User login
'An Organization in Turmoil': Ken Kizer on the Challenges Facing the VA
'An Organization in Turmoil': Ken Kizer on the Challenges Facing the VA

Kenneth W. Kizer, MD, MPH, knows a thing or two about transition at the US Department of Veterans Affairs (VA). He served as VA Under Secretary of Health from 1994 to 1999, stepping in during an era of crisis with a mandate for transformation.
Kizer, a Distinguished Professor Emeritus at the University of California, Davis School of Medicine, is among the top thinkers about the VA and its future. He recently spoke with Federal Practitioner about community care, the electronic health record transition, and other challenges facing the Veterans Health Administration (VHA).
At stake, Kizer explained, is an invaluable service for veterans—and much more. “VA is the largest provider of training for... multiple types of health professionals that people use every day,” he said. “There’s also the research, the direct care provided to veterans, and the contingency support the VA provides, which was very well demonstrated during the COVID pandemic. These are things that benefit all Americans, not just veterans.”
When you look at the VA, what do you see?
I see an organization in turmoil, a great health care system struggling with multiple major challenges simultaneously. The VHA is becoming a very large health insurance program without the necessary infrastructure, and costs are rising rapidly. And it is trying to roll out a new EHR and implement new third-party administrator contracts while suffering from significant staffing reductions and very depressed morale.
There are a host of other high-visibility and high-impact issues, including a major reorganization. There’s been a paucity of details about exactly what is going to change, who is going to be doing what, and how the changes will affect staffing and workflow.
How will the loss of 35,000 health care positions affect veterans' care?
If you don’t have enough people, then you’re not going to be able to provide the care that is needed. Years ago, I led a project assessing the Roseburg VA Medical Center in Central Oregon. Among other things, there were a lot of problems with cardiology care. The biggest complaint the cardiologists had, and why the hospital couldn’t keep cardiologists on staff, was that there weren’t enough support staff to do the electrocardiograms. The cardiologists had to do the electrocardiograms themselves, which meant they weren’t doing other things they should be doing. You can amplify that example in a hundred different ways in VA today. If physicians don’t have adequate support, they get frustrated and disenfranchised. And they leave.
One of the fallacies I’ve heard mentioned in some congressional hearings is that it’s mainly a matter of lower pay in the VA. Pay may be an issue somewhere on the list of recruiting challenges, but more important issues higher up are things like the support clinicians receive, the work environment, whether they feel valued, and how easy it is for them to do their work. Case in point: If you put in a new EHR that doesn’t work as well as the existing one, then some doctors are going to leave.
Is VA being pushed toward privatization?
At some point it becomes a self-fulfilling prophecy. If you don’t have the staff to provide the services, then you refer more veterans to the community, and you get in a downward spiral. Patients are going to the community, you lose more staff, you continue to be unable to provide services, and more care goes to the community.
A part of this equation that hasn’t been given adequate attention is VA’s teaching mission. If care is increasingly going to the community, those patients won’t be available for the trainees in teaching programs. That in turn impacts the pipeline of clinicians who will be available to serve the population at large. The negative effects will be seen far beyond the VA.
Why have you expressed concern over VA care fragmentation?1
Greater than 80% of VA ICU [intensive care unit] care is now being provided in community hospitals. When patients are discharged from those hospitals, they often continue getting follow-up care in the community because VA doesn’t have good mechanisms to reconnect those patients back to VA care.2
[Other researchers] found that the majority of emergency department care for enrolled veterans in New York State was being paid for by entities other than the VA, most commonly Medicare but also Medicaid and private insurance. Where follow-up care occurred often depended on who paid for the emergency department visit, not necessarily what was best for the patient.3
The core problem is that the VA has very little insight into what’s happening when its enrollees get care that is paid for by another payer. VA doesn’t know when their patients are in a private hospital emergency department, so they can’t reach out in real time, and they can’t reconnect with them afterward.
That is very different than for commercial health plans. They know when one of their enrollees is admitted to an out-of-network hospital, and when they are discharged, and they follow up immediately. VA doesn’t have the infrastructure in place to do that.
Why did the VA spend $44 billion on Medicare Advantage double-payments from 2018 to 2021?4
That number is much larger now—$87 billion from 2019 to 2023. Here’s the problem: When VA enrollees are also enrolled in a Medicare Advantage plan, the Medicare plan gets paid to provide the care for those veterans. But when those enrollees come to the VA, the VA provides and pays for the care but cannot bill Medicare for the costs. So the federal government ends up paying twice for care of the same person.
In a paper I coauthored last December we showed that in 2023 alone VA spent $23 billion for care of veterans enrolled in Medicare Advantage plan. Those duplicative payments accounted for almost 20% of VA's entire medical care budget.5
How can fragmented care be reduced?
Two things really stand out. First, real-time health insurance data sharing across payers is foundational. VA has to know when its patients get care by non-VA providers if it is going to coordinate and provide follow-up care. As a first step, VA and the Centers for Medicare & Medicaid Services need to create a data sharing platform for veterans dually enrolled in VA and Medicare or Medicaid.
This is not a new idea. I tried to do it when I was Under Secretary for Health in the late 1990s, but it never happened for various political reasons. Others have tried since. Maybe now, given how much money is at stake, it will finally get done.
Second, the VA needs to implement rigorous case management for high utilizers. The costs are not evenly distributed across enrollees. Approximately 10% of community care users account for almost 90% of community care expenditures. Common sense says you should intensely manage the care of those high-need patients who account for so much of the costs, try to avoid out-of-network ICU and emergency department care as much as possible, and build relationships with other providers so there are clear mechanisms to reconnect those patients back to VA care after an acute episode is treated outside the VA health system.
Is community care itself the problem?
No. Community care is a good thing for many veterans. It has increased access and made it easier for enrolled veterans to get care in some situations. The problem is that the VA hasn’t built in the mechanisms and processes to share information, manage complex patients, provide follow-up care, or oversee quality in community care.
Historically, VA has been an integrated delivery system that provided the overwhelming majority of care within its own facilities. However, over the last decade it has become a hybrid purchaser-provider system. It has become a very large purchaser of non-VA care, going from about $7 billion to $50 billion in community care spending over the past decade. But the VA hasn’t built the infrastructure—information exchange, case management, utilization review, quality oversight—that a hybrid purchaser-provider system needs to be a prudent purchaser.
What is your perspective on VHA's EHR transition?
The many problems with the rollout of the Oracle/Cerner EHR have been well-documented by the Inspector General, frontline clinicians, and others. The problems have been so bad that implementation has been halted a couple times. They’re now moving forward again, but it remains to be seen whether the problems truly have been fixed.
Still unaddressed is the more fundamental question of whether VistA could have been upgraded and modernized at far less cost and disruption of care. No thorough, deliberative analysis of that was ever done. And some of the ostensible problems with upgrading VistA in years past are no longer an issue.
Given the challenges VA faces, are you optimistic about its future?
While there definitely are problems, they are all solvable. Every challenge the VA is facing can be addressed. The question is when and how, and whether the VA is going to be given a fair chance to work through its challenges.
As for those who look to the private sector and think that’s the solution: They haven’t looked closely enough. The private sector is also struggling with staffing and financing issues, many of the same issues VA is dealing with, just in a somewhat different way. The problems in the private sector will be an increasing challenge for community care going forward.
Overall, my life experience is that dark times are always followed by daylight, so I am confident there are brighter days ahead for VA.
1. Kizer KW. Curbing the growing fragmentation of veterans’ health care. JAMA Health Forum. 2025;6:e254148. doi:10.1001/jamahealthforum.2025.4148
2. Hahn Z, Naiditch H, Talisa V, et al. Intensive care unit admissions purchased or delivered by veterans in the VA health care system. JAMA Health Forum. 2025;6:e255605. doi:10.1001/jamahealthforum.2025.5605
3. Vashi AA, Urech T, Wu S, Asch S. Fragmented financing in emergency department use among US veterans. JAMA Health Forum. 2025;6:e255635. doi:10.1001/jamahealthforum.2025.5635
4. Maremont M, Weaver C, McGinty T. Insurers collected billions from medicare for veterans who cost them almost nothing. The Wall Street Journal. December 2, 2024. Accessed March 17, 2026. https://www.wsj.com/health/healthcare /veterans-medicare-insurers-collect-billions-bfd47d27
5. Trivedi AN, Jiang L, Meyers DJ, et al. Spending by the Veterans Affairs health care system for Medicare Advantage Enrollees. JAMA Health Forum. 2025;6:e255653. doi:10.1001/jamahealthforum.2025.5653
Kenneth W. Kizer, MD, MPH, knows a thing or two about transition at the US Department of Veterans Affairs (VA). He served as VA Under Secretary of Health from 1994 to 1999, stepping in during an era of crisis with a mandate for transformation.
Kizer, a Distinguished Professor Emeritus at the University of California, Davis School of Medicine, is among the top thinkers about the VA and its future. He recently spoke with Federal Practitioner about community care, the electronic health record transition, and other challenges facing the Veterans Health Administration (VHA).
At stake, Kizer explained, is an invaluable service for veterans—and much more. “VA is the largest provider of training for... multiple types of health professionals that people use every day,” he said. “There’s also the research, the direct care provided to veterans, and the contingency support the VA provides, which was very well demonstrated during the COVID pandemic. These are things that benefit all Americans, not just veterans.”
When you look at the VA, what do you see?
I see an organization in turmoil, a great health care system struggling with multiple major challenges simultaneously. The VHA is becoming a very large health insurance program without the necessary infrastructure, and costs are rising rapidly. And it is trying to roll out a new EHR and implement new third-party administrator contracts while suffering from significant staffing reductions and very depressed morale.
There are a host of other high-visibility and high-impact issues, including a major reorganization. There’s been a paucity of details about exactly what is going to change, who is going to be doing what, and how the changes will affect staffing and workflow.
How will the loss of 35,000 health care positions affect veterans' care?
If you don’t have enough people, then you’re not going to be able to provide the care that is needed. Years ago, I led a project assessing the Roseburg VA Medical Center in Central Oregon. Among other things, there were a lot of problems with cardiology care. The biggest complaint the cardiologists had, and why the hospital couldn’t keep cardiologists on staff, was that there weren’t enough support staff to do the electrocardiograms. The cardiologists had to do the electrocardiograms themselves, which meant they weren’t doing other things they should be doing. You can amplify that example in a hundred different ways in VA today. If physicians don’t have adequate support, they get frustrated and disenfranchised. And they leave.
One of the fallacies I’ve heard mentioned in some congressional hearings is that it’s mainly a matter of lower pay in the VA. Pay may be an issue somewhere on the list of recruiting challenges, but more important issues higher up are things like the support clinicians receive, the work environment, whether they feel valued, and how easy it is for them to do their work. Case in point: If you put in a new EHR that doesn’t work as well as the existing one, then some doctors are going to leave.
Is VA being pushed toward privatization?
At some point it becomes a self-fulfilling prophecy. If you don’t have the staff to provide the services, then you refer more veterans to the community, and you get in a downward spiral. Patients are going to the community, you lose more staff, you continue to be unable to provide services, and more care goes to the community.
A part of this equation that hasn’t been given adequate attention is VA’s teaching mission. If care is increasingly going to the community, those patients won’t be available for the trainees in teaching programs. That in turn impacts the pipeline of clinicians who will be available to serve the population at large. The negative effects will be seen far beyond the VA.
Why have you expressed concern over VA care fragmentation?1
Greater than 80% of VA ICU [intensive care unit] care is now being provided in community hospitals. When patients are discharged from those hospitals, they often continue getting follow-up care in the community because VA doesn’t have good mechanisms to reconnect those patients back to VA care.2
[Other researchers] found that the majority of emergency department care for enrolled veterans in New York State was being paid for by entities other than the VA, most commonly Medicare but also Medicaid and private insurance. Where follow-up care occurred often depended on who paid for the emergency department visit, not necessarily what was best for the patient.3
The core problem is that the VA has very little insight into what’s happening when its enrollees get care that is paid for by another payer. VA doesn’t know when their patients are in a private hospital emergency department, so they can’t reach out in real time, and they can’t reconnect with them afterward.
That is very different than for commercial health plans. They know when one of their enrollees is admitted to an out-of-network hospital, and when they are discharged, and they follow up immediately. VA doesn’t have the infrastructure in place to do that.
Why did the VA spend $44 billion on Medicare Advantage double-payments from 2018 to 2021?4
That number is much larger now—$87 billion from 2019 to 2023. Here’s the problem: When VA enrollees are also enrolled in a Medicare Advantage plan, the Medicare plan gets paid to provide the care for those veterans. But when those enrollees come to the VA, the VA provides and pays for the care but cannot bill Medicare for the costs. So the federal government ends up paying twice for care of the same person.
In a paper I coauthored last December we showed that in 2023 alone VA spent $23 billion for care of veterans enrolled in Medicare Advantage plan. Those duplicative payments accounted for almost 20% of VA's entire medical care budget.5
How can fragmented care be reduced?
Two things really stand out. First, real-time health insurance data sharing across payers is foundational. VA has to know when its patients get care by non-VA providers if it is going to coordinate and provide follow-up care. As a first step, VA and the Centers for Medicare & Medicaid Services need to create a data sharing platform for veterans dually enrolled in VA and Medicare or Medicaid.
This is not a new idea. I tried to do it when I was Under Secretary for Health in the late 1990s, but it never happened for various political reasons. Others have tried since. Maybe now, given how much money is at stake, it will finally get done.
Second, the VA needs to implement rigorous case management for high utilizers. The costs are not evenly distributed across enrollees. Approximately 10% of community care users account for almost 90% of community care expenditures. Common sense says you should intensely manage the care of those high-need patients who account for so much of the costs, try to avoid out-of-network ICU and emergency department care as much as possible, and build relationships with other providers so there are clear mechanisms to reconnect those patients back to VA care after an acute episode is treated outside the VA health system.
Is community care itself the problem?
No. Community care is a good thing for many veterans. It has increased access and made it easier for enrolled veterans to get care in some situations. The problem is that the VA hasn’t built in the mechanisms and processes to share information, manage complex patients, provide follow-up care, or oversee quality in community care.
Historically, VA has been an integrated delivery system that provided the overwhelming majority of care within its own facilities. However, over the last decade it has become a hybrid purchaser-provider system. It has become a very large purchaser of non-VA care, going from about $7 billion to $50 billion in community care spending over the past decade. But the VA hasn’t built the infrastructure—information exchange, case management, utilization review, quality oversight—that a hybrid purchaser-provider system needs to be a prudent purchaser.
What is your perspective on VHA's EHR transition?
The many problems with the rollout of the Oracle/Cerner EHR have been well-documented by the Inspector General, frontline clinicians, and others. The problems have been so bad that implementation has been halted a couple times. They’re now moving forward again, but it remains to be seen whether the problems truly have been fixed.
Still unaddressed is the more fundamental question of whether VistA could have been upgraded and modernized at far less cost and disruption of care. No thorough, deliberative analysis of that was ever done. And some of the ostensible problems with upgrading VistA in years past are no longer an issue.
Given the challenges VA faces, are you optimistic about its future?
While there definitely are problems, they are all solvable. Every challenge the VA is facing can be addressed. The question is when and how, and whether the VA is going to be given a fair chance to work through its challenges.
As for those who look to the private sector and think that’s the solution: They haven’t looked closely enough. The private sector is also struggling with staffing and financing issues, many of the same issues VA is dealing with, just in a somewhat different way. The problems in the private sector will be an increasing challenge for community care going forward.
Overall, my life experience is that dark times are always followed by daylight, so I am confident there are brighter days ahead for VA.
Kenneth W. Kizer, MD, MPH, knows a thing or two about transition at the US Department of Veterans Affairs (VA). He served as VA Under Secretary of Health from 1994 to 1999, stepping in during an era of crisis with a mandate for transformation.
Kizer, a Distinguished Professor Emeritus at the University of California, Davis School of Medicine, is among the top thinkers about the VA and its future. He recently spoke with Federal Practitioner about community care, the electronic health record transition, and other challenges facing the Veterans Health Administration (VHA).
At stake, Kizer explained, is an invaluable service for veterans—and much more. “VA is the largest provider of training for... multiple types of health professionals that people use every day,” he said. “There’s also the research, the direct care provided to veterans, and the contingency support the VA provides, which was very well demonstrated during the COVID pandemic. These are things that benefit all Americans, not just veterans.”
When you look at the VA, what do you see?
I see an organization in turmoil, a great health care system struggling with multiple major challenges simultaneously. The VHA is becoming a very large health insurance program without the necessary infrastructure, and costs are rising rapidly. And it is trying to roll out a new EHR and implement new third-party administrator contracts while suffering from significant staffing reductions and very depressed morale.
There are a host of other high-visibility and high-impact issues, including a major reorganization. There’s been a paucity of details about exactly what is going to change, who is going to be doing what, and how the changes will affect staffing and workflow.
How will the loss of 35,000 health care positions affect veterans' care?
If you don’t have enough people, then you’re not going to be able to provide the care that is needed. Years ago, I led a project assessing the Roseburg VA Medical Center in Central Oregon. Among other things, there were a lot of problems with cardiology care. The biggest complaint the cardiologists had, and why the hospital couldn’t keep cardiologists on staff, was that there weren’t enough support staff to do the electrocardiograms. The cardiologists had to do the electrocardiograms themselves, which meant they weren’t doing other things they should be doing. You can amplify that example in a hundred different ways in VA today. If physicians don’t have adequate support, they get frustrated and disenfranchised. And they leave.
One of the fallacies I’ve heard mentioned in some congressional hearings is that it’s mainly a matter of lower pay in the VA. Pay may be an issue somewhere on the list of recruiting challenges, but more important issues higher up are things like the support clinicians receive, the work environment, whether they feel valued, and how easy it is for them to do their work. Case in point: If you put in a new EHR that doesn’t work as well as the existing one, then some doctors are going to leave.
Is VA being pushed toward privatization?
At some point it becomes a self-fulfilling prophecy. If you don’t have the staff to provide the services, then you refer more veterans to the community, and you get in a downward spiral. Patients are going to the community, you lose more staff, you continue to be unable to provide services, and more care goes to the community.
A part of this equation that hasn’t been given adequate attention is VA’s teaching mission. If care is increasingly going to the community, those patients won’t be available for the trainees in teaching programs. That in turn impacts the pipeline of clinicians who will be available to serve the population at large. The negative effects will be seen far beyond the VA.
Why have you expressed concern over VA care fragmentation?1
Greater than 80% of VA ICU [intensive care unit] care is now being provided in community hospitals. When patients are discharged from those hospitals, they often continue getting follow-up care in the community because VA doesn’t have good mechanisms to reconnect those patients back to VA care.2
[Other researchers] found that the majority of emergency department care for enrolled veterans in New York State was being paid for by entities other than the VA, most commonly Medicare but also Medicaid and private insurance. Where follow-up care occurred often depended on who paid for the emergency department visit, not necessarily what was best for the patient.3
The core problem is that the VA has very little insight into what’s happening when its enrollees get care that is paid for by another payer. VA doesn’t know when their patients are in a private hospital emergency department, so they can’t reach out in real time, and they can’t reconnect with them afterward.
That is very different than for commercial health plans. They know when one of their enrollees is admitted to an out-of-network hospital, and when they are discharged, and they follow up immediately. VA doesn’t have the infrastructure in place to do that.
Why did the VA spend $44 billion on Medicare Advantage double-payments from 2018 to 2021?4
That number is much larger now—$87 billion from 2019 to 2023. Here’s the problem: When VA enrollees are also enrolled in a Medicare Advantage plan, the Medicare plan gets paid to provide the care for those veterans. But when those enrollees come to the VA, the VA provides and pays for the care but cannot bill Medicare for the costs. So the federal government ends up paying twice for care of the same person.
In a paper I coauthored last December we showed that in 2023 alone VA spent $23 billion for care of veterans enrolled in Medicare Advantage plan. Those duplicative payments accounted for almost 20% of VA's entire medical care budget.5
How can fragmented care be reduced?
Two things really stand out. First, real-time health insurance data sharing across payers is foundational. VA has to know when its patients get care by non-VA providers if it is going to coordinate and provide follow-up care. As a first step, VA and the Centers for Medicare & Medicaid Services need to create a data sharing platform for veterans dually enrolled in VA and Medicare or Medicaid.
This is not a new idea. I tried to do it when I was Under Secretary for Health in the late 1990s, but it never happened for various political reasons. Others have tried since. Maybe now, given how much money is at stake, it will finally get done.
Second, the VA needs to implement rigorous case management for high utilizers. The costs are not evenly distributed across enrollees. Approximately 10% of community care users account for almost 90% of community care expenditures. Common sense says you should intensely manage the care of those high-need patients who account for so much of the costs, try to avoid out-of-network ICU and emergency department care as much as possible, and build relationships with other providers so there are clear mechanisms to reconnect those patients back to VA care after an acute episode is treated outside the VA health system.
Is community care itself the problem?
No. Community care is a good thing for many veterans. It has increased access and made it easier for enrolled veterans to get care in some situations. The problem is that the VA hasn’t built in the mechanisms and processes to share information, manage complex patients, provide follow-up care, or oversee quality in community care.
Historically, VA has been an integrated delivery system that provided the overwhelming majority of care within its own facilities. However, over the last decade it has become a hybrid purchaser-provider system. It has become a very large purchaser of non-VA care, going from about $7 billion to $50 billion in community care spending over the past decade. But the VA hasn’t built the infrastructure—information exchange, case management, utilization review, quality oversight—that a hybrid purchaser-provider system needs to be a prudent purchaser.
What is your perspective on VHA's EHR transition?
The many problems with the rollout of the Oracle/Cerner EHR have been well-documented by the Inspector General, frontline clinicians, and others. The problems have been so bad that implementation has been halted a couple times. They’re now moving forward again, but it remains to be seen whether the problems truly have been fixed.
Still unaddressed is the more fundamental question of whether VistA could have been upgraded and modernized at far less cost and disruption of care. No thorough, deliberative analysis of that was ever done. And some of the ostensible problems with upgrading VistA in years past are no longer an issue.
Given the challenges VA faces, are you optimistic about its future?
While there definitely are problems, they are all solvable. Every challenge the VA is facing can be addressed. The question is when and how, and whether the VA is going to be given a fair chance to work through its challenges.
As for those who look to the private sector and think that’s the solution: They haven’t looked closely enough. The private sector is also struggling with staffing and financing issues, many of the same issues VA is dealing with, just in a somewhat different way. The problems in the private sector will be an increasing challenge for community care going forward.
Overall, my life experience is that dark times are always followed by daylight, so I am confident there are brighter days ahead for VA.
1. Kizer KW. Curbing the growing fragmentation of veterans’ health care. JAMA Health Forum. 2025;6:e254148. doi:10.1001/jamahealthforum.2025.4148
2. Hahn Z, Naiditch H, Talisa V, et al. Intensive care unit admissions purchased or delivered by veterans in the VA health care system. JAMA Health Forum. 2025;6:e255605. doi:10.1001/jamahealthforum.2025.5605
3. Vashi AA, Urech T, Wu S, Asch S. Fragmented financing in emergency department use among US veterans. JAMA Health Forum. 2025;6:e255635. doi:10.1001/jamahealthforum.2025.5635
4. Maremont M, Weaver C, McGinty T. Insurers collected billions from medicare for veterans who cost them almost nothing. The Wall Street Journal. December 2, 2024. Accessed March 17, 2026. https://www.wsj.com/health/healthcare /veterans-medicare-insurers-collect-billions-bfd47d27
5. Trivedi AN, Jiang L, Meyers DJ, et al. Spending by the Veterans Affairs health care system for Medicare Advantage Enrollees. JAMA Health Forum. 2025;6:e255653. doi:10.1001/jamahealthforum.2025.5653
1. Kizer KW. Curbing the growing fragmentation of veterans’ health care. JAMA Health Forum. 2025;6:e254148. doi:10.1001/jamahealthforum.2025.4148
2. Hahn Z, Naiditch H, Talisa V, et al. Intensive care unit admissions purchased or delivered by veterans in the VA health care system. JAMA Health Forum. 2025;6:e255605. doi:10.1001/jamahealthforum.2025.5605
3. Vashi AA, Urech T, Wu S, Asch S. Fragmented financing in emergency department use among US veterans. JAMA Health Forum. 2025;6:e255635. doi:10.1001/jamahealthforum.2025.5635
4. Maremont M, Weaver C, McGinty T. Insurers collected billions from medicare for veterans who cost them almost nothing. The Wall Street Journal. December 2, 2024. Accessed March 17, 2026. https://www.wsj.com/health/healthcare /veterans-medicare-insurers-collect-billions-bfd47d27
5. Trivedi AN, Jiang L, Meyers DJ, et al. Spending by the Veterans Affairs health care system for Medicare Advantage Enrollees. JAMA Health Forum. 2025;6:e255653. doi:10.1001/jamahealthforum.2025.5653
'An Organization in Turmoil': Ken Kizer on the Challenges Facing the VA
'An Organization in Turmoil': Ken Kizer on the Challenges Facing the VA

Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
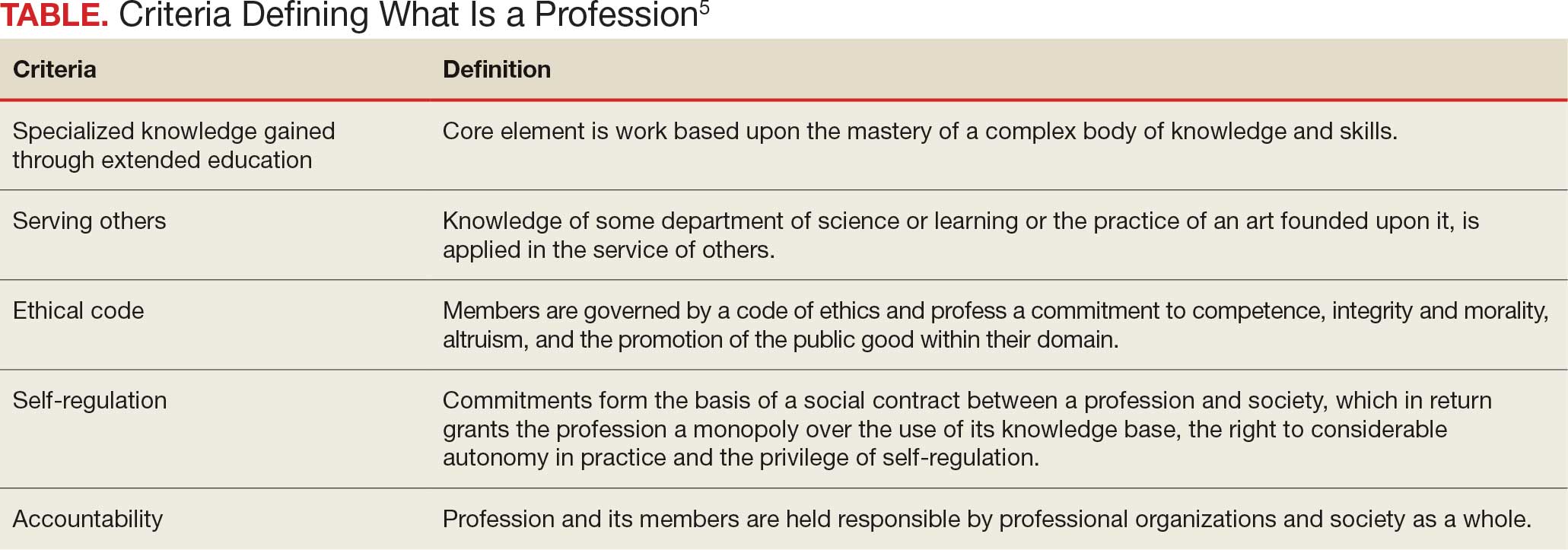
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?

The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
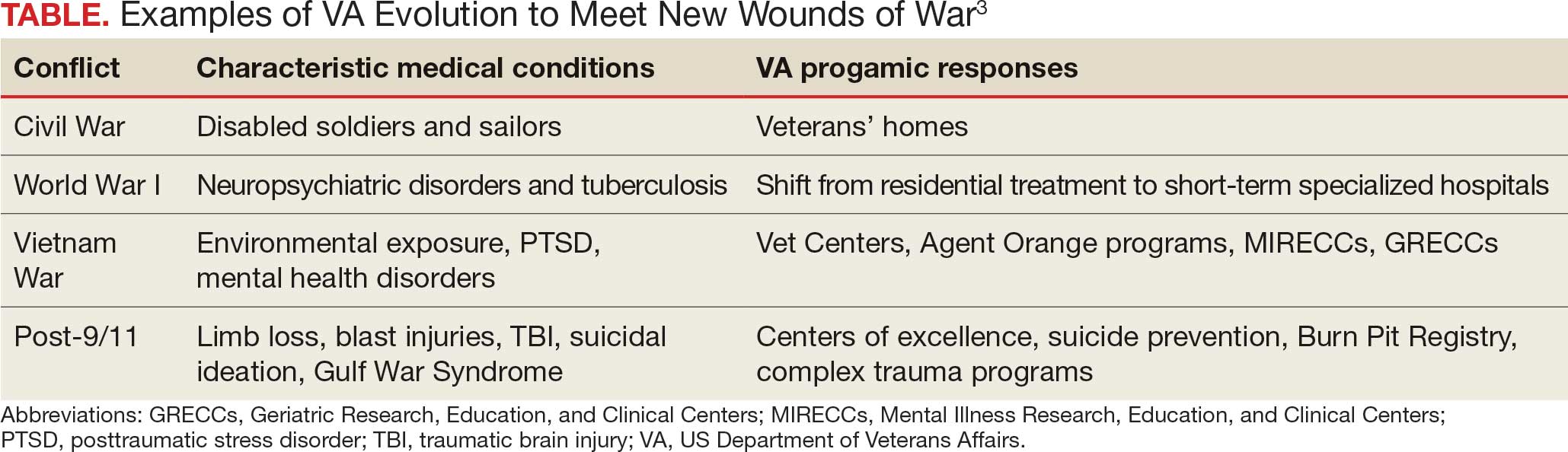
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration

VHA Facilities Report Severe Staffing Shortages
VHA Facilities Report Severe Staffing Shortages
For > 10 years, the US Department of Veterans Affairs (VA) Office of Inspector General (OIG) has annually surveyed Veterans Health Administration (VHA) facilities about staffing. Its recently released report is the 8th to find severe shortages—in this case, across the board. There were 4434 severe staffing shortages reported across all 139 VHA facilities in fiscal year (FY) 2025, a 50% increase from FY 2024.
In the OIG report lexicon, a severe shortage refers to "particular occupations that are difficult to fill," and is not necessarily an indication of vacancies. Vacancy refers to a "specific unoccupied position and is distinct from the designation of a severe shortage." For example, a facility could identify an occupation as a severe occupational shortage, which could have no vacant positions or 100 vacant positions.
Nearly all facilities (94%) had severe shortages for medical officers, and 79% had severe shortages for nurses even with VHA's ability to make noncompetitive appointments for those occupations. Psychology was the most frequently reported severe clinical occupational staffing shortage, reported by 79 facilities (57%), down slightly from FY 2024 (61%). One facility reported 116 clinical occupational shortages.
The report notes that the OIG does not verify or otherwise confirm the questionnaire responses, but it appears to support other data. In the first 9 months of FY 2024, the VA added 223 physicians and 3196 nurses compared with a deficit of 781 physicians and 2129 nurses over the same period in FY 2025.
VHA facilities are finding it hard to reverse the trend. According to internal documents examined by ProPublica, nearly 4 in 10 of the roughly 2000 doctors offered jobs from January through March 2025 turned them down, 4 times the rate in the same time period in 2024. VHA also lost twice as many nurses as it hired between January and June. Many potential candidates reportedly were worried about the stability of VA employment.
VA spokesperson Peter Kasperowicz did not dispute the ProPublica findings but accused the news outlet of bias and "cherry-picking issues that are mostly routine." A nationwide shortage of health care workers has made hiring and retention difficult, he said.
Kasperowicz said the VA is "working to address" the number of doctors declining job offers by speeding up the hiring process and that the agency "has several strategies to navigate shortages." Those include referring veterans to telehealth and private clinicians.
In a statement released Aug. 12, Sen Richard Blumenthal (D-CT), ranking member of the Senate Committee on Veterans' Affairs, said, "This report confirms what we've warned for months—this Administration is driving dedicated VA employees to the private sector at untenable rates."
The OIG survey did not ask about facilities' rationales for identifying shortages. Moreover, the OIG says the responses don't reflect the possible impacts of "workforce reshaping efforts," such as the Deferred Resignation Program announced on January 28, 2025.
In response to the OIG report, Kasperowicz said it is "not based on actual VA health care facility vacancies and therefore is not a reliable indicator of staffing shortages." In a statement to CBS News, he added, "The report simply lists occupations facilities feel are difficult for which to recruit and retain, so the results are completely subjective, not standardized, and unreliable." According to Kasperowicz, the system-wide vacancy rates for doctors and nurses are 14% and 10%, respectively, which are in line with historical averages.
The OIG made no recommendations but "encourages VA leaders to use these review results to inform staffing initiatives and organizational change."
For > 10 years, the US Department of Veterans Affairs (VA) Office of Inspector General (OIG) has annually surveyed Veterans Health Administration (VHA) facilities about staffing. Its recently released report is the 8th to find severe shortages—in this case, across the board. There were 4434 severe staffing shortages reported across all 139 VHA facilities in fiscal year (FY) 2025, a 50% increase from FY 2024.
In the OIG report lexicon, a severe shortage refers to "particular occupations that are difficult to fill," and is not necessarily an indication of vacancies. Vacancy refers to a "specific unoccupied position and is distinct from the designation of a severe shortage." For example, a facility could identify an occupation as a severe occupational shortage, which could have no vacant positions or 100 vacant positions.
Nearly all facilities (94%) had severe shortages for medical officers, and 79% had severe shortages for nurses even with VHA's ability to make noncompetitive appointments for those occupations. Psychology was the most frequently reported severe clinical occupational staffing shortage, reported by 79 facilities (57%), down slightly from FY 2024 (61%). One facility reported 116 clinical occupational shortages.
The report notes that the OIG does not verify or otherwise confirm the questionnaire responses, but it appears to support other data. In the first 9 months of FY 2024, the VA added 223 physicians and 3196 nurses compared with a deficit of 781 physicians and 2129 nurses over the same period in FY 2025.
VHA facilities are finding it hard to reverse the trend. According to internal documents examined by ProPublica, nearly 4 in 10 of the roughly 2000 doctors offered jobs from January through March 2025 turned them down, 4 times the rate in the same time period in 2024. VHA also lost twice as many nurses as it hired between January and June. Many potential candidates reportedly were worried about the stability of VA employment.
VA spokesperson Peter Kasperowicz did not dispute the ProPublica findings but accused the news outlet of bias and "cherry-picking issues that are mostly routine." A nationwide shortage of health care workers has made hiring and retention difficult, he said.
Kasperowicz said the VA is "working to address" the number of doctors declining job offers by speeding up the hiring process and that the agency "has several strategies to navigate shortages." Those include referring veterans to telehealth and private clinicians.
In a statement released Aug. 12, Sen Richard Blumenthal (D-CT), ranking member of the Senate Committee on Veterans' Affairs, said, "This report confirms what we've warned for months—this Administration is driving dedicated VA employees to the private sector at untenable rates."
The OIG survey did not ask about facilities' rationales for identifying shortages. Moreover, the OIG says the responses don't reflect the possible impacts of "workforce reshaping efforts," such as the Deferred Resignation Program announced on January 28, 2025.
In response to the OIG report, Kasperowicz said it is "not based on actual VA health care facility vacancies and therefore is not a reliable indicator of staffing shortages." In a statement to CBS News, he added, "The report simply lists occupations facilities feel are difficult for which to recruit and retain, so the results are completely subjective, not standardized, and unreliable." According to Kasperowicz, the system-wide vacancy rates for doctors and nurses are 14% and 10%, respectively, which are in line with historical averages.
The OIG made no recommendations but "encourages VA leaders to use these review results to inform staffing initiatives and organizational change."
For > 10 years, the US Department of Veterans Affairs (VA) Office of Inspector General (OIG) has annually surveyed Veterans Health Administration (VHA) facilities about staffing. Its recently released report is the 8th to find severe shortages—in this case, across the board. There were 4434 severe staffing shortages reported across all 139 VHA facilities in fiscal year (FY) 2025, a 50% increase from FY 2024.
In the OIG report lexicon, a severe shortage refers to "particular occupations that are difficult to fill," and is not necessarily an indication of vacancies. Vacancy refers to a "specific unoccupied position and is distinct from the designation of a severe shortage." For example, a facility could identify an occupation as a severe occupational shortage, which could have no vacant positions or 100 vacant positions.
Nearly all facilities (94%) had severe shortages for medical officers, and 79% had severe shortages for nurses even with VHA's ability to make noncompetitive appointments for those occupations. Psychology was the most frequently reported severe clinical occupational staffing shortage, reported by 79 facilities (57%), down slightly from FY 2024 (61%). One facility reported 116 clinical occupational shortages.
The report notes that the OIG does not verify or otherwise confirm the questionnaire responses, but it appears to support other data. In the first 9 months of FY 2024, the VA added 223 physicians and 3196 nurses compared with a deficit of 781 physicians and 2129 nurses over the same period in FY 2025.
VHA facilities are finding it hard to reverse the trend. According to internal documents examined by ProPublica, nearly 4 in 10 of the roughly 2000 doctors offered jobs from January through March 2025 turned them down, 4 times the rate in the same time period in 2024. VHA also lost twice as many nurses as it hired between January and June. Many potential candidates reportedly were worried about the stability of VA employment.
VA spokesperson Peter Kasperowicz did not dispute the ProPublica findings but accused the news outlet of bias and "cherry-picking issues that are mostly routine." A nationwide shortage of health care workers has made hiring and retention difficult, he said.
Kasperowicz said the VA is "working to address" the number of doctors declining job offers by speeding up the hiring process and that the agency "has several strategies to navigate shortages." Those include referring veterans to telehealth and private clinicians.
In a statement released Aug. 12, Sen Richard Blumenthal (D-CT), ranking member of the Senate Committee on Veterans' Affairs, said, "This report confirms what we've warned for months—this Administration is driving dedicated VA employees to the private sector at untenable rates."
The OIG survey did not ask about facilities' rationales for identifying shortages. Moreover, the OIG says the responses don't reflect the possible impacts of "workforce reshaping efforts," such as the Deferred Resignation Program announced on January 28, 2025.
In response to the OIG report, Kasperowicz said it is "not based on actual VA health care facility vacancies and therefore is not a reliable indicator of staffing shortages." In a statement to CBS News, he added, "The report simply lists occupations facilities feel are difficult for which to recruit and retain, so the results are completely subjective, not standardized, and unreliable." According to Kasperowicz, the system-wide vacancy rates for doctors and nurses are 14% and 10%, respectively, which are in line with historical averages.
The OIG made no recommendations but "encourages VA leaders to use these review results to inform staffing initiatives and organizational change."
VHA Facilities Report Severe Staffing Shortages
VHA Facilities Report Severe Staffing Shortages

VA Workforce Shrinking as it Loses Collective Bargaining Rights
VA Workforce Shrinking as it Loses Collective Bargaining Rights
The US Department of Veterans Affairs (VA) is on pace to cut nearly 30,000 positions by the end of fiscal year 2025, an initiative driven by a federal hiring freeze, deferred resignations, retirements, and normal attrition. According to the VA Workforce Dashboard, health care experienced the most significant net change through the first 9 months of fiscal year 2025. That included 2129 fewer registered nurses, 751 fewer physicians, and drops of 565 licensed practical nurses, 564 nurse assistants, and 1294 medical support assistants. In total, nearly 17,000 VA employees have left their jobs and 12,000 more are expected to leave by the end of September 2025.
According to VA Secretary Doug Collins, the departures have eliminated the need for the "large-scale" reduction-in-force that he proposed earlier in 2025.
The VA also announced that in accordance with an Executive Order issued by President Donald Trump, it is terminating collective bargaining rights for most of its employees, including most clinical staff not in leadership positions. The order includes the National Nurses Organizing Committee/National Nurses United, which represents 16,000 VA nurses, and the American Federation of Government Employees, which represents 320,000 VA employees. The order exempted police officers, firefighters, and security guards. The Unions have indicated they will continue to fight the changes.
VA staffing has undergone significant reversals over the past year. The VA added 223 physicians and 3196 nurses in the first 9 months of fiscal year 2024 before reversing course this year. According to the Workforce Dashboard, the VA and Veterans Health Administration combined to hire 26,984 employees in fiscal year 2025. Cumulative losses, however, totaled 54,308.
During exit interviews, VA employees noted a variety of reasons for their departure. "Personal/family matters" and "geographic relocation" were cited by many job categories. In addition, medical and dental workers also noted "poor working relationship with supervisor or coworker(s)," "desired work schedule not offered," and "job stress/pressure" among the causes. The VA has lost 148 psychologists in fiscal year 2025 who cited "lack of trust/confidence in senior leaders," as well as "policy or technology barriers to getting the work done," and "job stress/pressure" among their reasons for departure.
The US Department of Veterans Affairs (VA) is on pace to cut nearly 30,000 positions by the end of fiscal year 2025, an initiative driven by a federal hiring freeze, deferred resignations, retirements, and normal attrition. According to the VA Workforce Dashboard, health care experienced the most significant net change through the first 9 months of fiscal year 2025. That included 2129 fewer registered nurses, 751 fewer physicians, and drops of 565 licensed practical nurses, 564 nurse assistants, and 1294 medical support assistants. In total, nearly 17,000 VA employees have left their jobs and 12,000 more are expected to leave by the end of September 2025.
According to VA Secretary Doug Collins, the departures have eliminated the need for the "large-scale" reduction-in-force that he proposed earlier in 2025.
The VA also announced that in accordance with an Executive Order issued by President Donald Trump, it is terminating collective bargaining rights for most of its employees, including most clinical staff not in leadership positions. The order includes the National Nurses Organizing Committee/National Nurses United, which represents 16,000 VA nurses, and the American Federation of Government Employees, which represents 320,000 VA employees. The order exempted police officers, firefighters, and security guards. The Unions have indicated they will continue to fight the changes.
VA staffing has undergone significant reversals over the past year. The VA added 223 physicians and 3196 nurses in the first 9 months of fiscal year 2024 before reversing course this year. According to the Workforce Dashboard, the VA and Veterans Health Administration combined to hire 26,984 employees in fiscal year 2025. Cumulative losses, however, totaled 54,308.
During exit interviews, VA employees noted a variety of reasons for their departure. "Personal/family matters" and "geographic relocation" were cited by many job categories. In addition, medical and dental workers also noted "poor working relationship with supervisor or coworker(s)," "desired work schedule not offered," and "job stress/pressure" among the causes. The VA has lost 148 psychologists in fiscal year 2025 who cited "lack of trust/confidence in senior leaders," as well as "policy or technology barriers to getting the work done," and "job stress/pressure" among their reasons for departure.
The US Department of Veterans Affairs (VA) is on pace to cut nearly 30,000 positions by the end of fiscal year 2025, an initiative driven by a federal hiring freeze, deferred resignations, retirements, and normal attrition. According to the VA Workforce Dashboard, health care experienced the most significant net change through the first 9 months of fiscal year 2025. That included 2129 fewer registered nurses, 751 fewer physicians, and drops of 565 licensed practical nurses, 564 nurse assistants, and 1294 medical support assistants. In total, nearly 17,000 VA employees have left their jobs and 12,000 more are expected to leave by the end of September 2025.
According to VA Secretary Doug Collins, the departures have eliminated the need for the "large-scale" reduction-in-force that he proposed earlier in 2025.
The VA also announced that in accordance with an Executive Order issued by President Donald Trump, it is terminating collective bargaining rights for most of its employees, including most clinical staff not in leadership positions. The order includes the National Nurses Organizing Committee/National Nurses United, which represents 16,000 VA nurses, and the American Federation of Government Employees, which represents 320,000 VA employees. The order exempted police officers, firefighters, and security guards. The Unions have indicated they will continue to fight the changes.
VA staffing has undergone significant reversals over the past year. The VA added 223 physicians and 3196 nurses in the first 9 months of fiscal year 2024 before reversing course this year. According to the Workforce Dashboard, the VA and Veterans Health Administration combined to hire 26,984 employees in fiscal year 2025. Cumulative losses, however, totaled 54,308.
During exit interviews, VA employees noted a variety of reasons for their departure. "Personal/family matters" and "geographic relocation" were cited by many job categories. In addition, medical and dental workers also noted "poor working relationship with supervisor or coworker(s)," "desired work schedule not offered," and "job stress/pressure" among the causes. The VA has lost 148 psychologists in fiscal year 2025 who cited "lack of trust/confidence in senior leaders," as well as "policy or technology barriers to getting the work done," and "job stress/pressure" among their reasons for departure.
VA Workforce Shrinking as it Loses Collective Bargaining Rights
VA Workforce Shrinking as it Loses Collective Bargaining Rights

AVAHO Encourages Members to Make Voices Heard
Advocacy for veterans with cancer has always been a central part of the Association for VA Hematology/Oncology (AVAHO) mission, but that advocacy has now taken on a new focus: the fate of US Department of Veterans Affairs (VA) employees. The advocacy portal provides templated letters, a search function to find local Senators and Members of Congress, a search function to find regional media outlets, updates on voting and elections, and information on key legislation relevant to VA health care.
To ensure its members’ concerns are heard, AVAHO is encouraging members, in their own time and as private citizens, to contact their local representatives to inform them about the real impact of recent policy changes on VA employees and the veterans they care for. Members can select any of 4 letters focused on reductions in force, cancellation of VA contracts, the return to office mandate, and the National Institutes of Health’s proposed cap on indirect cost for research grants: “AVAHO recognizes the power of the individual voice. Our members have an important role in shaping the health care services provided to veterans across our nation.”
"The contracts that have been canceled and continue to be canceled included critical services related to cancer care," AVAHO notes on its Advocacy page. "We know these impacted contracts have hindered the VA’s ability to implement research protocols, process and report pharmacogenomic results, manage Electronic Health Record Modernization workgroups responsible for safety improvements, and execute new oncology services through the Close to Me initiative, just to name a few."
Advocacy for veterans with cancer has always been a central part of the Association for VA Hematology/Oncology (AVAHO) mission, but that advocacy has now taken on a new focus: the fate of US Department of Veterans Affairs (VA) employees. The advocacy portal provides templated letters, a search function to find local Senators and Members of Congress, a search function to find regional media outlets, updates on voting and elections, and information on key legislation relevant to VA health care.
To ensure its members’ concerns are heard, AVAHO is encouraging members, in their own time and as private citizens, to contact their local representatives to inform them about the real impact of recent policy changes on VA employees and the veterans they care for. Members can select any of 4 letters focused on reductions in force, cancellation of VA contracts, the return to office mandate, and the National Institutes of Health’s proposed cap on indirect cost for research grants: “AVAHO recognizes the power of the individual voice. Our members have an important role in shaping the health care services provided to veterans across our nation.”
"The contracts that have been canceled and continue to be canceled included critical services related to cancer care," AVAHO notes on its Advocacy page. "We know these impacted contracts have hindered the VA’s ability to implement research protocols, process and report pharmacogenomic results, manage Electronic Health Record Modernization workgroups responsible for safety improvements, and execute new oncology services through the Close to Me initiative, just to name a few."
Advocacy for veterans with cancer has always been a central part of the Association for VA Hematology/Oncology (AVAHO) mission, but that advocacy has now taken on a new focus: the fate of US Department of Veterans Affairs (VA) employees. The advocacy portal provides templated letters, a search function to find local Senators and Members of Congress, a search function to find regional media outlets, updates on voting and elections, and information on key legislation relevant to VA health care.
To ensure its members’ concerns are heard, AVAHO is encouraging members, in their own time and as private citizens, to contact their local representatives to inform them about the real impact of recent policy changes on VA employees and the veterans they care for. Members can select any of 4 letters focused on reductions in force, cancellation of VA contracts, the return to office mandate, and the National Institutes of Health’s proposed cap on indirect cost for research grants: “AVAHO recognizes the power of the individual voice. Our members have an important role in shaping the health care services provided to veterans across our nation.”
"The contracts that have been canceled and continue to be canceled included critical services related to cancer care," AVAHO notes on its Advocacy page. "We know these impacted contracts have hindered the VA’s ability to implement research protocols, process and report pharmacogenomic results, manage Electronic Health Record Modernization workgroups responsible for safety improvements, and execute new oncology services through the Close to Me initiative, just to name a few."

VA Choice Bill Defeated in the House
A U.S. House of Representatives appropriation to fund the Veterans Choice Program surprisingly went down to defeat on Monday. The VA Choice Program is set to run out of money in September, and VA officials have been calling for Congress to provide additional funding for the program. Republican leaders, hoping to expedite the bill’s passage and thinking that it was not controversial, submitted the bill in a process that required the votes of two-thirds of the representatives. The 219-186 vote fell well short of the necessary two-thirds, and voting fell largely along party lines.
Many veterans service organizations (VSOs) were critical of the bill and called on the House to make substantial changes to it. Seven VSOs signed a joint statement calling for the bill’s defeat. “As organizations who represent and support the interests of America’s 21 million veterans, and in fulfillment of our mandate to ensure that the men and women who served are able to receive the health care and benefits they need and deserve, we are calling on Members of Congress to defeat the House vote on unacceptable choice funding legislation (S. 114, with amendments),” the statement read.
AMVETS, Disabled American Veterans , Military Officers Association of America, Military Order of the Purple Heart, Veterans of Foreign Wars, Vietnam Veterans of America, and Wounded Warrior Project all signed on to the statement. The chief complaint was that the legislation “includes funding only for the ‘choice’ program which provides additional community care options, but makes no investment in VA and uses ‘savings’ from other veterans benefits or services to ‘pay’ for the ‘choice’ program.”
The bill would have allocated $2 billion for the Veterans Choice Program, taken funding for veteran housing loan fees, and would reduce the pensions for some veterans living in nursing facilities that also could be paid for under the Medicaid program.
The fate of the bill and funding for the Veterans Choice Program remains unclear. Senate and House veterans committees seem to be far apart on how to fund the program and for efforts to make more substantive changes to the program. Although House Republicans eventually may be able to pass a bill without Democrats, in the Senate, they will need the support of at least a handful of Democrats to move the bill to the President’s desk.
A U.S. House of Representatives appropriation to fund the Veterans Choice Program surprisingly went down to defeat on Monday. The VA Choice Program is set to run out of money in September, and VA officials have been calling for Congress to provide additional funding for the program. Republican leaders, hoping to expedite the bill’s passage and thinking that it was not controversial, submitted the bill in a process that required the votes of two-thirds of the representatives. The 219-186 vote fell well short of the necessary two-thirds, and voting fell largely along party lines.
Many veterans service organizations (VSOs) were critical of the bill and called on the House to make substantial changes to it. Seven VSOs signed a joint statement calling for the bill’s defeat. “As organizations who represent and support the interests of America’s 21 million veterans, and in fulfillment of our mandate to ensure that the men and women who served are able to receive the health care and benefits they need and deserve, we are calling on Members of Congress to defeat the House vote on unacceptable choice funding legislation (S. 114, with amendments),” the statement read.
AMVETS, Disabled American Veterans , Military Officers Association of America, Military Order of the Purple Heart, Veterans of Foreign Wars, Vietnam Veterans of America, and Wounded Warrior Project all signed on to the statement. The chief complaint was that the legislation “includes funding only for the ‘choice’ program which provides additional community care options, but makes no investment in VA and uses ‘savings’ from other veterans benefits or services to ‘pay’ for the ‘choice’ program.”
The bill would have allocated $2 billion for the Veterans Choice Program, taken funding for veteran housing loan fees, and would reduce the pensions for some veterans living in nursing facilities that also could be paid for under the Medicaid program.
The fate of the bill and funding for the Veterans Choice Program remains unclear. Senate and House veterans committees seem to be far apart on how to fund the program and for efforts to make more substantive changes to the program. Although House Republicans eventually may be able to pass a bill without Democrats, in the Senate, they will need the support of at least a handful of Democrats to move the bill to the President’s desk.
A U.S. House of Representatives appropriation to fund the Veterans Choice Program surprisingly went down to defeat on Monday. The VA Choice Program is set to run out of money in September, and VA officials have been calling for Congress to provide additional funding for the program. Republican leaders, hoping to expedite the bill’s passage and thinking that it was not controversial, submitted the bill in a process that required the votes of two-thirds of the representatives. The 219-186 vote fell well short of the necessary two-thirds, and voting fell largely along party lines.
Many veterans service organizations (VSOs) were critical of the bill and called on the House to make substantial changes to it. Seven VSOs signed a joint statement calling for the bill’s defeat. “As organizations who represent and support the interests of America’s 21 million veterans, and in fulfillment of our mandate to ensure that the men and women who served are able to receive the health care and benefits they need and deserve, we are calling on Members of Congress to defeat the House vote on unacceptable choice funding legislation (S. 114, with amendments),” the statement read.
AMVETS, Disabled American Veterans , Military Officers Association of America, Military Order of the Purple Heart, Veterans of Foreign Wars, Vietnam Veterans of America, and Wounded Warrior Project all signed on to the statement. The chief complaint was that the legislation “includes funding only for the ‘choice’ program which provides additional community care options, but makes no investment in VA and uses ‘savings’ from other veterans benefits or services to ‘pay’ for the ‘choice’ program.”
The bill would have allocated $2 billion for the Veterans Choice Program, taken funding for veteran housing loan fees, and would reduce the pensions for some veterans living in nursing facilities that also could be paid for under the Medicaid program.
The fate of the bill and funding for the Veterans Choice Program remains unclear. Senate and House veterans committees seem to be far apart on how to fund the program and for efforts to make more substantive changes to the program. Although House Republicans eventually may be able to pass a bill without Democrats, in the Senate, they will need the support of at least a handful of Democrats to move the bill to the President’s desk.
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health

The Home Improvements and Structural Alterations Program: Overview and Future Implications
The Home Improvements and Structural Alterations Program: Overview and Future Implications
The Veterans Health Administration (VHA) Home Improvements and Structural Alterations (HISA) program is a primary means through which veterans can obtain home modifications necessary to continue safe and independent living in their home, including fall risk reduction and accessibility to essential parts of the home. However, not all eligible veterans who may benefit from this program participate, for a variety of reasons.1-6 Historically, the HISA program has been administered in a decentralized and nonstandardized fashion dictated by the organizational structure of each US Department of Veterans Affairs (VA) medical center (VAMC) within a certain region or Veterans Integrated Service Network (VISN). Previous research found differential access to the HISA program by younger veterans, women, minorities, veterans with certain disability types, and veterans living in rural vs urban settings. These disparities in access and use of benefits conferred by the HISA program suggests an area of unmet need, which may improve veterans’ health care outcomes and reduce costs associated with their care.2-8
The purpose of this article is to provide information to improve equitable provision and effective eligible use of resources available through the HISA program in a more generalizable manner by providing insight to highlight common program process deficiencies and care provision gaps relevant to VAMCs nationwide. This information can be used to inform the VA Physical Medicine and Rehabilitation (PM&R) and Prosthetic and Sensory Aid Service (PSAS) national policy initiatives, as well as hiring practices, clinic organization, specific care provision, and administrative goals and metrics at each VISN and at the VA Healthcare System level.
Methods
Veterans who participated in the HISA program, VHA administrators, and VHA clinicians from select VAMCs were identified and interviewed to better understand what helps increase access to the program, barriers to access, and how existing program components and processes impact use of the service. These interviews were taken from a directed convenience sample of selected VAMCs. To obtain this directed convenience sample, 167 VAMCs that participated in the HISA program were categorized as facilities that provided either a high or low number of HISA program prescriptions based on data from 2010 to 2018. Ten facilities from the top quartiles and 10 from the bottom quartiles of prescribing locations were selected. This facility selection was driven by the proportion of rural veterans served by each facility, favoring those serving a greater proportion of rural veterans, as well geographic location, with the aim of avoiding overrepresentation of any specific region. The convenience sample included 45 individuals (20 VHA employees and 25 veterans) across 22 states from the Northeast, West, South, and Midwest US Census regions.
Interview Process
Interviews underwent a coding process. The development of topical themes followed a systematic, 2-phase approach. Initially, researchers analyzed responses to semistructured interview questions addressing specific aspects of the HISA program, such as program awareness and accessibility. These responses naturally clustered into preliminary categories based on the interview guide structure. For example, responses related to program discovery formed a marketing-related category, while recommendations about program implementation contributed to a training and development category.
Following this initial categorization, the research team conducted a more rigorous coding process. A team of 3 researchers systematically reviewed assigned interview transcripts to extract practical recommendations for the guide. The researchers first identified relevant responses individually and then convened during group meetings to discuss and finalize selections. This second phase refined the preliminary categorization while maintaining alignment with the original interview structure.
This approach allowed the team to preserve the practical utility of participant feedback while ensuring methodological rigor in the analysis process. Resulting themes reflect both the structured nature of the original inquiry and the practical recommendations identified for improving the HISA program. Information on the following areas were collected: education about the HISA program, the contracting process, use of telehealth, interaction between VHA clinical care and the PSAS, marketing of the program, program funding, and revising the application process.
Results
Interview respondents provided several recommendations for improving the HISA program (Table). Regarding training and education, respondents noted deficiencies in VHA employee communication about the HISA program to veterans. Some employees did not know details or were unaware the HISA program existed. Additionally, a lack of knowledge about HISA program alternatives, including other available programs for obtaining home modifications or other durable medical equipment alternatives (eg, provision of a portable ramp rather than construction of a permanent one), was apparent. It was strongly recommended to provide additional education to effectively disseminate knowledge about the HISA program. Specifically, VHA employees, especially those in Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services, require greater awareness of the program and its processes.
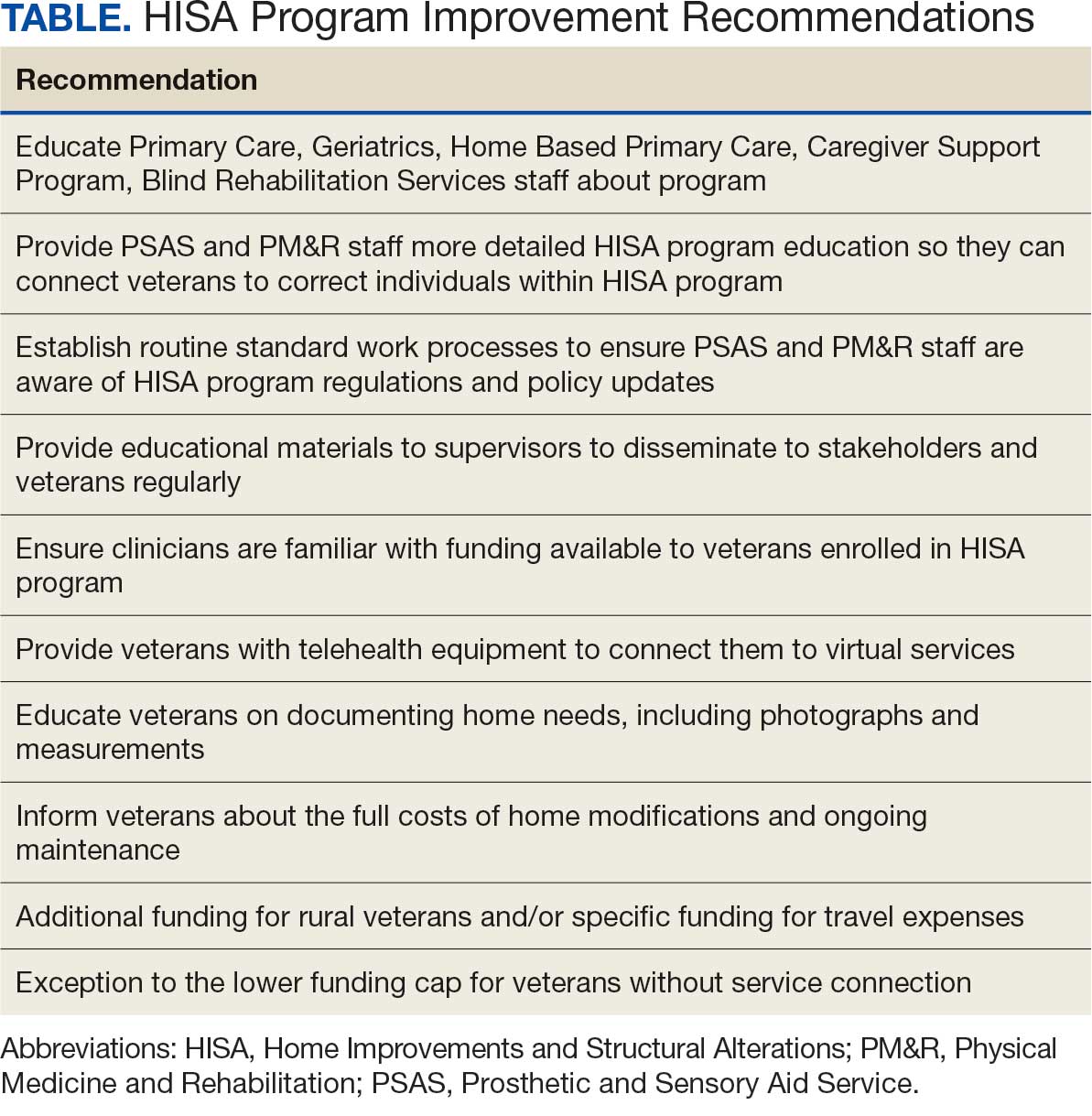
PSAS and PM&R professionals, including physicians, nurse practitioners, physician assistants, and physical and occupational therapists, would be expected to have some knowledge of the HISA program, and therefore be more likely to connect a veteran with it. However, they may lack specific details about the program such as correct contact persons in the other service (PSAS or PM&R, respectively), facility- specific processes, such as how to enter a HISA consultation within the veteran’s electronic health record, how the entered consultation would progress through the system and avoid cancellation, and what should routinely be done to avoid HISA consultation cancellation, such as referral to Occupational Therapy for a functional assessment so appropriate durable medical equipment can be trialed with the veteran prior to proceeding with more costly and time-consuming home modifications.
In addition, there is no routine standard work process to ensure that PM&R staff are aware of updates in HISA program regulations and policy. Further recommendations in this area include having supervisory employees in PSAS and PM&R work both individually and together to develop effective information dissemination methods for key stakeholders. These include targeted in-services (ie, educational trainings often scheduled and conducted during recurring meetings), whether faceto- face or virtually in real time, or recorded, that occur on an ongoing and regular basis with sister services such as Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services (eg, the facility Vision Impairment Services Team coordinator). Regularly updated educational materials should be provided to veterans and VHA adjacent stakeholders such as Veteran Service Organizations and Veteran County Service Officers, via a variety of platforms.
Successfully navigating the provision of home modifications via the HISA program involves identifying a contractor to perform the home modification and obtaining service and construction plan pricing. A key barrier in this area is that veterans and VHA clinicians perceive the funds available through HISA as insufficient, regardless of whether they have serviceconnected status or not. Service connection refers to designation of ≥ 1 medical conditions determined to be related to military service and thus eligible to receive VHA care.9 Service-connected veterans receive a lifetime maximum award of $6800 from HISA while veterans without service connection receive a lifetime maximum award of $2000.1,2
Rural veterans face a greater challenge than urban veterans, as there are fewer contractors located nearby. Thus, providing higher funding for rural veterans, or specific funding such as for travel expenses, would be especially helpful to find a willing contractor to perform home medications.1 The current requirement of working with a licensed contractor was also a barrier, especially for smaller jobs, and could result in VHA employees (including clinicians) feeling pressured to become overly involved to assist veterans to move through the process.
To that point, respondents requested resources such as a regularly updated list of licensed contractors in the area, especially those familiar with working with the HISA program, be provided to veterans and their assisting groups. In addition, respondents asked that VHA take on greater responsibility and liability with regard to contractors accessing HISA funding, such as not releasing final payment until VHA approved the completed home modification. On the other hand, respondents also expressed concerns about the length of time associated with HISA program payment and noted it should be sped up to allow contractors who participate to receive payment sooner, which many believed would increase the number of contractors willing to take on this work.
The role of telehealth was noted as a great facilitator of increased access to care, especially following the COVID-19 pandemic. Telehealth modalities adapted for the HISA program could help increase access to the program and improve processing speed. Barriers include lack of appropriate veteran telehealth equipment and poor understanding of information needed to move the process forward. Recommendations included providing veterans tablets to connect to virtual services, and developing information on home measurements needed, assistance in obtaining and sending photographs, and detailed information on successfully using telehealth for the HISA application process. Of note, some clinicians, representing home-based primary care, prosthetics services, geriatrics, rehabilitation therapy, mobile clinic, and the telehealth division, and including both clinical staff (eg, occupational therapists) and nonclinical staff (eg, prosthetics representatives and administrative personnel), have found patients expressed comparable satisfaction with the process whether faceto- face or via telehealth.
The essential relationship between PSAS and PM&R regarding the HISA program was a key finding. Both services are integral to helping veterans successfully obtain home modifications via the HISA program.1,2 Barriers include insufficient communication and a lack of clearly defined points of contact for each service, poorly defined roles, and inefficiencies because 2 services are involved in navigating the process. Recommendations therefore include addressing these issues, such as adopting a case management or liaison model between the services to better manage the process.
Respondents indicated that insufficient program funding was a concern. Veterans living in poorer quality housing, such as older homes, often require more expensive home modifications, necessitating greater out-of-pocket expenses. Veterans and VHA employees advocated for the creation of an exception to the lower funding cap for veterans without service connection in cases of financial hardship. Overall, the funding limits for both service-connected veterans and those without service connection were thought to be insufficient, especially as the COVID-19 pandemic increased the cost of construction materials.
Respondents also noted that veterans would benefit from clear messaging that receiving HISA funds does not impact eligibility for other VA benefits and services. Veterans must understand that home modifications work must be approved by VHA before being started and should be aware that if their disability rating increases so that they become eligible for the higher level service-connected benefits, they would then become eligible for the higher maximum benefit. Respondents recommended veterans should receive assistance in understanding the full costs of the home modification and ongoing maintenance, and the HISA research team recommended that the National Program develop a fact sheet that can be used to advise veterans.
Respondents consistently indicated that information about the HISA program was not disseminated effectively to key internal and external stakeholders, and opportunities to highlight the program on VHA websites, brochures throughout VHA facilities, and other outlets such as direct mailing should be used. Veterans who have used the program are overwhelmingly older (mean age 71 years), White, and male, suggesting missed opportunities and unmet need for underrepresented groups. Therefore, targeted marketing interventions would especially benefit these groups.
Respondents also noted inefficiencies throughout the HISA program application process and advocated for changes such as national standard operating procedures (SOPs) to guide navigation through the HISA process. The national SOPs could include home evaluation prior to HISA application submission, clearly identified points of contact for the HISA program in PSAS and PM&R, and standardized documentation.
Future Directions
Information from respondents provided several avenues for future studies. Recommendations were obtained from each of the 7 broad topical areas: training and educational needs, potential, contracting challenges and opportunities, telehealth as a conduit to facilitate the availability of the HISA program, PSAS, and clinical services collaboration, marketing, need for increased funding, and revision of the application process. Input from stakeholders can help direct efficient use of resources to guide future studies for the greatest impact and highlight current and future priorities. Easy areas of intervention indicated by respondents include creating a national standard work process regarding the HISA program with standardized educational materials for key stakeholders, revised at regular intervals, and readily available on national websites. A pre- and postimplementation survey could help provide quantifiable information about the benefits of such an intervention.
Conclusions
A qualitative analysis of interviews with veterans and VHA clinicians provides evidence of potential barriers for the HISA program. Addressing these barriers could allow HISA to better meet the VHA goal of providing home modifications that allow veterans to live safely and independently in their homes. There is a need for ongoing review and assessment of the program to ensure optimization and efficient use of resources across the spectrum of veteran needs.
- Semeah LM, Ahrentzen S, Jia H, et al. The Home Improvements and Structural Alterations Benefits Program: veterans with disabilities and home accessibility. J Disabil Policy Stud. 2017;28:43-51. doi:10.1177/1044207317696275
- Semeah LM, Wang X, Cowper Ripley DC, et al. Improving health through a home modification service for veterans. In: Fiedler BA, ed. Three Facets of Public Health and Paths to Improvements. 2020:381-416. doi:10.1016/B978-0-12-819008-1.00014-6
- Semeah LM, Ganesh SP, Wang X, et al. Home modification and health services utilization by rural and urban veterans with disabilities. Housing Policy Debate. 2021;31:862-874. doi:10.1080/10511482.2020.1858923
- Semeah LM, Orozco T, Wang X, et al. Home modifications for rural veterans with disabilities. Fed Pract. 2021;38:300- 310. doi:10.12788/fp.0153
- Semeah LM, Orozco T, Wang X, et al. Predictors of countylevel home modification use across the US. Fed Pract. 2022;39:274-280. doi:10.12788/fp.0279
- Semeah LM, Orozco T, Wang X, et al. Rural and urban home modification program users: a comparative study. HERD. 2023;16:223-235. doi:10.1177/19375867221142627
- US Department of of Veterans Affairs. Home Improvements and Structural Alterations (HISA) benefits program: final rule. Fed Regist. 2014;79:71658-71663
- US Department of Veterans Affairs. Home Improvement and Structural Alterations (HISA): increase in the limit for home improvement and structural alterations (HISA)-VA: final regulations. Fed Regist. 1993;58:25565.
- US Department of Veterans Affairs. Eligibility for VA disability benefits. Updated April 25, 2025. Accessed April 1, 2026. https://www.va.gov/disability/eligibility
The Veterans Health Administration (VHA) Home Improvements and Structural Alterations (HISA) program is a primary means through which veterans can obtain home modifications necessary to continue safe and independent living in their home, including fall risk reduction and accessibility to essential parts of the home. However, not all eligible veterans who may benefit from this program participate, for a variety of reasons.1-6 Historically, the HISA program has been administered in a decentralized and nonstandardized fashion dictated by the organizational structure of each US Department of Veterans Affairs (VA) medical center (VAMC) within a certain region or Veterans Integrated Service Network (VISN). Previous research found differential access to the HISA program by younger veterans, women, minorities, veterans with certain disability types, and veterans living in rural vs urban settings. These disparities in access and use of benefits conferred by the HISA program suggests an area of unmet need, which may improve veterans’ health care outcomes and reduce costs associated with their care.2-8
The purpose of this article is to provide information to improve equitable provision and effective eligible use of resources available through the HISA program in a more generalizable manner by providing insight to highlight common program process deficiencies and care provision gaps relevant to VAMCs nationwide. This information can be used to inform the VA Physical Medicine and Rehabilitation (PM&R) and Prosthetic and Sensory Aid Service (PSAS) national policy initiatives, as well as hiring practices, clinic organization, specific care provision, and administrative goals and metrics at each VISN and at the VA Healthcare System level.
Methods
Veterans who participated in the HISA program, VHA administrators, and VHA clinicians from select VAMCs were identified and interviewed to better understand what helps increase access to the program, barriers to access, and how existing program components and processes impact use of the service. These interviews were taken from a directed convenience sample of selected VAMCs. To obtain this directed convenience sample, 167 VAMCs that participated in the HISA program were categorized as facilities that provided either a high or low number of HISA program prescriptions based on data from 2010 to 2018. Ten facilities from the top quartiles and 10 from the bottom quartiles of prescribing locations were selected. This facility selection was driven by the proportion of rural veterans served by each facility, favoring those serving a greater proportion of rural veterans, as well geographic location, with the aim of avoiding overrepresentation of any specific region. The convenience sample included 45 individuals (20 VHA employees and 25 veterans) across 22 states from the Northeast, West, South, and Midwest US Census regions.
Interview Process
Interviews underwent a coding process. The development of topical themes followed a systematic, 2-phase approach. Initially, researchers analyzed responses to semistructured interview questions addressing specific aspects of the HISA program, such as program awareness and accessibility. These responses naturally clustered into preliminary categories based on the interview guide structure. For example, responses related to program discovery formed a marketing-related category, while recommendations about program implementation contributed to a training and development category.
Following this initial categorization, the research team conducted a more rigorous coding process. A team of 3 researchers systematically reviewed assigned interview transcripts to extract practical recommendations for the guide. The researchers first identified relevant responses individually and then convened during group meetings to discuss and finalize selections. This second phase refined the preliminary categorization while maintaining alignment with the original interview structure.
This approach allowed the team to preserve the practical utility of participant feedback while ensuring methodological rigor in the analysis process. Resulting themes reflect both the structured nature of the original inquiry and the practical recommendations identified for improving the HISA program. Information on the following areas were collected: education about the HISA program, the contracting process, use of telehealth, interaction between VHA clinical care and the PSAS, marketing of the program, program funding, and revising the application process.
Results
Interview respondents provided several recommendations for improving the HISA program (Table). Regarding training and education, respondents noted deficiencies in VHA employee communication about the HISA program to veterans. Some employees did not know details or were unaware the HISA program existed. Additionally, a lack of knowledge about HISA program alternatives, including other available programs for obtaining home modifications or other durable medical equipment alternatives (eg, provision of a portable ramp rather than construction of a permanent one), was apparent. It was strongly recommended to provide additional education to effectively disseminate knowledge about the HISA program. Specifically, VHA employees, especially those in Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services, require greater awareness of the program and its processes.
PSAS and PM&R professionals, including physicians, nurse practitioners, physician assistants, and physical and occupational therapists, would be expected to have some knowledge of the HISA program, and therefore be more likely to connect a veteran with it. However, they may lack specific details about the program such as correct contact persons in the other service (PSAS or PM&R, respectively), facility- specific processes, such as how to enter a HISA consultation within the veteran’s electronic health record, how the entered consultation would progress through the system and avoid cancellation, and what should routinely be done to avoid HISA consultation cancellation, such as referral to Occupational Therapy for a functional assessment so appropriate durable medical equipment can be trialed with the veteran prior to proceeding with more costly and time-consuming home modifications.
In addition, there is no routine standard work process to ensure that PM&R staff are aware of updates in HISA program regulations and policy. Further recommendations in this area include having supervisory employees in PSAS and PM&R work both individually and together to develop effective information dissemination methods for key stakeholders. These include targeted in-services (ie, educational trainings often scheduled and conducted during recurring meetings), whether faceto- face or virtually in real time, or recorded, that occur on an ongoing and regular basis with sister services such as Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services (eg, the facility Vision Impairment Services Team coordinator). Regularly updated educational materials should be provided to veterans and VHA adjacent stakeholders such as Veteran Service Organizations and Veteran County Service Officers, via a variety of platforms.
Successfully navigating the provision of home modifications via the HISA program involves identifying a contractor to perform the home modification and obtaining service and construction plan pricing. A key barrier in this area is that veterans and VHA clinicians perceive the funds available through HISA as insufficient, regardless of whether they have serviceconnected status or not. Service connection refers to designation of ≥ 1 medical conditions determined to be related to military service and thus eligible to receive VHA care.9 Service-connected veterans receive a lifetime maximum award of $6800 from HISA while veterans without service connection receive a lifetime maximum award of $2000.1,2
Rural veterans face a greater challenge than urban veterans, as there are fewer contractors located nearby. Thus, providing higher funding for rural veterans, or specific funding such as for travel expenses, would be especially helpful to find a willing contractor to perform home medications.1 The current requirement of working with a licensed contractor was also a barrier, especially for smaller jobs, and could result in VHA employees (including clinicians) feeling pressured to become overly involved to assist veterans to move through the process.
To that point, respondents requested resources such as a regularly updated list of licensed contractors in the area, especially those familiar with working with the HISA program, be provided to veterans and their assisting groups. In addition, respondents asked that VHA take on greater responsibility and liability with regard to contractors accessing HISA funding, such as not releasing final payment until VHA approved the completed home modification. On the other hand, respondents also expressed concerns about the length of time associated with HISA program payment and noted it should be sped up to allow contractors who participate to receive payment sooner, which many believed would increase the number of contractors willing to take on this work.
The role of telehealth was noted as a great facilitator of increased access to care, especially following the COVID-19 pandemic. Telehealth modalities adapted for the HISA program could help increase access to the program and improve processing speed. Barriers include lack of appropriate veteran telehealth equipment and poor understanding of information needed to move the process forward. Recommendations included providing veterans tablets to connect to virtual services, and developing information on home measurements needed, assistance in obtaining and sending photographs, and detailed information on successfully using telehealth for the HISA application process. Of note, some clinicians, representing home-based primary care, prosthetics services, geriatrics, rehabilitation therapy, mobile clinic, and the telehealth division, and including both clinical staff (eg, occupational therapists) and nonclinical staff (eg, prosthetics representatives and administrative personnel), have found patients expressed comparable satisfaction with the process whether faceto- face or via telehealth.
The essential relationship between PSAS and PM&R regarding the HISA program was a key finding. Both services are integral to helping veterans successfully obtain home modifications via the HISA program.1,2 Barriers include insufficient communication and a lack of clearly defined points of contact for each service, poorly defined roles, and inefficiencies because 2 services are involved in navigating the process. Recommendations therefore include addressing these issues, such as adopting a case management or liaison model between the services to better manage the process.
Respondents indicated that insufficient program funding was a concern. Veterans living in poorer quality housing, such as older homes, often require more expensive home modifications, necessitating greater out-of-pocket expenses. Veterans and VHA employees advocated for the creation of an exception to the lower funding cap for veterans without service connection in cases of financial hardship. Overall, the funding limits for both service-connected veterans and those without service connection were thought to be insufficient, especially as the COVID-19 pandemic increased the cost of construction materials.
Respondents also noted that veterans would benefit from clear messaging that receiving HISA funds does not impact eligibility for other VA benefits and services. Veterans must understand that home modifications work must be approved by VHA before being started and should be aware that if their disability rating increases so that they become eligible for the higher level service-connected benefits, they would then become eligible for the higher maximum benefit. Respondents recommended veterans should receive assistance in understanding the full costs of the home modification and ongoing maintenance, and the HISA research team recommended that the National Program develop a fact sheet that can be used to advise veterans.
Respondents consistently indicated that information about the HISA program was not disseminated effectively to key internal and external stakeholders, and opportunities to highlight the program on VHA websites, brochures throughout VHA facilities, and other outlets such as direct mailing should be used. Veterans who have used the program are overwhelmingly older (mean age 71 years), White, and male, suggesting missed opportunities and unmet need for underrepresented groups. Therefore, targeted marketing interventions would especially benefit these groups.
Respondents also noted inefficiencies throughout the HISA program application process and advocated for changes such as national standard operating procedures (SOPs) to guide navigation through the HISA process. The national SOPs could include home evaluation prior to HISA application submission, clearly identified points of contact for the HISA program in PSAS and PM&R, and standardized documentation.
Future Directions
Information from respondents provided several avenues for future studies. Recommendations were obtained from each of the 7 broad topical areas: training and educational needs, potential, contracting challenges and opportunities, telehealth as a conduit to facilitate the availability of the HISA program, PSAS, and clinical services collaboration, marketing, need for increased funding, and revision of the application process. Input from stakeholders can help direct efficient use of resources to guide future studies for the greatest impact and highlight current and future priorities. Easy areas of intervention indicated by respondents include creating a national standard work process regarding the HISA program with standardized educational materials for key stakeholders, revised at regular intervals, and readily available on national websites. A pre- and postimplementation survey could help provide quantifiable information about the benefits of such an intervention.
Conclusions
A qualitative analysis of interviews with veterans and VHA clinicians provides evidence of potential barriers for the HISA program. Addressing these barriers could allow HISA to better meet the VHA goal of providing home modifications that allow veterans to live safely and independently in their homes. There is a need for ongoing review and assessment of the program to ensure optimization and efficient use of resources across the spectrum of veteran needs.
The Veterans Health Administration (VHA) Home Improvements and Structural Alterations (HISA) program is a primary means through which veterans can obtain home modifications necessary to continue safe and independent living in their home, including fall risk reduction and accessibility to essential parts of the home. However, not all eligible veterans who may benefit from this program participate, for a variety of reasons.1-6 Historically, the HISA program has been administered in a decentralized and nonstandardized fashion dictated by the organizational structure of each US Department of Veterans Affairs (VA) medical center (VAMC) within a certain region or Veterans Integrated Service Network (VISN). Previous research found differential access to the HISA program by younger veterans, women, minorities, veterans with certain disability types, and veterans living in rural vs urban settings. These disparities in access and use of benefits conferred by the HISA program suggests an area of unmet need, which may improve veterans’ health care outcomes and reduce costs associated with their care.2-8
The purpose of this article is to provide information to improve equitable provision and effective eligible use of resources available through the HISA program in a more generalizable manner by providing insight to highlight common program process deficiencies and care provision gaps relevant to VAMCs nationwide. This information can be used to inform the VA Physical Medicine and Rehabilitation (PM&R) and Prosthetic and Sensory Aid Service (PSAS) national policy initiatives, as well as hiring practices, clinic organization, specific care provision, and administrative goals and metrics at each VISN and at the VA Healthcare System level.
Methods
Veterans who participated in the HISA program, VHA administrators, and VHA clinicians from select VAMCs were identified and interviewed to better understand what helps increase access to the program, barriers to access, and how existing program components and processes impact use of the service. These interviews were taken from a directed convenience sample of selected VAMCs. To obtain this directed convenience sample, 167 VAMCs that participated in the HISA program were categorized as facilities that provided either a high or low number of HISA program prescriptions based on data from 2010 to 2018. Ten facilities from the top quartiles and 10 from the bottom quartiles of prescribing locations were selected. This facility selection was driven by the proportion of rural veterans served by each facility, favoring those serving a greater proportion of rural veterans, as well geographic location, with the aim of avoiding overrepresentation of any specific region. The convenience sample included 45 individuals (20 VHA employees and 25 veterans) across 22 states from the Northeast, West, South, and Midwest US Census regions.
Interview Process
Interviews underwent a coding process. The development of topical themes followed a systematic, 2-phase approach. Initially, researchers analyzed responses to semistructured interview questions addressing specific aspects of the HISA program, such as program awareness and accessibility. These responses naturally clustered into preliminary categories based on the interview guide structure. For example, responses related to program discovery formed a marketing-related category, while recommendations about program implementation contributed to a training and development category.
Following this initial categorization, the research team conducted a more rigorous coding process. A team of 3 researchers systematically reviewed assigned interview transcripts to extract practical recommendations for the guide. The researchers first identified relevant responses individually and then convened during group meetings to discuss and finalize selections. This second phase refined the preliminary categorization while maintaining alignment with the original interview structure.
This approach allowed the team to preserve the practical utility of participant feedback while ensuring methodological rigor in the analysis process. Resulting themes reflect both the structured nature of the original inquiry and the practical recommendations identified for improving the HISA program. Information on the following areas were collected: education about the HISA program, the contracting process, use of telehealth, interaction between VHA clinical care and the PSAS, marketing of the program, program funding, and revising the application process.
Results
Interview respondents provided several recommendations for improving the HISA program (Table). Regarding training and education, respondents noted deficiencies in VHA employee communication about the HISA program to veterans. Some employees did not know details or were unaware the HISA program existed. Additionally, a lack of knowledge about HISA program alternatives, including other available programs for obtaining home modifications or other durable medical equipment alternatives (eg, provision of a portable ramp rather than construction of a permanent one), was apparent. It was strongly recommended to provide additional education to effectively disseminate knowledge about the HISA program. Specifically, VHA employees, especially those in Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services, require greater awareness of the program and its processes.
PSAS and PM&R professionals, including physicians, nurse practitioners, physician assistants, and physical and occupational therapists, would be expected to have some knowledge of the HISA program, and therefore be more likely to connect a veteran with it. However, they may lack specific details about the program such as correct contact persons in the other service (PSAS or PM&R, respectively), facility- specific processes, such as how to enter a HISA consultation within the veteran’s electronic health record, how the entered consultation would progress through the system and avoid cancellation, and what should routinely be done to avoid HISA consultation cancellation, such as referral to Occupational Therapy for a functional assessment so appropriate durable medical equipment can be trialed with the veteran prior to proceeding with more costly and time-consuming home modifications.
In addition, there is no routine standard work process to ensure that PM&R staff are aware of updates in HISA program regulations and policy. Further recommendations in this area include having supervisory employees in PSAS and PM&R work both individually and together to develop effective information dissemination methods for key stakeholders. These include targeted in-services (ie, educational trainings often scheduled and conducted during recurring meetings), whether faceto- face or virtually in real time, or recorded, that occur on an ongoing and regular basis with sister services such as Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services (eg, the facility Vision Impairment Services Team coordinator). Regularly updated educational materials should be provided to veterans and VHA adjacent stakeholders such as Veteran Service Organizations and Veteran County Service Officers, via a variety of platforms.
Successfully navigating the provision of home modifications via the HISA program involves identifying a contractor to perform the home modification and obtaining service and construction plan pricing. A key barrier in this area is that veterans and VHA clinicians perceive the funds available through HISA as insufficient, regardless of whether they have serviceconnected status or not. Service connection refers to designation of ≥ 1 medical conditions determined to be related to military service and thus eligible to receive VHA care.9 Service-connected veterans receive a lifetime maximum award of $6800 from HISA while veterans without service connection receive a lifetime maximum award of $2000.1,2
Rural veterans face a greater challenge than urban veterans, as there are fewer contractors located nearby. Thus, providing higher funding for rural veterans, or specific funding such as for travel expenses, would be especially helpful to find a willing contractor to perform home medications.1 The current requirement of working with a licensed contractor was also a barrier, especially for smaller jobs, and could result in VHA employees (including clinicians) feeling pressured to become overly involved to assist veterans to move through the process.
To that point, respondents requested resources such as a regularly updated list of licensed contractors in the area, especially those familiar with working with the HISA program, be provided to veterans and their assisting groups. In addition, respondents asked that VHA take on greater responsibility and liability with regard to contractors accessing HISA funding, such as not releasing final payment until VHA approved the completed home modification. On the other hand, respondents also expressed concerns about the length of time associated with HISA program payment and noted it should be sped up to allow contractors who participate to receive payment sooner, which many believed would increase the number of contractors willing to take on this work.
The role of telehealth was noted as a great facilitator of increased access to care, especially following the COVID-19 pandemic. Telehealth modalities adapted for the HISA program could help increase access to the program and improve processing speed. Barriers include lack of appropriate veteran telehealth equipment and poor understanding of information needed to move the process forward. Recommendations included providing veterans tablets to connect to virtual services, and developing information on home measurements needed, assistance in obtaining and sending photographs, and detailed information on successfully using telehealth for the HISA application process. Of note, some clinicians, representing home-based primary care, prosthetics services, geriatrics, rehabilitation therapy, mobile clinic, and the telehealth division, and including both clinical staff (eg, occupational therapists) and nonclinical staff (eg, prosthetics representatives and administrative personnel), have found patients expressed comparable satisfaction with the process whether faceto- face or via telehealth.
The essential relationship between PSAS and PM&R regarding the HISA program was a key finding. Both services are integral to helping veterans successfully obtain home modifications via the HISA program.1,2 Barriers include insufficient communication and a lack of clearly defined points of contact for each service, poorly defined roles, and inefficiencies because 2 services are involved in navigating the process. Recommendations therefore include addressing these issues, such as adopting a case management or liaison model between the services to better manage the process.
Respondents indicated that insufficient program funding was a concern. Veterans living in poorer quality housing, such as older homes, often require more expensive home modifications, necessitating greater out-of-pocket expenses. Veterans and VHA employees advocated for the creation of an exception to the lower funding cap for veterans without service connection in cases of financial hardship. Overall, the funding limits for both service-connected veterans and those without service connection were thought to be insufficient, especially as the COVID-19 pandemic increased the cost of construction materials.
Respondents also noted that veterans would benefit from clear messaging that receiving HISA funds does not impact eligibility for other VA benefits and services. Veterans must understand that home modifications work must be approved by VHA before being started and should be aware that if their disability rating increases so that they become eligible for the higher level service-connected benefits, they would then become eligible for the higher maximum benefit. Respondents recommended veterans should receive assistance in understanding the full costs of the home modification and ongoing maintenance, and the HISA research team recommended that the National Program develop a fact sheet that can be used to advise veterans.
Respondents consistently indicated that information about the HISA program was not disseminated effectively to key internal and external stakeholders, and opportunities to highlight the program on VHA websites, brochures throughout VHA facilities, and other outlets such as direct mailing should be used. Veterans who have used the program are overwhelmingly older (mean age 71 years), White, and male, suggesting missed opportunities and unmet need for underrepresented groups. Therefore, targeted marketing interventions would especially benefit these groups.
Respondents also noted inefficiencies throughout the HISA program application process and advocated for changes such as national standard operating procedures (SOPs) to guide navigation through the HISA process. The national SOPs could include home evaluation prior to HISA application submission, clearly identified points of contact for the HISA program in PSAS and PM&R, and standardized documentation.
Future Directions
Information from respondents provided several avenues for future studies. Recommendations were obtained from each of the 7 broad topical areas: training and educational needs, potential, contracting challenges and opportunities, telehealth as a conduit to facilitate the availability of the HISA program, PSAS, and clinical services collaboration, marketing, need for increased funding, and revision of the application process. Input from stakeholders can help direct efficient use of resources to guide future studies for the greatest impact and highlight current and future priorities. Easy areas of intervention indicated by respondents include creating a national standard work process regarding the HISA program with standardized educational materials for key stakeholders, revised at regular intervals, and readily available on national websites. A pre- and postimplementation survey could help provide quantifiable information about the benefits of such an intervention.
Conclusions
A qualitative analysis of interviews with veterans and VHA clinicians provides evidence of potential barriers for the HISA program. Addressing these barriers could allow HISA to better meet the VHA goal of providing home modifications that allow veterans to live safely and independently in their homes. There is a need for ongoing review and assessment of the program to ensure optimization and efficient use of resources across the spectrum of veteran needs.
- Semeah LM, Ahrentzen S, Jia H, et al. The Home Improvements and Structural Alterations Benefits Program: veterans with disabilities and home accessibility. J Disabil Policy Stud. 2017;28:43-51. doi:10.1177/1044207317696275
- Semeah LM, Wang X, Cowper Ripley DC, et al. Improving health through a home modification service for veterans. In: Fiedler BA, ed. Three Facets of Public Health and Paths to Improvements. 2020:381-416. doi:10.1016/B978-0-12-819008-1.00014-6
- Semeah LM, Ganesh SP, Wang X, et al. Home modification and health services utilization by rural and urban veterans with disabilities. Housing Policy Debate. 2021;31:862-874. doi:10.1080/10511482.2020.1858923
- Semeah LM, Orozco T, Wang X, et al. Home modifications for rural veterans with disabilities. Fed Pract. 2021;38:300- 310. doi:10.12788/fp.0153
- Semeah LM, Orozco T, Wang X, et al. Predictors of countylevel home modification use across the US. Fed Pract. 2022;39:274-280. doi:10.12788/fp.0279
- Semeah LM, Orozco T, Wang X, et al. Rural and urban home modification program users: a comparative study. HERD. 2023;16:223-235. doi:10.1177/19375867221142627
- US Department of of Veterans Affairs. Home Improvements and Structural Alterations (HISA) benefits program: final rule. Fed Regist. 2014;79:71658-71663
- US Department of Veterans Affairs. Home Improvement and Structural Alterations (HISA): increase in the limit for home improvement and structural alterations (HISA)-VA: final regulations. Fed Regist. 1993;58:25565.
- US Department of Veterans Affairs. Eligibility for VA disability benefits. Updated April 25, 2025. Accessed April 1, 2026. https://www.va.gov/disability/eligibility
- Semeah LM, Ahrentzen S, Jia H, et al. The Home Improvements and Structural Alterations Benefits Program: veterans with disabilities and home accessibility. J Disabil Policy Stud. 2017;28:43-51. doi:10.1177/1044207317696275
- Semeah LM, Wang X, Cowper Ripley DC, et al. Improving health through a home modification service for veterans. In: Fiedler BA, ed. Three Facets of Public Health and Paths to Improvements. 2020:381-416. doi:10.1016/B978-0-12-819008-1.00014-6
- Semeah LM, Ganesh SP, Wang X, et al. Home modification and health services utilization by rural and urban veterans with disabilities. Housing Policy Debate. 2021;31:862-874. doi:10.1080/10511482.2020.1858923
- Semeah LM, Orozco T, Wang X, et al. Home modifications for rural veterans with disabilities. Fed Pract. 2021;38:300- 310. doi:10.12788/fp.0153
- Semeah LM, Orozco T, Wang X, et al. Predictors of countylevel home modification use across the US. Fed Pract. 2022;39:274-280. doi:10.12788/fp.0279
- Semeah LM, Orozco T, Wang X, et al. Rural and urban home modification program users: a comparative study. HERD. 2023;16:223-235. doi:10.1177/19375867221142627
- US Department of of Veterans Affairs. Home Improvements and Structural Alterations (HISA) benefits program: final rule. Fed Regist. 2014;79:71658-71663
- US Department of Veterans Affairs. Home Improvement and Structural Alterations (HISA): increase in the limit for home improvement and structural alterations (HISA)-VA: final regulations. Fed Regist. 1993;58:25565.
- US Department of Veterans Affairs. Eligibility for VA disability benefits. Updated April 25, 2025. Accessed April 1, 2026. https://www.va.gov/disability/eligibility
The Home Improvements and Structural Alterations Program: Overview and Future Implications
The Home Improvements and Structural Alterations Program: Overview and Future Implications

Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program
Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program
The US Department of Veterans Affairs (VA) Home Loan Program, administered by the Veterans Benefits Administration (VBA), is a unique benefit for veterans, active-duty service members, National Guard and Reserve members, and eligible surviving spouses. Established in 1944, the program aims to help these individuals achieve homeownership by leveraging a third-party guarantee, typically from a government agency, to enhance access to credit and improve loan terms for borrowers who may not meet conventional loan qualifications.1 Since its inception, the VA has guaranteed > 28.5 million loans, enabling millions of veterans to buy, build, repair, retain, or adapt homes for personal occupancy.2 The program is designed to support veterans and eligible individuals to become homeowners, recognizing homeownership as a pathway to financial stability and community integration. VA home loans are provided by private lenders (eg, banks, mortgage companies) with a portion guaranteed by the VA, which reduces the risk for lenders and enables them to offer competitive terms, such as no down payment and lower interest rates, making homeownership more accessible to veterans.2
Eligibility criteria for the VA Home Loan Program include military service criteria such as active-duty service members with ≥ 90 continuous days of service; veterans with an honorable discharge meeting minimum service requirements; individuals who served in the National Guard/Reserve for ≥ 90 days of active service or 6 years of service with an honorable discharge; and surviving spouses of veterans who died in service or from a service-connected disability, were designated as missing in action/ prisoner of war, and the spouse is receiving Dependency and Indemnity Compensation. Financial criteria also apply: borrowers must meet lender requirements for credit and income (although VA loans are more flexible than conventional loans) and the home must be for personal occupancy rather than an investment property.3
A June 2025 PubMed literature search did not reveal any prior research on the VA Home Loan Program, although a limited number of studies tackled a wide range of issues related to federal and private home loans.4-12 To our knowledge, there is no prior published examination of the VA Home Loan Program. Understanding VA Home Loan Program usage among Veterans Health Administration (VHA) users can inform the future direction of the program. The VHA operates the largest integrated US health care system, serving > 9 million enrolled veterans annually at 1321 facilities, including 172 medical centers and 1138 outpatient clinics, providing primary and specialized health care, and related medical and social support services for enrolled veterans, including those who are experiencing housing instability or homelessness.13 Specialized VHA programs for homeless veterans include housing, employment, health care, justice, and re-entryrelated services in collaboration with federal and community partners.14 Housing instability has been defined as the state of being at risk of losing housing due to challenges such as difficulties paying rent, overcrowding, frequent relocation, and a substantial proportion of income spent on housing.15,16 Homelessness is a severe manifestation of housing instability that has been defined as the lack of stable, safe, and functioning housing.17,18
Health care and social services, including those that address housing instability and homelessness, are major priorities for the VHA and VBA.19 The VA Home Loan Program may represent an important resource to help veterans achieve long-term housing stability through home ownership. There has been wide public concern about housing affordability and the ability of many Americans, including veterans, to achieve home ownership.20 Homeownership is considered an important part of developing financial assets and achieving financial stability. Lowincome veterans, in particular, may benefit from this program as a national study found that 8.0% of low-income veterans and 13.9% of veterans with a history of homelessness have previously experienced a home foreclosure. 21 A greater understanding of who applies for and receives assistance from the VA Home Loan Program would inform homelessness prevention services and future planning for this program.
We conducted a quality improvement (QI) project on behalf of the VHA Homeless Programs Office and in partnership with the VBA. Our goals were to: (1) describe the annual number of applicants and recipients of the VA Home Loan Program by age group, sex, race/ethnicity, presence of any diagnosed substance use and/or mental health disorder, and history of homelessness; and (2) compare demographic, clinical, and homelessness characteristics among individuals who apply and are granted a loan through this program, individuals who apply and are denied a loan through this program, and individuals who do not apply for a loan through this program.
Methods
This project involved linked VA administrative national databases and was undertaken by the VHA Homeless Programs Office in partnership with the VBA. Specifically, VHA and VBA databases were linked together using veteran identifiers and all data were managed and analyzed on secure VA servers. The project followed VA’s Program Guide 1200.21 for nonresearch activities and institutional review board approval was waived through sponsorship by the VA Homeless Programs Office. The VHA Corporate Data Warehouse (CDW) was accessed to obtain data from the Homeless Operations Management and Evaluation System (HOMES) and other clinical data systems used by VHA clinicians and administrators that capture diagnoses, workload, and other health care data.22,23 HOMES collects intake, progress, and outcome data on homeless veterans within its care system that enables the VA to assess the effectiveness of programs and strategically allocate resources to prevent homelessness.24,25
A list of veterans who filed disability compensation and pension claims was obtained from the VBA Office of Performance Analysis and Integrity, including Social Security number, name, city and state, date of claim submission, grant or increase in benefits, homeless status, VA home loan approval, and homeless aid for dependent children from fiscal year (FY) 2022 through FY 2024. VBA data were linked to VHA CDW electronic health record data from veterans who sought VA health care services and HOMES data on veteran participation in homeless programs who were also experiencing homelessness. VHA data included demographic characteristics (eg, sex, age, race, marital status, combat service) at an index date (earliest visit to the VHA between October 1, 2021, and September 30, 2024); military sexual trauma; clinical characteristics within 12 months prior to the index date (VHA disability rating, substance use disorder [SUD] diagnosis, mental health disorder diagnosis, Charlson Comorbidity Index [CCI] score), and homelessness experience ≤ 5 years prior to the index date.
History of homelessness ≤ 5 years prior to the index date was determined using an operational definition of homelessness based on multiple indicators, including International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic code Z59.0; clinic stop codes or HOMES records indicating VA homeless programs clinical encounters; or a positive screen on an annual homelessness screener.16 US Department of Housing and Urban Development-VA Supportive Housing enrollees were excluded because they are considered to no longer be experiencing homelessness, and Veterans Justice Program enrollees were excluded because the program primarily focuses on serving criminal justice-involved veterans. The CCI predicts the risk of death ≤ 1 year by assessing the number and severity of a patient’s coexisting health conditions and is a valuable tool for understanding a patient’s overall health burden, aiding in clinical decision-making and evaluation research studies.26-29 Diagnoses based on ICD-10-CM codes were used to determine SUDs, mental health disorders, and CCI score, using methods that have been described in other publications.30
Population
The VBA cohort of veterans requesting benefits was further restricted to those who met the following eligibility criteria: (1) requested VA benefits FYs 2022 to 2024; (2) sought VHA services ≥ 1 time between FY 2022 and 2024; (3) had matching VBA/VHA records; (4) had no missing data on claim status and/ or demographic, clinical, and homelessness characteristics; and (5) had known home loan status FYs 2022 to 2024. The original VBA dataset consisted of 4,219,755 records and the original VHA dataset consisted of 7,170,199 records (Figure 1). The final linked VBA/VHA dataset after excluding 29 records with missing data on sex, 7 with missing data on age, 6 with missing data on marital status, and an additional 143,444 with unknown VBA claim status, consisted of 3,089,295 records corresponding to 2,260,851 unique veterans. Specifically, 251,796 records corresponded to veterans who had applied and received a loan, 84,751 to veterans who had applied and were nonrecipients of a loan, and 2,752,748 to veterans who did not apply for a loan.
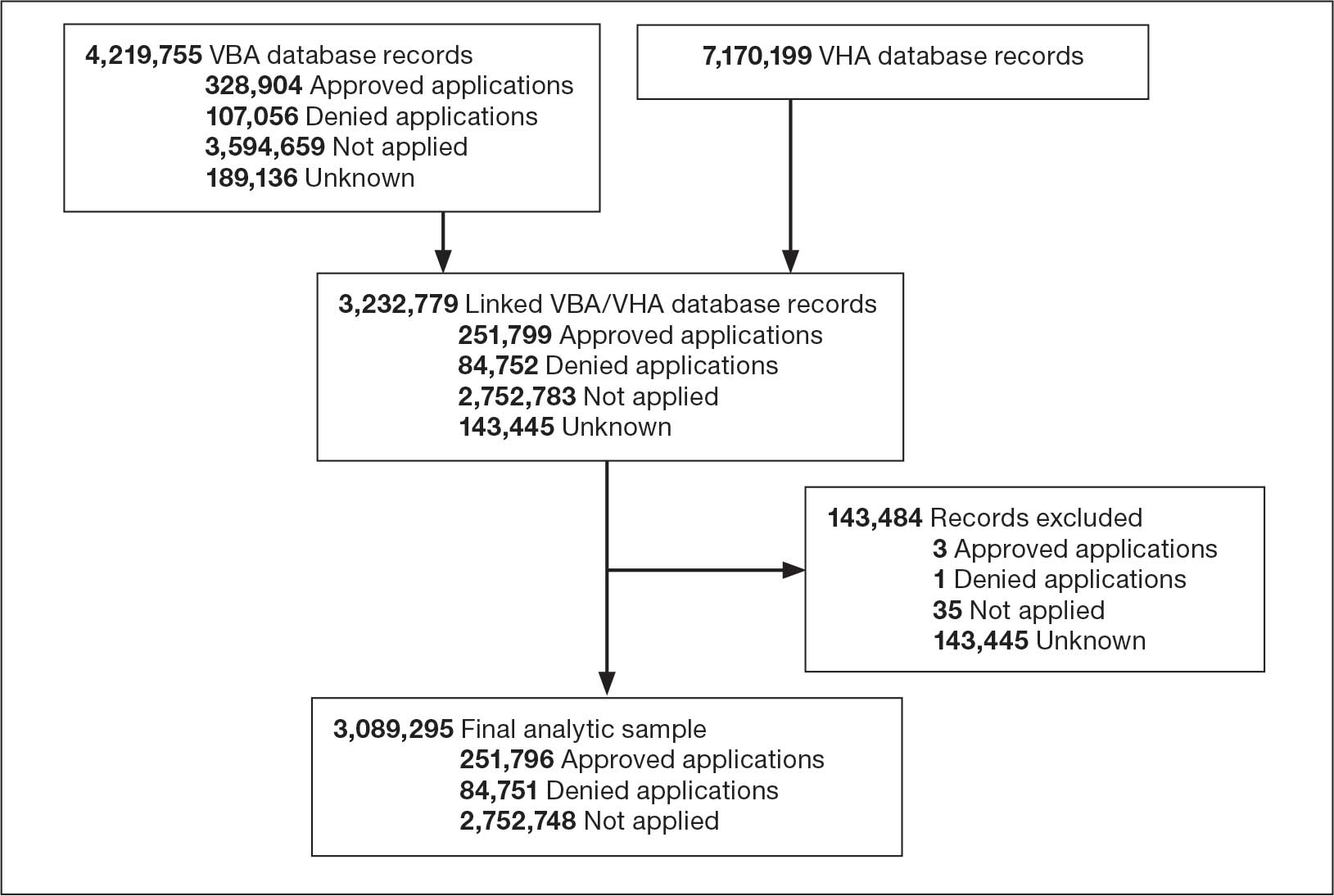
Abbreviations: FY, fiscal year; VBA, Veterans Benefits Administration; VHA, Veterans Health Administration.
Statistical Analysis
All statistical analyses were performed using SAS Enterprise Guide, an application that provides a point-and-click interface for data access, analysis, and management, accommodating both code-based and visual programming. 31 First, we relied on the final analytic sample to calculate the annual proportions of veterans who applied for and/or received a loan through the VA Home Loan Program. We also generated descriptive statistics stratified by age group, sex, race/ethnicity, SUD, mental health disorder, and homelessness, overall and within each FY. Pearson χ2 and Cochran-Armitage trend tests were applied to examine differences in application and receipt of a home loan by baseline characteristics and FY, respectively. Second, we conducted bivariate and multivariable analyses to compare demographic, clinical, and homelessness characteristics between 3 groups of veterans as they pertain to the VA Home Loan Program. Veterans who applied and were nonrecipients of a loan (group 1), veterans who applied and were recipients of a loan (group 2), and veterans who did not apply for a loan (group 3). Similar analyses compared VA Home Loan Program applicants who were recipients of a home loan vs VA Home Loan Program applicants who were nonrecipients of a home loan. Multinomial and binary logistic regression models were constructed to estimate the relative risk ratio (RR) and odds ratio (OR) with 95% CIs for comparisons between these distinct groups on demographic, clinical, and homelessness characteristics. Two-sided statistical tests were evaluated at α = 0.05.
Results
Tables 1 and 2 present the number of VBA applicants, including those who applied for and received benefits through the VA Home Loan Program, by age group, sex, race/ethnicity, as well as histories of SUDs, mental health disorders, and homelessness, overall, and by FY. As shown in Figure 2, 336,547 of 3,089,295 VBA applications (10.9%) pertained to the VA Home Loan Program, with a statistically significant decline in application rates, from 12.2% in FY 2022 to 9.9% in FY 2024 (P < .001 for trend). Among 336,547 veterans who applied for the VA Home Loan Program, 251,796 (74.8%) received a home loan during FYs 2022 to 2024, ranging between 73.8% for FY 2024 and 75.5% for FY 2023 (P < .001 for trend).
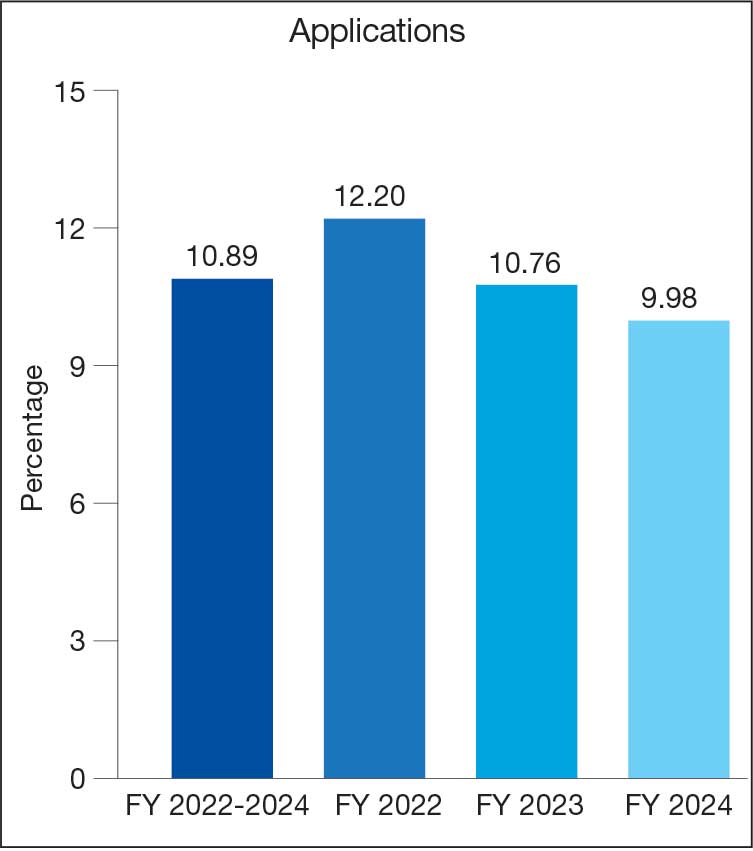
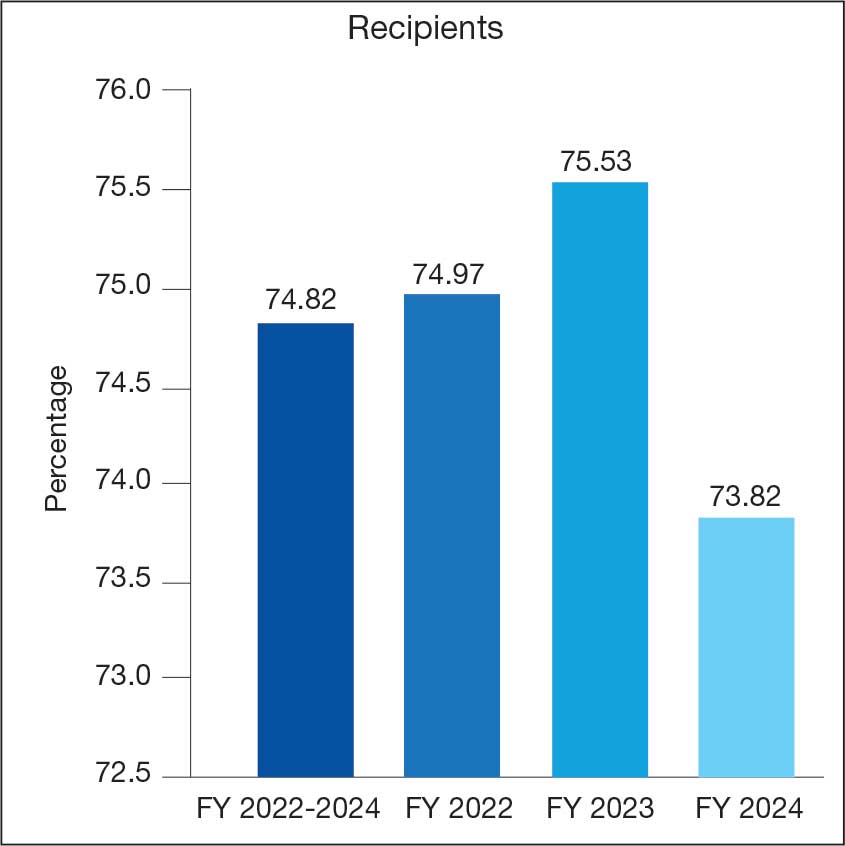
Veterans Affairs Home Loan Program, fiscal years (FY) 2022-2024.
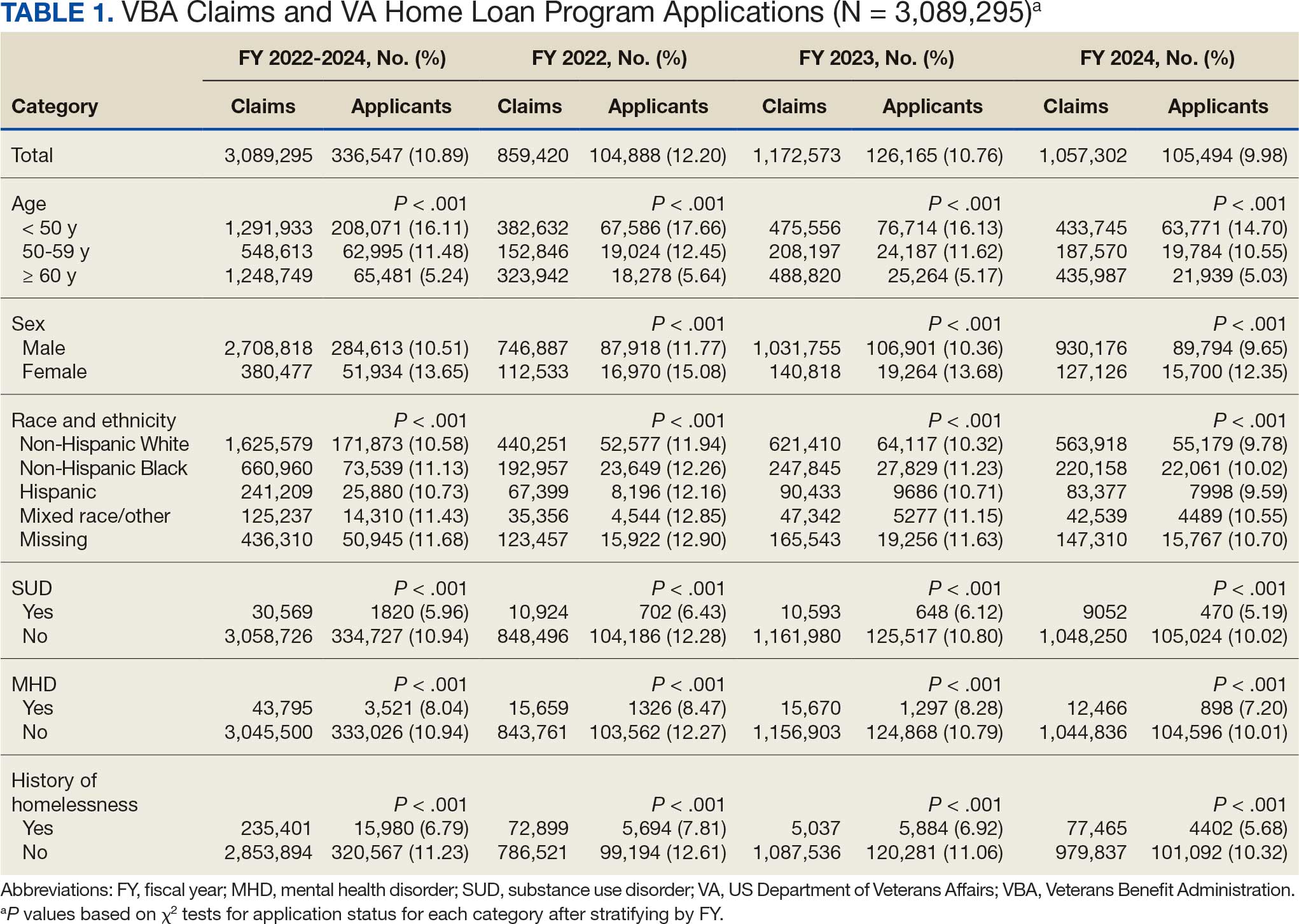
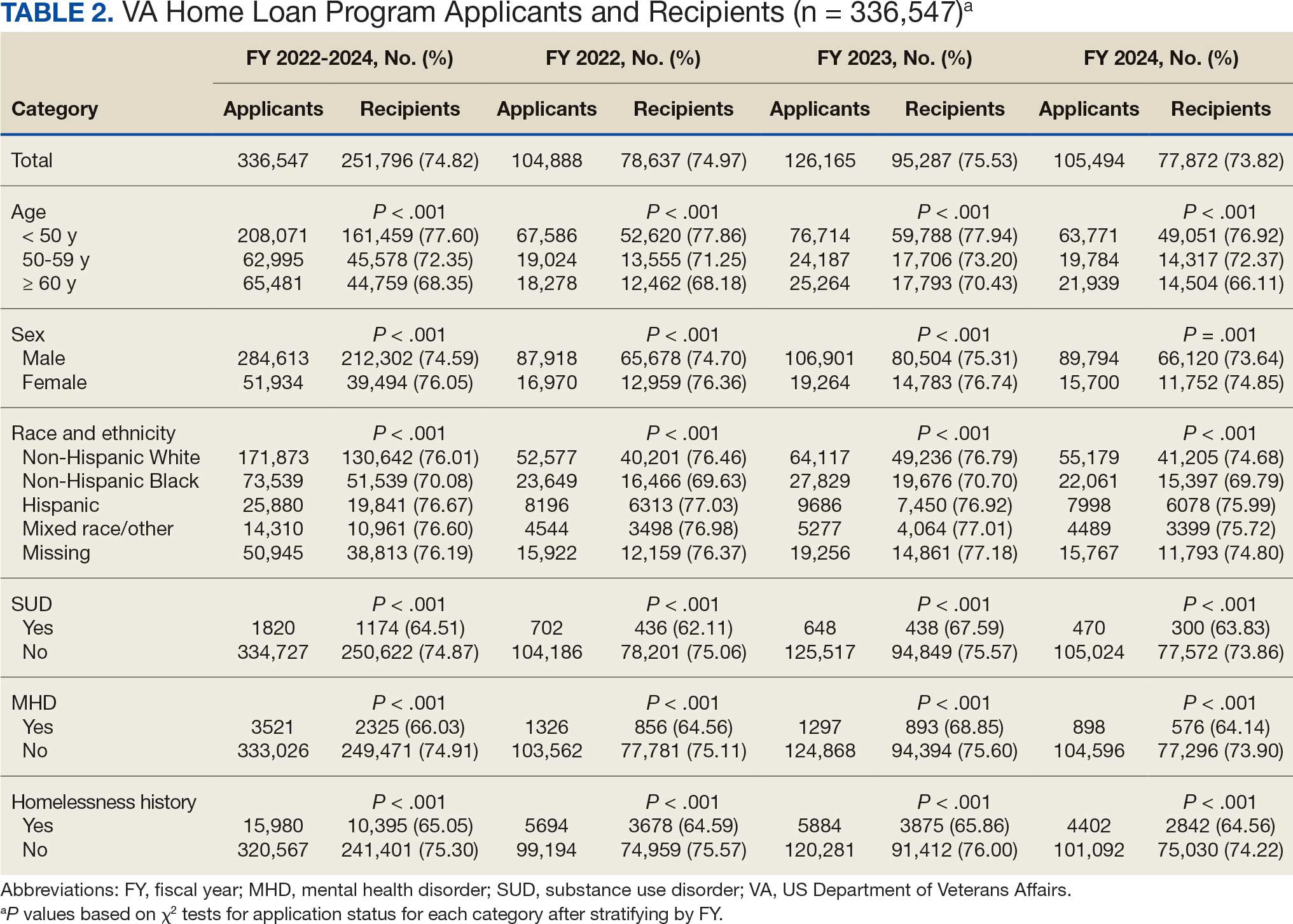
Multinomial logistic regression models for demographic, clinical, and homelessness characteristics as predictors of VA Home Loan Program status are provided in Appendix 1. Based on the fully adjusted model, compared with veterans who did not apply to the VA Home Loan Program, those who applied for a home loan were less likely to be aged ≥ 50 years, unmarried, Hispanic ethnicity, mixed race, or other race, diagnosed with a SUD, or history of homelessness. Veterans with higher VA service-connected disability ratings were more frequently recipients of VA home loans, whereas those who self-identified as non-Hispanic Black and those with higher CCI scores were less frequently recipients of VA home loans. Finally, those with mental health disorders were more likely than their counterparts to be applicants (recipients or nonrecipients) of VA home loans.
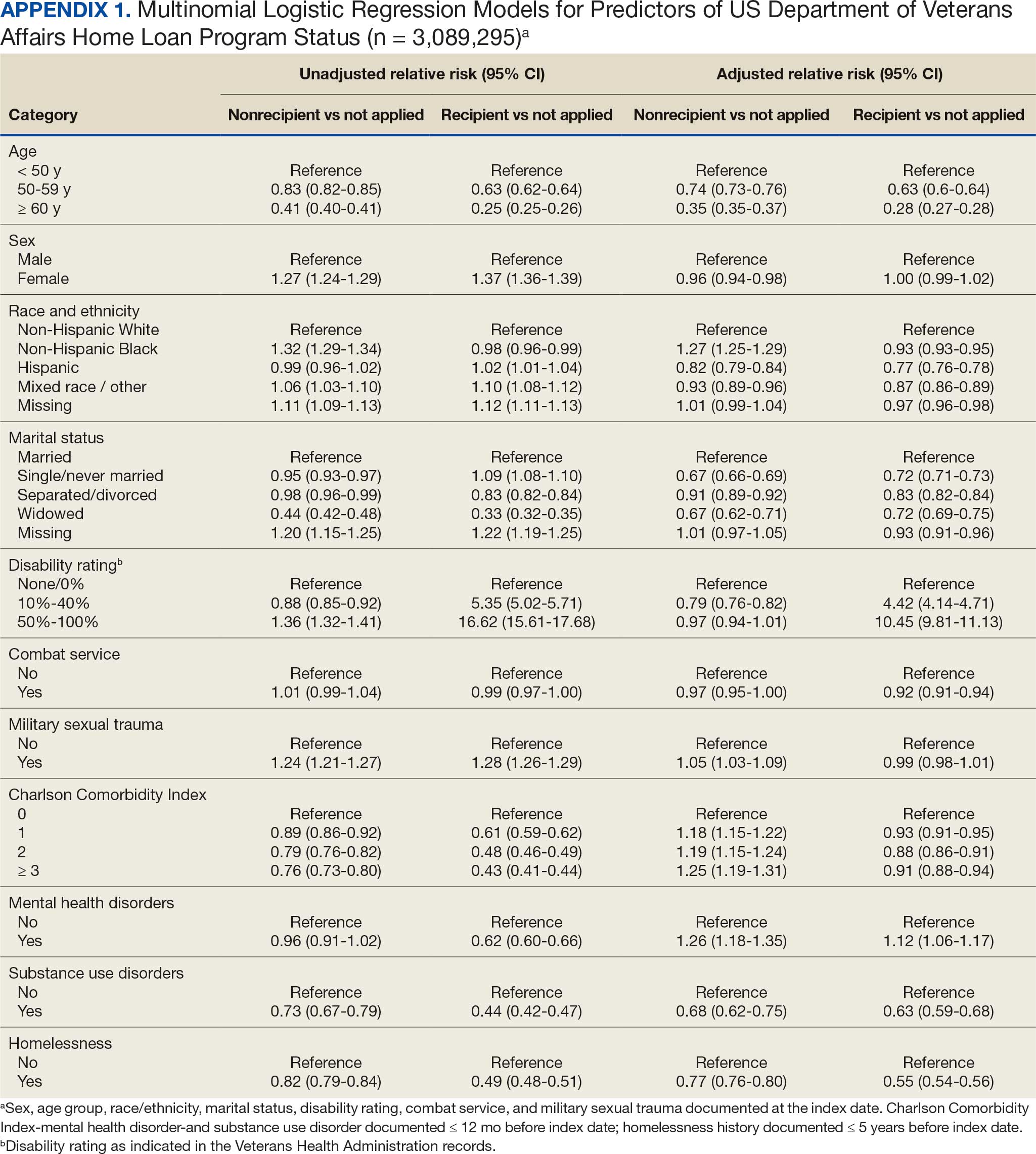
Binary logistic regression models for demographic, clinical, and homelessness characteristics as predictors of receipt status among applicants to the VA Home Loan Program are provided in Appendix 2. Among applicants, those who were granted a VA home loan were less likely to be aged ≥ 50 years; have a CCI score > 0; have experienced combat service and/or military sexual trauma; be diagnosed with a SUD and/or mental health disorder; or to have a history of homelessness compared with those denied a VA home loan. Applicants granted a VA home loan were also more likely to be female, non-Hispanic White, single or never married, and/or have a VA service-connected disability ratings > 0%.
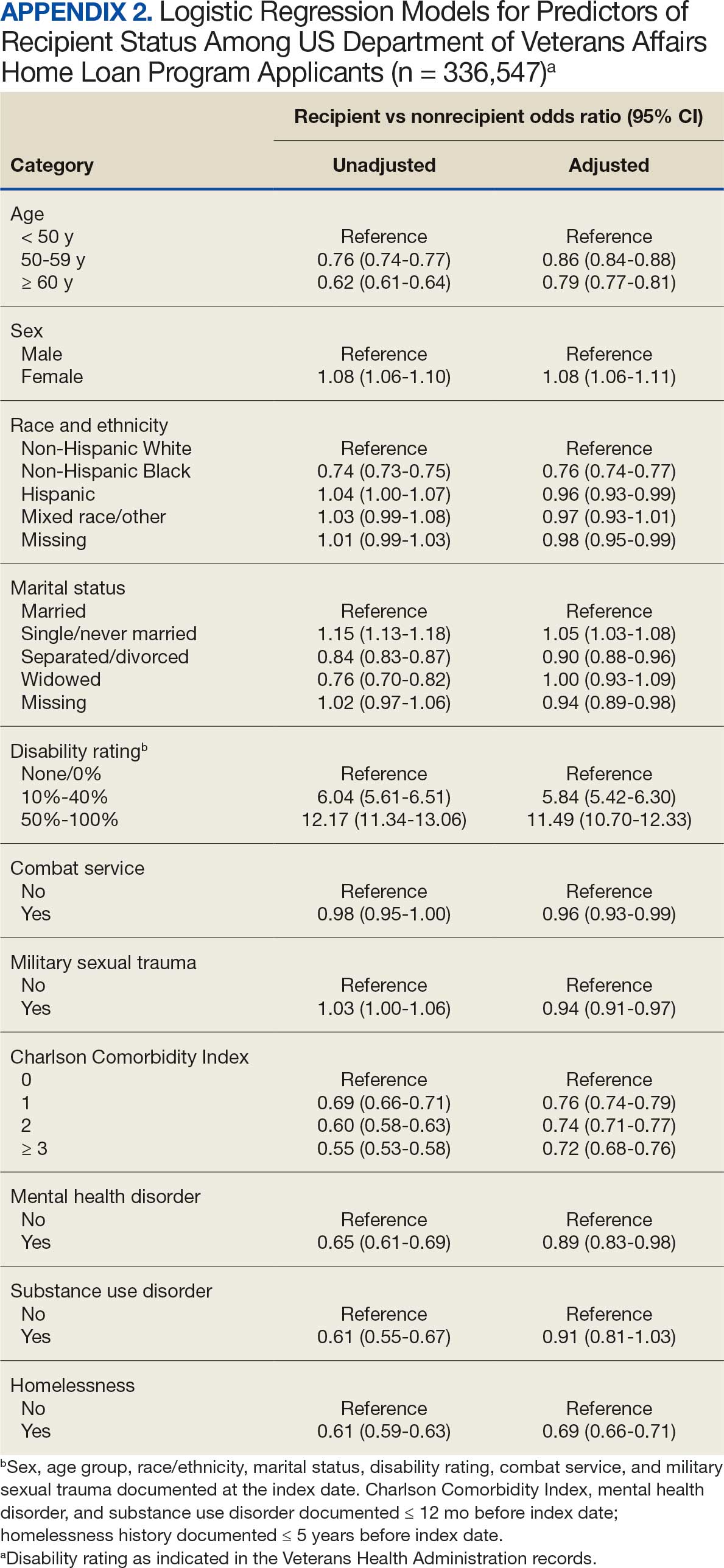
Discussion
The VA Home Loan Program is a unique benefit and resource for eligible veterans that may be increasingly important in a time of growing concern about the affordability of housing for many Americans. Research on other federally-supported home loan programs as well as private home mortgage programs has been mostly conducted in the economic realm, and studies focused on understanding these programs from a health care system perspective have been sparse.32,33 However, there is a large body of literature documenting the importance of stable, safe, and secure housing on health and well-being.34-37 This study did not focus on evaluating the effects of the VA Home Loan Program, because we wanted to first examine the characteristics of veterans who benefited from the program and how they differed from veterans who did not apply or did apply but had a denied application.
Our findings suggest that several thousands of veterans benefit from the VA Home Loan Program each year. For historical context, the time period examined was one of economic downturn with rising costs of living, including housing, and steady increases in homelessness as reported in the annual point-in-time count of sheltered and unsheltered people experiencing homelessness on a single night as mandated by the US Department of Housing and Urban Development.38-40 The Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded health care and benefits for veterans exposed to burn pits, Agent Orange, and other toxic substances, resulting in more VA disability benefit claims, including large retroactive payments.41-43 Anecdotally, the VBA has noted that the PACT Act helped some homeless veterans with funds and stability to exit homelessness and enroll in the VA Home Loan Program.
Our analysis suggests that beneficiaries of the VA Home Loan Program were frequently aged < 50 years, female, of non-Hispanic White race, and did not have histories of psychiatric disorders or homelessness. Most of these demographic and clinical characteristics were not surprising given the composition of the veteran population, although in-depth analyses are needed to examine sex differences that may have led to more females than males benefiting from the VA Home Loan Program. In addition, it was notable that many younger and non-Hispanic Black veterans had applied. While relatively few veterans with SUDs benefited from the VA Home Loan Program, few had applied. Research is warranted into why veterans with SUDs are less likely to apply for home loans. Quite surprisingly, a sizable proportion of veterans with histories of homelessness reported they had applied to the VA Home Loan Program, although they were less likely than veterans who had not experienced homelessness to be granted a loan.
The examination of differences between veterans who did not apply, were granted, and denied a loan through the VA Home Loan Program revealed several key predictors of application outcomes in multivariable models. Specifically, veterans who applied for home loans were less likely to be aged ≥ 50 years, unmarried, of Hispanic, mixed, or other race/ethnicity, diagnosed with an SUD, or have a history of homelessness. Veterans with higher disability ratings were less frequently denied and more frequently approved, while non-Hispanic Black veterans and those with higher CCI scores were more frequently denied and less frequently approved. VBA applicants with mental health disorders were also more likely to apply for a home loan. Conversely, those granted a home loan were more likely than those denied a home loan to be female, non-Hispanic White, single/unmarried, or to have > 0% VA service-connected disability rating, but less likely to be aged ≥ 50 years, have CCI score > 0, be diagnosed with psychiatric disorders, or have a history of homelessness.
Limitations
This analysis was restricted to a subset of FY 2022 to FY 2024 linked VBA/VHA databases (ie, to veterans who had both VBA and VHA records and met prespecified eligibility criteria). Despite the large number of linked records, a small percentage of these records corresponded to veterans who were applicants or recipients of the VA Home Loan Program. Future studies should expand the time frame to examine variations in application outcomes over time and by background characteristics of veterans enrolled in VHA care who applied for VBA benefits. In addition, we relied on data and ICD-10-CM diagnostic codes from existing electronic health records and claims data to define histories of homelessness, comorbidities, SUDs, and mental health disorders. Given the time-varying nature of these conditions, the temporal sequence of events was difficult to ascertain. Third, it is worth noting that these findings can only be generalized to veterans who applied for VBA benefits and met eligibility criteria, and that these veterans may differ in terms of their demographic and clinical characteristics from those who did not apply for these benefits.
Conclusions
This study analyzed data from 251,796 individuals who applied for and received a VA home loan, 84,751 who were denied a VA home loan, and 2,752,748 veterans who did not apply for a VA home loan from FY 2022 to FY 2024. Accordingly, 11% of applications pertained to the VA Home Loan Program, and 75% of VA Home Loan Program applicants received a home loan. Distinct demographic and clinical characteristics were observed for applicants and recipients of the VA Home Loan Program, which can set the stage for future planning and evaluation of the program. Despite the broad accessibility of veterans to the VA Home Loan Program, there were differences in approval rates among applicants based on sociodemographic and clinical characteristics. Further evaluation, perhaps using qualitative methods, is needed to better understand opportunities and challenges to achieving a VA home loan, especially among underserved veteran populations. Investigation and research can guide future recommendations for any development or corrective actions that can help increase access to veterans who can benefit from the program. Future analyses are also needed to compare veterans enrolled and not enrolled in the VA Home Loan Program on health care-related outcomes.
- US Department of Veterans Affairs. Home loans. Accessed April 1, 2026. https://www.benefits.va.gov/homeloans/
- Veterans United Home Loans. VA loans: the complete guide. Accessed April 1, 2026. https://www.veteransunited.com/va-loans/
- US Department of Veterans Affairs. VA-backed veterans home loans. Accessed April 1, 2026. https://www.va.gov/housing-assistance/home-loans/
- Choplin JM, Stark DP. Whispering sweet nothings: a review of verbal behaviors that undermine the effectiveness of government-mandated home-loan disclosures. Cogn Res Princ Implic. 2019;4:6. doi:10.1186/s41235-019-0154-7
- Evans M. Borrowing boon. More explore federal home loan banks backing. Mod Healthc. 2009;39:14.
- Hogarth M. A home loan: how—and how much? Nurs Times. 1973;69:908-909.
- Jacoby SF. Home Owners’ Loan Corporation maps and place-based injury risks: a complex history. Am J Public Health. 2023;113:356-358. doi:10.2105/AJPH.2023.307242
- Merrell C. Finance. Home: a loan. Nurs Times. 1996;92:61-64.
- Namin S, Xu W, Zhou Y, et al. The legacy of the Home Owners’ Loan Corporation and the political ecology of urban trees and air pollution in the United States. Soc Sci Med. 2020;246:112758. doi:10.1016/j.socscimed.2019.112758
- Namin S, Zhou Y, Xu W, et al. Persistence of mortgage lending bias in the United States: 80 years after the Home Owners’ Loan Corporation security maps. J Race Ethn City. 2022;3:70-94. doi:10.1080/26884674.2021.2019568
- Slottow R. The home loan program. J Natl Assoc Hosp Dev. 1990:43-45.
- Wang M, Chen H, Wang L. Locus of control and home mortgage loan behaviour. Int J Psychol. 2008;43:125-129. doi:10.1080/00207590801888760
- US Dept of Veterans Affairs. Veterans Health Administration. About VHA. Updated January 20, 2025. Accessed April 1, 2026. https://www.va.gov/health/aboutvha.asp
- US Dept of Veterans Affairs. VA homeless programs. Updated May 7, 2026. Accessed May 8, 2026. https://department.va.gov/homeless/
- DiTosto JD, Holder K, Soyemi E, et al. Housing instability and adverse perinatal outcomes: a systematic review. Am J Obstet Gynecol MFM. 2021;3:100477. doi:10.1016/j.ajogmf.2021.100477
- Tsai J, Szymkowiak D, Jutkowitz E. Developing an operational definition of housing instability and homelessness in Veterans Health Administration medical records. PLoS One. 2022;17:e0279973. doi:10.1371/journal.pone.0279973
- Fowler PJ, Hovmand PS, Marcal KE, et al. Solving homelessness from a complex systems perspective: insights for prevention responses. Annu Rev Public Health. 2019;40: 465-486. doi:10.1146/annurev-publhealth-040617-013553
- US Department of Health and Human Services. Healthy People 2030: housing instability. Accessed April 1, 2026. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability
- US Department of Veterans Affairs. VA health care priorities. Accessed April 1, 2026. https://www.va.gov/health/priorities/index.asp
- Tsai J. Federal priorities to address homelessness as a community health problem. Fam Community Health. 2025;48:57-69.
- Tsai J, Hooshyar D. Prevalence of eviction, home foreclosure, and homelessness among low-income US veterans: the National Veteran Homeless and Other Poverty Experiences study. Public Health. 2022;213:181-188. doi:10.1016/j.puhe.2022.10.017
- US Department of Veterans Affairs. Corporate Data Warehouse (CDW). Accessed April 1, 2026. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Price LE, Shea K, Gephart S. The Veterans Affairs Corporate Data Warehouse: uses and implications for nursing research and practice. Nurs Adm Q. 2015;39:311-318. doi:10.1097/NAQ.0000000000000118
- US Department of Veterans Affairs. Homeless Operations Management and Evaluation System (HOMES) User Manual—Phase 1. April 19, 2011. Accessed April 1, 2026. https://www.adldata.org/wp-content/uploads/2016/07/homes.pdf
- Tsai J, Kasprow WJ, Rosenheck RA. Latent homeless risk profiles of a national sample of homeless veterans and their relation to program referral and admission patterns. Am J Public Health. 2013;103:S239-S247. doi:10.2105/AJPH.2013.301322
- Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted inhospital mortality. J Clin Epidemiol. 2004;57:1288-1294. doi:10.1016/j.jclinepi.2004.03.012
- Beydoun HA, Szymkowiak D, Beydoun MA, et al. Comparing major comorbidity indices as predictors of all-cause mortality in the Veterans Affairs health care system. J Clin Epidemiol. 2025;182:111778. doi:10.1016/j.jclinepi.2025.111778
- Charlson ME, Carrozzino D, Guidi J, et al. Charlson Comorbidity Index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91:8-35. doi:10.1159/000521288
- Glasheen WP, Cordier T, Gumpina R, et al. Charlson Comorbidity Index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12:188-197.
- Beydoun HA, Szymkowiak D, Kinney R, et al. Is the risk of Alzheimer’s disease and related dementias among US veterans influenced by the intersectionality of housing status, HIV/AIDS, hepatitis C, and psychiatric disorders? J Gerontol A Biol Sci Med Sci. 2024;79:glae153. doi:10.1093/gerona/glae153
- SAS Institute. SAS Enterprise Guide. Accessed April 1, 2026. https://www.sas.com/en_us/software/enterprise-guide/features-list.html
- Agarwal S, Amromin G, Chomsisengphet S, et al. Mortgage refinancing, consumer spending, and competition: evidence from the Home Affordable Refinance Program. Rev Econ Stud. 2023;90:499-537.
- Ashcraft A, Bech ML, Frame WS. The Federal Home Loan Bank System: the lender of next-to-last resort? J Money Credit Bank. 2010;42:551-583.
- Gibson M, Petticrew M, Bambra C, et al. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17:175-184. doi:10.1016/j.healthplace.2010.09.011
- Shaw M. Housing and public health. Annu Rev Public Health. 2004; 25:397-418. doi:10.1146/annurev.publhealth.25.101802.123036
- Thomson H, Petticrew M, Morrison D. Health effects of housing improvement: systematic review of intervention studies. BMJ. 2001;323:187-190. doi:10.1136/bmj.323.7306.187
- Tsai J. Theorizing pathways between eviction filings and increased mortality risk. JAMA. 2024;331:570-571. doi:10.1001/jama.2023.27978
- Bernanke B, Blanchard O. What caused the US pandemicera inflation? Am Econ J Macroecon. 2025;17:1-35.
- Hall SG, Tavlas GS, Wang Y. Drivers and spillover effects of inflation: the United States, the euro area, and the United Kingdom. J Int Money Finance. 2023;131:1-13.
- US Department of Housing and Urban Development. Point-in-Time Count and Housing Inventory Count. Accessed April 1, 2026. https://www.hudexchange.info/programs/hdx/pit-hic/
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act: expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Zychowicz ME. The PACT Act: enhancing health care access for military personnel and veterans. N C Med J. 2023;84:379-380. doi:10.18043/001c.89208
- US Department of Veterans Affairs. The PACT Act and your VA benefits. April 2, 2026. https://www.va.gov/resources/the-pact-act-and-your-va-benefits/
The US Department of Veterans Affairs (VA) Home Loan Program, administered by the Veterans Benefits Administration (VBA), is a unique benefit for veterans, active-duty service members, National Guard and Reserve members, and eligible surviving spouses. Established in 1944, the program aims to help these individuals achieve homeownership by leveraging a third-party guarantee, typically from a government agency, to enhance access to credit and improve loan terms for borrowers who may not meet conventional loan qualifications.1 Since its inception, the VA has guaranteed > 28.5 million loans, enabling millions of veterans to buy, build, repair, retain, or adapt homes for personal occupancy.2 The program is designed to support veterans and eligible individuals to become homeowners, recognizing homeownership as a pathway to financial stability and community integration. VA home loans are provided by private lenders (eg, banks, mortgage companies) with a portion guaranteed by the VA, which reduces the risk for lenders and enables them to offer competitive terms, such as no down payment and lower interest rates, making homeownership more accessible to veterans.2
Eligibility criteria for the VA Home Loan Program include military service criteria such as active-duty service members with ≥ 90 continuous days of service; veterans with an honorable discharge meeting minimum service requirements; individuals who served in the National Guard/Reserve for ≥ 90 days of active service or 6 years of service with an honorable discharge; and surviving spouses of veterans who died in service or from a service-connected disability, were designated as missing in action/ prisoner of war, and the spouse is receiving Dependency and Indemnity Compensation. Financial criteria also apply: borrowers must meet lender requirements for credit and income (although VA loans are more flexible than conventional loans) and the home must be for personal occupancy rather than an investment property.3
A June 2025 PubMed literature search did not reveal any prior research on the VA Home Loan Program, although a limited number of studies tackled a wide range of issues related to federal and private home loans.4-12 To our knowledge, there is no prior published examination of the VA Home Loan Program. Understanding VA Home Loan Program usage among Veterans Health Administration (VHA) users can inform the future direction of the program. The VHA operates the largest integrated US health care system, serving > 9 million enrolled veterans annually at 1321 facilities, including 172 medical centers and 1138 outpatient clinics, providing primary and specialized health care, and related medical and social support services for enrolled veterans, including those who are experiencing housing instability or homelessness.13 Specialized VHA programs for homeless veterans include housing, employment, health care, justice, and re-entryrelated services in collaboration with federal and community partners.14 Housing instability has been defined as the state of being at risk of losing housing due to challenges such as difficulties paying rent, overcrowding, frequent relocation, and a substantial proportion of income spent on housing.15,16 Homelessness is a severe manifestation of housing instability that has been defined as the lack of stable, safe, and functioning housing.17,18
Health care and social services, including those that address housing instability and homelessness, are major priorities for the VHA and VBA.19 The VA Home Loan Program may represent an important resource to help veterans achieve long-term housing stability through home ownership. There has been wide public concern about housing affordability and the ability of many Americans, including veterans, to achieve home ownership.20 Homeownership is considered an important part of developing financial assets and achieving financial stability. Lowincome veterans, in particular, may benefit from this program as a national study found that 8.0% of low-income veterans and 13.9% of veterans with a history of homelessness have previously experienced a home foreclosure. 21 A greater understanding of who applies for and receives assistance from the VA Home Loan Program would inform homelessness prevention services and future planning for this program.
We conducted a quality improvement (QI) project on behalf of the VHA Homeless Programs Office and in partnership with the VBA. Our goals were to: (1) describe the annual number of applicants and recipients of the VA Home Loan Program by age group, sex, race/ethnicity, presence of any diagnosed substance use and/or mental health disorder, and history of homelessness; and (2) compare demographic, clinical, and homelessness characteristics among individuals who apply and are granted a loan through this program, individuals who apply and are denied a loan through this program, and individuals who do not apply for a loan through this program.
Methods
This project involved linked VA administrative national databases and was undertaken by the VHA Homeless Programs Office in partnership with the VBA. Specifically, VHA and VBA databases were linked together using veteran identifiers and all data were managed and analyzed on secure VA servers. The project followed VA’s Program Guide 1200.21 for nonresearch activities and institutional review board approval was waived through sponsorship by the VA Homeless Programs Office. The VHA Corporate Data Warehouse (CDW) was accessed to obtain data from the Homeless Operations Management and Evaluation System (HOMES) and other clinical data systems used by VHA clinicians and administrators that capture diagnoses, workload, and other health care data.22,23 HOMES collects intake, progress, and outcome data on homeless veterans within its care system that enables the VA to assess the effectiveness of programs and strategically allocate resources to prevent homelessness.24,25
A list of veterans who filed disability compensation and pension claims was obtained from the VBA Office of Performance Analysis and Integrity, including Social Security number, name, city and state, date of claim submission, grant or increase in benefits, homeless status, VA home loan approval, and homeless aid for dependent children from fiscal year (FY) 2022 through FY 2024. VBA data were linked to VHA CDW electronic health record data from veterans who sought VA health care services and HOMES data on veteran participation in homeless programs who were also experiencing homelessness. VHA data included demographic characteristics (eg, sex, age, race, marital status, combat service) at an index date (earliest visit to the VHA between October 1, 2021, and September 30, 2024); military sexual trauma; clinical characteristics within 12 months prior to the index date (VHA disability rating, substance use disorder [SUD] diagnosis, mental health disorder diagnosis, Charlson Comorbidity Index [CCI] score), and homelessness experience ≤ 5 years prior to the index date.
History of homelessness ≤ 5 years prior to the index date was determined using an operational definition of homelessness based on multiple indicators, including International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic code Z59.0; clinic stop codes or HOMES records indicating VA homeless programs clinical encounters; or a positive screen on an annual homelessness screener.16 US Department of Housing and Urban Development-VA Supportive Housing enrollees were excluded because they are considered to no longer be experiencing homelessness, and Veterans Justice Program enrollees were excluded because the program primarily focuses on serving criminal justice-involved veterans. The CCI predicts the risk of death ≤ 1 year by assessing the number and severity of a patient’s coexisting health conditions and is a valuable tool for understanding a patient’s overall health burden, aiding in clinical decision-making and evaluation research studies.26-29 Diagnoses based on ICD-10-CM codes were used to determine SUDs, mental health disorders, and CCI score, using methods that have been described in other publications.30
Population
The VBA cohort of veterans requesting benefits was further restricted to those who met the following eligibility criteria: (1) requested VA benefits FYs 2022 to 2024; (2) sought VHA services ≥ 1 time between FY 2022 and 2024; (3) had matching VBA/VHA records; (4) had no missing data on claim status and/ or demographic, clinical, and homelessness characteristics; and (5) had known home loan status FYs 2022 to 2024. The original VBA dataset consisted of 4,219,755 records and the original VHA dataset consisted of 7,170,199 records (Figure 1). The final linked VBA/VHA dataset after excluding 29 records with missing data on sex, 7 with missing data on age, 6 with missing data on marital status, and an additional 143,444 with unknown VBA claim status, consisted of 3,089,295 records corresponding to 2,260,851 unique veterans. Specifically, 251,796 records corresponded to veterans who had applied and received a loan, 84,751 to veterans who had applied and were nonrecipients of a loan, and 2,752,748 to veterans who did not apply for a loan.
Abbreviations: FY, fiscal year; VBA, Veterans Benefits Administration; VHA, Veterans Health Administration.
Statistical Analysis
All statistical analyses were performed using SAS Enterprise Guide, an application that provides a point-and-click interface for data access, analysis, and management, accommodating both code-based and visual programming. 31 First, we relied on the final analytic sample to calculate the annual proportions of veterans who applied for and/or received a loan through the VA Home Loan Program. We also generated descriptive statistics stratified by age group, sex, race/ethnicity, SUD, mental health disorder, and homelessness, overall and within each FY. Pearson χ2 and Cochran-Armitage trend tests were applied to examine differences in application and receipt of a home loan by baseline characteristics and FY, respectively. Second, we conducted bivariate and multivariable analyses to compare demographic, clinical, and homelessness characteristics between 3 groups of veterans as they pertain to the VA Home Loan Program. Veterans who applied and were nonrecipients of a loan (group 1), veterans who applied and were recipients of a loan (group 2), and veterans who did not apply for a loan (group 3). Similar analyses compared VA Home Loan Program applicants who were recipients of a home loan vs VA Home Loan Program applicants who were nonrecipients of a home loan. Multinomial and binary logistic regression models were constructed to estimate the relative risk ratio (RR) and odds ratio (OR) with 95% CIs for comparisons between these distinct groups on demographic, clinical, and homelessness characteristics. Two-sided statistical tests were evaluated at α = 0.05.
Results
Tables 1 and 2 present the number of VBA applicants, including those who applied for and received benefits through the VA Home Loan Program, by age group, sex, race/ethnicity, as well as histories of SUDs, mental health disorders, and homelessness, overall, and by FY. As shown in Figure 2, 336,547 of 3,089,295 VBA applications (10.9%) pertained to the VA Home Loan Program, with a statistically significant decline in application rates, from 12.2% in FY 2022 to 9.9% in FY 2024 (P < .001 for trend). Among 336,547 veterans who applied for the VA Home Loan Program, 251,796 (74.8%) received a home loan during FYs 2022 to 2024, ranging between 73.8% for FY 2024 and 75.5% for FY 2023 (P < .001 for trend).
Veterans Affairs Home Loan Program, fiscal years (FY) 2022-2024.
Multinomial logistic regression models for demographic, clinical, and homelessness characteristics as predictors of VA Home Loan Program status are provided in Appendix 1. Based on the fully adjusted model, compared with veterans who did not apply to the VA Home Loan Program, those who applied for a home loan were less likely to be aged ≥ 50 years, unmarried, Hispanic ethnicity, mixed race, or other race, diagnosed with a SUD, or history of homelessness. Veterans with higher VA service-connected disability ratings were more frequently recipients of VA home loans, whereas those who self-identified as non-Hispanic Black and those with higher CCI scores were less frequently recipients of VA home loans. Finally, those with mental health disorders were more likely than their counterparts to be applicants (recipients or nonrecipients) of VA home loans.
Binary logistic regression models for demographic, clinical, and homelessness characteristics as predictors of receipt status among applicants to the VA Home Loan Program are provided in Appendix 2. Among applicants, those who were granted a VA home loan were less likely to be aged ≥ 50 years; have a CCI score > 0; have experienced combat service and/or military sexual trauma; be diagnosed with a SUD and/or mental health disorder; or to have a history of homelessness compared with those denied a VA home loan. Applicants granted a VA home loan were also more likely to be female, non-Hispanic White, single or never married, and/or have a VA service-connected disability ratings > 0%.
Discussion
The VA Home Loan Program is a unique benefit and resource for eligible veterans that may be increasingly important in a time of growing concern about the affordability of housing for many Americans. Research on other federally-supported home loan programs as well as private home mortgage programs has been mostly conducted in the economic realm, and studies focused on understanding these programs from a health care system perspective have been sparse.32,33 However, there is a large body of literature documenting the importance of stable, safe, and secure housing on health and well-being.34-37 This study did not focus on evaluating the effects of the VA Home Loan Program, because we wanted to first examine the characteristics of veterans who benefited from the program and how they differed from veterans who did not apply or did apply but had a denied application.
Our findings suggest that several thousands of veterans benefit from the VA Home Loan Program each year. For historical context, the time period examined was one of economic downturn with rising costs of living, including housing, and steady increases in homelessness as reported in the annual point-in-time count of sheltered and unsheltered people experiencing homelessness on a single night as mandated by the US Department of Housing and Urban Development.38-40 The Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded health care and benefits for veterans exposed to burn pits, Agent Orange, and other toxic substances, resulting in more VA disability benefit claims, including large retroactive payments.41-43 Anecdotally, the VBA has noted that the PACT Act helped some homeless veterans with funds and stability to exit homelessness and enroll in the VA Home Loan Program.
Our analysis suggests that beneficiaries of the VA Home Loan Program were frequently aged < 50 years, female, of non-Hispanic White race, and did not have histories of psychiatric disorders or homelessness. Most of these demographic and clinical characteristics were not surprising given the composition of the veteran population, although in-depth analyses are needed to examine sex differences that may have led to more females than males benefiting from the VA Home Loan Program. In addition, it was notable that many younger and non-Hispanic Black veterans had applied. While relatively few veterans with SUDs benefited from the VA Home Loan Program, few had applied. Research is warranted into why veterans with SUDs are less likely to apply for home loans. Quite surprisingly, a sizable proportion of veterans with histories of homelessness reported they had applied to the VA Home Loan Program, although they were less likely than veterans who had not experienced homelessness to be granted a loan.
The examination of differences between veterans who did not apply, were granted, and denied a loan through the VA Home Loan Program revealed several key predictors of application outcomes in multivariable models. Specifically, veterans who applied for home loans were less likely to be aged ≥ 50 years, unmarried, of Hispanic, mixed, or other race/ethnicity, diagnosed with an SUD, or have a history of homelessness. Veterans with higher disability ratings were less frequently denied and more frequently approved, while non-Hispanic Black veterans and those with higher CCI scores were more frequently denied and less frequently approved. VBA applicants with mental health disorders were also more likely to apply for a home loan. Conversely, those granted a home loan were more likely than those denied a home loan to be female, non-Hispanic White, single/unmarried, or to have > 0% VA service-connected disability rating, but less likely to be aged ≥ 50 years, have CCI score > 0, be diagnosed with psychiatric disorders, or have a history of homelessness.
Limitations
This analysis was restricted to a subset of FY 2022 to FY 2024 linked VBA/VHA databases (ie, to veterans who had both VBA and VHA records and met prespecified eligibility criteria). Despite the large number of linked records, a small percentage of these records corresponded to veterans who were applicants or recipients of the VA Home Loan Program. Future studies should expand the time frame to examine variations in application outcomes over time and by background characteristics of veterans enrolled in VHA care who applied for VBA benefits. In addition, we relied on data and ICD-10-CM diagnostic codes from existing electronic health records and claims data to define histories of homelessness, comorbidities, SUDs, and mental health disorders. Given the time-varying nature of these conditions, the temporal sequence of events was difficult to ascertain. Third, it is worth noting that these findings can only be generalized to veterans who applied for VBA benefits and met eligibility criteria, and that these veterans may differ in terms of their demographic and clinical characteristics from those who did not apply for these benefits.
Conclusions
This study analyzed data from 251,796 individuals who applied for and received a VA home loan, 84,751 who were denied a VA home loan, and 2,752,748 veterans who did not apply for a VA home loan from FY 2022 to FY 2024. Accordingly, 11% of applications pertained to the VA Home Loan Program, and 75% of VA Home Loan Program applicants received a home loan. Distinct demographic and clinical characteristics were observed for applicants and recipients of the VA Home Loan Program, which can set the stage for future planning and evaluation of the program. Despite the broad accessibility of veterans to the VA Home Loan Program, there were differences in approval rates among applicants based on sociodemographic and clinical characteristics. Further evaluation, perhaps using qualitative methods, is needed to better understand opportunities and challenges to achieving a VA home loan, especially among underserved veteran populations. Investigation and research can guide future recommendations for any development or corrective actions that can help increase access to veterans who can benefit from the program. Future analyses are also needed to compare veterans enrolled and not enrolled in the VA Home Loan Program on health care-related outcomes.
The US Department of Veterans Affairs (VA) Home Loan Program, administered by the Veterans Benefits Administration (VBA), is a unique benefit for veterans, active-duty service members, National Guard and Reserve members, and eligible surviving spouses. Established in 1944, the program aims to help these individuals achieve homeownership by leveraging a third-party guarantee, typically from a government agency, to enhance access to credit and improve loan terms for borrowers who may not meet conventional loan qualifications.1 Since its inception, the VA has guaranteed > 28.5 million loans, enabling millions of veterans to buy, build, repair, retain, or adapt homes for personal occupancy.2 The program is designed to support veterans and eligible individuals to become homeowners, recognizing homeownership as a pathway to financial stability and community integration. VA home loans are provided by private lenders (eg, banks, mortgage companies) with a portion guaranteed by the VA, which reduces the risk for lenders and enables them to offer competitive terms, such as no down payment and lower interest rates, making homeownership more accessible to veterans.2
Eligibility criteria for the VA Home Loan Program include military service criteria such as active-duty service members with ≥ 90 continuous days of service; veterans with an honorable discharge meeting minimum service requirements; individuals who served in the National Guard/Reserve for ≥ 90 days of active service or 6 years of service with an honorable discharge; and surviving spouses of veterans who died in service or from a service-connected disability, were designated as missing in action/ prisoner of war, and the spouse is receiving Dependency and Indemnity Compensation. Financial criteria also apply: borrowers must meet lender requirements for credit and income (although VA loans are more flexible than conventional loans) and the home must be for personal occupancy rather than an investment property.3
A June 2025 PubMed literature search did not reveal any prior research on the VA Home Loan Program, although a limited number of studies tackled a wide range of issues related to federal and private home loans.4-12 To our knowledge, there is no prior published examination of the VA Home Loan Program. Understanding VA Home Loan Program usage among Veterans Health Administration (VHA) users can inform the future direction of the program. The VHA operates the largest integrated US health care system, serving > 9 million enrolled veterans annually at 1321 facilities, including 172 medical centers and 1138 outpatient clinics, providing primary and specialized health care, and related medical and social support services for enrolled veterans, including those who are experiencing housing instability or homelessness.13 Specialized VHA programs for homeless veterans include housing, employment, health care, justice, and re-entryrelated services in collaboration with federal and community partners.14 Housing instability has been defined as the state of being at risk of losing housing due to challenges such as difficulties paying rent, overcrowding, frequent relocation, and a substantial proportion of income spent on housing.15,16 Homelessness is a severe manifestation of housing instability that has been defined as the lack of stable, safe, and functioning housing.17,18
Health care and social services, including those that address housing instability and homelessness, are major priorities for the VHA and VBA.19 The VA Home Loan Program may represent an important resource to help veterans achieve long-term housing stability through home ownership. There has been wide public concern about housing affordability and the ability of many Americans, including veterans, to achieve home ownership.20 Homeownership is considered an important part of developing financial assets and achieving financial stability. Lowincome veterans, in particular, may benefit from this program as a national study found that 8.0% of low-income veterans and 13.9% of veterans with a history of homelessness have previously experienced a home foreclosure. 21 A greater understanding of who applies for and receives assistance from the VA Home Loan Program would inform homelessness prevention services and future planning for this program.
We conducted a quality improvement (QI) project on behalf of the VHA Homeless Programs Office and in partnership with the VBA. Our goals were to: (1) describe the annual number of applicants and recipients of the VA Home Loan Program by age group, sex, race/ethnicity, presence of any diagnosed substance use and/or mental health disorder, and history of homelessness; and (2) compare demographic, clinical, and homelessness characteristics among individuals who apply and are granted a loan through this program, individuals who apply and are denied a loan through this program, and individuals who do not apply for a loan through this program.
Methods
This project involved linked VA administrative national databases and was undertaken by the VHA Homeless Programs Office in partnership with the VBA. Specifically, VHA and VBA databases were linked together using veteran identifiers and all data were managed and analyzed on secure VA servers. The project followed VA’s Program Guide 1200.21 for nonresearch activities and institutional review board approval was waived through sponsorship by the VA Homeless Programs Office. The VHA Corporate Data Warehouse (CDW) was accessed to obtain data from the Homeless Operations Management and Evaluation System (HOMES) and other clinical data systems used by VHA clinicians and administrators that capture diagnoses, workload, and other health care data.22,23 HOMES collects intake, progress, and outcome data on homeless veterans within its care system that enables the VA to assess the effectiveness of programs and strategically allocate resources to prevent homelessness.24,25
A list of veterans who filed disability compensation and pension claims was obtained from the VBA Office of Performance Analysis and Integrity, including Social Security number, name, city and state, date of claim submission, grant or increase in benefits, homeless status, VA home loan approval, and homeless aid for dependent children from fiscal year (FY) 2022 through FY 2024. VBA data were linked to VHA CDW electronic health record data from veterans who sought VA health care services and HOMES data on veteran participation in homeless programs who were also experiencing homelessness. VHA data included demographic characteristics (eg, sex, age, race, marital status, combat service) at an index date (earliest visit to the VHA between October 1, 2021, and September 30, 2024); military sexual trauma; clinical characteristics within 12 months prior to the index date (VHA disability rating, substance use disorder [SUD] diagnosis, mental health disorder diagnosis, Charlson Comorbidity Index [CCI] score), and homelessness experience ≤ 5 years prior to the index date.
History of homelessness ≤ 5 years prior to the index date was determined using an operational definition of homelessness based on multiple indicators, including International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic code Z59.0; clinic stop codes or HOMES records indicating VA homeless programs clinical encounters; or a positive screen on an annual homelessness screener.16 US Department of Housing and Urban Development-VA Supportive Housing enrollees were excluded because they are considered to no longer be experiencing homelessness, and Veterans Justice Program enrollees were excluded because the program primarily focuses on serving criminal justice-involved veterans. The CCI predicts the risk of death ≤ 1 year by assessing the number and severity of a patient’s coexisting health conditions and is a valuable tool for understanding a patient’s overall health burden, aiding in clinical decision-making and evaluation research studies.26-29 Diagnoses based on ICD-10-CM codes were used to determine SUDs, mental health disorders, and CCI score, using methods that have been described in other publications.30
Population
The VBA cohort of veterans requesting benefits was further restricted to those who met the following eligibility criteria: (1) requested VA benefits FYs 2022 to 2024; (2) sought VHA services ≥ 1 time between FY 2022 and 2024; (3) had matching VBA/VHA records; (4) had no missing data on claim status and/ or demographic, clinical, and homelessness characteristics; and (5) had known home loan status FYs 2022 to 2024. The original VBA dataset consisted of 4,219,755 records and the original VHA dataset consisted of 7,170,199 records (Figure 1). The final linked VBA/VHA dataset after excluding 29 records with missing data on sex, 7 with missing data on age, 6 with missing data on marital status, and an additional 143,444 with unknown VBA claim status, consisted of 3,089,295 records corresponding to 2,260,851 unique veterans. Specifically, 251,796 records corresponded to veterans who had applied and received a loan, 84,751 to veterans who had applied and were nonrecipients of a loan, and 2,752,748 to veterans who did not apply for a loan.
Abbreviations: FY, fiscal year; VBA, Veterans Benefits Administration; VHA, Veterans Health Administration.
Statistical Analysis
All statistical analyses were performed using SAS Enterprise Guide, an application that provides a point-and-click interface for data access, analysis, and management, accommodating both code-based and visual programming. 31 First, we relied on the final analytic sample to calculate the annual proportions of veterans who applied for and/or received a loan through the VA Home Loan Program. We also generated descriptive statistics stratified by age group, sex, race/ethnicity, SUD, mental health disorder, and homelessness, overall and within each FY. Pearson χ2 and Cochran-Armitage trend tests were applied to examine differences in application and receipt of a home loan by baseline characteristics and FY, respectively. Second, we conducted bivariate and multivariable analyses to compare demographic, clinical, and homelessness characteristics between 3 groups of veterans as they pertain to the VA Home Loan Program. Veterans who applied and were nonrecipients of a loan (group 1), veterans who applied and were recipients of a loan (group 2), and veterans who did not apply for a loan (group 3). Similar analyses compared VA Home Loan Program applicants who were recipients of a home loan vs VA Home Loan Program applicants who were nonrecipients of a home loan. Multinomial and binary logistic regression models were constructed to estimate the relative risk ratio (RR) and odds ratio (OR) with 95% CIs for comparisons between these distinct groups on demographic, clinical, and homelessness characteristics. Two-sided statistical tests were evaluated at α = 0.05.
Results
Tables 1 and 2 present the number of VBA applicants, including those who applied for and received benefits through the VA Home Loan Program, by age group, sex, race/ethnicity, as well as histories of SUDs, mental health disorders, and homelessness, overall, and by FY. As shown in Figure 2, 336,547 of 3,089,295 VBA applications (10.9%) pertained to the VA Home Loan Program, with a statistically significant decline in application rates, from 12.2% in FY 2022 to 9.9% in FY 2024 (P < .001 for trend). Among 336,547 veterans who applied for the VA Home Loan Program, 251,796 (74.8%) received a home loan during FYs 2022 to 2024, ranging between 73.8% for FY 2024 and 75.5% for FY 2023 (P < .001 for trend).
Veterans Affairs Home Loan Program, fiscal years (FY) 2022-2024.
Multinomial logistic regression models for demographic, clinical, and homelessness characteristics as predictors of VA Home Loan Program status are provided in Appendix 1. Based on the fully adjusted model, compared with veterans who did not apply to the VA Home Loan Program, those who applied for a home loan were less likely to be aged ≥ 50 years, unmarried, Hispanic ethnicity, mixed race, or other race, diagnosed with a SUD, or history of homelessness. Veterans with higher VA service-connected disability ratings were more frequently recipients of VA home loans, whereas those who self-identified as non-Hispanic Black and those with higher CCI scores were less frequently recipients of VA home loans. Finally, those with mental health disorders were more likely than their counterparts to be applicants (recipients or nonrecipients) of VA home loans.
Binary logistic regression models for demographic, clinical, and homelessness characteristics as predictors of receipt status among applicants to the VA Home Loan Program are provided in Appendix 2. Among applicants, those who were granted a VA home loan were less likely to be aged ≥ 50 years; have a CCI score > 0; have experienced combat service and/or military sexual trauma; be diagnosed with a SUD and/or mental health disorder; or to have a history of homelessness compared with those denied a VA home loan. Applicants granted a VA home loan were also more likely to be female, non-Hispanic White, single or never married, and/or have a VA service-connected disability ratings > 0%.
Discussion
The VA Home Loan Program is a unique benefit and resource for eligible veterans that may be increasingly important in a time of growing concern about the affordability of housing for many Americans. Research on other federally-supported home loan programs as well as private home mortgage programs has been mostly conducted in the economic realm, and studies focused on understanding these programs from a health care system perspective have been sparse.32,33 However, there is a large body of literature documenting the importance of stable, safe, and secure housing on health and well-being.34-37 This study did not focus on evaluating the effects of the VA Home Loan Program, because we wanted to first examine the characteristics of veterans who benefited from the program and how they differed from veterans who did not apply or did apply but had a denied application.
Our findings suggest that several thousands of veterans benefit from the VA Home Loan Program each year. For historical context, the time period examined was one of economic downturn with rising costs of living, including housing, and steady increases in homelessness as reported in the annual point-in-time count of sheltered and unsheltered people experiencing homelessness on a single night as mandated by the US Department of Housing and Urban Development.38-40 The Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded health care and benefits for veterans exposed to burn pits, Agent Orange, and other toxic substances, resulting in more VA disability benefit claims, including large retroactive payments.41-43 Anecdotally, the VBA has noted that the PACT Act helped some homeless veterans with funds and stability to exit homelessness and enroll in the VA Home Loan Program.
Our analysis suggests that beneficiaries of the VA Home Loan Program were frequently aged < 50 years, female, of non-Hispanic White race, and did not have histories of psychiatric disorders or homelessness. Most of these demographic and clinical characteristics were not surprising given the composition of the veteran population, although in-depth analyses are needed to examine sex differences that may have led to more females than males benefiting from the VA Home Loan Program. In addition, it was notable that many younger and non-Hispanic Black veterans had applied. While relatively few veterans with SUDs benefited from the VA Home Loan Program, few had applied. Research is warranted into why veterans with SUDs are less likely to apply for home loans. Quite surprisingly, a sizable proportion of veterans with histories of homelessness reported they had applied to the VA Home Loan Program, although they were less likely than veterans who had not experienced homelessness to be granted a loan.
The examination of differences between veterans who did not apply, were granted, and denied a loan through the VA Home Loan Program revealed several key predictors of application outcomes in multivariable models. Specifically, veterans who applied for home loans were less likely to be aged ≥ 50 years, unmarried, of Hispanic, mixed, or other race/ethnicity, diagnosed with an SUD, or have a history of homelessness. Veterans with higher disability ratings were less frequently denied and more frequently approved, while non-Hispanic Black veterans and those with higher CCI scores were more frequently denied and less frequently approved. VBA applicants with mental health disorders were also more likely to apply for a home loan. Conversely, those granted a home loan were more likely than those denied a home loan to be female, non-Hispanic White, single/unmarried, or to have > 0% VA service-connected disability rating, but less likely to be aged ≥ 50 years, have CCI score > 0, be diagnosed with psychiatric disorders, or have a history of homelessness.
Limitations
This analysis was restricted to a subset of FY 2022 to FY 2024 linked VBA/VHA databases (ie, to veterans who had both VBA and VHA records and met prespecified eligibility criteria). Despite the large number of linked records, a small percentage of these records corresponded to veterans who were applicants or recipients of the VA Home Loan Program. Future studies should expand the time frame to examine variations in application outcomes over time and by background characteristics of veterans enrolled in VHA care who applied for VBA benefits. In addition, we relied on data and ICD-10-CM diagnostic codes from existing electronic health records and claims data to define histories of homelessness, comorbidities, SUDs, and mental health disorders. Given the time-varying nature of these conditions, the temporal sequence of events was difficult to ascertain. Third, it is worth noting that these findings can only be generalized to veterans who applied for VBA benefits and met eligibility criteria, and that these veterans may differ in terms of their demographic and clinical characteristics from those who did not apply for these benefits.
Conclusions
This study analyzed data from 251,796 individuals who applied for and received a VA home loan, 84,751 who were denied a VA home loan, and 2,752,748 veterans who did not apply for a VA home loan from FY 2022 to FY 2024. Accordingly, 11% of applications pertained to the VA Home Loan Program, and 75% of VA Home Loan Program applicants received a home loan. Distinct demographic and clinical characteristics were observed for applicants and recipients of the VA Home Loan Program, which can set the stage for future planning and evaluation of the program. Despite the broad accessibility of veterans to the VA Home Loan Program, there were differences in approval rates among applicants based on sociodemographic and clinical characteristics. Further evaluation, perhaps using qualitative methods, is needed to better understand opportunities and challenges to achieving a VA home loan, especially among underserved veteran populations. Investigation and research can guide future recommendations for any development or corrective actions that can help increase access to veterans who can benefit from the program. Future analyses are also needed to compare veterans enrolled and not enrolled in the VA Home Loan Program on health care-related outcomes.
- US Department of Veterans Affairs. Home loans. Accessed April 1, 2026. https://www.benefits.va.gov/homeloans/
- Veterans United Home Loans. VA loans: the complete guide. Accessed April 1, 2026. https://www.veteransunited.com/va-loans/
- US Department of Veterans Affairs. VA-backed veterans home loans. Accessed April 1, 2026. https://www.va.gov/housing-assistance/home-loans/
- Choplin JM, Stark DP. Whispering sweet nothings: a review of verbal behaviors that undermine the effectiveness of government-mandated home-loan disclosures. Cogn Res Princ Implic. 2019;4:6. doi:10.1186/s41235-019-0154-7
- Evans M. Borrowing boon. More explore federal home loan banks backing. Mod Healthc. 2009;39:14.
- Hogarth M. A home loan: how—and how much? Nurs Times. 1973;69:908-909.
- Jacoby SF. Home Owners’ Loan Corporation maps and place-based injury risks: a complex history. Am J Public Health. 2023;113:356-358. doi:10.2105/AJPH.2023.307242
- Merrell C. Finance. Home: a loan. Nurs Times. 1996;92:61-64.
- Namin S, Xu W, Zhou Y, et al. The legacy of the Home Owners’ Loan Corporation and the political ecology of urban trees and air pollution in the United States. Soc Sci Med. 2020;246:112758. doi:10.1016/j.socscimed.2019.112758
- Namin S, Zhou Y, Xu W, et al. Persistence of mortgage lending bias in the United States: 80 years after the Home Owners’ Loan Corporation security maps. J Race Ethn City. 2022;3:70-94. doi:10.1080/26884674.2021.2019568
- Slottow R. The home loan program. J Natl Assoc Hosp Dev. 1990:43-45.
- Wang M, Chen H, Wang L. Locus of control and home mortgage loan behaviour. Int J Psychol. 2008;43:125-129. doi:10.1080/00207590801888760
- US Dept of Veterans Affairs. Veterans Health Administration. About VHA. Updated January 20, 2025. Accessed April 1, 2026. https://www.va.gov/health/aboutvha.asp
- US Dept of Veterans Affairs. VA homeless programs. Updated May 7, 2026. Accessed May 8, 2026. https://department.va.gov/homeless/
- DiTosto JD, Holder K, Soyemi E, et al. Housing instability and adverse perinatal outcomes: a systematic review. Am J Obstet Gynecol MFM. 2021;3:100477. doi:10.1016/j.ajogmf.2021.100477
- Tsai J, Szymkowiak D, Jutkowitz E. Developing an operational definition of housing instability and homelessness in Veterans Health Administration medical records. PLoS One. 2022;17:e0279973. doi:10.1371/journal.pone.0279973
- Fowler PJ, Hovmand PS, Marcal KE, et al. Solving homelessness from a complex systems perspective: insights for prevention responses. Annu Rev Public Health. 2019;40: 465-486. doi:10.1146/annurev-publhealth-040617-013553
- US Department of Health and Human Services. Healthy People 2030: housing instability. Accessed April 1, 2026. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability
- US Department of Veterans Affairs. VA health care priorities. Accessed April 1, 2026. https://www.va.gov/health/priorities/index.asp
- Tsai J. Federal priorities to address homelessness as a community health problem. Fam Community Health. 2025;48:57-69.
- Tsai J, Hooshyar D. Prevalence of eviction, home foreclosure, and homelessness among low-income US veterans: the National Veteran Homeless and Other Poverty Experiences study. Public Health. 2022;213:181-188. doi:10.1016/j.puhe.2022.10.017
- US Department of Veterans Affairs. Corporate Data Warehouse (CDW). Accessed April 1, 2026. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Price LE, Shea K, Gephart S. The Veterans Affairs Corporate Data Warehouse: uses and implications for nursing research and practice. Nurs Adm Q. 2015;39:311-318. doi:10.1097/NAQ.0000000000000118
- US Department of Veterans Affairs. Homeless Operations Management and Evaluation System (HOMES) User Manual—Phase 1. April 19, 2011. Accessed April 1, 2026. https://www.adldata.org/wp-content/uploads/2016/07/homes.pdf
- Tsai J, Kasprow WJ, Rosenheck RA. Latent homeless risk profiles of a national sample of homeless veterans and their relation to program referral and admission patterns. Am J Public Health. 2013;103:S239-S247. doi:10.2105/AJPH.2013.301322
- Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted inhospital mortality. J Clin Epidemiol. 2004;57:1288-1294. doi:10.1016/j.jclinepi.2004.03.012
- Beydoun HA, Szymkowiak D, Beydoun MA, et al. Comparing major comorbidity indices as predictors of all-cause mortality in the Veterans Affairs health care system. J Clin Epidemiol. 2025;182:111778. doi:10.1016/j.jclinepi.2025.111778
- Charlson ME, Carrozzino D, Guidi J, et al. Charlson Comorbidity Index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91:8-35. doi:10.1159/000521288
- Glasheen WP, Cordier T, Gumpina R, et al. Charlson Comorbidity Index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12:188-197.
- Beydoun HA, Szymkowiak D, Kinney R, et al. Is the risk of Alzheimer’s disease and related dementias among US veterans influenced by the intersectionality of housing status, HIV/AIDS, hepatitis C, and psychiatric disorders? J Gerontol A Biol Sci Med Sci. 2024;79:glae153. doi:10.1093/gerona/glae153
- SAS Institute. SAS Enterprise Guide. Accessed April 1, 2026. https://www.sas.com/en_us/software/enterprise-guide/features-list.html
- Agarwal S, Amromin G, Chomsisengphet S, et al. Mortgage refinancing, consumer spending, and competition: evidence from the Home Affordable Refinance Program. Rev Econ Stud. 2023;90:499-537.
- Ashcraft A, Bech ML, Frame WS. The Federal Home Loan Bank System: the lender of next-to-last resort? J Money Credit Bank. 2010;42:551-583.
- Gibson M, Petticrew M, Bambra C, et al. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17:175-184. doi:10.1016/j.healthplace.2010.09.011
- Shaw M. Housing and public health. Annu Rev Public Health. 2004; 25:397-418. doi:10.1146/annurev.publhealth.25.101802.123036
- Thomson H, Petticrew M, Morrison D. Health effects of housing improvement: systematic review of intervention studies. BMJ. 2001;323:187-190. doi:10.1136/bmj.323.7306.187
- Tsai J. Theorizing pathways between eviction filings and increased mortality risk. JAMA. 2024;331:570-571. doi:10.1001/jama.2023.27978
- Bernanke B, Blanchard O. What caused the US pandemicera inflation? Am Econ J Macroecon. 2025;17:1-35.
- Hall SG, Tavlas GS, Wang Y. Drivers and spillover effects of inflation: the United States, the euro area, and the United Kingdom. J Int Money Finance. 2023;131:1-13.
- US Department of Housing and Urban Development. Point-in-Time Count and Housing Inventory Count. Accessed April 1, 2026. https://www.hudexchange.info/programs/hdx/pit-hic/
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act: expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Zychowicz ME. The PACT Act: enhancing health care access for military personnel and veterans. N C Med J. 2023;84:379-380. doi:10.18043/001c.89208
- US Department of Veterans Affairs. The PACT Act and your VA benefits. April 2, 2026. https://www.va.gov/resources/the-pact-act-and-your-va-benefits/
- US Department of Veterans Affairs. Home loans. Accessed April 1, 2026. https://www.benefits.va.gov/homeloans/
- Veterans United Home Loans. VA loans: the complete guide. Accessed April 1, 2026. https://www.veteransunited.com/va-loans/
- US Department of Veterans Affairs. VA-backed veterans home loans. Accessed April 1, 2026. https://www.va.gov/housing-assistance/home-loans/
- Choplin JM, Stark DP. Whispering sweet nothings: a review of verbal behaviors that undermine the effectiveness of government-mandated home-loan disclosures. Cogn Res Princ Implic. 2019;4:6. doi:10.1186/s41235-019-0154-7
- Evans M. Borrowing boon. More explore federal home loan banks backing. Mod Healthc. 2009;39:14.
- Hogarth M. A home loan: how—and how much? Nurs Times. 1973;69:908-909.
- Jacoby SF. Home Owners’ Loan Corporation maps and place-based injury risks: a complex history. Am J Public Health. 2023;113:356-358. doi:10.2105/AJPH.2023.307242
- Merrell C. Finance. Home: a loan. Nurs Times. 1996;92:61-64.
- Namin S, Xu W, Zhou Y, et al. The legacy of the Home Owners’ Loan Corporation and the political ecology of urban trees and air pollution in the United States. Soc Sci Med. 2020;246:112758. doi:10.1016/j.socscimed.2019.112758
- Namin S, Zhou Y, Xu W, et al. Persistence of mortgage lending bias in the United States: 80 years after the Home Owners’ Loan Corporation security maps. J Race Ethn City. 2022;3:70-94. doi:10.1080/26884674.2021.2019568
- Slottow R. The home loan program. J Natl Assoc Hosp Dev. 1990:43-45.
- Wang M, Chen H, Wang L. Locus of control and home mortgage loan behaviour. Int J Psychol. 2008;43:125-129. doi:10.1080/00207590801888760
- US Dept of Veterans Affairs. Veterans Health Administration. About VHA. Updated January 20, 2025. Accessed April 1, 2026. https://www.va.gov/health/aboutvha.asp
- US Dept of Veterans Affairs. VA homeless programs. Updated May 7, 2026. Accessed May 8, 2026. https://department.va.gov/homeless/
- DiTosto JD, Holder K, Soyemi E, et al. Housing instability and adverse perinatal outcomes: a systematic review. Am J Obstet Gynecol MFM. 2021;3:100477. doi:10.1016/j.ajogmf.2021.100477
- Tsai J, Szymkowiak D, Jutkowitz E. Developing an operational definition of housing instability and homelessness in Veterans Health Administration medical records. PLoS One. 2022;17:e0279973. doi:10.1371/journal.pone.0279973
- Fowler PJ, Hovmand PS, Marcal KE, et al. Solving homelessness from a complex systems perspective: insights for prevention responses. Annu Rev Public Health. 2019;40: 465-486. doi:10.1146/annurev-publhealth-040617-013553
- US Department of Health and Human Services. Healthy People 2030: housing instability. Accessed April 1, 2026. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability
- US Department of Veterans Affairs. VA health care priorities. Accessed April 1, 2026. https://www.va.gov/health/priorities/index.asp
- Tsai J. Federal priorities to address homelessness as a community health problem. Fam Community Health. 2025;48:57-69.
- Tsai J, Hooshyar D. Prevalence of eviction, home foreclosure, and homelessness among low-income US veterans: the National Veteran Homeless and Other Poverty Experiences study. Public Health. 2022;213:181-188. doi:10.1016/j.puhe.2022.10.017
- US Department of Veterans Affairs. Corporate Data Warehouse (CDW). Accessed April 1, 2026. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Price LE, Shea K, Gephart S. The Veterans Affairs Corporate Data Warehouse: uses and implications for nursing research and practice. Nurs Adm Q. 2015;39:311-318. doi:10.1097/NAQ.0000000000000118
- US Department of Veterans Affairs. Homeless Operations Management and Evaluation System (HOMES) User Manual—Phase 1. April 19, 2011. Accessed April 1, 2026. https://www.adldata.org/wp-content/uploads/2016/07/homes.pdf
- Tsai J, Kasprow WJ, Rosenheck RA. Latent homeless risk profiles of a national sample of homeless veterans and their relation to program referral and admission patterns. Am J Public Health. 2013;103:S239-S247. doi:10.2105/AJPH.2013.301322
- Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted inhospital mortality. J Clin Epidemiol. 2004;57:1288-1294. doi:10.1016/j.jclinepi.2004.03.012
- Beydoun HA, Szymkowiak D, Beydoun MA, et al. Comparing major comorbidity indices as predictors of all-cause mortality in the Veterans Affairs health care system. J Clin Epidemiol. 2025;182:111778. doi:10.1016/j.jclinepi.2025.111778
- Charlson ME, Carrozzino D, Guidi J, et al. Charlson Comorbidity Index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91:8-35. doi:10.1159/000521288
- Glasheen WP, Cordier T, Gumpina R, et al. Charlson Comorbidity Index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12:188-197.
- Beydoun HA, Szymkowiak D, Kinney R, et al. Is the risk of Alzheimer’s disease and related dementias among US veterans influenced by the intersectionality of housing status, HIV/AIDS, hepatitis C, and psychiatric disorders? J Gerontol A Biol Sci Med Sci. 2024;79:glae153. doi:10.1093/gerona/glae153
- SAS Institute. SAS Enterprise Guide. Accessed April 1, 2026. https://www.sas.com/en_us/software/enterprise-guide/features-list.html
- Agarwal S, Amromin G, Chomsisengphet S, et al. Mortgage refinancing, consumer spending, and competition: evidence from the Home Affordable Refinance Program. Rev Econ Stud. 2023;90:499-537.
- Ashcraft A, Bech ML, Frame WS. The Federal Home Loan Bank System: the lender of next-to-last resort? J Money Credit Bank. 2010;42:551-583.
- Gibson M, Petticrew M, Bambra C, et al. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17:175-184. doi:10.1016/j.healthplace.2010.09.011
- Shaw M. Housing and public health. Annu Rev Public Health. 2004; 25:397-418. doi:10.1146/annurev.publhealth.25.101802.123036
- Thomson H, Petticrew M, Morrison D. Health effects of housing improvement: systematic review of intervention studies. BMJ. 2001;323:187-190. doi:10.1136/bmj.323.7306.187
- Tsai J. Theorizing pathways between eviction filings and increased mortality risk. JAMA. 2024;331:570-571. doi:10.1001/jama.2023.27978
- Bernanke B, Blanchard O. What caused the US pandemicera inflation? Am Econ J Macroecon. 2025;17:1-35.
- Hall SG, Tavlas GS, Wang Y. Drivers and spillover effects of inflation: the United States, the euro area, and the United Kingdom. J Int Money Finance. 2023;131:1-13.
- US Department of Housing and Urban Development. Point-in-Time Count and Housing Inventory Count. Accessed April 1, 2026. https://www.hudexchange.info/programs/hdx/pit-hic/
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act: expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Zychowicz ME. The PACT Act: enhancing health care access for military personnel and veterans. N C Med J. 2023;84:379-380. doi:10.18043/001c.89208
- US Department of Veterans Affairs. The PACT Act and your VA benefits. April 2, 2026. https://www.va.gov/resources/the-pact-act-and-your-va-benefits/
Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program
Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program
