User login
Stroke and Preventable Hospitalization: Who Is Most At Risk?
Bite of the Brown Recluse Spider
The brown recluse spider (Loxosceles reclusa) is a small arachnid with great potential to inflict physical harm. More potent than a rattlesnake’s venom, the toxin emitted by the brown recluse has the ability to rupture cell membranes and destroy regional nerves, blood vessels, and fatty tissue. Envenomation by the brown recluse can lead to severe necrosis of the cutaneous tissues.1,2
In the United States, L reclusa is one of 13 species of Loxosceles—five of which have been associated with necrotic lesions resulting from bites and envenomation.3 Though rare, and virtually nonexistent across significant portions of North America,4 the brown recluse is often cited as the offending creature in reported bites involving envenomation5 (with reports sometimes outnumbering estimated numbers of specimens in a given area6). Considering the limited range within which the spider is considered endemic, any patient who presents reporting a possible brown recluse spider bite (or who presents with a wound suspected of being such a bite) must be questioned quickly and carefully. The first and foremost question: where, geographically, was the patient bitten?
Endemic Areas
Brown recluse spiders are known to be present in the subtropical areas of North America—but not in areas with high humidity. According to arachnologists in the southeastern United States, the closer one is to the Gulf of Mexico, the less likely one is to encounter a brown recluse.7 This spider is most commonly found in eastern Texas, Arkansas, areas west of the Appalachian Mountains, and northern areas of the Gulf Coast states (see Figure 18). They are virtually nonexistent along the Atlantic seaboard and the Gulf Coast,4 although lone specimens of Loxosceles species have been reported in numerous nonendemic areas, suggesting possible transport through commerce or family relocation.9 One suspected case of brown recluse envenomation was recently reported in New York State.10
If it is determined that the geographic area in question is indeed populated by brown recluse spiders, more detailed history must then be elicited from the patient regarding recent activities. The brown recluse may reside indoors and often hides in bed sheets, blankets, and stored clothing. This spider also may be found behind furniture, in basements and cupboards, or in other small, tight areas. It is commonly found in cardboard boxes stored in a closet or an attic,11 and boxes with folded flaps are a preferred dwelling place.7 (Thus, a remote chance that L reclusa can be inadvertently transported to a nonendemic area9 does exist.)
In the outdoors, the brown recluse may be found in woodpiles, piles of leaves or other natural debris, in outdoor sheds or garages, under rocks, and in other places that are relatively dark and seldom used.12
Patient Presentation/Patient History
Initially, patients with a brown recluse spider bite may present to a primary care provider with complaints of mild pain and itching, presumably around the bite site. Within eight hours, the pain becomes stabbing and penetrating and may give way to a burning sensation.7
Patients with a positive pertinent history who are at increased risk for a bite are those who live in areas where these spiders are endemic and who have been performing tasks in areas where these spiders might reside. Not wearing long pants and long-sleeved shirts contributes to the probability that a patient has sustained a bite.
Physical Examination
The site of the suspected bite and surrounding skin should be examined carefully. A pustule, generally small and white, may appear, surrounded by erythema. For as long as 24 hours following the time of the initial bite, a volcano-like lesion may be present, with a sunken central “crater” that has raised edges. While the center of the lesion is free of inflammation, the surrounding skin is typically red and inflamed.12
Pathologically, a specified sequence occurs following a bite with envenomation. Initially, platelets aggregate, followed by endothelial swelling and destruction (see Figure 2a). Gradually, this leads to the blocking of capillaries with white blood cells, which results in ischemia and ultimately necrosis.1
The clinical manifestations of the brown recluse spider bite may vary, based on the amount of venom injected and the age and overall health of the patient. One who has been bitten with minimal envenomation may experience little more than mild erythema, localized urticaria, and generalized discomfort that resolves spontaneously in three to five days.1
In patients who experience more significant envenomation, a “bull’s-eye” lesion may appear. The center of the wound may be bluish in hue, with concentric rings—an inner pale ring, and an outer reddened ring. The center of the wound subsequently forms a hemorrhagic bleb that will typically become necrotic. Eventually, as the eschar matures, the necrotic tissue will slough off, and an area of granulation will develop. Full healing of the wound may take from four weeks to as long as six months.1
Laboratory Workup
A complete blood count, including platelet count and differential, will allow the provider to observe for disseminated intravascular coagulation, hemolysis, and thrombocytopenia. The abnormal results most commonly found in patients who have sustained a brown recluse spider bite are leukocytosis and an elevated erythrocyte sedimentation rate. A skin biopsy of the site may reveal the presence of eosinophils, neutrophils, and thrombosis, all of which support the diagnosis of a brown recluse spider bite.2
A valid, reliable test to detect Loxosceles venom is needed in the clinical setting; the differential diagnosis for brown recluse spider bites is broad (see the table1,6,11,13-15 below), and diagnostic error can occur, delaying appropriate treatment for the actual presenting condition—which could be debilitating or in rare cases, fatal.16 One test for Loxosceles venom, though not currently marketed for use in humans, shows potential. It is a polyclonal enzyme-linked immunosorbent assay (ELISA) with a demonstrated ability to detect venom in rabbits for as long as seven days after injection.7 Further refinement of the polyclonal ELISA is under way in efforts to increase its sensitivity and specificity.17
Diagnosis
Diagnosis of a brown recluse spider bite is difficult at best. Other potential causes of the associated presenting symptoms should be excluded before a brown recluse spider bite is considered confirmed.
Several factors add to the difficulty of diagnosing a brown recluse bite. Oftentimes it may take the patients days or weeks after the bite to see a health care provider, and they rarely present with the spider that bit them (or that they believe bit them).1 Currently, the only true standard for proof of envenomation by a brown recluse is to collect the spider and have its identify verified by an entomologist or other expert—not necessarily the health care provider.
One condition that is frequently misdiagnosed as a brown recluse bite is methicillin-resistant Staphylococcus aureus infection (MRSA; see Figure 2b). Misdiagnosis as a bite will delay appropriate treatment for MRSA and possibly lead to transmission of infection to others, as the unaware patient does not take proper precautions to avoid spreading MRSA to others.7 Patients with MRSA who experience significant tissue eradication or tissue death, or who have developed systemic symptoms, are candidates for hospitalization and possibly surgical debridement.2
Treatment/Management
Even without proper verification that the lesion is the bite of a brown recluse, it remains essential to provide basic treatment—initially, to wash the area with mild soap and water, then elevate the affected extremity and apply ice; rest is recommended.12 The patient’s tetanus immunization status should be verified, with tetanus vaccine administered if appropriate.7,11
While most brown recluse bites will resolve without major treatment within two to three months, disabling manifestations warrant treatment. Treatment goals are to keep the skin intact, decrease the likelihood that infection will spread, and maintain circulation to the affected area.
Several treatment options are possible for a confirmed brown recluse spider bite with envenomation. Oral dapsone, initiated within 36 hours, has been shown to reduce or delay the need for surgical intervention in cases of severe necrotic arachnidism.2,13,18,19 Dosage ranges from 50 mg/d to 100 mg/d, divided bid for adults; and for children, 1.0 to 2.0 mg/kg/d, not to exceed 100 mg/d.3
Before dapsone is prescribed or administered, the patient must be tested for glucose-6-phosphate dehydrogenase (G6PD) deficiency, as dapsone use in such individuals can lead to hemolysis.3,20 Clinicians unfamiliar with this medication should request a consultation with an expert (eg, in infectious disease, wound care, pharmacology) regarding treatment and the need for monitoring potential adverse effects. Additionally, although dapsone has been recommended for this indication for longer than 20 years, few human studies have been reported to support its use.19
The anti-inflammatory effects of steroids may be useful in some cases, as they may provide red blood cell membrane–stabilizing effects in patients with systemic loxoscelism.7 Although no guideline currently exists for dosing of glucocorticoids in spider bite treatment, a shorter period of eschar duration was reported in one animal study involving methylprednisolone administered within two hours of inoculation, dosed at 2 mg/kg of body weight initially, then daily for two days longer.11
Antibiotics may minimize the inflammatory reaction at the bite site, although generally, antibiotics are reserved for infections and not recommended for prophylaxis. Antihistamines may be used to relieve minor symptoms related to histamine release (eg, itching) and also for treatment of anaphylaxis.3 Analgesics, such as acetaminophen, may be prescribed for minor discomfort. Clinicians should individualize medication use (both drug and dose) based on the needs of the patient.
Hyperbaric oxygen therapy, a modality commonly used in wound healing, has been theorized to break down sphingomyelinase-D, thus preventing further spread of venom.1,21 In patients treated with this modality for brown recluse bites, reported results have been mixed.7
Follow-Up
Daily wound checks should be performed until the lesion is noted to be improving or no longer worsening. At each follow-up for the initial 72 hours, it is recommended that patients undergo a CBC, including platelet level, to detect progression of the infection or systemic involvement, and urinalysis to check for hematuria. Renal function should be monitored as needed.1,2
Patient Education
Regarding brown recluse spider bites, patients should be advised to keep five points in mind:
• Diagnosis is made by confirmation that the spider is a brown recluse, ideally with the capture and expert evaluation of the spider22
• Workup will focus on history, geographic locale, and environ of patient when supposed bite occurred4,7,8
• Treatment varies but may include a tetanus shot, antibiotics, dapsone, steroids, hyperbaric oxygen therapy, and in severe cases of necrosis, surgery1,2,7,19,20
• Follow-up will occur routinely during the initial 72 hours1,2
• Prevention of bites includes avoiding piles of clutter in garages, sheds, and under beds; and wearing long sleeves when working in these areas.12
Finally, because the venom of the brown recluse spider is poisonous, the NIH encourages exposed persons to contact the National Poison Control Center at (800) 222-1222.23
Conclusion
Brown recluse spider bites, though most likely overdiagnosed, do occasionally occur in areas where the creature is endemic. However, a brown recluse spider bite should be considered a diagnosis of exclusion and other possibilities considered first in light of their limited presence in North America and their nonaggressive nature.
Any patient who calls to report a suspected brown recluse spider bite should be instructed to bring the spider to the office, if possible, for identification. The spider should then be identified with certainty as a brown recluse by the appropriate expert so that treatment for the patient can be based on a correct diagnosis rather than one of presumption.
1. Wilson JR, Hagood CO Jr, Prather ID. Brown recluse spider bites: a complex problem wound. A brief review and case study. Ostomy Wound Manage. 2005;51(3):59-66.
2. Rhoads J. Epidemiology of the brown recluse spider bite. J Am Acad Nurse Pract. 2007; 19(2):79-85.
3. Arnold TC. Spider envenomation, brown recluse. http://emedicine.medscape.com/article/772295-overview. Accessed November 23, 2010.
4. Vetter RS, Hinkle NC, Ames LM. Distribution of the brown recluse spider (Araneae: Sicariidae) in Georgia with comparison to poison center reports of envenomations. J Med Entomol. 2009;46(1):15-20.
5. Pagac BB, Reiland RW, Bolesh DT, Swanson DL. Skin lesions in barracks: consider community-acquired methicillin-resistant Staphylococcus aureus infection instead of spider bites. Mil Med. 2006;171(9):830-832.
6. Frithsen IL, Vetter RS, Stocks IC. Reports of envenomation by brown recluse spiders exceed verified specimens of Loxosceles spiders in South Carolina. J Am Board Fam Med. 2007;20(5):483-488.
7. Swanson DL, Vetter RS. Loxoscelism. Clin Dermatol. 2006;24(3):213-221.
8. CDC. Necrotic arachnidism: Pacific Northwest, 1988-1996. MMWR Morb Mortal Wkly Rep. 1996;45(21):433-436.
9. Gertsch WJ, Ennik F. The spider genus Loxosceles in North America, Central America, and the West Indies (Araneae, Loxoscelidae). Bull Am Museum of Nat Hist. 1983;175:265-360.
10. Andersen RJ, Campoli J, Johar SK, et al. Suspected brown recluse envenomation: a case report and review of different treatment modalities. J Emerg Med. 2010 Apr 2. [Epub ahead of print]
11. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352(7):700-709.
12. Nunnelee JD. Brown recluse spider bites: a case report. J Perianesth Nurs. 2006;21(1):12-15.
13. Naidu DK, Ghurani R, Salas RE, et al. Osteomyelitis of the mandibular symphysis caused by brown recluse spider bite. Eplasty. 2008 Aug 28;8:428-433.
14. Osterhoudt KC, Zaoutis T, Zorc JJ. Lyme disease masquerading as brown recluse spider bite. Ann Emerg Med. 2002;39(5):558-561.
15. Russell FE, Gertsch WJ. For those who treat spider or suspected spider bites. Toxicon. 1983;21(3):337-339.
16. Vetter RS, Bush SP. Reports of presumptive brown recluse spider bites reinforce improbably diagnosis in regions of North America where the spider is not endemic. Clin Infect Dis. 2002;35(4):442-445.
17. McGlasson DL, Green JA, Stoecker WV, et al. Duration of Loxosceles reclusa venom detection by ELISA from swabs. Clin Lab Sci. 2009;22(4):216-222.
18. Wendell RP. Brown recluse spiders: a review to help guide physicians in non-endemic areas. South Med J. 2003;96(5):486–90.
19. Rees RS, Altenbern DP, Lynch JB, King LE Jr. Brown recluse spider bites: a comparison of early surgical excision versus dapsone and delayed surgical excision. Ann Surg. 1985;202 (5):659-663.
20. Webster GF. Is topical dapsone safe in glucose-6-phosphate dehydrogenase-deficient and sulfonamide-allergic patients? J Drugs Dermatol. 2010;9(5):532-536.
21. Merchant ML, Hinton JF, Geren CR. Effect of hyperbaric oxygen on sphingomyelinase D activity of brown recluse spider (Loxosceles reclusa) venom as studied by 31P nuclear magnetic resonance spectroscopy. Am J Trop Med Hyg. 1997;56(3):335-338.
22. Bennett RG, Vetter RS. An approach to spider bites: erroneous attribution of dermonecrotic lesions to brown recluse or hobo spider bites in Canada. Can Fam Physician. 2004;50:1098-1101.
23. MedlinePlus, US National Library of Medicine, NIH. Brown recluse spider. www.mdconsult.com/das/patient/body/225048384-2/0/10041/32560.html. Accessed November 23, 2010.
The brown recluse spider (Loxosceles reclusa) is a small arachnid with great potential to inflict physical harm. More potent than a rattlesnake’s venom, the toxin emitted by the brown recluse has the ability to rupture cell membranes and destroy regional nerves, blood vessels, and fatty tissue. Envenomation by the brown recluse can lead to severe necrosis of the cutaneous tissues.1,2
In the United States, L reclusa is one of 13 species of Loxosceles—five of which have been associated with necrotic lesions resulting from bites and envenomation.3 Though rare, and virtually nonexistent across significant portions of North America,4 the brown recluse is often cited as the offending creature in reported bites involving envenomation5 (with reports sometimes outnumbering estimated numbers of specimens in a given area6). Considering the limited range within which the spider is considered endemic, any patient who presents reporting a possible brown recluse spider bite (or who presents with a wound suspected of being such a bite) must be questioned quickly and carefully. The first and foremost question: where, geographically, was the patient bitten?
Endemic Areas
Brown recluse spiders are known to be present in the subtropical areas of North America—but not in areas with high humidity. According to arachnologists in the southeastern United States, the closer one is to the Gulf of Mexico, the less likely one is to encounter a brown recluse.7 This spider is most commonly found in eastern Texas, Arkansas, areas west of the Appalachian Mountains, and northern areas of the Gulf Coast states (see Figure 18). They are virtually nonexistent along the Atlantic seaboard and the Gulf Coast,4 although lone specimens of Loxosceles species have been reported in numerous nonendemic areas, suggesting possible transport through commerce or family relocation.9 One suspected case of brown recluse envenomation was recently reported in New York State.10
If it is determined that the geographic area in question is indeed populated by brown recluse spiders, more detailed history must then be elicited from the patient regarding recent activities. The brown recluse may reside indoors and often hides in bed sheets, blankets, and stored clothing. This spider also may be found behind furniture, in basements and cupboards, or in other small, tight areas. It is commonly found in cardboard boxes stored in a closet or an attic,11 and boxes with folded flaps are a preferred dwelling place.7 (Thus, a remote chance that L reclusa can be inadvertently transported to a nonendemic area9 does exist.)
In the outdoors, the brown recluse may be found in woodpiles, piles of leaves or other natural debris, in outdoor sheds or garages, under rocks, and in other places that are relatively dark and seldom used.12
Patient Presentation/Patient History
Initially, patients with a brown recluse spider bite may present to a primary care provider with complaints of mild pain and itching, presumably around the bite site. Within eight hours, the pain becomes stabbing and penetrating and may give way to a burning sensation.7
Patients with a positive pertinent history who are at increased risk for a bite are those who live in areas where these spiders are endemic and who have been performing tasks in areas where these spiders might reside. Not wearing long pants and long-sleeved shirts contributes to the probability that a patient has sustained a bite.
Physical Examination
The site of the suspected bite and surrounding skin should be examined carefully. A pustule, generally small and white, may appear, surrounded by erythema. For as long as 24 hours following the time of the initial bite, a volcano-like lesion may be present, with a sunken central “crater” that has raised edges. While the center of the lesion is free of inflammation, the surrounding skin is typically red and inflamed.12
Pathologically, a specified sequence occurs following a bite with envenomation. Initially, platelets aggregate, followed by endothelial swelling and destruction (see Figure 2a). Gradually, this leads to the blocking of capillaries with white blood cells, which results in ischemia and ultimately necrosis.1
The clinical manifestations of the brown recluse spider bite may vary, based on the amount of venom injected and the age and overall health of the patient. One who has been bitten with minimal envenomation may experience little more than mild erythema, localized urticaria, and generalized discomfort that resolves spontaneously in three to five days.1
In patients who experience more significant envenomation, a “bull’s-eye” lesion may appear. The center of the wound may be bluish in hue, with concentric rings—an inner pale ring, and an outer reddened ring. The center of the wound subsequently forms a hemorrhagic bleb that will typically become necrotic. Eventually, as the eschar matures, the necrotic tissue will slough off, and an area of granulation will develop. Full healing of the wound may take from four weeks to as long as six months.1
Laboratory Workup
A complete blood count, including platelet count and differential, will allow the provider to observe for disseminated intravascular coagulation, hemolysis, and thrombocytopenia. The abnormal results most commonly found in patients who have sustained a brown recluse spider bite are leukocytosis and an elevated erythrocyte sedimentation rate. A skin biopsy of the site may reveal the presence of eosinophils, neutrophils, and thrombosis, all of which support the diagnosis of a brown recluse spider bite.2
A valid, reliable test to detect Loxosceles venom is needed in the clinical setting; the differential diagnosis for brown recluse spider bites is broad (see the table1,6,11,13-15 below), and diagnostic error can occur, delaying appropriate treatment for the actual presenting condition—which could be debilitating or in rare cases, fatal.16 One test for Loxosceles venom, though not currently marketed for use in humans, shows potential. It is a polyclonal enzyme-linked immunosorbent assay (ELISA) with a demonstrated ability to detect venom in rabbits for as long as seven days after injection.7 Further refinement of the polyclonal ELISA is under way in efforts to increase its sensitivity and specificity.17
Diagnosis
Diagnosis of a brown recluse spider bite is difficult at best. Other potential causes of the associated presenting symptoms should be excluded before a brown recluse spider bite is considered confirmed.
Several factors add to the difficulty of diagnosing a brown recluse bite. Oftentimes it may take the patients days or weeks after the bite to see a health care provider, and they rarely present with the spider that bit them (or that they believe bit them).1 Currently, the only true standard for proof of envenomation by a brown recluse is to collect the spider and have its identify verified by an entomologist or other expert—not necessarily the health care provider.
One condition that is frequently misdiagnosed as a brown recluse bite is methicillin-resistant Staphylococcus aureus infection (MRSA; see Figure 2b). Misdiagnosis as a bite will delay appropriate treatment for MRSA and possibly lead to transmission of infection to others, as the unaware patient does not take proper precautions to avoid spreading MRSA to others.7 Patients with MRSA who experience significant tissue eradication or tissue death, or who have developed systemic symptoms, are candidates for hospitalization and possibly surgical debridement.2
Treatment/Management
Even without proper verification that the lesion is the bite of a brown recluse, it remains essential to provide basic treatment—initially, to wash the area with mild soap and water, then elevate the affected extremity and apply ice; rest is recommended.12 The patient’s tetanus immunization status should be verified, with tetanus vaccine administered if appropriate.7,11
While most brown recluse bites will resolve without major treatment within two to three months, disabling manifestations warrant treatment. Treatment goals are to keep the skin intact, decrease the likelihood that infection will spread, and maintain circulation to the affected area.
Several treatment options are possible for a confirmed brown recluse spider bite with envenomation. Oral dapsone, initiated within 36 hours, has been shown to reduce or delay the need for surgical intervention in cases of severe necrotic arachnidism.2,13,18,19 Dosage ranges from 50 mg/d to 100 mg/d, divided bid for adults; and for children, 1.0 to 2.0 mg/kg/d, not to exceed 100 mg/d.3
Before dapsone is prescribed or administered, the patient must be tested for glucose-6-phosphate dehydrogenase (G6PD) deficiency, as dapsone use in such individuals can lead to hemolysis.3,20 Clinicians unfamiliar with this medication should request a consultation with an expert (eg, in infectious disease, wound care, pharmacology) regarding treatment and the need for monitoring potential adverse effects. Additionally, although dapsone has been recommended for this indication for longer than 20 years, few human studies have been reported to support its use.19
The anti-inflammatory effects of steroids may be useful in some cases, as they may provide red blood cell membrane–stabilizing effects in patients with systemic loxoscelism.7 Although no guideline currently exists for dosing of glucocorticoids in spider bite treatment, a shorter period of eschar duration was reported in one animal study involving methylprednisolone administered within two hours of inoculation, dosed at 2 mg/kg of body weight initially, then daily for two days longer.11
Antibiotics may minimize the inflammatory reaction at the bite site, although generally, antibiotics are reserved for infections and not recommended for prophylaxis. Antihistamines may be used to relieve minor symptoms related to histamine release (eg, itching) and also for treatment of anaphylaxis.3 Analgesics, such as acetaminophen, may be prescribed for minor discomfort. Clinicians should individualize medication use (both drug and dose) based on the needs of the patient.
Hyperbaric oxygen therapy, a modality commonly used in wound healing, has been theorized to break down sphingomyelinase-D, thus preventing further spread of venom.1,21 In patients treated with this modality for brown recluse bites, reported results have been mixed.7
Follow-Up
Daily wound checks should be performed until the lesion is noted to be improving or no longer worsening. At each follow-up for the initial 72 hours, it is recommended that patients undergo a CBC, including platelet level, to detect progression of the infection or systemic involvement, and urinalysis to check for hematuria. Renal function should be monitored as needed.1,2
Patient Education
Regarding brown recluse spider bites, patients should be advised to keep five points in mind:
• Diagnosis is made by confirmation that the spider is a brown recluse, ideally with the capture and expert evaluation of the spider22
• Workup will focus on history, geographic locale, and environ of patient when supposed bite occurred4,7,8
• Treatment varies but may include a tetanus shot, antibiotics, dapsone, steroids, hyperbaric oxygen therapy, and in severe cases of necrosis, surgery1,2,7,19,20
• Follow-up will occur routinely during the initial 72 hours1,2
• Prevention of bites includes avoiding piles of clutter in garages, sheds, and under beds; and wearing long sleeves when working in these areas.12
Finally, because the venom of the brown recluse spider is poisonous, the NIH encourages exposed persons to contact the National Poison Control Center at (800) 222-1222.23
Conclusion
Brown recluse spider bites, though most likely overdiagnosed, do occasionally occur in areas where the creature is endemic. However, a brown recluse spider bite should be considered a diagnosis of exclusion and other possibilities considered first in light of their limited presence in North America and their nonaggressive nature.
Any patient who calls to report a suspected brown recluse spider bite should be instructed to bring the spider to the office, if possible, for identification. The spider should then be identified with certainty as a brown recluse by the appropriate expert so that treatment for the patient can be based on a correct diagnosis rather than one of presumption.
The brown recluse spider (Loxosceles reclusa) is a small arachnid with great potential to inflict physical harm. More potent than a rattlesnake’s venom, the toxin emitted by the brown recluse has the ability to rupture cell membranes and destroy regional nerves, blood vessels, and fatty tissue. Envenomation by the brown recluse can lead to severe necrosis of the cutaneous tissues.1,2
In the United States, L reclusa is one of 13 species of Loxosceles—five of which have been associated with necrotic lesions resulting from bites and envenomation.3 Though rare, and virtually nonexistent across significant portions of North America,4 the brown recluse is often cited as the offending creature in reported bites involving envenomation5 (with reports sometimes outnumbering estimated numbers of specimens in a given area6). Considering the limited range within which the spider is considered endemic, any patient who presents reporting a possible brown recluse spider bite (or who presents with a wound suspected of being such a bite) must be questioned quickly and carefully. The first and foremost question: where, geographically, was the patient bitten?
Endemic Areas
Brown recluse spiders are known to be present in the subtropical areas of North America—but not in areas with high humidity. According to arachnologists in the southeastern United States, the closer one is to the Gulf of Mexico, the less likely one is to encounter a brown recluse.7 This spider is most commonly found in eastern Texas, Arkansas, areas west of the Appalachian Mountains, and northern areas of the Gulf Coast states (see Figure 18). They are virtually nonexistent along the Atlantic seaboard and the Gulf Coast,4 although lone specimens of Loxosceles species have been reported in numerous nonendemic areas, suggesting possible transport through commerce or family relocation.9 One suspected case of brown recluse envenomation was recently reported in New York State.10
If it is determined that the geographic area in question is indeed populated by brown recluse spiders, more detailed history must then be elicited from the patient regarding recent activities. The brown recluse may reside indoors and often hides in bed sheets, blankets, and stored clothing. This spider also may be found behind furniture, in basements and cupboards, or in other small, tight areas. It is commonly found in cardboard boxes stored in a closet or an attic,11 and boxes with folded flaps are a preferred dwelling place.7 (Thus, a remote chance that L reclusa can be inadvertently transported to a nonendemic area9 does exist.)
In the outdoors, the brown recluse may be found in woodpiles, piles of leaves or other natural debris, in outdoor sheds or garages, under rocks, and in other places that are relatively dark and seldom used.12
Patient Presentation/Patient History
Initially, patients with a brown recluse spider bite may present to a primary care provider with complaints of mild pain and itching, presumably around the bite site. Within eight hours, the pain becomes stabbing and penetrating and may give way to a burning sensation.7
Patients with a positive pertinent history who are at increased risk for a bite are those who live in areas where these spiders are endemic and who have been performing tasks in areas where these spiders might reside. Not wearing long pants and long-sleeved shirts contributes to the probability that a patient has sustained a bite.
Physical Examination
The site of the suspected bite and surrounding skin should be examined carefully. A pustule, generally small and white, may appear, surrounded by erythema. For as long as 24 hours following the time of the initial bite, a volcano-like lesion may be present, with a sunken central “crater” that has raised edges. While the center of the lesion is free of inflammation, the surrounding skin is typically red and inflamed.12
Pathologically, a specified sequence occurs following a bite with envenomation. Initially, platelets aggregate, followed by endothelial swelling and destruction (see Figure 2a). Gradually, this leads to the blocking of capillaries with white blood cells, which results in ischemia and ultimately necrosis.1
The clinical manifestations of the brown recluse spider bite may vary, based on the amount of venom injected and the age and overall health of the patient. One who has been bitten with minimal envenomation may experience little more than mild erythema, localized urticaria, and generalized discomfort that resolves spontaneously in three to five days.1
In patients who experience more significant envenomation, a “bull’s-eye” lesion may appear. The center of the wound may be bluish in hue, with concentric rings—an inner pale ring, and an outer reddened ring. The center of the wound subsequently forms a hemorrhagic bleb that will typically become necrotic. Eventually, as the eschar matures, the necrotic tissue will slough off, and an area of granulation will develop. Full healing of the wound may take from four weeks to as long as six months.1
Laboratory Workup
A complete blood count, including platelet count and differential, will allow the provider to observe for disseminated intravascular coagulation, hemolysis, and thrombocytopenia. The abnormal results most commonly found in patients who have sustained a brown recluse spider bite are leukocytosis and an elevated erythrocyte sedimentation rate. A skin biopsy of the site may reveal the presence of eosinophils, neutrophils, and thrombosis, all of which support the diagnosis of a brown recluse spider bite.2
A valid, reliable test to detect Loxosceles venom is needed in the clinical setting; the differential diagnosis for brown recluse spider bites is broad (see the table1,6,11,13-15 below), and diagnostic error can occur, delaying appropriate treatment for the actual presenting condition—which could be debilitating or in rare cases, fatal.16 One test for Loxosceles venom, though not currently marketed for use in humans, shows potential. It is a polyclonal enzyme-linked immunosorbent assay (ELISA) with a demonstrated ability to detect venom in rabbits for as long as seven days after injection.7 Further refinement of the polyclonal ELISA is under way in efforts to increase its sensitivity and specificity.17
Diagnosis
Diagnosis of a brown recluse spider bite is difficult at best. Other potential causes of the associated presenting symptoms should be excluded before a brown recluse spider bite is considered confirmed.
Several factors add to the difficulty of diagnosing a brown recluse bite. Oftentimes it may take the patients days or weeks after the bite to see a health care provider, and they rarely present with the spider that bit them (or that they believe bit them).1 Currently, the only true standard for proof of envenomation by a brown recluse is to collect the spider and have its identify verified by an entomologist or other expert—not necessarily the health care provider.
One condition that is frequently misdiagnosed as a brown recluse bite is methicillin-resistant Staphylococcus aureus infection (MRSA; see Figure 2b). Misdiagnosis as a bite will delay appropriate treatment for MRSA and possibly lead to transmission of infection to others, as the unaware patient does not take proper precautions to avoid spreading MRSA to others.7 Patients with MRSA who experience significant tissue eradication or tissue death, or who have developed systemic symptoms, are candidates for hospitalization and possibly surgical debridement.2
Treatment/Management
Even without proper verification that the lesion is the bite of a brown recluse, it remains essential to provide basic treatment—initially, to wash the area with mild soap and water, then elevate the affected extremity and apply ice; rest is recommended.12 The patient’s tetanus immunization status should be verified, with tetanus vaccine administered if appropriate.7,11
While most brown recluse bites will resolve without major treatment within two to three months, disabling manifestations warrant treatment. Treatment goals are to keep the skin intact, decrease the likelihood that infection will spread, and maintain circulation to the affected area.
Several treatment options are possible for a confirmed brown recluse spider bite with envenomation. Oral dapsone, initiated within 36 hours, has been shown to reduce or delay the need for surgical intervention in cases of severe necrotic arachnidism.2,13,18,19 Dosage ranges from 50 mg/d to 100 mg/d, divided bid for adults; and for children, 1.0 to 2.0 mg/kg/d, not to exceed 100 mg/d.3
Before dapsone is prescribed or administered, the patient must be tested for glucose-6-phosphate dehydrogenase (G6PD) deficiency, as dapsone use in such individuals can lead to hemolysis.3,20 Clinicians unfamiliar with this medication should request a consultation with an expert (eg, in infectious disease, wound care, pharmacology) regarding treatment and the need for monitoring potential adverse effects. Additionally, although dapsone has been recommended for this indication for longer than 20 years, few human studies have been reported to support its use.19
The anti-inflammatory effects of steroids may be useful in some cases, as they may provide red blood cell membrane–stabilizing effects in patients with systemic loxoscelism.7 Although no guideline currently exists for dosing of glucocorticoids in spider bite treatment, a shorter period of eschar duration was reported in one animal study involving methylprednisolone administered within two hours of inoculation, dosed at 2 mg/kg of body weight initially, then daily for two days longer.11
Antibiotics may minimize the inflammatory reaction at the bite site, although generally, antibiotics are reserved for infections and not recommended for prophylaxis. Antihistamines may be used to relieve minor symptoms related to histamine release (eg, itching) and also for treatment of anaphylaxis.3 Analgesics, such as acetaminophen, may be prescribed for minor discomfort. Clinicians should individualize medication use (both drug and dose) based on the needs of the patient.
Hyperbaric oxygen therapy, a modality commonly used in wound healing, has been theorized to break down sphingomyelinase-D, thus preventing further spread of venom.1,21 In patients treated with this modality for brown recluse bites, reported results have been mixed.7
Follow-Up
Daily wound checks should be performed until the lesion is noted to be improving or no longer worsening. At each follow-up for the initial 72 hours, it is recommended that patients undergo a CBC, including platelet level, to detect progression of the infection or systemic involvement, and urinalysis to check for hematuria. Renal function should be monitored as needed.1,2
Patient Education
Regarding brown recluse spider bites, patients should be advised to keep five points in mind:
• Diagnosis is made by confirmation that the spider is a brown recluse, ideally with the capture and expert evaluation of the spider22
• Workup will focus on history, geographic locale, and environ of patient when supposed bite occurred4,7,8
• Treatment varies but may include a tetanus shot, antibiotics, dapsone, steroids, hyperbaric oxygen therapy, and in severe cases of necrosis, surgery1,2,7,19,20
• Follow-up will occur routinely during the initial 72 hours1,2
• Prevention of bites includes avoiding piles of clutter in garages, sheds, and under beds; and wearing long sleeves when working in these areas.12
Finally, because the venom of the brown recluse spider is poisonous, the NIH encourages exposed persons to contact the National Poison Control Center at (800) 222-1222.23
Conclusion
Brown recluse spider bites, though most likely overdiagnosed, do occasionally occur in areas where the creature is endemic. However, a brown recluse spider bite should be considered a diagnosis of exclusion and other possibilities considered first in light of their limited presence in North America and their nonaggressive nature.
Any patient who calls to report a suspected brown recluse spider bite should be instructed to bring the spider to the office, if possible, for identification. The spider should then be identified with certainty as a brown recluse by the appropriate expert so that treatment for the patient can be based on a correct diagnosis rather than one of presumption.
1. Wilson JR, Hagood CO Jr, Prather ID. Brown recluse spider bites: a complex problem wound. A brief review and case study. Ostomy Wound Manage. 2005;51(3):59-66.
2. Rhoads J. Epidemiology of the brown recluse spider bite. J Am Acad Nurse Pract. 2007; 19(2):79-85.
3. Arnold TC. Spider envenomation, brown recluse. http://emedicine.medscape.com/article/772295-overview. Accessed November 23, 2010.
4. Vetter RS, Hinkle NC, Ames LM. Distribution of the brown recluse spider (Araneae: Sicariidae) in Georgia with comparison to poison center reports of envenomations. J Med Entomol. 2009;46(1):15-20.
5. Pagac BB, Reiland RW, Bolesh DT, Swanson DL. Skin lesions in barracks: consider community-acquired methicillin-resistant Staphylococcus aureus infection instead of spider bites. Mil Med. 2006;171(9):830-832.
6. Frithsen IL, Vetter RS, Stocks IC. Reports of envenomation by brown recluse spiders exceed verified specimens of Loxosceles spiders in South Carolina. J Am Board Fam Med. 2007;20(5):483-488.
7. Swanson DL, Vetter RS. Loxoscelism. Clin Dermatol. 2006;24(3):213-221.
8. CDC. Necrotic arachnidism: Pacific Northwest, 1988-1996. MMWR Morb Mortal Wkly Rep. 1996;45(21):433-436.
9. Gertsch WJ, Ennik F. The spider genus Loxosceles in North America, Central America, and the West Indies (Araneae, Loxoscelidae). Bull Am Museum of Nat Hist. 1983;175:265-360.
10. Andersen RJ, Campoli J, Johar SK, et al. Suspected brown recluse envenomation: a case report and review of different treatment modalities. J Emerg Med. 2010 Apr 2. [Epub ahead of print]
11. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352(7):700-709.
12. Nunnelee JD. Brown recluse spider bites: a case report. J Perianesth Nurs. 2006;21(1):12-15.
13. Naidu DK, Ghurani R, Salas RE, et al. Osteomyelitis of the mandibular symphysis caused by brown recluse spider bite. Eplasty. 2008 Aug 28;8:428-433.
14. Osterhoudt KC, Zaoutis T, Zorc JJ. Lyme disease masquerading as brown recluse spider bite. Ann Emerg Med. 2002;39(5):558-561.
15. Russell FE, Gertsch WJ. For those who treat spider or suspected spider bites. Toxicon. 1983;21(3):337-339.
16. Vetter RS, Bush SP. Reports of presumptive brown recluse spider bites reinforce improbably diagnosis in regions of North America where the spider is not endemic. Clin Infect Dis. 2002;35(4):442-445.
17. McGlasson DL, Green JA, Stoecker WV, et al. Duration of Loxosceles reclusa venom detection by ELISA from swabs. Clin Lab Sci. 2009;22(4):216-222.
18. Wendell RP. Brown recluse spiders: a review to help guide physicians in non-endemic areas. South Med J. 2003;96(5):486–90.
19. Rees RS, Altenbern DP, Lynch JB, King LE Jr. Brown recluse spider bites: a comparison of early surgical excision versus dapsone and delayed surgical excision. Ann Surg. 1985;202 (5):659-663.
20. Webster GF. Is topical dapsone safe in glucose-6-phosphate dehydrogenase-deficient and sulfonamide-allergic patients? J Drugs Dermatol. 2010;9(5):532-536.
21. Merchant ML, Hinton JF, Geren CR. Effect of hyperbaric oxygen on sphingomyelinase D activity of brown recluse spider (Loxosceles reclusa) venom as studied by 31P nuclear magnetic resonance spectroscopy. Am J Trop Med Hyg. 1997;56(3):335-338.
22. Bennett RG, Vetter RS. An approach to spider bites: erroneous attribution of dermonecrotic lesions to brown recluse or hobo spider bites in Canada. Can Fam Physician. 2004;50:1098-1101.
23. MedlinePlus, US National Library of Medicine, NIH. Brown recluse spider. www.mdconsult.com/das/patient/body/225048384-2/0/10041/32560.html. Accessed November 23, 2010.
1. Wilson JR, Hagood CO Jr, Prather ID. Brown recluse spider bites: a complex problem wound. A brief review and case study. Ostomy Wound Manage. 2005;51(3):59-66.
2. Rhoads J. Epidemiology of the brown recluse spider bite. J Am Acad Nurse Pract. 2007; 19(2):79-85.
3. Arnold TC. Spider envenomation, brown recluse. http://emedicine.medscape.com/article/772295-overview. Accessed November 23, 2010.
4. Vetter RS, Hinkle NC, Ames LM. Distribution of the brown recluse spider (Araneae: Sicariidae) in Georgia with comparison to poison center reports of envenomations. J Med Entomol. 2009;46(1):15-20.
5. Pagac BB, Reiland RW, Bolesh DT, Swanson DL. Skin lesions in barracks: consider community-acquired methicillin-resistant Staphylococcus aureus infection instead of spider bites. Mil Med. 2006;171(9):830-832.
6. Frithsen IL, Vetter RS, Stocks IC. Reports of envenomation by brown recluse spiders exceed verified specimens of Loxosceles spiders in South Carolina. J Am Board Fam Med. 2007;20(5):483-488.
7. Swanson DL, Vetter RS. Loxoscelism. Clin Dermatol. 2006;24(3):213-221.
8. CDC. Necrotic arachnidism: Pacific Northwest, 1988-1996. MMWR Morb Mortal Wkly Rep. 1996;45(21):433-436.
9. Gertsch WJ, Ennik F. The spider genus Loxosceles in North America, Central America, and the West Indies (Araneae, Loxoscelidae). Bull Am Museum of Nat Hist. 1983;175:265-360.
10. Andersen RJ, Campoli J, Johar SK, et al. Suspected brown recluse envenomation: a case report and review of different treatment modalities. J Emerg Med. 2010 Apr 2. [Epub ahead of print]
11. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352(7):700-709.
12. Nunnelee JD. Brown recluse spider bites: a case report. J Perianesth Nurs. 2006;21(1):12-15.
13. Naidu DK, Ghurani R, Salas RE, et al. Osteomyelitis of the mandibular symphysis caused by brown recluse spider bite. Eplasty. 2008 Aug 28;8:428-433.
14. Osterhoudt KC, Zaoutis T, Zorc JJ. Lyme disease masquerading as brown recluse spider bite. Ann Emerg Med. 2002;39(5):558-561.
15. Russell FE, Gertsch WJ. For those who treat spider or suspected spider bites. Toxicon. 1983;21(3):337-339.
16. Vetter RS, Bush SP. Reports of presumptive brown recluse spider bites reinforce improbably diagnosis in regions of North America where the spider is not endemic. Clin Infect Dis. 2002;35(4):442-445.
17. McGlasson DL, Green JA, Stoecker WV, et al. Duration of Loxosceles reclusa venom detection by ELISA from swabs. Clin Lab Sci. 2009;22(4):216-222.
18. Wendell RP. Brown recluse spiders: a review to help guide physicians in non-endemic areas. South Med J. 2003;96(5):486–90.
19. Rees RS, Altenbern DP, Lynch JB, King LE Jr. Brown recluse spider bites: a comparison of early surgical excision versus dapsone and delayed surgical excision. Ann Surg. 1985;202 (5):659-663.
20. Webster GF. Is topical dapsone safe in glucose-6-phosphate dehydrogenase-deficient and sulfonamide-allergic patients? J Drugs Dermatol. 2010;9(5):532-536.
21. Merchant ML, Hinton JF, Geren CR. Effect of hyperbaric oxygen on sphingomyelinase D activity of brown recluse spider (Loxosceles reclusa) venom as studied by 31P nuclear magnetic resonance spectroscopy. Am J Trop Med Hyg. 1997;56(3):335-338.
22. Bennett RG, Vetter RS. An approach to spider bites: erroneous attribution of dermonecrotic lesions to brown recluse or hobo spider bites in Canada. Can Fam Physician. 2004;50:1098-1101.
23. MedlinePlus, US National Library of Medicine, NIH. Brown recluse spider. www.mdconsult.com/das/patient/body/225048384-2/0/10041/32560.html. Accessed November 23, 2010.
Oncologic Emergencies: Endocrinologic/Metabolic, Hematologic, Renal/Urologic, Dermatologic/Immunologic, GI, and Pain
Illuminating Community-Acquired Pneumonia
Minimizing Blood Loss in Major Spinal Surgery: A Review of the Current Literature
Outcomes of Arthroscopic Versus Open Rotator Cuff Repair: A Systematic Review of the Literature
UPDATE: URINARY INCONTINENCE
Pelvic organ prolapse (POP) is no small problem. With a prevalence thought to range as high as 30%, the condition challenges us to manage resources in a way that is mindful of cost—both financial expense and cost to the patient in terms of recovery and quality of life.
Although a large percentage of women who have POP also complain of symptomatic incontinence, a substantial number of continent women who have severe POP become incontinent after surgical repair. One reason may be that advanced POP sometimes causes urethral kinking and external urethral compression, fixing a hypermobile urethra in place. Once normal anatomy is restored and the urethra is no longer kinked, the urinary incontinence is “unmasked.”
Women who develop de novo incontinence after POP repair are thought to have “occult” urinary incontinence. Occult stress incontinence is urinary leakage that is prevented by POP and becomes symptomatic only after restoration of pelvic anatomy.1 It has been reported that 36% to 80% of continent women who have POP will develop stress urinary incontinence once the prolapse is reduced, either preoperatively with a pessary or vaginal pack, or after surgical correction.2
This information prompts important questions: If a woman who has POP is continent at the time of her surgical repair, should she undergo a concomitant incontinence procedure “just in case”? Or should she be reevaluated postoperatively for a possible continence procedure at a later time?
The colpopexy and urinary reduction efforts (CARE) trial concluded that postoperative stress incontinence in continent women is significantly reduced when sacrocolpopexy is combined with Burch urethropexy (FIGURE).3 When women who underwent a concomitant Burch procedure were compared with those who didn’t, de novo stress incontinence after prolapse repair occurred in 24% and 44% of women, respectively.3,4 This finding suggests that Burch urethropexy provides a protective benefit for continent women when it is performed at the time of abdominal sacrocolpopexy, eliminating the need for an additional procedure in the future.
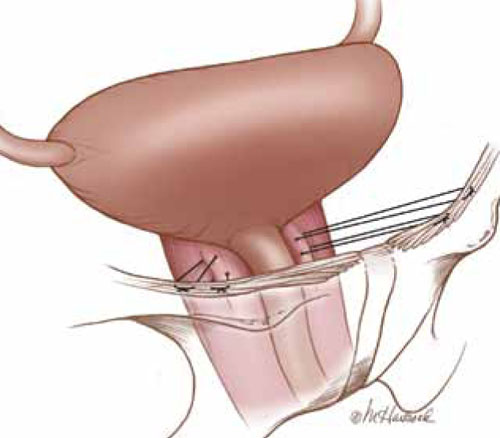
FIGURE: Burch urethropexy
Sutures are placed at the level of the bladder neck and passed through the Cooper’s ligaments to support the urethra and eliminate stress urinary incontinence.
Publication of the CARE findings sparked debate among pelvic surgeons. According to a recent survey of pelvic surgeons, only 50% changed their practice as a result of the CARE trial.5 Some argue that the addition of a continence procedure adds unnecessary surgical risk when the patient lacks subjective or objective evidence of stress incontinence. Besides the surgical risks—which, one might argue, are low—continence surgery may lead to new symptoms of urinary dysfunction, such as urinary obstruction or new-onset urge incontinence. The development of such symptoms can create significant dissatisfaction in a patient who was previously asymptomatic.
This article explores the issue in more depth, focusing on two recent studies:
- analysis of CARE trial data to determine the positive predictive value of preoperative prolapse reduction and urodynamic testing among continent women who have POP
- a retrospective comparison of women who had urodynamically confirmed occult incontinence with those who didn’t, along with their response to different interventions.
What’s the best way to assess women for occult stress incontinence?
Visco AG, Brubaker L, Nygaard I, et al; for Pelvic Floor Disorders Network. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):607–614.
Elser DM, Moen MD, Stanford EJ, et al. Abdominal sacrocolpopexy and urinary incontinence: surgical planning based on urodynamics. Am J Obstet Gynecol. 2010;202(4):375.e1–5.
Preoperative urodynamic testing is often used to evaluate women undergoing pelvic and continence surgery. For adequate evaluation, the prolapse must be reduced sufficiently to simulate the support achieved with the planned surgery. The techniques used to reduce the prolapse during the testing are variable, as is the predictive value of the urodynamic evaluation.
Prolapse may be reduced using a large cotton swab, ring forceps, pessary, or split speculum. When these methods and the utility of urodynamics were evaluated as part of the CARE trial, Visco and colleagues demonstrated that reduction of the prolapse with a large swab yielded the highest positive predictive value. Women who had urodynamically confirmed stress incontinence after the prolapse was reduced with a swab were more likely to develop symptomatic stress incontinence after sacrocolpopexy.
In this study, 35% of women who did not demonstrate occult incontinence during preoperative testing with the swab also went on to develop postoperative incontinence. Overall, urodynamic testing was not helpful in the evaluation of women who had POP. However, asymptomatic women who leaked during preoperative evaluation were more likely to experience incontinence postoperatively, even if they underwent Burch urethropexy.
1. Long CY, Hsu SC, Wu TP, Sun DJ, Su JH, Tsai EM. Urodynamic comparison of continent and incontinent women with severe uterovaginal prolapse. J Reprod Med. 2004;49(1):33-37.
2. Roovers JP, Oelke M. Clinical relevance of urodynamic investigation tests prior to surgical correction of genital prolapse: a literature review. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(4):455-460.
3. Brubaker L, Cundiff GW, Fine P, et al. Abdominal sacrocolpopexy with Burch colposuspension to reduce urinary stress incontinence. N Engl J Med. 2006;354(15):1557-1566.
4. Brubaker L, Nygaard I, Richter HE, et al. Two-year outcomes after sacrocolpopexy with and without Burch to prevent stress urinary incontinence. Obstet Gynecol. 2008;112(1):49-55.
5. Aungst MJ, Mamienski TD, Albright TS, Zahn CM, Fischer JR. Prophylactic Burch colposuspension at the time of abdominal sacrocolpopexy: a survey of current practice patterns. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(8):897-904.
6. Ward KL, Hilton P. Prospective multicentre randomised trial of tension-free vaginal tape and colposuspension as primary treatment for stress incontinence. BMJ. 2002;325(735):67-70.
7. Barber MD, Kleeman S, Karram MM, et al. Transobturator tape compared with tension-free vaginal tape for the treatment of stress urinary incontinence. Obstet Gynecol. 2008;111(3):611-621.
8. Kennelly MJ, Moore R, Nguyen JN, Lukban JC, Siegel S. Prospective evaluation of a single incision sling for stress urinary incontinence. J Urol. 2010;184(2):604-609.
Pelvic organ prolapse (POP) is no small problem. With a prevalence thought to range as high as 30%, the condition challenges us to manage resources in a way that is mindful of cost—both financial expense and cost to the patient in terms of recovery and quality of life.
Although a large percentage of women who have POP also complain of symptomatic incontinence, a substantial number of continent women who have severe POP become incontinent after surgical repair. One reason may be that advanced POP sometimes causes urethral kinking and external urethral compression, fixing a hypermobile urethra in place. Once normal anatomy is restored and the urethra is no longer kinked, the urinary incontinence is “unmasked.”
Women who develop de novo incontinence after POP repair are thought to have “occult” urinary incontinence. Occult stress incontinence is urinary leakage that is prevented by POP and becomes symptomatic only after restoration of pelvic anatomy.1 It has been reported that 36% to 80% of continent women who have POP will develop stress urinary incontinence once the prolapse is reduced, either preoperatively with a pessary or vaginal pack, or after surgical correction.2
This information prompts important questions: If a woman who has POP is continent at the time of her surgical repair, should she undergo a concomitant incontinence procedure “just in case”? Or should she be reevaluated postoperatively for a possible continence procedure at a later time?
The colpopexy and urinary reduction efforts (CARE) trial concluded that postoperative stress incontinence in continent women is significantly reduced when sacrocolpopexy is combined with Burch urethropexy (FIGURE).3 When women who underwent a concomitant Burch procedure were compared with those who didn’t, de novo stress incontinence after prolapse repair occurred in 24% and 44% of women, respectively.3,4 This finding suggests that Burch urethropexy provides a protective benefit for continent women when it is performed at the time of abdominal sacrocolpopexy, eliminating the need for an additional procedure in the future.
FIGURE: Burch urethropexy
Sutures are placed at the level of the bladder neck and passed through the Cooper’s ligaments to support the urethra and eliminate stress urinary incontinence.
Publication of the CARE findings sparked debate among pelvic surgeons. According to a recent survey of pelvic surgeons, only 50% changed their practice as a result of the CARE trial.5 Some argue that the addition of a continence procedure adds unnecessary surgical risk when the patient lacks subjective or objective evidence of stress incontinence. Besides the surgical risks—which, one might argue, are low—continence surgery may lead to new symptoms of urinary dysfunction, such as urinary obstruction or new-onset urge incontinence. The development of such symptoms can create significant dissatisfaction in a patient who was previously asymptomatic.
This article explores the issue in more depth, focusing on two recent studies:
- analysis of CARE trial data to determine the positive predictive value of preoperative prolapse reduction and urodynamic testing among continent women who have POP
- a retrospective comparison of women who had urodynamically confirmed occult incontinence with those who didn’t, along with their response to different interventions.
What’s the best way to assess women for occult stress incontinence?
Visco AG, Brubaker L, Nygaard I, et al; for Pelvic Floor Disorders Network. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):607–614.
Elser DM, Moen MD, Stanford EJ, et al. Abdominal sacrocolpopexy and urinary incontinence: surgical planning based on urodynamics. Am J Obstet Gynecol. 2010;202(4):375.e1–5.
Preoperative urodynamic testing is often used to evaluate women undergoing pelvic and continence surgery. For adequate evaluation, the prolapse must be reduced sufficiently to simulate the support achieved with the planned surgery. The techniques used to reduce the prolapse during the testing are variable, as is the predictive value of the urodynamic evaluation.
Prolapse may be reduced using a large cotton swab, ring forceps, pessary, or split speculum. When these methods and the utility of urodynamics were evaluated as part of the CARE trial, Visco and colleagues demonstrated that reduction of the prolapse with a large swab yielded the highest positive predictive value. Women who had urodynamically confirmed stress incontinence after the prolapse was reduced with a swab were more likely to develop symptomatic stress incontinence after sacrocolpopexy.
In this study, 35% of women who did not demonstrate occult incontinence during preoperative testing with the swab also went on to develop postoperative incontinence. Overall, urodynamic testing was not helpful in the evaluation of women who had POP. However, asymptomatic women who leaked during preoperative evaluation were more likely to experience incontinence postoperatively, even if they underwent Burch urethropexy.
Pelvic organ prolapse (POP) is no small problem. With a prevalence thought to range as high as 30%, the condition challenges us to manage resources in a way that is mindful of cost—both financial expense and cost to the patient in terms of recovery and quality of life.
Although a large percentage of women who have POP also complain of symptomatic incontinence, a substantial number of continent women who have severe POP become incontinent after surgical repair. One reason may be that advanced POP sometimes causes urethral kinking and external urethral compression, fixing a hypermobile urethra in place. Once normal anatomy is restored and the urethra is no longer kinked, the urinary incontinence is “unmasked.”
Women who develop de novo incontinence after POP repair are thought to have “occult” urinary incontinence. Occult stress incontinence is urinary leakage that is prevented by POP and becomes symptomatic only after restoration of pelvic anatomy.1 It has been reported that 36% to 80% of continent women who have POP will develop stress urinary incontinence once the prolapse is reduced, either preoperatively with a pessary or vaginal pack, or after surgical correction.2
This information prompts important questions: If a woman who has POP is continent at the time of her surgical repair, should she undergo a concomitant incontinence procedure “just in case”? Or should she be reevaluated postoperatively for a possible continence procedure at a later time?
The colpopexy and urinary reduction efforts (CARE) trial concluded that postoperative stress incontinence in continent women is significantly reduced when sacrocolpopexy is combined with Burch urethropexy (FIGURE).3 When women who underwent a concomitant Burch procedure were compared with those who didn’t, de novo stress incontinence after prolapse repair occurred in 24% and 44% of women, respectively.3,4 This finding suggests that Burch urethropexy provides a protective benefit for continent women when it is performed at the time of abdominal sacrocolpopexy, eliminating the need for an additional procedure in the future.
FIGURE: Burch urethropexy
Sutures are placed at the level of the bladder neck and passed through the Cooper’s ligaments to support the urethra and eliminate stress urinary incontinence.
Publication of the CARE findings sparked debate among pelvic surgeons. According to a recent survey of pelvic surgeons, only 50% changed their practice as a result of the CARE trial.5 Some argue that the addition of a continence procedure adds unnecessary surgical risk when the patient lacks subjective or objective evidence of stress incontinence. Besides the surgical risks—which, one might argue, are low—continence surgery may lead to new symptoms of urinary dysfunction, such as urinary obstruction or new-onset urge incontinence. The development of such symptoms can create significant dissatisfaction in a patient who was previously asymptomatic.
This article explores the issue in more depth, focusing on two recent studies:
- analysis of CARE trial data to determine the positive predictive value of preoperative prolapse reduction and urodynamic testing among continent women who have POP
- a retrospective comparison of women who had urodynamically confirmed occult incontinence with those who didn’t, along with their response to different interventions.
What’s the best way to assess women for occult stress incontinence?
Visco AG, Brubaker L, Nygaard I, et al; for Pelvic Floor Disorders Network. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):607–614.
Elser DM, Moen MD, Stanford EJ, et al. Abdominal sacrocolpopexy and urinary incontinence: surgical planning based on urodynamics. Am J Obstet Gynecol. 2010;202(4):375.e1–5.
Preoperative urodynamic testing is often used to evaluate women undergoing pelvic and continence surgery. For adequate evaluation, the prolapse must be reduced sufficiently to simulate the support achieved with the planned surgery. The techniques used to reduce the prolapse during the testing are variable, as is the predictive value of the urodynamic evaluation.
Prolapse may be reduced using a large cotton swab, ring forceps, pessary, or split speculum. When these methods and the utility of urodynamics were evaluated as part of the CARE trial, Visco and colleagues demonstrated that reduction of the prolapse with a large swab yielded the highest positive predictive value. Women who had urodynamically confirmed stress incontinence after the prolapse was reduced with a swab were more likely to develop symptomatic stress incontinence after sacrocolpopexy.
In this study, 35% of women who did not demonstrate occult incontinence during preoperative testing with the swab also went on to develop postoperative incontinence. Overall, urodynamic testing was not helpful in the evaluation of women who had POP. However, asymptomatic women who leaked during preoperative evaluation were more likely to experience incontinence postoperatively, even if they underwent Burch urethropexy.
1. Long CY, Hsu SC, Wu TP, Sun DJ, Su JH, Tsai EM. Urodynamic comparison of continent and incontinent women with severe uterovaginal prolapse. J Reprod Med. 2004;49(1):33-37.
2. Roovers JP, Oelke M. Clinical relevance of urodynamic investigation tests prior to surgical correction of genital prolapse: a literature review. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(4):455-460.
3. Brubaker L, Cundiff GW, Fine P, et al. Abdominal sacrocolpopexy with Burch colposuspension to reduce urinary stress incontinence. N Engl J Med. 2006;354(15):1557-1566.
4. Brubaker L, Nygaard I, Richter HE, et al. Two-year outcomes after sacrocolpopexy with and without Burch to prevent stress urinary incontinence. Obstet Gynecol. 2008;112(1):49-55.
5. Aungst MJ, Mamienski TD, Albright TS, Zahn CM, Fischer JR. Prophylactic Burch colposuspension at the time of abdominal sacrocolpopexy: a survey of current practice patterns. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(8):897-904.
6. Ward KL, Hilton P. Prospective multicentre randomised trial of tension-free vaginal tape and colposuspension as primary treatment for stress incontinence. BMJ. 2002;325(735):67-70.
7. Barber MD, Kleeman S, Karram MM, et al. Transobturator tape compared with tension-free vaginal tape for the treatment of stress urinary incontinence. Obstet Gynecol. 2008;111(3):611-621.
8. Kennelly MJ, Moore R, Nguyen JN, Lukban JC, Siegel S. Prospective evaluation of a single incision sling for stress urinary incontinence. J Urol. 2010;184(2):604-609.
1. Long CY, Hsu SC, Wu TP, Sun DJ, Su JH, Tsai EM. Urodynamic comparison of continent and incontinent women with severe uterovaginal prolapse. J Reprod Med. 2004;49(1):33-37.
2. Roovers JP, Oelke M. Clinical relevance of urodynamic investigation tests prior to surgical correction of genital prolapse: a literature review. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(4):455-460.
3. Brubaker L, Cundiff GW, Fine P, et al. Abdominal sacrocolpopexy with Burch colposuspension to reduce urinary stress incontinence. N Engl J Med. 2006;354(15):1557-1566.
4. Brubaker L, Nygaard I, Richter HE, et al. Two-year outcomes after sacrocolpopexy with and without Burch to prevent stress urinary incontinence. Obstet Gynecol. 2008;112(1):49-55.
5. Aungst MJ, Mamienski TD, Albright TS, Zahn CM, Fischer JR. Prophylactic Burch colposuspension at the time of abdominal sacrocolpopexy: a survey of current practice patterns. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(8):897-904.
6. Ward KL, Hilton P. Prospective multicentre randomised trial of tension-free vaginal tape and colposuspension as primary treatment for stress incontinence. BMJ. 2002;325(735):67-70.
7. Barber MD, Kleeman S, Karram MM, et al. Transobturator tape compared with tension-free vaginal tape for the treatment of stress urinary incontinence. Obstet Gynecol. 2008;111(3):611-621.
8. Kennelly MJ, Moore R, Nguyen JN, Lukban JC, Siegel S. Prospective evaluation of a single incision sling for stress urinary incontinence. J Urol. 2010;184(2):604-609.
Sound strategies to avoid malpractice hazards on labor and delivery
CASE: Is TOLAC feasible?
Your patient is a 33-year-old gravida 3, para 2002, with a previous cesarean delivery who was admitted to labor and delivery with premature ruptured membranes at term. She is not contracting. Fetal status is reassuring.
Her obstetric history is of one normal, spontaneous delivery followed by one cesarean delivery, both occurring at term.
She wants to know if she can safely undergo a trial of labor, or if she must have a repeat cesarean delivery. How should you counsel her?
At the start of any discussion about how to reduce your risk of being sued for malpractice because of your work as an obstetrician, in particular during labor and delivery, two distinct, underlying avenues of concern need to be addressed. Before moving on to discuss strategy, then, let’s consider what they are and how they arise: Allegation (perception). You are at risk of an allegation of malpractice (or of a perception of malpractice) because of an unexpected event or outcome for mother or baby. Allegation and perception can arise apart from any specific clinical action you undertook, or did not undertake. An example? Counseling about options for care that falls short of full understanding by the patient.
Allegation and perception are the subjects of this first installment of our two-part article on strategies for avoiding claims of malpractice in L & D that begin with the first prenatal visit.
Causation. Your actions—what you do in the course of providing prenatal care and delivering a baby—put you at risk of a charge of malpractice when you have provided medical care that 1) is inconsistent with current medical practice and thus 2) harmed the mother or newborn.
For a medical malpractice case to go forward, it must meet a well-defined paradigm that teases apart components of causation, beginning with your duty to the patient (TABLE 1).
TABLE 1 Signposts in the medical malpractice paradigm
| When the clinical issue at hand is … | … Then the legal term is … |
|---|---|
| A health-care professional’s obligation to provide care | “Duty” |
| A deviation in the care that was provided | “Standard of care” |
| An allegation that a breach in the standard of care resulted in injury | “Proximate cause” |
| An assertion or finding that an injury is “compensable” | “Damages” |
| Source: Yale New Haven Medical Center, 1997.5 | |
Allegation of malpractice arises from a range of sources, as we’ll discuss, but it is causation that reflects the actual, hands-on practice of medicine. We’ll examine strategies for avoiding charges of causation in the second part of this article.
(For now, we’ll just note that a recent excellent review of intrapartum interventions and their basis in evidence1 offers a model for evaluating a number of widely utilized practices in obstetrics. The goal, of course, is to minimize bad outcomes that follow from causation. Regrettably, that evidence-based approach is a limited one, because of a paucity of adequately controlled studies about OB practice.)
CASE: Continued
You consider your patient’s comment that she would like to avoid a repeat cesarean delivery, and advise her that she may safely attempt vaginal birth.
When spontaneous labor does not occur in 6 hours, oxytocin is administered. She dilates to 9 cm and begins to push spontaneously.
The fetal heart rate then drops to 70/min; fetal station, which had been +2, is now -1. A Stat cesarean delivery is performed. Uterine rupture with partial fetal expulsion is found. Apgar scores are 1, 3, and 5 at 1, 5, and 10 minutes.
Your patient requires a hysterectomy to control bleeding.
Some broad considerations for the physician arising from this CASE
- The counseling that you provide to a patient should be nondirective; it should include your opinion, however, about the best option available to her. Insert yourself into this hypothetical case, for discussion’s sake: Did you provide that important opinion to her?
- You must make certain that she clearly understands the risks and benefits of a procedure or other action, and the available alternatives. Did you undertake a check of her comprehension, given the anxiety and confusion of the moment?
- When an adverse outcome ensues—however unlikely it was to occur—it is necessary for you to review the circumstances with the patient as soon as clinically possible. Did you “debrief” and counsel her before and after the hysterectomy?
No more “perfect outcomes”: Our role changed, so did our risk
From the moment an OB patient enters triage, until her arrival home with her infant, this crucial period of her life is colored by concern, curiosity, myth, and fear.
Every woman anticipates the birth of a healthy infant. In an earlier era, the patient and her family relied on the sage advice of their physician to ensure this outcome. To an extent, physicians themselves reinforced this reliance, embracing the notion that they were, in fact, able to provide such a perfect outcome.
With advances that have been made in reproductive medicine, pregnancy has become more readily available to women with increasingly advanced disease; this has made labor and delivery more challenging to them and to their physicians. Realistically, our role as physicians is now better expressed as providing advice to help a woman achieve the best possible outcome, recognizing her individual clinical circumstances, instead of ensuring a perfect outcome.
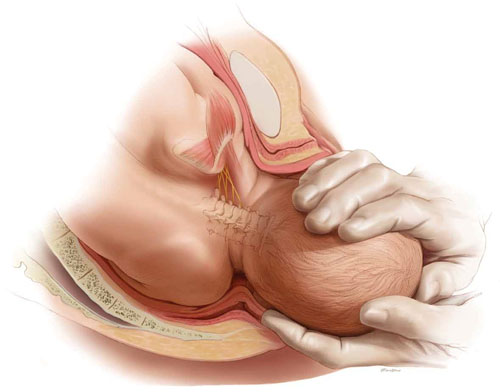
Every woman anticipates the birth of a healthy baby. But the role of the OB is better expressed as helping her achieve the best possible outcome, not a perfect outcome. ABOVE: Shoulder dystocia is one of the most treacherous and frightening—and litigated—complications of childbirth, yet it is, for the most part, unpredictable and unpreventable in the course of even routine delivery.
Key concept #1
COMMUNICATION
Communication is central to patients’ comprehension about the care that you provide to them. But to enter a genuine dialogue with a patient under your care, and with her family, can challenge your communication skills.
First, you need written and verbal skills. Second, you need to know how to read visual cues.
Third, the messages that you deliver to the patient are influenced by:
- your style of communication
- your cultural background
- the setting in which you’re providing care (office, hospital).
Where are such skills developed? For one, biopsychosocial models that are employed in medical student education and resident training aid the physician in developing appropriate communication skills.
But training alone cannot overcome the fact that communication is a double-sided activity: Patients bring many of their own variables to a dialogue. How patients understand and interact with you—and with other providers and the health-care system—is not, therefore, directly or strictly within your sphere of influence.
Yet your sensitivity to a patient’s issues can go a long way toward ameliorating her misconceptions and prejudices. Here are several suggestions, developed by others, to optimize patients’ understanding of their care2,3:
- Apply what’s known as flip default. Assume the patient does not understand the information that you’re providing. Ask her to repeat your instructions back to you (as is done with a verbal order in the hospital).
- Manage face-to-face time effectively. Don’t attempt to teach a patient everything about her care at once. Focus on the critical aspects of her case and on providing understanding; use a strategy of sequential learning.
- Reduce the “overwhelm” factor. Periodically, stop and ask the patient if she has questions. Don’t wait until the end of the appointment to do this.
- Eliminate jargon. When you notify a patient about the results of testing, for example, clarify what the results say about her health and mean for her care. Do so in plain language.
- Recognize her preconceptions. Discuss any psychosocial issues head on with the patient. Use an interpreter or a social worker, or counselors from other fields, as appropriate.
Remember: All health-care personnel need to understand the importance of making the patient comfortable in the often foreign, and sometimes sterile, milieu of the medical office and hospital.
Key concept #2
TRUST
Trust between patient and clinician is, we believe, the most basic necessity for ameliorating allegations of malpractice—secondary only, perhaps, to your knowledge of medicine.
Trust can be enhanced by interactions that demonstrate to both parties the advisability of working together to resolve a problem. Any aspect of the physician-patient interaction that is potentially adversarial does not serve the interests of either.
We encourage you to construct a communication bridge, so to speak, with your patient. Begin by:
- introducing yourself to her and explaining your role in her care
- making appropriate eye contact with her
- maintaining a positive attitude
- dressing appropriately
- making her feel that she is your No. 1 priority.
There is more.
Recognize the duality of respect
- Ask the patient how she wishes to be addressed
- Ask about her belief system
- Explain the specifics of her care without arrogance.
Engender trust
- Be honest with her
- Be on her side
- Take time with her
- Allow her the right that she has to select from the options or to refuse treatment
- Disclose to the patient your status as a student or resident, if that is your rank.
Recognize the benefits of partnership
Forging a partnership with the patient:
- improves the accuracy of information
- eases ongoing communication
- facilitates informed consent
- provides an opportunity for you to educate her.
TABLE 2 When building trust, both patient and physician
are charged with responsibilities
| In regard to … | The patient’s responsibility is to … | The physician’s responsibility is to … |
|---|---|---|
| Gathering an honest and complete medical history | Know and report | Question completely |
| Being adherent to prescribed care | Follow through | Make reasonable demands |
| Making decisions about care | Ask questions and actively participate in choices Make realistic requests | Be knowledgeable about available alternatives Individualize options |
Key concept #3
SHARED RESPONSIBILITY
Patient and physician both have responsibilities that are important to achieving an optimal outcome; so does the hospital (TABLE 2 and TABLE 3). Both patient and physician should practice full disclosure throughout the course of care; this will benefit both of you.4 Here are a few select examples.
TABLE 3 Relative degrees of responsibility for a good outcome
vary across interested parties, but none are exempt
| Area of emphasis | Hospital’s responsibility | Physician’s responsibility | Patient’s responsibility |
|---|---|---|---|
| Creating a positive environment for care | 3+ | 2+ | 1+ |
| Providing clear communication | 3+ | 3+ | 3+ |
| Obtaining informed consent | 3+ | 3+ | 3+ |
| Making reasonable requests | 1+ | 1+ | 3+ |
| Compliance | 3+ | 3+ | 3+ |
| Key to the relative scale: 1+: at the least, minimally responsible; 2+: at the least, somewhat responsible; 3+, responsible to the greatest degree. | |||
The importance of the intake form
At the outset of OB care, in most practices, the patient provides the initial detailed medical history by completing a form in the waiting room. In reviewing and completing this survey with her during the appointment, pay particular attention to those questions for which the response has been left blank.
Patients need to understand that key recommendations about their care, and a proper analysis of their concerns, are based on the information that they provide on this survey. In our practices, we find that patients answer most of these early questions without difficulty—even inquiries of a personal nature, such as the number of prior pregnancies, or drug, alcohol, and smoking habits—as long as they understand why it’s in their best interests for you to have this information. If they leave a question blank and you do not follow up verbally, you may have lost invaluable information that can affect the outcome of her pregnancy.
What should you do when, occasionally, a patient refuses to answer one of your questions? We recommend that you record her refusal on the form itself, where the note remains part of the record.
Keep in mind that all necessary and useful information about a patient may not be available, or may not be appropriate to consider, at the initial prenatal visit. In that case, you have an ongoing opportunity—at subsequent visits during the pregnancy—to develop her full medical profile and algorithm.
The necessity of adherence
It almost goes without saying: To provide the care that our patients need, we sometimes require the unpleasant of them—to undergo evaluations, or testing, or to take medications that may be inconvenient or costly.
After you explain the specific course of care to a patient—whether you’re ordering a test or writing a prescription—your follow-up must include notation in the record of adherence. The fact is that both of you share responsibility for having her understand the importance of adherence to your instructions and the consequences of limited adherence or nonadherence.
Recall one of the lessons from the case that introduced this article: For the patient to make an informed decision about her care, the clinician must have thorough knowledge of 1) the risks and benefits of whatever intervention is being proposed in the particular clinical scenario and 2) the available alternatives. It is key that you communicate your risk-benefit assessment accurately to the patient.
Follow-up
Sometimes, new medical problems arise during subsequent prenatal visits. Follow-up appointments also provide an opportunity for you to expand your attention to problems identified earlier. Regardless of what the patient reported about her history and current health at the initial prenatal visit, listen for her to bring new issues to light for resolution later in the pregnancy that will have an impact on L & D. Again, it goes without saying but needs to be said: The OB clinician needs to have whatever skills are necessary to 1) fully evaluate the progress of a pregnancy and 2) make recommendations for care in light of changes in the status of mother and fetus along the way.
TABLE 4 Examples of the cardinal rule of “Be specific”
when you document care
| Instead of noting … | … Use alternative wording |
|---|---|
| “Mild vaginal bleeding” | “Vaginal bleeding requiring two pads an hour” |
| “Gentle traction” | “The shoulders were rotated before assisting the patient’s expulsive efforts” |
| “Patient refuses…” [or “declines…”] | “Patient voiced the nature of the problem and the alternatives that i have explained to her” |
| “Expedited cesarean section” | “The time from decision to incision was 35 minutes” |
Basic principles of documentation
The medical record is the best witness to interactions between a physician and a patient. In the record, we’re required to write a “5-C” description of events—namely, one that is:
- correct
- comprehensive
- conscientious
- clear
- contemporaneous.
Avoid medical jargon in the record. Be careful not to use vague terminology or descriptions, such as “mild vaginal bleeding,” “gentle traction,” or “patient refuses and accepts the consequences.” Specificity is the key to accuracy with respect to documentation (TABLE 4).
Editor’s note: Part 2 of this article will appear in the January 2011 issue of OBG Management. The authors’ analysis of L & D malpractice claims moves to a discussion of causation—by way of 4 troubling cases.
You’ll find a rich, useful archive of expert analysis of your professional liability and malpractice risk, at www.obgmanagement.com
• 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
• After a patient’s unexpected death, First Aid for the emotionally wounded
Ronald A. Chez, MD, and Wayne Fortin, MS (April 2010)
• Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates, Senior Editor, with Lewis Laska, JD, PhD (October 2009)
• Can a change in practice patterns reduce the number of OB malpractice claims?
Jason K. Baxter, MD, MSCP, and Louis Weinstein, MD (April 2009)
• Strategies for breaking bad news to patients
Barry Bub, MD (September 2008)
• Stuff of nightmares: Criminal prosecution for malpractice
Gary Steinman, MD, PhD (August 2008)
• Deposition Dos and Don’ts: How to answer 8 tricky questions
James L. Knoll, IV, MD, and Phillip J. Resnick, MD (May 2008)
• Playing high-stakes poker: Do you fight—or settle—that malpractice lawsuit?
Jeffrey Segal, MD (April 2008)
We want to hear from you! Tell us what you think.
1. Berghella V, Baxter JK, Chauhan SP. Evidence-based labor and delivery management. Am J Obstet Gynecol. 2008;199(5):445-454.
2. Paasche-Orlow MK, Riekert KA, Bilderback A, et al. Tailored education may reduce health literacy disparities in asthma self-management. Am J Respir Crit Care Med. 2005;172:980-986.
3. Huvane K. Health literacy: reading is just the beginning. Focus on multicultural healthcare. 2007;3(4):16-19.
4. Giordano K. Legal Principles. In: O’Grady JP, Gimovsky ML, Bayer-Zwirello L, Giordano K, eds. Operative Obstetrics. 2nd ed. New York: Cambridge University Press; 2008.
5. The Four Elements of Medical Malpractice Yale New Haven Medical Center: Issues in Risk Management. 1997.
CASE: Is TOLAC feasible?
Your patient is a 33-year-old gravida 3, para 2002, with a previous cesarean delivery who was admitted to labor and delivery with premature ruptured membranes at term. She is not contracting. Fetal status is reassuring.
Her obstetric history is of one normal, spontaneous delivery followed by one cesarean delivery, both occurring at term.
She wants to know if she can safely undergo a trial of labor, or if she must have a repeat cesarean delivery. How should you counsel her?
At the start of any discussion about how to reduce your risk of being sued for malpractice because of your work as an obstetrician, in particular during labor and delivery, two distinct, underlying avenues of concern need to be addressed. Before moving on to discuss strategy, then, let’s consider what they are and how they arise: Allegation (perception). You are at risk of an allegation of malpractice (or of a perception of malpractice) because of an unexpected event or outcome for mother or baby. Allegation and perception can arise apart from any specific clinical action you undertook, or did not undertake. An example? Counseling about options for care that falls short of full understanding by the patient.
Allegation and perception are the subjects of this first installment of our two-part article on strategies for avoiding claims of malpractice in L & D that begin with the first prenatal visit.
Causation. Your actions—what you do in the course of providing prenatal care and delivering a baby—put you at risk of a charge of malpractice when you have provided medical care that 1) is inconsistent with current medical practice and thus 2) harmed the mother or newborn.
For a medical malpractice case to go forward, it must meet a well-defined paradigm that teases apart components of causation, beginning with your duty to the patient (TABLE 1).
TABLE 1 Signposts in the medical malpractice paradigm
| When the clinical issue at hand is … | … Then the legal term is … |
|---|---|
| A health-care professional’s obligation to provide care | “Duty” |
| A deviation in the care that was provided | “Standard of care” |
| An allegation that a breach in the standard of care resulted in injury | “Proximate cause” |
| An assertion or finding that an injury is “compensable” | “Damages” |
| Source: Yale New Haven Medical Center, 1997.5 | |
Allegation of malpractice arises from a range of sources, as we’ll discuss, but it is causation that reflects the actual, hands-on practice of medicine. We’ll examine strategies for avoiding charges of causation in the second part of this article.
(For now, we’ll just note that a recent excellent review of intrapartum interventions and their basis in evidence1 offers a model for evaluating a number of widely utilized practices in obstetrics. The goal, of course, is to minimize bad outcomes that follow from causation. Regrettably, that evidence-based approach is a limited one, because of a paucity of adequately controlled studies about OB practice.)
CASE: Continued
You consider your patient’s comment that she would like to avoid a repeat cesarean delivery, and advise her that she may safely attempt vaginal birth.
When spontaneous labor does not occur in 6 hours, oxytocin is administered. She dilates to 9 cm and begins to push spontaneously.
The fetal heart rate then drops to 70/min; fetal station, which had been +2, is now -1. A Stat cesarean delivery is performed. Uterine rupture with partial fetal expulsion is found. Apgar scores are 1, 3, and 5 at 1, 5, and 10 minutes.
Your patient requires a hysterectomy to control bleeding.
Some broad considerations for the physician arising from this CASE
- The counseling that you provide to a patient should be nondirective; it should include your opinion, however, about the best option available to her. Insert yourself into this hypothetical case, for discussion’s sake: Did you provide that important opinion to her?
- You must make certain that she clearly understands the risks and benefits of a procedure or other action, and the available alternatives. Did you undertake a check of her comprehension, given the anxiety and confusion of the moment?
- When an adverse outcome ensues—however unlikely it was to occur—it is necessary for you to review the circumstances with the patient as soon as clinically possible. Did you “debrief” and counsel her before and after the hysterectomy?
No more “perfect outcomes”: Our role changed, so did our risk
From the moment an OB patient enters triage, until her arrival home with her infant, this crucial period of her life is colored by concern, curiosity, myth, and fear.
Every woman anticipates the birth of a healthy infant. In an earlier era, the patient and her family relied on the sage advice of their physician to ensure this outcome. To an extent, physicians themselves reinforced this reliance, embracing the notion that they were, in fact, able to provide such a perfect outcome.
With advances that have been made in reproductive medicine, pregnancy has become more readily available to women with increasingly advanced disease; this has made labor and delivery more challenging to them and to their physicians. Realistically, our role as physicians is now better expressed as providing advice to help a woman achieve the best possible outcome, recognizing her individual clinical circumstances, instead of ensuring a perfect outcome.
Every woman anticipates the birth of a healthy baby. But the role of the OB is better expressed as helping her achieve the best possible outcome, not a perfect outcome. ABOVE: Shoulder dystocia is one of the most treacherous and frightening—and litigated—complications of childbirth, yet it is, for the most part, unpredictable and unpreventable in the course of even routine delivery.
Key concept #1
COMMUNICATION
Communication is central to patients’ comprehension about the care that you provide to them. But to enter a genuine dialogue with a patient under your care, and with her family, can challenge your communication skills.
First, you need written and verbal skills. Second, you need to know how to read visual cues.
Third, the messages that you deliver to the patient are influenced by:
- your style of communication
- your cultural background
- the setting in which you’re providing care (office, hospital).
Where are such skills developed? For one, biopsychosocial models that are employed in medical student education and resident training aid the physician in developing appropriate communication skills.
But training alone cannot overcome the fact that communication is a double-sided activity: Patients bring many of their own variables to a dialogue. How patients understand and interact with you—and with other providers and the health-care system—is not, therefore, directly or strictly within your sphere of influence.
Yet your sensitivity to a patient’s issues can go a long way toward ameliorating her misconceptions and prejudices. Here are several suggestions, developed by others, to optimize patients’ understanding of their care2,3:
- Apply what’s known as flip default. Assume the patient does not understand the information that you’re providing. Ask her to repeat your instructions back to you (as is done with a verbal order in the hospital).
- Manage face-to-face time effectively. Don’t attempt to teach a patient everything about her care at once. Focus on the critical aspects of her case and on providing understanding; use a strategy of sequential learning.
- Reduce the “overwhelm” factor. Periodically, stop and ask the patient if she has questions. Don’t wait until the end of the appointment to do this.
- Eliminate jargon. When you notify a patient about the results of testing, for example, clarify what the results say about her health and mean for her care. Do so in plain language.
- Recognize her preconceptions. Discuss any psychosocial issues head on with the patient. Use an interpreter or a social worker, or counselors from other fields, as appropriate.
Remember: All health-care personnel need to understand the importance of making the patient comfortable in the often foreign, and sometimes sterile, milieu of the medical office and hospital.
Key concept #2
TRUST
Trust between patient and clinician is, we believe, the most basic necessity for ameliorating allegations of malpractice—secondary only, perhaps, to your knowledge of medicine.
Trust can be enhanced by interactions that demonstrate to both parties the advisability of working together to resolve a problem. Any aspect of the physician-patient interaction that is potentially adversarial does not serve the interests of either.
We encourage you to construct a communication bridge, so to speak, with your patient. Begin by:
- introducing yourself to her and explaining your role in her care
- making appropriate eye contact with her
- maintaining a positive attitude
- dressing appropriately
- making her feel that she is your No. 1 priority.
There is more.
Recognize the duality of respect
- Ask the patient how she wishes to be addressed
- Ask about her belief system
- Explain the specifics of her care without arrogance.
Engender trust
- Be honest with her
- Be on her side
- Take time with her
- Allow her the right that she has to select from the options or to refuse treatment
- Disclose to the patient your status as a student or resident, if that is your rank.
Recognize the benefits of partnership
Forging a partnership with the patient:
- improves the accuracy of information
- eases ongoing communication
- facilitates informed consent
- provides an opportunity for you to educate her.
TABLE 2 When building trust, both patient and physician
are charged with responsibilities
| In regard to … | The patient’s responsibility is to … | The physician’s responsibility is to … |
|---|---|---|
| Gathering an honest and complete medical history | Know and report | Question completely |
| Being adherent to prescribed care | Follow through | Make reasonable demands |
| Making decisions about care | Ask questions and actively participate in choices Make realistic requests | Be knowledgeable about available alternatives Individualize options |
Key concept #3
SHARED RESPONSIBILITY
Patient and physician both have responsibilities that are important to achieving an optimal outcome; so does the hospital (TABLE 2 and TABLE 3). Both patient and physician should practice full disclosure throughout the course of care; this will benefit both of you.4 Here are a few select examples.
TABLE 3 Relative degrees of responsibility for a good outcome
vary across interested parties, but none are exempt
| Area of emphasis | Hospital’s responsibility | Physician’s responsibility | Patient’s responsibility |
|---|---|---|---|
| Creating a positive environment for care | 3+ | 2+ | 1+ |
| Providing clear communication | 3+ | 3+ | 3+ |
| Obtaining informed consent | 3+ | 3+ | 3+ |
| Making reasonable requests | 1+ | 1+ | 3+ |
| Compliance | 3+ | 3+ | 3+ |
| Key to the relative scale: 1+: at the least, minimally responsible; 2+: at the least, somewhat responsible; 3+, responsible to the greatest degree. | |||
The importance of the intake form
At the outset of OB care, in most practices, the patient provides the initial detailed medical history by completing a form in the waiting room. In reviewing and completing this survey with her during the appointment, pay particular attention to those questions for which the response has been left blank.
Patients need to understand that key recommendations about their care, and a proper analysis of their concerns, are based on the information that they provide on this survey. In our practices, we find that patients answer most of these early questions without difficulty—even inquiries of a personal nature, such as the number of prior pregnancies, or drug, alcohol, and smoking habits—as long as they understand why it’s in their best interests for you to have this information. If they leave a question blank and you do not follow up verbally, you may have lost invaluable information that can affect the outcome of her pregnancy.
What should you do when, occasionally, a patient refuses to answer one of your questions? We recommend that you record her refusal on the form itself, where the note remains part of the record.
Keep in mind that all necessary and useful information about a patient may not be available, or may not be appropriate to consider, at the initial prenatal visit. In that case, you have an ongoing opportunity—at subsequent visits during the pregnancy—to develop her full medical profile and algorithm.
The necessity of adherence
It almost goes without saying: To provide the care that our patients need, we sometimes require the unpleasant of them—to undergo evaluations, or testing, or to take medications that may be inconvenient or costly.
After you explain the specific course of care to a patient—whether you’re ordering a test or writing a prescription—your follow-up must include notation in the record of adherence. The fact is that both of you share responsibility for having her understand the importance of adherence to your instructions and the consequences of limited adherence or nonadherence.
Recall one of the lessons from the case that introduced this article: For the patient to make an informed decision about her care, the clinician must have thorough knowledge of 1) the risks and benefits of whatever intervention is being proposed in the particular clinical scenario and 2) the available alternatives. It is key that you communicate your risk-benefit assessment accurately to the patient.
Follow-up
Sometimes, new medical problems arise during subsequent prenatal visits. Follow-up appointments also provide an opportunity for you to expand your attention to problems identified earlier. Regardless of what the patient reported about her history and current health at the initial prenatal visit, listen for her to bring new issues to light for resolution later in the pregnancy that will have an impact on L & D. Again, it goes without saying but needs to be said: The OB clinician needs to have whatever skills are necessary to 1) fully evaluate the progress of a pregnancy and 2) make recommendations for care in light of changes in the status of mother and fetus along the way.
TABLE 4 Examples of the cardinal rule of “Be specific”
when you document care
| Instead of noting … | … Use alternative wording |
|---|---|
| “Mild vaginal bleeding” | “Vaginal bleeding requiring two pads an hour” |
| “Gentle traction” | “The shoulders were rotated before assisting the patient’s expulsive efforts” |
| “Patient refuses…” [or “declines…”] | “Patient voiced the nature of the problem and the alternatives that i have explained to her” |
| “Expedited cesarean section” | “The time from decision to incision was 35 minutes” |
Basic principles of documentation
The medical record is the best witness to interactions between a physician and a patient. In the record, we’re required to write a “5-C” description of events—namely, one that is:
- correct
- comprehensive
- conscientious
- clear
- contemporaneous.
Avoid medical jargon in the record. Be careful not to use vague terminology or descriptions, such as “mild vaginal bleeding,” “gentle traction,” or “patient refuses and accepts the consequences.” Specificity is the key to accuracy with respect to documentation (TABLE 4).
Editor’s note: Part 2 of this article will appear in the January 2011 issue of OBG Management. The authors’ analysis of L & D malpractice claims moves to a discussion of causation—by way of 4 troubling cases.
You’ll find a rich, useful archive of expert analysis of your professional liability and malpractice risk, at www.obgmanagement.com
• 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
• After a patient’s unexpected death, First Aid for the emotionally wounded
Ronald A. Chez, MD, and Wayne Fortin, MS (April 2010)
• Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates, Senior Editor, with Lewis Laska, JD, PhD (October 2009)
• Can a change in practice patterns reduce the number of OB malpractice claims?
Jason K. Baxter, MD, MSCP, and Louis Weinstein, MD (April 2009)
• Strategies for breaking bad news to patients
Barry Bub, MD (September 2008)
• Stuff of nightmares: Criminal prosecution for malpractice
Gary Steinman, MD, PhD (August 2008)
• Deposition Dos and Don’ts: How to answer 8 tricky questions
James L. Knoll, IV, MD, and Phillip J. Resnick, MD (May 2008)
• Playing high-stakes poker: Do you fight—or settle—that malpractice lawsuit?
Jeffrey Segal, MD (April 2008)
We want to hear from you! Tell us what you think.
CASE: Is TOLAC feasible?
Your patient is a 33-year-old gravida 3, para 2002, with a previous cesarean delivery who was admitted to labor and delivery with premature ruptured membranes at term. She is not contracting. Fetal status is reassuring.
Her obstetric history is of one normal, spontaneous delivery followed by one cesarean delivery, both occurring at term.
She wants to know if she can safely undergo a trial of labor, or if she must have a repeat cesarean delivery. How should you counsel her?
At the start of any discussion about how to reduce your risk of being sued for malpractice because of your work as an obstetrician, in particular during labor and delivery, two distinct, underlying avenues of concern need to be addressed. Before moving on to discuss strategy, then, let’s consider what they are and how they arise: Allegation (perception). You are at risk of an allegation of malpractice (or of a perception of malpractice) because of an unexpected event or outcome for mother or baby. Allegation and perception can arise apart from any specific clinical action you undertook, or did not undertake. An example? Counseling about options for care that falls short of full understanding by the patient.
Allegation and perception are the subjects of this first installment of our two-part article on strategies for avoiding claims of malpractice in L & D that begin with the first prenatal visit.
Causation. Your actions—what you do in the course of providing prenatal care and delivering a baby—put you at risk of a charge of malpractice when you have provided medical care that 1) is inconsistent with current medical practice and thus 2) harmed the mother or newborn.
For a medical malpractice case to go forward, it must meet a well-defined paradigm that teases apart components of causation, beginning with your duty to the patient (TABLE 1).
TABLE 1 Signposts in the medical malpractice paradigm
| When the clinical issue at hand is … | … Then the legal term is … |
|---|---|
| A health-care professional’s obligation to provide care | “Duty” |
| A deviation in the care that was provided | “Standard of care” |
| An allegation that a breach in the standard of care resulted in injury | “Proximate cause” |
| An assertion or finding that an injury is “compensable” | “Damages” |
| Source: Yale New Haven Medical Center, 1997.5 | |
Allegation of malpractice arises from a range of sources, as we’ll discuss, but it is causation that reflects the actual, hands-on practice of medicine. We’ll examine strategies for avoiding charges of causation in the second part of this article.
(For now, we’ll just note that a recent excellent review of intrapartum interventions and their basis in evidence1 offers a model for evaluating a number of widely utilized practices in obstetrics. The goal, of course, is to minimize bad outcomes that follow from causation. Regrettably, that evidence-based approach is a limited one, because of a paucity of adequately controlled studies about OB practice.)
CASE: Continued
You consider your patient’s comment that she would like to avoid a repeat cesarean delivery, and advise her that she may safely attempt vaginal birth.
When spontaneous labor does not occur in 6 hours, oxytocin is administered. She dilates to 9 cm and begins to push spontaneously.
The fetal heart rate then drops to 70/min; fetal station, which had been +2, is now -1. A Stat cesarean delivery is performed. Uterine rupture with partial fetal expulsion is found. Apgar scores are 1, 3, and 5 at 1, 5, and 10 minutes.
Your patient requires a hysterectomy to control bleeding.
Some broad considerations for the physician arising from this CASE
- The counseling that you provide to a patient should be nondirective; it should include your opinion, however, about the best option available to her. Insert yourself into this hypothetical case, for discussion’s sake: Did you provide that important opinion to her?
- You must make certain that she clearly understands the risks and benefits of a procedure or other action, and the available alternatives. Did you undertake a check of her comprehension, given the anxiety and confusion of the moment?
- When an adverse outcome ensues—however unlikely it was to occur—it is necessary for you to review the circumstances with the patient as soon as clinically possible. Did you “debrief” and counsel her before and after the hysterectomy?
No more “perfect outcomes”: Our role changed, so did our risk
From the moment an OB patient enters triage, until her arrival home with her infant, this crucial period of her life is colored by concern, curiosity, myth, and fear.
Every woman anticipates the birth of a healthy infant. In an earlier era, the patient and her family relied on the sage advice of their physician to ensure this outcome. To an extent, physicians themselves reinforced this reliance, embracing the notion that they were, in fact, able to provide such a perfect outcome.
With advances that have been made in reproductive medicine, pregnancy has become more readily available to women with increasingly advanced disease; this has made labor and delivery more challenging to them and to their physicians. Realistically, our role as physicians is now better expressed as providing advice to help a woman achieve the best possible outcome, recognizing her individual clinical circumstances, instead of ensuring a perfect outcome.
Every woman anticipates the birth of a healthy baby. But the role of the OB is better expressed as helping her achieve the best possible outcome, not a perfect outcome. ABOVE: Shoulder dystocia is one of the most treacherous and frightening—and litigated—complications of childbirth, yet it is, for the most part, unpredictable and unpreventable in the course of even routine delivery.
Key concept #1
COMMUNICATION
Communication is central to patients’ comprehension about the care that you provide to them. But to enter a genuine dialogue with a patient under your care, and with her family, can challenge your communication skills.
First, you need written and verbal skills. Second, you need to know how to read visual cues.
Third, the messages that you deliver to the patient are influenced by:
- your style of communication
- your cultural background
- the setting in which you’re providing care (office, hospital).
Where are such skills developed? For one, biopsychosocial models that are employed in medical student education and resident training aid the physician in developing appropriate communication skills.
But training alone cannot overcome the fact that communication is a double-sided activity: Patients bring many of their own variables to a dialogue. How patients understand and interact with you—and with other providers and the health-care system—is not, therefore, directly or strictly within your sphere of influence.
Yet your sensitivity to a patient’s issues can go a long way toward ameliorating her misconceptions and prejudices. Here are several suggestions, developed by others, to optimize patients’ understanding of their care2,3:
- Apply what’s known as flip default. Assume the patient does not understand the information that you’re providing. Ask her to repeat your instructions back to you (as is done with a verbal order in the hospital).
- Manage face-to-face time effectively. Don’t attempt to teach a patient everything about her care at once. Focus on the critical aspects of her case and on providing understanding; use a strategy of sequential learning.
- Reduce the “overwhelm” factor. Periodically, stop and ask the patient if she has questions. Don’t wait until the end of the appointment to do this.
- Eliminate jargon. When you notify a patient about the results of testing, for example, clarify what the results say about her health and mean for her care. Do so in plain language.
- Recognize her preconceptions. Discuss any psychosocial issues head on with the patient. Use an interpreter or a social worker, or counselors from other fields, as appropriate.
Remember: All health-care personnel need to understand the importance of making the patient comfortable in the often foreign, and sometimes sterile, milieu of the medical office and hospital.
Key concept #2
TRUST
Trust between patient and clinician is, we believe, the most basic necessity for ameliorating allegations of malpractice—secondary only, perhaps, to your knowledge of medicine.
Trust can be enhanced by interactions that demonstrate to both parties the advisability of working together to resolve a problem. Any aspect of the physician-patient interaction that is potentially adversarial does not serve the interests of either.
We encourage you to construct a communication bridge, so to speak, with your patient. Begin by:
- introducing yourself to her and explaining your role in her care
- making appropriate eye contact with her
- maintaining a positive attitude
- dressing appropriately
- making her feel that she is your No. 1 priority.
There is more.
Recognize the duality of respect
- Ask the patient how she wishes to be addressed
- Ask about her belief system
- Explain the specifics of her care without arrogance.
Engender trust
- Be honest with her
- Be on her side
- Take time with her
- Allow her the right that she has to select from the options or to refuse treatment
- Disclose to the patient your status as a student or resident, if that is your rank.
Recognize the benefits of partnership
Forging a partnership with the patient:
- improves the accuracy of information
- eases ongoing communication
- facilitates informed consent
- provides an opportunity for you to educate her.
TABLE 2 When building trust, both patient and physician
are charged with responsibilities
| In regard to … | The patient’s responsibility is to … | The physician’s responsibility is to … |
|---|---|---|
| Gathering an honest and complete medical history | Know and report | Question completely |
| Being adherent to prescribed care | Follow through | Make reasonable demands |
| Making decisions about care | Ask questions and actively participate in choices Make realistic requests | Be knowledgeable about available alternatives Individualize options |
Key concept #3
SHARED RESPONSIBILITY
Patient and physician both have responsibilities that are important to achieving an optimal outcome; so does the hospital (TABLE 2 and TABLE 3). Both patient and physician should practice full disclosure throughout the course of care; this will benefit both of you.4 Here are a few select examples.
TABLE 3 Relative degrees of responsibility for a good outcome
vary across interested parties, but none are exempt
| Area of emphasis | Hospital’s responsibility | Physician’s responsibility | Patient’s responsibility |
|---|---|---|---|
| Creating a positive environment for care | 3+ | 2+ | 1+ |
| Providing clear communication | 3+ | 3+ | 3+ |
| Obtaining informed consent | 3+ | 3+ | 3+ |
| Making reasonable requests | 1+ | 1+ | 3+ |
| Compliance | 3+ | 3+ | 3+ |
| Key to the relative scale: 1+: at the least, minimally responsible; 2+: at the least, somewhat responsible; 3+, responsible to the greatest degree. | |||
The importance of the intake form
At the outset of OB care, in most practices, the patient provides the initial detailed medical history by completing a form in the waiting room. In reviewing and completing this survey with her during the appointment, pay particular attention to those questions for which the response has been left blank.
Patients need to understand that key recommendations about their care, and a proper analysis of their concerns, are based on the information that they provide on this survey. In our practices, we find that patients answer most of these early questions without difficulty—even inquiries of a personal nature, such as the number of prior pregnancies, or drug, alcohol, and smoking habits—as long as they understand why it’s in their best interests for you to have this information. If they leave a question blank and you do not follow up verbally, you may have lost invaluable information that can affect the outcome of her pregnancy.
What should you do when, occasionally, a patient refuses to answer one of your questions? We recommend that you record her refusal on the form itself, where the note remains part of the record.
Keep in mind that all necessary and useful information about a patient may not be available, or may not be appropriate to consider, at the initial prenatal visit. In that case, you have an ongoing opportunity—at subsequent visits during the pregnancy—to develop her full medical profile and algorithm.
The necessity of adherence
It almost goes without saying: To provide the care that our patients need, we sometimes require the unpleasant of them—to undergo evaluations, or testing, or to take medications that may be inconvenient or costly.
After you explain the specific course of care to a patient—whether you’re ordering a test or writing a prescription—your follow-up must include notation in the record of adherence. The fact is that both of you share responsibility for having her understand the importance of adherence to your instructions and the consequences of limited adherence or nonadherence.
Recall one of the lessons from the case that introduced this article: For the patient to make an informed decision about her care, the clinician must have thorough knowledge of 1) the risks and benefits of whatever intervention is being proposed in the particular clinical scenario and 2) the available alternatives. It is key that you communicate your risk-benefit assessment accurately to the patient.
Follow-up
Sometimes, new medical problems arise during subsequent prenatal visits. Follow-up appointments also provide an opportunity for you to expand your attention to problems identified earlier. Regardless of what the patient reported about her history and current health at the initial prenatal visit, listen for her to bring new issues to light for resolution later in the pregnancy that will have an impact on L & D. Again, it goes without saying but needs to be said: The OB clinician needs to have whatever skills are necessary to 1) fully evaluate the progress of a pregnancy and 2) make recommendations for care in light of changes in the status of mother and fetus along the way.
TABLE 4 Examples of the cardinal rule of “Be specific”
when you document care
| Instead of noting … | … Use alternative wording |
|---|---|
| “Mild vaginal bleeding” | “Vaginal bleeding requiring two pads an hour” |
| “Gentle traction” | “The shoulders were rotated before assisting the patient’s expulsive efforts” |
| “Patient refuses…” [or “declines…”] | “Patient voiced the nature of the problem and the alternatives that i have explained to her” |
| “Expedited cesarean section” | “The time from decision to incision was 35 minutes” |
Basic principles of documentation
The medical record is the best witness to interactions between a physician and a patient. In the record, we’re required to write a “5-C” description of events—namely, one that is:
- correct
- comprehensive
- conscientious
- clear
- contemporaneous.
Avoid medical jargon in the record. Be careful not to use vague terminology or descriptions, such as “mild vaginal bleeding,” “gentle traction,” or “patient refuses and accepts the consequences.” Specificity is the key to accuracy with respect to documentation (TABLE 4).
Editor’s note: Part 2 of this article will appear in the January 2011 issue of OBG Management. The authors’ analysis of L & D malpractice claims moves to a discussion of causation—by way of 4 troubling cases.
You’ll find a rich, useful archive of expert analysis of your professional liability and malpractice risk, at www.obgmanagement.com
• 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
• After a patient’s unexpected death, First Aid for the emotionally wounded
Ronald A. Chez, MD, and Wayne Fortin, MS (April 2010)
• Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates, Senior Editor, with Lewis Laska, JD, PhD (October 2009)
• Can a change in practice patterns reduce the number of OB malpractice claims?
Jason K. Baxter, MD, MSCP, and Louis Weinstein, MD (April 2009)
• Strategies for breaking bad news to patients
Barry Bub, MD (September 2008)
• Stuff of nightmares: Criminal prosecution for malpractice
Gary Steinman, MD, PhD (August 2008)
• Deposition Dos and Don’ts: How to answer 8 tricky questions
James L. Knoll, IV, MD, and Phillip J. Resnick, MD (May 2008)
• Playing high-stakes poker: Do you fight—or settle—that malpractice lawsuit?
Jeffrey Segal, MD (April 2008)
We want to hear from you! Tell us what you think.
1. Berghella V, Baxter JK, Chauhan SP. Evidence-based labor and delivery management. Am J Obstet Gynecol. 2008;199(5):445-454.
2. Paasche-Orlow MK, Riekert KA, Bilderback A, et al. Tailored education may reduce health literacy disparities in asthma self-management. Am J Respir Crit Care Med. 2005;172:980-986.
3. Huvane K. Health literacy: reading is just the beginning. Focus on multicultural healthcare. 2007;3(4):16-19.
4. Giordano K. Legal Principles. In: O’Grady JP, Gimovsky ML, Bayer-Zwirello L, Giordano K, eds. Operative Obstetrics. 2nd ed. New York: Cambridge University Press; 2008.
5. The Four Elements of Medical Malpractice Yale New Haven Medical Center: Issues in Risk Management. 1997.
1. Berghella V, Baxter JK, Chauhan SP. Evidence-based labor and delivery management. Am J Obstet Gynecol. 2008;199(5):445-454.
2. Paasche-Orlow MK, Riekert KA, Bilderback A, et al. Tailored education may reduce health literacy disparities in asthma self-management. Am J Respir Crit Care Med. 2005;172:980-986.
3. Huvane K. Health literacy: reading is just the beginning. Focus on multicultural healthcare. 2007;3(4):16-19.
4. Giordano K. Legal Principles. In: O’Grady JP, Gimovsky ML, Bayer-Zwirello L, Giordano K, eds. Operative Obstetrics. 2nd ed. New York: Cambridge University Press; 2008.
5. The Four Elements of Medical Malpractice Yale New Haven Medical Center: Issues in Risk Management. 1997.
Skilled US imaging of the adnexae: The fallopian tubes
Part 1 A Starting Point (September 2010)
Part 2 The non-neoplastic ovarian mass (October 2010)
Part 3 Ovarian neoplasms (November 2010)
An imaging study of the adnexae would not be complete without thorough assessment of the fallopian tubes. Among the pathologies that may be identified or confirmed by ultrasonography are:
- ectopic pregnancy
- tubal inflammatory disease, or salpingitis
- chronic tubal disease, or hydrosalpinx
- tubo-ovarian complex
- tubo-ovarian abscess
- tubal and ovarian torsion
- cancer.
In this final installment of our four-part series on ultrasonographic (US) imaging of the adnexae, we take these entities as our focus.
Suspect ectopic pregnancy even if the hCG level is not yet available
A detailed discussion of ectopic pregnancy far exceeds the framework of this article. Suffice it to say that ectopic pregnancy should always be considered in a woman of reproductive age, especially one who complains of abdominal or pelvic pain, vaginal bleeding, or both. However, these signs and symptoms are present in only about 25% of women who have this condition. When these signs and symptoms are present, it is wise to be suspicious even if the results of human chorionic gonadotropin (hCG) measurement are not yet available.
A complete history is important in the diagnosis of ectopic pregnancy. Risk factors include a history of ectopic pregnancy, pelvic inflammatory disease (PID), or tubal surgery, or use of an intrauterine device.
Unequivocal US diagnosis of ectopic pregnancy is possible in only about 20% of cases, and depends on identification of an extrauterine pregnancy, which may not be visible in the early days of gestation. However, some grayscale ultrasonographic findings that may suggest ectopic pregnancy include:
- an empty uterus in a woman who has an hCG level above 1,000 to 1,500 mIu/mL (the discriminatory level)
- a thick, hyperechoic endometrial echo (decidualization)
- an adnexal mass other than a simple cyst
- echogenic fluid in the cul-de-sac (FIGURE 1A–1D).
Power Doppler can help the sonographer localize the ectopic pregnancy in the tubes by demonstrating the circular vascularization of the more or less typical “tubal ring” (FIGURE 1E–1G).
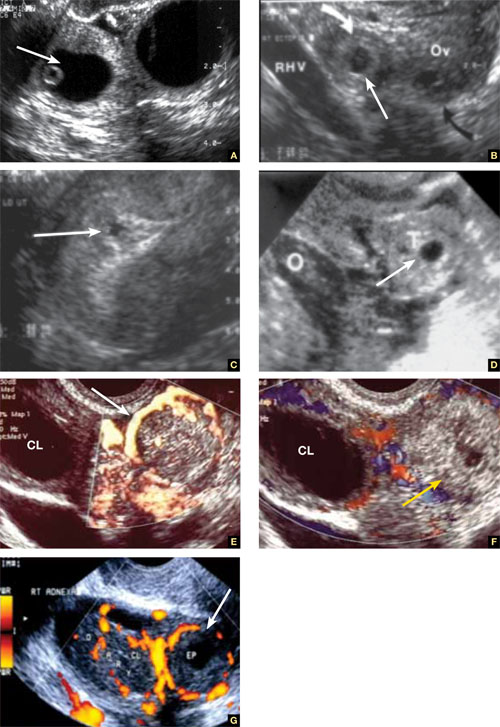
FIGURE 1 Ectopic pregnancy
A–D. Various cases of tubal ectopic gestation (arrows point to each gestation). E–G. Power Doppler localizes the ectopic pregnancy (arrows), side by side with the corpus luteum (CL).
A patient’s history may yield clues to tubal inflammatory disease
The diagnosis of acute salpingitis begins with a thorough patient history. Look for any report of PID, unexplained fever, foul vaginal discharge, sexually transmitted infection, or recent intrauterine procedures such as hysteroscopy, IUD insertion, endometrial biopsy, or saline infusion sonohysterography.
US diagnosis is based on the findings of a slightly dilated fallopian tube with low-level echogenic fluid content, thick tubal walls, and tenderness to the touch of the transvaginal probe.1
In cross section, the tube forms the “cogwheel sign” (FIGURE 2C). Power Doppler shows the subserosal blood vessels characteristic of this entity (FIGURE 2D).
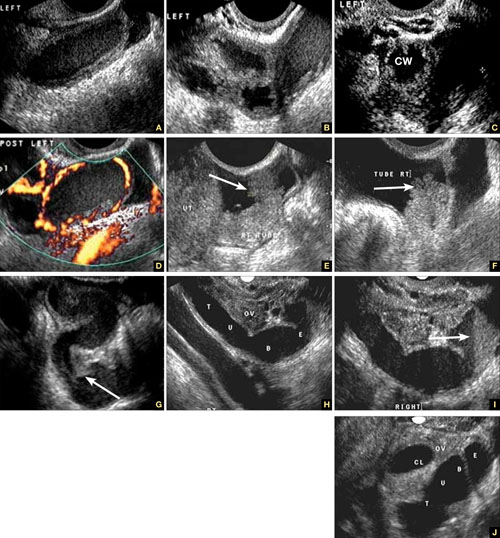
FIGURE 2 Tubal disease
A–C. Grayscale images showing thick walls, low-level echoic fluid (pus?) and the “cogwheel sign” (CW). D. Subserosal vascularization typical of an inflammatory response in hollow abdominal viscera. E,F. Edematous fimbrial end (arrow) of the inflamed tubes, floating in a small amount of free pelvic fluid. G. Low-level echoic, fluid-filled, thick-walled tubes with incomplete septae (arrow) are the hallmarks of hydrosalpinx. H–J. Bilateral hydrosalpinx. Note the thin walls and anechoic fluid-filled forms (sausage-shaped) (CL = corpus luteum; OV = ovary; UT = uterus).
Look for fluid dilating the tube in chronic tubal disease
Hydrosalpinx is characterized on US by thin tubal walls with a relatively anechoic but large amount of fluid dilating the tube (FIGURE 2G–2J). The interior wall is studded with shallow, echogenic, mural nodules (without blood vessels) that assume the appearance of a tube or sausage. The small, shallow internal papillae give the cross section of the tube the appearance of beads on a string.
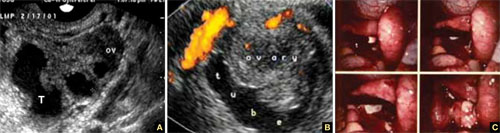
FIGURE 3 Tubo-ovarian complex
A. The tube (T) and ovary (OV) form an infectious conglomerate. B. Power Doppler appearance. C. Laparoscopic view.
Tubo-ovarian complex
When this complex arises, the anatomy and shape of the tube and the involved ovary are somewhat distorted but still largely discernible (FIGURE 3A AND 3B).
Tubo-ovarian abscess is a more advanced stage of a fast-progressing or neglected pelvic inflammatory process. In it, the tube and the ovary can barely be distinguished, and US signs of abscess appear, among them low-level echoic fluid and linear echogenicity (FIGURE 4).
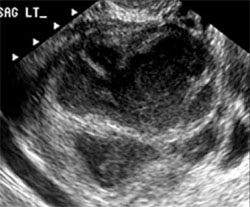
FIGURE 4 Tubo-ovarian abscess
The tube and ovary are indistinguishable. The fluid is of low-level echogenicity (pus), and the walls are thick.
In ovarian torsion, the follicles press outward
Although torsion has distinct sonographic signs, it remains a clinical diagnosis that US findings may or may not support. Correct diagnosis often is the purview of expert sonographers and sonologists.
When ovarian torsion is present, the ovaries are enlarged and hyperechoic, their follicles pushed toward the surface (FIGURE 5A–5C). The ovaries are also tender to the touch and typically demonstrate no blood flow by Doppler interrogation. On occasion, when arterial flow is still present (venous flow is usually the first characteristic to vanish), a twisted arterial pattern may result, similar to the coil of a telephone cord. Some pelvic fluid may also appear.
Tubal torsion is harder to diagnose. US recognition depends on the finding of a normal ovary with intact blood flow beside a fluid-filled, thin-walled, tender, cystic structure with some of the previously mentioned sonomarkers of tubal occlusion such as the bead-on-a-string or cogwheel sign (FIGURE 5D–5G).
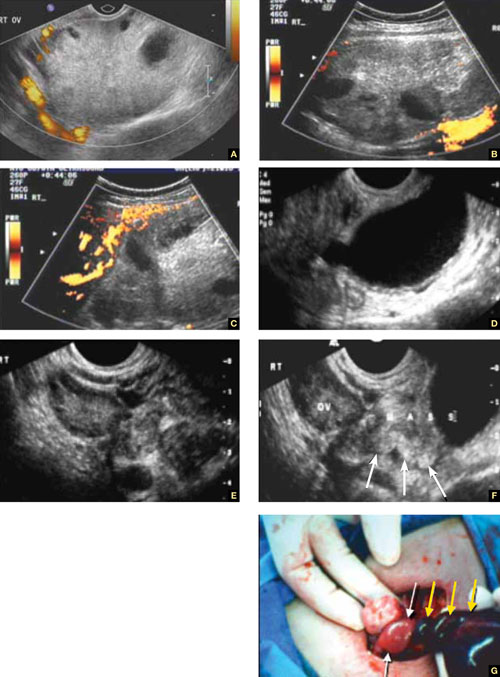
FIGURE 5 Torsion
A–C. Ovarian torsion. Hyperechoic, large ovary with follicles pushed toward the surface. Power Doppler reveals no blood flow in the ovary. D–F. Tubal torsion. Cystic dilatation with a small beak and a normal ovary. G. Intraoperative view of the tube (twisted three times; yellow arrows) and the normal ovary (white arrows).
Fluid in the cul-de-sac
In many cases, fluid may be present or trapped in the lesser pelvis, surrounded or blocked by the pelvic organs. If this fluid is the result or sequela of PID, thin, thread-like adhesive strands will be visible between the organs on US, betraying its pathogenesis (FIGURE 6). The “walls” of such loculated fluid are the pelvic wall itself and the surrounding organs.
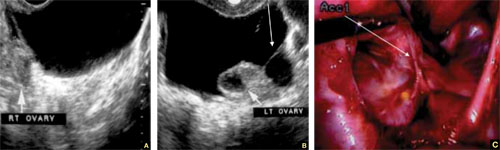
FIGURE 6 Fluid in the cul-de-sac
Sequelae of acute PID. A. Free pelvic fluid, also known as pelvic, peritoneal, loculated fluid. B. A normal ovary and an adhesive strand (arrow). C. Laparoscopic image of the adhesion (arrow).
Cancer of the tubes is unlikely, but it’s best to keep it in mind
Primary cancer of the fallopian tubes accounts for only 1% to 2% of all gynecologic cancers.2 Only 300 to 400 women are given this diagnosis each year in the United States— most of them postmenopausal.
Despite its rarity, fallopian-tube cancer is a major concern when a tubal mass is identified by palpation or imaging. In most cases, however, no palpable mass is found at the time of first examination, and tubal malignancy is diagnosed perioperatively or postoperatively.
US characteristics of tubal cancer are similar to those of ovarian cancer: a bizarre appearance, with extremely vascular tissue. At times, US attributes of tubal pathology, such as incomplete septae and tube-like fluid-filled structures, are apparent (FIGURE 7).
Consider cancer of the fallopian tube whenever an unexplained solid mass is palpated or imaged in the area of the tubes in conjunction with apparently normal ovaries.
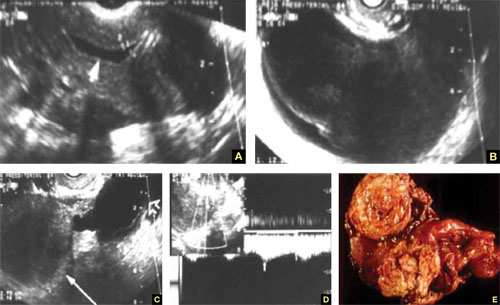
FIGURE 7 Fallopian tube cancer
A. Fluid-filled uterine cavity. B. Large cystic dilatation of the tube. C. A thickened tubal wall (arrow). D. Doppler interrogation reveals high diastolic flow (arrows). E. Macroscopic gross appearance.
The long view
As technology has advanced, so has ultrasonography. High-resolution transducers, color and power Doppler, and three-dimensional imaging make it possible for an experienced practitioner to identify and confirm the diagnosis of many adnexal masses and pathologies, from the corpus luteum to fallopian tube torsion. As the field continues to evolve, we expect that this modality will facilitate the diagnosis of adnexal abnormalities to an even greater degree.
In the meantime, this four-part tutorial offers guidance on the identification of adnexal masses. If we’ve helped ease coordination of care between the generalist ObGyn and the expert sonographer, we’ve accomplished our goal.
We want to hear from you! Tell us what you think.
1. Timor-Tritsch IE, Lerner JP, Monteagudo A, Murphy KE, Heller DS. Transvaginal sonographic markers of tubal inflammatory disease. Ultrasound Obstet Gynecol. 1998;12(1):56-66.
2. Goswami PK, Kerr-Wilson R, McCarthy K. Cancer of the fallopian tube. The Obstetrician & Gynaecologist. 2006;8(3):147-152.doi: 10.1576/toag.8.3.147.27249.
| Dr. Timor-Tritsch sums up this series on imaging |
Ilan E. Timor-Tritsch, MD
Dr. Timor-Tritsch is Professor of ObGyn and Director of ObGyn Ultrasound at New York University Medical Center in New York City.
Steven R. Goldstein, MD
Dr. Goldstein is Professor of ObGyn, Director of Gynecologic Ultrasound, and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the Board of Editors.
Dr. Timor-Tritsch reports no financial relationships relevant to this article. Dr. Goldstein reports that he is an advisor to Amgen, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Merck, and Pfizer. He also serves as a consultant to Cook ObGyn and Philips Ultrasound and as a speaker for Eli Lilly and Warner Chilcott. He is a director of Sonosite, Inc.
| Dr. Timor-Tritsch sums up this series on imaging |
Ilan E. Timor-Tritsch, MD
Dr. Timor-Tritsch is Professor of ObGyn and Director of ObGyn Ultrasound at New York University Medical Center in New York City.
Steven R. Goldstein, MD
Dr. Goldstein is Professor of ObGyn, Director of Gynecologic Ultrasound, and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the Board of Editors.
Dr. Timor-Tritsch reports no financial relationships relevant to this article. Dr. Goldstein reports that he is an advisor to Amgen, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Merck, and Pfizer. He also serves as a consultant to Cook ObGyn and Philips Ultrasound and as a speaker for Eli Lilly and Warner Chilcott. He is a director of Sonosite, Inc.
| Dr. Timor-Tritsch sums up this series on imaging |
Ilan E. Timor-Tritsch, MD
Dr. Timor-Tritsch is Professor of ObGyn and Director of ObGyn Ultrasound at New York University Medical Center in New York City.
Steven R. Goldstein, MD
Dr. Goldstein is Professor of ObGyn, Director of Gynecologic Ultrasound, and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the Board of Editors.
Dr. Timor-Tritsch reports no financial relationships relevant to this article. Dr. Goldstein reports that he is an advisor to Amgen, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Merck, and Pfizer. He also serves as a consultant to Cook ObGyn and Philips Ultrasound and as a speaker for Eli Lilly and Warner Chilcott. He is a director of Sonosite, Inc.
Part 1 A Starting Point (September 2010)
Part 2 The non-neoplastic ovarian mass (October 2010)
Part 3 Ovarian neoplasms (November 2010)
An imaging study of the adnexae would not be complete without thorough assessment of the fallopian tubes. Among the pathologies that may be identified or confirmed by ultrasonography are:
- ectopic pregnancy
- tubal inflammatory disease, or salpingitis
- chronic tubal disease, or hydrosalpinx
- tubo-ovarian complex
- tubo-ovarian abscess
- tubal and ovarian torsion
- cancer.
In this final installment of our four-part series on ultrasonographic (US) imaging of the adnexae, we take these entities as our focus.
Suspect ectopic pregnancy even if the hCG level is not yet available
A detailed discussion of ectopic pregnancy far exceeds the framework of this article. Suffice it to say that ectopic pregnancy should always be considered in a woman of reproductive age, especially one who complains of abdominal or pelvic pain, vaginal bleeding, or both. However, these signs and symptoms are present in only about 25% of women who have this condition. When these signs and symptoms are present, it is wise to be suspicious even if the results of human chorionic gonadotropin (hCG) measurement are not yet available.
A complete history is important in the diagnosis of ectopic pregnancy. Risk factors include a history of ectopic pregnancy, pelvic inflammatory disease (PID), or tubal surgery, or use of an intrauterine device.
Unequivocal US diagnosis of ectopic pregnancy is possible in only about 20% of cases, and depends on identification of an extrauterine pregnancy, which may not be visible in the early days of gestation. However, some grayscale ultrasonographic findings that may suggest ectopic pregnancy include:
- an empty uterus in a woman who has an hCG level above 1,000 to 1,500 mIu/mL (the discriminatory level)
- a thick, hyperechoic endometrial echo (decidualization)
- an adnexal mass other than a simple cyst
- echogenic fluid in the cul-de-sac (FIGURE 1A–1D).
Power Doppler can help the sonographer localize the ectopic pregnancy in the tubes by demonstrating the circular vascularization of the more or less typical “tubal ring” (FIGURE 1E–1G).
FIGURE 1 Ectopic pregnancy
A–D. Various cases of tubal ectopic gestation (arrows point to each gestation). E–G. Power Doppler localizes the ectopic pregnancy (arrows), side by side with the corpus luteum (CL).
A patient’s history may yield clues to tubal inflammatory disease
The diagnosis of acute salpingitis begins with a thorough patient history. Look for any report of PID, unexplained fever, foul vaginal discharge, sexually transmitted infection, or recent intrauterine procedures such as hysteroscopy, IUD insertion, endometrial biopsy, or saline infusion sonohysterography.
US diagnosis is based on the findings of a slightly dilated fallopian tube with low-level echogenic fluid content, thick tubal walls, and tenderness to the touch of the transvaginal probe.1
In cross section, the tube forms the “cogwheel sign” (FIGURE 2C). Power Doppler shows the subserosal blood vessels characteristic of this entity (FIGURE 2D).
FIGURE 2 Tubal disease
A–C. Grayscale images showing thick walls, low-level echoic fluid (pus?) and the “cogwheel sign” (CW). D. Subserosal vascularization typical of an inflammatory response in hollow abdominal viscera. E,F. Edematous fimbrial end (arrow) of the inflamed tubes, floating in a small amount of free pelvic fluid. G. Low-level echoic, fluid-filled, thick-walled tubes with incomplete septae (arrow) are the hallmarks of hydrosalpinx. H–J. Bilateral hydrosalpinx. Note the thin walls and anechoic fluid-filled forms (sausage-shaped) (CL = corpus luteum; OV = ovary; UT = uterus).
Look for fluid dilating the tube in chronic tubal disease
Hydrosalpinx is characterized on US by thin tubal walls with a relatively anechoic but large amount of fluid dilating the tube (FIGURE 2G–2J). The interior wall is studded with shallow, echogenic, mural nodules (without blood vessels) that assume the appearance of a tube or sausage. The small, shallow internal papillae give the cross section of the tube the appearance of beads on a string.
FIGURE 3 Tubo-ovarian complex
A. The tube (T) and ovary (OV) form an infectious conglomerate. B. Power Doppler appearance. C. Laparoscopic view.
Tubo-ovarian complex
When this complex arises, the anatomy and shape of the tube and the involved ovary are somewhat distorted but still largely discernible (FIGURE 3A AND 3B).
Tubo-ovarian abscess is a more advanced stage of a fast-progressing or neglected pelvic inflammatory process. In it, the tube and the ovary can barely be distinguished, and US signs of abscess appear, among them low-level echoic fluid and linear echogenicity (FIGURE 4).
FIGURE 4 Tubo-ovarian abscess
The tube and ovary are indistinguishable. The fluid is of low-level echogenicity (pus), and the walls are thick.
In ovarian torsion, the follicles press outward
Although torsion has distinct sonographic signs, it remains a clinical diagnosis that US findings may or may not support. Correct diagnosis often is the purview of expert sonographers and sonologists.
When ovarian torsion is present, the ovaries are enlarged and hyperechoic, their follicles pushed toward the surface (FIGURE 5A–5C). The ovaries are also tender to the touch and typically demonstrate no blood flow by Doppler interrogation. On occasion, when arterial flow is still present (venous flow is usually the first characteristic to vanish), a twisted arterial pattern may result, similar to the coil of a telephone cord. Some pelvic fluid may also appear.
Tubal torsion is harder to diagnose. US recognition depends on the finding of a normal ovary with intact blood flow beside a fluid-filled, thin-walled, tender, cystic structure with some of the previously mentioned sonomarkers of tubal occlusion such as the bead-on-a-string or cogwheel sign (FIGURE 5D–5G).
FIGURE 5 Torsion
A–C. Ovarian torsion. Hyperechoic, large ovary with follicles pushed toward the surface. Power Doppler reveals no blood flow in the ovary. D–F. Tubal torsion. Cystic dilatation with a small beak and a normal ovary. G. Intraoperative view of the tube (twisted three times; yellow arrows) and the normal ovary (white arrows).
Fluid in the cul-de-sac
In many cases, fluid may be present or trapped in the lesser pelvis, surrounded or blocked by the pelvic organs. If this fluid is the result or sequela of PID, thin, thread-like adhesive strands will be visible between the organs on US, betraying its pathogenesis (FIGURE 6). The “walls” of such loculated fluid are the pelvic wall itself and the surrounding organs.
FIGURE 6 Fluid in the cul-de-sac
Sequelae of acute PID. A. Free pelvic fluid, also known as pelvic, peritoneal, loculated fluid. B. A normal ovary and an adhesive strand (arrow). C. Laparoscopic image of the adhesion (arrow).
Cancer of the tubes is unlikely, but it’s best to keep it in mind
Primary cancer of the fallopian tubes accounts for only 1% to 2% of all gynecologic cancers.2 Only 300 to 400 women are given this diagnosis each year in the United States— most of them postmenopausal.
Despite its rarity, fallopian-tube cancer is a major concern when a tubal mass is identified by palpation or imaging. In most cases, however, no palpable mass is found at the time of first examination, and tubal malignancy is diagnosed perioperatively or postoperatively.
US characteristics of tubal cancer are similar to those of ovarian cancer: a bizarre appearance, with extremely vascular tissue. At times, US attributes of tubal pathology, such as incomplete septae and tube-like fluid-filled structures, are apparent (FIGURE 7).
Consider cancer of the fallopian tube whenever an unexplained solid mass is palpated or imaged in the area of the tubes in conjunction with apparently normal ovaries.
FIGURE 7 Fallopian tube cancer
A. Fluid-filled uterine cavity. B. Large cystic dilatation of the tube. C. A thickened tubal wall (arrow). D. Doppler interrogation reveals high diastolic flow (arrows). E. Macroscopic gross appearance.
The long view
As technology has advanced, so has ultrasonography. High-resolution transducers, color and power Doppler, and three-dimensional imaging make it possible for an experienced practitioner to identify and confirm the diagnosis of many adnexal masses and pathologies, from the corpus luteum to fallopian tube torsion. As the field continues to evolve, we expect that this modality will facilitate the diagnosis of adnexal abnormalities to an even greater degree.
In the meantime, this four-part tutorial offers guidance on the identification of adnexal masses. If we’ve helped ease coordination of care between the generalist ObGyn and the expert sonographer, we’ve accomplished our goal.
We want to hear from you! Tell us what you think.
Part 1 A Starting Point (September 2010)
Part 2 The non-neoplastic ovarian mass (October 2010)
Part 3 Ovarian neoplasms (November 2010)
An imaging study of the adnexae would not be complete without thorough assessment of the fallopian tubes. Among the pathologies that may be identified or confirmed by ultrasonography are:
- ectopic pregnancy
- tubal inflammatory disease, or salpingitis
- chronic tubal disease, or hydrosalpinx
- tubo-ovarian complex
- tubo-ovarian abscess
- tubal and ovarian torsion
- cancer.
In this final installment of our four-part series on ultrasonographic (US) imaging of the adnexae, we take these entities as our focus.
Suspect ectopic pregnancy even if the hCG level is not yet available
A detailed discussion of ectopic pregnancy far exceeds the framework of this article. Suffice it to say that ectopic pregnancy should always be considered in a woman of reproductive age, especially one who complains of abdominal or pelvic pain, vaginal bleeding, or both. However, these signs and symptoms are present in only about 25% of women who have this condition. When these signs and symptoms are present, it is wise to be suspicious even if the results of human chorionic gonadotropin (hCG) measurement are not yet available.
A complete history is important in the diagnosis of ectopic pregnancy. Risk factors include a history of ectopic pregnancy, pelvic inflammatory disease (PID), or tubal surgery, or use of an intrauterine device.
Unequivocal US diagnosis of ectopic pregnancy is possible in only about 20% of cases, and depends on identification of an extrauterine pregnancy, which may not be visible in the early days of gestation. However, some grayscale ultrasonographic findings that may suggest ectopic pregnancy include:
- an empty uterus in a woman who has an hCG level above 1,000 to 1,500 mIu/mL (the discriminatory level)
- a thick, hyperechoic endometrial echo (decidualization)
- an adnexal mass other than a simple cyst
- echogenic fluid in the cul-de-sac (FIGURE 1A–1D).
Power Doppler can help the sonographer localize the ectopic pregnancy in the tubes by demonstrating the circular vascularization of the more or less typical “tubal ring” (FIGURE 1E–1G).
FIGURE 1 Ectopic pregnancy
A–D. Various cases of tubal ectopic gestation (arrows point to each gestation). E–G. Power Doppler localizes the ectopic pregnancy (arrows), side by side with the corpus luteum (CL).
A patient’s history may yield clues to tubal inflammatory disease
The diagnosis of acute salpingitis begins with a thorough patient history. Look for any report of PID, unexplained fever, foul vaginal discharge, sexually transmitted infection, or recent intrauterine procedures such as hysteroscopy, IUD insertion, endometrial biopsy, or saline infusion sonohysterography.
US diagnosis is based on the findings of a slightly dilated fallopian tube with low-level echogenic fluid content, thick tubal walls, and tenderness to the touch of the transvaginal probe.1
In cross section, the tube forms the “cogwheel sign” (FIGURE 2C). Power Doppler shows the subserosal blood vessels characteristic of this entity (FIGURE 2D).
FIGURE 2 Tubal disease
A–C. Grayscale images showing thick walls, low-level echoic fluid (pus?) and the “cogwheel sign” (CW). D. Subserosal vascularization typical of an inflammatory response in hollow abdominal viscera. E,F. Edematous fimbrial end (arrow) of the inflamed tubes, floating in a small amount of free pelvic fluid. G. Low-level echoic, fluid-filled, thick-walled tubes with incomplete septae (arrow) are the hallmarks of hydrosalpinx. H–J. Bilateral hydrosalpinx. Note the thin walls and anechoic fluid-filled forms (sausage-shaped) (CL = corpus luteum; OV = ovary; UT = uterus).
Look for fluid dilating the tube in chronic tubal disease
Hydrosalpinx is characterized on US by thin tubal walls with a relatively anechoic but large amount of fluid dilating the tube (FIGURE 2G–2J). The interior wall is studded with shallow, echogenic, mural nodules (without blood vessels) that assume the appearance of a tube or sausage. The small, shallow internal papillae give the cross section of the tube the appearance of beads on a string.
FIGURE 3 Tubo-ovarian complex
A. The tube (T) and ovary (OV) form an infectious conglomerate. B. Power Doppler appearance. C. Laparoscopic view.
Tubo-ovarian complex
When this complex arises, the anatomy and shape of the tube and the involved ovary are somewhat distorted but still largely discernible (FIGURE 3A AND 3B).
Tubo-ovarian abscess is a more advanced stage of a fast-progressing or neglected pelvic inflammatory process. In it, the tube and the ovary can barely be distinguished, and US signs of abscess appear, among them low-level echoic fluid and linear echogenicity (FIGURE 4).
FIGURE 4 Tubo-ovarian abscess
The tube and ovary are indistinguishable. The fluid is of low-level echogenicity (pus), and the walls are thick.
In ovarian torsion, the follicles press outward
Although torsion has distinct sonographic signs, it remains a clinical diagnosis that US findings may or may not support. Correct diagnosis often is the purview of expert sonographers and sonologists.
When ovarian torsion is present, the ovaries are enlarged and hyperechoic, their follicles pushed toward the surface (FIGURE 5A–5C). The ovaries are also tender to the touch and typically demonstrate no blood flow by Doppler interrogation. On occasion, when arterial flow is still present (venous flow is usually the first characteristic to vanish), a twisted arterial pattern may result, similar to the coil of a telephone cord. Some pelvic fluid may also appear.
Tubal torsion is harder to diagnose. US recognition depends on the finding of a normal ovary with intact blood flow beside a fluid-filled, thin-walled, tender, cystic structure with some of the previously mentioned sonomarkers of tubal occlusion such as the bead-on-a-string or cogwheel sign (FIGURE 5D–5G).
FIGURE 5 Torsion
A–C. Ovarian torsion. Hyperechoic, large ovary with follicles pushed toward the surface. Power Doppler reveals no blood flow in the ovary. D–F. Tubal torsion. Cystic dilatation with a small beak and a normal ovary. G. Intraoperative view of the tube (twisted three times; yellow arrows) and the normal ovary (white arrows).
Fluid in the cul-de-sac
In many cases, fluid may be present or trapped in the lesser pelvis, surrounded or blocked by the pelvic organs. If this fluid is the result or sequela of PID, thin, thread-like adhesive strands will be visible between the organs on US, betraying its pathogenesis (FIGURE 6). The “walls” of such loculated fluid are the pelvic wall itself and the surrounding organs.
FIGURE 6 Fluid in the cul-de-sac
Sequelae of acute PID. A. Free pelvic fluid, also known as pelvic, peritoneal, loculated fluid. B. A normal ovary and an adhesive strand (arrow). C. Laparoscopic image of the adhesion (arrow).
Cancer of the tubes is unlikely, but it’s best to keep it in mind
Primary cancer of the fallopian tubes accounts for only 1% to 2% of all gynecologic cancers.2 Only 300 to 400 women are given this diagnosis each year in the United States— most of them postmenopausal.
Despite its rarity, fallopian-tube cancer is a major concern when a tubal mass is identified by palpation or imaging. In most cases, however, no palpable mass is found at the time of first examination, and tubal malignancy is diagnosed perioperatively or postoperatively.
US characteristics of tubal cancer are similar to those of ovarian cancer: a bizarre appearance, with extremely vascular tissue. At times, US attributes of tubal pathology, such as incomplete septae and tube-like fluid-filled structures, are apparent (FIGURE 7).
Consider cancer of the fallopian tube whenever an unexplained solid mass is palpated or imaged in the area of the tubes in conjunction with apparently normal ovaries.
FIGURE 7 Fallopian tube cancer
A. Fluid-filled uterine cavity. B. Large cystic dilatation of the tube. C. A thickened tubal wall (arrow). D. Doppler interrogation reveals high diastolic flow (arrows). E. Macroscopic gross appearance.
The long view
As technology has advanced, so has ultrasonography. High-resolution transducers, color and power Doppler, and three-dimensional imaging make it possible for an experienced practitioner to identify and confirm the diagnosis of many adnexal masses and pathologies, from the corpus luteum to fallopian tube torsion. As the field continues to evolve, we expect that this modality will facilitate the diagnosis of adnexal abnormalities to an even greater degree.
In the meantime, this four-part tutorial offers guidance on the identification of adnexal masses. If we’ve helped ease coordination of care between the generalist ObGyn and the expert sonographer, we’ve accomplished our goal.
We want to hear from you! Tell us what you think.
1. Timor-Tritsch IE, Lerner JP, Monteagudo A, Murphy KE, Heller DS. Transvaginal sonographic markers of tubal inflammatory disease. Ultrasound Obstet Gynecol. 1998;12(1):56-66.
2. Goswami PK, Kerr-Wilson R, McCarthy K. Cancer of the fallopian tube. The Obstetrician & Gynaecologist. 2006;8(3):147-152.doi: 10.1576/toag.8.3.147.27249.
1. Timor-Tritsch IE, Lerner JP, Monteagudo A, Murphy KE, Heller DS. Transvaginal sonographic markers of tubal inflammatory disease. Ultrasound Obstet Gynecol. 1998;12(1):56-66.
2. Goswami PK, Kerr-Wilson R, McCarthy K. Cancer of the fallopian tube. The Obstetrician & Gynaecologist. 2006;8(3):147-152.doi: 10.1576/toag.8.3.147.27249.