User login
Vigilant Awareness
In hospitals, clinicians constantly encounter conflicting and ambiguous information,” says Ronald M. Epstein, MD, professor of family medicine, psychiatry, and oncology at the University of Rochester Medical Center (URMC) N.Y. “This information often gets processed tacitly, outside of awareness, and often results in various undesired consequences. For example, premature closure of diagnostic thinking or ordering a test rather than inquiring further of the patient.” In the average hospital, distractions and sensory inputs, including smells, sights, sounds, and tactile sensations, as well as multiple tasks to complete, can all seem pretty overwhelming. Faced with so much data, says Dr. Epstein, the tendency of the mind is to simplify and reduce it in some way. And that’s when error can rear its ugly head.
“Simplification is often arbitrary and unconscious,” he says, and thus “the trick of working in hospital is to develop a vigilant awareness of the ambient stimuli that are all around you, making choices as to what you attend to, relegating other stimuli to the background, and in that way avoiding becoming overwhelmed or controlled by them. In that way, you have the capacity for making better judgments.”
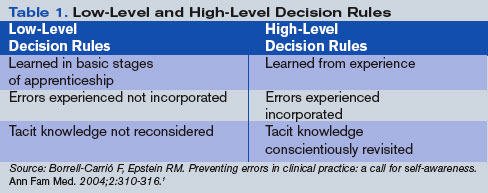
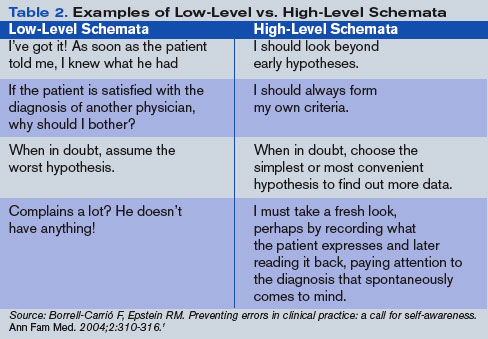
Some clinical decisions can be made fairly easily and routinely (low-level decisions), he says, whereas other patient situations require a fair bit of deliberation (high-level decisions). (See Tables 1 and 2, right.) The human mind tends to avoid the unpleasant and to give more attention to what is compelling. Also, the ambiguity of role and responsibility—especially in large hospitals—may further confound a hospitalist’s mental capacity. Keen attention to each moment also boosts physician well being.
“Hospitalists are often working in crowded, stressful, high-paced, windowless environments in which there is no natural form of respite,” says Dr. Epstein. Therefore, all physicians need ways of keeping themselves from being overwhelmed by the challenges of sensory input and intense emotions caused by exposure to suffering, conflicts, imperatives for critical thinking, and so on.
“If practitioners were able to be more mindful,” he says, “they might experience greater well-being, because they would be able to make more choices about what they attend to and how they react to them.”
Dr. Epstein and his colleagues at the University of Rochester Medical Center—Timothy Quill, MD, Michael Krasner, MD, and Howard Beckman, MD—have studied the qualities of mind required to exercise that awareness extensively, especially as they relate to clinical practice and education.2 They were recently awarded three complementary grants to teach mindfulness to physicians: one from the Arthur Vining Davis Foundations, another from the Physicians’ Foundation for Health Systems Excellence, and the Mannix Award for Excellence in Medical Education.
But just what does mindfulness in medicine entail?
Defining Mindful Practice
“Mindful practice is recognizing where you are at every moment. If you’re distressed, if you’re content or unhappy, if you’re comfortable or in pain, if you’re experiencing some kind of positive or negative effect, if you’re feeling in tune or disconnected from yourself. It’s that monitoring function to be able to say, I’m angry or I’m uncomfortable, or, possibly, I’m in the flow,” says Dr. Epstein.
For physicians to be able to exercise those qualities of mind, to watch and deconstruct their own behavior (what Dr. Epstein describes as “the ability to observe the observer observing the observed”) is something that goes back a long way for him.3 “There’s nothing really mystical about it,” he says. “People do this all the time. It’s part of being an excellent professional in lots of fields. It’s just that no one has organized the science of doing so in the context of medical training.”
In the late 1990s, Dr. Epstein and his coworkers implemented a curriculum reform process at URMC, and his particular charge was to assess the competence of medical students. To accomplish this, he did two things. First, he reviewed the literature on the assessment and definitions of special competence. Second, he turned the magnifying glass on himself. “I thought that it might be a useful exercise to try to understand what made me practice at my best and what barriers there were to doing so.”
The resulting article from this self-monitoring and evaluation was published in JAMA in 1999, before the review article on defining and assessing professional competence appeared in that same journal.3,4 Exploring the nature of his own mindful practice reacquainted him with two areas in which he had participated as a teenager: music and the study of mind—particularly the use of meditation to enhance mental capacities. Those inquiries led him to explore the psychology of a number of qualities of mind: attentiveness, curiosity, decision-making, and the use of cognitive knowledge. The literature was convergent in a number of ways, he says, and “seemed to point to the fact that a lot of competence is not a matter of book knowledge or the kind of knowledge we can explain but tacit knowledge, things we do semi-automatically that really take some effort to deconstruct.”
He realized that “what distinguished an excellent clinician from someone who wasn’t quite so excellent had to do with some of those same qualities that one sees in accomplished musicians, athletes, and meditators, which is the ability to make fine distinctions, lower one’s own level of reactivity, respond in a more conscious way, and pay attention to the unexpected—the surprises that are part of everyday work but that we often ignore.”
All of this rather radicalized his view of what medical education should be doing. He came to believe that—on top of a foundation of knowledge and skills—physicians need to be attentive to their own mental processes and alert to the effects of bias or prior experience.
Writing about excellent clinical practice in this way drew a crescendo of response from readers of the JAMA. The JAMA editors had thoroughly engaged in helping him refine and present the ideas in a way that would really speak to clinical practitioners and educators.3 After publication, he was amazed to receive hundreds of letters from all over the world from physicians in different specialties expressing their appreciation “for having articulated something that was really at the heart of medicine,” he says. “For me, that was incredibly gratifying.”
Hospitalist Qualities of Mind
What qualities of mind are important for a hospitalist to have?
“You have to be enthusiastic, fast-paced individuals,” says Yousaf Ali, MD, hospitalist at URMC and assistant professor of medicine in the Hospital Medicine Division. You also have to be able to immediately connect with patients and families and to have the knowledge and passion that makes that possible. Further, he says, you need to quickly access knowledge pertaining to caring for patients with multiple problems.
Traci Ferguson, MD, is a hospitalist at Boca Raton Community Hospital in Florida, which, by affiliating with Florida Atlantic University (the regional campus for the University of Miami School of Medicine), is moving from community hospital to teaching hospital. Dr. Ferguson believes the qualities of mind necessary to be a good hospitalist are the capacity to be aware of reactions and biases toward patients in order to avoid being judgmental.
“I think the major thing is being present and being attentive when you are caring for patients,” she says, “and that occurs when you’re writing a chart, when you’re talking to family members, [and] when you’re talking to nurses, just as it does when you’re at the bedside.”
Other qualities of mind, in Dr. Ferguson’s view, include the whole spectrum of empathy and compassion, being personable in the sense of being open to what patients and families have to say, and being patient. She also believes the quality of mind necessary to express a human touch is sometimes missing.
Valerie Lang, MD, is also a hospitalist at URMC and has studied mindfulness with Dr. Epstein. She is enrolled in Dr. Krasner’s class for healthcare providers on being mindful. What qualities of mind does she think are important for a hospitalist to have?
“I want to say an open mind, but that’s such a broad term,” she says. “Dr. Epstein uses the term ‘beginner’s mind’ [to refer to] when you’re willing to consider many alternatives, where you don’t necessarily jump to a conclusion and then just stick with it. As a hospitalist, you start making those conclusions as soon as you hear what the patient’s chief complaint is. I think that having [a] beginner’s mind … is so important because we don’t know these patients, and it’s easy to jump to conclusions because we have to make decisions very quickly and … repeatedly.” She also believes that “being able to reflect on how you are communicating with another person is incredibly important to their care.”
—Valerie Lang, MD, hospitalist, University of Rochester Medical Center
Operationalizing Mindfulness
In 2004, after the publication of two of Dr. Epstein’s articles on mindful practice in action, the Arthur Vining Davis Foundation approached him and requested a proposal.5,6 At that time, he was in the process of writing an article on reflection and mindfulness in the context of preventing errors.1 (See Table 3, left.)
“This [proposal] was an intriguing possibility,” says Dr. Epstein, “and galvanized my putting together a curriculum that would not just be elective experiences for preclinical students, which is what the offerings related to mindfulness currently are, but something that was really going to influence clinical training.”
In Dr. Epstein’s view, placing educational reform in the first two years of medical school is teaching it when it matters the least. “Where it matters the most is when students are interacting with patients and using the knowledge and skills and doing work that they’ll ultimately end up doing for the next 30 or 40 years,” says Dr. Epstein.
One project plan is to train practicing primary care physicians to communicate more mindfully with their patients. Outcomes of the intervention will be measured by how it has affected the physicians as well as the patients’ ratings of their physicians and their practice styles.
The second project is a series of annual workshops for 100 third-year medical students and about 250 residents in the nine largest programs at the medical center. All participants will take five seminars that include mindfulness techniques to improve the capacity for paying attention and observing, and narrative exercises, whose themes will include, for instance, suffering, meaningful experience, professionalism, physician self-care, and avoiding burnout. The coursework, which will include both cognitive and experiential content, will also involve training a cadre of about 20 faculty members to teach these sessions, and educational outcomes will ultimately be measured for all participants.
Focus on Metacognition
Dr. Epstein, director of The Rochester Center to Improve Communication in Health Care, says metacognition builds on other approaches, such as the Healer’s Art, a course designed by Rachel Remen, MD, and colleagues, which a number of medical centers are incorporating into their curricula.7
“We are building on Dr. Remen’s wonderful work,” he says. Both curricula include self-awareness, humanism, caring, compassion, meaningful experiences, and physician well being. Both address the “informal curriculum”—a term used to refer to the social environment in which medical trainees adopt values, expectations, and clinical habits. In addition, Dr. Epstein and his colleagues focus on quality of clinical care, including medical decision-making and preventing errors.
“Importantly, our initiative is part of the required curriculum,” says Dr. Epstein. “It targets students and residents working in clinical settings at an advanced level, and it also has a faculty component. … We are trying to transform and heal the informal curriculum, not just immunize students against its toxicity.”
In the Thick of It
All this sounds as if it might benefit hospital practice, according to the hospitalists interviewed for this story. All three believe that mindfulness can be cultivated. Dr. Ali believes the aforementioned forces acting on hospitalists require that hospitalists work at their top capacities, but prioritizing remains essential. He believes one way a hospitalist can cultivate mindfulness in the patient-physician relationship is to avoid burnout in any way that works. Having been a hospitalist for almost 10 years, he discusses this with his medical students and residents. In addition to his hospitalist practice and teaching, Dr. Ali does patient-related quality work, which refreshes his energy.
Dr. Ferguson also thinks mindful practice can be cultivated. “I took cues from the nursing profession in realizing that you do have to care for all aspects of the patient,” she says. “But you can learn this from mentors and people who are successful: people you can emulate, shadow, and follow.”
For her, such a person is Lisa Cooper, MD, MPH, an associate professor in the department of medicine at Johns Hopkins University School of Medicine. Dr. Cooper, both a practicing internist and a researcher, studies and teaches about communication between physicians and minorities—that is, how physicians interact with people of the same or different races and ethnicities. Dr. Ferguson says she feels fortunate to have adopted a mindful awareness in that regard.
As director of the medicine clerkship, Dr. Lang came into contact with Dr. Epstein’s project through her Dean’s Teaching Fellowship, a competitive program at the URSM for faculty members who have a special interest in education.
“The discussions with other educators and clinicians really got me thinking about how my own feelings, whether they had to do with a patient or anything else in life, affect my decision-making,” says Dr. Lang. “You see the phenomenon in residency where you’re in morning report when the residents present a patient and everyone is sitting around a table—not involved with the patient—making judgments about what they should have done. It’s so much easier when you’re not involved [in the situation].”
Though Dr. Lang thinks there are a lot of reasons for that, “part of it is that you are not in the excitement of the moment. And the other factor is that when you’re presenting a patient to a group, you wouldn’t convey your own emotions, what else was going on, what were the competing pressures. Even if you have a wonderful intellect and clinical reasoning skills, you might make the wrong decision when you’re in the thick of the situation.”
Mindful Hospital Practice
Dr. Lang has seen a number of outcomes from her study of mindful practice. It has made her aware of her biases and has taught her to say, in certain cases, “OK, I need to think through the problem again to make sure I’m not changing my judgment about what we should be doing clinically based on how I’m feeling about a patient.”
Dr. Lang sometimes asks herself, “How am I feeling about this? Did that wear me down?” Or, sometimes the opposite can occur. A patient can make you feel “puffed up, where they are so complimentary and make you feel so good that you think that every decision you make is perfect,” she explains.
What Dr. Lang has learned about herself has helped her recognize when she might have prematurely closed a differential diagnosis or come to a conclusion too quickly simply because the patient appeared to agree with her clinical assessment.
Dr. Lang also thinks being a mindful physician has made her a better physician and that she is providing better care that results in better outcomes. “I definitely communicate better with my patients. … I think my relationships with my patients have significantly improved.”
What is her recommendation for how her hospitalist colleagues can learn to practice mindfully? “It’s a practice, and it’s a matter of practice,” says Dr. Lang. “It’s not something you get overnight. It’s a matter of every day, every encounter, taking the time before entering the patient’s room to pause, put things aside, and be present with the patient. And then, at the end of the day, take some time to reflect.”
How does education for mindfulness differ from her original medical training? “I don’t think you’re really ever taught how to manage your emotions when you’ve just made a medical error and you are distraught,” says Dr. Lang, “or how to manage doing that when your pager is going off like crazy and yet you need to sit down and be present with your patient. And that’s the kind of thing that ends up being in your way of being the best physician you can be.” TH
References
- Borrell-Carrió F, Epstein RM. Preventing errors in clinical practice: a call for self-awareness. Ann Fam Med. 2004;2:310-316.
- Epstein RM. Assessment in medical education. N Engl J Med. 2007;356(4):387-396.
- Epstein RM. Mindful practice. JAMA. 1999 Sep;282(9):833-839.
- Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002 Jan 9;287(2):226-235.
- Epstein RM. Mindful practice in action (I): technical competence, evidence-based medicine and relationship-centered care. Fam Syst Health. 2003;21:1-9.
- Epstein RM. Mindful practice in action (II): cultivating habits of mind. Fam Syst Health. 2003;21:11-17.
- O’Donnell JF, Rabow MW, Remen RN. The healer’s art: awakening the heart of medicine. Medical Encounter: Newsletter of the American Academy on Communication in Healthcare. 2007;21, No 1.
In hospitals, clinicians constantly encounter conflicting and ambiguous information,” says Ronald M. Epstein, MD, professor of family medicine, psychiatry, and oncology at the University of Rochester Medical Center (URMC) N.Y. “This information often gets processed tacitly, outside of awareness, and often results in various undesired consequences. For example, premature closure of diagnostic thinking or ordering a test rather than inquiring further of the patient.” In the average hospital, distractions and sensory inputs, including smells, sights, sounds, and tactile sensations, as well as multiple tasks to complete, can all seem pretty overwhelming. Faced with so much data, says Dr. Epstein, the tendency of the mind is to simplify and reduce it in some way. And that’s when error can rear its ugly head.
“Simplification is often arbitrary and unconscious,” he says, and thus “the trick of working in hospital is to develop a vigilant awareness of the ambient stimuli that are all around you, making choices as to what you attend to, relegating other stimuli to the background, and in that way avoiding becoming overwhelmed or controlled by them. In that way, you have the capacity for making better judgments.”
Some clinical decisions can be made fairly easily and routinely (low-level decisions), he says, whereas other patient situations require a fair bit of deliberation (high-level decisions). (See Tables 1 and 2, right.) The human mind tends to avoid the unpleasant and to give more attention to what is compelling. Also, the ambiguity of role and responsibility—especially in large hospitals—may further confound a hospitalist’s mental capacity. Keen attention to each moment also boosts physician well being.
“Hospitalists are often working in crowded, stressful, high-paced, windowless environments in which there is no natural form of respite,” says Dr. Epstein. Therefore, all physicians need ways of keeping themselves from being overwhelmed by the challenges of sensory input and intense emotions caused by exposure to suffering, conflicts, imperatives for critical thinking, and so on.
“If practitioners were able to be more mindful,” he says, “they might experience greater well-being, because they would be able to make more choices about what they attend to and how they react to them.”
Dr. Epstein and his colleagues at the University of Rochester Medical Center—Timothy Quill, MD, Michael Krasner, MD, and Howard Beckman, MD—have studied the qualities of mind required to exercise that awareness extensively, especially as they relate to clinical practice and education.2 They were recently awarded three complementary grants to teach mindfulness to physicians: one from the Arthur Vining Davis Foundations, another from the Physicians’ Foundation for Health Systems Excellence, and the Mannix Award for Excellence in Medical Education.
But just what does mindfulness in medicine entail?
Defining Mindful Practice
“Mindful practice is recognizing where you are at every moment. If you’re distressed, if you’re content or unhappy, if you’re comfortable or in pain, if you’re experiencing some kind of positive or negative effect, if you’re feeling in tune or disconnected from yourself. It’s that monitoring function to be able to say, I’m angry or I’m uncomfortable, or, possibly, I’m in the flow,” says Dr. Epstein.
For physicians to be able to exercise those qualities of mind, to watch and deconstruct their own behavior (what Dr. Epstein describes as “the ability to observe the observer observing the observed”) is something that goes back a long way for him.3 “There’s nothing really mystical about it,” he says. “People do this all the time. It’s part of being an excellent professional in lots of fields. It’s just that no one has organized the science of doing so in the context of medical training.”
In the late 1990s, Dr. Epstein and his coworkers implemented a curriculum reform process at URMC, and his particular charge was to assess the competence of medical students. To accomplish this, he did two things. First, he reviewed the literature on the assessment and definitions of special competence. Second, he turned the magnifying glass on himself. “I thought that it might be a useful exercise to try to understand what made me practice at my best and what barriers there were to doing so.”
The resulting article from this self-monitoring and evaluation was published in JAMA in 1999, before the review article on defining and assessing professional competence appeared in that same journal.3,4 Exploring the nature of his own mindful practice reacquainted him with two areas in which he had participated as a teenager: music and the study of mind—particularly the use of meditation to enhance mental capacities. Those inquiries led him to explore the psychology of a number of qualities of mind: attentiveness, curiosity, decision-making, and the use of cognitive knowledge. The literature was convergent in a number of ways, he says, and “seemed to point to the fact that a lot of competence is not a matter of book knowledge or the kind of knowledge we can explain but tacit knowledge, things we do semi-automatically that really take some effort to deconstruct.”
He realized that “what distinguished an excellent clinician from someone who wasn’t quite so excellent had to do with some of those same qualities that one sees in accomplished musicians, athletes, and meditators, which is the ability to make fine distinctions, lower one’s own level of reactivity, respond in a more conscious way, and pay attention to the unexpected—the surprises that are part of everyday work but that we often ignore.”
All of this rather radicalized his view of what medical education should be doing. He came to believe that—on top of a foundation of knowledge and skills—physicians need to be attentive to their own mental processes and alert to the effects of bias or prior experience.
Writing about excellent clinical practice in this way drew a crescendo of response from readers of the JAMA. The JAMA editors had thoroughly engaged in helping him refine and present the ideas in a way that would really speak to clinical practitioners and educators.3 After publication, he was amazed to receive hundreds of letters from all over the world from physicians in different specialties expressing their appreciation “for having articulated something that was really at the heart of medicine,” he says. “For me, that was incredibly gratifying.”
Hospitalist Qualities of Mind
What qualities of mind are important for a hospitalist to have?
“You have to be enthusiastic, fast-paced individuals,” says Yousaf Ali, MD, hospitalist at URMC and assistant professor of medicine in the Hospital Medicine Division. You also have to be able to immediately connect with patients and families and to have the knowledge and passion that makes that possible. Further, he says, you need to quickly access knowledge pertaining to caring for patients with multiple problems.
Traci Ferguson, MD, is a hospitalist at Boca Raton Community Hospital in Florida, which, by affiliating with Florida Atlantic University (the regional campus for the University of Miami School of Medicine), is moving from community hospital to teaching hospital. Dr. Ferguson believes the qualities of mind necessary to be a good hospitalist are the capacity to be aware of reactions and biases toward patients in order to avoid being judgmental.
“I think the major thing is being present and being attentive when you are caring for patients,” she says, “and that occurs when you’re writing a chart, when you’re talking to family members, [and] when you’re talking to nurses, just as it does when you’re at the bedside.”
Other qualities of mind, in Dr. Ferguson’s view, include the whole spectrum of empathy and compassion, being personable in the sense of being open to what patients and families have to say, and being patient. She also believes the quality of mind necessary to express a human touch is sometimes missing.
Valerie Lang, MD, is also a hospitalist at URMC and has studied mindfulness with Dr. Epstein. She is enrolled in Dr. Krasner’s class for healthcare providers on being mindful. What qualities of mind does she think are important for a hospitalist to have?
“I want to say an open mind, but that’s such a broad term,” she says. “Dr. Epstein uses the term ‘beginner’s mind’ [to refer to] when you’re willing to consider many alternatives, where you don’t necessarily jump to a conclusion and then just stick with it. As a hospitalist, you start making those conclusions as soon as you hear what the patient’s chief complaint is. I think that having [a] beginner’s mind … is so important because we don’t know these patients, and it’s easy to jump to conclusions because we have to make decisions very quickly and … repeatedly.” She also believes that “being able to reflect on how you are communicating with another person is incredibly important to their care.”
—Valerie Lang, MD, hospitalist, University of Rochester Medical Center
Operationalizing Mindfulness
In 2004, after the publication of two of Dr. Epstein’s articles on mindful practice in action, the Arthur Vining Davis Foundation approached him and requested a proposal.5,6 At that time, he was in the process of writing an article on reflection and mindfulness in the context of preventing errors.1 (See Table 3, left.)
“This [proposal] was an intriguing possibility,” says Dr. Epstein, “and galvanized my putting together a curriculum that would not just be elective experiences for preclinical students, which is what the offerings related to mindfulness currently are, but something that was really going to influence clinical training.”
In Dr. Epstein’s view, placing educational reform in the first two years of medical school is teaching it when it matters the least. “Where it matters the most is when students are interacting with patients and using the knowledge and skills and doing work that they’ll ultimately end up doing for the next 30 or 40 years,” says Dr. Epstein.
One project plan is to train practicing primary care physicians to communicate more mindfully with their patients. Outcomes of the intervention will be measured by how it has affected the physicians as well as the patients’ ratings of their physicians and their practice styles.
The second project is a series of annual workshops for 100 third-year medical students and about 250 residents in the nine largest programs at the medical center. All participants will take five seminars that include mindfulness techniques to improve the capacity for paying attention and observing, and narrative exercises, whose themes will include, for instance, suffering, meaningful experience, professionalism, physician self-care, and avoiding burnout. The coursework, which will include both cognitive and experiential content, will also involve training a cadre of about 20 faculty members to teach these sessions, and educational outcomes will ultimately be measured for all participants.
Focus on Metacognition
Dr. Epstein, director of The Rochester Center to Improve Communication in Health Care, says metacognition builds on other approaches, such as the Healer’s Art, a course designed by Rachel Remen, MD, and colleagues, which a number of medical centers are incorporating into their curricula.7
“We are building on Dr. Remen’s wonderful work,” he says. Both curricula include self-awareness, humanism, caring, compassion, meaningful experiences, and physician well being. Both address the “informal curriculum”—a term used to refer to the social environment in which medical trainees adopt values, expectations, and clinical habits. In addition, Dr. Epstein and his colleagues focus on quality of clinical care, including medical decision-making and preventing errors.
“Importantly, our initiative is part of the required curriculum,” says Dr. Epstein. “It targets students and residents working in clinical settings at an advanced level, and it also has a faculty component. … We are trying to transform and heal the informal curriculum, not just immunize students against its toxicity.”
In the Thick of It
All this sounds as if it might benefit hospital practice, according to the hospitalists interviewed for this story. All three believe that mindfulness can be cultivated. Dr. Ali believes the aforementioned forces acting on hospitalists require that hospitalists work at their top capacities, but prioritizing remains essential. He believes one way a hospitalist can cultivate mindfulness in the patient-physician relationship is to avoid burnout in any way that works. Having been a hospitalist for almost 10 years, he discusses this with his medical students and residents. In addition to his hospitalist practice and teaching, Dr. Ali does patient-related quality work, which refreshes his energy.
Dr. Ferguson also thinks mindful practice can be cultivated. “I took cues from the nursing profession in realizing that you do have to care for all aspects of the patient,” she says. “But you can learn this from mentors and people who are successful: people you can emulate, shadow, and follow.”
For her, such a person is Lisa Cooper, MD, MPH, an associate professor in the department of medicine at Johns Hopkins University School of Medicine. Dr. Cooper, both a practicing internist and a researcher, studies and teaches about communication between physicians and minorities—that is, how physicians interact with people of the same or different races and ethnicities. Dr. Ferguson says she feels fortunate to have adopted a mindful awareness in that regard.
As director of the medicine clerkship, Dr. Lang came into contact with Dr. Epstein’s project through her Dean’s Teaching Fellowship, a competitive program at the URSM for faculty members who have a special interest in education.
“The discussions with other educators and clinicians really got me thinking about how my own feelings, whether they had to do with a patient or anything else in life, affect my decision-making,” says Dr. Lang. “You see the phenomenon in residency where you’re in morning report when the residents present a patient and everyone is sitting around a table—not involved with the patient—making judgments about what they should have done. It’s so much easier when you’re not involved [in the situation].”
Though Dr. Lang thinks there are a lot of reasons for that, “part of it is that you are not in the excitement of the moment. And the other factor is that when you’re presenting a patient to a group, you wouldn’t convey your own emotions, what else was going on, what were the competing pressures. Even if you have a wonderful intellect and clinical reasoning skills, you might make the wrong decision when you’re in the thick of the situation.”
Mindful Hospital Practice
Dr. Lang has seen a number of outcomes from her study of mindful practice. It has made her aware of her biases and has taught her to say, in certain cases, “OK, I need to think through the problem again to make sure I’m not changing my judgment about what we should be doing clinically based on how I’m feeling about a patient.”
Dr. Lang sometimes asks herself, “How am I feeling about this? Did that wear me down?” Or, sometimes the opposite can occur. A patient can make you feel “puffed up, where they are so complimentary and make you feel so good that you think that every decision you make is perfect,” she explains.
What Dr. Lang has learned about herself has helped her recognize when she might have prematurely closed a differential diagnosis or come to a conclusion too quickly simply because the patient appeared to agree with her clinical assessment.
Dr. Lang also thinks being a mindful physician has made her a better physician and that she is providing better care that results in better outcomes. “I definitely communicate better with my patients. … I think my relationships with my patients have significantly improved.”
What is her recommendation for how her hospitalist colleagues can learn to practice mindfully? “It’s a practice, and it’s a matter of practice,” says Dr. Lang. “It’s not something you get overnight. It’s a matter of every day, every encounter, taking the time before entering the patient’s room to pause, put things aside, and be present with the patient. And then, at the end of the day, take some time to reflect.”
How does education for mindfulness differ from her original medical training? “I don’t think you’re really ever taught how to manage your emotions when you’ve just made a medical error and you are distraught,” says Dr. Lang, “or how to manage doing that when your pager is going off like crazy and yet you need to sit down and be present with your patient. And that’s the kind of thing that ends up being in your way of being the best physician you can be.” TH
References
- Borrell-Carrió F, Epstein RM. Preventing errors in clinical practice: a call for self-awareness. Ann Fam Med. 2004;2:310-316.
- Epstein RM. Assessment in medical education. N Engl J Med. 2007;356(4):387-396.
- Epstein RM. Mindful practice. JAMA. 1999 Sep;282(9):833-839.
- Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002 Jan 9;287(2):226-235.
- Epstein RM. Mindful practice in action (I): technical competence, evidence-based medicine and relationship-centered care. Fam Syst Health. 2003;21:1-9.
- Epstein RM. Mindful practice in action (II): cultivating habits of mind. Fam Syst Health. 2003;21:11-17.
- O’Donnell JF, Rabow MW, Remen RN. The healer’s art: awakening the heart of medicine. Medical Encounter: Newsletter of the American Academy on Communication in Healthcare. 2007;21, No 1.
In hospitals, clinicians constantly encounter conflicting and ambiguous information,” says Ronald M. Epstein, MD, professor of family medicine, psychiatry, and oncology at the University of Rochester Medical Center (URMC) N.Y. “This information often gets processed tacitly, outside of awareness, and often results in various undesired consequences. For example, premature closure of diagnostic thinking or ordering a test rather than inquiring further of the patient.” In the average hospital, distractions and sensory inputs, including smells, sights, sounds, and tactile sensations, as well as multiple tasks to complete, can all seem pretty overwhelming. Faced with so much data, says Dr. Epstein, the tendency of the mind is to simplify and reduce it in some way. And that’s when error can rear its ugly head.
“Simplification is often arbitrary and unconscious,” he says, and thus “the trick of working in hospital is to develop a vigilant awareness of the ambient stimuli that are all around you, making choices as to what you attend to, relegating other stimuli to the background, and in that way avoiding becoming overwhelmed or controlled by them. In that way, you have the capacity for making better judgments.”
Some clinical decisions can be made fairly easily and routinely (low-level decisions), he says, whereas other patient situations require a fair bit of deliberation (high-level decisions). (See Tables 1 and 2, right.) The human mind tends to avoid the unpleasant and to give more attention to what is compelling. Also, the ambiguity of role and responsibility—especially in large hospitals—may further confound a hospitalist’s mental capacity. Keen attention to each moment also boosts physician well being.
“Hospitalists are often working in crowded, stressful, high-paced, windowless environments in which there is no natural form of respite,” says Dr. Epstein. Therefore, all physicians need ways of keeping themselves from being overwhelmed by the challenges of sensory input and intense emotions caused by exposure to suffering, conflicts, imperatives for critical thinking, and so on.
“If practitioners were able to be more mindful,” he says, “they might experience greater well-being, because they would be able to make more choices about what they attend to and how they react to them.”
Dr. Epstein and his colleagues at the University of Rochester Medical Center—Timothy Quill, MD, Michael Krasner, MD, and Howard Beckman, MD—have studied the qualities of mind required to exercise that awareness extensively, especially as they relate to clinical practice and education.2 They were recently awarded three complementary grants to teach mindfulness to physicians: one from the Arthur Vining Davis Foundations, another from the Physicians’ Foundation for Health Systems Excellence, and the Mannix Award for Excellence in Medical Education.
But just what does mindfulness in medicine entail?
Defining Mindful Practice
“Mindful practice is recognizing where you are at every moment. If you’re distressed, if you’re content or unhappy, if you’re comfortable or in pain, if you’re experiencing some kind of positive or negative effect, if you’re feeling in tune or disconnected from yourself. It’s that monitoring function to be able to say, I’m angry or I’m uncomfortable, or, possibly, I’m in the flow,” says Dr. Epstein.
For physicians to be able to exercise those qualities of mind, to watch and deconstruct their own behavior (what Dr. Epstein describes as “the ability to observe the observer observing the observed”) is something that goes back a long way for him.3 “There’s nothing really mystical about it,” he says. “People do this all the time. It’s part of being an excellent professional in lots of fields. It’s just that no one has organized the science of doing so in the context of medical training.”
In the late 1990s, Dr. Epstein and his coworkers implemented a curriculum reform process at URMC, and his particular charge was to assess the competence of medical students. To accomplish this, he did two things. First, he reviewed the literature on the assessment and definitions of special competence. Second, he turned the magnifying glass on himself. “I thought that it might be a useful exercise to try to understand what made me practice at my best and what barriers there were to doing so.”
The resulting article from this self-monitoring and evaluation was published in JAMA in 1999, before the review article on defining and assessing professional competence appeared in that same journal.3,4 Exploring the nature of his own mindful practice reacquainted him with two areas in which he had participated as a teenager: music and the study of mind—particularly the use of meditation to enhance mental capacities. Those inquiries led him to explore the psychology of a number of qualities of mind: attentiveness, curiosity, decision-making, and the use of cognitive knowledge. The literature was convergent in a number of ways, he says, and “seemed to point to the fact that a lot of competence is not a matter of book knowledge or the kind of knowledge we can explain but tacit knowledge, things we do semi-automatically that really take some effort to deconstruct.”
He realized that “what distinguished an excellent clinician from someone who wasn’t quite so excellent had to do with some of those same qualities that one sees in accomplished musicians, athletes, and meditators, which is the ability to make fine distinctions, lower one’s own level of reactivity, respond in a more conscious way, and pay attention to the unexpected—the surprises that are part of everyday work but that we often ignore.”
All of this rather radicalized his view of what medical education should be doing. He came to believe that—on top of a foundation of knowledge and skills—physicians need to be attentive to their own mental processes and alert to the effects of bias or prior experience.
Writing about excellent clinical practice in this way drew a crescendo of response from readers of the JAMA. The JAMA editors had thoroughly engaged in helping him refine and present the ideas in a way that would really speak to clinical practitioners and educators.3 After publication, he was amazed to receive hundreds of letters from all over the world from physicians in different specialties expressing their appreciation “for having articulated something that was really at the heart of medicine,” he says. “For me, that was incredibly gratifying.”
Hospitalist Qualities of Mind
What qualities of mind are important for a hospitalist to have?
“You have to be enthusiastic, fast-paced individuals,” says Yousaf Ali, MD, hospitalist at URMC and assistant professor of medicine in the Hospital Medicine Division. You also have to be able to immediately connect with patients and families and to have the knowledge and passion that makes that possible. Further, he says, you need to quickly access knowledge pertaining to caring for patients with multiple problems.
Traci Ferguson, MD, is a hospitalist at Boca Raton Community Hospital in Florida, which, by affiliating with Florida Atlantic University (the regional campus for the University of Miami School of Medicine), is moving from community hospital to teaching hospital. Dr. Ferguson believes the qualities of mind necessary to be a good hospitalist are the capacity to be aware of reactions and biases toward patients in order to avoid being judgmental.
“I think the major thing is being present and being attentive when you are caring for patients,” she says, “and that occurs when you’re writing a chart, when you’re talking to family members, [and] when you’re talking to nurses, just as it does when you’re at the bedside.”
Other qualities of mind, in Dr. Ferguson’s view, include the whole spectrum of empathy and compassion, being personable in the sense of being open to what patients and families have to say, and being patient. She also believes the quality of mind necessary to express a human touch is sometimes missing.
Valerie Lang, MD, is also a hospitalist at URMC and has studied mindfulness with Dr. Epstein. She is enrolled in Dr. Krasner’s class for healthcare providers on being mindful. What qualities of mind does she think are important for a hospitalist to have?
“I want to say an open mind, but that’s such a broad term,” she says. “Dr. Epstein uses the term ‘beginner’s mind’ [to refer to] when you’re willing to consider many alternatives, where you don’t necessarily jump to a conclusion and then just stick with it. As a hospitalist, you start making those conclusions as soon as you hear what the patient’s chief complaint is. I think that having [a] beginner’s mind … is so important because we don’t know these patients, and it’s easy to jump to conclusions because we have to make decisions very quickly and … repeatedly.” She also believes that “being able to reflect on how you are communicating with another person is incredibly important to their care.”
—Valerie Lang, MD, hospitalist, University of Rochester Medical Center
Operationalizing Mindfulness
In 2004, after the publication of two of Dr. Epstein’s articles on mindful practice in action, the Arthur Vining Davis Foundation approached him and requested a proposal.5,6 At that time, he was in the process of writing an article on reflection and mindfulness in the context of preventing errors.1 (See Table 3, left.)
“This [proposal] was an intriguing possibility,” says Dr. Epstein, “and galvanized my putting together a curriculum that would not just be elective experiences for preclinical students, which is what the offerings related to mindfulness currently are, but something that was really going to influence clinical training.”
In Dr. Epstein’s view, placing educational reform in the first two years of medical school is teaching it when it matters the least. “Where it matters the most is when students are interacting with patients and using the knowledge and skills and doing work that they’ll ultimately end up doing for the next 30 or 40 years,” says Dr. Epstein.
One project plan is to train practicing primary care physicians to communicate more mindfully with their patients. Outcomes of the intervention will be measured by how it has affected the physicians as well as the patients’ ratings of their physicians and their practice styles.
The second project is a series of annual workshops for 100 third-year medical students and about 250 residents in the nine largest programs at the medical center. All participants will take five seminars that include mindfulness techniques to improve the capacity for paying attention and observing, and narrative exercises, whose themes will include, for instance, suffering, meaningful experience, professionalism, physician self-care, and avoiding burnout. The coursework, which will include both cognitive and experiential content, will also involve training a cadre of about 20 faculty members to teach these sessions, and educational outcomes will ultimately be measured for all participants.
Focus on Metacognition
Dr. Epstein, director of The Rochester Center to Improve Communication in Health Care, says metacognition builds on other approaches, such as the Healer’s Art, a course designed by Rachel Remen, MD, and colleagues, which a number of medical centers are incorporating into their curricula.7
“We are building on Dr. Remen’s wonderful work,” he says. Both curricula include self-awareness, humanism, caring, compassion, meaningful experiences, and physician well being. Both address the “informal curriculum”—a term used to refer to the social environment in which medical trainees adopt values, expectations, and clinical habits. In addition, Dr. Epstein and his colleagues focus on quality of clinical care, including medical decision-making and preventing errors.
“Importantly, our initiative is part of the required curriculum,” says Dr. Epstein. “It targets students and residents working in clinical settings at an advanced level, and it also has a faculty component. … We are trying to transform and heal the informal curriculum, not just immunize students against its toxicity.”
In the Thick of It
All this sounds as if it might benefit hospital practice, according to the hospitalists interviewed for this story. All three believe that mindfulness can be cultivated. Dr. Ali believes the aforementioned forces acting on hospitalists require that hospitalists work at their top capacities, but prioritizing remains essential. He believes one way a hospitalist can cultivate mindfulness in the patient-physician relationship is to avoid burnout in any way that works. Having been a hospitalist for almost 10 years, he discusses this with his medical students and residents. In addition to his hospitalist practice and teaching, Dr. Ali does patient-related quality work, which refreshes his energy.
Dr. Ferguson also thinks mindful practice can be cultivated. “I took cues from the nursing profession in realizing that you do have to care for all aspects of the patient,” she says. “But you can learn this from mentors and people who are successful: people you can emulate, shadow, and follow.”
For her, such a person is Lisa Cooper, MD, MPH, an associate professor in the department of medicine at Johns Hopkins University School of Medicine. Dr. Cooper, both a practicing internist and a researcher, studies and teaches about communication between physicians and minorities—that is, how physicians interact with people of the same or different races and ethnicities. Dr. Ferguson says she feels fortunate to have adopted a mindful awareness in that regard.
As director of the medicine clerkship, Dr. Lang came into contact with Dr. Epstein’s project through her Dean’s Teaching Fellowship, a competitive program at the URSM for faculty members who have a special interest in education.
“The discussions with other educators and clinicians really got me thinking about how my own feelings, whether they had to do with a patient or anything else in life, affect my decision-making,” says Dr. Lang. “You see the phenomenon in residency where you’re in morning report when the residents present a patient and everyone is sitting around a table—not involved with the patient—making judgments about what they should have done. It’s so much easier when you’re not involved [in the situation].”
Though Dr. Lang thinks there are a lot of reasons for that, “part of it is that you are not in the excitement of the moment. And the other factor is that when you’re presenting a patient to a group, you wouldn’t convey your own emotions, what else was going on, what were the competing pressures. Even if you have a wonderful intellect and clinical reasoning skills, you might make the wrong decision when you’re in the thick of the situation.”
Mindful Hospital Practice
Dr. Lang has seen a number of outcomes from her study of mindful practice. It has made her aware of her biases and has taught her to say, in certain cases, “OK, I need to think through the problem again to make sure I’m not changing my judgment about what we should be doing clinically based on how I’m feeling about a patient.”
Dr. Lang sometimes asks herself, “How am I feeling about this? Did that wear me down?” Or, sometimes the opposite can occur. A patient can make you feel “puffed up, where they are so complimentary and make you feel so good that you think that every decision you make is perfect,” she explains.
What Dr. Lang has learned about herself has helped her recognize when she might have prematurely closed a differential diagnosis or come to a conclusion too quickly simply because the patient appeared to agree with her clinical assessment.
Dr. Lang also thinks being a mindful physician has made her a better physician and that she is providing better care that results in better outcomes. “I definitely communicate better with my patients. … I think my relationships with my patients have significantly improved.”
What is her recommendation for how her hospitalist colleagues can learn to practice mindfully? “It’s a practice, and it’s a matter of practice,” says Dr. Lang. “It’s not something you get overnight. It’s a matter of every day, every encounter, taking the time before entering the patient’s room to pause, put things aside, and be present with the patient. And then, at the end of the day, take some time to reflect.”
How does education for mindfulness differ from her original medical training? “I don’t think you’re really ever taught how to manage your emotions when you’ve just made a medical error and you are distraught,” says Dr. Lang, “or how to manage doing that when your pager is going off like crazy and yet you need to sit down and be present with your patient. And that’s the kind of thing that ends up being in your way of being the best physician you can be.” TH
References
- Borrell-Carrió F, Epstein RM. Preventing errors in clinical practice: a call for self-awareness. Ann Fam Med. 2004;2:310-316.
- Epstein RM. Assessment in medical education. N Engl J Med. 2007;356(4):387-396.
- Epstein RM. Mindful practice. JAMA. 1999 Sep;282(9):833-839.
- Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002 Jan 9;287(2):226-235.
- Epstein RM. Mindful practice in action (I): technical competence, evidence-based medicine and relationship-centered care. Fam Syst Health. 2003;21:1-9.
- Epstein RM. Mindful practice in action (II): cultivating habits of mind. Fam Syst Health. 2003;21:11-17.
- O’Donnell JF, Rabow MW, Remen RN. The healer’s art: awakening the heart of medicine. Medical Encounter: Newsletter of the American Academy on Communication in Healthcare. 2007;21, No 1.
Pitfalls in Pain Treatment
Note: This is Part 2 of The Hospitalist’s series on pain and hospital medicine. Part 1 appeared on p. 45 of the April issue.
Welcome to Part 2 of our three-part series on managing the pain of hospitalized patients. Last month’s article presented the context for pain management in the hospital—a core competency identified by SHM. It emphasized techniques for assessing patients’ pain, ranging from a zero-to-10 pain score to more complex pain histories addressing type, source, duration, and intensity as well as psychosocial and spiritual factors.
Part 2 delves into some difficult cases and dilemmas of pain management—situations that can take hospitalists out of their comfort zone and challenge their confidence in managing their patients’ pain.
Some of these dilemmas arise from misconceptions about pain and pain treatments and from the fact that, historically, physicians have not been well trained in optimal pain management. General barriers to pain management in the U.S. healthcare system, as identified by the National Association of Attorneys General, include patients’ beliefs, physician and institutional practices, restrictive state polices, and racial and socioeconomic disparities.1
Many of these issues relate specifically to the most common treatments for severe pain, opioid analgesics, which have all sorts of negative associations based on misconceptions about abuse, addiction, and overdose. In other cases, physicians face real challenges in balancing analgesic benefits with side effects and in determining the right medication, dose, and schedule to meet the patient’s need for pain relief.
Hospitalists confronting difficult pain cases work under the added pressure of trying to bring their patients’ acute illnesses under control so they can discharge them to a lower level of care as soon as prudently possible. This time pressure, along with demands arising from the rest of the hospitalist’s caseload, may impose limits on what can be accomplished in difficult situations or with medications that require time to stabilize.
Challenges also arise when the customary approach to pain management—the drug and dosing schedule the hospitalist is most comfortable using for most patients—fails to bring the pain under control. This is often a red flag for the need to try something new, says Stephen Bekanich, MD, a hospitalist at the University of Utah Medical Center in Salt Lake City and a consultant on the medical center’s palliative care service. In some cases, that means calling in a specialist in pain treatment, palliative medicine, psychiatry, or substance abuse.
“You need to work into the equation that there are pitfalls and caveats to everything we say about pain,” Dr. Bekanich observes. “Plus, the common pain treatments are controlled substances, with obvious legal implications and a professional duty for physicians to handle them safely and appropriately.”
When Dr. Bekanich finds himself confronting a difficult pain situation that has caused a conflict with a patient, he often involves one of the hospital’s customer service patient advocates. They are trained to mediate disagreements between patients and the treatment team.
Is This Patient’s Pain Real?
Physicians sometimes wonder if their patients’ reports of pain are accurate. Is the pain really as bad as the patient says it is? “Residents, frequently, are more skeptical of patients’ claims of pain, doubting whether they are truly experiencing that level of pain,” reports Jean Youngwerth, MD, a hospitalist, palliative care consultant, and fellowship associate program director at the University of Colorado Health Sciences Center in Aurora.
“I tell my residents that malingering is rare, and those few cases where it happens really tend to stand out,” Dr. Youngwerth says. “I also tell them that our default position is always to trust the patient, unless given a good reason not to. I have been burned more often when I questioned my patients’ reports of pain than when I didn’t.”
Pain experts emphasize that the patient’s self-report is the most reliable source of information on pain—based on an understanding of pain as a complex, subjective phenomenon associated with actual or potential tissue damage and the patient’s perception of and emotional reaction to that sensation. The phenomenon of pain also includes emotional, social, psychological, even spiritual components and can be mediated by a host of other factors. But that doesn’t mean it isn’t real to the patient.
“Often, younger physicians take the attitude that if the pain is real, then administration of morphine will make it go away,” says Porter Storey, MD, FACP, FAAHPM. “In reality, pain doesn’t always respond to opioids, for all sorts of reasons. Hospitalists value clarity, and they use pain as a screen for all sorts of other problems. Their goal, often, is not so much the comfort of the patient as it is diagnosing, treating, and then discharging the patient from the hospital.” Dr. Storey is a palliative care physician in Boulder, Colo., and executive vice president for Medical Affairs at the American Academy of Hospice and Palliative Medicine (AAHPM).
Physicians need to be reminded, however, that unresolved pain in hospitalized patients has many negative consequences. These range from resistance to rehabilitation to depression to delayed hospital discharge, as well as reduced job satisfaction for the healthcare professionals who care for them.
Will Prescribing Analgesics Cause Addiction?
Fears about causing addiction haunt many pain management discussions. Requests for more medications, obsessing over the next scheduled analgesic dose, and even manipulative or drug-seeking behaviors can be misunderstood by physicians who lack training in the real nature of drug addiction. Actual cases of drug addiction created by appropriate, sufficient, and well-monitored opioid analgesic treatment are rare, pain experts say. There is an important caveat: the patient who brings a prior history of drug abuse to the current acute medical episode.
“There are no good data about iatrogenic addiction,” says Robert Brody, MD, chief of the pain consultation clinic at San Francisco General Hospital and a frequent presenter on pain management topics at clinical workshops for hospitalists. “People who do pain management, certainly including hospice and palliative care physicians, don’t really believe in it. In my own clinical experience, most patients don’t like pain medications and stop them as soon as they can.”
Addiction is more accurately understood as the inappropriate use of a drug for non-medical purposes. It refers to disruptive, drug-seeking behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving.2 Addiction experts also describe addiction as a disease syndrome in its own right. Although that concept can sometimes be hard to accept by those who don’t have a lot of experience working with it, it is a useful paradigm to treat addiction as if it were a disease, says Ronald Crossno, MD, Rockdale, Texas-based area medical director for the VistaCare hospice chain.
Pain experts use the term pseudoaddiction for behaviors that are reminiscent of addiction but in fact reflect the pursuit of pain relief. Examples might include hoarding drugs, clock-watching, and exaggerated complaints of pain, such as moaning or crying. If it is pseudoaddiction, once the pain is brought under control, these behaviors cease. The term was coined in 1989 to describe an iatrogenic syndrome resulting from poorly treated pain.3-5
“Pseudoaddiction is a term you need to know,” Dr. Crossno asserted during a presentation on addiction pain at the recent annual conference of AAHPM in Salt Lake City in February. “It is at least as prevalent as addiction—and an indictment of how our healthcare system deals with pain.”
Dr. Youngwerth offers some advice.“We often see pseudoaddiction in response to undertreatment and inadequately managed pain,” she says. “If you treat the pain appropriately, these behaviors go away.” She tries to teach this concept to residents and hospital staff, who sometimes find it hard to put themselves in the shoes of patients experiencing severe pain.
“If you have a 68-year-old patient with no history of addiction or substance abuse who is in the hospital [with the] status post-hip replacement and is now clock-watching and routinely pressing the call button before her next dose of opioids is due, staff may feel that she is displaying addictive behaviors,” Dr. Youngwerth says. “Why would they think that this situation evolved into addiction during her brief hospital stay? It’s more likely that she’s just afraid of having pain.”
The solution to pseudoaddiction is to prescribe opioids at pharmacologically appropriate doses and schedules. Then, titrate up until analgesia is achieved or toxicities necessitate alternative approaches. Use all the techniques described in the first article of this series. It is also important to restore trust and the patient’s confidence in the medical system’s ability to manage his or her pain. Opioid pain regimens in the hospital should also be coordinated with plans for post-discharge medications and with the patient’s primary-care physician.
Two other concepts that often come up in discussions of opioid treatments are tolerance, which is a diminution of the drug’s effects over time, resulting in a need to increase doses of the medication to achieve the same analgesic effect, and physical dependence, in which the abrupt discontinuation of an analgesic after a period of continuous use causes physical symptoms of withdrawal from the drug. Both of these issues can be addressed with proper assessment and management, and neither is diagnostic of addiction.
Pain experts say tolerance, though a real phenomenon of opioids, is not often a serious problem with pain management in the hospital. Instead, the need for escalating analgesic doses may reflect changes in the underlying disease process. Tolerance can also include positive benefits such as its emergence for opioid side effects like nausea or sedation. Physical dependence on opioids is predictable but can be managed if the original cause of the pain is resolved and the analgesic is no longer needed. Most opioids can be gradually reduced, with each day’s dose at 75% of the previous day’s dose, until the drug is tapered off.6
What if the Patient Is an Addict?
Although pain experts believe that drug addiction caused by appropriate and adequate prescribing of opioids for analgesia is rare, this does not mean that hospitalists won’t face the problem of patients who are addicted to pain medications. “You are already treating patients with addiction,” said Dr. Crossno in his presentation at the AAHPM meeting in Salt Lake City.
Given that pre-existing addictions are relatively common in American society (estimates range from 5% to 17% of the population, depending on whether alcohol abuse is included), it is reasonable to expect this segment of the population will be represented among acutely ill, hospitalized patients.7 Sometimes, the substance abuse problem of a friend or family member affects the patient’s care, such as when pain medications are stolen from the patient.
“Some hospitalized patients do abuse opioids,” says Dr. Bekanich. “We catch people with drug paraphernalia or actually shooting up in their rooms.” Providers can exercise some control over what patients do in the hospital, but it is probably not realistic to expect that a hospitalist will be able to resolve long-standing substance abuse problems during the patient’s brief stay in the hospital.
As part of a comprehensive pain assessment, it is appropriate to ask if the patient has a history of drug use. Many patients will freely admit to such a history, may be actively in recovery or on a methadone maintenance program, or may even resist opioid analgesics despite severe pain because of their commitment to recovery. Without the benefit of such candor, however, it will be difficult to reach a conclusive diagnosis of drug addiction during the patient’s acute inpatient stay, because that ordinarily requires observations over time.
“It is not our job as hospitalists to get patients off opioids; there are other institutions and services for that,” Dr. Bekanich adds. “For us to try to do it in a few days in the hospital seems like a hopeless task. That is not to say we shouldn’t be mindful of the issues involved, talking to the patient or even offering a referral to a drug rehabilitation program. But we should not be trying to do drug rehab.”
The basic principles of believing patients’ reports of pain and providing analgesic doses sufficient to relieve the pain still apply—unless side effects or the patient’s problematic behavior demand a modification in this approach. Pain physicians often cite the maxim “trust but verify.” There are various screening tools that can be used for indicating the possibility of substance abuse, and it is imperative the use of controlled substances always be closely monitored.
Urine drug screening tests are easy to order in the hospital and may encourage compliance for patients who have a drug history when presented up front as a routine aspect of pain management. The urine test can detect prescribed medicines that are being taken by the patient as well as non-prescribed opioids, but it is important to be aware of false positives and negatives and opportunities for gaming the system by those who are determined to do so.
“Just as it is a myth that treating pain appropriately leads to addiction, it is also a myth that people with drug histories can’t have their pain treated effectively,” says Scott Irwin, MD, PhD, medical director of palliative care psychiatry at San Diego Hospice and Palliative Care. “The first thing to ask these patients is what are their goals for pain management. Get as much objective information as you can about the pain and the patient’s history. Fully inform the patient about options. Treat the pain just as you would for anyone else.”
Then, if things don’t add up, Dr. Irwin says, it may be necessary to go back and reassess the patient’s pain and history. Is there psychological distress? Perhaps the analgesic dose isn’t adequate. Maybe financial pressures or complicated social relationships are leading to drug diversion.
If the patient is participating in a methadone maintenance program or similar protocol, it is advisable for the hospitalist to speak to the medical director of that program. But effective pain control also supports maintenance. Emphasize long-acting analgesics, add non-opioid adjuvants and, when possible, find alternatives to intravenous administration. But if the patient is addicted, trying to minimize adverse effects from analgesic treatments might be the best the hospitalist can do.
Another approach to managing the patient with a history of drug abuse is the use of a contract or opioid agreement, in which the patient promises to do certain things with a clear understanding of the consequences for not doing so. Establish the rules early and be prepared to enforce them. Explain expectations for the patient and the physician’s role, designate a single pharmacy and a single physician responsible for pain prescribing, and get consent for treatment and drug testing. If a repeat offender breaks the agreement, it may be time to call in an addiction specialist. Such agreements should be negotiated in person by the physician, not delegated to nurses or other professionals, but then make sure other team members are in the loop. For an example of such an agreement, see http://tinyurl.com/y2bbh6.
Will Pain Medications Cause Respiratory Suppression?
Another common fear related to opioid use is that prescribing sufficient analgesic doses for patients with advanced illnesses could lead to toxicities, suppress their breathing, cause an overdose, or even prematurely end their lives. This scenario is often luridly presented as turning up the morphine drip. Pain management experts question the truth of this scenario, arguing that morphine often is falsely credited with deaths that result from advanced disease processes. Morphine is a common treatment for the sensation of dyspnea, while morphine-related toxicity likely will present with drowsiness, confusion, and loss of consciousness before respiratory compromise.8
A main concern of hospitalists is appreciating the need to balance pain relief with the side effects of analgesics, including opioid toxicities, which can be addressed through careful titration and frequent assessments. Respiratory suppression can be a side effect of opioids, and there are special groups of patients for whom any sedation is a major concern. An example is a lung transplant patient, for whom somnolence may suppress the important cough reflex.
Respiratory suppression from morphine is an area without a large evidence base. But a recent study of 725 patients nearing death in 13 hospice programs analyzed those who were receiving opioids and had at least one change in opioid dose prior to death to see if escalating opioid doses was associated with premature death.9 The authors conclude that “final opioid dose, but not percentage change in dose, was one of several factors associated with survival, but the association is very weak … (and explains) only a very small percentage in variation in survival.” They also found support for their conclusion that opioid use is not a major contributor to premature death in the few other published studies on the subject.
“I tell residents that the fear of respiratory suppression is overrated,” Dr. Youngwerth says. “As long as you follow World Health Organization and other recognized guidelines for dosing and titrating opioids, you can safely prescribe pain medications and control the patient’s pain. They get this fear ingrained during residency. In reality, it is not very common. I remind them that there is much more evidence of under-dosing.”
Dr. Bekanich describes a recent patient, a young woman suffering from severe abdominal pain following the birth of her baby. The pain was so difficult to manage that her hospital in rural Idaho transferred her to his medical center in Salt Lake City. She had also experienced respiratory arrest twice secondary to the application of fentanyl analgesic patches. “But she was relatively easy to manage once we tried a different drug, appropriately titrated,” he relates.
Dr. Bekanich spent two hours in the patient’s room adjusting the intravenous analgesic dose and monitoring the patient’s pulse oxygen level and neurological status. “These medicines don’t have to cause respiratory suppression, although it will happen occasionally, especially when there are multiple co-morbidities,” he says. “Hospitalists don’t realize that most of these problems can be avoided if you are meticulous in prescribing.”
Does Regulatory Scrutiny Chill Pain Treatment?
The ubiquitous fear of opioids and their potential side effects, including some unfounded or unrealistic fears, is also reflected in the regulation of controlled substances and physicians’ fears that they will be subjected to oppressive regulatory scrutiny.
Widely publicized cases of physicians being disciplined or prosecuted for over-prescribing opioids have only added to these fears, while the rare case of a physician being sued or sanctioned for under-prescribing pain medications does little to allay them.10
Growing attention to the inadequacies of and barriers to pain management—and the role of controlled substances regulation in those barriers—led to the 1998 promulgation of “Model Guidelines for the Use of Controlled Substances for the Treatment of Pain” by the Federation of State Medical Boards.11 These guidelines, promoting the legitimate role of opioids in relieving pain and acknowledging providers’ concerns about being disciplined, were revised in 2004 and have been adopted by 21 states.12
The effect remains, however. “For decades, physicians have reported being reluctant to prescribe opioids because of the fear of the stress, expense, and consequences of being investigated by licensing agencies or law enforcement,” states a 2006 state report card issued by the Pain & Policy Studies Group at the University of Wisconsin in Madison.13 “Some states—but far from all—have adopted policies which recognize that controlled substances are necessary for public health. … But in some states, pain treatment using opioids is unduly restricted by policies reflecting medical opinions that were discarded decades ago.”
The Pain & Policy Studies Group’s report card, which advocates for a balanced approach to the regulation and prescribing of controlled substances, has given every state a grade for how well it meets this goal. According to the 2006 report card, Michigan and Virginia get top grades for achieving balance in pain policy, while Georgia gets the lowest grade.
“Regulation is a real concern,” says Daniel Burkhardt, MD, associate professor and director of the Acute Pain Service at the University of California-San Francisco. “Every time a prosecutor arrests someone for prescribing too much pain medication, these things travel, adding to the extra regulatory burden on physicians.”
Carol Jessop, MD, a hospitalist and palliative care consultant at Alta Bates Summit Medical Center in Berkeley, Calif., says the burden has lessened somewhat in California because that state eliminated its requirements for triplicate paper prescribing forms for controlled substances.
A related concern involves the potential diversion of controlled substances by impaired healthcare professionals for personal use and abuse. This is another of the fears that have driven archaic pain regulation in many states. In fact, current estimates suggest that a substance abuse-related impairment will affect between 8% and 18% percent of physicians sometime in their lives, and that 2% of physicians are dealing with an active substance abuse problem.14
A recent medical journal letter to the editor from the Wisconsin Pain & Policy Studies Group suggests public policies on opioid diversion should focus more on sources of diversion such as “thefts, including armed robberies, night break-ins, and employee and customer pilferage,” rather than just the doctor-patient prescribing relationship.15
Physician diversion data don’t break out hospital medicine as a category, but some hospitalists say they have not heard of diversion problems involving hospitalist colleagues. That may reflect the fact that hospitalists, unlike some other health professionals, generally don’t administer controlled substances directly to the patient or have ready access to hospital drug storage facilities. TH
Larry Beresford is a regular contributor to The Hospitalist.
References
- Joranson D, Payne R. Will my pain be managed? In Improving End-of-Life Care: The Role of Attorneys General. National Association of Attorneys General. Washington, D.C. 2003. Available at www.naag.org/end-of-life_healthcare.php. Last accessed April 13, 2007.
- American Pain Society. Definitions related to the use of opioids for the treatment of pain: a consensus document from the American Academy of Pain Medicine, American Pain Society, and American Society of Addiction Medicine. Available at www.ampainsoc.org/advocacy/opioids2.htm. Last accessed April 13, 2007.
- Weissman DE, Haddox JD. Opioid pseudoaddiction. Pain. 1989 Mar;36(3):363-366.
- Weissman DE. Fast Fact and Concept #68: Is it pain or addiction? [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_68.htm. Last accessed April 13, 2007.
- Weissman DE. Fast Fact and Concept #69: Pseudoaddiction. [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_69.htm. Last accessed April 13, 2007.
- Doyle D, Hanks G, Cherny N, et al, eds. The Oxford Textbook of Palliative Medicine. 3rd ed. Oxford, England: Oxford University Press;2005:336.
- Passik SD, Kirsh KL. Chapter 56: Pain in patients with alcohol and drug dependence. In Bruera E, Higginson I, von Gunten C, et al. Textbook of Palliative Medicine. London, England: Hodder Arnold;2006:517-524.
- Von Gunten CF. Fast Fact and Concept #8: Morphine and hastened death. [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_008.htm. Last accessed April 13, 2007.
- Portenoy RK, Siberceva U, Smout R, et al. Opioid use and survival at the end of life: a survey of a hospice population. J Pain Symptom Manage. 2006;32:532-540.
- Warm EJ, Weissman DE. Fast Fact and Concept #63: The legal liability of under-treatment of pain. [The End of Life/Palliative Education Resource Center.] Available at: www.eperc.mcw.edu/fastFact/ff_63.htm. Last accessed April 13, 2007.
- Federation of the State Medical Boards of the United States. Dallas, Texas. Available at www.fsmb.org. Accessed April 13, 2007.
- National Association of Attorneys General. Improving End-of-Life Care: The Role of Attorneys General. National Association of Attorneys General. Washington, D.C. 2003. Available at www.naag.org/end-of-life_healthcare.php. Last accessed April 13, 2007.
- Pain & Policy Studies Group. University of Wisconsin Paul P. Carbone Comprehensive Cancer Center. Available at: www.painpolicy.wisc.edu. Accessed April 13, 2007.
- Blondell RD. Taking a proactive approach to physician impairment. Postgrad Med. 2005 Jul;118(1):16-18.
- Joranson DE, Gilson AM. Drug crime is a source of abused pain medications in the United States. J Pain Symptom Manage. 2005 Oct;30(4):299-301.
Note: This is Part 2 of The Hospitalist’s series on pain and hospital medicine. Part 1 appeared on p. 45 of the April issue.
Welcome to Part 2 of our three-part series on managing the pain of hospitalized patients. Last month’s article presented the context for pain management in the hospital—a core competency identified by SHM. It emphasized techniques for assessing patients’ pain, ranging from a zero-to-10 pain score to more complex pain histories addressing type, source, duration, and intensity as well as psychosocial and spiritual factors.
Part 2 delves into some difficult cases and dilemmas of pain management—situations that can take hospitalists out of their comfort zone and challenge their confidence in managing their patients’ pain.
Some of these dilemmas arise from misconceptions about pain and pain treatments and from the fact that, historically, physicians have not been well trained in optimal pain management. General barriers to pain management in the U.S. healthcare system, as identified by the National Association of Attorneys General, include patients’ beliefs, physician and institutional practices, restrictive state polices, and racial and socioeconomic disparities.1
Many of these issues relate specifically to the most common treatments for severe pain, opioid analgesics, which have all sorts of negative associations based on misconceptions about abuse, addiction, and overdose. In other cases, physicians face real challenges in balancing analgesic benefits with side effects and in determining the right medication, dose, and schedule to meet the patient’s need for pain relief.
Hospitalists confronting difficult pain cases work under the added pressure of trying to bring their patients’ acute illnesses under control so they can discharge them to a lower level of care as soon as prudently possible. This time pressure, along with demands arising from the rest of the hospitalist’s caseload, may impose limits on what can be accomplished in difficult situations or with medications that require time to stabilize.
Challenges also arise when the customary approach to pain management—the drug and dosing schedule the hospitalist is most comfortable using for most patients—fails to bring the pain under control. This is often a red flag for the need to try something new, says Stephen Bekanich, MD, a hospitalist at the University of Utah Medical Center in Salt Lake City and a consultant on the medical center’s palliative care service. In some cases, that means calling in a specialist in pain treatment, palliative medicine, psychiatry, or substance abuse.
“You need to work into the equation that there are pitfalls and caveats to everything we say about pain,” Dr. Bekanich observes. “Plus, the common pain treatments are controlled substances, with obvious legal implications and a professional duty for physicians to handle them safely and appropriately.”
When Dr. Bekanich finds himself confronting a difficult pain situation that has caused a conflict with a patient, he often involves one of the hospital’s customer service patient advocates. They are trained to mediate disagreements between patients and the treatment team.
Is This Patient’s Pain Real?
Physicians sometimes wonder if their patients’ reports of pain are accurate. Is the pain really as bad as the patient says it is? “Residents, frequently, are more skeptical of patients’ claims of pain, doubting whether they are truly experiencing that level of pain,” reports Jean Youngwerth, MD, a hospitalist, palliative care consultant, and fellowship associate program director at the University of Colorado Health Sciences Center in Aurora.
“I tell my residents that malingering is rare, and those few cases where it happens really tend to stand out,” Dr. Youngwerth says. “I also tell them that our default position is always to trust the patient, unless given a good reason not to. I have been burned more often when I questioned my patients’ reports of pain than when I didn’t.”
Pain experts emphasize that the patient’s self-report is the most reliable source of information on pain—based on an understanding of pain as a complex, subjective phenomenon associated with actual or potential tissue damage and the patient’s perception of and emotional reaction to that sensation. The phenomenon of pain also includes emotional, social, psychological, even spiritual components and can be mediated by a host of other factors. But that doesn’t mean it isn’t real to the patient.
“Often, younger physicians take the attitude that if the pain is real, then administration of morphine will make it go away,” says Porter Storey, MD, FACP, FAAHPM. “In reality, pain doesn’t always respond to opioids, for all sorts of reasons. Hospitalists value clarity, and they use pain as a screen for all sorts of other problems. Their goal, often, is not so much the comfort of the patient as it is diagnosing, treating, and then discharging the patient from the hospital.” Dr. Storey is a palliative care physician in Boulder, Colo., and executive vice president for Medical Affairs at the American Academy of Hospice and Palliative Medicine (AAHPM).
Physicians need to be reminded, however, that unresolved pain in hospitalized patients has many negative consequences. These range from resistance to rehabilitation to depression to delayed hospital discharge, as well as reduced job satisfaction for the healthcare professionals who care for them.
Will Prescribing Analgesics Cause Addiction?
Fears about causing addiction haunt many pain management discussions. Requests for more medications, obsessing over the next scheduled analgesic dose, and even manipulative or drug-seeking behaviors can be misunderstood by physicians who lack training in the real nature of drug addiction. Actual cases of drug addiction created by appropriate, sufficient, and well-monitored opioid analgesic treatment are rare, pain experts say. There is an important caveat: the patient who brings a prior history of drug abuse to the current acute medical episode.
“There are no good data about iatrogenic addiction,” says Robert Brody, MD, chief of the pain consultation clinic at San Francisco General Hospital and a frequent presenter on pain management topics at clinical workshops for hospitalists. “People who do pain management, certainly including hospice and palliative care physicians, don’t really believe in it. In my own clinical experience, most patients don’t like pain medications and stop them as soon as they can.”
Addiction is more accurately understood as the inappropriate use of a drug for non-medical purposes. It refers to disruptive, drug-seeking behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving.2 Addiction experts also describe addiction as a disease syndrome in its own right. Although that concept can sometimes be hard to accept by those who don’t have a lot of experience working with it, it is a useful paradigm to treat addiction as if it were a disease, says Ronald Crossno, MD, Rockdale, Texas-based area medical director for the VistaCare hospice chain.
Pain experts use the term pseudoaddiction for behaviors that are reminiscent of addiction but in fact reflect the pursuit of pain relief. Examples might include hoarding drugs, clock-watching, and exaggerated complaints of pain, such as moaning or crying. If it is pseudoaddiction, once the pain is brought under control, these behaviors cease. The term was coined in 1989 to describe an iatrogenic syndrome resulting from poorly treated pain.3-5
“Pseudoaddiction is a term you need to know,” Dr. Crossno asserted during a presentation on addiction pain at the recent annual conference of AAHPM in Salt Lake City in February. “It is at least as prevalent as addiction—and an indictment of how our healthcare system deals with pain.”
Dr. Youngwerth offers some advice.“We often see pseudoaddiction in response to undertreatment and inadequately managed pain,” she says. “If you treat the pain appropriately, these behaviors go away.” She tries to teach this concept to residents and hospital staff, who sometimes find it hard to put themselves in the shoes of patients experiencing severe pain.
“If you have a 68-year-old patient with no history of addiction or substance abuse who is in the hospital [with the] status post-hip replacement and is now clock-watching and routinely pressing the call button before her next dose of opioids is due, staff may feel that she is displaying addictive behaviors,” Dr. Youngwerth says. “Why would they think that this situation evolved into addiction during her brief hospital stay? It’s more likely that she’s just afraid of having pain.”
The solution to pseudoaddiction is to prescribe opioids at pharmacologically appropriate doses and schedules. Then, titrate up until analgesia is achieved or toxicities necessitate alternative approaches. Use all the techniques described in the first article of this series. It is also important to restore trust and the patient’s confidence in the medical system’s ability to manage his or her pain. Opioid pain regimens in the hospital should also be coordinated with plans for post-discharge medications and with the patient’s primary-care physician.
Two other concepts that often come up in discussions of opioid treatments are tolerance, which is a diminution of the drug’s effects over time, resulting in a need to increase doses of the medication to achieve the same analgesic effect, and physical dependence, in which the abrupt discontinuation of an analgesic after a period of continuous use causes physical symptoms of withdrawal from the drug. Both of these issues can be addressed with proper assessment and management, and neither is diagnostic of addiction.
Pain experts say tolerance, though a real phenomenon of opioids, is not often a serious problem with pain management in the hospital. Instead, the need for escalating analgesic doses may reflect changes in the underlying disease process. Tolerance can also include positive benefits such as its emergence for opioid side effects like nausea or sedation. Physical dependence on opioids is predictable but can be managed if the original cause of the pain is resolved and the analgesic is no longer needed. Most opioids can be gradually reduced, with each day’s dose at 75% of the previous day’s dose, until the drug is tapered off.6
What if the Patient Is an Addict?
Although pain experts believe that drug addiction caused by appropriate and adequate prescribing of opioids for analgesia is rare, this does not mean that hospitalists won’t face the problem of patients who are addicted to pain medications. “You are already treating patients with addiction,” said Dr. Crossno in his presentation at the AAHPM meeting in Salt Lake City.
Given that pre-existing addictions are relatively common in American society (estimates range from 5% to 17% of the population, depending on whether alcohol abuse is included), it is reasonable to expect this segment of the population will be represented among acutely ill, hospitalized patients.7 Sometimes, the substance abuse problem of a friend or family member affects the patient’s care, such as when pain medications are stolen from the patient.
“Some hospitalized patients do abuse opioids,” says Dr. Bekanich. “We catch people with drug paraphernalia or actually shooting up in their rooms.” Providers can exercise some control over what patients do in the hospital, but it is probably not realistic to expect that a hospitalist will be able to resolve long-standing substance abuse problems during the patient’s brief stay in the hospital.
As part of a comprehensive pain assessment, it is appropriate to ask if the patient has a history of drug use. Many patients will freely admit to such a history, may be actively in recovery or on a methadone maintenance program, or may even resist opioid analgesics despite severe pain because of their commitment to recovery. Without the benefit of such candor, however, it will be difficult to reach a conclusive diagnosis of drug addiction during the patient’s acute inpatient stay, because that ordinarily requires observations over time.
“It is not our job as hospitalists to get patients off opioids; there are other institutions and services for that,” Dr. Bekanich adds. “For us to try to do it in a few days in the hospital seems like a hopeless task. That is not to say we shouldn’t be mindful of the issues involved, talking to the patient or even offering a referral to a drug rehabilitation program. But we should not be trying to do drug rehab.”
The basic principles of believing patients’ reports of pain and providing analgesic doses sufficient to relieve the pain still apply—unless side effects or the patient’s problematic behavior demand a modification in this approach. Pain physicians often cite the maxim “trust but verify.” There are various screening tools that can be used for indicating the possibility of substance abuse, and it is imperative the use of controlled substances always be closely monitored.
Urine drug screening tests are easy to order in the hospital and may encourage compliance for patients who have a drug history when presented up front as a routine aspect of pain management. The urine test can detect prescribed medicines that are being taken by the patient as well as non-prescribed opioids, but it is important to be aware of false positives and negatives and opportunities for gaming the system by those who are determined to do so.
“Just as it is a myth that treating pain appropriately leads to addiction, it is also a myth that people with drug histories can’t have their pain treated effectively,” says Scott Irwin, MD, PhD, medical director of palliative care psychiatry at San Diego Hospice and Palliative Care. “The first thing to ask these patients is what are their goals for pain management. Get as much objective information as you can about the pain and the patient’s history. Fully inform the patient about options. Treat the pain just as you would for anyone else.”
Then, if things don’t add up, Dr. Irwin says, it may be necessary to go back and reassess the patient’s pain and history. Is there psychological distress? Perhaps the analgesic dose isn’t adequate. Maybe financial pressures or complicated social relationships are leading to drug diversion.
If the patient is participating in a methadone maintenance program or similar protocol, it is advisable for the hospitalist to speak to the medical director of that program. But effective pain control also supports maintenance. Emphasize long-acting analgesics, add non-opioid adjuvants and, when possible, find alternatives to intravenous administration. But if the patient is addicted, trying to minimize adverse effects from analgesic treatments might be the best the hospitalist can do.
Another approach to managing the patient with a history of drug abuse is the use of a contract or opioid agreement, in which the patient promises to do certain things with a clear understanding of the consequences for not doing so. Establish the rules early and be prepared to enforce them. Explain expectations for the patient and the physician’s role, designate a single pharmacy and a single physician responsible for pain prescribing, and get consent for treatment and drug testing. If a repeat offender breaks the agreement, it may be time to call in an addiction specialist. Such agreements should be negotiated in person by the physician, not delegated to nurses or other professionals, but then make sure other team members are in the loop. For an example of such an agreement, see http://tinyurl.com/y2bbh6.
Will Pain Medications Cause Respiratory Suppression?
Another common fear related to opioid use is that prescribing sufficient analgesic doses for patients with advanced illnesses could lead to toxicities, suppress their breathing, cause an overdose, or even prematurely end their lives. This scenario is often luridly presented as turning up the morphine drip. Pain management experts question the truth of this scenario, arguing that morphine often is falsely credited with deaths that result from advanced disease processes. Morphine is a common treatment for the sensation of dyspnea, while morphine-related toxicity likely will present with drowsiness, confusion, and loss of consciousness before respiratory compromise.8
A main concern of hospitalists is appreciating the need to balance pain relief with the side effects of analgesics, including opioid toxicities, which can be addressed through careful titration and frequent assessments. Respiratory suppression can be a side effect of opioids, and there are special groups of patients for whom any sedation is a major concern. An example is a lung transplant patient, for whom somnolence may suppress the important cough reflex.
Respiratory suppression from morphine is an area without a large evidence base. But a recent study of 725 patients nearing death in 13 hospice programs analyzed those who were receiving opioids and had at least one change in opioid dose prior to death to see if escalating opioid doses was associated with premature death.9 The authors conclude that “final opioid dose, but not percentage change in dose, was one of several factors associated with survival, but the association is very weak … (and explains) only a very small percentage in variation in survival.” They also found support for their conclusion that opioid use is not a major contributor to premature death in the few other published studies on the subject.
“I tell residents that the fear of respiratory suppression is overrated,” Dr. Youngwerth says. “As long as you follow World Health Organization and other recognized guidelines for dosing and titrating opioids, you can safely prescribe pain medications and control the patient’s pain. They get this fear ingrained during residency. In reality, it is not very common. I remind them that there is much more evidence of under-dosing.”
Dr. Bekanich describes a recent patient, a young woman suffering from severe abdominal pain following the birth of her baby. The pain was so difficult to manage that her hospital in rural Idaho transferred her to his medical center in Salt Lake City. She had also experienced respiratory arrest twice secondary to the application of fentanyl analgesic patches. “But she was relatively easy to manage once we tried a different drug, appropriately titrated,” he relates.
Dr. Bekanich spent two hours in the patient’s room adjusting the intravenous analgesic dose and monitoring the patient’s pulse oxygen level and neurological status. “These medicines don’t have to cause respiratory suppression, although it will happen occasionally, especially when there are multiple co-morbidities,” he says. “Hospitalists don’t realize that most of these problems can be avoided if you are meticulous in prescribing.”
Does Regulatory Scrutiny Chill Pain Treatment?
The ubiquitous fear of opioids and their potential side effects, including some unfounded or unrealistic fears, is also reflected in the regulation of controlled substances and physicians’ fears that they will be subjected to oppressive regulatory scrutiny.
Widely publicized cases of physicians being disciplined or prosecuted for over-prescribing opioids have only added to these fears, while the rare case of a physician being sued or sanctioned for under-prescribing pain medications does little to allay them.10
Growing attention to the inadequacies of and barriers to pain management—and the role of controlled substances regulation in those barriers—led to the 1998 promulgation of “Model Guidelines for the Use of Controlled Substances for the Treatment of Pain” by the Federation of State Medical Boards.11 These guidelines, promoting the legitimate role of opioids in relieving pain and acknowledging providers’ concerns about being disciplined, were revised in 2004 and have been adopted by 21 states.12
The effect remains, however. “For decades, physicians have reported being reluctant to prescribe opioids because of the fear of the stress, expense, and consequences of being investigated by licensing agencies or law enforcement,” states a 2006 state report card issued by the Pain & Policy Studies Group at the University of Wisconsin in Madison.13 “Some states—but far from all—have adopted policies which recognize that controlled substances are necessary for public health. … But in some states, pain treatment using opioids is unduly restricted by policies reflecting medical opinions that were discarded decades ago.”
The Pain & Policy Studies Group’s report card, which advocates for a balanced approach to the regulation and prescribing of controlled substances, has given every state a grade for how well it meets this goal. According to the 2006 report card, Michigan and Virginia get top grades for achieving balance in pain policy, while Georgia gets the lowest grade.
“Regulation is a real concern,” says Daniel Burkhardt, MD, associate professor and director of the Acute Pain Service at the University of California-San Francisco. “Every time a prosecutor arrests someone for prescribing too much pain medication, these things travel, adding to the extra regulatory burden on physicians.”
Carol Jessop, MD, a hospitalist and palliative care consultant at Alta Bates Summit Medical Center in Berkeley, Calif., says the burden has lessened somewhat in California because that state eliminated its requirements for triplicate paper prescribing forms for controlled substances.
A related concern involves the potential diversion of controlled substances by impaired healthcare professionals for personal use and abuse. This is another of the fears that have driven archaic pain regulation in many states. In fact, current estimates suggest that a substance abuse-related impairment will affect between 8% and 18% percent of physicians sometime in their lives, and that 2% of physicians are dealing with an active substance abuse problem.14
A recent medical journal letter to the editor from the Wisconsin Pain & Policy Studies Group suggests public policies on opioid diversion should focus more on sources of diversion such as “thefts, including armed robberies, night break-ins, and employee and customer pilferage,” rather than just the doctor-patient prescribing relationship.15
Physician diversion data don’t break out hospital medicine as a category, but some hospitalists say they have not heard of diversion problems involving hospitalist colleagues. That may reflect the fact that hospitalists, unlike some other health professionals, generally don’t administer controlled substances directly to the patient or have ready access to hospital drug storage facilities. TH
Larry Beresford is a regular contributor to The Hospitalist.
References
- Joranson D, Payne R. Will my pain be managed? In Improving End-of-Life Care: The Role of Attorneys General. National Association of Attorneys General. Washington, D.C. 2003. Available at www.naag.org/end-of-life_healthcare.php. Last accessed April 13, 2007.
- American Pain Society. Definitions related to the use of opioids for the treatment of pain: a consensus document from the American Academy of Pain Medicine, American Pain Society, and American Society of Addiction Medicine. Available at www.ampainsoc.org/advocacy/opioids2.htm. Last accessed April 13, 2007.
- Weissman DE, Haddox JD. Opioid pseudoaddiction. Pain. 1989 Mar;36(3):363-366.
- Weissman DE. Fast Fact and Concept #68: Is it pain or addiction? [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_68.htm. Last accessed April 13, 2007.
- Weissman DE. Fast Fact and Concept #69: Pseudoaddiction. [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_69.htm. Last accessed April 13, 2007.
- Doyle D, Hanks G, Cherny N, et al, eds. The Oxford Textbook of Palliative Medicine. 3rd ed. Oxford, England: Oxford University Press;2005:336.
- Passik SD, Kirsh KL. Chapter 56: Pain in patients with alcohol and drug dependence. In Bruera E, Higginson I, von Gunten C, et al. Textbook of Palliative Medicine. London, England: Hodder Arnold;2006:517-524.
- Von Gunten CF. Fast Fact and Concept #8: Morphine and hastened death. [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_008.htm. Last accessed April 13, 2007.
- Portenoy RK, Siberceva U, Smout R, et al. Opioid use and survival at the end of life: a survey of a hospice population. J Pain Symptom Manage. 2006;32:532-540.
- Warm EJ, Weissman DE. Fast Fact and Concept #63: The legal liability of under-treatment of pain. [The End of Life/Palliative Education Resource Center.] Available at: www.eperc.mcw.edu/fastFact/ff_63.htm. Last accessed April 13, 2007.
- Federation of the State Medical Boards of the United States. Dallas, Texas. Available at www.fsmb.org. Accessed April 13, 2007.
- National Association of Attorneys General. Improving End-of-Life Care: The Role of Attorneys General. National Association of Attorneys General. Washington, D.C. 2003. Available at www.naag.org/end-of-life_healthcare.php. Last accessed April 13, 2007.
- Pain & Policy Studies Group. University of Wisconsin Paul P. Carbone Comprehensive Cancer Center. Available at: www.painpolicy.wisc.edu. Accessed April 13, 2007.
- Blondell RD. Taking a proactive approach to physician impairment. Postgrad Med. 2005 Jul;118(1):16-18.
- Joranson DE, Gilson AM. Drug crime is a source of abused pain medications in the United States. J Pain Symptom Manage. 2005 Oct;30(4):299-301.
Note: This is Part 2 of The Hospitalist’s series on pain and hospital medicine. Part 1 appeared on p. 45 of the April issue.
Welcome to Part 2 of our three-part series on managing the pain of hospitalized patients. Last month’s article presented the context for pain management in the hospital—a core competency identified by SHM. It emphasized techniques for assessing patients’ pain, ranging from a zero-to-10 pain score to more complex pain histories addressing type, source, duration, and intensity as well as psychosocial and spiritual factors.
Part 2 delves into some difficult cases and dilemmas of pain management—situations that can take hospitalists out of their comfort zone and challenge their confidence in managing their patients’ pain.
Some of these dilemmas arise from misconceptions about pain and pain treatments and from the fact that, historically, physicians have not been well trained in optimal pain management. General barriers to pain management in the U.S. healthcare system, as identified by the National Association of Attorneys General, include patients’ beliefs, physician and institutional practices, restrictive state polices, and racial and socioeconomic disparities.1
Many of these issues relate specifically to the most common treatments for severe pain, opioid analgesics, which have all sorts of negative associations based on misconceptions about abuse, addiction, and overdose. In other cases, physicians face real challenges in balancing analgesic benefits with side effects and in determining the right medication, dose, and schedule to meet the patient’s need for pain relief.
Hospitalists confronting difficult pain cases work under the added pressure of trying to bring their patients’ acute illnesses under control so they can discharge them to a lower level of care as soon as prudently possible. This time pressure, along with demands arising from the rest of the hospitalist’s caseload, may impose limits on what can be accomplished in difficult situations or with medications that require time to stabilize.
Challenges also arise when the customary approach to pain management—the drug and dosing schedule the hospitalist is most comfortable using for most patients—fails to bring the pain under control. This is often a red flag for the need to try something new, says Stephen Bekanich, MD, a hospitalist at the University of Utah Medical Center in Salt Lake City and a consultant on the medical center’s palliative care service. In some cases, that means calling in a specialist in pain treatment, palliative medicine, psychiatry, or substance abuse.
“You need to work into the equation that there are pitfalls and caveats to everything we say about pain,” Dr. Bekanich observes. “Plus, the common pain treatments are controlled substances, with obvious legal implications and a professional duty for physicians to handle them safely and appropriately.”
When Dr. Bekanich finds himself confronting a difficult pain situation that has caused a conflict with a patient, he often involves one of the hospital’s customer service patient advocates. They are trained to mediate disagreements between patients and the treatment team.
Is This Patient’s Pain Real?
Physicians sometimes wonder if their patients’ reports of pain are accurate. Is the pain really as bad as the patient says it is? “Residents, frequently, are more skeptical of patients’ claims of pain, doubting whether they are truly experiencing that level of pain,” reports Jean Youngwerth, MD, a hospitalist, palliative care consultant, and fellowship associate program director at the University of Colorado Health Sciences Center in Aurora.
“I tell my residents that malingering is rare, and those few cases where it happens really tend to stand out,” Dr. Youngwerth says. “I also tell them that our default position is always to trust the patient, unless given a good reason not to. I have been burned more often when I questioned my patients’ reports of pain than when I didn’t.”
Pain experts emphasize that the patient’s self-report is the most reliable source of information on pain—based on an understanding of pain as a complex, subjective phenomenon associated with actual or potential tissue damage and the patient’s perception of and emotional reaction to that sensation. The phenomenon of pain also includes emotional, social, psychological, even spiritual components and can be mediated by a host of other factors. But that doesn’t mean it isn’t real to the patient.
“Often, younger physicians take the attitude that if the pain is real, then administration of morphine will make it go away,” says Porter Storey, MD, FACP, FAAHPM. “In reality, pain doesn’t always respond to opioids, for all sorts of reasons. Hospitalists value clarity, and they use pain as a screen for all sorts of other problems. Their goal, often, is not so much the comfort of the patient as it is diagnosing, treating, and then discharging the patient from the hospital.” Dr. Storey is a palliative care physician in Boulder, Colo., and executive vice president for Medical Affairs at the American Academy of Hospice and Palliative Medicine (AAHPM).
Physicians need to be reminded, however, that unresolved pain in hospitalized patients has many negative consequences. These range from resistance to rehabilitation to depression to delayed hospital discharge, as well as reduced job satisfaction for the healthcare professionals who care for them.
Will Prescribing Analgesics Cause Addiction?
Fears about causing addiction haunt many pain management discussions. Requests for more medications, obsessing over the next scheduled analgesic dose, and even manipulative or drug-seeking behaviors can be misunderstood by physicians who lack training in the real nature of drug addiction. Actual cases of drug addiction created by appropriate, sufficient, and well-monitored opioid analgesic treatment are rare, pain experts say. There is an important caveat: the patient who brings a prior history of drug abuse to the current acute medical episode.
“There are no good data about iatrogenic addiction,” says Robert Brody, MD, chief of the pain consultation clinic at San Francisco General Hospital and a frequent presenter on pain management topics at clinical workshops for hospitalists. “People who do pain management, certainly including hospice and palliative care physicians, don’t really believe in it. In my own clinical experience, most patients don’t like pain medications and stop them as soon as they can.”
Addiction is more accurately understood as the inappropriate use of a drug for non-medical purposes. It refers to disruptive, drug-seeking behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving.2 Addiction experts also describe addiction as a disease syndrome in its own right. Although that concept can sometimes be hard to accept by those who don’t have a lot of experience working with it, it is a useful paradigm to treat addiction as if it were a disease, says Ronald Crossno, MD, Rockdale, Texas-based area medical director for the VistaCare hospice chain.
Pain experts use the term pseudoaddiction for behaviors that are reminiscent of addiction but in fact reflect the pursuit of pain relief. Examples might include hoarding drugs, clock-watching, and exaggerated complaints of pain, such as moaning or crying. If it is pseudoaddiction, once the pain is brought under control, these behaviors cease. The term was coined in 1989 to describe an iatrogenic syndrome resulting from poorly treated pain.3-5
“Pseudoaddiction is a term you need to know,” Dr. Crossno asserted during a presentation on addiction pain at the recent annual conference of AAHPM in Salt Lake City in February. “It is at least as prevalent as addiction—and an indictment of how our healthcare system deals with pain.”
Dr. Youngwerth offers some advice.“We often see pseudoaddiction in response to undertreatment and inadequately managed pain,” she says. “If you treat the pain appropriately, these behaviors go away.” She tries to teach this concept to residents and hospital staff, who sometimes find it hard to put themselves in the shoes of patients experiencing severe pain.
“If you have a 68-year-old patient with no history of addiction or substance abuse who is in the hospital [with the] status post-hip replacement and is now clock-watching and routinely pressing the call button before her next dose of opioids is due, staff may feel that she is displaying addictive behaviors,” Dr. Youngwerth says. “Why would they think that this situation evolved into addiction during her brief hospital stay? It’s more likely that she’s just afraid of having pain.”
The solution to pseudoaddiction is to prescribe opioids at pharmacologically appropriate doses and schedules. Then, titrate up until analgesia is achieved or toxicities necessitate alternative approaches. Use all the techniques described in the first article of this series. It is also important to restore trust and the patient’s confidence in the medical system’s ability to manage his or her pain. Opioid pain regimens in the hospital should also be coordinated with plans for post-discharge medications and with the patient’s primary-care physician.
Two other concepts that often come up in discussions of opioid treatments are tolerance, which is a diminution of the drug’s effects over time, resulting in a need to increase doses of the medication to achieve the same analgesic effect, and physical dependence, in which the abrupt discontinuation of an analgesic after a period of continuous use causes physical symptoms of withdrawal from the drug. Both of these issues can be addressed with proper assessment and management, and neither is diagnostic of addiction.
Pain experts say tolerance, though a real phenomenon of opioids, is not often a serious problem with pain management in the hospital. Instead, the need for escalating analgesic doses may reflect changes in the underlying disease process. Tolerance can also include positive benefits such as its emergence for opioid side effects like nausea or sedation. Physical dependence on opioids is predictable but can be managed if the original cause of the pain is resolved and the analgesic is no longer needed. Most opioids can be gradually reduced, with each day’s dose at 75% of the previous day’s dose, until the drug is tapered off.6
What if the Patient Is an Addict?
Although pain experts believe that drug addiction caused by appropriate and adequate prescribing of opioids for analgesia is rare, this does not mean that hospitalists won’t face the problem of patients who are addicted to pain medications. “You are already treating patients with addiction,” said Dr. Crossno in his presentation at the AAHPM meeting in Salt Lake City.
Given that pre-existing addictions are relatively common in American society (estimates range from 5% to 17% of the population, depending on whether alcohol abuse is included), it is reasonable to expect this segment of the population will be represented among acutely ill, hospitalized patients.7 Sometimes, the substance abuse problem of a friend or family member affects the patient’s care, such as when pain medications are stolen from the patient.
“Some hospitalized patients do abuse opioids,” says Dr. Bekanich. “We catch people with drug paraphernalia or actually shooting up in their rooms.” Providers can exercise some control over what patients do in the hospital, but it is probably not realistic to expect that a hospitalist will be able to resolve long-standing substance abuse problems during the patient’s brief stay in the hospital.
As part of a comprehensive pain assessment, it is appropriate to ask if the patient has a history of drug use. Many patients will freely admit to such a history, may be actively in recovery or on a methadone maintenance program, or may even resist opioid analgesics despite severe pain because of their commitment to recovery. Without the benefit of such candor, however, it will be difficult to reach a conclusive diagnosis of drug addiction during the patient’s acute inpatient stay, because that ordinarily requires observations over time.
“It is not our job as hospitalists to get patients off opioids; there are other institutions and services for that,” Dr. Bekanich adds. “For us to try to do it in a few days in the hospital seems like a hopeless task. That is not to say we shouldn’t be mindful of the issues involved, talking to the patient or even offering a referral to a drug rehabilitation program. But we should not be trying to do drug rehab.”
The basic principles of believing patients’ reports of pain and providing analgesic doses sufficient to relieve the pain still apply—unless side effects or the patient’s problematic behavior demand a modification in this approach. Pain physicians often cite the maxim “trust but verify.” There are various screening tools that can be used for indicating the possibility of substance abuse, and it is imperative the use of controlled substances always be closely monitored.
Urine drug screening tests are easy to order in the hospital and may encourage compliance for patients who have a drug history when presented up front as a routine aspect of pain management. The urine test can detect prescribed medicines that are being taken by the patient as well as non-prescribed opioids, but it is important to be aware of false positives and negatives and opportunities for gaming the system by those who are determined to do so.
“Just as it is a myth that treating pain appropriately leads to addiction, it is also a myth that people with drug histories can’t have their pain treated effectively,” says Scott Irwin, MD, PhD, medical director of palliative care psychiatry at San Diego Hospice and Palliative Care. “The first thing to ask these patients is what are their goals for pain management. Get as much objective information as you can about the pain and the patient’s history. Fully inform the patient about options. Treat the pain just as you would for anyone else.”
Then, if things don’t add up, Dr. Irwin says, it may be necessary to go back and reassess the patient’s pain and history. Is there psychological distress? Perhaps the analgesic dose isn’t adequate. Maybe financial pressures or complicated social relationships are leading to drug diversion.
If the patient is participating in a methadone maintenance program or similar protocol, it is advisable for the hospitalist to speak to the medical director of that program. But effective pain control also supports maintenance. Emphasize long-acting analgesics, add non-opioid adjuvants and, when possible, find alternatives to intravenous administration. But if the patient is addicted, trying to minimize adverse effects from analgesic treatments might be the best the hospitalist can do.
Another approach to managing the patient with a history of drug abuse is the use of a contract or opioid agreement, in which the patient promises to do certain things with a clear understanding of the consequences for not doing so. Establish the rules early and be prepared to enforce them. Explain expectations for the patient and the physician’s role, designate a single pharmacy and a single physician responsible for pain prescribing, and get consent for treatment and drug testing. If a repeat offender breaks the agreement, it may be time to call in an addiction specialist. Such agreements should be negotiated in person by the physician, not delegated to nurses or other professionals, but then make sure other team members are in the loop. For an example of such an agreement, see http://tinyurl.com/y2bbh6.
Will Pain Medications Cause Respiratory Suppression?
Another common fear related to opioid use is that prescribing sufficient analgesic doses for patients with advanced illnesses could lead to toxicities, suppress their breathing, cause an overdose, or even prematurely end their lives. This scenario is often luridly presented as turning up the morphine drip. Pain management experts question the truth of this scenario, arguing that morphine often is falsely credited with deaths that result from advanced disease processes. Morphine is a common treatment for the sensation of dyspnea, while morphine-related toxicity likely will present with drowsiness, confusion, and loss of consciousness before respiratory compromise.8
A main concern of hospitalists is appreciating the need to balance pain relief with the side effects of analgesics, including opioid toxicities, which can be addressed through careful titration and frequent assessments. Respiratory suppression can be a side effect of opioids, and there are special groups of patients for whom any sedation is a major concern. An example is a lung transplant patient, for whom somnolence may suppress the important cough reflex.
Respiratory suppression from morphine is an area without a large evidence base. But a recent study of 725 patients nearing death in 13 hospice programs analyzed those who were receiving opioids and had at least one change in opioid dose prior to death to see if escalating opioid doses was associated with premature death.9 The authors conclude that “final opioid dose, but not percentage change in dose, was one of several factors associated with survival, but the association is very weak … (and explains) only a very small percentage in variation in survival.” They also found support for their conclusion that opioid use is not a major contributor to premature death in the few other published studies on the subject.
“I tell residents that the fear of respiratory suppression is overrated,” Dr. Youngwerth says. “As long as you follow World Health Organization and other recognized guidelines for dosing and titrating opioids, you can safely prescribe pain medications and control the patient’s pain. They get this fear ingrained during residency. In reality, it is not very common. I remind them that there is much more evidence of under-dosing.”
Dr. Bekanich describes a recent patient, a young woman suffering from severe abdominal pain following the birth of her baby. The pain was so difficult to manage that her hospital in rural Idaho transferred her to his medical center in Salt Lake City. She had also experienced respiratory arrest twice secondary to the application of fentanyl analgesic patches. “But she was relatively easy to manage once we tried a different drug, appropriately titrated,” he relates.
Dr. Bekanich spent two hours in the patient’s room adjusting the intravenous analgesic dose and monitoring the patient’s pulse oxygen level and neurological status. “These medicines don’t have to cause respiratory suppression, although it will happen occasionally, especially when there are multiple co-morbidities,” he says. “Hospitalists don’t realize that most of these problems can be avoided if you are meticulous in prescribing.”
Does Regulatory Scrutiny Chill Pain Treatment?
The ubiquitous fear of opioids and their potential side effects, including some unfounded or unrealistic fears, is also reflected in the regulation of controlled substances and physicians’ fears that they will be subjected to oppressive regulatory scrutiny.
Widely publicized cases of physicians being disciplined or prosecuted for over-prescribing opioids have only added to these fears, while the rare case of a physician being sued or sanctioned for under-prescribing pain medications does little to allay them.10
Growing attention to the inadequacies of and barriers to pain management—and the role of controlled substances regulation in those barriers—led to the 1998 promulgation of “Model Guidelines for the Use of Controlled Substances for the Treatment of Pain” by the Federation of State Medical Boards.11 These guidelines, promoting the legitimate role of opioids in relieving pain and acknowledging providers’ concerns about being disciplined, were revised in 2004 and have been adopted by 21 states.12
The effect remains, however. “For decades, physicians have reported being reluctant to prescribe opioids because of the fear of the stress, expense, and consequences of being investigated by licensing agencies or law enforcement,” states a 2006 state report card issued by the Pain & Policy Studies Group at the University of Wisconsin in Madison.13 “Some states—but far from all—have adopted policies which recognize that controlled substances are necessary for public health. … But in some states, pain treatment using opioids is unduly restricted by policies reflecting medical opinions that were discarded decades ago.”
The Pain & Policy Studies Group’s report card, which advocates for a balanced approach to the regulation and prescribing of controlled substances, has given every state a grade for how well it meets this goal. According to the 2006 report card, Michigan and Virginia get top grades for achieving balance in pain policy, while Georgia gets the lowest grade.
“Regulation is a real concern,” says Daniel Burkhardt, MD, associate professor and director of the Acute Pain Service at the University of California-San Francisco. “Every time a prosecutor arrests someone for prescribing too much pain medication, these things travel, adding to the extra regulatory burden on physicians.”
Carol Jessop, MD, a hospitalist and palliative care consultant at Alta Bates Summit Medical Center in Berkeley, Calif., says the burden has lessened somewhat in California because that state eliminated its requirements for triplicate paper prescribing forms for controlled substances.
A related concern involves the potential diversion of controlled substances by impaired healthcare professionals for personal use and abuse. This is another of the fears that have driven archaic pain regulation in many states. In fact, current estimates suggest that a substance abuse-related impairment will affect between 8% and 18% percent of physicians sometime in their lives, and that 2% of physicians are dealing with an active substance abuse problem.14
A recent medical journal letter to the editor from the Wisconsin Pain & Policy Studies Group suggests public policies on opioid diversion should focus more on sources of diversion such as “thefts, including armed robberies, night break-ins, and employee and customer pilferage,” rather than just the doctor-patient prescribing relationship.15
Physician diversion data don’t break out hospital medicine as a category, but some hospitalists say they have not heard of diversion problems involving hospitalist colleagues. That may reflect the fact that hospitalists, unlike some other health professionals, generally don’t administer controlled substances directly to the patient or have ready access to hospital drug storage facilities. TH
Larry Beresford is a regular contributor to The Hospitalist.
References
- Joranson D, Payne R. Will my pain be managed? In Improving End-of-Life Care: The Role of Attorneys General. National Association of Attorneys General. Washington, D.C. 2003. Available at www.naag.org/end-of-life_healthcare.php. Last accessed April 13, 2007.
- American Pain Society. Definitions related to the use of opioids for the treatment of pain: a consensus document from the American Academy of Pain Medicine, American Pain Society, and American Society of Addiction Medicine. Available at www.ampainsoc.org/advocacy/opioids2.htm. Last accessed April 13, 2007.
- Weissman DE, Haddox JD. Opioid pseudoaddiction. Pain. 1989 Mar;36(3):363-366.
- Weissman DE. Fast Fact and Concept #68: Is it pain or addiction? [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_68.htm. Last accessed April 13, 2007.
- Weissman DE. Fast Fact and Concept #69: Pseudoaddiction. [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_69.htm. Last accessed April 13, 2007.
- Doyle D, Hanks G, Cherny N, et al, eds. The Oxford Textbook of Palliative Medicine. 3rd ed. Oxford, England: Oxford University Press;2005:336.
- Passik SD, Kirsh KL. Chapter 56: Pain in patients with alcohol and drug dependence. In Bruera E, Higginson I, von Gunten C, et al. Textbook of Palliative Medicine. London, England: Hodder Arnold;2006:517-524.
- Von Gunten CF. Fast Fact and Concept #8: Morphine and hastened death. [The End of Life/Palliative Education Resource Center.] Available at www.eperc.mcw.edu/fastFact/ff_008.htm. Last accessed April 13, 2007.
- Portenoy RK, Siberceva U, Smout R, et al. Opioid use and survival at the end of life: a survey of a hospice population. J Pain Symptom Manage. 2006;32:532-540.
- Warm EJ, Weissman DE. Fast Fact and Concept #63: The legal liability of under-treatment of pain. [The End of Life/Palliative Education Resource Center.] Available at: www.eperc.mcw.edu/fastFact/ff_63.htm. Last accessed April 13, 2007.
- Federation of the State Medical Boards of the United States. Dallas, Texas. Available at www.fsmb.org. Accessed April 13, 2007.
- National Association of Attorneys General. Improving End-of-Life Care: The Role of Attorneys General. National Association of Attorneys General. Washington, D.C. 2003. Available at www.naag.org/end-of-life_healthcare.php. Last accessed April 13, 2007.
- Pain & Policy Studies Group. University of Wisconsin Paul P. Carbone Comprehensive Cancer Center. Available at: www.painpolicy.wisc.edu. Accessed April 13, 2007.
- Blondell RD. Taking a proactive approach to physician impairment. Postgrad Med. 2005 Jul;118(1):16-18.
- Joranson DE, Gilson AM. Drug crime is a source of abused pain medications in the United States. J Pain Symptom Manage. 2005 Oct;30(4):299-301.
A Wolf in Sheep's Clothing
Adverse drug reactions are a major clinical problem, accounting for 2%-6% of all hospital admissions. And, 6%-15% of hospitalized patients experience a serious adverse drug reaction that contributes to longer hospital stays and higher costs. It is crucial for clinicians to detect, diagnose, and report adverse drug reactions to ensure safe prescribing and continued drug safety monitoring, as illustrated by this brief case presentation.
The Patient
A 72-year-old male presented to the emergency department in acute respiratory distress due to severe angioedema of the face and tongue; the patient required intubation. He denied prior episodes of angioedema. A careful evaluation of all possible causes of angioedema, including a thorough assessment of the medications used by the patient, led to the conclusion that this life-threatening incident could be attributed only to a reaction to an angiotensin-converting enzyme (ACE) inhibitor. The patient had been on ACE inhibitor therapy for hypertension for more than five years and at the time of admission had been taking a combination of benazepril and amlodipine for more than two years. This medication was immediately discontinued, and he recovered fully after five days in the ICU on mechanical ventilation.
ACE Inhibitor-Associated Angioedema
ACE inhibitors are used by more than 35 million people worldwide to treat hypertension, heart failure, and diabetes mellitus; still, many physicians believe they are underprescribed.1 Angioedema is a serious complication of ACE inhibitor therapy that occurs in 0.1% to 0.68% of patients taking ACE inhibitors.2,3
Angioedema presents with a non-pitting swelling of subcutaneous or submucosal tissue without desquamation. Angioedema associated with ACE inhibitor use is rapid in onset, occurring minutes to hours after ingestion, does not present with urticaria, and usually lasts no more than 48 hours.4 At times, angioedema related to ACE inhibitor therapy occurs in the intestine, causing abdominal pain, diarrhea, and vomiting without mucocutaneous signs.1,4
Certain risk factors for developing ACE inhibitor-related angioedema include age older than 65, seasonal allergies, and black ethnicity. Another risk factor pertinent to our case presentation is the patient’s length of time on ACE inhibitor therapy. One study found that ACE inhibitor-associated angioedema occurred at a rate that was nine times higher during the first month of therapy than during subsequent months of therapy.2 Agostoni and colleagues found that ACE inhibitor-associated angioedema could occur in patients who had been on ACE inhibitor therapy for as long as eight years.5
The Process
ACE inhibitor-induced angioedema is probably a multifactorial process. Angiotensin-converting enzyme (ACE) metabolizes angiotensin I to angiotensin II in vivo and is a major inactivator of bradykinin. ACE and aminopeptidase P are the major pathways of bradykinin metabolism. A minor pathway uses carboxypeptidase N, which metabolizes bradykinin to its active metabolite, des-Arg-bradykinin. Des-Arg-bradykinin can then be inactivated by ACE and aminopeptidase P. In patients who had angioedema caused by ACE inhibitors, higher levels of des-Arg-bradykinin were found due to decreased activity of aminopeptidase P, which normally plays a major role in bradykinin breakdown when an ACE inhibitor is present.6
Bradykinin is a beta2 receptor agonist, but, when it is metabolized by carboxypeptidase N to des-Arg-bradykinin, it becomes a beta1 receptor agonist.6
During ACE inhibitor therapy, bradykinin can be inactivated by aminopeptidase P or metabolized into a beta1 receptor agonist by carboxypeptidase N, which is then broken down by aminopeptidase P. If aminopeptidase P is not active, then bradykinin can be converted to des-Arg-bradykinin, which can then act on upregulated beta1 receptors in the oropharynx and tongue, producing vasodilation, increased capillary permeability, and pain.
Treatment
Treatment of ACE inhibitor-induced angioedema includes discontinuing the ACE inhibitor and providing symptomatic support. Although some ACE inhibitors are more likely than others to cause angioedema, a patient who has had an episode of ACE inhibitor-associated angioedema should never again use any ACE inhibitor.3 Angiotensin receptor blockers (ARBs) do not affect the bradykinin system; however, they can cause angioedema (0.13% in one trial of ARBs), and it is not known if ARBs should be avoided in patients who have had ACE inhibitor-induced angioedema.7 Therapy with a bradykinin receptor antagonist to prevent or resolve ACE inhibitor-associated angioedema has not yet been studied in detail.1
Summary
Adverse drug reactions can present clinically in many different ways, and, indeed, these reactions have deposed syphilis and tuberculosis as the mimic of disease. Many adverse drug reactions are mild, but others can be severe and, occasionally, life-threatening. This variability in manifestations means clinicians always have to consider that the drug may be the cause of the patient’s symptoms. TH
Johnson is a medical student at the Kansas City University of Medicine and Biosciences, Kansas City, Mo. Dr. Egger is a consultant in general internal medicine at the Mayo Clinic, Rochester, Minn.
References
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26(4):725-737.
- Kostis JB, Kim HJ, Rusnak J, et al. Incidence and characteristics of angioedema associated with enalapril. Arch Intern Med. 2005 Jul;165(14):1637-1642.
- Kostis JB, Packer M, Black HR, et al. Omapatrilat and enalapril in patients with hypertension: the Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am J Hypertens. 2004 Feb;17(2):103-111.
- Kaplan AP, Greaves MW. Angioedema. J Am Acad Dermatol. 2005;53:373-388.
- Agostoni A, Cicardi M, Cugno M, et al. Angioedema due to angiotensin-converting enzyme inhibitors. Immunopharmacology. 1999;44:21-25.
- Molinaro G, Cugno M, Perez M, et al. Angiotensin-converting enzyme inhibitor-associated angioedema is characterized by a slower degradation of des-arginine(9)-bradykinin. J Pharmacol Exp Ther. 2002;303:232-237.
- Ward KE, Hume AL. Olmesartan (benicar) for hypertension. Am Fam Physician. 2005;72:673-674.
Adverse drug reactions are a major clinical problem, accounting for 2%-6% of all hospital admissions. And, 6%-15% of hospitalized patients experience a serious adverse drug reaction that contributes to longer hospital stays and higher costs. It is crucial for clinicians to detect, diagnose, and report adverse drug reactions to ensure safe prescribing and continued drug safety monitoring, as illustrated by this brief case presentation.
The Patient
A 72-year-old male presented to the emergency department in acute respiratory distress due to severe angioedema of the face and tongue; the patient required intubation. He denied prior episodes of angioedema. A careful evaluation of all possible causes of angioedema, including a thorough assessment of the medications used by the patient, led to the conclusion that this life-threatening incident could be attributed only to a reaction to an angiotensin-converting enzyme (ACE) inhibitor. The patient had been on ACE inhibitor therapy for hypertension for more than five years and at the time of admission had been taking a combination of benazepril and amlodipine for more than two years. This medication was immediately discontinued, and he recovered fully after five days in the ICU on mechanical ventilation.
ACE Inhibitor-Associated Angioedema
ACE inhibitors are used by more than 35 million people worldwide to treat hypertension, heart failure, and diabetes mellitus; still, many physicians believe they are underprescribed.1 Angioedema is a serious complication of ACE inhibitor therapy that occurs in 0.1% to 0.68% of patients taking ACE inhibitors.2,3
Angioedema presents with a non-pitting swelling of subcutaneous or submucosal tissue without desquamation. Angioedema associated with ACE inhibitor use is rapid in onset, occurring minutes to hours after ingestion, does not present with urticaria, and usually lasts no more than 48 hours.4 At times, angioedema related to ACE inhibitor therapy occurs in the intestine, causing abdominal pain, diarrhea, and vomiting without mucocutaneous signs.1,4
Certain risk factors for developing ACE inhibitor-related angioedema include age older than 65, seasonal allergies, and black ethnicity. Another risk factor pertinent to our case presentation is the patient’s length of time on ACE inhibitor therapy. One study found that ACE inhibitor-associated angioedema occurred at a rate that was nine times higher during the first month of therapy than during subsequent months of therapy.2 Agostoni and colleagues found that ACE inhibitor-associated angioedema could occur in patients who had been on ACE inhibitor therapy for as long as eight years.5
The Process
ACE inhibitor-induced angioedema is probably a multifactorial process. Angiotensin-converting enzyme (ACE) metabolizes angiotensin I to angiotensin II in vivo and is a major inactivator of bradykinin. ACE and aminopeptidase P are the major pathways of bradykinin metabolism. A minor pathway uses carboxypeptidase N, which metabolizes bradykinin to its active metabolite, des-Arg-bradykinin. Des-Arg-bradykinin can then be inactivated by ACE and aminopeptidase P. In patients who had angioedema caused by ACE inhibitors, higher levels of des-Arg-bradykinin were found due to decreased activity of aminopeptidase P, which normally plays a major role in bradykinin breakdown when an ACE inhibitor is present.6
Bradykinin is a beta2 receptor agonist, but, when it is metabolized by carboxypeptidase N to des-Arg-bradykinin, it becomes a beta1 receptor agonist.6
During ACE inhibitor therapy, bradykinin can be inactivated by aminopeptidase P or metabolized into a beta1 receptor agonist by carboxypeptidase N, which is then broken down by aminopeptidase P. If aminopeptidase P is not active, then bradykinin can be converted to des-Arg-bradykinin, which can then act on upregulated beta1 receptors in the oropharynx and tongue, producing vasodilation, increased capillary permeability, and pain.
Treatment
Treatment of ACE inhibitor-induced angioedema includes discontinuing the ACE inhibitor and providing symptomatic support. Although some ACE inhibitors are more likely than others to cause angioedema, a patient who has had an episode of ACE inhibitor-associated angioedema should never again use any ACE inhibitor.3 Angiotensin receptor blockers (ARBs) do not affect the bradykinin system; however, they can cause angioedema (0.13% in one trial of ARBs), and it is not known if ARBs should be avoided in patients who have had ACE inhibitor-induced angioedema.7 Therapy with a bradykinin receptor antagonist to prevent or resolve ACE inhibitor-associated angioedema has not yet been studied in detail.1
Summary
Adverse drug reactions can present clinically in many different ways, and, indeed, these reactions have deposed syphilis and tuberculosis as the mimic of disease. Many adverse drug reactions are mild, but others can be severe and, occasionally, life-threatening. This variability in manifestations means clinicians always have to consider that the drug may be the cause of the patient’s symptoms. TH
Johnson is a medical student at the Kansas City University of Medicine and Biosciences, Kansas City, Mo. Dr. Egger is a consultant in general internal medicine at the Mayo Clinic, Rochester, Minn.
References
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26(4):725-737.
- Kostis JB, Kim HJ, Rusnak J, et al. Incidence and characteristics of angioedema associated with enalapril. Arch Intern Med. 2005 Jul;165(14):1637-1642.
- Kostis JB, Packer M, Black HR, et al. Omapatrilat and enalapril in patients with hypertension: the Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am J Hypertens. 2004 Feb;17(2):103-111.
- Kaplan AP, Greaves MW. Angioedema. J Am Acad Dermatol. 2005;53:373-388.
- Agostoni A, Cicardi M, Cugno M, et al. Angioedema due to angiotensin-converting enzyme inhibitors. Immunopharmacology. 1999;44:21-25.
- Molinaro G, Cugno M, Perez M, et al. Angiotensin-converting enzyme inhibitor-associated angioedema is characterized by a slower degradation of des-arginine(9)-bradykinin. J Pharmacol Exp Ther. 2002;303:232-237.
- Ward KE, Hume AL. Olmesartan (benicar) for hypertension. Am Fam Physician. 2005;72:673-674.
Adverse drug reactions are a major clinical problem, accounting for 2%-6% of all hospital admissions. And, 6%-15% of hospitalized patients experience a serious adverse drug reaction that contributes to longer hospital stays and higher costs. It is crucial for clinicians to detect, diagnose, and report adverse drug reactions to ensure safe prescribing and continued drug safety monitoring, as illustrated by this brief case presentation.
The Patient
A 72-year-old male presented to the emergency department in acute respiratory distress due to severe angioedema of the face and tongue; the patient required intubation. He denied prior episodes of angioedema. A careful evaluation of all possible causes of angioedema, including a thorough assessment of the medications used by the patient, led to the conclusion that this life-threatening incident could be attributed only to a reaction to an angiotensin-converting enzyme (ACE) inhibitor. The patient had been on ACE inhibitor therapy for hypertension for more than five years and at the time of admission had been taking a combination of benazepril and amlodipine for more than two years. This medication was immediately discontinued, and he recovered fully after five days in the ICU on mechanical ventilation.
ACE Inhibitor-Associated Angioedema
ACE inhibitors are used by more than 35 million people worldwide to treat hypertension, heart failure, and diabetes mellitus; still, many physicians believe they are underprescribed.1 Angioedema is a serious complication of ACE inhibitor therapy that occurs in 0.1% to 0.68% of patients taking ACE inhibitors.2,3
Angioedema presents with a non-pitting swelling of subcutaneous or submucosal tissue without desquamation. Angioedema associated with ACE inhibitor use is rapid in onset, occurring minutes to hours after ingestion, does not present with urticaria, and usually lasts no more than 48 hours.4 At times, angioedema related to ACE inhibitor therapy occurs in the intestine, causing abdominal pain, diarrhea, and vomiting without mucocutaneous signs.1,4
Certain risk factors for developing ACE inhibitor-related angioedema include age older than 65, seasonal allergies, and black ethnicity. Another risk factor pertinent to our case presentation is the patient’s length of time on ACE inhibitor therapy. One study found that ACE inhibitor-associated angioedema occurred at a rate that was nine times higher during the first month of therapy than during subsequent months of therapy.2 Agostoni and colleagues found that ACE inhibitor-associated angioedema could occur in patients who had been on ACE inhibitor therapy for as long as eight years.5
The Process
ACE inhibitor-induced angioedema is probably a multifactorial process. Angiotensin-converting enzyme (ACE) metabolizes angiotensin I to angiotensin II in vivo and is a major inactivator of bradykinin. ACE and aminopeptidase P are the major pathways of bradykinin metabolism. A minor pathway uses carboxypeptidase N, which metabolizes bradykinin to its active metabolite, des-Arg-bradykinin. Des-Arg-bradykinin can then be inactivated by ACE and aminopeptidase P. In patients who had angioedema caused by ACE inhibitors, higher levels of des-Arg-bradykinin were found due to decreased activity of aminopeptidase P, which normally plays a major role in bradykinin breakdown when an ACE inhibitor is present.6
Bradykinin is a beta2 receptor agonist, but, when it is metabolized by carboxypeptidase N to des-Arg-bradykinin, it becomes a beta1 receptor agonist.6
During ACE inhibitor therapy, bradykinin can be inactivated by aminopeptidase P or metabolized into a beta1 receptor agonist by carboxypeptidase N, which is then broken down by aminopeptidase P. If aminopeptidase P is not active, then bradykinin can be converted to des-Arg-bradykinin, which can then act on upregulated beta1 receptors in the oropharynx and tongue, producing vasodilation, increased capillary permeability, and pain.
Treatment
Treatment of ACE inhibitor-induced angioedema includes discontinuing the ACE inhibitor and providing symptomatic support. Although some ACE inhibitors are more likely than others to cause angioedema, a patient who has had an episode of ACE inhibitor-associated angioedema should never again use any ACE inhibitor.3 Angiotensin receptor blockers (ARBs) do not affect the bradykinin system; however, they can cause angioedema (0.13% in one trial of ARBs), and it is not known if ARBs should be avoided in patients who have had ACE inhibitor-induced angioedema.7 Therapy with a bradykinin receptor antagonist to prevent or resolve ACE inhibitor-associated angioedema has not yet been studied in detail.1
Summary
Adverse drug reactions can present clinically in many different ways, and, indeed, these reactions have deposed syphilis and tuberculosis as the mimic of disease. Many adverse drug reactions are mild, but others can be severe and, occasionally, life-threatening. This variability in manifestations means clinicians always have to consider that the drug may be the cause of the patient’s symptoms. TH
Johnson is a medical student at the Kansas City University of Medicine and Biosciences, Kansas City, Mo. Dr. Egger is a consultant in general internal medicine at the Mayo Clinic, Rochester, Minn.
References
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26(4):725-737.
- Kostis JB, Kim HJ, Rusnak J, et al. Incidence and characteristics of angioedema associated with enalapril. Arch Intern Med. 2005 Jul;165(14):1637-1642.
- Kostis JB, Packer M, Black HR, et al. Omapatrilat and enalapril in patients with hypertension: the Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am J Hypertens. 2004 Feb;17(2):103-111.
- Kaplan AP, Greaves MW. Angioedema. J Am Acad Dermatol. 2005;53:373-388.
- Agostoni A, Cicardi M, Cugno M, et al. Angioedema due to angiotensin-converting enzyme inhibitors. Immunopharmacology. 1999;44:21-25.
- Molinaro G, Cugno M, Perez M, et al. Angiotensin-converting enzyme inhibitor-associated angioedema is characterized by a slower degradation of des-arginine(9)-bradykinin. J Pharmacol Exp Ther. 2002;303:232-237.
- Ward KE, Hume AL. Olmesartan (benicar) for hypertension. Am Fam Physician. 2005;72:673-674.
The New Institutional Leadership
Dr. Z has practiced hospital medicine at his local community hospital for the past three years. When he came on staff he quickly volunteered for a committee, and today he is its chair. Though he has a heavy workload, he has found the time to take several business courses at a nearby college, and he rarely turns down an opportunity to address a group.
Since he began his practice, he has never missed a local or national meeting of the professional associations to which he belongs. Dr. Z is a hospitalist with an ardent desire to make a difference. He believes he can be most effective in a hospital-wide administrative position, and he is preparing himself.
Dr. Z is a hypothetical example of a growing number of practicing hospitalists who are moving—or desire to move—into hospital-wide decision-making positions. What is the likelihood for their advancement to the higher echelons of hospital administration? Very good for those who have the right stuff for leadership, according to Larry Wellikson, MD, CEO of SHM.
Consider this: Just a decade ago, there were about 100 pioneering hospitalists caring for patients in 20 hospitals. Today there are 20,000 hospitalists serving patients in 2,500 hospitals across the country. Hospital medicine is the fastest growing medical specialty in the United States. The time is right for hospitalists to rise to the fore—not just as leaders of their hospitalist groups but also as system-wide decision makers.
Stacy Goldsholl, MD, represents the new breed: hospitalist as leader. Dr. Goldsholl has been a hospitalist for 12 years. “I got my first job as a community hospitalist before the term was even coined,” she says. “After about five years, I really hit a low point in my career. I was dissatisfied with the way the system was working; I didn’t feel there was enough emphasis on quality patient care. I was at a crossroad. I even considered giving up medicine altogether and going to rabbinical school,” she says, laughing. “But I was very passionate about making things better, so instead of quitting medicine, I embarked on a solo jaunt around the country trying to interest people in improving hospital medicine.”
Today Dr. Goldsholl is president of the Hospital Medicine Division of TeamHealth (Knoxville, Tenn.), a nationwide outsourcing provider of hospitalists in areas as far flung as Puerto Rico and Hawaii.
Though there are no hard-and-fast statistics on how many hospitalists now have leadership roles, Dr. Wellikson says the numbers are swelling. “It’s getting harder and harder to find someone who has strong leadership skills who’s five years into practice who is still just seeing patients,” he says. “There’s such a crying need for leadership in managing the team, leading the hospital medicine group, improving the hospital, improving the quality of care … there’s an enormous void. The first time somebody shows up who has an interest or an aptitude, someone will say, ‘Why don’t you be in charge?’ ”
What Hospitalists Bring to the Leadership Table
Study after study indicates hospitals employing hospitalists experience an improvement in the bottom line that is due, in part, to greater efficiency. This is an important consideration in the current economic crunch in which many hospitals find themselves, but today there is an increased focus on improving patient care as well.
In both efficiency and patient care, hospitalists are uniquely positioned to bring something to the leadership table that other candidates might not. “Hospitalists have a holistic view of the hospital,” says Dr. Goldsholl. “Private physicians don’t have the same connectedness to all the parts. That kind of experience is very valuable. After all, that’s what the hospital is all about.”
Jack M. Percelay, MD, a member of SHM’s Board of Directors, puts it another way. “Clearly, administrative positions require some knowledge of hospital function,” he says. “On-site physicians are certainly more aware of where the problems are. They face them on a daily basis.”
Dr. Wellikson adds, “From the very beginning of their medical careers, even when their main role is seeing patients, hospitalists are looking at the hospital as a system as an institution. They may be members of a quality-improvement team or a group that looks at the flow of patients from the emergency room to the hospital. It becomes sort of second nature to them. Our doctors learn these competencies from the beginning. In their training and their involvement with SHM, whole sections are devoted to systems improvement, leadership, and things like that.”
Dr. Wellikson suggests a demographic reason so many hospitalists look forward to climbing the administrative ladder: “It’s the times. Older doctors may be counting the days till retirement, whereas most hospitalists are younger—the average age is 37—and they say, ‘Hey, I’m going to have 20 more years of this. If I don’t change things, who will?’
“I’ll give you an analogy. When you go to a hotel and your towels aren’t delivered, you might complain until you get them, but you don’t try to manage the hotel. That’s the way practicing doctors felt 20 years ago. But hospitalists, because they’re going to go to work every day in that hospital, if it’s not working tip-top, they’re going to get involved. It’s an evolution in healthcare.”
How to Become a Hospitalist Leader
We asked our experts what advice they would give hospitalists who aspire to critical decision-making positions. “Even if you have natural skills as a leader—you’re charismatic, you take on responsibility—leadership is a skill like any other,” says Dr. Wellikson. “Take the time early in your career to develop that skill. Get involved in some project you feel passionate about. Part of leadership is getting other people to move in the right direction and part is dealing with the people who won’t follow. That can be frustrating. See how this feels to you. Get the education you need, and don’t be afraid to fail. Everybody has failures.”
Dr. Percelay suggests finding activities in your group where you can take initiative. “Clinical legitimacy is key, too, together with a systems viewpoint,” he says. “I would also recommend CME [continuing medical education]-type activities to develop leadership skills. There are the [SHM] Leadership Academy, local business schools, and the American College of Physician Executives, but learn mostly by doing and participating. Joining national organizations is also helpful because you will interact with other like-minded individuals.”
Dr. Goldsholl advises hospitalists to be passionate about their beliefs and to have confidence in what they do. She remembers a seminar she attended at which the speaker—a prominent business executive—gave this advice: “If you’ve never been fired, you are afraid to stand up for what you believe.”
Decision-making positions require hard work and long hours, Dr. Goldsholl cautions. “You have to keep a balance between your personal life and your career. And never underestimate the power of networking at regional and national levels as well as locally. Make your voice heard in print and [at] speaking engagements too. Get published in the Journal of Hospital Medicine. People do read these articles.”
Trends for Hospitalists as Decision Makers
Everyone with whom we spoke predicts a bright future for hospitalists who want to become critical decision makers. “Hospitalists understand the important manifestations of the way all pieces fit together to impact even a single event,” says Dr. Goldsholl. “Already hospitalists are vice presidents of medical affairs, chief operating officers, and so forth. This trend toward placing hospitalists in management roles is being driven, in large part, by the institutional knowledge that hospitalists have. I expect the trend will only expand.”
“There is so much overlap in medicine that what I see developing is a spirit of collaboration,” says Dr. Percelay. “What’s good for the hospitalist is good for the hospital and ultimately good for the patient. I believe that an alignment of incentives is driving the trend toward the appointment of hospitalists to general leadership positions.”
Hospitalists can create a healthcare system driven by teams of healthcare professionals and based on delivering measurable quality, according to Dr. Wellikson, who says hospitalists will play a major role in leading the quality revolution in this country. “We are moving to a time when business and Medicare are driving toward pay for performance,” he says. “Not just, ‘Did you do the surgery?’ but, ‘How well did you do the surgery?’ ”
Most importantly, Dr. Wellikson believes hospitalists are positioned incredibly well to be leaders in this movement. “The first thing people have to do is agree there is a problem. Then they have to measure the performance, try to improve the situation, and then measure the performance again. This is the wave of the future. We [hospitalists] are working with the government, with the National Quality Forum, with the Institute for Healthcare Improvement. Improvement in quality of care is the number one trend upon which hospitalist leaders will have an impact.”
Another emerging trend: Hospitalist decision makers will influence a redesigned hospital of the future. (Dr. Wellikson is one of 20 people on the Joint Commission Hospital of the Future Work Group.) “The hospital of the future will be very different,” explains Dr. Wellikson. “There’s going to be a home team in the new hospital. It will consist of the ED doctors, critical-care doctors, and hospitalists, working with nurses, pharmacists, and the administration as a team to deliver more technology and do more for sicker people.”
These efforts will be on a collision course with the hospital’s ability to afford them, he believes, so hospitalist leadership will be key to creating an efficient hospital that uses its resources in the best way possible and works as a team.
As more and more hospitalists gravitate toward hospitalwide leadership positions, they will confront some of their own. “It’s going to be very interesting,” says Dr. Percelay, “when the hospital medicine group leader differs with the vice president of medical affairs and they both share the same background. The hospital medicine group leader will no longer be able to say, ‘You don’t know where I’m coming from.’ ” TH
Joen Kinnan is a medical journalist based in Chicago.
Dr. Z has practiced hospital medicine at his local community hospital for the past three years. When he came on staff he quickly volunteered for a committee, and today he is its chair. Though he has a heavy workload, he has found the time to take several business courses at a nearby college, and he rarely turns down an opportunity to address a group.
Since he began his practice, he has never missed a local or national meeting of the professional associations to which he belongs. Dr. Z is a hospitalist with an ardent desire to make a difference. He believes he can be most effective in a hospital-wide administrative position, and he is preparing himself.
Dr. Z is a hypothetical example of a growing number of practicing hospitalists who are moving—or desire to move—into hospital-wide decision-making positions. What is the likelihood for their advancement to the higher echelons of hospital administration? Very good for those who have the right stuff for leadership, according to Larry Wellikson, MD, CEO of SHM.
Consider this: Just a decade ago, there were about 100 pioneering hospitalists caring for patients in 20 hospitals. Today there are 20,000 hospitalists serving patients in 2,500 hospitals across the country. Hospital medicine is the fastest growing medical specialty in the United States. The time is right for hospitalists to rise to the fore—not just as leaders of their hospitalist groups but also as system-wide decision makers.
Stacy Goldsholl, MD, represents the new breed: hospitalist as leader. Dr. Goldsholl has been a hospitalist for 12 years. “I got my first job as a community hospitalist before the term was even coined,” she says. “After about five years, I really hit a low point in my career. I was dissatisfied with the way the system was working; I didn’t feel there was enough emphasis on quality patient care. I was at a crossroad. I even considered giving up medicine altogether and going to rabbinical school,” she says, laughing. “But I was very passionate about making things better, so instead of quitting medicine, I embarked on a solo jaunt around the country trying to interest people in improving hospital medicine.”
Today Dr. Goldsholl is president of the Hospital Medicine Division of TeamHealth (Knoxville, Tenn.), a nationwide outsourcing provider of hospitalists in areas as far flung as Puerto Rico and Hawaii.
Though there are no hard-and-fast statistics on how many hospitalists now have leadership roles, Dr. Wellikson says the numbers are swelling. “It’s getting harder and harder to find someone who has strong leadership skills who’s five years into practice who is still just seeing patients,” he says. “There’s such a crying need for leadership in managing the team, leading the hospital medicine group, improving the hospital, improving the quality of care … there’s an enormous void. The first time somebody shows up who has an interest or an aptitude, someone will say, ‘Why don’t you be in charge?’ ”
What Hospitalists Bring to the Leadership Table
Study after study indicates hospitals employing hospitalists experience an improvement in the bottom line that is due, in part, to greater efficiency. This is an important consideration in the current economic crunch in which many hospitals find themselves, but today there is an increased focus on improving patient care as well.
In both efficiency and patient care, hospitalists are uniquely positioned to bring something to the leadership table that other candidates might not. “Hospitalists have a holistic view of the hospital,” says Dr. Goldsholl. “Private physicians don’t have the same connectedness to all the parts. That kind of experience is very valuable. After all, that’s what the hospital is all about.”
Jack M. Percelay, MD, a member of SHM’s Board of Directors, puts it another way. “Clearly, administrative positions require some knowledge of hospital function,” he says. “On-site physicians are certainly more aware of where the problems are. They face them on a daily basis.”
Dr. Wellikson adds, “From the very beginning of their medical careers, even when their main role is seeing patients, hospitalists are looking at the hospital as a system as an institution. They may be members of a quality-improvement team or a group that looks at the flow of patients from the emergency room to the hospital. It becomes sort of second nature to them. Our doctors learn these competencies from the beginning. In their training and their involvement with SHM, whole sections are devoted to systems improvement, leadership, and things like that.”
Dr. Wellikson suggests a demographic reason so many hospitalists look forward to climbing the administrative ladder: “It’s the times. Older doctors may be counting the days till retirement, whereas most hospitalists are younger—the average age is 37—and they say, ‘Hey, I’m going to have 20 more years of this. If I don’t change things, who will?’
“I’ll give you an analogy. When you go to a hotel and your towels aren’t delivered, you might complain until you get them, but you don’t try to manage the hotel. That’s the way practicing doctors felt 20 years ago. But hospitalists, because they’re going to go to work every day in that hospital, if it’s not working tip-top, they’re going to get involved. It’s an evolution in healthcare.”
How to Become a Hospitalist Leader
We asked our experts what advice they would give hospitalists who aspire to critical decision-making positions. “Even if you have natural skills as a leader—you’re charismatic, you take on responsibility—leadership is a skill like any other,” says Dr. Wellikson. “Take the time early in your career to develop that skill. Get involved in some project you feel passionate about. Part of leadership is getting other people to move in the right direction and part is dealing with the people who won’t follow. That can be frustrating. See how this feels to you. Get the education you need, and don’t be afraid to fail. Everybody has failures.”
Dr. Percelay suggests finding activities in your group where you can take initiative. “Clinical legitimacy is key, too, together with a systems viewpoint,” he says. “I would also recommend CME [continuing medical education]-type activities to develop leadership skills. There are the [SHM] Leadership Academy, local business schools, and the American College of Physician Executives, but learn mostly by doing and participating. Joining national organizations is also helpful because you will interact with other like-minded individuals.”
Dr. Goldsholl advises hospitalists to be passionate about their beliefs and to have confidence in what they do. She remembers a seminar she attended at which the speaker—a prominent business executive—gave this advice: “If you’ve never been fired, you are afraid to stand up for what you believe.”
Decision-making positions require hard work and long hours, Dr. Goldsholl cautions. “You have to keep a balance between your personal life and your career. And never underestimate the power of networking at regional and national levels as well as locally. Make your voice heard in print and [at] speaking engagements too. Get published in the Journal of Hospital Medicine. People do read these articles.”
Trends for Hospitalists as Decision Makers
Everyone with whom we spoke predicts a bright future for hospitalists who want to become critical decision makers. “Hospitalists understand the important manifestations of the way all pieces fit together to impact even a single event,” says Dr. Goldsholl. “Already hospitalists are vice presidents of medical affairs, chief operating officers, and so forth. This trend toward placing hospitalists in management roles is being driven, in large part, by the institutional knowledge that hospitalists have. I expect the trend will only expand.”
“There is so much overlap in medicine that what I see developing is a spirit of collaboration,” says Dr. Percelay. “What’s good for the hospitalist is good for the hospital and ultimately good for the patient. I believe that an alignment of incentives is driving the trend toward the appointment of hospitalists to general leadership positions.”
Hospitalists can create a healthcare system driven by teams of healthcare professionals and based on delivering measurable quality, according to Dr. Wellikson, who says hospitalists will play a major role in leading the quality revolution in this country. “We are moving to a time when business and Medicare are driving toward pay for performance,” he says. “Not just, ‘Did you do the surgery?’ but, ‘How well did you do the surgery?’ ”
Most importantly, Dr. Wellikson believes hospitalists are positioned incredibly well to be leaders in this movement. “The first thing people have to do is agree there is a problem. Then they have to measure the performance, try to improve the situation, and then measure the performance again. This is the wave of the future. We [hospitalists] are working with the government, with the National Quality Forum, with the Institute for Healthcare Improvement. Improvement in quality of care is the number one trend upon which hospitalist leaders will have an impact.”
Another emerging trend: Hospitalist decision makers will influence a redesigned hospital of the future. (Dr. Wellikson is one of 20 people on the Joint Commission Hospital of the Future Work Group.) “The hospital of the future will be very different,” explains Dr. Wellikson. “There’s going to be a home team in the new hospital. It will consist of the ED doctors, critical-care doctors, and hospitalists, working with nurses, pharmacists, and the administration as a team to deliver more technology and do more for sicker people.”
These efforts will be on a collision course with the hospital’s ability to afford them, he believes, so hospitalist leadership will be key to creating an efficient hospital that uses its resources in the best way possible and works as a team.
As more and more hospitalists gravitate toward hospitalwide leadership positions, they will confront some of their own. “It’s going to be very interesting,” says Dr. Percelay, “when the hospital medicine group leader differs with the vice president of medical affairs and they both share the same background. The hospital medicine group leader will no longer be able to say, ‘You don’t know where I’m coming from.’ ” TH
Joen Kinnan is a medical journalist based in Chicago.
Dr. Z has practiced hospital medicine at his local community hospital for the past three years. When he came on staff he quickly volunteered for a committee, and today he is its chair. Though he has a heavy workload, he has found the time to take several business courses at a nearby college, and he rarely turns down an opportunity to address a group.
Since he began his practice, he has never missed a local or national meeting of the professional associations to which he belongs. Dr. Z is a hospitalist with an ardent desire to make a difference. He believes he can be most effective in a hospital-wide administrative position, and he is preparing himself.
Dr. Z is a hypothetical example of a growing number of practicing hospitalists who are moving—or desire to move—into hospital-wide decision-making positions. What is the likelihood for their advancement to the higher echelons of hospital administration? Very good for those who have the right stuff for leadership, according to Larry Wellikson, MD, CEO of SHM.
Consider this: Just a decade ago, there were about 100 pioneering hospitalists caring for patients in 20 hospitals. Today there are 20,000 hospitalists serving patients in 2,500 hospitals across the country. Hospital medicine is the fastest growing medical specialty in the United States. The time is right for hospitalists to rise to the fore—not just as leaders of their hospitalist groups but also as system-wide decision makers.
Stacy Goldsholl, MD, represents the new breed: hospitalist as leader. Dr. Goldsholl has been a hospitalist for 12 years. “I got my first job as a community hospitalist before the term was even coined,” she says. “After about five years, I really hit a low point in my career. I was dissatisfied with the way the system was working; I didn’t feel there was enough emphasis on quality patient care. I was at a crossroad. I even considered giving up medicine altogether and going to rabbinical school,” she says, laughing. “But I was very passionate about making things better, so instead of quitting medicine, I embarked on a solo jaunt around the country trying to interest people in improving hospital medicine.”
Today Dr. Goldsholl is president of the Hospital Medicine Division of TeamHealth (Knoxville, Tenn.), a nationwide outsourcing provider of hospitalists in areas as far flung as Puerto Rico and Hawaii.
Though there are no hard-and-fast statistics on how many hospitalists now have leadership roles, Dr. Wellikson says the numbers are swelling. “It’s getting harder and harder to find someone who has strong leadership skills who’s five years into practice who is still just seeing patients,” he says. “There’s such a crying need for leadership in managing the team, leading the hospital medicine group, improving the hospital, improving the quality of care … there’s an enormous void. The first time somebody shows up who has an interest or an aptitude, someone will say, ‘Why don’t you be in charge?’ ”
What Hospitalists Bring to the Leadership Table
Study after study indicates hospitals employing hospitalists experience an improvement in the bottom line that is due, in part, to greater efficiency. This is an important consideration in the current economic crunch in which many hospitals find themselves, but today there is an increased focus on improving patient care as well.
In both efficiency and patient care, hospitalists are uniquely positioned to bring something to the leadership table that other candidates might not. “Hospitalists have a holistic view of the hospital,” says Dr. Goldsholl. “Private physicians don’t have the same connectedness to all the parts. That kind of experience is very valuable. After all, that’s what the hospital is all about.”
Jack M. Percelay, MD, a member of SHM’s Board of Directors, puts it another way. “Clearly, administrative positions require some knowledge of hospital function,” he says. “On-site physicians are certainly more aware of where the problems are. They face them on a daily basis.”
Dr. Wellikson adds, “From the very beginning of their medical careers, even when their main role is seeing patients, hospitalists are looking at the hospital as a system as an institution. They may be members of a quality-improvement team or a group that looks at the flow of patients from the emergency room to the hospital. It becomes sort of second nature to them. Our doctors learn these competencies from the beginning. In their training and their involvement with SHM, whole sections are devoted to systems improvement, leadership, and things like that.”
Dr. Wellikson suggests a demographic reason so many hospitalists look forward to climbing the administrative ladder: “It’s the times. Older doctors may be counting the days till retirement, whereas most hospitalists are younger—the average age is 37—and they say, ‘Hey, I’m going to have 20 more years of this. If I don’t change things, who will?’
“I’ll give you an analogy. When you go to a hotel and your towels aren’t delivered, you might complain until you get them, but you don’t try to manage the hotel. That’s the way practicing doctors felt 20 years ago. But hospitalists, because they’re going to go to work every day in that hospital, if it’s not working tip-top, they’re going to get involved. It’s an evolution in healthcare.”
How to Become a Hospitalist Leader
We asked our experts what advice they would give hospitalists who aspire to critical decision-making positions. “Even if you have natural skills as a leader—you’re charismatic, you take on responsibility—leadership is a skill like any other,” says Dr. Wellikson. “Take the time early in your career to develop that skill. Get involved in some project you feel passionate about. Part of leadership is getting other people to move in the right direction and part is dealing with the people who won’t follow. That can be frustrating. See how this feels to you. Get the education you need, and don’t be afraid to fail. Everybody has failures.”
Dr. Percelay suggests finding activities in your group where you can take initiative. “Clinical legitimacy is key, too, together with a systems viewpoint,” he says. “I would also recommend CME [continuing medical education]-type activities to develop leadership skills. There are the [SHM] Leadership Academy, local business schools, and the American College of Physician Executives, but learn mostly by doing and participating. Joining national organizations is also helpful because you will interact with other like-minded individuals.”
Dr. Goldsholl advises hospitalists to be passionate about their beliefs and to have confidence in what they do. She remembers a seminar she attended at which the speaker—a prominent business executive—gave this advice: “If you’ve never been fired, you are afraid to stand up for what you believe.”
Decision-making positions require hard work and long hours, Dr. Goldsholl cautions. “You have to keep a balance between your personal life and your career. And never underestimate the power of networking at regional and national levels as well as locally. Make your voice heard in print and [at] speaking engagements too. Get published in the Journal of Hospital Medicine. People do read these articles.”
Trends for Hospitalists as Decision Makers
Everyone with whom we spoke predicts a bright future for hospitalists who want to become critical decision makers. “Hospitalists understand the important manifestations of the way all pieces fit together to impact even a single event,” says Dr. Goldsholl. “Already hospitalists are vice presidents of medical affairs, chief operating officers, and so forth. This trend toward placing hospitalists in management roles is being driven, in large part, by the institutional knowledge that hospitalists have. I expect the trend will only expand.”
“There is so much overlap in medicine that what I see developing is a spirit of collaboration,” says Dr. Percelay. “What’s good for the hospitalist is good for the hospital and ultimately good for the patient. I believe that an alignment of incentives is driving the trend toward the appointment of hospitalists to general leadership positions.”
Hospitalists can create a healthcare system driven by teams of healthcare professionals and based on delivering measurable quality, according to Dr. Wellikson, who says hospitalists will play a major role in leading the quality revolution in this country. “We are moving to a time when business and Medicare are driving toward pay for performance,” he says. “Not just, ‘Did you do the surgery?’ but, ‘How well did you do the surgery?’ ”
Most importantly, Dr. Wellikson believes hospitalists are positioned incredibly well to be leaders in this movement. “The first thing people have to do is agree there is a problem. Then they have to measure the performance, try to improve the situation, and then measure the performance again. This is the wave of the future. We [hospitalists] are working with the government, with the National Quality Forum, with the Institute for Healthcare Improvement. Improvement in quality of care is the number one trend upon which hospitalist leaders will have an impact.”
Another emerging trend: Hospitalist decision makers will influence a redesigned hospital of the future. (Dr. Wellikson is one of 20 people on the Joint Commission Hospital of the Future Work Group.) “The hospital of the future will be very different,” explains Dr. Wellikson. “There’s going to be a home team in the new hospital. It will consist of the ED doctors, critical-care doctors, and hospitalists, working with nurses, pharmacists, and the administration as a team to deliver more technology and do more for sicker people.”
These efforts will be on a collision course with the hospital’s ability to afford them, he believes, so hospitalist leadership will be key to creating an efficient hospital that uses its resources in the best way possible and works as a team.
As more and more hospitalists gravitate toward hospitalwide leadership positions, they will confront some of their own. “It’s going to be very interesting,” says Dr. Percelay, “when the hospital medicine group leader differs with the vice president of medical affairs and they both share the same background. The hospital medicine group leader will no longer be able to say, ‘You don’t know where I’m coming from.’ ” TH
Joen Kinnan is a medical journalist based in Chicago.
A Night with Venus, a Lifetime with Mercury
When you think of mercury, what comes to mind? Do you think about the small, hot planet in our solar system nearest the sun? Perhaps the Roman god with winged feet?
I know some people who would surely think about the car. But how about heavy metal?
No, not rock music; the transition metal with the atomic number 80. Mercury is one of only five elements that is a liquid at room temperature.1 The periodic table symbol for mercury, Hg, comes from the Greek name hydrargyrum, a combination of the words for water (hydro) and silver (argyros) forming a word meaning “watery silver.’’ It’s an apt physical description of elemental mercury. The other common name for mercury is quicksilver.
Mercury, an element with a storied past, still presents dangers hospitalists must be aware of.
Organic compounds of mercury especially are toxic at even low levels. Human exposure must be limited when possible. Many elements and heavy metals are used by living organisms in trace amounts. Not mercury. Mercury is a toxin at any dose. Pure elemental mercury is less toxic than the organic compounds and salts. Exposed to water, mercury is quickly converted to the more toxic form, methylmercury. Because of its volatility, any open container of mercury is a biohazard and presents a risk of poisoning from mercury vapor. Inhaled vaporized mercury is readily absorbed through the alveoli.2
Historical Uses
Mankind has used mercury-containing products for a long time. Some of the red color in ancient cave drawings is cinnabar, or mercury sulfide (HgS). Cinnabar has also been used as the red pigment in tattoos. When I was in the Navy, we were told any skin rash that spared the red color in a tattoo was sure to be syphilis; according to the information we were given, the red pigment in a tattoo was created by mercury. Actually, tattoo parlors use several forms of red pigment, but mercury sulfide is certainly one of the choices.
Historically, many cultures used mercury in a variety of ways. More than two millennia ago, Greeks used mercury in medicines; Romans incorporated the element in their cosmetics.3 Medicinal uses of mercury have included the treatment of syphilis and use as a diuretic, antiseptic, and laxative.4 In the mid-20th century, mercury-containing compounds were popular as a remedy for infant-teething pain.
From the 17th to 19th centuries, mercury was used in the process of making felt for hats; hat makers were subjected to excessive exposure to the element. Mercury toxicity manifested as psychiatric illness and was widely recognized as an occupational hazard of hat-making.4,5 Reflecting this observation, “mad as a hatter” became a figure of speech and even found its way into the famous book “Through the Looking Glass (And What Alice Found There)’’ by Lewis Carroll.
Gold mining presents another occupational exposure to mercury. During 19th-century gold mining in California, mercury was used to extract gold from ore. Today, much controversy and ecological protest is focused on the South American gold mining industry, particularly in Brazil. In the past 20 years or so, it is estimated that 2,000 tons of mercury have been released into the environment in the Brazilian Amazon.6 Watchdog groups have been sounding the alarm for people who live in the villages along the Amazon River and consume a diet of fish caught from the river. Hair samples of those villagers revealed high levels of mercury.7 To date, clinical disease has not been reported there.
Infamous Occurrences
The most noted occurrence of clinical mercury poisoning was in Minamata, Japan. Starting before World War II and continuing until 1968, industrial mercury-containing waste was dumped into the sea near Minamata. The townspeople’s diet consisted of locally caught fish; the fish were heavily contaminated with mercury. Many people suffered permanent disability, and more than a thousand died.8 The effect of mercury poisoning was so great the disease was called Minamata’s disease.
Another epidemic occurred in the early 1970s in Iraq. Grain intended for use as seed for planting was treated with a mercury-containing fungicide. Accidentally, the local population used the grain for making bread, resulting in many cases of clinical mercury poisoning.8
One of the most historically interesting stories of mercury poisoning involves the first emperor of the Qin Dynasty in China, Qin Shi Huang Di, who lived from 259 to 210 B.C. At age 12 when Qin Shi Huang ascended to the throne, China was divided into warring feudal states. By asserting ruthless power, he succeeded in conquering the last warring province and unified China in 221 B.C. Although his rule was brutal and tyrannical, his accomplishments included standardization of the systems of measurement and weights, currency, and Chinese script. He was also a builder, conscripting labor for the development of roads, canals, and—most famously—his own mausoleum. The tomb of Qin Shi Huang at Xian is famous for its size and contents, including the army of more than 8,000 life-size, terracotta warriors.9
Qin Shi Huang Di (Di means supreme god) set out on a tour in 210 B.C. seeking eternal life in the “Islands of the Immortals.” It is not clear if his entourage found the site, but he was given a potion or pills, made by his court scientists, to make him immortal. The medication contained a toxic compound of mercury, and he died.9 The mausoleum was completed just in time to accommodate the emperor.
Exposure and Toxicity
Other than occupational exposure to mercury, the most important mercury exposures in the United States are dietary, the use of mercury amalgam in dentistry, and mercury used as a stabilizing agent in vaccines. The risk of toxicity depends on the form of mercury involved. Elemental mercury is poorly absorbed through the gastrointestinal tract; methylmercury, on the other hand, is readily absorbed if ingested. As previously noted, inhaled elemental mercury vapor is easily absorbed in the lungs.
Consensus supports the fact that dietary ingestion of methylmercury as found in large game fish—tuna, swordfish, shark, king mackerel, and tilefish—is the most important exposure to organic mercury. Small fish eat the mercury-contaminated plant life on the ocean bottom and are consumed by larger fish, and those fish are consumed by larger fish. Thus, the large game fish in the food chain accumulate high concentrations of mercury. It is recommended that children and pregnant women limit consumption of these types of fish.8
Dental silver for tooth fillings is a mixture of 50% mercury and 50% metal powder, such as silver, copper, or zinc. Because dental amalgam uses elemental mercury, gastrointestinal absorption is limited. Two studies examining more than 500 children each followed the neuro-psychiatric development of children with mercury amalgam fillings with a control group. No statistical differences were identified in IQ, memory, visual/motor, and renal function between the two groups over five- and seven-year follow-ups. Yet, doubts linger concerning long-term follow-up and questions raised with respect to the incidence of multiple sclerosis and Alzheimer’s disease.10 Overall, dental mercury amalgam is believed to be relatively safe with no evidence of acute toxicity.
Controversy has swirled around the use of thimerosal, a mercury-containing stabilizer and antibacterial agent used in vaccines. Used since the 1930s, thimerosal is metabolized to ethyl mercury in the body and has been implicated in a host of ailments, including the marked increase in incidences of autism. Although no dose-dependent toxicity has been established, questions concerning genetic vulnerability to mercury have been raised and considered significant.11-12 In 1999, the Department of Health and Human Services recommended thimerosal be decreased or eliminated from childhood vaccines.
Telltale Signs
Clinical symptoms of mercury toxicity are often insidious in onset and nonspecific, making diagnosis difficult without a high index of suspicion. Complaints may include gastrointestinal symptoms, headaches, insomnia, visual disturbances, peripheral neuropathy, or ataxia.2 Exposure to inorganic mercury from mercurial salves (merthiolate) or the chronic use of mercury-based cathartics may present with the constellation of symptoms known as acrodynia or pink disease, Feer disease, Feer’s disease, Swift syndrome, Swift’s disease, Swift disease, Swift-Feer disease, vegetative neurosis, dermatopolyneuritis, erythredema polyneuritis, and trophodermatoneurosis. This is characterized by a desquamating rash, hair loss, erythema of the palms and soles, anorexia, and gastrointestinal complaints. Elemental mercury does not readily cross the blood-brain barrier, so neurological complaints are not dominant.2
Organic mercury poisoning typically presents with neurological symptoms. In-utero exposure may result in spontaneous abortion; or the infant, if delivered, may suffer mental retardation. Adult toxicity presents with sensory and motor-neurological complaints, visual field loss, hearing loss, dysarthria, or cerebellar symptoms of ataxia. Severe toxicity results in movement disorders, paralysis, and seizures.2 Evidence of kidney damage and reproductive failure are also commonly associated.
In suspected cases, obtain blood and urine levels of mercury. Levels of mercury in hair may be helpful in some instances, but false-positive findings make this method of testing less reliable.
Treatment is supportive. Employ chelating agents if the patient is acutely symptomatic. The agent of choice is BAL (dimercaprol). Administer it as directed by consultation with a poison control team. BAL is not recommended for children. TH
References
- Wikipedia. The mercury element page. Available at http://en.wikipedia.org/wiki/Mercury_%28element%29. Last accessed April 19, 2007.
- Diner B. Toxicity, mercury. Available at http://emedicine.com/EMERGE/topic813.htm.
- WebElements. Periodic table. www.webelements.com
- Elinder CG. Epidemiology and toxicity of mercury. UpToDate, Nov. 2006. Available at member. www.patients.uptodate.com/topic.asp?file=renldis/14240]
- Mercury: useful metal or toxic chemical? Available at www.ci.vancouver.wa.us/solidwaste/pbt_site/usefulmetal.asp. Last accessed April 19, 2007.
- Malm O. Gold mining as a source of mercury exposure in the Brazilian Amazon. Environ Res 1998 May;77(2):73-78.
- Harada M, Nakanishi J, Yasoda E, et al. Mercury pollution in the Tapajos River basin, Amazon: mercury level of head hair and health effects. Environ Int. 2001;27(4):285-290
- Wikipedia. Mercury poisoning. Available at http://en.wikipedia.org/wiki/Mercury_poisoning. Last accessed April 19, 2007.
- Answers.com. Qin Shi Huang. Available at www.answers.com/topic/qin-shi-huang. Last accessed April 19, 2007.
- Needleman HL. Mercury in dental amalgam—a neurotoxic risk? JAMA. 2006 Apr 19;295(15):1835-1836.
- National Institutes of Allergy and Infectious Diseases. NAID research on thimerosal. December 2006. Available at www.niaid.nih.gov/factsheets/thimerosal.htm. Last accessed April 19, 2007.
- Environmental Working Group. Executive summary. December 13, 2004. Available at www.ewg.org/reports/autism/execsumm.php. Last accessed April 19, 2007.
When you think of mercury, what comes to mind? Do you think about the small, hot planet in our solar system nearest the sun? Perhaps the Roman god with winged feet?
I know some people who would surely think about the car. But how about heavy metal?
No, not rock music; the transition metal with the atomic number 80. Mercury is one of only five elements that is a liquid at room temperature.1 The periodic table symbol for mercury, Hg, comes from the Greek name hydrargyrum, a combination of the words for water (hydro) and silver (argyros) forming a word meaning “watery silver.’’ It’s an apt physical description of elemental mercury. The other common name for mercury is quicksilver.
Mercury, an element with a storied past, still presents dangers hospitalists must be aware of.
Organic compounds of mercury especially are toxic at even low levels. Human exposure must be limited when possible. Many elements and heavy metals are used by living organisms in trace amounts. Not mercury. Mercury is a toxin at any dose. Pure elemental mercury is less toxic than the organic compounds and salts. Exposed to water, mercury is quickly converted to the more toxic form, methylmercury. Because of its volatility, any open container of mercury is a biohazard and presents a risk of poisoning from mercury vapor. Inhaled vaporized mercury is readily absorbed through the alveoli.2
Historical Uses
Mankind has used mercury-containing products for a long time. Some of the red color in ancient cave drawings is cinnabar, or mercury sulfide (HgS). Cinnabar has also been used as the red pigment in tattoos. When I was in the Navy, we were told any skin rash that spared the red color in a tattoo was sure to be syphilis; according to the information we were given, the red pigment in a tattoo was created by mercury. Actually, tattoo parlors use several forms of red pigment, but mercury sulfide is certainly one of the choices.
Historically, many cultures used mercury in a variety of ways. More than two millennia ago, Greeks used mercury in medicines; Romans incorporated the element in their cosmetics.3 Medicinal uses of mercury have included the treatment of syphilis and use as a diuretic, antiseptic, and laxative.4 In the mid-20th century, mercury-containing compounds were popular as a remedy for infant-teething pain.
From the 17th to 19th centuries, mercury was used in the process of making felt for hats; hat makers were subjected to excessive exposure to the element. Mercury toxicity manifested as psychiatric illness and was widely recognized as an occupational hazard of hat-making.4,5 Reflecting this observation, “mad as a hatter” became a figure of speech and even found its way into the famous book “Through the Looking Glass (And What Alice Found There)’’ by Lewis Carroll.
Gold mining presents another occupational exposure to mercury. During 19th-century gold mining in California, mercury was used to extract gold from ore. Today, much controversy and ecological protest is focused on the South American gold mining industry, particularly in Brazil. In the past 20 years or so, it is estimated that 2,000 tons of mercury have been released into the environment in the Brazilian Amazon.6 Watchdog groups have been sounding the alarm for people who live in the villages along the Amazon River and consume a diet of fish caught from the river. Hair samples of those villagers revealed high levels of mercury.7 To date, clinical disease has not been reported there.
Infamous Occurrences
The most noted occurrence of clinical mercury poisoning was in Minamata, Japan. Starting before World War II and continuing until 1968, industrial mercury-containing waste was dumped into the sea near Minamata. The townspeople’s diet consisted of locally caught fish; the fish were heavily contaminated with mercury. Many people suffered permanent disability, and more than a thousand died.8 The effect of mercury poisoning was so great the disease was called Minamata’s disease.
Another epidemic occurred in the early 1970s in Iraq. Grain intended for use as seed for planting was treated with a mercury-containing fungicide. Accidentally, the local population used the grain for making bread, resulting in many cases of clinical mercury poisoning.8
One of the most historically interesting stories of mercury poisoning involves the first emperor of the Qin Dynasty in China, Qin Shi Huang Di, who lived from 259 to 210 B.C. At age 12 when Qin Shi Huang ascended to the throne, China was divided into warring feudal states. By asserting ruthless power, he succeeded in conquering the last warring province and unified China in 221 B.C. Although his rule was brutal and tyrannical, his accomplishments included standardization of the systems of measurement and weights, currency, and Chinese script. He was also a builder, conscripting labor for the development of roads, canals, and—most famously—his own mausoleum. The tomb of Qin Shi Huang at Xian is famous for its size and contents, including the army of more than 8,000 life-size, terracotta warriors.9
Qin Shi Huang Di (Di means supreme god) set out on a tour in 210 B.C. seeking eternal life in the “Islands of the Immortals.” It is not clear if his entourage found the site, but he was given a potion or pills, made by his court scientists, to make him immortal. The medication contained a toxic compound of mercury, and he died.9 The mausoleum was completed just in time to accommodate the emperor.
Exposure and Toxicity
Other than occupational exposure to mercury, the most important mercury exposures in the United States are dietary, the use of mercury amalgam in dentistry, and mercury used as a stabilizing agent in vaccines. The risk of toxicity depends on the form of mercury involved. Elemental mercury is poorly absorbed through the gastrointestinal tract; methylmercury, on the other hand, is readily absorbed if ingested. As previously noted, inhaled elemental mercury vapor is easily absorbed in the lungs.
Consensus supports the fact that dietary ingestion of methylmercury as found in large game fish—tuna, swordfish, shark, king mackerel, and tilefish—is the most important exposure to organic mercury. Small fish eat the mercury-contaminated plant life on the ocean bottom and are consumed by larger fish, and those fish are consumed by larger fish. Thus, the large game fish in the food chain accumulate high concentrations of mercury. It is recommended that children and pregnant women limit consumption of these types of fish.8
Dental silver for tooth fillings is a mixture of 50% mercury and 50% metal powder, such as silver, copper, or zinc. Because dental amalgam uses elemental mercury, gastrointestinal absorption is limited. Two studies examining more than 500 children each followed the neuro-psychiatric development of children with mercury amalgam fillings with a control group. No statistical differences were identified in IQ, memory, visual/motor, and renal function between the two groups over five- and seven-year follow-ups. Yet, doubts linger concerning long-term follow-up and questions raised with respect to the incidence of multiple sclerosis and Alzheimer’s disease.10 Overall, dental mercury amalgam is believed to be relatively safe with no evidence of acute toxicity.
Controversy has swirled around the use of thimerosal, a mercury-containing stabilizer and antibacterial agent used in vaccines. Used since the 1930s, thimerosal is metabolized to ethyl mercury in the body and has been implicated in a host of ailments, including the marked increase in incidences of autism. Although no dose-dependent toxicity has been established, questions concerning genetic vulnerability to mercury have been raised and considered significant.11-12 In 1999, the Department of Health and Human Services recommended thimerosal be decreased or eliminated from childhood vaccines.
Telltale Signs
Clinical symptoms of mercury toxicity are often insidious in onset and nonspecific, making diagnosis difficult without a high index of suspicion. Complaints may include gastrointestinal symptoms, headaches, insomnia, visual disturbances, peripheral neuropathy, or ataxia.2 Exposure to inorganic mercury from mercurial salves (merthiolate) or the chronic use of mercury-based cathartics may present with the constellation of symptoms known as acrodynia or pink disease, Feer disease, Feer’s disease, Swift syndrome, Swift’s disease, Swift disease, Swift-Feer disease, vegetative neurosis, dermatopolyneuritis, erythredema polyneuritis, and trophodermatoneurosis. This is characterized by a desquamating rash, hair loss, erythema of the palms and soles, anorexia, and gastrointestinal complaints. Elemental mercury does not readily cross the blood-brain barrier, so neurological complaints are not dominant.2
Organic mercury poisoning typically presents with neurological symptoms. In-utero exposure may result in spontaneous abortion; or the infant, if delivered, may suffer mental retardation. Adult toxicity presents with sensory and motor-neurological complaints, visual field loss, hearing loss, dysarthria, or cerebellar symptoms of ataxia. Severe toxicity results in movement disorders, paralysis, and seizures.2 Evidence of kidney damage and reproductive failure are also commonly associated.
In suspected cases, obtain blood and urine levels of mercury. Levels of mercury in hair may be helpful in some instances, but false-positive findings make this method of testing less reliable.
Treatment is supportive. Employ chelating agents if the patient is acutely symptomatic. The agent of choice is BAL (dimercaprol). Administer it as directed by consultation with a poison control team. BAL is not recommended for children. TH
References
- Wikipedia. The mercury element page. Available at http://en.wikipedia.org/wiki/Mercury_%28element%29. Last accessed April 19, 2007.
- Diner B. Toxicity, mercury. Available at http://emedicine.com/EMERGE/topic813.htm.
- WebElements. Periodic table. www.webelements.com
- Elinder CG. Epidemiology and toxicity of mercury. UpToDate, Nov. 2006. Available at member. www.patients.uptodate.com/topic.asp?file=renldis/14240]
- Mercury: useful metal or toxic chemical? Available at www.ci.vancouver.wa.us/solidwaste/pbt_site/usefulmetal.asp. Last accessed April 19, 2007.
- Malm O. Gold mining as a source of mercury exposure in the Brazilian Amazon. Environ Res 1998 May;77(2):73-78.
- Harada M, Nakanishi J, Yasoda E, et al. Mercury pollution in the Tapajos River basin, Amazon: mercury level of head hair and health effects. Environ Int. 2001;27(4):285-290
- Wikipedia. Mercury poisoning. Available at http://en.wikipedia.org/wiki/Mercury_poisoning. Last accessed April 19, 2007.
- Answers.com. Qin Shi Huang. Available at www.answers.com/topic/qin-shi-huang. Last accessed April 19, 2007.
- Needleman HL. Mercury in dental amalgam—a neurotoxic risk? JAMA. 2006 Apr 19;295(15):1835-1836.
- National Institutes of Allergy and Infectious Diseases. NAID research on thimerosal. December 2006. Available at www.niaid.nih.gov/factsheets/thimerosal.htm. Last accessed April 19, 2007.
- Environmental Working Group. Executive summary. December 13, 2004. Available at www.ewg.org/reports/autism/execsumm.php. Last accessed April 19, 2007.
When you think of mercury, what comes to mind? Do you think about the small, hot planet in our solar system nearest the sun? Perhaps the Roman god with winged feet?
I know some people who would surely think about the car. But how about heavy metal?
No, not rock music; the transition metal with the atomic number 80. Mercury is one of only five elements that is a liquid at room temperature.1 The periodic table symbol for mercury, Hg, comes from the Greek name hydrargyrum, a combination of the words for water (hydro) and silver (argyros) forming a word meaning “watery silver.’’ It’s an apt physical description of elemental mercury. The other common name for mercury is quicksilver.
Mercury, an element with a storied past, still presents dangers hospitalists must be aware of.
Organic compounds of mercury especially are toxic at even low levels. Human exposure must be limited when possible. Many elements and heavy metals are used by living organisms in trace amounts. Not mercury. Mercury is a toxin at any dose. Pure elemental mercury is less toxic than the organic compounds and salts. Exposed to water, mercury is quickly converted to the more toxic form, methylmercury. Because of its volatility, any open container of mercury is a biohazard and presents a risk of poisoning from mercury vapor. Inhaled vaporized mercury is readily absorbed through the alveoli.2
Historical Uses
Mankind has used mercury-containing products for a long time. Some of the red color in ancient cave drawings is cinnabar, or mercury sulfide (HgS). Cinnabar has also been used as the red pigment in tattoos. When I was in the Navy, we were told any skin rash that spared the red color in a tattoo was sure to be syphilis; according to the information we were given, the red pigment in a tattoo was created by mercury. Actually, tattoo parlors use several forms of red pigment, but mercury sulfide is certainly one of the choices.
Historically, many cultures used mercury in a variety of ways. More than two millennia ago, Greeks used mercury in medicines; Romans incorporated the element in their cosmetics.3 Medicinal uses of mercury have included the treatment of syphilis and use as a diuretic, antiseptic, and laxative.4 In the mid-20th century, mercury-containing compounds were popular as a remedy for infant-teething pain.
From the 17th to 19th centuries, mercury was used in the process of making felt for hats; hat makers were subjected to excessive exposure to the element. Mercury toxicity manifested as psychiatric illness and was widely recognized as an occupational hazard of hat-making.4,5 Reflecting this observation, “mad as a hatter” became a figure of speech and even found its way into the famous book “Through the Looking Glass (And What Alice Found There)’’ by Lewis Carroll.
Gold mining presents another occupational exposure to mercury. During 19th-century gold mining in California, mercury was used to extract gold from ore. Today, much controversy and ecological protest is focused on the South American gold mining industry, particularly in Brazil. In the past 20 years or so, it is estimated that 2,000 tons of mercury have been released into the environment in the Brazilian Amazon.6 Watchdog groups have been sounding the alarm for people who live in the villages along the Amazon River and consume a diet of fish caught from the river. Hair samples of those villagers revealed high levels of mercury.7 To date, clinical disease has not been reported there.
Infamous Occurrences
The most noted occurrence of clinical mercury poisoning was in Minamata, Japan. Starting before World War II and continuing until 1968, industrial mercury-containing waste was dumped into the sea near Minamata. The townspeople’s diet consisted of locally caught fish; the fish were heavily contaminated with mercury. Many people suffered permanent disability, and more than a thousand died.8 The effect of mercury poisoning was so great the disease was called Minamata’s disease.
Another epidemic occurred in the early 1970s in Iraq. Grain intended for use as seed for planting was treated with a mercury-containing fungicide. Accidentally, the local population used the grain for making bread, resulting in many cases of clinical mercury poisoning.8
One of the most historically interesting stories of mercury poisoning involves the first emperor of the Qin Dynasty in China, Qin Shi Huang Di, who lived from 259 to 210 B.C. At age 12 when Qin Shi Huang ascended to the throne, China was divided into warring feudal states. By asserting ruthless power, he succeeded in conquering the last warring province and unified China in 221 B.C. Although his rule was brutal and tyrannical, his accomplishments included standardization of the systems of measurement and weights, currency, and Chinese script. He was also a builder, conscripting labor for the development of roads, canals, and—most famously—his own mausoleum. The tomb of Qin Shi Huang at Xian is famous for its size and contents, including the army of more than 8,000 life-size, terracotta warriors.9
Qin Shi Huang Di (Di means supreme god) set out on a tour in 210 B.C. seeking eternal life in the “Islands of the Immortals.” It is not clear if his entourage found the site, but he was given a potion or pills, made by his court scientists, to make him immortal. The medication contained a toxic compound of mercury, and he died.9 The mausoleum was completed just in time to accommodate the emperor.
Exposure and Toxicity
Other than occupational exposure to mercury, the most important mercury exposures in the United States are dietary, the use of mercury amalgam in dentistry, and mercury used as a stabilizing agent in vaccines. The risk of toxicity depends on the form of mercury involved. Elemental mercury is poorly absorbed through the gastrointestinal tract; methylmercury, on the other hand, is readily absorbed if ingested. As previously noted, inhaled elemental mercury vapor is easily absorbed in the lungs.
Consensus supports the fact that dietary ingestion of methylmercury as found in large game fish—tuna, swordfish, shark, king mackerel, and tilefish—is the most important exposure to organic mercury. Small fish eat the mercury-contaminated plant life on the ocean bottom and are consumed by larger fish, and those fish are consumed by larger fish. Thus, the large game fish in the food chain accumulate high concentrations of mercury. It is recommended that children and pregnant women limit consumption of these types of fish.8
Dental silver for tooth fillings is a mixture of 50% mercury and 50% metal powder, such as silver, copper, or zinc. Because dental amalgam uses elemental mercury, gastrointestinal absorption is limited. Two studies examining more than 500 children each followed the neuro-psychiatric development of children with mercury amalgam fillings with a control group. No statistical differences were identified in IQ, memory, visual/motor, and renal function between the two groups over five- and seven-year follow-ups. Yet, doubts linger concerning long-term follow-up and questions raised with respect to the incidence of multiple sclerosis and Alzheimer’s disease.10 Overall, dental mercury amalgam is believed to be relatively safe with no evidence of acute toxicity.
Controversy has swirled around the use of thimerosal, a mercury-containing stabilizer and antibacterial agent used in vaccines. Used since the 1930s, thimerosal is metabolized to ethyl mercury in the body and has been implicated in a host of ailments, including the marked increase in incidences of autism. Although no dose-dependent toxicity has been established, questions concerning genetic vulnerability to mercury have been raised and considered significant.11-12 In 1999, the Department of Health and Human Services recommended thimerosal be decreased or eliminated from childhood vaccines.
Telltale Signs
Clinical symptoms of mercury toxicity are often insidious in onset and nonspecific, making diagnosis difficult without a high index of suspicion. Complaints may include gastrointestinal symptoms, headaches, insomnia, visual disturbances, peripheral neuropathy, or ataxia.2 Exposure to inorganic mercury from mercurial salves (merthiolate) or the chronic use of mercury-based cathartics may present with the constellation of symptoms known as acrodynia or pink disease, Feer disease, Feer’s disease, Swift syndrome, Swift’s disease, Swift disease, Swift-Feer disease, vegetative neurosis, dermatopolyneuritis, erythredema polyneuritis, and trophodermatoneurosis. This is characterized by a desquamating rash, hair loss, erythema of the palms and soles, anorexia, and gastrointestinal complaints. Elemental mercury does not readily cross the blood-brain barrier, so neurological complaints are not dominant.2
Organic mercury poisoning typically presents with neurological symptoms. In-utero exposure may result in spontaneous abortion; or the infant, if delivered, may suffer mental retardation. Adult toxicity presents with sensory and motor-neurological complaints, visual field loss, hearing loss, dysarthria, or cerebellar symptoms of ataxia. Severe toxicity results in movement disorders, paralysis, and seizures.2 Evidence of kidney damage and reproductive failure are also commonly associated.
In suspected cases, obtain blood and urine levels of mercury. Levels of mercury in hair may be helpful in some instances, but false-positive findings make this method of testing less reliable.
Treatment is supportive. Employ chelating agents if the patient is acutely symptomatic. The agent of choice is BAL (dimercaprol). Administer it as directed by consultation with a poison control team. BAL is not recommended for children. TH
References
- Wikipedia. The mercury element page. Available at http://en.wikipedia.org/wiki/Mercury_%28element%29. Last accessed April 19, 2007.
- Diner B. Toxicity, mercury. Available at http://emedicine.com/EMERGE/topic813.htm.
- WebElements. Periodic table. www.webelements.com
- Elinder CG. Epidemiology and toxicity of mercury. UpToDate, Nov. 2006. Available at member. www.patients.uptodate.com/topic.asp?file=renldis/14240]
- Mercury: useful metal or toxic chemical? Available at www.ci.vancouver.wa.us/solidwaste/pbt_site/usefulmetal.asp. Last accessed April 19, 2007.
- Malm O. Gold mining as a source of mercury exposure in the Brazilian Amazon. Environ Res 1998 May;77(2):73-78.
- Harada M, Nakanishi J, Yasoda E, et al. Mercury pollution in the Tapajos River basin, Amazon: mercury level of head hair and health effects. Environ Int. 2001;27(4):285-290
- Wikipedia. Mercury poisoning. Available at http://en.wikipedia.org/wiki/Mercury_poisoning. Last accessed April 19, 2007.
- Answers.com. Qin Shi Huang. Available at www.answers.com/topic/qin-shi-huang. Last accessed April 19, 2007.
- Needleman HL. Mercury in dental amalgam—a neurotoxic risk? JAMA. 2006 Apr 19;295(15):1835-1836.
- National Institutes of Allergy and Infectious Diseases. NAID research on thimerosal. December 2006. Available at www.niaid.nih.gov/factsheets/thimerosal.htm. Last accessed April 19, 2007.
- Environmental Working Group. Executive summary. December 13, 2004. Available at www.ewg.org/reports/autism/execsumm.php. Last accessed April 19, 2007.
The Sumter Tornado
On the evening of March 1, severe thunderstorms rumbled over southwestern Georgia, spawning a tornado that ripped through seven counties. Classified an EF 3 with winds ranging from approximately 136 to 165 miles per hour, the twister tore a path of destruction 37 miles long and as much as a mile wide, reaching its maximum strength and width as it reached Americus, the seat of Sumter county. Along the way, the Sumter tornado—part of a storm system that killed eight in a high school in Enterprise, Ala.—demolished or seriously damaged more than 200 homes and dozens of businesses in Americus and the surrounding area, causing two deaths and many more injuries.
Not only did it leave the local Winn-Dixie grocery store without its façade, but it also reduced a 1,600-foot-tall public television tower to a 150-foot stump, sheared the tops off trees, downed power lines, knocked out telephone service, and deposited a burning tractor in the middle of Highway 520.
More important, it destroyed Sumter Regional Hospital in Americus, a rural city of 17,000 residents. Thanks to Sumter Regional’s staff, including its four hospitalists, all 70 patients were evacuated from the 265,000-square-foot, 143-bed complex.
The Terror Begins
The tornado, which struck Americus between 9 and 9:30 p.m., did not arrive without warning—but the town did not sound its tornado siren. A firefighter dispatched to activate the warning was called back because it was too late to do any good. Sumter Regional’s staff was alerted a tornado might strike, and they had moved patients away from the windows.
Hospitalist Mukesh Kumar, MD, who had joined Sumter Regional two weeks before the tornado struck, rode the storm out in the hospitalists’ office—a small space on the same corridor with a number of patient rooms.
“[Dr. Kumar] was the poor guy on duty that night,” says Amanda Davis, MD, head of the hospitalist program, who was not in town that evening.
As soon as the storm passed, an emergency call went out via the local broadcast media, requesting that physicians and nurses report to the severely damaged hospital to aid in the evacuation and treat the injured.
Hospitalists Kathy Hudson, MD, and Rick Oster, MD, among others, rushed to help. Getting to the hospital wasn’t easy. The surrounding area had become a maze of downed trees and power lines. First responders who could use their cars had to park outside the devastated area and hike to the hospital in the dark. Others arrived on bicycles. Some could not make it because they were trapped in their driveways.

With the power out at the tornado-ravaged hospital, as it was in much of Americus, first responders helped those on duty carry many of the 70 patients down the stairs of the four-story complex. Outside, Dr. Hudson worked with the staff, suturing the injured. Sumter Regional Hospital was evacuated by about 1:30 the following morning.
Patients were loaded into the town’s four ambulances and others from around the region and transferred to facilities in southwest Georgia. The closest of these was Phoebe Putney Memorial Hospital in Albany, about 40 miles from Americus.
Taking Stock
Wind and water had compromised nearly every part of Sumter Regional, leaving only the chapel intact. Much of the roof was ripped off, nearly all the windows were blown out, and part of the complex collapsed. Damage was so severe the entire health center was rendered unsafe.
Not only did the storm leave Americus without its hospital, it also devastated virtually all the town’s private doctor offices, as well as the Sumter HealthPlex—a new, 8,000-square-foot, $3.1 million facility owned by the hospital. The HealthPlex provided outpatient imaging and laboratory services to the community.
In the days immediately following the tornado, the Middle Flint chapter of the American Red Cross—whose headquarters were also badly damaged—set up an emergency response center in the First Baptist Church of Americus that featured a makeshift emergency room. Dr. Davis and her staff of hospitalists, employed by TeamHealth’s Hospital Medicine Division, helped get the Red Cross center up and running. They also played a significant role in setting up a temporary urgent-care center in tents provided by the Federal Emergency Management Agency (FEMA), supplemented by two tents belonging to the Boy Scouts.
By Any Means Necessary
Although local physicians with their own practices were well represented among the first responders, they were (for the most part) not involved with staffing the tent hospital, according to Dr. Davis. Most of the work in the tents was done by the emergency department (ED) physicians and TeamHealth doctors, in conjunction with Sumter Regional’s four hospitalists.
As soon as the tents opened, the ED “regulars” started showing up in droves,” explains Dr. Davis. Because a significant number of private physicians’ offices in town were destroyed there were no other healthcare options for many residents.
“It’s a difficult situation,” says Dr. Davis. “There are people in the community without cars, for example, whose cars were destroyed. So they have no other way to get to another hospital. They were astonishingly grateful to have us there.”
As residents cleaned up more than a month after the disaster, the urgent-care facility in the tents still functions as Sumter Regional’s ED. Routine lab work and X-rays were provided, and staff also monitored patients on blood thinners and gave injections to cancer patients.
In a pinch, the tents have served as an impromptu obstetrics suite. One woman delivered her child there after being unable to travel to Phoebe Putney Memorial Hospital, which is providing obstetrical services to mothers who would have gone to Sumter Regional.

Care of the center’s cancer patients—a number of whom must take a bus to Albany for treatment—is now overseen by Phoebe Putney’s oncology department. Surgeons, too, have had to travel to other hospitals in order to operate. “It is a logistical nightmare,” says Dr. Davis.
While the urgent-care unit has been able to provide basic services, it has not been an easy task for the physicians and nurses who work there. Telephone lines have not been restored, making it virtually impossible to send faxes. Hospitalists and ED physicians staffing the tents have had to read their own films, essentially serving as their own radiologists. As Dr Davis notes, “You have to do the best with what you have.” Often, that is a bare minimum. Indeed, she once had to put in a central line to stabilize a patient. “It was pretty surreal treating (the patient) in a tent,” she says.
What’s Next?
FEMA Director David Paulison, who toured the devastated hospital with President Bush, says the immediate response was indicative of the “new FEMA.”

Bush declared Sumter County a disaster area the day after the tornado. Residents were urged to apply as quickly as possible for grants and low-cost loans to aid in recovery. Local, state, and federal officials opened a disaster recovery center March 5 in Americus, staffed by representatives of FEMA, the Georgia Emergency Management Agency (GEMA), and a number of other agencies. As of April 4, FEMA, GEMA, and the U.S. Small Business Association (SBA), had approved more than $6.58 million for disaster recovery.
A May 16 update by Sumter Regional on its Web site indicated progress in the construction of modular care facilities.
“By the end of May, there will be five modular buildings in the Mayo Street parking lot for use by physicians, each consisting of two single-wide modular buildings joined together,” the memo stated. “Currently, two of the five physician modular buildings are in place with both halves assembled, and three of the single units are on site ready for placement and assembly. The other three halves that will be used to construct the remaining three buildings are on the way. We are still seeking bids from contractors to do the plumbing, electrical and other utility work, and anticipate having the buildings functional by the end of May for physicians to begin seeing patients.”
On April 30, Sumter Regional opened its Sumter Regional East facility. Sumter East provides 24-hour urgent care, radiology services, clinical lab services, physical therapy, speech therapy, occupational therapy, and cardiopulmonary services, according to the hospital’s Web site.
An interim hospital is slated to open in mid-September, according to a May 10 statement by the hospital. The facility, to be built on the former site of the HealthPlex, is to include approximately 65 inpatient rooms, nine LDRP/obstetrics/nursery rooms, eight CCU rooms, four operating suites, and a fully functional ER.
Whether or not the center’s hospitalists will have a place in the modular health center is unclear. Maintaining the hospitalist program is expensive, explained Dr. Davis. Although she has been assured Sumter Regional’s hospitalist program will continue in some capacity, she is still unsure of the program’s status. Currently, Sumter Regional’s four TeamHealth hospitalists are without a hospital.

Eventually, Sumter Regional Hospital will be rebuilt. Shortly after the tornado destroyed the health center, its president and CEO, David Seagraves issued the following message to the community: “Sumter Regional Hospital is not closing. We are currently assessing the damage to our facility from the tornado, and we are also looking at temporary alternative sites to provide services. We will update our situation in the current days, but I repeat that we fully intend for Sumter Regional Hospital to be back better than ever as soon as humanly possible.”
But reconstructing the hospital will be costly, with damage estimated at more than $100 million. The center and its equipment are covered by a $90 million insurance policy, as well as $37 million in service interruption insurance—some of which is slated to pay the hospital’s 700 employees. The state Senate has authorized $11 million in emergency funding for the town, some of which may go toward re-establishing healthcare in the region. It will take far more than that to restore a fully functional hospital. Sumter Regional is seeking financial donations through its Web site (www.sumterregional.org) to help community members and to go toward rebuilding. Citizen’s Bank of Americus has donated $100,000, half to the hospital and half to aid the community. Wachovia is also active in the reconstruction effort.
Dr. Davis could not be more pleased with how Sumter Regional’s hospitalists responded to the disaster. “I am real proud of the doctors I work with,” she says. “They really stepped up to the plate—above and beyond the call of duty. No one complained. No one worried about getting paid. No one worried about their malpractice insurance. I am very proud.” TH
Roberta Newman is a frequent contributor to The Hospitalist.
On the evening of March 1, severe thunderstorms rumbled over southwestern Georgia, spawning a tornado that ripped through seven counties. Classified an EF 3 with winds ranging from approximately 136 to 165 miles per hour, the twister tore a path of destruction 37 miles long and as much as a mile wide, reaching its maximum strength and width as it reached Americus, the seat of Sumter county. Along the way, the Sumter tornado—part of a storm system that killed eight in a high school in Enterprise, Ala.—demolished or seriously damaged more than 200 homes and dozens of businesses in Americus and the surrounding area, causing two deaths and many more injuries.
Not only did it leave the local Winn-Dixie grocery store without its façade, but it also reduced a 1,600-foot-tall public television tower to a 150-foot stump, sheared the tops off trees, downed power lines, knocked out telephone service, and deposited a burning tractor in the middle of Highway 520.
More important, it destroyed Sumter Regional Hospital in Americus, a rural city of 17,000 residents. Thanks to Sumter Regional’s staff, including its four hospitalists, all 70 patients were evacuated from the 265,000-square-foot, 143-bed complex.
The Terror Begins
The tornado, which struck Americus between 9 and 9:30 p.m., did not arrive without warning—but the town did not sound its tornado siren. A firefighter dispatched to activate the warning was called back because it was too late to do any good. Sumter Regional’s staff was alerted a tornado might strike, and they had moved patients away from the windows.
Hospitalist Mukesh Kumar, MD, who had joined Sumter Regional two weeks before the tornado struck, rode the storm out in the hospitalists’ office—a small space on the same corridor with a number of patient rooms.
“[Dr. Kumar] was the poor guy on duty that night,” says Amanda Davis, MD, head of the hospitalist program, who was not in town that evening.
As soon as the storm passed, an emergency call went out via the local broadcast media, requesting that physicians and nurses report to the severely damaged hospital to aid in the evacuation and treat the injured.
Hospitalists Kathy Hudson, MD, and Rick Oster, MD, among others, rushed to help. Getting to the hospital wasn’t easy. The surrounding area had become a maze of downed trees and power lines. First responders who could use their cars had to park outside the devastated area and hike to the hospital in the dark. Others arrived on bicycles. Some could not make it because they were trapped in their driveways.
With the power out at the tornado-ravaged hospital, as it was in much of Americus, first responders helped those on duty carry many of the 70 patients down the stairs of the four-story complex. Outside, Dr. Hudson worked with the staff, suturing the injured. Sumter Regional Hospital was evacuated by about 1:30 the following morning.
Patients were loaded into the town’s four ambulances and others from around the region and transferred to facilities in southwest Georgia. The closest of these was Phoebe Putney Memorial Hospital in Albany, about 40 miles from Americus.
Taking Stock
Wind and water had compromised nearly every part of Sumter Regional, leaving only the chapel intact. Much of the roof was ripped off, nearly all the windows were blown out, and part of the complex collapsed. Damage was so severe the entire health center was rendered unsafe.
Not only did the storm leave Americus without its hospital, it also devastated virtually all the town’s private doctor offices, as well as the Sumter HealthPlex—a new, 8,000-square-foot, $3.1 million facility owned by the hospital. The HealthPlex provided outpatient imaging and laboratory services to the community.
In the days immediately following the tornado, the Middle Flint chapter of the American Red Cross—whose headquarters were also badly damaged—set up an emergency response center in the First Baptist Church of Americus that featured a makeshift emergency room. Dr. Davis and her staff of hospitalists, employed by TeamHealth’s Hospital Medicine Division, helped get the Red Cross center up and running. They also played a significant role in setting up a temporary urgent-care center in tents provided by the Federal Emergency Management Agency (FEMA), supplemented by two tents belonging to the Boy Scouts.
By Any Means Necessary
Although local physicians with their own practices were well represented among the first responders, they were (for the most part) not involved with staffing the tent hospital, according to Dr. Davis. Most of the work in the tents was done by the emergency department (ED) physicians and TeamHealth doctors, in conjunction with Sumter Regional’s four hospitalists.
As soon as the tents opened, the ED “regulars” started showing up in droves,” explains Dr. Davis. Because a significant number of private physicians’ offices in town were destroyed there were no other healthcare options for many residents.
“It’s a difficult situation,” says Dr. Davis. “There are people in the community without cars, for example, whose cars were destroyed. So they have no other way to get to another hospital. They were astonishingly grateful to have us there.”
As residents cleaned up more than a month after the disaster, the urgent-care facility in the tents still functions as Sumter Regional’s ED. Routine lab work and X-rays were provided, and staff also monitored patients on blood thinners and gave injections to cancer patients.
In a pinch, the tents have served as an impromptu obstetrics suite. One woman delivered her child there after being unable to travel to Phoebe Putney Memorial Hospital, which is providing obstetrical services to mothers who would have gone to Sumter Regional.
Care of the center’s cancer patients—a number of whom must take a bus to Albany for treatment—is now overseen by Phoebe Putney’s oncology department. Surgeons, too, have had to travel to other hospitals in order to operate. “It is a logistical nightmare,” says Dr. Davis.
While the urgent-care unit has been able to provide basic services, it has not been an easy task for the physicians and nurses who work there. Telephone lines have not been restored, making it virtually impossible to send faxes. Hospitalists and ED physicians staffing the tents have had to read their own films, essentially serving as their own radiologists. As Dr Davis notes, “You have to do the best with what you have.” Often, that is a bare minimum. Indeed, she once had to put in a central line to stabilize a patient. “It was pretty surreal treating (the patient) in a tent,” she says.
What’s Next?
FEMA Director David Paulison, who toured the devastated hospital with President Bush, says the immediate response was indicative of the “new FEMA.”
Bush declared Sumter County a disaster area the day after the tornado. Residents were urged to apply as quickly as possible for grants and low-cost loans to aid in recovery. Local, state, and federal officials opened a disaster recovery center March 5 in Americus, staffed by representatives of FEMA, the Georgia Emergency Management Agency (GEMA), and a number of other agencies. As of April 4, FEMA, GEMA, and the U.S. Small Business Association (SBA), had approved more than $6.58 million for disaster recovery.
A May 16 update by Sumter Regional on its Web site indicated progress in the construction of modular care facilities.
“By the end of May, there will be five modular buildings in the Mayo Street parking lot for use by physicians, each consisting of two single-wide modular buildings joined together,” the memo stated. “Currently, two of the five physician modular buildings are in place with both halves assembled, and three of the single units are on site ready for placement and assembly. The other three halves that will be used to construct the remaining three buildings are on the way. We are still seeking bids from contractors to do the plumbing, electrical and other utility work, and anticipate having the buildings functional by the end of May for physicians to begin seeing patients.”
On April 30, Sumter Regional opened its Sumter Regional East facility. Sumter East provides 24-hour urgent care, radiology services, clinical lab services, physical therapy, speech therapy, occupational therapy, and cardiopulmonary services, according to the hospital’s Web site.
An interim hospital is slated to open in mid-September, according to a May 10 statement by the hospital. The facility, to be built on the former site of the HealthPlex, is to include approximately 65 inpatient rooms, nine LDRP/obstetrics/nursery rooms, eight CCU rooms, four operating suites, and a fully functional ER.
Whether or not the center’s hospitalists will have a place in the modular health center is unclear. Maintaining the hospitalist program is expensive, explained Dr. Davis. Although she has been assured Sumter Regional’s hospitalist program will continue in some capacity, she is still unsure of the program’s status. Currently, Sumter Regional’s four TeamHealth hospitalists are without a hospital.
Eventually, Sumter Regional Hospital will be rebuilt. Shortly after the tornado destroyed the health center, its president and CEO, David Seagraves issued the following message to the community: “Sumter Regional Hospital is not closing. We are currently assessing the damage to our facility from the tornado, and we are also looking at temporary alternative sites to provide services. We will update our situation in the current days, but I repeat that we fully intend for Sumter Regional Hospital to be back better than ever as soon as humanly possible.”
But reconstructing the hospital will be costly, with damage estimated at more than $100 million. The center and its equipment are covered by a $90 million insurance policy, as well as $37 million in service interruption insurance—some of which is slated to pay the hospital’s 700 employees. The state Senate has authorized $11 million in emergency funding for the town, some of which may go toward re-establishing healthcare in the region. It will take far more than that to restore a fully functional hospital. Sumter Regional is seeking financial donations through its Web site (www.sumterregional.org) to help community members and to go toward rebuilding. Citizen’s Bank of Americus has donated $100,000, half to the hospital and half to aid the community. Wachovia is also active in the reconstruction effort.
Dr. Davis could not be more pleased with how Sumter Regional’s hospitalists responded to the disaster. “I am real proud of the doctors I work with,” she says. “They really stepped up to the plate—above and beyond the call of duty. No one complained. No one worried about getting paid. No one worried about their malpractice insurance. I am very proud.” TH
Roberta Newman is a frequent contributor to The Hospitalist.
On the evening of March 1, severe thunderstorms rumbled over southwestern Georgia, spawning a tornado that ripped through seven counties. Classified an EF 3 with winds ranging from approximately 136 to 165 miles per hour, the twister tore a path of destruction 37 miles long and as much as a mile wide, reaching its maximum strength and width as it reached Americus, the seat of Sumter county. Along the way, the Sumter tornado—part of a storm system that killed eight in a high school in Enterprise, Ala.—demolished or seriously damaged more than 200 homes and dozens of businesses in Americus and the surrounding area, causing two deaths and many more injuries.
Not only did it leave the local Winn-Dixie grocery store without its façade, but it also reduced a 1,600-foot-tall public television tower to a 150-foot stump, sheared the tops off trees, downed power lines, knocked out telephone service, and deposited a burning tractor in the middle of Highway 520.
More important, it destroyed Sumter Regional Hospital in Americus, a rural city of 17,000 residents. Thanks to Sumter Regional’s staff, including its four hospitalists, all 70 patients were evacuated from the 265,000-square-foot, 143-bed complex.
The Terror Begins
The tornado, which struck Americus between 9 and 9:30 p.m., did not arrive without warning—but the town did not sound its tornado siren. A firefighter dispatched to activate the warning was called back because it was too late to do any good. Sumter Regional’s staff was alerted a tornado might strike, and they had moved patients away from the windows.
Hospitalist Mukesh Kumar, MD, who had joined Sumter Regional two weeks before the tornado struck, rode the storm out in the hospitalists’ office—a small space on the same corridor with a number of patient rooms.
“[Dr. Kumar] was the poor guy on duty that night,” says Amanda Davis, MD, head of the hospitalist program, who was not in town that evening.
As soon as the storm passed, an emergency call went out via the local broadcast media, requesting that physicians and nurses report to the severely damaged hospital to aid in the evacuation and treat the injured.
Hospitalists Kathy Hudson, MD, and Rick Oster, MD, among others, rushed to help. Getting to the hospital wasn’t easy. The surrounding area had become a maze of downed trees and power lines. First responders who could use their cars had to park outside the devastated area and hike to the hospital in the dark. Others arrived on bicycles. Some could not make it because they were trapped in their driveways.
With the power out at the tornado-ravaged hospital, as it was in much of Americus, first responders helped those on duty carry many of the 70 patients down the stairs of the four-story complex. Outside, Dr. Hudson worked with the staff, suturing the injured. Sumter Regional Hospital was evacuated by about 1:30 the following morning.
Patients were loaded into the town’s four ambulances and others from around the region and transferred to facilities in southwest Georgia. The closest of these was Phoebe Putney Memorial Hospital in Albany, about 40 miles from Americus.
Taking Stock
Wind and water had compromised nearly every part of Sumter Regional, leaving only the chapel intact. Much of the roof was ripped off, nearly all the windows were blown out, and part of the complex collapsed. Damage was so severe the entire health center was rendered unsafe.
Not only did the storm leave Americus without its hospital, it also devastated virtually all the town’s private doctor offices, as well as the Sumter HealthPlex—a new, 8,000-square-foot, $3.1 million facility owned by the hospital. The HealthPlex provided outpatient imaging and laboratory services to the community.
In the days immediately following the tornado, the Middle Flint chapter of the American Red Cross—whose headquarters were also badly damaged—set up an emergency response center in the First Baptist Church of Americus that featured a makeshift emergency room. Dr. Davis and her staff of hospitalists, employed by TeamHealth’s Hospital Medicine Division, helped get the Red Cross center up and running. They also played a significant role in setting up a temporary urgent-care center in tents provided by the Federal Emergency Management Agency (FEMA), supplemented by two tents belonging to the Boy Scouts.
By Any Means Necessary
Although local physicians with their own practices were well represented among the first responders, they were (for the most part) not involved with staffing the tent hospital, according to Dr. Davis. Most of the work in the tents was done by the emergency department (ED) physicians and TeamHealth doctors, in conjunction with Sumter Regional’s four hospitalists.
As soon as the tents opened, the ED “regulars” started showing up in droves,” explains Dr. Davis. Because a significant number of private physicians’ offices in town were destroyed there were no other healthcare options for many residents.
“It’s a difficult situation,” says Dr. Davis. “There are people in the community without cars, for example, whose cars were destroyed. So they have no other way to get to another hospital. They were astonishingly grateful to have us there.”
As residents cleaned up more than a month after the disaster, the urgent-care facility in the tents still functions as Sumter Regional’s ED. Routine lab work and X-rays were provided, and staff also monitored patients on blood thinners and gave injections to cancer patients.
In a pinch, the tents have served as an impromptu obstetrics suite. One woman delivered her child there after being unable to travel to Phoebe Putney Memorial Hospital, which is providing obstetrical services to mothers who would have gone to Sumter Regional.
Care of the center’s cancer patients—a number of whom must take a bus to Albany for treatment—is now overseen by Phoebe Putney’s oncology department. Surgeons, too, have had to travel to other hospitals in order to operate. “It is a logistical nightmare,” says Dr. Davis.
While the urgent-care unit has been able to provide basic services, it has not been an easy task for the physicians and nurses who work there. Telephone lines have not been restored, making it virtually impossible to send faxes. Hospitalists and ED physicians staffing the tents have had to read their own films, essentially serving as their own radiologists. As Dr Davis notes, “You have to do the best with what you have.” Often, that is a bare minimum. Indeed, she once had to put in a central line to stabilize a patient. “It was pretty surreal treating (the patient) in a tent,” she says.
What’s Next?
FEMA Director David Paulison, who toured the devastated hospital with President Bush, says the immediate response was indicative of the “new FEMA.”
Bush declared Sumter County a disaster area the day after the tornado. Residents were urged to apply as quickly as possible for grants and low-cost loans to aid in recovery. Local, state, and federal officials opened a disaster recovery center March 5 in Americus, staffed by representatives of FEMA, the Georgia Emergency Management Agency (GEMA), and a number of other agencies. As of April 4, FEMA, GEMA, and the U.S. Small Business Association (SBA), had approved more than $6.58 million for disaster recovery.
A May 16 update by Sumter Regional on its Web site indicated progress in the construction of modular care facilities.
“By the end of May, there will be five modular buildings in the Mayo Street parking lot for use by physicians, each consisting of two single-wide modular buildings joined together,” the memo stated. “Currently, two of the five physician modular buildings are in place with both halves assembled, and three of the single units are on site ready for placement and assembly. The other three halves that will be used to construct the remaining three buildings are on the way. We are still seeking bids from contractors to do the plumbing, electrical and other utility work, and anticipate having the buildings functional by the end of May for physicians to begin seeing patients.”
On April 30, Sumter Regional opened its Sumter Regional East facility. Sumter East provides 24-hour urgent care, radiology services, clinical lab services, physical therapy, speech therapy, occupational therapy, and cardiopulmonary services, according to the hospital’s Web site.
An interim hospital is slated to open in mid-September, according to a May 10 statement by the hospital. The facility, to be built on the former site of the HealthPlex, is to include approximately 65 inpatient rooms, nine LDRP/obstetrics/nursery rooms, eight CCU rooms, four operating suites, and a fully functional ER.
Whether or not the center’s hospitalists will have a place in the modular health center is unclear. Maintaining the hospitalist program is expensive, explained Dr. Davis. Although she has been assured Sumter Regional’s hospitalist program will continue in some capacity, she is still unsure of the program’s status. Currently, Sumter Regional’s four TeamHealth hospitalists are without a hospital.
Eventually, Sumter Regional Hospital will be rebuilt. Shortly after the tornado destroyed the health center, its president and CEO, David Seagraves issued the following message to the community: “Sumter Regional Hospital is not closing. We are currently assessing the damage to our facility from the tornado, and we are also looking at temporary alternative sites to provide services. We will update our situation in the current days, but I repeat that we fully intend for Sumter Regional Hospital to be back better than ever as soon as humanly possible.”
But reconstructing the hospital will be costly, with damage estimated at more than $100 million. The center and its equipment are covered by a $90 million insurance policy, as well as $37 million in service interruption insurance—some of which is slated to pay the hospital’s 700 employees. The state Senate has authorized $11 million in emergency funding for the town, some of which may go toward re-establishing healthcare in the region. It will take far more than that to restore a fully functional hospital. Sumter Regional is seeking financial donations through its Web site (www.sumterregional.org) to help community members and to go toward rebuilding. Citizen’s Bank of Americus has donated $100,000, half to the hospital and half to aid the community. Wachovia is also active in the reconstruction effort.
Dr. Davis could not be more pleased with how Sumter Regional’s hospitalists responded to the disaster. “I am real proud of the doctors I work with,” she says. “They really stepped up to the plate—above and beyond the call of duty. No one complained. No one worried about getting paid. No one worried about their malpractice insurance. I am very proud.” TH
Roberta Newman is a frequent contributor to The Hospitalist.
Enchondromatosis

Patient history: A 53-year-old female admits with a history of multiple orthopedic, dermatologic, and plastic-surgical procedures. The physical exam is notable for multiple cutaneous hemangiomas.


Salient findings: The images show old fracture deformities of the left fibular shaft and proximal tibia as well as a deformity of the distal femur. The patient has had a left total knee arthroplasty. There are multiple lucent lesions involving the left second, fourth, and fifth rays, with bone deformities. Findings are consistent with multiple chondromas. There is no evidence for malignant degeneration.
Patient population and natural history of disease: Enchondromatosis is a condition of multiple benign ectopic rests of cartilage growing within intramedullary bone, forming lucent lesions and bone expansion on radiographs. The enchondromas can deform and shorten a limb and can predispose the patient to a pathologic fracture. Enchondromas account for 12%-14% of benign bone neoplasms. When associated with cutaneous and visceral hemangiomas, the condition is called Maffucci’s syndrome.
Most patients with Maffucci’s syndrome will develop malignant transformation of at least one enchondroma into a chondrosarcoma (malignant cartilage tumor). Enchondromatosis without hemangiomas is known as Ollier’s disease; about 25% of patients with Ollier’s disease will develop chondrosarcoma by age 40. Both Maffucci’s syndrome and Ollier’s disease are nonhereditary. Metachondromatosis, a condition characterized by multiple enchondromas, is an autosomal dominant condition uniquely associated with osteochondromas.
Management: The physician who evaluates a patient with Maffucci’s syndrome must have a high suspicion for pathologic fracture and malignant degeneration. All bone pain and swelling should be evaluated with plain radiographs. Bone expansion, cortical breakthrough, soft-tissue mass, and deep endosteal scalloping of the cortex are indicative of malignant transformation. These findings are unreliable in the smaller bones of the hands, however, and features of low-grade chondrosarcoma are often indistinguishable from benign enchondromas. Even in the absence of worrisome features on plain radiographs, if clinical suspicion is high, a CT scan and/or an MRI should be performed for further evaluation. Biopsy is often indicated on clinical findings, despite imaging characteristics. Hemangiomas can undergo rapid expansion and are often treated with surgery.
Take-home points:
- Enchondromas are the most common primary neoplasm of the bones in the hand and are benign;
- There is an increased risk of malignant transformation of enchondromas in patients with Ollier’s disease or Maffucci’s syndrome; and
- Biopsy of a lesion may be indicated if clinical suspicion for malignancy is high. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine in Rochester, Minn.
Bibliography
- Sun TC, Swee RG, Shives TC, et al. Chondrosarcoma in Maffucci’s syndrome. J Bone Joint Surg Am. 1985 Oct;67(8):1214-1219.
- Schwartz HS, Zimmerman NB, Simon MA, et al. The malignant potential of enchondromatosis. J Bone Joint Surg Am. 1987 Feb;69(2):269-274.
- Chew FS, Maldjian C. Enchondroma and enchondromatosis. emedicine. June 10, 2005. Available at: www.emedicine.com/radio/topic247.htm. Last accessed on March 14, 2007.
Patient history: A 53-year-old female admits with a history of multiple orthopedic, dermatologic, and plastic-surgical procedures. The physical exam is notable for multiple cutaneous hemangiomas.
Salient findings: The images show old fracture deformities of the left fibular shaft and proximal tibia as well as a deformity of the distal femur. The patient has had a left total knee arthroplasty. There are multiple lucent lesions involving the left second, fourth, and fifth rays, with bone deformities. Findings are consistent with multiple chondromas. There is no evidence for malignant degeneration.
Patient population and natural history of disease: Enchondromatosis is a condition of multiple benign ectopic rests of cartilage growing within intramedullary bone, forming lucent lesions and bone expansion on radiographs. The enchondromas can deform and shorten a limb and can predispose the patient to a pathologic fracture. Enchondromas account for 12%-14% of benign bone neoplasms. When associated with cutaneous and visceral hemangiomas, the condition is called Maffucci’s syndrome.
Most patients with Maffucci’s syndrome will develop malignant transformation of at least one enchondroma into a chondrosarcoma (malignant cartilage tumor). Enchondromatosis without hemangiomas is known as Ollier’s disease; about 25% of patients with Ollier’s disease will develop chondrosarcoma by age 40. Both Maffucci’s syndrome and Ollier’s disease are nonhereditary. Metachondromatosis, a condition characterized by multiple enchondromas, is an autosomal dominant condition uniquely associated with osteochondromas.
Management: The physician who evaluates a patient with Maffucci’s syndrome must have a high suspicion for pathologic fracture and malignant degeneration. All bone pain and swelling should be evaluated with plain radiographs. Bone expansion, cortical breakthrough, soft-tissue mass, and deep endosteal scalloping of the cortex are indicative of malignant transformation. These findings are unreliable in the smaller bones of the hands, however, and features of low-grade chondrosarcoma are often indistinguishable from benign enchondromas. Even in the absence of worrisome features on plain radiographs, if clinical suspicion is high, a CT scan and/or an MRI should be performed for further evaluation. Biopsy is often indicated on clinical findings, despite imaging characteristics. Hemangiomas can undergo rapid expansion and are often treated with surgery.
Take-home points:
- Enchondromas are the most common primary neoplasm of the bones in the hand and are benign;
- There is an increased risk of malignant transformation of enchondromas in patients with Ollier’s disease or Maffucci’s syndrome; and
- Biopsy of a lesion may be indicated if clinical suspicion for malignancy is high. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine in Rochester, Minn.
Bibliography
- Sun TC, Swee RG, Shives TC, et al. Chondrosarcoma in Maffucci’s syndrome. J Bone Joint Surg Am. 1985 Oct;67(8):1214-1219.
- Schwartz HS, Zimmerman NB, Simon MA, et al. The malignant potential of enchondromatosis. J Bone Joint Surg Am. 1987 Feb;69(2):269-274.
- Chew FS, Maldjian C. Enchondroma and enchondromatosis. emedicine. June 10, 2005. Available at: www.emedicine.com/radio/topic247.htm. Last accessed on March 14, 2007.
Patient history: A 53-year-old female admits with a history of multiple orthopedic, dermatologic, and plastic-surgical procedures. The physical exam is notable for multiple cutaneous hemangiomas.
Salient findings: The images show old fracture deformities of the left fibular shaft and proximal tibia as well as a deformity of the distal femur. The patient has had a left total knee arthroplasty. There are multiple lucent lesions involving the left second, fourth, and fifth rays, with bone deformities. Findings are consistent with multiple chondromas. There is no evidence for malignant degeneration.
Patient population and natural history of disease: Enchondromatosis is a condition of multiple benign ectopic rests of cartilage growing within intramedullary bone, forming lucent lesions and bone expansion on radiographs. The enchondromas can deform and shorten a limb and can predispose the patient to a pathologic fracture. Enchondromas account for 12%-14% of benign bone neoplasms. When associated with cutaneous and visceral hemangiomas, the condition is called Maffucci’s syndrome.
Most patients with Maffucci’s syndrome will develop malignant transformation of at least one enchondroma into a chondrosarcoma (malignant cartilage tumor). Enchondromatosis without hemangiomas is known as Ollier’s disease; about 25% of patients with Ollier’s disease will develop chondrosarcoma by age 40. Both Maffucci’s syndrome and Ollier’s disease are nonhereditary. Metachondromatosis, a condition characterized by multiple enchondromas, is an autosomal dominant condition uniquely associated with osteochondromas.
Management: The physician who evaluates a patient with Maffucci’s syndrome must have a high suspicion for pathologic fracture and malignant degeneration. All bone pain and swelling should be evaluated with plain radiographs. Bone expansion, cortical breakthrough, soft-tissue mass, and deep endosteal scalloping of the cortex are indicative of malignant transformation. These findings are unreliable in the smaller bones of the hands, however, and features of low-grade chondrosarcoma are often indistinguishable from benign enchondromas. Even in the absence of worrisome features on plain radiographs, if clinical suspicion is high, a CT scan and/or an MRI should be performed for further evaluation. Biopsy is often indicated on clinical findings, despite imaging characteristics. Hemangiomas can undergo rapid expansion and are often treated with surgery.
Take-home points:
- Enchondromas are the most common primary neoplasm of the bones in the hand and are benign;
- There is an increased risk of malignant transformation of enchondromas in patients with Ollier’s disease or Maffucci’s syndrome; and
- Biopsy of a lesion may be indicated if clinical suspicion for malignancy is high. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine in Rochester, Minn.
Bibliography
- Sun TC, Swee RG, Shives TC, et al. Chondrosarcoma in Maffucci’s syndrome. J Bone Joint Surg Am. 1985 Oct;67(8):1214-1219.
- Schwartz HS, Zimmerman NB, Simon MA, et al. The malignant potential of enchondromatosis. J Bone Joint Surg Am. 1987 Feb;69(2):269-274.
- Chew FS, Maldjian C. Enchondroma and enchondromatosis. emedicine. June 10, 2005. Available at: www.emedicine.com/radio/topic247.htm. Last accessed on March 14, 2007.
The Anorectic Heart

Patient history: A 40-year-old male with a history of anorexia, depression, and recent weight loss presents for a general medical evaluation prompted by his concerned father. A computed tomography (CT) scan of his chest shows a moderate amount of pneumomediastinum (PM) extending superiorly into the tissues of the neck. He also has a moderate-size pericardial effusion. The patient denies symptoms of chest pain, shortness of breath, nausea, vomiting, or recreational drug use. Specifically, the patient admits to a depressed mood, but denies any vomiting, retching, or auto-destructive behavior. He has no history or evidence of underlying pulmonary disease.
Other notable findings consistent with the patient’s eating disorder are a body mass index (BMI) of 15, leukopenia, hyponatremia, bradycardia, and low blood pressure. A subsequent gastrograffin esophagram shows no obvious leaks or abnormalities. The patient is admitted to the hospital, allowed nothing by mouth, and placed on intravenous piperacillin and tazobactam, and nutrition. A transthoracic echocardiogram to evaluate the pericardial effusion on the first hospital day shows early tamponade physiology. Repeat evaluation two days later shows mild right atrial collapse but no evidence of hemodynamic compromise. Inpatient psychiatry consultation is obtained regarding his depression and eating disorder. On the fifth hospital day, a repeat CT scan shows moderate improvement of the PM. The patient is discharged home with outpatient follow-up.
Discussion: PM is defined as free air or gas in the mediastinum and is an uncommon finding. The etiology is usually from the airway, esophagus, or external trauma/surgery. Spontaneous PM occurs in the absence of an apparent identifiable cause and can exist in isolation or in conjunction with pneumothorax and soft-tissue emphysema. Elevated intraalveolar pressures related to mechanical ventilation or activities involving Valsalva maneuvers, along with pre-existing lung disease, account for the majority of pulmonary-related PM.1 Esophageal tear or rupture is another, less common cause of PM. Several case reports of PM in patients with anorexia nervosa exist, and some experts have postulated that one possible mechanism is vomiting or some other auto-destructive behavior.2-4 Loss of pulmonary connective tissue related to prolonged starvation leading to spontaneous pneumothorax and PM has also been postulated using rat models.5
The most common symptoms associated with PM are chest pain, voice change, and cough. In rare cases, PM can lead to decreased cardiac output. Common triggers of spontaneous PM, such as cough, physical exercise, and drug abuse, have been reported. A high percentage of patients with spontaneous PM have underlying pulmonary disease, including asthma and COPD.1 PM in conjunction with Boerhaave’s syndrome may have a mortality rate as high as 50% to 70%. In patients with anorexia nervosa, PM is often seen in conjunction with other advanced findings, including pancytopenia, electrolyte disturbances, bradycardia, and hypotension.
The age and gender of the patient are atypical for anorexia nervosa, although he does indeed have a restrictive eating disorder. The PM and pericardial effusion are additive unique findings that likely relate to his malnourished state and possible auto-destructive behavior.
Management: Spontaneous PM has been managed in a variety of ways, ranging from outpatient radiographic follow-up to close, inpatient monitoring. Identifying the etiology and monitoring for further progression or complications is important. For patients in whom esophageal tear or microperforation is suspected, early surgical consultation is recommended. An acceptable algorithm for patients with suspected esophageal perforation after endoscopy is to begin with a contrast CT scan of the neck and chest with oral contrast or to use a water-soluble contrast (gastrograffin) esophagram followed by a barium swallow if the water-soluble study is negative.6,7 When imaging reveals no leakage, the PM can be followed radiographically—typically after 48 hours and thereafter slowly advancing the diet. TH
Mackram Eleid, MD, works in the Division of Internal Medicine at the Mayo Clinic Arizona (Scottsdale/Phoenix). Joseph Charles, MD, FACP, is an assistant professor of Medicine and division education coordinator in the Mayo Clinic Hospital Arizona, Scottsdale/Phoenix.
References
- Campillo-Soto A, Coll-Salinas A, Soria-Aledo V, et al. [Spontaneous pneumomediastinum: descriptive study of our experience with 36 cases.] [in Spanish] Arch Bronconeumol. 2005;41:528-531.
- Danzer G, Mulzer J, Weber G, et al. Advanced anorexia nervosa, associated with pneumomediastinum, pneumothorax, and soft-tissue emphysema without esophageal lesion. Int J Eat Disord. 2005 Nov;38(3):281-284.
- Brooks AP, Martyn C. Pneumomediastinum in anorexia nervosa. Br Med J. 1979;1:125.
- Chatfield WR, Bowditch JD, Forrest CA. Spontaneous pneumomediastinum complicating anorexia nervosa. Br Med J. 1979 Jan 13;1(6156):200-201.
- Sahebjami H, MacGee J. Changes in connective tissue composition of the lung in starvation and refeeding. Am Rev Respir Dis. 1983;128:644-647.
- Dodds WJ, Stewart ET, Vlymen WJ. Appropriate contrast media for the evaluation of esophageal disruption. Radiology. 1982 Jul;144(2):439-441.
- Ghahremani GG. Radiologic evaluation of suspected gastrointestinal perforations. Radiol Clin North Am. 1993 Nov;31(6):1219-1234.
Patient history: A 40-year-old male with a history of anorexia, depression, and recent weight loss presents for a general medical evaluation prompted by his concerned father. A computed tomography (CT) scan of his chest shows a moderate amount of pneumomediastinum (PM) extending superiorly into the tissues of the neck. He also has a moderate-size pericardial effusion. The patient denies symptoms of chest pain, shortness of breath, nausea, vomiting, or recreational drug use. Specifically, the patient admits to a depressed mood, but denies any vomiting, retching, or auto-destructive behavior. He has no history or evidence of underlying pulmonary disease.
Other notable findings consistent with the patient’s eating disorder are a body mass index (BMI) of 15, leukopenia, hyponatremia, bradycardia, and low blood pressure. A subsequent gastrograffin esophagram shows no obvious leaks or abnormalities. The patient is admitted to the hospital, allowed nothing by mouth, and placed on intravenous piperacillin and tazobactam, and nutrition. A transthoracic echocardiogram to evaluate the pericardial effusion on the first hospital day shows early tamponade physiology. Repeat evaluation two days later shows mild right atrial collapse but no evidence of hemodynamic compromise. Inpatient psychiatry consultation is obtained regarding his depression and eating disorder. On the fifth hospital day, a repeat CT scan shows moderate improvement of the PM. The patient is discharged home with outpatient follow-up.
Discussion: PM is defined as free air or gas in the mediastinum and is an uncommon finding. The etiology is usually from the airway, esophagus, or external trauma/surgery. Spontaneous PM occurs in the absence of an apparent identifiable cause and can exist in isolation or in conjunction with pneumothorax and soft-tissue emphysema. Elevated intraalveolar pressures related to mechanical ventilation or activities involving Valsalva maneuvers, along with pre-existing lung disease, account for the majority of pulmonary-related PM.1 Esophageal tear or rupture is another, less common cause of PM. Several case reports of PM in patients with anorexia nervosa exist, and some experts have postulated that one possible mechanism is vomiting or some other auto-destructive behavior.2-4 Loss of pulmonary connective tissue related to prolonged starvation leading to spontaneous pneumothorax and PM has also been postulated using rat models.5
The most common symptoms associated with PM are chest pain, voice change, and cough. In rare cases, PM can lead to decreased cardiac output. Common triggers of spontaneous PM, such as cough, physical exercise, and drug abuse, have been reported. A high percentage of patients with spontaneous PM have underlying pulmonary disease, including asthma and COPD.1 PM in conjunction with Boerhaave’s syndrome may have a mortality rate as high as 50% to 70%. In patients with anorexia nervosa, PM is often seen in conjunction with other advanced findings, including pancytopenia, electrolyte disturbances, bradycardia, and hypotension.
The age and gender of the patient are atypical for anorexia nervosa, although he does indeed have a restrictive eating disorder. The PM and pericardial effusion are additive unique findings that likely relate to his malnourished state and possible auto-destructive behavior.
Management: Spontaneous PM has been managed in a variety of ways, ranging from outpatient radiographic follow-up to close, inpatient monitoring. Identifying the etiology and monitoring for further progression or complications is important. For patients in whom esophageal tear or microperforation is suspected, early surgical consultation is recommended. An acceptable algorithm for patients with suspected esophageal perforation after endoscopy is to begin with a contrast CT scan of the neck and chest with oral contrast or to use a water-soluble contrast (gastrograffin) esophagram followed by a barium swallow if the water-soluble study is negative.6,7 When imaging reveals no leakage, the PM can be followed radiographically—typically after 48 hours and thereafter slowly advancing the diet. TH
Mackram Eleid, MD, works in the Division of Internal Medicine at the Mayo Clinic Arizona (Scottsdale/Phoenix). Joseph Charles, MD, FACP, is an assistant professor of Medicine and division education coordinator in the Mayo Clinic Hospital Arizona, Scottsdale/Phoenix.
References
- Campillo-Soto A, Coll-Salinas A, Soria-Aledo V, et al. [Spontaneous pneumomediastinum: descriptive study of our experience with 36 cases.] [in Spanish] Arch Bronconeumol. 2005;41:528-531.
- Danzer G, Mulzer J, Weber G, et al. Advanced anorexia nervosa, associated with pneumomediastinum, pneumothorax, and soft-tissue emphysema without esophageal lesion. Int J Eat Disord. 2005 Nov;38(3):281-284.
- Brooks AP, Martyn C. Pneumomediastinum in anorexia nervosa. Br Med J. 1979;1:125.
- Chatfield WR, Bowditch JD, Forrest CA. Spontaneous pneumomediastinum complicating anorexia nervosa. Br Med J. 1979 Jan 13;1(6156):200-201.
- Sahebjami H, MacGee J. Changes in connective tissue composition of the lung in starvation and refeeding. Am Rev Respir Dis. 1983;128:644-647.
- Dodds WJ, Stewart ET, Vlymen WJ. Appropriate contrast media for the evaluation of esophageal disruption. Radiology. 1982 Jul;144(2):439-441.
- Ghahremani GG. Radiologic evaluation of suspected gastrointestinal perforations. Radiol Clin North Am. 1993 Nov;31(6):1219-1234.
Patient history: A 40-year-old male with a history of anorexia, depression, and recent weight loss presents for a general medical evaluation prompted by his concerned father. A computed tomography (CT) scan of his chest shows a moderate amount of pneumomediastinum (PM) extending superiorly into the tissues of the neck. He also has a moderate-size pericardial effusion. The patient denies symptoms of chest pain, shortness of breath, nausea, vomiting, or recreational drug use. Specifically, the patient admits to a depressed mood, but denies any vomiting, retching, or auto-destructive behavior. He has no history or evidence of underlying pulmonary disease.
Other notable findings consistent with the patient’s eating disorder are a body mass index (BMI) of 15, leukopenia, hyponatremia, bradycardia, and low blood pressure. A subsequent gastrograffin esophagram shows no obvious leaks or abnormalities. The patient is admitted to the hospital, allowed nothing by mouth, and placed on intravenous piperacillin and tazobactam, and nutrition. A transthoracic echocardiogram to evaluate the pericardial effusion on the first hospital day shows early tamponade physiology. Repeat evaluation two days later shows mild right atrial collapse but no evidence of hemodynamic compromise. Inpatient psychiatry consultation is obtained regarding his depression and eating disorder. On the fifth hospital day, a repeat CT scan shows moderate improvement of the PM. The patient is discharged home with outpatient follow-up.
Discussion: PM is defined as free air or gas in the mediastinum and is an uncommon finding. The etiology is usually from the airway, esophagus, or external trauma/surgery. Spontaneous PM occurs in the absence of an apparent identifiable cause and can exist in isolation or in conjunction with pneumothorax and soft-tissue emphysema. Elevated intraalveolar pressures related to mechanical ventilation or activities involving Valsalva maneuvers, along with pre-existing lung disease, account for the majority of pulmonary-related PM.1 Esophageal tear or rupture is another, less common cause of PM. Several case reports of PM in patients with anorexia nervosa exist, and some experts have postulated that one possible mechanism is vomiting or some other auto-destructive behavior.2-4 Loss of pulmonary connective tissue related to prolonged starvation leading to spontaneous pneumothorax and PM has also been postulated using rat models.5
The most common symptoms associated with PM are chest pain, voice change, and cough. In rare cases, PM can lead to decreased cardiac output. Common triggers of spontaneous PM, such as cough, physical exercise, and drug abuse, have been reported. A high percentage of patients with spontaneous PM have underlying pulmonary disease, including asthma and COPD.1 PM in conjunction with Boerhaave’s syndrome may have a mortality rate as high as 50% to 70%. In patients with anorexia nervosa, PM is often seen in conjunction with other advanced findings, including pancytopenia, electrolyte disturbances, bradycardia, and hypotension.
The age and gender of the patient are atypical for anorexia nervosa, although he does indeed have a restrictive eating disorder. The PM and pericardial effusion are additive unique findings that likely relate to his malnourished state and possible auto-destructive behavior.
Management: Spontaneous PM has been managed in a variety of ways, ranging from outpatient radiographic follow-up to close, inpatient monitoring. Identifying the etiology and monitoring for further progression or complications is important. For patients in whom esophageal tear or microperforation is suspected, early surgical consultation is recommended. An acceptable algorithm for patients with suspected esophageal perforation after endoscopy is to begin with a contrast CT scan of the neck and chest with oral contrast or to use a water-soluble contrast (gastrograffin) esophagram followed by a barium swallow if the water-soluble study is negative.6,7 When imaging reveals no leakage, the PM can be followed radiographically—typically after 48 hours and thereafter slowly advancing the diet. TH
Mackram Eleid, MD, works in the Division of Internal Medicine at the Mayo Clinic Arizona (Scottsdale/Phoenix). Joseph Charles, MD, FACP, is an assistant professor of Medicine and division education coordinator in the Mayo Clinic Hospital Arizona, Scottsdale/Phoenix.
References
- Campillo-Soto A, Coll-Salinas A, Soria-Aledo V, et al. [Spontaneous pneumomediastinum: descriptive study of our experience with 36 cases.] [in Spanish] Arch Bronconeumol. 2005;41:528-531.
- Danzer G, Mulzer J, Weber G, et al. Advanced anorexia nervosa, associated with pneumomediastinum, pneumothorax, and soft-tissue emphysema without esophageal lesion. Int J Eat Disord. 2005 Nov;38(3):281-284.
- Brooks AP, Martyn C. Pneumomediastinum in anorexia nervosa. Br Med J. 1979;1:125.
- Chatfield WR, Bowditch JD, Forrest CA. Spontaneous pneumomediastinum complicating anorexia nervosa. Br Med J. 1979 Jan 13;1(6156):200-201.
- Sahebjami H, MacGee J. Changes in connective tissue composition of the lung in starvation and refeeding. Am Rev Respir Dis. 1983;128:644-647.
- Dodds WJ, Stewart ET, Vlymen WJ. Appropriate contrast media for the evaluation of esophageal disruption. Radiology. 1982 Jul;144(2):439-441.
- Ghahremani GG. Radiologic evaluation of suspected gastrointestinal perforations. Radiol Clin North Am. 1993 Nov;31(6):1219-1234.
Get Control

This is the first in a series of articles on the four pillars of career satisfaction in hospital medicine.
How do you feel about the hours, compensation, responsibilities, and stresses of your present position? Do you think your job is sustainable—that is, would you be happy to continue your current work for years to come?
Many of today’s hospitalists might not answer the last question with a resounding “yes” because of one or more common factors that lead to chronic dissatisfaction with their careers.
In 2005, SHM formed the Career Satisfaction Task Force (CSTF) to combat this dissatisfaction, charging it with a three-pronged mission: to identify working conditions in hospital medicine that promote success and wellness; to provide resources to enhance career satisfaction; and to promote research into hospitalist career satisfaction and burnout.
“Originally, we were concerned with burnout in hospital medicine,” says CSTF co-chair Sylvia C. W. McKean, MD, FACP, medical director at Brigham and Women's Hospital/Faulkner Hospitalist Service and associate professor of medicine, Harvard Medical School, Boston. “The task force was charged to examine the factors that lead to a long, satisfactory career in hospital medicine.”
New White Paper Available
After reviewing the literature on physician burnout and general career satisfaction, the CSTF created a comprehensive document, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available at www.hospitalmedicine.org), which can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction.
The white paper outlines the four pillars of career satisfaction: autonomy/control, workload/schedule, reward/recognition, and community/environment. It includes a Job Fit self-evaluation questionnaire and other tools and advice that can be used to gather information and take steps to improve problems identified by the survey.
While the information in the white paper can best be used to improve an entire hospital medicine program, individual hospitalists can also benefit from it. The paper clearly states that an individual hospitalist has the power to influence change within his or her job, perhaps by majority rule. They can find a niche of expertise within their practice; pursue continuing medical education opportunities to promote their areas of expertise; nurture networks with peers; and find a mentor and regularly seek advice.
The First Pillar: Autonomy/Control
Control, or autonomy, refers to the need to be able to affect the key factors that influence job performance. For example, do you have control over when, how, and how quickly you perform a specific task? Do you have some say in task assignment and policies? What about the availability of support staff, supplies, and materials?
“Doctors expect to have control in their jobs, control over the tasks they do, how and when they do those tasks,” says CSTF member Tosha Wetterneck, MD, University of Wisconsin Hospital/Clinics in Madison. “This control helps them cope with stress; take that control away, and they can’t cope as well.”
Autonomy is a problem in hospital medicine because the field is still new and not widely understood. Consequently, hospitalists may end up responsible for additional duties and hours—especially on weekends—that other physicians dump on them.
“In some hospitals, the only doctors who can’t cap [their workloads] are the hospitalists,” reports Dr. McKean.
The best way to ensure you’re comfortable with the autonomy offered by your position is to be aware of what you want—and what you get—when you take your job.
“An individual hospitalist always has a choice of taking a job with the clear understanding of what they’ll have control over,” says Dr. Wetterneck. “However, you have to understand what you as a person need to have control over. You don’t want to get yourself into a position where you don’t have control over the specific areas that matter the most to you.”
An Example of Autonomy
To help clarify how lack of autonomy can make career satisfaction plummet, here is a fictional example of a hospitalist who suddenly lost control in her job:
“I love working in hospital medicine and take my job very seriously. However, two months ago my hospital medicine group assumed responsibility for care of neurosurgical patients, and all hospitalists are now required to provide care to these patients. I find this upsetting—I feel like this is one more step in relegating my colleagues and I to the status of ‘super-residents’ who are responsible for everything that other physicians don’t want to do. I want to have control over which type of patients I see.”
According to the CSTF research, this individual should take the following steps:
Step 1: Assess the situation in the manner outlined in the white paper. The hospitalist should:
- Use the Job Fit questionnaire to profile the control elements of the hospitalist practice;
- Become familiar with the hospital’s leadership and committee structure;
- Understand key payer issues that might affect inpatient care; and
- Review her job description.
After reviewing the role personal autonomy plays within her practice, the hospitalist must consider whether she’s in a position to request a change of duties, or whether her new responsibilities are non-negotiable.
“There are different facets of control,” says Dr. Wetterneck. “Some could make the argument that a hospitalist doesn’t have the skills to take care of neurosurgical patients, that this is out of the realm of reasonable expectations for the job. Others might say that there is reasonable expectation, as long as the hospitalists would get extra learning and extra support from other [subspecialists] that they’d be available for consult.”
Regardless of where you stand on the argument of reasonable expectation of a hospitalist’s responsibilities, what if a new job task simply rubs you the wrong way—to the point where you no longer enjoy your work?
“If it’s truly an issue of ‘I don’t want to do this,’ then it becomes an issue of your fit with your group,” Dr. Wetterneck continues. “If everyone in the group is doing it and you don’t want to, then you need to understand how important this control is for you. Is it important enough to change jobs?”
Step 2: If the answer to that last question is “Yes,” this hospitalist should keep autonomy in mind as she begins a job search. The white paper includes questions to ask herself and her potential employers to ensure she has control in her next position. The diversity of hospitalist responsibilities works in her favor—assuming she’s willing to move to another part of the country.
“You can list all the things that make you happy in a job, and you can probably find every single thing on your list in a hospitalist job somewhere in the U.S.,” speculates Dr. Wetterneck.
Next Month
A discussion of the workload/schedule pillar, which refers to the type, volume, and intensity of a hospitalist's work.
The Only Constant
Working in hospital medicine practically guarantees your job will continually change. Whether it’s a change in responsibilities like the example above, the steady growth of your practice, or even a change in leadership or ownership, hospitalists must go with the flow.
“I definitely think that the job requires a certain amount of flexibility,” says Dr. Wetterneck. “Hospitalists have to understand that their job role will continue to change over time. Therefore, people have to really understand what’s important to them.”
The cost of lack of autonomy—or other job stressors—can be severe.
“If a change [in your job] throws you out of control, this can lead to stress,” Dr. Wetterneck points out. “We know from recent studies that stress has an impact on your health, specifically on cardiovascular disease and mortality.” TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the first in a series of articles on the four pillars of career satisfaction in hospital medicine.
How do you feel about the hours, compensation, responsibilities, and stresses of your present position? Do you think your job is sustainable—that is, would you be happy to continue your current work for years to come?
Many of today’s hospitalists might not answer the last question with a resounding “yes” because of one or more common factors that lead to chronic dissatisfaction with their careers.
In 2005, SHM formed the Career Satisfaction Task Force (CSTF) to combat this dissatisfaction, charging it with a three-pronged mission: to identify working conditions in hospital medicine that promote success and wellness; to provide resources to enhance career satisfaction; and to promote research into hospitalist career satisfaction and burnout.
“Originally, we were concerned with burnout in hospital medicine,” says CSTF co-chair Sylvia C. W. McKean, MD, FACP, medical director at Brigham and Women's Hospital/Faulkner Hospitalist Service and associate professor of medicine, Harvard Medical School, Boston. “The task force was charged to examine the factors that lead to a long, satisfactory career in hospital medicine.”
New White Paper Available
After reviewing the literature on physician burnout and general career satisfaction, the CSTF created a comprehensive document, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available at www.hospitalmedicine.org), which can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction.
The white paper outlines the four pillars of career satisfaction: autonomy/control, workload/schedule, reward/recognition, and community/environment. It includes a Job Fit self-evaluation questionnaire and other tools and advice that can be used to gather information and take steps to improve problems identified by the survey.
While the information in the white paper can best be used to improve an entire hospital medicine program, individual hospitalists can also benefit from it. The paper clearly states that an individual hospitalist has the power to influence change within his or her job, perhaps by majority rule. They can find a niche of expertise within their practice; pursue continuing medical education opportunities to promote their areas of expertise; nurture networks with peers; and find a mentor and regularly seek advice.
The First Pillar: Autonomy/Control
Control, or autonomy, refers to the need to be able to affect the key factors that influence job performance. For example, do you have control over when, how, and how quickly you perform a specific task? Do you have some say in task assignment and policies? What about the availability of support staff, supplies, and materials?
“Doctors expect to have control in their jobs, control over the tasks they do, how and when they do those tasks,” says CSTF member Tosha Wetterneck, MD, University of Wisconsin Hospital/Clinics in Madison. “This control helps them cope with stress; take that control away, and they can’t cope as well.”
Autonomy is a problem in hospital medicine because the field is still new and not widely understood. Consequently, hospitalists may end up responsible for additional duties and hours—especially on weekends—that other physicians dump on them.
“In some hospitals, the only doctors who can’t cap [their workloads] are the hospitalists,” reports Dr. McKean.
The best way to ensure you’re comfortable with the autonomy offered by your position is to be aware of what you want—and what you get—when you take your job.
“An individual hospitalist always has a choice of taking a job with the clear understanding of what they’ll have control over,” says Dr. Wetterneck. “However, you have to understand what you as a person need to have control over. You don’t want to get yourself into a position where you don’t have control over the specific areas that matter the most to you.”
An Example of Autonomy
To help clarify how lack of autonomy can make career satisfaction plummet, here is a fictional example of a hospitalist who suddenly lost control in her job:
“I love working in hospital medicine and take my job very seriously. However, two months ago my hospital medicine group assumed responsibility for care of neurosurgical patients, and all hospitalists are now required to provide care to these patients. I find this upsetting—I feel like this is one more step in relegating my colleagues and I to the status of ‘super-residents’ who are responsible for everything that other physicians don’t want to do. I want to have control over which type of patients I see.”
According to the CSTF research, this individual should take the following steps:
Step 1: Assess the situation in the manner outlined in the white paper. The hospitalist should:
- Use the Job Fit questionnaire to profile the control elements of the hospitalist practice;
- Become familiar with the hospital’s leadership and committee structure;
- Understand key payer issues that might affect inpatient care; and
- Review her job description.
After reviewing the role personal autonomy plays within her practice, the hospitalist must consider whether she’s in a position to request a change of duties, or whether her new responsibilities are non-negotiable.
“There are different facets of control,” says Dr. Wetterneck. “Some could make the argument that a hospitalist doesn’t have the skills to take care of neurosurgical patients, that this is out of the realm of reasonable expectations for the job. Others might say that there is reasonable expectation, as long as the hospitalists would get extra learning and extra support from other [subspecialists] that they’d be available for consult.”
Regardless of where you stand on the argument of reasonable expectation of a hospitalist’s responsibilities, what if a new job task simply rubs you the wrong way—to the point where you no longer enjoy your work?
“If it’s truly an issue of ‘I don’t want to do this,’ then it becomes an issue of your fit with your group,” Dr. Wetterneck continues. “If everyone in the group is doing it and you don’t want to, then you need to understand how important this control is for you. Is it important enough to change jobs?”
Step 2: If the answer to that last question is “Yes,” this hospitalist should keep autonomy in mind as she begins a job search. The white paper includes questions to ask herself and her potential employers to ensure she has control in her next position. The diversity of hospitalist responsibilities works in her favor—assuming she’s willing to move to another part of the country.
“You can list all the things that make you happy in a job, and you can probably find every single thing on your list in a hospitalist job somewhere in the U.S.,” speculates Dr. Wetterneck.
Next Month
A discussion of the workload/schedule pillar, which refers to the type, volume, and intensity of a hospitalist's work.
The Only Constant
Working in hospital medicine practically guarantees your job will continually change. Whether it’s a change in responsibilities like the example above, the steady growth of your practice, or even a change in leadership or ownership, hospitalists must go with the flow.
“I definitely think that the job requires a certain amount of flexibility,” says Dr. Wetterneck. “Hospitalists have to understand that their job role will continue to change over time. Therefore, people have to really understand what’s important to them.”
The cost of lack of autonomy—or other job stressors—can be severe.
“If a change [in your job] throws you out of control, this can lead to stress,” Dr. Wetterneck points out. “We know from recent studies that stress has an impact on your health, specifically on cardiovascular disease and mortality.” TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the first in a series of articles on the four pillars of career satisfaction in hospital medicine.
How do you feel about the hours, compensation, responsibilities, and stresses of your present position? Do you think your job is sustainable—that is, would you be happy to continue your current work for years to come?
Many of today’s hospitalists might not answer the last question with a resounding “yes” because of one or more common factors that lead to chronic dissatisfaction with their careers.
In 2005, SHM formed the Career Satisfaction Task Force (CSTF) to combat this dissatisfaction, charging it with a three-pronged mission: to identify working conditions in hospital medicine that promote success and wellness; to provide resources to enhance career satisfaction; and to promote research into hospitalist career satisfaction and burnout.
“Originally, we were concerned with burnout in hospital medicine,” says CSTF co-chair Sylvia C. W. McKean, MD, FACP, medical director at Brigham and Women's Hospital/Faulkner Hospitalist Service and associate professor of medicine, Harvard Medical School, Boston. “The task force was charged to examine the factors that lead to a long, satisfactory career in hospital medicine.”
New White Paper Available
After reviewing the literature on physician burnout and general career satisfaction, the CSTF created a comprehensive document, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available at www.hospitalmedicine.org), which can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction.
The white paper outlines the four pillars of career satisfaction: autonomy/control, workload/schedule, reward/recognition, and community/environment. It includes a Job Fit self-evaluation questionnaire and other tools and advice that can be used to gather information and take steps to improve problems identified by the survey.
While the information in the white paper can best be used to improve an entire hospital medicine program, individual hospitalists can also benefit from it. The paper clearly states that an individual hospitalist has the power to influence change within his or her job, perhaps by majority rule. They can find a niche of expertise within their practice; pursue continuing medical education opportunities to promote their areas of expertise; nurture networks with peers; and find a mentor and regularly seek advice.
The First Pillar: Autonomy/Control
Control, or autonomy, refers to the need to be able to affect the key factors that influence job performance. For example, do you have control over when, how, and how quickly you perform a specific task? Do you have some say in task assignment and policies? What about the availability of support staff, supplies, and materials?
“Doctors expect to have control in their jobs, control over the tasks they do, how and when they do those tasks,” says CSTF member Tosha Wetterneck, MD, University of Wisconsin Hospital/Clinics in Madison. “This control helps them cope with stress; take that control away, and they can’t cope as well.”
Autonomy is a problem in hospital medicine because the field is still new and not widely understood. Consequently, hospitalists may end up responsible for additional duties and hours—especially on weekends—that other physicians dump on them.
“In some hospitals, the only doctors who can’t cap [their workloads] are the hospitalists,” reports Dr. McKean.
The best way to ensure you’re comfortable with the autonomy offered by your position is to be aware of what you want—and what you get—when you take your job.
“An individual hospitalist always has a choice of taking a job with the clear understanding of what they’ll have control over,” says Dr. Wetterneck. “However, you have to understand what you as a person need to have control over. You don’t want to get yourself into a position where you don’t have control over the specific areas that matter the most to you.”
An Example of Autonomy
To help clarify how lack of autonomy can make career satisfaction plummet, here is a fictional example of a hospitalist who suddenly lost control in her job:
“I love working in hospital medicine and take my job very seriously. However, two months ago my hospital medicine group assumed responsibility for care of neurosurgical patients, and all hospitalists are now required to provide care to these patients. I find this upsetting—I feel like this is one more step in relegating my colleagues and I to the status of ‘super-residents’ who are responsible for everything that other physicians don’t want to do. I want to have control over which type of patients I see.”
According to the CSTF research, this individual should take the following steps:
Step 1: Assess the situation in the manner outlined in the white paper. The hospitalist should:
- Use the Job Fit questionnaire to profile the control elements of the hospitalist practice;
- Become familiar with the hospital’s leadership and committee structure;
- Understand key payer issues that might affect inpatient care; and
- Review her job description.
After reviewing the role personal autonomy plays within her practice, the hospitalist must consider whether she’s in a position to request a change of duties, or whether her new responsibilities are non-negotiable.
“There are different facets of control,” says Dr. Wetterneck. “Some could make the argument that a hospitalist doesn’t have the skills to take care of neurosurgical patients, that this is out of the realm of reasonable expectations for the job. Others might say that there is reasonable expectation, as long as the hospitalists would get extra learning and extra support from other [subspecialists] that they’d be available for consult.”
Regardless of where you stand on the argument of reasonable expectation of a hospitalist’s responsibilities, what if a new job task simply rubs you the wrong way—to the point where you no longer enjoy your work?
“If it’s truly an issue of ‘I don’t want to do this,’ then it becomes an issue of your fit with your group,” Dr. Wetterneck continues. “If everyone in the group is doing it and you don’t want to, then you need to understand how important this control is for you. Is it important enough to change jobs?”
Step 2: If the answer to that last question is “Yes,” this hospitalist should keep autonomy in mind as she begins a job search. The white paper includes questions to ask herself and her potential employers to ensure she has control in her next position. The diversity of hospitalist responsibilities works in her favor—assuming she’s willing to move to another part of the country.
“You can list all the things that make you happy in a job, and you can probably find every single thing on your list in a hospitalist job somewhere in the U.S.,” speculates Dr. Wetterneck.
Next Month
A discussion of the workload/schedule pillar, which refers to the type, volume, and intensity of a hospitalist's work.
The Only Constant
Working in hospital medicine practically guarantees your job will continually change. Whether it’s a change in responsibilities like the example above, the steady growth of your practice, or even a change in leadership or ownership, hospitalists must go with the flow.
“I definitely think that the job requires a certain amount of flexibility,” says Dr. Wetterneck. “Hospitalists have to understand that their job role will continue to change over time. Therefore, people have to really understand what’s important to them.”
The cost of lack of autonomy—or other job stressors—can be severe.
“If a change [in your job] throws you out of control, this can lead to stress,” Dr. Wetterneck points out. “We know from recent studies that stress has an impact on your health, specifically on cardiovascular disease and mortality.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Capitol Gains

Nine members of SHM’s Public Policy Committee (PPC), accompanied by several SHM staff members, paid a visit to Capitol Hill early this year.
The group spent Feb. 28 calling on senators, representatives, and congressional staff, as they participated in meetings similar to those included in SHM’s Legislative Advocacy Day, held during the 2006 Annual Meeting. In fact, many of the PPC members had second meetings with legislative staff they had met last May.
“We had already broken some ground with Legislative Day, so some people were familiar with us,” says Ron Angus, MD, Department of Medicine, Presbyterian Hospital of Dallas. “We had a little more time to talk about the issues.”
During their meetings, “We emphasized the different roles that SHM can play, and we tried to get a feel for what it means to have a Democrat-led Congress,” says Jack Percelay, MD, MPH, FAAP, Virtua Health, Ridgewood, N.J.
SHM’s senior adviser for advocacy and government affairs, Laura Allendorf, pronounces it “a very productive day.”

Building on a Foundation
The PPC visits were successful partly because this was the second time SHM had visited representatives, allowing the hospitalists to build on their introductory meetings and spend more time discussing issues and offering help. The committee hopes to continue this trend.
“In the long term, we want to see if we can meet with the same people more frequently,” explains Dr. Angus. Allendorf agrees, saying, “The more often we’re up there, the better.”
There may be many more visits or communications. “I think we’re building something long-term, and it’s going to take a while to do that,” says Dr. Angus. “As we get more comfortable talking to these folks, we’ll work on getting them to contact us when issues first come up. Our goal is to be there at the beginning of the process, rather than the end, when it’s too late to have much impact.”
Another reason the February visits were deemed a success involves whom the PPC met with.
“These meetings were more productive because we were meeting with key staff, people on key committees,” recounts Allendorf. “And [participants] had more visits during the day—each had between five and eight. We made a point to meet with committee staff, staff for key committees, including the House Ways and Means Health Subcommittee, the Senate Finance Committee, the Senate Committee on Appropriations, and the Senate Committee on Health, Education, Labor, and Pensions. We met with committee aides hired to handle special issues like Medicare Part B.”
Targeting these influential offices—particularly the powerful Ways and Means Committee—should have greater impact on healthcare legislation and funding.
Making Inroads with Ways and Means
The entire group ended the day in a meeting with Rep. Shelley Berkley, D-Nev., and her health legislative aide Jeff Davis. Berkley serves on the House Ways and Means Committee and is perceived as “physician-friendly.” Her husband is a nephrologist, and Allendorf describes the lawmaker as “very knowledgeable about the issues” in healthcare. “She’s now in a position to do something; she’ll be a major player,” predicts Allendorf.
“We met with Berkley for five or 10 minutes, then had a roundtable with Jeff Davis from her office,” says Dr. Angus. “We talked about increased funding for AHRQ [Agency for Healthcare Research and Quality] and coordinating quality initiatives being brought to bear in hospitals. We tried to emphasize that when you talk about quality in hospitals, you’re talking about hospitalists.”
With her majority role on a key committee, Berkley is one example of the newly empowered Democrats in office—Democrats who may make a difference in pushing through SHM-sponsored legislation.
Democratic Differences?
Did the PPC members notice a difference since May, with the change of majority party in Congress?
“I could feel it,” says Dr. Angus. “There’s been a huge sea change. Those who felt unempowered last year now feel that there’s a clean slate.”
Dr. Percelay saw a difference in priorities among healthcare issues. “In general, the access issue is much more prominent,” he says. “There’s a sense that we need to do something about healthcare expenses and access for everyone. There’s a recognition of big-picture issues—by both Democrats and Republicans—that we aren’t providing coverage for everyone, and we’re spending too much on it.”
Future Advocacy
The PPC counts its Capitol Hill visit a success. Members want to broaden the influence of SHM and hospitalists by enlisting the help of others.
“We want to identify members who are interested in public policy who live in key areas—areas served by legislators on key committees,” explains Dr. Percelay, “so that they can lobby from a local perspective.” Dr. Angus adds, “Ideally, they’ll interact with their national officials when they’re in their local offices. Also, we’d like members to keep an eye on state and local issues.”
Allendorf points out that these members can be identified and reached though SHM’s online Legislative Action Center at capwiz.com/hospitalmedicine/home. If you receive an e-mail asking you to contact one of your representatives regarding a specific issue, you can take part in the advocacy efforts.
In other plans, says Dr. Angus, “We hope to construct some body of resources that hospitalists who go to D.C. on their own can use to go up to the Hill with information in hand and talk to their Congress people.”
PPC members understand they have their work cut out for them when it comes to increasing awareness of SHM and hospitalists on Capitol Hill.
“This is a long-term investment process,” Dr. Percelay says. “We’re learning as an organization how to conduct our public policy efforts. We’re at the beginning stages of meeting with these people and letting them know what hospitalists can do.” TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Nine members of SHM’s Public Policy Committee (PPC), accompanied by several SHM staff members, paid a visit to Capitol Hill early this year.
The group spent Feb. 28 calling on senators, representatives, and congressional staff, as they participated in meetings similar to those included in SHM’s Legislative Advocacy Day, held during the 2006 Annual Meeting. In fact, many of the PPC members had second meetings with legislative staff they had met last May.
“We had already broken some ground with Legislative Day, so some people were familiar with us,” says Ron Angus, MD, Department of Medicine, Presbyterian Hospital of Dallas. “We had a little more time to talk about the issues.”
During their meetings, “We emphasized the different roles that SHM can play, and we tried to get a feel for what it means to have a Democrat-led Congress,” says Jack Percelay, MD, MPH, FAAP, Virtua Health, Ridgewood, N.J.
SHM’s senior adviser for advocacy and government affairs, Laura Allendorf, pronounces it “a very productive day.”
Building on a Foundation
The PPC visits were successful partly because this was the second time SHM had visited representatives, allowing the hospitalists to build on their introductory meetings and spend more time discussing issues and offering help. The committee hopes to continue this trend.
“In the long term, we want to see if we can meet with the same people more frequently,” explains Dr. Angus. Allendorf agrees, saying, “The more often we’re up there, the better.”
There may be many more visits or communications. “I think we’re building something long-term, and it’s going to take a while to do that,” says Dr. Angus. “As we get more comfortable talking to these folks, we’ll work on getting them to contact us when issues first come up. Our goal is to be there at the beginning of the process, rather than the end, when it’s too late to have much impact.”
Another reason the February visits were deemed a success involves whom the PPC met with.
“These meetings were more productive because we were meeting with key staff, people on key committees,” recounts Allendorf. “And [participants] had more visits during the day—each had between five and eight. We made a point to meet with committee staff, staff for key committees, including the House Ways and Means Health Subcommittee, the Senate Finance Committee, the Senate Committee on Appropriations, and the Senate Committee on Health, Education, Labor, and Pensions. We met with committee aides hired to handle special issues like Medicare Part B.”
Targeting these influential offices—particularly the powerful Ways and Means Committee—should have greater impact on healthcare legislation and funding.
Making Inroads with Ways and Means
The entire group ended the day in a meeting with Rep. Shelley Berkley, D-Nev., and her health legislative aide Jeff Davis. Berkley serves on the House Ways and Means Committee and is perceived as “physician-friendly.” Her husband is a nephrologist, and Allendorf describes the lawmaker as “very knowledgeable about the issues” in healthcare. “She’s now in a position to do something; she’ll be a major player,” predicts Allendorf.
“We met with Berkley for five or 10 minutes, then had a roundtable with Jeff Davis from her office,” says Dr. Angus. “We talked about increased funding for AHRQ [Agency for Healthcare Research and Quality] and coordinating quality initiatives being brought to bear in hospitals. We tried to emphasize that when you talk about quality in hospitals, you’re talking about hospitalists.”
With her majority role on a key committee, Berkley is one example of the newly empowered Democrats in office—Democrats who may make a difference in pushing through SHM-sponsored legislation.
Democratic Differences?
Did the PPC members notice a difference since May, with the change of majority party in Congress?
“I could feel it,” says Dr. Angus. “There’s been a huge sea change. Those who felt unempowered last year now feel that there’s a clean slate.”
Dr. Percelay saw a difference in priorities among healthcare issues. “In general, the access issue is much more prominent,” he says. “There’s a sense that we need to do something about healthcare expenses and access for everyone. There’s a recognition of big-picture issues—by both Democrats and Republicans—that we aren’t providing coverage for everyone, and we’re spending too much on it.”
Future Advocacy
The PPC counts its Capitol Hill visit a success. Members want to broaden the influence of SHM and hospitalists by enlisting the help of others.
“We want to identify members who are interested in public policy who live in key areas—areas served by legislators on key committees,” explains Dr. Percelay, “so that they can lobby from a local perspective.” Dr. Angus adds, “Ideally, they’ll interact with their national officials when they’re in their local offices. Also, we’d like members to keep an eye on state and local issues.”
Allendorf points out that these members can be identified and reached though SHM’s online Legislative Action Center at capwiz.com/hospitalmedicine/home. If you receive an e-mail asking you to contact one of your representatives regarding a specific issue, you can take part in the advocacy efforts.
In other plans, says Dr. Angus, “We hope to construct some body of resources that hospitalists who go to D.C. on their own can use to go up to the Hill with information in hand and talk to their Congress people.”
PPC members understand they have their work cut out for them when it comes to increasing awareness of SHM and hospitalists on Capitol Hill.
“This is a long-term investment process,” Dr. Percelay says. “We’re learning as an organization how to conduct our public policy efforts. We’re at the beginning stages of meeting with these people and letting them know what hospitalists can do.” TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Nine members of SHM’s Public Policy Committee (PPC), accompanied by several SHM staff members, paid a visit to Capitol Hill early this year.
The group spent Feb. 28 calling on senators, representatives, and congressional staff, as they participated in meetings similar to those included in SHM’s Legislative Advocacy Day, held during the 2006 Annual Meeting. In fact, many of the PPC members had second meetings with legislative staff they had met last May.
“We had already broken some ground with Legislative Day, so some people were familiar with us,” says Ron Angus, MD, Department of Medicine, Presbyterian Hospital of Dallas. “We had a little more time to talk about the issues.”
During their meetings, “We emphasized the different roles that SHM can play, and we tried to get a feel for what it means to have a Democrat-led Congress,” says Jack Percelay, MD, MPH, FAAP, Virtua Health, Ridgewood, N.J.
SHM’s senior adviser for advocacy and government affairs, Laura Allendorf, pronounces it “a very productive day.”
Building on a Foundation
The PPC visits were successful partly because this was the second time SHM had visited representatives, allowing the hospitalists to build on their introductory meetings and spend more time discussing issues and offering help. The committee hopes to continue this trend.
“In the long term, we want to see if we can meet with the same people more frequently,” explains Dr. Angus. Allendorf agrees, saying, “The more often we’re up there, the better.”
There may be many more visits or communications. “I think we’re building something long-term, and it’s going to take a while to do that,” says Dr. Angus. “As we get more comfortable talking to these folks, we’ll work on getting them to contact us when issues first come up. Our goal is to be there at the beginning of the process, rather than the end, when it’s too late to have much impact.”
Another reason the February visits were deemed a success involves whom the PPC met with.
“These meetings were more productive because we were meeting with key staff, people on key committees,” recounts Allendorf. “And [participants] had more visits during the day—each had between five and eight. We made a point to meet with committee staff, staff for key committees, including the House Ways and Means Health Subcommittee, the Senate Finance Committee, the Senate Committee on Appropriations, and the Senate Committee on Health, Education, Labor, and Pensions. We met with committee aides hired to handle special issues like Medicare Part B.”
Targeting these influential offices—particularly the powerful Ways and Means Committee—should have greater impact on healthcare legislation and funding.
Making Inroads with Ways and Means
The entire group ended the day in a meeting with Rep. Shelley Berkley, D-Nev., and her health legislative aide Jeff Davis. Berkley serves on the House Ways and Means Committee and is perceived as “physician-friendly.” Her husband is a nephrologist, and Allendorf describes the lawmaker as “very knowledgeable about the issues” in healthcare. “She’s now in a position to do something; she’ll be a major player,” predicts Allendorf.
“We met with Berkley for five or 10 minutes, then had a roundtable with Jeff Davis from her office,” says Dr. Angus. “We talked about increased funding for AHRQ [Agency for Healthcare Research and Quality] and coordinating quality initiatives being brought to bear in hospitals. We tried to emphasize that when you talk about quality in hospitals, you’re talking about hospitalists.”
With her majority role on a key committee, Berkley is one example of the newly empowered Democrats in office—Democrats who may make a difference in pushing through SHM-sponsored legislation.
Democratic Differences?
Did the PPC members notice a difference since May, with the change of majority party in Congress?
“I could feel it,” says Dr. Angus. “There’s been a huge sea change. Those who felt unempowered last year now feel that there’s a clean slate.”
Dr. Percelay saw a difference in priorities among healthcare issues. “In general, the access issue is much more prominent,” he says. “There’s a sense that we need to do something about healthcare expenses and access for everyone. There’s a recognition of big-picture issues—by both Democrats and Republicans—that we aren’t providing coverage for everyone, and we’re spending too much on it.”
Future Advocacy
The PPC counts its Capitol Hill visit a success. Members want to broaden the influence of SHM and hospitalists by enlisting the help of others.
“We want to identify members who are interested in public policy who live in key areas—areas served by legislators on key committees,” explains Dr. Percelay, “so that they can lobby from a local perspective.” Dr. Angus adds, “Ideally, they’ll interact with their national officials when they’re in their local offices. Also, we’d like members to keep an eye on state and local issues.”
Allendorf points out that these members can be identified and reached though SHM’s online Legislative Action Center at capwiz.com/hospitalmedicine/home. If you receive an e-mail asking you to contact one of your representatives regarding a specific issue, you can take part in the advocacy efforts.
In other plans, says Dr. Angus, “We hope to construct some body of resources that hospitalists who go to D.C. on their own can use to go up to the Hill with information in hand and talk to their Congress people.”
PPC members understand they have their work cut out for them when it comes to increasing awareness of SHM and hospitalists on Capitol Hill.
“This is a long-term investment process,” Dr. Percelay says. “We’re learning as an organization how to conduct our public policy efforts. We’re at the beginning stages of meeting with these people and letting them know what hospitalists can do.” TH
Jane Jerrard writes “Public Policy” for The Hospitalist.