User login
Asthma or Anaphylaxis?
The VA Disability Compensation Program: What Providers Should Know
Minimal to mild endometriosis: 4 treatment options
- Signs of minimal or mild endometriosis include tenderness or nodularity in the posterior cul-de-sac, especially at the uterosacral ligaments, and anterior cul-de-sac nodularity.
- Endometriosis can be associated with infertility at all stages of disease.
- Indications for laparoscopy include infertility of more than 1 year without other symptoms or after 6 months if the patient has other symptoms or is more than 35 years of age. Patients with pelvic pain that has not responded after 3 months of nonsteroidal anti-inflammatory drugs and/or oral contraceptives also are candidates.
- Following adequate surgical extirpation of disease, no further postoperative medical treatment is necessary for patients with either pain or infertility. However, oral contraceptives have benefits for many patients who are not attempting to conceive.
This case represents 1 of the challenges of treating minimal to mild endometriosis—disease without adhesions, invasive lesions, or endometriomas. Endometriosis is suggested in this patient by tenderness or nodularity in the posterior cul-de-sac, especially at the uterosacral ligaments, and anterior cul-de-sac nodularity. The patient’s complaint of pain does not necessarily indicate severe disease. Rather, the relationship between minimal or mild disease and symptoms is unclear. The patient may report significant pain when only superficial implants and minimal adhesions are present.
Although hysterectomy is the definitive treatment for patients with recurrent or intractable pain associated with endometriosis, I make every effort to avoid this operation in young women with minimal to mild disease. This article describes 4 other options—no treatment, ovarian suppression, surgical treatment, and combined treatment—and points out potential pitfalls associated with each approach.
Diagnosis
The diagnosis of endometriosis often can be difficult, and the extent of disease is thought to be underestimated in as many as 50% of patients.1-3
Clinical presentation. Endometriosis presents as pelvic pain in about 50% of patients, infertility in about 25%, pain and infertility in about 25%, and as ovarian endometrioma in less than 5% of cases.1-3 Asymptomatic disease is frequent: from 1% to 40%.1-3 The disease may occur any time after puberty, including adolescence. For other symptoms and characteristics, see “Endometriosis: A snapshot”.
Physical examination. Pelvic examination should be performed at the time of menses, when disease is more easily identified. The location of tenderness often corresponds to the location of the pain. As in the example case, signs of minimal or mild disease include:
- tenderness or nodularity in the posterior culde-sac, especially at the uterosacral ligaments
- anterior cul-de-sac nodularity
Indications for laparoscopy include infertility of more than 1 year without other symptoms or after 6 months if the patient has other symptoms or is more than 35 years of age. Evaluation for other female factors and sperm quality should be conducted prior to laparoscopy. Patients with pelvic pain that has not responded after 3 months of NSAIDs and/or oral contraceptives (OCs) also are candidates for laparoscopy. In the case described above, I would recommend at least a 3-month trial of OCs and NSAIDs before performing laparoscopy.
Staging the disease. The American Society for Reproductive Medicine has developed a staging system with scores from 1 to 150. Minimal and mild disease ranges from 1 to 15.4
Management options. Depending on the woman’s reproductive goals, 1 of the 4 options discussed below may be recommended.
Prevalence. Endometriosis affects about 7% of reproductive-aged women—approximately 5 million Americans. Most of these women are unaware that they have the disease, although many may suffer symptoms ranging from pelvic pain to infertility.
Symptoms. Endometriosis is suggested by a variety of symptoms, including dysmenorrhea, dyspareunia (especially with aching following coitus, as in the case described at the opening of this article), dyschezia, dysuria, mittelschmerz, or focal or generalized pelvic pain. Hematuria and hematochezia also may be present. About 30% of patients with endometriosis have no pain.1
Diagnostic challenges. Deeply invasive endometriosis that is overlooked or develops outside the posterior cul-de-sac can be inappropriately staged as minimal or mild disease.
Causes of pain. Pain symptoms often do not correlate well with disease severity. Pain may be due to secretion of irritating factors (eg, histamine), adhesions that cause scarring or retraction, immunologic reactivity, or other unknown entities.
Infertility can occur at any stage. Not surprisingly, patients who have severe or extensive disease have a poorer prognosis than those with minimal or mild disease.
Endometriosis is a progressive disease, but the rate of progression and nature of lesions vary from patient to patient. Adhesions develop due to the inflammatory process caused by longstanding endometriosis, becoming more extensive and dense over time. Complete cul-de-sac obliteration can result from longstanding invasive and adhesive disease or may stem from abnormal mullerian development.
Option 1No treatment
This option includes expectant management and/or limited use of analgesics and NSAIDs, which may be especially helpful for women with dysmenorrhea, particularly when infertility is the primary complaint. In other instances, this approach may fail to provide adequate relief from pain.
Almost all patients should undergo an initial trial of NSAIDs and/or OCs, using NSAIDs no more than 3 days per month and taking OCs continuously for 12 weeks followed by 1 week of withdrawal. Repeat the OC regimen so that the patient has only 4 withdrawal “periods” per year.
Monitor patients every 3 to 6 months the first year and annually thereafter if they are doing well. If this approach fails, laparoscopy usually is the next step, although a 3-month trial of gonadotropin-releasing hormone (GnRH) agonists may be attempted.
Option 2Ovarian suppression
Achieve this using OCs, progestins, danazol, or GnRH agonists or antagonists.
Oral contraceptives can be given cyclically, but many patients do better with continuous active-ingredient tablets for 3 months, followed by withdrawal for 1 week and then repetition. Monophasic OCs are superior to triphasic formulations.
The best beginning dosage usually is 35 μg of ethinyl estradiol, but this can be decreased if the patient is symptomatic with headaches; it also can be increased for breakthrough bleeding. Norethindrone 0.35 to 0.5 mg daily may be added if the patient is still symptomatic with bleeding.
Transdermal estradiol (0.05 mg or 0.1 mg twice weekly) also may be used if it is better tolerated. Treatment lasts 3 to 6 months.
Progestins alone such as medroxyprogesterone acetate (20 to 30 mg daily) or depot medroxyprogesterone acetate (150 mg every 3 months) suppress gonadotropin secretion and ovarian function but can be associated with breakthrough bleeding, mastalgia, bloating, weight gain, and depression.
Danazol (200 to 400 mg twice daily) functions primarily by suppressing follicle-stimulating hormone and luteinizing hormone from the pituitary gland, thereby creating a hypoestrogenic state. Unfortunately, danazol also is associated with androgenic side effects and for that reason is rarely used today. Still, it can be an effective second-line drug.
Laparoscopic treatment is sometimes combined with ovarian suppression to improve success or facilitate surgery.
GnRH agonists include nafarelin acetate nasal spray (200 μg twice daily), leuprolide acetate as an intramuscular injection (3.75 mg monthly), and goserelin implant (for 3-month release).
GnRH agonists cause hypoestrogenemia (ie, estradiol less than 40 pg/mL) and resultant amenorrhea, which permits regression of endometriosis and relief of symptoms. Side effects include hot flashes in about 90% of patients, decreased libido, vaginal dryness, headaches, emotional lability, and insomnia.
- The problem of bone loss. The major concern with GnRH agonists is the loss of bone density—about 3% to 8%—which occurs over 6 months of drug therapy, with a 2% to 3% loss persisting approximately 1 year after treatment.5 While only one 6-month course of GnRH agonist is approved by the US Food and Drug Administration, studies have shown that 3 months of treatment—both initially and for subsequent retreatment (if symptoms recur)—is as effective as 6 months of treatment and is associated with less bone loss.6,7 Patients generally should undergo dual-photon absorptiometry to confirm that they have normal bone density before beginning GnRH-agonist retreatment. In addition, patients should be fully informed of the potential risks of therapy. Subsequent symptoms also may be treated with OCs, danazol, and/or surgery.
- Hot flashes can be effectively managed with norethindrone (2.5 mg daily). Low doses of estrogen (conjugated estrogen 0.6 mg or estradiol 1 mg per day) have also been used as “add-back” therapy to reduce bone loss. More recently, add-back therapy for 6 to 12 months with norethindrone (2.5 mg daily) and alendronate (10 mg daily) has been suggested, along with calcium (1,000 mg per day).8 While these appear to be effective, the long-term impact of such add-back therapy is still being evaluated.
Option 3Surgical treatment
Laparoscopy enables treatment to be initiated, when appropriate, and possibly completed at the same time as diagnosis. Surgical therapy usually is conservative, consisting of excision, laser vaporization, or electrosurgical coagulation of endometriosis. Adjunctive procedures such as salpingo-ovariolysis also may be performed.
Other controversial but occasionally indicated procedures for pain include uterosacral nerve ablation and, for severe midline dysmenorrhea, presacral neurectomy.
Medical and surgical treatments sometimes have the same results, but surgical treatment completed at the time of diagnosis has a distinct advantage over medical therapy because of the decreased time, cost, and side effects associated with it.
Option 4Combined treatment
Laparoscopic treatment of endometriosis is sometimes combined with ovarian suppression to improve success or facilitate surgical procedures.
Preoperative medical therapy, for example, suppresses ovulation so that functional cysts are not present, since they may be confused with endometriosis. Metastatic or extensive superficial disease is suppressed and becomes atrophic. Other uses of GnRH agonists prior to surgery include reducing symptoms, increasing the time available for adequate preoperative evaluation, facilitating scheduling, and even delaying or avoiding surgery for a woman nearing menopause.
Potential disadvantages of preoperative medical treatment include the changed appearance of endometriosis, which may make the disease more difficult to diagnose; drug cost and side effects; delay of diagnosis; and delay in attempting pregnancy.
Postoperative medical treatment. GnRH agonists may be indicated postoperatively if complete resection of disease has not been accomplished or for treatment of pain. Preoperative or postoperative treatment usually is given for 2 to 6 months, but 3 months is adequate for most women. An especially successful treatment approach for patients who do not desire pregnancy is to give OCs continuously for 2 to 3 months after surgery, withdraw for 1 week, and repeat the 2 to 3 months of treatment. In a few cases, where indicated, OCs can be continued until menopause or until the patient wishes to attempt pregnancy. It is the most cost-effective approach for many patients.
Treatment outcomes
Pain. If a woman has persistent pain after several months of expectant management, such as the patient described at the opening of this article, continuous OCs (3 months on, 1 week off) and GnRH agonists appear to be similarly effective. Approximately 80% to 90% of patients experience significant relief while on OCs or GnRH agonists, but more than 50% have some dysmenorrhea by 6 months after the agent is discontinued.9
- Laparoscopic treatment also is effective in treating pelvic pain, with approximately 60% to 100% of patients showing significant clinical improvement following complete resection of disease.10 Of patients who have relief of pain at 6 months after conservative surgery, 90% continue to have decreased pain at 1 year.11
- Hysterectomy with oophorectomy results in a very high probability of “cure,” but should be avoided, if possible, in young women with minimal or mild disease. There is a small recurrence rate after hysterectomy, in the range of 5% to 8%.12 This rate may be reduced by meticulous resection of all endometriosis at the time of hysterectomy and by performing concomitant oophorectomy.
- Fertility treatment. Controlled ovarian hyperstimulation with clomiphene citrate (150 mg every day from cycle day 3 to 7) or gonadotropins and intrauterine insemination improves pregnancy rates in this group. Most patients will conceive within 3 to 6 cycles of clomiphene treatment; thus, therapy should not continue past that time.
- Medical treatment delays conception. Ovarian suppression for minimal and mild endometriosis merely delays the possibility of pregnancy by the duration of the therapy and is associated with additional cost and undesirable side effects. For that reason, medical therapy should not be used to treat minimal and mild endometriosis when the only symptom is infertility.
- Pregnancy after laparoscopy. A review of laparoscopic treatment of endometriosis reported pregnancy rates for minimal and mild disease of 58% whether treated by electrocoagulation or by CO2laser.17
Choosing a management approach
Treat disease at time of diagnosis. Endometriosis cannot be fully diagnosed without laparoscopy. Whether the patient’s symptoms involve pain or infertility, surgical treatment involving complete laparoscopic resection of the disease should be performed at the time of diagnosis, provided the surgeon is sufficiently skilled.18 The only exceptions to this approach are:
- patients given a presumptive diagnosis of endometriosis who plan to undergo a trial of medical therapy for pain, and
- young women with infertility as the sole symptom and extensive superficial peritoneal and/or ovarian disease. Treatment of such lesions may increase pregnancy rates, but also can lead to pelvic adhesions.
If the patient has adequate surgical extirpation of the disease, no further postoperative medical treatment is indicated (except for OCs), for either pain or infertility. If pain recurs, GnRH agonists usually should be the first line of treatment.
For infertile patients who fail to conceive, a second-look laparoscopy at 6 to 18 months is occasionally indicated, although in vitro fertilization may be more cost-effective, especially if other infertility factors are present.19
When no operative laparoscopy is performed or when resection of endometriosis is incomplete, pain patients are usually best managed with GnRH agonists or danazol for 3 to 6 months (TABLE). (GnRH agonists are generally preferred because of their more favorable side-effect profile.) If pain continues despite surgical and/or medical treatment, refer the patient to pain specialists for a comprehensive management approach. Discuss this option with the patient at her first consultation and integrate it into the treatment plan.
For infertility patients who have not undergone operative resection or who have had inadequate resection, minimal and mild disease needs no further treatment. Ovarian suppression should be avoided. Patients who do not conceive within approximately 6 to 15 months should generally move on to in vitro fertilization, although repeat laparoscopy is occasionally indicated if there is residual disease and pain associated with the infertility.
TABLE
Reports of pain in patients with laparoscopically diagnosed endometriosis treated with nafarelin acetate or danazol
| TREATMENT | DYSMENORRHEA | DYSPAREUNIA | PELVIC | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NO. | % | NO. | % | NO. | % | |||||
| ABSENT | PRESENT | ABSENT | PRESENT | NOT REPORTED | ABSENT | PRESENT | ||||
| Nafarelin 800 μg daily | 45 | 26 | 40 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 100 | 0 | 62 | 31 | 8 | 65 | 35 | |||
| Posttreatment† | 36 | 64 | 62 | 35 | 4 | 45 | 55 | |||
| Nafarelin 400 μg daily | 45 | 31 | 37 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 98 | 2 | 65 | 32 | 3 | 57 | 43 | |||
| Posttreatment† | 33 | 67 | 71 | 29 | 0 | 49 | 51 | |||
| Danazol 400 mg bid | 34 | 23 | 28 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 94 | 6 | 70 | 17 | 13 | 64 | 36 | |||
| Posttreatment† | 50 | 50 | 65 | 30 | 4 | 50 | 50 | |||
| bid = twice a day | ||||||||||
| All subjects reported pain on admission. | ||||||||||
| *Treatment was continued for 6 months | ||||||||||
| †Posttreatment period was 6 months follow-up | ||||||||||
| Source: Adamson and Kwei20 | ||||||||||
Treat the whole patient: Lifestyle and other factors
It is critical that physicians recognize the degree to which endometriosis can physically and emotionally disrupt patients’ lives. Understanding, empathy, and a comprehensive management approach are valuable components of successful treatment.
The patient also should be encouraged to develop a healthy lifestyle with respect to diet, exercise, and sleep. Stress reduction through mind-body techniques can be very helpful, as well.
If pain continues despite surgical or medical treatment, refer the patient to pain specialists for comprehensive management.
Information about the disease can serve as psychological support and is available from organizations such as the Endometriosis Association (www.endometriosisassn.org), RESOLVE (www.resolve.org), and the American Society for Reproductive Medicine (www.asrm.org). Personal or group counseling also may be helpful, especially for the patient with chronic pain.
Some patients may seek nontraditional and unproven approaches to treatment, such as acupuncture, herbal medicine, or special diets. Management in these chronic, complex situations should focus on alleviation of symptoms and improved quality of life.
A comprehensive evaluation of gastrointestinal, genitourinary, musculoskeletal, neurologic, and psychological systems may be indicated. Referral to a pain clinic may be helpful for further treatment, including biofeed back strategies, nerve blocks, psychotherapy, or other pain-management techniques.
Treatment of reactive depression frequently is necessary and often requires a multidisciplinary approach.
A comprehensive long-range treatment approach should be individualized to the patient. A complete cure can sometimes be achieved only by total hysterectomy and bilateral salpingo-oophorectomy.
Dr. Adamson reports no financial relationships relevant to this article.
1. Wheeler JM. Epidemiology of endometriosis-associated infertility. J Reprod Med. 1989;34:41-46.
2. Olive DL, Blackwell RE, Copperman AB. Endometriosis and pelvic pain. In: Blackwell RE, Olive DL, eds. Chronic Pelvic Pain. New York: Springer-Verlag; 1998;61-83.
3. Witz CA, Shenken RS. Pathogenesis. In: Speroff L, Adamson GD, eds. Seminar in Reproductive Endocrinology: Endometriosis. Vol. 15. New York: Thieme; 1997;199-200.
4. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997;67:817-821.
5. Lupron Depot 3.75 mg (leuprolide acetate for depot suspension). Physician’s Desk Reference. Montvale, NJ: Medical Economics; 1992;2311.-
6. Hornstein MD, Yuzpe AA, Burry KA, Heinrichs LR, Buttram VL, Jr, Orwall ES. Prospective randomized double-blind trial of 3 versus 6 months of nafarelin therapy for endometriosis associated pelvic pain. Fertil Steril. 1995;63:955-962.
7. Adamson GD, Heinrichs WC, Henzl MR, et al. Therapeutic efficacy and bone mineral density (BMD) response during and following a 3-month retreatment of endometriosis with nafarelin (Synarel). Am J Obstet Gynecol. 1997;177:1413-1418.
8. Surrey ES. and the Add-Bac, Consensus Working Group. Add-back therapy and gonadotrophin-releasing hormone agonists in the treatment of patients with endometriosis: can a consensus be reached? Fertil Steril. 1999;71:420-424.
9. Adamson GD, Kwei L, Edgren RA. Pain of endometriosis. Effects of nafarelin and danazol therapy. Int J Fertil. 1994;39:215-217.
10. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized double-blind controls: trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild and moderate endometriosis. Fertil Steril. 1994;62:969-970.
11. Jones KD, Haines F, Sutton CJG. Long-term follow-up of a controlled trial of laser laparoscopy for pelvic pain. JSLS. 2002;5:111-115.
12. Walters MD. Definitive surgery. In: Schenken RS, ed. Endometriosis: Contemporary Concepts in Clinical Management. Philadelphia: JB Lippincott; 1989;267-278.
13. Marcoux S, Maheux R, Berube S, et al. Laparoscopic surgery in infertile women with minimal or mild endometriosis. N Engl J Med. 1997;337:217-222.
14. Adamson GD, Hurd SJ, Pasta DJ, Rodriguez BD. Laparoscopic endometriosis treatment: is it better? Fertil Steril. 1993;59(1):35-44.
15. Adamson GD, Pasta DJ. Surgical treatment of endometriosis associated infertility: meta-analysis compared with survival analysis. Am J Obstet Gynecol. 1994;171:1488-1505.
16. Society for Assisted Reproductive Technology and the American Society for Reproductive Medicine. Assisted reproductive technology in the United States: 1999 results generated from the American Society for Reproductive Medicine/Society for Assisted Reproductive Technology Registry. Fertil Steril. 2002;78:918-931.
17. Kim AH, Adamson GD. Does therapy for minimal/mild endometriosis enhance conception? Inf Reprod Med Clin North Am. 1997;8:632-637.
18. Adamson GD. Laparoscopic treatment of endometriosis. In: Adamson GD, Martin DC, eds. Endoscopic Management of Gynecologic Disease. Philadelphia: Lippincott-Raven; 1995;147-148.
19. Adamson GD. A 36-year-old woman with endometriosis, pelvic pain and infertility. JAMA. 1999;282:2347-2354.
20. Adamson GD, Kwei L, Edgren RA. Pain of endometriosis: effects of nafarelin and danazol therapy. Int J Fertil. 1994;39:215-217.
- Signs of minimal or mild endometriosis include tenderness or nodularity in the posterior cul-de-sac, especially at the uterosacral ligaments, and anterior cul-de-sac nodularity.
- Endometriosis can be associated with infertility at all stages of disease.
- Indications for laparoscopy include infertility of more than 1 year without other symptoms or after 6 months if the patient has other symptoms or is more than 35 years of age. Patients with pelvic pain that has not responded after 3 months of nonsteroidal anti-inflammatory drugs and/or oral contraceptives also are candidates.
- Following adequate surgical extirpation of disease, no further postoperative medical treatment is necessary for patients with either pain or infertility. However, oral contraceptives have benefits for many patients who are not attempting to conceive.
This case represents 1 of the challenges of treating minimal to mild endometriosis—disease without adhesions, invasive lesions, or endometriomas. Endometriosis is suggested in this patient by tenderness or nodularity in the posterior cul-de-sac, especially at the uterosacral ligaments, and anterior cul-de-sac nodularity. The patient’s complaint of pain does not necessarily indicate severe disease. Rather, the relationship between minimal or mild disease and symptoms is unclear. The patient may report significant pain when only superficial implants and minimal adhesions are present.
Although hysterectomy is the definitive treatment for patients with recurrent or intractable pain associated with endometriosis, I make every effort to avoid this operation in young women with minimal to mild disease. This article describes 4 other options—no treatment, ovarian suppression, surgical treatment, and combined treatment—and points out potential pitfalls associated with each approach.
Diagnosis
The diagnosis of endometriosis often can be difficult, and the extent of disease is thought to be underestimated in as many as 50% of patients.1-3
Clinical presentation. Endometriosis presents as pelvic pain in about 50% of patients, infertility in about 25%, pain and infertility in about 25%, and as ovarian endometrioma in less than 5% of cases.1-3 Asymptomatic disease is frequent: from 1% to 40%.1-3 The disease may occur any time after puberty, including adolescence. For other symptoms and characteristics, see “Endometriosis: A snapshot”.
Physical examination. Pelvic examination should be performed at the time of menses, when disease is more easily identified. The location of tenderness often corresponds to the location of the pain. As in the example case, signs of minimal or mild disease include:
- tenderness or nodularity in the posterior culde-sac, especially at the uterosacral ligaments
- anterior cul-de-sac nodularity
Indications for laparoscopy include infertility of more than 1 year without other symptoms or after 6 months if the patient has other symptoms or is more than 35 years of age. Evaluation for other female factors and sperm quality should be conducted prior to laparoscopy. Patients with pelvic pain that has not responded after 3 months of NSAIDs and/or oral contraceptives (OCs) also are candidates for laparoscopy. In the case described above, I would recommend at least a 3-month trial of OCs and NSAIDs before performing laparoscopy.
Staging the disease. The American Society for Reproductive Medicine has developed a staging system with scores from 1 to 150. Minimal and mild disease ranges from 1 to 15.4
Management options. Depending on the woman’s reproductive goals, 1 of the 4 options discussed below may be recommended.
Prevalence. Endometriosis affects about 7% of reproductive-aged women—approximately 5 million Americans. Most of these women are unaware that they have the disease, although many may suffer symptoms ranging from pelvic pain to infertility.
Symptoms. Endometriosis is suggested by a variety of symptoms, including dysmenorrhea, dyspareunia (especially with aching following coitus, as in the case described at the opening of this article), dyschezia, dysuria, mittelschmerz, or focal or generalized pelvic pain. Hematuria and hematochezia also may be present. About 30% of patients with endometriosis have no pain.1
Diagnostic challenges. Deeply invasive endometriosis that is overlooked or develops outside the posterior cul-de-sac can be inappropriately staged as minimal or mild disease.
Causes of pain. Pain symptoms often do not correlate well with disease severity. Pain may be due to secretion of irritating factors (eg, histamine), adhesions that cause scarring or retraction, immunologic reactivity, or other unknown entities.
Infertility can occur at any stage. Not surprisingly, patients who have severe or extensive disease have a poorer prognosis than those with minimal or mild disease.
Endometriosis is a progressive disease, but the rate of progression and nature of lesions vary from patient to patient. Adhesions develop due to the inflammatory process caused by longstanding endometriosis, becoming more extensive and dense over time. Complete cul-de-sac obliteration can result from longstanding invasive and adhesive disease or may stem from abnormal mullerian development.
Option 1No treatment
This option includes expectant management and/or limited use of analgesics and NSAIDs, which may be especially helpful for women with dysmenorrhea, particularly when infertility is the primary complaint. In other instances, this approach may fail to provide adequate relief from pain.
Almost all patients should undergo an initial trial of NSAIDs and/or OCs, using NSAIDs no more than 3 days per month and taking OCs continuously for 12 weeks followed by 1 week of withdrawal. Repeat the OC regimen so that the patient has only 4 withdrawal “periods” per year.
Monitor patients every 3 to 6 months the first year and annually thereafter if they are doing well. If this approach fails, laparoscopy usually is the next step, although a 3-month trial of gonadotropin-releasing hormone (GnRH) agonists may be attempted.
Option 2Ovarian suppression
Achieve this using OCs, progestins, danazol, or GnRH agonists or antagonists.
Oral contraceptives can be given cyclically, but many patients do better with continuous active-ingredient tablets for 3 months, followed by withdrawal for 1 week and then repetition. Monophasic OCs are superior to triphasic formulations.
The best beginning dosage usually is 35 μg of ethinyl estradiol, but this can be decreased if the patient is symptomatic with headaches; it also can be increased for breakthrough bleeding. Norethindrone 0.35 to 0.5 mg daily may be added if the patient is still symptomatic with bleeding.
Transdermal estradiol (0.05 mg or 0.1 mg twice weekly) also may be used if it is better tolerated. Treatment lasts 3 to 6 months.
Progestins alone such as medroxyprogesterone acetate (20 to 30 mg daily) or depot medroxyprogesterone acetate (150 mg every 3 months) suppress gonadotropin secretion and ovarian function but can be associated with breakthrough bleeding, mastalgia, bloating, weight gain, and depression.
Danazol (200 to 400 mg twice daily) functions primarily by suppressing follicle-stimulating hormone and luteinizing hormone from the pituitary gland, thereby creating a hypoestrogenic state. Unfortunately, danazol also is associated with androgenic side effects and for that reason is rarely used today. Still, it can be an effective second-line drug.
Laparoscopic treatment is sometimes combined with ovarian suppression to improve success or facilitate surgery.
GnRH agonists include nafarelin acetate nasal spray (200 μg twice daily), leuprolide acetate as an intramuscular injection (3.75 mg monthly), and goserelin implant (for 3-month release).
GnRH agonists cause hypoestrogenemia (ie, estradiol less than 40 pg/mL) and resultant amenorrhea, which permits regression of endometriosis and relief of symptoms. Side effects include hot flashes in about 90% of patients, decreased libido, vaginal dryness, headaches, emotional lability, and insomnia.
- The problem of bone loss. The major concern with GnRH agonists is the loss of bone density—about 3% to 8%—which occurs over 6 months of drug therapy, with a 2% to 3% loss persisting approximately 1 year after treatment.5 While only one 6-month course of GnRH agonist is approved by the US Food and Drug Administration, studies have shown that 3 months of treatment—both initially and for subsequent retreatment (if symptoms recur)—is as effective as 6 months of treatment and is associated with less bone loss.6,7 Patients generally should undergo dual-photon absorptiometry to confirm that they have normal bone density before beginning GnRH-agonist retreatment. In addition, patients should be fully informed of the potential risks of therapy. Subsequent symptoms also may be treated with OCs, danazol, and/or surgery.
- Hot flashes can be effectively managed with norethindrone (2.5 mg daily). Low doses of estrogen (conjugated estrogen 0.6 mg or estradiol 1 mg per day) have also been used as “add-back” therapy to reduce bone loss. More recently, add-back therapy for 6 to 12 months with norethindrone (2.5 mg daily) and alendronate (10 mg daily) has been suggested, along with calcium (1,000 mg per day).8 While these appear to be effective, the long-term impact of such add-back therapy is still being evaluated.
Option 3Surgical treatment
Laparoscopy enables treatment to be initiated, when appropriate, and possibly completed at the same time as diagnosis. Surgical therapy usually is conservative, consisting of excision, laser vaporization, or electrosurgical coagulation of endometriosis. Adjunctive procedures such as salpingo-ovariolysis also may be performed.
Other controversial but occasionally indicated procedures for pain include uterosacral nerve ablation and, for severe midline dysmenorrhea, presacral neurectomy.
Medical and surgical treatments sometimes have the same results, but surgical treatment completed at the time of diagnosis has a distinct advantage over medical therapy because of the decreased time, cost, and side effects associated with it.
Option 4Combined treatment
Laparoscopic treatment of endometriosis is sometimes combined with ovarian suppression to improve success or facilitate surgical procedures.
Preoperative medical therapy, for example, suppresses ovulation so that functional cysts are not present, since they may be confused with endometriosis. Metastatic or extensive superficial disease is suppressed and becomes atrophic. Other uses of GnRH agonists prior to surgery include reducing symptoms, increasing the time available for adequate preoperative evaluation, facilitating scheduling, and even delaying or avoiding surgery for a woman nearing menopause.
Potential disadvantages of preoperative medical treatment include the changed appearance of endometriosis, which may make the disease more difficult to diagnose; drug cost and side effects; delay of diagnosis; and delay in attempting pregnancy.
Postoperative medical treatment. GnRH agonists may be indicated postoperatively if complete resection of disease has not been accomplished or for treatment of pain. Preoperative or postoperative treatment usually is given for 2 to 6 months, but 3 months is adequate for most women. An especially successful treatment approach for patients who do not desire pregnancy is to give OCs continuously for 2 to 3 months after surgery, withdraw for 1 week, and repeat the 2 to 3 months of treatment. In a few cases, where indicated, OCs can be continued until menopause or until the patient wishes to attempt pregnancy. It is the most cost-effective approach for many patients.
Treatment outcomes
Pain. If a woman has persistent pain after several months of expectant management, such as the patient described at the opening of this article, continuous OCs (3 months on, 1 week off) and GnRH agonists appear to be similarly effective. Approximately 80% to 90% of patients experience significant relief while on OCs or GnRH agonists, but more than 50% have some dysmenorrhea by 6 months after the agent is discontinued.9
- Laparoscopic treatment also is effective in treating pelvic pain, with approximately 60% to 100% of patients showing significant clinical improvement following complete resection of disease.10 Of patients who have relief of pain at 6 months after conservative surgery, 90% continue to have decreased pain at 1 year.11
- Hysterectomy with oophorectomy results in a very high probability of “cure,” but should be avoided, if possible, in young women with minimal or mild disease. There is a small recurrence rate after hysterectomy, in the range of 5% to 8%.12 This rate may be reduced by meticulous resection of all endometriosis at the time of hysterectomy and by performing concomitant oophorectomy.
- Fertility treatment. Controlled ovarian hyperstimulation with clomiphene citrate (150 mg every day from cycle day 3 to 7) or gonadotropins and intrauterine insemination improves pregnancy rates in this group. Most patients will conceive within 3 to 6 cycles of clomiphene treatment; thus, therapy should not continue past that time.
- Medical treatment delays conception. Ovarian suppression for minimal and mild endometriosis merely delays the possibility of pregnancy by the duration of the therapy and is associated with additional cost and undesirable side effects. For that reason, medical therapy should not be used to treat minimal and mild endometriosis when the only symptom is infertility.
- Pregnancy after laparoscopy. A review of laparoscopic treatment of endometriosis reported pregnancy rates for minimal and mild disease of 58% whether treated by electrocoagulation or by CO2laser.17
Choosing a management approach
Treat disease at time of diagnosis. Endometriosis cannot be fully diagnosed without laparoscopy. Whether the patient’s symptoms involve pain or infertility, surgical treatment involving complete laparoscopic resection of the disease should be performed at the time of diagnosis, provided the surgeon is sufficiently skilled.18 The only exceptions to this approach are:
- patients given a presumptive diagnosis of endometriosis who plan to undergo a trial of medical therapy for pain, and
- young women with infertility as the sole symptom and extensive superficial peritoneal and/or ovarian disease. Treatment of such lesions may increase pregnancy rates, but also can lead to pelvic adhesions.
If the patient has adequate surgical extirpation of the disease, no further postoperative medical treatment is indicated (except for OCs), for either pain or infertility. If pain recurs, GnRH agonists usually should be the first line of treatment.
For infertile patients who fail to conceive, a second-look laparoscopy at 6 to 18 months is occasionally indicated, although in vitro fertilization may be more cost-effective, especially if other infertility factors are present.19
When no operative laparoscopy is performed or when resection of endometriosis is incomplete, pain patients are usually best managed with GnRH agonists or danazol for 3 to 6 months (TABLE). (GnRH agonists are generally preferred because of their more favorable side-effect profile.) If pain continues despite surgical and/or medical treatment, refer the patient to pain specialists for a comprehensive management approach. Discuss this option with the patient at her first consultation and integrate it into the treatment plan.
For infertility patients who have not undergone operative resection or who have had inadequate resection, minimal and mild disease needs no further treatment. Ovarian suppression should be avoided. Patients who do not conceive within approximately 6 to 15 months should generally move on to in vitro fertilization, although repeat laparoscopy is occasionally indicated if there is residual disease and pain associated with the infertility.
TABLE
Reports of pain in patients with laparoscopically diagnosed endometriosis treated with nafarelin acetate or danazol
| TREATMENT | DYSMENORRHEA | DYSPAREUNIA | PELVIC | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NO. | % | NO. | % | NO. | % | |||||
| ABSENT | PRESENT | ABSENT | PRESENT | NOT REPORTED | ABSENT | PRESENT | ||||
| Nafarelin 800 μg daily | 45 | 26 | 40 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 100 | 0 | 62 | 31 | 8 | 65 | 35 | |||
| Posttreatment† | 36 | 64 | 62 | 35 | 4 | 45 | 55 | |||
| Nafarelin 400 μg daily | 45 | 31 | 37 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 98 | 2 | 65 | 32 | 3 | 57 | 43 | |||
| Posttreatment† | 33 | 67 | 71 | 29 | 0 | 49 | 51 | |||
| Danazol 400 mg bid | 34 | 23 | 28 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 94 | 6 | 70 | 17 | 13 | 64 | 36 | |||
| Posttreatment† | 50 | 50 | 65 | 30 | 4 | 50 | 50 | |||
| bid = twice a day | ||||||||||
| All subjects reported pain on admission. | ||||||||||
| *Treatment was continued for 6 months | ||||||||||
| †Posttreatment period was 6 months follow-up | ||||||||||
| Source: Adamson and Kwei20 | ||||||||||
Treat the whole patient: Lifestyle and other factors
It is critical that physicians recognize the degree to which endometriosis can physically and emotionally disrupt patients’ lives. Understanding, empathy, and a comprehensive management approach are valuable components of successful treatment.
The patient also should be encouraged to develop a healthy lifestyle with respect to diet, exercise, and sleep. Stress reduction through mind-body techniques can be very helpful, as well.
If pain continues despite surgical or medical treatment, refer the patient to pain specialists for comprehensive management.
Information about the disease can serve as psychological support and is available from organizations such as the Endometriosis Association (www.endometriosisassn.org), RESOLVE (www.resolve.org), and the American Society for Reproductive Medicine (www.asrm.org). Personal or group counseling also may be helpful, especially for the patient with chronic pain.
Some patients may seek nontraditional and unproven approaches to treatment, such as acupuncture, herbal medicine, or special diets. Management in these chronic, complex situations should focus on alleviation of symptoms and improved quality of life.
A comprehensive evaluation of gastrointestinal, genitourinary, musculoskeletal, neurologic, and psychological systems may be indicated. Referral to a pain clinic may be helpful for further treatment, including biofeed back strategies, nerve blocks, psychotherapy, or other pain-management techniques.
Treatment of reactive depression frequently is necessary and often requires a multidisciplinary approach.
A comprehensive long-range treatment approach should be individualized to the patient. A complete cure can sometimes be achieved only by total hysterectomy and bilateral salpingo-oophorectomy.
Dr. Adamson reports no financial relationships relevant to this article.
- Signs of minimal or mild endometriosis include tenderness or nodularity in the posterior cul-de-sac, especially at the uterosacral ligaments, and anterior cul-de-sac nodularity.
- Endometriosis can be associated with infertility at all stages of disease.
- Indications for laparoscopy include infertility of more than 1 year without other symptoms or after 6 months if the patient has other symptoms or is more than 35 years of age. Patients with pelvic pain that has not responded after 3 months of nonsteroidal anti-inflammatory drugs and/or oral contraceptives also are candidates.
- Following adequate surgical extirpation of disease, no further postoperative medical treatment is necessary for patients with either pain or infertility. However, oral contraceptives have benefits for many patients who are not attempting to conceive.
This case represents 1 of the challenges of treating minimal to mild endometriosis—disease without adhesions, invasive lesions, or endometriomas. Endometriosis is suggested in this patient by tenderness or nodularity in the posterior cul-de-sac, especially at the uterosacral ligaments, and anterior cul-de-sac nodularity. The patient’s complaint of pain does not necessarily indicate severe disease. Rather, the relationship between minimal or mild disease and symptoms is unclear. The patient may report significant pain when only superficial implants and minimal adhesions are present.
Although hysterectomy is the definitive treatment for patients with recurrent or intractable pain associated with endometriosis, I make every effort to avoid this operation in young women with minimal to mild disease. This article describes 4 other options—no treatment, ovarian suppression, surgical treatment, and combined treatment—and points out potential pitfalls associated with each approach.
Diagnosis
The diagnosis of endometriosis often can be difficult, and the extent of disease is thought to be underestimated in as many as 50% of patients.1-3
Clinical presentation. Endometriosis presents as pelvic pain in about 50% of patients, infertility in about 25%, pain and infertility in about 25%, and as ovarian endometrioma in less than 5% of cases.1-3 Asymptomatic disease is frequent: from 1% to 40%.1-3 The disease may occur any time after puberty, including adolescence. For other symptoms and characteristics, see “Endometriosis: A snapshot”.
Physical examination. Pelvic examination should be performed at the time of menses, when disease is more easily identified. The location of tenderness often corresponds to the location of the pain. As in the example case, signs of minimal or mild disease include:
- tenderness or nodularity in the posterior culde-sac, especially at the uterosacral ligaments
- anterior cul-de-sac nodularity
Indications for laparoscopy include infertility of more than 1 year without other symptoms or after 6 months if the patient has other symptoms or is more than 35 years of age. Evaluation for other female factors and sperm quality should be conducted prior to laparoscopy. Patients with pelvic pain that has not responded after 3 months of NSAIDs and/or oral contraceptives (OCs) also are candidates for laparoscopy. In the case described above, I would recommend at least a 3-month trial of OCs and NSAIDs before performing laparoscopy.
Staging the disease. The American Society for Reproductive Medicine has developed a staging system with scores from 1 to 150. Minimal and mild disease ranges from 1 to 15.4
Management options. Depending on the woman’s reproductive goals, 1 of the 4 options discussed below may be recommended.
Prevalence. Endometriosis affects about 7% of reproductive-aged women—approximately 5 million Americans. Most of these women are unaware that they have the disease, although many may suffer symptoms ranging from pelvic pain to infertility.
Symptoms. Endometriosis is suggested by a variety of symptoms, including dysmenorrhea, dyspareunia (especially with aching following coitus, as in the case described at the opening of this article), dyschezia, dysuria, mittelschmerz, or focal or generalized pelvic pain. Hematuria and hematochezia also may be present. About 30% of patients with endometriosis have no pain.1
Diagnostic challenges. Deeply invasive endometriosis that is overlooked or develops outside the posterior cul-de-sac can be inappropriately staged as minimal or mild disease.
Causes of pain. Pain symptoms often do not correlate well with disease severity. Pain may be due to secretion of irritating factors (eg, histamine), adhesions that cause scarring or retraction, immunologic reactivity, or other unknown entities.
Infertility can occur at any stage. Not surprisingly, patients who have severe or extensive disease have a poorer prognosis than those with minimal or mild disease.
Endometriosis is a progressive disease, but the rate of progression and nature of lesions vary from patient to patient. Adhesions develop due to the inflammatory process caused by longstanding endometriosis, becoming more extensive and dense over time. Complete cul-de-sac obliteration can result from longstanding invasive and adhesive disease or may stem from abnormal mullerian development.
Option 1No treatment
This option includes expectant management and/or limited use of analgesics and NSAIDs, which may be especially helpful for women with dysmenorrhea, particularly when infertility is the primary complaint. In other instances, this approach may fail to provide adequate relief from pain.
Almost all patients should undergo an initial trial of NSAIDs and/or OCs, using NSAIDs no more than 3 days per month and taking OCs continuously for 12 weeks followed by 1 week of withdrawal. Repeat the OC regimen so that the patient has only 4 withdrawal “periods” per year.
Monitor patients every 3 to 6 months the first year and annually thereafter if they are doing well. If this approach fails, laparoscopy usually is the next step, although a 3-month trial of gonadotropin-releasing hormone (GnRH) agonists may be attempted.
Option 2Ovarian suppression
Achieve this using OCs, progestins, danazol, or GnRH agonists or antagonists.
Oral contraceptives can be given cyclically, but many patients do better with continuous active-ingredient tablets for 3 months, followed by withdrawal for 1 week and then repetition. Monophasic OCs are superior to triphasic formulations.
The best beginning dosage usually is 35 μg of ethinyl estradiol, but this can be decreased if the patient is symptomatic with headaches; it also can be increased for breakthrough bleeding. Norethindrone 0.35 to 0.5 mg daily may be added if the patient is still symptomatic with bleeding.
Transdermal estradiol (0.05 mg or 0.1 mg twice weekly) also may be used if it is better tolerated. Treatment lasts 3 to 6 months.
Progestins alone such as medroxyprogesterone acetate (20 to 30 mg daily) or depot medroxyprogesterone acetate (150 mg every 3 months) suppress gonadotropin secretion and ovarian function but can be associated with breakthrough bleeding, mastalgia, bloating, weight gain, and depression.
Danazol (200 to 400 mg twice daily) functions primarily by suppressing follicle-stimulating hormone and luteinizing hormone from the pituitary gland, thereby creating a hypoestrogenic state. Unfortunately, danazol also is associated with androgenic side effects and for that reason is rarely used today. Still, it can be an effective second-line drug.
Laparoscopic treatment is sometimes combined with ovarian suppression to improve success or facilitate surgery.
GnRH agonists include nafarelin acetate nasal spray (200 μg twice daily), leuprolide acetate as an intramuscular injection (3.75 mg monthly), and goserelin implant (for 3-month release).
GnRH agonists cause hypoestrogenemia (ie, estradiol less than 40 pg/mL) and resultant amenorrhea, which permits regression of endometriosis and relief of symptoms. Side effects include hot flashes in about 90% of patients, decreased libido, vaginal dryness, headaches, emotional lability, and insomnia.
- The problem of bone loss. The major concern with GnRH agonists is the loss of bone density—about 3% to 8%—which occurs over 6 months of drug therapy, with a 2% to 3% loss persisting approximately 1 year after treatment.5 While only one 6-month course of GnRH agonist is approved by the US Food and Drug Administration, studies have shown that 3 months of treatment—both initially and for subsequent retreatment (if symptoms recur)—is as effective as 6 months of treatment and is associated with less bone loss.6,7 Patients generally should undergo dual-photon absorptiometry to confirm that they have normal bone density before beginning GnRH-agonist retreatment. In addition, patients should be fully informed of the potential risks of therapy. Subsequent symptoms also may be treated with OCs, danazol, and/or surgery.
- Hot flashes can be effectively managed with norethindrone (2.5 mg daily). Low doses of estrogen (conjugated estrogen 0.6 mg or estradiol 1 mg per day) have also been used as “add-back” therapy to reduce bone loss. More recently, add-back therapy for 6 to 12 months with norethindrone (2.5 mg daily) and alendronate (10 mg daily) has been suggested, along with calcium (1,000 mg per day).8 While these appear to be effective, the long-term impact of such add-back therapy is still being evaluated.
Option 3Surgical treatment
Laparoscopy enables treatment to be initiated, when appropriate, and possibly completed at the same time as diagnosis. Surgical therapy usually is conservative, consisting of excision, laser vaporization, or electrosurgical coagulation of endometriosis. Adjunctive procedures such as salpingo-ovariolysis also may be performed.
Other controversial but occasionally indicated procedures for pain include uterosacral nerve ablation and, for severe midline dysmenorrhea, presacral neurectomy.
Medical and surgical treatments sometimes have the same results, but surgical treatment completed at the time of diagnosis has a distinct advantage over medical therapy because of the decreased time, cost, and side effects associated with it.
Option 4Combined treatment
Laparoscopic treatment of endometriosis is sometimes combined with ovarian suppression to improve success or facilitate surgical procedures.
Preoperative medical therapy, for example, suppresses ovulation so that functional cysts are not present, since they may be confused with endometriosis. Metastatic or extensive superficial disease is suppressed and becomes atrophic. Other uses of GnRH agonists prior to surgery include reducing symptoms, increasing the time available for adequate preoperative evaluation, facilitating scheduling, and even delaying or avoiding surgery for a woman nearing menopause.
Potential disadvantages of preoperative medical treatment include the changed appearance of endometriosis, which may make the disease more difficult to diagnose; drug cost and side effects; delay of diagnosis; and delay in attempting pregnancy.
Postoperative medical treatment. GnRH agonists may be indicated postoperatively if complete resection of disease has not been accomplished or for treatment of pain. Preoperative or postoperative treatment usually is given for 2 to 6 months, but 3 months is adequate for most women. An especially successful treatment approach for patients who do not desire pregnancy is to give OCs continuously for 2 to 3 months after surgery, withdraw for 1 week, and repeat the 2 to 3 months of treatment. In a few cases, where indicated, OCs can be continued until menopause or until the patient wishes to attempt pregnancy. It is the most cost-effective approach for many patients.
Treatment outcomes
Pain. If a woman has persistent pain after several months of expectant management, such as the patient described at the opening of this article, continuous OCs (3 months on, 1 week off) and GnRH agonists appear to be similarly effective. Approximately 80% to 90% of patients experience significant relief while on OCs or GnRH agonists, but more than 50% have some dysmenorrhea by 6 months after the agent is discontinued.9
- Laparoscopic treatment also is effective in treating pelvic pain, with approximately 60% to 100% of patients showing significant clinical improvement following complete resection of disease.10 Of patients who have relief of pain at 6 months after conservative surgery, 90% continue to have decreased pain at 1 year.11
- Hysterectomy with oophorectomy results in a very high probability of “cure,” but should be avoided, if possible, in young women with minimal or mild disease. There is a small recurrence rate after hysterectomy, in the range of 5% to 8%.12 This rate may be reduced by meticulous resection of all endometriosis at the time of hysterectomy and by performing concomitant oophorectomy.
- Fertility treatment. Controlled ovarian hyperstimulation with clomiphene citrate (150 mg every day from cycle day 3 to 7) or gonadotropins and intrauterine insemination improves pregnancy rates in this group. Most patients will conceive within 3 to 6 cycles of clomiphene treatment; thus, therapy should not continue past that time.
- Medical treatment delays conception. Ovarian suppression for minimal and mild endometriosis merely delays the possibility of pregnancy by the duration of the therapy and is associated with additional cost and undesirable side effects. For that reason, medical therapy should not be used to treat minimal and mild endometriosis when the only symptom is infertility.
- Pregnancy after laparoscopy. A review of laparoscopic treatment of endometriosis reported pregnancy rates for minimal and mild disease of 58% whether treated by electrocoagulation or by CO2laser.17
Choosing a management approach
Treat disease at time of diagnosis. Endometriosis cannot be fully diagnosed without laparoscopy. Whether the patient’s symptoms involve pain or infertility, surgical treatment involving complete laparoscopic resection of the disease should be performed at the time of diagnosis, provided the surgeon is sufficiently skilled.18 The only exceptions to this approach are:
- patients given a presumptive diagnosis of endometriosis who plan to undergo a trial of medical therapy for pain, and
- young women with infertility as the sole symptom and extensive superficial peritoneal and/or ovarian disease. Treatment of such lesions may increase pregnancy rates, but also can lead to pelvic adhesions.
If the patient has adequate surgical extirpation of the disease, no further postoperative medical treatment is indicated (except for OCs), for either pain or infertility. If pain recurs, GnRH agonists usually should be the first line of treatment.
For infertile patients who fail to conceive, a second-look laparoscopy at 6 to 18 months is occasionally indicated, although in vitro fertilization may be more cost-effective, especially if other infertility factors are present.19
When no operative laparoscopy is performed or when resection of endometriosis is incomplete, pain patients are usually best managed with GnRH agonists or danazol for 3 to 6 months (TABLE). (GnRH agonists are generally preferred because of their more favorable side-effect profile.) If pain continues despite surgical and/or medical treatment, refer the patient to pain specialists for a comprehensive management approach. Discuss this option with the patient at her first consultation and integrate it into the treatment plan.
For infertility patients who have not undergone operative resection or who have had inadequate resection, minimal and mild disease needs no further treatment. Ovarian suppression should be avoided. Patients who do not conceive within approximately 6 to 15 months should generally move on to in vitro fertilization, although repeat laparoscopy is occasionally indicated if there is residual disease and pain associated with the infertility.
TABLE
Reports of pain in patients with laparoscopically diagnosed endometriosis treated with nafarelin acetate or danazol
| TREATMENT | DYSMENORRHEA | DYSPAREUNIA | PELVIC | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NO. | % | NO. | % | NO. | % | |||||
| ABSENT | PRESENT | ABSENT | PRESENT | NOT REPORTED | ABSENT | PRESENT | ||||
| Nafarelin 800 μg daily | 45 | 26 | 40 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 100 | 0 | 62 | 31 | 8 | 65 | 35 | |||
| Posttreatment† | 36 | 64 | 62 | 35 | 4 | 45 | 55 | |||
| Nafarelin 400 μg daily | 45 | 31 | 37 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 98 | 2 | 65 | 32 | 3 | 57 | 43 | |||
| Posttreatment† | 33 | 67 | 71 | 29 | 0 | 49 | 51 | |||
| Danazol 400 mg bid | 34 | 23 | 28 | |||||||
| Admission | 0 | 100 | 0 | 100 | 0 | 0 | 100 | |||
| Treatment* | 94 | 6 | 70 | 17 | 13 | 64 | 36 | |||
| Posttreatment† | 50 | 50 | 65 | 30 | 4 | 50 | 50 | |||
| bid = twice a day | ||||||||||
| All subjects reported pain on admission. | ||||||||||
| *Treatment was continued for 6 months | ||||||||||
| †Posttreatment period was 6 months follow-up | ||||||||||
| Source: Adamson and Kwei20 | ||||||||||
Treat the whole patient: Lifestyle and other factors
It is critical that physicians recognize the degree to which endometriosis can physically and emotionally disrupt patients’ lives. Understanding, empathy, and a comprehensive management approach are valuable components of successful treatment.
The patient also should be encouraged to develop a healthy lifestyle with respect to diet, exercise, and sleep. Stress reduction through mind-body techniques can be very helpful, as well.
If pain continues despite surgical or medical treatment, refer the patient to pain specialists for comprehensive management.
Information about the disease can serve as psychological support and is available from organizations such as the Endometriosis Association (www.endometriosisassn.org), RESOLVE (www.resolve.org), and the American Society for Reproductive Medicine (www.asrm.org). Personal or group counseling also may be helpful, especially for the patient with chronic pain.
Some patients may seek nontraditional and unproven approaches to treatment, such as acupuncture, herbal medicine, or special diets. Management in these chronic, complex situations should focus on alleviation of symptoms and improved quality of life.
A comprehensive evaluation of gastrointestinal, genitourinary, musculoskeletal, neurologic, and psychological systems may be indicated. Referral to a pain clinic may be helpful for further treatment, including biofeed back strategies, nerve blocks, psychotherapy, or other pain-management techniques.
Treatment of reactive depression frequently is necessary and often requires a multidisciplinary approach.
A comprehensive long-range treatment approach should be individualized to the patient. A complete cure can sometimes be achieved only by total hysterectomy and bilateral salpingo-oophorectomy.
Dr. Adamson reports no financial relationships relevant to this article.
1. Wheeler JM. Epidemiology of endometriosis-associated infertility. J Reprod Med. 1989;34:41-46.
2. Olive DL, Blackwell RE, Copperman AB. Endometriosis and pelvic pain. In: Blackwell RE, Olive DL, eds. Chronic Pelvic Pain. New York: Springer-Verlag; 1998;61-83.
3. Witz CA, Shenken RS. Pathogenesis. In: Speroff L, Adamson GD, eds. Seminar in Reproductive Endocrinology: Endometriosis. Vol. 15. New York: Thieme; 1997;199-200.
4. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997;67:817-821.
5. Lupron Depot 3.75 mg (leuprolide acetate for depot suspension). Physician’s Desk Reference. Montvale, NJ: Medical Economics; 1992;2311.-
6. Hornstein MD, Yuzpe AA, Burry KA, Heinrichs LR, Buttram VL, Jr, Orwall ES. Prospective randomized double-blind trial of 3 versus 6 months of nafarelin therapy for endometriosis associated pelvic pain. Fertil Steril. 1995;63:955-962.
7. Adamson GD, Heinrichs WC, Henzl MR, et al. Therapeutic efficacy and bone mineral density (BMD) response during and following a 3-month retreatment of endometriosis with nafarelin (Synarel). Am J Obstet Gynecol. 1997;177:1413-1418.
8. Surrey ES. and the Add-Bac, Consensus Working Group. Add-back therapy and gonadotrophin-releasing hormone agonists in the treatment of patients with endometriosis: can a consensus be reached? Fertil Steril. 1999;71:420-424.
9. Adamson GD, Kwei L, Edgren RA. Pain of endometriosis. Effects of nafarelin and danazol therapy. Int J Fertil. 1994;39:215-217.
10. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized double-blind controls: trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild and moderate endometriosis. Fertil Steril. 1994;62:969-970.
11. Jones KD, Haines F, Sutton CJG. Long-term follow-up of a controlled trial of laser laparoscopy for pelvic pain. JSLS. 2002;5:111-115.
12. Walters MD. Definitive surgery. In: Schenken RS, ed. Endometriosis: Contemporary Concepts in Clinical Management. Philadelphia: JB Lippincott; 1989;267-278.
13. Marcoux S, Maheux R, Berube S, et al. Laparoscopic surgery in infertile women with minimal or mild endometriosis. N Engl J Med. 1997;337:217-222.
14. Adamson GD, Hurd SJ, Pasta DJ, Rodriguez BD. Laparoscopic endometriosis treatment: is it better? Fertil Steril. 1993;59(1):35-44.
15. Adamson GD, Pasta DJ. Surgical treatment of endometriosis associated infertility: meta-analysis compared with survival analysis. Am J Obstet Gynecol. 1994;171:1488-1505.
16. Society for Assisted Reproductive Technology and the American Society for Reproductive Medicine. Assisted reproductive technology in the United States: 1999 results generated from the American Society for Reproductive Medicine/Society for Assisted Reproductive Technology Registry. Fertil Steril. 2002;78:918-931.
17. Kim AH, Adamson GD. Does therapy for minimal/mild endometriosis enhance conception? Inf Reprod Med Clin North Am. 1997;8:632-637.
18. Adamson GD. Laparoscopic treatment of endometriosis. In: Adamson GD, Martin DC, eds. Endoscopic Management of Gynecologic Disease. Philadelphia: Lippincott-Raven; 1995;147-148.
19. Adamson GD. A 36-year-old woman with endometriosis, pelvic pain and infertility. JAMA. 1999;282:2347-2354.
20. Adamson GD, Kwei L, Edgren RA. Pain of endometriosis: effects of nafarelin and danazol therapy. Int J Fertil. 1994;39:215-217.
1. Wheeler JM. Epidemiology of endometriosis-associated infertility. J Reprod Med. 1989;34:41-46.
2. Olive DL, Blackwell RE, Copperman AB. Endometriosis and pelvic pain. In: Blackwell RE, Olive DL, eds. Chronic Pelvic Pain. New York: Springer-Verlag; 1998;61-83.
3. Witz CA, Shenken RS. Pathogenesis. In: Speroff L, Adamson GD, eds. Seminar in Reproductive Endocrinology: Endometriosis. Vol. 15. New York: Thieme; 1997;199-200.
4. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997;67:817-821.
5. Lupron Depot 3.75 mg (leuprolide acetate for depot suspension). Physician’s Desk Reference. Montvale, NJ: Medical Economics; 1992;2311.-
6. Hornstein MD, Yuzpe AA, Burry KA, Heinrichs LR, Buttram VL, Jr, Orwall ES. Prospective randomized double-blind trial of 3 versus 6 months of nafarelin therapy for endometriosis associated pelvic pain. Fertil Steril. 1995;63:955-962.
7. Adamson GD, Heinrichs WC, Henzl MR, et al. Therapeutic efficacy and bone mineral density (BMD) response during and following a 3-month retreatment of endometriosis with nafarelin (Synarel). Am J Obstet Gynecol. 1997;177:1413-1418.
8. Surrey ES. and the Add-Bac, Consensus Working Group. Add-back therapy and gonadotrophin-releasing hormone agonists in the treatment of patients with endometriosis: can a consensus be reached? Fertil Steril. 1999;71:420-424.
9. Adamson GD, Kwei L, Edgren RA. Pain of endometriosis. Effects of nafarelin and danazol therapy. Int J Fertil. 1994;39:215-217.
10. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized double-blind controls: trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild and moderate endometriosis. Fertil Steril. 1994;62:969-970.
11. Jones KD, Haines F, Sutton CJG. Long-term follow-up of a controlled trial of laser laparoscopy for pelvic pain. JSLS. 2002;5:111-115.
12. Walters MD. Definitive surgery. In: Schenken RS, ed. Endometriosis: Contemporary Concepts in Clinical Management. Philadelphia: JB Lippincott; 1989;267-278.
13. Marcoux S, Maheux R, Berube S, et al. Laparoscopic surgery in infertile women with minimal or mild endometriosis. N Engl J Med. 1997;337:217-222.
14. Adamson GD, Hurd SJ, Pasta DJ, Rodriguez BD. Laparoscopic endometriosis treatment: is it better? Fertil Steril. 1993;59(1):35-44.
15. Adamson GD, Pasta DJ. Surgical treatment of endometriosis associated infertility: meta-analysis compared with survival analysis. Am J Obstet Gynecol. 1994;171:1488-1505.
16. Society for Assisted Reproductive Technology and the American Society for Reproductive Medicine. Assisted reproductive technology in the United States: 1999 results generated from the American Society for Reproductive Medicine/Society for Assisted Reproductive Technology Registry. Fertil Steril. 2002;78:918-931.
17. Kim AH, Adamson GD. Does therapy for minimal/mild endometriosis enhance conception? Inf Reprod Med Clin North Am. 1997;8:632-637.
18. Adamson GD. Laparoscopic treatment of endometriosis. In: Adamson GD, Martin DC, eds. Endoscopic Management of Gynecologic Disease. Philadelphia: Lippincott-Raven; 1995;147-148.
19. Adamson GD. A 36-year-old woman with endometriosis, pelvic pain and infertility. JAMA. 1999;282:2347-2354.
20. Adamson GD, Kwei L, Edgren RA. Pain of endometriosis: effects of nafarelin and danazol therapy. Int J Fertil. 1994;39:215-217.
Hypothyroidism: Should we screen all pregnant women?
Emerging research indicates that thyroid hormones play a key role in fetal brain development, and asymptomatic hypothyroidism during pregnancy may have an adverse effect on fetal growth and neurologic development. Findings published in the past year call our attention to the importance of identifying and adequately treating thyroid-deficient gravidas:
- Maternal free thyroxine (FT4) concentration below the 10th percentile at 12 weeks is associated with significant impairment of psychomotor development at ages 1 and 2 years.1
- The average serum thyroid-stimulating hormone (TSH) and FT4 levels of neonates born to hypothyroid mothers were significantly higher than those of controls; birth weight and head circumference were significantly lower.2
But given the paucity of data on how maternal hypothyroidism affects the offspring, is universal screening justified? We review the evidence to date, present the current positions of 3 organizations, and offer recommendations for current clinical practice.
Maternal thyroid status is important throughout gestation
The fetal thyroid gland begins to develop at 3 weeks’ gestation; it concentrates iodine and synthesizes thyroid hormone after 10 to 12 weeks.
Prior to this, the mother provides the thyroid hormones through placental diffusion (see “How thyroid needs change during pregnancy”). Indeed, thyroid hormones have been detected in human coelomic and amniotic fluids as early as 8 weeks’ gestation, before the fetal thyroid starts to function.3
New perspective on role of maternal thyroid function. It was previously believed that the mother’s thyroid hormone supply to the fetus was irrelevant after 10 to 12 weeks. However, Vulsma et al4 demonstrated that substantial amounts of thyroxine (T4) are transferred from mother to fetus during late gestation. They discovered T4 in the cord blood of fetuses at term who were unable to synthesize T4 due to organification defects or thyroid agenesis. The T4 in these cases (noted at concentrations 25% to 50% of normal) was obviously of maternal origin.
Thyroid hormone requirement increases during pregnancy in normal women, to provide for the added maternal and fetal needs. Thyroxine (T4) requirement also may grow as a result of placental degradation and increased maternal T4 clearance.20
Thyroid hormone turnover is altered during pregnancy, mainly in association with:
- lowered iodide availability to the maternal thyroid gland,
- increased serum thyroid-binding globulin (TBG) concentration, and
- increased production of thyroid-stimulating factors by the placenta.
- Maternal serum inorganic iodide levels decrease during pregnancy, possibly due to increased renal clearance of iodide—which stems from increased glomerular filtration rate, and transplacental transfer of iodide and iodothyronines.8,21 The reduced circulating concentration of iodide leads to decreased availability of iodide to the thyroid gland, and results in a 10% to 20% increase of thyroid volume.21 This iodide loss has no clinical importance where iodine intake is sufficient, but may lead to hypothyroidism and goiter in regions of overt iodine deficiency.
- The increase in the TBG serum concentration in pregnancy results from estrogen-induced increased synthesis and reduced hepatic clearance of TBG.
Most pregnant women are euthyroid by laboratory evaluation, and their TSH, free T4, and free T3 levels remain within normal values.
Thyroid hormones: Important to brain differentiation and development
In the mammalian embryo, thyroid hormones appear to regulate processes of neuronal proliferation, migration, synaptogenesis and myelination, though the precise mechanism is not fully understood.
Unlike T4, triiodothyronine (T3, the most potent thyroid hormone) does not readily penetrate the brain. Indeed, most brain T3 is produced locally from T4, after which it binds to nuclear thyroid hormone receptors. These in turn bind to specific DNA sequences in the regulatory region of target genes.5 A sufficient level of such receptors has been observed in the human fetus as early as 9 weeks’ gestation.
Information comes mostly from animal models, mainly rats. We must thus remain aware that the transfer of thyroid hormones from mother to embryo or fetus may differ between species,6 as may the stages of brain development before and after birth.
Hypothyroidism during pregnancy
The frequency of thyroid deficiency in pregnancy varies from 0.19% in Japan7 to 2.2% in Belgium8 and 2.5% in the United States.9
Hypothyroidism in pregnancy may be due to preexisting illness or a disease that evolves during pregnancy; in developed nations, the most common causes are Hashimoto’s thyroiditis, subacute thyroiditis, and surgical or radioactive ablation of the thyroid gland.
The hypothyroid state may be subclinical and can remain undiagnosed throughout pregnancy. The clinical manifestations of hypothyroidism (fatigue, sensitivity to cold, muscle irritability, cramps, constipation, paresthesia of the distal portion of the extremities, dry skin, and hair loss) may be masked in gestation as symptoms of pregnancy. Gestational hypothyroidism can be classified as overt (low FT4 values and elevated TSH) or subclinical (normal FT4 values and elevated TSH).
The IQ scores of children of hypothyroid women averaged 4 points lower than those of controls at age 7 to 9 years.
Increased rates of fetal death have also been associated with subclinical disorder (see “The importance of adequate supplementation: 2 case studies”).10
Monitoring thyroid hormone levels in hypothyroid women is performed several times during gestation (every 4 to 6 weeks), and the dosage of T4 supplementation adjusted as needed. Mandel et al, who studied women with primary hypothyroidism, noted that the replacement dosage had to be increased by 45% during pregnancy.11 This trend was apparent in the first trimester and persisted throughout gestation.
The following cases underscore the importance of:
- knowledge of maternal thyroid status during periconception,
- thyroid hormone supplementation for subclinical hypothyroidism, and
- close follow-up and appropriate adjustment of replacement therapy throughout pregnancy.
Case 1
Elevated TSH discovered after successive pregnancy losses
A woman suffered 2 consecutive pregnancy losses. Subsequent work-up revealed subclinical hypothyroidism: Her thyroid-stimulating hormone (TSH) value was moderately elevated and free thyroxine (FT4) was normal. Thyroid hormone supplementation was initiated.
Four months later the patient conceived spontaneously. Levothyroxine therapy in the prepregnant dosage was continued. The mother’s general physician monitored her levels during gestation.
TSH value was normal at 5 weeks but elevated again at 9 weeks. The dosage of thyroid hormone supplementation was increased and the TSH value returned to normal—and remained so in all subsequent studies, every 4 to 6 weeks until labor.
The child was born at 40 weeks’ gestation, with a birth weight of 3,680 g, a head circumference of 36 cm, and normal neonatal thyroid functions. Presently 7 years old, he is healthy and well developed.
Case 2
The perils of unmonitored supplementation
A year after her thyroid function was found to be normal, a woman became pregnant. At the 5th gestational week, fatigue and constipation prompted reexamination of her thyroid function. TSH values were elevated; FT4 was borderline low.
According to her endocrinologist she was given levothyroxine 100 μg daily throughout pregnancy, but no follow-up was conducted. At 39 weeks’ gestation the patient delivered a male newborn weighing 2,890 g with a head circumference of 33.7 cm. Neonatal thyroid function was:
- at 52 hours of age, TSH = 14.3 μIU/mL, FT4 = 37.4 pmol/L;
- at 132 hours of age, TSH = 8.0 μIU/mL, FT4 = 31.5 pmol/L.
Spontaneous normalization of the pituitary-thyroid axis was evident at age 17 days. The child, now 9 years old, displays problems with fine motor coordination and mild learning impairment.
How does maternal thyroid status affect fetal brain development?
Data on the impact of maternal hypothyroidism on the offspring’s mental development come from interventional experimental studies in animals, and, in humans, from observational studies only.
Animal studies show permanent cortical changes. Hypothyroidism in rats causes a reduction in brain size of the newborn pups and a lower total body mass of the embryos.12
Lavado-Autric et al13 recently reported that subtle T4 insufficiency in the pregnant rat disrupts migration of neurons in the fetal cortex and hippocampus, leading to the presence of neurons in aberrant locations in the adult offspring’s brain and “blurring” of cortical layers. These alterations in cortical cytoarchitecture seem to be permanent, not simply a reflection of delayed maturation.
Recent human studies point to neurologic impairment. It is well recognized that severe iodine deficiency during pregnancy may be associated with impaired psycho-neuro-intellectual outcome in progeny. However, since thyroid hormone deficiency can occur in both mother and fetus, it is difficultto determine whether any mental retardation is caused by maternal or fetal hypothyroidism, or both.
- Elevated maternal TSH associated with lower child IQ scores. Man and Jones14 first suggested in 1969 that mild maternal hypothyroidism with no iodine deficiency was associated with lower infant IQ scores.
- First trimester hypothyroidism linked to impaired psychomotor development. A 2003 study by Pop et al1 investigated the relationship between maternal hypothyroxinemia in the first trimester and neurodevelopment of the offspring. They showed that low maternal FT4 (below the 10th percentile) with normal TSH at 12 weeks’ gestation was associated with significant impairment of the child’s psychomotor development at 1 and 2 years of age.
- Alterations in the pituitary-thyroid axis noted in the early neonatal period. Recently, we prospectively compared thyroid function in 2 groups of full-term newborns: 259 infants born to 250 hypothyroid mothers who received thyroid replacement therapy during pregnancy, and 139 healthy newborns of women who had at least 2 normal thyroid function tests during their pregnancy.2 Maternal thyroid function tests were assessed 2.3±0.7 (mean±standard deviation) times during pregnancy.
Official guidelines are unclear
Considering the adverse effects that maternal hypothyroidism, even subclinical, can have on the offspring, the question arises: Is universal periconceptional screening for thyroid dysfunction appropriate? The current recommendations on this subject are unclear:
The Endocrine Society in 1999 called for a cost-effective screening program for hypothyroidism in all women before conception or in early pregnancy.16
The American Association of Clinical Endocrinologists recommended in 2002 that routine TSH measurement be performed before pregnancy or during the first trimester in all women.17
The American College of Obstetricians and Gynecologists, in contrast, stated in 2002 that data are insufficient to warrant routine screening of asymptomatic pregnant women; thyroid function tests should be performed only in gravidas with symptoms or a personal history of thyroid disease.18
Why routine screening is not yet justified
In view of the findings of adverse events associated with maternal hypothyroidism, a universal screening program appears warranted for timely initiation of therapy. However, data on the efficacy of T4 replacement in averting such effects is insufficient. Thus, it is premature to implement routine screening for thyroid function of all women contemplating pregnancy or early in gestation.
Well-designed clinical trials are needed to determine method and timing of testing, precise diagnostic criteria for maternal hypothyroidism, and ways to assure the adequacy and efficacy of therapy.
A randomized controlled antenatal screening study19 underway in South Wales aims to recruit 22,000 pregnant women.
Is current treatment inadequate?
These observations call into question the adequacy of current therapeutic regimens:
- no significant differences were seen in the IQ scores of children of untreated and treated hypothyroid mothers,15 and
- infants of treated hypothyroid women demonstrated restricted intrauterine growth and abnormal neonatal thyroid function.2
- In the general population, thyroid function testing—specifically, thyroid-stimulating hormone (TSH) and free thyroxine (FT4) studies—prior to conception or in early pregnancy is reasonable, but the decision should be left to the individual patient and her physician.
- TSH and FT4 testing should be performed prior to conception and during pregnancy in women with a family history of thyroid disease, symptoms of thyroid disease, or an immune disorder.
- For women with a personal history of hypothyroidism who are taking thyroxine (T4) replacement, serum TSH should be closely monitored in early pregnancy. Most of these patients will become hypothyroid as detected by a rise in TSH unless the T4 dose is increased in early pregnancy.
- For pregnant women found to be hypothyroid, close monitoring (4 to 6 week intervals) of TSH and FT4 throughout pregnancy and careful adjustment of the thyroid supplementation dosage are warranted.
1. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol(Oxf). 2003;59:282-288.
2. Blazer S, Moreh-Waterman Y, Miller-Lotan R, Tamir A, Hochberg Z. Maternal hypothyroidism may affect fetal growth and neonatal thyroid function. Obstet Gynecol. 2003;102:232-241.
3. Contempre B, Jauniaux E, Calvo R, Jurkovic D, Campbell S, de Escobar GM. Detection of thyroid hormones in human embryonic cavities during the first trimester of pregnancy. J Clin Endocrinol Metab. 1993;77:1719-1722.
4. Vulsma T, Gons MH, de Vijlder JJ. Maternal-fetal transfer of thyroxine in congenital hypothyroidism due to total organification defect or thyroid agenesis. N Engl J Med. 1989;321:13-16.
5. Oppenheimer JH, Schwartz HL. Molecular basis of thyroid hormone-dependent brain development. Endocr Rev. 1997;18:462-475.
6. Morreale De Escobar G, Obregon MJ, Escobar del Rey F. Is neurodevelopment related to maternal hypothyroidism or to maternal hypothyroxinemia? J Clin Endocrinol Metab. 2000;85:3975-3987.
7. Kamijo K, Saito T, Sato M, et al. Transient subclinical hypothyroidism in early pregnancy. Endocrinol Jpn. 1990;37:397-403.
8. Glinoer D. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocr Rev. 1997;18:404-433.
9. Utiger RD. Maternal hypothyroidism and fetal development. N Engl J Med. 1999;341:601-602.
10. Allan WC, Haddow JE, Palomaki GE, et al. Maternal thyroid deficiency and pregnancy complications: implications for population screening. J Med Screen. 2000;7:127-130.
11. Mandel SJ, Larsen PR, Seely EW, Brent GA. Increased need for thyroxine during pregnancy in women with primary hypothyroidism. N Engl J Med. 1990;323:91-96.
12. Usenko V, Lepekhin E, Lyzogubov V, Kornilovska I, Ushakova G, Witt M. The influence of low doses 131I-induced maternal hypothyroidism on the development of rat embryos. Exp Toxicol Pathol. 1999;51:223-227.
13. Lavado-Autric R, Auso E, Garcia-Velasco JV, et al. Early maternal hypothyroxinemia alters histogenesis and cerebral cortex cytoarchitecture of the progeny. J Clin Invest. 2003;111:1073-1082.
14. Man EB, Jones WS. Thyroid function in human pregnancy. V. Incidence of maternal serum low butanol-extractable iodines and of normal gestational TBG and TBPA capacities; retardation of 8-month-old infants. Am J Obstet Gynecol. 1969;104:898-908.
15. Haddow JE, Palomaki GE, Allan WC, et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999;341:549-555.
16. The Endocrine Society. The Endocrine Society issues recommendations in response to major hypothyroidism study. August 1999. Available at: www.endosociety.org/pubrelations/pressreleases/archives/1999/hypothyroid.cfm. Accessed March 26, 2004.
17. AACE Thyroid Task Force. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. Endocr Pract. 2002;8:457-469.
18. American College of Obstetricians and Gynecologists. Thyroid disease in pregnancy. Clinical management guidelines for obstetrician-gynecologists. ACOG practice bulletin No. 37. Obstet Gynecol. 2002;100:387-396.
19. Lazarus JH, Wald NJ, Angele C, et al. The controlled antenatal thyroid screening study (CATS): first observations. Endocrine Abstracts. 2003;5:P262.-
20. Brent GA. Maternal thyroid function: interpretation of thyroid function tests in pregnancy. Clin Obstet Gynecol. 1997;40:3-15.
21. Burrow GN, Fisher DA, Larsen PR. Maternal and fetal thyroid function. N Engl J Med. 1994;311:1072-1078.
Emerging research indicates that thyroid hormones play a key role in fetal brain development, and asymptomatic hypothyroidism during pregnancy may have an adverse effect on fetal growth and neurologic development. Findings published in the past year call our attention to the importance of identifying and adequately treating thyroid-deficient gravidas:
- Maternal free thyroxine (FT4) concentration below the 10th percentile at 12 weeks is associated with significant impairment of psychomotor development at ages 1 and 2 years.1
- The average serum thyroid-stimulating hormone (TSH) and FT4 levels of neonates born to hypothyroid mothers were significantly higher than those of controls; birth weight and head circumference were significantly lower.2
But given the paucity of data on how maternal hypothyroidism affects the offspring, is universal screening justified? We review the evidence to date, present the current positions of 3 organizations, and offer recommendations for current clinical practice.
Maternal thyroid status is important throughout gestation
The fetal thyroid gland begins to develop at 3 weeks’ gestation; it concentrates iodine and synthesizes thyroid hormone after 10 to 12 weeks.
Prior to this, the mother provides the thyroid hormones through placental diffusion (see “How thyroid needs change during pregnancy”). Indeed, thyroid hormones have been detected in human coelomic and amniotic fluids as early as 8 weeks’ gestation, before the fetal thyroid starts to function.3
New perspective on role of maternal thyroid function. It was previously believed that the mother’s thyroid hormone supply to the fetus was irrelevant after 10 to 12 weeks. However, Vulsma et al4 demonstrated that substantial amounts of thyroxine (T4) are transferred from mother to fetus during late gestation. They discovered T4 in the cord blood of fetuses at term who were unable to synthesize T4 due to organification defects or thyroid agenesis. The T4 in these cases (noted at concentrations 25% to 50% of normal) was obviously of maternal origin.
Thyroid hormone requirement increases during pregnancy in normal women, to provide for the added maternal and fetal needs. Thyroxine (T4) requirement also may grow as a result of placental degradation and increased maternal T4 clearance.20
Thyroid hormone turnover is altered during pregnancy, mainly in association with:
- lowered iodide availability to the maternal thyroid gland,
- increased serum thyroid-binding globulin (TBG) concentration, and
- increased production of thyroid-stimulating factors by the placenta.
- Maternal serum inorganic iodide levels decrease during pregnancy, possibly due to increased renal clearance of iodide—which stems from increased glomerular filtration rate, and transplacental transfer of iodide and iodothyronines.8,21 The reduced circulating concentration of iodide leads to decreased availability of iodide to the thyroid gland, and results in a 10% to 20% increase of thyroid volume.21 This iodide loss has no clinical importance where iodine intake is sufficient, but may lead to hypothyroidism and goiter in regions of overt iodine deficiency.
- The increase in the TBG serum concentration in pregnancy results from estrogen-induced increased synthesis and reduced hepatic clearance of TBG.
Most pregnant women are euthyroid by laboratory evaluation, and their TSH, free T4, and free T3 levels remain within normal values.
Thyroid hormones: Important to brain differentiation and development
In the mammalian embryo, thyroid hormones appear to regulate processes of neuronal proliferation, migration, synaptogenesis and myelination, though the precise mechanism is not fully understood.
Unlike T4, triiodothyronine (T3, the most potent thyroid hormone) does not readily penetrate the brain. Indeed, most brain T3 is produced locally from T4, after which it binds to nuclear thyroid hormone receptors. These in turn bind to specific DNA sequences in the regulatory region of target genes.5 A sufficient level of such receptors has been observed in the human fetus as early as 9 weeks’ gestation.
Information comes mostly from animal models, mainly rats. We must thus remain aware that the transfer of thyroid hormones from mother to embryo or fetus may differ between species,6 as may the stages of brain development before and after birth.
Hypothyroidism during pregnancy
The frequency of thyroid deficiency in pregnancy varies from 0.19% in Japan7 to 2.2% in Belgium8 and 2.5% in the United States.9
Hypothyroidism in pregnancy may be due to preexisting illness or a disease that evolves during pregnancy; in developed nations, the most common causes are Hashimoto’s thyroiditis, subacute thyroiditis, and surgical or radioactive ablation of the thyroid gland.
The hypothyroid state may be subclinical and can remain undiagnosed throughout pregnancy. The clinical manifestations of hypothyroidism (fatigue, sensitivity to cold, muscle irritability, cramps, constipation, paresthesia of the distal portion of the extremities, dry skin, and hair loss) may be masked in gestation as symptoms of pregnancy. Gestational hypothyroidism can be classified as overt (low FT4 values and elevated TSH) or subclinical (normal FT4 values and elevated TSH).
The IQ scores of children of hypothyroid women averaged 4 points lower than those of controls at age 7 to 9 years.
Increased rates of fetal death have also been associated with subclinical disorder (see “The importance of adequate supplementation: 2 case studies”).10
Monitoring thyroid hormone levels in hypothyroid women is performed several times during gestation (every 4 to 6 weeks), and the dosage of T4 supplementation adjusted as needed. Mandel et al, who studied women with primary hypothyroidism, noted that the replacement dosage had to be increased by 45% during pregnancy.11 This trend was apparent in the first trimester and persisted throughout gestation.
The following cases underscore the importance of:
- knowledge of maternal thyroid status during periconception,
- thyroid hormone supplementation for subclinical hypothyroidism, and
- close follow-up and appropriate adjustment of replacement therapy throughout pregnancy.
Case 1
Elevated TSH discovered after successive pregnancy losses
A woman suffered 2 consecutive pregnancy losses. Subsequent work-up revealed subclinical hypothyroidism: Her thyroid-stimulating hormone (TSH) value was moderately elevated and free thyroxine (FT4) was normal. Thyroid hormone supplementation was initiated.
Four months later the patient conceived spontaneously. Levothyroxine therapy in the prepregnant dosage was continued. The mother’s general physician monitored her levels during gestation.
TSH value was normal at 5 weeks but elevated again at 9 weeks. The dosage of thyroid hormone supplementation was increased and the TSH value returned to normal—and remained so in all subsequent studies, every 4 to 6 weeks until labor.
The child was born at 40 weeks’ gestation, with a birth weight of 3,680 g, a head circumference of 36 cm, and normal neonatal thyroid functions. Presently 7 years old, he is healthy and well developed.
Case 2
The perils of unmonitored supplementation
A year after her thyroid function was found to be normal, a woman became pregnant. At the 5th gestational week, fatigue and constipation prompted reexamination of her thyroid function. TSH values were elevated; FT4 was borderline low.
According to her endocrinologist she was given levothyroxine 100 μg daily throughout pregnancy, but no follow-up was conducted. At 39 weeks’ gestation the patient delivered a male newborn weighing 2,890 g with a head circumference of 33.7 cm. Neonatal thyroid function was:
- at 52 hours of age, TSH = 14.3 μIU/mL, FT4 = 37.4 pmol/L;
- at 132 hours of age, TSH = 8.0 μIU/mL, FT4 = 31.5 pmol/L.
Spontaneous normalization of the pituitary-thyroid axis was evident at age 17 days. The child, now 9 years old, displays problems with fine motor coordination and mild learning impairment.
How does maternal thyroid status affect fetal brain development?
Data on the impact of maternal hypothyroidism on the offspring’s mental development come from interventional experimental studies in animals, and, in humans, from observational studies only.
Animal studies show permanent cortical changes. Hypothyroidism in rats causes a reduction in brain size of the newborn pups and a lower total body mass of the embryos.12
Lavado-Autric et al13 recently reported that subtle T4 insufficiency in the pregnant rat disrupts migration of neurons in the fetal cortex and hippocampus, leading to the presence of neurons in aberrant locations in the adult offspring’s brain and “blurring” of cortical layers. These alterations in cortical cytoarchitecture seem to be permanent, not simply a reflection of delayed maturation.
Recent human studies point to neurologic impairment. It is well recognized that severe iodine deficiency during pregnancy may be associated with impaired psycho-neuro-intellectual outcome in progeny. However, since thyroid hormone deficiency can occur in both mother and fetus, it is difficultto determine whether any mental retardation is caused by maternal or fetal hypothyroidism, or both.
- Elevated maternal TSH associated with lower child IQ scores. Man and Jones14 first suggested in 1969 that mild maternal hypothyroidism with no iodine deficiency was associated with lower infant IQ scores.
- First trimester hypothyroidism linked to impaired psychomotor development. A 2003 study by Pop et al1 investigated the relationship between maternal hypothyroxinemia in the first trimester and neurodevelopment of the offspring. They showed that low maternal FT4 (below the 10th percentile) with normal TSH at 12 weeks’ gestation was associated with significant impairment of the child’s psychomotor development at 1 and 2 years of age.
- Alterations in the pituitary-thyroid axis noted in the early neonatal period. Recently, we prospectively compared thyroid function in 2 groups of full-term newborns: 259 infants born to 250 hypothyroid mothers who received thyroid replacement therapy during pregnancy, and 139 healthy newborns of women who had at least 2 normal thyroid function tests during their pregnancy.2 Maternal thyroid function tests were assessed 2.3±0.7 (mean±standard deviation) times during pregnancy.
Official guidelines are unclear
Considering the adverse effects that maternal hypothyroidism, even subclinical, can have on the offspring, the question arises: Is universal periconceptional screening for thyroid dysfunction appropriate? The current recommendations on this subject are unclear:
The Endocrine Society in 1999 called for a cost-effective screening program for hypothyroidism in all women before conception or in early pregnancy.16
The American Association of Clinical Endocrinologists recommended in 2002 that routine TSH measurement be performed before pregnancy or during the first trimester in all women.17
The American College of Obstetricians and Gynecologists, in contrast, stated in 2002 that data are insufficient to warrant routine screening of asymptomatic pregnant women; thyroid function tests should be performed only in gravidas with symptoms or a personal history of thyroid disease.18
Why routine screening is not yet justified
In view of the findings of adverse events associated with maternal hypothyroidism, a universal screening program appears warranted for timely initiation of therapy. However, data on the efficacy of T4 replacement in averting such effects is insufficient. Thus, it is premature to implement routine screening for thyroid function of all women contemplating pregnancy or early in gestation.
Well-designed clinical trials are needed to determine method and timing of testing, precise diagnostic criteria for maternal hypothyroidism, and ways to assure the adequacy and efficacy of therapy.
A randomized controlled antenatal screening study19 underway in South Wales aims to recruit 22,000 pregnant women.
Is current treatment inadequate?
These observations call into question the adequacy of current therapeutic regimens:
- no significant differences were seen in the IQ scores of children of untreated and treated hypothyroid mothers,15 and
- infants of treated hypothyroid women demonstrated restricted intrauterine growth and abnormal neonatal thyroid function.2
- In the general population, thyroid function testing—specifically, thyroid-stimulating hormone (TSH) and free thyroxine (FT4) studies—prior to conception or in early pregnancy is reasonable, but the decision should be left to the individual patient and her physician.
- TSH and FT4 testing should be performed prior to conception and during pregnancy in women with a family history of thyroid disease, symptoms of thyroid disease, or an immune disorder.
- For women with a personal history of hypothyroidism who are taking thyroxine (T4) replacement, serum TSH should be closely monitored in early pregnancy. Most of these patients will become hypothyroid as detected by a rise in TSH unless the T4 dose is increased in early pregnancy.
- For pregnant women found to be hypothyroid, close monitoring (4 to 6 week intervals) of TSH and FT4 throughout pregnancy and careful adjustment of the thyroid supplementation dosage are warranted.
Emerging research indicates that thyroid hormones play a key role in fetal brain development, and asymptomatic hypothyroidism during pregnancy may have an adverse effect on fetal growth and neurologic development. Findings published in the past year call our attention to the importance of identifying and adequately treating thyroid-deficient gravidas:
- Maternal free thyroxine (FT4) concentration below the 10th percentile at 12 weeks is associated with significant impairment of psychomotor development at ages 1 and 2 years.1
- The average serum thyroid-stimulating hormone (TSH) and FT4 levels of neonates born to hypothyroid mothers were significantly higher than those of controls; birth weight and head circumference were significantly lower.2
But given the paucity of data on how maternal hypothyroidism affects the offspring, is universal screening justified? We review the evidence to date, present the current positions of 3 organizations, and offer recommendations for current clinical practice.
Maternal thyroid status is important throughout gestation
The fetal thyroid gland begins to develop at 3 weeks’ gestation; it concentrates iodine and synthesizes thyroid hormone after 10 to 12 weeks.
Prior to this, the mother provides the thyroid hormones through placental diffusion (see “How thyroid needs change during pregnancy”). Indeed, thyroid hormones have been detected in human coelomic and amniotic fluids as early as 8 weeks’ gestation, before the fetal thyroid starts to function.3
New perspective on role of maternal thyroid function. It was previously believed that the mother’s thyroid hormone supply to the fetus was irrelevant after 10 to 12 weeks. However, Vulsma et al4 demonstrated that substantial amounts of thyroxine (T4) are transferred from mother to fetus during late gestation. They discovered T4 in the cord blood of fetuses at term who were unable to synthesize T4 due to organification defects or thyroid agenesis. The T4 in these cases (noted at concentrations 25% to 50% of normal) was obviously of maternal origin.
Thyroid hormone requirement increases during pregnancy in normal women, to provide for the added maternal and fetal needs. Thyroxine (T4) requirement also may grow as a result of placental degradation and increased maternal T4 clearance.20
Thyroid hormone turnover is altered during pregnancy, mainly in association with:
- lowered iodide availability to the maternal thyroid gland,
- increased serum thyroid-binding globulin (TBG) concentration, and
- increased production of thyroid-stimulating factors by the placenta.
- Maternal serum inorganic iodide levels decrease during pregnancy, possibly due to increased renal clearance of iodide—which stems from increased glomerular filtration rate, and transplacental transfer of iodide and iodothyronines.8,21 The reduced circulating concentration of iodide leads to decreased availability of iodide to the thyroid gland, and results in a 10% to 20% increase of thyroid volume.21 This iodide loss has no clinical importance where iodine intake is sufficient, but may lead to hypothyroidism and goiter in regions of overt iodine deficiency.
- The increase in the TBG serum concentration in pregnancy results from estrogen-induced increased synthesis and reduced hepatic clearance of TBG.
Most pregnant women are euthyroid by laboratory evaluation, and their TSH, free T4, and free T3 levels remain within normal values.
Thyroid hormones: Important to brain differentiation and development
In the mammalian embryo, thyroid hormones appear to regulate processes of neuronal proliferation, migration, synaptogenesis and myelination, though the precise mechanism is not fully understood.
Unlike T4, triiodothyronine (T3, the most potent thyroid hormone) does not readily penetrate the brain. Indeed, most brain T3 is produced locally from T4, after which it binds to nuclear thyroid hormone receptors. These in turn bind to specific DNA sequences in the regulatory region of target genes.5 A sufficient level of such receptors has been observed in the human fetus as early as 9 weeks’ gestation.
Information comes mostly from animal models, mainly rats. We must thus remain aware that the transfer of thyroid hormones from mother to embryo or fetus may differ between species,6 as may the stages of brain development before and after birth.
Hypothyroidism during pregnancy
The frequency of thyroid deficiency in pregnancy varies from 0.19% in Japan7 to 2.2% in Belgium8 and 2.5% in the United States.9
Hypothyroidism in pregnancy may be due to preexisting illness or a disease that evolves during pregnancy; in developed nations, the most common causes are Hashimoto’s thyroiditis, subacute thyroiditis, and surgical or radioactive ablation of the thyroid gland.
The hypothyroid state may be subclinical and can remain undiagnosed throughout pregnancy. The clinical manifestations of hypothyroidism (fatigue, sensitivity to cold, muscle irritability, cramps, constipation, paresthesia of the distal portion of the extremities, dry skin, and hair loss) may be masked in gestation as symptoms of pregnancy. Gestational hypothyroidism can be classified as overt (low FT4 values and elevated TSH) or subclinical (normal FT4 values and elevated TSH).
The IQ scores of children of hypothyroid women averaged 4 points lower than those of controls at age 7 to 9 years.
Increased rates of fetal death have also been associated with subclinical disorder (see “The importance of adequate supplementation: 2 case studies”).10
Monitoring thyroid hormone levels in hypothyroid women is performed several times during gestation (every 4 to 6 weeks), and the dosage of T4 supplementation adjusted as needed. Mandel et al, who studied women with primary hypothyroidism, noted that the replacement dosage had to be increased by 45% during pregnancy.11 This trend was apparent in the first trimester and persisted throughout gestation.
The following cases underscore the importance of:
- knowledge of maternal thyroid status during periconception,
- thyroid hormone supplementation for subclinical hypothyroidism, and
- close follow-up and appropriate adjustment of replacement therapy throughout pregnancy.
Case 1
Elevated TSH discovered after successive pregnancy losses
A woman suffered 2 consecutive pregnancy losses. Subsequent work-up revealed subclinical hypothyroidism: Her thyroid-stimulating hormone (TSH) value was moderately elevated and free thyroxine (FT4) was normal. Thyroid hormone supplementation was initiated.
Four months later the patient conceived spontaneously. Levothyroxine therapy in the prepregnant dosage was continued. The mother’s general physician monitored her levels during gestation.
TSH value was normal at 5 weeks but elevated again at 9 weeks. The dosage of thyroid hormone supplementation was increased and the TSH value returned to normal—and remained so in all subsequent studies, every 4 to 6 weeks until labor.
The child was born at 40 weeks’ gestation, with a birth weight of 3,680 g, a head circumference of 36 cm, and normal neonatal thyroid functions. Presently 7 years old, he is healthy and well developed.
Case 2
The perils of unmonitored supplementation
A year after her thyroid function was found to be normal, a woman became pregnant. At the 5th gestational week, fatigue and constipation prompted reexamination of her thyroid function. TSH values were elevated; FT4 was borderline low.
According to her endocrinologist she was given levothyroxine 100 μg daily throughout pregnancy, but no follow-up was conducted. At 39 weeks’ gestation the patient delivered a male newborn weighing 2,890 g with a head circumference of 33.7 cm. Neonatal thyroid function was:
- at 52 hours of age, TSH = 14.3 μIU/mL, FT4 = 37.4 pmol/L;
- at 132 hours of age, TSH = 8.0 μIU/mL, FT4 = 31.5 pmol/L.
Spontaneous normalization of the pituitary-thyroid axis was evident at age 17 days. The child, now 9 years old, displays problems with fine motor coordination and mild learning impairment.
How does maternal thyroid status affect fetal brain development?
Data on the impact of maternal hypothyroidism on the offspring’s mental development come from interventional experimental studies in animals, and, in humans, from observational studies only.
Animal studies show permanent cortical changes. Hypothyroidism in rats causes a reduction in brain size of the newborn pups and a lower total body mass of the embryos.12
Lavado-Autric et al13 recently reported that subtle T4 insufficiency in the pregnant rat disrupts migration of neurons in the fetal cortex and hippocampus, leading to the presence of neurons in aberrant locations in the adult offspring’s brain and “blurring” of cortical layers. These alterations in cortical cytoarchitecture seem to be permanent, not simply a reflection of delayed maturation.
Recent human studies point to neurologic impairment. It is well recognized that severe iodine deficiency during pregnancy may be associated with impaired psycho-neuro-intellectual outcome in progeny. However, since thyroid hormone deficiency can occur in both mother and fetus, it is difficultto determine whether any mental retardation is caused by maternal or fetal hypothyroidism, or both.
- Elevated maternal TSH associated with lower child IQ scores. Man and Jones14 first suggested in 1969 that mild maternal hypothyroidism with no iodine deficiency was associated with lower infant IQ scores.
- First trimester hypothyroidism linked to impaired psychomotor development. A 2003 study by Pop et al1 investigated the relationship between maternal hypothyroxinemia in the first trimester and neurodevelopment of the offspring. They showed that low maternal FT4 (below the 10th percentile) with normal TSH at 12 weeks’ gestation was associated with significant impairment of the child’s psychomotor development at 1 and 2 years of age.
- Alterations in the pituitary-thyroid axis noted in the early neonatal period. Recently, we prospectively compared thyroid function in 2 groups of full-term newborns: 259 infants born to 250 hypothyroid mothers who received thyroid replacement therapy during pregnancy, and 139 healthy newborns of women who had at least 2 normal thyroid function tests during their pregnancy.2 Maternal thyroid function tests were assessed 2.3±0.7 (mean±standard deviation) times during pregnancy.
Official guidelines are unclear
Considering the adverse effects that maternal hypothyroidism, even subclinical, can have on the offspring, the question arises: Is universal periconceptional screening for thyroid dysfunction appropriate? The current recommendations on this subject are unclear:
The Endocrine Society in 1999 called for a cost-effective screening program for hypothyroidism in all women before conception or in early pregnancy.16
The American Association of Clinical Endocrinologists recommended in 2002 that routine TSH measurement be performed before pregnancy or during the first trimester in all women.17
The American College of Obstetricians and Gynecologists, in contrast, stated in 2002 that data are insufficient to warrant routine screening of asymptomatic pregnant women; thyroid function tests should be performed only in gravidas with symptoms or a personal history of thyroid disease.18
Why routine screening is not yet justified
In view of the findings of adverse events associated with maternal hypothyroidism, a universal screening program appears warranted for timely initiation of therapy. However, data on the efficacy of T4 replacement in averting such effects is insufficient. Thus, it is premature to implement routine screening for thyroid function of all women contemplating pregnancy or early in gestation.
Well-designed clinical trials are needed to determine method and timing of testing, precise diagnostic criteria for maternal hypothyroidism, and ways to assure the adequacy and efficacy of therapy.
A randomized controlled antenatal screening study19 underway in South Wales aims to recruit 22,000 pregnant women.
Is current treatment inadequate?
These observations call into question the adequacy of current therapeutic regimens:
- no significant differences were seen in the IQ scores of children of untreated and treated hypothyroid mothers,15 and
- infants of treated hypothyroid women demonstrated restricted intrauterine growth and abnormal neonatal thyroid function.2
- In the general population, thyroid function testing—specifically, thyroid-stimulating hormone (TSH) and free thyroxine (FT4) studies—prior to conception or in early pregnancy is reasonable, but the decision should be left to the individual patient and her physician.
- TSH and FT4 testing should be performed prior to conception and during pregnancy in women with a family history of thyroid disease, symptoms of thyroid disease, or an immune disorder.
- For women with a personal history of hypothyroidism who are taking thyroxine (T4) replacement, serum TSH should be closely monitored in early pregnancy. Most of these patients will become hypothyroid as detected by a rise in TSH unless the T4 dose is increased in early pregnancy.
- For pregnant women found to be hypothyroid, close monitoring (4 to 6 week intervals) of TSH and FT4 throughout pregnancy and careful adjustment of the thyroid supplementation dosage are warranted.
1. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol(Oxf). 2003;59:282-288.
2. Blazer S, Moreh-Waterman Y, Miller-Lotan R, Tamir A, Hochberg Z. Maternal hypothyroidism may affect fetal growth and neonatal thyroid function. Obstet Gynecol. 2003;102:232-241.
3. Contempre B, Jauniaux E, Calvo R, Jurkovic D, Campbell S, de Escobar GM. Detection of thyroid hormones in human embryonic cavities during the first trimester of pregnancy. J Clin Endocrinol Metab. 1993;77:1719-1722.
4. Vulsma T, Gons MH, de Vijlder JJ. Maternal-fetal transfer of thyroxine in congenital hypothyroidism due to total organification defect or thyroid agenesis. N Engl J Med. 1989;321:13-16.
5. Oppenheimer JH, Schwartz HL. Molecular basis of thyroid hormone-dependent brain development. Endocr Rev. 1997;18:462-475.
6. Morreale De Escobar G, Obregon MJ, Escobar del Rey F. Is neurodevelopment related to maternal hypothyroidism or to maternal hypothyroxinemia? J Clin Endocrinol Metab. 2000;85:3975-3987.
7. Kamijo K, Saito T, Sato M, et al. Transient subclinical hypothyroidism in early pregnancy. Endocrinol Jpn. 1990;37:397-403.
8. Glinoer D. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocr Rev. 1997;18:404-433.
9. Utiger RD. Maternal hypothyroidism and fetal development. N Engl J Med. 1999;341:601-602.
10. Allan WC, Haddow JE, Palomaki GE, et al. Maternal thyroid deficiency and pregnancy complications: implications for population screening. J Med Screen. 2000;7:127-130.
11. Mandel SJ, Larsen PR, Seely EW, Brent GA. Increased need for thyroxine during pregnancy in women with primary hypothyroidism. N Engl J Med. 1990;323:91-96.
12. Usenko V, Lepekhin E, Lyzogubov V, Kornilovska I, Ushakova G, Witt M. The influence of low doses 131I-induced maternal hypothyroidism on the development of rat embryos. Exp Toxicol Pathol. 1999;51:223-227.
13. Lavado-Autric R, Auso E, Garcia-Velasco JV, et al. Early maternal hypothyroxinemia alters histogenesis and cerebral cortex cytoarchitecture of the progeny. J Clin Invest. 2003;111:1073-1082.
14. Man EB, Jones WS. Thyroid function in human pregnancy. V. Incidence of maternal serum low butanol-extractable iodines and of normal gestational TBG and TBPA capacities; retardation of 8-month-old infants. Am J Obstet Gynecol. 1969;104:898-908.
15. Haddow JE, Palomaki GE, Allan WC, et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999;341:549-555.
16. The Endocrine Society. The Endocrine Society issues recommendations in response to major hypothyroidism study. August 1999. Available at: www.endosociety.org/pubrelations/pressreleases/archives/1999/hypothyroid.cfm. Accessed March 26, 2004.
17. AACE Thyroid Task Force. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. Endocr Pract. 2002;8:457-469.
18. American College of Obstetricians and Gynecologists. Thyroid disease in pregnancy. Clinical management guidelines for obstetrician-gynecologists. ACOG practice bulletin No. 37. Obstet Gynecol. 2002;100:387-396.
19. Lazarus JH, Wald NJ, Angele C, et al. The controlled antenatal thyroid screening study (CATS): first observations. Endocrine Abstracts. 2003;5:P262.-
20. Brent GA. Maternal thyroid function: interpretation of thyroid function tests in pregnancy. Clin Obstet Gynecol. 1997;40:3-15.
21. Burrow GN, Fisher DA, Larsen PR. Maternal and fetal thyroid function. N Engl J Med. 1994;311:1072-1078.
1. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol(Oxf). 2003;59:282-288.
2. Blazer S, Moreh-Waterman Y, Miller-Lotan R, Tamir A, Hochberg Z. Maternal hypothyroidism may affect fetal growth and neonatal thyroid function. Obstet Gynecol. 2003;102:232-241.
3. Contempre B, Jauniaux E, Calvo R, Jurkovic D, Campbell S, de Escobar GM. Detection of thyroid hormones in human embryonic cavities during the first trimester of pregnancy. J Clin Endocrinol Metab. 1993;77:1719-1722.
4. Vulsma T, Gons MH, de Vijlder JJ. Maternal-fetal transfer of thyroxine in congenital hypothyroidism due to total organification defect or thyroid agenesis. N Engl J Med. 1989;321:13-16.
5. Oppenheimer JH, Schwartz HL. Molecular basis of thyroid hormone-dependent brain development. Endocr Rev. 1997;18:462-475.
6. Morreale De Escobar G, Obregon MJ, Escobar del Rey F. Is neurodevelopment related to maternal hypothyroidism or to maternal hypothyroxinemia? J Clin Endocrinol Metab. 2000;85:3975-3987.
7. Kamijo K, Saito T, Sato M, et al. Transient subclinical hypothyroidism in early pregnancy. Endocrinol Jpn. 1990;37:397-403.
8. Glinoer D. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocr Rev. 1997;18:404-433.
9. Utiger RD. Maternal hypothyroidism and fetal development. N Engl J Med. 1999;341:601-602.
10. Allan WC, Haddow JE, Palomaki GE, et al. Maternal thyroid deficiency and pregnancy complications: implications for population screening. J Med Screen. 2000;7:127-130.
11. Mandel SJ, Larsen PR, Seely EW, Brent GA. Increased need for thyroxine during pregnancy in women with primary hypothyroidism. N Engl J Med. 1990;323:91-96.
12. Usenko V, Lepekhin E, Lyzogubov V, Kornilovska I, Ushakova G, Witt M. The influence of low doses 131I-induced maternal hypothyroidism on the development of rat embryos. Exp Toxicol Pathol. 1999;51:223-227.
13. Lavado-Autric R, Auso E, Garcia-Velasco JV, et al. Early maternal hypothyroxinemia alters histogenesis and cerebral cortex cytoarchitecture of the progeny. J Clin Invest. 2003;111:1073-1082.
14. Man EB, Jones WS. Thyroid function in human pregnancy. V. Incidence of maternal serum low butanol-extractable iodines and of normal gestational TBG and TBPA capacities; retardation of 8-month-old infants. Am J Obstet Gynecol. 1969;104:898-908.
15. Haddow JE, Palomaki GE, Allan WC, et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999;341:549-555.
16. The Endocrine Society. The Endocrine Society issues recommendations in response to major hypothyroidism study. August 1999. Available at: www.endosociety.org/pubrelations/pressreleases/archives/1999/hypothyroid.cfm. Accessed March 26, 2004.
17. AACE Thyroid Task Force. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. Endocr Pract. 2002;8:457-469.
18. American College of Obstetricians and Gynecologists. Thyroid disease in pregnancy. Clinical management guidelines for obstetrician-gynecologists. ACOG practice bulletin No. 37. Obstet Gynecol. 2002;100:387-396.
19. Lazarus JH, Wald NJ, Angele C, et al. The controlled antenatal thyroid screening study (CATS): first observations. Endocrine Abstracts. 2003;5:P262.-
20. Brent GA. Maternal thyroid function: interpretation of thyroid function tests in pregnancy. Clin Obstet Gynecol. 1997;40:3-15.
21. Burrow GN, Fisher DA, Larsen PR. Maternal and fetal thyroid function. N Engl J Med. 1994;311:1072-1078.
Update on menopause: An expert’s insight on pivotal studies
The past 2 years have witnessed a flurry of scientific publications on menopause and related therapies, particularly use of the sex steroid hormones. In turn, attitudes about menopause and hormone therapy have changed. Perhaps the greatest consequence of all the attention is the confusion about what to do, on the part of both provider and patient.
Many organizations responded with considered, evidence-based, practical guidelines. The most detailed and practice-oriented of these guidelines is the North American Menopause Society’s (NAMS’s) September 2003 Position Statement on use of estrogen and progestogen in peri- and postmenopausal women (www.menopause.org). Even as this Update on Menopause is being written, the report of the terminated estrogen-only arm of the Women’s Health Initiative (WHI) is in press and may further change clinical practice. NAMS will present an updated report on all these developments at the 2004 scientific meeting in Washington, DC, October 6 to 9, 2004. In the interim, the current recommendations hold, and the following publications are of clinical relevance.
WHIHigher levels of exercise reduce breast cancer risk
McTiernan A, Kooperberg C, White E, et al. Recreational physical activity and the risk of breast cancer in postmenopausal women: the Women’s Health Initiative Cohort Study. JAMA. 2003;290:1331–1336.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED TRIAL
A total of 74,171 postmenopausal women aged 50 to 79, with no history of breast cancer, were enrolled. At a mean follow-up of 4.7 years, an increasing total current physical activity score was associated with a statistically significant reduced risk for breast cancer (P = .03 for trend). The women in whom the 18% (95% confidence interval [CI], 0.68-0.97) reduced risk of breast cancer was observed exercised the equivalent of 1.25 to 2.5 hours per week of brisk walking (5.1-10.0 metabolic hours). Women who exercised the equivalent of 10 or more hours of brisk walking per week had slightly greater reductions.
The greatest benefit was in women with a body mass index (BMI) below 24.1, but benefits were seen in women with BMIs ranging from 24.1 to 28.4. In evaluating the effect of previous strenuous-intensity exercise, a statistically significant decreased risk of breast cancer was seen for women who had engaged in strenuous exercise at age 35 (relative risk [RR], 0.86; 95% CI, 0.78-0.95); no significant associations were found for strenuous exercise at ages 18 or 50.
COMMENT
Modest protection, but encourage exercise anyway
This large, prospective cohort study performed in the mid-1990s strengthens the growing body of evidence that higher levels of physical activity afford modest protection against breast cancer. Recreational physical activity appears to be associated with reduced risk for breast cancer in postmenopausal women; longer exercise durations showed only slightly greater reduction in risk.
The strengths of this study are its large numbers, prospective nature, and detailed reporting of breast cancer outcomes. Limitations include possible confounders such as prior oral contraceptive use, and use of self-administered questionnaires to estimate physical activity.
One very important question is raised by this study: Given the low increase in absolute risk of breast cancer reported by the WHI with estrogen plus progestin1—which barely reached statistical significance (total breast cancer RR, 1.24; 95% CI, 1.02-1.50)—and given the statement in the McTiernan study that “the reduced risk associated with increased levels of total physical activity was seen across all the categories of these variables” (including current or past use, or no previous use of hormone therapy), does the reduction of incidence with physical activity in hormone therapy users lower the level of risk to non-significance or to that of nonexercisers in the placebo group? The answer cannot be determined from this report, but it would be illuminating.
These findings are preliminary, and confirming studies are needed. There is little harm in encouraging women to exercise, however.
1. Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative Randomized Trial. JAMA. 2003;289:3243-3253.
WHIEstrogen-progestin has no significant effect on gynecologic cancers
Anderson GL, Judd HL, Kaunitz AM, et al, for the Women’s Health Initiative Investigators. Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: the Women’s Health Initiative randomized trial. JAMA. 2003;290:1739–1748.
- LEVEL I EVIDENCE: RANDOMIZED, CONTROLLED TRIAL
In this randomized, double-blind, placebo-controlled trial, 16,608 women were assigned to either EPT (0.625 mg/day conjugated equine estrogens plus 2.5 mg/day medroxyprogesterone acetate) or placebo; none of the women had undergone a hysterectomy.
After an average follow-up of 5.6 years:
- There were 20 cases of invasive ovarian cancer in the EPT group (n = 8,506) and 12 cases in the placebo group (n = 8,102). Compared with placebo, the hazard ratio (HR) for invasive ovarian cancer among EPT recipients was a nonsignificant 1.58 (95% CI, 0.77-3.24 [adjusted 95% CI, 0.59-4.23]).
- For endometrial cancer, 27 and 31 cases occurred, respectively, which translated statistically to a nonsignificant hazard ratio for EPT recipients of 0.81 (95% CI, 0.48-1.36).
- For cervical cancers, 8 and 5 cases were reported, respectively, with a nonsignificant HR of 1.44 (95% CI, 0.47-4.42).
COMMENT
Bias against hormone therapy?
The authors concluded that EPT may increase the risk of ovarian cancer but has no significant effect on the risk of endometrial cancer. They commented, however, that, since the EPT arm of the trial was prematurely stopped, the precision of the results is limited and examination of longer-term exposure is precluded.
This paper once again raises the question of whether the writers of the WHI trial have a bias against hormone therapy. In this report, the EPT arm of the WHI trial had an observed annual incidence of 34 ovarian cancer cases per 100,000 person-years—somewhat less than the anticipated population-based rate of 45 per 100,000 person-years. In the authors’ words, the ovarian cancer rate in the EPT group “was elevated (HR 1.58; 95% CI 0.77-3.24 [adjusted 95% CI, 0.59-4.23]) but not statistically significant.” The Kaplan-Meier estimates of cumulative hazards also did not reach statistical significance. Yet in the conclusion of the abstract, the authors state that continuous combined EPT “may increase the risk of ovarian cancer while producing endometrial cancer rates similar to placebo.”
Regarding the conclusion on endometrial cancer risk, the observed incidence for EPT users was 62 per 100,000 person-years, which is also lower than the anticipated population-based rate of 83 per 100,000 person-years. The authors state that this was a “small, nonsignificant reduction” in endometrial cancer risk (HR 0.81; 95% CI, 0.48-1.36). Yet, in the conclusion, while claiming that the nonsignificant difference in ovarian cancer suggests an increased risk, the authors do not state that the nonsignificant reduction in endometrial cancer suggests a decreased risk.
What do the authors expect us to believe, their data or their conclusions? My interpretation of the data in this article is that ovarian and uterine cancers need not be of major concern when determining a woman’s risk-benefit ratio for hormone therapy.
A retraction. Of interest, when this issue was raised in subsequent JAMA correspondence, the WHI authors agreed—representing perhaps the first time that a WHI report publicly retracted a potentially biased conclusion.1,2
Fewer biopsies will be needed with lower dosage. It is not surprising that women taking hormonal therapy containing estrogen had more bleeding and, therefore, more endometrial biopsies than women taking placebo, because a known effect of estrogen is proliferation of the endometrial lining. With the lower-dose hormonal preparations currently available (which result in lower systemic estrogen levels and less endometrial stimulation), uterine bleeding episodes in menopausal hormone therapy users should diminish, along with the number of endometrial biopsies.
1. Utian WH. Hormone therapy and risk of gynecologic cancers [letter]. JAMA. 2004;291:42.-
2. Anderson GL, Judd HL, Kaunitz AM, et al. Hormone therapy and risk of gynecologic cancers—Reply. JAMA. 2004;291:43.-
MILLION WOMEN STUDYBreast cancer risks increased by estrogen plus progestogen
Beral V; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2003;362:419–427.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED
A total of 1,084,110 women aged 50 to 64 were enrolled between May 1996 and March 2001 and followed to the study finish (end of 2002). Mean follow-up was 2.6 years for breast cancer incidence and 4.1 years for mortality. Nearly half of the women had used postmenopausal hormone therapy, either estrogen therapy alone (ET) or EPT. Primary endpoints were diagnosis of breast cancer and death from breast cancer.
Current ET or EPT use (compared with nonuse) was associated with a statistically significant increased risk of both breast cancer incidence (RR, 1.66; 95% CI, 1.58-1.75) and breast cancer mortality (RR, 1.22; 95% CI, 1.00-1.48). Past use did not increase the risk of incident (RR, 1.01; 95% CI, 0.94-1.09) or fatal disease (RR, 1.05; 95% CI, 0.82-1.34), and the risk decreased with time since last use.
The risks associated with ET and with EPT differed significantly. Current ET users had a 30% increased risk for breast cancer (95% CI, 1.21-1.40) while current EPT users had a 100% increased risk (95% CI, 1.88-2.12). However, vaginal or other local EPT formulations did not increase the risk (RR 0.67, 95% CI, 0.30-1.49). No significant differences in risk were found between specific types or doses of EPT or between continuous combined and continuous cyclic regimens.
COMMENT
Limitations of observational studies
This extremely large observational study found levels of breast cancer risk associated with ET and EPT similar to those reported by the WHI and as predicted in 1997 by the Collaborative Group on Hormonal Factors in Breast Cancer study.1 The Million Women Study implicates an expanded number of ET and EPT products and routes of administration.
Acting as devil’s advocate, I will point out that this is an observational study with large potential for error. The major weakness is that it is a snapshot of hormone therapy use taken at the time of the women’s entry into the study, which was at the time of their 3-year mammogram. No further information was gleaned from the women regarding subsequent changes in hormone therapy use, such as whether they terminated use or changed the dose or route.
Also, the patient-provided data at entry showed a 96% agreement with the actual prescription written by the physician. The 4% variance, although it seems small, is of some concern given the narrow difference in relative risks and the large number of study participants. This is a weakness of any observational study; even if the prescription is filled, evidence that it was actually taken is inadequate.
Finally, the authors report that current use of hormone therapy at baseline increased the risk of breast cancer, although the relative risk was not as large as for disease incidence. They were not able to come up with reliable estimates of mortality attributable to breast cancer.
“Million Women” can be accepted only as an observational confirmation of a small increase in absolute risk of breast cancer.
In conclusion, the Million Women Study can be accepted only as an observational study providing confirmation of a small increase in the absolute risk for breast cancer in women on hormone therapy.
Further implications. The suggestion that these results apply to products beyond those tested in the WHI is in agreement with the NAMS Advisory Panel’s 2003 statement on Postmenopausal Hormone Therapy, which supports the view that although it is not possible to make general conclusions about all members of the estrogen and progestogen families, an improved benefit-risk profile of other EPT agents cannot be assumed.
1. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet. 1997;350:1047-1059.
Transdermal estrogen/progestogen had no effect on risk of venous thromboembolism in postmenopausal women.
ESTHER STUDYOral and transdermal EPT have different effects on risk of thromboembolism
Scarabin PY, Oger E, Plu-Bureau G, for the EStrogen and THromboEmbolism Risk (ESTHER) Study Group. Differential association of oral and transdermal oestrogen-replacement therapy with venous thromboembolism risk. Lancet 2003;362:428–432.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED STUDY
Investigators enrolled 155 women aged 45 to 70 years who had been diagnosed with VTE, defined as either pulmonary embolism or deep vein thrombosis, and 381 matched controls. In women with VTE, 21% were using oral EPT and 19% were using transdermal EPT. In controls, 7% and 24% were using oral or transdermal EPT, respectively. An adjusted analysis showed that, compared with nonuse, current use of oral EPT significantly increased the VTE risk (adjusted odds ratio, [OR] 3.5; 95% CI, 1.8-6.8); transdermal EPT did not increase the VTE risk (OR, 0.9; 95% CI, 0.5-1.6). A between-group comparison showed that current oral EPT users had a significantly increased VTE risk (OR, 4.0; 95% CI, 1.9-8.3) over transdermal EPT users.
COMMENT
More studies needed but unlikely
A prime consideration for nonoral EPT for postmenopausal women is avoidance of the first-pass hepatic effect of oral medications, thereby reducing potential for the adverse effects associated with oral therapies. This study demonstrates a difference between oral and transdermal therapy, but the number of patients is small and, while promising, it is probably not a final answer to the problem.
The reduced incidence of VTE in postmenopausal women on transdermal EPT does justify further randomized controlled clinical trials; however, given the low prevalence of VTE, conducting such a study would be nearly impossible. It would be interesting if data from the Million Women Study were analyzed for effects of different routes of ET/EPT administration on VTE.
3 RANDOMIZED, CONTROLLED TRIALSIsoflavones are no better than placebo for hot flashes
Soy 40%, placebo 40%
Penotti M, Fabio E, Modena AB, Rinaldi M, Omodei U, Vigano P. Effect of soy-derived isoflavones on hot flushes, endometrial thickness, and the pulsatility index of the uterine and cerebral arteries. Fertil Steril. 2003;79:1112–1117.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
Effects in women with breast cancer
Nikander E, Kikkinen A, Metsa-Heikkila M, et al. A randomized placebo-controlled crossover trial with phytoestrogens in treatment of menopause in breast cancer patients. Obstet Gynecol. 2003;101:1213–1220.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
Menopause-related symptoms, including hot flashes, were recorded on the Kupperman index. At study end, the overall Kupperman index score was reduced by 15.5% in the phytoestrogen group (mean drop, 4.2) and by 14.7% in the placebo group (mean, 4.0); the between-group difference was not statistically significant.
When evaluated separately from the rest of the Kupperman index, the hot flash component was reduced more in the placebo group (14.3%) than in the study group (10%), although the difference was not statistically significant.
The quality of life parameters measured—capacity to work and mood changes—were not affected by phytoestrogen therapy.
Phytoestrogen treatment was well tolerated and caused no significant changes in liver enzymes, creatinine, body mass index, or blood pressure. In a subset analysis, investigators evaluated results based on high and low levels of endogenous equol; results did not differ between the groups.
Red clover vs placebo
Tice JA, Ettinger B, Ensrud K, Wallace R, Blackwell T, Cummings SR. Phytoestrogen supplements for the treatment of hot flashes: the Isoflavone Clover Extract (ICE) study. JAMA. 2003;290:207–214.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
COMMENT
The clinical implications
These 3 negative trials of isoflavones (2 extracted from soy, 1 from red clover) confirm previous reports of their essential inefficacy. The clinical implications:
- Women with mild hot flashes might consider either no pharmacotherapy or low-dose selective serotonin-reuptake inhibitors.
- Women with moderate to severe hot flashes that disrupt quality of life may continue to benefit from short-term, low-dose hormone therapy.
The past 2 years have witnessed a flurry of scientific publications on menopause and related therapies, particularly use of the sex steroid hormones. In turn, attitudes about menopause and hormone therapy have changed. Perhaps the greatest consequence of all the attention is the confusion about what to do, on the part of both provider and patient.
Many organizations responded with considered, evidence-based, practical guidelines. The most detailed and practice-oriented of these guidelines is the North American Menopause Society’s (NAMS’s) September 2003 Position Statement on use of estrogen and progestogen in peri- and postmenopausal women (www.menopause.org). Even as this Update on Menopause is being written, the report of the terminated estrogen-only arm of the Women’s Health Initiative (WHI) is in press and may further change clinical practice. NAMS will present an updated report on all these developments at the 2004 scientific meeting in Washington, DC, October 6 to 9, 2004. In the interim, the current recommendations hold, and the following publications are of clinical relevance.
WHIHigher levels of exercise reduce breast cancer risk
McTiernan A, Kooperberg C, White E, et al. Recreational physical activity and the risk of breast cancer in postmenopausal women: the Women’s Health Initiative Cohort Study. JAMA. 2003;290:1331–1336.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED TRIAL
A total of 74,171 postmenopausal women aged 50 to 79, with no history of breast cancer, were enrolled. At a mean follow-up of 4.7 years, an increasing total current physical activity score was associated with a statistically significant reduced risk for breast cancer (P = .03 for trend). The women in whom the 18% (95% confidence interval [CI], 0.68-0.97) reduced risk of breast cancer was observed exercised the equivalent of 1.25 to 2.5 hours per week of brisk walking (5.1-10.0 metabolic hours). Women who exercised the equivalent of 10 or more hours of brisk walking per week had slightly greater reductions.
The greatest benefit was in women with a body mass index (BMI) below 24.1, but benefits were seen in women with BMIs ranging from 24.1 to 28.4. In evaluating the effect of previous strenuous-intensity exercise, a statistically significant decreased risk of breast cancer was seen for women who had engaged in strenuous exercise at age 35 (relative risk [RR], 0.86; 95% CI, 0.78-0.95); no significant associations were found for strenuous exercise at ages 18 or 50.
COMMENT
Modest protection, but encourage exercise anyway
This large, prospective cohort study performed in the mid-1990s strengthens the growing body of evidence that higher levels of physical activity afford modest protection against breast cancer. Recreational physical activity appears to be associated with reduced risk for breast cancer in postmenopausal women; longer exercise durations showed only slightly greater reduction in risk.
The strengths of this study are its large numbers, prospective nature, and detailed reporting of breast cancer outcomes. Limitations include possible confounders such as prior oral contraceptive use, and use of self-administered questionnaires to estimate physical activity.
One very important question is raised by this study: Given the low increase in absolute risk of breast cancer reported by the WHI with estrogen plus progestin1—which barely reached statistical significance (total breast cancer RR, 1.24; 95% CI, 1.02-1.50)—and given the statement in the McTiernan study that “the reduced risk associated with increased levels of total physical activity was seen across all the categories of these variables” (including current or past use, or no previous use of hormone therapy), does the reduction of incidence with physical activity in hormone therapy users lower the level of risk to non-significance or to that of nonexercisers in the placebo group? The answer cannot be determined from this report, but it would be illuminating.
These findings are preliminary, and confirming studies are needed. There is little harm in encouraging women to exercise, however.
1. Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative Randomized Trial. JAMA. 2003;289:3243-3253.
WHIEstrogen-progestin has no significant effect on gynecologic cancers
Anderson GL, Judd HL, Kaunitz AM, et al, for the Women’s Health Initiative Investigators. Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: the Women’s Health Initiative randomized trial. JAMA. 2003;290:1739–1748.
- LEVEL I EVIDENCE: RANDOMIZED, CONTROLLED TRIAL
In this randomized, double-blind, placebo-controlled trial, 16,608 women were assigned to either EPT (0.625 mg/day conjugated equine estrogens plus 2.5 mg/day medroxyprogesterone acetate) or placebo; none of the women had undergone a hysterectomy.
After an average follow-up of 5.6 years:
- There were 20 cases of invasive ovarian cancer in the EPT group (n = 8,506) and 12 cases in the placebo group (n = 8,102). Compared with placebo, the hazard ratio (HR) for invasive ovarian cancer among EPT recipients was a nonsignificant 1.58 (95% CI, 0.77-3.24 [adjusted 95% CI, 0.59-4.23]).
- For endometrial cancer, 27 and 31 cases occurred, respectively, which translated statistically to a nonsignificant hazard ratio for EPT recipients of 0.81 (95% CI, 0.48-1.36).
- For cervical cancers, 8 and 5 cases were reported, respectively, with a nonsignificant HR of 1.44 (95% CI, 0.47-4.42).
COMMENT
Bias against hormone therapy?
The authors concluded that EPT may increase the risk of ovarian cancer but has no significant effect on the risk of endometrial cancer. They commented, however, that, since the EPT arm of the trial was prematurely stopped, the precision of the results is limited and examination of longer-term exposure is precluded.
This paper once again raises the question of whether the writers of the WHI trial have a bias against hormone therapy. In this report, the EPT arm of the WHI trial had an observed annual incidence of 34 ovarian cancer cases per 100,000 person-years—somewhat less than the anticipated population-based rate of 45 per 100,000 person-years. In the authors’ words, the ovarian cancer rate in the EPT group “was elevated (HR 1.58; 95% CI 0.77-3.24 [adjusted 95% CI, 0.59-4.23]) but not statistically significant.” The Kaplan-Meier estimates of cumulative hazards also did not reach statistical significance. Yet in the conclusion of the abstract, the authors state that continuous combined EPT “may increase the risk of ovarian cancer while producing endometrial cancer rates similar to placebo.”
Regarding the conclusion on endometrial cancer risk, the observed incidence for EPT users was 62 per 100,000 person-years, which is also lower than the anticipated population-based rate of 83 per 100,000 person-years. The authors state that this was a “small, nonsignificant reduction” in endometrial cancer risk (HR 0.81; 95% CI, 0.48-1.36). Yet, in the conclusion, while claiming that the nonsignificant difference in ovarian cancer suggests an increased risk, the authors do not state that the nonsignificant reduction in endometrial cancer suggests a decreased risk.
What do the authors expect us to believe, their data or their conclusions? My interpretation of the data in this article is that ovarian and uterine cancers need not be of major concern when determining a woman’s risk-benefit ratio for hormone therapy.
A retraction. Of interest, when this issue was raised in subsequent JAMA correspondence, the WHI authors agreed—representing perhaps the first time that a WHI report publicly retracted a potentially biased conclusion.1,2
Fewer biopsies will be needed with lower dosage. It is not surprising that women taking hormonal therapy containing estrogen had more bleeding and, therefore, more endometrial biopsies than women taking placebo, because a known effect of estrogen is proliferation of the endometrial lining. With the lower-dose hormonal preparations currently available (which result in lower systemic estrogen levels and less endometrial stimulation), uterine bleeding episodes in menopausal hormone therapy users should diminish, along with the number of endometrial biopsies.
1. Utian WH. Hormone therapy and risk of gynecologic cancers [letter]. JAMA. 2004;291:42.-
2. Anderson GL, Judd HL, Kaunitz AM, et al. Hormone therapy and risk of gynecologic cancers—Reply. JAMA. 2004;291:43.-
MILLION WOMEN STUDYBreast cancer risks increased by estrogen plus progestogen
Beral V; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2003;362:419–427.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED
A total of 1,084,110 women aged 50 to 64 were enrolled between May 1996 and March 2001 and followed to the study finish (end of 2002). Mean follow-up was 2.6 years for breast cancer incidence and 4.1 years for mortality. Nearly half of the women had used postmenopausal hormone therapy, either estrogen therapy alone (ET) or EPT. Primary endpoints were diagnosis of breast cancer and death from breast cancer.
Current ET or EPT use (compared with nonuse) was associated with a statistically significant increased risk of both breast cancer incidence (RR, 1.66; 95% CI, 1.58-1.75) and breast cancer mortality (RR, 1.22; 95% CI, 1.00-1.48). Past use did not increase the risk of incident (RR, 1.01; 95% CI, 0.94-1.09) or fatal disease (RR, 1.05; 95% CI, 0.82-1.34), and the risk decreased with time since last use.
The risks associated with ET and with EPT differed significantly. Current ET users had a 30% increased risk for breast cancer (95% CI, 1.21-1.40) while current EPT users had a 100% increased risk (95% CI, 1.88-2.12). However, vaginal or other local EPT formulations did not increase the risk (RR 0.67, 95% CI, 0.30-1.49). No significant differences in risk were found between specific types or doses of EPT or between continuous combined and continuous cyclic regimens.
COMMENT
Limitations of observational studies
This extremely large observational study found levels of breast cancer risk associated with ET and EPT similar to those reported by the WHI and as predicted in 1997 by the Collaborative Group on Hormonal Factors in Breast Cancer study.1 The Million Women Study implicates an expanded number of ET and EPT products and routes of administration.
Acting as devil’s advocate, I will point out that this is an observational study with large potential for error. The major weakness is that it is a snapshot of hormone therapy use taken at the time of the women’s entry into the study, which was at the time of their 3-year mammogram. No further information was gleaned from the women regarding subsequent changes in hormone therapy use, such as whether they terminated use or changed the dose or route.
Also, the patient-provided data at entry showed a 96% agreement with the actual prescription written by the physician. The 4% variance, although it seems small, is of some concern given the narrow difference in relative risks and the large number of study participants. This is a weakness of any observational study; even if the prescription is filled, evidence that it was actually taken is inadequate.
Finally, the authors report that current use of hormone therapy at baseline increased the risk of breast cancer, although the relative risk was not as large as for disease incidence. They were not able to come up with reliable estimates of mortality attributable to breast cancer.
“Million Women” can be accepted only as an observational confirmation of a small increase in absolute risk of breast cancer.
In conclusion, the Million Women Study can be accepted only as an observational study providing confirmation of a small increase in the absolute risk for breast cancer in women on hormone therapy.
Further implications. The suggestion that these results apply to products beyond those tested in the WHI is in agreement with the NAMS Advisory Panel’s 2003 statement on Postmenopausal Hormone Therapy, which supports the view that although it is not possible to make general conclusions about all members of the estrogen and progestogen families, an improved benefit-risk profile of other EPT agents cannot be assumed.
1. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet. 1997;350:1047-1059.
Transdermal estrogen/progestogen had no effect on risk of venous thromboembolism in postmenopausal women.
ESTHER STUDYOral and transdermal EPT have different effects on risk of thromboembolism
Scarabin PY, Oger E, Plu-Bureau G, for the EStrogen and THromboEmbolism Risk (ESTHER) Study Group. Differential association of oral and transdermal oestrogen-replacement therapy with venous thromboembolism risk. Lancet 2003;362:428–432.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED STUDY
Investigators enrolled 155 women aged 45 to 70 years who had been diagnosed with VTE, defined as either pulmonary embolism or deep vein thrombosis, and 381 matched controls. In women with VTE, 21% were using oral EPT and 19% were using transdermal EPT. In controls, 7% and 24% were using oral or transdermal EPT, respectively. An adjusted analysis showed that, compared with nonuse, current use of oral EPT significantly increased the VTE risk (adjusted odds ratio, [OR] 3.5; 95% CI, 1.8-6.8); transdermal EPT did not increase the VTE risk (OR, 0.9; 95% CI, 0.5-1.6). A between-group comparison showed that current oral EPT users had a significantly increased VTE risk (OR, 4.0; 95% CI, 1.9-8.3) over transdermal EPT users.
COMMENT
More studies needed but unlikely
A prime consideration for nonoral EPT for postmenopausal women is avoidance of the first-pass hepatic effect of oral medications, thereby reducing potential for the adverse effects associated with oral therapies. This study demonstrates a difference between oral and transdermal therapy, but the number of patients is small and, while promising, it is probably not a final answer to the problem.
The reduced incidence of VTE in postmenopausal women on transdermal EPT does justify further randomized controlled clinical trials; however, given the low prevalence of VTE, conducting such a study would be nearly impossible. It would be interesting if data from the Million Women Study were analyzed for effects of different routes of ET/EPT administration on VTE.
3 RANDOMIZED, CONTROLLED TRIALSIsoflavones are no better than placebo for hot flashes
Soy 40%, placebo 40%
Penotti M, Fabio E, Modena AB, Rinaldi M, Omodei U, Vigano P. Effect of soy-derived isoflavones on hot flushes, endometrial thickness, and the pulsatility index of the uterine and cerebral arteries. Fertil Steril. 2003;79:1112–1117.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
Effects in women with breast cancer
Nikander E, Kikkinen A, Metsa-Heikkila M, et al. A randomized placebo-controlled crossover trial with phytoestrogens in treatment of menopause in breast cancer patients. Obstet Gynecol. 2003;101:1213–1220.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
Menopause-related symptoms, including hot flashes, were recorded on the Kupperman index. At study end, the overall Kupperman index score was reduced by 15.5% in the phytoestrogen group (mean drop, 4.2) and by 14.7% in the placebo group (mean, 4.0); the between-group difference was not statistically significant.
When evaluated separately from the rest of the Kupperman index, the hot flash component was reduced more in the placebo group (14.3%) than in the study group (10%), although the difference was not statistically significant.
The quality of life parameters measured—capacity to work and mood changes—were not affected by phytoestrogen therapy.
Phytoestrogen treatment was well tolerated and caused no significant changes in liver enzymes, creatinine, body mass index, or blood pressure. In a subset analysis, investigators evaluated results based on high and low levels of endogenous equol; results did not differ between the groups.
Red clover vs placebo
Tice JA, Ettinger B, Ensrud K, Wallace R, Blackwell T, Cummings SR. Phytoestrogen supplements for the treatment of hot flashes: the Isoflavone Clover Extract (ICE) study. JAMA. 2003;290:207–214.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
COMMENT
The clinical implications
These 3 negative trials of isoflavones (2 extracted from soy, 1 from red clover) confirm previous reports of their essential inefficacy. The clinical implications:
- Women with mild hot flashes might consider either no pharmacotherapy or low-dose selective serotonin-reuptake inhibitors.
- Women with moderate to severe hot flashes that disrupt quality of life may continue to benefit from short-term, low-dose hormone therapy.
The past 2 years have witnessed a flurry of scientific publications on menopause and related therapies, particularly use of the sex steroid hormones. In turn, attitudes about menopause and hormone therapy have changed. Perhaps the greatest consequence of all the attention is the confusion about what to do, on the part of both provider and patient.
Many organizations responded with considered, evidence-based, practical guidelines. The most detailed and practice-oriented of these guidelines is the North American Menopause Society’s (NAMS’s) September 2003 Position Statement on use of estrogen and progestogen in peri- and postmenopausal women (www.menopause.org). Even as this Update on Menopause is being written, the report of the terminated estrogen-only arm of the Women’s Health Initiative (WHI) is in press and may further change clinical practice. NAMS will present an updated report on all these developments at the 2004 scientific meeting in Washington, DC, October 6 to 9, 2004. In the interim, the current recommendations hold, and the following publications are of clinical relevance.
WHIHigher levels of exercise reduce breast cancer risk
McTiernan A, Kooperberg C, White E, et al. Recreational physical activity and the risk of breast cancer in postmenopausal women: the Women’s Health Initiative Cohort Study. JAMA. 2003;290:1331–1336.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED TRIAL
A total of 74,171 postmenopausal women aged 50 to 79, with no history of breast cancer, were enrolled. At a mean follow-up of 4.7 years, an increasing total current physical activity score was associated with a statistically significant reduced risk for breast cancer (P = .03 for trend). The women in whom the 18% (95% confidence interval [CI], 0.68-0.97) reduced risk of breast cancer was observed exercised the equivalent of 1.25 to 2.5 hours per week of brisk walking (5.1-10.0 metabolic hours). Women who exercised the equivalent of 10 or more hours of brisk walking per week had slightly greater reductions.
The greatest benefit was in women with a body mass index (BMI) below 24.1, but benefits were seen in women with BMIs ranging from 24.1 to 28.4. In evaluating the effect of previous strenuous-intensity exercise, a statistically significant decreased risk of breast cancer was seen for women who had engaged in strenuous exercise at age 35 (relative risk [RR], 0.86; 95% CI, 0.78-0.95); no significant associations were found for strenuous exercise at ages 18 or 50.
COMMENT
Modest protection, but encourage exercise anyway
This large, prospective cohort study performed in the mid-1990s strengthens the growing body of evidence that higher levels of physical activity afford modest protection against breast cancer. Recreational physical activity appears to be associated with reduced risk for breast cancer in postmenopausal women; longer exercise durations showed only slightly greater reduction in risk.
The strengths of this study are its large numbers, prospective nature, and detailed reporting of breast cancer outcomes. Limitations include possible confounders such as prior oral contraceptive use, and use of self-administered questionnaires to estimate physical activity.
One very important question is raised by this study: Given the low increase in absolute risk of breast cancer reported by the WHI with estrogen plus progestin1—which barely reached statistical significance (total breast cancer RR, 1.24; 95% CI, 1.02-1.50)—and given the statement in the McTiernan study that “the reduced risk associated with increased levels of total physical activity was seen across all the categories of these variables” (including current or past use, or no previous use of hormone therapy), does the reduction of incidence with physical activity in hormone therapy users lower the level of risk to non-significance or to that of nonexercisers in the placebo group? The answer cannot be determined from this report, but it would be illuminating.
These findings are preliminary, and confirming studies are needed. There is little harm in encouraging women to exercise, however.
1. Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative Randomized Trial. JAMA. 2003;289:3243-3253.
WHIEstrogen-progestin has no significant effect on gynecologic cancers
Anderson GL, Judd HL, Kaunitz AM, et al, for the Women’s Health Initiative Investigators. Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: the Women’s Health Initiative randomized trial. JAMA. 2003;290:1739–1748.
- LEVEL I EVIDENCE: RANDOMIZED, CONTROLLED TRIAL
In this randomized, double-blind, placebo-controlled trial, 16,608 women were assigned to either EPT (0.625 mg/day conjugated equine estrogens plus 2.5 mg/day medroxyprogesterone acetate) or placebo; none of the women had undergone a hysterectomy.
After an average follow-up of 5.6 years:
- There were 20 cases of invasive ovarian cancer in the EPT group (n = 8,506) and 12 cases in the placebo group (n = 8,102). Compared with placebo, the hazard ratio (HR) for invasive ovarian cancer among EPT recipients was a nonsignificant 1.58 (95% CI, 0.77-3.24 [adjusted 95% CI, 0.59-4.23]).
- For endometrial cancer, 27 and 31 cases occurred, respectively, which translated statistically to a nonsignificant hazard ratio for EPT recipients of 0.81 (95% CI, 0.48-1.36).
- For cervical cancers, 8 and 5 cases were reported, respectively, with a nonsignificant HR of 1.44 (95% CI, 0.47-4.42).
COMMENT
Bias against hormone therapy?
The authors concluded that EPT may increase the risk of ovarian cancer but has no significant effect on the risk of endometrial cancer. They commented, however, that, since the EPT arm of the trial was prematurely stopped, the precision of the results is limited and examination of longer-term exposure is precluded.
This paper once again raises the question of whether the writers of the WHI trial have a bias against hormone therapy. In this report, the EPT arm of the WHI trial had an observed annual incidence of 34 ovarian cancer cases per 100,000 person-years—somewhat less than the anticipated population-based rate of 45 per 100,000 person-years. In the authors’ words, the ovarian cancer rate in the EPT group “was elevated (HR 1.58; 95% CI 0.77-3.24 [adjusted 95% CI, 0.59-4.23]) but not statistically significant.” The Kaplan-Meier estimates of cumulative hazards also did not reach statistical significance. Yet in the conclusion of the abstract, the authors state that continuous combined EPT “may increase the risk of ovarian cancer while producing endometrial cancer rates similar to placebo.”
Regarding the conclusion on endometrial cancer risk, the observed incidence for EPT users was 62 per 100,000 person-years, which is also lower than the anticipated population-based rate of 83 per 100,000 person-years. The authors state that this was a “small, nonsignificant reduction” in endometrial cancer risk (HR 0.81; 95% CI, 0.48-1.36). Yet, in the conclusion, while claiming that the nonsignificant difference in ovarian cancer suggests an increased risk, the authors do not state that the nonsignificant reduction in endometrial cancer suggests a decreased risk.
What do the authors expect us to believe, their data or their conclusions? My interpretation of the data in this article is that ovarian and uterine cancers need not be of major concern when determining a woman’s risk-benefit ratio for hormone therapy.
A retraction. Of interest, when this issue was raised in subsequent JAMA correspondence, the WHI authors agreed—representing perhaps the first time that a WHI report publicly retracted a potentially biased conclusion.1,2
Fewer biopsies will be needed with lower dosage. It is not surprising that women taking hormonal therapy containing estrogen had more bleeding and, therefore, more endometrial biopsies than women taking placebo, because a known effect of estrogen is proliferation of the endometrial lining. With the lower-dose hormonal preparations currently available (which result in lower systemic estrogen levels and less endometrial stimulation), uterine bleeding episodes in menopausal hormone therapy users should diminish, along with the number of endometrial biopsies.
1. Utian WH. Hormone therapy and risk of gynecologic cancers [letter]. JAMA. 2004;291:42.-
2. Anderson GL, Judd HL, Kaunitz AM, et al. Hormone therapy and risk of gynecologic cancers—Reply. JAMA. 2004;291:43.-
MILLION WOMEN STUDYBreast cancer risks increased by estrogen plus progestogen
Beral V; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2003;362:419–427.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED
A total of 1,084,110 women aged 50 to 64 were enrolled between May 1996 and March 2001 and followed to the study finish (end of 2002). Mean follow-up was 2.6 years for breast cancer incidence and 4.1 years for mortality. Nearly half of the women had used postmenopausal hormone therapy, either estrogen therapy alone (ET) or EPT. Primary endpoints were diagnosis of breast cancer and death from breast cancer.
Current ET or EPT use (compared with nonuse) was associated with a statistically significant increased risk of both breast cancer incidence (RR, 1.66; 95% CI, 1.58-1.75) and breast cancer mortality (RR, 1.22; 95% CI, 1.00-1.48). Past use did not increase the risk of incident (RR, 1.01; 95% CI, 0.94-1.09) or fatal disease (RR, 1.05; 95% CI, 0.82-1.34), and the risk decreased with time since last use.
The risks associated with ET and with EPT differed significantly. Current ET users had a 30% increased risk for breast cancer (95% CI, 1.21-1.40) while current EPT users had a 100% increased risk (95% CI, 1.88-2.12). However, vaginal or other local EPT formulations did not increase the risk (RR 0.67, 95% CI, 0.30-1.49). No significant differences in risk were found between specific types or doses of EPT or between continuous combined and continuous cyclic regimens.
COMMENT
Limitations of observational studies
This extremely large observational study found levels of breast cancer risk associated with ET and EPT similar to those reported by the WHI and as predicted in 1997 by the Collaborative Group on Hormonal Factors in Breast Cancer study.1 The Million Women Study implicates an expanded number of ET and EPT products and routes of administration.
Acting as devil’s advocate, I will point out that this is an observational study with large potential for error. The major weakness is that it is a snapshot of hormone therapy use taken at the time of the women’s entry into the study, which was at the time of their 3-year mammogram. No further information was gleaned from the women regarding subsequent changes in hormone therapy use, such as whether they terminated use or changed the dose or route.
Also, the patient-provided data at entry showed a 96% agreement with the actual prescription written by the physician. The 4% variance, although it seems small, is of some concern given the narrow difference in relative risks and the large number of study participants. This is a weakness of any observational study; even if the prescription is filled, evidence that it was actually taken is inadequate.
Finally, the authors report that current use of hormone therapy at baseline increased the risk of breast cancer, although the relative risk was not as large as for disease incidence. They were not able to come up with reliable estimates of mortality attributable to breast cancer.
“Million Women” can be accepted only as an observational confirmation of a small increase in absolute risk of breast cancer.
In conclusion, the Million Women Study can be accepted only as an observational study providing confirmation of a small increase in the absolute risk for breast cancer in women on hormone therapy.
Further implications. The suggestion that these results apply to products beyond those tested in the WHI is in agreement with the NAMS Advisory Panel’s 2003 statement on Postmenopausal Hormone Therapy, which supports the view that although it is not possible to make general conclusions about all members of the estrogen and progestogen families, an improved benefit-risk profile of other EPT agents cannot be assumed.
1. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet. 1997;350:1047-1059.
Transdermal estrogen/progestogen had no effect on risk of venous thromboembolism in postmenopausal women.
ESTHER STUDYOral and transdermal EPT have different effects on risk of thromboembolism
Scarabin PY, Oger E, Plu-Bureau G, for the EStrogen and THromboEmbolism Risk (ESTHER) Study Group. Differential association of oral and transdermal oestrogen-replacement therapy with venous thromboembolism risk. Lancet 2003;362:428–432.
- LEVEL II-2 EVIDENCE: COHORT OR CASE-CONTROLLED STUDY
Investigators enrolled 155 women aged 45 to 70 years who had been diagnosed with VTE, defined as either pulmonary embolism or deep vein thrombosis, and 381 matched controls. In women with VTE, 21% were using oral EPT and 19% were using transdermal EPT. In controls, 7% and 24% were using oral or transdermal EPT, respectively. An adjusted analysis showed that, compared with nonuse, current use of oral EPT significantly increased the VTE risk (adjusted odds ratio, [OR] 3.5; 95% CI, 1.8-6.8); transdermal EPT did not increase the VTE risk (OR, 0.9; 95% CI, 0.5-1.6). A between-group comparison showed that current oral EPT users had a significantly increased VTE risk (OR, 4.0; 95% CI, 1.9-8.3) over transdermal EPT users.
COMMENT
More studies needed but unlikely
A prime consideration for nonoral EPT for postmenopausal women is avoidance of the first-pass hepatic effect of oral medications, thereby reducing potential for the adverse effects associated with oral therapies. This study demonstrates a difference between oral and transdermal therapy, but the number of patients is small and, while promising, it is probably not a final answer to the problem.
The reduced incidence of VTE in postmenopausal women on transdermal EPT does justify further randomized controlled clinical trials; however, given the low prevalence of VTE, conducting such a study would be nearly impossible. It would be interesting if data from the Million Women Study were analyzed for effects of different routes of ET/EPT administration on VTE.
3 RANDOMIZED, CONTROLLED TRIALSIsoflavones are no better than placebo for hot flashes
Soy 40%, placebo 40%
Penotti M, Fabio E, Modena AB, Rinaldi M, Omodei U, Vigano P. Effect of soy-derived isoflavones on hot flushes, endometrial thickness, and the pulsatility index of the uterine and cerebral arteries. Fertil Steril. 2003;79:1112–1117.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
Effects in women with breast cancer
Nikander E, Kikkinen A, Metsa-Heikkila M, et al. A randomized placebo-controlled crossover trial with phytoestrogens in treatment of menopause in breast cancer patients. Obstet Gynecol. 2003;101:1213–1220.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
Menopause-related symptoms, including hot flashes, were recorded on the Kupperman index. At study end, the overall Kupperman index score was reduced by 15.5% in the phytoestrogen group (mean drop, 4.2) and by 14.7% in the placebo group (mean, 4.0); the between-group difference was not statistically significant.
When evaluated separately from the rest of the Kupperman index, the hot flash component was reduced more in the placebo group (14.3%) than in the study group (10%), although the difference was not statistically significant.
The quality of life parameters measured—capacity to work and mood changes—were not affected by phytoestrogen therapy.
Phytoestrogen treatment was well tolerated and caused no significant changes in liver enzymes, creatinine, body mass index, or blood pressure. In a subset analysis, investigators evaluated results based on high and low levels of endogenous equol; results did not differ between the groups.
Red clover vs placebo
Tice JA, Ettinger B, Ensrud K, Wallace R, Blackwell T, Cummings SR. Phytoestrogen supplements for the treatment of hot flashes: the Isoflavone Clover Extract (ICE) study. JAMA. 2003;290:207–214.
- LEVEL I EVIDENCE: RANDOMIZED CONTROLLED TRIAL
COMMENT
The clinical implications
These 3 negative trials of isoflavones (2 extracted from soy, 1 from red clover) confirm previous reports of their essential inefficacy. The clinical implications:
- Women with mild hot flashes might consider either no pharmacotherapy or low-dose selective serotonin-reuptake inhibitors.
- Women with moderate to severe hot flashes that disrupt quality of life may continue to benefit from short-term, low-dose hormone therapy.
Is There Cost Justification for Decentralized Clinical Pharmacists?
Reconnection Through Dialectical Behavior Therapy
Argyria in the Silver State
New insight on an enduring enigma
The most important new advance in chronic pelvic pain is recognition that this complaint often does not represent an anatomical disorder that can be seen, photographed, or excised away. It is a syndrome—a group of related disorders associated with abnormal pain processing. The abnormal pain processing may relate to other symptoms affecting mood, sleep, and autonomic function. The term for this array of complaints—chronic pelvic pain syndrome–reinforces the concept that a group of disorders produces the subjective experience of pain.
This new understanding is steering us toward therapeutic strategies that may be more helpful than multiple uncoordinated treatments at the hands of different specialists—the unfortunate experience of too many women.
Clinicians have long understood that for many patients, there is no clear diagnosis. Patients become frustrated with clinicians’ apparent inability to help, or even take their complaints seriously. Doctor-shopping results in multiple tests, medication trials, and surgery. This chain of events stems from the traditional anatomic model of disease, which attributes pain to an organ or tissue abnormality that surgical correction might resolve.
Key findings. Clues that the anatomic model is inadequate have been a part of gynecologic teaching for decades, but recent studies confirm these impressions about chronic pelvic pain:
- Anatomic features noted at surgery may not give reliable information about the cause;
- The effect of surgical treatment is similar to placebo, at least short-term;
- A history of abuse is common.
‘Difficult’ patient or other disease was blamed when surgery failed. The traditional approach was to seek an anatomic abnormality such as endometriosis, adhesions, or pelvic congestion, and treat the abnormality with surgical removal of implants, scar tissue, or the pelvic organs altogether.
(The anatomic model still applies to acute pelvic pain; ruptured ovarian cyst, ectopic pregnancy, and appendicitis are highest on the list of diagnostic possibilities.)
Surgeons were convinced that their operations were successful, largely because they characterized cases that failed to get better as evidence of nongynecologic disease or a patient who simply wanted to be difficult.
Pivotal study: ‘Integrated’ treatment achieved better results. One of the earliest clues that surgery might not be the best approach to chronic pelvic pain came from a study of 106 patients randomized to 2 different strategies1:
- In the “standard” approach, laparoscopy was used early, and patients with no anatomic abnormalities were then evaluated for other problems, such as psychological disorders.
- In the “integrated” approach, the pain experience was thought to have 4 components: nociception, pain sensation (which includes processing), suffering, and pain behavior. This approach included psychological and physical therapy as well as evaluation for anatomic abnormalities, generally using nonsurgical methods.
Among the 57 women randomized to the integrated approach, 5 (9%) underwent surgery, compared with 100% of the group randomized to standard therapy. One year later, 75% of the women assigned to the integrated approach reported improvement in pain, compared with 41% of those in the standard group.
In both groups, associated symptoms were common at the onset of therapy, including backache, nausea, malaise, headache, and insomnia. These symptoms were more likely to improve with the integrated approach.
Initial strategy: Avoid surgery
Winkel CA. Evaluation and management of women with endometriosis. Obstet Gynecol. 2003;102:397-408.
Avoidance of surgery can be recommended except perhaps in patients with a mass or discrete and localized abnormalities (eg, tender uterosacral nodule with deep dyspareunia as the only complaint). This strategy challenges the anatomic model of chronic pelvic pain, but is consistent with challenges to the anatomic model of chronic pain at other sites, such as chronic back pain.
Empiric medical therapy may be preferable in women believed, clinically, to have endometriosis without a mass or who wish to get pregnant right away, Dr. Winkel noted.
Many diagnoses can be made in women with chronic pelvic pain, in addition to endometriosis (eg, irritable bowel syndrome, interstitial cystitis, vulvodynia, fibromyalgia, and somatization disorder); these may reflect different manifestations of the same disorder of pain processing, which is often associated with mood and sleep abnormalities. Therapy to improve sleep, physical conditioning, and coping strategies appears to be more helpful than surgery as an initial approach.
Visual and histologic diagnoses of endometriosis at odds
Walter AJ, Hentz JG, Magtibay PM, Cornella JL, Magrina JF. Endometriosis: correlation between histologic and visual findings at laparoscopy. Am J Obstet Gynecol. 2001;184:1407-1413.
Stratton P, Winkel CA, Sinaii N, Merino MJ, Zimmer C, Nieman LK. Location, color, size, depth and volume may predict endometriosis in lesions resected at surgery. Fertil Steril. 2002;78:743-749.
Stratton P, Winkel C, Premkumar A, et al. Diagnostic accuracy of laparoscopy, magnetic resonance imaging, and histopathologic examination for the detection of endometriosis. Fertil Steril. 2003;79:1078-1085.
Three recent studies assess the discrepancies between visual and histologic evidence of endometriosis in women with chronic pelvic pain. Earlier studies had indicated that visual diagnosis is not equivalent to histologic diagnosis, and that failure to see endometriosis does not mean it is not there.
In all 3 studies, visible lesions that appeared to be endometriosis were excised and evaluated by a pathologist.
- Walter et al found that 12 of 37 women with visible lesions had no histologic evidence of endometriosis; the positive predictive value of visualized endometriosis was 62%.
- Stratton et al found a similar 61% of 314 lesions believed on visual inspection to be endometriosis were histologically confirmed. Of 44 women with visual criteria suggesting endometriosis, 6 (14%) were unconfirmed by histology. This discrepancy was noted in women considered upon inspection to have “mild” disease, of whom 5 of 13 (38%) had no histologic evidence.
Does a diagnosis benefit the patient? In a commentary, Dr. Frank Ling2 questioned whether histologic or visual diagnoses are useful. After all, he argued, histologic diagnosis of endometriosis does not prove it caused the pain—prior studies showed a high prevalence of endometriosis in asymptomatic women.
Focusing on what the inside of the pelvis looks like, whether through a laparoscope or the pathologist’s microscope, may leave the woman with chronic pain without relief. Ling made a case for empiric medical treatment of endometriosis, without surgery.
Sham surgery: A potent placebo
Swank DJ, Swank-Bordewijk SC, Hop WC, et al. Laparoscopic adhesiolysis in patients with chronic abdominal pain: a blinded randomised controlled multi-centre trial. Lancet. 2003;361:1247-1251.
In chronic pelvic pain, the placebo effect can be potent—another indication that the anatomic model is not the answer. In the mid-90s, Sutton et al3 found equal responses to sham surgery and laser laparoscopy at 3 months postoperatively in patients with endometriosis-associated pain—but laser laparoscopy had an advantage over sham surgery at 6 months postoperatively.
Swank et al compared laparoscopic adhesiolysis with sham surgery in 100 adults (87% women) with chronic abdominal pain without intestinal stricture. At 1 year, 27% were pain-free or much improved, and there was no difference in visual analog score improvement, regardless of type of surgery. They concluded that abdominal pain can improve after surgery, but the benefit is not likely due to adhesiolysis.
In both groups, as in the Sutton study, reduced pain was maximal at 3 months and somewhat less by 6 months after surgery, supporting the likelihood of a placebo effect.
Possibly, the response to surgery was due in part to reduced anxiety after surgery excluded cancer, yet the mean number of prior operations was almost 3, suggesting that many of these patients had already had the opportunity to be reassured by benign operative findings.
Past abuse: The mind-body link
Lampe A, Doering S, Rumpold G, et al. Childhood pain syndromes and their relation to childhood abuse and stressful life events. J Psychosom Res. 2003;54:361-367.
It has been noted for years that women with chronic pelvic pain are more likely to have a history of sexual abuse than women without chronic pelvic pain. In a study of the chronic pain/abuse relationship, Lampe et al found “complex mutual interactions among childhood abuse, stressful life events, depression, and the occurrence of chronic pain,” and urged clinicians to consider these factors when treating patients.
It is clear that chronic pain syndromes and abuse are linked, but there is disagreement on whether pelvic pain is associated with sexual abuse more than other abuse, or if sexual abuse is associated more with pelvic pain than chronic pain at other sites.
These associations were once explained as physically and psychologically traumatic events being reenacted through illness behaviors. A theory more consistent with current views of pain-processing disorders is that physical or psychological trauma may “kindle” abnormalities of neurotransmitter function to which a patient is genetically predisposed. This model is analogous to the view that depression is a genetic disorder kindled by a major loss or adverse life event.
Such a view requires that we relinquish the mind-body dualism first proposed by Descartes in the 17th century, long before we recognized that neurotransmitters mediate mood as well as motor function, and that life events can alter the chemistry of the brain.
Dr. Scialli reports no financial relationships relevant to this article.
1. Peters AAW, van Dorst E, Jellis B, van Zuuren E, Hermans J, Trimbos JB. A randomized trial to compare 2 different approaches in women with chronic pelvic pain. Obstet Gynecol. 1991;77:740-744.
2. Ling FW. Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Obstet Gynecol. 1999;93:51-58.
3. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized, double-blind, controlled trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild and moderate endometriosis. Fertil Steril. 1994;62:696-700.
The most important new advance in chronic pelvic pain is recognition that this complaint often does not represent an anatomical disorder that can be seen, photographed, or excised away. It is a syndrome—a group of related disorders associated with abnormal pain processing. The abnormal pain processing may relate to other symptoms affecting mood, sleep, and autonomic function. The term for this array of complaints—chronic pelvic pain syndrome–reinforces the concept that a group of disorders produces the subjective experience of pain.
This new understanding is steering us toward therapeutic strategies that may be more helpful than multiple uncoordinated treatments at the hands of different specialists—the unfortunate experience of too many women.
Clinicians have long understood that for many patients, there is no clear diagnosis. Patients become frustrated with clinicians’ apparent inability to help, or even take their complaints seriously. Doctor-shopping results in multiple tests, medication trials, and surgery. This chain of events stems from the traditional anatomic model of disease, which attributes pain to an organ or tissue abnormality that surgical correction might resolve.
Key findings. Clues that the anatomic model is inadequate have been a part of gynecologic teaching for decades, but recent studies confirm these impressions about chronic pelvic pain:
- Anatomic features noted at surgery may not give reliable information about the cause;
- The effect of surgical treatment is similar to placebo, at least short-term;
- A history of abuse is common.
‘Difficult’ patient or other disease was blamed when surgery failed. The traditional approach was to seek an anatomic abnormality such as endometriosis, adhesions, or pelvic congestion, and treat the abnormality with surgical removal of implants, scar tissue, or the pelvic organs altogether.
(The anatomic model still applies to acute pelvic pain; ruptured ovarian cyst, ectopic pregnancy, and appendicitis are highest on the list of diagnostic possibilities.)
Surgeons were convinced that their operations were successful, largely because they characterized cases that failed to get better as evidence of nongynecologic disease or a patient who simply wanted to be difficult.
Pivotal study: ‘Integrated’ treatment achieved better results. One of the earliest clues that surgery might not be the best approach to chronic pelvic pain came from a study of 106 patients randomized to 2 different strategies1:
- In the “standard” approach, laparoscopy was used early, and patients with no anatomic abnormalities were then evaluated for other problems, such as psychological disorders.
- In the “integrated” approach, the pain experience was thought to have 4 components: nociception, pain sensation (which includes processing), suffering, and pain behavior. This approach included psychological and physical therapy as well as evaluation for anatomic abnormalities, generally using nonsurgical methods.
Among the 57 women randomized to the integrated approach, 5 (9%) underwent surgery, compared with 100% of the group randomized to standard therapy. One year later, 75% of the women assigned to the integrated approach reported improvement in pain, compared with 41% of those in the standard group.
In both groups, associated symptoms were common at the onset of therapy, including backache, nausea, malaise, headache, and insomnia. These symptoms were more likely to improve with the integrated approach.
Initial strategy: Avoid surgery
Winkel CA. Evaluation and management of women with endometriosis. Obstet Gynecol. 2003;102:397-408.
Avoidance of surgery can be recommended except perhaps in patients with a mass or discrete and localized abnormalities (eg, tender uterosacral nodule with deep dyspareunia as the only complaint). This strategy challenges the anatomic model of chronic pelvic pain, but is consistent with challenges to the anatomic model of chronic pain at other sites, such as chronic back pain.
Empiric medical therapy may be preferable in women believed, clinically, to have endometriosis without a mass or who wish to get pregnant right away, Dr. Winkel noted.
Many diagnoses can be made in women with chronic pelvic pain, in addition to endometriosis (eg, irritable bowel syndrome, interstitial cystitis, vulvodynia, fibromyalgia, and somatization disorder); these may reflect different manifestations of the same disorder of pain processing, which is often associated with mood and sleep abnormalities. Therapy to improve sleep, physical conditioning, and coping strategies appears to be more helpful than surgery as an initial approach.
Visual and histologic diagnoses of endometriosis at odds
Walter AJ, Hentz JG, Magtibay PM, Cornella JL, Magrina JF. Endometriosis: correlation between histologic and visual findings at laparoscopy. Am J Obstet Gynecol. 2001;184:1407-1413.
Stratton P, Winkel CA, Sinaii N, Merino MJ, Zimmer C, Nieman LK. Location, color, size, depth and volume may predict endometriosis in lesions resected at surgery. Fertil Steril. 2002;78:743-749.
Stratton P, Winkel C, Premkumar A, et al. Diagnostic accuracy of laparoscopy, magnetic resonance imaging, and histopathologic examination for the detection of endometriosis. Fertil Steril. 2003;79:1078-1085.
Three recent studies assess the discrepancies between visual and histologic evidence of endometriosis in women with chronic pelvic pain. Earlier studies had indicated that visual diagnosis is not equivalent to histologic diagnosis, and that failure to see endometriosis does not mean it is not there.
In all 3 studies, visible lesions that appeared to be endometriosis were excised and evaluated by a pathologist.
- Walter et al found that 12 of 37 women with visible lesions had no histologic evidence of endometriosis; the positive predictive value of visualized endometriosis was 62%.
- Stratton et al found a similar 61% of 314 lesions believed on visual inspection to be endometriosis were histologically confirmed. Of 44 women with visual criteria suggesting endometriosis, 6 (14%) were unconfirmed by histology. This discrepancy was noted in women considered upon inspection to have “mild” disease, of whom 5 of 13 (38%) had no histologic evidence.
Does a diagnosis benefit the patient? In a commentary, Dr. Frank Ling2 questioned whether histologic or visual diagnoses are useful. After all, he argued, histologic diagnosis of endometriosis does not prove it caused the pain—prior studies showed a high prevalence of endometriosis in asymptomatic women.
Focusing on what the inside of the pelvis looks like, whether through a laparoscope or the pathologist’s microscope, may leave the woman with chronic pain without relief. Ling made a case for empiric medical treatment of endometriosis, without surgery.
Sham surgery: A potent placebo
Swank DJ, Swank-Bordewijk SC, Hop WC, et al. Laparoscopic adhesiolysis in patients with chronic abdominal pain: a blinded randomised controlled multi-centre trial. Lancet. 2003;361:1247-1251.
In chronic pelvic pain, the placebo effect can be potent—another indication that the anatomic model is not the answer. In the mid-90s, Sutton et al3 found equal responses to sham surgery and laser laparoscopy at 3 months postoperatively in patients with endometriosis-associated pain—but laser laparoscopy had an advantage over sham surgery at 6 months postoperatively.
Swank et al compared laparoscopic adhesiolysis with sham surgery in 100 adults (87% women) with chronic abdominal pain without intestinal stricture. At 1 year, 27% were pain-free or much improved, and there was no difference in visual analog score improvement, regardless of type of surgery. They concluded that abdominal pain can improve after surgery, but the benefit is not likely due to adhesiolysis.
In both groups, as in the Sutton study, reduced pain was maximal at 3 months and somewhat less by 6 months after surgery, supporting the likelihood of a placebo effect.
Possibly, the response to surgery was due in part to reduced anxiety after surgery excluded cancer, yet the mean number of prior operations was almost 3, suggesting that many of these patients had already had the opportunity to be reassured by benign operative findings.
Past abuse: The mind-body link
Lampe A, Doering S, Rumpold G, et al. Childhood pain syndromes and their relation to childhood abuse and stressful life events. J Psychosom Res. 2003;54:361-367.
It has been noted for years that women with chronic pelvic pain are more likely to have a history of sexual abuse than women without chronic pelvic pain. In a study of the chronic pain/abuse relationship, Lampe et al found “complex mutual interactions among childhood abuse, stressful life events, depression, and the occurrence of chronic pain,” and urged clinicians to consider these factors when treating patients.
It is clear that chronic pain syndromes and abuse are linked, but there is disagreement on whether pelvic pain is associated with sexual abuse more than other abuse, or if sexual abuse is associated more with pelvic pain than chronic pain at other sites.
These associations were once explained as physically and psychologically traumatic events being reenacted through illness behaviors. A theory more consistent with current views of pain-processing disorders is that physical or psychological trauma may “kindle” abnormalities of neurotransmitter function to which a patient is genetically predisposed. This model is analogous to the view that depression is a genetic disorder kindled by a major loss or adverse life event.
Such a view requires that we relinquish the mind-body dualism first proposed by Descartes in the 17th century, long before we recognized that neurotransmitters mediate mood as well as motor function, and that life events can alter the chemistry of the brain.
Dr. Scialli reports no financial relationships relevant to this article.
The most important new advance in chronic pelvic pain is recognition that this complaint often does not represent an anatomical disorder that can be seen, photographed, or excised away. It is a syndrome—a group of related disorders associated with abnormal pain processing. The abnormal pain processing may relate to other symptoms affecting mood, sleep, and autonomic function. The term for this array of complaints—chronic pelvic pain syndrome–reinforces the concept that a group of disorders produces the subjective experience of pain.
This new understanding is steering us toward therapeutic strategies that may be more helpful than multiple uncoordinated treatments at the hands of different specialists—the unfortunate experience of too many women.
Clinicians have long understood that for many patients, there is no clear diagnosis. Patients become frustrated with clinicians’ apparent inability to help, or even take their complaints seriously. Doctor-shopping results in multiple tests, medication trials, and surgery. This chain of events stems from the traditional anatomic model of disease, which attributes pain to an organ or tissue abnormality that surgical correction might resolve.
Key findings. Clues that the anatomic model is inadequate have been a part of gynecologic teaching for decades, but recent studies confirm these impressions about chronic pelvic pain:
- Anatomic features noted at surgery may not give reliable information about the cause;
- The effect of surgical treatment is similar to placebo, at least short-term;
- A history of abuse is common.
‘Difficult’ patient or other disease was blamed when surgery failed. The traditional approach was to seek an anatomic abnormality such as endometriosis, adhesions, or pelvic congestion, and treat the abnormality with surgical removal of implants, scar tissue, or the pelvic organs altogether.
(The anatomic model still applies to acute pelvic pain; ruptured ovarian cyst, ectopic pregnancy, and appendicitis are highest on the list of diagnostic possibilities.)
Surgeons were convinced that their operations were successful, largely because they characterized cases that failed to get better as evidence of nongynecologic disease or a patient who simply wanted to be difficult.
Pivotal study: ‘Integrated’ treatment achieved better results. One of the earliest clues that surgery might not be the best approach to chronic pelvic pain came from a study of 106 patients randomized to 2 different strategies1:
- In the “standard” approach, laparoscopy was used early, and patients with no anatomic abnormalities were then evaluated for other problems, such as psychological disorders.
- In the “integrated” approach, the pain experience was thought to have 4 components: nociception, pain sensation (which includes processing), suffering, and pain behavior. This approach included psychological and physical therapy as well as evaluation for anatomic abnormalities, generally using nonsurgical methods.
Among the 57 women randomized to the integrated approach, 5 (9%) underwent surgery, compared with 100% of the group randomized to standard therapy. One year later, 75% of the women assigned to the integrated approach reported improvement in pain, compared with 41% of those in the standard group.
In both groups, associated symptoms were common at the onset of therapy, including backache, nausea, malaise, headache, and insomnia. These symptoms were more likely to improve with the integrated approach.
Initial strategy: Avoid surgery
Winkel CA. Evaluation and management of women with endometriosis. Obstet Gynecol. 2003;102:397-408.
Avoidance of surgery can be recommended except perhaps in patients with a mass or discrete and localized abnormalities (eg, tender uterosacral nodule with deep dyspareunia as the only complaint). This strategy challenges the anatomic model of chronic pelvic pain, but is consistent with challenges to the anatomic model of chronic pain at other sites, such as chronic back pain.
Empiric medical therapy may be preferable in women believed, clinically, to have endometriosis without a mass or who wish to get pregnant right away, Dr. Winkel noted.
Many diagnoses can be made in women with chronic pelvic pain, in addition to endometriosis (eg, irritable bowel syndrome, interstitial cystitis, vulvodynia, fibromyalgia, and somatization disorder); these may reflect different manifestations of the same disorder of pain processing, which is often associated with mood and sleep abnormalities. Therapy to improve sleep, physical conditioning, and coping strategies appears to be more helpful than surgery as an initial approach.
Visual and histologic diagnoses of endometriosis at odds
Walter AJ, Hentz JG, Magtibay PM, Cornella JL, Magrina JF. Endometriosis: correlation between histologic and visual findings at laparoscopy. Am J Obstet Gynecol. 2001;184:1407-1413.
Stratton P, Winkel CA, Sinaii N, Merino MJ, Zimmer C, Nieman LK. Location, color, size, depth and volume may predict endometriosis in lesions resected at surgery. Fertil Steril. 2002;78:743-749.
Stratton P, Winkel C, Premkumar A, et al. Diagnostic accuracy of laparoscopy, magnetic resonance imaging, and histopathologic examination for the detection of endometriosis. Fertil Steril. 2003;79:1078-1085.
Three recent studies assess the discrepancies between visual and histologic evidence of endometriosis in women with chronic pelvic pain. Earlier studies had indicated that visual diagnosis is not equivalent to histologic diagnosis, and that failure to see endometriosis does not mean it is not there.
In all 3 studies, visible lesions that appeared to be endometriosis were excised and evaluated by a pathologist.
- Walter et al found that 12 of 37 women with visible lesions had no histologic evidence of endometriosis; the positive predictive value of visualized endometriosis was 62%.
- Stratton et al found a similar 61% of 314 lesions believed on visual inspection to be endometriosis were histologically confirmed. Of 44 women with visual criteria suggesting endometriosis, 6 (14%) were unconfirmed by histology. This discrepancy was noted in women considered upon inspection to have “mild” disease, of whom 5 of 13 (38%) had no histologic evidence.
Does a diagnosis benefit the patient? In a commentary, Dr. Frank Ling2 questioned whether histologic or visual diagnoses are useful. After all, he argued, histologic diagnosis of endometriosis does not prove it caused the pain—prior studies showed a high prevalence of endometriosis in asymptomatic women.
Focusing on what the inside of the pelvis looks like, whether through a laparoscope or the pathologist’s microscope, may leave the woman with chronic pain without relief. Ling made a case for empiric medical treatment of endometriosis, without surgery.
Sham surgery: A potent placebo
Swank DJ, Swank-Bordewijk SC, Hop WC, et al. Laparoscopic adhesiolysis in patients with chronic abdominal pain: a blinded randomised controlled multi-centre trial. Lancet. 2003;361:1247-1251.
In chronic pelvic pain, the placebo effect can be potent—another indication that the anatomic model is not the answer. In the mid-90s, Sutton et al3 found equal responses to sham surgery and laser laparoscopy at 3 months postoperatively in patients with endometriosis-associated pain—but laser laparoscopy had an advantage over sham surgery at 6 months postoperatively.
Swank et al compared laparoscopic adhesiolysis with sham surgery in 100 adults (87% women) with chronic abdominal pain without intestinal stricture. At 1 year, 27% were pain-free or much improved, and there was no difference in visual analog score improvement, regardless of type of surgery. They concluded that abdominal pain can improve after surgery, but the benefit is not likely due to adhesiolysis.
In both groups, as in the Sutton study, reduced pain was maximal at 3 months and somewhat less by 6 months after surgery, supporting the likelihood of a placebo effect.
Possibly, the response to surgery was due in part to reduced anxiety after surgery excluded cancer, yet the mean number of prior operations was almost 3, suggesting that many of these patients had already had the opportunity to be reassured by benign operative findings.
Past abuse: The mind-body link
Lampe A, Doering S, Rumpold G, et al. Childhood pain syndromes and their relation to childhood abuse and stressful life events. J Psychosom Res. 2003;54:361-367.
It has been noted for years that women with chronic pelvic pain are more likely to have a history of sexual abuse than women without chronic pelvic pain. In a study of the chronic pain/abuse relationship, Lampe et al found “complex mutual interactions among childhood abuse, stressful life events, depression, and the occurrence of chronic pain,” and urged clinicians to consider these factors when treating patients.
It is clear that chronic pain syndromes and abuse are linked, but there is disagreement on whether pelvic pain is associated with sexual abuse more than other abuse, or if sexual abuse is associated more with pelvic pain than chronic pain at other sites.
These associations were once explained as physically and psychologically traumatic events being reenacted through illness behaviors. A theory more consistent with current views of pain-processing disorders is that physical or psychological trauma may “kindle” abnormalities of neurotransmitter function to which a patient is genetically predisposed. This model is analogous to the view that depression is a genetic disorder kindled by a major loss or adverse life event.
Such a view requires that we relinquish the mind-body dualism first proposed by Descartes in the 17th century, long before we recognized that neurotransmitters mediate mood as well as motor function, and that life events can alter the chemistry of the brain.
Dr. Scialli reports no financial relationships relevant to this article.
1. Peters AAW, van Dorst E, Jellis B, van Zuuren E, Hermans J, Trimbos JB. A randomized trial to compare 2 different approaches in women with chronic pelvic pain. Obstet Gynecol. 1991;77:740-744.
2. Ling FW. Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Obstet Gynecol. 1999;93:51-58.
3. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized, double-blind, controlled trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild and moderate endometriosis. Fertil Steril. 1994;62:696-700.
1. Peters AAW, van Dorst E, Jellis B, van Zuuren E, Hermans J, Trimbos JB. A randomized trial to compare 2 different approaches in women with chronic pelvic pain. Obstet Gynecol. 1991;77:740-744.
2. Ling FW. Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Obstet Gynecol. 1999;93:51-58.
3. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized, double-blind, controlled trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild and moderate endometriosis. Fertil Steril. 1994;62:696-700.
Anticoagulation in pregnancy: Q&A on low molecular weight heparin
- Low molecular weight heparin appears to be as safe as unfractionated heparin in pregnancy, with longer-lasting effects and reduced need for monitoring. Both the American College pregnancy with appropriate counseling.
- Although warfarin is the anticoagulant of choice in the nonpregnant state, it crosses the placenta and has been linked to structural birth defects known as “warfarin embryopathy.”
- A single subcutaneous, prophylactic 40-mg dose of the low molecular weight heparin enoxaparin costs about $30, compared with about $1 for an equivalent dose of unfractionated heparin.
What are the attributes of the ideal anticoagulant in pregnancy? Low molecular weight heparin fills the bill in many ways: It is safe for both mother and fetus, as effective in pregnancy as in the nongravid population, and side effects are minimal. It also has a favorable dosing route and interval, with less need for monitoring than with unfractionated heparin (UH).
In other ways, low molecular weight heparin (LMWH) is distinctly inferior. This article describes its strengths and weaknesses, addressing 10 common clinical questions.
Assessing the heightened risks of pregnancy
Pregnant women have 5 times the risk of venous thromboembolism (VTE) of nongravid patients.1 The increased risk is due to physiologic, mechanical and, sometimes, iatrogenic factors (TABLE 1):
- Gravidas have greater concentrations of factors I, VII, VIII, IX, and X; decreased fibrinolytic activity; and increased platelet activation. These changes in the coagulation system predispose the gravida to clot formation. Although they may protect against hemorrhage, they also heighten the risk for VTE during pregnancy and the postpartum period.
- The enlarging uterus can compress venous drainage from the lower extremities, resulting in stasis. Further, prolonged immobilization in the form of bed rest is often prescribed for obstetric complications such as hypertension, preterm labor, hemorrhage, and preterm premature rupture of membranes.
- Both abdominal and vaginal operative delivery can predispose to vascular endothelial injury.
LMWH deactivates more slowly than UH, exposing patients to fewer periods of subtherapeutic anticoagulation.
These factors—singularly or in combination–can lead to a thrombotic or embolic event.2
TABLE 1
Pregnancy-associated risk factors for venous thromboembolism
| RISK FACTOR | CAUSES |
|---|---|
| Changes in the coagulation system | Increased factors I, VII, VIII, IX, X |
| Decreased fibrinolytic activity | |
| Increased platelet activation | |
| Venous stasis | Enlarging uterus compresses venous return from lower extremities |
| Endothelial injury | Vacuum delivery |
| Forceps delivery | |
| Cesarean delivery | |
| Prolonged immobilization | Preterm labor |
| Preterm premature rupture of membranes | |
| Obstetric hemorrhage | |
| Hypertensive disorders of pregnancy |
Question 1When is anticoagulation warranted in pregnancy?
It is indicated in women who:
- experience a thromboembolic event,
- become pregnant while being treated for VTE,
- have a previous history of unprovoked VTE (unrelated to trauma, immobilization, etc),
- have a known hereditary thrombophilia such as antithrombin III deficiency, factor V Leiden mutation, or the prothrombin G20210A mutation, with or without a personal history of thrombosis, or
- have a connective tissue disorder such as antiphospholipid syndrome.
Anticoagulation in pregnancy is common, and usually is given for the duration of pregnancy, into the postpartum period.
Question 2What are the options for anticoagulation?
Heparin is the sole choice for long-term anticoagulation, since warfarin is contraindicated in pregnancy.3 (See “Dangers of warfarin”.)
Unfortunately, heparin has disadvantages that render it a second-line agent in the nonpregnant population. For example, because of enzymatic degradation, heparins cannot be given orally. In addition, because of its large size and strongly positive charge, the parent heparin molecule—known as “unfractionated” heparin—is rapidly deactivated by tissue proteins, making for an unpredictable anticoagulation response. Underdosing and overdosing are typical, and frequent monitoring is necessary.
For these and other reasons, investigators have sought a more predictable, reliable agent for long-term anticoagulation in patients who cannot take warfarin. Interest has focused on a derivative of the parent heparin molecule: LMWH.
Snapshot of LMWH. This agent is produced by the controlled enzymatic degradation of unfractionated heparin (molecular weight of approximately 10,000 to 15,000 daltons) into approximately 5,000-dalton molecules. Although they are much smaller than the parent molecule, these polymers still carry a strong positive charge.
This polarity is probably why LMWH does not cross the placenta—a major advantage over warfarin for anticoagulation during pregnancy.5
In addition, accumulating evidence6,7 suggests that LMWH is at least as safe and effective as UH in pregnancy, although more research is needed. As with UH, there appears to be no transplacental passage.8
Pregnancy category. According to the manufacturer, the LMWH enoxaparin falls into pregnancy category B.9 Another LMWH, dalteparin, also falls into pregnancy category B. Both the American College of Obstetricians and Gynecologists2 and the Society for Maternal-Fetal Medicine10 endorse the use of LMWH in pregnancy with appropriate counseling.8
Although it is the drug of choice in the nonpregnant population, warfarin is contraindicated in pregnancy because it can cross the placenta and has been linked to adverse pregnancy outcomes.
Several studies have demonstrated an association between first-trimester warfarin exposure and a constellation of structural birth defects, termed “warfarin embryopathy,” which includes craniofacial and skeletal defects. Exposure in any trimester is associated with fetal and neonatal intracranial hemorrhage.3
For these reasons, warfarin is contraindicated in pregnancy with the rare exception of women with mechanical prosthetic heart valves.4
Question 3How does LMWH differ from unfractionated heparin?
LMWH is more efficient. Both UH and LMWH contain an essential pentasaccharide within their polymer structure that binds to and enhances antithrombin III, which in turn inhibits thrombin and activated factor X (Xa). Because of its smaller size, LMWH preferentially inhibits Xa, which is higher in the coagulation cascade. Inhibition of a single molecule of Xa prevents the formation of many molecules of thrombin. Molecule for molecule, LMWH is a more efficient anticoagulant than UH (FIGURE).11
The second way that LMWH differs from UH also relates to the molecule’s size. Smaller heparin molecules are less likely to be deactivated by tissue proteins. This results in improved bioavailability of the administered dose. Greater bioavailability translates to a more predictable dose-response relationship, a long half-life, and better anticoagulation.12
FIGURE Simplified schematic of the coagulation cascade
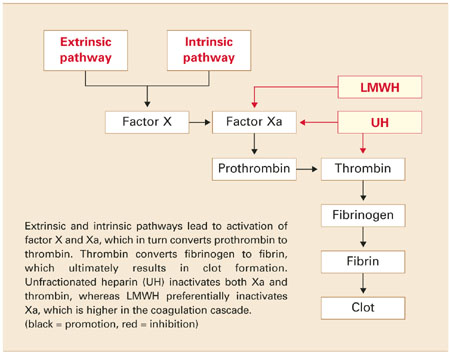
Question 4What are the clinical advantages of LMWH?
LMWH has longer-lasting effects and subcutaneous dosing. It also has fewer side effects than UH.
Because of its large size and positive charge, UH has an unfavorable pharmacokinetic profile. Tissue proteins interfere with and deactivate it, and many of these proteins increase in pregnancy and with advancing gestation. Heparin tissue levels are therefore erratic and unpredictable and often lead to periods of subtherapeutic coverage. This is true even with intravenous (IV) dosing.
Rapid absorption, no intravenous dosing. In contrast, because of its smaller size, LMWH is rapidly and predictably absorbed from a subcutaneous injection. Intravenous dosing is not necessary to obtain adequate tissue levels. Once in tissue, it is deactivated more slowly and therefore maintains its anticoagulation effect longer. Consequently, patients are exposed to fewer periods of subtherapeutic anticoagulation. A longer half-life also translates to more favorable dosing routes (subcutaneous rather than IV) and regimens (daily versus twice daily). Similarly, since the dose-response is predictable and tissue levels are more constant, frequent monitoring of treatment response is not routinely necessary.
Fewer side effects. Another advantage of LMWH over UH is the improved side-effect profile. Patients on LMWH have decreased risk of hemorrhage, osteoporosis, and antibody-mediated thrombocytopenia.11 Although most data regarding these advantages come from the nonpregnant population, it is plausible to speculate that these traits also are present in pregnant women (TABLE 2).
TABLE 2
Advantages and disadvantages of LMWH in pregnancy
| ADVANTAGES |
| More effective anticoagulation |
| Better dose-response |
| Longer half-life |
| Better dosing route |
| Decreased need for monitoring |
| Fewer side effects |
| DISADVANTAGES |
| Longer half-life |
| Risk of hematoma with epidural anesthesia |
| Not fully reversible with protamine sulfate |
| Anticoagulation effect difficult to monitor |
| Higher cost |
Question 5What are the disadvantages?
They include the long half-life, risk of hematoma with epidural anesthesia, lower efficacy of the antidote, monitoring difficulty, and higher cost.
The long half-life of LMWH is both an advantage and disadvantage. For example, when UH is administered intravenously, it has a half-life of 30 to 60 minutes. When it is given subcutaneously, the half-life is 1 to 2 hours. This means that a patient can undergo vaginal delivery or even surgery within hours of her last subcutaneous UH injection.
In contrast, LMWH has a half-life of approximately 4 hours. A recent dose may increase the risk of operative morbidity in the form of overt or delayed hemorrhage, hematoma, or wound dehiscence.
Not for use with epidural anesthesia. Case reports of epidural hematomas after regional anesthesia during orthopedic procedures have caused considerable concern about the use of LMWH and the placement of a neuraxial block such as a spinal or epidural.13 Many anesthesiologists will not place an epidural or spinal within 24 hours of a LMWH dose.14 However, as experience with these agents in the nonpregnant population expands, a more evidence-based approach is likely to develop.
Antidote less effective. Protamine sulfate is a strong base that binds with the positively charged UH molecule, thereby serving as an antidote through competitive inhibition. Because of its smaller size, LMWH is reversed by protamine to a lesser degree (approximately 60% effective).14 Therefore, hemorrhage associated with LMWH may require replacement of blood components, which carries the risks of infection and transfusion reactions.
Difficult to monitor. The anticoagulation effect of UH can be reliably monitored by the activated partial thromboplastin time (aPTT), which is a widely available test with a rapid turnaround. However, the anticoagulation effect of LMWH is not reflected by the aPTT. Assessment of LMWH activity requires assessment of the antifactor Xa level, a test that is not universally available and has a longer turnaround.
Higher cost. Another limitation of LMWH is its cost. A single, subcutaneous, prophylactic 40-mg dose of enoxaparin costs about $30, compared with about $1 for an equivalent dose of unfractionated heparin (5,000 U subcutaneously twice a day). Because of its increased cost, many insurance companies do not authorize the use of LMWH for prolonged periods such as pregnancy and the postpartum period. However, studies in the nonpregnant population have demonstrated overall decreased cost over UH due to the reduced need for monitoring, shorter length of hospital stay, and diminished treatment failure.
Question 6What is the dose for prophylaxis and treatment?
The standard dose of enoxaparin for prophylaxis in pregnancy and the postpartum period is 40 mg administered subcutaneously every 24 hours (TABLE 3). Therapeutic anticoagulation (sometimes referred to as a “weightadjusted” dose) is usually achieved with 1 mg/kg every 12 hours.
Dalteparin can be given in a prophylactic dose of 5,000 U subcutaneously every 24 hours and a therapeutic dose of 200 U/kg every 24 hours.15 Dosing may need to be adjusted with advancing gestation as plasma volume, renal clearance, and tissue proteins increase.
The various LMWH preparations are not equivalent in their pharmacokinetics. Generally, clinicians familiarize themselves with a single agent. It also is important to note that dosing regimens in pregnancy are not evidence-based but largely “borrowed” from nonpregnant regimens. They also vary widely in the available literature.
TABLE 3
Common low molecular weight heparins
| BRAND NAME | GENERIC NAME | PROPHYLACTIC DOSE | THERAPEUTIC DOSE |
|---|---|---|---|
| Lovenox | Enoxaparin | 40 mg every 24 hours | 1 mg/kg every 12 hours |
| Fragmin | Dalteparin | 5,000 U every 24 hours | 200 U/kg every 24 hours |
| Note: All doses are subcutaneous | |||
Question 7Under what conditions can LMWH be given?
Generally, LMWH can replace UH in any condition that warrants prophylactic or therapeutic anticoagulation in pregnancy, except the acute management of pulmonary embolism and in women with mechanical heart valves.
Prophylactic dosing can be offered to women with a previous thromboembolic event such as deep vein thrombosis (DVT) or pulmonary embolism that was not associated with a reversible and temporary predisposing risk factor such as immobilization or trauma. (In general, pregnancy is not seen as a reversible or temporary risk factor.)
Prophylactic or therapeutic dosing is sometimes offered to women with a hereditary thrombophilia, antiphospholipid syndrome, or other vasculopathies and connective-tissue diseases. In addition, LMWH is an accepted first-line therapeutic anticoagulant for acute DVT in pregnancy.
Not for use in treating acute pulmonary embolism. Evidence is insufficient to support the use of LMWH as a first-line anticoagulant for acute pulmonary embolism. To date, IV loading with UH is the standard of care, with conversion to LMWH after 4 to 5 days of therapeutic UH anticoagulation. This may change as experience with LMWH increases.
Not for use with mechanical prosthetic heart valves. Because of case reports of recurrent thromboembolism resulting in maternal and fetal death in pregnant women with mechanical prosthetic heart valves on therapeutic LMWH, the manufacturer of enoxaparin warns against its use in pregnancy in these women.9 However, similar outcomes have been reported with UH and warfarin. This forces clinicians to consider potentially less effective and more problematic agents for anticoagulation in this fortunately rare circumstance.
Contemporary management involves converting from warfarin to subcutaneous heparin or the heparin pump once pregnancy is established and before organogenesis (at approximately 6 weeks’ gestation), followed by frequent monitoring of aPTT. Alternatively, warfarin can be resumed after organogenesis (at about 12 weeks) and continued into the third trimester, followed by conversion to heparin pump, subcutaneous injections, or an IV drip near term. Both options carry significant maternal and fetal risk and should be performed in a multidisciplinary fashion along with cardiology and vascular medicine.16
Question 8How do I start and stop LMWH?
Start LMWH as a subcutaneous injection without IV loading. A baseline complete blood count for platelet count is reasonable. Patient education is straightforward.
Prophylactic dosing can be initiated on an outpatient basis immediately after patient education and procurement of the medicine.
Therapeutic dosing for DVT usually is begun during hospitalization, with 1 mg per kilogram given subcutaneously every 12 hours. Barring other comorbidities, discharge can be achieved after patient education. The exception is treatment of acute pulmonary embolism.Conversion to LMWH is achieved once the patient is fully anticoagulated.
Discontinuation. Pregnancy is a period of shifting maternal and fetal status, when indications for delivery can develop suddenly and with little warning (eg, abruptio placenta, nonreassuring antenatal testing).
LMWH dosing regimens in pregnancy are not evidence-based but largely “borrowed” from nonpregnant regimens.
A major consideration is the long half-life of LMWH. If a patient has had a recent subcutaneous injection of LMWH followed by an urgent indication for delivery, she may be anticoagulated during her delivery and be at increased risk for hemorrhage. Similarly, she may not be a candidate for epidural or spinal anesthesia because of the risk of epidural hematoma. If cesarean section is indicated, she may need general anesthesia, which is associated with increased maternal morbidity. If hemorrhage occurs, she may require transfusion of blood products, which carries the risks of infection and transfusion reactions.
Three strategies for peripartum management with LMWH are:
- Leave the patient on LMWH until the onset of labor. Depending on the timing and dose of her last injection, she may or may not be a candidate for regional anesthesia in labor. With prophylactic dosing, the risk of significant hemorrhage is low.
- Time delivery so that the patient withholds her PMinjection and presents for delivery the following morning, 24 hours after her last dose. This option is attractive when cesarean delivery is planned. The advantage of this approach is that it keeps the window of thrombosis as narrow as possible. The disadvantage is that the patient may enter labor or require delivery before the chosen delivery date, in which case she may be at risk for hemorrhage.
- Convert the patient to UH at approximately 36 to 37 weeks’ gestation. The advantage? The shorter half-life of UH increases the possibility for regional anesthesia and decreases the risk for hemorrhage. The disadvantage: The risk for thrombosis as well as complications (thrombocytopenia, osteoporosis, thrombosis) may be greater with UH for the reasons described earlier.
Restarting after delivery. Strategies for continued thromboprophylaxis in the postpartum period include continuing LMWH for an additional 6 to 8 weeks or converting to warfarin. Warfarin can be taken orally but requires frequent monitoring and adjustment of dosing, which is unnecessary with LMWH. Many patients choose to continue LMWH because they are familiar with the routine of daily injections. There is little data to support or refute either approach.
There also is little data to guide the decision of when to reinitiate prophylactic or therapeutic doses of LMWH after vaginal or cesarean delivery. Translating from other surgical subspecialties, most obstetricians are comfortable resuming both prophylactic and therapeutic doses at 6 hours after vaginal delivery and 8 hours after cesarean section.
Question 9How do I monitor the effectiveness of LMWH?
The frequent monitoring necessary with UH is not required with LMWH, since the increased bioavailability of LMWH leads to reliable tissue levels. The aPTT level does not correlate well with the anticoagulation effect of LMWH.
Antifactor Xa levels—sometimes referred to as the LMWH assay—of 0.5 to 1.2 IU/mL are considered adequate for therapeutic anticoagulation in the nonpregnant population. Peak anti-Xa activity is achieved approximately 4 hours after subcutaneous injection. AntiXa levels should therefore be drawn 4 hours after the last dose.17 Prophylactic subcutaneous dosing of enoxaparin 40 mg daily generally does not require monitoring of anti-Xa levels.
In nonpregnant women, routine monitoring is seldom necessary. Gravidas, however, are constantly changing in terms of weight, plasma volume, renal clearance, and amount of heparin-binding proteins. Because of this, periodic monitoring (every 4 weeks) is reasonable until an evidence-based recommendation can be made.
Question 10When can I provide neuraxial anesthesia?
Most anesthesiologists are reluctant to perform neuraxial anesthesia within 12 hours of the last prophylactic dose or 24 hours of the last therapeutic dose of LMWH because of the risk of epidural and spinal hematoma.
The American Society of Regional Anesthesia recommends that neuraxial anesthesia be withheld for 24 hours after the last therapeutic dose and 12 hours after a prophylactic dose. That organization did not recommend checking anti-Xa levels, since they do not adequately predict the risk of bleeding.9 However, as experience with LMWH broadens in nonobstetric surgical cases, such as orthopedic and cardiac procedures, it is likely that greater familiarity with the medication will lead to better evidence and broader acceptance.
Dr. Emery reports no financial relationships relevant to this article.
1. Gherman RB, Goodwin TM, Leung JD, Byrne JD, Hethumumi R, Montoro M. Incidence, clinical characteristics, and timing of objectively diagnosed venous thromboembolism during pregnancy. Obstet Gynecol. 1999;94:730-734.
2. American College of Obstetricians and Gynecologists. Practice Bulletin #19: Thromboembolism in Pregnancy. Washington, DC: ACOG; 2000.
3. Hall JG, Pauli RM, Wilson KM. Maternal and fetal sequelae of anticoagulation during pregnancy. Am J Med. 1980;68:122-140.
4. Born D, Martinez EE, Almeida PAM, et al. Pregnancy in patients with mechanical heart valves: the effects of anticoagulation on mother, fetus and neonate. Am Heart J. 1992;124:413-417.
5. Omri A, Delayoye JF, Anderson H, Bachmann F. Low molecular weight heparin Novo (LHN-1) does not cross the placenta during the second trimester of pregnancy. Thromb Haemost. 1989;61:55-56.
6. Sanson BJ, Lensing AWA, Prins MH, et al. Safety of low molecular weight heparin in pregnancy: a systematic review. Thromb Haemost. 1999;81:668-672.
7. Nelson-Piercy C, Letsky EA, de Sweit M. Low molecular weight heparin for obstetric thromboprophylaxis: experience of sixty-nine pregnancies in sixty-one women at risk. Am J Obstet Gynecol. 1997;176:1062-1068.
8. Forestier F, Daffos F, Rainaut M, et al. Low molecular weight heparin (CY 216) does not cross the placenta during the third trimester of pregnancy. Thromb Haemost. 1987;57:234.-
9. Lovenox injection [package insert]. Bridgewater, NJ: Aventis; 2003.
10. Enoxaprin sodium (Lovenox) and pregnancy. SMFM Practice Committee Announcement posted at http://www.smfm.org
11. Hirsh J, Warkentin TE, Raschke R, Granger C, Ohman EM, Dalen JE. Heparin and low molecular weight heparin: mechanisms of action, pharmacokinetics, dosing considerations, monitoring, efficacy and safety. Chest. 1998;114:489S-510S.
12. Weitz JI. Low-molecular-weight heparins. N Engl J Med. 1997;337:688-698.
13. US Department of Health and Human Services. FDA Public Health Advisory. Reports of Epidural and Spinal Hematomas with Concurrent Use of Low Molecular Weight Heparin and Spinal/Epidural Anesthesia or Spinal Puncture. Rockville, MD: Food and Drug Administration; December 1997.
14. American Society of Regional Anesthesia. Recommendations for Neuraxial Anesthesia and Anticoagulation. Richmond, Va: ASRA; 1998.
15. Hirsh J, Raschke R, Warkentin TE, et al. Heparin: mechanism of action, pharmacokinetics, dosing considerations, efficacy, and safety. Chest. 1995;108:258S-275S.
16. Anticoagulation and Enoxaparin Use in Patients with Prosthetic Heart Valves and/or Pregnancy. Clinical Cardiology Consensus Reports. Atlanta, Ga: American Health Consultants; 2002.
17. Ginsberg JS, Greer I, Hirsh J. Use of antithrombotic agents during pregnancy. Chest. 2001;119:122S-131S.
- Low molecular weight heparin appears to be as safe as unfractionated heparin in pregnancy, with longer-lasting effects and reduced need for monitoring. Both the American College pregnancy with appropriate counseling.
- Although warfarin is the anticoagulant of choice in the nonpregnant state, it crosses the placenta and has been linked to structural birth defects known as “warfarin embryopathy.”
- A single subcutaneous, prophylactic 40-mg dose of the low molecular weight heparin enoxaparin costs about $30, compared with about $1 for an equivalent dose of unfractionated heparin.
What are the attributes of the ideal anticoagulant in pregnancy? Low molecular weight heparin fills the bill in many ways: It is safe for both mother and fetus, as effective in pregnancy as in the nongravid population, and side effects are minimal. It also has a favorable dosing route and interval, with less need for monitoring than with unfractionated heparin (UH).
In other ways, low molecular weight heparin (LMWH) is distinctly inferior. This article describes its strengths and weaknesses, addressing 10 common clinical questions.
Assessing the heightened risks of pregnancy
Pregnant women have 5 times the risk of venous thromboembolism (VTE) of nongravid patients.1 The increased risk is due to physiologic, mechanical and, sometimes, iatrogenic factors (TABLE 1):
- Gravidas have greater concentrations of factors I, VII, VIII, IX, and X; decreased fibrinolytic activity; and increased platelet activation. These changes in the coagulation system predispose the gravida to clot formation. Although they may protect against hemorrhage, they also heighten the risk for VTE during pregnancy and the postpartum period.
- The enlarging uterus can compress venous drainage from the lower extremities, resulting in stasis. Further, prolonged immobilization in the form of bed rest is often prescribed for obstetric complications such as hypertension, preterm labor, hemorrhage, and preterm premature rupture of membranes.
- Both abdominal and vaginal operative delivery can predispose to vascular endothelial injury.
LMWH deactivates more slowly than UH, exposing patients to fewer periods of subtherapeutic anticoagulation.
These factors—singularly or in combination–can lead to a thrombotic or embolic event.2
TABLE 1
Pregnancy-associated risk factors for venous thromboembolism
| RISK FACTOR | CAUSES |
|---|---|
| Changes in the coagulation system | Increased factors I, VII, VIII, IX, X |
| Decreased fibrinolytic activity | |
| Increased platelet activation | |
| Venous stasis | Enlarging uterus compresses venous return from lower extremities |
| Endothelial injury | Vacuum delivery |
| Forceps delivery | |
| Cesarean delivery | |
| Prolonged immobilization | Preterm labor |
| Preterm premature rupture of membranes | |
| Obstetric hemorrhage | |
| Hypertensive disorders of pregnancy |
Question 1When is anticoagulation warranted in pregnancy?
It is indicated in women who:
- experience a thromboembolic event,
- become pregnant while being treated for VTE,
- have a previous history of unprovoked VTE (unrelated to trauma, immobilization, etc),
- have a known hereditary thrombophilia such as antithrombin III deficiency, factor V Leiden mutation, or the prothrombin G20210A mutation, with or without a personal history of thrombosis, or
- have a connective tissue disorder such as antiphospholipid syndrome.
Anticoagulation in pregnancy is common, and usually is given for the duration of pregnancy, into the postpartum period.
Question 2What are the options for anticoagulation?
Heparin is the sole choice for long-term anticoagulation, since warfarin is contraindicated in pregnancy.3 (See “Dangers of warfarin”.)
Unfortunately, heparin has disadvantages that render it a second-line agent in the nonpregnant population. For example, because of enzymatic degradation, heparins cannot be given orally. In addition, because of its large size and strongly positive charge, the parent heparin molecule—known as “unfractionated” heparin—is rapidly deactivated by tissue proteins, making for an unpredictable anticoagulation response. Underdosing and overdosing are typical, and frequent monitoring is necessary.
For these and other reasons, investigators have sought a more predictable, reliable agent for long-term anticoagulation in patients who cannot take warfarin. Interest has focused on a derivative of the parent heparin molecule: LMWH.
Snapshot of LMWH. This agent is produced by the controlled enzymatic degradation of unfractionated heparin (molecular weight of approximately 10,000 to 15,000 daltons) into approximately 5,000-dalton molecules. Although they are much smaller than the parent molecule, these polymers still carry a strong positive charge.
This polarity is probably why LMWH does not cross the placenta—a major advantage over warfarin for anticoagulation during pregnancy.5
In addition, accumulating evidence6,7 suggests that LMWH is at least as safe and effective as UH in pregnancy, although more research is needed. As with UH, there appears to be no transplacental passage.8
Pregnancy category. According to the manufacturer, the LMWH enoxaparin falls into pregnancy category B.9 Another LMWH, dalteparin, also falls into pregnancy category B. Both the American College of Obstetricians and Gynecologists2 and the Society for Maternal-Fetal Medicine10 endorse the use of LMWH in pregnancy with appropriate counseling.8
Although it is the drug of choice in the nonpregnant population, warfarin is contraindicated in pregnancy because it can cross the placenta and has been linked to adverse pregnancy outcomes.
Several studies have demonstrated an association between first-trimester warfarin exposure and a constellation of structural birth defects, termed “warfarin embryopathy,” which includes craniofacial and skeletal defects. Exposure in any trimester is associated with fetal and neonatal intracranial hemorrhage.3
For these reasons, warfarin is contraindicated in pregnancy with the rare exception of women with mechanical prosthetic heart valves.4
Question 3How does LMWH differ from unfractionated heparin?
LMWH is more efficient. Both UH and LMWH contain an essential pentasaccharide within their polymer structure that binds to and enhances antithrombin III, which in turn inhibits thrombin and activated factor X (Xa). Because of its smaller size, LMWH preferentially inhibits Xa, which is higher in the coagulation cascade. Inhibition of a single molecule of Xa prevents the formation of many molecules of thrombin. Molecule for molecule, LMWH is a more efficient anticoagulant than UH (FIGURE).11
The second way that LMWH differs from UH also relates to the molecule’s size. Smaller heparin molecules are less likely to be deactivated by tissue proteins. This results in improved bioavailability of the administered dose. Greater bioavailability translates to a more predictable dose-response relationship, a long half-life, and better anticoagulation.12
FIGURE Simplified schematic of the coagulation cascade
Question 4What are the clinical advantages of LMWH?
LMWH has longer-lasting effects and subcutaneous dosing. It also has fewer side effects than UH.
Because of its large size and positive charge, UH has an unfavorable pharmacokinetic profile. Tissue proteins interfere with and deactivate it, and many of these proteins increase in pregnancy and with advancing gestation. Heparin tissue levels are therefore erratic and unpredictable and often lead to periods of subtherapeutic coverage. This is true even with intravenous (IV) dosing.
Rapid absorption, no intravenous dosing. In contrast, because of its smaller size, LMWH is rapidly and predictably absorbed from a subcutaneous injection. Intravenous dosing is not necessary to obtain adequate tissue levels. Once in tissue, it is deactivated more slowly and therefore maintains its anticoagulation effect longer. Consequently, patients are exposed to fewer periods of subtherapeutic anticoagulation. A longer half-life also translates to more favorable dosing routes (subcutaneous rather than IV) and regimens (daily versus twice daily). Similarly, since the dose-response is predictable and tissue levels are more constant, frequent monitoring of treatment response is not routinely necessary.
Fewer side effects. Another advantage of LMWH over UH is the improved side-effect profile. Patients on LMWH have decreased risk of hemorrhage, osteoporosis, and antibody-mediated thrombocytopenia.11 Although most data regarding these advantages come from the nonpregnant population, it is plausible to speculate that these traits also are present in pregnant women (TABLE 2).
TABLE 2
Advantages and disadvantages of LMWH in pregnancy
| ADVANTAGES |
| More effective anticoagulation |
| Better dose-response |
| Longer half-life |
| Better dosing route |
| Decreased need for monitoring |
| Fewer side effects |
| DISADVANTAGES |
| Longer half-life |
| Risk of hematoma with epidural anesthesia |
| Not fully reversible with protamine sulfate |
| Anticoagulation effect difficult to monitor |
| Higher cost |
Question 5What are the disadvantages?
They include the long half-life, risk of hematoma with epidural anesthesia, lower efficacy of the antidote, monitoring difficulty, and higher cost.
The long half-life of LMWH is both an advantage and disadvantage. For example, when UH is administered intravenously, it has a half-life of 30 to 60 minutes. When it is given subcutaneously, the half-life is 1 to 2 hours. This means that a patient can undergo vaginal delivery or even surgery within hours of her last subcutaneous UH injection.
In contrast, LMWH has a half-life of approximately 4 hours. A recent dose may increase the risk of operative morbidity in the form of overt or delayed hemorrhage, hematoma, or wound dehiscence.
Not for use with epidural anesthesia. Case reports of epidural hematomas after regional anesthesia during orthopedic procedures have caused considerable concern about the use of LMWH and the placement of a neuraxial block such as a spinal or epidural.13 Many anesthesiologists will not place an epidural or spinal within 24 hours of a LMWH dose.14 However, as experience with these agents in the nonpregnant population expands, a more evidence-based approach is likely to develop.
Antidote less effective. Protamine sulfate is a strong base that binds with the positively charged UH molecule, thereby serving as an antidote through competitive inhibition. Because of its smaller size, LMWH is reversed by protamine to a lesser degree (approximately 60% effective).14 Therefore, hemorrhage associated with LMWH may require replacement of blood components, which carries the risks of infection and transfusion reactions.
Difficult to monitor. The anticoagulation effect of UH can be reliably monitored by the activated partial thromboplastin time (aPTT), which is a widely available test with a rapid turnaround. However, the anticoagulation effect of LMWH is not reflected by the aPTT. Assessment of LMWH activity requires assessment of the antifactor Xa level, a test that is not universally available and has a longer turnaround.
Higher cost. Another limitation of LMWH is its cost. A single, subcutaneous, prophylactic 40-mg dose of enoxaparin costs about $30, compared with about $1 for an equivalent dose of unfractionated heparin (5,000 U subcutaneously twice a day). Because of its increased cost, many insurance companies do not authorize the use of LMWH for prolonged periods such as pregnancy and the postpartum period. However, studies in the nonpregnant population have demonstrated overall decreased cost over UH due to the reduced need for monitoring, shorter length of hospital stay, and diminished treatment failure.
Question 6What is the dose for prophylaxis and treatment?
The standard dose of enoxaparin for prophylaxis in pregnancy and the postpartum period is 40 mg administered subcutaneously every 24 hours (TABLE 3). Therapeutic anticoagulation (sometimes referred to as a “weightadjusted” dose) is usually achieved with 1 mg/kg every 12 hours.
Dalteparin can be given in a prophylactic dose of 5,000 U subcutaneously every 24 hours and a therapeutic dose of 200 U/kg every 24 hours.15 Dosing may need to be adjusted with advancing gestation as plasma volume, renal clearance, and tissue proteins increase.
The various LMWH preparations are not equivalent in their pharmacokinetics. Generally, clinicians familiarize themselves with a single agent. It also is important to note that dosing regimens in pregnancy are not evidence-based but largely “borrowed” from nonpregnant regimens. They also vary widely in the available literature.
TABLE 3
Common low molecular weight heparins
| BRAND NAME | GENERIC NAME | PROPHYLACTIC DOSE | THERAPEUTIC DOSE |
|---|---|---|---|
| Lovenox | Enoxaparin | 40 mg every 24 hours | 1 mg/kg every 12 hours |
| Fragmin | Dalteparin | 5,000 U every 24 hours | 200 U/kg every 24 hours |
| Note: All doses are subcutaneous | |||
Question 7Under what conditions can LMWH be given?
Generally, LMWH can replace UH in any condition that warrants prophylactic or therapeutic anticoagulation in pregnancy, except the acute management of pulmonary embolism and in women with mechanical heart valves.
Prophylactic dosing can be offered to women with a previous thromboembolic event such as deep vein thrombosis (DVT) or pulmonary embolism that was not associated with a reversible and temporary predisposing risk factor such as immobilization or trauma. (In general, pregnancy is not seen as a reversible or temporary risk factor.)
Prophylactic or therapeutic dosing is sometimes offered to women with a hereditary thrombophilia, antiphospholipid syndrome, or other vasculopathies and connective-tissue diseases. In addition, LMWH is an accepted first-line therapeutic anticoagulant for acute DVT in pregnancy.
Not for use in treating acute pulmonary embolism. Evidence is insufficient to support the use of LMWH as a first-line anticoagulant for acute pulmonary embolism. To date, IV loading with UH is the standard of care, with conversion to LMWH after 4 to 5 days of therapeutic UH anticoagulation. This may change as experience with LMWH increases.
Not for use with mechanical prosthetic heart valves. Because of case reports of recurrent thromboembolism resulting in maternal and fetal death in pregnant women with mechanical prosthetic heart valves on therapeutic LMWH, the manufacturer of enoxaparin warns against its use in pregnancy in these women.9 However, similar outcomes have been reported with UH and warfarin. This forces clinicians to consider potentially less effective and more problematic agents for anticoagulation in this fortunately rare circumstance.
Contemporary management involves converting from warfarin to subcutaneous heparin or the heparin pump once pregnancy is established and before organogenesis (at approximately 6 weeks’ gestation), followed by frequent monitoring of aPTT. Alternatively, warfarin can be resumed after organogenesis (at about 12 weeks) and continued into the third trimester, followed by conversion to heparin pump, subcutaneous injections, or an IV drip near term. Both options carry significant maternal and fetal risk and should be performed in a multidisciplinary fashion along with cardiology and vascular medicine.16
Question 8How do I start and stop LMWH?
Start LMWH as a subcutaneous injection without IV loading. A baseline complete blood count for platelet count is reasonable. Patient education is straightforward.
Prophylactic dosing can be initiated on an outpatient basis immediately after patient education and procurement of the medicine.
Therapeutic dosing for DVT usually is begun during hospitalization, with 1 mg per kilogram given subcutaneously every 12 hours. Barring other comorbidities, discharge can be achieved after patient education. The exception is treatment of acute pulmonary embolism.Conversion to LMWH is achieved once the patient is fully anticoagulated.
Discontinuation. Pregnancy is a period of shifting maternal and fetal status, when indications for delivery can develop suddenly and with little warning (eg, abruptio placenta, nonreassuring antenatal testing).
LMWH dosing regimens in pregnancy are not evidence-based but largely “borrowed” from nonpregnant regimens.
A major consideration is the long half-life of LMWH. If a patient has had a recent subcutaneous injection of LMWH followed by an urgent indication for delivery, she may be anticoagulated during her delivery and be at increased risk for hemorrhage. Similarly, she may not be a candidate for epidural or spinal anesthesia because of the risk of epidural hematoma. If cesarean section is indicated, she may need general anesthesia, which is associated with increased maternal morbidity. If hemorrhage occurs, she may require transfusion of blood products, which carries the risks of infection and transfusion reactions.
Three strategies for peripartum management with LMWH are:
- Leave the patient on LMWH until the onset of labor. Depending on the timing and dose of her last injection, she may or may not be a candidate for regional anesthesia in labor. With prophylactic dosing, the risk of significant hemorrhage is low.
- Time delivery so that the patient withholds her PMinjection and presents for delivery the following morning, 24 hours after her last dose. This option is attractive when cesarean delivery is planned. The advantage of this approach is that it keeps the window of thrombosis as narrow as possible. The disadvantage is that the patient may enter labor or require delivery before the chosen delivery date, in which case she may be at risk for hemorrhage.
- Convert the patient to UH at approximately 36 to 37 weeks’ gestation. The advantage? The shorter half-life of UH increases the possibility for regional anesthesia and decreases the risk for hemorrhage. The disadvantage: The risk for thrombosis as well as complications (thrombocytopenia, osteoporosis, thrombosis) may be greater with UH for the reasons described earlier.
Restarting after delivery. Strategies for continued thromboprophylaxis in the postpartum period include continuing LMWH for an additional 6 to 8 weeks or converting to warfarin. Warfarin can be taken orally but requires frequent monitoring and adjustment of dosing, which is unnecessary with LMWH. Many patients choose to continue LMWH because they are familiar with the routine of daily injections. There is little data to support or refute either approach.
There also is little data to guide the decision of when to reinitiate prophylactic or therapeutic doses of LMWH after vaginal or cesarean delivery. Translating from other surgical subspecialties, most obstetricians are comfortable resuming both prophylactic and therapeutic doses at 6 hours after vaginal delivery and 8 hours after cesarean section.
Question 9How do I monitor the effectiveness of LMWH?
The frequent monitoring necessary with UH is not required with LMWH, since the increased bioavailability of LMWH leads to reliable tissue levels. The aPTT level does not correlate well with the anticoagulation effect of LMWH.
Antifactor Xa levels—sometimes referred to as the LMWH assay—of 0.5 to 1.2 IU/mL are considered adequate for therapeutic anticoagulation in the nonpregnant population. Peak anti-Xa activity is achieved approximately 4 hours after subcutaneous injection. AntiXa levels should therefore be drawn 4 hours after the last dose.17 Prophylactic subcutaneous dosing of enoxaparin 40 mg daily generally does not require monitoring of anti-Xa levels.
In nonpregnant women, routine monitoring is seldom necessary. Gravidas, however, are constantly changing in terms of weight, plasma volume, renal clearance, and amount of heparin-binding proteins. Because of this, periodic monitoring (every 4 weeks) is reasonable until an evidence-based recommendation can be made.
Question 10When can I provide neuraxial anesthesia?
Most anesthesiologists are reluctant to perform neuraxial anesthesia within 12 hours of the last prophylactic dose or 24 hours of the last therapeutic dose of LMWH because of the risk of epidural and spinal hematoma.
The American Society of Regional Anesthesia recommends that neuraxial anesthesia be withheld for 24 hours after the last therapeutic dose and 12 hours after a prophylactic dose. That organization did not recommend checking anti-Xa levels, since they do not adequately predict the risk of bleeding.9 However, as experience with LMWH broadens in nonobstetric surgical cases, such as orthopedic and cardiac procedures, it is likely that greater familiarity with the medication will lead to better evidence and broader acceptance.
Dr. Emery reports no financial relationships relevant to this article.
- Low molecular weight heparin appears to be as safe as unfractionated heparin in pregnancy, with longer-lasting effects and reduced need for monitoring. Both the American College pregnancy with appropriate counseling.
- Although warfarin is the anticoagulant of choice in the nonpregnant state, it crosses the placenta and has been linked to structural birth defects known as “warfarin embryopathy.”
- A single subcutaneous, prophylactic 40-mg dose of the low molecular weight heparin enoxaparin costs about $30, compared with about $1 for an equivalent dose of unfractionated heparin.
What are the attributes of the ideal anticoagulant in pregnancy? Low molecular weight heparin fills the bill in many ways: It is safe for both mother and fetus, as effective in pregnancy as in the nongravid population, and side effects are minimal. It also has a favorable dosing route and interval, with less need for monitoring than with unfractionated heparin (UH).
In other ways, low molecular weight heparin (LMWH) is distinctly inferior. This article describes its strengths and weaknesses, addressing 10 common clinical questions.
Assessing the heightened risks of pregnancy
Pregnant women have 5 times the risk of venous thromboembolism (VTE) of nongravid patients.1 The increased risk is due to physiologic, mechanical and, sometimes, iatrogenic factors (TABLE 1):
- Gravidas have greater concentrations of factors I, VII, VIII, IX, and X; decreased fibrinolytic activity; and increased platelet activation. These changes in the coagulation system predispose the gravida to clot formation. Although they may protect against hemorrhage, they also heighten the risk for VTE during pregnancy and the postpartum period.
- The enlarging uterus can compress venous drainage from the lower extremities, resulting in stasis. Further, prolonged immobilization in the form of bed rest is often prescribed for obstetric complications such as hypertension, preterm labor, hemorrhage, and preterm premature rupture of membranes.
- Both abdominal and vaginal operative delivery can predispose to vascular endothelial injury.
LMWH deactivates more slowly than UH, exposing patients to fewer periods of subtherapeutic anticoagulation.
These factors—singularly or in combination–can lead to a thrombotic or embolic event.2
TABLE 1
Pregnancy-associated risk factors for venous thromboembolism
| RISK FACTOR | CAUSES |
|---|---|
| Changes in the coagulation system | Increased factors I, VII, VIII, IX, X |
| Decreased fibrinolytic activity | |
| Increased platelet activation | |
| Venous stasis | Enlarging uterus compresses venous return from lower extremities |
| Endothelial injury | Vacuum delivery |
| Forceps delivery | |
| Cesarean delivery | |
| Prolonged immobilization | Preterm labor |
| Preterm premature rupture of membranes | |
| Obstetric hemorrhage | |
| Hypertensive disorders of pregnancy |
Question 1When is anticoagulation warranted in pregnancy?
It is indicated in women who:
- experience a thromboembolic event,
- become pregnant while being treated for VTE,
- have a previous history of unprovoked VTE (unrelated to trauma, immobilization, etc),
- have a known hereditary thrombophilia such as antithrombin III deficiency, factor V Leiden mutation, or the prothrombin G20210A mutation, with or without a personal history of thrombosis, or
- have a connective tissue disorder such as antiphospholipid syndrome.
Anticoagulation in pregnancy is common, and usually is given for the duration of pregnancy, into the postpartum period.
Question 2What are the options for anticoagulation?
Heparin is the sole choice for long-term anticoagulation, since warfarin is contraindicated in pregnancy.3 (See “Dangers of warfarin”.)
Unfortunately, heparin has disadvantages that render it a second-line agent in the nonpregnant population. For example, because of enzymatic degradation, heparins cannot be given orally. In addition, because of its large size and strongly positive charge, the parent heparin molecule—known as “unfractionated” heparin—is rapidly deactivated by tissue proteins, making for an unpredictable anticoagulation response. Underdosing and overdosing are typical, and frequent monitoring is necessary.
For these and other reasons, investigators have sought a more predictable, reliable agent for long-term anticoagulation in patients who cannot take warfarin. Interest has focused on a derivative of the parent heparin molecule: LMWH.
Snapshot of LMWH. This agent is produced by the controlled enzymatic degradation of unfractionated heparin (molecular weight of approximately 10,000 to 15,000 daltons) into approximately 5,000-dalton molecules. Although they are much smaller than the parent molecule, these polymers still carry a strong positive charge.
This polarity is probably why LMWH does not cross the placenta—a major advantage over warfarin for anticoagulation during pregnancy.5
In addition, accumulating evidence6,7 suggests that LMWH is at least as safe and effective as UH in pregnancy, although more research is needed. As with UH, there appears to be no transplacental passage.8
Pregnancy category. According to the manufacturer, the LMWH enoxaparin falls into pregnancy category B.9 Another LMWH, dalteparin, also falls into pregnancy category B. Both the American College of Obstetricians and Gynecologists2 and the Society for Maternal-Fetal Medicine10 endorse the use of LMWH in pregnancy with appropriate counseling.8
Although it is the drug of choice in the nonpregnant population, warfarin is contraindicated in pregnancy because it can cross the placenta and has been linked to adverse pregnancy outcomes.
Several studies have demonstrated an association between first-trimester warfarin exposure and a constellation of structural birth defects, termed “warfarin embryopathy,” which includes craniofacial and skeletal defects. Exposure in any trimester is associated with fetal and neonatal intracranial hemorrhage.3
For these reasons, warfarin is contraindicated in pregnancy with the rare exception of women with mechanical prosthetic heart valves.4
Question 3How does LMWH differ from unfractionated heparin?
LMWH is more efficient. Both UH and LMWH contain an essential pentasaccharide within their polymer structure that binds to and enhances antithrombin III, which in turn inhibits thrombin and activated factor X (Xa). Because of its smaller size, LMWH preferentially inhibits Xa, which is higher in the coagulation cascade. Inhibition of a single molecule of Xa prevents the formation of many molecules of thrombin. Molecule for molecule, LMWH is a more efficient anticoagulant than UH (FIGURE).11
The second way that LMWH differs from UH also relates to the molecule’s size. Smaller heparin molecules are less likely to be deactivated by tissue proteins. This results in improved bioavailability of the administered dose. Greater bioavailability translates to a more predictable dose-response relationship, a long half-life, and better anticoagulation.12
FIGURE Simplified schematic of the coagulation cascade
Question 4What are the clinical advantages of LMWH?
LMWH has longer-lasting effects and subcutaneous dosing. It also has fewer side effects than UH.
Because of its large size and positive charge, UH has an unfavorable pharmacokinetic profile. Tissue proteins interfere with and deactivate it, and many of these proteins increase in pregnancy and with advancing gestation. Heparin tissue levels are therefore erratic and unpredictable and often lead to periods of subtherapeutic coverage. This is true even with intravenous (IV) dosing.
Rapid absorption, no intravenous dosing. In contrast, because of its smaller size, LMWH is rapidly and predictably absorbed from a subcutaneous injection. Intravenous dosing is not necessary to obtain adequate tissue levels. Once in tissue, it is deactivated more slowly and therefore maintains its anticoagulation effect longer. Consequently, patients are exposed to fewer periods of subtherapeutic anticoagulation. A longer half-life also translates to more favorable dosing routes (subcutaneous rather than IV) and regimens (daily versus twice daily). Similarly, since the dose-response is predictable and tissue levels are more constant, frequent monitoring of treatment response is not routinely necessary.
Fewer side effects. Another advantage of LMWH over UH is the improved side-effect profile. Patients on LMWH have decreased risk of hemorrhage, osteoporosis, and antibody-mediated thrombocytopenia.11 Although most data regarding these advantages come from the nonpregnant population, it is plausible to speculate that these traits also are present in pregnant women (TABLE 2).
TABLE 2
Advantages and disadvantages of LMWH in pregnancy
| ADVANTAGES |
| More effective anticoagulation |
| Better dose-response |
| Longer half-life |
| Better dosing route |
| Decreased need for monitoring |
| Fewer side effects |
| DISADVANTAGES |
| Longer half-life |
| Risk of hematoma with epidural anesthesia |
| Not fully reversible with protamine sulfate |
| Anticoagulation effect difficult to monitor |
| Higher cost |
Question 5What are the disadvantages?
They include the long half-life, risk of hematoma with epidural anesthesia, lower efficacy of the antidote, monitoring difficulty, and higher cost.
The long half-life of LMWH is both an advantage and disadvantage. For example, when UH is administered intravenously, it has a half-life of 30 to 60 minutes. When it is given subcutaneously, the half-life is 1 to 2 hours. This means that a patient can undergo vaginal delivery or even surgery within hours of her last subcutaneous UH injection.
In contrast, LMWH has a half-life of approximately 4 hours. A recent dose may increase the risk of operative morbidity in the form of overt or delayed hemorrhage, hematoma, or wound dehiscence.
Not for use with epidural anesthesia. Case reports of epidural hematomas after regional anesthesia during orthopedic procedures have caused considerable concern about the use of LMWH and the placement of a neuraxial block such as a spinal or epidural.13 Many anesthesiologists will not place an epidural or spinal within 24 hours of a LMWH dose.14 However, as experience with these agents in the nonpregnant population expands, a more evidence-based approach is likely to develop.
Antidote less effective. Protamine sulfate is a strong base that binds with the positively charged UH molecule, thereby serving as an antidote through competitive inhibition. Because of its smaller size, LMWH is reversed by protamine to a lesser degree (approximately 60% effective).14 Therefore, hemorrhage associated with LMWH may require replacement of blood components, which carries the risks of infection and transfusion reactions.
Difficult to monitor. The anticoagulation effect of UH can be reliably monitored by the activated partial thromboplastin time (aPTT), which is a widely available test with a rapid turnaround. However, the anticoagulation effect of LMWH is not reflected by the aPTT. Assessment of LMWH activity requires assessment of the antifactor Xa level, a test that is not universally available and has a longer turnaround.
Higher cost. Another limitation of LMWH is its cost. A single, subcutaneous, prophylactic 40-mg dose of enoxaparin costs about $30, compared with about $1 for an equivalent dose of unfractionated heparin (5,000 U subcutaneously twice a day). Because of its increased cost, many insurance companies do not authorize the use of LMWH for prolonged periods such as pregnancy and the postpartum period. However, studies in the nonpregnant population have demonstrated overall decreased cost over UH due to the reduced need for monitoring, shorter length of hospital stay, and diminished treatment failure.
Question 6What is the dose for prophylaxis and treatment?
The standard dose of enoxaparin for prophylaxis in pregnancy and the postpartum period is 40 mg administered subcutaneously every 24 hours (TABLE 3). Therapeutic anticoagulation (sometimes referred to as a “weightadjusted” dose) is usually achieved with 1 mg/kg every 12 hours.
Dalteparin can be given in a prophylactic dose of 5,000 U subcutaneously every 24 hours and a therapeutic dose of 200 U/kg every 24 hours.15 Dosing may need to be adjusted with advancing gestation as plasma volume, renal clearance, and tissue proteins increase.
The various LMWH preparations are not equivalent in their pharmacokinetics. Generally, clinicians familiarize themselves with a single agent. It also is important to note that dosing regimens in pregnancy are not evidence-based but largely “borrowed” from nonpregnant regimens. They also vary widely in the available literature.
TABLE 3
Common low molecular weight heparins
| BRAND NAME | GENERIC NAME | PROPHYLACTIC DOSE | THERAPEUTIC DOSE |
|---|---|---|---|
| Lovenox | Enoxaparin | 40 mg every 24 hours | 1 mg/kg every 12 hours |
| Fragmin | Dalteparin | 5,000 U every 24 hours | 200 U/kg every 24 hours |
| Note: All doses are subcutaneous | |||
Question 7Under what conditions can LMWH be given?
Generally, LMWH can replace UH in any condition that warrants prophylactic or therapeutic anticoagulation in pregnancy, except the acute management of pulmonary embolism and in women with mechanical heart valves.
Prophylactic dosing can be offered to women with a previous thromboembolic event such as deep vein thrombosis (DVT) or pulmonary embolism that was not associated with a reversible and temporary predisposing risk factor such as immobilization or trauma. (In general, pregnancy is not seen as a reversible or temporary risk factor.)
Prophylactic or therapeutic dosing is sometimes offered to women with a hereditary thrombophilia, antiphospholipid syndrome, or other vasculopathies and connective-tissue diseases. In addition, LMWH is an accepted first-line therapeutic anticoagulant for acute DVT in pregnancy.
Not for use in treating acute pulmonary embolism. Evidence is insufficient to support the use of LMWH as a first-line anticoagulant for acute pulmonary embolism. To date, IV loading with UH is the standard of care, with conversion to LMWH after 4 to 5 days of therapeutic UH anticoagulation. This may change as experience with LMWH increases.
Not for use with mechanical prosthetic heart valves. Because of case reports of recurrent thromboembolism resulting in maternal and fetal death in pregnant women with mechanical prosthetic heart valves on therapeutic LMWH, the manufacturer of enoxaparin warns against its use in pregnancy in these women.9 However, similar outcomes have been reported with UH and warfarin. This forces clinicians to consider potentially less effective and more problematic agents for anticoagulation in this fortunately rare circumstance.
Contemporary management involves converting from warfarin to subcutaneous heparin or the heparin pump once pregnancy is established and before organogenesis (at approximately 6 weeks’ gestation), followed by frequent monitoring of aPTT. Alternatively, warfarin can be resumed after organogenesis (at about 12 weeks) and continued into the third trimester, followed by conversion to heparin pump, subcutaneous injections, or an IV drip near term. Both options carry significant maternal and fetal risk and should be performed in a multidisciplinary fashion along with cardiology and vascular medicine.16
Question 8How do I start and stop LMWH?
Start LMWH as a subcutaneous injection without IV loading. A baseline complete blood count for platelet count is reasonable. Patient education is straightforward.
Prophylactic dosing can be initiated on an outpatient basis immediately after patient education and procurement of the medicine.
Therapeutic dosing for DVT usually is begun during hospitalization, with 1 mg per kilogram given subcutaneously every 12 hours. Barring other comorbidities, discharge can be achieved after patient education. The exception is treatment of acute pulmonary embolism.Conversion to LMWH is achieved once the patient is fully anticoagulated.
Discontinuation. Pregnancy is a period of shifting maternal and fetal status, when indications for delivery can develop suddenly and with little warning (eg, abruptio placenta, nonreassuring antenatal testing).
LMWH dosing regimens in pregnancy are not evidence-based but largely “borrowed” from nonpregnant regimens.
A major consideration is the long half-life of LMWH. If a patient has had a recent subcutaneous injection of LMWH followed by an urgent indication for delivery, she may be anticoagulated during her delivery and be at increased risk for hemorrhage. Similarly, she may not be a candidate for epidural or spinal anesthesia because of the risk of epidural hematoma. If cesarean section is indicated, she may need general anesthesia, which is associated with increased maternal morbidity. If hemorrhage occurs, she may require transfusion of blood products, which carries the risks of infection and transfusion reactions.
Three strategies for peripartum management with LMWH are:
- Leave the patient on LMWH until the onset of labor. Depending on the timing and dose of her last injection, she may or may not be a candidate for regional anesthesia in labor. With prophylactic dosing, the risk of significant hemorrhage is low.
- Time delivery so that the patient withholds her PMinjection and presents for delivery the following morning, 24 hours after her last dose. This option is attractive when cesarean delivery is planned. The advantage of this approach is that it keeps the window of thrombosis as narrow as possible. The disadvantage is that the patient may enter labor or require delivery before the chosen delivery date, in which case she may be at risk for hemorrhage.
- Convert the patient to UH at approximately 36 to 37 weeks’ gestation. The advantage? The shorter half-life of UH increases the possibility for regional anesthesia and decreases the risk for hemorrhage. The disadvantage: The risk for thrombosis as well as complications (thrombocytopenia, osteoporosis, thrombosis) may be greater with UH for the reasons described earlier.
Restarting after delivery. Strategies for continued thromboprophylaxis in the postpartum period include continuing LMWH for an additional 6 to 8 weeks or converting to warfarin. Warfarin can be taken orally but requires frequent monitoring and adjustment of dosing, which is unnecessary with LMWH. Many patients choose to continue LMWH because they are familiar with the routine of daily injections. There is little data to support or refute either approach.
There also is little data to guide the decision of when to reinitiate prophylactic or therapeutic doses of LMWH after vaginal or cesarean delivery. Translating from other surgical subspecialties, most obstetricians are comfortable resuming both prophylactic and therapeutic doses at 6 hours after vaginal delivery and 8 hours after cesarean section.
Question 9How do I monitor the effectiveness of LMWH?
The frequent monitoring necessary with UH is not required with LMWH, since the increased bioavailability of LMWH leads to reliable tissue levels. The aPTT level does not correlate well with the anticoagulation effect of LMWH.
Antifactor Xa levels—sometimes referred to as the LMWH assay—of 0.5 to 1.2 IU/mL are considered adequate for therapeutic anticoagulation in the nonpregnant population. Peak anti-Xa activity is achieved approximately 4 hours after subcutaneous injection. AntiXa levels should therefore be drawn 4 hours after the last dose.17 Prophylactic subcutaneous dosing of enoxaparin 40 mg daily generally does not require monitoring of anti-Xa levels.
In nonpregnant women, routine monitoring is seldom necessary. Gravidas, however, are constantly changing in terms of weight, plasma volume, renal clearance, and amount of heparin-binding proteins. Because of this, periodic monitoring (every 4 weeks) is reasonable until an evidence-based recommendation can be made.
Question 10When can I provide neuraxial anesthesia?
Most anesthesiologists are reluctant to perform neuraxial anesthesia within 12 hours of the last prophylactic dose or 24 hours of the last therapeutic dose of LMWH because of the risk of epidural and spinal hematoma.
The American Society of Regional Anesthesia recommends that neuraxial anesthesia be withheld for 24 hours after the last therapeutic dose and 12 hours after a prophylactic dose. That organization did not recommend checking anti-Xa levels, since they do not adequately predict the risk of bleeding.9 However, as experience with LMWH broadens in nonobstetric surgical cases, such as orthopedic and cardiac procedures, it is likely that greater familiarity with the medication will lead to better evidence and broader acceptance.
Dr. Emery reports no financial relationships relevant to this article.
1. Gherman RB, Goodwin TM, Leung JD, Byrne JD, Hethumumi R, Montoro M. Incidence, clinical characteristics, and timing of objectively diagnosed venous thromboembolism during pregnancy. Obstet Gynecol. 1999;94:730-734.
2. American College of Obstetricians and Gynecologists. Practice Bulletin #19: Thromboembolism in Pregnancy. Washington, DC: ACOG; 2000.
3. Hall JG, Pauli RM, Wilson KM. Maternal and fetal sequelae of anticoagulation during pregnancy. Am J Med. 1980;68:122-140.
4. Born D, Martinez EE, Almeida PAM, et al. Pregnancy in patients with mechanical heart valves: the effects of anticoagulation on mother, fetus and neonate. Am Heart J. 1992;124:413-417.
5. Omri A, Delayoye JF, Anderson H, Bachmann F. Low molecular weight heparin Novo (LHN-1) does not cross the placenta during the second trimester of pregnancy. Thromb Haemost. 1989;61:55-56.
6. Sanson BJ, Lensing AWA, Prins MH, et al. Safety of low molecular weight heparin in pregnancy: a systematic review. Thromb Haemost. 1999;81:668-672.
7. Nelson-Piercy C, Letsky EA, de Sweit M. Low molecular weight heparin for obstetric thromboprophylaxis: experience of sixty-nine pregnancies in sixty-one women at risk. Am J Obstet Gynecol. 1997;176:1062-1068.
8. Forestier F, Daffos F, Rainaut M, et al. Low molecular weight heparin (CY 216) does not cross the placenta during the third trimester of pregnancy. Thromb Haemost. 1987;57:234.-
9. Lovenox injection [package insert]. Bridgewater, NJ: Aventis; 2003.
10. Enoxaprin sodium (Lovenox) and pregnancy. SMFM Practice Committee Announcement posted at http://www.smfm.org
11. Hirsh J, Warkentin TE, Raschke R, Granger C, Ohman EM, Dalen JE. Heparin and low molecular weight heparin: mechanisms of action, pharmacokinetics, dosing considerations, monitoring, efficacy and safety. Chest. 1998;114:489S-510S.
12. Weitz JI. Low-molecular-weight heparins. N Engl J Med. 1997;337:688-698.
13. US Department of Health and Human Services. FDA Public Health Advisory. Reports of Epidural and Spinal Hematomas with Concurrent Use of Low Molecular Weight Heparin and Spinal/Epidural Anesthesia or Spinal Puncture. Rockville, MD: Food and Drug Administration; December 1997.
14. American Society of Regional Anesthesia. Recommendations for Neuraxial Anesthesia and Anticoagulation. Richmond, Va: ASRA; 1998.
15. Hirsh J, Raschke R, Warkentin TE, et al. Heparin: mechanism of action, pharmacokinetics, dosing considerations, efficacy, and safety. Chest. 1995;108:258S-275S.
16. Anticoagulation and Enoxaparin Use in Patients with Prosthetic Heart Valves and/or Pregnancy. Clinical Cardiology Consensus Reports. Atlanta, Ga: American Health Consultants; 2002.
17. Ginsberg JS, Greer I, Hirsh J. Use of antithrombotic agents during pregnancy. Chest. 2001;119:122S-131S.
1. Gherman RB, Goodwin TM, Leung JD, Byrne JD, Hethumumi R, Montoro M. Incidence, clinical characteristics, and timing of objectively diagnosed venous thromboembolism during pregnancy. Obstet Gynecol. 1999;94:730-734.
2. American College of Obstetricians and Gynecologists. Practice Bulletin #19: Thromboembolism in Pregnancy. Washington, DC: ACOG; 2000.
3. Hall JG, Pauli RM, Wilson KM. Maternal and fetal sequelae of anticoagulation during pregnancy. Am J Med. 1980;68:122-140.
4. Born D, Martinez EE, Almeida PAM, et al. Pregnancy in patients with mechanical heart valves: the effects of anticoagulation on mother, fetus and neonate. Am Heart J. 1992;124:413-417.
5. Omri A, Delayoye JF, Anderson H, Bachmann F. Low molecular weight heparin Novo (LHN-1) does not cross the placenta during the second trimester of pregnancy. Thromb Haemost. 1989;61:55-56.
6. Sanson BJ, Lensing AWA, Prins MH, et al. Safety of low molecular weight heparin in pregnancy: a systematic review. Thromb Haemost. 1999;81:668-672.
7. Nelson-Piercy C, Letsky EA, de Sweit M. Low molecular weight heparin for obstetric thromboprophylaxis: experience of sixty-nine pregnancies in sixty-one women at risk. Am J Obstet Gynecol. 1997;176:1062-1068.
8. Forestier F, Daffos F, Rainaut M, et al. Low molecular weight heparin (CY 216) does not cross the placenta during the third trimester of pregnancy. Thromb Haemost. 1987;57:234.-
9. Lovenox injection [package insert]. Bridgewater, NJ: Aventis; 2003.
10. Enoxaprin sodium (Lovenox) and pregnancy. SMFM Practice Committee Announcement posted at http://www.smfm.org
11. Hirsh J, Warkentin TE, Raschke R, Granger C, Ohman EM, Dalen JE. Heparin and low molecular weight heparin: mechanisms of action, pharmacokinetics, dosing considerations, monitoring, efficacy and safety. Chest. 1998;114:489S-510S.
12. Weitz JI. Low-molecular-weight heparins. N Engl J Med. 1997;337:688-698.
13. US Department of Health and Human Services. FDA Public Health Advisory. Reports of Epidural and Spinal Hematomas with Concurrent Use of Low Molecular Weight Heparin and Spinal/Epidural Anesthesia or Spinal Puncture. Rockville, MD: Food and Drug Administration; December 1997.
14. American Society of Regional Anesthesia. Recommendations for Neuraxial Anesthesia and Anticoagulation. Richmond, Va: ASRA; 1998.
15. Hirsh J, Raschke R, Warkentin TE, et al. Heparin: mechanism of action, pharmacokinetics, dosing considerations, efficacy, and safety. Chest. 1995;108:258S-275S.
16. Anticoagulation and Enoxaparin Use in Patients with Prosthetic Heart Valves and/or Pregnancy. Clinical Cardiology Consensus Reports. Atlanta, Ga: American Health Consultants; 2002.
17. Ginsberg JS, Greer I, Hirsh J. Use of antithrombotic agents during pregnancy. Chest. 2001;119:122S-131S.