User login
'The whitest specialty,' revisited
A recent STAT article by Usha Lee McFarling identified orthopedic surgery as “the whitest specialty.” That’s a problem many, perhaps most, orthopedic surgeons are aware of. But seeing it stated so bluntly is jolting. It’s disconcerting to think that the orthopedic community is making so little progress toward achieving the principal ideal articulated in our country’s fundamental declaration of moral values: that all people are created equal and that they have inalienable rights – in our case, that everyone, Black, brown, as well as White, has the right to the same high level of medical care.
Unfortunately, as study after study has shown, minorities do not enjoy the right to equitable care. Instead, they are subject to disparities in treatment and outcomes that speak to the prejudices that are built into the health care system and are present – sometimes consciously, but most often subconsciously – in the minds of physicians. One important contributing element to these disparities is the paucity of minority practitioners. Studies have also shown that Black patients, for example, respond better to Black physicians, who so often share a psychological and cultural sympathy unavailable to most White physicians. It’s for that reason that being identified as “the whitest specialty” is so immensely troubling.
In researching her STAT article, Ms. McFarling spoke with American Academy of Orthopaedic Surgeons leaders, practicing surgeons, residents, and med students about the dearth of minority and female orthopedic surgeons. What she heard was perplexity and frustration about why better progress hasn’t been made toward correcting the gross underrepresentation of everyone other than White men. The AAOS, she noted, was one of the first specialties to recognize the lack of diversity and over the years has put in great effort to address the problem, creating task forces, committees, and diversity awards and sponsoring conferences and discussions. Yet progress has been glacial, at best.
From her respondents, Ms. McFarling heard an array of reasons for this. Black, Hispanic, and Native American persons are underrepresented in medical schools, so the pool of potential applicants for orthopedic residencies is shallow to begin with. STEM studies are notoriously inadequate in poorer primary and secondary schools, in which so many minority students are educated. The MCAT and USMLE Step 1 test, which play a role in acceptance to residencies, have been shown to be biased. The specialty has few Black or brown role models and, consequently, few advocates and a lack of mentorship. Overt bias may be fairly rare (though microaggressions are still a common and ongoing problem), but most minority and female orthopedic surgeons feel strongly that implicit or subconscious bias is entrenched and works against acceptance to residencies, success in residencies, and advancement in the field.
One of this article’s authors (AW) saw all these factors at work as a resident, then as an admissions committee member at both Yale and Harvard. But the fact is that other medical specialties face exactly these problems and barriers, and yet have been substantially more successful in overcoming them.
What seems to be distinctive about orthopedics is that the mindset which perpetuated (and still perpetuates) In this regard, Kristy Weber, MD, the first female president of the AAOS, told Ms. McFarling that the critical first step to bringing in more women or people of color is changing the culture. There seems to be a consensus about that.
So, what does that mean, given that the AAOS has made serious efforts in that regard that have clearly been less than effective?
The answer, as we see it, is first – to not give in to frustration. The time frames involved in changing customary states of mind are typically elongated, and the deeper the habituation, the longer transformation takes. Deep changes always mean a long, hard slog. For transformations of this sort to take place, the requirements are a general agreement on the value of the transformation, exposure to the destructive consequences of the customary modus operandi, and persuasion for why change needs to happen.
In orthopedics, the first requirement has been met. The AAOS espouses diversity and inclusion as a high-level value. In terms of the second two requirements – exposure and persuasion – orthopedic surgeons have been witness to events, campaigns, conferences, et cetera. But these have not been enough, which means that efforts need to be focused, enlarged, sustained, determined, and innovative.
Does the orthopedic surgery community have the ability to do that?
The answer is: Yes, it does.
Currently the orthopedic surgeon community boasts a number of organizations, groups, and individuals pushing for change, in addition to the AAOS’s Diversity Advisory Board. The predominantly African American J. Robert Gladden Orthopaedic Society, the Ruth Jackson Orthopaedic Society of female orthopedic physicians, and the Association of Latino Orthopaedic Surgeons are all energetic advocates, as is Nth Dimensions, the Perry Initiative, and various ad hoc and individual endeavors.
These are all strong proponents for their own groups in their own way. But history has shown in so many cases that concerted rather than individual action empowers advocacy, and what orthopedic surgery needs in its current situation of gross underrepresentation of minorities and women is an enhanced campaign to raise awareness and redouble persuasion.
One of many examples of the power of collective action is the Association of Minority Health Professions Schools founded by Dr. Louis Sullivan in 1977.* Dr. Sullivan (later secretary of the Department of Health & Human Services) was at that time the founding dean of Morehouse School of Medicine. Morehouse had been launched on a shoestring and needed funding urgently. Other Black health schools, such as Meharry Medical College and Tuskegee College of Veterinary Medicine, were in even more pressing financial need. The coalition of schools that Dr. Sullivan organized became a powerful force in Congress and the National Institutes of Health, magnitudes more effective in raising funds from government and other sources than the best individual efforts of the separate institutions.
Dr. Sullivan’s association is only one of a multitude of historical examples of the effectiveness of unified action. AAOS currently has no single officer charged with bringing together the efforts of the change assets that already exist. It could, perhaps should, have someone in that position. AAOS could invest that same office with a mandate to survey the other medical specialties and bring to bear the most effective diversity, equity, and inclusion (DEI) practices in their arsenals.
Finally, despite the attention AAOS has brought to DEI needs, a look at the organization’s strategic goals, its core values, and its “key enablers” finds not a single mention of diversity or inclusion. Given the country’s current focus on the need for equality, given the poor performance of the orthopedic surgery specialty in terms of inclusion, the obvious question is: Should there not be an official declaration positing diversity as a primary AAOS desideratum?
There is recent precedent for this in the American College of Physicians/American Board of Internal Medicine’s Physician Charter on Professionalism, which includes “social justice” as a primary goal of medical practice. This highlights and reinforces the humanitarian strivings of the profession. In light of the paralysis illuminated by Ms. McFarling’s STAT article, a clear, concise declaration by the AAOS of the value and need for DEI as a central component of the organization’s values should be high on the AAOS order of business. A commitment in that form would serve as a powerful catalyst for bringing orthopedic surgery into step with its sister specialties, as well as affirming the core egalitarian principle that underlies all of medical care.
Dr. White is the Ellen and Melvin Gordon Distinguished Professor of Medical Education and Professor of Orthopedic Surgery at Harvard Medical School, Boston. Dr. Chanoff is a founding board member of the Augustus A. White III Institute for Healthcare Equity. Neither Dr. White nor Dr. Chanoff reported any conflicts of interest. A version of this article first appeared on Medscape.com.
Correction, 2/1/22: An earlier version of this article omitted the title of "Dr." before Dr. Louis Sullivan's name.
A recent STAT article by Usha Lee McFarling identified orthopedic surgery as “the whitest specialty.” That’s a problem many, perhaps most, orthopedic surgeons are aware of. But seeing it stated so bluntly is jolting. It’s disconcerting to think that the orthopedic community is making so little progress toward achieving the principal ideal articulated in our country’s fundamental declaration of moral values: that all people are created equal and that they have inalienable rights – in our case, that everyone, Black, brown, as well as White, has the right to the same high level of medical care.
Unfortunately, as study after study has shown, minorities do not enjoy the right to equitable care. Instead, they are subject to disparities in treatment and outcomes that speak to the prejudices that are built into the health care system and are present – sometimes consciously, but most often subconsciously – in the minds of physicians. One important contributing element to these disparities is the paucity of minority practitioners. Studies have also shown that Black patients, for example, respond better to Black physicians, who so often share a psychological and cultural sympathy unavailable to most White physicians. It’s for that reason that being identified as “the whitest specialty” is so immensely troubling.
In researching her STAT article, Ms. McFarling spoke with American Academy of Orthopaedic Surgeons leaders, practicing surgeons, residents, and med students about the dearth of minority and female orthopedic surgeons. What she heard was perplexity and frustration about why better progress hasn’t been made toward correcting the gross underrepresentation of everyone other than White men. The AAOS, she noted, was one of the first specialties to recognize the lack of diversity and over the years has put in great effort to address the problem, creating task forces, committees, and diversity awards and sponsoring conferences and discussions. Yet progress has been glacial, at best.
From her respondents, Ms. McFarling heard an array of reasons for this. Black, Hispanic, and Native American persons are underrepresented in medical schools, so the pool of potential applicants for orthopedic residencies is shallow to begin with. STEM studies are notoriously inadequate in poorer primary and secondary schools, in which so many minority students are educated. The MCAT and USMLE Step 1 test, which play a role in acceptance to residencies, have been shown to be biased. The specialty has few Black or brown role models and, consequently, few advocates and a lack of mentorship. Overt bias may be fairly rare (though microaggressions are still a common and ongoing problem), but most minority and female orthopedic surgeons feel strongly that implicit or subconscious bias is entrenched and works against acceptance to residencies, success in residencies, and advancement in the field.
One of this article’s authors (AW) saw all these factors at work as a resident, then as an admissions committee member at both Yale and Harvard. But the fact is that other medical specialties face exactly these problems and barriers, and yet have been substantially more successful in overcoming them.
What seems to be distinctive about orthopedics is that the mindset which perpetuated (and still perpetuates) In this regard, Kristy Weber, MD, the first female president of the AAOS, told Ms. McFarling that the critical first step to bringing in more women or people of color is changing the culture. There seems to be a consensus about that.
So, what does that mean, given that the AAOS has made serious efforts in that regard that have clearly been less than effective?
The answer, as we see it, is first – to not give in to frustration. The time frames involved in changing customary states of mind are typically elongated, and the deeper the habituation, the longer transformation takes. Deep changes always mean a long, hard slog. For transformations of this sort to take place, the requirements are a general agreement on the value of the transformation, exposure to the destructive consequences of the customary modus operandi, and persuasion for why change needs to happen.
In orthopedics, the first requirement has been met. The AAOS espouses diversity and inclusion as a high-level value. In terms of the second two requirements – exposure and persuasion – orthopedic surgeons have been witness to events, campaigns, conferences, et cetera. But these have not been enough, which means that efforts need to be focused, enlarged, sustained, determined, and innovative.
Does the orthopedic surgery community have the ability to do that?
The answer is: Yes, it does.
Currently the orthopedic surgeon community boasts a number of organizations, groups, and individuals pushing for change, in addition to the AAOS’s Diversity Advisory Board. The predominantly African American J. Robert Gladden Orthopaedic Society, the Ruth Jackson Orthopaedic Society of female orthopedic physicians, and the Association of Latino Orthopaedic Surgeons are all energetic advocates, as is Nth Dimensions, the Perry Initiative, and various ad hoc and individual endeavors.
These are all strong proponents for their own groups in their own way. But history has shown in so many cases that concerted rather than individual action empowers advocacy, and what orthopedic surgery needs in its current situation of gross underrepresentation of minorities and women is an enhanced campaign to raise awareness and redouble persuasion.
One of many examples of the power of collective action is the Association of Minority Health Professions Schools founded by Dr. Louis Sullivan in 1977.* Dr. Sullivan (later secretary of the Department of Health & Human Services) was at that time the founding dean of Morehouse School of Medicine. Morehouse had been launched on a shoestring and needed funding urgently. Other Black health schools, such as Meharry Medical College and Tuskegee College of Veterinary Medicine, were in even more pressing financial need. The coalition of schools that Dr. Sullivan organized became a powerful force in Congress and the National Institutes of Health, magnitudes more effective in raising funds from government and other sources than the best individual efforts of the separate institutions.
Dr. Sullivan’s association is only one of a multitude of historical examples of the effectiveness of unified action. AAOS currently has no single officer charged with bringing together the efforts of the change assets that already exist. It could, perhaps should, have someone in that position. AAOS could invest that same office with a mandate to survey the other medical specialties and bring to bear the most effective diversity, equity, and inclusion (DEI) practices in their arsenals.
Finally, despite the attention AAOS has brought to DEI needs, a look at the organization’s strategic goals, its core values, and its “key enablers” finds not a single mention of diversity or inclusion. Given the country’s current focus on the need for equality, given the poor performance of the orthopedic surgery specialty in terms of inclusion, the obvious question is: Should there not be an official declaration positing diversity as a primary AAOS desideratum?
There is recent precedent for this in the American College of Physicians/American Board of Internal Medicine’s Physician Charter on Professionalism, which includes “social justice” as a primary goal of medical practice. This highlights and reinforces the humanitarian strivings of the profession. In light of the paralysis illuminated by Ms. McFarling’s STAT article, a clear, concise declaration by the AAOS of the value and need for DEI as a central component of the organization’s values should be high on the AAOS order of business. A commitment in that form would serve as a powerful catalyst for bringing orthopedic surgery into step with its sister specialties, as well as affirming the core egalitarian principle that underlies all of medical care.
Dr. White is the Ellen and Melvin Gordon Distinguished Professor of Medical Education and Professor of Orthopedic Surgery at Harvard Medical School, Boston. Dr. Chanoff is a founding board member of the Augustus A. White III Institute for Healthcare Equity. Neither Dr. White nor Dr. Chanoff reported any conflicts of interest. A version of this article first appeared on Medscape.com.
Correction, 2/1/22: An earlier version of this article omitted the title of "Dr." before Dr. Louis Sullivan's name.
A recent STAT article by Usha Lee McFarling identified orthopedic surgery as “the whitest specialty.” That’s a problem many, perhaps most, orthopedic surgeons are aware of. But seeing it stated so bluntly is jolting. It’s disconcerting to think that the orthopedic community is making so little progress toward achieving the principal ideal articulated in our country’s fundamental declaration of moral values: that all people are created equal and that they have inalienable rights – in our case, that everyone, Black, brown, as well as White, has the right to the same high level of medical care.
Unfortunately, as study after study has shown, minorities do not enjoy the right to equitable care. Instead, they are subject to disparities in treatment and outcomes that speak to the prejudices that are built into the health care system and are present – sometimes consciously, but most often subconsciously – in the minds of physicians. One important contributing element to these disparities is the paucity of minority practitioners. Studies have also shown that Black patients, for example, respond better to Black physicians, who so often share a psychological and cultural sympathy unavailable to most White physicians. It’s for that reason that being identified as “the whitest specialty” is so immensely troubling.
In researching her STAT article, Ms. McFarling spoke with American Academy of Orthopaedic Surgeons leaders, practicing surgeons, residents, and med students about the dearth of minority and female orthopedic surgeons. What she heard was perplexity and frustration about why better progress hasn’t been made toward correcting the gross underrepresentation of everyone other than White men. The AAOS, she noted, was one of the first specialties to recognize the lack of diversity and over the years has put in great effort to address the problem, creating task forces, committees, and diversity awards and sponsoring conferences and discussions. Yet progress has been glacial, at best.
From her respondents, Ms. McFarling heard an array of reasons for this. Black, Hispanic, and Native American persons are underrepresented in medical schools, so the pool of potential applicants for orthopedic residencies is shallow to begin with. STEM studies are notoriously inadequate in poorer primary and secondary schools, in which so many minority students are educated. The MCAT and USMLE Step 1 test, which play a role in acceptance to residencies, have been shown to be biased. The specialty has few Black or brown role models and, consequently, few advocates and a lack of mentorship. Overt bias may be fairly rare (though microaggressions are still a common and ongoing problem), but most minority and female orthopedic surgeons feel strongly that implicit or subconscious bias is entrenched and works against acceptance to residencies, success in residencies, and advancement in the field.
One of this article’s authors (AW) saw all these factors at work as a resident, then as an admissions committee member at both Yale and Harvard. But the fact is that other medical specialties face exactly these problems and barriers, and yet have been substantially more successful in overcoming them.
What seems to be distinctive about orthopedics is that the mindset which perpetuated (and still perpetuates) In this regard, Kristy Weber, MD, the first female president of the AAOS, told Ms. McFarling that the critical first step to bringing in more women or people of color is changing the culture. There seems to be a consensus about that.
So, what does that mean, given that the AAOS has made serious efforts in that regard that have clearly been less than effective?
The answer, as we see it, is first – to not give in to frustration. The time frames involved in changing customary states of mind are typically elongated, and the deeper the habituation, the longer transformation takes. Deep changes always mean a long, hard slog. For transformations of this sort to take place, the requirements are a general agreement on the value of the transformation, exposure to the destructive consequences of the customary modus operandi, and persuasion for why change needs to happen.
In orthopedics, the first requirement has been met. The AAOS espouses diversity and inclusion as a high-level value. In terms of the second two requirements – exposure and persuasion – orthopedic surgeons have been witness to events, campaigns, conferences, et cetera. But these have not been enough, which means that efforts need to be focused, enlarged, sustained, determined, and innovative.
Does the orthopedic surgery community have the ability to do that?
The answer is: Yes, it does.
Currently the orthopedic surgeon community boasts a number of organizations, groups, and individuals pushing for change, in addition to the AAOS’s Diversity Advisory Board. The predominantly African American J. Robert Gladden Orthopaedic Society, the Ruth Jackson Orthopaedic Society of female orthopedic physicians, and the Association of Latino Orthopaedic Surgeons are all energetic advocates, as is Nth Dimensions, the Perry Initiative, and various ad hoc and individual endeavors.
These are all strong proponents for their own groups in their own way. But history has shown in so many cases that concerted rather than individual action empowers advocacy, and what orthopedic surgery needs in its current situation of gross underrepresentation of minorities and women is an enhanced campaign to raise awareness and redouble persuasion.
One of many examples of the power of collective action is the Association of Minority Health Professions Schools founded by Dr. Louis Sullivan in 1977.* Dr. Sullivan (later secretary of the Department of Health & Human Services) was at that time the founding dean of Morehouse School of Medicine. Morehouse had been launched on a shoestring and needed funding urgently. Other Black health schools, such as Meharry Medical College and Tuskegee College of Veterinary Medicine, were in even more pressing financial need. The coalition of schools that Dr. Sullivan organized became a powerful force in Congress and the National Institutes of Health, magnitudes more effective in raising funds from government and other sources than the best individual efforts of the separate institutions.
Dr. Sullivan’s association is only one of a multitude of historical examples of the effectiveness of unified action. AAOS currently has no single officer charged with bringing together the efforts of the change assets that already exist. It could, perhaps should, have someone in that position. AAOS could invest that same office with a mandate to survey the other medical specialties and bring to bear the most effective diversity, equity, and inclusion (DEI) practices in their arsenals.
Finally, despite the attention AAOS has brought to DEI needs, a look at the organization’s strategic goals, its core values, and its “key enablers” finds not a single mention of diversity or inclusion. Given the country’s current focus on the need for equality, given the poor performance of the orthopedic surgery specialty in terms of inclusion, the obvious question is: Should there not be an official declaration positing diversity as a primary AAOS desideratum?
There is recent precedent for this in the American College of Physicians/American Board of Internal Medicine’s Physician Charter on Professionalism, which includes “social justice” as a primary goal of medical practice. This highlights and reinforces the humanitarian strivings of the profession. In light of the paralysis illuminated by Ms. McFarling’s STAT article, a clear, concise declaration by the AAOS of the value and need for DEI as a central component of the organization’s values should be high on the AAOS order of business. A commitment in that form would serve as a powerful catalyst for bringing orthopedic surgery into step with its sister specialties, as well as affirming the core egalitarian principle that underlies all of medical care.
Dr. White is the Ellen and Melvin Gordon Distinguished Professor of Medical Education and Professor of Orthopedic Surgery at Harvard Medical School, Boston. Dr. Chanoff is a founding board member of the Augustus A. White III Institute for Healthcare Equity. Neither Dr. White nor Dr. Chanoff reported any conflicts of interest. A version of this article first appeared on Medscape.com.
Correction, 2/1/22: An earlier version of this article omitted the title of "Dr." before Dr. Louis Sullivan's name.
We’re dying to tell you about fatigability
Are you tired? Or are you death tired?
When we’re feeling that burnout monster creep in we sometimes say that we’re being worked to death or that we’re dead tired, but what if that feeling could predict when it’s your actual time to go?
In a recent study published in the Journals of Gerontology: Series A, epidemiologists from the University of Pittsburgh were able to associate a level of “physical fatigability” with mortality.
The researchers administered the Pittsburgh Fatigability Scale to almost 3,000 participants aged ≥ 60 years, who ranked from 0 to 5 on how tired they thought they would be after doing activities like light housework or a leisurely 30-minute walk. After accounting for factors such as preexisting conditions and mental health, the researchers found that people who scored 25 or more points were 2.3 times more likely to die in the next 2.7 years, compared with those who scored under 25.
So what does that tell us about the importance of being continuously active? It’s pretty important.
“Previous research indicates that getting more physical activity can reduce a person’s fatigability. Our study is the first to link more severe physical fatigability to an earlier death,” lead author Nancy W. Glynn, PhD, said in a separate statement. The best way to keep physically active, she suggested, is to set manageable goals and a routine.
A nice walk around the neighborhood during golden hour or a little bit of yoga before breakfast could be a great way to keep the body moving, because you know what they say: Use it or lose it.
This work is NFT protected: Do not screenshot
If you’ve been following the nonmedical news, you’ve likely heard the term “NFT” explode in the past few months. Standing for nonfungible token, NFTs are, at least theoretically, a proof of ownership for digital creations that prevents anyone other than the buyer from reselling the artwork. Sounds like a great idea: It protects artists and buyers alike.

Much like its cousin cryptocurrency, however, the NFT world is rife with speculation, scams, misunderstanding, and drawings of bored monkeys. It’s the Wild West out there in the digital art universe: One poor unfortunate accidentally sold a $300k NFT image for $3,000, a group of investors spent $3 million buying an NFT for a rare version of Dune believing it gave them the copyright (it did not), and an Indonesian engineering student’s 5-year series of expressionless selfies is now worth a million dollars.
This is a column detailing weird medical news, however, so with our setup complete (though our understanding of NFTs is very much not), we move to France and meet our hero (?), Emmanuel Masmejean, an orthopedic surgeon who apparently wasn’t making enough money in his lucrative medical career.
In a move of apocalyptic madness, he threw ethics out the window, delved into his archive, and found an x-ray of a young woman with a bullet lodged in her arm. The woman was a survivor of the Bataclan mass shooting and bombing in 2015, and don’t you worry, our intrepid entrepreneur made sure to identify her as such when he tried selling the x-ray as an NFT on an online art website for $2,776. Yes, this is very much a violation of doctor-patient confidentiality, and no, that’s not a lot of money to risk your medical career on.
Naturally, the woman was horrified and shocked to learn that the image was being sold, her lawyer told the Guardian. When the doctor called her, he merely attempted to justify his action, rather than apologizing or showing any remorse. Dr. Masmejean is now facing legal action and a disciplinary charge for his attempted entry into the NFT world for publishing the image without permission, and the NFT has been removed from the website. Should have stuck with the bored monkeys.
Avatars could be the future
Zoom, FaceTime, and Skype are great when people can’t be together in the same room, state, or country. Not the same as being somewhere in person, but a pretty good replacement during a global pandemic. But what if you had a robot that could be present for you?
Seven-year-old Joshua Martinangeli of Berlin has a severe lung disease and needs to wear a tube in his neck, so he cannot attend school. A robot avatar, donated to Joshua through a private initiative, sits in his seat in the classroom and is able to interact with the students and teacher, according to Reuters. A light on the avatar blinks when Joshua wants to speak and the children can talk with him too. Joshua and his classmates agree that it’s not the same as him really being there to talk and learn, but it’s a great way to keep him included.
“We are the only district in Berlin that has bought four avatars for its schools. The impetus was COVID-19, but I think this will be the future well beyond the pandemic,” Torsten Kuehne, district education councilor, told Reuters.
So where do we get an avatar to go out and run errands? Can we send it to the office instead of Zooming the next meeting? Or maybe our avatar could go to the gym for us. But how do we get the results to show up on our bodies? C’mon science, figure this out.
Futility, thy name is Kiribati
Before we get to the rest of our regularly scheduled hilarity, a brief geography lesson is in order: Kiribati is an island nation – actually 32 atolls and one coral island – in the central Pacific Ocean. Those atolls are spread out across 1.4 million square miles around the intersection of the equator and the International Date Line, so Kiribati is the only country in the world located in all four hemispheres.

Now, back to the news.
Kiribati closed its borders early in the COVID-19 pandemic and recorded only two cases in almost 2 years. Things were going so well that the authorities recently decided to reopen the country to international travelers. Silly authorities.
The first plane was set to arrive on Jan. 14 from Fiji. This being the age of COVID, plans were made and precautions were taken. All 54 passengers quarantined for 2 weeks before the flight and underwent regular testing, the Guardian noted, and “they were only allowed on the flight after returning negative tests.”
You guessed it. Two-thirds of those 54 people tested positive for COVID-19 after landing in Kiribati.
All of the passengers were quarantined, but since then a security guard at the quarantine center has tested positive, as has someone who was not involved in the quarantine. According to NPR, the government said that “there is now an assumption that COVID-19 is now spreading in the community on South Tarawa and Betio.”
Moral of the story? You can’t beat COVID, so never try.
[EDITOR: Is that really the message we want to send to our readers?]
If you can’t beat them, join them.
[EDITOR: Nope. Try again.]
Resistance is futile?
[EDITOR: Sigh. Close enough.]
Are you tired? Or are you death tired?
When we’re feeling that burnout monster creep in we sometimes say that we’re being worked to death or that we’re dead tired, but what if that feeling could predict when it’s your actual time to go?
In a recent study published in the Journals of Gerontology: Series A, epidemiologists from the University of Pittsburgh were able to associate a level of “physical fatigability” with mortality.
The researchers administered the Pittsburgh Fatigability Scale to almost 3,000 participants aged ≥ 60 years, who ranked from 0 to 5 on how tired they thought they would be after doing activities like light housework or a leisurely 30-minute walk. After accounting for factors such as preexisting conditions and mental health, the researchers found that people who scored 25 or more points were 2.3 times more likely to die in the next 2.7 years, compared with those who scored under 25.
So what does that tell us about the importance of being continuously active? It’s pretty important.
“Previous research indicates that getting more physical activity can reduce a person’s fatigability. Our study is the first to link more severe physical fatigability to an earlier death,” lead author Nancy W. Glynn, PhD, said in a separate statement. The best way to keep physically active, she suggested, is to set manageable goals and a routine.
A nice walk around the neighborhood during golden hour or a little bit of yoga before breakfast could be a great way to keep the body moving, because you know what they say: Use it or lose it.
This work is NFT protected: Do not screenshot
If you’ve been following the nonmedical news, you’ve likely heard the term “NFT” explode in the past few months. Standing for nonfungible token, NFTs are, at least theoretically, a proof of ownership for digital creations that prevents anyone other than the buyer from reselling the artwork. Sounds like a great idea: It protects artists and buyers alike.
Much like its cousin cryptocurrency, however, the NFT world is rife with speculation, scams, misunderstanding, and drawings of bored monkeys. It’s the Wild West out there in the digital art universe: One poor unfortunate accidentally sold a $300k NFT image for $3,000, a group of investors spent $3 million buying an NFT for a rare version of Dune believing it gave them the copyright (it did not), and an Indonesian engineering student’s 5-year series of expressionless selfies is now worth a million dollars.
This is a column detailing weird medical news, however, so with our setup complete (though our understanding of NFTs is very much not), we move to France and meet our hero (?), Emmanuel Masmejean, an orthopedic surgeon who apparently wasn’t making enough money in his lucrative medical career.
In a move of apocalyptic madness, he threw ethics out the window, delved into his archive, and found an x-ray of a young woman with a bullet lodged in her arm. The woman was a survivor of the Bataclan mass shooting and bombing in 2015, and don’t you worry, our intrepid entrepreneur made sure to identify her as such when he tried selling the x-ray as an NFT on an online art website for $2,776. Yes, this is very much a violation of doctor-patient confidentiality, and no, that’s not a lot of money to risk your medical career on.
Naturally, the woman was horrified and shocked to learn that the image was being sold, her lawyer told the Guardian. When the doctor called her, he merely attempted to justify his action, rather than apologizing or showing any remorse. Dr. Masmejean is now facing legal action and a disciplinary charge for his attempted entry into the NFT world for publishing the image without permission, and the NFT has been removed from the website. Should have stuck with the bored monkeys.
Avatars could be the future
Zoom, FaceTime, and Skype are great when people can’t be together in the same room, state, or country. Not the same as being somewhere in person, but a pretty good replacement during a global pandemic. But what if you had a robot that could be present for you?
Seven-year-old Joshua Martinangeli of Berlin has a severe lung disease and needs to wear a tube in his neck, so he cannot attend school. A robot avatar, donated to Joshua through a private initiative, sits in his seat in the classroom and is able to interact with the students and teacher, according to Reuters. A light on the avatar blinks when Joshua wants to speak and the children can talk with him too. Joshua and his classmates agree that it’s not the same as him really being there to talk and learn, but it’s a great way to keep him included.
“We are the only district in Berlin that has bought four avatars for its schools. The impetus was COVID-19, but I think this will be the future well beyond the pandemic,” Torsten Kuehne, district education councilor, told Reuters.
So where do we get an avatar to go out and run errands? Can we send it to the office instead of Zooming the next meeting? Or maybe our avatar could go to the gym for us. But how do we get the results to show up on our bodies? C’mon science, figure this out.
Futility, thy name is Kiribati
Before we get to the rest of our regularly scheduled hilarity, a brief geography lesson is in order: Kiribati is an island nation – actually 32 atolls and one coral island – in the central Pacific Ocean. Those atolls are spread out across 1.4 million square miles around the intersection of the equator and the International Date Line, so Kiribati is the only country in the world located in all four hemispheres.
Now, back to the news.
Kiribati closed its borders early in the COVID-19 pandemic and recorded only two cases in almost 2 years. Things were going so well that the authorities recently decided to reopen the country to international travelers. Silly authorities.
The first plane was set to arrive on Jan. 14 from Fiji. This being the age of COVID, plans were made and precautions were taken. All 54 passengers quarantined for 2 weeks before the flight and underwent regular testing, the Guardian noted, and “they were only allowed on the flight after returning negative tests.”
You guessed it. Two-thirds of those 54 people tested positive for COVID-19 after landing in Kiribati.
All of the passengers were quarantined, but since then a security guard at the quarantine center has tested positive, as has someone who was not involved in the quarantine. According to NPR, the government said that “there is now an assumption that COVID-19 is now spreading in the community on South Tarawa and Betio.”
Moral of the story? You can’t beat COVID, so never try.
[EDITOR: Is that really the message we want to send to our readers?]
If you can’t beat them, join them.
[EDITOR: Nope. Try again.]
Resistance is futile?
[EDITOR: Sigh. Close enough.]
Are you tired? Or are you death tired?
When we’re feeling that burnout monster creep in we sometimes say that we’re being worked to death or that we’re dead tired, but what if that feeling could predict when it’s your actual time to go?
In a recent study published in the Journals of Gerontology: Series A, epidemiologists from the University of Pittsburgh were able to associate a level of “physical fatigability” with mortality.
The researchers administered the Pittsburgh Fatigability Scale to almost 3,000 participants aged ≥ 60 years, who ranked from 0 to 5 on how tired they thought they would be after doing activities like light housework or a leisurely 30-minute walk. After accounting for factors such as preexisting conditions and mental health, the researchers found that people who scored 25 or more points were 2.3 times more likely to die in the next 2.7 years, compared with those who scored under 25.
So what does that tell us about the importance of being continuously active? It’s pretty important.
“Previous research indicates that getting more physical activity can reduce a person’s fatigability. Our study is the first to link more severe physical fatigability to an earlier death,” lead author Nancy W. Glynn, PhD, said in a separate statement. The best way to keep physically active, she suggested, is to set manageable goals and a routine.
A nice walk around the neighborhood during golden hour or a little bit of yoga before breakfast could be a great way to keep the body moving, because you know what they say: Use it or lose it.
This work is NFT protected: Do not screenshot
If you’ve been following the nonmedical news, you’ve likely heard the term “NFT” explode in the past few months. Standing for nonfungible token, NFTs are, at least theoretically, a proof of ownership for digital creations that prevents anyone other than the buyer from reselling the artwork. Sounds like a great idea: It protects artists and buyers alike.
Much like its cousin cryptocurrency, however, the NFT world is rife with speculation, scams, misunderstanding, and drawings of bored monkeys. It’s the Wild West out there in the digital art universe: One poor unfortunate accidentally sold a $300k NFT image for $3,000, a group of investors spent $3 million buying an NFT for a rare version of Dune believing it gave them the copyright (it did not), and an Indonesian engineering student’s 5-year series of expressionless selfies is now worth a million dollars.
This is a column detailing weird medical news, however, so with our setup complete (though our understanding of NFTs is very much not), we move to France and meet our hero (?), Emmanuel Masmejean, an orthopedic surgeon who apparently wasn’t making enough money in his lucrative medical career.
In a move of apocalyptic madness, he threw ethics out the window, delved into his archive, and found an x-ray of a young woman with a bullet lodged in her arm. The woman was a survivor of the Bataclan mass shooting and bombing in 2015, and don’t you worry, our intrepid entrepreneur made sure to identify her as such when he tried selling the x-ray as an NFT on an online art website for $2,776. Yes, this is very much a violation of doctor-patient confidentiality, and no, that’s not a lot of money to risk your medical career on.
Naturally, the woman was horrified and shocked to learn that the image was being sold, her lawyer told the Guardian. When the doctor called her, he merely attempted to justify his action, rather than apologizing or showing any remorse. Dr. Masmejean is now facing legal action and a disciplinary charge for his attempted entry into the NFT world for publishing the image without permission, and the NFT has been removed from the website. Should have stuck with the bored monkeys.
Avatars could be the future
Zoom, FaceTime, and Skype are great when people can’t be together in the same room, state, or country. Not the same as being somewhere in person, but a pretty good replacement during a global pandemic. But what if you had a robot that could be present for you?
Seven-year-old Joshua Martinangeli of Berlin has a severe lung disease and needs to wear a tube in his neck, so he cannot attend school. A robot avatar, donated to Joshua through a private initiative, sits in his seat in the classroom and is able to interact with the students and teacher, according to Reuters. A light on the avatar blinks when Joshua wants to speak and the children can talk with him too. Joshua and his classmates agree that it’s not the same as him really being there to talk and learn, but it’s a great way to keep him included.
“We are the only district in Berlin that has bought four avatars for its schools. The impetus was COVID-19, but I think this will be the future well beyond the pandemic,” Torsten Kuehne, district education councilor, told Reuters.
So where do we get an avatar to go out and run errands? Can we send it to the office instead of Zooming the next meeting? Or maybe our avatar could go to the gym for us. But how do we get the results to show up on our bodies? C’mon science, figure this out.
Futility, thy name is Kiribati
Before we get to the rest of our regularly scheduled hilarity, a brief geography lesson is in order: Kiribati is an island nation – actually 32 atolls and one coral island – in the central Pacific Ocean. Those atolls are spread out across 1.4 million square miles around the intersection of the equator and the International Date Line, so Kiribati is the only country in the world located in all four hemispheres.
Now, back to the news.
Kiribati closed its borders early in the COVID-19 pandemic and recorded only two cases in almost 2 years. Things were going so well that the authorities recently decided to reopen the country to international travelers. Silly authorities.
The first plane was set to arrive on Jan. 14 from Fiji. This being the age of COVID, plans were made and precautions were taken. All 54 passengers quarantined for 2 weeks before the flight and underwent regular testing, the Guardian noted, and “they were only allowed on the flight after returning negative tests.”
You guessed it. Two-thirds of those 54 people tested positive for COVID-19 after landing in Kiribati.
All of the passengers were quarantined, but since then a security guard at the quarantine center has tested positive, as has someone who was not involved in the quarantine. According to NPR, the government said that “there is now an assumption that COVID-19 is now spreading in the community on South Tarawa and Betio.”
Moral of the story? You can’t beat COVID, so never try.
[EDITOR: Is that really the message we want to send to our readers?]
If you can’t beat them, join them.
[EDITOR: Nope. Try again.]
Resistance is futile?
[EDITOR: Sigh. Close enough.]
One in five female oncologists considering leaving academia, survey finds
More than half of respondents in academic medicine said they believe their gender adversely affects their likelihood for promotion, and 1 in 5 said they were considering leaving academia in the next 5 years.
Given the percentage of female oncologists planning to exit academia, “gender inequality is at high risk of continuing if the culture is not addressed,” write the authors in their study, published online Dec. 30 in JAMA Network Open.
Although women currently outnumber men in U.S. medical schools – a shift that first occurred in 2019 – female representation in academic oncology dwindles at more senior levels. Women represent 45% of hematology and oncology residents, only about 36% of academic faculty, and an even smaller percentage of leadership positions in academic medicine. Women, for instance, occupy about 31% of the chair positions in medical oncology, 17.4% in radiation oncology, and 11% in surgical oncology.
A team of researchers led by Emily C. Merfeld, MD, of the University of Wisconsin Hospitals and Clinics, Madison, set out to understand the factors influencing female oncologists’ decisions to pursue academic versus nonacademic career paths.
Dr. Merfeld and colleagues analyzed survey responses from 667 female oncologists between August 1 and Oct. 31, 2020 – 422 (63.2%) in academic medicine and 245 (36.8%) in nonacademic practice.
Overall, 1 in 4 oncologists said their spouse or partner and family “extremely or moderately” affected their decision to pursue academic practice.
Almost 43% of academic oncologists perceived time spent with loved ones as the biggest sacrifice related to pursuing a career in academic medicine. Approximately the same percentage (41.6%) of nonacademic oncologists perceived the pressure to achieve academic promotion as the most significant sacrifice associated with academic oncology, whereas only 22.4% perceived less time with loved ones as the biggest sacrifice.
“Although work-life balance was a concern for academic oncologists and may be a factor in female oncologists leaving academia, survey data suggested that women in nonacademic practice faced similar challenges,” the authors write.
More specifically, women in academic oncology reported working 2 more hours on the weekends compared to women not in academic medicine; however, both groups worked a similar number of hours during the week.
On the hiring front, almost 24% of academic oncologists said their gender had a “negative or somewhat negative” impact on their ability to get a job, compared with 21% of nonacademic oncologists. Conversely, nearly 28% of academic oncologists said their gender had a “positive or somewhat positive” influence on whether they were hired compared with 41.2% of nonacademic oncologists.
Respondents, however, perceived that gender strongly influenced promotion opportunities. More than half of the respondents – 54.6% of academic oncologists and 50.6% of nonacademic oncologists – believed they were less likely to be promoted than their male colleagues.
This perception aligns with findings from prior studies, which “found women were less likely than men to be promoted to associate professor, full professor, or department chair positions,” the authors write.
Overall, most respondents in each group – 71.3% in academic medicine and 68.6% in nonacademic practice – said they would choose the same career path again. But almost 22% of those in academia said they were “likely or very likely” to leave academic oncology in the next 5 years. Of these women, 28.2% said they would switch to industry employment and 25% would move to community practice.
“Contrary to popular assumptions,” the researchers note, “a spouse or partner and/or family were not a major factor in female oncologists favoring nonacademic careers, because this factor was similarly important to both academic and nonacademic oncologists.”
However, they note, “the increased financial compensation in nonacademic oncology may play a large role in some women’s career decisions.”
Making headway on gender equality?
In 2013, oncologist Katherine Reeder-Hayes, MD, MBA, now an associate at the University of North Carolina, Chapel Hill, published a study on gender equality in oncology in which she concluded that despite “an increasingly significant presence in the oncology physician workforce” women remained “under-represented in leadership positions and at the senior levels of academic medicine.”
Since then, Dr. Reeder-Hayes says that she has seen progress but recognizes the need for more.
“To some extent, I think that representation is improving over time due to factors outside the workplace – women are entering medical school in large numbers and may have more supportive partners and more social support for pursuing a professional career in general, [compared with] a decade or two ago,” Dr. Reeder-Hayes told this news organization.
On a personal level, she noted, “I do see many midcareer women assuming key leadership roles in my own institution.” However, she added, “I think the translation of those good candidates into increased representation in leadership probably varies widely across different institutions.”
In a 2019 editorial, researchers highlighted this variation while calling attention to the “notable progress” made by the American Association for Cancer Research (AACR). Specifically, the editorialists reported that women represent 40% of AACR members, 45% of the AACR Board of Directors, and half of the last 10 association presidents.
Editorial coauthor Elizabeth Jaffee, MD, deputy director of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and former AACR president, told this news organization that she attributes this progress to “concrete measures to ensure equality throughout the organization,” which include gender balance on nominating and program committees as well as research meetings and providing opportunities for mentoring, leadership training, and networking.
Despite this positive change, the COVID-19 pandemic threatens to widen the gender imbalance. In a recent article, Julie Silver, MD, an expert in gender equity in medicine, told this news organization that she anticipates trouble ahead.
“There are many indications that women are leaving medicine in disproportionately high numbers,” said Dr. Silver, associate chair and director of cancer rehabilitation in the department of physical medicine and rehabilitation at Harvard Medical School, Boston. “A lack of fair pay and promotion opportunities that were present before COVID-19 are now combined with a host of pandemic-related challenges.”
In addition to salary and promotion disparities, the U.S. continues to suffer from “a chronic shortage of available, affordable, and high-quality childcare and a lack of federal-level policy initiatives or employer initiatives to broaden paid family leave and develop childcare infrastructure and workforce,” Dr. Reeder-Hayes said. Providing extended leave for new parents and on-site childcare could go a long way to improving this problem, she said.
However, Dr. Reeder-Hayes noted that perhaps the “leaky pipeline” problem in oncology highlights the fact that women “are making good decisions that reflect balanced life priorities, [and that] if we don’t structure job responsibilities, childcare, and pacing of promotion and tenure in ways that allow people to nurture other parts of their lives, employees will feel they’re being asked to sacrifice key things.”
In other words, she said, “it’s the workplace that needs to change if we’re going to convince [women], and many men with similar values, to stay.”
A version of this article first appeared on Medscape.com.
More than half of respondents in academic medicine said they believe their gender adversely affects their likelihood for promotion, and 1 in 5 said they were considering leaving academia in the next 5 years.
Given the percentage of female oncologists planning to exit academia, “gender inequality is at high risk of continuing if the culture is not addressed,” write the authors in their study, published online Dec. 30 in JAMA Network Open.
Although women currently outnumber men in U.S. medical schools – a shift that first occurred in 2019 – female representation in academic oncology dwindles at more senior levels. Women represent 45% of hematology and oncology residents, only about 36% of academic faculty, and an even smaller percentage of leadership positions in academic medicine. Women, for instance, occupy about 31% of the chair positions in medical oncology, 17.4% in radiation oncology, and 11% in surgical oncology.
A team of researchers led by Emily C. Merfeld, MD, of the University of Wisconsin Hospitals and Clinics, Madison, set out to understand the factors influencing female oncologists’ decisions to pursue academic versus nonacademic career paths.
Dr. Merfeld and colleagues analyzed survey responses from 667 female oncologists between August 1 and Oct. 31, 2020 – 422 (63.2%) in academic medicine and 245 (36.8%) in nonacademic practice.
Overall, 1 in 4 oncologists said their spouse or partner and family “extremely or moderately” affected their decision to pursue academic practice.
Almost 43% of academic oncologists perceived time spent with loved ones as the biggest sacrifice related to pursuing a career in academic medicine. Approximately the same percentage (41.6%) of nonacademic oncologists perceived the pressure to achieve academic promotion as the most significant sacrifice associated with academic oncology, whereas only 22.4% perceived less time with loved ones as the biggest sacrifice.
“Although work-life balance was a concern for academic oncologists and may be a factor in female oncologists leaving academia, survey data suggested that women in nonacademic practice faced similar challenges,” the authors write.
More specifically, women in academic oncology reported working 2 more hours on the weekends compared to women not in academic medicine; however, both groups worked a similar number of hours during the week.
On the hiring front, almost 24% of academic oncologists said their gender had a “negative or somewhat negative” impact on their ability to get a job, compared with 21% of nonacademic oncologists. Conversely, nearly 28% of academic oncologists said their gender had a “positive or somewhat positive” influence on whether they were hired compared with 41.2% of nonacademic oncologists.
Respondents, however, perceived that gender strongly influenced promotion opportunities. More than half of the respondents – 54.6% of academic oncologists and 50.6% of nonacademic oncologists – believed they were less likely to be promoted than their male colleagues.
This perception aligns with findings from prior studies, which “found women were less likely than men to be promoted to associate professor, full professor, or department chair positions,” the authors write.
Overall, most respondents in each group – 71.3% in academic medicine and 68.6% in nonacademic practice – said they would choose the same career path again. But almost 22% of those in academia said they were “likely or very likely” to leave academic oncology in the next 5 years. Of these women, 28.2% said they would switch to industry employment and 25% would move to community practice.
“Contrary to popular assumptions,” the researchers note, “a spouse or partner and/or family were not a major factor in female oncologists favoring nonacademic careers, because this factor was similarly important to both academic and nonacademic oncologists.”
However, they note, “the increased financial compensation in nonacademic oncology may play a large role in some women’s career decisions.”
Making headway on gender equality?
In 2013, oncologist Katherine Reeder-Hayes, MD, MBA, now an associate at the University of North Carolina, Chapel Hill, published a study on gender equality in oncology in which she concluded that despite “an increasingly significant presence in the oncology physician workforce” women remained “under-represented in leadership positions and at the senior levels of academic medicine.”
Since then, Dr. Reeder-Hayes says that she has seen progress but recognizes the need for more.
“To some extent, I think that representation is improving over time due to factors outside the workplace – women are entering medical school in large numbers and may have more supportive partners and more social support for pursuing a professional career in general, [compared with] a decade or two ago,” Dr. Reeder-Hayes told this news organization.
On a personal level, she noted, “I do see many midcareer women assuming key leadership roles in my own institution.” However, she added, “I think the translation of those good candidates into increased representation in leadership probably varies widely across different institutions.”
In a 2019 editorial, researchers highlighted this variation while calling attention to the “notable progress” made by the American Association for Cancer Research (AACR). Specifically, the editorialists reported that women represent 40% of AACR members, 45% of the AACR Board of Directors, and half of the last 10 association presidents.
Editorial coauthor Elizabeth Jaffee, MD, deputy director of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and former AACR president, told this news organization that she attributes this progress to “concrete measures to ensure equality throughout the organization,” which include gender balance on nominating and program committees as well as research meetings and providing opportunities for mentoring, leadership training, and networking.
Despite this positive change, the COVID-19 pandemic threatens to widen the gender imbalance. In a recent article, Julie Silver, MD, an expert in gender equity in medicine, told this news organization that she anticipates trouble ahead.
“There are many indications that women are leaving medicine in disproportionately high numbers,” said Dr. Silver, associate chair and director of cancer rehabilitation in the department of physical medicine and rehabilitation at Harvard Medical School, Boston. “A lack of fair pay and promotion opportunities that were present before COVID-19 are now combined with a host of pandemic-related challenges.”
In addition to salary and promotion disparities, the U.S. continues to suffer from “a chronic shortage of available, affordable, and high-quality childcare and a lack of federal-level policy initiatives or employer initiatives to broaden paid family leave and develop childcare infrastructure and workforce,” Dr. Reeder-Hayes said. Providing extended leave for new parents and on-site childcare could go a long way to improving this problem, she said.
However, Dr. Reeder-Hayes noted that perhaps the “leaky pipeline” problem in oncology highlights the fact that women “are making good decisions that reflect balanced life priorities, [and that] if we don’t structure job responsibilities, childcare, and pacing of promotion and tenure in ways that allow people to nurture other parts of their lives, employees will feel they’re being asked to sacrifice key things.”
In other words, she said, “it’s the workplace that needs to change if we’re going to convince [women], and many men with similar values, to stay.”
A version of this article first appeared on Medscape.com.
More than half of respondents in academic medicine said they believe their gender adversely affects their likelihood for promotion, and 1 in 5 said they were considering leaving academia in the next 5 years.
Given the percentage of female oncologists planning to exit academia, “gender inequality is at high risk of continuing if the culture is not addressed,” write the authors in their study, published online Dec. 30 in JAMA Network Open.
Although women currently outnumber men in U.S. medical schools – a shift that first occurred in 2019 – female representation in academic oncology dwindles at more senior levels. Women represent 45% of hematology and oncology residents, only about 36% of academic faculty, and an even smaller percentage of leadership positions in academic medicine. Women, for instance, occupy about 31% of the chair positions in medical oncology, 17.4% in radiation oncology, and 11% in surgical oncology.
A team of researchers led by Emily C. Merfeld, MD, of the University of Wisconsin Hospitals and Clinics, Madison, set out to understand the factors influencing female oncologists’ decisions to pursue academic versus nonacademic career paths.
Dr. Merfeld and colleagues analyzed survey responses from 667 female oncologists between August 1 and Oct. 31, 2020 – 422 (63.2%) in academic medicine and 245 (36.8%) in nonacademic practice.
Overall, 1 in 4 oncologists said their spouse or partner and family “extremely or moderately” affected their decision to pursue academic practice.
Almost 43% of academic oncologists perceived time spent with loved ones as the biggest sacrifice related to pursuing a career in academic medicine. Approximately the same percentage (41.6%) of nonacademic oncologists perceived the pressure to achieve academic promotion as the most significant sacrifice associated with academic oncology, whereas only 22.4% perceived less time with loved ones as the biggest sacrifice.
“Although work-life balance was a concern for academic oncologists and may be a factor in female oncologists leaving academia, survey data suggested that women in nonacademic practice faced similar challenges,” the authors write.
More specifically, women in academic oncology reported working 2 more hours on the weekends compared to women not in academic medicine; however, both groups worked a similar number of hours during the week.
On the hiring front, almost 24% of academic oncologists said their gender had a “negative or somewhat negative” impact on their ability to get a job, compared with 21% of nonacademic oncologists. Conversely, nearly 28% of academic oncologists said their gender had a “positive or somewhat positive” influence on whether they were hired compared with 41.2% of nonacademic oncologists.
Respondents, however, perceived that gender strongly influenced promotion opportunities. More than half of the respondents – 54.6% of academic oncologists and 50.6% of nonacademic oncologists – believed they were less likely to be promoted than their male colleagues.
This perception aligns with findings from prior studies, which “found women were less likely than men to be promoted to associate professor, full professor, or department chair positions,” the authors write.
Overall, most respondents in each group – 71.3% in academic medicine and 68.6% in nonacademic practice – said they would choose the same career path again. But almost 22% of those in academia said they were “likely or very likely” to leave academic oncology in the next 5 years. Of these women, 28.2% said they would switch to industry employment and 25% would move to community practice.
“Contrary to popular assumptions,” the researchers note, “a spouse or partner and/or family were not a major factor in female oncologists favoring nonacademic careers, because this factor was similarly important to both academic and nonacademic oncologists.”
However, they note, “the increased financial compensation in nonacademic oncology may play a large role in some women’s career decisions.”
Making headway on gender equality?
In 2013, oncologist Katherine Reeder-Hayes, MD, MBA, now an associate at the University of North Carolina, Chapel Hill, published a study on gender equality in oncology in which she concluded that despite “an increasingly significant presence in the oncology physician workforce” women remained “under-represented in leadership positions and at the senior levels of academic medicine.”
Since then, Dr. Reeder-Hayes says that she has seen progress but recognizes the need for more.
“To some extent, I think that representation is improving over time due to factors outside the workplace – women are entering medical school in large numbers and may have more supportive partners and more social support for pursuing a professional career in general, [compared with] a decade or two ago,” Dr. Reeder-Hayes told this news organization.
On a personal level, she noted, “I do see many midcareer women assuming key leadership roles in my own institution.” However, she added, “I think the translation of those good candidates into increased representation in leadership probably varies widely across different institutions.”
In a 2019 editorial, researchers highlighted this variation while calling attention to the “notable progress” made by the American Association for Cancer Research (AACR). Specifically, the editorialists reported that women represent 40% of AACR members, 45% of the AACR Board of Directors, and half of the last 10 association presidents.
Editorial coauthor Elizabeth Jaffee, MD, deputy director of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and former AACR president, told this news organization that she attributes this progress to “concrete measures to ensure equality throughout the organization,” which include gender balance on nominating and program committees as well as research meetings and providing opportunities for mentoring, leadership training, and networking.
Despite this positive change, the COVID-19 pandemic threatens to widen the gender imbalance. In a recent article, Julie Silver, MD, an expert in gender equity in medicine, told this news organization that she anticipates trouble ahead.
“There are many indications that women are leaving medicine in disproportionately high numbers,” said Dr. Silver, associate chair and director of cancer rehabilitation in the department of physical medicine and rehabilitation at Harvard Medical School, Boston. “A lack of fair pay and promotion opportunities that were present before COVID-19 are now combined with a host of pandemic-related challenges.”
In addition to salary and promotion disparities, the U.S. continues to suffer from “a chronic shortage of available, affordable, and high-quality childcare and a lack of federal-level policy initiatives or employer initiatives to broaden paid family leave and develop childcare infrastructure and workforce,” Dr. Reeder-Hayes said. Providing extended leave for new parents and on-site childcare could go a long way to improving this problem, she said.
However, Dr. Reeder-Hayes noted that perhaps the “leaky pipeline” problem in oncology highlights the fact that women “are making good decisions that reflect balanced life priorities, [and that] if we don’t structure job responsibilities, childcare, and pacing of promotion and tenure in ways that allow people to nurture other parts of their lives, employees will feel they’re being asked to sacrifice key things.”
In other words, she said, “it’s the workplace that needs to change if we’re going to convince [women], and many men with similar values, to stay.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Doctor’s illegal opioid prescriptions lead to five deaths
According to court documents, between January 2014 and October 2019, family physician David Chisholm, MD, 64, of Wasilla, Alaska, wrote more than 20,000 prescriptions to approximately 350 patients for oxycodone, methadone, and hydrocodone, often prescribing the pills using variations of patients’ names in an attempt to avoid being red-flagged by payers.
When Walmart refused to continue filling the prescriptions, Dr. Chisholm told his staff to advise the patients to use other pharmacies. In addition, he often prescribed combinations of medications, such as concurrent opioids, benzodiazepines, sedatives, and carisoprodol, thus increasing the chances that his patients would become addicted to or overdose on the drugs. Chisholm, who pleaded guilty in June, acknowledged to federal officials that his prescriptions were a significant contributing factor to the overdose deaths of five of his patients during this time, according to a statement by the U.S. Attorney’s Office for the District of Alaska.
According to the Anchorage Daily News, Dr. Chisholm, who was not board certified in pain medicine, said his reason for prescribing the drugs was not to make money but to help patients suffering from chronic pain and because he enjoyed the challenge.
Dr. Chisholm’s attorney, Nick Oberheiden, told CNN his client “sacrificed his reputation as a patient advocate and his years of service to the Alaskan community” in overprescribing opioids. “He expressed his sincere remorse in open court and he accepts the consequences of his misconduct. He hopes that his case serves as a warning to other physicians facing the same dilemma when treating chronic pain.”
He surrendered his medical license in November 2020 before being formally charged in April 2021.
Texas hospital CEO, seven doctors settle kickback
A hospital executive and seven physicians have agreed to pay a total of $1.1 million to settle allegations that they violated the Anti-Kickback Statute and Stark Law. The eight have also agreed to cooperate in investigations and litigation involving other parties.
The Texas physicians involved in the settlement are internist Jaspaul Bhangoo, MD, of Denton; family physician Robert Megna, DO, of Ferris; cardiologist Baxter Montgomery, MD, of Houston; internist Murtaza Mussaji, DO, of Houston; family physician David Sneed, DO, of Austin; family physician Kevin Lewis, DO, of Houston; and family physician Angela Mosley-Nunnery, MD, of Kingwood.
Also settling was Richard DeFoore, former CEO of Jones County Regional Healthcare (dba Stamford Memorial Hospital).
The physicians were accused of accepting payments from organizations in exchange for ordering lab tests from True Health Diagnostics, Little River Healthcare, and Boston Heart. The payments to the physicians were disguised as investment returns but, according to the allegations, were in fact offered in exchange for the doctors’ referrals. Mr. DeFoore, the hospital executive involved in the settlement, allegedly oversaw a similar scheme that benefited the now-defunct Stamford Memorial.
“Paying kickbacks to physicians distorts the medical decision-making process, corrupts our health care system, and increases the cost of healthcare funded by the taxpayer,” Brit Featherston, U.S. attorney for the Eastern District of Texas, said in a statement announcing the agreement. “Laboratories, marketers, and physicians cannot immunize their conduct by attempting to disguise the kickbacks as some sort of investment arrangement.”
Practice administrative assistant sentenced for fraudulent prescriptions
An administrative assistant at an Illinois orthopedics office was sentenced to a year and a day in federal prison for writing fraudulent prescriptions for opioids.
Amanda Biesiada, 39, of Alsip, Ill., who worked as an administrative assistant at Hinsdale Orthopaedics in Westmont, Ill., was not a licensed physician and could not legally write the prescriptions unless instructed to do so and supervised by licensed doctors.
According to a statement by the U.S. Attorney’s Office for the Northern District of Illinois, the prescriptions for hydrocodone, oxycodone, and other controlled substances – 85 prescriptions in all from 2017 to 2019 – were made out to an acquaintance of Biesiada’s and written without the knowledge or approval of the providers in whose names she wrote them.
Federal officials said Ms. Biesiada attempted to conceal the fraudulent prescriptions by marking them “filed in error” in the practice’s prescription system.
Lab owner pleads guilty to $6.9 million testing fraud scheme
A Florida lab owner has pleaded guilty to conspiracy to defraud Medicare through false and fraudulent claims totaling more than $6.9 million.
According to court documents, Christopher Licata, 45, of Delray Beach, Fla., admitted to bribing patient brokers to refer orders for medically unnecessary genetic testing to his lab. The tests were then billed to Medicare.
Mr. Licata and the patient brokers entered sham agreements meant to disguise the true purpose of the payments, according to a statement from the Department of Justice. The 45-year-old owner of Boca Toxicology (dba Lab Dynamics) pleaded guilty to one count of conspiring to commit health care fraud.
The scheme began in 2018; however, once the pandemic began, Mr. Licata shifted strategies, playing on patients’ fears of COVID-19 to bundle inexpensive COVID tests with more expensive medically unnecessary tests. These tests included respiratory pathogen panels and genetic testing for cardiovascular disease, cancer, diabetes, Alzheimer’s disease, and other illnesses. In all, Mr. Licata’s laboratory submitted over $6.9 million in false and fraudulent claims to Medicare for these unnecessary tests, according to the DOJ statement.
The case is a part of the U.S. Attorney General’s COVID-19 Fraud Enforcement Task Force that was established to enhance the efforts of agencies and governments across the country to combat and prevent pandemic-related fraud.
Mr. Licata faces a maximum penalty of 10 years in prison. His sentencing is scheduled for March 24.
A version of this article first appeared on Medscape.com.
According to court documents, between January 2014 and October 2019, family physician David Chisholm, MD, 64, of Wasilla, Alaska, wrote more than 20,000 prescriptions to approximately 350 patients for oxycodone, methadone, and hydrocodone, often prescribing the pills using variations of patients’ names in an attempt to avoid being red-flagged by payers.
When Walmart refused to continue filling the prescriptions, Dr. Chisholm told his staff to advise the patients to use other pharmacies. In addition, he often prescribed combinations of medications, such as concurrent opioids, benzodiazepines, sedatives, and carisoprodol, thus increasing the chances that his patients would become addicted to or overdose on the drugs. Chisholm, who pleaded guilty in June, acknowledged to federal officials that his prescriptions were a significant contributing factor to the overdose deaths of five of his patients during this time, according to a statement by the U.S. Attorney’s Office for the District of Alaska.
According to the Anchorage Daily News, Dr. Chisholm, who was not board certified in pain medicine, said his reason for prescribing the drugs was not to make money but to help patients suffering from chronic pain and because he enjoyed the challenge.
Dr. Chisholm’s attorney, Nick Oberheiden, told CNN his client “sacrificed his reputation as a patient advocate and his years of service to the Alaskan community” in overprescribing opioids. “He expressed his sincere remorse in open court and he accepts the consequences of his misconduct. He hopes that his case serves as a warning to other physicians facing the same dilemma when treating chronic pain.”
He surrendered his medical license in November 2020 before being formally charged in April 2021.
Texas hospital CEO, seven doctors settle kickback
A hospital executive and seven physicians have agreed to pay a total of $1.1 million to settle allegations that they violated the Anti-Kickback Statute and Stark Law. The eight have also agreed to cooperate in investigations and litigation involving other parties.
The Texas physicians involved in the settlement are internist Jaspaul Bhangoo, MD, of Denton; family physician Robert Megna, DO, of Ferris; cardiologist Baxter Montgomery, MD, of Houston; internist Murtaza Mussaji, DO, of Houston; family physician David Sneed, DO, of Austin; family physician Kevin Lewis, DO, of Houston; and family physician Angela Mosley-Nunnery, MD, of Kingwood.
Also settling was Richard DeFoore, former CEO of Jones County Regional Healthcare (dba Stamford Memorial Hospital).
The physicians were accused of accepting payments from organizations in exchange for ordering lab tests from True Health Diagnostics, Little River Healthcare, and Boston Heart. The payments to the physicians were disguised as investment returns but, according to the allegations, were in fact offered in exchange for the doctors’ referrals. Mr. DeFoore, the hospital executive involved in the settlement, allegedly oversaw a similar scheme that benefited the now-defunct Stamford Memorial.
“Paying kickbacks to physicians distorts the medical decision-making process, corrupts our health care system, and increases the cost of healthcare funded by the taxpayer,” Brit Featherston, U.S. attorney for the Eastern District of Texas, said in a statement announcing the agreement. “Laboratories, marketers, and physicians cannot immunize their conduct by attempting to disguise the kickbacks as some sort of investment arrangement.”
Practice administrative assistant sentenced for fraudulent prescriptions
An administrative assistant at an Illinois orthopedics office was sentenced to a year and a day in federal prison for writing fraudulent prescriptions for opioids.
Amanda Biesiada, 39, of Alsip, Ill., who worked as an administrative assistant at Hinsdale Orthopaedics in Westmont, Ill., was not a licensed physician and could not legally write the prescriptions unless instructed to do so and supervised by licensed doctors.
According to a statement by the U.S. Attorney’s Office for the Northern District of Illinois, the prescriptions for hydrocodone, oxycodone, and other controlled substances – 85 prescriptions in all from 2017 to 2019 – were made out to an acquaintance of Biesiada’s and written without the knowledge or approval of the providers in whose names she wrote them.
Federal officials said Ms. Biesiada attempted to conceal the fraudulent prescriptions by marking them “filed in error” in the practice’s prescription system.
Lab owner pleads guilty to $6.9 million testing fraud scheme
A Florida lab owner has pleaded guilty to conspiracy to defraud Medicare through false and fraudulent claims totaling more than $6.9 million.
According to court documents, Christopher Licata, 45, of Delray Beach, Fla., admitted to bribing patient brokers to refer orders for medically unnecessary genetic testing to his lab. The tests were then billed to Medicare.
Mr. Licata and the patient brokers entered sham agreements meant to disguise the true purpose of the payments, according to a statement from the Department of Justice. The 45-year-old owner of Boca Toxicology (dba Lab Dynamics) pleaded guilty to one count of conspiring to commit health care fraud.
The scheme began in 2018; however, once the pandemic began, Mr. Licata shifted strategies, playing on patients’ fears of COVID-19 to bundle inexpensive COVID tests with more expensive medically unnecessary tests. These tests included respiratory pathogen panels and genetic testing for cardiovascular disease, cancer, diabetes, Alzheimer’s disease, and other illnesses. In all, Mr. Licata’s laboratory submitted over $6.9 million in false and fraudulent claims to Medicare for these unnecessary tests, according to the DOJ statement.
The case is a part of the U.S. Attorney General’s COVID-19 Fraud Enforcement Task Force that was established to enhance the efforts of agencies and governments across the country to combat and prevent pandemic-related fraud.
Mr. Licata faces a maximum penalty of 10 years in prison. His sentencing is scheduled for March 24.
A version of this article first appeared on Medscape.com.
According to court documents, between January 2014 and October 2019, family physician David Chisholm, MD, 64, of Wasilla, Alaska, wrote more than 20,000 prescriptions to approximately 350 patients for oxycodone, methadone, and hydrocodone, often prescribing the pills using variations of patients’ names in an attempt to avoid being red-flagged by payers.
When Walmart refused to continue filling the prescriptions, Dr. Chisholm told his staff to advise the patients to use other pharmacies. In addition, he often prescribed combinations of medications, such as concurrent opioids, benzodiazepines, sedatives, and carisoprodol, thus increasing the chances that his patients would become addicted to or overdose on the drugs. Chisholm, who pleaded guilty in June, acknowledged to federal officials that his prescriptions were a significant contributing factor to the overdose deaths of five of his patients during this time, according to a statement by the U.S. Attorney’s Office for the District of Alaska.
According to the Anchorage Daily News, Dr. Chisholm, who was not board certified in pain medicine, said his reason for prescribing the drugs was not to make money but to help patients suffering from chronic pain and because he enjoyed the challenge.
Dr. Chisholm’s attorney, Nick Oberheiden, told CNN his client “sacrificed his reputation as a patient advocate and his years of service to the Alaskan community” in overprescribing opioids. “He expressed his sincere remorse in open court and he accepts the consequences of his misconduct. He hopes that his case serves as a warning to other physicians facing the same dilemma when treating chronic pain.”
He surrendered his medical license in November 2020 before being formally charged in April 2021.
Texas hospital CEO, seven doctors settle kickback
A hospital executive and seven physicians have agreed to pay a total of $1.1 million to settle allegations that they violated the Anti-Kickback Statute and Stark Law. The eight have also agreed to cooperate in investigations and litigation involving other parties.
The Texas physicians involved in the settlement are internist Jaspaul Bhangoo, MD, of Denton; family physician Robert Megna, DO, of Ferris; cardiologist Baxter Montgomery, MD, of Houston; internist Murtaza Mussaji, DO, of Houston; family physician David Sneed, DO, of Austin; family physician Kevin Lewis, DO, of Houston; and family physician Angela Mosley-Nunnery, MD, of Kingwood.
Also settling was Richard DeFoore, former CEO of Jones County Regional Healthcare (dba Stamford Memorial Hospital).
The physicians were accused of accepting payments from organizations in exchange for ordering lab tests from True Health Diagnostics, Little River Healthcare, and Boston Heart. The payments to the physicians were disguised as investment returns but, according to the allegations, were in fact offered in exchange for the doctors’ referrals. Mr. DeFoore, the hospital executive involved in the settlement, allegedly oversaw a similar scheme that benefited the now-defunct Stamford Memorial.
“Paying kickbacks to physicians distorts the medical decision-making process, corrupts our health care system, and increases the cost of healthcare funded by the taxpayer,” Brit Featherston, U.S. attorney for the Eastern District of Texas, said in a statement announcing the agreement. “Laboratories, marketers, and physicians cannot immunize their conduct by attempting to disguise the kickbacks as some sort of investment arrangement.”
Practice administrative assistant sentenced for fraudulent prescriptions
An administrative assistant at an Illinois orthopedics office was sentenced to a year and a day in federal prison for writing fraudulent prescriptions for opioids.
Amanda Biesiada, 39, of Alsip, Ill., who worked as an administrative assistant at Hinsdale Orthopaedics in Westmont, Ill., was not a licensed physician and could not legally write the prescriptions unless instructed to do so and supervised by licensed doctors.
According to a statement by the U.S. Attorney’s Office for the Northern District of Illinois, the prescriptions for hydrocodone, oxycodone, and other controlled substances – 85 prescriptions in all from 2017 to 2019 – were made out to an acquaintance of Biesiada’s and written without the knowledge or approval of the providers in whose names she wrote them.
Federal officials said Ms. Biesiada attempted to conceal the fraudulent prescriptions by marking them “filed in error” in the practice’s prescription system.
Lab owner pleads guilty to $6.9 million testing fraud scheme
A Florida lab owner has pleaded guilty to conspiracy to defraud Medicare through false and fraudulent claims totaling more than $6.9 million.
According to court documents, Christopher Licata, 45, of Delray Beach, Fla., admitted to bribing patient brokers to refer orders for medically unnecessary genetic testing to his lab. The tests were then billed to Medicare.
Mr. Licata and the patient brokers entered sham agreements meant to disguise the true purpose of the payments, according to a statement from the Department of Justice. The 45-year-old owner of Boca Toxicology (dba Lab Dynamics) pleaded guilty to one count of conspiring to commit health care fraud.
The scheme began in 2018; however, once the pandemic began, Mr. Licata shifted strategies, playing on patients’ fears of COVID-19 to bundle inexpensive COVID tests with more expensive medically unnecessary tests. These tests included respiratory pathogen panels and genetic testing for cardiovascular disease, cancer, diabetes, Alzheimer’s disease, and other illnesses. In all, Mr. Licata’s laboratory submitted over $6.9 million in false and fraudulent claims to Medicare for these unnecessary tests, according to the DOJ statement.
The case is a part of the U.S. Attorney General’s COVID-19 Fraud Enforcement Task Force that was established to enhance the efforts of agencies and governments across the country to combat and prevent pandemic-related fraud.
Mr. Licata faces a maximum penalty of 10 years in prison. His sentencing is scheduled for March 24.
A version of this article first appeared on Medscape.com.
The doctor didn’t show up, but the hospital ED still charged $1,012
Dhaval Bhatt had been warned about hospital emergency departments.
“People always told me to avoid the ER in America unless you are really dying,” said Dr. Bhatt, an immigrant from India who got a PhD in pharmacology in the United States and is now a research scientist at Washington University, St. Louis.
But when Dr. Bhatt’s 2-year-old son burned his hand on the kitchen stove on a Wednesday morning in April, the family’s pediatrician directed them the next day to the local children’s hospital.
Dr. Bhatt was traveling. So, his wife, Mansi Bhatt, took their son to the hospital and was sent to the ED. A nurse practitioner took the toddler’s vitals and looked at the wound. She said a surgeon would inspect it more closely.
When the surgeon didn’t appear after more than an hour, Dr. Bhatt’s wife took her son home. The hospital told her to make a follow-up appointment with a doctor, which turned out to be unnecessary because the burn healed quickly.
Then the bill came.
The patient: Martand Bhatt, a toddler covered by a UnitedHealthcare insurance plan provided by the employer of his father, Dhaval Bhatt.
Medical service: An ED visit for a burn sustained when Martand touched an electric stove.
Total bill: $1,012. UnitedHealthcare’s negotiated rate was $858.92, all of which the Bhatts were responsible for because their plan had a $3,000 deductible.
Service provider: SSM Health Cardinal Glennon Children’s Hospital, one of 23 hospitals owned by SSM Health, a Catholic, nonprofit health system with more than $8 billion in annual revenue.
What gives: Many patients don’t understand that they can rack up huge bills almost as soon as they walk through the doors of an ED.
Unlike a restaurant or a mechanic who won’t charge if someone gets tired of waiting for a table or an inspection of a rattling engine,
Martand Bhatt received almost no medical service. A nurse practitioner looked over the toddler, listened to his heart and stomach, and looked in his nose, mouth and ears, according to provider notes prepared by the hospital and shared with KHN by Dr. Bhatt.
The nurse didn’t change the dressing on the wound or order any testing.
“My objection to this is that there was no care provided,” Dr. Bhatt wrote to Bill of the Month.
“My wife did not drive for 45 minutes to get to an ER and wait for an additional 1½ hours for someone to tell me that our child’s vitals – weight, height, temperature and blood pressure – were okay,” Dr. Bhatt continued. “We already knew that. ... It is absolutely ridiculous and unethical.”
When the Bhatts left the ED, Martand was “alert, active and well appearing,” according to the notes.
The nurse’s assessment of Martand cost $192, which was discounted by UnitedHealthcare to a negotiated rate of $38.92. The bulk of the Bhatts’ bill – $820 – was something called a facility fee.
Hospital officials defend these fees as necessary to keep the ED open 24 hours a day as a community asset.
SSM Health spokesperson Stephanie Zoller Mueller declined to discuss the details of Martand’s medical condition even though the Bhatts gave their permission for the hospital to do so.
In an email, Ms. Zoller Mueller said the charges were “appropriate” based on the “acuity of condition, discharge instructions, vital sign monitoring, traumatic wound care, [and] numerous assessments.”
She added: “A patient does not have to receive additional treatment – procedure, labs, x-rays, etc. – to validate an ED-level charge.”
But some patient advocates say these facility fees are applied much too widely and should be limited to patients who actually receive medical care.
“It’s just not appropriate for someone to be charged if they’re not provided treatment,” said Adam Fox, deputy director of the Colorado Consumer Health Initiative. “Patients aren’t availing themselves of a facility if they don’t get care.”
At the very least, hospitals could communicate more clearly to patients about the fees they may be charged for coming to an ED, said Maureen Hensley-Quinn, senior program director at the National Academy for State Health Policy.
“People should know that when they walk in to receive care, there is this fee that they will be assessed,” Ms. Hensley-Quinn said.
Hospitals could also post at the entrance to the ED standard fees for different levels of emergency care.
Dr. Bhatt’s fee still could have been lower if the hospital had classified his son’s injury as minor. But, again, the hospital billing process worked against the family and in favor of the hospital’s bottom line.
Emergency visits are usually classified for billing on a scale from 1 to 5. Level 1 is minor and routine; level 5 requires complex care for life-threatening conditions. And hospitals are increasingly using the highest-severity codes to classify emergency visits, research shows.
“There are financial incentives for billing at a higher severity,” said Aditi Sen, who directs policy and research at the nonprofit Health Care Cost Institute, which has studied ED coding.
Despite the lack of severity of Martand’s wound and the absence of medical care, his visit was classified as level 3, a moderate-severity problem.
Resolution: Incensed that he’d been charged so much, Dr. Bhatt made numerous attempts to get the hospital to reduce the charges. He also appealed to UnitedHealthcare to review the charges.
His efforts failed. In August, Dr. Bhatt received a letter from an SSM Health “patient advocate” informing him that the hospital would not adjust the bill and instructing him to contact patient billing to arrange for payment.
While Dr. Bhatt was trying to reach the patient advocate by phone, his bill was sent to Medicredit, a collection agency, which began sending him notices and calling him.
After KHN contacted SSM Health, Dr. Bhatt received a call from someone who worked on “patient financial experience” issues at the hospital.
The hospital agreed to forgive the $820 facility fee. Dr. Bhatt agreed to pay the remaining $38.92, the professional fee for the ED nurse’s work. Dr. Bhatt also received a notice from Medicredit that it would take no further action against him.
The takeaway: The Bhatts did what most parents would do when a pediatrician advises them to take their child to the hospital.
But EDs are among the most expensive places to get care in the U.S. health system.
If you have a relatively low-level issue, think twice before even registering at the front desk, the act that initiates the billing process. If your doctor doesn’t have same-day appointments or after-hours service, think about urgent care, which is often much cheaper if the center isn’t attached to a hospital.
And remember that if you go to a hospital ED with a relatively minor issue, chances are that you’ll have to wait, as the Bhatts did. Patients with more serious problems will be seen first.
Once you’re taken past the front desk, you will almost certainly be hit with a substantial facility fee even if you don’t receive care.
Appealing that fee to the hospital can occasionally be successful, but there are no guarantees. And, as Dr. Bhatt learned, don’t expect the health insurer to offer much help. Most insurers won’t challenge how a medical visit is coded except on extremely expensive medical claims that will cost them money.
In this case, Dr. Bhatt was on the hook for the whole fee because he had a high-deductible plan, so the insurer had little incentive to take up his cause.
For now, patients’ best hope, many advocates believe, is to publicize the high prices that hospitals charge for their services, inside and outside the ED.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Dhaval Bhatt had been warned about hospital emergency departments.
“People always told me to avoid the ER in America unless you are really dying,” said Dr. Bhatt, an immigrant from India who got a PhD in pharmacology in the United States and is now a research scientist at Washington University, St. Louis.
But when Dr. Bhatt’s 2-year-old son burned his hand on the kitchen stove on a Wednesday morning in April, the family’s pediatrician directed them the next day to the local children’s hospital.
Dr. Bhatt was traveling. So, his wife, Mansi Bhatt, took their son to the hospital and was sent to the ED. A nurse practitioner took the toddler’s vitals and looked at the wound. She said a surgeon would inspect it more closely.
When the surgeon didn’t appear after more than an hour, Dr. Bhatt’s wife took her son home. The hospital told her to make a follow-up appointment with a doctor, which turned out to be unnecessary because the burn healed quickly.
Then the bill came.
The patient: Martand Bhatt, a toddler covered by a UnitedHealthcare insurance plan provided by the employer of his father, Dhaval Bhatt.
Medical service: An ED visit for a burn sustained when Martand touched an electric stove.
Total bill: $1,012. UnitedHealthcare’s negotiated rate was $858.92, all of which the Bhatts were responsible for because their plan had a $3,000 deductible.
Service provider: SSM Health Cardinal Glennon Children’s Hospital, one of 23 hospitals owned by SSM Health, a Catholic, nonprofit health system with more than $8 billion in annual revenue.
What gives: Many patients don’t understand that they can rack up huge bills almost as soon as they walk through the doors of an ED.
Unlike a restaurant or a mechanic who won’t charge if someone gets tired of waiting for a table or an inspection of a rattling engine,
Martand Bhatt received almost no medical service. A nurse practitioner looked over the toddler, listened to his heart and stomach, and looked in his nose, mouth and ears, according to provider notes prepared by the hospital and shared with KHN by Dr. Bhatt.
The nurse didn’t change the dressing on the wound or order any testing.
“My objection to this is that there was no care provided,” Dr. Bhatt wrote to Bill of the Month.
“My wife did not drive for 45 minutes to get to an ER and wait for an additional 1½ hours for someone to tell me that our child’s vitals – weight, height, temperature and blood pressure – were okay,” Dr. Bhatt continued. “We already knew that. ... It is absolutely ridiculous and unethical.”
When the Bhatts left the ED, Martand was “alert, active and well appearing,” according to the notes.
The nurse’s assessment of Martand cost $192, which was discounted by UnitedHealthcare to a negotiated rate of $38.92. The bulk of the Bhatts’ bill – $820 – was something called a facility fee.
Hospital officials defend these fees as necessary to keep the ED open 24 hours a day as a community asset.
SSM Health spokesperson Stephanie Zoller Mueller declined to discuss the details of Martand’s medical condition even though the Bhatts gave their permission for the hospital to do so.
In an email, Ms. Zoller Mueller said the charges were “appropriate” based on the “acuity of condition, discharge instructions, vital sign monitoring, traumatic wound care, [and] numerous assessments.”
She added: “A patient does not have to receive additional treatment – procedure, labs, x-rays, etc. – to validate an ED-level charge.”
But some patient advocates say these facility fees are applied much too widely and should be limited to patients who actually receive medical care.
“It’s just not appropriate for someone to be charged if they’re not provided treatment,” said Adam Fox, deputy director of the Colorado Consumer Health Initiative. “Patients aren’t availing themselves of a facility if they don’t get care.”
At the very least, hospitals could communicate more clearly to patients about the fees they may be charged for coming to an ED, said Maureen Hensley-Quinn, senior program director at the National Academy for State Health Policy.
“People should know that when they walk in to receive care, there is this fee that they will be assessed,” Ms. Hensley-Quinn said.
Hospitals could also post at the entrance to the ED standard fees for different levels of emergency care.
Dr. Bhatt’s fee still could have been lower if the hospital had classified his son’s injury as minor. But, again, the hospital billing process worked against the family and in favor of the hospital’s bottom line.
Emergency visits are usually classified for billing on a scale from 1 to 5. Level 1 is minor and routine; level 5 requires complex care for life-threatening conditions. And hospitals are increasingly using the highest-severity codes to classify emergency visits, research shows.
“There are financial incentives for billing at a higher severity,” said Aditi Sen, who directs policy and research at the nonprofit Health Care Cost Institute, which has studied ED coding.
Despite the lack of severity of Martand’s wound and the absence of medical care, his visit was classified as level 3, a moderate-severity problem.
Resolution: Incensed that he’d been charged so much, Dr. Bhatt made numerous attempts to get the hospital to reduce the charges. He also appealed to UnitedHealthcare to review the charges.
His efforts failed. In August, Dr. Bhatt received a letter from an SSM Health “patient advocate” informing him that the hospital would not adjust the bill and instructing him to contact patient billing to arrange for payment.
While Dr. Bhatt was trying to reach the patient advocate by phone, his bill was sent to Medicredit, a collection agency, which began sending him notices and calling him.
After KHN contacted SSM Health, Dr. Bhatt received a call from someone who worked on “patient financial experience” issues at the hospital.
The hospital agreed to forgive the $820 facility fee. Dr. Bhatt agreed to pay the remaining $38.92, the professional fee for the ED nurse’s work. Dr. Bhatt also received a notice from Medicredit that it would take no further action against him.
The takeaway: The Bhatts did what most parents would do when a pediatrician advises them to take their child to the hospital.
But EDs are among the most expensive places to get care in the U.S. health system.
If you have a relatively low-level issue, think twice before even registering at the front desk, the act that initiates the billing process. If your doctor doesn’t have same-day appointments or after-hours service, think about urgent care, which is often much cheaper if the center isn’t attached to a hospital.
And remember that if you go to a hospital ED with a relatively minor issue, chances are that you’ll have to wait, as the Bhatts did. Patients with more serious problems will be seen first.
Once you’re taken past the front desk, you will almost certainly be hit with a substantial facility fee even if you don’t receive care.
Appealing that fee to the hospital can occasionally be successful, but there are no guarantees. And, as Dr. Bhatt learned, don’t expect the health insurer to offer much help. Most insurers won’t challenge how a medical visit is coded except on extremely expensive medical claims that will cost them money.
In this case, Dr. Bhatt was on the hook for the whole fee because he had a high-deductible plan, so the insurer had little incentive to take up his cause.
For now, patients’ best hope, many advocates believe, is to publicize the high prices that hospitals charge for their services, inside and outside the ED.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Dhaval Bhatt had been warned about hospital emergency departments.
“People always told me to avoid the ER in America unless you are really dying,” said Dr. Bhatt, an immigrant from India who got a PhD in pharmacology in the United States and is now a research scientist at Washington University, St. Louis.
But when Dr. Bhatt’s 2-year-old son burned his hand on the kitchen stove on a Wednesday morning in April, the family’s pediatrician directed them the next day to the local children’s hospital.
Dr. Bhatt was traveling. So, his wife, Mansi Bhatt, took their son to the hospital and was sent to the ED. A nurse practitioner took the toddler’s vitals and looked at the wound. She said a surgeon would inspect it more closely.
When the surgeon didn’t appear after more than an hour, Dr. Bhatt’s wife took her son home. The hospital told her to make a follow-up appointment with a doctor, which turned out to be unnecessary because the burn healed quickly.
Then the bill came.
The patient: Martand Bhatt, a toddler covered by a UnitedHealthcare insurance plan provided by the employer of his father, Dhaval Bhatt.
Medical service: An ED visit for a burn sustained when Martand touched an electric stove.
Total bill: $1,012. UnitedHealthcare’s negotiated rate was $858.92, all of which the Bhatts were responsible for because their plan had a $3,000 deductible.
Service provider: SSM Health Cardinal Glennon Children’s Hospital, one of 23 hospitals owned by SSM Health, a Catholic, nonprofit health system with more than $8 billion in annual revenue.
What gives: Many patients don’t understand that they can rack up huge bills almost as soon as they walk through the doors of an ED.
Unlike a restaurant or a mechanic who won’t charge if someone gets tired of waiting for a table or an inspection of a rattling engine,
Martand Bhatt received almost no medical service. A nurse practitioner looked over the toddler, listened to his heart and stomach, and looked in his nose, mouth and ears, according to provider notes prepared by the hospital and shared with KHN by Dr. Bhatt.
The nurse didn’t change the dressing on the wound or order any testing.
“My objection to this is that there was no care provided,” Dr. Bhatt wrote to Bill of the Month.
“My wife did not drive for 45 minutes to get to an ER and wait for an additional 1½ hours for someone to tell me that our child’s vitals – weight, height, temperature and blood pressure – were okay,” Dr. Bhatt continued. “We already knew that. ... It is absolutely ridiculous and unethical.”
When the Bhatts left the ED, Martand was “alert, active and well appearing,” according to the notes.
The nurse’s assessment of Martand cost $192, which was discounted by UnitedHealthcare to a negotiated rate of $38.92. The bulk of the Bhatts’ bill – $820 – was something called a facility fee.
Hospital officials defend these fees as necessary to keep the ED open 24 hours a day as a community asset.
SSM Health spokesperson Stephanie Zoller Mueller declined to discuss the details of Martand’s medical condition even though the Bhatts gave their permission for the hospital to do so.
In an email, Ms. Zoller Mueller said the charges were “appropriate” based on the “acuity of condition, discharge instructions, vital sign monitoring, traumatic wound care, [and] numerous assessments.”
She added: “A patient does not have to receive additional treatment – procedure, labs, x-rays, etc. – to validate an ED-level charge.”
But some patient advocates say these facility fees are applied much too widely and should be limited to patients who actually receive medical care.
“It’s just not appropriate for someone to be charged if they’re not provided treatment,” said Adam Fox, deputy director of the Colorado Consumer Health Initiative. “Patients aren’t availing themselves of a facility if they don’t get care.”
At the very least, hospitals could communicate more clearly to patients about the fees they may be charged for coming to an ED, said Maureen Hensley-Quinn, senior program director at the National Academy for State Health Policy.
“People should know that when they walk in to receive care, there is this fee that they will be assessed,” Ms. Hensley-Quinn said.
Hospitals could also post at the entrance to the ED standard fees for different levels of emergency care.
Dr. Bhatt’s fee still could have been lower if the hospital had classified his son’s injury as minor. But, again, the hospital billing process worked against the family and in favor of the hospital’s bottom line.
Emergency visits are usually classified for billing on a scale from 1 to 5. Level 1 is minor and routine; level 5 requires complex care for life-threatening conditions. And hospitals are increasingly using the highest-severity codes to classify emergency visits, research shows.
“There are financial incentives for billing at a higher severity,” said Aditi Sen, who directs policy and research at the nonprofit Health Care Cost Institute, which has studied ED coding.
Despite the lack of severity of Martand’s wound and the absence of medical care, his visit was classified as level 3, a moderate-severity problem.
Resolution: Incensed that he’d been charged so much, Dr. Bhatt made numerous attempts to get the hospital to reduce the charges. He also appealed to UnitedHealthcare to review the charges.
His efforts failed. In August, Dr. Bhatt received a letter from an SSM Health “patient advocate” informing him that the hospital would not adjust the bill and instructing him to contact patient billing to arrange for payment.
While Dr. Bhatt was trying to reach the patient advocate by phone, his bill was sent to Medicredit, a collection agency, which began sending him notices and calling him.
After KHN contacted SSM Health, Dr. Bhatt received a call from someone who worked on “patient financial experience” issues at the hospital.
The hospital agreed to forgive the $820 facility fee. Dr. Bhatt agreed to pay the remaining $38.92, the professional fee for the ED nurse’s work. Dr. Bhatt also received a notice from Medicredit that it would take no further action against him.
The takeaway: The Bhatts did what most parents would do when a pediatrician advises them to take their child to the hospital.
But EDs are among the most expensive places to get care in the U.S. health system.
If you have a relatively low-level issue, think twice before even registering at the front desk, the act that initiates the billing process. If your doctor doesn’t have same-day appointments or after-hours service, think about urgent care, which is often much cheaper if the center isn’t attached to a hospital.
And remember that if you go to a hospital ED with a relatively minor issue, chances are that you’ll have to wait, as the Bhatts did. Patients with more serious problems will be seen first.
Once you’re taken past the front desk, you will almost certainly be hit with a substantial facility fee even if you don’t receive care.
Appealing that fee to the hospital can occasionally be successful, but there are no guarantees. And, as Dr. Bhatt learned, don’t expect the health insurer to offer much help. Most insurers won’t challenge how a medical visit is coded except on extremely expensive medical claims that will cost them money.
In this case, Dr. Bhatt was on the hook for the whole fee because he had a high-deductible plan, so the insurer had little incentive to take up his cause.
For now, patients’ best hope, many advocates believe, is to publicize the high prices that hospitals charge for their services, inside and outside the ED.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
An unwelcome second opinion
“Why did the other doctor say that?”
I get that question here and there, and it’s always irritating. How should I know?
Generally it’s referring to something they say their family doctor told them: A scan that showed normal pressure hydrocephalus or multiple sclerosis, but when I actually get the neuroradiologist’s report it was normal. Sometimes it’s an alleged side effect from a drug for which I can find nothing in the literature or something that requires urgent surgery in spite of all objective evidence to the contrary.

These appointments are always frustrating. The patient is upset that what they’ve been told (or at least think they’ve been told) is incorrect. They’ve spent a few weeks doing medical research on Google for a condition they don’t have. They’re angry at me for shooting them down. They’re angry at the person who referred them for not being right. They’re angry that they wasted their time coming to me.
And then they ask me why the other doctor said that. I wasn’t there. I don’t know. Medicine is a less-than-perfect science. Maybe they were looking at the wrong report. Maybe they’d gotten an incorrect “wet read” by phone. (How many doctors today even know where the term came from?) Maybe they were having a bad day, were overwhelmed, and misread something.
There’s also the possibility that the other doctor didn’t say it at all. Many people will only hear what they want to hear. Or they’ve already decided what they have and are claiming “the other doctor” told them just to give credence to it, even if it’s not true.
Such visits often end on an ugly note. The patient doesn’t want to be billed because I didn’t say what they wanted me to say. Or pay a copay. Or just get up and leave.
I try, very hard, to be polite when this happens. I don’t know what really went on at the other office – if what’s claimed even happened at all. Even if the patient is telling the truth, It’s not like they were trying to be wrong or deceptive. I don’t fault my colleagues if they make an error, and hope they feel the same way about me.
But it’s still frustrating when it occurs. In many cases I’m left dictating a polite note back to the referring physician, explaining what happened. I chalk it up to a communication error, or experience, or even just a difficult patient. I never really know for sure.
I don’t think any of us are here to willfully deceive patients. We want to do our best for them. It’s frustrating when something happens to lead them to believe otherwise.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
“Why did the other doctor say that?”
I get that question here and there, and it’s always irritating. How should I know?
Generally it’s referring to something they say their family doctor told them: A scan that showed normal pressure hydrocephalus or multiple sclerosis, but when I actually get the neuroradiologist’s report it was normal. Sometimes it’s an alleged side effect from a drug for which I can find nothing in the literature or something that requires urgent surgery in spite of all objective evidence to the contrary.
These appointments are always frustrating. The patient is upset that what they’ve been told (or at least think they’ve been told) is incorrect. They’ve spent a few weeks doing medical research on Google for a condition they don’t have. They’re angry at me for shooting them down. They’re angry at the person who referred them for not being right. They’re angry that they wasted their time coming to me.
And then they ask me why the other doctor said that. I wasn’t there. I don’t know. Medicine is a less-than-perfect science. Maybe they were looking at the wrong report. Maybe they’d gotten an incorrect “wet read” by phone. (How many doctors today even know where the term came from?) Maybe they were having a bad day, were overwhelmed, and misread something.
There’s also the possibility that the other doctor didn’t say it at all. Many people will only hear what they want to hear. Or they’ve already decided what they have and are claiming “the other doctor” told them just to give credence to it, even if it’s not true.
Such visits often end on an ugly note. The patient doesn’t want to be billed because I didn’t say what they wanted me to say. Or pay a copay. Or just get up and leave.
I try, very hard, to be polite when this happens. I don’t know what really went on at the other office – if what’s claimed even happened at all. Even if the patient is telling the truth, It’s not like they were trying to be wrong or deceptive. I don’t fault my colleagues if they make an error, and hope they feel the same way about me.
But it’s still frustrating when it occurs. In many cases I’m left dictating a polite note back to the referring physician, explaining what happened. I chalk it up to a communication error, or experience, or even just a difficult patient. I never really know for sure.
I don’t think any of us are here to willfully deceive patients. We want to do our best for them. It’s frustrating when something happens to lead them to believe otherwise.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
“Why did the other doctor say that?”
I get that question here and there, and it’s always irritating. How should I know?
Generally it’s referring to something they say their family doctor told them: A scan that showed normal pressure hydrocephalus or multiple sclerosis, but when I actually get the neuroradiologist’s report it was normal. Sometimes it’s an alleged side effect from a drug for which I can find nothing in the literature or something that requires urgent surgery in spite of all objective evidence to the contrary.
These appointments are always frustrating. The patient is upset that what they’ve been told (or at least think they’ve been told) is incorrect. They’ve spent a few weeks doing medical research on Google for a condition they don’t have. They’re angry at me for shooting them down. They’re angry at the person who referred them for not being right. They’re angry that they wasted their time coming to me.
And then they ask me why the other doctor said that. I wasn’t there. I don’t know. Medicine is a less-than-perfect science. Maybe they were looking at the wrong report. Maybe they’d gotten an incorrect “wet read” by phone. (How many doctors today even know where the term came from?) Maybe they were having a bad day, were overwhelmed, and misread something.
There’s also the possibility that the other doctor didn’t say it at all. Many people will only hear what they want to hear. Or they’ve already decided what they have and are claiming “the other doctor” told them just to give credence to it, even if it’s not true.
Such visits often end on an ugly note. The patient doesn’t want to be billed because I didn’t say what they wanted me to say. Or pay a copay. Or just get up and leave.
I try, very hard, to be polite when this happens. I don’t know what really went on at the other office – if what’s claimed even happened at all. Even if the patient is telling the truth, It’s not like they were trying to be wrong or deceptive. I don’t fault my colleagues if they make an error, and hope they feel the same way about me.
But it’s still frustrating when it occurs. In many cases I’m left dictating a polite note back to the referring physician, explaining what happened. I chalk it up to a communication error, or experience, or even just a difficult patient. I never really know for sure.
I don’t think any of us are here to willfully deceive patients. We want to do our best for them. It’s frustrating when something happens to lead them to believe otherwise.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This doc still supports NP/PA-led care ... with caveats
Two years ago, I argued that independent care from nurse practitioners (NPs) and physician assistants (PAs) would not have ill effects on health outcomes. To the surprise of no one, NPs and PAs embraced the argument; physicians clobbered it.
My case had three pegs: One was that medicine isn’t rocket science and clinicians control a lot less than we think we do. The second peg was that technology levels the playing field of clinical care. High-sensitivity troponin assays, for instance, make missing MI a lot less likely. The third peg was empirical: Studies have found little difference in MD versus non–MD-led care. Looking back, I now see empiricism as the weakest part of the argument because the studies had so many limitations.
I update this viewpoint now because health care is increasingly delivered by NPs and PAs. And there are two concerning trends regarding NP education and experience. First is that nurses are turning to advanced practitioner training earlier in their careers – without gathering much bedside experience. And these training programs are increasingly likely to be online, with minimal hands-on clinical tutoring.
Education and experience pop in my head often. Not every day, but many days I think back to my lucky 7 years in Indiana learning under the supervision of master clinicians – at a time when trainees were allowed the leeway to make decisions ... and mistakes. Then, when I joined private practice, I continued to learn from experienced practitioners.
It would be foolish to argue that training and experience aren’t important.
But here’s the thing:
I will make three points: First, I will bolster two of my old arguments as to why we shouldn’t be worried about non-MD clinicians, then I will propose some ideas to increase confidence in NP and PA care.
Health care does not equal health
On the matter of how much clinicians affect outcomes, a recently published randomized controlled trial performed in India found that subsidizing insurance care led to increased utilization of hospital services but had no significant effect on health outcomes. This follows the RAND and Oregon Health Insurance studies in the United States, which largely reported similar results.
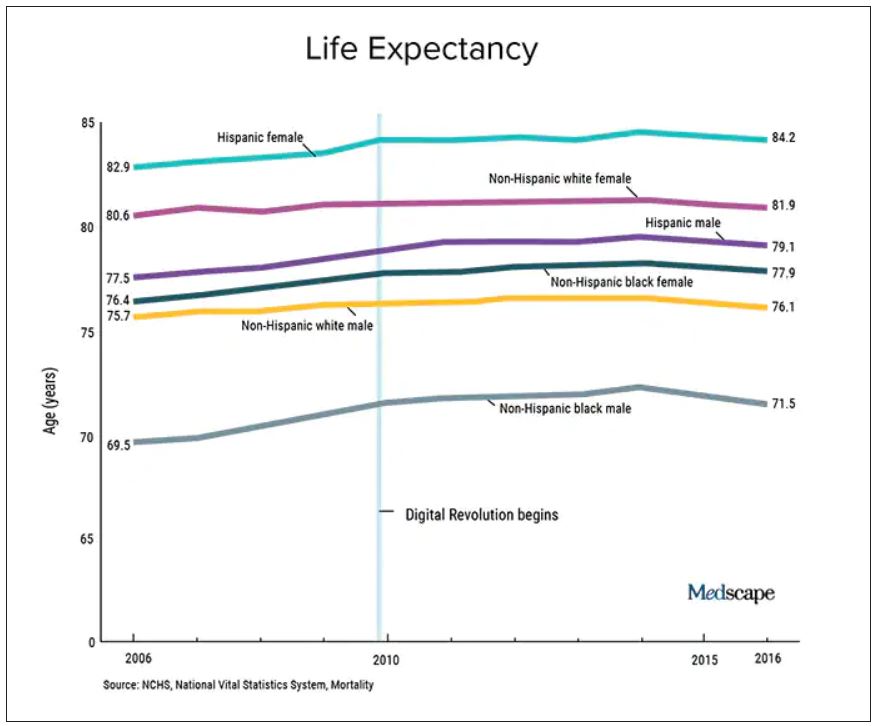
We should also not dismiss the fact that – despite the massive technology gains over the past half-century in digital health and artificial intelligence and increased use of quality measures, new drugs and procedures, and mega-medical centers – the average lifespan of Americans is flat to declining (in most ethnic and racial groups). Worse than no gains in longevity, perhaps, is that death from diseases like dementia and Parkinson’s disease are on the rise.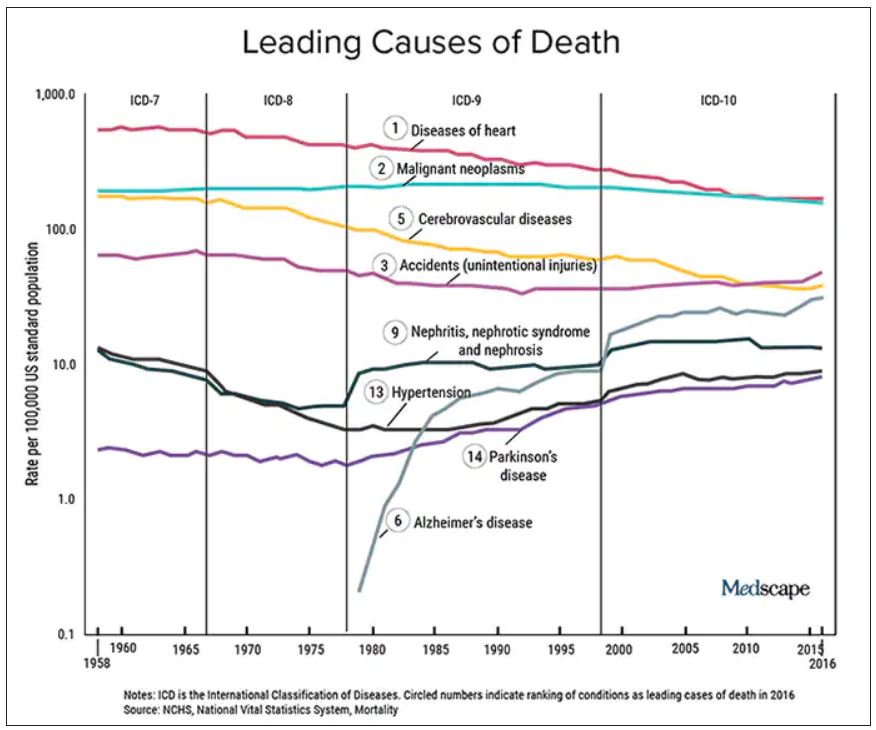
A neutral Martian would look down and wonder why all this health care hasn’t translated to longer and better lives. The causes of this paradox remain speculative, and are for another column, but the point remains that – on average – more health care is clearly not delivering more health. And if that is true, one may deduce that much of U.S. health care is marginal when it comes to affecting major outcomes.
It’s about the delta
Logos trumps pathos. Sure, my physician colleagues can tell scary anecdotes of bad outcomes caused by an inexperienced NP or PA. I would counter that by saying I have sat on our hospital’s peer review committee for 2 decades, including the era before NPs or PAs were practicing, and I have plenty of stories of physician errors. These include, of course, my own errors.
Logos: We must consider the difference between non–MD-led care and MD-led care.
My arguments from 2020 remain relevant today. Most medical problems are not engineering puzzles. Many, perhaps most, patients fall into an easy protocol – say, chest pain, dyspnea, or atrial fibrillation. With basic training, a motivated serious person quickly gains skill in recognizing and treating everyday problems.
And just 2 years on, technology further levels the playing field. Consider radiology in 2022 – it’s easy to take for granted the speed of the CT scan, the fidelity of the MRI, and the easy access to both in the U.S. hospital system. Less experienced clinicians have never had more tools to assist with diagnostics and therapeutics.
The expansion of team-based care has also mitigated the effects of inexperience. It took Americans longer than Canadians to figure out how helpful pharmacists could be. Pharmacists in my hospital now help us dose complicated medicines and protect us against prescribing errors.
Then there is the immediate access to online information. Gone are the days when you had to memorize long-QT syndromes. Book knowledge – that I spent years acquiring – now comes in seconds. The other day an NP corrected me. I asked, Are you sure? Boom, she took out her phone and showed me the evidence.
In sum, if it were even possible to measure the clinical competence of care from NP and PA versus physicians, there would be two bell-shaped curves with a tremendous amount of overlap. And that overlap would steadily increase as a given NP or PA gathered experience. (The NP in our electrophysiology division has more than 25 years’ experience in heart rhythm care, and it is common for colleagues to call her before one of us docs. Rightly so.)
Three basic proposals regarding NP and PA care
To ensure quality of care, I have three proposals.
It has always seemed strange to me that an NP or PA can flip from one field to another without a period of training. I can’t just change practice from electrophysiology to dermatology without doing a residency. But NPs and PAs can.
My first proposal would be that NPs and PAs spend a substantial period of training in a field before practice – a legit apprenticeship. The duration of this period is a matter of debate, but it ought to be standardized.
My second proposal is that, if physicians are required to pass certification exams, so should NPs. (PAs have an exam every 10 years.) The exam should be the same as (or very similar to) the physician exam, and it should be specific to their field of practice.
While I have argued (and still feel) that the American Board of Internal Medicine brand of certification is dubious, the fact remains that physicians must maintain proficiency in their field. Requiring NPs and PAs to do the same would help foster specialization. And while I can’t cite empirical evidence, specialization seems super-important. We have NPs at my hospital who have been in the same area for years, and they exude clinical competence.
Finally, I have come to believe that the best way for nearly any clinician to practice medicine is as part of a team. (The exception being primary care in rural areas where there are clinician shortages.)
On the matter of team care, I’ve practiced for a long time, but nearly every day I run situations by a colleague; often this person is an NP. The economist Friedrich Hayek proposed that dispersed knowledge always outpaces the wisdom of any individual. That notion pertains well to the increasing complexities and specialization of modern medical practice.
A person who commits to learning one area of medicine, enjoys helping people, asks often for help, and has the support of colleagues is set up to be a successful clinician – whether the letters after their name are APRN, PA, DO, or MD.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Ky. He did not report any relevant financial disclosures. A version of this article first appeared on Medscape.com.
Two years ago, I argued that independent care from nurse practitioners (NPs) and physician assistants (PAs) would not have ill effects on health outcomes. To the surprise of no one, NPs and PAs embraced the argument; physicians clobbered it.
My case had three pegs: One was that medicine isn’t rocket science and clinicians control a lot less than we think we do. The second peg was that technology levels the playing field of clinical care. High-sensitivity troponin assays, for instance, make missing MI a lot less likely. The third peg was empirical: Studies have found little difference in MD versus non–MD-led care. Looking back, I now see empiricism as the weakest part of the argument because the studies had so many limitations.
I update this viewpoint now because health care is increasingly delivered by NPs and PAs. And there are two concerning trends regarding NP education and experience. First is that nurses are turning to advanced practitioner training earlier in their careers – without gathering much bedside experience. And these training programs are increasingly likely to be online, with minimal hands-on clinical tutoring.
Education and experience pop in my head often. Not every day, but many days I think back to my lucky 7 years in Indiana learning under the supervision of master clinicians – at a time when trainees were allowed the leeway to make decisions ... and mistakes. Then, when I joined private practice, I continued to learn from experienced practitioners.
It would be foolish to argue that training and experience aren’t important.
But here’s the thing:
I will make three points: First, I will bolster two of my old arguments as to why we shouldn’t be worried about non-MD clinicians, then I will propose some ideas to increase confidence in NP and PA care.
Health care does not equal health
On the matter of how much clinicians affect outcomes, a recently published randomized controlled trial performed in India found that subsidizing insurance care led to increased utilization of hospital services but had no significant effect on health outcomes. This follows the RAND and Oregon Health Insurance studies in the United States, which largely reported similar results.
We should also not dismiss the fact that – despite the massive technology gains over the past half-century in digital health and artificial intelligence and increased use of quality measures, new drugs and procedures, and mega-medical centers – the average lifespan of Americans is flat to declining (in most ethnic and racial groups). Worse than no gains in longevity, perhaps, is that death from diseases like dementia and Parkinson’s disease are on the rise.
A neutral Martian would look down and wonder why all this health care hasn’t translated to longer and better lives. The causes of this paradox remain speculative, and are for another column, but the point remains that – on average – more health care is clearly not delivering more health. And if that is true, one may deduce that much of U.S. health care is marginal when it comes to affecting major outcomes.
It’s about the delta
Logos trumps pathos. Sure, my physician colleagues can tell scary anecdotes of bad outcomes caused by an inexperienced NP or PA. I would counter that by saying I have sat on our hospital’s peer review committee for 2 decades, including the era before NPs or PAs were practicing, and I have plenty of stories of physician errors. These include, of course, my own errors.
Logos: We must consider the difference between non–MD-led care and MD-led care.
My arguments from 2020 remain relevant today. Most medical problems are not engineering puzzles. Many, perhaps most, patients fall into an easy protocol – say, chest pain, dyspnea, or atrial fibrillation. With basic training, a motivated serious person quickly gains skill in recognizing and treating everyday problems.
And just 2 years on, technology further levels the playing field. Consider radiology in 2022 – it’s easy to take for granted the speed of the CT scan, the fidelity of the MRI, and the easy access to both in the U.S. hospital system. Less experienced clinicians have never had more tools to assist with diagnostics and therapeutics.
The expansion of team-based care has also mitigated the effects of inexperience. It took Americans longer than Canadians to figure out how helpful pharmacists could be. Pharmacists in my hospital now help us dose complicated medicines and protect us against prescribing errors.
Then there is the immediate access to online information. Gone are the days when you had to memorize long-QT syndromes. Book knowledge – that I spent years acquiring – now comes in seconds. The other day an NP corrected me. I asked, Are you sure? Boom, she took out her phone and showed me the evidence.
In sum, if it were even possible to measure the clinical competence of care from NP and PA versus physicians, there would be two bell-shaped curves with a tremendous amount of overlap. And that overlap would steadily increase as a given NP or PA gathered experience. (The NP in our electrophysiology division has more than 25 years’ experience in heart rhythm care, and it is common for colleagues to call her before one of us docs. Rightly so.)
Three basic proposals regarding NP and PA care
To ensure quality of care, I have three proposals.
It has always seemed strange to me that an NP or PA can flip from one field to another without a period of training. I can’t just change practice from electrophysiology to dermatology without doing a residency. But NPs and PAs can.
My first proposal would be that NPs and PAs spend a substantial period of training in a field before practice – a legit apprenticeship. The duration of this period is a matter of debate, but it ought to be standardized.
My second proposal is that, if physicians are required to pass certification exams, so should NPs. (PAs have an exam every 10 years.) The exam should be the same as (or very similar to) the physician exam, and it should be specific to their field of practice.
While I have argued (and still feel) that the American Board of Internal Medicine brand of certification is dubious, the fact remains that physicians must maintain proficiency in their field. Requiring NPs and PAs to do the same would help foster specialization. And while I can’t cite empirical evidence, specialization seems super-important. We have NPs at my hospital who have been in the same area for years, and they exude clinical competence.
Finally, I have come to believe that the best way for nearly any clinician to practice medicine is as part of a team. (The exception being primary care in rural areas where there are clinician shortages.)
On the matter of team care, I’ve practiced for a long time, but nearly every day I run situations by a colleague; often this person is an NP. The economist Friedrich Hayek proposed that dispersed knowledge always outpaces the wisdom of any individual. That notion pertains well to the increasing complexities and specialization of modern medical practice.
A person who commits to learning one area of medicine, enjoys helping people, asks often for help, and has the support of colleagues is set up to be a successful clinician – whether the letters after their name are APRN, PA, DO, or MD.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Ky. He did not report any relevant financial disclosures. A version of this article first appeared on Medscape.com.
Two years ago, I argued that independent care from nurse practitioners (NPs) and physician assistants (PAs) would not have ill effects on health outcomes. To the surprise of no one, NPs and PAs embraced the argument; physicians clobbered it.
My case had three pegs: One was that medicine isn’t rocket science and clinicians control a lot less than we think we do. The second peg was that technology levels the playing field of clinical care. High-sensitivity troponin assays, for instance, make missing MI a lot less likely. The third peg was empirical: Studies have found little difference in MD versus non–MD-led care. Looking back, I now see empiricism as the weakest part of the argument because the studies had so many limitations.
I update this viewpoint now because health care is increasingly delivered by NPs and PAs. And there are two concerning trends regarding NP education and experience. First is that nurses are turning to advanced practitioner training earlier in their careers – without gathering much bedside experience. And these training programs are increasingly likely to be online, with minimal hands-on clinical tutoring.
Education and experience pop in my head often. Not every day, but many days I think back to my lucky 7 years in Indiana learning under the supervision of master clinicians – at a time when trainees were allowed the leeway to make decisions ... and mistakes. Then, when I joined private practice, I continued to learn from experienced practitioners.
It would be foolish to argue that training and experience aren’t important.
But here’s the thing:
I will make three points: First, I will bolster two of my old arguments as to why we shouldn’t be worried about non-MD clinicians, then I will propose some ideas to increase confidence in NP and PA care.
Health care does not equal health
On the matter of how much clinicians affect outcomes, a recently published randomized controlled trial performed in India found that subsidizing insurance care led to increased utilization of hospital services but had no significant effect on health outcomes. This follows the RAND and Oregon Health Insurance studies in the United States, which largely reported similar results.
We should also not dismiss the fact that – despite the massive technology gains over the past half-century in digital health and artificial intelligence and increased use of quality measures, new drugs and procedures, and mega-medical centers – the average lifespan of Americans is flat to declining (in most ethnic and racial groups). Worse than no gains in longevity, perhaps, is that death from diseases like dementia and Parkinson’s disease are on the rise.
A neutral Martian would look down and wonder why all this health care hasn’t translated to longer and better lives. The causes of this paradox remain speculative, and are for another column, but the point remains that – on average – more health care is clearly not delivering more health. And if that is true, one may deduce that much of U.S. health care is marginal when it comes to affecting major outcomes.
It’s about the delta
Logos trumps pathos. Sure, my physician colleagues can tell scary anecdotes of bad outcomes caused by an inexperienced NP or PA. I would counter that by saying I have sat on our hospital’s peer review committee for 2 decades, including the era before NPs or PAs were practicing, and I have plenty of stories of physician errors. These include, of course, my own errors.
Logos: We must consider the difference between non–MD-led care and MD-led care.
My arguments from 2020 remain relevant today. Most medical problems are not engineering puzzles. Many, perhaps most, patients fall into an easy protocol – say, chest pain, dyspnea, or atrial fibrillation. With basic training, a motivated serious person quickly gains skill in recognizing and treating everyday problems.
And just 2 years on, technology further levels the playing field. Consider radiology in 2022 – it’s easy to take for granted the speed of the CT scan, the fidelity of the MRI, and the easy access to both in the U.S. hospital system. Less experienced clinicians have never had more tools to assist with diagnostics and therapeutics.
The expansion of team-based care has also mitigated the effects of inexperience. It took Americans longer than Canadians to figure out how helpful pharmacists could be. Pharmacists in my hospital now help us dose complicated medicines and protect us against prescribing errors.
Then there is the immediate access to online information. Gone are the days when you had to memorize long-QT syndromes. Book knowledge – that I spent years acquiring – now comes in seconds. The other day an NP corrected me. I asked, Are you sure? Boom, she took out her phone and showed me the evidence.
In sum, if it were even possible to measure the clinical competence of care from NP and PA versus physicians, there would be two bell-shaped curves with a tremendous amount of overlap. And that overlap would steadily increase as a given NP or PA gathered experience. (The NP in our electrophysiology division has more than 25 years’ experience in heart rhythm care, and it is common for colleagues to call her before one of us docs. Rightly so.)
Three basic proposals regarding NP and PA care
To ensure quality of care, I have three proposals.
It has always seemed strange to me that an NP or PA can flip from one field to another without a period of training. I can’t just change practice from electrophysiology to dermatology without doing a residency. But NPs and PAs can.
My first proposal would be that NPs and PAs spend a substantial period of training in a field before practice – a legit apprenticeship. The duration of this period is a matter of debate, but it ought to be standardized.
My second proposal is that, if physicians are required to pass certification exams, so should NPs. (PAs have an exam every 10 years.) The exam should be the same as (or very similar to) the physician exam, and it should be specific to their field of practice.
While I have argued (and still feel) that the American Board of Internal Medicine brand of certification is dubious, the fact remains that physicians must maintain proficiency in their field. Requiring NPs and PAs to do the same would help foster specialization. And while I can’t cite empirical evidence, specialization seems super-important. We have NPs at my hospital who have been in the same area for years, and they exude clinical competence.
Finally, I have come to believe that the best way for nearly any clinician to practice medicine is as part of a team. (The exception being primary care in rural areas where there are clinician shortages.)
On the matter of team care, I’ve practiced for a long time, but nearly every day I run situations by a colleague; often this person is an NP. The economist Friedrich Hayek proposed that dispersed knowledge always outpaces the wisdom of any individual. That notion pertains well to the increasing complexities and specialization of modern medical practice.
A person who commits to learning one area of medicine, enjoys helping people, asks often for help, and has the support of colleagues is set up to be a successful clinician – whether the letters after their name are APRN, PA, DO, or MD.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Ky. He did not report any relevant financial disclosures. A version of this article first appeared on Medscape.com.
Seven ways doctors could get better payment from insurers
, say experts in physician-payer contracts.
Many doctors sign long-term agreements and then forget about them, says Marcia Brauchler, president and founder of Physicians’ Ally, Littleton, Colorado, a health care consulting company. “The average doctor is trying to run a practice on 2010 rates because they haven’t touched their insurance contracts for 10 years,” she says.
Payers also make a lot of money by adopting dozens of unilateral policy and procedure changes every year that they know physicians are too busy to read. They are counting on the fact that few doctors will understand what the policy changes are and that even fewer will contest them, says Greg Brodek, JD, chair of the health law practice group and head of the managed care litigation practice at Duane Morris, who represents doctors in disputes with payers.
These experts say doctors can push back on one-sided payer contracts and negotiate changes. Mr. Brodek says some practices have more leverage than others to influence payers – if they are larger, in a specialty that the payer needs in its network, or located in a remote area where the payer has limited options.
Here are seven key areas to pay attention to:
1. Long-term contracts. Most doctors sign multiyear “evergreen” contracts that renew automatically every year. This allows insurers to continue to pay doctors the same rate for years.
To avoid this, doctors should negotiate new rates when their agreements renew or, if they prefer, ask that a cost-of-living adjustment be included in the multiyear contract that applies to subsequent years, says Ms. Brauchler.
2. Fee schedules. Payers will “whitewash” what they’re paying you by saying it’s 100% of the payer fee schedule. When it comes to Medicare, they may be paying you a lot less, says Ms. Brauchler.
“My biggest takeaway is to compare the CPT codes of the payer’s fee schedule against what Medicare allows. For example, for CPT code 99213, a 15-minute established office visit, if Medicare pays you $100 and Aetna pays you $75.00, you’re getting 75% of Medicare,” says Ms. Brauchler. To avoid this, doctors should ask that the contract state that reimbursement be made according to Medicare’s medical policies rather than the payer’s.
3. Audits. Commercial payers will claim they have a contractual right to conduct pre- and post-payment audits of physicians’ claims that can result in reduced payments. The contract only states that if doctors correctly submit claims, they will get paid, not that they will have to go through extra steps, which is a breach of their agreement, says Mr. Brodek.
In his experience, 90% of payers back down when asked to provide the contractual basis to conduct these audits. “Or, they take the position that it’s not in the contract but that they have a policy.”
4. Contract amendments versus policies and procedures. This is a huge area that needs to be clarified in contracts and monitored by providers throughout their relationships with payers. Contracts have three elements: the parties, the services provided, and the payment. Changing any one of those terms requires an amendment and advance written notice that has to be delivered to the other party in a certain way, such as by overnight delivery, says Mr. Brodek.
In addition, both parties have to sign that they agree to an amendment. “But, that’s too cumbersome and complicated for payers who have decided to adopt policies instead. These are unilateral changes made with no advance notice given, since the payer typically posts the change on its website,” says Mr. Brodek.
5. Recoupment efforts. Payers will review claims after they’re paid and contact the doctor saying they found a mistake, such as inappropriate coding. They will claim that the doctor now owes them a large sum of money based on a percentage of claims reviewed. “They typically send the doctor a letter that ends with, ‘If you do not pay this amount within 30 days, we will offset the amount due against future payments that we would otherwise make to you,’” says Mr. Brodek.
He recommends that contracts include the doctors’ right to contest an audit so the “payer doesn’t have the unilateral right to disregard the initial coding that the doctor appropriately assigned to the claim and recoup the money anyway,” says Mr. Brodek.
6. Medical network rentals and products. Most contracts say that payers can rent out their medical networks to other health plans, such as HMOs, and that the clinicians agree to comply with all of their policies and procedures. The agreement may also cover the products of other plans.
“The problem is that physicians are not given information about the other plans, including their terms and conditions for getting paid,” says Mr. Brodek. If a problem with payment arises, they have no written agreement with that plan, which makes it harder to enforce.
“That’s why we recommend that doctors negotiate agreements that only cover the main payer. Most of the time, the payer is amenable to putting that language in the contract,” he says.
7. Payer products. In the past several years, a typical contract has included appendices that list the payer’s products, such as Medicare, workers compensation, auto insurance liability, or health care exchange products. Many clinicians don’t realize they can pick the plans they want to participate in by accepting or opting out, says Mr. Brodek.
“We advise clients to limit the contract to what you want covered and to make informed decisions, because some products have low fees set by the states, such as workers compensation and health care exchanges,” says Mr. Brodek.
A version of this article first appeared on Medscape.com.
, say experts in physician-payer contracts.
Many doctors sign long-term agreements and then forget about them, says Marcia Brauchler, president and founder of Physicians’ Ally, Littleton, Colorado, a health care consulting company. “The average doctor is trying to run a practice on 2010 rates because they haven’t touched their insurance contracts for 10 years,” she says.
Payers also make a lot of money by adopting dozens of unilateral policy and procedure changes every year that they know physicians are too busy to read. They are counting on the fact that few doctors will understand what the policy changes are and that even fewer will contest them, says Greg Brodek, JD, chair of the health law practice group and head of the managed care litigation practice at Duane Morris, who represents doctors in disputes with payers.
These experts say doctors can push back on one-sided payer contracts and negotiate changes. Mr. Brodek says some practices have more leverage than others to influence payers – if they are larger, in a specialty that the payer needs in its network, or located in a remote area where the payer has limited options.
Here are seven key areas to pay attention to:
1. Long-term contracts. Most doctors sign multiyear “evergreen” contracts that renew automatically every year. This allows insurers to continue to pay doctors the same rate for years.
To avoid this, doctors should negotiate new rates when their agreements renew or, if they prefer, ask that a cost-of-living adjustment be included in the multiyear contract that applies to subsequent years, says Ms. Brauchler.
2. Fee schedules. Payers will “whitewash” what they’re paying you by saying it’s 100% of the payer fee schedule. When it comes to Medicare, they may be paying you a lot less, says Ms. Brauchler.
“My biggest takeaway is to compare the CPT codes of the payer’s fee schedule against what Medicare allows. For example, for CPT code 99213, a 15-minute established office visit, if Medicare pays you $100 and Aetna pays you $75.00, you’re getting 75% of Medicare,” says Ms. Brauchler. To avoid this, doctors should ask that the contract state that reimbursement be made according to Medicare’s medical policies rather than the payer’s.
3. Audits. Commercial payers will claim they have a contractual right to conduct pre- and post-payment audits of physicians’ claims that can result in reduced payments. The contract only states that if doctors correctly submit claims, they will get paid, not that they will have to go through extra steps, which is a breach of their agreement, says Mr. Brodek.
In his experience, 90% of payers back down when asked to provide the contractual basis to conduct these audits. “Or, they take the position that it’s not in the contract but that they have a policy.”
4. Contract amendments versus policies and procedures. This is a huge area that needs to be clarified in contracts and monitored by providers throughout their relationships with payers. Contracts have three elements: the parties, the services provided, and the payment. Changing any one of those terms requires an amendment and advance written notice that has to be delivered to the other party in a certain way, such as by overnight delivery, says Mr. Brodek.
In addition, both parties have to sign that they agree to an amendment. “But, that’s too cumbersome and complicated for payers who have decided to adopt policies instead. These are unilateral changes made with no advance notice given, since the payer typically posts the change on its website,” says Mr. Brodek.
5. Recoupment efforts. Payers will review claims after they’re paid and contact the doctor saying they found a mistake, such as inappropriate coding. They will claim that the doctor now owes them a large sum of money based on a percentage of claims reviewed. “They typically send the doctor a letter that ends with, ‘If you do not pay this amount within 30 days, we will offset the amount due against future payments that we would otherwise make to you,’” says Mr. Brodek.
He recommends that contracts include the doctors’ right to contest an audit so the “payer doesn’t have the unilateral right to disregard the initial coding that the doctor appropriately assigned to the claim and recoup the money anyway,” says Mr. Brodek.
6. Medical network rentals and products. Most contracts say that payers can rent out their medical networks to other health plans, such as HMOs, and that the clinicians agree to comply with all of their policies and procedures. The agreement may also cover the products of other plans.
“The problem is that physicians are not given information about the other plans, including their terms and conditions for getting paid,” says Mr. Brodek. If a problem with payment arises, they have no written agreement with that plan, which makes it harder to enforce.
“That’s why we recommend that doctors negotiate agreements that only cover the main payer. Most of the time, the payer is amenable to putting that language in the contract,” he says.
7. Payer products. In the past several years, a typical contract has included appendices that list the payer’s products, such as Medicare, workers compensation, auto insurance liability, or health care exchange products. Many clinicians don’t realize they can pick the plans they want to participate in by accepting or opting out, says Mr. Brodek.
“We advise clients to limit the contract to what you want covered and to make informed decisions, because some products have low fees set by the states, such as workers compensation and health care exchanges,” says Mr. Brodek.
A version of this article first appeared on Medscape.com.
, say experts in physician-payer contracts.
Many doctors sign long-term agreements and then forget about them, says Marcia Brauchler, president and founder of Physicians’ Ally, Littleton, Colorado, a health care consulting company. “The average doctor is trying to run a practice on 2010 rates because they haven’t touched their insurance contracts for 10 years,” she says.
Payers also make a lot of money by adopting dozens of unilateral policy and procedure changes every year that they know physicians are too busy to read. They are counting on the fact that few doctors will understand what the policy changes are and that even fewer will contest them, says Greg Brodek, JD, chair of the health law practice group and head of the managed care litigation practice at Duane Morris, who represents doctors in disputes with payers.
These experts say doctors can push back on one-sided payer contracts and negotiate changes. Mr. Brodek says some practices have more leverage than others to influence payers – if they are larger, in a specialty that the payer needs in its network, or located in a remote area where the payer has limited options.
Here are seven key areas to pay attention to:
1. Long-term contracts. Most doctors sign multiyear “evergreen” contracts that renew automatically every year. This allows insurers to continue to pay doctors the same rate for years.
To avoid this, doctors should negotiate new rates when their agreements renew or, if they prefer, ask that a cost-of-living adjustment be included in the multiyear contract that applies to subsequent years, says Ms. Brauchler.
2. Fee schedules. Payers will “whitewash” what they’re paying you by saying it’s 100% of the payer fee schedule. When it comes to Medicare, they may be paying you a lot less, says Ms. Brauchler.
“My biggest takeaway is to compare the CPT codes of the payer’s fee schedule against what Medicare allows. For example, for CPT code 99213, a 15-minute established office visit, if Medicare pays you $100 and Aetna pays you $75.00, you’re getting 75% of Medicare,” says Ms. Brauchler. To avoid this, doctors should ask that the contract state that reimbursement be made according to Medicare’s medical policies rather than the payer’s.
3. Audits. Commercial payers will claim they have a contractual right to conduct pre- and post-payment audits of physicians’ claims that can result in reduced payments. The contract only states that if doctors correctly submit claims, they will get paid, not that they will have to go through extra steps, which is a breach of their agreement, says Mr. Brodek.
In his experience, 90% of payers back down when asked to provide the contractual basis to conduct these audits. “Or, they take the position that it’s not in the contract but that they have a policy.”
4. Contract amendments versus policies and procedures. This is a huge area that needs to be clarified in contracts and monitored by providers throughout their relationships with payers. Contracts have three elements: the parties, the services provided, and the payment. Changing any one of those terms requires an amendment and advance written notice that has to be delivered to the other party in a certain way, such as by overnight delivery, says Mr. Brodek.
In addition, both parties have to sign that they agree to an amendment. “But, that’s too cumbersome and complicated for payers who have decided to adopt policies instead. These are unilateral changes made with no advance notice given, since the payer typically posts the change on its website,” says Mr. Brodek.
5. Recoupment efforts. Payers will review claims after they’re paid and contact the doctor saying they found a mistake, such as inappropriate coding. They will claim that the doctor now owes them a large sum of money based on a percentage of claims reviewed. “They typically send the doctor a letter that ends with, ‘If you do not pay this amount within 30 days, we will offset the amount due against future payments that we would otherwise make to you,’” says Mr. Brodek.
He recommends that contracts include the doctors’ right to contest an audit so the “payer doesn’t have the unilateral right to disregard the initial coding that the doctor appropriately assigned to the claim and recoup the money anyway,” says Mr. Brodek.
6. Medical network rentals and products. Most contracts say that payers can rent out their medical networks to other health plans, such as HMOs, and that the clinicians agree to comply with all of their policies and procedures. The agreement may also cover the products of other plans.
“The problem is that physicians are not given information about the other plans, including their terms and conditions for getting paid,” says Mr. Brodek. If a problem with payment arises, they have no written agreement with that plan, which makes it harder to enforce.
“That’s why we recommend that doctors negotiate agreements that only cover the main payer. Most of the time, the payer is amenable to putting that language in the contract,” he says.
7. Payer products. In the past several years, a typical contract has included appendices that list the payer’s products, such as Medicare, workers compensation, auto insurance liability, or health care exchange products. Many clinicians don’t realize they can pick the plans they want to participate in by accepting or opting out, says Mr. Brodek.
“We advise clients to limit the contract to what you want covered and to make informed decisions, because some products have low fees set by the states, such as workers compensation and health care exchanges,” says Mr. Brodek.
A version of this article first appeared on Medscape.com.
Physician burnout, depression compounded by COVID: Survey
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
Doc’s botched surgery leads to incontinence and $10 million judgment; more
Early in December 2021 a jury awarded a couple $10 million in a case involving a hysterectomy that went badly wrong, according to a story in the New York Post, among other news sites.
In October 2018, Michele Nugent, 41, of New York, underwent the procedure at Richmond University Medical Center. After giving birth to four children via cesarean delivery, she had developed scarring and was suffering from excessive and painful uterine bleeding.
A few days after her hysterectomy, however, Ms. Nugent experienced what she described as the worst pain of her life, along with nausea, vomiting, and urinary leakage. She was brought to the hospital emergency department, where she was reportedly told by staff there that her symptoms were normal complications of her surgery and that the treating gynecologist, Eli Serur, MD, would soon be in touch.
Despite these reassurances, Ms. Nugent’s postsurgical issues continued to worsen over the next 10 days. Among other things, she lost almost complete control of her bladder, which required her to wear adult diapers. Still, her doctor’s office told her to put off visiting until her next scheduled appointment.
At that meeting, which took place 13 days after Ms. Nugent’s surgery, Dr. Serur diagnosed a urinary tract infection and placed her on antibiotics. He also encouraged her to return to work the following week.
Ms. Nugent’s problems persisted, however. At an office meeting that included 20 men, she suddenly lost complete control of her bladder, despite going regularly to the bathroom and wearing adult diapers. “Out of nowhere,” she testified at trial, “I urinated all over myself and had to leave.” The experience left her humiliated and embarrassed.
Several weeks later, Ms. Nugent consulted with a urologist, who soon repaired the cause of her urinary problems – a fistula between her vagina and bladder.
Though successful, the procedure still left Ms. Nugent with, what are for now at least, intractable symptoms. At night, she’s forced to make multiple trips to the bathroom, and sex with her husband has become all but impossible because of the pain it elicits.
In reaching its verdict, the jury of four women and two men faulted Dr. Serur for not only performing a faulty surgery but for failing to identify and correct his mistake. In so doing, it concluded, he had departed “from good and accepted medical practice.”
Jurors divided the $10 million judgment against him into two parts: $6.5 million for Ms. Nugent’s past and future suffering, and $3.5 million to her husband for his past and future loss of consortium – that is, his loss of intimacy with his wife.
As for the medical center, the Nugents agreed to dismiss it from the case prior to trial.
Physician accused of gross negligence finally surrenders his license
A California doctor under investigation multiple times during the past 2 decades has surrendered his medical license, as a story reported by Valley Public Radio indicates.
Since 1999, the Medical Board of California has opened three investigations against Bakersfield ob.gyn. Arthur Park, MD, each involving accusations of gross negligence “following the deaths of mothers and/or their babies during childbirth.” In 2000, and again in 2020, the board voted that Dr. Park should lose his license but then suspended its decision, which enabled Dr. Park to continue practicing under probation and on condition that he complete remedial education.
Early in 2021, however, the board filed yet another accusation against him, this one involving the 2019 death of Demi Dominguez and her newborn baby. According to the accusation, Ms. Dominguez died of preeclampsia because Dr. Park and a colleague failed to treat her high blood pressure prior to delivery. While doctors attempted to resuscitate her, Ms. Dominguez’s son was delivered by emergency cesarean but died only a few hours later. The board said that Dr. Park was “grossly negligent in his care and treatment” and that his actions constituted “an extreme departure from the applicable standard of care.”
Early in December 2021, even before the board and attorney general’s office had completed their investigations, Dr. Park agreed to surrender his medical license.
Patient advocates were pleased by the doctor’s decision but also disappointed that he’d no longer be compelled to stand before a judge, as he had been scheduled to do in connection with the Dominguez case.
A review of public records by Valley Public Radio indicates that – between the various board accusations against him and an additional nine lawsuits alleging malpractice and other issues – at least two mothers and five children have died while under Dr. Park’s care. Others whose delivery he oversaw claim their children were permanently injured during childbirth.
Although Dr. Park will be eligible to reapply for his license after 2 years, a representative of his medical office said Dr. Park had decided to retire from practicing medicine.
Delayed cancer diagnosis prompts med-mal suit
An Illinois woman who claims her doctor and his staff failed to follow up on her abnormal Pap smear has filed a malpractice suit against them and their medical group, reports a story in the Madison-St. Clair Record.
In early 2019, Lisa Albright visited the medical group after she had experienced pain during intercourse. A family nurse practitioner at the practice performed a Pap smear, and Ms. Albright was instructed to wait a few days and check her patient portal for the results. In her suit, Ms. Albright claims those results were abnormal. Despite this, neither the nurse practitioner nor anyone else at the practice scheduled a follow-up test or other diagnostic assessment.
Approximately 5 months later, Ms. Albright consulted a new physician, whose follow-up testing indicated that Ms. Albright had a cervical squamous cell carcinoma.
Ms. Albright’s suit alleges that the diagnostic delay has, among other things, caused her to undergo multiple surgical procedures and treatments, face a shorter life expectancy, and endure a loss in the quality of her life.
At press time, Ms. Albright and her legal representative have not yet determined the amount they will ask for – it will be set after the severity and permanency of Ms. Albright’s injuries have been more thoroughly investigated. But it’s expected that they will seek damages, along with all legal and court expenses.
The defendants haven’t responded to the plaintiff’s suit.
A version of this article first appeared on Medscape.com.
Early in December 2021 a jury awarded a couple $10 million in a case involving a hysterectomy that went badly wrong, according to a story in the New York Post, among other news sites.
In October 2018, Michele Nugent, 41, of New York, underwent the procedure at Richmond University Medical Center. After giving birth to four children via cesarean delivery, she had developed scarring and was suffering from excessive and painful uterine bleeding.
A few days after her hysterectomy, however, Ms. Nugent experienced what she described as the worst pain of her life, along with nausea, vomiting, and urinary leakage. She was brought to the hospital emergency department, where she was reportedly told by staff there that her symptoms were normal complications of her surgery and that the treating gynecologist, Eli Serur, MD, would soon be in touch.
Despite these reassurances, Ms. Nugent’s postsurgical issues continued to worsen over the next 10 days. Among other things, she lost almost complete control of her bladder, which required her to wear adult diapers. Still, her doctor’s office told her to put off visiting until her next scheduled appointment.
At that meeting, which took place 13 days after Ms. Nugent’s surgery, Dr. Serur diagnosed a urinary tract infection and placed her on antibiotics. He also encouraged her to return to work the following week.
Ms. Nugent’s problems persisted, however. At an office meeting that included 20 men, she suddenly lost complete control of her bladder, despite going regularly to the bathroom and wearing adult diapers. “Out of nowhere,” she testified at trial, “I urinated all over myself and had to leave.” The experience left her humiliated and embarrassed.
Several weeks later, Ms. Nugent consulted with a urologist, who soon repaired the cause of her urinary problems – a fistula between her vagina and bladder.
Though successful, the procedure still left Ms. Nugent with, what are for now at least, intractable symptoms. At night, she’s forced to make multiple trips to the bathroom, and sex with her husband has become all but impossible because of the pain it elicits.
In reaching its verdict, the jury of four women and two men faulted Dr. Serur for not only performing a faulty surgery but for failing to identify and correct his mistake. In so doing, it concluded, he had departed “from good and accepted medical practice.”
Jurors divided the $10 million judgment against him into two parts: $6.5 million for Ms. Nugent’s past and future suffering, and $3.5 million to her husband for his past and future loss of consortium – that is, his loss of intimacy with his wife.
As for the medical center, the Nugents agreed to dismiss it from the case prior to trial.
Physician accused of gross negligence finally surrenders his license
A California doctor under investigation multiple times during the past 2 decades has surrendered his medical license, as a story reported by Valley Public Radio indicates.
Since 1999, the Medical Board of California has opened three investigations against Bakersfield ob.gyn. Arthur Park, MD, each involving accusations of gross negligence “following the deaths of mothers and/or their babies during childbirth.” In 2000, and again in 2020, the board voted that Dr. Park should lose his license but then suspended its decision, which enabled Dr. Park to continue practicing under probation and on condition that he complete remedial education.
Early in 2021, however, the board filed yet another accusation against him, this one involving the 2019 death of Demi Dominguez and her newborn baby. According to the accusation, Ms. Dominguez died of preeclampsia because Dr. Park and a colleague failed to treat her high blood pressure prior to delivery. While doctors attempted to resuscitate her, Ms. Dominguez’s son was delivered by emergency cesarean but died only a few hours later. The board said that Dr. Park was “grossly negligent in his care and treatment” and that his actions constituted “an extreme departure from the applicable standard of care.”
Early in December 2021, even before the board and attorney general’s office had completed their investigations, Dr. Park agreed to surrender his medical license.
Patient advocates were pleased by the doctor’s decision but also disappointed that he’d no longer be compelled to stand before a judge, as he had been scheduled to do in connection with the Dominguez case.
A review of public records by Valley Public Radio indicates that – between the various board accusations against him and an additional nine lawsuits alleging malpractice and other issues – at least two mothers and five children have died while under Dr. Park’s care. Others whose delivery he oversaw claim their children were permanently injured during childbirth.
Although Dr. Park will be eligible to reapply for his license after 2 years, a representative of his medical office said Dr. Park had decided to retire from practicing medicine.
Delayed cancer diagnosis prompts med-mal suit
An Illinois woman who claims her doctor and his staff failed to follow up on her abnormal Pap smear has filed a malpractice suit against them and their medical group, reports a story in the Madison-St. Clair Record.
In early 2019, Lisa Albright visited the medical group after she had experienced pain during intercourse. A family nurse practitioner at the practice performed a Pap smear, and Ms. Albright was instructed to wait a few days and check her patient portal for the results. In her suit, Ms. Albright claims those results were abnormal. Despite this, neither the nurse practitioner nor anyone else at the practice scheduled a follow-up test or other diagnostic assessment.
Approximately 5 months later, Ms. Albright consulted a new physician, whose follow-up testing indicated that Ms. Albright had a cervical squamous cell carcinoma.
Ms. Albright’s suit alleges that the diagnostic delay has, among other things, caused her to undergo multiple surgical procedures and treatments, face a shorter life expectancy, and endure a loss in the quality of her life.
At press time, Ms. Albright and her legal representative have not yet determined the amount they will ask for – it will be set after the severity and permanency of Ms. Albright’s injuries have been more thoroughly investigated. But it’s expected that they will seek damages, along with all legal and court expenses.
The defendants haven’t responded to the plaintiff’s suit.
A version of this article first appeared on Medscape.com.
Early in December 2021 a jury awarded a couple $10 million in a case involving a hysterectomy that went badly wrong, according to a story in the New York Post, among other news sites.
In October 2018, Michele Nugent, 41, of New York, underwent the procedure at Richmond University Medical Center. After giving birth to four children via cesarean delivery, she had developed scarring and was suffering from excessive and painful uterine bleeding.
A few days after her hysterectomy, however, Ms. Nugent experienced what she described as the worst pain of her life, along with nausea, vomiting, and urinary leakage. She was brought to the hospital emergency department, where she was reportedly told by staff there that her symptoms were normal complications of her surgery and that the treating gynecologist, Eli Serur, MD, would soon be in touch.
Despite these reassurances, Ms. Nugent’s postsurgical issues continued to worsen over the next 10 days. Among other things, she lost almost complete control of her bladder, which required her to wear adult diapers. Still, her doctor’s office told her to put off visiting until her next scheduled appointment.
At that meeting, which took place 13 days after Ms. Nugent’s surgery, Dr. Serur diagnosed a urinary tract infection and placed her on antibiotics. He also encouraged her to return to work the following week.
Ms. Nugent’s problems persisted, however. At an office meeting that included 20 men, she suddenly lost complete control of her bladder, despite going regularly to the bathroom and wearing adult diapers. “Out of nowhere,” she testified at trial, “I urinated all over myself and had to leave.” The experience left her humiliated and embarrassed.
Several weeks later, Ms. Nugent consulted with a urologist, who soon repaired the cause of her urinary problems – a fistula between her vagina and bladder.
Though successful, the procedure still left Ms. Nugent with, what are for now at least, intractable symptoms. At night, she’s forced to make multiple trips to the bathroom, and sex with her husband has become all but impossible because of the pain it elicits.
In reaching its verdict, the jury of four women and two men faulted Dr. Serur for not only performing a faulty surgery but for failing to identify and correct his mistake. In so doing, it concluded, he had departed “from good and accepted medical practice.”
Jurors divided the $10 million judgment against him into two parts: $6.5 million for Ms. Nugent’s past and future suffering, and $3.5 million to her husband for his past and future loss of consortium – that is, his loss of intimacy with his wife.
As for the medical center, the Nugents agreed to dismiss it from the case prior to trial.
Physician accused of gross negligence finally surrenders his license
A California doctor under investigation multiple times during the past 2 decades has surrendered his medical license, as a story reported by Valley Public Radio indicates.
Since 1999, the Medical Board of California has opened three investigations against Bakersfield ob.gyn. Arthur Park, MD, each involving accusations of gross negligence “following the deaths of mothers and/or their babies during childbirth.” In 2000, and again in 2020, the board voted that Dr. Park should lose his license but then suspended its decision, which enabled Dr. Park to continue practicing under probation and on condition that he complete remedial education.
Early in 2021, however, the board filed yet another accusation against him, this one involving the 2019 death of Demi Dominguez and her newborn baby. According to the accusation, Ms. Dominguez died of preeclampsia because Dr. Park and a colleague failed to treat her high blood pressure prior to delivery. While doctors attempted to resuscitate her, Ms. Dominguez’s son was delivered by emergency cesarean but died only a few hours later. The board said that Dr. Park was “grossly negligent in his care and treatment” and that his actions constituted “an extreme departure from the applicable standard of care.”
Early in December 2021, even before the board and attorney general’s office had completed their investigations, Dr. Park agreed to surrender his medical license.
Patient advocates were pleased by the doctor’s decision but also disappointed that he’d no longer be compelled to stand before a judge, as he had been scheduled to do in connection with the Dominguez case.
A review of public records by Valley Public Radio indicates that – between the various board accusations against him and an additional nine lawsuits alleging malpractice and other issues – at least two mothers and five children have died while under Dr. Park’s care. Others whose delivery he oversaw claim their children were permanently injured during childbirth.
Although Dr. Park will be eligible to reapply for his license after 2 years, a representative of his medical office said Dr. Park had decided to retire from practicing medicine.
Delayed cancer diagnosis prompts med-mal suit
An Illinois woman who claims her doctor and his staff failed to follow up on her abnormal Pap smear has filed a malpractice suit against them and their medical group, reports a story in the Madison-St. Clair Record.
In early 2019, Lisa Albright visited the medical group after she had experienced pain during intercourse. A family nurse practitioner at the practice performed a Pap smear, and Ms. Albright was instructed to wait a few days and check her patient portal for the results. In her suit, Ms. Albright claims those results were abnormal. Despite this, neither the nurse practitioner nor anyone else at the practice scheduled a follow-up test or other diagnostic assessment.
Approximately 5 months later, Ms. Albright consulted a new physician, whose follow-up testing indicated that Ms. Albright had a cervical squamous cell carcinoma.
Ms. Albright’s suit alleges that the diagnostic delay has, among other things, caused her to undergo multiple surgical procedures and treatments, face a shorter life expectancy, and endure a loss in the quality of her life.
At press time, Ms. Albright and her legal representative have not yet determined the amount they will ask for – it will be set after the severity and permanency of Ms. Albright’s injuries have been more thoroughly investigated. But it’s expected that they will seek damages, along with all legal and court expenses.
The defendants haven’t responded to the plaintiff’s suit.
A version of this article first appeared on Medscape.com.