User login
Metformin & glitazones: Do they really help PCOS patients?
- There is no evidence to support the routine use of either metformin or a thiazolidenedione as first-line therapy for treatment of polycystic ovarian syndrome. (C)
- Diet and exercise are a better approach to PCOS treatment. A weight reduction of as little as 5% can help regulate the menstrual cycle and improve fertility, decrease insulin resistance, and reduce associated symptoms and comorbidities. (B)
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
A 35-year-old woman with no past medical or surgical history presents to your office with complaints consistent with oligomenorrhea. She also reports a 15-pound weight gain over this past year.
Your patient is married and sexually active, but has never been pregnant. Her menarche was at age 12, and she says she has had irregular, infrequent menses over the past year, with 4 to 5 days of medium flow. Her social/family history is unremarkable.
She denies using any drugs, medications, supplements, or herbs. She had a recent TSH, fasting blood glucose, CBC, basic metabolic panel, and Pap smear done by her previous physician during a routine physical and all were normal.
On exam, your patient is clinically obese (abdominal adiposity) and notably hirsute. Her skin exam is also positive for hyperpigmented lichenified plaques around her neck and axilla, consistent with acanthosis nigricans. The rest of her exam is unremarkable.
Her signs and symptoms prompt you to suspect polycystic ovarian syndrome (PCOS), which you confirm after ruling out type 2 diabetes mellitus, thyroid disease, hyperprolactinemia, congenital adrenal hyperplasia, and androgen secreting tumors.
Your next step, of course, is treatment and you consider your options. Would pharmacological treatment with metformin or a thiazolidenedione (TZD) be appropriate?
An answer that may surprise you
There is no evidence to support the routine use of either metformin or a TZD as first-line therapy for the treatment of PCOS, based on a meta-analysis of randomized controlled clinical trials (strength of recommendation [SOR]: C). Instead, you should individualize your approach to achieve the patient’s short- and long-term goals, as well as to minimize complications and comorbidities. A good approach at this time would be to educate your patient on lifestyle changes, such as diet and exercise, since the evidence supports their use (SOR: B).1-4 A weight reduction of as little as 5% can help regulate the menstrual cycle and improve fertility, decrease insulin resistance, and reduce associated symptoms and comorbidities.4

PCOS is associated with features of insulin resistance, hyperandrogenism, and oligomenorrhea leading to anovulatory bleeding and infertility. Many—though not all—PCOS patients have ovarian cysts.
Why the shift away from metformin or a TZD?
This recommendation is based on a meta-analysis that we, the authors, recently conducted. The following review provides a more detailed look at our analysis of the evidence to date. But before we get to the study, let’s look at the syndrome that sparked our research.
Background Polycystic ovarian syndrome (PCOS) leads to a multitude of clinical and biochemical alterations in patients. Metformin and the thiazolidenediones (TZDs)—which have insulin sensitizing properties—are believed to be effective in minimizing the changes caused by this syndrome.
Objectives Our goal was to assess the evidence for the use of TZDs or metformin in the treatment of PCOS patients. In addition, we sought to assess and compare the effectiveness of metformin vs TZDs in the clinical and biochemical regression of PCOS based on available randomized controlled trials (RCTs).
Search strategy We searched Medline (January 1966 to January 2007), PubMed (January 1954 to January 2007), Google Scholar search engine (through January 2007), and reference lists of articles. We also contacted researchers and clinicians in the field.
Selection criteria We reviewed RCTs involving women diagnosed with PCOS (based on 1990 the National Institutes of Health Criteria) who were treated with either metformin or TZDs. Trials were limited to those that were testing only the effects of either of these agents as their primary endpoint.
Main results A total of 115 trials were obtained, of which only 33 trials met the inclusion criteria. Ultimately, 31 trials involving total 1892 patients were included in the analysis (23 metformin, 2 rosiglitazone, 1 pioglitazone, 5 troglitazone) with 2 unobtainable trials.
There was insufficient data to compare metformin to the TZDs in any parameter because the literature often contained inadequate quantitative data, or there were too few published trials. As a result, we performed the meta-analysis for metformin only.
Among the outcomes examined, the only statistically significant changes were minimal decreases with metformin in ovulation rates and luteinizing hormone to follicle stimulating hormone ratio (LH/FSH), and an increase in fasting insulin.
There was no clinically significant change with metformin in ovulation rate, pregnancy rate, body mass index, waist-to-hip ratio, hirsutism (F-G score), LH/FSH, fasting insulin, fasting blood glucose, total testosterone, free testosterone, androstenedione, and dehydroepiandrosterone sulfate.
Authors’ conclusions There is a paucity of data from RCTs to compare the effectiveness of metformin vs TZDs as well as the effects of either agent in treating the clinical and biochemical features of PCOS. Further research involving RCTs with larger sample sizes is needed before any recommendation can be made on the usefulness of these agents in the treatment of PCOS.
Background
A syndrome with extensive variability
PCOS (also known as Stein-Leventhal syndrome) is associated with features of insulin resistance (obesity, acanthosis nigricans); hyperandrogenism (hirsutism, elevated androgen levels), and oligomenorrhea leading to anovulatory bleeding and infertility. PCOS has a prevalence of approximately 5% to 10% in women of reproductive age. Patients may have high serum concentrations of androgenic hormones, such as testosterone, androstenedione, and dehydroepiandrosterone sulfate (DHEAS). However, much variation exists clinically and a specific patient may have normal androgen levels.3 In addition, despite the syndrome’s name, not all women with PCOS have ovarian cysts.
The features of peripheral insulin resistance, hyperinsulinemia, oligomenorrhea, and infertility can be magnified in the presence of obesity. Insulin resistance is not due to defects in insulin binding to the insulin receptors; rather, it involves post-binding signaling pathways. The elevated insulin levels may have gonadotropin-augmenting effects on ovarian function.3
Numerous comorbidities play a role
There is a great deal of frustration for both physicians and patients regarding the various comorbidities associated with this syndrome. For patients, the problems include androgenic features, menstrual irregularities, and infertility. For clinicians, however, the concerns include cardiovascular risks4 (obesity, lipid abnormalities, elevated C-reactive protein and leptin levels, blood pressure changes), hyperinsulinemia, insulin resistance, and the theoretical risks for endometrial hyperplasia due to a hyperestrogenic state.
NIH criteria is used for diagnosis in trials
Although there are no definitive consensus criteria for the diagnosis of PCOS, the 1990 National Institutes of Health (NIH) criteria and its revision in 2003, the Rotterdam Criteria, have been used to make the diagnosis in clinical trials. Most trials however use the NIH criteria as there is disagreement regarding the Rotterdam Criteria.
The NIH criteria use the following for the diagnosis of PCOS:
- oligomenorrhea
- hyperandrogenism (clinical or laboratory evidence), and
- absence of other endocrine disorders (congenital adrenal hyperplasia, hyperprolactinemia, thyroid dysfunction, and androgen secreting tumors).
In reviewing the literature, most clinicians and researchers have noted that PCOS has been associated with various outcomes such as elevated body mass index (BMI),5 waist-to-hip ratio,5,6 fasting blood glucose,7 insulin levels,7 testosterone levels,8 androstenedione levels,8 DHEAS levels,9 hirsutism scores,9 lipids,5 blood pressure,9 luteinizing hormone to follicle-stimulating hormone ratio (LH/FSH),9 C-peptide,5 and leptin,6 as well as decreased ovulatory and pregnancy rates.4,5,10
Metformin/TZDs are used, but what about the evidence?
Both metformin and the TZDs (glitazones) including troglitazone—which was withdrawn from the market—pioglitazone, and rosiglitazone, are antidiabetic agents that also work as insulin sensitizers. These agents—especially metformin—are widely used by primary care physicians and specialists to treat the clinical and biochemical features of PCOS. However, the evidence-based data supporting this use is lacking. Although much research has been done on this topic, most published trials are of less than ideal quality and involve methodological issues. Often times they are nonrandomized, not controlled, involve a low number of subjects, provide no long-term follow up, and use nonstudy agents or ancillary treatments that were not randomized and could yield confounding results.
Objectives
Our primary objective was to assess whether there is evidence to support the use of metformin or TZDs, as well as to suggest any differences among the drugs. The secondary objective was to ascertain if, and to what extent, the studied drugs affected the studied parameters.
Methods
Search Strategy
We searched MD Consult, PubMed, Medline, Ovid, and Google Scholar through January 2007 with the following terms: “PCOS and metformin,” “PCOS and Glucophage,” “PCOS and troglitazone,” “PCOS and pioglitazone,” “PCOS and rosiglitazone,” “PCOS and thiazolidenediones.” These searches were also done by substituting “+” instead of the word “and,” as well as by using full form of the abbreviation PCOS—polycystic ovarian syndrome.
The following limits were placed on the search: randomized controlled trials, English language, human, and female subjects. We also searched articles from reference lists and made additional efforts to contact clinicians and researchers in this field.
Selection criteria
Our search resulted in 115 articles. From these articles, we included only those trials that:
- Used the NIH 1990 criteria for the diagnosis of PCOS
- Studied the effect of any of the following drugs: metformin, troglitazone, rosiglitazone, or pioglitazone
- Did not use or advocate adjunctive therapy—ie, diet or exercise
- Were randomized and controlled (based on a review of the methods section).
We also excluded studies that permitted confounding or concomitant treatments if it made it difficult to estimate the true effect of the medications studied.
This criteria resulted in 33 trials and ultimately 31 trials were included in the analysis (23 metformin, 2 rosiglitazone, 1 pioglitazone, 5 troglitazone) with a total of 1892 patients. Two metformin trials were unobtainable.
Outcome measures
We studied the parameters that are needed for the diagnosis of PCOS, as well as parameters that are associated with the syndrome’s comorbidities. The measured variables included: ovulation rates, pregnancy rates, BMI, waist-to-hip ratio, lipid panel, blood pressure, fasting insulin levels, fasting blood glucose, C-peptide, glycosylated hemoglobin (Hb A1c), LH/FSH, total testosterone, free testosterone, androstenedione, DHEAS, leptin, C-reactive protein, hirsutism (based on the Ferriman-Gallwey [F-G] score), and weight.
Methods of the review
Each included trial was evaluated in detail regarding how well it met the inclusion and exclusion criteria, the number of participants, the follow-up period, quantitative reporting of the data, and the overall methodology. The principal author rated methodological quality as good, fair, or poor on the basis of an overall assessment of these features. We did not use explicit validity checklists with summary scores because they have not been shown to predict the effect of bias on treatment differences or to provide more reliable assessments of validity.11,12
Description of studies
All included studies met the inclusion criteria. However, it is important to note that most of the studies had low numbers of participants (only 4 studies had a sample size [n] >50, 3 studies with n >100). Some of the trials shared the same patients but analyzed different end points so the fundamental “independence” assumption required for most standard statistical analyses, including meta-analysis, was likely violated.
A few of the trials used another pharmacological agent or invasive procedure as control treatment. Some trials had designs such that in the end, the treatment and control groups both received ovulation induction agents for the patients who failed to ovulate. Even with the strict inclusion and exclusion criteria, many of the included trials still were of less than satisfactory design quality for our purposes.
Data collection/extraction
The principal author reviewed the text, tables, and figures and then collected and extracted the data from relevant publications. The data set was reviewed by the secondary authors for errors in data entry, format, outliers, or implausible values.
Statistical analysis
For each analysis, we converted all data to the same metric based on conversion formulas provided by each individual trial. We also verified the conversion factors online via data provided by standard clinical and reference laboratory values.
Some trials provided standard deviations (SD), while others provided standard error (SE) or standard error of the mean (SEM). We derived pooled variances accordingly. We converted all SDs to SE using the equation SE=SD/square root (N), where N denotes the sample size. We created data sets in the above fashion for each parameter.
Trials that did not report SD, SE, or sample variance for a given parameter were not included in the corresponding meta-analysis. We did not conduct a statistical analysis if only a small number of trials existed (ie, n <5), as it would result in less reliable conclusions.
No article provided individual level data or SD/SE for the “change” in the selected endpoint before and after treatment in the control and treatment arm. Instead, most publications presented the summary statistics separately for before and after treatment.
Since covariance (or correlation) between before and after values was not available and variability of the difference measure could not be estimated from the majority of the trials, it was not possible to perform methodologically sound meta-analysis by addressing the absolute or percent change before and after treatment and comparing this difference measure between 2 competing treatments. This is an inherent problem in many meta-analyses due to limited raw data.
However, as all the trials were randomized, we felt justified in performing the statistical analysis using the mean difference after treatment in the control and intervention arms. Our assumption: the values before treatment should be reasonably balanced between the 2 arms. Thus, we calculated the pooled estimates of treatment effect with 95% confidence intervals (CIs) for the mean differences between the control and intervention arms after treatment. We adopted the random effects model approach.13
Next, statistical significance was evaluated for treatment effect and heterogeneity. Publication bias was also examined by two different tests.14,15 Sensitivity analysis was also performed to assess the impact of the identification of potential hidden studies by the trim and fill method.16
A 2-sided hypothesis with type I error of 5% was employed in all statistical testing and CI construction. Statistical analyses were carried out by STATA version 8.2.17
Results
Of the 31 trials included for the meta-analysis, we judged that 7 were of good quality, 6 were of fair quality, and 18 were of poor quality.2,5-10,18-41 (See TABLE W1.)
Not enough data to compare TZD vs metformin
As the TZDs had few trials for each drug (5 troglitazone, 2 rosiglitazone, 1 pioglitazone) and not enough of the TZD trials reported data on most parameters, it became unrealistic to perform a statistical comparison of the treatment effect between metformin and the TZDs. Moreover, there were not enough data from TZD trials to analyze the effect of TZDs on any studied parameter. Thus, only data from metformin trials were used in the meta-analysis.
Metformin linked to changes in 3 outcomes
Of the outcomes we evaluated, there were statistically significant changes in three: ovulation rate, LH/FSH ratio, and fasting insulin. (For complete details of our findings, see TABLE.)
After analyzing the ovulation rate in 9 trials, we found a change of –0.18% (95% CI, –0.35 to –0.01; P=.03) from the control group. Our analysis of the LH/FSH ratio in 7 trials revealed a change in value of –0.21 (–0.30 to –0.13; P<.001). We evaluated the fasting insulin levels in 14 trials and found an increase of 30.4 pmol/L (13.9 to 46.8; P<.001).
Insufficient trials (n ≤5) reported on total cholesterol, triglycerides, HDL, LDL, systolic blood pressure, diastolic blood pressure, C-peptide, C-reactive protein, leptin, and Hb A1c. Thus, we did not conduct a meta-analysis for these outcomes.
We intentionally used type I error of 5% for individual tests, not for overall test. If we had adopted multiple testing adjustments, we would have had more conservative results with much wider CIs, which makes it harder to reject the null hypothesis. Specifically, only 2 comparisons (LH/FSH and fasting insulin) would still be significant after multiple testing adjustments, while all marginally significant results would no longer be significant. A second reason to use type I error of 5% for individual (not overall) test is that endpoints are expected to be correlated, since most data were from the same trials.42,43
We did not find any major change in results in the sensitivity analyses we performed. It is worth mentioning, though, that there was significant heterogeneity and variability in the treatment effects from virtually all comparisons we made, though most comparisons revealed no publication bias. When heterogeneity is detected, combining the effects is not always advisable; and when effects are combined, they should be viewed with extreme caution.44-46
At a minimum, we failed to find any homogeneous or consistent treatment effects. Our sensitivity analysis offers additional protection against publication bias or file drawer problems.47
TABLE
Meta-analysis results by outcome
| OUTCOME | NUMBER OF TRIALS | POOLED ESTIMATE OF TREATMENT EFFECT (95% CI)* | P VALUES | SENSITIVITY ANALYSIS** | ||
|---|---|---|---|---|---|---|
| TREATMENT EFFECT* | HETEROGENEITY† | PUBLICATION BIAS‡ | ||||
| Ovulation rate (%) | 9 | –0.18 (–0.35 to –0.01) | .03 | .001 | .92 | –0.18/0.03 |
| Pregnancy rate (%) | 8 | –0.09 (–0.18 to 0.01) | .08 | <.001 | .90 | Unchanged |
| BMI (kg/m2) | 16 | 0.70 (–0.08 to 1.48) | .08 | .05 | .01 | –0.001/1 |
| Waist-to-hip ratio | 13 | –0.02 (–0.05 to 0.02) | .38 | <.001 | .20 | –0.03/0.06 |
| Hirsutism (F-G score) | 7 | –0.26 (–1.64 to 1.12) | .71 | .09 | .76 | Unchanged |
| LH/FSH | 7 | –0.21 (–0.30 to –0.13) | <.001 | .72 | 1 | –0.22/<0.001 |
| Fasting insulin (pmol/L) | 14 | 30.4 (13.9 to 46.8) | <.001 | <.001 | .51 | Unchanged |
| FBG (mmol/L) | 13 | 0.21 (–0.10 to 0.52) | .19 | <.001 | .43 | Unchanged |
| Total testosterone (nmol/L) | 13 | 0.01 (–0.38 to 0.40) | .95 | <.001 | 1 | Unchanged |
| Free testosterone (pg/mL) | 8 | 1.40 (–0.04 to 2.85) | .06 | <.001 | .71 | Unchanged |
| Androstenedione (nmol/L) | 11 | 0.09 (–0.25 to 0.42) | .60 | <.001 | .53 | Unchanged |
| DHEAS (μmol/L) | 14 | –0.48 (–1.20 to 0.24) | .19 | .004 | .58 | –0.91/0.03 |
| *Using Dersimonian and Laird’s random effects model, uncorrected for multiple testing. | ||||||
| †Using Cochran’s Q statistics. | ||||||
| ‡Using Begg and Mazumdar test. | ||||||
| **Pooled estimate/P value, using the trim and fill method. | ||||||
| We did not conduct meta-analysis for endpoints with number of studies ≤5: total cholesterol, triglycerides, HDL, LDL, C-peptide, Hb A1c, leptin, C-reactive protein, systolic blood pressure, and diastolic blood pressure. | ||||||
| LH/FSH, luteinizing hormone to follicle-stimulating hormone ratio; FBG, fasting blood glucose; DHEAS, dehydroepiandrosterone sulfate. | ||||||
Findings don’t support a common practice
Much has been reported in the literature, as well as by the media, regarding the large role that metformin and the TZDs can play in helping to alleviate the alterations caused by the polycystic ovarian syndrome. However, this systematic review of the literature, focusing on randomized controlled trials, failed to find evidence supporting the claims made in the literature, by the media, or offered anecdotally.
Based on our analysis, there is insufficient evidence to assess a difference in effect sizes between the TZDs and metformin. There is also insufficient evidence to assess if either the TZDs or metformin have an effect on lipids, blood pressure, C-peptide, C-reactive protein, leptin, or Hb A1c.
With regard to the analyzed parameters, there were minimal decreases of statistical significance in ovulation rates and LH/FSH, and minimal increase of statistical significance in fasting insulin with metformin. (We cannot account for the paradoxical and unexpected finding of an increase of fasting insulin with metformin, especially since metformin works as an insulin sensitizer.) There was, however, no clinically significant change with metformin in any of the parameters we studied (ovulation rate, pregnancy rate, body mass index, waist-to-hip ratio, hirsutism score, LH/FSH, total cholesterol, fasting insulin, fasting blood glucose, total testosterone, free testosterone, androstenedione, and DHEAS).
This systematic review provides a strong message that many of the trials were not of adequate methodological quality to make a definitive statement for clinical practice. In addition, most trials had a low sample size and used additional treatments with gonadotropins or ovulation induction agents that can yield altered results.
The primary aim of this study was to ascertain the evidence for the use of either TZDs or metformin in the treatment of patients with PCOS. This systematic review with the meta-analysis has found insufficient evidence to support the routine use of either. The secondary aim of this study was to obtain evidence to assess if either agent was superior in clinically reducing the various biochemical and clinical alterations due to this condition. Based on our analysis, we cannot claim either agent as superior.
Limitations
Few trials, sparse data
Any systematic review and meta-analysis will have inherent limitations as data from multiple trials, that might not be directly comparable, are combined to give an overview. Another limitation is that trials published in other languages were not included. We cannot exclude the possibility of selection or information bias because only one person reviewed all the articles to decide which would be included. However, we set the inclusion/exclusion criteria as well as endpoints very carefully prior to the study and literature search and had independent reviews by other authors during statistical analyses to minimize this problem.
The quality assessment of each trial is also subjective, even though strict inclusion/exclusion criteria were utilized. Assessing the efficacy of the TZDs could not be done as there were very few trials. Moreover, most of the TZD trials did not study or report on all the parameters. It is difficult to assess for publication bias or outliers and to justify combining the results when only a small number of trials are available or the data are sparse. In addition, although 5 trials with good sample size were available for troglitazone, this agent is no longer on the market, thus limiting clinical utility.
As most trials were not truly blinded upon careful review of the article, this may provide some bias. Furthermore, we could not conduct the meta-analysis for the gold standard method based on difference measures (before, after, and between treatment) due to data unavailability. Our alternative choice of analysis is justified based on the assumption that randomization will allow for baseline values in both groups to be approximately similar.
Finally, we used the SD or SE (or SEM) information as the original authors reported. Although SE is a function of sample size, SD is the population parameter so its variability should not be high. However, we found that the SDs varied considerably. It may be that the authors inadvertently used SD and SE interchangeably, thus leading to the heterogeneity of effect size.
Conclusions
Further study is needed
Carefully designed and sufficiently powered PCOS studies with large sample sizes, followed by the proper reporting of the study findings, are warranted. These studies, evaluating drug effects, should be done in a randomized placebo controlled fashion. Such trials should not be interfered with by using hormonal or ovulation induction agents other than the medication being studied. Diet and exercise should not be a part of the study’s design as these have been independently validated in similar contexts.4
For now, focus on lifestyle, and symptom-based treatment
PCOS encompasses a myriad of clinical and biochemical features, where each component adds to morbidity. The data, as per our study, are not sufficient to support the use of either of the studied agents in altering either the clinical or biochemical changes associated with the condition.
Thus, clinicians should tailor their treatment regimen to the individual patient’s short- and long-term goals. Clinicians should also educate patients regarding lifestyle changes, such as diet and exercise, since multiple trials1-4 have justified their use. Other options include symptom-based treatment, such as oral contraceptives for the regulation of menses or hirsutism.4
Acknowledgments
We wish to thank Dr Jan Groft, Dr Zakia Niruddin, Dr Marc Silverstein, and Dr Madhu Mazumdar for their efforts and guidance.
Funding/Support
This research was conducted without any outside funding or support.
Correspondence
Anush S. Pillai, DO, 424 Hahlo, Houston, TX, 77020; [email protected].
1. Pasquali R, Gambineri A, Biscotti D, et al. Effect of long-term treatment with metformin added to hypocaloric diet on body composition, fat distribution, and androgen and insulin levels in abdominally obese women with and without the polycystic ovary syndrome. J Clin Endocrinol Metab 2000;85:2767-2774.
2. Moghetti P, Castello R, Negri C, et al. Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double-blind, placebo-controlled 6-month trial, followed by open, long-term clinical evaluation. J Clin Endocrinol Metab 2000;85:139-146.
3. Khan MI, Klachko DM. Polycystic ovarian syndrome. June 27, 2006. Available at: www.emedicine.com/med/topic2173.htm. Accessed on May 10, 2007.
4. Polycystic ovary syndrome. ACOG Practice Bulletin Number 41. Obstet Gynecol 2002;100:1389-1402.
5. Eisenhardt S, Schwarzmann N, Henschel V. Early effects of metformin in women with polycystic ovarian syndrome: a prospective randomized, double-blind, placebo-controlled trial. J Clin Endocrinol Metab 2006;91:946-952.
6. Mantzoros CS, Dunaif A, Flier JS. Leptin concentrations in the polycystic ovary syndrome. J Clin Endocrinol Metab 1997;82:1687-1691.
7. Brettenthaler N, De Geyter C, Huber PR, Keller U. Effect of the insulin sensitizer pioglitazone on insulin resistance, hyperandrogenism, and ovulatory dysfunction in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2004;89:3835-3840.
8. Ortega-González C, Luna S, Hernandez L. Responses of serum androgen and insulin resistance to metformin and pioglitazone in obese, insulin-resistant women with polycystic ovarian syndrome. J Clin Endocrinol Metab 2005;90:1360-1365.
9. Cicek MN, Bala A, Celik C, Akyurek C. The comparison of clinical and hormonal parameters in PCOS patients treated with metformin and GnRH analogue. Arch Gynecol Obstet 2003;268:107-112.
10. Palomba S, Orio F, Jr, Nardo LG. Metformin administration versus laparoscopic ovarian diathermy in clomiphene citrate-resistant women with polycystic ovary syndrome: a prospective parallel randomized double-blind placebo-controlled trial. J Clin Endocrinol Metab 2004;89:4801-2809.
11. Emerson JD, Burdick E, Hoaglin DC, Mosteller F, Chalmers TC. An empirical study of the possible relation of treatment differences to quality scores in controlled randomized clinical trials. Control Clin Trials 1990;11:339-352.
12. Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions in The Cochrane Library. Chichester, UK: John Wiley & Sons; 2006. Issue 4 [updated September 2006].
13. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-188.
14. Begg CB, Mazumda M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088-1101.
15. Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-634.
16. Duval SJ, Tweedie RL. Trim and fill: A simple funnel plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000;56:276-284.
17. Stata Version 8.2 Intercooled, Stata Corporation, College Station, Texas, USA, 2005.
18. Azziz R, Ehrmann DA, Legro RS, Fereshetian AG, O’Keefe M, Ghazzi MN. Troglitazone decreases adrenal androgen levels in women with polycystic ovary syndrome. Fertil Steril 2003;79:932-937.
19. Azziz R, Ehrmann D, Legro RS, et al. Troglitazone improves ovulation and hirsutism in the polycystic ovary syndrome: a multicenter, double blind, placebo-controlled trial. J Clin Endocrinol Metab 2001;86:1626-1632.
20. Legro RS, Azziz R, Ehrmann D, Fereshetian AG, O’Keefe M, Ghazzi MN. Minimal response of circulating lipids in women with polycystic ovary syndrome to improvement in insulin sensitivity with troglitazone. J Clin Endocrinol Metab 2003;88:5137-5144.
21. Dunaif A, Scott D, Finegood D, Quintana B, Whitcomb R. The insulin-sensitizing agent troglitazone improves metabolic and reproductive abnormalities in the polycystic ovary syndrome. J Clin Endocrinol Metab 1996;81:3299-3306.
22. Ghazeeri G, Kutteh WH, Bryer-Ash M, Haas D, Ke RW. Effect of rosiglitazone on spontaneous and clomiphene citrate-induced ovulation in women with polycystic ovary syndrome. Fertil Steril 2003;79:562-566.
23. Shobokshi A, Shaarawy M. Correction of insulin resistance and hyperandrogenism in polycystic ovary syndrome by combined rosiglitazone and clomiphene citrate therapy. J Soc Gynecol Investig 2003;10:99-104.
24. Chou KH, von Eye Corleta H, Capp E, Spritzer PM. Clinical, metabolic and endocrine parameters in response to metformin in obese women with polycystic ovary syndrome: a randomized, double-blind and placebo-controlled trial. Horm Metab Res 2003;35:86-91.
25. Kelly CJ, Gordon D. The effect of metformin on hirsutism in polycystic ovary syndrome. Eur J Endocrinol 2002;147:217-221.
26. Baillargeon JP, Iuorno MJ, Jakubowicz DJ, Apridonidze T, He N, Nestler JE. Metformin therapy increases insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2004;89:242-249.
27. Sturrock ND, Lannon B, Fay TN. Metformin does not enhance ovulation induction in clomiphene resistant polycystic ovary syndrome in clinical practice. Br J Clin Pharmacol 2002;53:469-473.
28. Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activity and serum free testosterone after reduction of insulin secretion in polycystic ovary syndrome. N Engl J Med 1996;335:617-623.
29. Ganie MA, Khurana ML, Eunice M. Comparison of efficacy of spironolactone with metformin in the management of polycystic ovary syndrome: an open-labelled study. J Clin Endocrinol Metab 2004;89:2756-2762.
30. George SS, George K, Irwin C, et al. Sequential treatment of metformin and clomiphene citrate in clomiphene-resistant women with polycystic ovary syndrome: a randomized, controlled trial. Hum Reprod 2003;18:299-304.
31. Harborne L, Fleming R, Lyall H, Sattar N, Norman J. Metformin or antiandrogen in the treatment of hirsutism in polycystic ovary syndrome. J Clin Endocrinol Metab 2003;88:4116-4123.
32. Malkawi HY, Qublan HS, Hamaideh AH. Medical vs. surgical treatment for clomiphene citrate-resistant women with polycystic ovary syndrome. J Obstet Gynaecol 2003;23:289-293.
33. Morin-Papunen L, Rautio K, Ruokonen A, Hedberg P, Puukka M, Tapanainen JS. Metformin reduces serum C-reactive protein levels in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2003;88:4649-4654.
34. Morin-Papunen L, Vauhkonen I, Koivunen R, Ruokonen A, Martikainen H. Tapanainen Metformin versus ethinyl estradiol-cyproterone acetate in the treatment of nonobese women with polycystic ovary syndrome: a randomized study. J Clin Endocrinol Metab 2003;88:148-156.
35. Elter K, Imir G, Durmusoglu F. Clinical, endocrine and metabolic effects of metformin added to ethinyl estradiol-cyproterone acetate in non-obese women with polycystic ovarian syndrome: a randomized controlled study. Hum Reprod 2002;17:1729-1737.
36. Kocak M, Caliskan E, Simsir C, Haberal A. Metformin therapy improves ovulatory rates, cervical scores, and pregnancy rates in clomiphene citrate-resistant women with polycystic ovary syndrome. Fertil Steril 2002;77:101-106.
37. Yarali H, Yildiz BO, Demirol A, et al. Co-administration of metformin during rFSH treatment in patients with clomiphene citrate-resistant polycystic ovarian syndrome: a prospective randomized trial. Hum Reprod 2002;17:289-294.
38. Jakubowicz DJ, Seppala M, Jakubowicz S, et al. Insulin reduction with metformin increases luteal phase serum glycodelin and insulin-like growth factor-binding protein 1 concentrations and enhances uterine vascularity and blood flow in the polycystic ovary syndrome. J Clin Endocrinol Metab 2001;86:1126-1133.
39. Ng EH, Wat NM, Ho PC. Effects of metformin on ovulation rate, hormonal and metabolic profiles in women with clomiphene-resistant polycystic ovaries: a randomized, double-blinded placebo-controlled trial. Hum Reprod 2001;16:1625-1631.
40. Vandermolen DT, Ratts VS, Evans WS, Stovall DW, Kauma SW, Nestler JE. Metformin increases the ovulatory rate and pregnancy rate from clomiphene citrate in patients with polycystic ovary syndrome who are resistant to clomiphene citrate alone. Fertil Steril 2001;75:310-315.
41. Morin-Papunen LC, Vauhkonen I, Koivunen RM, Ruokonen A, Martikainen HK, Tapanainen JS. Endocrine and metabolic effects of metformin versus ethinyl estradiol-cyproterone acetate in obese women with polycystic ovary syndrome: a randomized study. J Clin Endocrinol Metab 2000;85:3161-3168.
42. Bang H, Jung S-H, George SL. Simulation-based multiple testing procedure and sample size calculation. J Biopharm Stat 2005;15:956-967.
43. Jung S-H, Bang H, Young SS. Sample size calculation for multiple testing in microarray data analysis. Biostatistics 2005;6:157-169.
44. Rothman K, Greenland S. Modern Epidemiology. 2nd ed. Philadelphia, Pa: Lippincott Williams and Wilkins;1998.
45. Colditz GA, Burdick E, Mosteller F. Heterogeneity in meta-analysis of data from epidemiologic studies: a commentary. Am J Epidemiol 1995;142:371-382.
46. Berlin JA. Invited commentary: benefits of heterogeneity in meta-analysis of data from epidemiologic studies. Am J Epidemiol 1995;142:383-387.
47. Young SS, Bang H. The file-drawer problem, revisited. Science 2004;306:1133-1134.
- There is no evidence to support the routine use of either metformin or a thiazolidenedione as first-line therapy for treatment of polycystic ovarian syndrome. (C)
- Diet and exercise are a better approach to PCOS treatment. A weight reduction of as little as 5% can help regulate the menstrual cycle and improve fertility, decrease insulin resistance, and reduce associated symptoms and comorbidities. (B)
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
A 35-year-old woman with no past medical or surgical history presents to your office with complaints consistent with oligomenorrhea. She also reports a 15-pound weight gain over this past year.
Your patient is married and sexually active, but has never been pregnant. Her menarche was at age 12, and she says she has had irregular, infrequent menses over the past year, with 4 to 5 days of medium flow. Her social/family history is unremarkable.
She denies using any drugs, medications, supplements, or herbs. She had a recent TSH, fasting blood glucose, CBC, basic metabolic panel, and Pap smear done by her previous physician during a routine physical and all were normal.
On exam, your patient is clinically obese (abdominal adiposity) and notably hirsute. Her skin exam is also positive for hyperpigmented lichenified plaques around her neck and axilla, consistent with acanthosis nigricans. The rest of her exam is unremarkable.
Her signs and symptoms prompt you to suspect polycystic ovarian syndrome (PCOS), which you confirm after ruling out type 2 diabetes mellitus, thyroid disease, hyperprolactinemia, congenital adrenal hyperplasia, and androgen secreting tumors.
Your next step, of course, is treatment and you consider your options. Would pharmacological treatment with metformin or a thiazolidenedione (TZD) be appropriate?
An answer that may surprise you
There is no evidence to support the routine use of either metformin or a TZD as first-line therapy for the treatment of PCOS, based on a meta-analysis of randomized controlled clinical trials (strength of recommendation [SOR]: C). Instead, you should individualize your approach to achieve the patient’s short- and long-term goals, as well as to minimize complications and comorbidities. A good approach at this time would be to educate your patient on lifestyle changes, such as diet and exercise, since the evidence supports their use (SOR: B).1-4 A weight reduction of as little as 5% can help regulate the menstrual cycle and improve fertility, decrease insulin resistance, and reduce associated symptoms and comorbidities.4
PCOS is associated with features of insulin resistance, hyperandrogenism, and oligomenorrhea leading to anovulatory bleeding and infertility. Many—though not all—PCOS patients have ovarian cysts.
Why the shift away from metformin or a TZD?
This recommendation is based on a meta-analysis that we, the authors, recently conducted. The following review provides a more detailed look at our analysis of the evidence to date. But before we get to the study, let’s look at the syndrome that sparked our research.
Background Polycystic ovarian syndrome (PCOS) leads to a multitude of clinical and biochemical alterations in patients. Metformin and the thiazolidenediones (TZDs)—which have insulin sensitizing properties—are believed to be effective in minimizing the changes caused by this syndrome.
Objectives Our goal was to assess the evidence for the use of TZDs or metformin in the treatment of PCOS patients. In addition, we sought to assess and compare the effectiveness of metformin vs TZDs in the clinical and biochemical regression of PCOS based on available randomized controlled trials (RCTs).
Search strategy We searched Medline (January 1966 to January 2007), PubMed (January 1954 to January 2007), Google Scholar search engine (through January 2007), and reference lists of articles. We also contacted researchers and clinicians in the field.
Selection criteria We reviewed RCTs involving women diagnosed with PCOS (based on 1990 the National Institutes of Health Criteria) who were treated with either metformin or TZDs. Trials were limited to those that were testing only the effects of either of these agents as their primary endpoint.
Main results A total of 115 trials were obtained, of which only 33 trials met the inclusion criteria. Ultimately, 31 trials involving total 1892 patients were included in the analysis (23 metformin, 2 rosiglitazone, 1 pioglitazone, 5 troglitazone) with 2 unobtainable trials.
There was insufficient data to compare metformin to the TZDs in any parameter because the literature often contained inadequate quantitative data, or there were too few published trials. As a result, we performed the meta-analysis for metformin only.
Among the outcomes examined, the only statistically significant changes were minimal decreases with metformin in ovulation rates and luteinizing hormone to follicle stimulating hormone ratio (LH/FSH), and an increase in fasting insulin.
There was no clinically significant change with metformin in ovulation rate, pregnancy rate, body mass index, waist-to-hip ratio, hirsutism (F-G score), LH/FSH, fasting insulin, fasting blood glucose, total testosterone, free testosterone, androstenedione, and dehydroepiandrosterone sulfate.
Authors’ conclusions There is a paucity of data from RCTs to compare the effectiveness of metformin vs TZDs as well as the effects of either agent in treating the clinical and biochemical features of PCOS. Further research involving RCTs with larger sample sizes is needed before any recommendation can be made on the usefulness of these agents in the treatment of PCOS.
Background
A syndrome with extensive variability
PCOS (also known as Stein-Leventhal syndrome) is associated with features of insulin resistance (obesity, acanthosis nigricans); hyperandrogenism (hirsutism, elevated androgen levels), and oligomenorrhea leading to anovulatory bleeding and infertility. PCOS has a prevalence of approximately 5% to 10% in women of reproductive age. Patients may have high serum concentrations of androgenic hormones, such as testosterone, androstenedione, and dehydroepiandrosterone sulfate (DHEAS). However, much variation exists clinically and a specific patient may have normal androgen levels.3 In addition, despite the syndrome’s name, not all women with PCOS have ovarian cysts.
The features of peripheral insulin resistance, hyperinsulinemia, oligomenorrhea, and infertility can be magnified in the presence of obesity. Insulin resistance is not due to defects in insulin binding to the insulin receptors; rather, it involves post-binding signaling pathways. The elevated insulin levels may have gonadotropin-augmenting effects on ovarian function.3
Numerous comorbidities play a role
There is a great deal of frustration for both physicians and patients regarding the various comorbidities associated with this syndrome. For patients, the problems include androgenic features, menstrual irregularities, and infertility. For clinicians, however, the concerns include cardiovascular risks4 (obesity, lipid abnormalities, elevated C-reactive protein and leptin levels, blood pressure changes), hyperinsulinemia, insulin resistance, and the theoretical risks for endometrial hyperplasia due to a hyperestrogenic state.
NIH criteria is used for diagnosis in trials
Although there are no definitive consensus criteria for the diagnosis of PCOS, the 1990 National Institutes of Health (NIH) criteria and its revision in 2003, the Rotterdam Criteria, have been used to make the diagnosis in clinical trials. Most trials however use the NIH criteria as there is disagreement regarding the Rotterdam Criteria.
The NIH criteria use the following for the diagnosis of PCOS:
- oligomenorrhea
- hyperandrogenism (clinical or laboratory evidence), and
- absence of other endocrine disorders (congenital adrenal hyperplasia, hyperprolactinemia, thyroid dysfunction, and androgen secreting tumors).
In reviewing the literature, most clinicians and researchers have noted that PCOS has been associated with various outcomes such as elevated body mass index (BMI),5 waist-to-hip ratio,5,6 fasting blood glucose,7 insulin levels,7 testosterone levels,8 androstenedione levels,8 DHEAS levels,9 hirsutism scores,9 lipids,5 blood pressure,9 luteinizing hormone to follicle-stimulating hormone ratio (LH/FSH),9 C-peptide,5 and leptin,6 as well as decreased ovulatory and pregnancy rates.4,5,10
Metformin/TZDs are used, but what about the evidence?
Both metformin and the TZDs (glitazones) including troglitazone—which was withdrawn from the market—pioglitazone, and rosiglitazone, are antidiabetic agents that also work as insulin sensitizers. These agents—especially metformin—are widely used by primary care physicians and specialists to treat the clinical and biochemical features of PCOS. However, the evidence-based data supporting this use is lacking. Although much research has been done on this topic, most published trials are of less than ideal quality and involve methodological issues. Often times they are nonrandomized, not controlled, involve a low number of subjects, provide no long-term follow up, and use nonstudy agents or ancillary treatments that were not randomized and could yield confounding results.
Objectives
Our primary objective was to assess whether there is evidence to support the use of metformin or TZDs, as well as to suggest any differences among the drugs. The secondary objective was to ascertain if, and to what extent, the studied drugs affected the studied parameters.
Methods
Search Strategy
We searched MD Consult, PubMed, Medline, Ovid, and Google Scholar through January 2007 with the following terms: “PCOS and metformin,” “PCOS and Glucophage,” “PCOS and troglitazone,” “PCOS and pioglitazone,” “PCOS and rosiglitazone,” “PCOS and thiazolidenediones.” These searches were also done by substituting “+” instead of the word “and,” as well as by using full form of the abbreviation PCOS—polycystic ovarian syndrome.
The following limits were placed on the search: randomized controlled trials, English language, human, and female subjects. We also searched articles from reference lists and made additional efforts to contact clinicians and researchers in this field.
Selection criteria
Our search resulted in 115 articles. From these articles, we included only those trials that:
- Used the NIH 1990 criteria for the diagnosis of PCOS
- Studied the effect of any of the following drugs: metformin, troglitazone, rosiglitazone, or pioglitazone
- Did not use or advocate adjunctive therapy—ie, diet or exercise
- Were randomized and controlled (based on a review of the methods section).
We also excluded studies that permitted confounding or concomitant treatments if it made it difficult to estimate the true effect of the medications studied.
This criteria resulted in 33 trials and ultimately 31 trials were included in the analysis (23 metformin, 2 rosiglitazone, 1 pioglitazone, 5 troglitazone) with a total of 1892 patients. Two metformin trials were unobtainable.
Outcome measures
We studied the parameters that are needed for the diagnosis of PCOS, as well as parameters that are associated with the syndrome’s comorbidities. The measured variables included: ovulation rates, pregnancy rates, BMI, waist-to-hip ratio, lipid panel, blood pressure, fasting insulin levels, fasting blood glucose, C-peptide, glycosylated hemoglobin (Hb A1c), LH/FSH, total testosterone, free testosterone, androstenedione, DHEAS, leptin, C-reactive protein, hirsutism (based on the Ferriman-Gallwey [F-G] score), and weight.
Methods of the review
Each included trial was evaluated in detail regarding how well it met the inclusion and exclusion criteria, the number of participants, the follow-up period, quantitative reporting of the data, and the overall methodology. The principal author rated methodological quality as good, fair, or poor on the basis of an overall assessment of these features. We did not use explicit validity checklists with summary scores because they have not been shown to predict the effect of bias on treatment differences or to provide more reliable assessments of validity.11,12
Description of studies
All included studies met the inclusion criteria. However, it is important to note that most of the studies had low numbers of participants (only 4 studies had a sample size [n] >50, 3 studies with n >100). Some of the trials shared the same patients but analyzed different end points so the fundamental “independence” assumption required for most standard statistical analyses, including meta-analysis, was likely violated.
A few of the trials used another pharmacological agent or invasive procedure as control treatment. Some trials had designs such that in the end, the treatment and control groups both received ovulation induction agents for the patients who failed to ovulate. Even with the strict inclusion and exclusion criteria, many of the included trials still were of less than satisfactory design quality for our purposes.
Data collection/extraction
The principal author reviewed the text, tables, and figures and then collected and extracted the data from relevant publications. The data set was reviewed by the secondary authors for errors in data entry, format, outliers, or implausible values.
Statistical analysis
For each analysis, we converted all data to the same metric based on conversion formulas provided by each individual trial. We also verified the conversion factors online via data provided by standard clinical and reference laboratory values.
Some trials provided standard deviations (SD), while others provided standard error (SE) or standard error of the mean (SEM). We derived pooled variances accordingly. We converted all SDs to SE using the equation SE=SD/square root (N), where N denotes the sample size. We created data sets in the above fashion for each parameter.
Trials that did not report SD, SE, or sample variance for a given parameter were not included in the corresponding meta-analysis. We did not conduct a statistical analysis if only a small number of trials existed (ie, n <5), as it would result in less reliable conclusions.
No article provided individual level data or SD/SE for the “change” in the selected endpoint before and after treatment in the control and treatment arm. Instead, most publications presented the summary statistics separately for before and after treatment.
Since covariance (or correlation) between before and after values was not available and variability of the difference measure could not be estimated from the majority of the trials, it was not possible to perform methodologically sound meta-analysis by addressing the absolute or percent change before and after treatment and comparing this difference measure between 2 competing treatments. This is an inherent problem in many meta-analyses due to limited raw data.
However, as all the trials were randomized, we felt justified in performing the statistical analysis using the mean difference after treatment in the control and intervention arms. Our assumption: the values before treatment should be reasonably balanced between the 2 arms. Thus, we calculated the pooled estimates of treatment effect with 95% confidence intervals (CIs) for the mean differences between the control and intervention arms after treatment. We adopted the random effects model approach.13
Next, statistical significance was evaluated for treatment effect and heterogeneity. Publication bias was also examined by two different tests.14,15 Sensitivity analysis was also performed to assess the impact of the identification of potential hidden studies by the trim and fill method.16
A 2-sided hypothesis with type I error of 5% was employed in all statistical testing and CI construction. Statistical analyses were carried out by STATA version 8.2.17
Results
Of the 31 trials included for the meta-analysis, we judged that 7 were of good quality, 6 were of fair quality, and 18 were of poor quality.2,5-10,18-41 (See TABLE W1.)
Not enough data to compare TZD vs metformin
As the TZDs had few trials for each drug (5 troglitazone, 2 rosiglitazone, 1 pioglitazone) and not enough of the TZD trials reported data on most parameters, it became unrealistic to perform a statistical comparison of the treatment effect between metformin and the TZDs. Moreover, there were not enough data from TZD trials to analyze the effect of TZDs on any studied parameter. Thus, only data from metformin trials were used in the meta-analysis.
Metformin linked to changes in 3 outcomes
Of the outcomes we evaluated, there were statistically significant changes in three: ovulation rate, LH/FSH ratio, and fasting insulin. (For complete details of our findings, see TABLE.)
After analyzing the ovulation rate in 9 trials, we found a change of –0.18% (95% CI, –0.35 to –0.01; P=.03) from the control group. Our analysis of the LH/FSH ratio in 7 trials revealed a change in value of –0.21 (–0.30 to –0.13; P<.001). We evaluated the fasting insulin levels in 14 trials and found an increase of 30.4 pmol/L (13.9 to 46.8; P<.001).
Insufficient trials (n ≤5) reported on total cholesterol, triglycerides, HDL, LDL, systolic blood pressure, diastolic blood pressure, C-peptide, C-reactive protein, leptin, and Hb A1c. Thus, we did not conduct a meta-analysis for these outcomes.
We intentionally used type I error of 5% for individual tests, not for overall test. If we had adopted multiple testing adjustments, we would have had more conservative results with much wider CIs, which makes it harder to reject the null hypothesis. Specifically, only 2 comparisons (LH/FSH and fasting insulin) would still be significant after multiple testing adjustments, while all marginally significant results would no longer be significant. A second reason to use type I error of 5% for individual (not overall) test is that endpoints are expected to be correlated, since most data were from the same trials.42,43
We did not find any major change in results in the sensitivity analyses we performed. It is worth mentioning, though, that there was significant heterogeneity and variability in the treatment effects from virtually all comparisons we made, though most comparisons revealed no publication bias. When heterogeneity is detected, combining the effects is not always advisable; and when effects are combined, they should be viewed with extreme caution.44-46
At a minimum, we failed to find any homogeneous or consistent treatment effects. Our sensitivity analysis offers additional protection against publication bias or file drawer problems.47
TABLE
Meta-analysis results by outcome
| OUTCOME | NUMBER OF TRIALS | POOLED ESTIMATE OF TREATMENT EFFECT (95% CI)* | P VALUES | SENSITIVITY ANALYSIS** | ||
|---|---|---|---|---|---|---|
| TREATMENT EFFECT* | HETEROGENEITY† | PUBLICATION BIAS‡ | ||||
| Ovulation rate (%) | 9 | –0.18 (–0.35 to –0.01) | .03 | .001 | .92 | –0.18/0.03 |
| Pregnancy rate (%) | 8 | –0.09 (–0.18 to 0.01) | .08 | <.001 | .90 | Unchanged |
| BMI (kg/m2) | 16 | 0.70 (–0.08 to 1.48) | .08 | .05 | .01 | –0.001/1 |
| Waist-to-hip ratio | 13 | –0.02 (–0.05 to 0.02) | .38 | <.001 | .20 | –0.03/0.06 |
| Hirsutism (F-G score) | 7 | –0.26 (–1.64 to 1.12) | .71 | .09 | .76 | Unchanged |
| LH/FSH | 7 | –0.21 (–0.30 to –0.13) | <.001 | .72 | 1 | –0.22/<0.001 |
| Fasting insulin (pmol/L) | 14 | 30.4 (13.9 to 46.8) | <.001 | <.001 | .51 | Unchanged |
| FBG (mmol/L) | 13 | 0.21 (–0.10 to 0.52) | .19 | <.001 | .43 | Unchanged |
| Total testosterone (nmol/L) | 13 | 0.01 (–0.38 to 0.40) | .95 | <.001 | 1 | Unchanged |
| Free testosterone (pg/mL) | 8 | 1.40 (–0.04 to 2.85) | .06 | <.001 | .71 | Unchanged |
| Androstenedione (nmol/L) | 11 | 0.09 (–0.25 to 0.42) | .60 | <.001 | .53 | Unchanged |
| DHEAS (μmol/L) | 14 | –0.48 (–1.20 to 0.24) | .19 | .004 | .58 | –0.91/0.03 |
| *Using Dersimonian and Laird’s random effects model, uncorrected for multiple testing. | ||||||
| †Using Cochran’s Q statistics. | ||||||
| ‡Using Begg and Mazumdar test. | ||||||
| **Pooled estimate/P value, using the trim and fill method. | ||||||
| We did not conduct meta-analysis for endpoints with number of studies ≤5: total cholesterol, triglycerides, HDL, LDL, C-peptide, Hb A1c, leptin, C-reactive protein, systolic blood pressure, and diastolic blood pressure. | ||||||
| LH/FSH, luteinizing hormone to follicle-stimulating hormone ratio; FBG, fasting blood glucose; DHEAS, dehydroepiandrosterone sulfate. | ||||||
Findings don’t support a common practice
Much has been reported in the literature, as well as by the media, regarding the large role that metformin and the TZDs can play in helping to alleviate the alterations caused by the polycystic ovarian syndrome. However, this systematic review of the literature, focusing on randomized controlled trials, failed to find evidence supporting the claims made in the literature, by the media, or offered anecdotally.
Based on our analysis, there is insufficient evidence to assess a difference in effect sizes between the TZDs and metformin. There is also insufficient evidence to assess if either the TZDs or metformin have an effect on lipids, blood pressure, C-peptide, C-reactive protein, leptin, or Hb A1c.
With regard to the analyzed parameters, there were minimal decreases of statistical significance in ovulation rates and LH/FSH, and minimal increase of statistical significance in fasting insulin with metformin. (We cannot account for the paradoxical and unexpected finding of an increase of fasting insulin with metformin, especially since metformin works as an insulin sensitizer.) There was, however, no clinically significant change with metformin in any of the parameters we studied (ovulation rate, pregnancy rate, body mass index, waist-to-hip ratio, hirsutism score, LH/FSH, total cholesterol, fasting insulin, fasting blood glucose, total testosterone, free testosterone, androstenedione, and DHEAS).
This systematic review provides a strong message that many of the trials were not of adequate methodological quality to make a definitive statement for clinical practice. In addition, most trials had a low sample size and used additional treatments with gonadotropins or ovulation induction agents that can yield altered results.
The primary aim of this study was to ascertain the evidence for the use of either TZDs or metformin in the treatment of patients with PCOS. This systematic review with the meta-analysis has found insufficient evidence to support the routine use of either. The secondary aim of this study was to obtain evidence to assess if either agent was superior in clinically reducing the various biochemical and clinical alterations due to this condition. Based on our analysis, we cannot claim either agent as superior.
Limitations
Few trials, sparse data
Any systematic review and meta-analysis will have inherent limitations as data from multiple trials, that might not be directly comparable, are combined to give an overview. Another limitation is that trials published in other languages were not included. We cannot exclude the possibility of selection or information bias because only one person reviewed all the articles to decide which would be included. However, we set the inclusion/exclusion criteria as well as endpoints very carefully prior to the study and literature search and had independent reviews by other authors during statistical analyses to minimize this problem.
The quality assessment of each trial is also subjective, even though strict inclusion/exclusion criteria were utilized. Assessing the efficacy of the TZDs could not be done as there were very few trials. Moreover, most of the TZD trials did not study or report on all the parameters. It is difficult to assess for publication bias or outliers and to justify combining the results when only a small number of trials are available or the data are sparse. In addition, although 5 trials with good sample size were available for troglitazone, this agent is no longer on the market, thus limiting clinical utility.
As most trials were not truly blinded upon careful review of the article, this may provide some bias. Furthermore, we could not conduct the meta-analysis for the gold standard method based on difference measures (before, after, and between treatment) due to data unavailability. Our alternative choice of analysis is justified based on the assumption that randomization will allow for baseline values in both groups to be approximately similar.
Finally, we used the SD or SE (or SEM) information as the original authors reported. Although SE is a function of sample size, SD is the population parameter so its variability should not be high. However, we found that the SDs varied considerably. It may be that the authors inadvertently used SD and SE interchangeably, thus leading to the heterogeneity of effect size.
Conclusions
Further study is needed
Carefully designed and sufficiently powered PCOS studies with large sample sizes, followed by the proper reporting of the study findings, are warranted. These studies, evaluating drug effects, should be done in a randomized placebo controlled fashion. Such trials should not be interfered with by using hormonal or ovulation induction agents other than the medication being studied. Diet and exercise should not be a part of the study’s design as these have been independently validated in similar contexts.4
For now, focus on lifestyle, and symptom-based treatment
PCOS encompasses a myriad of clinical and biochemical features, where each component adds to morbidity. The data, as per our study, are not sufficient to support the use of either of the studied agents in altering either the clinical or biochemical changes associated with the condition.
Thus, clinicians should tailor their treatment regimen to the individual patient’s short- and long-term goals. Clinicians should also educate patients regarding lifestyle changes, such as diet and exercise, since multiple trials1-4 have justified their use. Other options include symptom-based treatment, such as oral contraceptives for the regulation of menses or hirsutism.4
Acknowledgments
We wish to thank Dr Jan Groft, Dr Zakia Niruddin, Dr Marc Silverstein, and Dr Madhu Mazumdar for their efforts and guidance.
Funding/Support
This research was conducted without any outside funding or support.
Correspondence
Anush S. Pillai, DO, 424 Hahlo, Houston, TX, 77020; [email protected].
- There is no evidence to support the routine use of either metformin or a thiazolidenedione as first-line therapy for treatment of polycystic ovarian syndrome. (C)
- Diet and exercise are a better approach to PCOS treatment. A weight reduction of as little as 5% can help regulate the menstrual cycle and improve fertility, decrease insulin resistance, and reduce associated symptoms and comorbidities. (B)
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
A 35-year-old woman with no past medical or surgical history presents to your office with complaints consistent with oligomenorrhea. She also reports a 15-pound weight gain over this past year.
Your patient is married and sexually active, but has never been pregnant. Her menarche was at age 12, and she says she has had irregular, infrequent menses over the past year, with 4 to 5 days of medium flow. Her social/family history is unremarkable.
She denies using any drugs, medications, supplements, or herbs. She had a recent TSH, fasting blood glucose, CBC, basic metabolic panel, and Pap smear done by her previous physician during a routine physical and all were normal.
On exam, your patient is clinically obese (abdominal adiposity) and notably hirsute. Her skin exam is also positive for hyperpigmented lichenified plaques around her neck and axilla, consistent with acanthosis nigricans. The rest of her exam is unremarkable.
Her signs and symptoms prompt you to suspect polycystic ovarian syndrome (PCOS), which you confirm after ruling out type 2 diabetes mellitus, thyroid disease, hyperprolactinemia, congenital adrenal hyperplasia, and androgen secreting tumors.
Your next step, of course, is treatment and you consider your options. Would pharmacological treatment with metformin or a thiazolidenedione (TZD) be appropriate?
An answer that may surprise you
There is no evidence to support the routine use of either metformin or a TZD as first-line therapy for the treatment of PCOS, based on a meta-analysis of randomized controlled clinical trials (strength of recommendation [SOR]: C). Instead, you should individualize your approach to achieve the patient’s short- and long-term goals, as well as to minimize complications and comorbidities. A good approach at this time would be to educate your patient on lifestyle changes, such as diet and exercise, since the evidence supports their use (SOR: B).1-4 A weight reduction of as little as 5% can help regulate the menstrual cycle and improve fertility, decrease insulin resistance, and reduce associated symptoms and comorbidities.4
PCOS is associated with features of insulin resistance, hyperandrogenism, and oligomenorrhea leading to anovulatory bleeding and infertility. Many—though not all—PCOS patients have ovarian cysts.
Why the shift away from metformin or a TZD?
This recommendation is based on a meta-analysis that we, the authors, recently conducted. The following review provides a more detailed look at our analysis of the evidence to date. But before we get to the study, let’s look at the syndrome that sparked our research.
Background Polycystic ovarian syndrome (PCOS) leads to a multitude of clinical and biochemical alterations in patients. Metformin and the thiazolidenediones (TZDs)—which have insulin sensitizing properties—are believed to be effective in minimizing the changes caused by this syndrome.
Objectives Our goal was to assess the evidence for the use of TZDs or metformin in the treatment of PCOS patients. In addition, we sought to assess and compare the effectiveness of metformin vs TZDs in the clinical and biochemical regression of PCOS based on available randomized controlled trials (RCTs).
Search strategy We searched Medline (January 1966 to January 2007), PubMed (January 1954 to January 2007), Google Scholar search engine (through January 2007), and reference lists of articles. We also contacted researchers and clinicians in the field.
Selection criteria We reviewed RCTs involving women diagnosed with PCOS (based on 1990 the National Institutes of Health Criteria) who were treated with either metformin or TZDs. Trials were limited to those that were testing only the effects of either of these agents as their primary endpoint.
Main results A total of 115 trials were obtained, of which only 33 trials met the inclusion criteria. Ultimately, 31 trials involving total 1892 patients were included in the analysis (23 metformin, 2 rosiglitazone, 1 pioglitazone, 5 troglitazone) with 2 unobtainable trials.
There was insufficient data to compare metformin to the TZDs in any parameter because the literature often contained inadequate quantitative data, or there were too few published trials. As a result, we performed the meta-analysis for metformin only.
Among the outcomes examined, the only statistically significant changes were minimal decreases with metformin in ovulation rates and luteinizing hormone to follicle stimulating hormone ratio (LH/FSH), and an increase in fasting insulin.
There was no clinically significant change with metformin in ovulation rate, pregnancy rate, body mass index, waist-to-hip ratio, hirsutism (F-G score), LH/FSH, fasting insulin, fasting blood glucose, total testosterone, free testosterone, androstenedione, and dehydroepiandrosterone sulfate.
Authors’ conclusions There is a paucity of data from RCTs to compare the effectiveness of metformin vs TZDs as well as the effects of either agent in treating the clinical and biochemical features of PCOS. Further research involving RCTs with larger sample sizes is needed before any recommendation can be made on the usefulness of these agents in the treatment of PCOS.
Background
A syndrome with extensive variability
PCOS (also known as Stein-Leventhal syndrome) is associated with features of insulin resistance (obesity, acanthosis nigricans); hyperandrogenism (hirsutism, elevated androgen levels), and oligomenorrhea leading to anovulatory bleeding and infertility. PCOS has a prevalence of approximately 5% to 10% in women of reproductive age. Patients may have high serum concentrations of androgenic hormones, such as testosterone, androstenedione, and dehydroepiandrosterone sulfate (DHEAS). However, much variation exists clinically and a specific patient may have normal androgen levels.3 In addition, despite the syndrome’s name, not all women with PCOS have ovarian cysts.
The features of peripheral insulin resistance, hyperinsulinemia, oligomenorrhea, and infertility can be magnified in the presence of obesity. Insulin resistance is not due to defects in insulin binding to the insulin receptors; rather, it involves post-binding signaling pathways. The elevated insulin levels may have gonadotropin-augmenting effects on ovarian function.3
Numerous comorbidities play a role
There is a great deal of frustration for both physicians and patients regarding the various comorbidities associated with this syndrome. For patients, the problems include androgenic features, menstrual irregularities, and infertility. For clinicians, however, the concerns include cardiovascular risks4 (obesity, lipid abnormalities, elevated C-reactive protein and leptin levels, blood pressure changes), hyperinsulinemia, insulin resistance, and the theoretical risks for endometrial hyperplasia due to a hyperestrogenic state.
NIH criteria is used for diagnosis in trials
Although there are no definitive consensus criteria for the diagnosis of PCOS, the 1990 National Institutes of Health (NIH) criteria and its revision in 2003, the Rotterdam Criteria, have been used to make the diagnosis in clinical trials. Most trials however use the NIH criteria as there is disagreement regarding the Rotterdam Criteria.
The NIH criteria use the following for the diagnosis of PCOS:
- oligomenorrhea
- hyperandrogenism (clinical or laboratory evidence), and
- absence of other endocrine disorders (congenital adrenal hyperplasia, hyperprolactinemia, thyroid dysfunction, and androgen secreting tumors).
In reviewing the literature, most clinicians and researchers have noted that PCOS has been associated with various outcomes such as elevated body mass index (BMI),5 waist-to-hip ratio,5,6 fasting blood glucose,7 insulin levels,7 testosterone levels,8 androstenedione levels,8 DHEAS levels,9 hirsutism scores,9 lipids,5 blood pressure,9 luteinizing hormone to follicle-stimulating hormone ratio (LH/FSH),9 C-peptide,5 and leptin,6 as well as decreased ovulatory and pregnancy rates.4,5,10
Metformin/TZDs are used, but what about the evidence?
Both metformin and the TZDs (glitazones) including troglitazone—which was withdrawn from the market—pioglitazone, and rosiglitazone, are antidiabetic agents that also work as insulin sensitizers. These agents—especially metformin—are widely used by primary care physicians and specialists to treat the clinical and biochemical features of PCOS. However, the evidence-based data supporting this use is lacking. Although much research has been done on this topic, most published trials are of less than ideal quality and involve methodological issues. Often times they are nonrandomized, not controlled, involve a low number of subjects, provide no long-term follow up, and use nonstudy agents or ancillary treatments that were not randomized and could yield confounding results.
Objectives
Our primary objective was to assess whether there is evidence to support the use of metformin or TZDs, as well as to suggest any differences among the drugs. The secondary objective was to ascertain if, and to what extent, the studied drugs affected the studied parameters.
Methods
Search Strategy
We searched MD Consult, PubMed, Medline, Ovid, and Google Scholar through January 2007 with the following terms: “PCOS and metformin,” “PCOS and Glucophage,” “PCOS and troglitazone,” “PCOS and pioglitazone,” “PCOS and rosiglitazone,” “PCOS and thiazolidenediones.” These searches were also done by substituting “+” instead of the word “and,” as well as by using full form of the abbreviation PCOS—polycystic ovarian syndrome.
The following limits were placed on the search: randomized controlled trials, English language, human, and female subjects. We also searched articles from reference lists and made additional efforts to contact clinicians and researchers in this field.
Selection criteria
Our search resulted in 115 articles. From these articles, we included only those trials that:
- Used the NIH 1990 criteria for the diagnosis of PCOS
- Studied the effect of any of the following drugs: metformin, troglitazone, rosiglitazone, or pioglitazone
- Did not use or advocate adjunctive therapy—ie, diet or exercise
- Were randomized and controlled (based on a review of the methods section).
We also excluded studies that permitted confounding or concomitant treatments if it made it difficult to estimate the true effect of the medications studied.
This criteria resulted in 33 trials and ultimately 31 trials were included in the analysis (23 metformin, 2 rosiglitazone, 1 pioglitazone, 5 troglitazone) with a total of 1892 patients. Two metformin trials were unobtainable.
Outcome measures
We studied the parameters that are needed for the diagnosis of PCOS, as well as parameters that are associated with the syndrome’s comorbidities. The measured variables included: ovulation rates, pregnancy rates, BMI, waist-to-hip ratio, lipid panel, blood pressure, fasting insulin levels, fasting blood glucose, C-peptide, glycosylated hemoglobin (Hb A1c), LH/FSH, total testosterone, free testosterone, androstenedione, DHEAS, leptin, C-reactive protein, hirsutism (based on the Ferriman-Gallwey [F-G] score), and weight.
Methods of the review
Each included trial was evaluated in detail regarding how well it met the inclusion and exclusion criteria, the number of participants, the follow-up period, quantitative reporting of the data, and the overall methodology. The principal author rated methodological quality as good, fair, or poor on the basis of an overall assessment of these features. We did not use explicit validity checklists with summary scores because they have not been shown to predict the effect of bias on treatment differences or to provide more reliable assessments of validity.11,12
Description of studies
All included studies met the inclusion criteria. However, it is important to note that most of the studies had low numbers of participants (only 4 studies had a sample size [n] >50, 3 studies with n >100). Some of the trials shared the same patients but analyzed different end points so the fundamental “independence” assumption required for most standard statistical analyses, including meta-analysis, was likely violated.
A few of the trials used another pharmacological agent or invasive procedure as control treatment. Some trials had designs such that in the end, the treatment and control groups both received ovulation induction agents for the patients who failed to ovulate. Even with the strict inclusion and exclusion criteria, many of the included trials still were of less than satisfactory design quality for our purposes.
Data collection/extraction
The principal author reviewed the text, tables, and figures and then collected and extracted the data from relevant publications. The data set was reviewed by the secondary authors for errors in data entry, format, outliers, or implausible values.
Statistical analysis
For each analysis, we converted all data to the same metric based on conversion formulas provided by each individual trial. We also verified the conversion factors online via data provided by standard clinical and reference laboratory values.
Some trials provided standard deviations (SD), while others provided standard error (SE) or standard error of the mean (SEM). We derived pooled variances accordingly. We converted all SDs to SE using the equation SE=SD/square root (N), where N denotes the sample size. We created data sets in the above fashion for each parameter.
Trials that did not report SD, SE, or sample variance for a given parameter were not included in the corresponding meta-analysis. We did not conduct a statistical analysis if only a small number of trials existed (ie, n <5), as it would result in less reliable conclusions.
No article provided individual level data or SD/SE for the “change” in the selected endpoint before and after treatment in the control and treatment arm. Instead, most publications presented the summary statistics separately for before and after treatment.
Since covariance (or correlation) between before and after values was not available and variability of the difference measure could not be estimated from the majority of the trials, it was not possible to perform methodologically sound meta-analysis by addressing the absolute or percent change before and after treatment and comparing this difference measure between 2 competing treatments. This is an inherent problem in many meta-analyses due to limited raw data.
However, as all the trials were randomized, we felt justified in performing the statistical analysis using the mean difference after treatment in the control and intervention arms. Our assumption: the values before treatment should be reasonably balanced between the 2 arms. Thus, we calculated the pooled estimates of treatment effect with 95% confidence intervals (CIs) for the mean differences between the control and intervention arms after treatment. We adopted the random effects model approach.13
Next, statistical significance was evaluated for treatment effect and heterogeneity. Publication bias was also examined by two different tests.14,15 Sensitivity analysis was also performed to assess the impact of the identification of potential hidden studies by the trim and fill method.16
A 2-sided hypothesis with type I error of 5% was employed in all statistical testing and CI construction. Statistical analyses were carried out by STATA version 8.2.17
Results
Of the 31 trials included for the meta-analysis, we judged that 7 were of good quality, 6 were of fair quality, and 18 were of poor quality.2,5-10,18-41 (See TABLE W1.)
Not enough data to compare TZD vs metformin
As the TZDs had few trials for each drug (5 troglitazone, 2 rosiglitazone, 1 pioglitazone) and not enough of the TZD trials reported data on most parameters, it became unrealistic to perform a statistical comparison of the treatment effect between metformin and the TZDs. Moreover, there were not enough data from TZD trials to analyze the effect of TZDs on any studied parameter. Thus, only data from metformin trials were used in the meta-analysis.
Metformin linked to changes in 3 outcomes
Of the outcomes we evaluated, there were statistically significant changes in three: ovulation rate, LH/FSH ratio, and fasting insulin. (For complete details of our findings, see TABLE.)
After analyzing the ovulation rate in 9 trials, we found a change of –0.18% (95% CI, –0.35 to –0.01; P=.03) from the control group. Our analysis of the LH/FSH ratio in 7 trials revealed a change in value of –0.21 (–0.30 to –0.13; P<.001). We evaluated the fasting insulin levels in 14 trials and found an increase of 30.4 pmol/L (13.9 to 46.8; P<.001).
Insufficient trials (n ≤5) reported on total cholesterol, triglycerides, HDL, LDL, systolic blood pressure, diastolic blood pressure, C-peptide, C-reactive protein, leptin, and Hb A1c. Thus, we did not conduct a meta-analysis for these outcomes.
We intentionally used type I error of 5% for individual tests, not for overall test. If we had adopted multiple testing adjustments, we would have had more conservative results with much wider CIs, which makes it harder to reject the null hypothesis. Specifically, only 2 comparisons (LH/FSH and fasting insulin) would still be significant after multiple testing adjustments, while all marginally significant results would no longer be significant. A second reason to use type I error of 5% for individual (not overall) test is that endpoints are expected to be correlated, since most data were from the same trials.42,43
We did not find any major change in results in the sensitivity analyses we performed. It is worth mentioning, though, that there was significant heterogeneity and variability in the treatment effects from virtually all comparisons we made, though most comparisons revealed no publication bias. When heterogeneity is detected, combining the effects is not always advisable; and when effects are combined, they should be viewed with extreme caution.44-46
At a minimum, we failed to find any homogeneous or consistent treatment effects. Our sensitivity analysis offers additional protection against publication bias or file drawer problems.47
TABLE
Meta-analysis results by outcome
| OUTCOME | NUMBER OF TRIALS | POOLED ESTIMATE OF TREATMENT EFFECT (95% CI)* | P VALUES | SENSITIVITY ANALYSIS** | ||
|---|---|---|---|---|---|---|
| TREATMENT EFFECT* | HETEROGENEITY† | PUBLICATION BIAS‡ | ||||
| Ovulation rate (%) | 9 | –0.18 (–0.35 to –0.01) | .03 | .001 | .92 | –0.18/0.03 |
| Pregnancy rate (%) | 8 | –0.09 (–0.18 to 0.01) | .08 | <.001 | .90 | Unchanged |
| BMI (kg/m2) | 16 | 0.70 (–0.08 to 1.48) | .08 | .05 | .01 | –0.001/1 |
| Waist-to-hip ratio | 13 | –0.02 (–0.05 to 0.02) | .38 | <.001 | .20 | –0.03/0.06 |
| Hirsutism (F-G score) | 7 | –0.26 (–1.64 to 1.12) | .71 | .09 | .76 | Unchanged |
| LH/FSH | 7 | –0.21 (–0.30 to –0.13) | <.001 | .72 | 1 | –0.22/<0.001 |
| Fasting insulin (pmol/L) | 14 | 30.4 (13.9 to 46.8) | <.001 | <.001 | .51 | Unchanged |
| FBG (mmol/L) | 13 | 0.21 (–0.10 to 0.52) | .19 | <.001 | .43 | Unchanged |
| Total testosterone (nmol/L) | 13 | 0.01 (–0.38 to 0.40) | .95 | <.001 | 1 | Unchanged |
| Free testosterone (pg/mL) | 8 | 1.40 (–0.04 to 2.85) | .06 | <.001 | .71 | Unchanged |
| Androstenedione (nmol/L) | 11 | 0.09 (–0.25 to 0.42) | .60 | <.001 | .53 | Unchanged |
| DHEAS (μmol/L) | 14 | –0.48 (–1.20 to 0.24) | .19 | .004 | .58 | –0.91/0.03 |
| *Using Dersimonian and Laird’s random effects model, uncorrected for multiple testing. | ||||||
| †Using Cochran’s Q statistics. | ||||||
| ‡Using Begg and Mazumdar test. | ||||||
| **Pooled estimate/P value, using the trim and fill method. | ||||||
| We did not conduct meta-analysis for endpoints with number of studies ≤5: total cholesterol, triglycerides, HDL, LDL, C-peptide, Hb A1c, leptin, C-reactive protein, systolic blood pressure, and diastolic blood pressure. | ||||||
| LH/FSH, luteinizing hormone to follicle-stimulating hormone ratio; FBG, fasting blood glucose; DHEAS, dehydroepiandrosterone sulfate. | ||||||
Findings don’t support a common practice
Much has been reported in the literature, as well as by the media, regarding the large role that metformin and the TZDs can play in helping to alleviate the alterations caused by the polycystic ovarian syndrome. However, this systematic review of the literature, focusing on randomized controlled trials, failed to find evidence supporting the claims made in the literature, by the media, or offered anecdotally.
Based on our analysis, there is insufficient evidence to assess a difference in effect sizes between the TZDs and metformin. There is also insufficient evidence to assess if either the TZDs or metformin have an effect on lipids, blood pressure, C-peptide, C-reactive protein, leptin, or Hb A1c.
With regard to the analyzed parameters, there were minimal decreases of statistical significance in ovulation rates and LH/FSH, and minimal increase of statistical significance in fasting insulin with metformin. (We cannot account for the paradoxical and unexpected finding of an increase of fasting insulin with metformin, especially since metformin works as an insulin sensitizer.) There was, however, no clinically significant change with metformin in any of the parameters we studied (ovulation rate, pregnancy rate, body mass index, waist-to-hip ratio, hirsutism score, LH/FSH, total cholesterol, fasting insulin, fasting blood glucose, total testosterone, free testosterone, androstenedione, and DHEAS).
This systematic review provides a strong message that many of the trials were not of adequate methodological quality to make a definitive statement for clinical practice. In addition, most trials had a low sample size and used additional treatments with gonadotropins or ovulation induction agents that can yield altered results.
The primary aim of this study was to ascertain the evidence for the use of either TZDs or metformin in the treatment of patients with PCOS. This systematic review with the meta-analysis has found insufficient evidence to support the routine use of either. The secondary aim of this study was to obtain evidence to assess if either agent was superior in clinically reducing the various biochemical and clinical alterations due to this condition. Based on our analysis, we cannot claim either agent as superior.
Limitations
Few trials, sparse data
Any systematic review and meta-analysis will have inherent limitations as data from multiple trials, that might not be directly comparable, are combined to give an overview. Another limitation is that trials published in other languages were not included. We cannot exclude the possibility of selection or information bias because only one person reviewed all the articles to decide which would be included. However, we set the inclusion/exclusion criteria as well as endpoints very carefully prior to the study and literature search and had independent reviews by other authors during statistical analyses to minimize this problem.
The quality assessment of each trial is also subjective, even though strict inclusion/exclusion criteria were utilized. Assessing the efficacy of the TZDs could not be done as there were very few trials. Moreover, most of the TZD trials did not study or report on all the parameters. It is difficult to assess for publication bias or outliers and to justify combining the results when only a small number of trials are available or the data are sparse. In addition, although 5 trials with good sample size were available for troglitazone, this agent is no longer on the market, thus limiting clinical utility.
As most trials were not truly blinded upon careful review of the article, this may provide some bias. Furthermore, we could not conduct the meta-analysis for the gold standard method based on difference measures (before, after, and between treatment) due to data unavailability. Our alternative choice of analysis is justified based on the assumption that randomization will allow for baseline values in both groups to be approximately similar.
Finally, we used the SD or SE (or SEM) information as the original authors reported. Although SE is a function of sample size, SD is the population parameter so its variability should not be high. However, we found that the SDs varied considerably. It may be that the authors inadvertently used SD and SE interchangeably, thus leading to the heterogeneity of effect size.
Conclusions
Further study is needed
Carefully designed and sufficiently powered PCOS studies with large sample sizes, followed by the proper reporting of the study findings, are warranted. These studies, evaluating drug effects, should be done in a randomized placebo controlled fashion. Such trials should not be interfered with by using hormonal or ovulation induction agents other than the medication being studied. Diet and exercise should not be a part of the study’s design as these have been independently validated in similar contexts.4
For now, focus on lifestyle, and symptom-based treatment
PCOS encompasses a myriad of clinical and biochemical features, where each component adds to morbidity. The data, as per our study, are not sufficient to support the use of either of the studied agents in altering either the clinical or biochemical changes associated with the condition.
Thus, clinicians should tailor their treatment regimen to the individual patient’s short- and long-term goals. Clinicians should also educate patients regarding lifestyle changes, such as diet and exercise, since multiple trials1-4 have justified their use. Other options include symptom-based treatment, such as oral contraceptives for the regulation of menses or hirsutism.4
Acknowledgments
We wish to thank Dr Jan Groft, Dr Zakia Niruddin, Dr Marc Silverstein, and Dr Madhu Mazumdar for their efforts and guidance.
Funding/Support
This research was conducted without any outside funding or support.
Correspondence
Anush S. Pillai, DO, 424 Hahlo, Houston, TX, 77020; [email protected].
1. Pasquali R, Gambineri A, Biscotti D, et al. Effect of long-term treatment with metformin added to hypocaloric diet on body composition, fat distribution, and androgen and insulin levels in abdominally obese women with and without the polycystic ovary syndrome. J Clin Endocrinol Metab 2000;85:2767-2774.
2. Moghetti P, Castello R, Negri C, et al. Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double-blind, placebo-controlled 6-month trial, followed by open, long-term clinical evaluation. J Clin Endocrinol Metab 2000;85:139-146.
3. Khan MI, Klachko DM. Polycystic ovarian syndrome. June 27, 2006. Available at: www.emedicine.com/med/topic2173.htm. Accessed on May 10, 2007.
4. Polycystic ovary syndrome. ACOG Practice Bulletin Number 41. Obstet Gynecol 2002;100:1389-1402.
5. Eisenhardt S, Schwarzmann N, Henschel V. Early effects of metformin in women with polycystic ovarian syndrome: a prospective randomized, double-blind, placebo-controlled trial. J Clin Endocrinol Metab 2006;91:946-952.
6. Mantzoros CS, Dunaif A, Flier JS. Leptin concentrations in the polycystic ovary syndrome. J Clin Endocrinol Metab 1997;82:1687-1691.
7. Brettenthaler N, De Geyter C, Huber PR, Keller U. Effect of the insulin sensitizer pioglitazone on insulin resistance, hyperandrogenism, and ovulatory dysfunction in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2004;89:3835-3840.
8. Ortega-González C, Luna S, Hernandez L. Responses of serum androgen and insulin resistance to metformin and pioglitazone in obese, insulin-resistant women with polycystic ovarian syndrome. J Clin Endocrinol Metab 2005;90:1360-1365.
9. Cicek MN, Bala A, Celik C, Akyurek C. The comparison of clinical and hormonal parameters in PCOS patients treated with metformin and GnRH analogue. Arch Gynecol Obstet 2003;268:107-112.
10. Palomba S, Orio F, Jr, Nardo LG. Metformin administration versus laparoscopic ovarian diathermy in clomiphene citrate-resistant women with polycystic ovary syndrome: a prospective parallel randomized double-blind placebo-controlled trial. J Clin Endocrinol Metab 2004;89:4801-2809.
11. Emerson JD, Burdick E, Hoaglin DC, Mosteller F, Chalmers TC. An empirical study of the possible relation of treatment differences to quality scores in controlled randomized clinical trials. Control Clin Trials 1990;11:339-352.
12. Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions in The Cochrane Library. Chichester, UK: John Wiley & Sons; 2006. Issue 4 [updated September 2006].
13. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-188.
14. Begg CB, Mazumda M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088-1101.
15. Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-634.
16. Duval SJ, Tweedie RL. Trim and fill: A simple funnel plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000;56:276-284.
17. Stata Version 8.2 Intercooled, Stata Corporation, College Station, Texas, USA, 2005.
18. Azziz R, Ehrmann DA, Legro RS, Fereshetian AG, O’Keefe M, Ghazzi MN. Troglitazone decreases adrenal androgen levels in women with polycystic ovary syndrome. Fertil Steril 2003;79:932-937.
19. Azziz R, Ehrmann D, Legro RS, et al. Troglitazone improves ovulation and hirsutism in the polycystic ovary syndrome: a multicenter, double blind, placebo-controlled trial. J Clin Endocrinol Metab 2001;86:1626-1632.
20. Legro RS, Azziz R, Ehrmann D, Fereshetian AG, O’Keefe M, Ghazzi MN. Minimal response of circulating lipids in women with polycystic ovary syndrome to improvement in insulin sensitivity with troglitazone. J Clin Endocrinol Metab 2003;88:5137-5144.
21. Dunaif A, Scott D, Finegood D, Quintana B, Whitcomb R. The insulin-sensitizing agent troglitazone improves metabolic and reproductive abnormalities in the polycystic ovary syndrome. J Clin Endocrinol Metab 1996;81:3299-3306.
22. Ghazeeri G, Kutteh WH, Bryer-Ash M, Haas D, Ke RW. Effect of rosiglitazone on spontaneous and clomiphene citrate-induced ovulation in women with polycystic ovary syndrome. Fertil Steril 2003;79:562-566.
23. Shobokshi A, Shaarawy M. Correction of insulin resistance and hyperandrogenism in polycystic ovary syndrome by combined rosiglitazone and clomiphene citrate therapy. J Soc Gynecol Investig 2003;10:99-104.
24. Chou KH, von Eye Corleta H, Capp E, Spritzer PM. Clinical, metabolic and endocrine parameters in response to metformin in obese women with polycystic ovary syndrome: a randomized, double-blind and placebo-controlled trial. Horm Metab Res 2003;35:86-91.
25. Kelly CJ, Gordon D. The effect of metformin on hirsutism in polycystic ovary syndrome. Eur J Endocrinol 2002;147:217-221.
26. Baillargeon JP, Iuorno MJ, Jakubowicz DJ, Apridonidze T, He N, Nestler JE. Metformin therapy increases insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2004;89:242-249.
27. Sturrock ND, Lannon B, Fay TN. Metformin does not enhance ovulation induction in clomiphene resistant polycystic ovary syndrome in clinical practice. Br J Clin Pharmacol 2002;53:469-473.
28. Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activity and serum free testosterone after reduction of insulin secretion in polycystic ovary syndrome. N Engl J Med 1996;335:617-623.
29. Ganie MA, Khurana ML, Eunice M. Comparison of efficacy of spironolactone with metformin in the management of polycystic ovary syndrome: an open-labelled study. J Clin Endocrinol Metab 2004;89:2756-2762.
30. George SS, George K, Irwin C, et al. Sequential treatment of metformin and clomiphene citrate in clomiphene-resistant women with polycystic ovary syndrome: a randomized, controlled trial. Hum Reprod 2003;18:299-304.
31. Harborne L, Fleming R, Lyall H, Sattar N, Norman J. Metformin or antiandrogen in the treatment of hirsutism in polycystic ovary syndrome. J Clin Endocrinol Metab 2003;88:4116-4123.
32. Malkawi HY, Qublan HS, Hamaideh AH. Medical vs. surgical treatment for clomiphene citrate-resistant women with polycystic ovary syndrome. J Obstet Gynaecol 2003;23:289-293.
33. Morin-Papunen L, Rautio K, Ruokonen A, Hedberg P, Puukka M, Tapanainen JS. Metformin reduces serum C-reactive protein levels in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2003;88:4649-4654.
34. Morin-Papunen L, Vauhkonen I, Koivunen R, Ruokonen A, Martikainen H. Tapanainen Metformin versus ethinyl estradiol-cyproterone acetate in the treatment of nonobese women with polycystic ovary syndrome: a randomized study. J Clin Endocrinol Metab 2003;88:148-156.
35. Elter K, Imir G, Durmusoglu F. Clinical, endocrine and metabolic effects of metformin added to ethinyl estradiol-cyproterone acetate in non-obese women with polycystic ovarian syndrome: a randomized controlled study. Hum Reprod 2002;17:1729-1737.
36. Kocak M, Caliskan E, Simsir C, Haberal A. Metformin therapy improves ovulatory rates, cervical scores, and pregnancy rates in clomiphene citrate-resistant women with polycystic ovary syndrome. Fertil Steril 2002;77:101-106.
37. Yarali H, Yildiz BO, Demirol A, et al. Co-administration of metformin during rFSH treatment in patients with clomiphene citrate-resistant polycystic ovarian syndrome: a prospective randomized trial. Hum Reprod 2002;17:289-294.
38. Jakubowicz DJ, Seppala M, Jakubowicz S, et al. Insulin reduction with metformin increases luteal phase serum glycodelin and insulin-like growth factor-binding protein 1 concentrations and enhances uterine vascularity and blood flow in the polycystic ovary syndrome. J Clin Endocrinol Metab 2001;86:1126-1133.
39. Ng EH, Wat NM, Ho PC. Effects of metformin on ovulation rate, hormonal and metabolic profiles in women with clomiphene-resistant polycystic ovaries: a randomized, double-blinded placebo-controlled trial. Hum Reprod 2001;16:1625-1631.
40. Vandermolen DT, Ratts VS, Evans WS, Stovall DW, Kauma SW, Nestler JE. Metformin increases the ovulatory rate and pregnancy rate from clomiphene citrate in patients with polycystic ovary syndrome who are resistant to clomiphene citrate alone. Fertil Steril 2001;75:310-315.
41. Morin-Papunen LC, Vauhkonen I, Koivunen RM, Ruokonen A, Martikainen HK, Tapanainen JS. Endocrine and metabolic effects of metformin versus ethinyl estradiol-cyproterone acetate in obese women with polycystic ovary syndrome: a randomized study. J Clin Endocrinol Metab 2000;85:3161-3168.
42. Bang H, Jung S-H, George SL. Simulation-based multiple testing procedure and sample size calculation. J Biopharm Stat 2005;15:956-967.
43. Jung S-H, Bang H, Young SS. Sample size calculation for multiple testing in microarray data analysis. Biostatistics 2005;6:157-169.
44. Rothman K, Greenland S. Modern Epidemiology. 2nd ed. Philadelphia, Pa: Lippincott Williams and Wilkins;1998.
45. Colditz GA, Burdick E, Mosteller F. Heterogeneity in meta-analysis of data from epidemiologic studies: a commentary. Am J Epidemiol 1995;142:371-382.
46. Berlin JA. Invited commentary: benefits of heterogeneity in meta-analysis of data from epidemiologic studies. Am J Epidemiol 1995;142:383-387.
47. Young SS, Bang H. The file-drawer problem, revisited. Science 2004;306:1133-1134.
1. Pasquali R, Gambineri A, Biscotti D, et al. Effect of long-term treatment with metformin added to hypocaloric diet on body composition, fat distribution, and androgen and insulin levels in abdominally obese women with and without the polycystic ovary syndrome. J Clin Endocrinol Metab 2000;85:2767-2774.
2. Moghetti P, Castello R, Negri C, et al. Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double-blind, placebo-controlled 6-month trial, followed by open, long-term clinical evaluation. J Clin Endocrinol Metab 2000;85:139-146.
3. Khan MI, Klachko DM. Polycystic ovarian syndrome. June 27, 2006. Available at: www.emedicine.com/med/topic2173.htm. Accessed on May 10, 2007.
4. Polycystic ovary syndrome. ACOG Practice Bulletin Number 41. Obstet Gynecol 2002;100:1389-1402.
5. Eisenhardt S, Schwarzmann N, Henschel V. Early effects of metformin in women with polycystic ovarian syndrome: a prospective randomized, double-blind, placebo-controlled trial. J Clin Endocrinol Metab 2006;91:946-952.
6. Mantzoros CS, Dunaif A, Flier JS. Leptin concentrations in the polycystic ovary syndrome. J Clin Endocrinol Metab 1997;82:1687-1691.
7. Brettenthaler N, De Geyter C, Huber PR, Keller U. Effect of the insulin sensitizer pioglitazone on insulin resistance, hyperandrogenism, and ovulatory dysfunction in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2004;89:3835-3840.
8. Ortega-González C, Luna S, Hernandez L. Responses of serum androgen and insulin resistance to metformin and pioglitazone in obese, insulin-resistant women with polycystic ovarian syndrome. J Clin Endocrinol Metab 2005;90:1360-1365.
9. Cicek MN, Bala A, Celik C, Akyurek C. The comparison of clinical and hormonal parameters in PCOS patients treated with metformin and GnRH analogue. Arch Gynecol Obstet 2003;268:107-112.
10. Palomba S, Orio F, Jr, Nardo LG. Metformin administration versus laparoscopic ovarian diathermy in clomiphene citrate-resistant women with polycystic ovary syndrome: a prospective parallel randomized double-blind placebo-controlled trial. J Clin Endocrinol Metab 2004;89:4801-2809.
11. Emerson JD, Burdick E, Hoaglin DC, Mosteller F, Chalmers TC. An empirical study of the possible relation of treatment differences to quality scores in controlled randomized clinical trials. Control Clin Trials 1990;11:339-352.
12. Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions in The Cochrane Library. Chichester, UK: John Wiley & Sons; 2006. Issue 4 [updated September 2006].
13. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-188.
14. Begg CB, Mazumda M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088-1101.
15. Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-634.
16. Duval SJ, Tweedie RL. Trim and fill: A simple funnel plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000;56:276-284.
17. Stata Version 8.2 Intercooled, Stata Corporation, College Station, Texas, USA, 2005.
18. Azziz R, Ehrmann DA, Legro RS, Fereshetian AG, O’Keefe M, Ghazzi MN. Troglitazone decreases adrenal androgen levels in women with polycystic ovary syndrome. Fertil Steril 2003;79:932-937.
19. Azziz R, Ehrmann D, Legro RS, et al. Troglitazone improves ovulation and hirsutism in the polycystic ovary syndrome: a multicenter, double blind, placebo-controlled trial. J Clin Endocrinol Metab 2001;86:1626-1632.
20. Legro RS, Azziz R, Ehrmann D, Fereshetian AG, O’Keefe M, Ghazzi MN. Minimal response of circulating lipids in women with polycystic ovary syndrome to improvement in insulin sensitivity with troglitazone. J Clin Endocrinol Metab 2003;88:5137-5144.
21. Dunaif A, Scott D, Finegood D, Quintana B, Whitcomb R. The insulin-sensitizing agent troglitazone improves metabolic and reproductive abnormalities in the polycystic ovary syndrome. J Clin Endocrinol Metab 1996;81:3299-3306.
22. Ghazeeri G, Kutteh WH, Bryer-Ash M, Haas D, Ke RW. Effect of rosiglitazone on spontaneous and clomiphene citrate-induced ovulation in women with polycystic ovary syndrome. Fertil Steril 2003;79:562-566.
23. Shobokshi A, Shaarawy M. Correction of insulin resistance and hyperandrogenism in polycystic ovary syndrome by combined rosiglitazone and clomiphene citrate therapy. J Soc Gynecol Investig 2003;10:99-104.
24. Chou KH, von Eye Corleta H, Capp E, Spritzer PM. Clinical, metabolic and endocrine parameters in response to metformin in obese women with polycystic ovary syndrome: a randomized, double-blind and placebo-controlled trial. Horm Metab Res 2003;35:86-91.
25. Kelly CJ, Gordon D. The effect of metformin on hirsutism in polycystic ovary syndrome. Eur J Endocrinol 2002;147:217-221.
26. Baillargeon JP, Iuorno MJ, Jakubowicz DJ, Apridonidze T, He N, Nestler JE. Metformin therapy increases insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2004;89:242-249.
27. Sturrock ND, Lannon B, Fay TN. Metformin does not enhance ovulation induction in clomiphene resistant polycystic ovary syndrome in clinical practice. Br J Clin Pharmacol 2002;53:469-473.
28. Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activity and serum free testosterone after reduction of insulin secretion in polycystic ovary syndrome. N Engl J Med 1996;335:617-623.
29. Ganie MA, Khurana ML, Eunice M. Comparison of efficacy of spironolactone with metformin in the management of polycystic ovary syndrome: an open-labelled study. J Clin Endocrinol Metab 2004;89:2756-2762.
30. George SS, George K, Irwin C, et al. Sequential treatment of metformin and clomiphene citrate in clomiphene-resistant women with polycystic ovary syndrome: a randomized, controlled trial. Hum Reprod 2003;18:299-304.
31. Harborne L, Fleming R, Lyall H, Sattar N, Norman J. Metformin or antiandrogen in the treatment of hirsutism in polycystic ovary syndrome. J Clin Endocrinol Metab 2003;88:4116-4123.
32. Malkawi HY, Qublan HS, Hamaideh AH. Medical vs. surgical treatment for clomiphene citrate-resistant women with polycystic ovary syndrome. J Obstet Gynaecol 2003;23:289-293.
33. Morin-Papunen L, Rautio K, Ruokonen A, Hedberg P, Puukka M, Tapanainen JS. Metformin reduces serum C-reactive protein levels in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2003;88:4649-4654.
34. Morin-Papunen L, Vauhkonen I, Koivunen R, Ruokonen A, Martikainen H. Tapanainen Metformin versus ethinyl estradiol-cyproterone acetate in the treatment of nonobese women with polycystic ovary syndrome: a randomized study. J Clin Endocrinol Metab 2003;88:148-156.
35. Elter K, Imir G, Durmusoglu F. Clinical, endocrine and metabolic effects of metformin added to ethinyl estradiol-cyproterone acetate in non-obese women with polycystic ovarian syndrome: a randomized controlled study. Hum Reprod 2002;17:1729-1737.
36. Kocak M, Caliskan E, Simsir C, Haberal A. Metformin therapy improves ovulatory rates, cervical scores, and pregnancy rates in clomiphene citrate-resistant women with polycystic ovary syndrome. Fertil Steril 2002;77:101-106.
37. Yarali H, Yildiz BO, Demirol A, et al. Co-administration of metformin during rFSH treatment in patients with clomiphene citrate-resistant polycystic ovarian syndrome: a prospective randomized trial. Hum Reprod 2002;17:289-294.
38. Jakubowicz DJ, Seppala M, Jakubowicz S, et al. Insulin reduction with metformin increases luteal phase serum glycodelin and insulin-like growth factor-binding protein 1 concentrations and enhances uterine vascularity and blood flow in the polycystic ovary syndrome. J Clin Endocrinol Metab 2001;86:1126-1133.
39. Ng EH, Wat NM, Ho PC. Effects of metformin on ovulation rate, hormonal and metabolic profiles in women with clomiphene-resistant polycystic ovaries: a randomized, double-blinded placebo-controlled trial. Hum Reprod 2001;16:1625-1631.
40. Vandermolen DT, Ratts VS, Evans WS, Stovall DW, Kauma SW, Nestler JE. Metformin increases the ovulatory rate and pregnancy rate from clomiphene citrate in patients with polycystic ovary syndrome who are resistant to clomiphene citrate alone. Fertil Steril 2001;75:310-315.
41. Morin-Papunen LC, Vauhkonen I, Koivunen RM, Ruokonen A, Martikainen HK, Tapanainen JS. Endocrine and metabolic effects of metformin versus ethinyl estradiol-cyproterone acetate in obese women with polycystic ovary syndrome: a randomized study. J Clin Endocrinol Metab 2000;85:3161-3168.
42. Bang H, Jung S-H, George SL. Simulation-based multiple testing procedure and sample size calculation. J Biopharm Stat 2005;15:956-967.
43. Jung S-H, Bang H, Young SS. Sample size calculation for multiple testing in microarray data analysis. Biostatistics 2005;6:157-169.
44. Rothman K, Greenland S. Modern Epidemiology. 2nd ed. Philadelphia, Pa: Lippincott Williams and Wilkins;1998.
45. Colditz GA, Burdick E, Mosteller F. Heterogeneity in meta-analysis of data from epidemiologic studies: a commentary. Am J Epidemiol 1995;142:371-382.
46. Berlin JA. Invited commentary: benefits of heterogeneity in meta-analysis of data from epidemiologic studies. Am J Epidemiol 1995;142:383-387.
47. Young SS, Bang H. The file-drawer problem, revisited. Science 2004;306:1133-1134.
Rx package inserts: Redesigned with fewer errors in mind
The package insert (PI) is getting an FDA-mandated “makeover”—one that should make it faster and easier to locate the piece of information you need before writing a prescription.
PIs for newly approved drugs will now feature a Highlights section at the top, a Contents section to help you find what you’re looking for, and a Patient Counseling section. Also new: manufacturer and FDA contact information near the top of the PI to facilitate adverse drug reaction reporting (FIGURE).
These revisions—the first that the FDA has mandated for the PI in 25 years1—are designed to save time and reduce adverse drug events. Evidence suggests that physicians could save approximately 15 seconds each time they refer to the new PI, thereby increasing the extent to which prescribing information is consulted.2
Additionally, the FDA anticipates healthcare system savings of approximately $400 million in the next 10 years resulting from adverse drug events avoided,2 presumably because prescribers will be better informed. The new format should also help increase adverse drug reaction reporting by providing toll-free contact information.3
Lack of Rx information caused many mistakes
Changing the PI became an FDA priority in 2000, after the Institute of Medicine (IOM) published its report, “To err is human: Building a safer health system.”4 In this report, the IOM indicated that medication errors accounted for almost 98,000 deaths annually and that some of these deaths were a result of confusing medical information.4 A July 2006 IOM report estimated that there are at least 1.5 million preventable adverse drug events resulting from medication errors in the US each year.5
One study demonstrated that the most common cause of medication errors was a lack of drug information at the time the prescription was written, resulting in 22% of the errors.6 A subsequent report released by the IOM in September 2006 identified the importance of improving the FDA’s role in monitoring drug safety in the postmarketing stage and conveying the risks and benefits of medications to the public.7
To help address this growing list of concerns, the FDA issued new regulations for the PI format in January 2006.1 Among its goals: Prompt pharmaceutical companies to create PIs that read more like a drug information reference, and less like a sophisticated legal document.
As PIs are revised to comply with the new regulations, the information in them will be used to populate a new online drug resource for clinicians (and the public) known as DailyMed.9 This free, online health information clearinghouse, developed by the FDA and National library of Medicine, can be found at dailymed. nlm.nih.gov/dailymed/about.cfm. It’s intended to provide wide access to prescribing information for physicians at the point of care.9 DailyMed features approved prescribing information, adverse event reporting information, and links to clinical articles.3,9 Additionally, DailyMed provides access to MedlinePlus, an online medication tool for consumers written in lay language.9
The new FDA regulations apply to all New Drug Applications (NDAs), supplemental NDAs, and Biologics License Applications (BLAs) submitted on or after June 30, 2006.1 In addition, drugs approved in the 5 years prior to the effective date, and older drugs for which there is a major change in the prescribing information (ie, new indication), will need to adopt the revised format over the next several years.2,8 Medications that are exempt from these requirements include over-the-counter products, generic drugs, and existing drugs with minor labeling changes.
To get the word out to the healthcare community, the FDA and Institute for Safe Medication Practices kicked off a national educational campaign last fall by providing an overview of the new labeling format during a live teleconference.8 In addition, this PI information is being posted on the Web. (See “New PI makes its way online”3,9)
Immediate access to important information
The revised PI contains 3 new sections: Highlights, Contents, and Patient Counseling Information.10
Highlights. The Highlights section is the most significant change to the PI, and provides immediate access to the most important prescribing information.1,11,12 It’s displayed prominently at the top of the PI and is a concise half-page summary that includes references to detailed sections in the Full Prescribing Information.2,3
The Highlights section is analogous to a structured abstract in a published clinical trial (FIGURE).13 It contains recent major changes to the following sections: Boxed Warning, Indications and Usage, Dosage and Administration, Contraindications, and Warnings and Precautions.12 Additionally, the original FDA drug approval date of the product is listed, enabling physicians to easily identify new medications.2,3 Manufacturer and FDA contact information is also provided to encourage and facilitate adverse drug reaction reporting.12
Contents. Physicians will be able to locate information more quickly with the Contents section. This section, which is analogous to the table of contents of a book, references all sections and subsections in the Full Prescribing Information section.12
Patient counseling. The new format now requires a Patient Counseling Information section that places a greater emphasis on the importance of communication between physicians and patients. This section provides key points, including information on dosing instructions, laboratory tests, and drug safety. This section is designed to help physicians by providing efficient and concise talking points involving drug usage.1
New design bids laundry lists farewell
The overall structure of the PI has been revised to allow easier access to important information and to group related sections.3 Information physicians frequently consult and consider most critical (ie, Boxed Warnings, Indications and Usage, Dosage Forms and Strengths, Dosage and Administration) are located at the beginning.3,12
The Adverse Reactions section no longer contains a laundry list of adverse reactions and is divided into 2 parts: clinical trials experience (adverse events identified during clinical trials) and postmarketing experience (adverse events reported spontaneously by physicians and patients).8 Additionally, the Warnings and Precautions are now consolidated into 1 section instead of being listed separately.8
The new regulations also require that the PI text be formatted in a certain way. The FDA requires that certain elements be in bold, and that there be a minimum font size to enhance the communication of important information.2,3 (Previously, there was no minimum font size requirement.) Type in the PI can now be no smaller than 6 points and labeling on promotional materials and product samples can be no smaller than 8 points.
Manufacturers worry that details will be overlooked
Manufacturers have expressed concern over the addition of the Highlights section to the PI, noting that physicians might rely too heavily on the condensed information when making prescribing decisions.2,14 Manufacturers are also concerned that they will be forced to choose certain information for the Highlights section while excluding other valuable points, increasing their liability.2,14 The FDA, though, seems to have addressed this issue: The Highlights section includes a limitation statement emphasizing that physicians should still refer to the complete prescribing information.2,14
Another concern: The revisions to the PI come at a price, albeit a relatively small one. Updating the PI is expected to cost manufacturers approximately $6190 for each new product and $8700 for each existing product.2
Overall, though, the revisions to the PI should lead to positive change by providing physicians with access to up-to-date information in a clear, concise, and easy-to-read format. Though not a panacea for medication errors, the new PI should serve as an improved tool in the physician’s arsenal.
Correspondence
Jennifer A. Fass, PharmD, Nova Southeastern University, College of Pharmacy, 3200 South university Drive, Fort lauderdale, FL 33328; [email protected].
1. US Food and Drug Administration. The FDA Announces New Prescription Drug Information Format. Available at: www.fda.gov/fdac/features/2006/206_format.html. Accessed on May 17, 2007.
2. Final Rule: Requirements on Content and Format of labeling for Human Prescription Drug and Biological Products 21 C.F.R. Sect 201, 314, 601 (2006).
3. US Food and Drug Administration. Questions and Answers About the New Content and Format Requirements for Prescribing Information. Available at: www.fda.gov/cder/regulatory/physLabel/physLabel_qa.htm. Accessed on May 17, 2007.
4. Institute of Medicine.To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press; 2000. Available at: www.nap.edu/catalog/9728.html. Accessed on May 17, 2007.
5. Institute of Medicine. Report Brief. Preventing Medication Errors. July 2006. Available at: www.iom.edu/CMS/3809/22526/35939/35943.aspx. Accessed on May 17, 2007.
6. Leape LL, Bates DW, Cullen D, et al. Systems analysis of adverse drug events. JAMA 1995;274:35-43.
7. Institute of Medicine. Report Brief. The Future of Drug Safety. Action Steps for Congress. September 2006. Available at www.iom.edu/CMS/3793/26341/37329/37331.aspx. Accessed on May 17, 2007.
8. Institute for Safe Medication Practices. An Introduction to the Improved FDA Prescription Drug labeling. Available at: www.ismp.org/fda/default.asp. Accessed on May 17, 2007.
9. National Library of Medicine. DailyMed Current Medication Information. Available at: dailymed.nlm.nih.gov/dailymed/about.cfm. Accessed on May 17, 2007.
10. U.S. Food and Drug Administration. FDA’s New Prescribing Information. Available at: www.fda.gov/cder/regulatory/physLabel/default.htm. Accessed on May 17, 2007.
11. US Food and Drug Administration. FDA Announces Final Rule on the Requirements for Prescribing Information for Drug and Biological Products. Available at: www.fda.gov/cder/regulatory/physLabel/summary.htm. Accessed on May 17, 2007.
12. US Food and Drug Administration. Information for Healthcare Professionals on the FDA’s New Prescribing Information for Drugs. Available at: www.fda.gov/cder/regulatory/physLabel/physLabel_HCP.htm. Accessed on May 17, 2007.
13. Merck & Co Inc.Prescribing information for Januvia. Available at: www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf. Accessed on May 17, 2007.
14. Barlas S. Easing information overload: new FDA rules make package inserts more reader-friendly P&T 2006; 31:134.
The package insert (PI) is getting an FDA-mandated “makeover”—one that should make it faster and easier to locate the piece of information you need before writing a prescription.
PIs for newly approved drugs will now feature a Highlights section at the top, a Contents section to help you find what you’re looking for, and a Patient Counseling section. Also new: manufacturer and FDA contact information near the top of the PI to facilitate adverse drug reaction reporting (FIGURE).
These revisions—the first that the FDA has mandated for the PI in 25 years1—are designed to save time and reduce adverse drug events. Evidence suggests that physicians could save approximately 15 seconds each time they refer to the new PI, thereby increasing the extent to which prescribing information is consulted.2
Additionally, the FDA anticipates healthcare system savings of approximately $400 million in the next 10 years resulting from adverse drug events avoided,2 presumably because prescribers will be better informed. The new format should also help increase adverse drug reaction reporting by providing toll-free contact information.3
Lack of Rx information caused many mistakes
Changing the PI became an FDA priority in 2000, after the Institute of Medicine (IOM) published its report, “To err is human: Building a safer health system.”4 In this report, the IOM indicated that medication errors accounted for almost 98,000 deaths annually and that some of these deaths were a result of confusing medical information.4 A July 2006 IOM report estimated that there are at least 1.5 million preventable adverse drug events resulting from medication errors in the US each year.5
One study demonstrated that the most common cause of medication errors was a lack of drug information at the time the prescription was written, resulting in 22% of the errors.6 A subsequent report released by the IOM in September 2006 identified the importance of improving the FDA’s role in monitoring drug safety in the postmarketing stage and conveying the risks and benefits of medications to the public.7
To help address this growing list of concerns, the FDA issued new regulations for the PI format in January 2006.1 Among its goals: Prompt pharmaceutical companies to create PIs that read more like a drug information reference, and less like a sophisticated legal document.
As PIs are revised to comply with the new regulations, the information in them will be used to populate a new online drug resource for clinicians (and the public) known as DailyMed.9 This free, online health information clearinghouse, developed by the FDA and National library of Medicine, can be found at dailymed. nlm.nih.gov/dailymed/about.cfm. It’s intended to provide wide access to prescribing information for physicians at the point of care.9 DailyMed features approved prescribing information, adverse event reporting information, and links to clinical articles.3,9 Additionally, DailyMed provides access to MedlinePlus, an online medication tool for consumers written in lay language.9
The new FDA regulations apply to all New Drug Applications (NDAs), supplemental NDAs, and Biologics License Applications (BLAs) submitted on or after June 30, 2006.1 In addition, drugs approved in the 5 years prior to the effective date, and older drugs for which there is a major change in the prescribing information (ie, new indication), will need to adopt the revised format over the next several years.2,8 Medications that are exempt from these requirements include over-the-counter products, generic drugs, and existing drugs with minor labeling changes.
To get the word out to the healthcare community, the FDA and Institute for Safe Medication Practices kicked off a national educational campaign last fall by providing an overview of the new labeling format during a live teleconference.8 In addition, this PI information is being posted on the Web. (See “New PI makes its way online”3,9)
Immediate access to important information
The revised PI contains 3 new sections: Highlights, Contents, and Patient Counseling Information.10
Highlights. The Highlights section is the most significant change to the PI, and provides immediate access to the most important prescribing information.1,11,12 It’s displayed prominently at the top of the PI and is a concise half-page summary that includes references to detailed sections in the Full Prescribing Information.2,3
The Highlights section is analogous to a structured abstract in a published clinical trial (FIGURE).13 It contains recent major changes to the following sections: Boxed Warning, Indications and Usage, Dosage and Administration, Contraindications, and Warnings and Precautions.12 Additionally, the original FDA drug approval date of the product is listed, enabling physicians to easily identify new medications.2,3 Manufacturer and FDA contact information is also provided to encourage and facilitate adverse drug reaction reporting.12
Contents. Physicians will be able to locate information more quickly with the Contents section. This section, which is analogous to the table of contents of a book, references all sections and subsections in the Full Prescribing Information section.12
Patient counseling. The new format now requires a Patient Counseling Information section that places a greater emphasis on the importance of communication between physicians and patients. This section provides key points, including information on dosing instructions, laboratory tests, and drug safety. This section is designed to help physicians by providing efficient and concise talking points involving drug usage.1
New design bids laundry lists farewell
The overall structure of the PI has been revised to allow easier access to important information and to group related sections.3 Information physicians frequently consult and consider most critical (ie, Boxed Warnings, Indications and Usage, Dosage Forms and Strengths, Dosage and Administration) are located at the beginning.3,12
The Adverse Reactions section no longer contains a laundry list of adverse reactions and is divided into 2 parts: clinical trials experience (adverse events identified during clinical trials) and postmarketing experience (adverse events reported spontaneously by physicians and patients).8 Additionally, the Warnings and Precautions are now consolidated into 1 section instead of being listed separately.8
The new regulations also require that the PI text be formatted in a certain way. The FDA requires that certain elements be in bold, and that there be a minimum font size to enhance the communication of important information.2,3 (Previously, there was no minimum font size requirement.) Type in the PI can now be no smaller than 6 points and labeling on promotional materials and product samples can be no smaller than 8 points.
Manufacturers worry that details will be overlooked
Manufacturers have expressed concern over the addition of the Highlights section to the PI, noting that physicians might rely too heavily on the condensed information when making prescribing decisions.2,14 Manufacturers are also concerned that they will be forced to choose certain information for the Highlights section while excluding other valuable points, increasing their liability.2,14 The FDA, though, seems to have addressed this issue: The Highlights section includes a limitation statement emphasizing that physicians should still refer to the complete prescribing information.2,14
Another concern: The revisions to the PI come at a price, albeit a relatively small one. Updating the PI is expected to cost manufacturers approximately $6190 for each new product and $8700 for each existing product.2
Overall, though, the revisions to the PI should lead to positive change by providing physicians with access to up-to-date information in a clear, concise, and easy-to-read format. Though not a panacea for medication errors, the new PI should serve as an improved tool in the physician’s arsenal.
Correspondence
Jennifer A. Fass, PharmD, Nova Southeastern University, College of Pharmacy, 3200 South university Drive, Fort lauderdale, FL 33328; [email protected].
The package insert (PI) is getting an FDA-mandated “makeover”—one that should make it faster and easier to locate the piece of information you need before writing a prescription.
PIs for newly approved drugs will now feature a Highlights section at the top, a Contents section to help you find what you’re looking for, and a Patient Counseling section. Also new: manufacturer and FDA contact information near the top of the PI to facilitate adverse drug reaction reporting (FIGURE).
These revisions—the first that the FDA has mandated for the PI in 25 years1—are designed to save time and reduce adverse drug events. Evidence suggests that physicians could save approximately 15 seconds each time they refer to the new PI, thereby increasing the extent to which prescribing information is consulted.2
Additionally, the FDA anticipates healthcare system savings of approximately $400 million in the next 10 years resulting from adverse drug events avoided,2 presumably because prescribers will be better informed. The new format should also help increase adverse drug reaction reporting by providing toll-free contact information.3
Lack of Rx information caused many mistakes
Changing the PI became an FDA priority in 2000, after the Institute of Medicine (IOM) published its report, “To err is human: Building a safer health system.”4 In this report, the IOM indicated that medication errors accounted for almost 98,000 deaths annually and that some of these deaths were a result of confusing medical information.4 A July 2006 IOM report estimated that there are at least 1.5 million preventable adverse drug events resulting from medication errors in the US each year.5
One study demonstrated that the most common cause of medication errors was a lack of drug information at the time the prescription was written, resulting in 22% of the errors.6 A subsequent report released by the IOM in September 2006 identified the importance of improving the FDA’s role in monitoring drug safety in the postmarketing stage and conveying the risks and benefits of medications to the public.7
To help address this growing list of concerns, the FDA issued new regulations for the PI format in January 2006.1 Among its goals: Prompt pharmaceutical companies to create PIs that read more like a drug information reference, and less like a sophisticated legal document.
As PIs are revised to comply with the new regulations, the information in them will be used to populate a new online drug resource for clinicians (and the public) known as DailyMed.9 This free, online health information clearinghouse, developed by the FDA and National library of Medicine, can be found at dailymed. nlm.nih.gov/dailymed/about.cfm. It’s intended to provide wide access to prescribing information for physicians at the point of care.9 DailyMed features approved prescribing information, adverse event reporting information, and links to clinical articles.3,9 Additionally, DailyMed provides access to MedlinePlus, an online medication tool for consumers written in lay language.9
The new FDA regulations apply to all New Drug Applications (NDAs), supplemental NDAs, and Biologics License Applications (BLAs) submitted on or after June 30, 2006.1 In addition, drugs approved in the 5 years prior to the effective date, and older drugs for which there is a major change in the prescribing information (ie, new indication), will need to adopt the revised format over the next several years.2,8 Medications that are exempt from these requirements include over-the-counter products, generic drugs, and existing drugs with minor labeling changes.
To get the word out to the healthcare community, the FDA and Institute for Safe Medication Practices kicked off a national educational campaign last fall by providing an overview of the new labeling format during a live teleconference.8 In addition, this PI information is being posted on the Web. (See “New PI makes its way online”3,9)
Immediate access to important information
The revised PI contains 3 new sections: Highlights, Contents, and Patient Counseling Information.10
Highlights. The Highlights section is the most significant change to the PI, and provides immediate access to the most important prescribing information.1,11,12 It’s displayed prominently at the top of the PI and is a concise half-page summary that includes references to detailed sections in the Full Prescribing Information.2,3
The Highlights section is analogous to a structured abstract in a published clinical trial (FIGURE).13 It contains recent major changes to the following sections: Boxed Warning, Indications and Usage, Dosage and Administration, Contraindications, and Warnings and Precautions.12 Additionally, the original FDA drug approval date of the product is listed, enabling physicians to easily identify new medications.2,3 Manufacturer and FDA contact information is also provided to encourage and facilitate adverse drug reaction reporting.12
Contents. Physicians will be able to locate information more quickly with the Contents section. This section, which is analogous to the table of contents of a book, references all sections and subsections in the Full Prescribing Information section.12
Patient counseling. The new format now requires a Patient Counseling Information section that places a greater emphasis on the importance of communication between physicians and patients. This section provides key points, including information on dosing instructions, laboratory tests, and drug safety. This section is designed to help physicians by providing efficient and concise talking points involving drug usage.1
New design bids laundry lists farewell
The overall structure of the PI has been revised to allow easier access to important information and to group related sections.3 Information physicians frequently consult and consider most critical (ie, Boxed Warnings, Indications and Usage, Dosage Forms and Strengths, Dosage and Administration) are located at the beginning.3,12
The Adverse Reactions section no longer contains a laundry list of adverse reactions and is divided into 2 parts: clinical trials experience (adverse events identified during clinical trials) and postmarketing experience (adverse events reported spontaneously by physicians and patients).8 Additionally, the Warnings and Precautions are now consolidated into 1 section instead of being listed separately.8
The new regulations also require that the PI text be formatted in a certain way. The FDA requires that certain elements be in bold, and that there be a minimum font size to enhance the communication of important information.2,3 (Previously, there was no minimum font size requirement.) Type in the PI can now be no smaller than 6 points and labeling on promotional materials and product samples can be no smaller than 8 points.
Manufacturers worry that details will be overlooked
Manufacturers have expressed concern over the addition of the Highlights section to the PI, noting that physicians might rely too heavily on the condensed information when making prescribing decisions.2,14 Manufacturers are also concerned that they will be forced to choose certain information for the Highlights section while excluding other valuable points, increasing their liability.2,14 The FDA, though, seems to have addressed this issue: The Highlights section includes a limitation statement emphasizing that physicians should still refer to the complete prescribing information.2,14
Another concern: The revisions to the PI come at a price, albeit a relatively small one. Updating the PI is expected to cost manufacturers approximately $6190 for each new product and $8700 for each existing product.2
Overall, though, the revisions to the PI should lead to positive change by providing physicians with access to up-to-date information in a clear, concise, and easy-to-read format. Though not a panacea for medication errors, the new PI should serve as an improved tool in the physician’s arsenal.
Correspondence
Jennifer A. Fass, PharmD, Nova Southeastern University, College of Pharmacy, 3200 South university Drive, Fort lauderdale, FL 33328; [email protected].
1. US Food and Drug Administration. The FDA Announces New Prescription Drug Information Format. Available at: www.fda.gov/fdac/features/2006/206_format.html. Accessed on May 17, 2007.
2. Final Rule: Requirements on Content and Format of labeling for Human Prescription Drug and Biological Products 21 C.F.R. Sect 201, 314, 601 (2006).
3. US Food and Drug Administration. Questions and Answers About the New Content and Format Requirements for Prescribing Information. Available at: www.fda.gov/cder/regulatory/physLabel/physLabel_qa.htm. Accessed on May 17, 2007.
4. Institute of Medicine.To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press; 2000. Available at: www.nap.edu/catalog/9728.html. Accessed on May 17, 2007.
5. Institute of Medicine. Report Brief. Preventing Medication Errors. July 2006. Available at: www.iom.edu/CMS/3809/22526/35939/35943.aspx. Accessed on May 17, 2007.
6. Leape LL, Bates DW, Cullen D, et al. Systems analysis of adverse drug events. JAMA 1995;274:35-43.
7. Institute of Medicine. Report Brief. The Future of Drug Safety. Action Steps for Congress. September 2006. Available at www.iom.edu/CMS/3793/26341/37329/37331.aspx. Accessed on May 17, 2007.
8. Institute for Safe Medication Practices. An Introduction to the Improved FDA Prescription Drug labeling. Available at: www.ismp.org/fda/default.asp. Accessed on May 17, 2007.
9. National Library of Medicine. DailyMed Current Medication Information. Available at: dailymed.nlm.nih.gov/dailymed/about.cfm. Accessed on May 17, 2007.
10. U.S. Food and Drug Administration. FDA’s New Prescribing Information. Available at: www.fda.gov/cder/regulatory/physLabel/default.htm. Accessed on May 17, 2007.
11. US Food and Drug Administration. FDA Announces Final Rule on the Requirements for Prescribing Information for Drug and Biological Products. Available at: www.fda.gov/cder/regulatory/physLabel/summary.htm. Accessed on May 17, 2007.
12. US Food and Drug Administration. Information for Healthcare Professionals on the FDA’s New Prescribing Information for Drugs. Available at: www.fda.gov/cder/regulatory/physLabel/physLabel_HCP.htm. Accessed on May 17, 2007.
13. Merck & Co Inc.Prescribing information for Januvia. Available at: www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf. Accessed on May 17, 2007.
14. Barlas S. Easing information overload: new FDA rules make package inserts more reader-friendly P&T 2006; 31:134.
1. US Food and Drug Administration. The FDA Announces New Prescription Drug Information Format. Available at: www.fda.gov/fdac/features/2006/206_format.html. Accessed on May 17, 2007.
2. Final Rule: Requirements on Content and Format of labeling for Human Prescription Drug and Biological Products 21 C.F.R. Sect 201, 314, 601 (2006).
3. US Food and Drug Administration. Questions and Answers About the New Content and Format Requirements for Prescribing Information. Available at: www.fda.gov/cder/regulatory/physLabel/physLabel_qa.htm. Accessed on May 17, 2007.
4. Institute of Medicine.To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press; 2000. Available at: www.nap.edu/catalog/9728.html. Accessed on May 17, 2007.
5. Institute of Medicine. Report Brief. Preventing Medication Errors. July 2006. Available at: www.iom.edu/CMS/3809/22526/35939/35943.aspx. Accessed on May 17, 2007.
6. Leape LL, Bates DW, Cullen D, et al. Systems analysis of adverse drug events. JAMA 1995;274:35-43.
7. Institute of Medicine. Report Brief. The Future of Drug Safety. Action Steps for Congress. September 2006. Available at www.iom.edu/CMS/3793/26341/37329/37331.aspx. Accessed on May 17, 2007.
8. Institute for Safe Medication Practices. An Introduction to the Improved FDA Prescription Drug labeling. Available at: www.ismp.org/fda/default.asp. Accessed on May 17, 2007.
9. National Library of Medicine. DailyMed Current Medication Information. Available at: dailymed.nlm.nih.gov/dailymed/about.cfm. Accessed on May 17, 2007.
10. U.S. Food and Drug Administration. FDA’s New Prescribing Information. Available at: www.fda.gov/cder/regulatory/physLabel/default.htm. Accessed on May 17, 2007.
11. US Food and Drug Administration. FDA Announces Final Rule on the Requirements for Prescribing Information for Drug and Biological Products. Available at: www.fda.gov/cder/regulatory/physLabel/summary.htm. Accessed on May 17, 2007.
12. US Food and Drug Administration. Information for Healthcare Professionals on the FDA’s New Prescribing Information for Drugs. Available at: www.fda.gov/cder/regulatory/physLabel/physLabel_HCP.htm. Accessed on May 17, 2007.
13. Merck & Co Inc.Prescribing information for Januvia. Available at: www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf. Accessed on May 17, 2007.
14. Barlas S. Easing information overload: new FDA rules make package inserts more reader-friendly P&T 2006; 31:134.
What’s the best approach to renal artery stenosis?
GRADE A RECOMMENDATIONS
- Blood pressure measurements improve after angioplasty—particularly in patients with bilateral disease.
- There is no difference in kidney function outcomes when medical and angioplasty treatments are compared.
- Worse baseline kidney function is associated with increased mortality and worse blood pressure measurements after angioplasty.
GRADE B RECOMMENDATIONS
- Patients with bilateral stenosis have larger decreases in blood pressure readings after angioplasty than with medical treatment. No such difference was found between treatment groups in patients with unilateral disease.
- There is no difference in mortality and cardiovascular event rates when medical and angioplasty treatments are compared.
- There is no difference in blood pressure and kidney outcomes between angioplasty patients with or without stent placement.
GRADE C RECOMMENDATIONS
- The evidence doesn’t support one treatment approach over the other (angioplasty with stent vs aggressive medical therapy) for the general population with atherosclerotic renal artery stenosis.
- The evidence is inconclusive about relative adverse events or complications from angioplasty compared with medical treatment.
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
- What treatment strategy is most effective at reducing mortality?
- What patient characteristics are associated with increased mortality?
- What are the indications for stent placement?
The answers to these questions are summarized below and in the Comparative Effectiveness Review: Comparative Effectiveness of Management Strategies for Renal Artery Stenosis, funded and published by Agency for Healthcare Research and Quality (AHRQ). The review summarizes the current evidence concerning the effectiveness and safety of angioplasty with stent placement compared with medical therapy in the treatment of atherosclerotic renal artery stenosis.
The review team accepted the patient population of original authors, without clearly defining the level of renal artery stenosis. “The population of interest for this report is adults with atherosclerotic renal artery stenosis that is of sufficient severity to warrant aggressive management, either due to resistant hypertension, evidence of kidney damage, or the high likelihood of poor outcomes.” The team considered the following outcomes: blood pressure control, preservation of kidney function, incidence of flash pulmonary edema, and survival rates. Adverse events associated with therapies were also considered.
Review is commissioned to tackle controversy
The Comparative Effectiveness Review notes that 12% to 14% of new dialysis patients in the United States have atherosclerotic renal artery stenosis. It also points out that the utilization of renal artery angioplasty has increased considerably over the last few years, from 7660 cases in 1996 to 18,520 in 2000. The review was commissioned because of the controversy regarding optimal strategies for the evaluation and management of patients with atherosclerotic renal artery stenosis. The Comparative Effectiveness Review is strengthened by excellent summary tables, a review of treatment-associated harm, and an extensive discussion of methods.
In addition to this review of the literature, the government is sponsoring a more definitive trial to determine which patients with atherosclerotic renal artery stenosis would most benefit from angioplasty with stent placement, as opposed to continued aggressive medical treatment. The results of the Cardiovascular Outcomes in Renal Atherosclerotic Lesion (CORAL) Trial, a large, multicenter trial sponsored by the National Institutes of Health, will not be available until 2010.
A review of nearly 40 years of research
The Tufts–New England Medical Center Evidence-Based Practice Center was commissioned by AHRQ to conduct the review. A comprehensive search of the literature included Medline from 1966 to September 6, 2005. A technical expert panel held teleconferences to refine key questions and define parameters for review of the evidence. Researchers gave priority to meta-analyses and systemic reviews. Abstracts of research presented at conferences and symposiums were not considered adequate to be considered. There were 76 references.
Quality assessment of the literature was designated by a 3-category grading system (A—good, B—fair/moderate, and C—poor). For our purposes, the evidence rating is updated to comply with the SORT taxonomy.1
A search of the literature did not identify any other guidelines for comparison.
Source for this guideline
Balk E, Raman G, Chung M, et al. Comparative Effectiveness Review: Comparative Effectiveness of Management Strategies for Renal Artery Stenosis. (Prepared by Tufts-New England Medical Center Evidence-based Practice Center under Contract No. 290-02-0022). Rockville, Md: Agency for Healthcare Research and Quality; October 2006. Available at: effectivehealthcare.ahrq.gov/repFiles/RAS_Final.pdf. Accessed on April 11, 2007.
Correspondence
Keith B. Holten, MD, 825 Locust Street, Wilmington, Ohio 45177; [email protected].
Reference
1. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. J Fam Pract 2004;53:111-120.
GRADE A RECOMMENDATIONS
- Blood pressure measurements improve after angioplasty—particularly in patients with bilateral disease.
- There is no difference in kidney function outcomes when medical and angioplasty treatments are compared.
- Worse baseline kidney function is associated with increased mortality and worse blood pressure measurements after angioplasty.
GRADE B RECOMMENDATIONS
- Patients with bilateral stenosis have larger decreases in blood pressure readings after angioplasty than with medical treatment. No such difference was found between treatment groups in patients with unilateral disease.
- There is no difference in mortality and cardiovascular event rates when medical and angioplasty treatments are compared.
- There is no difference in blood pressure and kidney outcomes between angioplasty patients with or without stent placement.
GRADE C RECOMMENDATIONS
- The evidence doesn’t support one treatment approach over the other (angioplasty with stent vs aggressive medical therapy) for the general population with atherosclerotic renal artery stenosis.
- The evidence is inconclusive about relative adverse events or complications from angioplasty compared with medical treatment.
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
- What treatment strategy is most effective at reducing mortality?
- What patient characteristics are associated with increased mortality?
- What are the indications for stent placement?
The answers to these questions are summarized below and in the Comparative Effectiveness Review: Comparative Effectiveness of Management Strategies for Renal Artery Stenosis, funded and published by Agency for Healthcare Research and Quality (AHRQ). The review summarizes the current evidence concerning the effectiveness and safety of angioplasty with stent placement compared with medical therapy in the treatment of atherosclerotic renal artery stenosis.
The review team accepted the patient population of original authors, without clearly defining the level of renal artery stenosis. “The population of interest for this report is adults with atherosclerotic renal artery stenosis that is of sufficient severity to warrant aggressive management, either due to resistant hypertension, evidence of kidney damage, or the high likelihood of poor outcomes.” The team considered the following outcomes: blood pressure control, preservation of kidney function, incidence of flash pulmonary edema, and survival rates. Adverse events associated with therapies were also considered.
Review is commissioned to tackle controversy
The Comparative Effectiveness Review notes that 12% to 14% of new dialysis patients in the United States have atherosclerotic renal artery stenosis. It also points out that the utilization of renal artery angioplasty has increased considerably over the last few years, from 7660 cases in 1996 to 18,520 in 2000. The review was commissioned because of the controversy regarding optimal strategies for the evaluation and management of patients with atherosclerotic renal artery stenosis. The Comparative Effectiveness Review is strengthened by excellent summary tables, a review of treatment-associated harm, and an extensive discussion of methods.
In addition to this review of the literature, the government is sponsoring a more definitive trial to determine which patients with atherosclerotic renal artery stenosis would most benefit from angioplasty with stent placement, as opposed to continued aggressive medical treatment. The results of the Cardiovascular Outcomes in Renal Atherosclerotic Lesion (CORAL) Trial, a large, multicenter trial sponsored by the National Institutes of Health, will not be available until 2010.
A review of nearly 40 years of research
The Tufts–New England Medical Center Evidence-Based Practice Center was commissioned by AHRQ to conduct the review. A comprehensive search of the literature included Medline from 1966 to September 6, 2005. A technical expert panel held teleconferences to refine key questions and define parameters for review of the evidence. Researchers gave priority to meta-analyses and systemic reviews. Abstracts of research presented at conferences and symposiums were not considered adequate to be considered. There were 76 references.
Quality assessment of the literature was designated by a 3-category grading system (A—good, B—fair/moderate, and C—poor). For our purposes, the evidence rating is updated to comply with the SORT taxonomy.1
A search of the literature did not identify any other guidelines for comparison.
Source for this guideline
Balk E, Raman G, Chung M, et al. Comparative Effectiveness Review: Comparative Effectiveness of Management Strategies for Renal Artery Stenosis. (Prepared by Tufts-New England Medical Center Evidence-based Practice Center under Contract No. 290-02-0022). Rockville, Md: Agency for Healthcare Research and Quality; October 2006. Available at: effectivehealthcare.ahrq.gov/repFiles/RAS_Final.pdf. Accessed on April 11, 2007.
Correspondence
Keith B. Holten, MD, 825 Locust Street, Wilmington, Ohio 45177; [email protected].
GRADE A RECOMMENDATIONS
- Blood pressure measurements improve after angioplasty—particularly in patients with bilateral disease.
- There is no difference in kidney function outcomes when medical and angioplasty treatments are compared.
- Worse baseline kidney function is associated with increased mortality and worse blood pressure measurements after angioplasty.
GRADE B RECOMMENDATIONS
- Patients with bilateral stenosis have larger decreases in blood pressure readings after angioplasty than with medical treatment. No such difference was found between treatment groups in patients with unilateral disease.
- There is no difference in mortality and cardiovascular event rates when medical and angioplasty treatments are compared.
- There is no difference in blood pressure and kidney outcomes between angioplasty patients with or without stent placement.
GRADE C RECOMMENDATIONS
- The evidence doesn’t support one treatment approach over the other (angioplasty with stent vs aggressive medical therapy) for the general population with atherosclerotic renal artery stenosis.
- The evidence is inconclusive about relative adverse events or complications from angioplasty compared with medical treatment.
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
- What treatment strategy is most effective at reducing mortality?
- What patient characteristics are associated with increased mortality?
- What are the indications for stent placement?
The answers to these questions are summarized below and in the Comparative Effectiveness Review: Comparative Effectiveness of Management Strategies for Renal Artery Stenosis, funded and published by Agency for Healthcare Research and Quality (AHRQ). The review summarizes the current evidence concerning the effectiveness and safety of angioplasty with stent placement compared with medical therapy in the treatment of atherosclerotic renal artery stenosis.
The review team accepted the patient population of original authors, without clearly defining the level of renal artery stenosis. “The population of interest for this report is adults with atherosclerotic renal artery stenosis that is of sufficient severity to warrant aggressive management, either due to resistant hypertension, evidence of kidney damage, or the high likelihood of poor outcomes.” The team considered the following outcomes: blood pressure control, preservation of kidney function, incidence of flash pulmonary edema, and survival rates. Adverse events associated with therapies were also considered.
Review is commissioned to tackle controversy
The Comparative Effectiveness Review notes that 12% to 14% of new dialysis patients in the United States have atherosclerotic renal artery stenosis. It also points out that the utilization of renal artery angioplasty has increased considerably over the last few years, from 7660 cases in 1996 to 18,520 in 2000. The review was commissioned because of the controversy regarding optimal strategies for the evaluation and management of patients with atherosclerotic renal artery stenosis. The Comparative Effectiveness Review is strengthened by excellent summary tables, a review of treatment-associated harm, and an extensive discussion of methods.
In addition to this review of the literature, the government is sponsoring a more definitive trial to determine which patients with atherosclerotic renal artery stenosis would most benefit from angioplasty with stent placement, as opposed to continued aggressive medical treatment. The results of the Cardiovascular Outcomes in Renal Atherosclerotic Lesion (CORAL) Trial, a large, multicenter trial sponsored by the National Institutes of Health, will not be available until 2010.
A review of nearly 40 years of research
The Tufts–New England Medical Center Evidence-Based Practice Center was commissioned by AHRQ to conduct the review. A comprehensive search of the literature included Medline from 1966 to September 6, 2005. A technical expert panel held teleconferences to refine key questions and define parameters for review of the evidence. Researchers gave priority to meta-analyses and systemic reviews. Abstracts of research presented at conferences and symposiums were not considered adequate to be considered. There were 76 references.
Quality assessment of the literature was designated by a 3-category grading system (A—good, B—fair/moderate, and C—poor). For our purposes, the evidence rating is updated to comply with the SORT taxonomy.1
A search of the literature did not identify any other guidelines for comparison.
Source for this guideline
Balk E, Raman G, Chung M, et al. Comparative Effectiveness Review: Comparative Effectiveness of Management Strategies for Renal Artery Stenosis. (Prepared by Tufts-New England Medical Center Evidence-based Practice Center under Contract No. 290-02-0022). Rockville, Md: Agency for Healthcare Research and Quality; October 2006. Available at: effectivehealthcare.ahrq.gov/repFiles/RAS_Final.pdf. Accessed on April 11, 2007.
Correspondence
Keith B. Holten, MD, 825 Locust Street, Wilmington, Ohio 45177; [email protected].
Reference
1. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. J Fam Pract 2004;53:111-120.
Reference
1. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. J Fam Pract 2004;53:111-120.
Beyond shy: When to suspect social anxiety disorder
- Cognitive Behavioral Therapy (CBT) is an effective treatment for social anxiety disorder. (B)
- Medication also helps patients with social anxiety disorder lead more functional lives. (B)
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Janice L, 41, comes into her physician’s office complaining that she’s “feeling anxious all the time” at her job at a local bank. She tells him that she’s been treated for depression in the past, though she’s not currently taking any antidepressants. As her physician takes a more thorough history, he notices that her alcohol consumption seems a bit excessive. Her demeanor, which he had previously chalked up to as “shyness,” comes into focus. He begins to suspect that his patient is more than just “quiet and unassuming” and may, in fact, be suffering from social anxiety disorder.
To confirm his suspicions, he excuses himself to retrieve an article he’d saved on the topic—one that identifies a quick screening tool for social anxiety disorder.1 He then asks his patient to rate the following statements on a scale of 0 to 4, with 0 being “not at all” and 4 being “extremely present”:
- Fear of embarrassment causes me to avoid doing things or speaking to people.
- I avoid activities in which I am the center of attention.
- Being embarrassed or looking stupid are among my worst fears.
His suspicions are confirmed when she scores a 10—well above the 6 that is highly suggestive of social anxiety disorder.
A debilitating disorder that’s all too common
Social anxiety, also known as social phobia, is the most common anxiety disorder, and is the third most common psychiatric disorder after depression and alcohol dependence.2 The Epidemiological Catchment Area Study revealed that 2% to 4% of the sample suffered from social anxiety with a lifetime prevalence of 2.8%. Other studies have found that as many at 10% of the sample suffer from social anxiety when a more appropriate diagnostic interview is used.3-5 Similarly, Kessler et al conducted a study investigating the prevalence of DSM-IV disorders and concluded that 6.8% of the entire sample suffered from social anxiety disorder.6
The difference between social anxiety disorder and shyness in children is that social anxiety debilitates the child’s ability to grow and develop socially in an appropriate manner. While children with—and without—social anxiety disorder may be uncomfortable around unfamiliar adults, children with this disorder will also be uncomfortable in a peer setting with unfamiliar kids their own age. Children with social anxiety may express their discomfort through crying, tantrums, or freezing from the social situation. In order for the child to meet full criteria for social anxiety, the duration of the symptoms must span at least 6 months.17
Social anxiety disorder is characterized as a persistent and debilitating fear of social interaction where patients fear negative evaluations by others. As a result, these patients may have trouble building and maintaining social relationships, which can result in a particularly isolated and depressed lifestyle.7
There are 2 subtypes of social anxiety disorder:
- Generalized social anxiety is generally more severe and more generalized and therefore, more disabling to patients. The majority of patients seen by the medical community tend to exhibit this sub-type of the disorder.
- Nongeneralized anxiety (also known as specific or discrete social phobia) is the less common and usually includes a fear associated with 1 or a few specific situations.
Although nongeneralized anxiety may be less likely to cause severe impairment in the patient’s life, it still may lead to significant underachievement in school or work.8 Still, patients with public speaking–only social anxiety are more likely to recover spontaneously, while patients with generalized social anxiety rarely recover spontaneously from the disorder.
The 2 subtypes also differ in their origin. Generalized social anxiety—the focus of this article—is significantly more prevalent among relatives who also suffer from the disorder, while patients with nongeneralized social anxiety disorder do not necessarily have relatives with the condition.9
“Shyness” in childhood that’s often overlooked
Social anxiety is a lifelong disorder that may begin as early as childhood, but is often described as beginning at age 13. At this age, though, the social anxiety is often mistaken for extreme shyness and therefore goes untreated.10 (See “Distinguishing shyness from social anxiety in kids,”.)
Overlooking shyness in such a young patient is particularly problematic as the avoidance that characterizes the social anxiety disorder can result in a lost opportunity to acquire social skills that are needed to ease the transition from adolescence to adulthood. This relative loss of social skills often facilitates the development of social dysfunction that is characteristic of this illness.11 As time goes by, sufferers eventually become accustomed to their fears and create a way of life that accommodates them.
Social anxiety can interrupt education or job success, cause financial dependence, and impair relationships.10 (See “Fear of embarrassment hinders relationships and careers”.) Sufferers tend to miss out on important social events and activities in their lives,12 and they begin to accumulate comorbidities such as depression and substance abuse.13 In fact, while many cases of social anxiety are overlooked as shyness, others are misdiagnosed as depression.
Patients suffering from social anxiety tend to have more difficulty in dating situations because of their constant fear of participating in social interactions.31 In fact, a large study in France found a connection between social anxiety and marriage rates. Forty-three percent of individuals who reported symptoms of social anxiety were married, compared with 65% of those who reported no symptoms.7
Careers also suffer because of the patient’s constant fear of embarrassment. Patients who have social anxiety record more sick days than those without the disorder.32 In addition, socially anxious patients have reduced work productivity compared with healthy controls.33 As a result of their inability to perform adequately in their career, many patients may have to rely on social assistance. In fact, one study indicates that 22% of patients with social anxiety were on social assistance compared with 10% of a matched controlled group.32
Complicating matters further is the issue of substance abuse. The Epidemiological Catchment Area Study found that alcohol abuse was reported in 17% of social anxiety cases and drug abuse was reported in 13%.5 In the study conducted by Kessler et al, results indicated that 8.8% of individuals suffering from a substance abuse problem also suffered from comorbid social anxiety.6
The substance abuse evolves slowly,14 and tends to arise as an inappropriate coping mechanism because so many cases of social anxiety go untreated.15
Symptoms to watch for, questions to ask
The primary indicator of social anxiety is intense fear of social situations. A patient suffering from social anxiety fears that he or she will act in a way that will be humiliating when confronted with unfamiliar situations or people or by the possibility of being scrutinized by others.16 While many people with social anxiety realize that their fears are excessive or unreasonable, they are unable to overcome them.17
There are also a number of physical, cognitive, and behavioral symptoms that are associated with social anxiety. The physical symptoms may include rapid heart rate, trembling, shortness of breath, sweating, and abdominal pain. The cognitive symptoms include maladaptive thoughts and beliefs about social situations (ie, irrational thought processes), that increase the anxiety when in the situation. Finally, behavioral symptoms include phobic avoidance of the feared situation.18
There are many screening devices that you can use to identify patients with social anxiety disorder or to assess the severity of symptoms. Some examples include the Liebowitz Social Phobia Scale,19 the Social Phobia Inventory (SPIN),20 Fear of Negative Evaluation Scale,21 and the Social Avoidance and Distress Scale.22 These tools, however, can be a bit time consuming.
A more handy—though admittedly less comprehensive—screening device is the “mini SPIN” that was used by the physician in our opener. In a study of 7165 managed care patients, 89% of the cases meeting criteria for social anxiety disorder were detected (with a score of 6 or better) using this screening method.1
To review, you’ll need to ask patients to rate the following statements on a scale of 0 “not at all” to 4 “extremely present”:
- Fear of embarrassment causes me to avoid doing things or speaking to people.
- I avoid activities in which I am the center of attention.
- Being embarrassed or looking stupid are among my worst fears.
TABLE
Pharmacologic options for treating social anxiety disorder
| INITIAL DAILY DOSE (MG) | MAXIMUM DAILY DOSE (MG) | |
|---|---|---|
| SSRIs | ||
| Citalopram (Celexa) | 20 | 40–60 |
| Escitalopram (Cipralex) | 5–10 | 20 |
| Fluoxetine (Prozac) | 20 | 80 |
| Fluvoxamine (Luvox) | 50 | 300 |
| Paroxetine (Paxil) | 20 | 60 |
| Paroxetine CR (Paxil CR) | 25 | 62.5 |
| Sertraline (Zoloft) | 50 | 200 |
| MAOIs/RIMAs | ||
| Moclobemide | 300 | 600 |
| Phenelzine (Nardil) | 15 | 90 |
| Tricyclics | ||
| Clomipramine | 25 | 200 |
| Imipramine | 25 | 150 |
| Other antidepressants | ||
| Bupropion SR (Wellbutrin SR) | 100–150 | 300 |
| Bupropion XL (Wellbutrin XL) | 150 | 300 |
| Mirtazapine (Remeron) | 15 | 45 |
| Mirtazapine RD (Remeron RD) | 15 | 45 |
| Venlafaxine XR (Effexor XR) | 37.5–75 | 225 |
| Benzodiazepines | ||
| Alprazolam | 0.25 | 1.5–3.0 |
| Bromazepam | 6 | 30 |
| Clonazepam | .25 | 4 |
| Diazepam | 2.5 | 10 |
| Lorazepam | 0.5 | 3–4 |
| Anticonvulsants | ||
| Gabapentin (Neurontin) | 900 | 3600 |
| Lamotrigine (Lamictal) | 25 | 200 |
| Pregabalin (Lyrica) | 150 | 600 |
| Topiramate (Topamax) | 25 | 800 |
| Atypical antipsychotics | ||
| Olanzapine (Zyprexa) | 2.5 | 20 |
| Risperidone (Risperdal) | 0.5 | 6 |
| Quetiapine (Seroquel) | 50 | 800 |
| SSRI, selective serotonin reuptake inhibitor; MAOI, monoamine oxidase inhibitor; RIMA, reverse inhibitor of monoamine oxidase A. | ||
A score of 6 or higher should prompt you to further evaluate the patient using one of the screening devices listed earlier.
Treatments of choice: CBT and drug therapy
Although social anxiety most commonly spans a lifetime, studies indicate that treatment—typically cognitive behavioral therapy (CBT) with drug therapy—can help sufferers deal with their fears and function more efficiently in their everyday lives. The best effects in treating social anxiety, therefore, are in combining the different treatment strategies.14
Cognitive begavioral therapy
Heimberg and colleagues found that 75% of social anxiety patients who participated in a cognitive behavioral therapy group experienced improved function and saw a reduction in symptoms of social anxiety.23 Successful CBT seems to not only alleviate symptomatic distress, but improve the patients’ perceptions of their general quality of life.24 Including behavioral components such as reinforcement or conditioning in CBT appears to be effective in helping sufferers minimize their symptoms. In addition, cognitive restructuring (ie, changing a patient’s thought process) has also been shown to be a helpful treatment.23
Some of the basic elements of CBT include anxiety management skills (ie, breathing and relaxation techniques), social skills training (ie, maintaining conversation with the patient while monitoring the patient’s eye contact), and gradual exposure to the feared situation (ie, exposure to social situations).
Drug therapy
Studies have also demonstrated the effectiveness of a variety of medications (including Venlafaxine XR [Effexor XR], Paroxetine [Paxil], Paroxetine CR [Paxil CR], Sertraline [Zoloft], and Fluvoxamine [Luvox]) in managing social anxiety disorder.25-28 If you are caring for a patient with social anxiety disorder, you’ll want to start him on a selective serotonin reuptake inhibitor (SSRI) or serotoninnorepinephrine reuptake inhibitor (SNRI).
If this doesn’t achieve the desired results, the next step is a monoamine oxidase inhibitor, such as phenelzine (Nardil), or a reverse inhibitor of monoamine oxidase A, such as moclobemide. Additionally, some benzodiazepines and anticonvulsants (clonazepam and pregabalin [Lyrica]) may also be effective if the other options do not achieve the desired results. The TABLE outlines common medications used to treat social anxiety, as well as recommended dosages.29
When putting your patient on any of these medications, patient teaching will be important. You’ll need to advise the patient that common antidepressant side effects include, but are not limited to, nausea, diarrhea, sexual dysfunction (ie, delayed orgasm), and headaches. These effects, however, typically disappear by the second week of intake.15 If the patient is taking a benzodiazepine, you’ll need to warn him about the risk of psychomotor or cognitive impairment.
If the patient has a comorbid substance abuse problem, you and the patient will also need to adjust your expectations somewhat. That’s because patients with a substance abuse problem are likely to have a poorer response to some of these medications than patients without a substance abuse problem.30
ON THE WEB…
- The anxiety Disorders association of Canada/association Canadienne des Troubles des anxieux www.anxietycanada.ca
- The Social anxiety Network www.social-anxiety-network.com
- The Social Phobia and Social anxiety association www.socialphobia.org
IN PRINT…
- Dying of Embarrassment: Help for Social Anxiety & Phobia (Barbara Markway, C. Alec Pollard, and Teresa Flynn), 1992
- Painfully Shy: How to Overcome Social Anxiety and Reclaim your Life (Barbara markway and Gregory markway), 2003
- The Shyness and Social Anxiety Workbook: Proven Techniques for Overcoming your Fears (Martin M. Anthony and Richard P. Swinson), 2000
Though the time it takes to manage the condition is variable, patients with social anxiety disorder can improve their situation and go on to live more fulfilling and happy lives. The trick, really, is spotting the disorder early, rather than assuming your patient is simply the “quiet type.”
Correspondence
Martin A. Katzman, MD, FRCPC, START Clinic for Mood and Anxiety Disorders, 790 Bay St, Toronto, Ontario, Canada M5G 1N8 [email protected]
1. Connor KM, Kobak KA, Churchill LE, Katzelnick D, Davidson JR. Mini-Spin: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety 2001;14:137-140.
2. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12 month prevalence of DSm III–R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51:8-19.
3. Robins LN, Regier DA. Psychiatric Disorders in America: The Epidemiological Catchment Area Study. New york: Free Press; 1990.
4. Eaton WW, Weissman M. Panic and phobias. In: Robins E, Da Regier, eds. Psychiatric Disorders in America: The Epidemiological Catchment Area Study. New york: Free Press; 1991:155-179.
5. Scheier FR, Johnson J, Hornig CD, Liebowitz MR, Weissman MM. Social phobia: Comorbidity and morbidity in an epidemiological sample. Arch Gen Psychiatry 1992;49:282-288.
6. Kessler RC, Chiu WT, Demier O, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry 2005;62:617-627.
7. Lepine JP, Pelissolo A. Why take social anxiety disorder seriously? Depress Anxiety 2000;11:87-92.
8. Wittchen HU, Fuetsch M, Sonntag H, Muller N, Liebowitz M. Disability and quality of life in pure and comorbid social phobia–findings from a controlled study. Eur Psychiatry 1999;14:118-131.
9. Stein MB, Chavira DA. Subtypes of social phobia and comorbidity with depression and other anxiety disorders. J Affect Disord 1998;50:S11-S16.
10. Valente S. Social phobia. J Am Psychiatric Nurses Assoc 2002;8:67-75.
11. Beidel DC. Social phobia: etiology and evolution. J Clin Psychiatry 1998;59(Suppl 17):27-31.
12. Greist JH. The diagnosis of social phobia. Clin Psychiatry 1995;56(5):5-12.
13. Den Boer JA, Baldwin D, Bobes J, Katschnig H, Westenberg H, Wittchen HU. Social anxiety disorder—our current understanding. Intl J Psychiatry Clin Pract 1999;3:S3-S12.
14. Montgomery SA. Social phobia: Diagnosis, severity and implications for treatment. Eur Arch Psychiatry Clin Neurosci 1999;249:S1-S6.
15. Davidson JR, Potts NL, Richichi E, et al. Treatment of social phobia with Clonazepan and placebo. J Clin Pharmacol 1993;13:423-428.
16. Kasper S. Social phobia: The nature of the disorder. J Affect Disord 1998;50:S3-S9.
17. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text rev. Washington, DC: APA; 2000.
18. Ross J. Social phobia: The consumer’s perspective. J Clin Psychiatry 1993;54:S5-S9.
19. Bruce TJ, Saeed SA. Social anxiety disorder: A common under recognized mental disorder. Am Fam Physician 1999;60:2311-2322.
20. Connor KT, Davidson JRT, Churchill E, Sherwood A, Foa E, Weisler RH. Psychometric properties of the Social Phobia Inventory (SPIN). Br J Psychiatry 2000;176:379-386.
21. Watson D, Friend R. Measurement of social-evaluative anxiety. J Consulting Clin Psychol 1969;33:448-457.
22. Heimberg RG, Hope DA, Rapee RM, Bruch MA. The validity of the Social avoidance and Distress Scale and the Fear of Negative Evaluation Scale with social phobic patients. Behav Res Ther 1988;26:407-410.
23. Antony M, Swinson R. The Shyness and Social Anxiety Workbook: Proven Techniques for Overcoming Your Fears. Oakland, Calif: New Harbinger; 2000.
24. Safren SA, Heimberg R, Brown E, Holle C. Quality of life in social phobia. Depress Anxiety 1996/1997;4:126-133.
25. Heimberg RG, Liebowitz MR, Hope DA, et al. Cognitive behavioral group therapy vs phenelzine therapy for social phobia. Arch Gen Psychiatry 1998;55:1133-1141.
26. Van V, Den Boer JA, Westenberg HG. Psychopharmacological treatment of social phobia: A double blind placebo controlled study with Fluvoxamine. Psychopharmacol 1994;115:128-134.
27. Kelsey JE. Venlafaxine in social phobia. Psychopharmacol Bull 1995;31:767-771.
28. Allgulander C. Paroxetine in social anxiety disorder: A randomized placebo controlled study. Acta Psychiatr Scand 1999;100:193-198.
29. Muller JE, Koen L, Seedat S, Stein DJ. Social anxiety disorder: current treatment recommendations. CNS Drugs 2005;19:377-391.
30. Sareen L, Stein M. A review of the epidemiology and approaches to the treatment of social anxiety disorder. Drugs 2000;3:497-509.
31. Lader M. The clinical relevance of treating social phobia. J Affect Disord 1998;50:S29-S34.
32. Dupont RL, Rice DP, Miller LS, Shiraki SS, Rowland CR, Harwood HJ. Economic costs of anxiety disorders. Anxiety 1996;2:167-172.
33. Wittchen HU, Fuetsch M, Sonntag H, Muller N, Liebowitz M. Disability and quality of life in pure and comorbid social phobia: findings from a controlled study. Eur Psychiatry 1999;14:118-131.
- Cognitive Behavioral Therapy (CBT) is an effective treatment for social anxiety disorder. (B)
- Medication also helps patients with social anxiety disorder lead more functional lives. (B)
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Janice L, 41, comes into her physician’s office complaining that she’s “feeling anxious all the time” at her job at a local bank. She tells him that she’s been treated for depression in the past, though she’s not currently taking any antidepressants. As her physician takes a more thorough history, he notices that her alcohol consumption seems a bit excessive. Her demeanor, which he had previously chalked up to as “shyness,” comes into focus. He begins to suspect that his patient is more than just “quiet and unassuming” and may, in fact, be suffering from social anxiety disorder.
To confirm his suspicions, he excuses himself to retrieve an article he’d saved on the topic—one that identifies a quick screening tool for social anxiety disorder.1 He then asks his patient to rate the following statements on a scale of 0 to 4, with 0 being “not at all” and 4 being “extremely present”:
- Fear of embarrassment causes me to avoid doing things or speaking to people.
- I avoid activities in which I am the center of attention.
- Being embarrassed or looking stupid are among my worst fears.
His suspicions are confirmed when she scores a 10—well above the 6 that is highly suggestive of social anxiety disorder.
A debilitating disorder that’s all too common
Social anxiety, also known as social phobia, is the most common anxiety disorder, and is the third most common psychiatric disorder after depression and alcohol dependence.2 The Epidemiological Catchment Area Study revealed that 2% to 4% of the sample suffered from social anxiety with a lifetime prevalence of 2.8%. Other studies have found that as many at 10% of the sample suffer from social anxiety when a more appropriate diagnostic interview is used.3-5 Similarly, Kessler et al conducted a study investigating the prevalence of DSM-IV disorders and concluded that 6.8% of the entire sample suffered from social anxiety disorder.6
The difference between social anxiety disorder and shyness in children is that social anxiety debilitates the child’s ability to grow and develop socially in an appropriate manner. While children with—and without—social anxiety disorder may be uncomfortable around unfamiliar adults, children with this disorder will also be uncomfortable in a peer setting with unfamiliar kids their own age. Children with social anxiety may express their discomfort through crying, tantrums, or freezing from the social situation. In order for the child to meet full criteria for social anxiety, the duration of the symptoms must span at least 6 months.17
Social anxiety disorder is characterized as a persistent and debilitating fear of social interaction where patients fear negative evaluations by others. As a result, these patients may have trouble building and maintaining social relationships, which can result in a particularly isolated and depressed lifestyle.7
There are 2 subtypes of social anxiety disorder:
- Generalized social anxiety is generally more severe and more generalized and therefore, more disabling to patients. The majority of patients seen by the medical community tend to exhibit this sub-type of the disorder.
- Nongeneralized anxiety (also known as specific or discrete social phobia) is the less common and usually includes a fear associated with 1 or a few specific situations.
Although nongeneralized anxiety may be less likely to cause severe impairment in the patient’s life, it still may lead to significant underachievement in school or work.8 Still, patients with public speaking–only social anxiety are more likely to recover spontaneously, while patients with generalized social anxiety rarely recover spontaneously from the disorder.
The 2 subtypes also differ in their origin. Generalized social anxiety—the focus of this article—is significantly more prevalent among relatives who also suffer from the disorder, while patients with nongeneralized social anxiety disorder do not necessarily have relatives with the condition.9
“Shyness” in childhood that’s often overlooked
Social anxiety is a lifelong disorder that may begin as early as childhood, but is often described as beginning at age 13. At this age, though, the social anxiety is often mistaken for extreme shyness and therefore goes untreated.10 (See “Distinguishing shyness from social anxiety in kids,”.)
Overlooking shyness in such a young patient is particularly problematic as the avoidance that characterizes the social anxiety disorder can result in a lost opportunity to acquire social skills that are needed to ease the transition from adolescence to adulthood. This relative loss of social skills often facilitates the development of social dysfunction that is characteristic of this illness.11 As time goes by, sufferers eventually become accustomed to their fears and create a way of life that accommodates them.
Social anxiety can interrupt education or job success, cause financial dependence, and impair relationships.10 (See “Fear of embarrassment hinders relationships and careers”.) Sufferers tend to miss out on important social events and activities in their lives,12 and they begin to accumulate comorbidities such as depression and substance abuse.13 In fact, while many cases of social anxiety are overlooked as shyness, others are misdiagnosed as depression.
Patients suffering from social anxiety tend to have more difficulty in dating situations because of their constant fear of participating in social interactions.31 In fact, a large study in France found a connection between social anxiety and marriage rates. Forty-three percent of individuals who reported symptoms of social anxiety were married, compared with 65% of those who reported no symptoms.7
Careers also suffer because of the patient’s constant fear of embarrassment. Patients who have social anxiety record more sick days than those without the disorder.32 In addition, socially anxious patients have reduced work productivity compared with healthy controls.33 As a result of their inability to perform adequately in their career, many patients may have to rely on social assistance. In fact, one study indicates that 22% of patients with social anxiety were on social assistance compared with 10% of a matched controlled group.32
Complicating matters further is the issue of substance abuse. The Epidemiological Catchment Area Study found that alcohol abuse was reported in 17% of social anxiety cases and drug abuse was reported in 13%.5 In the study conducted by Kessler et al, results indicated that 8.8% of individuals suffering from a substance abuse problem also suffered from comorbid social anxiety.6
The substance abuse evolves slowly,14 and tends to arise as an inappropriate coping mechanism because so many cases of social anxiety go untreated.15
Symptoms to watch for, questions to ask
The primary indicator of social anxiety is intense fear of social situations. A patient suffering from social anxiety fears that he or she will act in a way that will be humiliating when confronted with unfamiliar situations or people or by the possibility of being scrutinized by others.16 While many people with social anxiety realize that their fears are excessive or unreasonable, they are unable to overcome them.17
There are also a number of physical, cognitive, and behavioral symptoms that are associated with social anxiety. The physical symptoms may include rapid heart rate, trembling, shortness of breath, sweating, and abdominal pain. The cognitive symptoms include maladaptive thoughts and beliefs about social situations (ie, irrational thought processes), that increase the anxiety when in the situation. Finally, behavioral symptoms include phobic avoidance of the feared situation.18
There are many screening devices that you can use to identify patients with social anxiety disorder or to assess the severity of symptoms. Some examples include the Liebowitz Social Phobia Scale,19 the Social Phobia Inventory (SPIN),20 Fear of Negative Evaluation Scale,21 and the Social Avoidance and Distress Scale.22 These tools, however, can be a bit time consuming.
A more handy—though admittedly less comprehensive—screening device is the “mini SPIN” that was used by the physician in our opener. In a study of 7165 managed care patients, 89% of the cases meeting criteria for social anxiety disorder were detected (with a score of 6 or better) using this screening method.1
To review, you’ll need to ask patients to rate the following statements on a scale of 0 “not at all” to 4 “extremely present”:
- Fear of embarrassment causes me to avoid doing things or speaking to people.
- I avoid activities in which I am the center of attention.
- Being embarrassed or looking stupid are among my worst fears.
TABLE
Pharmacologic options for treating social anxiety disorder
| INITIAL DAILY DOSE (MG) | MAXIMUM DAILY DOSE (MG) | |
|---|---|---|
| SSRIs | ||
| Citalopram (Celexa) | 20 | 40–60 |
| Escitalopram (Cipralex) | 5–10 | 20 |
| Fluoxetine (Prozac) | 20 | 80 |
| Fluvoxamine (Luvox) | 50 | 300 |
| Paroxetine (Paxil) | 20 | 60 |
| Paroxetine CR (Paxil CR) | 25 | 62.5 |
| Sertraline (Zoloft) | 50 | 200 |
| MAOIs/RIMAs | ||
| Moclobemide | 300 | 600 |
| Phenelzine (Nardil) | 15 | 90 |
| Tricyclics | ||
| Clomipramine | 25 | 200 |
| Imipramine | 25 | 150 |
| Other antidepressants | ||
| Bupropion SR (Wellbutrin SR) | 100–150 | 300 |
| Bupropion XL (Wellbutrin XL) | 150 | 300 |
| Mirtazapine (Remeron) | 15 | 45 |
| Mirtazapine RD (Remeron RD) | 15 | 45 |
| Venlafaxine XR (Effexor XR) | 37.5–75 | 225 |
| Benzodiazepines | ||
| Alprazolam | 0.25 | 1.5–3.0 |
| Bromazepam | 6 | 30 |
| Clonazepam | .25 | 4 |
| Diazepam | 2.5 | 10 |
| Lorazepam | 0.5 | 3–4 |
| Anticonvulsants | ||
| Gabapentin (Neurontin) | 900 | 3600 |
| Lamotrigine (Lamictal) | 25 | 200 |
| Pregabalin (Lyrica) | 150 | 600 |
| Topiramate (Topamax) | 25 | 800 |
| Atypical antipsychotics | ||
| Olanzapine (Zyprexa) | 2.5 | 20 |
| Risperidone (Risperdal) | 0.5 | 6 |
| Quetiapine (Seroquel) | 50 | 800 |
| SSRI, selective serotonin reuptake inhibitor; MAOI, monoamine oxidase inhibitor; RIMA, reverse inhibitor of monoamine oxidase A. | ||
A score of 6 or higher should prompt you to further evaluate the patient using one of the screening devices listed earlier.
Treatments of choice: CBT and drug therapy
Although social anxiety most commonly spans a lifetime, studies indicate that treatment—typically cognitive behavioral therapy (CBT) with drug therapy—can help sufferers deal with their fears and function more efficiently in their everyday lives. The best effects in treating social anxiety, therefore, are in combining the different treatment strategies.14
Cognitive begavioral therapy
Heimberg and colleagues found that 75% of social anxiety patients who participated in a cognitive behavioral therapy group experienced improved function and saw a reduction in symptoms of social anxiety.23 Successful CBT seems to not only alleviate symptomatic distress, but improve the patients’ perceptions of their general quality of life.24 Including behavioral components such as reinforcement or conditioning in CBT appears to be effective in helping sufferers minimize their symptoms. In addition, cognitive restructuring (ie, changing a patient’s thought process) has also been shown to be a helpful treatment.23
Some of the basic elements of CBT include anxiety management skills (ie, breathing and relaxation techniques), social skills training (ie, maintaining conversation with the patient while monitoring the patient’s eye contact), and gradual exposure to the feared situation (ie, exposure to social situations).
Drug therapy
Studies have also demonstrated the effectiveness of a variety of medications (including Venlafaxine XR [Effexor XR], Paroxetine [Paxil], Paroxetine CR [Paxil CR], Sertraline [Zoloft], and Fluvoxamine [Luvox]) in managing social anxiety disorder.25-28 If you are caring for a patient with social anxiety disorder, you’ll want to start him on a selective serotonin reuptake inhibitor (SSRI) or serotoninnorepinephrine reuptake inhibitor (SNRI).
If this doesn’t achieve the desired results, the next step is a monoamine oxidase inhibitor, such as phenelzine (Nardil), or a reverse inhibitor of monoamine oxidase A, such as moclobemide. Additionally, some benzodiazepines and anticonvulsants (clonazepam and pregabalin [Lyrica]) may also be effective if the other options do not achieve the desired results. The TABLE outlines common medications used to treat social anxiety, as well as recommended dosages.29
When putting your patient on any of these medications, patient teaching will be important. You’ll need to advise the patient that common antidepressant side effects include, but are not limited to, nausea, diarrhea, sexual dysfunction (ie, delayed orgasm), and headaches. These effects, however, typically disappear by the second week of intake.15 If the patient is taking a benzodiazepine, you’ll need to warn him about the risk of psychomotor or cognitive impairment.
If the patient has a comorbid substance abuse problem, you and the patient will also need to adjust your expectations somewhat. That’s because patients with a substance abuse problem are likely to have a poorer response to some of these medications than patients without a substance abuse problem.30
ON THE WEB…
- The anxiety Disorders association of Canada/association Canadienne des Troubles des anxieux www.anxietycanada.ca
- The Social anxiety Network www.social-anxiety-network.com
- The Social Phobia and Social anxiety association www.socialphobia.org
IN PRINT…
- Dying of Embarrassment: Help for Social Anxiety & Phobia (Barbara Markway, C. Alec Pollard, and Teresa Flynn), 1992
- Painfully Shy: How to Overcome Social Anxiety and Reclaim your Life (Barbara markway and Gregory markway), 2003
- The Shyness and Social Anxiety Workbook: Proven Techniques for Overcoming your Fears (Martin M. Anthony and Richard P. Swinson), 2000
Though the time it takes to manage the condition is variable, patients with social anxiety disorder can improve their situation and go on to live more fulfilling and happy lives. The trick, really, is spotting the disorder early, rather than assuming your patient is simply the “quiet type.”
Correspondence
Martin A. Katzman, MD, FRCPC, START Clinic for Mood and Anxiety Disorders, 790 Bay St, Toronto, Ontario, Canada M5G 1N8 [email protected]
- Cognitive Behavioral Therapy (CBT) is an effective treatment for social anxiety disorder. (B)
- Medication also helps patients with social anxiety disorder lead more functional lives. (B)
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Janice L, 41, comes into her physician’s office complaining that she’s “feeling anxious all the time” at her job at a local bank. She tells him that she’s been treated for depression in the past, though she’s not currently taking any antidepressants. As her physician takes a more thorough history, he notices that her alcohol consumption seems a bit excessive. Her demeanor, which he had previously chalked up to as “shyness,” comes into focus. He begins to suspect that his patient is more than just “quiet and unassuming” and may, in fact, be suffering from social anxiety disorder.
To confirm his suspicions, he excuses himself to retrieve an article he’d saved on the topic—one that identifies a quick screening tool for social anxiety disorder.1 He then asks his patient to rate the following statements on a scale of 0 to 4, with 0 being “not at all” and 4 being “extremely present”:
- Fear of embarrassment causes me to avoid doing things or speaking to people.
- I avoid activities in which I am the center of attention.
- Being embarrassed or looking stupid are among my worst fears.
His suspicions are confirmed when she scores a 10—well above the 6 that is highly suggestive of social anxiety disorder.
A debilitating disorder that’s all too common
Social anxiety, also known as social phobia, is the most common anxiety disorder, and is the third most common psychiatric disorder after depression and alcohol dependence.2 The Epidemiological Catchment Area Study revealed that 2% to 4% of the sample suffered from social anxiety with a lifetime prevalence of 2.8%. Other studies have found that as many at 10% of the sample suffer from social anxiety when a more appropriate diagnostic interview is used.3-5 Similarly, Kessler et al conducted a study investigating the prevalence of DSM-IV disorders and concluded that 6.8% of the entire sample suffered from social anxiety disorder.6
The difference between social anxiety disorder and shyness in children is that social anxiety debilitates the child’s ability to grow and develop socially in an appropriate manner. While children with—and without—social anxiety disorder may be uncomfortable around unfamiliar adults, children with this disorder will also be uncomfortable in a peer setting with unfamiliar kids their own age. Children with social anxiety may express their discomfort through crying, tantrums, or freezing from the social situation. In order for the child to meet full criteria for social anxiety, the duration of the symptoms must span at least 6 months.17
Social anxiety disorder is characterized as a persistent and debilitating fear of social interaction where patients fear negative evaluations by others. As a result, these patients may have trouble building and maintaining social relationships, which can result in a particularly isolated and depressed lifestyle.7
There are 2 subtypes of social anxiety disorder:
- Generalized social anxiety is generally more severe and more generalized and therefore, more disabling to patients. The majority of patients seen by the medical community tend to exhibit this sub-type of the disorder.
- Nongeneralized anxiety (also known as specific or discrete social phobia) is the less common and usually includes a fear associated with 1 or a few specific situations.
Although nongeneralized anxiety may be less likely to cause severe impairment in the patient’s life, it still may lead to significant underachievement in school or work.8 Still, patients with public speaking–only social anxiety are more likely to recover spontaneously, while patients with generalized social anxiety rarely recover spontaneously from the disorder.
The 2 subtypes also differ in their origin. Generalized social anxiety—the focus of this article—is significantly more prevalent among relatives who also suffer from the disorder, while patients with nongeneralized social anxiety disorder do not necessarily have relatives with the condition.9
“Shyness” in childhood that’s often overlooked
Social anxiety is a lifelong disorder that may begin as early as childhood, but is often described as beginning at age 13. At this age, though, the social anxiety is often mistaken for extreme shyness and therefore goes untreated.10 (See “Distinguishing shyness from social anxiety in kids,”.)
Overlooking shyness in such a young patient is particularly problematic as the avoidance that characterizes the social anxiety disorder can result in a lost opportunity to acquire social skills that are needed to ease the transition from adolescence to adulthood. This relative loss of social skills often facilitates the development of social dysfunction that is characteristic of this illness.11 As time goes by, sufferers eventually become accustomed to their fears and create a way of life that accommodates them.
Social anxiety can interrupt education or job success, cause financial dependence, and impair relationships.10 (See “Fear of embarrassment hinders relationships and careers”.) Sufferers tend to miss out on important social events and activities in their lives,12 and they begin to accumulate comorbidities such as depression and substance abuse.13 In fact, while many cases of social anxiety are overlooked as shyness, others are misdiagnosed as depression.
Patients suffering from social anxiety tend to have more difficulty in dating situations because of their constant fear of participating in social interactions.31 In fact, a large study in France found a connection between social anxiety and marriage rates. Forty-three percent of individuals who reported symptoms of social anxiety were married, compared with 65% of those who reported no symptoms.7
Careers also suffer because of the patient’s constant fear of embarrassment. Patients who have social anxiety record more sick days than those without the disorder.32 In addition, socially anxious patients have reduced work productivity compared with healthy controls.33 As a result of their inability to perform adequately in their career, many patients may have to rely on social assistance. In fact, one study indicates that 22% of patients with social anxiety were on social assistance compared with 10% of a matched controlled group.32
Complicating matters further is the issue of substance abuse. The Epidemiological Catchment Area Study found that alcohol abuse was reported in 17% of social anxiety cases and drug abuse was reported in 13%.5 In the study conducted by Kessler et al, results indicated that 8.8% of individuals suffering from a substance abuse problem also suffered from comorbid social anxiety.6
The substance abuse evolves slowly,14 and tends to arise as an inappropriate coping mechanism because so many cases of social anxiety go untreated.15
Symptoms to watch for, questions to ask
The primary indicator of social anxiety is intense fear of social situations. A patient suffering from social anxiety fears that he or she will act in a way that will be humiliating when confronted with unfamiliar situations or people or by the possibility of being scrutinized by others.16 While many people with social anxiety realize that their fears are excessive or unreasonable, they are unable to overcome them.17
There are also a number of physical, cognitive, and behavioral symptoms that are associated with social anxiety. The physical symptoms may include rapid heart rate, trembling, shortness of breath, sweating, and abdominal pain. The cognitive symptoms include maladaptive thoughts and beliefs about social situations (ie, irrational thought processes), that increase the anxiety when in the situation. Finally, behavioral symptoms include phobic avoidance of the feared situation.18
There are many screening devices that you can use to identify patients with social anxiety disorder or to assess the severity of symptoms. Some examples include the Liebowitz Social Phobia Scale,19 the Social Phobia Inventory (SPIN),20 Fear of Negative Evaluation Scale,21 and the Social Avoidance and Distress Scale.22 These tools, however, can be a bit time consuming.
A more handy—though admittedly less comprehensive—screening device is the “mini SPIN” that was used by the physician in our opener. In a study of 7165 managed care patients, 89% of the cases meeting criteria for social anxiety disorder were detected (with a score of 6 or better) using this screening method.1
To review, you’ll need to ask patients to rate the following statements on a scale of 0 “not at all” to 4 “extremely present”:
- Fear of embarrassment causes me to avoid doing things or speaking to people.
- I avoid activities in which I am the center of attention.
- Being embarrassed or looking stupid are among my worst fears.
TABLE
Pharmacologic options for treating social anxiety disorder
| INITIAL DAILY DOSE (MG) | MAXIMUM DAILY DOSE (MG) | |
|---|---|---|
| SSRIs | ||
| Citalopram (Celexa) | 20 | 40–60 |
| Escitalopram (Cipralex) | 5–10 | 20 |
| Fluoxetine (Prozac) | 20 | 80 |
| Fluvoxamine (Luvox) | 50 | 300 |
| Paroxetine (Paxil) | 20 | 60 |
| Paroxetine CR (Paxil CR) | 25 | 62.5 |
| Sertraline (Zoloft) | 50 | 200 |
| MAOIs/RIMAs | ||
| Moclobemide | 300 | 600 |
| Phenelzine (Nardil) | 15 | 90 |
| Tricyclics | ||
| Clomipramine | 25 | 200 |
| Imipramine | 25 | 150 |
| Other antidepressants | ||
| Bupropion SR (Wellbutrin SR) | 100–150 | 300 |
| Bupropion XL (Wellbutrin XL) | 150 | 300 |
| Mirtazapine (Remeron) | 15 | 45 |
| Mirtazapine RD (Remeron RD) | 15 | 45 |
| Venlafaxine XR (Effexor XR) | 37.5–75 | 225 |
| Benzodiazepines | ||
| Alprazolam | 0.25 | 1.5–3.0 |
| Bromazepam | 6 | 30 |
| Clonazepam | .25 | 4 |
| Diazepam | 2.5 | 10 |
| Lorazepam | 0.5 | 3–4 |
| Anticonvulsants | ||
| Gabapentin (Neurontin) | 900 | 3600 |
| Lamotrigine (Lamictal) | 25 | 200 |
| Pregabalin (Lyrica) | 150 | 600 |
| Topiramate (Topamax) | 25 | 800 |
| Atypical antipsychotics | ||
| Olanzapine (Zyprexa) | 2.5 | 20 |
| Risperidone (Risperdal) | 0.5 | 6 |
| Quetiapine (Seroquel) | 50 | 800 |
| SSRI, selective serotonin reuptake inhibitor; MAOI, monoamine oxidase inhibitor; RIMA, reverse inhibitor of monoamine oxidase A. | ||
A score of 6 or higher should prompt you to further evaluate the patient using one of the screening devices listed earlier.
Treatments of choice: CBT and drug therapy
Although social anxiety most commonly spans a lifetime, studies indicate that treatment—typically cognitive behavioral therapy (CBT) with drug therapy—can help sufferers deal with their fears and function more efficiently in their everyday lives. The best effects in treating social anxiety, therefore, are in combining the different treatment strategies.14
Cognitive begavioral therapy
Heimberg and colleagues found that 75% of social anxiety patients who participated in a cognitive behavioral therapy group experienced improved function and saw a reduction in symptoms of social anxiety.23 Successful CBT seems to not only alleviate symptomatic distress, but improve the patients’ perceptions of their general quality of life.24 Including behavioral components such as reinforcement or conditioning in CBT appears to be effective in helping sufferers minimize their symptoms. In addition, cognitive restructuring (ie, changing a patient’s thought process) has also been shown to be a helpful treatment.23
Some of the basic elements of CBT include anxiety management skills (ie, breathing and relaxation techniques), social skills training (ie, maintaining conversation with the patient while monitoring the patient’s eye contact), and gradual exposure to the feared situation (ie, exposure to social situations).
Drug therapy
Studies have also demonstrated the effectiveness of a variety of medications (including Venlafaxine XR [Effexor XR], Paroxetine [Paxil], Paroxetine CR [Paxil CR], Sertraline [Zoloft], and Fluvoxamine [Luvox]) in managing social anxiety disorder.25-28 If you are caring for a patient with social anxiety disorder, you’ll want to start him on a selective serotonin reuptake inhibitor (SSRI) or serotoninnorepinephrine reuptake inhibitor (SNRI).
If this doesn’t achieve the desired results, the next step is a monoamine oxidase inhibitor, such as phenelzine (Nardil), or a reverse inhibitor of monoamine oxidase A, such as moclobemide. Additionally, some benzodiazepines and anticonvulsants (clonazepam and pregabalin [Lyrica]) may also be effective if the other options do not achieve the desired results. The TABLE outlines common medications used to treat social anxiety, as well as recommended dosages.29
When putting your patient on any of these medications, patient teaching will be important. You’ll need to advise the patient that common antidepressant side effects include, but are not limited to, nausea, diarrhea, sexual dysfunction (ie, delayed orgasm), and headaches. These effects, however, typically disappear by the second week of intake.15 If the patient is taking a benzodiazepine, you’ll need to warn him about the risk of psychomotor or cognitive impairment.
If the patient has a comorbid substance abuse problem, you and the patient will also need to adjust your expectations somewhat. That’s because patients with a substance abuse problem are likely to have a poorer response to some of these medications than patients without a substance abuse problem.30
ON THE WEB…
- The anxiety Disorders association of Canada/association Canadienne des Troubles des anxieux www.anxietycanada.ca
- The Social anxiety Network www.social-anxiety-network.com
- The Social Phobia and Social anxiety association www.socialphobia.org
IN PRINT…
- Dying of Embarrassment: Help for Social Anxiety & Phobia (Barbara Markway, C. Alec Pollard, and Teresa Flynn), 1992
- Painfully Shy: How to Overcome Social Anxiety and Reclaim your Life (Barbara markway and Gregory markway), 2003
- The Shyness and Social Anxiety Workbook: Proven Techniques for Overcoming your Fears (Martin M. Anthony and Richard P. Swinson), 2000
Though the time it takes to manage the condition is variable, patients with social anxiety disorder can improve their situation and go on to live more fulfilling and happy lives. The trick, really, is spotting the disorder early, rather than assuming your patient is simply the “quiet type.”
Correspondence
Martin A. Katzman, MD, FRCPC, START Clinic for Mood and Anxiety Disorders, 790 Bay St, Toronto, Ontario, Canada M5G 1N8 [email protected]
1. Connor KM, Kobak KA, Churchill LE, Katzelnick D, Davidson JR. Mini-Spin: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety 2001;14:137-140.
2. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12 month prevalence of DSm III–R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51:8-19.
3. Robins LN, Regier DA. Psychiatric Disorders in America: The Epidemiological Catchment Area Study. New york: Free Press; 1990.
4. Eaton WW, Weissman M. Panic and phobias. In: Robins E, Da Regier, eds. Psychiatric Disorders in America: The Epidemiological Catchment Area Study. New york: Free Press; 1991:155-179.
5. Scheier FR, Johnson J, Hornig CD, Liebowitz MR, Weissman MM. Social phobia: Comorbidity and morbidity in an epidemiological sample. Arch Gen Psychiatry 1992;49:282-288.
6. Kessler RC, Chiu WT, Demier O, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry 2005;62:617-627.
7. Lepine JP, Pelissolo A. Why take social anxiety disorder seriously? Depress Anxiety 2000;11:87-92.
8. Wittchen HU, Fuetsch M, Sonntag H, Muller N, Liebowitz M. Disability and quality of life in pure and comorbid social phobia–findings from a controlled study. Eur Psychiatry 1999;14:118-131.
9. Stein MB, Chavira DA. Subtypes of social phobia and comorbidity with depression and other anxiety disorders. J Affect Disord 1998;50:S11-S16.
10. Valente S. Social phobia. J Am Psychiatric Nurses Assoc 2002;8:67-75.
11. Beidel DC. Social phobia: etiology and evolution. J Clin Psychiatry 1998;59(Suppl 17):27-31.
12. Greist JH. The diagnosis of social phobia. Clin Psychiatry 1995;56(5):5-12.
13. Den Boer JA, Baldwin D, Bobes J, Katschnig H, Westenberg H, Wittchen HU. Social anxiety disorder—our current understanding. Intl J Psychiatry Clin Pract 1999;3:S3-S12.
14. Montgomery SA. Social phobia: Diagnosis, severity and implications for treatment. Eur Arch Psychiatry Clin Neurosci 1999;249:S1-S6.
15. Davidson JR, Potts NL, Richichi E, et al. Treatment of social phobia with Clonazepan and placebo. J Clin Pharmacol 1993;13:423-428.
16. Kasper S. Social phobia: The nature of the disorder. J Affect Disord 1998;50:S3-S9.
17. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text rev. Washington, DC: APA; 2000.
18. Ross J. Social phobia: The consumer’s perspective. J Clin Psychiatry 1993;54:S5-S9.
19. Bruce TJ, Saeed SA. Social anxiety disorder: A common under recognized mental disorder. Am Fam Physician 1999;60:2311-2322.
20. Connor KT, Davidson JRT, Churchill E, Sherwood A, Foa E, Weisler RH. Psychometric properties of the Social Phobia Inventory (SPIN). Br J Psychiatry 2000;176:379-386.
21. Watson D, Friend R. Measurement of social-evaluative anxiety. J Consulting Clin Psychol 1969;33:448-457.
22. Heimberg RG, Hope DA, Rapee RM, Bruch MA. The validity of the Social avoidance and Distress Scale and the Fear of Negative Evaluation Scale with social phobic patients. Behav Res Ther 1988;26:407-410.
23. Antony M, Swinson R. The Shyness and Social Anxiety Workbook: Proven Techniques for Overcoming Your Fears. Oakland, Calif: New Harbinger; 2000.
24. Safren SA, Heimberg R, Brown E, Holle C. Quality of life in social phobia. Depress Anxiety 1996/1997;4:126-133.
25. Heimberg RG, Liebowitz MR, Hope DA, et al. Cognitive behavioral group therapy vs phenelzine therapy for social phobia. Arch Gen Psychiatry 1998;55:1133-1141.
26. Van V, Den Boer JA, Westenberg HG. Psychopharmacological treatment of social phobia: A double blind placebo controlled study with Fluvoxamine. Psychopharmacol 1994;115:128-134.
27. Kelsey JE. Venlafaxine in social phobia. Psychopharmacol Bull 1995;31:767-771.
28. Allgulander C. Paroxetine in social anxiety disorder: A randomized placebo controlled study. Acta Psychiatr Scand 1999;100:193-198.
29. Muller JE, Koen L, Seedat S, Stein DJ. Social anxiety disorder: current treatment recommendations. CNS Drugs 2005;19:377-391.
30. Sareen L, Stein M. A review of the epidemiology and approaches to the treatment of social anxiety disorder. Drugs 2000;3:497-509.
31. Lader M. The clinical relevance of treating social phobia. J Affect Disord 1998;50:S29-S34.
32. Dupont RL, Rice DP, Miller LS, Shiraki SS, Rowland CR, Harwood HJ. Economic costs of anxiety disorders. Anxiety 1996;2:167-172.
33. Wittchen HU, Fuetsch M, Sonntag H, Muller N, Liebowitz M. Disability and quality of life in pure and comorbid social phobia: findings from a controlled study. Eur Psychiatry 1999;14:118-131.
1. Connor KM, Kobak KA, Churchill LE, Katzelnick D, Davidson JR. Mini-Spin: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety 2001;14:137-140.
2. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12 month prevalence of DSm III–R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51:8-19.
3. Robins LN, Regier DA. Psychiatric Disorders in America: The Epidemiological Catchment Area Study. New york: Free Press; 1990.
4. Eaton WW, Weissman M. Panic and phobias. In: Robins E, Da Regier, eds. Psychiatric Disorders in America: The Epidemiological Catchment Area Study. New york: Free Press; 1991:155-179.
5. Scheier FR, Johnson J, Hornig CD, Liebowitz MR, Weissman MM. Social phobia: Comorbidity and morbidity in an epidemiological sample. Arch Gen Psychiatry 1992;49:282-288.
6. Kessler RC, Chiu WT, Demier O, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry 2005;62:617-627.
7. Lepine JP, Pelissolo A. Why take social anxiety disorder seriously? Depress Anxiety 2000;11:87-92.
8. Wittchen HU, Fuetsch M, Sonntag H, Muller N, Liebowitz M. Disability and quality of life in pure and comorbid social phobia–findings from a controlled study. Eur Psychiatry 1999;14:118-131.
9. Stein MB, Chavira DA. Subtypes of social phobia and comorbidity with depression and other anxiety disorders. J Affect Disord 1998;50:S11-S16.
10. Valente S. Social phobia. J Am Psychiatric Nurses Assoc 2002;8:67-75.
11. Beidel DC. Social phobia: etiology and evolution. J Clin Psychiatry 1998;59(Suppl 17):27-31.
12. Greist JH. The diagnosis of social phobia. Clin Psychiatry 1995;56(5):5-12.
13. Den Boer JA, Baldwin D, Bobes J, Katschnig H, Westenberg H, Wittchen HU. Social anxiety disorder—our current understanding. Intl J Psychiatry Clin Pract 1999;3:S3-S12.
14. Montgomery SA. Social phobia: Diagnosis, severity and implications for treatment. Eur Arch Psychiatry Clin Neurosci 1999;249:S1-S6.
15. Davidson JR, Potts NL, Richichi E, et al. Treatment of social phobia with Clonazepan and placebo. J Clin Pharmacol 1993;13:423-428.
16. Kasper S. Social phobia: The nature of the disorder. J Affect Disord 1998;50:S3-S9.
17. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text rev. Washington, DC: APA; 2000.
18. Ross J. Social phobia: The consumer’s perspective. J Clin Psychiatry 1993;54:S5-S9.
19. Bruce TJ, Saeed SA. Social anxiety disorder: A common under recognized mental disorder. Am Fam Physician 1999;60:2311-2322.
20. Connor KT, Davidson JRT, Churchill E, Sherwood A, Foa E, Weisler RH. Psychometric properties of the Social Phobia Inventory (SPIN). Br J Psychiatry 2000;176:379-386.
21. Watson D, Friend R. Measurement of social-evaluative anxiety. J Consulting Clin Psychol 1969;33:448-457.
22. Heimberg RG, Hope DA, Rapee RM, Bruch MA. The validity of the Social avoidance and Distress Scale and the Fear of Negative Evaluation Scale with social phobic patients. Behav Res Ther 1988;26:407-410.
23. Antony M, Swinson R. The Shyness and Social Anxiety Workbook: Proven Techniques for Overcoming Your Fears. Oakland, Calif: New Harbinger; 2000.
24. Safren SA, Heimberg R, Brown E, Holle C. Quality of life in social phobia. Depress Anxiety 1996/1997;4:126-133.
25. Heimberg RG, Liebowitz MR, Hope DA, et al. Cognitive behavioral group therapy vs phenelzine therapy for social phobia. Arch Gen Psychiatry 1998;55:1133-1141.
26. Van V, Den Boer JA, Westenberg HG. Psychopharmacological treatment of social phobia: A double blind placebo controlled study with Fluvoxamine. Psychopharmacol 1994;115:128-134.
27. Kelsey JE. Venlafaxine in social phobia. Psychopharmacol Bull 1995;31:767-771.
28. Allgulander C. Paroxetine in social anxiety disorder: A randomized placebo controlled study. Acta Psychiatr Scand 1999;100:193-198.
29. Muller JE, Koen L, Seedat S, Stein DJ. Social anxiety disorder: current treatment recommendations. CNS Drugs 2005;19:377-391.
30. Sareen L, Stein M. A review of the epidemiology and approaches to the treatment of social anxiety disorder. Drugs 2000;3:497-509.
31. Lader M. The clinical relevance of treating social phobia. J Affect Disord 1998;50:S29-S34.
32. Dupont RL, Rice DP, Miller LS, Shiraki SS, Rowland CR, Harwood HJ. Economic costs of anxiety disorders. Anxiety 1996;2:167-172.
33. Wittchen HU, Fuetsch M, Sonntag H, Muller N, Liebowitz M. Disability and quality of life in pure and comorbid social phobia: findings from a controlled study. Eur Psychiatry 1999;14:118-131.
Calcaneal apophysitis: Simple diagnosis, simpler treatment
- The true origin of the heel pain of calcaneal apophysitis is a stress microfracture (invisible on x-ray) due to chronic repetitive microtrauma—it’s an overuse syndrome that resolves without surgery in nearly all cases. (C)
- Most patients experience pain relief and can resume full activities while using a simple in-shoe wedge-shaped orthotic. (C)
- The most distinguishing feature on physical exam is the exquisite heel pain produced by lateral and medial compression (“squeezing”) of the heel. (C)
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Two things about calcaneal “apophysitis” are a bit misleading. The first is its name. Although this common cause of heel pain in adolescents and teenagers was once considered a true osteochondritis, we now know that it’s actually a mechanical overuse pain syndrome with a self-limited, benign prognosis.1-3 The second area of confusion is what you’ll see on x-ray: an increased density and irregular fragmentation that was once viewed with suspicion, but is actually a normal pattern of ossification for this particular apophysis.
Don’t let the x-ray fool you
Primary care physicians can properly manage this common pain condition, given an understanding of the features, natural history, and treatment principles presented here.
Orthopedic referral is indicated for only a few recalcitrant cases.
Shoes aren’t to blame, but activity level is
Adolescents with calcaneal apophysitis—also known as Sever’s disease—will typically come into the office complaining of pain, often in both heels, particularly with mechanical activities such as running, jumping, and long-distance walking. Patients may walk on tiptoe to avoid the pain.4
The condition is common in both boys and girls, although personal experience indicates it’s more common in boys. The typical age of the patient is 8 to 15 years. The condition is most commonly seen in patients who are engaged in athletic endeavors,5,6 including soccer, basketball, and gymnastics,7,8 though no specific athletic endeavor has been directly implicated in the pathogenesis. Likewise, no specific foot structure or type of shoe wear has been directly related to the symptomatology.
An otherwise healthy boy, age 12, walks into your office—on tiptoe. His problem is pain in both heels, especially when running. It’s his first season on his school track team, and he says he’s been practicing hard for the 50-yard dash, “my best event.” his parents express to you their concern about possible sports-related injuries or underlying disease, and their son’s distress about the possibilty of “letting down the team” if he quits. You find no swelling, no skin changes, no erythema, and no other local abnormalities. Symptoms of marked pain are produced by medial and lateral compression (squeezing) of the heel at the site where the calcaneal apophysis attaches to the main body of the os calcis. There is no pain on plantar, posterior, or retrocalcaneal pressure, or adjacent to the Achilles tendon.
Exquisite heel pain produced by medial and lateral compression of the heel is the most distinguishing feature of calcaneal apophysitis
Is this x-ray normal? You order a lateral x-ray of the calcaneus to exclude other pathology. You observe a pattern of increased density and apparent irregular fragmentation on the x-ray. The radiologist reports no abnormal findings. The above x-ray typifies calcaneal apophysitis, an overuse syndrome often seen in children 8 to 15 years of age. The “dense” area is actually a secondary ossification center of the calcaneus, not an indication of pathology.
The ossification of the calcaneus is different from that of the tarsal bones, which are each ossified from a single center. In the case of the calcaneus, a secondary center of ossification typically appears in girls by age 6, and in boys by age 8.14,15 During adolescence, a C-shaped cartilage develops between the metaphyseal bone of the body of the calcaneus and the secondary center (or centers) of ossification. Then, at around age 10 or 11, a more superior tertiary ossification center appears in the apophysis of the calcaneus.
As the calcaneal apophysis progressively ossifies, it presents as a very dense radiographic pattern in an adolescent. For years, this was thought to represent a form of osteochondritis.16 In fact, this is a normal pattern of ossification for this particular apophysis.17-22
What do you tell the patient and parents? You advise an in-shoe orthotic, no limits on physical activity, and no surgery. You explain that the pain is due to recurrent impact (overuse), and that the orthotic will “unload” the heel and permit symtoms to resolve, typically within 60 days. If asked about discomfort, you may advise anti-inflammatories and ice/heat.
Patients typically have no swelling, skin changes, erythema, or other local abnormalities.8 The most characteristic distinguishing feature on physical examination is exquisite pain produced on medial and lateral compression (“squeezing”) of the heel at the site where the calcaneal apophysis attaches to the main body of the os calcis. The pain is not on plantar pressure (as you would see with plantar fasciitis), or posterior, retrocalcaneal, or adjacent to the Achilles tendon (as you would see on Achilles tendinitis), but on medial and lateral compression.3
I’ve noticed a number of trends over the years while caring for patients with calcaneal apophysitis. My chart review of the 227 patients I cared for between 1971 and 1997 revealed the following:
- 60% (137) of patients had bilateral involvement.
- 78% of the patients were male. The reason for the male preponderance remains unclear.
- All but 3 of the 364 feet obtained eventual complete symptom resolution with the prescribed sponge-leather heel orthotic.
- Symptoms typically resolved within 60 days.
- The 3 cases that were recalcitrant to orthotic treatment required an equinus-type cast for 4 to 6 weeks. Those patients treated with a cast also had resolution of their symptoms.
- Roughly 30% of the cases encountered a recurrence of symptoms with similar resolution with the previously described retreatment. Recurrences were unrelated to gender.
- No case ever required any other treatment type beyond the orthotic or cast.—Dennis Weiner, MD
Researchers found microfractures. Magnetic resonance imaging (MRI) evidence suggests that the true pathogenesis of calcaneal apophysitis is a stress microfracture related to chronic repetitive microtrauma.9 In addition, MRI evidence suggests that the location of the stress microfractures is in the metaphysis of the body of the calcaneus adjacent to—but not directly involving—the apophysis.1,7 This more recent evidence replaces the historical hypotheses that the condition is primarily an inflammatory process. As a consequence of the microtrauma, however, it’s possible that an inflammatory process may occur secondarily.
Should you order x-rays? X-rays are not essential to the diagnosis, though they may be used to rule out other conditions, such as fracture, infection, or a bone cyst. Keep in mind, though, that patients with calcaneal pain will have a normal x-ray.7 What is normal, however, is another matter, and has been the subject of confusion in the past.
Pain stops in a few weeks
Usually, the symptoms of calcaneal apophysitis resolve fairly quickly, and with relatively simple treatment. (The symptoms also disappear as the child gets older and the calcaneal apophysis amalgamates with the main body of the calcaneus.)
Physiotherapy, forced ankle dorsiflexion stretching, gastrocsoleus stretching, ice, heat, heel cups and pads,1,10-13 and anti-inflammatories have all been used in the management of the condition.3,8 Clinicians have also historically restricted the patients’ activity, but this is unnecessary.

An in-shoe soft orthotic is helpful in treating calcaneal apophysitis. The prescription that the lead author writes is for a ⅝″ compressible, sponge-filled leather orthotic that is made in the form of a heel wedge or heel pad. Pain relief is believed to occur as a result of relaxation of the tension on the gastrocsoleus complex inserting onto the calcaneal apophysis and by “cushioning” the impact of heel strike.3 The orthotic, which typically lasts for 3 to 6 months, generally abrogates the need for anti-inflammatories as a primary treatment. However, relief of discomfort during this period may include use of antiflammatories.
For many years, the lead author has utilized a simple in-shoe, wedge-shaped orthotic consisting of a sponge material covered by leather, and compressible down to ⅝″. It raises the heel and cushions the impact of weightbearing. It can be transferred from shoe to shoe, and the patient can resume full activities while wearing the orthotic. Pain relief is generally achieved within 6 weeks to 3 months. Recalcitrant cases may require a 4 to 6 week period of casting in a plantar flexed position. Surgery is not necessary, nor are there any surgical cases reported in the literature. Orthopaedic referral is indicated for recalcitrant cases.
Acknowledgments
The Audio-Visual Department, Children’s Hospital Medical Center, Akron and Adeline Weiner assisted in preparing this paper.
Correspondence
Dennis S. Weiner, MD, 300 Locust Street, Suite 160, Akron, OH 44302-1821. [email protected]
1. Ogden J. Skeletal Injury in the Child. 3rd ed. New York: Springer-Verlag; 2000:1118–1120.
2. Orava S, Virtanen K. Osteochondroses in athletes. Br J Sports Med 1982;16:161-168.
3. Weiner DS. Pediatric Orthopedics for Primary Care Physicians. 2nd ed. Cambridge: Cambridge University Press; 2004.
4. Ishikawa SN. Conditions of the calcaneus in skeletally immature patients. Foot Ankle Clin N Am 2005;10:503-513.
5. Allison N. Apophysitis of the os calcis. J Bone Joint Surg 1924;6:91-94.
6. Brantigan CO. Calcaneal apophysitis. One of the growing pains of adolescence. Rocky Mt Med J 1972;69(8):59-60.
7. Ogden J, Ganey T, Hill JD, Jaakkola JI. Sever’s injury: a stress fracture of the immature calcaneal metaphysis. J Pediatr Orthop 2004;24:488-492.
8. Micheli LJ, Ireland LM. Prevention and management of calcaneal apophysitis in children; an overuse syndrome. J Pediatr Orthop 1987;7:34-38.
9. Liberson A, Lieberson S, Mendes DG, Shajrawi I, Ben Haim Y, Boss JH. Remodeling of the calcaneus apophysis in the growing child. J Pediatr Orthop 1995;4:74-79.
10. Contompasis JP. The management of heel pain in the athlete. Clin Podiatr Med Surg 1986;3:705-711.
11. McKenzie DC, Taunton JE, Clement DB, Smart GW, McNicol KL. Calcaneal epiphysitis in adolescent athletes. Can J Appl Sport Sci 1981;6:123-125.
12. Madden C, Mellion M. Sever’s disease and other causes of heel pain in adolescents. Am Fam Physician 1996;54:1995-2000.
13. Meyerding HW, Stuck WG. Painful heels among children (apophysitis). JAMA 1934;102:1658-1660.
14. Rhine I, Locke R. Apophysitis of the calcaneus. J Am Osteopath Assoc 1952;51:441-447.
15. Ross SE, Caffey J. Ossification of the calcaneal apophysis in healthy children. Stanford Med Bull 1957;15:224-226.
16. Sever JW. Apophysitis of the os calcis. NY State J Med 1912;95:1025-1029.
17. Volpon JB, de Carvalho Filho G. Calcaneal apophysitis a quantitative radiographic evaluation of the secondary ossification center. Arch Orthop Trauma Surg 2002;122:338-341.
18. Hughes ASR. Painful heels in children. Surg Gynecol Obstet 1948;86:64-68.
19. Kohler A, Zimmer EA. Borderlands of the Normal and Early Pathologic and Skeletal Roentgenology. 3rd ed. New York: Grune and Stratton; 1968.
20. Shopfner CE, Coin CG. Effect of weightbearing on the appearance and development of the secondary calcaneal epiphysis. Radiology 1966;86:201-206.
21. Krantz MK. Calcaneal apophysitis a clinical and roentgenologic study. J Am Podiatry Assoc 1965;55:801-807.
22. Lerner LH. Radiographic evaluation of calcaneal apophysitis. J Natl Assoc Chiropodists 1957;47:451-459.
- The true origin of the heel pain of calcaneal apophysitis is a stress microfracture (invisible on x-ray) due to chronic repetitive microtrauma—it’s an overuse syndrome that resolves without surgery in nearly all cases. (C)
- Most patients experience pain relief and can resume full activities while using a simple in-shoe wedge-shaped orthotic. (C)
- The most distinguishing feature on physical exam is the exquisite heel pain produced by lateral and medial compression (“squeezing”) of the heel. (C)
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Two things about calcaneal “apophysitis” are a bit misleading. The first is its name. Although this common cause of heel pain in adolescents and teenagers was once considered a true osteochondritis, we now know that it’s actually a mechanical overuse pain syndrome with a self-limited, benign prognosis.1-3 The second area of confusion is what you’ll see on x-ray: an increased density and irregular fragmentation that was once viewed with suspicion, but is actually a normal pattern of ossification for this particular apophysis.
Don’t let the x-ray fool you
Primary care physicians can properly manage this common pain condition, given an understanding of the features, natural history, and treatment principles presented here.
Orthopedic referral is indicated for only a few recalcitrant cases.
Shoes aren’t to blame, but activity level is
Adolescents with calcaneal apophysitis—also known as Sever’s disease—will typically come into the office complaining of pain, often in both heels, particularly with mechanical activities such as running, jumping, and long-distance walking. Patients may walk on tiptoe to avoid the pain.4
The condition is common in both boys and girls, although personal experience indicates it’s more common in boys. The typical age of the patient is 8 to 15 years. The condition is most commonly seen in patients who are engaged in athletic endeavors,5,6 including soccer, basketball, and gymnastics,7,8 though no specific athletic endeavor has been directly implicated in the pathogenesis. Likewise, no specific foot structure or type of shoe wear has been directly related to the symptomatology.
An otherwise healthy boy, age 12, walks into your office—on tiptoe. His problem is pain in both heels, especially when running. It’s his first season on his school track team, and he says he’s been practicing hard for the 50-yard dash, “my best event.” his parents express to you their concern about possible sports-related injuries or underlying disease, and their son’s distress about the possibilty of “letting down the team” if he quits. You find no swelling, no skin changes, no erythema, and no other local abnormalities. Symptoms of marked pain are produced by medial and lateral compression (squeezing) of the heel at the site where the calcaneal apophysis attaches to the main body of the os calcis. There is no pain on plantar, posterior, or retrocalcaneal pressure, or adjacent to the Achilles tendon.
Exquisite heel pain produced by medial and lateral compression of the heel is the most distinguishing feature of calcaneal apophysitis
Is this x-ray normal? You order a lateral x-ray of the calcaneus to exclude other pathology. You observe a pattern of increased density and apparent irregular fragmentation on the x-ray. The radiologist reports no abnormal findings. The above x-ray typifies calcaneal apophysitis, an overuse syndrome often seen in children 8 to 15 years of age. The “dense” area is actually a secondary ossification center of the calcaneus, not an indication of pathology.
The ossification of the calcaneus is different from that of the tarsal bones, which are each ossified from a single center. In the case of the calcaneus, a secondary center of ossification typically appears in girls by age 6, and in boys by age 8.14,15 During adolescence, a C-shaped cartilage develops between the metaphyseal bone of the body of the calcaneus and the secondary center (or centers) of ossification. Then, at around age 10 or 11, a more superior tertiary ossification center appears in the apophysis of the calcaneus.
As the calcaneal apophysis progressively ossifies, it presents as a very dense radiographic pattern in an adolescent. For years, this was thought to represent a form of osteochondritis.16 In fact, this is a normal pattern of ossification for this particular apophysis.17-22
What do you tell the patient and parents? You advise an in-shoe orthotic, no limits on physical activity, and no surgery. You explain that the pain is due to recurrent impact (overuse), and that the orthotic will “unload” the heel and permit symtoms to resolve, typically within 60 days. If asked about discomfort, you may advise anti-inflammatories and ice/heat.
Patients typically have no swelling, skin changes, erythema, or other local abnormalities.8 The most characteristic distinguishing feature on physical examination is exquisite pain produced on medial and lateral compression (“squeezing”) of the heel at the site where the calcaneal apophysis attaches to the main body of the os calcis. The pain is not on plantar pressure (as you would see with plantar fasciitis), or posterior, retrocalcaneal, or adjacent to the Achilles tendon (as you would see on Achilles tendinitis), but on medial and lateral compression.3
I’ve noticed a number of trends over the years while caring for patients with calcaneal apophysitis. My chart review of the 227 patients I cared for between 1971 and 1997 revealed the following:
- 60% (137) of patients had bilateral involvement.
- 78% of the patients were male. The reason for the male preponderance remains unclear.
- All but 3 of the 364 feet obtained eventual complete symptom resolution with the prescribed sponge-leather heel orthotic.
- Symptoms typically resolved within 60 days.
- The 3 cases that were recalcitrant to orthotic treatment required an equinus-type cast for 4 to 6 weeks. Those patients treated with a cast also had resolution of their symptoms.
- Roughly 30% of the cases encountered a recurrence of symptoms with similar resolution with the previously described retreatment. Recurrences were unrelated to gender.
- No case ever required any other treatment type beyond the orthotic or cast.—Dennis Weiner, MD
Researchers found microfractures. Magnetic resonance imaging (MRI) evidence suggests that the true pathogenesis of calcaneal apophysitis is a stress microfracture related to chronic repetitive microtrauma.9 In addition, MRI evidence suggests that the location of the stress microfractures is in the metaphysis of the body of the calcaneus adjacent to—but not directly involving—the apophysis.1,7 This more recent evidence replaces the historical hypotheses that the condition is primarily an inflammatory process. As a consequence of the microtrauma, however, it’s possible that an inflammatory process may occur secondarily.
Should you order x-rays? X-rays are not essential to the diagnosis, though they may be used to rule out other conditions, such as fracture, infection, or a bone cyst. Keep in mind, though, that patients with calcaneal pain will have a normal x-ray.7 What is normal, however, is another matter, and has been the subject of confusion in the past.
Pain stops in a few weeks
Usually, the symptoms of calcaneal apophysitis resolve fairly quickly, and with relatively simple treatment. (The symptoms also disappear as the child gets older and the calcaneal apophysis amalgamates with the main body of the calcaneus.)
Physiotherapy, forced ankle dorsiflexion stretching, gastrocsoleus stretching, ice, heat, heel cups and pads,1,10-13 and anti-inflammatories have all been used in the management of the condition.3,8 Clinicians have also historically restricted the patients’ activity, but this is unnecessary.
An in-shoe soft orthotic is helpful in treating calcaneal apophysitis. The prescription that the lead author writes is for a ⅝″ compressible, sponge-filled leather orthotic that is made in the form of a heel wedge or heel pad. Pain relief is believed to occur as a result of relaxation of the tension on the gastrocsoleus complex inserting onto the calcaneal apophysis and by “cushioning” the impact of heel strike.3 The orthotic, which typically lasts for 3 to 6 months, generally abrogates the need for anti-inflammatories as a primary treatment. However, relief of discomfort during this period may include use of antiflammatories.
For many years, the lead author has utilized a simple in-shoe, wedge-shaped orthotic consisting of a sponge material covered by leather, and compressible down to ⅝″. It raises the heel and cushions the impact of weightbearing. It can be transferred from shoe to shoe, and the patient can resume full activities while wearing the orthotic. Pain relief is generally achieved within 6 weeks to 3 months. Recalcitrant cases may require a 4 to 6 week period of casting in a plantar flexed position. Surgery is not necessary, nor are there any surgical cases reported in the literature. Orthopaedic referral is indicated for recalcitrant cases.
Acknowledgments
The Audio-Visual Department, Children’s Hospital Medical Center, Akron and Adeline Weiner assisted in preparing this paper.
Correspondence
Dennis S. Weiner, MD, 300 Locust Street, Suite 160, Akron, OH 44302-1821. [email protected]
- The true origin of the heel pain of calcaneal apophysitis is a stress microfracture (invisible on x-ray) due to chronic repetitive microtrauma—it’s an overuse syndrome that resolves without surgery in nearly all cases. (C)
- Most patients experience pain relief and can resume full activities while using a simple in-shoe wedge-shaped orthotic. (C)
- The most distinguishing feature on physical exam is the exquisite heel pain produced by lateral and medial compression (“squeezing”) of the heel. (C)
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Two things about calcaneal “apophysitis” are a bit misleading. The first is its name. Although this common cause of heel pain in adolescents and teenagers was once considered a true osteochondritis, we now know that it’s actually a mechanical overuse pain syndrome with a self-limited, benign prognosis.1-3 The second area of confusion is what you’ll see on x-ray: an increased density and irregular fragmentation that was once viewed with suspicion, but is actually a normal pattern of ossification for this particular apophysis.
Don’t let the x-ray fool you
Primary care physicians can properly manage this common pain condition, given an understanding of the features, natural history, and treatment principles presented here.
Orthopedic referral is indicated for only a few recalcitrant cases.
Shoes aren’t to blame, but activity level is
Adolescents with calcaneal apophysitis—also known as Sever’s disease—will typically come into the office complaining of pain, often in both heels, particularly with mechanical activities such as running, jumping, and long-distance walking. Patients may walk on tiptoe to avoid the pain.4
The condition is common in both boys and girls, although personal experience indicates it’s more common in boys. The typical age of the patient is 8 to 15 years. The condition is most commonly seen in patients who are engaged in athletic endeavors,5,6 including soccer, basketball, and gymnastics,7,8 though no specific athletic endeavor has been directly implicated in the pathogenesis. Likewise, no specific foot structure or type of shoe wear has been directly related to the symptomatology.
An otherwise healthy boy, age 12, walks into your office—on tiptoe. His problem is pain in both heels, especially when running. It’s his first season on his school track team, and he says he’s been practicing hard for the 50-yard dash, “my best event.” his parents express to you their concern about possible sports-related injuries or underlying disease, and their son’s distress about the possibilty of “letting down the team” if he quits. You find no swelling, no skin changes, no erythema, and no other local abnormalities. Symptoms of marked pain are produced by medial and lateral compression (squeezing) of the heel at the site where the calcaneal apophysis attaches to the main body of the os calcis. There is no pain on plantar, posterior, or retrocalcaneal pressure, or adjacent to the Achilles tendon.
Exquisite heel pain produced by medial and lateral compression of the heel is the most distinguishing feature of calcaneal apophysitis
Is this x-ray normal? You order a lateral x-ray of the calcaneus to exclude other pathology. You observe a pattern of increased density and apparent irregular fragmentation on the x-ray. The radiologist reports no abnormal findings. The above x-ray typifies calcaneal apophysitis, an overuse syndrome often seen in children 8 to 15 years of age. The “dense” area is actually a secondary ossification center of the calcaneus, not an indication of pathology.
The ossification of the calcaneus is different from that of the tarsal bones, which are each ossified from a single center. In the case of the calcaneus, a secondary center of ossification typically appears in girls by age 6, and in boys by age 8.14,15 During adolescence, a C-shaped cartilage develops between the metaphyseal bone of the body of the calcaneus and the secondary center (or centers) of ossification. Then, at around age 10 or 11, a more superior tertiary ossification center appears in the apophysis of the calcaneus.
As the calcaneal apophysis progressively ossifies, it presents as a very dense radiographic pattern in an adolescent. For years, this was thought to represent a form of osteochondritis.16 In fact, this is a normal pattern of ossification for this particular apophysis.17-22
What do you tell the patient and parents? You advise an in-shoe orthotic, no limits on physical activity, and no surgery. You explain that the pain is due to recurrent impact (overuse), and that the orthotic will “unload” the heel and permit symtoms to resolve, typically within 60 days. If asked about discomfort, you may advise anti-inflammatories and ice/heat.
Patients typically have no swelling, skin changes, erythema, or other local abnormalities.8 The most characteristic distinguishing feature on physical examination is exquisite pain produced on medial and lateral compression (“squeezing”) of the heel at the site where the calcaneal apophysis attaches to the main body of the os calcis. The pain is not on plantar pressure (as you would see with plantar fasciitis), or posterior, retrocalcaneal, or adjacent to the Achilles tendon (as you would see on Achilles tendinitis), but on medial and lateral compression.3
I’ve noticed a number of trends over the years while caring for patients with calcaneal apophysitis. My chart review of the 227 patients I cared for between 1971 and 1997 revealed the following:
- 60% (137) of patients had bilateral involvement.
- 78% of the patients were male. The reason for the male preponderance remains unclear.
- All but 3 of the 364 feet obtained eventual complete symptom resolution with the prescribed sponge-leather heel orthotic.
- Symptoms typically resolved within 60 days.
- The 3 cases that were recalcitrant to orthotic treatment required an equinus-type cast for 4 to 6 weeks. Those patients treated with a cast also had resolution of their symptoms.
- Roughly 30% of the cases encountered a recurrence of symptoms with similar resolution with the previously described retreatment. Recurrences were unrelated to gender.
- No case ever required any other treatment type beyond the orthotic or cast.—Dennis Weiner, MD
Researchers found microfractures. Magnetic resonance imaging (MRI) evidence suggests that the true pathogenesis of calcaneal apophysitis is a stress microfracture related to chronic repetitive microtrauma.9 In addition, MRI evidence suggests that the location of the stress microfractures is in the metaphysis of the body of the calcaneus adjacent to—but not directly involving—the apophysis.1,7 This more recent evidence replaces the historical hypotheses that the condition is primarily an inflammatory process. As a consequence of the microtrauma, however, it’s possible that an inflammatory process may occur secondarily.
Should you order x-rays? X-rays are not essential to the diagnosis, though they may be used to rule out other conditions, such as fracture, infection, or a bone cyst. Keep in mind, though, that patients with calcaneal pain will have a normal x-ray.7 What is normal, however, is another matter, and has been the subject of confusion in the past.
Pain stops in a few weeks
Usually, the symptoms of calcaneal apophysitis resolve fairly quickly, and with relatively simple treatment. (The symptoms also disappear as the child gets older and the calcaneal apophysis amalgamates with the main body of the calcaneus.)
Physiotherapy, forced ankle dorsiflexion stretching, gastrocsoleus stretching, ice, heat, heel cups and pads,1,10-13 and anti-inflammatories have all been used in the management of the condition.3,8 Clinicians have also historically restricted the patients’ activity, but this is unnecessary.
An in-shoe soft orthotic is helpful in treating calcaneal apophysitis. The prescription that the lead author writes is for a ⅝″ compressible, sponge-filled leather orthotic that is made in the form of a heel wedge or heel pad. Pain relief is believed to occur as a result of relaxation of the tension on the gastrocsoleus complex inserting onto the calcaneal apophysis and by “cushioning” the impact of heel strike.3 The orthotic, which typically lasts for 3 to 6 months, generally abrogates the need for anti-inflammatories as a primary treatment. However, relief of discomfort during this period may include use of antiflammatories.
For many years, the lead author has utilized a simple in-shoe, wedge-shaped orthotic consisting of a sponge material covered by leather, and compressible down to ⅝″. It raises the heel and cushions the impact of weightbearing. It can be transferred from shoe to shoe, and the patient can resume full activities while wearing the orthotic. Pain relief is generally achieved within 6 weeks to 3 months. Recalcitrant cases may require a 4 to 6 week period of casting in a plantar flexed position. Surgery is not necessary, nor are there any surgical cases reported in the literature. Orthopaedic referral is indicated for recalcitrant cases.
Acknowledgments
The Audio-Visual Department, Children’s Hospital Medical Center, Akron and Adeline Weiner assisted in preparing this paper.
Correspondence
Dennis S. Weiner, MD, 300 Locust Street, Suite 160, Akron, OH 44302-1821. [email protected]
1. Ogden J. Skeletal Injury in the Child. 3rd ed. New York: Springer-Verlag; 2000:1118–1120.
2. Orava S, Virtanen K. Osteochondroses in athletes. Br J Sports Med 1982;16:161-168.
3. Weiner DS. Pediatric Orthopedics for Primary Care Physicians. 2nd ed. Cambridge: Cambridge University Press; 2004.
4. Ishikawa SN. Conditions of the calcaneus in skeletally immature patients. Foot Ankle Clin N Am 2005;10:503-513.
5. Allison N. Apophysitis of the os calcis. J Bone Joint Surg 1924;6:91-94.
6. Brantigan CO. Calcaneal apophysitis. One of the growing pains of adolescence. Rocky Mt Med J 1972;69(8):59-60.
7. Ogden J, Ganey T, Hill JD, Jaakkola JI. Sever’s injury: a stress fracture of the immature calcaneal metaphysis. J Pediatr Orthop 2004;24:488-492.
8. Micheli LJ, Ireland LM. Prevention and management of calcaneal apophysitis in children; an overuse syndrome. J Pediatr Orthop 1987;7:34-38.
9. Liberson A, Lieberson S, Mendes DG, Shajrawi I, Ben Haim Y, Boss JH. Remodeling of the calcaneus apophysis in the growing child. J Pediatr Orthop 1995;4:74-79.
10. Contompasis JP. The management of heel pain in the athlete. Clin Podiatr Med Surg 1986;3:705-711.
11. McKenzie DC, Taunton JE, Clement DB, Smart GW, McNicol KL. Calcaneal epiphysitis in adolescent athletes. Can J Appl Sport Sci 1981;6:123-125.
12. Madden C, Mellion M. Sever’s disease and other causes of heel pain in adolescents. Am Fam Physician 1996;54:1995-2000.
13. Meyerding HW, Stuck WG. Painful heels among children (apophysitis). JAMA 1934;102:1658-1660.
14. Rhine I, Locke R. Apophysitis of the calcaneus. J Am Osteopath Assoc 1952;51:441-447.
15. Ross SE, Caffey J. Ossification of the calcaneal apophysis in healthy children. Stanford Med Bull 1957;15:224-226.
16. Sever JW. Apophysitis of the os calcis. NY State J Med 1912;95:1025-1029.
17. Volpon JB, de Carvalho Filho G. Calcaneal apophysitis a quantitative radiographic evaluation of the secondary ossification center. Arch Orthop Trauma Surg 2002;122:338-341.
18. Hughes ASR. Painful heels in children. Surg Gynecol Obstet 1948;86:64-68.
19. Kohler A, Zimmer EA. Borderlands of the Normal and Early Pathologic and Skeletal Roentgenology. 3rd ed. New York: Grune and Stratton; 1968.
20. Shopfner CE, Coin CG. Effect of weightbearing on the appearance and development of the secondary calcaneal epiphysis. Radiology 1966;86:201-206.
21. Krantz MK. Calcaneal apophysitis a clinical and roentgenologic study. J Am Podiatry Assoc 1965;55:801-807.
22. Lerner LH. Radiographic evaluation of calcaneal apophysitis. J Natl Assoc Chiropodists 1957;47:451-459.
1. Ogden J. Skeletal Injury in the Child. 3rd ed. New York: Springer-Verlag; 2000:1118–1120.
2. Orava S, Virtanen K. Osteochondroses in athletes. Br J Sports Med 1982;16:161-168.
3. Weiner DS. Pediatric Orthopedics for Primary Care Physicians. 2nd ed. Cambridge: Cambridge University Press; 2004.
4. Ishikawa SN. Conditions of the calcaneus in skeletally immature patients. Foot Ankle Clin N Am 2005;10:503-513.
5. Allison N. Apophysitis of the os calcis. J Bone Joint Surg 1924;6:91-94.
6. Brantigan CO. Calcaneal apophysitis. One of the growing pains of adolescence. Rocky Mt Med J 1972;69(8):59-60.
7. Ogden J, Ganey T, Hill JD, Jaakkola JI. Sever’s injury: a stress fracture of the immature calcaneal metaphysis. J Pediatr Orthop 2004;24:488-492.
8. Micheli LJ, Ireland LM. Prevention and management of calcaneal apophysitis in children; an overuse syndrome. J Pediatr Orthop 1987;7:34-38.
9. Liberson A, Lieberson S, Mendes DG, Shajrawi I, Ben Haim Y, Boss JH. Remodeling of the calcaneus apophysis in the growing child. J Pediatr Orthop 1995;4:74-79.
10. Contompasis JP. The management of heel pain in the athlete. Clin Podiatr Med Surg 1986;3:705-711.
11. McKenzie DC, Taunton JE, Clement DB, Smart GW, McNicol KL. Calcaneal epiphysitis in adolescent athletes. Can J Appl Sport Sci 1981;6:123-125.
12. Madden C, Mellion M. Sever’s disease and other causes of heel pain in adolescents. Am Fam Physician 1996;54:1995-2000.
13. Meyerding HW, Stuck WG. Painful heels among children (apophysitis). JAMA 1934;102:1658-1660.
14. Rhine I, Locke R. Apophysitis of the calcaneus. J Am Osteopath Assoc 1952;51:441-447.
15. Ross SE, Caffey J. Ossification of the calcaneal apophysis in healthy children. Stanford Med Bull 1957;15:224-226.
16. Sever JW. Apophysitis of the os calcis. NY State J Med 1912;95:1025-1029.
17. Volpon JB, de Carvalho Filho G. Calcaneal apophysitis a quantitative radiographic evaluation of the secondary ossification center. Arch Orthop Trauma Surg 2002;122:338-341.
18. Hughes ASR. Painful heels in children. Surg Gynecol Obstet 1948;86:64-68.
19. Kohler A, Zimmer EA. Borderlands of the Normal and Early Pathologic and Skeletal Roentgenology. 3rd ed. New York: Grune and Stratton; 1968.
20. Shopfner CE, Coin CG. Effect of weightbearing on the appearance and development of the secondary calcaneal epiphysis. Radiology 1966;86:201-206.
21. Krantz MK. Calcaneal apophysitis a clinical and roentgenologic study. J Am Podiatry Assoc 1965;55:801-807.
22. Lerner LH. Radiographic evaluation of calcaneal apophysitis. J Natl Assoc Chiropodists 1957;47:451-459.
Stress tests: How to make a calculated choice
- Estimate pretest probability of CAD in patients with chest pain on the basis of age, sex, pain characteristics, and cardiovascular risk factors (B).
- Low pretest probability patients should undergo an exercise treadmill test alone (C).
- Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging (B). Patients with an electronically paced ventricular rhythm (C) or left bundle-branch block (B) require myocardial perfusion imaging.
- In high pretest probability patients, coronary angiography is an appropriate initial strategy for CAD diagnosis (C).
- In women, the data are insufficient to justify routine stress imaging tests as the initial test for CAD (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Are you a wise “consumer” of stress tests? That is: Do you consider your patient’s CAD probability score before ordering an exercise treadmill test or pharmacologic stress myocardial imaging (PSMI)? Are you as well-versed as you’d like to be on the predictive value of things like the Duke Treadmill Score?
If your answer is No to either question, this review may help guide your use of stress tests, based on evidence.
What is the pretest probability of CAD?
The decision to order an exercise stress test or a PSMI should be based on history, physical examination, and pretest probability for CAD. You can estimate the pretest probability for CAD in a chest pain patient based on the patient’s age, sex, and pain characteristics.1
Determine whether symptoms are typical, atypical, or nonanginal, based on whether the chest pain is substernal, brought on by exertion, or relieved by rest or nitroglycerin.2
To recap:
- Typical angina requires all 3 pain characteristics
- Atypical angina, only 2
- Nonanginal chest pain, 1.2
Use this information (along with the patient’s age) to determine whether he has a high, intermediate, low, or very low likelihood of CAD (TABLE 1). From the low, to the intermediate, to the high pretest probability levels, the positive predictive value increases progressively (21%, 62%, and 92%) and the negative predictive value decreases progressively (94%, 72%, and 28%).3 (These values are based on a review of symptomatic patients who had angiography following stress testing.)
TABLE 1
How to determine pretest probability of coronary artery disease
| STEP 1 | STEP 2 | STEP 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Ask 3 questions: | Total the number of “yes” answers to identify symptom pattern: | Find the cell in the matrix (below) where age, gender, and symptom pattern converge: | ||||||
| 0 of 3=Asymptomatic | High probability | >90% | |||||
| 1 of 3=Nonanginal chest pain | Intermediate | 10%–90% | ||||||
| 2 of 3=Atypical angina | Low | <10% | ||||||
| 3 of 3=Typical angina | Very low | <5% | ||||||
| AGE (YRS) | SYMPTOMS | |||||||
| ASYMPTOMATIC | NONANGINAL CHEST PAIN | ATYPICAL ANGINA | TYPICAL ANGINA | |||||
| MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | |
| 35–45 | Very low | Very low | Intermediate | Very low | Intermediate | Intermediate | Intermediate | Intermediate |
| 45–55 | Low | Very low | Intermediate | Low | Intermediate | Intermediate | High | Intermediate |
| 55–65 | Intermediate | Low | Intermediate | Intermediate | Intermediate | Intermediate | High | Intermediate |
| 65–75 | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | High | High |
| Adapted from Diamond GA.2 | ||||||||
Your patients’ score dictates whether testing is required, and if so what kind.
Very low pretest probability patients should not have an exercise test, since they have a high risk of false-positive results. Evaluate and treat them for noncardiac causes of chest pain and begin primary prevention of CAD.
Low pretest probability patients should undergo exercise treadmill testing alone since negative results carry a high negative predictive value in both men and women, but positive test results may be false and can be evaluated by more studies.3
Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging modality.3-5 However, intermediate pretest probability patients with baseline ECG abnormalities such as electronically paced ventricular rhythm or left bundle-branch block will require myocardial perfusion imaging.5
High pretest probability patients should have coronary angiography as an initial strategy for diagnosis of CAD.3
History, exam, and ECG determine test suitability
Can your patient take an exercise stress test, or will he need a pharmacologic stress test instead? (See “A guide to sensitivity, specificity, and likelihood ratios for stress tests.”) Can he pedal a bicycle, walk, or exercise for 6 minutes? On physical examination, take note of his gait, mobility, and limb strength.
What medications is the patient taking? Digoxin may cause false ST changes, beta-blockers may prevent attaining maximum heart rate, and antihypertensive agents and vasodilators may alter the blood pressure response, producing a false negative result. Nitrates attenuate angina and the associated ST depression of ischemia.6 In addition, metabolic abnormalities and cocaine or alcohol use may affect heart rate, metabolic oxygen demand and the ability to perform the exercise treadmill testing.
On examination, document murmurs, rhythm abnormalities, vascular bruits, and abnormal pulses. Limit laboratory studies to recent cardiac damage screening if indicated. Screen with a resting ECG for arrhythmias, conduction abnormalities or preexisting cardiac damage. ST-segment (≥1 mm) and T-wave changes such as inversions secondary to strain or old injury or conduction abnormalities such as bundle branch blocks and prolonged QT interval may obscure exercise treadmill testing findings. Consider spirometry for patients with asthma or chronic lung disease.
Exercise treadmill testing
Sensitivity varies from 45% to 67% and specificity 72% to 90% with operator and patient variables.6 An abnormal test in a man at a heart rate of 85% of predicted maximum for age has a sensitivity of about 65% and a specificity of 85% for CAD. In women, one meta-analysis demonstrated a sensitivity of only 61% and a specificity of only 70%.8
PSMI
Pharmacologic stress myocardial imaging is similar to exercise treadmill testing. Dipyridamole and adenosine PSMI with thallium T1 201 or technetium Tc 99m have a similar sensitivity of 90%, and specificity of 70% for detection of CAD.6
Echocardiography
Overall sensitivity for exercise echocardiography was about 85% and for dobutamine stress echocardiography 82%. Dobutamine has a higher sensitivity than vasodilator echocardiography.6
Likelihood ratios (LR) for exercise treadmill testing and PSMI
Based on a review of coronary artery disease with chest pain as the symptom and a reference standard of a coronary angiogram with >70% narrowing of one or more arteries, or >50% left main, the LR varies for sex and for each different study. The positive LR (LR+) for exercise treadmill testing is 3.00 for men and 2.00 for women. The negative LR (LR–) for exercise treadmill testing is 0.650 for men and 0.560 for women. LR+ for exercise treadmill testing with thallium imaging is 5.9 (generally), but 2.20 for women; LR–is 0.200 and is 0.340 for women. Dipyridamole PSMI, LR+ is 3.30 and LR- is 0.180.16
The decisive factors
Absolute contraindications to exercise treadmill testing include recent MI; significant aortic stenosis,7 and weight exceeding equipment capacity. Relative contraindications to exercise treadmill testing (which can be superseded if the benefits of exercise outweigh the risks) include: hypertension (systolic >200 mm Hg/diastolic >110 mm Hg),5 left main coronary stenosis and stenotic valvular disease. (For more on “Contraindications to exercise testing,” see TABLE 2.)
The role of imaging: Important, yes—routine, no
An important element of stress testing is, of course, the imaging method(s) that will be used. The options include myocardial perfusion imaging with thallium Tl 201 or technetium Tc 99m, and echocardiography.
Indications for myocardial perfusion imaging with exercise treadmill testing are a high pretest probability for CAD, an abnormal baseline ECG such as left bundle branch block, previous myocardial damage or coronary revascularization, or a previous equivocal or unexpected exercise ECG result. In women with an intermediate pretest probability for CAD, the sensitivity and specificity of an exercise treadmill testing is less than in men, which suggests that nuclear imaging would improve this test.8 There is, however, insufficient data to justify initial routine stress imaging tests in women.1
TABLE 2
Contraindications to exercise testing
| ABSOLUTE |
|---|
|
| RELATIVE CONTRAINDICATIONS (CAN BE SUPERSEDED IF THE BENEFITS OF EXERCISE OUTWEIGH THE RISKS) |
|
| Source: Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf Accessed: March 6, 2007. |
Of the 2 agents used for myocardial perfusion imaging, technetium Tc 99m has more favorable imaging characteristics.9 It has a shorter half-life (6 hours) than thallium Tl 201 (73 hours), and larger doses of technetium Tc99m may be used, permitting the assessment of ventricular function.10
Echocardiography may also be done with either exercise treadmill testing or PSMI to evaluate relative myocardial perfusion. While radionuclide technique assesses relative myocardial perfusion, echocardiography also evaluates global and regional function. Indications for echocardiography are similar to myocardial perfusion imaging but also include the need for prognostic information after MI, and to assess physiologic significance of a lesion or to determine the success of an intervention.
Time for the test: Selecting the protocol
While the Bruce exercise treadmill testing protocol is the most commonly used (82% of tests)11 in healthy adults, it may not be appropriate for women or the elderly as most protocols were developed for the evaluation of men.12 A ramp method with gradual increase in grade each minute is preferred by some clinicians when patients are unable to perform a standard Bruce protocol. Another option, the Modified Bruce protocol, which is more gradual than the standard Bruce protocol; it has two 3-minute warm-up stages.12
The 3 PSMI protocols include adenosine, dipyridamole, and dobutamine. Each has a different administration routine,9 though ECG, blood pressure and pulse are taken every minute for all 3.
- Adenosine is infused with a pump over 6 minutes and technetium Tc99m is injected 3 minutes into the infusion.
- Dipyridamole is infused over 4 minutes and technetium Tc99m is injected 2 to no more than 5 minutes after the infusion. Theophylline is injected, after dipyridamole if necessary, no earlier than 1 minute after technetium Tc99m is administered to avoid interference with the uptake.
- Dobutamine is titrated with a dose increase every 3 minutes. Tc99m is injected after the first minute at the highest concentration. (Typically dobutamine is used with echocardiography.6)
Adenosine
A potent vasodilator, this endogenous nucleoside is rapidly cleared (half-life, <10 seconds) along with its side effects of flushing, headache, and nausea.
Dipyridamole
This coronary vasodilator inhibits the uptake of adenosine. The same side effects as adenosine—flushing, headache, nausea—may last longer with dipyridamole (half-life,13 hours) but they are more common with adenosine and are relieved by administering theophylline.
All methylxanthines may interfere with either dipyridamole or adenosine and should be held for 24 to 48 hours prior to examination.
- Avoid both adenosine and dipyridamole in patients with asthma, severe COPD (FEV1<30%), second- or third-degree heart block, hypotension, or those who are on oral dipyridamole.
Dobutamine
This synthetic catecholamine increases heart rate, systolic blood pressure, and myocardial contractility, thereby provoking ischemia. Dobutamine (half-life 2 minutes) is not affected by methylxanthines.
- It is preferred in patients who are unable to use adenosine or dipyridamole.
- Caution is needed in patients with systolic BP less than 100 mm Hg, hypertension, ventricular ectopy, and glaucoma.
- Side effects can be reversed with beta-blockers.
Ideal endpoints and the realities that may creep in
The ideal endpoint in an exercise treadmill testing is 100% of the age-predicted maximum heart rate (220–age). Eighty-five percent of maximum heart rate is the minimum for an acceptable test.
Absolute contraindications
Absolute indicators for stopping an exercise treadmill test are either a 10 mm Hg systolic drop in blood pressure from standing baseline, moderate to severe angina symptoms, feelings of syncope, skin color changes suggestive of hypoxia or hypotension, ischemic ST changes, or the patient’s desire to stop.
Relative contraindications
Relative indicators to stop include fatigue, shortness of breath, leg pain, increased arrhythmias—particularly PVCs that increase with the exercise level—and blood pressure ≥250 systolic or 115 diastolic.6
Ideally, PSMI evaluations are terminated according to the prescribed length of infusions. They will also be terminated if a patient develops wheezing, severe or increasing chest pain or hypotension, neurological symptoms, ST-segment elevation abnormalities, or arrhythmias. To reverse the side effects of adenosine or dipyridamole, aminophylline IV will be administered (1–2 mg/kg slowly, up to 250 mg).
Heart of the matter: What a report should cover
Assuming you have ordered the stress test (and not done it yourself), a complete report should include
- ST changes
- symptoms during testing
- reason for ending the test
- estimation of exercise capacity
- blood pressure response
- the presence and frequency of arrhythmias or ectopy.
Abnormal. ST segment change is the most important ECG finding in a positive test; it’s defined as >1 mm horizontal or down sloping depression or elevation, at least 60 to 80 milliseconds after the end of the QRS complex and should prompt further workup to confirm CAD.5 An abnormal ECG during a PSMI test indicates an elevated risk of multivessel CAD and should prompt further evaluation regardless of normal myocardial perfusion imaging.13
Duke Treadmill Score
Duke Treadmill Score (DTS)=exercise time–(5 × ST deviation) - (4 × exercise angina), with 0=no angina during exercise, 1=nonlimiting angina, and 2=exercise-limiting angina.
The score typically ranges from –25 to +15.4
- Low risk: > +5
- Moderate risk: –10 to +4
- High risk: < –11
Elderly Alternative Treadmill Score (for patients over 65 years of age)
This score has 2 variables in common with the Duke Treadmill Score (exercise duration or the MET equivalent and millimeters of ST changes). It also has 2 different variables (drop in exercise systolic blood pressure below resting value and history of congestive heart failure [CHF] or use of digoxin [Dig]).17,18
The score is calculated as follows: 5 × (CHF/Dig [yes=1; no=0]) + exercise-induced ST depression in millimeters + change in systolic blood pressure score–METs
Systolic blood pressure score:
- 0 for an increase >40 mm Hg
- 1 for an increase of 31–40 mm Hg
- 2 for an increase of 21–30 mm Hg
- 3 for an increase of 11–20 mm Hg
- 4 for an increase of 0–10 mm Hg
- 5 for a reduction below standing systolic pre-exercise blood pressure.
A score of < –2 is low risk, –2 to 2 is moderate risk, and >2 is high risk.
Equivocal. Reports that come back as equivocal will have ECG changes nondiagnostic of ischemia such as alterations in P- or T-wave morphology and nondiagnostic changes in AV conduction, particularly if changes revert to baseline during the rest period. Unifocal PACs or PVCs (<5/min) are not specific indicators for CAD and the development of bundle branch blocks are nondiagnostic findings. Equivocal results need additional testing such as myocardial perfusion imaging or angiography to document ischemia if the pretest probability is high.
Incomplete or failure. If your patient’s test involves equipment failure or if he (or the operator) was unable to complete the test, you should get a report to that effect. Depending on the nature of the failure, you may need to repeat the test, consider PSMI, or make a cardiology referral.
Duke Treadmill Score
A helpful calculation following treadmill testing
If your patient had a positive or negative exercise treadmill test, consider calculating his Duke Treadmill Score (DTS), which is predictive of 5-year survival and significant severe CAD for patients who are younger than 75 years.4,14
DTS helps you to exclude low-risk patients from further invasive testing and ensure high-risk patients receive further evaluation and appropriate treatment. DTS appears to be more useful in women with an intermediate pretest score but not with a low pretest score.15
The DTS score typically ranges from –25 to +15.5 Patients at low risk will have a score of > +5), moderate risk will have scores ranging from –10 to +4, and those at high risk will have a score of ≤–11.4
A modified DTS is used for patients older than 65 years who may have a limited exercise capacity, controlled asymptomatic congestive heart failure, or be on digoxin, which may affect their ability to perform a maximal exercise treadmill test.5 The values for the Elderly Alternative Treadmill Score are as follows: low risk (< –2); moderate risk (–2 to 2); and high risk (>2). (See “The calculations behind the scores.”)
Bottom line
DTS scores, Elderly Alternative Treadmill Scores, and pre–stress test CAD probability scores are all extremely useful. Integrating them into your practice can ensure that patients get the prompt care they may need, while sparing them unnecessary tests along the way.
FIGURE
Template for dictating noninvasive cardiac tests
Correspondence
Dennis P. Breen, MD, Eau Claire Family Medicine Clinic, 617 Clairemont Avenue, Eau Claire, WI 54701. [email protected]
1. Snow V, Barry P, Fihn SD, et al. Evaluation of primary care patients with chronic stable angina: guidelines from the American College of Physicians. Ann Intern Med 2004;141:57-64.
2. Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol 1983;1:574-575.
3. Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct? Chest 2000;118:535-541.
4. Shaw LJ, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying diagnostic coronary disease subgroups. Circulation 1998;98:1622-1630.
5. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf. Accessed on March 6, 2007.
6. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on Management of Patients with Chronic Stable Angina). J Am Coll Cardiol 1999;33:2092-2197.
7. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111:3290-3295.
8. Lewis JF, McGorray S, Lin L, et al. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: Findings from the national heart, lung and blood institute-sponsored women’s ischemia syndrome evaluation (WISE). Am Heart J 2005;149:527-533.
9. Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (ACC/AHA/ASNC committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging). J Am Coll Cardiol 2003;42:1318-1333.
10. Lee TH, Boucher CA. Clinical practice. noninvasive tests in patients with stable coronary artery disease. N Engl J Med 2001;344:1840-1845.
11. Myers J, Voodi L, Umann T, Froelicher VF. A survey of exercise testing: Methods, utilization, interpretation, and safety in the VAHCS. J Cardiopulm Rehabil 2000;20:251-258.
12. Ashley EA, Myers J, Froelicher V. Exercise testing in clinical medicine. Lancet 2000;356:1592-1597.
13. Cosmai EM, Heller GV. The clinical importance of electrocardiographic changes during pharmacologic stress testing with radionuclide myocardial perfusion imaging. J Nucl Cardiol 2005;12:466-472.
14. Kwok JM, Miller TD, Hodge DO, Gibbons RJ. Prognostic value of the duke treadmill score in the elderly. J Am Coll Cardiol 2002;39:1475-1481.
15. Morise AP, Olson MB, Merz NB, et al. Validation of the accuracy of pretest and exercise test scores in women with a low prevalence of coronary disease. The NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study. Am Heart J 2004;147:1085-1092.
16. InfoRetriever [web site] Clinical Rules and Calculators (2007). InfoRetriever Search Results, Exercise Testing, Diagnostic Tests, Chest Pain. Available at: www.infopoems.com/irsearch/display_article.cfm?resource=D&article=34. Accessed on January 26, 2007.
17. Morrow K, Morris CK, Froelicher VF, et al. Prediction of cardiovascular death in men undergoing noninvasive evaluation for coronary artery disease. Ann Intern Med 1993;118:689-695.
18. Kwok JF, Christian TE. Effective use of the exercise stress test to detect and predict coronary artery disease. Emerg Med 2001;33:12-22.Available at: www.emedmag.com/html/pre/fea/features/051501.asp. Accessed on March 7, 2007.
- Estimate pretest probability of CAD in patients with chest pain on the basis of age, sex, pain characteristics, and cardiovascular risk factors (B).
- Low pretest probability patients should undergo an exercise treadmill test alone (C).
- Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging (B). Patients with an electronically paced ventricular rhythm (C) or left bundle-branch block (B) require myocardial perfusion imaging.
- In high pretest probability patients, coronary angiography is an appropriate initial strategy for CAD diagnosis (C).
- In women, the data are insufficient to justify routine stress imaging tests as the initial test for CAD (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Are you a wise “consumer” of stress tests? That is: Do you consider your patient’s CAD probability score before ordering an exercise treadmill test or pharmacologic stress myocardial imaging (PSMI)? Are you as well-versed as you’d like to be on the predictive value of things like the Duke Treadmill Score?
If your answer is No to either question, this review may help guide your use of stress tests, based on evidence.
What is the pretest probability of CAD?
The decision to order an exercise stress test or a PSMI should be based on history, physical examination, and pretest probability for CAD. You can estimate the pretest probability for CAD in a chest pain patient based on the patient’s age, sex, and pain characteristics.1
Determine whether symptoms are typical, atypical, or nonanginal, based on whether the chest pain is substernal, brought on by exertion, or relieved by rest or nitroglycerin.2
To recap:
- Typical angina requires all 3 pain characteristics
- Atypical angina, only 2
- Nonanginal chest pain, 1.2
Use this information (along with the patient’s age) to determine whether he has a high, intermediate, low, or very low likelihood of CAD (TABLE 1). From the low, to the intermediate, to the high pretest probability levels, the positive predictive value increases progressively (21%, 62%, and 92%) and the negative predictive value decreases progressively (94%, 72%, and 28%).3 (These values are based on a review of symptomatic patients who had angiography following stress testing.)
TABLE 1
How to determine pretest probability of coronary artery disease
| STEP 1 | STEP 2 | STEP 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Ask 3 questions: | Total the number of “yes” answers to identify symptom pattern: | Find the cell in the matrix (below) where age, gender, and symptom pattern converge: | ||||||
| 0 of 3=Asymptomatic | High probability | >90% | |||||
| 1 of 3=Nonanginal chest pain | Intermediate | 10%–90% | ||||||
| 2 of 3=Atypical angina | Low | <10% | ||||||
| 3 of 3=Typical angina | Very low | <5% | ||||||
| AGE (YRS) | SYMPTOMS | |||||||
| ASYMPTOMATIC | NONANGINAL CHEST PAIN | ATYPICAL ANGINA | TYPICAL ANGINA | |||||
| MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | |
| 35–45 | Very low | Very low | Intermediate | Very low | Intermediate | Intermediate | Intermediate | Intermediate |
| 45–55 | Low | Very low | Intermediate | Low | Intermediate | Intermediate | High | Intermediate |
| 55–65 | Intermediate | Low | Intermediate | Intermediate | Intermediate | Intermediate | High | Intermediate |
| 65–75 | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | High | High |
| Adapted from Diamond GA.2 | ||||||||
Your patients’ score dictates whether testing is required, and if so what kind.
Very low pretest probability patients should not have an exercise test, since they have a high risk of false-positive results. Evaluate and treat them for noncardiac causes of chest pain and begin primary prevention of CAD.
Low pretest probability patients should undergo exercise treadmill testing alone since negative results carry a high negative predictive value in both men and women, but positive test results may be false and can be evaluated by more studies.3
Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging modality.3-5 However, intermediate pretest probability patients with baseline ECG abnormalities such as electronically paced ventricular rhythm or left bundle-branch block will require myocardial perfusion imaging.5
High pretest probability patients should have coronary angiography as an initial strategy for diagnosis of CAD.3
History, exam, and ECG determine test suitability
Can your patient take an exercise stress test, or will he need a pharmacologic stress test instead? (See “A guide to sensitivity, specificity, and likelihood ratios for stress tests.”) Can he pedal a bicycle, walk, or exercise for 6 minutes? On physical examination, take note of his gait, mobility, and limb strength.
What medications is the patient taking? Digoxin may cause false ST changes, beta-blockers may prevent attaining maximum heart rate, and antihypertensive agents and vasodilators may alter the blood pressure response, producing a false negative result. Nitrates attenuate angina and the associated ST depression of ischemia.6 In addition, metabolic abnormalities and cocaine or alcohol use may affect heart rate, metabolic oxygen demand and the ability to perform the exercise treadmill testing.
On examination, document murmurs, rhythm abnormalities, vascular bruits, and abnormal pulses. Limit laboratory studies to recent cardiac damage screening if indicated. Screen with a resting ECG for arrhythmias, conduction abnormalities or preexisting cardiac damage. ST-segment (≥1 mm) and T-wave changes such as inversions secondary to strain or old injury or conduction abnormalities such as bundle branch blocks and prolonged QT interval may obscure exercise treadmill testing findings. Consider spirometry for patients with asthma or chronic lung disease.
Exercise treadmill testing
Sensitivity varies from 45% to 67% and specificity 72% to 90% with operator and patient variables.6 An abnormal test in a man at a heart rate of 85% of predicted maximum for age has a sensitivity of about 65% and a specificity of 85% for CAD. In women, one meta-analysis demonstrated a sensitivity of only 61% and a specificity of only 70%.8
PSMI
Pharmacologic stress myocardial imaging is similar to exercise treadmill testing. Dipyridamole and adenosine PSMI with thallium T1 201 or technetium Tc 99m have a similar sensitivity of 90%, and specificity of 70% for detection of CAD.6
Echocardiography
Overall sensitivity for exercise echocardiography was about 85% and for dobutamine stress echocardiography 82%. Dobutamine has a higher sensitivity than vasodilator echocardiography.6
Likelihood ratios (LR) for exercise treadmill testing and PSMI
Based on a review of coronary artery disease with chest pain as the symptom and a reference standard of a coronary angiogram with >70% narrowing of one or more arteries, or >50% left main, the LR varies for sex and for each different study. The positive LR (LR+) for exercise treadmill testing is 3.00 for men and 2.00 for women. The negative LR (LR–) for exercise treadmill testing is 0.650 for men and 0.560 for women. LR+ for exercise treadmill testing with thallium imaging is 5.9 (generally), but 2.20 for women; LR–is 0.200 and is 0.340 for women. Dipyridamole PSMI, LR+ is 3.30 and LR- is 0.180.16
The decisive factors
Absolute contraindications to exercise treadmill testing include recent MI; significant aortic stenosis,7 and weight exceeding equipment capacity. Relative contraindications to exercise treadmill testing (which can be superseded if the benefits of exercise outweigh the risks) include: hypertension (systolic >200 mm Hg/diastolic >110 mm Hg),5 left main coronary stenosis and stenotic valvular disease. (For more on “Contraindications to exercise testing,” see TABLE 2.)
The role of imaging: Important, yes—routine, no
An important element of stress testing is, of course, the imaging method(s) that will be used. The options include myocardial perfusion imaging with thallium Tl 201 or technetium Tc 99m, and echocardiography.
Indications for myocardial perfusion imaging with exercise treadmill testing are a high pretest probability for CAD, an abnormal baseline ECG such as left bundle branch block, previous myocardial damage or coronary revascularization, or a previous equivocal or unexpected exercise ECG result. In women with an intermediate pretest probability for CAD, the sensitivity and specificity of an exercise treadmill testing is less than in men, which suggests that nuclear imaging would improve this test.8 There is, however, insufficient data to justify initial routine stress imaging tests in women.1
TABLE 2
Contraindications to exercise testing
| ABSOLUTE |
|---|
|
| RELATIVE CONTRAINDICATIONS (CAN BE SUPERSEDED IF THE BENEFITS OF EXERCISE OUTWEIGH THE RISKS) |
|
| Source: Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf Accessed: March 6, 2007. |
Of the 2 agents used for myocardial perfusion imaging, technetium Tc 99m has more favorable imaging characteristics.9 It has a shorter half-life (6 hours) than thallium Tl 201 (73 hours), and larger doses of technetium Tc99m may be used, permitting the assessment of ventricular function.10
Echocardiography may also be done with either exercise treadmill testing or PSMI to evaluate relative myocardial perfusion. While radionuclide technique assesses relative myocardial perfusion, echocardiography also evaluates global and regional function. Indications for echocardiography are similar to myocardial perfusion imaging but also include the need for prognostic information after MI, and to assess physiologic significance of a lesion or to determine the success of an intervention.
Time for the test: Selecting the protocol
While the Bruce exercise treadmill testing protocol is the most commonly used (82% of tests)11 in healthy adults, it may not be appropriate for women or the elderly as most protocols were developed for the evaluation of men.12 A ramp method with gradual increase in grade each minute is preferred by some clinicians when patients are unable to perform a standard Bruce protocol. Another option, the Modified Bruce protocol, which is more gradual than the standard Bruce protocol; it has two 3-minute warm-up stages.12
The 3 PSMI protocols include adenosine, dipyridamole, and dobutamine. Each has a different administration routine,9 though ECG, blood pressure and pulse are taken every minute for all 3.
- Adenosine is infused with a pump over 6 minutes and technetium Tc99m is injected 3 minutes into the infusion.
- Dipyridamole is infused over 4 minutes and technetium Tc99m is injected 2 to no more than 5 minutes after the infusion. Theophylline is injected, after dipyridamole if necessary, no earlier than 1 minute after technetium Tc99m is administered to avoid interference with the uptake.
- Dobutamine is titrated with a dose increase every 3 minutes. Tc99m is injected after the first minute at the highest concentration. (Typically dobutamine is used with echocardiography.6)
Adenosine
A potent vasodilator, this endogenous nucleoside is rapidly cleared (half-life, <10 seconds) along with its side effects of flushing, headache, and nausea.
Dipyridamole
This coronary vasodilator inhibits the uptake of adenosine. The same side effects as adenosine—flushing, headache, nausea—may last longer with dipyridamole (half-life,13 hours) but they are more common with adenosine and are relieved by administering theophylline.
All methylxanthines may interfere with either dipyridamole or adenosine and should be held for 24 to 48 hours prior to examination.
- Avoid both adenosine and dipyridamole in patients with asthma, severe COPD (FEV1<30%), second- or third-degree heart block, hypotension, or those who are on oral dipyridamole.
Dobutamine
This synthetic catecholamine increases heart rate, systolic blood pressure, and myocardial contractility, thereby provoking ischemia. Dobutamine (half-life 2 minutes) is not affected by methylxanthines.
- It is preferred in patients who are unable to use adenosine or dipyridamole.
- Caution is needed in patients with systolic BP less than 100 mm Hg, hypertension, ventricular ectopy, and glaucoma.
- Side effects can be reversed with beta-blockers.
Ideal endpoints and the realities that may creep in
The ideal endpoint in an exercise treadmill testing is 100% of the age-predicted maximum heart rate (220–age). Eighty-five percent of maximum heart rate is the minimum for an acceptable test.
Absolute contraindications
Absolute indicators for stopping an exercise treadmill test are either a 10 mm Hg systolic drop in blood pressure from standing baseline, moderate to severe angina symptoms, feelings of syncope, skin color changes suggestive of hypoxia or hypotension, ischemic ST changes, or the patient’s desire to stop.
Relative contraindications
Relative indicators to stop include fatigue, shortness of breath, leg pain, increased arrhythmias—particularly PVCs that increase with the exercise level—and blood pressure ≥250 systolic or 115 diastolic.6
Ideally, PSMI evaluations are terminated according to the prescribed length of infusions. They will also be terminated if a patient develops wheezing, severe or increasing chest pain or hypotension, neurological symptoms, ST-segment elevation abnormalities, or arrhythmias. To reverse the side effects of adenosine or dipyridamole, aminophylline IV will be administered (1–2 mg/kg slowly, up to 250 mg).
Heart of the matter: What a report should cover
Assuming you have ordered the stress test (and not done it yourself), a complete report should include
- ST changes
- symptoms during testing
- reason for ending the test
- estimation of exercise capacity
- blood pressure response
- the presence and frequency of arrhythmias or ectopy.
Abnormal. ST segment change is the most important ECG finding in a positive test; it’s defined as >1 mm horizontal or down sloping depression or elevation, at least 60 to 80 milliseconds after the end of the QRS complex and should prompt further workup to confirm CAD.5 An abnormal ECG during a PSMI test indicates an elevated risk of multivessel CAD and should prompt further evaluation regardless of normal myocardial perfusion imaging.13
Duke Treadmill Score
Duke Treadmill Score (DTS)=exercise time–(5 × ST deviation) - (4 × exercise angina), with 0=no angina during exercise, 1=nonlimiting angina, and 2=exercise-limiting angina.
The score typically ranges from –25 to +15.4
- Low risk: > +5
- Moderate risk: –10 to +4
- High risk: < –11
Elderly Alternative Treadmill Score (for patients over 65 years of age)
This score has 2 variables in common with the Duke Treadmill Score (exercise duration or the MET equivalent and millimeters of ST changes). It also has 2 different variables (drop in exercise systolic blood pressure below resting value and history of congestive heart failure [CHF] or use of digoxin [Dig]).17,18
The score is calculated as follows: 5 × (CHF/Dig [yes=1; no=0]) + exercise-induced ST depression in millimeters + change in systolic blood pressure score–METs
Systolic blood pressure score:
- 0 for an increase >40 mm Hg
- 1 for an increase of 31–40 mm Hg
- 2 for an increase of 21–30 mm Hg
- 3 for an increase of 11–20 mm Hg
- 4 for an increase of 0–10 mm Hg
- 5 for a reduction below standing systolic pre-exercise blood pressure.
A score of < –2 is low risk, –2 to 2 is moderate risk, and >2 is high risk.
Equivocal. Reports that come back as equivocal will have ECG changes nondiagnostic of ischemia such as alterations in P- or T-wave morphology and nondiagnostic changes in AV conduction, particularly if changes revert to baseline during the rest period. Unifocal PACs or PVCs (<5/min) are not specific indicators for CAD and the development of bundle branch blocks are nondiagnostic findings. Equivocal results need additional testing such as myocardial perfusion imaging or angiography to document ischemia if the pretest probability is high.
Incomplete or failure. If your patient’s test involves equipment failure or if he (or the operator) was unable to complete the test, you should get a report to that effect. Depending on the nature of the failure, you may need to repeat the test, consider PSMI, or make a cardiology referral.
Duke Treadmill Score
A helpful calculation following treadmill testing
If your patient had a positive or negative exercise treadmill test, consider calculating his Duke Treadmill Score (DTS), which is predictive of 5-year survival and significant severe CAD for patients who are younger than 75 years.4,14
DTS helps you to exclude low-risk patients from further invasive testing and ensure high-risk patients receive further evaluation and appropriate treatment. DTS appears to be more useful in women with an intermediate pretest score but not with a low pretest score.15
The DTS score typically ranges from –25 to +15.5 Patients at low risk will have a score of > +5), moderate risk will have scores ranging from –10 to +4, and those at high risk will have a score of ≤–11.4
A modified DTS is used for patients older than 65 years who may have a limited exercise capacity, controlled asymptomatic congestive heart failure, or be on digoxin, which may affect their ability to perform a maximal exercise treadmill test.5 The values for the Elderly Alternative Treadmill Score are as follows: low risk (< –2); moderate risk (–2 to 2); and high risk (>2). (See “The calculations behind the scores.”)
Bottom line
DTS scores, Elderly Alternative Treadmill Scores, and pre–stress test CAD probability scores are all extremely useful. Integrating them into your practice can ensure that patients get the prompt care they may need, while sparing them unnecessary tests along the way.
FIGURE
Template for dictating noninvasive cardiac tests
Correspondence
Dennis P. Breen, MD, Eau Claire Family Medicine Clinic, 617 Clairemont Avenue, Eau Claire, WI 54701. [email protected]
- Estimate pretest probability of CAD in patients with chest pain on the basis of age, sex, pain characteristics, and cardiovascular risk factors (B).
- Low pretest probability patients should undergo an exercise treadmill test alone (C).
- Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging (B). Patients with an electronically paced ventricular rhythm (C) or left bundle-branch block (B) require myocardial perfusion imaging.
- In high pretest probability patients, coronary angiography is an appropriate initial strategy for CAD diagnosis (C).
- In women, the data are insufficient to justify routine stress imaging tests as the initial test for CAD (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Are you a wise “consumer” of stress tests? That is: Do you consider your patient’s CAD probability score before ordering an exercise treadmill test or pharmacologic stress myocardial imaging (PSMI)? Are you as well-versed as you’d like to be on the predictive value of things like the Duke Treadmill Score?
If your answer is No to either question, this review may help guide your use of stress tests, based on evidence.
What is the pretest probability of CAD?
The decision to order an exercise stress test or a PSMI should be based on history, physical examination, and pretest probability for CAD. You can estimate the pretest probability for CAD in a chest pain patient based on the patient’s age, sex, and pain characteristics.1
Determine whether symptoms are typical, atypical, or nonanginal, based on whether the chest pain is substernal, brought on by exertion, or relieved by rest or nitroglycerin.2
To recap:
- Typical angina requires all 3 pain characteristics
- Atypical angina, only 2
- Nonanginal chest pain, 1.2
Use this information (along with the patient’s age) to determine whether he has a high, intermediate, low, or very low likelihood of CAD (TABLE 1). From the low, to the intermediate, to the high pretest probability levels, the positive predictive value increases progressively (21%, 62%, and 92%) and the negative predictive value decreases progressively (94%, 72%, and 28%).3 (These values are based on a review of symptomatic patients who had angiography following stress testing.)
TABLE 1
How to determine pretest probability of coronary artery disease
| STEP 1 | STEP 2 | STEP 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Ask 3 questions: | Total the number of “yes” answers to identify symptom pattern: | Find the cell in the matrix (below) where age, gender, and symptom pattern converge: | ||||||
| 0 of 3=Asymptomatic | High probability | >90% | |||||
| 1 of 3=Nonanginal chest pain | Intermediate | 10%–90% | ||||||
| 2 of 3=Atypical angina | Low | <10% | ||||||
| 3 of 3=Typical angina | Very low | <5% | ||||||
| AGE (YRS) | SYMPTOMS | |||||||
| ASYMPTOMATIC | NONANGINAL CHEST PAIN | ATYPICAL ANGINA | TYPICAL ANGINA | |||||
| MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | |
| 35–45 | Very low | Very low | Intermediate | Very low | Intermediate | Intermediate | Intermediate | Intermediate |
| 45–55 | Low | Very low | Intermediate | Low | Intermediate | Intermediate | High | Intermediate |
| 55–65 | Intermediate | Low | Intermediate | Intermediate | Intermediate | Intermediate | High | Intermediate |
| 65–75 | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | High | High |
| Adapted from Diamond GA.2 | ||||||||
Your patients’ score dictates whether testing is required, and if so what kind.
Very low pretest probability patients should not have an exercise test, since they have a high risk of false-positive results. Evaluate and treat them for noncardiac causes of chest pain and begin primary prevention of CAD.
Low pretest probability patients should undergo exercise treadmill testing alone since negative results carry a high negative predictive value in both men and women, but positive test results may be false and can be evaluated by more studies.3
Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging modality.3-5 However, intermediate pretest probability patients with baseline ECG abnormalities such as electronically paced ventricular rhythm or left bundle-branch block will require myocardial perfusion imaging.5
High pretest probability patients should have coronary angiography as an initial strategy for diagnosis of CAD.3
History, exam, and ECG determine test suitability
Can your patient take an exercise stress test, or will he need a pharmacologic stress test instead? (See “A guide to sensitivity, specificity, and likelihood ratios for stress tests.”) Can he pedal a bicycle, walk, or exercise for 6 minutes? On physical examination, take note of his gait, mobility, and limb strength.
What medications is the patient taking? Digoxin may cause false ST changes, beta-blockers may prevent attaining maximum heart rate, and antihypertensive agents and vasodilators may alter the blood pressure response, producing a false negative result. Nitrates attenuate angina and the associated ST depression of ischemia.6 In addition, metabolic abnormalities and cocaine or alcohol use may affect heart rate, metabolic oxygen demand and the ability to perform the exercise treadmill testing.
On examination, document murmurs, rhythm abnormalities, vascular bruits, and abnormal pulses. Limit laboratory studies to recent cardiac damage screening if indicated. Screen with a resting ECG for arrhythmias, conduction abnormalities or preexisting cardiac damage. ST-segment (≥1 mm) and T-wave changes such as inversions secondary to strain or old injury or conduction abnormalities such as bundle branch blocks and prolonged QT interval may obscure exercise treadmill testing findings. Consider spirometry for patients with asthma or chronic lung disease.
Exercise treadmill testing
Sensitivity varies from 45% to 67% and specificity 72% to 90% with operator and patient variables.6 An abnormal test in a man at a heart rate of 85% of predicted maximum for age has a sensitivity of about 65% and a specificity of 85% for CAD. In women, one meta-analysis demonstrated a sensitivity of only 61% and a specificity of only 70%.8
PSMI
Pharmacologic stress myocardial imaging is similar to exercise treadmill testing. Dipyridamole and adenosine PSMI with thallium T1 201 or technetium Tc 99m have a similar sensitivity of 90%, and specificity of 70% for detection of CAD.6
Echocardiography
Overall sensitivity for exercise echocardiography was about 85% and for dobutamine stress echocardiography 82%. Dobutamine has a higher sensitivity than vasodilator echocardiography.6
Likelihood ratios (LR) for exercise treadmill testing and PSMI
Based on a review of coronary artery disease with chest pain as the symptom and a reference standard of a coronary angiogram with >70% narrowing of one or more arteries, or >50% left main, the LR varies for sex and for each different study. The positive LR (LR+) for exercise treadmill testing is 3.00 for men and 2.00 for women. The negative LR (LR–) for exercise treadmill testing is 0.650 for men and 0.560 for women. LR+ for exercise treadmill testing with thallium imaging is 5.9 (generally), but 2.20 for women; LR–is 0.200 and is 0.340 for women. Dipyridamole PSMI, LR+ is 3.30 and LR- is 0.180.16
The decisive factors
Absolute contraindications to exercise treadmill testing include recent MI; significant aortic stenosis,7 and weight exceeding equipment capacity. Relative contraindications to exercise treadmill testing (which can be superseded if the benefits of exercise outweigh the risks) include: hypertension (systolic >200 mm Hg/diastolic >110 mm Hg),5 left main coronary stenosis and stenotic valvular disease. (For more on “Contraindications to exercise testing,” see TABLE 2.)
The role of imaging: Important, yes—routine, no
An important element of stress testing is, of course, the imaging method(s) that will be used. The options include myocardial perfusion imaging with thallium Tl 201 or technetium Tc 99m, and echocardiography.
Indications for myocardial perfusion imaging with exercise treadmill testing are a high pretest probability for CAD, an abnormal baseline ECG such as left bundle branch block, previous myocardial damage or coronary revascularization, or a previous equivocal or unexpected exercise ECG result. In women with an intermediate pretest probability for CAD, the sensitivity and specificity of an exercise treadmill testing is less than in men, which suggests that nuclear imaging would improve this test.8 There is, however, insufficient data to justify initial routine stress imaging tests in women.1
TABLE 2
Contraindications to exercise testing
| ABSOLUTE |
|---|
|
| RELATIVE CONTRAINDICATIONS (CAN BE SUPERSEDED IF THE BENEFITS OF EXERCISE OUTWEIGH THE RISKS) |
|
| Source: Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf Accessed: March 6, 2007. |
Of the 2 agents used for myocardial perfusion imaging, technetium Tc 99m has more favorable imaging characteristics.9 It has a shorter half-life (6 hours) than thallium Tl 201 (73 hours), and larger doses of technetium Tc99m may be used, permitting the assessment of ventricular function.10
Echocardiography may also be done with either exercise treadmill testing or PSMI to evaluate relative myocardial perfusion. While radionuclide technique assesses relative myocardial perfusion, echocardiography also evaluates global and regional function. Indications for echocardiography are similar to myocardial perfusion imaging but also include the need for prognostic information after MI, and to assess physiologic significance of a lesion or to determine the success of an intervention.
Time for the test: Selecting the protocol
While the Bruce exercise treadmill testing protocol is the most commonly used (82% of tests)11 in healthy adults, it may not be appropriate for women or the elderly as most protocols were developed for the evaluation of men.12 A ramp method with gradual increase in grade each minute is preferred by some clinicians when patients are unable to perform a standard Bruce protocol. Another option, the Modified Bruce protocol, which is more gradual than the standard Bruce protocol; it has two 3-minute warm-up stages.12
The 3 PSMI protocols include adenosine, dipyridamole, and dobutamine. Each has a different administration routine,9 though ECG, blood pressure and pulse are taken every minute for all 3.
- Adenosine is infused with a pump over 6 minutes and technetium Tc99m is injected 3 minutes into the infusion.
- Dipyridamole is infused over 4 minutes and technetium Tc99m is injected 2 to no more than 5 minutes after the infusion. Theophylline is injected, after dipyridamole if necessary, no earlier than 1 minute after technetium Tc99m is administered to avoid interference with the uptake.
- Dobutamine is titrated with a dose increase every 3 minutes. Tc99m is injected after the first minute at the highest concentration. (Typically dobutamine is used with echocardiography.6)
Adenosine
A potent vasodilator, this endogenous nucleoside is rapidly cleared (half-life, <10 seconds) along with its side effects of flushing, headache, and nausea.
Dipyridamole
This coronary vasodilator inhibits the uptake of adenosine. The same side effects as adenosine—flushing, headache, nausea—may last longer with dipyridamole (half-life,13 hours) but they are more common with adenosine and are relieved by administering theophylline.
All methylxanthines may interfere with either dipyridamole or adenosine and should be held for 24 to 48 hours prior to examination.
- Avoid both adenosine and dipyridamole in patients with asthma, severe COPD (FEV1<30%), second- or third-degree heart block, hypotension, or those who are on oral dipyridamole.
Dobutamine
This synthetic catecholamine increases heart rate, systolic blood pressure, and myocardial contractility, thereby provoking ischemia. Dobutamine (half-life 2 minutes) is not affected by methylxanthines.
- It is preferred in patients who are unable to use adenosine or dipyridamole.
- Caution is needed in patients with systolic BP less than 100 mm Hg, hypertension, ventricular ectopy, and glaucoma.
- Side effects can be reversed with beta-blockers.
Ideal endpoints and the realities that may creep in
The ideal endpoint in an exercise treadmill testing is 100% of the age-predicted maximum heart rate (220–age). Eighty-five percent of maximum heart rate is the minimum for an acceptable test.
Absolute contraindications
Absolute indicators for stopping an exercise treadmill test are either a 10 mm Hg systolic drop in blood pressure from standing baseline, moderate to severe angina symptoms, feelings of syncope, skin color changes suggestive of hypoxia or hypotension, ischemic ST changes, or the patient’s desire to stop.
Relative contraindications
Relative indicators to stop include fatigue, shortness of breath, leg pain, increased arrhythmias—particularly PVCs that increase with the exercise level—and blood pressure ≥250 systolic or 115 diastolic.6
Ideally, PSMI evaluations are terminated according to the prescribed length of infusions. They will also be terminated if a patient develops wheezing, severe or increasing chest pain or hypotension, neurological symptoms, ST-segment elevation abnormalities, or arrhythmias. To reverse the side effects of adenosine or dipyridamole, aminophylline IV will be administered (1–2 mg/kg slowly, up to 250 mg).
Heart of the matter: What a report should cover
Assuming you have ordered the stress test (and not done it yourself), a complete report should include
- ST changes
- symptoms during testing
- reason for ending the test
- estimation of exercise capacity
- blood pressure response
- the presence and frequency of arrhythmias or ectopy.
Abnormal. ST segment change is the most important ECG finding in a positive test; it’s defined as >1 mm horizontal or down sloping depression or elevation, at least 60 to 80 milliseconds after the end of the QRS complex and should prompt further workup to confirm CAD.5 An abnormal ECG during a PSMI test indicates an elevated risk of multivessel CAD and should prompt further evaluation regardless of normal myocardial perfusion imaging.13
Duke Treadmill Score
Duke Treadmill Score (DTS)=exercise time–(5 × ST deviation) - (4 × exercise angina), with 0=no angina during exercise, 1=nonlimiting angina, and 2=exercise-limiting angina.
The score typically ranges from –25 to +15.4
- Low risk: > +5
- Moderate risk: –10 to +4
- High risk: < –11
Elderly Alternative Treadmill Score (for patients over 65 years of age)
This score has 2 variables in common with the Duke Treadmill Score (exercise duration or the MET equivalent and millimeters of ST changes). It also has 2 different variables (drop in exercise systolic blood pressure below resting value and history of congestive heart failure [CHF] or use of digoxin [Dig]).17,18
The score is calculated as follows: 5 × (CHF/Dig [yes=1; no=0]) + exercise-induced ST depression in millimeters + change in systolic blood pressure score–METs
Systolic blood pressure score:
- 0 for an increase >40 mm Hg
- 1 for an increase of 31–40 mm Hg
- 2 for an increase of 21–30 mm Hg
- 3 for an increase of 11–20 mm Hg
- 4 for an increase of 0–10 mm Hg
- 5 for a reduction below standing systolic pre-exercise blood pressure.
A score of < –2 is low risk, –2 to 2 is moderate risk, and >2 is high risk.
Equivocal. Reports that come back as equivocal will have ECG changes nondiagnostic of ischemia such as alterations in P- or T-wave morphology and nondiagnostic changes in AV conduction, particularly if changes revert to baseline during the rest period. Unifocal PACs or PVCs (<5/min) are not specific indicators for CAD and the development of bundle branch blocks are nondiagnostic findings. Equivocal results need additional testing such as myocardial perfusion imaging or angiography to document ischemia if the pretest probability is high.
Incomplete or failure. If your patient’s test involves equipment failure or if he (or the operator) was unable to complete the test, you should get a report to that effect. Depending on the nature of the failure, you may need to repeat the test, consider PSMI, or make a cardiology referral.
Duke Treadmill Score
A helpful calculation following treadmill testing
If your patient had a positive or negative exercise treadmill test, consider calculating his Duke Treadmill Score (DTS), which is predictive of 5-year survival and significant severe CAD for patients who are younger than 75 years.4,14
DTS helps you to exclude low-risk patients from further invasive testing and ensure high-risk patients receive further evaluation and appropriate treatment. DTS appears to be more useful in women with an intermediate pretest score but not with a low pretest score.15
The DTS score typically ranges from –25 to +15.5 Patients at low risk will have a score of > +5), moderate risk will have scores ranging from –10 to +4, and those at high risk will have a score of ≤–11.4
A modified DTS is used for patients older than 65 years who may have a limited exercise capacity, controlled asymptomatic congestive heart failure, or be on digoxin, which may affect their ability to perform a maximal exercise treadmill test.5 The values for the Elderly Alternative Treadmill Score are as follows: low risk (< –2); moderate risk (–2 to 2); and high risk (>2). (See “The calculations behind the scores.”)
Bottom line
DTS scores, Elderly Alternative Treadmill Scores, and pre–stress test CAD probability scores are all extremely useful. Integrating them into your practice can ensure that patients get the prompt care they may need, while sparing them unnecessary tests along the way.
FIGURE
Template for dictating noninvasive cardiac tests
Correspondence
Dennis P. Breen, MD, Eau Claire Family Medicine Clinic, 617 Clairemont Avenue, Eau Claire, WI 54701. [email protected]
1. Snow V, Barry P, Fihn SD, et al. Evaluation of primary care patients with chronic stable angina: guidelines from the American College of Physicians. Ann Intern Med 2004;141:57-64.
2. Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol 1983;1:574-575.
3. Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct? Chest 2000;118:535-541.
4. Shaw LJ, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying diagnostic coronary disease subgroups. Circulation 1998;98:1622-1630.
5. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf. Accessed on March 6, 2007.
6. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on Management of Patients with Chronic Stable Angina). J Am Coll Cardiol 1999;33:2092-2197.
7. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111:3290-3295.
8. Lewis JF, McGorray S, Lin L, et al. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: Findings from the national heart, lung and blood institute-sponsored women’s ischemia syndrome evaluation (WISE). Am Heart J 2005;149:527-533.
9. Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (ACC/AHA/ASNC committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging). J Am Coll Cardiol 2003;42:1318-1333.
10. Lee TH, Boucher CA. Clinical practice. noninvasive tests in patients with stable coronary artery disease. N Engl J Med 2001;344:1840-1845.
11. Myers J, Voodi L, Umann T, Froelicher VF. A survey of exercise testing: Methods, utilization, interpretation, and safety in the VAHCS. J Cardiopulm Rehabil 2000;20:251-258.
12. Ashley EA, Myers J, Froelicher V. Exercise testing in clinical medicine. Lancet 2000;356:1592-1597.
13. Cosmai EM, Heller GV. The clinical importance of electrocardiographic changes during pharmacologic stress testing with radionuclide myocardial perfusion imaging. J Nucl Cardiol 2005;12:466-472.
14. Kwok JM, Miller TD, Hodge DO, Gibbons RJ. Prognostic value of the duke treadmill score in the elderly. J Am Coll Cardiol 2002;39:1475-1481.
15. Morise AP, Olson MB, Merz NB, et al. Validation of the accuracy of pretest and exercise test scores in women with a low prevalence of coronary disease. The NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study. Am Heart J 2004;147:1085-1092.
16. InfoRetriever [web site] Clinical Rules and Calculators (2007). InfoRetriever Search Results, Exercise Testing, Diagnostic Tests, Chest Pain. Available at: www.infopoems.com/irsearch/display_article.cfm?resource=D&article=34. Accessed on January 26, 2007.
17. Morrow K, Morris CK, Froelicher VF, et al. Prediction of cardiovascular death in men undergoing noninvasive evaluation for coronary artery disease. Ann Intern Med 1993;118:689-695.
18. Kwok JF, Christian TE. Effective use of the exercise stress test to detect and predict coronary artery disease. Emerg Med 2001;33:12-22.Available at: www.emedmag.com/html/pre/fea/features/051501.asp. Accessed on March 7, 2007.
1. Snow V, Barry P, Fihn SD, et al. Evaluation of primary care patients with chronic stable angina: guidelines from the American College of Physicians. Ann Intern Med 2004;141:57-64.
2. Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol 1983;1:574-575.
3. Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct? Chest 2000;118:535-541.
4. Shaw LJ, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying diagnostic coronary disease subgroups. Circulation 1998;98:1622-1630.
5. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf. Accessed on March 6, 2007.
6. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on Management of Patients with Chronic Stable Angina). J Am Coll Cardiol 1999;33:2092-2197.
7. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111:3290-3295.
8. Lewis JF, McGorray S, Lin L, et al. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: Findings from the national heart, lung and blood institute-sponsored women’s ischemia syndrome evaluation (WISE). Am Heart J 2005;149:527-533.
9. Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (ACC/AHA/ASNC committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging). J Am Coll Cardiol 2003;42:1318-1333.
10. Lee TH, Boucher CA. Clinical practice. noninvasive tests in patients with stable coronary artery disease. N Engl J Med 2001;344:1840-1845.
11. Myers J, Voodi L, Umann T, Froelicher VF. A survey of exercise testing: Methods, utilization, interpretation, and safety in the VAHCS. J Cardiopulm Rehabil 2000;20:251-258.
12. Ashley EA, Myers J, Froelicher V. Exercise testing in clinical medicine. Lancet 2000;356:1592-1597.
13. Cosmai EM, Heller GV. The clinical importance of electrocardiographic changes during pharmacologic stress testing with radionuclide myocardial perfusion imaging. J Nucl Cardiol 2005;12:466-472.
14. Kwok JM, Miller TD, Hodge DO, Gibbons RJ. Prognostic value of the duke treadmill score in the elderly. J Am Coll Cardiol 2002;39:1475-1481.
15. Morise AP, Olson MB, Merz NB, et al. Validation of the accuracy of pretest and exercise test scores in women with a low prevalence of coronary disease. The NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study. Am Heart J 2004;147:1085-1092.
16. InfoRetriever [web site] Clinical Rules and Calculators (2007). InfoRetriever Search Results, Exercise Testing, Diagnostic Tests, Chest Pain. Available at: www.infopoems.com/irsearch/display_article.cfm?resource=D&article=34. Accessed on January 26, 2007.
17. Morrow K, Morris CK, Froelicher VF, et al. Prediction of cardiovascular death in men undergoing noninvasive evaluation for coronary artery disease. Ann Intern Med 1993;118:689-695.
18. Kwok JF, Christian TE. Effective use of the exercise stress test to detect and predict coronary artery disease. Emerg Med 2001;33:12-22.Available at: www.emedmag.com/html/pre/fea/features/051501.asp. Accessed on March 7, 2007.
Diabetes drug update: How 4 new options stack up
- Inhaled insulin, a short-acting insulin for type 1 and type 2 diabetes, is comparable with traditional subcutaneous regimens in terms of hemoglobin A1c and postprandial glucose reductions. It can also reduce the number of daily injections (B).
- Exenatide, which is indicated for type 2 diabetes in those uncontrolled on a sulfonylurea or metformin, provides a modest reduction in A1c and fasting glucose and is best suited for those whose A1c is within 1% of their goal. Among its advantages: weight loss and the potential to slow the progression of the disease (B).
- Sitagliptin is indicated for type 2 diabetes alone or in combination with metformin or a thiazolidinedione. It provides A1c reductions that are comparable to exenatide and does not have high rates of gastrointestinal side effects. It may also improve beta-cell function (B).
- Pramlintide, which is indicated for type 1 or type 2 diabetes uncontrolled with mealtime insulin, provides modest reductions in A1c and postprandial glucose—although it's more effective for those with postprandial hyperglycemia. It may reduce insulin dose requirements and the associated weight gain (B).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
The battle over glycemic control begins when you write out that first script for a patient for a sulfonylurea, metformin, or insulin. But it continues during every encounter thereafter, as you monitor your patient's progress, adjust dosages, and take advantage of new pharmacologic options. Recently, that list of options has expanded by 4: Three are new classes of agents, and the fourth is essentially a new delivery system for insulin. Inhaled insulin (Exubera) was approved by the Food and Drug Administration in January 2006, exenatide (Byetta) in April 2005, sitagliptin (Januvia) in October 2006, and pramlintide (Symlin) in March 2005 ( TABLE 1 ).
Staying abreast of new agents like these is essential if we are ever going to get the upper hand on a disease that in 2002 affected 18.2 million people.1 This review provides an at-a-glance summary of the key aspects of each agent, followed by a topline summary of their advantages and disadvantages.
TABLE 1
New therapeutic options for diabetes
| DRUG | INDICATIONS | DOSE | COST (AWP)* |
|---|---|---|---|
| Insulin, inhaled powder (Exubera) | Type 1 or type 2 diabetes mellitus | Administer 2-3 times a day just prior to meals. Dose (mg)=weight (kg)×0.05 mg/kg. Calculated dose should be rounded down to nearest whole milligram | Kit (includes inhaler plus 270 1- and 3-mg doses): $180 combination pack (180 1- and 3-mg doses): $134 combination pack (270 1- and 3-mg doses): $168 |
| Exenatide (Byetta) | Adjunct therapy for type 2 diabetes uncontrolled with metformin or sulfonylurea | Initial: 5 mcg sc twice daily. May be increased to 10 mcg sc twice daily after 1 month (max dose) | 5 mcg: $176.40/month 10 mcg: $207.00/month |
| Sitagliptin (Januvia) | Type 2 diabetes as monotherapy or in combination with metformin or thiazolidinedione | 100 mg orally once daily | $174.96/month |
| Pramlintide (Symlin) | Adjunct therapy for type 1 or type 2 diabetes in uncontrolled patients using mealtime insulin (with or without sulfonylurea or metformin in type 2 diabetes) | Type 1 diabetes: Initial: 15 mcg sc prior to each meal. Titrate to 30-60 mcg prior to each meal as tolerated. Type 2 diabetes: Initial: 60 mcg sc prior to each meal. Titrate to 120 mcg sc prior to each meal. | $95.40/month |
| AWP=average wholesale price; sc=subcutaneously | |||
| *Cost from Red Book Update 2006; 25(9) (Montvale, NJ: Thomson PDR; 2006). | |||
Exubera: A new twist on insulin
The first dry powder inhaled insulin, which can be used in lieu of rapid- or short-acting injectable insulins, is now available. The question is: How does it stack up? Inhaled insulin has been studied in several clinical trials in both type 1 and type 2 diabetes ( TABLE 2 ).2-8 In type 1 diabetes it's been combined with NPH insulin or ultralente insulin and compared with subcutaneous regimens of regular insulin with NPH insulin or ultralente insulin.2,3,6 These studies showed a similar decrease in glycosylated hemoglobin (Hb A1c) and 2-hour postprandial glucose between the inhaled and subcutaneous regimens. No studies comparing inhaled insulin powder containing regimens with subcutaneous regimens utilizing rapid acting insulin have been published.
In type 2 diabetes, inhaled insulin powder has been studied in combination with ultralente insulin, a sulfonylurea, and metformin.4,5,7,8 For patients with uncontrolled type 2 diabetes on a sulfonylurea or metformin, the addition of inhaled insulin powder has been shown to reduce A1c by 1.9% to 2.3%.4,8 When combined with ultralente in type 2 diabetes, reductions in A1c were comparable with traditional subcutaneous insulin regimens.
In addition, a few studies have looked at patient satisfaction with inhaled insulin. The findings: Inhaled insulin powder was linked to better satisfaction, convenience, ease of use, and social comfort in type 1 and 2 diabetes when compared to entirely subcutaneous regimens.6,9,10
TABLE 2
Inhaled insulin studies
| STUDY | TYPE | DESIGN | A1C CHANGE FROM BASELINE (%) |
|---|---|---|---|
| Skyler (2001) 3 | Type 1 | RCT, 12 weeks | -0.6 (INH); -0.8 (INJ) |
| Weiss (2003) 4 | Type 2 | RCT, 12 weeks INH + preexisting OHA vs preexisting OHA | -2.3 (INH+OHA) -0.1 (OHA)* |
| Quattrin (2004) 2 | Type 1 | RCT, 6 months INH + U vs R + NPH | -0.2 (INH + U) -0.4 (R + NPH) |
| Hollander (2004) 5 | Type 2 | RCT, 6 months INH + U vs R + NPH | -0.7 (INH + U) -0.6 (R + NPH) |
| Rosenstock (2004) 6 | Type 1 or type 2 | RCT, 12 weeks INH + U vs conventional split/mixed regimen | Type 1 diabetes: -0.69 (INH + U) -0.85 (split/mixed) Type 2 diabetes: -0.61 (INH + U) -0.79 (split/mixed) |
| DeFronzo (2005) 7 | Type 2 | RCT, 3 months INH vs rosiglitazone | -2.3 (INH) -1.4 (rosiglitazone) |
| Rosenstock (2005) 8 | Type 2 | RCT, 12 weeks INH alone, INH + OHA, or OHA alone (all after OHA failure) | -1.4 (INH alone) -1.9 (INH + OHA) -0.2 (OHA alone) |
| A1c, glycosylated hemoglobin; RCT, randomized controlled trial; INH, inhaled insulin; INJ, injected insulin; OHA, oral hypoglycemic agent; U, ultralente; R, regular insulin; NPH, NPH insulin | |||
| *P<.05 | |||
Not an option for smokers or those with pulmonary disease
The most common side effects of inhaled insulin include hypoglycemia, weight gain, cough, and bitter taste. The risk of hypoglycemia appears to be about the same or less than that seen with subcutaneous insulin.2 The same is true for weight gain, based on limited data.11 Other potential concerns include the formation of insulin antibodies. Antibody formation is higher with inhaled insulin than with subcutaneous insulin, but the clinical significance at this point is not clear.12
The drug's effect on lung function is also an issue. Inhaled insulin powder should not be used in patients who smoke (or those who have quit within the past 6 months) or who have underlying pulmonary disease. Smoking increases the drug's absorption and can lead to hypoglycemia.13 The safety and efficacy of inhaled insulin in patients with underlying pulmonary disease remains unclear. Some short-term studies in those without underlying pulmonary disease found no effects on pulmonary function, while others showed a decline in lung function.2-5
The manufacturer reports that in trials lasting less than 2 years, both individual patients on inhaled insulin or a comparative agent experienced a decrease in pulmonary function.14 Forced expiratory volume in 1 second (FEV1) declined by =20% in 1.5% of inhaled insulin treated patients and in 1.3% of those on another agent. Carbon monoxide diffusing capacity (DLCO) decreased by =20% in 5.1% of those on inhaled insulin and 3.6% of those on a comparative agent. Thus, the manufacturer recommends a baseline spirometry (FEV1) and possibly DLCO. The manufacturer does not recommend the use of inhaled insulin if FEV1 or DLCO is <70% predicted.
A patient's pulmonary function should be assessed after 6 months on the drug and then annually thereafter. Should FEV1 decline by =20% from baseline or pulmonary symptoms develop while on therapy, you'll need to discontinue the inhaled insulin. Two longer-term trials of up to 4 years in duration did not show any significant effect on pulmonary function.15,16
A convenience with a price tag
Inhaled insulin powder is available in single-dose 1-mg and 3-mg blister packs and should be used no more than 10 minutes before meals. To administer the insulin, the patient breathes out, inhales the dose, and then holds his breath for 5 seconds. The patient will, however, need to load each dose.
Each milligram of the inhaled insulin is equivalent to 2 to 3 units of regular subcutaneous insulin. Inhaled insulin powder is a bolus insulin that targets postprandial glucose and thus can be used in place of rapid- or short-acting injectable insulins.
Patients with type 1 diabetes will require an injectable basal insulin (intermediate or long acting) in conjunction with the inhaled insulin. In type 2 diabetes, inhaled insulin can be used in conjunction with a basal insulin or oral therapy. In patients who are currently using an injectable bolus insulin, the package insert contains a dose conversion table. Initial doses can also be estimated based on weight.
Inhaled insulin may reduce the number of daily insulin injections to 1 to 2 times a day, and that could translate into improved patient compliance, although this has not been directly evaluated. The cost of Exubera is significantly higher than traditional subcutaneous insulin. An Exubera kit costs $180, which includes an inhaler and 270 1 mg and 3 mg doses.
The take-home message is... While inhaled insulin offers comparative efficacy to subcutaneous regimens, there's a potential for short-term decreases in pulmonary function. The long-term effects are largely unknown. As a result, rapid or short-acting injectable insulins may be a safer alternative. Inhaled insulin's role in type 2 diabetes is less clear at this time. In patients with type 2 disease, it would be an option when considering the addition of insulin. However, there's limited data on using inhaled insulin in place of an oral agent.
Exenatide (Byetta): From the mouths of (gila) monsters
Exenatide is synthetic exendin-4, originally isolated from the saliva of the gila monster lizard. It binds to and activates the pancreatic GLP-1 (glucagon like peptide-1) receptor resulting in an increase in insulin secretion from beta cells in the presence of hyperglycemia. It also suppresses glucagon secretion, slows gastric emptying, and decreases food intake. Its use is limited to type 2 diabetes; it has no role in the management of type 1 diabetes.
In 2002 diabetes affected 18.2 million individuals, or 6.3% of the US population.1 The prevalence is expected to double within the next 20 years along with significant increases in cardiovascular disease.1
There are 2 theories as to how diabetes increases cardiovascular mortality.35,36 The first suggests that beta-cell dysfunction and subsequent failure leads to elevated glucose that causes an increase in oxidative stress, and thus leads to cardiovascular disease. The second theory suggests that insulin resistance causes endothelial dysfunction along with inflammation and fibrinolysis and this leads to cardiovascular disease. It's likely that both of these theories are at work, since we know that elevated blood glucose levels can lead to elevated insulin levels and insulin resistance can cause beta-cell dysfunction.
The research on the diabetes/CVD link is intriguing. For instance, there is data suggesting that insulin sensitizing agents may have a positive effect on cardiovascular disease.37 In addition, trials are being conducted between sulfonylureas and thiazolidinediones to evaluate reductions in CVD.38 It may not be long before reducing cardiovascular morbidity and mortality becomes a goal of treatment in the management of our patients with diabetes.
Three large placebo-controlled trials evaluated the use of exenatide as adjunct therapy to a sulfonylurea or metformin in patients unable to achieve glycemic control ( TABLE 3 ).17-19 Hemoglobin A1c was reduced by 0.4% to 0.6% with 5 mcg twice daily and 0.8% to 0.9% with 10 mcg twice daily. The effects on fasting plasma glucose were less impressive, though not surprising due to the drug's mechanism of action.
One other trial compared exenatide, 10 mcg twice daily, to insulin glargine, one daily dose titrated to achieve fasting glucose less than 100 mg/dL in patients with type 2 diabetes uncontrolled on a sulfonylurea and metformin, which represents a relatively common clinical scenario.20 The reduction in A1c after 26 weeks was comparable between the 2 groups (1.11% for both).
Exenatide was more effective at reducing postprandial glucose, while glargine more effectively reduced fasting glucose. Weight increased by an average of 1.8 kg in the glargine group and decreased by 2.3 kg with exenatide. Rates of symptomatic hypoglycemia were similar between the 2 groups. Gastrointestinal symptoms were more common in the exenatide group, including nausea (57.1% vs 8.6%), vomiting (17.4% vs 3.7%), and diarrhea (8.5% vs 3%). This led to a significant difference in the number of subjects who withdrew from the study (19.4% for exenatide vs 9.7% for glargine). It's important to note that the mean baseline A1c values were only moderately elevated (8.2% in exenatide vs 8.3% in glargine) and thus not representative of those with very poor control.
One other research finding is worth mentioning here. GLP-1 administration has been shown to result in beta-cell proliferation and increased beta-cell mass in animals and in vitro studies.21 Thus, in theory, exenatide could slow the progression of type 2 diabetes. However, long-term studies are needed to address this.
TABLE 3
Exenatide studies
| VARIABLE | BUSE (2004)17 | DEFRONZO (2005)18 | KENDALL (2005)19 |
|---|---|---|---|
| BASELINE DATA | |||
| Number of patients | 377 | 336 | 733 |
| Age (yrs) | 55 | 53 | 55 |
| BMI (kg/m2) | 33 | 34 | 34 |
| A1c (%) | 8.6 | 8.2 | 8.5 |
| FPG (mg/dL) | 184 | 172 | 180 |
| Concomitant therapy | Sulfonylurea | metformin | Sulfonylurea + metformin |
| RESULTS—CHANGE FROM BASELINE | |||
| A1c (%) | 5 mcg dose: -0.5 | 5 mcg dose: -0.4 | 5 mcg dose: -0.6 |
| 10 mcg dose: -0.9 | 10 mcg dose: -0.8 | 10 mcg dose: -0.8 | |
| FPG (mg/dL) | 5 mcg dose: -5.4 | 5 mcg dose: -7.2 | 5 mcg dose: -9 |
| 10 mcg dose: -10.8 | 10 mcg dose: -10.1 | 10 mcg dose: -11 | |
| Weight (kg) | 5 mcg dose: -0.9 | 5 mcg dose: -1.6 | 5 mcg dose: -1.6 |
| 10 mcg dose: -1.6 | 10 mcg dose: -2.8 | 10 mcg dose: -1.6 | |
| BMI, body mass index; A1c, glycosylated hemoglobin; FPG, fasting plasma glucose. | |||
Bad news: Transient nausea; Good news: Unrelated weight loss
Nausea is the most common side effect and occurs in 36% to 39% of patients with the 5-mcg dose and 45% to 50% of those with the 10-mcg dose, although it's usually transient.17-19,22 Exenatide results in a moderate reduction in weight (approximately 2-4 pounds), which does not appear to be related to the adverse gastrointestinal effects. There's a risk of mild to moderate hypoglycemia when exenatide is used with a sulfonylurea, which is most likely due to the effects of the sulfonylurea.
Exenatide reportedly results in low levels of antibodies in approximately 40% of patients but had no affect on glucose control.22 About 6% of patients may develop high antibody levels, which could result in a diminished response.22
Exenatide is dispensed as a injection pen containing a 30-day supply of medicine. The patient will need to administer it subcutaneously in the thigh, abdomen, or upper arm no more than 60 minutes before morning and evening meals. The cost of exenatide is substantially higher than sulfonylureas, metformin, or insulin but comparable with pioglitazone and rosiglitazone.
The take-home message is... Exenatide is not currently recommended for use as initial therapy in type 2 diabetes. In clinical trials, exenatide 10 mcg twice daily achieved A1c reductions of about 1%. Oral agents typically produce reductions of 1% to 2%, although the effects of combining oral agents may not always be additive.23,24
At this point, exenatide is best suited for those whose A1c is within 1% of their treatment goal, especially in those unable to take another oral agent or insulin (eg, due to renal or hepatic impairment or congestive heart failure) and those who have elevated postprandial glucose. Otherwise, adding an oral agent or insulin would likely produce the best results.
Sitagliptin (Januvia): It, too, focuses on GlP-1
Sitagliptin (Januvia), the first drug in a new class of agents called dipeptidyl-peptidase-4 (DPP-4) inhibitors, was just approved in October 2006 for the treatment of type 2 diabetes. This drug, like exenatide, focuses on the actions of GLP-1. Active GLP-1 is rapidly degraded by the DPP-4 enzyme. Inhibiting this enzyme results in an increased concentration and prolonged action of GLP-1.
There are some key differences between DPP-4 inhibitors and GLP-1 agonists such as exenatide. Specifically, DPP-4 inhibitors do not appear to have significant rates of nausea and vomiting, can be given orally, have no effect on gastric emptying, and are weight neutral. Limited evidence suggests that, like GLP-1 agonists, they may also improve chronic beta-cell function.25 Side effects include stuffy or runny nose and sore throat, upper respiratory infection, and headache.
Published studies are sparse at this point. One dose finding study randomized 552 patients to one of five treatments: placebo, sitagliptin (25, 50, or 100 mg once daily), or 50 mg twice daily. Baseline A1c ranged from 5.8% to 10.4% and after 12 weeks of treatment, the sitagliptin 100 mg once daily group had the largest reduction in A1c. Reductions were dependent on baseline A1c: Those with a baseline A1c <7%, 7% to 8.5%, or 8.5% to 10% had reductions of 0.4%, 0.6%, and 0.8%, respectively.26
Renal patients require a change in dose
The recommended dose of sitagliptin is 100 mg by mouth once a day as monotherapy or in combination with metformin or a thiazolidinedione. You'll need to reduce the dose in those patients with renal impairment.
The take-home message is... This newest class of medications exhibits some potential advantages and disadvantages when compared to the GLP-1 agonists. On the plus side, it does not appear to cause nausea and vomiting and can be given orally. On the downside, it has no effect on gastric emptying, which means it may not reduce postprandial glucose as much. In addition, it does not cause weight loss (although it does not cause weight gain either).
Pramlintide (Symlin): Shoring up deficiencies
Pramlintide is a synthetic analog of human amylin, a neuroendocrine hormone secreted by pancreatic beta cells. Amylin works in concert with insulin to suppress postprandial glucagon secretion and slow carbohydrate absorption by delaying gastric emptying. Amylin is cosecreted with insulin so patients with type 1 diabetes have an absolute deficiency of amylin while those with type 2 diabetes have a progressively declining production. Thus, pramlintide may be used in either type of diabetes.
In clinical trials, pramlintide produced modest reductions in A1c (0.1-0.62%) and more impressive reductions in postprandial glucose (64.8-126 mg/dL) in adults with type 1 or 2 diabetes ( TABLE 4 ).27-34 In addition, it has been shown to minimize insulin dose increases and the weight gain associated with insulin.27,29-31,34
Inhaled insulin, exenatide, sitagliptin, and pramlintide are exciting developments in the management of diabetes. They offer potential advantages over currently available therapies, but also have their share of limitations. As we gain further experience with them, their roles may increase.
Other agents are also on the horizon and worth noting. Vildagliptin (Galvus), a DPP-4 inhibitor, is expected to become available shortly. Another drug, liraglutide, a synthetic GlP-1 analog with a longer half-life than exenatide, is currently in phase III trials. A long-acting exenatide, given once weekly, is in phase II trials.
Time will tell as to how these agents—both the recently approved ones and those in the pipeline—will aid in our battle against diabetes. What is clear is that our arsenal will continue to grow, and we we'll continue to make inroads—one patient encounter at a time.
TABLE 4
Pramlintide studies
| STUDY | TYPE OF DIABETES | DESIGN | A1C CHANGE FROM BASELINE (%) | PPG CHANGE FROM BASELINE (MG/DL) |
|---|---|---|---|---|
| Fineman (1999) 30 | Type 1 | DB, PC, 26 wk | -0.2* (60 mcg 3x/day) -0.1 (90 mcg 2x/day) -0.1 (90 mcg 3x/day) 0.1 (placebo) | NA |
| Gottlieb (1999) 31 | Type 2 | DB, PC, 26 wk | -0.3 (90 mcg 2x/day) -0.4 (90 mcg 3x/day) -0.4* (120 mcg 2x/day) -0.1 (placebo) | NA |
| Nyholm (1999) 32 | Type 1 | DB, PC, 4 wk | NA | -126 (1-hr) -72 (2-hr) (30 mcg 4x/day) |
| Whitehouse (2002) 27 | Type 1 | R, DB, PC, 52 weeks | -0.39* (30-60 mcg 4x/day) -0.12 (placebo) | NA |
| Ratner (2002) 28 | Type 2 | R, DB, PC, 52 weeks | -0.3 (30 mcg 3x/day) -0.5 (75 mcg 3x/day) -0.6* (150 mcg 3x/day) -0.2 (placebo) | NA |
| Hollander (2003) 29 | Type 2 | R, DB, PC, 52 weeks | -0.35 (90 mcg 2x/day) -0.62* (120 mcg 2x/day) -0.22 (placebo) | NA |
| Levetan (2003) 33 | Type 1 | R, DB, PC, 4 weeks | NA | -79.2 (1-hr) -64.8 (2-hr) (30 mcg 3x/day) |
| Ratner (2004) 34 | Type 1 | R, DB, PC, 52 weeks | -0.29* (60 mcg 3x/day) -0.34* (60 mcg 4x/day) -0.04 (placebo) | NA |
| A1c, glycosylated hemoglobin; PPG, postprandial glucose; DB, double-blind; PC, placebo-controlled; R, randomized; NA, not accessed. | ||||
| *P<.05 vs placebo. | ||||
Nausea is a factor, as is slowed gastric emptying
The most common adverse effects include nausea, vomiting, and anorexia. Rates of nausea in studies have ranged from 9.5% to 59% with most cases being mild to moderate in nature and resolving in 2 to 8 weeks.27-29
Pramlintide in itself does not cause hypoglycemia, however when administered with insulin, it does increase the risk of insulin-induced hypoglycemia. Pramlintide should not be used in patients with gastroparesis since it slows gastric emptying. Pramlintide should not be mixed with insulin in the same syringe as there is insufficient data to support the safety of doing so. Thus, it may increase the number of daily injections for patients.
Pramlintide may also interfere with agents that stimulate gastric motility and slow the absorption of other drugs. The manufacturer recommends separating the administration of analgesics and pramlintide by 1 to 2 hours since coadministration could delay the analgesic onset.
Starting pramlintide means reductions elsewhere
Pramlintide is supplied as a 5 mL vial containing 0.6 mg/mL. Immediately prior to each major meal, the patient will need to administer it subcutaneously into the abdomen or thigh (arm administration is not recommended due to varying absorption). When initiating pramlintide in a patient, you'll need to reduce the patient's rapid/short insulin (including fixed-mixed insulin such as 70/30) by 50%.
In type 1 diabetes, the pramlintide dose may be increased in 15-mcg increments, provided that the patient has not experienced clinically significant nausea for at least 3 days and his glycemic goals are not met. In type 2 diabetes, the initial pramlintide dose may be doubled, provided that the patient has not experienced clinically significant nausea for 3 to 7 days and his glycemic goals are not met. In either case, should the increase in dose result in intolerable nausea, you may need to drop the dose back to the previous dose.
The take-home message is... While pramlinitide offers a different approach (as compared with insulin) to lowering postprandial glucose, there is no evidence that it offers any distinct advantage to the patient. Thus, it may be best to simply increase the premeal insulin dose. Should continued weight gain be a major concern, then pramlintide could play a role as adjunct therapy to mealtime insulin. Further studies evaluating quality of life and patient acceptance are needed.
CORRESPONDENCE
James R. Taylor, PharmD, CDE University of Florida, College of Pharmacy, PO Box 100486, Gainesville, FL 32610-0486 [email protected]
1. Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitis in the United States. JAMA 2003;290:1884-1890.
2. Quattrin T, Belanger A, Bohannon NJV, Schwartz SL. for the Exubera phase III Study Group. Efficacy and safety of inhaled insulin (Exubera) compared to subcuatenous insulin therapy in patients with type 1 diabetes: results of a 6-month, randomized, comparative trial. Diabetes Care 2004;27:2622-2627.
3. Skyler JS, Cefalu WT, Kourides IA, Landschulz WH, Balagtas CC, Cheng S-L, et al. for the Inhaled Insulin Phase II Study Group. Efficacy of inhaled human insulin in type 1 diabetes mellitus: a randomized proof-of-concept study. Lancet 2001;357:331-335.
4. Weiss SR, Cheng S-L, Kourides IA, Gelfand RA, Land-Schulz WH. for the Inhaled Insulin Phase II Study Group. Inhaled insulin provides improved glycemic control in patients with type 2 diabetes mellitus inadequately controlled with oral agents:a randomized controlled trial. Arch Intern Med 2003;163:2277-2282.
5. Hollander PA, Blonde L, Rowe R, Mehta ME, Milburn JL, Hershon KS. for the Exubera Phase III Study Group. Efficacy and safety of inhaled insulin (Exubera) compared with subcutaneous insulint eharpy in patients with type 2 diabetes: results of a 6-month, randomized comparative trial. Diabetes Care 2004;27:2356-2362.
6. Rosenstock J, Bolinder B, Cappeleri JC, Gerber R. Patient satisfaction and glycemic control after 1 year with inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes. Diabetes Care 2004;27:1318-1323.
7. DeFronzo RA, Bergenstal RM, Cefalu WT, Pullman J, Lerman S, Bode BW, et al. for the Exubera Phase III Study Group. Efficacy of inhaled insulin in patients with type 2 diabetes not controlled with diet and exercise. Diabetes Care 2005;28:1922-1928.
8. Rosenstock J, Zinman B, Murphy LJ, Clement SC, Moore P, Bowering K, Hendler R, Lan S-P, Cefalu WT. Inhaled insulin improves glycemic control when substituted for or added to oral combination therapy in type 2 diabetes. Ann Intern Med 2005;143:549-558.
9. Gerber RA, Cappalleri JC, Kourides IA, Gelfand RA. Treatment satisfaction with inhaled insulin in patients with type 1 diabetes: a randomized controlled trial. Diabetes Care 2001;24:1556-1559.
10. Cappalerri JC, Cefalu WT, Rosenstock J, Kourides IA, Gerber RA. Treatment satisfaction in type 2 diabetes: a comparison between an inhaled insulin regimen and a subcutaneous insulin regimen. Clin Ther 2002;24:552-564.
11. Odegard PS, Capoccia KL. Inhaled insulin: exubera. Ann Pharmacother 2005;39:843-853.
12. Fineberg SE, Schatz D, Krasner A. Results of insulin antibody monitoring during phase II and phase III clinical studies of inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes (abstract 46). Diabetes 2002;51(suppl):A17.-
13. Himmelman A, Jende J, Mellen A, Petersen AH, Dahl UL, Wollmer P. The impact of smoking on inhaled insulin. Diabetes Care 2003;26:677-682.
14. Pfizer. Exubera (insulin human inhalation opwder) package insert. New York, NY; 2006.
15. Barnett AH. for the Exubera Phase III Study group. Efficacy and one-year pulmonary safety of inhaled insulin (Exubera) as adjunctive therapy with metformin or glibenclamide in type 2 diabetes patients poorly controlled on oral agent monotherapy (abstract 454-P). Diabetes 2004;53:A107.-
16. Skyler J. for the Exubera Phase II Study Group. Sustained long-term efficacy and safety of inhaled insulin during 4 years continuous therapy (abstract 486-P). Diabetes 2004;53:A115.-
17. Buse JB, Henry RR, Han J, Kim DD, Fineman MS, Baron AD. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 2004;27:2628-2635.
18. DeFronzo RA, Ratner R, Han J, Kim D, Fineman MS, Baron AD. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes mellitus. Diabetes Care 2005;28:1092-1100.
19. Kendall DM, Riddle MC, Rosenstock J, et al. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes mellitus treated with metformin and a sulfonylurea. Diabetes Care 2005;28:1083-1091.
20. Heine RJ, Van Gaal LF, Johns D, Mihm MJ, Widel MH, Brodows RG. for the GWAA Study group. Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes. Ann Intern Med 2005;143:559-569.
21. Gallwitz B. Glucagon-like peptide-1 as a treatment option for type 2 diabetes and its role in restoring beta-cell mass. Diabetes Technol Ther 2005;7:651-657.
22. Triplitt C, Wright A, Chiquette E. Incretin mimetics and dipeptidyl peptidase-IV inhibitors: potential new therapies for type 2 diabetes mellitus. Pharmacotherapy 2006;26:360-374.
23. Willms B, Ruge D. Comparison of acarbose and metformin in patients with type 2 diabetes mellitus insufficiently controlled with diet and sulphonylureas: a randomized, placebo-controlled study. Diabetes Med 1999;16:755-761.
24. Rosenstock J, Sugimoto D, Strange P, Stewart JA, Soltesrak E, Dailey J. Triple therapy in type 2 diabetes: insulin glargine or rosiglitazone added to combination therapy of sulfonylurea plus metformin in insulin-naïve patients. Diabetes Care 2006;29:554-559.
25. Miller SA, St. Onge EL. Sitagliptin: a dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes. Ann Pharmacother 2006;40:1336-1343.
26. Herman G, Hanefeld M, Wu M, Chen X, Zhao P, Stein P. Effect of MK-0431, a dipeptidyl peptidase IV (DPP-IV) inhibitor, on glycemic control after 12 weeks in patients with T2DM (abstract 541-P). Diabetes 2005;54(suppl 1):A134.-
27. Whitehouse F, Kruger DF, Fineman M, Shen L, Ruggles JA, Maggs DG, et al. A randomized study and open-label extension evaluating the long-term efficacy of pramlintide as an adjunct to insulin therapy in type 1 diabetes. Diabetes Care 2002;25:724-730.
28. Ratner RE, Want LL, Fineman MS, Velte MJ, Ruggles JA, Gottlieb A, et al. Adjunctive therapy with the amylin analogue pramlintide leads to a combined improvement in glycemic and weight control in insulin-treated subjects with type 2 diabetes. Diabetes Technol Ther 2002;4:51-61.
29. Hollander PA, Levy P, Fineman MS, Maggs DG, Shen LZ, Strobel SA, et al. Pramlintide as an adjunct to insulin therapy improves long-term glycemic and weight control in patients with type 2 diabetes. Diabetes Care 2003;26:784-790.
30. Fineman M, Bahner A, Gottlieb A, Kolterman OG. Effects of six months administration of pramlintide as anadjunct to insulin therapy on metabolic control in people with type 1 diabetes (abstract). Diabetes 1999;48(suppl 1):A113.-
31. Gottlieb A, Fineman M, Bahner A, Parker J, Waite G, Kolterman O. Pramlintide therapy in addition to insulin in type 2 diabetes: effect on metabolic control after 6 months (abstract). Diabetologia 1999;42(suppl 1):A232.-
32. Nyholm B, Orskov L, Hove K, Gravholt CH, Moller N, Alberti GMN, et al. The amylin analog pramlintide improves glycemic control and reduces postprandial glucagons concentrations in patients wih type 1 diabetes mellitus. Metabolism 1999;48:935-941.
33. Levetan C, Want LL, Weyer C, Strobel SA, Crean J, Wang Y, et al. Impact of pramlintide on glucose fluctuations and postprandial glucose, glucagons, and triglyceride excursions among patients with type 1 diabetes intensively treated with insulin pumps. Diabetes Care 2003;26:1-8.
34. Ratner RE, Dickey R, Fineman M, et al. Amylin replacement with pramlintide as an adjunct to insulin therapy improves long-term glycemic and weight control in type 1 diabetes mellitus: a 1-year, randomized controlled trial. Diabet Med 2004;21:1204-1212.
35. Lillioja S, Mott DM, Spraul M, Ferraro R, Foley JE, Ravussin E. Insulin resistance and insulin and insulin secretory dysfunction as precursors of non-insulin-dependent diabetes mellitus. N Engl J Med 1993;329:1988-1992.
36. Ferrannini E. Insulin resistance versus insulin deficiency in non-insulin-dependent diabetes mellitus: problems and prospects. Endocr Rev 1998;19:477-490.
37. Jawa AA, Fonseca VA. Role of insulin secretagogues and insulin sensitizing agents in the prevention of cardiovascular disease in patients who have diabetes. Cardiol Clin 2005;23:119-138.
38. Mazzone T, Meyer PM, Feinstein SB, et al. Effect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes:a randomized trial. JAMA 2006;296:2572-2581.
- Inhaled insulin, a short-acting insulin for type 1 and type 2 diabetes, is comparable with traditional subcutaneous regimens in terms of hemoglobin A1c and postprandial glucose reductions. It can also reduce the number of daily injections (B).
- Exenatide, which is indicated for type 2 diabetes in those uncontrolled on a sulfonylurea or metformin, provides a modest reduction in A1c and fasting glucose and is best suited for those whose A1c is within 1% of their goal. Among its advantages: weight loss and the potential to slow the progression of the disease (B).
- Sitagliptin is indicated for type 2 diabetes alone or in combination with metformin or a thiazolidinedione. It provides A1c reductions that are comparable to exenatide and does not have high rates of gastrointestinal side effects. It may also improve beta-cell function (B).
- Pramlintide, which is indicated for type 1 or type 2 diabetes uncontrolled with mealtime insulin, provides modest reductions in A1c and postprandial glucose—although it's more effective for those with postprandial hyperglycemia. It may reduce insulin dose requirements and the associated weight gain (B).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
The battle over glycemic control begins when you write out that first script for a patient for a sulfonylurea, metformin, or insulin. But it continues during every encounter thereafter, as you monitor your patient's progress, adjust dosages, and take advantage of new pharmacologic options. Recently, that list of options has expanded by 4: Three are new classes of agents, and the fourth is essentially a new delivery system for insulin. Inhaled insulin (Exubera) was approved by the Food and Drug Administration in January 2006, exenatide (Byetta) in April 2005, sitagliptin (Januvia) in October 2006, and pramlintide (Symlin) in March 2005 ( TABLE 1 ).
Staying abreast of new agents like these is essential if we are ever going to get the upper hand on a disease that in 2002 affected 18.2 million people.1 This review provides an at-a-glance summary of the key aspects of each agent, followed by a topline summary of their advantages and disadvantages.
TABLE 1
New therapeutic options for diabetes
| DRUG | INDICATIONS | DOSE | COST (AWP)* |
|---|---|---|---|
| Insulin, inhaled powder (Exubera) | Type 1 or type 2 diabetes mellitus | Administer 2-3 times a day just prior to meals. Dose (mg)=weight (kg)×0.05 mg/kg. Calculated dose should be rounded down to nearest whole milligram | Kit (includes inhaler plus 270 1- and 3-mg doses): $180 combination pack (180 1- and 3-mg doses): $134 combination pack (270 1- and 3-mg doses): $168 |
| Exenatide (Byetta) | Adjunct therapy for type 2 diabetes uncontrolled with metformin or sulfonylurea | Initial: 5 mcg sc twice daily. May be increased to 10 mcg sc twice daily after 1 month (max dose) | 5 mcg: $176.40/month 10 mcg: $207.00/month |
| Sitagliptin (Januvia) | Type 2 diabetes as monotherapy or in combination with metformin or thiazolidinedione | 100 mg orally once daily | $174.96/month |
| Pramlintide (Symlin) | Adjunct therapy for type 1 or type 2 diabetes in uncontrolled patients using mealtime insulin (with or without sulfonylurea or metformin in type 2 diabetes) | Type 1 diabetes: Initial: 15 mcg sc prior to each meal. Titrate to 30-60 mcg prior to each meal as tolerated. Type 2 diabetes: Initial: 60 mcg sc prior to each meal. Titrate to 120 mcg sc prior to each meal. | $95.40/month |
| AWP=average wholesale price; sc=subcutaneously | |||
| *Cost from Red Book Update 2006; 25(9) (Montvale, NJ: Thomson PDR; 2006). | |||
Exubera: A new twist on insulin
The first dry powder inhaled insulin, which can be used in lieu of rapid- or short-acting injectable insulins, is now available. The question is: How does it stack up? Inhaled insulin has been studied in several clinical trials in both type 1 and type 2 diabetes ( TABLE 2 ).2-8 In type 1 diabetes it's been combined with NPH insulin or ultralente insulin and compared with subcutaneous regimens of regular insulin with NPH insulin or ultralente insulin.2,3,6 These studies showed a similar decrease in glycosylated hemoglobin (Hb A1c) and 2-hour postprandial glucose between the inhaled and subcutaneous regimens. No studies comparing inhaled insulin powder containing regimens with subcutaneous regimens utilizing rapid acting insulin have been published.
In type 2 diabetes, inhaled insulin powder has been studied in combination with ultralente insulin, a sulfonylurea, and metformin.4,5,7,8 For patients with uncontrolled type 2 diabetes on a sulfonylurea or metformin, the addition of inhaled insulin powder has been shown to reduce A1c by 1.9% to 2.3%.4,8 When combined with ultralente in type 2 diabetes, reductions in A1c were comparable with traditional subcutaneous insulin regimens.
In addition, a few studies have looked at patient satisfaction with inhaled insulin. The findings: Inhaled insulin powder was linked to better satisfaction, convenience, ease of use, and social comfort in type 1 and 2 diabetes when compared to entirely subcutaneous regimens.6,9,10
TABLE 2
Inhaled insulin studies
| STUDY | TYPE | DESIGN | A1C CHANGE FROM BASELINE (%) |
|---|---|---|---|
| Skyler (2001) 3 | Type 1 | RCT, 12 weeks | -0.6 (INH); -0.8 (INJ) |
| Weiss (2003) 4 | Type 2 | RCT, 12 weeks INH + preexisting OHA vs preexisting OHA | -2.3 (INH+OHA) -0.1 (OHA)* |
| Quattrin (2004) 2 | Type 1 | RCT, 6 months INH + U vs R + NPH | -0.2 (INH + U) -0.4 (R + NPH) |
| Hollander (2004) 5 | Type 2 | RCT, 6 months INH + U vs R + NPH | -0.7 (INH + U) -0.6 (R + NPH) |
| Rosenstock (2004) 6 | Type 1 or type 2 | RCT, 12 weeks INH + U vs conventional split/mixed regimen | Type 1 diabetes: -0.69 (INH + U) -0.85 (split/mixed) Type 2 diabetes: -0.61 (INH + U) -0.79 (split/mixed) |
| DeFronzo (2005) 7 | Type 2 | RCT, 3 months INH vs rosiglitazone | -2.3 (INH) -1.4 (rosiglitazone) |
| Rosenstock (2005) 8 | Type 2 | RCT, 12 weeks INH alone, INH + OHA, or OHA alone (all after OHA failure) | -1.4 (INH alone) -1.9 (INH + OHA) -0.2 (OHA alone) |
| A1c, glycosylated hemoglobin; RCT, randomized controlled trial; INH, inhaled insulin; INJ, injected insulin; OHA, oral hypoglycemic agent; U, ultralente; R, regular insulin; NPH, NPH insulin | |||
| *P<.05 | |||
Not an option for smokers or those with pulmonary disease
The most common side effects of inhaled insulin include hypoglycemia, weight gain, cough, and bitter taste. The risk of hypoglycemia appears to be about the same or less than that seen with subcutaneous insulin.2 The same is true for weight gain, based on limited data.11 Other potential concerns include the formation of insulin antibodies. Antibody formation is higher with inhaled insulin than with subcutaneous insulin, but the clinical significance at this point is not clear.12
The drug's effect on lung function is also an issue. Inhaled insulin powder should not be used in patients who smoke (or those who have quit within the past 6 months) or who have underlying pulmonary disease. Smoking increases the drug's absorption and can lead to hypoglycemia.13 The safety and efficacy of inhaled insulin in patients with underlying pulmonary disease remains unclear. Some short-term studies in those without underlying pulmonary disease found no effects on pulmonary function, while others showed a decline in lung function.2-5
The manufacturer reports that in trials lasting less than 2 years, both individual patients on inhaled insulin or a comparative agent experienced a decrease in pulmonary function.14 Forced expiratory volume in 1 second (FEV1) declined by =20% in 1.5% of inhaled insulin treated patients and in 1.3% of those on another agent. Carbon monoxide diffusing capacity (DLCO) decreased by =20% in 5.1% of those on inhaled insulin and 3.6% of those on a comparative agent. Thus, the manufacturer recommends a baseline spirometry (FEV1) and possibly DLCO. The manufacturer does not recommend the use of inhaled insulin if FEV1 or DLCO is <70% predicted.
A patient's pulmonary function should be assessed after 6 months on the drug and then annually thereafter. Should FEV1 decline by =20% from baseline or pulmonary symptoms develop while on therapy, you'll need to discontinue the inhaled insulin. Two longer-term trials of up to 4 years in duration did not show any significant effect on pulmonary function.15,16
A convenience with a price tag
Inhaled insulin powder is available in single-dose 1-mg and 3-mg blister packs and should be used no more than 10 minutes before meals. To administer the insulin, the patient breathes out, inhales the dose, and then holds his breath for 5 seconds. The patient will, however, need to load each dose.
Each milligram of the inhaled insulin is equivalent to 2 to 3 units of regular subcutaneous insulin. Inhaled insulin powder is a bolus insulin that targets postprandial glucose and thus can be used in place of rapid- or short-acting injectable insulins.
Patients with type 1 diabetes will require an injectable basal insulin (intermediate or long acting) in conjunction with the inhaled insulin. In type 2 diabetes, inhaled insulin can be used in conjunction with a basal insulin or oral therapy. In patients who are currently using an injectable bolus insulin, the package insert contains a dose conversion table. Initial doses can also be estimated based on weight.
Inhaled insulin may reduce the number of daily insulin injections to 1 to 2 times a day, and that could translate into improved patient compliance, although this has not been directly evaluated. The cost of Exubera is significantly higher than traditional subcutaneous insulin. An Exubera kit costs $180, which includes an inhaler and 270 1 mg and 3 mg doses.
The take-home message is... While inhaled insulin offers comparative efficacy to subcutaneous regimens, there's a potential for short-term decreases in pulmonary function. The long-term effects are largely unknown. As a result, rapid or short-acting injectable insulins may be a safer alternative. Inhaled insulin's role in type 2 diabetes is less clear at this time. In patients with type 2 disease, it would be an option when considering the addition of insulin. However, there's limited data on using inhaled insulin in place of an oral agent.
Exenatide (Byetta): From the mouths of (gila) monsters
Exenatide is synthetic exendin-4, originally isolated from the saliva of the gila monster lizard. It binds to and activates the pancreatic GLP-1 (glucagon like peptide-1) receptor resulting in an increase in insulin secretion from beta cells in the presence of hyperglycemia. It also suppresses glucagon secretion, slows gastric emptying, and decreases food intake. Its use is limited to type 2 diabetes; it has no role in the management of type 1 diabetes.
In 2002 diabetes affected 18.2 million individuals, or 6.3% of the US population.1 The prevalence is expected to double within the next 20 years along with significant increases in cardiovascular disease.1
There are 2 theories as to how diabetes increases cardiovascular mortality.35,36 The first suggests that beta-cell dysfunction and subsequent failure leads to elevated glucose that causes an increase in oxidative stress, and thus leads to cardiovascular disease. The second theory suggests that insulin resistance causes endothelial dysfunction along with inflammation and fibrinolysis and this leads to cardiovascular disease. It's likely that both of these theories are at work, since we know that elevated blood glucose levels can lead to elevated insulin levels and insulin resistance can cause beta-cell dysfunction.
The research on the diabetes/CVD link is intriguing. For instance, there is data suggesting that insulin sensitizing agents may have a positive effect on cardiovascular disease.37 In addition, trials are being conducted between sulfonylureas and thiazolidinediones to evaluate reductions in CVD.38 It may not be long before reducing cardiovascular morbidity and mortality becomes a goal of treatment in the management of our patients with diabetes.
Three large placebo-controlled trials evaluated the use of exenatide as adjunct therapy to a sulfonylurea or metformin in patients unable to achieve glycemic control ( TABLE 3 ).17-19 Hemoglobin A1c was reduced by 0.4% to 0.6% with 5 mcg twice daily and 0.8% to 0.9% with 10 mcg twice daily. The effects on fasting plasma glucose were less impressive, though not surprising due to the drug's mechanism of action.
One other trial compared exenatide, 10 mcg twice daily, to insulin glargine, one daily dose titrated to achieve fasting glucose less than 100 mg/dL in patients with type 2 diabetes uncontrolled on a sulfonylurea and metformin, which represents a relatively common clinical scenario.20 The reduction in A1c after 26 weeks was comparable between the 2 groups (1.11% for both).
Exenatide was more effective at reducing postprandial glucose, while glargine more effectively reduced fasting glucose. Weight increased by an average of 1.8 kg in the glargine group and decreased by 2.3 kg with exenatide. Rates of symptomatic hypoglycemia were similar between the 2 groups. Gastrointestinal symptoms were more common in the exenatide group, including nausea (57.1% vs 8.6%), vomiting (17.4% vs 3.7%), and diarrhea (8.5% vs 3%). This led to a significant difference in the number of subjects who withdrew from the study (19.4% for exenatide vs 9.7% for glargine). It's important to note that the mean baseline A1c values were only moderately elevated (8.2% in exenatide vs 8.3% in glargine) and thus not representative of those with very poor control.
One other research finding is worth mentioning here. GLP-1 administration has been shown to result in beta-cell proliferation and increased beta-cell mass in animals and in vitro studies.21 Thus, in theory, exenatide could slow the progression of type 2 diabetes. However, long-term studies are needed to address this.
TABLE 3
Exenatide studies
| VARIABLE | BUSE (2004)17 | DEFRONZO (2005)18 | KENDALL (2005)19 |
|---|---|---|---|
| BASELINE DATA | |||
| Number of patients | 377 | 336 | 733 |
| Age (yrs) | 55 | 53 | 55 |
| BMI (kg/m2) | 33 | 34 | 34 |
| A1c (%) | 8.6 | 8.2 | 8.5 |
| FPG (mg/dL) | 184 | 172 | 180 |
| Concomitant therapy | Sulfonylurea | metformin | Sulfonylurea + metformin |
| RESULTS—CHANGE FROM BASELINE | |||
| A1c (%) | 5 mcg dose: -0.5 | 5 mcg dose: -0.4 | 5 mcg dose: -0.6 |
| 10 mcg dose: -0.9 | 10 mcg dose: -0.8 | 10 mcg dose: -0.8 | |
| FPG (mg/dL) | 5 mcg dose: -5.4 | 5 mcg dose: -7.2 | 5 mcg dose: -9 |
| 10 mcg dose: -10.8 | 10 mcg dose: -10.1 | 10 mcg dose: -11 | |
| Weight (kg) | 5 mcg dose: -0.9 | 5 mcg dose: -1.6 | 5 mcg dose: -1.6 |
| 10 mcg dose: -1.6 | 10 mcg dose: -2.8 | 10 mcg dose: -1.6 | |
| BMI, body mass index; A1c, glycosylated hemoglobin; FPG, fasting plasma glucose. | |||
Bad news: Transient nausea; Good news: Unrelated weight loss
Nausea is the most common side effect and occurs in 36% to 39% of patients with the 5-mcg dose and 45% to 50% of those with the 10-mcg dose, although it's usually transient.17-19,22 Exenatide results in a moderate reduction in weight (approximately 2-4 pounds), which does not appear to be related to the adverse gastrointestinal effects. There's a risk of mild to moderate hypoglycemia when exenatide is used with a sulfonylurea, which is most likely due to the effects of the sulfonylurea.
Exenatide reportedly results in low levels of antibodies in approximately 40% of patients but had no affect on glucose control.22 About 6% of patients may develop high antibody levels, which could result in a diminished response.22
Exenatide is dispensed as a injection pen containing a 30-day supply of medicine. The patient will need to administer it subcutaneously in the thigh, abdomen, or upper arm no more than 60 minutes before morning and evening meals. The cost of exenatide is substantially higher than sulfonylureas, metformin, or insulin but comparable with pioglitazone and rosiglitazone.
The take-home message is... Exenatide is not currently recommended for use as initial therapy in type 2 diabetes. In clinical trials, exenatide 10 mcg twice daily achieved A1c reductions of about 1%. Oral agents typically produce reductions of 1% to 2%, although the effects of combining oral agents may not always be additive.23,24
At this point, exenatide is best suited for those whose A1c is within 1% of their treatment goal, especially in those unable to take another oral agent or insulin (eg, due to renal or hepatic impairment or congestive heart failure) and those who have elevated postprandial glucose. Otherwise, adding an oral agent or insulin would likely produce the best results.
Sitagliptin (Januvia): It, too, focuses on GlP-1
Sitagliptin (Januvia), the first drug in a new class of agents called dipeptidyl-peptidase-4 (DPP-4) inhibitors, was just approved in October 2006 for the treatment of type 2 diabetes. This drug, like exenatide, focuses on the actions of GLP-1. Active GLP-1 is rapidly degraded by the DPP-4 enzyme. Inhibiting this enzyme results in an increased concentration and prolonged action of GLP-1.
There are some key differences between DPP-4 inhibitors and GLP-1 agonists such as exenatide. Specifically, DPP-4 inhibitors do not appear to have significant rates of nausea and vomiting, can be given orally, have no effect on gastric emptying, and are weight neutral. Limited evidence suggests that, like GLP-1 agonists, they may also improve chronic beta-cell function.25 Side effects include stuffy or runny nose and sore throat, upper respiratory infection, and headache.
Published studies are sparse at this point. One dose finding study randomized 552 patients to one of five treatments: placebo, sitagliptin (25, 50, or 100 mg once daily), or 50 mg twice daily. Baseline A1c ranged from 5.8% to 10.4% and after 12 weeks of treatment, the sitagliptin 100 mg once daily group had the largest reduction in A1c. Reductions were dependent on baseline A1c: Those with a baseline A1c <7%, 7% to 8.5%, or 8.5% to 10% had reductions of 0.4%, 0.6%, and 0.8%, respectively.26
Renal patients require a change in dose
The recommended dose of sitagliptin is 100 mg by mouth once a day as monotherapy or in combination with metformin or a thiazolidinedione. You'll need to reduce the dose in those patients with renal impairment.
The take-home message is... This newest class of medications exhibits some potential advantages and disadvantages when compared to the GLP-1 agonists. On the plus side, it does not appear to cause nausea and vomiting and can be given orally. On the downside, it has no effect on gastric emptying, which means it may not reduce postprandial glucose as much. In addition, it does not cause weight loss (although it does not cause weight gain either).
Pramlintide (Symlin): Shoring up deficiencies
Pramlintide is a synthetic analog of human amylin, a neuroendocrine hormone secreted by pancreatic beta cells. Amylin works in concert with insulin to suppress postprandial glucagon secretion and slow carbohydrate absorption by delaying gastric emptying. Amylin is cosecreted with insulin so patients with type 1 diabetes have an absolute deficiency of amylin while those with type 2 diabetes have a progressively declining production. Thus, pramlintide may be used in either type of diabetes.
In clinical trials, pramlintide produced modest reductions in A1c (0.1-0.62%) and more impressive reductions in postprandial glucose (64.8-126 mg/dL) in adults with type 1 or 2 diabetes ( TABLE 4 ).27-34 In addition, it has been shown to minimize insulin dose increases and the weight gain associated with insulin.27,29-31,34
Inhaled insulin, exenatide, sitagliptin, and pramlintide are exciting developments in the management of diabetes. They offer potential advantages over currently available therapies, but also have their share of limitations. As we gain further experience with them, their roles may increase.
Other agents are also on the horizon and worth noting. Vildagliptin (Galvus), a DPP-4 inhibitor, is expected to become available shortly. Another drug, liraglutide, a synthetic GlP-1 analog with a longer half-life than exenatide, is currently in phase III trials. A long-acting exenatide, given once weekly, is in phase II trials.
Time will tell as to how these agents—both the recently approved ones and those in the pipeline—will aid in our battle against diabetes. What is clear is that our arsenal will continue to grow, and we we'll continue to make inroads—one patient encounter at a time.
TABLE 4
Pramlintide studies
| STUDY | TYPE OF DIABETES | DESIGN | A1C CHANGE FROM BASELINE (%) | PPG CHANGE FROM BASELINE (MG/DL) |
|---|---|---|---|---|
| Fineman (1999) 30 | Type 1 | DB, PC, 26 wk | -0.2* (60 mcg 3x/day) -0.1 (90 mcg 2x/day) -0.1 (90 mcg 3x/day) 0.1 (placebo) | NA |
| Gottlieb (1999) 31 | Type 2 | DB, PC, 26 wk | -0.3 (90 mcg 2x/day) -0.4 (90 mcg 3x/day) -0.4* (120 mcg 2x/day) -0.1 (placebo) | NA |
| Nyholm (1999) 32 | Type 1 | DB, PC, 4 wk | NA | -126 (1-hr) -72 (2-hr) (30 mcg 4x/day) |
| Whitehouse (2002) 27 | Type 1 | R, DB, PC, 52 weeks | -0.39* (30-60 mcg 4x/day) -0.12 (placebo) | NA |
| Ratner (2002) 28 | Type 2 | R, DB, PC, 52 weeks | -0.3 (30 mcg 3x/day) -0.5 (75 mcg 3x/day) -0.6* (150 mcg 3x/day) -0.2 (placebo) | NA |
| Hollander (2003) 29 | Type 2 | R, DB, PC, 52 weeks | -0.35 (90 mcg 2x/day) -0.62* (120 mcg 2x/day) -0.22 (placebo) | NA |
| Levetan (2003) 33 | Type 1 | R, DB, PC, 4 weeks | NA | -79.2 (1-hr) -64.8 (2-hr) (30 mcg 3x/day) |
| Ratner (2004) 34 | Type 1 | R, DB, PC, 52 weeks | -0.29* (60 mcg 3x/day) -0.34* (60 mcg 4x/day) -0.04 (placebo) | NA |
| A1c, glycosylated hemoglobin; PPG, postprandial glucose; DB, double-blind; PC, placebo-controlled; R, randomized; NA, not accessed. | ||||
| *P<.05 vs placebo. | ||||
Nausea is a factor, as is slowed gastric emptying
The most common adverse effects include nausea, vomiting, and anorexia. Rates of nausea in studies have ranged from 9.5% to 59% with most cases being mild to moderate in nature and resolving in 2 to 8 weeks.27-29
Pramlintide in itself does not cause hypoglycemia, however when administered with insulin, it does increase the risk of insulin-induced hypoglycemia. Pramlintide should not be used in patients with gastroparesis since it slows gastric emptying. Pramlintide should not be mixed with insulin in the same syringe as there is insufficient data to support the safety of doing so. Thus, it may increase the number of daily injections for patients.
Pramlintide may also interfere with agents that stimulate gastric motility and slow the absorption of other drugs. The manufacturer recommends separating the administration of analgesics and pramlintide by 1 to 2 hours since coadministration could delay the analgesic onset.
Starting pramlintide means reductions elsewhere
Pramlintide is supplied as a 5 mL vial containing 0.6 mg/mL. Immediately prior to each major meal, the patient will need to administer it subcutaneously into the abdomen or thigh (arm administration is not recommended due to varying absorption). When initiating pramlintide in a patient, you'll need to reduce the patient's rapid/short insulin (including fixed-mixed insulin such as 70/30) by 50%.
In type 1 diabetes, the pramlintide dose may be increased in 15-mcg increments, provided that the patient has not experienced clinically significant nausea for at least 3 days and his glycemic goals are not met. In type 2 diabetes, the initial pramlintide dose may be doubled, provided that the patient has not experienced clinically significant nausea for 3 to 7 days and his glycemic goals are not met. In either case, should the increase in dose result in intolerable nausea, you may need to drop the dose back to the previous dose.
The take-home message is... While pramlinitide offers a different approach (as compared with insulin) to lowering postprandial glucose, there is no evidence that it offers any distinct advantage to the patient. Thus, it may be best to simply increase the premeal insulin dose. Should continued weight gain be a major concern, then pramlintide could play a role as adjunct therapy to mealtime insulin. Further studies evaluating quality of life and patient acceptance are needed.
CORRESPONDENCE
James R. Taylor, PharmD, CDE University of Florida, College of Pharmacy, PO Box 100486, Gainesville, FL 32610-0486 [email protected]
- Inhaled insulin, a short-acting insulin for type 1 and type 2 diabetes, is comparable with traditional subcutaneous regimens in terms of hemoglobin A1c and postprandial glucose reductions. It can also reduce the number of daily injections (B).
- Exenatide, which is indicated for type 2 diabetes in those uncontrolled on a sulfonylurea or metformin, provides a modest reduction in A1c and fasting glucose and is best suited for those whose A1c is within 1% of their goal. Among its advantages: weight loss and the potential to slow the progression of the disease (B).
- Sitagliptin is indicated for type 2 diabetes alone or in combination with metformin or a thiazolidinedione. It provides A1c reductions that are comparable to exenatide and does not have high rates of gastrointestinal side effects. It may also improve beta-cell function (B).
- Pramlintide, which is indicated for type 1 or type 2 diabetes uncontrolled with mealtime insulin, provides modest reductions in A1c and postprandial glucose—although it's more effective for those with postprandial hyperglycemia. It may reduce insulin dose requirements and the associated weight gain (B).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
The battle over glycemic control begins when you write out that first script for a patient for a sulfonylurea, metformin, or insulin. But it continues during every encounter thereafter, as you monitor your patient's progress, adjust dosages, and take advantage of new pharmacologic options. Recently, that list of options has expanded by 4: Three are new classes of agents, and the fourth is essentially a new delivery system for insulin. Inhaled insulin (Exubera) was approved by the Food and Drug Administration in January 2006, exenatide (Byetta) in April 2005, sitagliptin (Januvia) in October 2006, and pramlintide (Symlin) in March 2005 ( TABLE 1 ).
Staying abreast of new agents like these is essential if we are ever going to get the upper hand on a disease that in 2002 affected 18.2 million people.1 This review provides an at-a-glance summary of the key aspects of each agent, followed by a topline summary of their advantages and disadvantages.
TABLE 1
New therapeutic options for diabetes
| DRUG | INDICATIONS | DOSE | COST (AWP)* |
|---|---|---|---|
| Insulin, inhaled powder (Exubera) | Type 1 or type 2 diabetes mellitus | Administer 2-3 times a day just prior to meals. Dose (mg)=weight (kg)×0.05 mg/kg. Calculated dose should be rounded down to nearest whole milligram | Kit (includes inhaler plus 270 1- and 3-mg doses): $180 combination pack (180 1- and 3-mg doses): $134 combination pack (270 1- and 3-mg doses): $168 |
| Exenatide (Byetta) | Adjunct therapy for type 2 diabetes uncontrolled with metformin or sulfonylurea | Initial: 5 mcg sc twice daily. May be increased to 10 mcg sc twice daily after 1 month (max dose) | 5 mcg: $176.40/month 10 mcg: $207.00/month |
| Sitagliptin (Januvia) | Type 2 diabetes as monotherapy or in combination with metformin or thiazolidinedione | 100 mg orally once daily | $174.96/month |
| Pramlintide (Symlin) | Adjunct therapy for type 1 or type 2 diabetes in uncontrolled patients using mealtime insulin (with or without sulfonylurea or metformin in type 2 diabetes) | Type 1 diabetes: Initial: 15 mcg sc prior to each meal. Titrate to 30-60 mcg prior to each meal as tolerated. Type 2 diabetes: Initial: 60 mcg sc prior to each meal. Titrate to 120 mcg sc prior to each meal. | $95.40/month |
| AWP=average wholesale price; sc=subcutaneously | |||
| *Cost from Red Book Update 2006; 25(9) (Montvale, NJ: Thomson PDR; 2006). | |||
Exubera: A new twist on insulin
The first dry powder inhaled insulin, which can be used in lieu of rapid- or short-acting injectable insulins, is now available. The question is: How does it stack up? Inhaled insulin has been studied in several clinical trials in both type 1 and type 2 diabetes ( TABLE 2 ).2-8 In type 1 diabetes it's been combined with NPH insulin or ultralente insulin and compared with subcutaneous regimens of regular insulin with NPH insulin or ultralente insulin.2,3,6 These studies showed a similar decrease in glycosylated hemoglobin (Hb A1c) and 2-hour postprandial glucose between the inhaled and subcutaneous regimens. No studies comparing inhaled insulin powder containing regimens with subcutaneous regimens utilizing rapid acting insulin have been published.
In type 2 diabetes, inhaled insulin powder has been studied in combination with ultralente insulin, a sulfonylurea, and metformin.4,5,7,8 For patients with uncontrolled type 2 diabetes on a sulfonylurea or metformin, the addition of inhaled insulin powder has been shown to reduce A1c by 1.9% to 2.3%.4,8 When combined with ultralente in type 2 diabetes, reductions in A1c were comparable with traditional subcutaneous insulin regimens.
In addition, a few studies have looked at patient satisfaction with inhaled insulin. The findings: Inhaled insulin powder was linked to better satisfaction, convenience, ease of use, and social comfort in type 1 and 2 diabetes when compared to entirely subcutaneous regimens.6,9,10
TABLE 2
Inhaled insulin studies
| STUDY | TYPE | DESIGN | A1C CHANGE FROM BASELINE (%) |
|---|---|---|---|
| Skyler (2001) 3 | Type 1 | RCT, 12 weeks | -0.6 (INH); -0.8 (INJ) |
| Weiss (2003) 4 | Type 2 | RCT, 12 weeks INH + preexisting OHA vs preexisting OHA | -2.3 (INH+OHA) -0.1 (OHA)* |
| Quattrin (2004) 2 | Type 1 | RCT, 6 months INH + U vs R + NPH | -0.2 (INH + U) -0.4 (R + NPH) |
| Hollander (2004) 5 | Type 2 | RCT, 6 months INH + U vs R + NPH | -0.7 (INH + U) -0.6 (R + NPH) |
| Rosenstock (2004) 6 | Type 1 or type 2 | RCT, 12 weeks INH + U vs conventional split/mixed regimen | Type 1 diabetes: -0.69 (INH + U) -0.85 (split/mixed) Type 2 diabetes: -0.61 (INH + U) -0.79 (split/mixed) |
| DeFronzo (2005) 7 | Type 2 | RCT, 3 months INH vs rosiglitazone | -2.3 (INH) -1.4 (rosiglitazone) |
| Rosenstock (2005) 8 | Type 2 | RCT, 12 weeks INH alone, INH + OHA, or OHA alone (all after OHA failure) | -1.4 (INH alone) -1.9 (INH + OHA) -0.2 (OHA alone) |
| A1c, glycosylated hemoglobin; RCT, randomized controlled trial; INH, inhaled insulin; INJ, injected insulin; OHA, oral hypoglycemic agent; U, ultralente; R, regular insulin; NPH, NPH insulin | |||
| *P<.05 | |||
Not an option for smokers or those with pulmonary disease
The most common side effects of inhaled insulin include hypoglycemia, weight gain, cough, and bitter taste. The risk of hypoglycemia appears to be about the same or less than that seen with subcutaneous insulin.2 The same is true for weight gain, based on limited data.11 Other potential concerns include the formation of insulin antibodies. Antibody formation is higher with inhaled insulin than with subcutaneous insulin, but the clinical significance at this point is not clear.12
The drug's effect on lung function is also an issue. Inhaled insulin powder should not be used in patients who smoke (or those who have quit within the past 6 months) or who have underlying pulmonary disease. Smoking increases the drug's absorption and can lead to hypoglycemia.13 The safety and efficacy of inhaled insulin in patients with underlying pulmonary disease remains unclear. Some short-term studies in those without underlying pulmonary disease found no effects on pulmonary function, while others showed a decline in lung function.2-5
The manufacturer reports that in trials lasting less than 2 years, both individual patients on inhaled insulin or a comparative agent experienced a decrease in pulmonary function.14 Forced expiratory volume in 1 second (FEV1) declined by =20% in 1.5% of inhaled insulin treated patients and in 1.3% of those on another agent. Carbon monoxide diffusing capacity (DLCO) decreased by =20% in 5.1% of those on inhaled insulin and 3.6% of those on a comparative agent. Thus, the manufacturer recommends a baseline spirometry (FEV1) and possibly DLCO. The manufacturer does not recommend the use of inhaled insulin if FEV1 or DLCO is <70% predicted.
A patient's pulmonary function should be assessed after 6 months on the drug and then annually thereafter. Should FEV1 decline by =20% from baseline or pulmonary symptoms develop while on therapy, you'll need to discontinue the inhaled insulin. Two longer-term trials of up to 4 years in duration did not show any significant effect on pulmonary function.15,16
A convenience with a price tag
Inhaled insulin powder is available in single-dose 1-mg and 3-mg blister packs and should be used no more than 10 minutes before meals. To administer the insulin, the patient breathes out, inhales the dose, and then holds his breath for 5 seconds. The patient will, however, need to load each dose.
Each milligram of the inhaled insulin is equivalent to 2 to 3 units of regular subcutaneous insulin. Inhaled insulin powder is a bolus insulin that targets postprandial glucose and thus can be used in place of rapid- or short-acting injectable insulins.
Patients with type 1 diabetes will require an injectable basal insulin (intermediate or long acting) in conjunction with the inhaled insulin. In type 2 diabetes, inhaled insulin can be used in conjunction with a basal insulin or oral therapy. In patients who are currently using an injectable bolus insulin, the package insert contains a dose conversion table. Initial doses can also be estimated based on weight.
Inhaled insulin may reduce the number of daily insulin injections to 1 to 2 times a day, and that could translate into improved patient compliance, although this has not been directly evaluated. The cost of Exubera is significantly higher than traditional subcutaneous insulin. An Exubera kit costs $180, which includes an inhaler and 270 1 mg and 3 mg doses.
The take-home message is... While inhaled insulin offers comparative efficacy to subcutaneous regimens, there's a potential for short-term decreases in pulmonary function. The long-term effects are largely unknown. As a result, rapid or short-acting injectable insulins may be a safer alternative. Inhaled insulin's role in type 2 diabetes is less clear at this time. In patients with type 2 disease, it would be an option when considering the addition of insulin. However, there's limited data on using inhaled insulin in place of an oral agent.
Exenatide (Byetta): From the mouths of (gila) monsters
Exenatide is synthetic exendin-4, originally isolated from the saliva of the gila monster lizard. It binds to and activates the pancreatic GLP-1 (glucagon like peptide-1) receptor resulting in an increase in insulin secretion from beta cells in the presence of hyperglycemia. It also suppresses glucagon secretion, slows gastric emptying, and decreases food intake. Its use is limited to type 2 diabetes; it has no role in the management of type 1 diabetes.
In 2002 diabetes affected 18.2 million individuals, or 6.3% of the US population.1 The prevalence is expected to double within the next 20 years along with significant increases in cardiovascular disease.1
There are 2 theories as to how diabetes increases cardiovascular mortality.35,36 The first suggests that beta-cell dysfunction and subsequent failure leads to elevated glucose that causes an increase in oxidative stress, and thus leads to cardiovascular disease. The second theory suggests that insulin resistance causes endothelial dysfunction along with inflammation and fibrinolysis and this leads to cardiovascular disease. It's likely that both of these theories are at work, since we know that elevated blood glucose levels can lead to elevated insulin levels and insulin resistance can cause beta-cell dysfunction.
The research on the diabetes/CVD link is intriguing. For instance, there is data suggesting that insulin sensitizing agents may have a positive effect on cardiovascular disease.37 In addition, trials are being conducted between sulfonylureas and thiazolidinediones to evaluate reductions in CVD.38 It may not be long before reducing cardiovascular morbidity and mortality becomes a goal of treatment in the management of our patients with diabetes.
Three large placebo-controlled trials evaluated the use of exenatide as adjunct therapy to a sulfonylurea or metformin in patients unable to achieve glycemic control ( TABLE 3 ).17-19 Hemoglobin A1c was reduced by 0.4% to 0.6% with 5 mcg twice daily and 0.8% to 0.9% with 10 mcg twice daily. The effects on fasting plasma glucose were less impressive, though not surprising due to the drug's mechanism of action.
One other trial compared exenatide, 10 mcg twice daily, to insulin glargine, one daily dose titrated to achieve fasting glucose less than 100 mg/dL in patients with type 2 diabetes uncontrolled on a sulfonylurea and metformin, which represents a relatively common clinical scenario.20 The reduction in A1c after 26 weeks was comparable between the 2 groups (1.11% for both).
Exenatide was more effective at reducing postprandial glucose, while glargine more effectively reduced fasting glucose. Weight increased by an average of 1.8 kg in the glargine group and decreased by 2.3 kg with exenatide. Rates of symptomatic hypoglycemia were similar between the 2 groups. Gastrointestinal symptoms were more common in the exenatide group, including nausea (57.1% vs 8.6%), vomiting (17.4% vs 3.7%), and diarrhea (8.5% vs 3%). This led to a significant difference in the number of subjects who withdrew from the study (19.4% for exenatide vs 9.7% for glargine). It's important to note that the mean baseline A1c values were only moderately elevated (8.2% in exenatide vs 8.3% in glargine) and thus not representative of those with very poor control.
One other research finding is worth mentioning here. GLP-1 administration has been shown to result in beta-cell proliferation and increased beta-cell mass in animals and in vitro studies.21 Thus, in theory, exenatide could slow the progression of type 2 diabetes. However, long-term studies are needed to address this.
TABLE 3
Exenatide studies
| VARIABLE | BUSE (2004)17 | DEFRONZO (2005)18 | KENDALL (2005)19 |
|---|---|---|---|
| BASELINE DATA | |||
| Number of patients | 377 | 336 | 733 |
| Age (yrs) | 55 | 53 | 55 |
| BMI (kg/m2) | 33 | 34 | 34 |
| A1c (%) | 8.6 | 8.2 | 8.5 |
| FPG (mg/dL) | 184 | 172 | 180 |
| Concomitant therapy | Sulfonylurea | metformin | Sulfonylurea + metformin |
| RESULTS—CHANGE FROM BASELINE | |||
| A1c (%) | 5 mcg dose: -0.5 | 5 mcg dose: -0.4 | 5 mcg dose: -0.6 |
| 10 mcg dose: -0.9 | 10 mcg dose: -0.8 | 10 mcg dose: -0.8 | |
| FPG (mg/dL) | 5 mcg dose: -5.4 | 5 mcg dose: -7.2 | 5 mcg dose: -9 |
| 10 mcg dose: -10.8 | 10 mcg dose: -10.1 | 10 mcg dose: -11 | |
| Weight (kg) | 5 mcg dose: -0.9 | 5 mcg dose: -1.6 | 5 mcg dose: -1.6 |
| 10 mcg dose: -1.6 | 10 mcg dose: -2.8 | 10 mcg dose: -1.6 | |
| BMI, body mass index; A1c, glycosylated hemoglobin; FPG, fasting plasma glucose. | |||
Bad news: Transient nausea; Good news: Unrelated weight loss
Nausea is the most common side effect and occurs in 36% to 39% of patients with the 5-mcg dose and 45% to 50% of those with the 10-mcg dose, although it's usually transient.17-19,22 Exenatide results in a moderate reduction in weight (approximately 2-4 pounds), which does not appear to be related to the adverse gastrointestinal effects. There's a risk of mild to moderate hypoglycemia when exenatide is used with a sulfonylurea, which is most likely due to the effects of the sulfonylurea.
Exenatide reportedly results in low levels of antibodies in approximately 40% of patients but had no affect on glucose control.22 About 6% of patients may develop high antibody levels, which could result in a diminished response.22
Exenatide is dispensed as a injection pen containing a 30-day supply of medicine. The patient will need to administer it subcutaneously in the thigh, abdomen, or upper arm no more than 60 minutes before morning and evening meals. The cost of exenatide is substantially higher than sulfonylureas, metformin, or insulin but comparable with pioglitazone and rosiglitazone.
The take-home message is... Exenatide is not currently recommended for use as initial therapy in type 2 diabetes. In clinical trials, exenatide 10 mcg twice daily achieved A1c reductions of about 1%. Oral agents typically produce reductions of 1% to 2%, although the effects of combining oral agents may not always be additive.23,24
At this point, exenatide is best suited for those whose A1c is within 1% of their treatment goal, especially in those unable to take another oral agent or insulin (eg, due to renal or hepatic impairment or congestive heart failure) and those who have elevated postprandial glucose. Otherwise, adding an oral agent or insulin would likely produce the best results.
Sitagliptin (Januvia): It, too, focuses on GlP-1
Sitagliptin (Januvia), the first drug in a new class of agents called dipeptidyl-peptidase-4 (DPP-4) inhibitors, was just approved in October 2006 for the treatment of type 2 diabetes. This drug, like exenatide, focuses on the actions of GLP-1. Active GLP-1 is rapidly degraded by the DPP-4 enzyme. Inhibiting this enzyme results in an increased concentration and prolonged action of GLP-1.
There are some key differences between DPP-4 inhibitors and GLP-1 agonists such as exenatide. Specifically, DPP-4 inhibitors do not appear to have significant rates of nausea and vomiting, can be given orally, have no effect on gastric emptying, and are weight neutral. Limited evidence suggests that, like GLP-1 agonists, they may also improve chronic beta-cell function.25 Side effects include stuffy or runny nose and sore throat, upper respiratory infection, and headache.
Published studies are sparse at this point. One dose finding study randomized 552 patients to one of five treatments: placebo, sitagliptin (25, 50, or 100 mg once daily), or 50 mg twice daily. Baseline A1c ranged from 5.8% to 10.4% and after 12 weeks of treatment, the sitagliptin 100 mg once daily group had the largest reduction in A1c. Reductions were dependent on baseline A1c: Those with a baseline A1c <7%, 7% to 8.5%, or 8.5% to 10% had reductions of 0.4%, 0.6%, and 0.8%, respectively.26
Renal patients require a change in dose
The recommended dose of sitagliptin is 100 mg by mouth once a day as monotherapy or in combination with metformin or a thiazolidinedione. You'll need to reduce the dose in those patients with renal impairment.
The take-home message is... This newest class of medications exhibits some potential advantages and disadvantages when compared to the GLP-1 agonists. On the plus side, it does not appear to cause nausea and vomiting and can be given orally. On the downside, it has no effect on gastric emptying, which means it may not reduce postprandial glucose as much. In addition, it does not cause weight loss (although it does not cause weight gain either).
Pramlintide (Symlin): Shoring up deficiencies
Pramlintide is a synthetic analog of human amylin, a neuroendocrine hormone secreted by pancreatic beta cells. Amylin works in concert with insulin to suppress postprandial glucagon secretion and slow carbohydrate absorption by delaying gastric emptying. Amylin is cosecreted with insulin so patients with type 1 diabetes have an absolute deficiency of amylin while those with type 2 diabetes have a progressively declining production. Thus, pramlintide may be used in either type of diabetes.
In clinical trials, pramlintide produced modest reductions in A1c (0.1-0.62%) and more impressive reductions in postprandial glucose (64.8-126 mg/dL) in adults with type 1 or 2 diabetes ( TABLE 4 ).27-34 In addition, it has been shown to minimize insulin dose increases and the weight gain associated with insulin.27,29-31,34
Inhaled insulin, exenatide, sitagliptin, and pramlintide are exciting developments in the management of diabetes. They offer potential advantages over currently available therapies, but also have their share of limitations. As we gain further experience with them, their roles may increase.
Other agents are also on the horizon and worth noting. Vildagliptin (Galvus), a DPP-4 inhibitor, is expected to become available shortly. Another drug, liraglutide, a synthetic GlP-1 analog with a longer half-life than exenatide, is currently in phase III trials. A long-acting exenatide, given once weekly, is in phase II trials.
Time will tell as to how these agents—both the recently approved ones and those in the pipeline—will aid in our battle against diabetes. What is clear is that our arsenal will continue to grow, and we we'll continue to make inroads—one patient encounter at a time.
TABLE 4
Pramlintide studies
| STUDY | TYPE OF DIABETES | DESIGN | A1C CHANGE FROM BASELINE (%) | PPG CHANGE FROM BASELINE (MG/DL) |
|---|---|---|---|---|
| Fineman (1999) 30 | Type 1 | DB, PC, 26 wk | -0.2* (60 mcg 3x/day) -0.1 (90 mcg 2x/day) -0.1 (90 mcg 3x/day) 0.1 (placebo) | NA |
| Gottlieb (1999) 31 | Type 2 | DB, PC, 26 wk | -0.3 (90 mcg 2x/day) -0.4 (90 mcg 3x/day) -0.4* (120 mcg 2x/day) -0.1 (placebo) | NA |
| Nyholm (1999) 32 | Type 1 | DB, PC, 4 wk | NA | -126 (1-hr) -72 (2-hr) (30 mcg 4x/day) |
| Whitehouse (2002) 27 | Type 1 | R, DB, PC, 52 weeks | -0.39* (30-60 mcg 4x/day) -0.12 (placebo) | NA |
| Ratner (2002) 28 | Type 2 | R, DB, PC, 52 weeks | -0.3 (30 mcg 3x/day) -0.5 (75 mcg 3x/day) -0.6* (150 mcg 3x/day) -0.2 (placebo) | NA |
| Hollander (2003) 29 | Type 2 | R, DB, PC, 52 weeks | -0.35 (90 mcg 2x/day) -0.62* (120 mcg 2x/day) -0.22 (placebo) | NA |
| Levetan (2003) 33 | Type 1 | R, DB, PC, 4 weeks | NA | -79.2 (1-hr) -64.8 (2-hr) (30 mcg 3x/day) |
| Ratner (2004) 34 | Type 1 | R, DB, PC, 52 weeks | -0.29* (60 mcg 3x/day) -0.34* (60 mcg 4x/day) -0.04 (placebo) | NA |
| A1c, glycosylated hemoglobin; PPG, postprandial glucose; DB, double-blind; PC, placebo-controlled; R, randomized; NA, not accessed. | ||||
| *P<.05 vs placebo. | ||||
Nausea is a factor, as is slowed gastric emptying
The most common adverse effects include nausea, vomiting, and anorexia. Rates of nausea in studies have ranged from 9.5% to 59% with most cases being mild to moderate in nature and resolving in 2 to 8 weeks.27-29
Pramlintide in itself does not cause hypoglycemia, however when administered with insulin, it does increase the risk of insulin-induced hypoglycemia. Pramlintide should not be used in patients with gastroparesis since it slows gastric emptying. Pramlintide should not be mixed with insulin in the same syringe as there is insufficient data to support the safety of doing so. Thus, it may increase the number of daily injections for patients.
Pramlintide may also interfere with agents that stimulate gastric motility and slow the absorption of other drugs. The manufacturer recommends separating the administration of analgesics and pramlintide by 1 to 2 hours since coadministration could delay the analgesic onset.
Starting pramlintide means reductions elsewhere
Pramlintide is supplied as a 5 mL vial containing 0.6 mg/mL. Immediately prior to each major meal, the patient will need to administer it subcutaneously into the abdomen or thigh (arm administration is not recommended due to varying absorption). When initiating pramlintide in a patient, you'll need to reduce the patient's rapid/short insulin (including fixed-mixed insulin such as 70/30) by 50%.
In type 1 diabetes, the pramlintide dose may be increased in 15-mcg increments, provided that the patient has not experienced clinically significant nausea for at least 3 days and his glycemic goals are not met. In type 2 diabetes, the initial pramlintide dose may be doubled, provided that the patient has not experienced clinically significant nausea for 3 to 7 days and his glycemic goals are not met. In either case, should the increase in dose result in intolerable nausea, you may need to drop the dose back to the previous dose.
The take-home message is... While pramlinitide offers a different approach (as compared with insulin) to lowering postprandial glucose, there is no evidence that it offers any distinct advantage to the patient. Thus, it may be best to simply increase the premeal insulin dose. Should continued weight gain be a major concern, then pramlintide could play a role as adjunct therapy to mealtime insulin. Further studies evaluating quality of life and patient acceptance are needed.
CORRESPONDENCE
James R. Taylor, PharmD, CDE University of Florida, College of Pharmacy, PO Box 100486, Gainesville, FL 32610-0486 [email protected]
1. Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitis in the United States. JAMA 2003;290:1884-1890.
2. Quattrin T, Belanger A, Bohannon NJV, Schwartz SL. for the Exubera phase III Study Group. Efficacy and safety of inhaled insulin (Exubera) compared to subcuatenous insulin therapy in patients with type 1 diabetes: results of a 6-month, randomized, comparative trial. Diabetes Care 2004;27:2622-2627.
3. Skyler JS, Cefalu WT, Kourides IA, Landschulz WH, Balagtas CC, Cheng S-L, et al. for the Inhaled Insulin Phase II Study Group. Efficacy of inhaled human insulin in type 1 diabetes mellitus: a randomized proof-of-concept study. Lancet 2001;357:331-335.
4. Weiss SR, Cheng S-L, Kourides IA, Gelfand RA, Land-Schulz WH. for the Inhaled Insulin Phase II Study Group. Inhaled insulin provides improved glycemic control in patients with type 2 diabetes mellitus inadequately controlled with oral agents:a randomized controlled trial. Arch Intern Med 2003;163:2277-2282.
5. Hollander PA, Blonde L, Rowe R, Mehta ME, Milburn JL, Hershon KS. for the Exubera Phase III Study Group. Efficacy and safety of inhaled insulin (Exubera) compared with subcutaneous insulint eharpy in patients with type 2 diabetes: results of a 6-month, randomized comparative trial. Diabetes Care 2004;27:2356-2362.
6. Rosenstock J, Bolinder B, Cappeleri JC, Gerber R. Patient satisfaction and glycemic control after 1 year with inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes. Diabetes Care 2004;27:1318-1323.
7. DeFronzo RA, Bergenstal RM, Cefalu WT, Pullman J, Lerman S, Bode BW, et al. for the Exubera Phase III Study Group. Efficacy of inhaled insulin in patients with type 2 diabetes not controlled with diet and exercise. Diabetes Care 2005;28:1922-1928.
8. Rosenstock J, Zinman B, Murphy LJ, Clement SC, Moore P, Bowering K, Hendler R, Lan S-P, Cefalu WT. Inhaled insulin improves glycemic control when substituted for or added to oral combination therapy in type 2 diabetes. Ann Intern Med 2005;143:549-558.
9. Gerber RA, Cappalleri JC, Kourides IA, Gelfand RA. Treatment satisfaction with inhaled insulin in patients with type 1 diabetes: a randomized controlled trial. Diabetes Care 2001;24:1556-1559.
10. Cappalerri JC, Cefalu WT, Rosenstock J, Kourides IA, Gerber RA. Treatment satisfaction in type 2 diabetes: a comparison between an inhaled insulin regimen and a subcutaneous insulin regimen. Clin Ther 2002;24:552-564.
11. Odegard PS, Capoccia KL. Inhaled insulin: exubera. Ann Pharmacother 2005;39:843-853.
12. Fineberg SE, Schatz D, Krasner A. Results of insulin antibody monitoring during phase II and phase III clinical studies of inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes (abstract 46). Diabetes 2002;51(suppl):A17.-
13. Himmelman A, Jende J, Mellen A, Petersen AH, Dahl UL, Wollmer P. The impact of smoking on inhaled insulin. Diabetes Care 2003;26:677-682.
14. Pfizer. Exubera (insulin human inhalation opwder) package insert. New York, NY; 2006.
15. Barnett AH. for the Exubera Phase III Study group. Efficacy and one-year pulmonary safety of inhaled insulin (Exubera) as adjunctive therapy with metformin or glibenclamide in type 2 diabetes patients poorly controlled on oral agent monotherapy (abstract 454-P). Diabetes 2004;53:A107.-
16. Skyler J. for the Exubera Phase II Study Group. Sustained long-term efficacy and safety of inhaled insulin during 4 years continuous therapy (abstract 486-P). Diabetes 2004;53:A115.-
17. Buse JB, Henry RR, Han J, Kim DD, Fineman MS, Baron AD. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 2004;27:2628-2635.
18. DeFronzo RA, Ratner R, Han J, Kim D, Fineman MS, Baron AD. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes mellitus. Diabetes Care 2005;28:1092-1100.
19. Kendall DM, Riddle MC, Rosenstock J, et al. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes mellitus treated with metformin and a sulfonylurea. Diabetes Care 2005;28:1083-1091.
20. Heine RJ, Van Gaal LF, Johns D, Mihm MJ, Widel MH, Brodows RG. for the GWAA Study group. Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes. Ann Intern Med 2005;143:559-569.
21. Gallwitz B. Glucagon-like peptide-1 as a treatment option for type 2 diabetes and its role in restoring beta-cell mass. Diabetes Technol Ther 2005;7:651-657.
22. Triplitt C, Wright A, Chiquette E. Incretin mimetics and dipeptidyl peptidase-IV inhibitors: potential new therapies for type 2 diabetes mellitus. Pharmacotherapy 2006;26:360-374.
23. Willms B, Ruge D. Comparison of acarbose and metformin in patients with type 2 diabetes mellitus insufficiently controlled with diet and sulphonylureas: a randomized, placebo-controlled study. Diabetes Med 1999;16:755-761.
24. Rosenstock J, Sugimoto D, Strange P, Stewart JA, Soltesrak E, Dailey J. Triple therapy in type 2 diabetes: insulin glargine or rosiglitazone added to combination therapy of sulfonylurea plus metformin in insulin-naïve patients. Diabetes Care 2006;29:554-559.
25. Miller SA, St. Onge EL. Sitagliptin: a dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes. Ann Pharmacother 2006;40:1336-1343.
26. Herman G, Hanefeld M, Wu M, Chen X, Zhao P, Stein P. Effect of MK-0431, a dipeptidyl peptidase IV (DPP-IV) inhibitor, on glycemic control after 12 weeks in patients with T2DM (abstract 541-P). Diabetes 2005;54(suppl 1):A134.-
27. Whitehouse F, Kruger DF, Fineman M, Shen L, Ruggles JA, Maggs DG, et al. A randomized study and open-label extension evaluating the long-term efficacy of pramlintide as an adjunct to insulin therapy in type 1 diabetes. Diabetes Care 2002;25:724-730.
28. Ratner RE, Want LL, Fineman MS, Velte MJ, Ruggles JA, Gottlieb A, et al. Adjunctive therapy with the amylin analogue pramlintide leads to a combined improvement in glycemic and weight control in insulin-treated subjects with type 2 diabetes. Diabetes Technol Ther 2002;4:51-61.
29. Hollander PA, Levy P, Fineman MS, Maggs DG, Shen LZ, Strobel SA, et al. Pramlintide as an adjunct to insulin therapy improves long-term glycemic and weight control in patients with type 2 diabetes. Diabetes Care 2003;26:784-790.
30. Fineman M, Bahner A, Gottlieb A, Kolterman OG. Effects of six months administration of pramlintide as anadjunct to insulin therapy on metabolic control in people with type 1 diabetes (abstract). Diabetes 1999;48(suppl 1):A113.-
31. Gottlieb A, Fineman M, Bahner A, Parker J, Waite G, Kolterman O. Pramlintide therapy in addition to insulin in type 2 diabetes: effect on metabolic control after 6 months (abstract). Diabetologia 1999;42(suppl 1):A232.-
32. Nyholm B, Orskov L, Hove K, Gravholt CH, Moller N, Alberti GMN, et al. The amylin analog pramlintide improves glycemic control and reduces postprandial glucagons concentrations in patients wih type 1 diabetes mellitus. Metabolism 1999;48:935-941.
33. Levetan C, Want LL, Weyer C, Strobel SA, Crean J, Wang Y, et al. Impact of pramlintide on glucose fluctuations and postprandial glucose, glucagons, and triglyceride excursions among patients with type 1 diabetes intensively treated with insulin pumps. Diabetes Care 2003;26:1-8.
34. Ratner RE, Dickey R, Fineman M, et al. Amylin replacement with pramlintide as an adjunct to insulin therapy improves long-term glycemic and weight control in type 1 diabetes mellitus: a 1-year, randomized controlled trial. Diabet Med 2004;21:1204-1212.
35. Lillioja S, Mott DM, Spraul M, Ferraro R, Foley JE, Ravussin E. Insulin resistance and insulin and insulin secretory dysfunction as precursors of non-insulin-dependent diabetes mellitus. N Engl J Med 1993;329:1988-1992.
36. Ferrannini E. Insulin resistance versus insulin deficiency in non-insulin-dependent diabetes mellitus: problems and prospects. Endocr Rev 1998;19:477-490.
37. Jawa AA, Fonseca VA. Role of insulin secretagogues and insulin sensitizing agents in the prevention of cardiovascular disease in patients who have diabetes. Cardiol Clin 2005;23:119-138.
38. Mazzone T, Meyer PM, Feinstein SB, et al. Effect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes:a randomized trial. JAMA 2006;296:2572-2581.
1. Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitis in the United States. JAMA 2003;290:1884-1890.
2. Quattrin T, Belanger A, Bohannon NJV, Schwartz SL. for the Exubera phase III Study Group. Efficacy and safety of inhaled insulin (Exubera) compared to subcuatenous insulin therapy in patients with type 1 diabetes: results of a 6-month, randomized, comparative trial. Diabetes Care 2004;27:2622-2627.
3. Skyler JS, Cefalu WT, Kourides IA, Landschulz WH, Balagtas CC, Cheng S-L, et al. for the Inhaled Insulin Phase II Study Group. Efficacy of inhaled human insulin in type 1 diabetes mellitus: a randomized proof-of-concept study. Lancet 2001;357:331-335.
4. Weiss SR, Cheng S-L, Kourides IA, Gelfand RA, Land-Schulz WH. for the Inhaled Insulin Phase II Study Group. Inhaled insulin provides improved glycemic control in patients with type 2 diabetes mellitus inadequately controlled with oral agents:a randomized controlled trial. Arch Intern Med 2003;163:2277-2282.
5. Hollander PA, Blonde L, Rowe R, Mehta ME, Milburn JL, Hershon KS. for the Exubera Phase III Study Group. Efficacy and safety of inhaled insulin (Exubera) compared with subcutaneous insulint eharpy in patients with type 2 diabetes: results of a 6-month, randomized comparative trial. Diabetes Care 2004;27:2356-2362.
6. Rosenstock J, Bolinder B, Cappeleri JC, Gerber R. Patient satisfaction and glycemic control after 1 year with inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes. Diabetes Care 2004;27:1318-1323.
7. DeFronzo RA, Bergenstal RM, Cefalu WT, Pullman J, Lerman S, Bode BW, et al. for the Exubera Phase III Study Group. Efficacy of inhaled insulin in patients with type 2 diabetes not controlled with diet and exercise. Diabetes Care 2005;28:1922-1928.
8. Rosenstock J, Zinman B, Murphy LJ, Clement SC, Moore P, Bowering K, Hendler R, Lan S-P, Cefalu WT. Inhaled insulin improves glycemic control when substituted for or added to oral combination therapy in type 2 diabetes. Ann Intern Med 2005;143:549-558.
9. Gerber RA, Cappalleri JC, Kourides IA, Gelfand RA. Treatment satisfaction with inhaled insulin in patients with type 1 diabetes: a randomized controlled trial. Diabetes Care 2001;24:1556-1559.
10. Cappalerri JC, Cefalu WT, Rosenstock J, Kourides IA, Gerber RA. Treatment satisfaction in type 2 diabetes: a comparison between an inhaled insulin regimen and a subcutaneous insulin regimen. Clin Ther 2002;24:552-564.
11. Odegard PS, Capoccia KL. Inhaled insulin: exubera. Ann Pharmacother 2005;39:843-853.
12. Fineberg SE, Schatz D, Krasner A. Results of insulin antibody monitoring during phase II and phase III clinical studies of inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes (abstract 46). Diabetes 2002;51(suppl):A17.-
13. Himmelman A, Jende J, Mellen A, Petersen AH, Dahl UL, Wollmer P. The impact of smoking on inhaled insulin. Diabetes Care 2003;26:677-682.
14. Pfizer. Exubera (insulin human inhalation opwder) package insert. New York, NY; 2006.
15. Barnett AH. for the Exubera Phase III Study group. Efficacy and one-year pulmonary safety of inhaled insulin (Exubera) as adjunctive therapy with metformin or glibenclamide in type 2 diabetes patients poorly controlled on oral agent monotherapy (abstract 454-P). Diabetes 2004;53:A107.-
16. Skyler J. for the Exubera Phase II Study Group. Sustained long-term efficacy and safety of inhaled insulin during 4 years continuous therapy (abstract 486-P). Diabetes 2004;53:A115.-
17. Buse JB, Henry RR, Han J, Kim DD, Fineman MS, Baron AD. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 2004;27:2628-2635.
18. DeFronzo RA, Ratner R, Han J, Kim D, Fineman MS, Baron AD. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes mellitus. Diabetes Care 2005;28:1092-1100.
19. Kendall DM, Riddle MC, Rosenstock J, et al. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes mellitus treated with metformin and a sulfonylurea. Diabetes Care 2005;28:1083-1091.
20. Heine RJ, Van Gaal LF, Johns D, Mihm MJ, Widel MH, Brodows RG. for the GWAA Study group. Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes. Ann Intern Med 2005;143:559-569.
21. Gallwitz B. Glucagon-like peptide-1 as a treatment option for type 2 diabetes and its role in restoring beta-cell mass. Diabetes Technol Ther 2005;7:651-657.
22. Triplitt C, Wright A, Chiquette E. Incretin mimetics and dipeptidyl peptidase-IV inhibitors: potential new therapies for type 2 diabetes mellitus. Pharmacotherapy 2006;26:360-374.
23. Willms B, Ruge D. Comparison of acarbose and metformin in patients with type 2 diabetes mellitus insufficiently controlled with diet and sulphonylureas: a randomized, placebo-controlled study. Diabetes Med 1999;16:755-761.
24. Rosenstock J, Sugimoto D, Strange P, Stewart JA, Soltesrak E, Dailey J. Triple therapy in type 2 diabetes: insulin glargine or rosiglitazone added to combination therapy of sulfonylurea plus metformin in insulin-naïve patients. Diabetes Care 2006;29:554-559.
25. Miller SA, St. Onge EL. Sitagliptin: a dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes. Ann Pharmacother 2006;40:1336-1343.
26. Herman G, Hanefeld M, Wu M, Chen X, Zhao P, Stein P. Effect of MK-0431, a dipeptidyl peptidase IV (DPP-IV) inhibitor, on glycemic control after 12 weeks in patients with T2DM (abstract 541-P). Diabetes 2005;54(suppl 1):A134.-
27. Whitehouse F, Kruger DF, Fineman M, Shen L, Ruggles JA, Maggs DG, et al. A randomized study and open-label extension evaluating the long-term efficacy of pramlintide as an adjunct to insulin therapy in type 1 diabetes. Diabetes Care 2002;25:724-730.
28. Ratner RE, Want LL, Fineman MS, Velte MJ, Ruggles JA, Gottlieb A, et al. Adjunctive therapy with the amylin analogue pramlintide leads to a combined improvement in glycemic and weight control in insulin-treated subjects with type 2 diabetes. Diabetes Technol Ther 2002;4:51-61.
29. Hollander PA, Levy P, Fineman MS, Maggs DG, Shen LZ, Strobel SA, et al. Pramlintide as an adjunct to insulin therapy improves long-term glycemic and weight control in patients with type 2 diabetes. Diabetes Care 2003;26:784-790.
30. Fineman M, Bahner A, Gottlieb A, Kolterman OG. Effects of six months administration of pramlintide as anadjunct to insulin therapy on metabolic control in people with type 1 diabetes (abstract). Diabetes 1999;48(suppl 1):A113.-
31. Gottlieb A, Fineman M, Bahner A, Parker J, Waite G, Kolterman O. Pramlintide therapy in addition to insulin in type 2 diabetes: effect on metabolic control after 6 months (abstract). Diabetologia 1999;42(suppl 1):A232.-
32. Nyholm B, Orskov L, Hove K, Gravholt CH, Moller N, Alberti GMN, et al. The amylin analog pramlintide improves glycemic control and reduces postprandial glucagons concentrations in patients wih type 1 diabetes mellitus. Metabolism 1999;48:935-941.
33. Levetan C, Want LL, Weyer C, Strobel SA, Crean J, Wang Y, et al. Impact of pramlintide on glucose fluctuations and postprandial glucose, glucagons, and triglyceride excursions among patients with type 1 diabetes intensively treated with insulin pumps. Diabetes Care 2003;26:1-8.
34. Ratner RE, Dickey R, Fineman M, et al. Amylin replacement with pramlintide as an adjunct to insulin therapy improves long-term glycemic and weight control in type 1 diabetes mellitus: a 1-year, randomized controlled trial. Diabet Med 2004;21:1204-1212.
35. Lillioja S, Mott DM, Spraul M, Ferraro R, Foley JE, Ravussin E. Insulin resistance and insulin and insulin secretory dysfunction as precursors of non-insulin-dependent diabetes mellitus. N Engl J Med 1993;329:1988-1992.
36. Ferrannini E. Insulin resistance versus insulin deficiency in non-insulin-dependent diabetes mellitus: problems and prospects. Endocr Rev 1998;19:477-490.
37. Jawa AA, Fonseca VA. Role of insulin secretagogues and insulin sensitizing agents in the prevention of cardiovascular disease in patients who have diabetes. Cardiol Clin 2005;23:119-138.
38. Mazzone T, Meyer PM, Feinstein SB, et al. Effect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes:a randomized trial. JAMA 2006;296:2572-2581.
Who should get the HPV vaccine?
- Consider recommending HPV vaccine for 11- and 12-year-old girls in your practice, before sexual activity puts them at risk of viral infection (A). The FDA has also approved the HPV vaccine for women up to 26 years of age.
- If women older than 26 years ask to be vaccinated, make sure they understand it is an off-label use for them (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Presexual adolescent girls and sexually active women can now lower their lifetime risk of cervical cancer, thanks to a newly available quadrivalent vaccine (Gardasil) directed at human papillomavirus (HPV). This gives us the opportunity to educate parents and adolescents (the primary target group for the vaccine), many of whom remain uninformed about the direct link between HPV infection and cervical cancer.
Ethical, cultural, social, and religious issues that will require attention1 are beyond the scope of this article.
Who should receive the HPV vaccine?
Pre-adolescent and adolescent girls
Girls ages 11 to 12 years—most of whom have not started sexual activity—are the primary targets of immunization. However, the US Food and Drug Administration also approved the use of Gardasil for girls as young as 9. Girls this age may require other vaccines, such as meningococcal conjugate and tetanus-diphtheria-acellular pertussis, and experience thus far indicates no negative immune effects with co-administration of vaccines.1,2
According to one study, vaccination of the entire US population of 12-year-old girls would prevent more than 200,000 HPV infections, 100,000 abnormal Pap tests, and 3300 cases of cervical cancer.3 Parental as well as health care provider acceptance of HPV vaccines for adolescents will be critical to the success of the vaccination effort (see “What makes FPs recommend the HPV vaccine” ).4
Practical issues. As with any new vaccine added to the childhood/adolescent vaccination schedule, a host of issues will need to be resolved to ensure adequate coverage. Factors likely to influence use of HPV vaccine among adolescents are cost and reimbursement, and adherence to the 3-dose regimen that spans 6 months.
The American Academy of Pediatrics’ Committee on Infectious Diseases and the Advisory Committee on Immunization Practices (ACIP) recommends universal use of the HPV vaccine for girls, with a focus on 11- to 12-year-olds. The vaccine is also recommended for 13- to 26-year-old girls and women who have received or completed the 3-dose vaccine series.
Why not vaccinate boys? HPV infection is highly prevalent in sexually active men.5 The efficacy of vaccinating boys against HPV infection is currently being explored.6 However, one model has suggested that vaccinating adolescent males with a bivalent HPV vaccine would only slightly reduce the incidence of cervical cancer cases beyond that achieved by vaccination of adolescent girls, and with an extremely high cost-effectiveness ratio compared with female-only vaccination.5
Women ≤26 years
Indications under FDA approval also include women up to 26 years. Even adults who have been sexually active for years may not have been exposed to all high-risk HPV covered by the vaccine.
Are women older than 26 years eligible?
Though FDA approval of the vaccine is for females aged 9 to 26 years, a recent working group on HPV prevention concluded that any sexually active person may benefit from vaccination and should have the opportunity to receive the vaccine.1 Importantly, women older than 26 years who request the vaccine should be made fully aware of its off-label application in their case.
The rationale behind the recommendations
HPV transmission occurs easily with skin-to-skin contact.8-11 HPV can infect the external genitalia during non-intercourse sexual activities, including manual and oral genital contact. Sexual intercourse is the most frequent mode of infection of the cervix. Condoms may help protect against transmission of HPV but are not fully effective.8,12
Adolescents are particularly vulnerable to HPV, but respond best to vaccine. The cervix is especially susceptible to HPV infection in adolescence because the squamous columnar cell junction transformation zone is more exposed. The adult cervix is less susceptible to HPV than the adolescent cervix because of the smaller area of cervical ectopy comprised of columnar epithelial cells.13 However, in adolescents, the immune response to HPV exposure is greater than in than adults.
Risk for acquiring HPV infection. Risk factors for acquiring HPV infection are listed in the TABLE .8,14,15 According to the Centers for Disease Control and Prevention, sexually active men and women have a 50% lifetime risk of acquiring HPV infection.16 An estimated 6.2 million people in the US become infected with HPV each year,16 and approximately 20 million currently harbor HPV infections.17 This estimate includes more than 9 million sexually active adolescents and young adults 15 to 24 years of age, the group in which nearly 75% of new HPV infections occur.18 Among women <25 years of age, between 28% and 46% are infected with HPV.19,20
Infection cannot always be cleared. Most HPV infections (whether high-risk or low-risk type) are asymptomatic and are efficiently cleared (ie, no detection of DNA for a specific HPV type) by the immune system.21,22 However, if the infection cannot be cleared or controlled by the immune system, it may become a persistent infection.
Persistent infection with HPV increases the probability of progression to high-grade cervical intraepithelial neoplasia (CIN) and invasive carcinoma ( FIGURE ).18-19 Evidence also increasingly shows that high-risk HPV types likely cause anal, penile, scrotal, vulvar, vaginal, and some head and neck cancers.25
After HPV vaccination, neutralizing antibodies are secreted from memory B cells, and bind to their target HPV type, preventing infection before it occurs, thereby blocking the initial step toward development of cervical cancer.
15 high-risk oncogenic types. Papillomaviruses such as HPV are nonenveloped, double-stranded, DNA viruses. They infect cutaneous and mucosal epithelial tissues. More than 100 HPV types have been identified,3 about 30 to 40 of which are spread by sexual contact.4 Of the many known HPVs, only 15 are high-risk oncogenic types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, and 73) that can cause cervical cancer.5.6 Of these high-risk oncogenic types, HPV 16 and 18 account for about 70% of all cervical cancers.7
The new HPV vaccines, Gardasil and Cervarix, (see Web table) both contain virosomal antigens to vaccinate against HPV types 16 and 18. Persistent infection with these high-risk HPV types is necessary for the development of cervical cancer. Chronic infection with low-risk HPV types (eg, HPV 6 or 11) may lead to the development of anogenital warts and other low-grade genital abnormalities, as well as laryngeal cancer or recurrent respiratory papillomatosis. Gardasil also contains virosome antigens for these 2 HPV types. Warts on the hands are usually attributable to HPV 7.8
Viral integration is a necessary step in the malignant transformation of HPV infection; infection may progress from residential to episomal, and, finally, to an integrated form. Residential infection typically occurs a minimum of 6 weeks from exposure, can persist without detection for decades, and can be low risk or high risk. In the episomal state, virally active HPV is located in the cell nucleus, separate from the human DNA. In the integrated form of infection, the HPV DNA circle has opened and joined the human DNA. Integrated HPV—always high risk—produces an abnormal Papanicolaou (Pap) test. If recognized on colposcopy, it must be treated to prevent progression to cervical cancer.
FIGURE
How HPV infection progresses to cervical cancer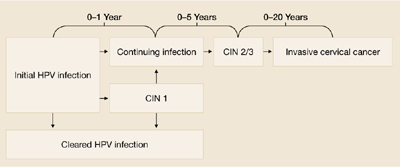
Adapted with permission from Pinto and Crum 200023 and Schlecht et al 2001.24
TABLE
Factors that put women at risk for HPV infection
| Young age (peak age group: 20–24 years) |
| Lifetime number of sexual partners |
| First sexual intercourse at early age |
| Male partner sexual behavior |
| Smoking |
| Oral contraceptive use |
| Uncircumcised male partners |
| Sources: Winer et al 2003;8 Schiffman and castle 2003;14 Insinga et al 2003.15 |
Why screening alone isn’t enough
New technologies for Pap testing, HPV DNA testing, and revisions in the Bethesda system for reporting cervical cytology have led to better treatment recommendations for patients with abnormal cytology results.26 But despite these advances, cervical screening is underused or not used at all for many women at risk.
For example, some women with abnormal cervical cytology—especially those of lower socioeconomic status, who often are medically underserved or lack insurance—may not receive adequate follow-up care.27 Though widespread cervical screening in the future may significantly decrease morbidity and mortality associated with cervical cancer, HPV vaccination can also help achieve this goal.
The case for vaccination plus screening
It will likely take at least a decade to assess the impact of HPV vaccination on invasive cervical cancer, and perhaps 20 to 30 years to achieve the maximum benefit from such a program. A computer-based model of the natural history of HPV and cervical cancer developed by the Harvard School of Public Health considered different cancer prevention policies, including vaccination against HPV types 16 and 18 (initiated at the age of 12 years), cytologic screening (initiated at 18, 21, 25, 30, or 35 years,) and combined vaccination and screening strategies. The model showed the combination strategy to be most effective.28
Dramatic reductions expected. The model predicts that with current screening and vaccination against HPV, low-grade cervical abnormalities associated with HPV-16 and HPV-18 infections would be reduced by 15% and high-grade lesions by 49%. Vaccination would decrease the number of cases of cervical cancer by about 66% in conjunction with screening. The vaccine, however, would not prevent cancers caused by other high-risk HPV types.
According to the model, HPV vaccination would produce health gains that are well worth the cost. Specifically, the cost per additional quality-adjusted life-year gained with vaccinating only females was estimated to be $21,000. This ratio compares favorably with many adult and pediatric vaccines currently used in the US.
A recent survey of attitudes about HPV vaccination among members of the American Academy of Family Physicians (AAFP) found that survey respondents would be more likely to administer an HPV vaccine to girls than to boys and to older rather than younger adolescents.4 Female gender, knowledge about HPV, and attitudes about vaccination were independently associated with family physicians’ intentions to recommend HPV vaccination.
It will take decades to see cervical cancer rates drop, but we will soon see fewer CIN 2/3 lesions once HPV 16/18 vaccination is routine.

HPV types 6 and 11 cause 90% of genital warts
Looking forward
The long-term efficacy of HPV vaccines remains to be determined. Sustained efficacy up to 4.5 years has been documented29 but it could be that boosters will be needed.
Research has shown that adolescents and parents, and even some providers of adolescent health care, may have a significant misunderstanding about HPV infection and its possible sequelae,30 suggesting the need for educational programs about the disease and its prevention. Education and vaccine advocacy from professional organizations such as the AAFP, the American Academy of Pediatrics, and the American College of Obstetricians and Gynecologists will be essential to foster acceptance of HPV vaccination.
CORRESPONDENCE
Michael E. Pichichero, MD, Elmwood Pediatric Group, 601 Elmwood Avenue, Box 672, Rochester, NY 14642. [email protected]
1. Frazer IH, Cox JT, Mayeaux Jr EJ, et al. advances in prevention of cervical cancer and other human papillomavirus-related diseases. Pediatr Infect Dis J 2006;25:S65-S81.
2. Bonnez W. Immunization against genital human papillomaviruses. J Infect Dis 2005;24:1005-1006.
3. Sanders GD, Taira AV. cost-effectiveness of a potential vaccine for human papillomavirus. Emerg Infect Dis 2003;9:37-48.
4. Riedesel JM, Rosenthal SL, Zimet GD, et al. Attitudes about HPV vaccine among family physicians. J Pediatr Adolesc Gynecol 2005;18:391-398.
5. Dunne EF, Nielson CM, Stone KM, Markowitz LE, Giuliano AR. Prevalence of HPV infection among men: A systematic review of the literature. J Infect Dis 2006;194:1044-1057.
6. Block SL, Nolan T, Sattler C, et al. Comparison of the immunogenicity and reactogenicity of a prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in mail and female adolescents and young adult women. Pediatrics 2006;118:2135-2145.
7. Taira AV, Neukermans CP, Sanders GD. Evaluating human papillomavirus vaccination programs. Emerg Infect Dis 2004;19:1915-1923.
8. Winer RL, Lee SK, Hughes JP, et al. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students. Am J Epidemiol 2003;157:218-226.
8. Kjaer SK, Chackerian B, van den Brule AJC, et al. High-risk human papillomavirus is sexually transmitted: Evidence from a follow-up study of virgins starting sexual activity (intercourse). Cancer Epidemiol Biomarkers Prev 2001;10:101-106.
10. Herrero R, Castellsague X, Pawlita M, et al. Human papillomavirus and oral cancer: the International Agency for Research on Cancer multicenter study. J Natl Cancer Inst 2003;95:1772-1783.
11. Smith EM, Ritchie JM, Yankowitz J, et al. Human papillomavirus prevalence and types in newborns and parents: concordance and modes of transmission. Sex Transm Dis 2004;31:57-62.
12. Winer RL, Hughes JP, Feng Q, et al. Condom use and the risk of genital human papillomavirus infection in young women. N Engl J Med 2006;354:2645-2654.
13. Kahn JA, Hillard PA. Human papillomavirus and cervical cytology in adolescents. Adolesc Med Clin 2004;15:301-321.
14. Schiffman M, Castle PE. Human papillomavirus: epidemiology and public health. Arch Pathol Lab Med 2003;127:930-934.
15. Insinga RP, Dasbach EF, Myers ER. The health and economic burden of genital warts in a set of private health plans in the United States. Clin Infect Dis 2003;36:1397-1403.
16. Centers for Disease Control and Prevention. Genital HPV Infection Fact Sheet. Rockville, Md: CDC National Prevention Information Network; 2004.
17. Cates W, Jr. and the American Social Health Association Panel. Estimates of the incidence and prevalence of sexually transmitted diseases in the United States. Sex Transm Dis 1999;26(suppl):S2-S7.
18. Weinstock H, Berman S, Cates W, Jr. Sexually transmitted diseases among American youth: incidence and prevalence estimates, 2000. Perspect Sex Reprod Health 2004;36:6-10.
19. Tarkowski TA, Koumans EH, Sawyer M, et al. Epidemiology of human papillomavirus infection and abnormal cytologic test results in an urban adolescent population. J Infect Dis 2004;189:46-50.
20. Revzina NV, Diclemente RJ. Prevalence and incidence of human papillomavirus infection in women in the USA: a systematic review. Int J STD AIDS 2005;16:528-537.
21. Brown DR, Shew ML, Qadadri B, et al. A longitudinal study of genital human papillomavirus infection in a cohort of closely followed adolescent women. J Infect Dis 2005;191:182-192.
22. Richardson H, Kelsall G, Tellier P, et al. The natural history of type-specific human papillomavirus infections in female university students. Cancer Epidemiol Biomarkers Prev 2003;12:485-490.
23. Pinto AP, Crum CP. Natural history of cervical neoplasia: defining progression and its consequence. Clin Obstet Gynecol 2000;43:352-362.
24. Schlecht NF, Kulaga S, Robitaille J, et al. Persistent human papillomavirus infection as a predictor of CIN. JAMA 2001;286:3106-3114.
25. Hernandez BY, McDuffie K, Zhu X, et al. Anal human papillomavirus infection in women and its relationship with cervical infection. Cancer Epidemiol Biomarkers Prev 2005;14:2550-2556.
26. Holcomb K, Runowicz CD. Cervical cancer screening. Surg Oncol Clin N Am 2005;14:777-797.
27. Benard VB, Lawson HW, Eheman CR, Anderson C, Helsel W. Adherence to guidelines for follow-up of low-grade cytologic abnormalities among medically underserved women. Obstet Gynecol 2005;105:1323-1328.
28. Goldie SJ, Kohli M, Grimm D, et al. Projected clinical benefits and cost-effectiveness of a human papillomavirus 16/18 vaccine. J Natl Cancer Inst 2004;96:604-615.
29. Harper DM, Franco EL, Wheeler CM, et al. Sustained efficacy up to 4.5 years of a bivalent L1 virus-like particle vaccine against human papillomavirus types 16 and 18: follow-up from a randomized control trial. Lancet 2006;367:1247-1255.
30. Dell DL, Chen H, Ahmad F, Stewart DE. Knowledge about human papillomavirus among adolescents. Obstet Gynecol 2000;96:653-656.
31. de Villiers EM, Fauquet C, Broker TR, Bernard HU, zur Hausen H. Classification of papillomaviruses. Virology 2004;324:17-27.
32. Howley PM. Papillomavirinae: The viruses and their replication. In: Fields BN, knipe DM, Howley PM, eds. Fields Virology. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1996:2045-2076.
33. Schiffman M, Castle PE. Human papillomavirus: epidemiology and public health. Arch Pathol Lab Med 2003;127:930-934.
34. Wiley DJ, Douglas J, Beutner K, et al. External genital warts: diagnosis, treatment, and prevention. Clin Infect Dis 2002;35:S210-S224.
35. Clifford GM, Smith JS, Aguadp T, Franceschi S. Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: a meta-analysis. Br J Cancer 2003;89:101-105.
36. de Villiers EM, Neumann C, Oltersdorf T, Fierlbeck G, zur Hausen H. Butcher’s wart virus (HPV 7) infections in non-butchers. J Invest Dermatol 1986;87:236-238.
- Consider recommending HPV vaccine for 11- and 12-year-old girls in your practice, before sexual activity puts them at risk of viral infection (A). The FDA has also approved the HPV vaccine for women up to 26 years of age.
- If women older than 26 years ask to be vaccinated, make sure they understand it is an off-label use for them (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Presexual adolescent girls and sexually active women can now lower their lifetime risk of cervical cancer, thanks to a newly available quadrivalent vaccine (Gardasil) directed at human papillomavirus (HPV). This gives us the opportunity to educate parents and adolescents (the primary target group for the vaccine), many of whom remain uninformed about the direct link between HPV infection and cervical cancer.
Ethical, cultural, social, and religious issues that will require attention1 are beyond the scope of this article.
Who should receive the HPV vaccine?
Pre-adolescent and adolescent girls
Girls ages 11 to 12 years—most of whom have not started sexual activity—are the primary targets of immunization. However, the US Food and Drug Administration also approved the use of Gardasil for girls as young as 9. Girls this age may require other vaccines, such as meningococcal conjugate and tetanus-diphtheria-acellular pertussis, and experience thus far indicates no negative immune effects with co-administration of vaccines.1,2
According to one study, vaccination of the entire US population of 12-year-old girls would prevent more than 200,000 HPV infections, 100,000 abnormal Pap tests, and 3300 cases of cervical cancer.3 Parental as well as health care provider acceptance of HPV vaccines for adolescents will be critical to the success of the vaccination effort (see “What makes FPs recommend the HPV vaccine” ).4
Practical issues. As with any new vaccine added to the childhood/adolescent vaccination schedule, a host of issues will need to be resolved to ensure adequate coverage. Factors likely to influence use of HPV vaccine among adolescents are cost and reimbursement, and adherence to the 3-dose regimen that spans 6 months.
The American Academy of Pediatrics’ Committee on Infectious Diseases and the Advisory Committee on Immunization Practices (ACIP) recommends universal use of the HPV vaccine for girls, with a focus on 11- to 12-year-olds. The vaccine is also recommended for 13- to 26-year-old girls and women who have received or completed the 3-dose vaccine series.
Why not vaccinate boys? HPV infection is highly prevalent in sexually active men.5 The efficacy of vaccinating boys against HPV infection is currently being explored.6 However, one model has suggested that vaccinating adolescent males with a bivalent HPV vaccine would only slightly reduce the incidence of cervical cancer cases beyond that achieved by vaccination of adolescent girls, and with an extremely high cost-effectiveness ratio compared with female-only vaccination.5
Women ≤26 years
Indications under FDA approval also include women up to 26 years. Even adults who have been sexually active for years may not have been exposed to all high-risk HPV covered by the vaccine.
Are women older than 26 years eligible?
Though FDA approval of the vaccine is for females aged 9 to 26 years, a recent working group on HPV prevention concluded that any sexually active person may benefit from vaccination and should have the opportunity to receive the vaccine.1 Importantly, women older than 26 years who request the vaccine should be made fully aware of its off-label application in their case.
The rationale behind the recommendations
HPV transmission occurs easily with skin-to-skin contact.8-11 HPV can infect the external genitalia during non-intercourse sexual activities, including manual and oral genital contact. Sexual intercourse is the most frequent mode of infection of the cervix. Condoms may help protect against transmission of HPV but are not fully effective.8,12
Adolescents are particularly vulnerable to HPV, but respond best to vaccine. The cervix is especially susceptible to HPV infection in adolescence because the squamous columnar cell junction transformation zone is more exposed. The adult cervix is less susceptible to HPV than the adolescent cervix because of the smaller area of cervical ectopy comprised of columnar epithelial cells.13 However, in adolescents, the immune response to HPV exposure is greater than in than adults.
Risk for acquiring HPV infection. Risk factors for acquiring HPV infection are listed in the TABLE .8,14,15 According to the Centers for Disease Control and Prevention, sexually active men and women have a 50% lifetime risk of acquiring HPV infection.16 An estimated 6.2 million people in the US become infected with HPV each year,16 and approximately 20 million currently harbor HPV infections.17 This estimate includes more than 9 million sexually active adolescents and young adults 15 to 24 years of age, the group in which nearly 75% of new HPV infections occur.18 Among women <25 years of age, between 28% and 46% are infected with HPV.19,20
Infection cannot always be cleared. Most HPV infections (whether high-risk or low-risk type) are asymptomatic and are efficiently cleared (ie, no detection of DNA for a specific HPV type) by the immune system.21,22 However, if the infection cannot be cleared or controlled by the immune system, it may become a persistent infection.
Persistent infection with HPV increases the probability of progression to high-grade cervical intraepithelial neoplasia (CIN) and invasive carcinoma ( FIGURE ).18-19 Evidence also increasingly shows that high-risk HPV types likely cause anal, penile, scrotal, vulvar, vaginal, and some head and neck cancers.25
After HPV vaccination, neutralizing antibodies are secreted from memory B cells, and bind to their target HPV type, preventing infection before it occurs, thereby blocking the initial step toward development of cervical cancer.
15 high-risk oncogenic types. Papillomaviruses such as HPV are nonenveloped, double-stranded, DNA viruses. They infect cutaneous and mucosal epithelial tissues. More than 100 HPV types have been identified,3 about 30 to 40 of which are spread by sexual contact.4 Of the many known HPVs, only 15 are high-risk oncogenic types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, and 73) that can cause cervical cancer.5.6 Of these high-risk oncogenic types, HPV 16 and 18 account for about 70% of all cervical cancers.7
The new HPV vaccines, Gardasil and Cervarix, (see Web table) both contain virosomal antigens to vaccinate against HPV types 16 and 18. Persistent infection with these high-risk HPV types is necessary for the development of cervical cancer. Chronic infection with low-risk HPV types (eg, HPV 6 or 11) may lead to the development of anogenital warts and other low-grade genital abnormalities, as well as laryngeal cancer or recurrent respiratory papillomatosis. Gardasil also contains virosome antigens for these 2 HPV types. Warts on the hands are usually attributable to HPV 7.8
Viral integration is a necessary step in the malignant transformation of HPV infection; infection may progress from residential to episomal, and, finally, to an integrated form. Residential infection typically occurs a minimum of 6 weeks from exposure, can persist without detection for decades, and can be low risk or high risk. In the episomal state, virally active HPV is located in the cell nucleus, separate from the human DNA. In the integrated form of infection, the HPV DNA circle has opened and joined the human DNA. Integrated HPV—always high risk—produces an abnormal Papanicolaou (Pap) test. If recognized on colposcopy, it must be treated to prevent progression to cervical cancer.
FIGURE
How HPV infection progresses to cervical cancer
Adapted with permission from Pinto and Crum 200023 and Schlecht et al 2001.24
TABLE
Factors that put women at risk for HPV infection
| Young age (peak age group: 20–24 years) |
| Lifetime number of sexual partners |
| First sexual intercourse at early age |
| Male partner sexual behavior |
| Smoking |
| Oral contraceptive use |
| Uncircumcised male partners |
| Sources: Winer et al 2003;8 Schiffman and castle 2003;14 Insinga et al 2003.15 |
Why screening alone isn’t enough
New technologies for Pap testing, HPV DNA testing, and revisions in the Bethesda system for reporting cervical cytology have led to better treatment recommendations for patients with abnormal cytology results.26 But despite these advances, cervical screening is underused or not used at all for many women at risk.
For example, some women with abnormal cervical cytology—especially those of lower socioeconomic status, who often are medically underserved or lack insurance—may not receive adequate follow-up care.27 Though widespread cervical screening in the future may significantly decrease morbidity and mortality associated with cervical cancer, HPV vaccination can also help achieve this goal.
The case for vaccination plus screening
It will likely take at least a decade to assess the impact of HPV vaccination on invasive cervical cancer, and perhaps 20 to 30 years to achieve the maximum benefit from such a program. A computer-based model of the natural history of HPV and cervical cancer developed by the Harvard School of Public Health considered different cancer prevention policies, including vaccination against HPV types 16 and 18 (initiated at the age of 12 years), cytologic screening (initiated at 18, 21, 25, 30, or 35 years,) and combined vaccination and screening strategies. The model showed the combination strategy to be most effective.28
Dramatic reductions expected. The model predicts that with current screening and vaccination against HPV, low-grade cervical abnormalities associated with HPV-16 and HPV-18 infections would be reduced by 15% and high-grade lesions by 49%. Vaccination would decrease the number of cases of cervical cancer by about 66% in conjunction with screening. The vaccine, however, would not prevent cancers caused by other high-risk HPV types.
According to the model, HPV vaccination would produce health gains that are well worth the cost. Specifically, the cost per additional quality-adjusted life-year gained with vaccinating only females was estimated to be $21,000. This ratio compares favorably with many adult and pediatric vaccines currently used in the US.
A recent survey of attitudes about HPV vaccination among members of the American Academy of Family Physicians (AAFP) found that survey respondents would be more likely to administer an HPV vaccine to girls than to boys and to older rather than younger adolescents.4 Female gender, knowledge about HPV, and attitudes about vaccination were independently associated with family physicians’ intentions to recommend HPV vaccination.
It will take decades to see cervical cancer rates drop, but we will soon see fewer CIN 2/3 lesions once HPV 16/18 vaccination is routine.
HPV types 6 and 11 cause 90% of genital warts
Looking forward
The long-term efficacy of HPV vaccines remains to be determined. Sustained efficacy up to 4.5 years has been documented29 but it could be that boosters will be needed.
Research has shown that adolescents and parents, and even some providers of adolescent health care, may have a significant misunderstanding about HPV infection and its possible sequelae,30 suggesting the need for educational programs about the disease and its prevention. Education and vaccine advocacy from professional organizations such as the AAFP, the American Academy of Pediatrics, and the American College of Obstetricians and Gynecologists will be essential to foster acceptance of HPV vaccination.
CORRESPONDENCE
Michael E. Pichichero, MD, Elmwood Pediatric Group, 601 Elmwood Avenue, Box 672, Rochester, NY 14642. [email protected]
- Consider recommending HPV vaccine for 11- and 12-year-old girls in your practice, before sexual activity puts them at risk of viral infection (A). The FDA has also approved the HPV vaccine for women up to 26 years of age.
- If women older than 26 years ask to be vaccinated, make sure they understand it is an off-label use for them (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Presexual adolescent girls and sexually active women can now lower their lifetime risk of cervical cancer, thanks to a newly available quadrivalent vaccine (Gardasil) directed at human papillomavirus (HPV). This gives us the opportunity to educate parents and adolescents (the primary target group for the vaccine), many of whom remain uninformed about the direct link between HPV infection and cervical cancer.
Ethical, cultural, social, and religious issues that will require attention1 are beyond the scope of this article.
Who should receive the HPV vaccine?
Pre-adolescent and adolescent girls
Girls ages 11 to 12 years—most of whom have not started sexual activity—are the primary targets of immunization. However, the US Food and Drug Administration also approved the use of Gardasil for girls as young as 9. Girls this age may require other vaccines, such as meningococcal conjugate and tetanus-diphtheria-acellular pertussis, and experience thus far indicates no negative immune effects with co-administration of vaccines.1,2
According to one study, vaccination of the entire US population of 12-year-old girls would prevent more than 200,000 HPV infections, 100,000 abnormal Pap tests, and 3300 cases of cervical cancer.3 Parental as well as health care provider acceptance of HPV vaccines for adolescents will be critical to the success of the vaccination effort (see “What makes FPs recommend the HPV vaccine” ).4
Practical issues. As with any new vaccine added to the childhood/adolescent vaccination schedule, a host of issues will need to be resolved to ensure adequate coverage. Factors likely to influence use of HPV vaccine among adolescents are cost and reimbursement, and adherence to the 3-dose regimen that spans 6 months.
The American Academy of Pediatrics’ Committee on Infectious Diseases and the Advisory Committee on Immunization Practices (ACIP) recommends universal use of the HPV vaccine for girls, with a focus on 11- to 12-year-olds. The vaccine is also recommended for 13- to 26-year-old girls and women who have received or completed the 3-dose vaccine series.
Why not vaccinate boys? HPV infection is highly prevalent in sexually active men.5 The efficacy of vaccinating boys against HPV infection is currently being explored.6 However, one model has suggested that vaccinating adolescent males with a bivalent HPV vaccine would only slightly reduce the incidence of cervical cancer cases beyond that achieved by vaccination of adolescent girls, and with an extremely high cost-effectiveness ratio compared with female-only vaccination.5
Women ≤26 years
Indications under FDA approval also include women up to 26 years. Even adults who have been sexually active for years may not have been exposed to all high-risk HPV covered by the vaccine.
Are women older than 26 years eligible?
Though FDA approval of the vaccine is for females aged 9 to 26 years, a recent working group on HPV prevention concluded that any sexually active person may benefit from vaccination and should have the opportunity to receive the vaccine.1 Importantly, women older than 26 years who request the vaccine should be made fully aware of its off-label application in their case.
The rationale behind the recommendations
HPV transmission occurs easily with skin-to-skin contact.8-11 HPV can infect the external genitalia during non-intercourse sexual activities, including manual and oral genital contact. Sexual intercourse is the most frequent mode of infection of the cervix. Condoms may help protect against transmission of HPV but are not fully effective.8,12
Adolescents are particularly vulnerable to HPV, but respond best to vaccine. The cervix is especially susceptible to HPV infection in adolescence because the squamous columnar cell junction transformation zone is more exposed. The adult cervix is less susceptible to HPV than the adolescent cervix because of the smaller area of cervical ectopy comprised of columnar epithelial cells.13 However, in adolescents, the immune response to HPV exposure is greater than in than adults.
Risk for acquiring HPV infection. Risk factors for acquiring HPV infection are listed in the TABLE .8,14,15 According to the Centers for Disease Control and Prevention, sexually active men and women have a 50% lifetime risk of acquiring HPV infection.16 An estimated 6.2 million people in the US become infected with HPV each year,16 and approximately 20 million currently harbor HPV infections.17 This estimate includes more than 9 million sexually active adolescents and young adults 15 to 24 years of age, the group in which nearly 75% of new HPV infections occur.18 Among women <25 years of age, between 28% and 46% are infected with HPV.19,20
Infection cannot always be cleared. Most HPV infections (whether high-risk or low-risk type) are asymptomatic and are efficiently cleared (ie, no detection of DNA for a specific HPV type) by the immune system.21,22 However, if the infection cannot be cleared or controlled by the immune system, it may become a persistent infection.
Persistent infection with HPV increases the probability of progression to high-grade cervical intraepithelial neoplasia (CIN) and invasive carcinoma ( FIGURE ).18-19 Evidence also increasingly shows that high-risk HPV types likely cause anal, penile, scrotal, vulvar, vaginal, and some head and neck cancers.25
After HPV vaccination, neutralizing antibodies are secreted from memory B cells, and bind to their target HPV type, preventing infection before it occurs, thereby blocking the initial step toward development of cervical cancer.
15 high-risk oncogenic types. Papillomaviruses such as HPV are nonenveloped, double-stranded, DNA viruses. They infect cutaneous and mucosal epithelial tissues. More than 100 HPV types have been identified,3 about 30 to 40 of which are spread by sexual contact.4 Of the many known HPVs, only 15 are high-risk oncogenic types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, and 73) that can cause cervical cancer.5.6 Of these high-risk oncogenic types, HPV 16 and 18 account for about 70% of all cervical cancers.7
The new HPV vaccines, Gardasil and Cervarix, (see Web table) both contain virosomal antigens to vaccinate against HPV types 16 and 18. Persistent infection with these high-risk HPV types is necessary for the development of cervical cancer. Chronic infection with low-risk HPV types (eg, HPV 6 or 11) may lead to the development of anogenital warts and other low-grade genital abnormalities, as well as laryngeal cancer or recurrent respiratory papillomatosis. Gardasil also contains virosome antigens for these 2 HPV types. Warts on the hands are usually attributable to HPV 7.8
Viral integration is a necessary step in the malignant transformation of HPV infection; infection may progress from residential to episomal, and, finally, to an integrated form. Residential infection typically occurs a minimum of 6 weeks from exposure, can persist without detection for decades, and can be low risk or high risk. In the episomal state, virally active HPV is located in the cell nucleus, separate from the human DNA. In the integrated form of infection, the HPV DNA circle has opened and joined the human DNA. Integrated HPV—always high risk—produces an abnormal Papanicolaou (Pap) test. If recognized on colposcopy, it must be treated to prevent progression to cervical cancer.
FIGURE
How HPV infection progresses to cervical cancer
Adapted with permission from Pinto and Crum 200023 and Schlecht et al 2001.24
TABLE
Factors that put women at risk for HPV infection
| Young age (peak age group: 20–24 years) |
| Lifetime number of sexual partners |
| First sexual intercourse at early age |
| Male partner sexual behavior |
| Smoking |
| Oral contraceptive use |
| Uncircumcised male partners |
| Sources: Winer et al 2003;8 Schiffman and castle 2003;14 Insinga et al 2003.15 |
Why screening alone isn’t enough
New technologies for Pap testing, HPV DNA testing, and revisions in the Bethesda system for reporting cervical cytology have led to better treatment recommendations for patients with abnormal cytology results.26 But despite these advances, cervical screening is underused or not used at all for many women at risk.
For example, some women with abnormal cervical cytology—especially those of lower socioeconomic status, who often are medically underserved or lack insurance—may not receive adequate follow-up care.27 Though widespread cervical screening in the future may significantly decrease morbidity and mortality associated with cervical cancer, HPV vaccination can also help achieve this goal.
The case for vaccination plus screening
It will likely take at least a decade to assess the impact of HPV vaccination on invasive cervical cancer, and perhaps 20 to 30 years to achieve the maximum benefit from such a program. A computer-based model of the natural history of HPV and cervical cancer developed by the Harvard School of Public Health considered different cancer prevention policies, including vaccination against HPV types 16 and 18 (initiated at the age of 12 years), cytologic screening (initiated at 18, 21, 25, 30, or 35 years,) and combined vaccination and screening strategies. The model showed the combination strategy to be most effective.28
Dramatic reductions expected. The model predicts that with current screening and vaccination against HPV, low-grade cervical abnormalities associated with HPV-16 and HPV-18 infections would be reduced by 15% and high-grade lesions by 49%. Vaccination would decrease the number of cases of cervical cancer by about 66% in conjunction with screening. The vaccine, however, would not prevent cancers caused by other high-risk HPV types.
According to the model, HPV vaccination would produce health gains that are well worth the cost. Specifically, the cost per additional quality-adjusted life-year gained with vaccinating only females was estimated to be $21,000. This ratio compares favorably with many adult and pediatric vaccines currently used in the US.
A recent survey of attitudes about HPV vaccination among members of the American Academy of Family Physicians (AAFP) found that survey respondents would be more likely to administer an HPV vaccine to girls than to boys and to older rather than younger adolescents.4 Female gender, knowledge about HPV, and attitudes about vaccination were independently associated with family physicians’ intentions to recommend HPV vaccination.
It will take decades to see cervical cancer rates drop, but we will soon see fewer CIN 2/3 lesions once HPV 16/18 vaccination is routine.
HPV types 6 and 11 cause 90% of genital warts
Looking forward
The long-term efficacy of HPV vaccines remains to be determined. Sustained efficacy up to 4.5 years has been documented29 but it could be that boosters will be needed.
Research has shown that adolescents and parents, and even some providers of adolescent health care, may have a significant misunderstanding about HPV infection and its possible sequelae,30 suggesting the need for educational programs about the disease and its prevention. Education and vaccine advocacy from professional organizations such as the AAFP, the American Academy of Pediatrics, and the American College of Obstetricians and Gynecologists will be essential to foster acceptance of HPV vaccination.
CORRESPONDENCE
Michael E. Pichichero, MD, Elmwood Pediatric Group, 601 Elmwood Avenue, Box 672, Rochester, NY 14642. [email protected]
1. Frazer IH, Cox JT, Mayeaux Jr EJ, et al. advances in prevention of cervical cancer and other human papillomavirus-related diseases. Pediatr Infect Dis J 2006;25:S65-S81.
2. Bonnez W. Immunization against genital human papillomaviruses. J Infect Dis 2005;24:1005-1006.
3. Sanders GD, Taira AV. cost-effectiveness of a potential vaccine for human papillomavirus. Emerg Infect Dis 2003;9:37-48.
4. Riedesel JM, Rosenthal SL, Zimet GD, et al. Attitudes about HPV vaccine among family physicians. J Pediatr Adolesc Gynecol 2005;18:391-398.
5. Dunne EF, Nielson CM, Stone KM, Markowitz LE, Giuliano AR. Prevalence of HPV infection among men: A systematic review of the literature. J Infect Dis 2006;194:1044-1057.
6. Block SL, Nolan T, Sattler C, et al. Comparison of the immunogenicity and reactogenicity of a prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in mail and female adolescents and young adult women. Pediatrics 2006;118:2135-2145.
7. Taira AV, Neukermans CP, Sanders GD. Evaluating human papillomavirus vaccination programs. Emerg Infect Dis 2004;19:1915-1923.
8. Winer RL, Lee SK, Hughes JP, et al. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students. Am J Epidemiol 2003;157:218-226.
8. Kjaer SK, Chackerian B, van den Brule AJC, et al. High-risk human papillomavirus is sexually transmitted: Evidence from a follow-up study of virgins starting sexual activity (intercourse). Cancer Epidemiol Biomarkers Prev 2001;10:101-106.
10. Herrero R, Castellsague X, Pawlita M, et al. Human papillomavirus and oral cancer: the International Agency for Research on Cancer multicenter study. J Natl Cancer Inst 2003;95:1772-1783.
11. Smith EM, Ritchie JM, Yankowitz J, et al. Human papillomavirus prevalence and types in newborns and parents: concordance and modes of transmission. Sex Transm Dis 2004;31:57-62.
12. Winer RL, Hughes JP, Feng Q, et al. Condom use and the risk of genital human papillomavirus infection in young women. N Engl J Med 2006;354:2645-2654.
13. Kahn JA, Hillard PA. Human papillomavirus and cervical cytology in adolescents. Adolesc Med Clin 2004;15:301-321.
14. Schiffman M, Castle PE. Human papillomavirus: epidemiology and public health. Arch Pathol Lab Med 2003;127:930-934.
15. Insinga RP, Dasbach EF, Myers ER. The health and economic burden of genital warts in a set of private health plans in the United States. Clin Infect Dis 2003;36:1397-1403.
16. Centers for Disease Control and Prevention. Genital HPV Infection Fact Sheet. Rockville, Md: CDC National Prevention Information Network; 2004.
17. Cates W, Jr. and the American Social Health Association Panel. Estimates of the incidence and prevalence of sexually transmitted diseases in the United States. Sex Transm Dis 1999;26(suppl):S2-S7.
18. Weinstock H, Berman S, Cates W, Jr. Sexually transmitted diseases among American youth: incidence and prevalence estimates, 2000. Perspect Sex Reprod Health 2004;36:6-10.
19. Tarkowski TA, Koumans EH, Sawyer M, et al. Epidemiology of human papillomavirus infection and abnormal cytologic test results in an urban adolescent population. J Infect Dis 2004;189:46-50.
20. Revzina NV, Diclemente RJ. Prevalence and incidence of human papillomavirus infection in women in the USA: a systematic review. Int J STD AIDS 2005;16:528-537.
21. Brown DR, Shew ML, Qadadri B, et al. A longitudinal study of genital human papillomavirus infection in a cohort of closely followed adolescent women. J Infect Dis 2005;191:182-192.
22. Richardson H, Kelsall G, Tellier P, et al. The natural history of type-specific human papillomavirus infections in female university students. Cancer Epidemiol Biomarkers Prev 2003;12:485-490.
23. Pinto AP, Crum CP. Natural history of cervical neoplasia: defining progression and its consequence. Clin Obstet Gynecol 2000;43:352-362.
24. Schlecht NF, Kulaga S, Robitaille J, et al. Persistent human papillomavirus infection as a predictor of CIN. JAMA 2001;286:3106-3114.
25. Hernandez BY, McDuffie K, Zhu X, et al. Anal human papillomavirus infection in women and its relationship with cervical infection. Cancer Epidemiol Biomarkers Prev 2005;14:2550-2556.
26. Holcomb K, Runowicz CD. Cervical cancer screening. Surg Oncol Clin N Am 2005;14:777-797.
27. Benard VB, Lawson HW, Eheman CR, Anderson C, Helsel W. Adherence to guidelines for follow-up of low-grade cytologic abnormalities among medically underserved women. Obstet Gynecol 2005;105:1323-1328.
28. Goldie SJ, Kohli M, Grimm D, et al. Projected clinical benefits and cost-effectiveness of a human papillomavirus 16/18 vaccine. J Natl Cancer Inst 2004;96:604-615.
29. Harper DM, Franco EL, Wheeler CM, et al. Sustained efficacy up to 4.5 years of a bivalent L1 virus-like particle vaccine against human papillomavirus types 16 and 18: follow-up from a randomized control trial. Lancet 2006;367:1247-1255.
30. Dell DL, Chen H, Ahmad F, Stewart DE. Knowledge about human papillomavirus among adolescents. Obstet Gynecol 2000;96:653-656.
31. de Villiers EM, Fauquet C, Broker TR, Bernard HU, zur Hausen H. Classification of papillomaviruses. Virology 2004;324:17-27.
32. Howley PM. Papillomavirinae: The viruses and their replication. In: Fields BN, knipe DM, Howley PM, eds. Fields Virology. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1996:2045-2076.
33. Schiffman M, Castle PE. Human papillomavirus: epidemiology and public health. Arch Pathol Lab Med 2003;127:930-934.
34. Wiley DJ, Douglas J, Beutner K, et al. External genital warts: diagnosis, treatment, and prevention. Clin Infect Dis 2002;35:S210-S224.
35. Clifford GM, Smith JS, Aguadp T, Franceschi S. Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: a meta-analysis. Br J Cancer 2003;89:101-105.
36. de Villiers EM, Neumann C, Oltersdorf T, Fierlbeck G, zur Hausen H. Butcher’s wart virus (HPV 7) infections in non-butchers. J Invest Dermatol 1986;87:236-238.
1. Frazer IH, Cox JT, Mayeaux Jr EJ, et al. advances in prevention of cervical cancer and other human papillomavirus-related diseases. Pediatr Infect Dis J 2006;25:S65-S81.
2. Bonnez W. Immunization against genital human papillomaviruses. J Infect Dis 2005;24:1005-1006.
3. Sanders GD, Taira AV. cost-effectiveness of a potential vaccine for human papillomavirus. Emerg Infect Dis 2003;9:37-48.
4. Riedesel JM, Rosenthal SL, Zimet GD, et al. Attitudes about HPV vaccine among family physicians. J Pediatr Adolesc Gynecol 2005;18:391-398.
5. Dunne EF, Nielson CM, Stone KM, Markowitz LE, Giuliano AR. Prevalence of HPV infection among men: A systematic review of the literature. J Infect Dis 2006;194:1044-1057.
6. Block SL, Nolan T, Sattler C, et al. Comparison of the immunogenicity and reactogenicity of a prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in mail and female adolescents and young adult women. Pediatrics 2006;118:2135-2145.
7. Taira AV, Neukermans CP, Sanders GD. Evaluating human papillomavirus vaccination programs. Emerg Infect Dis 2004;19:1915-1923.
8. Winer RL, Lee SK, Hughes JP, et al. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students. Am J Epidemiol 2003;157:218-226.
8. Kjaer SK, Chackerian B, van den Brule AJC, et al. High-risk human papillomavirus is sexually transmitted: Evidence from a follow-up study of virgins starting sexual activity (intercourse). Cancer Epidemiol Biomarkers Prev 2001;10:101-106.
10. Herrero R, Castellsague X, Pawlita M, et al. Human papillomavirus and oral cancer: the International Agency for Research on Cancer multicenter study. J Natl Cancer Inst 2003;95:1772-1783.
11. Smith EM, Ritchie JM, Yankowitz J, et al. Human papillomavirus prevalence and types in newborns and parents: concordance and modes of transmission. Sex Transm Dis 2004;31:57-62.
12. Winer RL, Hughes JP, Feng Q, et al. Condom use and the risk of genital human papillomavirus infection in young women. N Engl J Med 2006;354:2645-2654.
13. Kahn JA, Hillard PA. Human papillomavirus and cervical cytology in adolescents. Adolesc Med Clin 2004;15:301-321.
14. Schiffman M, Castle PE. Human papillomavirus: epidemiology and public health. Arch Pathol Lab Med 2003;127:930-934.
15. Insinga RP, Dasbach EF, Myers ER. The health and economic burden of genital warts in a set of private health plans in the United States. Clin Infect Dis 2003;36:1397-1403.
16. Centers for Disease Control and Prevention. Genital HPV Infection Fact Sheet. Rockville, Md: CDC National Prevention Information Network; 2004.
17. Cates W, Jr. and the American Social Health Association Panel. Estimates of the incidence and prevalence of sexually transmitted diseases in the United States. Sex Transm Dis 1999;26(suppl):S2-S7.
18. Weinstock H, Berman S, Cates W, Jr. Sexually transmitted diseases among American youth: incidence and prevalence estimates, 2000. Perspect Sex Reprod Health 2004;36:6-10.
19. Tarkowski TA, Koumans EH, Sawyer M, et al. Epidemiology of human papillomavirus infection and abnormal cytologic test results in an urban adolescent population. J Infect Dis 2004;189:46-50.
20. Revzina NV, Diclemente RJ. Prevalence and incidence of human papillomavirus infection in women in the USA: a systematic review. Int J STD AIDS 2005;16:528-537.
21. Brown DR, Shew ML, Qadadri B, et al. A longitudinal study of genital human papillomavirus infection in a cohort of closely followed adolescent women. J Infect Dis 2005;191:182-192.
22. Richardson H, Kelsall G, Tellier P, et al. The natural history of type-specific human papillomavirus infections in female university students. Cancer Epidemiol Biomarkers Prev 2003;12:485-490.
23. Pinto AP, Crum CP. Natural history of cervical neoplasia: defining progression and its consequence. Clin Obstet Gynecol 2000;43:352-362.
24. Schlecht NF, Kulaga S, Robitaille J, et al. Persistent human papillomavirus infection as a predictor of CIN. JAMA 2001;286:3106-3114.
25. Hernandez BY, McDuffie K, Zhu X, et al. Anal human papillomavirus infection in women and its relationship with cervical infection. Cancer Epidemiol Biomarkers Prev 2005;14:2550-2556.
26. Holcomb K, Runowicz CD. Cervical cancer screening. Surg Oncol Clin N Am 2005;14:777-797.
27. Benard VB, Lawson HW, Eheman CR, Anderson C, Helsel W. Adherence to guidelines for follow-up of low-grade cytologic abnormalities among medically underserved women. Obstet Gynecol 2005;105:1323-1328.
28. Goldie SJ, Kohli M, Grimm D, et al. Projected clinical benefits and cost-effectiveness of a human papillomavirus 16/18 vaccine. J Natl Cancer Inst 2004;96:604-615.
29. Harper DM, Franco EL, Wheeler CM, et al. Sustained efficacy up to 4.5 years of a bivalent L1 virus-like particle vaccine against human papillomavirus types 16 and 18: follow-up from a randomized control trial. Lancet 2006;367:1247-1255.
30. Dell DL, Chen H, Ahmad F, Stewart DE. Knowledge about human papillomavirus among adolescents. Obstet Gynecol 2000;96:653-656.
31. de Villiers EM, Fauquet C, Broker TR, Bernard HU, zur Hausen H. Classification of papillomaviruses. Virology 2004;324:17-27.
32. Howley PM. Papillomavirinae: The viruses and their replication. In: Fields BN, knipe DM, Howley PM, eds. Fields Virology. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1996:2045-2076.
33. Schiffman M, Castle PE. Human papillomavirus: epidemiology and public health. Arch Pathol Lab Med 2003;127:930-934.
34. Wiley DJ, Douglas J, Beutner K, et al. External genital warts: diagnosis, treatment, and prevention. Clin Infect Dis 2002;35:S210-S224.
35. Clifford GM, Smith JS, Aguadp T, Franceschi S. Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: a meta-analysis. Br J Cancer 2003;89:101-105.
36. de Villiers EM, Neumann C, Oltersdorf T, Fierlbeck G, zur Hausen H. Butcher’s wart virus (HPV 7) infections in non-butchers. J Invest Dermatol 1986;87:236-238.
Virtual colonoscopy: What is its role in cancer screening?
- Computed tomography colonography should be evaluated on a case-by-case basis, given the lack of consensus over the number of false positive/negative results it generates, and its lack of widespread acceptance by major insurance companies (C).
- CTC is a useful screening alternative for patients who have had an incomplete colonoscopy or who have an obstructing carcinoma (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
The virtual colonoscopy (CT colonography, or CTC) could make life just a little bit easier when it comes to discussing colorectal cancer screening options with your patients. After all, what patient wouldn’t like to hear that there is an alternative to the colonoscopy that doesn’t require sedation, IV injections, or a scope?
The reality, though, is that a number of roadblocks stand between the CTC and its inclusion in the battery of colorectal screening tools we typically discuss with our patients. Among the barriers: Mixed results from research studies evaluating the sensitivity and specificity of the CTC1-3 and a decision by many insurance plans not to cover the procedure, deeming it “experimental.”4
More research is undoubtedly needed, and some is already underway. The American College of Radiology Imaging Network has conducted a large scale, double-blind study,5 with results expected later this year. In the meantime, though, counseling your patients on their options will hinge on your knowledge of the advantages and disadvantages of the CTC and what the research—to date—tells us about its usefulness.
Like a colonoscopy, it offers a fly-through view
The CTC, which uses helical CT to capture 2D axial images that can be converted into a 3D view, allows the radiologist the same type of colon “fly through” view that a gastroenterologist would see using a colonoscopy (FIGURE).6 Among its pluses: It requires no anesthesia and is noninvasive, so it’s likely to appeal to patients who have a strong fear of colonoscopy. (See “What patients can expect during a CTC”) Another potential plus: While full bowel cleansing is still required, recent investigations have studied new “prep-less” CTC options consisting of a low residue diet with multiple doses of liquid barium without catharsis.7-9
CTC also offers a viable screening option for certain patient populations. Specifically, it’s already regularly being used in those who have had an incomplete colonoscopy or who have an obstructing carcinoma.10-12 CTC can also be used to screen elderly patients who have contraindications to conscious sedation or medical problems that preclude them from invasive procedures.
FIGURE
“Fly-through” via virtual colonoscopy
A 2D color reconstruction “fly-through” showing a large pedunculated polyp (left) and a large sessile polyp (right).On the downside, there is always a concern about the possible deleterious effects of radiation whenever an imaging technology is involved. The average person in the US gets about 3 mSv of radiation per year from the environment. This compares with about 10 mSv from a CT of the abdomen, 0.1 mSv from a chest x-ray, 0.7 mSv from mammography, or 5 to 7.8 mSv from CTC.13,14 Even though the radiation dosage currently used in CTC is safe, studies examining CTC with lower ionization have produced very hopeful results.15 In fact, a recent study by Brenner et al found that in terms of radiation from CTC and its ability to detect polyps, the benefits far outweigh any risks.16
As you might expect, the cost of a CTC is on the higher end of the colorectal cancer screening spectrum, though it is comparable with a colonoscopy. Fecal occult blood testing is the cheapest, with a cost, on average, of $10 to $20. Flexible sigmoidoscopy is about $150 to $300, double-contrast barium enema is about $250 to $500, and both colonoscopy and CTC are about $800 to $1600. However, CTC is currently not covered under most insurance plans, but it’s starting to gain acceptance as a reimbursable procedure. In fact, the Centers for Medicare and Medicaid Services has recently published CPT codes for CTC and even more recently made the professional components of both diagnostic and screening CTC fully reimbursible.
The protocol for CT colonography has become considerably more standardized over the past few years, and official American College of Radiology standards will soon be in place. Typically, though, a patient getting a screening CTC can expect the following:
The night before the procedure, he’ll need to cleanse the bowel completely, using an enema. The next day in the CT suite, a tube will be inserted into his rectum, and the rectum will be insufflated with carbon dioxide (about 1.5 L).29,30 Usually, the CT scans will be done while the patient is in both the supine and prone positions. The amount of radiation is comparable to that of a double-contrast barium enema.30 The 2D data is then analyzed using specialized workstations that can create both 2D and 3D views.
The entire exam takes less than 20 minutes and the scanning sessions last only a few minutes and require two 10-second breath holds.29,30
Widespread reimbursement in the private sector is not here yet, however, since many major insurance companies consider CTC an experimental procedure.4 This hesitance on the part of the private sector is understandable, as we found when we undertook a search of the literature.
Methods
We conducted a thorough and systematic search of PubMed for English-language articles from 1994 to 2006. Search terms included “CT colonography,” “virtual colonoscopy,” “CT colonoscopy,” “colography,” and “CT pneumocolon.”17 The general focus was on original research articles, but meta-analyses and review articles were also considered. In addition, we conducted general Internet searches to discern the general public’s view on this technology.
The research is mixed—specificity/sensitivity values vary
Research has shown that colorectal cancer arises in adenomatous polyps and that detection and removal reduces mortality for this cancer.18,19 Since 1994, when Vining et al first described the concept of CTC,6 numerous studies have compared its polyp detection rate with the gold standard, colonoscopy. The most recent are 3 large, multicenter prospective trials comparing the sensitivity and specificity of CTC against colonoscopy for adenomatous polyp detection.1-3 These 3 studies have not been consistent in their findings. One study showed very favorable results,1 but the other 2 showed unfavorable results (TABLE).
In December 2003, Dr Perry Pickhardt and his colleagues published the first multicenter prospective study comparing CTC with colonoscopy on a large, asymptomatic population.1 That study was performed in 3 medical centers and included 1233 subjects with a mean age of 57.8 years. All of the subjects underwent same-day CTC and colonoscopy. Each CTC was interpreted using both 2D and 3D imaging techniques. The results were very encouraging. CTC had a 93.8% sensitivity for adenomatous polyps at least 10 mm in diameter, 93.9% sensitivity for those at least 8 mm in diameter, and 88.7% sensitivity for those at least 6 mm in diameter. (For more on polyp size, see “Remove that polyp? With virtual colonoscopy, it’s not automatic,”.) The specificity for those polyp size categories was 96.0%, 92.2%, and 79.6%, respectively. The study concluded that CTC compared well with colonoscopy in the detection of adenomatous polyps in asymptomatic adults.
In April 2004, Dr Peter Cotton and his colleagues published the second multicenter, prospective study comparing CTC and colonoscopy in terms of adenomatous polyp detection for a screening population.2 The study took place at 9 medical centers and had 615 patients ages 50 and older who had both CTC and colonoscopy done on the same day. The researchers found that CTC had a sensitivity of 55% for those at least 10 mm in size and 39% for polyps at least 6 mm in size. They concluded that CTC technology was not ready for mainstream clinical use until a significant amount of enhancement took place in the use of this technology.
In January 2005, Dr Don Rockey and his colleagues published a multicenter study comparing CTC and colonoscopy at 14 sites.3 They had 614 patients with an average age of 57.4. They also found CTC to be significantly less sensitive for detecting polyps both >10 mm and >6 mm when compared with colonoscopy.
TABLE
Multicenter trials compared colonoscopy and virtual colonoscopy polyp detection rates
| PB COTTON ET AL2 (JAMA) | PJ PICKHARDT ET AL1 (NEJM) | DC ROCKEY ET AL3 (LANCET) | |
|---|---|---|---|
| Number of sites | 9 | 3 | 14 |
| Dates of study | April 2000–Oct 2001 | May 2002–June 2003 | Dec 2000–Feb 2004 |
| Number of patients | 615 | 1233 | 614 |
| Patient age (mean) | 61 | 57.8 | 57.4 |
| Sensitivity & specificity of detecting lesions ≥6 mm | Sensitivity: 39.0% Specificity: 90.5% | Sensitivity: 88.7% Specificity: 79.6% | Sensitivity: 51.0% Specificity: 89.0% |
| Sensitivity & specificity of detecting lesions ≥10 mm | Sensitivity: 55.0% Specificity: 96.0% | Sensitivity: 93.8% Specificity: 96.0% | Sensitivity: 59.0% Specificity: 96.0% |
The discrepancy may be a matter of software and protocols
Dr Pickhardt and his colleagues attribute part of their success in CTC to the particular software they used, which can render 3D images better than almost any other program available.20 A report issued by the American Gastroenterological Association says that Pickhardt et al’s use of primary 3D interpretation differs from most currently performed protocols.21 If Pickhardt et al’s results can even partly be attributed to use of new software, then it seems prudent to change the protocols to whatever works best in light of the evolving technology. The protocols must remain flexible until appropriate results are achieved and repeatable.
In addition, there are many other variables that could account for these results including a younger screening population, mostly composed of military families, the use of stool and fluid tagging (advanced techniques that improve accuracy and decrease the need for a completely clean bowel), or the aggressive, double-bowel preparations given before the procedure.1
Both Dr Pickhardt and Dr Joseph Ferrucci criticize the Cotton et al study because it primarily used 2D images and their trial ended in October 2001, whereas Pickhardt et al’s started in May 2002.22 With so much dependent on software issues, the interval is significant. In addition, the study by Dr Cotton and his colleagues used older CT and insufflation technology and several of the centers involved in the studies only had to show familiarity with the procedure, but no demonstrated ability in reading CTC images.22 Thus, both technical and reader issues were significant. Similarly, in the study by Rockey et al, the issue of reader inexperience was present, as was the fact that neither stool nor fluid tagging was used.22
When an adenomatous polyp of any size is found during a colonoscopy, the polyp is removed. Thus the diagnostic and therapeutic functions are married in colonoscopy. However, CTC only allows detection of these polyps, thus raising the question as to which size polyps should be reported and then removed by doing an additional colonoscopy. The issue of what size polyps have malignancy potential has been discussed extensively in the literature.31-33
It’s also a hotly debated topic in the literature for colorectal cancer screening, especially when any mention of CTC comes up. Every year, about 1% of polyps larger than 10 mm progress to colorectal cancer and there is agreement that these should be removed.34 However, there is considerable debate over the 6 to 9 mm category.34-36 Several trials have shown that the incidence of polyps between 6 to 9 mm progressing into colorectal cancer approaches, but is definitely less than 1%.37 Even the American Gastroenterological Association acknowledges that the risk of developing colorectal cancer from a polyp 6 to 9 mm remains uncertain.21
Thus, while it’s clear that polyps larger than 10 mm pose a significant enough risk to warrant removal, the data is equivocal—or absent—on what to do about polyps in the 6 to 9 mm category.
Another important variation between Pickhardt et al’s study and those by Drs Cotton and Rockey and their colleagues is the use of oral contrasts for stool tagging.23 A unique aspects of Pickhardt et al’s study was the aggressive bowel preparation using 2 types of oral contrast (water soluble and barium) for stool tagging. This allowed the computer to electronically separate and subtract residual stool from soft tissue structures improving image quality dramatically.1 This elaborate patient preparation has not been done by anyone else. Many contend that what Pickhardt et al achieved was a paradigm of the best CTC can be under ideal circumstances, technology, and expert interpretations and if not done in this manner, the results would get murky with diffuse application.23 This again emphasizes the importance of recognizing the evolving technology and protocol for CTC.
Much-needed research is underway
Until results of the caliber that Pickhardt et al achieved are reproducible locally, many insurance companies will delay coverage for screening CTC. For most areas, CTC would be about $1000 out of pocket cost for the patient. It seems likely that most patients would not opt for CTC when insurance companies cover other screening procedures.
The American College of Radiology Imaging Network has conducted a very large-scale double-blind study of CTC effectiveness in a screening population involving 15 institutions and 2300 participants.5 The results of this trial, expected out this summer, will surely influence CTC’s acceptance both by the medical community and by third party payers. Until then, family physicians will need to consider the use of CTC on a case-by-case basis.
Colorectal cancer mortality can be significantly reduced through proper screening.18,24-27 The American Cancer Society’s guidelines for screening28 indicate that beginning at age 50, both men and women with average risk factors should have one of the following:
- yearly fecal occult blood test
- flexible sigmoidoscopy every 5 years
- yearly fecal occult blood testing and flexible sigmoidoscopy every 5 years
- double-contrast barium enema every 5 years, or
- colonoscopy every 10 years.
A positive finding for any of the first 4 should prompt a colonoscopy.
CORRESPONDENCE
Jaspal Singh Ahluwalia, MD Walter Reed Army Medical Center, 6900 Georgia Avenue NW, Washington, D.C. 20307 E-mail: [email protected]
1. Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 2003;349:2191-2200.
2. Cotton PB, Durkalski VL, Pineau BC, et al. Computed tomographic colonography (virtual colonoscopy); a multicenter comparison with standard colonoscopy for detection of colorectal neoplasia. JAMA 2004;291:1713-1719.
3. Rockey DC, Paulson E, Niedzwiecki D. Analysis of air contrast barium enema, computed tomographic colonography, and colonoscopy: prospective comparison. Lancet 2005;365:305-311.
4. CT Colonography (“virtual colonoscopy”) for colon cancer screening. Technology Evaluation Center, Blue Cross and Blue Shield Associaiton assessment program, 2004 (July), vol 19. Chicago, Ill: Blue Cross and Blue Shield Association, 2004.
5. American College of Radiology website. ACRIN seeks institutions for CTC trial. Available at: www.acr.org/s_acr/doc.asp?DID=18669. Accessed on February 15, 2007.
6. Vining DJ, Gelfand DW, Bechtold RE, et al. Technological feasibility of colon imaging with helical CT and virtual reality. AJR 1994;162(suppl):S104.-
7. Lefere P, Gryspeerdt S, et al. Technical innovation: laxative-free CT colonograpy. ARJ 2004;183:945-948.
8. Lefere PA, Bryspeerdt SS, Dewyspelaere J, et al. Dietary fecal tagging as a cleansing method before CT colonography: initial results: polyp detection and patient acceptance. Radiology 2002;224:393-403.
9. Zalis ME, Perumpillichira J, Del Frate C, et al. CT colonography: digital subtraction and bowel cleansing with mucosal reconstruction—initial observations. Radiology 2003;226:911-917.
10. Macari M, Megibow AJ, Berman P, et al. CT colonography in patients with failed colonoscopy. AJR 1999;173:561-564.
11. Morrin MM, Kruskal JB, Farrell RJ, et al. Endoluminal CT colonography after incomplete endoscopic colonoscopy. AJR 1999;172:913-918.
12. Fenlon HM, McAneny DB, Nunes DP, et al. Occlusive colon carcinoma: virtual colonoscopy in the preoperative evaluation of the proximal colon. Radiology 1999;210:423-428.
13. RadiologyInfo website. Safety in medical imaging procedures. Radiological Society on North America. Available at: www.radiologyinfo.org/content/safety. Accessed on February 15, 2007.
14. Macari M, Milano A, Lavelle M, et al. Comparison of time-efficient CT colonography with two- and three-dimensional colonic evaluation for detecting colorectal polyps. AJR 2000;174:1543-1549.
15. Cohnen M, Vogt C, Beck A, et al. Feasibility of MDCT colonography in ultra-low-dose technique in the detection of colorectal lesions: comparison with high-resolution video colonoscopy. AJR 2004;183:1355-1359.
16. Brenner DJ, Georgsson MA. Mass screening with CT colonography: should the radiation exposure be of concern? Gastroenterology 2005;129:328-337.
17. Johnson CD. Virtual endoscopy: what’s in a name? AJR 1998;171:1201-1202.
18. Winawer SJ, Zauber AG, Ho MN. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med 1993;329:1977-1981.
19. Bond JH. Clinical evidence for the adenoma-carcinoma sequence, and the management of patients with colorectal adenomas. Gastrointest Dis 2000;11:176-184.
20. Pickhardt PJ. Author’s response. RadioGraphics 2004;24:1557-1559.
21. Van Dam J, Cotton P, Johnson CD, et al. AGA future trends report: CT colonography. Gastroenterology 2004;127:970-984.
22. Pickhardt PJ, Ferrucci J. Letters. JAMA 2004;292:431-433.
23. Ransohoff DF. Virtual colonoscopy—what it can do vs. what it will do. JAMA 2004;291:1772-1774.
24. Ransohoff DF, Sandler RS. Clinical practice: screening for colorectal cancer. N Engl J Med 2002;346:40-44.
25. Winawer SJ, Fletcher RH, Rex DK, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale—update based on new evidence. Gastroenterology 2003;124:544-560.
26. Mandel JS, Bond JH, Church TR, et al. Reducing the mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med 1993;328:1365-1371.
27. Muller AD, Sonnenberg A. Protection by endoscopy against death from colorectal cancer: a case control study among veterans. Arch Intern Med 1995;155:1741-1748.
28. Cancer Facts & Figures—2006. Atlanta, Ga: American Cancer Society, 2006. Available at: www.cancer.org/downloads/STT/caFF2006PWSecured.pdf. Accessed on February 15, 2007.
29. Morrin MM, LaMont JT. Screening virtual colonoscopy—ready for prime time? N Engl J Med 2003;349:2261-2264.
30. Johnson CD, Dachman AH. CT colonography: the next colon screening examination? Radiology 2000;216:331-341.
31. Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to screen asymptomatic adults for colorectal cancer. N Engl J Med 2000;343:162-168.
32. Imperiale TF, Wagner DR, Lin CY, et al. Risk of advanced proximal neoplasms in asymptomatic adults according to the distal colorectal finds. N Engl J Med 2000;343:169-174.
33. Hofstad B, Vatn MH, Anderen SN, et al. Growth of colorectal polyps: redetection and evaluation of unresected polyps for a period of three years. Gut 1996;39:449-456.
34. Stryker SJ, Wolff BG, Culp CE, et al. Natural history of untreated colonic polyps. Gastroenterology 1987;93:1009-1013.
35. Waye JD, Lewis BS, Frankel A, et al. Small colon polyps. Am J Gastroenterology 1988;83:120-122.
36. Nusko G, Mansmann U, Partzsch U, et al. Invasive carcinoma in colorectal adenomas: multivariate analysis of patient and adenoma characteristics. Endoscopy 1997;29:626-631.
37. Morson B. The polyp-cancer sequence in the large bowel. Proc R Soc Med 1974;67:451-457.
- Computed tomography colonography should be evaluated on a case-by-case basis, given the lack of consensus over the number of false positive/negative results it generates, and its lack of widespread acceptance by major insurance companies (C).
- CTC is a useful screening alternative for patients who have had an incomplete colonoscopy or who have an obstructing carcinoma (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
The virtual colonoscopy (CT colonography, or CTC) could make life just a little bit easier when it comes to discussing colorectal cancer screening options with your patients. After all, what patient wouldn’t like to hear that there is an alternative to the colonoscopy that doesn’t require sedation, IV injections, or a scope?
The reality, though, is that a number of roadblocks stand between the CTC and its inclusion in the battery of colorectal screening tools we typically discuss with our patients. Among the barriers: Mixed results from research studies evaluating the sensitivity and specificity of the CTC1-3 and a decision by many insurance plans not to cover the procedure, deeming it “experimental.”4
More research is undoubtedly needed, and some is already underway. The American College of Radiology Imaging Network has conducted a large scale, double-blind study,5 with results expected later this year. In the meantime, though, counseling your patients on their options will hinge on your knowledge of the advantages and disadvantages of the CTC and what the research—to date—tells us about its usefulness.
Like a colonoscopy, it offers a fly-through view
The CTC, which uses helical CT to capture 2D axial images that can be converted into a 3D view, allows the radiologist the same type of colon “fly through” view that a gastroenterologist would see using a colonoscopy (FIGURE).6 Among its pluses: It requires no anesthesia and is noninvasive, so it’s likely to appeal to patients who have a strong fear of colonoscopy. (See “What patients can expect during a CTC”) Another potential plus: While full bowel cleansing is still required, recent investigations have studied new “prep-less” CTC options consisting of a low residue diet with multiple doses of liquid barium without catharsis.7-9
CTC also offers a viable screening option for certain patient populations. Specifically, it’s already regularly being used in those who have had an incomplete colonoscopy or who have an obstructing carcinoma.10-12 CTC can also be used to screen elderly patients who have contraindications to conscious sedation or medical problems that preclude them from invasive procedures.
FIGURE
“Fly-through” via virtual colonoscopy
A 2D color reconstruction “fly-through” showing a large pedunculated polyp (left) and a large sessile polyp (right).On the downside, there is always a concern about the possible deleterious effects of radiation whenever an imaging technology is involved. The average person in the US gets about 3 mSv of radiation per year from the environment. This compares with about 10 mSv from a CT of the abdomen, 0.1 mSv from a chest x-ray, 0.7 mSv from mammography, or 5 to 7.8 mSv from CTC.13,14 Even though the radiation dosage currently used in CTC is safe, studies examining CTC with lower ionization have produced very hopeful results.15 In fact, a recent study by Brenner et al found that in terms of radiation from CTC and its ability to detect polyps, the benefits far outweigh any risks.16
As you might expect, the cost of a CTC is on the higher end of the colorectal cancer screening spectrum, though it is comparable with a colonoscopy. Fecal occult blood testing is the cheapest, with a cost, on average, of $10 to $20. Flexible sigmoidoscopy is about $150 to $300, double-contrast barium enema is about $250 to $500, and both colonoscopy and CTC are about $800 to $1600. However, CTC is currently not covered under most insurance plans, but it’s starting to gain acceptance as a reimbursable procedure. In fact, the Centers for Medicare and Medicaid Services has recently published CPT codes for CTC and even more recently made the professional components of both diagnostic and screening CTC fully reimbursible.
The protocol for CT colonography has become considerably more standardized over the past few years, and official American College of Radiology standards will soon be in place. Typically, though, a patient getting a screening CTC can expect the following:
The night before the procedure, he’ll need to cleanse the bowel completely, using an enema. The next day in the CT suite, a tube will be inserted into his rectum, and the rectum will be insufflated with carbon dioxide (about 1.5 L).29,30 Usually, the CT scans will be done while the patient is in both the supine and prone positions. The amount of radiation is comparable to that of a double-contrast barium enema.30 The 2D data is then analyzed using specialized workstations that can create both 2D and 3D views.
The entire exam takes less than 20 minutes and the scanning sessions last only a few minutes and require two 10-second breath holds.29,30
Widespread reimbursement in the private sector is not here yet, however, since many major insurance companies consider CTC an experimental procedure.4 This hesitance on the part of the private sector is understandable, as we found when we undertook a search of the literature.
Methods
We conducted a thorough and systematic search of PubMed for English-language articles from 1994 to 2006. Search terms included “CT colonography,” “virtual colonoscopy,” “CT colonoscopy,” “colography,” and “CT pneumocolon.”17 The general focus was on original research articles, but meta-analyses and review articles were also considered. In addition, we conducted general Internet searches to discern the general public’s view on this technology.
The research is mixed—specificity/sensitivity values vary
Research has shown that colorectal cancer arises in adenomatous polyps and that detection and removal reduces mortality for this cancer.18,19 Since 1994, when Vining et al first described the concept of CTC,6 numerous studies have compared its polyp detection rate with the gold standard, colonoscopy. The most recent are 3 large, multicenter prospective trials comparing the sensitivity and specificity of CTC against colonoscopy for adenomatous polyp detection.1-3 These 3 studies have not been consistent in their findings. One study showed very favorable results,1 but the other 2 showed unfavorable results (TABLE).
In December 2003, Dr Perry Pickhardt and his colleagues published the first multicenter prospective study comparing CTC with colonoscopy on a large, asymptomatic population.1 That study was performed in 3 medical centers and included 1233 subjects with a mean age of 57.8 years. All of the subjects underwent same-day CTC and colonoscopy. Each CTC was interpreted using both 2D and 3D imaging techniques. The results were very encouraging. CTC had a 93.8% sensitivity for adenomatous polyps at least 10 mm in diameter, 93.9% sensitivity for those at least 8 mm in diameter, and 88.7% sensitivity for those at least 6 mm in diameter. (For more on polyp size, see “Remove that polyp? With virtual colonoscopy, it’s not automatic,”.) The specificity for those polyp size categories was 96.0%, 92.2%, and 79.6%, respectively. The study concluded that CTC compared well with colonoscopy in the detection of adenomatous polyps in asymptomatic adults.
In April 2004, Dr Peter Cotton and his colleagues published the second multicenter, prospective study comparing CTC and colonoscopy in terms of adenomatous polyp detection for a screening population.2 The study took place at 9 medical centers and had 615 patients ages 50 and older who had both CTC and colonoscopy done on the same day. The researchers found that CTC had a sensitivity of 55% for those at least 10 mm in size and 39% for polyps at least 6 mm in size. They concluded that CTC technology was not ready for mainstream clinical use until a significant amount of enhancement took place in the use of this technology.
In January 2005, Dr Don Rockey and his colleagues published a multicenter study comparing CTC and colonoscopy at 14 sites.3 They had 614 patients with an average age of 57.4. They also found CTC to be significantly less sensitive for detecting polyps both >10 mm and >6 mm when compared with colonoscopy.
TABLE
Multicenter trials compared colonoscopy and virtual colonoscopy polyp detection rates
| PB COTTON ET AL2 (JAMA) | PJ PICKHARDT ET AL1 (NEJM) | DC ROCKEY ET AL3 (LANCET) | |
|---|---|---|---|
| Number of sites | 9 | 3 | 14 |
| Dates of study | April 2000–Oct 2001 | May 2002–June 2003 | Dec 2000–Feb 2004 |
| Number of patients | 615 | 1233 | 614 |
| Patient age (mean) | 61 | 57.8 | 57.4 |
| Sensitivity & specificity of detecting lesions ≥6 mm | Sensitivity: 39.0% Specificity: 90.5% | Sensitivity: 88.7% Specificity: 79.6% | Sensitivity: 51.0% Specificity: 89.0% |
| Sensitivity & specificity of detecting lesions ≥10 mm | Sensitivity: 55.0% Specificity: 96.0% | Sensitivity: 93.8% Specificity: 96.0% | Sensitivity: 59.0% Specificity: 96.0% |
The discrepancy may be a matter of software and protocols
Dr Pickhardt and his colleagues attribute part of their success in CTC to the particular software they used, which can render 3D images better than almost any other program available.20 A report issued by the American Gastroenterological Association says that Pickhardt et al’s use of primary 3D interpretation differs from most currently performed protocols.21 If Pickhardt et al’s results can even partly be attributed to use of new software, then it seems prudent to change the protocols to whatever works best in light of the evolving technology. The protocols must remain flexible until appropriate results are achieved and repeatable.
In addition, there are many other variables that could account for these results including a younger screening population, mostly composed of military families, the use of stool and fluid tagging (advanced techniques that improve accuracy and decrease the need for a completely clean bowel), or the aggressive, double-bowel preparations given before the procedure.1
Both Dr Pickhardt and Dr Joseph Ferrucci criticize the Cotton et al study because it primarily used 2D images and their trial ended in October 2001, whereas Pickhardt et al’s started in May 2002.22 With so much dependent on software issues, the interval is significant. In addition, the study by Dr Cotton and his colleagues used older CT and insufflation technology and several of the centers involved in the studies only had to show familiarity with the procedure, but no demonstrated ability in reading CTC images.22 Thus, both technical and reader issues were significant. Similarly, in the study by Rockey et al, the issue of reader inexperience was present, as was the fact that neither stool nor fluid tagging was used.22
When an adenomatous polyp of any size is found during a colonoscopy, the polyp is removed. Thus the diagnostic and therapeutic functions are married in colonoscopy. However, CTC only allows detection of these polyps, thus raising the question as to which size polyps should be reported and then removed by doing an additional colonoscopy. The issue of what size polyps have malignancy potential has been discussed extensively in the literature.31-33
It’s also a hotly debated topic in the literature for colorectal cancer screening, especially when any mention of CTC comes up. Every year, about 1% of polyps larger than 10 mm progress to colorectal cancer and there is agreement that these should be removed.34 However, there is considerable debate over the 6 to 9 mm category.34-36 Several trials have shown that the incidence of polyps between 6 to 9 mm progressing into colorectal cancer approaches, but is definitely less than 1%.37 Even the American Gastroenterological Association acknowledges that the risk of developing colorectal cancer from a polyp 6 to 9 mm remains uncertain.21
Thus, while it’s clear that polyps larger than 10 mm pose a significant enough risk to warrant removal, the data is equivocal—or absent—on what to do about polyps in the 6 to 9 mm category.
Another important variation between Pickhardt et al’s study and those by Drs Cotton and Rockey and their colleagues is the use of oral contrasts for stool tagging.23 A unique aspects of Pickhardt et al’s study was the aggressive bowel preparation using 2 types of oral contrast (water soluble and barium) for stool tagging. This allowed the computer to electronically separate and subtract residual stool from soft tissue structures improving image quality dramatically.1 This elaborate patient preparation has not been done by anyone else. Many contend that what Pickhardt et al achieved was a paradigm of the best CTC can be under ideal circumstances, technology, and expert interpretations and if not done in this manner, the results would get murky with diffuse application.23 This again emphasizes the importance of recognizing the evolving technology and protocol for CTC.
Much-needed research is underway
Until results of the caliber that Pickhardt et al achieved are reproducible locally, many insurance companies will delay coverage for screening CTC. For most areas, CTC would be about $1000 out of pocket cost for the patient. It seems likely that most patients would not opt for CTC when insurance companies cover other screening procedures.
The American College of Radiology Imaging Network has conducted a very large-scale double-blind study of CTC effectiveness in a screening population involving 15 institutions and 2300 participants.5 The results of this trial, expected out this summer, will surely influence CTC’s acceptance both by the medical community and by third party payers. Until then, family physicians will need to consider the use of CTC on a case-by-case basis.
Colorectal cancer mortality can be significantly reduced through proper screening.18,24-27 The American Cancer Society’s guidelines for screening28 indicate that beginning at age 50, both men and women with average risk factors should have one of the following:
- yearly fecal occult blood test
- flexible sigmoidoscopy every 5 years
- yearly fecal occult blood testing and flexible sigmoidoscopy every 5 years
- double-contrast barium enema every 5 years, or
- colonoscopy every 10 years.
A positive finding for any of the first 4 should prompt a colonoscopy.
CORRESPONDENCE
Jaspal Singh Ahluwalia, MD Walter Reed Army Medical Center, 6900 Georgia Avenue NW, Washington, D.C. 20307 E-mail: [email protected]
- Computed tomography colonography should be evaluated on a case-by-case basis, given the lack of consensus over the number of false positive/negative results it generates, and its lack of widespread acceptance by major insurance companies (C).
- CTC is a useful screening alternative for patients who have had an incomplete colonoscopy or who have an obstructing carcinoma (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
The virtual colonoscopy (CT colonography, or CTC) could make life just a little bit easier when it comes to discussing colorectal cancer screening options with your patients. After all, what patient wouldn’t like to hear that there is an alternative to the colonoscopy that doesn’t require sedation, IV injections, or a scope?
The reality, though, is that a number of roadblocks stand between the CTC and its inclusion in the battery of colorectal screening tools we typically discuss with our patients. Among the barriers: Mixed results from research studies evaluating the sensitivity and specificity of the CTC1-3 and a decision by many insurance plans not to cover the procedure, deeming it “experimental.”4
More research is undoubtedly needed, and some is already underway. The American College of Radiology Imaging Network has conducted a large scale, double-blind study,5 with results expected later this year. In the meantime, though, counseling your patients on their options will hinge on your knowledge of the advantages and disadvantages of the CTC and what the research—to date—tells us about its usefulness.
Like a colonoscopy, it offers a fly-through view
The CTC, which uses helical CT to capture 2D axial images that can be converted into a 3D view, allows the radiologist the same type of colon “fly through” view that a gastroenterologist would see using a colonoscopy (FIGURE).6 Among its pluses: It requires no anesthesia and is noninvasive, so it’s likely to appeal to patients who have a strong fear of colonoscopy. (See “What patients can expect during a CTC”) Another potential plus: While full bowel cleansing is still required, recent investigations have studied new “prep-less” CTC options consisting of a low residue diet with multiple doses of liquid barium without catharsis.7-9
CTC also offers a viable screening option for certain patient populations. Specifically, it’s already regularly being used in those who have had an incomplete colonoscopy or who have an obstructing carcinoma.10-12 CTC can also be used to screen elderly patients who have contraindications to conscious sedation or medical problems that preclude them from invasive procedures.
FIGURE
“Fly-through” via virtual colonoscopy
A 2D color reconstruction “fly-through” showing a large pedunculated polyp (left) and a large sessile polyp (right).On the downside, there is always a concern about the possible deleterious effects of radiation whenever an imaging technology is involved. The average person in the US gets about 3 mSv of radiation per year from the environment. This compares with about 10 mSv from a CT of the abdomen, 0.1 mSv from a chest x-ray, 0.7 mSv from mammography, or 5 to 7.8 mSv from CTC.13,14 Even though the radiation dosage currently used in CTC is safe, studies examining CTC with lower ionization have produced very hopeful results.15 In fact, a recent study by Brenner et al found that in terms of radiation from CTC and its ability to detect polyps, the benefits far outweigh any risks.16
As you might expect, the cost of a CTC is on the higher end of the colorectal cancer screening spectrum, though it is comparable with a colonoscopy. Fecal occult blood testing is the cheapest, with a cost, on average, of $10 to $20. Flexible sigmoidoscopy is about $150 to $300, double-contrast barium enema is about $250 to $500, and both colonoscopy and CTC are about $800 to $1600. However, CTC is currently not covered under most insurance plans, but it’s starting to gain acceptance as a reimbursable procedure. In fact, the Centers for Medicare and Medicaid Services has recently published CPT codes for CTC and even more recently made the professional components of both diagnostic and screening CTC fully reimbursible.
The protocol for CT colonography has become considerably more standardized over the past few years, and official American College of Radiology standards will soon be in place. Typically, though, a patient getting a screening CTC can expect the following:
The night before the procedure, he’ll need to cleanse the bowel completely, using an enema. The next day in the CT suite, a tube will be inserted into his rectum, and the rectum will be insufflated with carbon dioxide (about 1.5 L).29,30 Usually, the CT scans will be done while the patient is in both the supine and prone positions. The amount of radiation is comparable to that of a double-contrast barium enema.30 The 2D data is then analyzed using specialized workstations that can create both 2D and 3D views.
The entire exam takes less than 20 minutes and the scanning sessions last only a few minutes and require two 10-second breath holds.29,30
Widespread reimbursement in the private sector is not here yet, however, since many major insurance companies consider CTC an experimental procedure.4 This hesitance on the part of the private sector is understandable, as we found when we undertook a search of the literature.
Methods
We conducted a thorough and systematic search of PubMed for English-language articles from 1994 to 2006. Search terms included “CT colonography,” “virtual colonoscopy,” “CT colonoscopy,” “colography,” and “CT pneumocolon.”17 The general focus was on original research articles, but meta-analyses and review articles were also considered. In addition, we conducted general Internet searches to discern the general public’s view on this technology.
The research is mixed—specificity/sensitivity values vary
Research has shown that colorectal cancer arises in adenomatous polyps and that detection and removal reduces mortality for this cancer.18,19 Since 1994, when Vining et al first described the concept of CTC,6 numerous studies have compared its polyp detection rate with the gold standard, colonoscopy. The most recent are 3 large, multicenter prospective trials comparing the sensitivity and specificity of CTC against colonoscopy for adenomatous polyp detection.1-3 These 3 studies have not been consistent in their findings. One study showed very favorable results,1 but the other 2 showed unfavorable results (TABLE).
In December 2003, Dr Perry Pickhardt and his colleagues published the first multicenter prospective study comparing CTC with colonoscopy on a large, asymptomatic population.1 That study was performed in 3 medical centers and included 1233 subjects with a mean age of 57.8 years. All of the subjects underwent same-day CTC and colonoscopy. Each CTC was interpreted using both 2D and 3D imaging techniques. The results were very encouraging. CTC had a 93.8% sensitivity for adenomatous polyps at least 10 mm in diameter, 93.9% sensitivity for those at least 8 mm in diameter, and 88.7% sensitivity for those at least 6 mm in diameter. (For more on polyp size, see “Remove that polyp? With virtual colonoscopy, it’s not automatic,”.) The specificity for those polyp size categories was 96.0%, 92.2%, and 79.6%, respectively. The study concluded that CTC compared well with colonoscopy in the detection of adenomatous polyps in asymptomatic adults.
In April 2004, Dr Peter Cotton and his colleagues published the second multicenter, prospective study comparing CTC and colonoscopy in terms of adenomatous polyp detection for a screening population.2 The study took place at 9 medical centers and had 615 patients ages 50 and older who had both CTC and colonoscopy done on the same day. The researchers found that CTC had a sensitivity of 55% for those at least 10 mm in size and 39% for polyps at least 6 mm in size. They concluded that CTC technology was not ready for mainstream clinical use until a significant amount of enhancement took place in the use of this technology.
In January 2005, Dr Don Rockey and his colleagues published a multicenter study comparing CTC and colonoscopy at 14 sites.3 They had 614 patients with an average age of 57.4. They also found CTC to be significantly less sensitive for detecting polyps both >10 mm and >6 mm when compared with colonoscopy.
TABLE
Multicenter trials compared colonoscopy and virtual colonoscopy polyp detection rates
| PB COTTON ET AL2 (JAMA) | PJ PICKHARDT ET AL1 (NEJM) | DC ROCKEY ET AL3 (LANCET) | |
|---|---|---|---|
| Number of sites | 9 | 3 | 14 |
| Dates of study | April 2000–Oct 2001 | May 2002–June 2003 | Dec 2000–Feb 2004 |
| Number of patients | 615 | 1233 | 614 |
| Patient age (mean) | 61 | 57.8 | 57.4 |
| Sensitivity & specificity of detecting lesions ≥6 mm | Sensitivity: 39.0% Specificity: 90.5% | Sensitivity: 88.7% Specificity: 79.6% | Sensitivity: 51.0% Specificity: 89.0% |
| Sensitivity & specificity of detecting lesions ≥10 mm | Sensitivity: 55.0% Specificity: 96.0% | Sensitivity: 93.8% Specificity: 96.0% | Sensitivity: 59.0% Specificity: 96.0% |
The discrepancy may be a matter of software and protocols
Dr Pickhardt and his colleagues attribute part of their success in CTC to the particular software they used, which can render 3D images better than almost any other program available.20 A report issued by the American Gastroenterological Association says that Pickhardt et al’s use of primary 3D interpretation differs from most currently performed protocols.21 If Pickhardt et al’s results can even partly be attributed to use of new software, then it seems prudent to change the protocols to whatever works best in light of the evolving technology. The protocols must remain flexible until appropriate results are achieved and repeatable.
In addition, there are many other variables that could account for these results including a younger screening population, mostly composed of military families, the use of stool and fluid tagging (advanced techniques that improve accuracy and decrease the need for a completely clean bowel), or the aggressive, double-bowel preparations given before the procedure.1
Both Dr Pickhardt and Dr Joseph Ferrucci criticize the Cotton et al study because it primarily used 2D images and their trial ended in October 2001, whereas Pickhardt et al’s started in May 2002.22 With so much dependent on software issues, the interval is significant. In addition, the study by Dr Cotton and his colleagues used older CT and insufflation technology and several of the centers involved in the studies only had to show familiarity with the procedure, but no demonstrated ability in reading CTC images.22 Thus, both technical and reader issues were significant. Similarly, in the study by Rockey et al, the issue of reader inexperience was present, as was the fact that neither stool nor fluid tagging was used.22
When an adenomatous polyp of any size is found during a colonoscopy, the polyp is removed. Thus the diagnostic and therapeutic functions are married in colonoscopy. However, CTC only allows detection of these polyps, thus raising the question as to which size polyps should be reported and then removed by doing an additional colonoscopy. The issue of what size polyps have malignancy potential has been discussed extensively in the literature.31-33
It’s also a hotly debated topic in the literature for colorectal cancer screening, especially when any mention of CTC comes up. Every year, about 1% of polyps larger than 10 mm progress to colorectal cancer and there is agreement that these should be removed.34 However, there is considerable debate over the 6 to 9 mm category.34-36 Several trials have shown that the incidence of polyps between 6 to 9 mm progressing into colorectal cancer approaches, but is definitely less than 1%.37 Even the American Gastroenterological Association acknowledges that the risk of developing colorectal cancer from a polyp 6 to 9 mm remains uncertain.21
Thus, while it’s clear that polyps larger than 10 mm pose a significant enough risk to warrant removal, the data is equivocal—or absent—on what to do about polyps in the 6 to 9 mm category.
Another important variation between Pickhardt et al’s study and those by Drs Cotton and Rockey and their colleagues is the use of oral contrasts for stool tagging.23 A unique aspects of Pickhardt et al’s study was the aggressive bowel preparation using 2 types of oral contrast (water soluble and barium) for stool tagging. This allowed the computer to electronically separate and subtract residual stool from soft tissue structures improving image quality dramatically.1 This elaborate patient preparation has not been done by anyone else. Many contend that what Pickhardt et al achieved was a paradigm of the best CTC can be under ideal circumstances, technology, and expert interpretations and if not done in this manner, the results would get murky with diffuse application.23 This again emphasizes the importance of recognizing the evolving technology and protocol for CTC.
Much-needed research is underway
Until results of the caliber that Pickhardt et al achieved are reproducible locally, many insurance companies will delay coverage for screening CTC. For most areas, CTC would be about $1000 out of pocket cost for the patient. It seems likely that most patients would not opt for CTC when insurance companies cover other screening procedures.
The American College of Radiology Imaging Network has conducted a very large-scale double-blind study of CTC effectiveness in a screening population involving 15 institutions and 2300 participants.5 The results of this trial, expected out this summer, will surely influence CTC’s acceptance both by the medical community and by third party payers. Until then, family physicians will need to consider the use of CTC on a case-by-case basis.
Colorectal cancer mortality can be significantly reduced through proper screening.18,24-27 The American Cancer Society’s guidelines for screening28 indicate that beginning at age 50, both men and women with average risk factors should have one of the following:
- yearly fecal occult blood test
- flexible sigmoidoscopy every 5 years
- yearly fecal occult blood testing and flexible sigmoidoscopy every 5 years
- double-contrast barium enema every 5 years, or
- colonoscopy every 10 years.
A positive finding for any of the first 4 should prompt a colonoscopy.
CORRESPONDENCE
Jaspal Singh Ahluwalia, MD Walter Reed Army Medical Center, 6900 Georgia Avenue NW, Washington, D.C. 20307 E-mail: [email protected]
1. Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 2003;349:2191-2200.
2. Cotton PB, Durkalski VL, Pineau BC, et al. Computed tomographic colonography (virtual colonoscopy); a multicenter comparison with standard colonoscopy for detection of colorectal neoplasia. JAMA 2004;291:1713-1719.
3. Rockey DC, Paulson E, Niedzwiecki D. Analysis of air contrast barium enema, computed tomographic colonography, and colonoscopy: prospective comparison. Lancet 2005;365:305-311.
4. CT Colonography (“virtual colonoscopy”) for colon cancer screening. Technology Evaluation Center, Blue Cross and Blue Shield Associaiton assessment program, 2004 (July), vol 19. Chicago, Ill: Blue Cross and Blue Shield Association, 2004.
5. American College of Radiology website. ACRIN seeks institutions for CTC trial. Available at: www.acr.org/s_acr/doc.asp?DID=18669. Accessed on February 15, 2007.
6. Vining DJ, Gelfand DW, Bechtold RE, et al. Technological feasibility of colon imaging with helical CT and virtual reality. AJR 1994;162(suppl):S104.-
7. Lefere P, Gryspeerdt S, et al. Technical innovation: laxative-free CT colonograpy. ARJ 2004;183:945-948.
8. Lefere PA, Bryspeerdt SS, Dewyspelaere J, et al. Dietary fecal tagging as a cleansing method before CT colonography: initial results: polyp detection and patient acceptance. Radiology 2002;224:393-403.
9. Zalis ME, Perumpillichira J, Del Frate C, et al. CT colonography: digital subtraction and bowel cleansing with mucosal reconstruction—initial observations. Radiology 2003;226:911-917.
10. Macari M, Megibow AJ, Berman P, et al. CT colonography in patients with failed colonoscopy. AJR 1999;173:561-564.
11. Morrin MM, Kruskal JB, Farrell RJ, et al. Endoluminal CT colonography after incomplete endoscopic colonoscopy. AJR 1999;172:913-918.
12. Fenlon HM, McAneny DB, Nunes DP, et al. Occlusive colon carcinoma: virtual colonoscopy in the preoperative evaluation of the proximal colon. Radiology 1999;210:423-428.
13. RadiologyInfo website. Safety in medical imaging procedures. Radiological Society on North America. Available at: www.radiologyinfo.org/content/safety. Accessed on February 15, 2007.
14. Macari M, Milano A, Lavelle M, et al. Comparison of time-efficient CT colonography with two- and three-dimensional colonic evaluation for detecting colorectal polyps. AJR 2000;174:1543-1549.
15. Cohnen M, Vogt C, Beck A, et al. Feasibility of MDCT colonography in ultra-low-dose technique in the detection of colorectal lesions: comparison with high-resolution video colonoscopy. AJR 2004;183:1355-1359.
16. Brenner DJ, Georgsson MA. Mass screening with CT colonography: should the radiation exposure be of concern? Gastroenterology 2005;129:328-337.
17. Johnson CD. Virtual endoscopy: what’s in a name? AJR 1998;171:1201-1202.
18. Winawer SJ, Zauber AG, Ho MN. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med 1993;329:1977-1981.
19. Bond JH. Clinical evidence for the adenoma-carcinoma sequence, and the management of patients with colorectal adenomas. Gastrointest Dis 2000;11:176-184.
20. Pickhardt PJ. Author’s response. RadioGraphics 2004;24:1557-1559.
21. Van Dam J, Cotton P, Johnson CD, et al. AGA future trends report: CT colonography. Gastroenterology 2004;127:970-984.
22. Pickhardt PJ, Ferrucci J. Letters. JAMA 2004;292:431-433.
23. Ransohoff DF. Virtual colonoscopy—what it can do vs. what it will do. JAMA 2004;291:1772-1774.
24. Ransohoff DF, Sandler RS. Clinical practice: screening for colorectal cancer. N Engl J Med 2002;346:40-44.
25. Winawer SJ, Fletcher RH, Rex DK, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale—update based on new evidence. Gastroenterology 2003;124:544-560.
26. Mandel JS, Bond JH, Church TR, et al. Reducing the mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med 1993;328:1365-1371.
27. Muller AD, Sonnenberg A. Protection by endoscopy against death from colorectal cancer: a case control study among veterans. Arch Intern Med 1995;155:1741-1748.
28. Cancer Facts & Figures—2006. Atlanta, Ga: American Cancer Society, 2006. Available at: www.cancer.org/downloads/STT/caFF2006PWSecured.pdf. Accessed on February 15, 2007.
29. Morrin MM, LaMont JT. Screening virtual colonoscopy—ready for prime time? N Engl J Med 2003;349:2261-2264.
30. Johnson CD, Dachman AH. CT colonography: the next colon screening examination? Radiology 2000;216:331-341.
31. Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to screen asymptomatic adults for colorectal cancer. N Engl J Med 2000;343:162-168.
32. Imperiale TF, Wagner DR, Lin CY, et al. Risk of advanced proximal neoplasms in asymptomatic adults according to the distal colorectal finds. N Engl J Med 2000;343:169-174.
33. Hofstad B, Vatn MH, Anderen SN, et al. Growth of colorectal polyps: redetection and evaluation of unresected polyps for a period of three years. Gut 1996;39:449-456.
34. Stryker SJ, Wolff BG, Culp CE, et al. Natural history of untreated colonic polyps. Gastroenterology 1987;93:1009-1013.
35. Waye JD, Lewis BS, Frankel A, et al. Small colon polyps. Am J Gastroenterology 1988;83:120-122.
36. Nusko G, Mansmann U, Partzsch U, et al. Invasive carcinoma in colorectal adenomas: multivariate analysis of patient and adenoma characteristics. Endoscopy 1997;29:626-631.
37. Morson B. The polyp-cancer sequence in the large bowel. Proc R Soc Med 1974;67:451-457.
1. Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 2003;349:2191-2200.
2. Cotton PB, Durkalski VL, Pineau BC, et al. Computed tomographic colonography (virtual colonoscopy); a multicenter comparison with standard colonoscopy for detection of colorectal neoplasia. JAMA 2004;291:1713-1719.
3. Rockey DC, Paulson E, Niedzwiecki D. Analysis of air contrast barium enema, computed tomographic colonography, and colonoscopy: prospective comparison. Lancet 2005;365:305-311.
4. CT Colonography (“virtual colonoscopy”) for colon cancer screening. Technology Evaluation Center, Blue Cross and Blue Shield Associaiton assessment program, 2004 (July), vol 19. Chicago, Ill: Blue Cross and Blue Shield Association, 2004.
5. American College of Radiology website. ACRIN seeks institutions for CTC trial. Available at: www.acr.org/s_acr/doc.asp?DID=18669. Accessed on February 15, 2007.
6. Vining DJ, Gelfand DW, Bechtold RE, et al. Technological feasibility of colon imaging with helical CT and virtual reality. AJR 1994;162(suppl):S104.-
7. Lefere P, Gryspeerdt S, et al. Technical innovation: laxative-free CT colonograpy. ARJ 2004;183:945-948.
8. Lefere PA, Bryspeerdt SS, Dewyspelaere J, et al. Dietary fecal tagging as a cleansing method before CT colonography: initial results: polyp detection and patient acceptance. Radiology 2002;224:393-403.
9. Zalis ME, Perumpillichira J, Del Frate C, et al. CT colonography: digital subtraction and bowel cleansing with mucosal reconstruction—initial observations. Radiology 2003;226:911-917.
10. Macari M, Megibow AJ, Berman P, et al. CT colonography in patients with failed colonoscopy. AJR 1999;173:561-564.
11. Morrin MM, Kruskal JB, Farrell RJ, et al. Endoluminal CT colonography after incomplete endoscopic colonoscopy. AJR 1999;172:913-918.
12. Fenlon HM, McAneny DB, Nunes DP, et al. Occlusive colon carcinoma: virtual colonoscopy in the preoperative evaluation of the proximal colon. Radiology 1999;210:423-428.
13. RadiologyInfo website. Safety in medical imaging procedures. Radiological Society on North America. Available at: www.radiologyinfo.org/content/safety. Accessed on February 15, 2007.
14. Macari M, Milano A, Lavelle M, et al. Comparison of time-efficient CT colonography with two- and three-dimensional colonic evaluation for detecting colorectal polyps. AJR 2000;174:1543-1549.
15. Cohnen M, Vogt C, Beck A, et al. Feasibility of MDCT colonography in ultra-low-dose technique in the detection of colorectal lesions: comparison with high-resolution video colonoscopy. AJR 2004;183:1355-1359.
16. Brenner DJ, Georgsson MA. Mass screening with CT colonography: should the radiation exposure be of concern? Gastroenterology 2005;129:328-337.
17. Johnson CD. Virtual endoscopy: what’s in a name? AJR 1998;171:1201-1202.
18. Winawer SJ, Zauber AG, Ho MN. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med 1993;329:1977-1981.
19. Bond JH. Clinical evidence for the adenoma-carcinoma sequence, and the management of patients with colorectal adenomas. Gastrointest Dis 2000;11:176-184.
20. Pickhardt PJ. Author’s response. RadioGraphics 2004;24:1557-1559.
21. Van Dam J, Cotton P, Johnson CD, et al. AGA future trends report: CT colonography. Gastroenterology 2004;127:970-984.
22. Pickhardt PJ, Ferrucci J. Letters. JAMA 2004;292:431-433.
23. Ransohoff DF. Virtual colonoscopy—what it can do vs. what it will do. JAMA 2004;291:1772-1774.
24. Ransohoff DF, Sandler RS. Clinical practice: screening for colorectal cancer. N Engl J Med 2002;346:40-44.
25. Winawer SJ, Fletcher RH, Rex DK, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale—update based on new evidence. Gastroenterology 2003;124:544-560.
26. Mandel JS, Bond JH, Church TR, et al. Reducing the mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med 1993;328:1365-1371.
27. Muller AD, Sonnenberg A. Protection by endoscopy against death from colorectal cancer: a case control study among veterans. Arch Intern Med 1995;155:1741-1748.
28. Cancer Facts & Figures—2006. Atlanta, Ga: American Cancer Society, 2006. Available at: www.cancer.org/downloads/STT/caFF2006PWSecured.pdf. Accessed on February 15, 2007.
29. Morrin MM, LaMont JT. Screening virtual colonoscopy—ready for prime time? N Engl J Med 2003;349:2261-2264.
30. Johnson CD, Dachman AH. CT colonography: the next colon screening examination? Radiology 2000;216:331-341.
31. Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to screen asymptomatic adults for colorectal cancer. N Engl J Med 2000;343:162-168.
32. Imperiale TF, Wagner DR, Lin CY, et al. Risk of advanced proximal neoplasms in asymptomatic adults according to the distal colorectal finds. N Engl J Med 2000;343:169-174.
33. Hofstad B, Vatn MH, Anderen SN, et al. Growth of colorectal polyps: redetection and evaluation of unresected polyps for a period of three years. Gut 1996;39:449-456.
34. Stryker SJ, Wolff BG, Culp CE, et al. Natural history of untreated colonic polyps. Gastroenterology 1987;93:1009-1013.
35. Waye JD, Lewis BS, Frankel A, et al. Small colon polyps. Am J Gastroenterology 1988;83:120-122.
36. Nusko G, Mansmann U, Partzsch U, et al. Invasive carcinoma in colorectal adenomas: multivariate analysis of patient and adenoma characteristics. Endoscopy 1997;29:626-631.
37. Morson B. The polyp-cancer sequence in the large bowel. Proc R Soc Med 1974;67:451-457.
Dysglycemia and fluoroquinolones: Are you putting patients at risk?
- Avoid giving gatifloxacin to patients.
- Consider selecting an antibiotic other than a fluoroquinolone for an elderly patient with diabetes mellitus (especially those taking sulfonylureas), hepatic insufficiency, or renal insufficiency (A).
- Discontinue fluoroquinolone therapy if a patient experiences symptoms of hypo- or hyperglycemia, or if blood glucose levels fall below 60 mg/dL or rise above 200 mg/dL (C).
When was the last time you checked a glucose level before prescribing a fluoroquinolone? Though most side effects of these drugs are mild and self-limited (nausea, anorexia, vomiting, abdominal pain, diarrhea, taste disturbance, dizziness, headache, and somnolence), dysglycemia—hypoor hyperglycemia—is another side effect that is potentially fatal.
From their inception, fluoroquinolones were known to upset glucose metabolism. However, recent publication of several case reports of gatifloxacin-associated dysglycemia, and Bristol-Myers Squibb’s announcement of a contraindication for gatifloxacin in diabetic patients, brought the matter of potentially severe dysglycemia to the forefront. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature,” in the February 2004 Journal of Family Practice. A retrospective chart review of more than 17,000 hospitalized patients receiving levofloxacin, gatifloxacin, or ceftriaxone, showed 101 patients with glucose concentrations >200 mg/dL or <50 mg/dL within 72 hours of receiving the drugs. Of these 101 patients, 92 experienced hyperglycemia. Most of these patients had underlying renal insufficiency. Eighty-nine percent had diabetes mellitus and 40% were taking oral hypoglycemics. Hyperglycemia rates were greater with levofloxacin and gatifloxacin than with ceftriaxone; no difference was found between levofloxacin and gatifloxacin.6
Finally, a second retrospective chart review of a VA population identified 64,076 prescriptions written for fluoroquinolones between 1998 and 2003. More than 10,000 glucose values were measured during treatment or within 7 days of treatment completion. Hyperglycemia occurred much more often than hypoglycemia—in 11.6% of 32,000 patients. The majority (59%) of hyperglycemic episodes occurred in diabetic patients, and it was not clear that fluoroquinolone use caused the hyperglycemia. In contrast to the data listed above, gatifloxacin had a lower rate of associated hyperglycemia than either levofloxacin or ciprofloxacin.23
Studies finding no hyperglycemic effect. The studies reviewed in the section on hypoglycemia found no clinically significant hyperglycemic effect of fluoroquinolones.
Take-home points
As with hypoglycemia, most cases of fluoroquinolone-associated hyperglycemia have occurred in patients with NIDDM and mild-to-moderate renal insufficiency. More definitive risk factors for hyperglycemia include decreased insulin secretion (eg, IDDM), decreased insulin sensitivity (eg, NIDDM), advanced age, high carbohydrate intake, acute infection, stress, and corticosteroid use.24 While an association with fluoroquinolone use appears to be multifactorial and dependent on these underlying host factors, strong evidence is lacking.11 As opposed to the timing of hypoglycemic events, review of several case reports revealed that fluoroquinolone-associated hyperglycemia has generally occurred later in treatment, usually after 4 days of therapy, and with higher doses.
Summary of practice recommendations
The following conclusions and recommendations can be made based on the studies reviewed.
First, because the rate of fluoroquinolone-associated dysglycemia is highest with gatifloxacin, and most patients who experience fluoroquinolone-associated dysglycemia have diabetes, gatifloxacin should be avoided in patients who have diabetes (SOR: A).
Second, it’s wise to not use any fluoroquinolone in elderly patients with diabetes mellitus (especially those taking sulfonylureas), hepatic insufficiency, and/or renal insufficiency (SOR: A). If a fluoroquinolone must be used in these patients, favor levofloxacin or moxifloxacin over gatifloxacin (SOR: B).
Third, discontinue fluoroquinolone therapy if a patient experiences symptoms of hypo- or hyperglycemia and/or blood glucose levels fall below 60 mg/dL or rise above 200 mg/dL (SOR: C). If symptomatic hypo- or hyperglycemia does occur, administer appropriate therapy, and if necessary, admit the patient to the hospital for appropriate treatment (SOR: C).
Acknowledgments
The author would like to thanks Barry Weiss, MD, and M. Moe Bell, MD, for their assistance in editing this manuscript, and Robert Marlow, MD, for his assistance in evidence ratings.
CORRESPONDENCE
Martin Catero, MD Heuser Family Medicine Center, 7301 East Second Street, Suite 210, Scottsdale, AZ 85251. E-mail: [email protected]
1. Bristol-Myers Squibb Company. Tequin (gatifloxacin) package insert. Princeton, NJ; 2006.
2. Bayer Pharmaceuticals. Avelox (moxifloxacin) tablets/injection package insert. West Haven, CT: Bayer Pharmaceuticals; 2004.
3. Ortho-McNeil Pharmaceuticals. Levaquin (levofloxacin) tablets/injection package insert. Raritan, NJ: Ortho-McNeil; 2004.
4. Bayer Corporation. Cipro (ciprofloxacin) package insert. West Haven, CT; 2003.
5. Park-Wyllie LY, Juurlink DL, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med 2006;354:1352-1361.Epub 2006 Mar 1.
6. Mohr JF, McKinnon PS, Peymann PJ, et al. A retrospective, comparative evaluation of dysglycemias in hospitalized patients receiving gatifloxacin, levofloxacin, ciprofloxacin, or ceftriaxone. Pharmacother 2005;25:1303-1309.
7. Akpunow B, Michaelis J, Uy CN, et al. Multicenter postmarketing assessment of levofloxacin in the treatment of adults with community-acquired pneumonia. Clin Infect Dis 2004;38:S5-S15.
8. Letourneau G, Morrison H, McMorran M. Gatifloxacin (Tequin): hypoglycemia and hyperglycemia. Can Adverse React Newsletter 2003;13:1-2.
9. Frothingham R. Gatifloxacin associated with a 56-fold higher rate of glucose homeostasis abnormalities than comparator quinolones in the FDA spontaneous reporting database. Presented at the 44th interscience conference on antimicrobial agents and chemotherapy. Washington, DC, October 3-November 2, 2004.
10. Smith KM, Lomaestro BM. What role do fluoroquinolone antimicrobial agents play in cardiac dysfunction and altered glycemic control? J Pharm Pract 2003;16:349-360.
11. Donaldson AR, Vandiver JF, Finch CK. Possible gatifloxacin-induced hyperglycemia. Ann Pharmacother 2004;38:602-605.
12. Saraga A, Yokokura M, Gonoi T, et al. Effects of fluoroquinolones on insulin secretion and ß-cell ATP-sensitive K+ channels. Eur J Pharm 2004;497:111-117.
13. Leblanc M, Belanger C, Cossette P. Severe and resistant hypoglycemia associated with concomitant gatifloxacin and glyburide therapy. Pharmacother 2004;24:926-931.
14. Menzies DJ, Dorsainvil PA, Cunha BA, et al. Severe and persistent hypoglycemia due to gatifloxacin interaction with oral hypoglycemic agents. Am J Med 2002;113:232-234.
15. Lin G, Hays DP, Spillane L. Refractory hypoglycemia from ciprofloxacin and glyburide interaction. J Toxicol Clin Toxicol 2004;42:295-297.
16. Graumlich JF, Habis S, Avelino RR, et al. Hypoglycemia in inpatients after gatifloxacin or levofloxacin therapy: nested case control study. Pharmacother 2005;25:1296-1302.
17. Gajjar DA, LaCreta FP, Kollia GD, et al. Effect of multiple-dose gatifloxacin or ciprofloxacin on glucose homeostasis and insulin production in patients with non-insulin-dependent diabetes mellitus maintained with diet and exercise. Pharmacother 2000;20:76S-86S.
18. Gajjar DA, LaCreta FP, Uderman HD, et al. A dose-escalation study of the safety, tolerability, and pharmacokinetics of intravenous gatifloxacin in healthy adult men. Pharmacother 2000;20:49S-58S.
19. Gavin JR, Kubin R, Choudri S, et al. Moxifloxacin and glucose homeostasis. Drug Saf 2004;27:671-686.
20. Pichichero ME, Arguelas A, Dagan R. Safety and efficacy of gatifloxacin therapy for children with recurrent acute otitis media (AOM) and/or AOM treatment failure. Clin Infect Dis 2005;41:470-478.
21. Lawrence KR, Adra M, Keir C. Hypoglycemia-induced anoxic brain injury possibly associated with levofloxacin. J Infect 2006;52:e177-180.Epub 2005 Nov 2.
22. Ambrose PG, Bhavnani SM, Cirincione BB, et al. Gatifloxacin and the elderly: pharmacokinetic-pharmacodynamic rationale for a potential age-related dose reduction. J Antimicrob Chemother 2003;S2:434-440.
23. Coblio NA, Mowrey K, McCright P, et al. Use of a data warehouse to examine the effect of fluoroquinolones on glucose metabolism. Am J Health Syst Pharm 2004;61:2545-2548.
24. Gaglia JL, Wyckoff J, Abrahamson MJ. Acute hyperglycemic crisis in the elderly. Med Clin North Am 2004;88:1063-1084, xii.
- Avoid giving gatifloxacin to patients.
- Consider selecting an antibiotic other than a fluoroquinolone for an elderly patient with diabetes mellitus (especially those taking sulfonylureas), hepatic insufficiency, or renal insufficiency (A).
- Discontinue fluoroquinolone therapy if a patient experiences symptoms of hypo- or hyperglycemia, or if blood glucose levels fall below 60 mg/dL or rise above 200 mg/dL (C).
When was the last time you checked a glucose level before prescribing a fluoroquinolone? Though most side effects of these drugs are mild and self-limited (nausea, anorexia, vomiting, abdominal pain, diarrhea, taste disturbance, dizziness, headache, and somnolence), dysglycemia—hypoor hyperglycemia—is another side effect that is potentially fatal.
From their inception, fluoroquinolones were known to upset glucose metabolism. However, recent publication of several case reports of gatifloxacin-associated dysglycemia, and Bristol-Myers Squibb’s announcement of a contraindication for gatifloxacin in diabetic patients, brought the matter of potentially severe dysglycemia to the forefront. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature,” in the February 2004 Journal of Family Practice. A retrospective chart review of more than 17,000 hospitalized patients receiving levofloxacin, gatifloxacin, or ceftriaxone, showed 101 patients with glucose concentrations >200 mg/dL or <50 mg/dL within 72 hours of receiving the drugs. Of these 101 patients, 92 experienced hyperglycemia. Most of these patients had underlying renal insufficiency. Eighty-nine percent had diabetes mellitus and 40% were taking oral hypoglycemics. Hyperglycemia rates were greater with levofloxacin and gatifloxacin than with ceftriaxone; no difference was found between levofloxacin and gatifloxacin.6
Finally, a second retrospective chart review of a VA population identified 64,076 prescriptions written for fluoroquinolones between 1998 and 2003. More than 10,000 glucose values were measured during treatment or within 7 days of treatment completion. Hyperglycemia occurred much more often than hypoglycemia—in 11.6% of 32,000 patients. The majority (59%) of hyperglycemic episodes occurred in diabetic patients, and it was not clear that fluoroquinolone use caused the hyperglycemia. In contrast to the data listed above, gatifloxacin had a lower rate of associated hyperglycemia than either levofloxacin or ciprofloxacin.23
Studies finding no hyperglycemic effect. The studies reviewed in the section on hypoglycemia found no clinically significant hyperglycemic effect of fluoroquinolones.
Take-home points
As with hypoglycemia, most cases of fluoroquinolone-associated hyperglycemia have occurred in patients with NIDDM and mild-to-moderate renal insufficiency. More definitive risk factors for hyperglycemia include decreased insulin secretion (eg, IDDM), decreased insulin sensitivity (eg, NIDDM), advanced age, high carbohydrate intake, acute infection, stress, and corticosteroid use.24 While an association with fluoroquinolone use appears to be multifactorial and dependent on these underlying host factors, strong evidence is lacking.11 As opposed to the timing of hypoglycemic events, review of several case reports revealed that fluoroquinolone-associated hyperglycemia has generally occurred later in treatment, usually after 4 days of therapy, and with higher doses.
Summary of practice recommendations
The following conclusions and recommendations can be made based on the studies reviewed.
First, because the rate of fluoroquinolone-associated dysglycemia is highest with gatifloxacin, and most patients who experience fluoroquinolone-associated dysglycemia have diabetes, gatifloxacin should be avoided in patients who have diabetes (SOR: A).
Second, it’s wise to not use any fluoroquinolone in elderly patients with diabetes mellitus (especially those taking sulfonylureas), hepatic insufficiency, and/or renal insufficiency (SOR: A). If a fluoroquinolone must be used in these patients, favor levofloxacin or moxifloxacin over gatifloxacin (SOR: B).
Third, discontinue fluoroquinolone therapy if a patient experiences symptoms of hypo- or hyperglycemia and/or blood glucose levels fall below 60 mg/dL or rise above 200 mg/dL (SOR: C). If symptomatic hypo- or hyperglycemia does occur, administer appropriate therapy, and if necessary, admit the patient to the hospital for appropriate treatment (SOR: C).
Acknowledgments
The author would like to thanks Barry Weiss, MD, and M. Moe Bell, MD, for their assistance in editing this manuscript, and Robert Marlow, MD, for his assistance in evidence ratings.
CORRESPONDENCE
Martin Catero, MD Heuser Family Medicine Center, 7301 East Second Street, Suite 210, Scottsdale, AZ 85251. E-mail: [email protected]
- Avoid giving gatifloxacin to patients.
- Consider selecting an antibiotic other than a fluoroquinolone for an elderly patient with diabetes mellitus (especially those taking sulfonylureas), hepatic insufficiency, or renal insufficiency (A).
- Discontinue fluoroquinolone therapy if a patient experiences symptoms of hypo- or hyperglycemia, or if blood glucose levels fall below 60 mg/dL or rise above 200 mg/dL (C).
When was the last time you checked a glucose level before prescribing a fluoroquinolone? Though most side effects of these drugs are mild and self-limited (nausea, anorexia, vomiting, abdominal pain, diarrhea, taste disturbance, dizziness, headache, and somnolence), dysglycemia—hypoor hyperglycemia—is another side effect that is potentially fatal.
From their inception, fluoroquinolones were known to upset glucose metabolism. However, recent publication of several case reports of gatifloxacin-associated dysglycemia, and Bristol-Myers Squibb’s announcement of a contraindication for gatifloxacin in diabetic patients, brought the matter of potentially severe dysglycemia to the forefront. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature,” in the February 2004 Journal of Family Practice. A retrospective chart review of more than 17,000 hospitalized patients receiving levofloxacin, gatifloxacin, or ceftriaxone, showed 101 patients with glucose concentrations >200 mg/dL or <50 mg/dL within 72 hours of receiving the drugs. Of these 101 patients, 92 experienced hyperglycemia. Most of these patients had underlying renal insufficiency. Eighty-nine percent had diabetes mellitus and 40% were taking oral hypoglycemics. Hyperglycemia rates were greater with levofloxacin and gatifloxacin than with ceftriaxone; no difference was found between levofloxacin and gatifloxacin.6
Finally, a second retrospective chart review of a VA population identified 64,076 prescriptions written for fluoroquinolones between 1998 and 2003. More than 10,000 glucose values were measured during treatment or within 7 days of treatment completion. Hyperglycemia occurred much more often than hypoglycemia—in 11.6% of 32,000 patients. The majority (59%) of hyperglycemic episodes occurred in diabetic patients, and it was not clear that fluoroquinolone use caused the hyperglycemia. In contrast to the data listed above, gatifloxacin had a lower rate of associated hyperglycemia than either levofloxacin or ciprofloxacin.23
Studies finding no hyperglycemic effect. The studies reviewed in the section on hypoglycemia found no clinically significant hyperglycemic effect of fluoroquinolones.
Take-home points
As with hypoglycemia, most cases of fluoroquinolone-associated hyperglycemia have occurred in patients with NIDDM and mild-to-moderate renal insufficiency. More definitive risk factors for hyperglycemia include decreased insulin secretion (eg, IDDM), decreased insulin sensitivity (eg, NIDDM), advanced age, high carbohydrate intake, acute infection, stress, and corticosteroid use.24 While an association with fluoroquinolone use appears to be multifactorial and dependent on these underlying host factors, strong evidence is lacking.11 As opposed to the timing of hypoglycemic events, review of several case reports revealed that fluoroquinolone-associated hyperglycemia has generally occurred later in treatment, usually after 4 days of therapy, and with higher doses.
Summary of practice recommendations
The following conclusions and recommendations can be made based on the studies reviewed.
First, because the rate of fluoroquinolone-associated dysglycemia is highest with gatifloxacin, and most patients who experience fluoroquinolone-associated dysglycemia have diabetes, gatifloxacin should be avoided in patients who have diabetes (SOR: A).
Second, it’s wise to not use any fluoroquinolone in elderly patients with diabetes mellitus (especially those taking sulfonylureas), hepatic insufficiency, and/or renal insufficiency (SOR: A). If a fluoroquinolone must be used in these patients, favor levofloxacin or moxifloxacin over gatifloxacin (SOR: B).
Third, discontinue fluoroquinolone therapy if a patient experiences symptoms of hypo- or hyperglycemia and/or blood glucose levels fall below 60 mg/dL or rise above 200 mg/dL (SOR: C). If symptomatic hypo- or hyperglycemia does occur, administer appropriate therapy, and if necessary, admit the patient to the hospital for appropriate treatment (SOR: C).
Acknowledgments
The author would like to thanks Barry Weiss, MD, and M. Moe Bell, MD, for their assistance in editing this manuscript, and Robert Marlow, MD, for his assistance in evidence ratings.
CORRESPONDENCE
Martin Catero, MD Heuser Family Medicine Center, 7301 East Second Street, Suite 210, Scottsdale, AZ 85251. E-mail: [email protected]
1. Bristol-Myers Squibb Company. Tequin (gatifloxacin) package insert. Princeton, NJ; 2006.
2. Bayer Pharmaceuticals. Avelox (moxifloxacin) tablets/injection package insert. West Haven, CT: Bayer Pharmaceuticals; 2004.
3. Ortho-McNeil Pharmaceuticals. Levaquin (levofloxacin) tablets/injection package insert. Raritan, NJ: Ortho-McNeil; 2004.
4. Bayer Corporation. Cipro (ciprofloxacin) package insert. West Haven, CT; 2003.
5. Park-Wyllie LY, Juurlink DL, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med 2006;354:1352-1361.Epub 2006 Mar 1.
6. Mohr JF, McKinnon PS, Peymann PJ, et al. A retrospective, comparative evaluation of dysglycemias in hospitalized patients receiving gatifloxacin, levofloxacin, ciprofloxacin, or ceftriaxone. Pharmacother 2005;25:1303-1309.
7. Akpunow B, Michaelis J, Uy CN, et al. Multicenter postmarketing assessment of levofloxacin in the treatment of adults with community-acquired pneumonia. Clin Infect Dis 2004;38:S5-S15.
8. Letourneau G, Morrison H, McMorran M. Gatifloxacin (Tequin): hypoglycemia and hyperglycemia. Can Adverse React Newsletter 2003;13:1-2.
9. Frothingham R. Gatifloxacin associated with a 56-fold higher rate of glucose homeostasis abnormalities than comparator quinolones in the FDA spontaneous reporting database. Presented at the 44th interscience conference on antimicrobial agents and chemotherapy. Washington, DC, October 3-November 2, 2004.
10. Smith KM, Lomaestro BM. What role do fluoroquinolone antimicrobial agents play in cardiac dysfunction and altered glycemic control? J Pharm Pract 2003;16:349-360.
11. Donaldson AR, Vandiver JF, Finch CK. Possible gatifloxacin-induced hyperglycemia. Ann Pharmacother 2004;38:602-605.
12. Saraga A, Yokokura M, Gonoi T, et al. Effects of fluoroquinolones on insulin secretion and ß-cell ATP-sensitive K+ channels. Eur J Pharm 2004;497:111-117.
13. Leblanc M, Belanger C, Cossette P. Severe and resistant hypoglycemia associated with concomitant gatifloxacin and glyburide therapy. Pharmacother 2004;24:926-931.
14. Menzies DJ, Dorsainvil PA, Cunha BA, et al. Severe and persistent hypoglycemia due to gatifloxacin interaction with oral hypoglycemic agents. Am J Med 2002;113:232-234.
15. Lin G, Hays DP, Spillane L. Refractory hypoglycemia from ciprofloxacin and glyburide interaction. J Toxicol Clin Toxicol 2004;42:295-297.
16. Graumlich JF, Habis S, Avelino RR, et al. Hypoglycemia in inpatients after gatifloxacin or levofloxacin therapy: nested case control study. Pharmacother 2005;25:1296-1302.
17. Gajjar DA, LaCreta FP, Kollia GD, et al. Effect of multiple-dose gatifloxacin or ciprofloxacin on glucose homeostasis and insulin production in patients with non-insulin-dependent diabetes mellitus maintained with diet and exercise. Pharmacother 2000;20:76S-86S.
18. Gajjar DA, LaCreta FP, Uderman HD, et al. A dose-escalation study of the safety, tolerability, and pharmacokinetics of intravenous gatifloxacin in healthy adult men. Pharmacother 2000;20:49S-58S.
19. Gavin JR, Kubin R, Choudri S, et al. Moxifloxacin and glucose homeostasis. Drug Saf 2004;27:671-686.
20. Pichichero ME, Arguelas A, Dagan R. Safety and efficacy of gatifloxacin therapy for children with recurrent acute otitis media (AOM) and/or AOM treatment failure. Clin Infect Dis 2005;41:470-478.
21. Lawrence KR, Adra M, Keir C. Hypoglycemia-induced anoxic brain injury possibly associated with levofloxacin. J Infect 2006;52:e177-180.Epub 2005 Nov 2.
22. Ambrose PG, Bhavnani SM, Cirincione BB, et al. Gatifloxacin and the elderly: pharmacokinetic-pharmacodynamic rationale for a potential age-related dose reduction. J Antimicrob Chemother 2003;S2:434-440.
23. Coblio NA, Mowrey K, McCright P, et al. Use of a data warehouse to examine the effect of fluoroquinolones on glucose metabolism. Am J Health Syst Pharm 2004;61:2545-2548.
24. Gaglia JL, Wyckoff J, Abrahamson MJ. Acute hyperglycemic crisis in the elderly. Med Clin North Am 2004;88:1063-1084, xii.
1. Bristol-Myers Squibb Company. Tequin (gatifloxacin) package insert. Princeton, NJ; 2006.
2. Bayer Pharmaceuticals. Avelox (moxifloxacin) tablets/injection package insert. West Haven, CT: Bayer Pharmaceuticals; 2004.
3. Ortho-McNeil Pharmaceuticals. Levaquin (levofloxacin) tablets/injection package insert. Raritan, NJ: Ortho-McNeil; 2004.
4. Bayer Corporation. Cipro (ciprofloxacin) package insert. West Haven, CT; 2003.
5. Park-Wyllie LY, Juurlink DL, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med 2006;354:1352-1361.Epub 2006 Mar 1.
6. Mohr JF, McKinnon PS, Peymann PJ, et al. A retrospective, comparative evaluation of dysglycemias in hospitalized patients receiving gatifloxacin, levofloxacin, ciprofloxacin, or ceftriaxone. Pharmacother 2005;25:1303-1309.
7. Akpunow B, Michaelis J, Uy CN, et al. Multicenter postmarketing assessment of levofloxacin in the treatment of adults with community-acquired pneumonia. Clin Infect Dis 2004;38:S5-S15.
8. Letourneau G, Morrison H, McMorran M. Gatifloxacin (Tequin): hypoglycemia and hyperglycemia. Can Adverse React Newsletter 2003;13:1-2.
9. Frothingham R. Gatifloxacin associated with a 56-fold higher rate of glucose homeostasis abnormalities than comparator quinolones in the FDA spontaneous reporting database. Presented at the 44th interscience conference on antimicrobial agents and chemotherapy. Washington, DC, October 3-November 2, 2004.
10. Smith KM, Lomaestro BM. What role do fluoroquinolone antimicrobial agents play in cardiac dysfunction and altered glycemic control? J Pharm Pract 2003;16:349-360.
11. Donaldson AR, Vandiver JF, Finch CK. Possible gatifloxacin-induced hyperglycemia. Ann Pharmacother 2004;38:602-605.
12. Saraga A, Yokokura M, Gonoi T, et al. Effects of fluoroquinolones on insulin secretion and ß-cell ATP-sensitive K+ channels. Eur J Pharm 2004;497:111-117.
13. Leblanc M, Belanger C, Cossette P. Severe and resistant hypoglycemia associated with concomitant gatifloxacin and glyburide therapy. Pharmacother 2004;24:926-931.
14. Menzies DJ, Dorsainvil PA, Cunha BA, et al. Severe and persistent hypoglycemia due to gatifloxacin interaction with oral hypoglycemic agents. Am J Med 2002;113:232-234.
15. Lin G, Hays DP, Spillane L. Refractory hypoglycemia from ciprofloxacin and glyburide interaction. J Toxicol Clin Toxicol 2004;42:295-297.
16. Graumlich JF, Habis S, Avelino RR, et al. Hypoglycemia in inpatients after gatifloxacin or levofloxacin therapy: nested case control study. Pharmacother 2005;25:1296-1302.
17. Gajjar DA, LaCreta FP, Kollia GD, et al. Effect of multiple-dose gatifloxacin or ciprofloxacin on glucose homeostasis and insulin production in patients with non-insulin-dependent diabetes mellitus maintained with diet and exercise. Pharmacother 2000;20:76S-86S.
18. Gajjar DA, LaCreta FP, Uderman HD, et al. A dose-escalation study of the safety, tolerability, and pharmacokinetics of intravenous gatifloxacin in healthy adult men. Pharmacother 2000;20:49S-58S.
19. Gavin JR, Kubin R, Choudri S, et al. Moxifloxacin and glucose homeostasis. Drug Saf 2004;27:671-686.
20. Pichichero ME, Arguelas A, Dagan R. Safety and efficacy of gatifloxacin therapy for children with recurrent acute otitis media (AOM) and/or AOM treatment failure. Clin Infect Dis 2005;41:470-478.
21. Lawrence KR, Adra M, Keir C. Hypoglycemia-induced anoxic brain injury possibly associated with levofloxacin. J Infect 2006;52:e177-180.Epub 2005 Nov 2.
22. Ambrose PG, Bhavnani SM, Cirincione BB, et al. Gatifloxacin and the elderly: pharmacokinetic-pharmacodynamic rationale for a potential age-related dose reduction. J Antimicrob Chemother 2003;S2:434-440.
23. Coblio NA, Mowrey K, McCright P, et al. Use of a data warehouse to examine the effect of fluoroquinolones on glucose metabolism. Am J Health Syst Pharm 2004;61:2545-2548.
24. Gaglia JL, Wyckoff J, Abrahamson MJ. Acute hyperglycemic crisis in the elderly. Med Clin North Am 2004;88:1063-1084, xii.