User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Proposed TNM update could shift staging for lung cancers
The updates for the 9th edition of the TNM Classification of Malignant Tumors: Lung Cancer were presented at the annual World Conference on Lung Cancer. The final version will be published Jan. 1, 2024.
The core proposed change, according to Hisao Asamura, MD, chair of the IASLC Staging and Prognostic Factors Committee, is to divide N2 and M1c disease into two subcategories, while leaving the T descriptors unchanged.
This update is based on large survival differences among patients with these tumor characteristics, following an analysis of outcomes in more than 87,000 individuals diagnosed with lung cancer.
Session cochair Ramón Rami-Porta, MD, PhD, explained that previous editions of the classification were based on “pathologic stage, not clinical stage” but ultimately “we could not validate those findings” clinically.
“This is the first time that some sort of very simple quantification” of lung tumors “could be validated at the clinical stage as well,” which means that clinical staging can improve all over the world, said Dr. Rami-Porta, medical oncologist at Hospital Universitari Mútua Terrassa (Spain).
Session cochair Paul Van Schil, MD, PhD, of Antwerp (the Netherlands) University Hospital explained that the proposed changes reflect what clinicians already see in their daily practice.
The latest TNM classification included data submitted on 124,581 patients diagnosed with lung cancer between 2011 and 2019, 56% of whom were from Asia/Australia, 25% from Europe, and 16% from North America.
Overall, 87,339 patients were included in the analysis – 83% with non–small cell lung cancer (NSCLC) and 7% with small cell lung cancer (SCLC). Most (62%) underwent surgery, either alone (47%), alongside chemotherapy (13%), or plus radiotherapy (2%). A minority (13%) received chemotherapy alone, and 13% received all three modalities.
The committee working on the update to the TNM classification had 112 members and comprised 14 subcommittees, which focused on different aspects of diagnosing and assessing the disease.
The committee agreed there should be no changes to the T category in the upcoming 9th Edition.
Evaluating the T category, some members expressed concern that patients with T3 disease embedded in the chest wall have worse survival outcomes than those with other forms of T3 disease. But, Dr. Asamura explained, the pathological versus clinical findings were inconsistent.
On pathological assessment, patients with T3 disease in the chest wall had a worse prognosis but clinical assessment indicated no survival difference. Given the lack of consensus, “we do not recommend any changes” to the current criteria, said Dr. Asamura.
Turning to the N category, Dr. Asamura explained that N2 disease will be divided into two subcategories: N2a, categorized by single N2 station involvement, and N2b, defined as multiple N2 station involvement.
Further analysis indicated that the estimated 5-year survival was significantly worse for patients with N2b disease on clinical assessment (31% vs. 42% with N2a disease; hazard ratio for death, 1.27; P < .0001) and on pathological assessment (HR, 1.46; P < .0001).
The committee also proposed a change to the M category, dividing M1c disease into two subcategories:
- M1c1 – defined as multiple extrathoracic metastases in a single organ system
- M1c2 – defined as multiple extrathoracic metastases in multiple organ systems
This change was driven by estimates of 5-year survival among patients with M1c1 (27%) versus M1c2 disease (19%). Compared with M1b disease, M1c1 was associated with a lower risk for death than M1c2 disease (HR, 1.27 vs. 1.39).
These changes, particularly those for the N category, will have a notable impact on how patients are staged, Dr. Asamura said.
Dividing the N2 category into N2a and N2b disease will push patients with T1, N1 disease from the IIB category (8th edition) to the IIA category (9th edition). The 8th edition categorized all T1, N2 patients as IIIA but the new edition would categorize patients with T1, N2a disease as IIB overall and those with N2b disease as IIIA. And patients with T2, N2a disease will be staged as IIIA — the same category as T2, N2 disease in the 8th edition – while those with N2b disease will be staged as IIIB.
By contrast, the division of M1c into M1c1 and M1c2 disease will not affect a patient’s overall stage, which will be IVB in all cases.
Upal Basu Roy, PhD, MPH, who was not part of the committee, said the TNM classification stage of cancers is “incredibly important in cataloguing the extent of disease” and to “decide the optimal treatment option.”
TNM classification is also “used to describe the burden of disease to be eligible for a clinical trial,” said Dr. Roy, executive director of research, LUNGevity Foundation, Chicago.
The changes in N staging may require sampling more lymph nodes than the current sampling frame of six, Dr. Roy said, adding that “surgeons and pathologists may need to be educated about the need for additional sampling.”
The subcategories for M1c disease will also need to be aligned with definitions of oligometastatic disease. “This is critical,” Dr. Roy said, as this staging may affect treatment choices.
No funding was declared. Dr. Asamura declares relationships with Medtronic, Taiho Pharmaceutical, Johnson & Johnson, Lily, Astellas, and Ono Pharmaceutical. Dr. Roy declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The updates for the 9th edition of the TNM Classification of Malignant Tumors: Lung Cancer were presented at the annual World Conference on Lung Cancer. The final version will be published Jan. 1, 2024.
The core proposed change, according to Hisao Asamura, MD, chair of the IASLC Staging and Prognostic Factors Committee, is to divide N2 and M1c disease into two subcategories, while leaving the T descriptors unchanged.
This update is based on large survival differences among patients with these tumor characteristics, following an analysis of outcomes in more than 87,000 individuals diagnosed with lung cancer.
Session cochair Ramón Rami-Porta, MD, PhD, explained that previous editions of the classification were based on “pathologic stage, not clinical stage” but ultimately “we could not validate those findings” clinically.
“This is the first time that some sort of very simple quantification” of lung tumors “could be validated at the clinical stage as well,” which means that clinical staging can improve all over the world, said Dr. Rami-Porta, medical oncologist at Hospital Universitari Mútua Terrassa (Spain).
Session cochair Paul Van Schil, MD, PhD, of Antwerp (the Netherlands) University Hospital explained that the proposed changes reflect what clinicians already see in their daily practice.
The latest TNM classification included data submitted on 124,581 patients diagnosed with lung cancer between 2011 and 2019, 56% of whom were from Asia/Australia, 25% from Europe, and 16% from North America.
Overall, 87,339 patients were included in the analysis – 83% with non–small cell lung cancer (NSCLC) and 7% with small cell lung cancer (SCLC). Most (62%) underwent surgery, either alone (47%), alongside chemotherapy (13%), or plus radiotherapy (2%). A minority (13%) received chemotherapy alone, and 13% received all three modalities.
The committee working on the update to the TNM classification had 112 members and comprised 14 subcommittees, which focused on different aspects of diagnosing and assessing the disease.
The committee agreed there should be no changes to the T category in the upcoming 9th Edition.
Evaluating the T category, some members expressed concern that patients with T3 disease embedded in the chest wall have worse survival outcomes than those with other forms of T3 disease. But, Dr. Asamura explained, the pathological versus clinical findings were inconsistent.
On pathological assessment, patients with T3 disease in the chest wall had a worse prognosis but clinical assessment indicated no survival difference. Given the lack of consensus, “we do not recommend any changes” to the current criteria, said Dr. Asamura.
Turning to the N category, Dr. Asamura explained that N2 disease will be divided into two subcategories: N2a, categorized by single N2 station involvement, and N2b, defined as multiple N2 station involvement.
Further analysis indicated that the estimated 5-year survival was significantly worse for patients with N2b disease on clinical assessment (31% vs. 42% with N2a disease; hazard ratio for death, 1.27; P < .0001) and on pathological assessment (HR, 1.46; P < .0001).
The committee also proposed a change to the M category, dividing M1c disease into two subcategories:
- M1c1 – defined as multiple extrathoracic metastases in a single organ system
- M1c2 – defined as multiple extrathoracic metastases in multiple organ systems
This change was driven by estimates of 5-year survival among patients with M1c1 (27%) versus M1c2 disease (19%). Compared with M1b disease, M1c1 was associated with a lower risk for death than M1c2 disease (HR, 1.27 vs. 1.39).
These changes, particularly those for the N category, will have a notable impact on how patients are staged, Dr. Asamura said.
Dividing the N2 category into N2a and N2b disease will push patients with T1, N1 disease from the IIB category (8th edition) to the IIA category (9th edition). The 8th edition categorized all T1, N2 patients as IIIA but the new edition would categorize patients with T1, N2a disease as IIB overall and those with N2b disease as IIIA. And patients with T2, N2a disease will be staged as IIIA — the same category as T2, N2 disease in the 8th edition – while those with N2b disease will be staged as IIIB.
By contrast, the division of M1c into M1c1 and M1c2 disease will not affect a patient’s overall stage, which will be IVB in all cases.
Upal Basu Roy, PhD, MPH, who was not part of the committee, said the TNM classification stage of cancers is “incredibly important in cataloguing the extent of disease” and to “decide the optimal treatment option.”
TNM classification is also “used to describe the burden of disease to be eligible for a clinical trial,” said Dr. Roy, executive director of research, LUNGevity Foundation, Chicago.
The changes in N staging may require sampling more lymph nodes than the current sampling frame of six, Dr. Roy said, adding that “surgeons and pathologists may need to be educated about the need for additional sampling.”
The subcategories for M1c disease will also need to be aligned with definitions of oligometastatic disease. “This is critical,” Dr. Roy said, as this staging may affect treatment choices.
No funding was declared. Dr. Asamura declares relationships with Medtronic, Taiho Pharmaceutical, Johnson & Johnson, Lily, Astellas, and Ono Pharmaceutical. Dr. Roy declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The updates for the 9th edition of the TNM Classification of Malignant Tumors: Lung Cancer were presented at the annual World Conference on Lung Cancer. The final version will be published Jan. 1, 2024.
The core proposed change, according to Hisao Asamura, MD, chair of the IASLC Staging and Prognostic Factors Committee, is to divide N2 and M1c disease into two subcategories, while leaving the T descriptors unchanged.
This update is based on large survival differences among patients with these tumor characteristics, following an analysis of outcomes in more than 87,000 individuals diagnosed with lung cancer.
Session cochair Ramón Rami-Porta, MD, PhD, explained that previous editions of the classification were based on “pathologic stage, not clinical stage” but ultimately “we could not validate those findings” clinically.
“This is the first time that some sort of very simple quantification” of lung tumors “could be validated at the clinical stage as well,” which means that clinical staging can improve all over the world, said Dr. Rami-Porta, medical oncologist at Hospital Universitari Mútua Terrassa (Spain).
Session cochair Paul Van Schil, MD, PhD, of Antwerp (the Netherlands) University Hospital explained that the proposed changes reflect what clinicians already see in their daily practice.
The latest TNM classification included data submitted on 124,581 patients diagnosed with lung cancer between 2011 and 2019, 56% of whom were from Asia/Australia, 25% from Europe, and 16% from North America.
Overall, 87,339 patients were included in the analysis – 83% with non–small cell lung cancer (NSCLC) and 7% with small cell lung cancer (SCLC). Most (62%) underwent surgery, either alone (47%), alongside chemotherapy (13%), or plus radiotherapy (2%). A minority (13%) received chemotherapy alone, and 13% received all three modalities.
The committee working on the update to the TNM classification had 112 members and comprised 14 subcommittees, which focused on different aspects of diagnosing and assessing the disease.
The committee agreed there should be no changes to the T category in the upcoming 9th Edition.
Evaluating the T category, some members expressed concern that patients with T3 disease embedded in the chest wall have worse survival outcomes than those with other forms of T3 disease. But, Dr. Asamura explained, the pathological versus clinical findings were inconsistent.
On pathological assessment, patients with T3 disease in the chest wall had a worse prognosis but clinical assessment indicated no survival difference. Given the lack of consensus, “we do not recommend any changes” to the current criteria, said Dr. Asamura.
Turning to the N category, Dr. Asamura explained that N2 disease will be divided into two subcategories: N2a, categorized by single N2 station involvement, and N2b, defined as multiple N2 station involvement.
Further analysis indicated that the estimated 5-year survival was significantly worse for patients with N2b disease on clinical assessment (31% vs. 42% with N2a disease; hazard ratio for death, 1.27; P < .0001) and on pathological assessment (HR, 1.46; P < .0001).
The committee also proposed a change to the M category, dividing M1c disease into two subcategories:
- M1c1 – defined as multiple extrathoracic metastases in a single organ system
- M1c2 – defined as multiple extrathoracic metastases in multiple organ systems
This change was driven by estimates of 5-year survival among patients with M1c1 (27%) versus M1c2 disease (19%). Compared with M1b disease, M1c1 was associated with a lower risk for death than M1c2 disease (HR, 1.27 vs. 1.39).
These changes, particularly those for the N category, will have a notable impact on how patients are staged, Dr. Asamura said.
Dividing the N2 category into N2a and N2b disease will push patients with T1, N1 disease from the IIB category (8th edition) to the IIA category (9th edition). The 8th edition categorized all T1, N2 patients as IIIA but the new edition would categorize patients with T1, N2a disease as IIB overall and those with N2b disease as IIIA. And patients with T2, N2a disease will be staged as IIIA — the same category as T2, N2 disease in the 8th edition – while those with N2b disease will be staged as IIIB.
By contrast, the division of M1c into M1c1 and M1c2 disease will not affect a patient’s overall stage, which will be IVB in all cases.
Upal Basu Roy, PhD, MPH, who was not part of the committee, said the TNM classification stage of cancers is “incredibly important in cataloguing the extent of disease” and to “decide the optimal treatment option.”
TNM classification is also “used to describe the burden of disease to be eligible for a clinical trial,” said Dr. Roy, executive director of research, LUNGevity Foundation, Chicago.
The changes in N staging may require sampling more lymph nodes than the current sampling frame of six, Dr. Roy said, adding that “surgeons and pathologists may need to be educated about the need for additional sampling.”
The subcategories for M1c disease will also need to be aligned with definitions of oligometastatic disease. “This is critical,” Dr. Roy said, as this staging may affect treatment choices.
No funding was declared. Dr. Asamura declares relationships with Medtronic, Taiho Pharmaceutical, Johnson & Johnson, Lily, Astellas, and Ono Pharmaceutical. Dr. Roy declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM WCLC 2023
Neoadjuvant durvalumab does not affect surgical outcomes in NSCLC: Study
, according to the most recent analysis of data from the phase 3 AEGEAN study.
“In terms of cancellation of surgery, surgical delay, surgically related adverse events, complications, operation time, and operation procedure, there was no difference between the durvalumab group and the placebo group. In addition, the R0 resection rate was numerically higher in the durvalumab group. These [results] indicate that adding perioperative durvalumab did not adversely affect surgical outcomes,” wrote Tetsuya Mitsudomi, MD, PhD, who presented the new results at the annual World Conference on Lung Cancer, in an email. The topline results of AEGEAN were presented earlier this year at AACR 2023, which showed that the regimen combined with adjuvant durvalumab improved event-free survival (EFS) and pathologic complete response (pCR), compared with chemotherapy plus placebo.
Dr. Mitsudomi also pointed out that AEGEAN is one of the first studies looking at immune checkpoint inhibitors (ICI) in the perioperative settings that demonstrated improved EFS and pCR with no effect on surgical outcomes. Previously, the CheckMate 816 study demonstrated efficacy of neoadjuvant ICI alone.
“The AEGEAN study showed that neoadjuvant plus adjuvant ICI is another option for these patients. However, no one knows who should receive the postoperative ICI in addition to neoadjuvant ICI, because there are no trials including ongoing ones that ask this question,” wrote Dr. Mitsudomi.
The phase 3 AEGEAN study included 740 patients who were randomized to durvalumab or placebo. The median age was 65.0 years in both groups, and 33.3% and 33.4% of patients in each group respectively had fewer than 1% of tumor cells that expressed PD-L1. Expression in 1-49% of tumor cells occurred in 36.9% and 38.0% respectively, and expression ≥ 50% occurred in 29.8% and 28.6%.
Prior to surgery, 84.7% of the durvalumab arm completed four cycles of chemotherapy, as did 87.2% in the placebo arm. The proportion of patients undergoing surgery was 80.6% and 80.7% in the two arms, respectively, and surgical completion was achieved in 77.6% and 76.7%. The durvalumab arm and placebo arm had similar median times from last neoadjuvant treatment to surgery (34.0 days for both) and median time from surgery to first adjuvant dose (50.0 versus 52.0 days).
Among patients with stage II NSCLC, 84.3% in the durvalumab arm underwent surgery, versus 88.9% in the placebo arm. Among patients with stage III disease, the numbers were 79.2% and 77.4%, respectively. There was no surgical delay in 82.7% of patients in the durvalumab arm, compared with 77.8% in the placebo arm. The most common reason for surgical delay was logistical reasons. Mediastinal lymph node dissection was completed in 86.6% of the durvalumab arm and 84.7% of the placebo arm. In both groups where surgery was completed, R0 resection rates were over 90% overall as well as in both stage I and stage II patients. Following surgery, adverse events possibly related to surgery occurred in 40.2% of the durvalumab group and 39.2% of the placebo group. The most common surgical adverse events occurred at similar frequency between groups.
After the presentation, Solange Peters, MD, PhD, served as a discussant. She pointed out other studies that have examined ICI therapy for NSCLC in both the neoadjuvant and adjuvant setting, including Keynote-671 (pembrolizumab), Neotorch (toripalimab), CheckMate 77T (nivolumab), and Impower030 (atezolizumab). She pointed out that AEGEAN, Keynote-671, CheckMate 816, and NeoTorch all had similar trial designs and showed similar magnitude of benefit. “We have a growing paradigm [for combining neoadjuvant and adjuvant ICI therapy]. We are quite all convinced in the community that there is a biological rationale to use neoadjuvant immunotherapy because of the fit immune system, because of the presence of the neoantigens within the tumor at the time of the start of neoadjuvant treatment, [leading to] better priming of immune cells,” said Dr. Peters, who is a professor of medical oncology at University Hospital of Lausanne, Switzerland.
About one in five patients across the trials who would be eligible for surgery never undergo it, but there is promising data from CheckMate 816 that neoadjuvant ICB may improve the odds of surgery, according to Dr. Solange. The AEGEAN data produced some “quite interesting” data about the reasons that patients don’t make it to surgery, as it showed that 8%-10% of patients don’t reach surgery because of progression, but 10%-15% may fall out because they turned out not to be a good candidate for surgery. “I think we probably have to blame the enthusiasm we have to add all these patients into the trial, hoping for the best for the patient but maybe making a wrong selection,” said Dr. Peters.
The study was funded by AstraZeneca. Dr. Mitsudomi has received speaker fees, honoraria, or research funding from AstraZeneca, Chugai, Ono, Bristol Myers Squibb, and MSD. Dr. Peters has financial relationships with AstraZeneca as well as a wide range of other pharmaceutical companies.
, according to the most recent analysis of data from the phase 3 AEGEAN study.
“In terms of cancellation of surgery, surgical delay, surgically related adverse events, complications, operation time, and operation procedure, there was no difference between the durvalumab group and the placebo group. In addition, the R0 resection rate was numerically higher in the durvalumab group. These [results] indicate that adding perioperative durvalumab did not adversely affect surgical outcomes,” wrote Tetsuya Mitsudomi, MD, PhD, who presented the new results at the annual World Conference on Lung Cancer, in an email. The topline results of AEGEAN were presented earlier this year at AACR 2023, which showed that the regimen combined with adjuvant durvalumab improved event-free survival (EFS) and pathologic complete response (pCR), compared with chemotherapy plus placebo.
Dr. Mitsudomi also pointed out that AEGEAN is one of the first studies looking at immune checkpoint inhibitors (ICI) in the perioperative settings that demonstrated improved EFS and pCR with no effect on surgical outcomes. Previously, the CheckMate 816 study demonstrated efficacy of neoadjuvant ICI alone.
“The AEGEAN study showed that neoadjuvant plus adjuvant ICI is another option for these patients. However, no one knows who should receive the postoperative ICI in addition to neoadjuvant ICI, because there are no trials including ongoing ones that ask this question,” wrote Dr. Mitsudomi.
The phase 3 AEGEAN study included 740 patients who were randomized to durvalumab or placebo. The median age was 65.0 years in both groups, and 33.3% and 33.4% of patients in each group respectively had fewer than 1% of tumor cells that expressed PD-L1. Expression in 1-49% of tumor cells occurred in 36.9% and 38.0% respectively, and expression ≥ 50% occurred in 29.8% and 28.6%.
Prior to surgery, 84.7% of the durvalumab arm completed four cycles of chemotherapy, as did 87.2% in the placebo arm. The proportion of patients undergoing surgery was 80.6% and 80.7% in the two arms, respectively, and surgical completion was achieved in 77.6% and 76.7%. The durvalumab arm and placebo arm had similar median times from last neoadjuvant treatment to surgery (34.0 days for both) and median time from surgery to first adjuvant dose (50.0 versus 52.0 days).
Among patients with stage II NSCLC, 84.3% in the durvalumab arm underwent surgery, versus 88.9% in the placebo arm. Among patients with stage III disease, the numbers were 79.2% and 77.4%, respectively. There was no surgical delay in 82.7% of patients in the durvalumab arm, compared with 77.8% in the placebo arm. The most common reason for surgical delay was logistical reasons. Mediastinal lymph node dissection was completed in 86.6% of the durvalumab arm and 84.7% of the placebo arm. In both groups where surgery was completed, R0 resection rates were over 90% overall as well as in both stage I and stage II patients. Following surgery, adverse events possibly related to surgery occurred in 40.2% of the durvalumab group and 39.2% of the placebo group. The most common surgical adverse events occurred at similar frequency between groups.
After the presentation, Solange Peters, MD, PhD, served as a discussant. She pointed out other studies that have examined ICI therapy for NSCLC in both the neoadjuvant and adjuvant setting, including Keynote-671 (pembrolizumab), Neotorch (toripalimab), CheckMate 77T (nivolumab), and Impower030 (atezolizumab). She pointed out that AEGEAN, Keynote-671, CheckMate 816, and NeoTorch all had similar trial designs and showed similar magnitude of benefit. “We have a growing paradigm [for combining neoadjuvant and adjuvant ICI therapy]. We are quite all convinced in the community that there is a biological rationale to use neoadjuvant immunotherapy because of the fit immune system, because of the presence of the neoantigens within the tumor at the time of the start of neoadjuvant treatment, [leading to] better priming of immune cells,” said Dr. Peters, who is a professor of medical oncology at University Hospital of Lausanne, Switzerland.
About one in five patients across the trials who would be eligible for surgery never undergo it, but there is promising data from CheckMate 816 that neoadjuvant ICB may improve the odds of surgery, according to Dr. Solange. The AEGEAN data produced some “quite interesting” data about the reasons that patients don’t make it to surgery, as it showed that 8%-10% of patients don’t reach surgery because of progression, but 10%-15% may fall out because they turned out not to be a good candidate for surgery. “I think we probably have to blame the enthusiasm we have to add all these patients into the trial, hoping for the best for the patient but maybe making a wrong selection,” said Dr. Peters.
The study was funded by AstraZeneca. Dr. Mitsudomi has received speaker fees, honoraria, or research funding from AstraZeneca, Chugai, Ono, Bristol Myers Squibb, and MSD. Dr. Peters has financial relationships with AstraZeneca as well as a wide range of other pharmaceutical companies.
, according to the most recent analysis of data from the phase 3 AEGEAN study.
“In terms of cancellation of surgery, surgical delay, surgically related adverse events, complications, operation time, and operation procedure, there was no difference between the durvalumab group and the placebo group. In addition, the R0 resection rate was numerically higher in the durvalumab group. These [results] indicate that adding perioperative durvalumab did not adversely affect surgical outcomes,” wrote Tetsuya Mitsudomi, MD, PhD, who presented the new results at the annual World Conference on Lung Cancer, in an email. The topline results of AEGEAN were presented earlier this year at AACR 2023, which showed that the regimen combined with adjuvant durvalumab improved event-free survival (EFS) and pathologic complete response (pCR), compared with chemotherapy plus placebo.
Dr. Mitsudomi also pointed out that AEGEAN is one of the first studies looking at immune checkpoint inhibitors (ICI) in the perioperative settings that demonstrated improved EFS and pCR with no effect on surgical outcomes. Previously, the CheckMate 816 study demonstrated efficacy of neoadjuvant ICI alone.
“The AEGEAN study showed that neoadjuvant plus adjuvant ICI is another option for these patients. However, no one knows who should receive the postoperative ICI in addition to neoadjuvant ICI, because there are no trials including ongoing ones that ask this question,” wrote Dr. Mitsudomi.
The phase 3 AEGEAN study included 740 patients who were randomized to durvalumab or placebo. The median age was 65.0 years in both groups, and 33.3% and 33.4% of patients in each group respectively had fewer than 1% of tumor cells that expressed PD-L1. Expression in 1-49% of tumor cells occurred in 36.9% and 38.0% respectively, and expression ≥ 50% occurred in 29.8% and 28.6%.
Prior to surgery, 84.7% of the durvalumab arm completed four cycles of chemotherapy, as did 87.2% in the placebo arm. The proportion of patients undergoing surgery was 80.6% and 80.7% in the two arms, respectively, and surgical completion was achieved in 77.6% and 76.7%. The durvalumab arm and placebo arm had similar median times from last neoadjuvant treatment to surgery (34.0 days for both) and median time from surgery to first adjuvant dose (50.0 versus 52.0 days).
Among patients with stage II NSCLC, 84.3% in the durvalumab arm underwent surgery, versus 88.9% in the placebo arm. Among patients with stage III disease, the numbers were 79.2% and 77.4%, respectively. There was no surgical delay in 82.7% of patients in the durvalumab arm, compared with 77.8% in the placebo arm. The most common reason for surgical delay was logistical reasons. Mediastinal lymph node dissection was completed in 86.6% of the durvalumab arm and 84.7% of the placebo arm. In both groups where surgery was completed, R0 resection rates were over 90% overall as well as in both stage I and stage II patients. Following surgery, adverse events possibly related to surgery occurred in 40.2% of the durvalumab group and 39.2% of the placebo group. The most common surgical adverse events occurred at similar frequency between groups.
After the presentation, Solange Peters, MD, PhD, served as a discussant. She pointed out other studies that have examined ICI therapy for NSCLC in both the neoadjuvant and adjuvant setting, including Keynote-671 (pembrolizumab), Neotorch (toripalimab), CheckMate 77T (nivolumab), and Impower030 (atezolizumab). She pointed out that AEGEAN, Keynote-671, CheckMate 816, and NeoTorch all had similar trial designs and showed similar magnitude of benefit. “We have a growing paradigm [for combining neoadjuvant and adjuvant ICI therapy]. We are quite all convinced in the community that there is a biological rationale to use neoadjuvant immunotherapy because of the fit immune system, because of the presence of the neoantigens within the tumor at the time of the start of neoadjuvant treatment, [leading to] better priming of immune cells,” said Dr. Peters, who is a professor of medical oncology at University Hospital of Lausanne, Switzerland.
About one in five patients across the trials who would be eligible for surgery never undergo it, but there is promising data from CheckMate 816 that neoadjuvant ICB may improve the odds of surgery, according to Dr. Solange. The AEGEAN data produced some “quite interesting” data about the reasons that patients don’t make it to surgery, as it showed that 8%-10% of patients don’t reach surgery because of progression, but 10%-15% may fall out because they turned out not to be a good candidate for surgery. “I think we probably have to blame the enthusiasm we have to add all these patients into the trial, hoping for the best for the patient but maybe making a wrong selection,” said Dr. Peters.
The study was funded by AstraZeneca. Dr. Mitsudomi has received speaker fees, honoraria, or research funding from AstraZeneca, Chugai, Ono, Bristol Myers Squibb, and MSD. Dr. Peters has financial relationships with AstraZeneca as well as a wide range of other pharmaceutical companies.
FROM WCLC 2023
Debate: Should smoldering myeloma be treated?
Hematologist Sagar Lonial, MD, a multiple myeloma specialist and researcher at Emory University, Atlanta, argued for treatment. Hematologist Angela Dispenzieri, MD, also a myeloma researcher and specialist at the Mayo Clinic in Rochester, Minn., took the opposing side, arguing for watchful waiting.
The two experts based their arguments largely on the same two studies, the only randomized trials to tackle the issue to date. While Dr. Dispenzieri focused on their shortcomings, Dr. Lonial focused on their strengths.
In a poll after the debate, about a third of audience members agreed that watchful waiting is the way to go, but about two-thirds favored a personalized approach to smoldering myeloma treatment based on patient risk.
“I’m taking this as a win,” Dr. Lonial said.
Different interpretations of two trials
The first of the two trials recruited from 2007 to 2010 and was conducted in Spain and Portugal. Fifty-seven high-risk patients were randomized to lenalidomide plus dexamethasone (Len-Dex) for up to 2 years; 62 others were randomized to observation.
At 3 years, 70% of observed patients had progressed to multiple myeloma versus only 20% in the Len-Dex group; 82% of Len-Dex patients were alive at data cut-off in 2015 versus 64% of observation patients.
The second, more recent trial, which was led by Dr. Lonial, randomized 92 intermediate or high-risk smoldering myeloma patients to lenalidomide alone for a median of 2 years and 90 others to observation. Three-year progression-free survival (PFS) was 91% in the treatment arm versus 66% with observation. Overall survival data have not yet been reported.
Dr. Dispenzieri acknowledged that the results from Spain and Portugal are impressive. “Treating with Len-Dex gives you a far superior freedom from progression. ... Overall survival was better too.” Results for Len-Dex were “fantastic,” she said.
However, the trial was done before myeloma-defining event criteria existed, so it’s very likely that the treatment arm in the Spanish study included actual myeloma cases, she said.
About 46% of treated patients in Dr. Lonial’s study met the current definition for high risk for progression based on the 2-20-20 rule, which Dr. Dispenzieri helped develop. Although there was an improvement in PFS in the high-risk group, there was no significant improvement for intermediate- and low-risk subjects. Also, more than 80% of observed patients hadn’t progressed by 2 years, and overall survival data are missing.
Meanwhile, treated patients in both trials had more adverse events, including secondary malignancies, and there’s the possibility that early treatment may make patients resistant to treatment later on when they progress to multiple myeloma, although that didn’t seem to happen in the Spanish trial.
“Of course, we want to prevent morbidity, of course we would love to cure the disease,” but “should we treat high-risk smoldering myeloma patients based on overall survival data from a trial of” just 119 “patients that may have been contaminated with actual myeloma” cases? Is it ethical to treat low- and intermediate-risk patients who have only a 50% chance of developing myeloma after 10 years?”
Her answer to both questions was “no and no. ... There’s just a lot of work to be done” to better understand the condition and when and how to intervene. In the meantime, “don’t treat smoldering melanoma patients” outside of a trial, she said.
“First, do no harm,” Dr. Dispenzieri cautioned in her final slide.
Dr. Lonial said he agreed with many of Dr. Dispenzieri’s points, but disagreed with her conclusion not to treat.
“Everybody can always be critical of randomized trials, but at the end of the day, we now have two randomized phase 3 trials comparing early intervention with no intervention demonstrating a significant delay in developing myeloma. I think it’s time to end the ‘we need more data; we need more trials.’ It’s time for us to take a stand.”
He argued for 2 years of lenalidomide for patients who meet the 2-20-20 high-risk definition, based on the median time people were treated in his trial.
He said he discusses the option “with every smoldering patient [who] walks in to see me” if they aren’t eligible for a trial.
Dr. Lonial mentioned his team is currently pulling together longer-term survival data for their trial.
Hematologist Sagar Lonial, MD, a multiple myeloma specialist and researcher at Emory University, Atlanta, argued for treatment. Hematologist Angela Dispenzieri, MD, also a myeloma researcher and specialist at the Mayo Clinic in Rochester, Minn., took the opposing side, arguing for watchful waiting.
The two experts based their arguments largely on the same two studies, the only randomized trials to tackle the issue to date. While Dr. Dispenzieri focused on their shortcomings, Dr. Lonial focused on their strengths.
In a poll after the debate, about a third of audience members agreed that watchful waiting is the way to go, but about two-thirds favored a personalized approach to smoldering myeloma treatment based on patient risk.
“I’m taking this as a win,” Dr. Lonial said.
Different interpretations of two trials
The first of the two trials recruited from 2007 to 2010 and was conducted in Spain and Portugal. Fifty-seven high-risk patients were randomized to lenalidomide plus dexamethasone (Len-Dex) for up to 2 years; 62 others were randomized to observation.
At 3 years, 70% of observed patients had progressed to multiple myeloma versus only 20% in the Len-Dex group; 82% of Len-Dex patients were alive at data cut-off in 2015 versus 64% of observation patients.
The second, more recent trial, which was led by Dr. Lonial, randomized 92 intermediate or high-risk smoldering myeloma patients to lenalidomide alone for a median of 2 years and 90 others to observation. Three-year progression-free survival (PFS) was 91% in the treatment arm versus 66% with observation. Overall survival data have not yet been reported.
Dr. Dispenzieri acknowledged that the results from Spain and Portugal are impressive. “Treating with Len-Dex gives you a far superior freedom from progression. ... Overall survival was better too.” Results for Len-Dex were “fantastic,” she said.
However, the trial was done before myeloma-defining event criteria existed, so it’s very likely that the treatment arm in the Spanish study included actual myeloma cases, she said.
About 46% of treated patients in Dr. Lonial’s study met the current definition for high risk for progression based on the 2-20-20 rule, which Dr. Dispenzieri helped develop. Although there was an improvement in PFS in the high-risk group, there was no significant improvement for intermediate- and low-risk subjects. Also, more than 80% of observed patients hadn’t progressed by 2 years, and overall survival data are missing.
Meanwhile, treated patients in both trials had more adverse events, including secondary malignancies, and there’s the possibility that early treatment may make patients resistant to treatment later on when they progress to multiple myeloma, although that didn’t seem to happen in the Spanish trial.
“Of course, we want to prevent morbidity, of course we would love to cure the disease,” but “should we treat high-risk smoldering myeloma patients based on overall survival data from a trial of” just 119 “patients that may have been contaminated with actual myeloma” cases? Is it ethical to treat low- and intermediate-risk patients who have only a 50% chance of developing myeloma after 10 years?”
Her answer to both questions was “no and no. ... There’s just a lot of work to be done” to better understand the condition and when and how to intervene. In the meantime, “don’t treat smoldering melanoma patients” outside of a trial, she said.
“First, do no harm,” Dr. Dispenzieri cautioned in her final slide.
Dr. Lonial said he agreed with many of Dr. Dispenzieri’s points, but disagreed with her conclusion not to treat.
“Everybody can always be critical of randomized trials, but at the end of the day, we now have two randomized phase 3 trials comparing early intervention with no intervention demonstrating a significant delay in developing myeloma. I think it’s time to end the ‘we need more data; we need more trials.’ It’s time for us to take a stand.”
He argued for 2 years of lenalidomide for patients who meet the 2-20-20 high-risk definition, based on the median time people were treated in his trial.
He said he discusses the option “with every smoldering patient [who] walks in to see me” if they aren’t eligible for a trial.
Dr. Lonial mentioned his team is currently pulling together longer-term survival data for their trial.
Hematologist Sagar Lonial, MD, a multiple myeloma specialist and researcher at Emory University, Atlanta, argued for treatment. Hematologist Angela Dispenzieri, MD, also a myeloma researcher and specialist at the Mayo Clinic in Rochester, Minn., took the opposing side, arguing for watchful waiting.
The two experts based their arguments largely on the same two studies, the only randomized trials to tackle the issue to date. While Dr. Dispenzieri focused on their shortcomings, Dr. Lonial focused on their strengths.
In a poll after the debate, about a third of audience members agreed that watchful waiting is the way to go, but about two-thirds favored a personalized approach to smoldering myeloma treatment based on patient risk.
“I’m taking this as a win,” Dr. Lonial said.
Different interpretations of two trials
The first of the two trials recruited from 2007 to 2010 and was conducted in Spain and Portugal. Fifty-seven high-risk patients were randomized to lenalidomide plus dexamethasone (Len-Dex) for up to 2 years; 62 others were randomized to observation.
At 3 years, 70% of observed patients had progressed to multiple myeloma versus only 20% in the Len-Dex group; 82% of Len-Dex patients were alive at data cut-off in 2015 versus 64% of observation patients.
The second, more recent trial, which was led by Dr. Lonial, randomized 92 intermediate or high-risk smoldering myeloma patients to lenalidomide alone for a median of 2 years and 90 others to observation. Three-year progression-free survival (PFS) was 91% in the treatment arm versus 66% with observation. Overall survival data have not yet been reported.
Dr. Dispenzieri acknowledged that the results from Spain and Portugal are impressive. “Treating with Len-Dex gives you a far superior freedom from progression. ... Overall survival was better too.” Results for Len-Dex were “fantastic,” she said.
However, the trial was done before myeloma-defining event criteria existed, so it’s very likely that the treatment arm in the Spanish study included actual myeloma cases, she said.
About 46% of treated patients in Dr. Lonial’s study met the current definition for high risk for progression based on the 2-20-20 rule, which Dr. Dispenzieri helped develop. Although there was an improvement in PFS in the high-risk group, there was no significant improvement for intermediate- and low-risk subjects. Also, more than 80% of observed patients hadn’t progressed by 2 years, and overall survival data are missing.
Meanwhile, treated patients in both trials had more adverse events, including secondary malignancies, and there’s the possibility that early treatment may make patients resistant to treatment later on when they progress to multiple myeloma, although that didn’t seem to happen in the Spanish trial.
“Of course, we want to prevent morbidity, of course we would love to cure the disease,” but “should we treat high-risk smoldering myeloma patients based on overall survival data from a trial of” just 119 “patients that may have been contaminated with actual myeloma” cases? Is it ethical to treat low- and intermediate-risk patients who have only a 50% chance of developing myeloma after 10 years?”
Her answer to both questions was “no and no. ... There’s just a lot of work to be done” to better understand the condition and when and how to intervene. In the meantime, “don’t treat smoldering melanoma patients” outside of a trial, she said.
“First, do no harm,” Dr. Dispenzieri cautioned in her final slide.
Dr. Lonial said he agreed with many of Dr. Dispenzieri’s points, but disagreed with her conclusion not to treat.
“Everybody can always be critical of randomized trials, but at the end of the day, we now have two randomized phase 3 trials comparing early intervention with no intervention demonstrating a significant delay in developing myeloma. I think it’s time to end the ‘we need more data; we need more trials.’ It’s time for us to take a stand.”
He argued for 2 years of lenalidomide for patients who meet the 2-20-20 high-risk definition, based on the median time people were treated in his trial.
He said he discusses the option “with every smoldering patient [who] walks in to see me” if they aren’t eligible for a trial.
Dr. Lonial mentioned his team is currently pulling together longer-term survival data for their trial.
FROM SOHO 2023
Osimertinib plus chemo ups PFS, toxicity in first line
(PFS), according to interim results from the FLAURA2 trial.
Combining the third-generation tyrosine kinase inhibitor (TKI) with platinum-based chemotherapy achieved “statistically significant and clinically meaningful improvement in PFS over osimertinib monotherapy,” said Pasi A. Jänne, MD, PhD, professor of medicine at Harvard Medical School and director of the Lowe Center for Thoracic Oncology, Dana-Farber Cancer Institute, both in Boston, who presented the interim findings at the annual World Conference on Lung Cancer.
However, experts raised some questions about whether the combination would also offer improved overall survival and whether the accompanying toxicity would be acceptable to patients.
Yi-Long Wu, MD, PhD, who was not involved in the research, said that although the combination regimen does appear to offer a benefit, it may come at a steep cost.
Patients who received the combination had an almost fourfold greater risk of grade 3 or higher adverse events related to treatment, said Dr. Wu, professor of oncology, Guangdong Lung Cancer Institute, Guangdong Provincial People’s Hospital, Guangzhou, China.
And, notably, because the overall survival data in the interim analysis are immature, it’s unclear whether the combination will offer an overall survival benefit over osimertinib monotherapy, Dr. Wu said.
The 2019 FLAURA trial, which compared TKI monotherapy, demonstrated an overall survival advantage among patients who received osimertinib vs. a first-generation EGFR TKI, such as gefitinib (Iressa) or erlotinib (Tarceva). These data established the third-generation TKI as the preferred first-line treatment for patients with advanced EGFR NSCLC.
But resistance to EGFR TKIs remains a problem, which has led experts to explore combination strategies that might overcome resistance and improve clinical outcomes. Recent data indicate that combining first-generation EGFR TKIs with chemotherapy may have an additive effect and further improve outcomes with the drugs. And a recent study of untreated EGFR-mutated advanced NSCLC found patients receiving osimertinib plus platinum-pemetrexed demonstrated a promising objective response rate; however, Dr. Jänne noted that the combination has not been tested in a randomized trial.
To better understand the potential additive benefit of osimertinib and chemotherapy, the team conduced a global, open-label study in patients with pathologically confirmed nonsquamous NSCLC who had received no prior systemic therapy for advanced NSCLC and had a performance status of 0 or 1.
The team randomly assigned 557 patients to daily osimertinib alone or osimertinib plus chemotherapy with pemetrexed and carboplatin or cisplatin every 3 weeks for four cycles, followed by maintenance osimertinib plus pemetrexed every 3 weeks.
Treatment was continued until radiological disease progression, as defined using the RECIST 1.1 criteria, or other withdrawal criteria were met. The patients were assessed at weeks 6 and 12, and again every 12 weeks.
The median age of the patients was about 61 years, approximately 61% were female, and about 25% were Asian. Around two-thirds were never-smokers, about 60% had either Ex19del or L858R EGFR mutations, and about 40% had central nervous system metastases.
At the data cutoff, the median follow-up was 16.5 months in the osimertinib monotherapy arm and 19.5 months in the combination arm. Overall, 45% of patients on monotherapy and 56% in the combination arm were still on treatment.
Dr. Jänne reported that osimertinib plus chemotherapy was associated with a greater objective response rate than monotherapy – 83.2% vs. 75.5% – and a longer median duration of response – 24 months vs. 15.3 months.
Patients receiving the combination showed significant improvements in PFS – 25.5 months vs. 16.7 months (hazard ratio, 0.62; P < .0001). At 24 months, 57% of the patients in the combination arm were disease-free vs. 41% in the monotherapy group.
The benefit held across all patient subgroups, including age, sex, smoking history, and EGFR mutation type at baseline.
The PFS benefit appeared most pronounced among patients with CNS metastases at baseline – a median of 24.9 months in the combination arm vs. 13.8 months with monotherapy (HR, 0.47). But patients without CNS metastases who received the combination therapy also showed improvements in PFS (HR, 0.75).
Should there be an overall survival improvement, then the regimen used in FLAURA2 could become the “new standard of care in EGFR-mutated NSCLC in the first-line setting,” particularly in patients with CNS metastases and/or an exon21 mutation, Dr. Wu said. If, however, further analysis indicates no overall survival benefit, then patients will have experienced chemotherapy side effects earlier and longer than those receiving monotherapy, with no life gain.
Dr. Wu pointed out that the future role and sequence of the combination will also hinge on understanding how patients become resistant to it as well as whether the toxicity is manageable.
The FLAURA2 safety data indicated that the combination led to higher rates of grade 3 or higher adverse events overall – 64% vs. 27% – and higher rates of grade 3 or higher adverse events possibly related to treatment – 53% vs. 11%.
Experts who commented on the study findings via X (formerly Twitter) echoed Dr. Wu’s sentiments about the study findings and implications.
Mohana Roy, MD, said she did not find the results surprising, given that “many of us are adding chemo on slow progression on osimertinib already,” but noted that “questions of sequencing” remain.
Christian Rolfo, MD, PhD, MBA, commented that questions about the “real benefit” of osimertinib plus chemotherapy in subgroups and degree of resistance remain. Further toxicity and overall survival data “will clarify the future of the combination,” said Dr. Rolfo, of Icahn School of Medicine at Mount Sinai, New York.
The study was funded by AstraZeneca. Dr. Jänne declared relationships with Gatekeeper Pharmaceuticals, Labcorp, Astellas Pharmaceuticals, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, PUMA, Revolution Medicines, Takeda Oncology, Biocartis, Mirati Therapeutics, Transcenta, ACEA Biosciences, Araxes, Bayer, Chugai Pharmaceuticals, Eisai, Ignyta, Novartis, Nuvalent, Pfizer, Roche/Genentech, Sanofi, SFJ Pharmaceuticals, Silicon Therapeutics, Syndax, and Voronoi.
A version of this article first appeared on Medscape.com.
(PFS), according to interim results from the FLAURA2 trial.
Combining the third-generation tyrosine kinase inhibitor (TKI) with platinum-based chemotherapy achieved “statistically significant and clinically meaningful improvement in PFS over osimertinib monotherapy,” said Pasi A. Jänne, MD, PhD, professor of medicine at Harvard Medical School and director of the Lowe Center for Thoracic Oncology, Dana-Farber Cancer Institute, both in Boston, who presented the interim findings at the annual World Conference on Lung Cancer.
However, experts raised some questions about whether the combination would also offer improved overall survival and whether the accompanying toxicity would be acceptable to patients.
Yi-Long Wu, MD, PhD, who was not involved in the research, said that although the combination regimen does appear to offer a benefit, it may come at a steep cost.
Patients who received the combination had an almost fourfold greater risk of grade 3 or higher adverse events related to treatment, said Dr. Wu, professor of oncology, Guangdong Lung Cancer Institute, Guangdong Provincial People’s Hospital, Guangzhou, China.
And, notably, because the overall survival data in the interim analysis are immature, it’s unclear whether the combination will offer an overall survival benefit over osimertinib monotherapy, Dr. Wu said.
The 2019 FLAURA trial, which compared TKI monotherapy, demonstrated an overall survival advantage among patients who received osimertinib vs. a first-generation EGFR TKI, such as gefitinib (Iressa) or erlotinib (Tarceva). These data established the third-generation TKI as the preferred first-line treatment for patients with advanced EGFR NSCLC.
But resistance to EGFR TKIs remains a problem, which has led experts to explore combination strategies that might overcome resistance and improve clinical outcomes. Recent data indicate that combining first-generation EGFR TKIs with chemotherapy may have an additive effect and further improve outcomes with the drugs. And a recent study of untreated EGFR-mutated advanced NSCLC found patients receiving osimertinib plus platinum-pemetrexed demonstrated a promising objective response rate; however, Dr. Jänne noted that the combination has not been tested in a randomized trial.
To better understand the potential additive benefit of osimertinib and chemotherapy, the team conduced a global, open-label study in patients with pathologically confirmed nonsquamous NSCLC who had received no prior systemic therapy for advanced NSCLC and had a performance status of 0 or 1.
The team randomly assigned 557 patients to daily osimertinib alone or osimertinib plus chemotherapy with pemetrexed and carboplatin or cisplatin every 3 weeks for four cycles, followed by maintenance osimertinib plus pemetrexed every 3 weeks.
Treatment was continued until radiological disease progression, as defined using the RECIST 1.1 criteria, or other withdrawal criteria were met. The patients were assessed at weeks 6 and 12, and again every 12 weeks.
The median age of the patients was about 61 years, approximately 61% were female, and about 25% were Asian. Around two-thirds were never-smokers, about 60% had either Ex19del or L858R EGFR mutations, and about 40% had central nervous system metastases.
At the data cutoff, the median follow-up was 16.5 months in the osimertinib monotherapy arm and 19.5 months in the combination arm. Overall, 45% of patients on monotherapy and 56% in the combination arm were still on treatment.
Dr. Jänne reported that osimertinib plus chemotherapy was associated with a greater objective response rate than monotherapy – 83.2% vs. 75.5% – and a longer median duration of response – 24 months vs. 15.3 months.
Patients receiving the combination showed significant improvements in PFS – 25.5 months vs. 16.7 months (hazard ratio, 0.62; P < .0001). At 24 months, 57% of the patients in the combination arm were disease-free vs. 41% in the monotherapy group.
The benefit held across all patient subgroups, including age, sex, smoking history, and EGFR mutation type at baseline.
The PFS benefit appeared most pronounced among patients with CNS metastases at baseline – a median of 24.9 months in the combination arm vs. 13.8 months with monotherapy (HR, 0.47). But patients without CNS metastases who received the combination therapy also showed improvements in PFS (HR, 0.75).
Should there be an overall survival improvement, then the regimen used in FLAURA2 could become the “new standard of care in EGFR-mutated NSCLC in the first-line setting,” particularly in patients with CNS metastases and/or an exon21 mutation, Dr. Wu said. If, however, further analysis indicates no overall survival benefit, then patients will have experienced chemotherapy side effects earlier and longer than those receiving monotherapy, with no life gain.
Dr. Wu pointed out that the future role and sequence of the combination will also hinge on understanding how patients become resistant to it as well as whether the toxicity is manageable.
The FLAURA2 safety data indicated that the combination led to higher rates of grade 3 or higher adverse events overall – 64% vs. 27% – and higher rates of grade 3 or higher adverse events possibly related to treatment – 53% vs. 11%.
Experts who commented on the study findings via X (formerly Twitter) echoed Dr. Wu’s sentiments about the study findings and implications.
Mohana Roy, MD, said she did not find the results surprising, given that “many of us are adding chemo on slow progression on osimertinib already,” but noted that “questions of sequencing” remain.
Christian Rolfo, MD, PhD, MBA, commented that questions about the “real benefit” of osimertinib plus chemotherapy in subgroups and degree of resistance remain. Further toxicity and overall survival data “will clarify the future of the combination,” said Dr. Rolfo, of Icahn School of Medicine at Mount Sinai, New York.
The study was funded by AstraZeneca. Dr. Jänne declared relationships with Gatekeeper Pharmaceuticals, Labcorp, Astellas Pharmaceuticals, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, PUMA, Revolution Medicines, Takeda Oncology, Biocartis, Mirati Therapeutics, Transcenta, ACEA Biosciences, Araxes, Bayer, Chugai Pharmaceuticals, Eisai, Ignyta, Novartis, Nuvalent, Pfizer, Roche/Genentech, Sanofi, SFJ Pharmaceuticals, Silicon Therapeutics, Syndax, and Voronoi.
A version of this article first appeared on Medscape.com.
(PFS), according to interim results from the FLAURA2 trial.
Combining the third-generation tyrosine kinase inhibitor (TKI) with platinum-based chemotherapy achieved “statistically significant and clinically meaningful improvement in PFS over osimertinib monotherapy,” said Pasi A. Jänne, MD, PhD, professor of medicine at Harvard Medical School and director of the Lowe Center for Thoracic Oncology, Dana-Farber Cancer Institute, both in Boston, who presented the interim findings at the annual World Conference on Lung Cancer.
However, experts raised some questions about whether the combination would also offer improved overall survival and whether the accompanying toxicity would be acceptable to patients.
Yi-Long Wu, MD, PhD, who was not involved in the research, said that although the combination regimen does appear to offer a benefit, it may come at a steep cost.
Patients who received the combination had an almost fourfold greater risk of grade 3 or higher adverse events related to treatment, said Dr. Wu, professor of oncology, Guangdong Lung Cancer Institute, Guangdong Provincial People’s Hospital, Guangzhou, China.
And, notably, because the overall survival data in the interim analysis are immature, it’s unclear whether the combination will offer an overall survival benefit over osimertinib monotherapy, Dr. Wu said.
The 2019 FLAURA trial, which compared TKI monotherapy, demonstrated an overall survival advantage among patients who received osimertinib vs. a first-generation EGFR TKI, such as gefitinib (Iressa) or erlotinib (Tarceva). These data established the third-generation TKI as the preferred first-line treatment for patients with advanced EGFR NSCLC.
But resistance to EGFR TKIs remains a problem, which has led experts to explore combination strategies that might overcome resistance and improve clinical outcomes. Recent data indicate that combining first-generation EGFR TKIs with chemotherapy may have an additive effect and further improve outcomes with the drugs. And a recent study of untreated EGFR-mutated advanced NSCLC found patients receiving osimertinib plus platinum-pemetrexed demonstrated a promising objective response rate; however, Dr. Jänne noted that the combination has not been tested in a randomized trial.
To better understand the potential additive benefit of osimertinib and chemotherapy, the team conduced a global, open-label study in patients with pathologically confirmed nonsquamous NSCLC who had received no prior systemic therapy for advanced NSCLC and had a performance status of 0 or 1.
The team randomly assigned 557 patients to daily osimertinib alone or osimertinib plus chemotherapy with pemetrexed and carboplatin or cisplatin every 3 weeks for four cycles, followed by maintenance osimertinib plus pemetrexed every 3 weeks.
Treatment was continued until radiological disease progression, as defined using the RECIST 1.1 criteria, or other withdrawal criteria were met. The patients were assessed at weeks 6 and 12, and again every 12 weeks.
The median age of the patients was about 61 years, approximately 61% were female, and about 25% were Asian. Around two-thirds were never-smokers, about 60% had either Ex19del or L858R EGFR mutations, and about 40% had central nervous system metastases.
At the data cutoff, the median follow-up was 16.5 months in the osimertinib monotherapy arm and 19.5 months in the combination arm. Overall, 45% of patients on monotherapy and 56% in the combination arm were still on treatment.
Dr. Jänne reported that osimertinib plus chemotherapy was associated with a greater objective response rate than monotherapy – 83.2% vs. 75.5% – and a longer median duration of response – 24 months vs. 15.3 months.
Patients receiving the combination showed significant improvements in PFS – 25.5 months vs. 16.7 months (hazard ratio, 0.62; P < .0001). At 24 months, 57% of the patients in the combination arm were disease-free vs. 41% in the monotherapy group.
The benefit held across all patient subgroups, including age, sex, smoking history, and EGFR mutation type at baseline.
The PFS benefit appeared most pronounced among patients with CNS metastases at baseline – a median of 24.9 months in the combination arm vs. 13.8 months with monotherapy (HR, 0.47). But patients without CNS metastases who received the combination therapy also showed improvements in PFS (HR, 0.75).
Should there be an overall survival improvement, then the regimen used in FLAURA2 could become the “new standard of care in EGFR-mutated NSCLC in the first-line setting,” particularly in patients with CNS metastases and/or an exon21 mutation, Dr. Wu said. If, however, further analysis indicates no overall survival benefit, then patients will have experienced chemotherapy side effects earlier and longer than those receiving monotherapy, with no life gain.
Dr. Wu pointed out that the future role and sequence of the combination will also hinge on understanding how patients become resistant to it as well as whether the toxicity is manageable.
The FLAURA2 safety data indicated that the combination led to higher rates of grade 3 or higher adverse events overall – 64% vs. 27% – and higher rates of grade 3 or higher adverse events possibly related to treatment – 53% vs. 11%.
Experts who commented on the study findings via X (formerly Twitter) echoed Dr. Wu’s sentiments about the study findings and implications.
Mohana Roy, MD, said she did not find the results surprising, given that “many of us are adding chemo on slow progression on osimertinib already,” but noted that “questions of sequencing” remain.
Christian Rolfo, MD, PhD, MBA, commented that questions about the “real benefit” of osimertinib plus chemotherapy in subgroups and degree of resistance remain. Further toxicity and overall survival data “will clarify the future of the combination,” said Dr. Rolfo, of Icahn School of Medicine at Mount Sinai, New York.
The study was funded by AstraZeneca. Dr. Jänne declared relationships with Gatekeeper Pharmaceuticals, Labcorp, Astellas Pharmaceuticals, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, PUMA, Revolution Medicines, Takeda Oncology, Biocartis, Mirati Therapeutics, Transcenta, ACEA Biosciences, Araxes, Bayer, Chugai Pharmaceuticals, Eisai, Ignyta, Novartis, Nuvalent, Pfizer, Roche/Genentech, Sanofi, SFJ Pharmaceuticals, Silicon Therapeutics, Syndax, and Voronoi.
A version of this article first appeared on Medscape.com.
FROM WCLC 2023
Sleep apnea diagnosis: Awareness and tools
Obstructive sleep apnea (OSA) remains a significantly underdiagnosed condition, despite its high prevalence. Primary care physicians play a pivotal role in identifying patients afflicted by this condition. To effectively diagnose OSA in primary care, increasing awareness and enhancing communication are imperative. Fortunately, several straightforward diagnostic tools are readily available, and even more sophisticated ones, driven by artificial intelligence, are on the horizon.
Recognize the problem
At the annual congress of the European Respiratory Society, Cláudia Sofia De Almeida Vicente Ferreira, MD, a family physician from Coimbra, Portugal, and coordinator of the Respiratory Diseases Interest Group of the Portuguese Association of General and Family Medicine, highlighted the challenges of diagnosing OSA.
People do not come to the doctor and complain about it. Sometimes you catch it in the middle of other things,” she said in an interview.
Moreover, physicians’ busy schedules and limited appointment times often lead to a focus on the symptoms reported by patients, and insufficient attention is paid to the quality of sleep. This may be compounded by a tendency among medical professionals to underestimate the risks associated with OSA, as it is not directly linked to mortality, despite its clear connection to cardiovascular risks.
Identifying and recognizing risk factors can facilitate OSA suspicion during patient evaluations. These factors encompass both structural (for example, craniofacial and upper airway anomalies) and nonstructural elements (for example, smoking, alcohol use, or sedative consumption). While men are at higher risk, postmenopausal women who are not receiving hormone replacement therapy face similar risks. Certain medical conditions, such as hypothyroidism, acromegaly, amyloidosis, Cushing syndrome, and Down syndrome, have also been associated with OSA. A comprehensive physical examination can provide additional clues. Factors might include obesity, neck circumference, Mallampati score, and nasal and pharyngeal problems.
Inquire actively
Once the possibility of OSA is considered, the next step is to ask patients about their symptoms. Questionnaires are simple yet valuable tools for this purpose. The STOP questionnaire comprises four key questions:
- Do you SNORE loudly (louder than talking or loud enough to be heard through closed doors)?
- Do you often feel TIRED, fatigued, or sleepy during daytime?
- Has anyone OBSERVED you stop breathing during your sleep?
- Do you have or are you being treated for high blood PRESSURE?
The STOP-BANG questionnaire adds four clinical attributes: obesity (body mass index > 35 kg/m2), age (> 50 years), neck size (> 40 cm, or 16 inches), and sex.
Patients are classified as being at low, intermediate, or high risk for OSA.
The Epworth Sleepiness Scale, which is self-administered, is also useful: patients rate the likelihood of falling asleep in various daytime contexts. These questionnaires can be seamlessly integrated into routine patient appointments.
Comorbidities and occupation
Primary care physicians should carefully assess comorbidities, especially those linked to cardiovascular risk. Patients with resistant hypertension, pulmonary hypertension, and recurrent atrial fibrillation following cardioversion/ablation should be prioritized for diagnostic testing for OSA. Patients with other conditions, such as coronary artery disease or cerebrovascular disease, should also be referred to a sleep center if OSA is suspected on the basis of comprehensive sleep assessment. OSA has also been associated with type 2 diabetes, metabolic syndrome, and asthma.
Gaining access to sleep study services and subsequent therapy, such as continuous positive airway pressure (CPAP), can be challenging. Primary care physicians should prioritize patients on the basis of their risk levels. Occupation plays a significant role in this prioritization, as sleep fragmentation and daytime sleepiness can lead to workplace and vehicular accidents.
“You should include the occupation in the patient’s profile. What is he doing? Is he sitting at a desk, or is he working at height, driving, or operating machines? These workers are high-risk patients,” continued Dr. De Almeida Vicente Ferreira.
“I think that the family physician has a key role in the follow-up. Nobody else will look for CPAP compliance and will verify if CPAP is working or not. If the patient is not using it or if it is not effective, still there is someone paying for the machine (the national health care system or an insurance company). More importantly, if CPAP is not working, we are not improving our patient’s life in terms of reducing cardiovascular risk and ameliorating the quality of life.”
Is home testing a viable option?
Diagnosing OSA typically relies on overnight polysomnography in specialized sleep clinics, which is often associated with long waiting lists. Researchers are actively working on innovative sensors and digital solutions for home-based sleep testing, but according to Dr. De Almeida Vicente Ferreira, they are not yet ready for prime time: “Home-based studies with fewer evaluation parameters (such as pulse and oxygen levels) are not so secure or sensitive to establish a correct and complete diagnosis. Actually, the architecture of sleep is very complex. The test must be performed and read by a specialized team.”
Still, according to Renaud Tamisier, MD, PhD, professor of clinical physiology at the Université Grenoble Alpes in La Tronche, France, simplified sleep testing could be very useful. “There are many patients that still are not diagnosed despite having severe sleep apnea, with symptoms and comorbidities. These patients usually are not aware of their disease but complain about changes in their quality of life with excessive tiredness and sleepiness. Also, they are not connected to the healthcare system, for different reasons, including no time for consulting a sleep physician and performing a polysomnography, health cost, negligence. Therefore, providing through primary care a simple diagnostic approach deserves efforts and research,” he said in an interview.
New technologies could enable diagnostic sleep tests to be conducted at home, with the added benefit of multiple-night recordings to overcome the challenges of night-to-night variability in the apnea-hypopnea index. These novel testing methods should be cost effective, easy to install, and user friendly. Dr. Tamisier continued: “The issue about sleep diagnosis is that up to now, there was no such devices available. Many physicians use type III sleep recording that are dedicated to highly trained sleep scorers, but they use automatic analysis which in many cases is unsuccessful. For a trained sleep physician, it is easy to see that the result is inaccurate. New devices are being built for automatic analysis using artificial intelligence algorithms. Because by design they are automatic, the rate of success is very high, and if used with the right purpose, they could be highly effective and quick.”
In conclusion, the diagnosis of sleep apnea in primary care is becoming more feasible with advancements in diagnostic tools and technology. However, it is crucial for primary care physicians to exercise caution in cases in which the clinical presentation is not straightforward or when OSA is associated with comorbidities. Care management and clear boundaries are vital to ensure effective treatment and improve patient outcomes.
Dr. De Almeida Vicente Ferreira and Dr. Tamisier disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Obstructive sleep apnea (OSA) remains a significantly underdiagnosed condition, despite its high prevalence. Primary care physicians play a pivotal role in identifying patients afflicted by this condition. To effectively diagnose OSA in primary care, increasing awareness and enhancing communication are imperative. Fortunately, several straightforward diagnostic tools are readily available, and even more sophisticated ones, driven by artificial intelligence, are on the horizon.
Recognize the problem
At the annual congress of the European Respiratory Society, Cláudia Sofia De Almeida Vicente Ferreira, MD, a family physician from Coimbra, Portugal, and coordinator of the Respiratory Diseases Interest Group of the Portuguese Association of General and Family Medicine, highlighted the challenges of diagnosing OSA.
People do not come to the doctor and complain about it. Sometimes you catch it in the middle of other things,” she said in an interview.
Moreover, physicians’ busy schedules and limited appointment times often lead to a focus on the symptoms reported by patients, and insufficient attention is paid to the quality of sleep. This may be compounded by a tendency among medical professionals to underestimate the risks associated with OSA, as it is not directly linked to mortality, despite its clear connection to cardiovascular risks.
Identifying and recognizing risk factors can facilitate OSA suspicion during patient evaluations. These factors encompass both structural (for example, craniofacial and upper airway anomalies) and nonstructural elements (for example, smoking, alcohol use, or sedative consumption). While men are at higher risk, postmenopausal women who are not receiving hormone replacement therapy face similar risks. Certain medical conditions, such as hypothyroidism, acromegaly, amyloidosis, Cushing syndrome, and Down syndrome, have also been associated with OSA. A comprehensive physical examination can provide additional clues. Factors might include obesity, neck circumference, Mallampati score, and nasal and pharyngeal problems.
Inquire actively
Once the possibility of OSA is considered, the next step is to ask patients about their symptoms. Questionnaires are simple yet valuable tools for this purpose. The STOP questionnaire comprises four key questions:
- Do you SNORE loudly (louder than talking or loud enough to be heard through closed doors)?
- Do you often feel TIRED, fatigued, or sleepy during daytime?
- Has anyone OBSERVED you stop breathing during your sleep?
- Do you have or are you being treated for high blood PRESSURE?
The STOP-BANG questionnaire adds four clinical attributes: obesity (body mass index > 35 kg/m2), age (> 50 years), neck size (> 40 cm, or 16 inches), and sex.
Patients are classified as being at low, intermediate, or high risk for OSA.
The Epworth Sleepiness Scale, which is self-administered, is also useful: patients rate the likelihood of falling asleep in various daytime contexts. These questionnaires can be seamlessly integrated into routine patient appointments.
Comorbidities and occupation
Primary care physicians should carefully assess comorbidities, especially those linked to cardiovascular risk. Patients with resistant hypertension, pulmonary hypertension, and recurrent atrial fibrillation following cardioversion/ablation should be prioritized for diagnostic testing for OSA. Patients with other conditions, such as coronary artery disease or cerebrovascular disease, should also be referred to a sleep center if OSA is suspected on the basis of comprehensive sleep assessment. OSA has also been associated with type 2 diabetes, metabolic syndrome, and asthma.
Gaining access to sleep study services and subsequent therapy, such as continuous positive airway pressure (CPAP), can be challenging. Primary care physicians should prioritize patients on the basis of their risk levels. Occupation plays a significant role in this prioritization, as sleep fragmentation and daytime sleepiness can lead to workplace and vehicular accidents.
“You should include the occupation in the patient’s profile. What is he doing? Is he sitting at a desk, or is he working at height, driving, or operating machines? These workers are high-risk patients,” continued Dr. De Almeida Vicente Ferreira.
“I think that the family physician has a key role in the follow-up. Nobody else will look for CPAP compliance and will verify if CPAP is working or not. If the patient is not using it or if it is not effective, still there is someone paying for the machine (the national health care system or an insurance company). More importantly, if CPAP is not working, we are not improving our patient’s life in terms of reducing cardiovascular risk and ameliorating the quality of life.”
Is home testing a viable option?
Diagnosing OSA typically relies on overnight polysomnography in specialized sleep clinics, which is often associated with long waiting lists. Researchers are actively working on innovative sensors and digital solutions for home-based sleep testing, but according to Dr. De Almeida Vicente Ferreira, they are not yet ready for prime time: “Home-based studies with fewer evaluation parameters (such as pulse and oxygen levels) are not so secure or sensitive to establish a correct and complete diagnosis. Actually, the architecture of sleep is very complex. The test must be performed and read by a specialized team.”
Still, according to Renaud Tamisier, MD, PhD, professor of clinical physiology at the Université Grenoble Alpes in La Tronche, France, simplified sleep testing could be very useful. “There are many patients that still are not diagnosed despite having severe sleep apnea, with symptoms and comorbidities. These patients usually are not aware of their disease but complain about changes in their quality of life with excessive tiredness and sleepiness. Also, they are not connected to the healthcare system, for different reasons, including no time for consulting a sleep physician and performing a polysomnography, health cost, negligence. Therefore, providing through primary care a simple diagnostic approach deserves efforts and research,” he said in an interview.
New technologies could enable diagnostic sleep tests to be conducted at home, with the added benefit of multiple-night recordings to overcome the challenges of night-to-night variability in the apnea-hypopnea index. These novel testing methods should be cost effective, easy to install, and user friendly. Dr. Tamisier continued: “The issue about sleep diagnosis is that up to now, there was no such devices available. Many physicians use type III sleep recording that are dedicated to highly trained sleep scorers, but they use automatic analysis which in many cases is unsuccessful. For a trained sleep physician, it is easy to see that the result is inaccurate. New devices are being built for automatic analysis using artificial intelligence algorithms. Because by design they are automatic, the rate of success is very high, and if used with the right purpose, they could be highly effective and quick.”
In conclusion, the diagnosis of sleep apnea in primary care is becoming more feasible with advancements in diagnostic tools and technology. However, it is crucial for primary care physicians to exercise caution in cases in which the clinical presentation is not straightforward or when OSA is associated with comorbidities. Care management and clear boundaries are vital to ensure effective treatment and improve patient outcomes.
Dr. De Almeida Vicente Ferreira and Dr. Tamisier disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Obstructive sleep apnea (OSA) remains a significantly underdiagnosed condition, despite its high prevalence. Primary care physicians play a pivotal role in identifying patients afflicted by this condition. To effectively diagnose OSA in primary care, increasing awareness and enhancing communication are imperative. Fortunately, several straightforward diagnostic tools are readily available, and even more sophisticated ones, driven by artificial intelligence, are on the horizon.
Recognize the problem
At the annual congress of the European Respiratory Society, Cláudia Sofia De Almeida Vicente Ferreira, MD, a family physician from Coimbra, Portugal, and coordinator of the Respiratory Diseases Interest Group of the Portuguese Association of General and Family Medicine, highlighted the challenges of diagnosing OSA.
People do not come to the doctor and complain about it. Sometimes you catch it in the middle of other things,” she said in an interview.
Moreover, physicians’ busy schedules and limited appointment times often lead to a focus on the symptoms reported by patients, and insufficient attention is paid to the quality of sleep. This may be compounded by a tendency among medical professionals to underestimate the risks associated with OSA, as it is not directly linked to mortality, despite its clear connection to cardiovascular risks.
Identifying and recognizing risk factors can facilitate OSA suspicion during patient evaluations. These factors encompass both structural (for example, craniofacial and upper airway anomalies) and nonstructural elements (for example, smoking, alcohol use, or sedative consumption). While men are at higher risk, postmenopausal women who are not receiving hormone replacement therapy face similar risks. Certain medical conditions, such as hypothyroidism, acromegaly, amyloidosis, Cushing syndrome, and Down syndrome, have also been associated with OSA. A comprehensive physical examination can provide additional clues. Factors might include obesity, neck circumference, Mallampati score, and nasal and pharyngeal problems.
Inquire actively
Once the possibility of OSA is considered, the next step is to ask patients about their symptoms. Questionnaires are simple yet valuable tools for this purpose. The STOP questionnaire comprises four key questions:
- Do you SNORE loudly (louder than talking or loud enough to be heard through closed doors)?
- Do you often feel TIRED, fatigued, or sleepy during daytime?
- Has anyone OBSERVED you stop breathing during your sleep?
- Do you have or are you being treated for high blood PRESSURE?
The STOP-BANG questionnaire adds four clinical attributes: obesity (body mass index > 35 kg/m2), age (> 50 years), neck size (> 40 cm, or 16 inches), and sex.
Patients are classified as being at low, intermediate, or high risk for OSA.
The Epworth Sleepiness Scale, which is self-administered, is also useful: patients rate the likelihood of falling asleep in various daytime contexts. These questionnaires can be seamlessly integrated into routine patient appointments.
Comorbidities and occupation
Primary care physicians should carefully assess comorbidities, especially those linked to cardiovascular risk. Patients with resistant hypertension, pulmonary hypertension, and recurrent atrial fibrillation following cardioversion/ablation should be prioritized for diagnostic testing for OSA. Patients with other conditions, such as coronary artery disease or cerebrovascular disease, should also be referred to a sleep center if OSA is suspected on the basis of comprehensive sleep assessment. OSA has also been associated with type 2 diabetes, metabolic syndrome, and asthma.
Gaining access to sleep study services and subsequent therapy, such as continuous positive airway pressure (CPAP), can be challenging. Primary care physicians should prioritize patients on the basis of their risk levels. Occupation plays a significant role in this prioritization, as sleep fragmentation and daytime sleepiness can lead to workplace and vehicular accidents.
“You should include the occupation in the patient’s profile. What is he doing? Is he sitting at a desk, or is he working at height, driving, or operating machines? These workers are high-risk patients,” continued Dr. De Almeida Vicente Ferreira.
“I think that the family physician has a key role in the follow-up. Nobody else will look for CPAP compliance and will verify if CPAP is working or not. If the patient is not using it or if it is not effective, still there is someone paying for the machine (the national health care system or an insurance company). More importantly, if CPAP is not working, we are not improving our patient’s life in terms of reducing cardiovascular risk and ameliorating the quality of life.”
Is home testing a viable option?
Diagnosing OSA typically relies on overnight polysomnography in specialized sleep clinics, which is often associated with long waiting lists. Researchers are actively working on innovative sensors and digital solutions for home-based sleep testing, but according to Dr. De Almeida Vicente Ferreira, they are not yet ready for prime time: “Home-based studies with fewer evaluation parameters (such as pulse and oxygen levels) are not so secure or sensitive to establish a correct and complete diagnosis. Actually, the architecture of sleep is very complex. The test must be performed and read by a specialized team.”
Still, according to Renaud Tamisier, MD, PhD, professor of clinical physiology at the Université Grenoble Alpes in La Tronche, France, simplified sleep testing could be very useful. “There are many patients that still are not diagnosed despite having severe sleep apnea, with symptoms and comorbidities. These patients usually are not aware of their disease but complain about changes in their quality of life with excessive tiredness and sleepiness. Also, they are not connected to the healthcare system, for different reasons, including no time for consulting a sleep physician and performing a polysomnography, health cost, negligence. Therefore, providing through primary care a simple diagnostic approach deserves efforts and research,” he said in an interview.
New technologies could enable diagnostic sleep tests to be conducted at home, with the added benefit of multiple-night recordings to overcome the challenges of night-to-night variability in the apnea-hypopnea index. These novel testing methods should be cost effective, easy to install, and user friendly. Dr. Tamisier continued: “The issue about sleep diagnosis is that up to now, there was no such devices available. Many physicians use type III sleep recording that are dedicated to highly trained sleep scorers, but they use automatic analysis which in many cases is unsuccessful. For a trained sleep physician, it is easy to see that the result is inaccurate. New devices are being built for automatic analysis using artificial intelligence algorithms. Because by design they are automatic, the rate of success is very high, and if used with the right purpose, they could be highly effective and quick.”
In conclusion, the diagnosis of sleep apnea in primary care is becoming more feasible with advancements in diagnostic tools and technology. However, it is crucial for primary care physicians to exercise caution in cases in which the clinical presentation is not straightforward or when OSA is associated with comorbidities. Care management and clear boundaries are vital to ensure effective treatment and improve patient outcomes.
Dr. De Almeida Vicente Ferreira and Dr. Tamisier disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ERS 2023
Diagnosing progressive pulmonary fibrosis
MILAN – The European Respiratory Society Congress 2023 dedicated an entire session to the multifaceted challenges and ongoing debates surrounding progressive pulmonary fibrosis (PPF). Renowned medical professionals and experts congregated in Milan to explore the current landscape and future prospects of diagnosing PPF, with a particular focus on expediting the diagnostic process.
Anna Podolanczuk, MD, assistant professor of medicine at Weill Cornell Medicine, New York, dissected the diagnostic intricacies of PPF, addressing not only the existing challenges but also the opportunities to streamline diagnosis.
As the session’s cochair, Michael Kreuter, MD, director of the Lung Center at University Hospital, Mainz, Germany, emphasized the importance of patients’ voices in understanding and addressing diseases. Joining him as a cochair was Marlies S. Wijsenbeek, a pulmonary physician and the head of the Interstitial Lung Disease Centre at Erasmus University Medical Centre in Rotterdam, the Netherlands.
The session commenced with a powerful testament from Elisabeth Robertson, a PPF patient representative from the United Kingdom. Diagnosed with PPF in 2011, her journey to diagnosis was far from straightforward, and she spoke in a video about the frustrations she encountered due to the lack of accessible information. Ms. Robertson called for a clearer diagnostic pathway.
Timely diagnosis: Key to better outcomes
Dr. Podolanczuk underscored the significance of early diagnosis, citing Ms. Robertson’s personal experience as a poignant example. An early diagnosis not only alleviates patients’ uncertainties and anxieties about their future but also enables the utilization of available treatments, such as antifibrotic therapies, which can slow the decline in forced vital capacity (FVC) in patients with progressive fibrotic interstitial lung diseases.
Data gleaned from the INBUILD trial was presented, revealing that patients in the placebo group experienced a nearly 200 mL decline in lung function over 52 weeks. Dr. Podolanczuk stressed that initiating antifibrotic therapies sooner could lead to better outcomes, as baseline conditions are likely to worsen over time.
“General practitioners can have a role in diagnosing and managing PPF. They are the frontline. We need to increase awareness, because they are generally not aware of this disease, and they usually think about COPD, asthma, or cardiovascular diseases whenever a patient presents with such symptoms,” Dr. Podolanczuk told this news organization.
Defining the challenge
The foundation of any diagnosis lies in a clear definition and established diagnostic criteria. During the session, it became apparent that different criteria could be employed for PPF diagnosis, leading to the identification of distinct patient populations.
In 2022, the Official ATS/ERS/JRS/ALAT Clinical Practice Guideline provided the first comprehensive definition of the PPF phenotype. According to this guideline, PPF is defined by the presence of at least two of three criteria: worsening symptoms, radiological progression, or physiologic progression defined as a ≥ 5% absolute decline in FVC or ≥ 10% absolute decline in diffusion lung CO (DLCO) within the past year in a patient with interstitial lung disease (ILD) and lung scarring other than idiopathic pulmonary fibrosis (IPF), with no alternative explanation.
“Definitions from the guidelines were based on the available trials at that moment. Registry data suggest that using different criteria will probably lead to the identification of different, but always progressive, populations,” Dr. Wijsenbeek commented to this news organization. “I think we should not worry too much about the details of the criteria and it is good that we have a multimodality assessment: We ask the patient, we look at the pictures, and we measure the lung function. Combining those data, you can have a robust indication of progression.”
The current landscape
Currently, PPF diagnosis hinges on a combination of CT scans, patient narratives, and, in some cases, histological examination. Dr. Wijsenbeek stressed the need to transition to novel diagnostic modalities, including tools that can be readily employed by GPs in their practices.
“GPs have to care about a lot of different diseases, and it makes it more complicated to be aware of conditions like PPF: Symptoms are in fact extremely unspecific” Dr. Kreuter told this news organization. “My suggestion to GPs is to pay attention to the so-called inspiratory crackles because they represent a very early and specific sign of lung fibrosis. This sound does not resemble any other sound that you can hear with your stethoscope: It is like the sound you make walking on fresh snow,” he added, recommending a referral to the pulmonologist in case of identification of inspiratory crackles.
Additionally, several biomarkers can contribute to early PPF diagnosis, including the identification of the usual interstitial pneumonia (UIP) pattern through biopsy or imaging. “We know that this pattern predicts poor outcomes regardless of ILD type,” Dr. Podolanczuk explained, underlining the possibility of using a molecular classifier to identify a UIP pattern on transbronchial lung biopsy. “This is an already existing technology used to identify a gene expression pattern that is strongly predictive of a UIP pattern,” she said.
Furthermore, blood biomarkers, such as high peripheral blood monocyte count and telomere length, hold promise for early PPF detection and prognosis assessment.
The road ahead
The diagnostic landscape for PPF is evolving rapidly, with various emerging biomarkers and tools showing promise. Proteomics, alongside home spirometry as a digital biomarker for frequent FVC monitoring, have demonstrated potential for identifying patients who may benefit from early treatment. A 2022 study defined a 12-proteomic biomarkers signature of progressive fibrosing ILD that can identify patients who may benefit from early treatment and is predictive of outcomes regardless of the underlying CT pattern.
The integration of artificial intelligence into the interpretation of CT and x-ray images represents another avenue of advancement in PPF diagnosis. Dr. Podolanczuk highlighted the role of AI and quantitative CTs in enhancing diagnostic accuracy. She also mentioned innovative imaging methods, such as hyperpolarized gas MRI and endobronchial optical coherence tomography (EB-OCT), which offer new insights into disease progression and treatment response.
Beyond imaging and AI, various research tools are entering the diagnostic arena, including real-time breath analysis for distinguishing between different respiratory conditions. These tools collectively promise to shorten the time from symptom presentation to PPF diagnosis, a vital step in improving patient outcomes. In the words of Dr. Podolanczuk, “How early is too early to identify these patients? Let me say that there’s no such thing as ‘too early’ in the diagnosis of PPF!”
Dr. Podolanczuk disclosed grant funding from NHLBI, ALA, and Three Lakes Foundation; consulting fees from Regeneron, Roche, Imvaria, Boehringer Ingelheim, Veracyte, United Therapeutics, and Eisai; and honoraria from NACE and EBSCO/DynaMed. Ms. Robertson disclosed having no conflict.
A version of this article first appeared on Medscape.com.
MILAN – The European Respiratory Society Congress 2023 dedicated an entire session to the multifaceted challenges and ongoing debates surrounding progressive pulmonary fibrosis (PPF). Renowned medical professionals and experts congregated in Milan to explore the current landscape and future prospects of diagnosing PPF, with a particular focus on expediting the diagnostic process.
Anna Podolanczuk, MD, assistant professor of medicine at Weill Cornell Medicine, New York, dissected the diagnostic intricacies of PPF, addressing not only the existing challenges but also the opportunities to streamline diagnosis.
As the session’s cochair, Michael Kreuter, MD, director of the Lung Center at University Hospital, Mainz, Germany, emphasized the importance of patients’ voices in understanding and addressing diseases. Joining him as a cochair was Marlies S. Wijsenbeek, a pulmonary physician and the head of the Interstitial Lung Disease Centre at Erasmus University Medical Centre in Rotterdam, the Netherlands.
The session commenced with a powerful testament from Elisabeth Robertson, a PPF patient representative from the United Kingdom. Diagnosed with PPF in 2011, her journey to diagnosis was far from straightforward, and she spoke in a video about the frustrations she encountered due to the lack of accessible information. Ms. Robertson called for a clearer diagnostic pathway.
Timely diagnosis: Key to better outcomes
Dr. Podolanczuk underscored the significance of early diagnosis, citing Ms. Robertson’s personal experience as a poignant example. An early diagnosis not only alleviates patients’ uncertainties and anxieties about their future but also enables the utilization of available treatments, such as antifibrotic therapies, which can slow the decline in forced vital capacity (FVC) in patients with progressive fibrotic interstitial lung diseases.
Data gleaned from the INBUILD trial was presented, revealing that patients in the placebo group experienced a nearly 200 mL decline in lung function over 52 weeks. Dr. Podolanczuk stressed that initiating antifibrotic therapies sooner could lead to better outcomes, as baseline conditions are likely to worsen over time.
“General practitioners can have a role in diagnosing and managing PPF. They are the frontline. We need to increase awareness, because they are generally not aware of this disease, and they usually think about COPD, asthma, or cardiovascular diseases whenever a patient presents with such symptoms,” Dr. Podolanczuk told this news organization.
Defining the challenge
The foundation of any diagnosis lies in a clear definition and established diagnostic criteria. During the session, it became apparent that different criteria could be employed for PPF diagnosis, leading to the identification of distinct patient populations.
In 2022, the Official ATS/ERS/JRS/ALAT Clinical Practice Guideline provided the first comprehensive definition of the PPF phenotype. According to this guideline, PPF is defined by the presence of at least two of three criteria: worsening symptoms, radiological progression, or physiologic progression defined as a ≥ 5% absolute decline in FVC or ≥ 10% absolute decline in diffusion lung CO (DLCO) within the past year in a patient with interstitial lung disease (ILD) and lung scarring other than idiopathic pulmonary fibrosis (IPF), with no alternative explanation.
“Definitions from the guidelines were based on the available trials at that moment. Registry data suggest that using different criteria will probably lead to the identification of different, but always progressive, populations,” Dr. Wijsenbeek commented to this news organization. “I think we should not worry too much about the details of the criteria and it is good that we have a multimodality assessment: We ask the patient, we look at the pictures, and we measure the lung function. Combining those data, you can have a robust indication of progression.”
The current landscape
Currently, PPF diagnosis hinges on a combination of CT scans, patient narratives, and, in some cases, histological examination. Dr. Wijsenbeek stressed the need to transition to novel diagnostic modalities, including tools that can be readily employed by GPs in their practices.
“GPs have to care about a lot of different diseases, and it makes it more complicated to be aware of conditions like PPF: Symptoms are in fact extremely unspecific” Dr. Kreuter told this news organization. “My suggestion to GPs is to pay attention to the so-called inspiratory crackles because they represent a very early and specific sign of lung fibrosis. This sound does not resemble any other sound that you can hear with your stethoscope: It is like the sound you make walking on fresh snow,” he added, recommending a referral to the pulmonologist in case of identification of inspiratory crackles.
Additionally, several biomarkers can contribute to early PPF diagnosis, including the identification of the usual interstitial pneumonia (UIP) pattern through biopsy or imaging. “We know that this pattern predicts poor outcomes regardless of ILD type,” Dr. Podolanczuk explained, underlining the possibility of using a molecular classifier to identify a UIP pattern on transbronchial lung biopsy. “This is an already existing technology used to identify a gene expression pattern that is strongly predictive of a UIP pattern,” she said.
Furthermore, blood biomarkers, such as high peripheral blood monocyte count and telomere length, hold promise for early PPF detection and prognosis assessment.
The road ahead
The diagnostic landscape for PPF is evolving rapidly, with various emerging biomarkers and tools showing promise. Proteomics, alongside home spirometry as a digital biomarker for frequent FVC monitoring, have demonstrated potential for identifying patients who may benefit from early treatment. A 2022 study defined a 12-proteomic biomarkers signature of progressive fibrosing ILD that can identify patients who may benefit from early treatment and is predictive of outcomes regardless of the underlying CT pattern.
The integration of artificial intelligence into the interpretation of CT and x-ray images represents another avenue of advancement in PPF diagnosis. Dr. Podolanczuk highlighted the role of AI and quantitative CTs in enhancing diagnostic accuracy. She also mentioned innovative imaging methods, such as hyperpolarized gas MRI and endobronchial optical coherence tomography (EB-OCT), which offer new insights into disease progression and treatment response.
Beyond imaging and AI, various research tools are entering the diagnostic arena, including real-time breath analysis for distinguishing between different respiratory conditions. These tools collectively promise to shorten the time from symptom presentation to PPF diagnosis, a vital step in improving patient outcomes. In the words of Dr. Podolanczuk, “How early is too early to identify these patients? Let me say that there’s no such thing as ‘too early’ in the diagnosis of PPF!”
Dr. Podolanczuk disclosed grant funding from NHLBI, ALA, and Three Lakes Foundation; consulting fees from Regeneron, Roche, Imvaria, Boehringer Ingelheim, Veracyte, United Therapeutics, and Eisai; and honoraria from NACE and EBSCO/DynaMed. Ms. Robertson disclosed having no conflict.
A version of this article first appeared on Medscape.com.
MILAN – The European Respiratory Society Congress 2023 dedicated an entire session to the multifaceted challenges and ongoing debates surrounding progressive pulmonary fibrosis (PPF). Renowned medical professionals and experts congregated in Milan to explore the current landscape and future prospects of diagnosing PPF, with a particular focus on expediting the diagnostic process.
Anna Podolanczuk, MD, assistant professor of medicine at Weill Cornell Medicine, New York, dissected the diagnostic intricacies of PPF, addressing not only the existing challenges but also the opportunities to streamline diagnosis.
As the session’s cochair, Michael Kreuter, MD, director of the Lung Center at University Hospital, Mainz, Germany, emphasized the importance of patients’ voices in understanding and addressing diseases. Joining him as a cochair was Marlies S. Wijsenbeek, a pulmonary physician and the head of the Interstitial Lung Disease Centre at Erasmus University Medical Centre in Rotterdam, the Netherlands.
The session commenced with a powerful testament from Elisabeth Robertson, a PPF patient representative from the United Kingdom. Diagnosed with PPF in 2011, her journey to diagnosis was far from straightforward, and she spoke in a video about the frustrations she encountered due to the lack of accessible information. Ms. Robertson called for a clearer diagnostic pathway.
Timely diagnosis: Key to better outcomes
Dr. Podolanczuk underscored the significance of early diagnosis, citing Ms. Robertson’s personal experience as a poignant example. An early diagnosis not only alleviates patients’ uncertainties and anxieties about their future but also enables the utilization of available treatments, such as antifibrotic therapies, which can slow the decline in forced vital capacity (FVC) in patients with progressive fibrotic interstitial lung diseases.
Data gleaned from the INBUILD trial was presented, revealing that patients in the placebo group experienced a nearly 200 mL decline in lung function over 52 weeks. Dr. Podolanczuk stressed that initiating antifibrotic therapies sooner could lead to better outcomes, as baseline conditions are likely to worsen over time.
“General practitioners can have a role in diagnosing and managing PPF. They are the frontline. We need to increase awareness, because they are generally not aware of this disease, and they usually think about COPD, asthma, or cardiovascular diseases whenever a patient presents with such symptoms,” Dr. Podolanczuk told this news organization.
Defining the challenge
The foundation of any diagnosis lies in a clear definition and established diagnostic criteria. During the session, it became apparent that different criteria could be employed for PPF diagnosis, leading to the identification of distinct patient populations.
In 2022, the Official ATS/ERS/JRS/ALAT Clinical Practice Guideline provided the first comprehensive definition of the PPF phenotype. According to this guideline, PPF is defined by the presence of at least two of three criteria: worsening symptoms, radiological progression, or physiologic progression defined as a ≥ 5% absolute decline in FVC or ≥ 10% absolute decline in diffusion lung CO (DLCO) within the past year in a patient with interstitial lung disease (ILD) and lung scarring other than idiopathic pulmonary fibrosis (IPF), with no alternative explanation.
“Definitions from the guidelines were based on the available trials at that moment. Registry data suggest that using different criteria will probably lead to the identification of different, but always progressive, populations,” Dr. Wijsenbeek commented to this news organization. “I think we should not worry too much about the details of the criteria and it is good that we have a multimodality assessment: We ask the patient, we look at the pictures, and we measure the lung function. Combining those data, you can have a robust indication of progression.”
The current landscape
Currently, PPF diagnosis hinges on a combination of CT scans, patient narratives, and, in some cases, histological examination. Dr. Wijsenbeek stressed the need to transition to novel diagnostic modalities, including tools that can be readily employed by GPs in their practices.
“GPs have to care about a lot of different diseases, and it makes it more complicated to be aware of conditions like PPF: Symptoms are in fact extremely unspecific” Dr. Kreuter told this news organization. “My suggestion to GPs is to pay attention to the so-called inspiratory crackles because they represent a very early and specific sign of lung fibrosis. This sound does not resemble any other sound that you can hear with your stethoscope: It is like the sound you make walking on fresh snow,” he added, recommending a referral to the pulmonologist in case of identification of inspiratory crackles.
Additionally, several biomarkers can contribute to early PPF diagnosis, including the identification of the usual interstitial pneumonia (UIP) pattern through biopsy or imaging. “We know that this pattern predicts poor outcomes regardless of ILD type,” Dr. Podolanczuk explained, underlining the possibility of using a molecular classifier to identify a UIP pattern on transbronchial lung biopsy. “This is an already existing technology used to identify a gene expression pattern that is strongly predictive of a UIP pattern,” she said.
Furthermore, blood biomarkers, such as high peripheral blood monocyte count and telomere length, hold promise for early PPF detection and prognosis assessment.
The road ahead
The diagnostic landscape for PPF is evolving rapidly, with various emerging biomarkers and tools showing promise. Proteomics, alongside home spirometry as a digital biomarker for frequent FVC monitoring, have demonstrated potential for identifying patients who may benefit from early treatment. A 2022 study defined a 12-proteomic biomarkers signature of progressive fibrosing ILD that can identify patients who may benefit from early treatment and is predictive of outcomes regardless of the underlying CT pattern.
The integration of artificial intelligence into the interpretation of CT and x-ray images represents another avenue of advancement in PPF diagnosis. Dr. Podolanczuk highlighted the role of AI and quantitative CTs in enhancing diagnostic accuracy. She also mentioned innovative imaging methods, such as hyperpolarized gas MRI and endobronchial optical coherence tomography (EB-OCT), which offer new insights into disease progression and treatment response.
Beyond imaging and AI, various research tools are entering the diagnostic arena, including real-time breath analysis for distinguishing between different respiratory conditions. These tools collectively promise to shorten the time from symptom presentation to PPF diagnosis, a vital step in improving patient outcomes. In the words of Dr. Podolanczuk, “How early is too early to identify these patients? Let me say that there’s no such thing as ‘too early’ in the diagnosis of PPF!”
Dr. Podolanczuk disclosed grant funding from NHLBI, ALA, and Three Lakes Foundation; consulting fees from Regeneron, Roche, Imvaria, Boehringer Ingelheim, Veracyte, United Therapeutics, and Eisai; and honoraria from NACE and EBSCO/DynaMed. Ms. Robertson disclosed having no conflict.
A version of this article first appeared on Medscape.com.
AT ERS 2023
SGLT2 inhibitors: No benefit or harm in hospitalized COVID-19
A new meta-analysis has shown that SGLT2 inhibitors do not lead to lower 28-day all-cause mortality, compared with usual care or placebo, in patients hospitalized with COVID-19.
However, no major safety issues were identified with the use of SGLT2 inhibitors in these acutely ill patients, the researchers report.
“While these findings do not support the use of SGLT2-inhibitors as standard of care for patients hospitalized with COVID-19, I think the most important take home message here is that the use of these medications appears to be safe even in really acutely ill hospitalized patients,” lead investigator of the meta-analysis, Mikhail Kosiborod, MD, Saint Luke’s Mid America Heart Institute, Kansas City, Mo., concluded.
He said this was important because the list of indications for SGLT2 inhibitors is rapidly growing.
“These medications are being used in more and more patients. And we know that when we discontinue medications in the hospital they frequently don’t get restarted, which can lead to real risks if SGLT2 inhibitors are stopped in patients with heart failure, chronic kidney disease, or diabetes. So, ,” he added.
The new meta-analysis was presented at the recent annual congress of the European Society of Cardiology, held in Amsterdam.
Discussant of the presentation at the ESC Hotline session, Muthiah Vaduganathan, MD, MPH, Brigham and Women’s Hospital, Boston, agreed with Dr. Kosiborod’s interpretation.
“Until today we have had very limited information on the safety of SGLT2-inhibitors in acute illness, as the pivotal trials which established the use of these drugs in diabetes and chronic kidney disease largely excluded patients who were hospitalized,” Dr. Vaduganathan said.
“While the overall results of this meta-analysis are neutral and SGLT2 inhibitors will not be added as drugs to be used in the primary care of patients with COVID-19, it certainly sends a strong message of safety in acutely ill patients,” he added.
Dr. Vaduganathan explained that from the beginning of the COVID-19 pandemic, there was great interest in repurposing established therapies for alternative indications for their use in the management of COVID-19.
“Conditions that strongly predispose to adverse COVID outcomes strongly overlap with established indications for SGLT2-inhibitors. So many wondered whether these drugs may be an ideal treatment candidate for the management of COVID-19. However, there have been many safety concerns about the use of SGLT2-inhibitors in this acute setting, with worries that they may induce hemodynamic changes such an excessive lowering of blood pressure, or metabolic changes such as ketoacidosis in acutely ill patients,” he noted.
The initial DARE-19 study investigating SGLT2-inhibitors in COVID-19, with 1,250 participants, found a 20% reduction in the primary outcome of organ dysfunction or death, but this did not reach statistical significance, and no safety issues were seen. This “intriguing” result led to two further larger trials – the ACTIV-4a and RECOVERY trials, Dr. Vaduganathan reported.
“Those early signals of benefit seen in DARE-19 were largely not substantiated in the ACTIV-4A and RECOVERY trials, or in this new meta-analysis, and now we have this much larger body of evidence and more stable estimates about the efficacy of these drugs in acutely ill COVID-19 patients,” he said.
“But the story that we will all take forward is one of safety. This set of trials was arguably conducted in some of the sickest patients we’ve seen who have been exposed to SGLT2-inhibitors, and they strongly affirm that these agents can be safely continued in the setting of acute illness, with very low rates of ketoacidosis and kidney injury, and there was no prolongation of hospital stay,” he commented.
In his presentation, Dr. Kosiborod explained that treatments targeting COVID-19 pathobiology such as dysregulated immune responses, endothelial damage, microvascular thrombosis, and inflammation have been shown to improve the key outcomes in this patient group.
SGLT2 inhibitors, which modulate similar pathobiology, provide cardiovascular protection and prevent the progression of kidney disease in patients at risk for these events, including those with type 2 diabetes, heart failure, and kidney disease, and may also lead to organ protection in a setting of acute illness such as COVID-19, he noted. However, the role of SGLT2 inhibitors in patients hospitalized with COVID-19 remains uncertain.
To address the need for more definitive efficacy data, the World Health Organization Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group conducted a prospective meta-analysis using data from the three randomized controlled trials, DARE-19, RECOVERY, and ACTIV-4a, evaluating SGLT2 inhibitors in patients hospitalized with COVID-19.
Overall, these trials randomized 6,096 participants: 3,025 to SGLT2 inhibitors and 3,071 to usual care or placebo. The average age of participants ranged between 62 and 73 years across the trials, 39% were women, and 25% had type 2 diabetes.
By 28 days after randomization, all-cause mortality, the primary endpoint, had occurred in 11.6% of the SGLT2-inhibitor patients, compared with 12.4% of those randomized to usual care or placebo, giving an odds ratio of 0.93 (95% confidence interval, 0.79-1.08; P = .33) for SGLT2 inhibitors, with consistency across trials.
Data on in-hospital and 90-day all-cause mortality were only available for two out of three trials (DARE-19 and ACTIV-4a), but the results were similar to the primary endpoint showing nonsignificant trends toward a possible benefit in the SGLT2-inhibitor group.
The results were also similar for the secondary outcomes of progression to acute kidney injury or requirement for dialysis or death, and progression to invasive mechanical ventilation, extracorporeal membrane oxygenation, or death, both assessed at 28 days.
The primary safety outcome of ketoacidosis by 28 days was observed in seven and two patients allocated to SGLT2 inhibitors and usual care or placebo, respectively, and overall, the incidence of reported serious adverse events was balanced between treatment groups.
The RECOVERY trial was supported by grants to the University of Oxford from UK Research and Innovation, the National Institute for Health and Care Research, and Wellcome. The ACTIV-4a platform was sponsored by the National Heart, Lung, and Blood Institute. DARE-19 was an investigator-initiated collaborative trial supported by AstraZeneca. Dr. Kosiborod reported numerous conflicts of interest.
A version of this article first appeared on Medscape.com.
A new meta-analysis has shown that SGLT2 inhibitors do not lead to lower 28-day all-cause mortality, compared with usual care or placebo, in patients hospitalized with COVID-19.
However, no major safety issues were identified with the use of SGLT2 inhibitors in these acutely ill patients, the researchers report.
“While these findings do not support the use of SGLT2-inhibitors as standard of care for patients hospitalized with COVID-19, I think the most important take home message here is that the use of these medications appears to be safe even in really acutely ill hospitalized patients,” lead investigator of the meta-analysis, Mikhail Kosiborod, MD, Saint Luke’s Mid America Heart Institute, Kansas City, Mo., concluded.
He said this was important because the list of indications for SGLT2 inhibitors is rapidly growing.
“These medications are being used in more and more patients. And we know that when we discontinue medications in the hospital they frequently don’t get restarted, which can lead to real risks if SGLT2 inhibitors are stopped in patients with heart failure, chronic kidney disease, or diabetes. So, ,” he added.
The new meta-analysis was presented at the recent annual congress of the European Society of Cardiology, held in Amsterdam.
Discussant of the presentation at the ESC Hotline session, Muthiah Vaduganathan, MD, MPH, Brigham and Women’s Hospital, Boston, agreed with Dr. Kosiborod’s interpretation.
“Until today we have had very limited information on the safety of SGLT2-inhibitors in acute illness, as the pivotal trials which established the use of these drugs in diabetes and chronic kidney disease largely excluded patients who were hospitalized,” Dr. Vaduganathan said.
“While the overall results of this meta-analysis are neutral and SGLT2 inhibitors will not be added as drugs to be used in the primary care of patients with COVID-19, it certainly sends a strong message of safety in acutely ill patients,” he added.
Dr. Vaduganathan explained that from the beginning of the COVID-19 pandemic, there was great interest in repurposing established therapies for alternative indications for their use in the management of COVID-19.
“Conditions that strongly predispose to adverse COVID outcomes strongly overlap with established indications for SGLT2-inhibitors. So many wondered whether these drugs may be an ideal treatment candidate for the management of COVID-19. However, there have been many safety concerns about the use of SGLT2-inhibitors in this acute setting, with worries that they may induce hemodynamic changes such an excessive lowering of blood pressure, or metabolic changes such as ketoacidosis in acutely ill patients,” he noted.
The initial DARE-19 study investigating SGLT2-inhibitors in COVID-19, with 1,250 participants, found a 20% reduction in the primary outcome of organ dysfunction or death, but this did not reach statistical significance, and no safety issues were seen. This “intriguing” result led to two further larger trials – the ACTIV-4a and RECOVERY trials, Dr. Vaduganathan reported.
“Those early signals of benefit seen in DARE-19 were largely not substantiated in the ACTIV-4A and RECOVERY trials, or in this new meta-analysis, and now we have this much larger body of evidence and more stable estimates about the efficacy of these drugs in acutely ill COVID-19 patients,” he said.
“But the story that we will all take forward is one of safety. This set of trials was arguably conducted in some of the sickest patients we’ve seen who have been exposed to SGLT2-inhibitors, and they strongly affirm that these agents can be safely continued in the setting of acute illness, with very low rates of ketoacidosis and kidney injury, and there was no prolongation of hospital stay,” he commented.
In his presentation, Dr. Kosiborod explained that treatments targeting COVID-19 pathobiology such as dysregulated immune responses, endothelial damage, microvascular thrombosis, and inflammation have been shown to improve the key outcomes in this patient group.
SGLT2 inhibitors, which modulate similar pathobiology, provide cardiovascular protection and prevent the progression of kidney disease in patients at risk for these events, including those with type 2 diabetes, heart failure, and kidney disease, and may also lead to organ protection in a setting of acute illness such as COVID-19, he noted. However, the role of SGLT2 inhibitors in patients hospitalized with COVID-19 remains uncertain.
To address the need for more definitive efficacy data, the World Health Organization Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group conducted a prospective meta-analysis using data from the three randomized controlled trials, DARE-19, RECOVERY, and ACTIV-4a, evaluating SGLT2 inhibitors in patients hospitalized with COVID-19.
Overall, these trials randomized 6,096 participants: 3,025 to SGLT2 inhibitors and 3,071 to usual care or placebo. The average age of participants ranged between 62 and 73 years across the trials, 39% were women, and 25% had type 2 diabetes.
By 28 days after randomization, all-cause mortality, the primary endpoint, had occurred in 11.6% of the SGLT2-inhibitor patients, compared with 12.4% of those randomized to usual care or placebo, giving an odds ratio of 0.93 (95% confidence interval, 0.79-1.08; P = .33) for SGLT2 inhibitors, with consistency across trials.
Data on in-hospital and 90-day all-cause mortality were only available for two out of three trials (DARE-19 and ACTIV-4a), but the results were similar to the primary endpoint showing nonsignificant trends toward a possible benefit in the SGLT2-inhibitor group.
The results were also similar for the secondary outcomes of progression to acute kidney injury or requirement for dialysis or death, and progression to invasive mechanical ventilation, extracorporeal membrane oxygenation, or death, both assessed at 28 days.
The primary safety outcome of ketoacidosis by 28 days was observed in seven and two patients allocated to SGLT2 inhibitors and usual care or placebo, respectively, and overall, the incidence of reported serious adverse events was balanced between treatment groups.
The RECOVERY trial was supported by grants to the University of Oxford from UK Research and Innovation, the National Institute for Health and Care Research, and Wellcome. The ACTIV-4a platform was sponsored by the National Heart, Lung, and Blood Institute. DARE-19 was an investigator-initiated collaborative trial supported by AstraZeneca. Dr. Kosiborod reported numerous conflicts of interest.
A version of this article first appeared on Medscape.com.
A new meta-analysis has shown that SGLT2 inhibitors do not lead to lower 28-day all-cause mortality, compared with usual care or placebo, in patients hospitalized with COVID-19.
However, no major safety issues were identified with the use of SGLT2 inhibitors in these acutely ill patients, the researchers report.
“While these findings do not support the use of SGLT2-inhibitors as standard of care for patients hospitalized with COVID-19, I think the most important take home message here is that the use of these medications appears to be safe even in really acutely ill hospitalized patients,” lead investigator of the meta-analysis, Mikhail Kosiborod, MD, Saint Luke’s Mid America Heart Institute, Kansas City, Mo., concluded.
He said this was important because the list of indications for SGLT2 inhibitors is rapidly growing.
“These medications are being used in more and more patients. And we know that when we discontinue medications in the hospital they frequently don’t get restarted, which can lead to real risks if SGLT2 inhibitors are stopped in patients with heart failure, chronic kidney disease, or diabetes. So, ,” he added.
The new meta-analysis was presented at the recent annual congress of the European Society of Cardiology, held in Amsterdam.
Discussant of the presentation at the ESC Hotline session, Muthiah Vaduganathan, MD, MPH, Brigham and Women’s Hospital, Boston, agreed with Dr. Kosiborod’s interpretation.
“Until today we have had very limited information on the safety of SGLT2-inhibitors in acute illness, as the pivotal trials which established the use of these drugs in diabetes and chronic kidney disease largely excluded patients who were hospitalized,” Dr. Vaduganathan said.
“While the overall results of this meta-analysis are neutral and SGLT2 inhibitors will not be added as drugs to be used in the primary care of patients with COVID-19, it certainly sends a strong message of safety in acutely ill patients,” he added.
Dr. Vaduganathan explained that from the beginning of the COVID-19 pandemic, there was great interest in repurposing established therapies for alternative indications for their use in the management of COVID-19.
“Conditions that strongly predispose to adverse COVID outcomes strongly overlap with established indications for SGLT2-inhibitors. So many wondered whether these drugs may be an ideal treatment candidate for the management of COVID-19. However, there have been many safety concerns about the use of SGLT2-inhibitors in this acute setting, with worries that they may induce hemodynamic changes such an excessive lowering of blood pressure, or metabolic changes such as ketoacidosis in acutely ill patients,” he noted.
The initial DARE-19 study investigating SGLT2-inhibitors in COVID-19, with 1,250 participants, found a 20% reduction in the primary outcome of organ dysfunction or death, but this did not reach statistical significance, and no safety issues were seen. This “intriguing” result led to two further larger trials – the ACTIV-4a and RECOVERY trials, Dr. Vaduganathan reported.
“Those early signals of benefit seen in DARE-19 were largely not substantiated in the ACTIV-4A and RECOVERY trials, or in this new meta-analysis, and now we have this much larger body of evidence and more stable estimates about the efficacy of these drugs in acutely ill COVID-19 patients,” he said.
“But the story that we will all take forward is one of safety. This set of trials was arguably conducted in some of the sickest patients we’ve seen who have been exposed to SGLT2-inhibitors, and they strongly affirm that these agents can be safely continued in the setting of acute illness, with very low rates of ketoacidosis and kidney injury, and there was no prolongation of hospital stay,” he commented.
In his presentation, Dr. Kosiborod explained that treatments targeting COVID-19 pathobiology such as dysregulated immune responses, endothelial damage, microvascular thrombosis, and inflammation have been shown to improve the key outcomes in this patient group.
SGLT2 inhibitors, which modulate similar pathobiology, provide cardiovascular protection and prevent the progression of kidney disease in patients at risk for these events, including those with type 2 diabetes, heart failure, and kidney disease, and may also lead to organ protection in a setting of acute illness such as COVID-19, he noted. However, the role of SGLT2 inhibitors in patients hospitalized with COVID-19 remains uncertain.
To address the need for more definitive efficacy data, the World Health Organization Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group conducted a prospective meta-analysis using data from the three randomized controlled trials, DARE-19, RECOVERY, and ACTIV-4a, evaluating SGLT2 inhibitors in patients hospitalized with COVID-19.
Overall, these trials randomized 6,096 participants: 3,025 to SGLT2 inhibitors and 3,071 to usual care or placebo. The average age of participants ranged between 62 and 73 years across the trials, 39% were women, and 25% had type 2 diabetes.
By 28 days after randomization, all-cause mortality, the primary endpoint, had occurred in 11.6% of the SGLT2-inhibitor patients, compared with 12.4% of those randomized to usual care or placebo, giving an odds ratio of 0.93 (95% confidence interval, 0.79-1.08; P = .33) for SGLT2 inhibitors, with consistency across trials.
Data on in-hospital and 90-day all-cause mortality were only available for two out of three trials (DARE-19 and ACTIV-4a), but the results were similar to the primary endpoint showing nonsignificant trends toward a possible benefit in the SGLT2-inhibitor group.
The results were also similar for the secondary outcomes of progression to acute kidney injury or requirement for dialysis or death, and progression to invasive mechanical ventilation, extracorporeal membrane oxygenation, or death, both assessed at 28 days.
The primary safety outcome of ketoacidosis by 28 days was observed in seven and two patients allocated to SGLT2 inhibitors and usual care or placebo, respectively, and overall, the incidence of reported serious adverse events was balanced between treatment groups.
The RECOVERY trial was supported by grants to the University of Oxford from UK Research and Innovation, the National Institute for Health and Care Research, and Wellcome. The ACTIV-4a platform was sponsored by the National Heart, Lung, and Blood Institute. DARE-19 was an investigator-initiated collaborative trial supported by AstraZeneca. Dr. Kosiborod reported numerous conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2023
Should intravascular imaging be almost routine in PCI?
A routine role for intravascular imaging (IVI) guidance for percutaneous coronary intervention (PCI) has long been favored by many of the technology’s researchers and enthusiasts. Now evidence from large, randomized trials may be catching up with such aspirations, though not without caveats.
One way IVI guidance may achieve that, the research suggests, albeit more speculatively, is by cutting risk for stent thrombosis, compared with the risk associated with angiography-only PCI.
The new studies, two large randomized IVI trials plus a meta-analysis of 20 such studies, were presented at the annual congress of the European Society of Cardiology.
In one, called ILUMIEN-4, PCI guided by optical coherence tomography (OCT) was associated with fewer procedural complications and better acute results – that is, larger post-PCI minimum stent area (MSA) – than in angiography-only procedures (P < .001). Poststenting MSA, an established predictor of clinical outcomes, was the primary imaging endpoint of the trial with almost 2,500 patients.
Yet the OCT group’s greater post-PCI MSA did not translate to reduced risk for the primary clinical endpoint of 2-year target-vessel failure. Among secondary endpoints, however, stent thrombosis at some point during the follow-up was 64% less likely (P = .02) with OCT guidance than angiography-only PCI.
ILUMIEN-4, despite its neutral clinical result, still “strongly advocates” for PCI guidance by OCT, at least among patients like those in the trial, said principal investigator Ziad Ali, MD, DPhil. He based that largely on the strategy’s greater postprocedure lumen areas in the trials, which are among “the strongest independent predictors for long term outcomes,” said Dr. Ali, of St. Francis Hospital & Heart Center, Roslyn, N.Y., at a press conference on IVI trials during the ESC Congress.
Selected complex lesion type
In contrast, the OCTOBER trial, presented at the sessions back to back with ILUMIEN-4, saw OCT guidance lead to better clinical outcomes than angiography alone after PCI of bifurcation lesions, which normally can be a special challenge for operators.
In the trial, which entered about 1,200 patients with such complex lesions, the 2-year risk for major adverse cardiac events (MACE) fell 60% after OCT-guided PCI, compared with angiography-only procedures (P = .035).
The finding is novel for showing that OCT guidance in bifurcation PCI can make a significant clinical difference, said OCTOBER investigator Niels R. Holm, MD, at the same media presentation on IVI trials.
“Multiple studies have shown that OCT allows for optimization of bifurcation PCI, and our results confirm that such optimization may improve the patient’s prognosis,” said Dr. Holm of Aarhus (Denmark) University Hospital.
ILUMIEN-4 and OCTOBER, both of which prespecified the Xience (Abbott) everolimus-eluting stent for the procedures, were published in the New England Journal of Medicine in tandem with their respective presentations at the ESC sessions.
Covering the spectrum
A meta-analysis presented at the same ESC session compared IVI using either OCT or intravascular ultrasound (IVUS) with angiography-only PCI across 20 randomized trials with a total of more than 12,000 patients.
Significant outcomes for IVI guidance versus angiography alone included a 31% drop in risk for target-lesion failure, the primary endpoint. And this study, as well, showed a steep 52% reduction in risk for in-stent thrombosis with the IVI-guided approach.

And “for the first time” in IVI studies, “we demonstrated reductions in all-myocardial-infarction and all-cause death, the latter by 25%,” Gregg Stone, MD, Icahn School of Medicine at Mount Sinai, New York, said in presenting the meta-analysis. Dr. Stone is also the ILUMIEN-4 study chairperson.
“The routine use of OCT or IVUS to guide most PCI procedures will substantially improve patient event-free survival,” he predicted, “enhancing both the long-term safety and effectiveness of the procedure.”
Dr. Stone said that IVI guidance “should be standard of care, if not in all patients, then in most patients.” Part of the rationale: PCI is unlikely to be improved much further by incremental gains in drug-eluting stent design. “That technology has almost plateaued.” But there’s yet room for “substantially improved outcomes” from adjunctive treatments and techniques such as IVI guidance.
The 20 studies in the meta-analysis encompassed an array of patients and lesions both complex and noncomplex, Dr. Stone observed, including bifurcation lesions, chronic total occlusions, left-main coronary stenoses, and MI culprit lesions.
“They really covered the spectrum of PCI,” he said. “I’m not recommending that intravascular imaging be used in every single case. But I do think it should be used in the majority of patients” and be standard of care for PCI in left-main lesions and “complex coronary disease, high-risk patients, and high-risk lesions.”
Unique advantage
The IVI-guidance groups in both ILUMIEN-4 and the meta-analysis showed a significant drop in risk for stent thrombosis – that is, abrupt thrombotic vessel closure, which typically occurs in 1% or fewer PCI cases but can trigger an MI and pose a mortality risk up to 45%.
Those risk reductions are consistent with a unique IVI advantage: the ability to guide optimization of stent deployments. When formally presenting ILUMIEN-4 at the ESC sessions, Ali observed that IVUS and OCT imaging allows operators to identify and often correct less-than-ideal results of an initial stent delivery – such as residual gaps between stent struts and vessel wall – that may encroach on the lumen, with possible clinical consequences.
Such imaging, said Dr. Ali, “lets you identify tissue protrusions, malappositions, dissections, and untreated reference-segment disease” that may potentially trigger thrombosis. That makes a strong argument for giving IVI guidance a more common, perhaps even routine role in PCI procedures.
Selling routine IVI-guided PCI in practice
“I think the study results are quite clear,” said Deepak L. Bhatt, MD, MPH, as session comoderator following the OCTOBER presentation. “The challenge, though, will be convincing the average interventional cardiologist worldwide that it was specifically the imaging and not the extra care that the patient getting OCT also inherently receives.”

Did OCT’s better trial outcomes stem from IVI itself or from greater operator attentiveness to procedural results – such as, for example, more high-pressure expansions to optimize stent placement, “the sort of thing that tends to occur when invasive imaging is added on to just plain old angiography?” Dr. Bhatt asked of Lene N. Andreasen, MD, who had just presented the OCTOBER trial. “There’s no way of uncoupling the two things.”
What can be said, “at this point, to convince interventional cardiologists that the extra time, energy, expense, is truly indicated,” that the data are “sufficient to change global practice?” asked Dr. Bhatt, Mount Sinai Hospital and Icahn School of Medicine at Mount Sinai.
That remains an open question,” acknowledged Dr. Andreasen of Aarhus University Hospital. The best argument in favor of selective IVI-guided PCI is that “we actually see a clinical benefit” in the trials. “But of course, it comes with a cost. It comes with longer procedures and more contrast.” How clinical practice responds to the new data remains to be seen, she proposed.
ILUMIEN-4 and OCTOBER in detail
Conducted at 80 centers in 18 countries, ILUMIEN-4 randomly assigned patients with diabetes or complex coronary lesions to undergo PCI guided by OCT or using standard angiography only, 1,233 and 1,254 patients, respectively.
Post-PCI MSA averaged 5.72 mm2 with OCT guidance and 5.36 mm2 in the angiography-only group (P < .001).
Their rates of target-vessel failure at 2 years were not significantly different at 7.4% and 8.2%, respectively. The 2-year composite endpoint included cardiac death, target vessel–related MI, or ischemia-driven target-vessel revascularization.
Definite or probable stent thrombosis was observed over 2 years in 0.5% of the OCT group and 1.4% of those with angiography-only PCI (hazard ratio, 0.36; 95% confidence interval, 0.14-0.91; P = .02) favoring OCT.
The OCTOBER trial, conducted at 38 centers in Europe, entered 1201 patients with stable angina or acute coronary syndromes and angiographically identified complex bifurcation lesions. They involved the left-main coronary artery in about one-fifth of cases.
Patients were randomly assigned to bifurcation PCI guided by OCT or under standard angiography, 600 and 601 patients, respectively. Rates for procedure-related complications were similar at 6.8% and 5.7%, respectively.
Over a median of 2 years, 10.1% of the OCT group and 14.1% of angiography-only patients developed a MACE event, including cardiac death, target-lesion MI, or ischemia-driven target-lesion revascularization. The adjusted HR was 0.71 (95% CI, 0.51-0.98; P = .035) in favor of OCT.
Meta-analysis, trials to date
The meta-analysis presented by Dr. Stone included ILUMIEN-4, OCTOBER, and 18 earlier outcomes trials comparing PCI guided by IVI, either OCT or IVUS, and angiography-only PCI. It covered 12,428 patients with chronic or acute coronary disease and followed them a mean of 26 months; the longest follow-up was 5 years. They were assigned to IVI-guided or angiography-only PCI, 7,038 and 5,390 patients, respectively.
Dr. Stone and colleagues conducted a network meta-analysis of the 20 studies, that is, a combined analysis that allowed both direct and indirect comparisons of standard angiography-only procedures to each of the other studied comparator interventions including OCT, IVUS, and either OCT or IVUS. They then derived network-estimate odds ratios for IVI-guided PCI vs angiography-only procedures.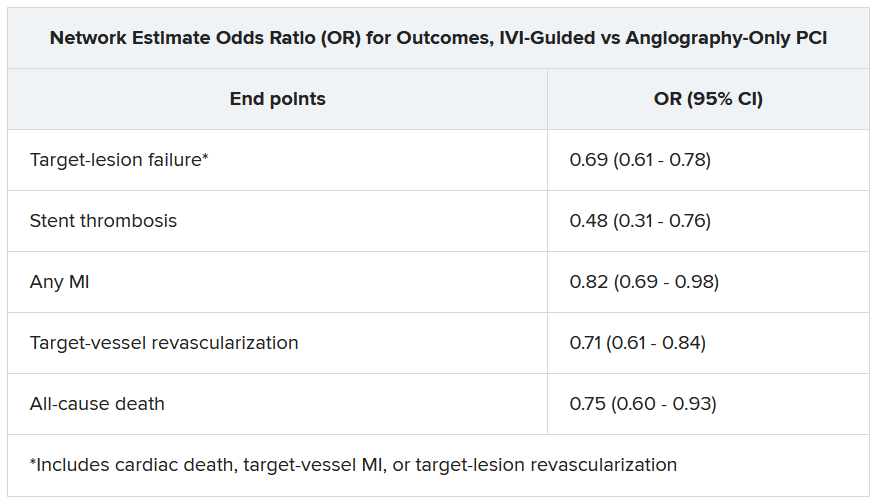
“Hopefully, this will impact the guidelines,” Dr. Stone said of the meta-analysis. Procedures guided by IVI might become more common in clinical practice if they were to garner a Class-I guideline recommendation, the strongest recommendation category.
“That would make a difference, but we’d also need to work to remove impediments to increasing intravascular imaging guidance” for most patients undergoing PCI, he said, referring to challenges in obtaining reimbursement for IVI-guided PCI and training enough operators to handle the projected demand.
ILUMIEN-4 was funded by Abbott. OCTOBER was supported by grants from Abbott Vascular, St. Jude Medical, and Aarhus University. The network meta-analysis received statistical support from Abbott. Dr. Ali disclosed institutional grant support from Abbott, Abiomed, Acist Medical, Boston Scientific, Cardiovascular Systems, Medtronic, the National Institutes of Health, Opsens Medical, Philips, and Teleflex; consulting fees from Astra Zeneca, Philips, Shockwave; and holding equity in Elucid, Spectrawave, Shockwave, and VitalConnect. Dr. Holm and Dr. Bhatt reported numerous conflicts of interest. Dr. Andreasen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A routine role for intravascular imaging (IVI) guidance for percutaneous coronary intervention (PCI) has long been favored by many of the technology’s researchers and enthusiasts. Now evidence from large, randomized trials may be catching up with such aspirations, though not without caveats.
One way IVI guidance may achieve that, the research suggests, albeit more speculatively, is by cutting risk for stent thrombosis, compared with the risk associated with angiography-only PCI.
The new studies, two large randomized IVI trials plus a meta-analysis of 20 such studies, were presented at the annual congress of the European Society of Cardiology.
In one, called ILUMIEN-4, PCI guided by optical coherence tomography (OCT) was associated with fewer procedural complications and better acute results – that is, larger post-PCI minimum stent area (MSA) – than in angiography-only procedures (P < .001). Poststenting MSA, an established predictor of clinical outcomes, was the primary imaging endpoint of the trial with almost 2,500 patients.
Yet the OCT group’s greater post-PCI MSA did not translate to reduced risk for the primary clinical endpoint of 2-year target-vessel failure. Among secondary endpoints, however, stent thrombosis at some point during the follow-up was 64% less likely (P = .02) with OCT guidance than angiography-only PCI.
ILUMIEN-4, despite its neutral clinical result, still “strongly advocates” for PCI guidance by OCT, at least among patients like those in the trial, said principal investigator Ziad Ali, MD, DPhil. He based that largely on the strategy’s greater postprocedure lumen areas in the trials, which are among “the strongest independent predictors for long term outcomes,” said Dr. Ali, of St. Francis Hospital & Heart Center, Roslyn, N.Y., at a press conference on IVI trials during the ESC Congress.
Selected complex lesion type
In contrast, the OCTOBER trial, presented at the sessions back to back with ILUMIEN-4, saw OCT guidance lead to better clinical outcomes than angiography alone after PCI of bifurcation lesions, which normally can be a special challenge for operators.
In the trial, which entered about 1,200 patients with such complex lesions, the 2-year risk for major adverse cardiac events (MACE) fell 60% after OCT-guided PCI, compared with angiography-only procedures (P = .035).
The finding is novel for showing that OCT guidance in bifurcation PCI can make a significant clinical difference, said OCTOBER investigator Niels R. Holm, MD, at the same media presentation on IVI trials.
“Multiple studies have shown that OCT allows for optimization of bifurcation PCI, and our results confirm that such optimization may improve the patient’s prognosis,” said Dr. Holm of Aarhus (Denmark) University Hospital.
ILUMIEN-4 and OCTOBER, both of which prespecified the Xience (Abbott) everolimus-eluting stent for the procedures, were published in the New England Journal of Medicine in tandem with their respective presentations at the ESC sessions.
Covering the spectrum
A meta-analysis presented at the same ESC session compared IVI using either OCT or intravascular ultrasound (IVUS) with angiography-only PCI across 20 randomized trials with a total of more than 12,000 patients.
Significant outcomes for IVI guidance versus angiography alone included a 31% drop in risk for target-lesion failure, the primary endpoint. And this study, as well, showed a steep 52% reduction in risk for in-stent thrombosis with the IVI-guided approach.
And “for the first time” in IVI studies, “we demonstrated reductions in all-myocardial-infarction and all-cause death, the latter by 25%,” Gregg Stone, MD, Icahn School of Medicine at Mount Sinai, New York, said in presenting the meta-analysis. Dr. Stone is also the ILUMIEN-4 study chairperson.
“The routine use of OCT or IVUS to guide most PCI procedures will substantially improve patient event-free survival,” he predicted, “enhancing both the long-term safety and effectiveness of the procedure.”
Dr. Stone said that IVI guidance “should be standard of care, if not in all patients, then in most patients.” Part of the rationale: PCI is unlikely to be improved much further by incremental gains in drug-eluting stent design. “That technology has almost plateaued.” But there’s yet room for “substantially improved outcomes” from adjunctive treatments and techniques such as IVI guidance.
The 20 studies in the meta-analysis encompassed an array of patients and lesions both complex and noncomplex, Dr. Stone observed, including bifurcation lesions, chronic total occlusions, left-main coronary stenoses, and MI culprit lesions.
“They really covered the spectrum of PCI,” he said. “I’m not recommending that intravascular imaging be used in every single case. But I do think it should be used in the majority of patients” and be standard of care for PCI in left-main lesions and “complex coronary disease, high-risk patients, and high-risk lesions.”
Unique advantage
The IVI-guidance groups in both ILUMIEN-4 and the meta-analysis showed a significant drop in risk for stent thrombosis – that is, abrupt thrombotic vessel closure, which typically occurs in 1% or fewer PCI cases but can trigger an MI and pose a mortality risk up to 45%.
Those risk reductions are consistent with a unique IVI advantage: the ability to guide optimization of stent deployments. When formally presenting ILUMIEN-4 at the ESC sessions, Ali observed that IVUS and OCT imaging allows operators to identify and often correct less-than-ideal results of an initial stent delivery – such as residual gaps between stent struts and vessel wall – that may encroach on the lumen, with possible clinical consequences.
Such imaging, said Dr. Ali, “lets you identify tissue protrusions, malappositions, dissections, and untreated reference-segment disease” that may potentially trigger thrombosis. That makes a strong argument for giving IVI guidance a more common, perhaps even routine role in PCI procedures.
Selling routine IVI-guided PCI in practice
“I think the study results are quite clear,” said Deepak L. Bhatt, MD, MPH, as session comoderator following the OCTOBER presentation. “The challenge, though, will be convincing the average interventional cardiologist worldwide that it was specifically the imaging and not the extra care that the patient getting OCT also inherently receives.”
Did OCT’s better trial outcomes stem from IVI itself or from greater operator attentiveness to procedural results – such as, for example, more high-pressure expansions to optimize stent placement, “the sort of thing that tends to occur when invasive imaging is added on to just plain old angiography?” Dr. Bhatt asked of Lene N. Andreasen, MD, who had just presented the OCTOBER trial. “There’s no way of uncoupling the two things.”
What can be said, “at this point, to convince interventional cardiologists that the extra time, energy, expense, is truly indicated,” that the data are “sufficient to change global practice?” asked Dr. Bhatt, Mount Sinai Hospital and Icahn School of Medicine at Mount Sinai.
That remains an open question,” acknowledged Dr. Andreasen of Aarhus University Hospital. The best argument in favor of selective IVI-guided PCI is that “we actually see a clinical benefit” in the trials. “But of course, it comes with a cost. It comes with longer procedures and more contrast.” How clinical practice responds to the new data remains to be seen, she proposed.
ILUMIEN-4 and OCTOBER in detail
Conducted at 80 centers in 18 countries, ILUMIEN-4 randomly assigned patients with diabetes or complex coronary lesions to undergo PCI guided by OCT or using standard angiography only, 1,233 and 1,254 patients, respectively.
Post-PCI MSA averaged 5.72 mm2 with OCT guidance and 5.36 mm2 in the angiography-only group (P < .001).
Their rates of target-vessel failure at 2 years were not significantly different at 7.4% and 8.2%, respectively. The 2-year composite endpoint included cardiac death, target vessel–related MI, or ischemia-driven target-vessel revascularization.
Definite or probable stent thrombosis was observed over 2 years in 0.5% of the OCT group and 1.4% of those with angiography-only PCI (hazard ratio, 0.36; 95% confidence interval, 0.14-0.91; P = .02) favoring OCT.
The OCTOBER trial, conducted at 38 centers in Europe, entered 1201 patients with stable angina or acute coronary syndromes and angiographically identified complex bifurcation lesions. They involved the left-main coronary artery in about one-fifth of cases.
Patients were randomly assigned to bifurcation PCI guided by OCT or under standard angiography, 600 and 601 patients, respectively. Rates for procedure-related complications were similar at 6.8% and 5.7%, respectively.
Over a median of 2 years, 10.1% of the OCT group and 14.1% of angiography-only patients developed a MACE event, including cardiac death, target-lesion MI, or ischemia-driven target-lesion revascularization. The adjusted HR was 0.71 (95% CI, 0.51-0.98; P = .035) in favor of OCT.
Meta-analysis, trials to date
The meta-analysis presented by Dr. Stone included ILUMIEN-4, OCTOBER, and 18 earlier outcomes trials comparing PCI guided by IVI, either OCT or IVUS, and angiography-only PCI. It covered 12,428 patients with chronic or acute coronary disease and followed them a mean of 26 months; the longest follow-up was 5 years. They were assigned to IVI-guided or angiography-only PCI, 7,038 and 5,390 patients, respectively.
Dr. Stone and colleagues conducted a network meta-analysis of the 20 studies, that is, a combined analysis that allowed both direct and indirect comparisons of standard angiography-only procedures to each of the other studied comparator interventions including OCT, IVUS, and either OCT or IVUS. They then derived network-estimate odds ratios for IVI-guided PCI vs angiography-only procedures.
“Hopefully, this will impact the guidelines,” Dr. Stone said of the meta-analysis. Procedures guided by IVI might become more common in clinical practice if they were to garner a Class-I guideline recommendation, the strongest recommendation category.
“That would make a difference, but we’d also need to work to remove impediments to increasing intravascular imaging guidance” for most patients undergoing PCI, he said, referring to challenges in obtaining reimbursement for IVI-guided PCI and training enough operators to handle the projected demand.
ILUMIEN-4 was funded by Abbott. OCTOBER was supported by grants from Abbott Vascular, St. Jude Medical, and Aarhus University. The network meta-analysis received statistical support from Abbott. Dr. Ali disclosed institutional grant support from Abbott, Abiomed, Acist Medical, Boston Scientific, Cardiovascular Systems, Medtronic, the National Institutes of Health, Opsens Medical, Philips, and Teleflex; consulting fees from Astra Zeneca, Philips, Shockwave; and holding equity in Elucid, Spectrawave, Shockwave, and VitalConnect. Dr. Holm and Dr. Bhatt reported numerous conflicts of interest. Dr. Andreasen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A routine role for intravascular imaging (IVI) guidance for percutaneous coronary intervention (PCI) has long been favored by many of the technology’s researchers and enthusiasts. Now evidence from large, randomized trials may be catching up with such aspirations, though not without caveats.
One way IVI guidance may achieve that, the research suggests, albeit more speculatively, is by cutting risk for stent thrombosis, compared with the risk associated with angiography-only PCI.
The new studies, two large randomized IVI trials plus a meta-analysis of 20 such studies, were presented at the annual congress of the European Society of Cardiology.
In one, called ILUMIEN-4, PCI guided by optical coherence tomography (OCT) was associated with fewer procedural complications and better acute results – that is, larger post-PCI minimum stent area (MSA) – than in angiography-only procedures (P < .001). Poststenting MSA, an established predictor of clinical outcomes, was the primary imaging endpoint of the trial with almost 2,500 patients.
Yet the OCT group’s greater post-PCI MSA did not translate to reduced risk for the primary clinical endpoint of 2-year target-vessel failure. Among secondary endpoints, however, stent thrombosis at some point during the follow-up was 64% less likely (P = .02) with OCT guidance than angiography-only PCI.
ILUMIEN-4, despite its neutral clinical result, still “strongly advocates” for PCI guidance by OCT, at least among patients like those in the trial, said principal investigator Ziad Ali, MD, DPhil. He based that largely on the strategy’s greater postprocedure lumen areas in the trials, which are among “the strongest independent predictors for long term outcomes,” said Dr. Ali, of St. Francis Hospital & Heart Center, Roslyn, N.Y., at a press conference on IVI trials during the ESC Congress.
Selected complex lesion type
In contrast, the OCTOBER trial, presented at the sessions back to back with ILUMIEN-4, saw OCT guidance lead to better clinical outcomes than angiography alone after PCI of bifurcation lesions, which normally can be a special challenge for operators.
In the trial, which entered about 1,200 patients with such complex lesions, the 2-year risk for major adverse cardiac events (MACE) fell 60% after OCT-guided PCI, compared with angiography-only procedures (P = .035).
The finding is novel for showing that OCT guidance in bifurcation PCI can make a significant clinical difference, said OCTOBER investigator Niels R. Holm, MD, at the same media presentation on IVI trials.
“Multiple studies have shown that OCT allows for optimization of bifurcation PCI, and our results confirm that such optimization may improve the patient’s prognosis,” said Dr. Holm of Aarhus (Denmark) University Hospital.
ILUMIEN-4 and OCTOBER, both of which prespecified the Xience (Abbott) everolimus-eluting stent for the procedures, were published in the New England Journal of Medicine in tandem with their respective presentations at the ESC sessions.
Covering the spectrum
A meta-analysis presented at the same ESC session compared IVI using either OCT or intravascular ultrasound (IVUS) with angiography-only PCI across 20 randomized trials with a total of more than 12,000 patients.
Significant outcomes for IVI guidance versus angiography alone included a 31% drop in risk for target-lesion failure, the primary endpoint. And this study, as well, showed a steep 52% reduction in risk for in-stent thrombosis with the IVI-guided approach.
And “for the first time” in IVI studies, “we demonstrated reductions in all-myocardial-infarction and all-cause death, the latter by 25%,” Gregg Stone, MD, Icahn School of Medicine at Mount Sinai, New York, said in presenting the meta-analysis. Dr. Stone is also the ILUMIEN-4 study chairperson.
“The routine use of OCT or IVUS to guide most PCI procedures will substantially improve patient event-free survival,” he predicted, “enhancing both the long-term safety and effectiveness of the procedure.”
Dr. Stone said that IVI guidance “should be standard of care, if not in all patients, then in most patients.” Part of the rationale: PCI is unlikely to be improved much further by incremental gains in drug-eluting stent design. “That technology has almost plateaued.” But there’s yet room for “substantially improved outcomes” from adjunctive treatments and techniques such as IVI guidance.
The 20 studies in the meta-analysis encompassed an array of patients and lesions both complex and noncomplex, Dr. Stone observed, including bifurcation lesions, chronic total occlusions, left-main coronary stenoses, and MI culprit lesions.
“They really covered the spectrum of PCI,” he said. “I’m not recommending that intravascular imaging be used in every single case. But I do think it should be used in the majority of patients” and be standard of care for PCI in left-main lesions and “complex coronary disease, high-risk patients, and high-risk lesions.”
Unique advantage
The IVI-guidance groups in both ILUMIEN-4 and the meta-analysis showed a significant drop in risk for stent thrombosis – that is, abrupt thrombotic vessel closure, which typically occurs in 1% or fewer PCI cases but can trigger an MI and pose a mortality risk up to 45%.
Those risk reductions are consistent with a unique IVI advantage: the ability to guide optimization of stent deployments. When formally presenting ILUMIEN-4 at the ESC sessions, Ali observed that IVUS and OCT imaging allows operators to identify and often correct less-than-ideal results of an initial stent delivery – such as residual gaps between stent struts and vessel wall – that may encroach on the lumen, with possible clinical consequences.
Such imaging, said Dr. Ali, “lets you identify tissue protrusions, malappositions, dissections, and untreated reference-segment disease” that may potentially trigger thrombosis. That makes a strong argument for giving IVI guidance a more common, perhaps even routine role in PCI procedures.
Selling routine IVI-guided PCI in practice
“I think the study results are quite clear,” said Deepak L. Bhatt, MD, MPH, as session comoderator following the OCTOBER presentation. “The challenge, though, will be convincing the average interventional cardiologist worldwide that it was specifically the imaging and not the extra care that the patient getting OCT also inherently receives.”
Did OCT’s better trial outcomes stem from IVI itself or from greater operator attentiveness to procedural results – such as, for example, more high-pressure expansions to optimize stent placement, “the sort of thing that tends to occur when invasive imaging is added on to just plain old angiography?” Dr. Bhatt asked of Lene N. Andreasen, MD, who had just presented the OCTOBER trial. “There’s no way of uncoupling the two things.”
What can be said, “at this point, to convince interventional cardiologists that the extra time, energy, expense, is truly indicated,” that the data are “sufficient to change global practice?” asked Dr. Bhatt, Mount Sinai Hospital and Icahn School of Medicine at Mount Sinai.
That remains an open question,” acknowledged Dr. Andreasen of Aarhus University Hospital. The best argument in favor of selective IVI-guided PCI is that “we actually see a clinical benefit” in the trials. “But of course, it comes with a cost. It comes with longer procedures and more contrast.” How clinical practice responds to the new data remains to be seen, she proposed.
ILUMIEN-4 and OCTOBER in detail
Conducted at 80 centers in 18 countries, ILUMIEN-4 randomly assigned patients with diabetes or complex coronary lesions to undergo PCI guided by OCT or using standard angiography only, 1,233 and 1,254 patients, respectively.
Post-PCI MSA averaged 5.72 mm2 with OCT guidance and 5.36 mm2 in the angiography-only group (P < .001).
Their rates of target-vessel failure at 2 years were not significantly different at 7.4% and 8.2%, respectively. The 2-year composite endpoint included cardiac death, target vessel–related MI, or ischemia-driven target-vessel revascularization.
Definite or probable stent thrombosis was observed over 2 years in 0.5% of the OCT group and 1.4% of those with angiography-only PCI (hazard ratio, 0.36; 95% confidence interval, 0.14-0.91; P = .02) favoring OCT.
The OCTOBER trial, conducted at 38 centers in Europe, entered 1201 patients with stable angina or acute coronary syndromes and angiographically identified complex bifurcation lesions. They involved the left-main coronary artery in about one-fifth of cases.
Patients were randomly assigned to bifurcation PCI guided by OCT or under standard angiography, 600 and 601 patients, respectively. Rates for procedure-related complications were similar at 6.8% and 5.7%, respectively.
Over a median of 2 years, 10.1% of the OCT group and 14.1% of angiography-only patients developed a MACE event, including cardiac death, target-lesion MI, or ischemia-driven target-lesion revascularization. The adjusted HR was 0.71 (95% CI, 0.51-0.98; P = .035) in favor of OCT.
Meta-analysis, trials to date
The meta-analysis presented by Dr. Stone included ILUMIEN-4, OCTOBER, and 18 earlier outcomes trials comparing PCI guided by IVI, either OCT or IVUS, and angiography-only PCI. It covered 12,428 patients with chronic or acute coronary disease and followed them a mean of 26 months; the longest follow-up was 5 years. They were assigned to IVI-guided or angiography-only PCI, 7,038 and 5,390 patients, respectively.
Dr. Stone and colleagues conducted a network meta-analysis of the 20 studies, that is, a combined analysis that allowed both direct and indirect comparisons of standard angiography-only procedures to each of the other studied comparator interventions including OCT, IVUS, and either OCT or IVUS. They then derived network-estimate odds ratios for IVI-guided PCI vs angiography-only procedures.
“Hopefully, this will impact the guidelines,” Dr. Stone said of the meta-analysis. Procedures guided by IVI might become more common in clinical practice if they were to garner a Class-I guideline recommendation, the strongest recommendation category.
“That would make a difference, but we’d also need to work to remove impediments to increasing intravascular imaging guidance” for most patients undergoing PCI, he said, referring to challenges in obtaining reimbursement for IVI-guided PCI and training enough operators to handle the projected demand.
ILUMIEN-4 was funded by Abbott. OCTOBER was supported by grants from Abbott Vascular, St. Jude Medical, and Aarhus University. The network meta-analysis received statistical support from Abbott. Dr. Ali disclosed institutional grant support from Abbott, Abiomed, Acist Medical, Boston Scientific, Cardiovascular Systems, Medtronic, the National Institutes of Health, Opsens Medical, Philips, and Teleflex; consulting fees from Astra Zeneca, Philips, Shockwave; and holding equity in Elucid, Spectrawave, Shockwave, and VitalConnect. Dr. Holm and Dr. Bhatt reported numerous conflicts of interest. Dr. Andreasen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE ESC CONGRESS 2023
Recent leaps in heart failure therapy spur ESC guideline–focused update
Two years is a long time in the world of heart failure (HF) management, enough to see publication of more than a dozen studies with insights that would supplant and expand key sections of a far-reaching European Society of Cardiology (ESC) clinical practice guideline on HF unveiled in 2021.
“Back in 2021, we had three and a half decades of data to consider,” but recent years have seen “an amazing amount of progress” that has necessitated some adjustments and key additions, including several Class I recommendations, observed Roy S. Gardner, MBChB, MD, Golden Jubilee National Hospital, Clydebank, United Kingdom.
, which Dr. Gardner helped unveil over several days at the annual congress of the European Society of Cardiology, held in Amsterdam.
The new document was also published in the European Heart Journal during the ESC sessions. Dr. Gardner is a co-author on both the 2021 and 2023 documents.
The task force that was charged with the focused update’s development “considered a large number of trials across the spectrum of acute chronic heart failure and the comorbidities associated with it,” Ultimately, it considered only those with “results that would lead to new or changed Class I or Class IIa recommendations,” noted Theresa A. McDonagh, MD, during the ESC sessions.
Dr. McDonagh, of King’s College Hospital, London, chaired the task force and led the document’s list of authors along with Marco Metra, MD, University of Brescia (Italy).
Chronic HF management
The 2021 document’s “beautiful algorithm” on managing HF with reduced ejection fraction, that is HF with an LVEF less than 40%, had helped enshrine the expeditious uptitration of the “four pillars” of drug therapy as a top management goal. That remains unchanged in the focused update, Dr. Gardner noted.
But the new document gives a boost to recommendations for HF with mildly reduced ejection fraction (HFmrEF), characterized by an LVEF greater than 40% to less than 50%. For that, the 2021 document recommended three of the four pillars of HF medical therapy: beta blockers, mineralocorticoid receptor antagonists (MRA), renin-angiotensin system (RAS) inhibitors.
The focused update, however, adds the fourth pillar – SGLT2 inhibitors – to core therapy for both HFmrEF and HF with preserved ejection fraction (HFpEF), the latter defined by an LVEF greater than 50%. Publication of trials supporting those new recommendations had narrowly missed availability for the 2021 document.
EMPEROR-Preserved, for example, was published during the same ESC 2021 sessions that introduced the 2021 guidelines. Its patients with HFpEF (which at the time included patients meeting the current definition of HFmrEF) assigned to the SGLT2 inhibitor empagliflozin (Jardiance) showed a 21% reduction in risk for a composite primary endpoint that was driven by the HF-hospitalization component.
“This wasn’t a fluke finding,” Dr. Gardner said, as the following year saw publication of the DELIVER trial, which resembled EMPEROR-Preserved in design and outcomes using the SGLT2 inhibitor dapagliflozin (Farxiga).
The two trials, backed up by meta-analyses that also included DAPA-HF and other studies, suggested as well that the two SGLT2 inhibitors “work across the spectrum of ejection fraction,” Dr. Gardner said.
The 2023 focused update indicates an SGLT2 inhibitor, either empagliflozin or dapagliflozin, for patients with either HFmrEF or HFpEF to reduce the risk of HF hospitalization or cardiovascular death. Both recommendations are of Class I, level of evidence A.
The new indications make SGLT2 inhibitors and diuretics (as needed for fluid retention) the only drugs for HFmrEF or HFpEF with a Class I recommendation. Previously established “rather weaker” Class IIb recommendation for RAS inhibitors, MRAs, and beta blockers that had been “based on subgroup analyses of neutral trials” remained unchanged in the focused update, Dr. McDonagh noted.
Patients hospitalized with HF
The 2021 guidelines had recommended that patients hospitalized with acute HF be started on evidence-based meds before discharge and that they return for evaluation 1 to 2 weeks after discharge. But the recommendation was unsupported by randomized trials.
That changed with the 2022 publication of STRONG-HF, in which a strategy of early and rapid uptitration of guideline-directed meds, initiated predischarge regardless of LVEF, led to a one-third reduced 6-month risk for death or HF readmission.
Based primarily on STRONG-HF, the focused update recommends “an intensive strategy of initiation and rapid up-titration of evidence-based treatment before discharge and during frequent and careful follow-up visits in the first 6 weeks after hospitalization” to reduce readmission and mortality: Class I, level of evidence B.
“There was a large consensus around this recommendation,” said STRONG-HF principal investigator Alexandre Mebazaa, MD, PhD, a co-author of both the 2021 and 2023 documents. Conducted before the advent of the four pillars of drug therapy, sometimes called quartet therapy, the trial’s requirement for evidence-based meds didn’t include SGLT2 inhibitors.
The new focused update considers the new status of those agents, especially with regard to their benefits independent of LVEF. So, it completed the quartet by adding empagliflozin or dapagliflozin to the agents that should be initiated predischarge, observed Dr. Mebazaa, University Hospitals Saint Louis‐Lariboisière, Paris, at the focused-update’s ESC 2023 sessions.
The new document also follows STRONG-HF with its emphasis on “frequent and careful follow-up” by recommending certain clinical and laboratory evaluations known to be prognostic in HF. They include congestion status, blood pressure, heart rate, natriuretic peptide (NT-proBNP) and potassium levels and estimated glomerular filtration rate.
Dr. Mebazaa stressed the importance of monitoring NT-proBNP after discharge. “What we saw in STRONG-HF is that sometimes the clinical signs do not necessarily tell you that the patient is still congested.”
After discharge, he said, NT-proBNP levels “should only go down.” So, knowing whether NT-proBNP levels “are stable or increasing” during the med optimization process can help guide diuretic dosing.
HF with comorbidities
The new document includes two new Class I recommendations for patients with HF and both type 2 diabetes and chronic kidney disease based on several recent randomized trials and meta-analyses.
The focused update recommends SGLT2 inhibitors as well as the selective, non-steroidal MRA finerenone (Kerendia) in HF patients with CKD and type-2 diabetes. Both Class I recommendations are supported by a level of evidence A.
The SGLT2 indication is based on DAPA-CKD and EMPA-KIDNEY plus meta-analyses that included those trials along with others. The recommendation for finerenone derives from the FIDELIO-DKD and FIGARO-DKD trials and a pooled analysis of the two studies.
The 2023 focused update also accounts for new clinical-trial insights for patients with HF and iron deficiency. The 2021 document featured recommendations for the diagnosis and iron-repletion therapy in such cases, but only as Class IIa or at lower low levels of evidence. The focused update considers more recent studies, especially IRONMAN and some meta-analyses.
The 2023 document indicates intravenous iron supplementation for symptomatic patients with iron deficiency and either HFrEF or HFmrEF to improve symptoms and quality of life (Class I, level of evidence A), and says it should be considered (Class IIa, level of evidence A) to reduce risk for HF hospitalization.
When the task force assembled to plan the 2023 focused update, Dr. Gardner observed, “the first thing we thought about was the nomenclature around the phenotyping of heart failure.”
Although the 2021 guidelines relied fundamentally on the distinctions between HFrEF, HFmrEF, and HFpEF, it had become apparent to some in the field that some meds, especially the SGLT2 inhibitors, were obscuring their LVEF-based boundaries, at least with respect to drug therapy.
The 2023 document’s developers, Dr. Gardner said, seriously considered changing the three categories to two, that is HFrEF and – to account for all other heart failure – HF with normal ejection fraction (HFnEF).
That didn’t happen, although the proposal was popular within the task force. Any changes to the 2021 document would require a 75% consensus on the matter, Dr. Gardner explained. When the task force took a vote on whether to change the nomenclature, he said, 71% favored the proposal.
Disclosures for members of the task force can be found in a supplement to the published 2023 Focused Update.
A version of this article first appeared on Medscape.com.
Two years is a long time in the world of heart failure (HF) management, enough to see publication of more than a dozen studies with insights that would supplant and expand key sections of a far-reaching European Society of Cardiology (ESC) clinical practice guideline on HF unveiled in 2021.
“Back in 2021, we had three and a half decades of data to consider,” but recent years have seen “an amazing amount of progress” that has necessitated some adjustments and key additions, including several Class I recommendations, observed Roy S. Gardner, MBChB, MD, Golden Jubilee National Hospital, Clydebank, United Kingdom.
, which Dr. Gardner helped unveil over several days at the annual congress of the European Society of Cardiology, held in Amsterdam.
The new document was also published in the European Heart Journal during the ESC sessions. Dr. Gardner is a co-author on both the 2021 and 2023 documents.
The task force that was charged with the focused update’s development “considered a large number of trials across the spectrum of acute chronic heart failure and the comorbidities associated with it,” Ultimately, it considered only those with “results that would lead to new or changed Class I or Class IIa recommendations,” noted Theresa A. McDonagh, MD, during the ESC sessions.
Dr. McDonagh, of King’s College Hospital, London, chaired the task force and led the document’s list of authors along with Marco Metra, MD, University of Brescia (Italy).
Chronic HF management
The 2021 document’s “beautiful algorithm” on managing HF with reduced ejection fraction, that is HF with an LVEF less than 40%, had helped enshrine the expeditious uptitration of the “four pillars” of drug therapy as a top management goal. That remains unchanged in the focused update, Dr. Gardner noted.
But the new document gives a boost to recommendations for HF with mildly reduced ejection fraction (HFmrEF), characterized by an LVEF greater than 40% to less than 50%. For that, the 2021 document recommended three of the four pillars of HF medical therapy: beta blockers, mineralocorticoid receptor antagonists (MRA), renin-angiotensin system (RAS) inhibitors.
The focused update, however, adds the fourth pillar – SGLT2 inhibitors – to core therapy for both HFmrEF and HF with preserved ejection fraction (HFpEF), the latter defined by an LVEF greater than 50%. Publication of trials supporting those new recommendations had narrowly missed availability for the 2021 document.
EMPEROR-Preserved, for example, was published during the same ESC 2021 sessions that introduced the 2021 guidelines. Its patients with HFpEF (which at the time included patients meeting the current definition of HFmrEF) assigned to the SGLT2 inhibitor empagliflozin (Jardiance) showed a 21% reduction in risk for a composite primary endpoint that was driven by the HF-hospitalization component.
“This wasn’t a fluke finding,” Dr. Gardner said, as the following year saw publication of the DELIVER trial, which resembled EMPEROR-Preserved in design and outcomes using the SGLT2 inhibitor dapagliflozin (Farxiga).
The two trials, backed up by meta-analyses that also included DAPA-HF and other studies, suggested as well that the two SGLT2 inhibitors “work across the spectrum of ejection fraction,” Dr. Gardner said.
The 2023 focused update indicates an SGLT2 inhibitor, either empagliflozin or dapagliflozin, for patients with either HFmrEF or HFpEF to reduce the risk of HF hospitalization or cardiovascular death. Both recommendations are of Class I, level of evidence A.
The new indications make SGLT2 inhibitors and diuretics (as needed for fluid retention) the only drugs for HFmrEF or HFpEF with a Class I recommendation. Previously established “rather weaker” Class IIb recommendation for RAS inhibitors, MRAs, and beta blockers that had been “based on subgroup analyses of neutral trials” remained unchanged in the focused update, Dr. McDonagh noted.
Patients hospitalized with HF
The 2021 guidelines had recommended that patients hospitalized with acute HF be started on evidence-based meds before discharge and that they return for evaluation 1 to 2 weeks after discharge. But the recommendation was unsupported by randomized trials.
That changed with the 2022 publication of STRONG-HF, in which a strategy of early and rapid uptitration of guideline-directed meds, initiated predischarge regardless of LVEF, led to a one-third reduced 6-month risk for death or HF readmission.
Based primarily on STRONG-HF, the focused update recommends “an intensive strategy of initiation and rapid up-titration of evidence-based treatment before discharge and during frequent and careful follow-up visits in the first 6 weeks after hospitalization” to reduce readmission and mortality: Class I, level of evidence B.
“There was a large consensus around this recommendation,” said STRONG-HF principal investigator Alexandre Mebazaa, MD, PhD, a co-author of both the 2021 and 2023 documents. Conducted before the advent of the four pillars of drug therapy, sometimes called quartet therapy, the trial’s requirement for evidence-based meds didn’t include SGLT2 inhibitors.
The new focused update considers the new status of those agents, especially with regard to their benefits independent of LVEF. So, it completed the quartet by adding empagliflozin or dapagliflozin to the agents that should be initiated predischarge, observed Dr. Mebazaa, University Hospitals Saint Louis‐Lariboisière, Paris, at the focused-update’s ESC 2023 sessions.
The new document also follows STRONG-HF with its emphasis on “frequent and careful follow-up” by recommending certain clinical and laboratory evaluations known to be prognostic in HF. They include congestion status, blood pressure, heart rate, natriuretic peptide (NT-proBNP) and potassium levels and estimated glomerular filtration rate.
Dr. Mebazaa stressed the importance of monitoring NT-proBNP after discharge. “What we saw in STRONG-HF is that sometimes the clinical signs do not necessarily tell you that the patient is still congested.”
After discharge, he said, NT-proBNP levels “should only go down.” So, knowing whether NT-proBNP levels “are stable or increasing” during the med optimization process can help guide diuretic dosing.
HF with comorbidities
The new document includes two new Class I recommendations for patients with HF and both type 2 diabetes and chronic kidney disease based on several recent randomized trials and meta-analyses.
The focused update recommends SGLT2 inhibitors as well as the selective, non-steroidal MRA finerenone (Kerendia) in HF patients with CKD and type-2 diabetes. Both Class I recommendations are supported by a level of evidence A.
The SGLT2 indication is based on DAPA-CKD and EMPA-KIDNEY plus meta-analyses that included those trials along with others. The recommendation for finerenone derives from the FIDELIO-DKD and FIGARO-DKD trials and a pooled analysis of the two studies.
The 2023 focused update also accounts for new clinical-trial insights for patients with HF and iron deficiency. The 2021 document featured recommendations for the diagnosis and iron-repletion therapy in such cases, but only as Class IIa or at lower low levels of evidence. The focused update considers more recent studies, especially IRONMAN and some meta-analyses.
The 2023 document indicates intravenous iron supplementation for symptomatic patients with iron deficiency and either HFrEF or HFmrEF to improve symptoms and quality of life (Class I, level of evidence A), and says it should be considered (Class IIa, level of evidence A) to reduce risk for HF hospitalization.
When the task force assembled to plan the 2023 focused update, Dr. Gardner observed, “the first thing we thought about was the nomenclature around the phenotyping of heart failure.”
Although the 2021 guidelines relied fundamentally on the distinctions between HFrEF, HFmrEF, and HFpEF, it had become apparent to some in the field that some meds, especially the SGLT2 inhibitors, were obscuring their LVEF-based boundaries, at least with respect to drug therapy.
The 2023 document’s developers, Dr. Gardner said, seriously considered changing the three categories to two, that is HFrEF and – to account for all other heart failure – HF with normal ejection fraction (HFnEF).
That didn’t happen, although the proposal was popular within the task force. Any changes to the 2021 document would require a 75% consensus on the matter, Dr. Gardner explained. When the task force took a vote on whether to change the nomenclature, he said, 71% favored the proposal.
Disclosures for members of the task force can be found in a supplement to the published 2023 Focused Update.
A version of this article first appeared on Medscape.com.
Two years is a long time in the world of heart failure (HF) management, enough to see publication of more than a dozen studies with insights that would supplant and expand key sections of a far-reaching European Society of Cardiology (ESC) clinical practice guideline on HF unveiled in 2021.
“Back in 2021, we had three and a half decades of data to consider,” but recent years have seen “an amazing amount of progress” that has necessitated some adjustments and key additions, including several Class I recommendations, observed Roy S. Gardner, MBChB, MD, Golden Jubilee National Hospital, Clydebank, United Kingdom.
, which Dr. Gardner helped unveil over several days at the annual congress of the European Society of Cardiology, held in Amsterdam.
The new document was also published in the European Heart Journal during the ESC sessions. Dr. Gardner is a co-author on both the 2021 and 2023 documents.
The task force that was charged with the focused update’s development “considered a large number of trials across the spectrum of acute chronic heart failure and the comorbidities associated with it,” Ultimately, it considered only those with “results that would lead to new or changed Class I or Class IIa recommendations,” noted Theresa A. McDonagh, MD, during the ESC sessions.
Dr. McDonagh, of King’s College Hospital, London, chaired the task force and led the document’s list of authors along with Marco Metra, MD, University of Brescia (Italy).
Chronic HF management
The 2021 document’s “beautiful algorithm” on managing HF with reduced ejection fraction, that is HF with an LVEF less than 40%, had helped enshrine the expeditious uptitration of the “four pillars” of drug therapy as a top management goal. That remains unchanged in the focused update, Dr. Gardner noted.
But the new document gives a boost to recommendations for HF with mildly reduced ejection fraction (HFmrEF), characterized by an LVEF greater than 40% to less than 50%. For that, the 2021 document recommended three of the four pillars of HF medical therapy: beta blockers, mineralocorticoid receptor antagonists (MRA), renin-angiotensin system (RAS) inhibitors.
The focused update, however, adds the fourth pillar – SGLT2 inhibitors – to core therapy for both HFmrEF and HF with preserved ejection fraction (HFpEF), the latter defined by an LVEF greater than 50%. Publication of trials supporting those new recommendations had narrowly missed availability for the 2021 document.
EMPEROR-Preserved, for example, was published during the same ESC 2021 sessions that introduced the 2021 guidelines. Its patients with HFpEF (which at the time included patients meeting the current definition of HFmrEF) assigned to the SGLT2 inhibitor empagliflozin (Jardiance) showed a 21% reduction in risk for a composite primary endpoint that was driven by the HF-hospitalization component.
“This wasn’t a fluke finding,” Dr. Gardner said, as the following year saw publication of the DELIVER trial, which resembled EMPEROR-Preserved in design and outcomes using the SGLT2 inhibitor dapagliflozin (Farxiga).
The two trials, backed up by meta-analyses that also included DAPA-HF and other studies, suggested as well that the two SGLT2 inhibitors “work across the spectrum of ejection fraction,” Dr. Gardner said.
The 2023 focused update indicates an SGLT2 inhibitor, either empagliflozin or dapagliflozin, for patients with either HFmrEF or HFpEF to reduce the risk of HF hospitalization or cardiovascular death. Both recommendations are of Class I, level of evidence A.
The new indications make SGLT2 inhibitors and diuretics (as needed for fluid retention) the only drugs for HFmrEF or HFpEF with a Class I recommendation. Previously established “rather weaker” Class IIb recommendation for RAS inhibitors, MRAs, and beta blockers that had been “based on subgroup analyses of neutral trials” remained unchanged in the focused update, Dr. McDonagh noted.
Patients hospitalized with HF
The 2021 guidelines had recommended that patients hospitalized with acute HF be started on evidence-based meds before discharge and that they return for evaluation 1 to 2 weeks after discharge. But the recommendation was unsupported by randomized trials.
That changed with the 2022 publication of STRONG-HF, in which a strategy of early and rapid uptitration of guideline-directed meds, initiated predischarge regardless of LVEF, led to a one-third reduced 6-month risk for death or HF readmission.
Based primarily on STRONG-HF, the focused update recommends “an intensive strategy of initiation and rapid up-titration of evidence-based treatment before discharge and during frequent and careful follow-up visits in the first 6 weeks after hospitalization” to reduce readmission and mortality: Class I, level of evidence B.
“There was a large consensus around this recommendation,” said STRONG-HF principal investigator Alexandre Mebazaa, MD, PhD, a co-author of both the 2021 and 2023 documents. Conducted before the advent of the four pillars of drug therapy, sometimes called quartet therapy, the trial’s requirement for evidence-based meds didn’t include SGLT2 inhibitors.
The new focused update considers the new status of those agents, especially with regard to their benefits independent of LVEF. So, it completed the quartet by adding empagliflozin or dapagliflozin to the agents that should be initiated predischarge, observed Dr. Mebazaa, University Hospitals Saint Louis‐Lariboisière, Paris, at the focused-update’s ESC 2023 sessions.
The new document also follows STRONG-HF with its emphasis on “frequent and careful follow-up” by recommending certain clinical and laboratory evaluations known to be prognostic in HF. They include congestion status, blood pressure, heart rate, natriuretic peptide (NT-proBNP) and potassium levels and estimated glomerular filtration rate.
Dr. Mebazaa stressed the importance of monitoring NT-proBNP after discharge. “What we saw in STRONG-HF is that sometimes the clinical signs do not necessarily tell you that the patient is still congested.”
After discharge, he said, NT-proBNP levels “should only go down.” So, knowing whether NT-proBNP levels “are stable or increasing” during the med optimization process can help guide diuretic dosing.
HF with comorbidities
The new document includes two new Class I recommendations for patients with HF and both type 2 diabetes and chronic kidney disease based on several recent randomized trials and meta-analyses.
The focused update recommends SGLT2 inhibitors as well as the selective, non-steroidal MRA finerenone (Kerendia) in HF patients with CKD and type-2 diabetes. Both Class I recommendations are supported by a level of evidence A.
The SGLT2 indication is based on DAPA-CKD and EMPA-KIDNEY plus meta-analyses that included those trials along with others. The recommendation for finerenone derives from the FIDELIO-DKD and FIGARO-DKD trials and a pooled analysis of the two studies.
The 2023 focused update also accounts for new clinical-trial insights for patients with HF and iron deficiency. The 2021 document featured recommendations for the diagnosis and iron-repletion therapy in such cases, but only as Class IIa or at lower low levels of evidence. The focused update considers more recent studies, especially IRONMAN and some meta-analyses.
The 2023 document indicates intravenous iron supplementation for symptomatic patients with iron deficiency and either HFrEF or HFmrEF to improve symptoms and quality of life (Class I, level of evidence A), and says it should be considered (Class IIa, level of evidence A) to reduce risk for HF hospitalization.
When the task force assembled to plan the 2023 focused update, Dr. Gardner observed, “the first thing we thought about was the nomenclature around the phenotyping of heart failure.”
Although the 2021 guidelines relied fundamentally on the distinctions between HFrEF, HFmrEF, and HFpEF, it had become apparent to some in the field that some meds, especially the SGLT2 inhibitors, were obscuring their LVEF-based boundaries, at least with respect to drug therapy.
The 2023 document’s developers, Dr. Gardner said, seriously considered changing the three categories to two, that is HFrEF and – to account for all other heart failure – HF with normal ejection fraction (HFnEF).
That didn’t happen, although the proposal was popular within the task force. Any changes to the 2021 document would require a 75% consensus on the matter, Dr. Gardner explained. When the task force took a vote on whether to change the nomenclature, he said, 71% favored the proposal.
Disclosures for members of the task force can be found in a supplement to the published 2023 Focused Update.
A version of this article first appeared on Medscape.com.
FROM THE ESC CONGRESS 2023
Safely skip PET2 after brentuximab in Hodgkin lymphoma?
FROM SOHO 2023
Data from four recent studies indicate that adding frontline brentuximab vedotin to AVD chemotherapy (doxorubicin, vinblastine, dacarbazine) improves outcomes for patients, regardless of PET2 scan results, according to lead investigator Ravand Samaeekia, MD, MSc, from Loma Linda (Calif.) University Medical Center.
These studies, including one conducted by Dr. Samaeekia’s team, provide “evidence for the safe omission of PET2 in treatment regimens that contain brentuximab vedotin,” Dr. Samaeekia, who presented the data, concluded.
Performing an interim PET-CT scan after two cycles of chemotherapy can help oncologists adapt treatment protocols for patients with Hodgkin lymphoma and has become the standard of care for these patients.
However, “there are obviously challenges associated with implementing a PET-guided approach,” said Dr. Samaeekia. Additional PET-CT scans can be costly, time consuming, and increase patients’ risk for toxicities when treatment is escalated based on the scan results.
Given these caveats, Dr. Samaeekia reviewed data exploring whether PET2 has predictive value for patients who receive the anti-CD30 antibody-drug conjugate, brentuximab vedotin, as part of first-line treatment alongside AVD chemotherapy.
Dr. Samaeekia’s team analyzed findings from three trials – ECHELON-1, AHOD1331, and BREACH – which assessed frontline standard of care chemotherapy with or without brentuximab. The team found that incorporating brentuximab into frontline treatment resulted in superior efficacy, and PET2 scans results generally did not change how patients were managed.
In ECHELON-1, 6-year overall survival favored patients with advanced Hodgkin lymphoma who received brentuximab and were PET2 negative (94.9% vs. 90.6%; hazard ratio for death, 0.54) as well as those who were PET2 positive (95% vs. 77%; HR, 0.16). Overall, just over 2% of patients who received the brentuximab regimen switched to an alternative chemotherapy and even fewer did so based on PET2 results.
In AHOD1331, 3-year event-free survival was significantly higher among adolescents and children with Hodgkin lymphoma who received brentuximab – 90.7% for those who had slow-responding lesions and 92.3% for those with rapid-responding lesions. Based on these results, the authors concluded that adding brentuximab “eliminated the predictive value of the interim PET assessment.” The BREACH trial echoed the findings from ECHELON-1 and AHOD1331.
Finally, in a retrospective study of 40 patients treated at Loma Linda with brentuximab vedotin plus AVD, Dr. Samaeekia and colleagues found that 24 were PET2 negative and 12 were PET2 positive. All patients who were PET2 negative remained negative on the end-of-treatment PET, indicating no cancer progression. Of the 12 PET2-positive patients, four (33%) remained PET positive at the end of treatment. Only one patient overall changed regimens following PET2.
Dr. Samaeekia’s team concluded that PET2 scan results “did not have any meaningful impact” on patient management or outcomes.
During the Q&A, Martin Hutchings, MD, PhD, challenged the idea that PET2 can be omitted. Dr. Hutchings, from the Rigshospitalet in Copenhagen, pointed out that 4 of the 12 PET2-positive patients treated at Loma Linda were still PET positive at the end of treatment.
Even so, Dr. Samaeekia explained, PET2 findings did not alter treatment for most patients, noting that doing a PET2 scan may make “us feel better,” but it ultimately doesn’t “make any difference in our management.”
In the AHOD1331 study, “the findings on the interim PET scan were not helpful in the ultimate outcome, whether it was either positive or negative,” added session comoderator Jonathan W. Friedberg, MD, MMSc, director of the James P. Wilmot Cancer Institute at the University of Rochester (N.Y.) Medical Center.
The study by Dr. Samaeekia and colleagues was internally funded. Dr. Samaeekia reports no relevant financial relationships. Dr. Hutchings has previously reported consultancy and research funding from numerous companies. Dr. Friedberg reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SOHO 2023
Data from four recent studies indicate that adding frontline brentuximab vedotin to AVD chemotherapy (doxorubicin, vinblastine, dacarbazine) improves outcomes for patients, regardless of PET2 scan results, according to lead investigator Ravand Samaeekia, MD, MSc, from Loma Linda (Calif.) University Medical Center.
These studies, including one conducted by Dr. Samaeekia’s team, provide “evidence for the safe omission of PET2 in treatment regimens that contain brentuximab vedotin,” Dr. Samaeekia, who presented the data, concluded.
Performing an interim PET-CT scan after two cycles of chemotherapy can help oncologists adapt treatment protocols for patients with Hodgkin lymphoma and has become the standard of care for these patients.
However, “there are obviously challenges associated with implementing a PET-guided approach,” said Dr. Samaeekia. Additional PET-CT scans can be costly, time consuming, and increase patients’ risk for toxicities when treatment is escalated based on the scan results.
Given these caveats, Dr. Samaeekia reviewed data exploring whether PET2 has predictive value for patients who receive the anti-CD30 antibody-drug conjugate, brentuximab vedotin, as part of first-line treatment alongside AVD chemotherapy.
Dr. Samaeekia’s team analyzed findings from three trials – ECHELON-1, AHOD1331, and BREACH – which assessed frontline standard of care chemotherapy with or without brentuximab. The team found that incorporating brentuximab into frontline treatment resulted in superior efficacy, and PET2 scans results generally did not change how patients were managed.
In ECHELON-1, 6-year overall survival favored patients with advanced Hodgkin lymphoma who received brentuximab and were PET2 negative (94.9% vs. 90.6%; hazard ratio for death, 0.54) as well as those who were PET2 positive (95% vs. 77%; HR, 0.16). Overall, just over 2% of patients who received the brentuximab regimen switched to an alternative chemotherapy and even fewer did so based on PET2 results.
In AHOD1331, 3-year event-free survival was significantly higher among adolescents and children with Hodgkin lymphoma who received brentuximab – 90.7% for those who had slow-responding lesions and 92.3% for those with rapid-responding lesions. Based on these results, the authors concluded that adding brentuximab “eliminated the predictive value of the interim PET assessment.” The BREACH trial echoed the findings from ECHELON-1 and AHOD1331.
Finally, in a retrospective study of 40 patients treated at Loma Linda with brentuximab vedotin plus AVD, Dr. Samaeekia and colleagues found that 24 were PET2 negative and 12 were PET2 positive. All patients who were PET2 negative remained negative on the end-of-treatment PET, indicating no cancer progression. Of the 12 PET2-positive patients, four (33%) remained PET positive at the end of treatment. Only one patient overall changed regimens following PET2.
Dr. Samaeekia’s team concluded that PET2 scan results “did not have any meaningful impact” on patient management or outcomes.
During the Q&A, Martin Hutchings, MD, PhD, challenged the idea that PET2 can be omitted. Dr. Hutchings, from the Rigshospitalet in Copenhagen, pointed out that 4 of the 12 PET2-positive patients treated at Loma Linda were still PET positive at the end of treatment.
Even so, Dr. Samaeekia explained, PET2 findings did not alter treatment for most patients, noting that doing a PET2 scan may make “us feel better,” but it ultimately doesn’t “make any difference in our management.”
In the AHOD1331 study, “the findings on the interim PET scan were not helpful in the ultimate outcome, whether it was either positive or negative,” added session comoderator Jonathan W. Friedberg, MD, MMSc, director of the James P. Wilmot Cancer Institute at the University of Rochester (N.Y.) Medical Center.
The study by Dr. Samaeekia and colleagues was internally funded. Dr. Samaeekia reports no relevant financial relationships. Dr. Hutchings has previously reported consultancy and research funding from numerous companies. Dr. Friedberg reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SOHO 2023
Data from four recent studies indicate that adding frontline brentuximab vedotin to AVD chemotherapy (doxorubicin, vinblastine, dacarbazine) improves outcomes for patients, regardless of PET2 scan results, according to lead investigator Ravand Samaeekia, MD, MSc, from Loma Linda (Calif.) University Medical Center.
These studies, including one conducted by Dr. Samaeekia’s team, provide “evidence for the safe omission of PET2 in treatment regimens that contain brentuximab vedotin,” Dr. Samaeekia, who presented the data, concluded.
Performing an interim PET-CT scan after two cycles of chemotherapy can help oncologists adapt treatment protocols for patients with Hodgkin lymphoma and has become the standard of care for these patients.
However, “there are obviously challenges associated with implementing a PET-guided approach,” said Dr. Samaeekia. Additional PET-CT scans can be costly, time consuming, and increase patients’ risk for toxicities when treatment is escalated based on the scan results.
Given these caveats, Dr. Samaeekia reviewed data exploring whether PET2 has predictive value for patients who receive the anti-CD30 antibody-drug conjugate, brentuximab vedotin, as part of first-line treatment alongside AVD chemotherapy.
Dr. Samaeekia’s team analyzed findings from three trials – ECHELON-1, AHOD1331, and BREACH – which assessed frontline standard of care chemotherapy with or without brentuximab. The team found that incorporating brentuximab into frontline treatment resulted in superior efficacy, and PET2 scans results generally did not change how patients were managed.
In ECHELON-1, 6-year overall survival favored patients with advanced Hodgkin lymphoma who received brentuximab and were PET2 negative (94.9% vs. 90.6%; hazard ratio for death, 0.54) as well as those who were PET2 positive (95% vs. 77%; HR, 0.16). Overall, just over 2% of patients who received the brentuximab regimen switched to an alternative chemotherapy and even fewer did so based on PET2 results.
In AHOD1331, 3-year event-free survival was significantly higher among adolescents and children with Hodgkin lymphoma who received brentuximab – 90.7% for those who had slow-responding lesions and 92.3% for those with rapid-responding lesions. Based on these results, the authors concluded that adding brentuximab “eliminated the predictive value of the interim PET assessment.” The BREACH trial echoed the findings from ECHELON-1 and AHOD1331.
Finally, in a retrospective study of 40 patients treated at Loma Linda with brentuximab vedotin plus AVD, Dr. Samaeekia and colleagues found that 24 were PET2 negative and 12 were PET2 positive. All patients who were PET2 negative remained negative on the end-of-treatment PET, indicating no cancer progression. Of the 12 PET2-positive patients, four (33%) remained PET positive at the end of treatment. Only one patient overall changed regimens following PET2.
Dr. Samaeekia’s team concluded that PET2 scan results “did not have any meaningful impact” on patient management or outcomes.
During the Q&A, Martin Hutchings, MD, PhD, challenged the idea that PET2 can be omitted. Dr. Hutchings, from the Rigshospitalet in Copenhagen, pointed out that 4 of the 12 PET2-positive patients treated at Loma Linda were still PET positive at the end of treatment.
Even so, Dr. Samaeekia explained, PET2 findings did not alter treatment for most patients, noting that doing a PET2 scan may make “us feel better,” but it ultimately doesn’t “make any difference in our management.”
In the AHOD1331 study, “the findings on the interim PET scan were not helpful in the ultimate outcome, whether it was either positive or negative,” added session comoderator Jonathan W. Friedberg, MD, MMSc, director of the James P. Wilmot Cancer Institute at the University of Rochester (N.Y.) Medical Center.
The study by Dr. Samaeekia and colleagues was internally funded. Dr. Samaeekia reports no relevant financial relationships. Dr. Hutchings has previously reported consultancy and research funding from numerous companies. Dr. Friedberg reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.