User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Children With Chronic Skin Disorders Face Substantial Stigma
TOPLINE:
METHODOLOGY:
- Stigmatization has been addressed for several chronic medical conditions, such as HIV/AIDS, obesity, and mental illness; however, it has received limited attention in children living with chronic skin disorders.
- This cross-sectional, single-visit study examined the prevalence of stigma, its dependence on disease visibility and severity, and its association with mental health and QoL in children with chronic skin disorders.
- A total of 1671 children aged 8-17 years (57.9% girls; mean age, 13.7 years) were recruited from 32 pediatric dermatology centers in the United States and Canada from November 2018 to November 2021. The most common conditions were acne, atopic dermatitis/eczematous disorders, alopecia, and psoriasis, but rare genetic disorders were also represented.
- The primary outcome was the extent of stigmatization in relation to disease visibility, assessed using the Patient-Reported Outcomes Measurement Instrumentation System Pediatric Stigma-Skin.
- Secondary outcomes were the extent of stigmatization in relation to disease severity, along with QoL, depression, anxiety, and poor peer relationships.
TAKEAWAY:
- Approximately half (56.4%) of the children self-reported their skin condition as highly visible; 50.5% reported their disease severity as moderate, while 21.3% reported it as severe.
- Stigma was experienced by 73% of children and adolescents with chronic skin disease, with 43.8% reporting moderate stigma.
- Stigma scores correlated strongly with impaired QOL (Spearman’s rank correlation coefficient = 0.73) and child-reported scores for depression (Spearman’s rank correlation coefficient = 0.61) and moderately with anxiety (Spearman’s rank correlation coefficient = 0.54) and peer relationships (Spearman’s rank correlation coefficient = −0.49; all P < .001).
- Although stigma is increased for children with higher disease visibility and severity, the relatively weak correlation between child-assessed disease visibility and stigma (Spearman’s rank correlation coefficient = 0.22) showed that stigma is common in children even when diseases are not highly visible.
IN PRACTICE:
“Better treatment approaches for chronic skin diseases in children remain an unmet need. Increased awareness and instituting medical and psychological interventions to identify and reduce stigma and disease severity are important directions for improving QOL,” the authors concluded.
SOURCE:
Amy S. Paller, MD, professor of pediatrics and dermatology, Northwestern University, Chicago, led the study, which was published online in JAMA Dermatology.
LIMITATIONS:
Stigmatization needs to be assessed in children from low- and middle-income countries. Investigators enrolled children who had physician-assessed moderate to severe disease severity and/or at least some visibility of skin disease while wearing clothing, which resulted in exclusion of children with mild chronic disease, and the pandemic limited enrollment.
DISCLOSURES:
This study was funded through a grant from the Pediatric Dermatology Research Alliance (PeDRA). The authors declared receiving grants, personal fees, and honorarium and having other ties with various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Stigmatization has been addressed for several chronic medical conditions, such as HIV/AIDS, obesity, and mental illness; however, it has received limited attention in children living with chronic skin disorders.
- This cross-sectional, single-visit study examined the prevalence of stigma, its dependence on disease visibility and severity, and its association with mental health and QoL in children with chronic skin disorders.
- A total of 1671 children aged 8-17 years (57.9% girls; mean age, 13.7 years) were recruited from 32 pediatric dermatology centers in the United States and Canada from November 2018 to November 2021. The most common conditions were acne, atopic dermatitis/eczematous disorders, alopecia, and psoriasis, but rare genetic disorders were also represented.
- The primary outcome was the extent of stigmatization in relation to disease visibility, assessed using the Patient-Reported Outcomes Measurement Instrumentation System Pediatric Stigma-Skin.
- Secondary outcomes were the extent of stigmatization in relation to disease severity, along with QoL, depression, anxiety, and poor peer relationships.
TAKEAWAY:
- Approximately half (56.4%) of the children self-reported their skin condition as highly visible; 50.5% reported their disease severity as moderate, while 21.3% reported it as severe.
- Stigma was experienced by 73% of children and adolescents with chronic skin disease, with 43.8% reporting moderate stigma.
- Stigma scores correlated strongly with impaired QOL (Spearman’s rank correlation coefficient = 0.73) and child-reported scores for depression (Spearman’s rank correlation coefficient = 0.61) and moderately with anxiety (Spearman’s rank correlation coefficient = 0.54) and peer relationships (Spearman’s rank correlation coefficient = −0.49; all P < .001).
- Although stigma is increased for children with higher disease visibility and severity, the relatively weak correlation between child-assessed disease visibility and stigma (Spearman’s rank correlation coefficient = 0.22) showed that stigma is common in children even when diseases are not highly visible.
IN PRACTICE:
“Better treatment approaches for chronic skin diseases in children remain an unmet need. Increased awareness and instituting medical and psychological interventions to identify and reduce stigma and disease severity are important directions for improving QOL,” the authors concluded.
SOURCE:
Amy S. Paller, MD, professor of pediatrics and dermatology, Northwestern University, Chicago, led the study, which was published online in JAMA Dermatology.
LIMITATIONS:
Stigmatization needs to be assessed in children from low- and middle-income countries. Investigators enrolled children who had physician-assessed moderate to severe disease severity and/or at least some visibility of skin disease while wearing clothing, which resulted in exclusion of children with mild chronic disease, and the pandemic limited enrollment.
DISCLOSURES:
This study was funded through a grant from the Pediatric Dermatology Research Alliance (PeDRA). The authors declared receiving grants, personal fees, and honorarium and having other ties with various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Stigmatization has been addressed for several chronic medical conditions, such as HIV/AIDS, obesity, and mental illness; however, it has received limited attention in children living with chronic skin disorders.
- This cross-sectional, single-visit study examined the prevalence of stigma, its dependence on disease visibility and severity, and its association with mental health and QoL in children with chronic skin disorders.
- A total of 1671 children aged 8-17 years (57.9% girls; mean age, 13.7 years) were recruited from 32 pediatric dermatology centers in the United States and Canada from November 2018 to November 2021. The most common conditions were acne, atopic dermatitis/eczematous disorders, alopecia, and psoriasis, but rare genetic disorders were also represented.
- The primary outcome was the extent of stigmatization in relation to disease visibility, assessed using the Patient-Reported Outcomes Measurement Instrumentation System Pediatric Stigma-Skin.
- Secondary outcomes were the extent of stigmatization in relation to disease severity, along with QoL, depression, anxiety, and poor peer relationships.
TAKEAWAY:
- Approximately half (56.4%) of the children self-reported their skin condition as highly visible; 50.5% reported their disease severity as moderate, while 21.3% reported it as severe.
- Stigma was experienced by 73% of children and adolescents with chronic skin disease, with 43.8% reporting moderate stigma.
- Stigma scores correlated strongly with impaired QOL (Spearman’s rank correlation coefficient = 0.73) and child-reported scores for depression (Spearman’s rank correlation coefficient = 0.61) and moderately with anxiety (Spearman’s rank correlation coefficient = 0.54) and peer relationships (Spearman’s rank correlation coefficient = −0.49; all P < .001).
- Although stigma is increased for children with higher disease visibility and severity, the relatively weak correlation between child-assessed disease visibility and stigma (Spearman’s rank correlation coefficient = 0.22) showed that stigma is common in children even when diseases are not highly visible.
IN PRACTICE:
“Better treatment approaches for chronic skin diseases in children remain an unmet need. Increased awareness and instituting medical and psychological interventions to identify and reduce stigma and disease severity are important directions for improving QOL,” the authors concluded.
SOURCE:
Amy S. Paller, MD, professor of pediatrics and dermatology, Northwestern University, Chicago, led the study, which was published online in JAMA Dermatology.
LIMITATIONS:
Stigmatization needs to be assessed in children from low- and middle-income countries. Investigators enrolled children who had physician-assessed moderate to severe disease severity and/or at least some visibility of skin disease while wearing clothing, which resulted in exclusion of children with mild chronic disease, and the pandemic limited enrollment.
DISCLOSURES:
This study was funded through a grant from the Pediatric Dermatology Research Alliance (PeDRA). The authors declared receiving grants, personal fees, and honorarium and having other ties with various sources.
A version of this article appeared on Medscape.com.
Primary Care Shortage Reshaping How Patients Seek Care
By February of 2022, Ella, a 25-year-old behavioral interventionist in Colorado Springs, Colorado, was sick with strep-like symptoms for the third time in 3 months. She didn’t bother to call her doctor.
The first two times she had strep throat, she’d tried to schedule an appointment with her newest primary care doctor but couldn’t get in. They only had available appointments 5 and even 10 days out, but she’d already had symptoms for 3 days.
Until she graduated college, Ella had only known easy-access primary care. Her childhood family doctor and the nurse practitioners at her college clinic knew her. They anticipated her yearly allergies and knew about her predisposition for strep throat. Appointments were easy to schedule, and providers responded to her messages. But since entering the workforce and leaving her parent’s insurance, the kind of primary care she’d come to rely on was nearly impossible to find.
“I went to urgent care, and that became my primary care,” she told this news organization.
Patients Can’t Get Appointments
Primary care is in crisis. A growing number of Americans, like Ella, can’t access care when they need it. According to a 2024 report, 29% of adults and 14% of children don’t have a regular source of care. Those looking for a new primary care provider face extensive research and 6- to 9-month waits for a new patient appointment — if they can get in at all.
But even those with a primary care provider face long wait times: Days to weeks for a sick visit and months for a wellness checkup. Over one third of Medicare beneficiaries wait more than a month to see a doctor. Accessing primary care is more difficult than access to surgery, physical therapy, or rehabilitative care, according to a survey of Medicare beneficiaries by the Commonwealth Fund.
“Shortages tend to be in rural and urban underserved areas, but now, you’re hearing about primary care shortages in Boston, which is a mecca of healthcare,” said Ann Greiner, president and CEO of the Primary Care Coalition.
While retail clinics, urgent care, and telehealth help close the gap in acute needs, they miss one of primary care’s most critical benefits: A doctor who knows you. There’s strong evidence that ongoing treatment from a primary care physician (PCP) who knows your history, family, and context results in better long-term outcomes and fewer hospitalizations and emergency room visits.
If patients continue to find it too hard to break into primary care or set up an appointment, experts are concerned that they’ll stop pursuing primary care altogether.
Doctors’ Hands Are Tied
“I want to highlight that this is not an issue of primary care doctors not wanting to be accessible,” said Lisa Rotenstein, MD, MBA, a PCP and medical director of Ambulatory Quality and Safety at the University of California San Francisco Health. “These access issues are symptoms of the design of primary care in the United States.”
Across the United States, there’s a dearth of family medicine doctors, pediatricians, and internists. And without significantly more primary care providers, there’s simply no way for all Americans to get optimal primary care. The Health Resources and Services administration estimates a current shortage of 13,000 primary care providers. And that shortage will skyrocket to 68,000 by 2036 as the number of Americans needing care balloons and existing PCPs retire with too few trainees to fill their shoes.
The American Association of Medical Colleges predicts a slightly lower shortage in 2036 — between 20,000 and 40,000 primary care physicians — only if more residency positions are funded nationwide.
However, even with more positions, medical trainees see little incentive to pursue primary care. Young doctors are avoiding primary care because of the pressures, Dr. Rotenstein said. There’s incredible pressure to get reimbursement for primary care doctors. And the added administrative burden makes “the work life of these specialties not really manageable,” she said.
Continued Shortages of PCPs
“We know there’s a documented pajama time,” Ms. Greiner said. For every 1 hour spent with a patient, primary care must spend nearly 2 additional hours on electronic health records and desk work, according to a study by the American Medical Association. Even with all those additional hours devoted to getting paid, primary care doctors make an average of $103,000 less annually compared with their counterparts in surgery and oncology.
It’s not an attractive combination for a new doctor with medical debt. This year, Ms. Greiner said that residency positions in internal medicine and pediatrics went unfilled. Of those trainees who do go into a primary care specialty, many won’t last. Only half of primary care residents practice in primary care 3-5 years later. The rest choose to subspecialize or become hospitalists.
These untenable demands on a primary care provider don’t go unnoticed by patients. In Ella’s attempts to invest in a new primary care relationship, she often doesn’t feel heard and can tell the doctor is rushed. “[Urgent care is] probably not the best care because they don’t know me, but it does seem like they are able to listen to me better,” Ella said.
Patients Want to Invest in Primary Care
Primary care should work like putting money in a bank account, Dr. Rotenstein said. Young patients invest in the relationship and reap the benefits of a doctor who knows them later in life when they need more complex care. But if seeing a doctor is so difficult, many young people may stop investing in their PCP relationship.
“One thing ... that I worry about in this kind of situation where patients really have to put in a lot of work to get the care they need is in inequities of care,” Dr. Rotenstein said. “We know some of our patients are more able to undertake that work.”
Alternatively, the primary care shortage could be reshaping how patients seek care. A 2023 study showed the proportion of primary care preventative visits increased over 20 years. Policies under the Affordable Care Act were the driving force. But it’s also true that sick visits are being diverted to urgent care.
Ella told this news organization she doesn’t even consider primary care for sick visits at this point. “I can’t wait 5 days or a week and a half. Unless I have bigger issues, like I need tests, I’m not even going to go to primary care.” It’s possible that other patients also see primary care as a place for testing and wellness checks and leave sick visits to retail and urgent care.
The Road Ahead
There’s no single fix for primary care, but experts agree that the fee-for-service model is a core issue for the specialty. In a 2021 report, the National Association of Engineering and Medicine said that primary care reform needs to include higher reimbursement rates for primary care and that US primary care should be restructured so that payers “pay primary care teams to care for people, not doctors to deliver services.”
In the current model, the doctor-patient clinic time is the only income-generating part of a primary care practice. A better model would consider the communication, administration, teams, and support doctors have to fund to provide the best primary care.
“We need to change how we pay and how much we pay, so [primary care doctors] are properly incentivized to build out a team to provide the comprehensive care you need,” Ms. Greiner said.
In the meantime, primary care doctors are adapting. Some drop down to part-time to account for the additional administrative workload. Others are transitioning to concierge services to offer the quality of care they want while getting the income they need. Still, others specialize their practice, offering primary care to a subset of the population, like older adults.
Employers are also looking to improve care access for their employees, hiring in-house doctors to provide primary care on site. Ms. Greiner recently met with a group of chief medical officers from major companies to discuss expanding primary care access via the workplace.
The efforts to adapt amid a broken system are admirable, Dr. Rotenstein said. And whatever a PCP has to do to keep practicing in primary care is laudable. The only problem with these adaptations is they largely limit a doctor’s patient pool and, therefore, limit access, she said. More significant reforms that adequately reimburse primary care and incentivize new doctors are still needed.
As for Ella, she got married. Her wife is in the military, so now she has Tricare, which comes with a more streamlined process to access primary care. However, doctor shortages are just as evident in that system. The couple called to schedule new patient appointments after their recent move to Virginia. The first available ones were 6 weeks out.
A version of this article appeared on Medscape.com.
By February of 2022, Ella, a 25-year-old behavioral interventionist in Colorado Springs, Colorado, was sick with strep-like symptoms for the third time in 3 months. She didn’t bother to call her doctor.
The first two times she had strep throat, she’d tried to schedule an appointment with her newest primary care doctor but couldn’t get in. They only had available appointments 5 and even 10 days out, but she’d already had symptoms for 3 days.
Until she graduated college, Ella had only known easy-access primary care. Her childhood family doctor and the nurse practitioners at her college clinic knew her. They anticipated her yearly allergies and knew about her predisposition for strep throat. Appointments were easy to schedule, and providers responded to her messages. But since entering the workforce and leaving her parent’s insurance, the kind of primary care she’d come to rely on was nearly impossible to find.
“I went to urgent care, and that became my primary care,” she told this news organization.
Patients Can’t Get Appointments
Primary care is in crisis. A growing number of Americans, like Ella, can’t access care when they need it. According to a 2024 report, 29% of adults and 14% of children don’t have a regular source of care. Those looking for a new primary care provider face extensive research and 6- to 9-month waits for a new patient appointment — if they can get in at all.
But even those with a primary care provider face long wait times: Days to weeks for a sick visit and months for a wellness checkup. Over one third of Medicare beneficiaries wait more than a month to see a doctor. Accessing primary care is more difficult than access to surgery, physical therapy, or rehabilitative care, according to a survey of Medicare beneficiaries by the Commonwealth Fund.
“Shortages tend to be in rural and urban underserved areas, but now, you’re hearing about primary care shortages in Boston, which is a mecca of healthcare,” said Ann Greiner, president and CEO of the Primary Care Coalition.
While retail clinics, urgent care, and telehealth help close the gap in acute needs, they miss one of primary care’s most critical benefits: A doctor who knows you. There’s strong evidence that ongoing treatment from a primary care physician (PCP) who knows your history, family, and context results in better long-term outcomes and fewer hospitalizations and emergency room visits.
If patients continue to find it too hard to break into primary care or set up an appointment, experts are concerned that they’ll stop pursuing primary care altogether.
Doctors’ Hands Are Tied
“I want to highlight that this is not an issue of primary care doctors not wanting to be accessible,” said Lisa Rotenstein, MD, MBA, a PCP and medical director of Ambulatory Quality and Safety at the University of California San Francisco Health. “These access issues are symptoms of the design of primary care in the United States.”
Across the United States, there’s a dearth of family medicine doctors, pediatricians, and internists. And without significantly more primary care providers, there’s simply no way for all Americans to get optimal primary care. The Health Resources and Services administration estimates a current shortage of 13,000 primary care providers. And that shortage will skyrocket to 68,000 by 2036 as the number of Americans needing care balloons and existing PCPs retire with too few trainees to fill their shoes.
The American Association of Medical Colleges predicts a slightly lower shortage in 2036 — between 20,000 and 40,000 primary care physicians — only if more residency positions are funded nationwide.
However, even with more positions, medical trainees see little incentive to pursue primary care. Young doctors are avoiding primary care because of the pressures, Dr. Rotenstein said. There’s incredible pressure to get reimbursement for primary care doctors. And the added administrative burden makes “the work life of these specialties not really manageable,” she said.
Continued Shortages of PCPs
“We know there’s a documented pajama time,” Ms. Greiner said. For every 1 hour spent with a patient, primary care must spend nearly 2 additional hours on electronic health records and desk work, according to a study by the American Medical Association. Even with all those additional hours devoted to getting paid, primary care doctors make an average of $103,000 less annually compared with their counterparts in surgery and oncology.
It’s not an attractive combination for a new doctor with medical debt. This year, Ms. Greiner said that residency positions in internal medicine and pediatrics went unfilled. Of those trainees who do go into a primary care specialty, many won’t last. Only half of primary care residents practice in primary care 3-5 years later. The rest choose to subspecialize or become hospitalists.
These untenable demands on a primary care provider don’t go unnoticed by patients. In Ella’s attempts to invest in a new primary care relationship, she often doesn’t feel heard and can tell the doctor is rushed. “[Urgent care is] probably not the best care because they don’t know me, but it does seem like they are able to listen to me better,” Ella said.
Patients Want to Invest in Primary Care
Primary care should work like putting money in a bank account, Dr. Rotenstein said. Young patients invest in the relationship and reap the benefits of a doctor who knows them later in life when they need more complex care. But if seeing a doctor is so difficult, many young people may stop investing in their PCP relationship.
“One thing ... that I worry about in this kind of situation where patients really have to put in a lot of work to get the care they need is in inequities of care,” Dr. Rotenstein said. “We know some of our patients are more able to undertake that work.”
Alternatively, the primary care shortage could be reshaping how patients seek care. A 2023 study showed the proportion of primary care preventative visits increased over 20 years. Policies under the Affordable Care Act were the driving force. But it’s also true that sick visits are being diverted to urgent care.
Ella told this news organization she doesn’t even consider primary care for sick visits at this point. “I can’t wait 5 days or a week and a half. Unless I have bigger issues, like I need tests, I’m not even going to go to primary care.” It’s possible that other patients also see primary care as a place for testing and wellness checks and leave sick visits to retail and urgent care.
The Road Ahead
There’s no single fix for primary care, but experts agree that the fee-for-service model is a core issue for the specialty. In a 2021 report, the National Association of Engineering and Medicine said that primary care reform needs to include higher reimbursement rates for primary care and that US primary care should be restructured so that payers “pay primary care teams to care for people, not doctors to deliver services.”
In the current model, the doctor-patient clinic time is the only income-generating part of a primary care practice. A better model would consider the communication, administration, teams, and support doctors have to fund to provide the best primary care.
“We need to change how we pay and how much we pay, so [primary care doctors] are properly incentivized to build out a team to provide the comprehensive care you need,” Ms. Greiner said.
In the meantime, primary care doctors are adapting. Some drop down to part-time to account for the additional administrative workload. Others are transitioning to concierge services to offer the quality of care they want while getting the income they need. Still, others specialize their practice, offering primary care to a subset of the population, like older adults.
Employers are also looking to improve care access for their employees, hiring in-house doctors to provide primary care on site. Ms. Greiner recently met with a group of chief medical officers from major companies to discuss expanding primary care access via the workplace.
The efforts to adapt amid a broken system are admirable, Dr. Rotenstein said. And whatever a PCP has to do to keep practicing in primary care is laudable. The only problem with these adaptations is they largely limit a doctor’s patient pool and, therefore, limit access, she said. More significant reforms that adequately reimburse primary care and incentivize new doctors are still needed.
As for Ella, she got married. Her wife is in the military, so now she has Tricare, which comes with a more streamlined process to access primary care. However, doctor shortages are just as evident in that system. The couple called to schedule new patient appointments after their recent move to Virginia. The first available ones were 6 weeks out.
A version of this article appeared on Medscape.com.
By February of 2022, Ella, a 25-year-old behavioral interventionist in Colorado Springs, Colorado, was sick with strep-like symptoms for the third time in 3 months. She didn’t bother to call her doctor.
The first two times she had strep throat, she’d tried to schedule an appointment with her newest primary care doctor but couldn’t get in. They only had available appointments 5 and even 10 days out, but she’d already had symptoms for 3 days.
Until she graduated college, Ella had only known easy-access primary care. Her childhood family doctor and the nurse practitioners at her college clinic knew her. They anticipated her yearly allergies and knew about her predisposition for strep throat. Appointments were easy to schedule, and providers responded to her messages. But since entering the workforce and leaving her parent’s insurance, the kind of primary care she’d come to rely on was nearly impossible to find.
“I went to urgent care, and that became my primary care,” she told this news organization.
Patients Can’t Get Appointments
Primary care is in crisis. A growing number of Americans, like Ella, can’t access care when they need it. According to a 2024 report, 29% of adults and 14% of children don’t have a regular source of care. Those looking for a new primary care provider face extensive research and 6- to 9-month waits for a new patient appointment — if they can get in at all.
But even those with a primary care provider face long wait times: Days to weeks for a sick visit and months for a wellness checkup. Over one third of Medicare beneficiaries wait more than a month to see a doctor. Accessing primary care is more difficult than access to surgery, physical therapy, or rehabilitative care, according to a survey of Medicare beneficiaries by the Commonwealth Fund.
“Shortages tend to be in rural and urban underserved areas, but now, you’re hearing about primary care shortages in Boston, which is a mecca of healthcare,” said Ann Greiner, president and CEO of the Primary Care Coalition.
While retail clinics, urgent care, and telehealth help close the gap in acute needs, they miss one of primary care’s most critical benefits: A doctor who knows you. There’s strong evidence that ongoing treatment from a primary care physician (PCP) who knows your history, family, and context results in better long-term outcomes and fewer hospitalizations and emergency room visits.
If patients continue to find it too hard to break into primary care or set up an appointment, experts are concerned that they’ll stop pursuing primary care altogether.
Doctors’ Hands Are Tied
“I want to highlight that this is not an issue of primary care doctors not wanting to be accessible,” said Lisa Rotenstein, MD, MBA, a PCP and medical director of Ambulatory Quality and Safety at the University of California San Francisco Health. “These access issues are symptoms of the design of primary care in the United States.”
Across the United States, there’s a dearth of family medicine doctors, pediatricians, and internists. And without significantly more primary care providers, there’s simply no way for all Americans to get optimal primary care. The Health Resources and Services administration estimates a current shortage of 13,000 primary care providers. And that shortage will skyrocket to 68,000 by 2036 as the number of Americans needing care balloons and existing PCPs retire with too few trainees to fill their shoes.
The American Association of Medical Colleges predicts a slightly lower shortage in 2036 — between 20,000 and 40,000 primary care physicians — only if more residency positions are funded nationwide.
However, even with more positions, medical trainees see little incentive to pursue primary care. Young doctors are avoiding primary care because of the pressures, Dr. Rotenstein said. There’s incredible pressure to get reimbursement for primary care doctors. And the added administrative burden makes “the work life of these specialties not really manageable,” she said.
Continued Shortages of PCPs
“We know there’s a documented pajama time,” Ms. Greiner said. For every 1 hour spent with a patient, primary care must spend nearly 2 additional hours on electronic health records and desk work, according to a study by the American Medical Association. Even with all those additional hours devoted to getting paid, primary care doctors make an average of $103,000 less annually compared with their counterparts in surgery and oncology.
It’s not an attractive combination for a new doctor with medical debt. This year, Ms. Greiner said that residency positions in internal medicine and pediatrics went unfilled. Of those trainees who do go into a primary care specialty, many won’t last. Only half of primary care residents practice in primary care 3-5 years later. The rest choose to subspecialize or become hospitalists.
These untenable demands on a primary care provider don’t go unnoticed by patients. In Ella’s attempts to invest in a new primary care relationship, she often doesn’t feel heard and can tell the doctor is rushed. “[Urgent care is] probably not the best care because they don’t know me, but it does seem like they are able to listen to me better,” Ella said.
Patients Want to Invest in Primary Care
Primary care should work like putting money in a bank account, Dr. Rotenstein said. Young patients invest in the relationship and reap the benefits of a doctor who knows them later in life when they need more complex care. But if seeing a doctor is so difficult, many young people may stop investing in their PCP relationship.
“One thing ... that I worry about in this kind of situation where patients really have to put in a lot of work to get the care they need is in inequities of care,” Dr. Rotenstein said. “We know some of our patients are more able to undertake that work.”
Alternatively, the primary care shortage could be reshaping how patients seek care. A 2023 study showed the proportion of primary care preventative visits increased over 20 years. Policies under the Affordable Care Act were the driving force. But it’s also true that sick visits are being diverted to urgent care.
Ella told this news organization she doesn’t even consider primary care for sick visits at this point. “I can’t wait 5 days or a week and a half. Unless I have bigger issues, like I need tests, I’m not even going to go to primary care.” It’s possible that other patients also see primary care as a place for testing and wellness checks and leave sick visits to retail and urgent care.
The Road Ahead
There’s no single fix for primary care, but experts agree that the fee-for-service model is a core issue for the specialty. In a 2021 report, the National Association of Engineering and Medicine said that primary care reform needs to include higher reimbursement rates for primary care and that US primary care should be restructured so that payers “pay primary care teams to care for people, not doctors to deliver services.”
In the current model, the doctor-patient clinic time is the only income-generating part of a primary care practice. A better model would consider the communication, administration, teams, and support doctors have to fund to provide the best primary care.
“We need to change how we pay and how much we pay, so [primary care doctors] are properly incentivized to build out a team to provide the comprehensive care you need,” Ms. Greiner said.
In the meantime, primary care doctors are adapting. Some drop down to part-time to account for the additional administrative workload. Others are transitioning to concierge services to offer the quality of care they want while getting the income they need. Still, others specialize their practice, offering primary care to a subset of the population, like older adults.
Employers are also looking to improve care access for their employees, hiring in-house doctors to provide primary care on site. Ms. Greiner recently met with a group of chief medical officers from major companies to discuss expanding primary care access via the workplace.
The efforts to adapt amid a broken system are admirable, Dr. Rotenstein said. And whatever a PCP has to do to keep practicing in primary care is laudable. The only problem with these adaptations is they largely limit a doctor’s patient pool and, therefore, limit access, she said. More significant reforms that adequately reimburse primary care and incentivize new doctors are still needed.
As for Ella, she got married. Her wife is in the military, so now she has Tricare, which comes with a more streamlined process to access primary care. However, doctor shortages are just as evident in that system. The couple called to schedule new patient appointments after their recent move to Virginia. The first available ones were 6 weeks out.
A version of this article appeared on Medscape.com.
Working Hard or Work Addiction — Have You Crossed the Line?
When child psychiatrist Javeed Sukhera, MD, PhD, was a few years into his career, he found himself doing it all. “I was in a leadership role academically at the medical school, I had a leadership role at the hospital, and I was seeing as many patients as I could. I could work all day every day.”
“It still wouldn’t have been enough,” he said.
Whenever there was a shift available, Dr. Sukhera would take it. His job was stressful, but as a new physician with a young family, he saw this obsession with work as necessary. “I began to cope with the stress from work by doing extra work and feeling like I needed to be everywhere. It was like I became a hamster on a spinning wheel. I was just running, running, running.”
Things shifted for Dr. Sukhera when he realized that while he was emotionally available for the children who were his patients, at home, his own children weren’t getting the best of him. “There was a specific moment when I thought my son was afraid of me,” he said. “I just stopped and realized that there was something happening that I needed to break. I needed to make a change.”
Dr. Sukhera, now chair of psychiatry at the Institute of Living and chief of the Department of Psychiatry at Hartford Hospital, Hartford, Connecticut, believes what he experienced was a steep fall into work addiction.
What Does Work Addiction Look Like for Doctors?
Behavioral addictions are fairly new in the addiction space. When gambling disorder, the first and only behavioral addiction in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, was added in 2013, it was seen as a “breakthrough addiction,” said Mark D. Griffiths, PhD, a leading behavioral addiction researcher and a distinguished professor at Nottingham Trent University.
Because there is not enough evidence yet to classify work addiction as a formal diagnosis, there is no clear consensus on how to define it. To further complicate things, the terms “workaholism” and “work addiction” can be used interchangeably, and some experts say the two are not the same, though they can overlap.
That said, a 2018 review of literature from several countries found that work addiction “fits very well into recently postulated criteria for conceptualization of a behavioral addiction.
“If you accept that gambling can be genuinely addictive, then there’s no reason to think that something like work, exercise, or video game playing couldn’t be an addiction as well,” said Dr. Griffiths.
“The neurobiology of addiction is that we get drawn to something that gives us a dopamine hit,” Dr. Sukhera added. “But to do that all day, every day, has consequences. It drains our emotional reserves, and it can greatly impact our relationships.”
On top of that, work addiction has been linked with poor sleep, poor cardiovascular health, high blood pressure, burnout, the development of autoimmune disorders, and other health issues.
Physicians are particularly susceptible. Doctors, after all, are expected to work long hours and put their patients’ needs first, even at the expense of their own health and well-being.
“Workaholism is not just socially acceptable in medicine,” said Dr. Sukhera. “It’s baked into the system and built into the structures. The healthcare system has largely functioned on the emotional labor of health workers, whose tendency to show up and work harder can, at times, in certain organizations, be exploited.”
Dr. Griffiths agreed that with the limited amount of data available, work addiction does appear to exist at higher rates in medicine than in other fields. As early as the 1970s, medical literature describes work as a “socially acceptable” addiction among doctors. A 2014 study published in Occupational Medicine reported that of 445 physicians who took part in the research, nearly half exhibited some level of work addiction with 13% “highly work addicted.”
Of course, working hard or even meeting unreasonable demands from work is not the same as work addiction, as Dr. Griffiths clarified in a 2023 editorial in BMJ Quality & Safety. The difference, as with other behavioral addictions, is when people obsess about work and use it to cope with stress. It can be easier to stay distracted and busy to gain a sense of control rather than learning to deal with complex emotions.
A 2021 study that Dr. Sukhera conducted with resident physicians found that working harder was one of the main ways they dealt with stress during the COVID-19 pandemic. “This idea that we deal with the stress of being burnt out by doing more and more of what burns us out is fairly ubiquitous at all stages of medical professionals’ careers,” he said.
Financial incentives also can fuel work addiction, said Dr. Sukhera. In residency, there are some safeguards around overwork and duty hours. When you become an attending, those limits no longer exist. As a young physician, Dr. Sukhera had student debt to pay off and a family to support. When he found opportunities to earn more by working more, his answer was always “yes.”
Pressure to produce medical research also can pose issues. Some physicians can become addicted to publishing studies, fearing that they might lose their professional status or position if they stop. It’s a cycle that can force a doctor to not only work long hours doing their job but also practically take on a second one.
How Physicians Can Recognize Work Addiction in Themselves
Work addiction can look and feel different for every person, said Malissa Clark, PhD, associate professor at the University of Georgia and author of the recent book Never Not Working: Why the Always-On Culture Is Bad for Business—and How to Fix It.
Dr. Clark noted that people who are highly engaged in their work tend to be driven by intrinsic motivation: “You work because you love it.” With work addiction, “you work because you feel like you ought to be working all the time.”
Of course, it’s not always so cut and dried; you can experience both forms of motivation and not necessarily become addicted to work. But if you are solely driven by the feeling that you ought to be working all the time, that can be a red flag.
Dr. Griffiths said that while many people may have problematic work habits or work too much, true work addicts must meet six criteria that apply to all addictions:
1. Salience: Work is the single most important thing in your life, to the point of neglecting everything else. Even if you’re on vacation, your mind might be flooded with work thoughts.
2. Mood modification: You use work to modify your mood, either to get a “high” or to cope with stress.
3. Tolerance: Over time, you’ve gone from working 8 or 10 hours a day to 12 hours a day, to a point where you’re working all the time.
4. Withdrawal: On a physiological level, you will have symptoms such as anxiety, nausea, or headaches when unable to work.
5. Conflict: You feel conflicted with yourself (you know you’re working too much) or with others (partners, friends, and children) about work, but you can’t stop.
6. Relapse: If you manage to cut down your hours but can’t resist overworking 1 day, you wind up right back where you were.
When It’s Time to Address Work Addiction
The lack of a formal diagnosis for work addiction makes getting treatment difficult. But there are ways to seek help. Unlike the drug and alcohol literature, abstinence is not the goal. “The therapeutic goal is getting a behavior under control and looking for the triggers of why you’re compulsively working,” said Dr. Griffiths.
Practice self-compassion
Dr. Sukhera eventually realized that his work addiction stemmed from the fear of being somehow excluded or unworthy. He actively corrected much of this through self-compassion and self-kindness, which helped him set boundaries. “Self-compassion is the root of everything,” he said. “Reminding ourselves that we’re doing our best is an important ingredient in breaking the cycle.”
Slowly expose yourself to relaxation
Many workaholics find rest very difficult. “When I conducted interviews with people [who considered themselves workaholics], a very common thing I heard was, ‘I have a very hard time being idle,’ ” said Dr. Clark. If rest feels hard, Dr. Sukhera suggests practicing relaxation for 2 minutes to start. Even small periods of downtime can challenge the belief that you must be constantly productive.
Reframe your to-do list
For work addicts, to-do lists can seem like they must be finished, which prolongs work hours. Instead, use to-do lists to help prioritize what is urgent, identify what can wait, and delegate out tasks to others, Dr. Clark recommends.
Pick up a mastery experience
Research from professor Sabine Sonnentag, Dr. rer. nat., at the University of Mannheim, Mannheim, Germany, suggests that mastery experiences — leisure activities that require thought and focus like learning a new language or taking a woodworking class — can help you actively disengage from work.
Try cognitive behavioral therapy
Widely used for other forms of addiction, cognitive behavioral therapy centers around recognizing emotions, challenging thought patterns, and changing behaviors. However, Dr. Clark admits the research on its impact on work addiction, in particular, is “pretty nascent.”
Shift your mindset
It seems logical to think that detaching from your feelings will allow you to “do more,” but experts say that idea is both untrue and dangerous. “The safest hospitals are the hospitals where people are attuned to their humanness,” said Dr. Sukhera. “It’s normal to overwork in medicine, and if you’re challenging a norm, you really have to be thoughtful about how you frame that for yourself.”
Most importantly: Seek support
Today, there is increased awareness about work addiction and more resources for physicians who are struggling, including programs such as Workaholics Anonymous or Physicians Anonymous and workplace wellness initiatives. But try not to overwhelm yourself with choosing whom to talk to or what specific resource to utilize, Dr. Sukhera advised. “Just talk to someone about it. You don’t have to carry this on your own.”
A version of this article appeared on Medscape.com.
When child psychiatrist Javeed Sukhera, MD, PhD, was a few years into his career, he found himself doing it all. “I was in a leadership role academically at the medical school, I had a leadership role at the hospital, and I was seeing as many patients as I could. I could work all day every day.”
“It still wouldn’t have been enough,” he said.
Whenever there was a shift available, Dr. Sukhera would take it. His job was stressful, but as a new physician with a young family, he saw this obsession with work as necessary. “I began to cope with the stress from work by doing extra work and feeling like I needed to be everywhere. It was like I became a hamster on a spinning wheel. I was just running, running, running.”
Things shifted for Dr. Sukhera when he realized that while he was emotionally available for the children who were his patients, at home, his own children weren’t getting the best of him. “There was a specific moment when I thought my son was afraid of me,” he said. “I just stopped and realized that there was something happening that I needed to break. I needed to make a change.”
Dr. Sukhera, now chair of psychiatry at the Institute of Living and chief of the Department of Psychiatry at Hartford Hospital, Hartford, Connecticut, believes what he experienced was a steep fall into work addiction.
What Does Work Addiction Look Like for Doctors?
Behavioral addictions are fairly new in the addiction space. When gambling disorder, the first and only behavioral addiction in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, was added in 2013, it was seen as a “breakthrough addiction,” said Mark D. Griffiths, PhD, a leading behavioral addiction researcher and a distinguished professor at Nottingham Trent University.
Because there is not enough evidence yet to classify work addiction as a formal diagnosis, there is no clear consensus on how to define it. To further complicate things, the terms “workaholism” and “work addiction” can be used interchangeably, and some experts say the two are not the same, though they can overlap.
That said, a 2018 review of literature from several countries found that work addiction “fits very well into recently postulated criteria for conceptualization of a behavioral addiction.
“If you accept that gambling can be genuinely addictive, then there’s no reason to think that something like work, exercise, or video game playing couldn’t be an addiction as well,” said Dr. Griffiths.
“The neurobiology of addiction is that we get drawn to something that gives us a dopamine hit,” Dr. Sukhera added. “But to do that all day, every day, has consequences. It drains our emotional reserves, and it can greatly impact our relationships.”
On top of that, work addiction has been linked with poor sleep, poor cardiovascular health, high blood pressure, burnout, the development of autoimmune disorders, and other health issues.
Physicians are particularly susceptible. Doctors, after all, are expected to work long hours and put their patients’ needs first, even at the expense of their own health and well-being.
“Workaholism is not just socially acceptable in medicine,” said Dr. Sukhera. “It’s baked into the system and built into the structures. The healthcare system has largely functioned on the emotional labor of health workers, whose tendency to show up and work harder can, at times, in certain organizations, be exploited.”
Dr. Griffiths agreed that with the limited amount of data available, work addiction does appear to exist at higher rates in medicine than in other fields. As early as the 1970s, medical literature describes work as a “socially acceptable” addiction among doctors. A 2014 study published in Occupational Medicine reported that of 445 physicians who took part in the research, nearly half exhibited some level of work addiction with 13% “highly work addicted.”
Of course, working hard or even meeting unreasonable demands from work is not the same as work addiction, as Dr. Griffiths clarified in a 2023 editorial in BMJ Quality & Safety. The difference, as with other behavioral addictions, is when people obsess about work and use it to cope with stress. It can be easier to stay distracted and busy to gain a sense of control rather than learning to deal with complex emotions.
A 2021 study that Dr. Sukhera conducted with resident physicians found that working harder was one of the main ways they dealt with stress during the COVID-19 pandemic. “This idea that we deal with the stress of being burnt out by doing more and more of what burns us out is fairly ubiquitous at all stages of medical professionals’ careers,” he said.
Financial incentives also can fuel work addiction, said Dr. Sukhera. In residency, there are some safeguards around overwork and duty hours. When you become an attending, those limits no longer exist. As a young physician, Dr. Sukhera had student debt to pay off and a family to support. When he found opportunities to earn more by working more, his answer was always “yes.”
Pressure to produce medical research also can pose issues. Some physicians can become addicted to publishing studies, fearing that they might lose their professional status or position if they stop. It’s a cycle that can force a doctor to not only work long hours doing their job but also practically take on a second one.
How Physicians Can Recognize Work Addiction in Themselves
Work addiction can look and feel different for every person, said Malissa Clark, PhD, associate professor at the University of Georgia and author of the recent book Never Not Working: Why the Always-On Culture Is Bad for Business—and How to Fix It.
Dr. Clark noted that people who are highly engaged in their work tend to be driven by intrinsic motivation: “You work because you love it.” With work addiction, “you work because you feel like you ought to be working all the time.”
Of course, it’s not always so cut and dried; you can experience both forms of motivation and not necessarily become addicted to work. But if you are solely driven by the feeling that you ought to be working all the time, that can be a red flag.
Dr. Griffiths said that while many people may have problematic work habits or work too much, true work addicts must meet six criteria that apply to all addictions:
1. Salience: Work is the single most important thing in your life, to the point of neglecting everything else. Even if you’re on vacation, your mind might be flooded with work thoughts.
2. Mood modification: You use work to modify your mood, either to get a “high” or to cope with stress.
3. Tolerance: Over time, you’ve gone from working 8 or 10 hours a day to 12 hours a day, to a point where you’re working all the time.
4. Withdrawal: On a physiological level, you will have symptoms such as anxiety, nausea, or headaches when unable to work.
5. Conflict: You feel conflicted with yourself (you know you’re working too much) or with others (partners, friends, and children) about work, but you can’t stop.
6. Relapse: If you manage to cut down your hours but can’t resist overworking 1 day, you wind up right back where you were.
When It’s Time to Address Work Addiction
The lack of a formal diagnosis for work addiction makes getting treatment difficult. But there are ways to seek help. Unlike the drug and alcohol literature, abstinence is not the goal. “The therapeutic goal is getting a behavior under control and looking for the triggers of why you’re compulsively working,” said Dr. Griffiths.
Practice self-compassion
Dr. Sukhera eventually realized that his work addiction stemmed from the fear of being somehow excluded or unworthy. He actively corrected much of this through self-compassion and self-kindness, which helped him set boundaries. “Self-compassion is the root of everything,” he said. “Reminding ourselves that we’re doing our best is an important ingredient in breaking the cycle.”
Slowly expose yourself to relaxation
Many workaholics find rest very difficult. “When I conducted interviews with people [who considered themselves workaholics], a very common thing I heard was, ‘I have a very hard time being idle,’ ” said Dr. Clark. If rest feels hard, Dr. Sukhera suggests practicing relaxation for 2 minutes to start. Even small periods of downtime can challenge the belief that you must be constantly productive.
Reframe your to-do list
For work addicts, to-do lists can seem like they must be finished, which prolongs work hours. Instead, use to-do lists to help prioritize what is urgent, identify what can wait, and delegate out tasks to others, Dr. Clark recommends.
Pick up a mastery experience
Research from professor Sabine Sonnentag, Dr. rer. nat., at the University of Mannheim, Mannheim, Germany, suggests that mastery experiences — leisure activities that require thought and focus like learning a new language or taking a woodworking class — can help you actively disengage from work.
Try cognitive behavioral therapy
Widely used for other forms of addiction, cognitive behavioral therapy centers around recognizing emotions, challenging thought patterns, and changing behaviors. However, Dr. Clark admits the research on its impact on work addiction, in particular, is “pretty nascent.”
Shift your mindset
It seems logical to think that detaching from your feelings will allow you to “do more,” but experts say that idea is both untrue and dangerous. “The safest hospitals are the hospitals where people are attuned to their humanness,” said Dr. Sukhera. “It’s normal to overwork in medicine, and if you’re challenging a norm, you really have to be thoughtful about how you frame that for yourself.”
Most importantly: Seek support
Today, there is increased awareness about work addiction and more resources for physicians who are struggling, including programs such as Workaholics Anonymous or Physicians Anonymous and workplace wellness initiatives. But try not to overwhelm yourself with choosing whom to talk to or what specific resource to utilize, Dr. Sukhera advised. “Just talk to someone about it. You don’t have to carry this on your own.”
A version of this article appeared on Medscape.com.
When child psychiatrist Javeed Sukhera, MD, PhD, was a few years into his career, he found himself doing it all. “I was in a leadership role academically at the medical school, I had a leadership role at the hospital, and I was seeing as many patients as I could. I could work all day every day.”
“It still wouldn’t have been enough,” he said.
Whenever there was a shift available, Dr. Sukhera would take it. His job was stressful, but as a new physician with a young family, he saw this obsession with work as necessary. “I began to cope with the stress from work by doing extra work and feeling like I needed to be everywhere. It was like I became a hamster on a spinning wheel. I was just running, running, running.”
Things shifted for Dr. Sukhera when he realized that while he was emotionally available for the children who were his patients, at home, his own children weren’t getting the best of him. “There was a specific moment when I thought my son was afraid of me,” he said. “I just stopped and realized that there was something happening that I needed to break. I needed to make a change.”
Dr. Sukhera, now chair of psychiatry at the Institute of Living and chief of the Department of Psychiatry at Hartford Hospital, Hartford, Connecticut, believes what he experienced was a steep fall into work addiction.
What Does Work Addiction Look Like for Doctors?
Behavioral addictions are fairly new in the addiction space. When gambling disorder, the first and only behavioral addiction in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, was added in 2013, it was seen as a “breakthrough addiction,” said Mark D. Griffiths, PhD, a leading behavioral addiction researcher and a distinguished professor at Nottingham Trent University.
Because there is not enough evidence yet to classify work addiction as a formal diagnosis, there is no clear consensus on how to define it. To further complicate things, the terms “workaholism” and “work addiction” can be used interchangeably, and some experts say the two are not the same, though they can overlap.
That said, a 2018 review of literature from several countries found that work addiction “fits very well into recently postulated criteria for conceptualization of a behavioral addiction.
“If you accept that gambling can be genuinely addictive, then there’s no reason to think that something like work, exercise, or video game playing couldn’t be an addiction as well,” said Dr. Griffiths.
“The neurobiology of addiction is that we get drawn to something that gives us a dopamine hit,” Dr. Sukhera added. “But to do that all day, every day, has consequences. It drains our emotional reserves, and it can greatly impact our relationships.”
On top of that, work addiction has been linked with poor sleep, poor cardiovascular health, high blood pressure, burnout, the development of autoimmune disorders, and other health issues.
Physicians are particularly susceptible. Doctors, after all, are expected to work long hours and put their patients’ needs first, even at the expense of their own health and well-being.
“Workaholism is not just socially acceptable in medicine,” said Dr. Sukhera. “It’s baked into the system and built into the structures. The healthcare system has largely functioned on the emotional labor of health workers, whose tendency to show up and work harder can, at times, in certain organizations, be exploited.”
Dr. Griffiths agreed that with the limited amount of data available, work addiction does appear to exist at higher rates in medicine than in other fields. As early as the 1970s, medical literature describes work as a “socially acceptable” addiction among doctors. A 2014 study published in Occupational Medicine reported that of 445 physicians who took part in the research, nearly half exhibited some level of work addiction with 13% “highly work addicted.”
Of course, working hard or even meeting unreasonable demands from work is not the same as work addiction, as Dr. Griffiths clarified in a 2023 editorial in BMJ Quality & Safety. The difference, as with other behavioral addictions, is when people obsess about work and use it to cope with stress. It can be easier to stay distracted and busy to gain a sense of control rather than learning to deal with complex emotions.
A 2021 study that Dr. Sukhera conducted with resident physicians found that working harder was one of the main ways they dealt with stress during the COVID-19 pandemic. “This idea that we deal with the stress of being burnt out by doing more and more of what burns us out is fairly ubiquitous at all stages of medical professionals’ careers,” he said.
Financial incentives also can fuel work addiction, said Dr. Sukhera. In residency, there are some safeguards around overwork and duty hours. When you become an attending, those limits no longer exist. As a young physician, Dr. Sukhera had student debt to pay off and a family to support. When he found opportunities to earn more by working more, his answer was always “yes.”
Pressure to produce medical research also can pose issues. Some physicians can become addicted to publishing studies, fearing that they might lose their professional status or position if they stop. It’s a cycle that can force a doctor to not only work long hours doing their job but also practically take on a second one.
How Physicians Can Recognize Work Addiction in Themselves
Work addiction can look and feel different for every person, said Malissa Clark, PhD, associate professor at the University of Georgia and author of the recent book Never Not Working: Why the Always-On Culture Is Bad for Business—and How to Fix It.
Dr. Clark noted that people who are highly engaged in their work tend to be driven by intrinsic motivation: “You work because you love it.” With work addiction, “you work because you feel like you ought to be working all the time.”
Of course, it’s not always so cut and dried; you can experience both forms of motivation and not necessarily become addicted to work. But if you are solely driven by the feeling that you ought to be working all the time, that can be a red flag.
Dr. Griffiths said that while many people may have problematic work habits or work too much, true work addicts must meet six criteria that apply to all addictions:
1. Salience: Work is the single most important thing in your life, to the point of neglecting everything else. Even if you’re on vacation, your mind might be flooded with work thoughts.
2. Mood modification: You use work to modify your mood, either to get a “high” or to cope with stress.
3. Tolerance: Over time, you’ve gone from working 8 or 10 hours a day to 12 hours a day, to a point where you’re working all the time.
4. Withdrawal: On a physiological level, you will have symptoms such as anxiety, nausea, or headaches when unable to work.
5. Conflict: You feel conflicted with yourself (you know you’re working too much) or with others (partners, friends, and children) about work, but you can’t stop.
6. Relapse: If you manage to cut down your hours but can’t resist overworking 1 day, you wind up right back where you were.
When It’s Time to Address Work Addiction
The lack of a formal diagnosis for work addiction makes getting treatment difficult. But there are ways to seek help. Unlike the drug and alcohol literature, abstinence is not the goal. “The therapeutic goal is getting a behavior under control and looking for the triggers of why you’re compulsively working,” said Dr. Griffiths.
Practice self-compassion
Dr. Sukhera eventually realized that his work addiction stemmed from the fear of being somehow excluded or unworthy. He actively corrected much of this through self-compassion and self-kindness, which helped him set boundaries. “Self-compassion is the root of everything,” he said. “Reminding ourselves that we’re doing our best is an important ingredient in breaking the cycle.”
Slowly expose yourself to relaxation
Many workaholics find rest very difficult. “When I conducted interviews with people [who considered themselves workaholics], a very common thing I heard was, ‘I have a very hard time being idle,’ ” said Dr. Clark. If rest feels hard, Dr. Sukhera suggests practicing relaxation for 2 minutes to start. Even small periods of downtime can challenge the belief that you must be constantly productive.
Reframe your to-do list
For work addicts, to-do lists can seem like they must be finished, which prolongs work hours. Instead, use to-do lists to help prioritize what is urgent, identify what can wait, and delegate out tasks to others, Dr. Clark recommends.
Pick up a mastery experience
Research from professor Sabine Sonnentag, Dr. rer. nat., at the University of Mannheim, Mannheim, Germany, suggests that mastery experiences — leisure activities that require thought and focus like learning a new language or taking a woodworking class — can help you actively disengage from work.
Try cognitive behavioral therapy
Widely used for other forms of addiction, cognitive behavioral therapy centers around recognizing emotions, challenging thought patterns, and changing behaviors. However, Dr. Clark admits the research on its impact on work addiction, in particular, is “pretty nascent.”
Shift your mindset
It seems logical to think that detaching from your feelings will allow you to “do more,” but experts say that idea is both untrue and dangerous. “The safest hospitals are the hospitals where people are attuned to their humanness,” said Dr. Sukhera. “It’s normal to overwork in medicine, and if you’re challenging a norm, you really have to be thoughtful about how you frame that for yourself.”
Most importantly: Seek support
Today, there is increased awareness about work addiction and more resources for physicians who are struggling, including programs such as Workaholics Anonymous or Physicians Anonymous and workplace wellness initiatives. But try not to overwhelm yourself with choosing whom to talk to or what specific resource to utilize, Dr. Sukhera advised. “Just talk to someone about it. You don’t have to carry this on your own.”
A version of this article appeared on Medscape.com.
PCP Compensation, Part 1
I recently read an op-ed piece in which the author wondered if any young people entering the practice of medicine felt that they were answering a “calling.” I suspect that there will continue to be, and will always be, idealists whose primary motivation for choosing medicine is that they will be healing the sick or at least providing comfort to the suffering. I occasionally hear that about a former patient who has been inspired by a personal or familial experience with a serious illness.
Unfortunately, I suspect those who feel called are the providers most likely to feel discouraged and frustrated by the current state of primary care. Luckily, I never felt a calling. For me, primary care pediatrics was a job. One that l felt obligated to perform to the best of my ability. Mine was not a calling but an inherited philosophy that work in itself was virtuous. A work ethic, if you will. Pediatrics offered the additional reward that, if well done, it might help some parents and their children feel a little better.

Fifty years ago I was not alone in treating medicine as a job. Most physicians were self-employed. Although there were exceptions like Albert Schweitzer, even those of us with a calling had to obey the basic rules of business as it applied to medicine. We were employer and employee and had to understand the critical factors of overhead, profit, and loss.
I have burdened you with this little history recitation not to suggest that things were better in the good old days, but to provide a stepping stone into the murky and uncomfortable topic of primary care physician (PCP) compensation. Because almost three quarters of you work for a hospital, health system, or corporate entity, I am going to illuminate our journey by leaning on the advice of an international company with 7000 employees and revenue of 2.5 billion dollars that considers itself a “global leader” in management consulting. Your employer is listening to some management consultant and it may help us to view your compensation from someone on their side of the table.
First, you should be aware that “most health systems lose money on their primary care operations — up to $200,000 or more per primary care physician.” This may help explain why despite being in short supply, you and most PCPs feel undervalued. However, if we are such losers, we must provide something(s) that the systems are seeking. It is likely that the system is looking to tout its ability to provide comprehensive care and demonstrate that it has a patient base broad enough to warrant attention and provide bargaining leverage on volume discounts.
The system also may want to minimize competition by absorbing the remaining PCPs in the community into their system. With you outside of the system, it had less control over your compensation than it does when you are under its umbrella.
Your employer may want to grow and feed its specialty care network, and it sees PCPs as having the fuel stored in their patient volume to do just that. In simplest and most cynical terms, the systems are willing to take a loss on us less profitable high-volume grunts in order to reap the profits of the lower-volume high-profitability specialties and subspecialties.
So that’s why you as a PCP have any value at all to a large healthcare system. But, it means that to maintain your value to the system you must continue to provide the volume it anticipates and needs. While the system may have been willing to accept some degrees of unprofitability when it hired you, there are limits. And, we shouldn’t be surprised if they continue to urge or demand that we narrow the gap between the revenue we generate and the costs that we incur, ie, our overhead.
In Part 2 of this series, I’m going to discuss the collateral damage that occurs when volume and overhead collide in an environment that claims to be committed to patient care.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I recently read an op-ed piece in which the author wondered if any young people entering the practice of medicine felt that they were answering a “calling.” I suspect that there will continue to be, and will always be, idealists whose primary motivation for choosing medicine is that they will be healing the sick or at least providing comfort to the suffering. I occasionally hear that about a former patient who has been inspired by a personal or familial experience with a serious illness.
Unfortunately, I suspect those who feel called are the providers most likely to feel discouraged and frustrated by the current state of primary care. Luckily, I never felt a calling. For me, primary care pediatrics was a job. One that l felt obligated to perform to the best of my ability. Mine was not a calling but an inherited philosophy that work in itself was virtuous. A work ethic, if you will. Pediatrics offered the additional reward that, if well done, it might help some parents and their children feel a little better.
Fifty years ago I was not alone in treating medicine as a job. Most physicians were self-employed. Although there were exceptions like Albert Schweitzer, even those of us with a calling had to obey the basic rules of business as it applied to medicine. We were employer and employee and had to understand the critical factors of overhead, profit, and loss.
I have burdened you with this little history recitation not to suggest that things were better in the good old days, but to provide a stepping stone into the murky and uncomfortable topic of primary care physician (PCP) compensation. Because almost three quarters of you work for a hospital, health system, or corporate entity, I am going to illuminate our journey by leaning on the advice of an international company with 7000 employees and revenue of 2.5 billion dollars that considers itself a “global leader” in management consulting. Your employer is listening to some management consultant and it may help us to view your compensation from someone on their side of the table.
First, you should be aware that “most health systems lose money on their primary care operations — up to $200,000 or more per primary care physician.” This may help explain why despite being in short supply, you and most PCPs feel undervalued. However, if we are such losers, we must provide something(s) that the systems are seeking. It is likely that the system is looking to tout its ability to provide comprehensive care and demonstrate that it has a patient base broad enough to warrant attention and provide bargaining leverage on volume discounts.
The system also may want to minimize competition by absorbing the remaining PCPs in the community into their system. With you outside of the system, it had less control over your compensation than it does when you are under its umbrella.
Your employer may want to grow and feed its specialty care network, and it sees PCPs as having the fuel stored in their patient volume to do just that. In simplest and most cynical terms, the systems are willing to take a loss on us less profitable high-volume grunts in order to reap the profits of the lower-volume high-profitability specialties and subspecialties.
So that’s why you as a PCP have any value at all to a large healthcare system. But, it means that to maintain your value to the system you must continue to provide the volume it anticipates and needs. While the system may have been willing to accept some degrees of unprofitability when it hired you, there are limits. And, we shouldn’t be surprised if they continue to urge or demand that we narrow the gap between the revenue we generate and the costs that we incur, ie, our overhead.
In Part 2 of this series, I’m going to discuss the collateral damage that occurs when volume and overhead collide in an environment that claims to be committed to patient care.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I recently read an op-ed piece in which the author wondered if any young people entering the practice of medicine felt that they were answering a “calling.” I suspect that there will continue to be, and will always be, idealists whose primary motivation for choosing medicine is that they will be healing the sick or at least providing comfort to the suffering. I occasionally hear that about a former patient who has been inspired by a personal or familial experience with a serious illness.
Unfortunately, I suspect those who feel called are the providers most likely to feel discouraged and frustrated by the current state of primary care. Luckily, I never felt a calling. For me, primary care pediatrics was a job. One that l felt obligated to perform to the best of my ability. Mine was not a calling but an inherited philosophy that work in itself was virtuous. A work ethic, if you will. Pediatrics offered the additional reward that, if well done, it might help some parents and their children feel a little better.
Fifty years ago I was not alone in treating medicine as a job. Most physicians were self-employed. Although there were exceptions like Albert Schweitzer, even those of us with a calling had to obey the basic rules of business as it applied to medicine. We were employer and employee and had to understand the critical factors of overhead, profit, and loss.
I have burdened you with this little history recitation not to suggest that things were better in the good old days, but to provide a stepping stone into the murky and uncomfortable topic of primary care physician (PCP) compensation. Because almost three quarters of you work for a hospital, health system, or corporate entity, I am going to illuminate our journey by leaning on the advice of an international company with 7000 employees and revenue of 2.5 billion dollars that considers itself a “global leader” in management consulting. Your employer is listening to some management consultant and it may help us to view your compensation from someone on their side of the table.
First, you should be aware that “most health systems lose money on their primary care operations — up to $200,000 or more per primary care physician.” This may help explain why despite being in short supply, you and most PCPs feel undervalued. However, if we are such losers, we must provide something(s) that the systems are seeking. It is likely that the system is looking to tout its ability to provide comprehensive care and demonstrate that it has a patient base broad enough to warrant attention and provide bargaining leverage on volume discounts.
The system also may want to minimize competition by absorbing the remaining PCPs in the community into their system. With you outside of the system, it had less control over your compensation than it does when you are under its umbrella.
Your employer may want to grow and feed its specialty care network, and it sees PCPs as having the fuel stored in their patient volume to do just that. In simplest and most cynical terms, the systems are willing to take a loss on us less profitable high-volume grunts in order to reap the profits of the lower-volume high-profitability specialties and subspecialties.
So that’s why you as a PCP have any value at all to a large healthcare system. But, it means that to maintain your value to the system you must continue to provide the volume it anticipates and needs. While the system may have been willing to accept some degrees of unprofitability when it hired you, there are limits. And, we shouldn’t be surprised if they continue to urge or demand that we narrow the gap between the revenue we generate and the costs that we incur, ie, our overhead.
In Part 2 of this series, I’m going to discuss the collateral damage that occurs when volume and overhead collide in an environment that claims to be committed to patient care.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Oregon Physician Assistants Get Name Change
On April 4, Oregon’s Governor Tina Kotek signed a bill into law that officially changed the title of “physician assistants” to “physician associates” in the state.
In the Medscape Physician Assistant Career Satisfaction Report 2023, a diverse range of opinions on the title switch was reflected. Only 40% of PAs favored the name change at the time, 45% neither opposed nor favored it, and 15% opposed the name change, reflecting the complexity of the issue.
According to the AAPA, the change came about to better reflect the work PAs do in not just “assisting” physicians but in working independently with patients. Some also felt that the word “assistant” implies dependence. However, despite associate’s more accurate reflection of the job, PAs mostly remain split on whether they want the new moniker.
Many say that the name change will be confusing for the public and their patients, while others say that physician assistant was already not well understood, as patients often thought of the profession as a doctor’s helper or an assistant, like a medical assistant.
Yet many long-time PAs say that they prefer the title they’ve always had and that explaining to patients the new associate title will be equally confusing. Some mentioned patients may think they’re a business associate of the physician.
Oregon PAs won’t immediately switch to the new name. The new law takes effect on June 6, 2024. The Oregon Medical Board will establish regulations and guidance before PAs adopt the new name in their practices.
The law only changes the name of PAs in Oregon, not in other states. In fact, prematurely using the title of physician associate could subject a PA to regulatory challenges or disciplinary actions.
A version of this article appeared on Medscape.com.
On April 4, Oregon’s Governor Tina Kotek signed a bill into law that officially changed the title of “physician assistants” to “physician associates” in the state.
In the Medscape Physician Assistant Career Satisfaction Report 2023, a diverse range of opinions on the title switch was reflected. Only 40% of PAs favored the name change at the time, 45% neither opposed nor favored it, and 15% opposed the name change, reflecting the complexity of the issue.
According to the AAPA, the change came about to better reflect the work PAs do in not just “assisting” physicians but in working independently with patients. Some also felt that the word “assistant” implies dependence. However, despite associate’s more accurate reflection of the job, PAs mostly remain split on whether they want the new moniker.
Many say that the name change will be confusing for the public and their patients, while others say that physician assistant was already not well understood, as patients often thought of the profession as a doctor’s helper or an assistant, like a medical assistant.
Yet many long-time PAs say that they prefer the title they’ve always had and that explaining to patients the new associate title will be equally confusing. Some mentioned patients may think they’re a business associate of the physician.
Oregon PAs won’t immediately switch to the new name. The new law takes effect on June 6, 2024. The Oregon Medical Board will establish regulations and guidance before PAs adopt the new name in their practices.
The law only changes the name of PAs in Oregon, not in other states. In fact, prematurely using the title of physician associate could subject a PA to regulatory challenges or disciplinary actions.
A version of this article appeared on Medscape.com.
On April 4, Oregon’s Governor Tina Kotek signed a bill into law that officially changed the title of “physician assistants” to “physician associates” in the state.
In the Medscape Physician Assistant Career Satisfaction Report 2023, a diverse range of opinions on the title switch was reflected. Only 40% of PAs favored the name change at the time, 45% neither opposed nor favored it, and 15% opposed the name change, reflecting the complexity of the issue.
According to the AAPA, the change came about to better reflect the work PAs do in not just “assisting” physicians but in working independently with patients. Some also felt that the word “assistant” implies dependence. However, despite associate’s more accurate reflection of the job, PAs mostly remain split on whether they want the new moniker.
Many say that the name change will be confusing for the public and their patients, while others say that physician assistant was already not well understood, as patients often thought of the profession as a doctor’s helper or an assistant, like a medical assistant.
Yet many long-time PAs say that they prefer the title they’ve always had and that explaining to patients the new associate title will be equally confusing. Some mentioned patients may think they’re a business associate of the physician.
Oregon PAs won’t immediately switch to the new name. The new law takes effect on June 6, 2024. The Oregon Medical Board will establish regulations and guidance before PAs adopt the new name in their practices.
The law only changes the name of PAs in Oregon, not in other states. In fact, prematurely using the title of physician associate could subject a PA to regulatory challenges or disciplinary actions.
A version of this article appeared on Medscape.com.
Microbiome Alterations Linked to Growth Hormone Deficiency
, said Chinese researchers.
The research, published recently in Pediatric Research, involved more than 80 children and showed that those with GHD had alterations in microbial populations that have been linked to longevity, as well as a microbial and metabolite signature that allowed accurate discrimination from ISS.
“These findings provide novel insights into potential early diagnosis and innovative treatment alternatives, such as fecal microbiota transplantation, for short stature with varying growth hormone levels,” the authors wrote.
Andrew Dauber, MD, MMSc, chief of endocrinology, Children’s National Hospital, Washington, who was not involved in the study, said that while this is “a really interesting area of research,” he expressed “hesitancy about getting too excited about this data yet.”
“One of the problems is how you define growth hormone deficiency,” as it is “not a black and white diagnosis,” and the etiology and child’s growth trajectory also need to be considered, Dr. Dauber told said.
He explained: “The problem is that, when you rely on the growth hormone stimulation test alone, there’s so many false positives and so much overlap between patients with true growth hormone deficiency and those without. And I think that this article fell prey to that.”
He added: “It would be really, really interesting and helpful to have a microbiome signature that allows you to distinguish between true growth hormone deficiency and patients with idiopathic short stature.”
“But you have to make sure that your groups are very well defined for this study to be really valid. And that’s one of my concerns here.”
Dr. Dauber continued: “Now, that being said, they did find some associations that correlated with growth hormone peak levels,” some which replicate previous findings, “so I do think that there are kernels of important findings here.”
‘Tease Out Influences’ to Isolate the Interaction
He pointed out that there are “many factors that influence the microbiome,” such as the use of antibiotics, diet, age, and geographic location. Therefore, a study that could truly tease out all these influences and isolate the interaction with growth hormone levels would need to be “very thoughtfully designed.”
A number of factors contribute to short stature, lead author Lan Li, MD, Department of Radiology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, China, and colleagues.
These include genetic factors, environmental factors, and conditions such as being small for gestational age at birth, familial short stature, and chronic systemic diseases, as well as GHD and ISS.
Recent animal studies have suggested that there may be a bidirectional relationship between the gut microbiota and the growth hormone/insulin-like growth factor 1 axis, and it has been shown that individuals with GHD have significant alterations in their gut microbiota compared with healthy controls.
To investigate, they studied 36 children diagnosed with GHD, 32 with ISS, and 16 age- and sex-matched healthy controls, all of whom were recruited between February 2019 and June 2021 from the Pediatric Endocrinology Department of The Second Affiliated Hospital of Wenzhou Medical University.
Fecal samples obtained from the children underwent microbiome analysis using 16S ribosomal RNA gene sequencing, alongside nuclear MRI analysis of the metabolome, or the entire complement of small molecules in the samples.
Patients with GHD had a significantly higher body mass index than those with ISS (P < .05), and their peak growth hormone level was significantly lower (P < .001). Patients with GHD also had significantly higher total cholesterol and low-density lipoprotein cholesterol levels than patients with ISS (P < .05).
The team reports that the alpha diversity of the fecal microbiome, which measures the microbial diversity within a fecal sample, was similar between the three groups.
However, there was significant variation between the groups in the beta diversity, which quantifies the similarity or dissimilarity between two samples, and allows the overall taxonomic or functional diversity pattern to be linked to environmental features.
Compared with the healthy control group, the abundance of Pelomonas, Rodentibacter, and Rothia was significantly decreased in GHD and patients with ISS, while the abundance of Prevotellaceae_NK3B31_group was increased in the two patient groups, particularly in those with GHD.
In addition, the researchers found a decreased Firmicutes/Bacteroidota (F/B) ratio in participants with short stature, particularly in the GHD group. They noted that “emerging evidence suggests the F/B ratio may play a role in longevity.”
Nocardioides was substantially more common in the ISS group vs both patients with GHD and healthy controls, while Fusobacterium mortiferum was characteristic of GHD. The team suggests this “may serve as a critical intestinal factor contributing to the short stature observed in GHD.”
The metabolome analysis revealed that glucose, pyruvate, and pyrimidine metabolism may also play a significant role in distinguishing between patients with GHD and ISS and healthy control groups.
Finally, the team demonstrated that a panel combining 13 microbiome and metabolome markers was able to discriminate between GHD and ISS at an area under the receiver operating characteristic curve of 0.945, with a sensitivity of 87% and a specificity of 91%.
The study was supported by grants from the National Natural Science Foundation of China and Wenzhou Science and Technology Bureau in China. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
, said Chinese researchers.
The research, published recently in Pediatric Research, involved more than 80 children and showed that those with GHD had alterations in microbial populations that have been linked to longevity, as well as a microbial and metabolite signature that allowed accurate discrimination from ISS.
“These findings provide novel insights into potential early diagnosis and innovative treatment alternatives, such as fecal microbiota transplantation, for short stature with varying growth hormone levels,” the authors wrote.
Andrew Dauber, MD, MMSc, chief of endocrinology, Children’s National Hospital, Washington, who was not involved in the study, said that while this is “a really interesting area of research,” he expressed “hesitancy about getting too excited about this data yet.”
“One of the problems is how you define growth hormone deficiency,” as it is “not a black and white diagnosis,” and the etiology and child’s growth trajectory also need to be considered, Dr. Dauber told said.
He explained: “The problem is that, when you rely on the growth hormone stimulation test alone, there’s so many false positives and so much overlap between patients with true growth hormone deficiency and those without. And I think that this article fell prey to that.”
He added: “It would be really, really interesting and helpful to have a microbiome signature that allows you to distinguish between true growth hormone deficiency and patients with idiopathic short stature.”
“But you have to make sure that your groups are very well defined for this study to be really valid. And that’s one of my concerns here.”
Dr. Dauber continued: “Now, that being said, they did find some associations that correlated with growth hormone peak levels,” some which replicate previous findings, “so I do think that there are kernels of important findings here.”
‘Tease Out Influences’ to Isolate the Interaction
He pointed out that there are “many factors that influence the microbiome,” such as the use of antibiotics, diet, age, and geographic location. Therefore, a study that could truly tease out all these influences and isolate the interaction with growth hormone levels would need to be “very thoughtfully designed.”
A number of factors contribute to short stature, lead author Lan Li, MD, Department of Radiology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, China, and colleagues.
These include genetic factors, environmental factors, and conditions such as being small for gestational age at birth, familial short stature, and chronic systemic diseases, as well as GHD and ISS.
Recent animal studies have suggested that there may be a bidirectional relationship between the gut microbiota and the growth hormone/insulin-like growth factor 1 axis, and it has been shown that individuals with GHD have significant alterations in their gut microbiota compared with healthy controls.
To investigate, they studied 36 children diagnosed with GHD, 32 with ISS, and 16 age- and sex-matched healthy controls, all of whom were recruited between February 2019 and June 2021 from the Pediatric Endocrinology Department of The Second Affiliated Hospital of Wenzhou Medical University.
Fecal samples obtained from the children underwent microbiome analysis using 16S ribosomal RNA gene sequencing, alongside nuclear MRI analysis of the metabolome, or the entire complement of small molecules in the samples.
Patients with GHD had a significantly higher body mass index than those with ISS (P < .05), and their peak growth hormone level was significantly lower (P < .001). Patients with GHD also had significantly higher total cholesterol and low-density lipoprotein cholesterol levels than patients with ISS (P < .05).
The team reports that the alpha diversity of the fecal microbiome, which measures the microbial diversity within a fecal sample, was similar between the three groups.
However, there was significant variation between the groups in the beta diversity, which quantifies the similarity or dissimilarity between two samples, and allows the overall taxonomic or functional diversity pattern to be linked to environmental features.
Compared with the healthy control group, the abundance of Pelomonas, Rodentibacter, and Rothia was significantly decreased in GHD and patients with ISS, while the abundance of Prevotellaceae_NK3B31_group was increased in the two patient groups, particularly in those with GHD.
In addition, the researchers found a decreased Firmicutes/Bacteroidota (F/B) ratio in participants with short stature, particularly in the GHD group. They noted that “emerging evidence suggests the F/B ratio may play a role in longevity.”
Nocardioides was substantially more common in the ISS group vs both patients with GHD and healthy controls, while Fusobacterium mortiferum was characteristic of GHD. The team suggests this “may serve as a critical intestinal factor contributing to the short stature observed in GHD.”
The metabolome analysis revealed that glucose, pyruvate, and pyrimidine metabolism may also play a significant role in distinguishing between patients with GHD and ISS and healthy control groups.
Finally, the team demonstrated that a panel combining 13 microbiome and metabolome markers was able to discriminate between GHD and ISS at an area under the receiver operating characteristic curve of 0.945, with a sensitivity of 87% and a specificity of 91%.
The study was supported by grants from the National Natural Science Foundation of China and Wenzhou Science and Technology Bureau in China. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
, said Chinese researchers.
The research, published recently in Pediatric Research, involved more than 80 children and showed that those with GHD had alterations in microbial populations that have been linked to longevity, as well as a microbial and metabolite signature that allowed accurate discrimination from ISS.
“These findings provide novel insights into potential early diagnosis and innovative treatment alternatives, such as fecal microbiota transplantation, for short stature with varying growth hormone levels,” the authors wrote.
Andrew Dauber, MD, MMSc, chief of endocrinology, Children’s National Hospital, Washington, who was not involved in the study, said that while this is “a really interesting area of research,” he expressed “hesitancy about getting too excited about this data yet.”
“One of the problems is how you define growth hormone deficiency,” as it is “not a black and white diagnosis,” and the etiology and child’s growth trajectory also need to be considered, Dr. Dauber told said.
He explained: “The problem is that, when you rely on the growth hormone stimulation test alone, there’s so many false positives and so much overlap between patients with true growth hormone deficiency and those without. And I think that this article fell prey to that.”
He added: “It would be really, really interesting and helpful to have a microbiome signature that allows you to distinguish between true growth hormone deficiency and patients with idiopathic short stature.”
“But you have to make sure that your groups are very well defined for this study to be really valid. And that’s one of my concerns here.”
Dr. Dauber continued: “Now, that being said, they did find some associations that correlated with growth hormone peak levels,” some which replicate previous findings, “so I do think that there are kernels of important findings here.”
‘Tease Out Influences’ to Isolate the Interaction
He pointed out that there are “many factors that influence the microbiome,” such as the use of antibiotics, diet, age, and geographic location. Therefore, a study that could truly tease out all these influences and isolate the interaction with growth hormone levels would need to be “very thoughtfully designed.”
A number of factors contribute to short stature, lead author Lan Li, MD, Department of Radiology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, China, and colleagues.
These include genetic factors, environmental factors, and conditions such as being small for gestational age at birth, familial short stature, and chronic systemic diseases, as well as GHD and ISS.
Recent animal studies have suggested that there may be a bidirectional relationship between the gut microbiota and the growth hormone/insulin-like growth factor 1 axis, and it has been shown that individuals with GHD have significant alterations in their gut microbiota compared with healthy controls.
To investigate, they studied 36 children diagnosed with GHD, 32 with ISS, and 16 age- and sex-matched healthy controls, all of whom were recruited between February 2019 and June 2021 from the Pediatric Endocrinology Department of The Second Affiliated Hospital of Wenzhou Medical University.
Fecal samples obtained from the children underwent microbiome analysis using 16S ribosomal RNA gene sequencing, alongside nuclear MRI analysis of the metabolome, or the entire complement of small molecules in the samples.
Patients with GHD had a significantly higher body mass index than those with ISS (P < .05), and their peak growth hormone level was significantly lower (P < .001). Patients with GHD also had significantly higher total cholesterol and low-density lipoprotein cholesterol levels than patients with ISS (P < .05).
The team reports that the alpha diversity of the fecal microbiome, which measures the microbial diversity within a fecal sample, was similar between the three groups.
However, there was significant variation between the groups in the beta diversity, which quantifies the similarity or dissimilarity between two samples, and allows the overall taxonomic or functional diversity pattern to be linked to environmental features.
Compared with the healthy control group, the abundance of Pelomonas, Rodentibacter, and Rothia was significantly decreased in GHD and patients with ISS, while the abundance of Prevotellaceae_NK3B31_group was increased in the two patient groups, particularly in those with GHD.
In addition, the researchers found a decreased Firmicutes/Bacteroidota (F/B) ratio in participants with short stature, particularly in the GHD group. They noted that “emerging evidence suggests the F/B ratio may play a role in longevity.”
Nocardioides was substantially more common in the ISS group vs both patients with GHD and healthy controls, while Fusobacterium mortiferum was characteristic of GHD. The team suggests this “may serve as a critical intestinal factor contributing to the short stature observed in GHD.”
The metabolome analysis revealed that glucose, pyruvate, and pyrimidine metabolism may also play a significant role in distinguishing between patients with GHD and ISS and healthy control groups.
Finally, the team demonstrated that a panel combining 13 microbiome and metabolome markers was able to discriminate between GHD and ISS at an area under the receiver operating characteristic curve of 0.945, with a sensitivity of 87% and a specificity of 91%.
The study was supported by grants from the National Natural Science Foundation of China and Wenzhou Science and Technology Bureau in China. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
FROM PEDIATRIC RESEARCH
How These Young MDs Impressed the Hell Out of Their Bosses
Safe to say that anyone undertaking the physician journey does so with intense motivation and book smarts. Still, it can be incredibly hard to stand out. Everyone’s a go-getter, but what’s the X factor?
Here’s what they said ...
Lesson #1: Never Be Scared to Ask
Brien Barnewolt, MD, chairman and chief of the Department of Emergency Medicine at Tufts Medical Center, was very much surprised when a resident named Scott G. Weiner did something unexpected: Go after a job in the fall of his junior year residency instead of following the typical senior year trajectory.
“It’s very unusual for a trainee to apply for a job virtually a year ahead of schedule. But he knew what he wanted,” said Dr. Barnewolt. “I’d never had anybody come to me in that same scenario, and I’ve been doing this a long time.”
Under normal circumstances it would’ve been easy for Dr. Barnewolt to say no. But the unexpected request made him and his colleagues take a closer look, and they were impressed with Dr. Weiner’s skills. That, paired with his ambition and demeanor, compelled them to offer him an early job. But there’s more.
As the next year approached, Dr. Weiner explained he had an opportunity to work in emergency medicine in Tuscany and asked if he could take a 1-year delayed start for the position he applied a year early for.
The department held his position, and upon his return, Dr. Weiner made a lasting impact at Tufts before eventually moving on. “He outgrew us, which is nice to see,” Dr. Barnewolt said. (Dr. Weiner is currently McGraw Distinguished Chair in Emergency Medicine at Brigham and Women’s Hospital and associate professor at Harvard Medical School.)
Bottom line: Why did Dr. Barnewolt and his colleagues do so much to accommodate a young candidate? Yes, Dr. Weiner was talented, but he was also up-front about his ambitions from the get-go. Dr. Barnewolt said that kind of initiative can only be looked at positively.
“My advice would be, if you see an opportunity or a potential place where you might want to work, put out those feelers, start those conversations,” he said. “It’s not too early, especially in certain specialties, where the job market is very tight. Then, when circumstances change, be open about it and have that conversation. The worst that somebody can say is no, so it never hurts to be honest and open about where you want to go and what you want to be.”
Lesson #2: Chase Your Passion ‘Relentlessly’
Vance G. Fowler, MD, MHS, an infectious disease specialist at Duke University School of Medicine, runs a laboratory that researches methicillin-resistant Staphylococcus aureus (MRSA). Over the years, he’s mentored many doctors but understands the ambitions of young trainees don’t always align with the little free time that they have. “Many of them drop away when you give them a [side] project,” he said.
So when Tori Kinamon asked him to work on an MRSA project — in her first year — he gave her one that focused on researching vertebral osteomyelitis, a bone infection that can coincide with S aureus. What Dr. Fowler didn’t know: Kinamon (now MD) had been a competitive gymnast at Brown and battled her own life-threatening infection with MRSA.
“To my absolute astonishment, not only did she stick to it, but she was able to compile a presentation on the science and gave an oral presentation within a year of walking in the door,” said Dr. Fowler.
She went on to lead an initiative between the National Institutes of Health and US Food and Drug Administration to create endpoints for clinical drug trials, all of which occurred before starting her residency, which she’s about to embark upon.
Dr. Kinamon’s a good example, he said, of what happens when you add genuine passion to book smarts. Those who do always stand out because you can’t fake that. “Find your passion, and then chase it down relentlessly,” he said. “Once you’ve found your passion, things get easy because it stops being work and it starts being something else.”
If you haven’t identified a focus area, Dr. Fowler said to “be agnostic and observant. Keep your eyes open and your options open because you may surprise yourself. It may turn out that you end up liking something a whole lot more than you thought you did.”
Lesson #3: When You Say You’ve Always Wanted to Do Something, Do Something
As the chief of pulmonary and critical care medicine at the Northwestern Medicine Canning Thoracic Institute, Scott Budinger, MD, often hears lip service from doctors who want to put their skills to use in their local communities. One of his students actually did it.
Justin Fiala, MD, a pulmonary, critical care, and sleep specialist at Northwestern Medicine, joined Northwestern as a pulmonary fellow with a big interest in addressing health equity issues.
Dr. Fiala began volunteering with CommunityHealth during his fellowship and saw that many patients of the free Chicago-area clinic needed help with sleep disorders. He launched the organization’s first sleep clinic and its Patient-Centered Apnea Protocols Initiative.
“He developed a plan with some of the partners of the sleep apnea equipment to do home sleep testing for these patients that’s free of cost,” said Dr. Budinger.
Dr. Fiala goes in on Saturdays and runs a free clinic conducting sleep studies for patients and outfits them with devices that they need to improve their conditions, said Dr. Budinger.
“And these patients are the severest of the severe patients,” he said. “These are people that have severe sleep apnea that are driving around the roads, oftentimes don’t have insurance because they’re also precluded from having auto insurance. So, this is really something that not just benefits these patients but benefits our whole community.”
The fact that Dr. Fiala followed through on something that all doctors aspire to do — and in the middle of a very busy training program — is something that Dr. Budinger said makes him stand out in a big way.
“If you talk to any of our trainees or young faculty, everybody’s interested in addressing the issue of health disparities,” said Dr. Budinger. “Justin looked at that and said, ‘Well, you know, I’m not interested in talking about it. What can I do about this problem? And how can I actually get boots on the ground and help?’ That requires a big activation energy that many people don’t have.”
Lesson #4: Be a People-Person and a Patient-Person
When hiring employees at American Family Care in Portland, Oregon, Andrew Miller, MD, director of provider training, is always on the lookout for young MDs with emotional intelligence and a good bedside manner. He has been recently blown away, however, by a young physician’s assistant named Joseph Van Bindsbergen, PA-C, who was described as “all-around wonderful” during his reference check.
“Having less than 6 months of experience out of school, he is our highest ranked provider, whether it’s a nurse practitioner, PA, or doctor, in terms of patient satisfaction,” said Dr. Miller. The young PA has an “unprecedented perfect score” on his NPS rating.
Why? Patients said they’ve never felt as heard as they felt with Van Bindsbergen.
“That’s the thing I think that the up-and-coming providers should be focusing on is making your patients feel heard,” explained Dr. Miller. Van Bindsbergen is great at building rapport with a patient, whether they are 6 or 96. “He doesn’t just ask about sore throat symptoms. He asks, ‘what is the impact on your life of the sore throat? How does it affect your family or your work? What do you think this could be besides just strep? What are your concerns?’ ”
Dr. Miller said the magic of Van Bindsbergen is that he has an innate ability to look at patients “not just as a diagnosis but as a person, which they love.”
Lesson #5: Remember to Make That Difference With Each Patient
Doctors are used to swooping in and seeing a patient, ordering further testing if needed, and then moving on to the next patient. But one young intern at the start of his medical career broke this mold by giving a very anxious patient some much-needed support.
“There was a resident who was working overnight, and this poor young woman came in who had a new diagnosis of an advanced illness and a lot of anxiety around her condition, the newness of it, and the impact this is going to have on her family and her life,” said Elizabeth Horn Prsic, MD, assistant professor at Yale School of Medicine and firm chief for medical oncology and the director of Adult Inpatient Palliative Care.
Dr. Prsic found out the next morning that this trainee accompanied the patient to the MRI and held her hand as much as he was allowed to throughout the entire experience. “I was like, ‘wait you went down with her to radiology?’ And he’s like, ‘Yes, I was there the whole time,’ ” she recalled.
This gesture not only helped the patient feel calmer after receiving a potentially life-altering diagnosis but also helped ensure the test results were as clear as possible.
“If the study is not done well and a patient is moving or uncomfortable, it has to be stopped early or paused,” said Dr. Prsic. “Then the study is not very useful. In situations like these, medical decisions may be made based on imperfect data. The fact that we had this full complete good quality scan helped us get the care that she needed in a much timelier manner to help her and to move along the care that she that was medically appropriate for her.”
Dr. Prsic got emotional reflecting on the experience. Working at Yale, she saw a ton of intelligent doctors come through the ranks. But this gesture, she said, should serve as a reminder that “you don’t need to be the smartest person in the room to just be there for a patient. It was pure empathic presence and human connection. It gave me hope in the next generation of physicians.”
A version of this article appeared on Medscape.com.
Safe to say that anyone undertaking the physician journey does so with intense motivation and book smarts. Still, it can be incredibly hard to stand out. Everyone’s a go-getter, but what’s the X factor?
Here’s what they said ...
Lesson #1: Never Be Scared to Ask
Brien Barnewolt, MD, chairman and chief of the Department of Emergency Medicine at Tufts Medical Center, was very much surprised when a resident named Scott G. Weiner did something unexpected: Go after a job in the fall of his junior year residency instead of following the typical senior year trajectory.
“It’s very unusual for a trainee to apply for a job virtually a year ahead of schedule. But he knew what he wanted,” said Dr. Barnewolt. “I’d never had anybody come to me in that same scenario, and I’ve been doing this a long time.”
Under normal circumstances it would’ve been easy for Dr. Barnewolt to say no. But the unexpected request made him and his colleagues take a closer look, and they were impressed with Dr. Weiner’s skills. That, paired with his ambition and demeanor, compelled them to offer him an early job. But there’s more.
As the next year approached, Dr. Weiner explained he had an opportunity to work in emergency medicine in Tuscany and asked if he could take a 1-year delayed start for the position he applied a year early for.
The department held his position, and upon his return, Dr. Weiner made a lasting impact at Tufts before eventually moving on. “He outgrew us, which is nice to see,” Dr. Barnewolt said. (Dr. Weiner is currently McGraw Distinguished Chair in Emergency Medicine at Brigham and Women’s Hospital and associate professor at Harvard Medical School.)
Bottom line: Why did Dr. Barnewolt and his colleagues do so much to accommodate a young candidate? Yes, Dr. Weiner was talented, but he was also up-front about his ambitions from the get-go. Dr. Barnewolt said that kind of initiative can only be looked at positively.
“My advice would be, if you see an opportunity or a potential place where you might want to work, put out those feelers, start those conversations,” he said. “It’s not too early, especially in certain specialties, where the job market is very tight. Then, when circumstances change, be open about it and have that conversation. The worst that somebody can say is no, so it never hurts to be honest and open about where you want to go and what you want to be.”
Lesson #2: Chase Your Passion ‘Relentlessly’
Vance G. Fowler, MD, MHS, an infectious disease specialist at Duke University School of Medicine, runs a laboratory that researches methicillin-resistant Staphylococcus aureus (MRSA). Over the years, he’s mentored many doctors but understands the ambitions of young trainees don’t always align with the little free time that they have. “Many of them drop away when you give them a [side] project,” he said.
So when Tori Kinamon asked him to work on an MRSA project — in her first year — he gave her one that focused on researching vertebral osteomyelitis, a bone infection that can coincide with S aureus. What Dr. Fowler didn’t know: Kinamon (now MD) had been a competitive gymnast at Brown and battled her own life-threatening infection with MRSA.
“To my absolute astonishment, not only did she stick to it, but she was able to compile a presentation on the science and gave an oral presentation within a year of walking in the door,” said Dr. Fowler.
She went on to lead an initiative between the National Institutes of Health and US Food and Drug Administration to create endpoints for clinical drug trials, all of which occurred before starting her residency, which she’s about to embark upon.
Dr. Kinamon’s a good example, he said, of what happens when you add genuine passion to book smarts. Those who do always stand out because you can’t fake that. “Find your passion, and then chase it down relentlessly,” he said. “Once you’ve found your passion, things get easy because it stops being work and it starts being something else.”
If you haven’t identified a focus area, Dr. Fowler said to “be agnostic and observant. Keep your eyes open and your options open because you may surprise yourself. It may turn out that you end up liking something a whole lot more than you thought you did.”
Lesson #3: When You Say You’ve Always Wanted to Do Something, Do Something
As the chief of pulmonary and critical care medicine at the Northwestern Medicine Canning Thoracic Institute, Scott Budinger, MD, often hears lip service from doctors who want to put their skills to use in their local communities. One of his students actually did it.
Justin Fiala, MD, a pulmonary, critical care, and sleep specialist at Northwestern Medicine, joined Northwestern as a pulmonary fellow with a big interest in addressing health equity issues.
Dr. Fiala began volunteering with CommunityHealth during his fellowship and saw that many patients of the free Chicago-area clinic needed help with sleep disorders. He launched the organization’s first sleep clinic and its Patient-Centered Apnea Protocols Initiative.
“He developed a plan with some of the partners of the sleep apnea equipment to do home sleep testing for these patients that’s free of cost,” said Dr. Budinger.
Dr. Fiala goes in on Saturdays and runs a free clinic conducting sleep studies for patients and outfits them with devices that they need to improve their conditions, said Dr. Budinger.
“And these patients are the severest of the severe patients,” he said. “These are people that have severe sleep apnea that are driving around the roads, oftentimes don’t have insurance because they’re also precluded from having auto insurance. So, this is really something that not just benefits these patients but benefits our whole community.”
The fact that Dr. Fiala followed through on something that all doctors aspire to do — and in the middle of a very busy training program — is something that Dr. Budinger said makes him stand out in a big way.
“If you talk to any of our trainees or young faculty, everybody’s interested in addressing the issue of health disparities,” said Dr. Budinger. “Justin looked at that and said, ‘Well, you know, I’m not interested in talking about it. What can I do about this problem? And how can I actually get boots on the ground and help?’ That requires a big activation energy that many people don’t have.”
Lesson #4: Be a People-Person and a Patient-Person
When hiring employees at American Family Care in Portland, Oregon, Andrew Miller, MD, director of provider training, is always on the lookout for young MDs with emotional intelligence and a good bedside manner. He has been recently blown away, however, by a young physician’s assistant named Joseph Van Bindsbergen, PA-C, who was described as “all-around wonderful” during his reference check.
“Having less than 6 months of experience out of school, he is our highest ranked provider, whether it’s a nurse practitioner, PA, or doctor, in terms of patient satisfaction,” said Dr. Miller. The young PA has an “unprecedented perfect score” on his NPS rating.
Why? Patients said they’ve never felt as heard as they felt with Van Bindsbergen.
“That’s the thing I think that the up-and-coming providers should be focusing on is making your patients feel heard,” explained Dr. Miller. Van Bindsbergen is great at building rapport with a patient, whether they are 6 or 96. “He doesn’t just ask about sore throat symptoms. He asks, ‘what is the impact on your life of the sore throat? How does it affect your family or your work? What do you think this could be besides just strep? What are your concerns?’ ”
Dr. Miller said the magic of Van Bindsbergen is that he has an innate ability to look at patients “not just as a diagnosis but as a person, which they love.”
Lesson #5: Remember to Make That Difference With Each Patient
Doctors are used to swooping in and seeing a patient, ordering further testing if needed, and then moving on to the next patient. But one young intern at the start of his medical career broke this mold by giving a very anxious patient some much-needed support.
“There was a resident who was working overnight, and this poor young woman came in who had a new diagnosis of an advanced illness and a lot of anxiety around her condition, the newness of it, and the impact this is going to have on her family and her life,” said Elizabeth Horn Prsic, MD, assistant professor at Yale School of Medicine and firm chief for medical oncology and the director of Adult Inpatient Palliative Care.
Dr. Prsic found out the next morning that this trainee accompanied the patient to the MRI and held her hand as much as he was allowed to throughout the entire experience. “I was like, ‘wait you went down with her to radiology?’ And he’s like, ‘Yes, I was there the whole time,’ ” she recalled.
This gesture not only helped the patient feel calmer after receiving a potentially life-altering diagnosis but also helped ensure the test results were as clear as possible.
“If the study is not done well and a patient is moving or uncomfortable, it has to be stopped early or paused,” said Dr. Prsic. “Then the study is not very useful. In situations like these, medical decisions may be made based on imperfect data. The fact that we had this full complete good quality scan helped us get the care that she needed in a much timelier manner to help her and to move along the care that she that was medically appropriate for her.”
Dr. Prsic got emotional reflecting on the experience. Working at Yale, she saw a ton of intelligent doctors come through the ranks. But this gesture, she said, should serve as a reminder that “you don’t need to be the smartest person in the room to just be there for a patient. It was pure empathic presence and human connection. It gave me hope in the next generation of physicians.”
A version of this article appeared on Medscape.com.
Safe to say that anyone undertaking the physician journey does so with intense motivation and book smarts. Still, it can be incredibly hard to stand out. Everyone’s a go-getter, but what’s the X factor?
Here’s what they said ...
Lesson #1: Never Be Scared to Ask
Brien Barnewolt, MD, chairman and chief of the Department of Emergency Medicine at Tufts Medical Center, was very much surprised when a resident named Scott G. Weiner did something unexpected: Go after a job in the fall of his junior year residency instead of following the typical senior year trajectory.
“It’s very unusual for a trainee to apply for a job virtually a year ahead of schedule. But he knew what he wanted,” said Dr. Barnewolt. “I’d never had anybody come to me in that same scenario, and I’ve been doing this a long time.”
Under normal circumstances it would’ve been easy for Dr. Barnewolt to say no. But the unexpected request made him and his colleagues take a closer look, and they were impressed with Dr. Weiner’s skills. That, paired with his ambition and demeanor, compelled them to offer him an early job. But there’s more.
As the next year approached, Dr. Weiner explained he had an opportunity to work in emergency medicine in Tuscany and asked if he could take a 1-year delayed start for the position he applied a year early for.
The department held his position, and upon his return, Dr. Weiner made a lasting impact at Tufts before eventually moving on. “He outgrew us, which is nice to see,” Dr. Barnewolt said. (Dr. Weiner is currently McGraw Distinguished Chair in Emergency Medicine at Brigham and Women’s Hospital and associate professor at Harvard Medical School.)
Bottom line: Why did Dr. Barnewolt and his colleagues do so much to accommodate a young candidate? Yes, Dr. Weiner was talented, but he was also up-front about his ambitions from the get-go. Dr. Barnewolt said that kind of initiative can only be looked at positively.
“My advice would be, if you see an opportunity or a potential place where you might want to work, put out those feelers, start those conversations,” he said. “It’s not too early, especially in certain specialties, where the job market is very tight. Then, when circumstances change, be open about it and have that conversation. The worst that somebody can say is no, so it never hurts to be honest and open about where you want to go and what you want to be.”
Lesson #2: Chase Your Passion ‘Relentlessly’
Vance G. Fowler, MD, MHS, an infectious disease specialist at Duke University School of Medicine, runs a laboratory that researches methicillin-resistant Staphylococcus aureus (MRSA). Over the years, he’s mentored many doctors but understands the ambitions of young trainees don’t always align with the little free time that they have. “Many of them drop away when you give them a [side] project,” he said.
So when Tori Kinamon asked him to work on an MRSA project — in her first year — he gave her one that focused on researching vertebral osteomyelitis, a bone infection that can coincide with S aureus. What Dr. Fowler didn’t know: Kinamon (now MD) had been a competitive gymnast at Brown and battled her own life-threatening infection with MRSA.
“To my absolute astonishment, not only did she stick to it, but she was able to compile a presentation on the science and gave an oral presentation within a year of walking in the door,” said Dr. Fowler.
She went on to lead an initiative between the National Institutes of Health and US Food and Drug Administration to create endpoints for clinical drug trials, all of which occurred before starting her residency, which she’s about to embark upon.
Dr. Kinamon’s a good example, he said, of what happens when you add genuine passion to book smarts. Those who do always stand out because you can’t fake that. “Find your passion, and then chase it down relentlessly,” he said. “Once you’ve found your passion, things get easy because it stops being work and it starts being something else.”
If you haven’t identified a focus area, Dr. Fowler said to “be agnostic and observant. Keep your eyes open and your options open because you may surprise yourself. It may turn out that you end up liking something a whole lot more than you thought you did.”
Lesson #3: When You Say You’ve Always Wanted to Do Something, Do Something
As the chief of pulmonary and critical care medicine at the Northwestern Medicine Canning Thoracic Institute, Scott Budinger, MD, often hears lip service from doctors who want to put their skills to use in their local communities. One of his students actually did it.
Justin Fiala, MD, a pulmonary, critical care, and sleep specialist at Northwestern Medicine, joined Northwestern as a pulmonary fellow with a big interest in addressing health equity issues.
Dr. Fiala began volunteering with CommunityHealth during his fellowship and saw that many patients of the free Chicago-area clinic needed help with sleep disorders. He launched the organization’s first sleep clinic and its Patient-Centered Apnea Protocols Initiative.
“He developed a plan with some of the partners of the sleep apnea equipment to do home sleep testing for these patients that’s free of cost,” said Dr. Budinger.
Dr. Fiala goes in on Saturdays and runs a free clinic conducting sleep studies for patients and outfits them with devices that they need to improve their conditions, said Dr. Budinger.
“And these patients are the severest of the severe patients,” he said. “These are people that have severe sleep apnea that are driving around the roads, oftentimes don’t have insurance because they’re also precluded from having auto insurance. So, this is really something that not just benefits these patients but benefits our whole community.”
The fact that Dr. Fiala followed through on something that all doctors aspire to do — and in the middle of a very busy training program — is something that Dr. Budinger said makes him stand out in a big way.
“If you talk to any of our trainees or young faculty, everybody’s interested in addressing the issue of health disparities,” said Dr. Budinger. “Justin looked at that and said, ‘Well, you know, I’m not interested in talking about it. What can I do about this problem? And how can I actually get boots on the ground and help?’ That requires a big activation energy that many people don’t have.”
Lesson #4: Be a People-Person and a Patient-Person
When hiring employees at American Family Care in Portland, Oregon, Andrew Miller, MD, director of provider training, is always on the lookout for young MDs with emotional intelligence and a good bedside manner. He has been recently blown away, however, by a young physician’s assistant named Joseph Van Bindsbergen, PA-C, who was described as “all-around wonderful” during his reference check.
“Having less than 6 months of experience out of school, he is our highest ranked provider, whether it’s a nurse practitioner, PA, or doctor, in terms of patient satisfaction,” said Dr. Miller. The young PA has an “unprecedented perfect score” on his NPS rating.
Why? Patients said they’ve never felt as heard as they felt with Van Bindsbergen.
“That’s the thing I think that the up-and-coming providers should be focusing on is making your patients feel heard,” explained Dr. Miller. Van Bindsbergen is great at building rapport with a patient, whether they are 6 or 96. “He doesn’t just ask about sore throat symptoms. He asks, ‘what is the impact on your life of the sore throat? How does it affect your family or your work? What do you think this could be besides just strep? What are your concerns?’ ”
Dr. Miller said the magic of Van Bindsbergen is that he has an innate ability to look at patients “not just as a diagnosis but as a person, which they love.”
Lesson #5: Remember to Make That Difference With Each Patient
Doctors are used to swooping in and seeing a patient, ordering further testing if needed, and then moving on to the next patient. But one young intern at the start of his medical career broke this mold by giving a very anxious patient some much-needed support.
“There was a resident who was working overnight, and this poor young woman came in who had a new diagnosis of an advanced illness and a lot of anxiety around her condition, the newness of it, and the impact this is going to have on her family and her life,” said Elizabeth Horn Prsic, MD, assistant professor at Yale School of Medicine and firm chief for medical oncology and the director of Adult Inpatient Palliative Care.
Dr. Prsic found out the next morning that this trainee accompanied the patient to the MRI and held her hand as much as he was allowed to throughout the entire experience. “I was like, ‘wait you went down with her to radiology?’ And he’s like, ‘Yes, I was there the whole time,’ ” she recalled.
This gesture not only helped the patient feel calmer after receiving a potentially life-altering diagnosis but also helped ensure the test results were as clear as possible.
“If the study is not done well and a patient is moving or uncomfortable, it has to be stopped early or paused,” said Dr. Prsic. “Then the study is not very useful. In situations like these, medical decisions may be made based on imperfect data. The fact that we had this full complete good quality scan helped us get the care that she needed in a much timelier manner to help her and to move along the care that she that was medically appropriate for her.”
Dr. Prsic got emotional reflecting on the experience. Working at Yale, she saw a ton of intelligent doctors come through the ranks. But this gesture, she said, should serve as a reminder that “you don’t need to be the smartest person in the room to just be there for a patient. It was pure empathic presence and human connection. It gave me hope in the next generation of physicians.”
A version of this article appeared on Medscape.com.
Federal Trade Commission Bans Noncompete Agreements, Urges More Protections for Healthcare Workers
But business groups have vowed to challenge the decision in court.
The proposed final rule passed on a 3-2 vote, with the dissenting commissioners disputing the FTC’s authority to broadly ban noncompetes.
Tensions around noncompetes have been building for years. In 2021, President Biden issued an executive order supporting measures to improve economic competition, in which he urged the FTC to consider its rulemaking authority to address noncompete clauses that unfairly limit workers’ mobility. In January 2023, per that directive, the agency proposed ending the restrictive covenants.
While the FTC estimates that the final rule will reduce healthcare costs by up to $194 billion over the next decade and increase worker earnings by $300 million annually, the ruling faces legal hurdles.
US Chamber of Commerce president and CEO Suzanne P. Clark said in a statement that the move is a “blatant power grab” that will undermine competitive business practices, adding that the Chamber will sue to block the measure.
The FTC received more than 26,000 comments on noncompetes during the public feedback period, with about 25,000 supporting the measure, said Benjamin Cady, JD, an FTC attorney.
Mr. Cady called the feedback “compelling,” citing instances of workers who were forced to commute long distances, uproot their families, or risk expensive litigation for wanting to pursue job opportunities.
For example, a comment from a physician working in Appalachia highlights the potential real-life implications of the agreements. “With hospital systems merging, providers with aggressive noncompetes must abandon the community that they serve if they [choose] to leave their employer. Healthcare providers feel trapped in their current employment situation, leading to significant burnout that can shorten their [career] longevity.”
Commissioner Alvaro Bedoya said physicians have had their lives upended by cumbersome noncompetes, often having to move out of state to practice. “A pandemic killed a million people in this country, and there are doctors who cannot work because of a noncompete,” he said.
It’s unclear whether physicians and others who work for nonprofit healthcare groups or hospitals will be covered by the new ban. FTC Commissioner Rebecca Slaughter acknowledged that the agency’s jurisdictional limitations mean that employees of “certain nonprofit organizations” may not benefit from the rule.
“We want to be transparent about the limitation and recognize there are workers, especially healthcare workers, who are bound by anticompetitive and unfair noncompete clauses, that our rule will struggle to reach,” she said. To cover nonprofit healthcare employees, Ms. Slaughter urged Congress to pass legislation banning noncompetes, such as the Workforce Mobility Act of 2021 and the Freedom to Compete Act of 2023.
The FTC final rule will take effect 120 days after it is published in the federal register, and new noncompete agreements will be banned as of this date. However, existing contracts for senior executives will remain in effect because these individuals are less likely to experience “acute harm” due to their ability to negotiate accordingly, said Mr. Cady.
States, AMA Take Aim at Noncompetes
Before the federal ban, several states had already passed legislation limiting the reach of noncompetes. According to a recent article in the Journal of the American College of Cardiology, 12 states prohibit noncompete clauses for physicians: Alabama, California, Colorado, Delaware, Massachusetts, Montana, New Hampshire, New Mexico, North Dakota, Oklahoma, Rhode Island, and South Dakota.
The remaining states allow noncompetes in some form, often excluding them for employees earning below a certain threshold. For example, in Oregon, noncompete agreements may apply to employees earning more than $113,241. Most states have provisions to adjust the threshold annually. The District of Columbia permits 2-year noncompetes for “medical specialists” earning over $250,000 annually.
Indiana employers can no longer enter into noncompete agreements with primary care providers. Other specialties may be subject to the clauses, except when the physician terminates the contract for cause or when an employer terminates the contract without cause.
Rachel Marcus, MD, a cardiologist in Washington, DC, found out how limiting her employment contract’s noncompete clause was when she wanted to leave a former position. Due to the restrictions, she told this news organization that she couldn’t work locally for a competitor for 2 years. The closest location she could seek employment without violating the agreement was Baltimore, approximately 40 miles away.
Dr. Marcus ultimately moved to another position within the same organization because of the company’s reputation for being “aggressive” in their enforcement actions.
Although the American Medical Association (AMA) does not support a total ban, its House of Delegates adopted policies last year to support the prohibition of noncompete contracts for physicians employed by for-profit or nonprofit hospitals, hospital systems, or staffing companies.
Challenges Await
The American Hospital Association, which opposed the proposed rule, called it “bad policy.” The decision “will likely be short-lived, with courts almost certain to stop it before it can do damage to hospitals’ ability to care for their patients and communities,” the association said in a statement.
To ease the transition to the new rule, the FTC also released a model language for employers to use when discussing the changes with their employees. “All employers need to do to comply with the rule is to stop enforcing existing noncompetes with workers other than senior executives and provide notice to such workers,” he said.
Dr. Marcus hopes the ban improves doctors’ lives. “Your employer is going to have to treat you better because they know that you can easily go across town to a place that has a higher salary, and your patient can go with you.”
A version of this article appeared on Medscape.com.
But business groups have vowed to challenge the decision in court.
The proposed final rule passed on a 3-2 vote, with the dissenting commissioners disputing the FTC’s authority to broadly ban noncompetes.
Tensions around noncompetes have been building for years. In 2021, President Biden issued an executive order supporting measures to improve economic competition, in which he urged the FTC to consider its rulemaking authority to address noncompete clauses that unfairly limit workers’ mobility. In January 2023, per that directive, the agency proposed ending the restrictive covenants.
While the FTC estimates that the final rule will reduce healthcare costs by up to $194 billion over the next decade and increase worker earnings by $300 million annually, the ruling faces legal hurdles.
US Chamber of Commerce president and CEO Suzanne P. Clark said in a statement that the move is a “blatant power grab” that will undermine competitive business practices, adding that the Chamber will sue to block the measure.
The FTC received more than 26,000 comments on noncompetes during the public feedback period, with about 25,000 supporting the measure, said Benjamin Cady, JD, an FTC attorney.
Mr. Cady called the feedback “compelling,” citing instances of workers who were forced to commute long distances, uproot their families, or risk expensive litigation for wanting to pursue job opportunities.
For example, a comment from a physician working in Appalachia highlights the potential real-life implications of the agreements. “With hospital systems merging, providers with aggressive noncompetes must abandon the community that they serve if they [choose] to leave their employer. Healthcare providers feel trapped in their current employment situation, leading to significant burnout that can shorten their [career] longevity.”
Commissioner Alvaro Bedoya said physicians have had their lives upended by cumbersome noncompetes, often having to move out of state to practice. “A pandemic killed a million people in this country, and there are doctors who cannot work because of a noncompete,” he said.
It’s unclear whether physicians and others who work for nonprofit healthcare groups or hospitals will be covered by the new ban. FTC Commissioner Rebecca Slaughter acknowledged that the agency’s jurisdictional limitations mean that employees of “certain nonprofit organizations” may not benefit from the rule.
“We want to be transparent about the limitation and recognize there are workers, especially healthcare workers, who are bound by anticompetitive and unfair noncompete clauses, that our rule will struggle to reach,” she said. To cover nonprofit healthcare employees, Ms. Slaughter urged Congress to pass legislation banning noncompetes, such as the Workforce Mobility Act of 2021 and the Freedom to Compete Act of 2023.
The FTC final rule will take effect 120 days after it is published in the federal register, and new noncompete agreements will be banned as of this date. However, existing contracts for senior executives will remain in effect because these individuals are less likely to experience “acute harm” due to their ability to negotiate accordingly, said Mr. Cady.
States, AMA Take Aim at Noncompetes
Before the federal ban, several states had already passed legislation limiting the reach of noncompetes. According to a recent article in the Journal of the American College of Cardiology, 12 states prohibit noncompete clauses for physicians: Alabama, California, Colorado, Delaware, Massachusetts, Montana, New Hampshire, New Mexico, North Dakota, Oklahoma, Rhode Island, and South Dakota.
The remaining states allow noncompetes in some form, often excluding them for employees earning below a certain threshold. For example, in Oregon, noncompete agreements may apply to employees earning more than $113,241. Most states have provisions to adjust the threshold annually. The District of Columbia permits 2-year noncompetes for “medical specialists” earning over $250,000 annually.
Indiana employers can no longer enter into noncompete agreements with primary care providers. Other specialties may be subject to the clauses, except when the physician terminates the contract for cause or when an employer terminates the contract without cause.
Rachel Marcus, MD, a cardiologist in Washington, DC, found out how limiting her employment contract’s noncompete clause was when she wanted to leave a former position. Due to the restrictions, she told this news organization that she couldn’t work locally for a competitor for 2 years. The closest location she could seek employment without violating the agreement was Baltimore, approximately 40 miles away.
Dr. Marcus ultimately moved to another position within the same organization because of the company’s reputation for being “aggressive” in their enforcement actions.
Although the American Medical Association (AMA) does not support a total ban, its House of Delegates adopted policies last year to support the prohibition of noncompete contracts for physicians employed by for-profit or nonprofit hospitals, hospital systems, or staffing companies.
Challenges Await
The American Hospital Association, which opposed the proposed rule, called it “bad policy.” The decision “will likely be short-lived, with courts almost certain to stop it before it can do damage to hospitals’ ability to care for their patients and communities,” the association said in a statement.
To ease the transition to the new rule, the FTC also released a model language for employers to use when discussing the changes with their employees. “All employers need to do to comply with the rule is to stop enforcing existing noncompetes with workers other than senior executives and provide notice to such workers,” he said.
Dr. Marcus hopes the ban improves doctors’ lives. “Your employer is going to have to treat you better because they know that you can easily go across town to a place that has a higher salary, and your patient can go with you.”
A version of this article appeared on Medscape.com.
But business groups have vowed to challenge the decision in court.
The proposed final rule passed on a 3-2 vote, with the dissenting commissioners disputing the FTC’s authority to broadly ban noncompetes.
Tensions around noncompetes have been building for years. In 2021, President Biden issued an executive order supporting measures to improve economic competition, in which he urged the FTC to consider its rulemaking authority to address noncompete clauses that unfairly limit workers’ mobility. In January 2023, per that directive, the agency proposed ending the restrictive covenants.
While the FTC estimates that the final rule will reduce healthcare costs by up to $194 billion over the next decade and increase worker earnings by $300 million annually, the ruling faces legal hurdles.
US Chamber of Commerce president and CEO Suzanne P. Clark said in a statement that the move is a “blatant power grab” that will undermine competitive business practices, adding that the Chamber will sue to block the measure.
The FTC received more than 26,000 comments on noncompetes during the public feedback period, with about 25,000 supporting the measure, said Benjamin Cady, JD, an FTC attorney.
Mr. Cady called the feedback “compelling,” citing instances of workers who were forced to commute long distances, uproot their families, or risk expensive litigation for wanting to pursue job opportunities.
For example, a comment from a physician working in Appalachia highlights the potential real-life implications of the agreements. “With hospital systems merging, providers with aggressive noncompetes must abandon the community that they serve if they [choose] to leave their employer. Healthcare providers feel trapped in their current employment situation, leading to significant burnout that can shorten their [career] longevity.”
Commissioner Alvaro Bedoya said physicians have had their lives upended by cumbersome noncompetes, often having to move out of state to practice. “A pandemic killed a million people in this country, and there are doctors who cannot work because of a noncompete,” he said.
It’s unclear whether physicians and others who work for nonprofit healthcare groups or hospitals will be covered by the new ban. FTC Commissioner Rebecca Slaughter acknowledged that the agency’s jurisdictional limitations mean that employees of “certain nonprofit organizations” may not benefit from the rule.
“We want to be transparent about the limitation and recognize there are workers, especially healthcare workers, who are bound by anticompetitive and unfair noncompete clauses, that our rule will struggle to reach,” she said. To cover nonprofit healthcare employees, Ms. Slaughter urged Congress to pass legislation banning noncompetes, such as the Workforce Mobility Act of 2021 and the Freedom to Compete Act of 2023.
The FTC final rule will take effect 120 days after it is published in the federal register, and new noncompete agreements will be banned as of this date. However, existing contracts for senior executives will remain in effect because these individuals are less likely to experience “acute harm” due to their ability to negotiate accordingly, said Mr. Cady.
States, AMA Take Aim at Noncompetes
Before the federal ban, several states had already passed legislation limiting the reach of noncompetes. According to a recent article in the Journal of the American College of Cardiology, 12 states prohibit noncompete clauses for physicians: Alabama, California, Colorado, Delaware, Massachusetts, Montana, New Hampshire, New Mexico, North Dakota, Oklahoma, Rhode Island, and South Dakota.
The remaining states allow noncompetes in some form, often excluding them for employees earning below a certain threshold. For example, in Oregon, noncompete agreements may apply to employees earning more than $113,241. Most states have provisions to adjust the threshold annually. The District of Columbia permits 2-year noncompetes for “medical specialists” earning over $250,000 annually.
Indiana employers can no longer enter into noncompete agreements with primary care providers. Other specialties may be subject to the clauses, except when the physician terminates the contract for cause or when an employer terminates the contract without cause.
Rachel Marcus, MD, a cardiologist in Washington, DC, found out how limiting her employment contract’s noncompete clause was when she wanted to leave a former position. Due to the restrictions, she told this news organization that she couldn’t work locally for a competitor for 2 years. The closest location she could seek employment without violating the agreement was Baltimore, approximately 40 miles away.
Dr. Marcus ultimately moved to another position within the same organization because of the company’s reputation for being “aggressive” in their enforcement actions.
Although the American Medical Association (AMA) does not support a total ban, its House of Delegates adopted policies last year to support the prohibition of noncompete contracts for physicians employed by for-profit or nonprofit hospitals, hospital systems, or staffing companies.
Challenges Await
The American Hospital Association, which opposed the proposed rule, called it “bad policy.” The decision “will likely be short-lived, with courts almost certain to stop it before it can do damage to hospitals’ ability to care for their patients and communities,” the association said in a statement.
To ease the transition to the new rule, the FTC also released a model language for employers to use when discussing the changes with their employees. “All employers need to do to comply with the rule is to stop enforcing existing noncompetes with workers other than senior executives and provide notice to such workers,” he said.
Dr. Marcus hopes the ban improves doctors’ lives. “Your employer is going to have to treat you better because they know that you can easily go across town to a place that has a higher salary, and your patient can go with you.”
A version of this article appeared on Medscape.com.
Are Women Better Doctors Than Men?
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.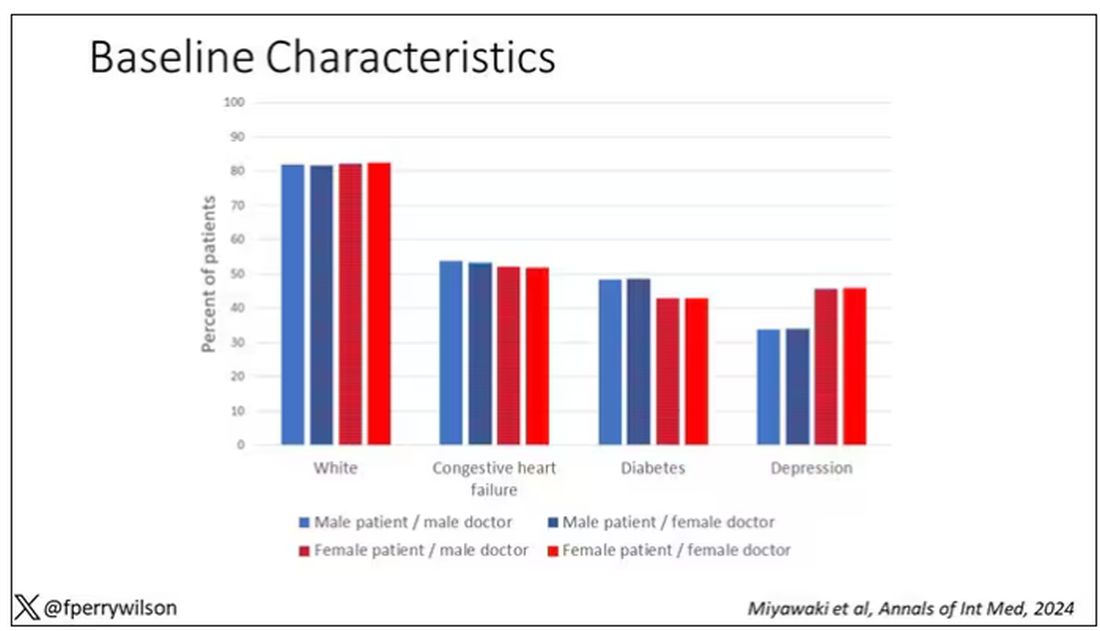
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here. 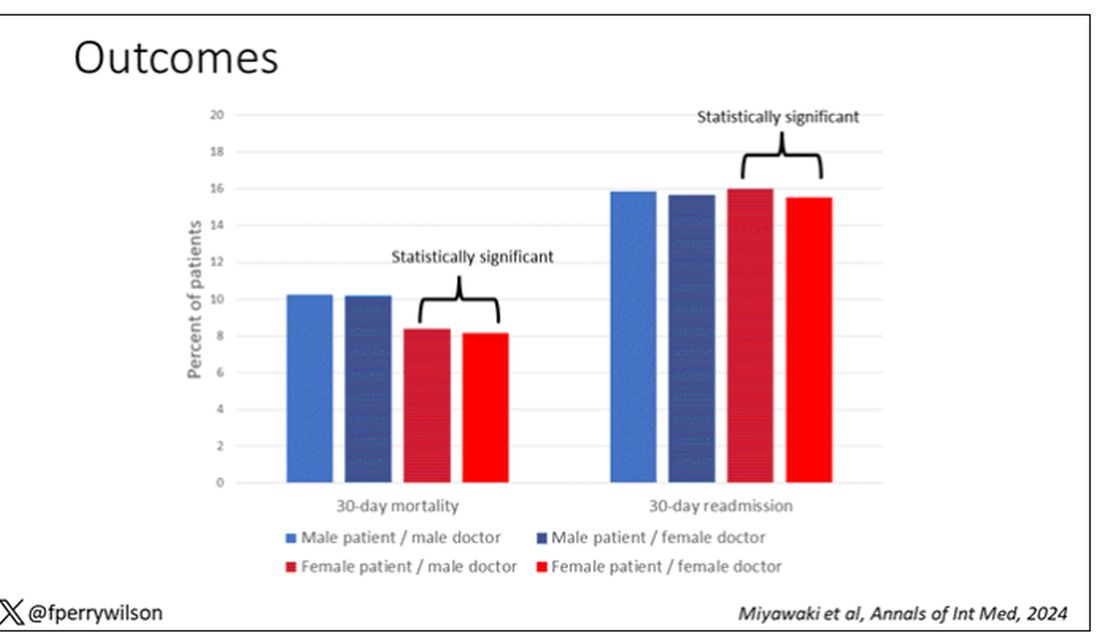
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here.
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here.
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
The Obesogenic Environment of Preschool and Day Care
Thirty years ago I had an experience in the office that influenced my approach to obesity for the rest of my career. The patient was a 4-year-old whom I had been seeing since her birth. At her annual well-child visit her weight had jumped up significantly from the previous year’s visit. She appeared well, but the change in her growth trajectory prompted a bit more in-depth history taking.
It turned out that finances had forced the family to employ one of the child’s grandmothers as the day care provider. Unfortunately, this grandmother’s passion was cooking and she was particularly adept at baking. She had no other hobbies and a sore hip limited her mobility, so she seldom went outside. When I eventually met her she was a cheerful, overweight, and delightful woman.
Deconstructing this obesogenic environment without disrupting this otherwise healthy family was an exercise that required tact, patience, and creativity. Fortunately, the young girl’s mother had already harbored some concerns about her child’s weight and was more than willing to participate in this environmental re-engineering project. It’s a long story, but she and I achieved our goals and the child eventually coasted back toward her previous growth curve.
I have always suspected that this scenario is being replayed hundreds of thousands of time across this country. But, sadly most don’t share this one’s happy ending. Parents don’t alway perceive the seriousness of the problem. The economic hurdles are often too steep to overcome, even when the most creative minds are involved.
How prevalent are obesogenic day care environments? We certainly know childhood obesity is a problem and the statistics in the preschool age group are particularly concerning. More than 14 million children are in non-parental early care and education programs; these environments would seem to be a logical place to target our prevention strategies. Understandably, there seems to be a hesitancy to point fingers, but how many day care providers are similar to the well-intentioned grandmother in the scenario I described? We must at least suspect that the example set by the adults in the preschool and day care environment might be having some influence on the children under their care.
There has been some research that sheds some light on this question. A paper from the University of Oklahoma has looked at the predictors of overweight and obesity in early care and education (ECE) teachers in hopes of “finding modifiable opportunities to enhance the health of this critical workforce.” In their paper, the investigators refer to other research that has found the prevalence of overweight and obesity among ECE teachers is higher than our national average and their waist circumference is significantly greater than the standard recommendation for women.
A study from Norway has looked at the association between preschool staff’s activity level and that of the children under their care using accelerometers. This particular investigation couldn’t determine whether it was the staff’s activity level that influenced the children or vice versa because it wasn’t an observational study. Common sense would lead one to believe it was the staff’s relative inactivity that was being reflected in the children’s.
It is interesting that in this Norwegian study when the teachers were asked about their attitudes toward activity and their self-perception of their own activity, there was no relationship between the staff’s and the children’s level of activity. In other words, the educators and caregivers bought into the importance of activity but had difficulty translating this philosophy into own behavior.
So where does this leave us? It turns out my experience decades ago was not a one-off event, but instead represents the tip of very large iceberg. Should we immediately create a system of day care provider boot camps? Let’s remember that each educator and caregiver is one of us. They may be slight outliers but not a group of individuals deserving of forced marches and half-rations to get them in shape.
ECEs have listened to the same message we have all heard about diet and activity and their importance for a child’s health. It’s for their own health and that of their charges. This could be as simple as providing accelerometers or step-counting smartwatches. Or, by having physical educators perform on-site audits that could then be used to create site-specific plans for increasing both teacher and student activity.
Modifying the educators’ diet is a more complex procedure and can quickly become entangled in the socio-economic background of each individual teacher. A healthy diet is not always equally available to everyone. The solution may involve providing the teachers with food to be eaten at work and to be prepared at home. But, creative answers can be found if we look for them.
Before we get too far down the obesity-is-a-disease pathway, we must take a closer look at the role the early care and early school milieu are playing in the obesity problem. A little common sense behavior modification when children are in the controlled environment of school/day care may allow us to be less reliant on the those new wonder drugs in the long run.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Thirty years ago I had an experience in the office that influenced my approach to obesity for the rest of my career. The patient was a 4-year-old whom I had been seeing since her birth. At her annual well-child visit her weight had jumped up significantly from the previous year’s visit. She appeared well, but the change in her growth trajectory prompted a bit more in-depth history taking.
It turned out that finances had forced the family to employ one of the child’s grandmothers as the day care provider. Unfortunately, this grandmother’s passion was cooking and she was particularly adept at baking. She had no other hobbies and a sore hip limited her mobility, so she seldom went outside. When I eventually met her she was a cheerful, overweight, and delightful woman.
Deconstructing this obesogenic environment without disrupting this otherwise healthy family was an exercise that required tact, patience, and creativity. Fortunately, the young girl’s mother had already harbored some concerns about her child’s weight and was more than willing to participate in this environmental re-engineering project. It’s a long story, but she and I achieved our goals and the child eventually coasted back toward her previous growth curve.
I have always suspected that this scenario is being replayed hundreds of thousands of time across this country. But, sadly most don’t share this one’s happy ending. Parents don’t alway perceive the seriousness of the problem. The economic hurdles are often too steep to overcome, even when the most creative minds are involved.
How prevalent are obesogenic day care environments? We certainly know childhood obesity is a problem and the statistics in the preschool age group are particularly concerning. More than 14 million children are in non-parental early care and education programs; these environments would seem to be a logical place to target our prevention strategies. Understandably, there seems to be a hesitancy to point fingers, but how many day care providers are similar to the well-intentioned grandmother in the scenario I described? We must at least suspect that the example set by the adults in the preschool and day care environment might be having some influence on the children under their care.
There has been some research that sheds some light on this question. A paper from the University of Oklahoma has looked at the predictors of overweight and obesity in early care and education (ECE) teachers in hopes of “finding modifiable opportunities to enhance the health of this critical workforce.” In their paper, the investigators refer to other research that has found the prevalence of overweight and obesity among ECE teachers is higher than our national average and their waist circumference is significantly greater than the standard recommendation for women.
A study from Norway has looked at the association between preschool staff’s activity level and that of the children under their care using accelerometers. This particular investigation couldn’t determine whether it was the staff’s activity level that influenced the children or vice versa because it wasn’t an observational study. Common sense would lead one to believe it was the staff’s relative inactivity that was being reflected in the children’s.
It is interesting that in this Norwegian study when the teachers were asked about their attitudes toward activity and their self-perception of their own activity, there was no relationship between the staff’s and the children’s level of activity. In other words, the educators and caregivers bought into the importance of activity but had difficulty translating this philosophy into own behavior.
So where does this leave us? It turns out my experience decades ago was not a one-off event, but instead represents the tip of very large iceberg. Should we immediately create a system of day care provider boot camps? Let’s remember that each educator and caregiver is one of us. They may be slight outliers but not a group of individuals deserving of forced marches and half-rations to get them in shape.
ECEs have listened to the same message we have all heard about diet and activity and their importance for a child’s health. It’s for their own health and that of their charges. This could be as simple as providing accelerometers or step-counting smartwatches. Or, by having physical educators perform on-site audits that could then be used to create site-specific plans for increasing both teacher and student activity.
Modifying the educators’ diet is a more complex procedure and can quickly become entangled in the socio-economic background of each individual teacher. A healthy diet is not always equally available to everyone. The solution may involve providing the teachers with food to be eaten at work and to be prepared at home. But, creative answers can be found if we look for them.
Before we get too far down the obesity-is-a-disease pathway, we must take a closer look at the role the early care and early school milieu are playing in the obesity problem. A little common sense behavior modification when children are in the controlled environment of school/day care may allow us to be less reliant on the those new wonder drugs in the long run.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Thirty years ago I had an experience in the office that influenced my approach to obesity for the rest of my career. The patient was a 4-year-old whom I had been seeing since her birth. At her annual well-child visit her weight had jumped up significantly from the previous year’s visit. She appeared well, but the change in her growth trajectory prompted a bit more in-depth history taking.
It turned out that finances had forced the family to employ one of the child’s grandmothers as the day care provider. Unfortunately, this grandmother’s passion was cooking and she was particularly adept at baking. She had no other hobbies and a sore hip limited her mobility, so she seldom went outside. When I eventually met her she was a cheerful, overweight, and delightful woman.
Deconstructing this obesogenic environment without disrupting this otherwise healthy family was an exercise that required tact, patience, and creativity. Fortunately, the young girl’s mother had already harbored some concerns about her child’s weight and was more than willing to participate in this environmental re-engineering project. It’s a long story, but she and I achieved our goals and the child eventually coasted back toward her previous growth curve.
I have always suspected that this scenario is being replayed hundreds of thousands of time across this country. But, sadly most don’t share this one’s happy ending. Parents don’t alway perceive the seriousness of the problem. The economic hurdles are often too steep to overcome, even when the most creative minds are involved.
How prevalent are obesogenic day care environments? We certainly know childhood obesity is a problem and the statistics in the preschool age group are particularly concerning. More than 14 million children are in non-parental early care and education programs; these environments would seem to be a logical place to target our prevention strategies. Understandably, there seems to be a hesitancy to point fingers, but how many day care providers are similar to the well-intentioned grandmother in the scenario I described? We must at least suspect that the example set by the adults in the preschool and day care environment might be having some influence on the children under their care.
There has been some research that sheds some light on this question. A paper from the University of Oklahoma has looked at the predictors of overweight and obesity in early care and education (ECE) teachers in hopes of “finding modifiable opportunities to enhance the health of this critical workforce.” In their paper, the investigators refer to other research that has found the prevalence of overweight and obesity among ECE teachers is higher than our national average and their waist circumference is significantly greater than the standard recommendation for women.
A study from Norway has looked at the association between preschool staff’s activity level and that of the children under their care using accelerometers. This particular investigation couldn’t determine whether it was the staff’s activity level that influenced the children or vice versa because it wasn’t an observational study. Common sense would lead one to believe it was the staff’s relative inactivity that was being reflected in the children’s.
It is interesting that in this Norwegian study when the teachers were asked about their attitudes toward activity and their self-perception of their own activity, there was no relationship between the staff’s and the children’s level of activity. In other words, the educators and caregivers bought into the importance of activity but had difficulty translating this philosophy into own behavior.
So where does this leave us? It turns out my experience decades ago was not a one-off event, but instead represents the tip of very large iceberg. Should we immediately create a system of day care provider boot camps? Let’s remember that each educator and caregiver is one of us. They may be slight outliers but not a group of individuals deserving of forced marches and half-rations to get them in shape.
ECEs have listened to the same message we have all heard about diet and activity and their importance for a child’s health. It’s for their own health and that of their charges. This could be as simple as providing accelerometers or step-counting smartwatches. Or, by having physical educators perform on-site audits that could then be used to create site-specific plans for increasing both teacher and student activity.
Modifying the educators’ diet is a more complex procedure and can quickly become entangled in the socio-economic background of each individual teacher. A healthy diet is not always equally available to everyone. The solution may involve providing the teachers with food to be eaten at work and to be prepared at home. But, creative answers can be found if we look for them.
Before we get too far down the obesity-is-a-disease pathway, we must take a closer look at the role the early care and early school milieu are playing in the obesity problem. A little common sense behavior modification when children are in the controlled environment of school/day care may allow us to be less reliant on the those new wonder drugs in the long run.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].