User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
USPSTF maintains ‘insufficient evidence’ for lipid disorder screenings in kids and teens
The group’s final recommendation and corresponding evidence report were published in the Journal of the American Medical Association, following a draft recommendation in January.
The organization reached a similar conclusion following its evaluation in 2016.
“There’s just not enough evidence to determine whether or not screening all children for high cholesterol improves their heart health into adulthood,” said Katrina Donahue, MD, MPH, a USPSTF member and a professor in the department of family medicine at the University of North Carolina at Chapel Hill. “We’re calling for additional research on the effectiveness of screening for and treatment of high cholesterol in children and adolescents to prevent heart attacks, strokes, and death in adulthood.”
The task force recommended other evidence-based strategies to promote heart health, such as screening for obesity and interventions to prevent tobacco use.
The recommendation was the result of a review of 43 studies from MEDLINE and the Cochrane Central Register of Controlled Trials through May 16, 2022. No randomized controlled trial directly addressed the effectiveness or harms of lipid screening for children and adolescents. The task force continued to use article alerts and targeted journal searches through March 24, 2023.
Conditions such as familial hypercholesterolemia and multifactorial dyslipidemia can cause abnormally high lipid levels in children, potentially leading to premature cardiovascular events such as myocardial infarction, stroke, and death in adulthood. According to the USPSTF, the prevalence of FH in U.S. children and adolescents ranges from 0.2% to 0.4% (one in every 250-500 youth). Multifactorial dyslipidemia is more common – the prevalence in children and adolescents ranges from 7.1% to 9.4%.
In an editorial response to the task force’s statement, the authors, including Sarah D. de Ferranti, MD, department of pediatrics at Harvard Medical School, Boston, question the impact of not screening children to identify FH and other conditions and caution against the subsequent delay in treatment.
“Treating FH during childhood slows the progression of vascular finding in atherosclerosis,” the authors write.
They note that the recommendation “leaves a void for clinicians seeking to provide care for patients today” while additional research is conducted.
Sarah Nosal, MD, a member of the board of directors of the American Academy of Family Physicians, said that despite the lack of a recommendation, primary care clinicians can still encourage proper nutrition and physical activity for patients.
Dr. Nosal said that even without clear recommendations from the USPSTF, in the rare case of a patient with a family history of FH, she would order a lipid test and discuss treatment plans with the patient and family, if needed.
“We really don’t want to do tests that we don’t know what to do with the information,” she said.
One USPSTF member reported receiving grants from Healthwise, a nonprofit organization, outside the submitted work.
A version of this article first appeared on Medscape.com.
The group’s final recommendation and corresponding evidence report were published in the Journal of the American Medical Association, following a draft recommendation in January.
The organization reached a similar conclusion following its evaluation in 2016.
“There’s just not enough evidence to determine whether or not screening all children for high cholesterol improves their heart health into adulthood,” said Katrina Donahue, MD, MPH, a USPSTF member and a professor in the department of family medicine at the University of North Carolina at Chapel Hill. “We’re calling for additional research on the effectiveness of screening for and treatment of high cholesterol in children and adolescents to prevent heart attacks, strokes, and death in adulthood.”
The task force recommended other evidence-based strategies to promote heart health, such as screening for obesity and interventions to prevent tobacco use.
The recommendation was the result of a review of 43 studies from MEDLINE and the Cochrane Central Register of Controlled Trials through May 16, 2022. No randomized controlled trial directly addressed the effectiveness or harms of lipid screening for children and adolescents. The task force continued to use article alerts and targeted journal searches through March 24, 2023.
Conditions such as familial hypercholesterolemia and multifactorial dyslipidemia can cause abnormally high lipid levels in children, potentially leading to premature cardiovascular events such as myocardial infarction, stroke, and death in adulthood. According to the USPSTF, the prevalence of FH in U.S. children and adolescents ranges from 0.2% to 0.4% (one in every 250-500 youth). Multifactorial dyslipidemia is more common – the prevalence in children and adolescents ranges from 7.1% to 9.4%.
In an editorial response to the task force’s statement, the authors, including Sarah D. de Ferranti, MD, department of pediatrics at Harvard Medical School, Boston, question the impact of not screening children to identify FH and other conditions and caution against the subsequent delay in treatment.
“Treating FH during childhood slows the progression of vascular finding in atherosclerosis,” the authors write.
They note that the recommendation “leaves a void for clinicians seeking to provide care for patients today” while additional research is conducted.
Sarah Nosal, MD, a member of the board of directors of the American Academy of Family Physicians, said that despite the lack of a recommendation, primary care clinicians can still encourage proper nutrition and physical activity for patients.
Dr. Nosal said that even without clear recommendations from the USPSTF, in the rare case of a patient with a family history of FH, she would order a lipid test and discuss treatment plans with the patient and family, if needed.
“We really don’t want to do tests that we don’t know what to do with the information,” she said.
One USPSTF member reported receiving grants from Healthwise, a nonprofit organization, outside the submitted work.
A version of this article first appeared on Medscape.com.
The group’s final recommendation and corresponding evidence report were published in the Journal of the American Medical Association, following a draft recommendation in January.
The organization reached a similar conclusion following its evaluation in 2016.
“There’s just not enough evidence to determine whether or not screening all children for high cholesterol improves their heart health into adulthood,” said Katrina Donahue, MD, MPH, a USPSTF member and a professor in the department of family medicine at the University of North Carolina at Chapel Hill. “We’re calling for additional research on the effectiveness of screening for and treatment of high cholesterol in children and adolescents to prevent heart attacks, strokes, and death in adulthood.”
The task force recommended other evidence-based strategies to promote heart health, such as screening for obesity and interventions to prevent tobacco use.
The recommendation was the result of a review of 43 studies from MEDLINE and the Cochrane Central Register of Controlled Trials through May 16, 2022. No randomized controlled trial directly addressed the effectiveness or harms of lipid screening for children and adolescents. The task force continued to use article alerts and targeted journal searches through March 24, 2023.
Conditions such as familial hypercholesterolemia and multifactorial dyslipidemia can cause abnormally high lipid levels in children, potentially leading to premature cardiovascular events such as myocardial infarction, stroke, and death in adulthood. According to the USPSTF, the prevalence of FH in U.S. children and adolescents ranges from 0.2% to 0.4% (one in every 250-500 youth). Multifactorial dyslipidemia is more common – the prevalence in children and adolescents ranges from 7.1% to 9.4%.
In an editorial response to the task force’s statement, the authors, including Sarah D. de Ferranti, MD, department of pediatrics at Harvard Medical School, Boston, question the impact of not screening children to identify FH and other conditions and caution against the subsequent delay in treatment.
“Treating FH during childhood slows the progression of vascular finding in atherosclerosis,” the authors write.
They note that the recommendation “leaves a void for clinicians seeking to provide care for patients today” while additional research is conducted.
Sarah Nosal, MD, a member of the board of directors of the American Academy of Family Physicians, said that despite the lack of a recommendation, primary care clinicians can still encourage proper nutrition and physical activity for patients.
Dr. Nosal said that even without clear recommendations from the USPSTF, in the rare case of a patient with a family history of FH, she would order a lipid test and discuss treatment plans with the patient and family, if needed.
“We really don’t want to do tests that we don’t know what to do with the information,” she said.
One USPSTF member reported receiving grants from Healthwise, a nonprofit organization, outside the submitted work.
A version of this article first appeared on Medscape.com.
Creating a fair time-off policy
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?

First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?
First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?
First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Summer diarrhea – Time to think outside the box
It’s “summertime and the livin’ is easy” according to the lyric from an old George Gershwin song. But sometimes, summer activities can lead to illnesses that can disrupt a child’s easy living.
Case: An otherwise healthy 11-year-old presents with four to five loose stools per day, mild nausea, excess flatulence, and cramps for 12 days with a 5-pound weight loss. His loose-to-mushy stools have no blood or mucous but smell worse than usual. He has had no fever, vomiting, rashes, or joint symptoms. A month ago, he went hiking/camping on the Appalachian Trail, drank boiled stream water. and slept in a common-use semi-enclosed shelter. He waded through streams and shared “Trail Magic” (soft drinks being cooled in a fresh mountain stream). Two other campers report similar symptoms.

Differential diagnosis: Broadly, we should consider bacteria, viruses, and parasites. But generally, bacteria are likely to produce more systemic symptoms and usually do not last 12 days. That said, this could be Clostridioides difficile, yet that seems unlikely because he is otherwise healthy and has no apparent risk factors. Salmonella spp., Campylobacter spp. and some Escherichia coli infections may drag on for more than a week but the lack of systemic symptoms or blood/mucous lowers the likelihood. Viral agents (rotavirus, norovirus, adenovirus, astrovirus, calicivirus, or sapovirus) seem unlikely because of the long symptom duration and the child’s preteen age.
The history and presentation seem more likely attributable to a parasite. Uncommonly detected protozoa include Microsporidium (mostly Enterocytozoon bieneusi) and amoeba. Microsporidium is very rare and seen mostly in immune compromised hosts, for example, those living with HIV. Amebiasis occurs mostly after travel to endemic areas, and stools usually contain blood or mucous. Some roundworm or tapeworm infestations cause abdominal pain and abnormal stools, but the usual exposures are absent. Giardia spp., Cryptosporidium spp., Cyclospora cayetanensis, and/or Cystoisospora belli best fit this presentation given his hiking/camping trip.
Workup. Laboratory testing of stool is warranted (because of weight loss and persistent diarrhea) despite a lack of systemic signs. Initially, bacterial culture, C. difficile testing, and viral testing seem unwarranted. The best initial approach, given our most likely suspects, is protozoan/parasite testing.
The Centers for Disease Control and Prevention recommends testing up to three stools collected on separate days.1 Initially, stool testing for giardia and cryptosporidium antigens by EIA assays could be done as a point-of-care test. Such antigen tests are often the first step because of their ease of use, relatively low expense, reasonably high sensitivity and specificity, and rapid turnaround (as little as 1 hour). Alternatively, direct examination of three stools for ova and parasites (O&P) and acid-fast stain or direct fluorescent antibody testing can usually detect our main suspects (giardia, cryptosporidium, cyclospora, and cystoisospora) along with other less likely parasites.
Some laboratories, however, use syndromic stool testing approaches (multiplex nucleic acid panels) that detect over 20 different bacteria, viruses, and select parasites. Multiplex testing has yielded increased detection rates, compared with microscopic examination alone in some settings. Further, they also share ease-of-use and rapid turnaround times with parasite antigen assays while requiring less hands-on time by laboratory personnel, compared with direct microscopic examination. However, multiplex assays are expensive and more readily detect commensal organisms, so they are not necessarily the ideal test in all diarrheal illnesses.
Diagnosis. You decide to first order giardia and cryptosporidium antigen testing because you are highly suspicious that giardia is the cause, based on wild-water exposure, the presentation, and symptom duration. You also order full microscopic O&P examination because you know that parasites can “run in packs.” Results of testing the first stool are positive for giardia. Microscopic examination on each of three stools is negative except for giardia trophozoites (the noninfectious form) in stools two and three.
Giardia overview. Giardia is the most common protozoan causing diarrhea in the United States, is fecal-oral spread, and like Shigella spp., is a low-inoculum infection (ingestion of as few as 10-100 cysts). Acquisition in the United States has been estimated as being 75% from contaminated water (streams are a classic source.2 Other sources are contaminated food (fresh produce is classic) and in some cases sexual encounters (mostly in men who have sex with men). Most detections are sporadic, but outbreaks can occur with case numbers usually below 20; 40% of outbreaks are attributable to contaminated water or food.3 Evaluating symptomatic household members can be important as transmission in families can occur.
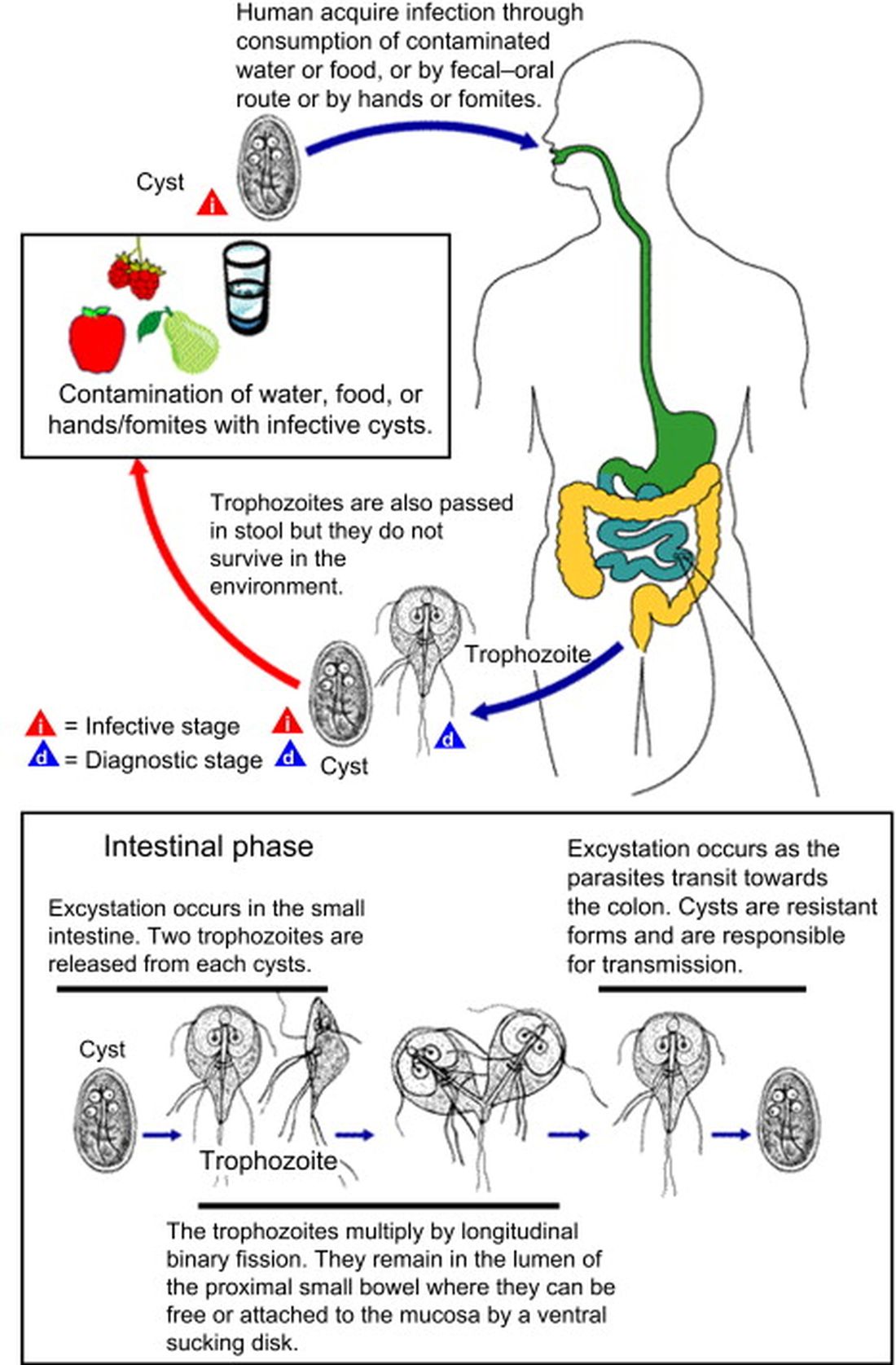
After ingestion, the cysts uncoat and form trophozoites, which reside mostly in the small bowel (Figure), causing inflammation and altering gut membrane permeability, thereby reducing nutrient absorption and circulating amino acids. Along with decreased food intake, altered absorption can lead to weight loss and potentially reduce growth in young children. Some trophozoites replicate while others encyst, eventually passing into stool. The cysts can survive for months in water or the environment (lakes, swimming pools, and clear mountain streams). Giardia has been linked to beavers’ feces contaminating wild-water sources, hence the moniker “Beaver fever” and warnings about stream water related to wilderness hiking.4
Management. Supportive therapy as with any diarrheal illness is the cornerstone of management. Specific antiparasitic treatment has traditionally been with metronidazole compounded into a liquid for young children, but the awful taste and frequent dosing often result in poor adherence. Nevertheless, published cure rates range from 80% to 100%. The taste issue, known adverse effects, and lack of FDA approval for giardia, have led to use of other drugs.5 One dose of tinidazole is as effective as metronidazole and can be prescribed for children 3 years old or older. But the drug nitazoxanide is becoming more standard. It is as effective as either alternative, and is FDA approved for children 1 year old and older. Nitazoxanide also is effective against other intestinal parasites (e.g., cryptosporidium). Nitazoxanide’s 3-day course involves every-12-hour dosing with food with each dose being 5 mL (100 mg) for 1- to 3-year-olds, 10 mL (200 mg) for 4- to 11-year-olds, and one tablet (500 mg) or 25 mL (500 mg) for children 12 years old or older.6
Key elements in this subacute nonsystemic diarrheal presentation were primitive camping history, multiple stream water contacts, nearly 2 weeks of symptoms, weight loss, and flatulence/cramping, but no fever or stool blood/mucous. Two friends also appear to be similarly symptomatic, so a common exposure seemed likely This is typical for several summertime activity–related parasites. So,
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital–Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines. The hospital also receives CDC funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus. Email Dr. Harrison at [email protected].
References
1. Diagnosis and Treatment Information for Medical Professionals, Giardia, Parasites. CDC.
2. Krumrie S et al. Curr Res Parasitol Vector Borne Dis. 2022;2:100084. doi: 10.1016/j.crpvbd.2022.100084.
3. Baldursson S and Karanis P. Water Res. 2011 Dec 15. doi: 10.1016/j.watres.2011.10.013.
4. “Water on the Appalachian Trail” AppalachianTrail.com.
5. Giardiasis: Treatment and prevention. UpToDate.
6. Kimberlin D et al. Red Book: 2021-2024 Report of the Committee on Infectious Diseases (Itasca, Ill.: American Academy of Pediatrics, 2021. 32nd ed.) Giardia duodenalis infections. pp. 335-8; and p. 961 (Table 4.11).
It’s “summertime and the livin’ is easy” according to the lyric from an old George Gershwin song. But sometimes, summer activities can lead to illnesses that can disrupt a child’s easy living.
Case: An otherwise healthy 11-year-old presents with four to five loose stools per day, mild nausea, excess flatulence, and cramps for 12 days with a 5-pound weight loss. His loose-to-mushy stools have no blood or mucous but smell worse than usual. He has had no fever, vomiting, rashes, or joint symptoms. A month ago, he went hiking/camping on the Appalachian Trail, drank boiled stream water. and slept in a common-use semi-enclosed shelter. He waded through streams and shared “Trail Magic” (soft drinks being cooled in a fresh mountain stream). Two other campers report similar symptoms.
Differential diagnosis: Broadly, we should consider bacteria, viruses, and parasites. But generally, bacteria are likely to produce more systemic symptoms and usually do not last 12 days. That said, this could be Clostridioides difficile, yet that seems unlikely because he is otherwise healthy and has no apparent risk factors. Salmonella spp., Campylobacter spp. and some Escherichia coli infections may drag on for more than a week but the lack of systemic symptoms or blood/mucous lowers the likelihood. Viral agents (rotavirus, norovirus, adenovirus, astrovirus, calicivirus, or sapovirus) seem unlikely because of the long symptom duration and the child’s preteen age.
The history and presentation seem more likely attributable to a parasite. Uncommonly detected protozoa include Microsporidium (mostly Enterocytozoon bieneusi) and amoeba. Microsporidium is very rare and seen mostly in immune compromised hosts, for example, those living with HIV. Amebiasis occurs mostly after travel to endemic areas, and stools usually contain blood or mucous. Some roundworm or tapeworm infestations cause abdominal pain and abnormal stools, but the usual exposures are absent. Giardia spp., Cryptosporidium spp., Cyclospora cayetanensis, and/or Cystoisospora belli best fit this presentation given his hiking/camping trip.
Workup. Laboratory testing of stool is warranted (because of weight loss and persistent diarrhea) despite a lack of systemic signs. Initially, bacterial culture, C. difficile testing, and viral testing seem unwarranted. The best initial approach, given our most likely suspects, is protozoan/parasite testing.
The Centers for Disease Control and Prevention recommends testing up to three stools collected on separate days.1 Initially, stool testing for giardia and cryptosporidium antigens by EIA assays could be done as a point-of-care test. Such antigen tests are often the first step because of their ease of use, relatively low expense, reasonably high sensitivity and specificity, and rapid turnaround (as little as 1 hour). Alternatively, direct examination of three stools for ova and parasites (O&P) and acid-fast stain or direct fluorescent antibody testing can usually detect our main suspects (giardia, cryptosporidium, cyclospora, and cystoisospora) along with other less likely parasites.
Some laboratories, however, use syndromic stool testing approaches (multiplex nucleic acid panels) that detect over 20 different bacteria, viruses, and select parasites. Multiplex testing has yielded increased detection rates, compared with microscopic examination alone in some settings. Further, they also share ease-of-use and rapid turnaround times with parasite antigen assays while requiring less hands-on time by laboratory personnel, compared with direct microscopic examination. However, multiplex assays are expensive and more readily detect commensal organisms, so they are not necessarily the ideal test in all diarrheal illnesses.
Diagnosis. You decide to first order giardia and cryptosporidium antigen testing because you are highly suspicious that giardia is the cause, based on wild-water exposure, the presentation, and symptom duration. You also order full microscopic O&P examination because you know that parasites can “run in packs.” Results of testing the first stool are positive for giardia. Microscopic examination on each of three stools is negative except for giardia trophozoites (the noninfectious form) in stools two and three.
Giardia overview. Giardia is the most common protozoan causing diarrhea in the United States, is fecal-oral spread, and like Shigella spp., is a low-inoculum infection (ingestion of as few as 10-100 cysts). Acquisition in the United States has been estimated as being 75% from contaminated water (streams are a classic source.2 Other sources are contaminated food (fresh produce is classic) and in some cases sexual encounters (mostly in men who have sex with men). Most detections are sporadic, but outbreaks can occur with case numbers usually below 20; 40% of outbreaks are attributable to contaminated water or food.3 Evaluating symptomatic household members can be important as transmission in families can occur.
After ingestion, the cysts uncoat and form trophozoites, which reside mostly in the small bowel (Figure), causing inflammation and altering gut membrane permeability, thereby reducing nutrient absorption and circulating amino acids. Along with decreased food intake, altered absorption can lead to weight loss and potentially reduce growth in young children. Some trophozoites replicate while others encyst, eventually passing into stool. The cysts can survive for months in water or the environment (lakes, swimming pools, and clear mountain streams). Giardia has been linked to beavers’ feces contaminating wild-water sources, hence the moniker “Beaver fever” and warnings about stream water related to wilderness hiking.4
Management. Supportive therapy as with any diarrheal illness is the cornerstone of management. Specific antiparasitic treatment has traditionally been with metronidazole compounded into a liquid for young children, but the awful taste and frequent dosing often result in poor adherence. Nevertheless, published cure rates range from 80% to 100%. The taste issue, known adverse effects, and lack of FDA approval for giardia, have led to use of other drugs.5 One dose of tinidazole is as effective as metronidazole and can be prescribed for children 3 years old or older. But the drug nitazoxanide is becoming more standard. It is as effective as either alternative, and is FDA approved for children 1 year old and older. Nitazoxanide also is effective against other intestinal parasites (e.g., cryptosporidium). Nitazoxanide’s 3-day course involves every-12-hour dosing with food with each dose being 5 mL (100 mg) for 1- to 3-year-olds, 10 mL (200 mg) for 4- to 11-year-olds, and one tablet (500 mg) or 25 mL (500 mg) for children 12 years old or older.6
Key elements in this subacute nonsystemic diarrheal presentation were primitive camping history, multiple stream water contacts, nearly 2 weeks of symptoms, weight loss, and flatulence/cramping, but no fever or stool blood/mucous. Two friends also appear to be similarly symptomatic, so a common exposure seemed likely This is typical for several summertime activity–related parasites. So,
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital–Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines. The hospital also receives CDC funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus. Email Dr. Harrison at [email protected].
References
1. Diagnosis and Treatment Information for Medical Professionals, Giardia, Parasites. CDC.
2. Krumrie S et al. Curr Res Parasitol Vector Borne Dis. 2022;2:100084. doi: 10.1016/j.crpvbd.2022.100084.
3. Baldursson S and Karanis P. Water Res. 2011 Dec 15. doi: 10.1016/j.watres.2011.10.013.
4. “Water on the Appalachian Trail” AppalachianTrail.com.
5. Giardiasis: Treatment and prevention. UpToDate.
6. Kimberlin D et al. Red Book: 2021-2024 Report of the Committee on Infectious Diseases (Itasca, Ill.: American Academy of Pediatrics, 2021. 32nd ed.) Giardia duodenalis infections. pp. 335-8; and p. 961 (Table 4.11).
It’s “summertime and the livin’ is easy” according to the lyric from an old George Gershwin song. But sometimes, summer activities can lead to illnesses that can disrupt a child’s easy living.
Case: An otherwise healthy 11-year-old presents with four to five loose stools per day, mild nausea, excess flatulence, and cramps for 12 days with a 5-pound weight loss. His loose-to-mushy stools have no blood or mucous but smell worse than usual. He has had no fever, vomiting, rashes, or joint symptoms. A month ago, he went hiking/camping on the Appalachian Trail, drank boiled stream water. and slept in a common-use semi-enclosed shelter. He waded through streams and shared “Trail Magic” (soft drinks being cooled in a fresh mountain stream). Two other campers report similar symptoms.
Differential diagnosis: Broadly, we should consider bacteria, viruses, and parasites. But generally, bacteria are likely to produce more systemic symptoms and usually do not last 12 days. That said, this could be Clostridioides difficile, yet that seems unlikely because he is otherwise healthy and has no apparent risk factors. Salmonella spp., Campylobacter spp. and some Escherichia coli infections may drag on for more than a week but the lack of systemic symptoms or blood/mucous lowers the likelihood. Viral agents (rotavirus, norovirus, adenovirus, astrovirus, calicivirus, or sapovirus) seem unlikely because of the long symptom duration and the child’s preteen age.
The history and presentation seem more likely attributable to a parasite. Uncommonly detected protozoa include Microsporidium (mostly Enterocytozoon bieneusi) and amoeba. Microsporidium is very rare and seen mostly in immune compromised hosts, for example, those living with HIV. Amebiasis occurs mostly after travel to endemic areas, and stools usually contain blood or mucous. Some roundworm or tapeworm infestations cause abdominal pain and abnormal stools, but the usual exposures are absent. Giardia spp., Cryptosporidium spp., Cyclospora cayetanensis, and/or Cystoisospora belli best fit this presentation given his hiking/camping trip.
Workup. Laboratory testing of stool is warranted (because of weight loss and persistent diarrhea) despite a lack of systemic signs. Initially, bacterial culture, C. difficile testing, and viral testing seem unwarranted. The best initial approach, given our most likely suspects, is protozoan/parasite testing.
The Centers for Disease Control and Prevention recommends testing up to three stools collected on separate days.1 Initially, stool testing for giardia and cryptosporidium antigens by EIA assays could be done as a point-of-care test. Such antigen tests are often the first step because of their ease of use, relatively low expense, reasonably high sensitivity and specificity, and rapid turnaround (as little as 1 hour). Alternatively, direct examination of three stools for ova and parasites (O&P) and acid-fast stain or direct fluorescent antibody testing can usually detect our main suspects (giardia, cryptosporidium, cyclospora, and cystoisospora) along with other less likely parasites.
Some laboratories, however, use syndromic stool testing approaches (multiplex nucleic acid panels) that detect over 20 different bacteria, viruses, and select parasites. Multiplex testing has yielded increased detection rates, compared with microscopic examination alone in some settings. Further, they also share ease-of-use and rapid turnaround times with parasite antigen assays while requiring less hands-on time by laboratory personnel, compared with direct microscopic examination. However, multiplex assays are expensive and more readily detect commensal organisms, so they are not necessarily the ideal test in all diarrheal illnesses.
Diagnosis. You decide to first order giardia and cryptosporidium antigen testing because you are highly suspicious that giardia is the cause, based on wild-water exposure, the presentation, and symptom duration. You also order full microscopic O&P examination because you know that parasites can “run in packs.” Results of testing the first stool are positive for giardia. Microscopic examination on each of three stools is negative except for giardia trophozoites (the noninfectious form) in stools two and three.
Giardia overview. Giardia is the most common protozoan causing diarrhea in the United States, is fecal-oral spread, and like Shigella spp., is a low-inoculum infection (ingestion of as few as 10-100 cysts). Acquisition in the United States has been estimated as being 75% from contaminated water (streams are a classic source.2 Other sources are contaminated food (fresh produce is classic) and in some cases sexual encounters (mostly in men who have sex with men). Most detections are sporadic, but outbreaks can occur with case numbers usually below 20; 40% of outbreaks are attributable to contaminated water or food.3 Evaluating symptomatic household members can be important as transmission in families can occur.
After ingestion, the cysts uncoat and form trophozoites, which reside mostly in the small bowel (Figure), causing inflammation and altering gut membrane permeability, thereby reducing nutrient absorption and circulating amino acids. Along with decreased food intake, altered absorption can lead to weight loss and potentially reduce growth in young children. Some trophozoites replicate while others encyst, eventually passing into stool. The cysts can survive for months in water or the environment (lakes, swimming pools, and clear mountain streams). Giardia has been linked to beavers’ feces contaminating wild-water sources, hence the moniker “Beaver fever” and warnings about stream water related to wilderness hiking.4
Management. Supportive therapy as with any diarrheal illness is the cornerstone of management. Specific antiparasitic treatment has traditionally been with metronidazole compounded into a liquid for young children, but the awful taste and frequent dosing often result in poor adherence. Nevertheless, published cure rates range from 80% to 100%. The taste issue, known adverse effects, and lack of FDA approval for giardia, have led to use of other drugs.5 One dose of tinidazole is as effective as metronidazole and can be prescribed for children 3 years old or older. But the drug nitazoxanide is becoming more standard. It is as effective as either alternative, and is FDA approved for children 1 year old and older. Nitazoxanide also is effective against other intestinal parasites (e.g., cryptosporidium). Nitazoxanide’s 3-day course involves every-12-hour dosing with food with each dose being 5 mL (100 mg) for 1- to 3-year-olds, 10 mL (200 mg) for 4- to 11-year-olds, and one tablet (500 mg) or 25 mL (500 mg) for children 12 years old or older.6
Key elements in this subacute nonsystemic diarrheal presentation were primitive camping history, multiple stream water contacts, nearly 2 weeks of symptoms, weight loss, and flatulence/cramping, but no fever or stool blood/mucous. Two friends also appear to be similarly symptomatic, so a common exposure seemed likely This is typical for several summertime activity–related parasites. So,
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital–Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines. The hospital also receives CDC funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus. Email Dr. Harrison at [email protected].
References
1. Diagnosis and Treatment Information for Medical Professionals, Giardia, Parasites. CDC.
2. Krumrie S et al. Curr Res Parasitol Vector Borne Dis. 2022;2:100084. doi: 10.1016/j.crpvbd.2022.100084.
3. Baldursson S and Karanis P. Water Res. 2011 Dec 15. doi: 10.1016/j.watres.2011.10.013.
4. “Water on the Appalachian Trail” AppalachianTrail.com.
5. Giardiasis: Treatment and prevention. UpToDate.
6. Kimberlin D et al. Red Book: 2021-2024 Report of the Committee on Infectious Diseases (Itasca, Ill.: American Academy of Pediatrics, 2021. 32nd ed.) Giardia duodenalis infections. pp. 335-8; and p. 961 (Table 4.11).
How the new depression screening guidelines in adults do little to address our mental health care crisis
According to the World Health Organization (WHO), approximately 5% of adults (or 280 million people) suffer from depression globally. Although depression is more common in women, it can affect anyone. It is seen in all socioeconomic classes, ages, and races. In response, the WHO developed the Mental Health Gap Action Programme to bring mental health care services to those in need.
Depression can lead to severe consequences, such as loss of employment, relationships difficulties, and suicide. In fact, suicide is the 10th leading cause of death in the United States.

The U.S. Preventive Services Task Force (USPSTF), in past years, concluded that there was insufficient evidence to screen adolescents and adults for depression, However, new guidelines were issued this year in which the task force concluded there was a moderate benefit to screening adults for depression but insufficient evidence to screen for suicide risk. The agency now recommends screening for depression in all adults, even in the absence of risk factors, by using brief screening instruments such as the PHQ (Patient Health Questionnaire).
As family doctors, we have witnessed the burden of depression in our practices. The previous recommendations neglected the fact that mental health disorders were often purposely hidden because of stigma. Many patients do not readily come for treatment for mental illness and sometimes do not even accept these diagnoses. It is good that screening is now recommended, but we need to do more to tear down the stigma attached to mental illness.
These new guidelines do not address the effect that the lack of available mental health services has on treatment. It can take months to get an appointment for a patient with a mental health disorder, even if that person is potentially suicidal. Primary care physicians are often left treating these disorders; sometimes we are treating mental illness whether we feel comfortable doing so or not. Patients may not receive the best care but it is better than no care at all.
Although treating anxiety and depression is common for primary care doctors, specialists should be contacted when cases get more complicated. Even a call to crisis intervention can lead to an emergency department visit with discharge back to the family doctor because there is nowhere else to send the patient. The burden falls on us when we are already burdened by many other things, such as the rising rates of obesity with the resultant consequences of diabetes and heart disease. We simply do not have the time or expertise to treat complicated mental illness.
Creating guidelines to diagnose more undetected cases of depression without increasing the infrastructure to handle it is only going to lead to more pressure on family doctors. Many of us are already burnt out and at our limits. Yes, we want to diagnose every case of depression we can and to treat these patients for these disorders, but we need help.
Another problem with the guidelines is the recommendation to screen for depression and not suicide risk. As family doctors, we ask all patients who are depressed if they have thoughts of hurting themselves or others. Also, some people who commit suicide are not clinically depressed. These questions are simple to ask on an intake form.
Screening for depression is a pretty simple process. A patient can complete a screening tool or the clinician can directly ask the questions. It is a quick, noninvasive process. The Diagnostic and Statistical Manual of Mental Disorders criteria for diagnosing depression are pretty rigid and straightforward so misdiagnoses are not likely to be common.
The new guidelines do not make recommendations for treatment. In the real world, we often see patients unable to get the medications we prescribe because their insurance won’t cover it. Having guidelines supporting medication use would be very helpful.
In the area where I practice, it is difficult to refer a patient for counseling despite there being a plethora of counselors, therapists, and psychologists. These mental health providers often take only cash-paying patients, which eliminates access for many patients.
If we truly want to address the ever-increasing rates of depression in our country, we need to do much more than create new screening guidelines (screening that many family doctors were already doing). We must remove stigma, especially in the health care setting, fund mental health services, make them more readily available, and provide care that is affordable and covered by insurance. Until then, we are just going to add to the load of family doctors until we either break or leave our profession. Patients deserve better.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. She was paid by Pfizer as a consultant on Paxlovid and is the editor in chief of Physician’s Weekly.
According to the World Health Organization (WHO), approximately 5% of adults (or 280 million people) suffer from depression globally. Although depression is more common in women, it can affect anyone. It is seen in all socioeconomic classes, ages, and races. In response, the WHO developed the Mental Health Gap Action Programme to bring mental health care services to those in need.
Depression can lead to severe consequences, such as loss of employment, relationships difficulties, and suicide. In fact, suicide is the 10th leading cause of death in the United States.
The U.S. Preventive Services Task Force (USPSTF), in past years, concluded that there was insufficient evidence to screen adolescents and adults for depression, However, new guidelines were issued this year in which the task force concluded there was a moderate benefit to screening adults for depression but insufficient evidence to screen for suicide risk. The agency now recommends screening for depression in all adults, even in the absence of risk factors, by using brief screening instruments such as the PHQ (Patient Health Questionnaire).
As family doctors, we have witnessed the burden of depression in our practices. The previous recommendations neglected the fact that mental health disorders were often purposely hidden because of stigma. Many patients do not readily come for treatment for mental illness and sometimes do not even accept these diagnoses. It is good that screening is now recommended, but we need to do more to tear down the stigma attached to mental illness.
These new guidelines do not address the effect that the lack of available mental health services has on treatment. It can take months to get an appointment for a patient with a mental health disorder, even if that person is potentially suicidal. Primary care physicians are often left treating these disorders; sometimes we are treating mental illness whether we feel comfortable doing so or not. Patients may not receive the best care but it is better than no care at all.
Although treating anxiety and depression is common for primary care doctors, specialists should be contacted when cases get more complicated. Even a call to crisis intervention can lead to an emergency department visit with discharge back to the family doctor because there is nowhere else to send the patient. The burden falls on us when we are already burdened by many other things, such as the rising rates of obesity with the resultant consequences of diabetes and heart disease. We simply do not have the time or expertise to treat complicated mental illness.
Creating guidelines to diagnose more undetected cases of depression without increasing the infrastructure to handle it is only going to lead to more pressure on family doctors. Many of us are already burnt out and at our limits. Yes, we want to diagnose every case of depression we can and to treat these patients for these disorders, but we need help.
Another problem with the guidelines is the recommendation to screen for depression and not suicide risk. As family doctors, we ask all patients who are depressed if they have thoughts of hurting themselves or others. Also, some people who commit suicide are not clinically depressed. These questions are simple to ask on an intake form.
Screening for depression is a pretty simple process. A patient can complete a screening tool or the clinician can directly ask the questions. It is a quick, noninvasive process. The Diagnostic and Statistical Manual of Mental Disorders criteria for diagnosing depression are pretty rigid and straightforward so misdiagnoses are not likely to be common.
The new guidelines do not make recommendations for treatment. In the real world, we often see patients unable to get the medications we prescribe because their insurance won’t cover it. Having guidelines supporting medication use would be very helpful.
In the area where I practice, it is difficult to refer a patient for counseling despite there being a plethora of counselors, therapists, and psychologists. These mental health providers often take only cash-paying patients, which eliminates access for many patients.
If we truly want to address the ever-increasing rates of depression in our country, we need to do much more than create new screening guidelines (screening that many family doctors were already doing). We must remove stigma, especially in the health care setting, fund mental health services, make them more readily available, and provide care that is affordable and covered by insurance. Until then, we are just going to add to the load of family doctors until we either break or leave our profession. Patients deserve better.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. She was paid by Pfizer as a consultant on Paxlovid and is the editor in chief of Physician’s Weekly.
According to the World Health Organization (WHO), approximately 5% of adults (or 280 million people) suffer from depression globally. Although depression is more common in women, it can affect anyone. It is seen in all socioeconomic classes, ages, and races. In response, the WHO developed the Mental Health Gap Action Programme to bring mental health care services to those in need.
Depression can lead to severe consequences, such as loss of employment, relationships difficulties, and suicide. In fact, suicide is the 10th leading cause of death in the United States.
The U.S. Preventive Services Task Force (USPSTF), in past years, concluded that there was insufficient evidence to screen adolescents and adults for depression, However, new guidelines were issued this year in which the task force concluded there was a moderate benefit to screening adults for depression but insufficient evidence to screen for suicide risk. The agency now recommends screening for depression in all adults, even in the absence of risk factors, by using brief screening instruments such as the PHQ (Patient Health Questionnaire).
As family doctors, we have witnessed the burden of depression in our practices. The previous recommendations neglected the fact that mental health disorders were often purposely hidden because of stigma. Many patients do not readily come for treatment for mental illness and sometimes do not even accept these diagnoses. It is good that screening is now recommended, but we need to do more to tear down the stigma attached to mental illness.
These new guidelines do not address the effect that the lack of available mental health services has on treatment. It can take months to get an appointment for a patient with a mental health disorder, even if that person is potentially suicidal. Primary care physicians are often left treating these disorders; sometimes we are treating mental illness whether we feel comfortable doing so or not. Patients may not receive the best care but it is better than no care at all.
Although treating anxiety and depression is common for primary care doctors, specialists should be contacted when cases get more complicated. Even a call to crisis intervention can lead to an emergency department visit with discharge back to the family doctor because there is nowhere else to send the patient. The burden falls on us when we are already burdened by many other things, such as the rising rates of obesity with the resultant consequences of diabetes and heart disease. We simply do not have the time or expertise to treat complicated mental illness.
Creating guidelines to diagnose more undetected cases of depression without increasing the infrastructure to handle it is only going to lead to more pressure on family doctors. Many of us are already burnt out and at our limits. Yes, we want to diagnose every case of depression we can and to treat these patients for these disorders, but we need help.
Another problem with the guidelines is the recommendation to screen for depression and not suicide risk. As family doctors, we ask all patients who are depressed if they have thoughts of hurting themselves or others. Also, some people who commit suicide are not clinically depressed. These questions are simple to ask on an intake form.
Screening for depression is a pretty simple process. A patient can complete a screening tool or the clinician can directly ask the questions. It is a quick, noninvasive process. The Diagnostic and Statistical Manual of Mental Disorders criteria for diagnosing depression are pretty rigid and straightforward so misdiagnoses are not likely to be common.
The new guidelines do not make recommendations for treatment. In the real world, we often see patients unable to get the medications we prescribe because their insurance won’t cover it. Having guidelines supporting medication use would be very helpful.
In the area where I practice, it is difficult to refer a patient for counseling despite there being a plethora of counselors, therapists, and psychologists. These mental health providers often take only cash-paying patients, which eliminates access for many patients.
If we truly want to address the ever-increasing rates of depression in our country, we need to do much more than create new screening guidelines (screening that many family doctors were already doing). We must remove stigma, especially in the health care setting, fund mental health services, make them more readily available, and provide care that is affordable and covered by insurance. Until then, we are just going to add to the load of family doctors until we either break or leave our profession. Patients deserve better.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. She was paid by Pfizer as a consultant on Paxlovid and is the editor in chief of Physician’s Weekly.
A primer on gender-affirming care for transgender youth
Over the past few years, there has been rampant misinformation regarding gender-affirming care for transgender youth. In particular, there has been confusion regarding how care is administered, and what types of care are considered at various stages of development. This primer will help you understand the developmental approach to supporting transgender youth.
While people generally think of medical and surgical aspects of gender-affirming care, other domains can be just as important. For example, a 2020 publication in The Lancet Public Health found that access to gender-congruent government identification documents was associated with lower odds of severe psychological distress and suicidality.1

Considerations for prepubertal children
The youngest developmental stage at which a young person may seek care regarding gender diversity is the prepubertal childhood stage. Guidelines set forth by The Endocrine Society and The World Professional Association for Transgender Health make it clear that no medical or surgical interventions are considered at this developmental stage.2,3 However, some young people may choose to pursue a “social transition.” Though this may sound like one thing, social transition can mean very different things for different people. It may include any combination of adopting a new name, pronouns, hairstyle, clothing, etc. Young people may also choose to pursue these various aspects of social transition in all settings, or sometimes only in some settings (for example, only at home if they don’t yet feel comfortable doing so at school). Research so far shows that prepubertal children who are allowed to socially transition have levels of anxiety and depression nearly indistinguishable from their cisgender peers.4 While some in the past have raised the question of whether a social transition increases a child’s degree of gender incongruence and thus their likelihood to “persist” in a transgender identity, research has suggested this is not the case, and that gender identity does not meaningfully differ before and after a social transition.5 It’s worth noting, that “desistance” of a young person’s transgender identity is generally not considered an ethical goal and that gender identity conversion efforts (that is, attempts to force transgender people to be cisgender) have been labeled unethical by the American Academy of Child & Adolescent Psychiatry.
Sadly, transgender children are victims of bullying at high rates in their schools and communities. Creating safe and affirming school and community environments can be some of the highest yield ways in which providers can support the mental health of gender-diverse youth at this stage. Gender Spectrum is an excellent nonprofit that provides resources to help families and communities with some of these nonmedical supports.
Early adolescence and pubertal suppression
The earliest gender-affirming medical intervention that may be considered is pubertal suppression. Pubertal suppression is achieved with gonadotropin-releasing hormone agonists. This class of medications is Food and Drug Administration approved in pediatrics for precocious puberty – a condition in which young people enter puberty much earlier than expected (sometimes as early as age 3). For that condition, the rationale is to delay puberty until the patient reaches a more developmentally normative age for puberty to begin. The rationale for pubertal suppression for adolescent gender dysphoria is somewhat similar – these medications allow for the temporary pausing of puberty, which can be particularly helpful for adolescents who are having severe negative psychological reactions to the ways in which their bodies are developing. The major advantage here is that pubertal suppression can be reversed (if the medication is stopped, endogenous puberty will proceed), whereas puberty itself cannot be easily reversed (resulting in adult transgender people needing surgery and other interventions later in life, if these changes can be fully undone at all). As with all medications, puberty blockers do carry known side effects, including falling behind on bone density (sex hormones are needed to mineralize bones). Because of this, it is generally recommended that adolescents have their bone density monitored during treatment, pursue avenues to improve bone health (for example, exercise), and either stop the puberty blocker to undergo endogenous puberty or start gender-affirming hormones (estrogen or testosterone) by around age 16.
It is also important to note that, under current guidelines, an adolescent must first undergo a comprehensive biopsychosocial mental health evaluation prior to starting pubertal suppression to ensure the clinical team has a comprehensive understanding of the adolescent’s mental health, that all potential gender supports that are needed are put into place, and that the adolescent and their guardians have a strong understanding of the medical intervention, its risks, side effects, and potential benefits. In addition, consent must be provided by parents or legal guardians, whereas adolescents themselves provide assent. Several studies have linked access to pubertal suppression, when indicated for gender dysphoria, to improved mental health outcomes (for example, van der Miesen and colleagues, Turban and colleagues, de Vries and colleagues, and Costa and colleagues).6-9
Later adolescence and gender-affirming hormones
Later in adolescence, transgender youth may be candidates for gender-affirming hormone treatment (for example, estrogen or testosterone) to induce pubertal changes that align with their gender identities. Once again, under current guidelines, a comprehensive mental health biopsychosocial evaluation must be conducted prior to initiation of these treatments. Part of this evaluation includes fertility counseling and consideration of fertility preservation (for example, oocyte or semen cryopreservation), given the potential for these medications to impact fertility. It also involves discussion of several of the physiologic changes from these medications that can be irreversible (for example, voice changes from testosterone are particularly difficult to reverse in the future). Tables of the physical changes from these medications, when they begin after starting, and when they generally reach their maximum are available in the Endocrine Society guidelines.2 The past endocrine society guidelines recommended not initiating gender-affirming hormones until age 16. The most recent guidelines note that there may be instances in which providers may consider starting them as early as age 13 (for example, to reduce risk of falling behind on bone density, or if a patient is having psychological distress related to their peers going through puberty while they are still in a prepubertal state). The latest World Professional Association for Transgender Health Standards of Care removed specific age cutoffs, highlighting the importance of a multidisciplinary team of mental health and hormone prescribing providers working together to understand the best course of action for a particular patient. As with pubertal suppression, several studies have linked access to gender-affirming hormones to improve mental health for adolescents with gender dysphoria (for example, Turban and colleagues, Chen and colleagues, de Vries and colleagues, Allen and colleagues, and Tordoff and colleagues).10-14
Gender-affirming surgeries
The vast majority of gender-affirming surgeries are not considered until adulthood. The most notable exception to this is masculinizing top surgery for trans masculine and nonbinary adolescents. As with all surgeries, this is a major decision, and requires agreement from a mental health provider, a medical provider, and the surgeon. Early research suggests such surgeries result in improved chest dysphoria and that regret rates appear to be low.15,16 While the latest World Professional Association for Transgender Health similarly removed strict age cutoffs for gender-affirming surgery, again noting the importance of individualized care, I suspect most will read this change in the context of the Endocrine Society guidelines and past WPATH guidelines that noted gender-affirming genital surgeries are not offered until adulthood (a rare exception perhaps being someone pursuing a gender-affirming vaginoplasty at say age 17 in the summer prior to college to avoid needing to take off from school for surgical recovery). Gender-affirming genital surgeries are generally much more involved surgeries with prolonged recovery times.
Given the substantial proportion of young people who openly identify as transgender,17 and the proliferation of misinformation, political rhetoric, and legislation that can impact gender-affirming care for adolescents with gender dysphoria,18 it is essential that providers have accurate, up-to-date information on what this care entails and how it is provided.
Dr. Turban is director of the gender psychiatry program at the University of California, San Francisco, where he is an assistant professor of child & adolescent psychiatry and affiliate faculty at the Philip R. Lee Institute for Health Policy Studies. He is on Twitter @jack_turban.
References
1. Malta M et al. Lancet Public Health. 2020 Apr;5(4):e178-9.
2. Hembree WC et al. J Clin Endocrinol Metab. 2017 Nov 1;102(11):3869-903.
3. Coleman E et al. Int J Transgend Health. 2022 Sep 6;23(Suppl 1):S1-259.
4. Durwood L et al. J Am Acad Child Adolesc Psychiatry. 2017 Feb;56(2):116-23.e2.
5. Rae JR et al. Psychol Sci. 2019 May;30(5):669-81.
6. van der Miesen AIR et al. J Adolesc Health. 2020 Jun;66(6):699-704.
7. Turban JL et al. Pediatrics. 2020 Feb;145(2):e20191725.
8. de Vries ALC et al. J Sex Med. 2011 Aug;8(8):2276-83.
9. Costa R et al. J Sex Med. 2015 Nov;12(11):2206-14.
10. Turban JL et al. PLoS One. 2022 Jan 12;17(1):e0261039.
11. Chen D et al. N Engl J Med. 2023;388:240-50.
12. de Vries ALC et al. Pediatrics. 2014 Oct;134(4):696-70.
13. Allen LR et al. Clin Pract Pediatr Psychol. 2019. doi: 10.1037/cpp0000288.
14. Tordoff DM et al. JAMA Netw Open. 2022 Feb 1;5(2):e220978.
15. Olson-Kennedy J et al. JAMA Pediatr. 2018;172(5):431-6.
16. Tang A et al. Ann Plast Surg. 2022 May;88(4 Suppl):S325-31
17. Johns MM et al. Morb Mortal Wkly Rep. 2019 Jan 25;68(3):67-71.
18. Turban JL et al. JAMA. 2021;325(22):2251-2.
Over the past few years, there has been rampant misinformation regarding gender-affirming care for transgender youth. In particular, there has been confusion regarding how care is administered, and what types of care are considered at various stages of development. This primer will help you understand the developmental approach to supporting transgender youth.
While people generally think of medical and surgical aspects of gender-affirming care, other domains can be just as important. For example, a 2020 publication in The Lancet Public Health found that access to gender-congruent government identification documents was associated with lower odds of severe psychological distress and suicidality.1
Considerations for prepubertal children
The youngest developmental stage at which a young person may seek care regarding gender diversity is the prepubertal childhood stage. Guidelines set forth by The Endocrine Society and The World Professional Association for Transgender Health make it clear that no medical or surgical interventions are considered at this developmental stage.2,3 However, some young people may choose to pursue a “social transition.” Though this may sound like one thing, social transition can mean very different things for different people. It may include any combination of adopting a new name, pronouns, hairstyle, clothing, etc. Young people may also choose to pursue these various aspects of social transition in all settings, or sometimes only in some settings (for example, only at home if they don’t yet feel comfortable doing so at school). Research so far shows that prepubertal children who are allowed to socially transition have levels of anxiety and depression nearly indistinguishable from their cisgender peers.4 While some in the past have raised the question of whether a social transition increases a child’s degree of gender incongruence and thus their likelihood to “persist” in a transgender identity, research has suggested this is not the case, and that gender identity does not meaningfully differ before and after a social transition.5 It’s worth noting, that “desistance” of a young person’s transgender identity is generally not considered an ethical goal and that gender identity conversion efforts (that is, attempts to force transgender people to be cisgender) have been labeled unethical by the American Academy of Child & Adolescent Psychiatry.
Sadly, transgender children are victims of bullying at high rates in their schools and communities. Creating safe and affirming school and community environments can be some of the highest yield ways in which providers can support the mental health of gender-diverse youth at this stage. Gender Spectrum is an excellent nonprofit that provides resources to help families and communities with some of these nonmedical supports.
Early adolescence and pubertal suppression
The earliest gender-affirming medical intervention that may be considered is pubertal suppression. Pubertal suppression is achieved with gonadotropin-releasing hormone agonists. This class of medications is Food and Drug Administration approved in pediatrics for precocious puberty – a condition in which young people enter puberty much earlier than expected (sometimes as early as age 3). For that condition, the rationale is to delay puberty until the patient reaches a more developmentally normative age for puberty to begin. The rationale for pubertal suppression for adolescent gender dysphoria is somewhat similar – these medications allow for the temporary pausing of puberty, which can be particularly helpful for adolescents who are having severe negative psychological reactions to the ways in which their bodies are developing. The major advantage here is that pubertal suppression can be reversed (if the medication is stopped, endogenous puberty will proceed), whereas puberty itself cannot be easily reversed (resulting in adult transgender people needing surgery and other interventions later in life, if these changes can be fully undone at all). As with all medications, puberty blockers do carry known side effects, including falling behind on bone density (sex hormones are needed to mineralize bones). Because of this, it is generally recommended that adolescents have their bone density monitored during treatment, pursue avenues to improve bone health (for example, exercise), and either stop the puberty blocker to undergo endogenous puberty or start gender-affirming hormones (estrogen or testosterone) by around age 16.
It is also important to note that, under current guidelines, an adolescent must first undergo a comprehensive biopsychosocial mental health evaluation prior to starting pubertal suppression to ensure the clinical team has a comprehensive understanding of the adolescent’s mental health, that all potential gender supports that are needed are put into place, and that the adolescent and their guardians have a strong understanding of the medical intervention, its risks, side effects, and potential benefits. In addition, consent must be provided by parents or legal guardians, whereas adolescents themselves provide assent. Several studies have linked access to pubertal suppression, when indicated for gender dysphoria, to improved mental health outcomes (for example, van der Miesen and colleagues, Turban and colleagues, de Vries and colleagues, and Costa and colleagues).6-9
Later adolescence and gender-affirming hormones
Later in adolescence, transgender youth may be candidates for gender-affirming hormone treatment (for example, estrogen or testosterone) to induce pubertal changes that align with their gender identities. Once again, under current guidelines, a comprehensive mental health biopsychosocial evaluation must be conducted prior to initiation of these treatments. Part of this evaluation includes fertility counseling and consideration of fertility preservation (for example, oocyte or semen cryopreservation), given the potential for these medications to impact fertility. It also involves discussion of several of the physiologic changes from these medications that can be irreversible (for example, voice changes from testosterone are particularly difficult to reverse in the future). Tables of the physical changes from these medications, when they begin after starting, and when they generally reach their maximum are available in the Endocrine Society guidelines.2 The past endocrine society guidelines recommended not initiating gender-affirming hormones until age 16. The most recent guidelines note that there may be instances in which providers may consider starting them as early as age 13 (for example, to reduce risk of falling behind on bone density, or if a patient is having psychological distress related to their peers going through puberty while they are still in a prepubertal state). The latest World Professional Association for Transgender Health Standards of Care removed specific age cutoffs, highlighting the importance of a multidisciplinary team of mental health and hormone prescribing providers working together to understand the best course of action for a particular patient. As with pubertal suppression, several studies have linked access to gender-affirming hormones to improve mental health for adolescents with gender dysphoria (for example, Turban and colleagues, Chen and colleagues, de Vries and colleagues, Allen and colleagues, and Tordoff and colleagues).10-14
Gender-affirming surgeries
The vast majority of gender-affirming surgeries are not considered until adulthood. The most notable exception to this is masculinizing top surgery for trans masculine and nonbinary adolescents. As with all surgeries, this is a major decision, and requires agreement from a mental health provider, a medical provider, and the surgeon. Early research suggests such surgeries result in improved chest dysphoria and that regret rates appear to be low.15,16 While the latest World Professional Association for Transgender Health similarly removed strict age cutoffs for gender-affirming surgery, again noting the importance of individualized care, I suspect most will read this change in the context of the Endocrine Society guidelines and past WPATH guidelines that noted gender-affirming genital surgeries are not offered until adulthood (a rare exception perhaps being someone pursuing a gender-affirming vaginoplasty at say age 17 in the summer prior to college to avoid needing to take off from school for surgical recovery). Gender-affirming genital surgeries are generally much more involved surgeries with prolonged recovery times.
Given the substantial proportion of young people who openly identify as transgender,17 and the proliferation of misinformation, political rhetoric, and legislation that can impact gender-affirming care for adolescents with gender dysphoria,18 it is essential that providers have accurate, up-to-date information on what this care entails and how it is provided.
Dr. Turban is director of the gender psychiatry program at the University of California, San Francisco, where he is an assistant professor of child & adolescent psychiatry and affiliate faculty at the Philip R. Lee Institute for Health Policy Studies. He is on Twitter @jack_turban.
References
1. Malta M et al. Lancet Public Health. 2020 Apr;5(4):e178-9.
2. Hembree WC et al. J Clin Endocrinol Metab. 2017 Nov 1;102(11):3869-903.
3. Coleman E et al. Int J Transgend Health. 2022 Sep 6;23(Suppl 1):S1-259.
4. Durwood L et al. J Am Acad Child Adolesc Psychiatry. 2017 Feb;56(2):116-23.e2.
5. Rae JR et al. Psychol Sci. 2019 May;30(5):669-81.
6. van der Miesen AIR et al. J Adolesc Health. 2020 Jun;66(6):699-704.
7. Turban JL et al. Pediatrics. 2020 Feb;145(2):e20191725.
8. de Vries ALC et al. J Sex Med. 2011 Aug;8(8):2276-83.
9. Costa R et al. J Sex Med. 2015 Nov;12(11):2206-14.
10. Turban JL et al. PLoS One. 2022 Jan 12;17(1):e0261039.
11. Chen D et al. N Engl J Med. 2023;388:240-50.
12. de Vries ALC et al. Pediatrics. 2014 Oct;134(4):696-70.
13. Allen LR et al. Clin Pract Pediatr Psychol. 2019. doi: 10.1037/cpp0000288.
14. Tordoff DM et al. JAMA Netw Open. 2022 Feb 1;5(2):e220978.
15. Olson-Kennedy J et al. JAMA Pediatr. 2018;172(5):431-6.
16. Tang A et al. Ann Plast Surg. 2022 May;88(4 Suppl):S325-31
17. Johns MM et al. Morb Mortal Wkly Rep. 2019 Jan 25;68(3):67-71.
18. Turban JL et al. JAMA. 2021;325(22):2251-2.
Over the past few years, there has been rampant misinformation regarding gender-affirming care for transgender youth. In particular, there has been confusion regarding how care is administered, and what types of care are considered at various stages of development. This primer will help you understand the developmental approach to supporting transgender youth.
While people generally think of medical and surgical aspects of gender-affirming care, other domains can be just as important. For example, a 2020 publication in The Lancet Public Health found that access to gender-congruent government identification documents was associated with lower odds of severe psychological distress and suicidality.1
Considerations for prepubertal children
The youngest developmental stage at which a young person may seek care regarding gender diversity is the prepubertal childhood stage. Guidelines set forth by The Endocrine Society and The World Professional Association for Transgender Health make it clear that no medical or surgical interventions are considered at this developmental stage.2,3 However, some young people may choose to pursue a “social transition.” Though this may sound like one thing, social transition can mean very different things for different people. It may include any combination of adopting a new name, pronouns, hairstyle, clothing, etc. Young people may also choose to pursue these various aspects of social transition in all settings, or sometimes only in some settings (for example, only at home if they don’t yet feel comfortable doing so at school). Research so far shows that prepubertal children who are allowed to socially transition have levels of anxiety and depression nearly indistinguishable from their cisgender peers.4 While some in the past have raised the question of whether a social transition increases a child’s degree of gender incongruence and thus their likelihood to “persist” in a transgender identity, research has suggested this is not the case, and that gender identity does not meaningfully differ before and after a social transition.5 It’s worth noting, that “desistance” of a young person’s transgender identity is generally not considered an ethical goal and that gender identity conversion efforts (that is, attempts to force transgender people to be cisgender) have been labeled unethical by the American Academy of Child & Adolescent Psychiatry.
Sadly, transgender children are victims of bullying at high rates in their schools and communities. Creating safe and affirming school and community environments can be some of the highest yield ways in which providers can support the mental health of gender-diverse youth at this stage. Gender Spectrum is an excellent nonprofit that provides resources to help families and communities with some of these nonmedical supports.
Early adolescence and pubertal suppression
The earliest gender-affirming medical intervention that may be considered is pubertal suppression. Pubertal suppression is achieved with gonadotropin-releasing hormone agonists. This class of medications is Food and Drug Administration approved in pediatrics for precocious puberty – a condition in which young people enter puberty much earlier than expected (sometimes as early as age 3). For that condition, the rationale is to delay puberty until the patient reaches a more developmentally normative age for puberty to begin. The rationale for pubertal suppression for adolescent gender dysphoria is somewhat similar – these medications allow for the temporary pausing of puberty, which can be particularly helpful for adolescents who are having severe negative psychological reactions to the ways in which their bodies are developing. The major advantage here is that pubertal suppression can be reversed (if the medication is stopped, endogenous puberty will proceed), whereas puberty itself cannot be easily reversed (resulting in adult transgender people needing surgery and other interventions later in life, if these changes can be fully undone at all). As with all medications, puberty blockers do carry known side effects, including falling behind on bone density (sex hormones are needed to mineralize bones). Because of this, it is generally recommended that adolescents have their bone density monitored during treatment, pursue avenues to improve bone health (for example, exercise), and either stop the puberty blocker to undergo endogenous puberty or start gender-affirming hormones (estrogen or testosterone) by around age 16.
It is also important to note that, under current guidelines, an adolescent must first undergo a comprehensive biopsychosocial mental health evaluation prior to starting pubertal suppression to ensure the clinical team has a comprehensive understanding of the adolescent’s mental health, that all potential gender supports that are needed are put into place, and that the adolescent and their guardians have a strong understanding of the medical intervention, its risks, side effects, and potential benefits. In addition, consent must be provided by parents or legal guardians, whereas adolescents themselves provide assent. Several studies have linked access to pubertal suppression, when indicated for gender dysphoria, to improved mental health outcomes (for example, van der Miesen and colleagues, Turban and colleagues, de Vries and colleagues, and Costa and colleagues).6-9
Later adolescence and gender-affirming hormones
Later in adolescence, transgender youth may be candidates for gender-affirming hormone treatment (for example, estrogen or testosterone) to induce pubertal changes that align with their gender identities. Once again, under current guidelines, a comprehensive mental health biopsychosocial evaluation must be conducted prior to initiation of these treatments. Part of this evaluation includes fertility counseling and consideration of fertility preservation (for example, oocyte or semen cryopreservation), given the potential for these medications to impact fertility. It also involves discussion of several of the physiologic changes from these medications that can be irreversible (for example, voice changes from testosterone are particularly difficult to reverse in the future). Tables of the physical changes from these medications, when they begin after starting, and when they generally reach their maximum are available in the Endocrine Society guidelines.2 The past endocrine society guidelines recommended not initiating gender-affirming hormones until age 16. The most recent guidelines note that there may be instances in which providers may consider starting them as early as age 13 (for example, to reduce risk of falling behind on bone density, or if a patient is having psychological distress related to their peers going through puberty while they are still in a prepubertal state). The latest World Professional Association for Transgender Health Standards of Care removed specific age cutoffs, highlighting the importance of a multidisciplinary team of mental health and hormone prescribing providers working together to understand the best course of action for a particular patient. As with pubertal suppression, several studies have linked access to gender-affirming hormones to improve mental health for adolescents with gender dysphoria (for example, Turban and colleagues, Chen and colleagues, de Vries and colleagues, Allen and colleagues, and Tordoff and colleagues).10-14
Gender-affirming surgeries
The vast majority of gender-affirming surgeries are not considered until adulthood. The most notable exception to this is masculinizing top surgery for trans masculine and nonbinary adolescents. As with all surgeries, this is a major decision, and requires agreement from a mental health provider, a medical provider, and the surgeon. Early research suggests such surgeries result in improved chest dysphoria and that regret rates appear to be low.15,16 While the latest World Professional Association for Transgender Health similarly removed strict age cutoffs for gender-affirming surgery, again noting the importance of individualized care, I suspect most will read this change in the context of the Endocrine Society guidelines and past WPATH guidelines that noted gender-affirming genital surgeries are not offered until adulthood (a rare exception perhaps being someone pursuing a gender-affirming vaginoplasty at say age 17 in the summer prior to college to avoid needing to take off from school for surgical recovery). Gender-affirming genital surgeries are generally much more involved surgeries with prolonged recovery times.
Given the substantial proportion of young people who openly identify as transgender,17 and the proliferation of misinformation, political rhetoric, and legislation that can impact gender-affirming care for adolescents with gender dysphoria,18 it is essential that providers have accurate, up-to-date information on what this care entails and how it is provided.
Dr. Turban is director of the gender psychiatry program at the University of California, San Francisco, where he is an assistant professor of child & adolescent psychiatry and affiliate faculty at the Philip R. Lee Institute for Health Policy Studies. He is on Twitter @jack_turban.
References
1. Malta M et al. Lancet Public Health. 2020 Apr;5(4):e178-9.
2. Hembree WC et al. J Clin Endocrinol Metab. 2017 Nov 1;102(11):3869-903.
3. Coleman E et al. Int J Transgend Health. 2022 Sep 6;23(Suppl 1):S1-259.
4. Durwood L et al. J Am Acad Child Adolesc Psychiatry. 2017 Feb;56(2):116-23.e2.
5. Rae JR et al. Psychol Sci. 2019 May;30(5):669-81.
6. van der Miesen AIR et al. J Adolesc Health. 2020 Jun;66(6):699-704.
7. Turban JL et al. Pediatrics. 2020 Feb;145(2):e20191725.
8. de Vries ALC et al. J Sex Med. 2011 Aug;8(8):2276-83.
9. Costa R et al. J Sex Med. 2015 Nov;12(11):2206-14.
10. Turban JL et al. PLoS One. 2022 Jan 12;17(1):e0261039.
11. Chen D et al. N Engl J Med. 2023;388:240-50.
12. de Vries ALC et al. Pediatrics. 2014 Oct;134(4):696-70.
13. Allen LR et al. Clin Pract Pediatr Psychol. 2019. doi: 10.1037/cpp0000288.
14. Tordoff DM et al. JAMA Netw Open. 2022 Feb 1;5(2):e220978.
15. Olson-Kennedy J et al. JAMA Pediatr. 2018;172(5):431-6.
16. Tang A et al. Ann Plast Surg. 2022 May;88(4 Suppl):S325-31
17. Johns MM et al. Morb Mortal Wkly Rep. 2019 Jan 25;68(3):67-71.
18. Turban JL et al. JAMA. 2021;325(22):2251-2.
FDA approves RSV monoclonal antibody for all infants
The monoclonal antibody Beyfortus (nirsevimab-alip), which already is approved for use in Europe and Canada, is indicated for newborns and infants born during or entering their first RSV season, and for children up to 24 months of age who are vulnerable to severe RSV through their second RSV season.
As many as 80,000 children under age 5 years are hospitalized with an RSV infection annually in the United States. Most cases are mild, but infants under 6 months, those born prematurely, and children with weakened immune systems or neuromuscular disorders are at an increased risk for severe illness, according to the Centers for Disease Control and Prevention.
The highly contagious virus is also a concern for immunocompromised adults and older people with underlying health conditions, who are at increased risk for severe disease.
Sanofi and AstraZeneca, which jointly developed the injectable agent, said in a press release that the companies plan to make it available by the fall of 2023. The long-acting antibody is given as a single intramuscular injection.
Beyfortus was approved in part based on data from the phase 3 MELODY trial, which found the shot reduced the incidence of medically attended lower respiratory tract infections associated with RSV by 74.9% versus placebo (95% confidence interval, 50.6-87.3; P < .001).
The phase 2/3 MEDLEY trial, conducted between July 2019 and May 2021, compared Beyfortus with palivizumab, another RSV antibody injection with more limited indications. The trial included more than 900 preterm infants less than 35 weeks’ gestational age and infants with congenital heart disease. Results were similar to the phase 3 MELODY trial, according to the manufacturers.
“Today’s approval marks an unprecedented moment for protecting infant health in the United States, following an RSV season that took a record toll on infants, their families, and the U.S. health care system,” said Thomas Triomphe, executive vice president for vaccines at Sanofi, in a press release about the FDA decision. “Beyfortus is the only monoclonal antibody approved for passive immunization to provide safe and effective protection for all infants during their first RSV season.”
A version of this article first appeared on Medscape.com.
The monoclonal antibody Beyfortus (nirsevimab-alip), which already is approved for use in Europe and Canada, is indicated for newborns and infants born during or entering their first RSV season, and for children up to 24 months of age who are vulnerable to severe RSV through their second RSV season.
As many as 80,000 children under age 5 years are hospitalized with an RSV infection annually in the United States. Most cases are mild, but infants under 6 months, those born prematurely, and children with weakened immune systems or neuromuscular disorders are at an increased risk for severe illness, according to the Centers for Disease Control and Prevention.
The highly contagious virus is also a concern for immunocompromised adults and older people with underlying health conditions, who are at increased risk for severe disease.
Sanofi and AstraZeneca, which jointly developed the injectable agent, said in a press release that the companies plan to make it available by the fall of 2023. The long-acting antibody is given as a single intramuscular injection.
Beyfortus was approved in part based on data from the phase 3 MELODY trial, which found the shot reduced the incidence of medically attended lower respiratory tract infections associated with RSV by 74.9% versus placebo (95% confidence interval, 50.6-87.3; P < .001).
The phase 2/3 MEDLEY trial, conducted between July 2019 and May 2021, compared Beyfortus with palivizumab, another RSV antibody injection with more limited indications. The trial included more than 900 preterm infants less than 35 weeks’ gestational age and infants with congenital heart disease. Results were similar to the phase 3 MELODY trial, according to the manufacturers.
“Today’s approval marks an unprecedented moment for protecting infant health in the United States, following an RSV season that took a record toll on infants, their families, and the U.S. health care system,” said Thomas Triomphe, executive vice president for vaccines at Sanofi, in a press release about the FDA decision. “Beyfortus is the only monoclonal antibody approved for passive immunization to provide safe and effective protection for all infants during their first RSV season.”
A version of this article first appeared on Medscape.com.
The monoclonal antibody Beyfortus (nirsevimab-alip), which already is approved for use in Europe and Canada, is indicated for newborns and infants born during or entering their first RSV season, and for children up to 24 months of age who are vulnerable to severe RSV through their second RSV season.
As many as 80,000 children under age 5 years are hospitalized with an RSV infection annually in the United States. Most cases are mild, but infants under 6 months, those born prematurely, and children with weakened immune systems or neuromuscular disorders are at an increased risk for severe illness, according to the Centers for Disease Control and Prevention.
The highly contagious virus is also a concern for immunocompromised adults and older people with underlying health conditions, who are at increased risk for severe disease.
Sanofi and AstraZeneca, which jointly developed the injectable agent, said in a press release that the companies plan to make it available by the fall of 2023. The long-acting antibody is given as a single intramuscular injection.
Beyfortus was approved in part based on data from the phase 3 MELODY trial, which found the shot reduced the incidence of medically attended lower respiratory tract infections associated with RSV by 74.9% versus placebo (95% confidence interval, 50.6-87.3; P < .001).
The phase 2/3 MEDLEY trial, conducted between July 2019 and May 2021, compared Beyfortus with palivizumab, another RSV antibody injection with more limited indications. The trial included more than 900 preterm infants less than 35 weeks’ gestational age and infants with congenital heart disease. Results were similar to the phase 3 MELODY trial, according to the manufacturers.
“Today’s approval marks an unprecedented moment for protecting infant health in the United States, following an RSV season that took a record toll on infants, their families, and the U.S. health care system,” said Thomas Triomphe, executive vice president for vaccines at Sanofi, in a press release about the FDA decision. “Beyfortus is the only monoclonal antibody approved for passive immunization to provide safe and effective protection for all infants during their first RSV season.”
A version of this article first appeared on Medscape.com.
For love or money: How do doctors choose their specialty?
Medical student loans top hundreds of thousands of dollars, so it’s understandable that physicians may want to select a specialty that pays well.
Moreover, most advised young doctors to follow their hearts rather than their wallets.
“There is no question that many young kids immediately think about money when deciding to pursue medicine, but the thought of a big paycheck will never sustain someone long enough to get them here,” says Sergio Alvarez, MD, a board-certified plastic surgeon based in Miami, Fla., and the CEO and medical director of Mia Aesthetics, which has several national locations.
“Getting into medicine is a long game, and there are many hurdles along the way that only the dedicated overcome,” says Dr. Alvarez.
Unfortunately, he says it may be late in that long game before some realize that the pay rate for certain specialties isn’t commensurate with the immense workload and responsibility they require.
“The short of it is that to become a happy doctor, medicine really needs to be a calling: a passion! There are far easier things to do to make money.”
Here is what physicians said about choosing between love or money.
The lowest-paying subspecialty in a low-paying specialty
Sophia Yen, MD, MPH, cofounder and CEO of Pandia Health, a women-founded, doctor-led birth control delivery service in Sunnyvale, Calif., and clinical associate professor at Stanford (Calif.) University, says you should pursue a specialty because you love the work.
“I chose the lowest-paying subspecialty (adolescent medicine) of a low-paying specialty (pediatrics), but I’d do it all again because I love the patient population – I love what I do.”
Dr. Yen says she chose adolescent medicine because she loves doing “outpatient gynecology” without going through the surgical training of a full ob.gyn. “I love the target population of young adults because you can talk to the patient versus in pediatrics, where you often talk to the parent. With young adults you can catch things – for example, teach a young person about consent, alcohol, marijuana’s effects on the growing brain, prevent unplanned pregnancies and sexually transmitted infections, instill healthy eating, and more.
“Do I wish that I got paid as much as a surgeon?” Dr. Yen says yes. “I hope that someday society will realize the time spent preventing future disease is worth it and pay us accordingly.”
Unfortunately, she says, since the health care system makes more money if you get pregnant, need a cardiac bypass, or need gastric surgery, those who deliver babies or do surgery get paid more than someone who prevents the need for those services.
Money doesn’t buy happiness
Stella Bard, MD, a rheumatologist in McKinney, Tex., says she eats, lives, and breathes rheumatology. “I never regret the decision of choosing this specialty for a single second,” says Dr. Bard. “I feel like it’s a rewarding experience with every single patient encounter.” Dr. Bard notes that money is no guarantee of happiness and that she feels blessed to wake up every morning doing what she loves.
Career or calling?
For Dr. Alvarez, inspiration came when watching his father help change people’s lives. “I saw how impactful a doctor is during a person’s most desperate moments, and that was enough to make medicine my life’s passion at the age of 10.”
He says once you’re in medical school, choosing a specialty is far easier than you think. “Each specialty requires a certain personality or specific characteristics, and some will call to you while others simply won’t.”
“For me, plastics was about finesse, art, and life-changing surgeries that affected people from kids to adults and involved every aspect of the human body. Changing someone’s outward appearance has a profoundly positive impact on their confidence and self-esteem, making plastic surgery a genuinely transformative experience.”
Patricia Celan, MD, a postgraduate psychiatry resident in Canada, also chose psychiatry for the love of the field. “I enjoy helping vulnerable people and exploring what makes a person tick, the source of their difficulties, and how to help people counteract and overcome the difficult cards they’ve been dealt in life.”
She says it’s incredibly rewarding to watch someone turn their life around from severe mental illness, especially those who have been victimized and traumatized, and learn to trust people again.
“I could have made more money in a higher-paying specialty, yes, but I’m not sure I would have felt as fulfilled as psychiatry can make me feel.”
Dr. Celan says everyone has their calling, and some lucky people find their deepest passion in higher-paying specialties. “My calling is psychiatry, and I am at peace with this no matter the money.”
For the love of surgery
“In my experience, most people don’t choose their specialty based on money,” says Nicole Aaronson, MD, MBA, an otolaryngologist and board-certified in the subspecialty of pediatric otolaryngology, an attending surgeon at Nemours Children’s Health of Delaware and clinical associate professor of otolaryngology and pediatrics at Sidney Kimmel Medical College, Philadelphia.
“The first decision point in medical school is usually figuring out if you are a surgery person or a medicine person. I knew very early that I wanted to be a surgeon and wanted to spend time in the OR fixing problems with my hands.”
Part of what attracted Dr. Aaronson to otolaryngology was the variety of conditions managed within the specialty, from head and neck cancer to voice problems to sleep disorders to sinus disease. “I chose my subspecialty because I enjoy working with children and making an impact that will help them live their best possible lives.”
She says a relatively simple surgery like placing ear tubes may help a child’s hearing and allow them to be more successful in school, opening up a new world of opportunities for the child’s future.
“While I don’t think most people choose their specialty based on prospective compensation, I do think all physicians want to be compensated fairly for their time, effort, and level of training,” says Dr. Aaronson.
Choosing a specialty for the money can lead to burnout and dissatisfaction
“For me, the decision to pursue gastroenterology went beyond financial considerations,” says Saurabh Sethi, MD, MPH, a gastroenterologist specializing in hepatology and interventional endoscopy. “While financial stability is undoubtedly important, no doctor enters this field solely for the love of money. The primary driving force for most medical professionals, myself included, is the passion to help people and make a positive difference in their lives.”
Dr. Sethi says the gratification that comes from providing quality care and witnessing patients’ improved well-being is priceless. Moreover, he believes that selecting a specialty based solely on financial gain is likely to lead to burnout and greater dissatisfaction over time.
“By following my love for gut health and prioritizing patient care, I have found a sense of fulfillment and purpose in my career. It has been a rewarding journey, and I’m grateful for the opportunity to contribute to the well-being of my patients through my expertise in gastroenterology.”
Key takeaways: Love or money?
Multiple factors influence doctors’ specialty choices, including genuine love for the work and the future of the specialty. Others include job prospects, hands-on experience they receive, mentors, childhood dreams, parental expectations, complexity of cases, the lifestyle of each specialty, including office hours worked, on-call requirements, and autonomy.
Physicians also mentioned other factors they considered when choosing their specialty:
- Personal interest.
- Intellectual stimulation.
- Work-life balance.
- Patient populations.
- Future opportunities.
- Desire to make a difference.
- Passion.
- Financial stability.
- Being personally fulfilled.
Overwhelmingly, doctors say to pick a specialty you can envision yourself loving 40 years from now and you won’t go wrong.
A version of this article first appeared on Medscape.com.
Medical student loans top hundreds of thousands of dollars, so it’s understandable that physicians may want to select a specialty that pays well.
Moreover, most advised young doctors to follow their hearts rather than their wallets.
“There is no question that many young kids immediately think about money when deciding to pursue medicine, but the thought of a big paycheck will never sustain someone long enough to get them here,” says Sergio Alvarez, MD, a board-certified plastic surgeon based in Miami, Fla., and the CEO and medical director of Mia Aesthetics, which has several national locations.
“Getting into medicine is a long game, and there are many hurdles along the way that only the dedicated overcome,” says Dr. Alvarez.
Unfortunately, he says it may be late in that long game before some realize that the pay rate for certain specialties isn’t commensurate with the immense workload and responsibility they require.
“The short of it is that to become a happy doctor, medicine really needs to be a calling: a passion! There are far easier things to do to make money.”
Here is what physicians said about choosing between love or money.
The lowest-paying subspecialty in a low-paying specialty
Sophia Yen, MD, MPH, cofounder and CEO of Pandia Health, a women-founded, doctor-led birth control delivery service in Sunnyvale, Calif., and clinical associate professor at Stanford (Calif.) University, says you should pursue a specialty because you love the work.
“I chose the lowest-paying subspecialty (adolescent medicine) of a low-paying specialty (pediatrics), but I’d do it all again because I love the patient population – I love what I do.”
Dr. Yen says she chose adolescent medicine because she loves doing “outpatient gynecology” without going through the surgical training of a full ob.gyn. “I love the target population of young adults because you can talk to the patient versus in pediatrics, where you often talk to the parent. With young adults you can catch things – for example, teach a young person about consent, alcohol, marijuana’s effects on the growing brain, prevent unplanned pregnancies and sexually transmitted infections, instill healthy eating, and more.
“Do I wish that I got paid as much as a surgeon?” Dr. Yen says yes. “I hope that someday society will realize the time spent preventing future disease is worth it and pay us accordingly.”
Unfortunately, she says, since the health care system makes more money if you get pregnant, need a cardiac bypass, or need gastric surgery, those who deliver babies or do surgery get paid more than someone who prevents the need for those services.
Money doesn’t buy happiness
Stella Bard, MD, a rheumatologist in McKinney, Tex., says she eats, lives, and breathes rheumatology. “I never regret the decision of choosing this specialty for a single second,” says Dr. Bard. “I feel like it’s a rewarding experience with every single patient encounter.” Dr. Bard notes that money is no guarantee of happiness and that she feels blessed to wake up every morning doing what she loves.
Career or calling?
For Dr. Alvarez, inspiration came when watching his father help change people’s lives. “I saw how impactful a doctor is during a person’s most desperate moments, and that was enough to make medicine my life’s passion at the age of 10.”
He says once you’re in medical school, choosing a specialty is far easier than you think. “Each specialty requires a certain personality or specific characteristics, and some will call to you while others simply won’t.”
“For me, plastics was about finesse, art, and life-changing surgeries that affected people from kids to adults and involved every aspect of the human body. Changing someone’s outward appearance has a profoundly positive impact on their confidence and self-esteem, making plastic surgery a genuinely transformative experience.”
Patricia Celan, MD, a postgraduate psychiatry resident in Canada, also chose psychiatry for the love of the field. “I enjoy helping vulnerable people and exploring what makes a person tick, the source of their difficulties, and how to help people counteract and overcome the difficult cards they’ve been dealt in life.”
She says it’s incredibly rewarding to watch someone turn their life around from severe mental illness, especially those who have been victimized and traumatized, and learn to trust people again.
“I could have made more money in a higher-paying specialty, yes, but I’m not sure I would have felt as fulfilled as psychiatry can make me feel.”
Dr. Celan says everyone has their calling, and some lucky people find their deepest passion in higher-paying specialties. “My calling is psychiatry, and I am at peace with this no matter the money.”
For the love of surgery
“In my experience, most people don’t choose their specialty based on money,” says Nicole Aaronson, MD, MBA, an otolaryngologist and board-certified in the subspecialty of pediatric otolaryngology, an attending surgeon at Nemours Children’s Health of Delaware and clinical associate professor of otolaryngology and pediatrics at Sidney Kimmel Medical College, Philadelphia.
“The first decision point in medical school is usually figuring out if you are a surgery person or a medicine person. I knew very early that I wanted to be a surgeon and wanted to spend time in the OR fixing problems with my hands.”
Part of what attracted Dr. Aaronson to otolaryngology was the variety of conditions managed within the specialty, from head and neck cancer to voice problems to sleep disorders to sinus disease. “I chose my subspecialty because I enjoy working with children and making an impact that will help them live their best possible lives.”
She says a relatively simple surgery like placing ear tubes may help a child’s hearing and allow them to be more successful in school, opening up a new world of opportunities for the child’s future.
“While I don’t think most people choose their specialty based on prospective compensation, I do think all physicians want to be compensated fairly for their time, effort, and level of training,” says Dr. Aaronson.
Choosing a specialty for the money can lead to burnout and dissatisfaction
“For me, the decision to pursue gastroenterology went beyond financial considerations,” says Saurabh Sethi, MD, MPH, a gastroenterologist specializing in hepatology and interventional endoscopy. “While financial stability is undoubtedly important, no doctor enters this field solely for the love of money. The primary driving force for most medical professionals, myself included, is the passion to help people and make a positive difference in their lives.”
Dr. Sethi says the gratification that comes from providing quality care and witnessing patients’ improved well-being is priceless. Moreover, he believes that selecting a specialty based solely on financial gain is likely to lead to burnout and greater dissatisfaction over time.
“By following my love for gut health and prioritizing patient care, I have found a sense of fulfillment and purpose in my career. It has been a rewarding journey, and I’m grateful for the opportunity to contribute to the well-being of my patients through my expertise in gastroenterology.”
Key takeaways: Love or money?
Multiple factors influence doctors’ specialty choices, including genuine love for the work and the future of the specialty. Others include job prospects, hands-on experience they receive, mentors, childhood dreams, parental expectations, complexity of cases, the lifestyle of each specialty, including office hours worked, on-call requirements, and autonomy.
Physicians also mentioned other factors they considered when choosing their specialty:
- Personal interest.
- Intellectual stimulation.
- Work-life balance.
- Patient populations.
- Future opportunities.
- Desire to make a difference.
- Passion.
- Financial stability.
- Being personally fulfilled.
Overwhelmingly, doctors say to pick a specialty you can envision yourself loving 40 years from now and you won’t go wrong.
A version of this article first appeared on Medscape.com.
Medical student loans top hundreds of thousands of dollars, so it’s understandable that physicians may want to select a specialty that pays well.
Moreover, most advised young doctors to follow their hearts rather than their wallets.
“There is no question that many young kids immediately think about money when deciding to pursue medicine, but the thought of a big paycheck will never sustain someone long enough to get them here,” says Sergio Alvarez, MD, a board-certified plastic surgeon based in Miami, Fla., and the CEO and medical director of Mia Aesthetics, which has several national locations.
“Getting into medicine is a long game, and there are many hurdles along the way that only the dedicated overcome,” says Dr. Alvarez.
Unfortunately, he says it may be late in that long game before some realize that the pay rate for certain specialties isn’t commensurate with the immense workload and responsibility they require.
“The short of it is that to become a happy doctor, medicine really needs to be a calling: a passion! There are far easier things to do to make money.”
Here is what physicians said about choosing between love or money.
The lowest-paying subspecialty in a low-paying specialty
Sophia Yen, MD, MPH, cofounder and CEO of Pandia Health, a women-founded, doctor-led birth control delivery service in Sunnyvale, Calif., and clinical associate professor at Stanford (Calif.) University, says you should pursue a specialty because you love the work.
“I chose the lowest-paying subspecialty (adolescent medicine) of a low-paying specialty (pediatrics), but I’d do it all again because I love the patient population – I love what I do.”
Dr. Yen says she chose adolescent medicine because she loves doing “outpatient gynecology” without going through the surgical training of a full ob.gyn. “I love the target population of young adults because you can talk to the patient versus in pediatrics, where you often talk to the parent. With young adults you can catch things – for example, teach a young person about consent, alcohol, marijuana’s effects on the growing brain, prevent unplanned pregnancies and sexually transmitted infections, instill healthy eating, and more.
“Do I wish that I got paid as much as a surgeon?” Dr. Yen says yes. “I hope that someday society will realize the time spent preventing future disease is worth it and pay us accordingly.”
Unfortunately, she says, since the health care system makes more money if you get pregnant, need a cardiac bypass, or need gastric surgery, those who deliver babies or do surgery get paid more than someone who prevents the need for those services.
Money doesn’t buy happiness
Stella Bard, MD, a rheumatologist in McKinney, Tex., says she eats, lives, and breathes rheumatology. “I never regret the decision of choosing this specialty for a single second,” says Dr. Bard. “I feel like it’s a rewarding experience with every single patient encounter.” Dr. Bard notes that money is no guarantee of happiness and that she feels blessed to wake up every morning doing what she loves.
Career or calling?
For Dr. Alvarez, inspiration came when watching his father help change people’s lives. “I saw how impactful a doctor is during a person’s most desperate moments, and that was enough to make medicine my life’s passion at the age of 10.”
He says once you’re in medical school, choosing a specialty is far easier than you think. “Each specialty requires a certain personality or specific characteristics, and some will call to you while others simply won’t.”
“For me, plastics was about finesse, art, and life-changing surgeries that affected people from kids to adults and involved every aspect of the human body. Changing someone’s outward appearance has a profoundly positive impact on their confidence and self-esteem, making plastic surgery a genuinely transformative experience.”
Patricia Celan, MD, a postgraduate psychiatry resident in Canada, also chose psychiatry for the love of the field. “I enjoy helping vulnerable people and exploring what makes a person tick, the source of their difficulties, and how to help people counteract and overcome the difficult cards they’ve been dealt in life.”
She says it’s incredibly rewarding to watch someone turn their life around from severe mental illness, especially those who have been victimized and traumatized, and learn to trust people again.
“I could have made more money in a higher-paying specialty, yes, but I’m not sure I would have felt as fulfilled as psychiatry can make me feel.”
Dr. Celan says everyone has their calling, and some lucky people find their deepest passion in higher-paying specialties. “My calling is psychiatry, and I am at peace with this no matter the money.”
For the love of surgery
“In my experience, most people don’t choose their specialty based on money,” says Nicole Aaronson, MD, MBA, an otolaryngologist and board-certified in the subspecialty of pediatric otolaryngology, an attending surgeon at Nemours Children’s Health of Delaware and clinical associate professor of otolaryngology and pediatrics at Sidney Kimmel Medical College, Philadelphia.
“The first decision point in medical school is usually figuring out if you are a surgery person or a medicine person. I knew very early that I wanted to be a surgeon and wanted to spend time in the OR fixing problems with my hands.”
Part of what attracted Dr. Aaronson to otolaryngology was the variety of conditions managed within the specialty, from head and neck cancer to voice problems to sleep disorders to sinus disease. “I chose my subspecialty because I enjoy working with children and making an impact that will help them live their best possible lives.”
She says a relatively simple surgery like placing ear tubes may help a child’s hearing and allow them to be more successful in school, opening up a new world of opportunities for the child’s future.
“While I don’t think most people choose their specialty based on prospective compensation, I do think all physicians want to be compensated fairly for their time, effort, and level of training,” says Dr. Aaronson.
Choosing a specialty for the money can lead to burnout and dissatisfaction
“For me, the decision to pursue gastroenterology went beyond financial considerations,” says Saurabh Sethi, MD, MPH, a gastroenterologist specializing in hepatology and interventional endoscopy. “While financial stability is undoubtedly important, no doctor enters this field solely for the love of money. The primary driving force for most medical professionals, myself included, is the passion to help people and make a positive difference in their lives.”
Dr. Sethi says the gratification that comes from providing quality care and witnessing patients’ improved well-being is priceless. Moreover, he believes that selecting a specialty based solely on financial gain is likely to lead to burnout and greater dissatisfaction over time.
“By following my love for gut health and prioritizing patient care, I have found a sense of fulfillment and purpose in my career. It has been a rewarding journey, and I’m grateful for the opportunity to contribute to the well-being of my patients through my expertise in gastroenterology.”
Key takeaways: Love or money?
Multiple factors influence doctors’ specialty choices, including genuine love for the work and the future of the specialty. Others include job prospects, hands-on experience they receive, mentors, childhood dreams, parental expectations, complexity of cases, the lifestyle of each specialty, including office hours worked, on-call requirements, and autonomy.
Physicians also mentioned other factors they considered when choosing their specialty:
- Personal interest.
- Intellectual stimulation.
- Work-life balance.
- Patient populations.
- Future opportunities.
- Desire to make a difference.
- Passion.
- Financial stability.
- Being personally fulfilled.
Overwhelmingly, doctors say to pick a specialty you can envision yourself loving 40 years from now and you won’t go wrong.
A version of this article first appeared on Medscape.com.
Anxiety screening
Anxiety symptoms in children are common, ranging from a toddler’s fear of the dark to an adolescent worrying about a major exam. The good news is that, if they are detected early and treated appropriately, they are curable. Unfortunately, they are often silent, or present with misleading symptoms. Screening for anxiety disorders, especially in the presence of the most common presenting concerns, can illuminate the true nature of a child’s challenge and point the way forward. In this month’s article, we will provide details on the prevalence of anxiety disorders in children, how they typically present, and how best to screen for them. We will offer some strategies for speaking about them with your patients and their parents, as well as introduce some of the strategies that can improve mild to moderate anxiety disorders. We will follow up with another piece on the evidence-based treatments for these common disorders, how to find appropriate referrals, and what you can do in your office to get treatment started.
Anxiety disorders: Common and treatable
Anxiety disorders – including separation anxiety disorder, social phobia, simple phobias, generalized anxiety disorder, panic disorder, and PTSD – affect between 15% and 20% of children before the age of 18, with some recent estimates as high as 31.9% of youth being affected. Indeed, the mean age of onset for most anxiety disorders (excluding panic disorder and PTSD) is between 5 and 9 years of age. Despite being so common, many anxiety disorders in childhood are never properly diagnosed, and most (as many as 80%) do not receive treatment from a mental health professional. With early diagnosis and evidence-based treatment, most anxiety disorders can be “cured” and no longer impair functioning. Untreated, anxiety disorders usually have a chronic course, causing significant behavioral problems and disruption of a child’s critical social, emotional, and identity development and their academic function. Untreated, they are frequently complicated in adolescence by mood, substance use, and eating disorders. With the passage of time, developmental consequences and comorbid illnesses, a curable childhood anxiety disorder can become a complex and entrenched psychiatric syndrome in young adulthood.

One of the reasons these illnesses frequently go unrecognized is that states of fearful distress, such as separation anxiety or social anxiety, are developmentally normal at different stages of childhood, and it can be difficult to discriminate between normal and pathological anxiety. Anxiety itself is an “internalizing” symptom, and is invisible except for the behaviors that can accompany it. Some behaviors suggest anxiety, such as fearful expressions, clinginess, excessive need for reassurance, or avoidance. But anxiety can also lead to obstinate refusal to do certain things. It might lead to explosive tantrums when a child is pushed to do something that makes them intensely anxious. It can lead to irritability and moody tantrums for a child exhausted after a long school day spent managing high levels of anxiety by themselves. Anxious children often appear inattentive in school. Anxiety disorders frequently disrupt restful sleep, leading to children who are irritable and moody as well as inattentive. These children may present to the pediatrician with frustrated parents concerned that they are oppositional or explosive, or because their teachers are concerned about ADHD, when the culprit is actually anxiety.
While anxiety is uncomfortable, these children are unlikely to experience their anxiety as unusual and foreign, like a sudden toothache. Instead, it feels to them like they are fearful for good reason, responding appropriately to something real. These children are more likely to respond to a novel or uncertain situation with worry rather than curiosity, and to a new challenge as a threat. For children who are managing their anxiety more internally, their parents are often unaware of their degree of distress. Indeed, these children are often careful, thoughtful, and attentive to detail. Parents and teachers may think they are doing wonderfully. They are typically very sensitive to physical discomforts, which are heightened by an anxious state. These are likely to present to the pediatrician’s office with parents very worried about a cluster of vague physical complaints (stomach ache, headache, “just not feeling good”), which coincides with a change, challenge, or anxious stimulus. In this situation, the parents may dismiss the possibility of anxiety, and the child may not even be aware of it. But it will get worse if they are pushed to bear the source of anxiety (going to school, sports practice, etc.).
Anxiety screening and treatment
When a child presents for a sick visit with vague symptoms, or a negative workup for specific ones, you should screen them for an anxiety disorder. When they present with concerns about inattention, insomnia, moodiness, obstinacy, and even explosive behaviors, you should screen them for an anxiety disorder. This is especially true if they are prepubertal, when anxiety disorders are far more common than mood disorders. But you should consider anxiety disorders alongside mood disorders in adolescents presenting with these complaints. While parents may be unaware of the presence of anxiety in their child, explain to them that anxiety disorders are very common and treatable in childhood to help them understand the value of screening. Asking children directly about their internal experience can also be helpful. Avoid asking about “anxiety,” instead asking if they ever worry about specific things, such as “talking to kids you don’t know at recess,” “being alone at home,” “getting robbed or kidnapped,” or “something bad happening to your parents.” Just asking helps children pay attention to their thoughts and feelings, and is a powerful screening instrument.

There are also real screening instruments that you might use routinely for sick visits in prepubertal children or when anxiety should be in the differential. These instruments can be prone to recall bias, but generally make it easier for (anxious) children to accurately describe their internal experience. An instrument like the GAD7 is brief, free, and sensitive, but not very specific. If it is positive, you can then offer a longer screen such as the SCARED, also free, which indicates likely diagnoses such as generalized anxiety disorder, separation anxiety disorder, panic disorder, and social phobia. There is a parent version and a self-report, and it is validated for youths 8-18 years old and takes approximately 20 minutes to complete and score.
A positive screen should lead to a more nuanced conversation with your patient and their parents about their anxiety symptoms. You may feel comfortable doing a more extensive interview to make the likely diagnosis or may prefer to refer to a psychiatrist or psychologist to assist with diagnosis and treatment recommendations. In either case, you can offer your patient and their parents meaningful reassurance that the intense discomfort of their anxiety will get better with effective treatment. In this visit, you can get treatment started by identifying what parents and their children can do right away to begin addressing anxiety symptoms. Offer strategies to protect and promote restful sleep and daily vigorous exercise, both of which can directly improve mild to moderate anxiety symptoms. Suggest to parents that they should help their children to notice what they are feeling, rather than rushing in to remove a source of anxiety. These measures can help their child to identify what is a thought, a feeling, a physical sensation, or a fact. They can offer support and validation around how uncomfortable these feelings are, but just being curious will reassure their child that they will be able to manage and master this feeling. This “practice” is akin to what their child will do in most effective treatments, and will have the added benefit of helping them to build skills that all children need to manage the challenges and worries that are a normal, but difficult part of growing up and of adult life. Finally, you can tell them that anxious temperaments come with advantages also, such as great powers of observation, attention to detail, and thoroughness, high levels of empathy, drive, and tenacity. By learning to manage anxiety early, these children can grow up to be engaged, resilient, successful, and satisfied adults.
Once identified, the range of effective treatments available include cognitive-behavioral therapy, graduated exposure, mindfulness/relaxation techniques, and medication, and we will discuss these in our next article.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Beesdo K et al. Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr Clin North Am. 2009 Sep. doi: 10.1016/j.psc.2009.06.002.
Anxiety symptoms in children are common, ranging from a toddler’s fear of the dark to an adolescent worrying about a major exam. The good news is that, if they are detected early and treated appropriately, they are curable. Unfortunately, they are often silent, or present with misleading symptoms. Screening for anxiety disorders, especially in the presence of the most common presenting concerns, can illuminate the true nature of a child’s challenge and point the way forward. In this month’s article, we will provide details on the prevalence of anxiety disorders in children, how they typically present, and how best to screen for them. We will offer some strategies for speaking about them with your patients and their parents, as well as introduce some of the strategies that can improve mild to moderate anxiety disorders. We will follow up with another piece on the evidence-based treatments for these common disorders, how to find appropriate referrals, and what you can do in your office to get treatment started.
Anxiety disorders: Common and treatable
Anxiety disorders – including separation anxiety disorder, social phobia, simple phobias, generalized anxiety disorder, panic disorder, and PTSD – affect between 15% and 20% of children before the age of 18, with some recent estimates as high as 31.9% of youth being affected. Indeed, the mean age of onset for most anxiety disorders (excluding panic disorder and PTSD) is between 5 and 9 years of age. Despite being so common, many anxiety disorders in childhood are never properly diagnosed, and most (as many as 80%) do not receive treatment from a mental health professional. With early diagnosis and evidence-based treatment, most anxiety disorders can be “cured” and no longer impair functioning. Untreated, anxiety disorders usually have a chronic course, causing significant behavioral problems and disruption of a child’s critical social, emotional, and identity development and their academic function. Untreated, they are frequently complicated in adolescence by mood, substance use, and eating disorders. With the passage of time, developmental consequences and comorbid illnesses, a curable childhood anxiety disorder can become a complex and entrenched psychiatric syndrome in young adulthood.
One of the reasons these illnesses frequently go unrecognized is that states of fearful distress, such as separation anxiety or social anxiety, are developmentally normal at different stages of childhood, and it can be difficult to discriminate between normal and pathological anxiety. Anxiety itself is an “internalizing” symptom, and is invisible except for the behaviors that can accompany it. Some behaviors suggest anxiety, such as fearful expressions, clinginess, excessive need for reassurance, or avoidance. But anxiety can also lead to obstinate refusal to do certain things. It might lead to explosive tantrums when a child is pushed to do something that makes them intensely anxious. It can lead to irritability and moody tantrums for a child exhausted after a long school day spent managing high levels of anxiety by themselves. Anxious children often appear inattentive in school. Anxiety disorders frequently disrupt restful sleep, leading to children who are irritable and moody as well as inattentive. These children may present to the pediatrician with frustrated parents concerned that they are oppositional or explosive, or because their teachers are concerned about ADHD, when the culprit is actually anxiety.
While anxiety is uncomfortable, these children are unlikely to experience their anxiety as unusual and foreign, like a sudden toothache. Instead, it feels to them like they are fearful for good reason, responding appropriately to something real. These children are more likely to respond to a novel or uncertain situation with worry rather than curiosity, and to a new challenge as a threat. For children who are managing their anxiety more internally, their parents are often unaware of their degree of distress. Indeed, these children are often careful, thoughtful, and attentive to detail. Parents and teachers may think they are doing wonderfully. They are typically very sensitive to physical discomforts, which are heightened by an anxious state. These are likely to present to the pediatrician’s office with parents very worried about a cluster of vague physical complaints (stomach ache, headache, “just not feeling good”), which coincides with a change, challenge, or anxious stimulus. In this situation, the parents may dismiss the possibility of anxiety, and the child may not even be aware of it. But it will get worse if they are pushed to bear the source of anxiety (going to school, sports practice, etc.).
Anxiety screening and treatment
When a child presents for a sick visit with vague symptoms, or a negative workup for specific ones, you should screen them for an anxiety disorder. When they present with concerns about inattention, insomnia, moodiness, obstinacy, and even explosive behaviors, you should screen them for an anxiety disorder. This is especially true if they are prepubertal, when anxiety disorders are far more common than mood disorders. But you should consider anxiety disorders alongside mood disorders in adolescents presenting with these complaints. While parents may be unaware of the presence of anxiety in their child, explain to them that anxiety disorders are very common and treatable in childhood to help them understand the value of screening. Asking children directly about their internal experience can also be helpful. Avoid asking about “anxiety,” instead asking if they ever worry about specific things, such as “talking to kids you don’t know at recess,” “being alone at home,” “getting robbed or kidnapped,” or “something bad happening to your parents.” Just asking helps children pay attention to their thoughts and feelings, and is a powerful screening instrument.
There are also real screening instruments that you might use routinely for sick visits in prepubertal children or when anxiety should be in the differential. These instruments can be prone to recall bias, but generally make it easier for (anxious) children to accurately describe their internal experience. An instrument like the GAD7 is brief, free, and sensitive, but not very specific. If it is positive, you can then offer a longer screen such as the SCARED, also free, which indicates likely diagnoses such as generalized anxiety disorder, separation anxiety disorder, panic disorder, and social phobia. There is a parent version and a self-report, and it is validated for youths 8-18 years old and takes approximately 20 minutes to complete and score.
A positive screen should lead to a more nuanced conversation with your patient and their parents about their anxiety symptoms. You may feel comfortable doing a more extensive interview to make the likely diagnosis or may prefer to refer to a psychiatrist or psychologist to assist with diagnosis and treatment recommendations. In either case, you can offer your patient and their parents meaningful reassurance that the intense discomfort of their anxiety will get better with effective treatment. In this visit, you can get treatment started by identifying what parents and their children can do right away to begin addressing anxiety symptoms. Offer strategies to protect and promote restful sleep and daily vigorous exercise, both of which can directly improve mild to moderate anxiety symptoms. Suggest to parents that they should help their children to notice what they are feeling, rather than rushing in to remove a source of anxiety. These measures can help their child to identify what is a thought, a feeling, a physical sensation, or a fact. They can offer support and validation around how uncomfortable these feelings are, but just being curious will reassure their child that they will be able to manage and master this feeling. This “practice” is akin to what their child will do in most effective treatments, and will have the added benefit of helping them to build skills that all children need to manage the challenges and worries that are a normal, but difficult part of growing up and of adult life. Finally, you can tell them that anxious temperaments come with advantages also, such as great powers of observation, attention to detail, and thoroughness, high levels of empathy, drive, and tenacity. By learning to manage anxiety early, these children can grow up to be engaged, resilient, successful, and satisfied adults.
Once identified, the range of effective treatments available include cognitive-behavioral therapy, graduated exposure, mindfulness/relaxation techniques, and medication, and we will discuss these in our next article.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Beesdo K et al. Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr Clin North Am. 2009 Sep. doi: 10.1016/j.psc.2009.06.002.
Anxiety symptoms in children are common, ranging from a toddler’s fear of the dark to an adolescent worrying about a major exam. The good news is that, if they are detected early and treated appropriately, they are curable. Unfortunately, they are often silent, or present with misleading symptoms. Screening for anxiety disorders, especially in the presence of the most common presenting concerns, can illuminate the true nature of a child’s challenge and point the way forward. In this month’s article, we will provide details on the prevalence of anxiety disorders in children, how they typically present, and how best to screen for them. We will offer some strategies for speaking about them with your patients and their parents, as well as introduce some of the strategies that can improve mild to moderate anxiety disorders. We will follow up with another piece on the evidence-based treatments for these common disorders, how to find appropriate referrals, and what you can do in your office to get treatment started.
Anxiety disorders: Common and treatable
Anxiety disorders – including separation anxiety disorder, social phobia, simple phobias, generalized anxiety disorder, panic disorder, and PTSD – affect between 15% and 20% of children before the age of 18, with some recent estimates as high as 31.9% of youth being affected. Indeed, the mean age of onset for most anxiety disorders (excluding panic disorder and PTSD) is between 5 and 9 years of age. Despite being so common, many anxiety disorders in childhood are never properly diagnosed, and most (as many as 80%) do not receive treatment from a mental health professional. With early diagnosis and evidence-based treatment, most anxiety disorders can be “cured” and no longer impair functioning. Untreated, anxiety disorders usually have a chronic course, causing significant behavioral problems and disruption of a child’s critical social, emotional, and identity development and their academic function. Untreated, they are frequently complicated in adolescence by mood, substance use, and eating disorders. With the passage of time, developmental consequences and comorbid illnesses, a curable childhood anxiety disorder can become a complex and entrenched psychiatric syndrome in young adulthood.
One of the reasons these illnesses frequently go unrecognized is that states of fearful distress, such as separation anxiety or social anxiety, are developmentally normal at different stages of childhood, and it can be difficult to discriminate between normal and pathological anxiety. Anxiety itself is an “internalizing” symptom, and is invisible except for the behaviors that can accompany it. Some behaviors suggest anxiety, such as fearful expressions, clinginess, excessive need for reassurance, or avoidance. But anxiety can also lead to obstinate refusal to do certain things. It might lead to explosive tantrums when a child is pushed to do something that makes them intensely anxious. It can lead to irritability and moody tantrums for a child exhausted after a long school day spent managing high levels of anxiety by themselves. Anxious children often appear inattentive in school. Anxiety disorders frequently disrupt restful sleep, leading to children who are irritable and moody as well as inattentive. These children may present to the pediatrician with frustrated parents concerned that they are oppositional or explosive, or because their teachers are concerned about ADHD, when the culprit is actually anxiety.
While anxiety is uncomfortable, these children are unlikely to experience their anxiety as unusual and foreign, like a sudden toothache. Instead, it feels to them like they are fearful for good reason, responding appropriately to something real. These children are more likely to respond to a novel or uncertain situation with worry rather than curiosity, and to a new challenge as a threat. For children who are managing their anxiety more internally, their parents are often unaware of their degree of distress. Indeed, these children are often careful, thoughtful, and attentive to detail. Parents and teachers may think they are doing wonderfully. They are typically very sensitive to physical discomforts, which are heightened by an anxious state. These are likely to present to the pediatrician’s office with parents very worried about a cluster of vague physical complaints (stomach ache, headache, “just not feeling good”), which coincides with a change, challenge, or anxious stimulus. In this situation, the parents may dismiss the possibility of anxiety, and the child may not even be aware of it. But it will get worse if they are pushed to bear the source of anxiety (going to school, sports practice, etc.).
Anxiety screening and treatment
When a child presents for a sick visit with vague symptoms, or a negative workup for specific ones, you should screen them for an anxiety disorder. When they present with concerns about inattention, insomnia, moodiness, obstinacy, and even explosive behaviors, you should screen them for an anxiety disorder. This is especially true if they are prepubertal, when anxiety disorders are far more common than mood disorders. But you should consider anxiety disorders alongside mood disorders in adolescents presenting with these complaints. While parents may be unaware of the presence of anxiety in their child, explain to them that anxiety disorders are very common and treatable in childhood to help them understand the value of screening. Asking children directly about their internal experience can also be helpful. Avoid asking about “anxiety,” instead asking if they ever worry about specific things, such as “talking to kids you don’t know at recess,” “being alone at home,” “getting robbed or kidnapped,” or “something bad happening to your parents.” Just asking helps children pay attention to their thoughts and feelings, and is a powerful screening instrument.
There are also real screening instruments that you might use routinely for sick visits in prepubertal children or when anxiety should be in the differential. These instruments can be prone to recall bias, but generally make it easier for (anxious) children to accurately describe their internal experience. An instrument like the GAD7 is brief, free, and sensitive, but not very specific. If it is positive, you can then offer a longer screen such as the SCARED, also free, which indicates likely diagnoses such as generalized anxiety disorder, separation anxiety disorder, panic disorder, and social phobia. There is a parent version and a self-report, and it is validated for youths 8-18 years old and takes approximately 20 minutes to complete and score.
A positive screen should lead to a more nuanced conversation with your patient and their parents about their anxiety symptoms. You may feel comfortable doing a more extensive interview to make the likely diagnosis or may prefer to refer to a psychiatrist or psychologist to assist with diagnosis and treatment recommendations. In either case, you can offer your patient and their parents meaningful reassurance that the intense discomfort of their anxiety will get better with effective treatment. In this visit, you can get treatment started by identifying what parents and their children can do right away to begin addressing anxiety symptoms. Offer strategies to protect and promote restful sleep and daily vigorous exercise, both of which can directly improve mild to moderate anxiety symptoms. Suggest to parents that they should help their children to notice what they are feeling, rather than rushing in to remove a source of anxiety. These measures can help their child to identify what is a thought, a feeling, a physical sensation, or a fact. They can offer support and validation around how uncomfortable these feelings are, but just being curious will reassure their child that they will be able to manage and master this feeling. This “practice” is akin to what their child will do in most effective treatments, and will have the added benefit of helping them to build skills that all children need to manage the challenges and worries that are a normal, but difficult part of growing up and of adult life. Finally, you can tell them that anxious temperaments come with advantages also, such as great powers of observation, attention to detail, and thoroughness, high levels of empathy, drive, and tenacity. By learning to manage anxiety early, these children can grow up to be engaged, resilient, successful, and satisfied adults.
Once identified, the range of effective treatments available include cognitive-behavioral therapy, graduated exposure, mindfulness/relaxation techniques, and medication, and we will discuss these in our next article.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Beesdo K et al. Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr Clin North Am. 2009 Sep. doi: 10.1016/j.psc.2009.06.002.
Camp Discovery: A place for children to be comfortable in their own skin
The talent show, the grand finale of the 1-week camp, was nearly 7 years ago, but Emily Haygood of Houston, now 17 and about to start her senior year, remembers it in detail. She sang “Death of a Bachelor,” an R&B pop song and Billboard No. 1 hit at the time about a former bachelor who had happily married. These days, she said, if she watched the video of her 10-year-old singing self, “I would probably throw up.” But she still treasures the audience response, “having all those people I’d gotten close to cheer for me.”
Emily was at , but share one feature: they are the kind of dermatologic issues that can make doing everyday kid or teen activities like swimming difficult and can elicit mean comments from classmates and other would-be friends.

Emily was first diagnosed with atopic dermatitis at age 4, her mother, Amber Haygood, says. By age 9, it had become severe. Emily remembers being teased some in elementary school. “I did feel bad a lot of the time, when asked insensitive questions.” Her mother still bristles that adults often could be cruel, too.
But at Camp Discovery, those issues were nonexistent. “Camp was so cool,” Emily said. Besides the usual camp activities, it had things that “normal” camp didn’t, like other kids who didn’t stare at your skin condition or make fun of it.
30th anniversary season begins
This year is the 30th anniversary of Camp Discovery. Sessions began July 23 and continue through Aug. 18, with locations in Crosslake, Minn.; Hebron, Conn.; and Millville, Pa., in addition to Burton, Tex. About 300 campers will attend this year, according to the AAD, and 6,151 campers have attended from 1993 to 2022.

The 1-week camp accepts youth with conditions ranging from eczema and psoriasis to vitiligo, alopecia, epidermolysis bullosa, and ichthyosis, according to the academy. A dermatologist first refers a child, downloading and completing the referral form and sending it to the academy.
The 1-week session, including travel, is free for the campers, thanks to donors. As a nonprofit and membership-based organization, the AAD does not release the detailed financial information about the operating budget for the camp. Dermatologists, nurses, and counselors volunteer their time.
In his presidential address at the AAD’s annual meeting in March, outgoing president Mark D. Kaufmann, MD, of the department of dermatology at the Icahn School of Medicine at Mount Sinai in New York, referred to camp volunteering as an antidote to professional burnout. Remembering why as a dermatologist one entered the profession can be one solution, he said, and described his own recent 3-day volunteer stint at the camp.
“Those 3 magical days, being with kids as they discovered they weren’t alone in the world, sharing their experiences and ideas, reminded me why I became a physician in the first place,” he told the audience of meeting attendees. He vowed to expand the program, with a goal of having every dermatology resident attend Camp Discovery.
Mental health effects of skin conditions
Much research has focused on the mental health fallout from living with chronic skin conditions, and even young children can be adversely affected. In one review of the literature, researchers concluded that pediatric skin disease, including acne, atopic dermatitis, and psoriasis, can affect quality of life, carry stigma, and lead to bullying and eventually even suicidal behavior. Another study, published earlier this year, found that atopic dermatitis affected children’s quality of life, impacting sleep and leading to feelings of being ashamed.

“It’s not necessarily about what their skin condition is and more about the psychosocial impact,’’ said Samantha Hill, MD, a pediatric and general dermatologist in Lynchburg, Va., who is the medical director of Camp Discovery in Minnesota this year.
Camp activities, reactions
The overriding theme of camp is allowing all the youth to be “just one of the kids at camp,” Dr. Hill said in an interview. “They come to do all kinds of things they don’t do in normal life because people don’t give them the credit to [be able to] do it.”

Every year, she said, “I tell my staff we are in the business of making things happen, so if there is a kid bandaged head to toe [because of a skin condition] and they want to go tubing and get in the lake, we figure out how to make it happen. We have done that multiple times.”
Newcomers are initially nervous, Dr. Hill acknowledged, but in time let their guard down. Returnees are a different story. “When kids who have been at camp before arrive, you can see them start breathing again, looking for their friends. You can see them relax right before your eyes.”
“The single most empowering thing is the realization you are not alone,” said Meena Julapalli, MD, a Houston dermatologist who is a medical team member and long-time volunteer at Camp Discovery. That, she said, and “You get to be a kid, and you don’t have to have people staring at you.”

Dr. Julapalli remembers one of her patients with keratitis-ichthyosis-deafness (KID) syndrome. “She needed more than what I could offer,” she said. “She needed camp.” At camp, the organizers found a counselor who knew sign language to accompany her. At first, she was quiet and didn’t smile much. By the end of the week, as she was about to observe her birthday, things changed. After breakfast, she was led to the stage, where fellow campers began singing – and signing the song they had just learned.
Camp staff gets it
Allyson Garin, who was diagnosed with vitiligo at age 6 months, is a camp program director at Camp Discovery in Crosslake, Minn. She first went to camp in 1990 at age 11, returning until she “aged out” at 16, then worked as a counselor. She gets it when campers tell her they hear rude comments about their skin conditions.

“I remember being in swimming pools, in lines at fairgrounds or amusement parks,” she said in an interview, “and hearing people say, ‘Don’t touch her,’ ’’ fearing contagion, perhaps. “People would make jokes about cows, since they are spotted,” she said, or people would simply step back.
All those years ago, her mother found out about the camp and decided to figure out how to get her there. She got there, and she met a fellow camper with vitiligo, and they became pen pals. “We still talk,” she said.
Meeting someone with the same skin condition, she said, isn’t just about commiserating. “There is a lot of information sharing,” on topics such as best treatments, strategies, and other conversations.
Other lessons
While campers can feel comfortable around others who also have skin conditions, and understand, the lesson extends beyond that, Ms. Garin said. “It gave me a perspective,” she said of her camp experience. “I always felt, ‘Woe is me.’ ” But when she met others with, as she said, conditions “way worse than vitiligo, it really grounds you.”
Dr. Hill agreed. Campers get the benefit of others accepting and including them, but also practicing that same attitude toward fellow campers, she said. “It insures that we are providing this environment of inclusion, but that they are practicing it as well. They need to practice it like everyone else.”
Getting parents on board
The idea of camp, especially for those at the younger end of the 8- to 16-years age range accepted for Camp Discovery, can take some getting used to for some parents. Ms. Haygood, Emily’s mother, relates to that. Her daughter’s dermatologist at the time, who is now retired, had first suggested the camp. Her first reaction? “I am not sending my chronically ill child to camp with strangers.” She also acknowledged that she, like other parents of children with a chronic illness, can be a helicopter parent.

Then, she noticed that Emily seemed interested, so she got more information, finding out that it was staffed by doctors. It all sounded good, she said, and the social interaction, she knew, would be beneficial. “Then my husband was a no,” she said, concerned about their daughter being with strangers. “Eventually he came around,” Ms. Haygood said. All along, Emily said, “it seemed fun. I was probably trying to talk them into it.” She admits she was very nervous at first, but calmed down when she realized her own dermatologist was going to be there.
Vanessa Hadley of Spring, Tex., was on board the moment she heard about Camp Discovery. “I just thought it was amazing,” she said. Her daughter Isabelle, 13, has been to the camp. “She has alopecia areata and severe eczema,” Ms. Hadley said. Now, Isabelle is returning to camp and coaching her sister Penelope, 8, who has eczema and mild alopecia and is a first-timer this summer.
One tip the 8-year-old has learned so far: Turn to your counselor for support if you’re nervous. That worked, Isabelle said, the first year when she was wary of the zipline – then surprised herself and conquered it.
Dr. Hill and Dr. Julapalli have no disclosures.
The talent show, the grand finale of the 1-week camp, was nearly 7 years ago, but Emily Haygood of Houston, now 17 and about to start her senior year, remembers it in detail. She sang “Death of a Bachelor,” an R&B pop song and Billboard No. 1 hit at the time about a former bachelor who had happily married. These days, she said, if she watched the video of her 10-year-old singing self, “I would probably throw up.” But she still treasures the audience response, “having all those people I’d gotten close to cheer for me.”
Emily was at , but share one feature: they are the kind of dermatologic issues that can make doing everyday kid or teen activities like swimming difficult and can elicit mean comments from classmates and other would-be friends.
Emily was first diagnosed with atopic dermatitis at age 4, her mother, Amber Haygood, says. By age 9, it had become severe. Emily remembers being teased some in elementary school. “I did feel bad a lot of the time, when asked insensitive questions.” Her mother still bristles that adults often could be cruel, too.
But at Camp Discovery, those issues were nonexistent. “Camp was so cool,” Emily said. Besides the usual camp activities, it had things that “normal” camp didn’t, like other kids who didn’t stare at your skin condition or make fun of it.
30th anniversary season begins
This year is the 30th anniversary of Camp Discovery. Sessions began July 23 and continue through Aug. 18, with locations in Crosslake, Minn.; Hebron, Conn.; and Millville, Pa., in addition to Burton, Tex. About 300 campers will attend this year, according to the AAD, and 6,151 campers have attended from 1993 to 2022.
The 1-week camp accepts youth with conditions ranging from eczema and psoriasis to vitiligo, alopecia, epidermolysis bullosa, and ichthyosis, according to the academy. A dermatologist first refers a child, downloading and completing the referral form and sending it to the academy.
The 1-week session, including travel, is free for the campers, thanks to donors. As a nonprofit and membership-based organization, the AAD does not release the detailed financial information about the operating budget for the camp. Dermatologists, nurses, and counselors volunteer their time.
In his presidential address at the AAD’s annual meeting in March, outgoing president Mark D. Kaufmann, MD, of the department of dermatology at the Icahn School of Medicine at Mount Sinai in New York, referred to camp volunteering as an antidote to professional burnout. Remembering why as a dermatologist one entered the profession can be one solution, he said, and described his own recent 3-day volunteer stint at the camp.
“Those 3 magical days, being with kids as they discovered they weren’t alone in the world, sharing their experiences and ideas, reminded me why I became a physician in the first place,” he told the audience of meeting attendees. He vowed to expand the program, with a goal of having every dermatology resident attend Camp Discovery.
Mental health effects of skin conditions
Much research has focused on the mental health fallout from living with chronic skin conditions, and even young children can be adversely affected. In one review of the literature, researchers concluded that pediatric skin disease, including acne, atopic dermatitis, and psoriasis, can affect quality of life, carry stigma, and lead to bullying and eventually even suicidal behavior. Another study, published earlier this year, found that atopic dermatitis affected children’s quality of life, impacting sleep and leading to feelings of being ashamed.
“It’s not necessarily about what their skin condition is and more about the psychosocial impact,’’ said Samantha Hill, MD, a pediatric and general dermatologist in Lynchburg, Va., who is the medical director of Camp Discovery in Minnesota this year.
Camp activities, reactions
The overriding theme of camp is allowing all the youth to be “just one of the kids at camp,” Dr. Hill said in an interview. “They come to do all kinds of things they don’t do in normal life because people don’t give them the credit to [be able to] do it.”
Every year, she said, “I tell my staff we are in the business of making things happen, so if there is a kid bandaged head to toe [because of a skin condition] and they want to go tubing and get in the lake, we figure out how to make it happen. We have done that multiple times.”
Newcomers are initially nervous, Dr. Hill acknowledged, but in time let their guard down. Returnees are a different story. “When kids who have been at camp before arrive, you can see them start breathing again, looking for their friends. You can see them relax right before your eyes.”
“The single most empowering thing is the realization you are not alone,” said Meena Julapalli, MD, a Houston dermatologist who is a medical team member and long-time volunteer at Camp Discovery. That, she said, and “You get to be a kid, and you don’t have to have people staring at you.”
Dr. Julapalli remembers one of her patients with keratitis-ichthyosis-deafness (KID) syndrome. “She needed more than what I could offer,” she said. “She needed camp.” At camp, the organizers found a counselor who knew sign language to accompany her. At first, she was quiet and didn’t smile much. By the end of the week, as she was about to observe her birthday, things changed. After breakfast, she was led to the stage, where fellow campers began singing – and signing the song they had just learned.
Camp staff gets it
Allyson Garin, who was diagnosed with vitiligo at age 6 months, is a camp program director at Camp Discovery in Crosslake, Minn. She first went to camp in 1990 at age 11, returning until she “aged out” at 16, then worked as a counselor. She gets it when campers tell her they hear rude comments about their skin conditions.
“I remember being in swimming pools, in lines at fairgrounds or amusement parks,” she said in an interview, “and hearing people say, ‘Don’t touch her,’ ’’ fearing contagion, perhaps. “People would make jokes about cows, since they are spotted,” she said, or people would simply step back.
All those years ago, her mother found out about the camp and decided to figure out how to get her there. She got there, and she met a fellow camper with vitiligo, and they became pen pals. “We still talk,” she said.
Meeting someone with the same skin condition, she said, isn’t just about commiserating. “There is a lot of information sharing,” on topics such as best treatments, strategies, and other conversations.
Other lessons
While campers can feel comfortable around others who also have skin conditions, and understand, the lesson extends beyond that, Ms. Garin said. “It gave me a perspective,” she said of her camp experience. “I always felt, ‘Woe is me.’ ” But when she met others with, as she said, conditions “way worse than vitiligo, it really grounds you.”
Dr. Hill agreed. Campers get the benefit of others accepting and including them, but also practicing that same attitude toward fellow campers, she said. “It insures that we are providing this environment of inclusion, but that they are practicing it as well. They need to practice it like everyone else.”
Getting parents on board
The idea of camp, especially for those at the younger end of the 8- to 16-years age range accepted for Camp Discovery, can take some getting used to for some parents. Ms. Haygood, Emily’s mother, relates to that. Her daughter’s dermatologist at the time, who is now retired, had first suggested the camp. Her first reaction? “I am not sending my chronically ill child to camp with strangers.” She also acknowledged that she, like other parents of children with a chronic illness, can be a helicopter parent.
Then, she noticed that Emily seemed interested, so she got more information, finding out that it was staffed by doctors. It all sounded good, she said, and the social interaction, she knew, would be beneficial. “Then my husband was a no,” she said, concerned about their daughter being with strangers. “Eventually he came around,” Ms. Haygood said. All along, Emily said, “it seemed fun. I was probably trying to talk them into it.” She admits she was very nervous at first, but calmed down when she realized her own dermatologist was going to be there.
Vanessa Hadley of Spring, Tex., was on board the moment she heard about Camp Discovery. “I just thought it was amazing,” she said. Her daughter Isabelle, 13, has been to the camp. “She has alopecia areata and severe eczema,” Ms. Hadley said. Now, Isabelle is returning to camp and coaching her sister Penelope, 8, who has eczema and mild alopecia and is a first-timer this summer.
One tip the 8-year-old has learned so far: Turn to your counselor for support if you’re nervous. That worked, Isabelle said, the first year when she was wary of the zipline – then surprised herself and conquered it.
Dr. Hill and Dr. Julapalli have no disclosures.
The talent show, the grand finale of the 1-week camp, was nearly 7 years ago, but Emily Haygood of Houston, now 17 and about to start her senior year, remembers it in detail. She sang “Death of a Bachelor,” an R&B pop song and Billboard No. 1 hit at the time about a former bachelor who had happily married. These days, she said, if she watched the video of her 10-year-old singing self, “I would probably throw up.” But she still treasures the audience response, “having all those people I’d gotten close to cheer for me.”
Emily was at , but share one feature: they are the kind of dermatologic issues that can make doing everyday kid or teen activities like swimming difficult and can elicit mean comments from classmates and other would-be friends.
Emily was first diagnosed with atopic dermatitis at age 4, her mother, Amber Haygood, says. By age 9, it had become severe. Emily remembers being teased some in elementary school. “I did feel bad a lot of the time, when asked insensitive questions.” Her mother still bristles that adults often could be cruel, too.
But at Camp Discovery, those issues were nonexistent. “Camp was so cool,” Emily said. Besides the usual camp activities, it had things that “normal” camp didn’t, like other kids who didn’t stare at your skin condition or make fun of it.
30th anniversary season begins
This year is the 30th anniversary of Camp Discovery. Sessions began July 23 and continue through Aug. 18, with locations in Crosslake, Minn.; Hebron, Conn.; and Millville, Pa., in addition to Burton, Tex. About 300 campers will attend this year, according to the AAD, and 6,151 campers have attended from 1993 to 2022.
The 1-week camp accepts youth with conditions ranging from eczema and psoriasis to vitiligo, alopecia, epidermolysis bullosa, and ichthyosis, according to the academy. A dermatologist first refers a child, downloading and completing the referral form and sending it to the academy.
The 1-week session, including travel, is free for the campers, thanks to donors. As a nonprofit and membership-based organization, the AAD does not release the detailed financial information about the operating budget for the camp. Dermatologists, nurses, and counselors volunteer their time.
In his presidential address at the AAD’s annual meeting in March, outgoing president Mark D. Kaufmann, MD, of the department of dermatology at the Icahn School of Medicine at Mount Sinai in New York, referred to camp volunteering as an antidote to professional burnout. Remembering why as a dermatologist one entered the profession can be one solution, he said, and described his own recent 3-day volunteer stint at the camp.
“Those 3 magical days, being with kids as they discovered they weren’t alone in the world, sharing their experiences and ideas, reminded me why I became a physician in the first place,” he told the audience of meeting attendees. He vowed to expand the program, with a goal of having every dermatology resident attend Camp Discovery.
Mental health effects of skin conditions
Much research has focused on the mental health fallout from living with chronic skin conditions, and even young children can be adversely affected. In one review of the literature, researchers concluded that pediatric skin disease, including acne, atopic dermatitis, and psoriasis, can affect quality of life, carry stigma, and lead to bullying and eventually even suicidal behavior. Another study, published earlier this year, found that atopic dermatitis affected children’s quality of life, impacting sleep and leading to feelings of being ashamed.
“It’s not necessarily about what their skin condition is and more about the psychosocial impact,’’ said Samantha Hill, MD, a pediatric and general dermatologist in Lynchburg, Va., who is the medical director of Camp Discovery in Minnesota this year.
Camp activities, reactions
The overriding theme of camp is allowing all the youth to be “just one of the kids at camp,” Dr. Hill said in an interview. “They come to do all kinds of things they don’t do in normal life because people don’t give them the credit to [be able to] do it.”
Every year, she said, “I tell my staff we are in the business of making things happen, so if there is a kid bandaged head to toe [because of a skin condition] and they want to go tubing and get in the lake, we figure out how to make it happen. We have done that multiple times.”
Newcomers are initially nervous, Dr. Hill acknowledged, but in time let their guard down. Returnees are a different story. “When kids who have been at camp before arrive, you can see them start breathing again, looking for their friends. You can see them relax right before your eyes.”
“The single most empowering thing is the realization you are not alone,” said Meena Julapalli, MD, a Houston dermatologist who is a medical team member and long-time volunteer at Camp Discovery. That, she said, and “You get to be a kid, and you don’t have to have people staring at you.”
Dr. Julapalli remembers one of her patients with keratitis-ichthyosis-deafness (KID) syndrome. “She needed more than what I could offer,” she said. “She needed camp.” At camp, the organizers found a counselor who knew sign language to accompany her. At first, she was quiet and didn’t smile much. By the end of the week, as she was about to observe her birthday, things changed. After breakfast, she was led to the stage, where fellow campers began singing – and signing the song they had just learned.
Camp staff gets it
Allyson Garin, who was diagnosed with vitiligo at age 6 months, is a camp program director at Camp Discovery in Crosslake, Minn. She first went to camp in 1990 at age 11, returning until she “aged out” at 16, then worked as a counselor. She gets it when campers tell her they hear rude comments about their skin conditions.
“I remember being in swimming pools, in lines at fairgrounds or amusement parks,” she said in an interview, “and hearing people say, ‘Don’t touch her,’ ’’ fearing contagion, perhaps. “People would make jokes about cows, since they are spotted,” she said, or people would simply step back.
All those years ago, her mother found out about the camp and decided to figure out how to get her there. She got there, and she met a fellow camper with vitiligo, and they became pen pals. “We still talk,” she said.
Meeting someone with the same skin condition, she said, isn’t just about commiserating. “There is a lot of information sharing,” on topics such as best treatments, strategies, and other conversations.
Other lessons
While campers can feel comfortable around others who also have skin conditions, and understand, the lesson extends beyond that, Ms. Garin said. “It gave me a perspective,” she said of her camp experience. “I always felt, ‘Woe is me.’ ” But when she met others with, as she said, conditions “way worse than vitiligo, it really grounds you.”
Dr. Hill agreed. Campers get the benefit of others accepting and including them, but also practicing that same attitude toward fellow campers, she said. “It insures that we are providing this environment of inclusion, but that they are practicing it as well. They need to practice it like everyone else.”
Getting parents on board
The idea of camp, especially for those at the younger end of the 8- to 16-years age range accepted for Camp Discovery, can take some getting used to for some parents. Ms. Haygood, Emily’s mother, relates to that. Her daughter’s dermatologist at the time, who is now retired, had first suggested the camp. Her first reaction? “I am not sending my chronically ill child to camp with strangers.” She also acknowledged that she, like other parents of children with a chronic illness, can be a helicopter parent.
Then, she noticed that Emily seemed interested, so she got more information, finding out that it was staffed by doctors. It all sounded good, she said, and the social interaction, she knew, would be beneficial. “Then my husband was a no,” she said, concerned about their daughter being with strangers. “Eventually he came around,” Ms. Haygood said. All along, Emily said, “it seemed fun. I was probably trying to talk them into it.” She admits she was very nervous at first, but calmed down when she realized her own dermatologist was going to be there.
Vanessa Hadley of Spring, Tex., was on board the moment she heard about Camp Discovery. “I just thought it was amazing,” she said. Her daughter Isabelle, 13, has been to the camp. “She has alopecia areata and severe eczema,” Ms. Hadley said. Now, Isabelle is returning to camp and coaching her sister Penelope, 8, who has eczema and mild alopecia and is a first-timer this summer.
One tip the 8-year-old has learned so far: Turn to your counselor for support if you’re nervous. That worked, Isabelle said, the first year when she was wary of the zipline – then surprised herself and conquered it.
Dr. Hill and Dr. Julapalli have no disclosures.
Setmelanotide offers significant, long-lasting weight loss
MARSEILLE, FRANCE – , according to results presented at the latest French Pediatric Society conference. The treatment is effective for adults and children alike.
Setmelanotide is the culmination of two decades of research involving the identification of genes involved in early-onset obesity and the characterization of the melanocortin 4 receptor. It became available via early access in 2021.
Currently limited to use in treating obesity linked to a biallelic POMC/PCSK1 or LEPR deficiency, setmelanotide is being tested with respect to other mutations responsible for severe obesity, raising hopes that it will soon be indicated for use in a larger number of patients.
Fewer than 1% of patients who suffer from severe obesity have monogenic forms of obesity. In recent years, the hope for a targeted treatment for patients with these monogenic forms has become a reality.
Although only a small number of patients currently meet the criteria for setmelanotide treatment (namely, those with obesity linked to a biallelic POMC/PCSK1 enzyme or LEPR deficiency and patients with Bardet-Biedl syndrome), there is a real hope that patients with other forms of severe obesity will be able to benefit from this product, including those with heterozygous (not just homozygous) monoallelic variants, who account for more than 10% of patients with severe early-onset obesity.
Restoring satiety signaling
“Setmelanotide is a melanocortin 4 receptor agonist,” said Béatrice Dubern, MD, PhD, pediatrician at Trousseau Hospital, Paris, and member of the French medical research institute (INSERM)/Sorbonne University team on nutrition and obesity. “Its mode of action rests on activation of the leptin-melanocortin signaling pathway in the hypothalamus, which regulates hunger, satiety, energy expenditure, and, therefore, body weight. Rare genetic variants in the leptin-melanocortin pathway are associated with polyphagia and severe early-onset obesity. It is believed that more than 60 genes involved in this leptin-melanocortin pathway are currently associated with obesity.”
In July 2021, the European Medicines Agency approved setmelanotide for daily use via subcutaneous administration.
Weight loss maintained
In phase 3 studies, setmelanotide (melanocortin 4 receptor agonist) demonstrated its effectiveness in reducing weight and hunger for patients with obesity caused by a POMC/PCSK1 or LEPR deficiency.
Twenty-four patients aged 6 years and older showed a significant response to setmelanotide after 1 year of treatment and were included in the extension study. “Significant response” was defined as a reduction in body weight greater than or equal to 10% after 52 weeks for patients aged 18 years and older or a reduction in body mass index (BMI) z-score greater than or equal to 0.3 after 52 weeks for patients younger than 18 years.
Among all patients, the mean variation (standard deviation) in BMI was −24.8% (8.2%, n = 24), −21% (13%, n = 23), and −24% (17.9%, n = 15) at 12, 24, and 36 months, respectively.
For patients aged greater than or equal to 18 years (n = 11), the mean variation (standard deviation) in weight was −25.1% (7.7%, n = 11), −22.9% (12.5%, n = 11), and −24.4% (13.2%, n = 8) at 12, 24, and 36 months, respectively.
For children and adolescents (patients aged < 18 years, n = 13), the mean reduction (standard deviation) in BMI z-score was −1.31 ([0.66], n = 13), −1.10 ([0.79], n = 11), and −1.01 (1.22], n = 4) at 12, 24, and 36 months, respectively.
For patients younger than 18 years, the mean variation in BMI z-score was −1.01 SD after three years on setmelanotide (standard deviation, 1.22 [n = 4]). The mean BMI z-score was +2.42 SD (standard deviation, 1.22 [n = 4]) after 3 years of treatment with setmelanotide.
In sum, the patients who achieved a reduction in body weight of at least 10% or greater than or equal to 0.3 mean variation in BMI z-score after 1 year experienced long-lasting, clinically significant benefit after 3 years. The finding supports the long-term use of setmelanotide for this group.
“We feared that setmelanotide’s effectiveness would decrease over time, but after 3 years, this had not happened, and we are hopeful that this sustained efficacy will be long lasting. The first two patients who took the drug in 2016 have not noticed any loss of efficacy as it stands,” said Dr. Dubern.
This is all the more encouraging. In the study presented at the 2023 pediatric conference, setmelanotide’s safety profile was reassuring, and it was consistent with previous studies. Side effects reported in greater than or equal to 15% of patients include injection site reactions, skin hyperpigmentation, nausea, diarrhea, mood disturbances, abdominal pain, vomiting, gastroenteritis, and spontaneous erection.
In addition to the lack of control group, Dr. Dubern acknowledged one other constraint of this study. “Only the patients who responded to treatment with setmelanotide during early-phase trials (85.7%) were enrolled.”
Dr. Dubern summarized the clinical implications: “In patients with early-onset obesity, starting before 5 years of age, doctors should really be considering the possibility that genetics might be involved in such cases. For confirmation and to seek expert opinion, specialist obesity clinics can be found throughout France. Additionally, the INSERM NutriOmics research team headed by Prof Karine Clément, MD, PhD, Sorbonne University, in conjunction with Prof Christine Poitou, MD, PhD, has developed a diagnostic tool [called] ObsGen for practitioners faced with patients with potentially genetic causes of obesity. We can answer any questions they have about the likelihood of a particular patient having a genetic form of obesity and guide their next steps. Treating patients with genetic obesity early on helps limit the condition worsening during adolescence, prevents related complications, and can reduce the stigmatization and suffering experienced by these people. It’s a huge issue. A clinical trial with setmelanotide is currently being carried out in children over 2 years of age.”
Hypothalamic obesity
During the pediatric conference, another speaker presented the results of a phase 2 study that evaluated the efficacy and tolerability of setmelanotide as a new treatment for hypothalamic obesity. Lesions in the hypothalamus can alter melanocortin 4 receptor pathway signaling and thus lead to hypothalamic obesity. Eighteen patients aged 6-40 years with a BMI greater than or equal to the 95th percentile (for patients aged 6-18 years) or greater than or equal to 35 kg/m2 (for adults aged ≥ 18 years) and hypothalamic obesity (craniopharyngioma or other benign brain tumors, surgical removal, and/or chemotherapy) were enrolled. A significant proportion of patients achieved a reduction of greater than or equal to 5% of their BMI (n = 16, 88.9%, CI 90%, 69%-89%, P < .0001), and 72.2% achieved a reduction of greater than or equal to 10% by week 16. The mean change in BMI was −14.9% (9.6%, n = 17). These early results may justify further studies of setmelanotide in treating hypothalamic obesity.
Dr. Dubern has collaborated with Rhythm Pharmaceuticals and Novo Nordisk.
This article was translated from the Medscape French Edition and a version appeared on Medscape.com.
MARSEILLE, FRANCE – , according to results presented at the latest French Pediatric Society conference. The treatment is effective for adults and children alike.
Setmelanotide is the culmination of two decades of research involving the identification of genes involved in early-onset obesity and the characterization of the melanocortin 4 receptor. It became available via early access in 2021.
Currently limited to use in treating obesity linked to a biallelic POMC/PCSK1 or LEPR deficiency, setmelanotide is being tested with respect to other mutations responsible for severe obesity, raising hopes that it will soon be indicated for use in a larger number of patients.
Fewer than 1% of patients who suffer from severe obesity have monogenic forms of obesity. In recent years, the hope for a targeted treatment for patients with these monogenic forms has become a reality.
Although only a small number of patients currently meet the criteria for setmelanotide treatment (namely, those with obesity linked to a biallelic POMC/PCSK1 enzyme or LEPR deficiency and patients with Bardet-Biedl syndrome), there is a real hope that patients with other forms of severe obesity will be able to benefit from this product, including those with heterozygous (not just homozygous) monoallelic variants, who account for more than 10% of patients with severe early-onset obesity.
Restoring satiety signaling
“Setmelanotide is a melanocortin 4 receptor agonist,” said Béatrice Dubern, MD, PhD, pediatrician at Trousseau Hospital, Paris, and member of the French medical research institute (INSERM)/Sorbonne University team on nutrition and obesity. “Its mode of action rests on activation of the leptin-melanocortin signaling pathway in the hypothalamus, which regulates hunger, satiety, energy expenditure, and, therefore, body weight. Rare genetic variants in the leptin-melanocortin pathway are associated with polyphagia and severe early-onset obesity. It is believed that more than 60 genes involved in this leptin-melanocortin pathway are currently associated with obesity.”
In July 2021, the European Medicines Agency approved setmelanotide for daily use via subcutaneous administration.
Weight loss maintained
In phase 3 studies, setmelanotide (melanocortin 4 receptor agonist) demonstrated its effectiveness in reducing weight and hunger for patients with obesity caused by a POMC/PCSK1 or LEPR deficiency.
Twenty-four patients aged 6 years and older showed a significant response to setmelanotide after 1 year of treatment and were included in the extension study. “Significant response” was defined as a reduction in body weight greater than or equal to 10% after 52 weeks for patients aged 18 years and older or a reduction in body mass index (BMI) z-score greater than or equal to 0.3 after 52 weeks for patients younger than 18 years.
Among all patients, the mean variation (standard deviation) in BMI was −24.8% (8.2%, n = 24), −21% (13%, n = 23), and −24% (17.9%, n = 15) at 12, 24, and 36 months, respectively.
For patients aged greater than or equal to 18 years (n = 11), the mean variation (standard deviation) in weight was −25.1% (7.7%, n = 11), −22.9% (12.5%, n = 11), and −24.4% (13.2%, n = 8) at 12, 24, and 36 months, respectively.
For children and adolescents (patients aged < 18 years, n = 13), the mean reduction (standard deviation) in BMI z-score was −1.31 ([0.66], n = 13), −1.10 ([0.79], n = 11), and −1.01 (1.22], n = 4) at 12, 24, and 36 months, respectively.
For patients younger than 18 years, the mean variation in BMI z-score was −1.01 SD after three years on setmelanotide (standard deviation, 1.22 [n = 4]). The mean BMI z-score was +2.42 SD (standard deviation, 1.22 [n = 4]) after 3 years of treatment with setmelanotide.
In sum, the patients who achieved a reduction in body weight of at least 10% or greater than or equal to 0.3 mean variation in BMI z-score after 1 year experienced long-lasting, clinically significant benefit after 3 years. The finding supports the long-term use of setmelanotide for this group.
“We feared that setmelanotide’s effectiveness would decrease over time, but after 3 years, this had not happened, and we are hopeful that this sustained efficacy will be long lasting. The first two patients who took the drug in 2016 have not noticed any loss of efficacy as it stands,” said Dr. Dubern.
This is all the more encouraging. In the study presented at the 2023 pediatric conference, setmelanotide’s safety profile was reassuring, and it was consistent with previous studies. Side effects reported in greater than or equal to 15% of patients include injection site reactions, skin hyperpigmentation, nausea, diarrhea, mood disturbances, abdominal pain, vomiting, gastroenteritis, and spontaneous erection.
In addition to the lack of control group, Dr. Dubern acknowledged one other constraint of this study. “Only the patients who responded to treatment with setmelanotide during early-phase trials (85.7%) were enrolled.”
Dr. Dubern summarized the clinical implications: “In patients with early-onset obesity, starting before 5 years of age, doctors should really be considering the possibility that genetics might be involved in such cases. For confirmation and to seek expert opinion, specialist obesity clinics can be found throughout France. Additionally, the INSERM NutriOmics research team headed by Prof Karine Clément, MD, PhD, Sorbonne University, in conjunction with Prof Christine Poitou, MD, PhD, has developed a diagnostic tool [called] ObsGen for practitioners faced with patients with potentially genetic causes of obesity. We can answer any questions they have about the likelihood of a particular patient having a genetic form of obesity and guide their next steps. Treating patients with genetic obesity early on helps limit the condition worsening during adolescence, prevents related complications, and can reduce the stigmatization and suffering experienced by these people. It’s a huge issue. A clinical trial with setmelanotide is currently being carried out in children over 2 years of age.”
Hypothalamic obesity
During the pediatric conference, another speaker presented the results of a phase 2 study that evaluated the efficacy and tolerability of setmelanotide as a new treatment for hypothalamic obesity. Lesions in the hypothalamus can alter melanocortin 4 receptor pathway signaling and thus lead to hypothalamic obesity. Eighteen patients aged 6-40 years with a BMI greater than or equal to the 95th percentile (for patients aged 6-18 years) or greater than or equal to 35 kg/m2 (for adults aged ≥ 18 years) and hypothalamic obesity (craniopharyngioma or other benign brain tumors, surgical removal, and/or chemotherapy) were enrolled. A significant proportion of patients achieved a reduction of greater than or equal to 5% of their BMI (n = 16, 88.9%, CI 90%, 69%-89%, P < .0001), and 72.2% achieved a reduction of greater than or equal to 10% by week 16. The mean change in BMI was −14.9% (9.6%, n = 17). These early results may justify further studies of setmelanotide in treating hypothalamic obesity.
Dr. Dubern has collaborated with Rhythm Pharmaceuticals and Novo Nordisk.
This article was translated from the Medscape French Edition and a version appeared on Medscape.com.
MARSEILLE, FRANCE – , according to results presented at the latest French Pediatric Society conference. The treatment is effective for adults and children alike.
Setmelanotide is the culmination of two decades of research involving the identification of genes involved in early-onset obesity and the characterization of the melanocortin 4 receptor. It became available via early access in 2021.
Currently limited to use in treating obesity linked to a biallelic POMC/PCSK1 or LEPR deficiency, setmelanotide is being tested with respect to other mutations responsible for severe obesity, raising hopes that it will soon be indicated for use in a larger number of patients.
Fewer than 1% of patients who suffer from severe obesity have monogenic forms of obesity. In recent years, the hope for a targeted treatment for patients with these monogenic forms has become a reality.
Although only a small number of patients currently meet the criteria for setmelanotide treatment (namely, those with obesity linked to a biallelic POMC/PCSK1 enzyme or LEPR deficiency and patients with Bardet-Biedl syndrome), there is a real hope that patients with other forms of severe obesity will be able to benefit from this product, including those with heterozygous (not just homozygous) monoallelic variants, who account for more than 10% of patients with severe early-onset obesity.
Restoring satiety signaling
“Setmelanotide is a melanocortin 4 receptor agonist,” said Béatrice Dubern, MD, PhD, pediatrician at Trousseau Hospital, Paris, and member of the French medical research institute (INSERM)/Sorbonne University team on nutrition and obesity. “Its mode of action rests on activation of the leptin-melanocortin signaling pathway in the hypothalamus, which regulates hunger, satiety, energy expenditure, and, therefore, body weight. Rare genetic variants in the leptin-melanocortin pathway are associated with polyphagia and severe early-onset obesity. It is believed that more than 60 genes involved in this leptin-melanocortin pathway are currently associated with obesity.”
In July 2021, the European Medicines Agency approved setmelanotide for daily use via subcutaneous administration.
Weight loss maintained
In phase 3 studies, setmelanotide (melanocortin 4 receptor agonist) demonstrated its effectiveness in reducing weight and hunger for patients with obesity caused by a POMC/PCSK1 or LEPR deficiency.
Twenty-four patients aged 6 years and older showed a significant response to setmelanotide after 1 year of treatment and were included in the extension study. “Significant response” was defined as a reduction in body weight greater than or equal to 10% after 52 weeks for patients aged 18 years and older or a reduction in body mass index (BMI) z-score greater than or equal to 0.3 after 52 weeks for patients younger than 18 years.
Among all patients, the mean variation (standard deviation) in BMI was −24.8% (8.2%, n = 24), −21% (13%, n = 23), and −24% (17.9%, n = 15) at 12, 24, and 36 months, respectively.
For patients aged greater than or equal to 18 years (n = 11), the mean variation (standard deviation) in weight was −25.1% (7.7%, n = 11), −22.9% (12.5%, n = 11), and −24.4% (13.2%, n = 8) at 12, 24, and 36 months, respectively.
For children and adolescents (patients aged < 18 years, n = 13), the mean reduction (standard deviation) in BMI z-score was −1.31 ([0.66], n = 13), −1.10 ([0.79], n = 11), and −1.01 (1.22], n = 4) at 12, 24, and 36 months, respectively.
For patients younger than 18 years, the mean variation in BMI z-score was −1.01 SD after three years on setmelanotide (standard deviation, 1.22 [n = 4]). The mean BMI z-score was +2.42 SD (standard deviation, 1.22 [n = 4]) after 3 years of treatment with setmelanotide.
In sum, the patients who achieved a reduction in body weight of at least 10% or greater than or equal to 0.3 mean variation in BMI z-score after 1 year experienced long-lasting, clinically significant benefit after 3 years. The finding supports the long-term use of setmelanotide for this group.
“We feared that setmelanotide’s effectiveness would decrease over time, but after 3 years, this had not happened, and we are hopeful that this sustained efficacy will be long lasting. The first two patients who took the drug in 2016 have not noticed any loss of efficacy as it stands,” said Dr. Dubern.
This is all the more encouraging. In the study presented at the 2023 pediatric conference, setmelanotide’s safety profile was reassuring, and it was consistent with previous studies. Side effects reported in greater than or equal to 15% of patients include injection site reactions, skin hyperpigmentation, nausea, diarrhea, mood disturbances, abdominal pain, vomiting, gastroenteritis, and spontaneous erection.
In addition to the lack of control group, Dr. Dubern acknowledged one other constraint of this study. “Only the patients who responded to treatment with setmelanotide during early-phase trials (85.7%) were enrolled.”
Dr. Dubern summarized the clinical implications: “In patients with early-onset obesity, starting before 5 years of age, doctors should really be considering the possibility that genetics might be involved in such cases. For confirmation and to seek expert opinion, specialist obesity clinics can be found throughout France. Additionally, the INSERM NutriOmics research team headed by Prof Karine Clément, MD, PhD, Sorbonne University, in conjunction with Prof Christine Poitou, MD, PhD, has developed a diagnostic tool [called] ObsGen for practitioners faced with patients with potentially genetic causes of obesity. We can answer any questions they have about the likelihood of a particular patient having a genetic form of obesity and guide their next steps. Treating patients with genetic obesity early on helps limit the condition worsening during adolescence, prevents related complications, and can reduce the stigmatization and suffering experienced by these people. It’s a huge issue. A clinical trial with setmelanotide is currently being carried out in children over 2 years of age.”
Hypothalamic obesity
During the pediatric conference, another speaker presented the results of a phase 2 study that evaluated the efficacy and tolerability of setmelanotide as a new treatment for hypothalamic obesity. Lesions in the hypothalamus can alter melanocortin 4 receptor pathway signaling and thus lead to hypothalamic obesity. Eighteen patients aged 6-40 years with a BMI greater than or equal to the 95th percentile (for patients aged 6-18 years) or greater than or equal to 35 kg/m2 (for adults aged ≥ 18 years) and hypothalamic obesity (craniopharyngioma or other benign brain tumors, surgical removal, and/or chemotherapy) were enrolled. A significant proportion of patients achieved a reduction of greater than or equal to 5% of their BMI (n = 16, 88.9%, CI 90%, 69%-89%, P < .0001), and 72.2% achieved a reduction of greater than or equal to 10% by week 16. The mean change in BMI was −14.9% (9.6%, n = 17). These early results may justify further studies of setmelanotide in treating hypothalamic obesity.
Dr. Dubern has collaborated with Rhythm Pharmaceuticals and Novo Nordisk.
This article was translated from the Medscape French Edition and a version appeared on Medscape.com.