User login
Single-dose psilocybin promising for resistant depression
PARIS –
Known as COMP360, the synthetic agent, a proprietary, purified form of psilocybin, improved symptoms related to mood and anhedonia while leaving aspects such as appetite and weight changes unaffected, reported investigators led by Guy M. Goodwin, PhD, emeritus professor of psychiatry, University of Oxford, England, and chief medical officer, COMPASS Pathways.
The study was presented at the European Psychiatric Association (EPA) 2023 Congress.
100 million affected
Affecting up to 100 million people globally, TRD is “not an official diagnosis,” although it is often defined as the failure to elicit a response with at least two antidepressant treatments, said Dr. Goodwin.

Compared to their counterparts with non-TRD, those with TRD experience higher relapse rates, higher rates of suicidal behavior, and more residual symptoms even when they do respond to treatment.
Previous results from the study known as P-TRD indicated that a single 25-mg dose of COMP360 significantly reduced depression scores for up to 12 weeks when given along with psychological support, although a later analysis suggested the effect subsequently dropped off.
The vast majority of the patients in the trial were naive to psychedelics, and so, Dr. Goodwin explained, they undergo a preparation phase during which they receive psychoeducation and have at least two visits with a therapist, who then stays with them during administration of the drug to offer support if they experience psychological distress.
Following the psilocybin session, participants go through a process known as integration, which involves two sessions with a therapist within 2 weeks.
“That, in our view, is essentially about safety, and about identifying problems that have arisen as a result of taking the drug,” said Dr. Goodwin.
The phase 2b trial examined changes in specific depression symptoms after psilocybin treatment in 233 patients with TRD. Participants were a mean age of 39.8 years and 59% were women. They were randomized to receive one of three doses of the drug: a 1-mg dose (n = 79), a 10-mg dose (n = 75), or a 25-mg dose (n = 79).
The primary outcome was changes in individual items on the Montgomery-Åsberg Depression Rating Scale (MADRS) and 16-item Quick Inventory of Depressive Symptomatology–Self Report (QIDS-SR-16) scale.
While the effect on overall depression scores is important, said Dr. Goodwin, many of the items included in the depression assessment scales are “uninformative.”
Reduction in ‘core’ symptoms
Participants were assessed by a blinded rater at baseline, day 1, day 2, and at 1, 2, 3, 6, 9, and 12 weeks after administration of COMP360. The primary endpoint was a reduction in individual items on MADRS and scores from baseline to 3 weeks. Individual items on the QIDS-SR-16 were rated by participants at the same time points.
Investigators found the largest mean changes from baseline were on reported and apparent sadness, lassitude, inability to feel, and concentration difficulties, with “very nice and clear dose-related differences,” Dr. Goodwin said.
The results indicate that the significant benefit with the largest dose at 3 weeks versus baseline was confined to items such as inability to feel and reported and apparent sadness on the MADRS and feeling sad and general interest on the QIDS-SR-16 (Table 1).
The results suggest the effect of COMP360 is “on the core symptoms of depression,” said Dr. Goodwin.
Results were similar for individual items on the QIDS-SR-16, with the greatest changes in items including feeling sad, general interest, energy level, falling asleep, view of myself, concentration/decision-making, and feeling down.
Other scale items, such as decreased appetite, feel restless, and weight changes, showed negligible changes in response to COMP360 therapy and were described by Dr. Goodwin as “inconsequential.”
“Essentially, these items are contributing nothing but noise to the signal,” he said.
He added the results of the study need to be replicated and that plans for phase 3 trials are underway. These studies, he said, are designed to convince the Food and Drug Administration that “this is not just a recreational drug, it’s a medicine.”
Enthusiasm running ahead of the data
Commenting on the findings, Bertha K. Madras, PhD, professor of psychobiology, department of psychiatry, Harvard Medical School, Boston, who was not involved in the study, said “hallucinogens are an intriguing class of drugs and I support ongoing high-quality research in this area.”
However, she told this news organization that the “breathtaking endorsement of this drug is far ahead of scientific data.”
She cited concerns such as the “narrow demographics” of participants, their previous experience with and expectations of hallucinogens, the “potential for symptom fluidity of enrollees,” such as depression evolving into psychosis, and the “undefined role” of the therapist during a hallucinogenic session.
“Finally, I am concerned that enthusiasm for therapeutic potential has been, and will continue to be, preempted and directed towards legalization and widespread access for vulnerable populations,” Dr. Madras said.
This, she said, “is occurring at breakneck speed in the U.S., with scant resistance or skepticism from the investigators engaged in therapeutic assessment.”
The study was funded by COMPASS Pathways. Dr. Goodwin has reported relationships with COMPASS Pathways, Buckley Psytech, Boehringer Ingelheim, Clerkenwell Health, EVA Pharma, Lundbeck, Janssen Global Services, Novartis, Ocean Neurosciences, P1vital, Sage Therapeutics, Servier, Takeda, and WebMD.
A version of this article first appeared on Medscape.com.
PARIS –
Known as COMP360, the synthetic agent, a proprietary, purified form of psilocybin, improved symptoms related to mood and anhedonia while leaving aspects such as appetite and weight changes unaffected, reported investigators led by Guy M. Goodwin, PhD, emeritus professor of psychiatry, University of Oxford, England, and chief medical officer, COMPASS Pathways.
The study was presented at the European Psychiatric Association (EPA) 2023 Congress.
100 million affected
Affecting up to 100 million people globally, TRD is “not an official diagnosis,” although it is often defined as the failure to elicit a response with at least two antidepressant treatments, said Dr. Goodwin.
Compared to their counterparts with non-TRD, those with TRD experience higher relapse rates, higher rates of suicidal behavior, and more residual symptoms even when they do respond to treatment.
Previous results from the study known as P-TRD indicated that a single 25-mg dose of COMP360 significantly reduced depression scores for up to 12 weeks when given along with psychological support, although a later analysis suggested the effect subsequently dropped off.
The vast majority of the patients in the trial were naive to psychedelics, and so, Dr. Goodwin explained, they undergo a preparation phase during which they receive psychoeducation and have at least two visits with a therapist, who then stays with them during administration of the drug to offer support if they experience psychological distress.
Following the psilocybin session, participants go through a process known as integration, which involves two sessions with a therapist within 2 weeks.
“That, in our view, is essentially about safety, and about identifying problems that have arisen as a result of taking the drug,” said Dr. Goodwin.
The phase 2b trial examined changes in specific depression symptoms after psilocybin treatment in 233 patients with TRD. Participants were a mean age of 39.8 years and 59% were women. They were randomized to receive one of three doses of the drug: a 1-mg dose (n = 79), a 10-mg dose (n = 75), or a 25-mg dose (n = 79).
The primary outcome was changes in individual items on the Montgomery-Åsberg Depression Rating Scale (MADRS) and 16-item Quick Inventory of Depressive Symptomatology–Self Report (QIDS-SR-16) scale.
While the effect on overall depression scores is important, said Dr. Goodwin, many of the items included in the depression assessment scales are “uninformative.”
Reduction in ‘core’ symptoms
Participants were assessed by a blinded rater at baseline, day 1, day 2, and at 1, 2, 3, 6, 9, and 12 weeks after administration of COMP360. The primary endpoint was a reduction in individual items on MADRS and scores from baseline to 3 weeks. Individual items on the QIDS-SR-16 were rated by participants at the same time points.
Investigators found the largest mean changes from baseline were on reported and apparent sadness, lassitude, inability to feel, and concentration difficulties, with “very nice and clear dose-related differences,” Dr. Goodwin said.
The results indicate that the significant benefit with the largest dose at 3 weeks versus baseline was confined to items such as inability to feel and reported and apparent sadness on the MADRS and feeling sad and general interest on the QIDS-SR-16 (Table 1).
The results suggest the effect of COMP360 is “on the core symptoms of depression,” said Dr. Goodwin.
Results were similar for individual items on the QIDS-SR-16, with the greatest changes in items including feeling sad, general interest, energy level, falling asleep, view of myself, concentration/decision-making, and feeling down.
Other scale items, such as decreased appetite, feel restless, and weight changes, showed negligible changes in response to COMP360 therapy and were described by Dr. Goodwin as “inconsequential.”
“Essentially, these items are contributing nothing but noise to the signal,” he said.
He added the results of the study need to be replicated and that plans for phase 3 trials are underway. These studies, he said, are designed to convince the Food and Drug Administration that “this is not just a recreational drug, it’s a medicine.”
Enthusiasm running ahead of the data
Commenting on the findings, Bertha K. Madras, PhD, professor of psychobiology, department of psychiatry, Harvard Medical School, Boston, who was not involved in the study, said “hallucinogens are an intriguing class of drugs and I support ongoing high-quality research in this area.”
However, she told this news organization that the “breathtaking endorsement of this drug is far ahead of scientific data.”
She cited concerns such as the “narrow demographics” of participants, their previous experience with and expectations of hallucinogens, the “potential for symptom fluidity of enrollees,” such as depression evolving into psychosis, and the “undefined role” of the therapist during a hallucinogenic session.
“Finally, I am concerned that enthusiasm for therapeutic potential has been, and will continue to be, preempted and directed towards legalization and widespread access for vulnerable populations,” Dr. Madras said.
This, she said, “is occurring at breakneck speed in the U.S., with scant resistance or skepticism from the investigators engaged in therapeutic assessment.”
The study was funded by COMPASS Pathways. Dr. Goodwin has reported relationships with COMPASS Pathways, Buckley Psytech, Boehringer Ingelheim, Clerkenwell Health, EVA Pharma, Lundbeck, Janssen Global Services, Novartis, Ocean Neurosciences, P1vital, Sage Therapeutics, Servier, Takeda, and WebMD.
A version of this article first appeared on Medscape.com.
PARIS –
Known as COMP360, the synthetic agent, a proprietary, purified form of psilocybin, improved symptoms related to mood and anhedonia while leaving aspects such as appetite and weight changes unaffected, reported investigators led by Guy M. Goodwin, PhD, emeritus professor of psychiatry, University of Oxford, England, and chief medical officer, COMPASS Pathways.
The study was presented at the European Psychiatric Association (EPA) 2023 Congress.
100 million affected
Affecting up to 100 million people globally, TRD is “not an official diagnosis,” although it is often defined as the failure to elicit a response with at least two antidepressant treatments, said Dr. Goodwin.
Compared to their counterparts with non-TRD, those with TRD experience higher relapse rates, higher rates of suicidal behavior, and more residual symptoms even when they do respond to treatment.
Previous results from the study known as P-TRD indicated that a single 25-mg dose of COMP360 significantly reduced depression scores for up to 12 weeks when given along with psychological support, although a later analysis suggested the effect subsequently dropped off.
The vast majority of the patients in the trial were naive to psychedelics, and so, Dr. Goodwin explained, they undergo a preparation phase during which they receive psychoeducation and have at least two visits with a therapist, who then stays with them during administration of the drug to offer support if they experience psychological distress.
Following the psilocybin session, participants go through a process known as integration, which involves two sessions with a therapist within 2 weeks.
“That, in our view, is essentially about safety, and about identifying problems that have arisen as a result of taking the drug,” said Dr. Goodwin.
The phase 2b trial examined changes in specific depression symptoms after psilocybin treatment in 233 patients with TRD. Participants were a mean age of 39.8 years and 59% were women. They were randomized to receive one of three doses of the drug: a 1-mg dose (n = 79), a 10-mg dose (n = 75), or a 25-mg dose (n = 79).
The primary outcome was changes in individual items on the Montgomery-Åsberg Depression Rating Scale (MADRS) and 16-item Quick Inventory of Depressive Symptomatology–Self Report (QIDS-SR-16) scale.
While the effect on overall depression scores is important, said Dr. Goodwin, many of the items included in the depression assessment scales are “uninformative.”
Reduction in ‘core’ symptoms
Participants were assessed by a blinded rater at baseline, day 1, day 2, and at 1, 2, 3, 6, 9, and 12 weeks after administration of COMP360. The primary endpoint was a reduction in individual items on MADRS and scores from baseline to 3 weeks. Individual items on the QIDS-SR-16 were rated by participants at the same time points.
Investigators found the largest mean changes from baseline were on reported and apparent sadness, lassitude, inability to feel, and concentration difficulties, with “very nice and clear dose-related differences,” Dr. Goodwin said.
The results indicate that the significant benefit with the largest dose at 3 weeks versus baseline was confined to items such as inability to feel and reported and apparent sadness on the MADRS and feeling sad and general interest on the QIDS-SR-16 (Table 1).
The results suggest the effect of COMP360 is “on the core symptoms of depression,” said Dr. Goodwin.
Results were similar for individual items on the QIDS-SR-16, with the greatest changes in items including feeling sad, general interest, energy level, falling asleep, view of myself, concentration/decision-making, and feeling down.
Other scale items, such as decreased appetite, feel restless, and weight changes, showed negligible changes in response to COMP360 therapy and were described by Dr. Goodwin as “inconsequential.”
“Essentially, these items are contributing nothing but noise to the signal,” he said.
He added the results of the study need to be replicated and that plans for phase 3 trials are underway. These studies, he said, are designed to convince the Food and Drug Administration that “this is not just a recreational drug, it’s a medicine.”
Enthusiasm running ahead of the data
Commenting on the findings, Bertha K. Madras, PhD, professor of psychobiology, department of psychiatry, Harvard Medical School, Boston, who was not involved in the study, said “hallucinogens are an intriguing class of drugs and I support ongoing high-quality research in this area.”
However, she told this news organization that the “breathtaking endorsement of this drug is far ahead of scientific data.”
She cited concerns such as the “narrow demographics” of participants, their previous experience with and expectations of hallucinogens, the “potential for symptom fluidity of enrollees,” such as depression evolving into psychosis, and the “undefined role” of the therapist during a hallucinogenic session.
“Finally, I am concerned that enthusiasm for therapeutic potential has been, and will continue to be, preempted and directed towards legalization and widespread access for vulnerable populations,” Dr. Madras said.
This, she said, “is occurring at breakneck speed in the U.S., with scant resistance or skepticism from the investigators engaged in therapeutic assessment.”
The study was funded by COMPASS Pathways. Dr. Goodwin has reported relationships with COMPASS Pathways, Buckley Psytech, Boehringer Ingelheim, Clerkenwell Health, EVA Pharma, Lundbeck, Janssen Global Services, Novartis, Ocean Neurosciences, P1vital, Sage Therapeutics, Servier, Takeda, and WebMD.
A version of this article first appeared on Medscape.com.
AT EPA 2023
Glutathione a potential biomarker for postpartum suicide
Approximately 10,000 suicide deaths are recorded in Brazil every year. The suicide risk is highest among patients with depressive disorders, particularly women (> 18% vs. 11% for men).
There are countless people who work to prevent suicide, and the challenges they face are many. But now, on the horizon, there are new tools that could prove invaluable to their efforts – tools such as biomarkers. In a study recently published in the journal Frontiers in Psychiatry, researchers from the Catholic University of Pelotas (UCPel), Brazil, reported an association of glutathione (GSH) with the degree of suicide risk in women at 18 months postpartum. Specifically, they found that reduced serum GSH levels were significantly lower for those with moderate to high suicide risk than for those without suicide risk. Their findings suggest that GSH may be a potential biomarker or etiologic factor among women at risk for suicide, with therapeutic implications.
This was a case-control study nested within a cohort study. From this cohort, 45 women were selected at 18 months postpartum. Thirty of them had mood disorders, such as major depression and bipolar disorder. The other 15 participants, none of whom had a mood disorder, made up the control group.
Depression and the risk for suicide were assessed using the Mini International Neuropsychiatric Interview Plus (MINI-Plus 5.0.0 Brazilian version), module A and module C, respectively. Blood samples were collected to evaluate serum levels of the following oxidative stress biomarkers: reactive oxygen species, superoxide dismutase, and GSH.
The prevalence of suicide risk observed in the women at 18 months postpartum was 24.4%. The prevalence of suicide risk in the mood disorder group was 36.7%.
In addition, the statistical analysis found that women with moderate to high suicide risk had cerebral redox imbalance, resulting in a decrease in blood GSH levels.
The study team was led by neuroscientist Adriano Martimbianco de Assis, PhD, the coordinator of UCPel’s postgraduate program in health and behavior. He said that the correlation identified between GSH serum levels and suicide risk gives rise to two possible applications: using GSH as a biomarker for suicide risk and using GSH therapeutically.
Regarding the former application, Dr. Martimbianco de Assis explained that additional studies are needed to take a step forward. “Although we believe that most of the GSH came from the brain – given that it’s the brain’s main antioxidant – as we analyze blood samples, we’re not yet able to rule out the possibility that it came from other organs,” he said in an interview. So, confirming that hypothesis will require studies that involve imaging brain tissue. According to Dr. Martimbianco de Assis, once there is confirmation, it will be possible to move to using the antioxidant as a biomarker for suicide risk.
He also shared his views about the second application: using GSH therapeutically. “We already know that there are very simple alternatives that can influence GSH levels, [and they] mostly have to do with exercise and [improving the quality of] the food one eats. But there are also drugs: for example, N-acetyl cysteine, which is a precursor of GSH.” Adopting strategies to increase the levels of this antioxidant in the body should reverse the imbalance identified in the study and, as a result, may lead to lowering the risk for suicide. But, he reiterated, “getting to a place where GSH [can be used] in clinical practice hinges on getting that confirmation that it did, in fact, come from the brain. Recall that our study found lower levels of GSH in women at risk for suicide.”
Even though the study evaluated postpartum women, it’s possible that the results can be extrapolated to other populations, said Dr. Martimbianco de Assis. This is because when the data were collected, 18 months had already passed since giving birth. The participants’ physiological condition at that point was more similar to the one prior to becoming pregnant.
The UCPel researchers continue to follow the cohort. “We intend to continue monitoring GSH levels at other times. Forty-eight months have now passed since the women gave birth, and the idea is to continue studying [the patients involved in the study],” said Dr. Martimbianco de Assis, adding that the team also intends to analyze brain tissue from in vitro studies using cell cultures.
This article was translated from the Medscape Portuguese Edition and a version appeared on Medscape.com.
Approximately 10,000 suicide deaths are recorded in Brazil every year. The suicide risk is highest among patients with depressive disorders, particularly women (> 18% vs. 11% for men).
There are countless people who work to prevent suicide, and the challenges they face are many. But now, on the horizon, there are new tools that could prove invaluable to their efforts – tools such as biomarkers. In a study recently published in the journal Frontiers in Psychiatry, researchers from the Catholic University of Pelotas (UCPel), Brazil, reported an association of glutathione (GSH) with the degree of suicide risk in women at 18 months postpartum. Specifically, they found that reduced serum GSH levels were significantly lower for those with moderate to high suicide risk than for those without suicide risk. Their findings suggest that GSH may be a potential biomarker or etiologic factor among women at risk for suicide, with therapeutic implications.
This was a case-control study nested within a cohort study. From this cohort, 45 women were selected at 18 months postpartum. Thirty of them had mood disorders, such as major depression and bipolar disorder. The other 15 participants, none of whom had a mood disorder, made up the control group.
Depression and the risk for suicide were assessed using the Mini International Neuropsychiatric Interview Plus (MINI-Plus 5.0.0 Brazilian version), module A and module C, respectively. Blood samples were collected to evaluate serum levels of the following oxidative stress biomarkers: reactive oxygen species, superoxide dismutase, and GSH.
The prevalence of suicide risk observed in the women at 18 months postpartum was 24.4%. The prevalence of suicide risk in the mood disorder group was 36.7%.
In addition, the statistical analysis found that women with moderate to high suicide risk had cerebral redox imbalance, resulting in a decrease in blood GSH levels.
The study team was led by neuroscientist Adriano Martimbianco de Assis, PhD, the coordinator of UCPel’s postgraduate program in health and behavior. He said that the correlation identified between GSH serum levels and suicide risk gives rise to two possible applications: using GSH as a biomarker for suicide risk and using GSH therapeutically.
Regarding the former application, Dr. Martimbianco de Assis explained that additional studies are needed to take a step forward. “Although we believe that most of the GSH came from the brain – given that it’s the brain’s main antioxidant – as we analyze blood samples, we’re not yet able to rule out the possibility that it came from other organs,” he said in an interview. So, confirming that hypothesis will require studies that involve imaging brain tissue. According to Dr. Martimbianco de Assis, once there is confirmation, it will be possible to move to using the antioxidant as a biomarker for suicide risk.
He also shared his views about the second application: using GSH therapeutically. “We already know that there are very simple alternatives that can influence GSH levels, [and they] mostly have to do with exercise and [improving the quality of] the food one eats. But there are also drugs: for example, N-acetyl cysteine, which is a precursor of GSH.” Adopting strategies to increase the levels of this antioxidant in the body should reverse the imbalance identified in the study and, as a result, may lead to lowering the risk for suicide. But, he reiterated, “getting to a place where GSH [can be used] in clinical practice hinges on getting that confirmation that it did, in fact, come from the brain. Recall that our study found lower levels of GSH in women at risk for suicide.”
Even though the study evaluated postpartum women, it’s possible that the results can be extrapolated to other populations, said Dr. Martimbianco de Assis. This is because when the data were collected, 18 months had already passed since giving birth. The participants’ physiological condition at that point was more similar to the one prior to becoming pregnant.
The UCPel researchers continue to follow the cohort. “We intend to continue monitoring GSH levels at other times. Forty-eight months have now passed since the women gave birth, and the idea is to continue studying [the patients involved in the study],” said Dr. Martimbianco de Assis, adding that the team also intends to analyze brain tissue from in vitro studies using cell cultures.
This article was translated from the Medscape Portuguese Edition and a version appeared on Medscape.com.
Approximately 10,000 suicide deaths are recorded in Brazil every year. The suicide risk is highest among patients with depressive disorders, particularly women (> 18% vs. 11% for men).
There are countless people who work to prevent suicide, and the challenges they face are many. But now, on the horizon, there are new tools that could prove invaluable to their efforts – tools such as biomarkers. In a study recently published in the journal Frontiers in Psychiatry, researchers from the Catholic University of Pelotas (UCPel), Brazil, reported an association of glutathione (GSH) with the degree of suicide risk in women at 18 months postpartum. Specifically, they found that reduced serum GSH levels were significantly lower for those with moderate to high suicide risk than for those without suicide risk. Their findings suggest that GSH may be a potential biomarker or etiologic factor among women at risk for suicide, with therapeutic implications.
This was a case-control study nested within a cohort study. From this cohort, 45 women were selected at 18 months postpartum. Thirty of them had mood disorders, such as major depression and bipolar disorder. The other 15 participants, none of whom had a mood disorder, made up the control group.
Depression and the risk for suicide were assessed using the Mini International Neuropsychiatric Interview Plus (MINI-Plus 5.0.0 Brazilian version), module A and module C, respectively. Blood samples were collected to evaluate serum levels of the following oxidative stress biomarkers: reactive oxygen species, superoxide dismutase, and GSH.
The prevalence of suicide risk observed in the women at 18 months postpartum was 24.4%. The prevalence of suicide risk in the mood disorder group was 36.7%.
In addition, the statistical analysis found that women with moderate to high suicide risk had cerebral redox imbalance, resulting in a decrease in blood GSH levels.
The study team was led by neuroscientist Adriano Martimbianco de Assis, PhD, the coordinator of UCPel’s postgraduate program in health and behavior. He said that the correlation identified between GSH serum levels and suicide risk gives rise to two possible applications: using GSH as a biomarker for suicide risk and using GSH therapeutically.
Regarding the former application, Dr. Martimbianco de Assis explained that additional studies are needed to take a step forward. “Although we believe that most of the GSH came from the brain – given that it’s the brain’s main antioxidant – as we analyze blood samples, we’re not yet able to rule out the possibility that it came from other organs,” he said in an interview. So, confirming that hypothesis will require studies that involve imaging brain tissue. According to Dr. Martimbianco de Assis, once there is confirmation, it will be possible to move to using the antioxidant as a biomarker for suicide risk.
He also shared his views about the second application: using GSH therapeutically. “We already know that there are very simple alternatives that can influence GSH levels, [and they] mostly have to do with exercise and [improving the quality of] the food one eats. But there are also drugs: for example, N-acetyl cysteine, which is a precursor of GSH.” Adopting strategies to increase the levels of this antioxidant in the body should reverse the imbalance identified in the study and, as a result, may lead to lowering the risk for suicide. But, he reiterated, “getting to a place where GSH [can be used] in clinical practice hinges on getting that confirmation that it did, in fact, come from the brain. Recall that our study found lower levels of GSH in women at risk for suicide.”
Even though the study evaluated postpartum women, it’s possible that the results can be extrapolated to other populations, said Dr. Martimbianco de Assis. This is because when the data were collected, 18 months had already passed since giving birth. The participants’ physiological condition at that point was more similar to the one prior to becoming pregnant.
The UCPel researchers continue to follow the cohort. “We intend to continue monitoring GSH levels at other times. Forty-eight months have now passed since the women gave birth, and the idea is to continue studying [the patients involved in the study],” said Dr. Martimbianco de Assis, adding that the team also intends to analyze brain tissue from in vitro studies using cell cultures.
This article was translated from the Medscape Portuguese Edition and a version appeared on Medscape.com.
A new way to gauge suicide risk?
Researchers found SDOH are risk factors for suicide among U.S. veterans and NLP can be leveraged to extract SDOH information from unstructured data in the EHR.
“Since SDOH is overwhelmingly described in EHR notes, the importance of NLP-extracted SDOH can be very significant, meaning that NLP can be used as an effective method for epidemiological and public health study,” senior investigator Hong Yu, PhD, from Miner School of Information and Computer Sciences, University of Massachusetts Lowell, told this news organization.
Although the study was conducted among U.S. veterans, the results likely hold for the general population as well.
“The NLP methods are generalizable. The SDOH categories are generalizable. There may be some variations in terms of the strength of associations in NLP-extracted SDOH and suicide death, but the overall findings are generalizable,” Dr. Yu said.
The study was published online JAMA Network Open.
Improved risk assessment
SDOH, which include factors such as socioeconomic status, access to healthy food, education, housing, and physical environment, are strong predictors of suicidal behaviors.
Several studies have identified a range of common risk factors for suicide using International Classification of Diseases (ICD) codes and other “structured” data from the EHR. However, the use of unstructured EHR data from clinician notes has received little attention in investigating potential associations between suicide and SDOH.
Using the large Veterans Health Administration EHR system, the researchers determined associations between veterans’ death by suicide and recent SDOH, identified using both structured data (ICD-10 codes and Veterans Health Administration stop codes) and unstructured data (NLP-processed clinical notes).
Participants included 8,821 veterans who committed suicide and 35,284 matched controls. The cohort was mostly male (96%) and White (79%). The mean age was 58 years.
The NLP-extracted SDOH were social isolation, job or financial insecurity, housing instability, legal problems, violence, barriers to care, transition of care, and food insecurity.
All of these unstructured clinical notes on SDOH were significantly associated with increased risk for death by suicide.
Legal problems had the largest estimated effect size, more than twice the risk of those with no exposure (adjusted odds ratio 2.62; 95% confidence interval, 2.38-2.89), followed by violence (aOR, 2.34; 95% CI, 2.17-2.52) and social isolation (aOR, 1.94; 95% CI, 1.83-2.06).
Similarly, all of the structured SDOH – social or family problems, employment or financial problems, housing instability, legal problems, violence, and nonspecific psychosocial needs – also showed significant associations with increased risk for suicide death, once again, with legal problems linked to the highest risk (aOR, 2.63; 95% CI, 2.37-2.91).
When combining the structured and NLP-extracted unstructured data, the top three risk factors for death by suicide were legal problems (aOR, 2.66; 95% CI 2.46-2.89), violence (aOR, 2.12; 95% CI, 1.98-2.27), and nonspecific psychosocial needs (aOR, 2.07; 95% CI, 1.92-2.23).
“To our knowledge, this the first large-scale study to implement and use an NLP system to extract SDOH information from unstructured EHR data,” the researchers write.
“We strongly believe that analyzing all available SDOH information, including those contained in clinical notes, can help develop a better system for risk assessment and suicide prevention. However, more studies are required to investigate ways of seamlessly incorporating SDOHs into existing health care systems,” they conclude.
Dr. Yu said it’s also important to note that their NLP system is built upon “the most advanced deep-learning technologies and therefore is more generalizable than most existing work that mainly used rule-based approaches or traditional machine learning for identifying social determinants of health.”
In an accompanying editorial, Ishanu Chattopadhyay, PhD, of the University of Chicago, said this suggests that unstructured clinical notes “may efficiently identify at-risk individuals even when structured data on the relevant variables are missing or incomplete.”
This work may provide “the foundation for addressing the key hurdles in enacting efficient universal assessment for suicide risk among the veterans and perhaps in the general population,” Dr. Chattopadhyay added.
This research was funded by a grant from the National Institute of Mental Health. The study authors and editorialist report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Researchers found SDOH are risk factors for suicide among U.S. veterans and NLP can be leveraged to extract SDOH information from unstructured data in the EHR.
“Since SDOH is overwhelmingly described in EHR notes, the importance of NLP-extracted SDOH can be very significant, meaning that NLP can be used as an effective method for epidemiological and public health study,” senior investigator Hong Yu, PhD, from Miner School of Information and Computer Sciences, University of Massachusetts Lowell, told this news organization.
Although the study was conducted among U.S. veterans, the results likely hold for the general population as well.
“The NLP methods are generalizable. The SDOH categories are generalizable. There may be some variations in terms of the strength of associations in NLP-extracted SDOH and suicide death, but the overall findings are generalizable,” Dr. Yu said.
The study was published online JAMA Network Open.
Improved risk assessment
SDOH, which include factors such as socioeconomic status, access to healthy food, education, housing, and physical environment, are strong predictors of suicidal behaviors.
Several studies have identified a range of common risk factors for suicide using International Classification of Diseases (ICD) codes and other “structured” data from the EHR. However, the use of unstructured EHR data from clinician notes has received little attention in investigating potential associations between suicide and SDOH.
Using the large Veterans Health Administration EHR system, the researchers determined associations between veterans’ death by suicide and recent SDOH, identified using both structured data (ICD-10 codes and Veterans Health Administration stop codes) and unstructured data (NLP-processed clinical notes).
Participants included 8,821 veterans who committed suicide and 35,284 matched controls. The cohort was mostly male (96%) and White (79%). The mean age was 58 years.
The NLP-extracted SDOH were social isolation, job or financial insecurity, housing instability, legal problems, violence, barriers to care, transition of care, and food insecurity.
All of these unstructured clinical notes on SDOH were significantly associated with increased risk for death by suicide.
Legal problems had the largest estimated effect size, more than twice the risk of those with no exposure (adjusted odds ratio 2.62; 95% confidence interval, 2.38-2.89), followed by violence (aOR, 2.34; 95% CI, 2.17-2.52) and social isolation (aOR, 1.94; 95% CI, 1.83-2.06).
Similarly, all of the structured SDOH – social or family problems, employment or financial problems, housing instability, legal problems, violence, and nonspecific psychosocial needs – also showed significant associations with increased risk for suicide death, once again, with legal problems linked to the highest risk (aOR, 2.63; 95% CI, 2.37-2.91).
When combining the structured and NLP-extracted unstructured data, the top three risk factors for death by suicide were legal problems (aOR, 2.66; 95% CI 2.46-2.89), violence (aOR, 2.12; 95% CI, 1.98-2.27), and nonspecific psychosocial needs (aOR, 2.07; 95% CI, 1.92-2.23).
“To our knowledge, this the first large-scale study to implement and use an NLP system to extract SDOH information from unstructured EHR data,” the researchers write.
“We strongly believe that analyzing all available SDOH information, including those contained in clinical notes, can help develop a better system for risk assessment and suicide prevention. However, more studies are required to investigate ways of seamlessly incorporating SDOHs into existing health care systems,” they conclude.
Dr. Yu said it’s also important to note that their NLP system is built upon “the most advanced deep-learning technologies and therefore is more generalizable than most existing work that mainly used rule-based approaches or traditional machine learning for identifying social determinants of health.”
In an accompanying editorial, Ishanu Chattopadhyay, PhD, of the University of Chicago, said this suggests that unstructured clinical notes “may efficiently identify at-risk individuals even when structured data on the relevant variables are missing or incomplete.”
This work may provide “the foundation for addressing the key hurdles in enacting efficient universal assessment for suicide risk among the veterans and perhaps in the general population,” Dr. Chattopadhyay added.
This research was funded by a grant from the National Institute of Mental Health. The study authors and editorialist report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Researchers found SDOH are risk factors for suicide among U.S. veterans and NLP can be leveraged to extract SDOH information from unstructured data in the EHR.
“Since SDOH is overwhelmingly described in EHR notes, the importance of NLP-extracted SDOH can be very significant, meaning that NLP can be used as an effective method for epidemiological and public health study,” senior investigator Hong Yu, PhD, from Miner School of Information and Computer Sciences, University of Massachusetts Lowell, told this news organization.
Although the study was conducted among U.S. veterans, the results likely hold for the general population as well.
“The NLP methods are generalizable. The SDOH categories are generalizable. There may be some variations in terms of the strength of associations in NLP-extracted SDOH and suicide death, but the overall findings are generalizable,” Dr. Yu said.
The study was published online JAMA Network Open.
Improved risk assessment
SDOH, which include factors such as socioeconomic status, access to healthy food, education, housing, and physical environment, are strong predictors of suicidal behaviors.
Several studies have identified a range of common risk factors for suicide using International Classification of Diseases (ICD) codes and other “structured” data from the EHR. However, the use of unstructured EHR data from clinician notes has received little attention in investigating potential associations between suicide and SDOH.
Using the large Veterans Health Administration EHR system, the researchers determined associations between veterans’ death by suicide and recent SDOH, identified using both structured data (ICD-10 codes and Veterans Health Administration stop codes) and unstructured data (NLP-processed clinical notes).
Participants included 8,821 veterans who committed suicide and 35,284 matched controls. The cohort was mostly male (96%) and White (79%). The mean age was 58 years.
The NLP-extracted SDOH were social isolation, job or financial insecurity, housing instability, legal problems, violence, barriers to care, transition of care, and food insecurity.
All of these unstructured clinical notes on SDOH were significantly associated with increased risk for death by suicide.
Legal problems had the largest estimated effect size, more than twice the risk of those with no exposure (adjusted odds ratio 2.62; 95% confidence interval, 2.38-2.89), followed by violence (aOR, 2.34; 95% CI, 2.17-2.52) and social isolation (aOR, 1.94; 95% CI, 1.83-2.06).
Similarly, all of the structured SDOH – social or family problems, employment or financial problems, housing instability, legal problems, violence, and nonspecific psychosocial needs – also showed significant associations with increased risk for suicide death, once again, with legal problems linked to the highest risk (aOR, 2.63; 95% CI, 2.37-2.91).
When combining the structured and NLP-extracted unstructured data, the top three risk factors for death by suicide were legal problems (aOR, 2.66; 95% CI 2.46-2.89), violence (aOR, 2.12; 95% CI, 1.98-2.27), and nonspecific psychosocial needs (aOR, 2.07; 95% CI, 1.92-2.23).
“To our knowledge, this the first large-scale study to implement and use an NLP system to extract SDOH information from unstructured EHR data,” the researchers write.
“We strongly believe that analyzing all available SDOH information, including those contained in clinical notes, can help develop a better system for risk assessment and suicide prevention. However, more studies are required to investigate ways of seamlessly incorporating SDOHs into existing health care systems,” they conclude.
Dr. Yu said it’s also important to note that their NLP system is built upon “the most advanced deep-learning technologies and therefore is more generalizable than most existing work that mainly used rule-based approaches or traditional machine learning for identifying social determinants of health.”
In an accompanying editorial, Ishanu Chattopadhyay, PhD, of the University of Chicago, said this suggests that unstructured clinical notes “may efficiently identify at-risk individuals even when structured data on the relevant variables are missing or incomplete.”
This work may provide “the foundation for addressing the key hurdles in enacting efficient universal assessment for suicide risk among the veterans and perhaps in the general population,” Dr. Chattopadhyay added.
This research was funded by a grant from the National Institute of Mental Health. The study authors and editorialist report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM JAMA NETWORK OPEN
‘Harm avoidance’ temperament predicts depression in adults
Temperament has been defined as “an individual’s propensity to react emotionally, learn behavior and to form attachments without conscious effort by associative conditioning,” wrote Aleksi Ahola, PhD, of the University of Oulu, Finland, and colleagues. “Temperament is a potential endophenotype for depression, as it is inheritable and genetically linked with depression,” they said. The Temperament and Character Inventory (TCI) includes four temperament traits: harm avoidance (HA), novelty seeking (NS), reward dependence (RD), and persistence (P); previous studies have shown associations between higher HA and depression, but long-term data are limited, they wrote.
In a population-based study published in Comprehensive Psychiatry, the researchers followed 3,999 adults from age 31 to 54 years. The participants were part of the Northern Finland Birth Cohort 1966 Study.
The primary outcome was the onset of depression in a previously mentally healthy adult population. Temperament was assessed using the TCI, and depression was based on the Hopkins system checklist-25 (SCL-25). Individuals with previous psychiatric disorders related to depression, bipolar disorder, or psychosis were excluded. Effect size was measured using the Cohen’s d test.
Overall, 240 individuals were diagnosed with depression over the follow-up period. Women later diagnosed with depression had higher baseline TCI scores for HA, compared with those without depression. After controlling for multiple variables, higher TCI scores for HA, NS, and P were significantly associated with increased risk of any depression.
Among men, the TCI HA score was associated with significantly increased risk of any depression after adjustments, but no association appeared for other TCI scores. However, higher RD was associated with a reduced risk of psychotic depression in men (odds ratio, 0.79), although the study was not designed to assess psychotic depression, the researchers noted.
In an additional analysis of temperament cluster groups, shy and pessimistic traits were associated with depression in men (OR, 1.89), but not in women. In women, the cluster group with no specific extreme personality traits (cluster III) appeared to show an association with depression, which may be related to the association of NS and P with depression, the researchers wrote in their discussion.
The study is the first known to show differences between genders in the prediction of depression based on temperament traits, notably the link between high persistence and the onset of any depression in women, they said.
The study findings were limited by several factors including the potential for missed cases of less severe depression not reported in a national register, and by the relatively small number of men in the study, the researchers noted. In addition, the TCI’s three character traits of self-directedness, cooperativeness, and self-transcendence were not part of the current study, they said.
However, the results were strengthened by the large sample size, premorbid temperament assessment, and long follow-up period, although more research is needed in larger populations using real-world personalities to confirm the findings, they said.
“Research regarding temperament is important as it may have clinical significance as predictor of psychiatric morbidity and even suicide risk,” they said.
“Understanding those potentially at risk of depression could help in preventing the onset of the disease, and creating cluster profiles to match real-world personas could offer a clinical tool for this kind of prevention,” they concluded.
The study was supported by the University of Oulu, Oulu University Hospital, the Ministry of Health and Social Affairs, the National Institute for Health and Welfare, and the Regional Institute of Occupational Health. The researchers had no financial conflicts to disclose.
Temperament has been defined as “an individual’s propensity to react emotionally, learn behavior and to form attachments without conscious effort by associative conditioning,” wrote Aleksi Ahola, PhD, of the University of Oulu, Finland, and colleagues. “Temperament is a potential endophenotype for depression, as it is inheritable and genetically linked with depression,” they said. The Temperament and Character Inventory (TCI) includes four temperament traits: harm avoidance (HA), novelty seeking (NS), reward dependence (RD), and persistence (P); previous studies have shown associations between higher HA and depression, but long-term data are limited, they wrote.
In a population-based study published in Comprehensive Psychiatry, the researchers followed 3,999 adults from age 31 to 54 years. The participants were part of the Northern Finland Birth Cohort 1966 Study.
The primary outcome was the onset of depression in a previously mentally healthy adult population. Temperament was assessed using the TCI, and depression was based on the Hopkins system checklist-25 (SCL-25). Individuals with previous psychiatric disorders related to depression, bipolar disorder, or psychosis were excluded. Effect size was measured using the Cohen’s d test.
Overall, 240 individuals were diagnosed with depression over the follow-up period. Women later diagnosed with depression had higher baseline TCI scores for HA, compared with those without depression. After controlling for multiple variables, higher TCI scores for HA, NS, and P were significantly associated with increased risk of any depression.
Among men, the TCI HA score was associated with significantly increased risk of any depression after adjustments, but no association appeared for other TCI scores. However, higher RD was associated with a reduced risk of psychotic depression in men (odds ratio, 0.79), although the study was not designed to assess psychotic depression, the researchers noted.
In an additional analysis of temperament cluster groups, shy and pessimistic traits were associated with depression in men (OR, 1.89), but not in women. In women, the cluster group with no specific extreme personality traits (cluster III) appeared to show an association with depression, which may be related to the association of NS and P with depression, the researchers wrote in their discussion.
The study is the first known to show differences between genders in the prediction of depression based on temperament traits, notably the link between high persistence and the onset of any depression in women, they said.
The study findings were limited by several factors including the potential for missed cases of less severe depression not reported in a national register, and by the relatively small number of men in the study, the researchers noted. In addition, the TCI’s three character traits of self-directedness, cooperativeness, and self-transcendence were not part of the current study, they said.
However, the results were strengthened by the large sample size, premorbid temperament assessment, and long follow-up period, although more research is needed in larger populations using real-world personalities to confirm the findings, they said.
“Research regarding temperament is important as it may have clinical significance as predictor of psychiatric morbidity and even suicide risk,” they said.
“Understanding those potentially at risk of depression could help in preventing the onset of the disease, and creating cluster profiles to match real-world personas could offer a clinical tool for this kind of prevention,” they concluded.
The study was supported by the University of Oulu, Oulu University Hospital, the Ministry of Health and Social Affairs, the National Institute for Health and Welfare, and the Regional Institute of Occupational Health. The researchers had no financial conflicts to disclose.
Temperament has been defined as “an individual’s propensity to react emotionally, learn behavior and to form attachments without conscious effort by associative conditioning,” wrote Aleksi Ahola, PhD, of the University of Oulu, Finland, and colleagues. “Temperament is a potential endophenotype for depression, as it is inheritable and genetically linked with depression,” they said. The Temperament and Character Inventory (TCI) includes four temperament traits: harm avoidance (HA), novelty seeking (NS), reward dependence (RD), and persistence (P); previous studies have shown associations between higher HA and depression, but long-term data are limited, they wrote.
In a population-based study published in Comprehensive Psychiatry, the researchers followed 3,999 adults from age 31 to 54 years. The participants were part of the Northern Finland Birth Cohort 1966 Study.
The primary outcome was the onset of depression in a previously mentally healthy adult population. Temperament was assessed using the TCI, and depression was based on the Hopkins system checklist-25 (SCL-25). Individuals with previous psychiatric disorders related to depression, bipolar disorder, or psychosis were excluded. Effect size was measured using the Cohen’s d test.
Overall, 240 individuals were diagnosed with depression over the follow-up period. Women later diagnosed with depression had higher baseline TCI scores for HA, compared with those without depression. After controlling for multiple variables, higher TCI scores for HA, NS, and P were significantly associated with increased risk of any depression.
Among men, the TCI HA score was associated with significantly increased risk of any depression after adjustments, but no association appeared for other TCI scores. However, higher RD was associated with a reduced risk of psychotic depression in men (odds ratio, 0.79), although the study was not designed to assess psychotic depression, the researchers noted.
In an additional analysis of temperament cluster groups, shy and pessimistic traits were associated with depression in men (OR, 1.89), but not in women. In women, the cluster group with no specific extreme personality traits (cluster III) appeared to show an association with depression, which may be related to the association of NS and P with depression, the researchers wrote in their discussion.
The study is the first known to show differences between genders in the prediction of depression based on temperament traits, notably the link between high persistence and the onset of any depression in women, they said.
The study findings were limited by several factors including the potential for missed cases of less severe depression not reported in a national register, and by the relatively small number of men in the study, the researchers noted. In addition, the TCI’s three character traits of self-directedness, cooperativeness, and self-transcendence were not part of the current study, they said.
However, the results were strengthened by the large sample size, premorbid temperament assessment, and long follow-up period, although more research is needed in larger populations using real-world personalities to confirm the findings, they said.
“Research regarding temperament is important as it may have clinical significance as predictor of psychiatric morbidity and even suicide risk,” they said.
“Understanding those potentially at risk of depression could help in preventing the onset of the disease, and creating cluster profiles to match real-world personas could offer a clinical tool for this kind of prevention,” they concluded.
The study was supported by the University of Oulu, Oulu University Hospital, the Ministry of Health and Social Affairs, the National Institute for Health and Welfare, and the Regional Institute of Occupational Health. The researchers had no financial conflicts to disclose.
FROM COMPREHENSIVE PSYCHIATRY
Cultivating strength: Psychological well-being after nonfatal suicide attempts
A study of three separate nationally representative samples of nearly 9,000 U.S. military veterans found psychological well-being – defined in terms of having a high sense of purpose, social connectedness, and happiness – to be significantly diminished among veteran suicide attempt survivors relative to nonattempters, even decades after their last attempt.1

Despite the trend toward diminished well-being, many veterans who survived a suicide attempt reported average to optimal levels of well-being. Specifically, 52%-60% of veterans reporting a prior suicide attempt also reported experiencing as much purpose, social connection, and happiness as veterans without a suicide attempt history. Remarkably, a small subset (2-7%) of veteran attempt survivors even reported higher levels of well-being than veterans without a suicide attempt history.
Thus,
These data are notable because, in 2021, approximately 1.4 million U.S. adults made a nonfatal suicide attempt. Historically, suicide research has understandably emphasized the study of risk factors that increase the likelihood that someone dies by suicide. Given that a prior suicide attempt is among the top risk factors for suicide, virtually all research on suicide attempt survivors has focused on their elevated risk for future suicidality. Yet, 9 out of 10 people who have made a nonfatal suicide attempt do not go on to die by suicide. It is thus critical to investigate the quality of life of the millions of suicide attempt survivors.
To date, we know little about a question keenly important to suicide attempt survivors and their loved ones: What is the possibility of rebuilding a meaningful, high-quality life after a suicide attempt?
In addition to reporting on the prevalence of high levels of psychological well-being after a nonfatal suicide attempt, it is pivotal to investigate factors that may help facilitate this outcome. To that end, we identified personal characteristics associated with high levels of well-being. Notably, it was malleable psychological strengths such as optimism and a curious mindset, more than the mere absence of symptoms, that were linked to higher levels of well-being among veteran suicide attempt survivors.
Current suicide prevention interventions and treatments, which often focus on mitigating immediate suicide risk by treating symptoms, may be overlooking the importance of cultivating and building psychological strengths that may help promote greater well-being and enriched lives. Moreover, treatments that emphasize such strengths might be particularly fruitful in mitigating suicide risk in veterans, as veterans may be more receptive to prevention and treatment initiatives that embrace the cultivation and bolstering of strengths that are inherent in military culture and values, such as resilience and perseverance in the face of life challenges.2
One notable caveat to this study is that the data were cross-sectional, meaning they were collected at a single time point. As such, the authors cannot conclude that factors such as curiosity necessarily caused higher levels of well-being in veterans, as opposed to well-being causing higher levels of curiosity.
Similarly, while one can infer that psychological well-being was near-absent at the time of a suicide attempt, well-being of attempt survivors was not assessed before their attempt. Longitudinal studies that follow attempt survivors over time are needed to understand how well-being changes over time for suicide attempt survivors and the causal chain in what predicts that change.
Nevertheless, the results of this large, multicohort study serve as an important first step toward a more comprehensive view of prognosis after a suicide attempt. Just as the process that leads to a suicide attempt is complex, so too is the process of recovery after an attempt. While this study provides sound estimates of well-being outcomes and some possible candidates that might facilitate these outcomes, a critical next step for future research is to replicate and extend these findings. To do so, it is pivotal to extend the assessment scope beyond symptom-based measures and include measures of well-being.
Additionally, the investment in resources into longer-term examinations following suicide attempts is essential to understand different pathways toward achieving greater well-being. Providing hope is vital and potentially lifesaving, as one of the most common experiences reported before a suicide attempt is an unremitting sense of hopelessness. Continued research on well-being has the potential to impart a more balanced, nuanced prognosis after a suicide attempt that challenges perceptions of an invariably bleak prospect of recovery after suicidality.
Collectively, these results highlight the importance of broadening the scope of how the mental health field views and treats psychiatric difficulties to include a greater focus on recovery-based outcomes and personal strengths that help facilitate recovery from adverse life experiences such as suicide attempts.
People desire lives that they enjoy and find meaningful, and having a history of suicide attempts does not preclude the prospect of such a life. It is time that suicide research reflects the vast landscape of potential outcomes after a suicide attempt that goes beyond the prediction of future suicide risk.
Mr. Brown is a doctoral student of clinical psychology at the University of South Florida, Tampa. Dr. Rottenberg is director of the Mood and Emotion Lab and area director of the department of clinical psychology, University of South Florida.
References
1. Brown BA et al. Psychological well-being in US veterans with non-fatal suicide attempts: A multi-cohort population-based study. J Affect Disord. 2022 Oct 1;314:34-43. doi: 10.1016/j.jad.2022.07.003.
2. Bryan CJ et al. Understanding and preventing military suicide. Arch Suicide Res. 2012;16(2):95-110. doi: 10.1080/13811118.2012.667321.
A study of three separate nationally representative samples of nearly 9,000 U.S. military veterans found psychological well-being – defined in terms of having a high sense of purpose, social connectedness, and happiness – to be significantly diminished among veteran suicide attempt survivors relative to nonattempters, even decades after their last attempt.1
Despite the trend toward diminished well-being, many veterans who survived a suicide attempt reported average to optimal levels of well-being. Specifically, 52%-60% of veterans reporting a prior suicide attempt also reported experiencing as much purpose, social connection, and happiness as veterans without a suicide attempt history. Remarkably, a small subset (2-7%) of veteran attempt survivors even reported higher levels of well-being than veterans without a suicide attempt history.
Thus,
These data are notable because, in 2021, approximately 1.4 million U.S. adults made a nonfatal suicide attempt. Historically, suicide research has understandably emphasized the study of risk factors that increase the likelihood that someone dies by suicide. Given that a prior suicide attempt is among the top risk factors for suicide, virtually all research on suicide attempt survivors has focused on their elevated risk for future suicidality. Yet, 9 out of 10 people who have made a nonfatal suicide attempt do not go on to die by suicide. It is thus critical to investigate the quality of life of the millions of suicide attempt survivors.
To date, we know little about a question keenly important to suicide attempt survivors and their loved ones: What is the possibility of rebuilding a meaningful, high-quality life after a suicide attempt?
In addition to reporting on the prevalence of high levels of psychological well-being after a nonfatal suicide attempt, it is pivotal to investigate factors that may help facilitate this outcome. To that end, we identified personal characteristics associated with high levels of well-being. Notably, it was malleable psychological strengths such as optimism and a curious mindset, more than the mere absence of symptoms, that were linked to higher levels of well-being among veteran suicide attempt survivors.
Current suicide prevention interventions and treatments, which often focus on mitigating immediate suicide risk by treating symptoms, may be overlooking the importance of cultivating and building psychological strengths that may help promote greater well-being and enriched lives. Moreover, treatments that emphasize such strengths might be particularly fruitful in mitigating suicide risk in veterans, as veterans may be more receptive to prevention and treatment initiatives that embrace the cultivation and bolstering of strengths that are inherent in military culture and values, such as resilience and perseverance in the face of life challenges.2
One notable caveat to this study is that the data were cross-sectional, meaning they were collected at a single time point. As such, the authors cannot conclude that factors such as curiosity necessarily caused higher levels of well-being in veterans, as opposed to well-being causing higher levels of curiosity.
Similarly, while one can infer that psychological well-being was near-absent at the time of a suicide attempt, well-being of attempt survivors was not assessed before their attempt. Longitudinal studies that follow attempt survivors over time are needed to understand how well-being changes over time for suicide attempt survivors and the causal chain in what predicts that change.
Nevertheless, the results of this large, multicohort study serve as an important first step toward a more comprehensive view of prognosis after a suicide attempt. Just as the process that leads to a suicide attempt is complex, so too is the process of recovery after an attempt. While this study provides sound estimates of well-being outcomes and some possible candidates that might facilitate these outcomes, a critical next step for future research is to replicate and extend these findings. To do so, it is pivotal to extend the assessment scope beyond symptom-based measures and include measures of well-being.
Additionally, the investment in resources into longer-term examinations following suicide attempts is essential to understand different pathways toward achieving greater well-being. Providing hope is vital and potentially lifesaving, as one of the most common experiences reported before a suicide attempt is an unremitting sense of hopelessness. Continued research on well-being has the potential to impart a more balanced, nuanced prognosis after a suicide attempt that challenges perceptions of an invariably bleak prospect of recovery after suicidality.
Collectively, these results highlight the importance of broadening the scope of how the mental health field views and treats psychiatric difficulties to include a greater focus on recovery-based outcomes and personal strengths that help facilitate recovery from adverse life experiences such as suicide attempts.
People desire lives that they enjoy and find meaningful, and having a history of suicide attempts does not preclude the prospect of such a life. It is time that suicide research reflects the vast landscape of potential outcomes after a suicide attempt that goes beyond the prediction of future suicide risk.
Mr. Brown is a doctoral student of clinical psychology at the University of South Florida, Tampa. Dr. Rottenberg is director of the Mood and Emotion Lab and area director of the department of clinical psychology, University of South Florida.
References
1. Brown BA et al. Psychological well-being in US veterans with non-fatal suicide attempts: A multi-cohort population-based study. J Affect Disord. 2022 Oct 1;314:34-43. doi: 10.1016/j.jad.2022.07.003.
2. Bryan CJ et al. Understanding and preventing military suicide. Arch Suicide Res. 2012;16(2):95-110. doi: 10.1080/13811118.2012.667321.
A study of three separate nationally representative samples of nearly 9,000 U.S. military veterans found psychological well-being – defined in terms of having a high sense of purpose, social connectedness, and happiness – to be significantly diminished among veteran suicide attempt survivors relative to nonattempters, even decades after their last attempt.1
Despite the trend toward diminished well-being, many veterans who survived a suicide attempt reported average to optimal levels of well-being. Specifically, 52%-60% of veterans reporting a prior suicide attempt also reported experiencing as much purpose, social connection, and happiness as veterans without a suicide attempt history. Remarkably, a small subset (2-7%) of veteran attempt survivors even reported higher levels of well-being than veterans without a suicide attempt history.
Thus,
These data are notable because, in 2021, approximately 1.4 million U.S. adults made a nonfatal suicide attempt. Historically, suicide research has understandably emphasized the study of risk factors that increase the likelihood that someone dies by suicide. Given that a prior suicide attempt is among the top risk factors for suicide, virtually all research on suicide attempt survivors has focused on their elevated risk for future suicidality. Yet, 9 out of 10 people who have made a nonfatal suicide attempt do not go on to die by suicide. It is thus critical to investigate the quality of life of the millions of suicide attempt survivors.
To date, we know little about a question keenly important to suicide attempt survivors and their loved ones: What is the possibility of rebuilding a meaningful, high-quality life after a suicide attempt?
In addition to reporting on the prevalence of high levels of psychological well-being after a nonfatal suicide attempt, it is pivotal to investigate factors that may help facilitate this outcome. To that end, we identified personal characteristics associated with high levels of well-being. Notably, it was malleable psychological strengths such as optimism and a curious mindset, more than the mere absence of symptoms, that were linked to higher levels of well-being among veteran suicide attempt survivors.
Current suicide prevention interventions and treatments, which often focus on mitigating immediate suicide risk by treating symptoms, may be overlooking the importance of cultivating and building psychological strengths that may help promote greater well-being and enriched lives. Moreover, treatments that emphasize such strengths might be particularly fruitful in mitigating suicide risk in veterans, as veterans may be more receptive to prevention and treatment initiatives that embrace the cultivation and bolstering of strengths that are inherent in military culture and values, such as resilience and perseverance in the face of life challenges.2
One notable caveat to this study is that the data were cross-sectional, meaning they were collected at a single time point. As such, the authors cannot conclude that factors such as curiosity necessarily caused higher levels of well-being in veterans, as opposed to well-being causing higher levels of curiosity.
Similarly, while one can infer that psychological well-being was near-absent at the time of a suicide attempt, well-being of attempt survivors was not assessed before their attempt. Longitudinal studies that follow attempt survivors over time are needed to understand how well-being changes over time for suicide attempt survivors and the causal chain in what predicts that change.
Nevertheless, the results of this large, multicohort study serve as an important first step toward a more comprehensive view of prognosis after a suicide attempt. Just as the process that leads to a suicide attempt is complex, so too is the process of recovery after an attempt. While this study provides sound estimates of well-being outcomes and some possible candidates that might facilitate these outcomes, a critical next step for future research is to replicate and extend these findings. To do so, it is pivotal to extend the assessment scope beyond symptom-based measures and include measures of well-being.
Additionally, the investment in resources into longer-term examinations following suicide attempts is essential to understand different pathways toward achieving greater well-being. Providing hope is vital and potentially lifesaving, as one of the most common experiences reported before a suicide attempt is an unremitting sense of hopelessness. Continued research on well-being has the potential to impart a more balanced, nuanced prognosis after a suicide attempt that challenges perceptions of an invariably bleak prospect of recovery after suicidality.
Collectively, these results highlight the importance of broadening the scope of how the mental health field views and treats psychiatric difficulties to include a greater focus on recovery-based outcomes and personal strengths that help facilitate recovery from adverse life experiences such as suicide attempts.
People desire lives that they enjoy and find meaningful, and having a history of suicide attempts does not preclude the prospect of such a life. It is time that suicide research reflects the vast landscape of potential outcomes after a suicide attempt that goes beyond the prediction of future suicide risk.
Mr. Brown is a doctoral student of clinical psychology at the University of South Florida, Tampa. Dr. Rottenberg is director of the Mood and Emotion Lab and area director of the department of clinical psychology, University of South Florida.
References
1. Brown BA et al. Psychological well-being in US veterans with non-fatal suicide attempts: A multi-cohort population-based study. J Affect Disord. 2022 Oct 1;314:34-43. doi: 10.1016/j.jad.2022.07.003.
2. Bryan CJ et al. Understanding and preventing military suicide. Arch Suicide Res. 2012;16(2):95-110. doi: 10.1080/13811118.2012.667321.
Antioxidants may ease anxiety and depression
The prevalence of anxiety and depression has increased worldwide, especially in the wake of the COVID-19 pandemic. “Therefore, identifying specific interventions that improve depressive status is critical for public health policy,” wrote Huan Wang, MD, of First Hospital of Jilin University, Changchun, China, and colleagues.
Recent evidence suggests that modifiable lifestyle factors, including nutrition, may have a positive impact on symptoms of anxiety and depression, and observational studies have shown that antioxidant supplements affect depressive status, but data from randomized, controlled trials are limited by small sample sizes, they wrote.
In a study published in the Journal of Affective Disorders, the researchers conducted a meta-analysis of 52 studies with a total of 4,049 patients. Of these, 2,004 received antioxidant supplements and 2,045 received a placebo supplement or no supplements. The median treatment duration was 11 weeks; treatment durations ranged from 2 weeks to 2 years. All 52 studies addressed the effect of antioxidants on depressive status, and 21 studies also assessed anxiety status. The studies used a range of depression scales, including the Beck Depression Inventory, the Edinburgh Postnatal Depression Scale, Montgomery-Asberg Depression Rating Scale, Hamilton Depression Rating Scale, Center for Epidemiologic Studies–Depression, and Hospital Anxiety and Depression Scale.
Overall, the meta-analysis revealed a statistically significant improvement in depressive status associated with antioxidant supplement use (standardized mean difference, 0.60; P < .00001). When broken down by supplement, significant positive effects appeared for magnesium (SMD = 0.16; P = .03), zinc (SMD = 0.59; P = .01), selenium (SMD = 0.33; P = .009), CoQ10 (SMD = 0.97; P = .05), tea and coffee (SMD = 1.15; P = .001) and crocin (MD = 6.04; P < .00001).
As a secondary outcome, antioxidant supplementation had a significantly positive effect on anxiety (SMD = 0.40; P < .00001).
The mechanism of action for the effect of antioxidants remains unclear, the researchers wrote in their discussion, but, “Depriving or boosting the supply of food components with antioxidant capabilities might worsen or lessen oxidative stress,” they said.
The researchers attempted a subgroup analysis across countries, and found that, while antioxidant supplementation improved depressive status in populations from Iran, China, and Italy, “no significant improvement was found in the United States, Australia, Italy and other countries.” The reasons for this difference might be related to fewer studies from these countries, or “the improvement brought about by antioxidants might be particularly pronounced in people with significant depression and higher depression scores,” they wrote. “Studies have shown that Asian countries have fewer psychiatrists and more expensive treatments,” they added.
The findings were limited by several factors including the inability to include all types of antioxidant supplements, the range of depression rating scales, and insufficient subgroup analysis of the range of populations from the included studies, the researchers noted.
“Additional data from large clinical trials are needed to confirm the efficacy and safety of antioxidant supplements in improving depressive status,” they said. However, the results suggest that antioxidants may play a role as an adjunct treatment to conventional antidepressants, they concluded.
The study was funded by the National Natural Science Foundation of China. The researchers had no financial conflicts to disclose.
The prevalence of anxiety and depression has increased worldwide, especially in the wake of the COVID-19 pandemic. “Therefore, identifying specific interventions that improve depressive status is critical for public health policy,” wrote Huan Wang, MD, of First Hospital of Jilin University, Changchun, China, and colleagues.
Recent evidence suggests that modifiable lifestyle factors, including nutrition, may have a positive impact on symptoms of anxiety and depression, and observational studies have shown that antioxidant supplements affect depressive status, but data from randomized, controlled trials are limited by small sample sizes, they wrote.
In a study published in the Journal of Affective Disorders, the researchers conducted a meta-analysis of 52 studies with a total of 4,049 patients. Of these, 2,004 received antioxidant supplements and 2,045 received a placebo supplement or no supplements. The median treatment duration was 11 weeks; treatment durations ranged from 2 weeks to 2 years. All 52 studies addressed the effect of antioxidants on depressive status, and 21 studies also assessed anxiety status. The studies used a range of depression scales, including the Beck Depression Inventory, the Edinburgh Postnatal Depression Scale, Montgomery-Asberg Depression Rating Scale, Hamilton Depression Rating Scale, Center for Epidemiologic Studies–Depression, and Hospital Anxiety and Depression Scale.
Overall, the meta-analysis revealed a statistically significant improvement in depressive status associated with antioxidant supplement use (standardized mean difference, 0.60; P < .00001). When broken down by supplement, significant positive effects appeared for magnesium (SMD = 0.16; P = .03), zinc (SMD = 0.59; P = .01), selenium (SMD = 0.33; P = .009), CoQ10 (SMD = 0.97; P = .05), tea and coffee (SMD = 1.15; P = .001) and crocin (MD = 6.04; P < .00001).
As a secondary outcome, antioxidant supplementation had a significantly positive effect on anxiety (SMD = 0.40; P < .00001).
The mechanism of action for the effect of antioxidants remains unclear, the researchers wrote in their discussion, but, “Depriving or boosting the supply of food components with antioxidant capabilities might worsen or lessen oxidative stress,” they said.
The researchers attempted a subgroup analysis across countries, and found that, while antioxidant supplementation improved depressive status in populations from Iran, China, and Italy, “no significant improvement was found in the United States, Australia, Italy and other countries.” The reasons for this difference might be related to fewer studies from these countries, or “the improvement brought about by antioxidants might be particularly pronounced in people with significant depression and higher depression scores,” they wrote. “Studies have shown that Asian countries have fewer psychiatrists and more expensive treatments,” they added.
The findings were limited by several factors including the inability to include all types of antioxidant supplements, the range of depression rating scales, and insufficient subgroup analysis of the range of populations from the included studies, the researchers noted.
“Additional data from large clinical trials are needed to confirm the efficacy and safety of antioxidant supplements in improving depressive status,” they said. However, the results suggest that antioxidants may play a role as an adjunct treatment to conventional antidepressants, they concluded.
The study was funded by the National Natural Science Foundation of China. The researchers had no financial conflicts to disclose.
The prevalence of anxiety and depression has increased worldwide, especially in the wake of the COVID-19 pandemic. “Therefore, identifying specific interventions that improve depressive status is critical for public health policy,” wrote Huan Wang, MD, of First Hospital of Jilin University, Changchun, China, and colleagues.
Recent evidence suggests that modifiable lifestyle factors, including nutrition, may have a positive impact on symptoms of anxiety and depression, and observational studies have shown that antioxidant supplements affect depressive status, but data from randomized, controlled trials are limited by small sample sizes, they wrote.
In a study published in the Journal of Affective Disorders, the researchers conducted a meta-analysis of 52 studies with a total of 4,049 patients. Of these, 2,004 received antioxidant supplements and 2,045 received a placebo supplement or no supplements. The median treatment duration was 11 weeks; treatment durations ranged from 2 weeks to 2 years. All 52 studies addressed the effect of antioxidants on depressive status, and 21 studies also assessed anxiety status. The studies used a range of depression scales, including the Beck Depression Inventory, the Edinburgh Postnatal Depression Scale, Montgomery-Asberg Depression Rating Scale, Hamilton Depression Rating Scale, Center for Epidemiologic Studies–Depression, and Hospital Anxiety and Depression Scale.
Overall, the meta-analysis revealed a statistically significant improvement in depressive status associated with antioxidant supplement use (standardized mean difference, 0.60; P < .00001). When broken down by supplement, significant positive effects appeared for magnesium (SMD = 0.16; P = .03), zinc (SMD = 0.59; P = .01), selenium (SMD = 0.33; P = .009), CoQ10 (SMD = 0.97; P = .05), tea and coffee (SMD = 1.15; P = .001) and crocin (MD = 6.04; P < .00001).
As a secondary outcome, antioxidant supplementation had a significantly positive effect on anxiety (SMD = 0.40; P < .00001).
The mechanism of action for the effect of antioxidants remains unclear, the researchers wrote in their discussion, but, “Depriving or boosting the supply of food components with antioxidant capabilities might worsen or lessen oxidative stress,” they said.
The researchers attempted a subgroup analysis across countries, and found that, while antioxidant supplementation improved depressive status in populations from Iran, China, and Italy, “no significant improvement was found in the United States, Australia, Italy and other countries.” The reasons for this difference might be related to fewer studies from these countries, or “the improvement brought about by antioxidants might be particularly pronounced in people with significant depression and higher depression scores,” they wrote. “Studies have shown that Asian countries have fewer psychiatrists and more expensive treatments,” they added.
The findings were limited by several factors including the inability to include all types of antioxidant supplements, the range of depression rating scales, and insufficient subgroup analysis of the range of populations from the included studies, the researchers noted.
“Additional data from large clinical trials are needed to confirm the efficacy and safety of antioxidant supplements in improving depressive status,” they said. However, the results suggest that antioxidants may play a role as an adjunct treatment to conventional antidepressants, they concluded.
The study was funded by the National Natural Science Foundation of China. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF AFFECTIVE DISORDERS
New data on IV ketamine for resistant depression in the elderly
NEW ORLEANS –
“These were patients with depression who had not responded even to intensive therapies or procedures, and we found that after a 6-week ketamine infusion regimen, there was no difference in the response to the treatment between the treatment-resistant geriatric and nongeriatric patients,” study investigator Jonathan Kim, of Emory University, Atlanta, the first author of one of two studies presented as part of the American Association for Geriatric Psychiatry annual meeting, said in an interview.
The findings are important because research on the effects of IV ketamine have not been well documented in geriatric patients, who have high rates of depression and TRD.
“There is a lack of data on IV ketamine in older adults with treatment-resistant depression, and there are some safety and tolerability concerns which may lead some older adults and their clinicians to be reluctant to pursue IV ketamine treatment,” study coinvestigator Hanadi Ajam Oughli, MD, a health sciences assistant clinical professor in the department of psychiatry and biobehavioral sciences, University of California, Los Angeles, told this news organization.
Nasal vs. IV administration
Ketamine has traditionally been used as an anesthetic that blocks N-methyl-D-aspartate (NMDA) glutamate receptors, Dr. Oughli and colleagues note.
In the treatment of TRD, an infusion of 0.5 mg/kg is typically administered over 40 minutes, producing a rapid antidepressant response. Recent research shows the drug reduces suicidality and improves mood and quality of life.
A more recent intranasal formulation of ketamine, esketamine, was approved by the U.S. Food and Drug Administration for TRD in 2019, and some experts questioned its path to approval. In addition, the drug’s high cost and poor bioavailability in comparison with IV ketamine remains an issue, said Dr. Oughli.
In the previous TRANSFORM-3 study, a placebo-controlled randomized trial, there was no difference between esketamine, used in conjunction with an antidepressant, and placebo for geriatric patients.
To better understand the effects of IV ketamine in this patient population, Mr. Kim’s team conducted a retrospective chart review of 91 older patients with TRD who received IV ketamine treatment between October 2016 and August 2022.
Patients were divided into two groups – those older than 60 years (n = 36; 44% women; mean age, 68.86) and those younger than 60 (n = 55; 49% women; mean age, 41.05). Participants in each age group received six ketamine infusions over 6 weeks.
Results showed that with regard to depression severity, as assessed using Beck Depression Inventory (BDI-II) scores, 27.8% of patients in the geriatric group had a 50% or greater improvement, vs. 25.4% of those younger than 60.
The average BDI-II scores represented a significant improvement for both groups (P < .01), and the difference in scores between the groups was not statistically significant (P = .973).
“It is important to note that our study was conducted in a real-world clinical setting with a treatment-resistant population; other clinical studies may not have such sick patients in their trials. Additional studies are therefore warranted to establish further treatment guidelines in this area,” Mr. Kim said.
Open-label trial results
In the second study, Dr. Oughli and colleagues evaluated additional key outcomes in geriatric patients treated with IV ketamine as part of a larger open-label late-life trial on TRD.
The secondary analysis of the trial focused on 23 patients (mean age, 71.5 years) who had been initially treated with twice-a-week IV ketamine for 4 weeks.
After the first 4 weeks, patients who had experienced a partial response received an additional 4 weeks of once-weekly IV ketamine.
Overall, 48% of participants achieved a response, and 24% achieved remission of depressive symptoms following the first 4 weeks of twice-weekly treatment. This effect was maintained during the continuation phase of the study.
These findings are consistent with research in younger adults and demonstrate that twice-weekly infusions yield a more sustained antidepressant response than once-weekly infusions, the authors note.
The analysis also showed important increases in psychological well-being scores on the Scale for Suicidal Ideation, improved sleep quality as measured by the Pittsburgh Sleep Quality Index, and overall psychological well-being as shown on the NIH Toolbox Positive Affect on happiness/contentment and the NIH Toolbox General Life Satisfaction scales.
In a previous analysis, published in The American Journal of Geriatric Psychiatry, the researchers also evaluated cognitive function using the NIH Cognitive Battery, which showed that geriatric patients with TRD had significant improvements in a composite of executive functioning and fluid cognition during the 4-week acute treatment period of twice-weekly IV ketamine infusions (Cohen’s d = 0.61) and that those improvements were sustained in the continuation phase of once-weekly infusions for 4 more weeks.
Those results are consistent with ketamine’s known potential procognitive effects in TRD, due to a putative antidepressant mechanism that rescues prefrontal circuit dysfunction through synaptogenesis, the researchers note.
Dr. Oughli said that in both analyses, patients tolerated ketamine well, and there were no serious adverse events.
“Adverse events, including hypertension, dissociated effects, and cravings, were rare and did not prevent the continued use of IV ketamine by older adults. We were able to use clonidine to help manage blood pressure changes seen during the infusions,” she noted.
“These findings are very promising and will need to be confirmed and extended in a larger randomized controlled trial.”
Unsettling for some older patients
George T. Grossberg, MD, director, geriatric psychiatry, Saint Louis University, noted that in his experience, IV ketamine treatment can be unsettling for some older geriatric patients, such as those in their 80s.
“Particularly with some of my older patients, the kind of psychotomimetic properties of ketamine and the out-of-body experiences [with the initial treatment] can be frightening,” he said. “They may be willing to try, but I’ve had more than one patient quit after one treatment because they became so frightened.”
However, the dire nature of TRD and failure to respond to multiple medications and combinations and other strategies may prompt patients to try ketamine as a measure with at least some potential, he noted.
“But there is a high bar for acceptance, especially on the part of older adults and their families, more than for younger people,” he said.
The investigators have disclosed no relevant financial relationships. Dr. Grossberg has received consulting fees from Acadia, Avanir, Biogen, BioXcel, Genentech, Karuna, Lundbeck, Otsuka, Roche, and Takeda.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
“These were patients with depression who had not responded even to intensive therapies or procedures, and we found that after a 6-week ketamine infusion regimen, there was no difference in the response to the treatment between the treatment-resistant geriatric and nongeriatric patients,” study investigator Jonathan Kim, of Emory University, Atlanta, the first author of one of two studies presented as part of the American Association for Geriatric Psychiatry annual meeting, said in an interview.
The findings are important because research on the effects of IV ketamine have not been well documented in geriatric patients, who have high rates of depression and TRD.
“There is a lack of data on IV ketamine in older adults with treatment-resistant depression, and there are some safety and tolerability concerns which may lead some older adults and their clinicians to be reluctant to pursue IV ketamine treatment,” study coinvestigator Hanadi Ajam Oughli, MD, a health sciences assistant clinical professor in the department of psychiatry and biobehavioral sciences, University of California, Los Angeles, told this news organization.
Nasal vs. IV administration
Ketamine has traditionally been used as an anesthetic that blocks N-methyl-D-aspartate (NMDA) glutamate receptors, Dr. Oughli and colleagues note.
In the treatment of TRD, an infusion of 0.5 mg/kg is typically administered over 40 minutes, producing a rapid antidepressant response. Recent research shows the drug reduces suicidality and improves mood and quality of life.
A more recent intranasal formulation of ketamine, esketamine, was approved by the U.S. Food and Drug Administration for TRD in 2019, and some experts questioned its path to approval. In addition, the drug’s high cost and poor bioavailability in comparison with IV ketamine remains an issue, said Dr. Oughli.
In the previous TRANSFORM-3 study, a placebo-controlled randomized trial, there was no difference between esketamine, used in conjunction with an antidepressant, and placebo for geriatric patients.
To better understand the effects of IV ketamine in this patient population, Mr. Kim’s team conducted a retrospective chart review of 91 older patients with TRD who received IV ketamine treatment between October 2016 and August 2022.
Patients were divided into two groups – those older than 60 years (n = 36; 44% women; mean age, 68.86) and those younger than 60 (n = 55; 49% women; mean age, 41.05). Participants in each age group received six ketamine infusions over 6 weeks.
Results showed that with regard to depression severity, as assessed using Beck Depression Inventory (BDI-II) scores, 27.8% of patients in the geriatric group had a 50% or greater improvement, vs. 25.4% of those younger than 60.
The average BDI-II scores represented a significant improvement for both groups (P < .01), and the difference in scores between the groups was not statistically significant (P = .973).
“It is important to note that our study was conducted in a real-world clinical setting with a treatment-resistant population; other clinical studies may not have such sick patients in their trials. Additional studies are therefore warranted to establish further treatment guidelines in this area,” Mr. Kim said.
Open-label trial results
In the second study, Dr. Oughli and colleagues evaluated additional key outcomes in geriatric patients treated with IV ketamine as part of a larger open-label late-life trial on TRD.
The secondary analysis of the trial focused on 23 patients (mean age, 71.5 years) who had been initially treated with twice-a-week IV ketamine for 4 weeks.
After the first 4 weeks, patients who had experienced a partial response received an additional 4 weeks of once-weekly IV ketamine.
Overall, 48% of participants achieved a response, and 24% achieved remission of depressive symptoms following the first 4 weeks of twice-weekly treatment. This effect was maintained during the continuation phase of the study.
These findings are consistent with research in younger adults and demonstrate that twice-weekly infusions yield a more sustained antidepressant response than once-weekly infusions, the authors note.
The analysis also showed important increases in psychological well-being scores on the Scale for Suicidal Ideation, improved sleep quality as measured by the Pittsburgh Sleep Quality Index, and overall psychological well-being as shown on the NIH Toolbox Positive Affect on happiness/contentment and the NIH Toolbox General Life Satisfaction scales.
In a previous analysis, published in The American Journal of Geriatric Psychiatry, the researchers also evaluated cognitive function using the NIH Cognitive Battery, which showed that geriatric patients with TRD had significant improvements in a composite of executive functioning and fluid cognition during the 4-week acute treatment period of twice-weekly IV ketamine infusions (Cohen’s d = 0.61) and that those improvements were sustained in the continuation phase of once-weekly infusions for 4 more weeks.
Those results are consistent with ketamine’s known potential procognitive effects in TRD, due to a putative antidepressant mechanism that rescues prefrontal circuit dysfunction through synaptogenesis, the researchers note.
Dr. Oughli said that in both analyses, patients tolerated ketamine well, and there were no serious adverse events.
“Adverse events, including hypertension, dissociated effects, and cravings, were rare and did not prevent the continued use of IV ketamine by older adults. We were able to use clonidine to help manage blood pressure changes seen during the infusions,” she noted.
“These findings are very promising and will need to be confirmed and extended in a larger randomized controlled trial.”
Unsettling for some older patients
George T. Grossberg, MD, director, geriatric psychiatry, Saint Louis University, noted that in his experience, IV ketamine treatment can be unsettling for some older geriatric patients, such as those in their 80s.
“Particularly with some of my older patients, the kind of psychotomimetic properties of ketamine and the out-of-body experiences [with the initial treatment] can be frightening,” he said. “They may be willing to try, but I’ve had more than one patient quit after one treatment because they became so frightened.”
However, the dire nature of TRD and failure to respond to multiple medications and combinations and other strategies may prompt patients to try ketamine as a measure with at least some potential, he noted.
“But there is a high bar for acceptance, especially on the part of older adults and their families, more than for younger people,” he said.
The investigators have disclosed no relevant financial relationships. Dr. Grossberg has received consulting fees from Acadia, Avanir, Biogen, BioXcel, Genentech, Karuna, Lundbeck, Otsuka, Roche, and Takeda.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
“These were patients with depression who had not responded even to intensive therapies or procedures, and we found that after a 6-week ketamine infusion regimen, there was no difference in the response to the treatment between the treatment-resistant geriatric and nongeriatric patients,” study investigator Jonathan Kim, of Emory University, Atlanta, the first author of one of two studies presented as part of the American Association for Geriatric Psychiatry annual meeting, said in an interview.
The findings are important because research on the effects of IV ketamine have not been well documented in geriatric patients, who have high rates of depression and TRD.
“There is a lack of data on IV ketamine in older adults with treatment-resistant depression, and there are some safety and tolerability concerns which may lead some older adults and their clinicians to be reluctant to pursue IV ketamine treatment,” study coinvestigator Hanadi Ajam Oughli, MD, a health sciences assistant clinical professor in the department of psychiatry and biobehavioral sciences, University of California, Los Angeles, told this news organization.
Nasal vs. IV administration
Ketamine has traditionally been used as an anesthetic that blocks N-methyl-D-aspartate (NMDA) glutamate receptors, Dr. Oughli and colleagues note.
In the treatment of TRD, an infusion of 0.5 mg/kg is typically administered over 40 minutes, producing a rapid antidepressant response. Recent research shows the drug reduces suicidality and improves mood and quality of life.
A more recent intranasal formulation of ketamine, esketamine, was approved by the U.S. Food and Drug Administration for TRD in 2019, and some experts questioned its path to approval. In addition, the drug’s high cost and poor bioavailability in comparison with IV ketamine remains an issue, said Dr. Oughli.
In the previous TRANSFORM-3 study, a placebo-controlled randomized trial, there was no difference between esketamine, used in conjunction with an antidepressant, and placebo for geriatric patients.
To better understand the effects of IV ketamine in this patient population, Mr. Kim’s team conducted a retrospective chart review of 91 older patients with TRD who received IV ketamine treatment between October 2016 and August 2022.
Patients were divided into two groups – those older than 60 years (n = 36; 44% women; mean age, 68.86) and those younger than 60 (n = 55; 49% women; mean age, 41.05). Participants in each age group received six ketamine infusions over 6 weeks.
Results showed that with regard to depression severity, as assessed using Beck Depression Inventory (BDI-II) scores, 27.8% of patients in the geriatric group had a 50% or greater improvement, vs. 25.4% of those younger than 60.
The average BDI-II scores represented a significant improvement for both groups (P < .01), and the difference in scores between the groups was not statistically significant (P = .973).
“It is important to note that our study was conducted in a real-world clinical setting with a treatment-resistant population; other clinical studies may not have such sick patients in their trials. Additional studies are therefore warranted to establish further treatment guidelines in this area,” Mr. Kim said.
Open-label trial results
In the second study, Dr. Oughli and colleagues evaluated additional key outcomes in geriatric patients treated with IV ketamine as part of a larger open-label late-life trial on TRD.
The secondary analysis of the trial focused on 23 patients (mean age, 71.5 years) who had been initially treated with twice-a-week IV ketamine for 4 weeks.
After the first 4 weeks, patients who had experienced a partial response received an additional 4 weeks of once-weekly IV ketamine.
Overall, 48% of participants achieved a response, and 24% achieved remission of depressive symptoms following the first 4 weeks of twice-weekly treatment. This effect was maintained during the continuation phase of the study.
These findings are consistent with research in younger adults and demonstrate that twice-weekly infusions yield a more sustained antidepressant response than once-weekly infusions, the authors note.
The analysis also showed important increases in psychological well-being scores on the Scale for Suicidal Ideation, improved sleep quality as measured by the Pittsburgh Sleep Quality Index, and overall psychological well-being as shown on the NIH Toolbox Positive Affect on happiness/contentment and the NIH Toolbox General Life Satisfaction scales.
In a previous analysis, published in The American Journal of Geriatric Psychiatry, the researchers also evaluated cognitive function using the NIH Cognitive Battery, which showed that geriatric patients with TRD had significant improvements in a composite of executive functioning and fluid cognition during the 4-week acute treatment period of twice-weekly IV ketamine infusions (Cohen’s d = 0.61) and that those improvements were sustained in the continuation phase of once-weekly infusions for 4 more weeks.
Those results are consistent with ketamine’s known potential procognitive effects in TRD, due to a putative antidepressant mechanism that rescues prefrontal circuit dysfunction through synaptogenesis, the researchers note.
Dr. Oughli said that in both analyses, patients tolerated ketamine well, and there were no serious adverse events.
“Adverse events, including hypertension, dissociated effects, and cravings, were rare and did not prevent the continued use of IV ketamine by older adults. We were able to use clonidine to help manage blood pressure changes seen during the infusions,” she noted.
“These findings are very promising and will need to be confirmed and extended in a larger randomized controlled trial.”
Unsettling for some older patients
George T. Grossberg, MD, director, geriatric psychiatry, Saint Louis University, noted that in his experience, IV ketamine treatment can be unsettling for some older geriatric patients, such as those in their 80s.
“Particularly with some of my older patients, the kind of psychotomimetic properties of ketamine and the out-of-body experiences [with the initial treatment] can be frightening,” he said. “They may be willing to try, but I’ve had more than one patient quit after one treatment because they became so frightened.”
However, the dire nature of TRD and failure to respond to multiple medications and combinations and other strategies may prompt patients to try ketamine as a measure with at least some potential, he noted.
“But there is a high bar for acceptance, especially on the part of older adults and their families, more than for younger people,” he said.
The investigators have disclosed no relevant financial relationships. Dr. Grossberg has received consulting fees from Acadia, Avanir, Biogen, BioXcel, Genentech, Karuna, Lundbeck, Otsuka, Roche, and Takeda.
A version of this article first appeared on Medscape.com.
AT AAGP 2023
Add-on antipsychotic beats switching meds in older adults with resistant depression
NEW ORLEANS –
“We found that adding aripiprazole led to higher rates of depression remission and greater improvements in psychological well-being – which means how positive and satisfied patients felt – and this is good news,” study investigator Eric J. Lenze, MD, of the department of psychiatry, Washington University, St. Louis, said in a press statement.

“However, even that approach helped only about 30% of people in the study with treatment-resistant depression, underscoring the need to find and develop more effective treatments that can help more people,” he added.
The findings were presented here as part of the American Association for Geriatric Psychiatry annual meeting, and published concurrently in the New England Journal of Medicine.
Need for safe treatment options
Treatment-resistant depression is common in older patients, but switching medications or adding other agents can be challenging. With higher rates of comorbidity and polypharmacy, treatment decisions in this patient population are more complex compared with those involving younger patients.
To compare the benefits of augmentation vs. drug-switching strategies, the researchers conducted a multicenter, two-step trial involving 619 patients with an average baseline age of 69 who had failed to respond to two courses of selective serotonin reuptake inhibitors (SSRIs).
Patients were randomly assigned to one of three groups. These included augmentation of existing antidepressant medication with either aripiprazole (n = 211) or the dopamine and norepinephrine–reuptake inhibitor bupropion (Wellbutrin, Zyban) (n = 206), or to taper off of their current antidepressant and switch to bupropion (n = 202).
After 10 weeks, patients’ psychological well-being was assessed via the National Institutes of Health Toolbox Positive Affect and General Life Satisfaction subscales. The researchers found patients in the aripiprazole and bupropion add-on groups improved by 4.83 points and 4.33 points, respectively. The bupropion switch group had a change of 2.04 points.
The difference between the aripiprazole augmentation group and the switch to bupropion group was significant (difference 2.79 points; P = .014). Other between-group differences were not significantly different.
Remission rates were similar in the aripiprazole and bupropion groups at 28.9% and 28.2%, respectively. The remission rate in the bupropion switch group was 19.3%.
The study results showed patients who received adjunctive bupropion had the highest fall rate at 0.55 falls per patient, vs. 0.33 falls per patient in the aripiprazole group, suggesting that among the three treatment options, adjunctive aripiprazole may be the best choice because of its superior efficacy and lower fall risk.
A total of 248 patients enrolled in the study showed no improvement and were further randomly assigned to receive adjunctive lithium (n = 127) or switch from current therapy to nortriptyline (n = 121).
Well-being scores in the lithium group improved by 3.17 points and 2.18 points in the nortriptyline group. Remission occurred in 18.9% of patients in the lithium group and 21.5% in the nortriptyline group. Fall rates were similar among the two groups.
Overall, “this large, randomized study demonstrated that adding aripiprazole was a superior option for older adults with treatment-resistant depression,” Dr. Lenze told this news organization.
“Since neither lithium nor nortriptyline were promising against treatment-resistant depression in older adults, those medications are unlikely to be helpful in most cases,” he added.
Practice changing?
In an accompanying editorial, Gemma Lewis, PhD, and Glyn Lewis, PhD, division of psychiatry, University of College London, noted the findings “support aripiprazole augmentation as a strategy for treatment-resistant depression in older persons, largely because of the lower risk of falls than with bupropion augmentation.”
However, “in clinical practice, [it] would be important to tailor treatment in light of potential adverse effects and the preferences of the patient,” they added.
Akathisia, for instance, is a common side effect of aripiprazole, shown in one recent trial to affect 11% of the patients. In addition, weight gain, though typically lower than seen with other antipsychotics, is a consideration with aripiprazole.
With respect to fall risk, they noted that bupropion was largely used in relatively high doses of 300 mg and 450 mg, despite some recent research showing little clinical benefit from increasing antidepressant doses above minimum recommendations.
“It is possible that smaller doses of bupropion than those used in the current trial would retain effectiveness while minimizing adverse effects such as falls,” the editorialists noted.
Commenting on the study, Jennifer R. Gatchel, MD, PhD, assistant psychiatrist at Massachusetts General Hospital/McLean Hospital and assistant professor of psychiatry at Harvard Medical School, Boston, said the findings have high clinical significance in the treatment of geriatric depression.

“These results are of great impact for clinicians managing older adults with treatment-resistant depression. They provide some of the first evidence of safety and efficacy of augmentation with aripiprazole as a strategy in clinical management of older adults who fail to initially respond to treatment,” said Dr. Gatchel, who was not associated with this research.
“Of particular significance, efficacy here is based on patient-centered outcomes and psychological well-being as a primary effectiveness outcome, which could translate into strengthened physician-patient alliance.”
While adjunctive aripiprazole is not necessarily a first-line strategy when older adults fail to respond to antidepressants, there is a lack of data on the risks and benefits of any other antipsychotic medications, she noted.
“Thus, this is evidence that will impact clinical practice and hopefully contribute to reduced societal burden of depression in older adults and the morbidity and mortality associated with it,” Dr. Gatchel said.
The study received support from a Patient-Centered Outcomes Research Institute (PCORI) Award (TRD-1511-33321). Dr. Lenze received additional support from the Taylor Family Institute for Innovative Psychiatric Research at Washington University School of Medicine, as well as the Washington University Institute of Clinical and Translational Sciences grant (UL1TR002345) from the National Center for Advancing Translational Sciences of the National Institutes of Health. Dr. Gatchel reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
“We found that adding aripiprazole led to higher rates of depression remission and greater improvements in psychological well-being – which means how positive and satisfied patients felt – and this is good news,” study investigator Eric J. Lenze, MD, of the department of psychiatry, Washington University, St. Louis, said in a press statement.
“However, even that approach helped only about 30% of people in the study with treatment-resistant depression, underscoring the need to find and develop more effective treatments that can help more people,” he added.
The findings were presented here as part of the American Association for Geriatric Psychiatry annual meeting, and published concurrently in the New England Journal of Medicine.
Need for safe treatment options
Treatment-resistant depression is common in older patients, but switching medications or adding other agents can be challenging. With higher rates of comorbidity and polypharmacy, treatment decisions in this patient population are more complex compared with those involving younger patients.
To compare the benefits of augmentation vs. drug-switching strategies, the researchers conducted a multicenter, two-step trial involving 619 patients with an average baseline age of 69 who had failed to respond to two courses of selective serotonin reuptake inhibitors (SSRIs).
Patients were randomly assigned to one of three groups. These included augmentation of existing antidepressant medication with either aripiprazole (n = 211) or the dopamine and norepinephrine–reuptake inhibitor bupropion (Wellbutrin, Zyban) (n = 206), or to taper off of their current antidepressant and switch to bupropion (n = 202).
After 10 weeks, patients’ psychological well-being was assessed via the National Institutes of Health Toolbox Positive Affect and General Life Satisfaction subscales. The researchers found patients in the aripiprazole and bupropion add-on groups improved by 4.83 points and 4.33 points, respectively. The bupropion switch group had a change of 2.04 points.
The difference between the aripiprazole augmentation group and the switch to bupropion group was significant (difference 2.79 points; P = .014). Other between-group differences were not significantly different.
Remission rates were similar in the aripiprazole and bupropion groups at 28.9% and 28.2%, respectively. The remission rate in the bupropion switch group was 19.3%.
The study results showed patients who received adjunctive bupropion had the highest fall rate at 0.55 falls per patient, vs. 0.33 falls per patient in the aripiprazole group, suggesting that among the three treatment options, adjunctive aripiprazole may be the best choice because of its superior efficacy and lower fall risk.
A total of 248 patients enrolled in the study showed no improvement and were further randomly assigned to receive adjunctive lithium (n = 127) or switch from current therapy to nortriptyline (n = 121).
Well-being scores in the lithium group improved by 3.17 points and 2.18 points in the nortriptyline group. Remission occurred in 18.9% of patients in the lithium group and 21.5% in the nortriptyline group. Fall rates were similar among the two groups.
Overall, “this large, randomized study demonstrated that adding aripiprazole was a superior option for older adults with treatment-resistant depression,” Dr. Lenze told this news organization.
“Since neither lithium nor nortriptyline were promising against treatment-resistant depression in older adults, those medications are unlikely to be helpful in most cases,” he added.
Practice changing?
In an accompanying editorial, Gemma Lewis, PhD, and Glyn Lewis, PhD, division of psychiatry, University of College London, noted the findings “support aripiprazole augmentation as a strategy for treatment-resistant depression in older persons, largely because of the lower risk of falls than with bupropion augmentation.”
However, “in clinical practice, [it] would be important to tailor treatment in light of potential adverse effects and the preferences of the patient,” they added.
Akathisia, for instance, is a common side effect of aripiprazole, shown in one recent trial to affect 11% of the patients. In addition, weight gain, though typically lower than seen with other antipsychotics, is a consideration with aripiprazole.
With respect to fall risk, they noted that bupropion was largely used in relatively high doses of 300 mg and 450 mg, despite some recent research showing little clinical benefit from increasing antidepressant doses above minimum recommendations.
“It is possible that smaller doses of bupropion than those used in the current trial would retain effectiveness while minimizing adverse effects such as falls,” the editorialists noted.
Commenting on the study, Jennifer R. Gatchel, MD, PhD, assistant psychiatrist at Massachusetts General Hospital/McLean Hospital and assistant professor of psychiatry at Harvard Medical School, Boston, said the findings have high clinical significance in the treatment of geriatric depression.
“These results are of great impact for clinicians managing older adults with treatment-resistant depression. They provide some of the first evidence of safety and efficacy of augmentation with aripiprazole as a strategy in clinical management of older adults who fail to initially respond to treatment,” said Dr. Gatchel, who was not associated with this research.
“Of particular significance, efficacy here is based on patient-centered outcomes and psychological well-being as a primary effectiveness outcome, which could translate into strengthened physician-patient alliance.”
While adjunctive aripiprazole is not necessarily a first-line strategy when older adults fail to respond to antidepressants, there is a lack of data on the risks and benefits of any other antipsychotic medications, she noted.
“Thus, this is evidence that will impact clinical practice and hopefully contribute to reduced societal burden of depression in older adults and the morbidity and mortality associated with it,” Dr. Gatchel said.
The study received support from a Patient-Centered Outcomes Research Institute (PCORI) Award (TRD-1511-33321). Dr. Lenze received additional support from the Taylor Family Institute for Innovative Psychiatric Research at Washington University School of Medicine, as well as the Washington University Institute of Clinical and Translational Sciences grant (UL1TR002345) from the National Center for Advancing Translational Sciences of the National Institutes of Health. Dr. Gatchel reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
“We found that adding aripiprazole led to higher rates of depression remission and greater improvements in psychological well-being – which means how positive and satisfied patients felt – and this is good news,” study investigator Eric J. Lenze, MD, of the department of psychiatry, Washington University, St. Louis, said in a press statement.
“However, even that approach helped only about 30% of people in the study with treatment-resistant depression, underscoring the need to find and develop more effective treatments that can help more people,” he added.
The findings were presented here as part of the American Association for Geriatric Psychiatry annual meeting, and published concurrently in the New England Journal of Medicine.
Need for safe treatment options
Treatment-resistant depression is common in older patients, but switching medications or adding other agents can be challenging. With higher rates of comorbidity and polypharmacy, treatment decisions in this patient population are more complex compared with those involving younger patients.
To compare the benefits of augmentation vs. drug-switching strategies, the researchers conducted a multicenter, two-step trial involving 619 patients with an average baseline age of 69 who had failed to respond to two courses of selective serotonin reuptake inhibitors (SSRIs).
Patients were randomly assigned to one of three groups. These included augmentation of existing antidepressant medication with either aripiprazole (n = 211) or the dopamine and norepinephrine–reuptake inhibitor bupropion (Wellbutrin, Zyban) (n = 206), or to taper off of their current antidepressant and switch to bupropion (n = 202).
After 10 weeks, patients’ psychological well-being was assessed via the National Institutes of Health Toolbox Positive Affect and General Life Satisfaction subscales. The researchers found patients in the aripiprazole and bupropion add-on groups improved by 4.83 points and 4.33 points, respectively. The bupropion switch group had a change of 2.04 points.
The difference between the aripiprazole augmentation group and the switch to bupropion group was significant (difference 2.79 points; P = .014). Other between-group differences were not significantly different.
Remission rates were similar in the aripiprazole and bupropion groups at 28.9% and 28.2%, respectively. The remission rate in the bupropion switch group was 19.3%.
The study results showed patients who received adjunctive bupropion had the highest fall rate at 0.55 falls per patient, vs. 0.33 falls per patient in the aripiprazole group, suggesting that among the three treatment options, adjunctive aripiprazole may be the best choice because of its superior efficacy and lower fall risk.
A total of 248 patients enrolled in the study showed no improvement and were further randomly assigned to receive adjunctive lithium (n = 127) or switch from current therapy to nortriptyline (n = 121).
Well-being scores in the lithium group improved by 3.17 points and 2.18 points in the nortriptyline group. Remission occurred in 18.9% of patients in the lithium group and 21.5% in the nortriptyline group. Fall rates were similar among the two groups.
Overall, “this large, randomized study demonstrated that adding aripiprazole was a superior option for older adults with treatment-resistant depression,” Dr. Lenze told this news organization.
“Since neither lithium nor nortriptyline were promising against treatment-resistant depression in older adults, those medications are unlikely to be helpful in most cases,” he added.
Practice changing?
In an accompanying editorial, Gemma Lewis, PhD, and Glyn Lewis, PhD, division of psychiatry, University of College London, noted the findings “support aripiprazole augmentation as a strategy for treatment-resistant depression in older persons, largely because of the lower risk of falls than with bupropion augmentation.”
However, “in clinical practice, [it] would be important to tailor treatment in light of potential adverse effects and the preferences of the patient,” they added.
Akathisia, for instance, is a common side effect of aripiprazole, shown in one recent trial to affect 11% of the patients. In addition, weight gain, though typically lower than seen with other antipsychotics, is a consideration with aripiprazole.
With respect to fall risk, they noted that bupropion was largely used in relatively high doses of 300 mg and 450 mg, despite some recent research showing little clinical benefit from increasing antidepressant doses above minimum recommendations.
“It is possible that smaller doses of bupropion than those used in the current trial would retain effectiveness while minimizing adverse effects such as falls,” the editorialists noted.
Commenting on the study, Jennifer R. Gatchel, MD, PhD, assistant psychiatrist at Massachusetts General Hospital/McLean Hospital and assistant professor of psychiatry at Harvard Medical School, Boston, said the findings have high clinical significance in the treatment of geriatric depression.
“These results are of great impact for clinicians managing older adults with treatment-resistant depression. They provide some of the first evidence of safety and efficacy of augmentation with aripiprazole as a strategy in clinical management of older adults who fail to initially respond to treatment,” said Dr. Gatchel, who was not associated with this research.
“Of particular significance, efficacy here is based on patient-centered outcomes and psychological well-being as a primary effectiveness outcome, which could translate into strengthened physician-patient alliance.”
While adjunctive aripiprazole is not necessarily a first-line strategy when older adults fail to respond to antidepressants, there is a lack of data on the risks and benefits of any other antipsychotic medications, she noted.
“Thus, this is evidence that will impact clinical practice and hopefully contribute to reduced societal burden of depression in older adults and the morbidity and mortality associated with it,” Dr. Gatchel said.
The study received support from a Patient-Centered Outcomes Research Institute (PCORI) Award (TRD-1511-33321). Dr. Lenze received additional support from the Taylor Family Institute for Innovative Psychiatric Research at Washington University School of Medicine, as well as the Washington University Institute of Clinical and Translational Sciences grant (UL1TR002345) from the National Center for Advancing Translational Sciences of the National Institutes of Health. Dr. Gatchel reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AAGP 2023
Modified ECT lowers dental, skeletal fracture risk

“ECT is associated with a very low risk of skeletal fractures, even in high-risk patients, and is also associated with a low risk of dental fractures,” said study investigator Chittaranjan Andrade, MD, noting that preexisting bone and dental disease increase this risk.
Overall, clinicians who provide ECT “need to be aware of rare adverse effects, as well as the common ones,” Dr. Andrade, senior professor of clinical psychopharmacology and neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India, told this news organization. He added they also “need data to be able to provide reassurance.”
The findings were published online in The Journal of Clinical Psychiatry.
Avoid unmodified ECT
Dr. Andrade conducted the study because the risk of skeletal and dental fractures associated with ECT is “not commonly discussed.”
Although ECT is perhaps the most effective available treatment for major mental illness, it is associated with several adverse effects, including those associated with delivery of an electrical stimulus to the brain, which results in central and peripheral seizure, he noted.
“The central seizure is essential for the efficacy of ECT,” said Dr. Andrade. In contrast, “the motor seizure has no therapeutic value, is cosmetically displeasing, and may rarely be associated with peripheral adverse effects affecting muscles, joints, teeth, and bones,” he added.
The musculoskeletal and dental injuries are caused by stretching, twisting, compression, or direct injury. Particularly during the motor seizure, the “sudden jerk” associated with the tonic contraction of muscles as well as the repeated jerks associated with each clonic contraction can result in injuries, including skeletal and dental fractures.
To address this concern, the motor seizure is “modified” or attenuated through use of an intravenous muscle relaxant administered with other ECT premedication.
“How effectively the musculoskeletal and dental adverse effects are minimized depends on how well the motor seizure is modified,” Dr. Andrade said. He emphasized that the “use of unmodified ECT is strongly discouraged.”
Dr. Andrade reviewed prior research into the skeletal and dental risks of ECT. The infrequency of cases and ethical difficulties in conducting randomized clinical trials with such patients require reliance on anecdotal reports, he said.
Bite blocks, seizure modifiers
Population-based data showed that the fracture risk with modified ECT is two events per 100,000 ECTs. However, the risk may be as low as 0.36 events per 100,000 ECTs if calculated only with recent data, Dr. Andrade noted.
Population-based studies also suggest that the dental fracture risk with modified ECT is .02% per ECT and .17% per ECT course.
Although fractures have been reported under “unusual circumstances” among patients receiving modified ECT, many other reports point to the safety of this treatment, even in ultrahigh-risk patients.
Such patients include those with severe osteoporosis, metastatic bone disease, osteogenesis imperfecta, Ehlers-Danlos syndrome, Harrington rod implants, recent long bone fractures, multiple bone fractures, surgical repair of hip fracture, vertebroplasty, and maxillofacial repair.
Dr. Andrade noted that oral health is “poor” among patients with major mental illness for multiple reasons, including poor nutrition, self-neglect, and decreased salivation caused by the anticholinergic effects of medications.
This places these patients at increased risk for dental adverse effects during ECT because the muscles of the jaw contract forcefully during the motor seizure, causing sudden impact and, subsequently, sustained pressure on the teeth, Dr. Andrade said.
Moreover, because ECT is typically administered through repeated sessions, dental injuries may accumulate over the course of treatment.
ECT-associated skeletal risks arise from the tonic-clonic contractions of the muscles of the trunk and limbs, which need to be addressed via use of succinylcholine or other muscle relaxants included in ECT premedication.
Dr. Andrade noted that succinylcholine is effective at modifying the motor seizure at the common dose of 0.5-1.0 mg/kg. However, about 5% of patients require a higher dose (>1.5 mg/kg). If the dose is 1-2 mg/kg for patients at high risk for orthopedic complications, “muscle relaxation during ECT could be expected to be reasonably complete,” he said.
“Because of wide interpersonal variation, a neurostimulator may need to be used to identify the ideal dose for an individual patient,” he added.
In addition, use of bite blocks and effective jaw immobilization during ECT can reduce the risk. “Careful assessment of preexisting risk and good ECT practice can minimize the risk of skeletal and dental complications during ECT,” Dr. Andrade said.
Risks vs. benefits
Commenting on the study, Mark S. George, MD, distinguished professor of psychiatry, radiology, and neurology, and director of the brain stimulation division, Medical University of South Carolina, Charleston, said this was a “well-written review of how frequently patients who are undergoing modern ECT have bone fractures or dental fractures during the procedure.”

Dr. George, who was not involved with the research, added that modern medications and management “make ECT a truly safe procedure.”
“It is not without some risk, but these risks are low, especially when compared to the risks of untreated or undertreated depression or catatonia, like suicide,” he said.
Dr. Andrade publishes an e-newsletter supported by Sun Pharmaceuticals, with payments made directly to registered charities, but does not benefit financially from the relationship. His travel expenses for delivering lectures and workshops have been supported by the organizers themselves or pharmaceutical companies at the behest of the organizers. He has provided advice to various pharmaceutical companies and has received “nominal compensation.” He has also received payments for developing educational materials for scientific initiatives and programs, such as for the Behavioral and Neurosciences Foundation of India, PsyBase India, Texas Tech University USA, the Nordic Association for Convulsive Therapy, and the American Society of Clinical Psychopharmacology. Dr. George reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“ECT is associated with a very low risk of skeletal fractures, even in high-risk patients, and is also associated with a low risk of dental fractures,” said study investigator Chittaranjan Andrade, MD, noting that preexisting bone and dental disease increase this risk.
Overall, clinicians who provide ECT “need to be aware of rare adverse effects, as well as the common ones,” Dr. Andrade, senior professor of clinical psychopharmacology and neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India, told this news organization. He added they also “need data to be able to provide reassurance.”
The findings were published online in The Journal of Clinical Psychiatry.
Avoid unmodified ECT
Dr. Andrade conducted the study because the risk of skeletal and dental fractures associated with ECT is “not commonly discussed.”
Although ECT is perhaps the most effective available treatment for major mental illness, it is associated with several adverse effects, including those associated with delivery of an electrical stimulus to the brain, which results in central and peripheral seizure, he noted.
“The central seizure is essential for the efficacy of ECT,” said Dr. Andrade. In contrast, “the motor seizure has no therapeutic value, is cosmetically displeasing, and may rarely be associated with peripheral adverse effects affecting muscles, joints, teeth, and bones,” he added.
The musculoskeletal and dental injuries are caused by stretching, twisting, compression, or direct injury. Particularly during the motor seizure, the “sudden jerk” associated with the tonic contraction of muscles as well as the repeated jerks associated with each clonic contraction can result in injuries, including skeletal and dental fractures.
To address this concern, the motor seizure is “modified” or attenuated through use of an intravenous muscle relaxant administered with other ECT premedication.
“How effectively the musculoskeletal and dental adverse effects are minimized depends on how well the motor seizure is modified,” Dr. Andrade said. He emphasized that the “use of unmodified ECT is strongly discouraged.”
Dr. Andrade reviewed prior research into the skeletal and dental risks of ECT. The infrequency of cases and ethical difficulties in conducting randomized clinical trials with such patients require reliance on anecdotal reports, he said.
Bite blocks, seizure modifiers
Population-based data showed that the fracture risk with modified ECT is two events per 100,000 ECTs. However, the risk may be as low as 0.36 events per 100,000 ECTs if calculated only with recent data, Dr. Andrade noted.
Population-based studies also suggest that the dental fracture risk with modified ECT is .02% per ECT and .17% per ECT course.
Although fractures have been reported under “unusual circumstances” among patients receiving modified ECT, many other reports point to the safety of this treatment, even in ultrahigh-risk patients.
Such patients include those with severe osteoporosis, metastatic bone disease, osteogenesis imperfecta, Ehlers-Danlos syndrome, Harrington rod implants, recent long bone fractures, multiple bone fractures, surgical repair of hip fracture, vertebroplasty, and maxillofacial repair.
Dr. Andrade noted that oral health is “poor” among patients with major mental illness for multiple reasons, including poor nutrition, self-neglect, and decreased salivation caused by the anticholinergic effects of medications.
This places these patients at increased risk for dental adverse effects during ECT because the muscles of the jaw contract forcefully during the motor seizure, causing sudden impact and, subsequently, sustained pressure on the teeth, Dr. Andrade said.
Moreover, because ECT is typically administered through repeated sessions, dental injuries may accumulate over the course of treatment.
ECT-associated skeletal risks arise from the tonic-clonic contractions of the muscles of the trunk and limbs, which need to be addressed via use of succinylcholine or other muscle relaxants included in ECT premedication.
Dr. Andrade noted that succinylcholine is effective at modifying the motor seizure at the common dose of 0.5-1.0 mg/kg. However, about 5% of patients require a higher dose (>1.5 mg/kg). If the dose is 1-2 mg/kg for patients at high risk for orthopedic complications, “muscle relaxation during ECT could be expected to be reasonably complete,” he said.
“Because of wide interpersonal variation, a neurostimulator may need to be used to identify the ideal dose for an individual patient,” he added.
In addition, use of bite blocks and effective jaw immobilization during ECT can reduce the risk. “Careful assessment of preexisting risk and good ECT practice can minimize the risk of skeletal and dental complications during ECT,” Dr. Andrade said.
Risks vs. benefits
Commenting on the study, Mark S. George, MD, distinguished professor of psychiatry, radiology, and neurology, and director of the brain stimulation division, Medical University of South Carolina, Charleston, said this was a “well-written review of how frequently patients who are undergoing modern ECT have bone fractures or dental fractures during the procedure.”
Dr. George, who was not involved with the research, added that modern medications and management “make ECT a truly safe procedure.”
“It is not without some risk, but these risks are low, especially when compared to the risks of untreated or undertreated depression or catatonia, like suicide,” he said.
Dr. Andrade publishes an e-newsletter supported by Sun Pharmaceuticals, with payments made directly to registered charities, but does not benefit financially from the relationship. His travel expenses for delivering lectures and workshops have been supported by the organizers themselves or pharmaceutical companies at the behest of the organizers. He has provided advice to various pharmaceutical companies and has received “nominal compensation.” He has also received payments for developing educational materials for scientific initiatives and programs, such as for the Behavioral and Neurosciences Foundation of India, PsyBase India, Texas Tech University USA, the Nordic Association for Convulsive Therapy, and the American Society of Clinical Psychopharmacology. Dr. George reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“ECT is associated with a very low risk of skeletal fractures, even in high-risk patients, and is also associated with a low risk of dental fractures,” said study investigator Chittaranjan Andrade, MD, noting that preexisting bone and dental disease increase this risk.
Overall, clinicians who provide ECT “need to be aware of rare adverse effects, as well as the common ones,” Dr. Andrade, senior professor of clinical psychopharmacology and neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India, told this news organization. He added they also “need data to be able to provide reassurance.”
The findings were published online in The Journal of Clinical Psychiatry.
Avoid unmodified ECT
Dr. Andrade conducted the study because the risk of skeletal and dental fractures associated with ECT is “not commonly discussed.”
Although ECT is perhaps the most effective available treatment for major mental illness, it is associated with several adverse effects, including those associated with delivery of an electrical stimulus to the brain, which results in central and peripheral seizure, he noted.
“The central seizure is essential for the efficacy of ECT,” said Dr. Andrade. In contrast, “the motor seizure has no therapeutic value, is cosmetically displeasing, and may rarely be associated with peripheral adverse effects affecting muscles, joints, teeth, and bones,” he added.
The musculoskeletal and dental injuries are caused by stretching, twisting, compression, or direct injury. Particularly during the motor seizure, the “sudden jerk” associated with the tonic contraction of muscles as well as the repeated jerks associated with each clonic contraction can result in injuries, including skeletal and dental fractures.
To address this concern, the motor seizure is “modified” or attenuated through use of an intravenous muscle relaxant administered with other ECT premedication.
“How effectively the musculoskeletal and dental adverse effects are minimized depends on how well the motor seizure is modified,” Dr. Andrade said. He emphasized that the “use of unmodified ECT is strongly discouraged.”
Dr. Andrade reviewed prior research into the skeletal and dental risks of ECT. The infrequency of cases and ethical difficulties in conducting randomized clinical trials with such patients require reliance on anecdotal reports, he said.
Bite blocks, seizure modifiers
Population-based data showed that the fracture risk with modified ECT is two events per 100,000 ECTs. However, the risk may be as low as 0.36 events per 100,000 ECTs if calculated only with recent data, Dr. Andrade noted.
Population-based studies also suggest that the dental fracture risk with modified ECT is .02% per ECT and .17% per ECT course.
Although fractures have been reported under “unusual circumstances” among patients receiving modified ECT, many other reports point to the safety of this treatment, even in ultrahigh-risk patients.
Such patients include those with severe osteoporosis, metastatic bone disease, osteogenesis imperfecta, Ehlers-Danlos syndrome, Harrington rod implants, recent long bone fractures, multiple bone fractures, surgical repair of hip fracture, vertebroplasty, and maxillofacial repair.
Dr. Andrade noted that oral health is “poor” among patients with major mental illness for multiple reasons, including poor nutrition, self-neglect, and decreased salivation caused by the anticholinergic effects of medications.
This places these patients at increased risk for dental adverse effects during ECT because the muscles of the jaw contract forcefully during the motor seizure, causing sudden impact and, subsequently, sustained pressure on the teeth, Dr. Andrade said.
Moreover, because ECT is typically administered through repeated sessions, dental injuries may accumulate over the course of treatment.
ECT-associated skeletal risks arise from the tonic-clonic contractions of the muscles of the trunk and limbs, which need to be addressed via use of succinylcholine or other muscle relaxants included in ECT premedication.
Dr. Andrade noted that succinylcholine is effective at modifying the motor seizure at the common dose of 0.5-1.0 mg/kg. However, about 5% of patients require a higher dose (>1.5 mg/kg). If the dose is 1-2 mg/kg for patients at high risk for orthopedic complications, “muscle relaxation during ECT could be expected to be reasonably complete,” he said.
“Because of wide interpersonal variation, a neurostimulator may need to be used to identify the ideal dose for an individual patient,” he added.
In addition, use of bite blocks and effective jaw immobilization during ECT can reduce the risk. “Careful assessment of preexisting risk and good ECT practice can minimize the risk of skeletal and dental complications during ECT,” Dr. Andrade said.
Risks vs. benefits
Commenting on the study, Mark S. George, MD, distinguished professor of psychiatry, radiology, and neurology, and director of the brain stimulation division, Medical University of South Carolina, Charleston, said this was a “well-written review of how frequently patients who are undergoing modern ECT have bone fractures or dental fractures during the procedure.”
Dr. George, who was not involved with the research, added that modern medications and management “make ECT a truly safe procedure.”
“It is not without some risk, but these risks are low, especially when compared to the risks of untreated or undertreated depression or catatonia, like suicide,” he said.
Dr. Andrade publishes an e-newsletter supported by Sun Pharmaceuticals, with payments made directly to registered charities, but does not benefit financially from the relationship. His travel expenses for delivering lectures and workshops have been supported by the organizers themselves or pharmaceutical companies at the behest of the organizers. He has provided advice to various pharmaceutical companies and has received “nominal compensation.” He has also received payments for developing educational materials for scientific initiatives and programs, such as for the Behavioral and Neurosciences Foundation of India, PsyBase India, Texas Tech University USA, the Nordic Association for Convulsive Therapy, and the American Society of Clinical Psychopharmacology. Dr. George reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Distinct suicidal thought patterns flag those at highest risk
Long-term assessment of suicide risk and ideation in older adults may help identify distinct ideation patterns and predict potential future suicidal behavior, new research suggests.
Investigators studied over 300 older adults, assessing suicidal ideation and behavior for up to 14 years at least once annually. They then identified four suicidal ideation profiles.
They found that In turn, fast-remitting ideators were at higher risk in comparison to low/nonideators with no attempts or suicide.
Chronic severe ideators also showed the most severe levels of dysfunction across personality, social characteristics, and impulsivity measures, while highly variable and fast-remitting ideators displayed more specific deficits.
“We identified longitudinal ideation profiles that convey differential risk of future suicidal behavior to help clinicians recognize high suicide risk patients for preventing suicide,” said lead author Hanga Galfalvy, PhD, associate professor, department of psychiatry, Columbia University Irving Medical Center, New York.
“Clinicians should repeatedly assess suicidal ideation and ask not only about current ideation but also about the worst ideation since the last visit [because] similar levels of ideation during a single assessment can belong to very different risk profiles,” said Dr. Galfalvy, also a professor of biostatistics and a coinvestigator in the Conte Center for Suicide Prevention at Columbia University.
The study was published online in the Journal of Clinical Psychiatry.
Vulnerable population
“Older adults in most countries, including the U.S., are at the highest risk of dying of suicide out of all age groups,” said Dr. Galfalvy. “A significant number of depressed older adults experience thoughts of killing themselves, but fortunately, only a few transition from suicidal thoughts to behavior.”
Senior author Katalin Szanto, MD, professor of psychiatry, University of Pittsburgh, said in an interview that currently established clinical and psychosocial suicide risk factors have “low predictive value and provide little insight into the high suicide rate in the elderly.”
These traditional risk factors “poorly distinguish between suicide ideators and suicide attempters and do not take into consideration the heterogeneity of suicidal behavior,” said Dr. Szanto, principal investigator at the University of Pittsburgh’s Longitudinal research Program in Late-Life Suicide, where the study was conducted.
“Suicidal ideation measured at one time point – current or lifetime – may not be enough to accurately predict suicide risk,” the investigators wrote.
The current study, a collaboration between investigators from the Longitudinal Research Program in Late-Life Suicide and the Conte Center for Suicide Prevention, investigates “profiles of suicidal thoughts and behavior in patients with late-life depression over a longer period of time,” Dr. Galfalvy said.
The researchers used latent profile analysis (LPA) in a cohort of adults with nonpsychotic unipolar depression (aged 50-93 years; n = 337; mean age, 65.12 years) to “identify distinct ideation profiles and their clinical correlates” and to “test the profiles’ association with the risk of suicidal behavior before and during follow-up.”
LPA is “a data-driven method of grouping individuals into subgroups, based on quantitative characteristics,” Dr. Galfalvy explained.
The LPA yielded four profiles of ideation.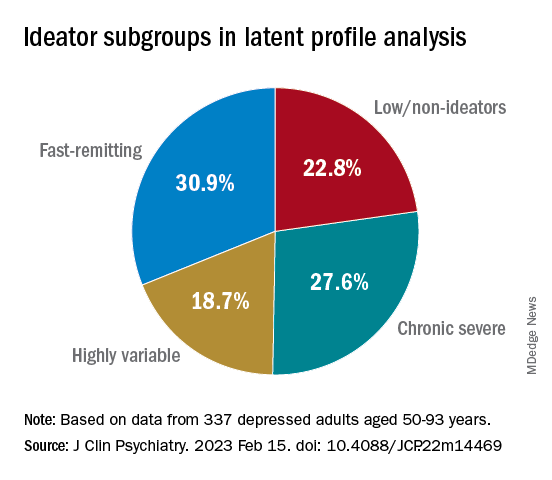
At baseline, the researchers assessed the presence or absence of suicidal behavior history and the number and lethality of attempts. They prospectively assessed suicidal ideation and attempts at least once annually thereafter over a period ranging from 3 months to 14 years (median, 3 years; IQR, 1.6-4 years).
At baseline and at follow-ups, they assessed ideation severity.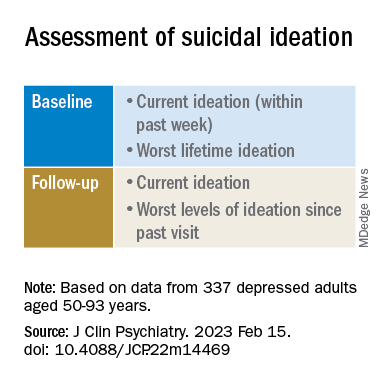
They also assessed depression severity, impulsivity, and personality measures, as well as perception of social support, social problem solving, cognitive performance, and physical comorbidities.
Personalized prevention
Of the original cohort, 92 patients died during the follow-up period, with 13 dying of suicide (or suspected suicide).
Over half (60%) of the chronic severe as well as the highly variable groups and almost half (48%) of the fast-remitting group had a history of past suicide attempt – all significantly higher than the low-nonideators (0%).
Despite comparable current ideation severity at baseline, the risk of suicide attempt/death was greater for chronic severe ideators versus fast-remitting ideators, but not greater than for highly variable ideators. On the other hand, highly variable ideators were at greater risk, compared with fast-remitting ideators.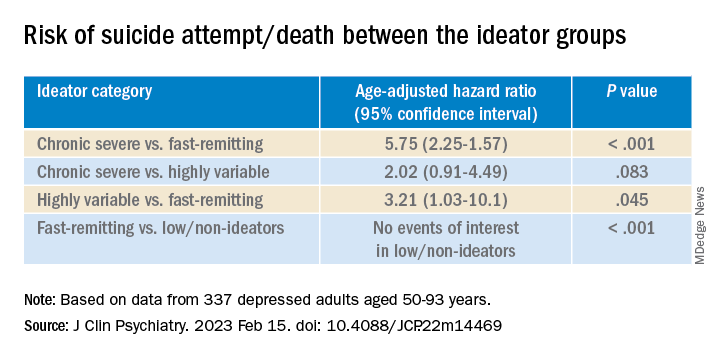
Cognitive factors “did not significantly discriminate between the ideation profiles, although ... lower global cognitive performance predicted suicidal behavior during follow-up,” the authors wrote.
This finding “aligns with prior studies indicating that late-life suicidal behavior but not ideation may be related to cognition ... and instead, ideation and cognition may act as independent risk factors for suicidal behavior,” they added.
“Patients in the fluctuating ideator group generally had moderate or high levels of worst suicidal ideation between visits, but not when asked about current ideation levels at the time of the follow-up assessment,” Dr. Galfalvy noted. “For them, the time frame of the question made a difference as to the level of ideation reported.”
The study “identified several clinical differences among these subgroups which could lead to more personalized suicide prevention efforts and further research into the heterogeneity of suicidal behavior,” she suggested.
New insight
Commenting on the study, Ari Cuperfain, MD, of the University of Toronto said the study “adds to the nuanced understanding of how changes in suicidal ideation over time can lead to suicidal actions and behavior.”
The study “sheds light on the notion of how older adults who die by suicide can demonstrate a greater degree of premeditated intent relative to younger cohorts, with chronic severe ideators portending the highest risk for suicide in this sample,” added Dr. Cuperfain, who was not involved with the current research.
“Overall, the paper highlights the importance of both screening for current levels of suicidal ideation in addition to the evolution of suicidal ideation in developing a risk assessment and in finding interventions to reduce this risk when it is most prominent,” he stated.
The research was supported by the National Institutes of Health. The authors and Dr. Cuperfain disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Long-term assessment of suicide risk and ideation in older adults may help identify distinct ideation patterns and predict potential future suicidal behavior, new research suggests.
Investigators studied over 300 older adults, assessing suicidal ideation and behavior for up to 14 years at least once annually. They then identified four suicidal ideation profiles.
They found that In turn, fast-remitting ideators were at higher risk in comparison to low/nonideators with no attempts or suicide.
Chronic severe ideators also showed the most severe levels of dysfunction across personality, social characteristics, and impulsivity measures, while highly variable and fast-remitting ideators displayed more specific deficits.
“We identified longitudinal ideation profiles that convey differential risk of future suicidal behavior to help clinicians recognize high suicide risk patients for preventing suicide,” said lead author Hanga Galfalvy, PhD, associate professor, department of psychiatry, Columbia University Irving Medical Center, New York.
“Clinicians should repeatedly assess suicidal ideation and ask not only about current ideation but also about the worst ideation since the last visit [because] similar levels of ideation during a single assessment can belong to very different risk profiles,” said Dr. Galfalvy, also a professor of biostatistics and a coinvestigator in the Conte Center for Suicide Prevention at Columbia University.
The study was published online in the Journal of Clinical Psychiatry.
Vulnerable population
“Older adults in most countries, including the U.S., are at the highest risk of dying of suicide out of all age groups,” said Dr. Galfalvy. “A significant number of depressed older adults experience thoughts of killing themselves, but fortunately, only a few transition from suicidal thoughts to behavior.”
Senior author Katalin Szanto, MD, professor of psychiatry, University of Pittsburgh, said in an interview that currently established clinical and psychosocial suicide risk factors have “low predictive value and provide little insight into the high suicide rate in the elderly.”
These traditional risk factors “poorly distinguish between suicide ideators and suicide attempters and do not take into consideration the heterogeneity of suicidal behavior,” said Dr. Szanto, principal investigator at the University of Pittsburgh’s Longitudinal research Program in Late-Life Suicide, where the study was conducted.
“Suicidal ideation measured at one time point – current or lifetime – may not be enough to accurately predict suicide risk,” the investigators wrote.
The current study, a collaboration between investigators from the Longitudinal Research Program in Late-Life Suicide and the Conte Center for Suicide Prevention, investigates “profiles of suicidal thoughts and behavior in patients with late-life depression over a longer period of time,” Dr. Galfalvy said.
The researchers used latent profile analysis (LPA) in a cohort of adults with nonpsychotic unipolar depression (aged 50-93 years; n = 337; mean age, 65.12 years) to “identify distinct ideation profiles and their clinical correlates” and to “test the profiles’ association with the risk of suicidal behavior before and during follow-up.”
LPA is “a data-driven method of grouping individuals into subgroups, based on quantitative characteristics,” Dr. Galfalvy explained.
The LPA yielded four profiles of ideation.
At baseline, the researchers assessed the presence or absence of suicidal behavior history and the number and lethality of attempts. They prospectively assessed suicidal ideation and attempts at least once annually thereafter over a period ranging from 3 months to 14 years (median, 3 years; IQR, 1.6-4 years).
At baseline and at follow-ups, they assessed ideation severity.
They also assessed depression severity, impulsivity, and personality measures, as well as perception of social support, social problem solving, cognitive performance, and physical comorbidities.
Personalized prevention
Of the original cohort, 92 patients died during the follow-up period, with 13 dying of suicide (or suspected suicide).
Over half (60%) of the chronic severe as well as the highly variable groups and almost half (48%) of the fast-remitting group had a history of past suicide attempt – all significantly higher than the low-nonideators (0%).
Despite comparable current ideation severity at baseline, the risk of suicide attempt/death was greater for chronic severe ideators versus fast-remitting ideators, but not greater than for highly variable ideators. On the other hand, highly variable ideators were at greater risk, compared with fast-remitting ideators.
Cognitive factors “did not significantly discriminate between the ideation profiles, although ... lower global cognitive performance predicted suicidal behavior during follow-up,” the authors wrote.
This finding “aligns with prior studies indicating that late-life suicidal behavior but not ideation may be related to cognition ... and instead, ideation and cognition may act as independent risk factors for suicidal behavior,” they added.
“Patients in the fluctuating ideator group generally had moderate or high levels of worst suicidal ideation between visits, but not when asked about current ideation levels at the time of the follow-up assessment,” Dr. Galfalvy noted. “For them, the time frame of the question made a difference as to the level of ideation reported.”
The study “identified several clinical differences among these subgroups which could lead to more personalized suicide prevention efforts and further research into the heterogeneity of suicidal behavior,” she suggested.
New insight
Commenting on the study, Ari Cuperfain, MD, of the University of Toronto said the study “adds to the nuanced understanding of how changes in suicidal ideation over time can lead to suicidal actions and behavior.”
The study “sheds light on the notion of how older adults who die by suicide can demonstrate a greater degree of premeditated intent relative to younger cohorts, with chronic severe ideators portending the highest risk for suicide in this sample,” added Dr. Cuperfain, who was not involved with the current research.
“Overall, the paper highlights the importance of both screening for current levels of suicidal ideation in addition to the evolution of suicidal ideation in developing a risk assessment and in finding interventions to reduce this risk when it is most prominent,” he stated.
The research was supported by the National Institutes of Health. The authors and Dr. Cuperfain disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Long-term assessment of suicide risk and ideation in older adults may help identify distinct ideation patterns and predict potential future suicidal behavior, new research suggests.
Investigators studied over 300 older adults, assessing suicidal ideation and behavior for up to 14 years at least once annually. They then identified four suicidal ideation profiles.
They found that In turn, fast-remitting ideators were at higher risk in comparison to low/nonideators with no attempts or suicide.
Chronic severe ideators also showed the most severe levels of dysfunction across personality, social characteristics, and impulsivity measures, while highly variable and fast-remitting ideators displayed more specific deficits.
“We identified longitudinal ideation profiles that convey differential risk of future suicidal behavior to help clinicians recognize high suicide risk patients for preventing suicide,” said lead author Hanga Galfalvy, PhD, associate professor, department of psychiatry, Columbia University Irving Medical Center, New York.
“Clinicians should repeatedly assess suicidal ideation and ask not only about current ideation but also about the worst ideation since the last visit [because] similar levels of ideation during a single assessment can belong to very different risk profiles,” said Dr. Galfalvy, also a professor of biostatistics and a coinvestigator in the Conte Center for Suicide Prevention at Columbia University.
The study was published online in the Journal of Clinical Psychiatry.
Vulnerable population
“Older adults in most countries, including the U.S., are at the highest risk of dying of suicide out of all age groups,” said Dr. Galfalvy. “A significant number of depressed older adults experience thoughts of killing themselves, but fortunately, only a few transition from suicidal thoughts to behavior.”
Senior author Katalin Szanto, MD, professor of psychiatry, University of Pittsburgh, said in an interview that currently established clinical and psychosocial suicide risk factors have “low predictive value and provide little insight into the high suicide rate in the elderly.”
These traditional risk factors “poorly distinguish between suicide ideators and suicide attempters and do not take into consideration the heterogeneity of suicidal behavior,” said Dr. Szanto, principal investigator at the University of Pittsburgh’s Longitudinal research Program in Late-Life Suicide, where the study was conducted.
“Suicidal ideation measured at one time point – current or lifetime – may not be enough to accurately predict suicide risk,” the investigators wrote.
The current study, a collaboration between investigators from the Longitudinal Research Program in Late-Life Suicide and the Conte Center for Suicide Prevention, investigates “profiles of suicidal thoughts and behavior in patients with late-life depression over a longer period of time,” Dr. Galfalvy said.
The researchers used latent profile analysis (LPA) in a cohort of adults with nonpsychotic unipolar depression (aged 50-93 years; n = 337; mean age, 65.12 years) to “identify distinct ideation profiles and their clinical correlates” and to “test the profiles’ association with the risk of suicidal behavior before and during follow-up.”
LPA is “a data-driven method of grouping individuals into subgroups, based on quantitative characteristics,” Dr. Galfalvy explained.
The LPA yielded four profiles of ideation.
At baseline, the researchers assessed the presence or absence of suicidal behavior history and the number and lethality of attempts. They prospectively assessed suicidal ideation and attempts at least once annually thereafter over a period ranging from 3 months to 14 years (median, 3 years; IQR, 1.6-4 years).
At baseline and at follow-ups, they assessed ideation severity.
They also assessed depression severity, impulsivity, and personality measures, as well as perception of social support, social problem solving, cognitive performance, and physical comorbidities.
Personalized prevention
Of the original cohort, 92 patients died during the follow-up period, with 13 dying of suicide (or suspected suicide).
Over half (60%) of the chronic severe as well as the highly variable groups and almost half (48%) of the fast-remitting group had a history of past suicide attempt – all significantly higher than the low-nonideators (0%).
Despite comparable current ideation severity at baseline, the risk of suicide attempt/death was greater for chronic severe ideators versus fast-remitting ideators, but not greater than for highly variable ideators. On the other hand, highly variable ideators were at greater risk, compared with fast-remitting ideators.
Cognitive factors “did not significantly discriminate between the ideation profiles, although ... lower global cognitive performance predicted suicidal behavior during follow-up,” the authors wrote.
This finding “aligns with prior studies indicating that late-life suicidal behavior but not ideation may be related to cognition ... and instead, ideation and cognition may act as independent risk factors for suicidal behavior,” they added.
“Patients in the fluctuating ideator group generally had moderate or high levels of worst suicidal ideation between visits, but not when asked about current ideation levels at the time of the follow-up assessment,” Dr. Galfalvy noted. “For them, the time frame of the question made a difference as to the level of ideation reported.”
The study “identified several clinical differences among these subgroups which could lead to more personalized suicide prevention efforts and further research into the heterogeneity of suicidal behavior,” she suggested.
New insight
Commenting on the study, Ari Cuperfain, MD, of the University of Toronto said the study “adds to the nuanced understanding of how changes in suicidal ideation over time can lead to suicidal actions and behavior.”
The study “sheds light on the notion of how older adults who die by suicide can demonstrate a greater degree of premeditated intent relative to younger cohorts, with chronic severe ideators portending the highest risk for suicide in this sample,” added Dr. Cuperfain, who was not involved with the current research.
“Overall, the paper highlights the importance of both screening for current levels of suicidal ideation in addition to the evolution of suicidal ideation in developing a risk assessment and in finding interventions to reduce this risk when it is most prominent,” he stated.
The research was supported by the National Institutes of Health. The authors and Dr. Cuperfain disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY