User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Can skin bleaching lead to cancer?
SINGAPORE –
This question was posed by Ousmane Faye, MD, PhD, director general of Mali’s Bamako Dermatology Hospital, at the World Congress of Dermatology.
Dr. Faye explored the issue during a hot topics session at the meeting, prefacing that it was an important question to ask because “in West Africa, skin bleaching is very common.”
“There are many local names” for skin bleaching, he said. “For example, in Senegal, it’s called xessal; in Mali and Ivory Coast, its name is caco; in South Africa, there are many names, like ukutsheyisa.”
Skin bleaching refers to the cosmetic misuse of topical agents to change one’s natural skin color. It’s a centuries-old practice that people, mainly women, adopt “to increase attractiveness and self-esteem,” explained Dr. Faye.
To demonstrate how pervasive skin bleaching is on the continent, he presented a slide that summarized figures from six studies spanning the past 2 decades. Prevalence ranged from 25% in Mali (based on a 1993 survey of 210 women) to a high of 79.25% in Benin (from a sample size of 511 women in 2019). In other studies of women in Burkina Faso and Togo, the figures were 44.3% and 58.9%, respectively. The most recently conducted study, which involved 2,689 Senegalese women and was published in 2022, found that nearly 6 in 10 (59.2%) respondents used skin-lightening products.
But skin bleaching isn’t just limited to Africa, said session moderator Omar Lupi, MD, PhD, associate professor of dermatology at the Federal University of the State of Rio de Janeiro, when approached for an independent comment. “It’s a traditional practice around the world. Maybe not in the developed countries, but it’s quite common in Africa, in South America, and in Asia.”
His sentiments are echoed in a meta-analysis that was published in the International Journal of Dermatology in 2019. The work examined 68 studies involving more than 67,000 people across Africa, Asia, Europe, the Middle East, and North America. It found that the pooled lifetime prevalence of skin bleaching was 27.7% (95% confidence interval, 19.6-37.5; P < .01).
“This is an important and interesting topic because our world is shrinking,” Dr. Lupi told this news organization. “Even in countries that don’t have bleaching as a common situation, we now have patients who are migrating from one part [of the world] to another, so bleaching is something that can knock on your door and you need to be prepared.”
Misuse leads to complications
The issue is pertinent to dermatologists because skin bleaching is associated with a wide range of complications. Take, for example, topical steroids, which are the most common products used for bleaching, said Dr. Faye in his talk.
“Clobetasol can suppress the hypothalamic-pituitary-adrenal (HPA) function,” he said, referring to the body’s main stress response system. “It can also foster skin infection, including bacterial, fungal, viral, and parasitic infection.”
In addition, topical steroids that are misused as skin lighteners have been reported to cause stretch marks, skin atrophy, inflammatory acne, and even metabolic disorders such as diabetes and hypertension, said Dr. Faye.
To further his point, he cited a 2021 prospective case-control study conducted across five sub-Saharan countries, which found that the use of “voluntary cosmetic depigmentation” significantly increased a person’s risk for necrotizing fasciitis of the lower limbs (odds ratio, 2.29; 95% CI, 1.19-3.73; P = .0226).
Similarly, mercury, another substance found in products commonly used to bleach skin, has been associated with problems ranging from rashes to renal toxicity. And because it’s so incredibly harmful, mercury is also known to cause neurologic abnormalities.
Apart from causing certain conditions, prolonged use of skin-lightening products can change the way existing diseases present themselves as well as their severity, added Dr. Faye.
An increased risk
But what about skin bleaching’s link with cancer? “Skin cancer on Black skin is uncommon, yet it occurs in skin-bleaching women,” said Dr. Faye.
“Since 2000, we have had some cases of skin cancer associated with skin bleaching,” he continued, adding that squamous cell carcinoma (SCC) is the most frequent type of cancer observed.
If you look at what’s been published on the topic so far, you’ll see that “all the cases of skin cancer are located over the neck or some exposed area when skin bleaching products are used for more than 10 years,” said Dr. Faye. “And most of the time, the age of the patient ranges from 30 to 60 years.”
The first known case in Africa was reported in a 58-year-old woman from Ghana, who had been using skin bleaching products for close to 30 years. The patient presented with tumors on her face, neck, and arms.
Dr. Faye then proceeded to share more than 10 such carcinoma cases. “These previous reports strongly suggest a relationship between skin bleaching and skin cancers,” said Dr. Faye.
Indeed, there have been reports and publications in the literature that support his observation, including one last year, which found that use of the tyrosinase inhibitor hydroquinone was associated with approximately a threefold increased risk for skin cancer.
For some, including Brazil’s Dr. Lupi, Dr. Faye’s talk was enlightening: “I didn’t know about this relationship [of bleaching] with skin cancer, it was something new for me.”
But the prevalence of SCC is very low, compared with that of skin bleaching, Dr. Faye acknowledged. Moreover, the cancer observed in the cases reported could have resulted from a number of reasons, including exposure to harmful ultraviolet rays from the sun and genetic predisposition in addition to the use of bleaching products such as hydroquinone. “Other causes of skin cancer are not excluded,” he said.
To further explore the link between skin bleaching and cancer, “we need case-control studies to provide more evidence,” he added. Until then, dermatologists “should keep on promoting messages” to prevent SCC from occurring. This includes encouraging the use of proper sun protection in addition to discouraging the practice of skin bleaching, which still persists despite more than 10 African nations banning the use of toxic skin-lightening products.
Dr. Faye and Dr. Lupi report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SINGAPORE –
This question was posed by Ousmane Faye, MD, PhD, director general of Mali’s Bamako Dermatology Hospital, at the World Congress of Dermatology.
Dr. Faye explored the issue during a hot topics session at the meeting, prefacing that it was an important question to ask because “in West Africa, skin bleaching is very common.”
“There are many local names” for skin bleaching, he said. “For example, in Senegal, it’s called xessal; in Mali and Ivory Coast, its name is caco; in South Africa, there are many names, like ukutsheyisa.”
Skin bleaching refers to the cosmetic misuse of topical agents to change one’s natural skin color. It’s a centuries-old practice that people, mainly women, adopt “to increase attractiveness and self-esteem,” explained Dr. Faye.
To demonstrate how pervasive skin bleaching is on the continent, he presented a slide that summarized figures from six studies spanning the past 2 decades. Prevalence ranged from 25% in Mali (based on a 1993 survey of 210 women) to a high of 79.25% in Benin (from a sample size of 511 women in 2019). In other studies of women in Burkina Faso and Togo, the figures were 44.3% and 58.9%, respectively. The most recently conducted study, which involved 2,689 Senegalese women and was published in 2022, found that nearly 6 in 10 (59.2%) respondents used skin-lightening products.
But skin bleaching isn’t just limited to Africa, said session moderator Omar Lupi, MD, PhD, associate professor of dermatology at the Federal University of the State of Rio de Janeiro, when approached for an independent comment. “It’s a traditional practice around the world. Maybe not in the developed countries, but it’s quite common in Africa, in South America, and in Asia.”
His sentiments are echoed in a meta-analysis that was published in the International Journal of Dermatology in 2019. The work examined 68 studies involving more than 67,000 people across Africa, Asia, Europe, the Middle East, and North America. It found that the pooled lifetime prevalence of skin bleaching was 27.7% (95% confidence interval, 19.6-37.5; P < .01).
“This is an important and interesting topic because our world is shrinking,” Dr. Lupi told this news organization. “Even in countries that don’t have bleaching as a common situation, we now have patients who are migrating from one part [of the world] to another, so bleaching is something that can knock on your door and you need to be prepared.”
Misuse leads to complications
The issue is pertinent to dermatologists because skin bleaching is associated with a wide range of complications. Take, for example, topical steroids, which are the most common products used for bleaching, said Dr. Faye in his talk.
“Clobetasol can suppress the hypothalamic-pituitary-adrenal (HPA) function,” he said, referring to the body’s main stress response system. “It can also foster skin infection, including bacterial, fungal, viral, and parasitic infection.”
In addition, topical steroids that are misused as skin lighteners have been reported to cause stretch marks, skin atrophy, inflammatory acne, and even metabolic disorders such as diabetes and hypertension, said Dr. Faye.
To further his point, he cited a 2021 prospective case-control study conducted across five sub-Saharan countries, which found that the use of “voluntary cosmetic depigmentation” significantly increased a person’s risk for necrotizing fasciitis of the lower limbs (odds ratio, 2.29; 95% CI, 1.19-3.73; P = .0226).
Similarly, mercury, another substance found in products commonly used to bleach skin, has been associated with problems ranging from rashes to renal toxicity. And because it’s so incredibly harmful, mercury is also known to cause neurologic abnormalities.
Apart from causing certain conditions, prolonged use of skin-lightening products can change the way existing diseases present themselves as well as their severity, added Dr. Faye.
An increased risk
But what about skin bleaching’s link with cancer? “Skin cancer on Black skin is uncommon, yet it occurs in skin-bleaching women,” said Dr. Faye.
“Since 2000, we have had some cases of skin cancer associated with skin bleaching,” he continued, adding that squamous cell carcinoma (SCC) is the most frequent type of cancer observed.
If you look at what’s been published on the topic so far, you’ll see that “all the cases of skin cancer are located over the neck or some exposed area when skin bleaching products are used for more than 10 years,” said Dr. Faye. “And most of the time, the age of the patient ranges from 30 to 60 years.”
The first known case in Africa was reported in a 58-year-old woman from Ghana, who had been using skin bleaching products for close to 30 years. The patient presented with tumors on her face, neck, and arms.
Dr. Faye then proceeded to share more than 10 such carcinoma cases. “These previous reports strongly suggest a relationship between skin bleaching and skin cancers,” said Dr. Faye.
Indeed, there have been reports and publications in the literature that support his observation, including one last year, which found that use of the tyrosinase inhibitor hydroquinone was associated with approximately a threefold increased risk for skin cancer.
For some, including Brazil’s Dr. Lupi, Dr. Faye’s talk was enlightening: “I didn’t know about this relationship [of bleaching] with skin cancer, it was something new for me.”
But the prevalence of SCC is very low, compared with that of skin bleaching, Dr. Faye acknowledged. Moreover, the cancer observed in the cases reported could have resulted from a number of reasons, including exposure to harmful ultraviolet rays from the sun and genetic predisposition in addition to the use of bleaching products such as hydroquinone. “Other causes of skin cancer are not excluded,” he said.
To further explore the link between skin bleaching and cancer, “we need case-control studies to provide more evidence,” he added. Until then, dermatologists “should keep on promoting messages” to prevent SCC from occurring. This includes encouraging the use of proper sun protection in addition to discouraging the practice of skin bleaching, which still persists despite more than 10 African nations banning the use of toxic skin-lightening products.
Dr. Faye and Dr. Lupi report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SINGAPORE –
This question was posed by Ousmane Faye, MD, PhD, director general of Mali’s Bamako Dermatology Hospital, at the World Congress of Dermatology.
Dr. Faye explored the issue during a hot topics session at the meeting, prefacing that it was an important question to ask because “in West Africa, skin bleaching is very common.”
“There are many local names” for skin bleaching, he said. “For example, in Senegal, it’s called xessal; in Mali and Ivory Coast, its name is caco; in South Africa, there are many names, like ukutsheyisa.”
Skin bleaching refers to the cosmetic misuse of topical agents to change one’s natural skin color. It’s a centuries-old practice that people, mainly women, adopt “to increase attractiveness and self-esteem,” explained Dr. Faye.
To demonstrate how pervasive skin bleaching is on the continent, he presented a slide that summarized figures from six studies spanning the past 2 decades. Prevalence ranged from 25% in Mali (based on a 1993 survey of 210 women) to a high of 79.25% in Benin (from a sample size of 511 women in 2019). In other studies of women in Burkina Faso and Togo, the figures were 44.3% and 58.9%, respectively. The most recently conducted study, which involved 2,689 Senegalese women and was published in 2022, found that nearly 6 in 10 (59.2%) respondents used skin-lightening products.
But skin bleaching isn’t just limited to Africa, said session moderator Omar Lupi, MD, PhD, associate professor of dermatology at the Federal University of the State of Rio de Janeiro, when approached for an independent comment. “It’s a traditional practice around the world. Maybe not in the developed countries, but it’s quite common in Africa, in South America, and in Asia.”
His sentiments are echoed in a meta-analysis that was published in the International Journal of Dermatology in 2019. The work examined 68 studies involving more than 67,000 people across Africa, Asia, Europe, the Middle East, and North America. It found that the pooled lifetime prevalence of skin bleaching was 27.7% (95% confidence interval, 19.6-37.5; P < .01).
“This is an important and interesting topic because our world is shrinking,” Dr. Lupi told this news organization. “Even in countries that don’t have bleaching as a common situation, we now have patients who are migrating from one part [of the world] to another, so bleaching is something that can knock on your door and you need to be prepared.”
Misuse leads to complications
The issue is pertinent to dermatologists because skin bleaching is associated with a wide range of complications. Take, for example, topical steroids, which are the most common products used for bleaching, said Dr. Faye in his talk.
“Clobetasol can suppress the hypothalamic-pituitary-adrenal (HPA) function,” he said, referring to the body’s main stress response system. “It can also foster skin infection, including bacterial, fungal, viral, and parasitic infection.”
In addition, topical steroids that are misused as skin lighteners have been reported to cause stretch marks, skin atrophy, inflammatory acne, and even metabolic disorders such as diabetes and hypertension, said Dr. Faye.
To further his point, he cited a 2021 prospective case-control study conducted across five sub-Saharan countries, which found that the use of “voluntary cosmetic depigmentation” significantly increased a person’s risk for necrotizing fasciitis of the lower limbs (odds ratio, 2.29; 95% CI, 1.19-3.73; P = .0226).
Similarly, mercury, another substance found in products commonly used to bleach skin, has been associated with problems ranging from rashes to renal toxicity. And because it’s so incredibly harmful, mercury is also known to cause neurologic abnormalities.
Apart from causing certain conditions, prolonged use of skin-lightening products can change the way existing diseases present themselves as well as their severity, added Dr. Faye.
An increased risk
But what about skin bleaching’s link with cancer? “Skin cancer on Black skin is uncommon, yet it occurs in skin-bleaching women,” said Dr. Faye.
“Since 2000, we have had some cases of skin cancer associated with skin bleaching,” he continued, adding that squamous cell carcinoma (SCC) is the most frequent type of cancer observed.
If you look at what’s been published on the topic so far, you’ll see that “all the cases of skin cancer are located over the neck or some exposed area when skin bleaching products are used for more than 10 years,” said Dr. Faye. “And most of the time, the age of the patient ranges from 30 to 60 years.”
The first known case in Africa was reported in a 58-year-old woman from Ghana, who had been using skin bleaching products for close to 30 years. The patient presented with tumors on her face, neck, and arms.
Dr. Faye then proceeded to share more than 10 such carcinoma cases. “These previous reports strongly suggest a relationship between skin bleaching and skin cancers,” said Dr. Faye.
Indeed, there have been reports and publications in the literature that support his observation, including one last year, which found that use of the tyrosinase inhibitor hydroquinone was associated with approximately a threefold increased risk for skin cancer.
For some, including Brazil’s Dr. Lupi, Dr. Faye’s talk was enlightening: “I didn’t know about this relationship [of bleaching] with skin cancer, it was something new for me.”
But the prevalence of SCC is very low, compared with that of skin bleaching, Dr. Faye acknowledged. Moreover, the cancer observed in the cases reported could have resulted from a number of reasons, including exposure to harmful ultraviolet rays from the sun and genetic predisposition in addition to the use of bleaching products such as hydroquinone. “Other causes of skin cancer are not excluded,” he said.
To further explore the link between skin bleaching and cancer, “we need case-control studies to provide more evidence,” he added. Until then, dermatologists “should keep on promoting messages” to prevent SCC from occurring. This includes encouraging the use of proper sun protection in addition to discouraging the practice of skin bleaching, which still persists despite more than 10 African nations banning the use of toxic skin-lightening products.
Dr. Faye and Dr. Lupi report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT WCD 2023
Surgery may worsen pleural mesothelioma survival outcomes
Pleural mesothelioma is generally treated by extended pleurectomy decortication, and there has been little improvement in systemic treatment of early-stage, resectable mesothelioma, which has led to the recommendations of maximum cytoreduction. U.S. and European guidelines, as well as an international consensus statement, support this approach, but it has never been tested in a randomized, controlled trial.
Now it has, and the result is surprising: The conclusion was uncomfortable for Eric Lim, MD, who presented the results of the MARS2 trial at the annual World Conference on Lung Cancer. “Ladies and gentlemen, as a surgeon standing here, you have no idea how much it pains me to conclude that extended pleurectomy decortication, an operation that we have been offering for over 70 years, has been associated with a higher risk of death, more serious complications, poorer quality of life, and higher costs, compared to mesothelioma patients who were randomized to chemotherapy alone,” said Dr. Lim of the Royal Brompton Hospital, London, during his presentation.
Although the line drew laughter and applause from the audience, Paula Ugalde Figueroa, MD, who served as a discussant, raised some concerns about the study. Disease presence in one hemithorax was assessed only by chest CT scan, which is notorious for underestimating the volume of disease during surgery. There was also no information on pleural effusion or how many patients received it prior to intervention. Existing guidelines suggest staging of mesothelioma should also use PET scans, and invasive mediastinal staging should be assessed with endobronchial ultrasound. “None of these were performed during the trial,” said Dr. Figueroa, who is an associate thoracic surgeon at Brigham and Women’s Hospital, Boston. “At this point, my question is, are the arms of this study well balanced in regard to tumor volume? We don’t know,” she added.
Dr. Figueroa noted that the 90-day mortality seemed higher than that seen in other studies. “So, does the surgeon’s experience and center volume affect the outcome of this study?” she asked. Dr. Figueroa personally made phone calls to the participating centers and found that 45% of the patients in the trial were treated at low-volume centers, defined by her as two to three patients per year. “Should we assume that their surgical outcomes are similar between those centers? In this trial, with approximately half of patients from low-volume centers, extended pleurectomy decortication for mesothelioma had no significant difference when compared to those patients that underwent chemotherapy alone. Would the outcome be different in exclusively high-volume centers?” she concluded.
The study randomized 335 patients to receive surgery and chemotherapy, or chemotherapy alone. They received two cycles of platinum-based chemotherapy and pemetrexed prior to surgery and up to four cycles after surgery. The average age was 69 years; 86.9% were male, and 85.7% of tumors were epithelioid only. Among those in the surgery group, 88.5% underwent extended pleurectomy/decortication, 8.3% underwent pleurectomy decortication, 1.9% underwent partial pleurectomy, 0.6% exploration with no pleurodesis, and 0.6% were classified as “other” surgery. Completeness of resection was R0 in 3.2% of surgeries, R1 in 80.9%, and R2 in 15.9%. In-hospital mortality occurred in 3.8% of patients, and postsurgical 90-day mortality was 8.9%.
Over the first 42 months of follow-up, the hazard ratio for overall survival was 1.28 in the no-surgery group (P = .03). “The survival was so good in this early-stage cohort that we had to extend the trial by 6 months to get the prerequisite number of deaths, underscoring the phenomenal importance of having a randomized comparative cohort for all future studies on surgery for mesothelioma,” said Dr. Lim.
After 42 months, there was no survival difference between the two groups (hazard ratio, 0.48; P = .15). Dr. Lim attributed the change at 42 months to the fact that only 15 patients remained in each arm at that stage. There was no significant difference between the two groups with respect to progression-free survival.
The survival benefit of the no-surgery group was sustained after additional analyses, including adjustment of the number of first-line chemotherapy cycles and immunotherapy received after completion of the trial protocol.
Adverse events were more common in the surgery group (incidence rate ratio, 3.6; P < .001), including any cardiac disorder (IRR, 2.73; 95% confidence interval, 1.11-6.67); any infection or infestation (IRR, 1.99; 95% CI, 1.33-2.99); any respiratory, thoracic, or mediastinal disorder (IRR, 2.40; 95% CI, 1.52-3.80); and any surgical or medical procedure (IRR, 2.23; 95% CI, 1.04-4.78). The EORTC quality of life score favored the nonsurgery group at 6 weeks, but there was no significant difference at other time points.
Dr. Lim and Dr. Figueroa have no relevant financial disclosures.
Pleural mesothelioma is generally treated by extended pleurectomy decortication, and there has been little improvement in systemic treatment of early-stage, resectable mesothelioma, which has led to the recommendations of maximum cytoreduction. U.S. and European guidelines, as well as an international consensus statement, support this approach, but it has never been tested in a randomized, controlled trial.
Now it has, and the result is surprising: The conclusion was uncomfortable for Eric Lim, MD, who presented the results of the MARS2 trial at the annual World Conference on Lung Cancer. “Ladies and gentlemen, as a surgeon standing here, you have no idea how much it pains me to conclude that extended pleurectomy decortication, an operation that we have been offering for over 70 years, has been associated with a higher risk of death, more serious complications, poorer quality of life, and higher costs, compared to mesothelioma patients who were randomized to chemotherapy alone,” said Dr. Lim of the Royal Brompton Hospital, London, during his presentation.
Although the line drew laughter and applause from the audience, Paula Ugalde Figueroa, MD, who served as a discussant, raised some concerns about the study. Disease presence in one hemithorax was assessed only by chest CT scan, which is notorious for underestimating the volume of disease during surgery. There was also no information on pleural effusion or how many patients received it prior to intervention. Existing guidelines suggest staging of mesothelioma should also use PET scans, and invasive mediastinal staging should be assessed with endobronchial ultrasound. “None of these were performed during the trial,” said Dr. Figueroa, who is an associate thoracic surgeon at Brigham and Women’s Hospital, Boston. “At this point, my question is, are the arms of this study well balanced in regard to tumor volume? We don’t know,” she added.
Dr. Figueroa noted that the 90-day mortality seemed higher than that seen in other studies. “So, does the surgeon’s experience and center volume affect the outcome of this study?” she asked. Dr. Figueroa personally made phone calls to the participating centers and found that 45% of the patients in the trial were treated at low-volume centers, defined by her as two to three patients per year. “Should we assume that their surgical outcomes are similar between those centers? In this trial, with approximately half of patients from low-volume centers, extended pleurectomy decortication for mesothelioma had no significant difference when compared to those patients that underwent chemotherapy alone. Would the outcome be different in exclusively high-volume centers?” she concluded.
The study randomized 335 patients to receive surgery and chemotherapy, or chemotherapy alone. They received two cycles of platinum-based chemotherapy and pemetrexed prior to surgery and up to four cycles after surgery. The average age was 69 years; 86.9% were male, and 85.7% of tumors were epithelioid only. Among those in the surgery group, 88.5% underwent extended pleurectomy/decortication, 8.3% underwent pleurectomy decortication, 1.9% underwent partial pleurectomy, 0.6% exploration with no pleurodesis, and 0.6% were classified as “other” surgery. Completeness of resection was R0 in 3.2% of surgeries, R1 in 80.9%, and R2 in 15.9%. In-hospital mortality occurred in 3.8% of patients, and postsurgical 90-day mortality was 8.9%.
Over the first 42 months of follow-up, the hazard ratio for overall survival was 1.28 in the no-surgery group (P = .03). “The survival was so good in this early-stage cohort that we had to extend the trial by 6 months to get the prerequisite number of deaths, underscoring the phenomenal importance of having a randomized comparative cohort for all future studies on surgery for mesothelioma,” said Dr. Lim.
After 42 months, there was no survival difference between the two groups (hazard ratio, 0.48; P = .15). Dr. Lim attributed the change at 42 months to the fact that only 15 patients remained in each arm at that stage. There was no significant difference between the two groups with respect to progression-free survival.
The survival benefit of the no-surgery group was sustained after additional analyses, including adjustment of the number of first-line chemotherapy cycles and immunotherapy received after completion of the trial protocol.
Adverse events were more common in the surgery group (incidence rate ratio, 3.6; P < .001), including any cardiac disorder (IRR, 2.73; 95% confidence interval, 1.11-6.67); any infection or infestation (IRR, 1.99; 95% CI, 1.33-2.99); any respiratory, thoracic, or mediastinal disorder (IRR, 2.40; 95% CI, 1.52-3.80); and any surgical or medical procedure (IRR, 2.23; 95% CI, 1.04-4.78). The EORTC quality of life score favored the nonsurgery group at 6 weeks, but there was no significant difference at other time points.
Dr. Lim and Dr. Figueroa have no relevant financial disclosures.
Pleural mesothelioma is generally treated by extended pleurectomy decortication, and there has been little improvement in systemic treatment of early-stage, resectable mesothelioma, which has led to the recommendations of maximum cytoreduction. U.S. and European guidelines, as well as an international consensus statement, support this approach, but it has never been tested in a randomized, controlled trial.
Now it has, and the result is surprising: The conclusion was uncomfortable for Eric Lim, MD, who presented the results of the MARS2 trial at the annual World Conference on Lung Cancer. “Ladies and gentlemen, as a surgeon standing here, you have no idea how much it pains me to conclude that extended pleurectomy decortication, an operation that we have been offering for over 70 years, has been associated with a higher risk of death, more serious complications, poorer quality of life, and higher costs, compared to mesothelioma patients who were randomized to chemotherapy alone,” said Dr. Lim of the Royal Brompton Hospital, London, during his presentation.
Although the line drew laughter and applause from the audience, Paula Ugalde Figueroa, MD, who served as a discussant, raised some concerns about the study. Disease presence in one hemithorax was assessed only by chest CT scan, which is notorious for underestimating the volume of disease during surgery. There was also no information on pleural effusion or how many patients received it prior to intervention. Existing guidelines suggest staging of mesothelioma should also use PET scans, and invasive mediastinal staging should be assessed with endobronchial ultrasound. “None of these were performed during the trial,” said Dr. Figueroa, who is an associate thoracic surgeon at Brigham and Women’s Hospital, Boston. “At this point, my question is, are the arms of this study well balanced in regard to tumor volume? We don’t know,” she added.
Dr. Figueroa noted that the 90-day mortality seemed higher than that seen in other studies. “So, does the surgeon’s experience and center volume affect the outcome of this study?” she asked. Dr. Figueroa personally made phone calls to the participating centers and found that 45% of the patients in the trial were treated at low-volume centers, defined by her as two to three patients per year. “Should we assume that their surgical outcomes are similar between those centers? In this trial, with approximately half of patients from low-volume centers, extended pleurectomy decortication for mesothelioma had no significant difference when compared to those patients that underwent chemotherapy alone. Would the outcome be different in exclusively high-volume centers?” she concluded.
The study randomized 335 patients to receive surgery and chemotherapy, or chemotherapy alone. They received two cycles of platinum-based chemotherapy and pemetrexed prior to surgery and up to four cycles after surgery. The average age was 69 years; 86.9% were male, and 85.7% of tumors were epithelioid only. Among those in the surgery group, 88.5% underwent extended pleurectomy/decortication, 8.3% underwent pleurectomy decortication, 1.9% underwent partial pleurectomy, 0.6% exploration with no pleurodesis, and 0.6% were classified as “other” surgery. Completeness of resection was R0 in 3.2% of surgeries, R1 in 80.9%, and R2 in 15.9%. In-hospital mortality occurred in 3.8% of patients, and postsurgical 90-day mortality was 8.9%.
Over the first 42 months of follow-up, the hazard ratio for overall survival was 1.28 in the no-surgery group (P = .03). “The survival was so good in this early-stage cohort that we had to extend the trial by 6 months to get the prerequisite number of deaths, underscoring the phenomenal importance of having a randomized comparative cohort for all future studies on surgery for mesothelioma,” said Dr. Lim.
After 42 months, there was no survival difference between the two groups (hazard ratio, 0.48; P = .15). Dr. Lim attributed the change at 42 months to the fact that only 15 patients remained in each arm at that stage. There was no significant difference between the two groups with respect to progression-free survival.
The survival benefit of the no-surgery group was sustained after additional analyses, including adjustment of the number of first-line chemotherapy cycles and immunotherapy received after completion of the trial protocol.
Adverse events were more common in the surgery group (incidence rate ratio, 3.6; P < .001), including any cardiac disorder (IRR, 2.73; 95% confidence interval, 1.11-6.67); any infection or infestation (IRR, 1.99; 95% CI, 1.33-2.99); any respiratory, thoracic, or mediastinal disorder (IRR, 2.40; 95% CI, 1.52-3.80); and any surgical or medical procedure (IRR, 2.23; 95% CI, 1.04-4.78). The EORTC quality of life score favored the nonsurgery group at 6 weeks, but there was no significant difference at other time points.
Dr. Lim and Dr. Figueroa have no relevant financial disclosures.
FROM WCLC 2023
Heart attack deaths static in those with type 1 diabetes
, new research shows.
Between 2006 and 2020, the annual incidences of overall mortality and major adverse cardiovascular events after a first-time myocardial infarction dropped significantly for people with type 2 diabetes and those without diabetes (controls).
However, the same trend was not seen for people with type 1 diabetes.
“There is an urgent need for further studies understanding cardiovascular disease in people with type 1 diabetes. Clinicians have to be aware of the absence of the declined mortality trend in people with type 1 diabetes having a first-time myocardial infarction,” lead author Thomas Nyström, MD, professor of medicine at the Karolinska Institute, Stockholm, said in an interview.
The findings are scheduled to be presented Oct. 5, 2023, at the annual meeting of the European Association for the Study of Diabetes.
Discussing potential reasons for the findings, the authors say that the standard care after a heart attack has improved with more availability of, for example, percutaneous coronary intervention and better overall medical treatment. However, this standard of care should have improved in all three groups.
“Although glycemic control and diabetes duration were much different between diabetes groups, in that those with type 1 had been exposed for a longer period of glycemia, the current study cannot tell whether glucose control is behind the association between mortality trends observed. Whether this is the case must be investigated with further studies,” Nyström said.
Data from Swedish health care registry
Among people with a first-time MI recorded in national Swedish health care registries between 2006 and 2020, there were 2,527 individuals with type 1 diabetes, 48,321 with type 2 diabetes, and 243,170 controls with neither form of diabetes.
Those with type 1 diabetes were younger than those with type 2 diabetes and controls (62 years vs. 75 and 73 years, respectively). The type 1 diabetes group also had a higher proportion of females (43.6% vs. 38.1% of both the type 2 diabetes and control groups).
The proportions of people with the most severe type of heart attack, ST-elevation MI (STEMI), versus non-STEMI were 29% versus 71% in the type 1 diabetes group, 30% versus 70% in the type 2 diabetes group, and 39% versus 61% in the control group, respectively.
After adjustment for covariates including age, sex, comorbidities, socioeconomic factors, and medication, there was a significant decreased annual incidence trend for all-cause death among the controls (–1.9%) and persons with type 2 diabetes (–1.3%), but there was no such decrease among those with type 1 diabetes.
For cardiovascular deaths, the annual incidence declines were –2.0% and –1.6% in the control group and the type 2 diabetes group, respectively, versus a nonsignificant –0.5% decline in the type 1 diabetes group. Similarly, for major adverse cardiovascular events, those decreases were –2.0% for controls and –1.6% for those with type 2 diabetes, but –0.6% for those with type 1 diabetes – again, a nonsignificant value.
“During the last 15 years, the risk of death and major cardiovascular events in people without diabetes and with type 2 diabetes after having a first-time heart attack has decreased significantly. In contrast, this decreasing trend was absent in people with type 1 diabetes. Our study highlights the urgent need for understanding the cardiovascular risk in people with type 1 diabetes,” the authors conclude.
Dr. Nyström has received honoraria from AstraZeneca, Merck Sharp & Dohme, Novo Nordisk, Eli Lilly , Boehringer Ingelheim, Abbott, and Amgen. The authors acknowledge the ALF agreement between Stockholm County Council and Karolinska Institutet.
A version of this article appeared on Medscape.com.
, new research shows.
Between 2006 and 2020, the annual incidences of overall mortality and major adverse cardiovascular events after a first-time myocardial infarction dropped significantly for people with type 2 diabetes and those without diabetes (controls).
However, the same trend was not seen for people with type 1 diabetes.
“There is an urgent need for further studies understanding cardiovascular disease in people with type 1 diabetes. Clinicians have to be aware of the absence of the declined mortality trend in people with type 1 diabetes having a first-time myocardial infarction,” lead author Thomas Nyström, MD, professor of medicine at the Karolinska Institute, Stockholm, said in an interview.
The findings are scheduled to be presented Oct. 5, 2023, at the annual meeting of the European Association for the Study of Diabetes.
Discussing potential reasons for the findings, the authors say that the standard care after a heart attack has improved with more availability of, for example, percutaneous coronary intervention and better overall medical treatment. However, this standard of care should have improved in all three groups.
“Although glycemic control and diabetes duration were much different between diabetes groups, in that those with type 1 had been exposed for a longer period of glycemia, the current study cannot tell whether glucose control is behind the association between mortality trends observed. Whether this is the case must be investigated with further studies,” Nyström said.
Data from Swedish health care registry
Among people with a first-time MI recorded in national Swedish health care registries between 2006 and 2020, there were 2,527 individuals with type 1 diabetes, 48,321 with type 2 diabetes, and 243,170 controls with neither form of diabetes.
Those with type 1 diabetes were younger than those with type 2 diabetes and controls (62 years vs. 75 and 73 years, respectively). The type 1 diabetes group also had a higher proportion of females (43.6% vs. 38.1% of both the type 2 diabetes and control groups).
The proportions of people with the most severe type of heart attack, ST-elevation MI (STEMI), versus non-STEMI were 29% versus 71% in the type 1 diabetes group, 30% versus 70% in the type 2 diabetes group, and 39% versus 61% in the control group, respectively.
After adjustment for covariates including age, sex, comorbidities, socioeconomic factors, and medication, there was a significant decreased annual incidence trend for all-cause death among the controls (–1.9%) and persons with type 2 diabetes (–1.3%), but there was no such decrease among those with type 1 diabetes.
For cardiovascular deaths, the annual incidence declines were –2.0% and –1.6% in the control group and the type 2 diabetes group, respectively, versus a nonsignificant –0.5% decline in the type 1 diabetes group. Similarly, for major adverse cardiovascular events, those decreases were –2.0% for controls and –1.6% for those with type 2 diabetes, but –0.6% for those with type 1 diabetes – again, a nonsignificant value.
“During the last 15 years, the risk of death and major cardiovascular events in people without diabetes and with type 2 diabetes after having a first-time heart attack has decreased significantly. In contrast, this decreasing trend was absent in people with type 1 diabetes. Our study highlights the urgent need for understanding the cardiovascular risk in people with type 1 diabetes,” the authors conclude.
Dr. Nyström has received honoraria from AstraZeneca, Merck Sharp & Dohme, Novo Nordisk, Eli Lilly , Boehringer Ingelheim, Abbott, and Amgen. The authors acknowledge the ALF agreement between Stockholm County Council and Karolinska Institutet.
A version of this article appeared on Medscape.com.
, new research shows.
Between 2006 and 2020, the annual incidences of overall mortality and major adverse cardiovascular events after a first-time myocardial infarction dropped significantly for people with type 2 diabetes and those without diabetes (controls).
However, the same trend was not seen for people with type 1 diabetes.
“There is an urgent need for further studies understanding cardiovascular disease in people with type 1 diabetes. Clinicians have to be aware of the absence of the declined mortality trend in people with type 1 diabetes having a first-time myocardial infarction,” lead author Thomas Nyström, MD, professor of medicine at the Karolinska Institute, Stockholm, said in an interview.
The findings are scheduled to be presented Oct. 5, 2023, at the annual meeting of the European Association for the Study of Diabetes.
Discussing potential reasons for the findings, the authors say that the standard care after a heart attack has improved with more availability of, for example, percutaneous coronary intervention and better overall medical treatment. However, this standard of care should have improved in all three groups.
“Although glycemic control and diabetes duration were much different between diabetes groups, in that those with type 1 had been exposed for a longer period of glycemia, the current study cannot tell whether glucose control is behind the association between mortality trends observed. Whether this is the case must be investigated with further studies,” Nyström said.
Data from Swedish health care registry
Among people with a first-time MI recorded in national Swedish health care registries between 2006 and 2020, there were 2,527 individuals with type 1 diabetes, 48,321 with type 2 diabetes, and 243,170 controls with neither form of diabetes.
Those with type 1 diabetes were younger than those with type 2 diabetes and controls (62 years vs. 75 and 73 years, respectively). The type 1 diabetes group also had a higher proportion of females (43.6% vs. 38.1% of both the type 2 diabetes and control groups).
The proportions of people with the most severe type of heart attack, ST-elevation MI (STEMI), versus non-STEMI were 29% versus 71% in the type 1 diabetes group, 30% versus 70% in the type 2 diabetes group, and 39% versus 61% in the control group, respectively.
After adjustment for covariates including age, sex, comorbidities, socioeconomic factors, and medication, there was a significant decreased annual incidence trend for all-cause death among the controls (–1.9%) and persons with type 2 diabetes (–1.3%), but there was no such decrease among those with type 1 diabetes.
For cardiovascular deaths, the annual incidence declines were –2.0% and –1.6% in the control group and the type 2 diabetes group, respectively, versus a nonsignificant –0.5% decline in the type 1 diabetes group. Similarly, for major adverse cardiovascular events, those decreases were –2.0% for controls and –1.6% for those with type 2 diabetes, but –0.6% for those with type 1 diabetes – again, a nonsignificant value.
“During the last 15 years, the risk of death and major cardiovascular events in people without diabetes and with type 2 diabetes after having a first-time heart attack has decreased significantly. In contrast, this decreasing trend was absent in people with type 1 diabetes. Our study highlights the urgent need for understanding the cardiovascular risk in people with type 1 diabetes,” the authors conclude.
Dr. Nyström has received honoraria from AstraZeneca, Merck Sharp & Dohme, Novo Nordisk, Eli Lilly , Boehringer Ingelheim, Abbott, and Amgen. The authors acknowledge the ALF agreement between Stockholm County Council and Karolinska Institutet.
A version of this article appeared on Medscape.com.
FROM EASD 2023
ADCs show early promise in NSCLC
This has led to a burgeoning interest in solid tumors, with over 100 clinical trials in progress. Non–small cell lung cancer (NSCLC) is no exception. In 2022, the Food and Drug Administration approved trastuzumab DXd for pretreated NSCLC patients with HER2-mutant tumors. Two others have lung cancer breakthrough therapy designations from the FDA, including patritumab deruxtecan (HER3-DXd) for EGFR-mutant NSCLC and telisotuzumab vedotin for NSCLC that overexpresses c-Met.
At the annual World Conference on Lung Cancer, researchers outlined some of the latest developments in ADCs targeting the antigens HER3, trophoblast cell-surface antigen 2 (TROP-2), and the B7-H3 immunoregulatory protein, as single agents or in combination with immunotherapy. Following the presentations, discussant Helena Linardou, MD, PhD, emphasized the need for pharmacogenomics to predict toxicity and studies to understand resistance mechanisms. “ADCs are a new, rapidly evolving class of therapeutics, and I think that we will all have to be prepared for the future that is coming,” said Dr. Linardou, who is director of the 4th oncology department and the Comprehensive Clinical Trials Center at Metropolitan Hospital in Athens.
Researchers presented four ADC clinical trial updates.
Patritumab deruxtecan
Patritumab deruxtecan (Daiichi Sankyo) links a HER3 antibody to the topoisomerase I inhibitor deruxtecan (HER3-DXd). In the open-label, phase 2 HERTHENA-Lung01 trial, it was tested in patients with NSCLC EGFR-activation mutations, which occurs in 14%-38% of NSCLC cases. There are few options for these patients following failure of EGFR tyrosine kinase inhibitor therapy.
The study included 225 patients previously treated with EGFR tyrosine kinase inhibitors and platinum-based chemotherapy who received 5.6 mg/kg of HER3-DXd every 3 weeks. Over a median follow-up of 13.1 months and a median treatment duration of 5.5 months), 29.8% had a confirmed overall response (95% confidence interval, 23.9%-36.2%) with a median duration of 6.4 months (95% CI, 4.9-7.8). The median progression-free survival was 5.5 months (95% CI, 5.1-5.9), and the median OS was 11.9 months (95% CI, 11.2-13.1). The researchers noted similar outcomes among patients with different mechanisms of EGFR TKI resistance. The frequency of adverse events was similar to previous studies, with drug-related adverse events linked to treatment discontinuation of 7.1% interstitial lung disease in 5.3%. Among 30 patients with brain metastases, the confirmed intracranial response rate was 33.3% (95% CI, 17.3%-52.8%).
The study was published simultaneously online in the Journal of Clinical Oncology. (Abstract)
Datopotamab deruxtecan
PD-1/PD-L1 inhibitors are the first-line therapy for metastatic NSCLC, but there are efforts to improve outcomes through combination therapy. Datopotamab deruxtecan (Dato-DXd, Daiichi Sankyo, AstraZeneca) is an ADC targeting TROP2, and it has been shown in preclinical studies to enhance tumor responses to PD-1/PD-L1 inhibitors. The ADC improved progression-free survival (PFS), compared with docetaxel, in previously treated advanced or metastatic NSCLC.
In an interim analysis of the phase 1b TROPION-Lung04 study, researchers reported results from the combination of Dato-DXd with durvalumab with or without carboplatin. The study included 38 patients, some of whom had previously undergone treatment with immune checkpoint inhibitors. Nineteen patients received the doublet, and 14 received the carboplatin triplet. Grade 3 or higher treatment-emergent adverse events occurred in 42.1% of the doublet group and 71.4% of the triplet group. Interstitial lung disease occurred in 15.8% and 7.1% of the two groups, respectively. The objective response rate was 50.0% in the doublet group and 76.9% in the triplet group. The disease control rate was 92.9% and 92.3%, respectively. Durable responses occurred in both the first-line setting and the overall population. (Abstract)
Sacituzumab govitecan
Another ADC being tested with PD-1/PD-L1 inhibitors is sacituzumab govitecan (Trodelvy, Gilead), which has already received FDA approval for metastatic triple-negative breast cancer, pretreated HR+/HER2- metastatic breast cancer, and metastatic urothelial cancer. Like datopotamab, sacituzumab targets TROP-2. Researchers reported preliminary results from the phase 2 EVOKE-02 study, in which the ADC was combined with pembrolizumab for the first-line treatment of metastatic NSCLC. The overall response rate was 56% (95% CI, 42%-69%). Among patients with PD-L1 tumor proportion score (TPS) ≥ 50%, the ORR was 69% (95% CI, 49%-85%) and 44% (95% CI, 26%-62%) among those with TPS < 50%. The disease control rate was 86% (95% CI, 68%-96%) and 78% (95% CI, 60%-91%), respectively. The most frequent treatment-emergent adverse events (TEAEs) were diarrhea, anemia, and asthenia, and 18% of patients discontinued the study drug because of TEAEs. (Abstract)
Ifinatamab deruxtecan
Ifinatamab deruxtecan (Daiichi Sankyo) targets the B7-H3 antigen, which is an immunoregulatory protein that is overexpressed in many tumors. In the DS7300-A-J101 study, it was tested in patients with advanced or metastatic solid tumors, without selection for B7-H3 expression. A subgroup analysis of 22 patients with small cell lung cancer (SCLC) showed an ORR of 52.4 (95% CI, 29.8-74.3), a complete response of 4.8%, and a partial response in 47.6%. The median PFS was 5.6 months (95% CI, 3.9-8.1) and median OS was 12.2 months (95% CI, 6.4-not applicable). The most common treatment-emergent adverse events were nausea (59.1%), fatigue (50.0%), anemia (27.3%), vomiting (27.3%), and decreased appetite (22.7%). (Abstract)
This has led to a burgeoning interest in solid tumors, with over 100 clinical trials in progress. Non–small cell lung cancer (NSCLC) is no exception. In 2022, the Food and Drug Administration approved trastuzumab DXd for pretreated NSCLC patients with HER2-mutant tumors. Two others have lung cancer breakthrough therapy designations from the FDA, including patritumab deruxtecan (HER3-DXd) for EGFR-mutant NSCLC and telisotuzumab vedotin for NSCLC that overexpresses c-Met.
At the annual World Conference on Lung Cancer, researchers outlined some of the latest developments in ADCs targeting the antigens HER3, trophoblast cell-surface antigen 2 (TROP-2), and the B7-H3 immunoregulatory protein, as single agents or in combination with immunotherapy. Following the presentations, discussant Helena Linardou, MD, PhD, emphasized the need for pharmacogenomics to predict toxicity and studies to understand resistance mechanisms. “ADCs are a new, rapidly evolving class of therapeutics, and I think that we will all have to be prepared for the future that is coming,” said Dr. Linardou, who is director of the 4th oncology department and the Comprehensive Clinical Trials Center at Metropolitan Hospital in Athens.
Researchers presented four ADC clinical trial updates.
Patritumab deruxtecan
Patritumab deruxtecan (Daiichi Sankyo) links a HER3 antibody to the topoisomerase I inhibitor deruxtecan (HER3-DXd). In the open-label, phase 2 HERTHENA-Lung01 trial, it was tested in patients with NSCLC EGFR-activation mutations, which occurs in 14%-38% of NSCLC cases. There are few options for these patients following failure of EGFR tyrosine kinase inhibitor therapy.
The study included 225 patients previously treated with EGFR tyrosine kinase inhibitors and platinum-based chemotherapy who received 5.6 mg/kg of HER3-DXd every 3 weeks. Over a median follow-up of 13.1 months and a median treatment duration of 5.5 months), 29.8% had a confirmed overall response (95% confidence interval, 23.9%-36.2%) with a median duration of 6.4 months (95% CI, 4.9-7.8). The median progression-free survival was 5.5 months (95% CI, 5.1-5.9), and the median OS was 11.9 months (95% CI, 11.2-13.1). The researchers noted similar outcomes among patients with different mechanisms of EGFR TKI resistance. The frequency of adverse events was similar to previous studies, with drug-related adverse events linked to treatment discontinuation of 7.1% interstitial lung disease in 5.3%. Among 30 patients with brain metastases, the confirmed intracranial response rate was 33.3% (95% CI, 17.3%-52.8%).
The study was published simultaneously online in the Journal of Clinical Oncology. (Abstract)
Datopotamab deruxtecan
PD-1/PD-L1 inhibitors are the first-line therapy for metastatic NSCLC, but there are efforts to improve outcomes through combination therapy. Datopotamab deruxtecan (Dato-DXd, Daiichi Sankyo, AstraZeneca) is an ADC targeting TROP2, and it has been shown in preclinical studies to enhance tumor responses to PD-1/PD-L1 inhibitors. The ADC improved progression-free survival (PFS), compared with docetaxel, in previously treated advanced or metastatic NSCLC.
In an interim analysis of the phase 1b TROPION-Lung04 study, researchers reported results from the combination of Dato-DXd with durvalumab with or without carboplatin. The study included 38 patients, some of whom had previously undergone treatment with immune checkpoint inhibitors. Nineteen patients received the doublet, and 14 received the carboplatin triplet. Grade 3 or higher treatment-emergent adverse events occurred in 42.1% of the doublet group and 71.4% of the triplet group. Interstitial lung disease occurred in 15.8% and 7.1% of the two groups, respectively. The objective response rate was 50.0% in the doublet group and 76.9% in the triplet group. The disease control rate was 92.9% and 92.3%, respectively. Durable responses occurred in both the first-line setting and the overall population. (Abstract)
Sacituzumab govitecan
Another ADC being tested with PD-1/PD-L1 inhibitors is sacituzumab govitecan (Trodelvy, Gilead), which has already received FDA approval for metastatic triple-negative breast cancer, pretreated HR+/HER2- metastatic breast cancer, and metastatic urothelial cancer. Like datopotamab, sacituzumab targets TROP-2. Researchers reported preliminary results from the phase 2 EVOKE-02 study, in which the ADC was combined with pembrolizumab for the first-line treatment of metastatic NSCLC. The overall response rate was 56% (95% CI, 42%-69%). Among patients with PD-L1 tumor proportion score (TPS) ≥ 50%, the ORR was 69% (95% CI, 49%-85%) and 44% (95% CI, 26%-62%) among those with TPS < 50%. The disease control rate was 86% (95% CI, 68%-96%) and 78% (95% CI, 60%-91%), respectively. The most frequent treatment-emergent adverse events (TEAEs) were diarrhea, anemia, and asthenia, and 18% of patients discontinued the study drug because of TEAEs. (Abstract)
Ifinatamab deruxtecan
Ifinatamab deruxtecan (Daiichi Sankyo) targets the B7-H3 antigen, which is an immunoregulatory protein that is overexpressed in many tumors. In the DS7300-A-J101 study, it was tested in patients with advanced or metastatic solid tumors, without selection for B7-H3 expression. A subgroup analysis of 22 patients with small cell lung cancer (SCLC) showed an ORR of 52.4 (95% CI, 29.8-74.3), a complete response of 4.8%, and a partial response in 47.6%. The median PFS was 5.6 months (95% CI, 3.9-8.1) and median OS was 12.2 months (95% CI, 6.4-not applicable). The most common treatment-emergent adverse events were nausea (59.1%), fatigue (50.0%), anemia (27.3%), vomiting (27.3%), and decreased appetite (22.7%). (Abstract)
This has led to a burgeoning interest in solid tumors, with over 100 clinical trials in progress. Non–small cell lung cancer (NSCLC) is no exception. In 2022, the Food and Drug Administration approved trastuzumab DXd for pretreated NSCLC patients with HER2-mutant tumors. Two others have lung cancer breakthrough therapy designations from the FDA, including patritumab deruxtecan (HER3-DXd) for EGFR-mutant NSCLC and telisotuzumab vedotin for NSCLC that overexpresses c-Met.
At the annual World Conference on Lung Cancer, researchers outlined some of the latest developments in ADCs targeting the antigens HER3, trophoblast cell-surface antigen 2 (TROP-2), and the B7-H3 immunoregulatory protein, as single agents or in combination with immunotherapy. Following the presentations, discussant Helena Linardou, MD, PhD, emphasized the need for pharmacogenomics to predict toxicity and studies to understand resistance mechanisms. “ADCs are a new, rapidly evolving class of therapeutics, and I think that we will all have to be prepared for the future that is coming,” said Dr. Linardou, who is director of the 4th oncology department and the Comprehensive Clinical Trials Center at Metropolitan Hospital in Athens.
Researchers presented four ADC clinical trial updates.
Patritumab deruxtecan
Patritumab deruxtecan (Daiichi Sankyo) links a HER3 antibody to the topoisomerase I inhibitor deruxtecan (HER3-DXd). In the open-label, phase 2 HERTHENA-Lung01 trial, it was tested in patients with NSCLC EGFR-activation mutations, which occurs in 14%-38% of NSCLC cases. There are few options for these patients following failure of EGFR tyrosine kinase inhibitor therapy.
The study included 225 patients previously treated with EGFR tyrosine kinase inhibitors and platinum-based chemotherapy who received 5.6 mg/kg of HER3-DXd every 3 weeks. Over a median follow-up of 13.1 months and a median treatment duration of 5.5 months), 29.8% had a confirmed overall response (95% confidence interval, 23.9%-36.2%) with a median duration of 6.4 months (95% CI, 4.9-7.8). The median progression-free survival was 5.5 months (95% CI, 5.1-5.9), and the median OS was 11.9 months (95% CI, 11.2-13.1). The researchers noted similar outcomes among patients with different mechanisms of EGFR TKI resistance. The frequency of adverse events was similar to previous studies, with drug-related adverse events linked to treatment discontinuation of 7.1% interstitial lung disease in 5.3%. Among 30 patients with brain metastases, the confirmed intracranial response rate was 33.3% (95% CI, 17.3%-52.8%).
The study was published simultaneously online in the Journal of Clinical Oncology. (Abstract)
Datopotamab deruxtecan
PD-1/PD-L1 inhibitors are the first-line therapy for metastatic NSCLC, but there are efforts to improve outcomes through combination therapy. Datopotamab deruxtecan (Dato-DXd, Daiichi Sankyo, AstraZeneca) is an ADC targeting TROP2, and it has been shown in preclinical studies to enhance tumor responses to PD-1/PD-L1 inhibitors. The ADC improved progression-free survival (PFS), compared with docetaxel, in previously treated advanced or metastatic NSCLC.
In an interim analysis of the phase 1b TROPION-Lung04 study, researchers reported results from the combination of Dato-DXd with durvalumab with or without carboplatin. The study included 38 patients, some of whom had previously undergone treatment with immune checkpoint inhibitors. Nineteen patients received the doublet, and 14 received the carboplatin triplet. Grade 3 or higher treatment-emergent adverse events occurred in 42.1% of the doublet group and 71.4% of the triplet group. Interstitial lung disease occurred in 15.8% and 7.1% of the two groups, respectively. The objective response rate was 50.0% in the doublet group and 76.9% in the triplet group. The disease control rate was 92.9% and 92.3%, respectively. Durable responses occurred in both the first-line setting and the overall population. (Abstract)
Sacituzumab govitecan
Another ADC being tested with PD-1/PD-L1 inhibitors is sacituzumab govitecan (Trodelvy, Gilead), which has already received FDA approval for metastatic triple-negative breast cancer, pretreated HR+/HER2- metastatic breast cancer, and metastatic urothelial cancer. Like datopotamab, sacituzumab targets TROP-2. Researchers reported preliminary results from the phase 2 EVOKE-02 study, in which the ADC was combined with pembrolizumab for the first-line treatment of metastatic NSCLC. The overall response rate was 56% (95% CI, 42%-69%). Among patients with PD-L1 tumor proportion score (TPS) ≥ 50%, the ORR was 69% (95% CI, 49%-85%) and 44% (95% CI, 26%-62%) among those with TPS < 50%. The disease control rate was 86% (95% CI, 68%-96%) and 78% (95% CI, 60%-91%), respectively. The most frequent treatment-emergent adverse events (TEAEs) were diarrhea, anemia, and asthenia, and 18% of patients discontinued the study drug because of TEAEs. (Abstract)
Ifinatamab deruxtecan
Ifinatamab deruxtecan (Daiichi Sankyo) targets the B7-H3 antigen, which is an immunoregulatory protein that is overexpressed in many tumors. In the DS7300-A-J101 study, it was tested in patients with advanced or metastatic solid tumors, without selection for B7-H3 expression. A subgroup analysis of 22 patients with small cell lung cancer (SCLC) showed an ORR of 52.4 (95% CI, 29.8-74.3), a complete response of 4.8%, and a partial response in 47.6%. The median PFS was 5.6 months (95% CI, 3.9-8.1) and median OS was 12.2 months (95% CI, 6.4-not applicable). The most common treatment-emergent adverse events were nausea (59.1%), fatigue (50.0%), anemia (27.3%), vomiting (27.3%), and decreased appetite (22.7%). (Abstract)
FROM WCLC 2023
Steady VKA therapy beats switch to NOAC in frail AFib patients: FRAIL-AF
Switching frail patients with atrial fibrillation (AFib) from anticoagulation therapy with vitamin K antagonists (VKAs) to a novel oral anticoagulant (NOAC) resulted in more bleeding without any reduction in thromboembolic complications or all-cause mortality, randomized trial results show.
The study, FRAIL-AF, is the first randomized NOAC trial to exclusively include frail older patients, said lead author Linda P.T. Joosten, MD, Julius Center for Health Sciences and Primary Care in Utrecht, the Netherlands, and these unexpected findings provide evidence that goes beyond what is currently available.
“Data from the FRAIL-AF trial showed that switching from a VKA to a NOAC should not be considered without a clear indication in frail older patients with AF[ib], as switching to a NOAC leads to 69% more bleeding,” she concluded, without any benefit on secondary clinical endpoints, including thromboembolic events and all-cause mortality.
“The results turned out different than we expected,” Dr. Joosten said. “The hypothesis of this superiority trial was that switching from VKA therapy to a NOAC would result in less bleeding. However, we observed the opposite. After the interim analysis, the data and safety monitoring board advised to stop inclusion because switching from a VKA to a NOAC was clearly contraindicated with a hazard ratio of 1.69 and a highly significant P value of .001.”
Results of FRAIL-AF were presented at the annual congress of the European Society of Cardiology and published online in the journal Circulation.
Session moderator Renate B. Schnabel, MD, interventional cardiologist with University Heart & Vascular Center Hamburg (Germany), congratulated the researchers on these “astonishing” data.
“The thing I want to emphasize here is that, in the absence of randomized controlled trial data, we should be very cautious in extrapolating data from the landmark trials to populations not enrolled in those, and to rely on observational data only,” Dr. Schnabel told Dr. Joosten. “We need randomized controlled trials that sometimes give astonishing results.”
Frailty a clinical syndrome
Frailty is “a lot more than just aging, multiple comorbidities and polypharmacy,” Dr. Joosten explained. “It’s really a clinical syndrome, with people with a high biological vulnerability, dependency on significant others, and a reduced capacity to resist stressors, all leading to a reduced homeostatic reserve.”
Frailty is common in the community, with a prevalence of about 12%, she noted, “and even more important, AF[ib] in frail older people is very common, with a prevalence of 18%. And “without any doubt, we have to adequately anticoagulate frail AF[ib] patients, as they have a high stroke risk, with an incidence of 12.4% per year,” Dr. Joosten noted, compared with 3.9% per year among nonfrail AFib patients.
NOACs are preferred over VKAs in nonfrail AFib patients, after four major trials, RE-LY with dabigatran, ROCKET-AF with rivaroxaban, ARISTOTLE with apixaban, and ENGAGE-AF with edoxaban, showed that NOAC treatment resulted in less major bleeding while stroke risk was comparable with treatment with warfarin, she noted.
The 2023 European Heart Rhythm Association consensus document on management of arrhythmias in frailty syndrome concludes that the advantages of NOACs relative to VKAs are “likely consistent” in frail and nonfrail AFib patients, but the level of evidence is low.
So it’s unknown if NOACs are preferred over VKAs in frail AFib patients, “and it’s even more questionable whether patients on VKAs should switch to NOAC therapy,” Dr. Joosten said.
This new trial aimed to answer the question of whether switching frail AFib patients currently managed on a VKA to a NOAC would reduce bleeding. FRAIL-AF was a pragmatic, multicenter, open-label, randomized, controlled superiority trial.
Older AFib patients were deemed frail if they were aged 75 years or older and had a score of 3 or more on the validated Groningen Frailty Indicator (GFI). Patients with a glomerular filtration rate of less than 30 mL/min per 1.73 m2 or with valvular AFib were excluded.
Eligible patients were then assigned randomly to switch from their international normalized ratio (INR)–guided VKA treatment with either 1 mg acenocoumarol or 3 mg phenprocoumon, to a NOAC, or to continue VKA treatment. They were followed for 12 months for the primary outcome – major bleeding or clinically relevant nonmajor bleeding complication, whichever came first – accounting for death as a competing risk.
A total of 1,330 patients were randomly assigned between January 2018 and June 2022. Their mean age was 83 years, and they had a median GFI of 4. After randomization, 6 patients in the switch-to-NOAC arm, and 1 in the continue-VKA arm were found to have exclusion criteria, so in the end, 662 patients were switched from a VKA to NOAC, while 661 continued on VKA therapy. The choice of NOAC was made by the treating physician.
Major bleeding was defined as a fatal bleeding; bleeding in a critical area or organ; bleeding leading to transfusion; and/or bleeding leading to a fall in hemoglobin level of 2 g/dL (1.24 mmol/L) or more. Nonmajor bleeding was bleeding not considered major but requiring face-to-face consultation, hospitalization or increased level of care, or medical intervention.
After a prespecified futility analysis planned after 163 primary outcome events, the trial was halted when it was seen that there were 101 primary outcome events in the switch arm compared to 62 in the continue arm, Dr. Joosten said. The difference appeared to be driven by clinically relevant nonmajor bleeding.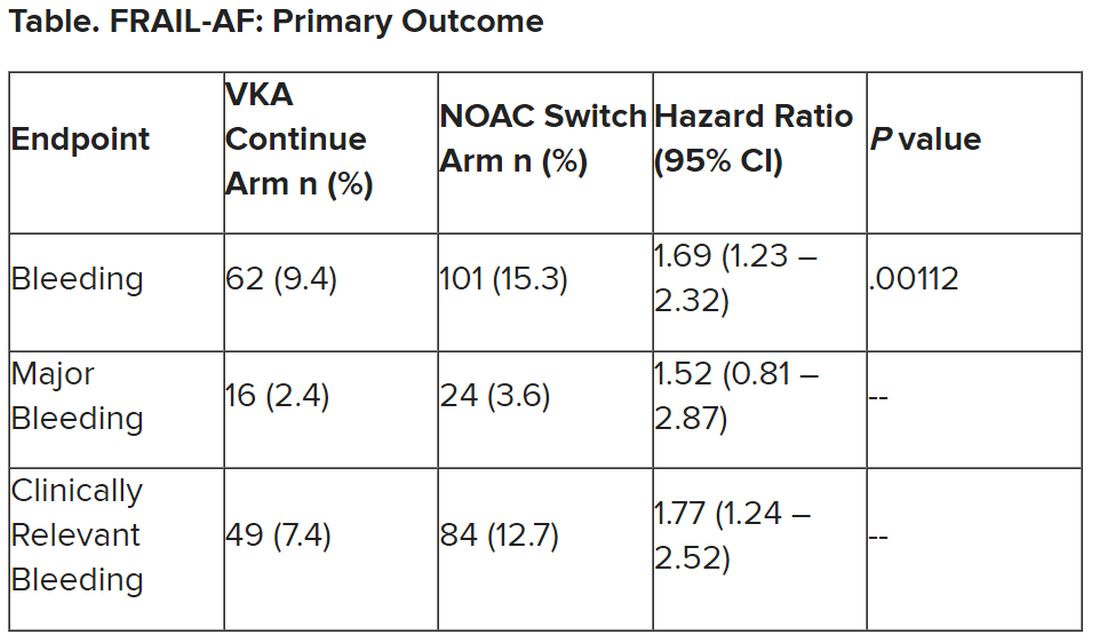
Secondary outcomes of thromboembolic events and all-cause mortality were similar between the groups.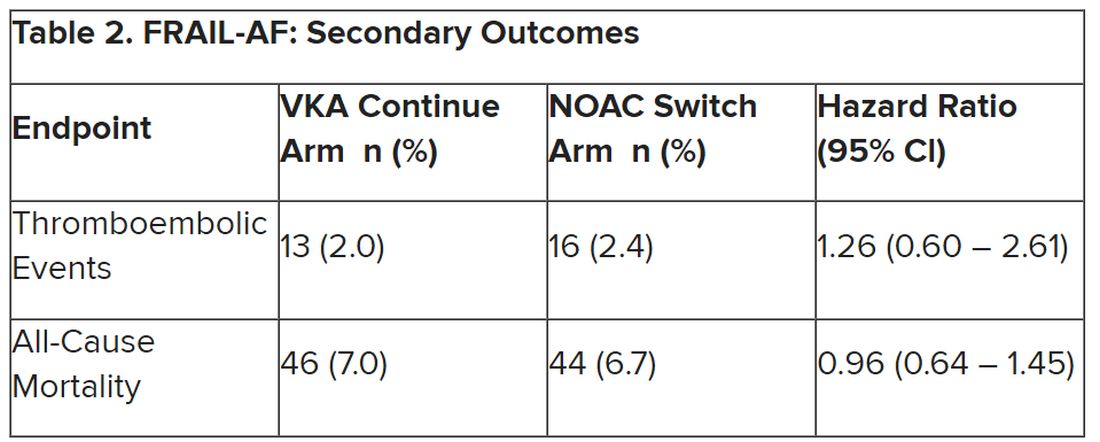
Completely different patients
Discussant at the meeting for the presentation was Isabelle C. Van Gelder, MD, University Medical Centre Groningen (the Netherlands). She said the results are important and relevant because it “provides data on an important gap of knowledge in our AF[ib] guidelines, and a note for all the cardiologists – this study was not done in the hospital. This trial was done in general practitioner practices, so that’s important to consider.”
Comparing FRAIL-AF patients with those of the four previous NOAC trials, “you see that enormous difference in age,” with an average age of 83 years versus 70-73 years in those trials. “These are completely different patients than have been included previously,” she said.
That GFI score of 4 or more includes patients on four or more different types of medication, as well as memory complaints, an inability to walk around the house, and problems with vision or hearing.
The finding of a 69% increase in bleeding with NOACs in FRAIL-AF was “completely unexpected, and I think that we as cardiologists and as NOAC believers did not expect it at all, but it is as clear as it is.” The curves don’t diverge immediately, but rather after 3 months or thereafter, “so it has nothing to do with the switching process. So why did it occur?”
The Netherlands has dedicated thrombosis services that might improve time in therapeutic range for VKA patients, but there is no real difference in TTRs in FRAIL-AF versus the other NOAC trials, Dr. Van Gelder noted.
The most likely suspect in her view is frailty itself, in particular the tendency for patients to be on a high number of medications. A previous study showed, for example, that polypharmacy could be used as a proxy for the effect of frailty on bleeding risk; patients on 10 or more medications had a higher risk for bleeding on treatment with rivaroxaban versus those on 4 or fewer medications.
“Therefore, in my view, why was there such a high risk of bleeding? It’s because these are other patients than we are normally used to treat, we as cardiologists,” although general practitioners see these patients all the time. “It’s all about frailty.”
NOACs are still relatively new drugs, with possible unknown interactions, she added. Because of their frailty and polypharmacy, these patients may benefit from INR control, Dr. Van Gelder speculated. “Therefore, I agree with them that we should be careful; if such old, frail patients survive on VKA, do not change medications and do not switch!”
The study was supported by the Dutch government with additional and unrestricted educational grants from Boehringer Ingelheim, BMS-Pfizer, Bayer, and Daiichi Sankyo. Dr. Joosten reported no relevant financial relationships. Dr. Van Gelder reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Switching frail patients with atrial fibrillation (AFib) from anticoagulation therapy with vitamin K antagonists (VKAs) to a novel oral anticoagulant (NOAC) resulted in more bleeding without any reduction in thromboembolic complications or all-cause mortality, randomized trial results show.
The study, FRAIL-AF, is the first randomized NOAC trial to exclusively include frail older patients, said lead author Linda P.T. Joosten, MD, Julius Center for Health Sciences and Primary Care in Utrecht, the Netherlands, and these unexpected findings provide evidence that goes beyond what is currently available.
“Data from the FRAIL-AF trial showed that switching from a VKA to a NOAC should not be considered without a clear indication in frail older patients with AF[ib], as switching to a NOAC leads to 69% more bleeding,” she concluded, without any benefit on secondary clinical endpoints, including thromboembolic events and all-cause mortality.
“The results turned out different than we expected,” Dr. Joosten said. “The hypothesis of this superiority trial was that switching from VKA therapy to a NOAC would result in less bleeding. However, we observed the opposite. After the interim analysis, the data and safety monitoring board advised to stop inclusion because switching from a VKA to a NOAC was clearly contraindicated with a hazard ratio of 1.69 and a highly significant P value of .001.”
Results of FRAIL-AF were presented at the annual congress of the European Society of Cardiology and published online in the journal Circulation.
Session moderator Renate B. Schnabel, MD, interventional cardiologist with University Heart & Vascular Center Hamburg (Germany), congratulated the researchers on these “astonishing” data.
“The thing I want to emphasize here is that, in the absence of randomized controlled trial data, we should be very cautious in extrapolating data from the landmark trials to populations not enrolled in those, and to rely on observational data only,” Dr. Schnabel told Dr. Joosten. “We need randomized controlled trials that sometimes give astonishing results.”
Frailty a clinical syndrome
Frailty is “a lot more than just aging, multiple comorbidities and polypharmacy,” Dr. Joosten explained. “It’s really a clinical syndrome, with people with a high biological vulnerability, dependency on significant others, and a reduced capacity to resist stressors, all leading to a reduced homeostatic reserve.”
Frailty is common in the community, with a prevalence of about 12%, she noted, “and even more important, AF[ib] in frail older people is very common, with a prevalence of 18%. And “without any doubt, we have to adequately anticoagulate frail AF[ib] patients, as they have a high stroke risk, with an incidence of 12.4% per year,” Dr. Joosten noted, compared with 3.9% per year among nonfrail AFib patients.
NOACs are preferred over VKAs in nonfrail AFib patients, after four major trials, RE-LY with dabigatran, ROCKET-AF with rivaroxaban, ARISTOTLE with apixaban, and ENGAGE-AF with edoxaban, showed that NOAC treatment resulted in less major bleeding while stroke risk was comparable with treatment with warfarin, she noted.
The 2023 European Heart Rhythm Association consensus document on management of arrhythmias in frailty syndrome concludes that the advantages of NOACs relative to VKAs are “likely consistent” in frail and nonfrail AFib patients, but the level of evidence is low.
So it’s unknown if NOACs are preferred over VKAs in frail AFib patients, “and it’s even more questionable whether patients on VKAs should switch to NOAC therapy,” Dr. Joosten said.
This new trial aimed to answer the question of whether switching frail AFib patients currently managed on a VKA to a NOAC would reduce bleeding. FRAIL-AF was a pragmatic, multicenter, open-label, randomized, controlled superiority trial.
Older AFib patients were deemed frail if they were aged 75 years or older and had a score of 3 or more on the validated Groningen Frailty Indicator (GFI). Patients with a glomerular filtration rate of less than 30 mL/min per 1.73 m2 or with valvular AFib were excluded.
Eligible patients were then assigned randomly to switch from their international normalized ratio (INR)–guided VKA treatment with either 1 mg acenocoumarol or 3 mg phenprocoumon, to a NOAC, or to continue VKA treatment. They were followed for 12 months for the primary outcome – major bleeding or clinically relevant nonmajor bleeding complication, whichever came first – accounting for death as a competing risk.
A total of 1,330 patients were randomly assigned between January 2018 and June 2022. Their mean age was 83 years, and they had a median GFI of 4. After randomization, 6 patients in the switch-to-NOAC arm, and 1 in the continue-VKA arm were found to have exclusion criteria, so in the end, 662 patients were switched from a VKA to NOAC, while 661 continued on VKA therapy. The choice of NOAC was made by the treating physician.
Major bleeding was defined as a fatal bleeding; bleeding in a critical area or organ; bleeding leading to transfusion; and/or bleeding leading to a fall in hemoglobin level of 2 g/dL (1.24 mmol/L) or more. Nonmajor bleeding was bleeding not considered major but requiring face-to-face consultation, hospitalization or increased level of care, or medical intervention.
After a prespecified futility analysis planned after 163 primary outcome events, the trial was halted when it was seen that there were 101 primary outcome events in the switch arm compared to 62 in the continue arm, Dr. Joosten said. The difference appeared to be driven by clinically relevant nonmajor bleeding.
Secondary outcomes of thromboembolic events and all-cause mortality were similar between the groups.
Completely different patients
Discussant at the meeting for the presentation was Isabelle C. Van Gelder, MD, University Medical Centre Groningen (the Netherlands). She said the results are important and relevant because it “provides data on an important gap of knowledge in our AF[ib] guidelines, and a note for all the cardiologists – this study was not done in the hospital. This trial was done in general practitioner practices, so that’s important to consider.”
Comparing FRAIL-AF patients with those of the four previous NOAC trials, “you see that enormous difference in age,” with an average age of 83 years versus 70-73 years in those trials. “These are completely different patients than have been included previously,” she said.
That GFI score of 4 or more includes patients on four or more different types of medication, as well as memory complaints, an inability to walk around the house, and problems with vision or hearing.
The finding of a 69% increase in bleeding with NOACs in FRAIL-AF was “completely unexpected, and I think that we as cardiologists and as NOAC believers did not expect it at all, but it is as clear as it is.” The curves don’t diverge immediately, but rather after 3 months or thereafter, “so it has nothing to do with the switching process. So why did it occur?”
The Netherlands has dedicated thrombosis services that might improve time in therapeutic range for VKA patients, but there is no real difference in TTRs in FRAIL-AF versus the other NOAC trials, Dr. Van Gelder noted.
The most likely suspect in her view is frailty itself, in particular the tendency for patients to be on a high number of medications. A previous study showed, for example, that polypharmacy could be used as a proxy for the effect of frailty on bleeding risk; patients on 10 or more medications had a higher risk for bleeding on treatment with rivaroxaban versus those on 4 or fewer medications.
“Therefore, in my view, why was there such a high risk of bleeding? It’s because these are other patients than we are normally used to treat, we as cardiologists,” although general practitioners see these patients all the time. “It’s all about frailty.”
NOACs are still relatively new drugs, with possible unknown interactions, she added. Because of their frailty and polypharmacy, these patients may benefit from INR control, Dr. Van Gelder speculated. “Therefore, I agree with them that we should be careful; if such old, frail patients survive on VKA, do not change medications and do not switch!”
The study was supported by the Dutch government with additional and unrestricted educational grants from Boehringer Ingelheim, BMS-Pfizer, Bayer, and Daiichi Sankyo. Dr. Joosten reported no relevant financial relationships. Dr. Van Gelder reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Switching frail patients with atrial fibrillation (AFib) from anticoagulation therapy with vitamin K antagonists (VKAs) to a novel oral anticoagulant (NOAC) resulted in more bleeding without any reduction in thromboembolic complications or all-cause mortality, randomized trial results show.
The study, FRAIL-AF, is the first randomized NOAC trial to exclusively include frail older patients, said lead author Linda P.T. Joosten, MD, Julius Center for Health Sciences and Primary Care in Utrecht, the Netherlands, and these unexpected findings provide evidence that goes beyond what is currently available.
“Data from the FRAIL-AF trial showed that switching from a VKA to a NOAC should not be considered without a clear indication in frail older patients with AF[ib], as switching to a NOAC leads to 69% more bleeding,” she concluded, without any benefit on secondary clinical endpoints, including thromboembolic events and all-cause mortality.
“The results turned out different than we expected,” Dr. Joosten said. “The hypothesis of this superiority trial was that switching from VKA therapy to a NOAC would result in less bleeding. However, we observed the opposite. After the interim analysis, the data and safety monitoring board advised to stop inclusion because switching from a VKA to a NOAC was clearly contraindicated with a hazard ratio of 1.69 and a highly significant P value of .001.”
Results of FRAIL-AF were presented at the annual congress of the European Society of Cardiology and published online in the journal Circulation.
Session moderator Renate B. Schnabel, MD, interventional cardiologist with University Heart & Vascular Center Hamburg (Germany), congratulated the researchers on these “astonishing” data.
“The thing I want to emphasize here is that, in the absence of randomized controlled trial data, we should be very cautious in extrapolating data from the landmark trials to populations not enrolled in those, and to rely on observational data only,” Dr. Schnabel told Dr. Joosten. “We need randomized controlled trials that sometimes give astonishing results.”
Frailty a clinical syndrome
Frailty is “a lot more than just aging, multiple comorbidities and polypharmacy,” Dr. Joosten explained. “It’s really a clinical syndrome, with people with a high biological vulnerability, dependency on significant others, and a reduced capacity to resist stressors, all leading to a reduced homeostatic reserve.”
Frailty is common in the community, with a prevalence of about 12%, she noted, “and even more important, AF[ib] in frail older people is very common, with a prevalence of 18%. And “without any doubt, we have to adequately anticoagulate frail AF[ib] patients, as they have a high stroke risk, with an incidence of 12.4% per year,” Dr. Joosten noted, compared with 3.9% per year among nonfrail AFib patients.
NOACs are preferred over VKAs in nonfrail AFib patients, after four major trials, RE-LY with dabigatran, ROCKET-AF with rivaroxaban, ARISTOTLE with apixaban, and ENGAGE-AF with edoxaban, showed that NOAC treatment resulted in less major bleeding while stroke risk was comparable with treatment with warfarin, she noted.
The 2023 European Heart Rhythm Association consensus document on management of arrhythmias in frailty syndrome concludes that the advantages of NOACs relative to VKAs are “likely consistent” in frail and nonfrail AFib patients, but the level of evidence is low.
So it’s unknown if NOACs are preferred over VKAs in frail AFib patients, “and it’s even more questionable whether patients on VKAs should switch to NOAC therapy,” Dr. Joosten said.
This new trial aimed to answer the question of whether switching frail AFib patients currently managed on a VKA to a NOAC would reduce bleeding. FRAIL-AF was a pragmatic, multicenter, open-label, randomized, controlled superiority trial.
Older AFib patients were deemed frail if they were aged 75 years or older and had a score of 3 or more on the validated Groningen Frailty Indicator (GFI). Patients with a glomerular filtration rate of less than 30 mL/min per 1.73 m2 or with valvular AFib were excluded.
Eligible patients were then assigned randomly to switch from their international normalized ratio (INR)–guided VKA treatment with either 1 mg acenocoumarol or 3 mg phenprocoumon, to a NOAC, or to continue VKA treatment. They were followed for 12 months for the primary outcome – major bleeding or clinically relevant nonmajor bleeding complication, whichever came first – accounting for death as a competing risk.
A total of 1,330 patients were randomly assigned between January 2018 and June 2022. Their mean age was 83 years, and they had a median GFI of 4. After randomization, 6 patients in the switch-to-NOAC arm, and 1 in the continue-VKA arm were found to have exclusion criteria, so in the end, 662 patients were switched from a VKA to NOAC, while 661 continued on VKA therapy. The choice of NOAC was made by the treating physician.
Major bleeding was defined as a fatal bleeding; bleeding in a critical area or organ; bleeding leading to transfusion; and/or bleeding leading to a fall in hemoglobin level of 2 g/dL (1.24 mmol/L) or more. Nonmajor bleeding was bleeding not considered major but requiring face-to-face consultation, hospitalization or increased level of care, or medical intervention.
After a prespecified futility analysis planned after 163 primary outcome events, the trial was halted when it was seen that there were 101 primary outcome events in the switch arm compared to 62 in the continue arm, Dr. Joosten said. The difference appeared to be driven by clinically relevant nonmajor bleeding.
Secondary outcomes of thromboembolic events and all-cause mortality were similar between the groups.
Completely different patients
Discussant at the meeting for the presentation was Isabelle C. Van Gelder, MD, University Medical Centre Groningen (the Netherlands). She said the results are important and relevant because it “provides data on an important gap of knowledge in our AF[ib] guidelines, and a note for all the cardiologists – this study was not done in the hospital. This trial was done in general practitioner practices, so that’s important to consider.”
Comparing FRAIL-AF patients with those of the four previous NOAC trials, “you see that enormous difference in age,” with an average age of 83 years versus 70-73 years in those trials. “These are completely different patients than have been included previously,” she said.
That GFI score of 4 or more includes patients on four or more different types of medication, as well as memory complaints, an inability to walk around the house, and problems with vision or hearing.
The finding of a 69% increase in bleeding with NOACs in FRAIL-AF was “completely unexpected, and I think that we as cardiologists and as NOAC believers did not expect it at all, but it is as clear as it is.” The curves don’t diverge immediately, but rather after 3 months or thereafter, “so it has nothing to do with the switching process. So why did it occur?”
The Netherlands has dedicated thrombosis services that might improve time in therapeutic range for VKA patients, but there is no real difference in TTRs in FRAIL-AF versus the other NOAC trials, Dr. Van Gelder noted.
The most likely suspect in her view is frailty itself, in particular the tendency for patients to be on a high number of medications. A previous study showed, for example, that polypharmacy could be used as a proxy for the effect of frailty on bleeding risk; patients on 10 or more medications had a higher risk for bleeding on treatment with rivaroxaban versus those on 4 or fewer medications.
“Therefore, in my view, why was there such a high risk of bleeding? It’s because these are other patients than we are normally used to treat, we as cardiologists,” although general practitioners see these patients all the time. “It’s all about frailty.”
NOACs are still relatively new drugs, with possible unknown interactions, she added. Because of their frailty and polypharmacy, these patients may benefit from INR control, Dr. Van Gelder speculated. “Therefore, I agree with them that we should be careful; if such old, frail patients survive on VKA, do not change medications and do not switch!”
The study was supported by the Dutch government with additional and unrestricted educational grants from Boehringer Ingelheim, BMS-Pfizer, Bayer, and Daiichi Sankyo. Dr. Joosten reported no relevant financial relationships. Dr. Van Gelder reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE ESC CONGRESS 2023
Novel ADC offers hope in heavily pretreated NSCLC
SINGAPORE – Heavily pretreated patients with EGFR-mutated non–small cell lung cancer (NSCLC) may experience a clinically meaningful benefit with the antibody-drug conjugate (ADC) patritumab deruxtecan (HER3-DXd), new phase 2 trial results suggest.
In the trial, almost 30% of patients receiving HER3-DXd achieved an objective response, and patients’ median overall survival approached 1 year.
HER3-DXd has “emerged as a promising therapy” in this patient population, “for whom available treatment options provide only limited efficacy,” concluded lead study author Helena A. Yu, MD, from Memorial Sloan Kettering Cancer Center, New York City, who presented findings from the HERTHENA-Lung01 trial at the 2023 World Conference on Lung Cancer.
The results were simultaneously published in the Journal of Clinical Oncology.
Acquired resistance to therapy among heavily pretreated patients with EGFR-mutated NSCLC is “universal,” Dr. Yu explained. The mechanisms of resistance to first-line osimertinib are also “diverse” and hard to identify. Salvage therapies after failed EGFR tyrosine kinase inhibitor (TKI) therapy and platinum-based chemotherapy offer “only a limited and transient and clinical benefit,” she said.
And with limited treatment options available to patients resistant to TKIs, there is a “high unmet medical need” for new therapies, said Helena Linardou, MD, PhD, who was not involved in the study.
HER3-DXd consists of a fully human anti-HER3 immunoglobulin G1 monoclonal antibody (patritumab) attached to a topoisomerase I inhibitor payload (DXd) via a tetrapeptide-based cleavable linker.
HER3, Dr. Linardou explained, is a “biologically and clinically important target” in NSCLC. It is highly expressed in NSCLC, upregulated in TKI-resistant EGFR-mutated NSCLC, and is associated with a poor prognosis.
After promising phase 1 data, Dr. Yu and colleagues conducted a phase 2 trial in patients with advanced EGFR-mutated NSCLC who had progressed on systematic therapy and had received EGFR TKI and platinum-based chemotherapy. Patients could have active or previously treated asymptomatic brain metastases.
Patients were initially randomized either to a fixed-dose arm of HER3-DXd 5.6 mg/kg once every 3 weeks or an uptitration arm with doses escalating from 3.2 mg/kg to 4.8 mg/kg to 6.4 mg/kg over three cycles. However, Dr. Yu noted, enrollment in the uptitration arm closed early based on a “benefit-risk assessment.”
The current findings focus on the 225 patients in the fixed-dose arm.
About half of patients had a history of central nervous system metastasis, and patients had a median of three prior lines of systemic therapy. Most patients (92.9%) had previously received a third-generation EGFR TKI, about 40% had received immunotherapy, and all had received platinum-based chemotherapy.
After a median follow-up of 18.9 months, the confirmed objective response rate with HER3-DXd across the whole patient population was 29.8%. The median duration of response was 6.4 months, median progression-free survival was 5.5 months, and median overall survival was 11.9 months.
The results were virtually identical when looking only at patients who had received a third-generation EGFR TKI versus any EGFR TKI. Response rates were also similar regardless of the driver of EGFR TKI resistance.
Among the 30 patients with measurable brain metastases at baseline, 33.3% had a confirmed objective response to therapy. In this group, the disease control rate was 76.7% and the intracranial duration of response was 8.4 months.
To identify biomarkers of response to HER3-DXd, the team stratified the patients by baseline tumor HER3 membrane H-scores. Dr. Yu and colleagues found no differences in the likelihood of having a complete or partial response, stable disease, or progressive disease based on HER3 expression at study entry.
Looking at the safety of the ADC, only 7.1% of patients experienced a treatment-emergent adverse event associated with treatment discontinuation, but close to half of patients (45.3%) experienced a grade 3 or higher treatment-emergent adverse event. Interstitial lung disease, for instance, occurred in 5.3% of patients, including one patient who died.
The safety profile of HER3-DXd in this population appeared to be consistent with previous reports, Dr. Yu noted.
Overall, the findings suggest that “HER3-DXd provided clinically meaningful and durable efficacy” in patients with advanced EGFR-mutant NSCLC that has progressed after EGFR TKI and platinum-based chemotherapy, Dr. Yu said.
“Efficacy was observed across diverse mechanisms of resistance and across a broad range of pretreatment tumor HER3 expression” and the ADC demonstrated “clinically meaningful intracranial antitumor activity,” she added.
Dr. Linardou agreed that the current results suggest that HER3-DXd was associated with a “meaningful and durable efficacy,” including in patients with intracranial metastases, and she pointed to its “easy dosing schedule” and activity across patient subgroups.
However, she noted that, despite the researchers’ best efforts with the data available, “we don’t have a biomarker of activity,” which is a “general issue with ADCs.”
Still, Dr. Linardou said, “HER3 is now a clinically actionable therapeutic target, and this is a great bonus.”
The study was sponsored by Daiichi Sankyo. Dr. Yu declared relationships with AstraZeneca, Daiichi Sankyo, Blueprint Medicines, Janssen, C4 Therapeutics, Cullinan Oncology, Black Diamond Therapeutics, Taiho Oncology, and others. Other authors declare numerous relationships.
A version of this article first appeared on Medscape.com.
SINGAPORE – Heavily pretreated patients with EGFR-mutated non–small cell lung cancer (NSCLC) may experience a clinically meaningful benefit with the antibody-drug conjugate (ADC) patritumab deruxtecan (HER3-DXd), new phase 2 trial results suggest.
In the trial, almost 30% of patients receiving HER3-DXd achieved an objective response, and patients’ median overall survival approached 1 year.
HER3-DXd has “emerged as a promising therapy” in this patient population, “for whom available treatment options provide only limited efficacy,” concluded lead study author Helena A. Yu, MD, from Memorial Sloan Kettering Cancer Center, New York City, who presented findings from the HERTHENA-Lung01 trial at the 2023 World Conference on Lung Cancer.
The results were simultaneously published in the Journal of Clinical Oncology.
Acquired resistance to therapy among heavily pretreated patients with EGFR-mutated NSCLC is “universal,” Dr. Yu explained. The mechanisms of resistance to first-line osimertinib are also “diverse” and hard to identify. Salvage therapies after failed EGFR tyrosine kinase inhibitor (TKI) therapy and platinum-based chemotherapy offer “only a limited and transient and clinical benefit,” she said.
And with limited treatment options available to patients resistant to TKIs, there is a “high unmet medical need” for new therapies, said Helena Linardou, MD, PhD, who was not involved in the study.
HER3-DXd consists of a fully human anti-HER3 immunoglobulin G1 monoclonal antibody (patritumab) attached to a topoisomerase I inhibitor payload (DXd) via a tetrapeptide-based cleavable linker.
HER3, Dr. Linardou explained, is a “biologically and clinically important target” in NSCLC. It is highly expressed in NSCLC, upregulated in TKI-resistant EGFR-mutated NSCLC, and is associated with a poor prognosis.
After promising phase 1 data, Dr. Yu and colleagues conducted a phase 2 trial in patients with advanced EGFR-mutated NSCLC who had progressed on systematic therapy and had received EGFR TKI and platinum-based chemotherapy. Patients could have active or previously treated asymptomatic brain metastases.
Patients were initially randomized either to a fixed-dose arm of HER3-DXd 5.6 mg/kg once every 3 weeks or an uptitration arm with doses escalating from 3.2 mg/kg to 4.8 mg/kg to 6.4 mg/kg over three cycles. However, Dr. Yu noted, enrollment in the uptitration arm closed early based on a “benefit-risk assessment.”
The current findings focus on the 225 patients in the fixed-dose arm.
About half of patients had a history of central nervous system metastasis, and patients had a median of three prior lines of systemic therapy. Most patients (92.9%) had previously received a third-generation EGFR TKI, about 40% had received immunotherapy, and all had received platinum-based chemotherapy.
After a median follow-up of 18.9 months, the confirmed objective response rate with HER3-DXd across the whole patient population was 29.8%. The median duration of response was 6.4 months, median progression-free survival was 5.5 months, and median overall survival was 11.9 months.
The results were virtually identical when looking only at patients who had received a third-generation EGFR TKI versus any EGFR TKI. Response rates were also similar regardless of the driver of EGFR TKI resistance.
Among the 30 patients with measurable brain metastases at baseline, 33.3% had a confirmed objective response to therapy. In this group, the disease control rate was 76.7% and the intracranial duration of response was 8.4 months.
To identify biomarkers of response to HER3-DXd, the team stratified the patients by baseline tumor HER3 membrane H-scores. Dr. Yu and colleagues found no differences in the likelihood of having a complete or partial response, stable disease, or progressive disease based on HER3 expression at study entry.
Looking at the safety of the ADC, only 7.1% of patients experienced a treatment-emergent adverse event associated with treatment discontinuation, but close to half of patients (45.3%) experienced a grade 3 or higher treatment-emergent adverse event. Interstitial lung disease, for instance, occurred in 5.3% of patients, including one patient who died.
The safety profile of HER3-DXd in this population appeared to be consistent with previous reports, Dr. Yu noted.
Overall, the findings suggest that “HER3-DXd provided clinically meaningful and durable efficacy” in patients with advanced EGFR-mutant NSCLC that has progressed after EGFR TKI and platinum-based chemotherapy, Dr. Yu said.
“Efficacy was observed across diverse mechanisms of resistance and across a broad range of pretreatment tumor HER3 expression” and the ADC demonstrated “clinically meaningful intracranial antitumor activity,” she added.
Dr. Linardou agreed that the current results suggest that HER3-DXd was associated with a “meaningful and durable efficacy,” including in patients with intracranial metastases, and she pointed to its “easy dosing schedule” and activity across patient subgroups.
However, she noted that, despite the researchers’ best efforts with the data available, “we don’t have a biomarker of activity,” which is a “general issue with ADCs.”
Still, Dr. Linardou said, “HER3 is now a clinically actionable therapeutic target, and this is a great bonus.”
The study was sponsored by Daiichi Sankyo. Dr. Yu declared relationships with AstraZeneca, Daiichi Sankyo, Blueprint Medicines, Janssen, C4 Therapeutics, Cullinan Oncology, Black Diamond Therapeutics, Taiho Oncology, and others. Other authors declare numerous relationships.
A version of this article first appeared on Medscape.com.
SINGAPORE – Heavily pretreated patients with EGFR-mutated non–small cell lung cancer (NSCLC) may experience a clinically meaningful benefit with the antibody-drug conjugate (ADC) patritumab deruxtecan (HER3-DXd), new phase 2 trial results suggest.
In the trial, almost 30% of patients receiving HER3-DXd achieved an objective response, and patients’ median overall survival approached 1 year.
HER3-DXd has “emerged as a promising therapy” in this patient population, “for whom available treatment options provide only limited efficacy,” concluded lead study author Helena A. Yu, MD, from Memorial Sloan Kettering Cancer Center, New York City, who presented findings from the HERTHENA-Lung01 trial at the 2023 World Conference on Lung Cancer.
The results were simultaneously published in the Journal of Clinical Oncology.
Acquired resistance to therapy among heavily pretreated patients with EGFR-mutated NSCLC is “universal,” Dr. Yu explained. The mechanisms of resistance to first-line osimertinib are also “diverse” and hard to identify. Salvage therapies after failed EGFR tyrosine kinase inhibitor (TKI) therapy and platinum-based chemotherapy offer “only a limited and transient and clinical benefit,” she said.
And with limited treatment options available to patients resistant to TKIs, there is a “high unmet medical need” for new therapies, said Helena Linardou, MD, PhD, who was not involved in the study.
HER3-DXd consists of a fully human anti-HER3 immunoglobulin G1 monoclonal antibody (patritumab) attached to a topoisomerase I inhibitor payload (DXd) via a tetrapeptide-based cleavable linker.
HER3, Dr. Linardou explained, is a “biologically and clinically important target” in NSCLC. It is highly expressed in NSCLC, upregulated in TKI-resistant EGFR-mutated NSCLC, and is associated with a poor prognosis.
After promising phase 1 data, Dr. Yu and colleagues conducted a phase 2 trial in patients with advanced EGFR-mutated NSCLC who had progressed on systematic therapy and had received EGFR TKI and platinum-based chemotherapy. Patients could have active or previously treated asymptomatic brain metastases.
Patients were initially randomized either to a fixed-dose arm of HER3-DXd 5.6 mg/kg once every 3 weeks or an uptitration arm with doses escalating from 3.2 mg/kg to 4.8 mg/kg to 6.4 mg/kg over three cycles. However, Dr. Yu noted, enrollment in the uptitration arm closed early based on a “benefit-risk assessment.”
The current findings focus on the 225 patients in the fixed-dose arm.
About half of patients had a history of central nervous system metastasis, and patients had a median of three prior lines of systemic therapy. Most patients (92.9%) had previously received a third-generation EGFR TKI, about 40% had received immunotherapy, and all had received platinum-based chemotherapy.
After a median follow-up of 18.9 months, the confirmed objective response rate with HER3-DXd across the whole patient population was 29.8%. The median duration of response was 6.4 months, median progression-free survival was 5.5 months, and median overall survival was 11.9 months.
The results were virtually identical when looking only at patients who had received a third-generation EGFR TKI versus any EGFR TKI. Response rates were also similar regardless of the driver of EGFR TKI resistance.
Among the 30 patients with measurable brain metastases at baseline, 33.3% had a confirmed objective response to therapy. In this group, the disease control rate was 76.7% and the intracranial duration of response was 8.4 months.
To identify biomarkers of response to HER3-DXd, the team stratified the patients by baseline tumor HER3 membrane H-scores. Dr. Yu and colleagues found no differences in the likelihood of having a complete or partial response, stable disease, or progressive disease based on HER3 expression at study entry.
Looking at the safety of the ADC, only 7.1% of patients experienced a treatment-emergent adverse event associated with treatment discontinuation, but close to half of patients (45.3%) experienced a grade 3 or higher treatment-emergent adverse event. Interstitial lung disease, for instance, occurred in 5.3% of patients, including one patient who died.
The safety profile of HER3-DXd in this population appeared to be consistent with previous reports, Dr. Yu noted.
Overall, the findings suggest that “HER3-DXd provided clinically meaningful and durable efficacy” in patients with advanced EGFR-mutant NSCLC that has progressed after EGFR TKI and platinum-based chemotherapy, Dr. Yu said.
“Efficacy was observed across diverse mechanisms of resistance and across a broad range of pretreatment tumor HER3 expression” and the ADC demonstrated “clinically meaningful intracranial antitumor activity,” she added.
Dr. Linardou agreed that the current results suggest that HER3-DXd was associated with a “meaningful and durable efficacy,” including in patients with intracranial metastases, and she pointed to its “easy dosing schedule” and activity across patient subgroups.
However, she noted that, despite the researchers’ best efforts with the data available, “we don’t have a biomarker of activity,” which is a “general issue with ADCs.”
Still, Dr. Linardou said, “HER3 is now a clinically actionable therapeutic target, and this is a great bonus.”
The study was sponsored by Daiichi Sankyo. Dr. Yu declared relationships with AstraZeneca, Daiichi Sankyo, Blueprint Medicines, Janssen, C4 Therapeutics, Cullinan Oncology, Black Diamond Therapeutics, Taiho Oncology, and others. Other authors declare numerous relationships.
A version of this article first appeared on Medscape.com.
AT IASLC 2023
‘New dawn’ for aldosterone as drug target in hypertension?
Once-daily treatment with the selective aldosterone synthase inhibitor lorundrostat (Mineralys Therapeutics) safely and significantly reduced blood pressure in adults with uncontrolled hypertension in a phase 2, randomized, controlled trial.
Eight weeks after adding lorundrostat (50 mg or 100 mg once daily) or placebo to background therapy, the medication lowered seated automated office systolic BP significantly more than placebo (−9.6 mm Hg with 50 mg; −7.8 mm Hg with 100 mg), with the greatest effects seen in adults with obesity.
“We need new drugs for treatment-resistant hypertension,” study investigator Steven Nissen, MD, chief academic officer at the Heart Vascular & Thoracic Institute at the Cleveland Clinic, said in an interview. Lorundrostat represents a “new class” of antihypertensive that “looks to be safe and we’re seeing very large reductions in blood pressure.”
Results of the Target-HTN trial were published online in JAMA to coincide with presentation at the Hypertension Scientific Sessions, sponsored by the American Heart Association.
Aldosterone’s contribution ‘vastly underappreciated’
Excess aldosterone production contributes to uncontrolled BP in patients with obesity and other associated diseases, such as obstructive sleep apnea and metabolic syndrome.
“Aldosterone’s contribution to uncontrolled hypertension is vastly underappreciated,” first author and study presenter Luke Laffin, MD, also with the Cleveland Clinic, said in an interview.
Aldosterone synthase inhibitors are a novel class of BP-lowering medications that decrease aldosterone production. Lorundrostat is one of two such agents in advanced clinical development. The other is baxdrostat (CinCor Pharma/AstraZeneca).
The Target-HTN randomized, placebo-controlled, dose-ranging trial enrolled 200 adults (mean age, 66 years; 60% women) with uncontrolled hypertension while taking two or more antihypertensive medications; 42% of participants were taking three or more antihypertensive medications, 48% were obese and 40% had diabetes.
The study population was divided into two cohorts: an initial cohort of 163 adults with suppressed plasma renin activity at baseline (PRA ≤ 1.0 ng/mL per hour) and elevated plasma aldosterone (≥ 1.0 ng/dL) and a second cohort of 37 adults with PRA greater than 1.0 ng/mL per hour.
Participants were randomly assigned to placebo or one of five doses of lorundrostat in the initial cohort (12.5 mg, 50 mg, or 100 mg once daily or 12.5 mg or 25 mg twice daily).
In the second cohort, participants were randomly assigned (1:6) to placebo or lorundrostat 100 mg once daily. The primary endpoint was change in automated office systolic BP from baseline to week 8.
Among participants with suppressed PRA, following 8 weeks of treatment, changes in office systolic BP of −14.1, −13.2, and −6.9 mm Hg were observed with 100 mg, 50 mg, and 12.5 mg once-daily lorundrostat, respectively, compared with a change of −4.1 mm Hg with placebo.
Reductions in systolic BP in individuals receiving twice-daily doses of 25 mg and 12.5 mg of lorundrostat were −10.1 and −13.8 mm Hg, respectively.
Among participants without suppressed PRA, lorundrostat 100 mg once daily decreased systolic BP by 11.4 mm Hg, similar to BP reduction in those with suppressed PRA receiving the same dose.
A prespecified subgroup analysis showed that participants with obesity demonstrated greater BP lowering in response to lorundrostat.
No instances of cortisol insufficiency occurred. Six participants had increases in serum potassium above 6.0 mEq/L (6.0 mmol/L) that corrected with dose reduction or drug discontinuation.
The increase in serum potassium is “expected and manageable,” Dr. Laffin said in an interview. “Anytime you disrupt aldosterone production, you’re going to have to have an increase in serum potassium, but it’s very manageable and not something that is worrisome.”
A phase 2 trial in 300 adults with uncontrolled hypertension is currently underway. The trial will evaluate the BP-lowering effects of lorundrostat, administered on a background of a standardized antihypertensive medication regimen. A larger phase 3 study will start before the end of the year.
‘New dawn’ for therapies targeting aldosterone
The author of an editorial in JAMA noted that more 70 years after the first isolation of aldosterone, then called electrocortin, “there is a new dawn for therapies targeting aldosterone.”
“There is now real potential to provide better-targeted treatment for patients in whom aldosterone excess is known to contribute to their clinical condition and influence their clinical outcome, notably those with difficult-to-control hypertension, obesity, heart failure, chronic kidney disease, and the many with yet-to-be-diagnosed primary aldosteronism,” said Bryan Williams, MD, University College London.
The trial was funded by Mineralys Therapeutics, which is developing lorundrostat. Dr. Laffin reported that the Cleveland Clinic, his employer, was a study site for the Target-HTN trial and that C5Research, the academic research organization of the Cleveland Clinic, receives payment for services related to other Mineralys clinical trials. Dr. Laffin also reported receipt of personal fees from Medtronic, Lilly, and Crispr Therapeutics, grants from AstraZeneca, and stock options for LucidAct Health and Gordy Health. Dr. Nissen reported receipt of grants from Mineralys during the conduct of the study and grants from AbbVie, AstraZeneca, Amgen, Bristol-Myers Squibb, Lilly, Esperion Therapeutics, Medtronic, grants from MyoKardia, New Amsterdam Pharmaceuticals, Novartis, and Silence Therapeutics. Dr. Williams reported being the unremunerated chair of the steering committee designing a phase 3 trial of the aldosterone synthase inhibitor baxdrostat for AstraZeneca.
A version of this article first appeared on Medscape.com.
Once-daily treatment with the selective aldosterone synthase inhibitor lorundrostat (Mineralys Therapeutics) safely and significantly reduced blood pressure in adults with uncontrolled hypertension in a phase 2, randomized, controlled trial.
Eight weeks after adding lorundrostat (50 mg or 100 mg once daily) or placebo to background therapy, the medication lowered seated automated office systolic BP significantly more than placebo (−9.6 mm Hg with 50 mg; −7.8 mm Hg with 100 mg), with the greatest effects seen in adults with obesity.
“We need new drugs for treatment-resistant hypertension,” study investigator Steven Nissen, MD, chief academic officer at the Heart Vascular & Thoracic Institute at the Cleveland Clinic, said in an interview. Lorundrostat represents a “new class” of antihypertensive that “looks to be safe and we’re seeing very large reductions in blood pressure.”
Results of the Target-HTN trial were published online in JAMA to coincide with presentation at the Hypertension Scientific Sessions, sponsored by the American Heart Association.
Aldosterone’s contribution ‘vastly underappreciated’
Excess aldosterone production contributes to uncontrolled BP in patients with obesity and other associated diseases, such as obstructive sleep apnea and metabolic syndrome.
“Aldosterone’s contribution to uncontrolled hypertension is vastly underappreciated,” first author and study presenter Luke Laffin, MD, also with the Cleveland Clinic, said in an interview.
Aldosterone synthase inhibitors are a novel class of BP-lowering medications that decrease aldosterone production. Lorundrostat is one of two such agents in advanced clinical development. The other is baxdrostat (CinCor Pharma/AstraZeneca).
The Target-HTN randomized, placebo-controlled, dose-ranging trial enrolled 200 adults (mean age, 66 years; 60% women) with uncontrolled hypertension while taking two or more antihypertensive medications; 42% of participants were taking three or more antihypertensive medications, 48% were obese and 40% had diabetes.
The study population was divided into two cohorts: an initial cohort of 163 adults with suppressed plasma renin activity at baseline (PRA ≤ 1.0 ng/mL per hour) and elevated plasma aldosterone (≥ 1.0 ng/dL) and a second cohort of 37 adults with PRA greater than 1.0 ng/mL per hour.
Participants were randomly assigned to placebo or one of five doses of lorundrostat in the initial cohort (12.5 mg, 50 mg, or 100 mg once daily or 12.5 mg or 25 mg twice daily).
In the second cohort, participants were randomly assigned (1:6) to placebo or lorundrostat 100 mg once daily. The primary endpoint was change in automated office systolic BP from baseline to week 8.
Among participants with suppressed PRA, following 8 weeks of treatment, changes in office systolic BP of −14.1, −13.2, and −6.9 mm Hg were observed with 100 mg, 50 mg, and 12.5 mg once-daily lorundrostat, respectively, compared with a change of −4.1 mm Hg with placebo.
Reductions in systolic BP in individuals receiving twice-daily doses of 25 mg and 12.5 mg of lorundrostat were −10.1 and −13.8 mm Hg, respectively.
Among participants without suppressed PRA, lorundrostat 100 mg once daily decreased systolic BP by 11.4 mm Hg, similar to BP reduction in those with suppressed PRA receiving the same dose.
A prespecified subgroup analysis showed that participants with obesity demonstrated greater BP lowering in response to lorundrostat.
No instances of cortisol insufficiency occurred. Six participants had increases in serum potassium above 6.0 mEq/L (6.0 mmol/L) that corrected with dose reduction or drug discontinuation.
The increase in serum potassium is “expected and manageable,” Dr. Laffin said in an interview. “Anytime you disrupt aldosterone production, you’re going to have to have an increase in serum potassium, but it’s very manageable and not something that is worrisome.”
A phase 2 trial in 300 adults with uncontrolled hypertension is currently underway. The trial will evaluate the BP-lowering effects of lorundrostat, administered on a background of a standardized antihypertensive medication regimen. A larger phase 3 study will start before the end of the year.
‘New dawn’ for therapies targeting aldosterone
The author of an editorial in JAMA noted that more 70 years after the first isolation of aldosterone, then called electrocortin, “there is a new dawn for therapies targeting aldosterone.”
“There is now real potential to provide better-targeted treatment for patients in whom aldosterone excess is known to contribute to their clinical condition and influence their clinical outcome, notably those with difficult-to-control hypertension, obesity, heart failure, chronic kidney disease, and the many with yet-to-be-diagnosed primary aldosteronism,” said Bryan Williams, MD, University College London.
The trial was funded by Mineralys Therapeutics, which is developing lorundrostat. Dr. Laffin reported that the Cleveland Clinic, his employer, was a study site for the Target-HTN trial and that C5Research, the academic research organization of the Cleveland Clinic, receives payment for services related to other Mineralys clinical trials. Dr. Laffin also reported receipt of personal fees from Medtronic, Lilly, and Crispr Therapeutics, grants from AstraZeneca, and stock options for LucidAct Health and Gordy Health. Dr. Nissen reported receipt of grants from Mineralys during the conduct of the study and grants from AbbVie, AstraZeneca, Amgen, Bristol-Myers Squibb, Lilly, Esperion Therapeutics, Medtronic, grants from MyoKardia, New Amsterdam Pharmaceuticals, Novartis, and Silence Therapeutics. Dr. Williams reported being the unremunerated chair of the steering committee designing a phase 3 trial of the aldosterone synthase inhibitor baxdrostat for AstraZeneca.
A version of this article first appeared on Medscape.com.
Once-daily treatment with the selective aldosterone synthase inhibitor lorundrostat (Mineralys Therapeutics) safely and significantly reduced blood pressure in adults with uncontrolled hypertension in a phase 2, randomized, controlled trial.
Eight weeks after adding lorundrostat (50 mg or 100 mg once daily) or placebo to background therapy, the medication lowered seated automated office systolic BP significantly more than placebo (−9.6 mm Hg with 50 mg; −7.8 mm Hg with 100 mg), with the greatest effects seen in adults with obesity.
“We need new drugs for treatment-resistant hypertension,” study investigator Steven Nissen, MD, chief academic officer at the Heart Vascular & Thoracic Institute at the Cleveland Clinic, said in an interview. Lorundrostat represents a “new class” of antihypertensive that “looks to be safe and we’re seeing very large reductions in blood pressure.”
Results of the Target-HTN trial were published online in JAMA to coincide with presentation at the Hypertension Scientific Sessions, sponsored by the American Heart Association.
Aldosterone’s contribution ‘vastly underappreciated’
Excess aldosterone production contributes to uncontrolled BP in patients with obesity and other associated diseases, such as obstructive sleep apnea and metabolic syndrome.
“Aldosterone’s contribution to uncontrolled hypertension is vastly underappreciated,” first author and study presenter Luke Laffin, MD, also with the Cleveland Clinic, said in an interview.
Aldosterone synthase inhibitors are a novel class of BP-lowering medications that decrease aldosterone production. Lorundrostat is one of two such agents in advanced clinical development. The other is baxdrostat (CinCor Pharma/AstraZeneca).
The Target-HTN randomized, placebo-controlled, dose-ranging trial enrolled 200 adults (mean age, 66 years; 60% women) with uncontrolled hypertension while taking two or more antihypertensive medications; 42% of participants were taking three or more antihypertensive medications, 48% were obese and 40% had diabetes.
The study population was divided into two cohorts: an initial cohort of 163 adults with suppressed plasma renin activity at baseline (PRA ≤ 1.0 ng/mL per hour) and elevated plasma aldosterone (≥ 1.0 ng/dL) and a second cohort of 37 adults with PRA greater than 1.0 ng/mL per hour.
Participants were randomly assigned to placebo or one of five doses of lorundrostat in the initial cohort (12.5 mg, 50 mg, or 100 mg once daily or 12.5 mg or 25 mg twice daily).
In the second cohort, participants were randomly assigned (1:6) to placebo or lorundrostat 100 mg once daily. The primary endpoint was change in automated office systolic BP from baseline to week 8.
Among participants with suppressed PRA, following 8 weeks of treatment, changes in office systolic BP of −14.1, −13.2, and −6.9 mm Hg were observed with 100 mg, 50 mg, and 12.5 mg once-daily lorundrostat, respectively, compared with a change of −4.1 mm Hg with placebo.
Reductions in systolic BP in individuals receiving twice-daily doses of 25 mg and 12.5 mg of lorundrostat were −10.1 and −13.8 mm Hg, respectively.
Among participants without suppressed PRA, lorundrostat 100 mg once daily decreased systolic BP by 11.4 mm Hg, similar to BP reduction in those with suppressed PRA receiving the same dose.
A prespecified subgroup analysis showed that participants with obesity demonstrated greater BP lowering in response to lorundrostat.
No instances of cortisol insufficiency occurred. Six participants had increases in serum potassium above 6.0 mEq/L (6.0 mmol/L) that corrected with dose reduction or drug discontinuation.
The increase in serum potassium is “expected and manageable,” Dr. Laffin said in an interview. “Anytime you disrupt aldosterone production, you’re going to have to have an increase in serum potassium, but it’s very manageable and not something that is worrisome.”
A phase 2 trial in 300 adults with uncontrolled hypertension is currently underway. The trial will evaluate the BP-lowering effects of lorundrostat, administered on a background of a standardized antihypertensive medication regimen. A larger phase 3 study will start before the end of the year.
‘New dawn’ for therapies targeting aldosterone
The author of an editorial in JAMA noted that more 70 years after the first isolation of aldosterone, then called electrocortin, “there is a new dawn for therapies targeting aldosterone.”
“There is now real potential to provide better-targeted treatment for patients in whom aldosterone excess is known to contribute to their clinical condition and influence their clinical outcome, notably those with difficult-to-control hypertension, obesity, heart failure, chronic kidney disease, and the many with yet-to-be-diagnosed primary aldosteronism,” said Bryan Williams, MD, University College London.
The trial was funded by Mineralys Therapeutics, which is developing lorundrostat. Dr. Laffin reported that the Cleveland Clinic, his employer, was a study site for the Target-HTN trial and that C5Research, the academic research organization of the Cleveland Clinic, receives payment for services related to other Mineralys clinical trials. Dr. Laffin also reported receipt of personal fees from Medtronic, Lilly, and Crispr Therapeutics, grants from AstraZeneca, and stock options for LucidAct Health and Gordy Health. Dr. Nissen reported receipt of grants from Mineralys during the conduct of the study and grants from AbbVie, AstraZeneca, Amgen, Bristol-Myers Squibb, Lilly, Esperion Therapeutics, Medtronic, grants from MyoKardia, New Amsterdam Pharmaceuticals, Novartis, and Silence Therapeutics. Dr. Williams reported being the unremunerated chair of the steering committee designing a phase 3 trial of the aldosterone synthase inhibitor baxdrostat for AstraZeneca.
A version of this article first appeared on Medscape.com.
FROM HYPERTENSION 2023
Is AFib ablation the fifth pillar in heart failure care? CASTLE-HTx
Recorded Aug. 28, 2023. This transcript has been edited for clarity.
John M. Mandrola, MD: I’m here at the European Society of Cardiology meeting, and I’m very excited to have two colleagues whom I met at the Western Atrial Fibrillation Symposium (Western AFib) and who presented the CASTLE-HTx study. This is Christian Sohns and Philipp Sommer, and the CASTLE-HTx study is very exciting.
Before I get into that, I really want to introduce the concept of atrial fibrillation in heart failure. I like to say that there are two big populations of patients with atrial fibrillation, and the vast majority can be treated slowly with reassurance and education. There is a group of patients who have heart failure who, when they develop atrial fibrillation, can degenerate rapidly. The CASTLE-HTx study looked at catheter ablation versus medical therapy in patients with advanced heart failure.
Christian, why don’t you tell us the top-line results and what you found.
CASTLE-HTx key findings
Christian Sohns, MD, PhD: Thanks, first of all, for mentioning this special cohort of patients in end-stage heart failure, which is very important. The endpoint of the study was a composite of death from any cause or left ventricular assist device (LVAD) implantation and heart transplantation. These are very hard, strong clinical endpoints, not the rate of rehospitalization or something like that.
Catheter ablation was superior to medical therapy alone in terms of this composite endpoint. That was driven by cardiovascular death and all-cause mortality, which highlights the fact that you should always consider atrial fibrillation ablation in the end-stage heart failure cohort. The findings were driven by the fact that we saw left ventricular reverse remodeling and the reduction of atrial fibrillation in these patients.
Dr. Mandrola: Tell me about how it came about. It was conducted at your center. Who were these patients?
Philipp Sommer, MD: As one of the biggest centers for heart transplantations all over Europe, with roughly 100 transplants per year, we had many patients being referred to our center with the questions of whether those patients are eligible for a heart transplantation. Not all of the patients in our study were listed for a transplant, but all of them were admitted in that end-stage heart failure status to evaluate their eligibility for transplant.
If we look at the baseline data of those patients, they had an ejection fraction of 29%. They had a 6-minute walk test as a functional capacity parameter of around 300 m. Approximately two thirds of them were New York Heart Association class III and IV, which is significantly worse than what we saw in the previous studies dealing with heart failure patients.
I think overall, if you also look at NT-proBNP levels, this is a really sick patient population where some people might doubt if they should admit and refer those patients for an ablation procedure. Therefore, it’s really interesting and fascinating to see the results.
Dr. Mandrola: I did read in the manuscript, and I heard from you, that these were recruited as outpatients. So they were stable outpatients who were referred to the center for consideration of an LVAD or transplant?
Dr. Sohns: The definition of stability is very difficult in these patients because they have hospital stays, they have a history of drug therapy, and they have a history of interventions also behind them – not atrial fibrillation ablation, but others. I think these patients are referred because the referring physicians are done with the case. They can no longer offer any option to the patients other than surgical treatment, assist device, pump implantation, or transplantation.
If you look at the guidelines, they do not comment on atrial fibrillation ablation in this cohort of patients. Also, they have different recommendations between the American societies and the European societies regarding what is end-stage heart failure and how to treat these patients. Therefore, it was a big benefit of CASTLE-HTx that we randomized a cohort of patients with advanced end-stage heart failure.
How can AFib ablation have such big, early effects?
Dr. Mandrola: These are very clinically significant findings, with large effect sizes and very early separation of the Kaplan-Meier curves. How do you explain how dramatic an effect that is, and how early of an effect?
Dr. Sommer: That’s one of the key questions at the end of the day. I think our job basically was to provide the data and to ensure that the data are clean and that it’s all perfectly done. The interpretation of these data is really kind of difficult, although we do not have the 100% perfect and obvious explanation why the curves separated so early. Our view on that is that we are talking about a pretty fragile patient population, so little differences like having a tachyarrhythmia of 110 day in, day out or being in sinus rhythm of 60 can make a huge difference. That’s obviously pretty early.
The one that remains in tachyarrhythmia will deteriorate and will require an LVAD after a couple of months, and the one that you may keep in sinus rhythm, even with reduced atrial fibrillation burden – not zero, but reduced atrial fibrillation burden – and improved LV function, all of a sudden this patient will still remain on a low level of being stable, but he or she will remain stable and will not require any surgical interventions for the next 1.5-2 years. If we can manage to do this, just postponing the natural cause of the disease, I think that is a great benefit for the patient.
Dr. Mandrola: One of the things that comes up in our center is that I look at some of these patients and think, there’s no way I can put this patient under general anesthetic and do all of this. Your ablation procedure wasn’t that extensive, was it?
Dr. Sohns: On the one hand, no. On the other hand, yes. You need to take into consideration that it has been performed by experienced physicians with experience in heart failure treatment and atrial fibrillation in heart transplantation centers, though it›s not sure that we can transfer these results one-to-one to all other centers in the world.
It is very clear that we have almost no major complications in these patients. We were able to do these ablation procedures without general anesthesia. We have 60% of patients who had pulmonary vein isolation only and 40% of patients who have PVI and additional therapy. We have a procedure duration of almost 90 minutes during radiofrequency ablation.
We have different categories. When you talk about the different patient cohorts, we also see different stages of myocardial tissue damage, which will be part of another publication for sure. It is, in part, surprising how normal some of the atria were despite having a volume of 180 mL, but they had no fibrosis. That was very interesting.
Dr. Mandrola: How did the persistent vs paroxysmal atrial fibrillation sort out? Were these mostly patients with persistent atrial fibrillation?
Dr. Sommer: Two-thirds were persistent. It would be expected in this patient population that you would not find so many paroxysmal cases. I think it›s very important what Christian was just mentioning that when we discussed the trial design, we were anticipating problems with the sedation, for example. With the follow-up of those procedures, would they decompensate because of the fluid that you have to deliver during such a procedure.
We were quite surprised at the end of the day that the procedures were quite straightforward. Fortunately, we had no major complications. I think there were four complications in the 100 ablated patients. I think we were really positive about how the procedures turned out.
I should mention that one of the exclusion criteria was a left atrial diameter of about 60 mm. The huge ones may be very diseased, and maybe the hopeless ones were excluded from the study. Below 60 mm, we did the ablation.
Rhythm control
Dr. Mandrola: One of my colleagues, who is even more skeptical than me, wanted me to ask you, why wouldn’t you take a patient with persistent atrial fibrillation who had heart failure and just cardiovert and use amiodarone and try and maintain sinus rhythm that way?
Dr. Sohns: It is important to mention that 50% of the patients have already had amiodarone before they were randomized and enrolled for the trial. It might bring you a couple of minutes or a couple of hours [of relief], but the patients would get recurrence.
It was very interesting also, and this is in line with the data from Jason Andrade, who demonstrated that we were able to reduce the percentage of patients with persistent atrial fibrillation to paroxysmal. We did a down-staging of the underlying disease. This is not possible with cardioversion or drugs, for example.
Dr. Sommer: What I really like about that question and that comment is the idea that rhythm control in this subset of patients obviously has a role and an importance. It may be a cardioversion initially, giving amiodarone if they didn’t have that before, and you can keep the patient in sinus rhythm with this therapy, I think we’re reaching the same goal.
I think the critical point to get into the mind of physicians who treat heart failure is that sinus rhythm is beneficial, however you get there. Ablation, of course, as in other studies, is the most powerful tool to get there. Cardioversion can be a really good thing to do; you just have to think about it and consider it.
Dr. Mandrola: I do want to say to everybody that there is a tension sometimes between the heart failure community and the electrophysiology community. I think the ideal situation is that we work together, because I think that we can help with the maintenance of sinus rhythm. The control group mortality at 1 year was 20%, and I’ve heard people say that that’s not advanced heart failure. Advanced heart failure patients have much higher mortality than that. My colleague who is a heart failure specialist was criticizing a selection bias in picking the best patients. How would you answer that?
Dr. Sohns: There are data available from Eurotransplant, for example, that the waiting list mortality is 18%, so I think we are almost in line with this 20% mortality in this conservative group. You cannot generalize it. All these patients have different histories. We have 60% dilated cardiomyopathy and 40% ischemic cardiomyopathy. I think it is a very representative group in contrast to your friend who suggests that it is not.
Dr. Sommer: What I like about the discussion is that some approach us to say that the mortality in the control group is much too high – like, what are you doing with those patients that you create so many endpoints? Then others say that it’s not high enough because that is not end-stage heart failure. Come on! We have a patient cohort that is very well described and very well characterized.
If the label is end-stage heart failure, advanced heart failure, or whatever, they are sicker than the patients that we had in earlier trials. The patients that we treated were mostly excluded from all other trials. We opened the door. We found a clear result. I think everyone can see whatever you like to see.
Dr. Mandrola: What would your take-home message be after having done this trial design, the trial was conducted in your single center, and you come up with these amazing results? What would your message be to the whole community?
Dr. Sohns: Taking into consideration how severely sick these patients are, I can just repeat it: They are one step away from death, more or less, or from surgical intervention that can prolong their life. You should also consider that there are options like atrial fibrillation ablation that can buy time, postpone the natural course, or even in some patients replace the destination therapy. Therefore, in my opinion the next guidelines should recommend that every patient should carefully be checked for sinus rhythm before bringing these patients into the environment of transplantation.
Dr. Sommer: My interpretation is that we have to try to bring into physicians’ minds that besides a well-established and well-documented effect of drug therapy with the fabulous four, we may now have the fabulous five, including an ablation option for patients with atrial fibrillation.
Dr. Mandrola is a clinical electrophysiologist at Baptist Medical Associates, Louisville, Ky. Dr. Sohns is deputy director of the Heart and Diabetes Center NRW, Ruhr University Bochum, Bad Oeynhausen, Germany. Dr. Sommer is professor of cardiology at the Heart and Diabetes Center NRW. Dr. Mandrola reported no conflicts of interest. Dr. Sohns reported receiving research funding from Else Kröner–Fresenius–Stiftung. Dr. Sommer reported consulting with Abbott, Biosense Webster, Boston Scientific, and Medtronic USA.
A version of this article first appeared on Medscape.com.
Recorded Aug. 28, 2023. This transcript has been edited for clarity.
John M. Mandrola, MD: I’m here at the European Society of Cardiology meeting, and I’m very excited to have two colleagues whom I met at the Western Atrial Fibrillation Symposium (Western AFib) and who presented the CASTLE-HTx study. This is Christian Sohns and Philipp Sommer, and the CASTLE-HTx study is very exciting.
Before I get into that, I really want to introduce the concept of atrial fibrillation in heart failure. I like to say that there are two big populations of patients with atrial fibrillation, and the vast majority can be treated slowly with reassurance and education. There is a group of patients who have heart failure who, when they develop atrial fibrillation, can degenerate rapidly. The CASTLE-HTx study looked at catheter ablation versus medical therapy in patients with advanced heart failure.
Christian, why don’t you tell us the top-line results and what you found.
CASTLE-HTx key findings
Christian Sohns, MD, PhD: Thanks, first of all, for mentioning this special cohort of patients in end-stage heart failure, which is very important. The endpoint of the study was a composite of death from any cause or left ventricular assist device (LVAD) implantation and heart transplantation. These are very hard, strong clinical endpoints, not the rate of rehospitalization or something like that.
Catheter ablation was superior to medical therapy alone in terms of this composite endpoint. That was driven by cardiovascular death and all-cause mortality, which highlights the fact that you should always consider atrial fibrillation ablation in the end-stage heart failure cohort. The findings were driven by the fact that we saw left ventricular reverse remodeling and the reduction of atrial fibrillation in these patients.
Dr. Mandrola: Tell me about how it came about. It was conducted at your center. Who were these patients?
Philipp Sommer, MD: As one of the biggest centers for heart transplantations all over Europe, with roughly 100 transplants per year, we had many patients being referred to our center with the questions of whether those patients are eligible for a heart transplantation. Not all of the patients in our study were listed for a transplant, but all of them were admitted in that end-stage heart failure status to evaluate their eligibility for transplant.
If we look at the baseline data of those patients, they had an ejection fraction of 29%. They had a 6-minute walk test as a functional capacity parameter of around 300 m. Approximately two thirds of them were New York Heart Association class III and IV, which is significantly worse than what we saw in the previous studies dealing with heart failure patients.
I think overall, if you also look at NT-proBNP levels, this is a really sick patient population where some people might doubt if they should admit and refer those patients for an ablation procedure. Therefore, it’s really interesting and fascinating to see the results.
Dr. Mandrola: I did read in the manuscript, and I heard from you, that these were recruited as outpatients. So they were stable outpatients who were referred to the center for consideration of an LVAD or transplant?
Dr. Sohns: The definition of stability is very difficult in these patients because they have hospital stays, they have a history of drug therapy, and they have a history of interventions also behind them – not atrial fibrillation ablation, but others. I think these patients are referred because the referring physicians are done with the case. They can no longer offer any option to the patients other than surgical treatment, assist device, pump implantation, or transplantation.
If you look at the guidelines, they do not comment on atrial fibrillation ablation in this cohort of patients. Also, they have different recommendations between the American societies and the European societies regarding what is end-stage heart failure and how to treat these patients. Therefore, it was a big benefit of CASTLE-HTx that we randomized a cohort of patients with advanced end-stage heart failure.
How can AFib ablation have such big, early effects?
Dr. Mandrola: These are very clinically significant findings, with large effect sizes and very early separation of the Kaplan-Meier curves. How do you explain how dramatic an effect that is, and how early of an effect?
Dr. Sommer: That’s one of the key questions at the end of the day. I think our job basically was to provide the data and to ensure that the data are clean and that it’s all perfectly done. The interpretation of these data is really kind of difficult, although we do not have the 100% perfect and obvious explanation why the curves separated so early. Our view on that is that we are talking about a pretty fragile patient population, so little differences like having a tachyarrhythmia of 110 day in, day out or being in sinus rhythm of 60 can make a huge difference. That’s obviously pretty early.
The one that remains in tachyarrhythmia will deteriorate and will require an LVAD after a couple of months, and the one that you may keep in sinus rhythm, even with reduced atrial fibrillation burden – not zero, but reduced atrial fibrillation burden – and improved LV function, all of a sudden this patient will still remain on a low level of being stable, but he or she will remain stable and will not require any surgical interventions for the next 1.5-2 years. If we can manage to do this, just postponing the natural cause of the disease, I think that is a great benefit for the patient.
Dr. Mandrola: One of the things that comes up in our center is that I look at some of these patients and think, there’s no way I can put this patient under general anesthetic and do all of this. Your ablation procedure wasn’t that extensive, was it?
Dr. Sohns: On the one hand, no. On the other hand, yes. You need to take into consideration that it has been performed by experienced physicians with experience in heart failure treatment and atrial fibrillation in heart transplantation centers, though it›s not sure that we can transfer these results one-to-one to all other centers in the world.
It is very clear that we have almost no major complications in these patients. We were able to do these ablation procedures without general anesthesia. We have 60% of patients who had pulmonary vein isolation only and 40% of patients who have PVI and additional therapy. We have a procedure duration of almost 90 minutes during radiofrequency ablation.
We have different categories. When you talk about the different patient cohorts, we also see different stages of myocardial tissue damage, which will be part of another publication for sure. It is, in part, surprising how normal some of the atria were despite having a volume of 180 mL, but they had no fibrosis. That was very interesting.
Dr. Mandrola: How did the persistent vs paroxysmal atrial fibrillation sort out? Were these mostly patients with persistent atrial fibrillation?
Dr. Sommer: Two-thirds were persistent. It would be expected in this patient population that you would not find so many paroxysmal cases. I think it›s very important what Christian was just mentioning that when we discussed the trial design, we were anticipating problems with the sedation, for example. With the follow-up of those procedures, would they decompensate because of the fluid that you have to deliver during such a procedure.
We were quite surprised at the end of the day that the procedures were quite straightforward. Fortunately, we had no major complications. I think there were four complications in the 100 ablated patients. I think we were really positive about how the procedures turned out.
I should mention that one of the exclusion criteria was a left atrial diameter of about 60 mm. The huge ones may be very diseased, and maybe the hopeless ones were excluded from the study. Below 60 mm, we did the ablation.
Rhythm control
Dr. Mandrola: One of my colleagues, who is even more skeptical than me, wanted me to ask you, why wouldn’t you take a patient with persistent atrial fibrillation who had heart failure and just cardiovert and use amiodarone and try and maintain sinus rhythm that way?
Dr. Sohns: It is important to mention that 50% of the patients have already had amiodarone before they were randomized and enrolled for the trial. It might bring you a couple of minutes or a couple of hours [of relief], but the patients would get recurrence.
It was very interesting also, and this is in line with the data from Jason Andrade, who demonstrated that we were able to reduce the percentage of patients with persistent atrial fibrillation to paroxysmal. We did a down-staging of the underlying disease. This is not possible with cardioversion or drugs, for example.
Dr. Sommer: What I really like about that question and that comment is the idea that rhythm control in this subset of patients obviously has a role and an importance. It may be a cardioversion initially, giving amiodarone if they didn’t have that before, and you can keep the patient in sinus rhythm with this therapy, I think we’re reaching the same goal.
I think the critical point to get into the mind of physicians who treat heart failure is that sinus rhythm is beneficial, however you get there. Ablation, of course, as in other studies, is the most powerful tool to get there. Cardioversion can be a really good thing to do; you just have to think about it and consider it.
Dr. Mandrola: I do want to say to everybody that there is a tension sometimes between the heart failure community and the electrophysiology community. I think the ideal situation is that we work together, because I think that we can help with the maintenance of sinus rhythm. The control group mortality at 1 year was 20%, and I’ve heard people say that that’s not advanced heart failure. Advanced heart failure patients have much higher mortality than that. My colleague who is a heart failure specialist was criticizing a selection bias in picking the best patients. How would you answer that?
Dr. Sohns: There are data available from Eurotransplant, for example, that the waiting list mortality is 18%, so I think we are almost in line with this 20% mortality in this conservative group. You cannot generalize it. All these patients have different histories. We have 60% dilated cardiomyopathy and 40% ischemic cardiomyopathy. I think it is a very representative group in contrast to your friend who suggests that it is not.
Dr. Sommer: What I like about the discussion is that some approach us to say that the mortality in the control group is much too high – like, what are you doing with those patients that you create so many endpoints? Then others say that it’s not high enough because that is not end-stage heart failure. Come on! We have a patient cohort that is very well described and very well characterized.
If the label is end-stage heart failure, advanced heart failure, or whatever, they are sicker than the patients that we had in earlier trials. The patients that we treated were mostly excluded from all other trials. We opened the door. We found a clear result. I think everyone can see whatever you like to see.
Dr. Mandrola: What would your take-home message be after having done this trial design, the trial was conducted in your single center, and you come up with these amazing results? What would your message be to the whole community?
Dr. Sohns: Taking into consideration how severely sick these patients are, I can just repeat it: They are one step away from death, more or less, or from surgical intervention that can prolong their life. You should also consider that there are options like atrial fibrillation ablation that can buy time, postpone the natural course, or even in some patients replace the destination therapy. Therefore, in my opinion the next guidelines should recommend that every patient should carefully be checked for sinus rhythm before bringing these patients into the environment of transplantation.
Dr. Sommer: My interpretation is that we have to try to bring into physicians’ minds that besides a well-established and well-documented effect of drug therapy with the fabulous four, we may now have the fabulous five, including an ablation option for patients with atrial fibrillation.
Dr. Mandrola is a clinical electrophysiologist at Baptist Medical Associates, Louisville, Ky. Dr. Sohns is deputy director of the Heart and Diabetes Center NRW, Ruhr University Bochum, Bad Oeynhausen, Germany. Dr. Sommer is professor of cardiology at the Heart and Diabetes Center NRW. Dr. Mandrola reported no conflicts of interest. Dr. Sohns reported receiving research funding from Else Kröner–Fresenius–Stiftung. Dr. Sommer reported consulting with Abbott, Biosense Webster, Boston Scientific, and Medtronic USA.
A version of this article first appeared on Medscape.com.
Recorded Aug. 28, 2023. This transcript has been edited for clarity.
John M. Mandrola, MD: I’m here at the European Society of Cardiology meeting, and I’m very excited to have two colleagues whom I met at the Western Atrial Fibrillation Symposium (Western AFib) and who presented the CASTLE-HTx study. This is Christian Sohns and Philipp Sommer, and the CASTLE-HTx study is very exciting.
Before I get into that, I really want to introduce the concept of atrial fibrillation in heart failure. I like to say that there are two big populations of patients with atrial fibrillation, and the vast majority can be treated slowly with reassurance and education. There is a group of patients who have heart failure who, when they develop atrial fibrillation, can degenerate rapidly. The CASTLE-HTx study looked at catheter ablation versus medical therapy in patients with advanced heart failure.
Christian, why don’t you tell us the top-line results and what you found.
CASTLE-HTx key findings
Christian Sohns, MD, PhD: Thanks, first of all, for mentioning this special cohort of patients in end-stage heart failure, which is very important. The endpoint of the study was a composite of death from any cause or left ventricular assist device (LVAD) implantation and heart transplantation. These are very hard, strong clinical endpoints, not the rate of rehospitalization or something like that.
Catheter ablation was superior to medical therapy alone in terms of this composite endpoint. That was driven by cardiovascular death and all-cause mortality, which highlights the fact that you should always consider atrial fibrillation ablation in the end-stage heart failure cohort. The findings were driven by the fact that we saw left ventricular reverse remodeling and the reduction of atrial fibrillation in these patients.
Dr. Mandrola: Tell me about how it came about. It was conducted at your center. Who were these patients?
Philipp Sommer, MD: As one of the biggest centers for heart transplantations all over Europe, with roughly 100 transplants per year, we had many patients being referred to our center with the questions of whether those patients are eligible for a heart transplantation. Not all of the patients in our study were listed for a transplant, but all of them were admitted in that end-stage heart failure status to evaluate their eligibility for transplant.
If we look at the baseline data of those patients, they had an ejection fraction of 29%. They had a 6-minute walk test as a functional capacity parameter of around 300 m. Approximately two thirds of them were New York Heart Association class III and IV, which is significantly worse than what we saw in the previous studies dealing with heart failure patients.
I think overall, if you also look at NT-proBNP levels, this is a really sick patient population where some people might doubt if they should admit and refer those patients for an ablation procedure. Therefore, it’s really interesting and fascinating to see the results.
Dr. Mandrola: I did read in the manuscript, and I heard from you, that these were recruited as outpatients. So they were stable outpatients who were referred to the center for consideration of an LVAD or transplant?
Dr. Sohns: The definition of stability is very difficult in these patients because they have hospital stays, they have a history of drug therapy, and they have a history of interventions also behind them – not atrial fibrillation ablation, but others. I think these patients are referred because the referring physicians are done with the case. They can no longer offer any option to the patients other than surgical treatment, assist device, pump implantation, or transplantation.
If you look at the guidelines, they do not comment on atrial fibrillation ablation in this cohort of patients. Also, they have different recommendations between the American societies and the European societies regarding what is end-stage heart failure and how to treat these patients. Therefore, it was a big benefit of CASTLE-HTx that we randomized a cohort of patients with advanced end-stage heart failure.
How can AFib ablation have such big, early effects?
Dr. Mandrola: These are very clinically significant findings, with large effect sizes and very early separation of the Kaplan-Meier curves. How do you explain how dramatic an effect that is, and how early of an effect?
Dr. Sommer: That’s one of the key questions at the end of the day. I think our job basically was to provide the data and to ensure that the data are clean and that it’s all perfectly done. The interpretation of these data is really kind of difficult, although we do not have the 100% perfect and obvious explanation why the curves separated so early. Our view on that is that we are talking about a pretty fragile patient population, so little differences like having a tachyarrhythmia of 110 day in, day out or being in sinus rhythm of 60 can make a huge difference. That’s obviously pretty early.
The one that remains in tachyarrhythmia will deteriorate and will require an LVAD after a couple of months, and the one that you may keep in sinus rhythm, even with reduced atrial fibrillation burden – not zero, but reduced atrial fibrillation burden – and improved LV function, all of a sudden this patient will still remain on a low level of being stable, but he or she will remain stable and will not require any surgical interventions for the next 1.5-2 years. If we can manage to do this, just postponing the natural cause of the disease, I think that is a great benefit for the patient.
Dr. Mandrola: One of the things that comes up in our center is that I look at some of these patients and think, there’s no way I can put this patient under general anesthetic and do all of this. Your ablation procedure wasn’t that extensive, was it?
Dr. Sohns: On the one hand, no. On the other hand, yes. You need to take into consideration that it has been performed by experienced physicians with experience in heart failure treatment and atrial fibrillation in heart transplantation centers, though it›s not sure that we can transfer these results one-to-one to all other centers in the world.
It is very clear that we have almost no major complications in these patients. We were able to do these ablation procedures without general anesthesia. We have 60% of patients who had pulmonary vein isolation only and 40% of patients who have PVI and additional therapy. We have a procedure duration of almost 90 minutes during radiofrequency ablation.
We have different categories. When you talk about the different patient cohorts, we also see different stages of myocardial tissue damage, which will be part of another publication for sure. It is, in part, surprising how normal some of the atria were despite having a volume of 180 mL, but they had no fibrosis. That was very interesting.
Dr. Mandrola: How did the persistent vs paroxysmal atrial fibrillation sort out? Were these mostly patients with persistent atrial fibrillation?
Dr. Sommer: Two-thirds were persistent. It would be expected in this patient population that you would not find so many paroxysmal cases. I think it›s very important what Christian was just mentioning that when we discussed the trial design, we were anticipating problems with the sedation, for example. With the follow-up of those procedures, would they decompensate because of the fluid that you have to deliver during such a procedure.
We were quite surprised at the end of the day that the procedures were quite straightforward. Fortunately, we had no major complications. I think there were four complications in the 100 ablated patients. I think we were really positive about how the procedures turned out.
I should mention that one of the exclusion criteria was a left atrial diameter of about 60 mm. The huge ones may be very diseased, and maybe the hopeless ones were excluded from the study. Below 60 mm, we did the ablation.
Rhythm control
Dr. Mandrola: One of my colleagues, who is even more skeptical than me, wanted me to ask you, why wouldn’t you take a patient with persistent atrial fibrillation who had heart failure and just cardiovert and use amiodarone and try and maintain sinus rhythm that way?
Dr. Sohns: It is important to mention that 50% of the patients have already had amiodarone before they were randomized and enrolled for the trial. It might bring you a couple of minutes or a couple of hours [of relief], but the patients would get recurrence.
It was very interesting also, and this is in line with the data from Jason Andrade, who demonstrated that we were able to reduce the percentage of patients with persistent atrial fibrillation to paroxysmal. We did a down-staging of the underlying disease. This is not possible with cardioversion or drugs, for example.
Dr. Sommer: What I really like about that question and that comment is the idea that rhythm control in this subset of patients obviously has a role and an importance. It may be a cardioversion initially, giving amiodarone if they didn’t have that before, and you can keep the patient in sinus rhythm with this therapy, I think we’re reaching the same goal.
I think the critical point to get into the mind of physicians who treat heart failure is that sinus rhythm is beneficial, however you get there. Ablation, of course, as in other studies, is the most powerful tool to get there. Cardioversion can be a really good thing to do; you just have to think about it and consider it.
Dr. Mandrola: I do want to say to everybody that there is a tension sometimes between the heart failure community and the electrophysiology community. I think the ideal situation is that we work together, because I think that we can help with the maintenance of sinus rhythm. The control group mortality at 1 year was 20%, and I’ve heard people say that that’s not advanced heart failure. Advanced heart failure patients have much higher mortality than that. My colleague who is a heart failure specialist was criticizing a selection bias in picking the best patients. How would you answer that?
Dr. Sohns: There are data available from Eurotransplant, for example, that the waiting list mortality is 18%, so I think we are almost in line with this 20% mortality in this conservative group. You cannot generalize it. All these patients have different histories. We have 60% dilated cardiomyopathy and 40% ischemic cardiomyopathy. I think it is a very representative group in contrast to your friend who suggests that it is not.
Dr. Sommer: What I like about the discussion is that some approach us to say that the mortality in the control group is much too high – like, what are you doing with those patients that you create so many endpoints? Then others say that it’s not high enough because that is not end-stage heart failure. Come on! We have a patient cohort that is very well described and very well characterized.
If the label is end-stage heart failure, advanced heart failure, or whatever, they are sicker than the patients that we had in earlier trials. The patients that we treated were mostly excluded from all other trials. We opened the door. We found a clear result. I think everyone can see whatever you like to see.
Dr. Mandrola: What would your take-home message be after having done this trial design, the trial was conducted in your single center, and you come up with these amazing results? What would your message be to the whole community?
Dr. Sohns: Taking into consideration how severely sick these patients are, I can just repeat it: They are one step away from death, more or less, or from surgical intervention that can prolong their life. You should also consider that there are options like atrial fibrillation ablation that can buy time, postpone the natural course, or even in some patients replace the destination therapy. Therefore, in my opinion the next guidelines should recommend that every patient should carefully be checked for sinus rhythm before bringing these patients into the environment of transplantation.
Dr. Sommer: My interpretation is that we have to try to bring into physicians’ minds that besides a well-established and well-documented effect of drug therapy with the fabulous four, we may now have the fabulous five, including an ablation option for patients with atrial fibrillation.
Dr. Mandrola is a clinical electrophysiologist at Baptist Medical Associates, Louisville, Ky. Dr. Sohns is deputy director of the Heart and Diabetes Center NRW, Ruhr University Bochum, Bad Oeynhausen, Germany. Dr. Sommer is professor of cardiology at the Heart and Diabetes Center NRW. Dr. Mandrola reported no conflicts of interest. Dr. Sohns reported receiving research funding from Else Kröner–Fresenius–Stiftung. Dr. Sommer reported consulting with Abbott, Biosense Webster, Boston Scientific, and Medtronic USA.
A version of this article first appeared on Medscape.com.
Heart failure guidelines update: What the ESC got right
This transcript has been edited for clarity.
This is my usual blog, except I am here from the absolutely beautiful city of Amsterdam, where the annual congress of the European Society of Cardiology has been going on.
SGLT2 inhibitors for HFpEF and HFrEF
I’m going to review very briefly the 2023 focused update to the ESC heart failure guidelines. Theresa McDonagh was the first author of this and of the previous ESC or European guidelines. These are a little bit different than the American guidelines, which were presented in 2022. We know that we need an update. The Europeans have gotten ahead of us, and now we have the European update, which I find incredibly well written and it really highlights the areas that I think the takeaways are for the clinicians.
First, we have been seeing now for several years – since 2018 – the benefits of the sodium-glucose cotransporter 2 (SGLT2) inhibitors. Every time we lift the veil on something, there they are in a positive light. We have learned about heart failure with reduced ejection fraction (HFrEF) for both empagliflozin and dapagliflozin. There are very similar results. One population may be enriched with a little of this and a little of that, but the basic messages are the same. In HFrEF, both of these drugs improve outcomes and it happens quickly. You don’t have to wait 1 or 2 years to see this. Within months, and actually within days, you start to see the curves split apart statistically.
The next logical ground was heart failure with preserved ejection fraction (HFpEF). The definition, when we started the HFpEF trials, was 45% or greater. I want the audience to realize that, in the midst of all these trials, we came out – we meaning the American Heart Association, the American College of Cardiology, and the Heart Failure Society – with the new definition of heart failure, which said that true HFpEF is 50% or greater. That in-between zone of 40%-50% or 41%-49% is mRF, or mid-range, what I call middle of the road. I think the Europeans have really emphasized that to us. I believe that those patients really behave much more like a HFrEF population.
Now that we have very positive findings with the SGLT2 inhibitors, both dapagliflozin and empagliflozin, in HFpEF – defined, as I said, as 40% or 45% or greater, not necessarily 50% – with excellent point estimates that just line up, one on top of the other. It doesn’t matter if patients have diabetes or not; the results are exactly the same.
This has been so promising that I am not surprised that the Europeans elevated the SGLT2 inhibitors to a class 1A indication. In the United States in 2022, we thought we were really way ahead by calling it a class 2A indication. Well, now it’s a class 1A indication in Europe, and I have a feeling that the AHA and the ACC are going to start talking about an update because the data are so strong.
Now, we even have data on initiating these drugs in the hospital. EMPULSE was a very large trial about the benefits of starting these drugs in the hospital. You do not have to wait until the patient is in the outpatient setting. You can start it in the hospital.
When? I have no specific day that I start it. I used to try to do a good diuresis first, get the patients somewhat decongested, and then start it. I don’t want to deprive the patients of the benefits of these drugs that happen very early by waiting until the patients are in the outpatient setting.
In the United States, we’ve had some issues with coverage of some of these drugs. In my institution, we now have both on the formulary, and I pick the drug depending upon the patient’s coverage. Medicare pretty much covers most of them. If the patient is older but not yet a Medicare patient, they may have a very large copay. I advise you to get your offices or your health system to look into this so that, when you give the prescription to the patient, whether they’re leaving the hospital or are now in your clinics, they can actually get the drug.
Finerenone and intravenous iron
There is an additional recommendation in these guidelines for finerenone, the mineralocorticoid receptor agonist that I’ve discussed before, that has some really promising data on type 2 diabetes with chronic kidney disease. They have called that a class 1A indication for finerenone. I think there is more to come.
One more: the iron deficiency. Giving intravenous iron actually does improve symptoms and quality of life. I have seen this in my own patients, so I have been very diligent at looking for iron deficiency.
It is a new era. We have more tools, obviously, for our patients. It means one more drug, and that’s always a challenge. We’ve already been doing the pillars of care. This is the fourth pillar of care, but now with a class 1A indication.
Take a look. They’re easy to read. Dr. McDonagh is the first author, and I think they’ve been extremely well done.
Dr. Piña is professor of medicine at Thomas Jefferson University Hospital in Philadelphia. She is a heart failure and cardiac transplantation expert. She disclosed serving as an adviser/consultant to the FDA’s Center for Devices and Radiological Health and has been a volunteer for the American Heart Association since 1982.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
This is my usual blog, except I am here from the absolutely beautiful city of Amsterdam, where the annual congress of the European Society of Cardiology has been going on.
SGLT2 inhibitors for HFpEF and HFrEF
I’m going to review very briefly the 2023 focused update to the ESC heart failure guidelines. Theresa McDonagh was the first author of this and of the previous ESC or European guidelines. These are a little bit different than the American guidelines, which were presented in 2022. We know that we need an update. The Europeans have gotten ahead of us, and now we have the European update, which I find incredibly well written and it really highlights the areas that I think the takeaways are for the clinicians.
First, we have been seeing now for several years – since 2018 – the benefits of the sodium-glucose cotransporter 2 (SGLT2) inhibitors. Every time we lift the veil on something, there they are in a positive light. We have learned about heart failure with reduced ejection fraction (HFrEF) for both empagliflozin and dapagliflozin. There are very similar results. One population may be enriched with a little of this and a little of that, but the basic messages are the same. In HFrEF, both of these drugs improve outcomes and it happens quickly. You don’t have to wait 1 or 2 years to see this. Within months, and actually within days, you start to see the curves split apart statistically.
The next logical ground was heart failure with preserved ejection fraction (HFpEF). The definition, when we started the HFpEF trials, was 45% or greater. I want the audience to realize that, in the midst of all these trials, we came out – we meaning the American Heart Association, the American College of Cardiology, and the Heart Failure Society – with the new definition of heart failure, which said that true HFpEF is 50% or greater. That in-between zone of 40%-50% or 41%-49% is mRF, or mid-range, what I call middle of the road. I think the Europeans have really emphasized that to us. I believe that those patients really behave much more like a HFrEF population.
Now that we have very positive findings with the SGLT2 inhibitors, both dapagliflozin and empagliflozin, in HFpEF – defined, as I said, as 40% or 45% or greater, not necessarily 50% – with excellent point estimates that just line up, one on top of the other. It doesn’t matter if patients have diabetes or not; the results are exactly the same.
This has been so promising that I am not surprised that the Europeans elevated the SGLT2 inhibitors to a class 1A indication. In the United States in 2022, we thought we were really way ahead by calling it a class 2A indication. Well, now it’s a class 1A indication in Europe, and I have a feeling that the AHA and the ACC are going to start talking about an update because the data are so strong.
Now, we even have data on initiating these drugs in the hospital. EMPULSE was a very large trial about the benefits of starting these drugs in the hospital. You do not have to wait until the patient is in the outpatient setting. You can start it in the hospital.
When? I have no specific day that I start it. I used to try to do a good diuresis first, get the patients somewhat decongested, and then start it. I don’t want to deprive the patients of the benefits of these drugs that happen very early by waiting until the patients are in the outpatient setting.
In the United States, we’ve had some issues with coverage of some of these drugs. In my institution, we now have both on the formulary, and I pick the drug depending upon the patient’s coverage. Medicare pretty much covers most of them. If the patient is older but not yet a Medicare patient, they may have a very large copay. I advise you to get your offices or your health system to look into this so that, when you give the prescription to the patient, whether they’re leaving the hospital or are now in your clinics, they can actually get the drug.
Finerenone and intravenous iron
There is an additional recommendation in these guidelines for finerenone, the mineralocorticoid receptor agonist that I’ve discussed before, that has some really promising data on type 2 diabetes with chronic kidney disease. They have called that a class 1A indication for finerenone. I think there is more to come.
One more: the iron deficiency. Giving intravenous iron actually does improve symptoms and quality of life. I have seen this in my own patients, so I have been very diligent at looking for iron deficiency.
It is a new era. We have more tools, obviously, for our patients. It means one more drug, and that’s always a challenge. We’ve already been doing the pillars of care. This is the fourth pillar of care, but now with a class 1A indication.
Take a look. They’re easy to read. Dr. McDonagh is the first author, and I think they’ve been extremely well done.
Dr. Piña is professor of medicine at Thomas Jefferson University Hospital in Philadelphia. She is a heart failure and cardiac transplantation expert. She disclosed serving as an adviser/consultant to the FDA’s Center for Devices and Radiological Health and has been a volunteer for the American Heart Association since 1982.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
This is my usual blog, except I am here from the absolutely beautiful city of Amsterdam, where the annual congress of the European Society of Cardiology has been going on.
SGLT2 inhibitors for HFpEF and HFrEF
I’m going to review very briefly the 2023 focused update to the ESC heart failure guidelines. Theresa McDonagh was the first author of this and of the previous ESC or European guidelines. These are a little bit different than the American guidelines, which were presented in 2022. We know that we need an update. The Europeans have gotten ahead of us, and now we have the European update, which I find incredibly well written and it really highlights the areas that I think the takeaways are for the clinicians.
First, we have been seeing now for several years – since 2018 – the benefits of the sodium-glucose cotransporter 2 (SGLT2) inhibitors. Every time we lift the veil on something, there they are in a positive light. We have learned about heart failure with reduced ejection fraction (HFrEF) for both empagliflozin and dapagliflozin. There are very similar results. One population may be enriched with a little of this and a little of that, but the basic messages are the same. In HFrEF, both of these drugs improve outcomes and it happens quickly. You don’t have to wait 1 or 2 years to see this. Within months, and actually within days, you start to see the curves split apart statistically.
The next logical ground was heart failure with preserved ejection fraction (HFpEF). The definition, when we started the HFpEF trials, was 45% or greater. I want the audience to realize that, in the midst of all these trials, we came out – we meaning the American Heart Association, the American College of Cardiology, and the Heart Failure Society – with the new definition of heart failure, which said that true HFpEF is 50% or greater. That in-between zone of 40%-50% or 41%-49% is mRF, or mid-range, what I call middle of the road. I think the Europeans have really emphasized that to us. I believe that those patients really behave much more like a HFrEF population.
Now that we have very positive findings with the SGLT2 inhibitors, both dapagliflozin and empagliflozin, in HFpEF – defined, as I said, as 40% or 45% or greater, not necessarily 50% – with excellent point estimates that just line up, one on top of the other. It doesn’t matter if patients have diabetes or not; the results are exactly the same.
This has been so promising that I am not surprised that the Europeans elevated the SGLT2 inhibitors to a class 1A indication. In the United States in 2022, we thought we were really way ahead by calling it a class 2A indication. Well, now it’s a class 1A indication in Europe, and I have a feeling that the AHA and the ACC are going to start talking about an update because the data are so strong.
Now, we even have data on initiating these drugs in the hospital. EMPULSE was a very large trial about the benefits of starting these drugs in the hospital. You do not have to wait until the patient is in the outpatient setting. You can start it in the hospital.
When? I have no specific day that I start it. I used to try to do a good diuresis first, get the patients somewhat decongested, and then start it. I don’t want to deprive the patients of the benefits of these drugs that happen very early by waiting until the patients are in the outpatient setting.
In the United States, we’ve had some issues with coverage of some of these drugs. In my institution, we now have both on the formulary, and I pick the drug depending upon the patient’s coverage. Medicare pretty much covers most of them. If the patient is older but not yet a Medicare patient, they may have a very large copay. I advise you to get your offices or your health system to look into this so that, when you give the prescription to the patient, whether they’re leaving the hospital or are now in your clinics, they can actually get the drug.
Finerenone and intravenous iron
There is an additional recommendation in these guidelines for finerenone, the mineralocorticoid receptor agonist that I’ve discussed before, that has some really promising data on type 2 diabetes with chronic kidney disease. They have called that a class 1A indication for finerenone. I think there is more to come.
One more: the iron deficiency. Giving intravenous iron actually does improve symptoms and quality of life. I have seen this in my own patients, so I have been very diligent at looking for iron deficiency.
It is a new era. We have more tools, obviously, for our patients. It means one more drug, and that’s always a challenge. We’ve already been doing the pillars of care. This is the fourth pillar of care, but now with a class 1A indication.
Take a look. They’re easy to read. Dr. McDonagh is the first author, and I think they’ve been extremely well done.
Dr. Piña is professor of medicine at Thomas Jefferson University Hospital in Philadelphia. She is a heart failure and cardiac transplantation expert. She disclosed serving as an adviser/consultant to the FDA’s Center for Devices and Radiological Health and has been a volunteer for the American Heart Association since 1982.
A version of this article appeared on Medscape.com.
New ESC ACS guideline combines STEMI and NSTE-ACS
AMSTERDAM –
The new guideline was released at the annual congress of the European Society of Cardiology, and was published online in the European Heart Journal.
“We found that it was realized by the cardiology community that patients with STEMI, NSTEMI, or unstable angina represent a spectrum,” the chair of the guideline task force, Robert Byrne, MD, chair of cardiovascular research at the RCSI University of Medicine and Health Sciences, Dublin, explained to this news organization. “After the initial triage and management decisions, then most of the rest of the care follows a common pathway so it would make sense to consider everything in one guideline.”
Dr. Byrne noted that for all patients with a suspected ACS, the guideline recommendation is to administer an ECG within 10 minutes of presentation. The time is critical particularly for those with an occluded epicardial vessel. If there are features on the ECG that suggest an acutely occluded epicardial vessel, then the patient needs immediate angiography or primary angioplasty.
“The 10-minute guidance has been maintained from previous guidelines, but the nuance in the new guideline is that typically when we think of an occluded epicardial vessel we think of ST-elevation on the ECG,” Byrne said. “While this captures most occluded epicardial vessels, it doesn’t capture all of them. So, we have provided some guidance on alternative ECG patterns which might be indicative of an acute occlusion of the epicardial vessel and should be dealt with in the same way as an ST-elevation MI. This is a new concept.”
This situation could arise when a patient has an occluded circumflex artery and the regular ECG may not show ST elevation but the patient has ongoing pain, he noted. “There are additional ECG leads that can be looked at that might identify patients who need an immediate invasive strategy.
“This is one more reason why all ACS patients should be considered as part of one spectrum, and while the ECG gives us important information, it is not the only thing to consider. Dividing the conditions up as to whether a patient has ST elevation or not does not always make pathophysiological sense,” he added.
Dr. Byrne noted that the new guidelines have tried to reach a wider stakeholder group that includes emergency doctors, internal medicine physicians, general practitioners, and surgeons, as well as cardiologists. The document includes animations in an effort to increase the reach of the guidelines to noncardiology stakeholders, and for the first time, the task force included a patient representative.
“As part of this strategy, we have put more structure in to emphasize the importance that at first contact, we already want to be thinking of antithrombotic therapy and whether the patient needs urgent transfer to the nearest cath lab. We also want to be thinking straight away about preventing the next heart attack by implementing strong secondary prevention measures,” he commented.
Dr. Byrne highlighted a few changes to individual recommendations in the new guidelines.
Invasive management in NSTE-ACS
He pointed out that a small change has been made in the advice on invasive management for patients with non–ST-elevation ACS.
Dr. Byrne explained that patients with ST elevation should be sent immediately to a cath lab for PCI. If this is not possible within 120 minutes, then the patient should receive thrombolysis. This recommendation is the same as in previous guidelines.
He added, however, that there is some novelty in recommendations for patients who don’t have ST elevation but do have a positive troponin. For this group, previous guidelines gave a Class I recommendation that all such patients undergo an angiogram within the first 24 hours. However, an additional meta-analysis that was published in 2022 showed that the evidence for triaging all patients to the cath lab within 24 hours is somewhat limited, Dr. Byrne noted.
“At the end of the day, the task force felt that a Class I recommendation to get all patients to the cath lab within 24 hours was too strong and couldn’t be sustained, so it has been downgraded to a Class IIa recommendation, which we thought was more appropriate,” he said.
“So, while all patients should still have an angiogram during the hospital admission, if they are high-risk ACS, the imperative to get everyone to the cath lab within 24 hours – which many of our colleagues were finding difficult to achieve – does not seem to be backed up by the evidence,” he added.
Antithrombotic therapy
Addressing administration of antithrombotics, the guidelines emphasize that at the time of initial diagnosis, all patients should receive antithrombotic therapy, usually aspirin and a parenteral antithrombotic, such as heparin, enoxaparin, bivalirudin, or fondaparinux. Dr. Byrne noted that the guidelines have a new algorithm as to which of these antithrombotics to give, depending on the clinical presentation of the patient.
On the use of upfront P2Y12 inhibitors, Dr. Byrne said the new guidelines only give a weak recommendation for this.
“Giving a P2Y12 inhibitor up front does not have a strong evidence base, and it’s not unreasonable to wait, do the angiogram, see where you are, and then start the P2Y12 inhibitor. This is something that’s not widely done in clinical practice,” he commented.
“The last 2020 guideline gave a Class III recommendation for upfront P2Y12 inhibitor therapy for ACS patients who do not have STEMI. We’ve generally maintained that with the introduction of the exception that if you are in a health care system where there is a long wait to get to the cath lab – 5 ,6 or 7 days – then it’s reasonable to make an exception and give a P2Y12 inhibitor, but otherwise we’ve sustained the Class III recommendation,” he noted.
Also, for patients who have STEMI, there is a new Class IIb recommendation that upfront P2Y12 inhibitors may be considered.
“This is also rather a weak recommendation. There isn’t a strong rationale to give a P2Y12 inhibitor it in ST elevation either. It’s also reasonable to wait,” he added.
Don’t rush cardiac arrest patients to the cath lab
Another update in the guidelines involves the management of patients with cardiac arrest who have been resuscitated. Dr. Byrne explained that these patients would all receive an immediate ECG, and if it is found that they have ST elevation, they would be sent immediately to the cath lab. But a series of randomized trials has suggested that for patients who don’t have ST elevation, it is not necessary to rush these patients to the cath lab.
“We’ve given a Class III recommendation for this, saying it may be better to stabilize the patients first in the ICU. This is in recognition that a large proportion of these patients turn out not to have an MI. They have had a cardiac arrest for another reason,” Dr. Byrne noted. “Moving them to the cath lab when they are still unstable could be harming these patients rather than helping them.”
Revascularization for multivessel disease
Dr. Byrne notes that revascularization remains a critical element in the care for patients with STEMI, and there is a new recommendation in this area for patients with multivessel disease.
“Up to half of patients presenting with STEMI have multivessel disease, and we now have five randomized trials to say that these patients should have complete revascularization rather than just the culprit vessel. There is a new Class I recommendation for this,” he said.
However, the optimal timing of revascularization (immediate vs. staged) has still not been investigated in adequately sized randomized trials, and no recommendation has been made on this, the task force notes.
Dr. Byrne commented: “If you want to do everything in one go, that’s fine, but it’s also okay to do the culprit lesion first and then the other vessels at a later date within 45 days. This might depend on individual circumstances. For example, if there are complex lesions or the vessels are heavily calcified, then it may be best to get the culprit lesion fixed first and let the patient recover, then bring them back in for the rest.”
He pointed out that the results of the MULTISTARS trial, which were not available when the task force was formulating the guidelines, were reported at the ESC Congress and confirmed their recommendation.
DAPT after PCI
On the duration of dual antiplatelet therapy (DAPT) after PCI, the new guidelines have largely retained prior recommendations for a default strategy of 12 months for the combination of aspirin and a P2Y12 inhibitor.
“This was the subject of some discussion, as there have been several trials now looking at shorter durations of DAPT and deescalating after a few months to just one of these treatments. And while there is a rationale to do this, we think it’s best to be kept as an alternative strategy rather than the default strategy,” Dr. Byrne said.
He explained that the trials of DAPT deescalation tended to enroll lower-risk patients, which reduced the generalizability of the results.
Most of the trials only randomly assigned patients to shorter durations of DAPT when they were event-free for some period, she said.
“This is a dynamic decision-making process and reflects the real world to some extent. We think it is best to recommend the standard aspirin and a P2Y12 inhibitor for the 12-month duration, but at 3 months, if the patient is doing well but you may be worried about bleeding risk, then you could decide to deescalate to single antiplatelet therapy,” she noted. “So, there is Class IIa recommendation that this can be considered, but it is not recommended as the default position.”
Polypill for secondary prevention
Another innovation in the new guidelines is a new Class IIa recommendation for prescription of a polypill containing secondary prevention medications for patients on discharge from hospital.
This recommendation follows a trial that showed that the use of such a polypill helps patients be more adherent to the therapies prescribed.
Byrne explains that such a polypill may contain aspirin, an ACE inhibitor, and a statin. Several varieties are available in most European countries, but they are not widely used.
On secondary prevention, he stressed, “Prevention of the next heart attack starts before the patient leaves hospital. It is important to make sure the patient has the right medication on board, including a high-dose, high-intensity statin, and has been referred to a cardiac rehabilitation program. These are largely maintained recommendations from previous guidelines, but they are very important.”
A version of this article appeared on Medscape.com.
AMSTERDAM –
The new guideline was released at the annual congress of the European Society of Cardiology, and was published online in the European Heart Journal.
“We found that it was realized by the cardiology community that patients with STEMI, NSTEMI, or unstable angina represent a spectrum,” the chair of the guideline task force, Robert Byrne, MD, chair of cardiovascular research at the RCSI University of Medicine and Health Sciences, Dublin, explained to this news organization. “After the initial triage and management decisions, then most of the rest of the care follows a common pathway so it would make sense to consider everything in one guideline.”
Dr. Byrne noted that for all patients with a suspected ACS, the guideline recommendation is to administer an ECG within 10 minutes of presentation. The time is critical particularly for those with an occluded epicardial vessel. If there are features on the ECG that suggest an acutely occluded epicardial vessel, then the patient needs immediate angiography or primary angioplasty.
“The 10-minute guidance has been maintained from previous guidelines, but the nuance in the new guideline is that typically when we think of an occluded epicardial vessel we think of ST-elevation on the ECG,” Byrne said. “While this captures most occluded epicardial vessels, it doesn’t capture all of them. So, we have provided some guidance on alternative ECG patterns which might be indicative of an acute occlusion of the epicardial vessel and should be dealt with in the same way as an ST-elevation MI. This is a new concept.”
This situation could arise when a patient has an occluded circumflex artery and the regular ECG may not show ST elevation but the patient has ongoing pain, he noted. “There are additional ECG leads that can be looked at that might identify patients who need an immediate invasive strategy.
“This is one more reason why all ACS patients should be considered as part of one spectrum, and while the ECG gives us important information, it is not the only thing to consider. Dividing the conditions up as to whether a patient has ST elevation or not does not always make pathophysiological sense,” he added.
Dr. Byrne noted that the new guidelines have tried to reach a wider stakeholder group that includes emergency doctors, internal medicine physicians, general practitioners, and surgeons, as well as cardiologists. The document includes animations in an effort to increase the reach of the guidelines to noncardiology stakeholders, and for the first time, the task force included a patient representative.
“As part of this strategy, we have put more structure in to emphasize the importance that at first contact, we already want to be thinking of antithrombotic therapy and whether the patient needs urgent transfer to the nearest cath lab. We also want to be thinking straight away about preventing the next heart attack by implementing strong secondary prevention measures,” he commented.
Dr. Byrne highlighted a few changes to individual recommendations in the new guidelines.
Invasive management in NSTE-ACS
He pointed out that a small change has been made in the advice on invasive management for patients with non–ST-elevation ACS.
Dr. Byrne explained that patients with ST elevation should be sent immediately to a cath lab for PCI. If this is not possible within 120 minutes, then the patient should receive thrombolysis. This recommendation is the same as in previous guidelines.
He added, however, that there is some novelty in recommendations for patients who don’t have ST elevation but do have a positive troponin. For this group, previous guidelines gave a Class I recommendation that all such patients undergo an angiogram within the first 24 hours. However, an additional meta-analysis that was published in 2022 showed that the evidence for triaging all patients to the cath lab within 24 hours is somewhat limited, Dr. Byrne noted.
“At the end of the day, the task force felt that a Class I recommendation to get all patients to the cath lab within 24 hours was too strong and couldn’t be sustained, so it has been downgraded to a Class IIa recommendation, which we thought was more appropriate,” he said.
“So, while all patients should still have an angiogram during the hospital admission, if they are high-risk ACS, the imperative to get everyone to the cath lab within 24 hours – which many of our colleagues were finding difficult to achieve – does not seem to be backed up by the evidence,” he added.
Antithrombotic therapy
Addressing administration of antithrombotics, the guidelines emphasize that at the time of initial diagnosis, all patients should receive antithrombotic therapy, usually aspirin and a parenteral antithrombotic, such as heparin, enoxaparin, bivalirudin, or fondaparinux. Dr. Byrne noted that the guidelines have a new algorithm as to which of these antithrombotics to give, depending on the clinical presentation of the patient.
On the use of upfront P2Y12 inhibitors, Dr. Byrne said the new guidelines only give a weak recommendation for this.
“Giving a P2Y12 inhibitor up front does not have a strong evidence base, and it’s not unreasonable to wait, do the angiogram, see where you are, and then start the P2Y12 inhibitor. This is something that’s not widely done in clinical practice,” he commented.
“The last 2020 guideline gave a Class III recommendation for upfront P2Y12 inhibitor therapy for ACS patients who do not have STEMI. We’ve generally maintained that with the introduction of the exception that if you are in a health care system where there is a long wait to get to the cath lab – 5 ,6 or 7 days – then it’s reasonable to make an exception and give a P2Y12 inhibitor, but otherwise we’ve sustained the Class III recommendation,” he noted.
Also, for patients who have STEMI, there is a new Class IIb recommendation that upfront P2Y12 inhibitors may be considered.
“This is also rather a weak recommendation. There isn’t a strong rationale to give a P2Y12 inhibitor it in ST elevation either. It’s also reasonable to wait,” he added.
Don’t rush cardiac arrest patients to the cath lab
Another update in the guidelines involves the management of patients with cardiac arrest who have been resuscitated. Dr. Byrne explained that these patients would all receive an immediate ECG, and if it is found that they have ST elevation, they would be sent immediately to the cath lab. But a series of randomized trials has suggested that for patients who don’t have ST elevation, it is not necessary to rush these patients to the cath lab.
“We’ve given a Class III recommendation for this, saying it may be better to stabilize the patients first in the ICU. This is in recognition that a large proportion of these patients turn out not to have an MI. They have had a cardiac arrest for another reason,” Dr. Byrne noted. “Moving them to the cath lab when they are still unstable could be harming these patients rather than helping them.”
Revascularization for multivessel disease
Dr. Byrne notes that revascularization remains a critical element in the care for patients with STEMI, and there is a new recommendation in this area for patients with multivessel disease.
“Up to half of patients presenting with STEMI have multivessel disease, and we now have five randomized trials to say that these patients should have complete revascularization rather than just the culprit vessel. There is a new Class I recommendation for this,” he said.
However, the optimal timing of revascularization (immediate vs. staged) has still not been investigated in adequately sized randomized trials, and no recommendation has been made on this, the task force notes.
Dr. Byrne commented: “If you want to do everything in one go, that’s fine, but it’s also okay to do the culprit lesion first and then the other vessels at a later date within 45 days. This might depend on individual circumstances. For example, if there are complex lesions or the vessels are heavily calcified, then it may be best to get the culprit lesion fixed first and let the patient recover, then bring them back in for the rest.”
He pointed out that the results of the MULTISTARS trial, which were not available when the task force was formulating the guidelines, were reported at the ESC Congress and confirmed their recommendation.
DAPT after PCI
On the duration of dual antiplatelet therapy (DAPT) after PCI, the new guidelines have largely retained prior recommendations for a default strategy of 12 months for the combination of aspirin and a P2Y12 inhibitor.
“This was the subject of some discussion, as there have been several trials now looking at shorter durations of DAPT and deescalating after a few months to just one of these treatments. And while there is a rationale to do this, we think it’s best to be kept as an alternative strategy rather than the default strategy,” Dr. Byrne said.
He explained that the trials of DAPT deescalation tended to enroll lower-risk patients, which reduced the generalizability of the results.
Most of the trials only randomly assigned patients to shorter durations of DAPT when they were event-free for some period, she said.
“This is a dynamic decision-making process and reflects the real world to some extent. We think it is best to recommend the standard aspirin and a P2Y12 inhibitor for the 12-month duration, but at 3 months, if the patient is doing well but you may be worried about bleeding risk, then you could decide to deescalate to single antiplatelet therapy,” she noted. “So, there is Class IIa recommendation that this can be considered, but it is not recommended as the default position.”
Polypill for secondary prevention
Another innovation in the new guidelines is a new Class IIa recommendation for prescription of a polypill containing secondary prevention medications for patients on discharge from hospital.
This recommendation follows a trial that showed that the use of such a polypill helps patients be more adherent to the therapies prescribed.
Byrne explains that such a polypill may contain aspirin, an ACE inhibitor, and a statin. Several varieties are available in most European countries, but they are not widely used.
On secondary prevention, he stressed, “Prevention of the next heart attack starts before the patient leaves hospital. It is important to make sure the patient has the right medication on board, including a high-dose, high-intensity statin, and has been referred to a cardiac rehabilitation program. These are largely maintained recommendations from previous guidelines, but they are very important.”
A version of this article appeared on Medscape.com.
AMSTERDAM –
The new guideline was released at the annual congress of the European Society of Cardiology, and was published online in the European Heart Journal.
“We found that it was realized by the cardiology community that patients with STEMI, NSTEMI, or unstable angina represent a spectrum,” the chair of the guideline task force, Robert Byrne, MD, chair of cardiovascular research at the RCSI University of Medicine and Health Sciences, Dublin, explained to this news organization. “After the initial triage and management decisions, then most of the rest of the care follows a common pathway so it would make sense to consider everything in one guideline.”
Dr. Byrne noted that for all patients with a suspected ACS, the guideline recommendation is to administer an ECG within 10 minutes of presentation. The time is critical particularly for those with an occluded epicardial vessel. If there are features on the ECG that suggest an acutely occluded epicardial vessel, then the patient needs immediate angiography or primary angioplasty.
“The 10-minute guidance has been maintained from previous guidelines, but the nuance in the new guideline is that typically when we think of an occluded epicardial vessel we think of ST-elevation on the ECG,” Byrne said. “While this captures most occluded epicardial vessels, it doesn’t capture all of them. So, we have provided some guidance on alternative ECG patterns which might be indicative of an acute occlusion of the epicardial vessel and should be dealt with in the same way as an ST-elevation MI. This is a new concept.”
This situation could arise when a patient has an occluded circumflex artery and the regular ECG may not show ST elevation but the patient has ongoing pain, he noted. “There are additional ECG leads that can be looked at that might identify patients who need an immediate invasive strategy.
“This is one more reason why all ACS patients should be considered as part of one spectrum, and while the ECG gives us important information, it is not the only thing to consider. Dividing the conditions up as to whether a patient has ST elevation or not does not always make pathophysiological sense,” he added.
Dr. Byrne noted that the new guidelines have tried to reach a wider stakeholder group that includes emergency doctors, internal medicine physicians, general practitioners, and surgeons, as well as cardiologists. The document includes animations in an effort to increase the reach of the guidelines to noncardiology stakeholders, and for the first time, the task force included a patient representative.
“As part of this strategy, we have put more structure in to emphasize the importance that at first contact, we already want to be thinking of antithrombotic therapy and whether the patient needs urgent transfer to the nearest cath lab. We also want to be thinking straight away about preventing the next heart attack by implementing strong secondary prevention measures,” he commented.
Dr. Byrne highlighted a few changes to individual recommendations in the new guidelines.
Invasive management in NSTE-ACS
He pointed out that a small change has been made in the advice on invasive management for patients with non–ST-elevation ACS.
Dr. Byrne explained that patients with ST elevation should be sent immediately to a cath lab for PCI. If this is not possible within 120 minutes, then the patient should receive thrombolysis. This recommendation is the same as in previous guidelines.
He added, however, that there is some novelty in recommendations for patients who don’t have ST elevation but do have a positive troponin. For this group, previous guidelines gave a Class I recommendation that all such patients undergo an angiogram within the first 24 hours. However, an additional meta-analysis that was published in 2022 showed that the evidence for triaging all patients to the cath lab within 24 hours is somewhat limited, Dr. Byrne noted.
“At the end of the day, the task force felt that a Class I recommendation to get all patients to the cath lab within 24 hours was too strong and couldn’t be sustained, so it has been downgraded to a Class IIa recommendation, which we thought was more appropriate,” he said.
“So, while all patients should still have an angiogram during the hospital admission, if they are high-risk ACS, the imperative to get everyone to the cath lab within 24 hours – which many of our colleagues were finding difficult to achieve – does not seem to be backed up by the evidence,” he added.
Antithrombotic therapy
Addressing administration of antithrombotics, the guidelines emphasize that at the time of initial diagnosis, all patients should receive antithrombotic therapy, usually aspirin and a parenteral antithrombotic, such as heparin, enoxaparin, bivalirudin, or fondaparinux. Dr. Byrne noted that the guidelines have a new algorithm as to which of these antithrombotics to give, depending on the clinical presentation of the patient.
On the use of upfront P2Y12 inhibitors, Dr. Byrne said the new guidelines only give a weak recommendation for this.
“Giving a P2Y12 inhibitor up front does not have a strong evidence base, and it’s not unreasonable to wait, do the angiogram, see where you are, and then start the P2Y12 inhibitor. This is something that’s not widely done in clinical practice,” he commented.
“The last 2020 guideline gave a Class III recommendation for upfront P2Y12 inhibitor therapy for ACS patients who do not have STEMI. We’ve generally maintained that with the introduction of the exception that if you are in a health care system where there is a long wait to get to the cath lab – 5 ,6 or 7 days – then it’s reasonable to make an exception and give a P2Y12 inhibitor, but otherwise we’ve sustained the Class III recommendation,” he noted.
Also, for patients who have STEMI, there is a new Class IIb recommendation that upfront P2Y12 inhibitors may be considered.
“This is also rather a weak recommendation. There isn’t a strong rationale to give a P2Y12 inhibitor it in ST elevation either. It’s also reasonable to wait,” he added.
Don’t rush cardiac arrest patients to the cath lab
Another update in the guidelines involves the management of patients with cardiac arrest who have been resuscitated. Dr. Byrne explained that these patients would all receive an immediate ECG, and if it is found that they have ST elevation, they would be sent immediately to the cath lab. But a series of randomized trials has suggested that for patients who don’t have ST elevation, it is not necessary to rush these patients to the cath lab.
“We’ve given a Class III recommendation for this, saying it may be better to stabilize the patients first in the ICU. This is in recognition that a large proportion of these patients turn out not to have an MI. They have had a cardiac arrest for another reason,” Dr. Byrne noted. “Moving them to the cath lab when they are still unstable could be harming these patients rather than helping them.”
Revascularization for multivessel disease
Dr. Byrne notes that revascularization remains a critical element in the care for patients with STEMI, and there is a new recommendation in this area for patients with multivessel disease.
“Up to half of patients presenting with STEMI have multivessel disease, and we now have five randomized trials to say that these patients should have complete revascularization rather than just the culprit vessel. There is a new Class I recommendation for this,” he said.
However, the optimal timing of revascularization (immediate vs. staged) has still not been investigated in adequately sized randomized trials, and no recommendation has been made on this, the task force notes.
Dr. Byrne commented: “If you want to do everything in one go, that’s fine, but it’s also okay to do the culprit lesion first and then the other vessels at a later date within 45 days. This might depend on individual circumstances. For example, if there are complex lesions or the vessels are heavily calcified, then it may be best to get the culprit lesion fixed first and let the patient recover, then bring them back in for the rest.”
He pointed out that the results of the MULTISTARS trial, which were not available when the task force was formulating the guidelines, were reported at the ESC Congress and confirmed their recommendation.
DAPT after PCI
On the duration of dual antiplatelet therapy (DAPT) after PCI, the new guidelines have largely retained prior recommendations for a default strategy of 12 months for the combination of aspirin and a P2Y12 inhibitor.
“This was the subject of some discussion, as there have been several trials now looking at shorter durations of DAPT and deescalating after a few months to just one of these treatments. And while there is a rationale to do this, we think it’s best to be kept as an alternative strategy rather than the default strategy,” Dr. Byrne said.
He explained that the trials of DAPT deescalation tended to enroll lower-risk patients, which reduced the generalizability of the results.
Most of the trials only randomly assigned patients to shorter durations of DAPT when they were event-free for some period, she said.
“This is a dynamic decision-making process and reflects the real world to some extent. We think it is best to recommend the standard aspirin and a P2Y12 inhibitor for the 12-month duration, but at 3 months, if the patient is doing well but you may be worried about bleeding risk, then you could decide to deescalate to single antiplatelet therapy,” she noted. “So, there is Class IIa recommendation that this can be considered, but it is not recommended as the default position.”
Polypill for secondary prevention
Another innovation in the new guidelines is a new Class IIa recommendation for prescription of a polypill containing secondary prevention medications for patients on discharge from hospital.
This recommendation follows a trial that showed that the use of such a polypill helps patients be more adherent to the therapies prescribed.
Byrne explains that such a polypill may contain aspirin, an ACE inhibitor, and a statin. Several varieties are available in most European countries, but they are not widely used.
On secondary prevention, he stressed, “Prevention of the next heart attack starts before the patient leaves hospital. It is important to make sure the patient has the right medication on board, including a high-dose, high-intensity statin, and has been referred to a cardiac rehabilitation program. These are largely maintained recommendations from previous guidelines, but they are very important.”
A version of this article appeared on Medscape.com.
AT ESC CONGRESS 2023