User login
How the New Vitamin D Guidelines Will, and Won’t, Change My Practice
Hi, everyone. I’m Dr. Kenny Lin. I am a family physician and associate director of the Lancaster General Hospital Family Medicine Residency, and I blog at Common Sense Family Doctor.
A few months ago, my health system added a clinical decision support function to our electronic health record to reduce inappropriate ordering of vitamin D levels. Clinicians are now required to select from a list of approved indications or diagnoses (including a history of vitamin D deficiency) before ordering the test.
Although I don’t know yet whether this process has had the desired effect, I felt that it was long overdue. Several years ago, I wrote an editorial that questioned the dramatic increase in vitamin D testing given the uncertainty about what level is adequate for good health and clinical trials showing that supplementing people with lower levels has no benefits for a variety of medical conditions. A more recent review of prospective studies of vitamin D supplements concluded that most correlations between vitamin D levels and outcomes in common and high-mortality conditions are unlikely to be causal.
A new Endocrine Society guideline recommends against routine measurement of vitamin D levels in healthy individuals. The guideline reinforces my current practice of not screening for vitamin D deficiency except in special situations, such as an individual with dark skin who works the night shift and rarely goes outdoors during daytime hours. But I haven’t been offering empirical vitamin D supplements to the four at-risk groups identified by the Endocrine Society: children, adults older than 75 years, pregnant patients, and adults with prediabetes. The evidence behind these recommendations merits a closer look.
In exclusively or primarily breastfed infants, I follow the American Academy of Pediatrics recommendation to prescribe a daily supplement containing 400 IU of vitamin D. However, the Endocrine Society found evidence from several studies conducted in other countries that continuing supplementation throughout childhood reduces the risk for rickets and possibly reduces the incidence of respiratory infections, with few adverse effects.
Many older women, and some older men, choose to take a calcium and vitamin D supplement for bone health, even though there is scant evidence that doing so prevents fractures in community-dwelling adults without osteoporosis. The Endocrine Society’s meta-analysis, however, found that 1000 adults aged 75 years or older who took an average of 900 IU of vitamin D daily for 2 years could expect to experience six fewer deaths than an identical group not taking supplements.
A typical prenatal vitamin contains 400 IU of vitamin D. Placebo-controlled trials reviewed by the Endocrine Society that gave an average of 2500 IU daily found statistically insignificant reductions in preeclampsia, intrauterine death, preterm birth, small for gestation age birth, and neonatal deaths.
Finally, the Endocrine Society’s recommendation for adults with prediabetes was based on 11 trials (three conducted in the United States) that tested a daily average of 3500 IU and found a slightly lower risk for progression to diabetes (24 fewer diagnoses of type 2 diabetes per 1000 persons) in the group who took supplements.
Of the four groups highlighted by the guideline, the strongest case for vitamin D supplements is in older adults — it’s hard to argue with lower mortality, even if the difference is small. Therefore, I will start suggesting that my patients over age 75 take a daily vitamin D supplement containing at least 800 IU if they aren’t already doing so.
On the other hand, I don’t plan to change my approach to pregnant patients (whose benefits in studies could have been due to chance), children after age 1 year (studies of children in other countries with different nutritional status may not apply to the United States), or adults with prediabetes (where we already have proven lifestyle interventions with much greater effects). In these cases, either I am unconvinced that the data support benefits for my patients, or I feel that the benefits of vitamin D supplements are small enough to be outweighed by potential harms, such as increased kidney stones.
Kenneth W. Lin, Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hi, everyone. I’m Dr. Kenny Lin. I am a family physician and associate director of the Lancaster General Hospital Family Medicine Residency, and I blog at Common Sense Family Doctor.
A few months ago, my health system added a clinical decision support function to our electronic health record to reduce inappropriate ordering of vitamin D levels. Clinicians are now required to select from a list of approved indications or diagnoses (including a history of vitamin D deficiency) before ordering the test.
Although I don’t know yet whether this process has had the desired effect, I felt that it was long overdue. Several years ago, I wrote an editorial that questioned the dramatic increase in vitamin D testing given the uncertainty about what level is adequate for good health and clinical trials showing that supplementing people with lower levels has no benefits for a variety of medical conditions. A more recent review of prospective studies of vitamin D supplements concluded that most correlations between vitamin D levels and outcomes in common and high-mortality conditions are unlikely to be causal.
A new Endocrine Society guideline recommends against routine measurement of vitamin D levels in healthy individuals. The guideline reinforces my current practice of not screening for vitamin D deficiency except in special situations, such as an individual with dark skin who works the night shift and rarely goes outdoors during daytime hours. But I haven’t been offering empirical vitamin D supplements to the four at-risk groups identified by the Endocrine Society: children, adults older than 75 years, pregnant patients, and adults with prediabetes. The evidence behind these recommendations merits a closer look.
In exclusively or primarily breastfed infants, I follow the American Academy of Pediatrics recommendation to prescribe a daily supplement containing 400 IU of vitamin D. However, the Endocrine Society found evidence from several studies conducted in other countries that continuing supplementation throughout childhood reduces the risk for rickets and possibly reduces the incidence of respiratory infections, with few adverse effects.
Many older women, and some older men, choose to take a calcium and vitamin D supplement for bone health, even though there is scant evidence that doing so prevents fractures in community-dwelling adults without osteoporosis. The Endocrine Society’s meta-analysis, however, found that 1000 adults aged 75 years or older who took an average of 900 IU of vitamin D daily for 2 years could expect to experience six fewer deaths than an identical group not taking supplements.
A typical prenatal vitamin contains 400 IU of vitamin D. Placebo-controlled trials reviewed by the Endocrine Society that gave an average of 2500 IU daily found statistically insignificant reductions in preeclampsia, intrauterine death, preterm birth, small for gestation age birth, and neonatal deaths.
Finally, the Endocrine Society’s recommendation for adults with prediabetes was based on 11 trials (three conducted in the United States) that tested a daily average of 3500 IU and found a slightly lower risk for progression to diabetes (24 fewer diagnoses of type 2 diabetes per 1000 persons) in the group who took supplements.
Of the four groups highlighted by the guideline, the strongest case for vitamin D supplements is in older adults — it’s hard to argue with lower mortality, even if the difference is small. Therefore, I will start suggesting that my patients over age 75 take a daily vitamin D supplement containing at least 800 IU if they aren’t already doing so.
On the other hand, I don’t plan to change my approach to pregnant patients (whose benefits in studies could have been due to chance), children after age 1 year (studies of children in other countries with different nutritional status may not apply to the United States), or adults with prediabetes (where we already have proven lifestyle interventions with much greater effects). In these cases, either I am unconvinced that the data support benefits for my patients, or I feel that the benefits of vitamin D supplements are small enough to be outweighed by potential harms, such as increased kidney stones.
Kenneth W. Lin, Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hi, everyone. I’m Dr. Kenny Lin. I am a family physician and associate director of the Lancaster General Hospital Family Medicine Residency, and I blog at Common Sense Family Doctor.
A few months ago, my health system added a clinical decision support function to our electronic health record to reduce inappropriate ordering of vitamin D levels. Clinicians are now required to select from a list of approved indications or diagnoses (including a history of vitamin D deficiency) before ordering the test.
Although I don’t know yet whether this process has had the desired effect, I felt that it was long overdue. Several years ago, I wrote an editorial that questioned the dramatic increase in vitamin D testing given the uncertainty about what level is adequate for good health and clinical trials showing that supplementing people with lower levels has no benefits for a variety of medical conditions. A more recent review of prospective studies of vitamin D supplements concluded that most correlations between vitamin D levels and outcomes in common and high-mortality conditions are unlikely to be causal.
A new Endocrine Society guideline recommends against routine measurement of vitamin D levels in healthy individuals. The guideline reinforces my current practice of not screening for vitamin D deficiency except in special situations, such as an individual with dark skin who works the night shift and rarely goes outdoors during daytime hours. But I haven’t been offering empirical vitamin D supplements to the four at-risk groups identified by the Endocrine Society: children, adults older than 75 years, pregnant patients, and adults with prediabetes. The evidence behind these recommendations merits a closer look.
In exclusively or primarily breastfed infants, I follow the American Academy of Pediatrics recommendation to prescribe a daily supplement containing 400 IU of vitamin D. However, the Endocrine Society found evidence from several studies conducted in other countries that continuing supplementation throughout childhood reduces the risk for rickets and possibly reduces the incidence of respiratory infections, with few adverse effects.
Many older women, and some older men, choose to take a calcium and vitamin D supplement for bone health, even though there is scant evidence that doing so prevents fractures in community-dwelling adults without osteoporosis. The Endocrine Society’s meta-analysis, however, found that 1000 adults aged 75 years or older who took an average of 900 IU of vitamin D daily for 2 years could expect to experience six fewer deaths than an identical group not taking supplements.
A typical prenatal vitamin contains 400 IU of vitamin D. Placebo-controlled trials reviewed by the Endocrine Society that gave an average of 2500 IU daily found statistically insignificant reductions in preeclampsia, intrauterine death, preterm birth, small for gestation age birth, and neonatal deaths.
Finally, the Endocrine Society’s recommendation for adults with prediabetes was based on 11 trials (three conducted in the United States) that tested a daily average of 3500 IU and found a slightly lower risk for progression to diabetes (24 fewer diagnoses of type 2 diabetes per 1000 persons) in the group who took supplements.
Of the four groups highlighted by the guideline, the strongest case for vitamin D supplements is in older adults — it’s hard to argue with lower mortality, even if the difference is small. Therefore, I will start suggesting that my patients over age 75 take a daily vitamin D supplement containing at least 800 IU if they aren’t already doing so.
On the other hand, I don’t plan to change my approach to pregnant patients (whose benefits in studies could have been due to chance), children after age 1 year (studies of children in other countries with different nutritional status may not apply to the United States), or adults with prediabetes (where we already have proven lifestyle interventions with much greater effects). In these cases, either I am unconvinced that the data support benefits for my patients, or I feel that the benefits of vitamin D supplements are small enough to be outweighed by potential harms, such as increased kidney stones.
Kenneth W. Lin, Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New Criteria Distinguish Memory Disorder Often Misdiagnosed as Alzheimer’s
Proposed clinical criteria for a memory loss disorder that is often misdiagnosed as Alzheimer’s disease (AD) have been published.
The new criteria for limbic-predominant amnestic neurodegenerative syndrome (LANS) provide a framework for neurologists and other experts to classify the condition and offer a more precise diagnosis and potential treatments.
“In our clinical work, we see patients whose memory symptoms appear to mimic Alzheimer’s disease, but when you look at their brain imaging or biomarkers, it’s clear they don’t have Alzheimer’s. Until now, there has not been a specific medical diagnosis to point to, but now we can offer them some answers,” senior investigator David T. Jones, MD, said in a release.
The proposed criteria and the research behind it were published online in Brain Communications and will be presented at the Alzheimer›s Association International Conference in Philadelphia.
Already in Use
Predominant limbic degeneration has been linked to various underlying etiologies, older age, predominant impairment of episodic memory, and slow clinical progression, the investigators noted. However, they added, the neurologic syndrome associated with predominant limbic degeneration is undefined.
Developing clinical criteria and validating them “is critical to distinguish such a syndrome from those originating from neocortical degeneration, which may differ in underlying etiology, disease course, and therapeutic needs,” the investigators wrote.
The newly proposed clinical criteria apply to LANS, which is “highly associated with limbic-predominant age-related TDP-43 encephalopathy but also other pathologic entities.”
The criteria incorporate core, standard, and advanced features including older age at evaluation, mild clinical syndrome, disproportionate hippocampal atrophy, impaired semantic memory, limbic hypometabolism, absence of endocortical degeneration, and low likelihood of neocortical tau with highest, high, moderate, and low degrees of certainty.
“A detailed history of the clinical symptoms, which may be supported by neuropsychological testing, with the observation of disproportionate hippocampal atrophy and limbic degeneration on MRI/FDG yields a high confidence in a diagnosis of LANS, where the most likely symptom-driving proteinopathy is TDP-43 and not Alzheimer’s associated proteins,” the first author, Nick Corriveau-Lecavalier, PhD, assistant professor of neurology and psychology at Mayo Clinic, Rochester, Minnesota, told this news organization.
To validate the criteria, the investigators screened autopsied patients from Mayo Clinic and Alzheimer’s Disease Neuroimaging Initiative cohorts and applied the criteria to those with a predominant amnestic syndrome and those who had AD neuropathologic change, limbic-predominant age-related TDP-43 encephalopathy, or both pathologies at autopsy.
“The criteria effectively categorized these cases, with Alzheimer’s disease having the lowest likelihoods, limbic-predominant age-related TDP-43 encephalopathy patients having the highest likelihoods, and patients with both pathologies having intermediate likelihoods,” the investigators reported.
“Patients with high likelihoods had a milder and slower clinical course and more severe temporo-limbic degeneration compared to those with low likelihoods,” they added.
Dr. Corriveau-Lecavalier said the team is currently analyzing longitudinal cognitive and imaging trajectories in LANS over several years. “This will help us better understand how LANS and Alzheimer’s differ in their sequence of symptoms over time.”
It is important to understand that memory symptoms in old age are not “unequivocally” driven by Alzheimer’s and that LANS progresses more slowly and has a better prognosis than AD, he noted.
In addition, in vivo markers of TDP-43 are “on the horizon and can hopefully make their way to human research settings soon. This will help better understand the underlying molecular etiologies causing LANS and associated symptoms,” he said.
Dr. Corriveau-Lecavalier said the LANS criteria are ready for clinical use by experts in neurologic care. These criteria can be used to inform not only diagnosis but also prognosis, where this syndrome is associated with slow and mild progression and a memory-dominant profile.
He added that “the new criteria are also routinely used in our practice to make decisions about anti-amyloid treatment eligibility.”
Commenting on the research for this news organization, Rebecca M. Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, said the research “exemplifies the great need to develop objective criteria for diagnosis and staging of Alzheimer’s and all other types of dementia and to create an integrated biological and clinical staging scheme that can be used effectively by physicians.”
“Advances in biomarkers will help to differentiate all types of dementia when incorporated into the diagnostic workup, but until those tools are available, a more succinct clinical criteria for diagnosis can be used to support a more personalized medicine approach to treatment, care, and enrollment into clinical studies,” said Dr. Edelmayer, who wasn’t involved in the research.
The research was funded in part by the National Institutes of Health and by the Robert Wood Johnson Foundation, the Elsie & Marvin Dekelboum Family Foundation, the Liston Family Foundation, the Edson Family, the Gerald A. and Henrietta Rauenhorst Foundation, and the Foundation Dr Corinne Schuler. Dr. Corriveau-Lecavalier and Dr. Edelmayer had no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Proposed clinical criteria for a memory loss disorder that is often misdiagnosed as Alzheimer’s disease (AD) have been published.
The new criteria for limbic-predominant amnestic neurodegenerative syndrome (LANS) provide a framework for neurologists and other experts to classify the condition and offer a more precise diagnosis and potential treatments.
“In our clinical work, we see patients whose memory symptoms appear to mimic Alzheimer’s disease, but when you look at their brain imaging or biomarkers, it’s clear they don’t have Alzheimer’s. Until now, there has not been a specific medical diagnosis to point to, but now we can offer them some answers,” senior investigator David T. Jones, MD, said in a release.
The proposed criteria and the research behind it were published online in Brain Communications and will be presented at the Alzheimer›s Association International Conference in Philadelphia.
Already in Use
Predominant limbic degeneration has been linked to various underlying etiologies, older age, predominant impairment of episodic memory, and slow clinical progression, the investigators noted. However, they added, the neurologic syndrome associated with predominant limbic degeneration is undefined.
Developing clinical criteria and validating them “is critical to distinguish such a syndrome from those originating from neocortical degeneration, which may differ in underlying etiology, disease course, and therapeutic needs,” the investigators wrote.
The newly proposed clinical criteria apply to LANS, which is “highly associated with limbic-predominant age-related TDP-43 encephalopathy but also other pathologic entities.”
The criteria incorporate core, standard, and advanced features including older age at evaluation, mild clinical syndrome, disproportionate hippocampal atrophy, impaired semantic memory, limbic hypometabolism, absence of endocortical degeneration, and low likelihood of neocortical tau with highest, high, moderate, and low degrees of certainty.
“A detailed history of the clinical symptoms, which may be supported by neuropsychological testing, with the observation of disproportionate hippocampal atrophy and limbic degeneration on MRI/FDG yields a high confidence in a diagnosis of LANS, where the most likely symptom-driving proteinopathy is TDP-43 and not Alzheimer’s associated proteins,” the first author, Nick Corriveau-Lecavalier, PhD, assistant professor of neurology and psychology at Mayo Clinic, Rochester, Minnesota, told this news organization.
To validate the criteria, the investigators screened autopsied patients from Mayo Clinic and Alzheimer’s Disease Neuroimaging Initiative cohorts and applied the criteria to those with a predominant amnestic syndrome and those who had AD neuropathologic change, limbic-predominant age-related TDP-43 encephalopathy, or both pathologies at autopsy.
“The criteria effectively categorized these cases, with Alzheimer’s disease having the lowest likelihoods, limbic-predominant age-related TDP-43 encephalopathy patients having the highest likelihoods, and patients with both pathologies having intermediate likelihoods,” the investigators reported.
“Patients with high likelihoods had a milder and slower clinical course and more severe temporo-limbic degeneration compared to those with low likelihoods,” they added.
Dr. Corriveau-Lecavalier said the team is currently analyzing longitudinal cognitive and imaging trajectories in LANS over several years. “This will help us better understand how LANS and Alzheimer’s differ in their sequence of symptoms over time.”
It is important to understand that memory symptoms in old age are not “unequivocally” driven by Alzheimer’s and that LANS progresses more slowly and has a better prognosis than AD, he noted.
In addition, in vivo markers of TDP-43 are “on the horizon and can hopefully make their way to human research settings soon. This will help better understand the underlying molecular etiologies causing LANS and associated symptoms,” he said.
Dr. Corriveau-Lecavalier said the LANS criteria are ready for clinical use by experts in neurologic care. These criteria can be used to inform not only diagnosis but also prognosis, where this syndrome is associated with slow and mild progression and a memory-dominant profile.
He added that “the new criteria are also routinely used in our practice to make decisions about anti-amyloid treatment eligibility.”
Commenting on the research for this news organization, Rebecca M. Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, said the research “exemplifies the great need to develop objective criteria for diagnosis and staging of Alzheimer’s and all other types of dementia and to create an integrated biological and clinical staging scheme that can be used effectively by physicians.”
“Advances in biomarkers will help to differentiate all types of dementia when incorporated into the diagnostic workup, but until those tools are available, a more succinct clinical criteria for diagnosis can be used to support a more personalized medicine approach to treatment, care, and enrollment into clinical studies,” said Dr. Edelmayer, who wasn’t involved in the research.
The research was funded in part by the National Institutes of Health and by the Robert Wood Johnson Foundation, the Elsie & Marvin Dekelboum Family Foundation, the Liston Family Foundation, the Edson Family, the Gerald A. and Henrietta Rauenhorst Foundation, and the Foundation Dr Corinne Schuler. Dr. Corriveau-Lecavalier and Dr. Edelmayer had no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Proposed clinical criteria for a memory loss disorder that is often misdiagnosed as Alzheimer’s disease (AD) have been published.
The new criteria for limbic-predominant amnestic neurodegenerative syndrome (LANS) provide a framework for neurologists and other experts to classify the condition and offer a more precise diagnosis and potential treatments.
“In our clinical work, we see patients whose memory symptoms appear to mimic Alzheimer’s disease, but when you look at their brain imaging or biomarkers, it’s clear they don’t have Alzheimer’s. Until now, there has not been a specific medical diagnosis to point to, but now we can offer them some answers,” senior investigator David T. Jones, MD, said in a release.
The proposed criteria and the research behind it were published online in Brain Communications and will be presented at the Alzheimer›s Association International Conference in Philadelphia.
Already in Use
Predominant limbic degeneration has been linked to various underlying etiologies, older age, predominant impairment of episodic memory, and slow clinical progression, the investigators noted. However, they added, the neurologic syndrome associated with predominant limbic degeneration is undefined.
Developing clinical criteria and validating them “is critical to distinguish such a syndrome from those originating from neocortical degeneration, which may differ in underlying etiology, disease course, and therapeutic needs,” the investigators wrote.
The newly proposed clinical criteria apply to LANS, which is “highly associated with limbic-predominant age-related TDP-43 encephalopathy but also other pathologic entities.”
The criteria incorporate core, standard, and advanced features including older age at evaluation, mild clinical syndrome, disproportionate hippocampal atrophy, impaired semantic memory, limbic hypometabolism, absence of endocortical degeneration, and low likelihood of neocortical tau with highest, high, moderate, and low degrees of certainty.
“A detailed history of the clinical symptoms, which may be supported by neuropsychological testing, with the observation of disproportionate hippocampal atrophy and limbic degeneration on MRI/FDG yields a high confidence in a diagnosis of LANS, where the most likely symptom-driving proteinopathy is TDP-43 and not Alzheimer’s associated proteins,” the first author, Nick Corriveau-Lecavalier, PhD, assistant professor of neurology and psychology at Mayo Clinic, Rochester, Minnesota, told this news organization.
To validate the criteria, the investigators screened autopsied patients from Mayo Clinic and Alzheimer’s Disease Neuroimaging Initiative cohorts and applied the criteria to those with a predominant amnestic syndrome and those who had AD neuropathologic change, limbic-predominant age-related TDP-43 encephalopathy, or both pathologies at autopsy.
“The criteria effectively categorized these cases, with Alzheimer’s disease having the lowest likelihoods, limbic-predominant age-related TDP-43 encephalopathy patients having the highest likelihoods, and patients with both pathologies having intermediate likelihoods,” the investigators reported.
“Patients with high likelihoods had a milder and slower clinical course and more severe temporo-limbic degeneration compared to those with low likelihoods,” they added.
Dr. Corriveau-Lecavalier said the team is currently analyzing longitudinal cognitive and imaging trajectories in LANS over several years. “This will help us better understand how LANS and Alzheimer’s differ in their sequence of symptoms over time.”
It is important to understand that memory symptoms in old age are not “unequivocally” driven by Alzheimer’s and that LANS progresses more slowly and has a better prognosis than AD, he noted.
In addition, in vivo markers of TDP-43 are “on the horizon and can hopefully make their way to human research settings soon. This will help better understand the underlying molecular etiologies causing LANS and associated symptoms,” he said.
Dr. Corriveau-Lecavalier said the LANS criteria are ready for clinical use by experts in neurologic care. These criteria can be used to inform not only diagnosis but also prognosis, where this syndrome is associated with slow and mild progression and a memory-dominant profile.
He added that “the new criteria are also routinely used in our practice to make decisions about anti-amyloid treatment eligibility.”
Commenting on the research for this news organization, Rebecca M. Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, said the research “exemplifies the great need to develop objective criteria for diagnosis and staging of Alzheimer’s and all other types of dementia and to create an integrated biological and clinical staging scheme that can be used effectively by physicians.”
“Advances in biomarkers will help to differentiate all types of dementia when incorporated into the diagnostic workup, but until those tools are available, a more succinct clinical criteria for diagnosis can be used to support a more personalized medicine approach to treatment, care, and enrollment into clinical studies,” said Dr. Edelmayer, who wasn’t involved in the research.
The research was funded in part by the National Institutes of Health and by the Robert Wood Johnson Foundation, the Elsie & Marvin Dekelboum Family Foundation, the Liston Family Foundation, the Edson Family, the Gerald A. and Henrietta Rauenhorst Foundation, and the Foundation Dr Corinne Schuler. Dr. Corriveau-Lecavalier and Dr. Edelmayer had no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Prognostication in Hospice Care: Challenges, Opportunities, and the Importance of Functional Status
Predicting life expectancy and providing an end-of-life diagnosis in hospice and palliative care is a challenge for most clinicians. Lack of training, limited communication skills, and relationships with patients are all contributing factors. These skills can improve with the use of functional scoring tools in conjunction with the patient’s comorbidities and physical/psychological symptoms. The Palliative Performance Scale (PPS), Karnofsky Performance Scale (KPS), and Eastern Cooperative Oncology Group Performance Status Scale (ECOG) are commonly used functional scoring tools.
The PPS measures 5 functional dimensions including ambulation, activity level, ability to administer self-care, oral intake, and level of consciousness.1 It has been shown to be valid for a broad range of palliative care patients, including those with advanced cancer or life-threatening noncancer diagnoses in hospitals or hospice care.2 The scale, measured in 10% increments, runs from 100% (completely functional) to 0% (dead). A PPS ≤ 70% helps meet hospice eligibility criteria.
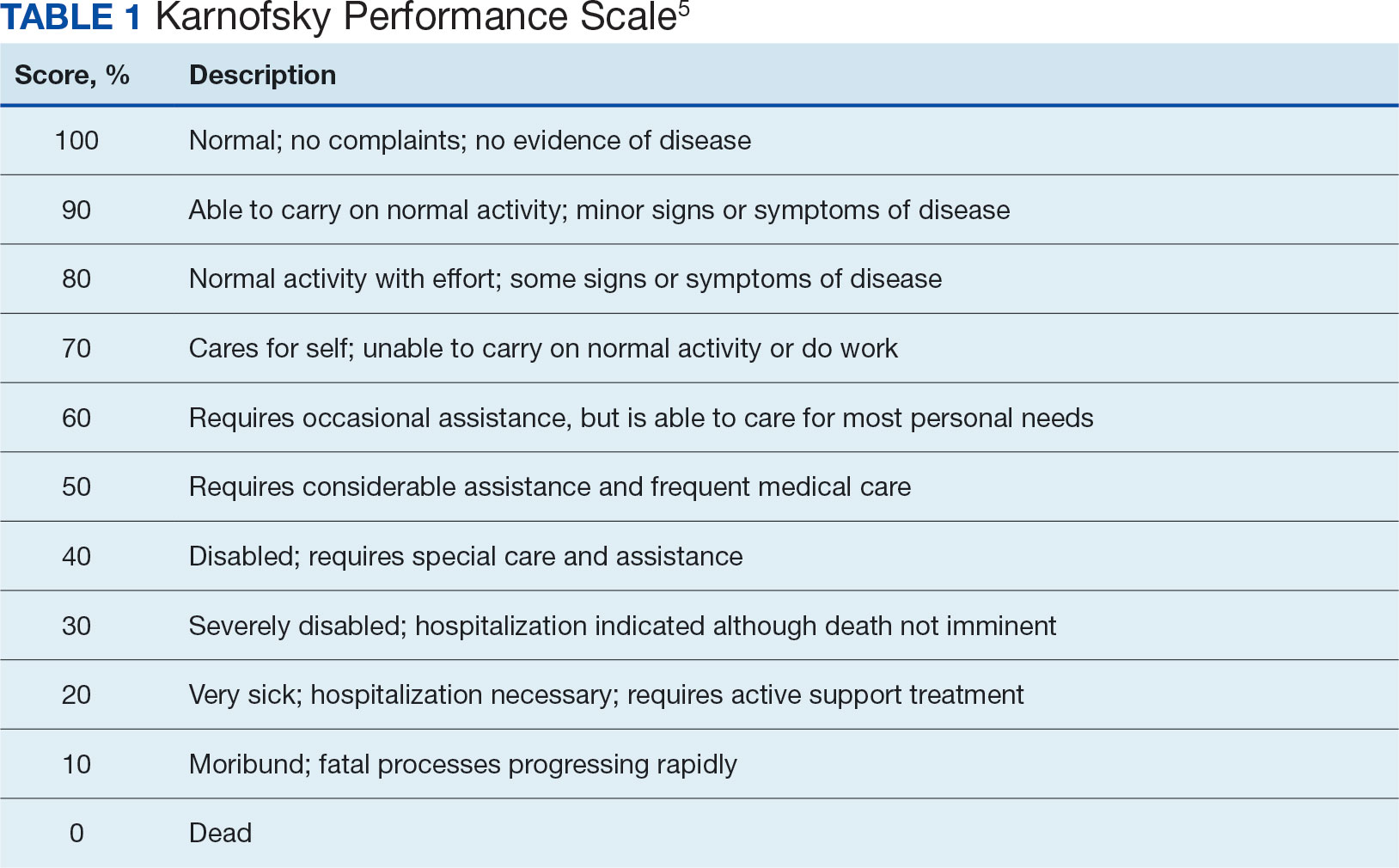
The KPS evaluates functional impairment and helps with prognostication. Developed in 1948, it evaluates a patient’s functional ability to tolerate chemotherapy, specifically in lung cancer, and has since been validated to predict mortality across older adults and in chronic disease populations.3,4 The KPS is also measured in 10% increments ranging from 100% (completely functional without assistance) to 0% (dead). A KPS ≤ 70% assists with hospice eligibility criteria (Table 1).5
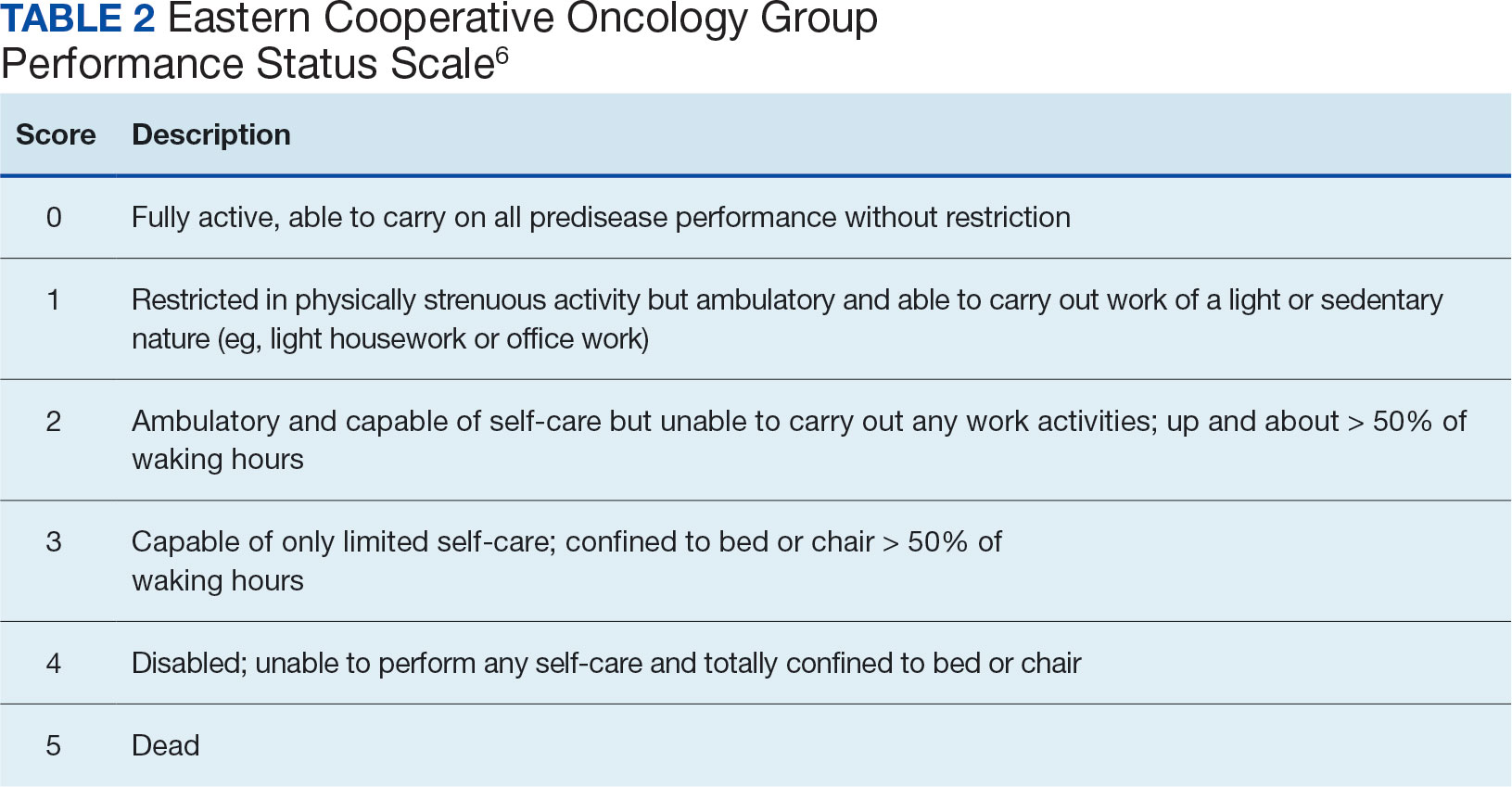
Developed in 1974, the ECOG has been identified as one of the most important functional status tools in adult cancer care.6 It describes a cancer patient’s functional ability, evaluating their ability to care for oneself and participate in daily activities.7 The ECOG is a 6-point scale; patients can receive scores ranging from 0 (fully active) to 5 (dead). An ECOG score of 4 (sometimes 3) is generally supportive of meeting hospice eligibility (Table 2).6
CASE Presentation
An 80-year-old patient was admitted to the hospice service at the Veterans Affairs Puget Sound Health Care System (VAPSHCS) community living center (CLC) in Tacoma, Washington, from a community-based acute care hospital. His medical history included prostate cancer with metastasis to his pelvis and type 2 diabetes mellitus, which was stable with treatment with oral medication. Six weeks earlier the patient reported a severe frontal headache that was not responding to over-the-counter analgesics. After 2 days with these symptoms, including a ground-level fall without injuries, he presented to the VAPSHCS emergency department (ED) where a complete neurological examination, including magnetic resonance imaging, revealed a left frontoparietal brain lesion that was 4.2 cm × 3.4 cm × 4.2 cm.
The patient experienced a seizure during his ED evaluation and was admitted for treatment. He underwent a craniotomy where most, but not all the lesions were successfully removed. Postoperatively, the patient exhibited right-sided neglect, gait instability, emotional lability, and cognitive communication disorder. The patient completed 15 of 20 planned radiation treatments but declined further radiation or chemotherapy. The patient decided to halt radiation treatments after being informed by the oncology service that the treatments would likely only add 1 to 2 months to his overall survival, which was < 6 months. The patient elected to focus his goals of care on comfort, dignity, and respect at the end of life and accepted recommendations to be placed into end-of-life hospice care. He was then transferred to the VAPSHCS CLC in Tacoma, Washington, for hospice care.
Upon admission, the patient weighed 94 kg, his vital signs were within reference range, and he reported no pain or headaches. His initial laboratory results revealed a 13.2 g/dL hemoglobin, 3.6 g/dL serum albumin, and a 5.5% hemoglobin A1c, all of which fall into a normal reference range. He had a reported ECOG score of 3 and a KPS score of 50% by the transferring medical team. The patient’s medications included scheduled dexamethasone, metformin, senna, levetiracetam, and as-needed midazolam nasal spray for breakthrough seizures. He also had as-needed acetaminophen for pain. He was alert, oriented ×3, and fully ambulatory but continuously used a 4-wheeled walker for safety and gait instability.
After the patient’s first night, the hospice team met with him to discuss his understanding of his health issues. The patient appeared to have low health literacy but told the team, “I know I am dying.” He had completed written advance directives and a Portable Order for Life-Sustaining Treatment indicating that life-sustaining treatments, including cardiopulmonary resuscitation, supplemental mechanical feeding, or intubation, were not to be used to keep him alive.
At his first 90-day recertification, the patient had gained 8 kg and laboratory results revealed a 14.6 g/dL hemoglobin, 3.8 g/dL serum albumin, and a 6.1% hemoglobin A1c. His ECOG score remained at 3, but his KPS score had increased to 60%. The patient exhibited no new neurologic symptoms or seizures and reported no headaches but had 2 ground-level falls without injury. On both occasions the patient chose not to use his walker to go to the bathroom because it was “too far from my bed.” Per VA policy, after discussions with the hospice team, he was recertified for 90 more days of hospice care. At the end of 6 months in CLC, the patient’s weight remained stable, as did his complete blood count and comprehensive medical panel. He had 1 additional noninjurious ground-level fall and again reported no pain and no use of as-needed acetaminophen. His only medical complication was testing positive for COVID-19, but he remained asymptomatic. The patient was graduated from hospice care and referred to a nearby non-VA adult family home in the community after 180 days. At that time his ECOG score was 2 and his KPS score had increased to 70%.
DISCUSSION
Primary brain tumors account for about 2% of all malignant neoplasms in adults. About half of them represent gliomas. Glioblastoma multiforme derived from neuroepithelial cells is the most frequent and deadly primary malignant central nervous system tumor in adults.8 About 50% of patients with glioblastomas are aged ≥ 65 years at diagnosis.9 A retrospective study of Centers for Medicare and Medicaid Services claims data paired with the Surveillance, Epidemiology, and End Results database indicated a median survival of 4 months for patients with glioblastoma multiforme aged > 65 years, including all treatment modalities.10 Surgical resection combined with radiation and chemotherapy offers the best prognosis for the preservation of neurologic function.11 However, comorbidities, adverse drug effects, and the potential for postoperative complications pose significant risks, especially for older patients. Ultimately, goals of care conversations and advance directives play a very important role in evaluating benefits vs risks with this malignancy.
Our patient was aged 80 years and had previously been diagnosed with metastatic prostate malignancy. His goals of care focused on spending time with his friends, leaving his room to eat in the facility dining area, and continuing his daily walks. He remained clear that he did not want his care team to institute life-sustaining treatments to be kept alive and felt the information regarding the risks vs benefits of accepting chemotherapy was not aligned with his goals of care. Over the 6 months that he received hospice care, he gained weight, improved his hemoglobin and serum albumin levels, and ambulated with the use of a 4-wheeled walker. As the patient exhibited no functional decline or new comorbidities and his functional status improved, the clinical staff felt he no longer needed hospice services. The patient had an ECOG score of 2 and a KPS score of 70% at his hospice graduation.
Medical prognostication is one of the biggest challenges clinicians face. Clinicians are generally “over prognosticators,” and their thoughts tend to be based on the patient relationship, overall experiences in health care, and desire to treat and cure patients.12 In hospice we are asked to define the usual, normal, or expected course of a disease, but what does that mean? Although metastatic malignancies usually have a predictable course in comparison to diagnoses such as dementia, chronic obstructive pulmonary disease, or congestive heart failure, the challenges to improve prognostic ability andpredict disease course continue.13-15 Focusing on functional status, goals of care, and comorbidities are keys to helping with prognosis. Given the challenge, we find the PPS, KPS, and ECOG scales important tools.
When prognosticating, we attempt to define quantity and quality of life (which our patients must define independently or from the voice of their surrogate) and their ability to perform daily activities. Quality of life in patients with glioblastoma is progressively and significantly impacted due to the emergence of debilitating neurologic symptoms arising from infiltrative tumor growth into functionally intact brain tissue that restricts and disrupts normal day-to-day activities. However, functional status plays a significant role in helping the hospice team improve its overall prognosis.
Conclusions
This case study illustrates the difficulty that comes with prognostication(s) despite a patient's severely morbid disease, history of metastatic prostate cancer, and advanced age. Although a diagnosis may be concerning, documenting a patient’s status using functional scales prior to hospice admission and during the recertification process is helpful in prognostication. Doing so will allow health care professionals to have an accepted medical standard to use regardless how distinct the patient's diagnosis. The expression, “as the disease does not read the textbook,” may serve as a helpful reminder in talking with patients and their families. This is important as most patient’s clinical disease courses are different and having the opportunity to use performance status scales may help improve prognostic skills.
1. Cleary TA. The Palliative Performance Scale (PPSv2) Version 2. In: Downing GM, ed. Medical Care of the Dying. 4th ed. Victoria Hospice Society, Learning Centre for Palliative Care; 2006:120.
2. Palliative Performance Scale. ePrognosis, University of California San Francisco. Accessed June 14, 2024. https://eprognosis.ucsf.edu/pps.php
3. Karnofsky DA, Burchenal JH. The Clinical Evaluation of Chemotherapeutic Agents in Cancer. In: MacLeod CM, ed. Evaluation of Chemotherapeutic Agents. Columbia University Press; 1949:191-205.
4. Khalid MA, Achakzai IK, Ahmed Khan S, et al. The use of Karnofsky Performance Status (KPS) as a predictor of 3 month post discharge mortality in cirrhotic patients. Gastroenterol Hepatol Bed Bench. 2018;11(4):301-305.
5. Karnofsky Performance Scale. US Dept of Veterans Affairs. Accessed June 14, 2024. https://www.hiv.va.gov/provider/tools/karnofsky-performance-scale.asp
6. Mischel A-M, Rosielle DA. Eastern Cooperative Oncology Group Performance Status. Palliative Care Network of Wisconsin. December 10, 2021. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/eastern-cooperative-oncology-group-performance-status/
7. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649-655.
8. Nizamutdinov D, Stock EM, Dandashi JA, et al. Prognostication of survival outcomes in patients diagnosed with glioblastoma. World Neurosurg. 2018;109:e67-e74. doi:10.1016/j.wneu.2017.09.104
9. Kita D Ciernik IFVaccarella S Age as a predictive factor in glioblastomas: population-based study. Neuroepidemiology. 2009;33(1):17-22. doi:10.1159/000210017
10. Jordan JT, Gerstner ER, Batchelor TT, Cahill DP, Plotkin SR. Glioblastoma care in the elderly. Cancer. 2016;122(2):189-197. doi:10.1002/cnr.29742
11. Brown, NF, Ottaviani D, Tazare J, et al. Survival outcomes and prognostic factors in glioblastoma. Cancers (Basel). 2022;14(13):3161. doi:10.3390/cancers14133161
12. Christalakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. University of Chicago Press; 2000.
13. Weissman DE. Determining Prognosis in Advanced Cancer. Palliative Care Network of Wisconsin. January 28, 2019. Accessed June 14, 2014. https://www.mypcnow.org/fast-fact/determining-prognosis-in-advanced-cancer/
14. Childers JW, Arnold R, Curtis JR. Prognosis in End-Stage COPD. Palliative Care Network of Wisconsin. February 11, 2019. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/prognosis-in-end-stage-copd/
15. Reisfield GM, Wilson GR. Prognostication in Heart Failure. Palliative Care Network of Wisconsin. February 11, 2019. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/prognostication-in-heart-failure/
Predicting life expectancy and providing an end-of-life diagnosis in hospice and palliative care is a challenge for most clinicians. Lack of training, limited communication skills, and relationships with patients are all contributing factors. These skills can improve with the use of functional scoring tools in conjunction with the patient’s comorbidities and physical/psychological symptoms. The Palliative Performance Scale (PPS), Karnofsky Performance Scale (KPS), and Eastern Cooperative Oncology Group Performance Status Scale (ECOG) are commonly used functional scoring tools.
The PPS measures 5 functional dimensions including ambulation, activity level, ability to administer self-care, oral intake, and level of consciousness.1 It has been shown to be valid for a broad range of palliative care patients, including those with advanced cancer or life-threatening noncancer diagnoses in hospitals or hospice care.2 The scale, measured in 10% increments, runs from 100% (completely functional) to 0% (dead). A PPS ≤ 70% helps meet hospice eligibility criteria.
The KPS evaluates functional impairment and helps with prognostication. Developed in 1948, it evaluates a patient’s functional ability to tolerate chemotherapy, specifically in lung cancer, and has since been validated to predict mortality across older adults and in chronic disease populations.3,4 The KPS is also measured in 10% increments ranging from 100% (completely functional without assistance) to 0% (dead). A KPS ≤ 70% assists with hospice eligibility criteria (Table 1).5
Developed in 1974, the ECOG has been identified as one of the most important functional status tools in adult cancer care.6 It describes a cancer patient’s functional ability, evaluating their ability to care for oneself and participate in daily activities.7 The ECOG is a 6-point scale; patients can receive scores ranging from 0 (fully active) to 5 (dead). An ECOG score of 4 (sometimes 3) is generally supportive of meeting hospice eligibility (Table 2).6
CASE Presentation
An 80-year-old patient was admitted to the hospice service at the Veterans Affairs Puget Sound Health Care System (VAPSHCS) community living center (CLC) in Tacoma, Washington, from a community-based acute care hospital. His medical history included prostate cancer with metastasis to his pelvis and type 2 diabetes mellitus, which was stable with treatment with oral medication. Six weeks earlier the patient reported a severe frontal headache that was not responding to over-the-counter analgesics. After 2 days with these symptoms, including a ground-level fall without injuries, he presented to the VAPSHCS emergency department (ED) where a complete neurological examination, including magnetic resonance imaging, revealed a left frontoparietal brain lesion that was 4.2 cm × 3.4 cm × 4.2 cm.
The patient experienced a seizure during his ED evaluation and was admitted for treatment. He underwent a craniotomy where most, but not all the lesions were successfully removed. Postoperatively, the patient exhibited right-sided neglect, gait instability, emotional lability, and cognitive communication disorder. The patient completed 15 of 20 planned radiation treatments but declined further radiation or chemotherapy. The patient decided to halt radiation treatments after being informed by the oncology service that the treatments would likely only add 1 to 2 months to his overall survival, which was < 6 months. The patient elected to focus his goals of care on comfort, dignity, and respect at the end of life and accepted recommendations to be placed into end-of-life hospice care. He was then transferred to the VAPSHCS CLC in Tacoma, Washington, for hospice care.
Upon admission, the patient weighed 94 kg, his vital signs were within reference range, and he reported no pain or headaches. His initial laboratory results revealed a 13.2 g/dL hemoglobin, 3.6 g/dL serum albumin, and a 5.5% hemoglobin A1c, all of which fall into a normal reference range. He had a reported ECOG score of 3 and a KPS score of 50% by the transferring medical team. The patient’s medications included scheduled dexamethasone, metformin, senna, levetiracetam, and as-needed midazolam nasal spray for breakthrough seizures. He also had as-needed acetaminophen for pain. He was alert, oriented ×3, and fully ambulatory but continuously used a 4-wheeled walker for safety and gait instability.
After the patient’s first night, the hospice team met with him to discuss his understanding of his health issues. The patient appeared to have low health literacy but told the team, “I know I am dying.” He had completed written advance directives and a Portable Order for Life-Sustaining Treatment indicating that life-sustaining treatments, including cardiopulmonary resuscitation, supplemental mechanical feeding, or intubation, were not to be used to keep him alive.
At his first 90-day recertification, the patient had gained 8 kg and laboratory results revealed a 14.6 g/dL hemoglobin, 3.8 g/dL serum albumin, and a 6.1% hemoglobin A1c. His ECOG score remained at 3, but his KPS score had increased to 60%. The patient exhibited no new neurologic symptoms or seizures and reported no headaches but had 2 ground-level falls without injury. On both occasions the patient chose not to use his walker to go to the bathroom because it was “too far from my bed.” Per VA policy, after discussions with the hospice team, he was recertified for 90 more days of hospice care. At the end of 6 months in CLC, the patient’s weight remained stable, as did his complete blood count and comprehensive medical panel. He had 1 additional noninjurious ground-level fall and again reported no pain and no use of as-needed acetaminophen. His only medical complication was testing positive for COVID-19, but he remained asymptomatic. The patient was graduated from hospice care and referred to a nearby non-VA adult family home in the community after 180 days. At that time his ECOG score was 2 and his KPS score had increased to 70%.
DISCUSSION
Primary brain tumors account for about 2% of all malignant neoplasms in adults. About half of them represent gliomas. Glioblastoma multiforme derived from neuroepithelial cells is the most frequent and deadly primary malignant central nervous system tumor in adults.8 About 50% of patients with glioblastomas are aged ≥ 65 years at diagnosis.9 A retrospective study of Centers for Medicare and Medicaid Services claims data paired with the Surveillance, Epidemiology, and End Results database indicated a median survival of 4 months for patients with glioblastoma multiforme aged > 65 years, including all treatment modalities.10 Surgical resection combined with radiation and chemotherapy offers the best prognosis for the preservation of neurologic function.11 However, comorbidities, adverse drug effects, and the potential for postoperative complications pose significant risks, especially for older patients. Ultimately, goals of care conversations and advance directives play a very important role in evaluating benefits vs risks with this malignancy.
Our patient was aged 80 years and had previously been diagnosed with metastatic prostate malignancy. His goals of care focused on spending time with his friends, leaving his room to eat in the facility dining area, and continuing his daily walks. He remained clear that he did not want his care team to institute life-sustaining treatments to be kept alive and felt the information regarding the risks vs benefits of accepting chemotherapy was not aligned with his goals of care. Over the 6 months that he received hospice care, he gained weight, improved his hemoglobin and serum albumin levels, and ambulated with the use of a 4-wheeled walker. As the patient exhibited no functional decline or new comorbidities and his functional status improved, the clinical staff felt he no longer needed hospice services. The patient had an ECOG score of 2 and a KPS score of 70% at his hospice graduation.
Medical prognostication is one of the biggest challenges clinicians face. Clinicians are generally “over prognosticators,” and their thoughts tend to be based on the patient relationship, overall experiences in health care, and desire to treat and cure patients.12 In hospice we are asked to define the usual, normal, or expected course of a disease, but what does that mean? Although metastatic malignancies usually have a predictable course in comparison to diagnoses such as dementia, chronic obstructive pulmonary disease, or congestive heart failure, the challenges to improve prognostic ability andpredict disease course continue.13-15 Focusing on functional status, goals of care, and comorbidities are keys to helping with prognosis. Given the challenge, we find the PPS, KPS, and ECOG scales important tools.
When prognosticating, we attempt to define quantity and quality of life (which our patients must define independently or from the voice of their surrogate) and their ability to perform daily activities. Quality of life in patients with glioblastoma is progressively and significantly impacted due to the emergence of debilitating neurologic symptoms arising from infiltrative tumor growth into functionally intact brain tissue that restricts and disrupts normal day-to-day activities. However, functional status plays a significant role in helping the hospice team improve its overall prognosis.
Conclusions
This case study illustrates the difficulty that comes with prognostication(s) despite a patient's severely morbid disease, history of metastatic prostate cancer, and advanced age. Although a diagnosis may be concerning, documenting a patient’s status using functional scales prior to hospice admission and during the recertification process is helpful in prognostication. Doing so will allow health care professionals to have an accepted medical standard to use regardless how distinct the patient's diagnosis. The expression, “as the disease does not read the textbook,” may serve as a helpful reminder in talking with patients and their families. This is important as most patient’s clinical disease courses are different and having the opportunity to use performance status scales may help improve prognostic skills.
Predicting life expectancy and providing an end-of-life diagnosis in hospice and palliative care is a challenge for most clinicians. Lack of training, limited communication skills, and relationships with patients are all contributing factors. These skills can improve with the use of functional scoring tools in conjunction with the patient’s comorbidities and physical/psychological symptoms. The Palliative Performance Scale (PPS), Karnofsky Performance Scale (KPS), and Eastern Cooperative Oncology Group Performance Status Scale (ECOG) are commonly used functional scoring tools.
The PPS measures 5 functional dimensions including ambulation, activity level, ability to administer self-care, oral intake, and level of consciousness.1 It has been shown to be valid for a broad range of palliative care patients, including those with advanced cancer or life-threatening noncancer diagnoses in hospitals or hospice care.2 The scale, measured in 10% increments, runs from 100% (completely functional) to 0% (dead). A PPS ≤ 70% helps meet hospice eligibility criteria.
The KPS evaluates functional impairment and helps with prognostication. Developed in 1948, it evaluates a patient’s functional ability to tolerate chemotherapy, specifically in lung cancer, and has since been validated to predict mortality across older adults and in chronic disease populations.3,4 The KPS is also measured in 10% increments ranging from 100% (completely functional without assistance) to 0% (dead). A KPS ≤ 70% assists with hospice eligibility criteria (Table 1).5
Developed in 1974, the ECOG has been identified as one of the most important functional status tools in adult cancer care.6 It describes a cancer patient’s functional ability, evaluating their ability to care for oneself and participate in daily activities.7 The ECOG is a 6-point scale; patients can receive scores ranging from 0 (fully active) to 5 (dead). An ECOG score of 4 (sometimes 3) is generally supportive of meeting hospice eligibility (Table 2).6
CASE Presentation
An 80-year-old patient was admitted to the hospice service at the Veterans Affairs Puget Sound Health Care System (VAPSHCS) community living center (CLC) in Tacoma, Washington, from a community-based acute care hospital. His medical history included prostate cancer with metastasis to his pelvis and type 2 diabetes mellitus, which was stable with treatment with oral medication. Six weeks earlier the patient reported a severe frontal headache that was not responding to over-the-counter analgesics. After 2 days with these symptoms, including a ground-level fall without injuries, he presented to the VAPSHCS emergency department (ED) where a complete neurological examination, including magnetic resonance imaging, revealed a left frontoparietal brain lesion that was 4.2 cm × 3.4 cm × 4.2 cm.
The patient experienced a seizure during his ED evaluation and was admitted for treatment. He underwent a craniotomy where most, but not all the lesions were successfully removed. Postoperatively, the patient exhibited right-sided neglect, gait instability, emotional lability, and cognitive communication disorder. The patient completed 15 of 20 planned radiation treatments but declined further radiation or chemotherapy. The patient decided to halt radiation treatments after being informed by the oncology service that the treatments would likely only add 1 to 2 months to his overall survival, which was < 6 months. The patient elected to focus his goals of care on comfort, dignity, and respect at the end of life and accepted recommendations to be placed into end-of-life hospice care. He was then transferred to the VAPSHCS CLC in Tacoma, Washington, for hospice care.
Upon admission, the patient weighed 94 kg, his vital signs were within reference range, and he reported no pain or headaches. His initial laboratory results revealed a 13.2 g/dL hemoglobin, 3.6 g/dL serum albumin, and a 5.5% hemoglobin A1c, all of which fall into a normal reference range. He had a reported ECOG score of 3 and a KPS score of 50% by the transferring medical team. The patient’s medications included scheduled dexamethasone, metformin, senna, levetiracetam, and as-needed midazolam nasal spray for breakthrough seizures. He also had as-needed acetaminophen for pain. He was alert, oriented ×3, and fully ambulatory but continuously used a 4-wheeled walker for safety and gait instability.
After the patient’s first night, the hospice team met with him to discuss his understanding of his health issues. The patient appeared to have low health literacy but told the team, “I know I am dying.” He had completed written advance directives and a Portable Order for Life-Sustaining Treatment indicating that life-sustaining treatments, including cardiopulmonary resuscitation, supplemental mechanical feeding, or intubation, were not to be used to keep him alive.
At his first 90-day recertification, the patient had gained 8 kg and laboratory results revealed a 14.6 g/dL hemoglobin, 3.8 g/dL serum albumin, and a 6.1% hemoglobin A1c. His ECOG score remained at 3, but his KPS score had increased to 60%. The patient exhibited no new neurologic symptoms or seizures and reported no headaches but had 2 ground-level falls without injury. On both occasions the patient chose not to use his walker to go to the bathroom because it was “too far from my bed.” Per VA policy, after discussions with the hospice team, he was recertified for 90 more days of hospice care. At the end of 6 months in CLC, the patient’s weight remained stable, as did his complete blood count and comprehensive medical panel. He had 1 additional noninjurious ground-level fall and again reported no pain and no use of as-needed acetaminophen. His only medical complication was testing positive for COVID-19, but he remained asymptomatic. The patient was graduated from hospice care and referred to a nearby non-VA adult family home in the community after 180 days. At that time his ECOG score was 2 and his KPS score had increased to 70%.
DISCUSSION
Primary brain tumors account for about 2% of all malignant neoplasms in adults. About half of them represent gliomas. Glioblastoma multiforme derived from neuroepithelial cells is the most frequent and deadly primary malignant central nervous system tumor in adults.8 About 50% of patients with glioblastomas are aged ≥ 65 years at diagnosis.9 A retrospective study of Centers for Medicare and Medicaid Services claims data paired with the Surveillance, Epidemiology, and End Results database indicated a median survival of 4 months for patients with glioblastoma multiforme aged > 65 years, including all treatment modalities.10 Surgical resection combined with radiation and chemotherapy offers the best prognosis for the preservation of neurologic function.11 However, comorbidities, adverse drug effects, and the potential for postoperative complications pose significant risks, especially for older patients. Ultimately, goals of care conversations and advance directives play a very important role in evaluating benefits vs risks with this malignancy.
Our patient was aged 80 years and had previously been diagnosed with metastatic prostate malignancy. His goals of care focused on spending time with his friends, leaving his room to eat in the facility dining area, and continuing his daily walks. He remained clear that he did not want his care team to institute life-sustaining treatments to be kept alive and felt the information regarding the risks vs benefits of accepting chemotherapy was not aligned with his goals of care. Over the 6 months that he received hospice care, he gained weight, improved his hemoglobin and serum albumin levels, and ambulated with the use of a 4-wheeled walker. As the patient exhibited no functional decline or new comorbidities and his functional status improved, the clinical staff felt he no longer needed hospice services. The patient had an ECOG score of 2 and a KPS score of 70% at his hospice graduation.
Medical prognostication is one of the biggest challenges clinicians face. Clinicians are generally “over prognosticators,” and their thoughts tend to be based on the patient relationship, overall experiences in health care, and desire to treat and cure patients.12 In hospice we are asked to define the usual, normal, or expected course of a disease, but what does that mean? Although metastatic malignancies usually have a predictable course in comparison to diagnoses such as dementia, chronic obstructive pulmonary disease, or congestive heart failure, the challenges to improve prognostic ability andpredict disease course continue.13-15 Focusing on functional status, goals of care, and comorbidities are keys to helping with prognosis. Given the challenge, we find the PPS, KPS, and ECOG scales important tools.
When prognosticating, we attempt to define quantity and quality of life (which our patients must define independently or from the voice of their surrogate) and their ability to perform daily activities. Quality of life in patients with glioblastoma is progressively and significantly impacted due to the emergence of debilitating neurologic symptoms arising from infiltrative tumor growth into functionally intact brain tissue that restricts and disrupts normal day-to-day activities. However, functional status plays a significant role in helping the hospice team improve its overall prognosis.
Conclusions
This case study illustrates the difficulty that comes with prognostication(s) despite a patient's severely morbid disease, history of metastatic prostate cancer, and advanced age. Although a diagnosis may be concerning, documenting a patient’s status using functional scales prior to hospice admission and during the recertification process is helpful in prognostication. Doing so will allow health care professionals to have an accepted medical standard to use regardless how distinct the patient's diagnosis. The expression, “as the disease does not read the textbook,” may serve as a helpful reminder in talking with patients and their families. This is important as most patient’s clinical disease courses are different and having the opportunity to use performance status scales may help improve prognostic skills.
1. Cleary TA. The Palliative Performance Scale (PPSv2) Version 2. In: Downing GM, ed. Medical Care of the Dying. 4th ed. Victoria Hospice Society, Learning Centre for Palliative Care; 2006:120.
2. Palliative Performance Scale. ePrognosis, University of California San Francisco. Accessed June 14, 2024. https://eprognosis.ucsf.edu/pps.php
3. Karnofsky DA, Burchenal JH. The Clinical Evaluation of Chemotherapeutic Agents in Cancer. In: MacLeod CM, ed. Evaluation of Chemotherapeutic Agents. Columbia University Press; 1949:191-205.
4. Khalid MA, Achakzai IK, Ahmed Khan S, et al. The use of Karnofsky Performance Status (KPS) as a predictor of 3 month post discharge mortality in cirrhotic patients. Gastroenterol Hepatol Bed Bench. 2018;11(4):301-305.
5. Karnofsky Performance Scale. US Dept of Veterans Affairs. Accessed June 14, 2024. https://www.hiv.va.gov/provider/tools/karnofsky-performance-scale.asp
6. Mischel A-M, Rosielle DA. Eastern Cooperative Oncology Group Performance Status. Palliative Care Network of Wisconsin. December 10, 2021. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/eastern-cooperative-oncology-group-performance-status/
7. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649-655.
8. Nizamutdinov D, Stock EM, Dandashi JA, et al. Prognostication of survival outcomes in patients diagnosed with glioblastoma. World Neurosurg. 2018;109:e67-e74. doi:10.1016/j.wneu.2017.09.104
9. Kita D Ciernik IFVaccarella S Age as a predictive factor in glioblastomas: population-based study. Neuroepidemiology. 2009;33(1):17-22. doi:10.1159/000210017
10. Jordan JT, Gerstner ER, Batchelor TT, Cahill DP, Plotkin SR. Glioblastoma care in the elderly. Cancer. 2016;122(2):189-197. doi:10.1002/cnr.29742
11. Brown, NF, Ottaviani D, Tazare J, et al. Survival outcomes and prognostic factors in glioblastoma. Cancers (Basel). 2022;14(13):3161. doi:10.3390/cancers14133161
12. Christalakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. University of Chicago Press; 2000.
13. Weissman DE. Determining Prognosis in Advanced Cancer. Palliative Care Network of Wisconsin. January 28, 2019. Accessed June 14, 2014. https://www.mypcnow.org/fast-fact/determining-prognosis-in-advanced-cancer/
14. Childers JW, Arnold R, Curtis JR. Prognosis in End-Stage COPD. Palliative Care Network of Wisconsin. February 11, 2019. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/prognosis-in-end-stage-copd/
15. Reisfield GM, Wilson GR. Prognostication in Heart Failure. Palliative Care Network of Wisconsin. February 11, 2019. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/prognostication-in-heart-failure/
1. Cleary TA. The Palliative Performance Scale (PPSv2) Version 2. In: Downing GM, ed. Medical Care of the Dying. 4th ed. Victoria Hospice Society, Learning Centre for Palliative Care; 2006:120.
2. Palliative Performance Scale. ePrognosis, University of California San Francisco. Accessed June 14, 2024. https://eprognosis.ucsf.edu/pps.php
3. Karnofsky DA, Burchenal JH. The Clinical Evaluation of Chemotherapeutic Agents in Cancer. In: MacLeod CM, ed. Evaluation of Chemotherapeutic Agents. Columbia University Press; 1949:191-205.
4. Khalid MA, Achakzai IK, Ahmed Khan S, et al. The use of Karnofsky Performance Status (KPS) as a predictor of 3 month post discharge mortality in cirrhotic patients. Gastroenterol Hepatol Bed Bench. 2018;11(4):301-305.
5. Karnofsky Performance Scale. US Dept of Veterans Affairs. Accessed June 14, 2024. https://www.hiv.va.gov/provider/tools/karnofsky-performance-scale.asp
6. Mischel A-M, Rosielle DA. Eastern Cooperative Oncology Group Performance Status. Palliative Care Network of Wisconsin. December 10, 2021. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/eastern-cooperative-oncology-group-performance-status/
7. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649-655.
8. Nizamutdinov D, Stock EM, Dandashi JA, et al. Prognostication of survival outcomes in patients diagnosed with glioblastoma. World Neurosurg. 2018;109:e67-e74. doi:10.1016/j.wneu.2017.09.104
9. Kita D Ciernik IFVaccarella S Age as a predictive factor in glioblastomas: population-based study. Neuroepidemiology. 2009;33(1):17-22. doi:10.1159/000210017
10. Jordan JT, Gerstner ER, Batchelor TT, Cahill DP, Plotkin SR. Glioblastoma care in the elderly. Cancer. 2016;122(2):189-197. doi:10.1002/cnr.29742
11. Brown, NF, Ottaviani D, Tazare J, et al. Survival outcomes and prognostic factors in glioblastoma. Cancers (Basel). 2022;14(13):3161. doi:10.3390/cancers14133161
12. Christalakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. University of Chicago Press; 2000.
13. Weissman DE. Determining Prognosis in Advanced Cancer. Palliative Care Network of Wisconsin. January 28, 2019. Accessed June 14, 2014. https://www.mypcnow.org/fast-fact/determining-prognosis-in-advanced-cancer/
14. Childers JW, Arnold R, Curtis JR. Prognosis in End-Stage COPD. Palliative Care Network of Wisconsin. February 11, 2019. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/prognosis-in-end-stage-copd/
15. Reisfield GM, Wilson GR. Prognostication in Heart Failure. Palliative Care Network of Wisconsin. February 11, 2019. Accessed June 14, 2024. https://www.mypcnow.org/fast-fact/prognostication-in-heart-failure/
Risk Stratification May Work Well for FIT-Based CRC Screening in Elderly
WASHINGTON — , according to a study presented at the annual Digestive Disease Week® (DDW).
In particular, interval CRC risk can vary substantially based on the fecal hemoglobin (f-Hb) concentration in the patient’s last fecal immunochemical test (FIT), as well as the number of prior screening rounds.
“Less is known about what happens after the upper age limit has been reached and individuals are not invited to participate in more screening rounds. This is important as life expectancy is increasing, and it is increasingly important to consider the most efficient way of screening the elderly,” said lead author Brenda van Stigt, a PhD candidate focused on cancer screening at Erasmus University Medical Center in Rotterdam, the Netherlands.
In the Netherlands, adults between ages 55 and 75 are invited to participate in stool-based CRC screening every 2 years. Based on a fecal immunochemical testing (FIT) threshold of 47 μg Hb/g, those who test positive are referred to colonoscopy, and those who test negative are invited to participate again after a 2-year period.
FIT can play a major role in risk stratification, Ms. van Stigt noted, along with other factors that influence CRC risk, such as age, sex, and CRC screening history. Although this is documented for ages 55-75, she and colleagues wanted to know more about what happens after age 75.
Ms. Van Stigt and colleagues conducted a population-based study by analyzing Dutch national cancer registry data and FIT results around the final screening at age 75, looking at those who were diagnosed with CRC within 24 months of their last negative FIT. The researchers assessed interval CRC risk and cancer stage, accounting for sex, last f-Hb concentration, and the number of screening rounds.
Among 305,761 people with a complete 24-month follow-up after a negative FIT, 661 patients were diagnosed with interval CRC, indicating an overall interval CRC risk of 21.6 per 10,000 individuals with a negative FIT. There were no significant differences by sex.
However, there were differences by screening rounds, with those who had participated in three or four screening rounds having a lower risk than those who participated only once (HR, .49).
In addition, those with detectable f-Hb (>0 μg Hb/g) in their last screening round had a much higher interval CRC risk (HR, 4.87), at 65.8 per 10,000 negative FITs, compared with 13.8 per 10,000 among those without detectable f-Hb. Interval CRC risk also increased over time for those with detectable f-Hb.
About 15% of the total population had detectable f-Hb, whereas 46% of those with interval CRC had detectable f-Hb, Ms. van Stigt said, meaning that nearly half of patients who were diagnosed with interval CRC already had detectable f-Hb in their prior FIT.
In a survival analysis, there was no association between interval CRC risk and sex. However, those who participated in three or four screening rounds were half as likely to be diagnosed than those who participated once or twice, and those with detectable f-Hb were five times as likely to be diagnosed.
For late-stage CRC, there was no association with sex or the number of screening rounds. Detectable f-Hb was associated with not only a higher risk of interval CRC but also a late-stage diagnosis.
“These findings indicate that one uniform age to stop screening is suboptimal,” Ms. van Stigt said. “Personalized screening strategies should, therefore, also ideally incorporate a risk-stratified age to stop screening.”
The US Preventive Services Task Force recommends that clinicians personalize screening for ages 76-85, accounting for overall health, prior screening history, and patient preferences.
“But we have no clear guidance on how to quantify or weigh these factors. This interesting study highlights how one of these factors (prior screening history) and fecal hemoglobin level (an emerging factor) are powerful stratifiers of subsequent colorectal cancer risk,” said Sameer D. Saini, MD, AGAF, director and research investigator at the VA Ann Arbor Healthcare System’s Center for Clinical Management Research. Dr. Saini wasn’t involved with the study.
At the clinical level, Dr. Saini said, sophisticated modeling is needed to understand the interaction with competing risks and identify the optimal screening strategies for patients at varying levels of cancer risk and life expectancy. Models could also help to quantify the population benefits and cost-effectiveness of personalized screening.
“Finally, it is important to note that, in many health systems, access to quantitative FIT may be limited,” he said. “These data may be less informative if colonoscopy is the primary mode of screening.”
Ms. van Stigt and Dr. Saini reported no relevant disclosures.
WASHINGTON — , according to a study presented at the annual Digestive Disease Week® (DDW).
In particular, interval CRC risk can vary substantially based on the fecal hemoglobin (f-Hb) concentration in the patient’s last fecal immunochemical test (FIT), as well as the number of prior screening rounds.
“Less is known about what happens after the upper age limit has been reached and individuals are not invited to participate in more screening rounds. This is important as life expectancy is increasing, and it is increasingly important to consider the most efficient way of screening the elderly,” said lead author Brenda van Stigt, a PhD candidate focused on cancer screening at Erasmus University Medical Center in Rotterdam, the Netherlands.
In the Netherlands, adults between ages 55 and 75 are invited to participate in stool-based CRC screening every 2 years. Based on a fecal immunochemical testing (FIT) threshold of 47 μg Hb/g, those who test positive are referred to colonoscopy, and those who test negative are invited to participate again after a 2-year period.
FIT can play a major role in risk stratification, Ms. van Stigt noted, along with other factors that influence CRC risk, such as age, sex, and CRC screening history. Although this is documented for ages 55-75, she and colleagues wanted to know more about what happens after age 75.
Ms. Van Stigt and colleagues conducted a population-based study by analyzing Dutch national cancer registry data and FIT results around the final screening at age 75, looking at those who were diagnosed with CRC within 24 months of their last negative FIT. The researchers assessed interval CRC risk and cancer stage, accounting for sex, last f-Hb concentration, and the number of screening rounds.
Among 305,761 people with a complete 24-month follow-up after a negative FIT, 661 patients were diagnosed with interval CRC, indicating an overall interval CRC risk of 21.6 per 10,000 individuals with a negative FIT. There were no significant differences by sex.
However, there were differences by screening rounds, with those who had participated in three or four screening rounds having a lower risk than those who participated only once (HR, .49).
In addition, those with detectable f-Hb (>0 μg Hb/g) in their last screening round had a much higher interval CRC risk (HR, 4.87), at 65.8 per 10,000 negative FITs, compared with 13.8 per 10,000 among those without detectable f-Hb. Interval CRC risk also increased over time for those with detectable f-Hb.
About 15% of the total population had detectable f-Hb, whereas 46% of those with interval CRC had detectable f-Hb, Ms. van Stigt said, meaning that nearly half of patients who were diagnosed with interval CRC already had detectable f-Hb in their prior FIT.
In a survival analysis, there was no association between interval CRC risk and sex. However, those who participated in three or four screening rounds were half as likely to be diagnosed than those who participated once or twice, and those with detectable f-Hb were five times as likely to be diagnosed.
For late-stage CRC, there was no association with sex or the number of screening rounds. Detectable f-Hb was associated with not only a higher risk of interval CRC but also a late-stage diagnosis.
“These findings indicate that one uniform age to stop screening is suboptimal,” Ms. van Stigt said. “Personalized screening strategies should, therefore, also ideally incorporate a risk-stratified age to stop screening.”
The US Preventive Services Task Force recommends that clinicians personalize screening for ages 76-85, accounting for overall health, prior screening history, and patient preferences.
“But we have no clear guidance on how to quantify or weigh these factors. This interesting study highlights how one of these factors (prior screening history) and fecal hemoglobin level (an emerging factor) are powerful stratifiers of subsequent colorectal cancer risk,” said Sameer D. Saini, MD, AGAF, director and research investigator at the VA Ann Arbor Healthcare System’s Center for Clinical Management Research. Dr. Saini wasn’t involved with the study.
At the clinical level, Dr. Saini said, sophisticated modeling is needed to understand the interaction with competing risks and identify the optimal screening strategies for patients at varying levels of cancer risk and life expectancy. Models could also help to quantify the population benefits and cost-effectiveness of personalized screening.
“Finally, it is important to note that, in many health systems, access to quantitative FIT may be limited,” he said. “These data may be less informative if colonoscopy is the primary mode of screening.”
Ms. van Stigt and Dr. Saini reported no relevant disclosures.
WASHINGTON — , according to a study presented at the annual Digestive Disease Week® (DDW).
In particular, interval CRC risk can vary substantially based on the fecal hemoglobin (f-Hb) concentration in the patient’s last fecal immunochemical test (FIT), as well as the number of prior screening rounds.
“Less is known about what happens after the upper age limit has been reached and individuals are not invited to participate in more screening rounds. This is important as life expectancy is increasing, and it is increasingly important to consider the most efficient way of screening the elderly,” said lead author Brenda van Stigt, a PhD candidate focused on cancer screening at Erasmus University Medical Center in Rotterdam, the Netherlands.
In the Netherlands, adults between ages 55 and 75 are invited to participate in stool-based CRC screening every 2 years. Based on a fecal immunochemical testing (FIT) threshold of 47 μg Hb/g, those who test positive are referred to colonoscopy, and those who test negative are invited to participate again after a 2-year period.
FIT can play a major role in risk stratification, Ms. van Stigt noted, along with other factors that influence CRC risk, such as age, sex, and CRC screening history. Although this is documented for ages 55-75, she and colleagues wanted to know more about what happens after age 75.
Ms. Van Stigt and colleagues conducted a population-based study by analyzing Dutch national cancer registry data and FIT results around the final screening at age 75, looking at those who were diagnosed with CRC within 24 months of their last negative FIT. The researchers assessed interval CRC risk and cancer stage, accounting for sex, last f-Hb concentration, and the number of screening rounds.
Among 305,761 people with a complete 24-month follow-up after a negative FIT, 661 patients were diagnosed with interval CRC, indicating an overall interval CRC risk of 21.6 per 10,000 individuals with a negative FIT. There were no significant differences by sex.
However, there were differences by screening rounds, with those who had participated in three or four screening rounds having a lower risk than those who participated only once (HR, .49).
In addition, those with detectable f-Hb (>0 μg Hb/g) in their last screening round had a much higher interval CRC risk (HR, 4.87), at 65.8 per 10,000 negative FITs, compared with 13.8 per 10,000 among those without detectable f-Hb. Interval CRC risk also increased over time for those with detectable f-Hb.
About 15% of the total population had detectable f-Hb, whereas 46% of those with interval CRC had detectable f-Hb, Ms. van Stigt said, meaning that nearly half of patients who were diagnosed with interval CRC already had detectable f-Hb in their prior FIT.
In a survival analysis, there was no association between interval CRC risk and sex. However, those who participated in three or four screening rounds were half as likely to be diagnosed than those who participated once or twice, and those with detectable f-Hb were five times as likely to be diagnosed.
For late-stage CRC, there was no association with sex or the number of screening rounds. Detectable f-Hb was associated with not only a higher risk of interval CRC but also a late-stage diagnosis.
“These findings indicate that one uniform age to stop screening is suboptimal,” Ms. van Stigt said. “Personalized screening strategies should, therefore, also ideally incorporate a risk-stratified age to stop screening.”
The US Preventive Services Task Force recommends that clinicians personalize screening for ages 76-85, accounting for overall health, prior screening history, and patient preferences.
“But we have no clear guidance on how to quantify or weigh these factors. This interesting study highlights how one of these factors (prior screening history) and fecal hemoglobin level (an emerging factor) are powerful stratifiers of subsequent colorectal cancer risk,” said Sameer D. Saini, MD, AGAF, director and research investigator at the VA Ann Arbor Healthcare System’s Center for Clinical Management Research. Dr. Saini wasn’t involved with the study.
At the clinical level, Dr. Saini said, sophisticated modeling is needed to understand the interaction with competing risks and identify the optimal screening strategies for patients at varying levels of cancer risk and life expectancy. Models could also help to quantify the population benefits and cost-effectiveness of personalized screening.
“Finally, it is important to note that, in many health systems, access to quantitative FIT may be limited,” he said. “These data may be less informative if colonoscopy is the primary mode of screening.”
Ms. van Stigt and Dr. Saini reported no relevant disclosures.
FROM DDW 2024
Statins, Vitamin D, and Exercise in Older Adults
In this article, I will review several recently published articles and guidelines relevant to the care of older adults in primary care. The articles of interest address statins for primary prevention, vitamin D supplementation and testing, and physical activity for healthy aging.
Statins for Primary Prevention of Cardiovascular Disease
A common conundrum in primary care is whether an older adult should be on a statin for primary prevention. This question has been difficult to answer because of the underrepresentation of older adults in clinical trials that examine the effect of statins for primary prevention. A recent study by Xu et al. published in Annals of Internal Medicine sought to address this gap in knowledge, investigating the risks and benefits of statins for primary prevention for older adults.1
This study stratified participants by “old” (aged 75-84 years) and “very old” (85 years or older). In this study, older adults who had an indication for statins were initiated on statins and studied over a 5-year period and compared with age-matched cohorts not initiated on statin therapy. Participants with known cardiovascular disease at baseline were excluded. The outcomes of interest were major cardiovascular disease (CVD) (a composite of myocardial infarction, stroke, or heart failure), all-cause mortality, and adverse effect of drug therapy (myopathy or liver dysfunction).
The study found that among older adults aged 75-84, initiation of statin therapy led to a 1.2% risk reduction in major CVD over a 5-year period. For older adults aged 85 and greater, initiation of statins had an even larger impact, leading to a 4.4% risk reduction in major CVD over a 5-year period. The study found that there was no significant difference in adverse effects including myopathy or liver dysfunction in both age groups.
Statins, the study suggests, are appropriate and safe to initiate for primary prevention in older adults and can lead to substantial benefits in reduction of CVD. While time to benefit was not explicitly examined in this study, a prior study by Yourman et al. suggested that the time to benefit for statins for primary prevention in adults aged 50-75 would be least 2.5 years.2
My takeaway from these findings is to discuss statin initiation for primary prevention for older patients who are focused on longevity, have good functional status (often used in geriatrics as a proxy for prognosis), and are willing to accept more medications.
Empiric Vitamin D Supplementation in Adults over 75 Years
Vitamin D is one of the most common supplements taken by older adults but evidence supporting vitamin D supplementation is variable in published literature, as most data comes from observational trials. New guidelines from the Endocrine Society focused on developing recommendations for healthy individuals with data obtained from randomized controlled trials (RCTs) and large longitudinal observational trials with comparison groups if RCTs were not available. These guidelines recommend against empiric supplementation of vitamin D for healthy adults aged 18-74, excluding pregnant women and patients with high-risk diabetes.3
For older adults aged 75 or greater, empiric vitamin D supplementation is recommended because of the possible reduction of risk in all-cause mortality in this population. Of note, this was a grade 2 recommendation by the panel, indicating that the benefits of the treatment probably outweigh the risks. The panel stated that vitamin D supplementation could be delivered through fortified foods, multivitamins with vitamin D, or as a separate vitamin D supplement.
The dosage should remain within the recommended daily allowance outlined by the Institute of Medicine of 800 IU daily for adults over 70, and the panel recommends low-dose daily vitamin D supplementation over high-dose interval supplementation. The panel noted that routine screening of vitamin D levels should not be used to guide decision-making on whether to start supplementation, but vitamin D levels should be obtained for patients who have an indication for evaluation.
The reviewers highlight that these guidelines were developed for healthy individuals and are not applicable to those with conditions that warrant vitamin D evaluation. In my clinical practice, many of my patients have bone-mineral conditions and cognitive impairment that warrant evaluation. Based on these guidelines, I will consider empiric vitamin D supplementation more often for healthy patients aged 75 and older.
Sedentary Behaviors and Healthy Aging
Engaging inactive older adults in regular physical activity can be challenging, particularly as the pandemic has led to more pervasive social isolation and affected the availability of in-person exercise activities in the community. Physical activity is a key component of healthy aging and cognition, and its benefits should be a part of routine counseling for older adults.
An interesting recent study published in JAMA Network Open by Shi et al. evaluated the association of health behaviors and aging in female US nurses over a 20-year period.4 Surveys were administered to capture time spent in each behavior, such as being sedentary (TV watching, sitting at home or at work), light activity (walking around the house or at work), and moderate to vigorous activity (walking for exercise, lawn mowing). “Healthy aging” was defined by the absence of chronic conditions such as heart failure, and lack of physical, mental, and cognitive impairment.
The study found that participants who were more sedentary were less likely to age healthfully, with each additional 2 hours of TV watching per day associated with a 12% reduction in likelihood of healthy aging. Light physical activity was associated with a significant increase in healthy aging, with a 6% increase in the likelihood of healthy aging for each additional 2 hours of light activity. Each additional 1 hour of moderate to vigorous activity was associated with a 14% increase in the likelihood of healthy aging. These findings support discussions with patients that behavior change, even in small increments, can be beneficial in healthy aging.
References
1. Xu W et al. Ann Intern Med. 2024 Jun;177(6):701-10.
2. Yourman LC et al. JAMA Intern Med. 2021;181:179-85.
3. Demay MB et al. J Clin Endocrinol Metab. August 2024;109(8):1907-47.
4. Shi H et al. JAMA Netw Open. 2024;7(6):e2416300.
In this article, I will review several recently published articles and guidelines relevant to the care of older adults in primary care. The articles of interest address statins for primary prevention, vitamin D supplementation and testing, and physical activity for healthy aging.
Statins for Primary Prevention of Cardiovascular Disease
A common conundrum in primary care is whether an older adult should be on a statin for primary prevention. This question has been difficult to answer because of the underrepresentation of older adults in clinical trials that examine the effect of statins for primary prevention. A recent study by Xu et al. published in Annals of Internal Medicine sought to address this gap in knowledge, investigating the risks and benefits of statins for primary prevention for older adults.1
This study stratified participants by “old” (aged 75-84 years) and “very old” (85 years or older). In this study, older adults who had an indication for statins were initiated on statins and studied over a 5-year period and compared with age-matched cohorts not initiated on statin therapy. Participants with known cardiovascular disease at baseline were excluded. The outcomes of interest were major cardiovascular disease (CVD) (a composite of myocardial infarction, stroke, or heart failure), all-cause mortality, and adverse effect of drug therapy (myopathy or liver dysfunction).
The study found that among older adults aged 75-84, initiation of statin therapy led to a 1.2% risk reduction in major CVD over a 5-year period. For older adults aged 85 and greater, initiation of statins had an even larger impact, leading to a 4.4% risk reduction in major CVD over a 5-year period. The study found that there was no significant difference in adverse effects including myopathy or liver dysfunction in both age groups.
Statins, the study suggests, are appropriate and safe to initiate for primary prevention in older adults and can lead to substantial benefits in reduction of CVD. While time to benefit was not explicitly examined in this study, a prior study by Yourman et al. suggested that the time to benefit for statins for primary prevention in adults aged 50-75 would be least 2.5 years.2
My takeaway from these findings is to discuss statin initiation for primary prevention for older patients who are focused on longevity, have good functional status (often used in geriatrics as a proxy for prognosis), and are willing to accept more medications.
Empiric Vitamin D Supplementation in Adults over 75 Years
Vitamin D is one of the most common supplements taken by older adults but evidence supporting vitamin D supplementation is variable in published literature, as most data comes from observational trials. New guidelines from the Endocrine Society focused on developing recommendations for healthy individuals with data obtained from randomized controlled trials (RCTs) and large longitudinal observational trials with comparison groups if RCTs were not available. These guidelines recommend against empiric supplementation of vitamin D for healthy adults aged 18-74, excluding pregnant women and patients with high-risk diabetes.3
For older adults aged 75 or greater, empiric vitamin D supplementation is recommended because of the possible reduction of risk in all-cause mortality in this population. Of note, this was a grade 2 recommendation by the panel, indicating that the benefits of the treatment probably outweigh the risks. The panel stated that vitamin D supplementation could be delivered through fortified foods, multivitamins with vitamin D, or as a separate vitamin D supplement.
The dosage should remain within the recommended daily allowance outlined by the Institute of Medicine of 800 IU daily for adults over 70, and the panel recommends low-dose daily vitamin D supplementation over high-dose interval supplementation. The panel noted that routine screening of vitamin D levels should not be used to guide decision-making on whether to start supplementation, but vitamin D levels should be obtained for patients who have an indication for evaluation.
The reviewers highlight that these guidelines were developed for healthy individuals and are not applicable to those with conditions that warrant vitamin D evaluation. In my clinical practice, many of my patients have bone-mineral conditions and cognitive impairment that warrant evaluation. Based on these guidelines, I will consider empiric vitamin D supplementation more often for healthy patients aged 75 and older.
Sedentary Behaviors and Healthy Aging
Engaging inactive older adults in regular physical activity can be challenging, particularly as the pandemic has led to more pervasive social isolation and affected the availability of in-person exercise activities in the community. Physical activity is a key component of healthy aging and cognition, and its benefits should be a part of routine counseling for older adults.
An interesting recent study published in JAMA Network Open by Shi et al. evaluated the association of health behaviors and aging in female US nurses over a 20-year period.4 Surveys were administered to capture time spent in each behavior, such as being sedentary (TV watching, sitting at home or at work), light activity (walking around the house or at work), and moderate to vigorous activity (walking for exercise, lawn mowing). “Healthy aging” was defined by the absence of chronic conditions such as heart failure, and lack of physical, mental, and cognitive impairment.
The study found that participants who were more sedentary were less likely to age healthfully, with each additional 2 hours of TV watching per day associated with a 12% reduction in likelihood of healthy aging. Light physical activity was associated with a significant increase in healthy aging, with a 6% increase in the likelihood of healthy aging for each additional 2 hours of light activity. Each additional 1 hour of moderate to vigorous activity was associated with a 14% increase in the likelihood of healthy aging. These findings support discussions with patients that behavior change, even in small increments, can be beneficial in healthy aging.
References
1. Xu W et al. Ann Intern Med. 2024 Jun;177(6):701-10.
2. Yourman LC et al. JAMA Intern Med. 2021;181:179-85.
3. Demay MB et al. J Clin Endocrinol Metab. August 2024;109(8):1907-47.
4. Shi H et al. JAMA Netw Open. 2024;7(6):e2416300.
In this article, I will review several recently published articles and guidelines relevant to the care of older adults in primary care. The articles of interest address statins for primary prevention, vitamin D supplementation and testing, and physical activity for healthy aging.
Statins for Primary Prevention of Cardiovascular Disease
A common conundrum in primary care is whether an older adult should be on a statin for primary prevention. This question has been difficult to answer because of the underrepresentation of older adults in clinical trials that examine the effect of statins for primary prevention. A recent study by Xu et al. published in Annals of Internal Medicine sought to address this gap in knowledge, investigating the risks and benefits of statins for primary prevention for older adults.1
This study stratified participants by “old” (aged 75-84 years) and “very old” (85 years or older). In this study, older adults who had an indication for statins were initiated on statins and studied over a 5-year period and compared with age-matched cohorts not initiated on statin therapy. Participants with known cardiovascular disease at baseline were excluded. The outcomes of interest were major cardiovascular disease (CVD) (a composite of myocardial infarction, stroke, or heart failure), all-cause mortality, and adverse effect of drug therapy (myopathy or liver dysfunction).
The study found that among older adults aged 75-84, initiation of statin therapy led to a 1.2% risk reduction in major CVD over a 5-year period. For older adults aged 85 and greater, initiation of statins had an even larger impact, leading to a 4.4% risk reduction in major CVD over a 5-year period. The study found that there was no significant difference in adverse effects including myopathy or liver dysfunction in both age groups.
Statins, the study suggests, are appropriate and safe to initiate for primary prevention in older adults and can lead to substantial benefits in reduction of CVD. While time to benefit was not explicitly examined in this study, a prior study by Yourman et al. suggested that the time to benefit for statins for primary prevention in adults aged 50-75 would be least 2.5 years.2
My takeaway from these findings is to discuss statin initiation for primary prevention for older patients who are focused on longevity, have good functional status (often used in geriatrics as a proxy for prognosis), and are willing to accept more medications.
Empiric Vitamin D Supplementation in Adults over 75 Years
Vitamin D is one of the most common supplements taken by older adults but evidence supporting vitamin D supplementation is variable in published literature, as most data comes from observational trials. New guidelines from the Endocrine Society focused on developing recommendations for healthy individuals with data obtained from randomized controlled trials (RCTs) and large longitudinal observational trials with comparison groups if RCTs were not available. These guidelines recommend against empiric supplementation of vitamin D for healthy adults aged 18-74, excluding pregnant women and patients with high-risk diabetes.3
For older adults aged 75 or greater, empiric vitamin D supplementation is recommended because of the possible reduction of risk in all-cause mortality in this population. Of note, this was a grade 2 recommendation by the panel, indicating that the benefits of the treatment probably outweigh the risks. The panel stated that vitamin D supplementation could be delivered through fortified foods, multivitamins with vitamin D, or as a separate vitamin D supplement.
The dosage should remain within the recommended daily allowance outlined by the Institute of Medicine of 800 IU daily for adults over 70, and the panel recommends low-dose daily vitamin D supplementation over high-dose interval supplementation. The panel noted that routine screening of vitamin D levels should not be used to guide decision-making on whether to start supplementation, but vitamin D levels should be obtained for patients who have an indication for evaluation.
The reviewers highlight that these guidelines were developed for healthy individuals and are not applicable to those with conditions that warrant vitamin D evaluation. In my clinical practice, many of my patients have bone-mineral conditions and cognitive impairment that warrant evaluation. Based on these guidelines, I will consider empiric vitamin D supplementation more often for healthy patients aged 75 and older.
Sedentary Behaviors and Healthy Aging
Engaging inactive older adults in regular physical activity can be challenging, particularly as the pandemic has led to more pervasive social isolation and affected the availability of in-person exercise activities in the community. Physical activity is a key component of healthy aging and cognition, and its benefits should be a part of routine counseling for older adults.
An interesting recent study published in JAMA Network Open by Shi et al. evaluated the association of health behaviors and aging in female US nurses over a 20-year period.4 Surveys were administered to capture time spent in each behavior, such as being sedentary (TV watching, sitting at home or at work), light activity (walking around the house or at work), and moderate to vigorous activity (walking for exercise, lawn mowing). “Healthy aging” was defined by the absence of chronic conditions such as heart failure, and lack of physical, mental, and cognitive impairment.
The study found that participants who were more sedentary were less likely to age healthfully, with each additional 2 hours of TV watching per day associated with a 12% reduction in likelihood of healthy aging. Light physical activity was associated with a significant increase in healthy aging, with a 6% increase in the likelihood of healthy aging for each additional 2 hours of light activity. Each additional 1 hour of moderate to vigorous activity was associated with a 14% increase in the likelihood of healthy aging. These findings support discussions with patients that behavior change, even in small increments, can be beneficial in healthy aging.
References
1. Xu W et al. Ann Intern Med. 2024 Jun;177(6):701-10.
2. Yourman LC et al. JAMA Intern Med. 2021;181:179-85.
3. Demay MB et al. J Clin Endocrinol Metab. August 2024;109(8):1907-47.
4. Shi H et al. JAMA Netw Open. 2024;7(6):e2416300.
Dermatoporosis in Older Adults: A Condition That Requires Holistic, Creative Management
WASHINGTON — and conveys the skin’s vulnerability to serious medical complications, said Adam Friedman, MD, at the ElderDerm conference on dermatology in the older patient.
Key features of dermatoporosis include atrophic skin, solar purpura, white pseudoscars, easily acquired skin lacerations and tears, bruises, and delayed healing. “We’re going to see more of this, and it will more and more be a chief complaint of patients,” said Dr. Friedman, professor and chair of dermatology at George Washington University (GWU) in Washington, and co-chair of the meeting. GWU hosted the conference, describing it as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.

Dermatoporosis was described in the literature in 2007 by dermatologists at the University of Geneva in Switzerland. “It is not only a cosmetic problem,” Dr. Friedman said. “This is a medical problem ... which can absolutely lead to comorbidities [such as deep dissecting hematomas] that are a huge strain on the healthcare system.”
Dermatologists can meet the moment with holistic, creative combination treatment and counseling approaches aimed at improving the mechanical strength of skin and preventing potential complications in older patients, Dr. Friedman said at the meeting.
He described the case of a 76-year-old woman who presented with dermatoporosis on her arms involving pronounced skin atrophy, solar purpura, and a small covered laceration. “This was a patient who was both devastated by the appearance” and impacted by the pain and burden of dressing frequent wounds, said Dr. Friedman, who is also the director of the Residency Program, of Translational Research, and of Supportive Oncodermatology, all within the Department of Dermatology at GWU.
With 11 months of topical treatment that included daily application of calcipotriene 0.05% ointment and nightly application of tazarotene 0.045% lotion and oral supplementation with 1000-mg vitamin C twice daily and 1000-mg citrus bioflavonoid complex daily, as well as no changes to the medications she took for various comorbidities, the solar purpura improved significantly and “we made a huge difference in the integrity of her skin,” he said.
Dr. Friedman also described this case in a recently published article in the Journal of Drugs in Dermatology titled “What’s Old Is New: An Emerging Focus on Dermatoporosis”.
Likely Pathophysiology
Advancing age and chronic ultraviolet (UV) radiation exposure are the chief drivers of dermatoporosis. In addition to UVA and UVB light, other secondary drivers include genetic susceptibility, topical and systematic corticosteroid use, and anticoagulant treatment.
Its pathogenesis is not well described in the literature but is easy to envision, Dr. Friedman said. For one, both advancing age and exposure to UV light lead to a reduction in hygroscopic glycosaminoglycans, including hyaluronate (HA), and the impact of this diminishment is believed to go “beyond [the loss of] buoyancy,” he noted. Researchers have “been showing these are not just water-loving molecules, they also have some biologic properties” relating to keratinocyte production and epidermal turnover that appear to be intricately linked to the pathogenesis of dermatoporosis.
HAs have been shown to interact with the cell surface receptor CD44 to stimulate keratinocyte proliferation, and low levels of CD44 have been reported in skin with dermatoporosis compared with a younger control population. (A newly characterized organelle, the hyaluronosome, serves as an HA factory and contains CD44 and heparin-binding epidermal growth factor, Dr. Friedman noted. Inadequate functioning may be involved in skin atrophy.)
Advancing age also brings an increase in matrix metalloproteinases (MMPs)–1, –2, and –3, which are “the demolition workers of the skin,” and downregulation of a tissue inhibitor of MMPs, he said.
Adding insult to injury, dermis-penetrating UVA also activates MMPs, “obliterating collagen and elastin.” UVB generates DNA photoproducts, including oxidative stress and damaging skin cell DNA. “That UV light induces breakdown [of the skin] through different mechanisms and inhibits buildup is a simple concept I think our patients can understand,” Dr. Friedman said.
Multifaceted Treatment
For an older adult, “there is never a wrong time to start sun-protective measures” to prevent or try to halt the progression of dermatoporosis, Dr. Friedman said, noting that “UV radiation is an immunosuppressant, so there are many good reasons to start” if the adult is not already taking measures on a regular basis.
Potential treatments for the syndrome of dermatoporosis are backed by few clinical studies, but dermatologists are skilled at translating the use of products from one disease state to another based on understandings of pathophysiology and mechanistic pathways, Dr. Friedman commented in an interview after the meeting.
For instance, “from decades of research, we know what retinoids will do to the skin,” he said in the interview. “We know they will turn on collagen-1 and -3 genes in the skin, and that they will increase the production of glycosaminoglycans ... By understanding the biology, we can translate this to dermatoporosis.” These changes were demonstrated, for instance, in a small study of topical retinol in older adults.
Studies of topical alpha hydroxy acid (AHA), moreover, have demonstrated epidermal thickening and firmness, and “some studies show they can limit steroid-induced atrophy,” Dr. Friedman said at the meeting. “And things like lactic acid and urea are super accessible.”
Topical dehydroepiandrosterone is backed by even less data than retinoids or AHAs are, “but it’s still something to consider” as part of a multimechanistic approach to dermatoporosis, Dr. Friedman shared, noting that a small study demonstrated beneficial effects on epidermal atrophy in aging skin.
The use of vitamin D analogues such as calcipotriene, which is approved for the treatment of psoriasis, may also be promising. “One concept is that [vitamin D analogues] increase calcium concentrations in the epidermis, and calcium is so central to keratinocyte differentiation” and epidermal function that calcipotriene in combination with topical steroid therapy has been shown to limit skin atrophy, he noted.
Nutritionally, low protein intake is a known problem in the older population and is associated with increased skin fragility and poorer healing. From a prevention and treatment standpoint, therefore, patients can be counseled to be attentive to their diets, Dr. Friedman said. Experts have recommended a higher protein intake for older adults than for younger adults; in 2013, an international group recommended a protein intake of 1-1.5 g/kg/d for healthy older adults and more for those with acute or chronic illness.
“Patients love talking about diet and skin disease ... and they love over-the-counter nutraceuticals as well because they want something natural,” Dr. Friedman said. “I like using bioflavonoids in combination with vitamin C, which can be effective especially for solar purpura.”

A 6-week randomized, placebo-controlled, double-blind trial involving 67 patients with purpura associated with aging found a 50% reduction in purpura lesions among those took a particular citrus bioflavonoid blend twice daily. “I thought this was a pretty well-done study,” he said, noting that patient self-assessment and investigator global assessment were utilized.
Skin Injury and Wound Prevention
In addition to recommending gentle skin cleansers and daily moisturizing, dermatologists should talk to their older patients with dermatoporosis about their home environments. “What is it like? Is there furniture with sharp edges?” Dr. Friedman advised. If so, could they use sleeves or protectors on their arms or legs “to protect against injury?”
In a later meeting session about lower-extremity wounds on geriatric patients, Michael Stempel, DPM, assistant professor of medicine and surgery and chief of podiatry at GWU, said that he was happy to hear the term dermatoporosis being used because like diabetes, it’s a risk factor for developing lower-extremity wounds and poor wound healing.
He shared the case of an older woman with dermatoporosis who “tripped and skinned her knee against a step and then self-treated it for over a month by pouring hydrogen peroxide over it and letting air get to it.” The wound developed into “full-thickness tissue loss,” said Dr. Stempel, also medical director of the Wound Healing and Limb Preservation Center at GWU Hospital.
Misperceptions are common among older patients about how a simple wound should be managed; for instance, the adage “just let it get air” is not uncommon. This makes anticipatory guidance about basic wound care — such as the importance of a moist and occlusive environment and the safe use of hydrogen peroxide — especially important for patients with dermatoporosis, Dr. Friedman commented after the meeting.
Dermatoporosis is quantifiable, Dr. Friedman said during the meeting, with a scoring system having been developed by the researchers in Switzerland who originally coined the term. Its use in practice is unnecessary, but its existence is “nice to share with patients who feel bothered because oftentimes, patients feel it’s been dismissed by other providers,” he said. “Telling your patients there’s an actual name for their problem, and that there are ways to quantify and measure changes over time, is validating.”
Its recognition as a medical condition, Dr. Friedman added, also enables the dermatologist to bring it up and counsel appropriately — without a patient feeling shame — when it is identified in the context of a skin excision, treatment of a primary inflammatory skin disease, or management of another dermatologic problem.
Dr. Friedman disclosed that he is a consultant/advisory board member for L’Oréal, La Roche-Posay, Galderma, and other companies; a speaker for Regeneron/Sanofi, Incyte, BMD, and Janssen; and has grants from Pfizer, Lilly, Incyte, and other companies. Dr. Stempel reported no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — and conveys the skin’s vulnerability to serious medical complications, said Adam Friedman, MD, at the ElderDerm conference on dermatology in the older patient.
Key features of dermatoporosis include atrophic skin, solar purpura, white pseudoscars, easily acquired skin lacerations and tears, bruises, and delayed healing. “We’re going to see more of this, and it will more and more be a chief complaint of patients,” said Dr. Friedman, professor and chair of dermatology at George Washington University (GWU) in Washington, and co-chair of the meeting. GWU hosted the conference, describing it as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.
Dermatoporosis was described in the literature in 2007 by dermatologists at the University of Geneva in Switzerland. “It is not only a cosmetic problem,” Dr. Friedman said. “This is a medical problem ... which can absolutely lead to comorbidities [such as deep dissecting hematomas] that are a huge strain on the healthcare system.”
Dermatologists can meet the moment with holistic, creative combination treatment and counseling approaches aimed at improving the mechanical strength of skin and preventing potential complications in older patients, Dr. Friedman said at the meeting.
He described the case of a 76-year-old woman who presented with dermatoporosis on her arms involving pronounced skin atrophy, solar purpura, and a small covered laceration. “This was a patient who was both devastated by the appearance” and impacted by the pain and burden of dressing frequent wounds, said Dr. Friedman, who is also the director of the Residency Program, of Translational Research, and of Supportive Oncodermatology, all within the Department of Dermatology at GWU.
With 11 months of topical treatment that included daily application of calcipotriene 0.05% ointment and nightly application of tazarotene 0.045% lotion and oral supplementation with 1000-mg vitamin C twice daily and 1000-mg citrus bioflavonoid complex daily, as well as no changes to the medications she took for various comorbidities, the solar purpura improved significantly and “we made a huge difference in the integrity of her skin,” he said.
Dr. Friedman also described this case in a recently published article in the Journal of Drugs in Dermatology titled “What’s Old Is New: An Emerging Focus on Dermatoporosis”.
Likely Pathophysiology
Advancing age and chronic ultraviolet (UV) radiation exposure are the chief drivers of dermatoporosis. In addition to UVA and UVB light, other secondary drivers include genetic susceptibility, topical and systematic corticosteroid use, and anticoagulant treatment.
Its pathogenesis is not well described in the literature but is easy to envision, Dr. Friedman said. For one, both advancing age and exposure to UV light lead to a reduction in hygroscopic glycosaminoglycans, including hyaluronate (HA), and the impact of this diminishment is believed to go “beyond [the loss of] buoyancy,” he noted. Researchers have “been showing these are not just water-loving molecules, they also have some biologic properties” relating to keratinocyte production and epidermal turnover that appear to be intricately linked to the pathogenesis of dermatoporosis.
HAs have been shown to interact with the cell surface receptor CD44 to stimulate keratinocyte proliferation, and low levels of CD44 have been reported in skin with dermatoporosis compared with a younger control population. (A newly characterized organelle, the hyaluronosome, serves as an HA factory and contains CD44 and heparin-binding epidermal growth factor, Dr. Friedman noted. Inadequate functioning may be involved in skin atrophy.)
Advancing age also brings an increase in matrix metalloproteinases (MMPs)–1, –2, and –3, which are “the demolition workers of the skin,” and downregulation of a tissue inhibitor of MMPs, he said.
Adding insult to injury, dermis-penetrating UVA also activates MMPs, “obliterating collagen and elastin.” UVB generates DNA photoproducts, including oxidative stress and damaging skin cell DNA. “That UV light induces breakdown [of the skin] through different mechanisms and inhibits buildup is a simple concept I think our patients can understand,” Dr. Friedman said.
Multifaceted Treatment
For an older adult, “there is never a wrong time to start sun-protective measures” to prevent or try to halt the progression of dermatoporosis, Dr. Friedman said, noting that “UV radiation is an immunosuppressant, so there are many good reasons to start” if the adult is not already taking measures on a regular basis.
Potential treatments for the syndrome of dermatoporosis are backed by few clinical studies, but dermatologists are skilled at translating the use of products from one disease state to another based on understandings of pathophysiology and mechanistic pathways, Dr. Friedman commented in an interview after the meeting.
For instance, “from decades of research, we know what retinoids will do to the skin,” he said in the interview. “We know they will turn on collagen-1 and -3 genes in the skin, and that they will increase the production of glycosaminoglycans ... By understanding the biology, we can translate this to dermatoporosis.” These changes were demonstrated, for instance, in a small study of topical retinol in older adults.
Studies of topical alpha hydroxy acid (AHA), moreover, have demonstrated epidermal thickening and firmness, and “some studies show they can limit steroid-induced atrophy,” Dr. Friedman said at the meeting. “And things like lactic acid and urea are super accessible.”
Topical dehydroepiandrosterone is backed by even less data than retinoids or AHAs are, “but it’s still something to consider” as part of a multimechanistic approach to dermatoporosis, Dr. Friedman shared, noting that a small study demonstrated beneficial effects on epidermal atrophy in aging skin.
The use of vitamin D analogues such as calcipotriene, which is approved for the treatment of psoriasis, may also be promising. “One concept is that [vitamin D analogues] increase calcium concentrations in the epidermis, and calcium is so central to keratinocyte differentiation” and epidermal function that calcipotriene in combination with topical steroid therapy has been shown to limit skin atrophy, he noted.
Nutritionally, low protein intake is a known problem in the older population and is associated with increased skin fragility and poorer healing. From a prevention and treatment standpoint, therefore, patients can be counseled to be attentive to their diets, Dr. Friedman said. Experts have recommended a higher protein intake for older adults than for younger adults; in 2013, an international group recommended a protein intake of 1-1.5 g/kg/d for healthy older adults and more for those with acute or chronic illness.
“Patients love talking about diet and skin disease ... and they love over-the-counter nutraceuticals as well because they want something natural,” Dr. Friedman said. “I like using bioflavonoids in combination with vitamin C, which can be effective especially for solar purpura.”
A 6-week randomized, placebo-controlled, double-blind trial involving 67 patients with purpura associated with aging found a 50% reduction in purpura lesions among those took a particular citrus bioflavonoid blend twice daily. “I thought this was a pretty well-done study,” he said, noting that patient self-assessment and investigator global assessment were utilized.
Skin Injury and Wound Prevention
In addition to recommending gentle skin cleansers and daily moisturizing, dermatologists should talk to their older patients with dermatoporosis about their home environments. “What is it like? Is there furniture with sharp edges?” Dr. Friedman advised. If so, could they use sleeves or protectors on their arms or legs “to protect against injury?”
In a later meeting session about lower-extremity wounds on geriatric patients, Michael Stempel, DPM, assistant professor of medicine and surgery and chief of podiatry at GWU, said that he was happy to hear the term dermatoporosis being used because like diabetes, it’s a risk factor for developing lower-extremity wounds and poor wound healing.
He shared the case of an older woman with dermatoporosis who “tripped and skinned her knee against a step and then self-treated it for over a month by pouring hydrogen peroxide over it and letting air get to it.” The wound developed into “full-thickness tissue loss,” said Dr. Stempel, also medical director of the Wound Healing and Limb Preservation Center at GWU Hospital.
Misperceptions are common among older patients about how a simple wound should be managed; for instance, the adage “just let it get air” is not uncommon. This makes anticipatory guidance about basic wound care — such as the importance of a moist and occlusive environment and the safe use of hydrogen peroxide — especially important for patients with dermatoporosis, Dr. Friedman commented after the meeting.
Dermatoporosis is quantifiable, Dr. Friedman said during the meeting, with a scoring system having been developed by the researchers in Switzerland who originally coined the term. Its use in practice is unnecessary, but its existence is “nice to share with patients who feel bothered because oftentimes, patients feel it’s been dismissed by other providers,” he said. “Telling your patients there’s an actual name for their problem, and that there are ways to quantify and measure changes over time, is validating.”
Its recognition as a medical condition, Dr. Friedman added, also enables the dermatologist to bring it up and counsel appropriately — without a patient feeling shame — when it is identified in the context of a skin excision, treatment of a primary inflammatory skin disease, or management of another dermatologic problem.
Dr. Friedman disclosed that he is a consultant/advisory board member for L’Oréal, La Roche-Posay, Galderma, and other companies; a speaker for Regeneron/Sanofi, Incyte, BMD, and Janssen; and has grants from Pfizer, Lilly, Incyte, and other companies. Dr. Stempel reported no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — and conveys the skin’s vulnerability to serious medical complications, said Adam Friedman, MD, at the ElderDerm conference on dermatology in the older patient.
Key features of dermatoporosis include atrophic skin, solar purpura, white pseudoscars, easily acquired skin lacerations and tears, bruises, and delayed healing. “We’re going to see more of this, and it will more and more be a chief complaint of patients,” said Dr. Friedman, professor and chair of dermatology at George Washington University (GWU) in Washington, and co-chair of the meeting. GWU hosted the conference, describing it as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.
Dermatoporosis was described in the literature in 2007 by dermatologists at the University of Geneva in Switzerland. “It is not only a cosmetic problem,” Dr. Friedman said. “This is a medical problem ... which can absolutely lead to comorbidities [such as deep dissecting hematomas] that are a huge strain on the healthcare system.”
Dermatologists can meet the moment with holistic, creative combination treatment and counseling approaches aimed at improving the mechanical strength of skin and preventing potential complications in older patients, Dr. Friedman said at the meeting.
He described the case of a 76-year-old woman who presented with dermatoporosis on her arms involving pronounced skin atrophy, solar purpura, and a small covered laceration. “This was a patient who was both devastated by the appearance” and impacted by the pain and burden of dressing frequent wounds, said Dr. Friedman, who is also the director of the Residency Program, of Translational Research, and of Supportive Oncodermatology, all within the Department of Dermatology at GWU.
With 11 months of topical treatment that included daily application of calcipotriene 0.05% ointment and nightly application of tazarotene 0.045% lotion and oral supplementation with 1000-mg vitamin C twice daily and 1000-mg citrus bioflavonoid complex daily, as well as no changes to the medications she took for various comorbidities, the solar purpura improved significantly and “we made a huge difference in the integrity of her skin,” he said.
Dr. Friedman also described this case in a recently published article in the Journal of Drugs in Dermatology titled “What’s Old Is New: An Emerging Focus on Dermatoporosis”.
Likely Pathophysiology
Advancing age and chronic ultraviolet (UV) radiation exposure are the chief drivers of dermatoporosis. In addition to UVA and UVB light, other secondary drivers include genetic susceptibility, topical and systematic corticosteroid use, and anticoagulant treatment.
Its pathogenesis is not well described in the literature but is easy to envision, Dr. Friedman said. For one, both advancing age and exposure to UV light lead to a reduction in hygroscopic glycosaminoglycans, including hyaluronate (HA), and the impact of this diminishment is believed to go “beyond [the loss of] buoyancy,” he noted. Researchers have “been showing these are not just water-loving molecules, they also have some biologic properties” relating to keratinocyte production and epidermal turnover that appear to be intricately linked to the pathogenesis of dermatoporosis.
HAs have been shown to interact with the cell surface receptor CD44 to stimulate keratinocyte proliferation, and low levels of CD44 have been reported in skin with dermatoporosis compared with a younger control population. (A newly characterized organelle, the hyaluronosome, serves as an HA factory and contains CD44 and heparin-binding epidermal growth factor, Dr. Friedman noted. Inadequate functioning may be involved in skin atrophy.)
Advancing age also brings an increase in matrix metalloproteinases (MMPs)–1, –2, and –3, which are “the demolition workers of the skin,” and downregulation of a tissue inhibitor of MMPs, he said.
Adding insult to injury, dermis-penetrating UVA also activates MMPs, “obliterating collagen and elastin.” UVB generates DNA photoproducts, including oxidative stress and damaging skin cell DNA. “That UV light induces breakdown [of the skin] through different mechanisms and inhibits buildup is a simple concept I think our patients can understand,” Dr. Friedman said.
Multifaceted Treatment
For an older adult, “there is never a wrong time to start sun-protective measures” to prevent or try to halt the progression of dermatoporosis, Dr. Friedman said, noting that “UV radiation is an immunosuppressant, so there are many good reasons to start” if the adult is not already taking measures on a regular basis.
Potential treatments for the syndrome of dermatoporosis are backed by few clinical studies, but dermatologists are skilled at translating the use of products from one disease state to another based on understandings of pathophysiology and mechanistic pathways, Dr. Friedman commented in an interview after the meeting.
For instance, “from decades of research, we know what retinoids will do to the skin,” he said in the interview. “We know they will turn on collagen-1 and -3 genes in the skin, and that they will increase the production of glycosaminoglycans ... By understanding the biology, we can translate this to dermatoporosis.” These changes were demonstrated, for instance, in a small study of topical retinol in older adults.
Studies of topical alpha hydroxy acid (AHA), moreover, have demonstrated epidermal thickening and firmness, and “some studies show they can limit steroid-induced atrophy,” Dr. Friedman said at the meeting. “And things like lactic acid and urea are super accessible.”
Topical dehydroepiandrosterone is backed by even less data than retinoids or AHAs are, “but it’s still something to consider” as part of a multimechanistic approach to dermatoporosis, Dr. Friedman shared, noting that a small study demonstrated beneficial effects on epidermal atrophy in aging skin.
The use of vitamin D analogues such as calcipotriene, which is approved for the treatment of psoriasis, may also be promising. “One concept is that [vitamin D analogues] increase calcium concentrations in the epidermis, and calcium is so central to keratinocyte differentiation” and epidermal function that calcipotriene in combination with topical steroid therapy has been shown to limit skin atrophy, he noted.
Nutritionally, low protein intake is a known problem in the older population and is associated with increased skin fragility and poorer healing. From a prevention and treatment standpoint, therefore, patients can be counseled to be attentive to their diets, Dr. Friedman said. Experts have recommended a higher protein intake for older adults than for younger adults; in 2013, an international group recommended a protein intake of 1-1.5 g/kg/d for healthy older adults and more for those with acute or chronic illness.
“Patients love talking about diet and skin disease ... and they love over-the-counter nutraceuticals as well because they want something natural,” Dr. Friedman said. “I like using bioflavonoids in combination with vitamin C, which can be effective especially for solar purpura.”
A 6-week randomized, placebo-controlled, double-blind trial involving 67 patients with purpura associated with aging found a 50% reduction in purpura lesions among those took a particular citrus bioflavonoid blend twice daily. “I thought this was a pretty well-done study,” he said, noting that patient self-assessment and investigator global assessment were utilized.
Skin Injury and Wound Prevention
In addition to recommending gentle skin cleansers and daily moisturizing, dermatologists should talk to their older patients with dermatoporosis about their home environments. “What is it like? Is there furniture with sharp edges?” Dr. Friedman advised. If so, could they use sleeves or protectors on their arms or legs “to protect against injury?”
In a later meeting session about lower-extremity wounds on geriatric patients, Michael Stempel, DPM, assistant professor of medicine and surgery and chief of podiatry at GWU, said that he was happy to hear the term dermatoporosis being used because like diabetes, it’s a risk factor for developing lower-extremity wounds and poor wound healing.
He shared the case of an older woman with dermatoporosis who “tripped and skinned her knee against a step and then self-treated it for over a month by pouring hydrogen peroxide over it and letting air get to it.” The wound developed into “full-thickness tissue loss,” said Dr. Stempel, also medical director of the Wound Healing and Limb Preservation Center at GWU Hospital.
Misperceptions are common among older patients about how a simple wound should be managed; for instance, the adage “just let it get air” is not uncommon. This makes anticipatory guidance about basic wound care — such as the importance of a moist and occlusive environment and the safe use of hydrogen peroxide — especially important for patients with dermatoporosis, Dr. Friedman commented after the meeting.
Dermatoporosis is quantifiable, Dr. Friedman said during the meeting, with a scoring system having been developed by the researchers in Switzerland who originally coined the term. Its use in practice is unnecessary, but its existence is “nice to share with patients who feel bothered because oftentimes, patients feel it’s been dismissed by other providers,” he said. “Telling your patients there’s an actual name for their problem, and that there are ways to quantify and measure changes over time, is validating.”
Its recognition as a medical condition, Dr. Friedman added, also enables the dermatologist to bring it up and counsel appropriately — without a patient feeling shame — when it is identified in the context of a skin excision, treatment of a primary inflammatory skin disease, or management of another dermatologic problem.
Dr. Friedman disclosed that he is a consultant/advisory board member for L’Oréal, La Roche-Posay, Galderma, and other companies; a speaker for Regeneron/Sanofi, Incyte, BMD, and Janssen; and has grants from Pfizer, Lilly, Incyte, and other companies. Dr. Stempel reported no disclosures.
A version of this article first appeared on Medscape.com.
FROM ELDERDERM 2024
Managing Atopic Dermatitis in Older Adults: A Common, Unique Challenge
WASHINGTON, DC — Jonathan I. Silverberg, MD, PhD, MPH, said at the ElderDerm Conference on dermatology in the older patient hosted by the George Washington University School of Medicine and Health Sciences, Washington, DC.
“I walked out of residency under the impression that if it didn’t start in the first year or two of life, it’s not AD,” said Dr. Silverberg, professor of dermatology and director of clinical research at George Washington University. “The numbers tell us a very different story.”

The prevalence of AD in the United States fluctuates between 6% and 8% through adulthood, including age categories up to 81-85 years, according to 2012 National Health Interview Survey data. And while persistence of childhood-onset AD is common, a systematic review and meta-analysis published in 2018 concluded that one in four adults with AD report adult-onset disease.
The investigators, including Dr. Silverberg, identified 25 observational studies — studies conducted across 16 countries and published during 1956-2017 — that included an analysis of age of onset beyond 10 years of age, and other inclusion criteria. Of the 25 studies, 17 reported age of onset after 16 years of age and had sufficient data for the meta-analysis. Using random-effects weighting, the investigators found a pooled proportion of adult-onset AD of 26.1% (95% CI, 16.5%-37.2%).
The research demonstrates that “the age of onset is distributed well throughout the lifespan,” Dr. Silverberg said, with the data “indicating there are many elderly-onset cases of true AD as well.” (Thirteen of the studies analyzed an age of onset from age ≥ 65, and several looked beyond age 80).
A 2021 study of a primary care database in the United Kingdom of 3.85 million children and adults found a “fascinating” bimodal distribution of incidence across the lifespan, with peaks in both infancy and older adulthood, he said. Incidence in adulthood was relatively stable from ages 18-49 years, after which, “into the 50s, 60s and beyond, you started to see a steady climb again.”
Also intriguing, Dr. Silverberg continued, are findings from a study of outpatient healthcare utilization for AD in which he and his coinvestigator analyzed data from the National Ambulatory Medical Care Survey (NAMCS). In the article, published in 2023 covering data from the 1993-2015 NAMCS, they reported that AD visits were more common among children aged 0-4 years (32.0%) and 5-9 years of age (10.6%), then decreased in adolescents aged 10-19 years (11.6%), remained fairly steady in patients aged 20-89 years (1.0%-4.7%), and increased in patients aged > 90 years (20.7%).
“The peak usage for dermatologists, primary care physicians, etc., is happening in the first few years of life, partially because that’s when the disease is more common and more severe but also partially because that’s when parents and caregivers are first learning [about] the disease and trying to understand how to gain control,” Dr. Silverberg said at the meeting, presenting data from an expanded, unpublished analysis of NAMCS data showing these same outpatient utilization patterns.
“It’s fascinating — there’s a much greater utilization in the elderly population. Why? The short answer is, we don’t know,” he said.
Risk Factors, Immune Differences
People with adult-onset AD were more likely to be women, smokers in adulthood, and have a lower childhood socioeconomic status than those whose AD started in childhood in a longitudinal study of two large birth cohorts from the United Kingdom , Dr. Silverberg pointed out.
Patients with childhood-onset AD, meanwhile, were more likely to have asthma, allergen-specific immunoglobulin E (IgE), and known genetic polymorphisms previously associated with AD. (Each cohort — the 1958 British Cohort Study and the 1970 British Cohort Study — had more than 17,000 participants who were followed from birth through middle age.)
Data is limited, but “mechanistically,” AD in much older adults appears to have a unique serum cytokine pattern, Dr. Silverberg said. He pointed to a cross-sectional study in China of 1312 children and adults with AD in which researchers analyzed clinical features, serum samples, and skin biopsy samples.
Adults aged > 60 years showed more lesions on the trunk and extensor sites of the extremities and lower levels of serum IgE and peripheral eosinophil counts than those in younger age groups. And “interestingly,” compared with healthy controls, older patients with AD had “higher levels of serum expression of a variety of cytokines, including IL [interleukin]-4 but also high TARC levels ... and a variety of cytokines related to the Th17, TH1 axes, etc.,” he said.
“So, we’re seeing a fascinating new profile that may be a little different than younger-onset cases,” he said, noting that TARC (thymus and activation-regulated chemokine) is regarded as a “decent biomarker” for AD.
In addition to higher levels of IL-4 and TARC, the study investigators reported significantly higher levels of IL-17A, IL-6, IL-22, IL-33, and thymic stromal lymphopoietin in older patients, compared with healthy controls.
Research also suggests that air pollution may play a role in the onset of AD in older age, Dr. Silverberg said, referencing a 2023 study that explored the association of air pollution and genetic risk with the onset of AD after age 50. The study analyzed 337,910 participants from the UK Biobank, with a median 12-year follow-up. Genetic risks were assessed as low, intermediate, and high, based on tertiles of polygenic risk scores. Exposure to various air pollutants was assessed using weighted quantile sum and also categorized into tertiles.
The incidence of older adult-onset AD was associated with medium and high air pollution compared with low air pollution, with hazard ratios (HRs) of 1.182 (P = .003) and 1.359 (P < .001), respectively. And “to a lesser extent,” Dr. Silverberg said, incidence was associated with medium and high genetic susceptibility, with HRs of 1.065 (P = .249) and 1.153 (P = .008).
The researchers calculated a greater population-attributable fraction of air pollution (15.5%) than genetic risk (6.4%). “This means that yes, genetics can contribute even to later-onset disease ... but environment may play an even more important role,” Dr. Silverberg said.
In the Clinic
In all patients, and especially in older adults, sleep disturbance associated with AD is a consideration for care. Data collected at the eczema clinic of Northwestern University, Chicago, Illinois, between 2014 and 2019 through previsit, self-administered questionnaires show that patients ≥ 65 years of age have more profound sleep disturbance (especially trouble staying asleep) than patients aged 18-64 years, despite having similar AD severity, said Dr. Silverberg, a coinvestigator of the study.
Older age was associated with having an increased number of nights of sleep disturbance (3-7 nights in the previous week) because of eczema (adjusted odds ratio [aOR], 2.14; 95% CI, 1.16-3.92). It was also associated with itching-attributed delays in falling asleep and nighttime awakenings in the prior 2 weeks (aOR, 1.88; 95% CI, 1.05-3.39).
“The aging population has dysregulated sleep patterns and altered circadian rhythms, so some of this is just natural predisposition,” Dr. Silverberg said. “But it’s amplified [with AD and itching], and it becomes a big clinical problem when we get into treatment because it’s our natural inclination to prescribe antihistamines for their sedative properties.”
Antihistamines can cause more profound sedation, more forgetfulness, and more anticholinergic side effects, he said, noting that “there’s some evidence that high-dose antihistamines may exacerbate dementia.”
Medication side effects and medication interactions, comorbidities, and decreased renal and hepatic clearance all can complicate treatment of AD in older adults. So can mobility, the extent of social/caregiving support, and other aspects of aging. For example, “I’m a big fan of ‘soak and smears’ ... but you have to ask, can you get out of a bathtub safely?” Dr. Silverberg said. “And you have to ask, can you reach the areas you need to [in order] to apply topicals?”
With oral Janus kinase inhibitors and other systemic medications, as with other drugs, “our older population is the most vulnerable from a safety perspective,” he said. A recently published post hoc analysis of four randomized trials of dupilumab in adults ≥ 60 years of age with moderate to severe AD demonstrated efficacy comparable with that in younger patients and “a really clean safety profile,” said Dr. Silverberg, the lead author. “We really need more of these types of post hocs to have some relative contextualization” for older adults.
Dr. Silverberg reported being a speaker for AbbVie, Eli Lilly, Leo Pharma, Pfizer, Regeneron, and Sanofi-Genzyme; a consultant and/or advisory board member for Regeneron, Sanofi-Genzyme, and other companies; and an investigator for several companies.
A version of this article first appeared on Medscape.com.
WASHINGTON, DC — Jonathan I. Silverberg, MD, PhD, MPH, said at the ElderDerm Conference on dermatology in the older patient hosted by the George Washington University School of Medicine and Health Sciences, Washington, DC.
“I walked out of residency under the impression that if it didn’t start in the first year or two of life, it’s not AD,” said Dr. Silverberg, professor of dermatology and director of clinical research at George Washington University. “The numbers tell us a very different story.”
The prevalence of AD in the United States fluctuates between 6% and 8% through adulthood, including age categories up to 81-85 years, according to 2012 National Health Interview Survey data. And while persistence of childhood-onset AD is common, a systematic review and meta-analysis published in 2018 concluded that one in four adults with AD report adult-onset disease.
The investigators, including Dr. Silverberg, identified 25 observational studies — studies conducted across 16 countries and published during 1956-2017 — that included an analysis of age of onset beyond 10 years of age, and other inclusion criteria. Of the 25 studies, 17 reported age of onset after 16 years of age and had sufficient data for the meta-analysis. Using random-effects weighting, the investigators found a pooled proportion of adult-onset AD of 26.1% (95% CI, 16.5%-37.2%).
The research demonstrates that “the age of onset is distributed well throughout the lifespan,” Dr. Silverberg said, with the data “indicating there are many elderly-onset cases of true AD as well.” (Thirteen of the studies analyzed an age of onset from age ≥ 65, and several looked beyond age 80).
A 2021 study of a primary care database in the United Kingdom of 3.85 million children and adults found a “fascinating” bimodal distribution of incidence across the lifespan, with peaks in both infancy and older adulthood, he said. Incidence in adulthood was relatively stable from ages 18-49 years, after which, “into the 50s, 60s and beyond, you started to see a steady climb again.”
Also intriguing, Dr. Silverberg continued, are findings from a study of outpatient healthcare utilization for AD in which he and his coinvestigator analyzed data from the National Ambulatory Medical Care Survey (NAMCS). In the article, published in 2023 covering data from the 1993-2015 NAMCS, they reported that AD visits were more common among children aged 0-4 years (32.0%) and 5-9 years of age (10.6%), then decreased in adolescents aged 10-19 years (11.6%), remained fairly steady in patients aged 20-89 years (1.0%-4.7%), and increased in patients aged > 90 years (20.7%).
“The peak usage for dermatologists, primary care physicians, etc., is happening in the first few years of life, partially because that’s when the disease is more common and more severe but also partially because that’s when parents and caregivers are first learning [about] the disease and trying to understand how to gain control,” Dr. Silverberg said at the meeting, presenting data from an expanded, unpublished analysis of NAMCS data showing these same outpatient utilization patterns.
“It’s fascinating — there’s a much greater utilization in the elderly population. Why? The short answer is, we don’t know,” he said.
Risk Factors, Immune Differences
People with adult-onset AD were more likely to be women, smokers in adulthood, and have a lower childhood socioeconomic status than those whose AD started in childhood in a longitudinal study of two large birth cohorts from the United Kingdom , Dr. Silverberg pointed out.
Patients with childhood-onset AD, meanwhile, were more likely to have asthma, allergen-specific immunoglobulin E (IgE), and known genetic polymorphisms previously associated with AD. (Each cohort — the 1958 British Cohort Study and the 1970 British Cohort Study — had more than 17,000 participants who were followed from birth through middle age.)
Data is limited, but “mechanistically,” AD in much older adults appears to have a unique serum cytokine pattern, Dr. Silverberg said. He pointed to a cross-sectional study in China of 1312 children and adults with AD in which researchers analyzed clinical features, serum samples, and skin biopsy samples.
Adults aged > 60 years showed more lesions on the trunk and extensor sites of the extremities and lower levels of serum IgE and peripheral eosinophil counts than those in younger age groups. And “interestingly,” compared with healthy controls, older patients with AD had “higher levels of serum expression of a variety of cytokines, including IL [interleukin]-4 but also high TARC levels ... and a variety of cytokines related to the Th17, TH1 axes, etc.,” he said.
“So, we’re seeing a fascinating new profile that may be a little different than younger-onset cases,” he said, noting that TARC (thymus and activation-regulated chemokine) is regarded as a “decent biomarker” for AD.
In addition to higher levels of IL-4 and TARC, the study investigators reported significantly higher levels of IL-17A, IL-6, IL-22, IL-33, and thymic stromal lymphopoietin in older patients, compared with healthy controls.
Research also suggests that air pollution may play a role in the onset of AD in older age, Dr. Silverberg said, referencing a 2023 study that explored the association of air pollution and genetic risk with the onset of AD after age 50. The study analyzed 337,910 participants from the UK Biobank, with a median 12-year follow-up. Genetic risks were assessed as low, intermediate, and high, based on tertiles of polygenic risk scores. Exposure to various air pollutants was assessed using weighted quantile sum and also categorized into tertiles.
The incidence of older adult-onset AD was associated with medium and high air pollution compared with low air pollution, with hazard ratios (HRs) of 1.182 (P = .003) and 1.359 (P < .001), respectively. And “to a lesser extent,” Dr. Silverberg said, incidence was associated with medium and high genetic susceptibility, with HRs of 1.065 (P = .249) and 1.153 (P = .008).
The researchers calculated a greater population-attributable fraction of air pollution (15.5%) than genetic risk (6.4%). “This means that yes, genetics can contribute even to later-onset disease ... but environment may play an even more important role,” Dr. Silverberg said.
In the Clinic
In all patients, and especially in older adults, sleep disturbance associated with AD is a consideration for care. Data collected at the eczema clinic of Northwestern University, Chicago, Illinois, between 2014 and 2019 through previsit, self-administered questionnaires show that patients ≥ 65 years of age have more profound sleep disturbance (especially trouble staying asleep) than patients aged 18-64 years, despite having similar AD severity, said Dr. Silverberg, a coinvestigator of the study.
Older age was associated with having an increased number of nights of sleep disturbance (3-7 nights in the previous week) because of eczema (adjusted odds ratio [aOR], 2.14; 95% CI, 1.16-3.92). It was also associated with itching-attributed delays in falling asleep and nighttime awakenings in the prior 2 weeks (aOR, 1.88; 95% CI, 1.05-3.39).
“The aging population has dysregulated sleep patterns and altered circadian rhythms, so some of this is just natural predisposition,” Dr. Silverberg said. “But it’s amplified [with AD and itching], and it becomes a big clinical problem when we get into treatment because it’s our natural inclination to prescribe antihistamines for their sedative properties.”
Antihistamines can cause more profound sedation, more forgetfulness, and more anticholinergic side effects, he said, noting that “there’s some evidence that high-dose antihistamines may exacerbate dementia.”
Medication side effects and medication interactions, comorbidities, and decreased renal and hepatic clearance all can complicate treatment of AD in older adults. So can mobility, the extent of social/caregiving support, and other aspects of aging. For example, “I’m a big fan of ‘soak and smears’ ... but you have to ask, can you get out of a bathtub safely?” Dr. Silverberg said. “And you have to ask, can you reach the areas you need to [in order] to apply topicals?”
With oral Janus kinase inhibitors and other systemic medications, as with other drugs, “our older population is the most vulnerable from a safety perspective,” he said. A recently published post hoc analysis of four randomized trials of dupilumab in adults ≥ 60 years of age with moderate to severe AD demonstrated efficacy comparable with that in younger patients and “a really clean safety profile,” said Dr. Silverberg, the lead author. “We really need more of these types of post hocs to have some relative contextualization” for older adults.
Dr. Silverberg reported being a speaker for AbbVie, Eli Lilly, Leo Pharma, Pfizer, Regeneron, and Sanofi-Genzyme; a consultant and/or advisory board member for Regeneron, Sanofi-Genzyme, and other companies; and an investigator for several companies.
A version of this article first appeared on Medscape.com.
WASHINGTON, DC — Jonathan I. Silverberg, MD, PhD, MPH, said at the ElderDerm Conference on dermatology in the older patient hosted by the George Washington University School of Medicine and Health Sciences, Washington, DC.
“I walked out of residency under the impression that if it didn’t start in the first year or two of life, it’s not AD,” said Dr. Silverberg, professor of dermatology and director of clinical research at George Washington University. “The numbers tell us a very different story.”
The prevalence of AD in the United States fluctuates between 6% and 8% through adulthood, including age categories up to 81-85 years, according to 2012 National Health Interview Survey data. And while persistence of childhood-onset AD is common, a systematic review and meta-analysis published in 2018 concluded that one in four adults with AD report adult-onset disease.
The investigators, including Dr. Silverberg, identified 25 observational studies — studies conducted across 16 countries and published during 1956-2017 — that included an analysis of age of onset beyond 10 years of age, and other inclusion criteria. Of the 25 studies, 17 reported age of onset after 16 years of age and had sufficient data for the meta-analysis. Using random-effects weighting, the investigators found a pooled proportion of adult-onset AD of 26.1% (95% CI, 16.5%-37.2%).
The research demonstrates that “the age of onset is distributed well throughout the lifespan,” Dr. Silverberg said, with the data “indicating there are many elderly-onset cases of true AD as well.” (Thirteen of the studies analyzed an age of onset from age ≥ 65, and several looked beyond age 80).
A 2021 study of a primary care database in the United Kingdom of 3.85 million children and adults found a “fascinating” bimodal distribution of incidence across the lifespan, with peaks in both infancy and older adulthood, he said. Incidence in adulthood was relatively stable from ages 18-49 years, after which, “into the 50s, 60s and beyond, you started to see a steady climb again.”
Also intriguing, Dr. Silverberg continued, are findings from a study of outpatient healthcare utilization for AD in which he and his coinvestigator analyzed data from the National Ambulatory Medical Care Survey (NAMCS). In the article, published in 2023 covering data from the 1993-2015 NAMCS, they reported that AD visits were more common among children aged 0-4 years (32.0%) and 5-9 years of age (10.6%), then decreased in adolescents aged 10-19 years (11.6%), remained fairly steady in patients aged 20-89 years (1.0%-4.7%), and increased in patients aged > 90 years (20.7%).
“The peak usage for dermatologists, primary care physicians, etc., is happening in the first few years of life, partially because that’s when the disease is more common and more severe but also partially because that’s when parents and caregivers are first learning [about] the disease and trying to understand how to gain control,” Dr. Silverberg said at the meeting, presenting data from an expanded, unpublished analysis of NAMCS data showing these same outpatient utilization patterns.
“It’s fascinating — there’s a much greater utilization in the elderly population. Why? The short answer is, we don’t know,” he said.
Risk Factors, Immune Differences
People with adult-onset AD were more likely to be women, smokers in adulthood, and have a lower childhood socioeconomic status than those whose AD started in childhood in a longitudinal study of two large birth cohorts from the United Kingdom , Dr. Silverberg pointed out.
Patients with childhood-onset AD, meanwhile, were more likely to have asthma, allergen-specific immunoglobulin E (IgE), and known genetic polymorphisms previously associated with AD. (Each cohort — the 1958 British Cohort Study and the 1970 British Cohort Study — had more than 17,000 participants who were followed from birth through middle age.)
Data is limited, but “mechanistically,” AD in much older adults appears to have a unique serum cytokine pattern, Dr. Silverberg said. He pointed to a cross-sectional study in China of 1312 children and adults with AD in which researchers analyzed clinical features, serum samples, and skin biopsy samples.
Adults aged > 60 years showed more lesions on the trunk and extensor sites of the extremities and lower levels of serum IgE and peripheral eosinophil counts than those in younger age groups. And “interestingly,” compared with healthy controls, older patients with AD had “higher levels of serum expression of a variety of cytokines, including IL [interleukin]-4 but also high TARC levels ... and a variety of cytokines related to the Th17, TH1 axes, etc.,” he said.
“So, we’re seeing a fascinating new profile that may be a little different than younger-onset cases,” he said, noting that TARC (thymus and activation-regulated chemokine) is regarded as a “decent biomarker” for AD.
In addition to higher levels of IL-4 and TARC, the study investigators reported significantly higher levels of IL-17A, IL-6, IL-22, IL-33, and thymic stromal lymphopoietin in older patients, compared with healthy controls.
Research also suggests that air pollution may play a role in the onset of AD in older age, Dr. Silverberg said, referencing a 2023 study that explored the association of air pollution and genetic risk with the onset of AD after age 50. The study analyzed 337,910 participants from the UK Biobank, with a median 12-year follow-up. Genetic risks were assessed as low, intermediate, and high, based on tertiles of polygenic risk scores. Exposure to various air pollutants was assessed using weighted quantile sum and also categorized into tertiles.
The incidence of older adult-onset AD was associated with medium and high air pollution compared with low air pollution, with hazard ratios (HRs) of 1.182 (P = .003) and 1.359 (P < .001), respectively. And “to a lesser extent,” Dr. Silverberg said, incidence was associated with medium and high genetic susceptibility, with HRs of 1.065 (P = .249) and 1.153 (P = .008).
The researchers calculated a greater population-attributable fraction of air pollution (15.5%) than genetic risk (6.4%). “This means that yes, genetics can contribute even to later-onset disease ... but environment may play an even more important role,” Dr. Silverberg said.
In the Clinic
In all patients, and especially in older adults, sleep disturbance associated with AD is a consideration for care. Data collected at the eczema clinic of Northwestern University, Chicago, Illinois, between 2014 and 2019 through previsit, self-administered questionnaires show that patients ≥ 65 years of age have more profound sleep disturbance (especially trouble staying asleep) than patients aged 18-64 years, despite having similar AD severity, said Dr. Silverberg, a coinvestigator of the study.
Older age was associated with having an increased number of nights of sleep disturbance (3-7 nights in the previous week) because of eczema (adjusted odds ratio [aOR], 2.14; 95% CI, 1.16-3.92). It was also associated with itching-attributed delays in falling asleep and nighttime awakenings in the prior 2 weeks (aOR, 1.88; 95% CI, 1.05-3.39).
“The aging population has dysregulated sleep patterns and altered circadian rhythms, so some of this is just natural predisposition,” Dr. Silverberg said. “But it’s amplified [with AD and itching], and it becomes a big clinical problem when we get into treatment because it’s our natural inclination to prescribe antihistamines for their sedative properties.”
Antihistamines can cause more profound sedation, more forgetfulness, and more anticholinergic side effects, he said, noting that “there’s some evidence that high-dose antihistamines may exacerbate dementia.”
Medication side effects and medication interactions, comorbidities, and decreased renal and hepatic clearance all can complicate treatment of AD in older adults. So can mobility, the extent of social/caregiving support, and other aspects of aging. For example, “I’m a big fan of ‘soak and smears’ ... but you have to ask, can you get out of a bathtub safely?” Dr. Silverberg said. “And you have to ask, can you reach the areas you need to [in order] to apply topicals?”
With oral Janus kinase inhibitors and other systemic medications, as with other drugs, “our older population is the most vulnerable from a safety perspective,” he said. A recently published post hoc analysis of four randomized trials of dupilumab in adults ≥ 60 years of age with moderate to severe AD demonstrated efficacy comparable with that in younger patients and “a really clean safety profile,” said Dr. Silverberg, the lead author. “We really need more of these types of post hocs to have some relative contextualization” for older adults.
Dr. Silverberg reported being a speaker for AbbVie, Eli Lilly, Leo Pharma, Pfizer, Regeneron, and Sanofi-Genzyme; a consultant and/or advisory board member for Regeneron, Sanofi-Genzyme, and other companies; and an investigator for several companies.
A version of this article first appeared on Medscape.com.
FROM ELDERDERM 2024
Over-the-Counter Hearing Aids as Effective as Traditional Models
Nearly 2 years ago, over-the-counter (OTC) hearing aids became available without a prescription. Audiologists and consumers have doubted their effectiveness, but OTC hearing aids can be as good as — and sometimes better — than traditional aids at half the cost.
A new study published in JAMA Otolaryngology–Head & Neck Surgery showed OTC hearing aids to be as or more effective in treating mild to moderate hearing loss.
“This means consumers with mild to moderate hearing loss can now access cost-effective devices without compromising on long-term benefits,” said De Wet Swanepoel, PhD, professor in the Department of Speech-Language Pathology and Audiology at the University of Pretoria in South Africa, and an author of the study.
Approximately 30% of people over the age of 70 who could benefit from hearing aids actually use them. In 2022, the US Food and Drug Administration (FDA) allowed the sale of nonprescription devices. But a year later, just 2% of people with hearing difficulty had purchased OTC hearing aids. Impaired hearing can increase the risk of developing dementia and decrease quality of life.
Dr. Swanepoel and his colleagues enrolled 44 individuals in the comparative effectiveness study, which was an extension of an initial randomized control trial lasting 6 weeks. Participants were tracked over an 8-month period, with about half using self-fitted OTC devices and the remaining with audiologist-fitted models. On the basis of users’ self-reported surveys, the results showed no clinically meaningful difference in effectiveness. The OTC hearing aids showed better satisfaction scores among users.
The typical pair of audiologist-fitted hearing aids costs $2000. OTC hearing aids, including the Lexi Lumen model used in the latest study and available in the United States, cost around $799.
“The cost savings combined with the effective performance of self-fit hearing aids make them a promising option for individuals with mild to moderate hearing loss,” Dr. Swanepoel said.
But many audiologists have reported they do not believe the nonprescription devices would provide the same benefit as a hearing aid provided by specialists, according to one survey in 2023.
OTC hearing aids may change the role of the primary care clinician, who may instead of referring patients to an audiologist, suggest a nonprescription version. They may also field questions from patients on which types are better, which Sharon Horesh Bergquist, MD, an internal medicine physician at Emory University in Atlanta, said she is already doing.
“Primary care physicians already evaluate patients with hearing loss to identify underlying causes and provide referrals to audiologists or ear, nose, and throat specialists; with the availability of OTC hearing aids, they can further support patients by informing them about these accessible options and help them understand when OTC aids may be appropriate,” Dr. Bergquist said.
When selecting a model, Dr. Bergquist recommends patients try them before buying. Certain models permit returns, but she advises patients to check the terms as not all models are the same.
“By removing the requirement to see an audiologist or ear, nose, and throat specialist, OTC hearing aids can increase use among individuals who might otherwise forgo them without eliminating the need for professional care,” Dr. Bergquist said.
She does refer some patients to visit an audiologist first to understand their type and cause of hearing impairment, which can help users select the best OTC model for them.
The study received funding from the hearX Pty Ltd Group and the National Institutes of Health. Various authors reported receiving personal fees from the hearX Group and Care Research Manchester Biomedical Research Centre.
A version of this article first appeared on Medscape.com.
Nearly 2 years ago, over-the-counter (OTC) hearing aids became available without a prescription. Audiologists and consumers have doubted their effectiveness, but OTC hearing aids can be as good as — and sometimes better — than traditional aids at half the cost.
A new study published in JAMA Otolaryngology–Head & Neck Surgery showed OTC hearing aids to be as or more effective in treating mild to moderate hearing loss.
“This means consumers with mild to moderate hearing loss can now access cost-effective devices without compromising on long-term benefits,” said De Wet Swanepoel, PhD, professor in the Department of Speech-Language Pathology and Audiology at the University of Pretoria in South Africa, and an author of the study.
Approximately 30% of people over the age of 70 who could benefit from hearing aids actually use them. In 2022, the US Food and Drug Administration (FDA) allowed the sale of nonprescription devices. But a year later, just 2% of people with hearing difficulty had purchased OTC hearing aids. Impaired hearing can increase the risk of developing dementia and decrease quality of life.
Dr. Swanepoel and his colleagues enrolled 44 individuals in the comparative effectiveness study, which was an extension of an initial randomized control trial lasting 6 weeks. Participants were tracked over an 8-month period, with about half using self-fitted OTC devices and the remaining with audiologist-fitted models. On the basis of users’ self-reported surveys, the results showed no clinically meaningful difference in effectiveness. The OTC hearing aids showed better satisfaction scores among users.
The typical pair of audiologist-fitted hearing aids costs $2000. OTC hearing aids, including the Lexi Lumen model used in the latest study and available in the United States, cost around $799.
“The cost savings combined with the effective performance of self-fit hearing aids make them a promising option for individuals with mild to moderate hearing loss,” Dr. Swanepoel said.
But many audiologists have reported they do not believe the nonprescription devices would provide the same benefit as a hearing aid provided by specialists, according to one survey in 2023.
OTC hearing aids may change the role of the primary care clinician, who may instead of referring patients to an audiologist, suggest a nonprescription version. They may also field questions from patients on which types are better, which Sharon Horesh Bergquist, MD, an internal medicine physician at Emory University in Atlanta, said she is already doing.
“Primary care physicians already evaluate patients with hearing loss to identify underlying causes and provide referrals to audiologists or ear, nose, and throat specialists; with the availability of OTC hearing aids, they can further support patients by informing them about these accessible options and help them understand when OTC aids may be appropriate,” Dr. Bergquist said.
When selecting a model, Dr. Bergquist recommends patients try them before buying. Certain models permit returns, but she advises patients to check the terms as not all models are the same.
“By removing the requirement to see an audiologist or ear, nose, and throat specialist, OTC hearing aids can increase use among individuals who might otherwise forgo them without eliminating the need for professional care,” Dr. Bergquist said.
She does refer some patients to visit an audiologist first to understand their type and cause of hearing impairment, which can help users select the best OTC model for them.
The study received funding from the hearX Pty Ltd Group and the National Institutes of Health. Various authors reported receiving personal fees from the hearX Group and Care Research Manchester Biomedical Research Centre.
A version of this article first appeared on Medscape.com.
Nearly 2 years ago, over-the-counter (OTC) hearing aids became available without a prescription. Audiologists and consumers have doubted their effectiveness, but OTC hearing aids can be as good as — and sometimes better — than traditional aids at half the cost.
A new study published in JAMA Otolaryngology–Head & Neck Surgery showed OTC hearing aids to be as or more effective in treating mild to moderate hearing loss.
“This means consumers with mild to moderate hearing loss can now access cost-effective devices without compromising on long-term benefits,” said De Wet Swanepoel, PhD, professor in the Department of Speech-Language Pathology and Audiology at the University of Pretoria in South Africa, and an author of the study.
Approximately 30% of people over the age of 70 who could benefit from hearing aids actually use them. In 2022, the US Food and Drug Administration (FDA) allowed the sale of nonprescription devices. But a year later, just 2% of people with hearing difficulty had purchased OTC hearing aids. Impaired hearing can increase the risk of developing dementia and decrease quality of life.
Dr. Swanepoel and his colleagues enrolled 44 individuals in the comparative effectiveness study, which was an extension of an initial randomized control trial lasting 6 weeks. Participants were tracked over an 8-month period, with about half using self-fitted OTC devices and the remaining with audiologist-fitted models. On the basis of users’ self-reported surveys, the results showed no clinically meaningful difference in effectiveness. The OTC hearing aids showed better satisfaction scores among users.
The typical pair of audiologist-fitted hearing aids costs $2000. OTC hearing aids, including the Lexi Lumen model used in the latest study and available in the United States, cost around $799.
“The cost savings combined with the effective performance of self-fit hearing aids make them a promising option for individuals with mild to moderate hearing loss,” Dr. Swanepoel said.
But many audiologists have reported they do not believe the nonprescription devices would provide the same benefit as a hearing aid provided by specialists, according to one survey in 2023.
OTC hearing aids may change the role of the primary care clinician, who may instead of referring patients to an audiologist, suggest a nonprescription version. They may also field questions from patients on which types are better, which Sharon Horesh Bergquist, MD, an internal medicine physician at Emory University in Atlanta, said she is already doing.
“Primary care physicians already evaluate patients with hearing loss to identify underlying causes and provide referrals to audiologists or ear, nose, and throat specialists; with the availability of OTC hearing aids, they can further support patients by informing them about these accessible options and help them understand when OTC aids may be appropriate,” Dr. Bergquist said.
When selecting a model, Dr. Bergquist recommends patients try them before buying. Certain models permit returns, but she advises patients to check the terms as not all models are the same.
“By removing the requirement to see an audiologist or ear, nose, and throat specialist, OTC hearing aids can increase use among individuals who might otherwise forgo them without eliminating the need for professional care,” Dr. Bergquist said.
She does refer some patients to visit an audiologist first to understand their type and cause of hearing impairment, which can help users select the best OTC model for them.
The study received funding from the hearX Pty Ltd Group and the National Institutes of Health. Various authors reported receiving personal fees from the hearX Group and Care Research Manchester Biomedical Research Centre.
A version of this article first appeared on Medscape.com.
FROM JAMA OTOLARYNGOLOGY–HEAD & NECK SURGERY
What Are the Ethics of Sex and Romance for Older Adults in Nursing Homes?
This transcript has been edited for clarity.
I had a case a couple years ago in which I found myself completely at odds with the person complaining. A daughter came to me and said [paraphrasing], look, my dad is in a nursing home, and he’s just there for care that he needs, but he’s mentally competent. He’s enjoying watching television, playing games. He plays bridge and does many things. The nursing home is letting him have a romantic relationship with a woman who’s also in the nursing home. I think you, ethicist, should both intervene and try to stop that, and write more about the immorality of facilities like nursing homes or other long-term care settings permitting romance or sexual relations to take place.
I was reminded of that case because a report recently appeared that sexually transmitted diseases are on the rise among the elderly, both in nursing homes and in other settings. This obviously is linked up to another technological advance: the erectile dysfunction drugs.
I’m sure there are many men who, at one point in their lives, could not engage in sexual activity due to impotence. We have found a treatment for erectile dysfunction. Loads and loads of men are using it, and we forget that some of them are going to be older. The rate of impotence goes up directly with aging. If you’re in a nursing home, home care, or wherever you are, you may find yourself able to engage in sex in a way that your dad or your granddad may not have been.
We also know — and I found this out when I was tracking sales of erectile dysfunction drugs — that some of these older men are going to visit prostitutes. That’s another route, unsafe sex, for sexual diseases to be spreading into various older communities.
Morally, I think every individual who is competent and wishes to engage in a romantic or sexual relationship should be able to do so. If they’re within a marriage and they want to resume sexual activity because they get better or they can use these drugs, well, that’s great. If they’re single and they’re just living with others and they form an interesting romantic relationship, why shouldn’t they be allowed to engage in sex?
It is not only something that I didn’t agree with the complaining daughter about, but also I think some of these facilities should make more rooms for privacy and more opportunity for intimacy. It’s not like we should tell granddad that he’s living in a college dorm and try to make sure that his roommate doesn’t come in if he’s going to have his girlfriend over.
Are there ethical issues? Sure. Obviously, we should remember, if we have older patients, to talk to them about sexually transmitted diseases as part of a discussion of their sex life. We shouldn’t presume that they’re not doing something. We should presume that they might be, and then remind them about safe sex, particularly if they’re going to use third parties like prostitutes.
Competency becomes important. It’s one thing to have a mutually agreed upon romantic relationship. It’s another thing if somebody is taking advantage of someone who has Alzheimer’s or severe mental dysfunction and they’re not consenting.
How do we determine that and how do we manage that? I think people who are incompetent need to be protected from sexual advances unless they have a relative or someone who says they can engage if they enjoy it and it brings them pleasure. I wouldn’t just have people who are vulnerable, exploited, or acting in a predatory way toward others.
As I said, we need to rethink the design of where older people are living, whether it’s assisted living, nursing home living, or wherever, just to give them the opportunity to have a full life, as any individual would have once they’re past the age of majority, no matter who they want to have romance with and what they want to do in terms of how far that intimacy goes.
Sadly, I didn’t agree with the daughter who came to me and asked me to stop it. I wouldn’t stop it nor would I publish against it. There are risks that we ought to be aware of, including exploiting vulnerable people if they can’t consent, and the danger of transmission of disease, as would be true in any group that might engage in high-risk behavior.
Another risk may be injury if someone is frail and can’t physically sustain sexual intimacy because they’re just too frail to do it. We also need to be sure to address the issue of sexuality with patients to make sure they know what’s going on, what risks there are, what rights they have, and so on.
At the end of the day, I’m not in the camp that says, “Just say no” when it comes to sex among the elderly.
Dr. Caplan is director, Division of Medical Ethics, New York University Langone Medical Center, New York. He has served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); he also serves as a contributing author and advisor for Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I had a case a couple years ago in which I found myself completely at odds with the person complaining. A daughter came to me and said [paraphrasing], look, my dad is in a nursing home, and he’s just there for care that he needs, but he’s mentally competent. He’s enjoying watching television, playing games. He plays bridge and does many things. The nursing home is letting him have a romantic relationship with a woman who’s also in the nursing home. I think you, ethicist, should both intervene and try to stop that, and write more about the immorality of facilities like nursing homes or other long-term care settings permitting romance or sexual relations to take place.
I was reminded of that case because a report recently appeared that sexually transmitted diseases are on the rise among the elderly, both in nursing homes and in other settings. This obviously is linked up to another technological advance: the erectile dysfunction drugs.
I’m sure there are many men who, at one point in their lives, could not engage in sexual activity due to impotence. We have found a treatment for erectile dysfunction. Loads and loads of men are using it, and we forget that some of them are going to be older. The rate of impotence goes up directly with aging. If you’re in a nursing home, home care, or wherever you are, you may find yourself able to engage in sex in a way that your dad or your granddad may not have been.
We also know — and I found this out when I was tracking sales of erectile dysfunction drugs — that some of these older men are going to visit prostitutes. That’s another route, unsafe sex, for sexual diseases to be spreading into various older communities.
Morally, I think every individual who is competent and wishes to engage in a romantic or sexual relationship should be able to do so. If they’re within a marriage and they want to resume sexual activity because they get better or they can use these drugs, well, that’s great. If they’re single and they’re just living with others and they form an interesting romantic relationship, why shouldn’t they be allowed to engage in sex?
It is not only something that I didn’t agree with the complaining daughter about, but also I think some of these facilities should make more rooms for privacy and more opportunity for intimacy. It’s not like we should tell granddad that he’s living in a college dorm and try to make sure that his roommate doesn’t come in if he’s going to have his girlfriend over.
Are there ethical issues? Sure. Obviously, we should remember, if we have older patients, to talk to them about sexually transmitted diseases as part of a discussion of their sex life. We shouldn’t presume that they’re not doing something. We should presume that they might be, and then remind them about safe sex, particularly if they’re going to use third parties like prostitutes.
Competency becomes important. It’s one thing to have a mutually agreed upon romantic relationship. It’s another thing if somebody is taking advantage of someone who has Alzheimer’s or severe mental dysfunction and they’re not consenting.
How do we determine that and how do we manage that? I think people who are incompetent need to be protected from sexual advances unless they have a relative or someone who says they can engage if they enjoy it and it brings them pleasure. I wouldn’t just have people who are vulnerable, exploited, or acting in a predatory way toward others.
As I said, we need to rethink the design of where older people are living, whether it’s assisted living, nursing home living, or wherever, just to give them the opportunity to have a full life, as any individual would have once they’re past the age of majority, no matter who they want to have romance with and what they want to do in terms of how far that intimacy goes.
Sadly, I didn’t agree with the daughter who came to me and asked me to stop it. I wouldn’t stop it nor would I publish against it. There are risks that we ought to be aware of, including exploiting vulnerable people if they can’t consent, and the danger of transmission of disease, as would be true in any group that might engage in high-risk behavior.
Another risk may be injury if someone is frail and can’t physically sustain sexual intimacy because they’re just too frail to do it. We also need to be sure to address the issue of sexuality with patients to make sure they know what’s going on, what risks there are, what rights they have, and so on.
At the end of the day, I’m not in the camp that says, “Just say no” when it comes to sex among the elderly.
Dr. Caplan is director, Division of Medical Ethics, New York University Langone Medical Center, New York. He has served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); he also serves as a contributing author and advisor for Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I had a case a couple years ago in which I found myself completely at odds with the person complaining. A daughter came to me and said [paraphrasing], look, my dad is in a nursing home, and he’s just there for care that he needs, but he’s mentally competent. He’s enjoying watching television, playing games. He plays bridge and does many things. The nursing home is letting him have a romantic relationship with a woman who’s also in the nursing home. I think you, ethicist, should both intervene and try to stop that, and write more about the immorality of facilities like nursing homes or other long-term care settings permitting romance or sexual relations to take place.
I was reminded of that case because a report recently appeared that sexually transmitted diseases are on the rise among the elderly, both in nursing homes and in other settings. This obviously is linked up to another technological advance: the erectile dysfunction drugs.
I’m sure there are many men who, at one point in their lives, could not engage in sexual activity due to impotence. We have found a treatment for erectile dysfunction. Loads and loads of men are using it, and we forget that some of them are going to be older. The rate of impotence goes up directly with aging. If you’re in a nursing home, home care, or wherever you are, you may find yourself able to engage in sex in a way that your dad or your granddad may not have been.
We also know — and I found this out when I was tracking sales of erectile dysfunction drugs — that some of these older men are going to visit prostitutes. That’s another route, unsafe sex, for sexual diseases to be spreading into various older communities.
Morally, I think every individual who is competent and wishes to engage in a romantic or sexual relationship should be able to do so. If they’re within a marriage and they want to resume sexual activity because they get better or they can use these drugs, well, that’s great. If they’re single and they’re just living with others and they form an interesting romantic relationship, why shouldn’t they be allowed to engage in sex?
It is not only something that I didn’t agree with the complaining daughter about, but also I think some of these facilities should make more rooms for privacy and more opportunity for intimacy. It’s not like we should tell granddad that he’s living in a college dorm and try to make sure that his roommate doesn’t come in if he’s going to have his girlfriend over.
Are there ethical issues? Sure. Obviously, we should remember, if we have older patients, to talk to them about sexually transmitted diseases as part of a discussion of their sex life. We shouldn’t presume that they’re not doing something. We should presume that they might be, and then remind them about safe sex, particularly if they’re going to use third parties like prostitutes.
Competency becomes important. It’s one thing to have a mutually agreed upon romantic relationship. It’s another thing if somebody is taking advantage of someone who has Alzheimer’s or severe mental dysfunction and they’re not consenting.
How do we determine that and how do we manage that? I think people who are incompetent need to be protected from sexual advances unless they have a relative or someone who says they can engage if they enjoy it and it brings them pleasure. I wouldn’t just have people who are vulnerable, exploited, or acting in a predatory way toward others.
As I said, we need to rethink the design of where older people are living, whether it’s assisted living, nursing home living, or wherever, just to give them the opportunity to have a full life, as any individual would have once they’re past the age of majority, no matter who they want to have romance with and what they want to do in terms of how far that intimacy goes.
Sadly, I didn’t agree with the daughter who came to me and asked me to stop it. I wouldn’t stop it nor would I publish against it. There are risks that we ought to be aware of, including exploiting vulnerable people if they can’t consent, and the danger of transmission of disease, as would be true in any group that might engage in high-risk behavior.
Another risk may be injury if someone is frail and can’t physically sustain sexual intimacy because they’re just too frail to do it. We also need to be sure to address the issue of sexuality with patients to make sure they know what’s going on, what risks there are, what rights they have, and so on.
At the end of the day, I’m not in the camp that says, “Just say no” when it comes to sex among the elderly.
Dr. Caplan is director, Division of Medical Ethics, New York University Langone Medical Center, New York. He has served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); he also serves as a contributing author and advisor for Medscape.
A version of this article first appeared on Medscape.com.
Guidance on How Best to Manage Opioid Risks in Older Adults
Polypharmacy and slow metabolism of drugs create a high risk among older adults for substance use disorder, raising the odds of intentional and unintentional overdoses. However, screening, assessment, and treatment for substance use disorder occurs less often in younger adults.
Rates of overdose from opioids increased the most among people aged 65 years and older from 2021 to 2022, compared with among younger age groups. Meanwhile, recent data show less than half older adults with opioid use disorder (OUD) receive care for the condition.
“Nobody is immune to developing some kind of use disorder, so don’t just assume that because someone’s 80 years old that there’s no way that they have a problem,” said Sara Meyer, PharmD, a medication safety pharmacist at Novant Health in Winston-Salem, North Carolina. “You never know who’s going to potentially have an issue.”
in an effort to reduce addiction and overdoses.
Older Adults Have Unique Needs
A major challenge of treating older adults is their high incidence of chronic pain and multiple complex chronic conditions. As a result, some of the nonopioid medications clinicians might otherwise prescribe, like nonsteroidal anti-inflammatory drugs, cannot be used, according to Caroline Goldzweig, MD, chief medical officer of the Cedars-Sinai Medical Network in Los Angeles, California.
“Before you know it, the only thing left is an opiate, so you can sometimes be between a rock and a hard place,” she said.
But for adults older than 65 years, opioids can carry problematic side effects, including sedation, cognitive impairment, falls, and fractures.
With those factors in mind, part of a yearly checkup or wellness visit should include time to discuss how a patient is managing their chronic pain, according to Timothy Anderson, MD, an assistant professor of medicine at the University of Pittsburgh, Pittsburgh, Pennsylvania, and codirector of the Prescribing Wisely Lab, a research collaboration between that institution and Beth Israel Deaconess Medical Center in Boston.
When considering a prescription for pain medication, Dr. Anderson said he evaluates the potential worst, best, and average outcomes for a patient. Nonopioid options should always be considered first-line treatment. Patients and physicians often struggle with balancing an option that meets a patient’s goals for pain relief but does not put them at a risk for adverse outcomes, he said.
Greater Risk
Older adults experience neurophysiologic effects different from younger people, said Benjamin Han, MD, a geriatrician and addiction medicine specialist at the University of California, San Diego.
Seniors also absorb, metabolize, and excrete drugs differently, sometimes affected by decreased production of gastric acid, lean body mass, and renal function. Coupled with complications of other chronic conditions or medications, diagnosing problematic opioid use or OUD can be one of the most challenging experiences in geriatrics, Dr. Han said.
As a result, OUD is often underdiagnosed in these patients, he said. Single-item screening tools like the TAPS and OWLS can be used to assess if the benefits of an opioid outweigh a patient’s risk for addiction.
Dr. Han finds medications like buprenorphine to be relatively safe and effective, along with nonpharmacologic interventions like physical therapy. He also advised clinicians to provide patients with opioid-overdose reversal agents.
“Naloxone is only used for reversing opioid withdrawal, but it is important to ensure that any patient at risk for an overdose, including being on chronic opioids, is provided naloxone and educated on preventing opioid overdoses,” he said.
Steroid injections and medications that target specific pathways, such as neuropathic pain, can be helpful in primary care for these older patients, according to Pooja Lagisetty, MD, an internal medicine physician at Michigan Medicine and a research scientist at VA Ann Arbor Health Care, Ann Arbor, Michigan.
She often recommends to her patients online programs that help them maintain strength and mobility, as well as low-impact exercises like tai chi, for pain management.
“This will ensure a much more balanced, patient-centered conversation with whatever decisions you and your patient come to,” Dr. Lagisetty said.
New Protocols for Pain Management in Older Adults
At the health system level, clinicians can use treatment agreements for patients taking opioids. At Novant, patients must attest they agree to take the medications only as prescribed and from a specified pharmacy. They promise not to seek opioids from other sources, to submit to random drug screenings, and to communicate regularly with their clinician about any health issues.
If a patient violates any part of this agreement, their clinician can stop the treatment. The system encourages clinicians to help patients find additional care for substance abuse disorder or pain management if it occurs.
Over the past 2 years, Novant also developed an AI prediction model, which generates a score for the risk a patient has in developing substance use disorder or experiencing an overdose within a year of initial opioid prescription. The model was validated by an internal team at the system but has not been independently certified.
If a patient has a high-risk score, their clinician considers additional risk mitigation strategies, such as seeing the patient more frequently or using an abuse deterrent formulation of an opioid. They also have the option of referring the patient to specialists in addiction medicine or neurology. Opioids are not necessarily withheld, according to Dr. Meyer. The tool is now used by clinicians during Medicare annual wellness visits.
And coming later this year are new protocols for pain management in patients aged 80 years and older. Clinicians will target a 50% dose reduction, compared with what a younger patient might receive to account for physiologic differences.
“We know that especially with some opioids like morphine, they’re not going to metabolize that the same way a young person with a young kidney will, so we’re trying to set the clinician up to select a lower starting dose for patients that are older,” Dr. Meyer said.
In 2017, the system implemented a program to reduce prescription of opioids to less than 350 morphine milligram equivalents (MME) per order following any kind of surgery. The health system compared numbers of prescriptions written among surgical colleagues and met with them to discuss alternative approaches. Novant said it continues to monitor the data and follow-up with surgeons who are not in alignment with the goal.
Between 2017 and 2019, patients switching to lower doses after surgeries rose by 20%.
Across the country at Cedars-Sinai Medical Network, leadership in 2016 made the move to deprescribe opioids or lower doses of the drugs to less than 90 MME per day, in accordance with Centers for Disease Control and Prevention guidelines established that year. Patients were referred to their pain program for support and for nonopioid interventions. Pharmacists worked closely with clinicians on safely tapering these medications in patients taking high doses.
The program worked, according to Dr. Goldzweig. Dr. Goldzweig could only find two patients currently taking high-dose opioids in the system’s database out of more than 7000 patients with Medicare Advantage insurance coverage.
“There will always be some patients who have no alternative than opioids, but we established some discipline with urine tox screens and pain agreements, and over time, we’ve been able to reduce the number of high-risk opioid prescriptions,” she said.
A version of this article first appeared on Medscape.com.
Polypharmacy and slow metabolism of drugs create a high risk among older adults for substance use disorder, raising the odds of intentional and unintentional overdoses. However, screening, assessment, and treatment for substance use disorder occurs less often in younger adults.
Rates of overdose from opioids increased the most among people aged 65 years and older from 2021 to 2022, compared with among younger age groups. Meanwhile, recent data show less than half older adults with opioid use disorder (OUD) receive care for the condition.
“Nobody is immune to developing some kind of use disorder, so don’t just assume that because someone’s 80 years old that there’s no way that they have a problem,” said Sara Meyer, PharmD, a medication safety pharmacist at Novant Health in Winston-Salem, North Carolina. “You never know who’s going to potentially have an issue.”
in an effort to reduce addiction and overdoses.
Older Adults Have Unique Needs
A major challenge of treating older adults is their high incidence of chronic pain and multiple complex chronic conditions. As a result, some of the nonopioid medications clinicians might otherwise prescribe, like nonsteroidal anti-inflammatory drugs, cannot be used, according to Caroline Goldzweig, MD, chief medical officer of the Cedars-Sinai Medical Network in Los Angeles, California.
“Before you know it, the only thing left is an opiate, so you can sometimes be between a rock and a hard place,” she said.
But for adults older than 65 years, opioids can carry problematic side effects, including sedation, cognitive impairment, falls, and fractures.
With those factors in mind, part of a yearly checkup or wellness visit should include time to discuss how a patient is managing their chronic pain, according to Timothy Anderson, MD, an assistant professor of medicine at the University of Pittsburgh, Pittsburgh, Pennsylvania, and codirector of the Prescribing Wisely Lab, a research collaboration between that institution and Beth Israel Deaconess Medical Center in Boston.
When considering a prescription for pain medication, Dr. Anderson said he evaluates the potential worst, best, and average outcomes for a patient. Nonopioid options should always be considered first-line treatment. Patients and physicians often struggle with balancing an option that meets a patient’s goals for pain relief but does not put them at a risk for adverse outcomes, he said.
Greater Risk
Older adults experience neurophysiologic effects different from younger people, said Benjamin Han, MD, a geriatrician and addiction medicine specialist at the University of California, San Diego.
Seniors also absorb, metabolize, and excrete drugs differently, sometimes affected by decreased production of gastric acid, lean body mass, and renal function. Coupled with complications of other chronic conditions or medications, diagnosing problematic opioid use or OUD can be one of the most challenging experiences in geriatrics, Dr. Han said.
As a result, OUD is often underdiagnosed in these patients, he said. Single-item screening tools like the TAPS and OWLS can be used to assess if the benefits of an opioid outweigh a patient’s risk for addiction.
Dr. Han finds medications like buprenorphine to be relatively safe and effective, along with nonpharmacologic interventions like physical therapy. He also advised clinicians to provide patients with opioid-overdose reversal agents.
“Naloxone is only used for reversing opioid withdrawal, but it is important to ensure that any patient at risk for an overdose, including being on chronic opioids, is provided naloxone and educated on preventing opioid overdoses,” he said.
Steroid injections and medications that target specific pathways, such as neuropathic pain, can be helpful in primary care for these older patients, according to Pooja Lagisetty, MD, an internal medicine physician at Michigan Medicine and a research scientist at VA Ann Arbor Health Care, Ann Arbor, Michigan.
She often recommends to her patients online programs that help them maintain strength and mobility, as well as low-impact exercises like tai chi, for pain management.
“This will ensure a much more balanced, patient-centered conversation with whatever decisions you and your patient come to,” Dr. Lagisetty said.
New Protocols for Pain Management in Older Adults
At the health system level, clinicians can use treatment agreements for patients taking opioids. At Novant, patients must attest they agree to take the medications only as prescribed and from a specified pharmacy. They promise not to seek opioids from other sources, to submit to random drug screenings, and to communicate regularly with their clinician about any health issues.
If a patient violates any part of this agreement, their clinician can stop the treatment. The system encourages clinicians to help patients find additional care for substance abuse disorder or pain management if it occurs.
Over the past 2 years, Novant also developed an AI prediction model, which generates a score for the risk a patient has in developing substance use disorder or experiencing an overdose within a year of initial opioid prescription. The model was validated by an internal team at the system but has not been independently certified.
If a patient has a high-risk score, their clinician considers additional risk mitigation strategies, such as seeing the patient more frequently or using an abuse deterrent formulation of an opioid. They also have the option of referring the patient to specialists in addiction medicine or neurology. Opioids are not necessarily withheld, according to Dr. Meyer. The tool is now used by clinicians during Medicare annual wellness visits.
And coming later this year are new protocols for pain management in patients aged 80 years and older. Clinicians will target a 50% dose reduction, compared with what a younger patient might receive to account for physiologic differences.
“We know that especially with some opioids like morphine, they’re not going to metabolize that the same way a young person with a young kidney will, so we’re trying to set the clinician up to select a lower starting dose for patients that are older,” Dr. Meyer said.
In 2017, the system implemented a program to reduce prescription of opioids to less than 350 morphine milligram equivalents (MME) per order following any kind of surgery. The health system compared numbers of prescriptions written among surgical colleagues and met with them to discuss alternative approaches. Novant said it continues to monitor the data and follow-up with surgeons who are not in alignment with the goal.
Between 2017 and 2019, patients switching to lower doses after surgeries rose by 20%.
Across the country at Cedars-Sinai Medical Network, leadership in 2016 made the move to deprescribe opioids or lower doses of the drugs to less than 90 MME per day, in accordance with Centers for Disease Control and Prevention guidelines established that year. Patients were referred to their pain program for support and for nonopioid interventions. Pharmacists worked closely with clinicians on safely tapering these medications in patients taking high doses.
The program worked, according to Dr. Goldzweig. Dr. Goldzweig could only find two patients currently taking high-dose opioids in the system’s database out of more than 7000 patients with Medicare Advantage insurance coverage.
“There will always be some patients who have no alternative than opioids, but we established some discipline with urine tox screens and pain agreements, and over time, we’ve been able to reduce the number of high-risk opioid prescriptions,” she said.
A version of this article first appeared on Medscape.com.
Polypharmacy and slow metabolism of drugs create a high risk among older adults for substance use disorder, raising the odds of intentional and unintentional overdoses. However, screening, assessment, and treatment for substance use disorder occurs less often in younger adults.
Rates of overdose from opioids increased the most among people aged 65 years and older from 2021 to 2022, compared with among younger age groups. Meanwhile, recent data show less than half older adults with opioid use disorder (OUD) receive care for the condition.
“Nobody is immune to developing some kind of use disorder, so don’t just assume that because someone’s 80 years old that there’s no way that they have a problem,” said Sara Meyer, PharmD, a medication safety pharmacist at Novant Health in Winston-Salem, North Carolina. “You never know who’s going to potentially have an issue.”
in an effort to reduce addiction and overdoses.
Older Adults Have Unique Needs
A major challenge of treating older adults is their high incidence of chronic pain and multiple complex chronic conditions. As a result, some of the nonopioid medications clinicians might otherwise prescribe, like nonsteroidal anti-inflammatory drugs, cannot be used, according to Caroline Goldzweig, MD, chief medical officer of the Cedars-Sinai Medical Network in Los Angeles, California.
“Before you know it, the only thing left is an opiate, so you can sometimes be between a rock and a hard place,” she said.
But for adults older than 65 years, opioids can carry problematic side effects, including sedation, cognitive impairment, falls, and fractures.
With those factors in mind, part of a yearly checkup or wellness visit should include time to discuss how a patient is managing their chronic pain, according to Timothy Anderson, MD, an assistant professor of medicine at the University of Pittsburgh, Pittsburgh, Pennsylvania, and codirector of the Prescribing Wisely Lab, a research collaboration between that institution and Beth Israel Deaconess Medical Center in Boston.
When considering a prescription for pain medication, Dr. Anderson said he evaluates the potential worst, best, and average outcomes for a patient. Nonopioid options should always be considered first-line treatment. Patients and physicians often struggle with balancing an option that meets a patient’s goals for pain relief but does not put them at a risk for adverse outcomes, he said.
Greater Risk
Older adults experience neurophysiologic effects different from younger people, said Benjamin Han, MD, a geriatrician and addiction medicine specialist at the University of California, San Diego.
Seniors also absorb, metabolize, and excrete drugs differently, sometimes affected by decreased production of gastric acid, lean body mass, and renal function. Coupled with complications of other chronic conditions or medications, diagnosing problematic opioid use or OUD can be one of the most challenging experiences in geriatrics, Dr. Han said.
As a result, OUD is often underdiagnosed in these patients, he said. Single-item screening tools like the TAPS and OWLS can be used to assess if the benefits of an opioid outweigh a patient’s risk for addiction.
Dr. Han finds medications like buprenorphine to be relatively safe and effective, along with nonpharmacologic interventions like physical therapy. He also advised clinicians to provide patients with opioid-overdose reversal agents.
“Naloxone is only used for reversing opioid withdrawal, but it is important to ensure that any patient at risk for an overdose, including being on chronic opioids, is provided naloxone and educated on preventing opioid overdoses,” he said.
Steroid injections and medications that target specific pathways, such as neuropathic pain, can be helpful in primary care for these older patients, according to Pooja Lagisetty, MD, an internal medicine physician at Michigan Medicine and a research scientist at VA Ann Arbor Health Care, Ann Arbor, Michigan.
She often recommends to her patients online programs that help them maintain strength and mobility, as well as low-impact exercises like tai chi, for pain management.
“This will ensure a much more balanced, patient-centered conversation with whatever decisions you and your patient come to,” Dr. Lagisetty said.
New Protocols for Pain Management in Older Adults
At the health system level, clinicians can use treatment agreements for patients taking opioids. At Novant, patients must attest they agree to take the medications only as prescribed and from a specified pharmacy. They promise not to seek opioids from other sources, to submit to random drug screenings, and to communicate regularly with their clinician about any health issues.
If a patient violates any part of this agreement, their clinician can stop the treatment. The system encourages clinicians to help patients find additional care for substance abuse disorder or pain management if it occurs.
Over the past 2 years, Novant also developed an AI prediction model, which generates a score for the risk a patient has in developing substance use disorder or experiencing an overdose within a year of initial opioid prescription. The model was validated by an internal team at the system but has not been independently certified.
If a patient has a high-risk score, their clinician considers additional risk mitigation strategies, such as seeing the patient more frequently or using an abuse deterrent formulation of an opioid. They also have the option of referring the patient to specialists in addiction medicine or neurology. Opioids are not necessarily withheld, according to Dr. Meyer. The tool is now used by clinicians during Medicare annual wellness visits.
And coming later this year are new protocols for pain management in patients aged 80 years and older. Clinicians will target a 50% dose reduction, compared with what a younger patient might receive to account for physiologic differences.
“We know that especially with some opioids like morphine, they’re not going to metabolize that the same way a young person with a young kidney will, so we’re trying to set the clinician up to select a lower starting dose for patients that are older,” Dr. Meyer said.
In 2017, the system implemented a program to reduce prescription of opioids to less than 350 morphine milligram equivalents (MME) per order following any kind of surgery. The health system compared numbers of prescriptions written among surgical colleagues and met with them to discuss alternative approaches. Novant said it continues to monitor the data and follow-up with surgeons who are not in alignment with the goal.
Between 2017 and 2019, patients switching to lower doses after surgeries rose by 20%.
Across the country at Cedars-Sinai Medical Network, leadership in 2016 made the move to deprescribe opioids or lower doses of the drugs to less than 90 MME per day, in accordance with Centers for Disease Control and Prevention guidelines established that year. Patients were referred to their pain program for support and for nonopioid interventions. Pharmacists worked closely with clinicians on safely tapering these medications in patients taking high doses.
The program worked, according to Dr. Goldzweig. Dr. Goldzweig could only find two patients currently taking high-dose opioids in the system’s database out of more than 7000 patients with Medicare Advantage insurance coverage.
“There will always be some patients who have no alternative than opioids, but we established some discipline with urine tox screens and pain agreements, and over time, we’ve been able to reduce the number of high-risk opioid prescriptions,” she said.
A version of this article first appeared on Medscape.com.