User login
Deoxycholic acid (Kybella) for treatment of submental fullness
We are so lucky to be part of a field of medicine where advances in patient treatment options continue to occur. Having been involved in the Kybella clinical trials, it is exciting and satisfactory to see a new successful aesthetic treatment come to fruition. Kybella is the first and only Food and Drug Administration–approved injectable drug to reduce the appearance of “double chin” (submental fullness associated with submental fat) in adult patients. It is a synthetic form of naturally occurring deoxycholic acid (DCA), which lyses adipocytes when properly injected into subcutaneous fat. The safe and effective use of Kybella for the treatment of subcutaneous fat outside of the submental region has not been established and is not recommended.

The drug received unanimous support from an FDA advisory panel in March based on two placebo-controlled phase III trials involving more than 1,000 adults. In over 1,600 patients treated, 79% saw great improvement. In the studies, safety and efficacy were demonstrated with treatment of up to 50 injections of 0.2 mL each of the 1% DCA solution administered in a single treatment. Up to six treatments were administered at least 1 month apart.
Serious side effects associated with injection of DCA may include injury to the marginal mandibular nerve and dysphagia, but the most common side effects are swelling, bruising, pain, numbness, redness, and areas of hardness in the treatment area. Other potential side effects include: tingling, nodule, itching, skin tightness, headache, alopecia, and skin ulceration. In the studies, all cases of marginal mandibular nerve injury, manifesting as an asymmetric smile or facial muscle weakness, resolved spontaneously (range 1-298 days, median 44 days). Dysphagia occurred in the clinical trials as a result of administration site reactions (for example, pain, swelling, and induration in the submental area). Cases of dysphagia resolved spontaneously (range 1-81 days, median 3 days).
Caution should be taken in patients with a history of medical conditions in the neck area, difficulty swallowing, bleeding problems, or who take blood thinners. Likewise, caution should be used in patients who are or plan to become pregnant or breastfeed as Kybella has not been studied in pregnant or breastfeeding patients. Injection is contraindicated in the presence of infection at injection sites. Kybella only should be administered by a trained health care professional.

In addition to assessing whether not the patient is an ideal candidate, setting realistic expectations, and counseling about potential side effects, consultation also should include preprocedure photographs in the Frankfurt plane. Patients with moderate to severe convexity or fullness of the submental area are ideal candidates for the procedure. Those with little submental fat and excessive skin laxity may not be good candidates for this procedure and should consider a neck lift surgery as an alternative. Patients with prominent platysmal bands prior to procedure still may notice these bands after the procedure and may consider botulinum toxin injections or platysmal banding to treat these. While the active ingredient targets fat, some beneficial skin tightening may occur as a result of inflammation and fibrosis.
After photographs are taken, it is highly recommended to mark out specific anatomic landmarks on the patient, to avoid injury to the marginal mandibular nerve, salivary glands, lymph nodes, and the subhyoid region.
The procedure takes about 15-20 minutes with a short preparation time involved. Antihistamines and anti-inflammatory medications such as loratadine and ibuprofen may be given before the procedure to help reduce risk of discomfort and edema often experienced after injection. Preprocedure injection with local anesthetic also is recommended.
Once the treatment area is demarcated with a grid placed on the patient’s skin, injections of 0.2 mL of DCA are performed with a 30-gauge ½ inch needle. The product is supplied in a box with four 2-mL vials (10 mg/mL). No refrigeration is required. Once a vial is opened, it should only be used on one patient. A maximum of up to 10 mL may be injected in one patient in one session. Ice may applied after treatment. Postprocedure swelling and throbbing can be expected for several days and may rarely last up to 1 month. Patients may require two to six treatments spaced at least 1 month apart.
Dr. Wesley and Dr. Talakoub are cocontributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley. Dr. Wesley was an investigator in the phase III Kybella clinical trials. E-mail her at [email protected].
We are so lucky to be part of a field of medicine where advances in patient treatment options continue to occur. Having been involved in the Kybella clinical trials, it is exciting and satisfactory to see a new successful aesthetic treatment come to fruition. Kybella is the first and only Food and Drug Administration–approved injectable drug to reduce the appearance of “double chin” (submental fullness associated with submental fat) in adult patients. It is a synthetic form of naturally occurring deoxycholic acid (DCA), which lyses adipocytes when properly injected into subcutaneous fat. The safe and effective use of Kybella for the treatment of subcutaneous fat outside of the submental region has not been established and is not recommended.
The drug received unanimous support from an FDA advisory panel in March based on two placebo-controlled phase III trials involving more than 1,000 adults. In over 1,600 patients treated, 79% saw great improvement. In the studies, safety and efficacy were demonstrated with treatment of up to 50 injections of 0.2 mL each of the 1% DCA solution administered in a single treatment. Up to six treatments were administered at least 1 month apart.
Serious side effects associated with injection of DCA may include injury to the marginal mandibular nerve and dysphagia, but the most common side effects are swelling, bruising, pain, numbness, redness, and areas of hardness in the treatment area. Other potential side effects include: tingling, nodule, itching, skin tightness, headache, alopecia, and skin ulceration. In the studies, all cases of marginal mandibular nerve injury, manifesting as an asymmetric smile or facial muscle weakness, resolved spontaneously (range 1-298 days, median 44 days). Dysphagia occurred in the clinical trials as a result of administration site reactions (for example, pain, swelling, and induration in the submental area). Cases of dysphagia resolved spontaneously (range 1-81 days, median 3 days).
Caution should be taken in patients with a history of medical conditions in the neck area, difficulty swallowing, bleeding problems, or who take blood thinners. Likewise, caution should be used in patients who are or plan to become pregnant or breastfeed as Kybella has not been studied in pregnant or breastfeeding patients. Injection is contraindicated in the presence of infection at injection sites. Kybella only should be administered by a trained health care professional.
In addition to assessing whether not the patient is an ideal candidate, setting realistic expectations, and counseling about potential side effects, consultation also should include preprocedure photographs in the Frankfurt plane. Patients with moderate to severe convexity or fullness of the submental area are ideal candidates for the procedure. Those with little submental fat and excessive skin laxity may not be good candidates for this procedure and should consider a neck lift surgery as an alternative. Patients with prominent platysmal bands prior to procedure still may notice these bands after the procedure and may consider botulinum toxin injections or platysmal banding to treat these. While the active ingredient targets fat, some beneficial skin tightening may occur as a result of inflammation and fibrosis.
After photographs are taken, it is highly recommended to mark out specific anatomic landmarks on the patient, to avoid injury to the marginal mandibular nerve, salivary glands, lymph nodes, and the subhyoid region.
The procedure takes about 15-20 minutes with a short preparation time involved. Antihistamines and anti-inflammatory medications such as loratadine and ibuprofen may be given before the procedure to help reduce risk of discomfort and edema often experienced after injection. Preprocedure injection with local anesthetic also is recommended.
Once the treatment area is demarcated with a grid placed on the patient’s skin, injections of 0.2 mL of DCA are performed with a 30-gauge ½ inch needle. The product is supplied in a box with four 2-mL vials (10 mg/mL). No refrigeration is required. Once a vial is opened, it should only be used on one patient. A maximum of up to 10 mL may be injected in one patient in one session. Ice may applied after treatment. Postprocedure swelling and throbbing can be expected for several days and may rarely last up to 1 month. Patients may require two to six treatments spaced at least 1 month apart.
Dr. Wesley and Dr. Talakoub are cocontributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley. Dr. Wesley was an investigator in the phase III Kybella clinical trials. E-mail her at [email protected].
We are so lucky to be part of a field of medicine where advances in patient treatment options continue to occur. Having been involved in the Kybella clinical trials, it is exciting and satisfactory to see a new successful aesthetic treatment come to fruition. Kybella is the first and only Food and Drug Administration–approved injectable drug to reduce the appearance of “double chin” (submental fullness associated with submental fat) in adult patients. It is a synthetic form of naturally occurring deoxycholic acid (DCA), which lyses adipocytes when properly injected into subcutaneous fat. The safe and effective use of Kybella for the treatment of subcutaneous fat outside of the submental region has not been established and is not recommended.
The drug received unanimous support from an FDA advisory panel in March based on two placebo-controlled phase III trials involving more than 1,000 adults. In over 1,600 patients treated, 79% saw great improvement. In the studies, safety and efficacy were demonstrated with treatment of up to 50 injections of 0.2 mL each of the 1% DCA solution administered in a single treatment. Up to six treatments were administered at least 1 month apart.
Serious side effects associated with injection of DCA may include injury to the marginal mandibular nerve and dysphagia, but the most common side effects are swelling, bruising, pain, numbness, redness, and areas of hardness in the treatment area. Other potential side effects include: tingling, nodule, itching, skin tightness, headache, alopecia, and skin ulceration. In the studies, all cases of marginal mandibular nerve injury, manifesting as an asymmetric smile or facial muscle weakness, resolved spontaneously (range 1-298 days, median 44 days). Dysphagia occurred in the clinical trials as a result of administration site reactions (for example, pain, swelling, and induration in the submental area). Cases of dysphagia resolved spontaneously (range 1-81 days, median 3 days).
Caution should be taken in patients with a history of medical conditions in the neck area, difficulty swallowing, bleeding problems, or who take blood thinners. Likewise, caution should be used in patients who are or plan to become pregnant or breastfeed as Kybella has not been studied in pregnant or breastfeeding patients. Injection is contraindicated in the presence of infection at injection sites. Kybella only should be administered by a trained health care professional.
In addition to assessing whether not the patient is an ideal candidate, setting realistic expectations, and counseling about potential side effects, consultation also should include preprocedure photographs in the Frankfurt plane. Patients with moderate to severe convexity or fullness of the submental area are ideal candidates for the procedure. Those with little submental fat and excessive skin laxity may not be good candidates for this procedure and should consider a neck lift surgery as an alternative. Patients with prominent platysmal bands prior to procedure still may notice these bands after the procedure and may consider botulinum toxin injections or platysmal banding to treat these. While the active ingredient targets fat, some beneficial skin tightening may occur as a result of inflammation and fibrosis.
After photographs are taken, it is highly recommended to mark out specific anatomic landmarks on the patient, to avoid injury to the marginal mandibular nerve, salivary glands, lymph nodes, and the subhyoid region.
The procedure takes about 15-20 minutes with a short preparation time involved. Antihistamines and anti-inflammatory medications such as loratadine and ibuprofen may be given before the procedure to help reduce risk of discomfort and edema often experienced after injection. Preprocedure injection with local anesthetic also is recommended.
Once the treatment area is demarcated with a grid placed on the patient’s skin, injections of 0.2 mL of DCA are performed with a 30-gauge ½ inch needle. The product is supplied in a box with four 2-mL vials (10 mg/mL). No refrigeration is required. Once a vial is opened, it should only be used on one patient. A maximum of up to 10 mL may be injected in one patient in one session. Ice may applied after treatment. Postprocedure swelling and throbbing can be expected for several days and may rarely last up to 1 month. Patients may require two to six treatments spaced at least 1 month apart.
Dr. Wesley and Dr. Talakoub are cocontributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley. Dr. Wesley was an investigator in the phase III Kybella clinical trials. E-mail her at [email protected].

‘Zebra’ hunting getting harder in general practice
I’m not a zebra hunter by nature. I see them here and there, but in a general practice the odds of finding them are pretty low. If I can’t solve the case, I refer to the more accomplished zebrologists at the tertiary centers.
That’s not to say I don’t look for them as best I can. Sometimes you get the vaguest hint you’re dealing with the unusual. Maybe because you’ve seen it before, or something the patient said triggered a distant memory from training.
One problem (among many) in diagnosing a zebra is time. It takes time to draw out a complex history and do an exam. There’s also time needed for the first, second, third … and later rounds of tests to come back, as well as time at appointments to note new symptoms, ask further questions, and discuss a diagnosis and plan. And, sometimes, you need time just to follow patients and see how their symptoms change.
Unfortunately, in medicine these days time is usually what you don’t have. Doctors are always under pressure to see a lot of patients and don’t have time to sort through the complex ones. This gets even worse for those employed by a health care system, when they may be working under quota requirements. After all, you can see four to five horses in the time needed for one zebra. And they pay about the same.
In solo practice, I don’t have quite the time constraints of an employed doctor meeting set numbers, but I still have the financial ones. I get the luxury of setting the schedule to give me more minutes when I know they’ll be needed, but at the back end it still comes with a financial penalty.
All of this makes it harder to find the zebras. They’re difficult enough to see as it is, and the financial pressure to shorten visits can keep even thorough docs from getting the whole story or turning over the case mentally. As one of my residency teachers (not Yogi Berra) said of differential diagnoses, “If you don’t think of it, you don’t think of it.”
Sadly, the nature of modern medicine is that it limits your ability to think of it, making it harder than ever to find the zebras in the herd.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m not a zebra hunter by nature. I see them here and there, but in a general practice the odds of finding them are pretty low. If I can’t solve the case, I refer to the more accomplished zebrologists at the tertiary centers.
That’s not to say I don’t look for them as best I can. Sometimes you get the vaguest hint you’re dealing with the unusual. Maybe because you’ve seen it before, or something the patient said triggered a distant memory from training.
One problem (among many) in diagnosing a zebra is time. It takes time to draw out a complex history and do an exam. There’s also time needed for the first, second, third … and later rounds of tests to come back, as well as time at appointments to note new symptoms, ask further questions, and discuss a diagnosis and plan. And, sometimes, you need time just to follow patients and see how their symptoms change.
Unfortunately, in medicine these days time is usually what you don’t have. Doctors are always under pressure to see a lot of patients and don’t have time to sort through the complex ones. This gets even worse for those employed by a health care system, when they may be working under quota requirements. After all, you can see four to five horses in the time needed for one zebra. And they pay about the same.
In solo practice, I don’t have quite the time constraints of an employed doctor meeting set numbers, but I still have the financial ones. I get the luxury of setting the schedule to give me more minutes when I know they’ll be needed, but at the back end it still comes with a financial penalty.
All of this makes it harder to find the zebras. They’re difficult enough to see as it is, and the financial pressure to shorten visits can keep even thorough docs from getting the whole story or turning over the case mentally. As one of my residency teachers (not Yogi Berra) said of differential diagnoses, “If you don’t think of it, you don’t think of it.”
Sadly, the nature of modern medicine is that it limits your ability to think of it, making it harder than ever to find the zebras in the herd.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m not a zebra hunter by nature. I see them here and there, but in a general practice the odds of finding them are pretty low. If I can’t solve the case, I refer to the more accomplished zebrologists at the tertiary centers.
That’s not to say I don’t look for them as best I can. Sometimes you get the vaguest hint you’re dealing with the unusual. Maybe because you’ve seen it before, or something the patient said triggered a distant memory from training.
One problem (among many) in diagnosing a zebra is time. It takes time to draw out a complex history and do an exam. There’s also time needed for the first, second, third … and later rounds of tests to come back, as well as time at appointments to note new symptoms, ask further questions, and discuss a diagnosis and plan. And, sometimes, you need time just to follow patients and see how their symptoms change.
Unfortunately, in medicine these days time is usually what you don’t have. Doctors are always under pressure to see a lot of patients and don’t have time to sort through the complex ones. This gets even worse for those employed by a health care system, when they may be working under quota requirements. After all, you can see four to five horses in the time needed for one zebra. And they pay about the same.
In solo practice, I don’t have quite the time constraints of an employed doctor meeting set numbers, but I still have the financial ones. I get the luxury of setting the schedule to give me more minutes when I know they’ll be needed, but at the back end it still comes with a financial penalty.
All of this makes it harder to find the zebras. They’re difficult enough to see as it is, and the financial pressure to shorten visits can keep even thorough docs from getting the whole story or turning over the case mentally. As one of my residency teachers (not Yogi Berra) said of differential diagnoses, “If you don’t think of it, you don’t think of it.”
Sadly, the nature of modern medicine is that it limits your ability to think of it, making it harder than ever to find the zebras in the herd.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

Naringenin
The flavanone naringenin (5,7,4-trihydroxyflavanone) is known to exhibit anticarcinogenic, antioxidative, antiatherogenic, estrogenic, and immunomodulatory activity (Nutr. Cancer. 2012;64:714-24; J. Nutr. 2001;131:235-41; Life Sci. 2013;93:516-24). Naringenin can be found in high concentrations in grapefruits, oranges, and other citrus fruits as well as tomatoes (skin), with grapefruit juice found to yield much higher levels in plasma than orange juice (J. Nutr. 2001;131:235-41; Am. J. Physiol. Gastrointest. Liver Physiol. 2000;279:G1148-54; Nutr. Cancer 2012;64:714-24). Naringenin has been shown, along with other flavanones such as hesperetin and ponciretin, to strongly inhibit IgE-induced beta-hexosaminidase release from RBL-2H3 cells. Sung-Hwan Park and associates have suggested that the glycosides of these substances have potential as agents for treating IgE-induced atopic allergies (Planta Med. 2005;71:24-7).
In 2012, Kushi Anand and associates also showed that the combination of curcumin and naringenin exerted antiangiogenic and antitumor effects in Swiss albino mice, adding that neither compound has been associated with reports of toxicity in animals or humans (Nutr. Cancer 2012;64:714-24).

Potential cutaneous benefits
Tae-Ho Kim and colleagues studied the effects of naringenin on 2,4-dinitrofluorobenzene (DNFB)-induced atomic dermatitis in NC/Nga mice in 2013. After repetitive skin contact with DNFB, mice received intraperitoneal injections of naringenin for 1 week, with the treatment with the fruit flavonoid significantly diminishing ear swelling and back skin lesions. The flavonoid also significantly inhibited interferon (IFN)-alpha production by activated CD4+ T cells and lowered serum IgE levels as well as DNFB-induced infiltration of eosinophils, mast cells, CD4+ T cells, and CD8+ T cells in skin lesions (Life Sci. 2013;93:516-24).
Also that year, a naringenin glucoside (naringenin-7-O-glucoside) was found in an industrial blanch water extract, a byproduct of almond processing, and believed to play a role in exerting or contributing to a photoprotective effect in a small in vivo study with 12 volunteers (Molecules 2013;18:12426-40).

In 2014, K. Murata and associates screened several Prunus species in a search for skin-whitening compounds. Using an antityrosinase assay, the investigators determined that P. persica exhibited the greatest inhibitory activity and, in additional evaluation, it was found to hinder melanogenesis in B16 rat melanoma cells. Further, they identified afzelin (3-O-alpha-L-rhamnosylkaempferol) and the flavanone naringenin as the active ingredients responsible for inhibition of tyrosinase and melanogenesis and concluded that these substances warrant attention as potential skin-whitening agents (Nat. Prod. Commun. 2014;9:185-8).
A 2014 study in the ophthalmologic literature may also shed light on the photoprotective properties of naringenin. Jun-Li Lin and colleagues, studying the effects of the flavanone in eye drops used to treat N-methyl-N-nitrosourea (MNU)-induced photoreceptor cell death in rats, found that topical naringenin dose-dependently shielded the outer nuclear layer, outer retina, and whole retina, and prevented structural and functional damages to retinal neurons (Int. J. Ophthalmol. 2014;7:391-6).
Conclusion
The antioxidative, antiatherogenic, anticarcinogenic, antiproliferative, antimutagenic, estrogenic, and immunomodulatory properties of naringenin have been established in the laboratory. It remains to be seen whether such activity can be harnessed for medical applications, particularly in the dermatologic arena. Nevertheless, this flavanone warrants watching as research into its potential cutaneous applications proceeds. Currently, there is a dearth of research, though, regarding the use of naringenin in topical products.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
The flavanone naringenin (5,7,4-trihydroxyflavanone) is known to exhibit anticarcinogenic, antioxidative, antiatherogenic, estrogenic, and immunomodulatory activity (Nutr. Cancer. 2012;64:714-24; J. Nutr. 2001;131:235-41; Life Sci. 2013;93:516-24). Naringenin can be found in high concentrations in grapefruits, oranges, and other citrus fruits as well as tomatoes (skin), with grapefruit juice found to yield much higher levels in plasma than orange juice (J. Nutr. 2001;131:235-41; Am. J. Physiol. Gastrointest. Liver Physiol. 2000;279:G1148-54; Nutr. Cancer 2012;64:714-24). Naringenin has been shown, along with other flavanones such as hesperetin and ponciretin, to strongly inhibit IgE-induced beta-hexosaminidase release from RBL-2H3 cells. Sung-Hwan Park and associates have suggested that the glycosides of these substances have potential as agents for treating IgE-induced atopic allergies (Planta Med. 2005;71:24-7).
In 2012, Kushi Anand and associates also showed that the combination of curcumin and naringenin exerted antiangiogenic and antitumor effects in Swiss albino mice, adding that neither compound has been associated with reports of toxicity in animals or humans (Nutr. Cancer 2012;64:714-24).
Potential cutaneous benefits
Tae-Ho Kim and colleagues studied the effects of naringenin on 2,4-dinitrofluorobenzene (DNFB)-induced atomic dermatitis in NC/Nga mice in 2013. After repetitive skin contact with DNFB, mice received intraperitoneal injections of naringenin for 1 week, with the treatment with the fruit flavonoid significantly diminishing ear swelling and back skin lesions. The flavonoid also significantly inhibited interferon (IFN)-alpha production by activated CD4+ T cells and lowered serum IgE levels as well as DNFB-induced infiltration of eosinophils, mast cells, CD4+ T cells, and CD8+ T cells in skin lesions (Life Sci. 2013;93:516-24).
Also that year, a naringenin glucoside (naringenin-7-O-glucoside) was found in an industrial blanch water extract, a byproduct of almond processing, and believed to play a role in exerting or contributing to a photoprotective effect in a small in vivo study with 12 volunteers (Molecules 2013;18:12426-40).
In 2014, K. Murata and associates screened several Prunus species in a search for skin-whitening compounds. Using an antityrosinase assay, the investigators determined that P. persica exhibited the greatest inhibitory activity and, in additional evaluation, it was found to hinder melanogenesis in B16 rat melanoma cells. Further, they identified afzelin (3-O-alpha-L-rhamnosylkaempferol) and the flavanone naringenin as the active ingredients responsible for inhibition of tyrosinase and melanogenesis and concluded that these substances warrant attention as potential skin-whitening agents (Nat. Prod. Commun. 2014;9:185-8).
A 2014 study in the ophthalmologic literature may also shed light on the photoprotective properties of naringenin. Jun-Li Lin and colleagues, studying the effects of the flavanone in eye drops used to treat N-methyl-N-nitrosourea (MNU)-induced photoreceptor cell death in rats, found that topical naringenin dose-dependently shielded the outer nuclear layer, outer retina, and whole retina, and prevented structural and functional damages to retinal neurons (Int. J. Ophthalmol. 2014;7:391-6).
Conclusion
The antioxidative, antiatherogenic, anticarcinogenic, antiproliferative, antimutagenic, estrogenic, and immunomodulatory properties of naringenin have been established in the laboratory. It remains to be seen whether such activity can be harnessed for medical applications, particularly in the dermatologic arena. Nevertheless, this flavanone warrants watching as research into its potential cutaneous applications proceeds. Currently, there is a dearth of research, though, regarding the use of naringenin in topical products.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
The flavanone naringenin (5,7,4-trihydroxyflavanone) is known to exhibit anticarcinogenic, antioxidative, antiatherogenic, estrogenic, and immunomodulatory activity (Nutr. Cancer. 2012;64:714-24; J. Nutr. 2001;131:235-41; Life Sci. 2013;93:516-24). Naringenin can be found in high concentrations in grapefruits, oranges, and other citrus fruits as well as tomatoes (skin), with grapefruit juice found to yield much higher levels in plasma than orange juice (J. Nutr. 2001;131:235-41; Am. J. Physiol. Gastrointest. Liver Physiol. 2000;279:G1148-54; Nutr. Cancer 2012;64:714-24). Naringenin has been shown, along with other flavanones such as hesperetin and ponciretin, to strongly inhibit IgE-induced beta-hexosaminidase release from RBL-2H3 cells. Sung-Hwan Park and associates have suggested that the glycosides of these substances have potential as agents for treating IgE-induced atopic allergies (Planta Med. 2005;71:24-7).
In 2012, Kushi Anand and associates also showed that the combination of curcumin and naringenin exerted antiangiogenic and antitumor effects in Swiss albino mice, adding that neither compound has been associated with reports of toxicity in animals or humans (Nutr. Cancer 2012;64:714-24).
Potential cutaneous benefits
Tae-Ho Kim and colleagues studied the effects of naringenin on 2,4-dinitrofluorobenzene (DNFB)-induced atomic dermatitis in NC/Nga mice in 2013. After repetitive skin contact with DNFB, mice received intraperitoneal injections of naringenin for 1 week, with the treatment with the fruit flavonoid significantly diminishing ear swelling and back skin lesions. The flavonoid also significantly inhibited interferon (IFN)-alpha production by activated CD4+ T cells and lowered serum IgE levels as well as DNFB-induced infiltration of eosinophils, mast cells, CD4+ T cells, and CD8+ T cells in skin lesions (Life Sci. 2013;93:516-24).
Also that year, a naringenin glucoside (naringenin-7-O-glucoside) was found in an industrial blanch water extract, a byproduct of almond processing, and believed to play a role in exerting or contributing to a photoprotective effect in a small in vivo study with 12 volunteers (Molecules 2013;18:12426-40).
In 2014, K. Murata and associates screened several Prunus species in a search for skin-whitening compounds. Using an antityrosinase assay, the investigators determined that P. persica exhibited the greatest inhibitory activity and, in additional evaluation, it was found to hinder melanogenesis in B16 rat melanoma cells. Further, they identified afzelin (3-O-alpha-L-rhamnosylkaempferol) and the flavanone naringenin as the active ingredients responsible for inhibition of tyrosinase and melanogenesis and concluded that these substances warrant attention as potential skin-whitening agents (Nat. Prod. Commun. 2014;9:185-8).
A 2014 study in the ophthalmologic literature may also shed light on the photoprotective properties of naringenin. Jun-Li Lin and colleagues, studying the effects of the flavanone in eye drops used to treat N-methyl-N-nitrosourea (MNU)-induced photoreceptor cell death in rats, found that topical naringenin dose-dependently shielded the outer nuclear layer, outer retina, and whole retina, and prevented structural and functional damages to retinal neurons (Int. J. Ophthalmol. 2014;7:391-6).
Conclusion
The antioxidative, antiatherogenic, anticarcinogenic, antiproliferative, antimutagenic, estrogenic, and immunomodulatory properties of naringenin have been established in the laboratory. It remains to be seen whether such activity can be harnessed for medical applications, particularly in the dermatologic arena. Nevertheless, this flavanone warrants watching as research into its potential cutaneous applications proceeds. Currently, there is a dearth of research, though, regarding the use of naringenin in topical products.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.

Nipping buds, kicking butts, being safer than sorry
Brad came in with his mother for me to treat a small wart on the sole of his left foot. “It doesn’t bother me,” he said.
“I had one of those when I was Brad’s age,” said his mother, Mary Lou. “We neglected it and it really grew! With a thing like that, you have to nip it in the bud.”
We all learn little maxims about how the world works and what to do about it. One of these is that to avoid trouble, you should nip things in the bud.

This sounds like it makes sense. Sometimes it’s actually true. But there are other times when what you’re trying to nip doesn’t have a bud.
If you have a plantar wart on the bottom of your foot and you don’t treat it, here are some things that can happen:
• It can grow and become painful.
• It can stay the same for years, never bother you, and go away.
• New ones can appear elsewhere on the sole.
• It can disappear tomorrow afternoon.
Which will happen? For the individual case, I have no idea. Like you, I’ve seen ‘em all.
There are reasons other than functional disability to treat plantar warts. For instance, they’re ugly and embarrassing. So if treatment is not too painful or expensive, why not? But sometimes we freeze it – a standard treatment – and it takes forever, visit after visit, and the wart is still there, grinning complacently. Some insurance plans don’t cover treatments unless the wart hurts, so therapy gets too expensive.
That’s when it might make sense to explain to the patient that you can nip some buds off plants to help them grow better, but you really can’t nip the buds off warts, which have neither roots nor buds.
Another maxim we all pick up is that it’s better to be safe than sorry. That sounds like plain common sense. “Can’t you take off that mole?” asks Annie. “I’m sure it’s bigger that it used to be.”
It’s just an ordinary mole, though, and it doesn’t look worrisome. All moles grow – they start out small and get a bit bigger before they stop. Plus, Annie is a young woman, and her mole is on her face. Even if a plastic surgeon takes it off, she’ll have a scar with no wrinkles to hide it in.
I explain this to Annie. “But isn’t it better to be safe than sorry?” she asks.
Well, sometimes maybe. Just not this time.
Ankur has eczema. He is really frustrated. “Doctors keep giving me creams,” he says. “The rash gets a little better,” but then it comes back. “I’d like you to give me a treatment that will kick it in the butt.”
What Ankur wants, of course, is for me to do something that will shove eczema out the door and then lock the door behind it so it can’t come back.
I would love to do that. Only I can’t. Like the many other recurring conditions we treat every day, nothing specific causes eczema, so nothing definitive gets rid of it once and for all.
In other words, eczema has no butt. So you can’t kick it.
The examples I’ve given are common and homely. There are bigger issues, in medicine and in life, to which common-sense maxims seem to apply but sometimes don’t.
The well-known public debates over prostate-specific antigen (PSA) screening for prostate cancer in older men and routine mammography in younger women attest to how tricky it is to decide whether catching things early is necessarily a good idea. It also shows how the public reacts when data contradict common sense. Of course you should catch cancer early, says the outraged public. Isn’t it always better to be safe than sorry?
No, actually it sometimes isn’t.
We all pick up maxims to live by. We hear them as children without realizing we’re learning them. That makes it hard to accept that not everything is a plant with a bud to be nipped. Or that there are situations when trying to be safe can make you sorrier.
Or that there are indeed butts, big and small. But not everything has one to kick.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.
Brad came in with his mother for me to treat a small wart on the sole of his left foot. “It doesn’t bother me,” he said.
“I had one of those when I was Brad’s age,” said his mother, Mary Lou. “We neglected it and it really grew! With a thing like that, you have to nip it in the bud.”
We all learn little maxims about how the world works and what to do about it. One of these is that to avoid trouble, you should nip things in the bud.
This sounds like it makes sense. Sometimes it’s actually true. But there are other times when what you’re trying to nip doesn’t have a bud.
If you have a plantar wart on the bottom of your foot and you don’t treat it, here are some things that can happen:
• It can grow and become painful.
• It can stay the same for years, never bother you, and go away.
• New ones can appear elsewhere on the sole.
• It can disappear tomorrow afternoon.
Which will happen? For the individual case, I have no idea. Like you, I’ve seen ‘em all.
There are reasons other than functional disability to treat plantar warts. For instance, they’re ugly and embarrassing. So if treatment is not too painful or expensive, why not? But sometimes we freeze it – a standard treatment – and it takes forever, visit after visit, and the wart is still there, grinning complacently. Some insurance plans don’t cover treatments unless the wart hurts, so therapy gets too expensive.
That’s when it might make sense to explain to the patient that you can nip some buds off plants to help them grow better, but you really can’t nip the buds off warts, which have neither roots nor buds.
Another maxim we all pick up is that it’s better to be safe than sorry. That sounds like plain common sense. “Can’t you take off that mole?” asks Annie. “I’m sure it’s bigger that it used to be.”
It’s just an ordinary mole, though, and it doesn’t look worrisome. All moles grow – they start out small and get a bit bigger before they stop. Plus, Annie is a young woman, and her mole is on her face. Even if a plastic surgeon takes it off, she’ll have a scar with no wrinkles to hide it in.
I explain this to Annie. “But isn’t it better to be safe than sorry?” she asks.
Well, sometimes maybe. Just not this time.
Ankur has eczema. He is really frustrated. “Doctors keep giving me creams,” he says. “The rash gets a little better,” but then it comes back. “I’d like you to give me a treatment that will kick it in the butt.”
What Ankur wants, of course, is for me to do something that will shove eczema out the door and then lock the door behind it so it can’t come back.
I would love to do that. Only I can’t. Like the many other recurring conditions we treat every day, nothing specific causes eczema, so nothing definitive gets rid of it once and for all.
In other words, eczema has no butt. So you can’t kick it.
The examples I’ve given are common and homely. There are bigger issues, in medicine and in life, to which common-sense maxims seem to apply but sometimes don’t.
The well-known public debates over prostate-specific antigen (PSA) screening for prostate cancer in older men and routine mammography in younger women attest to how tricky it is to decide whether catching things early is necessarily a good idea. It also shows how the public reacts when data contradict common sense. Of course you should catch cancer early, says the outraged public. Isn’t it always better to be safe than sorry?
No, actually it sometimes isn’t.
We all pick up maxims to live by. We hear them as children without realizing we’re learning them. That makes it hard to accept that not everything is a plant with a bud to be nipped. Or that there are situations when trying to be safe can make you sorrier.
Or that there are indeed butts, big and small. But not everything has one to kick.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.
Brad came in with his mother for me to treat a small wart on the sole of his left foot. “It doesn’t bother me,” he said.
“I had one of those when I was Brad’s age,” said his mother, Mary Lou. “We neglected it and it really grew! With a thing like that, you have to nip it in the bud.”
We all learn little maxims about how the world works and what to do about it. One of these is that to avoid trouble, you should nip things in the bud.
This sounds like it makes sense. Sometimes it’s actually true. But there are other times when what you’re trying to nip doesn’t have a bud.
If you have a plantar wart on the bottom of your foot and you don’t treat it, here are some things that can happen:
• It can grow and become painful.
• It can stay the same for years, never bother you, and go away.
• New ones can appear elsewhere on the sole.
• It can disappear tomorrow afternoon.
Which will happen? For the individual case, I have no idea. Like you, I’ve seen ‘em all.
There are reasons other than functional disability to treat plantar warts. For instance, they’re ugly and embarrassing. So if treatment is not too painful or expensive, why not? But sometimes we freeze it – a standard treatment – and it takes forever, visit after visit, and the wart is still there, grinning complacently. Some insurance plans don’t cover treatments unless the wart hurts, so therapy gets too expensive.
That’s when it might make sense to explain to the patient that you can nip some buds off plants to help them grow better, but you really can’t nip the buds off warts, which have neither roots nor buds.
Another maxim we all pick up is that it’s better to be safe than sorry. That sounds like plain common sense. “Can’t you take off that mole?” asks Annie. “I’m sure it’s bigger that it used to be.”
It’s just an ordinary mole, though, and it doesn’t look worrisome. All moles grow – they start out small and get a bit bigger before they stop. Plus, Annie is a young woman, and her mole is on her face. Even if a plastic surgeon takes it off, she’ll have a scar with no wrinkles to hide it in.
I explain this to Annie. “But isn’t it better to be safe than sorry?” she asks.
Well, sometimes maybe. Just not this time.
Ankur has eczema. He is really frustrated. “Doctors keep giving me creams,” he says. “The rash gets a little better,” but then it comes back. “I’d like you to give me a treatment that will kick it in the butt.”
What Ankur wants, of course, is for me to do something that will shove eczema out the door and then lock the door behind it so it can’t come back.
I would love to do that. Only I can’t. Like the many other recurring conditions we treat every day, nothing specific causes eczema, so nothing definitive gets rid of it once and for all.
In other words, eczema has no butt. So you can’t kick it.
The examples I’ve given are common and homely. There are bigger issues, in medicine and in life, to which common-sense maxims seem to apply but sometimes don’t.
The well-known public debates over prostate-specific antigen (PSA) screening for prostate cancer in older men and routine mammography in younger women attest to how tricky it is to decide whether catching things early is necessarily a good idea. It also shows how the public reacts when data contradict common sense. Of course you should catch cancer early, says the outraged public. Isn’t it always better to be safe than sorry?
No, actually it sometimes isn’t.
We all pick up maxims to live by. We hear them as children without realizing we’re learning them. That makes it hard to accept that not everything is a plant with a bud to be nipped. Or that there are situations when trying to be safe can make you sorrier.
Or that there are indeed butts, big and small. But not everything has one to kick.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.

Full transparency comes to medical records
Transparency, until recently, was rarely associated with health care. Not anymore. For better and sometimes worse, there is a revolutionary movement toward transparency in all facets of health care: transparency of costs, outcomes, quality, service, and reputation. Full transparency now has come to medical records in the form of OpenNotes. This is a patient-centered initiative that allows patients full access to their chart including all their providers’ notes.
Patients always have had the right to see their record. Ordinarily though, they would be required to go to the medical records office, fill out paperwork, and request copies of their chart. They would have to supply a reason and often pay a fee. OpenNotes changes that. Open patient charts are free and easy to access, usually digitally. OpenNotes programs are still rare, and before we go any further, it’s important to examine what we’ve learned about them.

In 2010, Beth Israel Deaconess Medical Center in Boston, Geisinger Health System in Pennsylvania, and Harborview Medical Center in Seattle invited 105 primary care physicians to open their notes to nearly 14,000 patients. The results were overwhelmingly (and to me, surprisingly) positive: More than 85% of patients accessed their notes at least once. Nearly 100% of patients wanted the program to continue. Patients reported a better understanding of their medical issues, better medication adherence, increased adoption of healthy habits, and less anxiety about their health. I would have expected more confusion and anxiety among the patients.
What about the physicians? According to the initiative, whereas one in three patients thought they should have unfettered access to their physicians’ notes, only 1 in 10 physicians did. That’s understandable. The physicians in the pilot shared many of the same concerns you and I have, namely that OpenNotes would lead to an increased workload to explain esoteric notes to patients and to allay anxieties.
Yet, this extra workload didn’t occur. Only 3% of physicians reported spending more time answering patients’ questions, although one-fifth did report that they changed the language they used when writing notes, primarily to avoid offending patients. Every physician in the initiative said he or she would continue using OpenNotes. Surprised? So was I.
Even the usually conservative SERMO physician audience responded in an unexpected manner. According to a poll conducted this June, SERMO asked 2,300 physicians if patients should have access to their medical records (including physician notes). Forty-nine percent said “only on a case-by-case basis,” 34% said “yes, always,” and 17% said “no, never.”
So, are OpenNotes a success? Let’s take a closer look at some of the challenges. First, we physicians use language that will confuse patients at best and lead them to incorrect conclusions at worst. “Acne necrotica?” Not as bad as it sounds. Or consider, “differential diagnosis includes neuroendocrine tumor.” It doesn’t mean you have it, but some patients will believe they do. Will we have to dumb down our charts then to appease them? Won’t this degrade note quality, one of the primary objectives we are trying to avoid? It’s unclear.
The purpose of a patient note is to inform other providers and to remind ourselves of the critical information needed to care for a patient. It must be pithy and honest. It often reflects our inchoate thoughts as much as our diagnoses. It also must include the sundry requirements we know and love that are needed only to bill for the visit. These are not characteristics that make for a good patient read.
Indeed, the benefits of transparency are not limitless. In some instances, more transparency is worse. Imagine if all your emails and texts were transparent to everyone. Or if everything you’ve ever said about your mother-in-law was viewable by her. Clearly, bad transparency, bad transparency. Not sharing everything doesn’t mean we are dishonest or duplicitous. It means we are civil. It doesn’t mean we don’t care; it means we do care. We care about our friends and family. We care about our patients and the best way to make them well.
Unless we make it clear to patients that the notes they are viewing are not written for them, I’m worried simply opening charts could damage the doctor-patient relationship as much as it fosters it. Interestingly, there are companies trying to build a technical solution for this conundrum. Others are advocating for standardization of pathology and lab reports that are patient friendly. I’ll research these topics and let you know what I find out in a future column.
Perhaps I shouldn’t have been surprised by the positive results from the OpenNotes initiative. After all, for the last several years, I have given patients their actual pathology report for every biopsy I’ve done (which numbers in the many thousands). I have had fewer than five follow-up questions from patients that I can remember. Pretty much all were legitimate, as I recall, including a wrong site error in a report.
Today, more than 5 million patients have access to their providers’ notes on OpenNotes. That number will grow. Our biggest risk is to not be involved. “Just say no” didn’t work for Nancy Reagan; it won’t do our cause any good either.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
Transparency, until recently, was rarely associated with health care. Not anymore. For better and sometimes worse, there is a revolutionary movement toward transparency in all facets of health care: transparency of costs, outcomes, quality, service, and reputation. Full transparency now has come to medical records in the form of OpenNotes. This is a patient-centered initiative that allows patients full access to their chart including all their providers’ notes.
Patients always have had the right to see their record. Ordinarily though, they would be required to go to the medical records office, fill out paperwork, and request copies of their chart. They would have to supply a reason and often pay a fee. OpenNotes changes that. Open patient charts are free and easy to access, usually digitally. OpenNotes programs are still rare, and before we go any further, it’s important to examine what we’ve learned about them.
In 2010, Beth Israel Deaconess Medical Center in Boston, Geisinger Health System in Pennsylvania, and Harborview Medical Center in Seattle invited 105 primary care physicians to open their notes to nearly 14,000 patients. The results were overwhelmingly (and to me, surprisingly) positive: More than 85% of patients accessed their notes at least once. Nearly 100% of patients wanted the program to continue. Patients reported a better understanding of their medical issues, better medication adherence, increased adoption of healthy habits, and less anxiety about their health. I would have expected more confusion and anxiety among the patients.
What about the physicians? According to the initiative, whereas one in three patients thought they should have unfettered access to their physicians’ notes, only 1 in 10 physicians did. That’s understandable. The physicians in the pilot shared many of the same concerns you and I have, namely that OpenNotes would lead to an increased workload to explain esoteric notes to patients and to allay anxieties.
Yet, this extra workload didn’t occur. Only 3% of physicians reported spending more time answering patients’ questions, although one-fifth did report that they changed the language they used when writing notes, primarily to avoid offending patients. Every physician in the initiative said he or she would continue using OpenNotes. Surprised? So was I.
Even the usually conservative SERMO physician audience responded in an unexpected manner. According to a poll conducted this June, SERMO asked 2,300 physicians if patients should have access to their medical records (including physician notes). Forty-nine percent said “only on a case-by-case basis,” 34% said “yes, always,” and 17% said “no, never.”
So, are OpenNotes a success? Let’s take a closer look at some of the challenges. First, we physicians use language that will confuse patients at best and lead them to incorrect conclusions at worst. “Acne necrotica?” Not as bad as it sounds. Or consider, “differential diagnosis includes neuroendocrine tumor.” It doesn’t mean you have it, but some patients will believe they do. Will we have to dumb down our charts then to appease them? Won’t this degrade note quality, one of the primary objectives we are trying to avoid? It’s unclear.
The purpose of a patient note is to inform other providers and to remind ourselves of the critical information needed to care for a patient. It must be pithy and honest. It often reflects our inchoate thoughts as much as our diagnoses. It also must include the sundry requirements we know and love that are needed only to bill for the visit. These are not characteristics that make for a good patient read.
Indeed, the benefits of transparency are not limitless. In some instances, more transparency is worse. Imagine if all your emails and texts were transparent to everyone. Or if everything you’ve ever said about your mother-in-law was viewable by her. Clearly, bad transparency, bad transparency. Not sharing everything doesn’t mean we are dishonest or duplicitous. It means we are civil. It doesn’t mean we don’t care; it means we do care. We care about our friends and family. We care about our patients and the best way to make them well.
Unless we make it clear to patients that the notes they are viewing are not written for them, I’m worried simply opening charts could damage the doctor-patient relationship as much as it fosters it. Interestingly, there are companies trying to build a technical solution for this conundrum. Others are advocating for standardization of pathology and lab reports that are patient friendly. I’ll research these topics and let you know what I find out in a future column.
Perhaps I shouldn’t have been surprised by the positive results from the OpenNotes initiative. After all, for the last several years, I have given patients their actual pathology report for every biopsy I’ve done (which numbers in the many thousands). I have had fewer than five follow-up questions from patients that I can remember. Pretty much all were legitimate, as I recall, including a wrong site error in a report.
Today, more than 5 million patients have access to their providers’ notes on OpenNotes. That number will grow. Our biggest risk is to not be involved. “Just say no” didn’t work for Nancy Reagan; it won’t do our cause any good either.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
Transparency, until recently, was rarely associated with health care. Not anymore. For better and sometimes worse, there is a revolutionary movement toward transparency in all facets of health care: transparency of costs, outcomes, quality, service, and reputation. Full transparency now has come to medical records in the form of OpenNotes. This is a patient-centered initiative that allows patients full access to their chart including all their providers’ notes.
Patients always have had the right to see their record. Ordinarily though, they would be required to go to the medical records office, fill out paperwork, and request copies of their chart. They would have to supply a reason and often pay a fee. OpenNotes changes that. Open patient charts are free and easy to access, usually digitally. OpenNotes programs are still rare, and before we go any further, it’s important to examine what we’ve learned about them.
In 2010, Beth Israel Deaconess Medical Center in Boston, Geisinger Health System in Pennsylvania, and Harborview Medical Center in Seattle invited 105 primary care physicians to open their notes to nearly 14,000 patients. The results were overwhelmingly (and to me, surprisingly) positive: More than 85% of patients accessed their notes at least once. Nearly 100% of patients wanted the program to continue. Patients reported a better understanding of their medical issues, better medication adherence, increased adoption of healthy habits, and less anxiety about their health. I would have expected more confusion and anxiety among the patients.
What about the physicians? According to the initiative, whereas one in three patients thought they should have unfettered access to their physicians’ notes, only 1 in 10 physicians did. That’s understandable. The physicians in the pilot shared many of the same concerns you and I have, namely that OpenNotes would lead to an increased workload to explain esoteric notes to patients and to allay anxieties.
Yet, this extra workload didn’t occur. Only 3% of physicians reported spending more time answering patients’ questions, although one-fifth did report that they changed the language they used when writing notes, primarily to avoid offending patients. Every physician in the initiative said he or she would continue using OpenNotes. Surprised? So was I.
Even the usually conservative SERMO physician audience responded in an unexpected manner. According to a poll conducted this June, SERMO asked 2,300 physicians if patients should have access to their medical records (including physician notes). Forty-nine percent said “only on a case-by-case basis,” 34% said “yes, always,” and 17% said “no, never.”
So, are OpenNotes a success? Let’s take a closer look at some of the challenges. First, we physicians use language that will confuse patients at best and lead them to incorrect conclusions at worst. “Acne necrotica?” Not as bad as it sounds. Or consider, “differential diagnosis includes neuroendocrine tumor.” It doesn’t mean you have it, but some patients will believe they do. Will we have to dumb down our charts then to appease them? Won’t this degrade note quality, one of the primary objectives we are trying to avoid? It’s unclear.
The purpose of a patient note is to inform other providers and to remind ourselves of the critical information needed to care for a patient. It must be pithy and honest. It often reflects our inchoate thoughts as much as our diagnoses. It also must include the sundry requirements we know and love that are needed only to bill for the visit. These are not characteristics that make for a good patient read.
Indeed, the benefits of transparency are not limitless. In some instances, more transparency is worse. Imagine if all your emails and texts were transparent to everyone. Or if everything you’ve ever said about your mother-in-law was viewable by her. Clearly, bad transparency, bad transparency. Not sharing everything doesn’t mean we are dishonest or duplicitous. It means we are civil. It doesn’t mean we don’t care; it means we do care. We care about our friends and family. We care about our patients and the best way to make them well.
Unless we make it clear to patients that the notes they are viewing are not written for them, I’m worried simply opening charts could damage the doctor-patient relationship as much as it fosters it. Interestingly, there are companies trying to build a technical solution for this conundrum. Others are advocating for standardization of pathology and lab reports that are patient friendly. I’ll research these topics and let you know what I find out in a future column.
Perhaps I shouldn’t have been surprised by the positive results from the OpenNotes initiative. After all, for the last several years, I have given patients their actual pathology report for every biopsy I’ve done (which numbers in the many thousands). I have had fewer than five follow-up questions from patients that I can remember. Pretty much all were legitimate, as I recall, including a wrong site error in a report.
Today, more than 5 million patients have access to their providers’ notes on OpenNotes. That number will grow. Our biggest risk is to not be involved. “Just say no” didn’t work for Nancy Reagan; it won’t do our cause any good either.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.

From the Washington Office
In the previous two editions of this column, I have written about the new Medicare Access and CHIP Reauthorization Act (MACRA) and the changes it will bring to Medicare physician payment beginning in January 2019 with the Merit-Based Incentive Payment System (MIPS). In June’s column, three of the four MIPS performance categories were outlined. Specifically, those include the Quality, Resource Use, and Electronic Health Record Meaningful Use components and encompass the Physician Quality Reporting System (PQRS), Value-Based Modifier (VBM), Physician Quality Reporting System (PQRS), and Electronic Health Record Meaningful Use (EHR-MU) programs with which Fellows are hopefully familiar. As promised, this month I will discuss the final performance category component, namely the Clinical Practice Improvement Activities (CPIA) as well as the Alternative Payment Models program (APMs). Lastly, I wish to bring to the attention of Fellows a new web-based resource developed by the ACS Division of Advocacy and Health Policy to assist them in avoiding current law Medicare penalties.
The CPIA are designed to assess and credit surgeons according to their effort toward improving their clinical practice OR their preparation toward participating in the APMs. The menu of specific, recognized activities will be established in collaboration with the Centers for Medicare & Medicaid Services and the providers to whom the activities will be applicable. Many of the specifics are yet to be determined and will be part of the rule-making process in coming years. However, the MACRA legislation specifies that the CPIA must be applicable to all specialties and be attainable for small practices and professionals in rural and underserved areas. To support the efforts of surgeons and other providers in small or rural practice, Congress set aside $20 million dollars for each year, 2016-2020, for technical assistance to support the efforts of practices with 15 or fewer professionals to improve MIPS performance or transition to APMs.

The new law takes concerted steps to incentivize and encourage the development of and participation in APMs. As with the CPIA outlined above, the details of APMs are not yet fully clear and will be established going forward. However, in general, these programs will base payment on quality measures, not volume or intensity, and will include an element of financial risk for providers. For those surgeons who receive a significant share of their revenue from an APM, an annual 5% bonus will be available for each of the years 2019-2024. To qualify for that bonus surgeons must receive 25% of their Medicare revenue from an APM in the years 2019 and 2020, with the requirement subsequently increasing to 50% in 2021 and ultimately to 75% beginning in 2023. Providers may qualify based on a combination of private APMs and Medicare APMs as well.
In recognition of the lack of APMs in many areas or applicability for many specialties, MACRA prioritizes development of models for small practices, models that are specialty specific, and model development in conjunction with private payers as well as Medicaid-based options, all with the ultimate goal of encouraging the development of new and innovative payment models. The legislative language in MACRA is broad enough that it may allow for creation of a model based on the ACS’ Clinical Affinity Group (CAG) concept whereby providers are grouped together based on the patients or conditions that they treat, not their specialty designation.
Surgeons who meet a threshold of payment received from a qualified APM will be exempted from participation in MIPS to include most EHR-MU requirements and also receive the 5% bonus as described above. Those who participate in an APM but fail to meet the threshold necessary to receive that bonus will receive credit for such in the CPIA portion of their MIPS composite score.
Finally, even though the permanent repeal of the SGR found in MACRA represents the successful culmination of long-standing, combined advocacy efforts of the American College of Surgeons (ACS) and other medical associations toward meaningful, future Medicare physician payment reform, Fellows should be well aware that the three current law Medicare quality programs, namely the PQRS, EHR-MU, and VBM and their corresponding requirements as well as their associated penalties remain in effect until January 2019.
Surgeons who do not successfully participate in the PQRS, EHR-MU, and VBM face significant penalties on future Medicare payments. Specifically, failure to meet the requirements imposed by these three programs in 2015 could result in total penalties of up to 9% in Medicare payments in 2017.
To assist Fellows in navigating the complexities of complying with current law quality program requirements and thus avoid Medicare penalties, the ACS Division of Advocacy and Health Policy has developed a new online interactive flowchart which can be found at [WEB ADDRESS]. Fellows may wish to refer to and bookmark this page as an ongoing reference in order to familiarize themselves with current law requirements, facilitate their individual compliance with same, and thus successfully avoid penalties. As always, Fellows with questions may contact the DAHP at 202-337-2701.
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
In the previous two editions of this column, I have written about the new Medicare Access and CHIP Reauthorization Act (MACRA) and the changes it will bring to Medicare physician payment beginning in January 2019 with the Merit-Based Incentive Payment System (MIPS). In June’s column, three of the four MIPS performance categories were outlined. Specifically, those include the Quality, Resource Use, and Electronic Health Record Meaningful Use components and encompass the Physician Quality Reporting System (PQRS), Value-Based Modifier (VBM), Physician Quality Reporting System (PQRS), and Electronic Health Record Meaningful Use (EHR-MU) programs with which Fellows are hopefully familiar. As promised, this month I will discuss the final performance category component, namely the Clinical Practice Improvement Activities (CPIA) as well as the Alternative Payment Models program (APMs). Lastly, I wish to bring to the attention of Fellows a new web-based resource developed by the ACS Division of Advocacy and Health Policy to assist them in avoiding current law Medicare penalties.
The CPIA are designed to assess and credit surgeons according to their effort toward improving their clinical practice OR their preparation toward participating in the APMs. The menu of specific, recognized activities will be established in collaboration with the Centers for Medicare & Medicaid Services and the providers to whom the activities will be applicable. Many of the specifics are yet to be determined and will be part of the rule-making process in coming years. However, the MACRA legislation specifies that the CPIA must be applicable to all specialties and be attainable for small practices and professionals in rural and underserved areas. To support the efforts of surgeons and other providers in small or rural practice, Congress set aside $20 million dollars for each year, 2016-2020, for technical assistance to support the efforts of practices with 15 or fewer professionals to improve MIPS performance or transition to APMs.
The new law takes concerted steps to incentivize and encourage the development of and participation in APMs. As with the CPIA outlined above, the details of APMs are not yet fully clear and will be established going forward. However, in general, these programs will base payment on quality measures, not volume or intensity, and will include an element of financial risk for providers. For those surgeons who receive a significant share of their revenue from an APM, an annual 5% bonus will be available for each of the years 2019-2024. To qualify for that bonus surgeons must receive 25% of their Medicare revenue from an APM in the years 2019 and 2020, with the requirement subsequently increasing to 50% in 2021 and ultimately to 75% beginning in 2023. Providers may qualify based on a combination of private APMs and Medicare APMs as well.
In recognition of the lack of APMs in many areas or applicability for many specialties, MACRA prioritizes development of models for small practices, models that are specialty specific, and model development in conjunction with private payers as well as Medicaid-based options, all with the ultimate goal of encouraging the development of new and innovative payment models. The legislative language in MACRA is broad enough that it may allow for creation of a model based on the ACS’ Clinical Affinity Group (CAG) concept whereby providers are grouped together based on the patients or conditions that they treat, not their specialty designation.
Surgeons who meet a threshold of payment received from a qualified APM will be exempted from participation in MIPS to include most EHR-MU requirements and also receive the 5% bonus as described above. Those who participate in an APM but fail to meet the threshold necessary to receive that bonus will receive credit for such in the CPIA portion of their MIPS composite score.
Finally, even though the permanent repeal of the SGR found in MACRA represents the successful culmination of long-standing, combined advocacy efforts of the American College of Surgeons (ACS) and other medical associations toward meaningful, future Medicare physician payment reform, Fellows should be well aware that the three current law Medicare quality programs, namely the PQRS, EHR-MU, and VBM and their corresponding requirements as well as their associated penalties remain in effect until January 2019.
Surgeons who do not successfully participate in the PQRS, EHR-MU, and VBM face significant penalties on future Medicare payments. Specifically, failure to meet the requirements imposed by these three programs in 2015 could result in total penalties of up to 9% in Medicare payments in 2017.
To assist Fellows in navigating the complexities of complying with current law quality program requirements and thus avoid Medicare penalties, the ACS Division of Advocacy and Health Policy has developed a new online interactive flowchart which can be found at [WEB ADDRESS]. Fellows may wish to refer to and bookmark this page as an ongoing reference in order to familiarize themselves with current law requirements, facilitate their individual compliance with same, and thus successfully avoid penalties. As always, Fellows with questions may contact the DAHP at 202-337-2701.
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
In the previous two editions of this column, I have written about the new Medicare Access and CHIP Reauthorization Act (MACRA) and the changes it will bring to Medicare physician payment beginning in January 2019 with the Merit-Based Incentive Payment System (MIPS). In June’s column, three of the four MIPS performance categories were outlined. Specifically, those include the Quality, Resource Use, and Electronic Health Record Meaningful Use components and encompass the Physician Quality Reporting System (PQRS), Value-Based Modifier (VBM), Physician Quality Reporting System (PQRS), and Electronic Health Record Meaningful Use (EHR-MU) programs with which Fellows are hopefully familiar. As promised, this month I will discuss the final performance category component, namely the Clinical Practice Improvement Activities (CPIA) as well as the Alternative Payment Models program (APMs). Lastly, I wish to bring to the attention of Fellows a new web-based resource developed by the ACS Division of Advocacy and Health Policy to assist them in avoiding current law Medicare penalties.
The CPIA are designed to assess and credit surgeons according to their effort toward improving their clinical practice OR their preparation toward participating in the APMs. The menu of specific, recognized activities will be established in collaboration with the Centers for Medicare & Medicaid Services and the providers to whom the activities will be applicable. Many of the specifics are yet to be determined and will be part of the rule-making process in coming years. However, the MACRA legislation specifies that the CPIA must be applicable to all specialties and be attainable for small practices and professionals in rural and underserved areas. To support the efforts of surgeons and other providers in small or rural practice, Congress set aside $20 million dollars for each year, 2016-2020, for technical assistance to support the efforts of practices with 15 or fewer professionals to improve MIPS performance or transition to APMs.
The new law takes concerted steps to incentivize and encourage the development of and participation in APMs. As with the CPIA outlined above, the details of APMs are not yet fully clear and will be established going forward. However, in general, these programs will base payment on quality measures, not volume or intensity, and will include an element of financial risk for providers. For those surgeons who receive a significant share of their revenue from an APM, an annual 5% bonus will be available for each of the years 2019-2024. To qualify for that bonus surgeons must receive 25% of their Medicare revenue from an APM in the years 2019 and 2020, with the requirement subsequently increasing to 50% in 2021 and ultimately to 75% beginning in 2023. Providers may qualify based on a combination of private APMs and Medicare APMs as well.
In recognition of the lack of APMs in many areas or applicability for many specialties, MACRA prioritizes development of models for small practices, models that are specialty specific, and model development in conjunction with private payers as well as Medicaid-based options, all with the ultimate goal of encouraging the development of new and innovative payment models. The legislative language in MACRA is broad enough that it may allow for creation of a model based on the ACS’ Clinical Affinity Group (CAG) concept whereby providers are grouped together based on the patients or conditions that they treat, not their specialty designation.
Surgeons who meet a threshold of payment received from a qualified APM will be exempted from participation in MIPS to include most EHR-MU requirements and also receive the 5% bonus as described above. Those who participate in an APM but fail to meet the threshold necessary to receive that bonus will receive credit for such in the CPIA portion of their MIPS composite score.
Finally, even though the permanent repeal of the SGR found in MACRA represents the successful culmination of long-standing, combined advocacy efforts of the American College of Surgeons (ACS) and other medical associations toward meaningful, future Medicare physician payment reform, Fellows should be well aware that the three current law Medicare quality programs, namely the PQRS, EHR-MU, and VBM and their corresponding requirements as well as their associated penalties remain in effect until January 2019.
Surgeons who do not successfully participate in the PQRS, EHR-MU, and VBM face significant penalties on future Medicare payments. Specifically, failure to meet the requirements imposed by these three programs in 2015 could result in total penalties of up to 9% in Medicare payments in 2017.
To assist Fellows in navigating the complexities of complying with current law quality program requirements and thus avoid Medicare penalties, the ACS Division of Advocacy and Health Policy has developed a new online interactive flowchart which can be found at [WEB ADDRESS]. Fellows may wish to refer to and bookmark this page as an ongoing reference in order to familiarize themselves with current law requirements, facilitate their individual compliance with same, and thus successfully avoid penalties. As always, Fellows with questions may contact the DAHP at 202-337-2701.
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.

ACS Communities: Bringing us together
I was in the surgeons’ lounge in the middle of the night – waiting, as we surgeons so often do. I plucked my phone from my pocket to see what was happening on the ACS Communities. Sure enough, another surgeon was up at night somewhere contemplating a case, another was railing against a CEO, and yet another was considering entering into an employment contract. All of them were asking the same question, “What do you think?” of their College. By College, I am not referring to the leadership or the staff but to that intangible entity that lives in the heart of every Fellow of the College. It consists of old residency friends, mentors, policy makers, new surgeons, and old surgeons. All share a common, decent desire to be not just a surgeon but also a great surgeon by whatever definition one happens to hold sacred.
I smiled to myself and shook my head. From the lonely moments before an emergency case, I had a quick dose of reassurance that I was not alone, that I was a part of something bigger than myself, and that many surgeons were and are doing exactly what I do every day. Those surgeons are truly a community.

As with any community, the participants of the ACS Communities are diverse and the viewpoints and knowledge among them vary widely. But all of them have a sense that their experience, knowledge, skills, tricks of the trade, and philosophic thoughts transcend to a common purpose for the good of the patients and the profession. One can lose sight of this in the hurly-burly world of surgery, which has so much drama inherently in its performance.
ACS Communities is about a year old now and almost all Fellows belong to at least one Community in the system. This project was in the pipeline for several years. The origin of the Communities idea extends back to the 1990s. It was the brainchild of Fellows George Sheldon, Tom Russell, and David Hoyt, who all realized that honest and open communication breeds understanding and mutual respect. But none of us involved in this effort to develop the Communities really knew what the impact would be on the American College of Surgeons or the surgical community at large. Reminiscent of the first telegraph message, as the system was turned on live I thought, “What hath God wrought?” For, in fact, communication at the speed of light among 60,000 surgeons is a bit like lighting a match in a dynamite factory. You might get to see what is in a previously dark room, but you could also get an explosive result.
As Editor in Chief of the system (with the able support of Jerry Schwartz at the Chicago ACS headquarters), I’ve read essentially every one of the now thousands of posts placed into the system. Having spent some time in the company of surgeons, I was prepared for their propensity for intense expression of their views. But I was amazed to discover that while discussions in the Communities are frequently very … ah … frank, foul language and nasty comments against individuals are rare. There have been a few exceptions but it is usually a surgeon writing in the heat of the moment and temporarily forgetting that once the send button activates, there’s no way to take it back. So, I would say the great majority of conversations have been frank without being unprofessional.
Just as you can’t believe many things you read on the Internet, you can’t believe everything you read from other surgeons. When clinical cases are discussed, one frequently sees widely divergent opinions. Some of the posts are of dubious value, while others are cutting-edge ideas from world-class experts. I would advise that when posting a case (always with an eye to avoiding a HIPAA violation) that participants look at the entire range of responses. From that variety of responses, you usually see the best course. Sometimes, it is obvious there isn’t a “right” answer but several reasonable ones.
Politics rears its ugly head frequently on the General Surgery Community. Interestingly, the specialty communities tend to be strictly professional in discussing cases, training, and surgical judgment. In the realm of the political, the discussions demonstrate some of the best and worst in us. One can see that College participants are similar to the general public in that they are usually about equally divided on any single issue. This means that inflexible positions taken by the College leadership favoring a particular point of view is likely to annoy about half of the Fellows. But a few opinions are almost universally voiced: a general hatred of EMR/EHRs (despite the knowledge that if they worked right as clinical documents, surgeons would love EHRs), dissatisfaction with government regulation no matter what the regulation, admiration of their mentors, and a shared belief that salaried employment is rapidly becoming the norm of surgical life.
A great aspect of the Communities is that College leadership is reading it. When a new issue or policy, such as EHR, employment, volume outcomes, etc., comes under discussion in the Communities, the Board of Governors and Board of Regents have access to unvarnished comments from front-line surgeons. At times, these views are a revelation and, at other times, they are a confirmation of leadership impressions. It is increasingly common to see the President of the ACS, the Chair of the Regents, or a Governor chime in directly or subsequently bring the matter up in a leadership conference. I would say to those who post that their thoughts published on the Communities are like ripples in a pond. You never know what great wave may eventually land on another shore.
There are dangers of instant communication in a written format. More than once a rumor that is without basis gets started. It becomes surgeon legend and then is very hard to displace with fact. Because inflection and tone are absent from written words, what is humorous to one can be unintentionally insulting to another. I’ve noted, however, that in most circumstances of misunderstanding or errors being posted, the system is remarkably self-correcting. Within a few hours, days at most, someone points out the error or the misunderstanding, and this leads to a resolution of the conflict.
ACS Communities is not a perfect system. No doubt, as technology advances, the software and hardware will change. What I hope remains constant is a way in which practically at any time and as often as a Fellow wishes, he or she can have a voice in the affairs of the College. At any time, thousands of colleagues are at the Fellow’s fingertips in ways that bring us all together as individuals who belong to a great organization. Ultimately, it is about relating to one another on a more personal, individual basis with mutual respect and support.
Dr. Hughes, an ACS Fellow, is a general surgeon practicing in McPherson, Kan., and Editor in Chief of the ACS Communities.
I was in the surgeons’ lounge in the middle of the night – waiting, as we surgeons so often do. I plucked my phone from my pocket to see what was happening on the ACS Communities. Sure enough, another surgeon was up at night somewhere contemplating a case, another was railing against a CEO, and yet another was considering entering into an employment contract. All of them were asking the same question, “What do you think?” of their College. By College, I am not referring to the leadership or the staff but to that intangible entity that lives in the heart of every Fellow of the College. It consists of old residency friends, mentors, policy makers, new surgeons, and old surgeons. All share a common, decent desire to be not just a surgeon but also a great surgeon by whatever definition one happens to hold sacred.
I smiled to myself and shook my head. From the lonely moments before an emergency case, I had a quick dose of reassurance that I was not alone, that I was a part of something bigger than myself, and that many surgeons were and are doing exactly what I do every day. Those surgeons are truly a community.
As with any community, the participants of the ACS Communities are diverse and the viewpoints and knowledge among them vary widely. But all of them have a sense that their experience, knowledge, skills, tricks of the trade, and philosophic thoughts transcend to a common purpose for the good of the patients and the profession. One can lose sight of this in the hurly-burly world of surgery, which has so much drama inherently in its performance.
ACS Communities is about a year old now and almost all Fellows belong to at least one Community in the system. This project was in the pipeline for several years. The origin of the Communities idea extends back to the 1990s. It was the brainchild of Fellows George Sheldon, Tom Russell, and David Hoyt, who all realized that honest and open communication breeds understanding and mutual respect. But none of us involved in this effort to develop the Communities really knew what the impact would be on the American College of Surgeons or the surgical community at large. Reminiscent of the first telegraph message, as the system was turned on live I thought, “What hath God wrought?” For, in fact, communication at the speed of light among 60,000 surgeons is a bit like lighting a match in a dynamite factory. You might get to see what is in a previously dark room, but you could also get an explosive result.
As Editor in Chief of the system (with the able support of Jerry Schwartz at the Chicago ACS headquarters), I’ve read essentially every one of the now thousands of posts placed into the system. Having spent some time in the company of surgeons, I was prepared for their propensity for intense expression of their views. But I was amazed to discover that while discussions in the Communities are frequently very … ah … frank, foul language and nasty comments against individuals are rare. There have been a few exceptions but it is usually a surgeon writing in the heat of the moment and temporarily forgetting that once the send button activates, there’s no way to take it back. So, I would say the great majority of conversations have been frank without being unprofessional.
Just as you can’t believe many things you read on the Internet, you can’t believe everything you read from other surgeons. When clinical cases are discussed, one frequently sees widely divergent opinions. Some of the posts are of dubious value, while others are cutting-edge ideas from world-class experts. I would advise that when posting a case (always with an eye to avoiding a HIPAA violation) that participants look at the entire range of responses. From that variety of responses, you usually see the best course. Sometimes, it is obvious there isn’t a “right” answer but several reasonable ones.
Politics rears its ugly head frequently on the General Surgery Community. Interestingly, the specialty communities tend to be strictly professional in discussing cases, training, and surgical judgment. In the realm of the political, the discussions demonstrate some of the best and worst in us. One can see that College participants are similar to the general public in that they are usually about equally divided on any single issue. This means that inflexible positions taken by the College leadership favoring a particular point of view is likely to annoy about half of the Fellows. But a few opinions are almost universally voiced: a general hatred of EMR/EHRs (despite the knowledge that if they worked right as clinical documents, surgeons would love EHRs), dissatisfaction with government regulation no matter what the regulation, admiration of their mentors, and a shared belief that salaried employment is rapidly becoming the norm of surgical life.
A great aspect of the Communities is that College leadership is reading it. When a new issue or policy, such as EHR, employment, volume outcomes, etc., comes under discussion in the Communities, the Board of Governors and Board of Regents have access to unvarnished comments from front-line surgeons. At times, these views are a revelation and, at other times, they are a confirmation of leadership impressions. It is increasingly common to see the President of the ACS, the Chair of the Regents, or a Governor chime in directly or subsequently bring the matter up in a leadership conference. I would say to those who post that their thoughts published on the Communities are like ripples in a pond. You never know what great wave may eventually land on another shore.
There are dangers of instant communication in a written format. More than once a rumor that is without basis gets started. It becomes surgeon legend and then is very hard to displace with fact. Because inflection and tone are absent from written words, what is humorous to one can be unintentionally insulting to another. I’ve noted, however, that in most circumstances of misunderstanding or errors being posted, the system is remarkably self-correcting. Within a few hours, days at most, someone points out the error or the misunderstanding, and this leads to a resolution of the conflict.
ACS Communities is not a perfect system. No doubt, as technology advances, the software and hardware will change. What I hope remains constant is a way in which practically at any time and as often as a Fellow wishes, he or she can have a voice in the affairs of the College. At any time, thousands of colleagues are at the Fellow’s fingertips in ways that bring us all together as individuals who belong to a great organization. Ultimately, it is about relating to one another on a more personal, individual basis with mutual respect and support.
Dr. Hughes, an ACS Fellow, is a general surgeon practicing in McPherson, Kan., and Editor in Chief of the ACS Communities.
I was in the surgeons’ lounge in the middle of the night – waiting, as we surgeons so often do. I plucked my phone from my pocket to see what was happening on the ACS Communities. Sure enough, another surgeon was up at night somewhere contemplating a case, another was railing against a CEO, and yet another was considering entering into an employment contract. All of them were asking the same question, “What do you think?” of their College. By College, I am not referring to the leadership or the staff but to that intangible entity that lives in the heart of every Fellow of the College. It consists of old residency friends, mentors, policy makers, new surgeons, and old surgeons. All share a common, decent desire to be not just a surgeon but also a great surgeon by whatever definition one happens to hold sacred.
I smiled to myself and shook my head. From the lonely moments before an emergency case, I had a quick dose of reassurance that I was not alone, that I was a part of something bigger than myself, and that many surgeons were and are doing exactly what I do every day. Those surgeons are truly a community.
As with any community, the participants of the ACS Communities are diverse and the viewpoints and knowledge among them vary widely. But all of them have a sense that their experience, knowledge, skills, tricks of the trade, and philosophic thoughts transcend to a common purpose for the good of the patients and the profession. One can lose sight of this in the hurly-burly world of surgery, which has so much drama inherently in its performance.
ACS Communities is about a year old now and almost all Fellows belong to at least one Community in the system. This project was in the pipeline for several years. The origin of the Communities idea extends back to the 1990s. It was the brainchild of Fellows George Sheldon, Tom Russell, and David Hoyt, who all realized that honest and open communication breeds understanding and mutual respect. But none of us involved in this effort to develop the Communities really knew what the impact would be on the American College of Surgeons or the surgical community at large. Reminiscent of the first telegraph message, as the system was turned on live I thought, “What hath God wrought?” For, in fact, communication at the speed of light among 60,000 surgeons is a bit like lighting a match in a dynamite factory. You might get to see what is in a previously dark room, but you could also get an explosive result.
As Editor in Chief of the system (with the able support of Jerry Schwartz at the Chicago ACS headquarters), I’ve read essentially every one of the now thousands of posts placed into the system. Having spent some time in the company of surgeons, I was prepared for their propensity for intense expression of their views. But I was amazed to discover that while discussions in the Communities are frequently very … ah … frank, foul language and nasty comments against individuals are rare. There have been a few exceptions but it is usually a surgeon writing in the heat of the moment and temporarily forgetting that once the send button activates, there’s no way to take it back. So, I would say the great majority of conversations have been frank without being unprofessional.
Just as you can’t believe many things you read on the Internet, you can’t believe everything you read from other surgeons. When clinical cases are discussed, one frequently sees widely divergent opinions. Some of the posts are of dubious value, while others are cutting-edge ideas from world-class experts. I would advise that when posting a case (always with an eye to avoiding a HIPAA violation) that participants look at the entire range of responses. From that variety of responses, you usually see the best course. Sometimes, it is obvious there isn’t a “right” answer but several reasonable ones.
Politics rears its ugly head frequently on the General Surgery Community. Interestingly, the specialty communities tend to be strictly professional in discussing cases, training, and surgical judgment. In the realm of the political, the discussions demonstrate some of the best and worst in us. One can see that College participants are similar to the general public in that they are usually about equally divided on any single issue. This means that inflexible positions taken by the College leadership favoring a particular point of view is likely to annoy about half of the Fellows. But a few opinions are almost universally voiced: a general hatred of EMR/EHRs (despite the knowledge that if they worked right as clinical documents, surgeons would love EHRs), dissatisfaction with government regulation no matter what the regulation, admiration of their mentors, and a shared belief that salaried employment is rapidly becoming the norm of surgical life.
A great aspect of the Communities is that College leadership is reading it. When a new issue or policy, such as EHR, employment, volume outcomes, etc., comes under discussion in the Communities, the Board of Governors and Board of Regents have access to unvarnished comments from front-line surgeons. At times, these views are a revelation and, at other times, they are a confirmation of leadership impressions. It is increasingly common to see the President of the ACS, the Chair of the Regents, or a Governor chime in directly or subsequently bring the matter up in a leadership conference. I would say to those who post that their thoughts published on the Communities are like ripples in a pond. You never know what great wave may eventually land on another shore.
There are dangers of instant communication in a written format. More than once a rumor that is without basis gets started. It becomes surgeon legend and then is very hard to displace with fact. Because inflection and tone are absent from written words, what is humorous to one can be unintentionally insulting to another. I’ve noted, however, that in most circumstances of misunderstanding or errors being posted, the system is remarkably self-correcting. Within a few hours, days at most, someone points out the error or the misunderstanding, and this leads to a resolution of the conflict.
ACS Communities is not a perfect system. No doubt, as technology advances, the software and hardware will change. What I hope remains constant is a way in which practically at any time and as often as a Fellow wishes, he or she can have a voice in the affairs of the College. At any time, thousands of colleagues are at the Fellow’s fingertips in ways that bring us all together as individuals who belong to a great organization. Ultimately, it is about relating to one another on a more personal, individual basis with mutual respect and support.
Dr. Hughes, an ACS Fellow, is a general surgeon practicing in McPherson, Kan., and Editor in Chief of the ACS Communities.

The Right Care at the Right Time and in the Right Place: The Role of Technology in the VHA
Embracing technology is nothing new for the VHA, whether it is telehealth, e-consults, or electronic health records. “The VHA is in a unique position to create the first truly national telemedicine network in the U.S.,” Adam W. Darkins, MD, then acting chief consultant of telemedicine at the VA wrote in a 2001 newsletter. “It is our collective task to make sure that if this happens, we have a system that can ‘plug and play.’”1
To better understand the progress in delivering health care, Federal Practitioner decided to devote this entire issue to the topic and to discuss the VHA and technology with Madhulika Agarwal, MD, MPH. As deputy under secretary for health for policy and services, Dr. Agarwal has been at the heart of the VHA’s embrace of many of these technologies for health care delivery and has been in a position to oversee their execution. More than anyone else at the VHA, she is familiar with the potential and limitations of telehealth.
Below is an edited and condensed version of the interview. To hear the complete interview, visit http://www.fedprac.com/multimedia/multimedia-library.html.
Importance of Telehealth to the VHA
Madhulika Agarwal, MD, MPH. Our goal is to ensure that veterans have optimal health and that we deliver the best health care with a focus on timely access and with an exceptional experience. And over the years, we have been building technologic tools so that we can provide the right care at the right time and in the right place. Telehealth affords veterans the convenience of accessing primary or specialized care services either from their local VA community clinic or from the privacy of their own home.
Now we have many virtual access solutions. The home telehealth, clinical video teleconferencing, store-and-forward technologies, e-consults, My HealtheVet, plus SCAN-ECHO [Specialty Care Access Network-Extension for Community Healthcare Outcomes]; and these all have demonstrated that they are mission-critical tools, which improve and expand the access for veterans who may have difficulty accessing care for multiple reasons.
It could be some clinical issues where there are transportation difficulties, such as for veterans with spinal cord injury, or mild traumatic brain injury, or geographic barriers. Many of our veterans, I would say roughly 40% to 45% of them, live in rural and highly rural areas where they may not have access to care nearby. Or it could be further exacerbated with geographic challenges by inclement weather or the drive times. And lastly, I would say it’s the lack of specialists in these rural communities where many of our veterans live.
VHA is successfully integrating into the existing technical administrative clinical infrastructures, and this infrastructure provides a reliable and robust IT network. We have an electronic health record. We provide national policy guidance regarding health information security, credentialing, privileging, etc. And our strategic goal has been to have personalized, proactive, patient-driven care; and telehealth supports that goal.
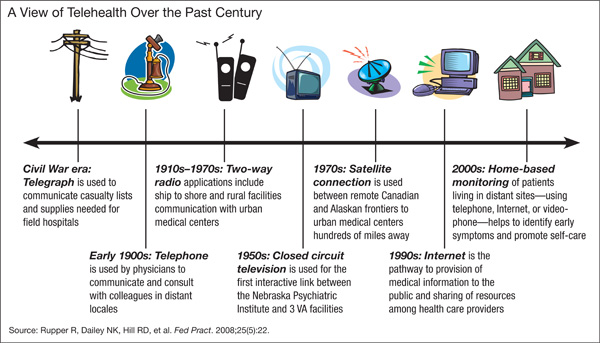
Improving Veteran Access
Dr. Agarwal. It’s interesting that both the Choice program, which is part of the Veterans Access, Choice, and Accountability Act of 2014, known as VACAA, and telehealth aim at improving veteran access to care. Under the Choice program, many veterans now have the option to access community partner health care rather than waiting for a VA appointment, or traveling to a VA facility when the geographic distance is more than 40 miles, or if the appointment in the VA is not available for 30 days.
The Choice program and telehealth are 2 very concrete examples of VHA’s transformation from a facility or provider-centric health care delivery model to a model that puts the veteran’s needs at the center and improving the veteran’s access to resources to meet their health care needs.
Related: Committed to Showing Results at the VA
More than 717,000 veterans have accessed VA care through telehealth in fiscal year [FY] 14, and 45% of these veterans live in rural and highly rural areas. In FY14, the total for veterans using telehealth represented about an 18% growth from the prior year; and the telehealth services provide access to help in more than 45 different specialty areas, including those areas where VHA has a particular expertise, especially, for example, in mental health that may not be available from the local community partner.
Telehealth Uses
Dr. Agarwal. A veteran who is living in a rural area, let’s just say in some rural part of Maryland, and has to commute to the Baltimore VA, which you know is an inner-city VA medical center, to keep his appointment for a mental health condition with his VA provider. Now, using telemental health, this veteran can access this provider from his or her own home through encrypted video conferencing and complete the telemental health visit in the comfort of his or her own home so that they are not subject to the traffic and other challenges that they would otherwise face and get even more stressed than what they started out with. The ability, the convenience of having the service of counseling or cognitive behavioral therapy into their own homes, is just remarkable.
Another example that I could cite for you would be an appointment in the hearing aid clinic. So a veteran who lives in the Florida Keys normally would have to travel 5 hours from the Florida Keys, go to Miami, stay in a hotel overnight so that they can go to their appointment at 8 am. Instead, the veteran now can visit the Key West clinic and have his hearing aid adjusted by a VA audiologist who’s located in Miami; and it saves the entire trip.
The third one I will cite you has to do with the C&P [Compensation & Pension] exams. Now, a veteran living even out of the country can access a VA provider in Connecticut or some [other] state, using the encrypted video conferencing; and they can have the whole clinical evaluation for C&P completed using the video conferencing. These are some of the examples of how telehealth has been used very successfully.
Technologic and Educational Challenges
Dr. Agarwal. We have been a pioneer of telehealth. And with that, of course, all those challenges come into play. And we certainly have implementation challenges that include provider and patient education and their buy-in into the use of technology and providing services as well as the technology itself and some administrative issues. They can all be very closely linked.
You know, one illustrative example that I just cited earlier about video conferencing is one such example into the veteran’s home. It is very convenient.… We started to implement this home telemental health program a couple of years ago. But since then, about 108,000 veterans have accessed using the video conferencing technology; but fewer than 2,000 or so have done it from their own home. And that’s largely because the current video visit from home is quite cumbersome. It requires passwords for each visit. It requires that the veteran download VA-licensed software on their own device. And in addition, there are restrictions because of the availability of the broadband Internet connectivity, which is required for the video visit—more so in the rural areas.
Related: Preparing the Military Health System for the 21st Century
Our general counsel is reviewing and attempting to resolve state licensure requirements that have been raised by some states, because the veterans here receive care at home and outside of our VA brick-and-mortar facility, as well as the legality of VA providers potentially prescribing a controlled substance for a veteran at home without a prior in-person office visit.
But to overcome the provider challenges, the national telehealth training and resource center has been working on training the providers in the use of telehealth. Roughly 11,400 VA staff have been trained in the use of telehealth in FY14. We have currently 144 facility telehealth coordinators and more than 1,100 telehealth clinical technicians who assist with training and outreach for both VA staff and veteran patients.
Legal/Security Challenges
Dr. Agarwal. High-speed connectivity happens to be one of the key ones.… Using 4G services, I think, is going to be essential for every veteran regardless of rurality. And when these 4G services are not available, that certainly hinders the ability to provide telehealth to all veterans. Having the right security with full data encryption is essential so that we can protect the private health information of the veterans.
But unfortunately, at this time, there is not an easy way to do that. I think a lot of innovation is required so that we can make it much easier for the veterans with 1-button access, both for the veterans as well as for the providers. And that’s going to require significant effort in the grid technology as well as overcoming certain legal requirements.
What Is Driving Telehealth?
Dr. Agarwal. The real driver here has to be the veterans’ needs, not the needs of telehealth nor the clinical services or operations. I think the whole goal here is that we must use technology to the extent possible. We have to move toward virtual access as the norm.
As much as possible, we should provide the virtual access in the veterans’ homes or wherever the veterans would like to receive their services. Make the connectivity as simple as possible for the veterans and move beyond the concept of the episodic visit so that the health information and self-care management tools are available to the veterans at all times. And that essentially needs to be the overarching strategy, and that should drive how we develop the technologies to provide the services.
Data Analysis
Dr. Agarwal. We have the general enrollee data. We look at access gaps in clinical services and the telehealth activity data for our program management and oversight as well as in developing an overarching strategy for the clinical services and telehealth services. It’s done somewhat in conjunction. And our outcome analysis shows that there has been significant reduction in admissions and bed days of care with the use of telehealth.
For example, in FY14, an analysis of 10,621 veterans who were newly enrolled in home telehealth with noninstitutional care needs and chronic care management categories had a decrease of about 54% of bed days of care. This was about a 32% decrease in the hospital admissions compared [with] the same patient data prior to the enrollment and home telehealth. The analysis of telemental health outcomes shows that there was a 35% reduction in acute psychiatric bed days of care for veterans receiving CBT [cognitive behavioral therapy] or the clinical video conferencing telemental health in FY14 when it was compared [with] the utilization in the prior year.
Telehealth Pilot Programs
Dr. Agarwal. I must admit that there are many more programs that begin in the facilities, but at the national level. The first one is the tele-ICU implementation, where VISN 23 is supporting VISN 15, 5 of the medical centers with clinical video teleconferencing capability for live interactive consults with ICU specialists; and it covers about 78 beds. VISN 10 is supporting VISN 7 in 7 of their medical centers, which covers about 72 beds.
Another program, which is in the pilot phase right now, is the telewound care pilot, which is being implemented in 6 VISNs and combines the use of home telehealth, clinical video teleconferencing, and store-and-forward telehealth technologies to create access to a continuum of wound care options across multiple patients and provider settings and locations, all with the goal of enhancing and improving wound care treatment and healing.… The initial phase has been that all the participating facilities have been identified, and some of the operations manuals have been developed.
Related: Acting Surgeon General Confident in Battle Against Tobacco, Ebola, and Preventable Diseases
The third quarter of this year, we will have a completion of the operations manual Provider Training and Treatment Template. The local sites are also working on the infrastructure and knowledge base so that this project can be completed by FY15.
And the last highlight that I’ll mention, which is in its very early stages, is a low-acuity/low-intensity pilot with the focus on health promotion and health prevention behaviors, such as tobacco cessation, weight management, and newly diagnosed but stable veterans with diabetes, high blood pressure, and heart failure, using a web-based browser technology.
VA Telehealth Leadership
Dr. Agarwal. Overall, when we start to look at the monumental impact of technology on other industries, such as banking, shopping, travel, and even personal communications, the emerging technologies continue to change the overall landscape of all these environments. This is an exciting time to be in the health care industry, because I think we have lagged somewhat behind in using technology. But as we look forward, the consumer-driven health care is going to become the norm.
As you know, VA has long been a pioneer with electronic medical records and with virtual modalities, such as telehealth both in the home and in the community, the use of patient web portals, such as My HealtheVet, secure messaging for various apps, kiosks; and we remain on the forefront of developing and utilizing these approaches to enhance health care delivery.
We all know that health care in the U.S. is complex and fragmented. VA is looking to become the benchmark in U.S. health care delivery, aiding in the transformation of the delivery of services for veterans and families, focusing on unified, integrated, and personalized virtual services that seamlessly connect them with the state-of-the-art health care system.
1. Darkins A. A message from the acting chief consultant: telemedicine grows throughout VHA. Telemedicine News. 2001;1(1):1. U.S. Department of Veterans Affairs Website. http://www.telehealth.va.gov/newsletter/2001/040201-newsletter_spring_01.pdf. Published April 2, 2001. Accessed June 23, 2015.
Embracing technology is nothing new for the VHA, whether it is telehealth, e-consults, or electronic health records. “The VHA is in a unique position to create the first truly national telemedicine network in the U.S.,” Adam W. Darkins, MD, then acting chief consultant of telemedicine at the VA wrote in a 2001 newsletter. “It is our collective task to make sure that if this happens, we have a system that can ‘plug and play.’”1
To better understand the progress in delivering health care, Federal Practitioner decided to devote this entire issue to the topic and to discuss the VHA and technology with Madhulika Agarwal, MD, MPH. As deputy under secretary for health for policy and services, Dr. Agarwal has been at the heart of the VHA’s embrace of many of these technologies for health care delivery and has been in a position to oversee their execution. More than anyone else at the VHA, she is familiar with the potential and limitations of telehealth.
Below is an edited and condensed version of the interview. To hear the complete interview, visit http://www.fedprac.com/multimedia/multimedia-library.html.
Importance of Telehealth to the VHA
Madhulika Agarwal, MD, MPH. Our goal is to ensure that veterans have optimal health and that we deliver the best health care with a focus on timely access and with an exceptional experience. And over the years, we have been building technologic tools so that we can provide the right care at the right time and in the right place. Telehealth affords veterans the convenience of accessing primary or specialized care services either from their local VA community clinic or from the privacy of their own home.
Now we have many virtual access solutions. The home telehealth, clinical video teleconferencing, store-and-forward technologies, e-consults, My HealtheVet, plus SCAN-ECHO [Specialty Care Access Network-Extension for Community Healthcare Outcomes]; and these all have demonstrated that they are mission-critical tools, which improve and expand the access for veterans who may have difficulty accessing care for multiple reasons.
It could be some clinical issues where there are transportation difficulties, such as for veterans with spinal cord injury, or mild traumatic brain injury, or geographic barriers. Many of our veterans, I would say roughly 40% to 45% of them, live in rural and highly rural areas where they may not have access to care nearby. Or it could be further exacerbated with geographic challenges by inclement weather or the drive times. And lastly, I would say it’s the lack of specialists in these rural communities where many of our veterans live.
VHA is successfully integrating into the existing technical administrative clinical infrastructures, and this infrastructure provides a reliable and robust IT network. We have an electronic health record. We provide national policy guidance regarding health information security, credentialing, privileging, etc. And our strategic goal has been to have personalized, proactive, patient-driven care; and telehealth supports that goal.
Improving Veteran Access
Dr. Agarwal. It’s interesting that both the Choice program, which is part of the Veterans Access, Choice, and Accountability Act of 2014, known as VACAA, and telehealth aim at improving veteran access to care. Under the Choice program, many veterans now have the option to access community partner health care rather than waiting for a VA appointment, or traveling to a VA facility when the geographic distance is more than 40 miles, or if the appointment in the VA is not available for 30 days.
The Choice program and telehealth are 2 very concrete examples of VHA’s transformation from a facility or provider-centric health care delivery model to a model that puts the veteran’s needs at the center and improving the veteran’s access to resources to meet their health care needs.
Related: Committed to Showing Results at the VA
More than 717,000 veterans have accessed VA care through telehealth in fiscal year [FY] 14, and 45% of these veterans live in rural and highly rural areas. In FY14, the total for veterans using telehealth represented about an 18% growth from the prior year; and the telehealth services provide access to help in more than 45 different specialty areas, including those areas where VHA has a particular expertise, especially, for example, in mental health that may not be available from the local community partner.
Telehealth Uses
Dr. Agarwal. A veteran who is living in a rural area, let’s just say in some rural part of Maryland, and has to commute to the Baltimore VA, which you know is an inner-city VA medical center, to keep his appointment for a mental health condition with his VA provider. Now, using telemental health, this veteran can access this provider from his or her own home through encrypted video conferencing and complete the telemental health visit in the comfort of his or her own home so that they are not subject to the traffic and other challenges that they would otherwise face and get even more stressed than what they started out with. The ability, the convenience of having the service of counseling or cognitive behavioral therapy into their own homes, is just remarkable.
Another example that I could cite for you would be an appointment in the hearing aid clinic. So a veteran who lives in the Florida Keys normally would have to travel 5 hours from the Florida Keys, go to Miami, stay in a hotel overnight so that they can go to their appointment at 8 am. Instead, the veteran now can visit the Key West clinic and have his hearing aid adjusted by a VA audiologist who’s located in Miami; and it saves the entire trip.
The third one I will cite you has to do with the C&P [Compensation & Pension] exams. Now, a veteran living even out of the country can access a VA provider in Connecticut or some [other] state, using the encrypted video conferencing; and they can have the whole clinical evaluation for C&P completed using the video conferencing. These are some of the examples of how telehealth has been used very successfully.
Technologic and Educational Challenges
Dr. Agarwal. We have been a pioneer of telehealth. And with that, of course, all those challenges come into play. And we certainly have implementation challenges that include provider and patient education and their buy-in into the use of technology and providing services as well as the technology itself and some administrative issues. They can all be very closely linked.
You know, one illustrative example that I just cited earlier about video conferencing is one such example into the veteran’s home. It is very convenient.… We started to implement this home telemental health program a couple of years ago. But since then, about 108,000 veterans have accessed using the video conferencing technology; but fewer than 2,000 or so have done it from their own home. And that’s largely because the current video visit from home is quite cumbersome. It requires passwords for each visit. It requires that the veteran download VA-licensed software on their own device. And in addition, there are restrictions because of the availability of the broadband Internet connectivity, which is required for the video visit—more so in the rural areas.
Related: Preparing the Military Health System for the 21st Century
Our general counsel is reviewing and attempting to resolve state licensure requirements that have been raised by some states, because the veterans here receive care at home and outside of our VA brick-and-mortar facility, as well as the legality of VA providers potentially prescribing a controlled substance for a veteran at home without a prior in-person office visit.
But to overcome the provider challenges, the national telehealth training and resource center has been working on training the providers in the use of telehealth. Roughly 11,400 VA staff have been trained in the use of telehealth in FY14. We have currently 144 facility telehealth coordinators and more than 1,100 telehealth clinical technicians who assist with training and outreach for both VA staff and veteran patients.
Legal/Security Challenges
Dr. Agarwal. High-speed connectivity happens to be one of the key ones.… Using 4G services, I think, is going to be essential for every veteran regardless of rurality. And when these 4G services are not available, that certainly hinders the ability to provide telehealth to all veterans. Having the right security with full data encryption is essential so that we can protect the private health information of the veterans.
But unfortunately, at this time, there is not an easy way to do that. I think a lot of innovation is required so that we can make it much easier for the veterans with 1-button access, both for the veterans as well as for the providers. And that’s going to require significant effort in the grid technology as well as overcoming certain legal requirements.
What Is Driving Telehealth?
Dr. Agarwal. The real driver here has to be the veterans’ needs, not the needs of telehealth nor the clinical services or operations. I think the whole goal here is that we must use technology to the extent possible. We have to move toward virtual access as the norm.
As much as possible, we should provide the virtual access in the veterans’ homes or wherever the veterans would like to receive their services. Make the connectivity as simple as possible for the veterans and move beyond the concept of the episodic visit so that the health information and self-care management tools are available to the veterans at all times. And that essentially needs to be the overarching strategy, and that should drive how we develop the technologies to provide the services.
Data Analysis
Dr. Agarwal. We have the general enrollee data. We look at access gaps in clinical services and the telehealth activity data for our program management and oversight as well as in developing an overarching strategy for the clinical services and telehealth services. It’s done somewhat in conjunction. And our outcome analysis shows that there has been significant reduction in admissions and bed days of care with the use of telehealth.
For example, in FY14, an analysis of 10,621 veterans who were newly enrolled in home telehealth with noninstitutional care needs and chronic care management categories had a decrease of about 54% of bed days of care. This was about a 32% decrease in the hospital admissions compared [with] the same patient data prior to the enrollment and home telehealth. The analysis of telemental health outcomes shows that there was a 35% reduction in acute psychiatric bed days of care for veterans receiving CBT [cognitive behavioral therapy] or the clinical video conferencing telemental health in FY14 when it was compared [with] the utilization in the prior year.
Telehealth Pilot Programs
Dr. Agarwal. I must admit that there are many more programs that begin in the facilities, but at the national level. The first one is the tele-ICU implementation, where VISN 23 is supporting VISN 15, 5 of the medical centers with clinical video teleconferencing capability for live interactive consults with ICU specialists; and it covers about 78 beds. VISN 10 is supporting VISN 7 in 7 of their medical centers, which covers about 72 beds.
Another program, which is in the pilot phase right now, is the telewound care pilot, which is being implemented in 6 VISNs and combines the use of home telehealth, clinical video teleconferencing, and store-and-forward telehealth technologies to create access to a continuum of wound care options across multiple patients and provider settings and locations, all with the goal of enhancing and improving wound care treatment and healing.… The initial phase has been that all the participating facilities have been identified, and some of the operations manuals have been developed.
Related: Acting Surgeon General Confident in Battle Against Tobacco, Ebola, and Preventable Diseases
The third quarter of this year, we will have a completion of the operations manual Provider Training and Treatment Template. The local sites are also working on the infrastructure and knowledge base so that this project can be completed by FY15.
And the last highlight that I’ll mention, which is in its very early stages, is a low-acuity/low-intensity pilot with the focus on health promotion and health prevention behaviors, such as tobacco cessation, weight management, and newly diagnosed but stable veterans with diabetes, high blood pressure, and heart failure, using a web-based browser technology.
VA Telehealth Leadership
Dr. Agarwal. Overall, when we start to look at the monumental impact of technology on other industries, such as banking, shopping, travel, and even personal communications, the emerging technologies continue to change the overall landscape of all these environments. This is an exciting time to be in the health care industry, because I think we have lagged somewhat behind in using technology. But as we look forward, the consumer-driven health care is going to become the norm.
As you know, VA has long been a pioneer with electronic medical records and with virtual modalities, such as telehealth both in the home and in the community, the use of patient web portals, such as My HealtheVet, secure messaging for various apps, kiosks; and we remain on the forefront of developing and utilizing these approaches to enhance health care delivery.
We all know that health care in the U.S. is complex and fragmented. VA is looking to become the benchmark in U.S. health care delivery, aiding in the transformation of the delivery of services for veterans and families, focusing on unified, integrated, and personalized virtual services that seamlessly connect them with the state-of-the-art health care system.
Embracing technology is nothing new for the VHA, whether it is telehealth, e-consults, or electronic health records. “The VHA is in a unique position to create the first truly national telemedicine network in the U.S.,” Adam W. Darkins, MD, then acting chief consultant of telemedicine at the VA wrote in a 2001 newsletter. “It is our collective task to make sure that if this happens, we have a system that can ‘plug and play.’”1
To better understand the progress in delivering health care, Federal Practitioner decided to devote this entire issue to the topic and to discuss the VHA and technology with Madhulika Agarwal, MD, MPH. As deputy under secretary for health for policy and services, Dr. Agarwal has been at the heart of the VHA’s embrace of many of these technologies for health care delivery and has been in a position to oversee their execution. More than anyone else at the VHA, she is familiar with the potential and limitations of telehealth.
Below is an edited and condensed version of the interview. To hear the complete interview, visit http://www.fedprac.com/multimedia/multimedia-library.html.
Importance of Telehealth to the VHA
Madhulika Agarwal, MD, MPH. Our goal is to ensure that veterans have optimal health and that we deliver the best health care with a focus on timely access and with an exceptional experience. And over the years, we have been building technologic tools so that we can provide the right care at the right time and in the right place. Telehealth affords veterans the convenience of accessing primary or specialized care services either from their local VA community clinic or from the privacy of their own home.
Now we have many virtual access solutions. The home telehealth, clinical video teleconferencing, store-and-forward technologies, e-consults, My HealtheVet, plus SCAN-ECHO [Specialty Care Access Network-Extension for Community Healthcare Outcomes]; and these all have demonstrated that they are mission-critical tools, which improve and expand the access for veterans who may have difficulty accessing care for multiple reasons.
It could be some clinical issues where there are transportation difficulties, such as for veterans with spinal cord injury, or mild traumatic brain injury, or geographic barriers. Many of our veterans, I would say roughly 40% to 45% of them, live in rural and highly rural areas where they may not have access to care nearby. Or it could be further exacerbated with geographic challenges by inclement weather or the drive times. And lastly, I would say it’s the lack of specialists in these rural communities where many of our veterans live.
VHA is successfully integrating into the existing technical administrative clinical infrastructures, and this infrastructure provides a reliable and robust IT network. We have an electronic health record. We provide national policy guidance regarding health information security, credentialing, privileging, etc. And our strategic goal has been to have personalized, proactive, patient-driven care; and telehealth supports that goal.
Improving Veteran Access
Dr. Agarwal. It’s interesting that both the Choice program, which is part of the Veterans Access, Choice, and Accountability Act of 2014, known as VACAA, and telehealth aim at improving veteran access to care. Under the Choice program, many veterans now have the option to access community partner health care rather than waiting for a VA appointment, or traveling to a VA facility when the geographic distance is more than 40 miles, or if the appointment in the VA is not available for 30 days.
The Choice program and telehealth are 2 very concrete examples of VHA’s transformation from a facility or provider-centric health care delivery model to a model that puts the veteran’s needs at the center and improving the veteran’s access to resources to meet their health care needs.
Related: Committed to Showing Results at the VA
More than 717,000 veterans have accessed VA care through telehealth in fiscal year [FY] 14, and 45% of these veterans live in rural and highly rural areas. In FY14, the total for veterans using telehealth represented about an 18% growth from the prior year; and the telehealth services provide access to help in more than 45 different specialty areas, including those areas where VHA has a particular expertise, especially, for example, in mental health that may not be available from the local community partner.
Telehealth Uses
Dr. Agarwal. A veteran who is living in a rural area, let’s just say in some rural part of Maryland, and has to commute to the Baltimore VA, which you know is an inner-city VA medical center, to keep his appointment for a mental health condition with his VA provider. Now, using telemental health, this veteran can access this provider from his or her own home through encrypted video conferencing and complete the telemental health visit in the comfort of his or her own home so that they are not subject to the traffic and other challenges that they would otherwise face and get even more stressed than what they started out with. The ability, the convenience of having the service of counseling or cognitive behavioral therapy into their own homes, is just remarkable.
Another example that I could cite for you would be an appointment in the hearing aid clinic. So a veteran who lives in the Florida Keys normally would have to travel 5 hours from the Florida Keys, go to Miami, stay in a hotel overnight so that they can go to their appointment at 8 am. Instead, the veteran now can visit the Key West clinic and have his hearing aid adjusted by a VA audiologist who’s located in Miami; and it saves the entire trip.
The third one I will cite you has to do with the C&P [Compensation & Pension] exams. Now, a veteran living even out of the country can access a VA provider in Connecticut or some [other] state, using the encrypted video conferencing; and they can have the whole clinical evaluation for C&P completed using the video conferencing. These are some of the examples of how telehealth has been used very successfully.
Technologic and Educational Challenges
Dr. Agarwal. We have been a pioneer of telehealth. And with that, of course, all those challenges come into play. And we certainly have implementation challenges that include provider and patient education and their buy-in into the use of technology and providing services as well as the technology itself and some administrative issues. They can all be very closely linked.
You know, one illustrative example that I just cited earlier about video conferencing is one such example into the veteran’s home. It is very convenient.… We started to implement this home telemental health program a couple of years ago. But since then, about 108,000 veterans have accessed using the video conferencing technology; but fewer than 2,000 or so have done it from their own home. And that’s largely because the current video visit from home is quite cumbersome. It requires passwords for each visit. It requires that the veteran download VA-licensed software on their own device. And in addition, there are restrictions because of the availability of the broadband Internet connectivity, which is required for the video visit—more so in the rural areas.
Related: Preparing the Military Health System for the 21st Century
Our general counsel is reviewing and attempting to resolve state licensure requirements that have been raised by some states, because the veterans here receive care at home and outside of our VA brick-and-mortar facility, as well as the legality of VA providers potentially prescribing a controlled substance for a veteran at home without a prior in-person office visit.
But to overcome the provider challenges, the national telehealth training and resource center has been working on training the providers in the use of telehealth. Roughly 11,400 VA staff have been trained in the use of telehealth in FY14. We have currently 144 facility telehealth coordinators and more than 1,100 telehealth clinical technicians who assist with training and outreach for both VA staff and veteran patients.
Legal/Security Challenges
Dr. Agarwal. High-speed connectivity happens to be one of the key ones.… Using 4G services, I think, is going to be essential for every veteran regardless of rurality. And when these 4G services are not available, that certainly hinders the ability to provide telehealth to all veterans. Having the right security with full data encryption is essential so that we can protect the private health information of the veterans.
But unfortunately, at this time, there is not an easy way to do that. I think a lot of innovation is required so that we can make it much easier for the veterans with 1-button access, both for the veterans as well as for the providers. And that’s going to require significant effort in the grid technology as well as overcoming certain legal requirements.
What Is Driving Telehealth?
Dr. Agarwal. The real driver here has to be the veterans’ needs, not the needs of telehealth nor the clinical services or operations. I think the whole goal here is that we must use technology to the extent possible. We have to move toward virtual access as the norm.
As much as possible, we should provide the virtual access in the veterans’ homes or wherever the veterans would like to receive their services. Make the connectivity as simple as possible for the veterans and move beyond the concept of the episodic visit so that the health information and self-care management tools are available to the veterans at all times. And that essentially needs to be the overarching strategy, and that should drive how we develop the technologies to provide the services.
Data Analysis
Dr. Agarwal. We have the general enrollee data. We look at access gaps in clinical services and the telehealth activity data for our program management and oversight as well as in developing an overarching strategy for the clinical services and telehealth services. It’s done somewhat in conjunction. And our outcome analysis shows that there has been significant reduction in admissions and bed days of care with the use of telehealth.
For example, in FY14, an analysis of 10,621 veterans who were newly enrolled in home telehealth with noninstitutional care needs and chronic care management categories had a decrease of about 54% of bed days of care. This was about a 32% decrease in the hospital admissions compared [with] the same patient data prior to the enrollment and home telehealth. The analysis of telemental health outcomes shows that there was a 35% reduction in acute psychiatric bed days of care for veterans receiving CBT [cognitive behavioral therapy] or the clinical video conferencing telemental health in FY14 when it was compared [with] the utilization in the prior year.
Telehealth Pilot Programs
Dr. Agarwal. I must admit that there are many more programs that begin in the facilities, but at the national level. The first one is the tele-ICU implementation, where VISN 23 is supporting VISN 15, 5 of the medical centers with clinical video teleconferencing capability for live interactive consults with ICU specialists; and it covers about 78 beds. VISN 10 is supporting VISN 7 in 7 of their medical centers, which covers about 72 beds.
Another program, which is in the pilot phase right now, is the telewound care pilot, which is being implemented in 6 VISNs and combines the use of home telehealth, clinical video teleconferencing, and store-and-forward telehealth technologies to create access to a continuum of wound care options across multiple patients and provider settings and locations, all with the goal of enhancing and improving wound care treatment and healing.… The initial phase has been that all the participating facilities have been identified, and some of the operations manuals have been developed.
Related: Acting Surgeon General Confident in Battle Against Tobacco, Ebola, and Preventable Diseases
The third quarter of this year, we will have a completion of the operations manual Provider Training and Treatment Template. The local sites are also working on the infrastructure and knowledge base so that this project can be completed by FY15.
And the last highlight that I’ll mention, which is in its very early stages, is a low-acuity/low-intensity pilot with the focus on health promotion and health prevention behaviors, such as tobacco cessation, weight management, and newly diagnosed but stable veterans with diabetes, high blood pressure, and heart failure, using a web-based browser technology.
VA Telehealth Leadership
Dr. Agarwal. Overall, when we start to look at the monumental impact of technology on other industries, such as banking, shopping, travel, and even personal communications, the emerging technologies continue to change the overall landscape of all these environments. This is an exciting time to be in the health care industry, because I think we have lagged somewhat behind in using technology. But as we look forward, the consumer-driven health care is going to become the norm.
As you know, VA has long been a pioneer with electronic medical records and with virtual modalities, such as telehealth both in the home and in the community, the use of patient web portals, such as My HealtheVet, secure messaging for various apps, kiosks; and we remain on the forefront of developing and utilizing these approaches to enhance health care delivery.
We all know that health care in the U.S. is complex and fragmented. VA is looking to become the benchmark in U.S. health care delivery, aiding in the transformation of the delivery of services for veterans and families, focusing on unified, integrated, and personalized virtual services that seamlessly connect them with the state-of-the-art health care system.
1. Darkins A. A message from the acting chief consultant: telemedicine grows throughout VHA. Telemedicine News. 2001;1(1):1. U.S. Department of Veterans Affairs Website. http://www.telehealth.va.gov/newsletter/2001/040201-newsletter_spring_01.pdf. Published April 2, 2001. Accessed June 23, 2015.
1. Darkins A. A message from the acting chief consultant: telemedicine grows throughout VHA. Telemedicine News. 2001;1(1):1. U.S. Department of Veterans Affairs Website. http://www.telehealth.va.gov/newsletter/2001/040201-newsletter_spring_01.pdf. Published April 2, 2001. Accessed June 23, 2015.

The precarious peril of pay for performance
As a primary care pediatrician, I am often on the front line of mental health care. Because child psychiatric referral services are sparse and overloaded, I often have to initiate counseling for anxiety in many of my patients. One thing that I have learned is that you can help someone with anxiety in a tremendous way by getting them to recognize a simple fact: It is counterproductive to worry about things that we cannot change. We need to acknowledge the things that we can change, the things that we have control over, and recognize that we cannot control everything. This simple truth can lift a tremendous weight.
The “new normal” for physicians entails that our livelihood will be increasingly based on things that we cannot control, thus increasing the anxiety level of an already frazzled profession. I am an advocate for complex case management: I think that it is wasteful to not coordinate resources in the care of a complicated patient. The problem is that, as pediatricians, the vast majority of the patients we treat do not have multiple chronic illnesses and do not fit a paradigm of complex case management. They do, however, have some pretty “nonalgorithmic” things happen to them that do not fit seamlessly into a treatment paradigm. As a primary care pediatrician in Eastern Kentucky, I have many patients whose parents prenatally chose to expose their developing infant to harmful substances and who postnatally continue to make unhealthy choices, despite caring and compassionate counseling.
This concern extends to physicians who take care of older patients who will not quit smoking or refuse to take prescribed medications regularly, etc. At some point, we as a society must acknowledge that there are consequences for our actions. However, we seem to want the freedom to make whatever choices we want and to have someone else bear the burden of the consequences.
Imagine that your local service station was contracted on a “capitated” basis to provide for your vehicle service needs. The station takes great care of your vehicle (and has extended service hours to “accommodate your busy schedule”), but you choose to fill the gas tank with dirty creek water and to randomly shift into reverse while cruising along. Is it the station’s “global package” responsibility to fund and staff an educational team to train you how to take proper care of your vehicle? Or should you bear at least a modicum of responsibility for your irresponsible behavior? In what I can survey, there is no mention of personal responsibility in the “new normal,” where everything is someone else’s fault. Our motto should not be “the patient is always right,” but instead should be “we will always do what is right for the patient.” This can lead to some uncomfortable discussions, that even though artfully and thoughtfully delivered by an “actively listening” physician some patients will not find to their liking and respond with negative “customer satisfaction” surveys.
Another concern with “rewarding” physicians for having “healthy” patients is that many physicians will not want to take care of really sick patients because these cases will “hurt their numbers.” So when the very patients who desperately need a medical home require care the most, where will they go? To the already overloaded emergency department (ED) to receive fragmented care. The same ED bound by Emergency Medical Treatment and Active Labor Act (EMTALA) laws to provide a screening exam or face penalties. Then, when the visit is judged retrospectively to be “nonemergent,” the ED is reimbursed a nonsustainable rate. This is killing rural hospitals. But I get the impression that “fly-over” country doesn’t matter much to the powers that be. This “new normal” looks oddly abnormal to me.
Ish Stevens, M.D.
Ashland Children’s Clinic
Ashland, Ky.
As a primary care pediatrician, I am often on the front line of mental health care. Because child psychiatric referral services are sparse and overloaded, I often have to initiate counseling for anxiety in many of my patients. One thing that I have learned is that you can help someone with anxiety in a tremendous way by getting them to recognize a simple fact: It is counterproductive to worry about things that we cannot change. We need to acknowledge the things that we can change, the things that we have control over, and recognize that we cannot control everything. This simple truth can lift a tremendous weight.
The “new normal” for physicians entails that our livelihood will be increasingly based on things that we cannot control, thus increasing the anxiety level of an already frazzled profession. I am an advocate for complex case management: I think that it is wasteful to not coordinate resources in the care of a complicated patient. The problem is that, as pediatricians, the vast majority of the patients we treat do not have multiple chronic illnesses and do not fit a paradigm of complex case management. They do, however, have some pretty “nonalgorithmic” things happen to them that do not fit seamlessly into a treatment paradigm. As a primary care pediatrician in Eastern Kentucky, I have many patients whose parents prenatally chose to expose their developing infant to harmful substances and who postnatally continue to make unhealthy choices, despite caring and compassionate counseling.
This concern extends to physicians who take care of older patients who will not quit smoking or refuse to take prescribed medications regularly, etc. At some point, we as a society must acknowledge that there are consequences for our actions. However, we seem to want the freedom to make whatever choices we want and to have someone else bear the burden of the consequences.
Imagine that your local service station was contracted on a “capitated” basis to provide for your vehicle service needs. The station takes great care of your vehicle (and has extended service hours to “accommodate your busy schedule”), but you choose to fill the gas tank with dirty creek water and to randomly shift into reverse while cruising along. Is it the station’s “global package” responsibility to fund and staff an educational team to train you how to take proper care of your vehicle? Or should you bear at least a modicum of responsibility for your irresponsible behavior? In what I can survey, there is no mention of personal responsibility in the “new normal,” where everything is someone else’s fault. Our motto should not be “the patient is always right,” but instead should be “we will always do what is right for the patient.” This can lead to some uncomfortable discussions, that even though artfully and thoughtfully delivered by an “actively listening” physician some patients will not find to their liking and respond with negative “customer satisfaction” surveys.
Another concern with “rewarding” physicians for having “healthy” patients is that many physicians will not want to take care of really sick patients because these cases will “hurt their numbers.” So when the very patients who desperately need a medical home require care the most, where will they go? To the already overloaded emergency department (ED) to receive fragmented care. The same ED bound by Emergency Medical Treatment and Active Labor Act (EMTALA) laws to provide a screening exam or face penalties. Then, when the visit is judged retrospectively to be “nonemergent,” the ED is reimbursed a nonsustainable rate. This is killing rural hospitals. But I get the impression that “fly-over” country doesn’t matter much to the powers that be. This “new normal” looks oddly abnormal to me.
Ish Stevens, M.D.
Ashland Children’s Clinic
Ashland, Ky.
As a primary care pediatrician, I am often on the front line of mental health care. Because child psychiatric referral services are sparse and overloaded, I often have to initiate counseling for anxiety in many of my patients. One thing that I have learned is that you can help someone with anxiety in a tremendous way by getting them to recognize a simple fact: It is counterproductive to worry about things that we cannot change. We need to acknowledge the things that we can change, the things that we have control over, and recognize that we cannot control everything. This simple truth can lift a tremendous weight.
The “new normal” for physicians entails that our livelihood will be increasingly based on things that we cannot control, thus increasing the anxiety level of an already frazzled profession. I am an advocate for complex case management: I think that it is wasteful to not coordinate resources in the care of a complicated patient. The problem is that, as pediatricians, the vast majority of the patients we treat do not have multiple chronic illnesses and do not fit a paradigm of complex case management. They do, however, have some pretty “nonalgorithmic” things happen to them that do not fit seamlessly into a treatment paradigm. As a primary care pediatrician in Eastern Kentucky, I have many patients whose parents prenatally chose to expose their developing infant to harmful substances and who postnatally continue to make unhealthy choices, despite caring and compassionate counseling.
This concern extends to physicians who take care of older patients who will not quit smoking or refuse to take prescribed medications regularly, etc. At some point, we as a society must acknowledge that there are consequences for our actions. However, we seem to want the freedom to make whatever choices we want and to have someone else bear the burden of the consequences.
Imagine that your local service station was contracted on a “capitated” basis to provide for your vehicle service needs. The station takes great care of your vehicle (and has extended service hours to “accommodate your busy schedule”), but you choose to fill the gas tank with dirty creek water and to randomly shift into reverse while cruising along. Is it the station’s “global package” responsibility to fund and staff an educational team to train you how to take proper care of your vehicle? Or should you bear at least a modicum of responsibility for your irresponsible behavior? In what I can survey, there is no mention of personal responsibility in the “new normal,” where everything is someone else’s fault. Our motto should not be “the patient is always right,” but instead should be “we will always do what is right for the patient.” This can lead to some uncomfortable discussions, that even though artfully and thoughtfully delivered by an “actively listening” physician some patients will not find to their liking and respond with negative “customer satisfaction” surveys.
Another concern with “rewarding” physicians for having “healthy” patients is that many physicians will not want to take care of really sick patients because these cases will “hurt their numbers.” So when the very patients who desperately need a medical home require care the most, where will they go? To the already overloaded emergency department (ED) to receive fragmented care. The same ED bound by Emergency Medical Treatment and Active Labor Act (EMTALA) laws to provide a screening exam or face penalties. Then, when the visit is judged retrospectively to be “nonemergent,” the ED is reimbursed a nonsustainable rate. This is killing rural hospitals. But I get the impression that “fly-over” country doesn’t matter much to the powers that be. This “new normal” looks oddly abnormal to me.
Ish Stevens, M.D.
Ashland Children’s Clinic
Ashland, Ky.
Sticks and stones: Navigating patient satisfaction scores
There is an old saying, “Sticks and stones may break my bones, but words will never hurt me.” When it comes to our patients’ impressions of us, nothing could be farther from the truth. As a matter of fact, their words, expressed in post-discharge patient satisfaction surveys, can play a tremendous role in the financial stability of our hospitals.
Throughout the years, hospitals have employed a wide variety of methods to evaluate their patients’ experiences, if only to improve their service and strengthen their brand. The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) initiative has taken patient satisfaction to a new level by creating the first national, standardized survey tool to measure patients’ perspectives of the care they received while hospitalized. In addition, HCAHPS was designed to provide objective, meaningful comparisons of hospitals, and these comparisons are publicly reported, which increases transparency of the quality of care provided to hospitalized patients.
The survey is administered between 48 hours and 6 weeks post discharge to a random sample of adult patients by mail, telephone, mail and telephone, or Interactive Voice Response (IVR). Discharged patients are asked 27 questions about their recent hospitalization including communication with doctors and nurses, pain management, discharge information, communication about medication, overall hospital rating, and whether they would recommend the hospital to others.
Four times per year, the Centers for Medicaid & Medicare Services publishes HCAHPS scores of participating hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov), though the survey is not restricted to Medicare patients. Patients can pick and choose which hospitals they like, and which ones they would avoid like the plague.
Of course, it’s not realistic to think that we are going to please all of our patients all of the time, but this initiative does have the potential to create a new sense of accountability, as well as competitiveness for hospital systems and providers alike. No one wants to be at the bottom of the pack.
So, how do we increase our scores? Many models and companies claim to help improve patient satisfaction. Just do an Internet search. Keep in mind, what works well for one group may be ineffective for another.
For instance, 5-minute per patient multidisciplinary bedside rounding – including the provider, nurse, pharmacist, and case manager – may be easy to implement and skyrocket patient satisfaction in some institutions. In others, getting appropriate staffing may be prohibitive. Regardless of the approach that may be right for your group, it is important to keep in mind that the tide of health care is ever changing. Patients are demanding, and receiving, a bigger role in their health care. We all want to be in the forefront, not at the tail end, of that tide.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at [email protected].
There is an old saying, “Sticks and stones may break my bones, but words will never hurt me.” When it comes to our patients’ impressions of us, nothing could be farther from the truth. As a matter of fact, their words, expressed in post-discharge patient satisfaction surveys, can play a tremendous role in the financial stability of our hospitals.
Throughout the years, hospitals have employed a wide variety of methods to evaluate their patients’ experiences, if only to improve their service and strengthen their brand. The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) initiative has taken patient satisfaction to a new level by creating the first national, standardized survey tool to measure patients’ perspectives of the care they received while hospitalized. In addition, HCAHPS was designed to provide objective, meaningful comparisons of hospitals, and these comparisons are publicly reported, which increases transparency of the quality of care provided to hospitalized patients.
The survey is administered between 48 hours and 6 weeks post discharge to a random sample of adult patients by mail, telephone, mail and telephone, or Interactive Voice Response (IVR). Discharged patients are asked 27 questions about their recent hospitalization including communication with doctors and nurses, pain management, discharge information, communication about medication, overall hospital rating, and whether they would recommend the hospital to others.
Four times per year, the Centers for Medicaid & Medicare Services publishes HCAHPS scores of participating hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov), though the survey is not restricted to Medicare patients. Patients can pick and choose which hospitals they like, and which ones they would avoid like the plague.
Of course, it’s not realistic to think that we are going to please all of our patients all of the time, but this initiative does have the potential to create a new sense of accountability, as well as competitiveness for hospital systems and providers alike. No one wants to be at the bottom of the pack.
So, how do we increase our scores? Many models and companies claim to help improve patient satisfaction. Just do an Internet search. Keep in mind, what works well for one group may be ineffective for another.
For instance, 5-minute per patient multidisciplinary bedside rounding – including the provider, nurse, pharmacist, and case manager – may be easy to implement and skyrocket patient satisfaction in some institutions. In others, getting appropriate staffing may be prohibitive. Regardless of the approach that may be right for your group, it is important to keep in mind that the tide of health care is ever changing. Patients are demanding, and receiving, a bigger role in their health care. We all want to be in the forefront, not at the tail end, of that tide.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at [email protected].
There is an old saying, “Sticks and stones may break my bones, but words will never hurt me.” When it comes to our patients’ impressions of us, nothing could be farther from the truth. As a matter of fact, their words, expressed in post-discharge patient satisfaction surveys, can play a tremendous role in the financial stability of our hospitals.
Throughout the years, hospitals have employed a wide variety of methods to evaluate their patients’ experiences, if only to improve their service and strengthen their brand. The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) initiative has taken patient satisfaction to a new level by creating the first national, standardized survey tool to measure patients’ perspectives of the care they received while hospitalized. In addition, HCAHPS was designed to provide objective, meaningful comparisons of hospitals, and these comparisons are publicly reported, which increases transparency of the quality of care provided to hospitalized patients.
The survey is administered between 48 hours and 6 weeks post discharge to a random sample of adult patients by mail, telephone, mail and telephone, or Interactive Voice Response (IVR). Discharged patients are asked 27 questions about their recent hospitalization including communication with doctors and nurses, pain management, discharge information, communication about medication, overall hospital rating, and whether they would recommend the hospital to others.
Four times per year, the Centers for Medicaid & Medicare Services publishes HCAHPS scores of participating hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov), though the survey is not restricted to Medicare patients. Patients can pick and choose which hospitals they like, and which ones they would avoid like the plague.
Of course, it’s not realistic to think that we are going to please all of our patients all of the time, but this initiative does have the potential to create a new sense of accountability, as well as competitiveness for hospital systems and providers alike. No one wants to be at the bottom of the pack.
So, how do we increase our scores? Many models and companies claim to help improve patient satisfaction. Just do an Internet search. Keep in mind, what works well for one group may be ineffective for another.
For instance, 5-minute per patient multidisciplinary bedside rounding – including the provider, nurse, pharmacist, and case manager – may be easy to implement and skyrocket patient satisfaction in some institutions. In others, getting appropriate staffing may be prohibitive. Regardless of the approach that may be right for your group, it is important to keep in mind that the tide of health care is ever changing. Patients are demanding, and receiving, a bigger role in their health care. We all want to be in the forefront, not at the tail end, of that tide.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at [email protected].
