User login
Practicing Medicine in Canada’s Far North
In 2019, we interviewed Andrea Prince, MD, who was completing her internship in the Inuit village of Puvirnituq, a town of 2000 inhabitants located in Nunavik, in the Canadian Far North. Five years later, still in her position, what perspective does she have on her practice? Have the challenges of practicing medicine in a remote region within the Inuit community affected her vocation? Would she recommend this experience to young doctors?
Question: What position do you currently hold?
Dr. Prince: I am a full-time general practitioner at Puvirnituq Hospital. My responsibilities range from following up on hospitalized patients to those seen in outpatient clinics for chronic illnesses. Within our medical team, I receive patients in the emergency department (day and night shifts), and I travel to smaller dispensaries nearby, especially to the village of Akulivik. So, it’s quite a varied practice.
More recently, I have been involved in remote continuing medical education projects in collaboration with specialists based in Montreal. In this context, we are increasingly trying to collaborate with doctors from other indigenous communities, such as the Grand Council of the Cree, because our practices are quite similar.
Q: What is the patient volume you see?
Dr. Prince: We see approximately 20-30 patients per day in the clinic, plus about 10 by appointment, and dozens of calls from dispensaries, in addition to patients transferred from other villages. There are four daytime doctors (one at night) and about 15 nurses stationed full-time at Puvirnituq Hospital.
Our practice relies heavily on collaboration with the nursing team, which has an expanded role — they can manage certain patients according to the treatment plan established by the doctor and prescribe treatments (eg, antibiotics for uncomplicated otitis).
Q: Access to care in these isolated regions is considered difficult. Have you observed any improvement in the situation over the past 5 years? What about new material and human resources?
Dr. Prince: For the past year, we have had a Starlink internet connection at the hospital, which facilitates telemedicine exchanges with specialists; we can now send data and medical images to Montreal to obtain expertise much more easily. Previously, everything was done by phone or with significant delays. We do not yet have a cellular network, and all records are currently in paper format.
But the challenges remain numerous. Progress is very slow. Like everywhere in the country, we are experiencing a shortage of staff, particularly an insufficient number of nurses. But the impact is even more dramatic in these isolated territories. We have had to close dispensaries on the coast due to a lack of personnel and only offer emergency services. However, patients have no other options; they cannot drive to another hospital. In Nunavik, the road network is practically nonexistent, and travel to other regions is by plane (about a 2.5-hour medical evacuation trip).
So, sometimes, patients do not seek care in time, and when we finally see them, unfortunately, the issue can be quite advanced.
Q: What are the most pressing logistical needs?
Dr. Prince: We still do not have a scanner in the Far North. This has a significant impact on mortality, especially in the case of accidents and trauma, which are very common in these regions. “Residents of Nunavik are four times more likely to suffer trauma than the rest of Quebec’s population and 40 times more likely to die from it,” as recently reported in La Presse.
There has also been much discussion about cancer mortality, with a risk for death about 70% higher following a lung cancer diagnosis (reported by Medscape Medical News). We do not have a mammogram machine to diagnose breast cancer. Before the COVID-19 pandemic, equipped diagnostic teams sometimes traveled to the region, but this is no longer the case. Today, a patient needing a mammogram will have to travel to Montreal. The same goes for colonoscopies, but visits are becoming less frequent. Therefore, campaigns to screen for certain common types of cancer are practically nonexistent.
As for urgent surgeries (appendicitis, cesarean sections, trauma, etc.), patients must be transferred to Montreal by medical evacuation. We have a visiting surgeon twice a year.
Q: What improvement strategies do you foresee despite the lack of resources?
Dr. Prince: The saying “prevention is better than cure” makes perfect sense in such remote regions under extreme conditions (it is impossible to fly a medevac when it is too windy or during a snowstorm!). That’s why my colleagues and I believe that prevention should be the top priority in terms of healthcare intervention. It may seem obvious, but nothing is simple in the Far North.
Q: In which areas should prevention campaigns be prioritized in your opinion?
Dr. Prince: An example is wearing helmets. Practically no one wears this type of protection in the Far North. They use all-terrain vehicles that are dangerous and for which helmet use is crucial. But they are simply not available in stores. So, communication is difficult: We tell people, “you need a helmet for the ATV, another for the bike, for the snowmobile, for playing hockey, etc.” when it is difficult to obtain one. With traumatologists in Montreal, we had a project to create multifunctional helmets for children — to protect them but also to develop a culture of helmet use, which is not common practice in the community — but these are projects that take a lot of time and are more complex than they seem.
Villages still do not have running water. Therefore, it is difficult to give recommendations to patients as they live in sanitary conditions that are unseen elsewhere in Canada. Without clean water, we cannot ensure that wound care is done properly. Not to mention the occurrence of hepatitis A epidemics, like the one we had to face.
Residents also grapple with significant alcohol and smoking problems, but there is no detox center or dedicated psychological help on site. To follow a detox program, patients would have to leave, move away from their families, and that can be psychologically very destabilizing. I try, in my practice, to talk to my patients about this, especially pregnant women — because many continue to smoke or drink during their pregnancy — but we need more resources.
Q: What about women’s health in this region?
Dr. Prince: We are fortunate to have a team of midwives, several of whom are Inuit, who are of great help in accessing contraception, performing cervical cancer screening tests, etc. But some patients with high-risk pregnancies who should be transferred to Montreal refuse to give birth away from their families. Again, if we had the means to allow high-risk women — or those for whom continuous monitoring or a cesarean section may be necessary — to give birth here safely, it would be a big step. As for abortion, it is feasible but remains a very taboo subject in the community.
Regarding violence against women, I have not observed any particularly encouraging developments in the past 5 years, but recently, we met with the mayor about this, hoping that concrete actions will be taken to help victims of violence.
Q: What is the predominant feeling in your daily life in a situation that is slow to evolve?
Dr. Prince: I remain hopeful for my patients. We must continue to fight! Initiatives must also come from the communities themselves; they must be involved in developing solutions. Because patients, too, need to have hope. They have the right to be cared for like other inhabitants of Canada.
On my part, I try to find a balance between feeling good about my caregiving profession and not burning out professionally. But burnout is a subject that concerns many doctors around the world and is increasingly being discussed. We should all have psychological support when entering medicine!
Q: Would you recommend colleagues to come and work in the Far North? What would you tell them?
Dr. Prince: I would tell them they will have no regrets! Yes, it’s difficult, but it’s a unique type of practice and very rewarding on a human level.
Professionally, it is a general practice that is no longer seen in the city today. The spectrum is very broad, ranging from neonatology to geriatrics, from the simplest to the most complex. It’s very stimulating. Diagnostically, practice is also very different from what is done in the metropolis. Without a scanner, you really have to question and investigate to evaluate whether a patient should be evacuated by plane to Montreal or not. It’s not trivial. Decisions must be made judiciously and quickly.
The human experience is also unique. Inuit communities are little known, and the aspects relayed in the media are often negative due to their increased risk for addiction. However, they are cheerful and very warm people, with an extraordinary culture. I have learned a lot from them, including reconsidering the notion of time, reviewing my priorities, and approaching life one day at a time.
I am very grateful to them for accepting me. I am sometimes even greeted with a “Welcome home!” when I return from vacation...Being told that in Nunavik, I am also “at home,” touches me immensely. I have seen children grow up, adolescents become adults. A bond of trust has developed.
Of course, all of this comes with sacrifices like being away from family and loved ones. We miss birthdays, weddings, etc. But without hesitation, it’s worth it!
Q: What are the next steps in your career in Nunavik? Will you stay for a long time?
Dr. Prince: I take it one day at a time, especially since I am about to take maternity leave very soon. But if a full-time return to Nunavik is difficult with a newborn, I know that the Nunavummiuts [inhabitants of Nunavik] will always be part of my life and my practice.
I want to remain involved with these communities, whether on-site (by practicing there a few months a year) or in Montreal where many patients are transferred. Coming to be treated in a big city (Montreal, 1.7M inhabitants), in very large hospitals, can be very stressful for them. They express themselves much less verbally than Westerners, so we must know how to listen to them, dedicate the necessary time to them, consider their culture and beliefs. I would like to be the familiar face they will encounter when they are cared for away from home. It’s a bond I want to preserve.
This story was translated from Medscape France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In 2019, we interviewed Andrea Prince, MD, who was completing her internship in the Inuit village of Puvirnituq, a town of 2000 inhabitants located in Nunavik, in the Canadian Far North. Five years later, still in her position, what perspective does she have on her practice? Have the challenges of practicing medicine in a remote region within the Inuit community affected her vocation? Would she recommend this experience to young doctors?
Question: What position do you currently hold?
Dr. Prince: I am a full-time general practitioner at Puvirnituq Hospital. My responsibilities range from following up on hospitalized patients to those seen in outpatient clinics for chronic illnesses. Within our medical team, I receive patients in the emergency department (day and night shifts), and I travel to smaller dispensaries nearby, especially to the village of Akulivik. So, it’s quite a varied practice.
More recently, I have been involved in remote continuing medical education projects in collaboration with specialists based in Montreal. In this context, we are increasingly trying to collaborate with doctors from other indigenous communities, such as the Grand Council of the Cree, because our practices are quite similar.
Q: What is the patient volume you see?
Dr. Prince: We see approximately 20-30 patients per day in the clinic, plus about 10 by appointment, and dozens of calls from dispensaries, in addition to patients transferred from other villages. There are four daytime doctors (one at night) and about 15 nurses stationed full-time at Puvirnituq Hospital.
Our practice relies heavily on collaboration with the nursing team, which has an expanded role — they can manage certain patients according to the treatment plan established by the doctor and prescribe treatments (eg, antibiotics for uncomplicated otitis).
Q: Access to care in these isolated regions is considered difficult. Have you observed any improvement in the situation over the past 5 years? What about new material and human resources?
Dr. Prince: For the past year, we have had a Starlink internet connection at the hospital, which facilitates telemedicine exchanges with specialists; we can now send data and medical images to Montreal to obtain expertise much more easily. Previously, everything was done by phone or with significant delays. We do not yet have a cellular network, and all records are currently in paper format.
But the challenges remain numerous. Progress is very slow. Like everywhere in the country, we are experiencing a shortage of staff, particularly an insufficient number of nurses. But the impact is even more dramatic in these isolated territories. We have had to close dispensaries on the coast due to a lack of personnel and only offer emergency services. However, patients have no other options; they cannot drive to another hospital. In Nunavik, the road network is practically nonexistent, and travel to other regions is by plane (about a 2.5-hour medical evacuation trip).
So, sometimes, patients do not seek care in time, and when we finally see them, unfortunately, the issue can be quite advanced.
Q: What are the most pressing logistical needs?
Dr. Prince: We still do not have a scanner in the Far North. This has a significant impact on mortality, especially in the case of accidents and trauma, which are very common in these regions. “Residents of Nunavik are four times more likely to suffer trauma than the rest of Quebec’s population and 40 times more likely to die from it,” as recently reported in La Presse.
There has also been much discussion about cancer mortality, with a risk for death about 70% higher following a lung cancer diagnosis (reported by Medscape Medical News). We do not have a mammogram machine to diagnose breast cancer. Before the COVID-19 pandemic, equipped diagnostic teams sometimes traveled to the region, but this is no longer the case. Today, a patient needing a mammogram will have to travel to Montreal. The same goes for colonoscopies, but visits are becoming less frequent. Therefore, campaigns to screen for certain common types of cancer are practically nonexistent.
As for urgent surgeries (appendicitis, cesarean sections, trauma, etc.), patients must be transferred to Montreal by medical evacuation. We have a visiting surgeon twice a year.
Q: What improvement strategies do you foresee despite the lack of resources?
Dr. Prince: The saying “prevention is better than cure” makes perfect sense in such remote regions under extreme conditions (it is impossible to fly a medevac when it is too windy or during a snowstorm!). That’s why my colleagues and I believe that prevention should be the top priority in terms of healthcare intervention. It may seem obvious, but nothing is simple in the Far North.
Q: In which areas should prevention campaigns be prioritized in your opinion?
Dr. Prince: An example is wearing helmets. Practically no one wears this type of protection in the Far North. They use all-terrain vehicles that are dangerous and for which helmet use is crucial. But they are simply not available in stores. So, communication is difficult: We tell people, “you need a helmet for the ATV, another for the bike, for the snowmobile, for playing hockey, etc.” when it is difficult to obtain one. With traumatologists in Montreal, we had a project to create multifunctional helmets for children — to protect them but also to develop a culture of helmet use, which is not common practice in the community — but these are projects that take a lot of time and are more complex than they seem.
Villages still do not have running water. Therefore, it is difficult to give recommendations to patients as they live in sanitary conditions that are unseen elsewhere in Canada. Without clean water, we cannot ensure that wound care is done properly. Not to mention the occurrence of hepatitis A epidemics, like the one we had to face.
Residents also grapple with significant alcohol and smoking problems, but there is no detox center or dedicated psychological help on site. To follow a detox program, patients would have to leave, move away from their families, and that can be psychologically very destabilizing. I try, in my practice, to talk to my patients about this, especially pregnant women — because many continue to smoke or drink during their pregnancy — but we need more resources.
Q: What about women’s health in this region?
Dr. Prince: We are fortunate to have a team of midwives, several of whom are Inuit, who are of great help in accessing contraception, performing cervical cancer screening tests, etc. But some patients with high-risk pregnancies who should be transferred to Montreal refuse to give birth away from their families. Again, if we had the means to allow high-risk women — or those for whom continuous monitoring or a cesarean section may be necessary — to give birth here safely, it would be a big step. As for abortion, it is feasible but remains a very taboo subject in the community.
Regarding violence against women, I have not observed any particularly encouraging developments in the past 5 years, but recently, we met with the mayor about this, hoping that concrete actions will be taken to help victims of violence.
Q: What is the predominant feeling in your daily life in a situation that is slow to evolve?
Dr. Prince: I remain hopeful for my patients. We must continue to fight! Initiatives must also come from the communities themselves; they must be involved in developing solutions. Because patients, too, need to have hope. They have the right to be cared for like other inhabitants of Canada.
On my part, I try to find a balance between feeling good about my caregiving profession and not burning out professionally. But burnout is a subject that concerns many doctors around the world and is increasingly being discussed. We should all have psychological support when entering medicine!
Q: Would you recommend colleagues to come and work in the Far North? What would you tell them?
Dr. Prince: I would tell them they will have no regrets! Yes, it’s difficult, but it’s a unique type of practice and very rewarding on a human level.
Professionally, it is a general practice that is no longer seen in the city today. The spectrum is very broad, ranging from neonatology to geriatrics, from the simplest to the most complex. It’s very stimulating. Diagnostically, practice is also very different from what is done in the metropolis. Without a scanner, you really have to question and investigate to evaluate whether a patient should be evacuated by plane to Montreal or not. It’s not trivial. Decisions must be made judiciously and quickly.
The human experience is also unique. Inuit communities are little known, and the aspects relayed in the media are often negative due to their increased risk for addiction. However, they are cheerful and very warm people, with an extraordinary culture. I have learned a lot from them, including reconsidering the notion of time, reviewing my priorities, and approaching life one day at a time.
I am very grateful to them for accepting me. I am sometimes even greeted with a “Welcome home!” when I return from vacation...Being told that in Nunavik, I am also “at home,” touches me immensely. I have seen children grow up, adolescents become adults. A bond of trust has developed.
Of course, all of this comes with sacrifices like being away from family and loved ones. We miss birthdays, weddings, etc. But without hesitation, it’s worth it!
Q: What are the next steps in your career in Nunavik? Will you stay for a long time?
Dr. Prince: I take it one day at a time, especially since I am about to take maternity leave very soon. But if a full-time return to Nunavik is difficult with a newborn, I know that the Nunavummiuts [inhabitants of Nunavik] will always be part of my life and my practice.
I want to remain involved with these communities, whether on-site (by practicing there a few months a year) or in Montreal where many patients are transferred. Coming to be treated in a big city (Montreal, 1.7M inhabitants), in very large hospitals, can be very stressful for them. They express themselves much less verbally than Westerners, so we must know how to listen to them, dedicate the necessary time to them, consider their culture and beliefs. I would like to be the familiar face they will encounter when they are cared for away from home. It’s a bond I want to preserve.
This story was translated from Medscape France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In 2019, we interviewed Andrea Prince, MD, who was completing her internship in the Inuit village of Puvirnituq, a town of 2000 inhabitants located in Nunavik, in the Canadian Far North. Five years later, still in her position, what perspective does she have on her practice? Have the challenges of practicing medicine in a remote region within the Inuit community affected her vocation? Would she recommend this experience to young doctors?
Question: What position do you currently hold?
Dr. Prince: I am a full-time general practitioner at Puvirnituq Hospital. My responsibilities range from following up on hospitalized patients to those seen in outpatient clinics for chronic illnesses. Within our medical team, I receive patients in the emergency department (day and night shifts), and I travel to smaller dispensaries nearby, especially to the village of Akulivik. So, it’s quite a varied practice.
More recently, I have been involved in remote continuing medical education projects in collaboration with specialists based in Montreal. In this context, we are increasingly trying to collaborate with doctors from other indigenous communities, such as the Grand Council of the Cree, because our practices are quite similar.
Q: What is the patient volume you see?
Dr. Prince: We see approximately 20-30 patients per day in the clinic, plus about 10 by appointment, and dozens of calls from dispensaries, in addition to patients transferred from other villages. There are four daytime doctors (one at night) and about 15 nurses stationed full-time at Puvirnituq Hospital.
Our practice relies heavily on collaboration with the nursing team, which has an expanded role — they can manage certain patients according to the treatment plan established by the doctor and prescribe treatments (eg, antibiotics for uncomplicated otitis).
Q: Access to care in these isolated regions is considered difficult. Have you observed any improvement in the situation over the past 5 years? What about new material and human resources?
Dr. Prince: For the past year, we have had a Starlink internet connection at the hospital, which facilitates telemedicine exchanges with specialists; we can now send data and medical images to Montreal to obtain expertise much more easily. Previously, everything was done by phone or with significant delays. We do not yet have a cellular network, and all records are currently in paper format.
But the challenges remain numerous. Progress is very slow. Like everywhere in the country, we are experiencing a shortage of staff, particularly an insufficient number of nurses. But the impact is even more dramatic in these isolated territories. We have had to close dispensaries on the coast due to a lack of personnel and only offer emergency services. However, patients have no other options; they cannot drive to another hospital. In Nunavik, the road network is practically nonexistent, and travel to other regions is by plane (about a 2.5-hour medical evacuation trip).
So, sometimes, patients do not seek care in time, and when we finally see them, unfortunately, the issue can be quite advanced.
Q: What are the most pressing logistical needs?
Dr. Prince: We still do not have a scanner in the Far North. This has a significant impact on mortality, especially in the case of accidents and trauma, which are very common in these regions. “Residents of Nunavik are four times more likely to suffer trauma than the rest of Quebec’s population and 40 times more likely to die from it,” as recently reported in La Presse.
There has also been much discussion about cancer mortality, with a risk for death about 70% higher following a lung cancer diagnosis (reported by Medscape Medical News). We do not have a mammogram machine to diagnose breast cancer. Before the COVID-19 pandemic, equipped diagnostic teams sometimes traveled to the region, but this is no longer the case. Today, a patient needing a mammogram will have to travel to Montreal. The same goes for colonoscopies, but visits are becoming less frequent. Therefore, campaigns to screen for certain common types of cancer are practically nonexistent.
As for urgent surgeries (appendicitis, cesarean sections, trauma, etc.), patients must be transferred to Montreal by medical evacuation. We have a visiting surgeon twice a year.
Q: What improvement strategies do you foresee despite the lack of resources?
Dr. Prince: The saying “prevention is better than cure” makes perfect sense in such remote regions under extreme conditions (it is impossible to fly a medevac when it is too windy or during a snowstorm!). That’s why my colleagues and I believe that prevention should be the top priority in terms of healthcare intervention. It may seem obvious, but nothing is simple in the Far North.
Q: In which areas should prevention campaigns be prioritized in your opinion?
Dr. Prince: An example is wearing helmets. Practically no one wears this type of protection in the Far North. They use all-terrain vehicles that are dangerous and for which helmet use is crucial. But they are simply not available in stores. So, communication is difficult: We tell people, “you need a helmet for the ATV, another for the bike, for the snowmobile, for playing hockey, etc.” when it is difficult to obtain one. With traumatologists in Montreal, we had a project to create multifunctional helmets for children — to protect them but also to develop a culture of helmet use, which is not common practice in the community — but these are projects that take a lot of time and are more complex than they seem.
Villages still do not have running water. Therefore, it is difficult to give recommendations to patients as they live in sanitary conditions that are unseen elsewhere in Canada. Without clean water, we cannot ensure that wound care is done properly. Not to mention the occurrence of hepatitis A epidemics, like the one we had to face.
Residents also grapple with significant alcohol and smoking problems, but there is no detox center or dedicated psychological help on site. To follow a detox program, patients would have to leave, move away from their families, and that can be psychologically very destabilizing. I try, in my practice, to talk to my patients about this, especially pregnant women — because many continue to smoke or drink during their pregnancy — but we need more resources.
Q: What about women’s health in this region?
Dr. Prince: We are fortunate to have a team of midwives, several of whom are Inuit, who are of great help in accessing contraception, performing cervical cancer screening tests, etc. But some patients with high-risk pregnancies who should be transferred to Montreal refuse to give birth away from their families. Again, if we had the means to allow high-risk women — or those for whom continuous monitoring or a cesarean section may be necessary — to give birth here safely, it would be a big step. As for abortion, it is feasible but remains a very taboo subject in the community.
Regarding violence against women, I have not observed any particularly encouraging developments in the past 5 years, but recently, we met with the mayor about this, hoping that concrete actions will be taken to help victims of violence.
Q: What is the predominant feeling in your daily life in a situation that is slow to evolve?
Dr. Prince: I remain hopeful for my patients. We must continue to fight! Initiatives must also come from the communities themselves; they must be involved in developing solutions. Because patients, too, need to have hope. They have the right to be cared for like other inhabitants of Canada.
On my part, I try to find a balance between feeling good about my caregiving profession and not burning out professionally. But burnout is a subject that concerns many doctors around the world and is increasingly being discussed. We should all have psychological support when entering medicine!
Q: Would you recommend colleagues to come and work in the Far North? What would you tell them?
Dr. Prince: I would tell them they will have no regrets! Yes, it’s difficult, but it’s a unique type of practice and very rewarding on a human level.
Professionally, it is a general practice that is no longer seen in the city today. The spectrum is very broad, ranging from neonatology to geriatrics, from the simplest to the most complex. It’s very stimulating. Diagnostically, practice is also very different from what is done in the metropolis. Without a scanner, you really have to question and investigate to evaluate whether a patient should be evacuated by plane to Montreal or not. It’s not trivial. Decisions must be made judiciously and quickly.
The human experience is also unique. Inuit communities are little known, and the aspects relayed in the media are often negative due to their increased risk for addiction. However, they are cheerful and very warm people, with an extraordinary culture. I have learned a lot from them, including reconsidering the notion of time, reviewing my priorities, and approaching life one day at a time.
I am very grateful to them for accepting me. I am sometimes even greeted with a “Welcome home!” when I return from vacation...Being told that in Nunavik, I am also “at home,” touches me immensely. I have seen children grow up, adolescents become adults. A bond of trust has developed.
Of course, all of this comes with sacrifices like being away from family and loved ones. We miss birthdays, weddings, etc. But without hesitation, it’s worth it!
Q: What are the next steps in your career in Nunavik? Will you stay for a long time?
Dr. Prince: I take it one day at a time, especially since I am about to take maternity leave very soon. But if a full-time return to Nunavik is difficult with a newborn, I know that the Nunavummiuts [inhabitants of Nunavik] will always be part of my life and my practice.
I want to remain involved with these communities, whether on-site (by practicing there a few months a year) or in Montreal where many patients are transferred. Coming to be treated in a big city (Montreal, 1.7M inhabitants), in very large hospitals, can be very stressful for them. They express themselves much less verbally than Westerners, so we must know how to listen to them, dedicate the necessary time to them, consider their culture and beliefs. I would like to be the familiar face they will encounter when they are cared for away from home. It’s a bond I want to preserve.
This story was translated from Medscape France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Vitamin D Supplements May Be a Double-Edged Sword
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.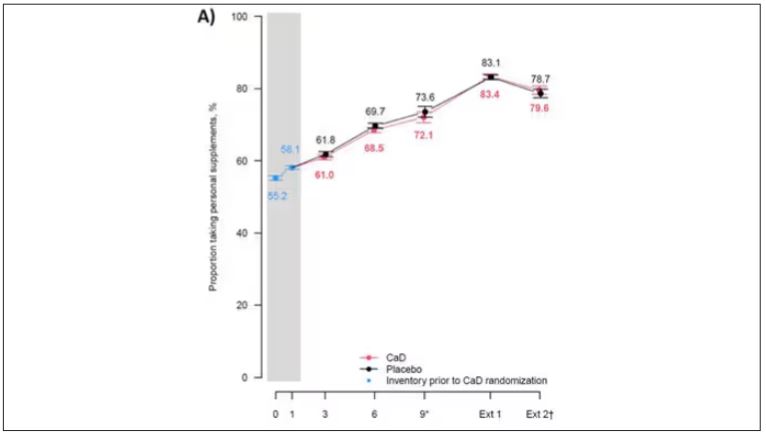
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.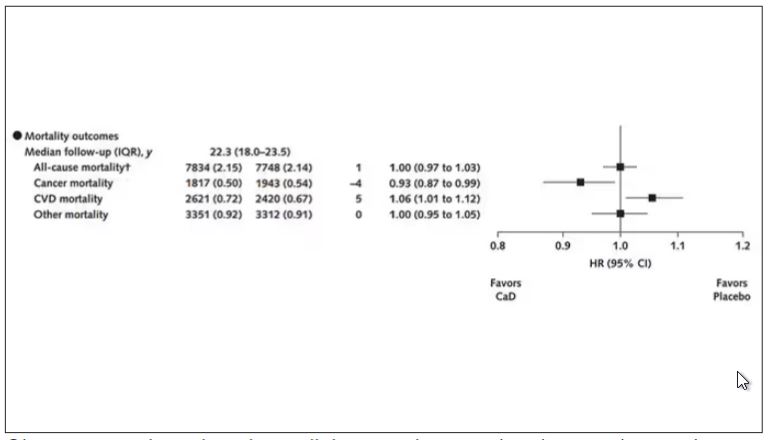
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.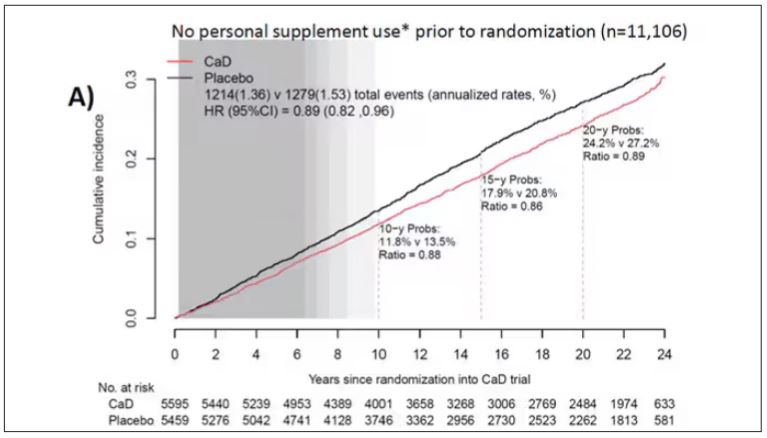
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.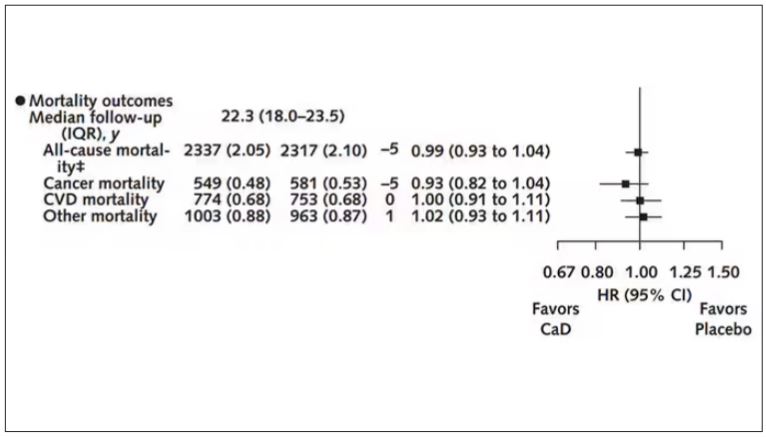
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
Long-Term Calcium and Vitamin D: Cancer Deaths Down, CVD Deaths Up in Older Women?
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.

“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.

“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”

Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.

“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.
“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.
“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”
Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.
“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.
“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.
“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”
Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.
“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
FROM ANNALS OF INTERNAL MEDICINE
Primary Care Physician’s Next Frontier: Palliative Care
Jason Black, MD, trained in family medicine, worked for Kaiser Permanente, and subsequently completed a fellowship in geriatrics. Today, he treats frail elderly patients, mostly residents of nursing homes and assisted living facilities or living in their own homes, for Gilchrist, a hospice and palliative care organization serving Baltimore and central Maryland.
“I’m practicing family medicine to the extent that I’m treating the family unit, including the anxieties of the adult children, and finding solutions for the parents,” said Dr. Black, one of Gilchrist’s 62 employed providers, one third of whom are physicians. One of his most important roles is medication reconciliation and deprescribing.
Palliative care, a medical specialty that focuses on clarifying the treatment goals of seriously ill patients, helping with end-of-life planning, and emphasizing pain and symptom management, has been growing in recent years. Already well-established in most US hospitals, it is expanding in community settings, often as an extension of hospice programs.
Now, by adding primary care physicians and practices to their service mix, palliative care groups are better meeting the needs of a neglected — and costly — population of frail elders. In doing so, they also are better able to find a niche in the rapidly evolving alphabet soup of value-based care and its varieties of shared savings for providers who post positive outcomes.
Most patients Dr. Black sees find it difficult to visit their doctors in a clinic setting, although they face a variety of medical needs and chronic conditions of aging. They may have a prognosis of several years to live and, thus, do not qualify for hospice care. To him, a palliative approach offers the satisfaction of focusing on what is most important to patients at this difficult time in their lives, rather than predetermined clinical metrics like blood pressure or blood glucose. “It takes a lot of work, but it feels important and rewarding,” he said.
A recent survey of community-dwelling older adults in Ontario, Canada, found most patients fail to receive this treatment homes in the final 3 months of life.
Continuums of Patients and Models
Gilchrist started as a nonprofit, hospital-affiliated hospice program in 1994 and in 2000 took on the management of a geriatric medicine practice for its parent, Greater Baltimore Medical Center. Today, its physicians and nurse practitioners see a range of patients in geriatric primary care, palliative medicine, and hospice, according to its chief medical officer, Mark J. Gloth, DO.
“As people progress in their disease, their location — where they call home — may change as well,” Dr. Gloth said. “We offer a continuum of care in order to not lose people through those transitions. That’s the core of our mission — making sure we are there to escort people through the difficult moments in their lives.”
Models for value-based care encompass accountable care organizations (ACOs), including the ACO REACH (Realizing Equity, Access, and Community Health) high-needs model for traditional Medicare patients, and Medicare Shared Savings Programs for fee-for-service beneficiaries. These value-based models offer a variety of opportunities for the palliative care organization to share in savings resulting from keeping the patient out of the hospital or emergency room and other quality and cost benchmarks.
Coming Together to Meet Needs
Gilchrist is one of nine hospice and palliative organizations that have joined to form their own multistate ACO, Responsive Care Solutions, focused on the clinical needs of frail elderly Medicare beneficiaries. Hospice of the Valley in Phoenix has Geriatric Solutions, a frail elder physician practice. And Capital Caring Health, a hospice and palliative care agency serving metro Washington, DC, has deployed several physicians and nurse practitioners on the road doing primary care at home, said Heidi Young, MD, its Primary Care at Home Lead Physician.
“Five years ago, we started our primary care practice under the umbrella of a 40-year-old hospice organization because we thought we needed to prepare for the changes that are coming to the hospice model,” Dr. Young said. “The thought was that we’re not just a hospice organization; we’re an advanced illness organization. We will come to your home, whatever that is, and provide your primary care.”
The greatest potential gains for a hospice organization are from assuming 100% risk for a large population of patients, keeping them out of the hospital to lower the costs of their care, then reaping those gains under a value-based profit-sharing model, Dr. Young said.
“Our program is still new and working toward getting more patients aligned into value-based models,” she said. “It’s a work in progress.”
A Foot in Each World
Agencies like Capital Caring and Gilchrist derive the largest share of their physician income from billing Medicare Part B and other insurers per visit. But that billing is not enough to break even on physician services.
With hopes for a value-based future, Gilchrist also gets grants from elder-facing charitable foundations to cover up to 40% of the costs of its home-based primary care, according to its president, Catherine Hamel. Hospice care continues to be paid on a per-diem basis by Medicare for eligible terminally ill patients, including Medicare Advantage patients, although the Centers for Medicare & Medicaid Services is reportedly considering new models for the hospice benefit.
The National Partnership for Healthcare and Hospice Innovation (NPHI) is a trade group representing more than 100 nonprofit, hospice-based organizations participating in palliative care and value-based care.
For a hospice to be successful in the evolving post–acute care/end-of-life care landscape, it can no longer rely solely on its hospice line of business, no matter how high-quality, said Ethan McChesney, policy director for the Washington, DC-based nonprofit.
NPHI members have developed their own palliative care programs, and perhaps, a quarter have primary care at home practices, Mr. McChesney said. Some of them acquired existing primary care practices in their service area with which they already had relationships; others created their own.
For hospice organizations building a continuum of services for the seriously ill, adding a primary care at home practice is a natural fit, he said. “You can provide all the services you would as a traditional primary care practice while you have the opportunity to establish long-term relationships with patients and their caregivers that lend themselves to palliative care referrals and then hospice referrals downstream [when the patient becomes eligible for hospice care].” Often, this primary medical care is a mix of in-person and telehealth.
Cameron Muir, MD, NPHI’s chief innovation officer, noted that the hamster wheel for primary care doctors has been spinning faster and faster, with reimbursement going down and costs going up.
But with home-based primary care for frail elders under value-based models, Dr. Muir said, the clinician is paid not for making more visits but for taking great care of the patient: “And I’m actually saving Medicare money and getting credit for the hospitalizations that were avoided.”
A version of this article appeared on Medscape.com.
Jason Black, MD, trained in family medicine, worked for Kaiser Permanente, and subsequently completed a fellowship in geriatrics. Today, he treats frail elderly patients, mostly residents of nursing homes and assisted living facilities or living in their own homes, for Gilchrist, a hospice and palliative care organization serving Baltimore and central Maryland.
“I’m practicing family medicine to the extent that I’m treating the family unit, including the anxieties of the adult children, and finding solutions for the parents,” said Dr. Black, one of Gilchrist’s 62 employed providers, one third of whom are physicians. One of his most important roles is medication reconciliation and deprescribing.
Palliative care, a medical specialty that focuses on clarifying the treatment goals of seriously ill patients, helping with end-of-life planning, and emphasizing pain and symptom management, has been growing in recent years. Already well-established in most US hospitals, it is expanding in community settings, often as an extension of hospice programs.
Now, by adding primary care physicians and practices to their service mix, palliative care groups are better meeting the needs of a neglected — and costly — population of frail elders. In doing so, they also are better able to find a niche in the rapidly evolving alphabet soup of value-based care and its varieties of shared savings for providers who post positive outcomes.
Most patients Dr. Black sees find it difficult to visit their doctors in a clinic setting, although they face a variety of medical needs and chronic conditions of aging. They may have a prognosis of several years to live and, thus, do not qualify for hospice care. To him, a palliative approach offers the satisfaction of focusing on what is most important to patients at this difficult time in their lives, rather than predetermined clinical metrics like blood pressure or blood glucose. “It takes a lot of work, but it feels important and rewarding,” he said.
A recent survey of community-dwelling older adults in Ontario, Canada, found most patients fail to receive this treatment homes in the final 3 months of life.
Continuums of Patients and Models
Gilchrist started as a nonprofit, hospital-affiliated hospice program in 1994 and in 2000 took on the management of a geriatric medicine practice for its parent, Greater Baltimore Medical Center. Today, its physicians and nurse practitioners see a range of patients in geriatric primary care, palliative medicine, and hospice, according to its chief medical officer, Mark J. Gloth, DO.
“As people progress in their disease, their location — where they call home — may change as well,” Dr. Gloth said. “We offer a continuum of care in order to not lose people through those transitions. That’s the core of our mission — making sure we are there to escort people through the difficult moments in their lives.”
Models for value-based care encompass accountable care organizations (ACOs), including the ACO REACH (Realizing Equity, Access, and Community Health) high-needs model for traditional Medicare patients, and Medicare Shared Savings Programs for fee-for-service beneficiaries. These value-based models offer a variety of opportunities for the palliative care organization to share in savings resulting from keeping the patient out of the hospital or emergency room and other quality and cost benchmarks.
Coming Together to Meet Needs
Gilchrist is one of nine hospice and palliative organizations that have joined to form their own multistate ACO, Responsive Care Solutions, focused on the clinical needs of frail elderly Medicare beneficiaries. Hospice of the Valley in Phoenix has Geriatric Solutions, a frail elder physician practice. And Capital Caring Health, a hospice and palliative care agency serving metro Washington, DC, has deployed several physicians and nurse practitioners on the road doing primary care at home, said Heidi Young, MD, its Primary Care at Home Lead Physician.
“Five years ago, we started our primary care practice under the umbrella of a 40-year-old hospice organization because we thought we needed to prepare for the changes that are coming to the hospice model,” Dr. Young said. “The thought was that we’re not just a hospice organization; we’re an advanced illness organization. We will come to your home, whatever that is, and provide your primary care.”
The greatest potential gains for a hospice organization are from assuming 100% risk for a large population of patients, keeping them out of the hospital to lower the costs of their care, then reaping those gains under a value-based profit-sharing model, Dr. Young said.
“Our program is still new and working toward getting more patients aligned into value-based models,” she said. “It’s a work in progress.”
A Foot in Each World
Agencies like Capital Caring and Gilchrist derive the largest share of their physician income from billing Medicare Part B and other insurers per visit. But that billing is not enough to break even on physician services.
With hopes for a value-based future, Gilchrist also gets grants from elder-facing charitable foundations to cover up to 40% of the costs of its home-based primary care, according to its president, Catherine Hamel. Hospice care continues to be paid on a per-diem basis by Medicare for eligible terminally ill patients, including Medicare Advantage patients, although the Centers for Medicare & Medicaid Services is reportedly considering new models for the hospice benefit.
The National Partnership for Healthcare and Hospice Innovation (NPHI) is a trade group representing more than 100 nonprofit, hospice-based organizations participating in palliative care and value-based care.
For a hospice to be successful in the evolving post–acute care/end-of-life care landscape, it can no longer rely solely on its hospice line of business, no matter how high-quality, said Ethan McChesney, policy director for the Washington, DC-based nonprofit.
NPHI members have developed their own palliative care programs, and perhaps, a quarter have primary care at home practices, Mr. McChesney said. Some of them acquired existing primary care practices in their service area with which they already had relationships; others created their own.
For hospice organizations building a continuum of services for the seriously ill, adding a primary care at home practice is a natural fit, he said. “You can provide all the services you would as a traditional primary care practice while you have the opportunity to establish long-term relationships with patients and their caregivers that lend themselves to palliative care referrals and then hospice referrals downstream [when the patient becomes eligible for hospice care].” Often, this primary medical care is a mix of in-person and telehealth.
Cameron Muir, MD, NPHI’s chief innovation officer, noted that the hamster wheel for primary care doctors has been spinning faster and faster, with reimbursement going down and costs going up.
But with home-based primary care for frail elders under value-based models, Dr. Muir said, the clinician is paid not for making more visits but for taking great care of the patient: “And I’m actually saving Medicare money and getting credit for the hospitalizations that were avoided.”
A version of this article appeared on Medscape.com.
Jason Black, MD, trained in family medicine, worked for Kaiser Permanente, and subsequently completed a fellowship in geriatrics. Today, he treats frail elderly patients, mostly residents of nursing homes and assisted living facilities or living in their own homes, for Gilchrist, a hospice and palliative care organization serving Baltimore and central Maryland.
“I’m practicing family medicine to the extent that I’m treating the family unit, including the anxieties of the adult children, and finding solutions for the parents,” said Dr. Black, one of Gilchrist’s 62 employed providers, one third of whom are physicians. One of his most important roles is medication reconciliation and deprescribing.
Palliative care, a medical specialty that focuses on clarifying the treatment goals of seriously ill patients, helping with end-of-life planning, and emphasizing pain and symptom management, has been growing in recent years. Already well-established in most US hospitals, it is expanding in community settings, often as an extension of hospice programs.
Now, by adding primary care physicians and practices to their service mix, palliative care groups are better meeting the needs of a neglected — and costly — population of frail elders. In doing so, they also are better able to find a niche in the rapidly evolving alphabet soup of value-based care and its varieties of shared savings for providers who post positive outcomes.
Most patients Dr. Black sees find it difficult to visit their doctors in a clinic setting, although they face a variety of medical needs and chronic conditions of aging. They may have a prognosis of several years to live and, thus, do not qualify for hospice care. To him, a palliative approach offers the satisfaction of focusing on what is most important to patients at this difficult time in their lives, rather than predetermined clinical metrics like blood pressure or blood glucose. “It takes a lot of work, but it feels important and rewarding,” he said.
A recent survey of community-dwelling older adults in Ontario, Canada, found most patients fail to receive this treatment homes in the final 3 months of life.
Continuums of Patients and Models
Gilchrist started as a nonprofit, hospital-affiliated hospice program in 1994 and in 2000 took on the management of a geriatric medicine practice for its parent, Greater Baltimore Medical Center. Today, its physicians and nurse practitioners see a range of patients in geriatric primary care, palliative medicine, and hospice, according to its chief medical officer, Mark J. Gloth, DO.
“As people progress in their disease, their location — where they call home — may change as well,” Dr. Gloth said. “We offer a continuum of care in order to not lose people through those transitions. That’s the core of our mission — making sure we are there to escort people through the difficult moments in their lives.”
Models for value-based care encompass accountable care organizations (ACOs), including the ACO REACH (Realizing Equity, Access, and Community Health) high-needs model for traditional Medicare patients, and Medicare Shared Savings Programs for fee-for-service beneficiaries. These value-based models offer a variety of opportunities for the palliative care organization to share in savings resulting from keeping the patient out of the hospital or emergency room and other quality and cost benchmarks.
Coming Together to Meet Needs
Gilchrist is one of nine hospice and palliative organizations that have joined to form their own multistate ACO, Responsive Care Solutions, focused on the clinical needs of frail elderly Medicare beneficiaries. Hospice of the Valley in Phoenix has Geriatric Solutions, a frail elder physician practice. And Capital Caring Health, a hospice and palliative care agency serving metro Washington, DC, has deployed several physicians and nurse practitioners on the road doing primary care at home, said Heidi Young, MD, its Primary Care at Home Lead Physician.
“Five years ago, we started our primary care practice under the umbrella of a 40-year-old hospice organization because we thought we needed to prepare for the changes that are coming to the hospice model,” Dr. Young said. “The thought was that we’re not just a hospice organization; we’re an advanced illness organization. We will come to your home, whatever that is, and provide your primary care.”
The greatest potential gains for a hospice organization are from assuming 100% risk for a large population of patients, keeping them out of the hospital to lower the costs of their care, then reaping those gains under a value-based profit-sharing model, Dr. Young said.
“Our program is still new and working toward getting more patients aligned into value-based models,” she said. “It’s a work in progress.”
A Foot in Each World
Agencies like Capital Caring and Gilchrist derive the largest share of their physician income from billing Medicare Part B and other insurers per visit. But that billing is not enough to break even on physician services.
With hopes for a value-based future, Gilchrist also gets grants from elder-facing charitable foundations to cover up to 40% of the costs of its home-based primary care, according to its president, Catherine Hamel. Hospice care continues to be paid on a per-diem basis by Medicare for eligible terminally ill patients, including Medicare Advantage patients, although the Centers for Medicare & Medicaid Services is reportedly considering new models for the hospice benefit.
The National Partnership for Healthcare and Hospice Innovation (NPHI) is a trade group representing more than 100 nonprofit, hospice-based organizations participating in palliative care and value-based care.
For a hospice to be successful in the evolving post–acute care/end-of-life care landscape, it can no longer rely solely on its hospice line of business, no matter how high-quality, said Ethan McChesney, policy director for the Washington, DC-based nonprofit.
NPHI members have developed their own palliative care programs, and perhaps, a quarter have primary care at home practices, Mr. McChesney said. Some of them acquired existing primary care practices in their service area with which they already had relationships; others created their own.
For hospice organizations building a continuum of services for the seriously ill, adding a primary care at home practice is a natural fit, he said. “You can provide all the services you would as a traditional primary care practice while you have the opportunity to establish long-term relationships with patients and their caregivers that lend themselves to palliative care referrals and then hospice referrals downstream [when the patient becomes eligible for hospice care].” Often, this primary medical care is a mix of in-person and telehealth.
Cameron Muir, MD, NPHI’s chief innovation officer, noted that the hamster wheel for primary care doctors has been spinning faster and faster, with reimbursement going down and costs going up.
But with home-based primary care for frail elders under value-based models, Dr. Muir said, the clinician is paid not for making more visits but for taking great care of the patient: “And I’m actually saving Medicare money and getting credit for the hospitalizations that were avoided.”
A version of this article appeared on Medscape.com.
Can Changes to Chemo Regimens Improve Drug Tolerability in Older Patients?
TOPLINE:
Treatment modifications, such as dose reductions, schedule changes, or use of less toxic regimens, can improve how well older patients with advanced cancer and aging-related conditions tolerate chemotherapy regimens.
METHODOLOGY:
- Older patients are underrepresented in clinical trials, which means the reported risks associated with standard-of-care regimens typically reflect outcomes in younger, healthier patients. This underrepresentation in clinical trials has also led to uncertainties about the safety of standard chemotherapy regimens in older patients who often have other health conditions to manage, alongside cancer.
- In this secondary analysis, researchers evaluated the association between primary treatment modifications to standard-of-care chemotherapy regimens and treatment tolerability.
- The trial included 609 patients aged ≥ 70 years who had advanced cancer alongside at least one age-related condition, such as impaired cognition, and planned to start a new palliative chemotherapy regimen in the community oncology setting. The most common cancer types were gastrointestinal cancer (37.4%) and lung cancer (28.6%).
- The primary outcome was grade 3-5 adverse events within 3 months of chemotherapy initiation.
- Secondary outcomes included patient-reported functional decline and combined adverse outcomes, which incorporated clinician-rated toxic effects, patient-reported functional decline, and 6-month overall survival.
TAKEAWAY:
- Overall, 281 patients (46.1%) received a primary treatment modification, most often a dose reduction (71.9%) or a scheduling change (11.7%).
- Patients who received primary treatment modifications had a 15% lower risk for grades 3-5 adverse effects (relative risk [RR], 0.85) and a 20% lower risk for patient-reported functional decline (RR, 0.80) than those who received standard treatment.
- Patients receiving treatment modifications had 32% lower risk for a worse combined adverse outcome (odds ratio, 0.68).
- Cancer type may matter as well. When looking at outcomes by cancer type, patients with gastrointestinal cancers who received a primary treatment modification had a lower risk for toxic effects (RR, 0.82), whereas patients with lung cancer did not (RR, 1.03; 95% CI, 0.88-1.20).
IN PRACTICE:
These findings “can help oncologists to choose the optimal drug regimen, select a safe and effective initial dose, and undertake appropriate monitoring strategies to manage the clinical care of older people with advanced cancer,” the authors said.
SOURCE:
This study, led by Mostafa R. Mohamed from University of Rochester, New York, was published February 15 in JAMA Network Open.
LIMITATIONS:
Residual confounding may be present. Extremely healthy older patients may have been excluded due to study criteria, limiting generalizability. There may be variation in toxicities due to inclusion of patients with multiple heterogeneous cancer.
DISCLOSURES:
This work was supported by the National Cancer Institute and the University of Rochester, New York. The authors disclosed financial relationships outside this work.
A version of this article first appeared on Medscape.com.
TOPLINE:
Treatment modifications, such as dose reductions, schedule changes, or use of less toxic regimens, can improve how well older patients with advanced cancer and aging-related conditions tolerate chemotherapy regimens.
METHODOLOGY:
- Older patients are underrepresented in clinical trials, which means the reported risks associated with standard-of-care regimens typically reflect outcomes in younger, healthier patients. This underrepresentation in clinical trials has also led to uncertainties about the safety of standard chemotherapy regimens in older patients who often have other health conditions to manage, alongside cancer.
- In this secondary analysis, researchers evaluated the association between primary treatment modifications to standard-of-care chemotherapy regimens and treatment tolerability.
- The trial included 609 patients aged ≥ 70 years who had advanced cancer alongside at least one age-related condition, such as impaired cognition, and planned to start a new palliative chemotherapy regimen in the community oncology setting. The most common cancer types were gastrointestinal cancer (37.4%) and lung cancer (28.6%).
- The primary outcome was grade 3-5 adverse events within 3 months of chemotherapy initiation.
- Secondary outcomes included patient-reported functional decline and combined adverse outcomes, which incorporated clinician-rated toxic effects, patient-reported functional decline, and 6-month overall survival.
TAKEAWAY:
- Overall, 281 patients (46.1%) received a primary treatment modification, most often a dose reduction (71.9%) or a scheduling change (11.7%).
- Patients who received primary treatment modifications had a 15% lower risk for grades 3-5 adverse effects (relative risk [RR], 0.85) and a 20% lower risk for patient-reported functional decline (RR, 0.80) than those who received standard treatment.
- Patients receiving treatment modifications had 32% lower risk for a worse combined adverse outcome (odds ratio, 0.68).
- Cancer type may matter as well. When looking at outcomes by cancer type, patients with gastrointestinal cancers who received a primary treatment modification had a lower risk for toxic effects (RR, 0.82), whereas patients with lung cancer did not (RR, 1.03; 95% CI, 0.88-1.20).
IN PRACTICE:
These findings “can help oncologists to choose the optimal drug regimen, select a safe and effective initial dose, and undertake appropriate monitoring strategies to manage the clinical care of older people with advanced cancer,” the authors said.
SOURCE:
This study, led by Mostafa R. Mohamed from University of Rochester, New York, was published February 15 in JAMA Network Open.
LIMITATIONS:
Residual confounding may be present. Extremely healthy older patients may have been excluded due to study criteria, limiting generalizability. There may be variation in toxicities due to inclusion of patients with multiple heterogeneous cancer.
DISCLOSURES:
This work was supported by the National Cancer Institute and the University of Rochester, New York. The authors disclosed financial relationships outside this work.
A version of this article first appeared on Medscape.com.
TOPLINE:
Treatment modifications, such as dose reductions, schedule changes, or use of less toxic regimens, can improve how well older patients with advanced cancer and aging-related conditions tolerate chemotherapy regimens.
METHODOLOGY:
- Older patients are underrepresented in clinical trials, which means the reported risks associated with standard-of-care regimens typically reflect outcomes in younger, healthier patients. This underrepresentation in clinical trials has also led to uncertainties about the safety of standard chemotherapy regimens in older patients who often have other health conditions to manage, alongside cancer.
- In this secondary analysis, researchers evaluated the association between primary treatment modifications to standard-of-care chemotherapy regimens and treatment tolerability.
- The trial included 609 patients aged ≥ 70 years who had advanced cancer alongside at least one age-related condition, such as impaired cognition, and planned to start a new palliative chemotherapy regimen in the community oncology setting. The most common cancer types were gastrointestinal cancer (37.4%) and lung cancer (28.6%).
- The primary outcome was grade 3-5 adverse events within 3 months of chemotherapy initiation.
- Secondary outcomes included patient-reported functional decline and combined adverse outcomes, which incorporated clinician-rated toxic effects, patient-reported functional decline, and 6-month overall survival.
TAKEAWAY:
- Overall, 281 patients (46.1%) received a primary treatment modification, most often a dose reduction (71.9%) or a scheduling change (11.7%).
- Patients who received primary treatment modifications had a 15% lower risk for grades 3-5 adverse effects (relative risk [RR], 0.85) and a 20% lower risk for patient-reported functional decline (RR, 0.80) than those who received standard treatment.
- Patients receiving treatment modifications had 32% lower risk for a worse combined adverse outcome (odds ratio, 0.68).
- Cancer type may matter as well. When looking at outcomes by cancer type, patients with gastrointestinal cancers who received a primary treatment modification had a lower risk for toxic effects (RR, 0.82), whereas patients with lung cancer did not (RR, 1.03; 95% CI, 0.88-1.20).
IN PRACTICE:
These findings “can help oncologists to choose the optimal drug regimen, select a safe and effective initial dose, and undertake appropriate monitoring strategies to manage the clinical care of older people with advanced cancer,” the authors said.
SOURCE:
This study, led by Mostafa R. Mohamed from University of Rochester, New York, was published February 15 in JAMA Network Open.
LIMITATIONS:
Residual confounding may be present. Extremely healthy older patients may have been excluded due to study criteria, limiting generalizability. There may be variation in toxicities due to inclusion of patients with multiple heterogeneous cancer.
DISCLOSURES:
This work was supported by the National Cancer Institute and the University of Rochester, New York. The authors disclosed financial relationships outside this work.
A version of this article first appeared on Medscape.com.
Older Age Confers a Higher Risk for Second Primary Melanoma: Study
TOPLINE:
.
METHODOLOGY:
- Knowledge about one’s risk for a second primary invasive melanoma over time remains incomplete.
- Using data from the Cancer Registry of Norway, researchers performed a cohort study of 19,196 individuals diagnosed with invasive melanomas during 2008-2020; 51% were women. The mean age at the first primary melanoma diagnosis was 62 years.
- The main outcome of interest was the incidence rate of second primary invasive melanoma after the first diagnosis.
- The researchers used accelerated failure time models to examine potential associations with patient and tumor characteristics. They also calculated the median time between first and second melanomas and the likelihood of second primary melanomas on the same or different site as the first primary melanoma.
TAKEAWAY:
- The incidence rate of a second primary melanoma in the year following a first primary melanoma was 16.8 (95% CI, 14.9-18.7) per 1000 person-years. This decreased to 7.3 (95% CI, 6.0-8.6) per 1000 person-years during the second year and remained stable after that.
- Patient age influenced the median time between first and second primaries. The median interval was 37 months (95% CI, 8-49) in patients aged < 40 years, 18 months (95% CI, 13-24) in patients aged 50-59 years, and 11 months (95% CI, 7-18) in patients aged ≥ 80 years.
- The body site of the second primary melanoma was the same as the first primary in 47% of patients but was located on a different body site in the remaining 53% of patients.
- Among patients who developed a second primary melanoma on the same site as the first, the median interval was shorter for men compared with women: A median of 12 (95% CI, 7-19) months vs 22 (95% CI, 11-35) months, respectively.
IN PRACTICE:
“Our findings suggest that increased surveillance may be considered for older patients, especially men, for at least the first 3 years after their initial diagnosis, regardless of the characteristics of their first melanoma,” the authors wrote.
SOURCE:
Corresponding author Reza Ghiasvand, PhD, of the Oslo Centre for Biostatistics and Epidemiology, Oslo University Hospital, Oslo, Norway, and colleagues conducted the research, published online on February 28, 2024, in JAMA Dermatology.
LIMITATIONS:
Information was lacking on phenotypic characteristics, personal ultraviolet radiation (UVR) exposure, genetic factors, and the number of follow-up skin examinations.
DISCLOSURES:
The study was supported by the South-Eastern Norway Regional Health Authority. The authors reported having no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Knowledge about one’s risk for a second primary invasive melanoma over time remains incomplete.
- Using data from the Cancer Registry of Norway, researchers performed a cohort study of 19,196 individuals diagnosed with invasive melanomas during 2008-2020; 51% were women. The mean age at the first primary melanoma diagnosis was 62 years.
- The main outcome of interest was the incidence rate of second primary invasive melanoma after the first diagnosis.
- The researchers used accelerated failure time models to examine potential associations with patient and tumor characteristics. They also calculated the median time between first and second melanomas and the likelihood of second primary melanomas on the same or different site as the first primary melanoma.
TAKEAWAY:
- The incidence rate of a second primary melanoma in the year following a first primary melanoma was 16.8 (95% CI, 14.9-18.7) per 1000 person-years. This decreased to 7.3 (95% CI, 6.0-8.6) per 1000 person-years during the second year and remained stable after that.
- Patient age influenced the median time between first and second primaries. The median interval was 37 months (95% CI, 8-49) in patients aged < 40 years, 18 months (95% CI, 13-24) in patients aged 50-59 years, and 11 months (95% CI, 7-18) in patients aged ≥ 80 years.
- The body site of the second primary melanoma was the same as the first primary in 47% of patients but was located on a different body site in the remaining 53% of patients.
- Among patients who developed a second primary melanoma on the same site as the first, the median interval was shorter for men compared with women: A median of 12 (95% CI, 7-19) months vs 22 (95% CI, 11-35) months, respectively.
IN PRACTICE:
“Our findings suggest that increased surveillance may be considered for older patients, especially men, for at least the first 3 years after their initial diagnosis, regardless of the characteristics of their first melanoma,” the authors wrote.
SOURCE:
Corresponding author Reza Ghiasvand, PhD, of the Oslo Centre for Biostatistics and Epidemiology, Oslo University Hospital, Oslo, Norway, and colleagues conducted the research, published online on February 28, 2024, in JAMA Dermatology.
LIMITATIONS:
Information was lacking on phenotypic characteristics, personal ultraviolet radiation (UVR) exposure, genetic factors, and the number of follow-up skin examinations.
DISCLOSURES:
The study was supported by the South-Eastern Norway Regional Health Authority. The authors reported having no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Knowledge about one’s risk for a second primary invasive melanoma over time remains incomplete.
- Using data from the Cancer Registry of Norway, researchers performed a cohort study of 19,196 individuals diagnosed with invasive melanomas during 2008-2020; 51% were women. The mean age at the first primary melanoma diagnosis was 62 years.
- The main outcome of interest was the incidence rate of second primary invasive melanoma after the first diagnosis.
- The researchers used accelerated failure time models to examine potential associations with patient and tumor characteristics. They also calculated the median time between first and second melanomas and the likelihood of second primary melanomas on the same or different site as the first primary melanoma.
TAKEAWAY:
- The incidence rate of a second primary melanoma in the year following a first primary melanoma was 16.8 (95% CI, 14.9-18.7) per 1000 person-years. This decreased to 7.3 (95% CI, 6.0-8.6) per 1000 person-years during the second year and remained stable after that.
- Patient age influenced the median time between first and second primaries. The median interval was 37 months (95% CI, 8-49) in patients aged < 40 years, 18 months (95% CI, 13-24) in patients aged 50-59 years, and 11 months (95% CI, 7-18) in patients aged ≥ 80 years.
- The body site of the second primary melanoma was the same as the first primary in 47% of patients but was located on a different body site in the remaining 53% of patients.
- Among patients who developed a second primary melanoma on the same site as the first, the median interval was shorter for men compared with women: A median of 12 (95% CI, 7-19) months vs 22 (95% CI, 11-35) months, respectively.
IN PRACTICE:
“Our findings suggest that increased surveillance may be considered for older patients, especially men, for at least the first 3 years after their initial diagnosis, regardless of the characteristics of their first melanoma,” the authors wrote.
SOURCE:
Corresponding author Reza Ghiasvand, PhD, of the Oslo Centre for Biostatistics and Epidemiology, Oslo University Hospital, Oslo, Norway, and colleagues conducted the research, published online on February 28, 2024, in JAMA Dermatology.
LIMITATIONS:
Information was lacking on phenotypic characteristics, personal ultraviolet radiation (UVR) exposure, genetic factors, and the number of follow-up skin examinations.
DISCLOSURES:
The study was supported by the South-Eastern Norway Regional Health Authority. The authors reported having no disclosures.
A version of this article appeared on Medscape.com.
Many Older Adults Don’t Receive Palliative Care Before Death
A prognostic tool may facilitate the early identification of older adults in the community who would benefit from palliative care in their final years, new research from Canada suggested.
The analysis of data from close to a quarter million community-dwelling older adults in Ontario with at least one interRAI (Resident Assessment Instrument) home care assessment showed that only half of those with an estimated survival of fewer than 3 months received at least one palliative home care visit before death.
“One of the challenges and a barrier to accessing palliative home care is the difficulty of predicting survival,” Amy Hsu, PhD, an investigator at the Bruyère Research Institute in Ottawa, Ontario, Canada, told this news organization. “Clinicians are good at prognosticating when a patient might be entering their last 3-6 weeks of life, but they have a harder time predicting if someone will survive 6 months or longer.”
The team developed the Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool (RESPECT) to see whether access to predicted survival data could inform conversations about a patient’s status and palliative care needs.
The study was published online in the Canadian Medical Association Journal.
Setting Care Goals
Researchers analyzed population health administrative data from Ontario involving home care clients who received at least one interRAI Home Care assessment between April 2018 and September 2019. The cohort included 247,377 adults (62% women) with a mean age of 80.1 years at the time of assessment. Comorbidities, including congestive heart failure, coronary artery disease, cancer, and chronic obstructive pulmonary disease, as well as symptoms of health instability, were more prevalent among those at higher risk of dying.
The team used an updated, validated version of RESPECT to predict survival.
Only 2.6% of home care clients had received a clinician diagnosis of an end-stage disease, which was more prevalent among those at highest mortality risk (77.9%). Most clients (74.5%) required extensive assistance in performing instrumental activities of daily living (ADLs, score ≤ 4), and half (50.3%) were less able to perform ADLs in the last 3 months of life.
Within the cohort, 75% of patients with a predicted median survival of fewer than 3 months, 55.4% of those with a predicted median survival between 3 and 6 months, and 40.7% of those with a predicted median survival between 6 and 12 months died within 6 months of the home care assessment.
Among decedents, 50.6% of those with a RESPECT-estimated median survival of fewer than 3 months received at least one nonphysician palliative home care visit before death. Less than a third (27.8%) received at least one palliative home care visit from a physician.
The proportion of those who received at least one nonphysician visit fell to 38.7% among those with a median survival of between 3 and 6 months and to 29.5% among those with a median survival of between 6 and 12 months.
Patients who received at least one palliative home care visit (from either physicians or nonphysician home care providers) within 6 months of an assessment had clinical characteristics similar to those who did not receive a visit. However, those who did not receive palliative home care were more likely to not have been identified by a clinician as being in their past 6 months of life.
“These results reinforce the role of clinicians in identifying older adults who may be in their last 6 months of life as an important component for the receipt of palliative home care and highlight the value of RESPECT in supplementing clinicians’ assessments of prognosis,” the authors wrote.
“Our goal is to use data and tools like RESPECT to help individuals living with a life-limiting illness have conversations about what their end-of-life care goals and wishes may be and discuss whether a referral to palliative care is appropriate or needed,” Dr. Hsu added. “Data about life expectancy could be helpful for framing these conversations.”
The researchers are working with partners in home, community care, and long-term care to implement RESPECT in their settings.
‘Valuable Tool’
Guohua Li, MD, DrPH, professor of epidemiology and anesthesiology at Columbia University Mailman School of Public Health and Vagelos College of Physicians and Surgeons in New York City, commented on the findings for this news organization. He noted that the study is “rigorously designed and meticulously analyzed. The findings are of high validity and population health significance.”
The findings are comparable with what is seen in the United States and Canada, he said, where about 50% of terminally ill patients die at home or in hospice. However, palliative care outside of North America “varies greatly, and in many developing countries, [it] is still in its infancy.”
As a mortality risk prediction algorithm, “RESPECT seems to perform reasonably well,” he said. “If incorporated into the electronic health record, it could be a valuable tool for clinicians to identify patients with less than 6 months of life expectancy and deliver palliative care to these patients. RESPECT appears to be particularly beneficial for home care patients without a clinically diagnosed terminal disease.”
That said, he added, “RESPECT should be viewed as a clinical decision support tool. It is no substitute for clinicians or clinical judgment. Based on the data presented in the paper, the algorithm tends to overestimate the short-term mortality risk for home care patients, therefore resulting in many false alarms.”
The study was supported by the Canadian Institutes of Health Research and the Associated Medical Services. Dr. Hsu is an executive lead on the steering committee of the Ontario Centres for Learning, Research, and Innovation in Long-Term Care. Funding for the centers comes from the Ontario Ministry of Health and Ministry of Long-Term Care and is partially administered by the Bruyère Research Institute. Dr. Li reported no relevant financial interests.
A version of this article appeared on Medscape.com.
A prognostic tool may facilitate the early identification of older adults in the community who would benefit from palliative care in their final years, new research from Canada suggested.
The analysis of data from close to a quarter million community-dwelling older adults in Ontario with at least one interRAI (Resident Assessment Instrument) home care assessment showed that only half of those with an estimated survival of fewer than 3 months received at least one palliative home care visit before death.
“One of the challenges and a barrier to accessing palliative home care is the difficulty of predicting survival,” Amy Hsu, PhD, an investigator at the Bruyère Research Institute in Ottawa, Ontario, Canada, told this news organization. “Clinicians are good at prognosticating when a patient might be entering their last 3-6 weeks of life, but they have a harder time predicting if someone will survive 6 months or longer.”
The team developed the Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool (RESPECT) to see whether access to predicted survival data could inform conversations about a patient’s status and palliative care needs.
The study was published online in the Canadian Medical Association Journal.
Setting Care Goals
Researchers analyzed population health administrative data from Ontario involving home care clients who received at least one interRAI Home Care assessment between April 2018 and September 2019. The cohort included 247,377 adults (62% women) with a mean age of 80.1 years at the time of assessment. Comorbidities, including congestive heart failure, coronary artery disease, cancer, and chronic obstructive pulmonary disease, as well as symptoms of health instability, were more prevalent among those at higher risk of dying.
The team used an updated, validated version of RESPECT to predict survival.
Only 2.6% of home care clients had received a clinician diagnosis of an end-stage disease, which was more prevalent among those at highest mortality risk (77.9%). Most clients (74.5%) required extensive assistance in performing instrumental activities of daily living (ADLs, score ≤ 4), and half (50.3%) were less able to perform ADLs in the last 3 months of life.
Within the cohort, 75% of patients with a predicted median survival of fewer than 3 months, 55.4% of those with a predicted median survival between 3 and 6 months, and 40.7% of those with a predicted median survival between 6 and 12 months died within 6 months of the home care assessment.
Among decedents, 50.6% of those with a RESPECT-estimated median survival of fewer than 3 months received at least one nonphysician palliative home care visit before death. Less than a third (27.8%) received at least one palliative home care visit from a physician.
The proportion of those who received at least one nonphysician visit fell to 38.7% among those with a median survival of between 3 and 6 months and to 29.5% among those with a median survival of between 6 and 12 months.
Patients who received at least one palliative home care visit (from either physicians or nonphysician home care providers) within 6 months of an assessment had clinical characteristics similar to those who did not receive a visit. However, those who did not receive palliative home care were more likely to not have been identified by a clinician as being in their past 6 months of life.
“These results reinforce the role of clinicians in identifying older adults who may be in their last 6 months of life as an important component for the receipt of palliative home care and highlight the value of RESPECT in supplementing clinicians’ assessments of prognosis,” the authors wrote.
“Our goal is to use data and tools like RESPECT to help individuals living with a life-limiting illness have conversations about what their end-of-life care goals and wishes may be and discuss whether a referral to palliative care is appropriate or needed,” Dr. Hsu added. “Data about life expectancy could be helpful for framing these conversations.”
The researchers are working with partners in home, community care, and long-term care to implement RESPECT in their settings.
‘Valuable Tool’
Guohua Li, MD, DrPH, professor of epidemiology and anesthesiology at Columbia University Mailman School of Public Health and Vagelos College of Physicians and Surgeons in New York City, commented on the findings for this news organization. He noted that the study is “rigorously designed and meticulously analyzed. The findings are of high validity and population health significance.”
The findings are comparable with what is seen in the United States and Canada, he said, where about 50% of terminally ill patients die at home or in hospice. However, palliative care outside of North America “varies greatly, and in many developing countries, [it] is still in its infancy.”
As a mortality risk prediction algorithm, “RESPECT seems to perform reasonably well,” he said. “If incorporated into the electronic health record, it could be a valuable tool for clinicians to identify patients with less than 6 months of life expectancy and deliver palliative care to these patients. RESPECT appears to be particularly beneficial for home care patients without a clinically diagnosed terminal disease.”
That said, he added, “RESPECT should be viewed as a clinical decision support tool. It is no substitute for clinicians or clinical judgment. Based on the data presented in the paper, the algorithm tends to overestimate the short-term mortality risk for home care patients, therefore resulting in many false alarms.”
The study was supported by the Canadian Institutes of Health Research and the Associated Medical Services. Dr. Hsu is an executive lead on the steering committee of the Ontario Centres for Learning, Research, and Innovation in Long-Term Care. Funding for the centers comes from the Ontario Ministry of Health and Ministry of Long-Term Care and is partially administered by the Bruyère Research Institute. Dr. Li reported no relevant financial interests.
A version of this article appeared on Medscape.com.
A prognostic tool may facilitate the early identification of older adults in the community who would benefit from palliative care in their final years, new research from Canada suggested.
The analysis of data from close to a quarter million community-dwelling older adults in Ontario with at least one interRAI (Resident Assessment Instrument) home care assessment showed that only half of those with an estimated survival of fewer than 3 months received at least one palliative home care visit before death.
“One of the challenges and a barrier to accessing palliative home care is the difficulty of predicting survival,” Amy Hsu, PhD, an investigator at the Bruyère Research Institute in Ottawa, Ontario, Canada, told this news organization. “Clinicians are good at prognosticating when a patient might be entering their last 3-6 weeks of life, but they have a harder time predicting if someone will survive 6 months or longer.”
The team developed the Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool (RESPECT) to see whether access to predicted survival data could inform conversations about a patient’s status and palliative care needs.
The study was published online in the Canadian Medical Association Journal.
Setting Care Goals
Researchers analyzed population health administrative data from Ontario involving home care clients who received at least one interRAI Home Care assessment between April 2018 and September 2019. The cohort included 247,377 adults (62% women) with a mean age of 80.1 years at the time of assessment. Comorbidities, including congestive heart failure, coronary artery disease, cancer, and chronic obstructive pulmonary disease, as well as symptoms of health instability, were more prevalent among those at higher risk of dying.
The team used an updated, validated version of RESPECT to predict survival.
Only 2.6% of home care clients had received a clinician diagnosis of an end-stage disease, which was more prevalent among those at highest mortality risk (77.9%). Most clients (74.5%) required extensive assistance in performing instrumental activities of daily living (ADLs, score ≤ 4), and half (50.3%) were less able to perform ADLs in the last 3 months of life.
Within the cohort, 75% of patients with a predicted median survival of fewer than 3 months, 55.4% of those with a predicted median survival between 3 and 6 months, and 40.7% of those with a predicted median survival between 6 and 12 months died within 6 months of the home care assessment.
Among decedents, 50.6% of those with a RESPECT-estimated median survival of fewer than 3 months received at least one nonphysician palliative home care visit before death. Less than a third (27.8%) received at least one palliative home care visit from a physician.
The proportion of those who received at least one nonphysician visit fell to 38.7% among those with a median survival of between 3 and 6 months and to 29.5% among those with a median survival of between 6 and 12 months.
Patients who received at least one palliative home care visit (from either physicians or nonphysician home care providers) within 6 months of an assessment had clinical characteristics similar to those who did not receive a visit. However, those who did not receive palliative home care were more likely to not have been identified by a clinician as being in their past 6 months of life.
“These results reinforce the role of clinicians in identifying older adults who may be in their last 6 months of life as an important component for the receipt of palliative home care and highlight the value of RESPECT in supplementing clinicians’ assessments of prognosis,” the authors wrote.
“Our goal is to use data and tools like RESPECT to help individuals living with a life-limiting illness have conversations about what their end-of-life care goals and wishes may be and discuss whether a referral to palliative care is appropriate or needed,” Dr. Hsu added. “Data about life expectancy could be helpful for framing these conversations.”
The researchers are working with partners in home, community care, and long-term care to implement RESPECT in their settings.
‘Valuable Tool’
Guohua Li, MD, DrPH, professor of epidemiology and anesthesiology at Columbia University Mailman School of Public Health and Vagelos College of Physicians and Surgeons in New York City, commented on the findings for this news organization. He noted that the study is “rigorously designed and meticulously analyzed. The findings are of high validity and population health significance.”
The findings are comparable with what is seen in the United States and Canada, he said, where about 50% of terminally ill patients die at home or in hospice. However, palliative care outside of North America “varies greatly, and in many developing countries, [it] is still in its infancy.”
As a mortality risk prediction algorithm, “RESPECT seems to perform reasonably well,” he said. “If incorporated into the electronic health record, it could be a valuable tool for clinicians to identify patients with less than 6 months of life expectancy and deliver palliative care to these patients. RESPECT appears to be particularly beneficial for home care patients without a clinically diagnosed terminal disease.”
That said, he added, “RESPECT should be viewed as a clinical decision support tool. It is no substitute for clinicians or clinical judgment. Based on the data presented in the paper, the algorithm tends to overestimate the short-term mortality risk for home care patients, therefore resulting in many false alarms.”
The study was supported by the Canadian Institutes of Health Research and the Associated Medical Services. Dr. Hsu is an executive lead on the steering committee of the Ontario Centres for Learning, Research, and Innovation in Long-Term Care. Funding for the centers comes from the Ontario Ministry of Health and Ministry of Long-Term Care and is partially administered by the Bruyère Research Institute. Dr. Li reported no relevant financial interests.
A version of this article appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
Study: Healthy Plant-Based Diets Do Not Raise Hip Fracture Risk
Long-term adherence to a plant-based diet was not tied to a greater risk of hip fracture and some plant-based regimens may actually reduce the risk, a large cohort study of postmenopausal women in the United States suggested.
Not all plant-centered regimens are healthful, however, and this study factored dietary quality into risk.
Writing in JAMA Network Open, the study authors compared the lowest to highest quintiles of Plant-Based Diet Index scores. They found the most recent intake of a healthy plant-based diet (hPDI) to be associated with a somewhat lower (21%) risk of fracture while the most recent intake of its unhealthy counterpart (uPDI) was linked to a somewhat higher (28%) risk.
“In addition, higher baseline scores in the uPDI were associated with higher risk of hip fracture,” wrote the researchers, led by Mercedes Sotos Prieto, PhD, a nutritional epidemiologist in the Department of Preventive Medicine and Public Health at the Autonomous University of Madrid.
Plant-based diets, characterized by higher consumption of plant foods and lower or no intake of animal foods, have raised concerns about their potential harm to bone health. In a recent meta-analysis, vegetarians, but particularly vegans with no consumption of any animal food, had a higher fracture risk and lower bone mineral density compared with omnivores.
Another study found that compared with meat eaters, fish eaters and vegetarians had a higher risk of hip fractures. These analyses, however, did not assess the quality of the plant-based diets.

“We hypothesized that the differences in the quality of the plant-based diets — whole grains, fruits, and vegetables vs refined carbohydrates or snacks, which are both plant-based but very different, would be important in the association for the risk of hip fracture,” Dr. Sotos Prieto said in an interview.
Study details
Her study drew on data from 70,285 postmenopausal White women who were in the US Nurses’ Health Study from 1984 through 2014; data were analyzed from Jan. 1 to July 31, 2023.
The mean age of the nurses was 54.92 years, and 2038 cases of hip fracture were reported during the study over as long as 30 years of follow-up.
Healthy plant foods included whole grains, fruits, vegetables, nuts, legumes, vegetable oils, and tea or coffee and received positive scores, whereas less healthy plant foods such as fruit juices, sweetened beverages, refined grains, potatoes, sweets, or desserts and animal foods received reversed scores. Dietary and lifestyle information was collected by self-reported questionnaires.
Individuals with higher hPDI scores were leaner, more physically active, less likely to be smokers, and more likely to use vitamin and calcium supplements. Not surprisingly, they also had higher intakes of dietary calcium and healthy plant foods and had lower intake of less healthy plant foods. “It’s plausible that reverse causation may account for the risk associations, as individuals with underlying health conditions that predisposed them to higher fracture risk may have changed their diet,” Dr. Sotos Prieto said. “In addition, baseline diet may reflect diet early on, which could be an important predictor of bone mineral density when there was more active bone turnover.”
Lack of information precluded adjustment for the use of anti-osteoporotic medication.
Neither the hPDI, with a hazard ratio (HR) for highest vs lowest quintile of 0.97 (95% confidence interval, 0.83-1.14) nor the uPDI, with an HR for highest vs lowest quintile of 1.02 (95% CI, 0.87-1.20) for diet adherence over the long term was associated with hip fracture risk.
For recent dietary intake in the highest vs lowest quintiles, however, the hPDI was associated with a 21% lower risk of hip fracture: HR, 0.79 (95% CI, 0.68-0.92; P = .02 for trend). In contrast, the uPDI was associated with a 28% higher risk: HR, 1.28 (95% CI, 1.09-1.51; P = .008 for trend).
Future studies in other populations are needed to confirm the results and enhance their generalizability, Dr. Sotos Prieto said. “Investigating the temporal dynamics of dietary patterns and their effects by examining how recent dietary changes may impact health outcomes over different timeframes is important.” In the meantime, people wishing to follow a plant-based diet should make sure it features high-quality foods.
This work was supported by Instituto de Salud Carlos III, State Secretary of Research, Development and Innovation of Spain, and the European Research Funds and European Social Fund, the Agencia Estatal de Investigación, the National Institutes of Health, and a Ramón y Cajal contract from the Ministry of Science, Innovation, and Universities. A coauthor reported a patent pending. No other disclosures were reported.
Long-term adherence to a plant-based diet was not tied to a greater risk of hip fracture and some plant-based regimens may actually reduce the risk, a large cohort study of postmenopausal women in the United States suggested.
Not all plant-centered regimens are healthful, however, and this study factored dietary quality into risk.
Writing in JAMA Network Open, the study authors compared the lowest to highest quintiles of Plant-Based Diet Index scores. They found the most recent intake of a healthy plant-based diet (hPDI) to be associated with a somewhat lower (21%) risk of fracture while the most recent intake of its unhealthy counterpart (uPDI) was linked to a somewhat higher (28%) risk.
“In addition, higher baseline scores in the uPDI were associated with higher risk of hip fracture,” wrote the researchers, led by Mercedes Sotos Prieto, PhD, a nutritional epidemiologist in the Department of Preventive Medicine and Public Health at the Autonomous University of Madrid.
Plant-based diets, characterized by higher consumption of plant foods and lower or no intake of animal foods, have raised concerns about their potential harm to bone health. In a recent meta-analysis, vegetarians, but particularly vegans with no consumption of any animal food, had a higher fracture risk and lower bone mineral density compared with omnivores.
Another study found that compared with meat eaters, fish eaters and vegetarians had a higher risk of hip fractures. These analyses, however, did not assess the quality of the plant-based diets.
“We hypothesized that the differences in the quality of the plant-based diets — whole grains, fruits, and vegetables vs refined carbohydrates or snacks, which are both plant-based but very different, would be important in the association for the risk of hip fracture,” Dr. Sotos Prieto said in an interview.
Study details
Her study drew on data from 70,285 postmenopausal White women who were in the US Nurses’ Health Study from 1984 through 2014; data were analyzed from Jan. 1 to July 31, 2023.
The mean age of the nurses was 54.92 years, and 2038 cases of hip fracture were reported during the study over as long as 30 years of follow-up.
Healthy plant foods included whole grains, fruits, vegetables, nuts, legumes, vegetable oils, and tea or coffee and received positive scores, whereas less healthy plant foods such as fruit juices, sweetened beverages, refined grains, potatoes, sweets, or desserts and animal foods received reversed scores. Dietary and lifestyle information was collected by self-reported questionnaires.
Individuals with higher hPDI scores were leaner, more physically active, less likely to be smokers, and more likely to use vitamin and calcium supplements. Not surprisingly, they also had higher intakes of dietary calcium and healthy plant foods and had lower intake of less healthy plant foods. “It’s plausible that reverse causation may account for the risk associations, as individuals with underlying health conditions that predisposed them to higher fracture risk may have changed their diet,” Dr. Sotos Prieto said. “In addition, baseline diet may reflect diet early on, which could be an important predictor of bone mineral density when there was more active bone turnover.”
Lack of information precluded adjustment for the use of anti-osteoporotic medication.
Neither the hPDI, with a hazard ratio (HR) for highest vs lowest quintile of 0.97 (95% confidence interval, 0.83-1.14) nor the uPDI, with an HR for highest vs lowest quintile of 1.02 (95% CI, 0.87-1.20) for diet adherence over the long term was associated with hip fracture risk.
For recent dietary intake in the highest vs lowest quintiles, however, the hPDI was associated with a 21% lower risk of hip fracture: HR, 0.79 (95% CI, 0.68-0.92; P = .02 for trend). In contrast, the uPDI was associated with a 28% higher risk: HR, 1.28 (95% CI, 1.09-1.51; P = .008 for trend).
Future studies in other populations are needed to confirm the results and enhance their generalizability, Dr. Sotos Prieto said. “Investigating the temporal dynamics of dietary patterns and their effects by examining how recent dietary changes may impact health outcomes over different timeframes is important.” In the meantime, people wishing to follow a plant-based diet should make sure it features high-quality foods.
This work was supported by Instituto de Salud Carlos III, State Secretary of Research, Development and Innovation of Spain, and the European Research Funds and European Social Fund, the Agencia Estatal de Investigación, the National Institutes of Health, and a Ramón y Cajal contract from the Ministry of Science, Innovation, and Universities. A coauthor reported a patent pending. No other disclosures were reported.
Long-term adherence to a plant-based diet was not tied to a greater risk of hip fracture and some plant-based regimens may actually reduce the risk, a large cohort study of postmenopausal women in the United States suggested.
Not all plant-centered regimens are healthful, however, and this study factored dietary quality into risk.
Writing in JAMA Network Open, the study authors compared the lowest to highest quintiles of Plant-Based Diet Index scores. They found the most recent intake of a healthy plant-based diet (hPDI) to be associated with a somewhat lower (21%) risk of fracture while the most recent intake of its unhealthy counterpart (uPDI) was linked to a somewhat higher (28%) risk.
“In addition, higher baseline scores in the uPDI were associated with higher risk of hip fracture,” wrote the researchers, led by Mercedes Sotos Prieto, PhD, a nutritional epidemiologist in the Department of Preventive Medicine and Public Health at the Autonomous University of Madrid.
Plant-based diets, characterized by higher consumption of plant foods and lower or no intake of animal foods, have raised concerns about their potential harm to bone health. In a recent meta-analysis, vegetarians, but particularly vegans with no consumption of any animal food, had a higher fracture risk and lower bone mineral density compared with omnivores.
Another study found that compared with meat eaters, fish eaters and vegetarians had a higher risk of hip fractures. These analyses, however, did not assess the quality of the plant-based diets.
“We hypothesized that the differences in the quality of the plant-based diets — whole grains, fruits, and vegetables vs refined carbohydrates or snacks, which are both plant-based but very different, would be important in the association for the risk of hip fracture,” Dr. Sotos Prieto said in an interview.
Study details
Her study drew on data from 70,285 postmenopausal White women who were in the US Nurses’ Health Study from 1984 through 2014; data were analyzed from Jan. 1 to July 31, 2023.
The mean age of the nurses was 54.92 years, and 2038 cases of hip fracture were reported during the study over as long as 30 years of follow-up.
Healthy plant foods included whole grains, fruits, vegetables, nuts, legumes, vegetable oils, and tea or coffee and received positive scores, whereas less healthy plant foods such as fruit juices, sweetened beverages, refined grains, potatoes, sweets, or desserts and animal foods received reversed scores. Dietary and lifestyle information was collected by self-reported questionnaires.
Individuals with higher hPDI scores were leaner, more physically active, less likely to be smokers, and more likely to use vitamin and calcium supplements. Not surprisingly, they also had higher intakes of dietary calcium and healthy plant foods and had lower intake of less healthy plant foods. “It’s plausible that reverse causation may account for the risk associations, as individuals with underlying health conditions that predisposed them to higher fracture risk may have changed their diet,” Dr. Sotos Prieto said. “In addition, baseline diet may reflect diet early on, which could be an important predictor of bone mineral density when there was more active bone turnover.”
Lack of information precluded adjustment for the use of anti-osteoporotic medication.
Neither the hPDI, with a hazard ratio (HR) for highest vs lowest quintile of 0.97 (95% confidence interval, 0.83-1.14) nor the uPDI, with an HR for highest vs lowest quintile of 1.02 (95% CI, 0.87-1.20) for diet adherence over the long term was associated with hip fracture risk.
For recent dietary intake in the highest vs lowest quintiles, however, the hPDI was associated with a 21% lower risk of hip fracture: HR, 0.79 (95% CI, 0.68-0.92; P = .02 for trend). In contrast, the uPDI was associated with a 28% higher risk: HR, 1.28 (95% CI, 1.09-1.51; P = .008 for trend).
Future studies in other populations are needed to confirm the results and enhance their generalizability, Dr. Sotos Prieto said. “Investigating the temporal dynamics of dietary patterns and their effects by examining how recent dietary changes may impact health outcomes over different timeframes is important.” In the meantime, people wishing to follow a plant-based diet should make sure it features high-quality foods.
This work was supported by Instituto de Salud Carlos III, State Secretary of Research, Development and Innovation of Spain, and the European Research Funds and European Social Fund, the Agencia Estatal de Investigación, the National Institutes of Health, and a Ramón y Cajal contract from the Ministry of Science, Innovation, and Universities. A coauthor reported a patent pending. No other disclosures were reported.
FROM JAMA NETWORK OPEN
Bariatric Surgery Yields Significant Cognitive Benefits
Bariatric surgery is associated with long-term improvements in cognition and brain structure in addition to general health benefits and expected weight loss, a large study found.
Among 133 adults with severe obesity who underwent bariatric surgery, roughly two in five showed > 20% improvement in global cognitive function at 24 months following the surgery.
“Notably, the temporal cortex exhibited not only higher cortical thickness but also higher vascular efficiency after surgery,” reported Amanda Kiliaan, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, and colleagues.
“These results highlight beneficial vascular responses occurring in conjunction with bariatric surgery,” the researchers wrote.
They also suggested that weight-loss surgery may represent a treatment option for patients with obesity and dementia.
The study was published online on February 9, 2024, in JAMA Network Open.
Obesity is associated with an increased risk of developing dementia. Bariatric surgery-induced weight loss has been associated with improvements in brain function and structure in some small cohort studies with short follow-up periods. However, long-term neurological outcomes associated with bariatric surgery are unclear.
To investigate, Dr. Kiliaan and colleagues studied 133 adults with severe obesity (mean age, 46 years; 84% women) who underwent Roux-en-Y gastric bypass. The researchers collected relevant data from laboratory tests, cognitive tests, and MRI brain scans before surgery and at 6 and 24 months after surgery.
Overall, mean body weight, body mass index, waist circumference, and blood pressure were significantly lower at 6 and 24 months after surgery. At 24 months, significantly fewer patients were taking antihypertensive medication (17% vs 36% before surgery).
Improvements in inflammatory markers, depressive symptoms, and physical activity were also evident after surgery.
Cognitive Improvements
Several cognitive domains showed significant improvement at 6 and 24 months after bariatric surgery. Based on the 20% change index, improvements in working memory, episodic memory, and verbal fluency were seen in 11%, 32%, and 24% of participants, respectively.
Forty percent of patients showed improvement in their able to shift their attention, and 43% showed improvements in global cognition after surgery.
Several changes in brain parameters were also noted. Despite lower cerebral blood flow (CBF) in several regions, volumes of hippocampus, nucleus accumbens, frontal cortex, white matter, and white matter hyperintensity remained stable after surgery.
The temporal cortex showed a greater thickness (mean, 2.724 mm vs 2.761 mm; P = .007) and lower spatial coefficient of variation (sCOV; median, 4.41% vs 3.97%; P = .02) after surgery.
Overall, the results suggest that cognitive improvements “begin shortly after bariatric surgery and are long lasting,” the authors wrote.
Various factors may be involved including remission of comorbidities, higher physical activity, lower depressive symptoms, and lower inflammatory factors, they suggest. Stabilization of volume, CBF, and sCOV in brain regions, coupled with gains in cortical thickness and vascular efficiency in the temporal cortex could also play a role.
‘Remarkable’ Results
“Taken together, the research intimates bariatric surgery’s potential protective effects against dementia manifest through both weight-related brain changes and reducing cardiovascular risk factors,” Shaheen Lakhan, MD, a neurologist and researcher based in Miami, who wasn’t involved in the study, told this news organization.
“These remarkable neurological transformations intimate this surgery represents a pivotal opportunity to combat the parallel public health crises of obesity and dementia threatening society,” he said.
“In demonstrating a durable cognitive and brain boost out years beyond surgery, patients now have an emphatic answer — these aren’t short-lived benefits but rather profound improvements propelling them positively for the rest of life,” he added.
This opens up questions on whether the new class of obesity medications targeting glucagon-like peptide 1 (GLP-1) and gastric inhibitory polypeptide pathways, that can achieve weight loss approaching that of bariatric surgery, could have similar benefits.
The use of GLP-1 drugs have also shown neuroprotective effects such as improvement in motor and cognitive deficits, reduction of neuroinflammation, prevention of neuronal loss, and possibly slowing of neurodegeneration across animal models of Parkinson’s disease, Alzheimer’s disease, and stroke, said Dr. Lakhan. However, the exact mechanisms and ability to cross the blood-brain barrier require further confirmation, especially in humans.
Large, long-term, randomized controlled trials looking into potential effects of semaglutide on early Alzheimer›s disease, including the EVOKE Plus trial, are currently underway, he noted.
“These game-changing obesity drugs may hand us medicine’s holy grail — a pill to rival surgery’s brain benefits without the scalpel, allowing patients a more accessible path to protecting their brain,” Dr. Lakhan said.
The study had no funding from industry. Dr. Kiliaan and Dr. Lakhan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Bariatric surgery is associated with long-term improvements in cognition and brain structure in addition to general health benefits and expected weight loss, a large study found.
Among 133 adults with severe obesity who underwent bariatric surgery, roughly two in five showed > 20% improvement in global cognitive function at 24 months following the surgery.
“Notably, the temporal cortex exhibited not only higher cortical thickness but also higher vascular efficiency after surgery,” reported Amanda Kiliaan, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, and colleagues.
“These results highlight beneficial vascular responses occurring in conjunction with bariatric surgery,” the researchers wrote.
They also suggested that weight-loss surgery may represent a treatment option for patients with obesity and dementia.
The study was published online on February 9, 2024, in JAMA Network Open.
Obesity is associated with an increased risk of developing dementia. Bariatric surgery-induced weight loss has been associated with improvements in brain function and structure in some small cohort studies with short follow-up periods. However, long-term neurological outcomes associated with bariatric surgery are unclear.
To investigate, Dr. Kiliaan and colleagues studied 133 adults with severe obesity (mean age, 46 years; 84% women) who underwent Roux-en-Y gastric bypass. The researchers collected relevant data from laboratory tests, cognitive tests, and MRI brain scans before surgery and at 6 and 24 months after surgery.
Overall, mean body weight, body mass index, waist circumference, and blood pressure were significantly lower at 6 and 24 months after surgery. At 24 months, significantly fewer patients were taking antihypertensive medication (17% vs 36% before surgery).
Improvements in inflammatory markers, depressive symptoms, and physical activity were also evident after surgery.
Cognitive Improvements
Several cognitive domains showed significant improvement at 6 and 24 months after bariatric surgery. Based on the 20% change index, improvements in working memory, episodic memory, and verbal fluency were seen in 11%, 32%, and 24% of participants, respectively.
Forty percent of patients showed improvement in their able to shift their attention, and 43% showed improvements in global cognition after surgery.
Several changes in brain parameters were also noted. Despite lower cerebral blood flow (CBF) in several regions, volumes of hippocampus, nucleus accumbens, frontal cortex, white matter, and white matter hyperintensity remained stable after surgery.
The temporal cortex showed a greater thickness (mean, 2.724 mm vs 2.761 mm; P = .007) and lower spatial coefficient of variation (sCOV; median, 4.41% vs 3.97%; P = .02) after surgery.
Overall, the results suggest that cognitive improvements “begin shortly after bariatric surgery and are long lasting,” the authors wrote.
Various factors may be involved including remission of comorbidities, higher physical activity, lower depressive symptoms, and lower inflammatory factors, they suggest. Stabilization of volume, CBF, and sCOV in brain regions, coupled with gains in cortical thickness and vascular efficiency in the temporal cortex could also play a role.
‘Remarkable’ Results
“Taken together, the research intimates bariatric surgery’s potential protective effects against dementia manifest through both weight-related brain changes and reducing cardiovascular risk factors,” Shaheen Lakhan, MD, a neurologist and researcher based in Miami, who wasn’t involved in the study, told this news organization.
“These remarkable neurological transformations intimate this surgery represents a pivotal opportunity to combat the parallel public health crises of obesity and dementia threatening society,” he said.
“In demonstrating a durable cognitive and brain boost out years beyond surgery, patients now have an emphatic answer — these aren’t short-lived benefits but rather profound improvements propelling them positively for the rest of life,” he added.
This opens up questions on whether the new class of obesity medications targeting glucagon-like peptide 1 (GLP-1) and gastric inhibitory polypeptide pathways, that can achieve weight loss approaching that of bariatric surgery, could have similar benefits.
The use of GLP-1 drugs have also shown neuroprotective effects such as improvement in motor and cognitive deficits, reduction of neuroinflammation, prevention of neuronal loss, and possibly slowing of neurodegeneration across animal models of Parkinson’s disease, Alzheimer’s disease, and stroke, said Dr. Lakhan. However, the exact mechanisms and ability to cross the blood-brain barrier require further confirmation, especially in humans.
Large, long-term, randomized controlled trials looking into potential effects of semaglutide on early Alzheimer›s disease, including the EVOKE Plus trial, are currently underway, he noted.
“These game-changing obesity drugs may hand us medicine’s holy grail — a pill to rival surgery’s brain benefits without the scalpel, allowing patients a more accessible path to protecting their brain,” Dr. Lakhan said.
The study had no funding from industry. Dr. Kiliaan and Dr. Lakhan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Bariatric surgery is associated with long-term improvements in cognition and brain structure in addition to general health benefits and expected weight loss, a large study found.
Among 133 adults with severe obesity who underwent bariatric surgery, roughly two in five showed > 20% improvement in global cognitive function at 24 months following the surgery.
“Notably, the temporal cortex exhibited not only higher cortical thickness but also higher vascular efficiency after surgery,” reported Amanda Kiliaan, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, and colleagues.
“These results highlight beneficial vascular responses occurring in conjunction with bariatric surgery,” the researchers wrote.
They also suggested that weight-loss surgery may represent a treatment option for patients with obesity and dementia.
The study was published online on February 9, 2024, in JAMA Network Open.
Obesity is associated with an increased risk of developing dementia. Bariatric surgery-induced weight loss has been associated with improvements in brain function and structure in some small cohort studies with short follow-up periods. However, long-term neurological outcomes associated with bariatric surgery are unclear.
To investigate, Dr. Kiliaan and colleagues studied 133 adults with severe obesity (mean age, 46 years; 84% women) who underwent Roux-en-Y gastric bypass. The researchers collected relevant data from laboratory tests, cognitive tests, and MRI brain scans before surgery and at 6 and 24 months after surgery.
Overall, mean body weight, body mass index, waist circumference, and blood pressure were significantly lower at 6 and 24 months after surgery. At 24 months, significantly fewer patients were taking antihypertensive medication (17% vs 36% before surgery).
Improvements in inflammatory markers, depressive symptoms, and physical activity were also evident after surgery.
Cognitive Improvements
Several cognitive domains showed significant improvement at 6 and 24 months after bariatric surgery. Based on the 20% change index, improvements in working memory, episodic memory, and verbal fluency were seen in 11%, 32%, and 24% of participants, respectively.
Forty percent of patients showed improvement in their able to shift their attention, and 43% showed improvements in global cognition after surgery.
Several changes in brain parameters were also noted. Despite lower cerebral blood flow (CBF) in several regions, volumes of hippocampus, nucleus accumbens, frontal cortex, white matter, and white matter hyperintensity remained stable after surgery.
The temporal cortex showed a greater thickness (mean, 2.724 mm vs 2.761 mm; P = .007) and lower spatial coefficient of variation (sCOV; median, 4.41% vs 3.97%; P = .02) after surgery.
Overall, the results suggest that cognitive improvements “begin shortly after bariatric surgery and are long lasting,” the authors wrote.
Various factors may be involved including remission of comorbidities, higher physical activity, lower depressive symptoms, and lower inflammatory factors, they suggest. Stabilization of volume, CBF, and sCOV in brain regions, coupled with gains in cortical thickness and vascular efficiency in the temporal cortex could also play a role.
‘Remarkable’ Results
“Taken together, the research intimates bariatric surgery’s potential protective effects against dementia manifest through both weight-related brain changes and reducing cardiovascular risk factors,” Shaheen Lakhan, MD, a neurologist and researcher based in Miami, who wasn’t involved in the study, told this news organization.
“These remarkable neurological transformations intimate this surgery represents a pivotal opportunity to combat the parallel public health crises of obesity and dementia threatening society,” he said.
“In demonstrating a durable cognitive and brain boost out years beyond surgery, patients now have an emphatic answer — these aren’t short-lived benefits but rather profound improvements propelling them positively for the rest of life,” he added.
This opens up questions on whether the new class of obesity medications targeting glucagon-like peptide 1 (GLP-1) and gastric inhibitory polypeptide pathways, that can achieve weight loss approaching that of bariatric surgery, could have similar benefits.
The use of GLP-1 drugs have also shown neuroprotective effects such as improvement in motor and cognitive deficits, reduction of neuroinflammation, prevention of neuronal loss, and possibly slowing of neurodegeneration across animal models of Parkinson’s disease, Alzheimer’s disease, and stroke, said Dr. Lakhan. However, the exact mechanisms and ability to cross the blood-brain barrier require further confirmation, especially in humans.
Large, long-term, randomized controlled trials looking into potential effects of semaglutide on early Alzheimer›s disease, including the EVOKE Plus trial, are currently underway, he noted.
“These game-changing obesity drugs may hand us medicine’s holy grail — a pill to rival surgery’s brain benefits without the scalpel, allowing patients a more accessible path to protecting their brain,” Dr. Lakhan said.
The study had no funding from industry. Dr. Kiliaan and Dr. Lakhan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
High Rate of Dementia Among Attendees in Adult Day Service Centers
About one-quarter of all adult day services center (ADSC) participants have dementia, and the prevalence of dementia in ADSCs that specialize in the disorder is more than 40%, a new US National Health Statistics Report revealed.
ADSCs are a growing sector of the US home- and community-based long-term care delivery system, providing daytime services to adults with disabilities who often have multiple chronic conditions, including various types of dementia, according to report authors Priyanka Singha, MPH, and colleagues at the US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics in Bethesda, Maryland.
Dementia often leads to the transition to receiving long-term care services, such as nursing home care. Delaying institutionalization is a primary goal of ADSCs, so they also try to meet the needs of a growing population of community-dwelling adults with dementia.
Survey responses from 1800 ADSCs across the United States showed that overall, 42.2% of participants had dementia in ADSCs specializing in dementia care, while 22.7% of participants in nonspecialized ADSCs also had dementia.
Dementia was more prevalent in the Midwest and West, where nearly one half of participants in specialized centers had dementia.
Nevertheless, the overall prevalence of dementia in ADSCs was similar across US regions, with a slightly lower percentage in the West.
Positive Outcomes
The new report used data from the ADSC component of the 2020 National Post-acute and Long-term Care Study collected from January 2020 through mid-July 2021. About 1800 ADSCs from a census of 5500 ADSCs were included and weighted to be nationally representative.
The authors compared dementia prevalence among participants in ADSCs that provide specialized care for dementia with other ADSCs by census region, metropolitan statistical area (MSA) status, chain affiliation, and ownership type.
MSA is a core urban area population of 50,000 or more. ADSCs that specialize in dementia care have specially trained staff, activities, and facilities. They offer social activities, including art and music therapy, dementia-appropriate games, and group exercises, as well as respite care for unpaid caregivers. The survey found that 14% of ADSCs reported specializing in dementia.
The investigators also found that the percentage of ADSC participants with dementia, regardless of center specialization, was higher in the Midwest (32.1%), Northeast (28.5%), and South (24.5%) than in the West (21.1%).
The percentage of participants with dementia in specialized centers was higher in the Midwest (49.5%) and West (48.8%) than in the Northeast (31.9%) and in nonchain centers (50.5%) than in chain-affiliated centers (30.4%).
In addition, the percentage of participants with dementia, regardless of specialization, was higher in nonchain ADSCs (25%) than in chain-affiliated centers (20.1%). In addition, the percentage of participants with dementia in nonspecialized centers was higher in nonchain centers (25%) than in chain-affiliated centers (20.1%).
Finally, the research revealed that the percentage of participants with dementia, regardless of specialization, was higher in nonprofit ADSCs (28.7%) than for-profit centers (21%).
“These findings indicate that ADSCs in MSAs, nonprofit organizations, and nonchain centers provide services to a higher proportion of participants with dementia, particularly among centers that specialize in dementia care,” the investigators wrote.
Whereas “caregivers manage prescription medications, help with activities of daily living, and offer nutritional diets, exercise, and social engagement, ADSCs play a role in providing this type of care for people with dementia while also offering respite for their unpaid caregivers,” they noted.
Overall, they concluded that ADSCs provide positive outcomes for both family caregivers and people with dementia.
They noted that the study’s limitations include the use of cross-sectional data, which cannot show effectiveness for participants receiving care in specialized centers or be used to analyze relationships between other participant-level sociodemographic or health characteristics and specialized dementia care.
A version of this article appeared on Medscape.com.
About one-quarter of all adult day services center (ADSC) participants have dementia, and the prevalence of dementia in ADSCs that specialize in the disorder is more than 40%, a new US National Health Statistics Report revealed.
ADSCs are a growing sector of the US home- and community-based long-term care delivery system, providing daytime services to adults with disabilities who often have multiple chronic conditions, including various types of dementia, according to report authors Priyanka Singha, MPH, and colleagues at the US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics in Bethesda, Maryland.
Dementia often leads to the transition to receiving long-term care services, such as nursing home care. Delaying institutionalization is a primary goal of ADSCs, so they also try to meet the needs of a growing population of community-dwelling adults with dementia.
Survey responses from 1800 ADSCs across the United States showed that overall, 42.2% of participants had dementia in ADSCs specializing in dementia care, while 22.7% of participants in nonspecialized ADSCs also had dementia.
Dementia was more prevalent in the Midwest and West, where nearly one half of participants in specialized centers had dementia.
Nevertheless, the overall prevalence of dementia in ADSCs was similar across US regions, with a slightly lower percentage in the West.
Positive Outcomes
The new report used data from the ADSC component of the 2020 National Post-acute and Long-term Care Study collected from January 2020 through mid-July 2021. About 1800 ADSCs from a census of 5500 ADSCs were included and weighted to be nationally representative.
The authors compared dementia prevalence among participants in ADSCs that provide specialized care for dementia with other ADSCs by census region, metropolitan statistical area (MSA) status, chain affiliation, and ownership type.
MSA is a core urban area population of 50,000 or more. ADSCs that specialize in dementia care have specially trained staff, activities, and facilities. They offer social activities, including art and music therapy, dementia-appropriate games, and group exercises, as well as respite care for unpaid caregivers. The survey found that 14% of ADSCs reported specializing in dementia.
The investigators also found that the percentage of ADSC participants with dementia, regardless of center specialization, was higher in the Midwest (32.1%), Northeast (28.5%), and South (24.5%) than in the West (21.1%).
The percentage of participants with dementia in specialized centers was higher in the Midwest (49.5%) and West (48.8%) than in the Northeast (31.9%) and in nonchain centers (50.5%) than in chain-affiliated centers (30.4%).
In addition, the percentage of participants with dementia, regardless of specialization, was higher in nonchain ADSCs (25%) than in chain-affiliated centers (20.1%). In addition, the percentage of participants with dementia in nonspecialized centers was higher in nonchain centers (25%) than in chain-affiliated centers (20.1%).
Finally, the research revealed that the percentage of participants with dementia, regardless of specialization, was higher in nonprofit ADSCs (28.7%) than for-profit centers (21%).
“These findings indicate that ADSCs in MSAs, nonprofit organizations, and nonchain centers provide services to a higher proportion of participants with dementia, particularly among centers that specialize in dementia care,” the investigators wrote.
Whereas “caregivers manage prescription medications, help with activities of daily living, and offer nutritional diets, exercise, and social engagement, ADSCs play a role in providing this type of care for people with dementia while also offering respite for their unpaid caregivers,” they noted.
Overall, they concluded that ADSCs provide positive outcomes for both family caregivers and people with dementia.
They noted that the study’s limitations include the use of cross-sectional data, which cannot show effectiveness for participants receiving care in specialized centers or be used to analyze relationships between other participant-level sociodemographic or health characteristics and specialized dementia care.
A version of this article appeared on Medscape.com.
About one-quarter of all adult day services center (ADSC) participants have dementia, and the prevalence of dementia in ADSCs that specialize in the disorder is more than 40%, a new US National Health Statistics Report revealed.
ADSCs are a growing sector of the US home- and community-based long-term care delivery system, providing daytime services to adults with disabilities who often have multiple chronic conditions, including various types of dementia, according to report authors Priyanka Singha, MPH, and colleagues at the US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics in Bethesda, Maryland.
Dementia often leads to the transition to receiving long-term care services, such as nursing home care. Delaying institutionalization is a primary goal of ADSCs, so they also try to meet the needs of a growing population of community-dwelling adults with dementia.
Survey responses from 1800 ADSCs across the United States showed that overall, 42.2% of participants had dementia in ADSCs specializing in dementia care, while 22.7% of participants in nonspecialized ADSCs also had dementia.
Dementia was more prevalent in the Midwest and West, where nearly one half of participants in specialized centers had dementia.
Nevertheless, the overall prevalence of dementia in ADSCs was similar across US regions, with a slightly lower percentage in the West.
Positive Outcomes
The new report used data from the ADSC component of the 2020 National Post-acute and Long-term Care Study collected from January 2020 through mid-July 2021. About 1800 ADSCs from a census of 5500 ADSCs were included and weighted to be nationally representative.
The authors compared dementia prevalence among participants in ADSCs that provide specialized care for dementia with other ADSCs by census region, metropolitan statistical area (MSA) status, chain affiliation, and ownership type.
MSA is a core urban area population of 50,000 or more. ADSCs that specialize in dementia care have specially trained staff, activities, and facilities. They offer social activities, including art and music therapy, dementia-appropriate games, and group exercises, as well as respite care for unpaid caregivers. The survey found that 14% of ADSCs reported specializing in dementia.
The investigators also found that the percentage of ADSC participants with dementia, regardless of center specialization, was higher in the Midwest (32.1%), Northeast (28.5%), and South (24.5%) than in the West (21.1%).
The percentage of participants with dementia in specialized centers was higher in the Midwest (49.5%) and West (48.8%) than in the Northeast (31.9%) and in nonchain centers (50.5%) than in chain-affiliated centers (30.4%).
In addition, the percentage of participants with dementia, regardless of specialization, was higher in nonchain ADSCs (25%) than in chain-affiliated centers (20.1%). In addition, the percentage of participants with dementia in nonspecialized centers was higher in nonchain centers (25%) than in chain-affiliated centers (20.1%).
Finally, the research revealed that the percentage of participants with dementia, regardless of specialization, was higher in nonprofit ADSCs (28.7%) than for-profit centers (21%).
“These findings indicate that ADSCs in MSAs, nonprofit organizations, and nonchain centers provide services to a higher proportion of participants with dementia, particularly among centers that specialize in dementia care,” the investigators wrote.
Whereas “caregivers manage prescription medications, help with activities of daily living, and offer nutritional diets, exercise, and social engagement, ADSCs play a role in providing this type of care for people with dementia while also offering respite for their unpaid caregivers,” they noted.
Overall, they concluded that ADSCs provide positive outcomes for both family caregivers and people with dementia.
They noted that the study’s limitations include the use of cross-sectional data, which cannot show effectiveness for participants receiving care in specialized centers or be used to analyze relationships between other participant-level sociodemographic or health characteristics and specialized dementia care.
A version of this article appeared on Medscape.com.