User login
Fibroids associated with lower chance of unsuspected malignancy
NATIONAL HARBOR, MD. – Women undergoing hysterectomy or myomectomy for benign indications, who also had fibroids, were less likely to have a malignant diagnosis, according to a study presented at the AAGL Global Congress.
These findings could change the conversation when it comes to counseling patients about the risks associated with morcellation, a procedure that was strongly discouraged by the FDA in 2014 due to the concern that it might have the potential to spread malignancy.
“There’s a lot of things going on in the media about morcellation and risk of malignancy at the time of benign fibroid surgery, but this research actually makes apparent the higher risk of malignancy when fibroids are not present,” Farah Alvi, MD, a second-year fellow at Northwestern University, Chicago, said in an interview. Despite the concerns regarding morcellation and malignancy, this research suggests that patients who have fibroids at time of surgery may have a lower chance of malignancy, compared with patients who have other indications for surgery, she explained.
Dr. Alvi and her colleagues studied 2,987 hysterectomy or myomectomy patients with benign indications between January 2005 and December 2014.
Among patients studied, researchers found 33 confirmed malignant or borderline tumors, 16 of 1,790 (0.89%) in the leiomyoma group and 17 of 1,197 (1.42%) in the group with other indications (P = 0.04). The malignancies/borderline tumors included three leiomyosarcomas, two endometrial sarcomas, two endometrioid adenocarcinomas, one granulose cell tumor, three smooth muscle tumors of uncertain malignant potential, three atypical leiomyoma, and one serous papillary borderline ovarian tumor.
Of those with leiomyomata, 1 in 600 patients were diagnosed with leiomyosarcoma, compared with a risk of 1 in 350 for unanticipated malignancy in general.
Patients with surgical indications of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) for diagnosis of an unanticipated malignancy, compared with those without leiomyoma, according to Dr. Alvi. The odds of malignancy were also reduced in patients with uterine sizes of 15-20 weeks (OR, 0.65; P = .43) and those with specimen sizes of 250-500 grams (OR, 0.68; P = .64).
These findings will have implications for how physicians counsel women undergoing minimally invasive hysterectomy or myomectomy, Dr. Alvi said.
“In counseling patients about morcellation, we often have quoted them an estimated risk of 1 in 458 for leiomyosarcoma, based on the FDA morcellation warnings, and one thing we can learn is that risk is actually much lower than we think it is,” Dr. Alvi said.
The findings also suggest a shift in focus toward identifying the factors that put women at higher risk for malignancy. For example, older age is one of the most significant risk factors identified in the study, she added.
Dr. Alvi reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Women undergoing hysterectomy or myomectomy for benign indications, who also had fibroids, were less likely to have a malignant diagnosis, according to a study presented at the AAGL Global Congress.
These findings could change the conversation when it comes to counseling patients about the risks associated with morcellation, a procedure that was strongly discouraged by the FDA in 2014 due to the concern that it might have the potential to spread malignancy.
“There’s a lot of things going on in the media about morcellation and risk of malignancy at the time of benign fibroid surgery, but this research actually makes apparent the higher risk of malignancy when fibroids are not present,” Farah Alvi, MD, a second-year fellow at Northwestern University, Chicago, said in an interview. Despite the concerns regarding morcellation and malignancy, this research suggests that patients who have fibroids at time of surgery may have a lower chance of malignancy, compared with patients who have other indications for surgery, she explained.
Dr. Alvi and her colleagues studied 2,987 hysterectomy or myomectomy patients with benign indications between January 2005 and December 2014.
Among patients studied, researchers found 33 confirmed malignant or borderline tumors, 16 of 1,790 (0.89%) in the leiomyoma group and 17 of 1,197 (1.42%) in the group with other indications (P = 0.04). The malignancies/borderline tumors included three leiomyosarcomas, two endometrial sarcomas, two endometrioid adenocarcinomas, one granulose cell tumor, three smooth muscle tumors of uncertain malignant potential, three atypical leiomyoma, and one serous papillary borderline ovarian tumor.
Of those with leiomyomata, 1 in 600 patients were diagnosed with leiomyosarcoma, compared with a risk of 1 in 350 for unanticipated malignancy in general.
Patients with surgical indications of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) for diagnosis of an unanticipated malignancy, compared with those without leiomyoma, according to Dr. Alvi. The odds of malignancy were also reduced in patients with uterine sizes of 15-20 weeks (OR, 0.65; P = .43) and those with specimen sizes of 250-500 grams (OR, 0.68; P = .64).
These findings will have implications for how physicians counsel women undergoing minimally invasive hysterectomy or myomectomy, Dr. Alvi said.
“In counseling patients about morcellation, we often have quoted them an estimated risk of 1 in 458 for leiomyosarcoma, based on the FDA morcellation warnings, and one thing we can learn is that risk is actually much lower than we think it is,” Dr. Alvi said.
The findings also suggest a shift in focus toward identifying the factors that put women at higher risk for malignancy. For example, older age is one of the most significant risk factors identified in the study, she added.
Dr. Alvi reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Women undergoing hysterectomy or myomectomy for benign indications, who also had fibroids, were less likely to have a malignant diagnosis, according to a study presented at the AAGL Global Congress.
These findings could change the conversation when it comes to counseling patients about the risks associated with morcellation, a procedure that was strongly discouraged by the FDA in 2014 due to the concern that it might have the potential to spread malignancy.
“There’s a lot of things going on in the media about morcellation and risk of malignancy at the time of benign fibroid surgery, but this research actually makes apparent the higher risk of malignancy when fibroids are not present,” Farah Alvi, MD, a second-year fellow at Northwestern University, Chicago, said in an interview. Despite the concerns regarding morcellation and malignancy, this research suggests that patients who have fibroids at time of surgery may have a lower chance of malignancy, compared with patients who have other indications for surgery, she explained.
Dr. Alvi and her colleagues studied 2,987 hysterectomy or myomectomy patients with benign indications between January 2005 and December 2014.
Among patients studied, researchers found 33 confirmed malignant or borderline tumors, 16 of 1,790 (0.89%) in the leiomyoma group and 17 of 1,197 (1.42%) in the group with other indications (P = 0.04). The malignancies/borderline tumors included three leiomyosarcomas, two endometrial sarcomas, two endometrioid adenocarcinomas, one granulose cell tumor, three smooth muscle tumors of uncertain malignant potential, three atypical leiomyoma, and one serous papillary borderline ovarian tumor.
Of those with leiomyomata, 1 in 600 patients were diagnosed with leiomyosarcoma, compared with a risk of 1 in 350 for unanticipated malignancy in general.
Patients with surgical indications of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) for diagnosis of an unanticipated malignancy, compared with those without leiomyoma, according to Dr. Alvi. The odds of malignancy were also reduced in patients with uterine sizes of 15-20 weeks (OR, 0.65; P = .43) and those with specimen sizes of 250-500 grams (OR, 0.68; P = .64).
These findings will have implications for how physicians counsel women undergoing minimally invasive hysterectomy or myomectomy, Dr. Alvi said.
“In counseling patients about morcellation, we often have quoted them an estimated risk of 1 in 458 for leiomyosarcoma, based on the FDA morcellation warnings, and one thing we can learn is that risk is actually much lower than we think it is,” Dr. Alvi said.
The findings also suggest a shift in focus toward identifying the factors that put women at higher risk for malignancy. For example, older age is one of the most significant risk factors identified in the study, she added.
Dr. Alvi reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
AT AAGL 2017
Key clinical point:
Major finding: Patients with preoperative indication of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) of having a diagnosis of malignancy.
Data source: Retrospective study of 2,987 hysterectomies or myomectomies between January 2005 and December 2014.
Disclosures: Dr. Alvi reported having no relevant financial disclosures.
Single-port laparoscopy has few complications but BMI matters
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.

“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.
“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.
“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
AT AAGL 2017
Key clinical point:
Major finding: Obese patients experienced a 1% increase in risk of surgical complications per unit value increase of BMI.
Data source: Retrospective cohort study of 587 consecutive patients undergoing single-port laparoscopy at a single academic institution.
Disclosures: Dr. Al-Niaimi reported having no financial disclosures.
ACOG updates guidance on pelvic organ prolapse
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
(POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
(POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
(POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
FROM OBSTETRICS & GYNECOLOGY
FDA: Ultrasound surgical devices are contraindicated for uterine fibroid removal
, according to the Food and Drug Administration.
These devices have the potential to disseminate undetected tumor tissue, and there are no proven preoperative screening methods for detecting uterine sarcoma in uterine fibroids that otherwise appear to be benign, FDA officials wrote in a guidance document issued Oct. 30. The FDA is calling for new product labeling for these devices within 120 days.
The devices deliver ultrasonic energy through an oscillating tip, which leads to tissue fragmentation. This can lead to tissue dissemination that cannot be eliminated by suction/aspiration. In advanced cancers, the risk of dissemination may be outweighed by the benefits of the devices, including the debulking effect with no thermal collateral damage, as well as avoidance of the need for organ removal or resection.
The devices are currently labeled in a way that suggests they could be used in removing uterine fibroids, though the agency said that it is not aware that they are used for this purpose.
The agency recommended against their use in uterine fibroids, in part because there are alternative treatment options available. But the American College of Obstetricians and Gynecologists has challenged that assertion. When the FDA first issued a draft notice of the labeling guidance in November 2016, ACOG commented that abdominal hysterectomy is the alternative treatment option and is associated with significant morbidity and mortality beyond that seen with minimally invasive techniques. ACOG urged the FDA to prioritize informed consent and the weighing of risks and benefits.
Ultrasonic surgical aspirator devices are used for a wide range of surgical applications, but the recommendations apply specifically to laparoscopic surgery, open surgery, and gynecologic surgery.
, according to the Food and Drug Administration.
These devices have the potential to disseminate undetected tumor tissue, and there are no proven preoperative screening methods for detecting uterine sarcoma in uterine fibroids that otherwise appear to be benign, FDA officials wrote in a guidance document issued Oct. 30. The FDA is calling for new product labeling for these devices within 120 days.
The devices deliver ultrasonic energy through an oscillating tip, which leads to tissue fragmentation. This can lead to tissue dissemination that cannot be eliminated by suction/aspiration. In advanced cancers, the risk of dissemination may be outweighed by the benefits of the devices, including the debulking effect with no thermal collateral damage, as well as avoidance of the need for organ removal or resection.
The devices are currently labeled in a way that suggests they could be used in removing uterine fibroids, though the agency said that it is not aware that they are used for this purpose.
The agency recommended against their use in uterine fibroids, in part because there are alternative treatment options available. But the American College of Obstetricians and Gynecologists has challenged that assertion. When the FDA first issued a draft notice of the labeling guidance in November 2016, ACOG commented that abdominal hysterectomy is the alternative treatment option and is associated with significant morbidity and mortality beyond that seen with minimally invasive techniques. ACOG urged the FDA to prioritize informed consent and the weighing of risks and benefits.
Ultrasonic surgical aspirator devices are used for a wide range of surgical applications, but the recommendations apply specifically to laparoscopic surgery, open surgery, and gynecologic surgery.
, according to the Food and Drug Administration.
These devices have the potential to disseminate undetected tumor tissue, and there are no proven preoperative screening methods for detecting uterine sarcoma in uterine fibroids that otherwise appear to be benign, FDA officials wrote in a guidance document issued Oct. 30. The FDA is calling for new product labeling for these devices within 120 days.
The devices deliver ultrasonic energy through an oscillating tip, which leads to tissue fragmentation. This can lead to tissue dissemination that cannot be eliminated by suction/aspiration. In advanced cancers, the risk of dissemination may be outweighed by the benefits of the devices, including the debulking effect with no thermal collateral damage, as well as avoidance of the need for organ removal or resection.
The devices are currently labeled in a way that suggests they could be used in removing uterine fibroids, though the agency said that it is not aware that they are used for this purpose.
The agency recommended against their use in uterine fibroids, in part because there are alternative treatment options available. But the American College of Obstetricians and Gynecologists has challenged that assertion. When the FDA first issued a draft notice of the labeling guidance in November 2016, ACOG commented that abdominal hysterectomy is the alternative treatment option and is associated with significant morbidity and mortality beyond that seen with minimally invasive techniques. ACOG urged the FDA to prioritize informed consent and the weighing of risks and benefits.
Ultrasonic surgical aspirator devices are used for a wide range of surgical applications, but the recommendations apply specifically to laparoscopic surgery, open surgery, and gynecologic surgery.
Use multimodal analgesia protocols after minimally invasive gynecologic surgery
Minimally invasive gynecologic surgeons can combat the opioid epidemic by devising creative, multimodal approaches to analgesia, according to the authors of an extensive narrative review.
Acetaminophen, NSAIDs, antiepileptics, and local anesthetic incision infiltration all significantly reduce postoperative pain, as does reducing laparoscopic trocar size to less than 10 mm and evacuating pneumoperitoneum at the end of a case, reported Marron Wong, MD, of Newton (Mass.)-Wellesley Hospital and her associates.
“In the midst of the opioid crisis currently affecting the United States, we believe that it is imperative for [minimally invasive gynecologic surgeons] to use these available tools,” Dr. Wong and her associates wrote in the Journal of Minimally Invasive Gynecology.
The experts reviewed studies identified through PubMed, EMBASE, and the Cochrane Database. They focused on randomized controlled trials and highlighted the role of multimodal approaches. “Reasonable evidence” supports the preemptive and postoperative use of NSAIDs and acetaminophen, as well as the preemptive use of gabapentin, pregabalin and dexamethasone, they concluded (J Minim Invasive Gynecol. 2017 Sep 27. doi: 10.1016/j.jmig.2017.09.016).
Preemptive liposomal bupivacaine also is promising, the reviewers said. In a randomized controlled trial, transverse abdominis plane (TAP) infiltration with liposomal bupivacaine was associated with significant and clinically meaningful reductions in pain, morphine use, and postoperative nausea and vomiting, compared with transverse abdominis plane infiltration with regular bupivacaine (Gynecol Oncol. 2015 Sep;138[3]:609-13).
“Local infiltration [also] has been shown to decrease pain as well as opioid intake,” the reviewers wrote. “Pre-closure infiltration has been shown to have more effect than pre-incisional dosing.” Bupivicaine has a longer duration of action (120-240 minutes) than lidocaine (30-60 minutes), which can be extended further by adding epinephrine, they noted.
The adverse effects of alpha-2 agonists (bradycardia and hypotension) and N-methyl-d-aspartate receptor antagonists (vivid dreams, hallucination, emergence confusion) limit their use, the reviewers found.
Another recent systematic review drew similar conclusions, recommending NSAIDs, acetaminophen, anti-epileptics, and dexamethasone for nonopioid pain management in benign minimally invasive hysterectomy (Am J Obstet Gynecol. 2017 Jun;216[6]:557-67). That review found no positive results for local anesthesia, suggesting that the benefits of local anesthesia are limited to minor procedures, Dr. Wong and her associates noted.
The authors reported having no financial disclosures.
Minimally invasive gynecologic surgeons can combat the opioid epidemic by devising creative, multimodal approaches to analgesia, according to the authors of an extensive narrative review.
Acetaminophen, NSAIDs, antiepileptics, and local anesthetic incision infiltration all significantly reduce postoperative pain, as does reducing laparoscopic trocar size to less than 10 mm and evacuating pneumoperitoneum at the end of a case, reported Marron Wong, MD, of Newton (Mass.)-Wellesley Hospital and her associates.
“In the midst of the opioid crisis currently affecting the United States, we believe that it is imperative for [minimally invasive gynecologic surgeons] to use these available tools,” Dr. Wong and her associates wrote in the Journal of Minimally Invasive Gynecology.
The experts reviewed studies identified through PubMed, EMBASE, and the Cochrane Database. They focused on randomized controlled trials and highlighted the role of multimodal approaches. “Reasonable evidence” supports the preemptive and postoperative use of NSAIDs and acetaminophen, as well as the preemptive use of gabapentin, pregabalin and dexamethasone, they concluded (J Minim Invasive Gynecol. 2017 Sep 27. doi: 10.1016/j.jmig.2017.09.016).
Preemptive liposomal bupivacaine also is promising, the reviewers said. In a randomized controlled trial, transverse abdominis plane (TAP) infiltration with liposomal bupivacaine was associated with significant and clinically meaningful reductions in pain, morphine use, and postoperative nausea and vomiting, compared with transverse abdominis plane infiltration with regular bupivacaine (Gynecol Oncol. 2015 Sep;138[3]:609-13).
“Local infiltration [also] has been shown to decrease pain as well as opioid intake,” the reviewers wrote. “Pre-closure infiltration has been shown to have more effect than pre-incisional dosing.” Bupivicaine has a longer duration of action (120-240 minutes) than lidocaine (30-60 minutes), which can be extended further by adding epinephrine, they noted.
The adverse effects of alpha-2 agonists (bradycardia and hypotension) and N-methyl-d-aspartate receptor antagonists (vivid dreams, hallucination, emergence confusion) limit their use, the reviewers found.
Another recent systematic review drew similar conclusions, recommending NSAIDs, acetaminophen, anti-epileptics, and dexamethasone for nonopioid pain management in benign minimally invasive hysterectomy (Am J Obstet Gynecol. 2017 Jun;216[6]:557-67). That review found no positive results for local anesthesia, suggesting that the benefits of local anesthesia are limited to minor procedures, Dr. Wong and her associates noted.
The authors reported having no financial disclosures.
Minimally invasive gynecologic surgeons can combat the opioid epidemic by devising creative, multimodal approaches to analgesia, according to the authors of an extensive narrative review.
Acetaminophen, NSAIDs, antiepileptics, and local anesthetic incision infiltration all significantly reduce postoperative pain, as does reducing laparoscopic trocar size to less than 10 mm and evacuating pneumoperitoneum at the end of a case, reported Marron Wong, MD, of Newton (Mass.)-Wellesley Hospital and her associates.
“In the midst of the opioid crisis currently affecting the United States, we believe that it is imperative for [minimally invasive gynecologic surgeons] to use these available tools,” Dr. Wong and her associates wrote in the Journal of Minimally Invasive Gynecology.
The experts reviewed studies identified through PubMed, EMBASE, and the Cochrane Database. They focused on randomized controlled trials and highlighted the role of multimodal approaches. “Reasonable evidence” supports the preemptive and postoperative use of NSAIDs and acetaminophen, as well as the preemptive use of gabapentin, pregabalin and dexamethasone, they concluded (J Minim Invasive Gynecol. 2017 Sep 27. doi: 10.1016/j.jmig.2017.09.016).
Preemptive liposomal bupivacaine also is promising, the reviewers said. In a randomized controlled trial, transverse abdominis plane (TAP) infiltration with liposomal bupivacaine was associated with significant and clinically meaningful reductions in pain, morphine use, and postoperative nausea and vomiting, compared with transverse abdominis plane infiltration with regular bupivacaine (Gynecol Oncol. 2015 Sep;138[3]:609-13).
“Local infiltration [also] has been shown to decrease pain as well as opioid intake,” the reviewers wrote. “Pre-closure infiltration has been shown to have more effect than pre-incisional dosing.” Bupivicaine has a longer duration of action (120-240 minutes) than lidocaine (30-60 minutes), which can be extended further by adding epinephrine, they noted.
The adverse effects of alpha-2 agonists (bradycardia and hypotension) and N-methyl-d-aspartate receptor antagonists (vivid dreams, hallucination, emergence confusion) limit their use, the reviewers found.
Another recent systematic review drew similar conclusions, recommending NSAIDs, acetaminophen, anti-epileptics, and dexamethasone for nonopioid pain management in benign minimally invasive hysterectomy (Am J Obstet Gynecol. 2017 Jun;216[6]:557-67). That review found no positive results for local anesthesia, suggesting that the benefits of local anesthesia are limited to minor procedures, Dr. Wong and her associates noted.
The authors reported having no financial disclosures.
FROM THE JOURNAL OF MINIMALLY INVASIVE GYNECOLOGY
Key clinical point:
Major finding: Medical options include acetaminophen, NSAIDs, antiepileptics, and local anesthetic incision infiltration. Surgical measures include reducing laparoscopic trocar size to less than 10 mm and evacuating pneumoperitoneum at the end of a case.
Data source: An extensive narrative review, primarily of randomized controlled trials.
Disclosures: The authors reported having no financial disclosures.
Approaching intraoperative bowel injury
Enterotomy can be a serious complication in abdominopelvic surgery, particularly if it is not immediately recognized and treated. Risk of visceral injury increases when complex dissection is required for treatment of cancer, resection of endometriosis, and extensive lysis of adhesions.
In a retrospective review from 1984 to 2003, investigators assessed intestinal injuries at the time of gynecologic operations. Of the 110 cases reported, about 37% occurred during the opening of the peritoneal cavity, 38% during adhesiolysis and pelvic dissection, 9% during laparoscopy, 9% during vaginal surgery, and 8% during dilation and curettage. Of the bowel injuries, more than 75% were minor.1 Mortality from unrecognized bowel injury is significant, and as such, appropriate recognition and management of these injuries is critical.2

Some basic principles are critical when surgeons face a bowel injury:
1. Recognize the extent of the injury, including the size of the breach, the depth (full or partial thickness), and the nature of the injury (thermal or cold).
2. Assess the integrity of the bowel, including adequacy of blood supply, prior bowel damage from radiation, and absence of downstream obstruction.
3. Ensure no other occult injuries exist in other segments.
4. Obtain adequate exposure and mobilization of the bowel beyond the site of injury, including the adjacent bowel. This involves releasing other adhesions so that adequate bowel length is available for a tension-free repair.
Methods of repair
The decision to employ each is influenced by multiple factors. Primary closure is best suited to small lesions (1 cm or less) that are a result of cold or sharp injury. However, thermal injury sustained via electrosurgical devices induces delayed tissue damage beyond the visible edges of the immediate defect, and surgeons should consider a resection of bowel to at least 1 cm beyond the immediately apparent injury site. Additionally, resection and re-anastamosis should also be considered if the damaged segment of bowel has poor blood supply, integrity, or the repair would result in tension along the suture/staple line or luminal narrowing.
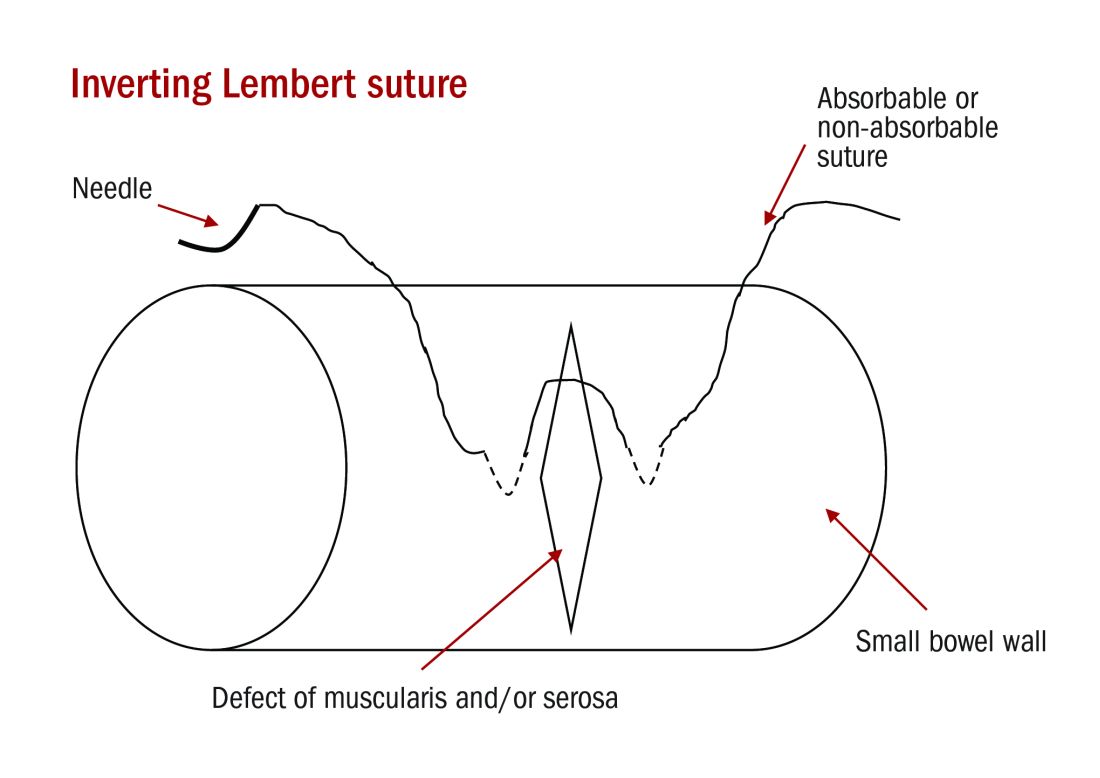
Simple small bowel closures
Serosal abrasions need not be repaired; however, small tears of the serosa and muscularis can be managed with a single layer of interrupted 3-0 absorbable or permanent silk suture on a tapered needle. The suture line should be perpendicular to the longitudinal axis of the bowel at 2-mm to 3-mm intervals in order to prevent narrowing of the lumen. The suture should pass through serosal and muscular layers in an imbricating (Lembert) stitch. For smaller defects of less than 6 mm, a single layer closure is typically adequate.
Small bowel resection
Some larger defects, thermal injuries, and segments with multiple enterotomies may be best repaired with resection and re-anastamosis technique. A segment of resectable bowel is chosen such that the afferent and efferent limbs to be re-anastamosed can be reapproximated in a tension-free fashion. A mesenterotomy is made at the proximal and distal portions of the involved bowel. A gastrointestinal anastomotic stapler is then inserted perpendicularly across the bowel. The remaining wedge of connected mesentery can then be efficiently excised with an electrothermal bipolar coagulator device ensuring that maximal mesentery and blood supply are preserved to the remaining limbs of intestine. The proximal and distal segments are then aligned at the antimesenteric sides.

Large bowel repair
Defects in the serosa and small lacerations can be managed with a primary closure, similar to the small intestine. For more extensive injuries that may require resection, diversion, or complicated repair, consultation with a gynecologic oncologist or general or colorectal surgeon may be indicated as colotomy repairs are associated with higher rates of breakdown and fistula. If fecal contamination is present, copious irrigation should be performed and placement of a peritoneal drain to reduce the likelihood of abscess formation should be considered. If appropriate antibiotic prophylaxis for colonic surgery has not been given prior to skin incision, it should be administered once the colotomy is identified.
Standard prophylaxis for hysterectomy (such as a first-generation cephalosporin like cefazolin) is not adequate for large bowel surgery, and either metronidazole should be added or a second-generation cephalosporin such as cefoxitin should be given. For patients with penicillin allergy, clindamycin or vancomycin with either gentamicin or a fluoroquinolone should be administered.6
Postoperative management
The potential for postoperative morbidity must be understood for appropriate management following bowel surgery. Ileus is common and the clinician should understand how to diagnose and manage it. Additionally, intra-abdominal abscess, anastomotic leak, fistula formation, and mechanical obstruction are complications that may require surgical intervention and must be vigilantly managed.
The routine use of postoperative nasogastric tube (NGT) does not hasten return of bowel function or prevent leak from sites of gastrointestinal repair. In fact, early feeding has been associated with reduced perioperative complications and earlier return of bowel function has been observed without the use of NGT.7 In general, for small and large intestinal injuries, early feeding is considered acceptable.8
Prolonged antibiotic prophylaxis, beyond 24 hours, is not recommended.6
Avoiding injury
Gynecologic surgeons should adhere to surgical principles with sharp dissection for adhesions, gentle tissue handling, adequate exposure, and light retraction to prevent bowel injury or minimize their extent. Laparoscopic entry sites should be chosen based on the likelihood of abdominal adhesions. When the patient’s history predicts a high likelihood of intraperitoneal adhesions, the left upper quadrant site should be strongly considered as the entry site. The likelihood of gastrointestinal injury is not influenced by open versus closed laparoscopic entry and surgeons should use the technique with which they have the greatest experience and skill.9 However, in patients who have had prior laparotomies, there is an increased risk of periumbilical adhesions, and consideration should be made for a nonumbilical entry site.10 Methodical sharp dissection and sparing use of thermal energy should be used with adhesiolysis. When injury occurs, prompt recognition, preparation, and methodical management can mitigate the impact.
Dr. Staley is a gynecologic oncology fellow at the University of North Carolina, Chapel Hill. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the university. They reported having no relevant financial disclosures.
References
1. Int Surg. 2006 Nov-Dec;91(6):336-40.
2. J Am Coll Surg. 2001 Jun;192(6):677-83.
3. Doherty, G. Current Diagnosis and Treatment: Surgery. Thirteenth Edition. New York: McGraw Hill, 2010.
4. Hoffman B. Williams Gynecology. Third Edition. New York: McGraw Hill, 2016.
5. Berek J, Hacker N. Berek & Hacker’s Gynecologic Oncology. Sixth Edition. Philadelphia: Wolters Kluwer, 2015.
6. Surg Infect (Larchmt). 2013 Feb;14(1):73-156.
7. Br J Surg. 2005 Jun;92(6):673-80.
8. Am J Obstet Gynecol. 2001 Jul;185(1):1-4.
9. Cochrane Database Syst Rev. 2015 Aug 31;8:CD006583.
10. Br J Obstet Gynaecol. 1997 May;104(5):595-600.
Enterotomy can be a serious complication in abdominopelvic surgery, particularly if it is not immediately recognized and treated. Risk of visceral injury increases when complex dissection is required for treatment of cancer, resection of endometriosis, and extensive lysis of adhesions.
In a retrospective review from 1984 to 2003, investigators assessed intestinal injuries at the time of gynecologic operations. Of the 110 cases reported, about 37% occurred during the opening of the peritoneal cavity, 38% during adhesiolysis and pelvic dissection, 9% during laparoscopy, 9% during vaginal surgery, and 8% during dilation and curettage. Of the bowel injuries, more than 75% were minor.1 Mortality from unrecognized bowel injury is significant, and as such, appropriate recognition and management of these injuries is critical.2
Some basic principles are critical when surgeons face a bowel injury:
1. Recognize the extent of the injury, including the size of the breach, the depth (full or partial thickness), and the nature of the injury (thermal or cold).
2. Assess the integrity of the bowel, including adequacy of blood supply, prior bowel damage from radiation, and absence of downstream obstruction.
3. Ensure no other occult injuries exist in other segments.
4. Obtain adequate exposure and mobilization of the bowel beyond the site of injury, including the adjacent bowel. This involves releasing other adhesions so that adequate bowel length is available for a tension-free repair.
Methods of repair
The decision to employ each is influenced by multiple factors. Primary closure is best suited to small lesions (1 cm or less) that are a result of cold or sharp injury. However, thermal injury sustained via electrosurgical devices induces delayed tissue damage beyond the visible edges of the immediate defect, and surgeons should consider a resection of bowel to at least 1 cm beyond the immediately apparent injury site. Additionally, resection and re-anastamosis should also be considered if the damaged segment of bowel has poor blood supply, integrity, or the repair would result in tension along the suture/staple line or luminal narrowing.
Simple small bowel closures
Serosal abrasions need not be repaired; however, small tears of the serosa and muscularis can be managed with a single layer of interrupted 3-0 absorbable or permanent silk suture on a tapered needle. The suture line should be perpendicular to the longitudinal axis of the bowel at 2-mm to 3-mm intervals in order to prevent narrowing of the lumen. The suture should pass through serosal and muscular layers in an imbricating (Lembert) stitch. For smaller defects of less than 6 mm, a single layer closure is typically adequate.
Small bowel resection
Some larger defects, thermal injuries, and segments with multiple enterotomies may be best repaired with resection and re-anastamosis technique. A segment of resectable bowel is chosen such that the afferent and efferent limbs to be re-anastamosed can be reapproximated in a tension-free fashion. A mesenterotomy is made at the proximal and distal portions of the involved bowel. A gastrointestinal anastomotic stapler is then inserted perpendicularly across the bowel. The remaining wedge of connected mesentery can then be efficiently excised with an electrothermal bipolar coagulator device ensuring that maximal mesentery and blood supply are preserved to the remaining limbs of intestine. The proximal and distal segments are then aligned at the antimesenteric sides.
Large bowel repair
Defects in the serosa and small lacerations can be managed with a primary closure, similar to the small intestine. For more extensive injuries that may require resection, diversion, or complicated repair, consultation with a gynecologic oncologist or general or colorectal surgeon may be indicated as colotomy repairs are associated with higher rates of breakdown and fistula. If fecal contamination is present, copious irrigation should be performed and placement of a peritoneal drain to reduce the likelihood of abscess formation should be considered. If appropriate antibiotic prophylaxis for colonic surgery has not been given prior to skin incision, it should be administered once the colotomy is identified.
Standard prophylaxis for hysterectomy (such as a first-generation cephalosporin like cefazolin) is not adequate for large bowel surgery, and either metronidazole should be added or a second-generation cephalosporin such as cefoxitin should be given. For patients with penicillin allergy, clindamycin or vancomycin with either gentamicin or a fluoroquinolone should be administered.6
Postoperative management
The potential for postoperative morbidity must be understood for appropriate management following bowel surgery. Ileus is common and the clinician should understand how to diagnose and manage it. Additionally, intra-abdominal abscess, anastomotic leak, fistula formation, and mechanical obstruction are complications that may require surgical intervention and must be vigilantly managed.
The routine use of postoperative nasogastric tube (NGT) does not hasten return of bowel function or prevent leak from sites of gastrointestinal repair. In fact, early feeding has been associated with reduced perioperative complications and earlier return of bowel function has been observed without the use of NGT.7 In general, for small and large intestinal injuries, early feeding is considered acceptable.8
Prolonged antibiotic prophylaxis, beyond 24 hours, is not recommended.6
Avoiding injury
Gynecologic surgeons should adhere to surgical principles with sharp dissection for adhesions, gentle tissue handling, adequate exposure, and light retraction to prevent bowel injury or minimize their extent. Laparoscopic entry sites should be chosen based on the likelihood of abdominal adhesions. When the patient’s history predicts a high likelihood of intraperitoneal adhesions, the left upper quadrant site should be strongly considered as the entry site. The likelihood of gastrointestinal injury is not influenced by open versus closed laparoscopic entry and surgeons should use the technique with which they have the greatest experience and skill.9 However, in patients who have had prior laparotomies, there is an increased risk of periumbilical adhesions, and consideration should be made for a nonumbilical entry site.10 Methodical sharp dissection and sparing use of thermal energy should be used with adhesiolysis. When injury occurs, prompt recognition, preparation, and methodical management can mitigate the impact.
Dr. Staley is a gynecologic oncology fellow at the University of North Carolina, Chapel Hill. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the university. They reported having no relevant financial disclosures.
References
1. Int Surg. 2006 Nov-Dec;91(6):336-40.
2. J Am Coll Surg. 2001 Jun;192(6):677-83.
3. Doherty, G. Current Diagnosis and Treatment: Surgery. Thirteenth Edition. New York: McGraw Hill, 2010.
4. Hoffman B. Williams Gynecology. Third Edition. New York: McGraw Hill, 2016.
5. Berek J, Hacker N. Berek & Hacker’s Gynecologic Oncology. Sixth Edition. Philadelphia: Wolters Kluwer, 2015.
6. Surg Infect (Larchmt). 2013 Feb;14(1):73-156.
7. Br J Surg. 2005 Jun;92(6):673-80.
8. Am J Obstet Gynecol. 2001 Jul;185(1):1-4.
9. Cochrane Database Syst Rev. 2015 Aug 31;8:CD006583.
10. Br J Obstet Gynaecol. 1997 May;104(5):595-600.
Enterotomy can be a serious complication in abdominopelvic surgery, particularly if it is not immediately recognized and treated. Risk of visceral injury increases when complex dissection is required for treatment of cancer, resection of endometriosis, and extensive lysis of adhesions.
In a retrospective review from 1984 to 2003, investigators assessed intestinal injuries at the time of gynecologic operations. Of the 110 cases reported, about 37% occurred during the opening of the peritoneal cavity, 38% during adhesiolysis and pelvic dissection, 9% during laparoscopy, 9% during vaginal surgery, and 8% during dilation and curettage. Of the bowel injuries, more than 75% were minor.1 Mortality from unrecognized bowel injury is significant, and as such, appropriate recognition and management of these injuries is critical.2
Some basic principles are critical when surgeons face a bowel injury:
1. Recognize the extent of the injury, including the size of the breach, the depth (full or partial thickness), and the nature of the injury (thermal or cold).
2. Assess the integrity of the bowel, including adequacy of blood supply, prior bowel damage from radiation, and absence of downstream obstruction.
3. Ensure no other occult injuries exist in other segments.
4. Obtain adequate exposure and mobilization of the bowel beyond the site of injury, including the adjacent bowel. This involves releasing other adhesions so that adequate bowel length is available for a tension-free repair.
Methods of repair
The decision to employ each is influenced by multiple factors. Primary closure is best suited to small lesions (1 cm or less) that are a result of cold or sharp injury. However, thermal injury sustained via electrosurgical devices induces delayed tissue damage beyond the visible edges of the immediate defect, and surgeons should consider a resection of bowel to at least 1 cm beyond the immediately apparent injury site. Additionally, resection and re-anastamosis should also be considered if the damaged segment of bowel has poor blood supply, integrity, or the repair would result in tension along the suture/staple line or luminal narrowing.
Simple small bowel closures
Serosal abrasions need not be repaired; however, small tears of the serosa and muscularis can be managed with a single layer of interrupted 3-0 absorbable or permanent silk suture on a tapered needle. The suture line should be perpendicular to the longitudinal axis of the bowel at 2-mm to 3-mm intervals in order to prevent narrowing of the lumen. The suture should pass through serosal and muscular layers in an imbricating (Lembert) stitch. For smaller defects of less than 6 mm, a single layer closure is typically adequate.
Small bowel resection
Some larger defects, thermal injuries, and segments with multiple enterotomies may be best repaired with resection and re-anastamosis technique. A segment of resectable bowel is chosen such that the afferent and efferent limbs to be re-anastamosed can be reapproximated in a tension-free fashion. A mesenterotomy is made at the proximal and distal portions of the involved bowel. A gastrointestinal anastomotic stapler is then inserted perpendicularly across the bowel. The remaining wedge of connected mesentery can then be efficiently excised with an electrothermal bipolar coagulator device ensuring that maximal mesentery and blood supply are preserved to the remaining limbs of intestine. The proximal and distal segments are then aligned at the antimesenteric sides.
Large bowel repair
Defects in the serosa and small lacerations can be managed with a primary closure, similar to the small intestine. For more extensive injuries that may require resection, diversion, or complicated repair, consultation with a gynecologic oncologist or general or colorectal surgeon may be indicated as colotomy repairs are associated with higher rates of breakdown and fistula. If fecal contamination is present, copious irrigation should be performed and placement of a peritoneal drain to reduce the likelihood of abscess formation should be considered. If appropriate antibiotic prophylaxis for colonic surgery has not been given prior to skin incision, it should be administered once the colotomy is identified.
Standard prophylaxis for hysterectomy (such as a first-generation cephalosporin like cefazolin) is not adequate for large bowel surgery, and either metronidazole should be added or a second-generation cephalosporin such as cefoxitin should be given. For patients with penicillin allergy, clindamycin or vancomycin with either gentamicin or a fluoroquinolone should be administered.6
Postoperative management
The potential for postoperative morbidity must be understood for appropriate management following bowel surgery. Ileus is common and the clinician should understand how to diagnose and manage it. Additionally, intra-abdominal abscess, anastomotic leak, fistula formation, and mechanical obstruction are complications that may require surgical intervention and must be vigilantly managed.
The routine use of postoperative nasogastric tube (NGT) does not hasten return of bowel function or prevent leak from sites of gastrointestinal repair. In fact, early feeding has been associated with reduced perioperative complications and earlier return of bowel function has been observed without the use of NGT.7 In general, for small and large intestinal injuries, early feeding is considered acceptable.8
Prolonged antibiotic prophylaxis, beyond 24 hours, is not recommended.6
Avoiding injury
Gynecologic surgeons should adhere to surgical principles with sharp dissection for adhesions, gentle tissue handling, adequate exposure, and light retraction to prevent bowel injury or minimize their extent. Laparoscopic entry sites should be chosen based on the likelihood of abdominal adhesions. When the patient’s history predicts a high likelihood of intraperitoneal adhesions, the left upper quadrant site should be strongly considered as the entry site. The likelihood of gastrointestinal injury is not influenced by open versus closed laparoscopic entry and surgeons should use the technique with which they have the greatest experience and skill.9 However, in patients who have had prior laparotomies, there is an increased risk of periumbilical adhesions, and consideration should be made for a nonumbilical entry site.10 Methodical sharp dissection and sparing use of thermal energy should be used with adhesiolysis. When injury occurs, prompt recognition, preparation, and methodical management can mitigate the impact.
Dr. Staley is a gynecologic oncology fellow at the University of North Carolina, Chapel Hill. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the university. They reported having no relevant financial disclosures.
References
1. Int Surg. 2006 Nov-Dec;91(6):336-40.
2. J Am Coll Surg. 2001 Jun;192(6):677-83.
3. Doherty, G. Current Diagnosis and Treatment: Surgery. Thirteenth Edition. New York: McGraw Hill, 2010.
4. Hoffman B. Williams Gynecology. Third Edition. New York: McGraw Hill, 2016.
5. Berek J, Hacker N. Berek & Hacker’s Gynecologic Oncology. Sixth Edition. Philadelphia: Wolters Kluwer, 2015.
6. Surg Infect (Larchmt). 2013 Feb;14(1):73-156.
7. Br J Surg. 2005 Jun;92(6):673-80.
8. Am J Obstet Gynecol. 2001 Jul;185(1):1-4.
9. Cochrane Database Syst Rev. 2015 Aug 31;8:CD006583.
10. Br J Obstet Gynaecol. 1997 May;104(5):595-600.
Consider routine penicillin allergy testing in obstetrics
PARK CITY, UTAH – When attendees at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology were asked if their institutions test to confirm alleged penicillin allergies, the only hands that went up were from clinicians at Duke University.
That’s a problem, according to Robert Heine, MD, a maternal-fetal medicine specialist at Duke, in Durham, N.C. “We, as a group, need to be doing [penicillin] allergy testing,” he said.
It’s become clear in recent years that patients who say they have a penicillin allergy often don’t have one, or remember a mild reaction from childhood that doesn’t preclude the use of beta-lactam antibiotics as adults. For decades, however, clinicians have taken those claims at face value, and duly noted them in charts and switched patients to non–beta-lactam antibiotics that don’t work as well.
That’s what happened at Duke in 2014. A total of 81 women with documented penicillin allergies were put on gentamicin and clindamycin to protect against cesarean wound infections and 16% ended up with infections anyway. Among the 864 women who received cefazolin – the first-line cesarean prophylaxis choice at Duke – the infection rate was 7%.
“Beta-lactam antibiotic prophylaxis reduced the risk of surgical site infections after cesareans by 60%,” said Benjamin Harris, MD, the lead investigator and an ob.gyn. resident at Duke, who presented the findings at the meeting.

When the investigators took a closer look at the 81 women who reported penicillin allergies, most of them had rashes and other mild reactions noted in their charts.
Findings such as those led Dr. Heine to push for routine testing. “I brought Duke into it kicking and screaming,” he said. The biggest obstacle was concern over liability, specifically that pregnant women would go into anaphylaxis and deliver prematurely, he said.
After a lot of lobbying, Dr. Heine and his colleagues started routine penicillin allergy testing in March 2016. There hasn’t been a single reaction among the 80-plus pregnant women tested so far, he reported.
Duke administrators were also concerned about reimbursement, but it hasn’t turned out to be a problem. Reimbursements from public and private payers “cover our costs,” a little over $100 per test, Dr. Heine said.
Dr. Heine said he can imagine outpatient testing at some point, but for now women are checked into triage. They get a fetal heart tone before 24 weeks, and a fetal heart rate monitor afterward. “We try to do it before 20 weeks so we don’t have to worry about the fetus,” he said.
When penicillin allergies are in the chart, or women say they are allergic, ask what type of reaction they had in the past. Type 1 reactions should be confirmed with testing. It’s okay to skip testing and give beta-lactams for non–type 1 reactions, but “if a woman has a non–type 1, and they’re already set up for testing, I’m going to do it anyway because getting the penicillin allergy off her chart is good for her and her life,” Dr. Heine said.
Dr. Heine and Dr. Harris reported having no financial disclosures.
PARK CITY, UTAH – When attendees at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology were asked if their institutions test to confirm alleged penicillin allergies, the only hands that went up were from clinicians at Duke University.
That’s a problem, according to Robert Heine, MD, a maternal-fetal medicine specialist at Duke, in Durham, N.C. “We, as a group, need to be doing [penicillin] allergy testing,” he said.
It’s become clear in recent years that patients who say they have a penicillin allergy often don’t have one, or remember a mild reaction from childhood that doesn’t preclude the use of beta-lactam antibiotics as adults. For decades, however, clinicians have taken those claims at face value, and duly noted them in charts and switched patients to non–beta-lactam antibiotics that don’t work as well.
That’s what happened at Duke in 2014. A total of 81 women with documented penicillin allergies were put on gentamicin and clindamycin to protect against cesarean wound infections and 16% ended up with infections anyway. Among the 864 women who received cefazolin – the first-line cesarean prophylaxis choice at Duke – the infection rate was 7%.
“Beta-lactam antibiotic prophylaxis reduced the risk of surgical site infections after cesareans by 60%,” said Benjamin Harris, MD, the lead investigator and an ob.gyn. resident at Duke, who presented the findings at the meeting.
When the investigators took a closer look at the 81 women who reported penicillin allergies, most of them had rashes and other mild reactions noted in their charts.
Findings such as those led Dr. Heine to push for routine testing. “I brought Duke into it kicking and screaming,” he said. The biggest obstacle was concern over liability, specifically that pregnant women would go into anaphylaxis and deliver prematurely, he said.
After a lot of lobbying, Dr. Heine and his colleagues started routine penicillin allergy testing in March 2016. There hasn’t been a single reaction among the 80-plus pregnant women tested so far, he reported.
Duke administrators were also concerned about reimbursement, but it hasn’t turned out to be a problem. Reimbursements from public and private payers “cover our costs,” a little over $100 per test, Dr. Heine said.
Dr. Heine said he can imagine outpatient testing at some point, but for now women are checked into triage. They get a fetal heart tone before 24 weeks, and a fetal heart rate monitor afterward. “We try to do it before 20 weeks so we don’t have to worry about the fetus,” he said.
When penicillin allergies are in the chart, or women say they are allergic, ask what type of reaction they had in the past. Type 1 reactions should be confirmed with testing. It’s okay to skip testing and give beta-lactams for non–type 1 reactions, but “if a woman has a non–type 1, and they’re already set up for testing, I’m going to do it anyway because getting the penicillin allergy off her chart is good for her and her life,” Dr. Heine said.
Dr. Heine and Dr. Harris reported having no financial disclosures.
PARK CITY, UTAH – When attendees at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology were asked if their institutions test to confirm alleged penicillin allergies, the only hands that went up were from clinicians at Duke University.
That’s a problem, according to Robert Heine, MD, a maternal-fetal medicine specialist at Duke, in Durham, N.C. “We, as a group, need to be doing [penicillin] allergy testing,” he said.
It’s become clear in recent years that patients who say they have a penicillin allergy often don’t have one, or remember a mild reaction from childhood that doesn’t preclude the use of beta-lactam antibiotics as adults. For decades, however, clinicians have taken those claims at face value, and duly noted them in charts and switched patients to non–beta-lactam antibiotics that don’t work as well.
That’s what happened at Duke in 2014. A total of 81 women with documented penicillin allergies were put on gentamicin and clindamycin to protect against cesarean wound infections and 16% ended up with infections anyway. Among the 864 women who received cefazolin – the first-line cesarean prophylaxis choice at Duke – the infection rate was 7%.
“Beta-lactam antibiotic prophylaxis reduced the risk of surgical site infections after cesareans by 60%,” said Benjamin Harris, MD, the lead investigator and an ob.gyn. resident at Duke, who presented the findings at the meeting.
When the investigators took a closer look at the 81 women who reported penicillin allergies, most of them had rashes and other mild reactions noted in their charts.
Findings such as those led Dr. Heine to push for routine testing. “I brought Duke into it kicking and screaming,” he said. The biggest obstacle was concern over liability, specifically that pregnant women would go into anaphylaxis and deliver prematurely, he said.
After a lot of lobbying, Dr. Heine and his colleagues started routine penicillin allergy testing in March 2016. There hasn’t been a single reaction among the 80-plus pregnant women tested so far, he reported.
Duke administrators were also concerned about reimbursement, but it hasn’t turned out to be a problem. Reimbursements from public and private payers “cover our costs,” a little over $100 per test, Dr. Heine said.
Dr. Heine said he can imagine outpatient testing at some point, but for now women are checked into triage. They get a fetal heart tone before 24 weeks, and a fetal heart rate monitor afterward. “We try to do it before 20 weeks so we don’t have to worry about the fetus,” he said.
When penicillin allergies are in the chart, or women say they are allergic, ask what type of reaction they had in the past. Type 1 reactions should be confirmed with testing. It’s okay to skip testing and give beta-lactams for non–type 1 reactions, but “if a woman has a non–type 1, and they’re already set up for testing, I’m going to do it anyway because getting the penicillin allergy off her chart is good for her and her life,” Dr. Heine said.
Dr. Heine and Dr. Harris reported having no financial disclosures.
AT IDSOG
Key clinical point:
Major finding: Among 81 women with documented penicillin allergies who received gentamicin and clindamycin, 16% developed surgical site infections. In contrast, among the 864 women who received cefazolin, the infection rate was 7%.
Data source: A single-center review at Duke University.
Disclosures: The investigators reported having no relevant financial disclosures.
VIDEO: How to catch postpartum necrotizing fasciitis in time
PARK CITY, UTAH – , and it’s easy to misdiagnose at first.
There’s no pus, and the skin can look mostly normal with just a little swelling. The tipoff is pain that seems out of proportion to the clinical signs.
David Eschenbach, MD, chair of the department of obstetrics and gynecology at the University of Washington, Seattle, knows the infection well. In an interview at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, he shared his insights on how physicians can recognize and treat postpartum necrotizing fasciitis in time to limit the damage.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PARK CITY, UTAH – , and it’s easy to misdiagnose at first.
There’s no pus, and the skin can look mostly normal with just a little swelling. The tipoff is pain that seems out of proportion to the clinical signs.
David Eschenbach, MD, chair of the department of obstetrics and gynecology at the University of Washington, Seattle, knows the infection well. In an interview at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, he shared his insights on how physicians can recognize and treat postpartum necrotizing fasciitis in time to limit the damage.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PARK CITY, UTAH – , and it’s easy to misdiagnose at first.
There’s no pus, and the skin can look mostly normal with just a little swelling. The tipoff is pain that seems out of proportion to the clinical signs.
David Eschenbach, MD, chair of the department of obstetrics and gynecology at the University of Washington, Seattle, knows the infection well. In an interview at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, he shared his insights on how physicians can recognize and treat postpartum necrotizing fasciitis in time to limit the damage.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT IDSOG

VIDEO: When to turn to surgery in postpartum uterine infection
PARK CITY, UTAH – When postpartum infections don’t respond to antibiotics, doctors and surgeons need to move fast; surgery – often hysterectomy – is the only thing that will save the woman’s life.
The problem is that with today’s antibiotics, doctors may have never encountered the situation, and sometimes continue to treat with antibiotics until it’s too late.
In Seattle, physicians turn to David Eschenbach, MD, chair of the department of obstetrics and gynecology at the University of Washington, for advice on when it’s time to give up on antibiotics and go to the OR. It’s a difficult decision, especially when patients are young.
In an interview at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, Dr. Eschenbach shared what he’s learned from decades of experience in dealing with one of the most devastating postpartum complications.
PARK CITY, UTAH – When postpartum infections don’t respond to antibiotics, doctors and surgeons need to move fast; surgery – often hysterectomy – is the only thing that will save the woman’s life.
The problem is that with today’s antibiotics, doctors may have never encountered the situation, and sometimes continue to treat with antibiotics until it’s too late.
In Seattle, physicians turn to David Eschenbach, MD, chair of the department of obstetrics and gynecology at the University of Washington, for advice on when it’s time to give up on antibiotics and go to the OR. It’s a difficult decision, especially when patients are young.
In an interview at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, Dr. Eschenbach shared what he’s learned from decades of experience in dealing with one of the most devastating postpartum complications.
PARK CITY, UTAH – When postpartum infections don’t respond to antibiotics, doctors and surgeons need to move fast; surgery – often hysterectomy – is the only thing that will save the woman’s life.
The problem is that with today’s antibiotics, doctors may have never encountered the situation, and sometimes continue to treat with antibiotics until it’s too late.
In Seattle, physicians turn to David Eschenbach, MD, chair of the department of obstetrics and gynecology at the University of Washington, for advice on when it’s time to give up on antibiotics and go to the OR. It’s a difficult decision, especially when patients are young.
In an interview at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, Dr. Eschenbach shared what he’s learned from decades of experience in dealing with one of the most devastating postpartum complications.
AT IDSOG

C-section raises hysterectomy complication risk later
Women who have at least one cesarean delivery have a more than 30% risk of a complication requiring reoperation after benign hysterectomy later in life, compared with women who have had vaginal deliveries only, according to a study of more than 7,600 women in a Danish patient registry.
Cesarean delivery is the most common major surgery performed in the world, and the rate is rapidly increasing, with the global average cesarean rate estimated at 18.6%, and rates as high as 52% in some European countries. However, the impact cesarean deliveries have on surgical complications later in life has not been thoroughly studied. The study authors said this might be the first population study of the association of cesarean delivery with hysterectomy complications.
Of the 388 women (5%) who had a hysterectomy and then a reoperation within 30 days, the risk increased with the number of previous cesarean deliveries. Those who had vaginal-only deliveries had reoperation rates of 4.4%, compared with 6.2% for those who had one cesarean delivery and 6.8% for those who had two or more. That represents increased risks of 31% and 35% for women who had one cesarean delivery and two or more cesarean deliveries, respectively, compared with women who had only vaginal deliveries.
Likewise, surgical complications were 16% more frequent in women who had one previous cesarean delivery and 30% more likely in women with two or more cesarean deliveries. Women who had two or more cesarean deliveries were almost twice as likely (odds ratio, 1.93) to receive a blood transfusion.
“Our results imply that information on long-term associations should be made more readily available to women, clinicians, and policymakers and suggest that decisions on cesarean delivery should take into account not only immediate maternal and neonatal influences, but also women’s health in the long term, including an increased risk of reoperation and complications associated with surgery later in life,” the researchers wrote. “The results support policies and clinical efforts to prevent cesarean deliveries that are not medically indicated.”
The study noted some limitations, including the observational design, which did not allow for elimination of all potential confounding factors.
The researchers reported having no relevant financial disclosures.
Women who have at least one cesarean delivery have a more than 30% risk of a complication requiring reoperation after benign hysterectomy later in life, compared with women who have had vaginal deliveries only, according to a study of more than 7,600 women in a Danish patient registry.
Cesarean delivery is the most common major surgery performed in the world, and the rate is rapidly increasing, with the global average cesarean rate estimated at 18.6%, and rates as high as 52% in some European countries. However, the impact cesarean deliveries have on surgical complications later in life has not been thoroughly studied. The study authors said this might be the first population study of the association of cesarean delivery with hysterectomy complications.
Of the 388 women (5%) who had a hysterectomy and then a reoperation within 30 days, the risk increased with the number of previous cesarean deliveries. Those who had vaginal-only deliveries had reoperation rates of 4.4%, compared with 6.2% for those who had one cesarean delivery and 6.8% for those who had two or more. That represents increased risks of 31% and 35% for women who had one cesarean delivery and two or more cesarean deliveries, respectively, compared with women who had only vaginal deliveries.
Likewise, surgical complications were 16% more frequent in women who had one previous cesarean delivery and 30% more likely in women with two or more cesarean deliveries. Women who had two or more cesarean deliveries were almost twice as likely (odds ratio, 1.93) to receive a blood transfusion.
“Our results imply that information on long-term associations should be made more readily available to women, clinicians, and policymakers and suggest that decisions on cesarean delivery should take into account not only immediate maternal and neonatal influences, but also women’s health in the long term, including an increased risk of reoperation and complications associated with surgery later in life,” the researchers wrote. “The results support policies and clinical efforts to prevent cesarean deliveries that are not medically indicated.”
The study noted some limitations, including the observational design, which did not allow for elimination of all potential confounding factors.
The researchers reported having no relevant financial disclosures.
Women who have at least one cesarean delivery have a more than 30% risk of a complication requiring reoperation after benign hysterectomy later in life, compared with women who have had vaginal deliveries only, according to a study of more than 7,600 women in a Danish patient registry.
Cesarean delivery is the most common major surgery performed in the world, and the rate is rapidly increasing, with the global average cesarean rate estimated at 18.6%, and rates as high as 52% in some European countries. However, the impact cesarean deliveries have on surgical complications later in life has not been thoroughly studied. The study authors said this might be the first population study of the association of cesarean delivery with hysterectomy complications.
Of the 388 women (5%) who had a hysterectomy and then a reoperation within 30 days, the risk increased with the number of previous cesarean deliveries. Those who had vaginal-only deliveries had reoperation rates of 4.4%, compared with 6.2% for those who had one cesarean delivery and 6.8% for those who had two or more. That represents increased risks of 31% and 35% for women who had one cesarean delivery and two or more cesarean deliveries, respectively, compared with women who had only vaginal deliveries.
Likewise, surgical complications were 16% more frequent in women who had one previous cesarean delivery and 30% more likely in women with two or more cesarean deliveries. Women who had two or more cesarean deliveries were almost twice as likely (odds ratio, 1.93) to receive a blood transfusion.
“Our results imply that information on long-term associations should be made more readily available to women, clinicians, and policymakers and suggest that decisions on cesarean delivery should take into account not only immediate maternal and neonatal influences, but also women’s health in the long term, including an increased risk of reoperation and complications associated with surgery later in life,” the researchers wrote. “The results support policies and clinical efforts to prevent cesarean deliveries that are not medically indicated.”
The study noted some limitations, including the observational design, which did not allow for elimination of all potential confounding factors.
The researchers reported having no relevant financial disclosures.
FROM JAMA SURGERY
Key clinical point:
Major finding: The rate of complications after hysterectomy was 4.4% for women who had vaginal birth only, 6.2% for those who had one cesarean delivery, and 6.8% for those who had two or more cesarean deliveries.
Data source: Danish National Patient Registry–based cohort study of 7,685 women who gave birth from 1993 to 2012.
Disclosures: The researchers reported having no financial disclosures.