
One example of this concerns an element in the policy for discharge bundles that institutions establish to better manage transfer of care. When lab results become available only after a patient’s discharge, it increases the risk for delays in diagnosis. Electronically placing the test results into the primary care physician’s e-mail inbox helps to “close the loop,” says Dr. Nagamine. “That information gets to somebody, and we’re clear on who that somebody is. We are putting in place those types of interventions—which are really the low-hanging fruit.”
Culture Change
Opening up about adverse events and providing feedback creates a different awareness about the risks surrounding the event.
“The look-alike, sound-alike medications are an example,” Dr. Nagamine says. “I went up to the unit and said, ‘A nurse recorded that she almost gave hydralazine instead of hydroxyzine—has that ever happened to you?’ The first three nurses I asked said, ‘Yes,’ ‘Yes,’ ‘Yes.’ Until I ask these types of questions, I don’t know. And until you can make it safe for your staff to talk, you will not have good information.”
Although this is the approach most of the safety world and quality world is embracing, it is not how most clinicians on the frontline view it.
“We are trying to educate people about a framework in which to think about this,” says Dr. Nagamine. “It is not constructive to point fingers, but it is important to give people feedback about how the event happened. It is far more constructive to look at the entire system and ask, ‘How did we fail here? What was your piece of it? What was the system’s piece of it?’ ”
Because of the connection between litigation and adverse events, changing the culture is a complex imperative. But providers must recognize that systems failures are involved in about 75% to 80% of medical malpractice cases—whether that involves communication breakdowns, inadequate availability of information, or a host of other factors. The individual, environment, and organization are linked.
Reducing negativity and sensitivity around the terms associated with error and reframing thinking toward prevention are important.
“There is a richness of information that comes once you change the culture from blaming to fixing,” says Dr. Nagamine. Providing feedback to frontline practitioners is key, as is thanking those who report. “It increases providers’ awareness about where the hot spots and vulnerabilities are and how to stay out of trouble. Simply by giving them information about an event raises their awareness of the magnitude of certain types of issues,” she explains.
When Dr. Nagamine led a safety initiative on the ICU floor consisting of human factors training and a new system for reporting events, the number of reports “went through roof,” she says. “My new problem was not that people were not reporting; it was being overwhelmed with the information that was coming in. We were able to create a culture of safety that made it safe to report and consequently had much better information from which we could devise prevention strategies.”
SHM, in planning to co-create standards for focused practice with the American Board of Internal Medicine, intends to promote the standards of professionalism along with other standards. The issue of personal accountability, although a part of that, has been less of a focus to date. In the future, all institutions may have technology hospitalists can use to learn whether the discharge diagnosis was correct in the months and years that followed. Will the culture be emotionally ready to handle what technology can offer?
“We will need to own it when things go well and when things don’t go well or when we are wrong,” says Dr. Halasyamani. “We need to be able to investigate the distribution of the reasons for misdiagnosis, determine how many of those problems are systems issues, and devise strategies to address them.” In a sense, she says, everything can be viewed as a system issue unless actions are egregious and malicious.
Yet when physicians are associated with an adverse event, research shows they feel they have little support to talk about it.
“The system we have in place has begun to try to address some of the issues related to system errors,” says Dr. Halasyamani. “But what if an individual does have an error? What systems do we have in place to support that person in the recovery? And along the way if we find people who are having these issues over and over again, we need to design processes to deal with that.”
One particular focus of SHM’s transfer-of-care initiative concerns communication surrounding handoffs. “We are setting those standards and thinking about what kinds of technology tools can help make those standards easier to adhere to and easier to implement,” says Dr. Halasyamani. TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
This is the second of a two-part series examining medical errors. Part 1 addressed thought processes hospitalists use that may lead to mistaken diagnoses (October 2007, p. 36). Part 2 examines what healthcare corporations are doing to improve diagnoses and reduce errors.
Pilots taking off, Swiss cheese, low-hanging fruit. Talk to hospitalists about the issue of medical errors and the analogies come quickly.
Ever since 2000’s landmark Institute of Medicine report “To Err is Human: Building a Safer Health System” found that anywhere from 40,000 to 100,000 patients incur injury or die every year because of medical errors, debate has been constant.
Medical literature is abundant on this topic. The Joint Commission, National Center for Patient Safety, Agency for Health Care Research and Quality, and myriad other organizations and institutions, including SHM, are all helping providers and hospitals solve the problems by establishing goals, standards, guidelines, and policies.
—Evan Falchuk, president, Best Doctors Inc., Boston
Definitions and Paradigms
Best-practice recommendations for reducing errors are generally based on two essential principles: using a systems-based approach to patient safety and creating an environment that supports open dialogue about errors, their causes, and strategies for prevention.
Terminology is a key factor. The terms “error” and “mistake” carry an emotional component associated with embarrassment and shame. Healthcare providers don’t like to be associated with errors. There is an accompanying fear of litigation, and people, perhaps especially physicians, don’t want to be known as someone who was sued.
“The language we use to talk about these issues is important,” says Janet Nagamine, MD, part-time hospitalist at Kaiser Permanente Santa Clara Medical Center in Calif. and current chair of SHM’s quality and patient safety committee. In fact, because of the negativity around the terms “misdiagnosis” and “delay in diagnosis” she advocates using the term “unintended adverse event” in order to appear more neutral.
“The term error is extremely threatening and scary to any health professional because it implies a personal failure,” says Dr. Nagamine. The goal when it comes to errors is essentially to look for the how—not the who.
Reporting medical errors is one thing, but reporting misdiagnoses is another, says Lakshmi Halasyamani, MD, vice chair for the department of internal medicine at St. Joseph’s Mercy Hospital in Ann Arbor, Mich., and SHM board member. “We don’t really talk about misdiagnosis,” she says. “That’s partly because we have tended to assign more individual blame for misdiagnoses.”
Drs. Nagamine and Halasyamani agree that altering the way of viewing errors means nurturing culture change.
“We have made very little headway helping physicians understand that in the course of their careers there will be misdiagnoses and the best of physicians have misdiagnoses,” says Dr. Halasyamani. “We are not developmentally at the same stage that we are with talking about medical errors.”
She believes this is largely a professionalism issue that first means normalizing the issue of misdiagnosis. “It is kind of ludicrous to think that you will practice medicine over 40 years and not have a misdiagnosis,” she says. “But we don’t look at it from that perspective when we begin to orient trainees.”
National Efforts
To the people at the U.S. Pharmacopeia Center for the Advancement of Patient Safety (USP), the arrival of universal electronic medical records (EMR) in the coming decade will be a boon to the error-reduction effort.
“Eventually we will all have our health information stored electronically for easy retrieval,” says Rodney W. Hicks, PhD, ARNP, manager, patient safety research and practice for the USP and first author on its most recent report. The beginning of regional networks for EMR is taking hold.
“Even before the IOM report, the USP was familiar with intensivists,” says Dr. Hicks. “We recognize hospitalists as experts who bring efficiency and effectiveness to the healthcare system.”
The USP maintains perhaps the largest database of medication errors in the world.1 Each year the USP issues a report that focuses on one topic and builds its knowledge base.
This year’s report focuses exclusively on the perioperative continuum of care. Last year’s covered ICU- and radiology-related errors. Two years ago the report was a five-year data summary of errors occurring primarily in hospitals.
“The area of errors due to breakdowns in handoffs remains a huge problem for diagnosis and the continuity of care,” says Shawn C. Becker, MS, BSN, RN, director of patient safety initiatives for the USP.
Classification
In general, errors are divided into those that stem from individual factors and those that are system-related, which include environmental and organizational factors.
Environmental risks are often related to human factors. Dr. Nagamine offers an aviation analogy to demonstrate the many pulls on caregivers’ attention.
“What happens in a cockpit at take off is that you are not allowed to talk about anything other than the take-off checklist,” she says. “In medicine, we have nurses’ stations or medication carts in the middle of the hallway, so nurses are preparing meds and people are tugging on their shoulder and interrupting them during a critical task.”
Organizational factors involve culture and priorities. If your organization says it values quality and safety but doesn’t put in place policies and processes to support it, that affects diagnostics and error-free performance.
Market Drivers
“The discussion about quality is driven by medical error,” says Evan Falchuk, president of Best Doctors Inc., based in Boston. “But the issue is more interesting than simply looking for mistakes.”
Best Doctors partners with employers and health plans to help members with serious illnesses make sure they have the right diagnosis and treatment. Members can consult with specialists who assess diagnoses and can recommend treatment. The firm believes this is the best way to measure quality, and consumers around the world increasingly agree: The company serves more than 10 million people in 30 countries.
Best Doctors was founded in 1989 by two internists: Falchuk’s father, Kenneth H. Falchuk, MD, a professor of medicine at Harvard University Medical School, and Jose Halperin, MD, an associate professor of medicine at Harvard. The service they created is one in which doctors review a patient’s medical information, identify the important issues, and consult with leading experts from their peer-reviewed database. The company then has clinicians work with the patient and his or her doctor to ensure that the patient is getting appropriate care. The process has identified incorrect diagnosis or treatment in more than half of reviewed cases.
“Hospitalists should think about quality in terms of things happening outside the hospital,” says Falchuk. “The informed, demanding consumer is coming to healthcare, and their expectations are clear: to be paid attention to, to have all of their questions answered, and to be certain that their diagnosis and treatment are correct.” These sentiments affect how hospitals do business.
The increasing amount of medical information patients can find on the Internet can raise questions in their minds. “Patients want to trust their doctors,” Falchuk says. “But when the patient has lots of information and questions and finds it difficult to spend as much time as they would like with their doctor, trust is eroded—and patients start to wonder if their doctor is doing the right thing.”
The complexity of modern medicine, with new diagnoses, treatments, and testing, and ultra-specialized experts, can sometimes—ironically—lead to lesser quality.
“It is more important than ever before that doctors with differing perspectives discuss each case,” says Falchuk. “But doctors complain that the system, often because of constraints imposed by managed care, only allows for episodic interactions like that. If that kind of interaction can be made the norm, it will give patients an extraordinary amount of comfort as to the quality of their care.”
Falchuk believes the tipping point for combating errors is being reached—at least from the business point of view.
“With major employers, as many as one in 200 employees call us for help,” he says. “That is close to the incidence rate of the illnesses we commonly see: cancer, heart problems, and undiagnosed situations. When you see this flood of demand, you say, ‘Something is going on that is driving this.’ ”
These market-based factors are driving hospitals to publish and compare rates for process of care and mortality, and many medical centers are publishing report cards. With the advent of advanced technology, hospital and provider performance will be increasingly apparent and transparent. Corporations and institutions will have to be less guarded about what they share publicly as their public accountability is increased.
Interventions, Feedback
The healthcare industry has embraced British psychologist James Reason’s 1990 Swiss cheese model of error as a means of tackling the cumulative effects that cause adverse events. The model conceptualizes the factors that contributed to an error as holes in slices of Swiss cheese. Only when the holes line up does the adverse event occur; placing barriers at one or more of the holes “traps the error” from being realized.
For instance, Best Doctors notes “potholes” in the reading stage of pathology.
“We see many cases of underdiagnosis or even misdiagnosis based on one of the most difficult steps: a pathology review,” says Falchuk. “With new, specifically targeted treatments, getting that right is extremely significant.” Best Doctors experts often recommend having pathology re-reviewed. “I wouldn’t call this error, but patients view it as a question of quality,” he says.
Integrating technology with observation skills is an important way hospitals are working to improve diagnostics and reduce error.
Because the same factors contribute to a near miss as to an actual event, studying the patterns of near misses can provide a wealth of information.
“I heard some statistics that for every 19 near misses, you’re going to have one event,” says Dr. Nagamine. If on a particular day, a provider was fatigued or overtaxed and didn’t catch a contributing factor that is a risk—termed a “latent condition”—that’s when the holes line up. “An event is never just the result of one thing or one person; it is a combination of factors,” says Dr. Nagamine.
One example of this concerns an element in the policy for discharge bundles that institutions establish to better manage transfer of care. When lab results become available only after a patient’s discharge, it increases the risk for delays in diagnosis. Electronically placing the test results into the primary care physician’s e-mail inbox helps to “close the loop,” says Dr. Nagamine. “That information gets to somebody, and we’re clear on who that somebody is. We are putting in place those types of interventions—which are really the low-hanging fruit.”
Culture Change
Opening up about adverse events and providing feedback creates a different awareness about the risks surrounding the event.
“The look-alike, sound-alike medications are an example,” Dr. Nagamine says. “I went up to the unit and said, ‘A nurse recorded that she almost gave hydralazine instead of hydroxyzine—has that ever happened to you?’ The first three nurses I asked said, ‘Yes,’ ‘Yes,’ ‘Yes.’ Until I ask these types of questions, I don’t know. And until you can make it safe for your staff to talk, you will not have good information.”
Although this is the approach most of the safety world and quality world is embracing, it is not how most clinicians on the frontline view it.
“We are trying to educate people about a framework in which to think about this,” says Dr. Nagamine. “It is not constructive to point fingers, but it is important to give people feedback about how the event happened. It is far more constructive to look at the entire system and ask, ‘How did we fail here? What was your piece of it? What was the system’s piece of it?’ ”
Because of the connection between litigation and adverse events, changing the culture is a complex imperative. But providers must recognize that systems failures are involved in about 75% to 80% of medical malpractice cases—whether that involves communication breakdowns, inadequate availability of information, or a host of other factors. The individual, environment, and organization are linked.
Reducing negativity and sensitivity around the terms associated with error and reframing thinking toward prevention are important.
“There is a richness of information that comes once you change the culture from blaming to fixing,” says Dr. Nagamine. Providing feedback to frontline practitioners is key, as is thanking those who report. “It increases providers’ awareness about where the hot spots and vulnerabilities are and how to stay out of trouble. Simply by giving them information about an event raises their awareness of the magnitude of certain types of issues,” she explains.
When Dr. Nagamine led a safety initiative on the ICU floor consisting of human factors training and a new system for reporting events, the number of reports “went through roof,” she says. “My new problem was not that people were not reporting; it was being overwhelmed with the information that was coming in. We were able to create a culture of safety that made it safe to report and consequently had much better information from which we could devise prevention strategies.”
SHM, in planning to co-create standards for focused practice with the American Board of Internal Medicine, intends to promote the standards of professionalism along with other standards. The issue of personal accountability, although a part of that, has been less of a focus to date. In the future, all institutions may have technology hospitalists can use to learn whether the discharge diagnosis was correct in the months and years that followed. Will the culture be emotionally ready to handle what technology can offer?
“We will need to own it when things go well and when things don’t go well or when we are wrong,” says Dr. Halasyamani. “We need to be able to investigate the distribution of the reasons for misdiagnosis, determine how many of those problems are systems issues, and devise strategies to address them.” In a sense, she says, everything can be viewed as a system issue unless actions are egregious and malicious.
Yet when physicians are associated with an adverse event, research shows they feel they have little support to talk about it.
“The system we have in place has begun to try to address some of the issues related to system errors,” says Dr. Halasyamani. “But what if an individual does have an error? What systems do we have in place to support that person in the recovery? And along the way if we find people who are having these issues over and over again, we need to design processes to deal with that.”
One particular focus of SHM’s transfer-of-care initiative concerns communication surrounding handoffs. “We are setting those standards and thinking about what kinds of technology tools can help make those standards easier to adhere to and easier to implement,” says Dr. Halasyamani. TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
This is the second of a two-part series examining medical errors. Part 1 addressed thought processes hospitalists use that may lead to mistaken diagnoses (October 2007, p. 36). Part 2 examines what healthcare corporations are doing to improve diagnoses and reduce errors.
Pilots taking off, Swiss cheese, low-hanging fruit. Talk to hospitalists about the issue of medical errors and the analogies come quickly.
Ever since 2000’s landmark Institute of Medicine report “To Err is Human: Building a Safer Health System” found that anywhere from 40,000 to 100,000 patients incur injury or die every year because of medical errors, debate has been constant.
Medical literature is abundant on this topic. The Joint Commission, National Center for Patient Safety, Agency for Health Care Research and Quality, and myriad other organizations and institutions, including SHM, are all helping providers and hospitals solve the problems by establishing goals, standards, guidelines, and policies.
—Evan Falchuk, president, Best Doctors Inc., Boston
Definitions and Paradigms
Best-practice recommendations for reducing errors are generally based on two essential principles: using a systems-based approach to patient safety and creating an environment that supports open dialogue about errors, their causes, and strategies for prevention.
Terminology is a key factor. The terms “error” and “mistake” carry an emotional component associated with embarrassment and shame. Healthcare providers don’t like to be associated with errors. There is an accompanying fear of litigation, and people, perhaps especially physicians, don’t want to be known as someone who was sued.
“The language we use to talk about these issues is important,” says Janet Nagamine, MD, part-time hospitalist at Kaiser Permanente Santa Clara Medical Center in Calif. and current chair of SHM’s quality and patient safety committee. In fact, because of the negativity around the terms “misdiagnosis” and “delay in diagnosis” she advocates using the term “unintended adverse event” in order to appear more neutral.
“The term error is extremely threatening and scary to any health professional because it implies a personal failure,” says Dr. Nagamine. The goal when it comes to errors is essentially to look for the how—not the who.
Reporting medical errors is one thing, but reporting misdiagnoses is another, says Lakshmi Halasyamani, MD, vice chair for the department of internal medicine at St. Joseph’s Mercy Hospital in Ann Arbor, Mich., and SHM board member. “We don’t really talk about misdiagnosis,” she says. “That’s partly because we have tended to assign more individual blame for misdiagnoses.”
Drs. Nagamine and Halasyamani agree that altering the way of viewing errors means nurturing culture change.
“We have made very little headway helping physicians understand that in the course of their careers there will be misdiagnoses and the best of physicians have misdiagnoses,” says Dr. Halasyamani. “We are not developmentally at the same stage that we are with talking about medical errors.”
She believes this is largely a professionalism issue that first means normalizing the issue of misdiagnosis. “It is kind of ludicrous to think that you will practice medicine over 40 years and not have a misdiagnosis,” she says. “But we don’t look at it from that perspective when we begin to orient trainees.”
National Efforts
To the people at the U.S. Pharmacopeia Center for the Advancement of Patient Safety (USP), the arrival of universal electronic medical records (EMR) in the coming decade will be a boon to the error-reduction effort.
“Eventually we will all have our health information stored electronically for easy retrieval,” says Rodney W. Hicks, PhD, ARNP, manager, patient safety research and practice for the USP and first author on its most recent report. The beginning of regional networks for EMR is taking hold.
“Even before the IOM report, the USP was familiar with intensivists,” says Dr. Hicks. “We recognize hospitalists as experts who bring efficiency and effectiveness to the healthcare system.”
The USP maintains perhaps the largest database of medication errors in the world.1 Each year the USP issues a report that focuses on one topic and builds its knowledge base.
This year’s report focuses exclusively on the perioperative continuum of care. Last year’s covered ICU- and radiology-related errors. Two years ago the report was a five-year data summary of errors occurring primarily in hospitals.
“The area of errors due to breakdowns in handoffs remains a huge problem for diagnosis and the continuity of care,” says Shawn C. Becker, MS, BSN, RN, director of patient safety initiatives for the USP.
Classification
In general, errors are divided into those that stem from individual factors and those that are system-related, which include environmental and organizational factors.
Environmental risks are often related to human factors. Dr. Nagamine offers an aviation analogy to demonstrate the many pulls on caregivers’ attention.
“What happens in a cockpit at take off is that you are not allowed to talk about anything other than the take-off checklist,” she says. “In medicine, we have nurses’ stations or medication carts in the middle of the hallway, so nurses are preparing meds and people are tugging on their shoulder and interrupting them during a critical task.”
Organizational factors involve culture and priorities. If your organization says it values quality and safety but doesn’t put in place policies and processes to support it, that affects diagnostics and error-free performance.
Market Drivers
“The discussion about quality is driven by medical error,” says Evan Falchuk, president of Best Doctors Inc., based in Boston. “But the issue is more interesting than simply looking for mistakes.”
Best Doctors partners with employers and health plans to help members with serious illnesses make sure they have the right diagnosis and treatment. Members can consult with specialists who assess diagnoses and can recommend treatment. The firm believes this is the best way to measure quality, and consumers around the world increasingly agree: The company serves more than 10 million people in 30 countries.
Best Doctors was founded in 1989 by two internists: Falchuk’s father, Kenneth H. Falchuk, MD, a professor of medicine at Harvard University Medical School, and Jose Halperin, MD, an associate professor of medicine at Harvard. The service they created is one in which doctors review a patient’s medical information, identify the important issues, and consult with leading experts from their peer-reviewed database. The company then has clinicians work with the patient and his or her doctor to ensure that the patient is getting appropriate care. The process has identified incorrect diagnosis or treatment in more than half of reviewed cases.
“Hospitalists should think about quality in terms of things happening outside the hospital,” says Falchuk. “The informed, demanding consumer is coming to healthcare, and their expectations are clear: to be paid attention to, to have all of their questions answered, and to be certain that their diagnosis and treatment are correct.” These sentiments affect how hospitals do business.
The increasing amount of medical information patients can find on the Internet can raise questions in their minds. “Patients want to trust their doctors,” Falchuk says. “But when the patient has lots of information and questions and finds it difficult to spend as much time as they would like with their doctor, trust is eroded—and patients start to wonder if their doctor is doing the right thing.”
The complexity of modern medicine, with new diagnoses, treatments, and testing, and ultra-specialized experts, can sometimes—ironically—lead to lesser quality.
“It is more important than ever before that doctors with differing perspectives discuss each case,” says Falchuk. “But doctors complain that the system, often because of constraints imposed by managed care, only allows for episodic interactions like that. If that kind of interaction can be made the norm, it will give patients an extraordinary amount of comfort as to the quality of their care.”
Falchuk believes the tipping point for combating errors is being reached—at least from the business point of view.
“With major employers, as many as one in 200 employees call us for help,” he says. “That is close to the incidence rate of the illnesses we commonly see: cancer, heart problems, and undiagnosed situations. When you see this flood of demand, you say, ‘Something is going on that is driving this.’ ”
These market-based factors are driving hospitals to publish and compare rates for process of care and mortality, and many medical centers are publishing report cards. With the advent of advanced technology, hospital and provider performance will be increasingly apparent and transparent. Corporations and institutions will have to be less guarded about what they share publicly as their public accountability is increased.
Interventions, Feedback
The healthcare industry has embraced British psychologist James Reason’s 1990 Swiss cheese model of error as a means of tackling the cumulative effects that cause adverse events. The model conceptualizes the factors that contributed to an error as holes in slices of Swiss cheese. Only when the holes line up does the adverse event occur; placing barriers at one or more of the holes “traps the error” from being realized.
For instance, Best Doctors notes “potholes” in the reading stage of pathology.
“We see many cases of underdiagnosis or even misdiagnosis based on one of the most difficult steps: a pathology review,” says Falchuk. “With new, specifically targeted treatments, getting that right is extremely significant.” Best Doctors experts often recommend having pathology re-reviewed. “I wouldn’t call this error, but patients view it as a question of quality,” he says.
Integrating technology with observation skills is an important way hospitals are working to improve diagnostics and reduce error.
Because the same factors contribute to a near miss as to an actual event, studying the patterns of near misses can provide a wealth of information.
“I heard some statistics that for every 19 near misses, you’re going to have one event,” says Dr. Nagamine. If on a particular day, a provider was fatigued or overtaxed and didn’t catch a contributing factor that is a risk—termed a “latent condition”—that’s when the holes line up. “An event is never just the result of one thing or one person; it is a combination of factors,” says Dr. Nagamine.
One example of this concerns an element in the policy for discharge bundles that institutions establish to better manage transfer of care. When lab results become available only after a patient’s discharge, it increases the risk for delays in diagnosis. Electronically placing the test results into the primary care physician’s e-mail inbox helps to “close the loop,” says Dr. Nagamine. “That information gets to somebody, and we’re clear on who that somebody is. We are putting in place those types of interventions—which are really the low-hanging fruit.”
Culture Change
Opening up about adverse events and providing feedback creates a different awareness about the risks surrounding the event.
“The look-alike, sound-alike medications are an example,” Dr. Nagamine says. “I went up to the unit and said, ‘A nurse recorded that she almost gave hydralazine instead of hydroxyzine—has that ever happened to you?’ The first three nurses I asked said, ‘Yes,’ ‘Yes,’ ‘Yes.’ Until I ask these types of questions, I don’t know. And until you can make it safe for your staff to talk, you will not have good information.”
Although this is the approach most of the safety world and quality world is embracing, it is not how most clinicians on the frontline view it.
“We are trying to educate people about a framework in which to think about this,” says Dr. Nagamine. “It is not constructive to point fingers, but it is important to give people feedback about how the event happened. It is far more constructive to look at the entire system and ask, ‘How did we fail here? What was your piece of it? What was the system’s piece of it?’ ”
Because of the connection between litigation and adverse events, changing the culture is a complex imperative. But providers must recognize that systems failures are involved in about 75% to 80% of medical malpractice cases—whether that involves communication breakdowns, inadequate availability of information, or a host of other factors. The individual, environment, and organization are linked.
Reducing negativity and sensitivity around the terms associated with error and reframing thinking toward prevention are important.
“There is a richness of information that comes once you change the culture from blaming to fixing,” says Dr. Nagamine. Providing feedback to frontline practitioners is key, as is thanking those who report. “It increases providers’ awareness about where the hot spots and vulnerabilities are and how to stay out of trouble. Simply by giving them information about an event raises their awareness of the magnitude of certain types of issues,” she explains.
When Dr. Nagamine led a safety initiative on the ICU floor consisting of human factors training and a new system for reporting events, the number of reports “went through roof,” she says. “My new problem was not that people were not reporting; it was being overwhelmed with the information that was coming in. We were able to create a culture of safety that made it safe to report and consequently had much better information from which we could devise prevention strategies.”
SHM, in planning to co-create standards for focused practice with the American Board of Internal Medicine, intends to promote the standards of professionalism along with other standards. The issue of personal accountability, although a part of that, has been less of a focus to date. In the future, all institutions may have technology hospitalists can use to learn whether the discharge diagnosis was correct in the months and years that followed. Will the culture be emotionally ready to handle what technology can offer?
“We will need to own it when things go well and when things don’t go well or when we are wrong,” says Dr. Halasyamani. “We need to be able to investigate the distribution of the reasons for misdiagnosis, determine how many of those problems are systems issues, and devise strategies to address them.” In a sense, she says, everything can be viewed as a system issue unless actions are egregious and malicious.
Yet when physicians are associated with an adverse event, research shows they feel they have little support to talk about it.
“The system we have in place has begun to try to address some of the issues related to system errors,” says Dr. Halasyamani. “But what if an individual does have an error? What systems do we have in place to support that person in the recovery? And along the way if we find people who are having these issues over and over again, we need to design processes to deal with that.”
One particular focus of SHM’s transfer-of-care initiative concerns communication surrounding handoffs. “We are setting those standards and thinking about what kinds of technology tools can help make those standards easier to adhere to and easier to implement,” says Dr. Halasyamani. TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
Prudent Partners
In an ideal world, the directors of hospitalist programs and residency programs would be perfectly aligned in their efforts to advance the hospital’s financial health, education initiatives, and quality of patient care. In reality, friction among them is common.
The roots of the tensions lie in their differing responsibilities.
“The goals for residency programs, which are governed by rules of the ACGME [Accreditation Council for Graduate Medical Education], don’t necessarily always match with those of the hospitalists for patient care delivery,” notes Alpesh Amin, MD, MBA, FACP, professor and chief, general internal medicine, executive director and founder of the hospitalist program at the University of California Irvine (UCI), and also associate program director of the UCI internal medicine residency program. Dr. Amin is also a member of SHM’s board of directors.
In teaching hospitals, residency program directors must ensure their residents comply with the ACGME work hour and patient load caps. These requirements limit residents to an 80-hour workweek and continuous on-site duty no longer than 24 consecutive hours, and multiresident internal medicine teams to no more than 24 patients at a time.
Compliance can pressure house staff hospitalists to pick up the slack. In addition, to advance the educational mission, a residency program director might want to have his or her residents read three hours a day. But the hospitalist, charged with caring for as many patients as possible, may want residents on his or her service to spend that time admitting, managing, and discharging patients.
William Iobst, MD, designated institutional official at Lehigh Valley Hospital in Allentown, Pa., and associate program director of the hospital medicine program, knows these issues firsthand. “The conflict usually comes up in that most hospitalist programs are put in place to provide streamlined and efficient service in the hospital,” he says. “To that end, they have targeted goals of improving efficiency, reducing length of stay, and using their expertise in repetitive treatments of the same condition [such as congestive heart failure or pneumonia] over time.”
Hospitalists, says Dr. Iobst, “get very efficient at providing care. In some ways, asking a hospitalist to serve as an educator potentially disrupts that charge of efficiency, quality, and rapid transit through the hospital. So, they may be put in a position of having conflicting bosses.”
—Alpesh Amin, MD, MBA, FACP, professor and chief, general internal medicine, executive director and founder of the hospitalist program at the University of California Irvine
Dual Roles
Some hospitalists work in both worlds: They serve as associate program directors for residency programs as well as directors of hospitalist programs. This can set the stage for conflicts.
Such is the case with Michael Pistoria, DO, chief of the division of hospital medicine at Lehigh Valley Hospital and associate program director for the free-standing medicine residency program.
“There are times when something in one area is impacting—sometimes adversely—the other areas for which I’m responsible,” he says. “One big issue that we really struggle with is how to deal with the [sometimes overwhelming] volume of patients when residents are able to do less and less according to ACGME rules.”
This is especially tricky, he says, when mapping coverage for overnight shifts. Not only are residents’ work hours capped, but the Residency Review Committee (RRC), which provides ACGME oversight, also stipulates that residents must have continuity with patients. They are not supposed to admit patients who won’t be seen by a resident the next day. This can create tension between the resident and hospitalist programs—especially when the latter face high patient loads.
One solution at Lehigh Valley has been to rotate resident teams admitting patients in the afternoon and evening hours, but only to their service. This ensures resident continuity for those patients and meets ACGME requirements. All other patients are admitted through the hospitalist service.
Capitalize on Uniqueness
It’s crucial to identify areas where hospitalists and program directors can dovetail efforts so the programs are not at loggerheads.
Program directors and medical directors can have a positive effect on meshing residency and private hospitalist programs. “We have to talk with our hospitalists, explain that we have no way around this [ACGME guideline], how it will impact them, and figure out a way [together] to help minimize that impact,” says Dr. Pistoria.
Dr. Amin believes the goals of the residency and hospital medicine programs can be mutually beneficial. “Some people may have inherent biases against the concept of hospital medicine,” he says. “But hopefully, as time goes on, you’ll find more and more hospitalists serving in program director or associate program director roles. My view is that the residency program ought to turn to the hospitalist when they’re looking for general inpatient, consultative, and perioperative curricular development. They could turn to hospitalists in the same way that they ask nephrology groups to help design a nephrology curriculum.”
The situation requires planning to make sure all stakeholders can accept the impact of having residents, Dr. Iobst points out. “The program director’s role is to work with the hospitalists and make sure that they understand that the residents have to adhere to their service caps,’’ he says. “The issue then would be to find other meaningful learning opportunities for residents that would not involve admitting patients.”
Dr. Iobst agrees with Dr. Amin. Some opportunities, he says, “are to ensure that a program director is capitalizing on what a hospitalist does.” If hospitalists are offering only “another general internal medicine inpatient service rotation to residents,” they are not capitalizing on their own uniqueness. Instead, hospitalists could offer hospital medicine as a senior rotation for residents. The residents could receive training and exposure to quality improvement; the business aspects of medicine, including the importance of length of stay and appropriate ICD-9 coding; and an evidence-based approach to care.
Embrace Teaching
Although ACGME work-hour caps sometimes create pressures, it’s up to hospitalists to be flexible with residents on their service, says Hasan Shabbir, MD, a hospitalist and associate medical director of quality at Emory Johns Creek Hospital in Duluth, Ga., and an assistant professor of medicine at Emory University in Atlanta.
This is especially true when particular residents are on night float rotation; admitting and managing patients into the early morning can bring them close to their work-hour caps. “We have to be cognizant of that [the ACGME guidelines], give them leeway, and let them go early whenever possible,” he says.
Having the right attitude toward residents is key. “I think we’ve approached [teaching residents] with the attitude that we’re quite fortunate to have residents to do a lot of the upfront work and to be able to help and teach them along the way,” explains Dr. Shabbir. “I think the negative feeling [about residents] is often tied to expectations. If one comes into our program, for example, and expects to just lie back and let the residents do all the work, that would be a bad expectation to have. All of us, having been [residents] at some point, can understand what residents go through. Not every hospitalist has the good fortune of having residents with them.”
There is value to having residents, agrees Dr. Iobst. “There’s the value of serving as a mentor; of training future colleagues; and the value for people who are enthused by the opportunity to teach. The key is to clearly establish all the boundaries and get them on the table to begin with, define which ones are absolutely required and are not flexible, and to ensure that the administration of the hospital that is supporting the hospitalists understands that need.”
Dr. Amin believes program directors need hospitalists to serve as faculty and that hospitalists need to take into account residency rules and regulations so the program can retain accreditation status.
“It’s a two-way street,” he says. “It doesn’t help anybody if the residency program is not accredited, and it doesn’t help anybody if the hospitalist faculty members don’t have good morale.” At UC Irvine, he says: “We try not to develop systems that overwhelm the residents; we also try not to develop systems that allow faculty to be overwhelmed. On the other hand, patient care is not predictable all the time, so some of the ACGME rules may put people into difficult situations.”
Goals and Relationships
Dr. Amin believes that if hospitalists and residency program directors can advocate for their own programs and work together for the greater good, they can craft an exponentially better team model.
One way to achieve this is to encourage more hospitalist directors to also serve as associate program directors/program directors of residency programs. This, he says, “could potentially help facilitate a stronger bridge between both programs.”
Within hospitalist groups, directors can encourage understanding about the dual sets of goals. It’s important for group leaders to involve everyone in the group when making decisions so people feel they are part of the process, says Alan L. Wang, MD, chief medical officer at Emory Johns Creek Hospital in Ga., and co-director of the hospitalist program.
Another tool for aligning hospitalists on their team with hospital goals, he says, is to share the patient workload. “One of the most important ways for medical directors to increase their credibility with the team members is to do shift work,” he asserts. “Getting in the trenches allows you to understand the day-to-day issues and problems that your hospitalists face.”
Dr. Shabbir notes that the burden of good relationship building should not fall solely to the group leaders. “There has to be an effort on all sides,” he says. “It can’t work with the leader alone trying. As a hospitalist, I think the focus has to be not only patient care, but also system efficiency, because, in the end, that makes for better overall patient care.”
Dr. Amin and others believe tensions between residency and hospitalist programs will resolve over time, in part due to hospitalists taking associate program director and program director roles, and in part to increased cooperation.
“The hospitalist could be the program director’s best friend and viewed as a vehicle for developing and training residents in system-based practice, competency-based learning and refinement of communication skills,” he says. TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
In an ideal world, the directors of hospitalist programs and residency programs would be perfectly aligned in their efforts to advance the hospital’s financial health, education initiatives, and quality of patient care. In reality, friction among them is common.
The roots of the tensions lie in their differing responsibilities.
“The goals for residency programs, which are governed by rules of the ACGME [Accreditation Council for Graduate Medical Education], don’t necessarily always match with those of the hospitalists for patient care delivery,” notes Alpesh Amin, MD, MBA, FACP, professor and chief, general internal medicine, executive director and founder of the hospitalist program at the University of California Irvine (UCI), and also associate program director of the UCI internal medicine residency program. Dr. Amin is also a member of SHM’s board of directors.
In teaching hospitals, residency program directors must ensure their residents comply with the ACGME work hour and patient load caps. These requirements limit residents to an 80-hour workweek and continuous on-site duty no longer than 24 consecutive hours, and multiresident internal medicine teams to no more than 24 patients at a time.
Compliance can pressure house staff hospitalists to pick up the slack. In addition, to advance the educational mission, a residency program director might want to have his or her residents read three hours a day. But the hospitalist, charged with caring for as many patients as possible, may want residents on his or her service to spend that time admitting, managing, and discharging patients.
William Iobst, MD, designated institutional official at Lehigh Valley Hospital in Allentown, Pa., and associate program director of the hospital medicine program, knows these issues firsthand. “The conflict usually comes up in that most hospitalist programs are put in place to provide streamlined and efficient service in the hospital,” he says. “To that end, they have targeted goals of improving efficiency, reducing length of stay, and using their expertise in repetitive treatments of the same condition [such as congestive heart failure or pneumonia] over time.”
Hospitalists, says Dr. Iobst, “get very efficient at providing care. In some ways, asking a hospitalist to serve as an educator potentially disrupts that charge of efficiency, quality, and rapid transit through the hospital. So, they may be put in a position of having conflicting bosses.”
—Alpesh Amin, MD, MBA, FACP, professor and chief, general internal medicine, executive director and founder of the hospitalist program at the University of California Irvine
Dual Roles
Some hospitalists work in both worlds: They serve as associate program directors for residency programs as well as directors of hospitalist programs. This can set the stage for conflicts.
Such is the case with Michael Pistoria, DO, chief of the division of hospital medicine at Lehigh Valley Hospital and associate program director for the free-standing medicine residency program.
“There are times when something in one area is impacting—sometimes adversely—the other areas for which I’m responsible,” he says. “One big issue that we really struggle with is how to deal with the [sometimes overwhelming] volume of patients when residents are able to do less and less according to ACGME rules.”
This is especially tricky, he says, when mapping coverage for overnight shifts. Not only are residents’ work hours capped, but the Residency Review Committee (RRC), which provides ACGME oversight, also stipulates that residents must have continuity with patients. They are not supposed to admit patients who won’t be seen by a resident the next day. This can create tension between the resident and hospitalist programs—especially when the latter face high patient loads.
One solution at Lehigh Valley has been to rotate resident teams admitting patients in the afternoon and evening hours, but only to their service. This ensures resident continuity for those patients and meets ACGME requirements. All other patients are admitted through the hospitalist service.
Capitalize on Uniqueness
It’s crucial to identify areas where hospitalists and program directors can dovetail efforts so the programs are not at loggerheads.
Program directors and medical directors can have a positive effect on meshing residency and private hospitalist programs. “We have to talk with our hospitalists, explain that we have no way around this [ACGME guideline], how it will impact them, and figure out a way [together] to help minimize that impact,” says Dr. Pistoria.
Dr. Amin believes the goals of the residency and hospital medicine programs can be mutually beneficial. “Some people may have inherent biases against the concept of hospital medicine,” he says. “But hopefully, as time goes on, you’ll find more and more hospitalists serving in program director or associate program director roles. My view is that the residency program ought to turn to the hospitalist when they’re looking for general inpatient, consultative, and perioperative curricular development. They could turn to hospitalists in the same way that they ask nephrology groups to help design a nephrology curriculum.”
The situation requires planning to make sure all stakeholders can accept the impact of having residents, Dr. Iobst points out. “The program director’s role is to work with the hospitalists and make sure that they understand that the residents have to adhere to their service caps,’’ he says. “The issue then would be to find other meaningful learning opportunities for residents that would not involve admitting patients.”
Dr. Iobst agrees with Dr. Amin. Some opportunities, he says, “are to ensure that a program director is capitalizing on what a hospitalist does.” If hospitalists are offering only “another general internal medicine inpatient service rotation to residents,” they are not capitalizing on their own uniqueness. Instead, hospitalists could offer hospital medicine as a senior rotation for residents. The residents could receive training and exposure to quality improvement; the business aspects of medicine, including the importance of length of stay and appropriate ICD-9 coding; and an evidence-based approach to care.
Embrace Teaching
Although ACGME work-hour caps sometimes create pressures, it’s up to hospitalists to be flexible with residents on their service, says Hasan Shabbir, MD, a hospitalist and associate medical director of quality at Emory Johns Creek Hospital in Duluth, Ga., and an assistant professor of medicine at Emory University in Atlanta.
This is especially true when particular residents are on night float rotation; admitting and managing patients into the early morning can bring them close to their work-hour caps. “We have to be cognizant of that [the ACGME guidelines], give them leeway, and let them go early whenever possible,” he says.
Having the right attitude toward residents is key. “I think we’ve approached [teaching residents] with the attitude that we’re quite fortunate to have residents to do a lot of the upfront work and to be able to help and teach them along the way,” explains Dr. Shabbir. “I think the negative feeling [about residents] is often tied to expectations. If one comes into our program, for example, and expects to just lie back and let the residents do all the work, that would be a bad expectation to have. All of us, having been [residents] at some point, can understand what residents go through. Not every hospitalist has the good fortune of having residents with them.”
There is value to having residents, agrees Dr. Iobst. “There’s the value of serving as a mentor; of training future colleagues; and the value for people who are enthused by the opportunity to teach. The key is to clearly establish all the boundaries and get them on the table to begin with, define which ones are absolutely required and are not flexible, and to ensure that the administration of the hospital that is supporting the hospitalists understands that need.”
Dr. Amin believes program directors need hospitalists to serve as faculty and that hospitalists need to take into account residency rules and regulations so the program can retain accreditation status.
“It’s a two-way street,” he says. “It doesn’t help anybody if the residency program is not accredited, and it doesn’t help anybody if the hospitalist faculty members don’t have good morale.” At UC Irvine, he says: “We try not to develop systems that overwhelm the residents; we also try not to develop systems that allow faculty to be overwhelmed. On the other hand, patient care is not predictable all the time, so some of the ACGME rules may put people into difficult situations.”
Goals and Relationships
Dr. Amin believes that if hospitalists and residency program directors can advocate for their own programs and work together for the greater good, they can craft an exponentially better team model.
One way to achieve this is to encourage more hospitalist directors to also serve as associate program directors/program directors of residency programs. This, he says, “could potentially help facilitate a stronger bridge between both programs.”
Within hospitalist groups, directors can encourage understanding about the dual sets of goals. It’s important for group leaders to involve everyone in the group when making decisions so people feel they are part of the process, says Alan L. Wang, MD, chief medical officer at Emory Johns Creek Hospital in Ga., and co-director of the hospitalist program.
Another tool for aligning hospitalists on their team with hospital goals, he says, is to share the patient workload. “One of the most important ways for medical directors to increase their credibility with the team members is to do shift work,” he asserts. “Getting in the trenches allows you to understand the day-to-day issues and problems that your hospitalists face.”
Dr. Shabbir notes that the burden of good relationship building should not fall solely to the group leaders. “There has to be an effort on all sides,” he says. “It can’t work with the leader alone trying. As a hospitalist, I think the focus has to be not only patient care, but also system efficiency, because, in the end, that makes for better overall patient care.”
Dr. Amin and others believe tensions between residency and hospitalist programs will resolve over time, in part due to hospitalists taking associate program director and program director roles, and in part to increased cooperation.
“The hospitalist could be the program director’s best friend and viewed as a vehicle for developing and training residents in system-based practice, competency-based learning and refinement of communication skills,” he says. TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
In an ideal world, the directors of hospitalist programs and residency programs would be perfectly aligned in their efforts to advance the hospital’s financial health, education initiatives, and quality of patient care. In reality, friction among them is common.
The roots of the tensions lie in their differing responsibilities.
“The goals for residency programs, which are governed by rules of the ACGME [Accreditation Council for Graduate Medical Education], don’t necessarily always match with those of the hospitalists for patient care delivery,” notes Alpesh Amin, MD, MBA, FACP, professor and chief, general internal medicine, executive director and founder of the hospitalist program at the University of California Irvine (UCI), and also associate program director of the UCI internal medicine residency program. Dr. Amin is also a member of SHM’s board of directors.
In teaching hospitals, residency program directors must ensure their residents comply with the ACGME work hour and patient load caps. These requirements limit residents to an 80-hour workweek and continuous on-site duty no longer than 24 consecutive hours, and multiresident internal medicine teams to no more than 24 patients at a time.
Compliance can pressure house staff hospitalists to pick up the slack. In addition, to advance the educational mission, a residency program director might want to have his or her residents read three hours a day. But the hospitalist, charged with caring for as many patients as possible, may want residents on his or her service to spend that time admitting, managing, and discharging patients.
William Iobst, MD, designated institutional official at Lehigh Valley Hospital in Allentown, Pa., and associate program director of the hospital medicine program, knows these issues firsthand. “The conflict usually comes up in that most hospitalist programs are put in place to provide streamlined and efficient service in the hospital,” he says. “To that end, they have targeted goals of improving efficiency, reducing length of stay, and using their expertise in repetitive treatments of the same condition [such as congestive heart failure or pneumonia] over time.”
Hospitalists, says Dr. Iobst, “get very efficient at providing care. In some ways, asking a hospitalist to serve as an educator potentially disrupts that charge of efficiency, quality, and rapid transit through the hospital. So, they may be put in a position of having conflicting bosses.”
—Alpesh Amin, MD, MBA, FACP, professor and chief, general internal medicine, executive director and founder of the hospitalist program at the University of California Irvine
Dual Roles
Some hospitalists work in both worlds: They serve as associate program directors for residency programs as well as directors of hospitalist programs. This can set the stage for conflicts.
Such is the case with Michael Pistoria, DO, chief of the division of hospital medicine at Lehigh Valley Hospital and associate program director for the free-standing medicine residency program.
“There are times when something in one area is impacting—sometimes adversely—the other areas for which I’m responsible,” he says. “One big issue that we really struggle with is how to deal with the [sometimes overwhelming] volume of patients when residents are able to do less and less according to ACGME rules.”
This is especially tricky, he says, when mapping coverage for overnight shifts. Not only are residents’ work hours capped, but the Residency Review Committee (RRC), which provides ACGME oversight, also stipulates that residents must have continuity with patients. They are not supposed to admit patients who won’t be seen by a resident the next day. This can create tension between the resident and hospitalist programs—especially when the latter face high patient loads.
One solution at Lehigh Valley has been to rotate resident teams admitting patients in the afternoon and evening hours, but only to their service. This ensures resident continuity for those patients and meets ACGME requirements. All other patients are admitted through the hospitalist service.
Capitalize on Uniqueness
It’s crucial to identify areas where hospitalists and program directors can dovetail efforts so the programs are not at loggerheads.
Program directors and medical directors can have a positive effect on meshing residency and private hospitalist programs. “We have to talk with our hospitalists, explain that we have no way around this [ACGME guideline], how it will impact them, and figure out a way [together] to help minimize that impact,” says Dr. Pistoria.
Dr. Amin believes the goals of the residency and hospital medicine programs can be mutually beneficial. “Some people may have inherent biases against the concept of hospital medicine,” he says. “But hopefully, as time goes on, you’ll find more and more hospitalists serving in program director or associate program director roles. My view is that the residency program ought to turn to the hospitalist when they’re looking for general inpatient, consultative, and perioperative curricular development. They could turn to hospitalists in the same way that they ask nephrology groups to help design a nephrology curriculum.”
The situation requires planning to make sure all stakeholders can accept the impact of having residents, Dr. Iobst points out. “The program director’s role is to work with the hospitalists and make sure that they understand that the residents have to adhere to their service caps,’’ he says. “The issue then would be to find other meaningful learning opportunities for residents that would not involve admitting patients.”
Dr. Iobst agrees with Dr. Amin. Some opportunities, he says, “are to ensure that a program director is capitalizing on what a hospitalist does.” If hospitalists are offering only “another general internal medicine inpatient service rotation to residents,” they are not capitalizing on their own uniqueness. Instead, hospitalists could offer hospital medicine as a senior rotation for residents. The residents could receive training and exposure to quality improvement; the business aspects of medicine, including the importance of length of stay and appropriate ICD-9 coding; and an evidence-based approach to care.
Embrace Teaching
Although ACGME work-hour caps sometimes create pressures, it’s up to hospitalists to be flexible with residents on their service, says Hasan Shabbir, MD, a hospitalist and associate medical director of quality at Emory Johns Creek Hospital in Duluth, Ga., and an assistant professor of medicine at Emory University in Atlanta.
This is especially true when particular residents are on night float rotation; admitting and managing patients into the early morning can bring them close to their work-hour caps. “We have to be cognizant of that [the ACGME guidelines], give them leeway, and let them go early whenever possible,” he says.
Having the right attitude toward residents is key. “I think we’ve approached [teaching residents] with the attitude that we’re quite fortunate to have residents to do a lot of the upfront work and to be able to help and teach them along the way,” explains Dr. Shabbir. “I think the negative feeling [about residents] is often tied to expectations. If one comes into our program, for example, and expects to just lie back and let the residents do all the work, that would be a bad expectation to have. All of us, having been [residents] at some point, can understand what residents go through. Not every hospitalist has the good fortune of having residents with them.”
There is value to having residents, agrees Dr. Iobst. “There’s the value of serving as a mentor; of training future colleagues; and the value for people who are enthused by the opportunity to teach. The key is to clearly establish all the boundaries and get them on the table to begin with, define which ones are absolutely required and are not flexible, and to ensure that the administration of the hospital that is supporting the hospitalists understands that need.”
Dr. Amin believes program directors need hospitalists to serve as faculty and that hospitalists need to take into account residency rules and regulations so the program can retain accreditation status.
“It’s a two-way street,” he says. “It doesn’t help anybody if the residency program is not accredited, and it doesn’t help anybody if the hospitalist faculty members don’t have good morale.” At UC Irvine, he says: “We try not to develop systems that overwhelm the residents; we also try not to develop systems that allow faculty to be overwhelmed. On the other hand, patient care is not predictable all the time, so some of the ACGME rules may put people into difficult situations.”
Goals and Relationships
Dr. Amin believes that if hospitalists and residency program directors can advocate for their own programs and work together for the greater good, they can craft an exponentially better team model.
One way to achieve this is to encourage more hospitalist directors to also serve as associate program directors/program directors of residency programs. This, he says, “could potentially help facilitate a stronger bridge between both programs.”
Within hospitalist groups, directors can encourage understanding about the dual sets of goals. It’s important for group leaders to involve everyone in the group when making decisions so people feel they are part of the process, says Alan L. Wang, MD, chief medical officer at Emory Johns Creek Hospital in Ga., and co-director of the hospitalist program.
Another tool for aligning hospitalists on their team with hospital goals, he says, is to share the patient workload. “One of the most important ways for medical directors to increase their credibility with the team members is to do shift work,” he asserts. “Getting in the trenches allows you to understand the day-to-day issues and problems that your hospitalists face.”
Dr. Shabbir notes that the burden of good relationship building should not fall solely to the group leaders. “There has to be an effort on all sides,” he says. “It can’t work with the leader alone trying. As a hospitalist, I think the focus has to be not only patient care, but also system efficiency, because, in the end, that makes for better overall patient care.”
Dr. Amin and others believe tensions between residency and hospitalist programs will resolve over time, in part due to hospitalists taking associate program director and program director roles, and in part to increased cooperation.
“The hospitalist could be the program director’s best friend and viewed as a vehicle for developing and training residents in system-based practice, competency-based learning and refinement of communication skills,” he says. TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
Tackle Technology
Dennis Deruelle, MD, a hospitalist at University Community Hospital in Tampa, Fla., once needed reliable medical information in a hurry while treating a young woman admitted to the hospital with cellulitis.
The woman was later diagnosed with methicillin-resistant staphylococcus aureus (MRSA). After Dr. Deruelle administered prochlorperazine (Compazine), she had a severe dystonic reaction.
“She was going rigid right before my eyes,” Dr. Deruelle says. There was no instantly accessible hospital clearinghouse of medical information, although he had called the pharmacy department and was waiting for a call back. So he opened his laptop and turned to an aid available to anyone with a computer and Internet access: Google. “I immediately looked up information on reactions to Compazine and the correct dose for counteracting it. I administered the dose, and within minutes [the patient] was getting better.”
Dr. Deruelle is not alone among physicians in answering medical questions with Google. (See The Hospitalist, July 2007, p. 33.)
He has been interested in medical applications of computer technology for years and serves on SHM’s advisory committee on technology. He receives tech support from his employer, IPC-The Hospitalist Company, based in North Hollywood, Calif. IPC offers its physicians a Web-accessible network called IPC Link—a “virtual office” to help with billing, medical decision support, reference software, continuing medical education, and even blogs written by company CEO Adam Singer, MD.
But Dr. Deruelle has also developed his own applications, including an off-the-shelf voice recognition software loaded onto his company-supplied, 2.5-lb. Tablet PC. He uses it to dictate brief notes to give attending physicians a heads-up about patients being discharged. These notes are uploaded to the company’s network, which automatically generates a fax to the attending within minutes.
The formal discharge summary, produced by the hospital’s medical transcription department, may take 48 hours to arrive.
Dr. Deruelle has wireless Internet access at four of the five hospitals he visits as a hospitalist practice leader.
“As soon as I walk in the door I’m ‘hot,’ ” he says. At the fifth hospital, he uses workstation computers to connect with IPC Link.
Array of Options
A dizzying range of communications technology is available to working hospitalists, typically accessed through personal digital assistants (PDAs), smartphones, computer tablets, pocket PCs, and laptops.
The Palm Pilot, introduced in 1996, is a well-known example of this technology, as are the Palm Treo and BlackBerry. PDAs combine the functions of cell phones, video phones, cameras, video recorders, media players, Web browsers, reference tools, bar code scanners, and global positioning system (GPS) devices—all in a palm-size package.
Hardware and supporting software vary in terms of ease of use, in particular, the ability to interface with the Web or the hospital, practice, or employer network the physician needs to connect with.
The technology is evolving rapidly. But anomalies abound, such as dependence on the fax machine as a staple of communication with attending physicians. Through all of these changes, hospitalists are responsible for learning what works and how best to take advantage of the technology to make their jobs easier.
Hospitalists also vary tremendously in terms of their comfort levels and openness to new technology.
“There is a considerable gap between those of us who ‘Palm’ and those who don’t,” says Timothy Hartzog, MD, pediatric hospitalist at Medical University of South Carolina (MUSC) in Charleston and a medical technology consultant. “Physicians want their patient data in different ways. Some want it printed out or in a paper chart.”
—Steven Liu, MD, of Emory University Medical Center in Atlanta
But implementation of technology, such as hospital electronic health records or computerized physician order entry, inevitably changes their relationships with information technology and patient information.
Some hospitalists, like Dr. Deruelle, are interested in what communication technology can bring their work and how to adapt it to their needs. Others, like Dr. Hartzog, medical director of Information Technology at MUSC, have taken added responsibilities for technology within their institutions.
And a few, such as Steven Liu, MD, of Emory University Medical Center in Atlanta, have taken their interest in computer technology a step further. In 1999, Dr. Liu founded Ingenious Med, an Atlanta software company that offers a suite of inpatient practice management applications to working hospitalists.
“Often the hospitalist is already on the forefront of technology,” Dr. Liu says. “The demographic is typically younger and techno-savvy. They may get tapped by their hospitals to help customize the electronic health record to make sure it satisfies the needs of clinicians. Conversely, if an electronic project does not involve strong physician feedback and collaboration, physicians can be the Achilles’ heel impeding successful implementation. Even though they are the ones who stand to gain most from the potential efficiency, physicians will not adopt technology that does not fit their workflow.”
State of the Art?
Russell Cucina, MD, MS, a hospitalist at the University of California-San Francisco Medical Center, San Francisco, is also the associate medical director for information technology at UCSF.
Dr. Cucina quips that a good example of a state-of-the-art, stand-alone patient data management system offering rapid data entry, long battery life, and high mobility is the paper index card, the longtime standard for making rounding notes.
“Plenty of doctors, including me, use it every day,” he says. But growing numbers of hospitalists also use PDAs, smartphones, and laptops to access information and support applications. Among the plethora of reference applications readily available to physicians by PDA or laptop are UpToDate, Epocrates, the Pocket Sanford Guide to Anti-Microbial Therapy, and Merck Medicus.
“I use many different resources as a hospitalist,” Dr. Cucina says. “I Google all the time.” Hospitalists still have opportunities to innovate, although increasingly their “home-grown” solutions will compete with multinational technology conglomerates entering the medical market.
The use of technology and equipment also varies depending on whether the hospitalist is employed by the hospital or part of an independent medical group.
Another factor is whether that hospital is academic, community-based, or part of a system like the Veterans Affairs or a staff-model HMO such as Kaiser Permanente. But all hospitalists are used to working on the run, Dr. Cucina says. And in their daily jobs, workflow is everything.
Tech in Use
“I use medical technology on the job to a moderate degree,” reports Latha Sivaprasad, MD, a hospitalist at Beth Israel Medical Center in New York City. “This is my sixth year working as a hospitalist, and for the first five years I didn’t use a specific device. Now I have a Palm-based program with MD Everywhere, Epocrates, UpToDate, and the ability to do billing. The hospital’s tech support staff trained us on the new system and how to use the PDA for tasks like developing rounding lists, accessing our colleagues’ lists and creating system-based memos.”
Dr. Sivaprasad also has GPS in her car, a cell phone, and a laptop at home. “We probably aren’t using medical technology as much as we could,” she says. “Many physicians still write prescriptions by hand. I’ve never used voice-recognition software. In a previous hospital, we used the hospital’s transcription service for dictated notes.”
Karim Godamunne, MD, MBA, a hospitalist with Eagle Hospital Physicians and a practice medical director at South Fulton Medical Center in Atlanta, uses a PDA at work for billing.
“I don’t use the PDA intensively,’’ he says. “I’d like to see our hospital create a wireless network like the one I have at home. Our sister hospital has wireless.” He notes, however, that there are computer workstations for him to use at his hospital.
Dr. Godamunne’s group has a practice coordinator who faxes discharge summaries to attending physicians.
“Fax is kind of what they expect these days,” he says. “I’m not sure e-mail would be as reliable for the community we serve. I’d be concerned that the attendings wouldn’t read their e-mails.” He says he sometimes gives written notes to patients at discharge with instructions to hand the note to their physician on their next office visit.
Michelle Pezzani, MD, is part of a 10-member hospital medicine group that practices at El Camino Hospital in Mountain View, Calif., in the heart of Silicon Valley. The hospital tries to stay on the cutting edge with technology, and its hospitalists were given Microsoft XP Tablet laptops a few years ago. “I access the Web two to four times a day at work,” Dr. Pezzani says. “It helps keep us current. The great thing about the laptop is I also take it home with me, and I can use it to check or reorder labs from home. We’re all connected to the hospital’s Intranet from home.”
“One of the issues we’re struggling with is how to achieve the best sign-out possible,” with up to four hospitalists on the day shift checking out and handing over patient responsibilities to the night shift, Dr. Pezzani says. For her, the ideal sign-out is face to face because it permits asking questions and reading nonverbal cues about how sick the patients really are. However, the logistics of multiple physicians and patients makes this ideal difficult to achieve.
Second best (if all group members used a Palm Pilot), would be to send sign-outs via text messaging—although that would also present logistical challenges. “Texting is easier,” she says. “You know who is sending the message. We could beam the written sign-out to each other in a matter of seconds, making it quick and easy. Furthermore, any day-to-day changes on a specific patient would be easy to amend and easy to send. It’s also a quick way to let a colleague know, ‘I need you right now!’ ”
The hospitalists at El Camino use voicemail to record sign-outs. But these messages can take a long time to record and play back, multiplied by the four physicians signing out. “Ideally, there would be a different voice mail for every patient, so I wouldn’t have to listen to patients A, B, C, D, and E to get to the pertinent information about patient F, who is crashing upstairs,” she says. Dr. Pezzani’s group is still exploring how to balance these considerations.
She says her hospitalist group is tight-knit and collaborative. “We leave our cell phones on all the time and answer each other’s calls after hours,” she says. “For example, I’m now on vacation with my family in San Diego and I have gotten at least two calls a day from my partners, either business related, or something like: ‘Do you remember that patient you admitted? Can you give me some information on them?’”
The Wired Hospital
Dr. Cucina is excited about the extra large, easy-to-grip handle on the 3-lb. Motion Computing C5 portable PC that UCSF hospitalists are field-testing. He’s also intrigued by the ever-expanding opportunities for interfacing with the hospital’s technology.
In August he gave a tour of Unit 13L at UCSF’s Moffitt/Long Hospital, a new ward that opened in June and is being used as a technology demonstration site.
The 32-bed unit has a narrow corridor lined with 10 computer workstations for the nurses. All 10 are in use. In an adjacent cubicle, several physicians are typing on their laptops.
On the unit, portable vital signs monitors are attached to rolling stands that also have docking ports for the laptops, offering real-time point-of-care acquisition of vital-signs data directly into the hospital’s medical record.
A nurse or physician can grab the big-handled Tablet PC and run to another room while remaining connected to the patient’s vital signs. The docking ports in patients’ rooms are also linked to a 37-inch, high-definition television. “A clinician can show the patient radiographic studies here or bring up interactive patient education programs,” he explains.
One of the most exciting potentials for this emerging technology is to find ways for embedding medical decision support in physicians’ workflow. “We know that the barriers to physicians routinely consulting decision support applications are high,” Dr. Cucina says.
For Dr. Deruelle, who had to look outside of hospital channels to answer his question about a dystonic patient, medicine has a serious information gap. “I believe we will move to where the technology will put that information at my fingertips,” he says. “Why aren’t we there yet? Not enough people are using the technology, and we don’t agree on what information should be included. But I think we can start with basic things and work up from there. What excites me is that we’re closing the information gap—although medicine is still in the Stone Age compared with other professions.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Dennis Deruelle, MD, a hospitalist at University Community Hospital in Tampa, Fla., once needed reliable medical information in a hurry while treating a young woman admitted to the hospital with cellulitis.
The woman was later diagnosed with methicillin-resistant staphylococcus aureus (MRSA). After Dr. Deruelle administered prochlorperazine (Compazine), she had a severe dystonic reaction.
“She was going rigid right before my eyes,” Dr. Deruelle says. There was no instantly accessible hospital clearinghouse of medical information, although he had called the pharmacy department and was waiting for a call back. So he opened his laptop and turned to an aid available to anyone with a computer and Internet access: Google. “I immediately looked up information on reactions to Compazine and the correct dose for counteracting it. I administered the dose, and within minutes [the patient] was getting better.”
Dr. Deruelle is not alone among physicians in answering medical questions with Google. (See The Hospitalist, July 2007, p. 33.)
He has been interested in medical applications of computer technology for years and serves on SHM’s advisory committee on technology. He receives tech support from his employer, IPC-The Hospitalist Company, based in North Hollywood, Calif. IPC offers its physicians a Web-accessible network called IPC Link—a “virtual office” to help with billing, medical decision support, reference software, continuing medical education, and even blogs written by company CEO Adam Singer, MD.
But Dr. Deruelle has also developed his own applications, including an off-the-shelf voice recognition software loaded onto his company-supplied, 2.5-lb. Tablet PC. He uses it to dictate brief notes to give attending physicians a heads-up about patients being discharged. These notes are uploaded to the company’s network, which automatically generates a fax to the attending within minutes.
The formal discharge summary, produced by the hospital’s medical transcription department, may take 48 hours to arrive.
Dr. Deruelle has wireless Internet access at four of the five hospitals he visits as a hospitalist practice leader.
“As soon as I walk in the door I’m ‘hot,’ ” he says. At the fifth hospital, he uses workstation computers to connect with IPC Link.
Array of Options
A dizzying range of communications technology is available to working hospitalists, typically accessed through personal digital assistants (PDAs), smartphones, computer tablets, pocket PCs, and laptops.
The Palm Pilot, introduced in 1996, is a well-known example of this technology, as are the Palm Treo and BlackBerry. PDAs combine the functions of cell phones, video phones, cameras, video recorders, media players, Web browsers, reference tools, bar code scanners, and global positioning system (GPS) devices—all in a palm-size package.
Hardware and supporting software vary in terms of ease of use, in particular, the ability to interface with the Web or the hospital, practice, or employer network the physician needs to connect with.
The technology is evolving rapidly. But anomalies abound, such as dependence on the fax machine as a staple of communication with attending physicians. Through all of these changes, hospitalists are responsible for learning what works and how best to take advantage of the technology to make their jobs easier.
Hospitalists also vary tremendously in terms of their comfort levels and openness to new technology.
“There is a considerable gap between those of us who ‘Palm’ and those who don’t,” says Timothy Hartzog, MD, pediatric hospitalist at Medical University of South Carolina (MUSC) in Charleston and a medical technology consultant. “Physicians want their patient data in different ways. Some want it printed out or in a paper chart.”
—Steven Liu, MD, of Emory University Medical Center in Atlanta
But implementation of technology, such as hospital electronic health records or computerized physician order entry, inevitably changes their relationships with information technology and patient information.
Some hospitalists, like Dr. Deruelle, are interested in what communication technology can bring their work and how to adapt it to their needs. Others, like Dr. Hartzog, medical director of Information Technology at MUSC, have taken added responsibilities for technology within their institutions.
And a few, such as Steven Liu, MD, of Emory University Medical Center in Atlanta, have taken their interest in computer technology a step further. In 1999, Dr. Liu founded Ingenious Med, an Atlanta software company that offers a suite of inpatient practice management applications to working hospitalists.
“Often the hospitalist is already on the forefront of technology,” Dr. Liu says. “The demographic is typically younger and techno-savvy. They may get tapped by their hospitals to help customize the electronic health record to make sure it satisfies the needs of clinicians. Conversely, if an electronic project does not involve strong physician feedback and collaboration, physicians can be the Achilles’ heel impeding successful implementation. Even though they are the ones who stand to gain most from the potential efficiency, physicians will not adopt technology that does not fit their workflow.”
State of the Art?
Russell Cucina, MD, MS, a hospitalist at the University of California-San Francisco Medical Center, San Francisco, is also the associate medical director for information technology at UCSF.
Dr. Cucina quips that a good example of a state-of-the-art, stand-alone patient data management system offering rapid data entry, long battery life, and high mobility is the paper index card, the longtime standard for making rounding notes.
“Plenty of doctors, including me, use it every day,” he says. But growing numbers of hospitalists also use PDAs, smartphones, and laptops to access information and support applications. Among the plethora of reference applications readily available to physicians by PDA or laptop are UpToDate, Epocrates, the Pocket Sanford Guide to Anti-Microbial Therapy, and Merck Medicus.
“I use many different resources as a hospitalist,” Dr. Cucina says. “I Google all the time.” Hospitalists still have opportunities to innovate, although increasingly their “home-grown” solutions will compete with multinational technology conglomerates entering the medical market.
The use of technology and equipment also varies depending on whether the hospitalist is employed by the hospital or part of an independent medical group.
Another factor is whether that hospital is academic, community-based, or part of a system like the Veterans Affairs or a staff-model HMO such as Kaiser Permanente. But all hospitalists are used to working on the run, Dr. Cucina says. And in their daily jobs, workflow is everything.
Tech in Use
“I use medical technology on the job to a moderate degree,” reports Latha Sivaprasad, MD, a hospitalist at Beth Israel Medical Center in New York City. “This is my sixth year working as a hospitalist, and for the first five years I didn’t use a specific device. Now I have a Palm-based program with MD Everywhere, Epocrates, UpToDate, and the ability to do billing. The hospital’s tech support staff trained us on the new system and how to use the PDA for tasks like developing rounding lists, accessing our colleagues’ lists and creating system-based memos.”
Dr. Sivaprasad also has GPS in her car, a cell phone, and a laptop at home. “We probably aren’t using medical technology as much as we could,” she says. “Many physicians still write prescriptions by hand. I’ve never used voice-recognition software. In a previous hospital, we used the hospital’s transcription service for dictated notes.”
Karim Godamunne, MD, MBA, a hospitalist with Eagle Hospital Physicians and a practice medical director at South Fulton Medical Center in Atlanta, uses a PDA at work for billing.
“I don’t use the PDA intensively,’’ he says. “I’d like to see our hospital create a wireless network like the one I have at home. Our sister hospital has wireless.” He notes, however, that there are computer workstations for him to use at his hospital.
Dr. Godamunne’s group has a practice coordinator who faxes discharge summaries to attending physicians.
“Fax is kind of what they expect these days,” he says. “I’m not sure e-mail would be as reliable for the community we serve. I’d be concerned that the attendings wouldn’t read their e-mails.” He says he sometimes gives written notes to patients at discharge with instructions to hand the note to their physician on their next office visit.
Michelle Pezzani, MD, is part of a 10-member hospital medicine group that practices at El Camino Hospital in Mountain View, Calif., in the heart of Silicon Valley. The hospital tries to stay on the cutting edge with technology, and its hospitalists were given Microsoft XP Tablet laptops a few years ago. “I access the Web two to four times a day at work,” Dr. Pezzani says. “It helps keep us current. The great thing about the laptop is I also take it home with me, and I can use it to check or reorder labs from home. We’re all connected to the hospital’s Intranet from home.”
“One of the issues we’re struggling with is how to achieve the best sign-out possible,” with up to four hospitalists on the day shift checking out and handing over patient responsibilities to the night shift, Dr. Pezzani says. For her, the ideal sign-out is face to face because it permits asking questions and reading nonverbal cues about how sick the patients really are. However, the logistics of multiple physicians and patients makes this ideal difficult to achieve.
Second best (if all group members used a Palm Pilot), would be to send sign-outs via text messaging—although that would also present logistical challenges. “Texting is easier,” she says. “You know who is sending the message. We could beam the written sign-out to each other in a matter of seconds, making it quick and easy. Furthermore, any day-to-day changes on a specific patient would be easy to amend and easy to send. It’s also a quick way to let a colleague know, ‘I need you right now!’ ”
The hospitalists at El Camino use voicemail to record sign-outs. But these messages can take a long time to record and play back, multiplied by the four physicians signing out. “Ideally, there would be a different voice mail for every patient, so I wouldn’t have to listen to patients A, B, C, D, and E to get to the pertinent information about patient F, who is crashing upstairs,” she says. Dr. Pezzani’s group is still exploring how to balance these considerations.
She says her hospitalist group is tight-knit and collaborative. “We leave our cell phones on all the time and answer each other’s calls after hours,” she says. “For example, I’m now on vacation with my family in San Diego and I have gotten at least two calls a day from my partners, either business related, or something like: ‘Do you remember that patient you admitted? Can you give me some information on them?’”
The Wired Hospital
Dr. Cucina is excited about the extra large, easy-to-grip handle on the 3-lb. Motion Computing C5 portable PC that UCSF hospitalists are field-testing. He’s also intrigued by the ever-expanding opportunities for interfacing with the hospital’s technology.
In August he gave a tour of Unit 13L at UCSF’s Moffitt/Long Hospital, a new ward that opened in June and is being used as a technology demonstration site.
The 32-bed unit has a narrow corridor lined with 10 computer workstations for the nurses. All 10 are in use. In an adjacent cubicle, several physicians are typing on their laptops.
On the unit, portable vital signs monitors are attached to rolling stands that also have docking ports for the laptops, offering real-time point-of-care acquisition of vital-signs data directly into the hospital’s medical record.
A nurse or physician can grab the big-handled Tablet PC and run to another room while remaining connected to the patient’s vital signs. The docking ports in patients’ rooms are also linked to a 37-inch, high-definition television. “A clinician can show the patient radiographic studies here or bring up interactive patient education programs,” he explains.
One of the most exciting potentials for this emerging technology is to find ways for embedding medical decision support in physicians’ workflow. “We know that the barriers to physicians routinely consulting decision support applications are high,” Dr. Cucina says.
For Dr. Deruelle, who had to look outside of hospital channels to answer his question about a dystonic patient, medicine has a serious information gap. “I believe we will move to where the technology will put that information at my fingertips,” he says. “Why aren’t we there yet? Not enough people are using the technology, and we don’t agree on what information should be included. But I think we can start with basic things and work up from there. What excites me is that we’re closing the information gap—although medicine is still in the Stone Age compared with other professions.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Dennis Deruelle, MD, a hospitalist at University Community Hospital in Tampa, Fla., once needed reliable medical information in a hurry while treating a young woman admitted to the hospital with cellulitis.
The woman was later diagnosed with methicillin-resistant staphylococcus aureus (MRSA). After Dr. Deruelle administered prochlorperazine (Compazine), she had a severe dystonic reaction.
“She was going rigid right before my eyes,” Dr. Deruelle says. There was no instantly accessible hospital clearinghouse of medical information, although he had called the pharmacy department and was waiting for a call back. So he opened his laptop and turned to an aid available to anyone with a computer and Internet access: Google. “I immediately looked up information on reactions to Compazine and the correct dose for counteracting it. I administered the dose, and within minutes [the patient] was getting better.”
Dr. Deruelle is not alone among physicians in answering medical questions with Google. (See The Hospitalist, July 2007, p. 33.)
He has been interested in medical applications of computer technology for years and serves on SHM’s advisory committee on technology. He receives tech support from his employer, IPC-The Hospitalist Company, based in North Hollywood, Calif. IPC offers its physicians a Web-accessible network called IPC Link—a “virtual office” to help with billing, medical decision support, reference software, continuing medical education, and even blogs written by company CEO Adam Singer, MD.
But Dr. Deruelle has also developed his own applications, including an off-the-shelf voice recognition software loaded onto his company-supplied, 2.5-lb. Tablet PC. He uses it to dictate brief notes to give attending physicians a heads-up about patients being discharged. These notes are uploaded to the company’s network, which automatically generates a fax to the attending within minutes.
The formal discharge summary, produced by the hospital’s medical transcription department, may take 48 hours to arrive.
Dr. Deruelle has wireless Internet access at four of the five hospitals he visits as a hospitalist practice leader.
“As soon as I walk in the door I’m ‘hot,’ ” he says. At the fifth hospital, he uses workstation computers to connect with IPC Link.
Array of Options
A dizzying range of communications technology is available to working hospitalists, typically accessed through personal digital assistants (PDAs), smartphones, computer tablets, pocket PCs, and laptops.
The Palm Pilot, introduced in 1996, is a well-known example of this technology, as are the Palm Treo and BlackBerry. PDAs combine the functions of cell phones, video phones, cameras, video recorders, media players, Web browsers, reference tools, bar code scanners, and global positioning system (GPS) devices—all in a palm-size package.
Hardware and supporting software vary in terms of ease of use, in particular, the ability to interface with the Web or the hospital, practice, or employer network the physician needs to connect with.
The technology is evolving rapidly. But anomalies abound, such as dependence on the fax machine as a staple of communication with attending physicians. Through all of these changes, hospitalists are responsible for learning what works and how best to take advantage of the technology to make their jobs easier.
Hospitalists also vary tremendously in terms of their comfort levels and openness to new technology.
“There is a considerable gap between those of us who ‘Palm’ and those who don’t,” says Timothy Hartzog, MD, pediatric hospitalist at Medical University of South Carolina (MUSC) in Charleston and a medical technology consultant. “Physicians want their patient data in different ways. Some want it printed out or in a paper chart.”
—Steven Liu, MD, of Emory University Medical Center in Atlanta
But implementation of technology, such as hospital electronic health records or computerized physician order entry, inevitably changes their relationships with information technology and patient information.
Some hospitalists, like Dr. Deruelle, are interested in what communication technology can bring their work and how to adapt it to their needs. Others, like Dr. Hartzog, medical director of Information Technology at MUSC, have taken added responsibilities for technology within their institutions.
And a few, such as Steven Liu, MD, of Emory University Medical Center in Atlanta, have taken their interest in computer technology a step further. In 1999, Dr. Liu founded Ingenious Med, an Atlanta software company that offers a suite of inpatient practice management applications to working hospitalists.
“Often the hospitalist is already on the forefront of technology,” Dr. Liu says. “The demographic is typically younger and techno-savvy. They may get tapped by their hospitals to help customize the electronic health record to make sure it satisfies the needs of clinicians. Conversely, if an electronic project does not involve strong physician feedback and collaboration, physicians can be the Achilles’ heel impeding successful implementation. Even though they are the ones who stand to gain most from the potential efficiency, physicians will not adopt technology that does not fit their workflow.”
State of the Art?
Russell Cucina, MD, MS, a hospitalist at the University of California-San Francisco Medical Center, San Francisco, is also the associate medical director for information technology at UCSF.
Dr. Cucina quips that a good example of a state-of-the-art, stand-alone patient data management system offering rapid data entry, long battery life, and high mobility is the paper index card, the longtime standard for making rounding notes.
“Plenty of doctors, including me, use it every day,” he says. But growing numbers of hospitalists also use PDAs, smartphones, and laptops to access information and support applications. Among the plethora of reference applications readily available to physicians by PDA or laptop are UpToDate, Epocrates, the Pocket Sanford Guide to Anti-Microbial Therapy, and Merck Medicus.
“I use many different resources as a hospitalist,” Dr. Cucina says. “I Google all the time.” Hospitalists still have opportunities to innovate, although increasingly their “home-grown” solutions will compete with multinational technology conglomerates entering the medical market.
The use of technology and equipment also varies depending on whether the hospitalist is employed by the hospital or part of an independent medical group.
Another factor is whether that hospital is academic, community-based, or part of a system like the Veterans Affairs or a staff-model HMO such as Kaiser Permanente. But all hospitalists are used to working on the run, Dr. Cucina says. And in their daily jobs, workflow is everything.
Tech in Use
“I use medical technology on the job to a moderate degree,” reports Latha Sivaprasad, MD, a hospitalist at Beth Israel Medical Center in New York City. “This is my sixth year working as a hospitalist, and for the first five years I didn’t use a specific device. Now I have a Palm-based program with MD Everywhere, Epocrates, UpToDate, and the ability to do billing. The hospital’s tech support staff trained us on the new system and how to use the PDA for tasks like developing rounding lists, accessing our colleagues’ lists and creating system-based memos.”
Dr. Sivaprasad also has GPS in her car, a cell phone, and a laptop at home. “We probably aren’t using medical technology as much as we could,” she says. “Many physicians still write prescriptions by hand. I’ve never used voice-recognition software. In a previous hospital, we used the hospital’s transcription service for dictated notes.”
Karim Godamunne, MD, MBA, a hospitalist with Eagle Hospital Physicians and a practice medical director at South Fulton Medical Center in Atlanta, uses a PDA at work for billing.
“I don’t use the PDA intensively,’’ he says. “I’d like to see our hospital create a wireless network like the one I have at home. Our sister hospital has wireless.” He notes, however, that there are computer workstations for him to use at his hospital.
Dr. Godamunne’s group has a practice coordinator who faxes discharge summaries to attending physicians.
“Fax is kind of what they expect these days,” he says. “I’m not sure e-mail would be as reliable for the community we serve. I’d be concerned that the attendings wouldn’t read their e-mails.” He says he sometimes gives written notes to patients at discharge with instructions to hand the note to their physician on their next office visit.
Michelle Pezzani, MD, is part of a 10-member hospital medicine group that practices at El Camino Hospital in Mountain View, Calif., in the heart of Silicon Valley. The hospital tries to stay on the cutting edge with technology, and its hospitalists were given Microsoft XP Tablet laptops a few years ago. “I access the Web two to four times a day at work,” Dr. Pezzani says. “It helps keep us current. The great thing about the laptop is I also take it home with me, and I can use it to check or reorder labs from home. We’re all connected to the hospital’s Intranet from home.”
“One of the issues we’re struggling with is how to achieve the best sign-out possible,” with up to four hospitalists on the day shift checking out and handing over patient responsibilities to the night shift, Dr. Pezzani says. For her, the ideal sign-out is face to face because it permits asking questions and reading nonverbal cues about how sick the patients really are. However, the logistics of multiple physicians and patients makes this ideal difficult to achieve.
Second best (if all group members used a Palm Pilot), would be to send sign-outs via text messaging—although that would also present logistical challenges. “Texting is easier,” she says. “You know who is sending the message. We could beam the written sign-out to each other in a matter of seconds, making it quick and easy. Furthermore, any day-to-day changes on a specific patient would be easy to amend and easy to send. It’s also a quick way to let a colleague know, ‘I need you right now!’ ”
The hospitalists at El Camino use voicemail to record sign-outs. But these messages can take a long time to record and play back, multiplied by the four physicians signing out. “Ideally, there would be a different voice mail for every patient, so I wouldn’t have to listen to patients A, B, C, D, and E to get to the pertinent information about patient F, who is crashing upstairs,” she says. Dr. Pezzani’s group is still exploring how to balance these considerations.
She says her hospitalist group is tight-knit and collaborative. “We leave our cell phones on all the time and answer each other’s calls after hours,” she says. “For example, I’m now on vacation with my family in San Diego and I have gotten at least two calls a day from my partners, either business related, or something like: ‘Do you remember that patient you admitted? Can you give me some information on them?’”
The Wired Hospital
Dr. Cucina is excited about the extra large, easy-to-grip handle on the 3-lb. Motion Computing C5 portable PC that UCSF hospitalists are field-testing. He’s also intrigued by the ever-expanding opportunities for interfacing with the hospital’s technology.
In August he gave a tour of Unit 13L at UCSF’s Moffitt/Long Hospital, a new ward that opened in June and is being used as a technology demonstration site.
The 32-bed unit has a narrow corridor lined with 10 computer workstations for the nurses. All 10 are in use. In an adjacent cubicle, several physicians are typing on their laptops.
On the unit, portable vital signs monitors are attached to rolling stands that also have docking ports for the laptops, offering real-time point-of-care acquisition of vital-signs data directly into the hospital’s medical record.
A nurse or physician can grab the big-handled Tablet PC and run to another room while remaining connected to the patient’s vital signs. The docking ports in patients’ rooms are also linked to a 37-inch, high-definition television. “A clinician can show the patient radiographic studies here or bring up interactive patient education programs,” he explains.
One of the most exciting potentials for this emerging technology is to find ways for embedding medical decision support in physicians’ workflow. “We know that the barriers to physicians routinely consulting decision support applications are high,” Dr. Cucina says.
For Dr. Deruelle, who had to look outside of hospital channels to answer his question about a dystonic patient, medicine has a serious information gap. “I believe we will move to where the technology will put that information at my fingertips,” he says. “Why aren’t we there yet? Not enough people are using the technology, and we don’t agree on what information should be included. But I think we can start with basic things and work up from there. What excites me is that we’re closing the information gap—although medicine is still in the Stone Age compared with other professions.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Demystify Admissions
Physicians may encounter patients in various ways during the first few days of a hospitalization: admission services, consultations, and medical-surgical co-management.
Submitting claims for these services is often inconsistent and inaccurate because billing education is not a standard part of medical education.
In an attempt to clarify the rules and reduce frustration, I will address billing, coding, and reimbursement guidelines for each type of initial hospital encounter over the next several issues.
Definition
Initial Hospital Care (IHC) comprises all services related to the patient’s admission to an acute care facility. An acute care facility is any that registers inpatients but does not have a corresponding Current Procedural Terminology (CPT) code category for claim reporting. Acute care facilities also include “partial hospitals.”
For example, admissions to inpatient rehabilitation are reported with IHC codes 99221-99223, while nursing facility admissions have a designated category and are best reported with CPT codes 99304-99306 for Initial Nursing Facility Care.
Code Use
IHC codes are reported once per hospitalization and reserved for the physician/group assuming primary responsibility for the patient’s care during that time.
If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99221-99223 are denied or rejected pending review of documentation to ascertain the correct service date and responsible party. This is common because physicians confuse code description IHC with its true intent. They mistakenly report these codes for their first inpatient encounter, regardless of the encounter date or the admitting physician/group.
Specialists assisting in the patient’s management and not primarily responsible for the entire hospitalization report the code category that best reflects the performed service and documentation—as long as the selected category requirements are met. The physician selects from either Inpatient Consultation codes 99251-99255 or Subsequent Hospital Care (SHC) codes 99231-99233. Any physician who provides patient services after the initial encounter, including those by the responsible attending physician/group or a specialist concurrently involved in the patient’s care, reports SHC codes for each date in which a face-to-face encounter occurs.
When services begin in one location (e.g., physician’s office, emergency department, or observation) and end with an inpatient admission on the same calendar day, the physician reports only the most appropriate initial hospital care code. It is not necessary for the physician to duplicate the information from the earlier encounter for the admission service. Instead, the physician can forward a copy of the progress note from the earlier encounter to the inpatient chart, along with the documented decision for admission and pertinent information obtained throughout the day. Auditors consider the culmination of all chart entries in a given date when reviewed. When services begin in one location but end with an admission on different calendar day, the physician separately reports each service provided on each date: 99220 on Day 1 and 99223 on Day 2.
Intrafacility Transfers
Patients may receive different components of inpatient services within the same (uninterrupted) episode of care, all within the same building but treated as separate facility admissions (e.g., rehabilitation or long-term acute care).
It is unlikely the attending physician of record during the acute care phase will also be the attending physician during the second phase of care. Should this occur, Medicare contractors and those payers who follow Medicare guidelines permit the attending physician to separately report the acute care discharge (99238-99239) and the secondary admission (99221-99223), but only in the absence of a shared medical record (see Section 30.6.9.1D,www.cms.hhs.gov/manuals/downloads/clm104c12.pdf). If a common chart is used, the physician reports the secondary admission services as ongoing care, using SHC codes 99231-99233 instead.
Similarly, transfers occur within a single phase of care, such as transfers to and from a medical intensive care unit and a standard medical-surgical unit. Such transfers are not treated as separate admissions, and the receiving physician reports only the SHC codes because the IHC service was previously reported by the admitting physician/group. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia.
Physicians may encounter patients in various ways during the first few days of a hospitalization: admission services, consultations, and medical-surgical co-management.
Submitting claims for these services is often inconsistent and inaccurate because billing education is not a standard part of medical education.
In an attempt to clarify the rules and reduce frustration, I will address billing, coding, and reimbursement guidelines for each type of initial hospital encounter over the next several issues.
Definition
Initial Hospital Care (IHC) comprises all services related to the patient’s admission to an acute care facility. An acute care facility is any that registers inpatients but does not have a corresponding Current Procedural Terminology (CPT) code category for claim reporting. Acute care facilities also include “partial hospitals.”
For example, admissions to inpatient rehabilitation are reported with IHC codes 99221-99223, while nursing facility admissions have a designated category and are best reported with CPT codes 99304-99306 for Initial Nursing Facility Care.
Code Use
IHC codes are reported once per hospitalization and reserved for the physician/group assuming primary responsibility for the patient’s care during that time.
If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99221-99223 are denied or rejected pending review of documentation to ascertain the correct service date and responsible party. This is common because physicians confuse code description IHC with its true intent. They mistakenly report these codes for their first inpatient encounter, regardless of the encounter date or the admitting physician/group.
Specialists assisting in the patient’s management and not primarily responsible for the entire hospitalization report the code category that best reflects the performed service and documentation—as long as the selected category requirements are met. The physician selects from either Inpatient Consultation codes 99251-99255 or Subsequent Hospital Care (SHC) codes 99231-99233. Any physician who provides patient services after the initial encounter, including those by the responsible attending physician/group or a specialist concurrently involved in the patient’s care, reports SHC codes for each date in which a face-to-face encounter occurs.
When services begin in one location (e.g., physician’s office, emergency department, or observation) and end with an inpatient admission on the same calendar day, the physician reports only the most appropriate initial hospital care code. It is not necessary for the physician to duplicate the information from the earlier encounter for the admission service. Instead, the physician can forward a copy of the progress note from the earlier encounter to the inpatient chart, along with the documented decision for admission and pertinent information obtained throughout the day. Auditors consider the culmination of all chart entries in a given date when reviewed. When services begin in one location but end with an admission on different calendar day, the physician separately reports each service provided on each date: 99220 on Day 1 and 99223 on Day 2.
Intrafacility Transfers
Patients may receive different components of inpatient services within the same (uninterrupted) episode of care, all within the same building but treated as separate facility admissions (e.g., rehabilitation or long-term acute care).
It is unlikely the attending physician of record during the acute care phase will also be the attending physician during the second phase of care. Should this occur, Medicare contractors and those payers who follow Medicare guidelines permit the attending physician to separately report the acute care discharge (99238-99239) and the secondary admission (99221-99223), but only in the absence of a shared medical record (see Section 30.6.9.1D,www.cms.hhs.gov/manuals/downloads/clm104c12.pdf). If a common chart is used, the physician reports the secondary admission services as ongoing care, using SHC codes 99231-99233 instead.
Similarly, transfers occur within a single phase of care, such as transfers to and from a medical intensive care unit and a standard medical-surgical unit. Such transfers are not treated as separate admissions, and the receiving physician reports only the SHC codes because the IHC service was previously reported by the admitting physician/group. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia.
Physicians may encounter patients in various ways during the first few days of a hospitalization: admission services, consultations, and medical-surgical co-management.
Submitting claims for these services is often inconsistent and inaccurate because billing education is not a standard part of medical education.
In an attempt to clarify the rules and reduce frustration, I will address billing, coding, and reimbursement guidelines for each type of initial hospital encounter over the next several issues.
Definition
Initial Hospital Care (IHC) comprises all services related to the patient’s admission to an acute care facility. An acute care facility is any that registers inpatients but does not have a corresponding Current Procedural Terminology (CPT) code category for claim reporting. Acute care facilities also include “partial hospitals.”
For example, admissions to inpatient rehabilitation are reported with IHC codes 99221-99223, while nursing facility admissions have a designated category and are best reported with CPT codes 99304-99306 for Initial Nursing Facility Care.
Code Use
IHC codes are reported once per hospitalization and reserved for the physician/group assuming primary responsibility for the patient’s care during that time.
If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99221-99223 are denied or rejected pending review of documentation to ascertain the correct service date and responsible party. This is common because physicians confuse code description IHC with its true intent. They mistakenly report these codes for their first inpatient encounter, regardless of the encounter date or the admitting physician/group.
Specialists assisting in the patient’s management and not primarily responsible for the entire hospitalization report the code category that best reflects the performed service and documentation—as long as the selected category requirements are met. The physician selects from either Inpatient Consultation codes 99251-99255 or Subsequent Hospital Care (SHC) codes 99231-99233. Any physician who provides patient services after the initial encounter, including those by the responsible attending physician/group or a specialist concurrently involved in the patient’s care, reports SHC codes for each date in which a face-to-face encounter occurs.
When services begin in one location (e.g., physician’s office, emergency department, or observation) and end with an inpatient admission on the same calendar day, the physician reports only the most appropriate initial hospital care code. It is not necessary for the physician to duplicate the information from the earlier encounter for the admission service. Instead, the physician can forward a copy of the progress note from the earlier encounter to the inpatient chart, along with the documented decision for admission and pertinent information obtained throughout the day. Auditors consider the culmination of all chart entries in a given date when reviewed. When services begin in one location but end with an admission on different calendar day, the physician separately reports each service provided on each date: 99220 on Day 1 and 99223 on Day 2.
Intrafacility Transfers
Patients may receive different components of inpatient services within the same (uninterrupted) episode of care, all within the same building but treated as separate facility admissions (e.g., rehabilitation or long-term acute care).
It is unlikely the attending physician of record during the acute care phase will also be the attending physician during the second phase of care. Should this occur, Medicare contractors and those payers who follow Medicare guidelines permit the attending physician to separately report the acute care discharge (99238-99239) and the secondary admission (99221-99223), but only in the absence of a shared medical record (see Section 30.6.9.1D,www.cms.hhs.gov/manuals/downloads/clm104c12.pdf). If a common chart is used, the physician reports the secondary admission services as ongoing care, using SHC codes 99231-99233 instead.
Similarly, transfers occur within a single phase of care, such as transfers to and from a medical intensive care unit and a standard medical-surgical unit. Such transfers are not treated as separate admissions, and the receiving physician reports only the SHC codes because the IHC service was previously reported by the admitting physician/group. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia.
Voters Weigh in Early
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.

—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.
—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.
—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
Administrative Ambition
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Drug Stents and Surgery

Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Manage Cancer Drugs
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs

Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs
Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs
Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.