User login
Higher Daily Buprenorphine Doses Help Manage OUD: AMA Recommends Policy Change
Higher daily buprenorphine doses may help patients better manage opioid use disorder (OUD), data from a National Institutes of Health (NIH) study suggested.
The new data highlight that the dose size currently recommended by the US Food and Drug Administration (FDA) and insurance caps on doses are outdated and harmful in the age of fentanyl overdoses, according to the American Medical Association (AMA) and physicians who have studied the issue.
Findings of the study, led by Sarah Axeen, PhD, with the Schaeffer Center for Health Policy & Economics, University of Southern California, Los Angeles, were published in JAMA Network Open.
The researchers reviewed insurance claims data from more than 35,000 people diagnosed with OUD who started on buprenorphine treatment between 2016 and 2021. They found that 12.5% had an emergency department (ED) or inpatient visit related to behavioral health within the study period.
They analyzed whether a patient’s buprenorphine dose was linked with the length of time between treatment start and an ED or inpatient visit.
Higher Doses, Better Outcomes
The FDA’s recommended target dose for buprenorphine is 16 mg/d. Dr. Axeen’s team found that those taking higher daily doses (> 16 to 24 mg) took 20% longer to have an ED or inpatient visit related to behavioral health within the first year after receiving treatment than those who took > 8 to 16 mg/d.
“Those taking daily doses of more than 24 mg of buprenorphine went 50% longer before having a subsequent emergency or inpatient healthcare visit related to behavioral health within the first year after receiving treatment, compared to those receiving > 8 to 16 mg a day,” the researchers said in a press release.
AMA Says the Findings Should Change Policies
Bobby Mukkamala, MD, president-elect of the AMA and Chair of the AMA Substance Use and Pain Care Task Force, said the association welcomed the study findings and urged policymakers and insurance providers to act on them with updated policies.
“The findings support AMA policy calling for flexibility in buprenorphine dosing, allowing patients to receive doses exceeding FDA-approved limits when clinically recommended by their prescriber,” he said in a statement. “Policymakers must take note of these findings and the growing body of evidence that further affirm buprenorphine as a safe, effective, and lifesaving tool in the fight against the illicit fentanyl overdose epidemic. It is also critically important for health insurance companies, Medicaid, and Medicare to remove dosage caps for buprenorphine.”
‘Tangible Economic Impact’
Lucinda Grande, MD, a family physician and addiction specialist with Pioneer Family Practice in Lacey, Washington, said in an interview that she was happy to see this study because “it is the first buprenorphine dose study that addresses an outcome with a tangible economic impact that would affect the bottom line of payers and healthcare systems” and may capture the attention of policymakers in changing what she says are outdated recommendations.
“This study is also unusual because it looked specifically at the dose range above 24 mg. Even though that top tier included only a tiny proportion (1.8%) of patients, it was the group that had the greatest long-term benefit from buprenorphine,” Dr. Grande said, adding that other studies have not included that high a dose.
Dr. Grande, who published on a related topic in 2023, noted that Medicaid patients were excluded from the current study, and they make up a substantial portion of those using buprenorphine for OUD. Had they been included, she said, she suspects the evidence would have been even stronger in favor of higher doses.
Physicians can prescribe higher doses off-label, but buprenorphine is expensive, and some insurers have caps based on the FDA recommendations. Dr. Grande says she rarely prescribes > 32 mg/d, and the patients who need the higher doses often have chronic pain. “In Washington State,” she said, “we have had the luxury of prescribing up to 32 mg daily to Medicaid patients for years. I have had a lot of opportunity to work in that dose rage for people who really need it, and I can really see a difference.”
As fentanyl has grown into the primary illicit opioid, she says, the FDA recommendations for buprenorphine have become progressively weaker.
“Fentanyl is 50 times more potent than heroin, the opioid prevalent when the FDA guidelines were written,” she said. “It’s like a popgun that you’re using against a cannon.”
This manuscript was prepared with support from the National Institute on Drug Abuse. Dr. Axeen reported no relevant financial disclosures. Coauthor Jessica S. Merlin, MD, reported grants from Cambia Health Foundation outside the submitted work. Adam J. Gordon, MD, reported grants from NIH and the Veterans Affairs (institution) during the conduct of the study; he reported service as editor-in-chief with the Association for Multidisciplinary Education and Research in Substance use and Addiction. Bradley D. Stein, MD, reported grants from the NIH during the conduct of the study. Dr. Mukkamala and Dr. Grande reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Higher daily buprenorphine doses may help patients better manage opioid use disorder (OUD), data from a National Institutes of Health (NIH) study suggested.
The new data highlight that the dose size currently recommended by the US Food and Drug Administration (FDA) and insurance caps on doses are outdated and harmful in the age of fentanyl overdoses, according to the American Medical Association (AMA) and physicians who have studied the issue.
Findings of the study, led by Sarah Axeen, PhD, with the Schaeffer Center for Health Policy & Economics, University of Southern California, Los Angeles, were published in JAMA Network Open.
The researchers reviewed insurance claims data from more than 35,000 people diagnosed with OUD who started on buprenorphine treatment between 2016 and 2021. They found that 12.5% had an emergency department (ED) or inpatient visit related to behavioral health within the study period.
They analyzed whether a patient’s buprenorphine dose was linked with the length of time between treatment start and an ED or inpatient visit.
Higher Doses, Better Outcomes
The FDA’s recommended target dose for buprenorphine is 16 mg/d. Dr. Axeen’s team found that those taking higher daily doses (> 16 to 24 mg) took 20% longer to have an ED or inpatient visit related to behavioral health within the first year after receiving treatment than those who took > 8 to 16 mg/d.
“Those taking daily doses of more than 24 mg of buprenorphine went 50% longer before having a subsequent emergency or inpatient healthcare visit related to behavioral health within the first year after receiving treatment, compared to those receiving > 8 to 16 mg a day,” the researchers said in a press release.
AMA Says the Findings Should Change Policies
Bobby Mukkamala, MD, president-elect of the AMA and Chair of the AMA Substance Use and Pain Care Task Force, said the association welcomed the study findings and urged policymakers and insurance providers to act on them with updated policies.
“The findings support AMA policy calling for flexibility in buprenorphine dosing, allowing patients to receive doses exceeding FDA-approved limits when clinically recommended by their prescriber,” he said in a statement. “Policymakers must take note of these findings and the growing body of evidence that further affirm buprenorphine as a safe, effective, and lifesaving tool in the fight against the illicit fentanyl overdose epidemic. It is also critically important for health insurance companies, Medicaid, and Medicare to remove dosage caps for buprenorphine.”
‘Tangible Economic Impact’
Lucinda Grande, MD, a family physician and addiction specialist with Pioneer Family Practice in Lacey, Washington, said in an interview that she was happy to see this study because “it is the first buprenorphine dose study that addresses an outcome with a tangible economic impact that would affect the bottom line of payers and healthcare systems” and may capture the attention of policymakers in changing what she says are outdated recommendations.
“This study is also unusual because it looked specifically at the dose range above 24 mg. Even though that top tier included only a tiny proportion (1.8%) of patients, it was the group that had the greatest long-term benefit from buprenorphine,” Dr. Grande said, adding that other studies have not included that high a dose.
Dr. Grande, who published on a related topic in 2023, noted that Medicaid patients were excluded from the current study, and they make up a substantial portion of those using buprenorphine for OUD. Had they been included, she said, she suspects the evidence would have been even stronger in favor of higher doses.
Physicians can prescribe higher doses off-label, but buprenorphine is expensive, and some insurers have caps based on the FDA recommendations. Dr. Grande says she rarely prescribes > 32 mg/d, and the patients who need the higher doses often have chronic pain. “In Washington State,” she said, “we have had the luxury of prescribing up to 32 mg daily to Medicaid patients for years. I have had a lot of opportunity to work in that dose rage for people who really need it, and I can really see a difference.”
As fentanyl has grown into the primary illicit opioid, she says, the FDA recommendations for buprenorphine have become progressively weaker.
“Fentanyl is 50 times more potent than heroin, the opioid prevalent when the FDA guidelines were written,” she said. “It’s like a popgun that you’re using against a cannon.”
This manuscript was prepared with support from the National Institute on Drug Abuse. Dr. Axeen reported no relevant financial disclosures. Coauthor Jessica S. Merlin, MD, reported grants from Cambia Health Foundation outside the submitted work. Adam J. Gordon, MD, reported grants from NIH and the Veterans Affairs (institution) during the conduct of the study; he reported service as editor-in-chief with the Association for Multidisciplinary Education and Research in Substance use and Addiction. Bradley D. Stein, MD, reported grants from the NIH during the conduct of the study. Dr. Mukkamala and Dr. Grande reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Higher daily buprenorphine doses may help patients better manage opioid use disorder (OUD), data from a National Institutes of Health (NIH) study suggested.
The new data highlight that the dose size currently recommended by the US Food and Drug Administration (FDA) and insurance caps on doses are outdated and harmful in the age of fentanyl overdoses, according to the American Medical Association (AMA) and physicians who have studied the issue.
Findings of the study, led by Sarah Axeen, PhD, with the Schaeffer Center for Health Policy & Economics, University of Southern California, Los Angeles, were published in JAMA Network Open.
The researchers reviewed insurance claims data from more than 35,000 people diagnosed with OUD who started on buprenorphine treatment between 2016 and 2021. They found that 12.5% had an emergency department (ED) or inpatient visit related to behavioral health within the study period.
They analyzed whether a patient’s buprenorphine dose was linked with the length of time between treatment start and an ED or inpatient visit.
Higher Doses, Better Outcomes
The FDA’s recommended target dose for buprenorphine is 16 mg/d. Dr. Axeen’s team found that those taking higher daily doses (> 16 to 24 mg) took 20% longer to have an ED or inpatient visit related to behavioral health within the first year after receiving treatment than those who took > 8 to 16 mg/d.
“Those taking daily doses of more than 24 mg of buprenorphine went 50% longer before having a subsequent emergency or inpatient healthcare visit related to behavioral health within the first year after receiving treatment, compared to those receiving > 8 to 16 mg a day,” the researchers said in a press release.
AMA Says the Findings Should Change Policies
Bobby Mukkamala, MD, president-elect of the AMA and Chair of the AMA Substance Use and Pain Care Task Force, said the association welcomed the study findings and urged policymakers and insurance providers to act on them with updated policies.
“The findings support AMA policy calling for flexibility in buprenorphine dosing, allowing patients to receive doses exceeding FDA-approved limits when clinically recommended by their prescriber,” he said in a statement. “Policymakers must take note of these findings and the growing body of evidence that further affirm buprenorphine as a safe, effective, and lifesaving tool in the fight against the illicit fentanyl overdose epidemic. It is also critically important for health insurance companies, Medicaid, and Medicare to remove dosage caps for buprenorphine.”
‘Tangible Economic Impact’
Lucinda Grande, MD, a family physician and addiction specialist with Pioneer Family Practice in Lacey, Washington, said in an interview that she was happy to see this study because “it is the first buprenorphine dose study that addresses an outcome with a tangible economic impact that would affect the bottom line of payers and healthcare systems” and may capture the attention of policymakers in changing what she says are outdated recommendations.
“This study is also unusual because it looked specifically at the dose range above 24 mg. Even though that top tier included only a tiny proportion (1.8%) of patients, it was the group that had the greatest long-term benefit from buprenorphine,” Dr. Grande said, adding that other studies have not included that high a dose.
Dr. Grande, who published on a related topic in 2023, noted that Medicaid patients were excluded from the current study, and they make up a substantial portion of those using buprenorphine for OUD. Had they been included, she said, she suspects the evidence would have been even stronger in favor of higher doses.
Physicians can prescribe higher doses off-label, but buprenorphine is expensive, and some insurers have caps based on the FDA recommendations. Dr. Grande says she rarely prescribes > 32 mg/d, and the patients who need the higher doses often have chronic pain. “In Washington State,” she said, “we have had the luxury of prescribing up to 32 mg daily to Medicaid patients for years. I have had a lot of opportunity to work in that dose rage for people who really need it, and I can really see a difference.”
As fentanyl has grown into the primary illicit opioid, she says, the FDA recommendations for buprenorphine have become progressively weaker.
“Fentanyl is 50 times more potent than heroin, the opioid prevalent when the FDA guidelines were written,” she said. “It’s like a popgun that you’re using against a cannon.”
This manuscript was prepared with support from the National Institute on Drug Abuse. Dr. Axeen reported no relevant financial disclosures. Coauthor Jessica S. Merlin, MD, reported grants from Cambia Health Foundation outside the submitted work. Adam J. Gordon, MD, reported grants from NIH and the Veterans Affairs (institution) during the conduct of the study; he reported service as editor-in-chief with the Association for Multidisciplinary Education and Research in Substance use and Addiction. Bradley D. Stein, MD, reported grants from the NIH during the conduct of the study. Dr. Mukkamala and Dr. Grande reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Which Medication Is Best? VA Genetic Tests May Have the Answer
The US Department of Veterans Affairs (VA) now has a permanent pharmacogenomics service that provides genetic tests to give clinicians insight into the best medication options for their patients.
The tests, which have no extra cost, are available to all veterans, said pharmacist Jill S. Bates, PharmD, MS, executive director of the VA National Pharmacogenomics Program, who spoke in an interview and a presentation at the annual meeting of the Association of VA Hematology/Oncology.
Genetic testing is “a tool that can help optimize care that we provide for veterans,” she said. “Pharmacogenomics is additional information to help the clinician make a decision. We know that most veterans—greater than 90%—carry a variant in a pharmacogenomics gene that is actionable.”
The genetic tests can provide insight into the optimal medication for multiple conditions such as mental illness, gastrointestinal disorders, cancer, pain, and heart disease. According to a 2019 analysis of over 6 years of data, more than half of the VA patient population used medications whose efficacy may have been affected by detectable genetic variants.
For instance, Bates said tests can let clinicians know whether patients are susceptible to statin-associated muscle adverse effects if they take simvastatin, the cholesterol medication. An estimated 25.6% of the VA population has this variant.
Elsewhere on the cardiac front, an estimated 58.3% of the VA population has a genetic variant that increases sensitivity to the blood thinner warfarin.
Testing could help psychiatrists determine whether certain medications should not be prescribed—or should be prescribed at lower doses—in patients who’ve had adverse reactions to antidepressants, Bates said.
In cancer, Bates said, genetic testing can identify patients who have a genetic variant that boosts toxicity from fluoropyrimidine chemotherapy treatments, which include capecitabine, floxuridine, and fluorouracil. Meanwhile, an estimated 0.9% will have no reaction or limited reaction to capecitabine and fluorouracil, and 4.8% will have hypersensitivity to carbamazepine and oxcarbazepine.
Tests can also identify a genetic variant that can lead to poor metabolism of the chemotherapy drug irinotecan, which is used to treat colon cancer. “In those patients, you’d want to reduce the dose by 20%,” Bates said. In other cases, alternate drugs may be the best strategy to address genetic variations.
Prior to 2019, clinicians had to order pharmacogenomic tests outside of the VA system, according to Bates. That year, a donation from Sanford Health brought VA pharmacogenomics to 40 pilot sites. Since then, more than 88,000 tests have been performed.
The VA has now made its pharmacogenomic program permanent, Bates said. As of early September, testing was available at 139 VA sites and is coming soon to 4 more. It’s not available at another 23 sites that are scattered across the country.
A tool in the VA electronic health record now reminds clinicians about the availability of genetic testing and allows them to order tests. However, testing isn’t available for patients who have had liver transplants or certain bone marrow transplants.
The VA is working on developing decision-making tools to help clinicians determine when the tests are appropriate, Bates said. It typically takes 2 to 3 weeks to get results, she said, adding that external laboratories provide results. “We eventually would like to bring in all pharmacogenomics testing to be conducted within the VA enterprise.”
Bates reported that she had no disclosures.
The US Department of Veterans Affairs (VA) now has a permanent pharmacogenomics service that provides genetic tests to give clinicians insight into the best medication options for their patients.
The tests, which have no extra cost, are available to all veterans, said pharmacist Jill S. Bates, PharmD, MS, executive director of the VA National Pharmacogenomics Program, who spoke in an interview and a presentation at the annual meeting of the Association of VA Hematology/Oncology.
Genetic testing is “a tool that can help optimize care that we provide for veterans,” she said. “Pharmacogenomics is additional information to help the clinician make a decision. We know that most veterans—greater than 90%—carry a variant in a pharmacogenomics gene that is actionable.”
The genetic tests can provide insight into the optimal medication for multiple conditions such as mental illness, gastrointestinal disorders, cancer, pain, and heart disease. According to a 2019 analysis of over 6 years of data, more than half of the VA patient population used medications whose efficacy may have been affected by detectable genetic variants.
For instance, Bates said tests can let clinicians know whether patients are susceptible to statin-associated muscle adverse effects if they take simvastatin, the cholesterol medication. An estimated 25.6% of the VA population has this variant.
Elsewhere on the cardiac front, an estimated 58.3% of the VA population has a genetic variant that increases sensitivity to the blood thinner warfarin.
Testing could help psychiatrists determine whether certain medications should not be prescribed—or should be prescribed at lower doses—in patients who’ve had adverse reactions to antidepressants, Bates said.
In cancer, Bates said, genetic testing can identify patients who have a genetic variant that boosts toxicity from fluoropyrimidine chemotherapy treatments, which include capecitabine, floxuridine, and fluorouracil. Meanwhile, an estimated 0.9% will have no reaction or limited reaction to capecitabine and fluorouracil, and 4.8% will have hypersensitivity to carbamazepine and oxcarbazepine.
Tests can also identify a genetic variant that can lead to poor metabolism of the chemotherapy drug irinotecan, which is used to treat colon cancer. “In those patients, you’d want to reduce the dose by 20%,” Bates said. In other cases, alternate drugs may be the best strategy to address genetic variations.
Prior to 2019, clinicians had to order pharmacogenomic tests outside of the VA system, according to Bates. That year, a donation from Sanford Health brought VA pharmacogenomics to 40 pilot sites. Since then, more than 88,000 tests have been performed.
The VA has now made its pharmacogenomic program permanent, Bates said. As of early September, testing was available at 139 VA sites and is coming soon to 4 more. It’s not available at another 23 sites that are scattered across the country.
A tool in the VA electronic health record now reminds clinicians about the availability of genetic testing and allows them to order tests. However, testing isn’t available for patients who have had liver transplants or certain bone marrow transplants.
The VA is working on developing decision-making tools to help clinicians determine when the tests are appropriate, Bates said. It typically takes 2 to 3 weeks to get results, she said, adding that external laboratories provide results. “We eventually would like to bring in all pharmacogenomics testing to be conducted within the VA enterprise.”
Bates reported that she had no disclosures.
The US Department of Veterans Affairs (VA) now has a permanent pharmacogenomics service that provides genetic tests to give clinicians insight into the best medication options for their patients.
The tests, which have no extra cost, are available to all veterans, said pharmacist Jill S. Bates, PharmD, MS, executive director of the VA National Pharmacogenomics Program, who spoke in an interview and a presentation at the annual meeting of the Association of VA Hematology/Oncology.
Genetic testing is “a tool that can help optimize care that we provide for veterans,” she said. “Pharmacogenomics is additional information to help the clinician make a decision. We know that most veterans—greater than 90%—carry a variant in a pharmacogenomics gene that is actionable.”
The genetic tests can provide insight into the optimal medication for multiple conditions such as mental illness, gastrointestinal disorders, cancer, pain, and heart disease. According to a 2019 analysis of over 6 years of data, more than half of the VA patient population used medications whose efficacy may have been affected by detectable genetic variants.
For instance, Bates said tests can let clinicians know whether patients are susceptible to statin-associated muscle adverse effects if they take simvastatin, the cholesterol medication. An estimated 25.6% of the VA population has this variant.
Elsewhere on the cardiac front, an estimated 58.3% of the VA population has a genetic variant that increases sensitivity to the blood thinner warfarin.
Testing could help psychiatrists determine whether certain medications should not be prescribed—or should be prescribed at lower doses—in patients who’ve had adverse reactions to antidepressants, Bates said.
In cancer, Bates said, genetic testing can identify patients who have a genetic variant that boosts toxicity from fluoropyrimidine chemotherapy treatments, which include capecitabine, floxuridine, and fluorouracil. Meanwhile, an estimated 0.9% will have no reaction or limited reaction to capecitabine and fluorouracil, and 4.8% will have hypersensitivity to carbamazepine and oxcarbazepine.
Tests can also identify a genetic variant that can lead to poor metabolism of the chemotherapy drug irinotecan, which is used to treat colon cancer. “In those patients, you’d want to reduce the dose by 20%,” Bates said. In other cases, alternate drugs may be the best strategy to address genetic variations.
Prior to 2019, clinicians had to order pharmacogenomic tests outside of the VA system, according to Bates. That year, a donation from Sanford Health brought VA pharmacogenomics to 40 pilot sites. Since then, more than 88,000 tests have been performed.
The VA has now made its pharmacogenomic program permanent, Bates said. As of early September, testing was available at 139 VA sites and is coming soon to 4 more. It’s not available at another 23 sites that are scattered across the country.
A tool in the VA electronic health record now reminds clinicians about the availability of genetic testing and allows them to order tests. However, testing isn’t available for patients who have had liver transplants or certain bone marrow transplants.
The VA is working on developing decision-making tools to help clinicians determine when the tests are appropriate, Bates said. It typically takes 2 to 3 weeks to get results, she said, adding that external laboratories provide results. “We eventually would like to bring in all pharmacogenomics testing to be conducted within the VA enterprise.”
Bates reported that she had no disclosures.
Heightened Amygdala Activity Tied to Postpartum Depression
MILAN, ITALY — Pregnant women with heightened amygdala activity have a reduced capacity to regulate emotions and report more symptoms of depression than those with lower activity in this brain region, a new imaging study suggested.
If validated, these findings could pave the way for identifying women at higher risk for postpartum depression, said lead researcher Franziska Weinmar, MSc, from the University of Tübingen in Germany.
The study was presented at the 37th European College of Neuropsychopharmacology Congress.
Differences in Brain Activity
During pregnancy and the peripartum period, rising hormone levels create a “psychoneuroendocrinological window of vulnerability” for mental health in which 80% of women can develop transitory “baby blues,” and about one in seven develop more serious postpartum depression, Ms. Weinmar told this news organization.
The study included 47 women — 15 pregnant women and 32 nonpregnant controls. The nonpregnant women had normal menstrual cycles; 16 were in the early follicular phase with low estradiol levels (231.7 pmol/L), and 16 had high estradiol levels (516.6 pmol/L) after administration of estradiol.
To examine brain activity, participants were asked to view negative emotional images while undergoing functional MRI. They were then asked to use cognitive reappraisal to regulate their emotional response to the images.
The findings showed that both pregnant and nonpregnant women were equally successful at emotional regulation, but this process involved different brain activity in pregnant vs their nonpregnant counterpart.
All women had increased left middle frontal gyrus activity when regulating their emotions, but there was a difference in the amygdala between the pregnancy group and controls, Ms. Weinmar noted.
This suggests that pregnant women may have to exert more neural effort in emotional regulation, she said. “And pregnant women with higher amygdala activity were less able to regulate their emotions successfully compared to those with less amygdala activity.”
Linear regression analyses were performed to assess the relation of brain activity during down-regulation, regulation success, and self-reported depression scores, and this showed that higher amygdala activity was also associated with higher depression scores.
“We need to be cautious in interpreting this,” said Ms. Weinmar. “This is a small sample, and we are the first to undertake this work.”
Nonetheless, she said that if the findings are confirmed by larger studies, pregnant women could be assessed “in the waiting room” using existing questionnaires that evaluate emotional regulation.
If a woman has difficulties with emotion regulation, “there are adaptive strategies, like cognitive reappraisal that a counseling psychotherapist can help with,” said Ms. Weinmar.
“I could also imagine group sessions, for example, or online courses,” she said, adding that obstetricians could also be trained to identify these women.
Commenting on the findings in a press release, Susana Carmona, PhD, from Gregorio Marañón Hospital in Madrid, Spain, said research like this is crucial for gaining insight into one of the most intense physiological processes a human can undergo: pregnancy. It’s remarkable how much remains unknown.
“Recently, the FDA [Food and Drug Administration] approved the first treatment for postpartum depression. However, we still have a long way to go in characterizing what happens in the brain during pregnancy, identifying biomarkers that can indicate the risk of developing perinatal mental disorders, and designing strategies to prevent mother and infant suffering during the delicate and critical peripartum period,” Dr. Carmona added.
The study was supported by the Center for Integrative Neuroscience in Tübingen, Germany, and the International Research Training Group “Women’s Mental Health Across the Reproductive Years” (IRTG 2804). Ms. Weinmar and Dr. Carmona reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN, ITALY — Pregnant women with heightened amygdala activity have a reduced capacity to regulate emotions and report more symptoms of depression than those with lower activity in this brain region, a new imaging study suggested.
If validated, these findings could pave the way for identifying women at higher risk for postpartum depression, said lead researcher Franziska Weinmar, MSc, from the University of Tübingen in Germany.
The study was presented at the 37th European College of Neuropsychopharmacology Congress.
Differences in Brain Activity
During pregnancy and the peripartum period, rising hormone levels create a “psychoneuroendocrinological window of vulnerability” for mental health in which 80% of women can develop transitory “baby blues,” and about one in seven develop more serious postpartum depression, Ms. Weinmar told this news organization.
The study included 47 women — 15 pregnant women and 32 nonpregnant controls. The nonpregnant women had normal menstrual cycles; 16 were in the early follicular phase with low estradiol levels (231.7 pmol/L), and 16 had high estradiol levels (516.6 pmol/L) after administration of estradiol.
To examine brain activity, participants were asked to view negative emotional images while undergoing functional MRI. They were then asked to use cognitive reappraisal to regulate their emotional response to the images.
The findings showed that both pregnant and nonpregnant women were equally successful at emotional regulation, but this process involved different brain activity in pregnant vs their nonpregnant counterpart.
All women had increased left middle frontal gyrus activity when regulating their emotions, but there was a difference in the amygdala between the pregnancy group and controls, Ms. Weinmar noted.
This suggests that pregnant women may have to exert more neural effort in emotional regulation, she said. “And pregnant women with higher amygdala activity were less able to regulate their emotions successfully compared to those with less amygdala activity.”
Linear regression analyses were performed to assess the relation of brain activity during down-regulation, regulation success, and self-reported depression scores, and this showed that higher amygdala activity was also associated with higher depression scores.
“We need to be cautious in interpreting this,” said Ms. Weinmar. “This is a small sample, and we are the first to undertake this work.”
Nonetheless, she said that if the findings are confirmed by larger studies, pregnant women could be assessed “in the waiting room” using existing questionnaires that evaluate emotional regulation.
If a woman has difficulties with emotion regulation, “there are adaptive strategies, like cognitive reappraisal that a counseling psychotherapist can help with,” said Ms. Weinmar.
“I could also imagine group sessions, for example, or online courses,” she said, adding that obstetricians could also be trained to identify these women.
Commenting on the findings in a press release, Susana Carmona, PhD, from Gregorio Marañón Hospital in Madrid, Spain, said research like this is crucial for gaining insight into one of the most intense physiological processes a human can undergo: pregnancy. It’s remarkable how much remains unknown.
“Recently, the FDA [Food and Drug Administration] approved the first treatment for postpartum depression. However, we still have a long way to go in characterizing what happens in the brain during pregnancy, identifying biomarkers that can indicate the risk of developing perinatal mental disorders, and designing strategies to prevent mother and infant suffering during the delicate and critical peripartum period,” Dr. Carmona added.
The study was supported by the Center for Integrative Neuroscience in Tübingen, Germany, and the International Research Training Group “Women’s Mental Health Across the Reproductive Years” (IRTG 2804). Ms. Weinmar and Dr. Carmona reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN, ITALY — Pregnant women with heightened amygdala activity have a reduced capacity to regulate emotions and report more symptoms of depression than those with lower activity in this brain region, a new imaging study suggested.
If validated, these findings could pave the way for identifying women at higher risk for postpartum depression, said lead researcher Franziska Weinmar, MSc, from the University of Tübingen in Germany.
The study was presented at the 37th European College of Neuropsychopharmacology Congress.
Differences in Brain Activity
During pregnancy and the peripartum period, rising hormone levels create a “psychoneuroendocrinological window of vulnerability” for mental health in which 80% of women can develop transitory “baby blues,” and about one in seven develop more serious postpartum depression, Ms. Weinmar told this news organization.
The study included 47 women — 15 pregnant women and 32 nonpregnant controls. The nonpregnant women had normal menstrual cycles; 16 were in the early follicular phase with low estradiol levels (231.7 pmol/L), and 16 had high estradiol levels (516.6 pmol/L) after administration of estradiol.
To examine brain activity, participants were asked to view negative emotional images while undergoing functional MRI. They were then asked to use cognitive reappraisal to regulate their emotional response to the images.
The findings showed that both pregnant and nonpregnant women were equally successful at emotional regulation, but this process involved different brain activity in pregnant vs their nonpregnant counterpart.
All women had increased left middle frontal gyrus activity when regulating their emotions, but there was a difference in the amygdala between the pregnancy group and controls, Ms. Weinmar noted.
This suggests that pregnant women may have to exert more neural effort in emotional regulation, she said. “And pregnant women with higher amygdala activity were less able to regulate their emotions successfully compared to those with less amygdala activity.”
Linear regression analyses were performed to assess the relation of brain activity during down-regulation, regulation success, and self-reported depression scores, and this showed that higher amygdala activity was also associated with higher depression scores.
“We need to be cautious in interpreting this,” said Ms. Weinmar. “This is a small sample, and we are the first to undertake this work.”
Nonetheless, she said that if the findings are confirmed by larger studies, pregnant women could be assessed “in the waiting room” using existing questionnaires that evaluate emotional regulation.
If a woman has difficulties with emotion regulation, “there are adaptive strategies, like cognitive reappraisal that a counseling psychotherapist can help with,” said Ms. Weinmar.
“I could also imagine group sessions, for example, or online courses,” she said, adding that obstetricians could also be trained to identify these women.
Commenting on the findings in a press release, Susana Carmona, PhD, from Gregorio Marañón Hospital in Madrid, Spain, said research like this is crucial for gaining insight into one of the most intense physiological processes a human can undergo: pregnancy. It’s remarkable how much remains unknown.
“Recently, the FDA [Food and Drug Administration] approved the first treatment for postpartum depression. However, we still have a long way to go in characterizing what happens in the brain during pregnancy, identifying biomarkers that can indicate the risk of developing perinatal mental disorders, and designing strategies to prevent mother and infant suffering during the delicate and critical peripartum period,” Dr. Carmona added.
The study was supported by the Center for Integrative Neuroscience in Tübingen, Germany, and the International Research Training Group “Women’s Mental Health Across the Reproductive Years” (IRTG 2804). Ms. Weinmar and Dr. Carmona reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ECNP 2024
Childhood-Onset Atopic Dermatitis Adds Burden in Adulthood
AMSTERDAM — There is a mountain of evidence that atopic dermatitis (AD) exerts a large negative impact on quality of life, but a unique study with
These data, drawn from the ambitious Scars of Life (SOL) project, “suggest that childhood AD persisting into adulthood is its own phenotype,” reported Jonathan I. Silverberg, MD, PhD, director of clinical research, Department of Dermatology, George Washington University, Washington, DC.

One reasonable message from these data is that the failure to achieve adequate control of AD in children, whether by a late start of systemic agents or other reasons, results in a greater lifetime burden of disease when the burden beyond physical symptoms is measured, according to Dr. Silverberg.
More Than 30,000 From Five Continents Participated
In the SOL project, which was designed to analyze how the age of AD onset affects the severity of symptoms and quality of life, completed questionnaires were collected from 30,801 individuals in 27 countries on five continents. The questions, which elicited data to measure the burden of AD, were developed in association with several professional and patient associations with an interest in AD, including the National Eczema Association.
The SOL project has produced an enormous amount of data in four distinct groups, but Dr. Silverberg, speaking in a late-breaking news session at the annual congress of the European Academy of Dermatology and Venereology, focused on a comparison between the 2875 participants who had AD in childhood that has persisted into adulthood and the 7383 adults with adult-onset AD. Data from the other two subsets in SOL — AD in childhood but not in adulthood and no AD in either phase of life — are expected to fuel an extended series of publications.
In the two groups, baseline characteristics were similar with about 60% reporting moderate to severe symptoms and a median age of about 37 years. The proportion of women was 61% in both groups.
Using the PUSH-D questionnaire, which Dr. Silverberg described as a validated tool for gauging a sense of stigmatization, the greater burden of AD was remarkably consistent for those with childhood-onset AD vs adult-onset AD. With higher scores representing a greater sense of stigmatization, the differences in the overall score (23.0 vs 18.1; P < .0001) were highly significant as was every other domain evaluated.
For all five social behavior domains, such as avoiding contact in public and wariness of approaching people spontaneously, having AD onset in childhood persisting into adulthood produced significantly higher scores than having AD onset in adulthood, with no exceptions (P < .001 for all).
AD From Childhood Consistently Results in Worse Outcomes
Providing examples for some of the other 12 domains, Dr. Silverberg maintained that feelings of shame and psychological discomfort were always greater in adults with AD persistent since childhood vs AD starting in adulthood. The P values for these outcomes, such as experiencing bias at work or reporting a sense that others avoided them, were typically highly significant (P < .001).
Compared with those whose AD started in adulthood, “adults with atopic eczema that started during childhood have significantly more difficulties in their life, including occupational relationships, daily life, personal life, and partner or family relationships,” Dr. Silverberg reported.
He said that the data were controlled for multiple confounders, particularly greater severity of AD. He acknowledged that childhood onset might be considered a surrogate for more severe disease, but the data were controlled for this possibility.
Despite the fact that there are “thousands of studies across all age groups showing the burden of AD,” Dr. Silverberg considers these data to be unique by emphasizing the burden of chronicity rather than the impact of AD in any single moment in time.
For those with chronic AD from childhood, “the effect is not just on physical health but a deep negative influence on psychological and social aspects of life,” Dr. Silverberg said, suggesting that the independent effects of chronicity might be worth studying across other dermatologic diseases.
“Regulatory agencies focus on what you can do in that moment of time, losing the bigger picture of how patients are affected chronically,” he said, adding that this is an area of clinical research that should be further explored.
What the data further suggest “is that the earlier we intervene, the more likely patients will do better long term,” he said.
Data Provide Evidence of Systemic Therapy in Kids
For Gudrun Ratzinger, MD, of the Department of Dermatology and Venerology at the Medical University of Innsbruck in Austria, these are valuable data.
“When I prescribe systemic therapies to children, I often get resistance from the healthcare system and even other colleagues,” said Dr. Ratzinger, who was asked to comment on the results. “We are at a teaching hospital, but I often find that when patients return to their home physician, the systemic therapies are stopped.”
In her own practice, she believes the most effective therapies should be introduced in children and adults when complete control is not achieved on first-line drugs. “These data are very helpful for me in explaining to others the importance of effective treatment of atopic dermatitis in children,” she said.
Dr. Silverberg reported financial relationships with more than 40 pharmaceutical companies, including those that make drugs for AD. Dr. Ratzinger reported financial relationships with AbbVie, Almirall, Boehringer Ingelheim, Eli Lilly, Janssen, Leo Pharma, Novartis, Pelpharma, Pfizer, and UCB.
A version of this article first appeared on Medscape.com.
AMSTERDAM — There is a mountain of evidence that atopic dermatitis (AD) exerts a large negative impact on quality of life, but a unique study with
These data, drawn from the ambitious Scars of Life (SOL) project, “suggest that childhood AD persisting into adulthood is its own phenotype,” reported Jonathan I. Silverberg, MD, PhD, director of clinical research, Department of Dermatology, George Washington University, Washington, DC.
One reasonable message from these data is that the failure to achieve adequate control of AD in children, whether by a late start of systemic agents or other reasons, results in a greater lifetime burden of disease when the burden beyond physical symptoms is measured, according to Dr. Silverberg.
More Than 30,000 From Five Continents Participated
In the SOL project, which was designed to analyze how the age of AD onset affects the severity of symptoms and quality of life, completed questionnaires were collected from 30,801 individuals in 27 countries on five continents. The questions, which elicited data to measure the burden of AD, were developed in association with several professional and patient associations with an interest in AD, including the National Eczema Association.
The SOL project has produced an enormous amount of data in four distinct groups, but Dr. Silverberg, speaking in a late-breaking news session at the annual congress of the European Academy of Dermatology and Venereology, focused on a comparison between the 2875 participants who had AD in childhood that has persisted into adulthood and the 7383 adults with adult-onset AD. Data from the other two subsets in SOL — AD in childhood but not in adulthood and no AD in either phase of life — are expected to fuel an extended series of publications.
In the two groups, baseline characteristics were similar with about 60% reporting moderate to severe symptoms and a median age of about 37 years. The proportion of women was 61% in both groups.
Using the PUSH-D questionnaire, which Dr. Silverberg described as a validated tool for gauging a sense of stigmatization, the greater burden of AD was remarkably consistent for those with childhood-onset AD vs adult-onset AD. With higher scores representing a greater sense of stigmatization, the differences in the overall score (23.0 vs 18.1; P < .0001) were highly significant as was every other domain evaluated.
For all five social behavior domains, such as avoiding contact in public and wariness of approaching people spontaneously, having AD onset in childhood persisting into adulthood produced significantly higher scores than having AD onset in adulthood, with no exceptions (P < .001 for all).
AD From Childhood Consistently Results in Worse Outcomes
Providing examples for some of the other 12 domains, Dr. Silverberg maintained that feelings of shame and psychological discomfort were always greater in adults with AD persistent since childhood vs AD starting in adulthood. The P values for these outcomes, such as experiencing bias at work or reporting a sense that others avoided them, were typically highly significant (P < .001).
Compared with those whose AD started in adulthood, “adults with atopic eczema that started during childhood have significantly more difficulties in their life, including occupational relationships, daily life, personal life, and partner or family relationships,” Dr. Silverberg reported.
He said that the data were controlled for multiple confounders, particularly greater severity of AD. He acknowledged that childhood onset might be considered a surrogate for more severe disease, but the data were controlled for this possibility.
Despite the fact that there are “thousands of studies across all age groups showing the burden of AD,” Dr. Silverberg considers these data to be unique by emphasizing the burden of chronicity rather than the impact of AD in any single moment in time.
For those with chronic AD from childhood, “the effect is not just on physical health but a deep negative influence on psychological and social aspects of life,” Dr. Silverberg said, suggesting that the independent effects of chronicity might be worth studying across other dermatologic diseases.
“Regulatory agencies focus on what you can do in that moment of time, losing the bigger picture of how patients are affected chronically,” he said, adding that this is an area of clinical research that should be further explored.
What the data further suggest “is that the earlier we intervene, the more likely patients will do better long term,” he said.
Data Provide Evidence of Systemic Therapy in Kids
For Gudrun Ratzinger, MD, of the Department of Dermatology and Venerology at the Medical University of Innsbruck in Austria, these are valuable data.
“When I prescribe systemic therapies to children, I often get resistance from the healthcare system and even other colleagues,” said Dr. Ratzinger, who was asked to comment on the results. “We are at a teaching hospital, but I often find that when patients return to their home physician, the systemic therapies are stopped.”
In her own practice, she believes the most effective therapies should be introduced in children and adults when complete control is not achieved on first-line drugs. “These data are very helpful for me in explaining to others the importance of effective treatment of atopic dermatitis in children,” she said.
Dr. Silverberg reported financial relationships with more than 40 pharmaceutical companies, including those that make drugs for AD. Dr. Ratzinger reported financial relationships with AbbVie, Almirall, Boehringer Ingelheim, Eli Lilly, Janssen, Leo Pharma, Novartis, Pelpharma, Pfizer, and UCB.
A version of this article first appeared on Medscape.com.
AMSTERDAM — There is a mountain of evidence that atopic dermatitis (AD) exerts a large negative impact on quality of life, but a unique study with
These data, drawn from the ambitious Scars of Life (SOL) project, “suggest that childhood AD persisting into adulthood is its own phenotype,” reported Jonathan I. Silverberg, MD, PhD, director of clinical research, Department of Dermatology, George Washington University, Washington, DC.
One reasonable message from these data is that the failure to achieve adequate control of AD in children, whether by a late start of systemic agents or other reasons, results in a greater lifetime burden of disease when the burden beyond physical symptoms is measured, according to Dr. Silverberg.
More Than 30,000 From Five Continents Participated
In the SOL project, which was designed to analyze how the age of AD onset affects the severity of symptoms and quality of life, completed questionnaires were collected from 30,801 individuals in 27 countries on five continents. The questions, which elicited data to measure the burden of AD, were developed in association with several professional and patient associations with an interest in AD, including the National Eczema Association.
The SOL project has produced an enormous amount of data in four distinct groups, but Dr. Silverberg, speaking in a late-breaking news session at the annual congress of the European Academy of Dermatology and Venereology, focused on a comparison between the 2875 participants who had AD in childhood that has persisted into adulthood and the 7383 adults with adult-onset AD. Data from the other two subsets in SOL — AD in childhood but not in adulthood and no AD in either phase of life — are expected to fuel an extended series of publications.
In the two groups, baseline characteristics were similar with about 60% reporting moderate to severe symptoms and a median age of about 37 years. The proportion of women was 61% in both groups.
Using the PUSH-D questionnaire, which Dr. Silverberg described as a validated tool for gauging a sense of stigmatization, the greater burden of AD was remarkably consistent for those with childhood-onset AD vs adult-onset AD. With higher scores representing a greater sense of stigmatization, the differences in the overall score (23.0 vs 18.1; P < .0001) were highly significant as was every other domain evaluated.
For all five social behavior domains, such as avoiding contact in public and wariness of approaching people spontaneously, having AD onset in childhood persisting into adulthood produced significantly higher scores than having AD onset in adulthood, with no exceptions (P < .001 for all).
AD From Childhood Consistently Results in Worse Outcomes
Providing examples for some of the other 12 domains, Dr. Silverberg maintained that feelings of shame and psychological discomfort were always greater in adults with AD persistent since childhood vs AD starting in adulthood. The P values for these outcomes, such as experiencing bias at work or reporting a sense that others avoided them, were typically highly significant (P < .001).
Compared with those whose AD started in adulthood, “adults with atopic eczema that started during childhood have significantly more difficulties in their life, including occupational relationships, daily life, personal life, and partner or family relationships,” Dr. Silverberg reported.
He said that the data were controlled for multiple confounders, particularly greater severity of AD. He acknowledged that childhood onset might be considered a surrogate for more severe disease, but the data were controlled for this possibility.
Despite the fact that there are “thousands of studies across all age groups showing the burden of AD,” Dr. Silverberg considers these data to be unique by emphasizing the burden of chronicity rather than the impact of AD in any single moment in time.
For those with chronic AD from childhood, “the effect is not just on physical health but a deep negative influence on psychological and social aspects of life,” Dr. Silverberg said, suggesting that the independent effects of chronicity might be worth studying across other dermatologic diseases.
“Regulatory agencies focus on what you can do in that moment of time, losing the bigger picture of how patients are affected chronically,” he said, adding that this is an area of clinical research that should be further explored.
What the data further suggest “is that the earlier we intervene, the more likely patients will do better long term,” he said.
Data Provide Evidence of Systemic Therapy in Kids
For Gudrun Ratzinger, MD, of the Department of Dermatology and Venerology at the Medical University of Innsbruck in Austria, these are valuable data.
“When I prescribe systemic therapies to children, I often get resistance from the healthcare system and even other colleagues,” said Dr. Ratzinger, who was asked to comment on the results. “We are at a teaching hospital, but I often find that when patients return to their home physician, the systemic therapies are stopped.”
In her own practice, she believes the most effective therapies should be introduced in children and adults when complete control is not achieved on first-line drugs. “These data are very helpful for me in explaining to others the importance of effective treatment of atopic dermatitis in children,” she said.
Dr. Silverberg reported financial relationships with more than 40 pharmaceutical companies, including those that make drugs for AD. Dr. Ratzinger reported financial relationships with AbbVie, Almirall, Boehringer Ingelheim, Eli Lilly, Janssen, Leo Pharma, Novartis, Pelpharma, Pfizer, and UCB.
A version of this article first appeared on Medscape.com.
FROM EADV 2024
Expert Calls for Research into GLP-1s for Mental Illness
MILAN — Recent research allaying concerns about suicidality linked to glucagon-like peptide 1 (GLP-1) receptor agonists, along with evidence of these agents’ potential psychiatric and cognitive benefits, has prompted the lead investigator of a major analysis to urge researchers to explore the potential of these drugs for mental illness.
“So far, we’ve been talking about the safety from a neuropsychiatric perspective in diabetes, but there is also the safety and benefit in people with mental disorders,” Riccardo De Giorgi, MD, PhD, from the Department of Psychiatry, University of Oxford in England, said in an interview.
The results of the meta-analysis were previously reported by this news organization and reviewed by Dr. De Giorgi at the 37th European College of Neuropsychopharmacology (ECNP) Congress. Dr. De Giorgi broached
Noting that GLP-1s are not approved for psychiatric disorders, Dr. De Giorgi said it can’t be assumed that the “metabolic or maybe even more general mechanisms that are being modified with these medications in diabetes or even in obesity are the same for people with psychiatric disorders. We’re talking about very different things. From a clinical perspective, you could do real harm,” he told this news organization.
Yet Dr. De Giorgi emphasized the importance of exploring the potential benefits of these medications in psychiatry.
“From a research perspective ... I am very worried about missing an opportunity here. This happened with rimonabant, a cannabis medication that was used for weight loss back in 2012 and was withdrawn quite dramatically in Europe immediately after licensing because it increased suicide risk. Since then, nobody has been touching the cannabinoid system, and that’s a shame because in psychiatry, we don’t have that much we can work on. So we don’t want to miss an opportunity with the GLP-1 system — that’s why we need to be cautious and look at safety first,” he said.
Signal of Efficacy?
Dr. De Giorgi’s research suggested several potential neurobiological effects of GLP-1 inhibition in diabetes research.
“There was a bit of a signal specifically for the big three dementias — vascular, Lewy Body, and frontotemporal — although there was not enough power,” he reported. “We also saw a reduced risk in nicotine misuse, especially amongst other substance use disorders ... and finally a more tentative association for reduced depression.”
He noted that GLP-1s for psychiatric illness likely have limitations and may not cure mental disorders but could help specific subsets of patients. Rather than aiming for large-scale studies, the focus should be on small, incremental studies to advance the research.
Asked by the session chair, John Cryan, PhD, from University College Cork in Ireland, and chair of the ECNP Scientific Committee whether improvement in patients’ mood could be attributed to weight loss, Dr. De Giorgi replied no.
“We now have quite a lot of studies that show that if there is an effect or association it is seen quite a bit earlier than any weight loss. Remember, weight loss takes quite a lot of time, and at quite high doses, but more provocatively, even if that’s the case, does it matter? We as psychiatrists do worry that we need to disentangle these things, but they don’t do that in cardiology, for example. If they see a benefit in mortality they don’t really care if it’s specifically an effect on heart failure or ischemic disease,” said Dr. De Giorgi.
Regardless of their neuropsychiatric potential, the cardiometabolic benefits of GLP-1 inhibitors are sorely needed in the psychiatric population, noted two experts in a recent JAMA Psychiatry viewpoint article.
Sri Mahavir Agarwal, MD, PhD, and Margaret Hahn, MD, PhD, from the University of Toronto and the Schizophrenia Division at the Centre for Addiction and Mental Health, in Toronto, Ontario, Canada, pointed out that “individuals with severe mental illness (SMI) have exceedingly high rates of metabolic comorbidity; three of four are overweight or obese, whereas the prevalence of type 2 diabetes (T2D) is several-fold higher than in the general population. Consequently, individuals with SMI die 15-20 years earlier from cardiovascular disease (CVD) than do those in the general population with CVD,” they noted.
“The arrival of semaglutide has infused significant enthusiasm in the field of mental health research. The proximal effects of weight and related CV comorbidities are significant in themselves. It is plausible that semaglutide could act through neurogenesis or secondary benefits of improving metabolic health on other important outcomes, such as cognitive health and quality of life, thereby filling an unmet need in the treatment of SMI,” Dr. Agarwal and Dr. Hahn added.
An Exciting Opportunity
Current research investigating GLP-1s in psychiatry and neurology is increasingly focused on neuroinflammation, said Dr. De Giorgi.
Research shows significant evidence that certain medications may help reduce dysfunctional inflammatory processes linked to various cognitive and psychiatric disorders, he added.
Many patients with established psychiatric conditions also have physical health issues, which contribute to increased mortality risk, said Dr. De Giorgi. It’s crucial to understand that, if these treatments improve mortality outcomes for psychiatric patients, the specific mechanisms involved are secondary to the results. Psychiatrists must be equipped to prescribe, manage, and initiate these therapies.
“While trials involving psychosis patients are ongoing, we are making progress and should seize this opportunity” said Dr. De Giorgi.
Dr. Cryan agreed: “I think we’ll get there. What these drugs have shown is that you can, through a single mechanism, have multitude effects related to brain-body interactions, and why not focus that on mood and anxiety and cognitive performance? It’s exciting no matter what. We now need to do longitudinal, cross-sectional, placebo-controlled trials in specific patient populations.”
This study received funding from the National Institute for Health and Care Research Oxford Health Biomedical Research Centre and Medical Research Council. Dr. De Giorgi’s coauthors reported receiving funding for other work from Novo Nordisk, Five Lives, Cognetivity Ltd., Cognex, P1vital, Lundbeck, Servier, UCB, Zogenix, Johnson & Johnson, and Syndesi. Dr. Cryan reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN — Recent research allaying concerns about suicidality linked to glucagon-like peptide 1 (GLP-1) receptor agonists, along with evidence of these agents’ potential psychiatric and cognitive benefits, has prompted the lead investigator of a major analysis to urge researchers to explore the potential of these drugs for mental illness.
“So far, we’ve been talking about the safety from a neuropsychiatric perspective in diabetes, but there is also the safety and benefit in people with mental disorders,” Riccardo De Giorgi, MD, PhD, from the Department of Psychiatry, University of Oxford in England, said in an interview.
The results of the meta-analysis were previously reported by this news organization and reviewed by Dr. De Giorgi at the 37th European College of Neuropsychopharmacology (ECNP) Congress. Dr. De Giorgi broached
Noting that GLP-1s are not approved for psychiatric disorders, Dr. De Giorgi said it can’t be assumed that the “metabolic or maybe even more general mechanisms that are being modified with these medications in diabetes or even in obesity are the same for people with psychiatric disorders. We’re talking about very different things. From a clinical perspective, you could do real harm,” he told this news organization.
Yet Dr. De Giorgi emphasized the importance of exploring the potential benefits of these medications in psychiatry.
“From a research perspective ... I am very worried about missing an opportunity here. This happened with rimonabant, a cannabis medication that was used for weight loss back in 2012 and was withdrawn quite dramatically in Europe immediately after licensing because it increased suicide risk. Since then, nobody has been touching the cannabinoid system, and that’s a shame because in psychiatry, we don’t have that much we can work on. So we don’t want to miss an opportunity with the GLP-1 system — that’s why we need to be cautious and look at safety first,” he said.
Signal of Efficacy?
Dr. De Giorgi’s research suggested several potential neurobiological effects of GLP-1 inhibition in diabetes research.
“There was a bit of a signal specifically for the big three dementias — vascular, Lewy Body, and frontotemporal — although there was not enough power,” he reported. “We also saw a reduced risk in nicotine misuse, especially amongst other substance use disorders ... and finally a more tentative association for reduced depression.”
He noted that GLP-1s for psychiatric illness likely have limitations and may not cure mental disorders but could help specific subsets of patients. Rather than aiming for large-scale studies, the focus should be on small, incremental studies to advance the research.
Asked by the session chair, John Cryan, PhD, from University College Cork in Ireland, and chair of the ECNP Scientific Committee whether improvement in patients’ mood could be attributed to weight loss, Dr. De Giorgi replied no.
“We now have quite a lot of studies that show that if there is an effect or association it is seen quite a bit earlier than any weight loss. Remember, weight loss takes quite a lot of time, and at quite high doses, but more provocatively, even if that’s the case, does it matter? We as psychiatrists do worry that we need to disentangle these things, but they don’t do that in cardiology, for example. If they see a benefit in mortality they don’t really care if it’s specifically an effect on heart failure or ischemic disease,” said Dr. De Giorgi.
Regardless of their neuropsychiatric potential, the cardiometabolic benefits of GLP-1 inhibitors are sorely needed in the psychiatric population, noted two experts in a recent JAMA Psychiatry viewpoint article.
Sri Mahavir Agarwal, MD, PhD, and Margaret Hahn, MD, PhD, from the University of Toronto and the Schizophrenia Division at the Centre for Addiction and Mental Health, in Toronto, Ontario, Canada, pointed out that “individuals with severe mental illness (SMI) have exceedingly high rates of metabolic comorbidity; three of four are overweight or obese, whereas the prevalence of type 2 diabetes (T2D) is several-fold higher than in the general population. Consequently, individuals with SMI die 15-20 years earlier from cardiovascular disease (CVD) than do those in the general population with CVD,” they noted.
“The arrival of semaglutide has infused significant enthusiasm in the field of mental health research. The proximal effects of weight and related CV comorbidities are significant in themselves. It is plausible that semaglutide could act through neurogenesis or secondary benefits of improving metabolic health on other important outcomes, such as cognitive health and quality of life, thereby filling an unmet need in the treatment of SMI,” Dr. Agarwal and Dr. Hahn added.
An Exciting Opportunity
Current research investigating GLP-1s in psychiatry and neurology is increasingly focused on neuroinflammation, said Dr. De Giorgi.
Research shows significant evidence that certain medications may help reduce dysfunctional inflammatory processes linked to various cognitive and psychiatric disorders, he added.
Many patients with established psychiatric conditions also have physical health issues, which contribute to increased mortality risk, said Dr. De Giorgi. It’s crucial to understand that, if these treatments improve mortality outcomes for psychiatric patients, the specific mechanisms involved are secondary to the results. Psychiatrists must be equipped to prescribe, manage, and initiate these therapies.
“While trials involving psychosis patients are ongoing, we are making progress and should seize this opportunity” said Dr. De Giorgi.
Dr. Cryan agreed: “I think we’ll get there. What these drugs have shown is that you can, through a single mechanism, have multitude effects related to brain-body interactions, and why not focus that on mood and anxiety and cognitive performance? It’s exciting no matter what. We now need to do longitudinal, cross-sectional, placebo-controlled trials in specific patient populations.”
This study received funding from the National Institute for Health and Care Research Oxford Health Biomedical Research Centre and Medical Research Council. Dr. De Giorgi’s coauthors reported receiving funding for other work from Novo Nordisk, Five Lives, Cognetivity Ltd., Cognex, P1vital, Lundbeck, Servier, UCB, Zogenix, Johnson & Johnson, and Syndesi. Dr. Cryan reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN — Recent research allaying concerns about suicidality linked to glucagon-like peptide 1 (GLP-1) receptor agonists, along with evidence of these agents’ potential psychiatric and cognitive benefits, has prompted the lead investigator of a major analysis to urge researchers to explore the potential of these drugs for mental illness.
“So far, we’ve been talking about the safety from a neuropsychiatric perspective in diabetes, but there is also the safety and benefit in people with mental disorders,” Riccardo De Giorgi, MD, PhD, from the Department of Psychiatry, University of Oxford in England, said in an interview.
The results of the meta-analysis were previously reported by this news organization and reviewed by Dr. De Giorgi at the 37th European College of Neuropsychopharmacology (ECNP) Congress. Dr. De Giorgi broached
Noting that GLP-1s are not approved for psychiatric disorders, Dr. De Giorgi said it can’t be assumed that the “metabolic or maybe even more general mechanisms that are being modified with these medications in diabetes or even in obesity are the same for people with psychiatric disorders. We’re talking about very different things. From a clinical perspective, you could do real harm,” he told this news organization.
Yet Dr. De Giorgi emphasized the importance of exploring the potential benefits of these medications in psychiatry.
“From a research perspective ... I am very worried about missing an opportunity here. This happened with rimonabant, a cannabis medication that was used for weight loss back in 2012 and was withdrawn quite dramatically in Europe immediately after licensing because it increased suicide risk. Since then, nobody has been touching the cannabinoid system, and that’s a shame because in psychiatry, we don’t have that much we can work on. So we don’t want to miss an opportunity with the GLP-1 system — that’s why we need to be cautious and look at safety first,” he said.
Signal of Efficacy?
Dr. De Giorgi’s research suggested several potential neurobiological effects of GLP-1 inhibition in diabetes research.
“There was a bit of a signal specifically for the big three dementias — vascular, Lewy Body, and frontotemporal — although there was not enough power,” he reported. “We also saw a reduced risk in nicotine misuse, especially amongst other substance use disorders ... and finally a more tentative association for reduced depression.”
He noted that GLP-1s for psychiatric illness likely have limitations and may not cure mental disorders but could help specific subsets of patients. Rather than aiming for large-scale studies, the focus should be on small, incremental studies to advance the research.
Asked by the session chair, John Cryan, PhD, from University College Cork in Ireland, and chair of the ECNP Scientific Committee whether improvement in patients’ mood could be attributed to weight loss, Dr. De Giorgi replied no.
“We now have quite a lot of studies that show that if there is an effect or association it is seen quite a bit earlier than any weight loss. Remember, weight loss takes quite a lot of time, and at quite high doses, but more provocatively, even if that’s the case, does it matter? We as psychiatrists do worry that we need to disentangle these things, but they don’t do that in cardiology, for example. If they see a benefit in mortality they don’t really care if it’s specifically an effect on heart failure or ischemic disease,” said Dr. De Giorgi.
Regardless of their neuropsychiatric potential, the cardiometabolic benefits of GLP-1 inhibitors are sorely needed in the psychiatric population, noted two experts in a recent JAMA Psychiatry viewpoint article.
Sri Mahavir Agarwal, MD, PhD, and Margaret Hahn, MD, PhD, from the University of Toronto and the Schizophrenia Division at the Centre for Addiction and Mental Health, in Toronto, Ontario, Canada, pointed out that “individuals with severe mental illness (SMI) have exceedingly high rates of metabolic comorbidity; three of four are overweight or obese, whereas the prevalence of type 2 diabetes (T2D) is several-fold higher than in the general population. Consequently, individuals with SMI die 15-20 years earlier from cardiovascular disease (CVD) than do those in the general population with CVD,” they noted.
“The arrival of semaglutide has infused significant enthusiasm in the field of mental health research. The proximal effects of weight and related CV comorbidities are significant in themselves. It is plausible that semaglutide could act through neurogenesis or secondary benefits of improving metabolic health on other important outcomes, such as cognitive health and quality of life, thereby filling an unmet need in the treatment of SMI,” Dr. Agarwal and Dr. Hahn added.
An Exciting Opportunity
Current research investigating GLP-1s in psychiatry and neurology is increasingly focused on neuroinflammation, said Dr. De Giorgi.
Research shows significant evidence that certain medications may help reduce dysfunctional inflammatory processes linked to various cognitive and psychiatric disorders, he added.
Many patients with established psychiatric conditions also have physical health issues, which contribute to increased mortality risk, said Dr. De Giorgi. It’s crucial to understand that, if these treatments improve mortality outcomes for psychiatric patients, the specific mechanisms involved are secondary to the results. Psychiatrists must be equipped to prescribe, manage, and initiate these therapies.
“While trials involving psychosis patients are ongoing, we are making progress and should seize this opportunity” said Dr. De Giorgi.
Dr. Cryan agreed: “I think we’ll get there. What these drugs have shown is that you can, through a single mechanism, have multitude effects related to brain-body interactions, and why not focus that on mood and anxiety and cognitive performance? It’s exciting no matter what. We now need to do longitudinal, cross-sectional, placebo-controlled trials in specific patient populations.”
This study received funding from the National Institute for Health and Care Research Oxford Health Biomedical Research Centre and Medical Research Council. Dr. De Giorgi’s coauthors reported receiving funding for other work from Novo Nordisk, Five Lives, Cognetivity Ltd., Cognex, P1vital, Lundbeck, Servier, UCB, Zogenix, Johnson & Johnson, and Syndesi. Dr. Cryan reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ECNP CONGRESS 2024
Treatment-Resistant Depression Linked to Increased Mortality
TOPLINE:
Treatment-resistant major depression (TRD) is associated with a 17% higher risk for all-cause mortality than non-TRD major depressive disorder (MDD), a new study shows. The increased mortality risk was driven largely by suicide and accidental overdose, which were nearly twice as high among people whose depression didn’t improve after two treatments.
METHODOLOGY:
- Data on 176,942 individuals diagnosed with MDD and treated with an antidepressant (median age at diagnosis, 40 years; 63% women) were obtained from Finnish nationwide registers.
- About 11% of the participants had TRD, defined as having more than two adequate treatment trials of at least 28 days, each within 2 years from the index antidepressant prescription.
- The outcomes were all-cause and cause-specific mortality, with demographic characteristics, psychiatric comorbidities, and treatment history included as covariates.
- The median follow-up period was 8.9 years.
TAKEAWAY:
- Median time to TRD was 8 months, and 959 and 7662 deaths were observed in the TRD and non-TRD groups, respectively.
- All-cause mortality was 17% higher among patients with TRD than among those with non-TRD (adjusted hazard ratio [aHR], 1.17; 95% CI, 1.09-1.25) because of higher mortality to external causes.
- Mortalities because of suicides (aHR, 1.90; 95% CI, 1.64-2.20) and accidental poisonings (aHR, 1.81; 95% CI, 1.48-2.22) were almost double in the TRD group, compared with the non-TRD group.
- No significant difference in mortality due to natural causes was observed between the TRD and non-TRD groups.
IN PRACTICE:
“The markedly increased mortality due to suicides and accidental overdoses suggests that persons with TRD may experience higher-intensity symptoms and more severe suicidal ideation than persons with non-TRD major depression,” the study authors wrote.
SOURCE:
The study was led by Tapio T. Gustafsson, University of Eastern Finland, Niuvanniemi Hospital, Kuopio, Finland. It was published online on September 11, 2024, in The Journal of Affective Disorders.
LIMITATIONS:
The definition of TRD lacked consensus. The study used routine data to define TRD, which may not have captured all relevant clinical nuances. Additionally, the reasons for medication changes were unavailable.
DISCLOSURES:
This study was funded by Johnson & Johnson Innovative Medicine and Niuvanniemi Hospital, with support from the Finnish Ministry of Social Affairs and Health. Several authors disclosed financial relationships with various pharmaceutical companies, and two are employees of Johnson & Johnson Innovative Medicine.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Treatment-resistant major depression (TRD) is associated with a 17% higher risk for all-cause mortality than non-TRD major depressive disorder (MDD), a new study shows. The increased mortality risk was driven largely by suicide and accidental overdose, which were nearly twice as high among people whose depression didn’t improve after two treatments.
METHODOLOGY:
- Data on 176,942 individuals diagnosed with MDD and treated with an antidepressant (median age at diagnosis, 40 years; 63% women) were obtained from Finnish nationwide registers.
- About 11% of the participants had TRD, defined as having more than two adequate treatment trials of at least 28 days, each within 2 years from the index antidepressant prescription.
- The outcomes were all-cause and cause-specific mortality, with demographic characteristics, psychiatric comorbidities, and treatment history included as covariates.
- The median follow-up period was 8.9 years.
TAKEAWAY:
- Median time to TRD was 8 months, and 959 and 7662 deaths were observed in the TRD and non-TRD groups, respectively.
- All-cause mortality was 17% higher among patients with TRD than among those with non-TRD (adjusted hazard ratio [aHR], 1.17; 95% CI, 1.09-1.25) because of higher mortality to external causes.
- Mortalities because of suicides (aHR, 1.90; 95% CI, 1.64-2.20) and accidental poisonings (aHR, 1.81; 95% CI, 1.48-2.22) were almost double in the TRD group, compared with the non-TRD group.
- No significant difference in mortality due to natural causes was observed between the TRD and non-TRD groups.
IN PRACTICE:
“The markedly increased mortality due to suicides and accidental overdoses suggests that persons with TRD may experience higher-intensity symptoms and more severe suicidal ideation than persons with non-TRD major depression,” the study authors wrote.
SOURCE:
The study was led by Tapio T. Gustafsson, University of Eastern Finland, Niuvanniemi Hospital, Kuopio, Finland. It was published online on September 11, 2024, in The Journal of Affective Disorders.
LIMITATIONS:
The definition of TRD lacked consensus. The study used routine data to define TRD, which may not have captured all relevant clinical nuances. Additionally, the reasons for medication changes were unavailable.
DISCLOSURES:
This study was funded by Johnson & Johnson Innovative Medicine and Niuvanniemi Hospital, with support from the Finnish Ministry of Social Affairs and Health. Several authors disclosed financial relationships with various pharmaceutical companies, and two are employees of Johnson & Johnson Innovative Medicine.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Treatment-resistant major depression (TRD) is associated with a 17% higher risk for all-cause mortality than non-TRD major depressive disorder (MDD), a new study shows. The increased mortality risk was driven largely by suicide and accidental overdose, which were nearly twice as high among people whose depression didn’t improve after two treatments.
METHODOLOGY:
- Data on 176,942 individuals diagnosed with MDD and treated with an antidepressant (median age at diagnosis, 40 years; 63% women) were obtained from Finnish nationwide registers.
- About 11% of the participants had TRD, defined as having more than two adequate treatment trials of at least 28 days, each within 2 years from the index antidepressant prescription.
- The outcomes were all-cause and cause-specific mortality, with demographic characteristics, psychiatric comorbidities, and treatment history included as covariates.
- The median follow-up period was 8.9 years.
TAKEAWAY:
- Median time to TRD was 8 months, and 959 and 7662 deaths were observed in the TRD and non-TRD groups, respectively.
- All-cause mortality was 17% higher among patients with TRD than among those with non-TRD (adjusted hazard ratio [aHR], 1.17; 95% CI, 1.09-1.25) because of higher mortality to external causes.
- Mortalities because of suicides (aHR, 1.90; 95% CI, 1.64-2.20) and accidental poisonings (aHR, 1.81; 95% CI, 1.48-2.22) were almost double in the TRD group, compared with the non-TRD group.
- No significant difference in mortality due to natural causes was observed between the TRD and non-TRD groups.
IN PRACTICE:
“The markedly increased mortality due to suicides and accidental overdoses suggests that persons with TRD may experience higher-intensity symptoms and more severe suicidal ideation than persons with non-TRD major depression,” the study authors wrote.
SOURCE:
The study was led by Tapio T. Gustafsson, University of Eastern Finland, Niuvanniemi Hospital, Kuopio, Finland. It was published online on September 11, 2024, in The Journal of Affective Disorders.
LIMITATIONS:
The definition of TRD lacked consensus. The study used routine data to define TRD, which may not have captured all relevant clinical nuances. Additionally, the reasons for medication changes were unavailable.
DISCLOSURES:
This study was funded by Johnson & Johnson Innovative Medicine and Niuvanniemi Hospital, with support from the Finnish Ministry of Social Affairs and Health. Several authors disclosed financial relationships with various pharmaceutical companies, and two are employees of Johnson & Johnson Innovative Medicine.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Considering Eating Disorder Potential When Prescribing Weight Loss Drugs to Teens
Now, with the rising popularity of medications like Ozempic for weight loss, she fears she will care for more teens with eating disorders who are seeking glucagon-like peptide 1 (GLP-1) agonists or who have developed a disorder while taking them.
“We haven’t seen patients yet, but I’m sure they are on their way,” said Dr. Dennis, a clinical assistant professor in the Department of Psychiatry at the University of Illinois College of Medicine in Chicago. She is also the cofounder and chief medical officer of SunCloud Health, an outpatient eating disorder treatment center in Illinois.
Dr. Dennis’ concerns reflect a growing unease among eating disorder specialists as obesity medications gain traction for adolescent use. A recent study published in JAMA Pediatrics showed nearly 80% of teens in treatment for obesity reported symptoms of disordered eating at the outset of an intervention. These included signs of binge eating and loss of control.
The randomized clinical trial, conducted from 2018 to 2023, examined 141 adolescents with obesity undergoing interventions like low-energy diets or intermittent energy restriction. Almost half scored as having risk for an undiagnosed eating disorder, as defined by the Eating Disorder Examination Questionnaire (EDE-Q).
At the end of the intervention, many teens continued to have symptoms of disordered eating, while a smaller group was newly scored as having a risk for an eating disorder.
Weight Loss and Eating Disorders: A Balancing Act
The findings illuminate a significant challenge for pediatricians and primary care clinicians: Balancing effective weight management with the risk of exacerbating or triggering eating disorders, said Hiba Jebeile, PhD, a research dietitian at The Children’s Hospital at Westmead in Australia, and the study’s lead author. Adding weight loss medication on top of the equation can further complicate care.
“It is helpful for obesity and eating disorder services to work together, with clear referral pathways, to manage these adolescents,” Dr. Jebeile said.
The US Food and Drug Administration approved semaglutide for weight loss in adolescents aged 12-17 years in December 2020. One study found that the number of adolescents prescribed GLP-1 receptor agonists (GLP-1 RAs) for type 2 diabetes and weight management rose from 8722 to 60,567 between 2020 and 2023 — a nearly sevenfold increase.
“The number of adolescents taking these medications is going up because they work,” said Suzanne Cuda, MD, medical director of Alamo City Healthy Kids and Families, a medical weight management clinic in San Antonio. The medications have been shown to treat type 2 diabetes, lower blood pressure, and reduce the risk for cardiovascular diseases.
“The younger you are, the better the outcome,” Dr. Cuda said.
How GLP-1 agonists may affect adolescents in the long run is not yet clear. Existing studies on GLP-1 medications in patients with eating disorders have shown mixed results. Some studies indicate that the drugs decrease binge episodes for those with binge eating disorder or bulimia nervosa. However, these studies had small sample sizes and measured only short-term effects, leaving long-term outcomes and risks unknown.
Traditional treatments for eating disorders emphasize regular eating patterns, body acceptance, addressing weight stigma, and improving attunement to hunger and fullness cues — approaches that may conflict with the effects of GLP-1 agonists. These drugs suppress appetite, alter metabolic signals, and may unintentionally reinforce weight loss as a primary goal, creating a potential disconnect between the aims of recovery from eating disorders and the biologic effects of the medication, experts said.
Dr. Cuda said she has cared for adolescents with diagnosed eating disorders in her practice who are seeking GLP-1 agonists. She said she first works with patients to treat the underlying disorder before prescribing medication.
“One of the concerns is the extreme reductions in calories that could be induced by GLP-1 RA in children and adolescents,” she said. Unlike adults, adolescents use caloric energy not just for physical activity but also for growing and developing, she said.
“They can’t catch up on that growth and development,” she added.
Advice for Screening and Monitoring
The National Eating Disorders Association raised concerns about the potential misuse of these medications and their potential to exacerbate eating disorder behaviors in people who are already at a higher risk of developing one of the conditions, including those with existing mental health disorders, stress, who have already dieted, and who have experienced weight-centric bullying.
Clinicians should be on the lookout for patients seeking GLP-1s who present with symptoms of an eating disorder that may be less apparent, such as picky eating, insomnia or difficulty sleeping, or, for girls, irregular menstrual periods, Dr. Dennis said. These patients may be more likely to go undiagnosed or misdiagnosed. Research also suggests that people of color are less likely to be diagnosed or receive specialty care for eating disorders.
Discussions between patients and clinicians about obesity treatment prior to prescribing provide a crucial opportunity to screen and monitor for disordered eating, which Dr. Dennis said does not universally occur currently.
Dr. Dennis recommended initial assessments using validated screening tools like the EDE-Q and the Center for Epidemiologic Studies Depression Scale Revised, 10-Item Version.
Ongoing monitoring throughout treatment is essential, with initial monthly check-ins that include dietary counseling to detect subtle changes in eating behaviors or attitudes toward food and body image, Dr. Cuda said.
The Obesity Medicine Association (OMA) has stressed the importance of a collaborative approach involving connections with mental health professionals specializing in eating disorders and dietitians.
“If you have a chance to send them to an obesity medicine specialist, you should do that,” said Dr. Cuda, who coauthored the OMA statement. “It’s impractical to expect a primary care physician to do everything: Screen for dietary disorders, do a full dietary counseling, follow up on their activity.”
For patients showing signs of disordered eating, clinicians should avoid recommending restrictive dietary approaches, like cutting out food groups such as carbohydrates or a restricted calorie goal. Instead, they can suggest focusing on healthier lifestyle habits and referring to a psychotherapist, the experts said. Clinicians also should be prepared to adjust or pause GLP-1 agonists if disordered eating disorder symptoms worsen.
“I think a weight-agnostic approach where the focus of care is not weight loss but increase in health protective behaviors and nutritional intake is safest for all kids, especially those with eating disorders or eating disorder risk factors,” Dr. Dennis said.
Various authors of the eating disorder study reported receiving grants, advisory board fees, and speaker fees from entities including the National Health and Medical Research Council of Australia, Eli Lilly, Novo Nordisk, Nu-Mega Ingredients, and the National Institutes of Health, among others.
A version of this article appeared on Medscape.com.
Now, with the rising popularity of medications like Ozempic for weight loss, she fears she will care for more teens with eating disorders who are seeking glucagon-like peptide 1 (GLP-1) agonists or who have developed a disorder while taking them.
“We haven’t seen patients yet, but I’m sure they are on their way,” said Dr. Dennis, a clinical assistant professor in the Department of Psychiatry at the University of Illinois College of Medicine in Chicago. She is also the cofounder and chief medical officer of SunCloud Health, an outpatient eating disorder treatment center in Illinois.
Dr. Dennis’ concerns reflect a growing unease among eating disorder specialists as obesity medications gain traction for adolescent use. A recent study published in JAMA Pediatrics showed nearly 80% of teens in treatment for obesity reported symptoms of disordered eating at the outset of an intervention. These included signs of binge eating and loss of control.
The randomized clinical trial, conducted from 2018 to 2023, examined 141 adolescents with obesity undergoing interventions like low-energy diets or intermittent energy restriction. Almost half scored as having risk for an undiagnosed eating disorder, as defined by the Eating Disorder Examination Questionnaire (EDE-Q).
At the end of the intervention, many teens continued to have symptoms of disordered eating, while a smaller group was newly scored as having a risk for an eating disorder.
Weight Loss and Eating Disorders: A Balancing Act
The findings illuminate a significant challenge for pediatricians and primary care clinicians: Balancing effective weight management with the risk of exacerbating or triggering eating disorders, said Hiba Jebeile, PhD, a research dietitian at The Children’s Hospital at Westmead in Australia, and the study’s lead author. Adding weight loss medication on top of the equation can further complicate care.
“It is helpful for obesity and eating disorder services to work together, with clear referral pathways, to manage these adolescents,” Dr. Jebeile said.
The US Food and Drug Administration approved semaglutide for weight loss in adolescents aged 12-17 years in December 2020. One study found that the number of adolescents prescribed GLP-1 receptor agonists (GLP-1 RAs) for type 2 diabetes and weight management rose from 8722 to 60,567 between 2020 and 2023 — a nearly sevenfold increase.
“The number of adolescents taking these medications is going up because they work,” said Suzanne Cuda, MD, medical director of Alamo City Healthy Kids and Families, a medical weight management clinic in San Antonio. The medications have been shown to treat type 2 diabetes, lower blood pressure, and reduce the risk for cardiovascular diseases.
“The younger you are, the better the outcome,” Dr. Cuda said.
How GLP-1 agonists may affect adolescents in the long run is not yet clear. Existing studies on GLP-1 medications in patients with eating disorders have shown mixed results. Some studies indicate that the drugs decrease binge episodes for those with binge eating disorder or bulimia nervosa. However, these studies had small sample sizes and measured only short-term effects, leaving long-term outcomes and risks unknown.
Traditional treatments for eating disorders emphasize regular eating patterns, body acceptance, addressing weight stigma, and improving attunement to hunger and fullness cues — approaches that may conflict with the effects of GLP-1 agonists. These drugs suppress appetite, alter metabolic signals, and may unintentionally reinforce weight loss as a primary goal, creating a potential disconnect between the aims of recovery from eating disorders and the biologic effects of the medication, experts said.
Dr. Cuda said she has cared for adolescents with diagnosed eating disorders in her practice who are seeking GLP-1 agonists. She said she first works with patients to treat the underlying disorder before prescribing medication.
“One of the concerns is the extreme reductions in calories that could be induced by GLP-1 RA in children and adolescents,” she said. Unlike adults, adolescents use caloric energy not just for physical activity but also for growing and developing, she said.
“They can’t catch up on that growth and development,” she added.
Advice for Screening and Monitoring
The National Eating Disorders Association raised concerns about the potential misuse of these medications and their potential to exacerbate eating disorder behaviors in people who are already at a higher risk of developing one of the conditions, including those with existing mental health disorders, stress, who have already dieted, and who have experienced weight-centric bullying.
Clinicians should be on the lookout for patients seeking GLP-1s who present with symptoms of an eating disorder that may be less apparent, such as picky eating, insomnia or difficulty sleeping, or, for girls, irregular menstrual periods, Dr. Dennis said. These patients may be more likely to go undiagnosed or misdiagnosed. Research also suggests that people of color are less likely to be diagnosed or receive specialty care for eating disorders.
Discussions between patients and clinicians about obesity treatment prior to prescribing provide a crucial opportunity to screen and monitor for disordered eating, which Dr. Dennis said does not universally occur currently.
Dr. Dennis recommended initial assessments using validated screening tools like the EDE-Q and the Center for Epidemiologic Studies Depression Scale Revised, 10-Item Version.
Ongoing monitoring throughout treatment is essential, with initial monthly check-ins that include dietary counseling to detect subtle changes in eating behaviors or attitudes toward food and body image, Dr. Cuda said.
The Obesity Medicine Association (OMA) has stressed the importance of a collaborative approach involving connections with mental health professionals specializing in eating disorders and dietitians.
“If you have a chance to send them to an obesity medicine specialist, you should do that,” said Dr. Cuda, who coauthored the OMA statement. “It’s impractical to expect a primary care physician to do everything: Screen for dietary disorders, do a full dietary counseling, follow up on their activity.”
For patients showing signs of disordered eating, clinicians should avoid recommending restrictive dietary approaches, like cutting out food groups such as carbohydrates or a restricted calorie goal. Instead, they can suggest focusing on healthier lifestyle habits and referring to a psychotherapist, the experts said. Clinicians also should be prepared to adjust or pause GLP-1 agonists if disordered eating disorder symptoms worsen.
“I think a weight-agnostic approach where the focus of care is not weight loss but increase in health protective behaviors and nutritional intake is safest for all kids, especially those with eating disorders or eating disorder risk factors,” Dr. Dennis said.
Various authors of the eating disorder study reported receiving grants, advisory board fees, and speaker fees from entities including the National Health and Medical Research Council of Australia, Eli Lilly, Novo Nordisk, Nu-Mega Ingredients, and the National Institutes of Health, among others.
A version of this article appeared on Medscape.com.
Now, with the rising popularity of medications like Ozempic for weight loss, she fears she will care for more teens with eating disorders who are seeking glucagon-like peptide 1 (GLP-1) agonists or who have developed a disorder while taking them.
“We haven’t seen patients yet, but I’m sure they are on their way,” said Dr. Dennis, a clinical assistant professor in the Department of Psychiatry at the University of Illinois College of Medicine in Chicago. She is also the cofounder and chief medical officer of SunCloud Health, an outpatient eating disorder treatment center in Illinois.
Dr. Dennis’ concerns reflect a growing unease among eating disorder specialists as obesity medications gain traction for adolescent use. A recent study published in JAMA Pediatrics showed nearly 80% of teens in treatment for obesity reported symptoms of disordered eating at the outset of an intervention. These included signs of binge eating and loss of control.
The randomized clinical trial, conducted from 2018 to 2023, examined 141 adolescents with obesity undergoing interventions like low-energy diets or intermittent energy restriction. Almost half scored as having risk for an undiagnosed eating disorder, as defined by the Eating Disorder Examination Questionnaire (EDE-Q).
At the end of the intervention, many teens continued to have symptoms of disordered eating, while a smaller group was newly scored as having a risk for an eating disorder.
Weight Loss and Eating Disorders: A Balancing Act
The findings illuminate a significant challenge for pediatricians and primary care clinicians: Balancing effective weight management with the risk of exacerbating or triggering eating disorders, said Hiba Jebeile, PhD, a research dietitian at The Children’s Hospital at Westmead in Australia, and the study’s lead author. Adding weight loss medication on top of the equation can further complicate care.
“It is helpful for obesity and eating disorder services to work together, with clear referral pathways, to manage these adolescents,” Dr. Jebeile said.
The US Food and Drug Administration approved semaglutide for weight loss in adolescents aged 12-17 years in December 2020. One study found that the number of adolescents prescribed GLP-1 receptor agonists (GLP-1 RAs) for type 2 diabetes and weight management rose from 8722 to 60,567 between 2020 and 2023 — a nearly sevenfold increase.
“The number of adolescents taking these medications is going up because they work,” said Suzanne Cuda, MD, medical director of Alamo City Healthy Kids and Families, a medical weight management clinic in San Antonio. The medications have been shown to treat type 2 diabetes, lower blood pressure, and reduce the risk for cardiovascular diseases.
“The younger you are, the better the outcome,” Dr. Cuda said.
How GLP-1 agonists may affect adolescents in the long run is not yet clear. Existing studies on GLP-1 medications in patients with eating disorders have shown mixed results. Some studies indicate that the drugs decrease binge episodes for those with binge eating disorder or bulimia nervosa. However, these studies had small sample sizes and measured only short-term effects, leaving long-term outcomes and risks unknown.
Traditional treatments for eating disorders emphasize regular eating patterns, body acceptance, addressing weight stigma, and improving attunement to hunger and fullness cues — approaches that may conflict with the effects of GLP-1 agonists. These drugs suppress appetite, alter metabolic signals, and may unintentionally reinforce weight loss as a primary goal, creating a potential disconnect between the aims of recovery from eating disorders and the biologic effects of the medication, experts said.
Dr. Cuda said she has cared for adolescents with diagnosed eating disorders in her practice who are seeking GLP-1 agonists. She said she first works with patients to treat the underlying disorder before prescribing medication.
“One of the concerns is the extreme reductions in calories that could be induced by GLP-1 RA in children and adolescents,” she said. Unlike adults, adolescents use caloric energy not just for physical activity but also for growing and developing, she said.
“They can’t catch up on that growth and development,” she added.
Advice for Screening and Monitoring
The National Eating Disorders Association raised concerns about the potential misuse of these medications and their potential to exacerbate eating disorder behaviors in people who are already at a higher risk of developing one of the conditions, including those with existing mental health disorders, stress, who have already dieted, and who have experienced weight-centric bullying.
Clinicians should be on the lookout for patients seeking GLP-1s who present with symptoms of an eating disorder that may be less apparent, such as picky eating, insomnia or difficulty sleeping, or, for girls, irregular menstrual periods, Dr. Dennis said. These patients may be more likely to go undiagnosed or misdiagnosed. Research also suggests that people of color are less likely to be diagnosed or receive specialty care for eating disorders.
Discussions between patients and clinicians about obesity treatment prior to prescribing provide a crucial opportunity to screen and monitor for disordered eating, which Dr. Dennis said does not universally occur currently.
Dr. Dennis recommended initial assessments using validated screening tools like the EDE-Q and the Center for Epidemiologic Studies Depression Scale Revised, 10-Item Version.
Ongoing monitoring throughout treatment is essential, with initial monthly check-ins that include dietary counseling to detect subtle changes in eating behaviors or attitudes toward food and body image, Dr. Cuda said.
The Obesity Medicine Association (OMA) has stressed the importance of a collaborative approach involving connections with mental health professionals specializing in eating disorders and dietitians.
“If you have a chance to send them to an obesity medicine specialist, you should do that,” said Dr. Cuda, who coauthored the OMA statement. “It’s impractical to expect a primary care physician to do everything: Screen for dietary disorders, do a full dietary counseling, follow up on their activity.”
For patients showing signs of disordered eating, clinicians should avoid recommending restrictive dietary approaches, like cutting out food groups such as carbohydrates or a restricted calorie goal. Instead, they can suggest focusing on healthier lifestyle habits and referring to a psychotherapist, the experts said. Clinicians also should be prepared to adjust or pause GLP-1 agonists if disordered eating disorder symptoms worsen.
“I think a weight-agnostic approach where the focus of care is not weight loss but increase in health protective behaviors and nutritional intake is safest for all kids, especially those with eating disorders or eating disorder risk factors,” Dr. Dennis said.
Various authors of the eating disorder study reported receiving grants, advisory board fees, and speaker fees from entities including the National Health and Medical Research Council of Australia, Eli Lilly, Novo Nordisk, Nu-Mega Ingredients, and the National Institutes of Health, among others.
A version of this article appeared on Medscape.com.
FROM JAMA PEDIATRICS
Hidden in Plain Sight: The Growing Epidemic of Ultraprocessed Food Addiction
Yet, even as this evidence mounted, these food items have become increasingly prominent in diets globally.
Now, recent studies are unlocking why cutting back on ultraprocessed foods can be so challenging. In their ability to fuel intense cravings, loss of control, and even withdrawal symptoms, ultraprocessed foods appear as capable of triggering addiction as traditional culprits like tobacco and alcohol.
This has driven efforts to better understand the addictive nature of these foods and identify strategies for combating it.
The Key Role of the Food Industry
Some foods are more likely to trigger addictions than others. For instance, in our studies, participants frequently mention chocolate, pizza, French fries, potato chips, and soda as some of the most addictive foods. What these foods all share is an ability to deliver high doses of refined carbohydrates, fat, or salt at levels exceeding those found in natural foods (eg, fruits, vegetables, beans).
Furthermore, ultraprocessed foods are industrially mass-produced in a process that relies on the heavy use of flavor enhancers and additives, as well as preservatives and packaging that make them shelf-stable. This has flooded our food supply with cheap, accessible, hyperrewarding foods that our brains are not well equipped to resist.
To add to these already substantial effects, the food industry often employs strategies reminiscent of Big Tobacco. They engineer foods to hit our “bliss points,” maximizing craving and fostering brand loyalty from a young age. This product engineering, coupled with aggressive marketing, makes these foods both attractive and seemingly ubiquitous.
How Many People Are Affected?
Addiction to ultraprocessed food is more common than you might think. According to the Yale Food Addiction Scale — a tool that uses the same criteria for diagnosing substance use disorders to assess ultraprocessed food addiction (UPFA) — about 14% of adults and 12% of children show clinically significant signs of addiction to such foods. This is quite similar to addiction rates among adults for legal substances like alcohol and tobacco.
Research has shown that behaviors and brain mechanisms contributing to addictive disorders, such as cravings and impulsivity, also apply to UPFA.
Many more people outside of those who meet the criteria for UPFA are influenced by their addictive properties. Picture a teenager craving a sugary drink after school, a child needing the morning cereal fix, or adults reaching for candy and fast food; these scenarios illustrate how addictive ultraprocessed foods permeate our daily lives.
From a public health standpoint, this comes at a significant cost. Even experiencing one or two symptoms of UPFA, such as intense cravings or a feeling of loss of control over intake, can lead to consuming too many calories, sugar, fat, and sodium in a way that puts health at risk.
Clinical Implications
Numerous studies have found that individuals who exhibit UPFA have more severe mental and physical health challenges. For example, UPFA is associated with higher rates of diet-related diseases (like type 2 diabetes), greater overall mental health issues, and generally poorer outcomes in weight loss treatments.
Despite the growing understanding of UPFA’s relevance in clinical settings, research is still limited on how to best treat, manage, or prevent it. Most of the existing work has focused on investigating whether UPFA is indeed a real condition, with efforts to create clinical guidelines only just beginning.
Of note, UPFA isn’t officially recognized as a diagnosis — yet. If it were, it could spark much more research into how to handle it clinically.
There is some debate about whether we really need this new diagnosis, given that eating disorders are already recognized. However, the statistics tell a different story: Around 14% of people might have UPFA compared with about 1% for binge-type eating disorders. This suggests that many individuals with problematic eating habits are currently flying under the radar with our existing diagnostic categories.
What’s even more concerning is that these individuals often suffer significant problems and exhibit distinct brain differences, even if they do not neatly fit into an existing eating disorder diagnosis. Officially recognizing UPFA could open up new avenues for support and lead to better treatments aimed at reducing compulsive eating patterns.
Treatment Options
Treatment options for UPFA are still being explored. Initial evidence suggests that medications used for treating substance addiction, such as naltrexone and bupropion, might help with highly processed food addiction as well. Newer drugs, like glucagon-like peptide-1 receptor agonists, which appear to curb food cravings and manage addictive behaviors, also look promising.
Psychosocial approaches can also be used to address UPFA. Strategies include:
- Helping individuals become more aware of their triggers for addictive patterns of intake. This often involves identifying certain types of food (eg, potato chips, candy), specific places or times of day (eg, sitting on the couch at night while watching TV), and particular emotional states (eg, anger, loneliness, boredom, sadness). Increasing awareness of personal triggers can help people minimize their exposure to these and develop coping strategies when they do arise.
- Many people use ultraprocessed foods to cope with challenging emotions. Helping individuals develop healthier strategies to regulate their emotions can be key. This may include seeking out social support, journaling, going for a walk, or practicing mindfulness.
- UPFA can be associated with erratic and inconsistent eating patterns. Stabilizing eating habits by consuming regular meals composed of more minimally processed foods (eg, vegetables, fruits, high-quality protein, beans) can help heal the body and reduce vulnerability to ultraprocessed food triggers.
- Many people with UPFA have other existing mental health conditions, including mood disorders, anxiety, substance use disorders, or trauma-related disorders. Addressing these co-occurring mental health conditions can help reduce reliance on ultraprocessed foods.
Public-policy interventions may also help safeguard vulnerable populations from developing UPFA. For instance, support exists for policies to protect children from cigarette marketing and to put clear addiction warning labels on cigarette packages. A similar approach could be applied to reduce the harms associated with ultraprocessed foods, particularly for children.
Combating this growing problem requires treating ultraprocessed foods like other addictive substances. By identifying the threat posed by these common food items, we can not only help patients with UPFA, but also potentially stave off the development of several diet-related conditions.
Dr. Gearhardt, professor of psychology, University of Michigan, Ann Arbor, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Yet, even as this evidence mounted, these food items have become increasingly prominent in diets globally.
Now, recent studies are unlocking why cutting back on ultraprocessed foods can be so challenging. In their ability to fuel intense cravings, loss of control, and even withdrawal symptoms, ultraprocessed foods appear as capable of triggering addiction as traditional culprits like tobacco and alcohol.
This has driven efforts to better understand the addictive nature of these foods and identify strategies for combating it.
The Key Role of the Food Industry
Some foods are more likely to trigger addictions than others. For instance, in our studies, participants frequently mention chocolate, pizza, French fries, potato chips, and soda as some of the most addictive foods. What these foods all share is an ability to deliver high doses of refined carbohydrates, fat, or salt at levels exceeding those found in natural foods (eg, fruits, vegetables, beans).
Furthermore, ultraprocessed foods are industrially mass-produced in a process that relies on the heavy use of flavor enhancers and additives, as well as preservatives and packaging that make them shelf-stable. This has flooded our food supply with cheap, accessible, hyperrewarding foods that our brains are not well equipped to resist.
To add to these already substantial effects, the food industry often employs strategies reminiscent of Big Tobacco. They engineer foods to hit our “bliss points,” maximizing craving and fostering brand loyalty from a young age. This product engineering, coupled with aggressive marketing, makes these foods both attractive and seemingly ubiquitous.
How Many People Are Affected?
Addiction to ultraprocessed food is more common than you might think. According to the Yale Food Addiction Scale — a tool that uses the same criteria for diagnosing substance use disorders to assess ultraprocessed food addiction (UPFA) — about 14% of adults and 12% of children show clinically significant signs of addiction to such foods. This is quite similar to addiction rates among adults for legal substances like alcohol and tobacco.
Research has shown that behaviors and brain mechanisms contributing to addictive disorders, such as cravings and impulsivity, also apply to UPFA.
Many more people outside of those who meet the criteria for UPFA are influenced by their addictive properties. Picture a teenager craving a sugary drink after school, a child needing the morning cereal fix, or adults reaching for candy and fast food; these scenarios illustrate how addictive ultraprocessed foods permeate our daily lives.
From a public health standpoint, this comes at a significant cost. Even experiencing one or two symptoms of UPFA, such as intense cravings or a feeling of loss of control over intake, can lead to consuming too many calories, sugar, fat, and sodium in a way that puts health at risk.
Clinical Implications
Numerous studies have found that individuals who exhibit UPFA have more severe mental and physical health challenges. For example, UPFA is associated with higher rates of diet-related diseases (like type 2 diabetes), greater overall mental health issues, and generally poorer outcomes in weight loss treatments.
Despite the growing understanding of UPFA’s relevance in clinical settings, research is still limited on how to best treat, manage, or prevent it. Most of the existing work has focused on investigating whether UPFA is indeed a real condition, with efforts to create clinical guidelines only just beginning.
Of note, UPFA isn’t officially recognized as a diagnosis — yet. If it were, it could spark much more research into how to handle it clinically.
There is some debate about whether we really need this new diagnosis, given that eating disorders are already recognized. However, the statistics tell a different story: Around 14% of people might have UPFA compared with about 1% for binge-type eating disorders. This suggests that many individuals with problematic eating habits are currently flying under the radar with our existing diagnostic categories.
What’s even more concerning is that these individuals often suffer significant problems and exhibit distinct brain differences, even if they do not neatly fit into an existing eating disorder diagnosis. Officially recognizing UPFA could open up new avenues for support and lead to better treatments aimed at reducing compulsive eating patterns.
Treatment Options
Treatment options for UPFA are still being explored. Initial evidence suggests that medications used for treating substance addiction, such as naltrexone and bupropion, might help with highly processed food addiction as well. Newer drugs, like glucagon-like peptide-1 receptor agonists, which appear to curb food cravings and manage addictive behaviors, also look promising.
Psychosocial approaches can also be used to address UPFA. Strategies include:
- Helping individuals become more aware of their triggers for addictive patterns of intake. This often involves identifying certain types of food (eg, potato chips, candy), specific places or times of day (eg, sitting on the couch at night while watching TV), and particular emotional states (eg, anger, loneliness, boredom, sadness). Increasing awareness of personal triggers can help people minimize their exposure to these and develop coping strategies when they do arise.
- Many people use ultraprocessed foods to cope with challenging emotions. Helping individuals develop healthier strategies to regulate their emotions can be key. This may include seeking out social support, journaling, going for a walk, or practicing mindfulness.
- UPFA can be associated with erratic and inconsistent eating patterns. Stabilizing eating habits by consuming regular meals composed of more minimally processed foods (eg, vegetables, fruits, high-quality protein, beans) can help heal the body and reduce vulnerability to ultraprocessed food triggers.
- Many people with UPFA have other existing mental health conditions, including mood disorders, anxiety, substance use disorders, or trauma-related disorders. Addressing these co-occurring mental health conditions can help reduce reliance on ultraprocessed foods.
Public-policy interventions may also help safeguard vulnerable populations from developing UPFA. For instance, support exists for policies to protect children from cigarette marketing and to put clear addiction warning labels on cigarette packages. A similar approach could be applied to reduce the harms associated with ultraprocessed foods, particularly for children.
Combating this growing problem requires treating ultraprocessed foods like other addictive substances. By identifying the threat posed by these common food items, we can not only help patients with UPFA, but also potentially stave off the development of several diet-related conditions.
Dr. Gearhardt, professor of psychology, University of Michigan, Ann Arbor, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Yet, even as this evidence mounted, these food items have become increasingly prominent in diets globally.
Now, recent studies are unlocking why cutting back on ultraprocessed foods can be so challenging. In their ability to fuel intense cravings, loss of control, and even withdrawal symptoms, ultraprocessed foods appear as capable of triggering addiction as traditional culprits like tobacco and alcohol.
This has driven efforts to better understand the addictive nature of these foods and identify strategies for combating it.
The Key Role of the Food Industry
Some foods are more likely to trigger addictions than others. For instance, in our studies, participants frequently mention chocolate, pizza, French fries, potato chips, and soda as some of the most addictive foods. What these foods all share is an ability to deliver high doses of refined carbohydrates, fat, or salt at levels exceeding those found in natural foods (eg, fruits, vegetables, beans).
Furthermore, ultraprocessed foods are industrially mass-produced in a process that relies on the heavy use of flavor enhancers and additives, as well as preservatives and packaging that make them shelf-stable. This has flooded our food supply with cheap, accessible, hyperrewarding foods that our brains are not well equipped to resist.
To add to these already substantial effects, the food industry often employs strategies reminiscent of Big Tobacco. They engineer foods to hit our “bliss points,” maximizing craving and fostering brand loyalty from a young age. This product engineering, coupled with aggressive marketing, makes these foods both attractive and seemingly ubiquitous.
How Many People Are Affected?
Addiction to ultraprocessed food is more common than you might think. According to the Yale Food Addiction Scale — a tool that uses the same criteria for diagnosing substance use disorders to assess ultraprocessed food addiction (UPFA) — about 14% of adults and 12% of children show clinically significant signs of addiction to such foods. This is quite similar to addiction rates among adults for legal substances like alcohol and tobacco.
Research has shown that behaviors and brain mechanisms contributing to addictive disorders, such as cravings and impulsivity, also apply to UPFA.
Many more people outside of those who meet the criteria for UPFA are influenced by their addictive properties. Picture a teenager craving a sugary drink after school, a child needing the morning cereal fix, or adults reaching for candy and fast food; these scenarios illustrate how addictive ultraprocessed foods permeate our daily lives.
From a public health standpoint, this comes at a significant cost. Even experiencing one or two symptoms of UPFA, such as intense cravings or a feeling of loss of control over intake, can lead to consuming too many calories, sugar, fat, and sodium in a way that puts health at risk.
Clinical Implications
Numerous studies have found that individuals who exhibit UPFA have more severe mental and physical health challenges. For example, UPFA is associated with higher rates of diet-related diseases (like type 2 diabetes), greater overall mental health issues, and generally poorer outcomes in weight loss treatments.
Despite the growing understanding of UPFA’s relevance in clinical settings, research is still limited on how to best treat, manage, or prevent it. Most of the existing work has focused on investigating whether UPFA is indeed a real condition, with efforts to create clinical guidelines only just beginning.
Of note, UPFA isn’t officially recognized as a diagnosis — yet. If it were, it could spark much more research into how to handle it clinically.
There is some debate about whether we really need this new diagnosis, given that eating disorders are already recognized. However, the statistics tell a different story: Around 14% of people might have UPFA compared with about 1% for binge-type eating disorders. This suggests that many individuals with problematic eating habits are currently flying under the radar with our existing diagnostic categories.
What’s even more concerning is that these individuals often suffer significant problems and exhibit distinct brain differences, even if they do not neatly fit into an existing eating disorder diagnosis. Officially recognizing UPFA could open up new avenues for support and lead to better treatments aimed at reducing compulsive eating patterns.
Treatment Options
Treatment options for UPFA are still being explored. Initial evidence suggests that medications used for treating substance addiction, such as naltrexone and bupropion, might help with highly processed food addiction as well. Newer drugs, like glucagon-like peptide-1 receptor agonists, which appear to curb food cravings and manage addictive behaviors, also look promising.
Psychosocial approaches can also be used to address UPFA. Strategies include:
- Helping individuals become more aware of their triggers for addictive patterns of intake. This often involves identifying certain types of food (eg, potato chips, candy), specific places or times of day (eg, sitting on the couch at night while watching TV), and particular emotional states (eg, anger, loneliness, boredom, sadness). Increasing awareness of personal triggers can help people minimize their exposure to these and develop coping strategies when they do arise.
- Many people use ultraprocessed foods to cope with challenging emotions. Helping individuals develop healthier strategies to regulate their emotions can be key. This may include seeking out social support, journaling, going for a walk, or practicing mindfulness.
- UPFA can be associated with erratic and inconsistent eating patterns. Stabilizing eating habits by consuming regular meals composed of more minimally processed foods (eg, vegetables, fruits, high-quality protein, beans) can help heal the body and reduce vulnerability to ultraprocessed food triggers.
- Many people with UPFA have other existing mental health conditions, including mood disorders, anxiety, substance use disorders, or trauma-related disorders. Addressing these co-occurring mental health conditions can help reduce reliance on ultraprocessed foods.
Public-policy interventions may also help safeguard vulnerable populations from developing UPFA. For instance, support exists for policies to protect children from cigarette marketing and to put clear addiction warning labels on cigarette packages. A similar approach could be applied to reduce the harms associated with ultraprocessed foods, particularly for children.
Combating this growing problem requires treating ultraprocessed foods like other addictive substances. By identifying the threat posed by these common food items, we can not only help patients with UPFA, but also potentially stave off the development of several diet-related conditions.
Dr. Gearhardt, professor of psychology, University of Michigan, Ann Arbor, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Impact of Expanded Eligibility for Veterans With Other Than Honorable Discharges on Treatment Courts and VA Mental Health Care
In April 2022, the US Department of Veterans Affairs (VA) revised its behavioral health care eligibility policies to provide comprehensive mental and behavioral health care to former service members who received an Other Than Honorable (OTH) discharge characterization upon separation from military service.1 This policy shift represents a marked expansion in eligibility practices (Table 1 includes amended eligibility criteria).
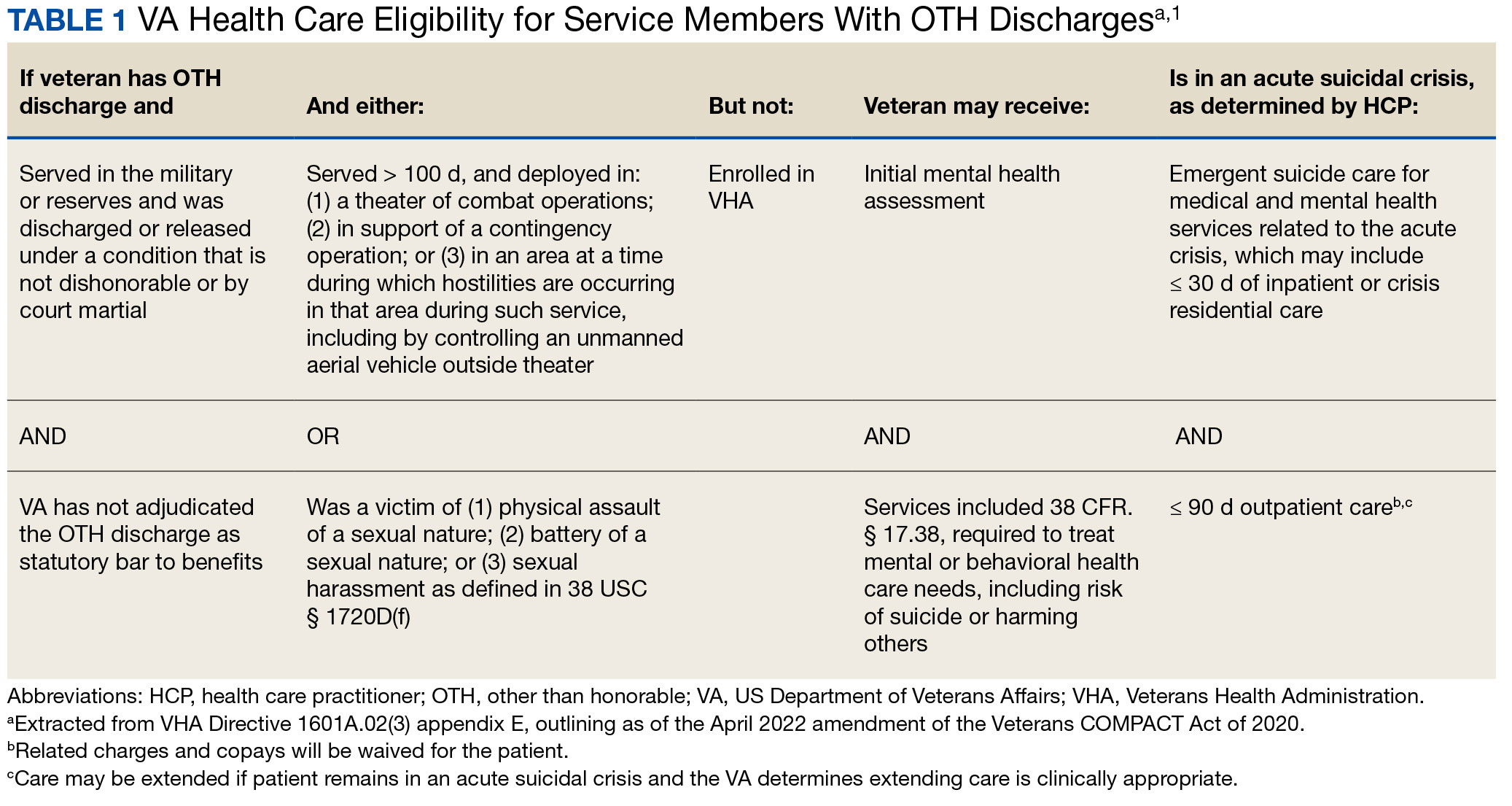
Since June 2017, eligibility policies allowed veterans with OTH discharges to receive “emergent mental health services” needed to stabilize acute mental health crises related to military service (eg, acute escalations in suicide risk).2,3 Previously, veterans with OTH discharges were largely ineligible for VA-based health care; these individuals were only able to access Veterans Health Administration (VHA) mental and behavioral health care through limited channels of eligibility (eg, for treatment of military sexual trauma or psychosis or other mental illness within 2 years of discharge).4,5 The impetus for expansions in eligibility stemmed from VA efforts to reduce the suicide rate among veterans.6-8 Implications of such expansion extend beyond suicide prevention efforts, with notable promised effects on the care of veterans with criminal-legal involvement. This article highlights potential effects of recent eligibility expansions on veterans with criminal-legal involvement and makes specific recommendations for agencies and organizations serving these veterans.
OTHER THAN HONORABLE DISCHARGE
The US Department of Defense delineates 6 discharge characterizations provided to service members upon separation from military service: honorable, general under honorable conditions, OTH, bad conduct, dishonorable, and uncharacterized. Honorable discharge characterizations are considered to reflect general concordance between service member behavior and military standards; general discharge characterizations reflect some disparity between the service member’s behavior and military standards; OTH, bad conduct, and dishonorable discharge characterizations reflect serious disparities between the service member’s behavior and military standards; and uncharacterized discharge characterizations are given when other discharge characterizations are deemed inappropriate.9,10 OTH discharge characterizations are typically issued under instances of misconduct, fraudulent entry, security reasons, or in lieu of trial by court martial.9,10
Recent research suggests that about 85% of service members receive an honorable discharge characterization upon separation from military service, 8% receive general, 6% receive OTH, and 1% receive bad conduct or dishonorable discharges.11 In 2017, the VA estimated there were > 500,000 prior service members with OTH discharge characterizations, which has grown over time (1.9% during the Korean Conflict, 2.5% during the Vietnam War Era, 3.9% during the Cold War, 4.8% in the Persian Gulf War, and 5.8% in the post-9/11 era).7,11
The OTH discharge characterization is 1 of 3 less than honorable discharges informally referred to as bad papers (ie, OTH, bad conduct, or dishonorable). Former service members receiving these discharge characterizations face significant social stigma and structural discrimination upon military discharge, including significant hurdles to employment and educational pursuits as well as notable social alienation.12 Due to their discharge characterization, some are viewed as less deserving of the veteran title, and until recently, many did not qualify for the complex legal definition of veteran as established by the Congress.11,13 Veterans with OTH discharge characterizations have also historically been excluded from services (eg, VHA care),3 benefits (eg, disability compensation),14 and protections (eg, Uniformed Services Employment and Reemployment Rights Act)15 offered to veterans with honorable or general discharge characterizations. However, eligibility policies have gradually expanded, providing veterans with OTH discharges with access to VHA-based mental and behavioral health services and VA supportive housing assistance.1,3,16
Perhaps due to their historical exclusion from VA services, there is limited research available on the behavioral health and associated needs of veterans with OTH discharges. Some scholars argue that historical exclusions have exacerbated underlying difficulties faced by this population, thereby contributing to stark health and social disparities across discharge types.14,15,17 Studies with large veteran samples, for example, reflect notable demographic and behavioral health differences across discharge types. Compared to routinely discharged veterans, veterans with OTH discharges are significantly more likely to be younger, have lower income, use substances, have a history of criminal-legal involvement, and have mental and physical health difficulties.18,19
Substantial evidence also suggests a historical racial bias, with service members of color being disproportionately more likely to receive an OTH discharge.12 Similarly, across all branches of military service, Black service members are significantly more likely to face general or special court martial in military justice proceedings when compared with White service members.20 Service members from gender and sexual minorities are also disproportionately impacted by the OTH designation. Historically, many have been discharged with bad papers due to discriminatory policies, such as Don’t Ask Don’t Tell, which discriminated on the basis of sexual orientation between December 1993 and September 2011, and Directive-type Memorandum-19-004, which banned transgender persons from military service between April 2019 and January 2021.21,22
There is also significant mental health bias in the provision of OTH discharges, such that OTH characterizations are disproportionately represented among individuals with mental health disorders.18-20 Veterans discharged from military service due to behavioral misconduct are significantly more likely to meet diagnostic criteria for various behavioral health conditions and to experience homelessness, criminal-legal involvement, and suicidal ideation and behavior compared with routinely-discharged veterans.23-28
Consistent with their comparatively higher rates of criminal-legal involvement relative to routinely discharged veterans, veterans with OTH discharges are disproportionately represented in criminal justice settings. While veterans with OTH discharges represent only 6% of discharging service members and 2.5% of community-based veterans, they represent 10% of incarcerated veterans.11,18,23,29 Preliminary research suggests veterans with OTH discharges may be at higher risk for lifetime incarceration, though the association between OTH discharge and frequency of lifetime arrests remains unclear.18,30
VETERANS TREATMENT COURTS
Given the overrepresentation of veterans with OTH discharges in criminal-legal settings, consideration for this subset of the veteran population and its unique needs is commonplace among problem-solving courts that service veterans. First conceptualized in 2004, Veterans Treatment Courts (VTCs) are specialized problem-solving courts that divert veterans away from traditional judicial court and penal systems and into community-based supervision and treatment (most commonly behavioral health services).31-34 Although each VTC program is unique in structure, policies, and procedures, most VTCs can be characterized by certain key elements, including voluntary participation, plea requirements, delayed sentencing (often including reduced or dismissed charges), integration of military culture into court proceedings, a rehabilitative vs adversarial approach to decreasing risk of future criminal behavior, mandated treatment and supervision during participation, and use of veteran mentors to provide peer support.32-35 Eligibility requirements vary; however, many restrict participation to veterans with honorable discharge types and charges for nonviolent offenses.32,33,35-37
VTCs connect veterans within the criminal-legal system to needed behavioral health, community, and social services.31-33,37 VTC participants are commonly connected to case management, behavioral health care, therapeutic journaling programs, and vocational rehabilitation.38,39 Accordingly, the most common difficulties faced by veterans participating in these courts include substance use, mental health, family issues, anger management and/or aggressive behavior, and homelessness.36,39 There is limited research on the effectiveness of VTCs. Evidence on their overall effectiveness is largely mixed, though some studies suggest VTC graduates tend to have lower recidivism rates than offenders more broadly or persons who terminate VTC programs prior to completion.40,41 Other studies suggest that VTC participants are more likely to have jail sanctions, new arrests, and new incarcerations relative to nontreatment court participants.42 Notably, experimental designs (considered the gold standard in assessing effectiveness) to date have not been applied to evaluate the effectiveness of VTCs; as such, the effectiveness of these programs remains an area in need of continued empirical investigation.
Like all problem-solving courts, VTCs occasionally struggle to connect participating defendants with appropriate care, particularly when encountering structural barriers (eg, insurance, transportation) and/or complex behavioral health needs (eg, personality disorders).34,43 As suicide rates among veterans experiencing criminal-legal involvement surge (about 150 per 100,000 in 2021, a 10% increase from 2020 to 2021 compared to about 40 per 100,000 and a 1.8% increase among other veterans), efficiency of adequate care coordination is vital.44 Many VTCs rely on VTC-VA partnerships and collaborations to navigate these difficulties and facilitate connection of participating veterans to needed services.32-34,45 For example, within the VHA, Veterans Justice Outreach (VJO) and Health Care for Re-Entry Veterans (HCRV) specialists assist and bridge the gap between the criminal-legal system (including, but not limited to VTCs) and VA services by engaging veterans involved in the criminal-legal system and connecting them to needed VA-based services (Table 2). Generally, VJO specialists support veterans involved with the front end of the criminallegal system (eg, arrest, pretrial incarceration, or participation in VTCs), while HCRV specialists tend to support veterans transitioning back into the community after a period of incarceration.46,47 Specific to VTCs, VJO specialists typically serve as liaisons between the courts and VA, coordinating VA services for defendants to fulfill their terms of VTC participation.46
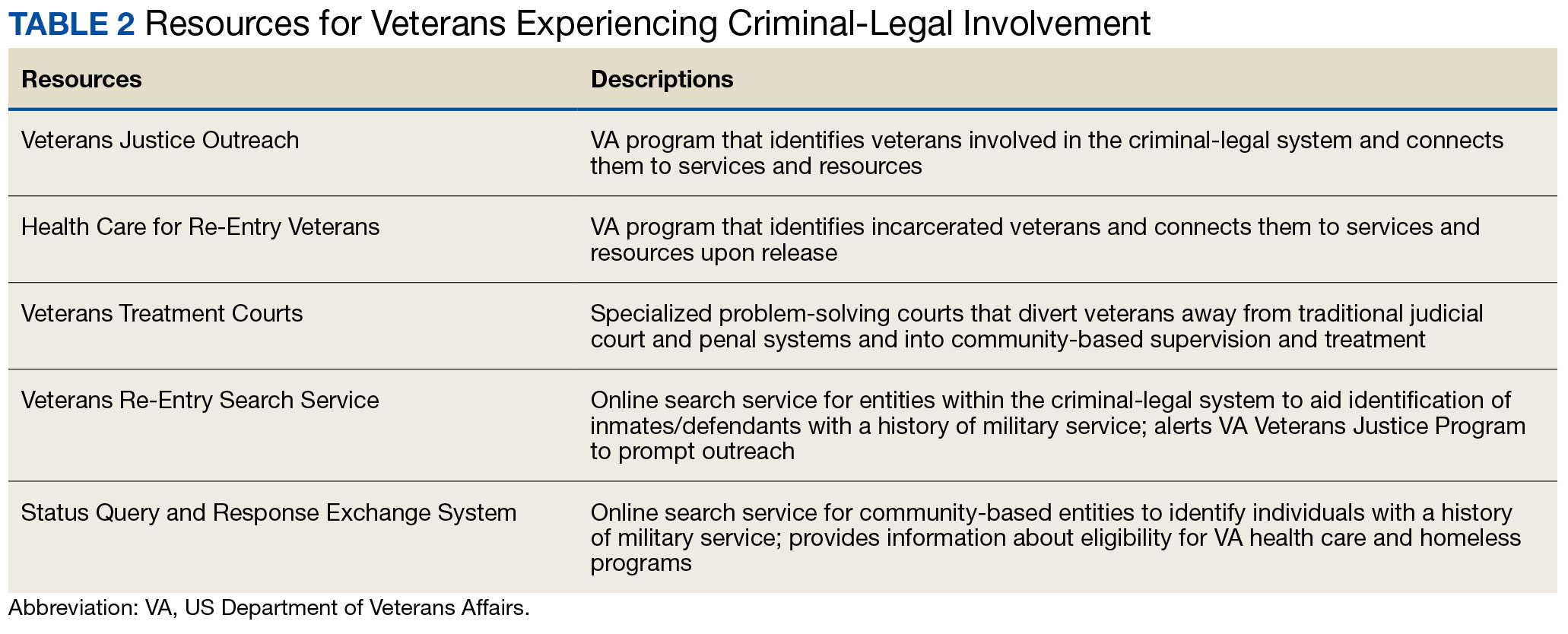
The historical exclusion of veterans with OTH discharge characterizations from VA-based services has restricted many from accessing VTC programs.32 Of 17 VTC programs active in Pennsylvania in 2014, only 5 accepted veterans with OTstayH discharges, and 3 required application to and eligibility for VA benefits.33 Similarly, in national surveys of VTC programs, about 1 in 3 report excluding veterans deemed ineligible for VA services.35,36 When veterans with OTH discharges have accessed VTC programs, they have historically relied on non-VA, community-based programming to fulfill treatment mandates, which may be less suited to addressing the unique needs of veterans.48
Veterans who utilize VTCs receive several benefits, namely peer support and mentorship, acceptance into a veteran-centric space, and connection with specially trained staff capable of supporting the veteran through applications for a range of VA benefits (eg, service connection, housing support).31-33,37 Given the disparate prevalence of OTH discharge characterizations among service members from racial, sexual, and gender minorities and among service members with mental health disorders, exclusion of veterans with OTH discharges from VTCs solely based on the type of discharge likely contributes to structural inequities among these already underserved groups by restricting access to these potential benefits. Such structural inequity stands in direct conflict with VTC best practice standards, which admonish programs to adjust eligibility requirements to facilitate access to treatment court programs for historically marginalized groups.49
ELIGIBILITY EXPANSIONS
Given the overrepresentation of veterans with OTH discharge characterizations within the criminal-legal system and historical barriers of these veterans to access needed mental and behavioral health care, expansions in VA eligibility policies could have immense implications for VTCs. First, these expansions could mitigate common barriers to connecting VTC-participating veterans with OTH discharges with needed behavioral health care by allowing these veterans to access established, VA-based services and programming. Expansion may also allow VTCs to serve as a key intercept point for identifying and engaging veterans with OTH discharges who may be unaware of their eligibility for VA-based behavioral health care.
Access to VA health care services is a major resource for VTC participants and a common requirement.32 Eligibility expansion should ease access barriers veterans with OTH discharges commonly face. By providing a potential source of treatment, expansions may also support OTH eligibility practices within VTCs, particularly practices that require participants to be eligible for VA health care.33,35,36 Some VTCs may continue to determine eligibility on the basis of discharge status and remain inaccessible to veterans with OTH discharge characterizations without program-level policy changes.32,36,37
Communicating changes in eligibility policies relevant to veterans with OTH discharges may be a challenge, because many of these individuals have no established channels of communication with the VA. Because veterans with OTH discharges are at increased risk for legal system involvement, VTCs may serve as a unique point of contact to help facilitate communication.18 For example, upon referral to a VTC, veterans with OTH discharges can be identified, VA health care eligibility can be verified, and veterans can connect to VA staff to facilitate enrollment in VA services and care.
VJO specialists are in a favorable position to serve a critical role in utilizing VTCs as a potential intercept point for engaging veterans with OTH discharge characterizations. As outlined in the STRONG Veterans Act of 2022, VJOs are mandated to “spread awareness and understanding of veteran eligibility for the [VJO] Program, including the eligibility of veterans who were discharged from service in the Armed Forces under conditions other than honorable.”50 The Act further requires VJOs to be annually trained in communicating eligibility changes as they arise. Accordingly, VJOs receive ongoing training in a wide variety of critical outreach topics, including changes in eligibility; while VJOs cannot make eligibility determinations, they are tasked with enrolling all veterans involved in the criminal-legal system with whom they interact into VHA services, whether through typical or special eligibility criteria (M. Stimmel, PhD, National Training Director for Veteran Justice Programming, oral communication, July 14, 2023). VJOs therefore routinely serve in this capacity of facilitating VA enrollment of veterans with OTH discharge characterizations.
Recommendations to Veteran-Servicing Judicial Programs
Considering these potential implications, professionals routinely interacting with veterans involved in the criminal-legal system should become familiarized with recent changes in VA eligibility policies. Such familiarization would support the identification of veterans previously considered ineligible for care; provision of education to these veterans regarding their new eligibility; and referral to appropriate VA-based behavioral health care options. Although conceptually simple, executing such an educational campaign may prove logistically difficult. Given their historical exclusion from VA services, veterans with OTH discharge characterizations are unlikely to seek VA-based services in times of need, instead relying on a broad swath of civilian community-based organizations and resources. Usual approaches to advertising VHA health care policy changes (eg, by notifying VA employees and/or departments providing corresponding services or by circulating information to veteran-focused mailing lists and organizations) likely would prove insufficient. Educational campaigns to disseminate information about recent OTH eligibility changes should instead consider partnering with traditionally civilian, communitybased organizations and institutions, such as state bar associations, legal aid networks, case management services, nonveteran treatment court programs (eg, drug courts, or domestic violence courts), or probation/ parole programs. Because national surveys suggest generally low military cultural competence among civilian populations, providing concurrent support in developing foundational veteran cultural competencies (eg, how to phrase questions about military service history, or understanding discharge characterizations) may be necessary to ensure effective identification and engagement of veteran clients.48
Programs that serve veterans with criminal-legal involvement should also consider potential relevance of recent OTH eligibility changes to program operations. VTC program staff and key partners (eg, judges, case managers, district attorneys, or defense attorneys), should revisit policies and procedures surrounding the engagement of veterans with OTH discharges within VTC programs and strategies for connecting these veterans with needed services. VTC programs that have historically excluded veterans with OTH discharges due to associated difficulties in locating and connecting with needed services should consider expanding eligibility policies considering recent shifts in VA behavioral health care eligibility.33,35,36 Within the VHA, VJO specialists can play a critical role in supporting these VTC eligibility and cultural shifts. Some evidence suggests a large proportion of VTC referrals are facilitated by VJO specialists and that many such referrals are identified when veterans involved with the criminal-legal system seek VA support and/or services.33 Given the historical exclusion of veterans with OTH discharges from VA care, strategies used by VJO specialists to identify, connect, and engage veterans with OTH discharges with VTCs and other services may be beneficial.
Even with knowledge of VA eligibility changes and considerations of these changes on local operations, many forensic settings and programs struggle to identify veterans. These difficulties are likely amplified among veterans with OTH discharge characterizations, who may be hesitant to self-disclose their military service history due to fear of stigma and/or views of OTH discharge characterizations as undeserving of the veteran title.12 The VA offers 2 tools to aid in identification of veterans for these settings: the Veterans Re-Entry Search Service (VRSS) and Status Query and Response Exchange System (SQUARES). For VRSS, correctional facilities, courts, and other criminal justice entities upload a simple spreadsheet that contains basic identifying information of inmates or defendants in their system. VRSS returns information about which inmates or defendants have a history of military service and alerts VA Veterans Justice Programs staff so they can conduct outreach. A pilot study conducted by the California Department of Corrections and Rehabilitation found that 2.7% of its inmate population self-identified as veterans, while VRSS identified 7.7% of inmates with a history of military service. This difference represented about 5000 previously unidentified veterans.51 Similarly, community entities that partner with the VA, such as law enforcement or homeless service programs, can be approved to become a SQUARES user and submit identifying information of individuals with whom they interact directly into the SQUARES search engine. SQUARES then directly returns information about the individual’s veteran status and eligibility for VA health care and homeless programs.
Other Eligibility Limitations
VTCs and other professionals looking to refer veterans with OTH discharge characterizations to VA-based behavioral health care should be aware of potential limitations in eligibility and access. Specifically, although veterans with OTH discharges are now broadly eligible for VA-based behavioral health care and homeless programs, they remain ineligible for other forms of health care, including primary care and nonbehavioral specialty care.1 Research has found a strong comorbidity between behavioral and nonbehavioral health concerns, particularly within historically marginalized demographic groups.52-55 Because these historically marginalized groups are often overrepresented among persons with criminal-legal involvement, veterans with OTH discharges, and VTC participants, such comorbidities require consideration by services or programming designed to support veterans with criminal-legal involvement.12,56-58 Connection with VA-based health care will therefore continue to fall short of addressing all health care needs of veterans with OTH discharges and effective case management will require considerable treatment coordination between VA behavioral health care practitioners (HCPs) and community-based HCPs (eg, primary care professionals or nonbehavioral HCPs).
Implications for VA Mental Health Care
Recent eligibility expansions will also have inevitable consequences for VA mental health care systems. For many years, these systems have been overburdened by high caseloads and clinician burnout.59,60 Given the generally elevated rates of mental health and substance use concerns among veterans with OTH discharge characterizations, expansions hold the potential to further burden caseloads with clinically complex, high-risk, high-need clients. Nevertheless, these expansions are also structured in a way that forces existing systems to absorb the responsibilities of providing necessary care to these veterans. To mitigate detrimental effects of eligibility expansions on the broader VA mental health system, clinicians should be explicitly trained in identifying veterans with OTH discharge characterizations and the implications of discharge status on broader health care eligibility. Treatment of veterans with OTH discharges may also benefit from close coordination between mental health professionals and behavioral health care coordinators to ensure appropriate coordination of care between VA- and non–VA-based HCPs.
CONCLUSIONS
Recent changes to VA eligibility policies now allow comprehensive mental and behavioral health care services to be provided to veterans with OTH discharges.1 Compared to routinely discharged veterans, veterans with OTH discharges are more likely to be persons of color, sexual or gender minorities, and experiencing mental health-related difficulties. Given the disproportionate mental health burden often faced by veterans with OTH discharges and relative overrepresentation of these veterans in judicial and correctional systems, these changes have considerable implications for programs and services designed to support veterans with criminallegal involvement. Professionals within these systems, particularly VTC programs, are therefore encouraged to familiarize themselves with recent changes in VA eligibility policies and to revisit strategies, policies, and procedures surrounding the engagement and enrollment of veterans with OTH discharge characterizations. Doing so may ensure veterans with OTH discharges are effectively connected to needed behavioral health care services.
- US Department of Veterans, Veterans Health Administration. VHA Directive 1601A.02(6): Eligibility Determination. Updated March 6, 2024. Accessed August 8, 2024. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=8908
- Mental and behavioral health care for certain former members of the Armed Forces. 38 USC §1720I (2018). Accessed August 5, 2024. https://uscode.house.gov/view.xhtml?req=(title:38%20section:1720I%20edition:prelim
- US Department of Veterans, Veterans Health Administration. VHA Directive 1601A.02, Eligibility Determination. June 7, 2017.
- US Department of Veterans, Veterans Health Administration. VHA Directive 1115(1), Military Sexual Trauma (MST) Program. May 8, 2018. Accessed August 5, 2024. https:// www.va.gov/vhapublications/viewpublication.asp?pub_ID=6402
- US Department of Veterans Affairs. Tentative Eligibility Determinations; Presumptive Eligibility for Psychosis and Other Mental Illness. 38 CFR §17.109. May 14, 2013. Accessed August 5, 2024. https://www.federalregister.gov/documents/2013/05/14/2013-11410/tentative-eligibility-determinations-presumptive-eligibility-for-psychosis-and-other-mental-illness
- US Department of Veterans Affairs, VA Office of Mental Health and Suicide Prevention. National strategy for preventing veteran suicide 2018-2028. Published September 2018. Accessed August 5, 2024. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
- US Department of Veterans Affairs. VA secretary announces intention to expand mental health care to former service members with other-than-honorable discharges and in crisis. Press Release. March 8, 2017. Accessed August 5, 2024. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=2867
- Smith C. Dramatic increase in mental health services to other-than-honorable discharge veterans. VA News. February 23, 2022. Accessed August 5, 2024. https://news.va.gov/100460/dramatic-increase-in-mental-health-services-to-other-than-honorable-discharge-veterans/
- US Department of Defense. DoD Instruction 1332.14. Enlisted administrative separations. Updated August 1, 2024. Accessed August 5, 2024. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/133214p.pdf
- US Department of Defense. DoD Instruction 1332.30. Commissioned officer administrative separations. Updated September 9, 2021. Accessed August 5, 2024. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/133230p.pdf
- OUTVETS, Legal Services Center of Harvard Law School, Veterans Legal Services. Turned away: how the VA unlawfully denies healthcare to veterans with bad paper discharges. 2020. Accessed August 5, 2024. https://legalservicescenter.org/wp-content/uploads/Turn-Away-Report.pdf
- McClean H. Discharged and discarded: the collateral consequences of a less-than-honorable military discharge. Columbia Law Rev. 2021;121(7):2203-2268.
- Veterans Benefits, General Provisions, Definitions. 38 USC §101(2) (1958). Accessed August 5, 2024. https://uscode.house.gov/view.xhtml?req=granuleid:USC-prelim-title38-section101&num=0&edition=prelim
- Bedford JR. Other than honorable discharges: unfair and unjust life sentences of decreased earning capacity. U Penn J Law Pub Affairs. 2021;6(4):687.
- Karin ML. Other than honorable discrimination. Case Western Reserve Law Rev. 2016;67(1):135-191. https://scholarlycommons.law.case.edu/caselrev/vol67/iss1/9
- Veteran HOUSE Act of 2020, HR 2398, 116th Cong, (2020). Accessed August 5, 2024. https://www.congress.gov/bill/116th-congress/house-bill/2398
- Scapardine D. Leaving other than honorable soldiers behind: how the Departments of Defense and Veterans Affairs inadvertently created a health and social crisis. Md Law Rev. 2017;76(4):1133-1165.
- Elbogen EB, Wagner HR, Brancu M, et al. Psychosocial risk factors and other than honorable military discharge: providing healthcare to previously ineligible veterans. Mil Med. 2018;183(9-10):e532-e538. doi:10.1093/milmed/usx128
- Tsai J, Rosenheck RA. Characteristics and health needs of veterans with other-than-honorable discharges: expanding eligibility in the Veterans Health Administration. Mil Med. 2018;183(5-6):e153-e157. doi:10.1093/milmed/usx110
- Christensen DM, Tsilker Y. Racial disparities in military justice: findings of substantial and persistent racial disparities within the United States military justice system. Accessed August 5, 2024. https://www.protectourdefenders.com/wp-content/uploads/2017/05/Report_20.pdf
- Don’t Ask Don’t Tell, 10 USC §654 (1993) (Repealed 2010). Accessed August 5, 2024. http://www.gpo.gov/fdsys/pkg/USCODE-2010-title10/pdf/USCODE-2010-title10-subtitleA-partII-chap37-sec654.pdf
- Palm Center. The making of a ban: how DTM-19-004 works to push transgender people out of military service. 2019. March 20, 2019. Accessed August 5, 2024. https://www.palmcenter.org/wp-content/uploads/2019/04/The-Making-of-a-Ban.pdf
- Edwards ER, Greene AL, Epshteyn G, Gromatsky M, Kinney AR, Holliday R. Mental health of incarcerated veterans and civilians: latent class analysis of the 2016 Survey of Prison Inmates. Crim Justice Behav. 2022;49(12):1800- 1821. doi:10.1177/00938548221121142
- Brignone E, Fargo JD, Blais RK, Carter ME, Samore MH, Gundlapalli AV. Non-routine discharge from military service: mental illness, substance use disorders, and suicidality. Am J Prev Med. 2017;52(5):557-565. doi:10.1016/j.amepre.2016.11.015
- Gamache G, Rosenheck R, Tessler R. Military discharge status of homeless veterans with mental illness. Mil Med. 2000;165(11):803-808. doi:10.1093/milmed/165.11.803
- Gundlapalli AV, Fargo JD, Metraux S, et al. Military Misconduct and Homelessness Among US Veterans Separated From Active Duty, 2001-2012. JAMA. 2015;314(8):832-834. doi:10.1001/jama.2015.8207
- Brooks Holliday S, Pedersen ER. The association between discharge status, mental health, and substance misuse among young adult veterans. Psychiatry Res. 2017;256:428-434. doi:10.1016/j.psychres.2017.07.011
- Williamson RB. DOD Health: Actions Needed to Ensure Post-Traumatic Stress Disorder and Traumatic Brain Injury are Considered in Misconduct Separations. US Government Accountability Office; 2017. Accessed August 5, 2024. https://apps.dtic.mil/sti/pdfs/AD1168610.pdf
- Maruschak LM, Bronson J, Alper M. Indicators of mental health problems reported by prisoners: survey of prison inmates. US Department of Justice Bureau of Justice Statistics. June 2021. Accessed August 5, 2024. https://bjs.ojp.gov/sites/g/files/xyckuh236/files/media/document/imhprpspi16st.pdf
- Brooke E, Gau J. Military service and lifetime arrests: examining the effects of the total military experience on arrests in a sample of prison inmates. Crim Justice Policy Rev. 2018;29(1):24-44. doi:10.1177/0887403415619007
- Russell RT. Veterans treatment court: a proactive approach. N Engl J Crim Civ Confin. 2009;35:357-372.
- Cartwright T. To care for him who shall have borne the battle: the recent development of Veterans Treatment Courts in America. Stanford Law Pol Rev. 2011;22:295-316.
- Douds AS, Ahlin EM, Howard D, Stigerwalt S. Varieties of veterans’ courts: a statewide assessment of veterans’ treatment court components. Crim Justice Policy Rev. 2017;28:740-769. doi:10.1177/0887403415620633
- Rowen J. Worthy of justice: a veterans treatment court in practice. Law Policy. 2020;42(1):78-100. doi:10.1111/lapo.12142
- Timko C, Flatley B, Tjemsland A, et al. A longitudinal examination of veterans treatment courts’ characteristics and eligibility criteria. Justice Res Policy. 2016;17(2):123-136.
- Baldwin JM. Executive summary: national survey of veterans treatment courts. SSRN. Preprint posted online June 5, 2013. Accessed August 5, 2024. doi:10.2139/ssrn.2274138
- Renz T. Veterans treatment court: a hand up rather than lock up. Richmond Public Interest Law Rev. 2013;17(3):697-705. https://scholarship.richmond.edu/pilr/vol17/iss3/6
- Knudsen KJ, Wingenfeld S. A specialized treatment court for veterans with trauma exposure: implications for the field. Community Ment Health J. 2016;52(2):127-135. doi:10.1007/s10597-015-9845-9
- McCall JD, Tsai J, Gordon AJ. Veterans treatment court research: participant characteristics, outcomes, and gaps in the literature. J Offender Rehabil. 2018;57:384-401. doi:10.1080/10509674.2018.1510864
- Smith JS. The Anchorage, Alaska veterans court and recidivism: July 6, 2004 – December 31, 2010. Alsk Law Rev. 2012;29(1):93-111.
- Hartley RD, Baldwin JM. Waging war on recidivism among justice-involved veterans: an impact evaluation of a large urban veterans treatment court. Crim Justice Policy Rev. 2019;30(1):52-78. doi:10.1177/0887403416650490
- Tsai J, Flatley B, Kasprow WJ, Clark S, Finlay A. Diversion of veterans with criminal justice involvement to treatment courts: participant characteristics and outcomes. Psychiatr Serv. 2017;68(4):375-383. doi:10.1176/appi.ps.201600233
- Edwards ER, Sissoko DR, Abrams D, Samost D, La Gamma S, Geraci J. Connecting mental health court participants with services: process, challenges, and recommendations. Psychol Public Policy Law. 2020;26(4):463-475. doi:10.1037/law0000236
- US Department of Veterans Affairs, VA Office of Mental Health and Suicide Prevention. 2023 National Veteran Suicide Prevention Annual Report. US Department of Veterans Affairs; November 2023. Accessed August 5, 2024. https://www.mentalhealth.va.gov/docs/data-sheets/2023/2023-National-Veteran-Suicide-Prevention-Annual-Report-FINAL-508.pdf
- Finlay AK, Clark S, Blue-Howells J, et al. Logic model of the Department of Veterans Affairs’ role in veterans treatment courts. Drug Court Rev. 2019;2:45-62.
- Finlay AK, Smelson D, Sawh L, et al. U.S. Department of Veterans Affairs veterans justice outreach program: connecting justice-involved veterans with mental health and substance use disorder treatment. Crim Justice Policy Rev. 2016;27(2):10.1177/0887403414562601. doi:10.1177/0887403414562601
- Finlay AK, Stimmel M, Blue-Howells J, et al. Use of Veterans Health Administration mental health and substance use disorder treatment after exiting prison: the health care for reentry veterans program. Adm Policy Ment Health. 2017;44(2):177-187. doi:10.1007/s10488-015-0708-z
- Meyer EG, Writer BW, Brim W. The Importance of Military Cultural Competence. Curr Psychiatry Rep. 2016;18(3):26. doi:10.1007/s11920-016-0662-9
- National Association of Drug Court Professionals. Adult Drug Court Best Practice Standards Volume I. National Association of Drug Court Professionals; 2013. Accessed August 5, 2024. https://allrise.org/publications/standards/
- STRONG Veterans Act of 2022, HR 6411, 117th Cong (2022). https://www.congress.gov/bill/117th-congress/house-bill/6411/text
- Pelletier D, Clark S, Davis L. Veterans reentry search service (VRSS) and the SQUARES application. Presented at: National Association of Drug Court Professionals Conference; August 15-18, 2021; National Harbor, Maryland.
- Scott KM, Lim C, Al-Hamzawi A, et al. Association of Mental Disorders With Subsequent Chronic Physical Conditions: World Mental Health Surveys From 17 Countries. JAMA Psychiatry. 2016;73(2):150-158. doi:10.1001/jamapsychiatry.2015.2688
- Ahmed N, Conway CA. Medical and mental health comorbidities among minority racial/ethnic groups in the United States. J Soc Beh Health Sci. 2020;14(1):153-168. doi:10.5590/JSBHS.2020.14.1.11
- Hanna B, Desai R, Parekh T, Guirguis E, Kumar G, Sachdeva R. Psychiatric disorders in the U.S. transgender population. Ann Epidemiol. 2019;39:1-7.e1. doi:10.1016/j.annepidem.2019.09.009
- Watkins DC, Assari S, Johnson-Lawrence V. Race and ethnic group differences in comorbid major depressive disorder, generalized anxiety disorder, and chronic medical conditions. J Racial Ethn Health Disparities. 2015;2(3):385- 394. doi:10.1007/s40615-015-0085-z
- Baldwin J. Whom do they serve? National examination of veterans treatment court participants and their challenges. Crim Justice Policy Rev. 2017;28(6):515-554. doi:10.1177/0887403415606184
- Beatty LG, Snell TL. Profile of prison inmates, 2016. US Department of Justice Bureau of Justice Statistics. December 2021. Accessed August 5, 2024. https://bjs.ojp.gov/content/pub/pdf/ppi16.pdf
- Al-Rousan T, Rubenstein L, Sieleni B, Deol H, Wallace RB. Inside the nation’s largest mental health institution: a prevalence study in a state prison system. BMC Public Health. 2017;17(1):342. doi:10.1186/s12889-017-4257-0
- Rosen CS, Kaplan AN, Nelson DB, et al. Implementation context and burnout among Department of Veterans Affairs psychotherapists prior to and during the COVID-19 pandemic. J Affect Disord. 2023;320:517-524. doi:10.1016/j.jad.2022.09.141
- Tsai J, Jones N, Klee A, Deegan D. Job burnout among mental health staff at a veterans affairs psychosocial rehabilitation center. Community Ment Health J. 2020;56(2):294- 297. doi:10.1007/s10597-019-00487-5
In April 2022, the US Department of Veterans Affairs (VA) revised its behavioral health care eligibility policies to provide comprehensive mental and behavioral health care to former service members who received an Other Than Honorable (OTH) discharge characterization upon separation from military service.1 This policy shift represents a marked expansion in eligibility practices (Table 1 includes amended eligibility criteria).
Since June 2017, eligibility policies allowed veterans with OTH discharges to receive “emergent mental health services” needed to stabilize acute mental health crises related to military service (eg, acute escalations in suicide risk).2,3 Previously, veterans with OTH discharges were largely ineligible for VA-based health care; these individuals were only able to access Veterans Health Administration (VHA) mental and behavioral health care through limited channels of eligibility (eg, for treatment of military sexual trauma or psychosis or other mental illness within 2 years of discharge).4,5 The impetus for expansions in eligibility stemmed from VA efforts to reduce the suicide rate among veterans.6-8 Implications of such expansion extend beyond suicide prevention efforts, with notable promised effects on the care of veterans with criminal-legal involvement. This article highlights potential effects of recent eligibility expansions on veterans with criminal-legal involvement and makes specific recommendations for agencies and organizations serving these veterans.
OTHER THAN HONORABLE DISCHARGE
The US Department of Defense delineates 6 discharge characterizations provided to service members upon separation from military service: honorable, general under honorable conditions, OTH, bad conduct, dishonorable, and uncharacterized. Honorable discharge characterizations are considered to reflect general concordance between service member behavior and military standards; general discharge characterizations reflect some disparity between the service member’s behavior and military standards; OTH, bad conduct, and dishonorable discharge characterizations reflect serious disparities between the service member’s behavior and military standards; and uncharacterized discharge characterizations are given when other discharge characterizations are deemed inappropriate.9,10 OTH discharge characterizations are typically issued under instances of misconduct, fraudulent entry, security reasons, or in lieu of trial by court martial.9,10
Recent research suggests that about 85% of service members receive an honorable discharge characterization upon separation from military service, 8% receive general, 6% receive OTH, and 1% receive bad conduct or dishonorable discharges.11 In 2017, the VA estimated there were > 500,000 prior service members with OTH discharge characterizations, which has grown over time (1.9% during the Korean Conflict, 2.5% during the Vietnam War Era, 3.9% during the Cold War, 4.8% in the Persian Gulf War, and 5.8% in the post-9/11 era).7,11
The OTH discharge characterization is 1 of 3 less than honorable discharges informally referred to as bad papers (ie, OTH, bad conduct, or dishonorable). Former service members receiving these discharge characterizations face significant social stigma and structural discrimination upon military discharge, including significant hurdles to employment and educational pursuits as well as notable social alienation.12 Due to their discharge characterization, some are viewed as less deserving of the veteran title, and until recently, many did not qualify for the complex legal definition of veteran as established by the Congress.11,13 Veterans with OTH discharge characterizations have also historically been excluded from services (eg, VHA care),3 benefits (eg, disability compensation),14 and protections (eg, Uniformed Services Employment and Reemployment Rights Act)15 offered to veterans with honorable or general discharge characterizations. However, eligibility policies have gradually expanded, providing veterans with OTH discharges with access to VHA-based mental and behavioral health services and VA supportive housing assistance.1,3,16
Perhaps due to their historical exclusion from VA services, there is limited research available on the behavioral health and associated needs of veterans with OTH discharges. Some scholars argue that historical exclusions have exacerbated underlying difficulties faced by this population, thereby contributing to stark health and social disparities across discharge types.14,15,17 Studies with large veteran samples, for example, reflect notable demographic and behavioral health differences across discharge types. Compared to routinely discharged veterans, veterans with OTH discharges are significantly more likely to be younger, have lower income, use substances, have a history of criminal-legal involvement, and have mental and physical health difficulties.18,19
Substantial evidence also suggests a historical racial bias, with service members of color being disproportionately more likely to receive an OTH discharge.12 Similarly, across all branches of military service, Black service members are significantly more likely to face general or special court martial in military justice proceedings when compared with White service members.20 Service members from gender and sexual minorities are also disproportionately impacted by the OTH designation. Historically, many have been discharged with bad papers due to discriminatory policies, such as Don’t Ask Don’t Tell, which discriminated on the basis of sexual orientation between December 1993 and September 2011, and Directive-type Memorandum-19-004, which banned transgender persons from military service between April 2019 and January 2021.21,22
There is also significant mental health bias in the provision of OTH discharges, such that OTH characterizations are disproportionately represented among individuals with mental health disorders.18-20 Veterans discharged from military service due to behavioral misconduct are significantly more likely to meet diagnostic criteria for various behavioral health conditions and to experience homelessness, criminal-legal involvement, and suicidal ideation and behavior compared with routinely-discharged veterans.23-28
Consistent with their comparatively higher rates of criminal-legal involvement relative to routinely discharged veterans, veterans with OTH discharges are disproportionately represented in criminal justice settings. While veterans with OTH discharges represent only 6% of discharging service members and 2.5% of community-based veterans, they represent 10% of incarcerated veterans.11,18,23,29 Preliminary research suggests veterans with OTH discharges may be at higher risk for lifetime incarceration, though the association between OTH discharge and frequency of lifetime arrests remains unclear.18,30
VETERANS TREATMENT COURTS
Given the overrepresentation of veterans with OTH discharges in criminal-legal settings, consideration for this subset of the veteran population and its unique needs is commonplace among problem-solving courts that service veterans. First conceptualized in 2004, Veterans Treatment Courts (VTCs) are specialized problem-solving courts that divert veterans away from traditional judicial court and penal systems and into community-based supervision and treatment (most commonly behavioral health services).31-34 Although each VTC program is unique in structure, policies, and procedures, most VTCs can be characterized by certain key elements, including voluntary participation, plea requirements, delayed sentencing (often including reduced or dismissed charges), integration of military culture into court proceedings, a rehabilitative vs adversarial approach to decreasing risk of future criminal behavior, mandated treatment and supervision during participation, and use of veteran mentors to provide peer support.32-35 Eligibility requirements vary; however, many restrict participation to veterans with honorable discharge types and charges for nonviolent offenses.32,33,35-37
VTCs connect veterans within the criminal-legal system to needed behavioral health, community, and social services.31-33,37 VTC participants are commonly connected to case management, behavioral health care, therapeutic journaling programs, and vocational rehabilitation.38,39 Accordingly, the most common difficulties faced by veterans participating in these courts include substance use, mental health, family issues, anger management and/or aggressive behavior, and homelessness.36,39 There is limited research on the effectiveness of VTCs. Evidence on their overall effectiveness is largely mixed, though some studies suggest VTC graduates tend to have lower recidivism rates than offenders more broadly or persons who terminate VTC programs prior to completion.40,41 Other studies suggest that VTC participants are more likely to have jail sanctions, new arrests, and new incarcerations relative to nontreatment court participants.42 Notably, experimental designs (considered the gold standard in assessing effectiveness) to date have not been applied to evaluate the effectiveness of VTCs; as such, the effectiveness of these programs remains an area in need of continued empirical investigation.
Like all problem-solving courts, VTCs occasionally struggle to connect participating defendants with appropriate care, particularly when encountering structural barriers (eg, insurance, transportation) and/or complex behavioral health needs (eg, personality disorders).34,43 As suicide rates among veterans experiencing criminal-legal involvement surge (about 150 per 100,000 in 2021, a 10% increase from 2020 to 2021 compared to about 40 per 100,000 and a 1.8% increase among other veterans), efficiency of adequate care coordination is vital.44 Many VTCs rely on VTC-VA partnerships and collaborations to navigate these difficulties and facilitate connection of participating veterans to needed services.32-34,45 For example, within the VHA, Veterans Justice Outreach (VJO) and Health Care for Re-Entry Veterans (HCRV) specialists assist and bridge the gap between the criminal-legal system (including, but not limited to VTCs) and VA services by engaging veterans involved in the criminal-legal system and connecting them to needed VA-based services (Table 2). Generally, VJO specialists support veterans involved with the front end of the criminallegal system (eg, arrest, pretrial incarceration, or participation in VTCs), while HCRV specialists tend to support veterans transitioning back into the community after a period of incarceration.46,47 Specific to VTCs, VJO specialists typically serve as liaisons between the courts and VA, coordinating VA services for defendants to fulfill their terms of VTC participation.46
The historical exclusion of veterans with OTH discharge characterizations from VA-based services has restricted many from accessing VTC programs.32 Of 17 VTC programs active in Pennsylvania in 2014, only 5 accepted veterans with OTstayH discharges, and 3 required application to and eligibility for VA benefits.33 Similarly, in national surveys of VTC programs, about 1 in 3 report excluding veterans deemed ineligible for VA services.35,36 When veterans with OTH discharges have accessed VTC programs, they have historically relied on non-VA, community-based programming to fulfill treatment mandates, which may be less suited to addressing the unique needs of veterans.48
Veterans who utilize VTCs receive several benefits, namely peer support and mentorship, acceptance into a veteran-centric space, and connection with specially trained staff capable of supporting the veteran through applications for a range of VA benefits (eg, service connection, housing support).31-33,37 Given the disparate prevalence of OTH discharge characterizations among service members from racial, sexual, and gender minorities and among service members with mental health disorders, exclusion of veterans with OTH discharges from VTCs solely based on the type of discharge likely contributes to structural inequities among these already underserved groups by restricting access to these potential benefits. Such structural inequity stands in direct conflict with VTC best practice standards, which admonish programs to adjust eligibility requirements to facilitate access to treatment court programs for historically marginalized groups.49
ELIGIBILITY EXPANSIONS
Given the overrepresentation of veterans with OTH discharge characterizations within the criminal-legal system and historical barriers of these veterans to access needed mental and behavioral health care, expansions in VA eligibility policies could have immense implications for VTCs. First, these expansions could mitigate common barriers to connecting VTC-participating veterans with OTH discharges with needed behavioral health care by allowing these veterans to access established, VA-based services and programming. Expansion may also allow VTCs to serve as a key intercept point for identifying and engaging veterans with OTH discharges who may be unaware of their eligibility for VA-based behavioral health care.
Access to VA health care services is a major resource for VTC participants and a common requirement.32 Eligibility expansion should ease access barriers veterans with OTH discharges commonly face. By providing a potential source of treatment, expansions may also support OTH eligibility practices within VTCs, particularly practices that require participants to be eligible for VA health care.33,35,36 Some VTCs may continue to determine eligibility on the basis of discharge status and remain inaccessible to veterans with OTH discharge characterizations without program-level policy changes.32,36,37
Communicating changes in eligibility policies relevant to veterans with OTH discharges may be a challenge, because many of these individuals have no established channels of communication with the VA. Because veterans with OTH discharges are at increased risk for legal system involvement, VTCs may serve as a unique point of contact to help facilitate communication.18 For example, upon referral to a VTC, veterans with OTH discharges can be identified, VA health care eligibility can be verified, and veterans can connect to VA staff to facilitate enrollment in VA services and care.
VJO specialists are in a favorable position to serve a critical role in utilizing VTCs as a potential intercept point for engaging veterans with OTH discharge characterizations. As outlined in the STRONG Veterans Act of 2022, VJOs are mandated to “spread awareness and understanding of veteran eligibility for the [VJO] Program, including the eligibility of veterans who were discharged from service in the Armed Forces under conditions other than honorable.”50 The Act further requires VJOs to be annually trained in communicating eligibility changes as they arise. Accordingly, VJOs receive ongoing training in a wide variety of critical outreach topics, including changes in eligibility; while VJOs cannot make eligibility determinations, they are tasked with enrolling all veterans involved in the criminal-legal system with whom they interact into VHA services, whether through typical or special eligibility criteria (M. Stimmel, PhD, National Training Director for Veteran Justice Programming, oral communication, July 14, 2023). VJOs therefore routinely serve in this capacity of facilitating VA enrollment of veterans with OTH discharge characterizations.
Recommendations to Veteran-Servicing Judicial Programs
Considering these potential implications, professionals routinely interacting with veterans involved in the criminal-legal system should become familiarized with recent changes in VA eligibility policies. Such familiarization would support the identification of veterans previously considered ineligible for care; provision of education to these veterans regarding their new eligibility; and referral to appropriate VA-based behavioral health care options. Although conceptually simple, executing such an educational campaign may prove logistically difficult. Given their historical exclusion from VA services, veterans with OTH discharge characterizations are unlikely to seek VA-based services in times of need, instead relying on a broad swath of civilian community-based organizations and resources. Usual approaches to advertising VHA health care policy changes (eg, by notifying VA employees and/or departments providing corresponding services or by circulating information to veteran-focused mailing lists and organizations) likely would prove insufficient. Educational campaigns to disseminate information about recent OTH eligibility changes should instead consider partnering with traditionally civilian, communitybased organizations and institutions, such as state bar associations, legal aid networks, case management services, nonveteran treatment court programs (eg, drug courts, or domestic violence courts), or probation/ parole programs. Because national surveys suggest generally low military cultural competence among civilian populations, providing concurrent support in developing foundational veteran cultural competencies (eg, how to phrase questions about military service history, or understanding discharge characterizations) may be necessary to ensure effective identification and engagement of veteran clients.48
Programs that serve veterans with criminal-legal involvement should also consider potential relevance of recent OTH eligibility changes to program operations. VTC program staff and key partners (eg, judges, case managers, district attorneys, or defense attorneys), should revisit policies and procedures surrounding the engagement of veterans with OTH discharges within VTC programs and strategies for connecting these veterans with needed services. VTC programs that have historically excluded veterans with OTH discharges due to associated difficulties in locating and connecting with needed services should consider expanding eligibility policies considering recent shifts in VA behavioral health care eligibility.33,35,36 Within the VHA, VJO specialists can play a critical role in supporting these VTC eligibility and cultural shifts. Some evidence suggests a large proportion of VTC referrals are facilitated by VJO specialists and that many such referrals are identified when veterans involved with the criminal-legal system seek VA support and/or services.33 Given the historical exclusion of veterans with OTH discharges from VA care, strategies used by VJO specialists to identify, connect, and engage veterans with OTH discharges with VTCs and other services may be beneficial.
Even with knowledge of VA eligibility changes and considerations of these changes on local operations, many forensic settings and programs struggle to identify veterans. These difficulties are likely amplified among veterans with OTH discharge characterizations, who may be hesitant to self-disclose their military service history due to fear of stigma and/or views of OTH discharge characterizations as undeserving of the veteran title.12 The VA offers 2 tools to aid in identification of veterans for these settings: the Veterans Re-Entry Search Service (VRSS) and Status Query and Response Exchange System (SQUARES). For VRSS, correctional facilities, courts, and other criminal justice entities upload a simple spreadsheet that contains basic identifying information of inmates or defendants in their system. VRSS returns information about which inmates or defendants have a history of military service and alerts VA Veterans Justice Programs staff so they can conduct outreach. A pilot study conducted by the California Department of Corrections and Rehabilitation found that 2.7% of its inmate population self-identified as veterans, while VRSS identified 7.7% of inmates with a history of military service. This difference represented about 5000 previously unidentified veterans.51 Similarly, community entities that partner with the VA, such as law enforcement or homeless service programs, can be approved to become a SQUARES user and submit identifying information of individuals with whom they interact directly into the SQUARES search engine. SQUARES then directly returns information about the individual’s veteran status and eligibility for VA health care and homeless programs.
Other Eligibility Limitations
VTCs and other professionals looking to refer veterans with OTH discharge characterizations to VA-based behavioral health care should be aware of potential limitations in eligibility and access. Specifically, although veterans with OTH discharges are now broadly eligible for VA-based behavioral health care and homeless programs, they remain ineligible for other forms of health care, including primary care and nonbehavioral specialty care.1 Research has found a strong comorbidity between behavioral and nonbehavioral health concerns, particularly within historically marginalized demographic groups.52-55 Because these historically marginalized groups are often overrepresented among persons with criminal-legal involvement, veterans with OTH discharges, and VTC participants, such comorbidities require consideration by services or programming designed to support veterans with criminal-legal involvement.12,56-58 Connection with VA-based health care will therefore continue to fall short of addressing all health care needs of veterans with OTH discharges and effective case management will require considerable treatment coordination between VA behavioral health care practitioners (HCPs) and community-based HCPs (eg, primary care professionals or nonbehavioral HCPs).
Implications for VA Mental Health Care
Recent eligibility expansions will also have inevitable consequences for VA mental health care systems. For many years, these systems have been overburdened by high caseloads and clinician burnout.59,60 Given the generally elevated rates of mental health and substance use concerns among veterans with OTH discharge characterizations, expansions hold the potential to further burden caseloads with clinically complex, high-risk, high-need clients. Nevertheless, these expansions are also structured in a way that forces existing systems to absorb the responsibilities of providing necessary care to these veterans. To mitigate detrimental effects of eligibility expansions on the broader VA mental health system, clinicians should be explicitly trained in identifying veterans with OTH discharge characterizations and the implications of discharge status on broader health care eligibility. Treatment of veterans with OTH discharges may also benefit from close coordination between mental health professionals and behavioral health care coordinators to ensure appropriate coordination of care between VA- and non–VA-based HCPs.
CONCLUSIONS
Recent changes to VA eligibility policies now allow comprehensive mental and behavioral health care services to be provided to veterans with OTH discharges.1 Compared to routinely discharged veterans, veterans with OTH discharges are more likely to be persons of color, sexual or gender minorities, and experiencing mental health-related difficulties. Given the disproportionate mental health burden often faced by veterans with OTH discharges and relative overrepresentation of these veterans in judicial and correctional systems, these changes have considerable implications for programs and services designed to support veterans with criminallegal involvement. Professionals within these systems, particularly VTC programs, are therefore encouraged to familiarize themselves with recent changes in VA eligibility policies and to revisit strategies, policies, and procedures surrounding the engagement and enrollment of veterans with OTH discharge characterizations. Doing so may ensure veterans with OTH discharges are effectively connected to needed behavioral health care services.
In April 2022, the US Department of Veterans Affairs (VA) revised its behavioral health care eligibility policies to provide comprehensive mental and behavioral health care to former service members who received an Other Than Honorable (OTH) discharge characterization upon separation from military service.1 This policy shift represents a marked expansion in eligibility practices (Table 1 includes amended eligibility criteria).
Since June 2017, eligibility policies allowed veterans with OTH discharges to receive “emergent mental health services” needed to stabilize acute mental health crises related to military service (eg, acute escalations in suicide risk).2,3 Previously, veterans with OTH discharges were largely ineligible for VA-based health care; these individuals were only able to access Veterans Health Administration (VHA) mental and behavioral health care through limited channels of eligibility (eg, for treatment of military sexual trauma or psychosis or other mental illness within 2 years of discharge).4,5 The impetus for expansions in eligibility stemmed from VA efforts to reduce the suicide rate among veterans.6-8 Implications of such expansion extend beyond suicide prevention efforts, with notable promised effects on the care of veterans with criminal-legal involvement. This article highlights potential effects of recent eligibility expansions on veterans with criminal-legal involvement and makes specific recommendations for agencies and organizations serving these veterans.
OTHER THAN HONORABLE DISCHARGE
The US Department of Defense delineates 6 discharge characterizations provided to service members upon separation from military service: honorable, general under honorable conditions, OTH, bad conduct, dishonorable, and uncharacterized. Honorable discharge characterizations are considered to reflect general concordance between service member behavior and military standards; general discharge characterizations reflect some disparity between the service member’s behavior and military standards; OTH, bad conduct, and dishonorable discharge characterizations reflect serious disparities between the service member’s behavior and military standards; and uncharacterized discharge characterizations are given when other discharge characterizations are deemed inappropriate.9,10 OTH discharge characterizations are typically issued under instances of misconduct, fraudulent entry, security reasons, or in lieu of trial by court martial.9,10
Recent research suggests that about 85% of service members receive an honorable discharge characterization upon separation from military service, 8% receive general, 6% receive OTH, and 1% receive bad conduct or dishonorable discharges.11 In 2017, the VA estimated there were > 500,000 prior service members with OTH discharge characterizations, which has grown over time (1.9% during the Korean Conflict, 2.5% during the Vietnam War Era, 3.9% during the Cold War, 4.8% in the Persian Gulf War, and 5.8% in the post-9/11 era).7,11
The OTH discharge characterization is 1 of 3 less than honorable discharges informally referred to as bad papers (ie, OTH, bad conduct, or dishonorable). Former service members receiving these discharge characterizations face significant social stigma and structural discrimination upon military discharge, including significant hurdles to employment and educational pursuits as well as notable social alienation.12 Due to their discharge characterization, some are viewed as less deserving of the veteran title, and until recently, many did not qualify for the complex legal definition of veteran as established by the Congress.11,13 Veterans with OTH discharge characterizations have also historically been excluded from services (eg, VHA care),3 benefits (eg, disability compensation),14 and protections (eg, Uniformed Services Employment and Reemployment Rights Act)15 offered to veterans with honorable or general discharge characterizations. However, eligibility policies have gradually expanded, providing veterans with OTH discharges with access to VHA-based mental and behavioral health services and VA supportive housing assistance.1,3,16
Perhaps due to their historical exclusion from VA services, there is limited research available on the behavioral health and associated needs of veterans with OTH discharges. Some scholars argue that historical exclusions have exacerbated underlying difficulties faced by this population, thereby contributing to stark health and social disparities across discharge types.14,15,17 Studies with large veteran samples, for example, reflect notable demographic and behavioral health differences across discharge types. Compared to routinely discharged veterans, veterans with OTH discharges are significantly more likely to be younger, have lower income, use substances, have a history of criminal-legal involvement, and have mental and physical health difficulties.18,19
Substantial evidence also suggests a historical racial bias, with service members of color being disproportionately more likely to receive an OTH discharge.12 Similarly, across all branches of military service, Black service members are significantly more likely to face general or special court martial in military justice proceedings when compared with White service members.20 Service members from gender and sexual minorities are also disproportionately impacted by the OTH designation. Historically, many have been discharged with bad papers due to discriminatory policies, such as Don’t Ask Don’t Tell, which discriminated on the basis of sexual orientation between December 1993 and September 2011, and Directive-type Memorandum-19-004, which banned transgender persons from military service between April 2019 and January 2021.21,22
There is also significant mental health bias in the provision of OTH discharges, such that OTH characterizations are disproportionately represented among individuals with mental health disorders.18-20 Veterans discharged from military service due to behavioral misconduct are significantly more likely to meet diagnostic criteria for various behavioral health conditions and to experience homelessness, criminal-legal involvement, and suicidal ideation and behavior compared with routinely-discharged veterans.23-28
Consistent with their comparatively higher rates of criminal-legal involvement relative to routinely discharged veterans, veterans with OTH discharges are disproportionately represented in criminal justice settings. While veterans with OTH discharges represent only 6% of discharging service members and 2.5% of community-based veterans, they represent 10% of incarcerated veterans.11,18,23,29 Preliminary research suggests veterans with OTH discharges may be at higher risk for lifetime incarceration, though the association between OTH discharge and frequency of lifetime arrests remains unclear.18,30
VETERANS TREATMENT COURTS
Given the overrepresentation of veterans with OTH discharges in criminal-legal settings, consideration for this subset of the veteran population and its unique needs is commonplace among problem-solving courts that service veterans. First conceptualized in 2004, Veterans Treatment Courts (VTCs) are specialized problem-solving courts that divert veterans away from traditional judicial court and penal systems and into community-based supervision and treatment (most commonly behavioral health services).31-34 Although each VTC program is unique in structure, policies, and procedures, most VTCs can be characterized by certain key elements, including voluntary participation, plea requirements, delayed sentencing (often including reduced or dismissed charges), integration of military culture into court proceedings, a rehabilitative vs adversarial approach to decreasing risk of future criminal behavior, mandated treatment and supervision during participation, and use of veteran mentors to provide peer support.32-35 Eligibility requirements vary; however, many restrict participation to veterans with honorable discharge types and charges for nonviolent offenses.32,33,35-37
VTCs connect veterans within the criminal-legal system to needed behavioral health, community, and social services.31-33,37 VTC participants are commonly connected to case management, behavioral health care, therapeutic journaling programs, and vocational rehabilitation.38,39 Accordingly, the most common difficulties faced by veterans participating in these courts include substance use, mental health, family issues, anger management and/or aggressive behavior, and homelessness.36,39 There is limited research on the effectiveness of VTCs. Evidence on their overall effectiveness is largely mixed, though some studies suggest VTC graduates tend to have lower recidivism rates than offenders more broadly or persons who terminate VTC programs prior to completion.40,41 Other studies suggest that VTC participants are more likely to have jail sanctions, new arrests, and new incarcerations relative to nontreatment court participants.42 Notably, experimental designs (considered the gold standard in assessing effectiveness) to date have not been applied to evaluate the effectiveness of VTCs; as such, the effectiveness of these programs remains an area in need of continued empirical investigation.
Like all problem-solving courts, VTCs occasionally struggle to connect participating defendants with appropriate care, particularly when encountering structural barriers (eg, insurance, transportation) and/or complex behavioral health needs (eg, personality disorders).34,43 As suicide rates among veterans experiencing criminal-legal involvement surge (about 150 per 100,000 in 2021, a 10% increase from 2020 to 2021 compared to about 40 per 100,000 and a 1.8% increase among other veterans), efficiency of adequate care coordination is vital.44 Many VTCs rely on VTC-VA partnerships and collaborations to navigate these difficulties and facilitate connection of participating veterans to needed services.32-34,45 For example, within the VHA, Veterans Justice Outreach (VJO) and Health Care for Re-Entry Veterans (HCRV) specialists assist and bridge the gap between the criminal-legal system (including, but not limited to VTCs) and VA services by engaging veterans involved in the criminal-legal system and connecting them to needed VA-based services (Table 2). Generally, VJO specialists support veterans involved with the front end of the criminallegal system (eg, arrest, pretrial incarceration, or participation in VTCs), while HCRV specialists tend to support veterans transitioning back into the community after a period of incarceration.46,47 Specific to VTCs, VJO specialists typically serve as liaisons between the courts and VA, coordinating VA services for defendants to fulfill their terms of VTC participation.46
The historical exclusion of veterans with OTH discharge characterizations from VA-based services has restricted many from accessing VTC programs.32 Of 17 VTC programs active in Pennsylvania in 2014, only 5 accepted veterans with OTstayH discharges, and 3 required application to and eligibility for VA benefits.33 Similarly, in national surveys of VTC programs, about 1 in 3 report excluding veterans deemed ineligible for VA services.35,36 When veterans with OTH discharges have accessed VTC programs, they have historically relied on non-VA, community-based programming to fulfill treatment mandates, which may be less suited to addressing the unique needs of veterans.48
Veterans who utilize VTCs receive several benefits, namely peer support and mentorship, acceptance into a veteran-centric space, and connection with specially trained staff capable of supporting the veteran through applications for a range of VA benefits (eg, service connection, housing support).31-33,37 Given the disparate prevalence of OTH discharge characterizations among service members from racial, sexual, and gender minorities and among service members with mental health disorders, exclusion of veterans with OTH discharges from VTCs solely based on the type of discharge likely contributes to structural inequities among these already underserved groups by restricting access to these potential benefits. Such structural inequity stands in direct conflict with VTC best practice standards, which admonish programs to adjust eligibility requirements to facilitate access to treatment court programs for historically marginalized groups.49
ELIGIBILITY EXPANSIONS
Given the overrepresentation of veterans with OTH discharge characterizations within the criminal-legal system and historical barriers of these veterans to access needed mental and behavioral health care, expansions in VA eligibility policies could have immense implications for VTCs. First, these expansions could mitigate common barriers to connecting VTC-participating veterans with OTH discharges with needed behavioral health care by allowing these veterans to access established, VA-based services and programming. Expansion may also allow VTCs to serve as a key intercept point for identifying and engaging veterans with OTH discharges who may be unaware of their eligibility for VA-based behavioral health care.
Access to VA health care services is a major resource for VTC participants and a common requirement.32 Eligibility expansion should ease access barriers veterans with OTH discharges commonly face. By providing a potential source of treatment, expansions may also support OTH eligibility practices within VTCs, particularly practices that require participants to be eligible for VA health care.33,35,36 Some VTCs may continue to determine eligibility on the basis of discharge status and remain inaccessible to veterans with OTH discharge characterizations without program-level policy changes.32,36,37
Communicating changes in eligibility policies relevant to veterans with OTH discharges may be a challenge, because many of these individuals have no established channels of communication with the VA. Because veterans with OTH discharges are at increased risk for legal system involvement, VTCs may serve as a unique point of contact to help facilitate communication.18 For example, upon referral to a VTC, veterans with OTH discharges can be identified, VA health care eligibility can be verified, and veterans can connect to VA staff to facilitate enrollment in VA services and care.
VJO specialists are in a favorable position to serve a critical role in utilizing VTCs as a potential intercept point for engaging veterans with OTH discharge characterizations. As outlined in the STRONG Veterans Act of 2022, VJOs are mandated to “spread awareness and understanding of veteran eligibility for the [VJO] Program, including the eligibility of veterans who were discharged from service in the Armed Forces under conditions other than honorable.”50 The Act further requires VJOs to be annually trained in communicating eligibility changes as they arise. Accordingly, VJOs receive ongoing training in a wide variety of critical outreach topics, including changes in eligibility; while VJOs cannot make eligibility determinations, they are tasked with enrolling all veterans involved in the criminal-legal system with whom they interact into VHA services, whether through typical or special eligibility criteria (M. Stimmel, PhD, National Training Director for Veteran Justice Programming, oral communication, July 14, 2023). VJOs therefore routinely serve in this capacity of facilitating VA enrollment of veterans with OTH discharge characterizations.
Recommendations to Veteran-Servicing Judicial Programs
Considering these potential implications, professionals routinely interacting with veterans involved in the criminal-legal system should become familiarized with recent changes in VA eligibility policies. Such familiarization would support the identification of veterans previously considered ineligible for care; provision of education to these veterans regarding their new eligibility; and referral to appropriate VA-based behavioral health care options. Although conceptually simple, executing such an educational campaign may prove logistically difficult. Given their historical exclusion from VA services, veterans with OTH discharge characterizations are unlikely to seek VA-based services in times of need, instead relying on a broad swath of civilian community-based organizations and resources. Usual approaches to advertising VHA health care policy changes (eg, by notifying VA employees and/or departments providing corresponding services or by circulating information to veteran-focused mailing lists and organizations) likely would prove insufficient. Educational campaigns to disseminate information about recent OTH eligibility changes should instead consider partnering with traditionally civilian, communitybased organizations and institutions, such as state bar associations, legal aid networks, case management services, nonveteran treatment court programs (eg, drug courts, or domestic violence courts), or probation/ parole programs. Because national surveys suggest generally low military cultural competence among civilian populations, providing concurrent support in developing foundational veteran cultural competencies (eg, how to phrase questions about military service history, or understanding discharge characterizations) may be necessary to ensure effective identification and engagement of veteran clients.48
Programs that serve veterans with criminal-legal involvement should also consider potential relevance of recent OTH eligibility changes to program operations. VTC program staff and key partners (eg, judges, case managers, district attorneys, or defense attorneys), should revisit policies and procedures surrounding the engagement of veterans with OTH discharges within VTC programs and strategies for connecting these veterans with needed services. VTC programs that have historically excluded veterans with OTH discharges due to associated difficulties in locating and connecting with needed services should consider expanding eligibility policies considering recent shifts in VA behavioral health care eligibility.33,35,36 Within the VHA, VJO specialists can play a critical role in supporting these VTC eligibility and cultural shifts. Some evidence suggests a large proportion of VTC referrals are facilitated by VJO specialists and that many such referrals are identified when veterans involved with the criminal-legal system seek VA support and/or services.33 Given the historical exclusion of veterans with OTH discharges from VA care, strategies used by VJO specialists to identify, connect, and engage veterans with OTH discharges with VTCs and other services may be beneficial.
Even with knowledge of VA eligibility changes and considerations of these changes on local operations, many forensic settings and programs struggle to identify veterans. These difficulties are likely amplified among veterans with OTH discharge characterizations, who may be hesitant to self-disclose their military service history due to fear of stigma and/or views of OTH discharge characterizations as undeserving of the veteran title.12 The VA offers 2 tools to aid in identification of veterans for these settings: the Veterans Re-Entry Search Service (VRSS) and Status Query and Response Exchange System (SQUARES). For VRSS, correctional facilities, courts, and other criminal justice entities upload a simple spreadsheet that contains basic identifying information of inmates or defendants in their system. VRSS returns information about which inmates or defendants have a history of military service and alerts VA Veterans Justice Programs staff so they can conduct outreach. A pilot study conducted by the California Department of Corrections and Rehabilitation found that 2.7% of its inmate population self-identified as veterans, while VRSS identified 7.7% of inmates with a history of military service. This difference represented about 5000 previously unidentified veterans.51 Similarly, community entities that partner with the VA, such as law enforcement or homeless service programs, can be approved to become a SQUARES user and submit identifying information of individuals with whom they interact directly into the SQUARES search engine. SQUARES then directly returns information about the individual’s veteran status and eligibility for VA health care and homeless programs.
Other Eligibility Limitations
VTCs and other professionals looking to refer veterans with OTH discharge characterizations to VA-based behavioral health care should be aware of potential limitations in eligibility and access. Specifically, although veterans with OTH discharges are now broadly eligible for VA-based behavioral health care and homeless programs, they remain ineligible for other forms of health care, including primary care and nonbehavioral specialty care.1 Research has found a strong comorbidity between behavioral and nonbehavioral health concerns, particularly within historically marginalized demographic groups.52-55 Because these historically marginalized groups are often overrepresented among persons with criminal-legal involvement, veterans with OTH discharges, and VTC participants, such comorbidities require consideration by services or programming designed to support veterans with criminal-legal involvement.12,56-58 Connection with VA-based health care will therefore continue to fall short of addressing all health care needs of veterans with OTH discharges and effective case management will require considerable treatment coordination between VA behavioral health care practitioners (HCPs) and community-based HCPs (eg, primary care professionals or nonbehavioral HCPs).
Implications for VA Mental Health Care
Recent eligibility expansions will also have inevitable consequences for VA mental health care systems. For many years, these systems have been overburdened by high caseloads and clinician burnout.59,60 Given the generally elevated rates of mental health and substance use concerns among veterans with OTH discharge characterizations, expansions hold the potential to further burden caseloads with clinically complex, high-risk, high-need clients. Nevertheless, these expansions are also structured in a way that forces existing systems to absorb the responsibilities of providing necessary care to these veterans. To mitigate detrimental effects of eligibility expansions on the broader VA mental health system, clinicians should be explicitly trained in identifying veterans with OTH discharge characterizations and the implications of discharge status on broader health care eligibility. Treatment of veterans with OTH discharges may also benefit from close coordination between mental health professionals and behavioral health care coordinators to ensure appropriate coordination of care between VA- and non–VA-based HCPs.
CONCLUSIONS
Recent changes to VA eligibility policies now allow comprehensive mental and behavioral health care services to be provided to veterans with OTH discharges.1 Compared to routinely discharged veterans, veterans with OTH discharges are more likely to be persons of color, sexual or gender minorities, and experiencing mental health-related difficulties. Given the disproportionate mental health burden often faced by veterans with OTH discharges and relative overrepresentation of these veterans in judicial and correctional systems, these changes have considerable implications for programs and services designed to support veterans with criminallegal involvement. Professionals within these systems, particularly VTC programs, are therefore encouraged to familiarize themselves with recent changes in VA eligibility policies and to revisit strategies, policies, and procedures surrounding the engagement and enrollment of veterans with OTH discharge characterizations. Doing so may ensure veterans with OTH discharges are effectively connected to needed behavioral health care services.
- US Department of Veterans, Veterans Health Administration. VHA Directive 1601A.02(6): Eligibility Determination. Updated March 6, 2024. Accessed August 8, 2024. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=8908
- Mental and behavioral health care for certain former members of the Armed Forces. 38 USC §1720I (2018). Accessed August 5, 2024. https://uscode.house.gov/view.xhtml?req=(title:38%20section:1720I%20edition:prelim
- US Department of Veterans, Veterans Health Administration. VHA Directive 1601A.02, Eligibility Determination. June 7, 2017.
- US Department of Veterans, Veterans Health Administration. VHA Directive 1115(1), Military Sexual Trauma (MST) Program. May 8, 2018. Accessed August 5, 2024. https:// www.va.gov/vhapublications/viewpublication.asp?pub_ID=6402
- US Department of Veterans Affairs. Tentative Eligibility Determinations; Presumptive Eligibility for Psychosis and Other Mental Illness. 38 CFR §17.109. May 14, 2013. Accessed August 5, 2024. https://www.federalregister.gov/documents/2013/05/14/2013-11410/tentative-eligibility-determinations-presumptive-eligibility-for-psychosis-and-other-mental-illness
- US Department of Veterans Affairs, VA Office of Mental Health and Suicide Prevention. National strategy for preventing veteran suicide 2018-2028. Published September 2018. Accessed August 5, 2024. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
- US Department of Veterans Affairs. VA secretary announces intention to expand mental health care to former service members with other-than-honorable discharges and in crisis. Press Release. March 8, 2017. Accessed August 5, 2024. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=2867
- Smith C. Dramatic increase in mental health services to other-than-honorable discharge veterans. VA News. February 23, 2022. Accessed August 5, 2024. https://news.va.gov/100460/dramatic-increase-in-mental-health-services-to-other-than-honorable-discharge-veterans/
- US Department of Defense. DoD Instruction 1332.14. Enlisted administrative separations. Updated August 1, 2024. Accessed August 5, 2024. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/133214p.pdf
- US Department of Defense. DoD Instruction 1332.30. Commissioned officer administrative separations. Updated September 9, 2021. Accessed August 5, 2024. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/133230p.pdf
- OUTVETS, Legal Services Center of Harvard Law School, Veterans Legal Services. Turned away: how the VA unlawfully denies healthcare to veterans with bad paper discharges. 2020. Accessed August 5, 2024. https://legalservicescenter.org/wp-content/uploads/Turn-Away-Report.pdf
- McClean H. Discharged and discarded: the collateral consequences of a less-than-honorable military discharge. Columbia Law Rev. 2021;121(7):2203-2268.
- Veterans Benefits, General Provisions, Definitions. 38 USC §101(2) (1958). Accessed August 5, 2024. https://uscode.house.gov/view.xhtml?req=granuleid:USC-prelim-title38-section101&num=0&edition=prelim
- Bedford JR. Other than honorable discharges: unfair and unjust life sentences of decreased earning capacity. U Penn J Law Pub Affairs. 2021;6(4):687.
- Karin ML. Other than honorable discrimination. Case Western Reserve Law Rev. 2016;67(1):135-191. https://scholarlycommons.law.case.edu/caselrev/vol67/iss1/9
- Veteran HOUSE Act of 2020, HR 2398, 116th Cong, (2020). Accessed August 5, 2024. https://www.congress.gov/bill/116th-congress/house-bill/2398
- Scapardine D. Leaving other than honorable soldiers behind: how the Departments of Defense and Veterans Affairs inadvertently created a health and social crisis. Md Law Rev. 2017;76(4):1133-1165.
- Elbogen EB, Wagner HR, Brancu M, et al. Psychosocial risk factors and other than honorable military discharge: providing healthcare to previously ineligible veterans. Mil Med. 2018;183(9-10):e532-e538. doi:10.1093/milmed/usx128
- Tsai J, Rosenheck RA. Characteristics and health needs of veterans with other-than-honorable discharges: expanding eligibility in the Veterans Health Administration. Mil Med. 2018;183(5-6):e153-e157. doi:10.1093/milmed/usx110
- Christensen DM, Tsilker Y. Racial disparities in military justice: findings of substantial and persistent racial disparities within the United States military justice system. Accessed August 5, 2024. https://www.protectourdefenders.com/wp-content/uploads/2017/05/Report_20.pdf
- Don’t Ask Don’t Tell, 10 USC §654 (1993) (Repealed 2010). Accessed August 5, 2024. http://www.gpo.gov/fdsys/pkg/USCODE-2010-title10/pdf/USCODE-2010-title10-subtitleA-partII-chap37-sec654.pdf
- Palm Center. The making of a ban: how DTM-19-004 works to push transgender people out of military service. 2019. March 20, 2019. Accessed August 5, 2024. https://www.palmcenter.org/wp-content/uploads/2019/04/The-Making-of-a-Ban.pdf
- Edwards ER, Greene AL, Epshteyn G, Gromatsky M, Kinney AR, Holliday R. Mental health of incarcerated veterans and civilians: latent class analysis of the 2016 Survey of Prison Inmates. Crim Justice Behav. 2022;49(12):1800- 1821. doi:10.1177/00938548221121142
- Brignone E, Fargo JD, Blais RK, Carter ME, Samore MH, Gundlapalli AV. Non-routine discharge from military service: mental illness, substance use disorders, and suicidality. Am J Prev Med. 2017;52(5):557-565. doi:10.1016/j.amepre.2016.11.015
- Gamache G, Rosenheck R, Tessler R. Military discharge status of homeless veterans with mental illness. Mil Med. 2000;165(11):803-808. doi:10.1093/milmed/165.11.803
- Gundlapalli AV, Fargo JD, Metraux S, et al. Military Misconduct and Homelessness Among US Veterans Separated From Active Duty, 2001-2012. JAMA. 2015;314(8):832-834. doi:10.1001/jama.2015.8207
- Brooks Holliday S, Pedersen ER. The association between discharge status, mental health, and substance misuse among young adult veterans. Psychiatry Res. 2017;256:428-434. doi:10.1016/j.psychres.2017.07.011
- Williamson RB. DOD Health: Actions Needed to Ensure Post-Traumatic Stress Disorder and Traumatic Brain Injury are Considered in Misconduct Separations. US Government Accountability Office; 2017. Accessed August 5, 2024. https://apps.dtic.mil/sti/pdfs/AD1168610.pdf
- Maruschak LM, Bronson J, Alper M. Indicators of mental health problems reported by prisoners: survey of prison inmates. US Department of Justice Bureau of Justice Statistics. June 2021. Accessed August 5, 2024. https://bjs.ojp.gov/sites/g/files/xyckuh236/files/media/document/imhprpspi16st.pdf
- Brooke E, Gau J. Military service and lifetime arrests: examining the effects of the total military experience on arrests in a sample of prison inmates. Crim Justice Policy Rev. 2018;29(1):24-44. doi:10.1177/0887403415619007
- Russell RT. Veterans treatment court: a proactive approach. N Engl J Crim Civ Confin. 2009;35:357-372.
- Cartwright T. To care for him who shall have borne the battle: the recent development of Veterans Treatment Courts in America. Stanford Law Pol Rev. 2011;22:295-316.
- Douds AS, Ahlin EM, Howard D, Stigerwalt S. Varieties of veterans’ courts: a statewide assessment of veterans’ treatment court components. Crim Justice Policy Rev. 2017;28:740-769. doi:10.1177/0887403415620633
- Rowen J. Worthy of justice: a veterans treatment court in practice. Law Policy. 2020;42(1):78-100. doi:10.1111/lapo.12142
- Timko C, Flatley B, Tjemsland A, et al. A longitudinal examination of veterans treatment courts’ characteristics and eligibility criteria. Justice Res Policy. 2016;17(2):123-136.
- Baldwin JM. Executive summary: national survey of veterans treatment courts. SSRN. Preprint posted online June 5, 2013. Accessed August 5, 2024. doi:10.2139/ssrn.2274138
- Renz T. Veterans treatment court: a hand up rather than lock up. Richmond Public Interest Law Rev. 2013;17(3):697-705. https://scholarship.richmond.edu/pilr/vol17/iss3/6
- Knudsen KJ, Wingenfeld S. A specialized treatment court for veterans with trauma exposure: implications for the field. Community Ment Health J. 2016;52(2):127-135. doi:10.1007/s10597-015-9845-9
- McCall JD, Tsai J, Gordon AJ. Veterans treatment court research: participant characteristics, outcomes, and gaps in the literature. J Offender Rehabil. 2018;57:384-401. doi:10.1080/10509674.2018.1510864
- Smith JS. The Anchorage, Alaska veterans court and recidivism: July 6, 2004 – December 31, 2010. Alsk Law Rev. 2012;29(1):93-111.
- Hartley RD, Baldwin JM. Waging war on recidivism among justice-involved veterans: an impact evaluation of a large urban veterans treatment court. Crim Justice Policy Rev. 2019;30(1):52-78. doi:10.1177/0887403416650490
- Tsai J, Flatley B, Kasprow WJ, Clark S, Finlay A. Diversion of veterans with criminal justice involvement to treatment courts: participant characteristics and outcomes. Psychiatr Serv. 2017;68(4):375-383. doi:10.1176/appi.ps.201600233
- Edwards ER, Sissoko DR, Abrams D, Samost D, La Gamma S, Geraci J. Connecting mental health court participants with services: process, challenges, and recommendations. Psychol Public Policy Law. 2020;26(4):463-475. doi:10.1037/law0000236
- US Department of Veterans Affairs, VA Office of Mental Health and Suicide Prevention. 2023 National Veteran Suicide Prevention Annual Report. US Department of Veterans Affairs; November 2023. Accessed August 5, 2024. https://www.mentalhealth.va.gov/docs/data-sheets/2023/2023-National-Veteran-Suicide-Prevention-Annual-Report-FINAL-508.pdf
- Finlay AK, Clark S, Blue-Howells J, et al. Logic model of the Department of Veterans Affairs’ role in veterans treatment courts. Drug Court Rev. 2019;2:45-62.
- Finlay AK, Smelson D, Sawh L, et al. U.S. Department of Veterans Affairs veterans justice outreach program: connecting justice-involved veterans with mental health and substance use disorder treatment. Crim Justice Policy Rev. 2016;27(2):10.1177/0887403414562601. doi:10.1177/0887403414562601
- Finlay AK, Stimmel M, Blue-Howells J, et al. Use of Veterans Health Administration mental health and substance use disorder treatment after exiting prison: the health care for reentry veterans program. Adm Policy Ment Health. 2017;44(2):177-187. doi:10.1007/s10488-015-0708-z
- Meyer EG, Writer BW, Brim W. The Importance of Military Cultural Competence. Curr Psychiatry Rep. 2016;18(3):26. doi:10.1007/s11920-016-0662-9
- National Association of Drug Court Professionals. Adult Drug Court Best Practice Standards Volume I. National Association of Drug Court Professionals; 2013. Accessed August 5, 2024. https://allrise.org/publications/standards/
- STRONG Veterans Act of 2022, HR 6411, 117th Cong (2022). https://www.congress.gov/bill/117th-congress/house-bill/6411/text
- Pelletier D, Clark S, Davis L. Veterans reentry search service (VRSS) and the SQUARES application. Presented at: National Association of Drug Court Professionals Conference; August 15-18, 2021; National Harbor, Maryland.
- Scott KM, Lim C, Al-Hamzawi A, et al. Association of Mental Disorders With Subsequent Chronic Physical Conditions: World Mental Health Surveys From 17 Countries. JAMA Psychiatry. 2016;73(2):150-158. doi:10.1001/jamapsychiatry.2015.2688
- Ahmed N, Conway CA. Medical and mental health comorbidities among minority racial/ethnic groups in the United States. J Soc Beh Health Sci. 2020;14(1):153-168. doi:10.5590/JSBHS.2020.14.1.11
- Hanna B, Desai R, Parekh T, Guirguis E, Kumar G, Sachdeva R. Psychiatric disorders in the U.S. transgender population. Ann Epidemiol. 2019;39:1-7.e1. doi:10.1016/j.annepidem.2019.09.009
- Watkins DC, Assari S, Johnson-Lawrence V. Race and ethnic group differences in comorbid major depressive disorder, generalized anxiety disorder, and chronic medical conditions. J Racial Ethn Health Disparities. 2015;2(3):385- 394. doi:10.1007/s40615-015-0085-z
- Baldwin J. Whom do they serve? National examination of veterans treatment court participants and their challenges. Crim Justice Policy Rev. 2017;28(6):515-554. doi:10.1177/0887403415606184
- Beatty LG, Snell TL. Profile of prison inmates, 2016. US Department of Justice Bureau of Justice Statistics. December 2021. Accessed August 5, 2024. https://bjs.ojp.gov/content/pub/pdf/ppi16.pdf
- Al-Rousan T, Rubenstein L, Sieleni B, Deol H, Wallace RB. Inside the nation’s largest mental health institution: a prevalence study in a state prison system. BMC Public Health. 2017;17(1):342. doi:10.1186/s12889-017-4257-0
- Rosen CS, Kaplan AN, Nelson DB, et al. Implementation context and burnout among Department of Veterans Affairs psychotherapists prior to and during the COVID-19 pandemic. J Affect Disord. 2023;320:517-524. doi:10.1016/j.jad.2022.09.141
- Tsai J, Jones N, Klee A, Deegan D. Job burnout among mental health staff at a veterans affairs psychosocial rehabilitation center. Community Ment Health J. 2020;56(2):294- 297. doi:10.1007/s10597-019-00487-5
- US Department of Veterans, Veterans Health Administration. VHA Directive 1601A.02(6): Eligibility Determination. Updated March 6, 2024. Accessed August 8, 2024. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=8908
- Mental and behavioral health care for certain former members of the Armed Forces. 38 USC §1720I (2018). Accessed August 5, 2024. https://uscode.house.gov/view.xhtml?req=(title:38%20section:1720I%20edition:prelim
- US Department of Veterans, Veterans Health Administration. VHA Directive 1601A.02, Eligibility Determination. June 7, 2017.
- US Department of Veterans, Veterans Health Administration. VHA Directive 1115(1), Military Sexual Trauma (MST) Program. May 8, 2018. Accessed August 5, 2024. https:// www.va.gov/vhapublications/viewpublication.asp?pub_ID=6402
- US Department of Veterans Affairs. Tentative Eligibility Determinations; Presumptive Eligibility for Psychosis and Other Mental Illness. 38 CFR §17.109. May 14, 2013. Accessed August 5, 2024. https://www.federalregister.gov/documents/2013/05/14/2013-11410/tentative-eligibility-determinations-presumptive-eligibility-for-psychosis-and-other-mental-illness
- US Department of Veterans Affairs, VA Office of Mental Health and Suicide Prevention. National strategy for preventing veteran suicide 2018-2028. Published September 2018. Accessed August 5, 2024. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
- US Department of Veterans Affairs. VA secretary announces intention to expand mental health care to former service members with other-than-honorable discharges and in crisis. Press Release. March 8, 2017. Accessed August 5, 2024. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=2867
- Smith C. Dramatic increase in mental health services to other-than-honorable discharge veterans. VA News. February 23, 2022. Accessed August 5, 2024. https://news.va.gov/100460/dramatic-increase-in-mental-health-services-to-other-than-honorable-discharge-veterans/
- US Department of Defense. DoD Instruction 1332.14. Enlisted administrative separations. Updated August 1, 2024. Accessed August 5, 2024. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/133214p.pdf
- US Department of Defense. DoD Instruction 1332.30. Commissioned officer administrative separations. Updated September 9, 2021. Accessed August 5, 2024. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/133230p.pdf
- OUTVETS, Legal Services Center of Harvard Law School, Veterans Legal Services. Turned away: how the VA unlawfully denies healthcare to veterans with bad paper discharges. 2020. Accessed August 5, 2024. https://legalservicescenter.org/wp-content/uploads/Turn-Away-Report.pdf
- McClean H. Discharged and discarded: the collateral consequences of a less-than-honorable military discharge. Columbia Law Rev. 2021;121(7):2203-2268.
- Veterans Benefits, General Provisions, Definitions. 38 USC §101(2) (1958). Accessed August 5, 2024. https://uscode.house.gov/view.xhtml?req=granuleid:USC-prelim-title38-section101&num=0&edition=prelim
- Bedford JR. Other than honorable discharges: unfair and unjust life sentences of decreased earning capacity. U Penn J Law Pub Affairs. 2021;6(4):687.
- Karin ML. Other than honorable discrimination. Case Western Reserve Law Rev. 2016;67(1):135-191. https://scholarlycommons.law.case.edu/caselrev/vol67/iss1/9
- Veteran HOUSE Act of 2020, HR 2398, 116th Cong, (2020). Accessed August 5, 2024. https://www.congress.gov/bill/116th-congress/house-bill/2398
- Scapardine D. Leaving other than honorable soldiers behind: how the Departments of Defense and Veterans Affairs inadvertently created a health and social crisis. Md Law Rev. 2017;76(4):1133-1165.
- Elbogen EB, Wagner HR, Brancu M, et al. Psychosocial risk factors and other than honorable military discharge: providing healthcare to previously ineligible veterans. Mil Med. 2018;183(9-10):e532-e538. doi:10.1093/milmed/usx128
- Tsai J, Rosenheck RA. Characteristics and health needs of veterans with other-than-honorable discharges: expanding eligibility in the Veterans Health Administration. Mil Med. 2018;183(5-6):e153-e157. doi:10.1093/milmed/usx110
- Christensen DM, Tsilker Y. Racial disparities in military justice: findings of substantial and persistent racial disparities within the United States military justice system. Accessed August 5, 2024. https://www.protectourdefenders.com/wp-content/uploads/2017/05/Report_20.pdf
- Don’t Ask Don’t Tell, 10 USC §654 (1993) (Repealed 2010). Accessed August 5, 2024. http://www.gpo.gov/fdsys/pkg/USCODE-2010-title10/pdf/USCODE-2010-title10-subtitleA-partII-chap37-sec654.pdf
- Palm Center. The making of a ban: how DTM-19-004 works to push transgender people out of military service. 2019. March 20, 2019. Accessed August 5, 2024. https://www.palmcenter.org/wp-content/uploads/2019/04/The-Making-of-a-Ban.pdf
- Edwards ER, Greene AL, Epshteyn G, Gromatsky M, Kinney AR, Holliday R. Mental health of incarcerated veterans and civilians: latent class analysis of the 2016 Survey of Prison Inmates. Crim Justice Behav. 2022;49(12):1800- 1821. doi:10.1177/00938548221121142
- Brignone E, Fargo JD, Blais RK, Carter ME, Samore MH, Gundlapalli AV. Non-routine discharge from military service: mental illness, substance use disorders, and suicidality. Am J Prev Med. 2017;52(5):557-565. doi:10.1016/j.amepre.2016.11.015
- Gamache G, Rosenheck R, Tessler R. Military discharge status of homeless veterans with mental illness. Mil Med. 2000;165(11):803-808. doi:10.1093/milmed/165.11.803
- Gundlapalli AV, Fargo JD, Metraux S, et al. Military Misconduct and Homelessness Among US Veterans Separated From Active Duty, 2001-2012. JAMA. 2015;314(8):832-834. doi:10.1001/jama.2015.8207
- Brooks Holliday S, Pedersen ER. The association between discharge status, mental health, and substance misuse among young adult veterans. Psychiatry Res. 2017;256:428-434. doi:10.1016/j.psychres.2017.07.011
- Williamson RB. DOD Health: Actions Needed to Ensure Post-Traumatic Stress Disorder and Traumatic Brain Injury are Considered in Misconduct Separations. US Government Accountability Office; 2017. Accessed August 5, 2024. https://apps.dtic.mil/sti/pdfs/AD1168610.pdf
- Maruschak LM, Bronson J, Alper M. Indicators of mental health problems reported by prisoners: survey of prison inmates. US Department of Justice Bureau of Justice Statistics. June 2021. Accessed August 5, 2024. https://bjs.ojp.gov/sites/g/files/xyckuh236/files/media/document/imhprpspi16st.pdf
- Brooke E, Gau J. Military service and lifetime arrests: examining the effects of the total military experience on arrests in a sample of prison inmates. Crim Justice Policy Rev. 2018;29(1):24-44. doi:10.1177/0887403415619007
- Russell RT. Veterans treatment court: a proactive approach. N Engl J Crim Civ Confin. 2009;35:357-372.
- Cartwright T. To care for him who shall have borne the battle: the recent development of Veterans Treatment Courts in America. Stanford Law Pol Rev. 2011;22:295-316.
- Douds AS, Ahlin EM, Howard D, Stigerwalt S. Varieties of veterans’ courts: a statewide assessment of veterans’ treatment court components. Crim Justice Policy Rev. 2017;28:740-769. doi:10.1177/0887403415620633
- Rowen J. Worthy of justice: a veterans treatment court in practice. Law Policy. 2020;42(1):78-100. doi:10.1111/lapo.12142
- Timko C, Flatley B, Tjemsland A, et al. A longitudinal examination of veterans treatment courts’ characteristics and eligibility criteria. Justice Res Policy. 2016;17(2):123-136.
- Baldwin JM. Executive summary: national survey of veterans treatment courts. SSRN. Preprint posted online June 5, 2013. Accessed August 5, 2024. doi:10.2139/ssrn.2274138
- Renz T. Veterans treatment court: a hand up rather than lock up. Richmond Public Interest Law Rev. 2013;17(3):697-705. https://scholarship.richmond.edu/pilr/vol17/iss3/6
- Knudsen KJ, Wingenfeld S. A specialized treatment court for veterans with trauma exposure: implications for the field. Community Ment Health J. 2016;52(2):127-135. doi:10.1007/s10597-015-9845-9
- McCall JD, Tsai J, Gordon AJ. Veterans treatment court research: participant characteristics, outcomes, and gaps in the literature. J Offender Rehabil. 2018;57:384-401. doi:10.1080/10509674.2018.1510864
- Smith JS. The Anchorage, Alaska veterans court and recidivism: July 6, 2004 – December 31, 2010. Alsk Law Rev. 2012;29(1):93-111.
- Hartley RD, Baldwin JM. Waging war on recidivism among justice-involved veterans: an impact evaluation of a large urban veterans treatment court. Crim Justice Policy Rev. 2019;30(1):52-78. doi:10.1177/0887403416650490
- Tsai J, Flatley B, Kasprow WJ, Clark S, Finlay A. Diversion of veterans with criminal justice involvement to treatment courts: participant characteristics and outcomes. Psychiatr Serv. 2017;68(4):375-383. doi:10.1176/appi.ps.201600233
- Edwards ER, Sissoko DR, Abrams D, Samost D, La Gamma S, Geraci J. Connecting mental health court participants with services: process, challenges, and recommendations. Psychol Public Policy Law. 2020;26(4):463-475. doi:10.1037/law0000236
- US Department of Veterans Affairs, VA Office of Mental Health and Suicide Prevention. 2023 National Veteran Suicide Prevention Annual Report. US Department of Veterans Affairs; November 2023. Accessed August 5, 2024. https://www.mentalhealth.va.gov/docs/data-sheets/2023/2023-National-Veteran-Suicide-Prevention-Annual-Report-FINAL-508.pdf
- Finlay AK, Clark S, Blue-Howells J, et al. Logic model of the Department of Veterans Affairs’ role in veterans treatment courts. Drug Court Rev. 2019;2:45-62.
- Finlay AK, Smelson D, Sawh L, et al. U.S. Department of Veterans Affairs veterans justice outreach program: connecting justice-involved veterans with mental health and substance use disorder treatment. Crim Justice Policy Rev. 2016;27(2):10.1177/0887403414562601. doi:10.1177/0887403414562601
- Finlay AK, Stimmel M, Blue-Howells J, et al. Use of Veterans Health Administration mental health and substance use disorder treatment after exiting prison: the health care for reentry veterans program. Adm Policy Ment Health. 2017;44(2):177-187. doi:10.1007/s10488-015-0708-z
- Meyer EG, Writer BW, Brim W. The Importance of Military Cultural Competence. Curr Psychiatry Rep. 2016;18(3):26. doi:10.1007/s11920-016-0662-9
- National Association of Drug Court Professionals. Adult Drug Court Best Practice Standards Volume I. National Association of Drug Court Professionals; 2013. Accessed August 5, 2024. https://allrise.org/publications/standards/
- STRONG Veterans Act of 2022, HR 6411, 117th Cong (2022). https://www.congress.gov/bill/117th-congress/house-bill/6411/text
- Pelletier D, Clark S, Davis L. Veterans reentry search service (VRSS) and the SQUARES application. Presented at: National Association of Drug Court Professionals Conference; August 15-18, 2021; National Harbor, Maryland.
- Scott KM, Lim C, Al-Hamzawi A, et al. Association of Mental Disorders With Subsequent Chronic Physical Conditions: World Mental Health Surveys From 17 Countries. JAMA Psychiatry. 2016;73(2):150-158. doi:10.1001/jamapsychiatry.2015.2688
- Ahmed N, Conway CA. Medical and mental health comorbidities among minority racial/ethnic groups in the United States. J Soc Beh Health Sci. 2020;14(1):153-168. doi:10.5590/JSBHS.2020.14.1.11
- Hanna B, Desai R, Parekh T, Guirguis E, Kumar G, Sachdeva R. Psychiatric disorders in the U.S. transgender population. Ann Epidemiol. 2019;39:1-7.e1. doi:10.1016/j.annepidem.2019.09.009
- Watkins DC, Assari S, Johnson-Lawrence V. Race and ethnic group differences in comorbid major depressive disorder, generalized anxiety disorder, and chronic medical conditions. J Racial Ethn Health Disparities. 2015;2(3):385- 394. doi:10.1007/s40615-015-0085-z
- Baldwin J. Whom do they serve? National examination of veterans treatment court participants and their challenges. Crim Justice Policy Rev. 2017;28(6):515-554. doi:10.1177/0887403415606184
- Beatty LG, Snell TL. Profile of prison inmates, 2016. US Department of Justice Bureau of Justice Statistics. December 2021. Accessed August 5, 2024. https://bjs.ojp.gov/content/pub/pdf/ppi16.pdf
- Al-Rousan T, Rubenstein L, Sieleni B, Deol H, Wallace RB. Inside the nation’s largest mental health institution: a prevalence study in a state prison system. BMC Public Health. 2017;17(1):342. doi:10.1186/s12889-017-4257-0
- Rosen CS, Kaplan AN, Nelson DB, et al. Implementation context and burnout among Department of Veterans Affairs psychotherapists prior to and during the COVID-19 pandemic. J Affect Disord. 2023;320:517-524. doi:10.1016/j.jad.2022.09.141
- Tsai J, Jones N, Klee A, Deegan D. Job burnout among mental health staff at a veterans affairs psychosocial rehabilitation center. Community Ment Health J. 2020;56(2):294- 297. doi:10.1007/s10597-019-00487-5
Stress Management
With the changing leaves and cooling temperatures, early autumn also brings the excitement of the new school year. While returning to sports, mastering new subjects, and spending time with old and new friends is exhilarating, this season can also be a time of intense stress.
For those high school students who are especially ambitious, the school year presents the challenge of a very high stakes performance, one whose success will be measured by admission to a prized college. Not only are there classes to study for, but schedules are packed with a maximum number of subjects, a maximum number of Advanced Placement courses and a maximum number of impressive extra-curricular activities. Varsity sports practice, SAT prep, Debate Club, volunteer hours, and on and on.
What is often missing is enough time for sleep, socializing, exploring new interests, and unwinding. When you hear your patients (or parents) describing the intense stress of their overloaded schedules compounded by a sense that “I have no choice,” you have an opportunity to complicate their thinking. Introduce the idea that there are smart approaches to performing your best under stress. Pushing themselves relentlessly will inevitably lead to burnout and exhaustion. This approach will help them learn to make wise choices and will better serve their healthy development.

Start by acknowledging the stress of high-stakes performance. Telling your patients that they need to lower the temperature by not putting so much pressure on themselves is likely to be experienced as a lack of confidence in them and is unlikely to get any traction. Instead, ask your patients what matters to them the most: Is it admission to the college of their choice? Achieving a certain score or GPA? Is it their competitiveness and drive to win? There is no wrong answer, but it is helpful for them to be able to reflect on what matters to them. Are they hoping to impress someone else? Are they worried about their future financial health and convinced that getting into a certain college will secure their financial success? Do they think this matters more to their parents than to themselves? Or have they discovered an intense interest in theoretical physics and want to be able to study at Caltech? If their ambition is meaningfully connected to an authentic interest or to their emerging identity, their sense of purpose will be much deeper and able to sustain them.
Even with talent and a strong sense of purpose, performing well is very difficult and demanding. It is important to consider the cycle of performance as including preparation, performance itself, and effective rest and recovery, just as with athletic performance. Whether the performance is the SATs, an AP test, a debate or big game, there were probably hours of preparation for every hour of performance. Help them to consider the importance of this practice or preparation time, and how to use that time effectively. Are they able to work in environments where there are few distractions? Do they have the support or useful feedback they need? How are they able to know when it is time for a break or when they are ready? It can be helpful for them to appreciate whether preparation or performance is more challenging for them, as the former requires focus and patience, while the latter requires courage and tenacity. If they are aware of which is harder for them, they can be thoughtful about how to effectively handle those challenges.

What can be most valuable for your patients is hearing from their pediatricians that they need to have time protected for rest and recharging, and not only for preparation and performance. Any athlete knows that failing to do so will lead to exhaustion and injury, and performance inevitably suffers. Rest is unwinding and slowing down, and a restful activity will leave them feeling calm, relaxed, and ready for sleep. A recharging activity is one that leaves them feeling refreshed and energized. Some common restful activities are a hot bath or shower, a distracting activity such as watching a show or surfing the web, playing a simple video game or puzzle or listening to music. Some recharging activities are creative ones (making art or music), engaging in hobbies, reading, or talking with a good friend. A few activities — sleep, exercise, and mindfulness meditation, are powerful in that they pack both rest and recharge into the same activity. Your patients should be discovering and learning which activities they find restful or recharging. The college application process or preparing for a varsity tryout will both add stress and give them an opportunity to learn what rests and recharges them. They should aim to have a list of at least five effective strategies that they can turn to when it’s time to rest or to recharge. Help them turn their work ethic to building a deeper well of self-knowledge that will serve them when they face challenges in high school or when they are on their own in college. This time of stress can be a time of growth, too.
Of course, remind your patients that this is a critical time to focus on basic self-care: They need consistently adequate, restful sleep, good nutrition, and physical activity. They will benefit from regular time in nature and time spent with friends that nourish them. They can find ways to compound these activities: Go for a walk with a friend, eat dinner with family, play a relaxing game while enjoying music. Lastly, ask your patients what is the last new thing they tried. It is easy to become so focused on an ambitious project that there is no time for exploration and play. Play is important throughout life, but adolescents are actively discovering their interests, talents, tastes, and values. To do this they need to be trying things that are new and maybe less purpose-driven. I call this type of activity “senseless fun.” Splashing in the pool is senseless fun, swimming laps is purposeful exercise that my contribute to recharging, and competing in a swim meet is often more on the stressful side. As they discover new talents, deeply engaging interests, what relaxes and recharges them, they will be learning who they are. Regardless of the outcome of a test, a big game, or where they go to college, it is this emerging knowledge about themselves that will carry them into adulthood. The pediatrician’s goal: Encouraging aspiration, exploration, and self-awareness in the context of giving permission for rest, recharging, and senseless fun.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
With the changing leaves and cooling temperatures, early autumn also brings the excitement of the new school year. While returning to sports, mastering new subjects, and spending time with old and new friends is exhilarating, this season can also be a time of intense stress.
For those high school students who are especially ambitious, the school year presents the challenge of a very high stakes performance, one whose success will be measured by admission to a prized college. Not only are there classes to study for, but schedules are packed with a maximum number of subjects, a maximum number of Advanced Placement courses and a maximum number of impressive extra-curricular activities. Varsity sports practice, SAT prep, Debate Club, volunteer hours, and on and on.
What is often missing is enough time for sleep, socializing, exploring new interests, and unwinding. When you hear your patients (or parents) describing the intense stress of their overloaded schedules compounded by a sense that “I have no choice,” you have an opportunity to complicate their thinking. Introduce the idea that there are smart approaches to performing your best under stress. Pushing themselves relentlessly will inevitably lead to burnout and exhaustion. This approach will help them learn to make wise choices and will better serve their healthy development.
Start by acknowledging the stress of high-stakes performance. Telling your patients that they need to lower the temperature by not putting so much pressure on themselves is likely to be experienced as a lack of confidence in them and is unlikely to get any traction. Instead, ask your patients what matters to them the most: Is it admission to the college of their choice? Achieving a certain score or GPA? Is it their competitiveness and drive to win? There is no wrong answer, but it is helpful for them to be able to reflect on what matters to them. Are they hoping to impress someone else? Are they worried about their future financial health and convinced that getting into a certain college will secure their financial success? Do they think this matters more to their parents than to themselves? Or have they discovered an intense interest in theoretical physics and want to be able to study at Caltech? If their ambition is meaningfully connected to an authentic interest or to their emerging identity, their sense of purpose will be much deeper and able to sustain them.
Even with talent and a strong sense of purpose, performing well is very difficult and demanding. It is important to consider the cycle of performance as including preparation, performance itself, and effective rest and recovery, just as with athletic performance. Whether the performance is the SATs, an AP test, a debate or big game, there were probably hours of preparation for every hour of performance. Help them to consider the importance of this practice or preparation time, and how to use that time effectively. Are they able to work in environments where there are few distractions? Do they have the support or useful feedback they need? How are they able to know when it is time for a break or when they are ready? It can be helpful for them to appreciate whether preparation or performance is more challenging for them, as the former requires focus and patience, while the latter requires courage and tenacity. If they are aware of which is harder for them, they can be thoughtful about how to effectively handle those challenges.
What can be most valuable for your patients is hearing from their pediatricians that they need to have time protected for rest and recharging, and not only for preparation and performance. Any athlete knows that failing to do so will lead to exhaustion and injury, and performance inevitably suffers. Rest is unwinding and slowing down, and a restful activity will leave them feeling calm, relaxed, and ready for sleep. A recharging activity is one that leaves them feeling refreshed and energized. Some common restful activities are a hot bath or shower, a distracting activity such as watching a show or surfing the web, playing a simple video game or puzzle or listening to music. Some recharging activities are creative ones (making art or music), engaging in hobbies, reading, or talking with a good friend. A few activities — sleep, exercise, and mindfulness meditation, are powerful in that they pack both rest and recharge into the same activity. Your patients should be discovering and learning which activities they find restful or recharging. The college application process or preparing for a varsity tryout will both add stress and give them an opportunity to learn what rests and recharges them. They should aim to have a list of at least five effective strategies that they can turn to when it’s time to rest or to recharge. Help them turn their work ethic to building a deeper well of self-knowledge that will serve them when they face challenges in high school or when they are on their own in college. This time of stress can be a time of growth, too.
Of course, remind your patients that this is a critical time to focus on basic self-care: They need consistently adequate, restful sleep, good nutrition, and physical activity. They will benefit from regular time in nature and time spent with friends that nourish them. They can find ways to compound these activities: Go for a walk with a friend, eat dinner with family, play a relaxing game while enjoying music. Lastly, ask your patients what is the last new thing they tried. It is easy to become so focused on an ambitious project that there is no time for exploration and play. Play is important throughout life, but adolescents are actively discovering their interests, talents, tastes, and values. To do this they need to be trying things that are new and maybe less purpose-driven. I call this type of activity “senseless fun.” Splashing in the pool is senseless fun, swimming laps is purposeful exercise that my contribute to recharging, and competing in a swim meet is often more on the stressful side. As they discover new talents, deeply engaging interests, what relaxes and recharges them, they will be learning who they are. Regardless of the outcome of a test, a big game, or where they go to college, it is this emerging knowledge about themselves that will carry them into adulthood. The pediatrician’s goal: Encouraging aspiration, exploration, and self-awareness in the context of giving permission for rest, recharging, and senseless fun.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
With the changing leaves and cooling temperatures, early autumn also brings the excitement of the new school year. While returning to sports, mastering new subjects, and spending time with old and new friends is exhilarating, this season can also be a time of intense stress.
For those high school students who are especially ambitious, the school year presents the challenge of a very high stakes performance, one whose success will be measured by admission to a prized college. Not only are there classes to study for, but schedules are packed with a maximum number of subjects, a maximum number of Advanced Placement courses and a maximum number of impressive extra-curricular activities. Varsity sports practice, SAT prep, Debate Club, volunteer hours, and on and on.
What is often missing is enough time for sleep, socializing, exploring new interests, and unwinding. When you hear your patients (or parents) describing the intense stress of their overloaded schedules compounded by a sense that “I have no choice,” you have an opportunity to complicate their thinking. Introduce the idea that there are smart approaches to performing your best under stress. Pushing themselves relentlessly will inevitably lead to burnout and exhaustion. This approach will help them learn to make wise choices and will better serve their healthy development.
Start by acknowledging the stress of high-stakes performance. Telling your patients that they need to lower the temperature by not putting so much pressure on themselves is likely to be experienced as a lack of confidence in them and is unlikely to get any traction. Instead, ask your patients what matters to them the most: Is it admission to the college of their choice? Achieving a certain score or GPA? Is it their competitiveness and drive to win? There is no wrong answer, but it is helpful for them to be able to reflect on what matters to them. Are they hoping to impress someone else? Are they worried about their future financial health and convinced that getting into a certain college will secure their financial success? Do they think this matters more to their parents than to themselves? Or have they discovered an intense interest in theoretical physics and want to be able to study at Caltech? If their ambition is meaningfully connected to an authentic interest or to their emerging identity, their sense of purpose will be much deeper and able to sustain them.
Even with talent and a strong sense of purpose, performing well is very difficult and demanding. It is important to consider the cycle of performance as including preparation, performance itself, and effective rest and recovery, just as with athletic performance. Whether the performance is the SATs, an AP test, a debate or big game, there were probably hours of preparation for every hour of performance. Help them to consider the importance of this practice or preparation time, and how to use that time effectively. Are they able to work in environments where there are few distractions? Do they have the support or useful feedback they need? How are they able to know when it is time for a break or when they are ready? It can be helpful for them to appreciate whether preparation or performance is more challenging for them, as the former requires focus and patience, while the latter requires courage and tenacity. If they are aware of which is harder for them, they can be thoughtful about how to effectively handle those challenges.
What can be most valuable for your patients is hearing from their pediatricians that they need to have time protected for rest and recharging, and not only for preparation and performance. Any athlete knows that failing to do so will lead to exhaustion and injury, and performance inevitably suffers. Rest is unwinding and slowing down, and a restful activity will leave them feeling calm, relaxed, and ready for sleep. A recharging activity is one that leaves them feeling refreshed and energized. Some common restful activities are a hot bath or shower, a distracting activity such as watching a show or surfing the web, playing a simple video game or puzzle or listening to music. Some recharging activities are creative ones (making art or music), engaging in hobbies, reading, or talking with a good friend. A few activities — sleep, exercise, and mindfulness meditation, are powerful in that they pack both rest and recharge into the same activity. Your patients should be discovering and learning which activities they find restful or recharging. The college application process or preparing for a varsity tryout will both add stress and give them an opportunity to learn what rests and recharges them. They should aim to have a list of at least five effective strategies that they can turn to when it’s time to rest or to recharge. Help them turn their work ethic to building a deeper well of self-knowledge that will serve them when they face challenges in high school or when they are on their own in college. This time of stress can be a time of growth, too.
Of course, remind your patients that this is a critical time to focus on basic self-care: They need consistently adequate, restful sleep, good nutrition, and physical activity. They will benefit from regular time in nature and time spent with friends that nourish them. They can find ways to compound these activities: Go for a walk with a friend, eat dinner with family, play a relaxing game while enjoying music. Lastly, ask your patients what is the last new thing they tried. It is easy to become so focused on an ambitious project that there is no time for exploration and play. Play is important throughout life, but adolescents are actively discovering their interests, talents, tastes, and values. To do this they need to be trying things that are new and maybe less purpose-driven. I call this type of activity “senseless fun.” Splashing in the pool is senseless fun, swimming laps is purposeful exercise that my contribute to recharging, and competing in a swim meet is often more on the stressful side. As they discover new talents, deeply engaging interests, what relaxes and recharges them, they will be learning who they are. Regardless of the outcome of a test, a big game, or where they go to college, it is this emerging knowledge about themselves that will carry them into adulthood. The pediatrician’s goal: Encouraging aspiration, exploration, and self-awareness in the context of giving permission for rest, recharging, and senseless fun.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].