User login
Efficacy, Diagnoses, Frequency Play Parts in Coverage Limitations
Under Section 1862(a)(1)(A) of the Social Security Act, the Medicare program may only pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g. colorectal cancer screening).1 Coverage limitations include:2
- Proven clinical efficacy. For example, Medicare deems acupuncture “experimental/investigational” in the diagnosis or treatment of illness or injury;
- Diagnoses. As an example, vitamin B-12 injections are covered, but only for such diagnoses as pernicious anemia and dementias secondary to vitamin B-12 deficiency; and
- Frequency/utilization parameters. For example, a screening colonoscopy (G0105) can be paid once every 24 months for beneficiaries who are at high risk for colorectal cancer; otherwise the service is limited to once every 10 years.
Beyond these factors, individual consideration might be granted. Supportive and unambiguous documentation (medical records, clinical studies, etc.) must be submitted when the clinical circumstances do not appear to support the medical necessity for the service.
Diagnoses Selection
Select the code that best represents the primary reason for the service or procedure on a given date. In the absence of a definitive diagnosis, the code may correspond to a sign or symptom. Physicians never should report a code that represents a probable, suspected, or “rule out” condition. Although facility billing might consider these unconfirmed circumstances (when necessary), physician billing prohibits this practice.
Reporting services for hospitalized patients is challenging when multiple services for the same patient are provided on the same date by the same or different physician, also known as concurrent care. Each physician manages a particular aspect while still considering the patient’s overall condition; each physician should report the corresponding diagnosis for that management. If billed correctly, each physician will have a different primary diagnosis code to justify their involvement, increasing their opportunity for payment.3
The non-primary diagnoses might also be listed on the claim if appropriately addressed in the documentation (i.e. “non-primary” conditions’ indirect role in the focused management of the primary condition). For example, a hospitalist, pulmonologist, and nephrologist manage a patient’s uncontrolled diabetes (250.02), COPD exacerbation (491.21), and CRI (585.9), respectively. Each may report subsequent hospital care (99231-99233) for medically necessary concurrent care:
- Hospitalist: 250.02, 491.21, 585.9;
- Pulmonologist: 491.21, 250.02, 585.9; and
- Nephrologist: 585.9, 492.21, 250.02.
Coverage Determinations
Code comparisons can be made after diagnosis code selection. Coverage determinations identify specific conditions (i.e. ICD-9-CM codes) for which services are considered medically necessary. They also outline the frequency interval at which services can be performed, when applicable.
For example, vascular studies (e.g. CPT 93971) are indicated for the preoperative examination (ICD-9-CM V72.83) of potential harvest vein grafts prior to bypass surgery.4 This is a covered service only when the results of the study are necessary to locate suitable graft vessels. The need for bypass surgery must be determined prior to performance of the test. V72.83 is “covered” only when reported for a unilateral study, not a bilateral study (CPT 93970). Frequency parameters allow for only one preoperative scan.4
Coverage determination can occur on two levels: national and local. The Centers for Medicare & Medicaid Services (CMS) develops national coverage determinations (NCDs) through an evidence-based process, with opportunities for public participation.5 All Medicare administrative contractors must abide by NCDs without imposing further limitations or guidelines. As example, the NCD “Consultations With a Beneficiary’s Family and Associates” permits a physician to provide counseling to family members. Family counseling services are covered only when the primary purpose of such counseling is the treatment of the patient’s condition.6
Non-Medicare payors do not have to follow federal guidelines unless the member participates in a Medicare managed-care plan.
In the absence of a national coverage policy, an item or service may be covered at the discretion of the Medicare contractors based on a local coverage determination (LCD).5 LCDs vary by state, creating an inconsistent approach to medical coverage. The vascular study guidelines listed above do not apply to all contractors. For example, Trailblazer Health Enterprises’ policy does not reference preoperative exams being limited to unilateral studies.7 (A listing of Medicare Contractor LCDs can be found at www.cms.hhs.gov/DeterminationProcess/04_LCDs.asp.)
Other Considerations
Investigate “medical necessity” denials. Do not take them at face value. Billing personnel often assume that the physician reported an incorrect diagnosis code. Consider the service when trying to formulate a response to the denial. Procedures (surgical or diagnostic services) may be denied for an invalid diagnosis. After reviewing the documentation to ensure that it supports the diagnosis, the claim may be resubmitted with a corrected diagnosis code, when applicable. Denials for frequency limitations can only be appealed with documentation that explicitly identifies the need for the service beyond the contractor-stated parameters.
If the “medical necessity” denial involves a covered evaluation and management (E/M) visit, it is less likely to be diagnosis-related. More likely, when dealing with Medicare contractors, the denial is the result of a failed response to a prepayment request for documentation. Medicare typically issues a request to review documentation prior to payment for the following inpatient E/M services: 99223, 99233, 99239, and 99292.
If the documentation is not provided to the Medicare prepayment review department within the designated time frame, the claim is automatically denied with a citation of “not deemed a medical necessity.” Acknowledge this remittance remark and do not assume that the physician assigned an incorrect diagnosis code. Although this is a possibility, it is more likely due to the failed request response. Appealing these claims requires submission of documentation to the Medicare appeals department. Reimbursement is provided once supportive documentation is received.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Social Security Administration. Exclusions from coverage and Medicare as a secondary payer. Social Security Administration website. Available at: http://www.ssa.gov/OP_Home/ssact/title18/1862.htm. Accessed March 1, 2012.
- Highmark Medicare Services. A/B Reference Manual: Chapter 6, Medical Coverage, Medical Necessity, and Medical Policy. Highmark Medicare Services website. Available at: http://www.highmarkmedicareservices.com/refman/chapter-6.html. Accessed March 1, 2012.
- Pohlig C. Daily care conundrums. The Hospitalist. 2008;12(12):18.
- Highmark Medicare Services. LCD L27506: Non-Invasive Peripheral Venous Studies. Highmark Medicare Services website. Available at: http://www.highmarkmedicareservices.com/policy/mac-ab/l27506-r10.html. Accessed March 1, 2012.
- Centers for Medicare & Medicaid Services. Medicare Coverage Determination Process: Overview. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/DeterminationProcess/01_Overview.asp#TopOfPage. Accessed March 1, 2012.
- Centers for Medicare & Medicaid Services. Medicare National Coverage Determination Manual: Chapter 1, Part 1, Section 70.1. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/ncd103c1_Part1.pdf. Accessed March 1, 2012.
- Trailblazer Health Enterprises. LCD 2866: Non-Invasive Venous Studies. Trailblazer Health Enterprises website. Available at: http://www.trailblazerhealth.com/Tools/LCDs.aspx?ID=2866. Accessed March 1, 2012.
Under Section 1862(a)(1)(A) of the Social Security Act, the Medicare program may only pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g. colorectal cancer screening).1 Coverage limitations include:2
- Proven clinical efficacy. For example, Medicare deems acupuncture “experimental/investigational” in the diagnosis or treatment of illness or injury;
- Diagnoses. As an example, vitamin B-12 injections are covered, but only for such diagnoses as pernicious anemia and dementias secondary to vitamin B-12 deficiency; and
- Frequency/utilization parameters. For example, a screening colonoscopy (G0105) can be paid once every 24 months for beneficiaries who are at high risk for colorectal cancer; otherwise the service is limited to once every 10 years.
Beyond these factors, individual consideration might be granted. Supportive and unambiguous documentation (medical records, clinical studies, etc.) must be submitted when the clinical circumstances do not appear to support the medical necessity for the service.
Diagnoses Selection
Select the code that best represents the primary reason for the service or procedure on a given date. In the absence of a definitive diagnosis, the code may correspond to a sign or symptom. Physicians never should report a code that represents a probable, suspected, or “rule out” condition. Although facility billing might consider these unconfirmed circumstances (when necessary), physician billing prohibits this practice.
Reporting services for hospitalized patients is challenging when multiple services for the same patient are provided on the same date by the same or different physician, also known as concurrent care. Each physician manages a particular aspect while still considering the patient’s overall condition; each physician should report the corresponding diagnosis for that management. If billed correctly, each physician will have a different primary diagnosis code to justify their involvement, increasing their opportunity for payment.3
The non-primary diagnoses might also be listed on the claim if appropriately addressed in the documentation (i.e. “non-primary” conditions’ indirect role in the focused management of the primary condition). For example, a hospitalist, pulmonologist, and nephrologist manage a patient’s uncontrolled diabetes (250.02), COPD exacerbation (491.21), and CRI (585.9), respectively. Each may report subsequent hospital care (99231-99233) for medically necessary concurrent care:
- Hospitalist: 250.02, 491.21, 585.9;
- Pulmonologist: 491.21, 250.02, 585.9; and
- Nephrologist: 585.9, 492.21, 250.02.
Coverage Determinations
Code comparisons can be made after diagnosis code selection. Coverage determinations identify specific conditions (i.e. ICD-9-CM codes) for which services are considered medically necessary. They also outline the frequency interval at which services can be performed, when applicable.
For example, vascular studies (e.g. CPT 93971) are indicated for the preoperative examination (ICD-9-CM V72.83) of potential harvest vein grafts prior to bypass surgery.4 This is a covered service only when the results of the study are necessary to locate suitable graft vessels. The need for bypass surgery must be determined prior to performance of the test. V72.83 is “covered” only when reported for a unilateral study, not a bilateral study (CPT 93970). Frequency parameters allow for only one preoperative scan.4
Coverage determination can occur on two levels: national and local. The Centers for Medicare & Medicaid Services (CMS) develops national coverage determinations (NCDs) through an evidence-based process, with opportunities for public participation.5 All Medicare administrative contractors must abide by NCDs without imposing further limitations or guidelines. As example, the NCD “Consultations With a Beneficiary’s Family and Associates” permits a physician to provide counseling to family members. Family counseling services are covered only when the primary purpose of such counseling is the treatment of the patient’s condition.6
Non-Medicare payors do not have to follow federal guidelines unless the member participates in a Medicare managed-care plan.
In the absence of a national coverage policy, an item or service may be covered at the discretion of the Medicare contractors based on a local coverage determination (LCD).5 LCDs vary by state, creating an inconsistent approach to medical coverage. The vascular study guidelines listed above do not apply to all contractors. For example, Trailblazer Health Enterprises’ policy does not reference preoperative exams being limited to unilateral studies.7 (A listing of Medicare Contractor LCDs can be found at www.cms.hhs.gov/DeterminationProcess/04_LCDs.asp.)
Other Considerations
Investigate “medical necessity” denials. Do not take them at face value. Billing personnel often assume that the physician reported an incorrect diagnosis code. Consider the service when trying to formulate a response to the denial. Procedures (surgical or diagnostic services) may be denied for an invalid diagnosis. After reviewing the documentation to ensure that it supports the diagnosis, the claim may be resubmitted with a corrected diagnosis code, when applicable. Denials for frequency limitations can only be appealed with documentation that explicitly identifies the need for the service beyond the contractor-stated parameters.
If the “medical necessity” denial involves a covered evaluation and management (E/M) visit, it is less likely to be diagnosis-related. More likely, when dealing with Medicare contractors, the denial is the result of a failed response to a prepayment request for documentation. Medicare typically issues a request to review documentation prior to payment for the following inpatient E/M services: 99223, 99233, 99239, and 99292.
If the documentation is not provided to the Medicare prepayment review department within the designated time frame, the claim is automatically denied with a citation of “not deemed a medical necessity.” Acknowledge this remittance remark and do not assume that the physician assigned an incorrect diagnosis code. Although this is a possibility, it is more likely due to the failed request response. Appealing these claims requires submission of documentation to the Medicare appeals department. Reimbursement is provided once supportive documentation is received.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Social Security Administration. Exclusions from coverage and Medicare as a secondary payer. Social Security Administration website. Available at: http://www.ssa.gov/OP_Home/ssact/title18/1862.htm. Accessed March 1, 2012.
- Highmark Medicare Services. A/B Reference Manual: Chapter 6, Medical Coverage, Medical Necessity, and Medical Policy. Highmark Medicare Services website. Available at: http://www.highmarkmedicareservices.com/refman/chapter-6.html. Accessed March 1, 2012.
- Pohlig C. Daily care conundrums. The Hospitalist. 2008;12(12):18.
- Highmark Medicare Services. LCD L27506: Non-Invasive Peripheral Venous Studies. Highmark Medicare Services website. Available at: http://www.highmarkmedicareservices.com/policy/mac-ab/l27506-r10.html. Accessed March 1, 2012.
- Centers for Medicare & Medicaid Services. Medicare Coverage Determination Process: Overview. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/DeterminationProcess/01_Overview.asp#TopOfPage. Accessed March 1, 2012.
- Centers for Medicare & Medicaid Services. Medicare National Coverage Determination Manual: Chapter 1, Part 1, Section 70.1. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/ncd103c1_Part1.pdf. Accessed March 1, 2012.
- Trailblazer Health Enterprises. LCD 2866: Non-Invasive Venous Studies. Trailblazer Health Enterprises website. Available at: http://www.trailblazerhealth.com/Tools/LCDs.aspx?ID=2866. Accessed March 1, 2012.
Under Section 1862(a)(1)(A) of the Social Security Act, the Medicare program may only pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g. colorectal cancer screening).1 Coverage limitations include:2
- Proven clinical efficacy. For example, Medicare deems acupuncture “experimental/investigational” in the diagnosis or treatment of illness or injury;
- Diagnoses. As an example, vitamin B-12 injections are covered, but only for such diagnoses as pernicious anemia and dementias secondary to vitamin B-12 deficiency; and
- Frequency/utilization parameters. For example, a screening colonoscopy (G0105) can be paid once every 24 months for beneficiaries who are at high risk for colorectal cancer; otherwise the service is limited to once every 10 years.
Beyond these factors, individual consideration might be granted. Supportive and unambiguous documentation (medical records, clinical studies, etc.) must be submitted when the clinical circumstances do not appear to support the medical necessity for the service.
Diagnoses Selection
Select the code that best represents the primary reason for the service or procedure on a given date. In the absence of a definitive diagnosis, the code may correspond to a sign or symptom. Physicians never should report a code that represents a probable, suspected, or “rule out” condition. Although facility billing might consider these unconfirmed circumstances (when necessary), physician billing prohibits this practice.
Reporting services for hospitalized patients is challenging when multiple services for the same patient are provided on the same date by the same or different physician, also known as concurrent care. Each physician manages a particular aspect while still considering the patient’s overall condition; each physician should report the corresponding diagnosis for that management. If billed correctly, each physician will have a different primary diagnosis code to justify their involvement, increasing their opportunity for payment.3
The non-primary diagnoses might also be listed on the claim if appropriately addressed in the documentation (i.e. “non-primary” conditions’ indirect role in the focused management of the primary condition). For example, a hospitalist, pulmonologist, and nephrologist manage a patient’s uncontrolled diabetes (250.02), COPD exacerbation (491.21), and CRI (585.9), respectively. Each may report subsequent hospital care (99231-99233) for medically necessary concurrent care:
- Hospitalist: 250.02, 491.21, 585.9;
- Pulmonologist: 491.21, 250.02, 585.9; and
- Nephrologist: 585.9, 492.21, 250.02.
Coverage Determinations
Code comparisons can be made after diagnosis code selection. Coverage determinations identify specific conditions (i.e. ICD-9-CM codes) for which services are considered medically necessary. They also outline the frequency interval at which services can be performed, when applicable.
For example, vascular studies (e.g. CPT 93971) are indicated for the preoperative examination (ICD-9-CM V72.83) of potential harvest vein grafts prior to bypass surgery.4 This is a covered service only when the results of the study are necessary to locate suitable graft vessels. The need for bypass surgery must be determined prior to performance of the test. V72.83 is “covered” only when reported for a unilateral study, not a bilateral study (CPT 93970). Frequency parameters allow for only one preoperative scan.4
Coverage determination can occur on two levels: national and local. The Centers for Medicare & Medicaid Services (CMS) develops national coverage determinations (NCDs) through an evidence-based process, with opportunities for public participation.5 All Medicare administrative contractors must abide by NCDs without imposing further limitations or guidelines. As example, the NCD “Consultations With a Beneficiary’s Family and Associates” permits a physician to provide counseling to family members. Family counseling services are covered only when the primary purpose of such counseling is the treatment of the patient’s condition.6
Non-Medicare payors do not have to follow federal guidelines unless the member participates in a Medicare managed-care plan.
In the absence of a national coverage policy, an item or service may be covered at the discretion of the Medicare contractors based on a local coverage determination (LCD).5 LCDs vary by state, creating an inconsistent approach to medical coverage. The vascular study guidelines listed above do not apply to all contractors. For example, Trailblazer Health Enterprises’ policy does not reference preoperative exams being limited to unilateral studies.7 (A listing of Medicare Contractor LCDs can be found at www.cms.hhs.gov/DeterminationProcess/04_LCDs.asp.)
Other Considerations
Investigate “medical necessity” denials. Do not take them at face value. Billing personnel often assume that the physician reported an incorrect diagnosis code. Consider the service when trying to formulate a response to the denial. Procedures (surgical or diagnostic services) may be denied for an invalid diagnosis. After reviewing the documentation to ensure that it supports the diagnosis, the claim may be resubmitted with a corrected diagnosis code, when applicable. Denials for frequency limitations can only be appealed with documentation that explicitly identifies the need for the service beyond the contractor-stated parameters.
If the “medical necessity” denial involves a covered evaluation and management (E/M) visit, it is less likely to be diagnosis-related. More likely, when dealing with Medicare contractors, the denial is the result of a failed response to a prepayment request for documentation. Medicare typically issues a request to review documentation prior to payment for the following inpatient E/M services: 99223, 99233, 99239, and 99292.
If the documentation is not provided to the Medicare prepayment review department within the designated time frame, the claim is automatically denied with a citation of “not deemed a medical necessity.” Acknowledge this remittance remark and do not assume that the physician assigned an incorrect diagnosis code. Although this is a possibility, it is more likely due to the failed request response. Appealing these claims requires submission of documentation to the Medicare appeals department. Reimbursement is provided once supportive documentation is received.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Social Security Administration. Exclusions from coverage and Medicare as a secondary payer. Social Security Administration website. Available at: http://www.ssa.gov/OP_Home/ssact/title18/1862.htm. Accessed March 1, 2012.
- Highmark Medicare Services. A/B Reference Manual: Chapter 6, Medical Coverage, Medical Necessity, and Medical Policy. Highmark Medicare Services website. Available at: http://www.highmarkmedicareservices.com/refman/chapter-6.html. Accessed March 1, 2012.
- Pohlig C. Daily care conundrums. The Hospitalist. 2008;12(12):18.
- Highmark Medicare Services. LCD L27506: Non-Invasive Peripheral Venous Studies. Highmark Medicare Services website. Available at: http://www.highmarkmedicareservices.com/policy/mac-ab/l27506-r10.html. Accessed March 1, 2012.
- Centers for Medicare & Medicaid Services. Medicare Coverage Determination Process: Overview. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/DeterminationProcess/01_Overview.asp#TopOfPage. Accessed March 1, 2012.
- Centers for Medicare & Medicaid Services. Medicare National Coverage Determination Manual: Chapter 1, Part 1, Section 70.1. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/ncd103c1_Part1.pdf. Accessed March 1, 2012.
- Trailblazer Health Enterprises. LCD 2866: Non-Invasive Venous Studies. Trailblazer Health Enterprises website. Available at: http://www.trailblazerhealth.com/Tools/LCDs.aspx?ID=2866. Accessed March 1, 2012.
Communication Vital to End-of-Life Care
A year ago in March, I looked my father in the eyes for the last time as he mouthed the words "help me" from his ICU bed. But despite being surrounded by teams of medical personnel and the latest healthcare technology, I felt utterly powerless to make a clear decision—and unclear to whom to turn for sound advice.
After 30 days of care in a well-known teaching hospital in the Northeast, my father was about to succumb to Stage 4 lung cancer, a tumor invading his spine. Moments before his plea, the ICU team had conducted a breathing test that apparently went awry—beginning the trial while my mother and I were downstairs receiving the latest round of conflicting information from a pair of doctors debating his outlook for discharge, physical rehabilitation, and hospice care. They casually informed us that a breathing test was about to occur; we rushed back to my father's side to learn the unfortunate outcome.
Prior to the episode that led to his being moved to the ICU, my father had been residing in a room directly across from a small hospitalist oncology office. What ensued was dizzying to behold: an endless parade of consultations; a narrowly averted million-dollar-plus spinal surgery in the wee hours; a too-zealous resident's further injuring of my father's right leg, which had already been compromised by a tumor degrading the femur.
My mother, my wife, and I struggled to maintain Dad's always-indomitable spirit while parsing the barrage of input regarding his potential for quality of life outside the hospital. We sat in numerous meetings, often with a pair of doctors espousing diametrically opposed outlooks. We tried to keep track of whom we were speaking with and who was in charge at any given moment; the lists we kept looked like the roster of a sports team, amply covered in scribbled-out names, phone numbers—and question marks.
It was only after my father tried feebly to speak his last words to me that the doctor who'd appeared to be most in charge pulled me aside at the door of the ICU. My mother and I hemmed and hawed in trying to decide whether to accede to another round of heroic measures. I was surprised by the somewhat terse tone of voice this senior physician used in dissuading us from allowing further life-extending efforts. I would have welcomed such honesty wholeheartedly far earlier in the process.
One of the value propositions hospitalists tout to their employers and patients is their expertise in coordinating care and facilitating communication among caregivers. Of course, there are nearly as many methods for doing so as there are hospitalist teams.
As the medical process grows more complex and specialized, with more "stakeholders" weighing in on the conversation, the hospitalist's role in taking charge of and energetically managing the flow of information for the benefit of beleaguered kin is more vital than ever. I can't speak for all loved ones who must witness the passage of a parent, a child, or a spouse, but for me, a hospitalist's firm hand would have made a world of difference in how we navigated this inevitable event.
Geoff Giordano was editor of The Hospitalist from 2007 to 2008. His father, Thomas, a lifelong journalist, wrote several articles for the magazine during that period.
A year ago in March, I looked my father in the eyes for the last time as he mouthed the words "help me" from his ICU bed. But despite being surrounded by teams of medical personnel and the latest healthcare technology, I felt utterly powerless to make a clear decision—and unclear to whom to turn for sound advice.
After 30 days of care in a well-known teaching hospital in the Northeast, my father was about to succumb to Stage 4 lung cancer, a tumor invading his spine. Moments before his plea, the ICU team had conducted a breathing test that apparently went awry—beginning the trial while my mother and I were downstairs receiving the latest round of conflicting information from a pair of doctors debating his outlook for discharge, physical rehabilitation, and hospice care. They casually informed us that a breathing test was about to occur; we rushed back to my father's side to learn the unfortunate outcome.
Prior to the episode that led to his being moved to the ICU, my father had been residing in a room directly across from a small hospitalist oncology office. What ensued was dizzying to behold: an endless parade of consultations; a narrowly averted million-dollar-plus spinal surgery in the wee hours; a too-zealous resident's further injuring of my father's right leg, which had already been compromised by a tumor degrading the femur.
My mother, my wife, and I struggled to maintain Dad's always-indomitable spirit while parsing the barrage of input regarding his potential for quality of life outside the hospital. We sat in numerous meetings, often with a pair of doctors espousing diametrically opposed outlooks. We tried to keep track of whom we were speaking with and who was in charge at any given moment; the lists we kept looked like the roster of a sports team, amply covered in scribbled-out names, phone numbers—and question marks.
It was only after my father tried feebly to speak his last words to me that the doctor who'd appeared to be most in charge pulled me aside at the door of the ICU. My mother and I hemmed and hawed in trying to decide whether to accede to another round of heroic measures. I was surprised by the somewhat terse tone of voice this senior physician used in dissuading us from allowing further life-extending efforts. I would have welcomed such honesty wholeheartedly far earlier in the process.
One of the value propositions hospitalists tout to their employers and patients is their expertise in coordinating care and facilitating communication among caregivers. Of course, there are nearly as many methods for doing so as there are hospitalist teams.
As the medical process grows more complex and specialized, with more "stakeholders" weighing in on the conversation, the hospitalist's role in taking charge of and energetically managing the flow of information for the benefit of beleaguered kin is more vital than ever. I can't speak for all loved ones who must witness the passage of a parent, a child, or a spouse, but for me, a hospitalist's firm hand would have made a world of difference in how we navigated this inevitable event.
Geoff Giordano was editor of The Hospitalist from 2007 to 2008. His father, Thomas, a lifelong journalist, wrote several articles for the magazine during that period.
A year ago in March, I looked my father in the eyes for the last time as he mouthed the words "help me" from his ICU bed. But despite being surrounded by teams of medical personnel and the latest healthcare technology, I felt utterly powerless to make a clear decision—and unclear to whom to turn for sound advice.
After 30 days of care in a well-known teaching hospital in the Northeast, my father was about to succumb to Stage 4 lung cancer, a tumor invading his spine. Moments before his plea, the ICU team had conducted a breathing test that apparently went awry—beginning the trial while my mother and I were downstairs receiving the latest round of conflicting information from a pair of doctors debating his outlook for discharge, physical rehabilitation, and hospice care. They casually informed us that a breathing test was about to occur; we rushed back to my father's side to learn the unfortunate outcome.
Prior to the episode that led to his being moved to the ICU, my father had been residing in a room directly across from a small hospitalist oncology office. What ensued was dizzying to behold: an endless parade of consultations; a narrowly averted million-dollar-plus spinal surgery in the wee hours; a too-zealous resident's further injuring of my father's right leg, which had already been compromised by a tumor degrading the femur.
My mother, my wife, and I struggled to maintain Dad's always-indomitable spirit while parsing the barrage of input regarding his potential for quality of life outside the hospital. We sat in numerous meetings, often with a pair of doctors espousing diametrically opposed outlooks. We tried to keep track of whom we were speaking with and who was in charge at any given moment; the lists we kept looked like the roster of a sports team, amply covered in scribbled-out names, phone numbers—and question marks.
It was only after my father tried feebly to speak his last words to me that the doctor who'd appeared to be most in charge pulled me aside at the door of the ICU. My mother and I hemmed and hawed in trying to decide whether to accede to another round of heroic measures. I was surprised by the somewhat terse tone of voice this senior physician used in dissuading us from allowing further life-extending efforts. I would have welcomed such honesty wholeheartedly far earlier in the process.
One of the value propositions hospitalists tout to their employers and patients is their expertise in coordinating care and facilitating communication among caregivers. Of course, there are nearly as many methods for doing so as there are hospitalist teams.
As the medical process grows more complex and specialized, with more "stakeholders" weighing in on the conversation, the hospitalist's role in taking charge of and energetically managing the flow of information for the benefit of beleaguered kin is more vital than ever. I can't speak for all loved ones who must witness the passage of a parent, a child, or a spouse, but for me, a hospitalist's firm hand would have made a world of difference in how we navigated this inevitable event.
Geoff Giordano was editor of The Hospitalist from 2007 to 2008. His father, Thomas, a lifelong journalist, wrote several articles for the magazine during that period.
Neonatal Team Absent at Difficult Birth
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Neonatal Team Absent at Difficult Birth
A Virginia woman was referred for an ultrasound by her obstetrician at 20 weeks’ gestation due to a suspicion of omphalocele or gastroschisis. The imaging revealed gastroschisis with a moderate amount of exposed bowel.
The mother presented to the hospital in labor at 38 weeks’ gestation. From the beginning, the electronic monitor tracing of the fetal heart rate exhibited a sinusoidal pattern. At the shift nurse’s request, the fetal monitor strip was reviewed with a physician who found it to be “almost” sinusoidal. When a second nurse started her shift, the fetal heart rate was 60 to 70 beats/min. A physician artificially ruptured the amniotic membranes. No personnel from the pediatric service, nursery, or neonatal ICU had yet been contacted.
Upon rupture of the membranes, thick meconium was found in the amniotic fluid. A fetal scalp electrode was placed, showing a fetal heart rate between 30 and 100 beats/min. A second fetal scalp electrode was placed, and it showed the same fetal heart rate range.
A baby boy delivered precipitously in critical condition, with Apgar scores of 1 at one minute, 2 at five minutes, and 4 at 10 minutes. The newborn was depressed, flaccid, blue, and unresponsive, with thick meconium below the vocal cords, obstructing his breathing at the time of birth.
The neonatal ICU team was called after delivery. When they arrived, the infant was making no respiratory effort and had a heart rate of 60 beats/min. He was suctioned, but the airway box was blocked by meconium. The baby was intubated at four minutes after birth, but ventilation was initially unsuccessful; he was extubated and reintubated at five minutes postdelivery.
Results of an arterial blood sample were consistent with severe metabolic acidosis from hypoxia in utero and during resuscitation. Fetal cooling, which might have ameliorated the infant’s ongoing brain injury, was ruled out by the presence of gastroschisis.
The child experienced hypoxic ischemic encephalopathy from intrapartum asphyxia, which resulted in microcephaly. He requires a feeding tube due to an inability to swallow and will need lifelong care.
OUTCOME
Two suits were filed, one on the infant’s behalf and one on the mother’s. The infant’s case was settled for $1.8 million, and the mother’s case for $1 million.
COMMENT
This fetus was clearly in distress during delivery, and based on the confirmed presence of gastroschisis, the neonatal team should have been at the bedside for delivery. Even assuming that the strip was read as a pseudosinusoidal pattern, the fetus was frankly bradycardic, and the certainty of caring for an infant with exposed bowel contents required the neonatal team’s presence.
Gastroschisis refers to the failure of the developing fetus’s abdominal wall to close, resulting in protrusion of a portion of fetal intestine outside the abdominal cavity. It is relatively rare, with an incidence of 1.4 to 2.5 per 10,000 live births. A sinusoidal fetal heart rate pattern is characterized by a regular, smooth, undulating form typical of a sine wave. It is rare and ominous, and is associated with high fetal morbidity and mortality. By contrast, a pseudosinusoidal pattern is a benign form showing long-term variability. A true sinusoidal pattern lacks the beat-to-beat variability of the more jagged-appearing pseudosinusoidal pattern.
In this case, problems at delivery were foreseeable. A jury would have little trouble understanding gastroschisis and would find it alarming. Given the fetal bradycardia and monitor pattern, most jurors would conclude that the standard of care was breached. —DML
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Neonatal Team Absent at Difficult Birth
A Virginia woman was referred for an ultrasound by her obstetrician at 20 weeks’ gestation due to a suspicion of omphalocele or gastroschisis. The imaging revealed gastroschisis with a moderate amount of exposed bowel.
The mother presented to the hospital in labor at 38 weeks’ gestation. From the beginning, the electronic monitor tracing of the fetal heart rate exhibited a sinusoidal pattern. At the shift nurse’s request, the fetal monitor strip was reviewed with a physician who found it to be “almost” sinusoidal. When a second nurse started her shift, the fetal heart rate was 60 to 70 beats/min. A physician artificially ruptured the amniotic membranes. No personnel from the pediatric service, nursery, or neonatal ICU had yet been contacted.
Upon rupture of the membranes, thick meconium was found in the amniotic fluid. A fetal scalp electrode was placed, showing a fetal heart rate between 30 and 100 beats/min. A second fetal scalp electrode was placed, and it showed the same fetal heart rate range.
A baby boy delivered precipitously in critical condition, with Apgar scores of 1 at one minute, 2 at five minutes, and 4 at 10 minutes. The newborn was depressed, flaccid, blue, and unresponsive, with thick meconium below the vocal cords, obstructing his breathing at the time of birth.
The neonatal ICU team was called after delivery. When they arrived, the infant was making no respiratory effort and had a heart rate of 60 beats/min. He was suctioned, but the airway box was blocked by meconium. The baby was intubated at four minutes after birth, but ventilation was initially unsuccessful; he was extubated and reintubated at five minutes postdelivery.
Results of an arterial blood sample were consistent with severe metabolic acidosis from hypoxia in utero and during resuscitation. Fetal cooling, which might have ameliorated the infant’s ongoing brain injury, was ruled out by the presence of gastroschisis.
The child experienced hypoxic ischemic encephalopathy from intrapartum asphyxia, which resulted in microcephaly. He requires a feeding tube due to an inability to swallow and will need lifelong care.
OUTCOME
Two suits were filed, one on the infant’s behalf and one on the mother’s. The infant’s case was settled for $1.8 million, and the mother’s case for $1 million.
COMMENT
This fetus was clearly in distress during delivery, and based on the confirmed presence of gastroschisis, the neonatal team should have been at the bedside for delivery. Even assuming that the strip was read as a pseudosinusoidal pattern, the fetus was frankly bradycardic, and the certainty of caring for an infant with exposed bowel contents required the neonatal team’s presence.
Gastroschisis refers to the failure of the developing fetus’s abdominal wall to close, resulting in protrusion of a portion of fetal intestine outside the abdominal cavity. It is relatively rare, with an incidence of 1.4 to 2.5 per 10,000 live births. A sinusoidal fetal heart rate pattern is characterized by a regular, smooth, undulating form typical of a sine wave. It is rare and ominous, and is associated with high fetal morbidity and mortality. By contrast, a pseudosinusoidal pattern is a benign form showing long-term variability. A true sinusoidal pattern lacks the beat-to-beat variability of the more jagged-appearing pseudosinusoidal pattern.
In this case, problems at delivery were foreseeable. A jury would have little trouble understanding gastroschisis and would find it alarming. Given the fetal bradycardia and monitor pattern, most jurors would conclude that the standard of care was breached. —DML
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Neonatal Team Absent at Difficult Birth
A Virginia woman was referred for an ultrasound by her obstetrician at 20 weeks’ gestation due to a suspicion of omphalocele or gastroschisis. The imaging revealed gastroschisis with a moderate amount of exposed bowel.
The mother presented to the hospital in labor at 38 weeks’ gestation. From the beginning, the electronic monitor tracing of the fetal heart rate exhibited a sinusoidal pattern. At the shift nurse’s request, the fetal monitor strip was reviewed with a physician who found it to be “almost” sinusoidal. When a second nurse started her shift, the fetal heart rate was 60 to 70 beats/min. A physician artificially ruptured the amniotic membranes. No personnel from the pediatric service, nursery, or neonatal ICU had yet been contacted.
Upon rupture of the membranes, thick meconium was found in the amniotic fluid. A fetal scalp electrode was placed, showing a fetal heart rate between 30 and 100 beats/min. A second fetal scalp electrode was placed, and it showed the same fetal heart rate range.
A baby boy delivered precipitously in critical condition, with Apgar scores of 1 at one minute, 2 at five minutes, and 4 at 10 minutes. The newborn was depressed, flaccid, blue, and unresponsive, with thick meconium below the vocal cords, obstructing his breathing at the time of birth.
The neonatal ICU team was called after delivery. When they arrived, the infant was making no respiratory effort and had a heart rate of 60 beats/min. He was suctioned, but the airway box was blocked by meconium. The baby was intubated at four minutes after birth, but ventilation was initially unsuccessful; he was extubated and reintubated at five minutes postdelivery.
Results of an arterial blood sample were consistent with severe metabolic acidosis from hypoxia in utero and during resuscitation. Fetal cooling, which might have ameliorated the infant’s ongoing brain injury, was ruled out by the presence of gastroschisis.
The child experienced hypoxic ischemic encephalopathy from intrapartum asphyxia, which resulted in microcephaly. He requires a feeding tube due to an inability to swallow and will need lifelong care.
OUTCOME
Two suits were filed, one on the infant’s behalf and one on the mother’s. The infant’s case was settled for $1.8 million, and the mother’s case for $1 million.
COMMENT
This fetus was clearly in distress during delivery, and based on the confirmed presence of gastroschisis, the neonatal team should have been at the bedside for delivery. Even assuming that the strip was read as a pseudosinusoidal pattern, the fetus was frankly bradycardic, and the certainty of caring for an infant with exposed bowel contents required the neonatal team’s presence.
Gastroschisis refers to the failure of the developing fetus’s abdominal wall to close, resulting in protrusion of a portion of fetal intestine outside the abdominal cavity. It is relatively rare, with an incidence of 1.4 to 2.5 per 10,000 live births. A sinusoidal fetal heart rate pattern is characterized by a regular, smooth, undulating form typical of a sine wave. It is rare and ominous, and is associated with high fetal morbidity and mortality. By contrast, a pseudosinusoidal pattern is a benign form showing long-term variability. A true sinusoidal pattern lacks the beat-to-beat variability of the more jagged-appearing pseudosinusoidal pattern.
In this case, problems at delivery were foreseeable. A jury would have little trouble understanding gastroschisis and would find it alarming. Given the fetal bradycardia and monitor pattern, most jurors would conclude that the standard of care was breached. —DML
Mother dies 10 h post-delivery … and more

AT 38 WEEKS’ GESTATION, a 20-year-old woman had preeclampsia and a borderline-low platelet count. She was admitted to a US Navy hospital for induction of labor.
When labor failed to progress after 53 hours, a cesarean delivery was performed. The patient suffered uncontrolled bleeding and developed HELLP syndrome (hemolysis, elevated liver enzymes, low platelet count). A platelet transfusion was needed, but the nearest supply was at a city hospital approximately 60 miles away. Because of bad weather, the patient could not be flown to the city. She died 10 hours after delivery.
ESTATE’S CLAIM A cesarean delivery should have been performed earlier. Lab results showing the severity of the mother’s condition at delivery were not read for 5 hours.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $2.1 million Missouri settlement was reached.
Did OB’s errors cause this child’s injuries?
A CHILD WAS BORN with a left brachial plexus injury and fractured left clavicle.
PATIENT’S CLAIM The ObGyn failed to diagnose shoulder dystocia, failed to perform appropriate maneuvers to free the entrapped anterior shoulder, and applied excessive lateral traction to deliver the child.
PHYSICIAN’S DEFENSE There was no shoulder dystocia. The child’s injuries were caused by the natural forces of labor.
VERDICT A $1,314,600 Iowa verdict was returned.
Sedation for surgery leads to brain damage
A 20-YEAR-OLD WOMAN with sickle-cell anemia (SCA) was sent to an ambulatory surgery center for surgical treatment of cervical dysplasia.
A certified nurse anesthetist (CRNA) sedated the patient at the surgery center. The patient went into cardiac arrest and was transferred to a hospital. She suffered a brain injury caused by oxygen deprivation. Her IQ dropped by 11 points; with the brain damage, she was unable to retain her driver’s license.
PATIENT’S CLAIM The procedure could have been performed safely in the doctor’s office under local anesthesia. The gynecologist had signed off on the anesthesia plan, although he knew of the risks of giving general anesthesia to someone with SCA. She was sent to the surgery center only because of the gynecologist’s desire to generate revenue.
DEFENDANTS’ DEFENSE The gynecologist blamed the CRNA, who, allegedly, allowed a kink to form in the IV anesthesia line. When the line cleared, sedative flooded into the patient, causing her heart to stop. The gynecologist admitted that general anesthesia was unnecessary; local anesthesia would have been safer. The CRNA argued that the surgery center was at fault; she had followed the center’s standard operating procedure. The surgery center denied negligence.
VERDICT An $851,000 South Carolina settlement was reached with the gynecologist, CRNA, and surgery center.
Pain from retained sponge, surgical ring
TWINS WERE BORN BY CESAREAN delivery to a 40-year-old woman. She developed abdominal pain and reported it to her ObGyn several times. Four months after delivery, the ObGyn found a retained sponge and surgical ring during exploratory laparotomy.
PATIENT’S CLAIM The ObGyn did not adequately inspect the operative area before closing. Although the patient reported abdominal pain immediately after delivery, her complaints were ignored for several months.
PHYSICIAN’S DEFENSE The nurses are responsible for any errors in the sponge count. The patient’s complaints were not brought to his attention until four months after delivery.
VERDICT The patient reached a confidential settlement with the delivery nurses, an assisting physician, and the hospital. A New York jury found the ObGyn 60% at fault; a $1.5 million verdict was returned. The patient agreed to a $550,000 posttrial settlement with the ObGyn’s insurer.
Patient falls from exam table during non-stress test
IN HER EIGHTH GESTATIONAL MONTH, a woman in her 30s underwent a non-stress test because of five prior miscarriages. She became ill just as the test was beginning, turned to her side to vomit, and fell off the examination table. She fractured her cervical spine.
An emergency cesarean delivery resulted in the birth of a healthy baby. The woman then underwent fusion surgery to repair the cervical fracture. She required physical therapy, and made a good recovery.
PATIENT’S CLAIM The examination table should have had side rails, which would have prevented the fall.
DEFENDANTS’ DEFENSE Side rails were not required on an examination table. This was an unforeseeable event that occurred while a nurse was setting up the procedure and reaching for a blood-pressure cuff.
VERDICT A Connecticut defense verdict was returned.
Sexually abused by nursing assistant: $67 million verdict
A 38-YEAR-OLD WOMAN UNDERWENT laparoscopic ovarian cyst removal. While hospitalized, a male nursing assistant sexually assaulted her by digital penetration of the vagina without wearing gloves. The employee was arrested for the assault, but allegedly fled the country after posting bail.
PATIENT’S CLAIM At least five similar incidents involving the same nursing assistant reportedly occurred in the hospital over a 16-month period. At trial, four patients and an employee testified that they had been similarly assaulted and had reported the incidents to hospital staff. The nursing assistant should have been removed from his position after the first reported incident, and a thorough investigation conducted. The patient suffered post-traumatic stress disorder because of her experience.
DEFENDANTS’ DEFENSE A proper investigation was made. Often, female patients are uncomfortable with male nurses. The hospital denied being notified of some incidents, and maintained it had suspended the male nursing assistant when it became aware of the incident under litigation.
VERDICT A $67,359,753 California verdict included $65 million in punitive damages against the hospital and its former corporate owner.
Salpingectomy results in death
TO INCREASE HER CHANCES of becoming pregnant using IVF, a woman in her 30s underwent adhesiolysis and salpingectomy. She was discharged the same day.
The next day, she complained of abdominal pain to her ObGyn. She died two days after surgery from septic shock due to a perforated bowel.
ESTATE’S CLAIM The ObGyn was negligent in discharging her, especially because the surgeon had identified a superficial injury to the bowel during surgery. She should have been examined the day after surgery when she first complained of abdominal pain.
PHYSICIANS’ DEFENSE The ObGyn acted appropriately in relying on the surgeon’s recommendation for discharge. He had contacted the patient twice after her initial call regarding abdominal pain, and was told both times that she was feeling better.
VERDICT A Virginia defense verdict was returned.
Disastrous D&C after miscarriage
A 29-YEAR-OLD WOMAN miscarried at 14 weeks’ gestation. An ObGyn recommended that she undergo dilation and curettage (D&C).
With the ObGyn in attendance, a resident sedated the patient and performed the D&C. When the resident perforated the uterus, the ObGyn took over, inserting ring forceps to remove the remains. The forceps went through the perforation and tore the top half of the rectum and a portion of bowel.
A rectal surgeon, called in to repair the injury, performed an ileostomy and created an ileostomy pouch. The ileo-stomy was later successfully reversed.
PATIENT’S CLAIM The woman was at risk of injury because her uterus was anteverted and she had under-gone a cesarean delivery; an experienced physician should have performed the procedure.
When the perforation first occurred, ultrasonography should have been used to identify the puncture and prevent in-jury to the rectum and bowel.
DEFENDANTS’ DEFENSE The patient gave informed consent. The injury is a known risk of the procedure.
VERDICT A $2.5 million Michigan verdict was returned against the ObGyn and hospital, but was reduced to $1.25 million under the statutory cap.
These cases were selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
AT 38 WEEKS’ GESTATION, a 20-year-old woman had preeclampsia and a borderline-low platelet count. She was admitted to a US Navy hospital for induction of labor.
When labor failed to progress after 53 hours, a cesarean delivery was performed. The patient suffered uncontrolled bleeding and developed HELLP syndrome (hemolysis, elevated liver enzymes, low platelet count). A platelet transfusion was needed, but the nearest supply was at a city hospital approximately 60 miles away. Because of bad weather, the patient could not be flown to the city. She died 10 hours after delivery.
ESTATE’S CLAIM A cesarean delivery should have been performed earlier. Lab results showing the severity of the mother’s condition at delivery were not read for 5 hours.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $2.1 million Missouri settlement was reached.
Did OB’s errors cause this child’s injuries?
A CHILD WAS BORN with a left brachial plexus injury and fractured left clavicle.
PATIENT’S CLAIM The ObGyn failed to diagnose shoulder dystocia, failed to perform appropriate maneuvers to free the entrapped anterior shoulder, and applied excessive lateral traction to deliver the child.
PHYSICIAN’S DEFENSE There was no shoulder dystocia. The child’s injuries were caused by the natural forces of labor.
VERDICT A $1,314,600 Iowa verdict was returned.
Sedation for surgery leads to brain damage
A 20-YEAR-OLD WOMAN with sickle-cell anemia (SCA) was sent to an ambulatory surgery center for surgical treatment of cervical dysplasia.
A certified nurse anesthetist (CRNA) sedated the patient at the surgery center. The patient went into cardiac arrest and was transferred to a hospital. She suffered a brain injury caused by oxygen deprivation. Her IQ dropped by 11 points; with the brain damage, she was unable to retain her driver’s license.
PATIENT’S CLAIM The procedure could have been performed safely in the doctor’s office under local anesthesia. The gynecologist had signed off on the anesthesia plan, although he knew of the risks of giving general anesthesia to someone with SCA. She was sent to the surgery center only because of the gynecologist’s desire to generate revenue.
DEFENDANTS’ DEFENSE The gynecologist blamed the CRNA, who, allegedly, allowed a kink to form in the IV anesthesia line. When the line cleared, sedative flooded into the patient, causing her heart to stop. The gynecologist admitted that general anesthesia was unnecessary; local anesthesia would have been safer. The CRNA argued that the surgery center was at fault; she had followed the center’s standard operating procedure. The surgery center denied negligence.
VERDICT An $851,000 South Carolina settlement was reached with the gynecologist, CRNA, and surgery center.
Pain from retained sponge, surgical ring
TWINS WERE BORN BY CESAREAN delivery to a 40-year-old woman. She developed abdominal pain and reported it to her ObGyn several times. Four months after delivery, the ObGyn found a retained sponge and surgical ring during exploratory laparotomy.
PATIENT’S CLAIM The ObGyn did not adequately inspect the operative area before closing. Although the patient reported abdominal pain immediately after delivery, her complaints were ignored for several months.
PHYSICIAN’S DEFENSE The nurses are responsible for any errors in the sponge count. The patient’s complaints were not brought to his attention until four months after delivery.
VERDICT The patient reached a confidential settlement with the delivery nurses, an assisting physician, and the hospital. A New York jury found the ObGyn 60% at fault; a $1.5 million verdict was returned. The patient agreed to a $550,000 posttrial settlement with the ObGyn’s insurer.
Patient falls from exam table during non-stress test
IN HER EIGHTH GESTATIONAL MONTH, a woman in her 30s underwent a non-stress test because of five prior miscarriages. She became ill just as the test was beginning, turned to her side to vomit, and fell off the examination table. She fractured her cervical spine.
An emergency cesarean delivery resulted in the birth of a healthy baby. The woman then underwent fusion surgery to repair the cervical fracture. She required physical therapy, and made a good recovery.
PATIENT’S CLAIM The examination table should have had side rails, which would have prevented the fall.
DEFENDANTS’ DEFENSE Side rails were not required on an examination table. This was an unforeseeable event that occurred while a nurse was setting up the procedure and reaching for a blood-pressure cuff.
VERDICT A Connecticut defense verdict was returned.
Sexually abused by nursing assistant: $67 million verdict
A 38-YEAR-OLD WOMAN UNDERWENT laparoscopic ovarian cyst removal. While hospitalized, a male nursing assistant sexually assaulted her by digital penetration of the vagina without wearing gloves. The employee was arrested for the assault, but allegedly fled the country after posting bail.
PATIENT’S CLAIM At least five similar incidents involving the same nursing assistant reportedly occurred in the hospital over a 16-month period. At trial, four patients and an employee testified that they had been similarly assaulted and had reported the incidents to hospital staff. The nursing assistant should have been removed from his position after the first reported incident, and a thorough investigation conducted. The patient suffered post-traumatic stress disorder because of her experience.
DEFENDANTS’ DEFENSE A proper investigation was made. Often, female patients are uncomfortable with male nurses. The hospital denied being notified of some incidents, and maintained it had suspended the male nursing assistant when it became aware of the incident under litigation.
VERDICT A $67,359,753 California verdict included $65 million in punitive damages against the hospital and its former corporate owner.
Salpingectomy results in death
TO INCREASE HER CHANCES of becoming pregnant using IVF, a woman in her 30s underwent adhesiolysis and salpingectomy. She was discharged the same day.
The next day, she complained of abdominal pain to her ObGyn. She died two days after surgery from septic shock due to a perforated bowel.
ESTATE’S CLAIM The ObGyn was negligent in discharging her, especially because the surgeon had identified a superficial injury to the bowel during surgery. She should have been examined the day after surgery when she first complained of abdominal pain.
PHYSICIANS’ DEFENSE The ObGyn acted appropriately in relying on the surgeon’s recommendation for discharge. He had contacted the patient twice after her initial call regarding abdominal pain, and was told both times that she was feeling better.
VERDICT A Virginia defense verdict was returned.
Disastrous D&C after miscarriage
A 29-YEAR-OLD WOMAN miscarried at 14 weeks’ gestation. An ObGyn recommended that she undergo dilation and curettage (D&C).
With the ObGyn in attendance, a resident sedated the patient and performed the D&C. When the resident perforated the uterus, the ObGyn took over, inserting ring forceps to remove the remains. The forceps went through the perforation and tore the top half of the rectum and a portion of bowel.
A rectal surgeon, called in to repair the injury, performed an ileostomy and created an ileostomy pouch. The ileo-stomy was later successfully reversed.
PATIENT’S CLAIM The woman was at risk of injury because her uterus was anteverted and she had under-gone a cesarean delivery; an experienced physician should have performed the procedure.
When the perforation first occurred, ultrasonography should have been used to identify the puncture and prevent in-jury to the rectum and bowel.
DEFENDANTS’ DEFENSE The patient gave informed consent. The injury is a known risk of the procedure.
VERDICT A $2.5 million Michigan verdict was returned against the ObGyn and hospital, but was reduced to $1.25 million under the statutory cap.
AT 38 WEEKS’ GESTATION, a 20-year-old woman had preeclampsia and a borderline-low platelet count. She was admitted to a US Navy hospital for induction of labor.
When labor failed to progress after 53 hours, a cesarean delivery was performed. The patient suffered uncontrolled bleeding and developed HELLP syndrome (hemolysis, elevated liver enzymes, low platelet count). A platelet transfusion was needed, but the nearest supply was at a city hospital approximately 60 miles away. Because of bad weather, the patient could not be flown to the city. She died 10 hours after delivery.
ESTATE’S CLAIM A cesarean delivery should have been performed earlier. Lab results showing the severity of the mother’s condition at delivery were not read for 5 hours.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $2.1 million Missouri settlement was reached.
Did OB’s errors cause this child’s injuries?
A CHILD WAS BORN with a left brachial plexus injury and fractured left clavicle.
PATIENT’S CLAIM The ObGyn failed to diagnose shoulder dystocia, failed to perform appropriate maneuvers to free the entrapped anterior shoulder, and applied excessive lateral traction to deliver the child.
PHYSICIAN’S DEFENSE There was no shoulder dystocia. The child’s injuries were caused by the natural forces of labor.
VERDICT A $1,314,600 Iowa verdict was returned.
Sedation for surgery leads to brain damage
A 20-YEAR-OLD WOMAN with sickle-cell anemia (SCA) was sent to an ambulatory surgery center for surgical treatment of cervical dysplasia.
A certified nurse anesthetist (CRNA) sedated the patient at the surgery center. The patient went into cardiac arrest and was transferred to a hospital. She suffered a brain injury caused by oxygen deprivation. Her IQ dropped by 11 points; with the brain damage, she was unable to retain her driver’s license.
PATIENT’S CLAIM The procedure could have been performed safely in the doctor’s office under local anesthesia. The gynecologist had signed off on the anesthesia plan, although he knew of the risks of giving general anesthesia to someone with SCA. She was sent to the surgery center only because of the gynecologist’s desire to generate revenue.
DEFENDANTS’ DEFENSE The gynecologist blamed the CRNA, who, allegedly, allowed a kink to form in the IV anesthesia line. When the line cleared, sedative flooded into the patient, causing her heart to stop. The gynecologist admitted that general anesthesia was unnecessary; local anesthesia would have been safer. The CRNA argued that the surgery center was at fault; she had followed the center’s standard operating procedure. The surgery center denied negligence.
VERDICT An $851,000 South Carolina settlement was reached with the gynecologist, CRNA, and surgery center.
Pain from retained sponge, surgical ring
TWINS WERE BORN BY CESAREAN delivery to a 40-year-old woman. She developed abdominal pain and reported it to her ObGyn several times. Four months after delivery, the ObGyn found a retained sponge and surgical ring during exploratory laparotomy.
PATIENT’S CLAIM The ObGyn did not adequately inspect the operative area before closing. Although the patient reported abdominal pain immediately after delivery, her complaints were ignored for several months.
PHYSICIAN’S DEFENSE The nurses are responsible for any errors in the sponge count. The patient’s complaints were not brought to his attention until four months after delivery.
VERDICT The patient reached a confidential settlement with the delivery nurses, an assisting physician, and the hospital. A New York jury found the ObGyn 60% at fault; a $1.5 million verdict was returned. The patient agreed to a $550,000 posttrial settlement with the ObGyn’s insurer.
Patient falls from exam table during non-stress test
IN HER EIGHTH GESTATIONAL MONTH, a woman in her 30s underwent a non-stress test because of five prior miscarriages. She became ill just as the test was beginning, turned to her side to vomit, and fell off the examination table. She fractured her cervical spine.
An emergency cesarean delivery resulted in the birth of a healthy baby. The woman then underwent fusion surgery to repair the cervical fracture. She required physical therapy, and made a good recovery.
PATIENT’S CLAIM The examination table should have had side rails, which would have prevented the fall.
DEFENDANTS’ DEFENSE Side rails were not required on an examination table. This was an unforeseeable event that occurred while a nurse was setting up the procedure and reaching for a blood-pressure cuff.
VERDICT A Connecticut defense verdict was returned.
Sexually abused by nursing assistant: $67 million verdict
A 38-YEAR-OLD WOMAN UNDERWENT laparoscopic ovarian cyst removal. While hospitalized, a male nursing assistant sexually assaulted her by digital penetration of the vagina without wearing gloves. The employee was arrested for the assault, but allegedly fled the country after posting bail.
PATIENT’S CLAIM At least five similar incidents involving the same nursing assistant reportedly occurred in the hospital over a 16-month period. At trial, four patients and an employee testified that they had been similarly assaulted and had reported the incidents to hospital staff. The nursing assistant should have been removed from his position after the first reported incident, and a thorough investigation conducted. The patient suffered post-traumatic stress disorder because of her experience.
DEFENDANTS’ DEFENSE A proper investigation was made. Often, female patients are uncomfortable with male nurses. The hospital denied being notified of some incidents, and maintained it had suspended the male nursing assistant when it became aware of the incident under litigation.
VERDICT A $67,359,753 California verdict included $65 million in punitive damages against the hospital and its former corporate owner.
Salpingectomy results in death
TO INCREASE HER CHANCES of becoming pregnant using IVF, a woman in her 30s underwent adhesiolysis and salpingectomy. She was discharged the same day.
The next day, she complained of abdominal pain to her ObGyn. She died two days after surgery from septic shock due to a perforated bowel.
ESTATE’S CLAIM The ObGyn was negligent in discharging her, especially because the surgeon had identified a superficial injury to the bowel during surgery. She should have been examined the day after surgery when she first complained of abdominal pain.
PHYSICIANS’ DEFENSE The ObGyn acted appropriately in relying on the surgeon’s recommendation for discharge. He had contacted the patient twice after her initial call regarding abdominal pain, and was told both times that she was feeling better.
VERDICT A Virginia defense verdict was returned.
Disastrous D&C after miscarriage
A 29-YEAR-OLD WOMAN miscarried at 14 weeks’ gestation. An ObGyn recommended that she undergo dilation and curettage (D&C).
With the ObGyn in attendance, a resident sedated the patient and performed the D&C. When the resident perforated the uterus, the ObGyn took over, inserting ring forceps to remove the remains. The forceps went through the perforation and tore the top half of the rectum and a portion of bowel.
A rectal surgeon, called in to repair the injury, performed an ileostomy and created an ileostomy pouch. The ileo-stomy was later successfully reversed.
PATIENT’S CLAIM The woman was at risk of injury because her uterus was anteverted and she had under-gone a cesarean delivery; an experienced physician should have performed the procedure.
When the perforation first occurred, ultrasonography should have been used to identify the puncture and prevent in-jury to the rectum and bowel.
DEFENDANTS’ DEFENSE The patient gave informed consent. The injury is a known risk of the procedure.
VERDICT A $2.5 million Michigan verdict was returned against the ObGyn and hospital, but was reduced to $1.25 million under the statutory cap.
These cases were selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Online calculator helps prevent post-op respiratory failure
- New drug for long-term treatment of PE
- Benefits of triple therapy for COPD
- Knee-length compression stockings as good as thigh-length for PTS
- Video monitoring improves hand hygiene
- Asymptomatic bacteriuria often misdiagnosed as UTI
- CT accurate for lower GI bleeding diagnosis
- Switch from albuterol to lavalbuterol to reduce tachycardia not recommended
Preoperative Risk Calculator Can Help Predict Postoperative Respiratory Failure
Clinical question: Can preoperative factors identify patients at risk for postoperative respiratory failure (PRF)?
Background: PRF—when a patient requires mechanical ventilation >48 hours after surgery or needs unplanned intubation within 30 days of surgery—is associated with high mortality, with 30-day mortality rates of 26%.
Study design: Analysis of multicenter, prospective databases of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP).
Setting: Analysis of NSQIP data from 2007 (training set) and 2008 (validation set).
Synopsis: PRF was seen in 3.1% of patients in the 2007 data set and 2.6% in the 2008 data set. Those with PRF had significantly higher mortality rates than those without PRF (25.62% vs. 0.98%; P<0.0001). Preoperative risk factors associated with significantly increased risk of PRF were American Society of Anesthesiologists’ class, functional status, emergent nature of procedure, type of surgery, and preoperative sepsis.
The 2007 data set was used to develop the model, and the 2008 data set was used as a validation set. The selected risk model showed similar results in both sets with a c-statistic of 0.91 in the training set and 0.90 in the validation set. This selected model was then used to develop an interactive calculator predicting PRF (available at www.surgicalriskcalculator.com/prf-risk-calculator).
Bottom line: The PRF risk calculator can identify patients at high risk for PRF, which can aid in tailoring preventive strategies for patients prior to surgery.
Citation: Gupta H, Gupta PK, Fang X, et al. Development and validation of a risk calculator predicting postoperative respiratory failure. Chest. 2011;140:1207-1215.
New Drug for Treatment of Acute Symptomatic Pulmonary Embolism
Clinical question: Is the incidence of recurrent venous thromboembolism (VTE) or bleeding with use of idrabiotaparinux comparable to warfarin for treatment of acute symptomatic pulmonary embolism (PE)?
Background: Warfarin is an effective treatment for PE; however, maintenance of effective and safe levels of anticoagulation is difficult to achieve. A straightforward treatment option would be an attractive alternative. Idrabiotaparinux, a factor Xa inhibitor bound with a biotin moiety, is a weekly subcutaneous injection proposed as an alternative to warfarin for treatment of PE.
Study design: Industry-sponsored double-blind, randomized controlled trial.
Setting: 291 centers in 37 countries.
Synopsis: A group of 3,202 patients aged 18 to 96 years were randomly assigned to receive enoxaparin, followed by idrabiotaparinux or enoxaparin, then overlapped and followed by warfarin for three or six months. The incidence of recurrent VTE (including fatal and nonfatal PE or deep vein thrombosis) did not differ between the two treatment arms.
Of the 1,599 patients treated with idrabiotaparinux, 48 (3%) had a recurrence; of the 1,603 treated with warfarin, 97 (6%) had a recurrence (odds ratio, 0.49). The rate of clinically relevant bleeding was also similar, with 72 (5%) in the idrabiotaparinux group versus 106 (7%) in the warfarin group. Much like warfarin, idrabiotaparinux requires bridging therapy with initial low-molecular-weight heparin.
Bottom line: Use of enoxaparin followed by weekly subcutaneous injection of idrabiotaparinux was as effective as enoxaparin followed by warfarin for preventing recurrent VTE, and may provide a suitable option for treatment of acute symptomatic PE.
Citation: Buller HR, Gallus AS, Pillion G, Prins MH, Raskob GE. Enoxaparin followed by once-weekly idrabiotaparinux versus enoxaparin plus warfarin for patients with acute symptomatic pulmonary embolism: a randomised, double-blind, double-dummy, non-inferiority trial. Lancet. 2012;379:123-129.
Triple Therapy Better than Double for COPD
Clinical question: Does addition of tiotropium to inhaled corticosteroids and long-acting beta-agonists (LABA) have an additive benefit in reducing mortality, hospital admissions, and exacerbations in COPD?
Background: Triple therapy in COPD involves adding LABA and long-acting antimuscarinics (LAMA), such as tiotropium, to inhaled corticosteroids (ICS). Despite the guidelines recommending triple therapy for severe COPD, most studies have evaluated either LAMA or LABA plus ICS, but not all three together.
Study design: Retrospective cohort.
Setting: Tayside, Scotland’s National Health Services database.
Synopsis: Patients with severe COPD were divided into two groups: 1,857 patients had received ICS+LABA (double therapy) and 996 had received ICS+LABA+tiotropium (triple therapy), with follow-up of 4.65 years.
All-cause mortality was 35% lower in the triple therapy group (HR 0.65, 95% CI 0.57-0.75). Corticosteroid use was 29% lower (HR 0.71, 95% CI 0.63-0.80), and hospital admissions were 15% lower (HR 0.85, 95% CI 0.73-0.99) in the triple-therapy group. These results were adjusted for smoking, age, sex, socioeconomic status, and history of diabetes, cardiovascular, and respiratory disease.
This study is limited by its observational retrospective design but provides good evidence of the need for randomized controlled trials to validate the clinical benefits of triple therapy.
Bottom line: Adding tiotropium to ICS plus LABA is associated with lower all-cause mortality, hospitalizations, and corticosteroid use when compared with ICS plus LABA, validating its current use in management of severe COPD.
Citation: Short PM, Williamson PA, Elder DHJ, Lipworth SIW, Schembi S, Lipworth BJ. The impact of tiotropium on mortality and exacerbations when added to inhaled corticosteroids and long-acting β-agonist therapy in COPD. Chest. 2012;141:81-86.
Above-Knee Compression Stockings Not Better than Below-Knee Stockings for Protection Against Post-Thrombotic Syndrome
Clinical question: Do above-knee compression elastic stockings prevent post-thrombotic syndrome (PTS) better than below-knee stockings?
Background: PTS—characterized by leg pain, cramps, edema, and hyperpigmentation—occurs in 25% to 50% of patients after an episode of deep venous thrombosis (DVT). Previous studies demonstrated a 50% reduction in the incidence of PTS when patients used below-knee stockings.
Study design: Open-label, randomized clinical trial.
Setting: Eight hospitals in Italy.
Synopsis: A total of 267 patients with their first episode of DVT were randomized to thigh-length or below-knee compression elastic stockings, as well as therapeutic anticoagulation, with a primary endpoint of three-year incidence of PTS. Assessment was done by study personnel who were blinded to the type of stocking the patients had been prescribed. Severity of PTS was graded by a scoring system incorporating objective and subjective criteria with an independent adjudicator.
The intention-to-treat analysis showed no significant difference in the three-year incidence of PTS between thigh- and knee-length stockings (32.6% vs. 35.6%, respectively). Compliance was better in the knee-length (82.6%) than in the thigh-length (66.7%) group due to the significantly lower rate of stockings-related side effects.
The study is limited by a lack of blinding in the study participants.
Bottom line: Knee-length stockings offer equal similar protection against PTS with better compliance when compared with thigh-length stockings.
Citation: Prandoni P, Noventa F, Quintavalla R, et al. Thigh-length versus below-knee compression elastic stockings for prevention of the post-thrombotic syndrome in patients with proximal-venous thrombosis: a randomized trial. Blood. 2012;119:1561-1565.
Video Auditing With Near- Real-Time Feedback Improves Hand Hygiene Practices
Clinical question: Does the use of direct video monitoring with continuous, multi-modal feedback promote improvement in healthcare workers’ compliance with hand hygiene?
Background: Appropriate hand hygiene is an effective means of infection control. Direct human observation of hand hygiene compliance does little more than provide a biased, temporary, and often overestimated assessment of compliance. The use of video-based monitoring technology in other aspects of society (e.g. traffic signal cameras) has been well demonstrated to modify behavior.
Study design: Prospective cohort study.
Setting: Tertiary-care hospital’s 17-bed medical ICU in the northeastern U.S.
Synopsis: Through the use of 21 motion-activated video cameras with continuous third-party auditing, the provision of near real-time feedback improved hand hygiene rates of healthcare workers from 6.5% to 81.6%. In the four months preceding feedback, only 3,933 hand-washing events out of 60,542 (6.5%) were considered “passing.” During the active feedback period, 59,627 events out of 73,080 (81.6%) passed.
The improvement was sustained in the maintenance period of the study with an average rate of hand hygiene compliance of 87.9%. The improvement in hand hygiene compliance required active provision of feedback as well as the presence of monitoring equipment, making the applicability of this study limited, based on the cost of the technology and the manpower to provide feedback.
Bottom line: Hand hygiene practices improve when healthcare workers are given immediate feedback on their compliance.
Citation: Rebellion D, Husain E, Schilling ME, et al. Using high-technology to enforce low-technology safety measures: the use of third-party remote video auditing and real-time feedback in healthcare. Clin Infect Dis. 2012:54(1):1-7.
Mismanagement of Enterococcal Bacteriuria
Clinical question: Are clinical providers following appropriate guidelines to identify and manage enterococcal bacteriuria?
Background: There are specific evidence-based guidelines for the diagnosis and treatment of urinary tract infections (UTI) and asymptomatic bacteriuria (ABU). ABU is often mistaken for a UTI, and incorrectly treated as one.
Study design: Retrospective cohort.
Setting: Two academic teaching hospitals in Houston, Texas.
Synopsis: Using the current Infectious Disease Society of America (IDSA) guidelines, 375 Enterococcus urine cultures were reviewed and determined to be either UTI or ABU. The cultures were initially reviewed for appropriate treatment and again 30 days later for complications. UTI was defined as bacteriuria with one or more sign or symptom (urgency, frequency, dysuria, suprapubic tenderness, flank pain, rigors, visible hematuria, delirium, or fevers) without another identifiable cause. ABU was defined as bacteriuria without any of the signs or symptoms, or a clear nonurinary source.
Of the 339 cultures matching inclusion criteria, 156 were classified as UTI and 183 classified as ABU. Sixty of the 183 ABU (32.8%) were inappropriately treated with antibiotics, while antibiotics were withheld in 23 of the 156 UTI (14.7%). Eighty-three of 339 cultures (24.5%) were incorrectly treated. The most common reason for ABU being inappropriately treated was the presence of pyuria, associated with a threefold higher use of antibiotics.
There was no significant difference in subsequent infections or infectious complications between UTI and ABU.
Bottom line: Enterococcal ABU is frequently treated with antibiotics, even though guidelines recommend against it; providers should resist overtreating enterococcal ABU.
Citation: Lin E, Bhusal Y, Horwitz D, Shelburne SA, Trautner BW. Overtreatment of enterococcal bacteriuria. Arch Intern Med. 2012;172:33-38.
CT Angiography for the Diagnosis of Acute Lower GI Bleeding in an Emergency Setting
Clinical question: Is CT angiography a reliable initial diagnostic procedure to identify the presence and location of an acute lower gastrointestinal (GI) bleed in the ED setting?
Background: CT angiography has been identified as a potentially useful procedure to identify acute GI bleeds; however, the specific role and timing of the procedure has not been clearly identified.
Study design: Prospective study.
Setting: ED of a university-based hospital in Madrid.
Synopsis: CT angiography was performed on 47 ED patients (27 men, 20 women, with a mean age of 68 years) with an acute lower GI bleed. Study protocol included a preliminary unenhanced CT scan followed by CT angiogram prior to the standard clinical protocol, which included colonoscopy, angiography, or laparotomy.
Images were reviewed by two different ED radiologists, who were blinded to the diagnosis, and compared with the standard protocol findings. CT angiography correctly identified active acute or recent GI bleeding in 46 of the 47 patients, with a sensitivity of 100% (19 of 19), NPV of 100% (27 of 27), specificity of 96% (27 of 28), and PPV of 95% (19 of 20). CT angiography also was 93% accurate in identifying the cause of the GI bleed when compared with the standard reference.
Limitations of the study include its small size and the lack of a control group.
Bottom line: CT angiography is an accurate and more readily available modality for the diagnosis of acute lower GI bleeding, though it does not provide a therapeutic option.
Citation: Martí M, Artigas JM, Garzón G, Alvarez-Sala R, Soto JA. Acute lower intestinal bleeding: feasibility and diagnostic performance of CT angiography. Radiology. 2012;262:109-116.
Substitution of Levalbuterol to Avoid Tachyarrhythmia Not Supported
Clinical question: Does substitution of levalbuterol for albuterol in critically ill adult patients result in decreased incidence of tachyarrhythmias?
Background: Studies have indicated an increased risk of mortality from tachycardia and tachyarrhythmias in ICU patients. Levalbuterol is the R-isomer of albuterol, and it has been proposed that it may mitigate cardiac side effects seen with beta-2 agonists. For this reason, some clinicians have advocated using nebulized levalbuterol in critically ill patients.
Study design: Prospective randomized controlled trial with patient crossover.
Setting: Single academic medical center.
Synopsis: All ICU patients in a single teaching hospital were screened, and 70 patients were included. Patients were randomly crossed over between albuterol and levalbuterol every four to six hours. This resulted in a total of 836 measurements of heart rate, the primary outcome measurement. The study showed no clinically significant differences in average heart rate when using levalbuterol versus albuterol. This was a small study of ICU patients, using a surrogate endpoint of heart rate rather than mortality. Furthermore, the assessment of tachyarrhythmias was limited given the study size and relative rarity of these events. Despite these limitations, the study casts significant doubt on the theory and practice of switching from albuterol to levalbuterol solely for the purpose of reducing or avoiding tachycardia or tachyarrhythmias.
Bottom line: Substitution of levalbuterol for albuterol to avert tachycardia in critically ill patients is not warranted.
Citation: Khorfan FM, Smith P, Watt S, Barber KR. Effects of nebulized bronchodilator therapy on heart rate and arrhythmias in critically ill adult patients. Chest. 2011;140:1466-1472.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Online calculator helps prevent post-op respiratory failure
- New drug for long-term treatment of PE
- Benefits of triple therapy for COPD
- Knee-length compression stockings as good as thigh-length for PTS
- Video monitoring improves hand hygiene
- Asymptomatic bacteriuria often misdiagnosed as UTI
- CT accurate for lower GI bleeding diagnosis
- Switch from albuterol to lavalbuterol to reduce tachycardia not recommended
Preoperative Risk Calculator Can Help Predict Postoperative Respiratory Failure
Clinical question: Can preoperative factors identify patients at risk for postoperative respiratory failure (PRF)?
Background: PRF—when a patient requires mechanical ventilation >48 hours after surgery or needs unplanned intubation within 30 days of surgery—is associated with high mortality, with 30-day mortality rates of 26%.
Study design: Analysis of multicenter, prospective databases of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP).
Setting: Analysis of NSQIP data from 2007 (training set) and 2008 (validation set).
Synopsis: PRF was seen in 3.1% of patients in the 2007 data set and 2.6% in the 2008 data set. Those with PRF had significantly higher mortality rates than those without PRF (25.62% vs. 0.98%; P<0.0001). Preoperative risk factors associated with significantly increased risk of PRF were American Society of Anesthesiologists’ class, functional status, emergent nature of procedure, type of surgery, and preoperative sepsis.
The 2007 data set was used to develop the model, and the 2008 data set was used as a validation set. The selected risk model showed similar results in both sets with a c-statistic of 0.91 in the training set and 0.90 in the validation set. This selected model was then used to develop an interactive calculator predicting PRF (available at www.surgicalriskcalculator.com/prf-risk-calculator).
Bottom line: The PRF risk calculator can identify patients at high risk for PRF, which can aid in tailoring preventive strategies for patients prior to surgery.
Citation: Gupta H, Gupta PK, Fang X, et al. Development and validation of a risk calculator predicting postoperative respiratory failure. Chest. 2011;140:1207-1215.
New Drug for Treatment of Acute Symptomatic Pulmonary Embolism
Clinical question: Is the incidence of recurrent venous thromboembolism (VTE) or bleeding with use of idrabiotaparinux comparable to warfarin for treatment of acute symptomatic pulmonary embolism (PE)?
Background: Warfarin is an effective treatment for PE; however, maintenance of effective and safe levels of anticoagulation is difficult to achieve. A straightforward treatment option would be an attractive alternative. Idrabiotaparinux, a factor Xa inhibitor bound with a biotin moiety, is a weekly subcutaneous injection proposed as an alternative to warfarin for treatment of PE.
Study design: Industry-sponsored double-blind, randomized controlled trial.
Setting: 291 centers in 37 countries.
Synopsis: A group of 3,202 patients aged 18 to 96 years were randomly assigned to receive enoxaparin, followed by idrabiotaparinux or enoxaparin, then overlapped and followed by warfarin for three or six months. The incidence of recurrent VTE (including fatal and nonfatal PE or deep vein thrombosis) did not differ between the two treatment arms.
Of the 1,599 patients treated with idrabiotaparinux, 48 (3%) had a recurrence; of the 1,603 treated with warfarin, 97 (6%) had a recurrence (odds ratio, 0.49). The rate of clinically relevant bleeding was also similar, with 72 (5%) in the idrabiotaparinux group versus 106 (7%) in the warfarin group. Much like warfarin, idrabiotaparinux requires bridging therapy with initial low-molecular-weight heparin.
Bottom line: Use of enoxaparin followed by weekly subcutaneous injection of idrabiotaparinux was as effective as enoxaparin followed by warfarin for preventing recurrent VTE, and may provide a suitable option for treatment of acute symptomatic PE.
Citation: Buller HR, Gallus AS, Pillion G, Prins MH, Raskob GE. Enoxaparin followed by once-weekly idrabiotaparinux versus enoxaparin plus warfarin for patients with acute symptomatic pulmonary embolism: a randomised, double-blind, double-dummy, non-inferiority trial. Lancet. 2012;379:123-129.
Triple Therapy Better than Double for COPD
Clinical question: Does addition of tiotropium to inhaled corticosteroids and long-acting beta-agonists (LABA) have an additive benefit in reducing mortality, hospital admissions, and exacerbations in COPD?
Background: Triple therapy in COPD involves adding LABA and long-acting antimuscarinics (LAMA), such as tiotropium, to inhaled corticosteroids (ICS). Despite the guidelines recommending triple therapy for severe COPD, most studies have evaluated either LAMA or LABA plus ICS, but not all three together.
Study design: Retrospective cohort.
Setting: Tayside, Scotland’s National Health Services database.
Synopsis: Patients with severe COPD were divided into two groups: 1,857 patients had received ICS+LABA (double therapy) and 996 had received ICS+LABA+tiotropium (triple therapy), with follow-up of 4.65 years.
All-cause mortality was 35% lower in the triple therapy group (HR 0.65, 95% CI 0.57-0.75). Corticosteroid use was 29% lower (HR 0.71, 95% CI 0.63-0.80), and hospital admissions were 15% lower (HR 0.85, 95% CI 0.73-0.99) in the triple-therapy group. These results were adjusted for smoking, age, sex, socioeconomic status, and history of diabetes, cardiovascular, and respiratory disease.
This study is limited by its observational retrospective design but provides good evidence of the need for randomized controlled trials to validate the clinical benefits of triple therapy.
Bottom line: Adding tiotropium to ICS plus LABA is associated with lower all-cause mortality, hospitalizations, and corticosteroid use when compared with ICS plus LABA, validating its current use in management of severe COPD.
Citation: Short PM, Williamson PA, Elder DHJ, Lipworth SIW, Schembi S, Lipworth BJ. The impact of tiotropium on mortality and exacerbations when added to inhaled corticosteroids and long-acting β-agonist therapy in COPD. Chest. 2012;141:81-86.
Above-Knee Compression Stockings Not Better than Below-Knee Stockings for Protection Against Post-Thrombotic Syndrome
Clinical question: Do above-knee compression elastic stockings prevent post-thrombotic syndrome (PTS) better than below-knee stockings?
Background: PTS—characterized by leg pain, cramps, edema, and hyperpigmentation—occurs in 25% to 50% of patients after an episode of deep venous thrombosis (DVT). Previous studies demonstrated a 50% reduction in the incidence of PTS when patients used below-knee stockings.
Study design: Open-label, randomized clinical trial.
Setting: Eight hospitals in Italy.
Synopsis: A total of 267 patients with their first episode of DVT were randomized to thigh-length or below-knee compression elastic stockings, as well as therapeutic anticoagulation, with a primary endpoint of three-year incidence of PTS. Assessment was done by study personnel who were blinded to the type of stocking the patients had been prescribed. Severity of PTS was graded by a scoring system incorporating objective and subjective criteria with an independent adjudicator.
The intention-to-treat analysis showed no significant difference in the three-year incidence of PTS between thigh- and knee-length stockings (32.6% vs. 35.6%, respectively). Compliance was better in the knee-length (82.6%) than in the thigh-length (66.7%) group due to the significantly lower rate of stockings-related side effects.
The study is limited by a lack of blinding in the study participants.
Bottom line: Knee-length stockings offer equal similar protection against PTS with better compliance when compared with thigh-length stockings.
Citation: Prandoni P, Noventa F, Quintavalla R, et al. Thigh-length versus below-knee compression elastic stockings for prevention of the post-thrombotic syndrome in patients with proximal-venous thrombosis: a randomized trial. Blood. 2012;119:1561-1565.
Video Auditing With Near- Real-Time Feedback Improves Hand Hygiene Practices
Clinical question: Does the use of direct video monitoring with continuous, multi-modal feedback promote improvement in healthcare workers’ compliance with hand hygiene?
Background: Appropriate hand hygiene is an effective means of infection control. Direct human observation of hand hygiene compliance does little more than provide a biased, temporary, and often overestimated assessment of compliance. The use of video-based monitoring technology in other aspects of society (e.g. traffic signal cameras) has been well demonstrated to modify behavior.
Study design: Prospective cohort study.
Setting: Tertiary-care hospital’s 17-bed medical ICU in the northeastern U.S.
Synopsis: Through the use of 21 motion-activated video cameras with continuous third-party auditing, the provision of near real-time feedback improved hand hygiene rates of healthcare workers from 6.5% to 81.6%. In the four months preceding feedback, only 3,933 hand-washing events out of 60,542 (6.5%) were considered “passing.” During the active feedback period, 59,627 events out of 73,080 (81.6%) passed.
The improvement was sustained in the maintenance period of the study with an average rate of hand hygiene compliance of 87.9%. The improvement in hand hygiene compliance required active provision of feedback as well as the presence of monitoring equipment, making the applicability of this study limited, based on the cost of the technology and the manpower to provide feedback.
Bottom line: Hand hygiene practices improve when healthcare workers are given immediate feedback on their compliance.
Citation: Rebellion D, Husain E, Schilling ME, et al. Using high-technology to enforce low-technology safety measures: the use of third-party remote video auditing and real-time feedback in healthcare. Clin Infect Dis. 2012:54(1):1-7.
Mismanagement of Enterococcal Bacteriuria
Clinical question: Are clinical providers following appropriate guidelines to identify and manage enterococcal bacteriuria?
Background: There are specific evidence-based guidelines for the diagnosis and treatment of urinary tract infections (UTI) and asymptomatic bacteriuria (ABU). ABU is often mistaken for a UTI, and incorrectly treated as one.
Study design: Retrospective cohort.
Setting: Two academic teaching hospitals in Houston, Texas.
Synopsis: Using the current Infectious Disease Society of America (IDSA) guidelines, 375 Enterococcus urine cultures were reviewed and determined to be either UTI or ABU. The cultures were initially reviewed for appropriate treatment and again 30 days later for complications. UTI was defined as bacteriuria with one or more sign or symptom (urgency, frequency, dysuria, suprapubic tenderness, flank pain, rigors, visible hematuria, delirium, or fevers) without another identifiable cause. ABU was defined as bacteriuria without any of the signs or symptoms, or a clear nonurinary source.
Of the 339 cultures matching inclusion criteria, 156 were classified as UTI and 183 classified as ABU. Sixty of the 183 ABU (32.8%) were inappropriately treated with antibiotics, while antibiotics were withheld in 23 of the 156 UTI (14.7%). Eighty-three of 339 cultures (24.5%) were incorrectly treated. The most common reason for ABU being inappropriately treated was the presence of pyuria, associated with a threefold higher use of antibiotics.
There was no significant difference in subsequent infections or infectious complications between UTI and ABU.
Bottom line: Enterococcal ABU is frequently treated with antibiotics, even though guidelines recommend against it; providers should resist overtreating enterococcal ABU.
Citation: Lin E, Bhusal Y, Horwitz D, Shelburne SA, Trautner BW. Overtreatment of enterococcal bacteriuria. Arch Intern Med. 2012;172:33-38.
CT Angiography for the Diagnosis of Acute Lower GI Bleeding in an Emergency Setting
Clinical question: Is CT angiography a reliable initial diagnostic procedure to identify the presence and location of an acute lower gastrointestinal (GI) bleed in the ED setting?
Background: CT angiography has been identified as a potentially useful procedure to identify acute GI bleeds; however, the specific role and timing of the procedure has not been clearly identified.
Study design: Prospective study.
Setting: ED of a university-based hospital in Madrid.
Synopsis: CT angiography was performed on 47 ED patients (27 men, 20 women, with a mean age of 68 years) with an acute lower GI bleed. Study protocol included a preliminary unenhanced CT scan followed by CT angiogram prior to the standard clinical protocol, which included colonoscopy, angiography, or laparotomy.
Images were reviewed by two different ED radiologists, who were blinded to the diagnosis, and compared with the standard protocol findings. CT angiography correctly identified active acute or recent GI bleeding in 46 of the 47 patients, with a sensitivity of 100% (19 of 19), NPV of 100% (27 of 27), specificity of 96% (27 of 28), and PPV of 95% (19 of 20). CT angiography also was 93% accurate in identifying the cause of the GI bleed when compared with the standard reference.
Limitations of the study include its small size and the lack of a control group.
Bottom line: CT angiography is an accurate and more readily available modality for the diagnosis of acute lower GI bleeding, though it does not provide a therapeutic option.
Citation: Martí M, Artigas JM, Garzón G, Alvarez-Sala R, Soto JA. Acute lower intestinal bleeding: feasibility and diagnostic performance of CT angiography. Radiology. 2012;262:109-116.
Substitution of Levalbuterol to Avoid Tachyarrhythmia Not Supported
Clinical question: Does substitution of levalbuterol for albuterol in critically ill adult patients result in decreased incidence of tachyarrhythmias?
Background: Studies have indicated an increased risk of mortality from tachycardia and tachyarrhythmias in ICU patients. Levalbuterol is the R-isomer of albuterol, and it has been proposed that it may mitigate cardiac side effects seen with beta-2 agonists. For this reason, some clinicians have advocated using nebulized levalbuterol in critically ill patients.
Study design: Prospective randomized controlled trial with patient crossover.
Setting: Single academic medical center.
Synopsis: All ICU patients in a single teaching hospital were screened, and 70 patients were included. Patients were randomly crossed over between albuterol and levalbuterol every four to six hours. This resulted in a total of 836 measurements of heart rate, the primary outcome measurement. The study showed no clinically significant differences in average heart rate when using levalbuterol versus albuterol. This was a small study of ICU patients, using a surrogate endpoint of heart rate rather than mortality. Furthermore, the assessment of tachyarrhythmias was limited given the study size and relative rarity of these events. Despite these limitations, the study casts significant doubt on the theory and practice of switching from albuterol to levalbuterol solely for the purpose of reducing or avoiding tachycardia or tachyarrhythmias.
Bottom line: Substitution of levalbuterol for albuterol to avert tachycardia in critically ill patients is not warranted.
Citation: Khorfan FM, Smith P, Watt S, Barber KR. Effects of nebulized bronchodilator therapy on heart rate and arrhythmias in critically ill adult patients. Chest. 2011;140:1466-1472.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Online calculator helps prevent post-op respiratory failure
- New drug for long-term treatment of PE
- Benefits of triple therapy for COPD
- Knee-length compression stockings as good as thigh-length for PTS
- Video monitoring improves hand hygiene
- Asymptomatic bacteriuria often misdiagnosed as UTI
- CT accurate for lower GI bleeding diagnosis
- Switch from albuterol to lavalbuterol to reduce tachycardia not recommended
Preoperative Risk Calculator Can Help Predict Postoperative Respiratory Failure
Clinical question: Can preoperative factors identify patients at risk for postoperative respiratory failure (PRF)?
Background: PRF—when a patient requires mechanical ventilation >48 hours after surgery or needs unplanned intubation within 30 days of surgery—is associated with high mortality, with 30-day mortality rates of 26%.
Study design: Analysis of multicenter, prospective databases of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP).
Setting: Analysis of NSQIP data from 2007 (training set) and 2008 (validation set).
Synopsis: PRF was seen in 3.1% of patients in the 2007 data set and 2.6% in the 2008 data set. Those with PRF had significantly higher mortality rates than those without PRF (25.62% vs. 0.98%; P<0.0001). Preoperative risk factors associated with significantly increased risk of PRF were American Society of Anesthesiologists’ class, functional status, emergent nature of procedure, type of surgery, and preoperative sepsis.
The 2007 data set was used to develop the model, and the 2008 data set was used as a validation set. The selected risk model showed similar results in both sets with a c-statistic of 0.91 in the training set and 0.90 in the validation set. This selected model was then used to develop an interactive calculator predicting PRF (available at www.surgicalriskcalculator.com/prf-risk-calculator).
Bottom line: The PRF risk calculator can identify patients at high risk for PRF, which can aid in tailoring preventive strategies for patients prior to surgery.
Citation: Gupta H, Gupta PK, Fang X, et al. Development and validation of a risk calculator predicting postoperative respiratory failure. Chest. 2011;140:1207-1215.
New Drug for Treatment of Acute Symptomatic Pulmonary Embolism
Clinical question: Is the incidence of recurrent venous thromboembolism (VTE) or bleeding with use of idrabiotaparinux comparable to warfarin for treatment of acute symptomatic pulmonary embolism (PE)?
Background: Warfarin is an effective treatment for PE; however, maintenance of effective and safe levels of anticoagulation is difficult to achieve. A straightforward treatment option would be an attractive alternative. Idrabiotaparinux, a factor Xa inhibitor bound with a biotin moiety, is a weekly subcutaneous injection proposed as an alternative to warfarin for treatment of PE.
Study design: Industry-sponsored double-blind, randomized controlled trial.
Setting: 291 centers in 37 countries.
Synopsis: A group of 3,202 patients aged 18 to 96 years were randomly assigned to receive enoxaparin, followed by idrabiotaparinux or enoxaparin, then overlapped and followed by warfarin for three or six months. The incidence of recurrent VTE (including fatal and nonfatal PE or deep vein thrombosis) did not differ between the two treatment arms.
Of the 1,599 patients treated with idrabiotaparinux, 48 (3%) had a recurrence; of the 1,603 treated with warfarin, 97 (6%) had a recurrence (odds ratio, 0.49). The rate of clinically relevant bleeding was also similar, with 72 (5%) in the idrabiotaparinux group versus 106 (7%) in the warfarin group. Much like warfarin, idrabiotaparinux requires bridging therapy with initial low-molecular-weight heparin.
Bottom line: Use of enoxaparin followed by weekly subcutaneous injection of idrabiotaparinux was as effective as enoxaparin followed by warfarin for preventing recurrent VTE, and may provide a suitable option for treatment of acute symptomatic PE.
Citation: Buller HR, Gallus AS, Pillion G, Prins MH, Raskob GE. Enoxaparin followed by once-weekly idrabiotaparinux versus enoxaparin plus warfarin for patients with acute symptomatic pulmonary embolism: a randomised, double-blind, double-dummy, non-inferiority trial. Lancet. 2012;379:123-129.
Triple Therapy Better than Double for COPD
Clinical question: Does addition of tiotropium to inhaled corticosteroids and long-acting beta-agonists (LABA) have an additive benefit in reducing mortality, hospital admissions, and exacerbations in COPD?
Background: Triple therapy in COPD involves adding LABA and long-acting antimuscarinics (LAMA), such as tiotropium, to inhaled corticosteroids (ICS). Despite the guidelines recommending triple therapy for severe COPD, most studies have evaluated either LAMA or LABA plus ICS, but not all three together.
Study design: Retrospective cohort.
Setting: Tayside, Scotland’s National Health Services database.
Synopsis: Patients with severe COPD were divided into two groups: 1,857 patients had received ICS+LABA (double therapy) and 996 had received ICS+LABA+tiotropium (triple therapy), with follow-up of 4.65 years.
All-cause mortality was 35% lower in the triple therapy group (HR 0.65, 95% CI 0.57-0.75). Corticosteroid use was 29% lower (HR 0.71, 95% CI 0.63-0.80), and hospital admissions were 15% lower (HR 0.85, 95% CI 0.73-0.99) in the triple-therapy group. These results were adjusted for smoking, age, sex, socioeconomic status, and history of diabetes, cardiovascular, and respiratory disease.
This study is limited by its observational retrospective design but provides good evidence of the need for randomized controlled trials to validate the clinical benefits of triple therapy.
Bottom line: Adding tiotropium to ICS plus LABA is associated with lower all-cause mortality, hospitalizations, and corticosteroid use when compared with ICS plus LABA, validating its current use in management of severe COPD.
Citation: Short PM, Williamson PA, Elder DHJ, Lipworth SIW, Schembi S, Lipworth BJ. The impact of tiotropium on mortality and exacerbations when added to inhaled corticosteroids and long-acting β-agonist therapy in COPD. Chest. 2012;141:81-86.
Above-Knee Compression Stockings Not Better than Below-Knee Stockings for Protection Against Post-Thrombotic Syndrome
Clinical question: Do above-knee compression elastic stockings prevent post-thrombotic syndrome (PTS) better than below-knee stockings?
Background: PTS—characterized by leg pain, cramps, edema, and hyperpigmentation—occurs in 25% to 50% of patients after an episode of deep venous thrombosis (DVT). Previous studies demonstrated a 50% reduction in the incidence of PTS when patients used below-knee stockings.
Study design: Open-label, randomized clinical trial.
Setting: Eight hospitals in Italy.
Synopsis: A total of 267 patients with their first episode of DVT were randomized to thigh-length or below-knee compression elastic stockings, as well as therapeutic anticoagulation, with a primary endpoint of three-year incidence of PTS. Assessment was done by study personnel who were blinded to the type of stocking the patients had been prescribed. Severity of PTS was graded by a scoring system incorporating objective and subjective criteria with an independent adjudicator.
The intention-to-treat analysis showed no significant difference in the three-year incidence of PTS between thigh- and knee-length stockings (32.6% vs. 35.6%, respectively). Compliance was better in the knee-length (82.6%) than in the thigh-length (66.7%) group due to the significantly lower rate of stockings-related side effects.
The study is limited by a lack of blinding in the study participants.
Bottom line: Knee-length stockings offer equal similar protection against PTS with better compliance when compared with thigh-length stockings.
Citation: Prandoni P, Noventa F, Quintavalla R, et al. Thigh-length versus below-knee compression elastic stockings for prevention of the post-thrombotic syndrome in patients with proximal-venous thrombosis: a randomized trial. Blood. 2012;119:1561-1565.
Video Auditing With Near- Real-Time Feedback Improves Hand Hygiene Practices
Clinical question: Does the use of direct video monitoring with continuous, multi-modal feedback promote improvement in healthcare workers’ compliance with hand hygiene?
Background: Appropriate hand hygiene is an effective means of infection control. Direct human observation of hand hygiene compliance does little more than provide a biased, temporary, and often overestimated assessment of compliance. The use of video-based monitoring technology in other aspects of society (e.g. traffic signal cameras) has been well demonstrated to modify behavior.
Study design: Prospective cohort study.
Setting: Tertiary-care hospital’s 17-bed medical ICU in the northeastern U.S.
Synopsis: Through the use of 21 motion-activated video cameras with continuous third-party auditing, the provision of near real-time feedback improved hand hygiene rates of healthcare workers from 6.5% to 81.6%. In the four months preceding feedback, only 3,933 hand-washing events out of 60,542 (6.5%) were considered “passing.” During the active feedback period, 59,627 events out of 73,080 (81.6%) passed.
The improvement was sustained in the maintenance period of the study with an average rate of hand hygiene compliance of 87.9%. The improvement in hand hygiene compliance required active provision of feedback as well as the presence of monitoring equipment, making the applicability of this study limited, based on the cost of the technology and the manpower to provide feedback.
Bottom line: Hand hygiene practices improve when healthcare workers are given immediate feedback on their compliance.
Citation: Rebellion D, Husain E, Schilling ME, et al. Using high-technology to enforce low-technology safety measures: the use of third-party remote video auditing and real-time feedback in healthcare. Clin Infect Dis. 2012:54(1):1-7.
Mismanagement of Enterococcal Bacteriuria
Clinical question: Are clinical providers following appropriate guidelines to identify and manage enterococcal bacteriuria?
Background: There are specific evidence-based guidelines for the diagnosis and treatment of urinary tract infections (UTI) and asymptomatic bacteriuria (ABU). ABU is often mistaken for a UTI, and incorrectly treated as one.
Study design: Retrospective cohort.
Setting: Two academic teaching hospitals in Houston, Texas.
Synopsis: Using the current Infectious Disease Society of America (IDSA) guidelines, 375 Enterococcus urine cultures were reviewed and determined to be either UTI or ABU. The cultures were initially reviewed for appropriate treatment and again 30 days later for complications. UTI was defined as bacteriuria with one or more sign or symptom (urgency, frequency, dysuria, suprapubic tenderness, flank pain, rigors, visible hematuria, delirium, or fevers) without another identifiable cause. ABU was defined as bacteriuria without any of the signs or symptoms, or a clear nonurinary source.
Of the 339 cultures matching inclusion criteria, 156 were classified as UTI and 183 classified as ABU. Sixty of the 183 ABU (32.8%) were inappropriately treated with antibiotics, while antibiotics were withheld in 23 of the 156 UTI (14.7%). Eighty-three of 339 cultures (24.5%) were incorrectly treated. The most common reason for ABU being inappropriately treated was the presence of pyuria, associated with a threefold higher use of antibiotics.
There was no significant difference in subsequent infections or infectious complications between UTI and ABU.
Bottom line: Enterococcal ABU is frequently treated with antibiotics, even though guidelines recommend against it; providers should resist overtreating enterococcal ABU.
Citation: Lin E, Bhusal Y, Horwitz D, Shelburne SA, Trautner BW. Overtreatment of enterococcal bacteriuria. Arch Intern Med. 2012;172:33-38.
CT Angiography for the Diagnosis of Acute Lower GI Bleeding in an Emergency Setting
Clinical question: Is CT angiography a reliable initial diagnostic procedure to identify the presence and location of an acute lower gastrointestinal (GI) bleed in the ED setting?
Background: CT angiography has been identified as a potentially useful procedure to identify acute GI bleeds; however, the specific role and timing of the procedure has not been clearly identified.
Study design: Prospective study.
Setting: ED of a university-based hospital in Madrid.
Synopsis: CT angiography was performed on 47 ED patients (27 men, 20 women, with a mean age of 68 years) with an acute lower GI bleed. Study protocol included a preliminary unenhanced CT scan followed by CT angiogram prior to the standard clinical protocol, which included colonoscopy, angiography, or laparotomy.
Images were reviewed by two different ED radiologists, who were blinded to the diagnosis, and compared with the standard protocol findings. CT angiography correctly identified active acute or recent GI bleeding in 46 of the 47 patients, with a sensitivity of 100% (19 of 19), NPV of 100% (27 of 27), specificity of 96% (27 of 28), and PPV of 95% (19 of 20). CT angiography also was 93% accurate in identifying the cause of the GI bleed when compared with the standard reference.
Limitations of the study include its small size and the lack of a control group.
Bottom line: CT angiography is an accurate and more readily available modality for the diagnosis of acute lower GI bleeding, though it does not provide a therapeutic option.
Citation: Martí M, Artigas JM, Garzón G, Alvarez-Sala R, Soto JA. Acute lower intestinal bleeding: feasibility and diagnostic performance of CT angiography. Radiology. 2012;262:109-116.
Substitution of Levalbuterol to Avoid Tachyarrhythmia Not Supported
Clinical question: Does substitution of levalbuterol for albuterol in critically ill adult patients result in decreased incidence of tachyarrhythmias?
Background: Studies have indicated an increased risk of mortality from tachycardia and tachyarrhythmias in ICU patients. Levalbuterol is the R-isomer of albuterol, and it has been proposed that it may mitigate cardiac side effects seen with beta-2 agonists. For this reason, some clinicians have advocated using nebulized levalbuterol in critically ill patients.
Study design: Prospective randomized controlled trial with patient crossover.
Setting: Single academic medical center.
Synopsis: All ICU patients in a single teaching hospital were screened, and 70 patients were included. Patients were randomly crossed over between albuterol and levalbuterol every four to six hours. This resulted in a total of 836 measurements of heart rate, the primary outcome measurement. The study showed no clinically significant differences in average heart rate when using levalbuterol versus albuterol. This was a small study of ICU patients, using a surrogate endpoint of heart rate rather than mortality. Furthermore, the assessment of tachyarrhythmias was limited given the study size and relative rarity of these events. Despite these limitations, the study casts significant doubt on the theory and practice of switching from albuterol to levalbuterol solely for the purpose of reducing or avoiding tachycardia or tachyarrhythmias.
Bottom line: Substitution of levalbuterol for albuterol to avert tachycardia in critically ill patients is not warranted.
Citation: Khorfan FM, Smith P, Watt S, Barber KR. Effects of nebulized bronchodilator therapy on heart rate and arrhythmias in critically ill adult patients. Chest. 2011;140:1466-1472.
Urinary Tract Infections Do Not Play a Significant Role in Chronic Kidney Disease

Clinical question: What is the association between childhood urinary tract infections (UTIs) and chronic kidney disease (CKD)?
Background: A traditional paradigm in pediatrics is that CKD might be caused by renal scarring as a result of recurrent UTIs, particularly in the presence of vesicoureteral reflux (VUR). Increasingly, this has been called into question as nonintervention for low-grade VUR has not impacted clinical outcomes.
Study design: Retrospective cohort and systematic literature review.
Setting: Tertiary-care hospital in Finland and PubMed database.
Synopsis: A search of the PubMed database for articles published from 1966 to 2009 relating to a potential association between CKD and UTIs yielded 10 studies reporting on 1,576 patients with UTIs and long-term evaluation for CKD. Only three of the 1,576 patients had childhood UTIs without structural kidney abnormalities as a potential cause of the CKD. VUR was not considered a structural abnormality. The authors note that no data on kidney morphology prior to UTI recurrence were available in these cases.
At the same time, the study authors reviewed the records of 366 patients with CKD at a tertiary-care hospital in Finland. They excluded 308 patients with defined noninfectious causes of CKD. Of the 58 remaining patients, three potentially had recurrent UTIs as a contributing cause to eventual CKD. All three patients had structurally abnormal kidneys on first radiologic examination, possibly suggesting pre-existing renal anomalies. The potential association between recurrent childhood UTIs without structural abnormalities and CKD appears to be less than 1%.
Limitations of this study include its retrospective design and incomplete characterization systematic review. Nevertheless, the study appears to support recent work that childhood UTIs without underlying kidney abnormalities are unlikely to result in permanent renal damage.
Bottom line: Childhood UTIs, without structural kidney abnormality, are not a significant cause of chronic kidney disease in adults.
Citation: Salo J, Ilkäheimo R, Tapiainen T, Uhari M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011;128:840-847.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the association between childhood urinary tract infections (UTIs) and chronic kidney disease (CKD)?
Background: A traditional paradigm in pediatrics is that CKD might be caused by renal scarring as a result of recurrent UTIs, particularly in the presence of vesicoureteral reflux (VUR). Increasingly, this has been called into question as nonintervention for low-grade VUR has not impacted clinical outcomes.
Study design: Retrospective cohort and systematic literature review.
Setting: Tertiary-care hospital in Finland and PubMed database.
Synopsis: A search of the PubMed database for articles published from 1966 to 2009 relating to a potential association between CKD and UTIs yielded 10 studies reporting on 1,576 patients with UTIs and long-term evaluation for CKD. Only three of the 1,576 patients had childhood UTIs without structural kidney abnormalities as a potential cause of the CKD. VUR was not considered a structural abnormality. The authors note that no data on kidney morphology prior to UTI recurrence were available in these cases.
At the same time, the study authors reviewed the records of 366 patients with CKD at a tertiary-care hospital in Finland. They excluded 308 patients with defined noninfectious causes of CKD. Of the 58 remaining patients, three potentially had recurrent UTIs as a contributing cause to eventual CKD. All three patients had structurally abnormal kidneys on first radiologic examination, possibly suggesting pre-existing renal anomalies. The potential association between recurrent childhood UTIs without structural abnormalities and CKD appears to be less than 1%.
Limitations of this study include its retrospective design and incomplete characterization systematic review. Nevertheless, the study appears to support recent work that childhood UTIs without underlying kidney abnormalities are unlikely to result in permanent renal damage.
Bottom line: Childhood UTIs, without structural kidney abnormality, are not a significant cause of chronic kidney disease in adults.
Citation: Salo J, Ilkäheimo R, Tapiainen T, Uhari M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011;128:840-847.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the association between childhood urinary tract infections (UTIs) and chronic kidney disease (CKD)?
Background: A traditional paradigm in pediatrics is that CKD might be caused by renal scarring as a result of recurrent UTIs, particularly in the presence of vesicoureteral reflux (VUR). Increasingly, this has been called into question as nonintervention for low-grade VUR has not impacted clinical outcomes.
Study design: Retrospective cohort and systematic literature review.
Setting: Tertiary-care hospital in Finland and PubMed database.
Synopsis: A search of the PubMed database for articles published from 1966 to 2009 relating to a potential association between CKD and UTIs yielded 10 studies reporting on 1,576 patients with UTIs and long-term evaluation for CKD. Only three of the 1,576 patients had childhood UTIs without structural kidney abnormalities as a potential cause of the CKD. VUR was not considered a structural abnormality. The authors note that no data on kidney morphology prior to UTI recurrence were available in these cases.
At the same time, the study authors reviewed the records of 366 patients with CKD at a tertiary-care hospital in Finland. They excluded 308 patients with defined noninfectious causes of CKD. Of the 58 remaining patients, three potentially had recurrent UTIs as a contributing cause to eventual CKD. All three patients had structurally abnormal kidneys on first radiologic examination, possibly suggesting pre-existing renal anomalies. The potential association between recurrent childhood UTIs without structural abnormalities and CKD appears to be less than 1%.
Limitations of this study include its retrospective design and incomplete characterization systematic review. Nevertheless, the study appears to support recent work that childhood UTIs without underlying kidney abnormalities are unlikely to result in permanent renal damage.
Bottom line: Childhood UTIs, without structural kidney abnormality, are not a significant cause of chronic kidney disease in adults.
Citation: Salo J, Ilkäheimo R, Tapiainen T, Uhari M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011;128:840-847.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Guidelines for Treatment of Uncomplicated Cystitis and Pyelonephritis in Healthy, Community-Dwelling Women

Background
Uncomplicated cystitis is one of the most common indications for prescribing antimicrobial therapy to otherwise healthy women, but wide variation in prescribing practices has been described.1-2 This has prompted the need for guidelines to help providers in their selection of empiric antimicrobial regimens. Antibiotic selection should take into consideration the efficacy of individual agents, as well as their propensity for inducing resistance, altering gut flora, and increasing the risk of colonization or infection with multi-drug resistant organisms.
Guideline Update
In March 2010, the Infectious Diseases Society of America (IDSA) and the European Society for Microbiology and Infectious Diseases (ESCMID) published new guidelines for the treatment of uncomplicated cystitis and pyelonephritis in healthy, community-dwelling women.3
First-line recommended agents for empiric treatment of uncomplicated cystitis are:
- nitrofurantoin for five days;
- trimethoprim-sulfamethoxazole for three days;
- fosfomycin in a single dose; or
- pivmecillinam (where available) for three to seven days.
Although highly efficacious, fluoroquinolones are not recommended as first-line treatment for acute cystitis because of their propensity for causing “collateral damage,” especially alteration of gut flora and increased risk of multi-drug resistant infection or colonization, including methicillin-resistant Staphylococcus aureus. Oral beta-lactams (other than pivmecillinam) have generally demonstrated inferior efficacy and more adverse effects when compared with the above agents, and should be used only if none of the preferred agents can be used. Specifically, amoxicillin and ampicillin are not recommended as empiric therapy due to their low efficacy in unselected patients, though may be appropriate when culture data is available to guide therapy. Narrow spectrum cephalosporins are also a potential agent for use in certain clinical situations, although the guidelines do not make any recommendation for or against their use, given a lack of studies.
For the treatment of acute pyelonephritis, the guidelines emphasize that all patients should have urine culture and susceptibility testing in order to tailor empiric therapy to the specific uropathogen. A 5-7 day course of an oral fluoroquinolone is appropriate when the prevalence of resistance in community uropathogens is ≤10%. Where resistance is more common, an initial intravenous dose of ceftriaxone or an aminoglycoside can be administered prior to starting oral therapy. Other alternatives include a 14-day course of trimethoprim-sulfamethoxazole or an oral beta-lactam.
Women requiring hospitalization for pyelonephritis should initially be treated with an intravenous antimicrobial regimen, the choice of which should be based on local resistance patterns. Recommended intravenous agents include fluoroquinolones, aminoglycosides (with or without ampicillin), extended-spectrum cephalosporins / penicillins, or carbapenems.
Analysis
Previous guidelines for the treatment of uncomplicated cystitis and pyelonephritis were published by the IDSA in 1999.4 The guidelines were updated based on the following factors:
- continued variability in prescribing practices;1-2
- increase in antimicrobial resistance among uropathogens;
- awareness of the unintended consequences of antimicrobial therapy, such as selection of drug-resistant organisms and colonization or infection with multi-drug resistant organisms; and
- study of newer agents and different durations of therapy.
Two important differences exist between the 1999 and 2010 guidelines:
- Nitrofurantoin has taken on more prominence in the 2010 guidelines for uncomplicated cystitis. The 1999 guidelines recommended trimethoprim-sulfamethoxazole as a first-line agent and mentioned nitrofurantoin and fosfomycin as potential alternative agents, but had few studies available to inform comparative efficacy or duration of therapy.
- For the outpatient treatment of mildly-ill patients with acute pyelonephritis, the 1999 guidelines recommended 14 days of therapy regardless of the agent used; in contrast, the 2010 guidelines recommend a five- to seven-day course for oral fluoroquinolones.
The American Congress of Obstetricians and Gynecologists, American Urological Association, Association of Medical Microbiology and Infectious Diseases-Canada, and the Society for Academic Emergency Medicine have endorsed the 2010 IDSA-ESCMID guidelines. The IDSA and ESCMID plan to evaluate the need for revisions to the 2010 guidelines based on an annual review of the current literature.
HM Takeaways
The 2010 IDSA-ESCMID guidelines are a resource available to hospitalists treating acute uncomplicated cystitis and pyelonephritis. As important differences exist between the target population and the hospitalist’s patient population, there are some key points to consider for clinicians treating cystitis or pyelonephritis in hospitalized patients.
Importantly, while nitrofurantoin is favored as a first-line antimicrobial agent for cystitis in the 2010 IDSA-ESCMID guidelines, it might be problematic in hospitalized patients for several reasons:
- it is not approved or recommended for the treatment of pyelonephritis;
- it is contraindicated in patients with creatinine clearance <60 ml/min; and
- it is generally not recommended for use in patients >65 years old because of the risk of renal impairment (Beers Criteria).5
Additionally, the treatment of acute cystitis in men requires special consideration. Notably, nitrofurantoin is not recommended in men because of poor prostatic tissue penetration, and although studies are limited, some sources recommend a longer treatment duration of at least 7 days.6 Finally, hospitalized patients commonly have other conditions, such as urological abnormalities, indwelling Foley catheters, recent urinary tract instrumentation, recent use of antibiotics, risk for multi-drug resistant organisms, potential interactions with other medications, and immunosuppression. The presence of any of these factors will influence the choice of empiric therapy and may warrant treatment for complicated cystitis or pyelonephritis, which are not addressed by these guidelines.
Drs. Tarvin and Sponsler are academic hospitalists at Vanderbilt University School of Medicine in Nashville, Tenn.
References
- Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2006;166:635-639.
- Kahan NR, Chinitz DP, Kahan E. Longer than recommended empiric antibiotic treatment of urinary tract infection in women: an avoidable waste of money. J Clin Pharm Therap. 2004;29:59-63.
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Inf Dis. 2011;52(5):e103-20.
- Warren JW, Abrutyn E, Hebel JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America. Clin Inf Dis. 1999;29(4):745-58.
- Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a U.S. consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
- Mehnert-Kay SA. Diagnosis and management of uncomplicated urinary tract infections. A Fam Phys. 2005;72(3):451-456.
Background
Uncomplicated cystitis is one of the most common indications for prescribing antimicrobial therapy to otherwise healthy women, but wide variation in prescribing practices has been described.1-2 This has prompted the need for guidelines to help providers in their selection of empiric antimicrobial regimens. Antibiotic selection should take into consideration the efficacy of individual agents, as well as their propensity for inducing resistance, altering gut flora, and increasing the risk of colonization or infection with multi-drug resistant organisms.
Guideline Update
In March 2010, the Infectious Diseases Society of America (IDSA) and the European Society for Microbiology and Infectious Diseases (ESCMID) published new guidelines for the treatment of uncomplicated cystitis and pyelonephritis in healthy, community-dwelling women.3
First-line recommended agents for empiric treatment of uncomplicated cystitis are:
- nitrofurantoin for five days;
- trimethoprim-sulfamethoxazole for three days;
- fosfomycin in a single dose; or
- pivmecillinam (where available) for three to seven days.
Although highly efficacious, fluoroquinolones are not recommended as first-line treatment for acute cystitis because of their propensity for causing “collateral damage,” especially alteration of gut flora and increased risk of multi-drug resistant infection or colonization, including methicillin-resistant Staphylococcus aureus. Oral beta-lactams (other than pivmecillinam) have generally demonstrated inferior efficacy and more adverse effects when compared with the above agents, and should be used only if none of the preferred agents can be used. Specifically, amoxicillin and ampicillin are not recommended as empiric therapy due to their low efficacy in unselected patients, though may be appropriate when culture data is available to guide therapy. Narrow spectrum cephalosporins are also a potential agent for use in certain clinical situations, although the guidelines do not make any recommendation for or against their use, given a lack of studies.
For the treatment of acute pyelonephritis, the guidelines emphasize that all patients should have urine culture and susceptibility testing in order to tailor empiric therapy to the specific uropathogen. A 5-7 day course of an oral fluoroquinolone is appropriate when the prevalence of resistance in community uropathogens is ≤10%. Where resistance is more common, an initial intravenous dose of ceftriaxone or an aminoglycoside can be administered prior to starting oral therapy. Other alternatives include a 14-day course of trimethoprim-sulfamethoxazole or an oral beta-lactam.
Women requiring hospitalization for pyelonephritis should initially be treated with an intravenous antimicrobial regimen, the choice of which should be based on local resistance patterns. Recommended intravenous agents include fluoroquinolones, aminoglycosides (with or without ampicillin), extended-spectrum cephalosporins / penicillins, or carbapenems.
Analysis
Previous guidelines for the treatment of uncomplicated cystitis and pyelonephritis were published by the IDSA in 1999.4 The guidelines were updated based on the following factors:
- continued variability in prescribing practices;1-2
- increase in antimicrobial resistance among uropathogens;
- awareness of the unintended consequences of antimicrobial therapy, such as selection of drug-resistant organisms and colonization or infection with multi-drug resistant organisms; and
- study of newer agents and different durations of therapy.
Two important differences exist between the 1999 and 2010 guidelines:
- Nitrofurantoin has taken on more prominence in the 2010 guidelines for uncomplicated cystitis. The 1999 guidelines recommended trimethoprim-sulfamethoxazole as a first-line agent and mentioned nitrofurantoin and fosfomycin as potential alternative agents, but had few studies available to inform comparative efficacy or duration of therapy.
- For the outpatient treatment of mildly-ill patients with acute pyelonephritis, the 1999 guidelines recommended 14 days of therapy regardless of the agent used; in contrast, the 2010 guidelines recommend a five- to seven-day course for oral fluoroquinolones.
The American Congress of Obstetricians and Gynecologists, American Urological Association, Association of Medical Microbiology and Infectious Diseases-Canada, and the Society for Academic Emergency Medicine have endorsed the 2010 IDSA-ESCMID guidelines. The IDSA and ESCMID plan to evaluate the need for revisions to the 2010 guidelines based on an annual review of the current literature.
HM Takeaways
The 2010 IDSA-ESCMID guidelines are a resource available to hospitalists treating acute uncomplicated cystitis and pyelonephritis. As important differences exist between the target population and the hospitalist’s patient population, there are some key points to consider for clinicians treating cystitis or pyelonephritis in hospitalized patients.
Importantly, while nitrofurantoin is favored as a first-line antimicrobial agent for cystitis in the 2010 IDSA-ESCMID guidelines, it might be problematic in hospitalized patients for several reasons:
- it is not approved or recommended for the treatment of pyelonephritis;
- it is contraindicated in patients with creatinine clearance <60 ml/min; and
- it is generally not recommended for use in patients >65 years old because of the risk of renal impairment (Beers Criteria).5
Additionally, the treatment of acute cystitis in men requires special consideration. Notably, nitrofurantoin is not recommended in men because of poor prostatic tissue penetration, and although studies are limited, some sources recommend a longer treatment duration of at least 7 days.6 Finally, hospitalized patients commonly have other conditions, such as urological abnormalities, indwelling Foley catheters, recent urinary tract instrumentation, recent use of antibiotics, risk for multi-drug resistant organisms, potential interactions with other medications, and immunosuppression. The presence of any of these factors will influence the choice of empiric therapy and may warrant treatment for complicated cystitis or pyelonephritis, which are not addressed by these guidelines.
Drs. Tarvin and Sponsler are academic hospitalists at Vanderbilt University School of Medicine in Nashville, Tenn.
References
- Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2006;166:635-639.
- Kahan NR, Chinitz DP, Kahan E. Longer than recommended empiric antibiotic treatment of urinary tract infection in women: an avoidable waste of money. J Clin Pharm Therap. 2004;29:59-63.
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Inf Dis. 2011;52(5):e103-20.
- Warren JW, Abrutyn E, Hebel JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America. Clin Inf Dis. 1999;29(4):745-58.
- Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a U.S. consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
- Mehnert-Kay SA. Diagnosis and management of uncomplicated urinary tract infections. A Fam Phys. 2005;72(3):451-456.
Background
Uncomplicated cystitis is one of the most common indications for prescribing antimicrobial therapy to otherwise healthy women, but wide variation in prescribing practices has been described.1-2 This has prompted the need for guidelines to help providers in their selection of empiric antimicrobial regimens. Antibiotic selection should take into consideration the efficacy of individual agents, as well as their propensity for inducing resistance, altering gut flora, and increasing the risk of colonization or infection with multi-drug resistant organisms.
Guideline Update
In March 2010, the Infectious Diseases Society of America (IDSA) and the European Society for Microbiology and Infectious Diseases (ESCMID) published new guidelines for the treatment of uncomplicated cystitis and pyelonephritis in healthy, community-dwelling women.3
First-line recommended agents for empiric treatment of uncomplicated cystitis are:
- nitrofurantoin for five days;
- trimethoprim-sulfamethoxazole for three days;
- fosfomycin in a single dose; or
- pivmecillinam (where available) for three to seven days.
Although highly efficacious, fluoroquinolones are not recommended as first-line treatment for acute cystitis because of their propensity for causing “collateral damage,” especially alteration of gut flora and increased risk of multi-drug resistant infection or colonization, including methicillin-resistant Staphylococcus aureus. Oral beta-lactams (other than pivmecillinam) have generally demonstrated inferior efficacy and more adverse effects when compared with the above agents, and should be used only if none of the preferred agents can be used. Specifically, amoxicillin and ampicillin are not recommended as empiric therapy due to their low efficacy in unselected patients, though may be appropriate when culture data is available to guide therapy. Narrow spectrum cephalosporins are also a potential agent for use in certain clinical situations, although the guidelines do not make any recommendation for or against their use, given a lack of studies.
For the treatment of acute pyelonephritis, the guidelines emphasize that all patients should have urine culture and susceptibility testing in order to tailor empiric therapy to the specific uropathogen. A 5-7 day course of an oral fluoroquinolone is appropriate when the prevalence of resistance in community uropathogens is ≤10%. Where resistance is more common, an initial intravenous dose of ceftriaxone or an aminoglycoside can be administered prior to starting oral therapy. Other alternatives include a 14-day course of trimethoprim-sulfamethoxazole or an oral beta-lactam.
Women requiring hospitalization for pyelonephritis should initially be treated with an intravenous antimicrobial regimen, the choice of which should be based on local resistance patterns. Recommended intravenous agents include fluoroquinolones, aminoglycosides (with or without ampicillin), extended-spectrum cephalosporins / penicillins, or carbapenems.
Analysis
Previous guidelines for the treatment of uncomplicated cystitis and pyelonephritis were published by the IDSA in 1999.4 The guidelines were updated based on the following factors:
- continued variability in prescribing practices;1-2
- increase in antimicrobial resistance among uropathogens;
- awareness of the unintended consequences of antimicrobial therapy, such as selection of drug-resistant organisms and colonization or infection with multi-drug resistant organisms; and
- study of newer agents and different durations of therapy.
Two important differences exist between the 1999 and 2010 guidelines:
- Nitrofurantoin has taken on more prominence in the 2010 guidelines for uncomplicated cystitis. The 1999 guidelines recommended trimethoprim-sulfamethoxazole as a first-line agent and mentioned nitrofurantoin and fosfomycin as potential alternative agents, but had few studies available to inform comparative efficacy or duration of therapy.
- For the outpatient treatment of mildly-ill patients with acute pyelonephritis, the 1999 guidelines recommended 14 days of therapy regardless of the agent used; in contrast, the 2010 guidelines recommend a five- to seven-day course for oral fluoroquinolones.
The American Congress of Obstetricians and Gynecologists, American Urological Association, Association of Medical Microbiology and Infectious Diseases-Canada, and the Society for Academic Emergency Medicine have endorsed the 2010 IDSA-ESCMID guidelines. The IDSA and ESCMID plan to evaluate the need for revisions to the 2010 guidelines based on an annual review of the current literature.
HM Takeaways
The 2010 IDSA-ESCMID guidelines are a resource available to hospitalists treating acute uncomplicated cystitis and pyelonephritis. As important differences exist between the target population and the hospitalist’s patient population, there are some key points to consider for clinicians treating cystitis or pyelonephritis in hospitalized patients.
Importantly, while nitrofurantoin is favored as a first-line antimicrobial agent for cystitis in the 2010 IDSA-ESCMID guidelines, it might be problematic in hospitalized patients for several reasons:
- it is not approved or recommended for the treatment of pyelonephritis;
- it is contraindicated in patients with creatinine clearance <60 ml/min; and
- it is generally not recommended for use in patients >65 years old because of the risk of renal impairment (Beers Criteria).5
Additionally, the treatment of acute cystitis in men requires special consideration. Notably, nitrofurantoin is not recommended in men because of poor prostatic tissue penetration, and although studies are limited, some sources recommend a longer treatment duration of at least 7 days.6 Finally, hospitalized patients commonly have other conditions, such as urological abnormalities, indwelling Foley catheters, recent urinary tract instrumentation, recent use of antibiotics, risk for multi-drug resistant organisms, potential interactions with other medications, and immunosuppression. The presence of any of these factors will influence the choice of empiric therapy and may warrant treatment for complicated cystitis or pyelonephritis, which are not addressed by these guidelines.
Drs. Tarvin and Sponsler are academic hospitalists at Vanderbilt University School of Medicine in Nashville, Tenn.
References
- Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2006;166:635-639.
- Kahan NR, Chinitz DP, Kahan E. Longer than recommended empiric antibiotic treatment of urinary tract infection in women: an avoidable waste of money. J Clin Pharm Therap. 2004;29:59-63.
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Inf Dis. 2011;52(5):e103-20.
- Warren JW, Abrutyn E, Hebel JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America. Clin Inf Dis. 1999;29(4):745-58.
- Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a U.S. consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
- Mehnert-Kay SA. Diagnosis and management of uncomplicated urinary tract infections. A Fam Phys. 2005;72(3):451-456.
SHM Offers Multitude of Educational, Professional Development Opportunities
In addition to the annual meeting, SHM and its partners bring hospitalists the very best in education, professional development, and networking in the form of in-person meetings.
July: Pediatric Hospital Medicine
Every year, hundreds of pediatric hospitalists come together to share their passion for caring for hospitalized children. This year, Pediatric Hospital Medicine 2012 will convene July 19-22 at the Northern Kentucky Convention Center, just outside Cincinnati. The meeting is co-sponsored by the Academic Pediatric Association, SHM, and the American Academy of Pediatrics.
For details and to register, visit www.hospitalmedicine.org/events.
October: Leadership Academy
SHM’s Leadership Academy continues to create the next generation of hospitalist leaders and sharpen the skills of existing leaders.
SHM will present its next industry-leading Leadership Academy Oct. 1-4 in Scottsdale, Ariz. The program will feature the popular “Foundations of Effective Leadership” course and the second-level “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” course.
Both courses build leadership skills for hospitalists, or, as more than one hospitalist has called the curriculum, “everything they don’t teach you in medical school.”
In the highly interactive, four-day “Foundations of Effective Leadership” course, hospitalists learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, and examine how hospital metrics are derived.
The “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” program provides skills building for hospitalists who want to drive culture change through specific leadership behaviors and actions. It also delves deep into financial storytelling, effective professional negotiation activities with proven techniques, and more.
“Advanced Leadership” is a second-level course and is open only to hospitalists who have completed the “Foundations of Effective Leadership” course, or who have earned an advanced management degree, such as an MBA.
Both courses are required for the new Leadership Certification program, which gives hospitalists the ability to demonstrate their leadership skills through certification.
Hospitalists planning to take any Leadership Academy course should note that, starting in 2013, Leadership Academy courses will be offered only in the fall.
For details and registration, visit www.hospitalmedicine.org/leadership.
Anytime: Online Education
Hospitalists working to demonstrate their expertise and commitment to HM through the Focused Practice in Hospital Medicine designation can earn Maintenance of Certification (MOC) self-evaluation points and CME credit online at www.hospitalmedicine.org/mkm.
SHM’s Medical Knowledge Modules are online learning and self-evaluation tools that provide the user with industry-leading instruction on quality-improvement (QI) theory; project design; system processes; measurement; chance science; tools for implementation; epidemiology of patient safety; and error types, disclosure, prevention strategies, and theory.
Three Medical Knowledge Modules are available: Hospital QI and Patient Safety, Hospital QI and Patient Safety II, and Pediatric Hospital QI and Patient Safety. Each online module consists of 25 multiple-choice questions. If the correct answer is chosen, the module provides a rationale explaining why that answer was correct. When an incorrect answer is selected, users are encouraged to try again.
Each module will earn hospitalists 10 self-evaluation points for diplomates enrolled in ABIM’s MOC program and three AMA PRA Category 1 CME Credits.
SHM will continue to roll out other topics throughout 2012.
Brendon Shank is SHM associate vice president of communications.
In addition to the annual meeting, SHM and its partners bring hospitalists the very best in education, professional development, and networking in the form of in-person meetings.
July: Pediatric Hospital Medicine
Every year, hundreds of pediatric hospitalists come together to share their passion for caring for hospitalized children. This year, Pediatric Hospital Medicine 2012 will convene July 19-22 at the Northern Kentucky Convention Center, just outside Cincinnati. The meeting is co-sponsored by the Academic Pediatric Association, SHM, and the American Academy of Pediatrics.
For details and to register, visit www.hospitalmedicine.org/events.
October: Leadership Academy
SHM’s Leadership Academy continues to create the next generation of hospitalist leaders and sharpen the skills of existing leaders.
SHM will present its next industry-leading Leadership Academy Oct. 1-4 in Scottsdale, Ariz. The program will feature the popular “Foundations of Effective Leadership” course and the second-level “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” course.
Both courses build leadership skills for hospitalists, or, as more than one hospitalist has called the curriculum, “everything they don’t teach you in medical school.”
In the highly interactive, four-day “Foundations of Effective Leadership” course, hospitalists learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, and examine how hospital metrics are derived.
The “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” program provides skills building for hospitalists who want to drive culture change through specific leadership behaviors and actions. It also delves deep into financial storytelling, effective professional negotiation activities with proven techniques, and more.
“Advanced Leadership” is a second-level course and is open only to hospitalists who have completed the “Foundations of Effective Leadership” course, or who have earned an advanced management degree, such as an MBA.
Both courses are required for the new Leadership Certification program, which gives hospitalists the ability to demonstrate their leadership skills through certification.
Hospitalists planning to take any Leadership Academy course should note that, starting in 2013, Leadership Academy courses will be offered only in the fall.
For details and registration, visit www.hospitalmedicine.org/leadership.
Anytime: Online Education
Hospitalists working to demonstrate their expertise and commitment to HM through the Focused Practice in Hospital Medicine designation can earn Maintenance of Certification (MOC) self-evaluation points and CME credit online at www.hospitalmedicine.org/mkm.
SHM’s Medical Knowledge Modules are online learning and self-evaluation tools that provide the user with industry-leading instruction on quality-improvement (QI) theory; project design; system processes; measurement; chance science; tools for implementation; epidemiology of patient safety; and error types, disclosure, prevention strategies, and theory.
Three Medical Knowledge Modules are available: Hospital QI and Patient Safety, Hospital QI and Patient Safety II, and Pediatric Hospital QI and Patient Safety. Each online module consists of 25 multiple-choice questions. If the correct answer is chosen, the module provides a rationale explaining why that answer was correct. When an incorrect answer is selected, users are encouraged to try again.
Each module will earn hospitalists 10 self-evaluation points for diplomates enrolled in ABIM’s MOC program and three AMA PRA Category 1 CME Credits.
SHM will continue to roll out other topics throughout 2012.
Brendon Shank is SHM associate vice president of communications.
In addition to the annual meeting, SHM and its partners bring hospitalists the very best in education, professional development, and networking in the form of in-person meetings.
July: Pediatric Hospital Medicine
Every year, hundreds of pediatric hospitalists come together to share their passion for caring for hospitalized children. This year, Pediatric Hospital Medicine 2012 will convene July 19-22 at the Northern Kentucky Convention Center, just outside Cincinnati. The meeting is co-sponsored by the Academic Pediatric Association, SHM, and the American Academy of Pediatrics.
For details and to register, visit www.hospitalmedicine.org/events.
October: Leadership Academy
SHM’s Leadership Academy continues to create the next generation of hospitalist leaders and sharpen the skills of existing leaders.
SHM will present its next industry-leading Leadership Academy Oct. 1-4 in Scottsdale, Ariz. The program will feature the popular “Foundations of Effective Leadership” course and the second-level “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” course.
Both courses build leadership skills for hospitalists, or, as more than one hospitalist has called the curriculum, “everything they don’t teach you in medical school.”
In the highly interactive, four-day “Foundations of Effective Leadership” course, hospitalists learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, and examine how hospital metrics are derived.
The “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” program provides skills building for hospitalists who want to drive culture change through specific leadership behaviors and actions. It also delves deep into financial storytelling, effective professional negotiation activities with proven techniques, and more.
“Advanced Leadership” is a second-level course and is open only to hospitalists who have completed the “Foundations of Effective Leadership” course, or who have earned an advanced management degree, such as an MBA.
Both courses are required for the new Leadership Certification program, which gives hospitalists the ability to demonstrate their leadership skills through certification.
Hospitalists planning to take any Leadership Academy course should note that, starting in 2013, Leadership Academy courses will be offered only in the fall.
For details and registration, visit www.hospitalmedicine.org/leadership.
Anytime: Online Education
Hospitalists working to demonstrate their expertise and commitment to HM through the Focused Practice in Hospital Medicine designation can earn Maintenance of Certification (MOC) self-evaluation points and CME credit online at www.hospitalmedicine.org/mkm.
SHM’s Medical Knowledge Modules are online learning and self-evaluation tools that provide the user with industry-leading instruction on quality-improvement (QI) theory; project design; system processes; measurement; chance science; tools for implementation; epidemiology of patient safety; and error types, disclosure, prevention strategies, and theory.
Three Medical Knowledge Modules are available: Hospital QI and Patient Safety, Hospital QI and Patient Safety II, and Pediatric Hospital QI and Patient Safety. Each online module consists of 25 multiple-choice questions. If the correct answer is chosen, the module provides a rationale explaining why that answer was correct. When an incorrect answer is selected, users are encouraged to try again.
Each module will earn hospitalists 10 self-evaluation points for diplomates enrolled in ABIM’s MOC program and three AMA PRA Category 1 CME Credits.
SHM will continue to roll out other topics throughout 2012.
Brendon Shank is SHM associate vice president of communications.
Survey Insights: The Unique Connection between Compensation and Productivity
Perhaps one of the most interesting concepts in the 2011 SHM/MGMA State of Hospital Medicine report is illustrated by the potentially confusing graph, at right, which is reproduced from the report. By taking a few minutes to fully understand what the graph portrays, users can gain valuable insights into the relationship between productivity and compensation.
Let’s say I’m a hospitalist and my annual work RVU (wRVU) productivity is in the bottom 25% (first quartile) of all of the hospitalists who responded to the survey. My total compensation is likely to be relatively low—a median of $188,800—but my compensation per unit of work is likely to be relatively high—a median of $73.85 per wRVU.
On the other hand, if I’m a hospitalist with productivity in the top 25% of all hospitalists (fourth quartile), my overall compensation will probably be much higher—a median of $260,283—but my average compensation per unit of work has probably gone down quite a bit (note the median of $40.82 per wRVU).
Why is it that my compensation has gone up, but not at the same rate as my productivity?
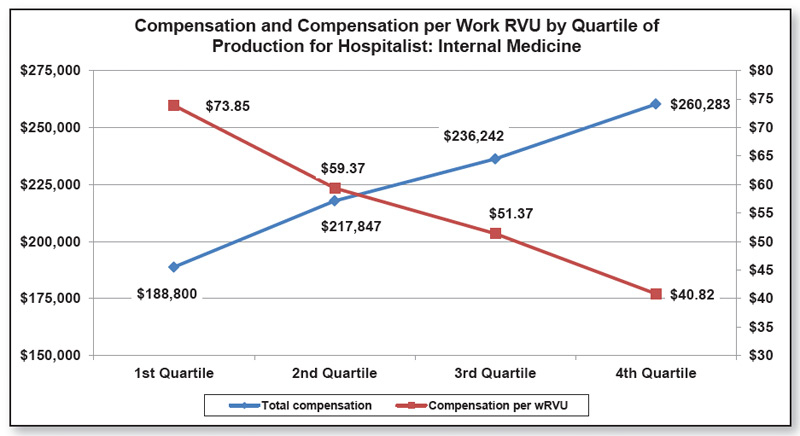
Well, despite the increasing popularity of productivity incentives among HM groups in recent years, the majority of hospitalists still receive most of their pay in the form of a fixed salary. In fact, the survey, at right, found that the average hospitalist compensation package consists of about 80% fixed-base compensation, 16% productivity incentive, and 4% quality/performance incentive. Such compensation models give clear advantages to hospitalists with low productivity, and disadvantages to those with very high productivity.
Yes, many hospitalists can earn at least a bit more if they increase their productivity, but it’s often pennies on the dollar because neither their base salary nor their quality bonus components increase as their productivity goes up. Some of you might argue that compensation should rise in a straight line along with productivity, as it does in a practice with a 100% productivity-based compensation plan (some know this as the “eat what you treat” plan).
But what rises in a straight line can also fall in a straight line, and few hospitalists are comfortable with the risk of significant drops in income if their volume decreases for some reason.
Others might argue that it’s a good thing for compensation increases to taper off at high productivity levels, since this provides at least some reward for working harder but is less likely to incentivize people to work at unreasonable levels. And a few might argue that compensation per unit of work should actually increase at high productivity levels because once a hospitalist has covered their base salary and contribution to practice overhead, any additional revenue they bring into the practice is pure profit.
I have my opinions about these things, and I’m sure you do, too. But one of the things I like best about HM is the wide variety of practices out there. With so many hospitalist practices and so much variety, there’s a compensation model out there somewhere to suit everyone.
Perhaps one of the most interesting concepts in the 2011 SHM/MGMA State of Hospital Medicine report is illustrated by the potentially confusing graph, at right, which is reproduced from the report. By taking a few minutes to fully understand what the graph portrays, users can gain valuable insights into the relationship between productivity and compensation.
Let’s say I’m a hospitalist and my annual work RVU (wRVU) productivity is in the bottom 25% (first quartile) of all of the hospitalists who responded to the survey. My total compensation is likely to be relatively low—a median of $188,800—but my compensation per unit of work is likely to be relatively high—a median of $73.85 per wRVU.
On the other hand, if I’m a hospitalist with productivity in the top 25% of all hospitalists (fourth quartile), my overall compensation will probably be much higher—a median of $260,283—but my average compensation per unit of work has probably gone down quite a bit (note the median of $40.82 per wRVU).
Why is it that my compensation has gone up, but not at the same rate as my productivity?
Well, despite the increasing popularity of productivity incentives among HM groups in recent years, the majority of hospitalists still receive most of their pay in the form of a fixed salary. In fact, the survey, at right, found that the average hospitalist compensation package consists of about 80% fixed-base compensation, 16% productivity incentive, and 4% quality/performance incentive. Such compensation models give clear advantages to hospitalists with low productivity, and disadvantages to those with very high productivity.
Yes, many hospitalists can earn at least a bit more if they increase their productivity, but it’s often pennies on the dollar because neither their base salary nor their quality bonus components increase as their productivity goes up. Some of you might argue that compensation should rise in a straight line along with productivity, as it does in a practice with a 100% productivity-based compensation plan (some know this as the “eat what you treat” plan).
But what rises in a straight line can also fall in a straight line, and few hospitalists are comfortable with the risk of significant drops in income if their volume decreases for some reason.
Others might argue that it’s a good thing for compensation increases to taper off at high productivity levels, since this provides at least some reward for working harder but is less likely to incentivize people to work at unreasonable levels. And a few might argue that compensation per unit of work should actually increase at high productivity levels because once a hospitalist has covered their base salary and contribution to practice overhead, any additional revenue they bring into the practice is pure profit.
I have my opinions about these things, and I’m sure you do, too. But one of the things I like best about HM is the wide variety of practices out there. With so many hospitalist practices and so much variety, there’s a compensation model out there somewhere to suit everyone.
Perhaps one of the most interesting concepts in the 2011 SHM/MGMA State of Hospital Medicine report is illustrated by the potentially confusing graph, at right, which is reproduced from the report. By taking a few minutes to fully understand what the graph portrays, users can gain valuable insights into the relationship between productivity and compensation.
Let’s say I’m a hospitalist and my annual work RVU (wRVU) productivity is in the bottom 25% (first quartile) of all of the hospitalists who responded to the survey. My total compensation is likely to be relatively low—a median of $188,800—but my compensation per unit of work is likely to be relatively high—a median of $73.85 per wRVU.
On the other hand, if I’m a hospitalist with productivity in the top 25% of all hospitalists (fourth quartile), my overall compensation will probably be much higher—a median of $260,283—but my average compensation per unit of work has probably gone down quite a bit (note the median of $40.82 per wRVU).
Why is it that my compensation has gone up, but not at the same rate as my productivity?
Well, despite the increasing popularity of productivity incentives among HM groups in recent years, the majority of hospitalists still receive most of their pay in the form of a fixed salary. In fact, the survey, at right, found that the average hospitalist compensation package consists of about 80% fixed-base compensation, 16% productivity incentive, and 4% quality/performance incentive. Such compensation models give clear advantages to hospitalists with low productivity, and disadvantages to those with very high productivity.
Yes, many hospitalists can earn at least a bit more if they increase their productivity, but it’s often pennies on the dollar because neither their base salary nor their quality bonus components increase as their productivity goes up. Some of you might argue that compensation should rise in a straight line along with productivity, as it does in a practice with a 100% productivity-based compensation plan (some know this as the “eat what you treat” plan).
But what rises in a straight line can also fall in a straight line, and few hospitalists are comfortable with the risk of significant drops in income if their volume decreases for some reason.
Others might argue that it’s a good thing for compensation increases to taper off at high productivity levels, since this provides at least some reward for working harder but is less likely to incentivize people to work at unreasonable levels. And a few might argue that compensation per unit of work should actually increase at high productivity levels because once a hospitalist has covered their base salary and contribution to practice overhead, any additional revenue they bring into the practice is pure profit.
I have my opinions about these things, and I’m sure you do, too. But one of the things I like best about HM is the wide variety of practices out there. With so many hospitalist practices and so much variety, there’s a compensation model out there somewhere to suit everyone.
HM On the Move


Meadowview Regional Medical Center in Maysville, Ky., recently added a hospitalist program as part of its renovation campaign. Jeff Dickerson, MD, Ignacio Calvo, MD, and nurse practitioner Abe Keating are heading up the new hospitalist team.
Eric McFarling, MD, a hospitalist at St. Cloud Hospital in St. Cloud, Minn., received the Physician of Excellence Award from employees and peers. The award recognizes commitment to patient satisfaction and teamwork.
Emily Hebert, MD, an internal-medicine hospitalist at Baylor University Medical Center in Waco, Texas, was awarded the 2011 Texas Medical Association’s Anson Jones, MD, Award in the Physician Excellence in Reporting category for her work as medical expert for the local ABC affiliate. She recently joined the staff at The Cooper Clinic in Dallas as a preventive- medicine physician, specializing in internal medicine and pediatrics.
Business Moves
IPC: the Hospitalist Co. has signed agreements to acquire Inpatient Clinical Solutions Inc. (ICS), an acute-care practice headquartered in Coral Springs, Fla., and the hospitalist practice of Lionel J. Gatien, DO, PA, based in Jacksonville, Fla. IPC expects to add approximately 116,000 patient visits on an annual basis from these acquisitions.
Glendale, Calif.-based Apollo Medical Holdings Inc., a hospitalist-, critical-care and multi-disciplinary care-management service, has appointed Edward “Ted” Schreck chairman of the board. Schreck is a senior healthcare executive with 37 years of experience in both the private and public healthcare sectors.
Carlisle (Pa.) Regional Medical Center has added a 12-member hospitalist team to its list of medical departments. The team will be known as Hospitalists of Central Pennsylvania. Michael Hilden, MD, will serve as group director.
—Alexandra Schultz
Meadowview Regional Medical Center in Maysville, Ky., recently added a hospitalist program as part of its renovation campaign. Jeff Dickerson, MD, Ignacio Calvo, MD, and nurse practitioner Abe Keating are heading up the new hospitalist team.
Eric McFarling, MD, a hospitalist at St. Cloud Hospital in St. Cloud, Minn., received the Physician of Excellence Award from employees and peers. The award recognizes commitment to patient satisfaction and teamwork.
Emily Hebert, MD, an internal-medicine hospitalist at Baylor University Medical Center in Waco, Texas, was awarded the 2011 Texas Medical Association’s Anson Jones, MD, Award in the Physician Excellence in Reporting category for her work as medical expert for the local ABC affiliate. She recently joined the staff at The Cooper Clinic in Dallas as a preventive- medicine physician, specializing in internal medicine and pediatrics.
Business Moves
IPC: the Hospitalist Co. has signed agreements to acquire Inpatient Clinical Solutions Inc. (ICS), an acute-care practice headquartered in Coral Springs, Fla., and the hospitalist practice of Lionel J. Gatien, DO, PA, based in Jacksonville, Fla. IPC expects to add approximately 116,000 patient visits on an annual basis from these acquisitions.
Glendale, Calif.-based Apollo Medical Holdings Inc., a hospitalist-, critical-care and multi-disciplinary care-management service, has appointed Edward “Ted” Schreck chairman of the board. Schreck is a senior healthcare executive with 37 years of experience in both the private and public healthcare sectors.
Carlisle (Pa.) Regional Medical Center has added a 12-member hospitalist team to its list of medical departments. The team will be known as Hospitalists of Central Pennsylvania. Michael Hilden, MD, will serve as group director.
—Alexandra Schultz
Meadowview Regional Medical Center in Maysville, Ky., recently added a hospitalist program as part of its renovation campaign. Jeff Dickerson, MD, Ignacio Calvo, MD, and nurse practitioner Abe Keating are heading up the new hospitalist team.
Eric McFarling, MD, a hospitalist at St. Cloud Hospital in St. Cloud, Minn., received the Physician of Excellence Award from employees and peers. The award recognizes commitment to patient satisfaction and teamwork.
Emily Hebert, MD, an internal-medicine hospitalist at Baylor University Medical Center in Waco, Texas, was awarded the 2011 Texas Medical Association’s Anson Jones, MD, Award in the Physician Excellence in Reporting category for her work as medical expert for the local ABC affiliate. She recently joined the staff at The Cooper Clinic in Dallas as a preventive- medicine physician, specializing in internal medicine and pediatrics.
Business Moves
IPC: the Hospitalist Co. has signed agreements to acquire Inpatient Clinical Solutions Inc. (ICS), an acute-care practice headquartered in Coral Springs, Fla., and the hospitalist practice of Lionel J. Gatien, DO, PA, based in Jacksonville, Fla. IPC expects to add approximately 116,000 patient visits on an annual basis from these acquisitions.
Glendale, Calif.-based Apollo Medical Holdings Inc., a hospitalist-, critical-care and multi-disciplinary care-management service, has appointed Edward “Ted” Schreck chairman of the board. Schreck is a senior healthcare executive with 37 years of experience in both the private and public healthcare sectors.
Carlisle (Pa.) Regional Medical Center has added a 12-member hospitalist team to its list of medical departments. The team will be known as Hospitalists of Central Pennsylvania. Michael Hilden, MD, will serve as group director.
—Alexandra Schultz