User login
Big D Births an HM Program

When hospitalists stepped into Parkland Hospital (Dallas) a few months ago, they knew they were taking up a new challenge. Initially, they were known as the doctors without a team in a place where everyone was used to seeing no fewer than six to eight physicians rounding in a group.
Soon our hospitalists realized that a lot of teaching and awareness was needed among the nursing and support staff of the hospital to get them ready for this new breed of physicians.
A Case of Nerves
After four years of administrative planning and developing, the hospitalist program finally started in July 2006. Parkland started a hospitalist program due to the new restrictions on resident work hours and the number of patients a resident can admit. There used to be a considerable delay in the admission process causing patients to wait in our emergency department (ED) for hours until an admitting team could see them. This led to higher patient load in the ED. This load not only affected our patient care adversely, but it also caused considerable financial loss to the hospital because we couldn’t bill for admission until the patients were assigned a bed.
Our hospitalists help ease this overcrowding because they don’t work under these restrictions and can increase the ED throughput of the patients. Parkland also instituted a hospital medicine program to decrease length of stay.
Initially there was a lot of excitement, nervousness, and anxiety about the program. When I say nervousness and anxiety, it was primarily related to the nursing and administrative staff’s skepticism about how they would deal with full-time attending physicians. They wondered whether hospitalists would be easily approachable or not. How would they compare with medical residents?
Fortunately, during the next few months, this anxiety gave way to a new trust between the nurses and the hospitalists as the nurses realized that their concerns were answered promptly. Nursing staff also enjoyed a new benefit: the ability to communicate directly with the attending physicians and, in the process, the potential to play a greater role in the medical management of their patients.
Initially we hired eight hospitalists (actually we started with two because the others were in the process of getting credentialed). We handled the workload in the beginning by limiting the number of admissions each day for each hospitalist until everyone was on board. One hospitalist was already a Parkland doc; the rest were hired from outside.

Details
Like many new hospital medicine programs, Parkland’s hospitalists were venturing into a place where the nursing staff’s involvement in patient care was different from that of their private counterparts.
Background: Parkland Hospital is the main teaching site for the University of Texas Southwestern Medical School and Residency Training Program. The residents and medical students are involved to a great extent in patient care. They assume most patient care responsibilities, including placing PPDs (tuberculosis skin tests), caring for wounds, taking arterial blood gases (ABGs), and removing peripherally inserted central catheter (PICC) lines—to name just a few.
As a result of the residents’ involvement, our nursing staff took a back seat in these aspects of care. But once our hospitalists entered the picture they didn’t have the support of medical students or residents. Therefore, to increase the hospitalists’ efficiency in seeing more patients, the onus of doing those procedures fell on the shoulders of the nursing and paramedic staff. Educating the nursing and paramedical staff to help them regain autonomy and play a great role in patient care was a new challenge for the hospitalists.
We achieved this goal by holding a series of meetings in which physicians, including hospitalists and administrators, worked continuously on these concerns. Also, more operational issues were identified. Among them:
- Giving telephonic verbal orders to nurses for medications, laboratory studies, and radiology procedures, which was not the case with residents;
- Easing restrictions on the use of different medicines that usually require approval of attending faculty for the resident teams; and
- Setting up new dictation lines for our hospitalists (residents have to write their own patient histories and physical assessments).
We resolved to ensure that the program would run like any other private hospitalist program.
Modifications and Scheduling
Other services, including pharmacy, wound care, medical records, and pathology, were also approached by the hospitalists—including the medical director and chief of general internal medicine. The pharmacy was approached to ease restrictions on the medicine prescribed by hospitalists (as opposed to rules for residents, who have to work under different restrictions because they are training.)
Wound-care nurses were asked to implement their orders after telephone approval by the hospitalists (again, this is not the case with resident services). The Medical Records Department created a separate way to handle incomplete medical records for hospitalists—one that takes into account their week-on/week-off schedule. All these requests are now in different phases of approval and implementation.
Overall Parkland has responded well to these changes by appointing senior leadership to fast-track several of these recommendations. Many more policies are under review to complete the transformation from a resident-run model to one that is run by hospitalists.
Scheduling
Like any other new program, the hospitalist program at Parkland went through the growing pains of choosing the right kind of schedule to meet the expectations of the hospital as well as the professional expectations of its doctors. As mentioned above, we currently employ eight hospitalists. Four hospitalists work a week of 12- to 13-hour shifts; they are then off the following week. At that time the other four hospitalists take over for their counterparts. We cover nights using nocturnists.
When the program was not fully staffed there were fewer teams, depending on the number of hospitalists on shift. After the first two hospitalists were hired, we added one team to bring the total number of teams to four. Our teams worked the week-on/week-off schedule. During our initial start-up, the odd-numbered hospitalist who didn’t have a partner to work in week-on/week-off mode worked Monday through Friday each week with weekends covered by one of the main teams.
One of the most important considerations in a hospitalist’s job is the need for flexibility in working hours as compared with the schedule used in a traditional internal medicine practice. At Parkland, hospitalists see 10 to 12 patients in a week. During their week off from patient duties, they are free from all clinical duties and can handle administrative duties, conduct research projects, and accomplish any other tasks awaiting their attention.
Dual Launch Benefits Both Hospitals
At the same time the Parkland Hospital Medicine Program was launched, the Southwestern University also started a hospitalist program at St. Paul University Hospital, Dallas. The Department of Medicine of the University of Texas Southwestern oversees both the programs. All hospitalists are hired by Southwestern University and are part of the Department of General Internal medicine.
The common leadership of both of these programs in the Department of Medicine led to the implementation of a variety of policies derived from the best practices of the two groups. The interaction between these programs has been fruitful. The exchange of physicians credentialed at both hospitals has also reduced the staffing problems that tend to occur due to vacations, holidays, and illness.
Working toward the Future
As we settle down, fully staffed with eight hospitalists, we have started participating in the hospital’s administration by joining various committees. Our hospitalists participate on the pathology clinical advisory committee, the antibiotic committee, the medical reconciliation committee, and the utilization review committee.
Every day brings new challenges and continuous hard work. To make a successful program, it is not only important to grow out of the teething problems, but also to provide exceptional care so that the idea of a hospitalist program is well thought of by the hospital administration. Two of our teething issues included:
- General acceptance of our hospitalists as attending physicians by nursing, support staff, and the other physicians—not as trainees interacting with residents for patient care; and
- Recognition of the distinction between residents who traditionally work under several restrictions as a part of their training as compared with hospitalists who have already undergone training in their field.
Naturally, the hospital wants improvements in both short-term and long-term quality of care. The advantages the hospitalists provide include rendering consistent quality of care, developing new clinical pathways to provide efficient care, and ensuring greater continuity of care.
Regarding specific expectations, for example, SHM advocates 10 to 12 patient encounters per day as adequate. And so we expect our hospitalists to see that number of patients. Other expectations we have:
- That our hospitalists be involved in research projects on patient safety and quality of care; and
- That our hospitalists be involved in developing clinical pathways.
Conclusion
The future of the hospitalist program at Parkland Hospital is bright. As part of the university’s teaching faculty, our hospitalists will be progressively more involved in resident and medical student teaching. As a result, as time goes on, the schedule will have to change in order to provide both continuity of patient care and continuity in the teaching service. While our schedule now works well, we expect to get involved in a resident teaching service to a greater extent, as well as medical consult service and perioperative consult and care. These additional responsibilities may change our schedule.
The hospitalists are actively involved in developing an inpatient curriculum for the residents, along with a new set of standard orders suited to hospitalist practice. Other areas the hospitalists will become more involved in include pre- and perioperative consultations and co-management of surgical and orthopedic patients. We are also working on special hospital projects, focusing on patient safety and hospital efficiency.
The hospitalists at the University of Texas Southwestern put in nothing less than their best efforts. After all, “High achievement always takes place in a framework of high expectation” (Jack Kinder, motivational author). TH
Dr. Mohan is the medical director of the hospital medicine program at Parkland Hospital, Dallas.
When hospitalists stepped into Parkland Hospital (Dallas) a few months ago, they knew they were taking up a new challenge. Initially, they were known as the doctors without a team in a place where everyone was used to seeing no fewer than six to eight physicians rounding in a group.
Soon our hospitalists realized that a lot of teaching and awareness was needed among the nursing and support staff of the hospital to get them ready for this new breed of physicians.
A Case of Nerves
After four years of administrative planning and developing, the hospitalist program finally started in July 2006. Parkland started a hospitalist program due to the new restrictions on resident work hours and the number of patients a resident can admit. There used to be a considerable delay in the admission process causing patients to wait in our emergency department (ED) for hours until an admitting team could see them. This led to higher patient load in the ED. This load not only affected our patient care adversely, but it also caused considerable financial loss to the hospital because we couldn’t bill for admission until the patients were assigned a bed.
Our hospitalists help ease this overcrowding because they don’t work under these restrictions and can increase the ED throughput of the patients. Parkland also instituted a hospital medicine program to decrease length of stay.
Initially there was a lot of excitement, nervousness, and anxiety about the program. When I say nervousness and anxiety, it was primarily related to the nursing and administrative staff’s skepticism about how they would deal with full-time attending physicians. They wondered whether hospitalists would be easily approachable or not. How would they compare with medical residents?
Fortunately, during the next few months, this anxiety gave way to a new trust between the nurses and the hospitalists as the nurses realized that their concerns were answered promptly. Nursing staff also enjoyed a new benefit: the ability to communicate directly with the attending physicians and, in the process, the potential to play a greater role in the medical management of their patients.
Initially we hired eight hospitalists (actually we started with two because the others were in the process of getting credentialed). We handled the workload in the beginning by limiting the number of admissions each day for each hospitalist until everyone was on board. One hospitalist was already a Parkland doc; the rest were hired from outside.
Details
Like many new hospital medicine programs, Parkland’s hospitalists were venturing into a place where the nursing staff’s involvement in patient care was different from that of their private counterparts.
Background: Parkland Hospital is the main teaching site for the University of Texas Southwestern Medical School and Residency Training Program. The residents and medical students are involved to a great extent in patient care. They assume most patient care responsibilities, including placing PPDs (tuberculosis skin tests), caring for wounds, taking arterial blood gases (ABGs), and removing peripherally inserted central catheter (PICC) lines—to name just a few.
As a result of the residents’ involvement, our nursing staff took a back seat in these aspects of care. But once our hospitalists entered the picture they didn’t have the support of medical students or residents. Therefore, to increase the hospitalists’ efficiency in seeing more patients, the onus of doing those procedures fell on the shoulders of the nursing and paramedic staff. Educating the nursing and paramedical staff to help them regain autonomy and play a great role in patient care was a new challenge for the hospitalists.
We achieved this goal by holding a series of meetings in which physicians, including hospitalists and administrators, worked continuously on these concerns. Also, more operational issues were identified. Among them:
- Giving telephonic verbal orders to nurses for medications, laboratory studies, and radiology procedures, which was not the case with residents;
- Easing restrictions on the use of different medicines that usually require approval of attending faculty for the resident teams; and
- Setting up new dictation lines for our hospitalists (residents have to write their own patient histories and physical assessments).
We resolved to ensure that the program would run like any other private hospitalist program.
Modifications and Scheduling
Other services, including pharmacy, wound care, medical records, and pathology, were also approached by the hospitalists—including the medical director and chief of general internal medicine. The pharmacy was approached to ease restrictions on the medicine prescribed by hospitalists (as opposed to rules for residents, who have to work under different restrictions because they are training.)
Wound-care nurses were asked to implement their orders after telephone approval by the hospitalists (again, this is not the case with resident services). The Medical Records Department created a separate way to handle incomplete medical records for hospitalists—one that takes into account their week-on/week-off schedule. All these requests are now in different phases of approval and implementation.
Overall Parkland has responded well to these changes by appointing senior leadership to fast-track several of these recommendations. Many more policies are under review to complete the transformation from a resident-run model to one that is run by hospitalists.
Scheduling
Like any other new program, the hospitalist program at Parkland went through the growing pains of choosing the right kind of schedule to meet the expectations of the hospital as well as the professional expectations of its doctors. As mentioned above, we currently employ eight hospitalists. Four hospitalists work a week of 12- to 13-hour shifts; they are then off the following week. At that time the other four hospitalists take over for their counterparts. We cover nights using nocturnists.
When the program was not fully staffed there were fewer teams, depending on the number of hospitalists on shift. After the first two hospitalists were hired, we added one team to bring the total number of teams to four. Our teams worked the week-on/week-off schedule. During our initial start-up, the odd-numbered hospitalist who didn’t have a partner to work in week-on/week-off mode worked Monday through Friday each week with weekends covered by one of the main teams.
One of the most important considerations in a hospitalist’s job is the need for flexibility in working hours as compared with the schedule used in a traditional internal medicine practice. At Parkland, hospitalists see 10 to 12 patients in a week. During their week off from patient duties, they are free from all clinical duties and can handle administrative duties, conduct research projects, and accomplish any other tasks awaiting their attention.
Dual Launch Benefits Both Hospitals
At the same time the Parkland Hospital Medicine Program was launched, the Southwestern University also started a hospitalist program at St. Paul University Hospital, Dallas. The Department of Medicine of the University of Texas Southwestern oversees both the programs. All hospitalists are hired by Southwestern University and are part of the Department of General Internal medicine.
The common leadership of both of these programs in the Department of Medicine led to the implementation of a variety of policies derived from the best practices of the two groups. The interaction between these programs has been fruitful. The exchange of physicians credentialed at both hospitals has also reduced the staffing problems that tend to occur due to vacations, holidays, and illness.
Working toward the Future
As we settle down, fully staffed with eight hospitalists, we have started participating in the hospital’s administration by joining various committees. Our hospitalists participate on the pathology clinical advisory committee, the antibiotic committee, the medical reconciliation committee, and the utilization review committee.
Every day brings new challenges and continuous hard work. To make a successful program, it is not only important to grow out of the teething problems, but also to provide exceptional care so that the idea of a hospitalist program is well thought of by the hospital administration. Two of our teething issues included:
- General acceptance of our hospitalists as attending physicians by nursing, support staff, and the other physicians—not as trainees interacting with residents for patient care; and
- Recognition of the distinction between residents who traditionally work under several restrictions as a part of their training as compared with hospitalists who have already undergone training in their field.
Naturally, the hospital wants improvements in both short-term and long-term quality of care. The advantages the hospitalists provide include rendering consistent quality of care, developing new clinical pathways to provide efficient care, and ensuring greater continuity of care.
Regarding specific expectations, for example, SHM advocates 10 to 12 patient encounters per day as adequate. And so we expect our hospitalists to see that number of patients. Other expectations we have:
- That our hospitalists be involved in research projects on patient safety and quality of care; and
- That our hospitalists be involved in developing clinical pathways.
Conclusion
The future of the hospitalist program at Parkland Hospital is bright. As part of the university’s teaching faculty, our hospitalists will be progressively more involved in resident and medical student teaching. As a result, as time goes on, the schedule will have to change in order to provide both continuity of patient care and continuity in the teaching service. While our schedule now works well, we expect to get involved in a resident teaching service to a greater extent, as well as medical consult service and perioperative consult and care. These additional responsibilities may change our schedule.
The hospitalists are actively involved in developing an inpatient curriculum for the residents, along with a new set of standard orders suited to hospitalist practice. Other areas the hospitalists will become more involved in include pre- and perioperative consultations and co-management of surgical and orthopedic patients. We are also working on special hospital projects, focusing on patient safety and hospital efficiency.
The hospitalists at the University of Texas Southwestern put in nothing less than their best efforts. After all, “High achievement always takes place in a framework of high expectation” (Jack Kinder, motivational author). TH
Dr. Mohan is the medical director of the hospital medicine program at Parkland Hospital, Dallas.
When hospitalists stepped into Parkland Hospital (Dallas) a few months ago, they knew they were taking up a new challenge. Initially, they were known as the doctors without a team in a place where everyone was used to seeing no fewer than six to eight physicians rounding in a group.
Soon our hospitalists realized that a lot of teaching and awareness was needed among the nursing and support staff of the hospital to get them ready for this new breed of physicians.
A Case of Nerves
After four years of administrative planning and developing, the hospitalist program finally started in July 2006. Parkland started a hospitalist program due to the new restrictions on resident work hours and the number of patients a resident can admit. There used to be a considerable delay in the admission process causing patients to wait in our emergency department (ED) for hours until an admitting team could see them. This led to higher patient load in the ED. This load not only affected our patient care adversely, but it also caused considerable financial loss to the hospital because we couldn’t bill for admission until the patients were assigned a bed.
Our hospitalists help ease this overcrowding because they don’t work under these restrictions and can increase the ED throughput of the patients. Parkland also instituted a hospital medicine program to decrease length of stay.
Initially there was a lot of excitement, nervousness, and anxiety about the program. When I say nervousness and anxiety, it was primarily related to the nursing and administrative staff’s skepticism about how they would deal with full-time attending physicians. They wondered whether hospitalists would be easily approachable or not. How would they compare with medical residents?
Fortunately, during the next few months, this anxiety gave way to a new trust between the nurses and the hospitalists as the nurses realized that their concerns were answered promptly. Nursing staff also enjoyed a new benefit: the ability to communicate directly with the attending physicians and, in the process, the potential to play a greater role in the medical management of their patients.
Initially we hired eight hospitalists (actually we started with two because the others were in the process of getting credentialed). We handled the workload in the beginning by limiting the number of admissions each day for each hospitalist until everyone was on board. One hospitalist was already a Parkland doc; the rest were hired from outside.
Details
Like many new hospital medicine programs, Parkland’s hospitalists were venturing into a place where the nursing staff’s involvement in patient care was different from that of their private counterparts.
Background: Parkland Hospital is the main teaching site for the University of Texas Southwestern Medical School and Residency Training Program. The residents and medical students are involved to a great extent in patient care. They assume most patient care responsibilities, including placing PPDs (tuberculosis skin tests), caring for wounds, taking arterial blood gases (ABGs), and removing peripherally inserted central catheter (PICC) lines—to name just a few.
As a result of the residents’ involvement, our nursing staff took a back seat in these aspects of care. But once our hospitalists entered the picture they didn’t have the support of medical students or residents. Therefore, to increase the hospitalists’ efficiency in seeing more patients, the onus of doing those procedures fell on the shoulders of the nursing and paramedic staff. Educating the nursing and paramedical staff to help them regain autonomy and play a great role in patient care was a new challenge for the hospitalists.
We achieved this goal by holding a series of meetings in which physicians, including hospitalists and administrators, worked continuously on these concerns. Also, more operational issues were identified. Among them:
- Giving telephonic verbal orders to nurses for medications, laboratory studies, and radiology procedures, which was not the case with residents;
- Easing restrictions on the use of different medicines that usually require approval of attending faculty for the resident teams; and
- Setting up new dictation lines for our hospitalists (residents have to write their own patient histories and physical assessments).
We resolved to ensure that the program would run like any other private hospitalist program.
Modifications and Scheduling
Other services, including pharmacy, wound care, medical records, and pathology, were also approached by the hospitalists—including the medical director and chief of general internal medicine. The pharmacy was approached to ease restrictions on the medicine prescribed by hospitalists (as opposed to rules for residents, who have to work under different restrictions because they are training.)
Wound-care nurses were asked to implement their orders after telephone approval by the hospitalists (again, this is not the case with resident services). The Medical Records Department created a separate way to handle incomplete medical records for hospitalists—one that takes into account their week-on/week-off schedule. All these requests are now in different phases of approval and implementation.
Overall Parkland has responded well to these changes by appointing senior leadership to fast-track several of these recommendations. Many more policies are under review to complete the transformation from a resident-run model to one that is run by hospitalists.
Scheduling
Like any other new program, the hospitalist program at Parkland went through the growing pains of choosing the right kind of schedule to meet the expectations of the hospital as well as the professional expectations of its doctors. As mentioned above, we currently employ eight hospitalists. Four hospitalists work a week of 12- to 13-hour shifts; they are then off the following week. At that time the other four hospitalists take over for their counterparts. We cover nights using nocturnists.
When the program was not fully staffed there were fewer teams, depending on the number of hospitalists on shift. After the first two hospitalists were hired, we added one team to bring the total number of teams to four. Our teams worked the week-on/week-off schedule. During our initial start-up, the odd-numbered hospitalist who didn’t have a partner to work in week-on/week-off mode worked Monday through Friday each week with weekends covered by one of the main teams.
One of the most important considerations in a hospitalist’s job is the need for flexibility in working hours as compared with the schedule used in a traditional internal medicine practice. At Parkland, hospitalists see 10 to 12 patients in a week. During their week off from patient duties, they are free from all clinical duties and can handle administrative duties, conduct research projects, and accomplish any other tasks awaiting their attention.
Dual Launch Benefits Both Hospitals
At the same time the Parkland Hospital Medicine Program was launched, the Southwestern University also started a hospitalist program at St. Paul University Hospital, Dallas. The Department of Medicine of the University of Texas Southwestern oversees both the programs. All hospitalists are hired by Southwestern University and are part of the Department of General Internal medicine.
The common leadership of both of these programs in the Department of Medicine led to the implementation of a variety of policies derived from the best practices of the two groups. The interaction between these programs has been fruitful. The exchange of physicians credentialed at both hospitals has also reduced the staffing problems that tend to occur due to vacations, holidays, and illness.
Working toward the Future
As we settle down, fully staffed with eight hospitalists, we have started participating in the hospital’s administration by joining various committees. Our hospitalists participate on the pathology clinical advisory committee, the antibiotic committee, the medical reconciliation committee, and the utilization review committee.
Every day brings new challenges and continuous hard work. To make a successful program, it is not only important to grow out of the teething problems, but also to provide exceptional care so that the idea of a hospitalist program is well thought of by the hospital administration. Two of our teething issues included:
- General acceptance of our hospitalists as attending physicians by nursing, support staff, and the other physicians—not as trainees interacting with residents for patient care; and
- Recognition of the distinction between residents who traditionally work under several restrictions as a part of their training as compared with hospitalists who have already undergone training in their field.
Naturally, the hospital wants improvements in both short-term and long-term quality of care. The advantages the hospitalists provide include rendering consistent quality of care, developing new clinical pathways to provide efficient care, and ensuring greater continuity of care.
Regarding specific expectations, for example, SHM advocates 10 to 12 patient encounters per day as adequate. And so we expect our hospitalists to see that number of patients. Other expectations we have:
- That our hospitalists be involved in research projects on patient safety and quality of care; and
- That our hospitalists be involved in developing clinical pathways.
Conclusion
The future of the hospitalist program at Parkland Hospital is bright. As part of the university’s teaching faculty, our hospitalists will be progressively more involved in resident and medical student teaching. As a result, as time goes on, the schedule will have to change in order to provide both continuity of patient care and continuity in the teaching service. While our schedule now works well, we expect to get involved in a resident teaching service to a greater extent, as well as medical consult service and perioperative consult and care. These additional responsibilities may change our schedule.
The hospitalists are actively involved in developing an inpatient curriculum for the residents, along with a new set of standard orders suited to hospitalist practice. Other areas the hospitalists will become more involved in include pre- and perioperative consultations and co-management of surgical and orthopedic patients. We are also working on special hospital projects, focusing on patient safety and hospital efficiency.
The hospitalists at the University of Texas Southwestern put in nothing less than their best efforts. After all, “High achievement always takes place in a framework of high expectation” (Jack Kinder, motivational author). TH
Dr. Mohan is the medical director of the hospital medicine program at Parkland Hospital, Dallas.
Town & Gown
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Scapular Pain
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).

Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.


Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.

Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)




Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Vacuum-Assisted Closure Therapy
Vacuum-assisted closure (VAC) therapy has been used to manage wounds for 20 years and has taken wound treatment to a higher level. Clinical applications include chronic and acute wounds. Wound treatment has become easier with VAC. It improves the quality of life of the patient and reduces hospitalization time and expenses.
With the development of a portable vacuum device, treating patients with wounds is possible even in the home. We have been treating admitted and home care patients with VAC for five years in our Wound Centre. In this article, we discuss our experiences with VAC and review the procedure’s current applications and complications.
Background
Before the introduction of VAC therapy, the treatment and management of difficult wounds mainly belonged in the arena of plastic and reconstructive surgery.1 When Morykwas and colleagues developed VAC, however, they could have hoped only that it would take the treatment of acute and chronic wounds to a higher level.2 VAC is also known as TNP (topical negative pressure), as SPD (sub-atmospheric pressure), as VST (vacuum sealing technique), and as SSS (sealed surface wound suction).3 It is a technique that is easy to use in a clinical setting, and it has a low complication rate.4 The portable VAC system has made wound treatment possible in a home care setting, a development that improves quality of life and reduces hospitalization time.5,6 The portable VAC system (V.A.C. Freedom) is the size of a regular handbag. (See Figure 1, left.)
In this paper, we will discuss the working mechanisms of VAC, its current clinical applications, and the complications that might occur during VAC treatment.
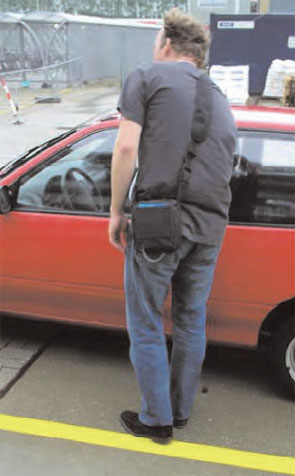
How Does It Work?
Normally, wounds heal by approximation of the wound edges—for example, by suturing or by the formation of a matrix of small blood vessels and connective tissue, when wound edges are not opposed, for the migration of keratinocytes across the surface and the re-epithelialization of the defect. This is a complex process; its main objectives can be considered minimization of blood loss, replacement of any defects with new tissue (granulation), and the restoration of an intact epithelial barrier. For this process to occur, healing debris must be removed, infection must be controlled, and inflammation must be cleared.4 Further disturbance of the rate of healing may occur due to inadequate vascular supply and incapacity of the wound to form new capillaries or matrix. Any disruption in the processes involved in wound healing, such as debridement, granulation, and epithelialization, can lead to the formation of a chronic wound. In our Wound Centre, VAC is mainly used in the granulation phase of a wound, as well as for securing split skin grafts.7
VAC uses medical-grade, open cell polyurethane ether foam.2,4 The pore size is generally 400-600 micrometers. This foam is cut to fit the wound bed before it is applied to the wound. If necessary, multiple pieces of foam can be used to connect separate wounds or to fill up any remaining gaps. Adhesive tape is then applied over an additional three to five cm border of intact skin to provide a seal.4 Then a track pad is placed over a small hole in the adhesive tape. A tube connects the track pad to an adjustable vacuum pump and a canister for collecting effluent fluids. The pump can be adjusted for both the timing (intermittent vs. continuous) and the magnitude of the vacuum effect.4 In general, an intermittent cycle (five minutes on, two minutes off) is used; this has been shown to be most beneficial.2 The VAC system is easy to apply, even on difficult wounds like the open abdomen. (See Figure 2, left.)

With the VAC technique, the open wound is converted into a controlled and temporarily closed environment. Animal studies have shown that VAC optimizes blood flow, decreases local edema, reduces bacteria levels, and removes excess fluids from the wound.2,8 (See Figure 3, above.) The cyclical application of sub-atmospheric pressure alters the cytoskeleton of the cells in the wound bed, triggering a cascade of intracellular signals that increases the rate of cell division and, thus, the formation of granulation tissue.9 This results in faster healing of the wounds than would have occurred with regular therapy; further, it significantly reduces hospitalization time and expenses.
Indications
VAC can be used on several types of wounds; however, before starting VAC therapy; adequate debridement for the formation of granulation tissue is essential.10 An overview of current clinical applications follows.
Chronic Wounds
The VAC system was originally designed to treat chronic wounds and to simplify the treatment of patients with chronic wounds both inside and outside the hospital.11 Around 10% of the general population will develop a chronic wound in the course of a lifetime; mortality resulting from these wounds amounts to 2.5%.12 VAC therapy has changed the clinical approach to and management of chronic wounds such as venous stasis ulcers, pressure ulcers, surgical dehisced wounds, arterial and diabetic ulcers, and a wide variety of other types of lingering wounds.12-15 Chronic wounds should be adequately debrided, either surgically or using another approach such as maggot debridement.16-18 This converts a chronic wound into a semi-acute wound. Such wounds respond better to VAC therapy than non-debrided wounds.11
Acute Wounds
VAC has become widely accepted in the treatment of large soft-tissue injuries with compromised tissue; it is also used for contaminated wounds, hematomas, and gunshot wounds. It has successfully been used in the treatment of extremities and orthopedic trauma and in treating degloving injuries and burns.19,21-25 (See Figure 4, p. 41.) When using VAC on traumatic injuries, nonviable tissue must be debrided, foreign bodies removed, and hemostasis obtained. Coverage of vital structures such as major vessels, viscera, and nerves by mobilization of local muscle or soft tissue is preferential. Wounds are then treated with VAC, and dressings are changed at appropriate intervals; if there is any suspicion of significant contamination, or if the patient develops signs of infection, adequate action, such as antibiotics or more dressing changes, must be taken.11
VAC therapy can also be used on a wide variety of surgical wounds and in treating surgical complications. It has successfully been used in sternal infections and mediastinitis, abdominal wall defects, enterocutaneous fistula, and perineal surgical wounds.11,26-35 The application of VAC in both chronic and acute wounds shows that it is a technique that facilitates wound management and wound healing for a wide variety of wound types.
Complications
When used within recommendations, complications resulting from VAC are infrequent.4 As the vacuum system device is more frequently adapted to multiple problems, however, the complication rate increases, probably due to co-morbidity and mortality.11 Localized superficial skin irritation is the most common complication reported in the literature.36 Further complications involve pain, infection, bleeding, and fluid depletion.4,12,35-37 Rare, severe complications, such as toxic shock syndrome, anaerobic sepsis, or thrombosis have been described as well.38-39(Also see M. Leijnen, MD, MSc, and colleagues, unpublished data, 2007.)
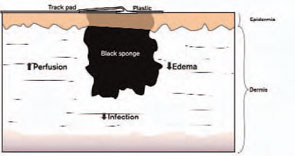
Conclusion
After 20 years of experience with vacuum-assisted closure, we can state that VAC therapy contributes positively to wound treatment. Wounds treated with this procedure are easier to manage, both in the hospital and at home. It can be used on a wide variety of chronic and acute wounds, and more applications are being developed. The procedure also reduces hospitalization time and expenses, and perhaps most important, it improves the patient’s quality of life. TH
M. Leijnen, MD, MSc, and S.A. da Costa, MD, PhD, practice in the Department of Surgery, Rijnland Hospital, Leiderdorp, The Netherlands. L. van Doorn, MA-NPA, practices in the Rijnland Wound Centre, Leiderdorp, The Netherlands. P. Steenvoorde, MD, MSc, and J. Oskam, MD, PhD practice in the Department of Surgery, Rijnland Hospital, Leiderdorp, The Netherlands, and in the Rijnland Wound Center, Leiderdorp, The Netherlands.

References
- Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997 Jun;38(6):563-576; discussion 577. Ann Plast Surg. 2000 Sep;45(3):332-334; discussion 335-336.
- Morykwas MJ, Argenta LC, Shelton-Brown EI, et al. Vacuum assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg. 1997 Jun;38(6):553-562. Comment in: Ann Plast Surg. 2000 Sep;45(3):332-334; discussion 335-336.
- Banwell PE, Teot L. Topical negative pressure (TNP): the evolution of a novel wound therapy. J Wound Care. 2003;12(1):22-28. Review.
- Lambert KV, Hayes P, McCarthy M. Vacuum assisted closure: a review of development and current applications. Eur J Vasc Endovasc Surg. 2005 Mar;29(3):219-226.
- Baradarian S, Stahovich M, Krause S, et al. Case series: clinical management of persistent mechanical assist device driveline drainage using vacuum-assisted closure therapy. ASAIO J. 2006;52:354-356.
- Sposato G, Molea G, Di Caprio G, et al. Ambulant vacuum-assisted closure of skin-graft dressing in the lower limbs using a portable mini-VAC device. Br J Plast Surg. 2001 Apr;54(3):235-237.
- Scherer LA, Shiver S, Chang M, et al. The vacuum assisted closure device: a method of securing skin grafts and improving graft survival. Arch Surg. 2002 Aug;137(8):930-933.
- Chen SZ, Li J, Li XY, et al. Effects of vacuum-assisted closure on wound microcirculation: an experimental study. Asian J Surg. 2005 Jul;28(3):211-217.
- Venturi ML, Attinger CE, Mesbahi AN, et al. Mechanisms and clinical applications of the vacuum-assisted closure (VAC) device: a review. Am J Clin Dermatol. 2005;6(3):185-194. Review.
- Philbeck TE Jr, Whittington KT, Millsap MH, et al. The clinical and cost effectiveness of externally applied negative pressure wound therapy in the treatment of wounds in home healthcare Medicare patients. Ostomy Wound Manage. 1999 Nov;45(11):41-50.
- Argenta LC, Morykwas MJ, Marks MW, et al. Vacuum-assisted closure: state of clinic art. Plast Reconstr Surg. 2006 Jun;117(7 Suppl):127S-142S.
- Karl T, Modic PK, Voss EU. Indications and results of VAC therapy treatments in vascular surgery - state of the art in the treatment of chronic wounds [in German]. Zentralbl Chir. 2004 May;129 Suppl 1:S74-S79.
- Ford CN, Reinhard ER, Yeh D, et al. Interim analysis of a prospective, randomized trial of vacuum-assisted closure versus the healthpoint system in the management of pressure ulcers. Ann Plast Surg. 2002 Jul;49(1):55-61.
- Joseph E, Hamori CA, Bergman S, et al. A prospective randomized trial of vacuum-assisted closure versus standard therapy of chronic non-healing wounds. Wounds. 2000;12:60-67.
- Rozeboom AL, Steenvoorde P, Hartgrink HH, et al. Necrotizing fasciitis of the leg following a simple pelvic fracture: case report and literature review. J Wound Care. 2006;15:117-120.
- Steenvoorde P, Calame JJ, Oskam J. Maggot-treated wounds follow normal wound healing phases. Int J Dermatol. 2006;45:1477-1479.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2(4):219-227.
- Attinger CE, Bulan EJ. Debridement. The key initial first step in wound healing. Foot Ankle Clin. 2001 Dec;6(4):627-660.
- Stannard JP, Robinson JT, Anderson ER, et al. Negative pressure wound therapy to treat hematomas and surgical incisions following high-energy trauma. J Trauma. 2006 Jun;60(6):1301-1306.
- Webb LX, Laver D, DeFranzo A. Negative pressure wound therapy in the management of orthopedic wounds. Ostomy Wound Manage. 2004 Apr;50(4A Suppl):26-27.
- Herscovici D Jr, Sanders RW, Scaduto JM, et al. Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J Orthop Trauma. 2003 Nov-Dec;17(10):683-688.
- Wong LK, Nesbit RD, Turner LA, et al. Management of a circumferential lower extremity degloving injury with the use of vacuum-assisted closure. South Med J. 2006;99:628-630.
- Josty IC, Ramaswamy R, Laing JH. Vacuum assisted closure: an alternative strategy in the management of degloving injuries of the foot. Br J Plast Surg. 2001 Jun;54(4):363-365.
- Adamkova M, Tymonova J, Zamecnikova I, et al. First experience with the use of vacuum assisted closure in the treatment of skin defects at the burn center. Acta Chir Plast. 2005;47(1):24-27.
- Kamolz LP, Andel H, Haslik W, et al. Use of subatmospheric pressure therapy to prevent burn wound progression in human: first experiences. Burns. 2004;30:253-258.
- Obdeijn MC, de Lange MY, Lichtendahl DH, et al. Vacuum-assisted closure in the treatment of poststernotomy mediastinitis. Ann Thorac Surg. 1999;68:2358-2360.
- Agarwal JP, Ogilvie M, Wu LC, et al. Vacuum-assisted closure for sternal wounds: a first-line therapeutic management approach. Plast Reconstr Surg. 2005;116:1035-1040.
- Scholl L, Chang E, Reitz B, et al. Sternal osteomyelitis: use of vacuum-assisted closure device as an adjunct to definitive closure with sternectomy and muscle flap reconstruction. J Card Surg. 2004 Sep-Oct;19(5):453-461.
- DeFranzo AJ, Argenta L. Vacuum-assisted closure for the treatment of abdominal wounds. Clin Plast Surg. 2006;33:213-224.
- Nienhuijs SW, Manupassa R, Strobbe LJ, et al. Can topical negative pressure be used to control complex enterocutaneous fistulae? J Wound Care. 2003;12:343-345.
- Alvarez AA, Maxwell GL, Rodriguez GC. Vacuum-assisted closure for cutaneous gastrointestinal fistula management. Gynecol Oncol. 2001;80:413-416.
- Erdmann D, Drye C, Heller L, et al. Abdominal wall defect and enterocutaneous fistula treatment with the Vacuum-Assisted Closure (V.A.C.) system. Plast Reconstr Surg. 2001;108:2066-2068.
- Schaffzin DM, Douglas JM, Stahl TJ, et al. Vacuum-assisted closure of complex perineal wounds. Dis Colon Rectum. 2004;47:1745-1748.
- Jethwa P, Lake SP. Using topical negative pressure therapy to resolve wound failure following perineal resection. J Wound Care. 2005;14:166-167.
- McGuinness JG, Winter DC, O’Connell PR. Vacuum-assisted closure of a complex pilonidal sinus. Dis Colon Rectum. 2003;46:274-276.
- Steenvoorde P, van Engeland A. Oskam J. Vacuum-assisted closure therapy and oral anticoagulation therapy. Plast Reconstr Surg. 2004;113:2220-2221.
- Negative pressure wound therapy: Morykwas approach [adverse events data]. Available at: www.npwt.com/morykwas.htm. Last accessed March 20, 2007.
- Carson SN, Overall K, Lee-Jahshan S, et al. Vacuum-assisted closure used for healing chronic wounds and skin grafts in the lower extremities. Ostomy Wound Manage. 2004;50:52-58.
- Gwan-Nulla D, Casal RS. Toxic shock syndrome associated with the use of the vacuum-assisted closure device. Ann Plast Surg. 2001;47:552-554.
Vacuum-assisted closure (VAC) therapy has been used to manage wounds for 20 years and has taken wound treatment to a higher level. Clinical applications include chronic and acute wounds. Wound treatment has become easier with VAC. It improves the quality of life of the patient and reduces hospitalization time and expenses.
With the development of a portable vacuum device, treating patients with wounds is possible even in the home. We have been treating admitted and home care patients with VAC for five years in our Wound Centre. In this article, we discuss our experiences with VAC and review the procedure’s current applications and complications.
Background
Before the introduction of VAC therapy, the treatment and management of difficult wounds mainly belonged in the arena of plastic and reconstructive surgery.1 When Morykwas and colleagues developed VAC, however, they could have hoped only that it would take the treatment of acute and chronic wounds to a higher level.2 VAC is also known as TNP (topical negative pressure), as SPD (sub-atmospheric pressure), as VST (vacuum sealing technique), and as SSS (sealed surface wound suction).3 It is a technique that is easy to use in a clinical setting, and it has a low complication rate.4 The portable VAC system has made wound treatment possible in a home care setting, a development that improves quality of life and reduces hospitalization time.5,6 The portable VAC system (V.A.C. Freedom) is the size of a regular handbag. (See Figure 1, left.)
In this paper, we will discuss the working mechanisms of VAC, its current clinical applications, and the complications that might occur during VAC treatment.
How Does It Work?
Normally, wounds heal by approximation of the wound edges—for example, by suturing or by the formation of a matrix of small blood vessels and connective tissue, when wound edges are not opposed, for the migration of keratinocytes across the surface and the re-epithelialization of the defect. This is a complex process; its main objectives can be considered minimization of blood loss, replacement of any defects with new tissue (granulation), and the restoration of an intact epithelial barrier. For this process to occur, healing debris must be removed, infection must be controlled, and inflammation must be cleared.4 Further disturbance of the rate of healing may occur due to inadequate vascular supply and incapacity of the wound to form new capillaries or matrix. Any disruption in the processes involved in wound healing, such as debridement, granulation, and epithelialization, can lead to the formation of a chronic wound. In our Wound Centre, VAC is mainly used in the granulation phase of a wound, as well as for securing split skin grafts.7
VAC uses medical-grade, open cell polyurethane ether foam.2,4 The pore size is generally 400-600 micrometers. This foam is cut to fit the wound bed before it is applied to the wound. If necessary, multiple pieces of foam can be used to connect separate wounds or to fill up any remaining gaps. Adhesive tape is then applied over an additional three to five cm border of intact skin to provide a seal.4 Then a track pad is placed over a small hole in the adhesive tape. A tube connects the track pad to an adjustable vacuum pump and a canister for collecting effluent fluids. The pump can be adjusted for both the timing (intermittent vs. continuous) and the magnitude of the vacuum effect.4 In general, an intermittent cycle (five minutes on, two minutes off) is used; this has been shown to be most beneficial.2 The VAC system is easy to apply, even on difficult wounds like the open abdomen. (See Figure 2, left.)
With the VAC technique, the open wound is converted into a controlled and temporarily closed environment. Animal studies have shown that VAC optimizes blood flow, decreases local edema, reduces bacteria levels, and removes excess fluids from the wound.2,8 (See Figure 3, above.) The cyclical application of sub-atmospheric pressure alters the cytoskeleton of the cells in the wound bed, triggering a cascade of intracellular signals that increases the rate of cell division and, thus, the formation of granulation tissue.9 This results in faster healing of the wounds than would have occurred with regular therapy; further, it significantly reduces hospitalization time and expenses.
Indications
VAC can be used on several types of wounds; however, before starting VAC therapy; adequate debridement for the formation of granulation tissue is essential.10 An overview of current clinical applications follows.
Chronic Wounds
The VAC system was originally designed to treat chronic wounds and to simplify the treatment of patients with chronic wounds both inside and outside the hospital.11 Around 10% of the general population will develop a chronic wound in the course of a lifetime; mortality resulting from these wounds amounts to 2.5%.12 VAC therapy has changed the clinical approach to and management of chronic wounds such as venous stasis ulcers, pressure ulcers, surgical dehisced wounds, arterial and diabetic ulcers, and a wide variety of other types of lingering wounds.12-15 Chronic wounds should be adequately debrided, either surgically or using another approach such as maggot debridement.16-18 This converts a chronic wound into a semi-acute wound. Such wounds respond better to VAC therapy than non-debrided wounds.11
Acute Wounds
VAC has become widely accepted in the treatment of large soft-tissue injuries with compromised tissue; it is also used for contaminated wounds, hematomas, and gunshot wounds. It has successfully been used in the treatment of extremities and orthopedic trauma and in treating degloving injuries and burns.19,21-25 (See Figure 4, p. 41.) When using VAC on traumatic injuries, nonviable tissue must be debrided, foreign bodies removed, and hemostasis obtained. Coverage of vital structures such as major vessels, viscera, and nerves by mobilization of local muscle or soft tissue is preferential. Wounds are then treated with VAC, and dressings are changed at appropriate intervals; if there is any suspicion of significant contamination, or if the patient develops signs of infection, adequate action, such as antibiotics or more dressing changes, must be taken.11
VAC therapy can also be used on a wide variety of surgical wounds and in treating surgical complications. It has successfully been used in sternal infections and mediastinitis, abdominal wall defects, enterocutaneous fistula, and perineal surgical wounds.11,26-35 The application of VAC in both chronic and acute wounds shows that it is a technique that facilitates wound management and wound healing for a wide variety of wound types.
Complications
When used within recommendations, complications resulting from VAC are infrequent.4 As the vacuum system device is more frequently adapted to multiple problems, however, the complication rate increases, probably due to co-morbidity and mortality.11 Localized superficial skin irritation is the most common complication reported in the literature.36 Further complications involve pain, infection, bleeding, and fluid depletion.4,12,35-37 Rare, severe complications, such as toxic shock syndrome, anaerobic sepsis, or thrombosis have been described as well.38-39(Also see M. Leijnen, MD, MSc, and colleagues, unpublished data, 2007.)
Conclusion
After 20 years of experience with vacuum-assisted closure, we can state that VAC therapy contributes positively to wound treatment. Wounds treated with this procedure are easier to manage, both in the hospital and at home. It can be used on a wide variety of chronic and acute wounds, and more applications are being developed. The procedure also reduces hospitalization time and expenses, and perhaps most important, it improves the patient’s quality of life. TH
M. Leijnen, MD, MSc, and S.A. da Costa, MD, PhD, practice in the Department of Surgery, Rijnland Hospital, Leiderdorp, The Netherlands. L. van Doorn, MA-NPA, practices in the Rijnland Wound Centre, Leiderdorp, The Netherlands. P. Steenvoorde, MD, MSc, and J. Oskam, MD, PhD practice in the Department of Surgery, Rijnland Hospital, Leiderdorp, The Netherlands, and in the Rijnland Wound Center, Leiderdorp, The Netherlands.
References
- Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997 Jun;38(6):563-576; discussion 577. Ann Plast Surg. 2000 Sep;45(3):332-334; discussion 335-336.
- Morykwas MJ, Argenta LC, Shelton-Brown EI, et al. Vacuum assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg. 1997 Jun;38(6):553-562. Comment in: Ann Plast Surg. 2000 Sep;45(3):332-334; discussion 335-336.
- Banwell PE, Teot L. Topical negative pressure (TNP): the evolution of a novel wound therapy. J Wound Care. 2003;12(1):22-28. Review.
- Lambert KV, Hayes P, McCarthy M. Vacuum assisted closure: a review of development and current applications. Eur J Vasc Endovasc Surg. 2005 Mar;29(3):219-226.
- Baradarian S, Stahovich M, Krause S, et al. Case series: clinical management of persistent mechanical assist device driveline drainage using vacuum-assisted closure therapy. ASAIO J. 2006;52:354-356.
- Sposato G, Molea G, Di Caprio G, et al. Ambulant vacuum-assisted closure of skin-graft dressing in the lower limbs using a portable mini-VAC device. Br J Plast Surg. 2001 Apr;54(3):235-237.
- Scherer LA, Shiver S, Chang M, et al. The vacuum assisted closure device: a method of securing skin grafts and improving graft survival. Arch Surg. 2002 Aug;137(8):930-933.
- Chen SZ, Li J, Li XY, et al. Effects of vacuum-assisted closure on wound microcirculation: an experimental study. Asian J Surg. 2005 Jul;28(3):211-217.
- Venturi ML, Attinger CE, Mesbahi AN, et al. Mechanisms and clinical applications of the vacuum-assisted closure (VAC) device: a review. Am J Clin Dermatol. 2005;6(3):185-194. Review.
- Philbeck TE Jr, Whittington KT, Millsap MH, et al. The clinical and cost effectiveness of externally applied negative pressure wound therapy in the treatment of wounds in home healthcare Medicare patients. Ostomy Wound Manage. 1999 Nov;45(11):41-50.
- Argenta LC, Morykwas MJ, Marks MW, et al. Vacuum-assisted closure: state of clinic art. Plast Reconstr Surg. 2006 Jun;117(7 Suppl):127S-142S.
- Karl T, Modic PK, Voss EU. Indications and results of VAC therapy treatments in vascular surgery - state of the art in the treatment of chronic wounds [in German]. Zentralbl Chir. 2004 May;129 Suppl 1:S74-S79.
- Ford CN, Reinhard ER, Yeh D, et al. Interim analysis of a prospective, randomized trial of vacuum-assisted closure versus the healthpoint system in the management of pressure ulcers. Ann Plast Surg. 2002 Jul;49(1):55-61.
- Joseph E, Hamori CA, Bergman S, et al. A prospective randomized trial of vacuum-assisted closure versus standard therapy of chronic non-healing wounds. Wounds. 2000;12:60-67.
- Rozeboom AL, Steenvoorde P, Hartgrink HH, et al. Necrotizing fasciitis of the leg following a simple pelvic fracture: case report and literature review. J Wound Care. 2006;15:117-120.
- Steenvoorde P, Calame JJ, Oskam J. Maggot-treated wounds follow normal wound healing phases. Int J Dermatol. 2006;45:1477-1479.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2(4):219-227.
- Attinger CE, Bulan EJ. Debridement. The key initial first step in wound healing. Foot Ankle Clin. 2001 Dec;6(4):627-660.
- Stannard JP, Robinson JT, Anderson ER, et al. Negative pressure wound therapy to treat hematomas and surgical incisions following high-energy trauma. J Trauma. 2006 Jun;60(6):1301-1306.
- Webb LX, Laver D, DeFranzo A. Negative pressure wound therapy in the management of orthopedic wounds. Ostomy Wound Manage. 2004 Apr;50(4A Suppl):26-27.
- Herscovici D Jr, Sanders RW, Scaduto JM, et al. Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J Orthop Trauma. 2003 Nov-Dec;17(10):683-688.
- Wong LK, Nesbit RD, Turner LA, et al. Management of a circumferential lower extremity degloving injury with the use of vacuum-assisted closure. South Med J. 2006;99:628-630.
- Josty IC, Ramaswamy R, Laing JH. Vacuum assisted closure: an alternative strategy in the management of degloving injuries of the foot. Br J Plast Surg. 2001 Jun;54(4):363-365.
- Adamkova M, Tymonova J, Zamecnikova I, et al. First experience with the use of vacuum assisted closure in the treatment of skin defects at the burn center. Acta Chir Plast. 2005;47(1):24-27.
- Kamolz LP, Andel H, Haslik W, et al. Use of subatmospheric pressure therapy to prevent burn wound progression in human: first experiences. Burns. 2004;30:253-258.
- Obdeijn MC, de Lange MY, Lichtendahl DH, et al. Vacuum-assisted closure in the treatment of poststernotomy mediastinitis. Ann Thorac Surg. 1999;68:2358-2360.
- Agarwal JP, Ogilvie M, Wu LC, et al. Vacuum-assisted closure for sternal wounds: a first-line therapeutic management approach. Plast Reconstr Surg. 2005;116:1035-1040.
- Scholl L, Chang E, Reitz B, et al. Sternal osteomyelitis: use of vacuum-assisted closure device as an adjunct to definitive closure with sternectomy and muscle flap reconstruction. J Card Surg. 2004 Sep-Oct;19(5):453-461.
- DeFranzo AJ, Argenta L. Vacuum-assisted closure for the treatment of abdominal wounds. Clin Plast Surg. 2006;33:213-224.
- Nienhuijs SW, Manupassa R, Strobbe LJ, et al. Can topical negative pressure be used to control complex enterocutaneous fistulae? J Wound Care. 2003;12:343-345.
- Alvarez AA, Maxwell GL, Rodriguez GC. Vacuum-assisted closure for cutaneous gastrointestinal fistula management. Gynecol Oncol. 2001;80:413-416.
- Erdmann D, Drye C, Heller L, et al. Abdominal wall defect and enterocutaneous fistula treatment with the Vacuum-Assisted Closure (V.A.C.) system. Plast Reconstr Surg. 2001;108:2066-2068.
- Schaffzin DM, Douglas JM, Stahl TJ, et al. Vacuum-assisted closure of complex perineal wounds. Dis Colon Rectum. 2004;47:1745-1748.
- Jethwa P, Lake SP. Using topical negative pressure therapy to resolve wound failure following perineal resection. J Wound Care. 2005;14:166-167.
- McGuinness JG, Winter DC, O’Connell PR. Vacuum-assisted closure of a complex pilonidal sinus. Dis Colon Rectum. 2003;46:274-276.
- Steenvoorde P, van Engeland A. Oskam J. Vacuum-assisted closure therapy and oral anticoagulation therapy. Plast Reconstr Surg. 2004;113:2220-2221.
- Negative pressure wound therapy: Morykwas approach [adverse events data]. Available at: www.npwt.com/morykwas.htm. Last accessed March 20, 2007.
- Carson SN, Overall K, Lee-Jahshan S, et al. Vacuum-assisted closure used for healing chronic wounds and skin grafts in the lower extremities. Ostomy Wound Manage. 2004;50:52-58.
- Gwan-Nulla D, Casal RS. Toxic shock syndrome associated with the use of the vacuum-assisted closure device. Ann Plast Surg. 2001;47:552-554.
Vacuum-assisted closure (VAC) therapy has been used to manage wounds for 20 years and has taken wound treatment to a higher level. Clinical applications include chronic and acute wounds. Wound treatment has become easier with VAC. It improves the quality of life of the patient and reduces hospitalization time and expenses.
With the development of a portable vacuum device, treating patients with wounds is possible even in the home. We have been treating admitted and home care patients with VAC for five years in our Wound Centre. In this article, we discuss our experiences with VAC and review the procedure’s current applications and complications.
Background
Before the introduction of VAC therapy, the treatment and management of difficult wounds mainly belonged in the arena of plastic and reconstructive surgery.1 When Morykwas and colleagues developed VAC, however, they could have hoped only that it would take the treatment of acute and chronic wounds to a higher level.2 VAC is also known as TNP (topical negative pressure), as SPD (sub-atmospheric pressure), as VST (vacuum sealing technique), and as SSS (sealed surface wound suction).3 It is a technique that is easy to use in a clinical setting, and it has a low complication rate.4 The portable VAC system has made wound treatment possible in a home care setting, a development that improves quality of life and reduces hospitalization time.5,6 The portable VAC system (V.A.C. Freedom) is the size of a regular handbag. (See Figure 1, left.)
In this paper, we will discuss the working mechanisms of VAC, its current clinical applications, and the complications that might occur during VAC treatment.
How Does It Work?
Normally, wounds heal by approximation of the wound edges—for example, by suturing or by the formation of a matrix of small blood vessels and connective tissue, when wound edges are not opposed, for the migration of keratinocytes across the surface and the re-epithelialization of the defect. This is a complex process; its main objectives can be considered minimization of blood loss, replacement of any defects with new tissue (granulation), and the restoration of an intact epithelial barrier. For this process to occur, healing debris must be removed, infection must be controlled, and inflammation must be cleared.4 Further disturbance of the rate of healing may occur due to inadequate vascular supply and incapacity of the wound to form new capillaries or matrix. Any disruption in the processes involved in wound healing, such as debridement, granulation, and epithelialization, can lead to the formation of a chronic wound. In our Wound Centre, VAC is mainly used in the granulation phase of a wound, as well as for securing split skin grafts.7
VAC uses medical-grade, open cell polyurethane ether foam.2,4 The pore size is generally 400-600 micrometers. This foam is cut to fit the wound bed before it is applied to the wound. If necessary, multiple pieces of foam can be used to connect separate wounds or to fill up any remaining gaps. Adhesive tape is then applied over an additional three to five cm border of intact skin to provide a seal.4 Then a track pad is placed over a small hole in the adhesive tape. A tube connects the track pad to an adjustable vacuum pump and a canister for collecting effluent fluids. The pump can be adjusted for both the timing (intermittent vs. continuous) and the magnitude of the vacuum effect.4 In general, an intermittent cycle (five minutes on, two minutes off) is used; this has been shown to be most beneficial.2 The VAC system is easy to apply, even on difficult wounds like the open abdomen. (See Figure 2, left.)
With the VAC technique, the open wound is converted into a controlled and temporarily closed environment. Animal studies have shown that VAC optimizes blood flow, decreases local edema, reduces bacteria levels, and removes excess fluids from the wound.2,8 (See Figure 3, above.) The cyclical application of sub-atmospheric pressure alters the cytoskeleton of the cells in the wound bed, triggering a cascade of intracellular signals that increases the rate of cell division and, thus, the formation of granulation tissue.9 This results in faster healing of the wounds than would have occurred with regular therapy; further, it significantly reduces hospitalization time and expenses.
Indications
VAC can be used on several types of wounds; however, before starting VAC therapy; adequate debridement for the formation of granulation tissue is essential.10 An overview of current clinical applications follows.
Chronic Wounds
The VAC system was originally designed to treat chronic wounds and to simplify the treatment of patients with chronic wounds both inside and outside the hospital.11 Around 10% of the general population will develop a chronic wound in the course of a lifetime; mortality resulting from these wounds amounts to 2.5%.12 VAC therapy has changed the clinical approach to and management of chronic wounds such as venous stasis ulcers, pressure ulcers, surgical dehisced wounds, arterial and diabetic ulcers, and a wide variety of other types of lingering wounds.12-15 Chronic wounds should be adequately debrided, either surgically or using another approach such as maggot debridement.16-18 This converts a chronic wound into a semi-acute wound. Such wounds respond better to VAC therapy than non-debrided wounds.11
Acute Wounds
VAC has become widely accepted in the treatment of large soft-tissue injuries with compromised tissue; it is also used for contaminated wounds, hematomas, and gunshot wounds. It has successfully been used in the treatment of extremities and orthopedic trauma and in treating degloving injuries and burns.19,21-25 (See Figure 4, p. 41.) When using VAC on traumatic injuries, nonviable tissue must be debrided, foreign bodies removed, and hemostasis obtained. Coverage of vital structures such as major vessels, viscera, and nerves by mobilization of local muscle or soft tissue is preferential. Wounds are then treated with VAC, and dressings are changed at appropriate intervals; if there is any suspicion of significant contamination, or if the patient develops signs of infection, adequate action, such as antibiotics or more dressing changes, must be taken.11
VAC therapy can also be used on a wide variety of surgical wounds and in treating surgical complications. It has successfully been used in sternal infections and mediastinitis, abdominal wall defects, enterocutaneous fistula, and perineal surgical wounds.11,26-35 The application of VAC in both chronic and acute wounds shows that it is a technique that facilitates wound management and wound healing for a wide variety of wound types.
Complications
When used within recommendations, complications resulting from VAC are infrequent.4 As the vacuum system device is more frequently adapted to multiple problems, however, the complication rate increases, probably due to co-morbidity and mortality.11 Localized superficial skin irritation is the most common complication reported in the literature.36 Further complications involve pain, infection, bleeding, and fluid depletion.4,12,35-37 Rare, severe complications, such as toxic shock syndrome, anaerobic sepsis, or thrombosis have been described as well.38-39(Also see M. Leijnen, MD, MSc, and colleagues, unpublished data, 2007.)
Conclusion
After 20 years of experience with vacuum-assisted closure, we can state that VAC therapy contributes positively to wound treatment. Wounds treated with this procedure are easier to manage, both in the hospital and at home. It can be used on a wide variety of chronic and acute wounds, and more applications are being developed. The procedure also reduces hospitalization time and expenses, and perhaps most important, it improves the patient’s quality of life. TH
M. Leijnen, MD, MSc, and S.A. da Costa, MD, PhD, practice in the Department of Surgery, Rijnland Hospital, Leiderdorp, The Netherlands. L. van Doorn, MA-NPA, practices in the Rijnland Wound Centre, Leiderdorp, The Netherlands. P. Steenvoorde, MD, MSc, and J. Oskam, MD, PhD practice in the Department of Surgery, Rijnland Hospital, Leiderdorp, The Netherlands, and in the Rijnland Wound Center, Leiderdorp, The Netherlands.
References
- Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997 Jun;38(6):563-576; discussion 577. Ann Plast Surg. 2000 Sep;45(3):332-334; discussion 335-336.
- Morykwas MJ, Argenta LC, Shelton-Brown EI, et al. Vacuum assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg. 1997 Jun;38(6):553-562. Comment in: Ann Plast Surg. 2000 Sep;45(3):332-334; discussion 335-336.
- Banwell PE, Teot L. Topical negative pressure (TNP): the evolution of a novel wound therapy. J Wound Care. 2003;12(1):22-28. Review.
- Lambert KV, Hayes P, McCarthy M. Vacuum assisted closure: a review of development and current applications. Eur J Vasc Endovasc Surg. 2005 Mar;29(3):219-226.
- Baradarian S, Stahovich M, Krause S, et al. Case series: clinical management of persistent mechanical assist device driveline drainage using vacuum-assisted closure therapy. ASAIO J. 2006;52:354-356.
- Sposato G, Molea G, Di Caprio G, et al. Ambulant vacuum-assisted closure of skin-graft dressing in the lower limbs using a portable mini-VAC device. Br J Plast Surg. 2001 Apr;54(3):235-237.
- Scherer LA, Shiver S, Chang M, et al. The vacuum assisted closure device: a method of securing skin grafts and improving graft survival. Arch Surg. 2002 Aug;137(8):930-933.
- Chen SZ, Li J, Li XY, et al. Effects of vacuum-assisted closure on wound microcirculation: an experimental study. Asian J Surg. 2005 Jul;28(3):211-217.
- Venturi ML, Attinger CE, Mesbahi AN, et al. Mechanisms and clinical applications of the vacuum-assisted closure (VAC) device: a review. Am J Clin Dermatol. 2005;6(3):185-194. Review.
- Philbeck TE Jr, Whittington KT, Millsap MH, et al. The clinical and cost effectiveness of externally applied negative pressure wound therapy in the treatment of wounds in home healthcare Medicare patients. Ostomy Wound Manage. 1999 Nov;45(11):41-50.
- Argenta LC, Morykwas MJ, Marks MW, et al. Vacuum-assisted closure: state of clinic art. Plast Reconstr Surg. 2006 Jun;117(7 Suppl):127S-142S.
- Karl T, Modic PK, Voss EU. Indications and results of VAC therapy treatments in vascular surgery - state of the art in the treatment of chronic wounds [in German]. Zentralbl Chir. 2004 May;129 Suppl 1:S74-S79.
- Ford CN, Reinhard ER, Yeh D, et al. Interim analysis of a prospective, randomized trial of vacuum-assisted closure versus the healthpoint system in the management of pressure ulcers. Ann Plast Surg. 2002 Jul;49(1):55-61.
- Joseph E, Hamori CA, Bergman S, et al. A prospective randomized trial of vacuum-assisted closure versus standard therapy of chronic non-healing wounds. Wounds. 2000;12:60-67.
- Rozeboom AL, Steenvoorde P, Hartgrink HH, et al. Necrotizing fasciitis of the leg following a simple pelvic fracture: case report and literature review. J Wound Care. 2006;15:117-120.
- Steenvoorde P, Calame JJ, Oskam J. Maggot-treated wounds follow normal wound healing phases. Int J Dermatol. 2006;45:1477-1479.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2(4):219-227.
- Attinger CE, Bulan EJ. Debridement. The key initial first step in wound healing. Foot Ankle Clin. 2001 Dec;6(4):627-660.
- Stannard JP, Robinson JT, Anderson ER, et al. Negative pressure wound therapy to treat hematomas and surgical incisions following high-energy trauma. J Trauma. 2006 Jun;60(6):1301-1306.
- Webb LX, Laver D, DeFranzo A. Negative pressure wound therapy in the management of orthopedic wounds. Ostomy Wound Manage. 2004 Apr;50(4A Suppl):26-27.
- Herscovici D Jr, Sanders RW, Scaduto JM, et al. Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J Orthop Trauma. 2003 Nov-Dec;17(10):683-688.
- Wong LK, Nesbit RD, Turner LA, et al. Management of a circumferential lower extremity degloving injury with the use of vacuum-assisted closure. South Med J. 2006;99:628-630.
- Josty IC, Ramaswamy R, Laing JH. Vacuum assisted closure: an alternative strategy in the management of degloving injuries of the foot. Br J Plast Surg. 2001 Jun;54(4):363-365.
- Adamkova M, Tymonova J, Zamecnikova I, et al. First experience with the use of vacuum assisted closure in the treatment of skin defects at the burn center. Acta Chir Plast. 2005;47(1):24-27.
- Kamolz LP, Andel H, Haslik W, et al. Use of subatmospheric pressure therapy to prevent burn wound progression in human: first experiences. Burns. 2004;30:253-258.
- Obdeijn MC, de Lange MY, Lichtendahl DH, et al. Vacuum-assisted closure in the treatment of poststernotomy mediastinitis. Ann Thorac Surg. 1999;68:2358-2360.
- Agarwal JP, Ogilvie M, Wu LC, et al. Vacuum-assisted closure for sternal wounds: a first-line therapeutic management approach. Plast Reconstr Surg. 2005;116:1035-1040.
- Scholl L, Chang E, Reitz B, et al. Sternal osteomyelitis: use of vacuum-assisted closure device as an adjunct to definitive closure with sternectomy and muscle flap reconstruction. J Card Surg. 2004 Sep-Oct;19(5):453-461.
- DeFranzo AJ, Argenta L. Vacuum-assisted closure for the treatment of abdominal wounds. Clin Plast Surg. 2006;33:213-224.
- Nienhuijs SW, Manupassa R, Strobbe LJ, et al. Can topical negative pressure be used to control complex enterocutaneous fistulae? J Wound Care. 2003;12:343-345.
- Alvarez AA, Maxwell GL, Rodriguez GC. Vacuum-assisted closure for cutaneous gastrointestinal fistula management. Gynecol Oncol. 2001;80:413-416.
- Erdmann D, Drye C, Heller L, et al. Abdominal wall defect and enterocutaneous fistula treatment with the Vacuum-Assisted Closure (V.A.C.) system. Plast Reconstr Surg. 2001;108:2066-2068.
- Schaffzin DM, Douglas JM, Stahl TJ, et al. Vacuum-assisted closure of complex perineal wounds. Dis Colon Rectum. 2004;47:1745-1748.
- Jethwa P, Lake SP. Using topical negative pressure therapy to resolve wound failure following perineal resection. J Wound Care. 2005;14:166-167.
- McGuinness JG, Winter DC, O’Connell PR. Vacuum-assisted closure of a complex pilonidal sinus. Dis Colon Rectum. 2003;46:274-276.
- Steenvoorde P, van Engeland A. Oskam J. Vacuum-assisted closure therapy and oral anticoagulation therapy. Plast Reconstr Surg. 2004;113:2220-2221.
- Negative pressure wound therapy: Morykwas approach [adverse events data]. Available at: www.npwt.com/morykwas.htm. Last accessed March 20, 2007.
- Carson SN, Overall K, Lee-Jahshan S, et al. Vacuum-assisted closure used for healing chronic wounds and skin grafts in the lower extremities. Ostomy Wound Manage. 2004;50:52-58.
- Gwan-Nulla D, Casal RS. Toxic shock syndrome associated with the use of the vacuum-assisted closure device. Ann Plast Surg. 2001;47:552-554.
New Moves
The transition from hospital to home or to another care site is a high-risk period for the patient for a number of reasons, as we have discussed in The Hospitalist this year. Ineffective communication with the patient and between healthcare practitioners at discharge is common. In addition, primary care providers increasingly delegate inpatient care to hospitalists. This delegation of care can lead to gaps in knowledge that present risks to patient safety.
Further, information transfer among healthcare practitioners—whether they be primary care providers or hospitalists—and their patients is often compromised by record inaccuracies, omissions, illegibility, information never delivered, and delays in generation or transmission.
The Agency for Healthcare Research and Quality (AHRQ) has identified recall error, increased clinician workloads, interface failures between physicians and clerical staff, and inadequate training of physicians to respect the discharge process as the root causes of deficiencies in the current process of information transfer at discharge. While an interoperable health information technology infrastructure for the nation could effectively address many issues related to discharge planning, such a solution is certainly many years away.
New Approaches
Given the fact that a nationwide, interoperable health information technology infrastructure is not yet a reality, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) is exploring multiple approaches for improving communication with patients and among practitioners in the discharge planning process. This article details those strategies and is meant to stimulate discussion and elicit suggestions for future approaches.
If you have any suggestions for improving the discharge planning process, e-mail us at [email protected]. We’ll publish the most effective and intriguing responses in a future issue of The Hospitalist.
Discharge Planning Standards
Patients may be discharged from the hospital entirely or transferred to another level of care, treatment, and services; they may be reassigned to different professionals or settings for continued services. JCAHO standards require that the hospital’s processes for transfer or discharge be based on the patient’s assessed needs. To facilitate discharge or transfer, the hospital should assess the patient’s needs, plan for discharge or transfer, facilitate the discharge or transfer process, and help to ensure that continuity of care, treatment, and services is maintained.
These standards (found in the Provision of Care (PC), Ethics, Rights and Responsibilities (RI), and Management of Information (IM) chapters of the hospital accreditation manual) will be updated in July 2007. The changes include both new language and new requirements meant to improve communication with patients and among providers during the discharge planning process. Rather than a significant overhaul, these changes can be viewed as refinements to the existing standards that will help hospitals ensure that the intent of each standard is actually carried out to benefit patients. For example, an element of performance for standard PC.4.10 that addresses development of a plan of care now specifies that this process should be individualized to the patient’s needs. Another example is standard IM.6.20, for which an element of performance will require that the medical record contain medications dispensed or prescribed at discharge.
It is also important to note that JCAHO standards underscore the importance of the patient retaining information. Today, JCAHO requires—through its National Patient Safety Goals—that a list of current medications be provided to the patient at discharge. For patients who have been treated by a hospitalist, this requirement is especially important when they return to their primary care physicians for follow-up treatment.
Discharge Planning During the On-Site Survey
JCAHO began more closely examining discharge planning in 2005 by piloting a new process that surveyors used to evaluate standards compliance in 2006. The first option tested is a concurrent review in which surveyors observe the discharge instructions as they are being taught to the patient and then interview the patient about the content. The second option is a retrospective review and entails calling patients 24 to 48 hours after discharge to ascertain their understanding of the medication regimen and other instructions provided. Both options are used by JCAHO surveyors to understand how practitioners, nurses, and other caregivers carry out the hospital’s policies.
To help hospitalists understand how surveyors approach this process, the following summary provides information about the two review options.
Discharge Planning—Active Review
- Ask for a list of patients who will be discharged during the survey.
- Review the patient’s medical/clinical record for discharge orders.
- Request that the organization obtain patient permission to observe the discharge process.
- Observe the clinician providing discharge instructions. Components of the discharge instruction may include:
- Activity;
- Diet;
- Medications (post-discharge);
- Plans for physician follow-up;
- Wound care, if applicable;
- Signs and symptoms to be aware of (i.e., elevated temperature, medication side effects);
- The name and telephone number of a physician to call should a problem or question arise following discharge; and
- Patient repetition of information to confirm understanding.
- Review the written discharge instructions given to the patient. The discharge instructions are written in a language the patient can read and understand.
- Interview the patient to determine the patient’s level of understanding of discharge instructions. If applicable to the instructions given to the patient being observed, the patient should understand:
- The purpose for taking any new medication;
- How to take the medication, including dose and frequency;
- Possible side effects of medication;
- The medication regimen, including continuation or discontinuation of medications taken prior to hospital admission;
- Contraindications between prescribed medications and over-the-counter medications and herbal remedies;
- Changes in diet and dietary restric- tions or supplements;
- Signs and symptoms of potential problems and who to call with questions and concerns;
- Information regarding continued self-care (i.e., wound care, activity);
- Follow-up process with physician(s); and
- Arrangements made for home-health needs (i.e., oxygen therapy, physical therapy).
- Interview the nurse/clinician to ascertain the origination of discharge information (physician-nurse communication regarding discharge instruction).
Discharge Planning—Retrospective Review
- Ask for a list of patients discharged during the past 48 hours.
- Review the patient’s old medical record for discharge orders.
- Request that the organization stay with the surveyor as phone calls are made. The organization should first talk with the patient to explain the purpose of the call and obtain permission for a phone interview.
- Interview the patient to determine understanding of discharge instructions provided. If applicable to the instructions given to the patient being observed, the patient should understand:
- The purpose for taking any new medication;
- How to take the medication, including dose and frequency;
- The medication regimen, including continuation or discontinuation of medications taken prior to hospital admission;
- Possible side effects of medication;
- Contraindications between prescribed medications and over-the-counter medications and herbal remedies;
- Changes in diet and dietary restrictions or supplements;
- Signs and symptoms of potential problems and whom to call with questions and concerns;
- Information regarding continued self-care (i.e., wound care, activity);
- Follow-up process with physician(s); and
- Arrangements made for home health needs (i.e., oxygen therapy, physical therapy).
- Explore the patient’s perception of the discharge instructions. Does the patient believe the necessary information was given?
Continuity of Care Record
Recognizing that patients remain the primary vehicle for transporting basic health information between providers, JCAHO is exploring strategies related to the Continuity of Care Record (CCR). This approach acknowledges that electronic health records are—at this time—a goal rather than the norm. Patients typically transport basic health information between providers in the context of completing a basic set of information on a registration form that is attached to a medical clipboard, prior to outpatient appointments and admissions.
An accurate minimum data set, containing such items as medication lists, allergies, conditions, and procedures, would provide substantial value to providers and patients. JCAHO already requires that an accurate medication list be updated at discharge and made available to the patient and the subsequent provider of care, but other key pieces of patient data, such as diagnosis and procedures, as well as the means required to make these data available to the patient or to the next caregiver, are not currently required.
JCAHO is now considering how hospitals and other healthcare organizations could provide or update a clinically relevant minimum data set of summarized health information, such as that contained in the CCR. The CCR is a standard specification being developed jointly by ASTM International, the Massachusetts Medical Society, the Healthcare Information Management Systems Society (HIMSS), the American Academy of Family Physicians, and the American Academy of Pediatrics.
JCAHO envisions a minimum data set that includes an accurate list of demographics, medical insurance, medications, diagnosis, past procedures, allergies, and current healthcare providers. It also desires a data set that can be provided to the patient or the patient’s authorized representatives—both as paper and in a fully transportable and interoperable digital format—that could be presented to subsequent caregivers. This summary health record would permit care providers within or outside the organization to review the patient’s important clinical information at the point of care and near the time of clinical decision-making. Subsequent care providers would then be able to update the patient’s minimum data set as appropriate.
In addition to providing caregivers with the most essential and relevant information necessary to ensure safe, quality care, such an approach would minimize the effort necessary to keep such information current. Healthcare providers would have easy access to the most recent patient assessment and the recommendations of the caregiver who last treated the patient.
Patient Involvement
JCAHO has sought to help healthcare organizations in assisting patients with the discharge planning process through its Speak Up education program, which urges people to take an active role in their own healthcare. “Planning Your Recovery” provides tips to help people get more involved in their care and obtain the information they need for the best possible recovery. Patients who understand and follow directions about their follow-up care have a greater chance of getting better faster; they are also less likely to go back to the hospital.
Specifically, the JCAHO education campaign advises patients to:
1. Find out about their condition. This includes knowing how soon they should feel better, getting information about their ability to do everyday activities such as walking or preparing meals, knowing warning signs and symptoms to watch for, enlisting the help of a family member of friend in the discharge process from the hospital, and getting the phone number of a person to call at the hospital if a problem arises.
2. Find out about new medicines. It is important to request written directions about new medicines and ask any questions before leaving the hospital. Other issues that JCAHO advises patients to consider include finding out whether other medicines, vitamins, and herbs could interfere with the new drugs and knowing whether there are any specific foods or drinks to avoid. Understanding the side effects of medications and any necessary restrictions on daily activities because of the potential for dizziness or sleepiness is also crucial.
3. Find out about follow-up care. This includes asking for written directions about cleaning and bandaging wounds, using special equipment, or doing any required exercises; finding out about follow-up visits to the hospital and making transportation arrangements for those visits; reviewing insurance to find out whether the cost of medicines and equipment needed for recovery will be covered; and determining whether home care services or a nursing home or assisted living center will be necessary for follow-up care.
JCAHO is joined in encouraging people to play an active role in planning their recovery by the National Alliance for Caregiving and the Centers for Medicare and Medicaid Services’ Care Planner. Practitioners who want to share this advice with their patients or wish to direct their patients to the information can go to JCAHO’s Web site, www.jointcommission.org, to download a free Speak Up brochure.
Conclusion
Ideally, discharge planning should be a smooth process facilitated by a personal health record that is controlled by the patient and that provides ready access to all of the patient’s health data that have been compiled from all the patient’s healthcare providers. Such a record would be accessible anywhere and at any time, over a lifetime. This concept remains in its infancy, however. Until such time as communication with patients and among providers is more transparent and less prone to error, The Joint Commission will continue to seek methods to better address this important aspect of providing safe, effective care. TH
Dr. Jacott, special advisor for professional relations at JCAHO, is the organization’s liaison to SHM. He also reaches out to state and specialty physician societies, hospital medical staffs, and other professional organizations.
The transition from hospital to home or to another care site is a high-risk period for the patient for a number of reasons, as we have discussed in The Hospitalist this year. Ineffective communication with the patient and between healthcare practitioners at discharge is common. In addition, primary care providers increasingly delegate inpatient care to hospitalists. This delegation of care can lead to gaps in knowledge that present risks to patient safety.
Further, information transfer among healthcare practitioners—whether they be primary care providers or hospitalists—and their patients is often compromised by record inaccuracies, omissions, illegibility, information never delivered, and delays in generation or transmission.
The Agency for Healthcare Research and Quality (AHRQ) has identified recall error, increased clinician workloads, interface failures between physicians and clerical staff, and inadequate training of physicians to respect the discharge process as the root causes of deficiencies in the current process of information transfer at discharge. While an interoperable health information technology infrastructure for the nation could effectively address many issues related to discharge planning, such a solution is certainly many years away.
New Approaches
Given the fact that a nationwide, interoperable health information technology infrastructure is not yet a reality, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) is exploring multiple approaches for improving communication with patients and among practitioners in the discharge planning process. This article details those strategies and is meant to stimulate discussion and elicit suggestions for future approaches.
If you have any suggestions for improving the discharge planning process, e-mail us at [email protected]. We’ll publish the most effective and intriguing responses in a future issue of The Hospitalist.
Discharge Planning Standards
Patients may be discharged from the hospital entirely or transferred to another level of care, treatment, and services; they may be reassigned to different professionals or settings for continued services. JCAHO standards require that the hospital’s processes for transfer or discharge be based on the patient’s assessed needs. To facilitate discharge or transfer, the hospital should assess the patient’s needs, plan for discharge or transfer, facilitate the discharge or transfer process, and help to ensure that continuity of care, treatment, and services is maintained.
These standards (found in the Provision of Care (PC), Ethics, Rights and Responsibilities (RI), and Management of Information (IM) chapters of the hospital accreditation manual) will be updated in July 2007. The changes include both new language and new requirements meant to improve communication with patients and among providers during the discharge planning process. Rather than a significant overhaul, these changes can be viewed as refinements to the existing standards that will help hospitals ensure that the intent of each standard is actually carried out to benefit patients. For example, an element of performance for standard PC.4.10 that addresses development of a plan of care now specifies that this process should be individualized to the patient’s needs. Another example is standard IM.6.20, for which an element of performance will require that the medical record contain medications dispensed or prescribed at discharge.
It is also important to note that JCAHO standards underscore the importance of the patient retaining information. Today, JCAHO requires—through its National Patient Safety Goals—that a list of current medications be provided to the patient at discharge. For patients who have been treated by a hospitalist, this requirement is especially important when they return to their primary care physicians for follow-up treatment.
Discharge Planning During the On-Site Survey
JCAHO began more closely examining discharge planning in 2005 by piloting a new process that surveyors used to evaluate standards compliance in 2006. The first option tested is a concurrent review in which surveyors observe the discharge instructions as they are being taught to the patient and then interview the patient about the content. The second option is a retrospective review and entails calling patients 24 to 48 hours after discharge to ascertain their understanding of the medication regimen and other instructions provided. Both options are used by JCAHO surveyors to understand how practitioners, nurses, and other caregivers carry out the hospital’s policies.
To help hospitalists understand how surveyors approach this process, the following summary provides information about the two review options.
Discharge Planning—Active Review
- Ask for a list of patients who will be discharged during the survey.
- Review the patient’s medical/clinical record for discharge orders.
- Request that the organization obtain patient permission to observe the discharge process.
- Observe the clinician providing discharge instructions. Components of the discharge instruction may include:
- Activity;
- Diet;
- Medications (post-discharge);
- Plans for physician follow-up;
- Wound care, if applicable;
- Signs and symptoms to be aware of (i.e., elevated temperature, medication side effects);
- The name and telephone number of a physician to call should a problem or question arise following discharge; and
- Patient repetition of information to confirm understanding.
- Review the written discharge instructions given to the patient. The discharge instructions are written in a language the patient can read and understand.
- Interview the patient to determine the patient’s level of understanding of discharge instructions. If applicable to the instructions given to the patient being observed, the patient should understand:
- The purpose for taking any new medication;
- How to take the medication, including dose and frequency;
- Possible side effects of medication;
- The medication regimen, including continuation or discontinuation of medications taken prior to hospital admission;
- Contraindications between prescribed medications and over-the-counter medications and herbal remedies;
- Changes in diet and dietary restric- tions or supplements;
- Signs and symptoms of potential problems and who to call with questions and concerns;
- Information regarding continued self-care (i.e., wound care, activity);
- Follow-up process with physician(s); and
- Arrangements made for home-health needs (i.e., oxygen therapy, physical therapy).
- Interview the nurse/clinician to ascertain the origination of discharge information (physician-nurse communication regarding discharge instruction).
Discharge Planning—Retrospective Review
- Ask for a list of patients discharged during the past 48 hours.
- Review the patient’s old medical record for discharge orders.
- Request that the organization stay with the surveyor as phone calls are made. The organization should first talk with the patient to explain the purpose of the call and obtain permission for a phone interview.
- Interview the patient to determine understanding of discharge instructions provided. If applicable to the instructions given to the patient being observed, the patient should understand:
- The purpose for taking any new medication;
- How to take the medication, including dose and frequency;
- The medication regimen, including continuation or discontinuation of medications taken prior to hospital admission;
- Possible side effects of medication;
- Contraindications between prescribed medications and over-the-counter medications and herbal remedies;
- Changes in diet and dietary restrictions or supplements;
- Signs and symptoms of potential problems and whom to call with questions and concerns;
- Information regarding continued self-care (i.e., wound care, activity);
- Follow-up process with physician(s); and
- Arrangements made for home health needs (i.e., oxygen therapy, physical therapy).
- Explore the patient’s perception of the discharge instructions. Does the patient believe the necessary information was given?
Continuity of Care Record
Recognizing that patients remain the primary vehicle for transporting basic health information between providers, JCAHO is exploring strategies related to the Continuity of Care Record (CCR). This approach acknowledges that electronic health records are—at this time—a goal rather than the norm. Patients typically transport basic health information between providers in the context of completing a basic set of information on a registration form that is attached to a medical clipboard, prior to outpatient appointments and admissions.
An accurate minimum data set, containing such items as medication lists, allergies, conditions, and procedures, would provide substantial value to providers and patients. JCAHO already requires that an accurate medication list be updated at discharge and made available to the patient and the subsequent provider of care, but other key pieces of patient data, such as diagnosis and procedures, as well as the means required to make these data available to the patient or to the next caregiver, are not currently required.
JCAHO is now considering how hospitals and other healthcare organizations could provide or update a clinically relevant minimum data set of summarized health information, such as that contained in the CCR. The CCR is a standard specification being developed jointly by ASTM International, the Massachusetts Medical Society, the Healthcare Information Management Systems Society (HIMSS), the American Academy of Family Physicians, and the American Academy of Pediatrics.
JCAHO envisions a minimum data set that includes an accurate list of demographics, medical insurance, medications, diagnosis, past procedures, allergies, and current healthcare providers. It also desires a data set that can be provided to the patient or the patient’s authorized representatives—both as paper and in a fully transportable and interoperable digital format—that could be presented to subsequent caregivers. This summary health record would permit care providers within or outside the organization to review the patient’s important clinical information at the point of care and near the time of clinical decision-making. Subsequent care providers would then be able to update the patient’s minimum data set as appropriate.
In addition to providing caregivers with the most essential and relevant information necessary to ensure safe, quality care, such an approach would minimize the effort necessary to keep such information current. Healthcare providers would have easy access to the most recent patient assessment and the recommendations of the caregiver who last treated the patient.
Patient Involvement
JCAHO has sought to help healthcare organizations in assisting patients with the discharge planning process through its Speak Up education program, which urges people to take an active role in their own healthcare. “Planning Your Recovery” provides tips to help people get more involved in their care and obtain the information they need for the best possible recovery. Patients who understand and follow directions about their follow-up care have a greater chance of getting better faster; they are also less likely to go back to the hospital.
Specifically, the JCAHO education campaign advises patients to:
1. Find out about their condition. This includes knowing how soon they should feel better, getting information about their ability to do everyday activities such as walking or preparing meals, knowing warning signs and symptoms to watch for, enlisting the help of a family member of friend in the discharge process from the hospital, and getting the phone number of a person to call at the hospital if a problem arises.
2. Find out about new medicines. It is important to request written directions about new medicines and ask any questions before leaving the hospital. Other issues that JCAHO advises patients to consider include finding out whether other medicines, vitamins, and herbs could interfere with the new drugs and knowing whether there are any specific foods or drinks to avoid. Understanding the side effects of medications and any necessary restrictions on daily activities because of the potential for dizziness or sleepiness is also crucial.
3. Find out about follow-up care. This includes asking for written directions about cleaning and bandaging wounds, using special equipment, or doing any required exercises; finding out about follow-up visits to the hospital and making transportation arrangements for those visits; reviewing insurance to find out whether the cost of medicines and equipment needed for recovery will be covered; and determining whether home care services or a nursing home or assisted living center will be necessary for follow-up care.
JCAHO is joined in encouraging people to play an active role in planning their recovery by the National Alliance for Caregiving and the Centers for Medicare and Medicaid Services’ Care Planner. Practitioners who want to share this advice with their patients or wish to direct their patients to the information can go to JCAHO’s Web site, www.jointcommission.org, to download a free Speak Up brochure.
Conclusion
Ideally, discharge planning should be a smooth process facilitated by a personal health record that is controlled by the patient and that provides ready access to all of the patient’s health data that have been compiled from all the patient’s healthcare providers. Such a record would be accessible anywhere and at any time, over a lifetime. This concept remains in its infancy, however. Until such time as communication with patients and among providers is more transparent and less prone to error, The Joint Commission will continue to seek methods to better address this important aspect of providing safe, effective care. TH
Dr. Jacott, special advisor for professional relations at JCAHO, is the organization’s liaison to SHM. He also reaches out to state and specialty physician societies, hospital medical staffs, and other professional organizations.
The transition from hospital to home or to another care site is a high-risk period for the patient for a number of reasons, as we have discussed in The Hospitalist this year. Ineffective communication with the patient and between healthcare practitioners at discharge is common. In addition, primary care providers increasingly delegate inpatient care to hospitalists. This delegation of care can lead to gaps in knowledge that present risks to patient safety.
Further, information transfer among healthcare practitioners—whether they be primary care providers or hospitalists—and their patients is often compromised by record inaccuracies, omissions, illegibility, information never delivered, and delays in generation or transmission.
The Agency for Healthcare Research and Quality (AHRQ) has identified recall error, increased clinician workloads, interface failures between physicians and clerical staff, and inadequate training of physicians to respect the discharge process as the root causes of deficiencies in the current process of information transfer at discharge. While an interoperable health information technology infrastructure for the nation could effectively address many issues related to discharge planning, such a solution is certainly many years away.
New Approaches
Given the fact that a nationwide, interoperable health information technology infrastructure is not yet a reality, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) is exploring multiple approaches for improving communication with patients and among practitioners in the discharge planning process. This article details those strategies and is meant to stimulate discussion and elicit suggestions for future approaches.
If you have any suggestions for improving the discharge planning process, e-mail us at [email protected]. We’ll publish the most effective and intriguing responses in a future issue of The Hospitalist.
Discharge Planning Standards
Patients may be discharged from the hospital entirely or transferred to another level of care, treatment, and services; they may be reassigned to different professionals or settings for continued services. JCAHO standards require that the hospital’s processes for transfer or discharge be based on the patient’s assessed needs. To facilitate discharge or transfer, the hospital should assess the patient’s needs, plan for discharge or transfer, facilitate the discharge or transfer process, and help to ensure that continuity of care, treatment, and services is maintained.
These standards (found in the Provision of Care (PC), Ethics, Rights and Responsibilities (RI), and Management of Information (IM) chapters of the hospital accreditation manual) will be updated in July 2007. The changes include both new language and new requirements meant to improve communication with patients and among providers during the discharge planning process. Rather than a significant overhaul, these changes can be viewed as refinements to the existing standards that will help hospitals ensure that the intent of each standard is actually carried out to benefit patients. For example, an element of performance for standard PC.4.10 that addresses development of a plan of care now specifies that this process should be individualized to the patient’s needs. Another example is standard IM.6.20, for which an element of performance will require that the medical record contain medications dispensed or prescribed at discharge.
It is also important to note that JCAHO standards underscore the importance of the patient retaining information. Today, JCAHO requires—through its National Patient Safety Goals—that a list of current medications be provided to the patient at discharge. For patients who have been treated by a hospitalist, this requirement is especially important when they return to their primary care physicians for follow-up treatment.
Discharge Planning During the On-Site Survey
JCAHO began more closely examining discharge planning in 2005 by piloting a new process that surveyors used to evaluate standards compliance in 2006. The first option tested is a concurrent review in which surveyors observe the discharge instructions as they are being taught to the patient and then interview the patient about the content. The second option is a retrospective review and entails calling patients 24 to 48 hours after discharge to ascertain their understanding of the medication regimen and other instructions provided. Both options are used by JCAHO surveyors to understand how practitioners, nurses, and other caregivers carry out the hospital’s policies.
To help hospitalists understand how surveyors approach this process, the following summary provides information about the two review options.
Discharge Planning—Active Review
- Ask for a list of patients who will be discharged during the survey.
- Review the patient’s medical/clinical record for discharge orders.
- Request that the organization obtain patient permission to observe the discharge process.
- Observe the clinician providing discharge instructions. Components of the discharge instruction may include:
- Activity;
- Diet;
- Medications (post-discharge);
- Plans for physician follow-up;
- Wound care, if applicable;
- Signs and symptoms to be aware of (i.e., elevated temperature, medication side effects);
- The name and telephone number of a physician to call should a problem or question arise following discharge; and
- Patient repetition of information to confirm understanding.
- Review the written discharge instructions given to the patient. The discharge instructions are written in a language the patient can read and understand.
- Interview the patient to determine the patient’s level of understanding of discharge instructions. If applicable to the instructions given to the patient being observed, the patient should understand:
- The purpose for taking any new medication;
- How to take the medication, including dose and frequency;
- Possible side effects of medication;
- The medication regimen, including continuation or discontinuation of medications taken prior to hospital admission;
- Contraindications between prescribed medications and over-the-counter medications and herbal remedies;
- Changes in diet and dietary restric- tions or supplements;
- Signs and symptoms of potential problems and who to call with questions and concerns;
- Information regarding continued self-care (i.e., wound care, activity);
- Follow-up process with physician(s); and
- Arrangements made for home-health needs (i.e., oxygen therapy, physical therapy).
- Interview the nurse/clinician to ascertain the origination of discharge information (physician-nurse communication regarding discharge instruction).
Discharge Planning—Retrospective Review
- Ask for a list of patients discharged during the past 48 hours.
- Review the patient’s old medical record for discharge orders.
- Request that the organization stay with the surveyor as phone calls are made. The organization should first talk with the patient to explain the purpose of the call and obtain permission for a phone interview.
- Interview the patient to determine understanding of discharge instructions provided. If applicable to the instructions given to the patient being observed, the patient should understand:
- The purpose for taking any new medication;
- How to take the medication, including dose and frequency;
- The medication regimen, including continuation or discontinuation of medications taken prior to hospital admission;
- Possible side effects of medication;
- Contraindications between prescribed medications and over-the-counter medications and herbal remedies;
- Changes in diet and dietary restrictions or supplements;
- Signs and symptoms of potential problems and whom to call with questions and concerns;
- Information regarding continued self-care (i.e., wound care, activity);
- Follow-up process with physician(s); and
- Arrangements made for home health needs (i.e., oxygen therapy, physical therapy).
- Explore the patient’s perception of the discharge instructions. Does the patient believe the necessary information was given?
Continuity of Care Record
Recognizing that patients remain the primary vehicle for transporting basic health information between providers, JCAHO is exploring strategies related to the Continuity of Care Record (CCR). This approach acknowledges that electronic health records are—at this time—a goal rather than the norm. Patients typically transport basic health information between providers in the context of completing a basic set of information on a registration form that is attached to a medical clipboard, prior to outpatient appointments and admissions.
An accurate minimum data set, containing such items as medication lists, allergies, conditions, and procedures, would provide substantial value to providers and patients. JCAHO already requires that an accurate medication list be updated at discharge and made available to the patient and the subsequent provider of care, but other key pieces of patient data, such as diagnosis and procedures, as well as the means required to make these data available to the patient or to the next caregiver, are not currently required.
JCAHO is now considering how hospitals and other healthcare organizations could provide or update a clinically relevant minimum data set of summarized health information, such as that contained in the CCR. The CCR is a standard specification being developed jointly by ASTM International, the Massachusetts Medical Society, the Healthcare Information Management Systems Society (HIMSS), the American Academy of Family Physicians, and the American Academy of Pediatrics.
JCAHO envisions a minimum data set that includes an accurate list of demographics, medical insurance, medications, diagnosis, past procedures, allergies, and current healthcare providers. It also desires a data set that can be provided to the patient or the patient’s authorized representatives—both as paper and in a fully transportable and interoperable digital format—that could be presented to subsequent caregivers. This summary health record would permit care providers within or outside the organization to review the patient’s important clinical information at the point of care and near the time of clinical decision-making. Subsequent care providers would then be able to update the patient’s minimum data set as appropriate.
In addition to providing caregivers with the most essential and relevant information necessary to ensure safe, quality care, such an approach would minimize the effort necessary to keep such information current. Healthcare providers would have easy access to the most recent patient assessment and the recommendations of the caregiver who last treated the patient.
Patient Involvement
JCAHO has sought to help healthcare organizations in assisting patients with the discharge planning process through its Speak Up education program, which urges people to take an active role in their own healthcare. “Planning Your Recovery” provides tips to help people get more involved in their care and obtain the information they need for the best possible recovery. Patients who understand and follow directions about their follow-up care have a greater chance of getting better faster; they are also less likely to go back to the hospital.
Specifically, the JCAHO education campaign advises patients to:
1. Find out about their condition. This includes knowing how soon they should feel better, getting information about their ability to do everyday activities such as walking or preparing meals, knowing warning signs and symptoms to watch for, enlisting the help of a family member of friend in the discharge process from the hospital, and getting the phone number of a person to call at the hospital if a problem arises.
2. Find out about new medicines. It is important to request written directions about new medicines and ask any questions before leaving the hospital. Other issues that JCAHO advises patients to consider include finding out whether other medicines, vitamins, and herbs could interfere with the new drugs and knowing whether there are any specific foods or drinks to avoid. Understanding the side effects of medications and any necessary restrictions on daily activities because of the potential for dizziness or sleepiness is also crucial.
3. Find out about follow-up care. This includes asking for written directions about cleaning and bandaging wounds, using special equipment, or doing any required exercises; finding out about follow-up visits to the hospital and making transportation arrangements for those visits; reviewing insurance to find out whether the cost of medicines and equipment needed for recovery will be covered; and determining whether home care services or a nursing home or assisted living center will be necessary for follow-up care.
JCAHO is joined in encouraging people to play an active role in planning their recovery by the National Alliance for Caregiving and the Centers for Medicare and Medicaid Services’ Care Planner. Practitioners who want to share this advice with their patients or wish to direct their patients to the information can go to JCAHO’s Web site, www.jointcommission.org, to download a free Speak Up brochure.
Conclusion
Ideally, discharge planning should be a smooth process facilitated by a personal health record that is controlled by the patient and that provides ready access to all of the patient’s health data that have been compiled from all the patient’s healthcare providers. Such a record would be accessible anywhere and at any time, over a lifetime. This concept remains in its infancy, however. Until such time as communication with patients and among providers is more transparent and less prone to error, The Joint Commission will continue to seek methods to better address this important aspect of providing safe, effective care. TH
Dr. Jacott, special advisor for professional relations at JCAHO, is the organization’s liaison to SHM. He also reaches out to state and specialty physician societies, hospital medical staffs, and other professional organizations.
How to Navigate Hospital Medicine
Each career path within hospital medicine offers distinct responsibilities, opportunities, and rewards. One of the biggest decisions you’ll make as a hospitalist is whether to enter an academic or a community-based hospital medicine field—but there are additional factors to take into account. Here’s an overview of the career paths within these two areas that may help you with your decision.
Choices in Academic Hospital Medicine
Only a small percentage of hospitalists go into academic jobs, and residents are—obviously—most familiar with these choices.
“[The environment] is familiar to you, and you’re able to grow professionally because … people are always asking you questions,” says Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine at the Ann Arbor Veterans Affairs Medical Center and the University of Michigan Medical School. “The opportunity to be around learners—residents and medical students—is very exciting to residents.”
There are other reasons you may prefer academic over community-based hospital medicine. “The types of patients you treat are different,” says Dr. Saint. “They may be more complicated, and thus you can improve your clinical skills. Also, there’s prestige in being associated with an academic medical center. That appeals to some people.”
The rigorousness of the schedule varies with the institution. “Theoretically, you have residents, so you don’t have to take calls,” explains Dr. Saint. “But when you’re on, say, for a month there’s often no attending coverage on weekends or holidays.”
Hospital medicine work in an academic setting falls into four categories:
1) Hospitalist clinician-investigator: “These hospitalists typically spend the minority of their time doing clinical work—maybe 20% to 40% of their time,” says Dr. Saint. “The rest is spent developing their research agenda, applying for and obtaining grants to fund their research. The investigative focus is usually inpatient-oriented to provide synergy between their clinical work and their research.” This track typically leads to tenure, and usually requires some type of fellowship.
2) Hospitalist-educator: “There are a large number of these positions in academic medical centers,” says Dr. Saint. “These hospitalists spend about 80% of their time seeing patients and teaching residents and medical students.”
Typical hospitalist-educator activities include ward attending, medical consultation, and preoperative evaluations. “They spend about 20% of their time doing some type of scholarly activity, whether writing articles or developing educational curricula that can be disseminated,” estimates Dr. Saint.
Hospitalist-educator is usually a non-tenured position and these academicians are promoted primarily based on their clinical expertise and perceived skills as teachers. You don’t need to have a fellowship for this position; usually, the hospitalist director will hire individuals from his or her program—often a former chief resident.
3) Hospitalist-clinician: “These hospitalists primarily focus on patient care,” explains Dr. Saint. “A lot of them have been hired recently because of the limits on work hours for residents. There is minimal teaching and scholarly activity.”
Often, people do this for one or two years between residency and a fellowship, or to pay off school loans.
4) Hospitalist-administrator: “A major portion of their day is spent on administrative tasks,” says Dr. Saint. “They may run the hospital medicine program, or have educational administrative tasks, like residency directors.” However, he warns, “a resident isn’t going to go straight into one of these positions; you have to pay your dues first. But this can be an opportunity to think about for the future.”
What is the job market like for these academic positions? “There are huge opportunities for residents wanting to become hospitalists, regardless of which track they want to follow,” says Dr. Saint. “There are only a handful of clinician-investigators in hospital medicine now, and I see tremendous growth in this field. There’s also a growing need for hospitalist-clinicians because of the restrictions imposed on the workweek [for residents]. And as the number of hospitalists grows, there will obviously be a need for more hospitalist-administrators. Of course, there will always be a need for hospitalist-educators—but many are already in those roles.”
Choices in Community-Based Hospital Medicine
The first thing to realize about community-based hospital medicine is that there are various employers involved.
“Programs will have different mandates; a lot depends on the financial drivers,” says Sanjiv Panwala, MD, hospitalist at Providence Medical Center, Portland, Ore. “If you’re paid by the hospital, your priorities will be theirs: coverage of uncovered patients, shorter length of stay, etc. It trickles down.”
Michael-Anthony Williams, MD, regional CMO of Sound Inpatient Physicians in Denver, agrees. “It’s important to understand who the employer is and what their values are,” he says. “Is it the hospital or a local, regional, or national practice? If you’re employed by a hospital, you may be one of several employed specialists.” That can impact what types of clinical work you handle.
Regardless of whom you work for, says Dr. Williams, “The biggest differences [from an academic institution] are a much greater focus on patient care, and the fact that community-based groups change and evolve more quickly than academic groups.”
But there can be more to community-based hospitalists than direct patient care. “Ask if the job is limited to clinical duties or if there are ways to branch out and expand, maybe by becoming a medical director for a hospital or by designing quality programs,” suggests Dr. Williams.
Working Within Managed Care
Cara Steinkeler, MD, a hospitalist at Kaiser Permanente Sunnyside Medical Center, Clackamas, Ore., worked in private practice before she signed on with managed-care giant Kaiser. “Overall, the schedules—in terms of number of days per month and shifts—are pretty similar” for managed care and private practice, she says. “In terms of quality of life, they’re also about equivalent.”
The difference may be in how hospitalists spend their time. “I’m relatively isolated from the business of medicine,” says Dr. Steinkeler. “We’re able to concentrate on treating patients. When I was in private practice, I’d spend 10 or 15 hours a week doing my own coding and billing; here, we [now] have coding experts that do that.”
Dr. Steinkeler’s group is primarily salary-based, so she isn’t tied to productivity. While the salaries may not always be as high as other hospitalist options, there are trade-offs. “I know that the starting salaries for hospitalists in private practices in Portland were a little higher than for HMOs,” says Dr. Steinkeler. “The financial payoff for working here is really when you stay long enough be vested; it’s in the benefits. But we tried to rectify that [starting salary discrepancy] because we were having trouble hiring.”
Size May Matter Most
Keep in mind that hospital medicine programs can vary widely, for both academic and community-based institutions. “Program differences are based on the size of the program,” explains Dr. Panwala. “In tertiary care centers, you won’t do much ICU work, but in a small or medium-sized hospital it’s very different. You can basically be the ICU doc.”
The plus side of working for a larger hospital medicine group is flexibility and opportunity for career growth. Dr. Steinkeler highlights another benefit: “One good thing about working in a large group … is the flexibility,” she says. “A large group has the ability to flex around people’s needs, so you can cut your hours or get time off if you have kids or aging parents.”
This basic information on the various employment options within hospital medicine should give you a good starting point in choosing the career path you’d like to take. Your decision, or preliminary preference, will influence how you prepare for, and go after, your first position as a working hospitalist. TH
Each career path within hospital medicine offers distinct responsibilities, opportunities, and rewards. One of the biggest decisions you’ll make as a hospitalist is whether to enter an academic or a community-based hospital medicine field—but there are additional factors to take into account. Here’s an overview of the career paths within these two areas that may help you with your decision.
Choices in Academic Hospital Medicine
Only a small percentage of hospitalists go into academic jobs, and residents are—obviously—most familiar with these choices.
“[The environment] is familiar to you, and you’re able to grow professionally because … people are always asking you questions,” says Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine at the Ann Arbor Veterans Affairs Medical Center and the University of Michigan Medical School. “The opportunity to be around learners—residents and medical students—is very exciting to residents.”
There are other reasons you may prefer academic over community-based hospital medicine. “The types of patients you treat are different,” says Dr. Saint. “They may be more complicated, and thus you can improve your clinical skills. Also, there’s prestige in being associated with an academic medical center. That appeals to some people.”
The rigorousness of the schedule varies with the institution. “Theoretically, you have residents, so you don’t have to take calls,” explains Dr. Saint. “But when you’re on, say, for a month there’s often no attending coverage on weekends or holidays.”
Hospital medicine work in an academic setting falls into four categories:
1) Hospitalist clinician-investigator: “These hospitalists typically spend the minority of their time doing clinical work—maybe 20% to 40% of their time,” says Dr. Saint. “The rest is spent developing their research agenda, applying for and obtaining grants to fund their research. The investigative focus is usually inpatient-oriented to provide synergy between their clinical work and their research.” This track typically leads to tenure, and usually requires some type of fellowship.
2) Hospitalist-educator: “There are a large number of these positions in academic medical centers,” says Dr. Saint. “These hospitalists spend about 80% of their time seeing patients and teaching residents and medical students.”
Typical hospitalist-educator activities include ward attending, medical consultation, and preoperative evaluations. “They spend about 20% of their time doing some type of scholarly activity, whether writing articles or developing educational curricula that can be disseminated,” estimates Dr. Saint.
Hospitalist-educator is usually a non-tenured position and these academicians are promoted primarily based on their clinical expertise and perceived skills as teachers. You don’t need to have a fellowship for this position; usually, the hospitalist director will hire individuals from his or her program—often a former chief resident.
3) Hospitalist-clinician: “These hospitalists primarily focus on patient care,” explains Dr. Saint. “A lot of them have been hired recently because of the limits on work hours for residents. There is minimal teaching and scholarly activity.”
Often, people do this for one or two years between residency and a fellowship, or to pay off school loans.
4) Hospitalist-administrator: “A major portion of their day is spent on administrative tasks,” says Dr. Saint. “They may run the hospital medicine program, or have educational administrative tasks, like residency directors.” However, he warns, “a resident isn’t going to go straight into one of these positions; you have to pay your dues first. But this can be an opportunity to think about for the future.”
What is the job market like for these academic positions? “There are huge opportunities for residents wanting to become hospitalists, regardless of which track they want to follow,” says Dr. Saint. “There are only a handful of clinician-investigators in hospital medicine now, and I see tremendous growth in this field. There’s also a growing need for hospitalist-clinicians because of the restrictions imposed on the workweek [for residents]. And as the number of hospitalists grows, there will obviously be a need for more hospitalist-administrators. Of course, there will always be a need for hospitalist-educators—but many are already in those roles.”
Choices in Community-Based Hospital Medicine
The first thing to realize about community-based hospital medicine is that there are various employers involved.
“Programs will have different mandates; a lot depends on the financial drivers,” says Sanjiv Panwala, MD, hospitalist at Providence Medical Center, Portland, Ore. “If you’re paid by the hospital, your priorities will be theirs: coverage of uncovered patients, shorter length of stay, etc. It trickles down.”
Michael-Anthony Williams, MD, regional CMO of Sound Inpatient Physicians in Denver, agrees. “It’s important to understand who the employer is and what their values are,” he says. “Is it the hospital or a local, regional, or national practice? If you’re employed by a hospital, you may be one of several employed specialists.” That can impact what types of clinical work you handle.
Regardless of whom you work for, says Dr. Williams, “The biggest differences [from an academic institution] are a much greater focus on patient care, and the fact that community-based groups change and evolve more quickly than academic groups.”
But there can be more to community-based hospitalists than direct patient care. “Ask if the job is limited to clinical duties or if there are ways to branch out and expand, maybe by becoming a medical director for a hospital or by designing quality programs,” suggests Dr. Williams.
Working Within Managed Care
Cara Steinkeler, MD, a hospitalist at Kaiser Permanente Sunnyside Medical Center, Clackamas, Ore., worked in private practice before she signed on with managed-care giant Kaiser. “Overall, the schedules—in terms of number of days per month and shifts—are pretty similar” for managed care and private practice, she says. “In terms of quality of life, they’re also about equivalent.”
The difference may be in how hospitalists spend their time. “I’m relatively isolated from the business of medicine,” says Dr. Steinkeler. “We’re able to concentrate on treating patients. When I was in private practice, I’d spend 10 or 15 hours a week doing my own coding and billing; here, we [now] have coding experts that do that.”
Dr. Steinkeler’s group is primarily salary-based, so she isn’t tied to productivity. While the salaries may not always be as high as other hospitalist options, there are trade-offs. “I know that the starting salaries for hospitalists in private practices in Portland were a little higher than for HMOs,” says Dr. Steinkeler. “The financial payoff for working here is really when you stay long enough be vested; it’s in the benefits. But we tried to rectify that [starting salary discrepancy] because we were having trouble hiring.”
Size May Matter Most
Keep in mind that hospital medicine programs can vary widely, for both academic and community-based institutions. “Program differences are based on the size of the program,” explains Dr. Panwala. “In tertiary care centers, you won’t do much ICU work, but in a small or medium-sized hospital it’s very different. You can basically be the ICU doc.”
The plus side of working for a larger hospital medicine group is flexibility and opportunity for career growth. Dr. Steinkeler highlights another benefit: “One good thing about working in a large group … is the flexibility,” she says. “A large group has the ability to flex around people’s needs, so you can cut your hours or get time off if you have kids or aging parents.”
This basic information on the various employment options within hospital medicine should give you a good starting point in choosing the career path you’d like to take. Your decision, or preliminary preference, will influence how you prepare for, and go after, your first position as a working hospitalist. TH
Each career path within hospital medicine offers distinct responsibilities, opportunities, and rewards. One of the biggest decisions you’ll make as a hospitalist is whether to enter an academic or a community-based hospital medicine field—but there are additional factors to take into account. Here’s an overview of the career paths within these two areas that may help you with your decision.
Choices in Academic Hospital Medicine
Only a small percentage of hospitalists go into academic jobs, and residents are—obviously—most familiar with these choices.
“[The environment] is familiar to you, and you’re able to grow professionally because … people are always asking you questions,” says Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine at the Ann Arbor Veterans Affairs Medical Center and the University of Michigan Medical School. “The opportunity to be around learners—residents and medical students—is very exciting to residents.”
There are other reasons you may prefer academic over community-based hospital medicine. “The types of patients you treat are different,” says Dr. Saint. “They may be more complicated, and thus you can improve your clinical skills. Also, there’s prestige in being associated with an academic medical center. That appeals to some people.”
The rigorousness of the schedule varies with the institution. “Theoretically, you have residents, so you don’t have to take calls,” explains Dr. Saint. “But when you’re on, say, for a month there’s often no attending coverage on weekends or holidays.”
Hospital medicine work in an academic setting falls into four categories:
1) Hospitalist clinician-investigator: “These hospitalists typically spend the minority of their time doing clinical work—maybe 20% to 40% of their time,” says Dr. Saint. “The rest is spent developing their research agenda, applying for and obtaining grants to fund their research. The investigative focus is usually inpatient-oriented to provide synergy between their clinical work and their research.” This track typically leads to tenure, and usually requires some type of fellowship.
2) Hospitalist-educator: “There are a large number of these positions in academic medical centers,” says Dr. Saint. “These hospitalists spend about 80% of their time seeing patients and teaching residents and medical students.”
Typical hospitalist-educator activities include ward attending, medical consultation, and preoperative evaluations. “They spend about 20% of their time doing some type of scholarly activity, whether writing articles or developing educational curricula that can be disseminated,” estimates Dr. Saint.
Hospitalist-educator is usually a non-tenured position and these academicians are promoted primarily based on their clinical expertise and perceived skills as teachers. You don’t need to have a fellowship for this position; usually, the hospitalist director will hire individuals from his or her program—often a former chief resident.
3) Hospitalist-clinician: “These hospitalists primarily focus on patient care,” explains Dr. Saint. “A lot of them have been hired recently because of the limits on work hours for residents. There is minimal teaching and scholarly activity.”
Often, people do this for one or two years between residency and a fellowship, or to pay off school loans.
4) Hospitalist-administrator: “A major portion of their day is spent on administrative tasks,” says Dr. Saint. “They may run the hospital medicine program, or have educational administrative tasks, like residency directors.” However, he warns, “a resident isn’t going to go straight into one of these positions; you have to pay your dues first. But this can be an opportunity to think about for the future.”
What is the job market like for these academic positions? “There are huge opportunities for residents wanting to become hospitalists, regardless of which track they want to follow,” says Dr. Saint. “There are only a handful of clinician-investigators in hospital medicine now, and I see tremendous growth in this field. There’s also a growing need for hospitalist-clinicians because of the restrictions imposed on the workweek [for residents]. And as the number of hospitalists grows, there will obviously be a need for more hospitalist-administrators. Of course, there will always be a need for hospitalist-educators—but many are already in those roles.”
Choices in Community-Based Hospital Medicine
The first thing to realize about community-based hospital medicine is that there are various employers involved.
“Programs will have different mandates; a lot depends on the financial drivers,” says Sanjiv Panwala, MD, hospitalist at Providence Medical Center, Portland, Ore. “If you’re paid by the hospital, your priorities will be theirs: coverage of uncovered patients, shorter length of stay, etc. It trickles down.”
Michael-Anthony Williams, MD, regional CMO of Sound Inpatient Physicians in Denver, agrees. “It’s important to understand who the employer is and what their values are,” he says. “Is it the hospital or a local, regional, or national practice? If you’re employed by a hospital, you may be one of several employed specialists.” That can impact what types of clinical work you handle.
Regardless of whom you work for, says Dr. Williams, “The biggest differences [from an academic institution] are a much greater focus on patient care, and the fact that community-based groups change and evolve more quickly than academic groups.”
But there can be more to community-based hospitalists than direct patient care. “Ask if the job is limited to clinical duties or if there are ways to branch out and expand, maybe by becoming a medical director for a hospital or by designing quality programs,” suggests Dr. Williams.
Working Within Managed Care
Cara Steinkeler, MD, a hospitalist at Kaiser Permanente Sunnyside Medical Center, Clackamas, Ore., worked in private practice before she signed on with managed-care giant Kaiser. “Overall, the schedules—in terms of number of days per month and shifts—are pretty similar” for managed care and private practice, she says. “In terms of quality of life, they’re also about equivalent.”
The difference may be in how hospitalists spend their time. “I’m relatively isolated from the business of medicine,” says Dr. Steinkeler. “We’re able to concentrate on treating patients. When I was in private practice, I’d spend 10 or 15 hours a week doing my own coding and billing; here, we [now] have coding experts that do that.”
Dr. Steinkeler’s group is primarily salary-based, so she isn’t tied to productivity. While the salaries may not always be as high as other hospitalist options, there are trade-offs. “I know that the starting salaries for hospitalists in private practices in Portland were a little higher than for HMOs,” says Dr. Steinkeler. “The financial payoff for working here is really when you stay long enough be vested; it’s in the benefits. But we tried to rectify that [starting salary discrepancy] because we were having trouble hiring.”
Size May Matter Most
Keep in mind that hospital medicine programs can vary widely, for both academic and community-based institutions. “Program differences are based on the size of the program,” explains Dr. Panwala. “In tertiary care centers, you won’t do much ICU work, but in a small or medium-sized hospital it’s very different. You can basically be the ICU doc.”
The plus side of working for a larger hospital medicine group is flexibility and opportunity for career growth. Dr. Steinkeler highlights another benefit: “One good thing about working in a large group … is the flexibility,” she says. “A large group has the ability to flex around people’s needs, so you can cut your hours or get time off if you have kids or aging parents.”
This basic information on the various employment options within hospital medicine should give you a good starting point in choosing the career path you’d like to take. Your decision, or preliminary preference, will influence how you prepare for, and go after, your first position as a working hospitalist. TH
SHM Behind the Scenes

Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
Dr. Hospitalist

Measure Up
Question: I’m a new graduate who just took a job as a hospitalist. I’m hearing a lot about the importance of compliance with the “Core Measures.” Can you explain to me what they are and why these seem to be so important?
Measure for Measure,
Austin, Texas
Dr. Hospitalist responds: As a federal agency, the Center for Medicare and Medicaid Services (CMS) is the largest payer of healthcare in the country. In 2003, it required hospitals that receive CMS payments to report data on the quality of care Medicare recipients received for several inpatient diagnoses (myocardial infarction, heart failure, and community-acquired pneumonia).
CMS enacted this requirement because there was evidence to suggest hospitalized patients were not uniformly receiving evidence-based care.
For example, I am unaware of any healthcare providers who would question the routine use of aspirin in patients who present with acute myocardial infarction. Despite this widespread knowledge, CMS audits found this practice was not uniform among hospitals nationwide. More detailed analysis suggested this inconsistency was not usually because of ignorant providers but more often a lack of systems to ensure uniform care for all patients at all times.
Since 2003, CMS has expanded the number of Core Quality Measures hospitals must report. For example, the present quality measures for community-acquired pneumonia include:
- Initial antibiotics within four hours of hospital presentation;
- Oxygen assessment;
- Blood culture before first antibiotic dose;
- Appropriate initial antibiotic selection;
- Smoking cessation counseling;
- Influenza vaccination for inpatients from October through February; and
- Pneumococcal vaccination for patients 65 and older.
This year, CMS raised the stakes by tying reimbursement to performance on these quality measures. I can assure you the few hospitals around the country that hadn’t addressed this issue have done so today. The risk of losing CMS funding is not an option for most hospitals. In many cases, the hospitals have turned to providers in location-based specialties (e.g., emergency department providers, hospitalists, and intensivists) as partners in the development, implementation, and enforcement of these quality measures. These providers are uniquely positioned to address performance on these quality measures.
Well Rounded
Question: Do you have any suggestions on how to improve communications between hospitalists and other inpatient providers like nurses and case managers?
Let’s Talk,
Madison, Wis.
Dr. Hospitalist responds: If your hospitalist program is not conducting multidisciplinary rounds, consider them.
The primary goal is interdisciplinary communication. Conduct these rounds at least once each morning, as early as possible after nursing shift change and hospitalist hand-off. Participants should include hospitalists, nurses, and case managers at a minimum. Some programs include other providers like nurses’ aides, pharmacists, physical/occupational therapists, social workers, and dietitians.
During rounds, the hospitalist leads a brief discussion about the plan of care for each patient, soliciting feedback from all participants. Discussions should last no longer than two-three minutes apiece and often are shorter. The occasional patient whose issues demand a longer discussion should be treated as an outlier and discussed at the end of rounds.
Nonphysician providers should solicit written physician orders during rounds. The team should consider barriers to discharge and identify ways to overcome those barriers. At the conclusion of rounds, each participant should leave with a clear understanding of each patient’s plan of care for that day and for the hospital stay. Hospitalists should leave rounds able to prioritize the order of patient care. They should see the sickest patients first, then potential early discharges, then everyone else.
Rounds can fail for several reasons. Watch for the signs and address them before the rounds spiral out of control:
- Participants are late: It is vital to set the expectation that everyone will show up on time. Without that, the start time for rounds will drift from day to day and waste time;
- Participants come unprepared: Taking part at rounds requires that the nurse leaves nursing hand-off with the necessary information to participate effectively. This is the same for the hospitalist with morning hand-off from the doctor who worked overnight. Without sufficient information, participants will find themselves with nothing to say—or worse, provide erroneous or useless information; or
- Participants stray off the topic: It is easy to digress during group discussions. As the rounds leader, the hospitalist must keep discussion pertinent so rounds are not prolonged with unnecessary discussion. Think of rounds as an investment. We are asking busy providers to take 30 minutes out of their busy schedule to talk about patient care. A wise investment saves providers more time than they invested.
A primary benefit of rounds is as a forum for communication. All providers should try to funnel communication toward rounds rather than stopping the doctor or nurse throughout the day with questions and comments. Minimizing interruptions will foster more efficient care. Some hospitalist programs even huddle briefly in the afternoon to review plans discussed at morning rounds. TH
Measure Up
Question: I’m a new graduate who just took a job as a hospitalist. I’m hearing a lot about the importance of compliance with the “Core Measures.” Can you explain to me what they are and why these seem to be so important?
Measure for Measure,
Austin, Texas
Dr. Hospitalist responds: As a federal agency, the Center for Medicare and Medicaid Services (CMS) is the largest payer of healthcare in the country. In 2003, it required hospitals that receive CMS payments to report data on the quality of care Medicare recipients received for several inpatient diagnoses (myocardial infarction, heart failure, and community-acquired pneumonia).
CMS enacted this requirement because there was evidence to suggest hospitalized patients were not uniformly receiving evidence-based care.
For example, I am unaware of any healthcare providers who would question the routine use of aspirin in patients who present with acute myocardial infarction. Despite this widespread knowledge, CMS audits found this practice was not uniform among hospitals nationwide. More detailed analysis suggested this inconsistency was not usually because of ignorant providers but more often a lack of systems to ensure uniform care for all patients at all times.
Since 2003, CMS has expanded the number of Core Quality Measures hospitals must report. For example, the present quality measures for community-acquired pneumonia include:
- Initial antibiotics within four hours of hospital presentation;
- Oxygen assessment;
- Blood culture before first antibiotic dose;
- Appropriate initial antibiotic selection;
- Smoking cessation counseling;
- Influenza vaccination for inpatients from October through February; and
- Pneumococcal vaccination for patients 65 and older.
This year, CMS raised the stakes by tying reimbursement to performance on these quality measures. I can assure you the few hospitals around the country that hadn’t addressed this issue have done so today. The risk of losing CMS funding is not an option for most hospitals. In many cases, the hospitals have turned to providers in location-based specialties (e.g., emergency department providers, hospitalists, and intensivists) as partners in the development, implementation, and enforcement of these quality measures. These providers are uniquely positioned to address performance on these quality measures.
Well Rounded
Question: Do you have any suggestions on how to improve communications between hospitalists and other inpatient providers like nurses and case managers?
Let’s Talk,
Madison, Wis.
Dr. Hospitalist responds: If your hospitalist program is not conducting multidisciplinary rounds, consider them.
The primary goal is interdisciplinary communication. Conduct these rounds at least once each morning, as early as possible after nursing shift change and hospitalist hand-off. Participants should include hospitalists, nurses, and case managers at a minimum. Some programs include other providers like nurses’ aides, pharmacists, physical/occupational therapists, social workers, and dietitians.
During rounds, the hospitalist leads a brief discussion about the plan of care for each patient, soliciting feedback from all participants. Discussions should last no longer than two-three minutes apiece and often are shorter. The occasional patient whose issues demand a longer discussion should be treated as an outlier and discussed at the end of rounds.
Nonphysician providers should solicit written physician orders during rounds. The team should consider barriers to discharge and identify ways to overcome those barriers. At the conclusion of rounds, each participant should leave with a clear understanding of each patient’s plan of care for that day and for the hospital stay. Hospitalists should leave rounds able to prioritize the order of patient care. They should see the sickest patients first, then potential early discharges, then everyone else.
Rounds can fail for several reasons. Watch for the signs and address them before the rounds spiral out of control:
- Participants are late: It is vital to set the expectation that everyone will show up on time. Without that, the start time for rounds will drift from day to day and waste time;
- Participants come unprepared: Taking part at rounds requires that the nurse leaves nursing hand-off with the necessary information to participate effectively. This is the same for the hospitalist with morning hand-off from the doctor who worked overnight. Without sufficient information, participants will find themselves with nothing to say—or worse, provide erroneous or useless information; or
- Participants stray off the topic: It is easy to digress during group discussions. As the rounds leader, the hospitalist must keep discussion pertinent so rounds are not prolonged with unnecessary discussion. Think of rounds as an investment. We are asking busy providers to take 30 minutes out of their busy schedule to talk about patient care. A wise investment saves providers more time than they invested.
A primary benefit of rounds is as a forum for communication. All providers should try to funnel communication toward rounds rather than stopping the doctor or nurse throughout the day with questions and comments. Minimizing interruptions will foster more efficient care. Some hospitalist programs even huddle briefly in the afternoon to review plans discussed at morning rounds. TH
Measure Up
Question: I’m a new graduate who just took a job as a hospitalist. I’m hearing a lot about the importance of compliance with the “Core Measures.” Can you explain to me what they are and why these seem to be so important?
Measure for Measure,
Austin, Texas
Dr. Hospitalist responds: As a federal agency, the Center for Medicare and Medicaid Services (CMS) is the largest payer of healthcare in the country. In 2003, it required hospitals that receive CMS payments to report data on the quality of care Medicare recipients received for several inpatient diagnoses (myocardial infarction, heart failure, and community-acquired pneumonia).
CMS enacted this requirement because there was evidence to suggest hospitalized patients were not uniformly receiving evidence-based care.
For example, I am unaware of any healthcare providers who would question the routine use of aspirin in patients who present with acute myocardial infarction. Despite this widespread knowledge, CMS audits found this practice was not uniform among hospitals nationwide. More detailed analysis suggested this inconsistency was not usually because of ignorant providers but more often a lack of systems to ensure uniform care for all patients at all times.
Since 2003, CMS has expanded the number of Core Quality Measures hospitals must report. For example, the present quality measures for community-acquired pneumonia include:
- Initial antibiotics within four hours of hospital presentation;
- Oxygen assessment;
- Blood culture before first antibiotic dose;
- Appropriate initial antibiotic selection;
- Smoking cessation counseling;
- Influenza vaccination for inpatients from October through February; and
- Pneumococcal vaccination for patients 65 and older.
This year, CMS raised the stakes by tying reimbursement to performance on these quality measures. I can assure you the few hospitals around the country that hadn’t addressed this issue have done so today. The risk of losing CMS funding is not an option for most hospitals. In many cases, the hospitals have turned to providers in location-based specialties (e.g., emergency department providers, hospitalists, and intensivists) as partners in the development, implementation, and enforcement of these quality measures. These providers are uniquely positioned to address performance on these quality measures.
Well Rounded
Question: Do you have any suggestions on how to improve communications between hospitalists and other inpatient providers like nurses and case managers?
Let’s Talk,
Madison, Wis.
Dr. Hospitalist responds: If your hospitalist program is not conducting multidisciplinary rounds, consider them.
The primary goal is interdisciplinary communication. Conduct these rounds at least once each morning, as early as possible after nursing shift change and hospitalist hand-off. Participants should include hospitalists, nurses, and case managers at a minimum. Some programs include other providers like nurses’ aides, pharmacists, physical/occupational therapists, social workers, and dietitians.
During rounds, the hospitalist leads a brief discussion about the plan of care for each patient, soliciting feedback from all participants. Discussions should last no longer than two-three minutes apiece and often are shorter. The occasional patient whose issues demand a longer discussion should be treated as an outlier and discussed at the end of rounds.
Nonphysician providers should solicit written physician orders during rounds. The team should consider barriers to discharge and identify ways to overcome those barriers. At the conclusion of rounds, each participant should leave with a clear understanding of each patient’s plan of care for that day and for the hospital stay. Hospitalists should leave rounds able to prioritize the order of patient care. They should see the sickest patients first, then potential early discharges, then everyone else.
Rounds can fail for several reasons. Watch for the signs and address them before the rounds spiral out of control:
- Participants are late: It is vital to set the expectation that everyone will show up on time. Without that, the start time for rounds will drift from day to day and waste time;
- Participants come unprepared: Taking part at rounds requires that the nurse leaves nursing hand-off with the necessary information to participate effectively. This is the same for the hospitalist with morning hand-off from the doctor who worked overnight. Without sufficient information, participants will find themselves with nothing to say—or worse, provide erroneous or useless information; or
- Participants stray off the topic: It is easy to digress during group discussions. As the rounds leader, the hospitalist must keep discussion pertinent so rounds are not prolonged with unnecessary discussion. Think of rounds as an investment. We are asking busy providers to take 30 minutes out of their busy schedule to talk about patient care. A wise investment saves providers more time than they invested.
A primary benefit of rounds is as a forum for communication. All providers should try to funnel communication toward rounds rather than stopping the doctor or nurse throughout the day with questions and comments. Minimizing interruptions will foster more efficient care. Some hospitalist programs even huddle briefly in the afternoon to review plans discussed at morning rounds. TH
With Liberty and Access for All

The latest estimates from the National Coalition on Health Care (www.nchc.org/facts/coverage.shtml) show that 46 million Americans—nearly 16% of the population—have no health insurance, and those numbers are increasing. The federal government has been flirting with addressing this growing problem for years, but 2007 may be the turning point, when key legislation may help turn the rising tide of uninsured and underinsured patients.
“A couple of things create a more favorable milieu for this,” explains Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis., and chair of SHM’s Public Policy Committee. “The first is that Massachusetts did it on their own—states are no longer waiting for Congress to do something. The second is that, with every passing year, there’s increased pressure to do something.”
Regardless of why this is happening now, some promising legislation has been introduced in Congress that may provide the beginnings of a solution.
The Health Partnership Act
Perhaps the most promising legislation on healthcare access is an innovative, bipartisan, bicameral effort known as the Health Partnership Act, which proposes a federal-state partnership to address the issue.
Identical bills have been introduced in each house. The Health Partnership Act (S. 325) was introduced in the Senate by Jeff Bingaman (D-N.M.) and George Voinovich (R-Ohio), and the Health Partnership Act through Creative Federalism (HR 506) was introduced in the House by Tammy Baldwin (D-Wis.), Tom Price (R-Ga.), and John Tierney (D-Mass.). Similar legislation was introduced by some of these same parties in the last Congress; though the bill died before action was taken, it was immediately reintroduced in the new Congress this January.
If enacted, the Health Partnership Act would give state and local governments the opportunity to implement their own solutions for providing coverage to uninsured populations, allowing them to address the unique needs that exist within their boundaries. Interested states, groups of states, or even parts of states would apply for five-year federal grants by submitting proposals that demonstrate how their plans would reduce the number of uninsured and improve healthcare quality. Each plan would include information on the appropriate use of information technology to improve the availability of evidence-based medical and outcomes data to providers and patients.
The act would establish a new bipartisan State Health Innovation Commission (SHIC), which would be part of the Department of Health and Human Services. This commission would review the state proposals and submit to Congress a list of recommended applications. It would also work with an established organization—possibly the Institute of Medicine—to develop performance measures and goals regarding coverage, quality, and cost of state programs.
Participating states would eventually report their progress to the SHIC, which would then report to Congress on whether each state was meeting the goals of the act and would then recommend further action.
Giving individual states the flexibility to create their own programs could generate new ideas and would ultimately reveal which programs work best. “We’re not expecting states to hit the ball out of the park the first time, but it’s a start,” says Dr. Siegal. “It’s a step in the right direction.”
SHM supports the Health Partnership Act and has sent a letter of support to Senate sponsors. “This [legislation] may or may not be the most expedient way to get it done,” says Dr. Siegal. “But SHM supports this legislation and is currently drafting a letter of support for the House version.”
The Healthy Americans Act
Another, more comprehensive, bill was introduced in the Senate by Ron Wyden (D-Ore.) in December 2006.
The Healthy Americans Act would require businesses to replace their current health benefits with an increase in wages equal to the amount spent on health insurance premiums. It would require all employees to use these increased wages to purchase their own health plans and would provide subsidies to low-income workers to help pay their premiums.
Those employers not currently providing any health benefits would be required to begin making phased-in “Employer Shared Responsibility Payments,” which would be used to ensure that everyone is able to afford their health plans by funding premium reductions.
Wyden’s bill would have each state establish a Health Help Agency to educate residents about private health plans, to administer enrollment, and to assist income-eligible enrollees with sliding scale premium reductions. These agencies would be funded by the federal government and insurance companies.
Finally, insurance companies would be required to cover every individual who chooses to enroll and would not be allowed to raise prices or deny coverage if individuals are sick.
Some State-Level Solutions
Some states—Massachusetts, for one—have already taken action, implementing their own innovative policies and programs to expand coverage for their populations. Maine, Massachusetts, and Vermont have instituted comprehensive healthcare reform; Arkansas, Montana, New Mexico, Oklahoma, Rhode Island, Tennessee, and Utah have all implemented some form of public-private partnerships; and Illinois and Pennsylvania have initiatives that cover all children.
Maine, Massachusetts, and Vermont all use Medicaid funds to partially subsidize healthcare coverage for families with annual incomes as high as $53,000.
For details on all current state initiatives for healthcare coverage, download the report “State of the States 2007: Building Hope, Raising Expectations” from the Web site of the State Coverage Initiatives at www.statecoverage.net.
Why Hospitalists Should Care
Providing healthcare coverage to the uninsured is one of SHM’s public policy priorities. “There really is a crisis out there, and hospitalists are on the front line of it every day,” says Dr. Siegal.
As former SHM President Mary Jo Gorman states in SHM’s letter of support for the Senate’s Health Partnership Act: “Many hospitalist programs exist to manage the burgeoning population of uninsured and underinsured patients who require hospitalization. These patients are more likely to delay seeking care until their illnesses deteriorate to the point that they need emergency care. In many communities, hospitalists have become the safety net for this vulnerable patient population.”
For further information about federal legislation for improved access and to see if your representatives are cosponsors, visit SHM’s Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
The latest estimates from the National Coalition on Health Care (www.nchc.org/facts/coverage.shtml) show that 46 million Americans—nearly 16% of the population—have no health insurance, and those numbers are increasing. The federal government has been flirting with addressing this growing problem for years, but 2007 may be the turning point, when key legislation may help turn the rising tide of uninsured and underinsured patients.
“A couple of things create a more favorable milieu for this,” explains Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis., and chair of SHM’s Public Policy Committee. “The first is that Massachusetts did it on their own—states are no longer waiting for Congress to do something. The second is that, with every passing year, there’s increased pressure to do something.”
Regardless of why this is happening now, some promising legislation has been introduced in Congress that may provide the beginnings of a solution.
The Health Partnership Act
Perhaps the most promising legislation on healthcare access is an innovative, bipartisan, bicameral effort known as the Health Partnership Act, which proposes a federal-state partnership to address the issue.
Identical bills have been introduced in each house. The Health Partnership Act (S. 325) was introduced in the Senate by Jeff Bingaman (D-N.M.) and George Voinovich (R-Ohio), and the Health Partnership Act through Creative Federalism (HR 506) was introduced in the House by Tammy Baldwin (D-Wis.), Tom Price (R-Ga.), and John Tierney (D-Mass.). Similar legislation was introduced by some of these same parties in the last Congress; though the bill died before action was taken, it was immediately reintroduced in the new Congress this January.
If enacted, the Health Partnership Act would give state and local governments the opportunity to implement their own solutions for providing coverage to uninsured populations, allowing them to address the unique needs that exist within their boundaries. Interested states, groups of states, or even parts of states would apply for five-year federal grants by submitting proposals that demonstrate how their plans would reduce the number of uninsured and improve healthcare quality. Each plan would include information on the appropriate use of information technology to improve the availability of evidence-based medical and outcomes data to providers and patients.
The act would establish a new bipartisan State Health Innovation Commission (SHIC), which would be part of the Department of Health and Human Services. This commission would review the state proposals and submit to Congress a list of recommended applications. It would also work with an established organization—possibly the Institute of Medicine—to develop performance measures and goals regarding coverage, quality, and cost of state programs.
Participating states would eventually report their progress to the SHIC, which would then report to Congress on whether each state was meeting the goals of the act and would then recommend further action.
Giving individual states the flexibility to create their own programs could generate new ideas and would ultimately reveal which programs work best. “We’re not expecting states to hit the ball out of the park the first time, but it’s a start,” says Dr. Siegal. “It’s a step in the right direction.”
SHM supports the Health Partnership Act and has sent a letter of support to Senate sponsors. “This [legislation] may or may not be the most expedient way to get it done,” says Dr. Siegal. “But SHM supports this legislation and is currently drafting a letter of support for the House version.”
The Healthy Americans Act
Another, more comprehensive, bill was introduced in the Senate by Ron Wyden (D-Ore.) in December 2006.
The Healthy Americans Act would require businesses to replace their current health benefits with an increase in wages equal to the amount spent on health insurance premiums. It would require all employees to use these increased wages to purchase their own health plans and would provide subsidies to low-income workers to help pay their premiums.
Those employers not currently providing any health benefits would be required to begin making phased-in “Employer Shared Responsibility Payments,” which would be used to ensure that everyone is able to afford their health plans by funding premium reductions.
Wyden’s bill would have each state establish a Health Help Agency to educate residents about private health plans, to administer enrollment, and to assist income-eligible enrollees with sliding scale premium reductions. These agencies would be funded by the federal government and insurance companies.
Finally, insurance companies would be required to cover every individual who chooses to enroll and would not be allowed to raise prices or deny coverage if individuals are sick.
Some State-Level Solutions
Some states—Massachusetts, for one—have already taken action, implementing their own innovative policies and programs to expand coverage for their populations. Maine, Massachusetts, and Vermont have instituted comprehensive healthcare reform; Arkansas, Montana, New Mexico, Oklahoma, Rhode Island, Tennessee, and Utah have all implemented some form of public-private partnerships; and Illinois and Pennsylvania have initiatives that cover all children.
Maine, Massachusetts, and Vermont all use Medicaid funds to partially subsidize healthcare coverage for families with annual incomes as high as $53,000.
For details on all current state initiatives for healthcare coverage, download the report “State of the States 2007: Building Hope, Raising Expectations” from the Web site of the State Coverage Initiatives at www.statecoverage.net.
Why Hospitalists Should Care
Providing healthcare coverage to the uninsured is one of SHM’s public policy priorities. “There really is a crisis out there, and hospitalists are on the front line of it every day,” says Dr. Siegal.
As former SHM President Mary Jo Gorman states in SHM’s letter of support for the Senate’s Health Partnership Act: “Many hospitalist programs exist to manage the burgeoning population of uninsured and underinsured patients who require hospitalization. These patients are more likely to delay seeking care until their illnesses deteriorate to the point that they need emergency care. In many communities, hospitalists have become the safety net for this vulnerable patient population.”
For further information about federal legislation for improved access and to see if your representatives are cosponsors, visit SHM’s Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
The latest estimates from the National Coalition on Health Care (www.nchc.org/facts/coverage.shtml) show that 46 million Americans—nearly 16% of the population—have no health insurance, and those numbers are increasing. The federal government has been flirting with addressing this growing problem for years, but 2007 may be the turning point, when key legislation may help turn the rising tide of uninsured and underinsured patients.
“A couple of things create a more favorable milieu for this,” explains Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis., and chair of SHM’s Public Policy Committee. “The first is that Massachusetts did it on their own—states are no longer waiting for Congress to do something. The second is that, with every passing year, there’s increased pressure to do something.”
Regardless of why this is happening now, some promising legislation has been introduced in Congress that may provide the beginnings of a solution.
The Health Partnership Act
Perhaps the most promising legislation on healthcare access is an innovative, bipartisan, bicameral effort known as the Health Partnership Act, which proposes a federal-state partnership to address the issue.
Identical bills have been introduced in each house. The Health Partnership Act (S. 325) was introduced in the Senate by Jeff Bingaman (D-N.M.) and George Voinovich (R-Ohio), and the Health Partnership Act through Creative Federalism (HR 506) was introduced in the House by Tammy Baldwin (D-Wis.), Tom Price (R-Ga.), and John Tierney (D-Mass.). Similar legislation was introduced by some of these same parties in the last Congress; though the bill died before action was taken, it was immediately reintroduced in the new Congress this January.
If enacted, the Health Partnership Act would give state and local governments the opportunity to implement their own solutions for providing coverage to uninsured populations, allowing them to address the unique needs that exist within their boundaries. Interested states, groups of states, or even parts of states would apply for five-year federal grants by submitting proposals that demonstrate how their plans would reduce the number of uninsured and improve healthcare quality. Each plan would include information on the appropriate use of information technology to improve the availability of evidence-based medical and outcomes data to providers and patients.
The act would establish a new bipartisan State Health Innovation Commission (SHIC), which would be part of the Department of Health and Human Services. This commission would review the state proposals and submit to Congress a list of recommended applications. It would also work with an established organization—possibly the Institute of Medicine—to develop performance measures and goals regarding coverage, quality, and cost of state programs.
Participating states would eventually report their progress to the SHIC, which would then report to Congress on whether each state was meeting the goals of the act and would then recommend further action.
Giving individual states the flexibility to create their own programs could generate new ideas and would ultimately reveal which programs work best. “We’re not expecting states to hit the ball out of the park the first time, but it’s a start,” says Dr. Siegal. “It’s a step in the right direction.”
SHM supports the Health Partnership Act and has sent a letter of support to Senate sponsors. “This [legislation] may or may not be the most expedient way to get it done,” says Dr. Siegal. “But SHM supports this legislation and is currently drafting a letter of support for the House version.”
The Healthy Americans Act
Another, more comprehensive, bill was introduced in the Senate by Ron Wyden (D-Ore.) in December 2006.
The Healthy Americans Act would require businesses to replace their current health benefits with an increase in wages equal to the amount spent on health insurance premiums. It would require all employees to use these increased wages to purchase their own health plans and would provide subsidies to low-income workers to help pay their premiums.
Those employers not currently providing any health benefits would be required to begin making phased-in “Employer Shared Responsibility Payments,” which would be used to ensure that everyone is able to afford their health plans by funding premium reductions.
Wyden’s bill would have each state establish a Health Help Agency to educate residents about private health plans, to administer enrollment, and to assist income-eligible enrollees with sliding scale premium reductions. These agencies would be funded by the federal government and insurance companies.
Finally, insurance companies would be required to cover every individual who chooses to enroll and would not be allowed to raise prices or deny coverage if individuals are sick.
Some State-Level Solutions
Some states—Massachusetts, for one—have already taken action, implementing their own innovative policies and programs to expand coverage for their populations. Maine, Massachusetts, and Vermont have instituted comprehensive healthcare reform; Arkansas, Montana, New Mexico, Oklahoma, Rhode Island, Tennessee, and Utah have all implemented some form of public-private partnerships; and Illinois and Pennsylvania have initiatives that cover all children.
Maine, Massachusetts, and Vermont all use Medicaid funds to partially subsidize healthcare coverage for families with annual incomes as high as $53,000.
For details on all current state initiatives for healthcare coverage, download the report “State of the States 2007: Building Hope, Raising Expectations” from the Web site of the State Coverage Initiatives at www.statecoverage.net.
Why Hospitalists Should Care
Providing healthcare coverage to the uninsured is one of SHM’s public policy priorities. “There really is a crisis out there, and hospitalists are on the front line of it every day,” says Dr. Siegal.
As former SHM President Mary Jo Gorman states in SHM’s letter of support for the Senate’s Health Partnership Act: “Many hospitalist programs exist to manage the burgeoning population of uninsured and underinsured patients who require hospitalization. These patients are more likely to delay seeking care until their illnesses deteriorate to the point that they need emergency care. In many communities, hospitalists have become the safety net for this vulnerable patient population.”
For further information about federal legislation for improved access and to see if your representatives are cosponsors, visit SHM’s Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
SHM Launches Geriatric Special Interest Group

At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck

It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
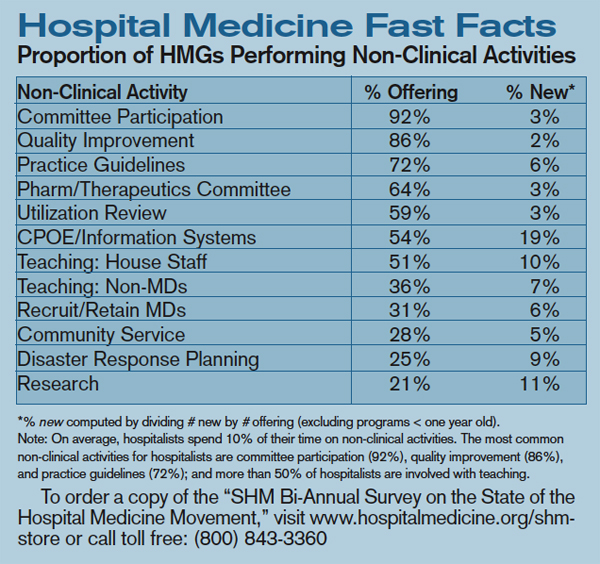
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck
It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck
It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH