User login
Why Scientists Are Linking More Diseases to Light at Night
This October, millions of Americans missed out on two of the most spectacular shows in the universe: the northern lights and a rare comet. Even if you were aware of them, light pollution made them difficult to see, unless you went to a dark area and let your eyes adjust.
It’s not getting any easier — the night sky over North America has been growing brighter by about 10% per year since 2011. More and more research is linking all that light pollution to a surprising range of health consequences: cancer, heart disease, diabetes, Alzheimer’s disease, and even low sperm quality, though the reasons for these troubling associations are not always clear.
“We’ve lost the contrast between light and dark, and we are confusing our physiology on a regular basis,” said John Hanifin, PhD, associate director of Thomas Jefferson University’s Light Research Program.
Our own galaxy is invisible to nearly 80% of people in North America. In 1994, an earthquake-triggered blackout in Los Angeles led to calls to the Griffith Observatory from people wondering about that hazy blob of light in the night sky. It was the Milky Way.
Glaring headlights, illuminated buildings, blazing billboards, and streetlights fill our urban skies with a glow that even affects rural residents. Inside, since the invention of the lightbulb, we’ve kept our homes bright at night. Now, we’ve also added blue light-emitting devices — smartphones, television screens, tablets — which have been linked to sleep problems.
But outdoor light may matter for our health, too. “Every photon counts,” Hanifin said.
Bright Lights, Big Problems
For one 2024 study researchers used satellite data to measure light pollution at residential addresses of over 13,000 people. They found that those who lived in places with the brightest skies at night had a 31% higher risk of high blood pressure. Another study out of Hong Kong showed a 29% higher risk of death from coronary heart disease. And yet another found a 17%higher risk of cerebrovascular disease, such as strokes or brain aneurysms.
Of course, urban areas also have air pollution, noise, and a lack of greenery. So, for some studies, scientists controlled for these factors, and the correlation remained strong (although air pollution with fine particulate matter appeared to be worse for heart health than outdoor light).
Research has found links between the nighttime glow outside and other diseases:
Breast cancer. “It’s a very strong correlation,” said Randy Nelson, PhD, a neuroscientist at West Virginia University. A study of over 100,000 teachers in California revealed that women living in areas with the most light pollution had a 12%higher risk. That effect is comparable to increasing your intake of ultra-processed foods by 10%.
Alzheimer’s disease. In a study published this fall, outdoor light at night was more strongly linked to the disease than even alcohol misuse or obesity.
Diabetes. In one recent study, people living in the most illuminated areas had a 28% higher risk of diabetes than those residing in much darker places. In a country like China, scientists concluded that 9 million cases of diabetes could be linked to light pollution.
What Happens in Your Body When You’re Exposed to Light at Night
, the “hormone of darkness.” “Darkness is very important,” Hanifin said. When he and his colleagues decades ago started studying the effects of light on human physiology, “people thought we were borderline crazy,” he said.
Nighttime illumination affects the health and behavior of species as diverse as Siberian hamsters, zebra finches, mice, crickets, and mosquitoes. Like most creatures on Earth, humans have internal clocks that are synced to the 24-hour cycle of day and night. The master clock is in your hypothalamus, a diamond-shaped part of the brain, but every cell in your body has its own clock, too. Many physiological processes run on circadian rhythms (a term derived from a Latin phrase meaning “about a day”), from sleep-wake cycle to hormone secretion, as well as processes involved in cancer progression, such as cell division.
“There are special photoreceptors in the eye that don’t deal with visual information. They just send light information,” Nelson said. “If you get light at the wrong time, you’re resetting the clocks.”
This internal clock “prepares the body for various recurrent challenges, such as eating,” said Christian Benedict, PhD, a sleep researcher at Uppsala University, Sweden. “Light exposure [at night] can mess up this very important system.” This could mean, for instance, that your insulin is released at the wrong time, Benedict said, causing “a jet lag-ish condition that will then impair the ability to handle blood sugar.” Animal studies confirm that exposure to light at night can reduce glucose tolerance and alter insulin secretion – potential pathways to diabetes.
The hormone melatonin, produced when it’s dark by the pineal gland in the brain, is a key player in this modern struggle. Melatonin helps you sleep, synchronizes the body’s circadian rhythms, protects neurons from damage, regulates the immune system, and fights inflammation. But even a sliver of light at night can suppress its secretion. Less than 30 lux of light, about the level of a pedestrian street at night, can slash melatonin by half.
When lab animals are exposed to nighttime light, they “show enormous neuroinflammation” — that is, inflammation of nervous tissue, Nelson said. In one experiment on humans, those who slept immersed in weak light had higher levels of C-reactive protein in their blood, a marker of inflammation.
Low melatonin has also been linked to cancer. It “allows the metabolic machinery of the cancer cells to be active,” Hanifin said. One of melatonin’s effects is stimulation of natural killer cells, which can recognize and destroy cancer cells. What’s more, when melatonin plunges, estrogen may go up, which could explain the link between light at night and breast cancer (estrogen fuels tumor growth in breast cancers).
Researchers concede that satellite data might be too coarse to estimate how much light people are actually exposed to while they sleep. Plus, many of us are staring at bright screens. “But the studies keep coming,” Nelson said, suggesting that outdoor light pollution does have an impact.
When researchers put wrist-worn light sensors on over 80,000 British people, they found that the more light the device registered between half-past midnight and 6 a.m., the more its wearer was at risk of having diabetes several years down the road — no matter how long they’ve actually slept. This, according to the study’s authors, supports the findings of satellite data.
A similar study that used actigraphy with built-in light sensors, measuring whether people had been sleeping in complete darkness for at least five hours, found that light pollution upped the risk of heart disease by 74%.
What Can You Do About This?
Not everyone’s melatonin is affected by nighttime light to the same degree. “Some people are very much sensitive to very dim light, whereas others are not as sensitive and need far, far more light stimulation [to impact melatonin],” Benedict said. In one study, some volunteers needed 350 lux to lower their melatonin by half. For such people, flipping on the light in the bathroom at night wouldn’t matter; for others, though, a mere 6 lux was already as harmful – which is darker than twilight.
You can protect yourself by keeping your bedroom lights off and your screens stashed away, but avoiding outdoor light pollution may be harder. You can invest in high-quality blackout curtains, of course, although some light may still seep inside. You can plant trees in front of your windows, reorient any motion-detector lights, and even petition your local government to reduce over-illumination of buildings and to choose better streetlights. You can support organizations, such as the International Dark-Sky Association, that work to preserve darkness.
Last but not least, you might want to change your habits. If you live in a particularly light-polluted area, such as the District of Columbia, America’s top place for urban blaze, you might reconsider late-night walks or drives around the neighborhood. Instead, Hanifin said, read a book in bed, while keeping the light “as dim as you can.” It’s “a much better idea versus being outside in midtown Manhattan,” he said. According to recent recommendations published by Hanifin and his colleagues, when you sleep, there should be no more than 1 lux of illumination at the level of your eyes — about as much as you’d get from having a lit candle 1 meter away.
And if we manage to preserve outdoor darkness, and the stars reappear (including the breathtaking Milky Way), we could reap more benefits — some research suggests that stargazing can elicit positive emotions, a sense of personal growth, and “a variety of transcendent thoughts and experiences.”
A version of this article appeared on WebMD.com.
This October, millions of Americans missed out on two of the most spectacular shows in the universe: the northern lights and a rare comet. Even if you were aware of them, light pollution made them difficult to see, unless you went to a dark area and let your eyes adjust.
It’s not getting any easier — the night sky over North America has been growing brighter by about 10% per year since 2011. More and more research is linking all that light pollution to a surprising range of health consequences: cancer, heart disease, diabetes, Alzheimer’s disease, and even low sperm quality, though the reasons for these troubling associations are not always clear.
“We’ve lost the contrast between light and dark, and we are confusing our physiology on a regular basis,” said John Hanifin, PhD, associate director of Thomas Jefferson University’s Light Research Program.
Our own galaxy is invisible to nearly 80% of people in North America. In 1994, an earthquake-triggered blackout in Los Angeles led to calls to the Griffith Observatory from people wondering about that hazy blob of light in the night sky. It was the Milky Way.
Glaring headlights, illuminated buildings, blazing billboards, and streetlights fill our urban skies with a glow that even affects rural residents. Inside, since the invention of the lightbulb, we’ve kept our homes bright at night. Now, we’ve also added blue light-emitting devices — smartphones, television screens, tablets — which have been linked to sleep problems.
But outdoor light may matter for our health, too. “Every photon counts,” Hanifin said.
Bright Lights, Big Problems
For one 2024 study researchers used satellite data to measure light pollution at residential addresses of over 13,000 people. They found that those who lived in places with the brightest skies at night had a 31% higher risk of high blood pressure. Another study out of Hong Kong showed a 29% higher risk of death from coronary heart disease. And yet another found a 17%higher risk of cerebrovascular disease, such as strokes or brain aneurysms.
Of course, urban areas also have air pollution, noise, and a lack of greenery. So, for some studies, scientists controlled for these factors, and the correlation remained strong (although air pollution with fine particulate matter appeared to be worse for heart health than outdoor light).
Research has found links between the nighttime glow outside and other diseases:
Breast cancer. “It’s a very strong correlation,” said Randy Nelson, PhD, a neuroscientist at West Virginia University. A study of over 100,000 teachers in California revealed that women living in areas with the most light pollution had a 12%higher risk. That effect is comparable to increasing your intake of ultra-processed foods by 10%.
Alzheimer’s disease. In a study published this fall, outdoor light at night was more strongly linked to the disease than even alcohol misuse or obesity.
Diabetes. In one recent study, people living in the most illuminated areas had a 28% higher risk of diabetes than those residing in much darker places. In a country like China, scientists concluded that 9 million cases of diabetes could be linked to light pollution.
What Happens in Your Body When You’re Exposed to Light at Night
, the “hormone of darkness.” “Darkness is very important,” Hanifin said. When he and his colleagues decades ago started studying the effects of light on human physiology, “people thought we were borderline crazy,” he said.
Nighttime illumination affects the health and behavior of species as diverse as Siberian hamsters, zebra finches, mice, crickets, and mosquitoes. Like most creatures on Earth, humans have internal clocks that are synced to the 24-hour cycle of day and night. The master clock is in your hypothalamus, a diamond-shaped part of the brain, but every cell in your body has its own clock, too. Many physiological processes run on circadian rhythms (a term derived from a Latin phrase meaning “about a day”), from sleep-wake cycle to hormone secretion, as well as processes involved in cancer progression, such as cell division.
“There are special photoreceptors in the eye that don’t deal with visual information. They just send light information,” Nelson said. “If you get light at the wrong time, you’re resetting the clocks.”
This internal clock “prepares the body for various recurrent challenges, such as eating,” said Christian Benedict, PhD, a sleep researcher at Uppsala University, Sweden. “Light exposure [at night] can mess up this very important system.” This could mean, for instance, that your insulin is released at the wrong time, Benedict said, causing “a jet lag-ish condition that will then impair the ability to handle blood sugar.” Animal studies confirm that exposure to light at night can reduce glucose tolerance and alter insulin secretion – potential pathways to diabetes.
The hormone melatonin, produced when it’s dark by the pineal gland in the brain, is a key player in this modern struggle. Melatonin helps you sleep, synchronizes the body’s circadian rhythms, protects neurons from damage, regulates the immune system, and fights inflammation. But even a sliver of light at night can suppress its secretion. Less than 30 lux of light, about the level of a pedestrian street at night, can slash melatonin by half.
When lab animals are exposed to nighttime light, they “show enormous neuroinflammation” — that is, inflammation of nervous tissue, Nelson said. In one experiment on humans, those who slept immersed in weak light had higher levels of C-reactive protein in their blood, a marker of inflammation.
Low melatonin has also been linked to cancer. It “allows the metabolic machinery of the cancer cells to be active,” Hanifin said. One of melatonin’s effects is stimulation of natural killer cells, which can recognize and destroy cancer cells. What’s more, when melatonin plunges, estrogen may go up, which could explain the link between light at night and breast cancer (estrogen fuels tumor growth in breast cancers).
Researchers concede that satellite data might be too coarse to estimate how much light people are actually exposed to while they sleep. Plus, many of us are staring at bright screens. “But the studies keep coming,” Nelson said, suggesting that outdoor light pollution does have an impact.
When researchers put wrist-worn light sensors on over 80,000 British people, they found that the more light the device registered between half-past midnight and 6 a.m., the more its wearer was at risk of having diabetes several years down the road — no matter how long they’ve actually slept. This, according to the study’s authors, supports the findings of satellite data.
A similar study that used actigraphy with built-in light sensors, measuring whether people had been sleeping in complete darkness for at least five hours, found that light pollution upped the risk of heart disease by 74%.
What Can You Do About This?
Not everyone’s melatonin is affected by nighttime light to the same degree. “Some people are very much sensitive to very dim light, whereas others are not as sensitive and need far, far more light stimulation [to impact melatonin],” Benedict said. In one study, some volunteers needed 350 lux to lower their melatonin by half. For such people, flipping on the light in the bathroom at night wouldn’t matter; for others, though, a mere 6 lux was already as harmful – which is darker than twilight.
You can protect yourself by keeping your bedroom lights off and your screens stashed away, but avoiding outdoor light pollution may be harder. You can invest in high-quality blackout curtains, of course, although some light may still seep inside. You can plant trees in front of your windows, reorient any motion-detector lights, and even petition your local government to reduce over-illumination of buildings and to choose better streetlights. You can support organizations, such as the International Dark-Sky Association, that work to preserve darkness.
Last but not least, you might want to change your habits. If you live in a particularly light-polluted area, such as the District of Columbia, America’s top place for urban blaze, you might reconsider late-night walks or drives around the neighborhood. Instead, Hanifin said, read a book in bed, while keeping the light “as dim as you can.” It’s “a much better idea versus being outside in midtown Manhattan,” he said. According to recent recommendations published by Hanifin and his colleagues, when you sleep, there should be no more than 1 lux of illumination at the level of your eyes — about as much as you’d get from having a lit candle 1 meter away.
And if we manage to preserve outdoor darkness, and the stars reappear (including the breathtaking Milky Way), we could reap more benefits — some research suggests that stargazing can elicit positive emotions, a sense of personal growth, and “a variety of transcendent thoughts and experiences.”
A version of this article appeared on WebMD.com.
This October, millions of Americans missed out on two of the most spectacular shows in the universe: the northern lights and a rare comet. Even if you were aware of them, light pollution made them difficult to see, unless you went to a dark area and let your eyes adjust.
It’s not getting any easier — the night sky over North America has been growing brighter by about 10% per year since 2011. More and more research is linking all that light pollution to a surprising range of health consequences: cancer, heart disease, diabetes, Alzheimer’s disease, and even low sperm quality, though the reasons for these troubling associations are not always clear.
“We’ve lost the contrast between light and dark, and we are confusing our physiology on a regular basis,” said John Hanifin, PhD, associate director of Thomas Jefferson University’s Light Research Program.
Our own galaxy is invisible to nearly 80% of people in North America. In 1994, an earthquake-triggered blackout in Los Angeles led to calls to the Griffith Observatory from people wondering about that hazy blob of light in the night sky. It was the Milky Way.
Glaring headlights, illuminated buildings, blazing billboards, and streetlights fill our urban skies with a glow that even affects rural residents. Inside, since the invention of the lightbulb, we’ve kept our homes bright at night. Now, we’ve also added blue light-emitting devices — smartphones, television screens, tablets — which have been linked to sleep problems.
But outdoor light may matter for our health, too. “Every photon counts,” Hanifin said.
Bright Lights, Big Problems
For one 2024 study researchers used satellite data to measure light pollution at residential addresses of over 13,000 people. They found that those who lived in places with the brightest skies at night had a 31% higher risk of high blood pressure. Another study out of Hong Kong showed a 29% higher risk of death from coronary heart disease. And yet another found a 17%higher risk of cerebrovascular disease, such as strokes or brain aneurysms.
Of course, urban areas also have air pollution, noise, and a lack of greenery. So, for some studies, scientists controlled for these factors, and the correlation remained strong (although air pollution with fine particulate matter appeared to be worse for heart health than outdoor light).
Research has found links between the nighttime glow outside and other diseases:
Breast cancer. “It’s a very strong correlation,” said Randy Nelson, PhD, a neuroscientist at West Virginia University. A study of over 100,000 teachers in California revealed that women living in areas with the most light pollution had a 12%higher risk. That effect is comparable to increasing your intake of ultra-processed foods by 10%.
Alzheimer’s disease. In a study published this fall, outdoor light at night was more strongly linked to the disease than even alcohol misuse or obesity.
Diabetes. In one recent study, people living in the most illuminated areas had a 28% higher risk of diabetes than those residing in much darker places. In a country like China, scientists concluded that 9 million cases of diabetes could be linked to light pollution.
What Happens in Your Body When You’re Exposed to Light at Night
, the “hormone of darkness.” “Darkness is very important,” Hanifin said. When he and his colleagues decades ago started studying the effects of light on human physiology, “people thought we were borderline crazy,” he said.
Nighttime illumination affects the health and behavior of species as diverse as Siberian hamsters, zebra finches, mice, crickets, and mosquitoes. Like most creatures on Earth, humans have internal clocks that are synced to the 24-hour cycle of day and night. The master clock is in your hypothalamus, a diamond-shaped part of the brain, but every cell in your body has its own clock, too. Many physiological processes run on circadian rhythms (a term derived from a Latin phrase meaning “about a day”), from sleep-wake cycle to hormone secretion, as well as processes involved in cancer progression, such as cell division.
“There are special photoreceptors in the eye that don’t deal with visual information. They just send light information,” Nelson said. “If you get light at the wrong time, you’re resetting the clocks.”
This internal clock “prepares the body for various recurrent challenges, such as eating,” said Christian Benedict, PhD, a sleep researcher at Uppsala University, Sweden. “Light exposure [at night] can mess up this very important system.” This could mean, for instance, that your insulin is released at the wrong time, Benedict said, causing “a jet lag-ish condition that will then impair the ability to handle blood sugar.” Animal studies confirm that exposure to light at night can reduce glucose tolerance and alter insulin secretion – potential pathways to diabetes.
The hormone melatonin, produced when it’s dark by the pineal gland in the brain, is a key player in this modern struggle. Melatonin helps you sleep, synchronizes the body’s circadian rhythms, protects neurons from damage, regulates the immune system, and fights inflammation. But even a sliver of light at night can suppress its secretion. Less than 30 lux of light, about the level of a pedestrian street at night, can slash melatonin by half.
When lab animals are exposed to nighttime light, they “show enormous neuroinflammation” — that is, inflammation of nervous tissue, Nelson said. In one experiment on humans, those who slept immersed in weak light had higher levels of C-reactive protein in their blood, a marker of inflammation.
Low melatonin has also been linked to cancer. It “allows the metabolic machinery of the cancer cells to be active,” Hanifin said. One of melatonin’s effects is stimulation of natural killer cells, which can recognize and destroy cancer cells. What’s more, when melatonin plunges, estrogen may go up, which could explain the link between light at night and breast cancer (estrogen fuels tumor growth in breast cancers).
Researchers concede that satellite data might be too coarse to estimate how much light people are actually exposed to while they sleep. Plus, many of us are staring at bright screens. “But the studies keep coming,” Nelson said, suggesting that outdoor light pollution does have an impact.
When researchers put wrist-worn light sensors on over 80,000 British people, they found that the more light the device registered between half-past midnight and 6 a.m., the more its wearer was at risk of having diabetes several years down the road — no matter how long they’ve actually slept. This, according to the study’s authors, supports the findings of satellite data.
A similar study that used actigraphy with built-in light sensors, measuring whether people had been sleeping in complete darkness for at least five hours, found that light pollution upped the risk of heart disease by 74%.
What Can You Do About This?
Not everyone’s melatonin is affected by nighttime light to the same degree. “Some people are very much sensitive to very dim light, whereas others are not as sensitive and need far, far more light stimulation [to impact melatonin],” Benedict said. In one study, some volunteers needed 350 lux to lower their melatonin by half. For such people, flipping on the light in the bathroom at night wouldn’t matter; for others, though, a mere 6 lux was already as harmful – which is darker than twilight.
You can protect yourself by keeping your bedroom lights off and your screens stashed away, but avoiding outdoor light pollution may be harder. You can invest in high-quality blackout curtains, of course, although some light may still seep inside. You can plant trees in front of your windows, reorient any motion-detector lights, and even petition your local government to reduce over-illumination of buildings and to choose better streetlights. You can support organizations, such as the International Dark-Sky Association, that work to preserve darkness.
Last but not least, you might want to change your habits. If you live in a particularly light-polluted area, such as the District of Columbia, America’s top place for urban blaze, you might reconsider late-night walks or drives around the neighborhood. Instead, Hanifin said, read a book in bed, while keeping the light “as dim as you can.” It’s “a much better idea versus being outside in midtown Manhattan,” he said. According to recent recommendations published by Hanifin and his colleagues, when you sleep, there should be no more than 1 lux of illumination at the level of your eyes — about as much as you’d get from having a lit candle 1 meter away.
And if we manage to preserve outdoor darkness, and the stars reappear (including the breathtaking Milky Way), we could reap more benefits — some research suggests that stargazing can elicit positive emotions, a sense of personal growth, and “a variety of transcendent thoughts and experiences.”
A version of this article appeared on WebMD.com.
The Rising Tide of Atrial Fibrillation: Is Primary Care Ready?
The incidence of atrial fibrillation (AF) is on the rise, and recent joint guidelines from the American College of Cardiology and American Heart Association (ACC/AHA) stress the role of primary care clinicians in prevention and management.
One in three White and one in five Black Americans will develop AF in their lifetime, and the projected number of individuals diagnosed with AF in the United States is expected to double by 2050.
Cardiologists who spoke to Medscape Medical News said primary care clinicians can help control AF by focusing on diabetes and hypertension, along with lifestyle factors such as diet, exercise, and alcohol intake.
“It’s not just a rhythm abnormality, but a complex disease that needs to be addressed in a multidisciplinary, holistic way,” said Jose Joglar, MD, a professor in the Department of Internal Medicine at the UT Southwestern Medical Center in Dallas and lead author of the guidelines.
Joglar said primary care clinicians can play an important role in counseling on lifestyle changes for patients with the most common etiologies such as poorly controlled hypertension, diabetes, and obesity.
The Primary Care Physicians ABCs: Risk Factors and Comorbidities
“As a primary care physician or as a cardiologist, I often think that if I do these things, I’m going to help with a lot of conditions, not just atrial fibrillation,” said Manesh Patel, MD, chief of the Divisions of Cardiology and Clinical Pharmacology at the Duke University School of Medicine in Durham, North Carolina.
Lifestyle choices such as sleeping habits can play a big part in AF outcomes. Although the guidelines specifically address obstructive sleep apnea as a risk factor, he said more data are needed on the effect of sleep hygiene — getting 8 hours of sleep a night — a goal few people attain.
“What we do know is people that can routinely try to go to sleep and sleep with some regularity seem to have less cardiovascular risk,” Patel said.
Although existing data are limited, literature reviews have found evidence that sleep disruptions, sleep duration, circadian rhythm, and insomnia are associated with heart disease, independent of obstructive sleep apnea.
Use of alcohol should also be discussed with patients, as many are unaware of the effects of the drug on cardiovascular disease, said Joglar, who is also the program director of the Clinical Cardiac Electrophysiology Fellowship program at the UT Southwestern Medical Center.
“Doctors can inform the patient that this is not a judgment call but simple medical fact,” he said.
Joglar also said many physicians need to become educated on a common misconception.
“Every time a patient develops palpitations or atrial fibrillation, the first thing every patient tells me is, I quit drinking coffee,” Joglar said.
However, as the guidelines point out, the link between caffeine and AF is uncertain at best.
Preventing AF
A newer class of drugs may help clinicians manage comorbidities that contribute to AF, such as hypertension, sleep apnea, and obesity, said John Mandrola, MD, an electrophysiologist in Louisville, Kentucky, who hosts This Week in Cardiology on Medscape.
Although originally approved for treatment of diabetes, sodium-glucose cotransporter-2 inhibitors are also approved for management of heart failure. Mandrola started prescribing these drugs 2 years ago for patients, given the links of both conditions with AF.
“I think the next frontier for us in cardiology and AF management will be the GLP-1 agonists,” Mandrola said. He hasn’t started prescribing these drugs for his patients yet but said they will likely play a role in the management of patients with AF with the common constellation of comorbidities such as obesity, hypertension, and sleep apnea.
“The GLP-1 agonists have a really good chance of competing with AF ablation for rhythm control over the long term,” he said.
Decisions, Decisions: Stroke Risk Scoring Systems
The risk for stroke varies widely among patients with AF, so primary care clinicians can pick among several scoring systems to estimate the risk for stroke and guide the decision on whether to initiate anticoagulation therapy.
The ACC/AHA guidelines do not state a preference for a particular instrument. The Congestive heart failure, Hypertension, Age, Diabetes mellitus, Stroke, Vascular disease, Sex (CHA2DS2-VASc) score is the most widely used and validated instrument, Joglar said. He usually recommends anticoagulation if the CHA2DS2-VASc score is > 2, dependent on individual patient factors.
“If you have a CHA2DS2-VASc score of 1, and you only had one episode of AF for a few hours a year ago, then your risk of stroke is not as high as somebody who has a score of 1 but has more frequent or persistent AF,” Joglar said.
None of the systems is perfect at predicting risk for stroke, so clinicians should discuss options with patients.
“The real message is, are you talking about the risk of stroke and systemic embolism to your patient, so that the patient understands that risk?” he said.
Patel also said measuring creatine clearance can be analogous to using an instrument like CHA2DS2-VASc.
“I often think about renal disease as a very good risk marker and something that does elevate your risk,” he said.
Which Anticoagulant?
Although the ACC/AHA guidelines still recommend warfarin for patients with AF with mechanical heart valves or moderate to severe rheumatic fever, direct oral anticoagulants (DOACs) are the first-line therapy for all other patients with AF.
In terms of which DOACs to use, the differences are subtle, according to Patel.
“I don’t know that they’re that different from each other,” he said. “All of the new drugs are better than warfarin by far.”
Patel pointed out that dabigatran at 150 mg is the only DOAC shown to reduce the incidence of ischemic stroke. For patients with renal dysfunction, he has a slight preference for a 15-mg dose of rivaroxaban.
Mandrola said he mainly prescribes apixaban and rivaroxaban, the latter of which requires only once a day dosing.
“We stopped using dabigatran because 10% of people get gastrointestinal upset,” he said.
Although studies suggest aspirin is less effective than either warfarin or DOACs for the prevention of stroke, Joglar said he still sees patients who come to him after being prescribed low-dose aspirin from primary care clinicians.
“We made it very clear that it should not be recommended just for mitigating stroke risk in atrial fibrillation,” Joglar said. “You could use it if the patient has another indication, such as a prior heart attack.”
Does My Patient Have to Be in Normal Sinus Rhythm?
The new guidelines present evidence maintaining sinus rhythm should be favored over controlling heart rate for managing AF.
“We’ve focused on rhythm control as a better strategy, especially catheter ablation, which seems to be particularly effective in parallel to lifestyle interventions and management of comorbidities,” Joglar said. Rhythm control is of particular benefit for patients with AF triggered by heart failure. Control of rhythm in these patients has been shown to improve multiple outcomes such as ejection fraction, symptoms, and survival.
Patel said as a patient’s symptoms increase, the more likely a clinician will be able to control sinus rhythm. Some patients do not notice their arrhythmia, but others feel dizzy or have chest pain.
“The less symptomatic the patient is, the more likely they’re going to tolerate it, especially if they’re older, and it’s hard to get them into sinus rhythm,” Patel said.
When to Refer for Catheter Ablation?
The new guidelines upgraded the recommendation for catheter ablation to class I (strong recommendation) for patients with symptomatic AF in whom anti-arrhythmic therapy is unsuccessful, not tolerated, or contraindicated; patients with symptomatic paroxysmal AF (typically younger patients with few comorbidities); and patients with symptomatic or clinically significant atrial flutter. The previous iteration recommended trying drug therapy first.
Multiple randomized clinical trials have demonstrated the effectiveness of catheter ablation.
“In somebody who is younger, with a healthy heart, the 1-year success rate of the procedure might be about 70%,” Joglar said. While 70% of patients receiving a catheter have no AF episodes in the following year, Joglar said 20%-25% of those who do have recurrences will experience fewer or shorter episodes.
Conversations about rate vs rhythm control and whether to pursue catheter ablation often come down to preference, Patel said. He would tend to intervene earlier using ablation in patients with heart failure or those experiencing symptoms of AF who cannot be controlled with a heart rate < 100 beats/min.
But he said he prefers using medication for rate control in many of his patients who are older, have chronic AF, and do not have heart failure.
Mandrola takes a more conservative approach, reserving catheter ablation for patients in whom risk factor management and anti-arrhythmic drugs have not been successful.
“In my hospital, it’s done for patients who have symptomatic AF that’s really impacting their quality of life,” he said. But for those with fewer symptoms, his advice is to provide education, reassurance, and time because AF can resolve on its own.
What About Data From Implantables and Wearables?
The guidelines provide an algorithm for when to treat non-symptomatic atrial high-rate episodes detected by a cardiovascular implantable electronic device such as a pacemaker or defibrillator. Episodes less than 5 minutes can be ignored, while treatment could be considered for those with episodes lasting 5 minutes up to 24 hours with a CHA2DS2-VASc score ≥ 3, or lasting longer than 24 hours with a CHA2DS2-VASc score ≥ 2.
But whether anticoagulation improves outcomes is unclear.
“That is a $64,000 question,” Mandrola said. “I would bet every day I get a notification in the electronic health record that says Mr. Smith had 2 hours of AFib 2 weeks ago.”
He also hears from patients who report their Apple Watch has detected an episode of AF.
Mandrola cited evidence from two recent studies of patients who had an atrial high-rate episode longer than 6 minutes detected by implantable devices. The NOAH-AFNET 6 trial randomized patients over 65 years with one or more risk factors for stroke to receive a DOAC or placebo, while the ARTESIA trial used similar inclusion criteria to assign patients to receive either DOAC or aspirin. Both studies reported modest reductions in stroke that were outweighed by a higher incidence of major bleeding in the group receiving anticoagulation.
Shared decision-making should play a role in deciding how aggressively to treat episodes of AF detected by implantable or wearable devices.
He said some patients fear having a stroke, while others are adamantly opposed to taking an anticoagulant.
For patients who present with a documented episode of AF but who otherwise have no symptoms, Patel said clinicians should consider risk for stroke and frequency and duration of episodes.
“One way clinicians should be thinking about it is, the more risk factors they have, the lower burden of AF I need to treat,” Patel said. Even for patients who are having only short episodes of AF, he has a low threshold for recommending an anticoagulation drug if the patient’s CHA2DS2-VASc score is high.
Patel reported research grants from Bayer, Novartis, Idorsia, NHLBI, and Janssen Pharmaceuticals and served as a consultant on the advisory boards of Bayer, Janssen Pharmaceuticals, and Esperion Therapeutics.
Joglar and Mandrola had no disclosures.
A version of this article appeared on Medscape.com.
The incidence of atrial fibrillation (AF) is on the rise, and recent joint guidelines from the American College of Cardiology and American Heart Association (ACC/AHA) stress the role of primary care clinicians in prevention and management.
One in three White and one in five Black Americans will develop AF in their lifetime, and the projected number of individuals diagnosed with AF in the United States is expected to double by 2050.
Cardiologists who spoke to Medscape Medical News said primary care clinicians can help control AF by focusing on diabetes and hypertension, along with lifestyle factors such as diet, exercise, and alcohol intake.
“It’s not just a rhythm abnormality, but a complex disease that needs to be addressed in a multidisciplinary, holistic way,” said Jose Joglar, MD, a professor in the Department of Internal Medicine at the UT Southwestern Medical Center in Dallas and lead author of the guidelines.
Joglar said primary care clinicians can play an important role in counseling on lifestyle changes for patients with the most common etiologies such as poorly controlled hypertension, diabetes, and obesity.
The Primary Care Physicians ABCs: Risk Factors and Comorbidities
“As a primary care physician or as a cardiologist, I often think that if I do these things, I’m going to help with a lot of conditions, not just atrial fibrillation,” said Manesh Patel, MD, chief of the Divisions of Cardiology and Clinical Pharmacology at the Duke University School of Medicine in Durham, North Carolina.
Lifestyle choices such as sleeping habits can play a big part in AF outcomes. Although the guidelines specifically address obstructive sleep apnea as a risk factor, he said more data are needed on the effect of sleep hygiene — getting 8 hours of sleep a night — a goal few people attain.
“What we do know is people that can routinely try to go to sleep and sleep with some regularity seem to have less cardiovascular risk,” Patel said.
Although existing data are limited, literature reviews have found evidence that sleep disruptions, sleep duration, circadian rhythm, and insomnia are associated with heart disease, independent of obstructive sleep apnea.
Use of alcohol should also be discussed with patients, as many are unaware of the effects of the drug on cardiovascular disease, said Joglar, who is also the program director of the Clinical Cardiac Electrophysiology Fellowship program at the UT Southwestern Medical Center.
“Doctors can inform the patient that this is not a judgment call but simple medical fact,” he said.
Joglar also said many physicians need to become educated on a common misconception.
“Every time a patient develops palpitations or atrial fibrillation, the first thing every patient tells me is, I quit drinking coffee,” Joglar said.
However, as the guidelines point out, the link between caffeine and AF is uncertain at best.
Preventing AF
A newer class of drugs may help clinicians manage comorbidities that contribute to AF, such as hypertension, sleep apnea, and obesity, said John Mandrola, MD, an electrophysiologist in Louisville, Kentucky, who hosts This Week in Cardiology on Medscape.
Although originally approved for treatment of diabetes, sodium-glucose cotransporter-2 inhibitors are also approved for management of heart failure. Mandrola started prescribing these drugs 2 years ago for patients, given the links of both conditions with AF.
“I think the next frontier for us in cardiology and AF management will be the GLP-1 agonists,” Mandrola said. He hasn’t started prescribing these drugs for his patients yet but said they will likely play a role in the management of patients with AF with the common constellation of comorbidities such as obesity, hypertension, and sleep apnea.
“The GLP-1 agonists have a really good chance of competing with AF ablation for rhythm control over the long term,” he said.
Decisions, Decisions: Stroke Risk Scoring Systems
The risk for stroke varies widely among patients with AF, so primary care clinicians can pick among several scoring systems to estimate the risk for stroke and guide the decision on whether to initiate anticoagulation therapy.
The ACC/AHA guidelines do not state a preference for a particular instrument. The Congestive heart failure, Hypertension, Age, Diabetes mellitus, Stroke, Vascular disease, Sex (CHA2DS2-VASc) score is the most widely used and validated instrument, Joglar said. He usually recommends anticoagulation if the CHA2DS2-VASc score is > 2, dependent on individual patient factors.
“If you have a CHA2DS2-VASc score of 1, and you only had one episode of AF for a few hours a year ago, then your risk of stroke is not as high as somebody who has a score of 1 but has more frequent or persistent AF,” Joglar said.
None of the systems is perfect at predicting risk for stroke, so clinicians should discuss options with patients.
“The real message is, are you talking about the risk of stroke and systemic embolism to your patient, so that the patient understands that risk?” he said.
Patel also said measuring creatine clearance can be analogous to using an instrument like CHA2DS2-VASc.
“I often think about renal disease as a very good risk marker and something that does elevate your risk,” he said.
Which Anticoagulant?
Although the ACC/AHA guidelines still recommend warfarin for patients with AF with mechanical heart valves or moderate to severe rheumatic fever, direct oral anticoagulants (DOACs) are the first-line therapy for all other patients with AF.
In terms of which DOACs to use, the differences are subtle, according to Patel.
“I don’t know that they’re that different from each other,” he said. “All of the new drugs are better than warfarin by far.”
Patel pointed out that dabigatran at 150 mg is the only DOAC shown to reduce the incidence of ischemic stroke. For patients with renal dysfunction, he has a slight preference for a 15-mg dose of rivaroxaban.
Mandrola said he mainly prescribes apixaban and rivaroxaban, the latter of which requires only once a day dosing.
“We stopped using dabigatran because 10% of people get gastrointestinal upset,” he said.
Although studies suggest aspirin is less effective than either warfarin or DOACs for the prevention of stroke, Joglar said he still sees patients who come to him after being prescribed low-dose aspirin from primary care clinicians.
“We made it very clear that it should not be recommended just for mitigating stroke risk in atrial fibrillation,” Joglar said. “You could use it if the patient has another indication, such as a prior heart attack.”
Does My Patient Have to Be in Normal Sinus Rhythm?
The new guidelines present evidence maintaining sinus rhythm should be favored over controlling heart rate for managing AF.
“We’ve focused on rhythm control as a better strategy, especially catheter ablation, which seems to be particularly effective in parallel to lifestyle interventions and management of comorbidities,” Joglar said. Rhythm control is of particular benefit for patients with AF triggered by heart failure. Control of rhythm in these patients has been shown to improve multiple outcomes such as ejection fraction, symptoms, and survival.
Patel said as a patient’s symptoms increase, the more likely a clinician will be able to control sinus rhythm. Some patients do not notice their arrhythmia, but others feel dizzy or have chest pain.
“The less symptomatic the patient is, the more likely they’re going to tolerate it, especially if they’re older, and it’s hard to get them into sinus rhythm,” Patel said.
When to Refer for Catheter Ablation?
The new guidelines upgraded the recommendation for catheter ablation to class I (strong recommendation) for patients with symptomatic AF in whom anti-arrhythmic therapy is unsuccessful, not tolerated, or contraindicated; patients with symptomatic paroxysmal AF (typically younger patients with few comorbidities); and patients with symptomatic or clinically significant atrial flutter. The previous iteration recommended trying drug therapy first.
Multiple randomized clinical trials have demonstrated the effectiveness of catheter ablation.
“In somebody who is younger, with a healthy heart, the 1-year success rate of the procedure might be about 70%,” Joglar said. While 70% of patients receiving a catheter have no AF episodes in the following year, Joglar said 20%-25% of those who do have recurrences will experience fewer or shorter episodes.
Conversations about rate vs rhythm control and whether to pursue catheter ablation often come down to preference, Patel said. He would tend to intervene earlier using ablation in patients with heart failure or those experiencing symptoms of AF who cannot be controlled with a heart rate < 100 beats/min.
But he said he prefers using medication for rate control in many of his patients who are older, have chronic AF, and do not have heart failure.
Mandrola takes a more conservative approach, reserving catheter ablation for patients in whom risk factor management and anti-arrhythmic drugs have not been successful.
“In my hospital, it’s done for patients who have symptomatic AF that’s really impacting their quality of life,” he said. But for those with fewer symptoms, his advice is to provide education, reassurance, and time because AF can resolve on its own.
What About Data From Implantables and Wearables?
The guidelines provide an algorithm for when to treat non-symptomatic atrial high-rate episodes detected by a cardiovascular implantable electronic device such as a pacemaker or defibrillator. Episodes less than 5 minutes can be ignored, while treatment could be considered for those with episodes lasting 5 minutes up to 24 hours with a CHA2DS2-VASc score ≥ 3, or lasting longer than 24 hours with a CHA2DS2-VASc score ≥ 2.
But whether anticoagulation improves outcomes is unclear.
“That is a $64,000 question,” Mandrola said. “I would bet every day I get a notification in the electronic health record that says Mr. Smith had 2 hours of AFib 2 weeks ago.”
He also hears from patients who report their Apple Watch has detected an episode of AF.
Mandrola cited evidence from two recent studies of patients who had an atrial high-rate episode longer than 6 minutes detected by implantable devices. The NOAH-AFNET 6 trial randomized patients over 65 years with one or more risk factors for stroke to receive a DOAC or placebo, while the ARTESIA trial used similar inclusion criteria to assign patients to receive either DOAC or aspirin. Both studies reported modest reductions in stroke that were outweighed by a higher incidence of major bleeding in the group receiving anticoagulation.
Shared decision-making should play a role in deciding how aggressively to treat episodes of AF detected by implantable or wearable devices.
He said some patients fear having a stroke, while others are adamantly opposed to taking an anticoagulant.
For patients who present with a documented episode of AF but who otherwise have no symptoms, Patel said clinicians should consider risk for stroke and frequency and duration of episodes.
“One way clinicians should be thinking about it is, the more risk factors they have, the lower burden of AF I need to treat,” Patel said. Even for patients who are having only short episodes of AF, he has a low threshold for recommending an anticoagulation drug if the patient’s CHA2DS2-VASc score is high.
Patel reported research grants from Bayer, Novartis, Idorsia, NHLBI, and Janssen Pharmaceuticals and served as a consultant on the advisory boards of Bayer, Janssen Pharmaceuticals, and Esperion Therapeutics.
Joglar and Mandrola had no disclosures.
A version of this article appeared on Medscape.com.
The incidence of atrial fibrillation (AF) is on the rise, and recent joint guidelines from the American College of Cardiology and American Heart Association (ACC/AHA) stress the role of primary care clinicians in prevention and management.
One in three White and one in five Black Americans will develop AF in their lifetime, and the projected number of individuals diagnosed with AF in the United States is expected to double by 2050.
Cardiologists who spoke to Medscape Medical News said primary care clinicians can help control AF by focusing on diabetes and hypertension, along with lifestyle factors such as diet, exercise, and alcohol intake.
“It’s not just a rhythm abnormality, but a complex disease that needs to be addressed in a multidisciplinary, holistic way,” said Jose Joglar, MD, a professor in the Department of Internal Medicine at the UT Southwestern Medical Center in Dallas and lead author of the guidelines.
Joglar said primary care clinicians can play an important role in counseling on lifestyle changes for patients with the most common etiologies such as poorly controlled hypertension, diabetes, and obesity.
The Primary Care Physicians ABCs: Risk Factors and Comorbidities
“As a primary care physician or as a cardiologist, I often think that if I do these things, I’m going to help with a lot of conditions, not just atrial fibrillation,” said Manesh Patel, MD, chief of the Divisions of Cardiology and Clinical Pharmacology at the Duke University School of Medicine in Durham, North Carolina.
Lifestyle choices such as sleeping habits can play a big part in AF outcomes. Although the guidelines specifically address obstructive sleep apnea as a risk factor, he said more data are needed on the effect of sleep hygiene — getting 8 hours of sleep a night — a goal few people attain.
“What we do know is people that can routinely try to go to sleep and sleep with some regularity seem to have less cardiovascular risk,” Patel said.
Although existing data are limited, literature reviews have found evidence that sleep disruptions, sleep duration, circadian rhythm, and insomnia are associated with heart disease, independent of obstructive sleep apnea.
Use of alcohol should also be discussed with patients, as many are unaware of the effects of the drug on cardiovascular disease, said Joglar, who is also the program director of the Clinical Cardiac Electrophysiology Fellowship program at the UT Southwestern Medical Center.
“Doctors can inform the patient that this is not a judgment call but simple medical fact,” he said.
Joglar also said many physicians need to become educated on a common misconception.
“Every time a patient develops palpitations or atrial fibrillation, the first thing every patient tells me is, I quit drinking coffee,” Joglar said.
However, as the guidelines point out, the link between caffeine and AF is uncertain at best.
Preventing AF
A newer class of drugs may help clinicians manage comorbidities that contribute to AF, such as hypertension, sleep apnea, and obesity, said John Mandrola, MD, an electrophysiologist in Louisville, Kentucky, who hosts This Week in Cardiology on Medscape.
Although originally approved for treatment of diabetes, sodium-glucose cotransporter-2 inhibitors are also approved for management of heart failure. Mandrola started prescribing these drugs 2 years ago for patients, given the links of both conditions with AF.
“I think the next frontier for us in cardiology and AF management will be the GLP-1 agonists,” Mandrola said. He hasn’t started prescribing these drugs for his patients yet but said they will likely play a role in the management of patients with AF with the common constellation of comorbidities such as obesity, hypertension, and sleep apnea.
“The GLP-1 agonists have a really good chance of competing with AF ablation for rhythm control over the long term,” he said.
Decisions, Decisions: Stroke Risk Scoring Systems
The risk for stroke varies widely among patients with AF, so primary care clinicians can pick among several scoring systems to estimate the risk for stroke and guide the decision on whether to initiate anticoagulation therapy.
The ACC/AHA guidelines do not state a preference for a particular instrument. The Congestive heart failure, Hypertension, Age, Diabetes mellitus, Stroke, Vascular disease, Sex (CHA2DS2-VASc) score is the most widely used and validated instrument, Joglar said. He usually recommends anticoagulation if the CHA2DS2-VASc score is > 2, dependent on individual patient factors.
“If you have a CHA2DS2-VASc score of 1, and you only had one episode of AF for a few hours a year ago, then your risk of stroke is not as high as somebody who has a score of 1 but has more frequent or persistent AF,” Joglar said.
None of the systems is perfect at predicting risk for stroke, so clinicians should discuss options with patients.
“The real message is, are you talking about the risk of stroke and systemic embolism to your patient, so that the patient understands that risk?” he said.
Patel also said measuring creatine clearance can be analogous to using an instrument like CHA2DS2-VASc.
“I often think about renal disease as a very good risk marker and something that does elevate your risk,” he said.
Which Anticoagulant?
Although the ACC/AHA guidelines still recommend warfarin for patients with AF with mechanical heart valves or moderate to severe rheumatic fever, direct oral anticoagulants (DOACs) are the first-line therapy for all other patients with AF.
In terms of which DOACs to use, the differences are subtle, according to Patel.
“I don’t know that they’re that different from each other,” he said. “All of the new drugs are better than warfarin by far.”
Patel pointed out that dabigatran at 150 mg is the only DOAC shown to reduce the incidence of ischemic stroke. For patients with renal dysfunction, he has a slight preference for a 15-mg dose of rivaroxaban.
Mandrola said he mainly prescribes apixaban and rivaroxaban, the latter of which requires only once a day dosing.
“We stopped using dabigatran because 10% of people get gastrointestinal upset,” he said.
Although studies suggest aspirin is less effective than either warfarin or DOACs for the prevention of stroke, Joglar said he still sees patients who come to him after being prescribed low-dose aspirin from primary care clinicians.
“We made it very clear that it should not be recommended just for mitigating stroke risk in atrial fibrillation,” Joglar said. “You could use it if the patient has another indication, such as a prior heart attack.”
Does My Patient Have to Be in Normal Sinus Rhythm?
The new guidelines present evidence maintaining sinus rhythm should be favored over controlling heart rate for managing AF.
“We’ve focused on rhythm control as a better strategy, especially catheter ablation, which seems to be particularly effective in parallel to lifestyle interventions and management of comorbidities,” Joglar said. Rhythm control is of particular benefit for patients with AF triggered by heart failure. Control of rhythm in these patients has been shown to improve multiple outcomes such as ejection fraction, symptoms, and survival.
Patel said as a patient’s symptoms increase, the more likely a clinician will be able to control sinus rhythm. Some patients do not notice their arrhythmia, but others feel dizzy or have chest pain.
“The less symptomatic the patient is, the more likely they’re going to tolerate it, especially if they’re older, and it’s hard to get them into sinus rhythm,” Patel said.
When to Refer for Catheter Ablation?
The new guidelines upgraded the recommendation for catheter ablation to class I (strong recommendation) for patients with symptomatic AF in whom anti-arrhythmic therapy is unsuccessful, not tolerated, or contraindicated; patients with symptomatic paroxysmal AF (typically younger patients with few comorbidities); and patients with symptomatic or clinically significant atrial flutter. The previous iteration recommended trying drug therapy first.
Multiple randomized clinical trials have demonstrated the effectiveness of catheter ablation.
“In somebody who is younger, with a healthy heart, the 1-year success rate of the procedure might be about 70%,” Joglar said. While 70% of patients receiving a catheter have no AF episodes in the following year, Joglar said 20%-25% of those who do have recurrences will experience fewer or shorter episodes.
Conversations about rate vs rhythm control and whether to pursue catheter ablation often come down to preference, Patel said. He would tend to intervene earlier using ablation in patients with heart failure or those experiencing symptoms of AF who cannot be controlled with a heart rate < 100 beats/min.
But he said he prefers using medication for rate control in many of his patients who are older, have chronic AF, and do not have heart failure.
Mandrola takes a more conservative approach, reserving catheter ablation for patients in whom risk factor management and anti-arrhythmic drugs have not been successful.
“In my hospital, it’s done for patients who have symptomatic AF that’s really impacting their quality of life,” he said. But for those with fewer symptoms, his advice is to provide education, reassurance, and time because AF can resolve on its own.
What About Data From Implantables and Wearables?
The guidelines provide an algorithm for when to treat non-symptomatic atrial high-rate episodes detected by a cardiovascular implantable electronic device such as a pacemaker or defibrillator. Episodes less than 5 minutes can be ignored, while treatment could be considered for those with episodes lasting 5 minutes up to 24 hours with a CHA2DS2-VASc score ≥ 3, or lasting longer than 24 hours with a CHA2DS2-VASc score ≥ 2.
But whether anticoagulation improves outcomes is unclear.
“That is a $64,000 question,” Mandrola said. “I would bet every day I get a notification in the electronic health record that says Mr. Smith had 2 hours of AFib 2 weeks ago.”
He also hears from patients who report their Apple Watch has detected an episode of AF.
Mandrola cited evidence from two recent studies of patients who had an atrial high-rate episode longer than 6 minutes detected by implantable devices. The NOAH-AFNET 6 trial randomized patients over 65 years with one or more risk factors for stroke to receive a DOAC or placebo, while the ARTESIA trial used similar inclusion criteria to assign patients to receive either DOAC or aspirin. Both studies reported modest reductions in stroke that were outweighed by a higher incidence of major bleeding in the group receiving anticoagulation.
Shared decision-making should play a role in deciding how aggressively to treat episodes of AF detected by implantable or wearable devices.
He said some patients fear having a stroke, while others are adamantly opposed to taking an anticoagulant.
For patients who present with a documented episode of AF but who otherwise have no symptoms, Patel said clinicians should consider risk for stroke and frequency and duration of episodes.
“One way clinicians should be thinking about it is, the more risk factors they have, the lower burden of AF I need to treat,” Patel said. Even for patients who are having only short episodes of AF, he has a low threshold for recommending an anticoagulation drug if the patient’s CHA2DS2-VASc score is high.
Patel reported research grants from Bayer, Novartis, Idorsia, NHLBI, and Janssen Pharmaceuticals and served as a consultant on the advisory boards of Bayer, Janssen Pharmaceuticals, and Esperion Therapeutics.
Joglar and Mandrola had no disclosures.
A version of this article appeared on Medscape.com.
The Genitals Are a Window Into Health: Sex as a Vital Sign
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, a urologist and sexual medicine specialist in the Washington, DC, area. And I am so thrilled because my co-fellow, the brilliant and famous Dr. Ashley Winter, a board-certified urologist and a certified menopause practitioner, who sees patients in our practice from Los Angeles, is joining us today to talk about sex as a vital sign.
Ashley Winter, MD: To have the best sexual function, you need many different systems to work. You need your hormones to be in the right place. You need your blood vessels to dilate when you want them to. You need your nerves to connect to your genitalia to make them responsive. The way people say, “The eyes are the window into the soul” — well, the genitals are the window into the cardiovascular system, the peripheral nervous system, and the hormonal system. It’s so dynamic. Patients can understand how this reflects their health. We just need healthcare providers to hammer home how those things connect.
Rubin: If you’re a primary care doctor seeing a patient and you want to educate them on diabetes or high blood pressure, how can you “ ‘sell it with ‘sex”? How can you use sex to educate them about these important medical conditions?
Winter: I hate using it as a fear tactic, but sometimes you have to. Time and again, I’ve seen men with severe profound erectile dysfunction at a young age, with chronically uncontrolled diabetes.
Diabetes can impair the peripheral nerves, resulting in peripheral neuropathy. The same way that it can affect the fingers and toes, diabetes can affect the penis, even before those other areas. Diabetes can also lead to other conditions such as low testosterone, which also affects the function of the penis.
I’m being brutally honest when I tell patients that diabetes control is critical to having a wonderful sexspan — the duration of your life where you’re able to be sexually active and have great sex and do it in the way that you want.
Chronic conditions such as high cholesterol or hypertension can affect your ability to become erect or aroused whether you have a penis or a vulva, and even your ability to have an orgasm.
Rubin: None of my doctors has ever asked me about these issues. But we have to bring them up with patients because they›re not going to bring them up to us. I always say in the review of systems, we shouldn›t just ask, “Do you have any sexual problems?” (which nobody ever does) and move past the question about men, women or both. We should be asking, “Do you have any issues with libido? Do you want to talk about it? Any issues with erection, arousal, orgasm, or sexual pain?”
When you can talk about those things, you can treat the patient from a whole physiologic perspective. For example, how does their sciatica affect their sexual pain? How does their antidepressant cause a delayed orgasm? How does their low testosterone level affect their energy level, their libido, and their desire?
We see so much shame and guilt in sexual health, to the extent that patients feel broken. We can help them understand the anatomy and physiology and explain that they aren’t broken. Instead, it’s “You need this medicine for your crippling anxiety, and that’s why your orgasm is delayed, and so can we augment it or add or subtract something to help you with it.”
Winter: In a primary care setting, where we are considering the patient›s overall health, we strive for medication compliance, but a huge part of medication noncompliance is sexual side effects, whether it›s antidepressants, beta-blockers, birth control, or this new world of GLP-1 agonists.
Rubin: I would add breast cancer treatments. Many patients go off their anastrozole or their tamoxifen because of the sexual side effects.
Winter: This is where we get to the crux of this discussion about sex being a vital sign — something you need to check routinely. We need to become comfortable with it, because then we are unlocking the ability to treat every patient like a whole person, give them better outcomes, improve their compliance, and have a really powerful tool for education.
Rubin: We have a growing toolbox for all genders when it comes to sexual health. We have FDA- approved medications for low libido in women. We use testosterone in men in an evidence-based way to safely improve libido. We use medications to help with the genitourinary syndrome of menopause. Orgasm is a challenging one, but we have devices that can help with those reflexes. And working with people who specialize in sexual pain can be extremely helpful for patients.
Dr. Winter, having practiced in different settings, what would you tell the primary care doctors who don’t want to talk about libido or who minimize sexual complaints because they don’t know how to navigate them?
Winter: I do not envy the challenge of being a primary care provider in the healthcare world we are living in. I think it is the hardest job. The ultimate takeaway is to just normalize the conversation and be able to validate what is happening. Have a few basic tools, and then have referrals. It›s not that you have to have all the time in the world or you have to treat every condition, but you have to start the conversation, be comfortable with it, and then get patients hooked up with the right resources.
Rubin: Every doctor of every kind can connect with patients and try to understand what they care about. What are their goals? What do they want for their families, for their relationships, for their quality of life? And how can we work collaboratively as a team to help them with those things?
Sex is a huge part of people’s lives. If we don’t ask about it; if we don’t look into it; and if we don’t admit that our physiology, our medications, and our surgeries can affect sexual health and functioning, how can we improve people’s lives? We can do so much as a team when we consider sex as a true vital sign.
Dr. Rubin, Assistant Clinical Professor, Department of Urology, Georgetown University, Washington, DC, has disclosed ties with Maternal Medical, Absorption Pharmaceuticals, GlaxoSmithKline, and Endo.
A version of this article first appeared on Medscape.com.
PCOS Linked to Hypertensive Blood Pressure in Teens
TOPLINE:
Adolescent girls with polycystic ovary syndrome (PCOS) have an increased risk for hypertension, according to a new study which underscores the importance of blood pressure surveillance in this population.
METHODOLOGY:
- The retrospective cohort study examined the association between PCOS and hypertension in adolescent girls within a diverse community-based US healthcare population.
- The researchers analyzed data from 224,418 adolescent girls (mean age at index visit, 14.9 years; 15.8% classified as having obesity) who had a well-child visit between 2013 and 2019, during which their systolic blood pressure and diastolic blood pressure were measured.
- Blood pressure in the hypertensive range was classified using the 2017 American Academy of Pediatrics Practice Guideline, with thresholds of 130/80 mm Hg or greater.
TAKEAWAY:
- The proportion of adolescent girls with high blood pressure was significantly greater among those with PCOS than among those without the condition (18.2% vs 7.1%; P < .001).
- Adolescent girls with PCOS had a 25% higher risk for hypertension than those without the disorder (adjusted odds ratio [aOR], 1.25; 95% CI, 1.10-1.42).
- Similarly, adolescent girls with obesity and PCOS had a 23% higher risk for high blood pressure than those without PCOS (aOR, 1.23; 95% CI, 1.06-1.42).
IN PRACTICE:
“The high prevalence of [hypertension] associated with PCOS emphasizes the key role of early [blood pressure] monitoring in this high-risk group,” the authors of the study wrote.
SOURCE:
The study was led by Sherry Zhang, MD, Kaiser Permanente Oakland Medical Center, Oakland, California, and was published online in the American Journal of Preventive Medicine.
LIMITATIONS:
The study relied on coded diagnoses of PCOS from clinical settings, which may have led to detection and referral biases. The findings may not be generalizable to an unselected population in which adolescent girls are systematically screened for both PCOS and hypertension.
DISCLOSURES:
This study was funded by the Cardiovascular and Metabolic Conditions Research Section and the Biostatistical Consulting Unit at the Division of Research, Kaiser Permanente Northern California and by the Kaiser Permanente Northern California Community Health Program. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Adolescent girls with polycystic ovary syndrome (PCOS) have an increased risk for hypertension, according to a new study which underscores the importance of blood pressure surveillance in this population.
METHODOLOGY:
- The retrospective cohort study examined the association between PCOS and hypertension in adolescent girls within a diverse community-based US healthcare population.
- The researchers analyzed data from 224,418 adolescent girls (mean age at index visit, 14.9 years; 15.8% classified as having obesity) who had a well-child visit between 2013 and 2019, during which their systolic blood pressure and diastolic blood pressure were measured.
- Blood pressure in the hypertensive range was classified using the 2017 American Academy of Pediatrics Practice Guideline, with thresholds of 130/80 mm Hg or greater.
TAKEAWAY:
- The proportion of adolescent girls with high blood pressure was significantly greater among those with PCOS than among those without the condition (18.2% vs 7.1%; P < .001).
- Adolescent girls with PCOS had a 25% higher risk for hypertension than those without the disorder (adjusted odds ratio [aOR], 1.25; 95% CI, 1.10-1.42).
- Similarly, adolescent girls with obesity and PCOS had a 23% higher risk for high blood pressure than those without PCOS (aOR, 1.23; 95% CI, 1.06-1.42).
IN PRACTICE:
“The high prevalence of [hypertension] associated with PCOS emphasizes the key role of early [blood pressure] monitoring in this high-risk group,” the authors of the study wrote.
SOURCE:
The study was led by Sherry Zhang, MD, Kaiser Permanente Oakland Medical Center, Oakland, California, and was published online in the American Journal of Preventive Medicine.
LIMITATIONS:
The study relied on coded diagnoses of PCOS from clinical settings, which may have led to detection and referral biases. The findings may not be generalizable to an unselected population in which adolescent girls are systematically screened for both PCOS and hypertension.
DISCLOSURES:
This study was funded by the Cardiovascular and Metabolic Conditions Research Section and the Biostatistical Consulting Unit at the Division of Research, Kaiser Permanente Northern California and by the Kaiser Permanente Northern California Community Health Program. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Adolescent girls with polycystic ovary syndrome (PCOS) have an increased risk for hypertension, according to a new study which underscores the importance of blood pressure surveillance in this population.
METHODOLOGY:
- The retrospective cohort study examined the association between PCOS and hypertension in adolescent girls within a diverse community-based US healthcare population.
- The researchers analyzed data from 224,418 adolescent girls (mean age at index visit, 14.9 years; 15.8% classified as having obesity) who had a well-child visit between 2013 and 2019, during which their systolic blood pressure and diastolic blood pressure were measured.
- Blood pressure in the hypertensive range was classified using the 2017 American Academy of Pediatrics Practice Guideline, with thresholds of 130/80 mm Hg or greater.
TAKEAWAY:
- The proportion of adolescent girls with high blood pressure was significantly greater among those with PCOS than among those without the condition (18.2% vs 7.1%; P < .001).
- Adolescent girls with PCOS had a 25% higher risk for hypertension than those without the disorder (adjusted odds ratio [aOR], 1.25; 95% CI, 1.10-1.42).
- Similarly, adolescent girls with obesity and PCOS had a 23% higher risk for high blood pressure than those without PCOS (aOR, 1.23; 95% CI, 1.06-1.42).
IN PRACTICE:
“The high prevalence of [hypertension] associated with PCOS emphasizes the key role of early [blood pressure] monitoring in this high-risk group,” the authors of the study wrote.
SOURCE:
The study was led by Sherry Zhang, MD, Kaiser Permanente Oakland Medical Center, Oakland, California, and was published online in the American Journal of Preventive Medicine.
LIMITATIONS:
The study relied on coded diagnoses of PCOS from clinical settings, which may have led to detection and referral biases. The findings may not be generalizable to an unselected population in which adolescent girls are systematically screened for both PCOS and hypertension.
DISCLOSURES:
This study was funded by the Cardiovascular and Metabolic Conditions Research Section and the Biostatistical Consulting Unit at the Division of Research, Kaiser Permanente Northern California and by the Kaiser Permanente Northern California Community Health Program. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Higher Doses of Vitamin D3 Do Not Reduce Cardiac Biomarkers in Older Adults
TOPLINE:
Higher doses of vitamin D3 supplementation did not significantly reduce cardiac biomarkers in older adults with low serum vitamin D levels. The STURDY trial found no significant differences in high-sensitivity cardiac troponin I (hs-cTnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) between low- and high-dose groups.
METHODOLOGY:
- A total of 688 participants aged 70 years or older with low serum 25-hydroxy vitamin D levels (10-29 ng/mL) were included in the STURDY trial.
- Participants were randomized to receive one of four doses of vitamin D3 supplementation: 200, 1000, 2000, or 4000 IU/d, with 200 IU/d as the reference dose.
- Cardiac biomarkers, including hs-cTnI and NT-proBNP, were measured at baseline, 3 months, 12 months, and 24 months.
- The trial was conducted at two community-based research institutions in the United States between July 2015 and March 2019.
- The effects of vitamin D3 dose on biomarkers were assessed via mixed-effects tobit models, with participants followed up to 24 months or until study termination.
TAKEAWAY:
- Higher doses of vitamin D3 supplementation did not significantly affect hs-cTnI levels compared with the low-dose group (1.6% difference; 95% CI, −5.3 to 8.9).
- No significant differences were observed in NT-proBNP levels between the high-dose and low-dose groups (−1.8% difference; 95% CI, −9.3 to 6.3).
- Both hs-cTnI and NT-proBNP levels increased in both low- and high-dose groups over time, with hs-cTnI increasing by 5.2% and 7.0%, respectively, and NT-proBNP increasing by 11.3% and 9.3%, respectively.
- The findings suggest that higher doses of vitamin D3 supplementation do not reduce markers of subclinical cardiovascular disease in older adults with low serum vitamin D levels.
IN PRACTICE:
“We can speculate that the systemic effects of vitamin D deficiency are more profound among the very old, and there may be an inverse relationship between supplementation and inflammation. It is also possible that serum vitamin D level is a risk marker but not a risk factor for CVD risk and related underlying mechanisms,” wrote the authors of the study.
SOURCE:
The study was led by Katharine W. Rainer, MD, Beth Israel Deaconess Medical Center in Boston. It was published online in the Journal of the American College of Cardiology.
LIMITATIONS:
The study’s community-based population may limit the generalizability of the findings to populations at higher risk for cardiovascular disease. Additionally, the baseline cardiac biomarkers were lower than those in some high-risk populations, which may affect the precision of the assay performance. The study may not have had adequate power for cross-sectional and subgroup analyses. Both groups received some vitamin D3 supplementation, making it difficult to determine the impact of lower-dose supplementation vs no supplementation.
DISCLOSURES:
The study was supported by grants from the National Institute on Aging, the Office of Dietary Supplements, the Mid-Atlantic Nutrition Obesity Research Center, and the Johns Hopkins Institute for Clinical and Translational Research. Rainer disclosed receiving grants from these organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Higher doses of vitamin D3 supplementation did not significantly reduce cardiac biomarkers in older adults with low serum vitamin D levels. The STURDY trial found no significant differences in high-sensitivity cardiac troponin I (hs-cTnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) between low- and high-dose groups.
METHODOLOGY:
- A total of 688 participants aged 70 years or older with low serum 25-hydroxy vitamin D levels (10-29 ng/mL) were included in the STURDY trial.
- Participants were randomized to receive one of four doses of vitamin D3 supplementation: 200, 1000, 2000, or 4000 IU/d, with 200 IU/d as the reference dose.
- Cardiac biomarkers, including hs-cTnI and NT-proBNP, were measured at baseline, 3 months, 12 months, and 24 months.
- The trial was conducted at two community-based research institutions in the United States between July 2015 and March 2019.
- The effects of vitamin D3 dose on biomarkers were assessed via mixed-effects tobit models, with participants followed up to 24 months or until study termination.
TAKEAWAY:
- Higher doses of vitamin D3 supplementation did not significantly affect hs-cTnI levels compared with the low-dose group (1.6% difference; 95% CI, −5.3 to 8.9).
- No significant differences were observed in NT-proBNP levels between the high-dose and low-dose groups (−1.8% difference; 95% CI, −9.3 to 6.3).
- Both hs-cTnI and NT-proBNP levels increased in both low- and high-dose groups over time, with hs-cTnI increasing by 5.2% and 7.0%, respectively, and NT-proBNP increasing by 11.3% and 9.3%, respectively.
- The findings suggest that higher doses of vitamin D3 supplementation do not reduce markers of subclinical cardiovascular disease in older adults with low serum vitamin D levels.
IN PRACTICE:
“We can speculate that the systemic effects of vitamin D deficiency are more profound among the very old, and there may be an inverse relationship between supplementation and inflammation. It is also possible that serum vitamin D level is a risk marker but not a risk factor for CVD risk and related underlying mechanisms,” wrote the authors of the study.
SOURCE:
The study was led by Katharine W. Rainer, MD, Beth Israel Deaconess Medical Center in Boston. It was published online in the Journal of the American College of Cardiology.
LIMITATIONS:
The study’s community-based population may limit the generalizability of the findings to populations at higher risk for cardiovascular disease. Additionally, the baseline cardiac biomarkers were lower than those in some high-risk populations, which may affect the precision of the assay performance. The study may not have had adequate power for cross-sectional and subgroup analyses. Both groups received some vitamin D3 supplementation, making it difficult to determine the impact of lower-dose supplementation vs no supplementation.
DISCLOSURES:
The study was supported by grants from the National Institute on Aging, the Office of Dietary Supplements, the Mid-Atlantic Nutrition Obesity Research Center, and the Johns Hopkins Institute for Clinical and Translational Research. Rainer disclosed receiving grants from these organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Higher doses of vitamin D3 supplementation did not significantly reduce cardiac biomarkers in older adults with low serum vitamin D levels. The STURDY trial found no significant differences in high-sensitivity cardiac troponin I (hs-cTnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) between low- and high-dose groups.
METHODOLOGY:
- A total of 688 participants aged 70 years or older with low serum 25-hydroxy vitamin D levels (10-29 ng/mL) were included in the STURDY trial.
- Participants were randomized to receive one of four doses of vitamin D3 supplementation: 200, 1000, 2000, or 4000 IU/d, with 200 IU/d as the reference dose.
- Cardiac biomarkers, including hs-cTnI and NT-proBNP, were measured at baseline, 3 months, 12 months, and 24 months.
- The trial was conducted at two community-based research institutions in the United States between July 2015 and March 2019.
- The effects of vitamin D3 dose on biomarkers were assessed via mixed-effects tobit models, with participants followed up to 24 months or until study termination.
TAKEAWAY:
- Higher doses of vitamin D3 supplementation did not significantly affect hs-cTnI levels compared with the low-dose group (1.6% difference; 95% CI, −5.3 to 8.9).
- No significant differences were observed in NT-proBNP levels between the high-dose and low-dose groups (−1.8% difference; 95% CI, −9.3 to 6.3).
- Both hs-cTnI and NT-proBNP levels increased in both low- and high-dose groups over time, with hs-cTnI increasing by 5.2% and 7.0%, respectively, and NT-proBNP increasing by 11.3% and 9.3%, respectively.
- The findings suggest that higher doses of vitamin D3 supplementation do not reduce markers of subclinical cardiovascular disease in older adults with low serum vitamin D levels.
IN PRACTICE:
“We can speculate that the systemic effects of vitamin D deficiency are more profound among the very old, and there may be an inverse relationship between supplementation and inflammation. It is also possible that serum vitamin D level is a risk marker but not a risk factor for CVD risk and related underlying mechanisms,” wrote the authors of the study.
SOURCE:
The study was led by Katharine W. Rainer, MD, Beth Israel Deaconess Medical Center in Boston. It was published online in the Journal of the American College of Cardiology.
LIMITATIONS:
The study’s community-based population may limit the generalizability of the findings to populations at higher risk for cardiovascular disease. Additionally, the baseline cardiac biomarkers were lower than those in some high-risk populations, which may affect the precision of the assay performance. The study may not have had adequate power for cross-sectional and subgroup analyses. Both groups received some vitamin D3 supplementation, making it difficult to determine the impact of lower-dose supplementation vs no supplementation.
DISCLOSURES:
The study was supported by grants from the National Institute on Aging, the Office of Dietary Supplements, the Mid-Atlantic Nutrition Obesity Research Center, and the Johns Hopkins Institute for Clinical and Translational Research. Rainer disclosed receiving grants from these organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
ASA Releases New Primary Stroke Prevention Guideline
The first update in a decade, the 2024 Guideline for the Primary Prevention of Stroke, replaces the 2014 version and is intended to be a resource for clinicians to help them implement a variety of prevention strategies in patients with no previous history of stroke. It aligns with the American Heart Association’s Life’s Essential 8.
“This guideline is an important and timely update from 2014 for multiple reasons. First, there have been groundbreaking clinical trials that have been published with new medications to not only treat the target disease [including] diabetes/obesity and high cholesterol], but also lower the risk of stroke and heart disease,” said chair of the guideline writing group, Cheryl D. Bushnell, MD, MHS, FAHA, and vice chair of the research, Department of Neurology, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
It was published online on October 21 in Stroke.
Up to 80% of Strokes Preventable
Estimates show that every year in the United States, more than 500,000 individuals have a first stroke. However, the guideline authors noted that up to 80% of strokes may be preventable. As a result, they called for better primary stroke prevention that includes improved screening and lifestyle changes.
This includes adoption of the Mediterranean diet, which has been shown to significantly reduce stroke risk, especially when supplemented with consumption of nuts and olive oil.
The guideline recommendations also emphasize the need for physical activity, which is “essential” for cardiovascular health and stroke reduction. The authors underscored this point and provided a new recommendation to screen for sedentary behavior and advise patients to avoid inactivity and engage in regular moderate to vigorous physical activity.
Another new recommendation is based on “robust” data that glucagon-like peptide 1 receptor agonists (GLP-1s) significantly improve the management of type 2 diabetes, weight loss, and lower the risk for cardiovascular disease. As a result, guideline authors called for the use of GLP-1s in patients with diabetes and high cardiovascular risk or established cardiovascular disease.
“The glucagon-like peptide receptor agonists have been shown to not only drastically reduce blood sugars in patients with diabetes, but they also lead to significant weight loss in these patients, which has many downstream benefits. Together, this reduces the risk of stroke and other complications of diabetes,” said Bushnell.
She also noted that another drug class introduced since the 2014 guidelines were published, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, have proven to be highly effective in lowering low-density lipoprotein cholesterol. These medications have also been shown to reduce the risk for stroke.
At Least Two Meds Needed to Reduce BP
Effective blood pressure (BP) management is crucial for stroke prevention. Randomized controlled trials show that a single antihypertensive medication helps only about 30% of participants reach their BP target.
Most patients only achieve the desired BP target with two to three medications. In line with these data, the committee recommends using at least two antihypertensives for primary stroke prevention in most patients who require BP-lowering medications for hypertension.
In patients with antiphospholipid syndrome or systemic lupus erythematosus and no history of stroke or unprovoked venous thromboembolism, the authors recommended antiplatelet therapy to prevent stroke. They added that patients with antiphospholipid syndrome who have had a prior unprovoked venous thrombosis will likely benefit from vitamin K antagonist therapy (target international normalized ratio, 2-3) over direct oral anticoagulants.
Emphasis on Women’s Health
Preventing pregnancy-related stroke is achieved primarily by managing hypertension, the guideline authors noted. They recommended treating verified systolic BP over 160 mm Hg or diastolic BP over 110 mm Hg during pregnancy and up to 6 weeks postpartum to lower the risk for fatal maternal intracerebral hemorrhage.
They noted that adverse pregnancy outcomes are also common and linked to chronic hypertension, which increases stroke risk later in life. Therefore, they recommended screening for these outcomes to assess and manage vascular risk factors. The guideline includes a screening tool to help with this in clinical practice.
Endometriosis, premature ovarian failure (before age 40 years), and early-onset menopause (before age 45 years) are all associated with increased stroke risk. As a result, the guideline authors said screening for all three of these conditions is a “reasonable step in the evaluation and management of vascular risk factors in these individuals to reduce stroke risk.”
Finally, the guideline authors addressed primary stroke prevention in transgender individuals, noting that transgender women undergoing estrogen therapy for gender affirmation are at increased risk. They emphasized that evaluating and modifying risk factors could be beneficial for reducing stroke risk in this patient population.
Challenges Lie Ahead
Now that the guideline has been published, the challenge lies in determining how best to implement “its screening recommendations in primary care and other practices when these clinicians are already pushed to see as many patients as possible,” Bushnell said.
Development of screening tools that can be easily incorporated into the clinic visit or the electronic health record, as well as additional personnel to provide counseling, are probably needed to disseminate them, she added.
Bushnell also emphasized that the guideline includes a strong focus on social determinants of health and related social needs.
“We worked hard to use inclusive language and to consider populations historically excluded from research. In acknowledging that social determinants of health including access to healthcare, access to education, economic stability, neighborhood and geographic location, and social and community context have a tremendous influence on stroke risk, we describe how these factors are closely tied to the prevalence and management of many medical risks like obesity, hypertension, and diabetes.
“Our recommendations offer practical steps for screening and addressing essential health-related social needs, including access to nutritious food, stable housing, and reliable transportation, within clinical practice. By considering these factors more comprehensively, we believe we can make meaningful strides toward reducing the disparities in stroke risk,” said Bushnell.
A version of this article appeared on Medscape.com.
The first update in a decade, the 2024 Guideline for the Primary Prevention of Stroke, replaces the 2014 version and is intended to be a resource for clinicians to help them implement a variety of prevention strategies in patients with no previous history of stroke. It aligns with the American Heart Association’s Life’s Essential 8.
“This guideline is an important and timely update from 2014 for multiple reasons. First, there have been groundbreaking clinical trials that have been published with new medications to not only treat the target disease [including] diabetes/obesity and high cholesterol], but also lower the risk of stroke and heart disease,” said chair of the guideline writing group, Cheryl D. Bushnell, MD, MHS, FAHA, and vice chair of the research, Department of Neurology, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
It was published online on October 21 in Stroke.
Up to 80% of Strokes Preventable
Estimates show that every year in the United States, more than 500,000 individuals have a first stroke. However, the guideline authors noted that up to 80% of strokes may be preventable. As a result, they called for better primary stroke prevention that includes improved screening and lifestyle changes.
This includes adoption of the Mediterranean diet, which has been shown to significantly reduce stroke risk, especially when supplemented with consumption of nuts and olive oil.
The guideline recommendations also emphasize the need for physical activity, which is “essential” for cardiovascular health and stroke reduction. The authors underscored this point and provided a new recommendation to screen for sedentary behavior and advise patients to avoid inactivity and engage in regular moderate to vigorous physical activity.
Another new recommendation is based on “robust” data that glucagon-like peptide 1 receptor agonists (GLP-1s) significantly improve the management of type 2 diabetes, weight loss, and lower the risk for cardiovascular disease. As a result, guideline authors called for the use of GLP-1s in patients with diabetes and high cardiovascular risk or established cardiovascular disease.
“The glucagon-like peptide receptor agonists have been shown to not only drastically reduce blood sugars in patients with diabetes, but they also lead to significant weight loss in these patients, which has many downstream benefits. Together, this reduces the risk of stroke and other complications of diabetes,” said Bushnell.
She also noted that another drug class introduced since the 2014 guidelines were published, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, have proven to be highly effective in lowering low-density lipoprotein cholesterol. These medications have also been shown to reduce the risk for stroke.
At Least Two Meds Needed to Reduce BP
Effective blood pressure (BP) management is crucial for stroke prevention. Randomized controlled trials show that a single antihypertensive medication helps only about 30% of participants reach their BP target.
Most patients only achieve the desired BP target with two to three medications. In line with these data, the committee recommends using at least two antihypertensives for primary stroke prevention in most patients who require BP-lowering medications for hypertension.
In patients with antiphospholipid syndrome or systemic lupus erythematosus and no history of stroke or unprovoked venous thromboembolism, the authors recommended antiplatelet therapy to prevent stroke. They added that patients with antiphospholipid syndrome who have had a prior unprovoked venous thrombosis will likely benefit from vitamin K antagonist therapy (target international normalized ratio, 2-3) over direct oral anticoagulants.
Emphasis on Women’s Health
Preventing pregnancy-related stroke is achieved primarily by managing hypertension, the guideline authors noted. They recommended treating verified systolic BP over 160 mm Hg or diastolic BP over 110 mm Hg during pregnancy and up to 6 weeks postpartum to lower the risk for fatal maternal intracerebral hemorrhage.
They noted that adverse pregnancy outcomes are also common and linked to chronic hypertension, which increases stroke risk later in life. Therefore, they recommended screening for these outcomes to assess and manage vascular risk factors. The guideline includes a screening tool to help with this in clinical practice.
Endometriosis, premature ovarian failure (before age 40 years), and early-onset menopause (before age 45 years) are all associated with increased stroke risk. As a result, the guideline authors said screening for all three of these conditions is a “reasonable step in the evaluation and management of vascular risk factors in these individuals to reduce stroke risk.”
Finally, the guideline authors addressed primary stroke prevention in transgender individuals, noting that transgender women undergoing estrogen therapy for gender affirmation are at increased risk. They emphasized that evaluating and modifying risk factors could be beneficial for reducing stroke risk in this patient population.
Challenges Lie Ahead
Now that the guideline has been published, the challenge lies in determining how best to implement “its screening recommendations in primary care and other practices when these clinicians are already pushed to see as many patients as possible,” Bushnell said.
Development of screening tools that can be easily incorporated into the clinic visit or the electronic health record, as well as additional personnel to provide counseling, are probably needed to disseminate them, she added.
Bushnell also emphasized that the guideline includes a strong focus on social determinants of health and related social needs.
“We worked hard to use inclusive language and to consider populations historically excluded from research. In acknowledging that social determinants of health including access to healthcare, access to education, economic stability, neighborhood and geographic location, and social and community context have a tremendous influence on stroke risk, we describe how these factors are closely tied to the prevalence and management of many medical risks like obesity, hypertension, and diabetes.
“Our recommendations offer practical steps for screening and addressing essential health-related social needs, including access to nutritious food, stable housing, and reliable transportation, within clinical practice. By considering these factors more comprehensively, we believe we can make meaningful strides toward reducing the disparities in stroke risk,” said Bushnell.
A version of this article appeared on Medscape.com.
The first update in a decade, the 2024 Guideline for the Primary Prevention of Stroke, replaces the 2014 version and is intended to be a resource for clinicians to help them implement a variety of prevention strategies in patients with no previous history of stroke. It aligns with the American Heart Association’s Life’s Essential 8.
“This guideline is an important and timely update from 2014 for multiple reasons. First, there have been groundbreaking clinical trials that have been published with new medications to not only treat the target disease [including] diabetes/obesity and high cholesterol], but also lower the risk of stroke and heart disease,” said chair of the guideline writing group, Cheryl D. Bushnell, MD, MHS, FAHA, and vice chair of the research, Department of Neurology, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
It was published online on October 21 in Stroke.
Up to 80% of Strokes Preventable
Estimates show that every year in the United States, more than 500,000 individuals have a first stroke. However, the guideline authors noted that up to 80% of strokes may be preventable. As a result, they called for better primary stroke prevention that includes improved screening and lifestyle changes.
This includes adoption of the Mediterranean diet, which has been shown to significantly reduce stroke risk, especially when supplemented with consumption of nuts and olive oil.
The guideline recommendations also emphasize the need for physical activity, which is “essential” for cardiovascular health and stroke reduction. The authors underscored this point and provided a new recommendation to screen for sedentary behavior and advise patients to avoid inactivity and engage in regular moderate to vigorous physical activity.
Another new recommendation is based on “robust” data that glucagon-like peptide 1 receptor agonists (GLP-1s) significantly improve the management of type 2 diabetes, weight loss, and lower the risk for cardiovascular disease. As a result, guideline authors called for the use of GLP-1s in patients with diabetes and high cardiovascular risk or established cardiovascular disease.
“The glucagon-like peptide receptor agonists have been shown to not only drastically reduce blood sugars in patients with diabetes, but they also lead to significant weight loss in these patients, which has many downstream benefits. Together, this reduces the risk of stroke and other complications of diabetes,” said Bushnell.
She also noted that another drug class introduced since the 2014 guidelines were published, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, have proven to be highly effective in lowering low-density lipoprotein cholesterol. These medications have also been shown to reduce the risk for stroke.
At Least Two Meds Needed to Reduce BP
Effective blood pressure (BP) management is crucial for stroke prevention. Randomized controlled trials show that a single antihypertensive medication helps only about 30% of participants reach their BP target.
Most patients only achieve the desired BP target with two to three medications. In line with these data, the committee recommends using at least two antihypertensives for primary stroke prevention in most patients who require BP-lowering medications for hypertension.
In patients with antiphospholipid syndrome or systemic lupus erythematosus and no history of stroke or unprovoked venous thromboembolism, the authors recommended antiplatelet therapy to prevent stroke. They added that patients with antiphospholipid syndrome who have had a prior unprovoked venous thrombosis will likely benefit from vitamin K antagonist therapy (target international normalized ratio, 2-3) over direct oral anticoagulants.
Emphasis on Women’s Health
Preventing pregnancy-related stroke is achieved primarily by managing hypertension, the guideline authors noted. They recommended treating verified systolic BP over 160 mm Hg or diastolic BP over 110 mm Hg during pregnancy and up to 6 weeks postpartum to lower the risk for fatal maternal intracerebral hemorrhage.
They noted that adverse pregnancy outcomes are also common and linked to chronic hypertension, which increases stroke risk later in life. Therefore, they recommended screening for these outcomes to assess and manage vascular risk factors. The guideline includes a screening tool to help with this in clinical practice.
Endometriosis, premature ovarian failure (before age 40 years), and early-onset menopause (before age 45 years) are all associated with increased stroke risk. As a result, the guideline authors said screening for all three of these conditions is a “reasonable step in the evaluation and management of vascular risk factors in these individuals to reduce stroke risk.”
Finally, the guideline authors addressed primary stroke prevention in transgender individuals, noting that transgender women undergoing estrogen therapy for gender affirmation are at increased risk. They emphasized that evaluating and modifying risk factors could be beneficial for reducing stroke risk in this patient population.
Challenges Lie Ahead
Now that the guideline has been published, the challenge lies in determining how best to implement “its screening recommendations in primary care and other practices when these clinicians are already pushed to see as many patients as possible,” Bushnell said.
Development of screening tools that can be easily incorporated into the clinic visit or the electronic health record, as well as additional personnel to provide counseling, are probably needed to disseminate them, she added.
Bushnell also emphasized that the guideline includes a strong focus on social determinants of health and related social needs.
“We worked hard to use inclusive language and to consider populations historically excluded from research. In acknowledging that social determinants of health including access to healthcare, access to education, economic stability, neighborhood and geographic location, and social and community context have a tremendous influence on stroke risk, we describe how these factors are closely tied to the prevalence and management of many medical risks like obesity, hypertension, and diabetes.
“Our recommendations offer practical steps for screening and addressing essential health-related social needs, including access to nutritious food, stable housing, and reliable transportation, within clinical practice. By considering these factors more comprehensively, we believe we can make meaningful strides toward reducing the disparities in stroke risk,” said Bushnell.
A version of this article appeared on Medscape.com.
State of Confusion: Should All Children Get Lipid Labs for High Cholesterol?
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
AHA Scientific Statement Links Three Common Cardiovascular Diseases to Cognitive Decline, Dementia
The statement includes an extensive research review and offers compelling evidence of the inextricable link between heart health and brain health, which investigators said underscores the benefit of early intervention.
The cumulative evidence “confirms that the trajectories of cardiac health and brain health are inextricably intertwined through modifiable and nonmodifiable factors,” the authors wrote.
Investigators say the findings reinforce the message that addressing cardiovascular health early in life may deter the onset or progression of cognitive impairment later on.
And the earlier this is done, the better, said lead author Fernando D. Testai, MD, PhD, a professor of neurology and the vascular neurology section head, Department of Neurology and Rehabilitation, University of Illinois, Chicago.
The statement was published online in Stroke.
Bridging the Research Gap
It’s well known that there’s a bidirectional relationship between heart and brain function. For example, heart failure can lead to decreased blood flow that can damage the brain, and stroke in some areas of the brain can affect the heart.
However, that’s only part of the puzzle and doesn’t address all the gaps in the understanding of how cardiovascular disease contributes to cognition, said Testai.
“What we’re trying to do here is to go one step further and describe other connections between the heart and the brain,” he said.
Investigators carried out an extensive PubMed search for heart failure, atrial fibrillation, and coronary heart disease. Researchers detailed the frequency of each condition, mechanisms by which they might cause cognitive impairment, and prospects for prevention and treatment to maintain brain health.
A recurring theme in the paper is the role of inflammation. Evidence shows there are “remarkable similarities in the inflammatory response that takes place,” with both cardiac disease and cognitive decline, said Testai.
Another potential shared mechanism relates to biomarkers, particularly amyloid, which is strongly linked to Alzheimer’s disease.
“But some studies show amyloid can also be present in the heart, especially in patients who have decreased ejection fraction,” said Testai.
Robust Heart-Brain Connection
The statement’s authors collected a substantial amount of evidence showing vascular risk factors such as hypertension and diabetes “can change how the brain processes and clears up amyloid,” Testai added.
The paper also provides a compilation of evidence of shared genetic predispositions when it comes to heart and brain disorders.
“We noticed that some genetic signatures that have historically been associated with heart disease seem to also correlate with structural changes in the brain. That means that at the end of the day, some patients may be born with a genetic predisposition to developing both conditions,” said Testai.
This indicates that the link between the two organs “begins as early as conception” and underscores the importance of adopting healthy lifestyle habits as early as possible, he added.
“That means you can avoid bad habits that eventually lead to hypertension, diabetes, and cholesterol, that eventually will lead to cardiac disease, which eventually will lead to stroke, which eventually will lead to cognitive decline,” Testai noted.
However, cardiovascular health is more complicated than having good genes and adhering to a healthy lifestyle. It’s not clear, for example, why some people who should be predisposed to developing heart disease do not develop it, something Testai refers to as enhanced “resilience.”
For example, Hispanic or Latino patients, who have relatively poor cardiovascular risk factor profiles, seem to be less susceptible to developing cardiac disease.
More Research Needed
While genetics may partly explain the paradox, Testai believes other protective factors are at play, including strong social support networks.
Testai referred to the AHA’s “Life’s Essential 8” — the eight components of cardiovascular health. These include a healthy diet, participation in physical activity, nicotine avoidance, healthy sleep, healthy weight, and healthy levels of blood lipids, blood glucose, and blood pressure.
More evidence is needed to show that effective management of cardiac disease positively affects cognition. Currently, cognitive measures are rarely included in studies examining various heart disease treatments, said Testai.
“There should probably be an effort to include brain health outcomes in some of the cardiac literature to make sure we can also measure whether the intervention in the heart leads to an advantage for the brain,” he said.
More research is also needed to determine whether immunomodulation has a beneficial effect on the cognitive trajectory, the statement’s authors noted.
They point out that the interpretation and generalizability of the studies described in the statement are confounded by disparate methodologies, including small sample sizes, cross-sectional designs, and underrepresentation of Black and Hispanic individuals.
‘An Important Step’
Reached for a comment, Natalia S. Rost, MD, Chief of the Stroke Division at Massachusetts General Hospital and professor of neurology at Harvard Medical School, both in Boston, said this paper “is an important step” in terms of pulling together pertinent information on the topic of heart-brain health.
She praised the authors for gathering evidence on risk factors related to atrial fibrillation, heart failure, and coronary heart disease, which is “the part of the puzzle that is controllable.”
This helps reinforce the message that controlling vascular risk factors helps with brain health, said Rost.
But brain health is “much more complex than just vascular health,” she said. It includes other elements such as freedom from epilepsy, migraine, traumatic brain injury, and adult learning disabilities.
No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
The statement includes an extensive research review and offers compelling evidence of the inextricable link between heart health and brain health, which investigators said underscores the benefit of early intervention.
The cumulative evidence “confirms that the trajectories of cardiac health and brain health are inextricably intertwined through modifiable and nonmodifiable factors,” the authors wrote.
Investigators say the findings reinforce the message that addressing cardiovascular health early in life may deter the onset or progression of cognitive impairment later on.
And the earlier this is done, the better, said lead author Fernando D. Testai, MD, PhD, a professor of neurology and the vascular neurology section head, Department of Neurology and Rehabilitation, University of Illinois, Chicago.
The statement was published online in Stroke.
Bridging the Research Gap
It’s well known that there’s a bidirectional relationship between heart and brain function. For example, heart failure can lead to decreased blood flow that can damage the brain, and stroke in some areas of the brain can affect the heart.
However, that’s only part of the puzzle and doesn’t address all the gaps in the understanding of how cardiovascular disease contributes to cognition, said Testai.
“What we’re trying to do here is to go one step further and describe other connections between the heart and the brain,” he said.
Investigators carried out an extensive PubMed search for heart failure, atrial fibrillation, and coronary heart disease. Researchers detailed the frequency of each condition, mechanisms by which they might cause cognitive impairment, and prospects for prevention and treatment to maintain brain health.
A recurring theme in the paper is the role of inflammation. Evidence shows there are “remarkable similarities in the inflammatory response that takes place,” with both cardiac disease and cognitive decline, said Testai.
Another potential shared mechanism relates to biomarkers, particularly amyloid, which is strongly linked to Alzheimer’s disease.
“But some studies show amyloid can also be present in the heart, especially in patients who have decreased ejection fraction,” said Testai.
Robust Heart-Brain Connection
The statement’s authors collected a substantial amount of evidence showing vascular risk factors such as hypertension and diabetes “can change how the brain processes and clears up amyloid,” Testai added.
The paper also provides a compilation of evidence of shared genetic predispositions when it comes to heart and brain disorders.
“We noticed that some genetic signatures that have historically been associated with heart disease seem to also correlate with structural changes in the brain. That means that at the end of the day, some patients may be born with a genetic predisposition to developing both conditions,” said Testai.
This indicates that the link between the two organs “begins as early as conception” and underscores the importance of adopting healthy lifestyle habits as early as possible, he added.
“That means you can avoid bad habits that eventually lead to hypertension, diabetes, and cholesterol, that eventually will lead to cardiac disease, which eventually will lead to stroke, which eventually will lead to cognitive decline,” Testai noted.
However, cardiovascular health is more complicated than having good genes and adhering to a healthy lifestyle. It’s not clear, for example, why some people who should be predisposed to developing heart disease do not develop it, something Testai refers to as enhanced “resilience.”
For example, Hispanic or Latino patients, who have relatively poor cardiovascular risk factor profiles, seem to be less susceptible to developing cardiac disease.
More Research Needed
While genetics may partly explain the paradox, Testai believes other protective factors are at play, including strong social support networks.
Testai referred to the AHA’s “Life’s Essential 8” — the eight components of cardiovascular health. These include a healthy diet, participation in physical activity, nicotine avoidance, healthy sleep, healthy weight, and healthy levels of blood lipids, blood glucose, and blood pressure.
More evidence is needed to show that effective management of cardiac disease positively affects cognition. Currently, cognitive measures are rarely included in studies examining various heart disease treatments, said Testai.
“There should probably be an effort to include brain health outcomes in some of the cardiac literature to make sure we can also measure whether the intervention in the heart leads to an advantage for the brain,” he said.
More research is also needed to determine whether immunomodulation has a beneficial effect on the cognitive trajectory, the statement’s authors noted.
They point out that the interpretation and generalizability of the studies described in the statement are confounded by disparate methodologies, including small sample sizes, cross-sectional designs, and underrepresentation of Black and Hispanic individuals.
‘An Important Step’
Reached for a comment, Natalia S. Rost, MD, Chief of the Stroke Division at Massachusetts General Hospital and professor of neurology at Harvard Medical School, both in Boston, said this paper “is an important step” in terms of pulling together pertinent information on the topic of heart-brain health.
She praised the authors for gathering evidence on risk factors related to atrial fibrillation, heart failure, and coronary heart disease, which is “the part of the puzzle that is controllable.”
This helps reinforce the message that controlling vascular risk factors helps with brain health, said Rost.
But brain health is “much more complex than just vascular health,” she said. It includes other elements such as freedom from epilepsy, migraine, traumatic brain injury, and adult learning disabilities.
No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
The statement includes an extensive research review and offers compelling evidence of the inextricable link between heart health and brain health, which investigators said underscores the benefit of early intervention.
The cumulative evidence “confirms that the trajectories of cardiac health and brain health are inextricably intertwined through modifiable and nonmodifiable factors,” the authors wrote.
Investigators say the findings reinforce the message that addressing cardiovascular health early in life may deter the onset or progression of cognitive impairment later on.
And the earlier this is done, the better, said lead author Fernando D. Testai, MD, PhD, a professor of neurology and the vascular neurology section head, Department of Neurology and Rehabilitation, University of Illinois, Chicago.
The statement was published online in Stroke.
Bridging the Research Gap
It’s well known that there’s a bidirectional relationship between heart and brain function. For example, heart failure can lead to decreased blood flow that can damage the brain, and stroke in some areas of the brain can affect the heart.
However, that’s only part of the puzzle and doesn’t address all the gaps in the understanding of how cardiovascular disease contributes to cognition, said Testai.
“What we’re trying to do here is to go one step further and describe other connections between the heart and the brain,” he said.
Investigators carried out an extensive PubMed search for heart failure, atrial fibrillation, and coronary heart disease. Researchers detailed the frequency of each condition, mechanisms by which they might cause cognitive impairment, and prospects for prevention and treatment to maintain brain health.
A recurring theme in the paper is the role of inflammation. Evidence shows there are “remarkable similarities in the inflammatory response that takes place,” with both cardiac disease and cognitive decline, said Testai.
Another potential shared mechanism relates to biomarkers, particularly amyloid, which is strongly linked to Alzheimer’s disease.
“But some studies show amyloid can also be present in the heart, especially in patients who have decreased ejection fraction,” said Testai.
Robust Heart-Brain Connection
The statement’s authors collected a substantial amount of evidence showing vascular risk factors such as hypertension and diabetes “can change how the brain processes and clears up amyloid,” Testai added.
The paper also provides a compilation of evidence of shared genetic predispositions when it comes to heart and brain disorders.
“We noticed that some genetic signatures that have historically been associated with heart disease seem to also correlate with structural changes in the brain. That means that at the end of the day, some patients may be born with a genetic predisposition to developing both conditions,” said Testai.
This indicates that the link between the two organs “begins as early as conception” and underscores the importance of adopting healthy lifestyle habits as early as possible, he added.
“That means you can avoid bad habits that eventually lead to hypertension, diabetes, and cholesterol, that eventually will lead to cardiac disease, which eventually will lead to stroke, which eventually will lead to cognitive decline,” Testai noted.
However, cardiovascular health is more complicated than having good genes and adhering to a healthy lifestyle. It’s not clear, for example, why some people who should be predisposed to developing heart disease do not develop it, something Testai refers to as enhanced “resilience.”
For example, Hispanic or Latino patients, who have relatively poor cardiovascular risk factor profiles, seem to be less susceptible to developing cardiac disease.
More Research Needed
While genetics may partly explain the paradox, Testai believes other protective factors are at play, including strong social support networks.
Testai referred to the AHA’s “Life’s Essential 8” — the eight components of cardiovascular health. These include a healthy diet, participation in physical activity, nicotine avoidance, healthy sleep, healthy weight, and healthy levels of blood lipids, blood glucose, and blood pressure.
More evidence is needed to show that effective management of cardiac disease positively affects cognition. Currently, cognitive measures are rarely included in studies examining various heart disease treatments, said Testai.
“There should probably be an effort to include brain health outcomes in some of the cardiac literature to make sure we can also measure whether the intervention in the heart leads to an advantage for the brain,” he said.
More research is also needed to determine whether immunomodulation has a beneficial effect on the cognitive trajectory, the statement’s authors noted.
They point out that the interpretation and generalizability of the studies described in the statement are confounded by disparate methodologies, including small sample sizes, cross-sectional designs, and underrepresentation of Black and Hispanic individuals.
‘An Important Step’
Reached for a comment, Natalia S. Rost, MD, Chief of the Stroke Division at Massachusetts General Hospital and professor of neurology at Harvard Medical School, both in Boston, said this paper “is an important step” in terms of pulling together pertinent information on the topic of heart-brain health.
She praised the authors for gathering evidence on risk factors related to atrial fibrillation, heart failure, and coronary heart disease, which is “the part of the puzzle that is controllable.”
This helps reinforce the message that controlling vascular risk factors helps with brain health, said Rost.
But brain health is “much more complex than just vascular health,” she said. It includes other elements such as freedom from epilepsy, migraine, traumatic brain injury, and adult learning disabilities.
No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
FROM STROKE
Ultraprocessed Foods and CVD: Myths vs Facts
I’d like to talk with you about ultraprocessed foods (UPFs) and risk for cardiovascular disease (CVD) and try to separate some of the facts from the myths. I’d like to discuss a recent report in The Lancet Regional Health that looks at this topic comprehensively and in detail.
This report includes three large-scale prospective cohort studies of US female and male health professionals, more than 200,000 participants in total. It also includes a meta-analysis of 22 international cohorts with about 1.2 million participants. I’d like to acknowledge that I’m a co-author of this study.
What are UPFs, and why are they important? Why do we care, and what are the knowledge gaps? UPFs are generally packaged foods that contain ingredients to extend shelf life and improve taste and palatability. It’s important because 60%-70% of the US diet, if not more, is made up of UPFs. So, the relationship between UPFs and CVD and other health outcomes is actually very important.
And the research to date on this subject has been quite limited.
In other studies, these UPFs have been linked to weight gain and dyslipidemia; some tissue glycation has been found, and some changes in the microbiome. Some studies have linked higher UPF intake with type 2 diabetes. A few have looked at certain selected UPF foods and found a higher risk for CVD, but a really comprehensive look at this question hasn’t been done.
So, that’s what we did in this paper and in the meta-analysis with the 22 cohorts, and we saw a very clear and distinct significant increase in coronary heart disease by 23%, total CVD by 17%, and stroke by 9% when comparing the highest vs the lowest category [of UPF intake]. When we drilled down deeply into the types of UPFs in the US health professional cohorts, we saw that there were some major differences in the relationship with CVD depending on the type of UPF.
In comparing the highest quintile vs the lowest quintile [of total UPF intake], we saw that some of the UPFs were associated with significant elevations in risk for CVD. These included sugar-sweetened beverages and processed meats. But some UPFs were linked with a lower risk for CVD. These included breakfast cereals, yogurt, some dairy desserts, and whole grains.
Overall, it seemed that UPFs are actually quite diverse in their association with health. It’s not one size fits all. They’re not all created equal, and some of these differences matter. Although overall we would recommend that our diets be focused on whole foods, primarily plant based, lots of fruits and vegetables, whole grains, fish, and other whole foods, it seems from this report and the meta-analysis that certain types of UPFs can be incorporated into a healthy diet and don’t need to be avoided entirely.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and Chief of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston, Massachusetts. She reported receiving donations and infrastructure support from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
I’d like to talk with you about ultraprocessed foods (UPFs) and risk for cardiovascular disease (CVD) and try to separate some of the facts from the myths. I’d like to discuss a recent report in The Lancet Regional Health that looks at this topic comprehensively and in detail.
This report includes three large-scale prospective cohort studies of US female and male health professionals, more than 200,000 participants in total. It also includes a meta-analysis of 22 international cohorts with about 1.2 million participants. I’d like to acknowledge that I’m a co-author of this study.
What are UPFs, and why are they important? Why do we care, and what are the knowledge gaps? UPFs are generally packaged foods that contain ingredients to extend shelf life and improve taste and palatability. It’s important because 60%-70% of the US diet, if not more, is made up of UPFs. So, the relationship between UPFs and CVD and other health outcomes is actually very important.
And the research to date on this subject has been quite limited.
In other studies, these UPFs have been linked to weight gain and dyslipidemia; some tissue glycation has been found, and some changes in the microbiome. Some studies have linked higher UPF intake with type 2 diabetes. A few have looked at certain selected UPF foods and found a higher risk for CVD, but a really comprehensive look at this question hasn’t been done.
So, that’s what we did in this paper and in the meta-analysis with the 22 cohorts, and we saw a very clear and distinct significant increase in coronary heart disease by 23%, total CVD by 17%, and stroke by 9% when comparing the highest vs the lowest category [of UPF intake]. When we drilled down deeply into the types of UPFs in the US health professional cohorts, we saw that there were some major differences in the relationship with CVD depending on the type of UPF.
In comparing the highest quintile vs the lowest quintile [of total UPF intake], we saw that some of the UPFs were associated with significant elevations in risk for CVD. These included sugar-sweetened beverages and processed meats. But some UPFs were linked with a lower risk for CVD. These included breakfast cereals, yogurt, some dairy desserts, and whole grains.
Overall, it seemed that UPFs are actually quite diverse in their association with health. It’s not one size fits all. They’re not all created equal, and some of these differences matter. Although overall we would recommend that our diets be focused on whole foods, primarily plant based, lots of fruits and vegetables, whole grains, fish, and other whole foods, it seems from this report and the meta-analysis that certain types of UPFs can be incorporated into a healthy diet and don’t need to be avoided entirely.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and Chief of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston, Massachusetts. She reported receiving donations and infrastructure support from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
I’d like to talk with you about ultraprocessed foods (UPFs) and risk for cardiovascular disease (CVD) and try to separate some of the facts from the myths. I’d like to discuss a recent report in The Lancet Regional Health that looks at this topic comprehensively and in detail.
This report includes three large-scale prospective cohort studies of US female and male health professionals, more than 200,000 participants in total. It also includes a meta-analysis of 22 international cohorts with about 1.2 million participants. I’d like to acknowledge that I’m a co-author of this study.
What are UPFs, and why are they important? Why do we care, and what are the knowledge gaps? UPFs are generally packaged foods that contain ingredients to extend shelf life and improve taste and palatability. It’s important because 60%-70% of the US diet, if not more, is made up of UPFs. So, the relationship between UPFs and CVD and other health outcomes is actually very important.
And the research to date on this subject has been quite limited.
In other studies, these UPFs have been linked to weight gain and dyslipidemia; some tissue glycation has been found, and some changes in the microbiome. Some studies have linked higher UPF intake with type 2 diabetes. A few have looked at certain selected UPF foods and found a higher risk for CVD, but a really comprehensive look at this question hasn’t been done.
So, that’s what we did in this paper and in the meta-analysis with the 22 cohorts, and we saw a very clear and distinct significant increase in coronary heart disease by 23%, total CVD by 17%, and stroke by 9% when comparing the highest vs the lowest category [of UPF intake]. When we drilled down deeply into the types of UPFs in the US health professional cohorts, we saw that there were some major differences in the relationship with CVD depending on the type of UPF.
In comparing the highest quintile vs the lowest quintile [of total UPF intake], we saw that some of the UPFs were associated with significant elevations in risk for CVD. These included sugar-sweetened beverages and processed meats. But some UPFs were linked with a lower risk for CVD. These included breakfast cereals, yogurt, some dairy desserts, and whole grains.
Overall, it seemed that UPFs are actually quite diverse in their association with health. It’s not one size fits all. They’re not all created equal, and some of these differences matter. Although overall we would recommend that our diets be focused on whole foods, primarily plant based, lots of fruits and vegetables, whole grains, fish, and other whole foods, it seems from this report and the meta-analysis that certain types of UPFs can be incorporated into a healthy diet and don’t need to be avoided entirely.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and Chief of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston, Massachusetts. She reported receiving donations and infrastructure support from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
Heard of ApoB Testing? New Guidelines
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
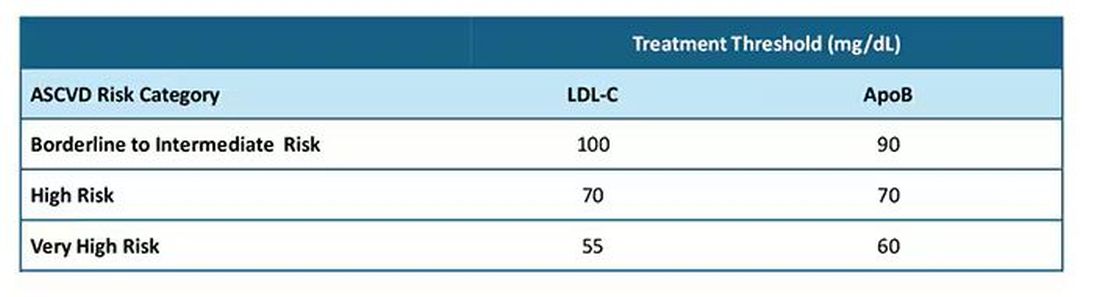
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.