User login
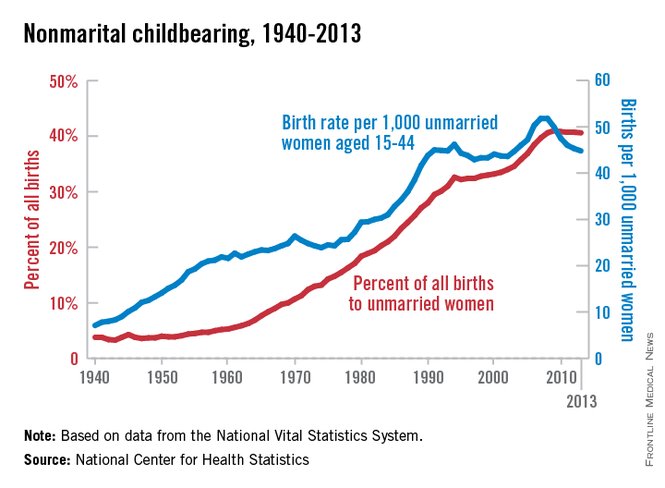
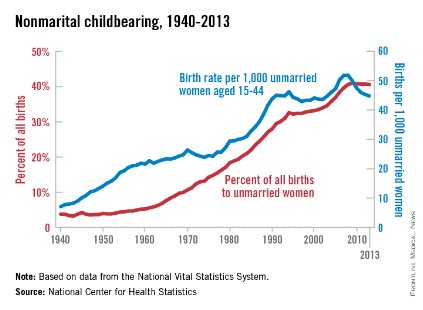
Births to unmarried women down since 2008
The nonmarital birth rate for women aged 15-44 years has declined 14% since peaking in 2007 and 2008, the National Center for Health Statistics reported.
The rate was 44.8 births per 1,000 unmarried women in 2013, compared with 51.8 in 2007-2008. The percentage of all births to unmarried women – 40.6% in 2013 – has leveled off since reaching a high of 41% in 2009, according to the analysis of data from the National Vital Statistics System.
The total number of births to unmarried women was 1,605,643 in 2013, a drop of 7% since 2008, when it reached a high of 1,726,566. "The recent declines in birth rates and numbers of births to unmarried women parallel to some extent the overall decline in birth rates during this period and also reflect the declines in teen birth rates," the report said, adding that "the majority of births to teenagers are to unmarried women."
Nonmarital birth rates since 2007 are down for all age groups under age 35 years, with the largest percentage declines coming among teenagers: 30% to 14/1,000 for those aged 15-17 years and 26% to 46/1,000 for those aged 18-19 years. The nonmarital birth rate has continued to increase for women aged 35 and over, the NCHS noted.
The nonmarital birth rate for women aged 15-44 years has declined 14% since peaking in 2007 and 2008, the National Center for Health Statistics reported.
The rate was 44.8 births per 1,000 unmarried women in 2013, compared with 51.8 in 2007-2008. The percentage of all births to unmarried women – 40.6% in 2013 – has leveled off since reaching a high of 41% in 2009, according to the analysis of data from the National Vital Statistics System.
The total number of births to unmarried women was 1,605,643 in 2013, a drop of 7% since 2008, when it reached a high of 1,726,566. "The recent declines in birth rates and numbers of births to unmarried women parallel to some extent the overall decline in birth rates during this period and also reflect the declines in teen birth rates," the report said, adding that "the majority of births to teenagers are to unmarried women."
Nonmarital birth rates since 2007 are down for all age groups under age 35 years, with the largest percentage declines coming among teenagers: 30% to 14/1,000 for those aged 15-17 years and 26% to 46/1,000 for those aged 18-19 years. The nonmarital birth rate has continued to increase for women aged 35 and over, the NCHS noted.
The nonmarital birth rate for women aged 15-44 years has declined 14% since peaking in 2007 and 2008, the National Center for Health Statistics reported.
The rate was 44.8 births per 1,000 unmarried women in 2013, compared with 51.8 in 2007-2008. The percentage of all births to unmarried women – 40.6% in 2013 – has leveled off since reaching a high of 41% in 2009, according to the analysis of data from the National Vital Statistics System.
The total number of births to unmarried women was 1,605,643 in 2013, a drop of 7% since 2008, when it reached a high of 1,726,566. "The recent declines in birth rates and numbers of births to unmarried women parallel to some extent the overall decline in birth rates during this period and also reflect the declines in teen birth rates," the report said, adding that "the majority of births to teenagers are to unmarried women."
Nonmarital birth rates since 2007 are down for all age groups under age 35 years, with the largest percentage declines coming among teenagers: 30% to 14/1,000 for those aged 15-17 years and 26% to 46/1,000 for those aged 18-19 years. The nonmarital birth rate has continued to increase for women aged 35 and over, the NCHS noted.
Mediolateral episiotomy shines in 10-year Netherlands analysis
WASHINGTON – The use of mediolateral episiotomy in women undergoing operative vaginal delivery – a common practice in the Netherlands – was associated with a large reduction in the risk of obstetrical anal sphincter injuries, according to an analysis of 10 years of data from the Netherlands Perinatal Registry.
For physicians and other obstetrical providers in the small European country, the findings reinforce current practice of favoring mediolateral episiotomies in operative vaginal deliveries as protection against obstetrical anal sphincter injuries (OASIS) – a risk factor for fecal incontinence, the investigators said.
"In the Netherlands, a mediolateral episiotomy is common practice. ... Our opinion is that the mediolateral episiotomies are causing less morbidity than an anal sphincter rupture would cause," Dr. Jeroen van Bavel reported during a press conference at the scientific meetings of the American Urogynecologic Society (AUGS) and the International Urogynecological Association.
But for physicians here in the United States, the risks are weighed differently. "It’s not that we don’t know that a mediolateral episiotomy decreases the risk of sphincter injury," Dr. Haywood Brown, professor and chair of obstetrics and gynecology at Duke University, Durham, N.C., said in a telephone interview after the conference.
"The problem is, mediolateral incisions are so uncomfortable," said Dr. Brown, who also is chair of the American College of Obstetricians and Gynecologists, District IV.
"They heal poorly, they heal with defects, ... and as a result the patient has more pain related to the mediolateral [episiotomy] than they would have with a third- or fourth-degree tear," he said. "Doing the mediolateral is really not the answer."
The Netherlands Perinatal Registry contains information on 96% of the 1.5 million deliveries that occurred during 2000-2009. Dr. van Bavel, of Amphia Hospital in Breda, the Netherlands, and his coinvestigators focused their analysis on the 170,974 women who had operative vaginal deliveries, comparing the rates of OASIS in women who had mediolateral episiotomies with those who did not.
Among primiparous women who had vacuum deliveries, OASIS occurred in 2.5% of those who had mediolateral episiotomies, compared with 14% who did not. Among multiparous women who had vacuum deliveries, OASIS rates were 2.1% with mediolateral episiotomy versus 7.5% without.
The differences were more striking with forceps deliveries. Anal sphincter injuries occurred in 3.4% versus 26.7% in primiparous women with and without mediolateral episiotomies, respectively. Among multiparous women, the risk of OASIS was 2.6% versus 14.2%.
For primiparous women, the number of mediolateral episiotomies needed to prevent one OASIS was 8 for vacuum delivery and 4 for forceps delivery, according to the analysis. For multiparous women, 18 mediolateral episiotomies were needed to prevent one OASIS for vacuum delivery, and 8 for forceps delivery.
ACOG’s Practice Bulletin No. 71 on episiotomy, which was written in 2006 (Obstet. Gynecol. 2006;107:957-62) and reaffirmed in 2013, states that median episiotomy is associated with higher rates of injury to the anal sphincter and rectum than mediolateral episiotomy (level A evidence), and that mediolateral episiotomy may be preferable in selected cases (level B evidence).
Overall, "restricted use of episiotomy is preferable to routine use of episiotomy," the guidelines say (level A evidence). Postpartum recovery, the guidelines note, is an area of obstetrics that lacks systematic study and analysis.
Dr. Brown said he stands firmly with his belief that mediolateral episiotomy as a routine prophylactic procedure in operative vaginal deliveries cannot be justified. "Having lived through an era of mediolaterals and seeing how long they take to heal, and the discomfort that patients have, I can’t justify it," he said.
"We’ve moved away from episiotomies [in the United States], period," he said. "We’ve moved away from them primarily because of the data showing that midline episiotomies increase the risk of sphincter injury. And the mediolateral episiotomies are just too painful."
The risk of OASIS can be minimized through good delivery technique, he noted.
"The trend here is toward more vacuum deliveries, which have [been shown to be less risky] than forceps deliveries, although its depends on the type of forceps used and the skill of the [obstetrician]," Dr. Brown said. "The challenge we face is that we don’t have enough forceps and vacuum deliveries to easily keep skill levels up."
Dr. Charles W. Nager, president of AUGS and director the urogynecological and reconstructive pelvic surgery division at the University of California, San Diego, said that rates of both episiotomy and operative vaginal delivery have been declining in the United States, and that simultaneously, "there’s been a parallel drop in OASIS."
There also is more training ongoing in U.S. hospitals on repairing third- and fourth-degree obstetric lacerations, he said in an interview at the meeting.
The Netherlands analysis excluded women with preterm delivery, stillbirth, multiple gestation, transverse position, and breech delivery, as well as women whose deliveries involved both forceps and vacuum and women who had a midline episiotomy.
Factors controlled for in the study included parity, fetal position, birth weight, augmentation with oxytocin, and duration of the second stage of labor.
Dr. van Bavel and all but one of his coinvestigators reported no disclosures.
WASHINGTON – The use of mediolateral episiotomy in women undergoing operative vaginal delivery – a common practice in the Netherlands – was associated with a large reduction in the risk of obstetrical anal sphincter injuries, according to an analysis of 10 years of data from the Netherlands Perinatal Registry.
For physicians and other obstetrical providers in the small European country, the findings reinforce current practice of favoring mediolateral episiotomies in operative vaginal deliveries as protection against obstetrical anal sphincter injuries (OASIS) – a risk factor for fecal incontinence, the investigators said.
"In the Netherlands, a mediolateral episiotomy is common practice. ... Our opinion is that the mediolateral episiotomies are causing less morbidity than an anal sphincter rupture would cause," Dr. Jeroen van Bavel reported during a press conference at the scientific meetings of the American Urogynecologic Society (AUGS) and the International Urogynecological Association.
But for physicians here in the United States, the risks are weighed differently. "It’s not that we don’t know that a mediolateral episiotomy decreases the risk of sphincter injury," Dr. Haywood Brown, professor and chair of obstetrics and gynecology at Duke University, Durham, N.C., said in a telephone interview after the conference.
"The problem is, mediolateral incisions are so uncomfortable," said Dr. Brown, who also is chair of the American College of Obstetricians and Gynecologists, District IV.
"They heal poorly, they heal with defects, ... and as a result the patient has more pain related to the mediolateral [episiotomy] than they would have with a third- or fourth-degree tear," he said. "Doing the mediolateral is really not the answer."
The Netherlands Perinatal Registry contains information on 96% of the 1.5 million deliveries that occurred during 2000-2009. Dr. van Bavel, of Amphia Hospital in Breda, the Netherlands, and his coinvestigators focused their analysis on the 170,974 women who had operative vaginal deliveries, comparing the rates of OASIS in women who had mediolateral episiotomies with those who did not.
Among primiparous women who had vacuum deliveries, OASIS occurred in 2.5% of those who had mediolateral episiotomies, compared with 14% who did not. Among multiparous women who had vacuum deliveries, OASIS rates were 2.1% with mediolateral episiotomy versus 7.5% without.
The differences were more striking with forceps deliveries. Anal sphincter injuries occurred in 3.4% versus 26.7% in primiparous women with and without mediolateral episiotomies, respectively. Among multiparous women, the risk of OASIS was 2.6% versus 14.2%.
For primiparous women, the number of mediolateral episiotomies needed to prevent one OASIS was 8 for vacuum delivery and 4 for forceps delivery, according to the analysis. For multiparous women, 18 mediolateral episiotomies were needed to prevent one OASIS for vacuum delivery, and 8 for forceps delivery.
ACOG’s Practice Bulletin No. 71 on episiotomy, which was written in 2006 (Obstet. Gynecol. 2006;107:957-62) and reaffirmed in 2013, states that median episiotomy is associated with higher rates of injury to the anal sphincter and rectum than mediolateral episiotomy (level A evidence), and that mediolateral episiotomy may be preferable in selected cases (level B evidence).
Overall, "restricted use of episiotomy is preferable to routine use of episiotomy," the guidelines say (level A evidence). Postpartum recovery, the guidelines note, is an area of obstetrics that lacks systematic study and analysis.
Dr. Brown said he stands firmly with his belief that mediolateral episiotomy as a routine prophylactic procedure in operative vaginal deliveries cannot be justified. "Having lived through an era of mediolaterals and seeing how long they take to heal, and the discomfort that patients have, I can’t justify it," he said.
"We’ve moved away from episiotomies [in the United States], period," he said. "We’ve moved away from them primarily because of the data showing that midline episiotomies increase the risk of sphincter injury. And the mediolateral episiotomies are just too painful."
The risk of OASIS can be minimized through good delivery technique, he noted.
"The trend here is toward more vacuum deliveries, which have [been shown to be less risky] than forceps deliveries, although its depends on the type of forceps used and the skill of the [obstetrician]," Dr. Brown said. "The challenge we face is that we don’t have enough forceps and vacuum deliveries to easily keep skill levels up."
Dr. Charles W. Nager, president of AUGS and director the urogynecological and reconstructive pelvic surgery division at the University of California, San Diego, said that rates of both episiotomy and operative vaginal delivery have been declining in the United States, and that simultaneously, "there’s been a parallel drop in OASIS."
There also is more training ongoing in U.S. hospitals on repairing third- and fourth-degree obstetric lacerations, he said in an interview at the meeting.
The Netherlands analysis excluded women with preterm delivery, stillbirth, multiple gestation, transverse position, and breech delivery, as well as women whose deliveries involved both forceps and vacuum and women who had a midline episiotomy.
Factors controlled for in the study included parity, fetal position, birth weight, augmentation with oxytocin, and duration of the second stage of labor.
Dr. van Bavel and all but one of his coinvestigators reported no disclosures.
WASHINGTON – The use of mediolateral episiotomy in women undergoing operative vaginal delivery – a common practice in the Netherlands – was associated with a large reduction in the risk of obstetrical anal sphincter injuries, according to an analysis of 10 years of data from the Netherlands Perinatal Registry.
For physicians and other obstetrical providers in the small European country, the findings reinforce current practice of favoring mediolateral episiotomies in operative vaginal deliveries as protection against obstetrical anal sphincter injuries (OASIS) – a risk factor for fecal incontinence, the investigators said.
"In the Netherlands, a mediolateral episiotomy is common practice. ... Our opinion is that the mediolateral episiotomies are causing less morbidity than an anal sphincter rupture would cause," Dr. Jeroen van Bavel reported during a press conference at the scientific meetings of the American Urogynecologic Society (AUGS) and the International Urogynecological Association.
But for physicians here in the United States, the risks are weighed differently. "It’s not that we don’t know that a mediolateral episiotomy decreases the risk of sphincter injury," Dr. Haywood Brown, professor and chair of obstetrics and gynecology at Duke University, Durham, N.C., said in a telephone interview after the conference.
"The problem is, mediolateral incisions are so uncomfortable," said Dr. Brown, who also is chair of the American College of Obstetricians and Gynecologists, District IV.
"They heal poorly, they heal with defects, ... and as a result the patient has more pain related to the mediolateral [episiotomy] than they would have with a third- or fourth-degree tear," he said. "Doing the mediolateral is really not the answer."
The Netherlands Perinatal Registry contains information on 96% of the 1.5 million deliveries that occurred during 2000-2009. Dr. van Bavel, of Amphia Hospital in Breda, the Netherlands, and his coinvestigators focused their analysis on the 170,974 women who had operative vaginal deliveries, comparing the rates of OASIS in women who had mediolateral episiotomies with those who did not.
Among primiparous women who had vacuum deliveries, OASIS occurred in 2.5% of those who had mediolateral episiotomies, compared with 14% who did not. Among multiparous women who had vacuum deliveries, OASIS rates were 2.1% with mediolateral episiotomy versus 7.5% without.
The differences were more striking with forceps deliveries. Anal sphincter injuries occurred in 3.4% versus 26.7% in primiparous women with and without mediolateral episiotomies, respectively. Among multiparous women, the risk of OASIS was 2.6% versus 14.2%.
For primiparous women, the number of mediolateral episiotomies needed to prevent one OASIS was 8 for vacuum delivery and 4 for forceps delivery, according to the analysis. For multiparous women, 18 mediolateral episiotomies were needed to prevent one OASIS for vacuum delivery, and 8 for forceps delivery.
ACOG’s Practice Bulletin No. 71 on episiotomy, which was written in 2006 (Obstet. Gynecol. 2006;107:957-62) and reaffirmed in 2013, states that median episiotomy is associated with higher rates of injury to the anal sphincter and rectum than mediolateral episiotomy (level A evidence), and that mediolateral episiotomy may be preferable in selected cases (level B evidence).
Overall, "restricted use of episiotomy is preferable to routine use of episiotomy," the guidelines say (level A evidence). Postpartum recovery, the guidelines note, is an area of obstetrics that lacks systematic study and analysis.
Dr. Brown said he stands firmly with his belief that mediolateral episiotomy as a routine prophylactic procedure in operative vaginal deliveries cannot be justified. "Having lived through an era of mediolaterals and seeing how long they take to heal, and the discomfort that patients have, I can’t justify it," he said.
"We’ve moved away from episiotomies [in the United States], period," he said. "We’ve moved away from them primarily because of the data showing that midline episiotomies increase the risk of sphincter injury. And the mediolateral episiotomies are just too painful."
The risk of OASIS can be minimized through good delivery technique, he noted.
"The trend here is toward more vacuum deliveries, which have [been shown to be less risky] than forceps deliveries, although its depends on the type of forceps used and the skill of the [obstetrician]," Dr. Brown said. "The challenge we face is that we don’t have enough forceps and vacuum deliveries to easily keep skill levels up."
Dr. Charles W. Nager, president of AUGS and director the urogynecological and reconstructive pelvic surgery division at the University of California, San Diego, said that rates of both episiotomy and operative vaginal delivery have been declining in the United States, and that simultaneously, "there’s been a parallel drop in OASIS."
There also is more training ongoing in U.S. hospitals on repairing third- and fourth-degree obstetric lacerations, he said in an interview at the meeting.
The Netherlands analysis excluded women with preterm delivery, stillbirth, multiple gestation, transverse position, and breech delivery, as well as women whose deliveries involved both forceps and vacuum and women who had a midline episiotomy.
Factors controlled for in the study included parity, fetal position, birth weight, augmentation with oxytocin, and duration of the second stage of labor.
Dr. van Bavel and all but one of his coinvestigators reported no disclosures.
AT AUGS/IUGA 2014
Key clinical point: The findings reinforce the Dutch practice of favoring mediolateral episiotomies in operative vaginal deliveries as protection against obstetrical anal sphincter injuries, but American obstetricians disagree on the basis that mediolateral episiotomies are quite painful and vacuum and forceps deliveries are becoming less common in the United States.
Major finding: The use of mediolateral episiotomy in vaginal operative deliveries is associated with significant reductions in the risk of obstetric anal sphincter injuries, across vacuum and forceps deliveries and primiparous and multiparous births.
Data source: A retrospective cohort study of 170,974 vaginal operative deliveries in the Netherlands.
Disclosures: Dr. Jeroen van Bavel and all but one of his coinvestigators reported no disclosures.
Pregnancy exposure registries confirmed useful in assessing product safety
BELLEVUE, WASH. – Registries that collect data on pregnant women’s exposures to medical products and outcomes are contributing to product safety in this population, as intended, suggests an exploratory review conducted by the Food and Drug Administration.
But they do have some shortcomings.
"Currently, pregnancy registries are the most common type of postapproval study in pregnant women that are either required or requested by FDA from pharmaceutical companies," first author Dr. Leyla Sahin, an FDA medical officer on the Pediatric and Maternal Health Staff of the Maternal Health Team, in Harvard, Mass., explained at the annual meeting of the Teratology Society.

"However, recently, the Agency has had a concern that pregnancy registries often fail to provide useful information, and usually this is due to low enrollment. ... Companies will come back to the agency a few years later and say, ‘We have been unable to recruit enough patients into our study, so please release us from our postmarketing requirement,’" she added. So, FDA sought to discover "what characteristics determine a successful registry so that we could then provide guidance to industry."
Dr. Sahin and her colleagues studied 38 pregnancy registries listed on the FDA’s Pregnancy Registry website that tracked 59 medical products–drugs, biologics, or vaccines.
Findings showed that for 12% of the products, registry results led to changes in the labeling for that product, as in the cases of the Bupropion Pregnancy Registry and the Pregnancy Registry for Varicella Zoster Virus–Containing Vaccines.
Similarly, for 12% of products, registry results had informed practice guidelines, as in the cases of the Pregnancy Registry for Gardasil and the Antiretroviral Pregnancy Registry.
Of the seven products that had registry data added to their approved labeling, 86% also had their results published in a peer-reviewed journal. Of the 59 products overall, 37% had interim or final registry results published in a peer-reviewed journal.
But the registries did struggle with enrollment. Overall, 17% had been closed for feasibility reasons, meaning they had not been able to enroll sufficient patients. And of the 22 products that had a target enrollment stated in the pregnancy registry protocol, just 14% had achieved that enrollment.
Additionally, for the 21 products having registries that provided information about loss to follow-up and that had at least moderate enrollment, the median rate of loss to follow-up of enrolled women was 23.4%.
"What we took away from this review is that basically, pregnancy registries have contributed safety data to labeling and to clinical guidelines, and have been published in the medical literature. However, there is room for improvement in terms of doing a better job with recruitment and enrollment into these studies," commented Dr. Sahin.
"Unfortunately, we are not able to draw conclusions from this review on the characteristics that result in a successful registry because of limitations" such as the lack of inclusion of disease-based registries, the review’s exploratory nature (as opposed to a comprehensive one), and no assessment of factors such as registries’ data quality, resources used, and expertise.
"Pregnancy registries by themselves may not be sufficient to collect data that inform product labeling, so we need to explore complementary study methods to do this," Dr. Sahin maintained. To address that and related issues, the agency held a public meeting in May.

"The key messages that we obtained from experts and stakeholders at the meeting are that pregnancy registries continue to have an important role in data collection, but that improvements are needed in the methodology and conduct," she reported. Participants suggested, for example, using a combination of approaches that include complementary study designs to overcome the limitations of individual study designs; developing personal connections with both patients and health care providers, using "champions" enthusiastic about registries to boost recruitment and enrollment; and harnessing electronic medical records to improve data collection.
"The next steps now for the agency are to review the transcripts from the public meeting, and then to develop future policies in terms of what to request as postmarketing requirements from companies. And then developing policy, and integrating what we got from the public meeting into revising the pregnancy registry guidance for industry," Dr. Sahin said. Plans additionally include "working on developing further communication and outreach, looking at the FDA Pregnancy Registry web page, and how that can be specifically designed to meet the needs of all stakeholders, and then also continuing to explore opportunities for collaboration through public-private partnership."
In an interview, session cochair Marlissa Campbell, Ph.D., said, "In general, I think FDA’s purpose in reviewing the registries in order to help manufacturers improve the process to obtain useful data is good, and potentially very important. I had not known that attaining enrollment goals for these registries was proving to be so difficult."
The feedback from the public meeting may go a long way toward improving data collection in these registries, she agreed. "Getting input from clinicians, as well as manufacturers and other registry programs should help the agency formulate next steps." Dr. Campbell is staff toxicologist with the Office of Environmental Health Hazard Assessment (OEHHA), California Environmental Protection Agency, Sacramento.
Dr. Sahin disclosed no relevant conflicts of interest.
Do you tell your pregnant patients about pregnancy exposure registries and suggest that they sign up? Take our Quick Poll on the ObGyn News homepage.
BELLEVUE, WASH. – Registries that collect data on pregnant women’s exposures to medical products and outcomes are contributing to product safety in this population, as intended, suggests an exploratory review conducted by the Food and Drug Administration.
But they do have some shortcomings.
"Currently, pregnancy registries are the most common type of postapproval study in pregnant women that are either required or requested by FDA from pharmaceutical companies," first author Dr. Leyla Sahin, an FDA medical officer on the Pediatric and Maternal Health Staff of the Maternal Health Team, in Harvard, Mass., explained at the annual meeting of the Teratology Society.
"However, recently, the Agency has had a concern that pregnancy registries often fail to provide useful information, and usually this is due to low enrollment. ... Companies will come back to the agency a few years later and say, ‘We have been unable to recruit enough patients into our study, so please release us from our postmarketing requirement,’" she added. So, FDA sought to discover "what characteristics determine a successful registry so that we could then provide guidance to industry."
Dr. Sahin and her colleagues studied 38 pregnancy registries listed on the FDA’s Pregnancy Registry website that tracked 59 medical products–drugs, biologics, or vaccines.
Findings showed that for 12% of the products, registry results led to changes in the labeling for that product, as in the cases of the Bupropion Pregnancy Registry and the Pregnancy Registry for Varicella Zoster Virus–Containing Vaccines.
Similarly, for 12% of products, registry results had informed practice guidelines, as in the cases of the Pregnancy Registry for Gardasil and the Antiretroviral Pregnancy Registry.
Of the seven products that had registry data added to their approved labeling, 86% also had their results published in a peer-reviewed journal. Of the 59 products overall, 37% had interim or final registry results published in a peer-reviewed journal.
But the registries did struggle with enrollment. Overall, 17% had been closed for feasibility reasons, meaning they had not been able to enroll sufficient patients. And of the 22 products that had a target enrollment stated in the pregnancy registry protocol, just 14% had achieved that enrollment.
Additionally, for the 21 products having registries that provided information about loss to follow-up and that had at least moderate enrollment, the median rate of loss to follow-up of enrolled women was 23.4%.
"What we took away from this review is that basically, pregnancy registries have contributed safety data to labeling and to clinical guidelines, and have been published in the medical literature. However, there is room for improvement in terms of doing a better job with recruitment and enrollment into these studies," commented Dr. Sahin.
"Unfortunately, we are not able to draw conclusions from this review on the characteristics that result in a successful registry because of limitations" such as the lack of inclusion of disease-based registries, the review’s exploratory nature (as opposed to a comprehensive one), and no assessment of factors such as registries’ data quality, resources used, and expertise.
"Pregnancy registries by themselves may not be sufficient to collect data that inform product labeling, so we need to explore complementary study methods to do this," Dr. Sahin maintained. To address that and related issues, the agency held a public meeting in May.
"The key messages that we obtained from experts and stakeholders at the meeting are that pregnancy registries continue to have an important role in data collection, but that improvements are needed in the methodology and conduct," she reported. Participants suggested, for example, using a combination of approaches that include complementary study designs to overcome the limitations of individual study designs; developing personal connections with both patients and health care providers, using "champions" enthusiastic about registries to boost recruitment and enrollment; and harnessing electronic medical records to improve data collection.
"The next steps now for the agency are to review the transcripts from the public meeting, and then to develop future policies in terms of what to request as postmarketing requirements from companies. And then developing policy, and integrating what we got from the public meeting into revising the pregnancy registry guidance for industry," Dr. Sahin said. Plans additionally include "working on developing further communication and outreach, looking at the FDA Pregnancy Registry web page, and how that can be specifically designed to meet the needs of all stakeholders, and then also continuing to explore opportunities for collaboration through public-private partnership."
In an interview, session cochair Marlissa Campbell, Ph.D., said, "In general, I think FDA’s purpose in reviewing the registries in order to help manufacturers improve the process to obtain useful data is good, and potentially very important. I had not known that attaining enrollment goals for these registries was proving to be so difficult."
The feedback from the public meeting may go a long way toward improving data collection in these registries, she agreed. "Getting input from clinicians, as well as manufacturers and other registry programs should help the agency formulate next steps." Dr. Campbell is staff toxicologist with the Office of Environmental Health Hazard Assessment (OEHHA), California Environmental Protection Agency, Sacramento.
Dr. Sahin disclosed no relevant conflicts of interest.
Do you tell your pregnant patients about pregnancy exposure registries and suggest that they sign up? Take our Quick Poll on the ObGyn News homepage.
BELLEVUE, WASH. – Registries that collect data on pregnant women’s exposures to medical products and outcomes are contributing to product safety in this population, as intended, suggests an exploratory review conducted by the Food and Drug Administration.
But they do have some shortcomings.
"Currently, pregnancy registries are the most common type of postapproval study in pregnant women that are either required or requested by FDA from pharmaceutical companies," first author Dr. Leyla Sahin, an FDA medical officer on the Pediatric and Maternal Health Staff of the Maternal Health Team, in Harvard, Mass., explained at the annual meeting of the Teratology Society.
"However, recently, the Agency has had a concern that pregnancy registries often fail to provide useful information, and usually this is due to low enrollment. ... Companies will come back to the agency a few years later and say, ‘We have been unable to recruit enough patients into our study, so please release us from our postmarketing requirement,’" she added. So, FDA sought to discover "what characteristics determine a successful registry so that we could then provide guidance to industry."
Dr. Sahin and her colleagues studied 38 pregnancy registries listed on the FDA’s Pregnancy Registry website that tracked 59 medical products–drugs, biologics, or vaccines.
Findings showed that for 12% of the products, registry results led to changes in the labeling for that product, as in the cases of the Bupropion Pregnancy Registry and the Pregnancy Registry for Varicella Zoster Virus–Containing Vaccines.
Similarly, for 12% of products, registry results had informed practice guidelines, as in the cases of the Pregnancy Registry for Gardasil and the Antiretroviral Pregnancy Registry.
Of the seven products that had registry data added to their approved labeling, 86% also had their results published in a peer-reviewed journal. Of the 59 products overall, 37% had interim or final registry results published in a peer-reviewed journal.
But the registries did struggle with enrollment. Overall, 17% had been closed for feasibility reasons, meaning they had not been able to enroll sufficient patients. And of the 22 products that had a target enrollment stated in the pregnancy registry protocol, just 14% had achieved that enrollment.
Additionally, for the 21 products having registries that provided information about loss to follow-up and that had at least moderate enrollment, the median rate of loss to follow-up of enrolled women was 23.4%.
"What we took away from this review is that basically, pregnancy registries have contributed safety data to labeling and to clinical guidelines, and have been published in the medical literature. However, there is room for improvement in terms of doing a better job with recruitment and enrollment into these studies," commented Dr. Sahin.
"Unfortunately, we are not able to draw conclusions from this review on the characteristics that result in a successful registry because of limitations" such as the lack of inclusion of disease-based registries, the review’s exploratory nature (as opposed to a comprehensive one), and no assessment of factors such as registries’ data quality, resources used, and expertise.
"Pregnancy registries by themselves may not be sufficient to collect data that inform product labeling, so we need to explore complementary study methods to do this," Dr. Sahin maintained. To address that and related issues, the agency held a public meeting in May.
"The key messages that we obtained from experts and stakeholders at the meeting are that pregnancy registries continue to have an important role in data collection, but that improvements are needed in the methodology and conduct," she reported. Participants suggested, for example, using a combination of approaches that include complementary study designs to overcome the limitations of individual study designs; developing personal connections with both patients and health care providers, using "champions" enthusiastic about registries to boost recruitment and enrollment; and harnessing electronic medical records to improve data collection.
"The next steps now for the agency are to review the transcripts from the public meeting, and then to develop future policies in terms of what to request as postmarketing requirements from companies. And then developing policy, and integrating what we got from the public meeting into revising the pregnancy registry guidance for industry," Dr. Sahin said. Plans additionally include "working on developing further communication and outreach, looking at the FDA Pregnancy Registry web page, and how that can be specifically designed to meet the needs of all stakeholders, and then also continuing to explore opportunities for collaboration through public-private partnership."
In an interview, session cochair Marlissa Campbell, Ph.D., said, "In general, I think FDA’s purpose in reviewing the registries in order to help manufacturers improve the process to obtain useful data is good, and potentially very important. I had not known that attaining enrollment goals for these registries was proving to be so difficult."
The feedback from the public meeting may go a long way toward improving data collection in these registries, she agreed. "Getting input from clinicians, as well as manufacturers and other registry programs should help the agency formulate next steps." Dr. Campbell is staff toxicologist with the Office of Environmental Health Hazard Assessment (OEHHA), California Environmental Protection Agency, Sacramento.
Dr. Sahin disclosed no relevant conflicts of interest.
Do you tell your pregnant patients about pregnancy exposure registries and suggest that they sign up? Take our Quick Poll on the ObGyn News homepage.
AT TERATOLOGY SOCIETY 2014
Key clinical point: Pregnancy exposure registry data contribute to product safety, but the registries have problems enrolling enough patients.
Major finding: Registry data led to labeling changes for 12% of products and contributed to practice guidelines for 12% of products. But a sizable share of registries struggled with enrollment and follow-up.
Data source: An exploratory review of 38 pregnancy registries that tracked 59 products
Disclosures: Dr. Sahin disclosed no relevant conflicts of interest.

Preconception Concerns: Diabetes and Pregnancy
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Link between autoimmune therapy, preterm birth is largely due to confounding
BELLEVUE, WASH. – Women with autoimmune diseases who take corticosteroids and disease-modifying antirheumatic drugs later in pregnancy have an increased risk of preterm birth, but this association is largely explained by confounding with sociodemographic and clinical factors and disease severity, a study showed.
Researchers prospectively studied 678 pregnant women from the MotherToBaby database who had rheumatoid arthritis, psoriasis or psoriatic arthritis, ankylosing spondylitis, or Crohn’s disease. They focused on steroid use and disease-modifying antirheumatic drug (DMARD) use in the 16 weeks before delivery.

The results presented at the annual meeting of the Teratology Society showed that the incidence of preterm birth (birth before 37 weeks of gestation) was 19.2% among women using only steroids, 11.9% among those using only DMARDs, and 25.0% among those using both, compared with 11.2% among women who used neither throughout pregnancy.
In unadjusted analyses, women taking both steroids and DMARDs had significantly higher odds of preterm birth relative to peers who took neither (relative risk, 2.23), reported lead author Kristin Palmsten, Sc.D., of the University of California, San Diego.
But this risk was attenuated and no longer significant after adjustment for sociodemographic and clinical factors, such as age, race/ethnicity, parity, prior preterm birth, twin pregnancy, prepregnancy hypertension, depression, and use of nonsteroidal anti-inflammatory drugs.
It was attenuated further still after additional adjustment for the severity of autoimmune disease earlier in pregnancy, as assessed with the Health Assessment Questionnaire Disability Index (HAQ-DI) in analyses that excluded patients with Crohn’s disease (because they were not asked about disease severity).
The use of steroids alone and the use of DMARDs alone were not associated with a significantly elevated risk of preterm birth in either unadjusted or adjusted analyses.
The findings showed that confounders at least partially explain the heightened risk of preterm birth associated with autoimmune therapy, according to Dr. Palmsten.
A major study strength was exposure ascertainment, as the women were directly asked about their medication use several times during pregnancy, she noted. A limitation was the potential lack of generalizability, as the women studied were predominantly white and had higher socioeconomic status and lower disease severity.
In ongoing analyses, the investigators are looking at the proportions of preterm births that were spontaneous and medically indicated, and at the specific gestational age of the preterm births.
"I’d like to confirm the results in a different population; I’d like to look at this association in the Medicaid population, which is a low-income population," Dr. Palmsten added. "And I think preterm birth subtypes should be considered in further investigation. I’d also like to explore the timing of exposure and dose as well."
Session attendee Dr. Jan M. Friedman of the University of British Columbia in Vancouver noted the wide confidence intervals seen in analyses. "Obviously, that’s partially a function of the fact that the groups are fairly small. Is this an ongoing study? Will you have more data, more patients to look at in a year or something?" he asked.
"It is ongoing," Dr. Palmsten replied. "I don’t think that we’ll have 500 women exposed even after a year. But I do hope to address that with the Medicaid data because that would have a very large population."
Dr. Palmsten disclosed no relevant conflicts of interest. The MotherToBaby Pregnancy Study is sponsored by AbbVie, Amgen, Sanofi-Aventis, Apotex, Barr, Par Pharmaceutical, Sandoz, Teva, Bristol-Myers Squibb, Roche/Genentech, UCB Pharma, Pfizer, and Janssen.
BELLEVUE, WASH. – Women with autoimmune diseases who take corticosteroids and disease-modifying antirheumatic drugs later in pregnancy have an increased risk of preterm birth, but this association is largely explained by confounding with sociodemographic and clinical factors and disease severity, a study showed.
Researchers prospectively studied 678 pregnant women from the MotherToBaby database who had rheumatoid arthritis, psoriasis or psoriatic arthritis, ankylosing spondylitis, or Crohn’s disease. They focused on steroid use and disease-modifying antirheumatic drug (DMARD) use in the 16 weeks before delivery.
The results presented at the annual meeting of the Teratology Society showed that the incidence of preterm birth (birth before 37 weeks of gestation) was 19.2% among women using only steroids, 11.9% among those using only DMARDs, and 25.0% among those using both, compared with 11.2% among women who used neither throughout pregnancy.
In unadjusted analyses, women taking both steroids and DMARDs had significantly higher odds of preterm birth relative to peers who took neither (relative risk, 2.23), reported lead author Kristin Palmsten, Sc.D., of the University of California, San Diego.
But this risk was attenuated and no longer significant after adjustment for sociodemographic and clinical factors, such as age, race/ethnicity, parity, prior preterm birth, twin pregnancy, prepregnancy hypertension, depression, and use of nonsteroidal anti-inflammatory drugs.
It was attenuated further still after additional adjustment for the severity of autoimmune disease earlier in pregnancy, as assessed with the Health Assessment Questionnaire Disability Index (HAQ-DI) in analyses that excluded patients with Crohn’s disease (because they were not asked about disease severity).
The use of steroids alone and the use of DMARDs alone were not associated with a significantly elevated risk of preterm birth in either unadjusted or adjusted analyses.
The findings showed that confounders at least partially explain the heightened risk of preterm birth associated with autoimmune therapy, according to Dr. Palmsten.
A major study strength was exposure ascertainment, as the women were directly asked about their medication use several times during pregnancy, she noted. A limitation was the potential lack of generalizability, as the women studied were predominantly white and had higher socioeconomic status and lower disease severity.
In ongoing analyses, the investigators are looking at the proportions of preterm births that were spontaneous and medically indicated, and at the specific gestational age of the preterm births.
"I’d like to confirm the results in a different population; I’d like to look at this association in the Medicaid population, which is a low-income population," Dr. Palmsten added. "And I think preterm birth subtypes should be considered in further investigation. I’d also like to explore the timing of exposure and dose as well."
Session attendee Dr. Jan M. Friedman of the University of British Columbia in Vancouver noted the wide confidence intervals seen in analyses. "Obviously, that’s partially a function of the fact that the groups are fairly small. Is this an ongoing study? Will you have more data, more patients to look at in a year or something?" he asked.
"It is ongoing," Dr. Palmsten replied. "I don’t think that we’ll have 500 women exposed even after a year. But I do hope to address that with the Medicaid data because that would have a very large population."
Dr. Palmsten disclosed no relevant conflicts of interest. The MotherToBaby Pregnancy Study is sponsored by AbbVie, Amgen, Sanofi-Aventis, Apotex, Barr, Par Pharmaceutical, Sandoz, Teva, Bristol-Myers Squibb, Roche/Genentech, UCB Pharma, Pfizer, and Janssen.
BELLEVUE, WASH. – Women with autoimmune diseases who take corticosteroids and disease-modifying antirheumatic drugs later in pregnancy have an increased risk of preterm birth, but this association is largely explained by confounding with sociodemographic and clinical factors and disease severity, a study showed.
Researchers prospectively studied 678 pregnant women from the MotherToBaby database who had rheumatoid arthritis, psoriasis or psoriatic arthritis, ankylosing spondylitis, or Crohn’s disease. They focused on steroid use and disease-modifying antirheumatic drug (DMARD) use in the 16 weeks before delivery.
The results presented at the annual meeting of the Teratology Society showed that the incidence of preterm birth (birth before 37 weeks of gestation) was 19.2% among women using only steroids, 11.9% among those using only DMARDs, and 25.0% among those using both, compared with 11.2% among women who used neither throughout pregnancy.
In unadjusted analyses, women taking both steroids and DMARDs had significantly higher odds of preterm birth relative to peers who took neither (relative risk, 2.23), reported lead author Kristin Palmsten, Sc.D., of the University of California, San Diego.
But this risk was attenuated and no longer significant after adjustment for sociodemographic and clinical factors, such as age, race/ethnicity, parity, prior preterm birth, twin pregnancy, prepregnancy hypertension, depression, and use of nonsteroidal anti-inflammatory drugs.
It was attenuated further still after additional adjustment for the severity of autoimmune disease earlier in pregnancy, as assessed with the Health Assessment Questionnaire Disability Index (HAQ-DI) in analyses that excluded patients with Crohn’s disease (because they were not asked about disease severity).
The use of steroids alone and the use of DMARDs alone were not associated with a significantly elevated risk of preterm birth in either unadjusted or adjusted analyses.
The findings showed that confounders at least partially explain the heightened risk of preterm birth associated with autoimmune therapy, according to Dr. Palmsten.
A major study strength was exposure ascertainment, as the women were directly asked about their medication use several times during pregnancy, she noted. A limitation was the potential lack of generalizability, as the women studied were predominantly white and had higher socioeconomic status and lower disease severity.
In ongoing analyses, the investigators are looking at the proportions of preterm births that were spontaneous and medically indicated, and at the specific gestational age of the preterm births.
"I’d like to confirm the results in a different population; I’d like to look at this association in the Medicaid population, which is a low-income population," Dr. Palmsten added. "And I think preterm birth subtypes should be considered in further investigation. I’d also like to explore the timing of exposure and dose as well."
Session attendee Dr. Jan M. Friedman of the University of British Columbia in Vancouver noted the wide confidence intervals seen in analyses. "Obviously, that’s partially a function of the fact that the groups are fairly small. Is this an ongoing study? Will you have more data, more patients to look at in a year or something?" he asked.
"It is ongoing," Dr. Palmsten replied. "I don’t think that we’ll have 500 women exposed even after a year. But I do hope to address that with the Medicaid data because that would have a very large population."
Dr. Palmsten disclosed no relevant conflicts of interest. The MotherToBaby Pregnancy Study is sponsored by AbbVie, Amgen, Sanofi-Aventis, Apotex, Barr, Par Pharmaceutical, Sandoz, Teva, Bristol-Myers Squibb, Roche/Genentech, UCB Pharma, Pfizer, and Janssen.
AT TERATOLOGY SOCIETY 2014
Key clinical point: Confounders at least partially explain the heightened risk of preterm birth associated with autoimmune therapy.
Major finding: Women taking both steroids and DMARDs had 2.23 times the risk of a preterm birth relative to peers taking neither, but the association was no longer significant after adjustment for confounders.
Data source: A prospective cohort study of 678 pregnant women with autoimmune diseases
Disclosures: Dr. Palmsten disclosed no relevant conflicts of interest. The MotherToBaby Pregnancy Study is sponsored by AbbVie, Amgen, Sanofi-Aventis, Apotex, Barr, Par Pharmaceutical, Sandoz, Teva, Bristol-Myers Squibb, Roche/Genentech, UCB Pharma, Pfizer, and Janssen.

Hispanic ethnicity is linked to congenital ear deformities
BELLEVUE, WASH. – Hispanic women are much more likely than white women to give birth to an infant with small or no ears, an analysis of data from the National Birth Defects Prevention Study found.
In the NBDPS study of more than 8,500 births in the United States, the incidence of congenital isolated anotia or microtia was about three times higher among U.S.-born Hispanic women and five times higher among foreign-born Hispanic women, compared with non-Hispanic white women.

The elevation of risk for Hispanic women was especially pronounced if they had not completed high school, were obese, or smoked around the time of conception, and if they were less acculturated to the U.S. lifestyle.
"Anotia/microtia represents an extreme example of a racial/ethnic disparity in birth defects, especially among Hispanics," commented lead investigator Adrienne T. Hoyt, an epidemiologist with the Texas Department of State Health Services in Austin.
"These differences may be due to a combination of environmental, cultural, and genetic factors, which I think point a way toward future research in this area," she added at the annual meeting of the Teratology Society.
Session attendee Dr. Jan M. Friedman, a medical geneticist at the University of British Columbia in Vancouver, commented, "I’m having a hard time trying to get my head around how these factors are related to microtia/anotia if it isn’t poverty. Do you think they could all be just surrogates for poverty? [Lack of money] obviously has an influence on diet, access to medical care, and many other things."
Session cochair Suzan L. Carmichael, Ph.D., of the department of pediatrics (neonatology) at Stanford (Calif.) University, concurred, saying, "That is a question I was going to ask. ... So I know education was part of the analysis, but what socioeconomic status variables did you adjust for?"
"We did adjust for household income in all of our models. Unfortunately, this is a variable collected by the NBDPS, and it has a high rate of ‘missing,’ mothers who elected not to give household income. I think we had over 10% missing for this particular variable, but we did include that in the models."
The investigators analyzed data for 8,786 births between 1997 and 2007. All analyses excluded women with diabetes as it has been shown to be a strong risk factor for anotia and microtia, noted Ms. Hoyt.
The incidence of birth of an infant with anotia or microtia was 7.2% among U.S.-born Hispanic women and 11.0% among foreign-born Hispanic women, dramatically higher than the 2.3% among non-Hispanic white women, she reported.
In adjusted analyses stratified by sociodemographic factors, the elevated risk of having an infant with anotia/microtia associated with Hispanic versus white ethnicity was especially marked among strata of women having less than 12 years of education (odds ratios, 4.9-8.8), those having a body mass index exceeding 30 kg/m2 before conceiving (OR, 3.7-11.9), those who smoked in the periconceptional period (OR, 8.2 for foreign-born women), and those who did not take folic acid supplements periconceptionally (OR, 2.7-5.2).
In further analyses looking at acculturation factors and including infants having both a non-Hispanic white mother and father as the comparator group, the risk was elevated for Hispanic mothers who predominantly spoke English (odds ratio, 2.4), but more so for those who predominantly spoke Spanish (OR, 4.5). Similarly, the risk was elevated for U.S.-born Hispanic women (OR, 2.5), but more so for Mexican-born women who immigrated after age 5 (OR, 4.9).
Ms. Hoyt disclosed no relevant financial conflicts.
BELLEVUE, WASH. – Hispanic women are much more likely than white women to give birth to an infant with small or no ears, an analysis of data from the National Birth Defects Prevention Study found.
In the NBDPS study of more than 8,500 births in the United States, the incidence of congenital isolated anotia or microtia was about three times higher among U.S.-born Hispanic women and five times higher among foreign-born Hispanic women, compared with non-Hispanic white women.
The elevation of risk for Hispanic women was especially pronounced if they had not completed high school, were obese, or smoked around the time of conception, and if they were less acculturated to the U.S. lifestyle.
"Anotia/microtia represents an extreme example of a racial/ethnic disparity in birth defects, especially among Hispanics," commented lead investigator Adrienne T. Hoyt, an epidemiologist with the Texas Department of State Health Services in Austin.
"These differences may be due to a combination of environmental, cultural, and genetic factors, which I think point a way toward future research in this area," she added at the annual meeting of the Teratology Society.
Session attendee Dr. Jan M. Friedman, a medical geneticist at the University of British Columbia in Vancouver, commented, "I’m having a hard time trying to get my head around how these factors are related to microtia/anotia if it isn’t poverty. Do you think they could all be just surrogates for poverty? [Lack of money] obviously has an influence on diet, access to medical care, and many other things."
Session cochair Suzan L. Carmichael, Ph.D., of the department of pediatrics (neonatology) at Stanford (Calif.) University, concurred, saying, "That is a question I was going to ask. ... So I know education was part of the analysis, but what socioeconomic status variables did you adjust for?"
"We did adjust for household income in all of our models. Unfortunately, this is a variable collected by the NBDPS, and it has a high rate of ‘missing,’ mothers who elected not to give household income. I think we had over 10% missing for this particular variable, but we did include that in the models."
The investigators analyzed data for 8,786 births between 1997 and 2007. All analyses excluded women with diabetes as it has been shown to be a strong risk factor for anotia and microtia, noted Ms. Hoyt.
The incidence of birth of an infant with anotia or microtia was 7.2% among U.S.-born Hispanic women and 11.0% among foreign-born Hispanic women, dramatically higher than the 2.3% among non-Hispanic white women, she reported.
In adjusted analyses stratified by sociodemographic factors, the elevated risk of having an infant with anotia/microtia associated with Hispanic versus white ethnicity was especially marked among strata of women having less than 12 years of education (odds ratios, 4.9-8.8), those having a body mass index exceeding 30 kg/m2 before conceiving (OR, 3.7-11.9), those who smoked in the periconceptional period (OR, 8.2 for foreign-born women), and those who did not take folic acid supplements periconceptionally (OR, 2.7-5.2).
In further analyses looking at acculturation factors and including infants having both a non-Hispanic white mother and father as the comparator group, the risk was elevated for Hispanic mothers who predominantly spoke English (odds ratio, 2.4), but more so for those who predominantly spoke Spanish (OR, 4.5). Similarly, the risk was elevated for U.S.-born Hispanic women (OR, 2.5), but more so for Mexican-born women who immigrated after age 5 (OR, 4.9).
Ms. Hoyt disclosed no relevant financial conflicts.
BELLEVUE, WASH. – Hispanic women are much more likely than white women to give birth to an infant with small or no ears, an analysis of data from the National Birth Defects Prevention Study found.
In the NBDPS study of more than 8,500 births in the United States, the incidence of congenital isolated anotia or microtia was about three times higher among U.S.-born Hispanic women and five times higher among foreign-born Hispanic women, compared with non-Hispanic white women.
The elevation of risk for Hispanic women was especially pronounced if they had not completed high school, were obese, or smoked around the time of conception, and if they were less acculturated to the U.S. lifestyle.
"Anotia/microtia represents an extreme example of a racial/ethnic disparity in birth defects, especially among Hispanics," commented lead investigator Adrienne T. Hoyt, an epidemiologist with the Texas Department of State Health Services in Austin.
"These differences may be due to a combination of environmental, cultural, and genetic factors, which I think point a way toward future research in this area," she added at the annual meeting of the Teratology Society.
Session attendee Dr. Jan M. Friedman, a medical geneticist at the University of British Columbia in Vancouver, commented, "I’m having a hard time trying to get my head around how these factors are related to microtia/anotia if it isn’t poverty. Do you think they could all be just surrogates for poverty? [Lack of money] obviously has an influence on diet, access to medical care, and many other things."
Session cochair Suzan L. Carmichael, Ph.D., of the department of pediatrics (neonatology) at Stanford (Calif.) University, concurred, saying, "That is a question I was going to ask. ... So I know education was part of the analysis, but what socioeconomic status variables did you adjust for?"
"We did adjust for household income in all of our models. Unfortunately, this is a variable collected by the NBDPS, and it has a high rate of ‘missing,’ mothers who elected not to give household income. I think we had over 10% missing for this particular variable, but we did include that in the models."
The investigators analyzed data for 8,786 births between 1997 and 2007. All analyses excluded women with diabetes as it has been shown to be a strong risk factor for anotia and microtia, noted Ms. Hoyt.
The incidence of birth of an infant with anotia or microtia was 7.2% among U.S.-born Hispanic women and 11.0% among foreign-born Hispanic women, dramatically higher than the 2.3% among non-Hispanic white women, she reported.
In adjusted analyses stratified by sociodemographic factors, the elevated risk of having an infant with anotia/microtia associated with Hispanic versus white ethnicity was especially marked among strata of women having less than 12 years of education (odds ratios, 4.9-8.8), those having a body mass index exceeding 30 kg/m2 before conceiving (OR, 3.7-11.9), those who smoked in the periconceptional period (OR, 8.2 for foreign-born women), and those who did not take folic acid supplements periconceptionally (OR, 2.7-5.2).
In further analyses looking at acculturation factors and including infants having both a non-Hispanic white mother and father as the comparator group, the risk was elevated for Hispanic mothers who predominantly spoke English (odds ratio, 2.4), but more so for those who predominantly spoke Spanish (OR, 4.5). Similarly, the risk was elevated for U.S.-born Hispanic women (OR, 2.5), but more so for Mexican-born women who immigrated after age 5 (OR, 4.9).
Ms. Hoyt disclosed no relevant financial conflicts.
AT TERATOLOGY SOCIETY 2014
Key clinical point: Risk of anotia or microtia is increased in Hispanic women, especially if they have not completed high school, are obese, or smoke around the time of conception.
Major finding: The incidence of birth of an infant with anotia or microtia was 7.2% among U.S.-born Hispanic women and 11.0% among foreign-born Hispanic women, compared with 2.3% among non-Hispanic white women.
Data source: A cohort study of 8,786 births from National Birth Defects Prevention Study for 1997-2007.
Disclosures: Ms. Hoyt disclosed no relevant financial conflicts.

Suctioning Neonates at Birth: Time to Change Our Approach
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing
after wiping or suctioning
Kelleher et al1 studied neonates born after at least 35 weeks gestation, excluding those who had major congenital anomalies or were non-vigorous (depressed muscle tone or respiration, heart rate <100 beats/min, or both) and born into meconium-stained amniotic fluid, as well as those whom they anticipated would need advanced resuscitation. Neonates were randomly assigned to receive either oronasopharyngeal suctioning with a bulb syringe or wiping of the face and mouth with a towel, starting immediately after the umbilical cord was cut and lasting as long as needed while in the delivery room. The primary outcome was the mean respiratory rate in the first 24 hours after birth. The predefined range of clinical equivalence between the 2 groups was a respiratory rate within 4 breaths/min.
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning,
but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best
if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
…..
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing
after wiping or suctioning
Kelleher et al1 studied neonates born after at least 35 weeks gestation, excluding those who had major congenital anomalies or were non-vigorous (depressed muscle tone or respiration, heart rate <100 beats/min, or both) and born into meconium-stained amniotic fluid, as well as those whom they anticipated would need advanced resuscitation. Neonates were randomly assigned to receive either oronasopharyngeal suctioning with a bulb syringe or wiping of the face and mouth with a towel, starting immediately after the umbilical cord was cut and lasting as long as needed while in the delivery room. The primary outcome was the mean respiratory rate in the first 24 hours after birth. The predefined range of clinical equivalence between the 2 groups was a respiratory rate within 4 breaths/min.
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning,
but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best
if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
…..
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing
after wiping or suctioning
Kelleher et al1 studied neonates born after at least 35 weeks gestation, excluding those who had major congenital anomalies or were non-vigorous (depressed muscle tone or respiration, heart rate <100 beats/min, or both) and born into meconium-stained amniotic fluid, as well as those whom they anticipated would need advanced resuscitation. Neonates were randomly assigned to receive either oronasopharyngeal suctioning with a bulb syringe or wiping of the face and mouth with a towel, starting immediately after the umbilical cord was cut and lasting as long as needed while in the delivery room. The primary outcome was the mean respiratory rate in the first 24 hours after birth. The predefined range of clinical equivalence between the 2 groups was a respiratory rate within 4 breaths/min.
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning,
but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best
if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
…..
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
Early ID of placenta accreta key to optimal management
SAN DIEGO – An early and accurate diagnosis of placenta accreta is crucial because maternal mortality can be as high as 7% and perinatal mortality can be as high as 10%.
"Historically, the clinical presentation of placenta accreta was a prolonged third-stage or retained placenta after delivery of the baby and subsequent onset of hemorrhage or the onset of hemorrhage at the time of the termination of pregnancy," Dr. Gladys Ramos said at the University of California, San Diego, Critical Care Summer Session. "Now, with predelivery diagnosis, we have changed the management and the clinical presentation."

Placenta accreta is defined as the abnormal presence of villi attached to the myometrium due to a defect in the decidua basalis. In the 1980s, placenta accreta was believed to be rare. However, a study from 2005 showed an increase in the rate of placenta accreta (Am. J. Obstet. Gynecol. 2005;192:1458-61). The condition now occurs in 1 in every 533 pregnancies.
"Mirroring this rise is a rise in cesarean deliveries," said Dr. Ramos, a perinatologist at the UCSD Medical Center. "We think these two conditions are related. At UCSD, we take care of about 3,200 deliveries per year, and from 1990 to 2008 we have seen a linear increase in the rate of placenta accreta. We take care of about two patients per month with this condition."
Risk factors for the placenta accreta are prior uterine surgery, placenta previa, advanced maternal age, parity, and smoking. The published rate of detection by ultrasound ranges from 80% to 100%, "with a low false-positive rate," Dr. Ramos said. Telltale signs on ultrasound include loss of myometrial interface, a heterogeneous "Swiss cheese–looking" appearance to the placenta, an increase in the vascularity of the placenta, and evidence of bladder invasion.
MRI can be used as an adjunct to ultrasound diagnosis. The published detection rate with MRI ranges from 80% to 88%, "with a very low false-positive rate, which is why we use it as an adjunct to an ultrasound," she said. "We see similar findings on MRI that we do on ultrasound: thickened, dark nodular contour to the placenta; extension of the dark bands within the placenta; and mass effect causing a bulge on T1."
Nurses and sonographers at UCSD have been trained to ask patients upon presentation about risk factors for the condition." Then we look for signs of placenta accreta on ultrasound, including endovaginal ultrasound," Dr. Ramos said. "If we are concerned, we plan ahead with a multidisciplinary approach. If we’re still not sure, we proceed with MRI for diagnosis."
In 1995, clinicians at UCSD developed a multidisciplinary approach to treating patients with placenta accreta, mindful that "it took a cast of thousands to be able to make sure our outcomes were optimal for both mom and baby," said Pat Inzano, R.N., an administrative nurse in labor and delivery at UCSD. "Over the years, we’ve recognized the risk factors and the importance of early and accurate diagnosis."
The approach includes detailed maternal counseling and meticulous planning with colleagues at every conceivable step along the way in the care of the mom and baby, from neonatology and gynecologic surgery to surgical ICU staff and social workers. "When a mother gets the news [of placenta accreta], not only does she probably not understand the pathophysiology of what’s going on, but it takes a long time for her to digest this information," Ms. Inzano explained. "One of the things that’s so important at every level is getting her and her family to understand the diagnosis and reminding her that she’s [receiving] the best possible care."
The multidisciplinary team stages a conference to discuss the patient’s hospital delivery and care; availability of blood products; the need for anesthesia, surgical, and radiological expertise in house; and intensive care capability. Proper consents are also required "because the surgery will involve removing the patient’s uterus and rendering her sterile," she said. "We want to get the patient and the family as comfortable as possible with what’s going to happen. We found that providing tours of every single area that she will be ‘parking in’ is stress-relieving for her and her family, including labor and delivery and the neonatal ICU. We also provide consultations with all of the specialties involved in the case. All of this is education and counseling on a lot of different levels."
The team develops a time-line and schedules a planned delivery, including admission to the hospital, cesarean section/hysterectomy in the main operating room (OR), and unit transfers for epidural, central lines, and femoral balloons. In addition, the team coordinates a hospital tour for the patient and family. Most recommended deliveries are at week 34 because "we don’t want her to get near term and go into labor, which would aggravate a bleed of the placenta accreta," Ms. Inzano said.
The team also crafts a "plan B" for emergent delivery, including a detailed list of whom to contact and their pager numbers. "If we need to emergency deliver this patient in the main OR at 3 in the morning, we have our attending physician call the attending trauma physician to put us on trauma bypass in case we need the blood products," she said. "If we don’t have the type and cross-matched blood available, we activate an [obstetric] hemorrhage protocol in order to obtain O-negative blood in massive quantities until she’s cross-matched."
Ms. Inzano said that the multidisciplinary approach to placenta accreta "has become a smooth operation at our institution, but we never drop our awareness of the severity of what can happen. With the multidisciplinary effort, it brings everyone together; everyone’s on the same page, and everyone knows what to anticipate."
Neither Dr. Ramos nor Ms. Inzano had relevant financial conflicts.
On Twitter @dougbrunk
SAN DIEGO – An early and accurate diagnosis of placenta accreta is crucial because maternal mortality can be as high as 7% and perinatal mortality can be as high as 10%.
"Historically, the clinical presentation of placenta accreta was a prolonged third-stage or retained placenta after delivery of the baby and subsequent onset of hemorrhage or the onset of hemorrhage at the time of the termination of pregnancy," Dr. Gladys Ramos said at the University of California, San Diego, Critical Care Summer Session. "Now, with predelivery diagnosis, we have changed the management and the clinical presentation."
Placenta accreta is defined as the abnormal presence of villi attached to the myometrium due to a defect in the decidua basalis. In the 1980s, placenta accreta was believed to be rare. However, a study from 2005 showed an increase in the rate of placenta accreta (Am. J. Obstet. Gynecol. 2005;192:1458-61). The condition now occurs in 1 in every 533 pregnancies.
"Mirroring this rise is a rise in cesarean deliveries," said Dr. Ramos, a perinatologist at the UCSD Medical Center. "We think these two conditions are related. At UCSD, we take care of about 3,200 deliveries per year, and from 1990 to 2008 we have seen a linear increase in the rate of placenta accreta. We take care of about two patients per month with this condition."
Risk factors for the placenta accreta are prior uterine surgery, placenta previa, advanced maternal age, parity, and smoking. The published rate of detection by ultrasound ranges from 80% to 100%, "with a low false-positive rate," Dr. Ramos said. Telltale signs on ultrasound include loss of myometrial interface, a heterogeneous "Swiss cheese–looking" appearance to the placenta, an increase in the vascularity of the placenta, and evidence of bladder invasion.
MRI can be used as an adjunct to ultrasound diagnosis. The published detection rate with MRI ranges from 80% to 88%, "with a very low false-positive rate, which is why we use it as an adjunct to an ultrasound," she said. "We see similar findings on MRI that we do on ultrasound: thickened, dark nodular contour to the placenta; extension of the dark bands within the placenta; and mass effect causing a bulge on T1."
Nurses and sonographers at UCSD have been trained to ask patients upon presentation about risk factors for the condition." Then we look for signs of placenta accreta on ultrasound, including endovaginal ultrasound," Dr. Ramos said. "If we are concerned, we plan ahead with a multidisciplinary approach. If we’re still not sure, we proceed with MRI for diagnosis."
In 1995, clinicians at UCSD developed a multidisciplinary approach to treating patients with placenta accreta, mindful that "it took a cast of thousands to be able to make sure our outcomes were optimal for both mom and baby," said Pat Inzano, R.N., an administrative nurse in labor and delivery at UCSD. "Over the years, we’ve recognized the risk factors and the importance of early and accurate diagnosis."
The approach includes detailed maternal counseling and meticulous planning with colleagues at every conceivable step along the way in the care of the mom and baby, from neonatology and gynecologic surgery to surgical ICU staff and social workers. "When a mother gets the news [of placenta accreta], not only does she probably not understand the pathophysiology of what’s going on, but it takes a long time for her to digest this information," Ms. Inzano explained. "One of the things that’s so important at every level is getting her and her family to understand the diagnosis and reminding her that she’s [receiving] the best possible care."
The multidisciplinary team stages a conference to discuss the patient’s hospital delivery and care; availability of blood products; the need for anesthesia, surgical, and radiological expertise in house; and intensive care capability. Proper consents are also required "because the surgery will involve removing the patient’s uterus and rendering her sterile," she said. "We want to get the patient and the family as comfortable as possible with what’s going to happen. We found that providing tours of every single area that she will be ‘parking in’ is stress-relieving for her and her family, including labor and delivery and the neonatal ICU. We also provide consultations with all of the specialties involved in the case. All of this is education and counseling on a lot of different levels."
The team develops a time-line and schedules a planned delivery, including admission to the hospital, cesarean section/hysterectomy in the main operating room (OR), and unit transfers for epidural, central lines, and femoral balloons. In addition, the team coordinates a hospital tour for the patient and family. Most recommended deliveries are at week 34 because "we don’t want her to get near term and go into labor, which would aggravate a bleed of the placenta accreta," Ms. Inzano said.
The team also crafts a "plan B" for emergent delivery, including a detailed list of whom to contact and their pager numbers. "If we need to emergency deliver this patient in the main OR at 3 in the morning, we have our attending physician call the attending trauma physician to put us on trauma bypass in case we need the blood products," she said. "If we don’t have the type and cross-matched blood available, we activate an [obstetric] hemorrhage protocol in order to obtain O-negative blood in massive quantities until she’s cross-matched."
Ms. Inzano said that the multidisciplinary approach to placenta accreta "has become a smooth operation at our institution, but we never drop our awareness of the severity of what can happen. With the multidisciplinary effort, it brings everyone together; everyone’s on the same page, and everyone knows what to anticipate."
Neither Dr. Ramos nor Ms. Inzano had relevant financial conflicts.
On Twitter @dougbrunk
SAN DIEGO – An early and accurate diagnosis of placenta accreta is crucial because maternal mortality can be as high as 7% and perinatal mortality can be as high as 10%.
"Historically, the clinical presentation of placenta accreta was a prolonged third-stage or retained placenta after delivery of the baby and subsequent onset of hemorrhage or the onset of hemorrhage at the time of the termination of pregnancy," Dr. Gladys Ramos said at the University of California, San Diego, Critical Care Summer Session. "Now, with predelivery diagnosis, we have changed the management and the clinical presentation."
Placenta accreta is defined as the abnormal presence of villi attached to the myometrium due to a defect in the decidua basalis. In the 1980s, placenta accreta was believed to be rare. However, a study from 2005 showed an increase in the rate of placenta accreta (Am. J. Obstet. Gynecol. 2005;192:1458-61). The condition now occurs in 1 in every 533 pregnancies.
"Mirroring this rise is a rise in cesarean deliveries," said Dr. Ramos, a perinatologist at the UCSD Medical Center. "We think these two conditions are related. At UCSD, we take care of about 3,200 deliveries per year, and from 1990 to 2008 we have seen a linear increase in the rate of placenta accreta. We take care of about two patients per month with this condition."
Risk factors for the placenta accreta are prior uterine surgery, placenta previa, advanced maternal age, parity, and smoking. The published rate of detection by ultrasound ranges from 80% to 100%, "with a low false-positive rate," Dr. Ramos said. Telltale signs on ultrasound include loss of myometrial interface, a heterogeneous "Swiss cheese–looking" appearance to the placenta, an increase in the vascularity of the placenta, and evidence of bladder invasion.
MRI can be used as an adjunct to ultrasound diagnosis. The published detection rate with MRI ranges from 80% to 88%, "with a very low false-positive rate, which is why we use it as an adjunct to an ultrasound," she said. "We see similar findings on MRI that we do on ultrasound: thickened, dark nodular contour to the placenta; extension of the dark bands within the placenta; and mass effect causing a bulge on T1."
Nurses and sonographers at UCSD have been trained to ask patients upon presentation about risk factors for the condition." Then we look for signs of placenta accreta on ultrasound, including endovaginal ultrasound," Dr. Ramos said. "If we are concerned, we plan ahead with a multidisciplinary approach. If we’re still not sure, we proceed with MRI for diagnosis."
In 1995, clinicians at UCSD developed a multidisciplinary approach to treating patients with placenta accreta, mindful that "it took a cast of thousands to be able to make sure our outcomes were optimal for both mom and baby," said Pat Inzano, R.N., an administrative nurse in labor and delivery at UCSD. "Over the years, we’ve recognized the risk factors and the importance of early and accurate diagnosis."
The approach includes detailed maternal counseling and meticulous planning with colleagues at every conceivable step along the way in the care of the mom and baby, from neonatology and gynecologic surgery to surgical ICU staff and social workers. "When a mother gets the news [of placenta accreta], not only does she probably not understand the pathophysiology of what’s going on, but it takes a long time for her to digest this information," Ms. Inzano explained. "One of the things that’s so important at every level is getting her and her family to understand the diagnosis and reminding her that she’s [receiving] the best possible care."
The multidisciplinary team stages a conference to discuss the patient’s hospital delivery and care; availability of blood products; the need for anesthesia, surgical, and radiological expertise in house; and intensive care capability. Proper consents are also required "because the surgery will involve removing the patient’s uterus and rendering her sterile," she said. "We want to get the patient and the family as comfortable as possible with what’s going to happen. We found that providing tours of every single area that she will be ‘parking in’ is stress-relieving for her and her family, including labor and delivery and the neonatal ICU. We also provide consultations with all of the specialties involved in the case. All of this is education and counseling on a lot of different levels."
The team develops a time-line and schedules a planned delivery, including admission to the hospital, cesarean section/hysterectomy in the main operating room (OR), and unit transfers for epidural, central lines, and femoral balloons. In addition, the team coordinates a hospital tour for the patient and family. Most recommended deliveries are at week 34 because "we don’t want her to get near term and go into labor, which would aggravate a bleed of the placenta accreta," Ms. Inzano said.
The team also crafts a "plan B" for emergent delivery, including a detailed list of whom to contact and their pager numbers. "If we need to emergency deliver this patient in the main OR at 3 in the morning, we have our attending physician call the attending trauma physician to put us on trauma bypass in case we need the blood products," she said. "If we don’t have the type and cross-matched blood available, we activate an [obstetric] hemorrhage protocol in order to obtain O-negative blood in massive quantities until she’s cross-matched."
Ms. Inzano said that the multidisciplinary approach to placenta accreta "has become a smooth operation at our institution, but we never drop our awareness of the severity of what can happen. With the multidisciplinary effort, it brings everyone together; everyone’s on the same page, and everyone knows what to anticipate."
Neither Dr. Ramos nor Ms. Inzano had relevant financial conflicts.
On Twitter @dougbrunk
EXPERT ANALYSIS AT THE UCSD CRITICAL CARE SUMMER SESSION

The High Cost of “Free Advice”
A couple had their first child in May 1998. The boy exhibited developmental delays and had chronic problems with eating and weight gain. In August 1999, he collapsed with uncontrollable seizures. He was placed in a drug-induced coma. A month later, when he emerged from the coma, he was neurologically compromised. He recovered somewhat but then regressed, experiencing another seizure episode. He died in January 2000. MRI of his brain showed a lesion on his thalamus.
The couple’s second child was born in April 2002. This child also had delays and developed seizures, was placed in a coma, and emerged neurologically impaired. She too was found to have an abnormality in her thalamus. She died in July 2004.
The couple was referred to Dr. S, a geneticist. They consulted Dr. S both before and after the second child’s death. After their daughter’s death, the couple asked Dr. S whether it was possible to have biological children who would not have the same problems. Dr. S told them that he could not identify the specific gene causing the defect but advised that it would be safe to conceive a child with a donor egg from the general population and the husband’s sperm through in vitro fertilization.
Dr. S allegedly advised the couple that a child conceived this way would have essentially the same risk for the unidentified disease as anyone in the general population. The couple asked in writing if it would be safer to use both a donor sperm and a donor egg to further reduce the risk, and Dr. S replied by letter that the difference was “negligible.”
In June 2007, the couple had a child who was conceived with a donated egg and the husband’s sperm. This child suffered the same fate as the two previous children, dying in September 2008. MRI of the child’s brain, like the others, showed an abnormality of the thalamus. The child was diagnosed with Alpers syndrome postmortem.
The plaintiffs claimed that the chances of having a child with Alpers syndrome are about 1:200,000 in the general population, but that the chances if one parent is a known carrier are about 1:1,000. The plaintiffs claimed that if they had known of this risk, they would have used a donor egg and donor sperm to conceive a child or would have adopted. The plaintiffs alleged negligence by Dr. S in failing to give them this information.
Continue for the outcome and David Lang's comment >>
OUTCOME
A $1,086,612 verdict was returned, with the jury finding Dr. S 25% at fault and the plaintiffs 75% at fault.
COMMENT
A skilled tax accountant will provide guidance on how to claim deductions. Many lawyers listen and advise but do little else. These people sit at a desk and provide advice—that is what they do. Dispensing advice from a seated position is their only stock in store.
By contrast, clinicians are kinetic people. They are on their feet, up and about. They perform workups and surgeries, procedures and treatments. Clinicians are people in motion accustomed to action.
Yet clinicians often forget: Dispensing advice is practicing medicine. They are conditioned to dispense this advice freely, and by freely I mean both casually and without compensation. As a result, clinicians often fail to realize the value and potential liability of the spoken word. Make no mistake: Giving medical advice incurs legal risk. Lawyers know this; how many give free advice while absorbing the risk for that advice? Yeah, I thought so ....
Clinicians can be held legally liable for misinformation as easily as they can for misdiagnosis. The key is detrimental reliance. When a clinician gives a patient incorrect information, there is no legal case. The patient has a legal case if, and only if, he or she relies on that information and is injured (detriment) based on that reliance.
Here, the standard of care required the geneticist to be familiar with Alpers syndrome and accurately convey the risk associated with different courses of action. Like an accountant or attorney, the service sought and tendered is advice. The plaintiff was told that the risk for having another child with Alpers syndrome was “negligible” and made a decision based on that risk assessment.
The risk, however, was not negligible; it was 200 times greater than that in the general population. Relying on the geneticist’s information, the plaintiffs decided to use the father’s sperm and suffered legally compensable injury when their third child was born with the same condition. There was clearly clinician error.
Nevertheless, the jurors found the parents 75% at fault (for attempting to have another child) and the physician 25% at fault. Some states only allow a plaintiff to recover damages if they have no fault at all (pure contributory negligence), while others permit recovery if the plaintiff is 50% or less at fault. A handful of states—including Florida, where this case occurred—allow a plaintiff to recover even if they are 99% at fault (pure comparative negligence). In those cases, the jury determines the damages and the parties’ respective fault percentages, and the plaintiff’s recovery is reduced by that percentage. Here, the physician was responsible for 25% of the $1,086,612 award and thus had to pay $271,653.
In sum: Don’t give “free advice” too freely. >>
IN SUM
Don’t give “free advice” too freely. Document advice and options, and make sure the patient understands them. Understand that providing advice establishes a clinician–patient relationship and that you are legally responsible for advice given.
Beware of dispensing advice electronically or over the phone, where you are off your turf and lack the usual preconditions to high quality care (eg, a chart, vital signs, a medication/allergy/problem list). Never provide advice in situations where you cannot do so (my recurring favorite: a request for telephone diagnosis of a rash you’ve never seen). Dispense advice as you would medication: cautiously and with documentation. —DML
A couple had their first child in May 1998. The boy exhibited developmental delays and had chronic problems with eating and weight gain. In August 1999, he collapsed with uncontrollable seizures. He was placed in a drug-induced coma. A month later, when he emerged from the coma, he was neurologically compromised. He recovered somewhat but then regressed, experiencing another seizure episode. He died in January 2000. MRI of his brain showed a lesion on his thalamus.
The couple’s second child was born in April 2002. This child also had delays and developed seizures, was placed in a coma, and emerged neurologically impaired. She too was found to have an abnormality in her thalamus. She died in July 2004.
The couple was referred to Dr. S, a geneticist. They consulted Dr. S both before and after the second child’s death. After their daughter’s death, the couple asked Dr. S whether it was possible to have biological children who would not have the same problems. Dr. S told them that he could not identify the specific gene causing the defect but advised that it would be safe to conceive a child with a donor egg from the general population and the husband’s sperm through in vitro fertilization.
Dr. S allegedly advised the couple that a child conceived this way would have essentially the same risk for the unidentified disease as anyone in the general population. The couple asked in writing if it would be safer to use both a donor sperm and a donor egg to further reduce the risk, and Dr. S replied by letter that the difference was “negligible.”
In June 2007, the couple had a child who was conceived with a donated egg and the husband’s sperm. This child suffered the same fate as the two previous children, dying in September 2008. MRI of the child’s brain, like the others, showed an abnormality of the thalamus. The child was diagnosed with Alpers syndrome postmortem.
The plaintiffs claimed that the chances of having a child with Alpers syndrome are about 1:200,000 in the general population, but that the chances if one parent is a known carrier are about 1:1,000. The plaintiffs claimed that if they had known of this risk, they would have used a donor egg and donor sperm to conceive a child or would have adopted. The plaintiffs alleged negligence by Dr. S in failing to give them this information.
Continue for the outcome and David Lang's comment >>
OUTCOME
A $1,086,612 verdict was returned, with the jury finding Dr. S 25% at fault and the plaintiffs 75% at fault.
COMMENT
A skilled tax accountant will provide guidance on how to claim deductions. Many lawyers listen and advise but do little else. These people sit at a desk and provide advice—that is what they do. Dispensing advice from a seated position is their only stock in store.
By contrast, clinicians are kinetic people. They are on their feet, up and about. They perform workups and surgeries, procedures and treatments. Clinicians are people in motion accustomed to action.
Yet clinicians often forget: Dispensing advice is practicing medicine. They are conditioned to dispense this advice freely, and by freely I mean both casually and without compensation. As a result, clinicians often fail to realize the value and potential liability of the spoken word. Make no mistake: Giving medical advice incurs legal risk. Lawyers know this; how many give free advice while absorbing the risk for that advice? Yeah, I thought so ....
Clinicians can be held legally liable for misinformation as easily as they can for misdiagnosis. The key is detrimental reliance. When a clinician gives a patient incorrect information, there is no legal case. The patient has a legal case if, and only if, he or she relies on that information and is injured (detriment) based on that reliance.
Here, the standard of care required the geneticist to be familiar with Alpers syndrome and accurately convey the risk associated with different courses of action. Like an accountant or attorney, the service sought and tendered is advice. The plaintiff was told that the risk for having another child with Alpers syndrome was “negligible” and made a decision based on that risk assessment.
The risk, however, was not negligible; it was 200 times greater than that in the general population. Relying on the geneticist’s information, the plaintiffs decided to use the father’s sperm and suffered legally compensable injury when their third child was born with the same condition. There was clearly clinician error.
Nevertheless, the jurors found the parents 75% at fault (for attempting to have another child) and the physician 25% at fault. Some states only allow a plaintiff to recover damages if they have no fault at all (pure contributory negligence), while others permit recovery if the plaintiff is 50% or less at fault. A handful of states—including Florida, where this case occurred—allow a plaintiff to recover even if they are 99% at fault (pure comparative negligence). In those cases, the jury determines the damages and the parties’ respective fault percentages, and the plaintiff’s recovery is reduced by that percentage. Here, the physician was responsible for 25% of the $1,086,612 award and thus had to pay $271,653.
In sum: Don’t give “free advice” too freely. >>
IN SUM
Don’t give “free advice” too freely. Document advice and options, and make sure the patient understands them. Understand that providing advice establishes a clinician–patient relationship and that you are legally responsible for advice given.
Beware of dispensing advice electronically or over the phone, where you are off your turf and lack the usual preconditions to high quality care (eg, a chart, vital signs, a medication/allergy/problem list). Never provide advice in situations where you cannot do so (my recurring favorite: a request for telephone diagnosis of a rash you’ve never seen). Dispense advice as you would medication: cautiously and with documentation. —DML
A couple had their first child in May 1998. The boy exhibited developmental delays and had chronic problems with eating and weight gain. In August 1999, he collapsed with uncontrollable seizures. He was placed in a drug-induced coma. A month later, when he emerged from the coma, he was neurologically compromised. He recovered somewhat but then regressed, experiencing another seizure episode. He died in January 2000. MRI of his brain showed a lesion on his thalamus.
The couple’s second child was born in April 2002. This child also had delays and developed seizures, was placed in a coma, and emerged neurologically impaired. She too was found to have an abnormality in her thalamus. She died in July 2004.
The couple was referred to Dr. S, a geneticist. They consulted Dr. S both before and after the second child’s death. After their daughter’s death, the couple asked Dr. S whether it was possible to have biological children who would not have the same problems. Dr. S told them that he could not identify the specific gene causing the defect but advised that it would be safe to conceive a child with a donor egg from the general population and the husband’s sperm through in vitro fertilization.
Dr. S allegedly advised the couple that a child conceived this way would have essentially the same risk for the unidentified disease as anyone in the general population. The couple asked in writing if it would be safer to use both a donor sperm and a donor egg to further reduce the risk, and Dr. S replied by letter that the difference was “negligible.”
In June 2007, the couple had a child who was conceived with a donated egg and the husband’s sperm. This child suffered the same fate as the two previous children, dying in September 2008. MRI of the child’s brain, like the others, showed an abnormality of the thalamus. The child was diagnosed with Alpers syndrome postmortem.
The plaintiffs claimed that the chances of having a child with Alpers syndrome are about 1:200,000 in the general population, but that the chances if one parent is a known carrier are about 1:1,000. The plaintiffs claimed that if they had known of this risk, they would have used a donor egg and donor sperm to conceive a child or would have adopted. The plaintiffs alleged negligence by Dr. S in failing to give them this information.
Continue for the outcome and David Lang's comment >>
OUTCOME
A $1,086,612 verdict was returned, with the jury finding Dr. S 25% at fault and the plaintiffs 75% at fault.
COMMENT
A skilled tax accountant will provide guidance on how to claim deductions. Many lawyers listen and advise but do little else. These people sit at a desk and provide advice—that is what they do. Dispensing advice from a seated position is their only stock in store.
By contrast, clinicians are kinetic people. They are on their feet, up and about. They perform workups and surgeries, procedures and treatments. Clinicians are people in motion accustomed to action.
Yet clinicians often forget: Dispensing advice is practicing medicine. They are conditioned to dispense this advice freely, and by freely I mean both casually and without compensation. As a result, clinicians often fail to realize the value and potential liability of the spoken word. Make no mistake: Giving medical advice incurs legal risk. Lawyers know this; how many give free advice while absorbing the risk for that advice? Yeah, I thought so ....
Clinicians can be held legally liable for misinformation as easily as they can for misdiagnosis. The key is detrimental reliance. When a clinician gives a patient incorrect information, there is no legal case. The patient has a legal case if, and only if, he or she relies on that information and is injured (detriment) based on that reliance.
Here, the standard of care required the geneticist to be familiar with Alpers syndrome and accurately convey the risk associated with different courses of action. Like an accountant or attorney, the service sought and tendered is advice. The plaintiff was told that the risk for having another child with Alpers syndrome was “negligible” and made a decision based on that risk assessment.
The risk, however, was not negligible; it was 200 times greater than that in the general population. Relying on the geneticist’s information, the plaintiffs decided to use the father’s sperm and suffered legally compensable injury when their third child was born with the same condition. There was clearly clinician error.
Nevertheless, the jurors found the parents 75% at fault (for attempting to have another child) and the physician 25% at fault. Some states only allow a plaintiff to recover damages if they have no fault at all (pure contributory negligence), while others permit recovery if the plaintiff is 50% or less at fault. A handful of states—including Florida, where this case occurred—allow a plaintiff to recover even if they are 99% at fault (pure comparative negligence). In those cases, the jury determines the damages and the parties’ respective fault percentages, and the plaintiff’s recovery is reduced by that percentage. Here, the physician was responsible for 25% of the $1,086,612 award and thus had to pay $271,653.
In sum: Don’t give “free advice” too freely. >>
IN SUM
Don’t give “free advice” too freely. Document advice and options, and make sure the patient understands them. Understand that providing advice establishes a clinician–patient relationship and that you are legally responsible for advice given.
Beware of dispensing advice electronically or over the phone, where you are off your turf and lack the usual preconditions to high quality care (eg, a chart, vital signs, a medication/allergy/problem list). Never provide advice in situations where you cannot do so (my recurring favorite: a request for telephone diagnosis of a rash you’ve never seen). Dispense advice as you would medication: cautiously and with documentation. —DML
Only weak link seen between gestational pesticide exposure and gastroschisis
BELLEVUE, WASH. – Early gestational exposure to agricultural pesticides is only weakly linked to the risk of gastroschisis in offspring, suggests a case-control study conducted in California’s San Joaquin Valley, an area having among the highest levels of pesticide use nationwide.
Using data from the state and the National Birth Defects Prevention Study for the years 1997-2012, investigators led by Gary M. Shaw, Dr.P.H., assessed maternal exposure during early pregnancy to hundreds of chemicals as ascertained from state pesticide reporting data by geographic area and the women’s address of residence, obtained during interviews.

Analyses were based on 156 live births, fetal deaths, or pregnancy terminations affected by gastroschisis and 785 unaffected matched controls.
"Gastroschisis is a rather unique birth defect. It has a very unique epidemiology," noted Dr. Shaw, who is a professor of clinical research and a doctor of public health in the pediatrics department at Stanford (Calif.) University. "It’s one of a few or perhaps the only one that has been increasing around the world for the last 20-30 years, and it really looks like it’s a disease of young women from what we observe." Teenagers, for example, have a seven to nine times higher risk than do older women.
Overall, 35% of cases and 38% of controls had maternal pesticide exposure in early pregnancy, Dr. Shaw reported at the annual meeting of the Teratology Society. The most common chemical groups to which women had been exposed were poly-alkyl-oxy compounds, glycophosphates, organophosphorus insecticides, alcohols/ethers, and pyrethroids.
However, in adjusted analyses of 52 chemical groups restricted to those for which more than four cases or controls were exposed, only one – the triazine group – was associated with an increased risk of gastroschisis (odds ratio, 1.7), and that association was merely borderline significant, with the confidence interval including unity.
Similarly, in adjusted analyses of 233 individual chemicals restricted to those for which more than four cases or controls were exposed, only two – oxyfluorfen (OR, 1.6) and petroleum distillates (OR, 2.5) – showed an association with this risk; in these cases, the confidence intervals did not include unity.

"We basically got a general lack of association in a discovery, hypothesis-generating study. We have a detailed exposure assessment. ... We conducted many comparisons, and we’ve got modest sample sizes," Dr. Shaw concluded. "And the kicker is that none of the associations we looked at seemed to stand up for young maternal age."
"This is a useful negative study, and it is noteworthy that, even without correcting for multiple comparisons, there were no impressive positive findings," commented session cochair Dr. James Mills, an investigator with the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Md.
In additional study results, analyses of exposure to those chemicals classified as reproductive toxicants, ones listed in California’s Proposition 65 (which aims to eliminate carcinogenic and teratogenic agents from drinking water and consumer products), and known endocrine disruptors, either alone or in combinations, did not alter the findings, according to Dr. Shaw.
Furthermore, there was no significant association of the combination of pesticide exposure and air pollution exposure (any of either vs. none) and the risk of gastroschisis.
Dr. Shaw had no relevant conflicts of interest.
BELLEVUE, WASH. – Early gestational exposure to agricultural pesticides is only weakly linked to the risk of gastroschisis in offspring, suggests a case-control study conducted in California’s San Joaquin Valley, an area having among the highest levels of pesticide use nationwide.
Using data from the state and the National Birth Defects Prevention Study for the years 1997-2012, investigators led by Gary M. Shaw, Dr.P.H., assessed maternal exposure during early pregnancy to hundreds of chemicals as ascertained from state pesticide reporting data by geographic area and the women’s address of residence, obtained during interviews.
Analyses were based on 156 live births, fetal deaths, or pregnancy terminations affected by gastroschisis and 785 unaffected matched controls.
"Gastroschisis is a rather unique birth defect. It has a very unique epidemiology," noted Dr. Shaw, who is a professor of clinical research and a doctor of public health in the pediatrics department at Stanford (Calif.) University. "It’s one of a few or perhaps the only one that has been increasing around the world for the last 20-30 years, and it really looks like it’s a disease of young women from what we observe." Teenagers, for example, have a seven to nine times higher risk than do older women.
Overall, 35% of cases and 38% of controls had maternal pesticide exposure in early pregnancy, Dr. Shaw reported at the annual meeting of the Teratology Society. The most common chemical groups to which women had been exposed were poly-alkyl-oxy compounds, glycophosphates, organophosphorus insecticides, alcohols/ethers, and pyrethroids.
However, in adjusted analyses of 52 chemical groups restricted to those for which more than four cases or controls were exposed, only one – the triazine group – was associated with an increased risk of gastroschisis (odds ratio, 1.7), and that association was merely borderline significant, with the confidence interval including unity.
Similarly, in adjusted analyses of 233 individual chemicals restricted to those for which more than four cases or controls were exposed, only two – oxyfluorfen (OR, 1.6) and petroleum distillates (OR, 2.5) – showed an association with this risk; in these cases, the confidence intervals did not include unity.
"We basically got a general lack of association in a discovery, hypothesis-generating study. We have a detailed exposure assessment. ... We conducted many comparisons, and we’ve got modest sample sizes," Dr. Shaw concluded. "And the kicker is that none of the associations we looked at seemed to stand up for young maternal age."
"This is a useful negative study, and it is noteworthy that, even without correcting for multiple comparisons, there were no impressive positive findings," commented session cochair Dr. James Mills, an investigator with the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Md.
In additional study results, analyses of exposure to those chemicals classified as reproductive toxicants, ones listed in California’s Proposition 65 (which aims to eliminate carcinogenic and teratogenic agents from drinking water and consumer products), and known endocrine disruptors, either alone or in combinations, did not alter the findings, according to Dr. Shaw.
Furthermore, there was no significant association of the combination of pesticide exposure and air pollution exposure (any of either vs. none) and the risk of gastroschisis.
Dr. Shaw had no relevant conflicts of interest.
BELLEVUE, WASH. – Early gestational exposure to agricultural pesticides is only weakly linked to the risk of gastroschisis in offspring, suggests a case-control study conducted in California’s San Joaquin Valley, an area having among the highest levels of pesticide use nationwide.
Using data from the state and the National Birth Defects Prevention Study for the years 1997-2012, investigators led by Gary M. Shaw, Dr.P.H., assessed maternal exposure during early pregnancy to hundreds of chemicals as ascertained from state pesticide reporting data by geographic area and the women’s address of residence, obtained during interviews.
Analyses were based on 156 live births, fetal deaths, or pregnancy terminations affected by gastroschisis and 785 unaffected matched controls.
"Gastroschisis is a rather unique birth defect. It has a very unique epidemiology," noted Dr. Shaw, who is a professor of clinical research and a doctor of public health in the pediatrics department at Stanford (Calif.) University. "It’s one of a few or perhaps the only one that has been increasing around the world for the last 20-30 years, and it really looks like it’s a disease of young women from what we observe." Teenagers, for example, have a seven to nine times higher risk than do older women.
Overall, 35% of cases and 38% of controls had maternal pesticide exposure in early pregnancy, Dr. Shaw reported at the annual meeting of the Teratology Society. The most common chemical groups to which women had been exposed were poly-alkyl-oxy compounds, glycophosphates, organophosphorus insecticides, alcohols/ethers, and pyrethroids.
However, in adjusted analyses of 52 chemical groups restricted to those for which more than four cases or controls were exposed, only one – the triazine group – was associated with an increased risk of gastroschisis (odds ratio, 1.7), and that association was merely borderline significant, with the confidence interval including unity.
Similarly, in adjusted analyses of 233 individual chemicals restricted to those for which more than four cases or controls were exposed, only two – oxyfluorfen (OR, 1.6) and petroleum distillates (OR, 2.5) – showed an association with this risk; in these cases, the confidence intervals did not include unity.
"We basically got a general lack of association in a discovery, hypothesis-generating study. We have a detailed exposure assessment. ... We conducted many comparisons, and we’ve got modest sample sizes," Dr. Shaw concluded. "And the kicker is that none of the associations we looked at seemed to stand up for young maternal age."
"This is a useful negative study, and it is noteworthy that, even without correcting for multiple comparisons, there were no impressive positive findings," commented session cochair Dr. James Mills, an investigator with the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Md.
In additional study results, analyses of exposure to those chemicals classified as reproductive toxicants, ones listed in California’s Proposition 65 (which aims to eliminate carcinogenic and teratogenic agents from drinking water and consumer products), and known endocrine disruptors, either alone or in combinations, did not alter the findings, according to Dr. Shaw.
Furthermore, there was no significant association of the combination of pesticide exposure and air pollution exposure (any of either vs. none) and the risk of gastroschisis.
Dr. Shaw had no relevant conflicts of interest.
AT TERATOLOGY SOCIETY 2014
Key clinical point: There does not appear to be a strong link between gestational pesticide exposure and gastroschisis.
Major finding: Only 1 of 52 chemical groups and 2 of 233 individual chemicals showed any borderline or significant association with gastroschisis.
Data source: A case-control study of 156 affected and 785 matched unaffected live births, fetal deaths, or pregnancy terminations.
Disclosures: Dr. Shaw had no relevant conflicts of interest.
