User login
Study found low rates, but significant risk factors, for incidental gallbladder cancer in cholecystectomy patients
Only 0.19% of cholecystectomy patients had incidental gallbladder cancer, and incidence was just 0.03% in patients who lacked risk factors for the malignancy, according to investigators. The report was published in Annals of Surgery.
The results were lower than historical reports, probably because cholecystectomy has been increasingly performed in younger patients, said Dr. Susan Pitt of Washington University, St. Louis, and her associates.
The investigators reported that significant risk factors for incidental gall bladder cancer (iGBC) included open (vs. laparoscopic) cholecystectomy, older age, Asian or African-American race, female sex, and an elevated alkaline phosphatase (ALP) level (Ann. Surg. 2014 Feb. 6 [doi:10.1097/SLA.0000000000000485]).
The retrospective cohort study included 91,260 patients aged 16 years and older who underwent laparoscopic (n = 80,924 [88.7%]) or open (n = 10,336 [11.3%]) cholecystectomy from 2005 to 2009. Patients were identified through the American College of Surgeons-National Surgical Quality Improvement Program Participant Use File.
Only 0.05% of laparoscopic patients had iGBC, vs. 0.60% of laparoscopic converted to open cholecystectomy patients (P less than .001) and 1.13% of open cholecystectomy patients (P less than .001), the researchers said. Multivariable predictors for iGBC included open vs. laparoscopic approach (odds ratio, 12.0; 95% confidence interval, 8.5-16.7); age 65 years or older (OR, 5.3; 95% CI, 3.7-7.4); Asian (OR, 2.2; 95% CI, 1.1-4.4) or African-American race (OR, 1.7; 95% CI, 1.1-2.6); alkaline phosphatase level 120 units/L or greater (OR, 1.7; 95% CI, 1.3-2.3); and female sex (OR, 1.6; 95% CI, 1.1-2.2).
"Even in the presence of all these risk factors, the incidence of iGBC is only 1.4%, although it is nearly 50-fold higher than a patient without any risk factors," Dr. Pitt and her associates wrote. Identifying patients at risk of iGBC before surgery "might allow a surgeon to be prepared to perform an adequate R0 resection at the initial procedure or refer the patient to a center with expertise in liver surgery, especially in the presence of a gallbladder polyp or mass on imaging," they added.
Within 30 days of surgery, patients with iGBC had significantly higher rates of death, serious morbidity, overall morbidity, surgical site infection, and organ space surgical site infection (P less than .001 for all outcomes), the researchers reported.
The study database lacked information on symptoms, preoperative diagnoses, or diagnostic studies specific to gallbladder disease, Dr. Pitt and her coworkers noted. The large sample size increased the possibility of type I error because small differences might reach statistical significance even if they lacked clinical importance, they added.
The authors received no funding for the study. One of the investigators, Dr. Bruce Hall, is a paid consultant for the American College of Surgeons.
Only 0.19% of cholecystectomy patients had incidental gallbladder cancer, and incidence was just 0.03% in patients who lacked risk factors for the malignancy, according to investigators. The report was published in Annals of Surgery.
The results were lower than historical reports, probably because cholecystectomy has been increasingly performed in younger patients, said Dr. Susan Pitt of Washington University, St. Louis, and her associates.
The investigators reported that significant risk factors for incidental gall bladder cancer (iGBC) included open (vs. laparoscopic) cholecystectomy, older age, Asian or African-American race, female sex, and an elevated alkaline phosphatase (ALP) level (Ann. Surg. 2014 Feb. 6 [doi:10.1097/SLA.0000000000000485]).
The retrospective cohort study included 91,260 patients aged 16 years and older who underwent laparoscopic (n = 80,924 [88.7%]) or open (n = 10,336 [11.3%]) cholecystectomy from 2005 to 2009. Patients were identified through the American College of Surgeons-National Surgical Quality Improvement Program Participant Use File.
Only 0.05% of laparoscopic patients had iGBC, vs. 0.60% of laparoscopic converted to open cholecystectomy patients (P less than .001) and 1.13% of open cholecystectomy patients (P less than .001), the researchers said. Multivariable predictors for iGBC included open vs. laparoscopic approach (odds ratio, 12.0; 95% confidence interval, 8.5-16.7); age 65 years or older (OR, 5.3; 95% CI, 3.7-7.4); Asian (OR, 2.2; 95% CI, 1.1-4.4) or African-American race (OR, 1.7; 95% CI, 1.1-2.6); alkaline phosphatase level 120 units/L or greater (OR, 1.7; 95% CI, 1.3-2.3); and female sex (OR, 1.6; 95% CI, 1.1-2.2).
"Even in the presence of all these risk factors, the incidence of iGBC is only 1.4%, although it is nearly 50-fold higher than a patient without any risk factors," Dr. Pitt and her associates wrote. Identifying patients at risk of iGBC before surgery "might allow a surgeon to be prepared to perform an adequate R0 resection at the initial procedure or refer the patient to a center with expertise in liver surgery, especially in the presence of a gallbladder polyp or mass on imaging," they added.
Within 30 days of surgery, patients with iGBC had significantly higher rates of death, serious morbidity, overall morbidity, surgical site infection, and organ space surgical site infection (P less than .001 for all outcomes), the researchers reported.
The study database lacked information on symptoms, preoperative diagnoses, or diagnostic studies specific to gallbladder disease, Dr. Pitt and her coworkers noted. The large sample size increased the possibility of type I error because small differences might reach statistical significance even if they lacked clinical importance, they added.
The authors received no funding for the study. One of the investigators, Dr. Bruce Hall, is a paid consultant for the American College of Surgeons.
Only 0.19% of cholecystectomy patients had incidental gallbladder cancer, and incidence was just 0.03% in patients who lacked risk factors for the malignancy, according to investigators. The report was published in Annals of Surgery.
The results were lower than historical reports, probably because cholecystectomy has been increasingly performed in younger patients, said Dr. Susan Pitt of Washington University, St. Louis, and her associates.
The investigators reported that significant risk factors for incidental gall bladder cancer (iGBC) included open (vs. laparoscopic) cholecystectomy, older age, Asian or African-American race, female sex, and an elevated alkaline phosphatase (ALP) level (Ann. Surg. 2014 Feb. 6 [doi:10.1097/SLA.0000000000000485]).
The retrospective cohort study included 91,260 patients aged 16 years and older who underwent laparoscopic (n = 80,924 [88.7%]) or open (n = 10,336 [11.3%]) cholecystectomy from 2005 to 2009. Patients were identified through the American College of Surgeons-National Surgical Quality Improvement Program Participant Use File.
Only 0.05% of laparoscopic patients had iGBC, vs. 0.60% of laparoscopic converted to open cholecystectomy patients (P less than .001) and 1.13% of open cholecystectomy patients (P less than .001), the researchers said. Multivariable predictors for iGBC included open vs. laparoscopic approach (odds ratio, 12.0; 95% confidence interval, 8.5-16.7); age 65 years or older (OR, 5.3; 95% CI, 3.7-7.4); Asian (OR, 2.2; 95% CI, 1.1-4.4) or African-American race (OR, 1.7; 95% CI, 1.1-2.6); alkaline phosphatase level 120 units/L or greater (OR, 1.7; 95% CI, 1.3-2.3); and female sex (OR, 1.6; 95% CI, 1.1-2.2).
"Even in the presence of all these risk factors, the incidence of iGBC is only 1.4%, although it is nearly 50-fold higher than a patient without any risk factors," Dr. Pitt and her associates wrote. Identifying patients at risk of iGBC before surgery "might allow a surgeon to be prepared to perform an adequate R0 resection at the initial procedure or refer the patient to a center with expertise in liver surgery, especially in the presence of a gallbladder polyp or mass on imaging," they added.
Within 30 days of surgery, patients with iGBC had significantly higher rates of death, serious morbidity, overall morbidity, surgical site infection, and organ space surgical site infection (P less than .001 for all outcomes), the researchers reported.
The study database lacked information on symptoms, preoperative diagnoses, or diagnostic studies specific to gallbladder disease, Dr. Pitt and her coworkers noted. The large sample size increased the possibility of type I error because small differences might reach statistical significance even if they lacked clinical importance, they added.
The authors received no funding for the study. One of the investigators, Dr. Bruce Hall, is a paid consultant for the American College of Surgeons.
FROM ANNALS OF SURGERY
Major finding: Overall incidence of incidental gallbladder cancer was 0.19%. Risk factors included open vs. laparoscopic approach (odds ratio, 12.0); age at least 65 years (OR, 5.3); Asian (OR, 2.2) or African-American race (OR, 1.7); alkaline phosphatase greater than 120 units/L (OR, 1.7); and female sex (OR, 1.6).
Data source: Retrospective cohort study of 91,260 patients aged 16 years or older who underwent laparoscopic (n = 80,924 [88.7%]) or open (n = 10,336 [11.3%]) cholecystectomy from 2005 to 2009.
Disclosures: The authors received no funding for the study. One of the investigators is a paid consultant for the American College of Surgeons.
Hold the immunomodulators for surgery? Maybe yes, maybe no
SCOTTSDALE, ARIZ. – When patients on immunosuppressive therapies need surgery, the risks of disease flare and compromised postoperative recovery and rehabilitation must be weighed against the risk of increased infections and impaired wound healing.
"I’m not sure that there is necessarily a right answer, but I think most people would stop biologic [agents] beforehand," Dr. Paul Grant said at a meeting on perioperative medicine sponsored by the University of Miami.
The decision whether to suspend a disease-modifying antirheumatic drug before surgery may depend on the individual drug and on the patient, said Dr. Grant, director of perioperative and consultative medicine at the University of Michigan Health System in Ann Arbor.
For example, it appears to be safe for patients on methotrexate to continue on therapy during elective orthopedic surgery. Evidence for this comes from a randomized clinical trial in which patients with rheumatoid arthritis (RA) were assigned to either continue on methotrexate (MTX) or suspend taking it for 2 weeks before and 2 weeks after surgery. The study also contained a control of patients with RA who were not on MTX (Ann. Rheum. Dis. 2001;60:214-7).
The investigators found that there were no significant differences in early complication rates or in complications up to 1 year of follow-up between patients who suspended or remained on MTX. Patients who stayed on the drug had significantly lower rates of RA flare.
Additionally, two systematic reviews, one looking at eight studies echoes the findings of the aforementioned randomized trial, and the other looking at four studies, in which the reviewer concluded that "continued MTX therapy appears to be safe perioperatively and seems also to be associated with a reduced risk of flares (Clin. Exp. Rheumatol. 2009;27:856-62) (Clin. Rheumatol. 2008;27:1217-20).None of the examined papers addresses the issue of safety in connection with comorbidities, age, or high doses of methotrexate."
"The bottom line here is that methotrexate should be continued for most surgeries. I think it might be reasonable to hold it in certain situations, for example if the patient has pretty bad kidney or liver disease, or if it’s surgery to treat a major infection," Dr. Grant said.
TNF-alpha antagonists
In contrast, the data on tumor necrosis factor–alpha (TNF-alpha) antagonists are fuzzier, with limited and conflicting information on perioperative use of these agents (etanercept, infliximab, adalimumab, certolizumab, golimumab).
"The major concern with these drugs is infection," Dr. Grant said. He pointed to a meta-analysis published in JAMA in 2006, which showed that taking the drugs doubled the risk of serious infections in general. The study did not specifically look at perioperative use of TNF-alpha antagonists (JAMA 2006;295:2275-85).
A retrospective cohort studyof 127 patients with RA who were undergoing various orthopedic procedures found that there were no differences in surgical site infections but more cases of wound dehiscence in patients who continued on the drugs, compared with those who interrupted their use perioperatively (Clin. Exp. Rheumatol. 2007;25:430-6).
A second, prospective study in 31 patients with RA undergoing foot/ankle surgery found that there were no significant differences in infection or healing between patients who interrupted therapy and those who did not (Foot Ankle Clin. 2007;12:509-24).
Other studies and systematic reviews in patients with RA or Crohn’s disease generally found no significant differences in serious infection rates, but they did detect a higher incidence of skin and soft-tissue infections among patients on anti-TNF-alpha agents vs. other disease-modifying antirheumatic drugs.
The risk of infections tends to be highest at the start of therapy with a TNF-alpha antagonist and stopping therapy is more likely to result in RA flares among patients with established disease, compared with those in the early stages of RA. Therefore, TNF blocker therapy should be restarted as soon as possible after surgery to prevent flare, Dr. Grant said.
The American College of Rheumatology and British Society of Rheumatology recommend holding TNF-alpha antagonists for one dosing cycle before major surgery. For etanercept (Enbrel), that translates to a 1-week before surgery hold, for infliximab (Remicade) 6-8 weeks, and for adalimumab (Humira) 2 weeks. These agents should also be held for 10-14 days after surgery or until wound healing is satisfactory.
"It’s probably safe to continue these medications for minor surgeries," Dr. Grant said.
Other agents
The anti-CD20 agent rituximab (Rituxan) – currently used to treat RA, vasculitis, hematologic malignancies, and other conditions – has a lower risk for bacterial infections than does TNF-alpha antagonists and has been shown to be safe in patients with a history of recurrent bacterial infections.
"Hydroxychloroquine (or Plaquenil) is felt to be safe during the preoperative period. It is recommended to continue this medication without stopping," Dr. Grant said.
There is conflicting information on infection risk with the use leflunomide (Arava), but it may be wise to stop therapy 2-4 weeks before nonurgent surgery in higher-risk patients.
There is consensus that sulfasalazine (Azulfidine) and azathioprine (Imuran) can be safely continued perioperatively, he said, although some advise holding sulfasalazine on the day of surgery.
Regarding perioperative steroids, Dr. Grant recommended determining the patient’s steroid exposure over the past year.
"Stress dose steroids are not routinely needed as long as the patients continue their normal dose. That’s really the important piece: If someone’s taking prednisone every day, make sure they take at least that dose on the day of surgery," he said.
Dr. Grant reported having no financial disclosures.
SCOTTSDALE, ARIZ. – When patients on immunosuppressive therapies need surgery, the risks of disease flare and compromised postoperative recovery and rehabilitation must be weighed against the risk of increased infections and impaired wound healing.
"I’m not sure that there is necessarily a right answer, but I think most people would stop biologic [agents] beforehand," Dr. Paul Grant said at a meeting on perioperative medicine sponsored by the University of Miami.
The decision whether to suspend a disease-modifying antirheumatic drug before surgery may depend on the individual drug and on the patient, said Dr. Grant, director of perioperative and consultative medicine at the University of Michigan Health System in Ann Arbor.
For example, it appears to be safe for patients on methotrexate to continue on therapy during elective orthopedic surgery. Evidence for this comes from a randomized clinical trial in which patients with rheumatoid arthritis (RA) were assigned to either continue on methotrexate (MTX) or suspend taking it for 2 weeks before and 2 weeks after surgery. The study also contained a control of patients with RA who were not on MTX (Ann. Rheum. Dis. 2001;60:214-7).
The investigators found that there were no significant differences in early complication rates or in complications up to 1 year of follow-up between patients who suspended or remained on MTX. Patients who stayed on the drug had significantly lower rates of RA flare.
Additionally, two systematic reviews, one looking at eight studies echoes the findings of the aforementioned randomized trial, and the other looking at four studies, in which the reviewer concluded that "continued MTX therapy appears to be safe perioperatively and seems also to be associated with a reduced risk of flares (Clin. Exp. Rheumatol. 2009;27:856-62) (Clin. Rheumatol. 2008;27:1217-20).None of the examined papers addresses the issue of safety in connection with comorbidities, age, or high doses of methotrexate."
"The bottom line here is that methotrexate should be continued for most surgeries. I think it might be reasonable to hold it in certain situations, for example if the patient has pretty bad kidney or liver disease, or if it’s surgery to treat a major infection," Dr. Grant said.
TNF-alpha antagonists
In contrast, the data on tumor necrosis factor–alpha (TNF-alpha) antagonists are fuzzier, with limited and conflicting information on perioperative use of these agents (etanercept, infliximab, adalimumab, certolizumab, golimumab).
"The major concern with these drugs is infection," Dr. Grant said. He pointed to a meta-analysis published in JAMA in 2006, which showed that taking the drugs doubled the risk of serious infections in general. The study did not specifically look at perioperative use of TNF-alpha antagonists (JAMA 2006;295:2275-85).
A retrospective cohort studyof 127 patients with RA who were undergoing various orthopedic procedures found that there were no differences in surgical site infections but more cases of wound dehiscence in patients who continued on the drugs, compared with those who interrupted their use perioperatively (Clin. Exp. Rheumatol. 2007;25:430-6).
A second, prospective study in 31 patients with RA undergoing foot/ankle surgery found that there were no significant differences in infection or healing between patients who interrupted therapy and those who did not (Foot Ankle Clin. 2007;12:509-24).
Other studies and systematic reviews in patients with RA or Crohn’s disease generally found no significant differences in serious infection rates, but they did detect a higher incidence of skin and soft-tissue infections among patients on anti-TNF-alpha agents vs. other disease-modifying antirheumatic drugs.
The risk of infections tends to be highest at the start of therapy with a TNF-alpha antagonist and stopping therapy is more likely to result in RA flares among patients with established disease, compared with those in the early stages of RA. Therefore, TNF blocker therapy should be restarted as soon as possible after surgery to prevent flare, Dr. Grant said.
The American College of Rheumatology and British Society of Rheumatology recommend holding TNF-alpha antagonists for one dosing cycle before major surgery. For etanercept (Enbrel), that translates to a 1-week before surgery hold, for infliximab (Remicade) 6-8 weeks, and for adalimumab (Humira) 2 weeks. These agents should also be held for 10-14 days after surgery or until wound healing is satisfactory.
"It’s probably safe to continue these medications for minor surgeries," Dr. Grant said.
Other agents
The anti-CD20 agent rituximab (Rituxan) – currently used to treat RA, vasculitis, hematologic malignancies, and other conditions – has a lower risk for bacterial infections than does TNF-alpha antagonists and has been shown to be safe in patients with a history of recurrent bacterial infections.
"Hydroxychloroquine (or Plaquenil) is felt to be safe during the preoperative period. It is recommended to continue this medication without stopping," Dr. Grant said.
There is conflicting information on infection risk with the use leflunomide (Arava), but it may be wise to stop therapy 2-4 weeks before nonurgent surgery in higher-risk patients.
There is consensus that sulfasalazine (Azulfidine) and azathioprine (Imuran) can be safely continued perioperatively, he said, although some advise holding sulfasalazine on the day of surgery.
Regarding perioperative steroids, Dr. Grant recommended determining the patient’s steroid exposure over the past year.
"Stress dose steroids are not routinely needed as long as the patients continue their normal dose. That’s really the important piece: If someone’s taking prednisone every day, make sure they take at least that dose on the day of surgery," he said.
Dr. Grant reported having no financial disclosures.
SCOTTSDALE, ARIZ. – When patients on immunosuppressive therapies need surgery, the risks of disease flare and compromised postoperative recovery and rehabilitation must be weighed against the risk of increased infections and impaired wound healing.
"I’m not sure that there is necessarily a right answer, but I think most people would stop biologic [agents] beforehand," Dr. Paul Grant said at a meeting on perioperative medicine sponsored by the University of Miami.
The decision whether to suspend a disease-modifying antirheumatic drug before surgery may depend on the individual drug and on the patient, said Dr. Grant, director of perioperative and consultative medicine at the University of Michigan Health System in Ann Arbor.
For example, it appears to be safe for patients on methotrexate to continue on therapy during elective orthopedic surgery. Evidence for this comes from a randomized clinical trial in which patients with rheumatoid arthritis (RA) were assigned to either continue on methotrexate (MTX) or suspend taking it for 2 weeks before and 2 weeks after surgery. The study also contained a control of patients with RA who were not on MTX (Ann. Rheum. Dis. 2001;60:214-7).
The investigators found that there were no significant differences in early complication rates or in complications up to 1 year of follow-up between patients who suspended or remained on MTX. Patients who stayed on the drug had significantly lower rates of RA flare.
Additionally, two systematic reviews, one looking at eight studies echoes the findings of the aforementioned randomized trial, and the other looking at four studies, in which the reviewer concluded that "continued MTX therapy appears to be safe perioperatively and seems also to be associated with a reduced risk of flares (Clin. Exp. Rheumatol. 2009;27:856-62) (Clin. Rheumatol. 2008;27:1217-20).None of the examined papers addresses the issue of safety in connection with comorbidities, age, or high doses of methotrexate."
"The bottom line here is that methotrexate should be continued for most surgeries. I think it might be reasonable to hold it in certain situations, for example if the patient has pretty bad kidney or liver disease, or if it’s surgery to treat a major infection," Dr. Grant said.
TNF-alpha antagonists
In contrast, the data on tumor necrosis factor–alpha (TNF-alpha) antagonists are fuzzier, with limited and conflicting information on perioperative use of these agents (etanercept, infliximab, adalimumab, certolizumab, golimumab).
"The major concern with these drugs is infection," Dr. Grant said. He pointed to a meta-analysis published in JAMA in 2006, which showed that taking the drugs doubled the risk of serious infections in general. The study did not specifically look at perioperative use of TNF-alpha antagonists (JAMA 2006;295:2275-85).
A retrospective cohort studyof 127 patients with RA who were undergoing various orthopedic procedures found that there were no differences in surgical site infections but more cases of wound dehiscence in patients who continued on the drugs, compared with those who interrupted their use perioperatively (Clin. Exp. Rheumatol. 2007;25:430-6).
A second, prospective study in 31 patients with RA undergoing foot/ankle surgery found that there were no significant differences in infection or healing between patients who interrupted therapy and those who did not (Foot Ankle Clin. 2007;12:509-24).
Other studies and systematic reviews in patients with RA or Crohn’s disease generally found no significant differences in serious infection rates, but they did detect a higher incidence of skin and soft-tissue infections among patients on anti-TNF-alpha agents vs. other disease-modifying antirheumatic drugs.
The risk of infections tends to be highest at the start of therapy with a TNF-alpha antagonist and stopping therapy is more likely to result in RA flares among patients with established disease, compared with those in the early stages of RA. Therefore, TNF blocker therapy should be restarted as soon as possible after surgery to prevent flare, Dr. Grant said.
The American College of Rheumatology and British Society of Rheumatology recommend holding TNF-alpha antagonists for one dosing cycle before major surgery. For etanercept (Enbrel), that translates to a 1-week before surgery hold, for infliximab (Remicade) 6-8 weeks, and for adalimumab (Humira) 2 weeks. These agents should also be held for 10-14 days after surgery or until wound healing is satisfactory.
"It’s probably safe to continue these medications for minor surgeries," Dr. Grant said.
Other agents
The anti-CD20 agent rituximab (Rituxan) – currently used to treat RA, vasculitis, hematologic malignancies, and other conditions – has a lower risk for bacterial infections than does TNF-alpha antagonists and has been shown to be safe in patients with a history of recurrent bacterial infections.
"Hydroxychloroquine (or Plaquenil) is felt to be safe during the preoperative period. It is recommended to continue this medication without stopping," Dr. Grant said.
There is conflicting information on infection risk with the use leflunomide (Arava), but it may be wise to stop therapy 2-4 weeks before nonurgent surgery in higher-risk patients.
There is consensus that sulfasalazine (Azulfidine) and azathioprine (Imuran) can be safely continued perioperatively, he said, although some advise holding sulfasalazine on the day of surgery.
Regarding perioperative steroids, Dr. Grant recommended determining the patient’s steroid exposure over the past year.
"Stress dose steroids are not routinely needed as long as the patients continue their normal dose. That’s really the important piece: If someone’s taking prednisone every day, make sure they take at least that dose on the day of surgery," he said.
Dr. Grant reported having no financial disclosures.
AT THE PERIOPERATIVE MEDICINE SUMMIT
Major finding: Some immunomodulating agents for inflammatory and autoimmune diseases can be safely continued in the perioperative period.
Data source: A review of evidence on the use of various immunomodulators.
Disclosures: Dr. Grant reported having no financial disclosures.
Defining patients’ risk helps prevent postop urinary retention
SCOTTSDALE, ARIZ. – Early hospital readmissions are not good for patients and can be terrible for a hospital’s bottom line, but at least one cause of readmission – urinary retention after surgery – can be significantly reduced.
"Postoperative urinary retention is a prevalent and mostly avoidable complication," said Dr. Sarita Khemani, a surgical comanagement hospitalist at Stanford (Calif.) University Medical Center.
Postoperative urinary retention can be defined as the inability to void in the presence of symptoms or bladder distension. However, as some patients may retain urine without feeling symptoms or the urge to void, it can also be defined as the inability to void with a bladder volume greater than 500 mL, or the presence of a postvoid residual volume greater than 200 mL on bladder scan, she said at a meeting on perioperative medicine sponsored by the University of Miami.
Identify high-risk patients
"For management, identifying the high-risk patient is very important," said Dr. Khemani.
She and her colleagues are working to develop a scoring system for identifying patients at risk for postoperative retention, she noted.
Depending on the risk factor, patients may require continued use of benign prostatic hyperplasia (BPH) medications (a strategy currently under clinical investigation), multimodal anesthesia, monitoring of IV fluids during and after surgery, and, when necessary, catheterization.

"There is really no consensus as to what is the best catheterization strategy we should use when it comes to urinary retention," Dr. Khemani said.
Low-risk patients undergoing outpatient procedures can be safely sent home without voiding, she said. High-risk patients undergoing ambulatory surgery can be managed with intermittent catheterization.
Patients who are undergoing major but uncomplicated surgery but are at low risk for postoperative retention do not generally need to have Foley catheters placed before surgery. Indwelling catheters should be limited, if possible, to 24 hours after surgery, and the patient can be managed with bladder scans every 6 hours if needed.
Patients scheduled for extensive, complicated procedures and those at high risk may require an indwelling catheter for up to 5 days after surgery. Studies have shown that in these patients early catheter removal actually increases the risk for postoperative urinary retention, Dr. Khemani said.
"It really needs to be followed by bladder scanning very closely, every 6 hours, to try to prevent overdistention and complications after that," she said.
The incidence of postoperative urinary retention among general surgery patients is 3.8%, but can range as high 70% after orthopedic surgery, 50% after anorectal procedures, 40% following spinal surgeries, and 38% after herniorrhaphy, Dr. Khemani said.
Preoperative risk factors for urinary retention after surgery include age over 50; male sex; history of retention; BPH; history of diabetes, stroke, or spinal lesions; or use of drugs such anticholinergic agents or beta-blockers.
Intraoperative and postoperative risk factors include the type and duration of surgery, anesthesia (especially spinal and epidural anethesias), systemic analgesia with opioids (especially patient-controlled analgesia, or PCA), and the use of intraoperative intravenous fluids. High IV fluid infusion causes rapid distention of the bladder detrusor muscles, leading to inability of the muscles to contract after surgery, Dr. Khemani noted.
Complications of postoperative urinary retention can include:
• Autonomic responses to bladder distention, leading to effects such as bradycardia, hypotension, vomiting, and delirium in some elderly patients.
• Infectious complications – urinary tract infections, sepsis, and joint infections.
• Prolonged need for catheterization.
• Bladder dysfunction.
A recent systematic review of drugs for treatment of urinary retention after surgery in adults found that of seven studies involving a total of 494 patients, neither cholinergic agents, alpha blockers, nor sedatives made a significant difference in reducing the incidence of retention. Only prostaglandins, and only when those agents were given intravesically, appeared to offer any benefit, the authors found.
"At this point we definitely need more studies to look at pharmacological alternatives to catheterization for treatment and prevention of this condition," Dr. Khemani concluded.
She reported having no financial disclosures.
SCOTTSDALE, ARIZ. – Early hospital readmissions are not good for patients and can be terrible for a hospital’s bottom line, but at least one cause of readmission – urinary retention after surgery – can be significantly reduced.
"Postoperative urinary retention is a prevalent and mostly avoidable complication," said Dr. Sarita Khemani, a surgical comanagement hospitalist at Stanford (Calif.) University Medical Center.
Postoperative urinary retention can be defined as the inability to void in the presence of symptoms or bladder distension. However, as some patients may retain urine without feeling symptoms or the urge to void, it can also be defined as the inability to void with a bladder volume greater than 500 mL, or the presence of a postvoid residual volume greater than 200 mL on bladder scan, she said at a meeting on perioperative medicine sponsored by the University of Miami.
Identify high-risk patients
"For management, identifying the high-risk patient is very important," said Dr. Khemani.
She and her colleagues are working to develop a scoring system for identifying patients at risk for postoperative retention, she noted.
Depending on the risk factor, patients may require continued use of benign prostatic hyperplasia (BPH) medications (a strategy currently under clinical investigation), multimodal anesthesia, monitoring of IV fluids during and after surgery, and, when necessary, catheterization.
"There is really no consensus as to what is the best catheterization strategy we should use when it comes to urinary retention," Dr. Khemani said.
Low-risk patients undergoing outpatient procedures can be safely sent home without voiding, she said. High-risk patients undergoing ambulatory surgery can be managed with intermittent catheterization.
Patients who are undergoing major but uncomplicated surgery but are at low risk for postoperative retention do not generally need to have Foley catheters placed before surgery. Indwelling catheters should be limited, if possible, to 24 hours after surgery, and the patient can be managed with bladder scans every 6 hours if needed.
Patients scheduled for extensive, complicated procedures and those at high risk may require an indwelling catheter for up to 5 days after surgery. Studies have shown that in these patients early catheter removal actually increases the risk for postoperative urinary retention, Dr. Khemani said.
"It really needs to be followed by bladder scanning very closely, every 6 hours, to try to prevent overdistention and complications after that," she said.
The incidence of postoperative urinary retention among general surgery patients is 3.8%, but can range as high 70% after orthopedic surgery, 50% after anorectal procedures, 40% following spinal surgeries, and 38% after herniorrhaphy, Dr. Khemani said.
Preoperative risk factors for urinary retention after surgery include age over 50; male sex; history of retention; BPH; history of diabetes, stroke, or spinal lesions; or use of drugs such anticholinergic agents or beta-blockers.
Intraoperative and postoperative risk factors include the type and duration of surgery, anesthesia (especially spinal and epidural anethesias), systemic analgesia with opioids (especially patient-controlled analgesia, or PCA), and the use of intraoperative intravenous fluids. High IV fluid infusion causes rapid distention of the bladder detrusor muscles, leading to inability of the muscles to contract after surgery, Dr. Khemani noted.
Complications of postoperative urinary retention can include:
• Autonomic responses to bladder distention, leading to effects such as bradycardia, hypotension, vomiting, and delirium in some elderly patients.
• Infectious complications – urinary tract infections, sepsis, and joint infections.
• Prolonged need for catheterization.
• Bladder dysfunction.
A recent systematic review of drugs for treatment of urinary retention after surgery in adults found that of seven studies involving a total of 494 patients, neither cholinergic agents, alpha blockers, nor sedatives made a significant difference in reducing the incidence of retention. Only prostaglandins, and only when those agents were given intravesically, appeared to offer any benefit, the authors found.
"At this point we definitely need more studies to look at pharmacological alternatives to catheterization for treatment and prevention of this condition," Dr. Khemani concluded.
She reported having no financial disclosures.
SCOTTSDALE, ARIZ. – Early hospital readmissions are not good for patients and can be terrible for a hospital’s bottom line, but at least one cause of readmission – urinary retention after surgery – can be significantly reduced.
"Postoperative urinary retention is a prevalent and mostly avoidable complication," said Dr. Sarita Khemani, a surgical comanagement hospitalist at Stanford (Calif.) University Medical Center.
Postoperative urinary retention can be defined as the inability to void in the presence of symptoms or bladder distension. However, as some patients may retain urine without feeling symptoms or the urge to void, it can also be defined as the inability to void with a bladder volume greater than 500 mL, or the presence of a postvoid residual volume greater than 200 mL on bladder scan, she said at a meeting on perioperative medicine sponsored by the University of Miami.
Identify high-risk patients
"For management, identifying the high-risk patient is very important," said Dr. Khemani.
She and her colleagues are working to develop a scoring system for identifying patients at risk for postoperative retention, she noted.
Depending on the risk factor, patients may require continued use of benign prostatic hyperplasia (BPH) medications (a strategy currently under clinical investigation), multimodal anesthesia, monitoring of IV fluids during and after surgery, and, when necessary, catheterization.
"There is really no consensus as to what is the best catheterization strategy we should use when it comes to urinary retention," Dr. Khemani said.
Low-risk patients undergoing outpatient procedures can be safely sent home without voiding, she said. High-risk patients undergoing ambulatory surgery can be managed with intermittent catheterization.
Patients who are undergoing major but uncomplicated surgery but are at low risk for postoperative retention do not generally need to have Foley catheters placed before surgery. Indwelling catheters should be limited, if possible, to 24 hours after surgery, and the patient can be managed with bladder scans every 6 hours if needed.
Patients scheduled for extensive, complicated procedures and those at high risk may require an indwelling catheter for up to 5 days after surgery. Studies have shown that in these patients early catheter removal actually increases the risk for postoperative urinary retention, Dr. Khemani said.
"It really needs to be followed by bladder scanning very closely, every 6 hours, to try to prevent overdistention and complications after that," she said.
The incidence of postoperative urinary retention among general surgery patients is 3.8%, but can range as high 70% after orthopedic surgery, 50% after anorectal procedures, 40% following spinal surgeries, and 38% after herniorrhaphy, Dr. Khemani said.
Preoperative risk factors for urinary retention after surgery include age over 50; male sex; history of retention; BPH; history of diabetes, stroke, or spinal lesions; or use of drugs such anticholinergic agents or beta-blockers.
Intraoperative and postoperative risk factors include the type and duration of surgery, anesthesia (especially spinal and epidural anethesias), systemic analgesia with opioids (especially patient-controlled analgesia, or PCA), and the use of intraoperative intravenous fluids. High IV fluid infusion causes rapid distention of the bladder detrusor muscles, leading to inability of the muscles to contract after surgery, Dr. Khemani noted.
Complications of postoperative urinary retention can include:
• Autonomic responses to bladder distention, leading to effects such as bradycardia, hypotension, vomiting, and delirium in some elderly patients.
• Infectious complications – urinary tract infections, sepsis, and joint infections.
• Prolonged need for catheterization.
• Bladder dysfunction.
A recent systematic review of drugs for treatment of urinary retention after surgery in adults found that of seven studies involving a total of 494 patients, neither cholinergic agents, alpha blockers, nor sedatives made a significant difference in reducing the incidence of retention. Only prostaglandins, and only when those agents were given intravesically, appeared to offer any benefit, the authors found.
"At this point we definitely need more studies to look at pharmacological alternatives to catheterization for treatment and prevention of this condition," Dr. Khemani concluded.
She reported having no financial disclosures.
AT THE PERIOPERATIVE MEDICINE SUMMIT
Major finding: The incidence of postoperative urinary retention may be as high as 70% after orthopedic procedures.
Data source: Review of evidence on the risk factors, prevention, and treatment of postoperative urinary retention.
Disclosures: Dr. Khemani reported having no financial disclosures.

Rising to the challenge of glucose control before and after surgery
SCOTTSDALE, ARIZ. – Controlling hyperglycemia before and after surgery in patients with diabetes is a balancing act, but when done properly, it can reduce infections and wound complications, according to Dr. David Baldwin.
The key to preoperative planning for patients with diabetes is a full list of medications and an understanding of how well (or how poorly) patients’ glycemia is controlled, said Dr. Baldwin, an endocrinologist at Rush University Medical Center in Chicago.
He discussed strategies for perioperative management of patients with diabetes and thyroid disorders at the Perioperative Medicine Summit 2014."You definitely want to write down exactly what they are and aren’t taking. We find that the medication list for people getting admitted for surgery is often fraught with a lack of little details," he said.
For patients with type 2 diabetes, it’s important to record an accurate description of antidiabetes medications, especially combination oral agents such as Actoplus MET (metformin and pioglitazone) or Janumet (sitagliptin and metformin). For patients with type 1 and 2 diabetes, it is important to record not just the type of insulin but the regimen the patient uses.

Dr. Baldwin noted that many intake staff make the mistake of reporting that patients take "Novolin" or "Humulin," which are brand families of insulin and not specific insulin types.
"We often find, probably at least half of the time, that until we actually go and ask the patients what they take for insulin post-op, the correct information won’t have been in the medical record," he said.
The best way to determine whether a patient has good control of chronic hyperglycemia is with a hemoglobin A1c (HbA1c) level. A value above 6.5% is diagnostic for diabetes; well-controlled patients have HbA1c levels from 6% to 8%. HbA1c values not more than 2 months old should be a routine part of preoperative evaluations for patients with diabetes or newly discovered hyperglycemia, Dr. Baldwin said.
Preoperative medications
The Rush University protocol for the preoperative management of antidiabetic therapies other than insulin notes that sulfonylureas, metformin, pioglitazone, exenatide, liraglutide, sitagliptin, linagliptin, saxagliptin, alogliptin, alpha-glucosidase inhibitors, and canagaflozin may all be taken with food on the eve of surgery, but none should be taken on the morning of surgery.
Specific rules also apply for patients who use insulin, depending on the insulin type, as follows:
• For long-acting insulins (glargine or detemir), the patient should take the full dose on the evening before surgery or the morning of surgery if the dose is prescribed for either morning or evening administration. Patients with prescriptions for a b.i.d. dose should take the full dose both the evening before and the morning of surgery.
• With intermediate-acting insulin (NPH), the patient should take the full dose on the evening before surgery and 80% of the morning dose on the morning of surgery.
• For rapid-acting insulins (aspart, lispro, glulisine, or regular) and premixed insulins (NPH or rapid acting), the patient should take the full dose with dinner the night before, and none on the morning of surgery.
Dr. Baldwin emphasized that except in rare circumstances, patients on subcutaneous insulin pumps should not use the pumps during surgery, and should get special instructions from their endocrinologists.
Ideally, the patient can convert to insulin glargine the night before surgery, with the dose equivalent to the total 24-hour basal insulin dose delivered by the pump. Two hours after the glargine dose is given, the patient should disconnect the pump and leave it at home.
Glycemic control in the hospital
As noted before, poor glycemic control can lead to poor wound healing from impaired leukocyte function, which can lead to decreased chemotaxis, phagocytosis, and bacteriocidal activity.
The risk of bacteremia is especially high among patients who are on total parenteral nutrition with poorly controlled glucose levels, he noted.
Forces conspiring against glucose control in the hospital can include elevated levels of hormones that counterregulate glucose; nausea/vomiting, anorexia, or nothing-by-mouth orders; erratic meal timing due to tests or interventions; intravenous glucose; glucocorticoid therapy; and "physician indifference and lack of attention to required adjustments in therapy," Dr. Baldwin noted.
Evidence from a randomized study showed that in patients with type 2 diabetes undergoing general surgery, basal-bolus treatment with insulin glargine once daily plus insulin glulisine before meals both improved glycemic control and reduced hospital complications compared with sliding-scale insulin therapy, he reported.
Hyper- and hypothyroid patients
Switching endocrinology hats, Dr. Baldwin said that patients who have significant weight loss or resting tachycardia before surgery should be evaluated for hyperthyroidism. A good rule of thumb is that in patients with hyperthyroidism, all but emergency procedures should be postponed until the condition can be controlled with methimazole.
Patients with undiagnosed or untreated hyperthyroidism who undergo anesthesia and surgery are at high risk for thyroid storm, a provoked crisis of multiorgan failure, he said.
If the surgery cannot be delayed until elevated levels of thyroxine are achieved, the team can initiate oral or intravenous beta-blockade, or if the patient is in critical condition, infusion with the beta-1 receptor blocker esmolol (Brevibloc) is preferred, he said.
Patients should also be started on methimazole 30-40 mg/day, and the patient should be given iodine if she has not already received iodinated radiologic contrast. Stress dose glucocorticoids and adequate volume resuscitation may also provide support in this situation.
In contrast, "hypothyroidism is usually not a big deal," Dr. Baldwin said.
Such patients usually tolerate major surgery without significant complications, he said, but patients with hypothyroidism may be more sensitive to sedatives, slower to wean from ventilation, and handle free-water excretion less well than euthyroid patients.
Patients who take levothyroxine (Synthroid and generics) should always have their free T4 and thyroid-stimulating hormone (thyrotropin) levels checked during preoperative evaluation, he said.
Dr. Baldwin reported having no relevant financial conflicts of interest.
SCOTTSDALE, ARIZ. – Controlling hyperglycemia before and after surgery in patients with diabetes is a balancing act, but when done properly, it can reduce infections and wound complications, according to Dr. David Baldwin.
The key to preoperative planning for patients with diabetes is a full list of medications and an understanding of how well (or how poorly) patients’ glycemia is controlled, said Dr. Baldwin, an endocrinologist at Rush University Medical Center in Chicago.
He discussed strategies for perioperative management of patients with diabetes and thyroid disorders at the Perioperative Medicine Summit 2014."You definitely want to write down exactly what they are and aren’t taking. We find that the medication list for people getting admitted for surgery is often fraught with a lack of little details," he said.
For patients with type 2 diabetes, it’s important to record an accurate description of antidiabetes medications, especially combination oral agents such as Actoplus MET (metformin and pioglitazone) or Janumet (sitagliptin and metformin). For patients with type 1 and 2 diabetes, it is important to record not just the type of insulin but the regimen the patient uses.
Dr. Baldwin noted that many intake staff make the mistake of reporting that patients take "Novolin" or "Humulin," which are brand families of insulin and not specific insulin types.
"We often find, probably at least half of the time, that until we actually go and ask the patients what they take for insulin post-op, the correct information won’t have been in the medical record," he said.
The best way to determine whether a patient has good control of chronic hyperglycemia is with a hemoglobin A1c (HbA1c) level. A value above 6.5% is diagnostic for diabetes; well-controlled patients have HbA1c levels from 6% to 8%. HbA1c values not more than 2 months old should be a routine part of preoperative evaluations for patients with diabetes or newly discovered hyperglycemia, Dr. Baldwin said.
Preoperative medications
The Rush University protocol for the preoperative management of antidiabetic therapies other than insulin notes that sulfonylureas, metformin, pioglitazone, exenatide, liraglutide, sitagliptin, linagliptin, saxagliptin, alogliptin, alpha-glucosidase inhibitors, and canagaflozin may all be taken with food on the eve of surgery, but none should be taken on the morning of surgery.
Specific rules also apply for patients who use insulin, depending on the insulin type, as follows:
• For long-acting insulins (glargine or detemir), the patient should take the full dose on the evening before surgery or the morning of surgery if the dose is prescribed for either morning or evening administration. Patients with prescriptions for a b.i.d. dose should take the full dose both the evening before and the morning of surgery.
• With intermediate-acting insulin (NPH), the patient should take the full dose on the evening before surgery and 80% of the morning dose on the morning of surgery.
• For rapid-acting insulins (aspart, lispro, glulisine, or regular) and premixed insulins (NPH or rapid acting), the patient should take the full dose with dinner the night before, and none on the morning of surgery.
Dr. Baldwin emphasized that except in rare circumstances, patients on subcutaneous insulin pumps should not use the pumps during surgery, and should get special instructions from their endocrinologists.
Ideally, the patient can convert to insulin glargine the night before surgery, with the dose equivalent to the total 24-hour basal insulin dose delivered by the pump. Two hours after the glargine dose is given, the patient should disconnect the pump and leave it at home.
Glycemic control in the hospital
As noted before, poor glycemic control can lead to poor wound healing from impaired leukocyte function, which can lead to decreased chemotaxis, phagocytosis, and bacteriocidal activity.
The risk of bacteremia is especially high among patients who are on total parenteral nutrition with poorly controlled glucose levels, he noted.
Forces conspiring against glucose control in the hospital can include elevated levels of hormones that counterregulate glucose; nausea/vomiting, anorexia, or nothing-by-mouth orders; erratic meal timing due to tests or interventions; intravenous glucose; glucocorticoid therapy; and "physician indifference and lack of attention to required adjustments in therapy," Dr. Baldwin noted.
Evidence from a randomized study showed that in patients with type 2 diabetes undergoing general surgery, basal-bolus treatment with insulin glargine once daily plus insulin glulisine before meals both improved glycemic control and reduced hospital complications compared with sliding-scale insulin therapy, he reported.
Hyper- and hypothyroid patients
Switching endocrinology hats, Dr. Baldwin said that patients who have significant weight loss or resting tachycardia before surgery should be evaluated for hyperthyroidism. A good rule of thumb is that in patients with hyperthyroidism, all but emergency procedures should be postponed until the condition can be controlled with methimazole.
Patients with undiagnosed or untreated hyperthyroidism who undergo anesthesia and surgery are at high risk for thyroid storm, a provoked crisis of multiorgan failure, he said.
If the surgery cannot be delayed until elevated levels of thyroxine are achieved, the team can initiate oral or intravenous beta-blockade, or if the patient is in critical condition, infusion with the beta-1 receptor blocker esmolol (Brevibloc) is preferred, he said.
Patients should also be started on methimazole 30-40 mg/day, and the patient should be given iodine if she has not already received iodinated radiologic contrast. Stress dose glucocorticoids and adequate volume resuscitation may also provide support in this situation.
In contrast, "hypothyroidism is usually not a big deal," Dr. Baldwin said.
Such patients usually tolerate major surgery without significant complications, he said, but patients with hypothyroidism may be more sensitive to sedatives, slower to wean from ventilation, and handle free-water excretion less well than euthyroid patients.
Patients who take levothyroxine (Synthroid and generics) should always have their free T4 and thyroid-stimulating hormone (thyrotropin) levels checked during preoperative evaluation, he said.
Dr. Baldwin reported having no relevant financial conflicts of interest.
SCOTTSDALE, ARIZ. – Controlling hyperglycemia before and after surgery in patients with diabetes is a balancing act, but when done properly, it can reduce infections and wound complications, according to Dr. David Baldwin.
The key to preoperative planning for patients with diabetes is a full list of medications and an understanding of how well (or how poorly) patients’ glycemia is controlled, said Dr. Baldwin, an endocrinologist at Rush University Medical Center in Chicago.
He discussed strategies for perioperative management of patients with diabetes and thyroid disorders at the Perioperative Medicine Summit 2014."You definitely want to write down exactly what they are and aren’t taking. We find that the medication list for people getting admitted for surgery is often fraught with a lack of little details," he said.
For patients with type 2 diabetes, it’s important to record an accurate description of antidiabetes medications, especially combination oral agents such as Actoplus MET (metformin and pioglitazone) or Janumet (sitagliptin and metformin). For patients with type 1 and 2 diabetes, it is important to record not just the type of insulin but the regimen the patient uses.
Dr. Baldwin noted that many intake staff make the mistake of reporting that patients take "Novolin" or "Humulin," which are brand families of insulin and not specific insulin types.
"We often find, probably at least half of the time, that until we actually go and ask the patients what they take for insulin post-op, the correct information won’t have been in the medical record," he said.
The best way to determine whether a patient has good control of chronic hyperglycemia is with a hemoglobin A1c (HbA1c) level. A value above 6.5% is diagnostic for diabetes; well-controlled patients have HbA1c levels from 6% to 8%. HbA1c values not more than 2 months old should be a routine part of preoperative evaluations for patients with diabetes or newly discovered hyperglycemia, Dr. Baldwin said.
Preoperative medications
The Rush University protocol for the preoperative management of antidiabetic therapies other than insulin notes that sulfonylureas, metformin, pioglitazone, exenatide, liraglutide, sitagliptin, linagliptin, saxagliptin, alogliptin, alpha-glucosidase inhibitors, and canagaflozin may all be taken with food on the eve of surgery, but none should be taken on the morning of surgery.
Specific rules also apply for patients who use insulin, depending on the insulin type, as follows:
• For long-acting insulins (glargine or detemir), the patient should take the full dose on the evening before surgery or the morning of surgery if the dose is prescribed for either morning or evening administration. Patients with prescriptions for a b.i.d. dose should take the full dose both the evening before and the morning of surgery.
• With intermediate-acting insulin (NPH), the patient should take the full dose on the evening before surgery and 80% of the morning dose on the morning of surgery.
• For rapid-acting insulins (aspart, lispro, glulisine, or regular) and premixed insulins (NPH or rapid acting), the patient should take the full dose with dinner the night before, and none on the morning of surgery.
Dr. Baldwin emphasized that except in rare circumstances, patients on subcutaneous insulin pumps should not use the pumps during surgery, and should get special instructions from their endocrinologists.
Ideally, the patient can convert to insulin glargine the night before surgery, with the dose equivalent to the total 24-hour basal insulin dose delivered by the pump. Two hours after the glargine dose is given, the patient should disconnect the pump and leave it at home.
Glycemic control in the hospital
As noted before, poor glycemic control can lead to poor wound healing from impaired leukocyte function, which can lead to decreased chemotaxis, phagocytosis, and bacteriocidal activity.
The risk of bacteremia is especially high among patients who are on total parenteral nutrition with poorly controlled glucose levels, he noted.
Forces conspiring against glucose control in the hospital can include elevated levels of hormones that counterregulate glucose; nausea/vomiting, anorexia, or nothing-by-mouth orders; erratic meal timing due to tests or interventions; intravenous glucose; glucocorticoid therapy; and "physician indifference and lack of attention to required adjustments in therapy," Dr. Baldwin noted.
Evidence from a randomized study showed that in patients with type 2 diabetes undergoing general surgery, basal-bolus treatment with insulin glargine once daily plus insulin glulisine before meals both improved glycemic control and reduced hospital complications compared with sliding-scale insulin therapy, he reported.
Hyper- and hypothyroid patients
Switching endocrinology hats, Dr. Baldwin said that patients who have significant weight loss or resting tachycardia before surgery should be evaluated for hyperthyroidism. A good rule of thumb is that in patients with hyperthyroidism, all but emergency procedures should be postponed until the condition can be controlled with methimazole.
Patients with undiagnosed or untreated hyperthyroidism who undergo anesthesia and surgery are at high risk for thyroid storm, a provoked crisis of multiorgan failure, he said.
If the surgery cannot be delayed until elevated levels of thyroxine are achieved, the team can initiate oral or intravenous beta-blockade, or if the patient is in critical condition, infusion with the beta-1 receptor blocker esmolol (Brevibloc) is preferred, he said.
Patients should also be started on methimazole 30-40 mg/day, and the patient should be given iodine if she has not already received iodinated radiologic contrast. Stress dose glucocorticoids and adequate volume resuscitation may also provide support in this situation.
In contrast, "hypothyroidism is usually not a big deal," Dr. Baldwin said.
Such patients usually tolerate major surgery without significant complications, he said, but patients with hypothyroidism may be more sensitive to sedatives, slower to wean from ventilation, and handle free-water excretion less well than euthyroid patients.
Patients who take levothyroxine (Synthroid and generics) should always have their free T4 and thyroid-stimulating hormone (thyrotropin) levels checked during preoperative evaluation, he said.
Dr. Baldwin reported having no relevant financial conflicts of interest.
AT THE PERIOPERATIVE MEDICINE SUMMIT 2014
Major finding: Patients with diabetes and thyroid disorder require special handling before, during, and after surgery.
Data source: A review of current practice.
Disclosures: Dr. Baldwin reported having no relevant financial conflicts of interest.

Surgical checklists failed to improve outcomes
The mandatory use of surgical safety checklists at hospitals across Ontario failed to improve operative mortality, surgical complications, readmissions, or emergency department visits within 30 days after hospital discharge, according to a report published March 12 in the New England Journal of Medicine.
In the 3 months following introduction of checklists at 101 hospitals, mortality remained the same across all subgroups studied, including high-risk groups such as elderly patients and those who required emergency procedures, said Dr. David R. Urbach of the Institute for Clinical Evaluative Sciences and the Institute of Health Policy, Management, and Evaluation, University of Toronto, and his associates.

"There may be value in the use of surgical safety checklists, such as enhanced communication and teamwork, and the promotion of a hospital culture in which safety is a high priority; however, these potential benefits did not translate into meaningful improvements in the outcomes we analyzed," they reported.
The investigators studied about 200,000 surgical procedures performed at "virtually all hospitals providing surgical care for the population of Ontario, [allowing] us to obtain an estimate of the effectiveness of surgical safety checklists that is less susceptible to biases from selective reporting."
Of the 92 hospitals that furnished copies of their checklist, 79 used that of the Canadian Patient Safety Institute, 9 used customized lists, and 4 used the World Health Organization checklist.
A total of 97 hospitals reported that they used a special intervention or educational program to implement the checklist, and almost every hospital reported that it achieved nearly 100% compliance. "The lowest reported compliance by a large community hospital during this period was 91.6%," the investigators said.
The primary outcome measure – overall operative mortality – was 0.71% before introduction of the surgical safety checklist and 0.65% afterward, a nonsignificant difference.
The risk of an emergency department visit within 1 month of hospital discharge was 10.44% before the checklist and 10.55% afterward, and the risk of readmission within 1 month of hospital discharge was 3.11% before the checklist and 3.14% afterward. These differences too were nonsignificant.
When the data were analyzed according to individual hospitals, "no hospital had a significant change in operative mortality after checklist introduction. Within-hospital changes in other surgical outcomes were mixed. For example, 6 hospitals had significantly fewer complications after introduction of the checklist, whereas 3 had significantly more complications," the investigators reported (N. Engl. J. Med. 2014;370:1029-38).
When the data were further adjusted to account for other factors that might contribute to surgical outcomes, such as patient income, gender, and urban vs. rural residence, the results did not change appreciably. Subgroup analyses also failed to identify any particular group of surgical patients who benefited from implementation of the checklist.
The study was supported by the Canadian Institutes of Health Research and the Institute for Clinical Evaluative Sciences. Dr. Urbach and his associates reported no financial conflicts of interest.
Gaming the system is universal, and true compliance cannot be determined, so "the likely reason for the failure of the surgical checklist in Ontario is that it was not actually used," Dr. Lucian L. Leape said.
An observational study in the United Kingdom revealed that compliance with presurgical checklists there was only 55% and compliance with postsurgical checklists only 9%; a Netherlands study reported full compliance with only 39% of operations. In the Ontario study, "even if full implementation did occur, it is unlikely that an effect would have been seen within 3 months," Dr. Leape noted.
Most hospitals struggle with implementing surgical checklists, and their use probably shouldn’t be mandated as it was in Ontario because "regulation works best when a practice of unquestioned value has become the norm. We are not there yet," Dr. Leape said.
Dr. Leape is at the Harvard School of Public Health, Boston. He reported no potential financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Urbach’s report (N. Engl. J. Med. 2014;370:1063-4).
Gaming the system is universal, and true compliance cannot be determined, so "the likely reason for the failure of the surgical checklist in Ontario is that it was not actually used," Dr. Lucian L. Leape said.
An observational study in the United Kingdom revealed that compliance with presurgical checklists there was only 55% and compliance with postsurgical checklists only 9%; a Netherlands study reported full compliance with only 39% of operations. In the Ontario study, "even if full implementation did occur, it is unlikely that an effect would have been seen within 3 months," Dr. Leape noted.
Most hospitals struggle with implementing surgical checklists, and their use probably shouldn’t be mandated as it was in Ontario because "regulation works best when a practice of unquestioned value has become the norm. We are not there yet," Dr. Leape said.
Dr. Leape is at the Harvard School of Public Health, Boston. He reported no potential financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Urbach’s report (N. Engl. J. Med. 2014;370:1063-4).
Gaming the system is universal, and true compliance cannot be determined, so "the likely reason for the failure of the surgical checklist in Ontario is that it was not actually used," Dr. Lucian L. Leape said.
An observational study in the United Kingdom revealed that compliance with presurgical checklists there was only 55% and compliance with postsurgical checklists only 9%; a Netherlands study reported full compliance with only 39% of operations. In the Ontario study, "even if full implementation did occur, it is unlikely that an effect would have been seen within 3 months," Dr. Leape noted.
Most hospitals struggle with implementing surgical checklists, and their use probably shouldn’t be mandated as it was in Ontario because "regulation works best when a practice of unquestioned value has become the norm. We are not there yet," Dr. Leape said.
Dr. Leape is at the Harvard School of Public Health, Boston. He reported no potential financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Urbach’s report (N. Engl. J. Med. 2014;370:1063-4).
The mandatory use of surgical safety checklists at hospitals across Ontario failed to improve operative mortality, surgical complications, readmissions, or emergency department visits within 30 days after hospital discharge, according to a report published March 12 in the New England Journal of Medicine.
In the 3 months following introduction of checklists at 101 hospitals, mortality remained the same across all subgroups studied, including high-risk groups such as elderly patients and those who required emergency procedures, said Dr. David R. Urbach of the Institute for Clinical Evaluative Sciences and the Institute of Health Policy, Management, and Evaluation, University of Toronto, and his associates.
"There may be value in the use of surgical safety checklists, such as enhanced communication and teamwork, and the promotion of a hospital culture in which safety is a high priority; however, these potential benefits did not translate into meaningful improvements in the outcomes we analyzed," they reported.
The investigators studied about 200,000 surgical procedures performed at "virtually all hospitals providing surgical care for the population of Ontario, [allowing] us to obtain an estimate of the effectiveness of surgical safety checklists that is less susceptible to biases from selective reporting."
Of the 92 hospitals that furnished copies of their checklist, 79 used that of the Canadian Patient Safety Institute, 9 used customized lists, and 4 used the World Health Organization checklist.
A total of 97 hospitals reported that they used a special intervention or educational program to implement the checklist, and almost every hospital reported that it achieved nearly 100% compliance. "The lowest reported compliance by a large community hospital during this period was 91.6%," the investigators said.
The primary outcome measure – overall operative mortality – was 0.71% before introduction of the surgical safety checklist and 0.65% afterward, a nonsignificant difference.
The risk of an emergency department visit within 1 month of hospital discharge was 10.44% before the checklist and 10.55% afterward, and the risk of readmission within 1 month of hospital discharge was 3.11% before the checklist and 3.14% afterward. These differences too were nonsignificant.
When the data were analyzed according to individual hospitals, "no hospital had a significant change in operative mortality after checklist introduction. Within-hospital changes in other surgical outcomes were mixed. For example, 6 hospitals had significantly fewer complications after introduction of the checklist, whereas 3 had significantly more complications," the investigators reported (N. Engl. J. Med. 2014;370:1029-38).
When the data were further adjusted to account for other factors that might contribute to surgical outcomes, such as patient income, gender, and urban vs. rural residence, the results did not change appreciably. Subgroup analyses also failed to identify any particular group of surgical patients who benefited from implementation of the checklist.
The study was supported by the Canadian Institutes of Health Research and the Institute for Clinical Evaluative Sciences. Dr. Urbach and his associates reported no financial conflicts of interest.
The mandatory use of surgical safety checklists at hospitals across Ontario failed to improve operative mortality, surgical complications, readmissions, or emergency department visits within 30 days after hospital discharge, according to a report published March 12 in the New England Journal of Medicine.
In the 3 months following introduction of checklists at 101 hospitals, mortality remained the same across all subgroups studied, including high-risk groups such as elderly patients and those who required emergency procedures, said Dr. David R. Urbach of the Institute for Clinical Evaluative Sciences and the Institute of Health Policy, Management, and Evaluation, University of Toronto, and his associates.
"There may be value in the use of surgical safety checklists, such as enhanced communication and teamwork, and the promotion of a hospital culture in which safety is a high priority; however, these potential benefits did not translate into meaningful improvements in the outcomes we analyzed," they reported.
The investigators studied about 200,000 surgical procedures performed at "virtually all hospitals providing surgical care for the population of Ontario, [allowing] us to obtain an estimate of the effectiveness of surgical safety checklists that is less susceptible to biases from selective reporting."
Of the 92 hospitals that furnished copies of their checklist, 79 used that of the Canadian Patient Safety Institute, 9 used customized lists, and 4 used the World Health Organization checklist.
A total of 97 hospitals reported that they used a special intervention or educational program to implement the checklist, and almost every hospital reported that it achieved nearly 100% compliance. "The lowest reported compliance by a large community hospital during this period was 91.6%," the investigators said.
The primary outcome measure – overall operative mortality – was 0.71% before introduction of the surgical safety checklist and 0.65% afterward, a nonsignificant difference.
The risk of an emergency department visit within 1 month of hospital discharge was 10.44% before the checklist and 10.55% afterward, and the risk of readmission within 1 month of hospital discharge was 3.11% before the checklist and 3.14% afterward. These differences too were nonsignificant.
When the data were analyzed according to individual hospitals, "no hospital had a significant change in operative mortality after checklist introduction. Within-hospital changes in other surgical outcomes were mixed. For example, 6 hospitals had significantly fewer complications after introduction of the checklist, whereas 3 had significantly more complications," the investigators reported (N. Engl. J. Med. 2014;370:1029-38).
When the data were further adjusted to account for other factors that might contribute to surgical outcomes, such as patient income, gender, and urban vs. rural residence, the results did not change appreciably. Subgroup analyses also failed to identify any particular group of surgical patients who benefited from implementation of the checklist.
The study was supported by the Canadian Institutes of Health Research and the Institute for Clinical Evaluative Sciences. Dr. Urbach and his associates reported no financial conflicts of interest.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major finding: Overall operative mortality was 0.71% before introduction of the surgical safety checklist and 0.65% afterward, a nonsignificant difference.
Data source: A population-based analysis comparing surgical outcomes at 101 Ontario hospitals during the 3 months before and the 3 months after mandatory use of a surgical safety checklist was introduced across the province.
Disclosures: This study was supported by the Canadian Institutes of Health Research and the Institute for Clinical Evaluative Sciences. Dr. Urbach and his associates reported no financial conflicts of interest.

Simultaneous colorectal/liver mets resection saves time and money
MIAMI BEACH – For patients with colorectal cancer and liver metastasis, one-stage surgery cuts hospital time and expense.
Compared to a staged approach, resecting both the primary and metastatic cancers shaved almost $28,000 off total hospital charges. Most of the savings came from the shortened hospital stay – an average of 6 fewer days than for patients with staged procedures, Dr. Aslam Ejaz said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
"The main driving factor [of costs] was the increasing length of stay," said Dr. Ejaz, a research fellow in surgical oncology at Johns Hopkins Hospital, Baltimore. "Each additional day resulted in a mean increase of $3,600."
Most studies have found similar clinical outcomes for such patients, regardless of whether their surgical treatment is staged or simultaneous. But there are few data comparing the techniques’ economic impact.
For the study, Dr. Ejaz used a Johns Hopkins database to examine the staged vs. the one-stage approach. His cohort included 224 patients who, from 1990 to 2012, underwent a liver resection with curative intent for synchronous colorectal liver metastasis. They had a simultaneous procedure (111) or a staged procedure (113).
Most of the patients were in their 50s. Preoperative chemotherapy was significantly more common among those who had staged surgery with liver resection first. Primary rectal cancers were significantly more common among patients who had staged surgery.
The overall hepatectomy-related morbidity rate was similar: 25% in the simultaneous surgery group and 27% in the staged surgery group. Major complications after hepatectomy occurred in 18% of the simultaneous and 13% of the staged group – not significantly different.
Clear margins were obtained in 85% of the simultaneous surgery group and 88% of the staged surgery group. Mortality was similar (1% vs. 2%). The total length of stay was significantly longer in the staged surgery group (13 vs. 7 days.).
When categorized into minor and major hepatectomies, the overall complication rate was similar. For minor hepatectomies, it was 25% in the simultaneous surgery group and 29% in the staged group. For major hepatectomies, the rates were 27% and 28%, respectively.
There were no deaths in the minor hepatectomy group. Among those who had major hepatectomy, 4% of each surgical group died.
The median overall survival was 33 months. In both groups, 5-year survival was about 28%. The median recurrence-free survival was 26 months. The median 5-year recurrence-free survival was 20% in both groups.
A multivariate analysis examined factors associated with complications. There were no significant associations with simultaneous resection, major hepatectomy, rectal tumor, bilateral hepatic disease, or extrahepatic metastasis. However, concurrent resection and ablation doubled the risk of a complication (odds ratio, 2.02).
Patients who had a simultaneous procedure had significantly shorter hospital stays than did those who underwent a staged procedure. Most who had simultaneous surgery went home in 6 days or less (48) or in 6-9 days (38). Just 12 stayed 9-11 days; 13 stayed for 11 or more days.
Among those who had staged procedures, none went home in 6 or fewer days, and only 7 went home in 6-9 days. All other staged surgery patients stayed longer: 26 stayed 9-11 days, 39 stayed 11-13 days, and 41 stayed more than 13 days.
This extra time translated into extra money, Dr. Ejaz said, with each hospital day costing a mean of $3,581. To tease out cost associations, he stratified patients by operative factors and disease-related characteristics.
Charges for patents with unilateral or bilateral disease were significantly different ($48,000 vs. $53,000). There also were significantly different charges for those who had resection only compared to resection plus ablation ($45,500 vs. $57,000), and minor hepatic surgery compared to major hepatic surgery ($44,300 vs. $54,500).
Surgery timing also significantly affected price. The mean total cost for those who had simultaneous surgery was $34,000, while it was $62,000 for those who had staged surgery – a 55% difference amounting to $28,000.
Since clinical outcomes were so similar, the study shows that patients with resectable synchronous colorectal liver metastasis can be safely managed with either simultaneous or staged approach, Dr. Ejaz said. "But a simultaneous approach results in fewer hospital days and overall lower hospital charges, and should be the preferred approach when it’s clinically appropriate and technically feasible."
Dr. Timothy Pawlik – Dr. Ejaz’s preceptor – said that the findings are useful to both patients and systems.
"This study can be used to explain to patients how a simultaneous operation is generally safe," he said in an interview. "It may, in fact, be more beneficial to surgeons and hospitals or health care systems, as it shows that a simultaneous operation can be performed safely and save on health care costs."
Neither Dr. Ejaz nor Dr. Pawlik had any financial disclosures.
MIAMI BEACH – For patients with colorectal cancer and liver metastasis, one-stage surgery cuts hospital time and expense.
Compared to a staged approach, resecting both the primary and metastatic cancers shaved almost $28,000 off total hospital charges. Most of the savings came from the shortened hospital stay – an average of 6 fewer days than for patients with staged procedures, Dr. Aslam Ejaz said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
"The main driving factor [of costs] was the increasing length of stay," said Dr. Ejaz, a research fellow in surgical oncology at Johns Hopkins Hospital, Baltimore. "Each additional day resulted in a mean increase of $3,600."
Most studies have found similar clinical outcomes for such patients, regardless of whether their surgical treatment is staged or simultaneous. But there are few data comparing the techniques’ economic impact.
For the study, Dr. Ejaz used a Johns Hopkins database to examine the staged vs. the one-stage approach. His cohort included 224 patients who, from 1990 to 2012, underwent a liver resection with curative intent for synchronous colorectal liver metastasis. They had a simultaneous procedure (111) or a staged procedure (113).
Most of the patients were in their 50s. Preoperative chemotherapy was significantly more common among those who had staged surgery with liver resection first. Primary rectal cancers were significantly more common among patients who had staged surgery.
The overall hepatectomy-related morbidity rate was similar: 25% in the simultaneous surgery group and 27% in the staged surgery group. Major complications after hepatectomy occurred in 18% of the simultaneous and 13% of the staged group – not significantly different.
Clear margins were obtained in 85% of the simultaneous surgery group and 88% of the staged surgery group. Mortality was similar (1% vs. 2%). The total length of stay was significantly longer in the staged surgery group (13 vs. 7 days.).
When categorized into minor and major hepatectomies, the overall complication rate was similar. For minor hepatectomies, it was 25% in the simultaneous surgery group and 29% in the staged group. For major hepatectomies, the rates were 27% and 28%, respectively.
There were no deaths in the minor hepatectomy group. Among those who had major hepatectomy, 4% of each surgical group died.
The median overall survival was 33 months. In both groups, 5-year survival was about 28%. The median recurrence-free survival was 26 months. The median 5-year recurrence-free survival was 20% in both groups.
A multivariate analysis examined factors associated with complications. There were no significant associations with simultaneous resection, major hepatectomy, rectal tumor, bilateral hepatic disease, or extrahepatic metastasis. However, concurrent resection and ablation doubled the risk of a complication (odds ratio, 2.02).
Patients who had a simultaneous procedure had significantly shorter hospital stays than did those who underwent a staged procedure. Most who had simultaneous surgery went home in 6 days or less (48) or in 6-9 days (38). Just 12 stayed 9-11 days; 13 stayed for 11 or more days.
Among those who had staged procedures, none went home in 6 or fewer days, and only 7 went home in 6-9 days. All other staged surgery patients stayed longer: 26 stayed 9-11 days, 39 stayed 11-13 days, and 41 stayed more than 13 days.
This extra time translated into extra money, Dr. Ejaz said, with each hospital day costing a mean of $3,581. To tease out cost associations, he stratified patients by operative factors and disease-related characteristics.
Charges for patents with unilateral or bilateral disease were significantly different ($48,000 vs. $53,000). There also were significantly different charges for those who had resection only compared to resection plus ablation ($45,500 vs. $57,000), and minor hepatic surgery compared to major hepatic surgery ($44,300 vs. $54,500).
Surgery timing also significantly affected price. The mean total cost for those who had simultaneous surgery was $34,000, while it was $62,000 for those who had staged surgery – a 55% difference amounting to $28,000.
Since clinical outcomes were so similar, the study shows that patients with resectable synchronous colorectal liver metastasis can be safely managed with either simultaneous or staged approach, Dr. Ejaz said. "But a simultaneous approach results in fewer hospital days and overall lower hospital charges, and should be the preferred approach when it’s clinically appropriate and technically feasible."
Dr. Timothy Pawlik – Dr. Ejaz’s preceptor – said that the findings are useful to both patients and systems.
"This study can be used to explain to patients how a simultaneous operation is generally safe," he said in an interview. "It may, in fact, be more beneficial to surgeons and hospitals or health care systems, as it shows that a simultaneous operation can be performed safely and save on health care costs."
Neither Dr. Ejaz nor Dr. Pawlik had any financial disclosures.
MIAMI BEACH – For patients with colorectal cancer and liver metastasis, one-stage surgery cuts hospital time and expense.
Compared to a staged approach, resecting both the primary and metastatic cancers shaved almost $28,000 off total hospital charges. Most of the savings came from the shortened hospital stay – an average of 6 fewer days than for patients with staged procedures, Dr. Aslam Ejaz said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
"The main driving factor [of costs] was the increasing length of stay," said Dr. Ejaz, a research fellow in surgical oncology at Johns Hopkins Hospital, Baltimore. "Each additional day resulted in a mean increase of $3,600."
Most studies have found similar clinical outcomes for such patients, regardless of whether their surgical treatment is staged or simultaneous. But there are few data comparing the techniques’ economic impact.
For the study, Dr. Ejaz used a Johns Hopkins database to examine the staged vs. the one-stage approach. His cohort included 224 patients who, from 1990 to 2012, underwent a liver resection with curative intent for synchronous colorectal liver metastasis. They had a simultaneous procedure (111) or a staged procedure (113).
Most of the patients were in their 50s. Preoperative chemotherapy was significantly more common among those who had staged surgery with liver resection first. Primary rectal cancers were significantly more common among patients who had staged surgery.
The overall hepatectomy-related morbidity rate was similar: 25% in the simultaneous surgery group and 27% in the staged surgery group. Major complications after hepatectomy occurred in 18% of the simultaneous and 13% of the staged group – not significantly different.
Clear margins were obtained in 85% of the simultaneous surgery group and 88% of the staged surgery group. Mortality was similar (1% vs. 2%). The total length of stay was significantly longer in the staged surgery group (13 vs. 7 days.).
When categorized into minor and major hepatectomies, the overall complication rate was similar. For minor hepatectomies, it was 25% in the simultaneous surgery group and 29% in the staged group. For major hepatectomies, the rates were 27% and 28%, respectively.
There were no deaths in the minor hepatectomy group. Among those who had major hepatectomy, 4% of each surgical group died.
The median overall survival was 33 months. In both groups, 5-year survival was about 28%. The median recurrence-free survival was 26 months. The median 5-year recurrence-free survival was 20% in both groups.
A multivariate analysis examined factors associated with complications. There were no significant associations with simultaneous resection, major hepatectomy, rectal tumor, bilateral hepatic disease, or extrahepatic metastasis. However, concurrent resection and ablation doubled the risk of a complication (odds ratio, 2.02).
Patients who had a simultaneous procedure had significantly shorter hospital stays than did those who underwent a staged procedure. Most who had simultaneous surgery went home in 6 days or less (48) or in 6-9 days (38). Just 12 stayed 9-11 days; 13 stayed for 11 or more days.
Among those who had staged procedures, none went home in 6 or fewer days, and only 7 went home in 6-9 days. All other staged surgery patients stayed longer: 26 stayed 9-11 days, 39 stayed 11-13 days, and 41 stayed more than 13 days.
This extra time translated into extra money, Dr. Ejaz said, with each hospital day costing a mean of $3,581. To tease out cost associations, he stratified patients by operative factors and disease-related characteristics.
Charges for patents with unilateral or bilateral disease were significantly different ($48,000 vs. $53,000). There also were significantly different charges for those who had resection only compared to resection plus ablation ($45,500 vs. $57,000), and minor hepatic surgery compared to major hepatic surgery ($44,300 vs. $54,500).
Surgery timing also significantly affected price. The mean total cost for those who had simultaneous surgery was $34,000, while it was $62,000 for those who had staged surgery – a 55% difference amounting to $28,000.
Since clinical outcomes were so similar, the study shows that patients with resectable synchronous colorectal liver metastasis can be safely managed with either simultaneous or staged approach, Dr. Ejaz said. "But a simultaneous approach results in fewer hospital days and overall lower hospital charges, and should be the preferred approach when it’s clinically appropriate and technically feasible."
Dr. Timothy Pawlik – Dr. Ejaz’s preceptor – said that the findings are useful to both patients and systems.
"This study can be used to explain to patients how a simultaneous operation is generally safe," he said in an interview. "It may, in fact, be more beneficial to surgeons and hospitals or health care systems, as it shows that a simultaneous operation can be performed safely and save on health care costs."
Neither Dr. Ejaz nor Dr. Pawlik had any financial disclosures.
AT AHPBA 2014
Major finding: Compared to a staged surgery, simultaneously resecting colorectal cancer and liver metastases saved about 6 days of hospital stay, with a 55% cost savings in total hospital charges.
Data source: A retrospective study of 224 patients.
Disclosures: Neither Dr. Ejaz nor Dr. Pawlik had any financial disclosures.
VIDEO: Despite privacy concerns, some physicians optimistic about Google Glass
ORLANDO – Google Glass will soon be available to the public, but its future role in medicine is still hazy.
Glass, which is among the growing number of wearable technologies, has several applications to health care settings, experts say. Just last year, a surgeon at Ohio State University’s Wexner Medical Center in Columbus live-streamed an ACL procedure via his Google Glass. And most recently, Rhode Island Hospital’s emergency department began using the device’s video capabilities to consult with off-site specialists.
But Glass is not HIPAA compliant, raising patient privacy concerns and dissuading hospitals from incorporating it into their growing list of mobile technologies. Still, technology enthusiasts are charging ahead, envisioning a future in which Glass could be yet another piece in physicians’ toolkits.
At the annual meeting of the Healthcare Information and Management Systems Society, Dr. Jonathan A. Handler, chief medical information officer for M*Modal, spoke about Glass's potential in medicine.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemsmiller
ORLANDO – Google Glass will soon be available to the public, but its future role in medicine is still hazy.
Glass, which is among the growing number of wearable technologies, has several applications to health care settings, experts say. Just last year, a surgeon at Ohio State University’s Wexner Medical Center in Columbus live-streamed an ACL procedure via his Google Glass. And most recently, Rhode Island Hospital’s emergency department began using the device’s video capabilities to consult with off-site specialists.
But Glass is not HIPAA compliant, raising patient privacy concerns and dissuading hospitals from incorporating it into their growing list of mobile technologies. Still, technology enthusiasts are charging ahead, envisioning a future in which Glass could be yet another piece in physicians’ toolkits.
At the annual meeting of the Healthcare Information and Management Systems Society, Dr. Jonathan A. Handler, chief medical information officer for M*Modal, spoke about Glass's potential in medicine.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemsmiller
ORLANDO – Google Glass will soon be available to the public, but its future role in medicine is still hazy.
Glass, which is among the growing number of wearable technologies, has several applications to health care settings, experts say. Just last year, a surgeon at Ohio State University’s Wexner Medical Center in Columbus live-streamed an ACL procedure via his Google Glass. And most recently, Rhode Island Hospital’s emergency department began using the device’s video capabilities to consult with off-site specialists.
But Glass is not HIPAA compliant, raising patient privacy concerns and dissuading hospitals from incorporating it into their growing list of mobile technologies. Still, technology enthusiasts are charging ahead, envisioning a future in which Glass could be yet another piece in physicians’ toolkits.
At the annual meeting of the Healthcare Information and Management Systems Society, Dr. Jonathan A. Handler, chief medical information officer for M*Modal, spoke about Glass's potential in medicine.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemsmiller
AT HIMSS14

Fluorescent cholangiography as effective as standard, but cheaper
MIAMI BEACH – Intraoperative fluorescent cholangiography is just as effective as traditional cholangiography but costs hundreds of dollars less and is significantly faster to perform.
It’s also a great teaching tool, Dr. Fernando Dip said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. In just one session, all of the third- and fourth-year surgical residents were able to correctly identify 100% of the biliary structures.

"It appears to be an additional tool for the laparoscopic surgeon," said Dr. Dip, chief of surgical research at the Cleveland Clinic in Weston, Fla. "It’s quick, inexpensive, real-time, there are no adverse events, and it’s an inciscionless procedure."
Common bile duct injury is the most frequent injury seen in laparoscopic cholecystectomy, he said, and although the overall incidence is low, the number of injuries each year is not inconsiderable, since more than 750,000 laparoscopic cholecystectomies are performed in the United States annually.
"Only 3% of these injuries are due to problems with technical skill," Dr. Dip said. "The other 97% are problems of visual perception – illusions of where the ducts are."
Intraoperative cholangiography helps surgeons visualize this anatomy, but its true usefulness is somewhat controversial. Dr. Dip cited a recent study of almost 93,000 patients – 40% of whom underwent the procedure. It showed that intraoperative cholangiography is not effective as a preventive strategy against common duct injury during cholecystectomy.
Intraoperative fluorescent cholangiography is sometimes used to identify biliary anatomy in extrahepatic surgery. Dr. Dip and his colleagues examined its usefulness in 45 patients undergoing laparoscopic cholecystectomy. Senior residents performed all of the procedures under the supervision of experienced laparoscopic surgeons. All patients underwent the investigational procedure, followed by standard cholangiography.
The patients had a mean age of 49 years and were evenly split between men and women. The mean body mass index was 28 kg/m2. Surgical indications were cholelithiasis (22), acute cholecystitis (17), chronic cholecystitis (5), and polyp (1). About 1 hour before surgery, patients received an infusion of indocyanine green 0.5 mg/kg. During the laparoscopic exploration, surgeons used near-infrared light to make the marker fluoresce as it was excreted by the liver.
In a picture review before surgery, all residents correctly identified 100% of the anatomic structures visualized by the fluorescent procedure. They were able to complete the fluorescent procedure in all of the patients. The completion rate for cholangiography was 93% (42 patients). In three patients, cholangiography failed because the cystic duct could not be cannulated.
The residents identified the cystic duct in 44 of the patients (98%), the common bile duct in 36 (80%), and the common hepatic ducts in 27 (60%). Neither technique identified any aberrant or accessory ducts.
Because fluorescent cholangiography is a real-time surgical procedure, it allowed checking of the transection and resection of the gallbladder pedicle before smooth dissection in all of the patients.
The procedure was significantly quicker than standard cholangiography (0.71 minutes vs. 7.15 minutes). It was also significantly cheaper, costing a mean of $14 vs. $778. There were no adverse surgical events, and no adverse reactions to the dye or at the infusion site, Dr. Dip said. Additionally, he noted, fluorescent cholangiography does not rely on x-rays, and so spared the patients any radiation exposure.
He added that the Cleveland Clinic, in conjunction with the University of Tokyo, will soon launch a randomized clinical trial comparing the two methods. An ongoing trial from another institution is evaluating fluorescent cholangiography compared with critical view technique in visualizing anatomy during laparoscopic cholecystectomy. It was set to wrap up in January, but according to the trial record on clinicaltrials.gov, is still recruiting patients.
Dr. Dip had no financial disclosures.
On Twitter @alz_gal
MIAMI BEACH – Intraoperative fluorescent cholangiography is just as effective as traditional cholangiography but costs hundreds of dollars less and is significantly faster to perform.
It’s also a great teaching tool, Dr. Fernando Dip said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. In just one session, all of the third- and fourth-year surgical residents were able to correctly identify 100% of the biliary structures.
"It appears to be an additional tool for the laparoscopic surgeon," said Dr. Dip, chief of surgical research at the Cleveland Clinic in Weston, Fla. "It’s quick, inexpensive, real-time, there are no adverse events, and it’s an inciscionless procedure."
Common bile duct injury is the most frequent injury seen in laparoscopic cholecystectomy, he said, and although the overall incidence is low, the number of injuries each year is not inconsiderable, since more than 750,000 laparoscopic cholecystectomies are performed in the United States annually.
"Only 3% of these injuries are due to problems with technical skill," Dr. Dip said. "The other 97% are problems of visual perception – illusions of where the ducts are."
Intraoperative cholangiography helps surgeons visualize this anatomy, but its true usefulness is somewhat controversial. Dr. Dip cited a recent study of almost 93,000 patients – 40% of whom underwent the procedure. It showed that intraoperative cholangiography is not effective as a preventive strategy against common duct injury during cholecystectomy.
Intraoperative fluorescent cholangiography is sometimes used to identify biliary anatomy in extrahepatic surgery. Dr. Dip and his colleagues examined its usefulness in 45 patients undergoing laparoscopic cholecystectomy. Senior residents performed all of the procedures under the supervision of experienced laparoscopic surgeons. All patients underwent the investigational procedure, followed by standard cholangiography.
The patients had a mean age of 49 years and were evenly split between men and women. The mean body mass index was 28 kg/m2. Surgical indications were cholelithiasis (22), acute cholecystitis (17), chronic cholecystitis (5), and polyp (1). About 1 hour before surgery, patients received an infusion of indocyanine green 0.5 mg/kg. During the laparoscopic exploration, surgeons used near-infrared light to make the marker fluoresce as it was excreted by the liver.
In a picture review before surgery, all residents correctly identified 100% of the anatomic structures visualized by the fluorescent procedure. They were able to complete the fluorescent procedure in all of the patients. The completion rate for cholangiography was 93% (42 patients). In three patients, cholangiography failed because the cystic duct could not be cannulated.
The residents identified the cystic duct in 44 of the patients (98%), the common bile duct in 36 (80%), and the common hepatic ducts in 27 (60%). Neither technique identified any aberrant or accessory ducts.
Because fluorescent cholangiography is a real-time surgical procedure, it allowed checking of the transection and resection of the gallbladder pedicle before smooth dissection in all of the patients.
The procedure was significantly quicker than standard cholangiography (0.71 minutes vs. 7.15 minutes). It was also significantly cheaper, costing a mean of $14 vs. $778. There were no adverse surgical events, and no adverse reactions to the dye or at the infusion site, Dr. Dip said. Additionally, he noted, fluorescent cholangiography does not rely on x-rays, and so spared the patients any radiation exposure.
He added that the Cleveland Clinic, in conjunction with the University of Tokyo, will soon launch a randomized clinical trial comparing the two methods. An ongoing trial from another institution is evaluating fluorescent cholangiography compared with critical view technique in visualizing anatomy during laparoscopic cholecystectomy. It was set to wrap up in January, but according to the trial record on clinicaltrials.gov, is still recruiting patients.
Dr. Dip had no financial disclosures.
On Twitter @alz_gal
MIAMI BEACH – Intraoperative fluorescent cholangiography is just as effective as traditional cholangiography but costs hundreds of dollars less and is significantly faster to perform.
It’s also a great teaching tool, Dr. Fernando Dip said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. In just one session, all of the third- and fourth-year surgical residents were able to correctly identify 100% of the biliary structures.
"It appears to be an additional tool for the laparoscopic surgeon," said Dr. Dip, chief of surgical research at the Cleveland Clinic in Weston, Fla. "It’s quick, inexpensive, real-time, there are no adverse events, and it’s an inciscionless procedure."
Common bile duct injury is the most frequent injury seen in laparoscopic cholecystectomy, he said, and although the overall incidence is low, the number of injuries each year is not inconsiderable, since more than 750,000 laparoscopic cholecystectomies are performed in the United States annually.
"Only 3% of these injuries are due to problems with technical skill," Dr. Dip said. "The other 97% are problems of visual perception – illusions of where the ducts are."
Intraoperative cholangiography helps surgeons visualize this anatomy, but its true usefulness is somewhat controversial. Dr. Dip cited a recent study of almost 93,000 patients – 40% of whom underwent the procedure. It showed that intraoperative cholangiography is not effective as a preventive strategy against common duct injury during cholecystectomy.
Intraoperative fluorescent cholangiography is sometimes used to identify biliary anatomy in extrahepatic surgery. Dr. Dip and his colleagues examined its usefulness in 45 patients undergoing laparoscopic cholecystectomy. Senior residents performed all of the procedures under the supervision of experienced laparoscopic surgeons. All patients underwent the investigational procedure, followed by standard cholangiography.
The patients had a mean age of 49 years and were evenly split between men and women. The mean body mass index was 28 kg/m2. Surgical indications were cholelithiasis (22), acute cholecystitis (17), chronic cholecystitis (5), and polyp (1). About 1 hour before surgery, patients received an infusion of indocyanine green 0.5 mg/kg. During the laparoscopic exploration, surgeons used near-infrared light to make the marker fluoresce as it was excreted by the liver.
In a picture review before surgery, all residents correctly identified 100% of the anatomic structures visualized by the fluorescent procedure. They were able to complete the fluorescent procedure in all of the patients. The completion rate for cholangiography was 93% (42 patients). In three patients, cholangiography failed because the cystic duct could not be cannulated.
The residents identified the cystic duct in 44 of the patients (98%), the common bile duct in 36 (80%), and the common hepatic ducts in 27 (60%). Neither technique identified any aberrant or accessory ducts.
Because fluorescent cholangiography is a real-time surgical procedure, it allowed checking of the transection and resection of the gallbladder pedicle before smooth dissection in all of the patients.
The procedure was significantly quicker than standard cholangiography (0.71 minutes vs. 7.15 minutes). It was also significantly cheaper, costing a mean of $14 vs. $778. There were no adverse surgical events, and no adverse reactions to the dye or at the infusion site, Dr. Dip said. Additionally, he noted, fluorescent cholangiography does not rely on x-rays, and so spared the patients any radiation exposure.
He added that the Cleveland Clinic, in conjunction with the University of Tokyo, will soon launch a randomized clinical trial comparing the two methods. An ongoing trial from another institution is evaluating fluorescent cholangiography compared with critical view technique in visualizing anatomy during laparoscopic cholecystectomy. It was set to wrap up in January, but according to the trial record on clinicaltrials.gov, is still recruiting patients.
Dr. Dip had no financial disclosures.
On Twitter @alz_gal
AT AHPBA 2014
Major finding: Fluorescent cholangiography identified 100% of relevant anatomy during laparoscopic cholecystectomy, while costing less than standard cholangiography ($14 vs. $778).
Data source: Prospective study of 45 patients.
Disclosures: Dr. Dip had no financial disclosures.

Intraoperative ultrasound can change approach to liver resection
MIAMI BEACH – Intraoperative ultrasound during resection of colorectal liver metastases changed operative management in 43% of cases, according to a retrospective study.
Ultrasound employed during surgery identified new lesions not seen on preoperative imaging, and gave additional details about known lesions, said Dr. Sarah Knowles, a surgical resident at the University of Western Ontario, London (Canada).
"Intraoperative ultrasound provided new information about the number, size, location, and appearance of the lesions," she said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. The procedure was associated with significantly more blood loss, however, and there were no differences in negative surgical margins between patients who had ultrasound during surgery and those who did not.

Dr. Knowles presented a retrospective study of 103 patients who, from 2009 to 2012, underwent liver resection of colorectal cancer metastases. Mean age of the patients was 62 years. Most (94%) had undergone preoperative computerized tomography; the rest had undergone magnetic resonance imaging. The mean time from preoperative imaging to surgery was 66 days. Most of the patients (72) had intraoperative ultrasound imaging.
There were 45 anatomic resections and 27 nonanatomic resections in the group that had intraoperative ultrasound. This was significantly different from the nonultrasound group, which had 25 anatomic and 6 nonanatomic resections.
Ultrasound changed surgical strategy in 43% (31) of those who had it. Surgical strategy changed in 10% of those who had no intraoperative imaging – a significant difference (P = less than .001). Blood loss was significantly greater in the ultrasound group (650 mL vs. 350 mL).
The bulk of the strategic changes in the ultrasound group (17) were due to additional information about the location of lesions – either deeper or more superficial than preoperative imaging suggested. Other reasons for a shift in strategy were the discovery of new lesions (13), a disappearing lesion (1), larger-than-expected lesions (5), smaller-than-expected lesions (2), or a difference in the lesions’ appearance (3).
Resection margins were similar in the two groups. In the ultrasound group, 85% had R0 margins and 15% had R1 margins. In the group without ultrasound, 87% had R0 margins and 13% had R1 margins. There was no significant difference in disease-free 5-year survival.
Dr. Knowles had no financial disclosures.
MIAMI BEACH – Intraoperative ultrasound during resection of colorectal liver metastases changed operative management in 43% of cases, according to a retrospective study.
Ultrasound employed during surgery identified new lesions not seen on preoperative imaging, and gave additional details about known lesions, said Dr. Sarah Knowles, a surgical resident at the University of Western Ontario, London (Canada).
"Intraoperative ultrasound provided new information about the number, size, location, and appearance of the lesions," she said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. The procedure was associated with significantly more blood loss, however, and there were no differences in negative surgical margins between patients who had ultrasound during surgery and those who did not.
Dr. Knowles presented a retrospective study of 103 patients who, from 2009 to 2012, underwent liver resection of colorectal cancer metastases. Mean age of the patients was 62 years. Most (94%) had undergone preoperative computerized tomography; the rest had undergone magnetic resonance imaging. The mean time from preoperative imaging to surgery was 66 days. Most of the patients (72) had intraoperative ultrasound imaging.
There were 45 anatomic resections and 27 nonanatomic resections in the group that had intraoperative ultrasound. This was significantly different from the nonultrasound group, which had 25 anatomic and 6 nonanatomic resections.
Ultrasound changed surgical strategy in 43% (31) of those who had it. Surgical strategy changed in 10% of those who had no intraoperative imaging – a significant difference (P = less than .001). Blood loss was significantly greater in the ultrasound group (650 mL vs. 350 mL).
The bulk of the strategic changes in the ultrasound group (17) were due to additional information about the location of lesions – either deeper or more superficial than preoperative imaging suggested. Other reasons for a shift in strategy were the discovery of new lesions (13), a disappearing lesion (1), larger-than-expected lesions (5), smaller-than-expected lesions (2), or a difference in the lesions’ appearance (3).
Resection margins were similar in the two groups. In the ultrasound group, 85% had R0 margins and 15% had R1 margins. In the group without ultrasound, 87% had R0 margins and 13% had R1 margins. There was no significant difference in disease-free 5-year survival.
Dr. Knowles had no financial disclosures.
MIAMI BEACH – Intraoperative ultrasound during resection of colorectal liver metastases changed operative management in 43% of cases, according to a retrospective study.
Ultrasound employed during surgery identified new lesions not seen on preoperative imaging, and gave additional details about known lesions, said Dr. Sarah Knowles, a surgical resident at the University of Western Ontario, London (Canada).
"Intraoperative ultrasound provided new information about the number, size, location, and appearance of the lesions," she said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. The procedure was associated with significantly more blood loss, however, and there were no differences in negative surgical margins between patients who had ultrasound during surgery and those who did not.
Dr. Knowles presented a retrospective study of 103 patients who, from 2009 to 2012, underwent liver resection of colorectal cancer metastases. Mean age of the patients was 62 years. Most (94%) had undergone preoperative computerized tomography; the rest had undergone magnetic resonance imaging. The mean time from preoperative imaging to surgery was 66 days. Most of the patients (72) had intraoperative ultrasound imaging.
There were 45 anatomic resections and 27 nonanatomic resections in the group that had intraoperative ultrasound. This was significantly different from the nonultrasound group, which had 25 anatomic and 6 nonanatomic resections.
Ultrasound changed surgical strategy in 43% (31) of those who had it. Surgical strategy changed in 10% of those who had no intraoperative imaging – a significant difference (P = less than .001). Blood loss was significantly greater in the ultrasound group (650 mL vs. 350 mL).
The bulk of the strategic changes in the ultrasound group (17) were due to additional information about the location of lesions – either deeper or more superficial than preoperative imaging suggested. Other reasons for a shift in strategy were the discovery of new lesions (13), a disappearing lesion (1), larger-than-expected lesions (5), smaller-than-expected lesions (2), or a difference in the lesions’ appearance (3).
Resection margins were similar in the two groups. In the ultrasound group, 85% had R0 margins and 15% had R1 margins. In the group without ultrasound, 87% had R0 margins and 13% had R1 margins. There was no significant difference in disease-free 5-year survival.
Dr. Knowles had no financial disclosures.
AT AHPBA 2014
Major finding: Intraoperative ultrasound changed surgical strategy in 43% of patients undergoing liver resections of colorectal cancer metastases.
Data source: A retrospective study of 103 patients.
Disclosures: Dr. Knowles had no financial disclosures.

CDC sounds alarm on hospital antibiotic use
A scathing new report by the Centers for Disease Control and Prevention found ample room for improvement in inpatient antibiotic prescribing.
Findings include continued overuse of antibiotics in hospitals, errors in prescribing, and the lifesaving potential of efforts to reduce antibiotic use:
• Physicians in some hospitals prescribed three times as many antibiotics as doctors in other hospitals, even though patients were being cared for in similar areas of each hospital.
• Antibiotic prescriptions contained an error in 37% of cases involving treatment for urinary tract infections or use of the common and critical drug, vancomycin (Vancocin).
• Models predicted that a 30% decrease in the use of broad-spectrum antibiotics would lead to a 26% reduction in Clostridium difficile infections, which kill roughly 14,000 hospitalized patients each year.

"Antibiotics are often lifesaving, and we have to protect them before our medicine chests run empty," CDC director Tom Frieden said during a press conference highlighting the report, released in the CDC’s March 4 Morbidity and Mortality Weekly Report (MMWR 2014 March 4;63:1-7).
Dr. Frieden announced that the CDC’s fiscal 2015 budget, part of President Obama’s budget initiative rolled out today, contains a $30 million increase in funds to establish a robust infrastructure in the United States to detect antibiotic threats and protect patients and communities.
The new monies would allow the CDC to extend the "detect and protect" strategy to combat antibiotic resistance outlined last year, help support state and hospital efforts to implement antibiotic stewardship programs, and improve rapid detection of antimicrobial threats and outbreaks.
"One of the things that makes us so focused on antimicrobial resistance is that not only is it a really serious problem, but [also] it’s not too late," Dr. Frieden said.
If funded, he anticipates the CDC and other stakeholders will be able to reverse drug resistance and cut in half the rate of C. difficile and the "nightmare" carbapenem-resistant Enterobacteriaceae infections.
It was noted that robust efforts to improve the use of antibiotics associated with C. difficile in the United Kingdom have resulted in more than a 50% reduction in use of those targeted agents and a roughly 70% reduction in C. difficile infections over the past 6 to 7 years.
The CDC is strongly recommending that every hospital in the United States have an antibiotic stewardship program and is providing a new checklist to help facilities with the task. The checklist contains seven core elements of an effective program: leadership commitment; accountability for outcomes under a single leader; drug expertise under a single pharmacist leader; taking action on at least one prescribing improvement practice; tracking antibiotic prescribing and resistance patterns; reporting regularly to staff about these patterns; and educating staff on antibiotic resistance and improving prescribing practices.
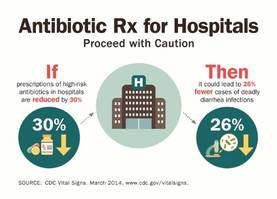
Specific advice was also given to clinicians to order recommended cultures before antibiotics are given and to start drugs promptly; make sure the indication, dose, and expected duration are specified in the patient record; and reassess patients within 48 hours and adjust treatment, if necessary, or stop treatment, if indicated.
Concerns were raised during the briefing over whether voluntary strategies will curb interfacility transmission caused by transfers of patients with multidrug-resistant infections and the failure to report outbreaks between facilities. Dr. John R. Combes, the American Hospital Association’s senior vice president said several groups are working to smooth out these transfers and that the AHA’s "Hospitals in Pursuit of Excellence" program provides best practices to facilitate transfers and foster cooperation with surrounding facilities to prevent infections.
The new CDC report is based on a review of data from all 323 hospitals in the MarketScan Hospital Drug Database and from hospitals in the CDC’s Emerging Infections Program.
Antibiotics were prescribed for 55.7% of patients hospitalized in 2010 in the MarketScan Hospital Drug Database, with 30% receiving at least one dose of broad-spectrum antibiotics.
One or more antibiotics were used to treat active infections in 37% of 11,282 patients treated in 2011 at 183 acute care hospitals evaluated by the Emerging Infections Program. Half of the antibiotics were prescribed for one of three scenarios: lower respiratory tract infections (22.2%), urinary tract infections (14%), and suspected drug-resistant Gram-positive infections such as methicillin-resistant Staphylococcus aureus (17.6%).
The CDC previously called on physicians to address antibiotic resistance in its Antibiotic Threats in the United States, 2013 report and the 2013 Get Smart About Antibiotics Week. The issue also will be tackled in the CDC’s forthcoming Transatlantic Taskforce on Antimicrobial Resistance 2013 report, with additional research expected to focus on contributing factors that led to such wide variances in antibiotic use between hospitals.
Dr. Frieden and Dr. Combes reported having no financial disclosures.

|
| Dr. Franklin A. Michota |
Dr. Franklin A. Michota is director of academic affairs, department of hospital medicine, Cleveland Clinic. He reports having no disclosures.
|
|
| Dr. Franklin A. Michota |
Dr. Franklin A. Michota is director of academic affairs, department of hospital medicine, Cleveland Clinic. He reports having no disclosures.
|
|
| Dr. Franklin A. Michota |
Dr. Franklin A. Michota is director of academic affairs, department of hospital medicine, Cleveland Clinic. He reports having no disclosures.
A scathing new report by the Centers for Disease Control and Prevention found ample room for improvement in inpatient antibiotic prescribing.
Findings include continued overuse of antibiotics in hospitals, errors in prescribing, and the lifesaving potential of efforts to reduce antibiotic use:
• Physicians in some hospitals prescribed three times as many antibiotics as doctors in other hospitals, even though patients were being cared for in similar areas of each hospital.
• Antibiotic prescriptions contained an error in 37% of cases involving treatment for urinary tract infections or use of the common and critical drug, vancomycin (Vancocin).
• Models predicted that a 30% decrease in the use of broad-spectrum antibiotics would lead to a 26% reduction in Clostridium difficile infections, which kill roughly 14,000 hospitalized patients each year.
"Antibiotics are often lifesaving, and we have to protect them before our medicine chests run empty," CDC director Tom Frieden said during a press conference highlighting the report, released in the CDC’s March 4 Morbidity and Mortality Weekly Report (MMWR 2014 March 4;63:1-7).
Dr. Frieden announced that the CDC’s fiscal 2015 budget, part of President Obama’s budget initiative rolled out today, contains a $30 million increase in funds to establish a robust infrastructure in the United States to detect antibiotic threats and protect patients and communities.
The new monies would allow the CDC to extend the "detect and protect" strategy to combat antibiotic resistance outlined last year, help support state and hospital efforts to implement antibiotic stewardship programs, and improve rapid detection of antimicrobial threats and outbreaks.
"One of the things that makes us so focused on antimicrobial resistance is that not only is it a really serious problem, but [also] it’s not too late," Dr. Frieden said.
If funded, he anticipates the CDC and other stakeholders will be able to reverse drug resistance and cut in half the rate of C. difficile and the "nightmare" carbapenem-resistant Enterobacteriaceae infections.
It was noted that robust efforts to improve the use of antibiotics associated with C. difficile in the United Kingdom have resulted in more than a 50% reduction in use of those targeted agents and a roughly 70% reduction in C. difficile infections over the past 6 to 7 years.
The CDC is strongly recommending that every hospital in the United States have an antibiotic stewardship program and is providing a new checklist to help facilities with the task. The checklist contains seven core elements of an effective program: leadership commitment; accountability for outcomes under a single leader; drug expertise under a single pharmacist leader; taking action on at least one prescribing improvement practice; tracking antibiotic prescribing and resistance patterns; reporting regularly to staff about these patterns; and educating staff on antibiotic resistance and improving prescribing practices.
Specific advice was also given to clinicians to order recommended cultures before antibiotics are given and to start drugs promptly; make sure the indication, dose, and expected duration are specified in the patient record; and reassess patients within 48 hours and adjust treatment, if necessary, or stop treatment, if indicated.
Concerns were raised during the briefing over whether voluntary strategies will curb interfacility transmission caused by transfers of patients with multidrug-resistant infections and the failure to report outbreaks between facilities. Dr. John R. Combes, the American Hospital Association’s senior vice president said several groups are working to smooth out these transfers and that the AHA’s "Hospitals in Pursuit of Excellence" program provides best practices to facilitate transfers and foster cooperation with surrounding facilities to prevent infections.
The new CDC report is based on a review of data from all 323 hospitals in the MarketScan Hospital Drug Database and from hospitals in the CDC’s Emerging Infections Program.
Antibiotics were prescribed for 55.7% of patients hospitalized in 2010 in the MarketScan Hospital Drug Database, with 30% receiving at least one dose of broad-spectrum antibiotics.
One or more antibiotics were used to treat active infections in 37% of 11,282 patients treated in 2011 at 183 acute care hospitals evaluated by the Emerging Infections Program. Half of the antibiotics were prescribed for one of three scenarios: lower respiratory tract infections (22.2%), urinary tract infections (14%), and suspected drug-resistant Gram-positive infections such as methicillin-resistant Staphylococcus aureus (17.6%).
The CDC previously called on physicians to address antibiotic resistance in its Antibiotic Threats in the United States, 2013 report and the 2013 Get Smart About Antibiotics Week. The issue also will be tackled in the CDC’s forthcoming Transatlantic Taskforce on Antimicrobial Resistance 2013 report, with additional research expected to focus on contributing factors that led to such wide variances in antibiotic use between hospitals.
Dr. Frieden and Dr. Combes reported having no financial disclosures.
A scathing new report by the Centers for Disease Control and Prevention found ample room for improvement in inpatient antibiotic prescribing.
Findings include continued overuse of antibiotics in hospitals, errors in prescribing, and the lifesaving potential of efforts to reduce antibiotic use:
• Physicians in some hospitals prescribed three times as many antibiotics as doctors in other hospitals, even though patients were being cared for in similar areas of each hospital.
• Antibiotic prescriptions contained an error in 37% of cases involving treatment for urinary tract infections or use of the common and critical drug, vancomycin (Vancocin).
• Models predicted that a 30% decrease in the use of broad-spectrum antibiotics would lead to a 26% reduction in Clostridium difficile infections, which kill roughly 14,000 hospitalized patients each year.
"Antibiotics are often lifesaving, and we have to protect them before our medicine chests run empty," CDC director Tom Frieden said during a press conference highlighting the report, released in the CDC’s March 4 Morbidity and Mortality Weekly Report (MMWR 2014 March 4;63:1-7).
Dr. Frieden announced that the CDC’s fiscal 2015 budget, part of President Obama’s budget initiative rolled out today, contains a $30 million increase in funds to establish a robust infrastructure in the United States to detect antibiotic threats and protect patients and communities.
The new monies would allow the CDC to extend the "detect and protect" strategy to combat antibiotic resistance outlined last year, help support state and hospital efforts to implement antibiotic stewardship programs, and improve rapid detection of antimicrobial threats and outbreaks.
"One of the things that makes us so focused on antimicrobial resistance is that not only is it a really serious problem, but [also] it’s not too late," Dr. Frieden said.
If funded, he anticipates the CDC and other stakeholders will be able to reverse drug resistance and cut in half the rate of C. difficile and the "nightmare" carbapenem-resistant Enterobacteriaceae infections.
It was noted that robust efforts to improve the use of antibiotics associated with C. difficile in the United Kingdom have resulted in more than a 50% reduction in use of those targeted agents and a roughly 70% reduction in C. difficile infections over the past 6 to 7 years.
The CDC is strongly recommending that every hospital in the United States have an antibiotic stewardship program and is providing a new checklist to help facilities with the task. The checklist contains seven core elements of an effective program: leadership commitment; accountability for outcomes under a single leader; drug expertise under a single pharmacist leader; taking action on at least one prescribing improvement practice; tracking antibiotic prescribing and resistance patterns; reporting regularly to staff about these patterns; and educating staff on antibiotic resistance and improving prescribing practices.
Specific advice was also given to clinicians to order recommended cultures before antibiotics are given and to start drugs promptly; make sure the indication, dose, and expected duration are specified in the patient record; and reassess patients within 48 hours and adjust treatment, if necessary, or stop treatment, if indicated.
Concerns were raised during the briefing over whether voluntary strategies will curb interfacility transmission caused by transfers of patients with multidrug-resistant infections and the failure to report outbreaks between facilities. Dr. John R. Combes, the American Hospital Association’s senior vice president said several groups are working to smooth out these transfers and that the AHA’s "Hospitals in Pursuit of Excellence" program provides best practices to facilitate transfers and foster cooperation with surrounding facilities to prevent infections.
The new CDC report is based on a review of data from all 323 hospitals in the MarketScan Hospital Drug Database and from hospitals in the CDC’s Emerging Infections Program.
Antibiotics were prescribed for 55.7% of patients hospitalized in 2010 in the MarketScan Hospital Drug Database, with 30% receiving at least one dose of broad-spectrum antibiotics.
One or more antibiotics were used to treat active infections in 37% of 11,282 patients treated in 2011 at 183 acute care hospitals evaluated by the Emerging Infections Program. Half of the antibiotics were prescribed for one of three scenarios: lower respiratory tract infections (22.2%), urinary tract infections (14%), and suspected drug-resistant Gram-positive infections such as methicillin-resistant Staphylococcus aureus (17.6%).
The CDC previously called on physicians to address antibiotic resistance in its Antibiotic Threats in the United States, 2013 report and the 2013 Get Smart About Antibiotics Week. The issue also will be tackled in the CDC’s forthcoming Transatlantic Taskforce on Antimicrobial Resistance 2013 report, with additional research expected to focus on contributing factors that led to such wide variances in antibiotic use between hospitals.
Dr. Frieden and Dr. Combes reported having no financial disclosures.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
