User login
Large dark discoloration on the back

The FP recognized that this child had a large bathing trunk nevus with multiple small melanocytic satellite lesions on her arms.
He explained to the worried parents that their daughter had a bathing trunk nevus and that a local expert was needed. The FP consulted a local dermatologist, who subsequently explained to the parents that there was a significant risk of cutaneous melanoma if nothing was done about this large congenital nevus. The dermatologist indicated that while removal could decrease that risk, the process would require multiple large surgeries by a plastic surgeon. She also explained that a magnetic resonance imaging scan of the brain would be needed at about 6 months to look for neurocutaneous melanosis, which can cause seizures, hydrocephalus, and a central nervous system melanoma.
The parents were conflicted about whether to put their child through a series of massive surgeries or to accept the higher risk of melanoma and proceed with careful monitoring by the dermatologist. (No additional details on how this case resolved are available—Editor.)
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith, M. Congenital nevi. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:953-957.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
The FP recognized that this child had a large bathing trunk nevus with multiple small melanocytic satellite lesions on her arms.
He explained to the worried parents that their daughter had a bathing trunk nevus and that a local expert was needed. The FP consulted a local dermatologist, who subsequently explained to the parents that there was a significant risk of cutaneous melanoma if nothing was done about this large congenital nevus. The dermatologist indicated that while removal could decrease that risk, the process would require multiple large surgeries by a plastic surgeon. She also explained that a magnetic resonance imaging scan of the brain would be needed at about 6 months to look for neurocutaneous melanosis, which can cause seizures, hydrocephalus, and a central nervous system melanoma.
The parents were conflicted about whether to put their child through a series of massive surgeries or to accept the higher risk of melanoma and proceed with careful monitoring by the dermatologist. (No additional details on how this case resolved are available—Editor.)
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith, M. Congenital nevi. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:953-957.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
The FP recognized that this child had a large bathing trunk nevus with multiple small melanocytic satellite lesions on her arms.
He explained to the worried parents that their daughter had a bathing trunk nevus and that a local expert was needed. The FP consulted a local dermatologist, who subsequently explained to the parents that there was a significant risk of cutaneous melanoma if nothing was done about this large congenital nevus. The dermatologist indicated that while removal could decrease that risk, the process would require multiple large surgeries by a plastic surgeon. She also explained that a magnetic resonance imaging scan of the brain would be needed at about 6 months to look for neurocutaneous melanosis, which can cause seizures, hydrocephalus, and a central nervous system melanoma.
The parents were conflicted about whether to put their child through a series of massive surgeries or to accept the higher risk of melanoma and proceed with careful monitoring by the dermatologist. (No additional details on how this case resolved are available—Editor.)
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith, M. Congenital nevi. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:953-957.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
Atopic eczema linked to cardiovascular disease risk
according to a case-control study published online May 23 in BMJ.
In a population-based cohort study, researchers compared the electronic health records of 387,439 adults with eczema and 1,528,477 patients without eczema in the United Kingddom, matched according to age, sex, general practice, and calendar time, during 1998-2015. Patients were followed up for a median of 5.1 years
With the exception of cardiovascular death, atopic eczema was associated with all cardiovascular outcomes (MI, unstable angina, heart failure, atrial fibrillation, and stroke). The associations were stronger for severe atopic eczema, with significantly higher risks of MI, unstable angina, atrial fibrillation, stroke, cardiovascular death, and coronary revascularization among individuals with severe atopic eczema, compared with controls.
After adjustment for potential mediators such as body mass index, smoking, hyperlipidemia, diabetes, and severe alcohol use, individuals with severe eczema had a significant 37% increased risk of MI, 67% greater risk of heart failure, 35% greater risk of atrial fibrillation, 30% greater risk of cardiovascular death, and 36% greater risk of coronary revascularization, compared with controls with no eczema.
Increased cardiovascular risks also were seen in individuals whose atopic eczema was active more than half the time at follow-up. This group had a 37% greater risk of heart failure, 36% greater risk of unstable angina, and 19% greater risk of stroke, as well as significantly elevated risks of MI, atrial fibrillation, cardiovascular death, and coronary revascularization, compared with those without eczema.
Overall, atopic eczema contributed around 2.4% of the population-attributable risk for unstable angina, and 1.9% for heart failure (the highest population attributable risks). Ethnicity or high-dose corticosteroid use did not significantly impact outcomes.
Richard J. Silverwood, PhD, from the London School of Hygiene and Tropical Medicine, and his coauthors wrote that previous work examining the relationship between atopic eczema and cardiovascular disease had shown inconsistent outcomes, with some studies even pointing to a possible protective effect of mild atopic eczema.
“Mechanistic work suggests that atopic eczema may be associated with increased platelet activation and decreased fibrinolysis, which may increase the risk of clotting, though a recent study found no association with metabolite levels,” the authors wrote.
They noted that the strengths of their study were that it was largest to examine the association between atopic eczema and cardiovascular risk, and that they had access to data on body mass index, smoking, and severe alcohol use for most of the study population, which enabled them to adjust for these potential mediators.
“Consideration should be given to developing prevention strategies to reduce the risk of cardiovascular disease among patients with severe or predominantly active atopic eczema, including awareness of and screening for conventional cardiovascular risk factors by those providing clinical care,” they wrote.
The study was supported by the Wellcome Trust, and no relevant conflicts of interest were declared.
SOURCE: Silverwood R et al. BMJ 2018 May 23;361:k1786. doi: 10.1136/bmj.k1786.
The evidence in favor of a link between chronic inflammatory conditions, such as rheumatoid arthritis, and cardiovascular disease is growing. However, there are conflicting data and some of the uncertainty may be a result of a dose-response effect, where the increased cardiovascular risk is seen only in people with more severe disease.
This study and its finding of increased cardiovascular risk in patients with severe or more active eczema supports the case for targeted screening of this group for standard cardiovascular disease risk factors. It also could prompt incorporation of severe eczema as an independent cardiovascular disease risk factor in calculation of thresholds for primary prevention interventions.
The findings also may have implications for health care resources allocated to treatment of eczema, as prevention of cardiovascular disease could contribute to the argument in favor of the more expensive next-generation biologic treatments for eczema that are becoming available.
John R. Ingram, MD, is senior lecturer and consultant dermatologist, dermatology and academic wound healing in the division of infection and immunity at Cardiff (U.K.) University. These comments are taken from an accompanying editorial No conflicts of interest were declared. (BMJ. 2018 May 23. doi: 10.1136/bmj.k2064).
The evidence in favor of a link between chronic inflammatory conditions, such as rheumatoid arthritis, and cardiovascular disease is growing. However, there are conflicting data and some of the uncertainty may be a result of a dose-response effect, where the increased cardiovascular risk is seen only in people with more severe disease.
This study and its finding of increased cardiovascular risk in patients with severe or more active eczema supports the case for targeted screening of this group for standard cardiovascular disease risk factors. It also could prompt incorporation of severe eczema as an independent cardiovascular disease risk factor in calculation of thresholds for primary prevention interventions.
The findings also may have implications for health care resources allocated to treatment of eczema, as prevention of cardiovascular disease could contribute to the argument in favor of the more expensive next-generation biologic treatments for eczema that are becoming available.
John R. Ingram, MD, is senior lecturer and consultant dermatologist, dermatology and academic wound healing in the division of infection and immunity at Cardiff (U.K.) University. These comments are taken from an accompanying editorial No conflicts of interest were declared. (BMJ. 2018 May 23. doi: 10.1136/bmj.k2064).
The evidence in favor of a link between chronic inflammatory conditions, such as rheumatoid arthritis, and cardiovascular disease is growing. However, there are conflicting data and some of the uncertainty may be a result of a dose-response effect, where the increased cardiovascular risk is seen only in people with more severe disease.
This study and its finding of increased cardiovascular risk in patients with severe or more active eczema supports the case for targeted screening of this group for standard cardiovascular disease risk factors. It also could prompt incorporation of severe eczema as an independent cardiovascular disease risk factor in calculation of thresholds for primary prevention interventions.
The findings also may have implications for health care resources allocated to treatment of eczema, as prevention of cardiovascular disease could contribute to the argument in favor of the more expensive next-generation biologic treatments for eczema that are becoming available.
John R. Ingram, MD, is senior lecturer and consultant dermatologist, dermatology and academic wound healing in the division of infection and immunity at Cardiff (U.K.) University. These comments are taken from an accompanying editorial No conflicts of interest were declared. (BMJ. 2018 May 23. doi: 10.1136/bmj.k2064).
according to a case-control study published online May 23 in BMJ.
In a population-based cohort study, researchers compared the electronic health records of 387,439 adults with eczema and 1,528,477 patients without eczema in the United Kingddom, matched according to age, sex, general practice, and calendar time, during 1998-2015. Patients were followed up for a median of 5.1 years
With the exception of cardiovascular death, atopic eczema was associated with all cardiovascular outcomes (MI, unstable angina, heart failure, atrial fibrillation, and stroke). The associations were stronger for severe atopic eczema, with significantly higher risks of MI, unstable angina, atrial fibrillation, stroke, cardiovascular death, and coronary revascularization among individuals with severe atopic eczema, compared with controls.
After adjustment for potential mediators such as body mass index, smoking, hyperlipidemia, diabetes, and severe alcohol use, individuals with severe eczema had a significant 37% increased risk of MI, 67% greater risk of heart failure, 35% greater risk of atrial fibrillation, 30% greater risk of cardiovascular death, and 36% greater risk of coronary revascularization, compared with controls with no eczema.
Increased cardiovascular risks also were seen in individuals whose atopic eczema was active more than half the time at follow-up. This group had a 37% greater risk of heart failure, 36% greater risk of unstable angina, and 19% greater risk of stroke, as well as significantly elevated risks of MI, atrial fibrillation, cardiovascular death, and coronary revascularization, compared with those without eczema.
Overall, atopic eczema contributed around 2.4% of the population-attributable risk for unstable angina, and 1.9% for heart failure (the highest population attributable risks). Ethnicity or high-dose corticosteroid use did not significantly impact outcomes.
Richard J. Silverwood, PhD, from the London School of Hygiene and Tropical Medicine, and his coauthors wrote that previous work examining the relationship between atopic eczema and cardiovascular disease had shown inconsistent outcomes, with some studies even pointing to a possible protective effect of mild atopic eczema.
“Mechanistic work suggests that atopic eczema may be associated with increased platelet activation and decreased fibrinolysis, which may increase the risk of clotting, though a recent study found no association with metabolite levels,” the authors wrote.
They noted that the strengths of their study were that it was largest to examine the association between atopic eczema and cardiovascular risk, and that they had access to data on body mass index, smoking, and severe alcohol use for most of the study population, which enabled them to adjust for these potential mediators.
“Consideration should be given to developing prevention strategies to reduce the risk of cardiovascular disease among patients with severe or predominantly active atopic eczema, including awareness of and screening for conventional cardiovascular risk factors by those providing clinical care,” they wrote.
The study was supported by the Wellcome Trust, and no relevant conflicts of interest were declared.
SOURCE: Silverwood R et al. BMJ 2018 May 23;361:k1786. doi: 10.1136/bmj.k1786.
according to a case-control study published online May 23 in BMJ.
In a population-based cohort study, researchers compared the electronic health records of 387,439 adults with eczema and 1,528,477 patients without eczema in the United Kingddom, matched according to age, sex, general practice, and calendar time, during 1998-2015. Patients were followed up for a median of 5.1 years
With the exception of cardiovascular death, atopic eczema was associated with all cardiovascular outcomes (MI, unstable angina, heart failure, atrial fibrillation, and stroke). The associations were stronger for severe atopic eczema, with significantly higher risks of MI, unstable angina, atrial fibrillation, stroke, cardiovascular death, and coronary revascularization among individuals with severe atopic eczema, compared with controls.
After adjustment for potential mediators such as body mass index, smoking, hyperlipidemia, diabetes, and severe alcohol use, individuals with severe eczema had a significant 37% increased risk of MI, 67% greater risk of heart failure, 35% greater risk of atrial fibrillation, 30% greater risk of cardiovascular death, and 36% greater risk of coronary revascularization, compared with controls with no eczema.
Increased cardiovascular risks also were seen in individuals whose atopic eczema was active more than half the time at follow-up. This group had a 37% greater risk of heart failure, 36% greater risk of unstable angina, and 19% greater risk of stroke, as well as significantly elevated risks of MI, atrial fibrillation, cardiovascular death, and coronary revascularization, compared with those without eczema.
Overall, atopic eczema contributed around 2.4% of the population-attributable risk for unstable angina, and 1.9% for heart failure (the highest population attributable risks). Ethnicity or high-dose corticosteroid use did not significantly impact outcomes.
Richard J. Silverwood, PhD, from the London School of Hygiene and Tropical Medicine, and his coauthors wrote that previous work examining the relationship between atopic eczema and cardiovascular disease had shown inconsistent outcomes, with some studies even pointing to a possible protective effect of mild atopic eczema.
“Mechanistic work suggests that atopic eczema may be associated with increased platelet activation and decreased fibrinolysis, which may increase the risk of clotting, though a recent study found no association with metabolite levels,” the authors wrote.
They noted that the strengths of their study were that it was largest to examine the association between atopic eczema and cardiovascular risk, and that they had access to data on body mass index, smoking, and severe alcohol use for most of the study population, which enabled them to adjust for these potential mediators.
“Consideration should be given to developing prevention strategies to reduce the risk of cardiovascular disease among patients with severe or predominantly active atopic eczema, including awareness of and screening for conventional cardiovascular risk factors by those providing clinical care,” they wrote.
The study was supported by the Wellcome Trust, and no relevant conflicts of interest were declared.
SOURCE: Silverwood R et al. BMJ 2018 May 23;361:k1786. doi: 10.1136/bmj.k1786.
FROM THE BMJ
Key clinical point: Severe atopic eczema may be associated with a significantly increased risk of cardiovascular disease.
Major finding: Individuals with severe atopic eczema were at increased for cardiovascular disease, including a 67% greater risk of heart failure.
Study details: A population-based case-control cohort study in 387,439 patients with atopic eczema, compared with more than 1 million controls.
Disclosures: The study was supported by the Wellcome Trust, and no relevant conflicts of interest were declared.
Source: Silverwood R et al. BMJ. 2018 May 23;361:k1786.
CBC values linked to CVD risk in psoriasis
ORLANDO – conducted by researchers at Case Western Reserve University, Cleveland.*
It’s generally accepted that psoriasis increases the risk of cardiovascular disease (CVD), but it’s not clear who’s most at risk. “We really wanted to find something that is cheap and easy to risk stratify these patients” said lead investigator Rosalynn Conic, MD, of Case Western’s department of dermatology.

What they found was “very impressive, for sure,” Dr. Conic said at the International Investigative Dermatology meeting.
The incidence of MI was highest among the 1,920 patients (5%) with elevated RDW and MPV (odds ratio, 3.4; 95% confidence interval, 2.7-4.2; P less than .001), followed by the 7,060 (18%) patients with high RDW and normal MPV (OR, 2.4; 95% CI, 2.1-2.8; P less than .001), as compared with normal/low MPV and RDW patients.
Elevated RDW or elevated RDW plus MPV increased the odds of atrial fibrillation, coronary artery disease, heart failure, and peripheral vascular disease anywhere from 2 to 8.3 times (P less than .001). Among psoriatic arthritis patients, elevated RDW almost doubled the risk of MI (OR, 1.8; P less than .001). Results were adjusted for age, gender, and hypertension.
In a subanalysis of treatment effects, 4 of 23 psoriasis patients at Case Western had elevated RDWs at baseline. Values normalized in the three patients who achieved a 75% reduction in the Psoriasis Area and Severity Index score after about a year of systemic treatment.
“We aim to validate [the study results] with a Veterans Administration data set,” Dr. Conic said. If it pans out, “one use would be to send [patients with elevated values] to a cardiologist earlier” so other CVD risk factors can be monitored and treated. The findings also add to the case for good control, she noted.
Systemic inflammation is the common denominator between the blood value elevations and CVD. The same inflammatory cytokines that cause skin problems in psoriasis also stimulate bone marrow to release immature red blood cells, which are larger than mature cells, leading to an increased RDW. Similarly, elevated MPV indicates a higher number of larger, younger platelets in the blood.
“It’s probably something along those lines, but I think we need to go back to basic science and really figure it out,” Dr. Conic said.
Patients were 18-65 years old. The study excluded patients with diabetes, Crohn’s disease, RA, and generalized atherosclerosis.
The National Institutes of Health funded the work. Dr. Conic reported no relevant financial disclosures.
*This article was updated on May 30, 2018.
SOURCE: Conic R et al. IID 2018, Abstract 550.
ORLANDO – conducted by researchers at Case Western Reserve University, Cleveland.*
It’s generally accepted that psoriasis increases the risk of cardiovascular disease (CVD), but it’s not clear who’s most at risk. “We really wanted to find something that is cheap and easy to risk stratify these patients” said lead investigator Rosalynn Conic, MD, of Case Western’s department of dermatology.
What they found was “very impressive, for sure,” Dr. Conic said at the International Investigative Dermatology meeting.
The incidence of MI was highest among the 1,920 patients (5%) with elevated RDW and MPV (odds ratio, 3.4; 95% confidence interval, 2.7-4.2; P less than .001), followed by the 7,060 (18%) patients with high RDW and normal MPV (OR, 2.4; 95% CI, 2.1-2.8; P less than .001), as compared with normal/low MPV and RDW patients.
Elevated RDW or elevated RDW plus MPV increased the odds of atrial fibrillation, coronary artery disease, heart failure, and peripheral vascular disease anywhere from 2 to 8.3 times (P less than .001). Among psoriatic arthritis patients, elevated RDW almost doubled the risk of MI (OR, 1.8; P less than .001). Results were adjusted for age, gender, and hypertension.
In a subanalysis of treatment effects, 4 of 23 psoriasis patients at Case Western had elevated RDWs at baseline. Values normalized in the three patients who achieved a 75% reduction in the Psoriasis Area and Severity Index score after about a year of systemic treatment.
“We aim to validate [the study results] with a Veterans Administration data set,” Dr. Conic said. If it pans out, “one use would be to send [patients with elevated values] to a cardiologist earlier” so other CVD risk factors can be monitored and treated. The findings also add to the case for good control, she noted.
Systemic inflammation is the common denominator between the blood value elevations and CVD. The same inflammatory cytokines that cause skin problems in psoriasis also stimulate bone marrow to release immature red blood cells, which are larger than mature cells, leading to an increased RDW. Similarly, elevated MPV indicates a higher number of larger, younger platelets in the blood.
“It’s probably something along those lines, but I think we need to go back to basic science and really figure it out,” Dr. Conic said.
Patients were 18-65 years old. The study excluded patients with diabetes, Crohn’s disease, RA, and generalized atherosclerosis.
The National Institutes of Health funded the work. Dr. Conic reported no relevant financial disclosures.
*This article was updated on May 30, 2018.
SOURCE: Conic R et al. IID 2018, Abstract 550.
ORLANDO – conducted by researchers at Case Western Reserve University, Cleveland.*
It’s generally accepted that psoriasis increases the risk of cardiovascular disease (CVD), but it’s not clear who’s most at risk. “We really wanted to find something that is cheap and easy to risk stratify these patients” said lead investigator Rosalynn Conic, MD, of Case Western’s department of dermatology.
What they found was “very impressive, for sure,” Dr. Conic said at the International Investigative Dermatology meeting.
The incidence of MI was highest among the 1,920 patients (5%) with elevated RDW and MPV (odds ratio, 3.4; 95% confidence interval, 2.7-4.2; P less than .001), followed by the 7,060 (18%) patients with high RDW and normal MPV (OR, 2.4; 95% CI, 2.1-2.8; P less than .001), as compared with normal/low MPV and RDW patients.
Elevated RDW or elevated RDW plus MPV increased the odds of atrial fibrillation, coronary artery disease, heart failure, and peripheral vascular disease anywhere from 2 to 8.3 times (P less than .001). Among psoriatic arthritis patients, elevated RDW almost doubled the risk of MI (OR, 1.8; P less than .001). Results were adjusted for age, gender, and hypertension.
In a subanalysis of treatment effects, 4 of 23 psoriasis patients at Case Western had elevated RDWs at baseline. Values normalized in the three patients who achieved a 75% reduction in the Psoriasis Area and Severity Index score after about a year of systemic treatment.
“We aim to validate [the study results] with a Veterans Administration data set,” Dr. Conic said. If it pans out, “one use would be to send [patients with elevated values] to a cardiologist earlier” so other CVD risk factors can be monitored and treated. The findings also add to the case for good control, she noted.
Systemic inflammation is the common denominator between the blood value elevations and CVD. The same inflammatory cytokines that cause skin problems in psoriasis also stimulate bone marrow to release immature red blood cells, which are larger than mature cells, leading to an increased RDW. Similarly, elevated MPV indicates a higher number of larger, younger platelets in the blood.
“It’s probably something along those lines, but I think we need to go back to basic science and really figure it out,” Dr. Conic said.
Patients were 18-65 years old. The study excluded patients with diabetes, Crohn’s disease, RA, and generalized atherosclerosis.
The National Institutes of Health funded the work. Dr. Conic reported no relevant financial disclosures.
*This article was updated on May 30, 2018.
SOURCE: Conic R et al. IID 2018, Abstract 550.
REPORTING FROM IID 2018
Key clinical point: Elevated red blood cell distribution width and mean platelet volume might identify psoriasis patients at risk for cardiovascular disease.
Major finding: The incidence of MI was highest among the 1,920 patients with elevated red cell distribution width and mean platelet volume (odds ratio, 3.4; 95% confidence interval, 2.7-4.2; P less than .001).
Study details: A database review of 39,510 patients with psoriasis.
Disclosures: The National Institutes of Health funded the work. The lead investigator had no disclosures to report.
Source: Conic R et al. IID 2018, Abstract 550.
Atopic dermatitis severity reduced by topical microbiome treatment
The Beginning Assessment of Cutaneous Treatment Efficacy of Roseomonas in Atopic Dermatitis trial; BACTERiAD I/II study, an open-label phase I/II trial, first looked at the therapeutic use of R. mucosa in 10 adults aged 18 years or older. Three sucrose mixtures with increasing doses of live R. mucosa bacteria were topically applied to two body areas – the antecubital fossae and a body surface of their choice – twice per week for 2 weeks per dose. At 6 weeks, the patients stopped using the mixtures and followed a 4-week washout phase.
Treatment was found to reduce mean antecubital SCORAD (SCORing Atopic Dermatitis) scores by 59.8%. Reduction in pruritus was even more pronounced, with a mean decrease of 78.5%. Treating the hands did not improve disease severity, even in patients whose symptoms improved in other body areas. One explanation may be the increased exposure of the hands to topical antimicrobials and environmental exposures, the researchers noted.
With the success in the adult cohort, the researchers enrolled five children aged 7-17 years in the study. These patients were treated twice weekly for 16 weeks. The pediatric patients experienced a mean decrease of 70.3% in their SCORAD scores. The mean decrease in pruritis was 78.8%.
All adults who responded continued to report improved symptoms after the washout period. The pediatric patients are now being evaluated in a washout period.
Four patients did not respond; three of them had a family history of AD persisting into adulthood. “The association between these complex medical histories and the lack of clinical response suggests that differences in heritable host and/or microbial factors may impact treatment responses,” wrote Ian A. Myles, MD, and his colleagues.
“Overall, our findings suggest the safety of topical R. mucosa therapy and justify continuation of our ongoing trial to assess safety and activity in a pediatric cohort of patients with AD. These studies will additionally assess changes in host serum markers, skin metabolomics, and the skin microbiota by culture and genomic methods.”
The researchers noted that expanding to the pediatric population will deepen understanding of topical microbiome transplantation and lay the foundation for placebo-controlled trials to assess efficacy.
This work was supported by the Intramural Research Program of the National Institutes of Allergy and Infectious Diseases and the National Institutes of Health. The researchers had no disclosures.
SOURCE: Myles IA et al. JCI Insight. 2018 May 3. doi: 10.1172/jci.insight.120608.
The Beginning Assessment of Cutaneous Treatment Efficacy of Roseomonas in Atopic Dermatitis trial; BACTERiAD I/II study, an open-label phase I/II trial, first looked at the therapeutic use of R. mucosa in 10 adults aged 18 years or older. Three sucrose mixtures with increasing doses of live R. mucosa bacteria were topically applied to two body areas – the antecubital fossae and a body surface of their choice – twice per week for 2 weeks per dose. At 6 weeks, the patients stopped using the mixtures and followed a 4-week washout phase.
Treatment was found to reduce mean antecubital SCORAD (SCORing Atopic Dermatitis) scores by 59.8%. Reduction in pruritus was even more pronounced, with a mean decrease of 78.5%. Treating the hands did not improve disease severity, even in patients whose symptoms improved in other body areas. One explanation may be the increased exposure of the hands to topical antimicrobials and environmental exposures, the researchers noted.
With the success in the adult cohort, the researchers enrolled five children aged 7-17 years in the study. These patients were treated twice weekly for 16 weeks. The pediatric patients experienced a mean decrease of 70.3% in their SCORAD scores. The mean decrease in pruritis was 78.8%.
All adults who responded continued to report improved symptoms after the washout period. The pediatric patients are now being evaluated in a washout period.
Four patients did not respond; three of them had a family history of AD persisting into adulthood. “The association between these complex medical histories and the lack of clinical response suggests that differences in heritable host and/or microbial factors may impact treatment responses,” wrote Ian A. Myles, MD, and his colleagues.
“Overall, our findings suggest the safety of topical R. mucosa therapy and justify continuation of our ongoing trial to assess safety and activity in a pediatric cohort of patients with AD. These studies will additionally assess changes in host serum markers, skin metabolomics, and the skin microbiota by culture and genomic methods.”
The researchers noted that expanding to the pediatric population will deepen understanding of topical microbiome transplantation and lay the foundation for placebo-controlled trials to assess efficacy.
This work was supported by the Intramural Research Program of the National Institutes of Allergy and Infectious Diseases and the National Institutes of Health. The researchers had no disclosures.
SOURCE: Myles IA et al. JCI Insight. 2018 May 3. doi: 10.1172/jci.insight.120608.
The Beginning Assessment of Cutaneous Treatment Efficacy of Roseomonas in Atopic Dermatitis trial; BACTERiAD I/II study, an open-label phase I/II trial, first looked at the therapeutic use of R. mucosa in 10 adults aged 18 years or older. Three sucrose mixtures with increasing doses of live R. mucosa bacteria were topically applied to two body areas – the antecubital fossae and a body surface of their choice – twice per week for 2 weeks per dose. At 6 weeks, the patients stopped using the mixtures and followed a 4-week washout phase.
Treatment was found to reduce mean antecubital SCORAD (SCORing Atopic Dermatitis) scores by 59.8%. Reduction in pruritus was even more pronounced, with a mean decrease of 78.5%. Treating the hands did not improve disease severity, even in patients whose symptoms improved in other body areas. One explanation may be the increased exposure of the hands to topical antimicrobials and environmental exposures, the researchers noted.
With the success in the adult cohort, the researchers enrolled five children aged 7-17 years in the study. These patients were treated twice weekly for 16 weeks. The pediatric patients experienced a mean decrease of 70.3% in their SCORAD scores. The mean decrease in pruritis was 78.8%.
All adults who responded continued to report improved symptoms after the washout period. The pediatric patients are now being evaluated in a washout period.
Four patients did not respond; three of them had a family history of AD persisting into adulthood. “The association between these complex medical histories and the lack of clinical response suggests that differences in heritable host and/or microbial factors may impact treatment responses,” wrote Ian A. Myles, MD, and his colleagues.
“Overall, our findings suggest the safety of topical R. mucosa therapy and justify continuation of our ongoing trial to assess safety and activity in a pediatric cohort of patients with AD. These studies will additionally assess changes in host serum markers, skin metabolomics, and the skin microbiota by culture and genomic methods.”
The researchers noted that expanding to the pediatric population will deepen understanding of topical microbiome transplantation and lay the foundation for placebo-controlled trials to assess efficacy.
This work was supported by the Intramural Research Program of the National Institutes of Allergy and Infectious Diseases and the National Institutes of Health. The researchers had no disclosures.
SOURCE: Myles IA et al. JCI Insight. 2018 May 3. doi: 10.1172/jci.insight.120608.
FROM JCI INSIGHT
Key clinical point: Roseomonas mucosa reduces disease severity.
Major finding: There were reductions in SCORAD scores of 78.5% and 70.3% in the adult and pediatric cohorts, respectively.
Study details: Case study of 10 adult and 5 pediatric patients with atopic dermatitis.
Disclosures: No relevant financial disclosures were reported.
Source: Myles IA et al. JCI Insight. 2018 May 3. doi: 10.1172/jci.insight.120608.
VIDEO: Characteristic flora define intestinal microbiome in scleroderma
SANDESTIN, FLA. – Scleroderma patients appear to have a characteristic microbiome composition, which is consistent in samples taken around the world.
These patients showed decreased populations of beneficial commensal flora and increased populations of proinflammatory species, Elizabeth Volkmann, MD, said at the annual Congress of Clinical Rheumatology.
Furthermore, specific species seem to correlate with specific gastrointestinal symptoms, said Dr. Volkmann of the University of California, Los Angeles. “Features also unexpectedly overlap with the consortium typical for Crohn’s disease, a disease with both inflammatory and fibrosing phenotype,” she said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Her recent exploration of this topic included 17 patients with scleroderma and GI symptoms and 17 matched healthy controls (BMJ Open Gastro. 2017;3:e000134). Everyone underwent a bowel prep and colonoscopy, during which cecum and sigmoid mucosal lavage samples were obtained. Those samples underwent RNA sequencing.
In addition to quantifying the species present, Dr. Volkmann sought to associate populations with symptoms. The primary assessment tool was the GIT 2.0, which measures distention/bloating; diarrhea; fecal soilage; constipation; emotional well-being; and social functioning.
Similar to the findings in inflammatory disease states, scleroderma patients had decreased levels of commensal Clostridia, a class of Firmicutes that is established in early infancy and very important in the maintenance of gut homeostasis. They also showed a decreased proportion of Faecalibacterium, a genus with anti-inflammatory activity; this finding has been observed in patients with Crohn’s disease.
Patients also showed relative increases in pathobionts. These are potentially pathological organisms that, under normal circumstances, live symbiotically. Janet Chow, PhD, who coined the term in a 2011 paper, said these species are typically proinflammatory (Curr Opin Immunol. 2011 Aug; 23[4]:473-80).
“Organisms proposed as pathobionts are associated with chronic inflammatory conditions – unlike opportunistic pathogens, which often cause acute infections and are typically acquired from the environment or other parts of the body. In addition, pathobionts are innocuous to the host under normal conditions,” wrote Dr. Chow of the California Institute of Technology, Pasadena.
In Dr. Volkmann’s study, Bifidobacterium and Lactobacillus, which are usually reduced in proinflammatory disorders, were relatively abundant in patients, compared with controls.
She noted specific associations with both symptoms. Parabacteroides and Enterobacteriaceae were associated with increased constipation. Prevotella was associated with increased diarrhea and increased distention/bloating.
Her results are consistent with a Swedish study (Arthritis Res Ther. 2016 Nov 1;18[1]:278) and three Italian studies conducted in Rome, Milan, and Piacenza.
“It’s fascinating that we seem to be identifying a consistent microbiome profile for scleroderma patients,” Dr. Volkmann said.
Dr. Volkmann had no relevant financial disclosures.
SANDESTIN, FLA. – Scleroderma patients appear to have a characteristic microbiome composition, which is consistent in samples taken around the world.
These patients showed decreased populations of beneficial commensal flora and increased populations of proinflammatory species, Elizabeth Volkmann, MD, said at the annual Congress of Clinical Rheumatology.
Furthermore, specific species seem to correlate with specific gastrointestinal symptoms, said Dr. Volkmann of the University of California, Los Angeles. “Features also unexpectedly overlap with the consortium typical for Crohn’s disease, a disease with both inflammatory and fibrosing phenotype,” she said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Her recent exploration of this topic included 17 patients with scleroderma and GI symptoms and 17 matched healthy controls (BMJ Open Gastro. 2017;3:e000134). Everyone underwent a bowel prep and colonoscopy, during which cecum and sigmoid mucosal lavage samples were obtained. Those samples underwent RNA sequencing.
In addition to quantifying the species present, Dr. Volkmann sought to associate populations with symptoms. The primary assessment tool was the GIT 2.0, which measures distention/bloating; diarrhea; fecal soilage; constipation; emotional well-being; and social functioning.
Similar to the findings in inflammatory disease states, scleroderma patients had decreased levels of commensal Clostridia, a class of Firmicutes that is established in early infancy and very important in the maintenance of gut homeostasis. They also showed a decreased proportion of Faecalibacterium, a genus with anti-inflammatory activity; this finding has been observed in patients with Crohn’s disease.
Patients also showed relative increases in pathobionts. These are potentially pathological organisms that, under normal circumstances, live symbiotically. Janet Chow, PhD, who coined the term in a 2011 paper, said these species are typically proinflammatory (Curr Opin Immunol. 2011 Aug; 23[4]:473-80).
“Organisms proposed as pathobionts are associated with chronic inflammatory conditions – unlike opportunistic pathogens, which often cause acute infections and are typically acquired from the environment or other parts of the body. In addition, pathobionts are innocuous to the host under normal conditions,” wrote Dr. Chow of the California Institute of Technology, Pasadena.
In Dr. Volkmann’s study, Bifidobacterium and Lactobacillus, which are usually reduced in proinflammatory disorders, were relatively abundant in patients, compared with controls.
She noted specific associations with both symptoms. Parabacteroides and Enterobacteriaceae were associated with increased constipation. Prevotella was associated with increased diarrhea and increased distention/bloating.
Her results are consistent with a Swedish study (Arthritis Res Ther. 2016 Nov 1;18[1]:278) and three Italian studies conducted in Rome, Milan, and Piacenza.
“It’s fascinating that we seem to be identifying a consistent microbiome profile for scleroderma patients,” Dr. Volkmann said.
Dr. Volkmann had no relevant financial disclosures.
SANDESTIN, FLA. – Scleroderma patients appear to have a characteristic microbiome composition, which is consistent in samples taken around the world.
These patients showed decreased populations of beneficial commensal flora and increased populations of proinflammatory species, Elizabeth Volkmann, MD, said at the annual Congress of Clinical Rheumatology.
Furthermore, specific species seem to correlate with specific gastrointestinal symptoms, said Dr. Volkmann of the University of California, Los Angeles. “Features also unexpectedly overlap with the consortium typical for Crohn’s disease, a disease with both inflammatory and fibrosing phenotype,” she said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Her recent exploration of this topic included 17 patients with scleroderma and GI symptoms and 17 matched healthy controls (BMJ Open Gastro. 2017;3:e000134). Everyone underwent a bowel prep and colonoscopy, during which cecum and sigmoid mucosal lavage samples were obtained. Those samples underwent RNA sequencing.
In addition to quantifying the species present, Dr. Volkmann sought to associate populations with symptoms. The primary assessment tool was the GIT 2.0, which measures distention/bloating; diarrhea; fecal soilage; constipation; emotional well-being; and social functioning.
Similar to the findings in inflammatory disease states, scleroderma patients had decreased levels of commensal Clostridia, a class of Firmicutes that is established in early infancy and very important in the maintenance of gut homeostasis. They also showed a decreased proportion of Faecalibacterium, a genus with anti-inflammatory activity; this finding has been observed in patients with Crohn’s disease.
Patients also showed relative increases in pathobionts. These are potentially pathological organisms that, under normal circumstances, live symbiotically. Janet Chow, PhD, who coined the term in a 2011 paper, said these species are typically proinflammatory (Curr Opin Immunol. 2011 Aug; 23[4]:473-80).
“Organisms proposed as pathobionts are associated with chronic inflammatory conditions – unlike opportunistic pathogens, which often cause acute infections and are typically acquired from the environment or other parts of the body. In addition, pathobionts are innocuous to the host under normal conditions,” wrote Dr. Chow of the California Institute of Technology, Pasadena.
In Dr. Volkmann’s study, Bifidobacterium and Lactobacillus, which are usually reduced in proinflammatory disorders, were relatively abundant in patients, compared with controls.
She noted specific associations with both symptoms. Parabacteroides and Enterobacteriaceae were associated with increased constipation. Prevotella was associated with increased diarrhea and increased distention/bloating.
Her results are consistent with a Swedish study (Arthritis Res Ther. 2016 Nov 1;18[1]:278) and three Italian studies conducted in Rome, Milan, and Piacenza.
“It’s fascinating that we seem to be identifying a consistent microbiome profile for scleroderma patients,” Dr. Volkmann said.
Dr. Volkmann had no relevant financial disclosures.
REPORTING FROM CCR 18
VIDEO: Skin exam crucial in rheumatic diseases, expert says
SANDESTIN, FLA. – Even when you know a patient’s serology and hear their symptoms and think you have a bead on their rheumatic disease, you might not. It’s vital to check the skin in patients with rheumatic disease to be sure the right disease is being treated and that they don’t actually have a more severe condition that might progress suddenly if left unchecked, said Alisa Femia, MD, assistant professor of dermatology at the annual Congress of Clinical Rheumatology.
In a session filled with pearls for rheumatologists on what to look for on their patients’ skin to help guide diagnosis and treatment, she told the story of a woman whom a rheumatologist colleague had correctly diagnosed with dermatomyositis. She was started on prednisone and mycophenolate mofetil, but her skin disease did not clear.
After examining her skin, Dr. Femia became immediately concerned.
“Despite prednisone, despite mycophenolate, here not only does she have Gottron’s papules, but she has erosions within her Gottron’s papules,” Dr. Femia said. The woman also had erosions within papules on her palms.
These were telltale signs of MDA5-associated dermatomyositis, which studies have found to be linked with interstitial lung disease (J Am Acad Dermatol. 2011 Jul;65[1]:25-34). Under her care, these patients ideally undergo lung monitoring every 3 months, Dr. Femia said.
“That is a form of dermatomyositis that you cannot miss,” she said.
The effects of discoid lupus are another reason to take special care in skin examination. Once the disease, which involves a scaling of the skin, is obvious, there can be permanent aesthetic effects that could have been avoided with earlier detection and treatment, Dr. Femia said.
Clinicians should also be on the lookout for volume loss, or contour change, in discoid lupus patients, because that’s a sign of lupus panniculitis, which involves deeper lesions mainly to fatty areas such as the cheeks or thighs. The disease can progress fast, with sudden, massive loss of body volume, so therapy should be escalated quickly, she said.
“We want to treat these patients aggressively in order to avoid this.”
SOURCE: Femia A. CCR 2018.
SANDESTIN, FLA. – Even when you know a patient’s serology and hear their symptoms and think you have a bead on their rheumatic disease, you might not. It’s vital to check the skin in patients with rheumatic disease to be sure the right disease is being treated and that they don’t actually have a more severe condition that might progress suddenly if left unchecked, said Alisa Femia, MD, assistant professor of dermatology at the annual Congress of Clinical Rheumatology.
In a session filled with pearls for rheumatologists on what to look for on their patients’ skin to help guide diagnosis and treatment, she told the story of a woman whom a rheumatologist colleague had correctly diagnosed with dermatomyositis. She was started on prednisone and mycophenolate mofetil, but her skin disease did not clear.
After examining her skin, Dr. Femia became immediately concerned.
“Despite prednisone, despite mycophenolate, here not only does she have Gottron’s papules, but she has erosions within her Gottron’s papules,” Dr. Femia said. The woman also had erosions within papules on her palms.
These were telltale signs of MDA5-associated dermatomyositis, which studies have found to be linked with interstitial lung disease (J Am Acad Dermatol. 2011 Jul;65[1]:25-34). Under her care, these patients ideally undergo lung monitoring every 3 months, Dr. Femia said.
“That is a form of dermatomyositis that you cannot miss,” she said.
The effects of discoid lupus are another reason to take special care in skin examination. Once the disease, which involves a scaling of the skin, is obvious, there can be permanent aesthetic effects that could have been avoided with earlier detection and treatment, Dr. Femia said.
Clinicians should also be on the lookout for volume loss, or contour change, in discoid lupus patients, because that’s a sign of lupus panniculitis, which involves deeper lesions mainly to fatty areas such as the cheeks or thighs. The disease can progress fast, with sudden, massive loss of body volume, so therapy should be escalated quickly, she said.
“We want to treat these patients aggressively in order to avoid this.”
SOURCE: Femia A. CCR 2018.
SANDESTIN, FLA. – Even when you know a patient’s serology and hear their symptoms and think you have a bead on their rheumatic disease, you might not. It’s vital to check the skin in patients with rheumatic disease to be sure the right disease is being treated and that they don’t actually have a more severe condition that might progress suddenly if left unchecked, said Alisa Femia, MD, assistant professor of dermatology at the annual Congress of Clinical Rheumatology.
In a session filled with pearls for rheumatologists on what to look for on their patients’ skin to help guide diagnosis and treatment, she told the story of a woman whom a rheumatologist colleague had correctly diagnosed with dermatomyositis. She was started on prednisone and mycophenolate mofetil, but her skin disease did not clear.
After examining her skin, Dr. Femia became immediately concerned.
“Despite prednisone, despite mycophenolate, here not only does she have Gottron’s papules, but she has erosions within her Gottron’s papules,” Dr. Femia said. The woman also had erosions within papules on her palms.
These were telltale signs of MDA5-associated dermatomyositis, which studies have found to be linked with interstitial lung disease (J Am Acad Dermatol. 2011 Jul;65[1]:25-34). Under her care, these patients ideally undergo lung monitoring every 3 months, Dr. Femia said.
“That is a form of dermatomyositis that you cannot miss,” she said.
The effects of discoid lupus are another reason to take special care in skin examination. Once the disease, which involves a scaling of the skin, is obvious, there can be permanent aesthetic effects that could have been avoided with earlier detection and treatment, Dr. Femia said.
Clinicians should also be on the lookout for volume loss, or contour change, in discoid lupus patients, because that’s a sign of lupus panniculitis, which involves deeper lesions mainly to fatty areas such as the cheeks or thighs. The disease can progress fast, with sudden, massive loss of body volume, so therapy should be escalated quickly, she said.
“We want to treat these patients aggressively in order to avoid this.”
SOURCE: Femia A. CCR 2018.
EXPERT ANALYSIS AT CCR 18
Guidelines-based intervention improves pediatrician management of acne
A guidelines-based educational program on treating acne in teenagers has led to significant improvements in pediatricians’ management of the condition and decreased referrals to dermatologists, new research suggests.
A research letter published online May in the Journal of the American Academy of Dermatology described the results of a study involving 116 pediatricians, who participated in an educational program, including brief live sessions, on how to manage acne in teenagers.
After 4 months, researchers saw that acne-coded visits to pediatricians increased by 18% (P less than .001), but this did not translate to more work for the physicians involved; instead, three-quarters of those involved said the treatment process involved “minimal to no work.”
At the same time, the intervention was associated with a 26% decrease in the percentage of acne referrals to dermatologists, reported Jenna Borok of the Rady Children’s Hospital in San Diego, and her coauthors.
The researchers saw a fivefold increase in the likelihood of pediatricians prescribing retinoids (P = .003), after controlling for confounding factors such as sex and insurance status, and significantly less topical clindamycin being prescribed.
The study was initiated to address what the authors described as a “practice gap” between pediatricians treating acne, compared with dermatologists treating acne, which included significantly lower prescribing rates of topical retinoids among pediatricians.
Ms. Borok and her coauthors wrote that their educational program and prescribing tool aimed to address this practice gap without increasing the workload for pediatricians or dermatologists. “Adherence to guidelines by pediatricians has the potential to improve treatment provided in the primary care setting, better patient satisfaction, and allow greater access to dermatologists and pediatric dermatologists for patients with more severe acne and other conditions.”
Acknowledging that the study took place over a relatively short period of time, the authors said future research would examine the impact of the educational program and ordering tool on patient acne outcomes.
No funding or conflicts of interest were declared.
SOURCE: Borok J et al. J Am Acad Dermatol. 2018 May 9. doi: 10.1016/j.jaad.2018.04.055.
A guidelines-based educational program on treating acne in teenagers has led to significant improvements in pediatricians’ management of the condition and decreased referrals to dermatologists, new research suggests.
A research letter published online May in the Journal of the American Academy of Dermatology described the results of a study involving 116 pediatricians, who participated in an educational program, including brief live sessions, on how to manage acne in teenagers.
After 4 months, researchers saw that acne-coded visits to pediatricians increased by 18% (P less than .001), but this did not translate to more work for the physicians involved; instead, three-quarters of those involved said the treatment process involved “minimal to no work.”
At the same time, the intervention was associated with a 26% decrease in the percentage of acne referrals to dermatologists, reported Jenna Borok of the Rady Children’s Hospital in San Diego, and her coauthors.
The researchers saw a fivefold increase in the likelihood of pediatricians prescribing retinoids (P = .003), after controlling for confounding factors such as sex and insurance status, and significantly less topical clindamycin being prescribed.
The study was initiated to address what the authors described as a “practice gap” between pediatricians treating acne, compared with dermatologists treating acne, which included significantly lower prescribing rates of topical retinoids among pediatricians.
Ms. Borok and her coauthors wrote that their educational program and prescribing tool aimed to address this practice gap without increasing the workload for pediatricians or dermatologists. “Adherence to guidelines by pediatricians has the potential to improve treatment provided in the primary care setting, better patient satisfaction, and allow greater access to dermatologists and pediatric dermatologists for patients with more severe acne and other conditions.”
Acknowledging that the study took place over a relatively short period of time, the authors said future research would examine the impact of the educational program and ordering tool on patient acne outcomes.
No funding or conflicts of interest were declared.
SOURCE: Borok J et al. J Am Acad Dermatol. 2018 May 9. doi: 10.1016/j.jaad.2018.04.055.
A guidelines-based educational program on treating acne in teenagers has led to significant improvements in pediatricians’ management of the condition and decreased referrals to dermatologists, new research suggests.
A research letter published online May in the Journal of the American Academy of Dermatology described the results of a study involving 116 pediatricians, who participated in an educational program, including brief live sessions, on how to manage acne in teenagers.
After 4 months, researchers saw that acne-coded visits to pediatricians increased by 18% (P less than .001), but this did not translate to more work for the physicians involved; instead, three-quarters of those involved said the treatment process involved “minimal to no work.”
At the same time, the intervention was associated with a 26% decrease in the percentage of acne referrals to dermatologists, reported Jenna Borok of the Rady Children’s Hospital in San Diego, and her coauthors.
The researchers saw a fivefold increase in the likelihood of pediatricians prescribing retinoids (P = .003), after controlling for confounding factors such as sex and insurance status, and significantly less topical clindamycin being prescribed.
The study was initiated to address what the authors described as a “practice gap” between pediatricians treating acne, compared with dermatologists treating acne, which included significantly lower prescribing rates of topical retinoids among pediatricians.
Ms. Borok and her coauthors wrote that their educational program and prescribing tool aimed to address this practice gap without increasing the workload for pediatricians or dermatologists. “Adherence to guidelines by pediatricians has the potential to improve treatment provided in the primary care setting, better patient satisfaction, and allow greater access to dermatologists and pediatric dermatologists for patients with more severe acne and other conditions.”
Acknowledging that the study took place over a relatively short period of time, the authors said future research would examine the impact of the educational program and ordering tool on patient acne outcomes.
No funding or conflicts of interest were declared.
SOURCE: Borok J et al. J Am Acad Dermatol. 2018 May 9. doi: 10.1016/j.jaad.2018.04.055.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point:
Major finding: An education program for pediatricians on acne treatment increased retinoid prescribing but decreased referrals to dermatologists.
Study details: Interventional study in 116 pediatricians.
Disclosures: No funding or conflicts of interest were declared.
Source: Borok J et al. J Am Acad Dermatol. 2018 May 9. doi: 10.1016/j.jaad.2018.04.055.

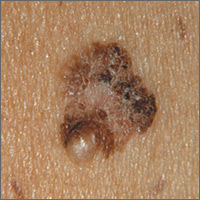
Changing mole on arm
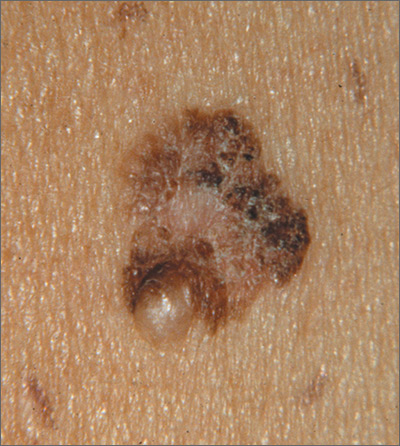
The FP suspected that this was a melanoma.
He thought through the ABCDEs of melanoma and saw that it was Asymmetric, had an irregular Border, had varied Colors, the Diameter was larger than 6 mm, and it was Evolving. The FP also noted that one area was elevated and another area (the center) seemed to be regressing. Using his dermatoscope, he noted strong evidence of regression in the center and an “atypical network.” He told the patient that this was very suspicious for melanoma and recommended a skin biopsy without delay. The patient agreed and after local anesthesia with lidocaine with epinephrine, a saucerization biopsy was performed using a DermaBlade. (See the Watch & Learn video on “Shave biopsy.”) The FP easily removed all of the visible tumor with the saucerization (deep shave). The bleeding was stopped with topical aluminum chloride, and the specimen was sent in formalin to the pathologist. The pathology report came back as a melanoma of 2.1 mm depth arising in a pre-existing nevus.
The patient was referred to a surgical oncologist for sentinel lymph node biopsy and excision with wide margins.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Congenital nevi. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine, 2nd ed. New York, NY: McGraw-Hill; 2013:953-957.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
The FP suspected that this was a melanoma.
He thought through the ABCDEs of melanoma and saw that it was Asymmetric, had an irregular Border, had varied Colors, the Diameter was larger than 6 mm, and it was Evolving. The FP also noted that one area was elevated and another area (the center) seemed to be regressing. Using his dermatoscope, he noted strong evidence of regression in the center and an “atypical network.” He told the patient that this was very suspicious for melanoma and recommended a skin biopsy without delay. The patient agreed and after local anesthesia with lidocaine with epinephrine, a saucerization biopsy was performed using a DermaBlade. (See the Watch & Learn video on “Shave biopsy.”) The FP easily removed all of the visible tumor with the saucerization (deep shave). The bleeding was stopped with topical aluminum chloride, and the specimen was sent in formalin to the pathologist. The pathology report came back as a melanoma of 2.1 mm depth arising in a pre-existing nevus.
The patient was referred to a surgical oncologist for sentinel lymph node biopsy and excision with wide margins.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Congenital nevi. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine, 2nd ed. New York, NY: McGraw-Hill; 2013:953-957.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
The FP suspected that this was a melanoma.
He thought through the ABCDEs of melanoma and saw that it was Asymmetric, had an irregular Border, had varied Colors, the Diameter was larger than 6 mm, and it was Evolving. The FP also noted that one area was elevated and another area (the center) seemed to be regressing. Using his dermatoscope, he noted strong evidence of regression in the center and an “atypical network.” He told the patient that this was very suspicious for melanoma and recommended a skin biopsy without delay. The patient agreed and after local anesthesia with lidocaine with epinephrine, a saucerization biopsy was performed using a DermaBlade. (See the Watch & Learn video on “Shave biopsy.”) The FP easily removed all of the visible tumor with the saucerization (deep shave). The bleeding was stopped with topical aluminum chloride, and the specimen was sent in formalin to the pathologist. The pathology report came back as a melanoma of 2.1 mm depth arising in a pre-existing nevus.
The patient was referred to a surgical oncologist for sentinel lymph node biopsy and excision with wide margins.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Congenital nevi. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine, 2nd ed. New York, NY: McGraw-Hill; 2013:953-957.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
Hyperpigmentation, paraparesis are signs of vitamin B12 deficiency
Vitamin B12 deficiency can cause skin hyperpigmentation and partial paralysis, but these issues can be easily treated early on with vitamin B12 shots, said Ashish Agarwal, MD, and his colleagues at the Postgraduate Institute of Medical Education and Research in Chandigarh, India.
A 6-year-old boy, who had been previously healthy, presented with darkening of his hands and feet over a 4-month period. It also was noted that the skin on his palms and soles was thin and shiny. His walking gait had become abnormal in the previous 2 weeks; his legs were stiff when he walked, which caused him to fall and led to difficulty climbing stairs. The boy had no personal or family history of muscle issues or neurological issues. The boy’s personal history revealed that he ate a vegetarian diet.
A clinical diagnosis was made of megaloblastic anemia with subacute degeneration of the cord caused by vitamin B12 deficiency, a diagnosis not uncommon among vegetarians. The boy was started on daily intramuscular injections of B12 for 2 weeks, followed by weekly injections for a month. Monthly injections then were administered for the next 2 months. In the first few weeks, the hyperpigmentation began improving. At his 4-month follow-up, the boy was asymptomatic with reversal of the hyperpigmentation.
Dr. Agarwal and his associates concluded that skin darkening is an important clue toward underlying hematologic and neurologic manifestations of B12 deficiency.
SOURCE: Agarwal A et al. J Pediatr. 2018. doi: 10.1016/j.jpeds.2018.03.073.
Vitamin B12 deficiency can cause skin hyperpigmentation and partial paralysis, but these issues can be easily treated early on with vitamin B12 shots, said Ashish Agarwal, MD, and his colleagues at the Postgraduate Institute of Medical Education and Research in Chandigarh, India.
A 6-year-old boy, who had been previously healthy, presented with darkening of his hands and feet over a 4-month period. It also was noted that the skin on his palms and soles was thin and shiny. His walking gait had become abnormal in the previous 2 weeks; his legs were stiff when he walked, which caused him to fall and led to difficulty climbing stairs. The boy had no personal or family history of muscle issues or neurological issues. The boy’s personal history revealed that he ate a vegetarian diet.
A clinical diagnosis was made of megaloblastic anemia with subacute degeneration of the cord caused by vitamin B12 deficiency, a diagnosis not uncommon among vegetarians. The boy was started on daily intramuscular injections of B12 for 2 weeks, followed by weekly injections for a month. Monthly injections then were administered for the next 2 months. In the first few weeks, the hyperpigmentation began improving. At his 4-month follow-up, the boy was asymptomatic with reversal of the hyperpigmentation.
Dr. Agarwal and his associates concluded that skin darkening is an important clue toward underlying hematologic and neurologic manifestations of B12 deficiency.
SOURCE: Agarwal A et al. J Pediatr. 2018. doi: 10.1016/j.jpeds.2018.03.073.
Vitamin B12 deficiency can cause skin hyperpigmentation and partial paralysis, but these issues can be easily treated early on with vitamin B12 shots, said Ashish Agarwal, MD, and his colleagues at the Postgraduate Institute of Medical Education and Research in Chandigarh, India.
A 6-year-old boy, who had been previously healthy, presented with darkening of his hands and feet over a 4-month period. It also was noted that the skin on his palms and soles was thin and shiny. His walking gait had become abnormal in the previous 2 weeks; his legs were stiff when he walked, which caused him to fall and led to difficulty climbing stairs. The boy had no personal or family history of muscle issues or neurological issues. The boy’s personal history revealed that he ate a vegetarian diet.
A clinical diagnosis was made of megaloblastic anemia with subacute degeneration of the cord caused by vitamin B12 deficiency, a diagnosis not uncommon among vegetarians. The boy was started on daily intramuscular injections of B12 for 2 weeks, followed by weekly injections for a month. Monthly injections then were administered for the next 2 months. In the first few weeks, the hyperpigmentation began improving. At his 4-month follow-up, the boy was asymptomatic with reversal of the hyperpigmentation.
Dr. Agarwal and his associates concluded that skin darkening is an important clue toward underlying hematologic and neurologic manifestations of B12 deficiency.
SOURCE: Agarwal A et al. J Pediatr. 2018. doi: 10.1016/j.jpeds.2018.03.073.
FROM THE JOURNAL OF PEDIATRICS
Pain relievers, bed rest may be sufficient to manage PEH
Although skin biopsy and the “presence of deep dermal mixed infiltrate with abundant neutrophils surrounding eccrine sweat glands” is considered the preferred method for diagnosing palmoplantar eccrine hidradenitis (PEH), Paola Piccini, MD, and her colleagues at the University of Florence (Italy) caution that biopsy frequently is not needed.
In the days prior to the appearance of erythematous and painful nodules on the soles of his feet, a healthy 8-year-old boy sustained “thermal and mechanical trauma playing football and cycling,” that made walking difficult. The week prior to the injury, he had complained of diarrhea in the absence of fever.
Given results of testing and the patient’s overall good health, he received a diagnosis of PEH. Dr. Piccini and her colleagues chose not to biopsy the nodules because they typically resolve on their own within a few weeks. Instead, he was prescribed pain relievers and bed rest. Within 2 weeks, the nodules were completely healed, and no further relapse was reported, the authors noted in the Journal of Pediatrics.
All previous case studies cited in the literature reported complete resolution without treatment within 4 weeks, said Dr. Piccini and her colleagues. They added that correct diagnosis is key to avoiding inappropriate medical treatments given the benign course of PEH.
Common presenting risk factors tend to include local thermal and mechanical trauma plus intense physical activity and recent infection. It is these risk factors that cause rupture of the eccrine gland and resulting infiltration of neutrophils to the site.
Conditions that share common symptoms with PEH include erythema multiforme, nodular erythema, cellulitis, and viral infections.
No disclosures were noted.
SOURCE: Piccini, P et al. J. Pediatr. 2018. doi: 10.1016/j.peds.2018.03.017.
Although skin biopsy and the “presence of deep dermal mixed infiltrate with abundant neutrophils surrounding eccrine sweat glands” is considered the preferred method for diagnosing palmoplantar eccrine hidradenitis (PEH), Paola Piccini, MD, and her colleagues at the University of Florence (Italy) caution that biopsy frequently is not needed.
In the days prior to the appearance of erythematous and painful nodules on the soles of his feet, a healthy 8-year-old boy sustained “thermal and mechanical trauma playing football and cycling,” that made walking difficult. The week prior to the injury, he had complained of diarrhea in the absence of fever.
Given results of testing and the patient’s overall good health, he received a diagnosis of PEH. Dr. Piccini and her colleagues chose not to biopsy the nodules because they typically resolve on their own within a few weeks. Instead, he was prescribed pain relievers and bed rest. Within 2 weeks, the nodules were completely healed, and no further relapse was reported, the authors noted in the Journal of Pediatrics.
All previous case studies cited in the literature reported complete resolution without treatment within 4 weeks, said Dr. Piccini and her colleagues. They added that correct diagnosis is key to avoiding inappropriate medical treatments given the benign course of PEH.
Common presenting risk factors tend to include local thermal and mechanical trauma plus intense physical activity and recent infection. It is these risk factors that cause rupture of the eccrine gland and resulting infiltration of neutrophils to the site.
Conditions that share common symptoms with PEH include erythema multiforme, nodular erythema, cellulitis, and viral infections.
No disclosures were noted.
SOURCE: Piccini, P et al. J. Pediatr. 2018. doi: 10.1016/j.peds.2018.03.017.
Although skin biopsy and the “presence of deep dermal mixed infiltrate with abundant neutrophils surrounding eccrine sweat glands” is considered the preferred method for diagnosing palmoplantar eccrine hidradenitis (PEH), Paola Piccini, MD, and her colleagues at the University of Florence (Italy) caution that biopsy frequently is not needed.
In the days prior to the appearance of erythematous and painful nodules on the soles of his feet, a healthy 8-year-old boy sustained “thermal and mechanical trauma playing football and cycling,” that made walking difficult. The week prior to the injury, he had complained of diarrhea in the absence of fever.
Given results of testing and the patient’s overall good health, he received a diagnosis of PEH. Dr. Piccini and her colleagues chose not to biopsy the nodules because they typically resolve on their own within a few weeks. Instead, he was prescribed pain relievers and bed rest. Within 2 weeks, the nodules were completely healed, and no further relapse was reported, the authors noted in the Journal of Pediatrics.
All previous case studies cited in the literature reported complete resolution without treatment within 4 weeks, said Dr. Piccini and her colleagues. They added that correct diagnosis is key to avoiding inappropriate medical treatments given the benign course of PEH.
Common presenting risk factors tend to include local thermal and mechanical trauma plus intense physical activity and recent infection. It is these risk factors that cause rupture of the eccrine gland and resulting infiltration of neutrophils to the site.
Conditions that share common symptoms with PEH include erythema multiforme, nodular erythema, cellulitis, and viral infections.
No disclosures were noted.
SOURCE: Piccini, P et al. J. Pediatr. 2018. doi: 10.1016/j.peds.2018.03.017.
FROM THE JOURNAL OF PEDIATRICS
Key clinical point: Complete resolution within 4 weeks is common without treatment.
Major finding: .
Study details: Case study.
Disclosures: No disclosures were noted.
Source: Lund, E et al. Ped. Dermatol. 2018. doi: 10.1111/pde.13508.