User login
Denosumab favored over alendronate for BMD protection in glucocorticoid-induced osteoporosis
Denosumab boosted bone mineral density (BMD) over 12 months to a greater extent than did alendronate in a randomized, 12-month study. The investigator-initiated research compared BMD at the lumbar spine and elsewhere among people with systemic lupus erythematosus (SLE) and other autoimmune conditions. Long-term glucocorticoid therapy places some people in this group at higher risk for adverse effects of bone density loss.

“Glucocorticoids remain the mainstay of treatment of rheumatic diseases, but [they are] a major risk factor for osteoporosis and fracture,” study author Chi Chiu Mok, MD, said in an interview.
Compared with baseline, adults randomly assigned to denosumab had a 3.5% increase in lumbar spine BMD at 12 months, compared with 2.5% among those taking alendronate, a significant difference. Dr. Mok, a consultant and honorary associate professor in the department of medicine and nuclear medicine at Tuen Mun Hospital in Hong Kong, presented the study results at the virtual annual meeting of the American College of Rheumatology.
“Given the knowledge that denosumab is more effective than alendronate in raising spinal BMD in chronic users of GCs without increasing adverse events, this drug may be considered as an alternative first-line therapy in higher-risk patients and in those who are contraindicated for the oral bisphosphonates,” he said.
Cost considerations
Denosumab is a human monoclonal antibody administered as a subcutaneous injection, available under the brand names Prolia and Xgeva. Alendronate is an oral agent available as both generic and brand name formulations.
“Yes, denosumab is more expensive, more costly than oral alendronate, but our study shows efficacy is better for steroid users,” Dr. Mok said in answer to a question about cost disparity between the two agents during his presentation at the meeting. “For patients who are contraindicated or have low compliance for bisphosphonate, or are high-risk patients, I recommend first-line use of denosumab.”
Researchers previously studied these agents, including a smaller study by Dr. Mok and colleagues that showed a BMD benefit after switching people on an oral bisphosphonate to denosumab. However, he said, “There is a paucity of data regarding comparative efficacy of denosumab and the bisphosphonates in long-term steroid users.”
To explore any differences in a larger patient population, the investigators randomly assigned adults with SLE and other autoimmune conditions to the two treatments: denosumab 60 mg subcutaneoulsy every 6 months or oral alendronate 70 mg/week. All patients also received 3,000 mg calcium and 1,000 IU vitamin D3 (cholecalciferol) each day.
After three discontinuations in denosumab cohort and four in the alendronate group, the researchers evaluated 69 people taking denosumab and 70 others taking alendronate. The discontinuations were caused by noncompliance, Dr. Mok said, not by adverse events.
Adverse events were reported, but the rate did not differ significantly between groups. Dr. Mok highlighted some notable differences, including more minor infections and arthralgias reported in the denosumab cohort. Chest discomfort was reported in one denosumab recipient versus no patients in the alendronate group. Dyspepsia/upper GI symptoms and dizziness/vertigo occurred more often in the alendronate group.
Women were 96% of the study population, and mean age was 50 years. A majority, 81%, had underlying SLE. Other diagnoses included rheumatoid arthritis, myositis, antineutrophil cytoplasmic antibody–associated vasculitis, and polymyalgia rheumatica. The mean dose of prednisolone at study entry was 5.1 mg/day.
Key BMD and biomarker findings
BMD increased significantly in the spine, hip, and femoral neck in both treatment groups by 12 months. However, after adjustment for baseline BMD and covariates including age, menopause, and history of fracture, the gains in the denosumab group were significantly higher.
The increase in lumbar spine BMD at 12 months of 3.5% in the denosumab group versus 2.5% in the alendronate group was statistically significant (P = .045). Less significant was a 0.9% increase at the hip in the denosumab patients versus 1.6% in the alendronate group (P = .10), as well as femoral neck BMD gains of 1% in the denosumab group versus 1.5% in the alendronate group (P = .86).
Furthermore, “denosumab was more potent in suppressing the bone markers at 12 months,” Dr. Mok said.
Specifically, the percentage decrease in serum PINP (procollagen type I N-terminal propeptide) levels in the denosumab group was significantly greater than in the alendronate group (P = .001). Likewise, the decrease in CTX (C-terminal telopeptide of type I collagen) was significantly greater in the denosumab cohort versus the alendronate cohort (P < .001).
“Dr. Mok’s study was a well-controlled investigation. The superiority of denosumab was impressive, especially given the small group sizes of 69 and 70,” session comoderator Gregg Silverman, MD, professor in the department of internal medicine and the department of pathology at New York University, said when asked for comment.
“However, bone density measurements may not tell the whole story. These results support a bigger and much larger-scale study to confirm that rates of fracture on denosumab are also reduced.”
No new symptomatic fractures occurred in either group during the study. The investigators are evaluating for any new radiologic fractures, with results pending.
Dr. Mok said “results of our study in Asian patients are largely confirmatory” of a previous 2018 comparison study and a 2019 comparison study, each sponsored by Amgen.
A small sample size, short duration of treatment, and the open-label design were limitations of the study.
The trial was an investigator-initiated study. Dr. Mok and colleagues had no relevant financial disclosures. Dr. Silverman had no relevant financial disclosures.
SOURCE: Mok CC et al. Arthritis Rheumatol. 2020;72(suppl 10). ACR 2020, Abstract 1442.
Denosumab boosted bone mineral density (BMD) over 12 months to a greater extent than did alendronate in a randomized, 12-month study. The investigator-initiated research compared BMD at the lumbar spine and elsewhere among people with systemic lupus erythematosus (SLE) and other autoimmune conditions. Long-term glucocorticoid therapy places some people in this group at higher risk for adverse effects of bone density loss.
“Glucocorticoids remain the mainstay of treatment of rheumatic diseases, but [they are] a major risk factor for osteoporosis and fracture,” study author Chi Chiu Mok, MD, said in an interview.
Compared with baseline, adults randomly assigned to denosumab had a 3.5% increase in lumbar spine BMD at 12 months, compared with 2.5% among those taking alendronate, a significant difference. Dr. Mok, a consultant and honorary associate professor in the department of medicine and nuclear medicine at Tuen Mun Hospital in Hong Kong, presented the study results at the virtual annual meeting of the American College of Rheumatology.
“Given the knowledge that denosumab is more effective than alendronate in raising spinal BMD in chronic users of GCs without increasing adverse events, this drug may be considered as an alternative first-line therapy in higher-risk patients and in those who are contraindicated for the oral bisphosphonates,” he said.
Cost considerations
Denosumab is a human monoclonal antibody administered as a subcutaneous injection, available under the brand names Prolia and Xgeva. Alendronate is an oral agent available as both generic and brand name formulations.
“Yes, denosumab is more expensive, more costly than oral alendronate, but our study shows efficacy is better for steroid users,” Dr. Mok said in answer to a question about cost disparity between the two agents during his presentation at the meeting. “For patients who are contraindicated or have low compliance for bisphosphonate, or are high-risk patients, I recommend first-line use of denosumab.”
Researchers previously studied these agents, including a smaller study by Dr. Mok and colleagues that showed a BMD benefit after switching people on an oral bisphosphonate to denosumab. However, he said, “There is a paucity of data regarding comparative efficacy of denosumab and the bisphosphonates in long-term steroid users.”
To explore any differences in a larger patient population, the investigators randomly assigned adults with SLE and other autoimmune conditions to the two treatments: denosumab 60 mg subcutaneoulsy every 6 months or oral alendronate 70 mg/week. All patients also received 3,000 mg calcium and 1,000 IU vitamin D3 (cholecalciferol) each day.
After three discontinuations in denosumab cohort and four in the alendronate group, the researchers evaluated 69 people taking denosumab and 70 others taking alendronate. The discontinuations were caused by noncompliance, Dr. Mok said, not by adverse events.
Adverse events were reported, but the rate did not differ significantly between groups. Dr. Mok highlighted some notable differences, including more minor infections and arthralgias reported in the denosumab cohort. Chest discomfort was reported in one denosumab recipient versus no patients in the alendronate group. Dyspepsia/upper GI symptoms and dizziness/vertigo occurred more often in the alendronate group.
Women were 96% of the study population, and mean age was 50 years. A majority, 81%, had underlying SLE. Other diagnoses included rheumatoid arthritis, myositis, antineutrophil cytoplasmic antibody–associated vasculitis, and polymyalgia rheumatica. The mean dose of prednisolone at study entry was 5.1 mg/day.
Key BMD and biomarker findings
BMD increased significantly in the spine, hip, and femoral neck in both treatment groups by 12 months. However, after adjustment for baseline BMD and covariates including age, menopause, and history of fracture, the gains in the denosumab group were significantly higher.
The increase in lumbar spine BMD at 12 months of 3.5% in the denosumab group versus 2.5% in the alendronate group was statistically significant (P = .045). Less significant was a 0.9% increase at the hip in the denosumab patients versus 1.6% in the alendronate group (P = .10), as well as femoral neck BMD gains of 1% in the denosumab group versus 1.5% in the alendronate group (P = .86).
Furthermore, “denosumab was more potent in suppressing the bone markers at 12 months,” Dr. Mok said.
Specifically, the percentage decrease in serum PINP (procollagen type I N-terminal propeptide) levels in the denosumab group was significantly greater than in the alendronate group (P = .001). Likewise, the decrease in CTX (C-terminal telopeptide of type I collagen) was significantly greater in the denosumab cohort versus the alendronate cohort (P < .001).
“Dr. Mok’s study was a well-controlled investigation. The superiority of denosumab was impressive, especially given the small group sizes of 69 and 70,” session comoderator Gregg Silverman, MD, professor in the department of internal medicine and the department of pathology at New York University, said when asked for comment.
“However, bone density measurements may not tell the whole story. These results support a bigger and much larger-scale study to confirm that rates of fracture on denosumab are also reduced.”
No new symptomatic fractures occurred in either group during the study. The investigators are evaluating for any new radiologic fractures, with results pending.
Dr. Mok said “results of our study in Asian patients are largely confirmatory” of a previous 2018 comparison study and a 2019 comparison study, each sponsored by Amgen.
A small sample size, short duration of treatment, and the open-label design were limitations of the study.
The trial was an investigator-initiated study. Dr. Mok and colleagues had no relevant financial disclosures. Dr. Silverman had no relevant financial disclosures.
SOURCE: Mok CC et al. Arthritis Rheumatol. 2020;72(suppl 10). ACR 2020, Abstract 1442.
Denosumab boosted bone mineral density (BMD) over 12 months to a greater extent than did alendronate in a randomized, 12-month study. The investigator-initiated research compared BMD at the lumbar spine and elsewhere among people with systemic lupus erythematosus (SLE) and other autoimmune conditions. Long-term glucocorticoid therapy places some people in this group at higher risk for adverse effects of bone density loss.
“Glucocorticoids remain the mainstay of treatment of rheumatic diseases, but [they are] a major risk factor for osteoporosis and fracture,” study author Chi Chiu Mok, MD, said in an interview.
Compared with baseline, adults randomly assigned to denosumab had a 3.5% increase in lumbar spine BMD at 12 months, compared with 2.5% among those taking alendronate, a significant difference. Dr. Mok, a consultant and honorary associate professor in the department of medicine and nuclear medicine at Tuen Mun Hospital in Hong Kong, presented the study results at the virtual annual meeting of the American College of Rheumatology.
“Given the knowledge that denosumab is more effective than alendronate in raising spinal BMD in chronic users of GCs without increasing adverse events, this drug may be considered as an alternative first-line therapy in higher-risk patients and in those who are contraindicated for the oral bisphosphonates,” he said.
Cost considerations
Denosumab is a human monoclonal antibody administered as a subcutaneous injection, available under the brand names Prolia and Xgeva. Alendronate is an oral agent available as both generic and brand name formulations.
“Yes, denosumab is more expensive, more costly than oral alendronate, but our study shows efficacy is better for steroid users,” Dr. Mok said in answer to a question about cost disparity between the two agents during his presentation at the meeting. “For patients who are contraindicated or have low compliance for bisphosphonate, or are high-risk patients, I recommend first-line use of denosumab.”
Researchers previously studied these agents, including a smaller study by Dr. Mok and colleagues that showed a BMD benefit after switching people on an oral bisphosphonate to denosumab. However, he said, “There is a paucity of data regarding comparative efficacy of denosumab and the bisphosphonates in long-term steroid users.”
To explore any differences in a larger patient population, the investigators randomly assigned adults with SLE and other autoimmune conditions to the two treatments: denosumab 60 mg subcutaneoulsy every 6 months or oral alendronate 70 mg/week. All patients also received 3,000 mg calcium and 1,000 IU vitamin D3 (cholecalciferol) each day.
After three discontinuations in denosumab cohort and four in the alendronate group, the researchers evaluated 69 people taking denosumab and 70 others taking alendronate. The discontinuations were caused by noncompliance, Dr. Mok said, not by adverse events.
Adverse events were reported, but the rate did not differ significantly between groups. Dr. Mok highlighted some notable differences, including more minor infections and arthralgias reported in the denosumab cohort. Chest discomfort was reported in one denosumab recipient versus no patients in the alendronate group. Dyspepsia/upper GI symptoms and dizziness/vertigo occurred more often in the alendronate group.
Women were 96% of the study population, and mean age was 50 years. A majority, 81%, had underlying SLE. Other diagnoses included rheumatoid arthritis, myositis, antineutrophil cytoplasmic antibody–associated vasculitis, and polymyalgia rheumatica. The mean dose of prednisolone at study entry was 5.1 mg/day.
Key BMD and biomarker findings
BMD increased significantly in the spine, hip, and femoral neck in both treatment groups by 12 months. However, after adjustment for baseline BMD and covariates including age, menopause, and history of fracture, the gains in the denosumab group were significantly higher.
The increase in lumbar spine BMD at 12 months of 3.5% in the denosumab group versus 2.5% in the alendronate group was statistically significant (P = .045). Less significant was a 0.9% increase at the hip in the denosumab patients versus 1.6% in the alendronate group (P = .10), as well as femoral neck BMD gains of 1% in the denosumab group versus 1.5% in the alendronate group (P = .86).
Furthermore, “denosumab was more potent in suppressing the bone markers at 12 months,” Dr. Mok said.
Specifically, the percentage decrease in serum PINP (procollagen type I N-terminal propeptide) levels in the denosumab group was significantly greater than in the alendronate group (P = .001). Likewise, the decrease in CTX (C-terminal telopeptide of type I collagen) was significantly greater in the denosumab cohort versus the alendronate cohort (P < .001).
“Dr. Mok’s study was a well-controlled investigation. The superiority of denosumab was impressive, especially given the small group sizes of 69 and 70,” session comoderator Gregg Silverman, MD, professor in the department of internal medicine and the department of pathology at New York University, said when asked for comment.
“However, bone density measurements may not tell the whole story. These results support a bigger and much larger-scale study to confirm that rates of fracture on denosumab are also reduced.”
No new symptomatic fractures occurred in either group during the study. The investigators are evaluating for any new radiologic fractures, with results pending.
Dr. Mok said “results of our study in Asian patients are largely confirmatory” of a previous 2018 comparison study and a 2019 comparison study, each sponsored by Amgen.
A small sample size, short duration of treatment, and the open-label design were limitations of the study.
The trial was an investigator-initiated study. Dr. Mok and colleagues had no relevant financial disclosures. Dr. Silverman had no relevant financial disclosures.
SOURCE: Mok CC et al. Arthritis Rheumatol. 2020;72(suppl 10). ACR 2020, Abstract 1442.
FROM ACR 2020
Osteoporosis underdiagnosed in older men with fracture
Osteoporosis is frequently underdiagnosed and undertreated in men before and even after they have experienced a fracture, according to research presented at the virtual annual meeting of the American College of Rheumatology.
“This is an important public health concern,” as fractures contribute significantly to morbidity and mortality, said Jeffrey Curtis, MD, MS, MPH, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham.
Men are often overlooked, he said, “because it’s misconstrued as a disease that mainly, if not only, affects Caucasian women,” despite the fact that 20%-25% of fractures occur in men.
Emerging evidence suggests that men who have bone fractures have worse outcomes than women, Dr. Curtis said.
Guidelines lacking
Consistent guidelines for osteoporosis screening among men are also lacking, leading to ambiguity and increased disease burden.
Researchers studied records for a 5% random sample of male Medicare fee-for-service beneficiaries (n = 9,876) aged at least 65 years with a closed fragility fracture between January 2010 and September 2014. Average age for the men with fractures was 77.9 years, and the most common sites of the fracture were the spine, hip, and ankle.
They looked back to see whether these men had been effectively screened and treated.
Very few had.
“We found that 92.8% of them did not have any diagnosis or treatment of osteoporosis at baseline,” Curtis said. On top of that, less than 6% of men had undergone any dual-energy x-ray absorptiometry (DEXA) or bone mineral testing in the 2 years prior to their fracture.
Even men who had high-risk factors for falls, such as those using beta-blockers, mobility impairment, or a history of opioid use, were unlikely to be screened, he said.
Dr. Curtis’s data show there was actually a decline in DEXA scans from 2012 to 2014, and that decline was particularly high in men aged 75 years and older who are more likely to be at risk for fracture.
In addition to underscreening and undertreating before the fracture, Dr. Curtis said, “The treatment patterns after the fracture were not much better.” In the year after the fracture, “only about 10% of these men had BMD [bone mineral density] testing. Only 9% were treated with an osteoporosis medication.”
“Importantly, about 7% of the men in this large cohort went on to have one or more fractures in the next year,” he added.
Reasons for undertreatment
Reasons for the poor rates of diagnosis and treatment may begin with patients not having symptoms. Therefore, they aren’t coming into doctors’ offices asking to be screened. “Even if they break bones, they may not know enough to ask how to prevent the next fracture,” Dr. Curtis said.
There’s a financial obstacle as well, Dr. Curtis explained. “U.S. legislation that provides population screening for Medicare patients really, for men, is quite dissimilar to the near-universal coverage for women. So many clinicians worry they won’t get reimbursed if they order DEXA in men for screening.”
Additionally, postfracture quality-of-care guidelines that are reimbursed as part of the Medicare Access and CHIP Reauthorization Act of 2015 and the Merit-based Incentive Payment System program specifically exclude men, he noted.
Better management of male osteoporosis, including early identification of at-risk individuals is clearly warranted, he said, so they can be screened and put on effective therapy.
Sonali Khandelwal, MD, a rheumatologist with Rush University Medical Center, Chicago, who was not part of the research, agreed.
She said in an interview that part of the problem is that diagnosis and treatment could come from a variety of specialists – endocrinologists, rheumatologists, orthopedists, and primary care physicians – and each may think it falls in another’s realm.
At Rush and some other sites nationally, she said, an alert is registered in electronic medical records flagging any patient who may need bone density screening based on age, medications, or history.
Rush University also has a fracture liaison service under which everyone hospitalized there who may have had a history of a fracture or is admitted with a fracture gets followed up with screening and treatment, “to capture those patients who may not have come through the system otherwise.”
She said guidelines have called for DEXA screening for men at age 70, but she said clinical screening should start younger – as young as 50 – for patients with conditions such as lupus, rheumatoid arthritis, hypogonadism, or those on chronic steroids.
Dr. Khandelwal said that, even when an insurance company doesn›t typically cover bone density screening for men, physicians can often make a case for reimbursement if the patient has a history of falls or fractures.
“In the long run, preventing a fracture is saving so much more money than when you get a fracture and end up in a hospital and have to go to a nursing home,” she said.
Dr. Curtis reported relationships with AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Janssen, Lilly, Myriad, Pfizer, Regeneron, Roche, UCB, Gilead Sciences, and Sanofi. Dr. Khandelwal reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Osteoporosis is frequently underdiagnosed and undertreated in men before and even after they have experienced a fracture, according to research presented at the virtual annual meeting of the American College of Rheumatology.
“This is an important public health concern,” as fractures contribute significantly to morbidity and mortality, said Jeffrey Curtis, MD, MS, MPH, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham.
Men are often overlooked, he said, “because it’s misconstrued as a disease that mainly, if not only, affects Caucasian women,” despite the fact that 20%-25% of fractures occur in men.
Emerging evidence suggests that men who have bone fractures have worse outcomes than women, Dr. Curtis said.
Guidelines lacking
Consistent guidelines for osteoporosis screening among men are also lacking, leading to ambiguity and increased disease burden.
Researchers studied records for a 5% random sample of male Medicare fee-for-service beneficiaries (n = 9,876) aged at least 65 years with a closed fragility fracture between January 2010 and September 2014. Average age for the men with fractures was 77.9 years, and the most common sites of the fracture were the spine, hip, and ankle.
They looked back to see whether these men had been effectively screened and treated.
Very few had.
“We found that 92.8% of them did not have any diagnosis or treatment of osteoporosis at baseline,” Curtis said. On top of that, less than 6% of men had undergone any dual-energy x-ray absorptiometry (DEXA) or bone mineral testing in the 2 years prior to their fracture.
Even men who had high-risk factors for falls, such as those using beta-blockers, mobility impairment, or a history of opioid use, were unlikely to be screened, he said.
Dr. Curtis’s data show there was actually a decline in DEXA scans from 2012 to 2014, and that decline was particularly high in men aged 75 years and older who are more likely to be at risk for fracture.
In addition to underscreening and undertreating before the fracture, Dr. Curtis said, “The treatment patterns after the fracture were not much better.” In the year after the fracture, “only about 10% of these men had BMD [bone mineral density] testing. Only 9% were treated with an osteoporosis medication.”
“Importantly, about 7% of the men in this large cohort went on to have one or more fractures in the next year,” he added.
Reasons for undertreatment
Reasons for the poor rates of diagnosis and treatment may begin with patients not having symptoms. Therefore, they aren’t coming into doctors’ offices asking to be screened. “Even if they break bones, they may not know enough to ask how to prevent the next fracture,” Dr. Curtis said.
There’s a financial obstacle as well, Dr. Curtis explained. “U.S. legislation that provides population screening for Medicare patients really, for men, is quite dissimilar to the near-universal coverage for women. So many clinicians worry they won’t get reimbursed if they order DEXA in men for screening.”
Additionally, postfracture quality-of-care guidelines that are reimbursed as part of the Medicare Access and CHIP Reauthorization Act of 2015 and the Merit-based Incentive Payment System program specifically exclude men, he noted.
Better management of male osteoporosis, including early identification of at-risk individuals is clearly warranted, he said, so they can be screened and put on effective therapy.
Sonali Khandelwal, MD, a rheumatologist with Rush University Medical Center, Chicago, who was not part of the research, agreed.
She said in an interview that part of the problem is that diagnosis and treatment could come from a variety of specialists – endocrinologists, rheumatologists, orthopedists, and primary care physicians – and each may think it falls in another’s realm.
At Rush and some other sites nationally, she said, an alert is registered in electronic medical records flagging any patient who may need bone density screening based on age, medications, or history.
Rush University also has a fracture liaison service under which everyone hospitalized there who may have had a history of a fracture or is admitted with a fracture gets followed up with screening and treatment, “to capture those patients who may not have come through the system otherwise.”
She said guidelines have called for DEXA screening for men at age 70, but she said clinical screening should start younger – as young as 50 – for patients with conditions such as lupus, rheumatoid arthritis, hypogonadism, or those on chronic steroids.
Dr. Khandelwal said that, even when an insurance company doesn›t typically cover bone density screening for men, physicians can often make a case for reimbursement if the patient has a history of falls or fractures.
“In the long run, preventing a fracture is saving so much more money than when you get a fracture and end up in a hospital and have to go to a nursing home,” she said.
Dr. Curtis reported relationships with AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Janssen, Lilly, Myriad, Pfizer, Regeneron, Roche, UCB, Gilead Sciences, and Sanofi. Dr. Khandelwal reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Osteoporosis is frequently underdiagnosed and undertreated in men before and even after they have experienced a fracture, according to research presented at the virtual annual meeting of the American College of Rheumatology.
“This is an important public health concern,” as fractures contribute significantly to morbidity and mortality, said Jeffrey Curtis, MD, MS, MPH, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham.
Men are often overlooked, he said, “because it’s misconstrued as a disease that mainly, if not only, affects Caucasian women,” despite the fact that 20%-25% of fractures occur in men.
Emerging evidence suggests that men who have bone fractures have worse outcomes than women, Dr. Curtis said.
Guidelines lacking
Consistent guidelines for osteoporosis screening among men are also lacking, leading to ambiguity and increased disease burden.
Researchers studied records for a 5% random sample of male Medicare fee-for-service beneficiaries (n = 9,876) aged at least 65 years with a closed fragility fracture between January 2010 and September 2014. Average age for the men with fractures was 77.9 years, and the most common sites of the fracture were the spine, hip, and ankle.
They looked back to see whether these men had been effectively screened and treated.
Very few had.
“We found that 92.8% of them did not have any diagnosis or treatment of osteoporosis at baseline,” Curtis said. On top of that, less than 6% of men had undergone any dual-energy x-ray absorptiometry (DEXA) or bone mineral testing in the 2 years prior to their fracture.
Even men who had high-risk factors for falls, such as those using beta-blockers, mobility impairment, or a history of opioid use, were unlikely to be screened, he said.
Dr. Curtis’s data show there was actually a decline in DEXA scans from 2012 to 2014, and that decline was particularly high in men aged 75 years and older who are more likely to be at risk for fracture.
In addition to underscreening and undertreating before the fracture, Dr. Curtis said, “The treatment patterns after the fracture were not much better.” In the year after the fracture, “only about 10% of these men had BMD [bone mineral density] testing. Only 9% were treated with an osteoporosis medication.”
“Importantly, about 7% of the men in this large cohort went on to have one or more fractures in the next year,” he added.
Reasons for undertreatment
Reasons for the poor rates of diagnosis and treatment may begin with patients not having symptoms. Therefore, they aren’t coming into doctors’ offices asking to be screened. “Even if they break bones, they may not know enough to ask how to prevent the next fracture,” Dr. Curtis said.
There’s a financial obstacle as well, Dr. Curtis explained. “U.S. legislation that provides population screening for Medicare patients really, for men, is quite dissimilar to the near-universal coverage for women. So many clinicians worry they won’t get reimbursed if they order DEXA in men for screening.”
Additionally, postfracture quality-of-care guidelines that are reimbursed as part of the Medicare Access and CHIP Reauthorization Act of 2015 and the Merit-based Incentive Payment System program specifically exclude men, he noted.
Better management of male osteoporosis, including early identification of at-risk individuals is clearly warranted, he said, so they can be screened and put on effective therapy.
Sonali Khandelwal, MD, a rheumatologist with Rush University Medical Center, Chicago, who was not part of the research, agreed.
She said in an interview that part of the problem is that diagnosis and treatment could come from a variety of specialists – endocrinologists, rheumatologists, orthopedists, and primary care physicians – and each may think it falls in another’s realm.
At Rush and some other sites nationally, she said, an alert is registered in electronic medical records flagging any patient who may need bone density screening based on age, medications, or history.
Rush University also has a fracture liaison service under which everyone hospitalized there who may have had a history of a fracture or is admitted with a fracture gets followed up with screening and treatment, “to capture those patients who may not have come through the system otherwise.”
She said guidelines have called for DEXA screening for men at age 70, but she said clinical screening should start younger – as young as 50 – for patients with conditions such as lupus, rheumatoid arthritis, hypogonadism, or those on chronic steroids.
Dr. Khandelwal said that, even when an insurance company doesn›t typically cover bone density screening for men, physicians can often make a case for reimbursement if the patient has a history of falls or fractures.
“In the long run, preventing a fracture is saving so much more money than when you get a fracture and end up in a hospital and have to go to a nursing home,” she said.
Dr. Curtis reported relationships with AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Janssen, Lilly, Myriad, Pfizer, Regeneron, Roche, UCB, Gilead Sciences, and Sanofi. Dr. Khandelwal reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Treatment sequence with romosozumab influences osteoporosis outcomes
Timing is everything when it comes to the use of the anabolic agent romosozumab (Evenity) for the treatment of advanced osteoporosis, a review of clinical trials suggests.

In four studies with treatment sequences in which romosozumab was administered either before or following the use of an antiresorptive agent, initial treatment with 1 year of romosozumab produced substantial bone mineral density (BMD) gains in the total hip and lumbar spine.
Transition from romosozumab to a potent resorptive agent, either alendronate or denosumab (Prolia) augmented the initial gains, reported Felicia Cosman, MD, professor of clinical medicine at Columbia University, New York.
Romosozumab was the third approved agent in its class, following teriparatide in 2002, and abaloparatide (Tymlos) in 2017, both of which have been shown to produce rapid reductions in fracture risk and large improvements in BMD when they were administered up front, followed by an antiresorptive agent.
“But since romosozumab has a very different mechanism of action compared to both teriparatide and abaloparatide, we didn’t know if treatment sequence would be as important for this agent as it was for teriparatide,” she said during a press briefing prior to her presentation of the data in an oral abstract session at the virtual annual meeting of the American College of Rheumatology.
Two-for-one
Romosozumab is unique in that it both increases bone formation and decreases bone resorption, and has been shown in treatment-naive postmenopausal women with osteoporosis to significantly improve BMD and reduce fracture risk, compared with either placebo or alendronate. Romosozumab has also been studied as sequential therapy in patients treated initially with either alendronate or denosumab.
To see whether treatment sequence could have differential effects on clinical outcomes for patients with osteoporosis, Dr. Cosman and colleagues looked at results from four clinical trials, using levels of bone turnover markers (procollagen type I N-terminal propeptide [PINP] and beta-isomer of the C-terminal telopeptide of type I collagen [beta-CTX]) and BMD gains in the total hip and spine as outcomes.
The two trials of romosozumab in treatment-naive women were the ARCH trial comparing romosozumab with alendronate in a double-blind phase for 1 year, followed by 1 year of open-label alendronate, and the FRAME trial, in which romosozumab was compared with placebo in a 1-year double-blind phase, followed by 1-year of open-label denosumab.
The two trials of romosozumab in women treated initially with antiresorptive agents were the STRUCTURE trial in which patients on oral bisphosphonates for at least 3 years or alendronate 70 mg weekly for 1 year were randomized to receive either romosozumab or teriparatide, and a phase 2 trial (NCT00896532) that included a 24-month romosozumab or placebo treatment phase followed by rerandomization to a 12-month extension phase with denosumab or placebo, followed by a 12-month retreatment phase with romosozumab, followed by a 24-month follow-on phase with zoledronic acid or no intervention.
Total hip BMD gains
In the ARCH trial, total hip BMD increased 6.2% with 1 year of romosozumab, and a cumulative total of 7.1% with the 2-year romosozumab/alendronate sequence. In the FRAME trial, patients gained 6.8% in total hip BMD after 1 year of romosozumab and a total of 8.8% after 2 years of romosozumab followed by denosumab.
In contrast, in the STRUCTURE trial, patients treated for 1 year or longer with alendronate and then with 1 year of romosozumab had a 2.9% BMD gain in the total hip. In the phase 2 trial, 1 year of romosozumab following 1 year of denosumab yielded a 0.9% BMD gain, for a total gain of 3.8% with the denosumab sequence.
Lumbar spine BMD gains
In ARCH, lumbar spine BMD increased 13.7% with 1 year of romosozumab, and a total of 15.2% with the 2-year sequence of romosozumab followed by alendronate. Similarly, in FRAME, patients gained 13.3% in BMD after a year of romosozumab, and total of 17.6% by the end of the 2-year romosozumab/denosumab sequence.
In contrast, in STRUCTURE, patients who had previously been on alendronate for at least 1 year had a gain of 9.8% after 1 year of romosozumab, and in the phase 2 study, patients who had been on denosumab for 1 year had an increase in lumbar spine BMD of 5.3% after 1 year on romosozumab, and a total gain of 11.5% at the end of the 2-year sequence.
Serum PINP and beta-CTX
Looking at the markers of bone turnover, the investigators saw that, in both ARCH and FRAME, PINP peaked at over 80% of baseline at 1 month, and then continued to steadily decline past 1 year. The beta-CTX nadir was 40%-50% below baseline at 1 year.
At the end of year 2, the PINP nadir was –67% with follow-on alendronate, and –69% with denosumab, and the beta-CTX nadir was –72% and –92%, respectively.
In the two trials where romosozumab was the follow-on therapy, however, the trends were distinctly different. In STRUCTURE, for example, PINP peaked at 141% of baseline at 1 month, and then returned toward baseline, whereas beta-CTX remained largely unchanged.
In the phase 2 trial, PINP peaked at 28% above baseline at 9 months, and then only slightly declined, and beta-CTX peaked at 211% at the end of 1 year of romosozumab.
Best used up front
“This study is important, because it suggests that for the three bone-building drugs that the best effects will really be attained on bone strength if the agents are used as initial therapy in very-high-risk patients. Those are people who have sustained fractures within the preceding 2 years, who had multiple fractures at any point in their adulthood, and who present with very low BMD, particularly if they have any associated clinical risk factors such as family history or other underlying diseases or medications that have detrimental effects on bone,” Dr. Cosman said at the briefing.
Marcy Bolster, MD, from the division of rheumatology, allergy, and immunology at Massachusetts General Hospital, Boston, and associate professor of medicine at Harvard Medical School in Boston, who was not involved in the study, commented that the study provides important information for clinicians who treat patients with osteoporosis.

“We have an increasing number of medications available for use in the treatment of patients with osteoporosis, and as we consider the importance of reducing fracture risk, the duration of therapy, the timing of a bisphosphonate holiday, it is essential that we consider any advantages to the order or sequence of our medications,” she said when asked for comment.
“This study provides evidence supporting the concept of the ‘anabolic window’ in which there is a demonstrated advantage in treating patients with an anabolic agent prior to treatment with an antiresorptive agent, and while gains in bone mineral density were achieved with either order of medication use, the gains were more dramatic with treatment with romosozumab as the first agent,” she added.
Dr. Bolster also noted it will be important to demonstrate reduction in fracture risk as well as gain in BMD.
The study was sponsored by Amgen, Astellas, and UCB. Dr. Cosman disclosed grants/research support from Amgen, and consulting fees and speaker activities for Amgen and Radius Health. Dr. Bolster disclosed relationships with AbbVie, Corbus, Cumberland, Gilead, Johnson & Johnson, and Pfizer.
SOURCE: Cosman F et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 1973.
Timing is everything when it comes to the use of the anabolic agent romosozumab (Evenity) for the treatment of advanced osteoporosis, a review of clinical trials suggests.
In four studies with treatment sequences in which romosozumab was administered either before or following the use of an antiresorptive agent, initial treatment with 1 year of romosozumab produced substantial bone mineral density (BMD) gains in the total hip and lumbar spine.
Transition from romosozumab to a potent resorptive agent, either alendronate or denosumab (Prolia) augmented the initial gains, reported Felicia Cosman, MD, professor of clinical medicine at Columbia University, New York.
Romosozumab was the third approved agent in its class, following teriparatide in 2002, and abaloparatide (Tymlos) in 2017, both of which have been shown to produce rapid reductions in fracture risk and large improvements in BMD when they were administered up front, followed by an antiresorptive agent.
“But since romosozumab has a very different mechanism of action compared to both teriparatide and abaloparatide, we didn’t know if treatment sequence would be as important for this agent as it was for teriparatide,” she said during a press briefing prior to her presentation of the data in an oral abstract session at the virtual annual meeting of the American College of Rheumatology.
Two-for-one
Romosozumab is unique in that it both increases bone formation and decreases bone resorption, and has been shown in treatment-naive postmenopausal women with osteoporosis to significantly improve BMD and reduce fracture risk, compared with either placebo or alendronate. Romosozumab has also been studied as sequential therapy in patients treated initially with either alendronate or denosumab.
To see whether treatment sequence could have differential effects on clinical outcomes for patients with osteoporosis, Dr. Cosman and colleagues looked at results from four clinical trials, using levels of bone turnover markers (procollagen type I N-terminal propeptide [PINP] and beta-isomer of the C-terminal telopeptide of type I collagen [beta-CTX]) and BMD gains in the total hip and spine as outcomes.
The two trials of romosozumab in treatment-naive women were the ARCH trial comparing romosozumab with alendronate in a double-blind phase for 1 year, followed by 1 year of open-label alendronate, and the FRAME trial, in which romosozumab was compared with placebo in a 1-year double-blind phase, followed by 1-year of open-label denosumab.
The two trials of romosozumab in women treated initially with antiresorptive agents were the STRUCTURE trial in which patients on oral bisphosphonates for at least 3 years or alendronate 70 mg weekly for 1 year were randomized to receive either romosozumab or teriparatide, and a phase 2 trial (NCT00896532) that included a 24-month romosozumab or placebo treatment phase followed by rerandomization to a 12-month extension phase with denosumab or placebo, followed by a 12-month retreatment phase with romosozumab, followed by a 24-month follow-on phase with zoledronic acid or no intervention.
Total hip BMD gains
In the ARCH trial, total hip BMD increased 6.2% with 1 year of romosozumab, and a cumulative total of 7.1% with the 2-year romosozumab/alendronate sequence. In the FRAME trial, patients gained 6.8% in total hip BMD after 1 year of romosozumab and a total of 8.8% after 2 years of romosozumab followed by denosumab.
In contrast, in the STRUCTURE trial, patients treated for 1 year or longer with alendronate and then with 1 year of romosozumab had a 2.9% BMD gain in the total hip. In the phase 2 trial, 1 year of romosozumab following 1 year of denosumab yielded a 0.9% BMD gain, for a total gain of 3.8% with the denosumab sequence.
Lumbar spine BMD gains
In ARCH, lumbar spine BMD increased 13.7% with 1 year of romosozumab, and a total of 15.2% with the 2-year sequence of romosozumab followed by alendronate. Similarly, in FRAME, patients gained 13.3% in BMD after a year of romosozumab, and total of 17.6% by the end of the 2-year romosozumab/denosumab sequence.
In contrast, in STRUCTURE, patients who had previously been on alendronate for at least 1 year had a gain of 9.8% after 1 year of romosozumab, and in the phase 2 study, patients who had been on denosumab for 1 year had an increase in lumbar spine BMD of 5.3% after 1 year on romosozumab, and a total gain of 11.5% at the end of the 2-year sequence.
Serum PINP and beta-CTX
Looking at the markers of bone turnover, the investigators saw that, in both ARCH and FRAME, PINP peaked at over 80% of baseline at 1 month, and then continued to steadily decline past 1 year. The beta-CTX nadir was 40%-50% below baseline at 1 year.
At the end of year 2, the PINP nadir was –67% with follow-on alendronate, and –69% with denosumab, and the beta-CTX nadir was –72% and –92%, respectively.
In the two trials where romosozumab was the follow-on therapy, however, the trends were distinctly different. In STRUCTURE, for example, PINP peaked at 141% of baseline at 1 month, and then returned toward baseline, whereas beta-CTX remained largely unchanged.
In the phase 2 trial, PINP peaked at 28% above baseline at 9 months, and then only slightly declined, and beta-CTX peaked at 211% at the end of 1 year of romosozumab.
Best used up front
“This study is important, because it suggests that for the three bone-building drugs that the best effects will really be attained on bone strength if the agents are used as initial therapy in very-high-risk patients. Those are people who have sustained fractures within the preceding 2 years, who had multiple fractures at any point in their adulthood, and who present with very low BMD, particularly if they have any associated clinical risk factors such as family history or other underlying diseases or medications that have detrimental effects on bone,” Dr. Cosman said at the briefing.
Marcy Bolster, MD, from the division of rheumatology, allergy, and immunology at Massachusetts General Hospital, Boston, and associate professor of medicine at Harvard Medical School in Boston, who was not involved in the study, commented that the study provides important information for clinicians who treat patients with osteoporosis.
“We have an increasing number of medications available for use in the treatment of patients with osteoporosis, and as we consider the importance of reducing fracture risk, the duration of therapy, the timing of a bisphosphonate holiday, it is essential that we consider any advantages to the order or sequence of our medications,” she said when asked for comment.
“This study provides evidence supporting the concept of the ‘anabolic window’ in which there is a demonstrated advantage in treating patients with an anabolic agent prior to treatment with an antiresorptive agent, and while gains in bone mineral density were achieved with either order of medication use, the gains were more dramatic with treatment with romosozumab as the first agent,” she added.
Dr. Bolster also noted it will be important to demonstrate reduction in fracture risk as well as gain in BMD.
The study was sponsored by Amgen, Astellas, and UCB. Dr. Cosman disclosed grants/research support from Amgen, and consulting fees and speaker activities for Amgen and Radius Health. Dr. Bolster disclosed relationships with AbbVie, Corbus, Cumberland, Gilead, Johnson & Johnson, and Pfizer.
SOURCE: Cosman F et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 1973.
Timing is everything when it comes to the use of the anabolic agent romosozumab (Evenity) for the treatment of advanced osteoporosis, a review of clinical trials suggests.
In four studies with treatment sequences in which romosozumab was administered either before or following the use of an antiresorptive agent, initial treatment with 1 year of romosozumab produced substantial bone mineral density (BMD) gains in the total hip and lumbar spine.
Transition from romosozumab to a potent resorptive agent, either alendronate or denosumab (Prolia) augmented the initial gains, reported Felicia Cosman, MD, professor of clinical medicine at Columbia University, New York.
Romosozumab was the third approved agent in its class, following teriparatide in 2002, and abaloparatide (Tymlos) in 2017, both of which have been shown to produce rapid reductions in fracture risk and large improvements in BMD when they were administered up front, followed by an antiresorptive agent.
“But since romosozumab has a very different mechanism of action compared to both teriparatide and abaloparatide, we didn’t know if treatment sequence would be as important for this agent as it was for teriparatide,” she said during a press briefing prior to her presentation of the data in an oral abstract session at the virtual annual meeting of the American College of Rheumatology.
Two-for-one
Romosozumab is unique in that it both increases bone formation and decreases bone resorption, and has been shown in treatment-naive postmenopausal women with osteoporosis to significantly improve BMD and reduce fracture risk, compared with either placebo or alendronate. Romosozumab has also been studied as sequential therapy in patients treated initially with either alendronate or denosumab.
To see whether treatment sequence could have differential effects on clinical outcomes for patients with osteoporosis, Dr. Cosman and colleagues looked at results from four clinical trials, using levels of bone turnover markers (procollagen type I N-terminal propeptide [PINP] and beta-isomer of the C-terminal telopeptide of type I collagen [beta-CTX]) and BMD gains in the total hip and spine as outcomes.
The two trials of romosozumab in treatment-naive women were the ARCH trial comparing romosozumab with alendronate in a double-blind phase for 1 year, followed by 1 year of open-label alendronate, and the FRAME trial, in which romosozumab was compared with placebo in a 1-year double-blind phase, followed by 1-year of open-label denosumab.
The two trials of romosozumab in women treated initially with antiresorptive agents were the STRUCTURE trial in which patients on oral bisphosphonates for at least 3 years or alendronate 70 mg weekly for 1 year were randomized to receive either romosozumab or teriparatide, and a phase 2 trial (NCT00896532) that included a 24-month romosozumab or placebo treatment phase followed by rerandomization to a 12-month extension phase with denosumab or placebo, followed by a 12-month retreatment phase with romosozumab, followed by a 24-month follow-on phase with zoledronic acid or no intervention.
Total hip BMD gains
In the ARCH trial, total hip BMD increased 6.2% with 1 year of romosozumab, and a cumulative total of 7.1% with the 2-year romosozumab/alendronate sequence. In the FRAME trial, patients gained 6.8% in total hip BMD after 1 year of romosozumab and a total of 8.8% after 2 years of romosozumab followed by denosumab.
In contrast, in the STRUCTURE trial, patients treated for 1 year or longer with alendronate and then with 1 year of romosozumab had a 2.9% BMD gain in the total hip. In the phase 2 trial, 1 year of romosozumab following 1 year of denosumab yielded a 0.9% BMD gain, for a total gain of 3.8% with the denosumab sequence.
Lumbar spine BMD gains
In ARCH, lumbar spine BMD increased 13.7% with 1 year of romosozumab, and a total of 15.2% with the 2-year sequence of romosozumab followed by alendronate. Similarly, in FRAME, patients gained 13.3% in BMD after a year of romosozumab, and total of 17.6% by the end of the 2-year romosozumab/denosumab sequence.
In contrast, in STRUCTURE, patients who had previously been on alendronate for at least 1 year had a gain of 9.8% after 1 year of romosozumab, and in the phase 2 study, patients who had been on denosumab for 1 year had an increase in lumbar spine BMD of 5.3% after 1 year on romosozumab, and a total gain of 11.5% at the end of the 2-year sequence.
Serum PINP and beta-CTX
Looking at the markers of bone turnover, the investigators saw that, in both ARCH and FRAME, PINP peaked at over 80% of baseline at 1 month, and then continued to steadily decline past 1 year. The beta-CTX nadir was 40%-50% below baseline at 1 year.
At the end of year 2, the PINP nadir was –67% with follow-on alendronate, and –69% with denosumab, and the beta-CTX nadir was –72% and –92%, respectively.
In the two trials where romosozumab was the follow-on therapy, however, the trends were distinctly different. In STRUCTURE, for example, PINP peaked at 141% of baseline at 1 month, and then returned toward baseline, whereas beta-CTX remained largely unchanged.
In the phase 2 trial, PINP peaked at 28% above baseline at 9 months, and then only slightly declined, and beta-CTX peaked at 211% at the end of 1 year of romosozumab.
Best used up front
“This study is important, because it suggests that for the three bone-building drugs that the best effects will really be attained on bone strength if the agents are used as initial therapy in very-high-risk patients. Those are people who have sustained fractures within the preceding 2 years, who had multiple fractures at any point in their adulthood, and who present with very low BMD, particularly if they have any associated clinical risk factors such as family history or other underlying diseases or medications that have detrimental effects on bone,” Dr. Cosman said at the briefing.
Marcy Bolster, MD, from the division of rheumatology, allergy, and immunology at Massachusetts General Hospital, Boston, and associate professor of medicine at Harvard Medical School in Boston, who was not involved in the study, commented that the study provides important information for clinicians who treat patients with osteoporosis.
“We have an increasing number of medications available for use in the treatment of patients with osteoporosis, and as we consider the importance of reducing fracture risk, the duration of therapy, the timing of a bisphosphonate holiday, it is essential that we consider any advantages to the order or sequence of our medications,” she said when asked for comment.
“This study provides evidence supporting the concept of the ‘anabolic window’ in which there is a demonstrated advantage in treating patients with an anabolic agent prior to treatment with an antiresorptive agent, and while gains in bone mineral density were achieved with either order of medication use, the gains were more dramatic with treatment with romosozumab as the first agent,” she added.
Dr. Bolster also noted it will be important to demonstrate reduction in fracture risk as well as gain in BMD.
The study was sponsored by Amgen, Astellas, and UCB. Dr. Cosman disclosed grants/research support from Amgen, and consulting fees and speaker activities for Amgen and Radius Health. Dr. Bolster disclosed relationships with AbbVie, Corbus, Cumberland, Gilead, Johnson & Johnson, and Pfizer.
SOURCE: Cosman F et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 1973.
FROM ACR 2020
.
‘Disordered eating’ drops after teens undergo bariatric surgery
Kristina M. Decker, PhD, a postdoctoral fellow at Cincinnati Children’s Hospital Medical Center, presented these findings during the virtual ObesityWeek 2020.
Dr. Decker and associates examined rates of disordered eating in more than 200 adolescents (aged 13-18 years) who were severely obese, of whom 141 underwent bariatric surgery and the remainder did not.
At baseline (presurgery), the teens in both groups had rates of disordered eating ranging from 11% to 50%, with higher rates in those who went on to have bariatric surgery.
Six years later, rates of disordered eating were much lower in those who had bariatric surgery.
The data nevertheless “underscore that young adults with persistent severe obesity are at high risk for poor health and well-being,” Dr. Decker said in an interview.
“This means disordered eating behaviors should be closely monitored” in all such patients, both those who undergo surgery and those who don’t, she stressed.
Robust findings because of long follow-up and controls
The findings are not unexpected, based on adult bariatric literature, but are “novel because of the age of the patients,” senior author Margaret H. Zeller, PhD, Cincinnati Children’s Hospital Medical Center and professor at the University of Cincinnati, added.
In a comment comment, psychologist Kajsa Järvholm, PhD, of the Childhood Obesity Unit at Skåne University Hospital, Malmö̈, Sweden, who has published related work, said that this is “a needed study.”
Notably, it had “long-term follow-up and a control group,” and it “confirms that adolescents are in better control of their eating after surgery.”
However, an important additional takeaway for clinicians is that “disordered eating is associated with other mental health problems and self-worth. Clinicians treating obesity must address problems related to eating disorders to improve outcomes and well-being,” she stressed.
How does bariatric surgery impact overeating, binge eating, in teens?
“For teens with severe obesity, metabolic and bariatric surgery is the most effective treatment for improved cardiometabolic functioning, weight loss, and improved quality of life,” Dr. Decker stressed.
However, pre- and postsurgical disordered eating behaviors have been associated with a lower percentage change in body mass index (BMI), although this has not been well studied.
To investigate how disordered eating is affected by bariatric surgery in adolescents with severe obesity, researchers used data from Teen-LABS, which enrolled 242 participants aged 19 years and under who mainly underwent Roux-en-Y gastric bypass (67%) or sleeve gastrectomy (28%) from 2007 to 2012 at five adolescent bariatric surgery centers.
The current analysis examined data from 141 participants in Teen-LABS who underwent bariatric surgery at a mean age of 16.8 years. Mean BMI was 51.5, most were girls (80%), and they had diverse race/ethnicity (66% were White).
Researchers also identified a control group of 83 adolescents of a similar age and gender who had diverse race/ethnicity (54% White) and a mean BMI of 46.9.
At year 6, data were available for 123 young adults in the surgery group (who by then had a mean BMI of 39.7) and 63 young adults in the nonsurgery group (who had a mean BMI of 52.6).
At baseline and year 6, participants replied to questionnaires that identified three eating disorders: continuous eating (eating in an unplanned and repetitious way between meals and snacks), objective overeating (eating a “large” amount of food without loss of control), and objective binge eating (eating a “large” amount of food with loss of control).
At baseline, rates of continuous eating, overeating, and binge eating were higher in the surgical group (50%, 40%, and 30%, respectively) than the nonsurgical group (40%, 22%, and 11%, respectively).
Six years later, when participants were aged 19-24 years, rates of continuous eating, overeating, and binge eating had declined in the surgical group (to 17%, 5%, and 1%, respectively). In the nonsurgical group, only continuous eating and overeating declined (to 24% and 7%, respectively), and binge eating increased slightly (to 13%).
Disordered eating associated with low self-worth, anxiety, and depression
In young adulthood in both groups, disordered eating was associated with lower self-worth. In the surgical group, it was also associated with lower weight-related quality of life, and in the nonsurgical group, it was also associated with anxiety and/or depression.
“The current findings cannot tell us whether disordered eating is a direct result or caused by anxiety, depression, low self-worth, or poor quality of life,” Dr. Decker said.
“These findings do give us insight about what other areas of clinical concern might present together [in] young adults (e.g., disordered eating, low self-esteem).”
Bariatric surgery affects the amount of food people can eat at one time, she noted in reply to a question from the audience. If people eat too much at a time they can experience vomiting, dumping syndrome (where certain food is “dumped” into the small intestine without being digested, causing nausea and vomiting), and plugging (a sense of food becoming stuck).
The home environment and transition to adulthood might impact disordered eating in young adults, she said in reply to another question, but these issues were not examined in this study.
A version of this article originally appeared on Medscape.com.
Kristina M. Decker, PhD, a postdoctoral fellow at Cincinnati Children’s Hospital Medical Center, presented these findings during the virtual ObesityWeek 2020.
Dr. Decker and associates examined rates of disordered eating in more than 200 adolescents (aged 13-18 years) who were severely obese, of whom 141 underwent bariatric surgery and the remainder did not.
At baseline (presurgery), the teens in both groups had rates of disordered eating ranging from 11% to 50%, with higher rates in those who went on to have bariatric surgery.
Six years later, rates of disordered eating were much lower in those who had bariatric surgery.
The data nevertheless “underscore that young adults with persistent severe obesity are at high risk for poor health and well-being,” Dr. Decker said in an interview.
“This means disordered eating behaviors should be closely monitored” in all such patients, both those who undergo surgery and those who don’t, she stressed.
Robust findings because of long follow-up and controls
The findings are not unexpected, based on adult bariatric literature, but are “novel because of the age of the patients,” senior author Margaret H. Zeller, PhD, Cincinnati Children’s Hospital Medical Center and professor at the University of Cincinnati, added.
In a comment comment, psychologist Kajsa Järvholm, PhD, of the Childhood Obesity Unit at Skåne University Hospital, Malmö̈, Sweden, who has published related work, said that this is “a needed study.”
Notably, it had “long-term follow-up and a control group,” and it “confirms that adolescents are in better control of their eating after surgery.”
However, an important additional takeaway for clinicians is that “disordered eating is associated with other mental health problems and self-worth. Clinicians treating obesity must address problems related to eating disorders to improve outcomes and well-being,” she stressed.
How does bariatric surgery impact overeating, binge eating, in teens?
“For teens with severe obesity, metabolic and bariatric surgery is the most effective treatment for improved cardiometabolic functioning, weight loss, and improved quality of life,” Dr. Decker stressed.
However, pre- and postsurgical disordered eating behaviors have been associated with a lower percentage change in body mass index (BMI), although this has not been well studied.
To investigate how disordered eating is affected by bariatric surgery in adolescents with severe obesity, researchers used data from Teen-LABS, which enrolled 242 participants aged 19 years and under who mainly underwent Roux-en-Y gastric bypass (67%) or sleeve gastrectomy (28%) from 2007 to 2012 at five adolescent bariatric surgery centers.
The current analysis examined data from 141 participants in Teen-LABS who underwent bariatric surgery at a mean age of 16.8 years. Mean BMI was 51.5, most were girls (80%), and they had diverse race/ethnicity (66% were White).
Researchers also identified a control group of 83 adolescents of a similar age and gender who had diverse race/ethnicity (54% White) and a mean BMI of 46.9.
At year 6, data were available for 123 young adults in the surgery group (who by then had a mean BMI of 39.7) and 63 young adults in the nonsurgery group (who had a mean BMI of 52.6).
At baseline and year 6, participants replied to questionnaires that identified three eating disorders: continuous eating (eating in an unplanned and repetitious way between meals and snacks), objective overeating (eating a “large” amount of food without loss of control), and objective binge eating (eating a “large” amount of food with loss of control).
At baseline, rates of continuous eating, overeating, and binge eating were higher in the surgical group (50%, 40%, and 30%, respectively) than the nonsurgical group (40%, 22%, and 11%, respectively).
Six years later, when participants were aged 19-24 years, rates of continuous eating, overeating, and binge eating had declined in the surgical group (to 17%, 5%, and 1%, respectively). In the nonsurgical group, only continuous eating and overeating declined (to 24% and 7%, respectively), and binge eating increased slightly (to 13%).
Disordered eating associated with low self-worth, anxiety, and depression
In young adulthood in both groups, disordered eating was associated with lower self-worth. In the surgical group, it was also associated with lower weight-related quality of life, and in the nonsurgical group, it was also associated with anxiety and/or depression.
“The current findings cannot tell us whether disordered eating is a direct result or caused by anxiety, depression, low self-worth, or poor quality of life,” Dr. Decker said.
“These findings do give us insight about what other areas of clinical concern might present together [in] young adults (e.g., disordered eating, low self-esteem).”
Bariatric surgery affects the amount of food people can eat at one time, she noted in reply to a question from the audience. If people eat too much at a time they can experience vomiting, dumping syndrome (where certain food is “dumped” into the small intestine without being digested, causing nausea and vomiting), and plugging (a sense of food becoming stuck).
The home environment and transition to adulthood might impact disordered eating in young adults, she said in reply to another question, but these issues were not examined in this study.
A version of this article originally appeared on Medscape.com.
Kristina M. Decker, PhD, a postdoctoral fellow at Cincinnati Children’s Hospital Medical Center, presented these findings during the virtual ObesityWeek 2020.
Dr. Decker and associates examined rates of disordered eating in more than 200 adolescents (aged 13-18 years) who were severely obese, of whom 141 underwent bariatric surgery and the remainder did not.
At baseline (presurgery), the teens in both groups had rates of disordered eating ranging from 11% to 50%, with higher rates in those who went on to have bariatric surgery.
Six years later, rates of disordered eating were much lower in those who had bariatric surgery.
The data nevertheless “underscore that young adults with persistent severe obesity are at high risk for poor health and well-being,” Dr. Decker said in an interview.
“This means disordered eating behaviors should be closely monitored” in all such patients, both those who undergo surgery and those who don’t, she stressed.
Robust findings because of long follow-up and controls
The findings are not unexpected, based on adult bariatric literature, but are “novel because of the age of the patients,” senior author Margaret H. Zeller, PhD, Cincinnati Children’s Hospital Medical Center and professor at the University of Cincinnati, added.
In a comment comment, psychologist Kajsa Järvholm, PhD, of the Childhood Obesity Unit at Skåne University Hospital, Malmö̈, Sweden, who has published related work, said that this is “a needed study.”
Notably, it had “long-term follow-up and a control group,” and it “confirms that adolescents are in better control of their eating after surgery.”
However, an important additional takeaway for clinicians is that “disordered eating is associated with other mental health problems and self-worth. Clinicians treating obesity must address problems related to eating disorders to improve outcomes and well-being,” she stressed.
How does bariatric surgery impact overeating, binge eating, in teens?
“For teens with severe obesity, metabolic and bariatric surgery is the most effective treatment for improved cardiometabolic functioning, weight loss, and improved quality of life,” Dr. Decker stressed.
However, pre- and postsurgical disordered eating behaviors have been associated with a lower percentage change in body mass index (BMI), although this has not been well studied.
To investigate how disordered eating is affected by bariatric surgery in adolescents with severe obesity, researchers used data from Teen-LABS, which enrolled 242 participants aged 19 years and under who mainly underwent Roux-en-Y gastric bypass (67%) or sleeve gastrectomy (28%) from 2007 to 2012 at five adolescent bariatric surgery centers.
The current analysis examined data from 141 participants in Teen-LABS who underwent bariatric surgery at a mean age of 16.8 years. Mean BMI was 51.5, most were girls (80%), and they had diverse race/ethnicity (66% were White).
Researchers also identified a control group of 83 adolescents of a similar age and gender who had diverse race/ethnicity (54% White) and a mean BMI of 46.9.
At year 6, data were available for 123 young adults in the surgery group (who by then had a mean BMI of 39.7) and 63 young adults in the nonsurgery group (who had a mean BMI of 52.6).
At baseline and year 6, participants replied to questionnaires that identified three eating disorders: continuous eating (eating in an unplanned and repetitious way between meals and snacks), objective overeating (eating a “large” amount of food without loss of control), and objective binge eating (eating a “large” amount of food with loss of control).
At baseline, rates of continuous eating, overeating, and binge eating were higher in the surgical group (50%, 40%, and 30%, respectively) than the nonsurgical group (40%, 22%, and 11%, respectively).
Six years later, when participants were aged 19-24 years, rates of continuous eating, overeating, and binge eating had declined in the surgical group (to 17%, 5%, and 1%, respectively). In the nonsurgical group, only continuous eating and overeating declined (to 24% and 7%, respectively), and binge eating increased slightly (to 13%).
Disordered eating associated with low self-worth, anxiety, and depression
In young adulthood in both groups, disordered eating was associated with lower self-worth. In the surgical group, it was also associated with lower weight-related quality of life, and in the nonsurgical group, it was also associated with anxiety and/or depression.
“The current findings cannot tell us whether disordered eating is a direct result or caused by anxiety, depression, low self-worth, or poor quality of life,” Dr. Decker said.
“These findings do give us insight about what other areas of clinical concern might present together [in] young adults (e.g., disordered eating, low self-esteem).”
Bariatric surgery affects the amount of food people can eat at one time, she noted in reply to a question from the audience. If people eat too much at a time they can experience vomiting, dumping syndrome (where certain food is “dumped” into the small intestine without being digested, causing nausea and vomiting), and plugging (a sense of food becoming stuck).
The home environment and transition to adulthood might impact disordered eating in young adults, she said in reply to another question, but these issues were not examined in this study.
A version of this article originally appeared on Medscape.com.
Medication adherence challenges and helpers
For most chronic diseases, up to 20%-30% of the pills that are prescribed are not taken. In the case of inhalers for asthma and COPD, patients miss over half of the prescribed doses.
There are many things that contribute to the problem of poor adherence, but people often just simply forget. Thankfully, there are tools designed to help remind patients of what they need to take and when. A survey of apps developed to help patients remember to take their medicines found more than 700 available in Apple and Android app stores.1 Most apps focus on medication alerts, reminders, and medication logs.2 A recent review showed that apps have some – yet limited – effectiveness in increasing adherence, with patient self-reported improvements of 7%-40%.3

Another perhaps more promising area of improving adherence involves high-tech advances in the way medications can be taken. Inhalers are a primary target as they are complicated devices. A patient has to breathe in at the correct time after the inhaler is actuated, and the inhaler works optimally only if the rate of inhalation is sufficient to carry the medication into the lungs.
A number of companies have developed attachments for inhalers (and even inhalers themselves) that can record when the medication is taken through a Bluetooth connection to a patient’s smartphone. These can also assess inspiratory flow. Reminders to take the medication are built into the app, and those reminders disappear if the medication is taken. Patients can receive feedback about the quality of their timing and inspiratory rate to maximize medication delivery to the lungs.4
We learned long ago that it is difficult to take medications three to four times a day, so extended-release tablets were developed to reduce the frequency to once or twice a day. A great deal of work is now being done behind the scenes to develop medications that decrease the need for patients to remember to take their medications. The best examples of this are the long-acting reversible contraception (LARC) devices, specifically IUDs and Nexplanon. Compared with traditional oral contraceptives that need to be taken daily, LARCs reduce the rate of pregnancy by five- to tenfold.
We also now have medications for osteoporosis that can be taken monthly, or even annually. When bisphosphonates were first developed for osteoporosis prevention, they needed to be taken daily. Then a weekly bisphosphonate was developed. Now there is a once-monthly oral bisphosphonate, Ibandronate, and even a once yearly IV bisphosphonate.
Exciting developments have also occurred in the management of diabetes. We may be tempted to take for granted how once-daily long-acting insulin, which releases insulin slowly over the course of a day, has revolutionized the diabetic treatment since its Food and Drug Administration approval in 2000. Yet progress did not end there. The first GLP-1 receptor agonist for diabetes was approved in 2005 and was a twice-a-day medicine. Shortly afterward, a daily GLP-1 was approved, and now there are three once-weekly GLP-1 receptor agonists.
Several pharmaceutical manufacturers are now working on a once-weekly insulin,5 as well as an implantable GLP-1 receptor agonist that will need to be replaced every 6-12 months.6 Imagine your patient coming in once a year to replace his or her potent glucose lowering medication – one that offers a low incidence of hypoglycemia, maintains glucose control all year long, and requires no adherence to a complicated medication regimen.
Similar technology is being used to develop a once-yearly anti-HIV prophylactic medication delivery system.7 This could help prevent the spread of HIV in areas of the world where it may be difficult for people to take daily medications.7
The many technological advances we have described may help us reduce our likelihood of missing a dose of a medication. We are hopeful that progress in this area will continue, and that one day medication adherence will require even less effort from patients than it does today.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Follow him on Twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
References
1. Tabi K et al. Mobile apps for medication management: Review and analysis. JMIR Mhealth Uhealth. 2019 Sep 7(9):13608.
2. Park JYE et al. Mobile phone apps targeting medication adherence: Quality assessment and content analysis of user reviews. JMIR Mhealth Uhealth. 2019 Jan 31;7(1):e11919.
3. Pérez-Jover V et al. Mobile apps for increasing treatment adherence: Systematic review. J Med Internet Res. 2019;21(6):e12505. doi: 10.2196/12505.
4. 4 Smart inhalers that could be lifesaving for people living with asthma & COPD. MyTherapy, July 11, 2019.
5. Rosenstock J et al. Once-weekly insulin for type 2 diabetes without previous insulin treatment. N Engl J Med. 2020 Sep 22. doi: 10.1056/NEJMoa2022474.
6. GLP-1 agonists: From 2 daily injections to 1 per week and beyond. DiaTribe, Jan. 10, 2018.
7. Long-acting HIV prevention tools. Hiv.gov, July 20, 2019.
For most chronic diseases, up to 20%-30% of the pills that are prescribed are not taken. In the case of inhalers for asthma and COPD, patients miss over half of the prescribed doses.
There are many things that contribute to the problem of poor adherence, but people often just simply forget. Thankfully, there are tools designed to help remind patients of what they need to take and when. A survey of apps developed to help patients remember to take their medicines found more than 700 available in Apple and Android app stores.1 Most apps focus on medication alerts, reminders, and medication logs.2 A recent review showed that apps have some – yet limited – effectiveness in increasing adherence, with patient self-reported improvements of 7%-40%.3
Another perhaps more promising area of improving adherence involves high-tech advances in the way medications can be taken. Inhalers are a primary target as they are complicated devices. A patient has to breathe in at the correct time after the inhaler is actuated, and the inhaler works optimally only if the rate of inhalation is sufficient to carry the medication into the lungs.
A number of companies have developed attachments for inhalers (and even inhalers themselves) that can record when the medication is taken through a Bluetooth connection to a patient’s smartphone. These can also assess inspiratory flow. Reminders to take the medication are built into the app, and those reminders disappear if the medication is taken. Patients can receive feedback about the quality of their timing and inspiratory rate to maximize medication delivery to the lungs.4
We learned long ago that it is difficult to take medications three to four times a day, so extended-release tablets were developed to reduce the frequency to once or twice a day. A great deal of work is now being done behind the scenes to develop medications that decrease the need for patients to remember to take their medications. The best examples of this are the long-acting reversible contraception (LARC) devices, specifically IUDs and Nexplanon. Compared with traditional oral contraceptives that need to be taken daily, LARCs reduce the rate of pregnancy by five- to tenfold.
We also now have medications for osteoporosis that can be taken monthly, or even annually. When bisphosphonates were first developed for osteoporosis prevention, they needed to be taken daily. Then a weekly bisphosphonate was developed. Now there is a once-monthly oral bisphosphonate, Ibandronate, and even a once yearly IV bisphosphonate.
Exciting developments have also occurred in the management of diabetes. We may be tempted to take for granted how once-daily long-acting insulin, which releases insulin slowly over the course of a day, has revolutionized the diabetic treatment since its Food and Drug Administration approval in 2000. Yet progress did not end there. The first GLP-1 receptor agonist for diabetes was approved in 2005 and was a twice-a-day medicine. Shortly afterward, a daily GLP-1 was approved, and now there are three once-weekly GLP-1 receptor agonists.
Several pharmaceutical manufacturers are now working on a once-weekly insulin,5 as well as an implantable GLP-1 receptor agonist that will need to be replaced every 6-12 months.6 Imagine your patient coming in once a year to replace his or her potent glucose lowering medication – one that offers a low incidence of hypoglycemia, maintains glucose control all year long, and requires no adherence to a complicated medication regimen.
Similar technology is being used to develop a once-yearly anti-HIV prophylactic medication delivery system.7 This could help prevent the spread of HIV in areas of the world where it may be difficult for people to take daily medications.7
The many technological advances we have described may help us reduce our likelihood of missing a dose of a medication. We are hopeful that progress in this area will continue, and that one day medication adherence will require even less effort from patients than it does today.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Follow him on Twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
References
1. Tabi K et al. Mobile apps for medication management: Review and analysis. JMIR Mhealth Uhealth. 2019 Sep 7(9):13608.
2. Park JYE et al. Mobile phone apps targeting medication adherence: Quality assessment and content analysis of user reviews. JMIR Mhealth Uhealth. 2019 Jan 31;7(1):e11919.
3. Pérez-Jover V et al. Mobile apps for increasing treatment adherence: Systematic review. J Med Internet Res. 2019;21(6):e12505. doi: 10.2196/12505.
4. 4 Smart inhalers that could be lifesaving for people living with asthma & COPD. MyTherapy, July 11, 2019.
5. Rosenstock J et al. Once-weekly insulin for type 2 diabetes without previous insulin treatment. N Engl J Med. 2020 Sep 22. doi: 10.1056/NEJMoa2022474.
6. GLP-1 agonists: From 2 daily injections to 1 per week and beyond. DiaTribe, Jan. 10, 2018.
7. Long-acting HIV prevention tools. Hiv.gov, July 20, 2019.
For most chronic diseases, up to 20%-30% of the pills that are prescribed are not taken. In the case of inhalers for asthma and COPD, patients miss over half of the prescribed doses.
There are many things that contribute to the problem of poor adherence, but people often just simply forget. Thankfully, there are tools designed to help remind patients of what they need to take and when. A survey of apps developed to help patients remember to take their medicines found more than 700 available in Apple and Android app stores.1 Most apps focus on medication alerts, reminders, and medication logs.2 A recent review showed that apps have some – yet limited – effectiveness in increasing adherence, with patient self-reported improvements of 7%-40%.3
Another perhaps more promising area of improving adherence involves high-tech advances in the way medications can be taken. Inhalers are a primary target as they are complicated devices. A patient has to breathe in at the correct time after the inhaler is actuated, and the inhaler works optimally only if the rate of inhalation is sufficient to carry the medication into the lungs.
A number of companies have developed attachments for inhalers (and even inhalers themselves) that can record when the medication is taken through a Bluetooth connection to a patient’s smartphone. These can also assess inspiratory flow. Reminders to take the medication are built into the app, and those reminders disappear if the medication is taken. Patients can receive feedback about the quality of their timing and inspiratory rate to maximize medication delivery to the lungs.4
We learned long ago that it is difficult to take medications three to four times a day, so extended-release tablets were developed to reduce the frequency to once or twice a day. A great deal of work is now being done behind the scenes to develop medications that decrease the need for patients to remember to take their medications. The best examples of this are the long-acting reversible contraception (LARC) devices, specifically IUDs and Nexplanon. Compared with traditional oral contraceptives that need to be taken daily, LARCs reduce the rate of pregnancy by five- to tenfold.
We also now have medications for osteoporosis that can be taken monthly, or even annually. When bisphosphonates were first developed for osteoporosis prevention, they needed to be taken daily. Then a weekly bisphosphonate was developed. Now there is a once-monthly oral bisphosphonate, Ibandronate, and even a once yearly IV bisphosphonate.
Exciting developments have also occurred in the management of diabetes. We may be tempted to take for granted how once-daily long-acting insulin, which releases insulin slowly over the course of a day, has revolutionized the diabetic treatment since its Food and Drug Administration approval in 2000. Yet progress did not end there. The first GLP-1 receptor agonist for diabetes was approved in 2005 and was a twice-a-day medicine. Shortly afterward, a daily GLP-1 was approved, and now there are three once-weekly GLP-1 receptor agonists.
Several pharmaceutical manufacturers are now working on a once-weekly insulin,5 as well as an implantable GLP-1 receptor agonist that will need to be replaced every 6-12 months.6 Imagine your patient coming in once a year to replace his or her potent glucose lowering medication – one that offers a low incidence of hypoglycemia, maintains glucose control all year long, and requires no adherence to a complicated medication regimen.
Similar technology is being used to develop a once-yearly anti-HIV prophylactic medication delivery system.7 This could help prevent the spread of HIV in areas of the world where it may be difficult for people to take daily medications.7
The many technological advances we have described may help us reduce our likelihood of missing a dose of a medication. We are hopeful that progress in this area will continue, and that one day medication adherence will require even less effort from patients than it does today.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Follow him on Twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
References
1. Tabi K et al. Mobile apps for medication management: Review and analysis. JMIR Mhealth Uhealth. 2019 Sep 7(9):13608.
2. Park JYE et al. Mobile phone apps targeting medication adherence: Quality assessment and content analysis of user reviews. JMIR Mhealth Uhealth. 2019 Jan 31;7(1):e11919.
3. Pérez-Jover V et al. Mobile apps for increasing treatment adherence: Systematic review. J Med Internet Res. 2019;21(6):e12505. doi: 10.2196/12505.
4. 4 Smart inhalers that could be lifesaving for people living with asthma & COPD. MyTherapy, July 11, 2019.
5. Rosenstock J et al. Once-weekly insulin for type 2 diabetes without previous insulin treatment. N Engl J Med. 2020 Sep 22. doi: 10.1056/NEJMoa2022474.
6. GLP-1 agonists: From 2 daily injections to 1 per week and beyond. DiaTribe, Jan. 10, 2018.
7. Long-acting HIV prevention tools. Hiv.gov, July 20, 2019.
First-of-its kind guideline on lipid monitoring in endocrine diseases
Endocrine diseases of any type – not just diabetes – can represent a cardiovascular risk and patients with those disorders should be screened for high cholesterol, according to a new clinical practice guideline from the Endocrine Society.
“The simple recommendation to check a lipid panel in patients with endocrine diseases and calculate cardiovascular risk may be practice changing because that is not done routinely,” Connie Newman, MD, chair of the Endocrine Society committee that developed the guideline, said in an interview.
“Usually the focus is on assessment and treatment of the endocrine disease, rather than on assessment and treatment of atherosclerotic cardiovascular disease risk,” said Newman, an adjunct professor of medicine in the department of medicine, division of endocrinology, diabetes & metabolism, at New York University.
Whereas diabetes, well-known for its increased cardiovascular risk profile, is commonly addressed in other cardiovascular and cholesterol practice management guidelines, the array of other endocrine diseases are not typically included.
“This guideline is the first of its kind,” Dr. Newman said. “The Endocrine Society has not previously issued a guideline on lipid management in endocrine disorders [and] other organizations have not written guidelines on this topic.
“Rather, guidelines have been written on cholesterol management, but these do not describe cholesterol management in patients with endocrine diseases such as thyroid disease [hypothyroidism and hyperthyroidism], Cushing’s syndrome, acromegaly, growth hormone deficiency, menopause, male hypogonadism, and obesity,” she noted.
But these conditions carry a host of cardiovascular risk factors that may require careful monitoring and management.
“Although endocrine hormones, such as thyroid hormone, cortisol, estrogen, testosterone, growth hormone, and insulin, affect pathways for lipid metabolism, physicians lack guidance on lipid abnormalities, cardiovascular risk, and treatment to reduce lipids and cardiovascular risk in patients with endocrine diseases,” she explained.
Vinaya Simha, MD, an internal medicine specialist at the Mayo Clinic in Rochester, Minn., agrees that the guideline is notable in addressing an unmet need.
Recommendations that stand out to Dr. Simha include the suggestion of adding eicosapentaenoic acid (EPA) ethyl ester to reduce the risk of cardiovascular disease in adults with diabetes or atherosclerotic cardiovascular disease who have elevated triglyceride levels despite statin treatment.
James L. Rosenzweig, MD, an endocrinologist at Hebrew SeniorLife in Boston, agreed that this is an important addition to an area that needs more guidance.
“Many of these clinical situations can exacerbate dyslipidemia and some also increase the cardiovascular risk to a greater extent in combination with elevated cholesterol and/or triglycerides,” he said in an interview.
“In many cases, treatment of the underlying disorder appropriately can have an important impact in resolving the lipid disorder. In others, more aggressive pharmacological treatment is indicated,” he said.
“I think that this will be a valuable resource, especially for endocrinologists, but it can be used as well by providers in other disciplines.”
Key recommendations for different endocrine conditions
The guideline, published in the Journal of Clinical Endocrinology & Metabolism, details those risks and provides evidence-based recommendations on their management and treatment.
Key recommendations include:
- Obtain a lipid panel and evaluate cardiovascular risk factors in all adults with endocrine disorders.
- In patients with and risk factors for cardiovascular disease, start statin therapy in addition to lifestyle modification to reduce cardiovascular risk. “This could mean earlier treatment because other guidelines recommend consideration of therapy at age 40,” Dr. Newman said.
- Statin therapy is also recommended for adults over 40 with with a duration of diabetes of more than 20 years and/or microvascular complications, regardless of their cardiovascular risk score. “This means earlier treatment of patients with type 1 diabetes with statins in order to reduce cardiovascular disease risk,” Dr. Newman noted.
- In patients with hyperlipidemia, rule out as the cause before treating with lipid-lowering medications. And among patients who are found to have hypothyroidism, reevaluate the lipid profile when the patient has thyroid hormone levels in the normal range.
- Adults with persistent endogenous Cushing’s syndrome should have their lipid profile monitored. Statin therapy should be considered in addition to lifestyle modifications, irrespective of the cardiovascular risk score.
- In postmenopausal women, high cholesterol or triglycerides should be treated with statins rather than hormone therapy.
- Evaluate and treat lipids and other cardiovascular risk factors in women who enter menopause early (before the age of 40-45 years).
Nice summary of ‘risk-enhancing’ endocrine disorders
Dr. Simha said in an interview that the new guideline is “probably the first comprehensive statement addressing lipid treatment in patients with a broad range of endocrine disorders besides diabetes.”
“Most of the treatment recommendations are congruent with other current guidelines such as the American College of Cardiology/American Heart Association [guidelines], but there is specific mention of which endocrine disorders represent enhanced cardiovascular risk,” she explained.
The new recommendations are notable for including “a nice summary of how different endocrine disorders affect lipid values, and also which endocrine disorders need to be considered as ‘risk-enhancing factors,’ ” Dr. Simha noted.
“The use of EPA in patients with hypertriglyceridemia is novel, compared to the ACC/AHA recommendation. This reflects new data which is now available,” she added.
The American Association of Clinical Endocrinologists also just issued a new algorithm on lipid management and prevention of cardiovascular disease in which treatment of hypertriglyceridemia is emphasized.
In addition, the new Endocrine Society guideline “also mentions an LDL [cholesterol] treatment threshold of 70 mg/dL, and 55 mg/dL in some patient categories, which previous guidelines have not,” Dr. Simha noted.
Overall, Dr. Newman added that the goal of the guideline is to increase awareness of key issues with endocrine diseases that may not necessarily be on clinicians’ radars.
“We hope that it will make a lipid panel and cardiovascular risk evaluation routine in adults with endocrine diseases and cause a greater focus on therapies to reduce heart disease and stroke,” she said.
Dr. Newman, Dr. Simha, and Dr. Rosenzweig reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Endocrine diseases of any type – not just diabetes – can represent a cardiovascular risk and patients with those disorders should be screened for high cholesterol, according to a new clinical practice guideline from the Endocrine Society.
“The simple recommendation to check a lipid panel in patients with endocrine diseases and calculate cardiovascular risk may be practice changing because that is not done routinely,” Connie Newman, MD, chair of the Endocrine Society committee that developed the guideline, said in an interview.
“Usually the focus is on assessment and treatment of the endocrine disease, rather than on assessment and treatment of atherosclerotic cardiovascular disease risk,” said Newman, an adjunct professor of medicine in the department of medicine, division of endocrinology, diabetes & metabolism, at New York University.
Whereas diabetes, well-known for its increased cardiovascular risk profile, is commonly addressed in other cardiovascular and cholesterol practice management guidelines, the array of other endocrine diseases are not typically included.
“This guideline is the first of its kind,” Dr. Newman said. “The Endocrine Society has not previously issued a guideline on lipid management in endocrine disorders [and] other organizations have not written guidelines on this topic.
“Rather, guidelines have been written on cholesterol management, but these do not describe cholesterol management in patients with endocrine diseases such as thyroid disease [hypothyroidism and hyperthyroidism], Cushing’s syndrome, acromegaly, growth hormone deficiency, menopause, male hypogonadism, and obesity,” she noted.
But these conditions carry a host of cardiovascular risk factors that may require careful monitoring and management.
“Although endocrine hormones, such as thyroid hormone, cortisol, estrogen, testosterone, growth hormone, and insulin, affect pathways for lipid metabolism, physicians lack guidance on lipid abnormalities, cardiovascular risk, and treatment to reduce lipids and cardiovascular risk in patients with endocrine diseases,” she explained.
Vinaya Simha, MD, an internal medicine specialist at the Mayo Clinic in Rochester, Minn., agrees that the guideline is notable in addressing an unmet need.
Recommendations that stand out to Dr. Simha include the suggestion of adding eicosapentaenoic acid (EPA) ethyl ester to reduce the risk of cardiovascular disease in adults with diabetes or atherosclerotic cardiovascular disease who have elevated triglyceride levels despite statin treatment.
James L. Rosenzweig, MD, an endocrinologist at Hebrew SeniorLife in Boston, agreed that this is an important addition to an area that needs more guidance.
“Many of these clinical situations can exacerbate dyslipidemia and some also increase the cardiovascular risk to a greater extent in combination with elevated cholesterol and/or triglycerides,” he said in an interview.
“In many cases, treatment of the underlying disorder appropriately can have an important impact in resolving the lipid disorder. In others, more aggressive pharmacological treatment is indicated,” he said.
“I think that this will be a valuable resource, especially for endocrinologists, but it can be used as well by providers in other disciplines.”
Key recommendations for different endocrine conditions
The guideline, published in the Journal of Clinical Endocrinology & Metabolism, details those risks and provides evidence-based recommendations on their management and treatment.
Key recommendations include:
- Obtain a lipid panel and evaluate cardiovascular risk factors in all adults with endocrine disorders.
- In patients with and risk factors for cardiovascular disease, start statin therapy in addition to lifestyle modification to reduce cardiovascular risk. “This could mean earlier treatment because other guidelines recommend consideration of therapy at age 40,” Dr. Newman said.
- Statin therapy is also recommended for adults over 40 with with a duration of diabetes of more than 20 years and/or microvascular complications, regardless of their cardiovascular risk score. “This means earlier treatment of patients with type 1 diabetes with statins in order to reduce cardiovascular disease risk,” Dr. Newman noted.
- In patients with hyperlipidemia, rule out as the cause before treating with lipid-lowering medications. And among patients who are found to have hypothyroidism, reevaluate the lipid profile when the patient has thyroid hormone levels in the normal range.
- Adults with persistent endogenous Cushing’s syndrome should have their lipid profile monitored. Statin therapy should be considered in addition to lifestyle modifications, irrespective of the cardiovascular risk score.
- In postmenopausal women, high cholesterol or triglycerides should be treated with statins rather than hormone therapy.
- Evaluate and treat lipids and other cardiovascular risk factors in women who enter menopause early (before the age of 40-45 years).
Nice summary of ‘risk-enhancing’ endocrine disorders
Dr. Simha said in an interview that the new guideline is “probably the first comprehensive statement addressing lipid treatment in patients with a broad range of endocrine disorders besides diabetes.”
“Most of the treatment recommendations are congruent with other current guidelines such as the American College of Cardiology/American Heart Association [guidelines], but there is specific mention of which endocrine disorders represent enhanced cardiovascular risk,” she explained.
The new recommendations are notable for including “a nice summary of how different endocrine disorders affect lipid values, and also which endocrine disorders need to be considered as ‘risk-enhancing factors,’ ” Dr. Simha noted.
“The use of EPA in patients with hypertriglyceridemia is novel, compared to the ACC/AHA recommendation. This reflects new data which is now available,” she added.
The American Association of Clinical Endocrinologists also just issued a new algorithm on lipid management and prevention of cardiovascular disease in which treatment of hypertriglyceridemia is emphasized.
In addition, the new Endocrine Society guideline “also mentions an LDL [cholesterol] treatment threshold of 70 mg/dL, and 55 mg/dL in some patient categories, which previous guidelines have not,” Dr. Simha noted.
Overall, Dr. Newman added that the goal of the guideline is to increase awareness of key issues with endocrine diseases that may not necessarily be on clinicians’ radars.
“We hope that it will make a lipid panel and cardiovascular risk evaluation routine in adults with endocrine diseases and cause a greater focus on therapies to reduce heart disease and stroke,” she said.
Dr. Newman, Dr. Simha, and Dr. Rosenzweig reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Endocrine diseases of any type – not just diabetes – can represent a cardiovascular risk and patients with those disorders should be screened for high cholesterol, according to a new clinical practice guideline from the Endocrine Society.
“The simple recommendation to check a lipid panel in patients with endocrine diseases and calculate cardiovascular risk may be practice changing because that is not done routinely,” Connie Newman, MD, chair of the Endocrine Society committee that developed the guideline, said in an interview.
“Usually the focus is on assessment and treatment of the endocrine disease, rather than on assessment and treatment of atherosclerotic cardiovascular disease risk,” said Newman, an adjunct professor of medicine in the department of medicine, division of endocrinology, diabetes & metabolism, at New York University.
Whereas diabetes, well-known for its increased cardiovascular risk profile, is commonly addressed in other cardiovascular and cholesterol practice management guidelines, the array of other endocrine diseases are not typically included.
“This guideline is the first of its kind,” Dr. Newman said. “The Endocrine Society has not previously issued a guideline on lipid management in endocrine disorders [and] other organizations have not written guidelines on this topic.
“Rather, guidelines have been written on cholesterol management, but these do not describe cholesterol management in patients with endocrine diseases such as thyroid disease [hypothyroidism and hyperthyroidism], Cushing’s syndrome, acromegaly, growth hormone deficiency, menopause, male hypogonadism, and obesity,” she noted.
But these conditions carry a host of cardiovascular risk factors that may require careful monitoring and management.
“Although endocrine hormones, such as thyroid hormone, cortisol, estrogen, testosterone, growth hormone, and insulin, affect pathways for lipid metabolism, physicians lack guidance on lipid abnormalities, cardiovascular risk, and treatment to reduce lipids and cardiovascular risk in patients with endocrine diseases,” she explained.
Vinaya Simha, MD, an internal medicine specialist at the Mayo Clinic in Rochester, Minn., agrees that the guideline is notable in addressing an unmet need.
Recommendations that stand out to Dr. Simha include the suggestion of adding eicosapentaenoic acid (EPA) ethyl ester to reduce the risk of cardiovascular disease in adults with diabetes or atherosclerotic cardiovascular disease who have elevated triglyceride levels despite statin treatment.
James L. Rosenzweig, MD, an endocrinologist at Hebrew SeniorLife in Boston, agreed that this is an important addition to an area that needs more guidance.
“Many of these clinical situations can exacerbate dyslipidemia and some also increase the cardiovascular risk to a greater extent in combination with elevated cholesterol and/or triglycerides,” he said in an interview.
“In many cases, treatment of the underlying disorder appropriately can have an important impact in resolving the lipid disorder. In others, more aggressive pharmacological treatment is indicated,” he said.
“I think that this will be a valuable resource, especially for endocrinologists, but it can be used as well by providers in other disciplines.”
Key recommendations for different endocrine conditions
The guideline, published in the Journal of Clinical Endocrinology & Metabolism, details those risks and provides evidence-based recommendations on their management and treatment.
Key recommendations include:
- Obtain a lipid panel and evaluate cardiovascular risk factors in all adults with endocrine disorders.
- In patients with and risk factors for cardiovascular disease, start statin therapy in addition to lifestyle modification to reduce cardiovascular risk. “This could mean earlier treatment because other guidelines recommend consideration of therapy at age 40,” Dr. Newman said.
- Statin therapy is also recommended for adults over 40 with with a duration of diabetes of more than 20 years and/or microvascular complications, regardless of their cardiovascular risk score. “This means earlier treatment of patients with type 1 diabetes with statins in order to reduce cardiovascular disease risk,” Dr. Newman noted.
- In patients with hyperlipidemia, rule out as the cause before treating with lipid-lowering medications. And among patients who are found to have hypothyroidism, reevaluate the lipid profile when the patient has thyroid hormone levels in the normal range.
- Adults with persistent endogenous Cushing’s syndrome should have their lipid profile monitored. Statin therapy should be considered in addition to lifestyle modifications, irrespective of the cardiovascular risk score.
- In postmenopausal women, high cholesterol or triglycerides should be treated with statins rather than hormone therapy.
- Evaluate and treat lipids and other cardiovascular risk factors in women who enter menopause early (before the age of 40-45 years).
Nice summary of ‘risk-enhancing’ endocrine disorders
Dr. Simha said in an interview that the new guideline is “probably the first comprehensive statement addressing lipid treatment in patients with a broad range of endocrine disorders besides diabetes.”
“Most of the treatment recommendations are congruent with other current guidelines such as the American College of Cardiology/American Heart Association [guidelines], but there is specific mention of which endocrine disorders represent enhanced cardiovascular risk,” she explained.
The new recommendations are notable for including “a nice summary of how different endocrine disorders affect lipid values, and also which endocrine disorders need to be considered as ‘risk-enhancing factors,’ ” Dr. Simha noted.
“The use of EPA in patients with hypertriglyceridemia is novel, compared to the ACC/AHA recommendation. This reflects new data which is now available,” she added.
The American Association of Clinical Endocrinologists also just issued a new algorithm on lipid management and prevention of cardiovascular disease in which treatment of hypertriglyceridemia is emphasized.
In addition, the new Endocrine Society guideline “also mentions an LDL [cholesterol] treatment threshold of 70 mg/dL, and 55 mg/dL in some patient categories, which previous guidelines have not,” Dr. Simha noted.
Overall, Dr. Newman added that the goal of the guideline is to increase awareness of key issues with endocrine diseases that may not necessarily be on clinicians’ radars.
“We hope that it will make a lipid panel and cardiovascular risk evaluation routine in adults with endocrine diseases and cause a greater focus on therapies to reduce heart disease and stroke,” she said.
Dr. Newman, Dr. Simha, and Dr. Rosenzweig reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Consensus guidelines address inpatient diabetes technology
A new consensus statement offers detailed guidelines for inpatient use of continuous glucose monitors (CGM) and automated insulin delivery (AID) systems.
Aimed at clinicians, researchers, and hospital administrators, the open-access document was recently published by a multidisciplinary international panel of 24 experts in the Journal of Diabetes Science and Technology.
The statement includes 77 separate recommendations under five headings: 1) continued use of CGM by patients already using them at home, 2) initiation of CGM in hospital, 3) continuation of AID systems in hospital by patients already using them at home, 4) logistics and hands-on care of hospitalized patients using CGM and AID systems, and 5) data management of CGM and AID systems in hospital.
“This is the most comprehensive and up-to-date guideline on the use of diabetes technology in the hospital now,” lead author Rodolfo J. Galindo, MD, told Medscape Medical News in an interview.
“Overall, most experts believe that CGM and AID have the potential to overcome the current limitations of glycemic monitoring in the hospital to improve patient outcomes, but we need research – first to get the approval and second to get widespread use,” said Galindo, medical chair of the hospital diabetes taskforce at Emory Healthcare System, Atlanta.
“COVID-19 changed everything”
The guideline is an update of a 2017 statement on hospital use of CGM. The new guideline adds AID systems (sometimes referred to as an artificial pancreas), which combines a CGM and insulin pump and uses an algorithm to guide insulin delivery, and is the first to be developed during the COVID-19 era.
The update had been planned prior to the pandemic, but the actual panel meeting took place in April 2020, after the US Food and Drug Administration allowed inpatient use of CGM despite lack of official approval.
“COVID-19 changed everything. ... We had to be more specific about how to implement CGM in these patients. The standard of care is hourly point-of-care glucose monitoring in the [ICU], and at least every 4 hours outside the ICU. With limited [personal protective equipment] and the burden on nursing it was unachievable,” Galindo explained.
In June 2020, Galindo and other guideline authors developed a COVID-19–specific document (also open-access), which goes more into detail about CGM and how to implement in-hospital use during the pandemic.
The current consensus guideline “provides a high-level review of the evidence by experts,” Galindo added.
Recommendations cover different technologies and hospital settings
The panel “strongly” advises that hospital providers consult with an inpatient diabetes team, if available, to help manage patients already using CGM prior to admission. Among other recommendations, they list several situations in which CGM data should not be relied upon for management decisions, including severe hyper- or hypoglycemia, diabetic ketoacidosis, or in patients with skin infections near the sensor site.
The panel also call for more research into outcomes for CGM continuation in the hospital and optimal implementation of both CGM and point-of-care glucose testing. For hospitals, strong recommendations include developing standard CGM data reports and workflows, as well as policies for CGM use.
Galindo pointed out: “A lot of hospitals have policies on that, but there aren’t many studies. It’s just that patients like it and it’s very hard to take it away from patients when they’re doing well.”
The section on CGM inpatient initiation is where COVID-19 plays the greatest role, which includes just one strong clinical practice recommendation: “Healthcare providers should consider prescribing CGM to reduce the need for frequent nurse contact for point-of-care glucose testing and the use of personal protective equipment for patients on isolation with highly contagious infectious diseases (eg, COVID-19).”
Strong recommendations also include a call for outcomes research and for hospitals to develop CGM protocols and educational tools for staff.
“We can do a study for approval but if administration and hospital policies aren’t there we’re not going to be able to use them,” Galindo noted.
For patients who already use AID systems – either the Medtronic 670G or Tandem Control IQ in the United States – the panel advises assessment to ensure the AID system is the most appropriate inpatient treatment, and the development of an alternative plan for diabetes management, if necessary. They also strongly recommend research in this area, and for hospitals to develop protocols for use of AID systems in various clinical situations.
Most detailed guidance addresses logistics and data management
Most of the strong recommendations regarding logistics are aimed at nursing staff, including receiving training in use of CGM and AID systems, confirming patient capacity, inspection of devices, and understanding when to administer a point-of-care glucose test.
Again, the panel calls for more data and for hospitals to develop policies and protocols for ensuring safe CGM and AID systems use, and when to avoid use.
Finally, they make one strong clinical recommendation regarding data management: “Healthcare providers should develop a set of core data elements and definitions for CGM data for inclusion in common data models and the electronic health record.”
That’s followed by a long list of relevant recommendations for research in the area, and for hospitals to integrate CGM and AID system data into their EHR systems.
This last area has proven particularly challenging, Galindo said. “Right now we do four point-of-care glucoses a day, and that goes right into the EHR, but with CGM it’s much more than that. How do we get all those data into the EHR and interpret it? Many steps need to be taken into consideration.”
Studies are being conducted in order to fulfill requirements for FDA approval of inpatient CGM use, he said, with data on implementation and inpatient AID system use to follow.
“More data will be available, triggered by the COVID-19 pandemic. However, the use of technology in the hospital goes beyond COVID-19,” he said
Galindo has reported receiving unrestricted research support to Emory for investigator-initiated studies from Novo Nordisk and Dexcom, and consulting fees from Abbott Diabetes Care, Sanofi, Novo Nordisk, Eli Lilly, and Valeritas. He is partially supported by research grants from the NIH/NIDDK.
This article first appeared on Medscape.com.
A new consensus statement offers detailed guidelines for inpatient use of continuous glucose monitors (CGM) and automated insulin delivery (AID) systems.
Aimed at clinicians, researchers, and hospital administrators, the open-access document was recently published by a multidisciplinary international panel of 24 experts in the Journal of Diabetes Science and Technology.
The statement includes 77 separate recommendations under five headings: 1) continued use of CGM by patients already using them at home, 2) initiation of CGM in hospital, 3) continuation of AID systems in hospital by patients already using them at home, 4) logistics and hands-on care of hospitalized patients using CGM and AID systems, and 5) data management of CGM and AID systems in hospital.
“This is the most comprehensive and up-to-date guideline on the use of diabetes technology in the hospital now,” lead author Rodolfo J. Galindo, MD, told Medscape Medical News in an interview.
“Overall, most experts believe that CGM and AID have the potential to overcome the current limitations of glycemic monitoring in the hospital to improve patient outcomes, but we need research – first to get the approval and second to get widespread use,” said Galindo, medical chair of the hospital diabetes taskforce at Emory Healthcare System, Atlanta.
“COVID-19 changed everything”
The guideline is an update of a 2017 statement on hospital use of CGM. The new guideline adds AID systems (sometimes referred to as an artificial pancreas), which combines a CGM and insulin pump and uses an algorithm to guide insulin delivery, and is the first to be developed during the COVID-19 era.
The update had been planned prior to the pandemic, but the actual panel meeting took place in April 2020, after the US Food and Drug Administration allowed inpatient use of CGM despite lack of official approval.
“COVID-19 changed everything. ... We had to be more specific about how to implement CGM in these patients. The standard of care is hourly point-of-care glucose monitoring in the [ICU], and at least every 4 hours outside the ICU. With limited [personal protective equipment] and the burden on nursing it was unachievable,” Galindo explained.
In June 2020, Galindo and other guideline authors developed a COVID-19–specific document (also open-access), which goes more into detail about CGM and how to implement in-hospital use during the pandemic.
The current consensus guideline “provides a high-level review of the evidence by experts,” Galindo added.
Recommendations cover different technologies and hospital settings
The panel “strongly” advises that hospital providers consult with an inpatient diabetes team, if available, to help manage patients already using CGM prior to admission. Among other recommendations, they list several situations in which CGM data should not be relied upon for management decisions, including severe hyper- or hypoglycemia, diabetic ketoacidosis, or in patients with skin infections near the sensor site.
The panel also call for more research into outcomes for CGM continuation in the hospital and optimal implementation of both CGM and point-of-care glucose testing. For hospitals, strong recommendations include developing standard CGM data reports and workflows, as well as policies for CGM use.
Galindo pointed out: “A lot of hospitals have policies on that, but there aren’t many studies. It’s just that patients like it and it’s very hard to take it away from patients when they’re doing well.”
The section on CGM inpatient initiation is where COVID-19 plays the greatest role, which includes just one strong clinical practice recommendation: “Healthcare providers should consider prescribing CGM to reduce the need for frequent nurse contact for point-of-care glucose testing and the use of personal protective equipment for patients on isolation with highly contagious infectious diseases (eg, COVID-19).”
Strong recommendations also include a call for outcomes research and for hospitals to develop CGM protocols and educational tools for staff.
“We can do a study for approval but if administration and hospital policies aren’t there we’re not going to be able to use them,” Galindo noted.
For patients who already use AID systems – either the Medtronic 670G or Tandem Control IQ in the United States – the panel advises assessment to ensure the AID system is the most appropriate inpatient treatment, and the development of an alternative plan for diabetes management, if necessary. They also strongly recommend research in this area, and for hospitals to develop protocols for use of AID systems in various clinical situations.
Most detailed guidance addresses logistics and data management
Most of the strong recommendations regarding logistics are aimed at nursing staff, including receiving training in use of CGM and AID systems, confirming patient capacity, inspection of devices, and understanding when to administer a point-of-care glucose test.
Again, the panel calls for more data and for hospitals to develop policies and protocols for ensuring safe CGM and AID systems use, and when to avoid use.
Finally, they make one strong clinical recommendation regarding data management: “Healthcare providers should develop a set of core data elements and definitions for CGM data for inclusion in common data models and the electronic health record.”
That’s followed by a long list of relevant recommendations for research in the area, and for hospitals to integrate CGM and AID system data into their EHR systems.
This last area has proven particularly challenging, Galindo said. “Right now we do four point-of-care glucoses a day, and that goes right into the EHR, but with CGM it’s much more than that. How do we get all those data into the EHR and interpret it? Many steps need to be taken into consideration.”
Studies are being conducted in order to fulfill requirements for FDA approval of inpatient CGM use, he said, with data on implementation and inpatient AID system use to follow.
“More data will be available, triggered by the COVID-19 pandemic. However, the use of technology in the hospital goes beyond COVID-19,” he said
Galindo has reported receiving unrestricted research support to Emory for investigator-initiated studies from Novo Nordisk and Dexcom, and consulting fees from Abbott Diabetes Care, Sanofi, Novo Nordisk, Eli Lilly, and Valeritas. He is partially supported by research grants from the NIH/NIDDK.
This article first appeared on Medscape.com.
A new consensus statement offers detailed guidelines for inpatient use of continuous glucose monitors (CGM) and automated insulin delivery (AID) systems.
Aimed at clinicians, researchers, and hospital administrators, the open-access document was recently published by a multidisciplinary international panel of 24 experts in the Journal of Diabetes Science and Technology.
The statement includes 77 separate recommendations under five headings: 1) continued use of CGM by patients already using them at home, 2) initiation of CGM in hospital, 3) continuation of AID systems in hospital by patients already using them at home, 4) logistics and hands-on care of hospitalized patients using CGM and AID systems, and 5) data management of CGM and AID systems in hospital.
“This is the most comprehensive and up-to-date guideline on the use of diabetes technology in the hospital now,” lead author Rodolfo J. Galindo, MD, told Medscape Medical News in an interview.
“Overall, most experts believe that CGM and AID have the potential to overcome the current limitations of glycemic monitoring in the hospital to improve patient outcomes, but we need research – first to get the approval and second to get widespread use,” said Galindo, medical chair of the hospital diabetes taskforce at Emory Healthcare System, Atlanta.
“COVID-19 changed everything”
The guideline is an update of a 2017 statement on hospital use of CGM. The new guideline adds AID systems (sometimes referred to as an artificial pancreas), which combines a CGM and insulin pump and uses an algorithm to guide insulin delivery, and is the first to be developed during the COVID-19 era.
The update had been planned prior to the pandemic, but the actual panel meeting took place in April 2020, after the US Food and Drug Administration allowed inpatient use of CGM despite lack of official approval.
“COVID-19 changed everything. ... We had to be more specific about how to implement CGM in these patients. The standard of care is hourly point-of-care glucose monitoring in the [ICU], and at least every 4 hours outside the ICU. With limited [personal protective equipment] and the burden on nursing it was unachievable,” Galindo explained.
In June 2020, Galindo and other guideline authors developed a COVID-19–specific document (also open-access), which goes more into detail about CGM and how to implement in-hospital use during the pandemic.
The current consensus guideline “provides a high-level review of the evidence by experts,” Galindo added.
Recommendations cover different technologies and hospital settings
The panel “strongly” advises that hospital providers consult with an inpatient diabetes team, if available, to help manage patients already using CGM prior to admission. Among other recommendations, they list several situations in which CGM data should not be relied upon for management decisions, including severe hyper- or hypoglycemia, diabetic ketoacidosis, or in patients with skin infections near the sensor site.
The panel also call for more research into outcomes for CGM continuation in the hospital and optimal implementation of both CGM and point-of-care glucose testing. For hospitals, strong recommendations include developing standard CGM data reports and workflows, as well as policies for CGM use.
Galindo pointed out: “A lot of hospitals have policies on that, but there aren’t many studies. It’s just that patients like it and it’s very hard to take it away from patients when they’re doing well.”
The section on CGM inpatient initiation is where COVID-19 plays the greatest role, which includes just one strong clinical practice recommendation: “Healthcare providers should consider prescribing CGM to reduce the need for frequent nurse contact for point-of-care glucose testing and the use of personal protective equipment for patients on isolation with highly contagious infectious diseases (eg, COVID-19).”
Strong recommendations also include a call for outcomes research and for hospitals to develop CGM protocols and educational tools for staff.
“We can do a study for approval but if administration and hospital policies aren’t there we’re not going to be able to use them,” Galindo noted.
For patients who already use AID systems – either the Medtronic 670G or Tandem Control IQ in the United States – the panel advises assessment to ensure the AID system is the most appropriate inpatient treatment, and the development of an alternative plan for diabetes management, if necessary. They also strongly recommend research in this area, and for hospitals to develop protocols for use of AID systems in various clinical situations.
Most detailed guidance addresses logistics and data management
Most of the strong recommendations regarding logistics are aimed at nursing staff, including receiving training in use of CGM and AID systems, confirming patient capacity, inspection of devices, and understanding when to administer a point-of-care glucose test.
Again, the panel calls for more data and for hospitals to develop policies and protocols for ensuring safe CGM and AID systems use, and when to avoid use.
Finally, they make one strong clinical recommendation regarding data management: “Healthcare providers should develop a set of core data elements and definitions for CGM data for inclusion in common data models and the electronic health record.”
That’s followed by a long list of relevant recommendations for research in the area, and for hospitals to integrate CGM and AID system data into their EHR systems.
This last area has proven particularly challenging, Galindo said. “Right now we do four point-of-care glucoses a day, and that goes right into the EHR, but with CGM it’s much more than that. How do we get all those data into the EHR and interpret it? Many steps need to be taken into consideration.”
Studies are being conducted in order to fulfill requirements for FDA approval of inpatient CGM use, he said, with data on implementation and inpatient AID system use to follow.
“More data will be available, triggered by the COVID-19 pandemic. However, the use of technology in the hospital goes beyond COVID-19,” he said
Galindo has reported receiving unrestricted research support to Emory for investigator-initiated studies from Novo Nordisk and Dexcom, and consulting fees from Abbott Diabetes Care, Sanofi, Novo Nordisk, Eli Lilly, and Valeritas. He is partially supported by research grants from the NIH/NIDDK.
This article first appeared on Medscape.com.
AACE issues ‘cookbook’ algorithm to manage dyslipidemia
A new algorithm on lipid management and prevention of cardiovascular disease from the American Association of Clinical Endocrinologists* (AACE) and the American College of Endocrinology (ACE) is “a nice cookbook” that many clinicians, especially those who are not lipid experts, will find useful, according to writing committee chair Yehuda Handelsman, MD.
The algorithm, published Oct. 10 in Endocrine Practice as 10 slides, or as part of a more detailed consensus statement, is a companion to the 2017 AACE/ACE guidelines for lipid management and includes more recent information about new therapies.
“What we’re trying to do here is to say, ‘focus on LDL-C, triglycerides, high-risk patients, and lifestyle. Understand all the medications available to you to reduce LDL-C and reduce triglycerides,’ ” Dr. Handelsman, of the Metabolic Institute of America, Tarzana, Calif., explained in an interview.
“We touch on lipoprotein(a), which we still don’t have medication for, but it identifies people at high risk, and we need that.”
Clinicians also need to know “that we’ve got some newer drugs in the market that can manage people who have statin intolerance,” Dr. Handelsman added.
“We introduced new therapies like icosapent ethyl” (Vascepa, Amarin) for hypertriglyceridemia, “when to use it, and how to use it. Even though it was not part of the 2017 guideline, we gave recommendations based on current data in the algorithm.”
Although there is no good evidence that lowering triglycerides reduces heart disease, he continued, many experts believe that the target triglyceride level should be less than 150 mg/dL, and the algorithm explains how to treat to this goal.
“Last, and most importantly, I cannot fail to underscore the fact that lifestyle is very important,” he emphasized.
Robert H. Eckel, MD, of the University of Colorado at Denver, Aurora, and president of medicine and science at the American Diabetes Association, who was not involved with this algorithm, said in an interview that the algorithm is important since it offers “the clinician or health care practitioner an approach, a kind of a cookbook or application of the guidelines, for how to manage lipid disorders in patients at risk ... It’s geared for the nonexperts too,” he said.

Dyslipidemia treatment summarized in 10 slides
The AACE/ACE algorithm comprises 10 slides, one each for dyslipidemic states, secondary causes of lipid disorders, screening for and assessing lipid disorders and atherosclerotic CVD (ASCVD) risk, ASCVD risk categories and treatment goals, lifestyle recommendations, treating LDL-C to goal, managing statin intolerance and safety, management of hypertriglyceridemia and the role of icosapent ethyl, assessment and management of elevated lipoprotein(a), and profiles of medications for dyslipidemia.
The algorithm defines five ASCVD risk categories and recommends increasingly lower LDL-C, non–HDL-C, and apo B target levels with increasing risk, but the same triglyceride target for all.
First, “treatment of lipid disorders begins with lifestyle therapy to improve nutrition, physical activity, weight, and other factors that affect lipids,” the consensus statement authors stress.
Next, “LDL-C has been, and remains, the main focus of efforts to improve lipid profiles in individuals at risk for ASCVD” (see table).
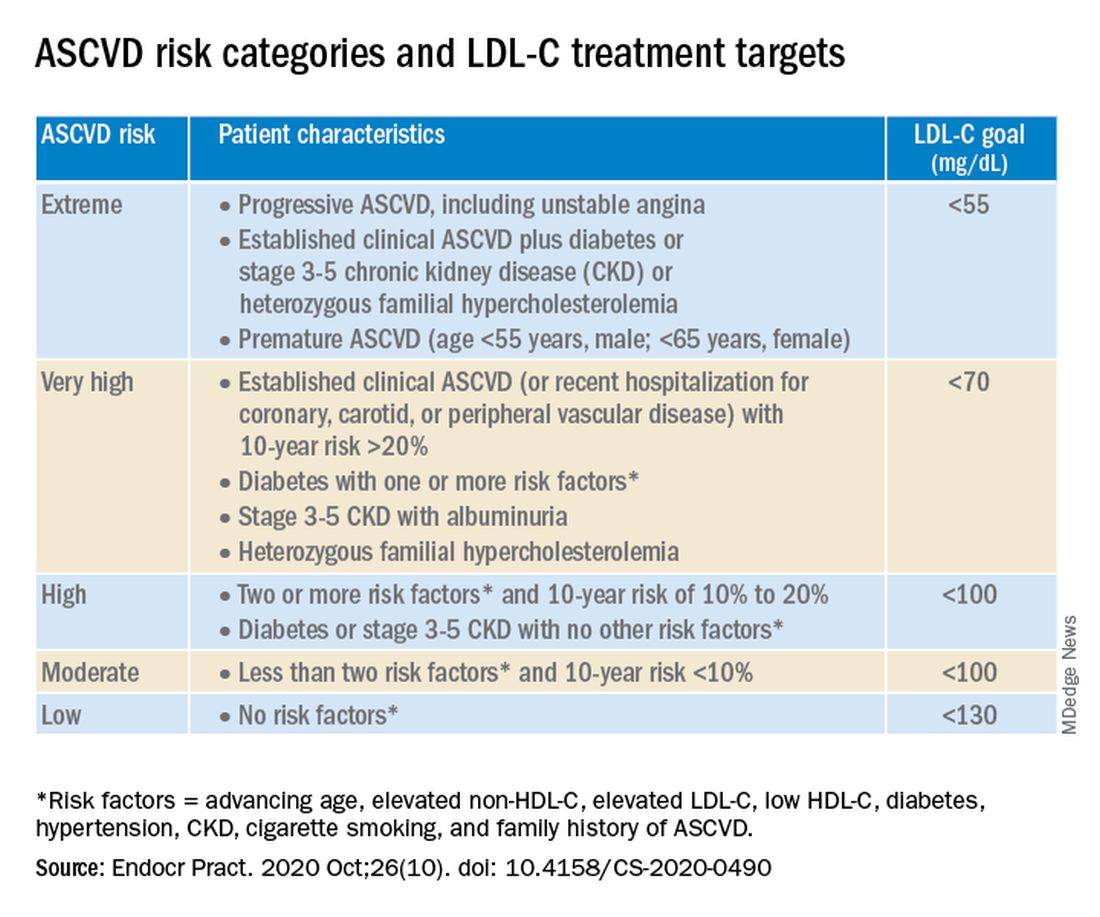
“We stratify [LDL-C] not as a one-treatment-target-for-all,” but rather as extreme, very high, high, moderate, and low ASCVD risk, Dr. Handelsman explained, with different treatment pathways (specified in another slide) to reach different risk-dependent goals.
“Unlike the ACC [American College of Cardiology] guideline, which shows if you want to further reduce LDL after statin give ezetimibe first, we say ‘no’,” he noted. “If somebody has an extreme risk, and you don’t think ezetimibe will get to a goal below 55 mg/dL, you should go first with a PCSK9 [proprotein convertase subtilisin/kexin type 9] inhibitor, and only then add ezetimibe or [colesevelam] or other drugs,” he said.
The consensus statement authors expand on this scenario. “Treatment for patients at extreme risk should begin with lifestyle therapy plus a high-intensity statin (atorvastatin 40 to 80 mg or rosuvastatin 20 to 40 mg, or the highest tolerated statin dose) to achieve an LDL-C goal of less than 55 mg/dL.”
“If LDL-C remains above goal after 3 months,” a PCSK9 inhibitor (evolocumab [Repatha, Amgen] or alirocumab [Praluent, Sanofi/Regeneron]), the cholesterol absorption inhibitor ezetimibe, or the bile acid sequestrant colesevelam (Welchol, Daiichi Sankyo) or the adenosine triphosphate-citrate lyase (ACL) inhibitor bempedoic acid (Nexletol, Esperion) “should be added, depending on required LDL-C lowering, and a third agent should be added if the combination fails to achieve the goal.”
However, “because the cost of ezetimibe is low, it may be preferred over PCSK9 inhibitors as second-line therapy to achieve an LDL-C below 70 mg/dL for patients who require no more than 15%-20% further reduction to reach goals.”
For patients at moderate or high risk, lipid management should begin with a moderate-intensity statin and be increased to a high-intensity statin before adding a second lipid-lowering medication to reach an LDL-C below 100 mg/dL.
According to the consensus statement, the desirable goal for triglycerides is less than 150 mg/dL.
In all patients with triglyceride levels of at least 500 mg/dL, statin therapy should be combined with a fibrate, prescription-grade omega-3 fatty acid, and/or niacin to reduce triglycerides.
In any patient with established ASCVD or diabetes with at least 2 ASCVD risk factors and triglycerides of 135-499 mg/dL, icosapent ethyl should be added to a statin to prevent ASCVD events.
Statement aligns with major guidelines
In general, the 2017 AACE/ACE guidelines and algorithm are “pretty similar” to other guidelines such as the 2018 ACC/American Heart Association (AHA) guidelines for cholesterol management, the 2019 ACC/AHA guidelines for primary prevention of CVD, and the 2019 European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) guidelines for the management of dyslipidemia, according to Dr. Eckel.
They have “all have now taken into consideration the evidence behind PCSK9 inhibitors,” he noted. “That’s important because those drugs have proven to be effective.”
Two differences, he pointed out, are that the 2019 ESC/EAS guidelines suggest that lipoprotein(a) measurement be considered at least once in every adult’s lifetime, and they recommend apo B analysis in people with high triglycerides but normal LDL (or no higher than 100 mg/dL), to identify additional risk.
*AACE changes its name, broadens focus
Shortly after its algorithm was published, AACE announced that it has a new organization name and brand, the American Association of Clinical Endocrinology, which “more clearly defines AACE as a community of individuals who work together to elevate the practice of clinical endocrinology,” according to an Oct. 20 statement.
The change is meant to acknowledge AACE’s “more modern, inclusive approach to endocrinology that supports multidisciplinary care teams – with endocrinologists leading the way.”
Along with the name change is a new global website. The statement notes that “health care professionals and community members can access all of the valuable clinical content such as guidelines, disease state networks and important education by visiting the pro portal in the top right corner of the site, or by going directly to pro.aace.com.”
Dr. Handelsman discloses that he receives research grant support from Amgen, Applied Therapeutics, AstraZeneca, BMS, Gan & Lee, Novo Nordisk, and Sanofi, and he is a consultant and/or speaker for Amarin, BI-Lilly, and Sanofi.
Dr. Eckel has received consultant/advisory board fees from Kowa, Novo Nordisk, and Provention Bio.
A new algorithm on lipid management and prevention of cardiovascular disease from the American Association of Clinical Endocrinologists* (AACE) and the American College of Endocrinology (ACE) is “a nice cookbook” that many clinicians, especially those who are not lipid experts, will find useful, according to writing committee chair Yehuda Handelsman, MD.
The algorithm, published Oct. 10 in Endocrine Practice as 10 slides, or as part of a more detailed consensus statement, is a companion to the 2017 AACE/ACE guidelines for lipid management and includes more recent information about new therapies.
“What we’re trying to do here is to say, ‘focus on LDL-C, triglycerides, high-risk patients, and lifestyle. Understand all the medications available to you to reduce LDL-C and reduce triglycerides,’ ” Dr. Handelsman, of the Metabolic Institute of America, Tarzana, Calif., explained in an interview.
“We touch on lipoprotein(a), which we still don’t have medication for, but it identifies people at high risk, and we need that.”
Clinicians also need to know “that we’ve got some newer drugs in the market that can manage people who have statin intolerance,” Dr. Handelsman added.
“We introduced new therapies like icosapent ethyl” (Vascepa, Amarin) for hypertriglyceridemia, “when to use it, and how to use it. Even though it was not part of the 2017 guideline, we gave recommendations based on current data in the algorithm.”
Although there is no good evidence that lowering triglycerides reduces heart disease, he continued, many experts believe that the target triglyceride level should be less than 150 mg/dL, and the algorithm explains how to treat to this goal.
“Last, and most importantly, I cannot fail to underscore the fact that lifestyle is very important,” he emphasized.
Robert H. Eckel, MD, of the University of Colorado at Denver, Aurora, and president of medicine and science at the American Diabetes Association, who was not involved with this algorithm, said in an interview that the algorithm is important since it offers “the clinician or health care practitioner an approach, a kind of a cookbook or application of the guidelines, for how to manage lipid disorders in patients at risk ... It’s geared for the nonexperts too,” he said.
Dyslipidemia treatment summarized in 10 slides
The AACE/ACE algorithm comprises 10 slides, one each for dyslipidemic states, secondary causes of lipid disorders, screening for and assessing lipid disorders and atherosclerotic CVD (ASCVD) risk, ASCVD risk categories and treatment goals, lifestyle recommendations, treating LDL-C to goal, managing statin intolerance and safety, management of hypertriglyceridemia and the role of icosapent ethyl, assessment and management of elevated lipoprotein(a), and profiles of medications for dyslipidemia.
The algorithm defines five ASCVD risk categories and recommends increasingly lower LDL-C, non–HDL-C, and apo B target levels with increasing risk, but the same triglyceride target for all.
First, “treatment of lipid disorders begins with lifestyle therapy to improve nutrition, physical activity, weight, and other factors that affect lipids,” the consensus statement authors stress.
Next, “LDL-C has been, and remains, the main focus of efforts to improve lipid profiles in individuals at risk for ASCVD” (see table).
“We stratify [LDL-C] not as a one-treatment-target-for-all,” but rather as extreme, very high, high, moderate, and low ASCVD risk, Dr. Handelsman explained, with different treatment pathways (specified in another slide) to reach different risk-dependent goals.
“Unlike the ACC [American College of Cardiology] guideline, which shows if you want to further reduce LDL after statin give ezetimibe first, we say ‘no’,” he noted. “If somebody has an extreme risk, and you don’t think ezetimibe will get to a goal below 55 mg/dL, you should go first with a PCSK9 [proprotein convertase subtilisin/kexin type 9] inhibitor, and only then add ezetimibe or [colesevelam] or other drugs,” he said.
The consensus statement authors expand on this scenario. “Treatment for patients at extreme risk should begin with lifestyle therapy plus a high-intensity statin (atorvastatin 40 to 80 mg or rosuvastatin 20 to 40 mg, or the highest tolerated statin dose) to achieve an LDL-C goal of less than 55 mg/dL.”
“If LDL-C remains above goal after 3 months,” a PCSK9 inhibitor (evolocumab [Repatha, Amgen] or alirocumab [Praluent, Sanofi/Regeneron]), the cholesterol absorption inhibitor ezetimibe, or the bile acid sequestrant colesevelam (Welchol, Daiichi Sankyo) or the adenosine triphosphate-citrate lyase (ACL) inhibitor bempedoic acid (Nexletol, Esperion) “should be added, depending on required LDL-C lowering, and a third agent should be added if the combination fails to achieve the goal.”
However, “because the cost of ezetimibe is low, it may be preferred over PCSK9 inhibitors as second-line therapy to achieve an LDL-C below 70 mg/dL for patients who require no more than 15%-20% further reduction to reach goals.”
For patients at moderate or high risk, lipid management should begin with a moderate-intensity statin and be increased to a high-intensity statin before adding a second lipid-lowering medication to reach an LDL-C below 100 mg/dL.
According to the consensus statement, the desirable goal for triglycerides is less than 150 mg/dL.
In all patients with triglyceride levels of at least 500 mg/dL, statin therapy should be combined with a fibrate, prescription-grade omega-3 fatty acid, and/or niacin to reduce triglycerides.
In any patient with established ASCVD or diabetes with at least 2 ASCVD risk factors and triglycerides of 135-499 mg/dL, icosapent ethyl should be added to a statin to prevent ASCVD events.
Statement aligns with major guidelines
In general, the 2017 AACE/ACE guidelines and algorithm are “pretty similar” to other guidelines such as the 2018 ACC/American Heart Association (AHA) guidelines for cholesterol management, the 2019 ACC/AHA guidelines for primary prevention of CVD, and the 2019 European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) guidelines for the management of dyslipidemia, according to Dr. Eckel.
They have “all have now taken into consideration the evidence behind PCSK9 inhibitors,” he noted. “That’s important because those drugs have proven to be effective.”
Two differences, he pointed out, are that the 2019 ESC/EAS guidelines suggest that lipoprotein(a) measurement be considered at least once in every adult’s lifetime, and they recommend apo B analysis in people with high triglycerides but normal LDL (or no higher than 100 mg/dL), to identify additional risk.
*AACE changes its name, broadens focus
Shortly after its algorithm was published, AACE announced that it has a new organization name and brand, the American Association of Clinical Endocrinology, which “more clearly defines AACE as a community of individuals who work together to elevate the practice of clinical endocrinology,” according to an Oct. 20 statement.
The change is meant to acknowledge AACE’s “more modern, inclusive approach to endocrinology that supports multidisciplinary care teams – with endocrinologists leading the way.”
Along with the name change is a new global website. The statement notes that “health care professionals and community members can access all of the valuable clinical content such as guidelines, disease state networks and important education by visiting the pro portal in the top right corner of the site, or by going directly to pro.aace.com.”
Dr. Handelsman discloses that he receives research grant support from Amgen, Applied Therapeutics, AstraZeneca, BMS, Gan & Lee, Novo Nordisk, and Sanofi, and he is a consultant and/or speaker for Amarin, BI-Lilly, and Sanofi.
Dr. Eckel has received consultant/advisory board fees from Kowa, Novo Nordisk, and Provention Bio.
A new algorithm on lipid management and prevention of cardiovascular disease from the American Association of Clinical Endocrinologists* (AACE) and the American College of Endocrinology (ACE) is “a nice cookbook” that many clinicians, especially those who are not lipid experts, will find useful, according to writing committee chair Yehuda Handelsman, MD.
The algorithm, published Oct. 10 in Endocrine Practice as 10 slides, or as part of a more detailed consensus statement, is a companion to the 2017 AACE/ACE guidelines for lipid management and includes more recent information about new therapies.
“What we’re trying to do here is to say, ‘focus on LDL-C, triglycerides, high-risk patients, and lifestyle. Understand all the medications available to you to reduce LDL-C and reduce triglycerides,’ ” Dr. Handelsman, of the Metabolic Institute of America, Tarzana, Calif., explained in an interview.
“We touch on lipoprotein(a), which we still don’t have medication for, but it identifies people at high risk, and we need that.”
Clinicians also need to know “that we’ve got some newer drugs in the market that can manage people who have statin intolerance,” Dr. Handelsman added.
“We introduced new therapies like icosapent ethyl” (Vascepa, Amarin) for hypertriglyceridemia, “when to use it, and how to use it. Even though it was not part of the 2017 guideline, we gave recommendations based on current data in the algorithm.”
Although there is no good evidence that lowering triglycerides reduces heart disease, he continued, many experts believe that the target triglyceride level should be less than 150 mg/dL, and the algorithm explains how to treat to this goal.
“Last, and most importantly, I cannot fail to underscore the fact that lifestyle is very important,” he emphasized.
Robert H. Eckel, MD, of the University of Colorado at Denver, Aurora, and president of medicine and science at the American Diabetes Association, who was not involved with this algorithm, said in an interview that the algorithm is important since it offers “the clinician or health care practitioner an approach, a kind of a cookbook or application of the guidelines, for how to manage lipid disorders in patients at risk ... It’s geared for the nonexperts too,” he said.
Dyslipidemia treatment summarized in 10 slides
The AACE/ACE algorithm comprises 10 slides, one each for dyslipidemic states, secondary causes of lipid disorders, screening for and assessing lipid disorders and atherosclerotic CVD (ASCVD) risk, ASCVD risk categories and treatment goals, lifestyle recommendations, treating LDL-C to goal, managing statin intolerance and safety, management of hypertriglyceridemia and the role of icosapent ethyl, assessment and management of elevated lipoprotein(a), and profiles of medications for dyslipidemia.
The algorithm defines five ASCVD risk categories and recommends increasingly lower LDL-C, non–HDL-C, and apo B target levels with increasing risk, but the same triglyceride target for all.
First, “treatment of lipid disorders begins with lifestyle therapy to improve nutrition, physical activity, weight, and other factors that affect lipids,” the consensus statement authors stress.
Next, “LDL-C has been, and remains, the main focus of efforts to improve lipid profiles in individuals at risk for ASCVD” (see table).
“We stratify [LDL-C] not as a one-treatment-target-for-all,” but rather as extreme, very high, high, moderate, and low ASCVD risk, Dr. Handelsman explained, with different treatment pathways (specified in another slide) to reach different risk-dependent goals.
“Unlike the ACC [American College of Cardiology] guideline, which shows if you want to further reduce LDL after statin give ezetimibe first, we say ‘no’,” he noted. “If somebody has an extreme risk, and you don’t think ezetimibe will get to a goal below 55 mg/dL, you should go first with a PCSK9 [proprotein convertase subtilisin/kexin type 9] inhibitor, and only then add ezetimibe or [colesevelam] or other drugs,” he said.
The consensus statement authors expand on this scenario. “Treatment for patients at extreme risk should begin with lifestyle therapy plus a high-intensity statin (atorvastatin 40 to 80 mg or rosuvastatin 20 to 40 mg, or the highest tolerated statin dose) to achieve an LDL-C goal of less than 55 mg/dL.”
“If LDL-C remains above goal after 3 months,” a PCSK9 inhibitor (evolocumab [Repatha, Amgen] or alirocumab [Praluent, Sanofi/Regeneron]), the cholesterol absorption inhibitor ezetimibe, or the bile acid sequestrant colesevelam (Welchol, Daiichi Sankyo) or the adenosine triphosphate-citrate lyase (ACL) inhibitor bempedoic acid (Nexletol, Esperion) “should be added, depending on required LDL-C lowering, and a third agent should be added if the combination fails to achieve the goal.”
However, “because the cost of ezetimibe is low, it may be preferred over PCSK9 inhibitors as second-line therapy to achieve an LDL-C below 70 mg/dL for patients who require no more than 15%-20% further reduction to reach goals.”
For patients at moderate or high risk, lipid management should begin with a moderate-intensity statin and be increased to a high-intensity statin before adding a second lipid-lowering medication to reach an LDL-C below 100 mg/dL.
According to the consensus statement, the desirable goal for triglycerides is less than 150 mg/dL.
In all patients with triglyceride levels of at least 500 mg/dL, statin therapy should be combined with a fibrate, prescription-grade omega-3 fatty acid, and/or niacin to reduce triglycerides.
In any patient with established ASCVD or diabetes with at least 2 ASCVD risk factors and triglycerides of 135-499 mg/dL, icosapent ethyl should be added to a statin to prevent ASCVD events.
Statement aligns with major guidelines
In general, the 2017 AACE/ACE guidelines and algorithm are “pretty similar” to other guidelines such as the 2018 ACC/American Heart Association (AHA) guidelines for cholesterol management, the 2019 ACC/AHA guidelines for primary prevention of CVD, and the 2019 European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) guidelines for the management of dyslipidemia, according to Dr. Eckel.
They have “all have now taken into consideration the evidence behind PCSK9 inhibitors,” he noted. “That’s important because those drugs have proven to be effective.”
Two differences, he pointed out, are that the 2019 ESC/EAS guidelines suggest that lipoprotein(a) measurement be considered at least once in every adult’s lifetime, and they recommend apo B analysis in people with high triglycerides but normal LDL (or no higher than 100 mg/dL), to identify additional risk.
*AACE changes its name, broadens focus
Shortly after its algorithm was published, AACE announced that it has a new organization name and brand, the American Association of Clinical Endocrinology, which “more clearly defines AACE as a community of individuals who work together to elevate the practice of clinical endocrinology,” according to an Oct. 20 statement.
The change is meant to acknowledge AACE’s “more modern, inclusive approach to endocrinology that supports multidisciplinary care teams – with endocrinologists leading the way.”
Along with the name change is a new global website. The statement notes that “health care professionals and community members can access all of the valuable clinical content such as guidelines, disease state networks and important education by visiting the pro portal in the top right corner of the site, or by going directly to pro.aace.com.”
Dr. Handelsman discloses that he receives research grant support from Amgen, Applied Therapeutics, AstraZeneca, BMS, Gan & Lee, Novo Nordisk, and Sanofi, and he is a consultant and/or speaker for Amarin, BI-Lilly, and Sanofi.
Dr. Eckel has received consultant/advisory board fees from Kowa, Novo Nordisk, and Provention Bio.
Avoid pituitary pitfalls in hyperprolactinemia
,” Ashlyn Smith, PA-C, of Endocrinology Associates, Scottsdale, Ariz., said in a presentation at the at the virtual meeting of the annual Metabolic and Endocrine Disease Summit held by Global Academy for Medical Education.
The most common demographic for pituitary disorders is women in their 30s and 40s, Ms. Smith said. Early red flags for pituitary problems include patients presenting with headaches and/or blurred or double vision, which could signal bitemporal hemianopsia, she said.
Roughly two-thirds of pituitary adenomas are functional, meaning that they secrete pituitary hormones and cause clinical syndromes, Ms. Smith said. The most common reason for hypersecretion is hyperprolactinemia, she said.
Hyperprolactinemia, like most pituitary conditions, is more common in women than men, Ms. Smith noted. However, symptoms may include not only galactorrhea, but also gynecomastia, and hypogonadism, which may be red flags in men, she noted.
“Prolactin inhibits the gonadal pathway, so we see low gonadal hormones. For example, if men present with atypical hypogonadism for their age, or women present with changes in the menstrual cycle, check the prolactin levels,” she said.
The etiologies of hyperprolactinemia include physiologic reasons such as breastfeeding and pregnancy, as well as intercourse and breast manipulation, stress, and sleep issues. Pathologic reasons for prolactin elevation include prolactinoma, gonad-hormone secreting tumor, hypothyroidism, and renal insufficiency, Ms. Smith said.
Evaluation of patients with suspected hyperprolactinemia includes screening for physiologic causes, renal function and thyroid function tests, and a thyroid-specific MRI. Ordering a dedicated MRI of the pituitary gland is important to help identify compression of the optic nerve, noted Ms. Smith.
A medication review also is essential in evaluating hyperprolactinemia, and especially in the setting of the COVID-19 pandemic, because patients may have made changes to psychiatric medications, said Ms. Smith. Neuroleptics and antipsychotics including risperidone, haloperidol, chlorpromazine, and thiothixene can be associated with hyperprolactinemia, as can benzodiazepines and various analgesics and antidepressants, she said.
Treatment in cases of medication-induced hyperprolactinemia can be challenging if the patients are unable to change a medication, said Ms. Smith. However, patients with hypogonadism or low bone mineral density who can’t change medications may benefit from exogenous gonadal hormones, she said.
Some patients with hyperprolactinemia benefit from treatment with dopamine agonists, which may ease symptoms and reduce the size of the prolactinoma, she explained. However, patients on dopamine agonists should be alert to side effects including constipation and orthostasis. Ms. Smith said she recommends that patients on dopamine agonists for hyperprolactinemia take the medication at night so they are lying down if orthostasis occurs.
Monitor prolactin levels at 1 month, and taper or discontinue if the prolactin returns to normal and the adenoma resolves, which can take approximately 2 years, she said. Ms. Smith then advised follow-up every 3 months for 1 year, then annual prolactin checks.
The risk of recurrence ranges from 26% to 69%, Ms. Smith said, and is higher in patients with higher prolactin levels and larger adenomas, she noted. Recurrence is most likely within a year of withdrawal from treatment, she said.
Ms. Smith disclosed serving as an adviser and speaker for Abbott Nutrition, a speaker for Xeris Pharmaceuticals, and an adviser for Sanofi and Radius.
Global Academy for Medical Education and this news organization are owned by the same parent company.
SOURCE: Smith A. MEDS 2020.
,” Ashlyn Smith, PA-C, of Endocrinology Associates, Scottsdale, Ariz., said in a presentation at the at the virtual meeting of the annual Metabolic and Endocrine Disease Summit held by Global Academy for Medical Education.
The most common demographic for pituitary disorders is women in their 30s and 40s, Ms. Smith said. Early red flags for pituitary problems include patients presenting with headaches and/or blurred or double vision, which could signal bitemporal hemianopsia, she said.
Roughly two-thirds of pituitary adenomas are functional, meaning that they secrete pituitary hormones and cause clinical syndromes, Ms. Smith said. The most common reason for hypersecretion is hyperprolactinemia, she said.
Hyperprolactinemia, like most pituitary conditions, is more common in women than men, Ms. Smith noted. However, symptoms may include not only galactorrhea, but also gynecomastia, and hypogonadism, which may be red flags in men, she noted.
“Prolactin inhibits the gonadal pathway, so we see low gonadal hormones. For example, if men present with atypical hypogonadism for their age, or women present with changes in the menstrual cycle, check the prolactin levels,” she said.
The etiologies of hyperprolactinemia include physiologic reasons such as breastfeeding and pregnancy, as well as intercourse and breast manipulation, stress, and sleep issues. Pathologic reasons for prolactin elevation include prolactinoma, gonad-hormone secreting tumor, hypothyroidism, and renal insufficiency, Ms. Smith said.
Evaluation of patients with suspected hyperprolactinemia includes screening for physiologic causes, renal function and thyroid function tests, and a thyroid-specific MRI. Ordering a dedicated MRI of the pituitary gland is important to help identify compression of the optic nerve, noted Ms. Smith.
A medication review also is essential in evaluating hyperprolactinemia, and especially in the setting of the COVID-19 pandemic, because patients may have made changes to psychiatric medications, said Ms. Smith. Neuroleptics and antipsychotics including risperidone, haloperidol, chlorpromazine, and thiothixene can be associated with hyperprolactinemia, as can benzodiazepines and various analgesics and antidepressants, she said.
Treatment in cases of medication-induced hyperprolactinemia can be challenging if the patients are unable to change a medication, said Ms. Smith. However, patients with hypogonadism or low bone mineral density who can’t change medications may benefit from exogenous gonadal hormones, she said.
Some patients with hyperprolactinemia benefit from treatment with dopamine agonists, which may ease symptoms and reduce the size of the prolactinoma, she explained. However, patients on dopamine agonists should be alert to side effects including constipation and orthostasis. Ms. Smith said she recommends that patients on dopamine agonists for hyperprolactinemia take the medication at night so they are lying down if orthostasis occurs.
Monitor prolactin levels at 1 month, and taper or discontinue if the prolactin returns to normal and the adenoma resolves, which can take approximately 2 years, she said. Ms. Smith then advised follow-up every 3 months for 1 year, then annual prolactin checks.
The risk of recurrence ranges from 26% to 69%, Ms. Smith said, and is higher in patients with higher prolactin levels and larger adenomas, she noted. Recurrence is most likely within a year of withdrawal from treatment, she said.
Ms. Smith disclosed serving as an adviser and speaker for Abbott Nutrition, a speaker for Xeris Pharmaceuticals, and an adviser for Sanofi and Radius.
Global Academy for Medical Education and this news organization are owned by the same parent company.
SOURCE: Smith A. MEDS 2020.
,” Ashlyn Smith, PA-C, of Endocrinology Associates, Scottsdale, Ariz., said in a presentation at the at the virtual meeting of the annual Metabolic and Endocrine Disease Summit held by Global Academy for Medical Education.
The most common demographic for pituitary disorders is women in their 30s and 40s, Ms. Smith said. Early red flags for pituitary problems include patients presenting with headaches and/or blurred or double vision, which could signal bitemporal hemianopsia, she said.
Roughly two-thirds of pituitary adenomas are functional, meaning that they secrete pituitary hormones and cause clinical syndromes, Ms. Smith said. The most common reason for hypersecretion is hyperprolactinemia, she said.
Hyperprolactinemia, like most pituitary conditions, is more common in women than men, Ms. Smith noted. However, symptoms may include not only galactorrhea, but also gynecomastia, and hypogonadism, which may be red flags in men, she noted.
“Prolactin inhibits the gonadal pathway, so we see low gonadal hormones. For example, if men present with atypical hypogonadism for their age, or women present with changes in the menstrual cycle, check the prolactin levels,” she said.
The etiologies of hyperprolactinemia include physiologic reasons such as breastfeeding and pregnancy, as well as intercourse and breast manipulation, stress, and sleep issues. Pathologic reasons for prolactin elevation include prolactinoma, gonad-hormone secreting tumor, hypothyroidism, and renal insufficiency, Ms. Smith said.
Evaluation of patients with suspected hyperprolactinemia includes screening for physiologic causes, renal function and thyroid function tests, and a thyroid-specific MRI. Ordering a dedicated MRI of the pituitary gland is important to help identify compression of the optic nerve, noted Ms. Smith.
A medication review also is essential in evaluating hyperprolactinemia, and especially in the setting of the COVID-19 pandemic, because patients may have made changes to psychiatric medications, said Ms. Smith. Neuroleptics and antipsychotics including risperidone, haloperidol, chlorpromazine, and thiothixene can be associated with hyperprolactinemia, as can benzodiazepines and various analgesics and antidepressants, she said.
Treatment in cases of medication-induced hyperprolactinemia can be challenging if the patients are unable to change a medication, said Ms. Smith. However, patients with hypogonadism or low bone mineral density who can’t change medications may benefit from exogenous gonadal hormones, she said.
Some patients with hyperprolactinemia benefit from treatment with dopamine agonists, which may ease symptoms and reduce the size of the prolactinoma, she explained. However, patients on dopamine agonists should be alert to side effects including constipation and orthostasis. Ms. Smith said she recommends that patients on dopamine agonists for hyperprolactinemia take the medication at night so they are lying down if orthostasis occurs.
Monitor prolactin levels at 1 month, and taper or discontinue if the prolactin returns to normal and the adenoma resolves, which can take approximately 2 years, she said. Ms. Smith then advised follow-up every 3 months for 1 year, then annual prolactin checks.
The risk of recurrence ranges from 26% to 69%, Ms. Smith said, and is higher in patients with higher prolactin levels and larger adenomas, she noted. Recurrence is most likely within a year of withdrawal from treatment, she said.
Ms. Smith disclosed serving as an adviser and speaker for Abbott Nutrition, a speaker for Xeris Pharmaceuticals, and an adviser for Sanofi and Radius.
Global Academy for Medical Education and this news organization are owned by the same parent company.
SOURCE: Smith A. MEDS 2020.
EXPERT ANALYSIS FROM MEDS 2020
Vertebral fractures in COVID-19 linked to mortality
Vertebral fractures appear to be common in people with severe COVID-19, and also raise the mortality risk, findings from a retrospective cohort suggest.
Among 114 patients with COVID-19 who underwent lateral chest x-rays at the San Raffaele Hospital ED in Milan, more than a third were found to have thoracic vertebral fractures. And, those individuals were more than twice as likely to die as were those without vertebral fractures.
“Morphometric vertebral fractures are one of the most common comorbidities among adults hospitalized with COVID-19, and the presence of such fractures may predict the severity of disease outcomes,” lead investigator Andrea Giustina, MD, said in an interview.
This is the first study to examine vertebral fracture prevalence in any coronavirus disease, but such fractures have been linked to an increased risk of pneumonia and impaired respiratory function, including restrictive pulmonary dysfunction. One possible mechanism may be that they cause anatomical changes, such as kyphosis, which negatively impact respiratory function by decreasing vital capacity, forced expiratory volume in 1 second, and inspiratory time, explained Dr. Giustina, professor of endocrinology, San Raffaele Vita Salute University, Milan, and president of the European Society of Endocrinology. The results were published in the Journal of Clinical Endocrinology and Metabolism.
Clinically, the findings suggest that all patients with COVID-19 who are undergoing chest x-rays should have morphometric vertebral x-ray evaluation, said Dr. Giustina.
“One interesting aspect of the study is that without morphometry, approximatively two thirds of vertebral fractures [would have been] missed. Therefore, they are largely underestimated in clinical practice,” he noted.
Thoracic vertebral fractures assessed via lateral chest x-rays
The 114 study subjects included were those whose lateral chest x-rays allowed for a high-quality assessment and in which all the thoracic tract of T4-T12 were viewable and assessable. None had been using glucocorticoids and only 3% had a prior diagnosis of osteoporosis.
The majority (75%) were male, and median age was 57 years. Most (79%) were hospitalized after evaluation in the ED. Of those, 12% (13) were admitted to the ICU and 15% (16) died.
Thoracic vertebral fractures were detected on the lateral chest x-rays in 36% (41) of the patients. In contrast, in studies of women aged 50 years and older from the general European population, morphometric vertebral fracture prevalence ranged from 18% to 26%, the investigators noted.
Of the total 65 vertebral fractures detected, 60% were classified as mild (height ratio decrease <25%), 33.3% as moderate (25%-40% decrease) and 7.7% as severe (>40%). Patients with more than one vertebral fracture were classified by their most severe one.
Those with versus without vertebral fractures didn’t differ by sex, body mass index, or clinical or biological parameters evaluated in the ED. But, compared with those without vertebral fractures, those with them were significantly older (68 vs. 54 years) and were more likely to have arterial hypertension (56% vs. 30%) and coronary artery disease (22% vs. 7%).
In multivariate analysis, age was the only statistically significant predictor of vertebral fractures (odds ratio, 1.04; P < .001).
Mortality doubled, though not significantly
Those with vertebral fractures were more likely to be hospitalized, although not significantly (88% vs. 74%). There was no significant difference in ICU admission (11% vs. 12.5%).
However, those with vertebral fractures required noninvasive mechanical ventilation significantly more often (48.8% vs. 27.4%; P = .02), and were more than twice as likely to die (22% vs. 10%; P = .07). While the difference in overall mortality wasn’t quite statistically significant, those with severe vertebral fractures were significantly more likely to die, compared with those with mild or moderate fractures (60%, 7%, 24%, respectively, for severe, moderate, and mild; P = .04), despite no significant differences in clinical or laboratory parameters.
“Our data from the field reinforce the need of implementing previously published recommendations concerning the importance of bone fragility care during the COVID pandemic with at least those patients already treated with antiosteoporotic drugs maintaining their adherence to treatments including vitamin D, which have also been suggested very recently to have no relevant predisposing effect on COVID-19,” Dr. Giustina and colleagues wrote.
Moreover, they added, “continuity of care should also include bone density monitoring despite very restricted access to clinical facilities, during the COVID-19 pandemic. Finally, all patients with fractures should start antiresorptive treatment right away, even during hospital stay.”
The authors reported having no disclosures.
SOURCE: Giustina A et al. J Clin Endocrinol Metab. 2020 Oct 21. doi: 10.1210/clinem/dgaa738.
Vertebral fractures appear to be common in people with severe COVID-19, and also raise the mortality risk, findings from a retrospective cohort suggest.
Among 114 patients with COVID-19 who underwent lateral chest x-rays at the San Raffaele Hospital ED in Milan, more than a third were found to have thoracic vertebral fractures. And, those individuals were more than twice as likely to die as were those without vertebral fractures.
“Morphometric vertebral fractures are one of the most common comorbidities among adults hospitalized with COVID-19, and the presence of such fractures may predict the severity of disease outcomes,” lead investigator Andrea Giustina, MD, said in an interview.
This is the first study to examine vertebral fracture prevalence in any coronavirus disease, but such fractures have been linked to an increased risk of pneumonia and impaired respiratory function, including restrictive pulmonary dysfunction. One possible mechanism may be that they cause anatomical changes, such as kyphosis, which negatively impact respiratory function by decreasing vital capacity, forced expiratory volume in 1 second, and inspiratory time, explained Dr. Giustina, professor of endocrinology, San Raffaele Vita Salute University, Milan, and president of the European Society of Endocrinology. The results were published in the Journal of Clinical Endocrinology and Metabolism.
Clinically, the findings suggest that all patients with COVID-19 who are undergoing chest x-rays should have morphometric vertebral x-ray evaluation, said Dr. Giustina.
“One interesting aspect of the study is that without morphometry, approximatively two thirds of vertebral fractures [would have been] missed. Therefore, they are largely underestimated in clinical practice,” he noted.
Thoracic vertebral fractures assessed via lateral chest x-rays
The 114 study subjects included were those whose lateral chest x-rays allowed for a high-quality assessment and in which all the thoracic tract of T4-T12 were viewable and assessable. None had been using glucocorticoids and only 3% had a prior diagnosis of osteoporosis.
The majority (75%) were male, and median age was 57 years. Most (79%) were hospitalized after evaluation in the ED. Of those, 12% (13) were admitted to the ICU and 15% (16) died.
Thoracic vertebral fractures were detected on the lateral chest x-rays in 36% (41) of the patients. In contrast, in studies of women aged 50 years and older from the general European population, morphometric vertebral fracture prevalence ranged from 18% to 26%, the investigators noted.
Of the total 65 vertebral fractures detected, 60% were classified as mild (height ratio decrease <25%), 33.3% as moderate (25%-40% decrease) and 7.7% as severe (>40%). Patients with more than one vertebral fracture were classified by their most severe one.
Those with versus without vertebral fractures didn’t differ by sex, body mass index, or clinical or biological parameters evaluated in the ED. But, compared with those without vertebral fractures, those with them were significantly older (68 vs. 54 years) and were more likely to have arterial hypertension (56% vs. 30%) and coronary artery disease (22% vs. 7%).
In multivariate analysis, age was the only statistically significant predictor of vertebral fractures (odds ratio, 1.04; P < .001).
Mortality doubled, though not significantly
Those with vertebral fractures were more likely to be hospitalized, although not significantly (88% vs. 74%). There was no significant difference in ICU admission (11% vs. 12.5%).
However, those with vertebral fractures required noninvasive mechanical ventilation significantly more often (48.8% vs. 27.4%; P = .02), and were more than twice as likely to die (22% vs. 10%; P = .07). While the difference in overall mortality wasn’t quite statistically significant, those with severe vertebral fractures were significantly more likely to die, compared with those with mild or moderate fractures (60%, 7%, 24%, respectively, for severe, moderate, and mild; P = .04), despite no significant differences in clinical or laboratory parameters.
“Our data from the field reinforce the need of implementing previously published recommendations concerning the importance of bone fragility care during the COVID pandemic with at least those patients already treated with antiosteoporotic drugs maintaining their adherence to treatments including vitamin D, which have also been suggested very recently to have no relevant predisposing effect on COVID-19,” Dr. Giustina and colleagues wrote.
Moreover, they added, “continuity of care should also include bone density monitoring despite very restricted access to clinical facilities, during the COVID-19 pandemic. Finally, all patients with fractures should start antiresorptive treatment right away, even during hospital stay.”
The authors reported having no disclosures.
SOURCE: Giustina A et al. J Clin Endocrinol Metab. 2020 Oct 21. doi: 10.1210/clinem/dgaa738.
Vertebral fractures appear to be common in people with severe COVID-19, and also raise the mortality risk, findings from a retrospective cohort suggest.
Among 114 patients with COVID-19 who underwent lateral chest x-rays at the San Raffaele Hospital ED in Milan, more than a third were found to have thoracic vertebral fractures. And, those individuals were more than twice as likely to die as were those without vertebral fractures.
“Morphometric vertebral fractures are one of the most common comorbidities among adults hospitalized with COVID-19, and the presence of such fractures may predict the severity of disease outcomes,” lead investigator Andrea Giustina, MD, said in an interview.
This is the first study to examine vertebral fracture prevalence in any coronavirus disease, but such fractures have been linked to an increased risk of pneumonia and impaired respiratory function, including restrictive pulmonary dysfunction. One possible mechanism may be that they cause anatomical changes, such as kyphosis, which negatively impact respiratory function by decreasing vital capacity, forced expiratory volume in 1 second, and inspiratory time, explained Dr. Giustina, professor of endocrinology, San Raffaele Vita Salute University, Milan, and president of the European Society of Endocrinology. The results were published in the Journal of Clinical Endocrinology and Metabolism.
Clinically, the findings suggest that all patients with COVID-19 who are undergoing chest x-rays should have morphometric vertebral x-ray evaluation, said Dr. Giustina.
“One interesting aspect of the study is that without morphometry, approximatively two thirds of vertebral fractures [would have been] missed. Therefore, they are largely underestimated in clinical practice,” he noted.
Thoracic vertebral fractures assessed via lateral chest x-rays
The 114 study subjects included were those whose lateral chest x-rays allowed for a high-quality assessment and in which all the thoracic tract of T4-T12 were viewable and assessable. None had been using glucocorticoids and only 3% had a prior diagnosis of osteoporosis.
The majority (75%) were male, and median age was 57 years. Most (79%) were hospitalized after evaluation in the ED. Of those, 12% (13) were admitted to the ICU and 15% (16) died.
Thoracic vertebral fractures were detected on the lateral chest x-rays in 36% (41) of the patients. In contrast, in studies of women aged 50 years and older from the general European population, morphometric vertebral fracture prevalence ranged from 18% to 26%, the investigators noted.
Of the total 65 vertebral fractures detected, 60% were classified as mild (height ratio decrease <25%), 33.3% as moderate (25%-40% decrease) and 7.7% as severe (>40%). Patients with more than one vertebral fracture were classified by their most severe one.
Those with versus without vertebral fractures didn’t differ by sex, body mass index, or clinical or biological parameters evaluated in the ED. But, compared with those without vertebral fractures, those with them were significantly older (68 vs. 54 years) and were more likely to have arterial hypertension (56% vs. 30%) and coronary artery disease (22% vs. 7%).
In multivariate analysis, age was the only statistically significant predictor of vertebral fractures (odds ratio, 1.04; P < .001).
Mortality doubled, though not significantly
Those with vertebral fractures were more likely to be hospitalized, although not significantly (88% vs. 74%). There was no significant difference in ICU admission (11% vs. 12.5%).
However, those with vertebral fractures required noninvasive mechanical ventilation significantly more often (48.8% vs. 27.4%; P = .02), and were more than twice as likely to die (22% vs. 10%; P = .07). While the difference in overall mortality wasn’t quite statistically significant, those with severe vertebral fractures were significantly more likely to die, compared with those with mild or moderate fractures (60%, 7%, 24%, respectively, for severe, moderate, and mild; P = .04), despite no significant differences in clinical or laboratory parameters.
“Our data from the field reinforce the need of implementing previously published recommendations concerning the importance of bone fragility care during the COVID pandemic with at least those patients already treated with antiosteoporotic drugs maintaining their adherence to treatments including vitamin D, which have also been suggested very recently to have no relevant predisposing effect on COVID-19,” Dr. Giustina and colleagues wrote.
Moreover, they added, “continuity of care should also include bone density monitoring despite very restricted access to clinical facilities, during the COVID-19 pandemic. Finally, all patients with fractures should start antiresorptive treatment right away, even during hospital stay.”
The authors reported having no disclosures.
SOURCE: Giustina A et al. J Clin Endocrinol Metab. 2020 Oct 21. doi: 10.1210/clinem/dgaa738.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM