User login
Novel mutation may be unrecognized cause of sudden infant death
A previously healthy infant who survived sudden cardiac arrest at home was later found to have a de novo likely pathogenic genetic mutation in the SOS1 gene, which might be an unrecognized cause of sudden infant death, report clinicians from Missouri.
SOS1 gene variants are associated with Noonan syndrome, a genetic disorder that affects the RAS/MAPK signaling pathway. However, on presentation, the infant had none of the usual structural cardiac findings typical of Noonan syndrome, such as valvular disease or hypertrophic cardiomyopathy.
“To date, this is the first case reported of a ventricular fibrillation arrest in a patient with a RASopathy-related variant prior to development of the typically associated structural cardiac phenotype and may represent a previously unrecognized etiology of sudden death during infancy,” write Christopher W. Follansbee, MD, and Lindsey Malloy-Walton, DO, from the Ward Family Heart Center, Children’s Mercy Kansas City, and the University of Missouri School of Medicine.
“Genetic testing in cases of unexplained aborted or sudden cardiac deaths, even in previously healthy children, can be valuable in establishing a diagnosis, determining the prognosis, and assessing risk to family members,” they add in a news release.
Dr. Follansbee and Dr. Malloy-Walton describe the case in a report published in the August issue of HeartRhythm Case Reports.
Case details
The case involved a 2-month-old girl who did not wake up as usual for her morning feeding. Her mother found her limp, pale, and having difficulty breathing.
When emergency medical services arrived, the infant had no pulse. Cardiopulmonary resuscitation was initiated and an external defibrillator revealed coarse ventricular fibrillation. An initial shock of 10 J was given with conversion to an atrial rhythm with aberrant ventricular conduction.
The infant developed increasing frequency of ectopy before degenerating to ventricular fibrillation. A second shock with 20 J was unsuccessful, but a third shock of 20 J successfully converted the rhythm to sinus with aberrant ventricular conduction and atrial ectopy with return of spontaneous circulation.
In the ICU, the infant displayed incessant, nonsustained ectopic atrial tachycardia, with rapid episodes of ectopic atrial tachycardia with ventricular rates up to 300 beats per minute in the setting of seizure activity, they report.
With intravenous lorazepam, seizure activity resolved and treatment with amiodarone boluses led to transient establishment of sinus rhythm.
The QTc was noted to be above 500 ms and Brugada positioning of leads was unrevealing, the authors note.
Transthoracic echocardiogram showed a structurally normal heart with normal valve morphology and a patent foramen ovale with left-to-right flow. The initial ejection fraction was 49%. There was no evidence of ventricular hypertrophy, dilation, or noncompaction.
The infant was started on an esmolol infusion titrated to 225 μg/kg per min with frequent, nonsustained breakthrough of ectopic atrial tachycardia. Over the next 24 hours, the QTc interval normalized with normal T-wave morphology.
A procainamide challenge was negative. Cardiac MRI revealed normalization of ventricular function.
The genetics team was called in and a standard three-generation family history was obtained. An older sibling, 2 years of age, had no known medical conditions. The child’s paternal grandfather had died of a presumed myocardial infarction in his 50s, but no autopsy had been performed.
There was no family history of congenital heart disease, arrhythmia, sudden death, cardiomyopathy, recurrent syncope, congenital deafness, seizure, miscarriage, or developmental delay. Electrocardiograms obtained on the parents were normal.
Genetic testing using a comprehensive arrhythmia and cardiomyopathy next-generation sequencing panel revealed a de novo likely pathogenetic variant of the SOS1 gene associated with Noonan syndrome.
Given the aborted sudden cardiac death, the patient underwent dual-chamber epicardial implantable cardioverter-defibrillator implantation prior to discharge.
Dr. Follansbee and Dr. Malloy-Walton say a limitation to the case report is the lack of definitive association of the SOS1 variant with the presentation.
However, knowing the infant has the SOS1 variant and a history of aborted sudden death will allow for “monitoring and early intervention on typical manifestations of Noonan syndrome as the patient grows,” they say.
This research had no specific funding. Dr. Follansbee and Dr. Malloy-Walton have disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A previously healthy infant who survived sudden cardiac arrest at home was later found to have a de novo likely pathogenic genetic mutation in the SOS1 gene, which might be an unrecognized cause of sudden infant death, report clinicians from Missouri.
SOS1 gene variants are associated with Noonan syndrome, a genetic disorder that affects the RAS/MAPK signaling pathway. However, on presentation, the infant had none of the usual structural cardiac findings typical of Noonan syndrome, such as valvular disease or hypertrophic cardiomyopathy.
“To date, this is the first case reported of a ventricular fibrillation arrest in a patient with a RASopathy-related variant prior to development of the typically associated structural cardiac phenotype and may represent a previously unrecognized etiology of sudden death during infancy,” write Christopher W. Follansbee, MD, and Lindsey Malloy-Walton, DO, from the Ward Family Heart Center, Children’s Mercy Kansas City, and the University of Missouri School of Medicine.
“Genetic testing in cases of unexplained aborted or sudden cardiac deaths, even in previously healthy children, can be valuable in establishing a diagnosis, determining the prognosis, and assessing risk to family members,” they add in a news release.
Dr. Follansbee and Dr. Malloy-Walton describe the case in a report published in the August issue of HeartRhythm Case Reports.
Case details
The case involved a 2-month-old girl who did not wake up as usual for her morning feeding. Her mother found her limp, pale, and having difficulty breathing.
When emergency medical services arrived, the infant had no pulse. Cardiopulmonary resuscitation was initiated and an external defibrillator revealed coarse ventricular fibrillation. An initial shock of 10 J was given with conversion to an atrial rhythm with aberrant ventricular conduction.
The infant developed increasing frequency of ectopy before degenerating to ventricular fibrillation. A second shock with 20 J was unsuccessful, but a third shock of 20 J successfully converted the rhythm to sinus with aberrant ventricular conduction and atrial ectopy with return of spontaneous circulation.
In the ICU, the infant displayed incessant, nonsustained ectopic atrial tachycardia, with rapid episodes of ectopic atrial tachycardia with ventricular rates up to 300 beats per minute in the setting of seizure activity, they report.
With intravenous lorazepam, seizure activity resolved and treatment with amiodarone boluses led to transient establishment of sinus rhythm.
The QTc was noted to be above 500 ms and Brugada positioning of leads was unrevealing, the authors note.
Transthoracic echocardiogram showed a structurally normal heart with normal valve morphology and a patent foramen ovale with left-to-right flow. The initial ejection fraction was 49%. There was no evidence of ventricular hypertrophy, dilation, or noncompaction.
The infant was started on an esmolol infusion titrated to 225 μg/kg per min with frequent, nonsustained breakthrough of ectopic atrial tachycardia. Over the next 24 hours, the QTc interval normalized with normal T-wave morphology.
A procainamide challenge was negative. Cardiac MRI revealed normalization of ventricular function.
The genetics team was called in and a standard three-generation family history was obtained. An older sibling, 2 years of age, had no known medical conditions. The child’s paternal grandfather had died of a presumed myocardial infarction in his 50s, but no autopsy had been performed.
There was no family history of congenital heart disease, arrhythmia, sudden death, cardiomyopathy, recurrent syncope, congenital deafness, seizure, miscarriage, or developmental delay. Electrocardiograms obtained on the parents were normal.
Genetic testing using a comprehensive arrhythmia and cardiomyopathy next-generation sequencing panel revealed a de novo likely pathogenetic variant of the SOS1 gene associated with Noonan syndrome.
Given the aborted sudden cardiac death, the patient underwent dual-chamber epicardial implantable cardioverter-defibrillator implantation prior to discharge.
Dr. Follansbee and Dr. Malloy-Walton say a limitation to the case report is the lack of definitive association of the SOS1 variant with the presentation.
However, knowing the infant has the SOS1 variant and a history of aborted sudden death will allow for “monitoring and early intervention on typical manifestations of Noonan syndrome as the patient grows,” they say.
This research had no specific funding. Dr. Follansbee and Dr. Malloy-Walton have disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A previously healthy infant who survived sudden cardiac arrest at home was later found to have a de novo likely pathogenic genetic mutation in the SOS1 gene, which might be an unrecognized cause of sudden infant death, report clinicians from Missouri.
SOS1 gene variants are associated with Noonan syndrome, a genetic disorder that affects the RAS/MAPK signaling pathway. However, on presentation, the infant had none of the usual structural cardiac findings typical of Noonan syndrome, such as valvular disease or hypertrophic cardiomyopathy.
“To date, this is the first case reported of a ventricular fibrillation arrest in a patient with a RASopathy-related variant prior to development of the typically associated structural cardiac phenotype and may represent a previously unrecognized etiology of sudden death during infancy,” write Christopher W. Follansbee, MD, and Lindsey Malloy-Walton, DO, from the Ward Family Heart Center, Children’s Mercy Kansas City, and the University of Missouri School of Medicine.
“Genetic testing in cases of unexplained aborted or sudden cardiac deaths, even in previously healthy children, can be valuable in establishing a diagnosis, determining the prognosis, and assessing risk to family members,” they add in a news release.
Dr. Follansbee and Dr. Malloy-Walton describe the case in a report published in the August issue of HeartRhythm Case Reports.
Case details
The case involved a 2-month-old girl who did not wake up as usual for her morning feeding. Her mother found her limp, pale, and having difficulty breathing.
When emergency medical services arrived, the infant had no pulse. Cardiopulmonary resuscitation was initiated and an external defibrillator revealed coarse ventricular fibrillation. An initial shock of 10 J was given with conversion to an atrial rhythm with aberrant ventricular conduction.
The infant developed increasing frequency of ectopy before degenerating to ventricular fibrillation. A second shock with 20 J was unsuccessful, but a third shock of 20 J successfully converted the rhythm to sinus with aberrant ventricular conduction and atrial ectopy with return of spontaneous circulation.
In the ICU, the infant displayed incessant, nonsustained ectopic atrial tachycardia, with rapid episodes of ectopic atrial tachycardia with ventricular rates up to 300 beats per minute in the setting of seizure activity, they report.
With intravenous lorazepam, seizure activity resolved and treatment with amiodarone boluses led to transient establishment of sinus rhythm.
The QTc was noted to be above 500 ms and Brugada positioning of leads was unrevealing, the authors note.
Transthoracic echocardiogram showed a structurally normal heart with normal valve morphology and a patent foramen ovale with left-to-right flow. The initial ejection fraction was 49%. There was no evidence of ventricular hypertrophy, dilation, or noncompaction.
The infant was started on an esmolol infusion titrated to 225 μg/kg per min with frequent, nonsustained breakthrough of ectopic atrial tachycardia. Over the next 24 hours, the QTc interval normalized with normal T-wave morphology.
A procainamide challenge was negative. Cardiac MRI revealed normalization of ventricular function.
The genetics team was called in and a standard three-generation family history was obtained. An older sibling, 2 years of age, had no known medical conditions. The child’s paternal grandfather had died of a presumed myocardial infarction in his 50s, but no autopsy had been performed.
There was no family history of congenital heart disease, arrhythmia, sudden death, cardiomyopathy, recurrent syncope, congenital deafness, seizure, miscarriage, or developmental delay. Electrocardiograms obtained on the parents were normal.
Genetic testing using a comprehensive arrhythmia and cardiomyopathy next-generation sequencing panel revealed a de novo likely pathogenetic variant of the SOS1 gene associated with Noonan syndrome.
Given the aborted sudden cardiac death, the patient underwent dual-chamber epicardial implantable cardioverter-defibrillator implantation prior to discharge.
Dr. Follansbee and Dr. Malloy-Walton say a limitation to the case report is the lack of definitive association of the SOS1 variant with the presentation.
However, knowing the infant has the SOS1 variant and a history of aborted sudden death will allow for “monitoring and early intervention on typical manifestations of Noonan syndrome as the patient grows,” they say.
This research had no specific funding. Dr. Follansbee and Dr. Malloy-Walton have disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Healing Haiti: The emotional trauma of repeat crises
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Study informs about risks of discontinuing meds in JIA
Flares are modest in preliminary data.
Many but not all children with juvenile idiopathic arthritis (JIA) can regain remission after stopping and then restarting treatment, according to preliminary data from the ongoing Recapture-JIA study that were presented in a symposium sponsored by the Rheumatology Research Foundation.

The aim of this study is to evaluate the risks of discontinuing treatment after a period when JIA has been well controlled. Such data are of increasing interest to parents now that many children with JIA are achieving sustained periods of remission, according to Sarah Ringold, MD, a pediatric rheumatologist and associate professor of pediatrics at Seattle Children’s Hospital.
In follow-up so far, “recapture rates range from 50% to 76%” depending on type of JIA, reported Dr. Ringold, who said that patients with systemic JIA have so far been the most likely to achieve a good response when treatment is restarted.
The study is being conducted through the Childhood Arthritis and Rheumatology Research Alliance, which has 71 participating centers and has accrued data on more than 10,000 children with rheumatic diseases. For the study, the researchers identified 384 children with JIA who were already enrolled in the CARRA registry and had discontinued medications and then subsequently restarted them, and they also enrolled a prospective cohort of patients new to the registry who presented with flare after discontinuing their medication. Dr. Ringold reported on 64 of the patients in the prospective cohort.
Median time to flare: 219 days
Of findings so far, disease recurrence after discontinuation has been generally characterized by flares “of moderate activity” several months to more than a year after treatment discontinuation, according to Dr. Ringold, who emphasized repeatedly that these data are preliminary. The median time to a flare after treatment discontinuation was approximately 7 months (219 days).
In the combined cohorts, the median age at onset of JIA was 4 years. The median age at time of discontinuation was 9 years. More than half (55%) were taking a conventional disease-modifying antirheumatic drug (DMARD) and 35% were taking a tumor necrosis factor inhibitor at the time that their therapy was discontinued.
Most JIA types are represented. The most common form is rheumatoid factor–negative oligoarticular JIA. The main outcome looked the rate of clinically inactive disease at 6 months in children who had discontinued therapy after a period of remission. They defined clinically inactive disease as a Physician’s Global Assessment of less than 1 and an active joint count of 0.
Systemic JIA recapture rate at 6 months: 76%
At the time of disease flare after treatment discontinuation across both the retrospective and prospective cohorts, the median clinical Juvenile Arthritis Disease Activity Score based on 10 joints (cJADAS10; score range of 0-30) was 3.5. The recapture rate to clinically inactive disease at 6 months was 76% in those with systemic JIA and 50% in those with rheumatoid factor–positive polyarticular JIA. Other subtypes fell within this range. Rates of inactive disease at 6 months according to cJADAS10 score were lower, ranging from 26% with enthesitis-related arthritis/juvenile psoriatic arthritis to 57% with systemic JIA.
About 40% of those who restarted on therapy after a flare took the same medication again. About one-third of patients were restarted on glucocorticoids, mostly involving injections to inflamed joints, and data are not yet in about whether these were restarted alone or with other drugs, according to Dr. Ringold.
The final analysis of this study will explore clinical and laboratory variables associated with disease recapture. In the prospective cohort, which did not reach its planned enrollment of 150 children because the COVID pandemic, a broad array of these variables was evaluated at baseline.
Numerous studies have already looked at predictors of sustained remission after stopping medications of JIA, according to Dr. Ringold, but she said that there is relatively little information about outcomes in children who stop medications, flare, and are retreated. Other experts agree.
“We know little about how successfully DMARDs can be discontinued and used again after a disease flare,” reported Jens Klotsche, MD, a researcher at the German Rheumatism Research Center, which is part of the Leibniz Institute in Berlin. Dr. Klotsche, who is an author of a recent study that found etanercept effective for retreatment when children with JIA had discontinued therapy, agreed that “data from large cohort studies are necessary to support the treatment decisions by clinicians, parents, and patients.”
JIA recurrence risk is unclear
In a systematic review published 2 years ago, rates of flare following discontinuation of treatment for JIA were relatively high, but there were some limitations to this analysis, according to the lead author, Olha Halyabar, MD, a pediatric rheumatologist at Boston Children’s Hospital.
“The data in our systematic review showed that overall quality of evidence was low, with large variations and sometimes very different conclusions,” Dr. Halyabar said in an interview. She believes that the data generated by the CARRA analysis will be valuable, particularly in evaluating outcomes across subtypes.
“Even though, at this point, [previously published] reports indicate overall high rates of recurrence (>50% for some JIA subtypes), there are some encouraging studies from early treat-to-target strategies,” she said, adding that large datasets like those from CARRA offer an opportunity to gather data likely to be clinically useful.
Dr. Ringold cautioned that there are some limitations to the CARRA analysis, including some missing data from the retrospective cohort. She also pointed out that patients have been assessed at routine clinical visits rather than at standardized intervals, introducing a potential for bias.
For parents concerned about the costs, inconvenience, and side effects from sustained JIA treatment once remission is achieved, data from CARRA will allow clinicians to provide evidence-based counseling on balancing the risks of discontinuing therapy, including the likelihood of regaining remission when disease returns, against the goals of stopping treatment.
“Parents are having more conversations about when to stop medications,” Dr. Ringold said. She indicated that these data should be helpful for providing guidance.
Dr. Ringold, Dr. Klotsche, and Dr. Halyabar reported having no potential conflicts of interest.
Flares are modest in preliminary data.
Flares are modest in preliminary data.
Many but not all children with juvenile idiopathic arthritis (JIA) can regain remission after stopping and then restarting treatment, according to preliminary data from the ongoing Recapture-JIA study that were presented in a symposium sponsored by the Rheumatology Research Foundation.
The aim of this study is to evaluate the risks of discontinuing treatment after a period when JIA has been well controlled. Such data are of increasing interest to parents now that many children with JIA are achieving sustained periods of remission, according to Sarah Ringold, MD, a pediatric rheumatologist and associate professor of pediatrics at Seattle Children’s Hospital.
In follow-up so far, “recapture rates range from 50% to 76%” depending on type of JIA, reported Dr. Ringold, who said that patients with systemic JIA have so far been the most likely to achieve a good response when treatment is restarted.
The study is being conducted through the Childhood Arthritis and Rheumatology Research Alliance, which has 71 participating centers and has accrued data on more than 10,000 children with rheumatic diseases. For the study, the researchers identified 384 children with JIA who were already enrolled in the CARRA registry and had discontinued medications and then subsequently restarted them, and they also enrolled a prospective cohort of patients new to the registry who presented with flare after discontinuing their medication. Dr. Ringold reported on 64 of the patients in the prospective cohort.
Median time to flare: 219 days
Of findings so far, disease recurrence after discontinuation has been generally characterized by flares “of moderate activity” several months to more than a year after treatment discontinuation, according to Dr. Ringold, who emphasized repeatedly that these data are preliminary. The median time to a flare after treatment discontinuation was approximately 7 months (219 days).
In the combined cohorts, the median age at onset of JIA was 4 years. The median age at time of discontinuation was 9 years. More than half (55%) were taking a conventional disease-modifying antirheumatic drug (DMARD) and 35% were taking a tumor necrosis factor inhibitor at the time that their therapy was discontinued.
Most JIA types are represented. The most common form is rheumatoid factor–negative oligoarticular JIA. The main outcome looked the rate of clinically inactive disease at 6 months in children who had discontinued therapy after a period of remission. They defined clinically inactive disease as a Physician’s Global Assessment of less than 1 and an active joint count of 0.
Systemic JIA recapture rate at 6 months: 76%
At the time of disease flare after treatment discontinuation across both the retrospective and prospective cohorts, the median clinical Juvenile Arthritis Disease Activity Score based on 10 joints (cJADAS10; score range of 0-30) was 3.5. The recapture rate to clinically inactive disease at 6 months was 76% in those with systemic JIA and 50% in those with rheumatoid factor–positive polyarticular JIA. Other subtypes fell within this range. Rates of inactive disease at 6 months according to cJADAS10 score were lower, ranging from 26% with enthesitis-related arthritis/juvenile psoriatic arthritis to 57% with systemic JIA.
About 40% of those who restarted on therapy after a flare took the same medication again. About one-third of patients were restarted on glucocorticoids, mostly involving injections to inflamed joints, and data are not yet in about whether these were restarted alone or with other drugs, according to Dr. Ringold.
The final analysis of this study will explore clinical and laboratory variables associated with disease recapture. In the prospective cohort, which did not reach its planned enrollment of 150 children because the COVID pandemic, a broad array of these variables was evaluated at baseline.
Numerous studies have already looked at predictors of sustained remission after stopping medications of JIA, according to Dr. Ringold, but she said that there is relatively little information about outcomes in children who stop medications, flare, and are retreated. Other experts agree.
“We know little about how successfully DMARDs can be discontinued and used again after a disease flare,” reported Jens Klotsche, MD, a researcher at the German Rheumatism Research Center, which is part of the Leibniz Institute in Berlin. Dr. Klotsche, who is an author of a recent study that found etanercept effective for retreatment when children with JIA had discontinued therapy, agreed that “data from large cohort studies are necessary to support the treatment decisions by clinicians, parents, and patients.”
JIA recurrence risk is unclear
In a systematic review published 2 years ago, rates of flare following discontinuation of treatment for JIA were relatively high, but there were some limitations to this analysis, according to the lead author, Olha Halyabar, MD, a pediatric rheumatologist at Boston Children’s Hospital.
“The data in our systematic review showed that overall quality of evidence was low, with large variations and sometimes very different conclusions,” Dr. Halyabar said in an interview. She believes that the data generated by the CARRA analysis will be valuable, particularly in evaluating outcomes across subtypes.
“Even though, at this point, [previously published] reports indicate overall high rates of recurrence (>50% for some JIA subtypes), there are some encouraging studies from early treat-to-target strategies,” she said, adding that large datasets like those from CARRA offer an opportunity to gather data likely to be clinically useful.
Dr. Ringold cautioned that there are some limitations to the CARRA analysis, including some missing data from the retrospective cohort. She also pointed out that patients have been assessed at routine clinical visits rather than at standardized intervals, introducing a potential for bias.
For parents concerned about the costs, inconvenience, and side effects from sustained JIA treatment once remission is achieved, data from CARRA will allow clinicians to provide evidence-based counseling on balancing the risks of discontinuing therapy, including the likelihood of regaining remission when disease returns, against the goals of stopping treatment.
“Parents are having more conversations about when to stop medications,” Dr. Ringold said. She indicated that these data should be helpful for providing guidance.
Dr. Ringold, Dr. Klotsche, and Dr. Halyabar reported having no potential conflicts of interest.
Many but not all children with juvenile idiopathic arthritis (JIA) can regain remission after stopping and then restarting treatment, according to preliminary data from the ongoing Recapture-JIA study that were presented in a symposium sponsored by the Rheumatology Research Foundation.
The aim of this study is to evaluate the risks of discontinuing treatment after a period when JIA has been well controlled. Such data are of increasing interest to parents now that many children with JIA are achieving sustained periods of remission, according to Sarah Ringold, MD, a pediatric rheumatologist and associate professor of pediatrics at Seattle Children’s Hospital.
In follow-up so far, “recapture rates range from 50% to 76%” depending on type of JIA, reported Dr. Ringold, who said that patients with systemic JIA have so far been the most likely to achieve a good response when treatment is restarted.
The study is being conducted through the Childhood Arthritis and Rheumatology Research Alliance, which has 71 participating centers and has accrued data on more than 10,000 children with rheumatic diseases. For the study, the researchers identified 384 children with JIA who were already enrolled in the CARRA registry and had discontinued medications and then subsequently restarted them, and they also enrolled a prospective cohort of patients new to the registry who presented with flare after discontinuing their medication. Dr. Ringold reported on 64 of the patients in the prospective cohort.
Median time to flare: 219 days
Of findings so far, disease recurrence after discontinuation has been generally characterized by flares “of moderate activity” several months to more than a year after treatment discontinuation, according to Dr. Ringold, who emphasized repeatedly that these data are preliminary. The median time to a flare after treatment discontinuation was approximately 7 months (219 days).
In the combined cohorts, the median age at onset of JIA was 4 years. The median age at time of discontinuation was 9 years. More than half (55%) were taking a conventional disease-modifying antirheumatic drug (DMARD) and 35% were taking a tumor necrosis factor inhibitor at the time that their therapy was discontinued.
Most JIA types are represented. The most common form is rheumatoid factor–negative oligoarticular JIA. The main outcome looked the rate of clinically inactive disease at 6 months in children who had discontinued therapy after a period of remission. They defined clinically inactive disease as a Physician’s Global Assessment of less than 1 and an active joint count of 0.
Systemic JIA recapture rate at 6 months: 76%
At the time of disease flare after treatment discontinuation across both the retrospective and prospective cohorts, the median clinical Juvenile Arthritis Disease Activity Score based on 10 joints (cJADAS10; score range of 0-30) was 3.5. The recapture rate to clinically inactive disease at 6 months was 76% in those with systemic JIA and 50% in those with rheumatoid factor–positive polyarticular JIA. Other subtypes fell within this range. Rates of inactive disease at 6 months according to cJADAS10 score were lower, ranging from 26% with enthesitis-related arthritis/juvenile psoriatic arthritis to 57% with systemic JIA.
About 40% of those who restarted on therapy after a flare took the same medication again. About one-third of patients were restarted on glucocorticoids, mostly involving injections to inflamed joints, and data are not yet in about whether these were restarted alone or with other drugs, according to Dr. Ringold.
The final analysis of this study will explore clinical and laboratory variables associated with disease recapture. In the prospective cohort, which did not reach its planned enrollment of 150 children because the COVID pandemic, a broad array of these variables was evaluated at baseline.
Numerous studies have already looked at predictors of sustained remission after stopping medications of JIA, according to Dr. Ringold, but she said that there is relatively little information about outcomes in children who stop medications, flare, and are retreated. Other experts agree.
“We know little about how successfully DMARDs can be discontinued and used again after a disease flare,” reported Jens Klotsche, MD, a researcher at the German Rheumatism Research Center, which is part of the Leibniz Institute in Berlin. Dr. Klotsche, who is an author of a recent study that found etanercept effective for retreatment when children with JIA had discontinued therapy, agreed that “data from large cohort studies are necessary to support the treatment decisions by clinicians, parents, and patients.”
JIA recurrence risk is unclear
In a systematic review published 2 years ago, rates of flare following discontinuation of treatment for JIA were relatively high, but there were some limitations to this analysis, according to the lead author, Olha Halyabar, MD, a pediatric rheumatologist at Boston Children’s Hospital.
“The data in our systematic review showed that overall quality of evidence was low, with large variations and sometimes very different conclusions,” Dr. Halyabar said in an interview. She believes that the data generated by the CARRA analysis will be valuable, particularly in evaluating outcomes across subtypes.
“Even though, at this point, [previously published] reports indicate overall high rates of recurrence (>50% for some JIA subtypes), there are some encouraging studies from early treat-to-target strategies,” she said, adding that large datasets like those from CARRA offer an opportunity to gather data likely to be clinically useful.
Dr. Ringold cautioned that there are some limitations to the CARRA analysis, including some missing data from the retrospective cohort. She also pointed out that patients have been assessed at routine clinical visits rather than at standardized intervals, introducing a potential for bias.
For parents concerned about the costs, inconvenience, and side effects from sustained JIA treatment once remission is achieved, data from CARRA will allow clinicians to provide evidence-based counseling on balancing the risks of discontinuing therapy, including the likelihood of regaining remission when disease returns, against the goals of stopping treatment.
“Parents are having more conversations about when to stop medications,” Dr. Ringold said. She indicated that these data should be helpful for providing guidance.
Dr. Ringold, Dr. Klotsche, and Dr. Halyabar reported having no potential conflicts of interest.
FROM RHEUMATOLOGY RESEARCH FOUNDATION SUMMER SERIES
AHA targets rising prevalence of obstructive sleep apnea in children
Obstructive sleep apnea is becoming more common in children and adolescents as the prevalence of obesity increases, but it may also be a preventable risk factor for cardiovascular disease, according to a new scientific statement from the American Heart Association.

The statement focuses on the links between OSA and CVD risk factors in children and adolescents, and reviews diagnostic strategies and treatments. The writing committee reported that 1%-6% of children and adolescents have OSA, as do up to 60% of adolescents considered obese.
The statement was created by the AHA’s Atherosclerosis, Hypertension, and Obesity in the Young subcommittee of the Council on Cardiovascular Disease in the Young and was published online in the Journal of the American Heart Association.
Carissa M. Baker-Smith, MD, chair of the writing group chair and director of pediatric preventive cardiology at Nemours Cardiac Center, Alfred I. duPont Hospital for Children, Wilmington, Del., explained the rationale for issuing the statement at this time, noting that the relationship between OSA and CVD in adults is well documented.
“There has been less focus on the importance of recognizing and treating sleep apnea in youth,” she said in an interview. “Thus, we felt that it was vitally important to get the word out to parents and to providers that paying attention to the quality and duration of your child’s sleep is vitally important to a child’s long-term heart health. Risk factors for heart disease, when present in childhood, can persist into adulthood.”
Clarity on polysomnography
For making the diagnosis of OSA in children, the statement provides clarity on the use of polysomnography and the role of the apnea-hypopnea index, which is lower in children with OSA than in adults. “One controversy, or at least as I saw it, was whether or not polysomnography testing is always required to make the diagnosis of OSA and before proceeding with tonsil and adenoid removal among children for whom enlarged tonsils and adenoids are present,” Dr. Baker-Smith said. “Polysomnography testing is not always needed before an ear, nose, and throat surgeon may recommend surgery.”
The statement also noted that history and physical examination may not yield enough reliable information to distinguish OSA from snoring.
In areas where sleep laboratories that work with children aren’t available, alternative tests such as daytime nap polysomnography, nocturnal oximetry, and nocturnal video recording may be used – with a caveat. “These alternative tests have weaker positive and negative predictive values when compared with polysomnography,” the writing committee noted. Home sleep apnea tests aren’t recommended in children. Questionnaires “are useful as screening, but not as diagnostic tools.”
Pediatric patients being evaluated for OSA should also be screened for hypertension and metabolic syndrome, as well as central nervous system and behavioral disorders. Diagnosing OSA in children and adolescents requires “a high index of suspicion,” the committee wrote.
Pediatricians and pediatric cardiologists should exercise that high index of suspicion when receiving referrals for cardiac evaluations for attention deficit hyperactivity disorder medication, Dr. Baker-Smith said. “Take the time to ask about a child’s sleep – snoring, apnea, etc. – especially if the child has obesity, difficulty focusing during the day, and if there is evidence of systemic hypertension or other signs of metabolic syndrome,” she said.
Risk factors for OSA in children
The statement also reviewed risk factors for OSA, among them obesity, particularly among children younger than 6 years. Other risk factors include upper and lower airway disease, hypotonia, parental history of hyperplasia of the adenoids and tonsils, craniofacial malformations, and neuromuscular disorders. However, the committee cited “limited data” to support that children with congenital heart disease may be at greater risk for OSA and sleep-disordered breathing (SDB).
Black children are at significantly greater risk, and socioeconomic factors “may be potential confounders,” the committee stated. Other risk factors include allergic rhinitis and sickle cell disease.
But the statement underscores that “obesity is the main risk factor” for OSA in children and adolescents, and that the presence of increased inflammation may explain this relationship. Steroids may alleviate these symptoms, even in nonobese children, and removal of the adenoids or tonsils is an option to reduce inflammation in children with OSA.
“Obesity is a significant risk factor for sleep disturbances and obstructive sleep apnea, and the severity of sleep apnea may be improved by weight-loss interventions, which then improves metabolic syndrome factors such as insulin sensitivity,” Dr. Baker-Smith said. “We need to increase awareness about how the rising prevalence of obesity may be impacting sleep quality in kids and recognize sleep-disordered breathing as something that could contribute to risks for hypertension and later cardiovascular disease.”
Children in whom OSA is suspected should also undergo screening for metabolic syndrome, and central nervous system and behavioral disorders.
Cardiovascular risks
The statement explores the connection between cardiovascular complications and SDB and OSA in depth.
“Inadequate sleep duration of < 5 hours per night in children and adolescents has been linked to an increased risk of hypertension and is also associated with an increased prevalence of obesity,” the committee wrote.
However, the statement left one question hanging: whether OSA alone or obesity cause higher BP in younger patients with OSA. But the committee concluded that BP levels increase with the severity of OSA, although the effects can vary with age. OSA in children peaks between ages 2 and 8, corresponding to the peak prevalence of hypertrophy of the tonsils and adenoids. Children aged 10-11 with more severe OSA may have BP dysregulation, while older adolescents develop higher sustained BP. Obesity may be a confounder for daytime BP elevations, while nighttime hypertension depends less on obesity and more on OSA severity.
“OSA is associated with abnormal BP in youth and, in particular, higher nighttime blood pressures and loss of the normal decline in BP that should occur during sleep,” Dr. Baker-Smith said. “Children with OSA appear to have higher BP than controls during both sleep and wake times, and BP levels increase with increasing severity of OSA.”
Nonetheless, children with OSA are at greater risk for other cardiovascular problems. Left ventricular hypertrophy may be a secondary outcome. “The presence of obstructive sleep apnea in children is associated with an 11-fold increased risk for LVH in children, a relationship not seen in the presence of primary snoring alone,” Dr. Baker-Smith said.
Dr. Baker-Smith had no relevant disclosures. Coauthor Amal Isaiah, MD, is coinventor of an imaging system for sleep apnea and receives royalties from the University of Maryland. The other coauthors have no relevant financial relationships to disclose.
Obstructive sleep apnea is becoming more common in children and adolescents as the prevalence of obesity increases, but it may also be a preventable risk factor for cardiovascular disease, according to a new scientific statement from the American Heart Association.
The statement focuses on the links between OSA and CVD risk factors in children and adolescents, and reviews diagnostic strategies and treatments. The writing committee reported that 1%-6% of children and adolescents have OSA, as do up to 60% of adolescents considered obese.
The statement was created by the AHA’s Atherosclerosis, Hypertension, and Obesity in the Young subcommittee of the Council on Cardiovascular Disease in the Young and was published online in the Journal of the American Heart Association.
Carissa M. Baker-Smith, MD, chair of the writing group chair and director of pediatric preventive cardiology at Nemours Cardiac Center, Alfred I. duPont Hospital for Children, Wilmington, Del., explained the rationale for issuing the statement at this time, noting that the relationship between OSA and CVD in adults is well documented.
“There has been less focus on the importance of recognizing and treating sleep apnea in youth,” she said in an interview. “Thus, we felt that it was vitally important to get the word out to parents and to providers that paying attention to the quality and duration of your child’s sleep is vitally important to a child’s long-term heart health. Risk factors for heart disease, when present in childhood, can persist into adulthood.”
Clarity on polysomnography
For making the diagnosis of OSA in children, the statement provides clarity on the use of polysomnography and the role of the apnea-hypopnea index, which is lower in children with OSA than in adults. “One controversy, or at least as I saw it, was whether or not polysomnography testing is always required to make the diagnosis of OSA and before proceeding with tonsil and adenoid removal among children for whom enlarged tonsils and adenoids are present,” Dr. Baker-Smith said. “Polysomnography testing is not always needed before an ear, nose, and throat surgeon may recommend surgery.”
The statement also noted that history and physical examination may not yield enough reliable information to distinguish OSA from snoring.
In areas where sleep laboratories that work with children aren’t available, alternative tests such as daytime nap polysomnography, nocturnal oximetry, and nocturnal video recording may be used – with a caveat. “These alternative tests have weaker positive and negative predictive values when compared with polysomnography,” the writing committee noted. Home sleep apnea tests aren’t recommended in children. Questionnaires “are useful as screening, but not as diagnostic tools.”
Pediatric patients being evaluated for OSA should also be screened for hypertension and metabolic syndrome, as well as central nervous system and behavioral disorders. Diagnosing OSA in children and adolescents requires “a high index of suspicion,” the committee wrote.
Pediatricians and pediatric cardiologists should exercise that high index of suspicion when receiving referrals for cardiac evaluations for attention deficit hyperactivity disorder medication, Dr. Baker-Smith said. “Take the time to ask about a child’s sleep – snoring, apnea, etc. – especially if the child has obesity, difficulty focusing during the day, and if there is evidence of systemic hypertension or other signs of metabolic syndrome,” she said.
Risk factors for OSA in children
The statement also reviewed risk factors for OSA, among them obesity, particularly among children younger than 6 years. Other risk factors include upper and lower airway disease, hypotonia, parental history of hyperplasia of the adenoids and tonsils, craniofacial malformations, and neuromuscular disorders. However, the committee cited “limited data” to support that children with congenital heart disease may be at greater risk for OSA and sleep-disordered breathing (SDB).
Black children are at significantly greater risk, and socioeconomic factors “may be potential confounders,” the committee stated. Other risk factors include allergic rhinitis and sickle cell disease.
But the statement underscores that “obesity is the main risk factor” for OSA in children and adolescents, and that the presence of increased inflammation may explain this relationship. Steroids may alleviate these symptoms, even in nonobese children, and removal of the adenoids or tonsils is an option to reduce inflammation in children with OSA.
“Obesity is a significant risk factor for sleep disturbances and obstructive sleep apnea, and the severity of sleep apnea may be improved by weight-loss interventions, which then improves metabolic syndrome factors such as insulin sensitivity,” Dr. Baker-Smith said. “We need to increase awareness about how the rising prevalence of obesity may be impacting sleep quality in kids and recognize sleep-disordered breathing as something that could contribute to risks for hypertension and later cardiovascular disease.”
Children in whom OSA is suspected should also undergo screening for metabolic syndrome, and central nervous system and behavioral disorders.
Cardiovascular risks
The statement explores the connection between cardiovascular complications and SDB and OSA in depth.
“Inadequate sleep duration of < 5 hours per night in children and adolescents has been linked to an increased risk of hypertension and is also associated with an increased prevalence of obesity,” the committee wrote.
However, the statement left one question hanging: whether OSA alone or obesity cause higher BP in younger patients with OSA. But the committee concluded that BP levels increase with the severity of OSA, although the effects can vary with age. OSA in children peaks between ages 2 and 8, corresponding to the peak prevalence of hypertrophy of the tonsils and adenoids. Children aged 10-11 with more severe OSA may have BP dysregulation, while older adolescents develop higher sustained BP. Obesity may be a confounder for daytime BP elevations, while nighttime hypertension depends less on obesity and more on OSA severity.
“OSA is associated with abnormal BP in youth and, in particular, higher nighttime blood pressures and loss of the normal decline in BP that should occur during sleep,” Dr. Baker-Smith said. “Children with OSA appear to have higher BP than controls during both sleep and wake times, and BP levels increase with increasing severity of OSA.”
Nonetheless, children with OSA are at greater risk for other cardiovascular problems. Left ventricular hypertrophy may be a secondary outcome. “The presence of obstructive sleep apnea in children is associated with an 11-fold increased risk for LVH in children, a relationship not seen in the presence of primary snoring alone,” Dr. Baker-Smith said.
Dr. Baker-Smith had no relevant disclosures. Coauthor Amal Isaiah, MD, is coinventor of an imaging system for sleep apnea and receives royalties from the University of Maryland. The other coauthors have no relevant financial relationships to disclose.
Obstructive sleep apnea is becoming more common in children and adolescents as the prevalence of obesity increases, but it may also be a preventable risk factor for cardiovascular disease, according to a new scientific statement from the American Heart Association.
The statement focuses on the links between OSA and CVD risk factors in children and adolescents, and reviews diagnostic strategies and treatments. The writing committee reported that 1%-6% of children and adolescents have OSA, as do up to 60% of adolescents considered obese.
The statement was created by the AHA’s Atherosclerosis, Hypertension, and Obesity in the Young subcommittee of the Council on Cardiovascular Disease in the Young and was published online in the Journal of the American Heart Association.
Carissa M. Baker-Smith, MD, chair of the writing group chair and director of pediatric preventive cardiology at Nemours Cardiac Center, Alfred I. duPont Hospital for Children, Wilmington, Del., explained the rationale for issuing the statement at this time, noting that the relationship between OSA and CVD in adults is well documented.
“There has been less focus on the importance of recognizing and treating sleep apnea in youth,” she said in an interview. “Thus, we felt that it was vitally important to get the word out to parents and to providers that paying attention to the quality and duration of your child’s sleep is vitally important to a child’s long-term heart health. Risk factors for heart disease, when present in childhood, can persist into adulthood.”
Clarity on polysomnography
For making the diagnosis of OSA in children, the statement provides clarity on the use of polysomnography and the role of the apnea-hypopnea index, which is lower in children with OSA than in adults. “One controversy, or at least as I saw it, was whether or not polysomnography testing is always required to make the diagnosis of OSA and before proceeding with tonsil and adenoid removal among children for whom enlarged tonsils and adenoids are present,” Dr. Baker-Smith said. “Polysomnography testing is not always needed before an ear, nose, and throat surgeon may recommend surgery.”
The statement also noted that history and physical examination may not yield enough reliable information to distinguish OSA from snoring.
In areas where sleep laboratories that work with children aren’t available, alternative tests such as daytime nap polysomnography, nocturnal oximetry, and nocturnal video recording may be used – with a caveat. “These alternative tests have weaker positive and negative predictive values when compared with polysomnography,” the writing committee noted. Home sleep apnea tests aren’t recommended in children. Questionnaires “are useful as screening, but not as diagnostic tools.”
Pediatric patients being evaluated for OSA should also be screened for hypertension and metabolic syndrome, as well as central nervous system and behavioral disorders. Diagnosing OSA in children and adolescents requires “a high index of suspicion,” the committee wrote.
Pediatricians and pediatric cardiologists should exercise that high index of suspicion when receiving referrals for cardiac evaluations for attention deficit hyperactivity disorder medication, Dr. Baker-Smith said. “Take the time to ask about a child’s sleep – snoring, apnea, etc. – especially if the child has obesity, difficulty focusing during the day, and if there is evidence of systemic hypertension or other signs of metabolic syndrome,” she said.
Risk factors for OSA in children
The statement also reviewed risk factors for OSA, among them obesity, particularly among children younger than 6 years. Other risk factors include upper and lower airway disease, hypotonia, parental history of hyperplasia of the adenoids and tonsils, craniofacial malformations, and neuromuscular disorders. However, the committee cited “limited data” to support that children with congenital heart disease may be at greater risk for OSA and sleep-disordered breathing (SDB).
Black children are at significantly greater risk, and socioeconomic factors “may be potential confounders,” the committee stated. Other risk factors include allergic rhinitis and sickle cell disease.
But the statement underscores that “obesity is the main risk factor” for OSA in children and adolescents, and that the presence of increased inflammation may explain this relationship. Steroids may alleviate these symptoms, even in nonobese children, and removal of the adenoids or tonsils is an option to reduce inflammation in children with OSA.
“Obesity is a significant risk factor for sleep disturbances and obstructive sleep apnea, and the severity of sleep apnea may be improved by weight-loss interventions, which then improves metabolic syndrome factors such as insulin sensitivity,” Dr. Baker-Smith said. “We need to increase awareness about how the rising prevalence of obesity may be impacting sleep quality in kids and recognize sleep-disordered breathing as something that could contribute to risks for hypertension and later cardiovascular disease.”
Children in whom OSA is suspected should also undergo screening for metabolic syndrome, and central nervous system and behavioral disorders.
Cardiovascular risks
The statement explores the connection between cardiovascular complications and SDB and OSA in depth.
“Inadequate sleep duration of < 5 hours per night in children and adolescents has been linked to an increased risk of hypertension and is also associated with an increased prevalence of obesity,” the committee wrote.
However, the statement left one question hanging: whether OSA alone or obesity cause higher BP in younger patients with OSA. But the committee concluded that BP levels increase with the severity of OSA, although the effects can vary with age. OSA in children peaks between ages 2 and 8, corresponding to the peak prevalence of hypertrophy of the tonsils and adenoids. Children aged 10-11 with more severe OSA may have BP dysregulation, while older adolescents develop higher sustained BP. Obesity may be a confounder for daytime BP elevations, while nighttime hypertension depends less on obesity and more on OSA severity.
“OSA is associated with abnormal BP in youth and, in particular, higher nighttime blood pressures and loss of the normal decline in BP that should occur during sleep,” Dr. Baker-Smith said. “Children with OSA appear to have higher BP than controls during both sleep and wake times, and BP levels increase with increasing severity of OSA.”
Nonetheless, children with OSA are at greater risk for other cardiovascular problems. Left ventricular hypertrophy may be a secondary outcome. “The presence of obstructive sleep apnea in children is associated with an 11-fold increased risk for LVH in children, a relationship not seen in the presence of primary snoring alone,” Dr. Baker-Smith said.
Dr. Baker-Smith had no relevant disclosures. Coauthor Amal Isaiah, MD, is coinventor of an imaging system for sleep apnea and receives royalties from the University of Maryland. The other coauthors have no relevant financial relationships to disclose.
FROM JOURNAL OF THE AMERICAN HEART ASSOCIATION
Not so fast food
As long as I can remember, children have been notoriously wasteful when dining in school cafeterias. Even those children who bring their own food often return home in the afternoon with their lunches half eaten. Not surprisingly, the food tossed out is often the healthier portion of the meal. Schools have tried a variety of strategies to curb this wastage, including using volunteer student monitors to police and encourage ecologically based recycling.

The authors of a recent study published on JAMA Network Open observed that when elementary and middle-school students were allowed a 20-minute seated lunch period they consumed more food and there was significantly less waste of fruits and vegetable compared with when the students’ lunch period was limited to 10 minutes. Interestingly, there was no difference in the beverage and entrée consumption when the lunch period was doubled.
The authors postulate that younger children may not have acquired the dexterity to feed themselves optimally in the shorter lunch period. I’m not sure I buy that argument. It may be simply that the children ate and drank their favorites first and needed a bit more time to allow their little guts to move things along. But, regardless of the explanation, the investigators’ observations deserve further study.
When I was in high school our lunch period was a full hour, which allowed me to make the half mile walk to home and back to eat a home-prepared meal. The noon hour was when school clubs and committees met and there was a full schedule of diversions to fill out the hour. I don’t recall the seated portion of the lunch period having any time restriction.
By the time my own children were in middle school, lunch periods lasted no longer than 20 minutes. I was not surprised to learn from this recent study that in some schools the seated lunch period has been shortened to 10 minutes. In some cases the truncated lunch periods are a response to space and time limitations. I fear that occasionally, educators and administrators have found it so difficult to keep young children who are accustomed to watching television while they eat engaged that the periods have been shortened to minimize the chaos.
Here in Maine, the governor has just announced plans to offer free breakfast and lunch to every student in response to a federal initiative. If we intend to make nutrition a cornerstone of the educational process this study from the University of Illinois at Urbana-Champaign suggests that we must do more than simply provide the food at no cost. We must somehow carve out more time in the day for the children to eat a healthy diet.
But, where is this time going to come from? Many school systems have already cannibalized physical education to the point that most children are not getting a healthy amount of exercise. It is unfortunate that we have come to expect public school systems to solve all of our societal ills and compensate for less-than-healthy home environments. But that is the reality. If we think nutrition and physical activity are important components of our children’s educations then we must make the time necessary to provide them.
Will this mean longer school days? And will those longer days cost money? You bet they will, but that may be the price we have to pay for healthier, better educated children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
As long as I can remember, children have been notoriously wasteful when dining in school cafeterias. Even those children who bring their own food often return home in the afternoon with their lunches half eaten. Not surprisingly, the food tossed out is often the healthier portion of the meal. Schools have tried a variety of strategies to curb this wastage, including using volunteer student monitors to police and encourage ecologically based recycling.
The authors of a recent study published on JAMA Network Open observed that when elementary and middle-school students were allowed a 20-minute seated lunch period they consumed more food and there was significantly less waste of fruits and vegetable compared with when the students’ lunch period was limited to 10 minutes. Interestingly, there was no difference in the beverage and entrée consumption when the lunch period was doubled.
The authors postulate that younger children may not have acquired the dexterity to feed themselves optimally in the shorter lunch period. I’m not sure I buy that argument. It may be simply that the children ate and drank their favorites first and needed a bit more time to allow their little guts to move things along. But, regardless of the explanation, the investigators’ observations deserve further study.
When I was in high school our lunch period was a full hour, which allowed me to make the half mile walk to home and back to eat a home-prepared meal. The noon hour was when school clubs and committees met and there was a full schedule of diversions to fill out the hour. I don’t recall the seated portion of the lunch period having any time restriction.
By the time my own children were in middle school, lunch periods lasted no longer than 20 minutes. I was not surprised to learn from this recent study that in some schools the seated lunch period has been shortened to 10 minutes. In some cases the truncated lunch periods are a response to space and time limitations. I fear that occasionally, educators and administrators have found it so difficult to keep young children who are accustomed to watching television while they eat engaged that the periods have been shortened to minimize the chaos.
Here in Maine, the governor has just announced plans to offer free breakfast and lunch to every student in response to a federal initiative. If we intend to make nutrition a cornerstone of the educational process this study from the University of Illinois at Urbana-Champaign suggests that we must do more than simply provide the food at no cost. We must somehow carve out more time in the day for the children to eat a healthy diet.
But, where is this time going to come from? Many school systems have already cannibalized physical education to the point that most children are not getting a healthy amount of exercise. It is unfortunate that we have come to expect public school systems to solve all of our societal ills and compensate for less-than-healthy home environments. But that is the reality. If we think nutrition and physical activity are important components of our children’s educations then we must make the time necessary to provide them.
Will this mean longer school days? And will those longer days cost money? You bet they will, but that may be the price we have to pay for healthier, better educated children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
As long as I can remember, children have been notoriously wasteful when dining in school cafeterias. Even those children who bring their own food often return home in the afternoon with their lunches half eaten. Not surprisingly, the food tossed out is often the healthier portion of the meal. Schools have tried a variety of strategies to curb this wastage, including using volunteer student monitors to police and encourage ecologically based recycling.
The authors of a recent study published on JAMA Network Open observed that when elementary and middle-school students were allowed a 20-minute seated lunch period they consumed more food and there was significantly less waste of fruits and vegetable compared with when the students’ lunch period was limited to 10 minutes. Interestingly, there was no difference in the beverage and entrée consumption when the lunch period was doubled.
The authors postulate that younger children may not have acquired the dexterity to feed themselves optimally in the shorter lunch period. I’m not sure I buy that argument. It may be simply that the children ate and drank their favorites first and needed a bit more time to allow their little guts to move things along. But, regardless of the explanation, the investigators’ observations deserve further study.
When I was in high school our lunch period was a full hour, which allowed me to make the half mile walk to home and back to eat a home-prepared meal. The noon hour was when school clubs and committees met and there was a full schedule of diversions to fill out the hour. I don’t recall the seated portion of the lunch period having any time restriction.
By the time my own children were in middle school, lunch periods lasted no longer than 20 minutes. I was not surprised to learn from this recent study that in some schools the seated lunch period has been shortened to 10 minutes. In some cases the truncated lunch periods are a response to space and time limitations. I fear that occasionally, educators and administrators have found it so difficult to keep young children who are accustomed to watching television while they eat engaged that the periods have been shortened to minimize the chaos.
Here in Maine, the governor has just announced plans to offer free breakfast and lunch to every student in response to a federal initiative. If we intend to make nutrition a cornerstone of the educational process this study from the University of Illinois at Urbana-Champaign suggests that we must do more than simply provide the food at no cost. We must somehow carve out more time in the day for the children to eat a healthy diet.
But, where is this time going to come from? Many school systems have already cannibalized physical education to the point that most children are not getting a healthy amount of exercise. It is unfortunate that we have come to expect public school systems to solve all of our societal ills and compensate for less-than-healthy home environments. But that is the reality. If we think nutrition and physical activity are important components of our children’s educations then we must make the time necessary to provide them.
Will this mean longer school days? And will those longer days cost money? You bet they will, but that may be the price we have to pay for healthier, better educated children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Children and COVID: New cases soar to near-record level
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
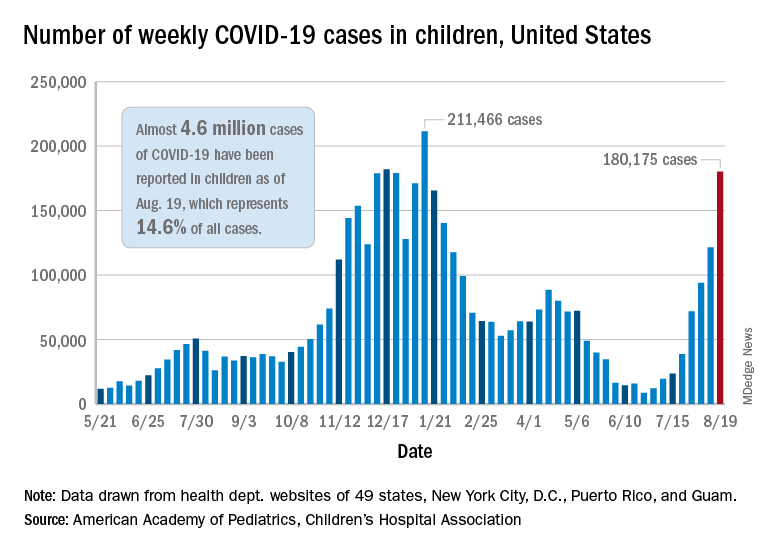
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.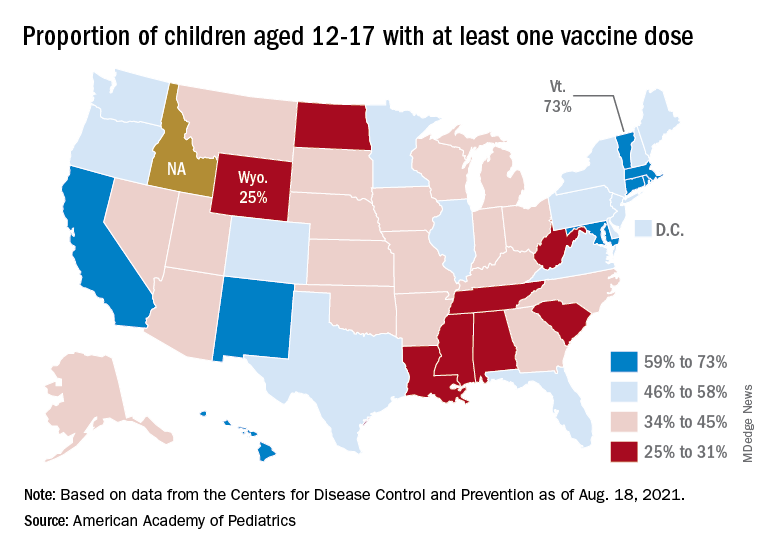
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Prevalence of youth-onset diabetes climbing, type 2 disease more so in racial/ethnic minorities
The prevalence of youth-onset diabetes in the United States rose significantly from 2001 to 2017, with rates of type 2 diabetes climbing disproportionately among racial/ethnic minorities, according to investigators.
In individuals aged 19 years or younger, prevalence rates of type 1 and type 2 diabetes increased 45.1% and 95.3%, respectively, reported lead author Jean M. Lawrence, ScD, MPH, MSSA, program director of the division of diabetes, endocrinology, and metabolic diseases at the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Md., and colleagues.
“Elucidating differences in diabetes prevalence trends by diabetes type and demographic characteristics is essential to describe the burden of disease and to estimate current and future resource needs,” Dr. Lawrence and colleagues wrote in JAMA.
The retrospective analysis was a part of the ongoing SEARCH study, which includes data from individuals in six areas across the United States: Colorado, California, Ohio, South Carolina, Washington state, and Arizona/New Mexico (Indian Health Services). In the present report, three prevalence years were evaluated: 2001, 2009, and 2017. For each year, approximately 3.5 million youths were included. Findings were reported in terms of diabetes type, race/ethnicity, age at diagnosis, and sex.
Absolute prevalence of type 1 diabetes per 1,000 youths increased from 1.48 in 2001, to 1.93 in 2009, and finally 2.15 in 2017. Across the 16-year period, this represents an absolute increase of 0.67 (95% confidence interval, 0.64-0.70), and a relative increase of 45.1% (95% CI, 40.0%-50.4%). In absolute terms, prevalence increased most among non-Hispanic White (0.93 per 1,000) and non-Hispanic Black (0.89 per 1,000) youths.
While type 2 diabetes was comparatively less common than type 1 diabetes, absolute prevalence per 1,000 youths increased to a greater degree, rising from 0.34 in 2001 to 0.46 in 2009 and to 0.67 in 2017. This amounts to relative increase across the period of 95.3% (95% CI, 77.0%-115.4%). Absolute increases were disproportionate among racial/ethnic minorities, particularly Black and Hispanic youths, who had absolute increases per 1,000 youths of 0.85 (95% CI, 0.74-0.97) and 0.57 (95% CI, 0.51-0.64), respectively, compared with 0.05 (95% CI, 0.03-0.07) for White youths.
“Increases [among Black and Hispanic youths] were not linear,” the investigators noted. “Hispanic youths had a significantly greater increase in the first interval compared with the second interval, while Black youths had no significant increase in the first interval and a significant increase in the second interval.”
Dr. Lawrence and colleagues offered several possible factors driving these trends in type 2 diabetes.
“Changes in anthropometric risk factors appear to play a significant role,” they wrote, noting that “Black and Mexican American teenagers experienced the greatest increase in prevalence of obesity/severe obesity from 1999 to 2018, which may contribute to race and ethnicity differences. Other contributing factors may include increases in exposure to maternal obesity and diabetes (gestational and type 2 diabetes) and exposure to environmental chemicals.”

According to Megan Kelsey, MD, associate professor of pediatric endocrinology, director of lifestyle medicine endocrinology, and medical director of the bariatric surgery center at Children’s Hospital Colorado, Aurora, the increased rates of type 2 diabetes reported by the study are alarming, yet they pale in comparison with what’s been happening since the pandemic began.
“Individual institutions have reported anywhere between a 50% – which is basically what we’re seeing at our hospital – to a 300% increase in new diagnoses [of type 2 diabetes] in a single-year time period,” Dr. Kelsey said in an interview. “So what is reported [in the present study] doesn’t even get at what’s been going on over the past year and a half.”
Dr. Kelsey offered some speculative drivers of this recent surge in cases, including stress, weight gain caused by sedentary behavior and more access to food, and the possibility that SARS-CoV-2 may infect pancreatic islet beta cells, thereby interfering with insulin production.
Type 2 diabetes is particularly concerning among young people, Dr. Kelsey noted, as it is more challenging to manage than adult-onset disease.
Young patients “also develop complications much sooner than you’d expect,” she added. “So we really need to understand why these rates are increasing, how we can identify kids at risk, and how we can better prevent it, so we aren’t stuck with a disease that’s really difficult to treat.”
To this end, the NIH recently opened applications for investigators to participate in a prospective longitudinal study of youth-onset type 2 diabetes. Young people at risk of diabetes will be followed through puberty, a period of increased risk, according to Dr. Kelsey.
“The goal will be to take kids who don’t yet have [type 2] diabetes, but are at risk, and try to better understand, as some of them progress to developing diabetes, what is going on,” Dr. Kelsey said. “What are other factors that we can use to better predict who’s going to develop diabetes? And can we use the information from this [upcoming] study to understand how to better prevent it? Because nothing that has been tried so far has worked.”
The study was supported by the Centers for Disease Control and Prevention, NIDDK, and others. The investigators and Dr. Kelsey reported no conflicts of interest.
The prevalence of youth-onset diabetes in the United States rose significantly from 2001 to 2017, with rates of type 2 diabetes climbing disproportionately among racial/ethnic minorities, according to investigators.
In individuals aged 19 years or younger, prevalence rates of type 1 and type 2 diabetes increased 45.1% and 95.3%, respectively, reported lead author Jean M. Lawrence, ScD, MPH, MSSA, program director of the division of diabetes, endocrinology, and metabolic diseases at the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Md., and colleagues.
“Elucidating differences in diabetes prevalence trends by diabetes type and demographic characteristics is essential to describe the burden of disease and to estimate current and future resource needs,” Dr. Lawrence and colleagues wrote in JAMA.
The retrospective analysis was a part of the ongoing SEARCH study, which includes data from individuals in six areas across the United States: Colorado, California, Ohio, South Carolina, Washington state, and Arizona/New Mexico (Indian Health Services). In the present report, three prevalence years were evaluated: 2001, 2009, and 2017. For each year, approximately 3.5 million youths were included. Findings were reported in terms of diabetes type, race/ethnicity, age at diagnosis, and sex.
Absolute prevalence of type 1 diabetes per 1,000 youths increased from 1.48 in 2001, to 1.93 in 2009, and finally 2.15 in 2017. Across the 16-year period, this represents an absolute increase of 0.67 (95% confidence interval, 0.64-0.70), and a relative increase of 45.1% (95% CI, 40.0%-50.4%). In absolute terms, prevalence increased most among non-Hispanic White (0.93 per 1,000) and non-Hispanic Black (0.89 per 1,000) youths.
While type 2 diabetes was comparatively less common than type 1 diabetes, absolute prevalence per 1,000 youths increased to a greater degree, rising from 0.34 in 2001 to 0.46 in 2009 and to 0.67 in 2017. This amounts to relative increase across the period of 95.3% (95% CI, 77.0%-115.4%). Absolute increases were disproportionate among racial/ethnic minorities, particularly Black and Hispanic youths, who had absolute increases per 1,000 youths of 0.85 (95% CI, 0.74-0.97) and 0.57 (95% CI, 0.51-0.64), respectively, compared with 0.05 (95% CI, 0.03-0.07) for White youths.
“Increases [among Black and Hispanic youths] were not linear,” the investigators noted. “Hispanic youths had a significantly greater increase in the first interval compared with the second interval, while Black youths had no significant increase in the first interval and a significant increase in the second interval.”
Dr. Lawrence and colleagues offered several possible factors driving these trends in type 2 diabetes.
“Changes in anthropometric risk factors appear to play a significant role,” they wrote, noting that “Black and Mexican American teenagers experienced the greatest increase in prevalence of obesity/severe obesity from 1999 to 2018, which may contribute to race and ethnicity differences. Other contributing factors may include increases in exposure to maternal obesity and diabetes (gestational and type 2 diabetes) and exposure to environmental chemicals.”
According to Megan Kelsey, MD, associate professor of pediatric endocrinology, director of lifestyle medicine endocrinology, and medical director of the bariatric surgery center at Children’s Hospital Colorado, Aurora, the increased rates of type 2 diabetes reported by the study are alarming, yet they pale in comparison with what’s been happening since the pandemic began.
“Individual institutions have reported anywhere between a 50% – which is basically what we’re seeing at our hospital – to a 300% increase in new diagnoses [of type 2 diabetes] in a single-year time period,” Dr. Kelsey said in an interview. “So what is reported [in the present study] doesn’t even get at what’s been going on over the past year and a half.”
Dr. Kelsey offered some speculative drivers of this recent surge in cases, including stress, weight gain caused by sedentary behavior and more access to food, and the possibility that SARS-CoV-2 may infect pancreatic islet beta cells, thereby interfering with insulin production.
Type 2 diabetes is particularly concerning among young people, Dr. Kelsey noted, as it is more challenging to manage than adult-onset disease.
Young patients “also develop complications much sooner than you’d expect,” she added. “So we really need to understand why these rates are increasing, how we can identify kids at risk, and how we can better prevent it, so we aren’t stuck with a disease that’s really difficult to treat.”
To this end, the NIH recently opened applications for investigators to participate in a prospective longitudinal study of youth-onset type 2 diabetes. Young people at risk of diabetes will be followed through puberty, a period of increased risk, according to Dr. Kelsey.
“The goal will be to take kids who don’t yet have [type 2] diabetes, but are at risk, and try to better understand, as some of them progress to developing diabetes, what is going on,” Dr. Kelsey said. “What are other factors that we can use to better predict who’s going to develop diabetes? And can we use the information from this [upcoming] study to understand how to better prevent it? Because nothing that has been tried so far has worked.”
The study was supported by the Centers for Disease Control and Prevention, NIDDK, and others. The investigators and Dr. Kelsey reported no conflicts of interest.
The prevalence of youth-onset diabetes in the United States rose significantly from 2001 to 2017, with rates of type 2 diabetes climbing disproportionately among racial/ethnic minorities, according to investigators.
In individuals aged 19 years or younger, prevalence rates of type 1 and type 2 diabetes increased 45.1% and 95.3%, respectively, reported lead author Jean M. Lawrence, ScD, MPH, MSSA, program director of the division of diabetes, endocrinology, and metabolic diseases at the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Md., and colleagues.
“Elucidating differences in diabetes prevalence trends by diabetes type and demographic characteristics is essential to describe the burden of disease and to estimate current and future resource needs,” Dr. Lawrence and colleagues wrote in JAMA.
The retrospective analysis was a part of the ongoing SEARCH study, which includes data from individuals in six areas across the United States: Colorado, California, Ohio, South Carolina, Washington state, and Arizona/New Mexico (Indian Health Services). In the present report, three prevalence years were evaluated: 2001, 2009, and 2017. For each year, approximately 3.5 million youths were included. Findings were reported in terms of diabetes type, race/ethnicity, age at diagnosis, and sex.
Absolute prevalence of type 1 diabetes per 1,000 youths increased from 1.48 in 2001, to 1.93 in 2009, and finally 2.15 in 2017. Across the 16-year period, this represents an absolute increase of 0.67 (95% confidence interval, 0.64-0.70), and a relative increase of 45.1% (95% CI, 40.0%-50.4%). In absolute terms, prevalence increased most among non-Hispanic White (0.93 per 1,000) and non-Hispanic Black (0.89 per 1,000) youths.
While type 2 diabetes was comparatively less common than type 1 diabetes, absolute prevalence per 1,000 youths increased to a greater degree, rising from 0.34 in 2001 to 0.46 in 2009 and to 0.67 in 2017. This amounts to relative increase across the period of 95.3% (95% CI, 77.0%-115.4%). Absolute increases were disproportionate among racial/ethnic minorities, particularly Black and Hispanic youths, who had absolute increases per 1,000 youths of 0.85 (95% CI, 0.74-0.97) and 0.57 (95% CI, 0.51-0.64), respectively, compared with 0.05 (95% CI, 0.03-0.07) for White youths.
“Increases [among Black and Hispanic youths] were not linear,” the investigators noted. “Hispanic youths had a significantly greater increase in the first interval compared with the second interval, while Black youths had no significant increase in the first interval and a significant increase in the second interval.”
Dr. Lawrence and colleagues offered several possible factors driving these trends in type 2 diabetes.
“Changes in anthropometric risk factors appear to play a significant role,” they wrote, noting that “Black and Mexican American teenagers experienced the greatest increase in prevalence of obesity/severe obesity from 1999 to 2018, which may contribute to race and ethnicity differences. Other contributing factors may include increases in exposure to maternal obesity and diabetes (gestational and type 2 diabetes) and exposure to environmental chemicals.”
According to Megan Kelsey, MD, associate professor of pediatric endocrinology, director of lifestyle medicine endocrinology, and medical director of the bariatric surgery center at Children’s Hospital Colorado, Aurora, the increased rates of type 2 diabetes reported by the study are alarming, yet they pale in comparison with what’s been happening since the pandemic began.
“Individual institutions have reported anywhere between a 50% – which is basically what we’re seeing at our hospital – to a 300% increase in new diagnoses [of type 2 diabetes] in a single-year time period,” Dr. Kelsey said in an interview. “So what is reported [in the present study] doesn’t even get at what’s been going on over the past year and a half.”
Dr. Kelsey offered some speculative drivers of this recent surge in cases, including stress, weight gain caused by sedentary behavior and more access to food, and the possibility that SARS-CoV-2 may infect pancreatic islet beta cells, thereby interfering with insulin production.
Type 2 diabetes is particularly concerning among young people, Dr. Kelsey noted, as it is more challenging to manage than adult-onset disease.
Young patients “also develop complications much sooner than you’d expect,” she added. “So we really need to understand why these rates are increasing, how we can identify kids at risk, and how we can better prevent it, so we aren’t stuck with a disease that’s really difficult to treat.”
To this end, the NIH recently opened applications for investigators to participate in a prospective longitudinal study of youth-onset type 2 diabetes. Young people at risk of diabetes will be followed through puberty, a period of increased risk, according to Dr. Kelsey.
“The goal will be to take kids who don’t yet have [type 2] diabetes, but are at risk, and try to better understand, as some of them progress to developing diabetes, what is going on,” Dr. Kelsey said. “What are other factors that we can use to better predict who’s going to develop diabetes? And can we use the information from this [upcoming] study to understand how to better prevent it? Because nothing that has been tried so far has worked.”
The study was supported by the Centers for Disease Control and Prevention, NIDDK, and others. The investigators and Dr. Kelsey reported no conflicts of interest.
FROM JAMA
Prevalence of high-risk HPV types dwindled since vaccine approval
Young women who received the quadrivalent human papillomavirus (HPV) vaccine had fewer and fewer infections with high-risk HPV strains covered by the vaccine year after year, but the incidence of high-risk strains that were not covered by the vaccine increased over the same 12-year period, researchers report in a study published August 23 in JAMA Open Network.
“One of the unique contributions that this study provides is the evaluation of a real-world example of the HPV infection rates following immunization in a population of adolescent girls and young adult women at a single health center in a large U.S. city, reflecting strong evidence of vaccine effectiveness,” write Nicolas F. Schlecht, PhD, a professor of oncology at Roswell Park Comprehensive Cancer Center, Buffalo, and his colleagues. “Previous surveillance studies from the U.S. have involved older women and populations with relatively low vaccine coverage.”
In addition to supporting the value of continuing to vaccinate teens against HPV, the findings underscore the importance of continuing to screen women for cervical cancer, Dr. Schlecht said in an interview.
“HPV has not and is not going away,” he said. “We need to keep on our toes with screening and other measures to continue to prevent the development of cervix cancer,” including monitoring different high-risk HPV types and keeping a close eye on cervical precancer rates, particularly CIN3 and cervix cancer, he said. “The vaccines are definitely a good thing. Just getting rid of HPV16 is an amazing accomplishment.”
Kevin Ault, MD, a professor of ob/gyn and academic specialist director of clinical and translational research at the University of Kansas, Kansas City, told this news organization that other studies have had similar findings, but this one is larger with longer follow-up.
“The take-home message is that vaccines work, and this is especially true for the HPV vaccine,” said Dr. Ault, who was not involved in the research. “The vaccine prevents HPV infections and the consequences of these infections, such as cervical cancer. The results are consistent with other studies in different settings, so they are likely generalizable.”
The researchers collected data from October 2007, shortly after the vaccine was approved, through September 2019 on sexually active adolescent and young women aged 13 to 21 years who had received the HPV vaccine and had agreed to follow-up assessments every 6 months until they turned 26. Each follow-up included the collecting of samples of cervical and anal cells for polymerase chain reaction testing for the presence of HPV types.
More than half of the 1,453 participants were Hispanic (58.8%), and half were Black (50.4%), including 15% Hispanic and Black patients. The average age of the participants was 18 years. They were tracked for a median 2.4 years. Nearly half the participants (48%) received the HPV vaccine prior to sexual debut.
For the longitudinal study, the researchers adjusted for participants’ age, the year they received the vaccine, and the years since they were vaccinated. They also tracked breakthrough infections for the four types of HPV covered by the vaccine in participants who received the vaccine before sexual debut.
“We evaluated whether infection rates for HPV have changed since the administration of the vaccine by assessing longitudinally the probability of HPV detection over time among vaccinated participants while adjusting for changes in cohort characteristics over time,” the researchers write. In their statistical analysis, they made adjustments for the number of vaccine doses participants received before their first study visit, age at sexual debut, age at first vaccine dose, number of sexual partners in the preceding 6 months, consistency of condom use during sex, history of a positive chlamydia test, and, for anal HPV analyses, whether the participants had had anal sex in the previous 6 months.
The average age at first intercourse remained steady at 15 years throughout the study, but the average age of vaccination dropped from 18 years in 2008 to 12 years in 2019 (P < .001). More than half the participants (64%) had had at least three lifetime sexual partners at baseline.
After adjustment for age, the researchers found that the incidence of the four HPV types covered by the vaccine – HPV-6, HPV-11, HPV-16, and HPV-18 – dropped more each year, shifting from 9.1% from 2008-2010 to 4.7% from 2017-2019. The effect was even greater among those vaccinated prior to sexual debut; for those patients, the incidence of the four vaccine types dropped from 8.8% to 1.7% over the course of the study. Declines over time also occurred for anal types HPV-31 (adjusted odds ratio [aOR] = 0.76) and HPV-45 (aOR = 0.77). Those vaccinated prior to any sexual intercourse had 19% lower odds of infection per year with a vaccine-covered HPV type.
“We were really excited to see that the types targeted by the vaccines were considerably lower over time in our population,” Dr. Schlecht told this news organization. “This is an important observation, since most of these types are the most worrisome for cervical cancer.”
They were surprised, however, to see overall HPV prevalence increase over time, particularly with the high-risk HPV types that were not covered by the quadrivalent vaccine.
Prevalence of cervical high-risk types not in the vaccine increased from 25.1% from 2008-2010 to 30.5% from 2017-2019. Odds of detection of high-risk HPV types not covered by the vaccine increased 8% each year, particularly for HPV-56 and HPV-68; anal HPV types increased 11% each year. Neither age nor recent number of sexual partners affected the findings.
“The underlying mechanisms for the observed increased detection of specific non-vaccine HPV types over time are not yet clear.”
“We hope this doesn’t translate into some increase in cervical neoplasia that is unanticipated,” Dr. Schlecht said. He noted that the attributable risks for cancer associated with nonvaccine high-risk HPV types remain low. “Theoretical concerns are one thing; actual data is what drives the show,” he said.
The research was funded by the National Institutes of Health and the Icahn School of Medicine at Mount Sinai, New York. Dr. Schlecht has served on advisory boards for Merck, GlaxoSmithKline (GSK), and PDS Biotechnology. One author previously served on a GSK advisory board, and another worked with Merck on an early vaccine trial. Dr. Ault has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Young women who received the quadrivalent human papillomavirus (HPV) vaccine had fewer and fewer infections with high-risk HPV strains covered by the vaccine year after year, but the incidence of high-risk strains that were not covered by the vaccine increased over the same 12-year period, researchers report in a study published August 23 in JAMA Open Network.
“One of the unique contributions that this study provides is the evaluation of a real-world example of the HPV infection rates following immunization in a population of adolescent girls and young adult women at a single health center in a large U.S. city, reflecting strong evidence of vaccine effectiveness,” write Nicolas F. Schlecht, PhD, a professor of oncology at Roswell Park Comprehensive Cancer Center, Buffalo, and his colleagues. “Previous surveillance studies from the U.S. have involved older women and populations with relatively low vaccine coverage.”
In addition to supporting the value of continuing to vaccinate teens against HPV, the findings underscore the importance of continuing to screen women for cervical cancer, Dr. Schlecht said in an interview.
“HPV has not and is not going away,” he said. “We need to keep on our toes with screening and other measures to continue to prevent the development of cervix cancer,” including monitoring different high-risk HPV types and keeping a close eye on cervical precancer rates, particularly CIN3 and cervix cancer, he said. “The vaccines are definitely a good thing. Just getting rid of HPV16 is an amazing accomplishment.”
Kevin Ault, MD, a professor of ob/gyn and academic specialist director of clinical and translational research at the University of Kansas, Kansas City, told this news organization that other studies have had similar findings, but this one is larger with longer follow-up.
“The take-home message is that vaccines work, and this is especially true for the HPV vaccine,” said Dr. Ault, who was not involved in the research. “The vaccine prevents HPV infections and the consequences of these infections, such as cervical cancer. The results are consistent with other studies in different settings, so they are likely generalizable.”
The researchers collected data from October 2007, shortly after the vaccine was approved, through September 2019 on sexually active adolescent and young women aged 13 to 21 years who had received the HPV vaccine and had agreed to follow-up assessments every 6 months until they turned 26. Each follow-up included the collecting of samples of cervical and anal cells for polymerase chain reaction testing for the presence of HPV types.
More than half of the 1,453 participants were Hispanic (58.8%), and half were Black (50.4%), including 15% Hispanic and Black patients. The average age of the participants was 18 years. They were tracked for a median 2.4 years. Nearly half the participants (48%) received the HPV vaccine prior to sexual debut.
For the longitudinal study, the researchers adjusted for participants’ age, the year they received the vaccine, and the years since they were vaccinated. They also tracked breakthrough infections for the four types of HPV covered by the vaccine in participants who received the vaccine before sexual debut.
“We evaluated whether infection rates for HPV have changed since the administration of the vaccine by assessing longitudinally the probability of HPV detection over time among vaccinated participants while adjusting for changes in cohort characteristics over time,” the researchers write. In their statistical analysis, they made adjustments for the number of vaccine doses participants received before their first study visit, age at sexual debut, age at first vaccine dose, number of sexual partners in the preceding 6 months, consistency of condom use during sex, history of a positive chlamydia test, and, for anal HPV analyses, whether the participants had had anal sex in the previous 6 months.
The average age at first intercourse remained steady at 15 years throughout the study, but the average age of vaccination dropped from 18 years in 2008 to 12 years in 2019 (P < .001). More than half the participants (64%) had had at least three lifetime sexual partners at baseline.
After adjustment for age, the researchers found that the incidence of the four HPV types covered by the vaccine – HPV-6, HPV-11, HPV-16, and HPV-18 – dropped more each year, shifting from 9.1% from 2008-2010 to 4.7% from 2017-2019. The effect was even greater among those vaccinated prior to sexual debut; for those patients, the incidence of the four vaccine types dropped from 8.8% to 1.7% over the course of the study. Declines over time also occurred for anal types HPV-31 (adjusted odds ratio [aOR] = 0.76) and HPV-45 (aOR = 0.77). Those vaccinated prior to any sexual intercourse had 19% lower odds of infection per year with a vaccine-covered HPV type.
“We were really excited to see that the types targeted by the vaccines were considerably lower over time in our population,” Dr. Schlecht told this news organization. “This is an important observation, since most of these types are the most worrisome for cervical cancer.”
They were surprised, however, to see overall HPV prevalence increase over time, particularly with the high-risk HPV types that were not covered by the quadrivalent vaccine.
Prevalence of cervical high-risk types not in the vaccine increased from 25.1% from 2008-2010 to 30.5% from 2017-2019. Odds of detection of high-risk HPV types not covered by the vaccine increased 8% each year, particularly for HPV-56 and HPV-68; anal HPV types increased 11% each year. Neither age nor recent number of sexual partners affected the findings.
“The underlying mechanisms for the observed increased detection of specific non-vaccine HPV types over time are not yet clear.”
“We hope this doesn’t translate into some increase in cervical neoplasia that is unanticipated,” Dr. Schlecht said. He noted that the attributable risks for cancer associated with nonvaccine high-risk HPV types remain low. “Theoretical concerns are one thing; actual data is what drives the show,” he said.
The research was funded by the National Institutes of Health and the Icahn School of Medicine at Mount Sinai, New York. Dr. Schlecht has served on advisory boards for Merck, GlaxoSmithKline (GSK), and PDS Biotechnology. One author previously served on a GSK advisory board, and another worked with Merck on an early vaccine trial. Dr. Ault has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Young women who received the quadrivalent human papillomavirus (HPV) vaccine had fewer and fewer infections with high-risk HPV strains covered by the vaccine year after year, but the incidence of high-risk strains that were not covered by the vaccine increased over the same 12-year period, researchers report in a study published August 23 in JAMA Open Network.
“One of the unique contributions that this study provides is the evaluation of a real-world example of the HPV infection rates following immunization in a population of adolescent girls and young adult women at a single health center in a large U.S. city, reflecting strong evidence of vaccine effectiveness,” write Nicolas F. Schlecht, PhD, a professor of oncology at Roswell Park Comprehensive Cancer Center, Buffalo, and his colleagues. “Previous surveillance studies from the U.S. have involved older women and populations with relatively low vaccine coverage.”
In addition to supporting the value of continuing to vaccinate teens against HPV, the findings underscore the importance of continuing to screen women for cervical cancer, Dr. Schlecht said in an interview.
“HPV has not and is not going away,” he said. “We need to keep on our toes with screening and other measures to continue to prevent the development of cervix cancer,” including monitoring different high-risk HPV types and keeping a close eye on cervical precancer rates, particularly CIN3 and cervix cancer, he said. “The vaccines are definitely a good thing. Just getting rid of HPV16 is an amazing accomplishment.”
Kevin Ault, MD, a professor of ob/gyn and academic specialist director of clinical and translational research at the University of Kansas, Kansas City, told this news organization that other studies have had similar findings, but this one is larger with longer follow-up.
“The take-home message is that vaccines work, and this is especially true for the HPV vaccine,” said Dr. Ault, who was not involved in the research. “The vaccine prevents HPV infections and the consequences of these infections, such as cervical cancer. The results are consistent with other studies in different settings, so they are likely generalizable.”
The researchers collected data from October 2007, shortly after the vaccine was approved, through September 2019 on sexually active adolescent and young women aged 13 to 21 years who had received the HPV vaccine and had agreed to follow-up assessments every 6 months until they turned 26. Each follow-up included the collecting of samples of cervical and anal cells for polymerase chain reaction testing for the presence of HPV types.
More than half of the 1,453 participants were Hispanic (58.8%), and half were Black (50.4%), including 15% Hispanic and Black patients. The average age of the participants was 18 years. They were tracked for a median 2.4 years. Nearly half the participants (48%) received the HPV vaccine prior to sexual debut.
For the longitudinal study, the researchers adjusted for participants’ age, the year they received the vaccine, and the years since they were vaccinated. They also tracked breakthrough infections for the four types of HPV covered by the vaccine in participants who received the vaccine before sexual debut.
“We evaluated whether infection rates for HPV have changed since the administration of the vaccine by assessing longitudinally the probability of HPV detection over time among vaccinated participants while adjusting for changes in cohort characteristics over time,” the researchers write. In their statistical analysis, they made adjustments for the number of vaccine doses participants received before their first study visit, age at sexual debut, age at first vaccine dose, number of sexual partners in the preceding 6 months, consistency of condom use during sex, history of a positive chlamydia test, and, for anal HPV analyses, whether the participants had had anal sex in the previous 6 months.
The average age at first intercourse remained steady at 15 years throughout the study, but the average age of vaccination dropped from 18 years in 2008 to 12 years in 2019 (P < .001). More than half the participants (64%) had had at least three lifetime sexual partners at baseline.
After adjustment for age, the researchers found that the incidence of the four HPV types covered by the vaccine – HPV-6, HPV-11, HPV-16, and HPV-18 – dropped more each year, shifting from 9.1% from 2008-2010 to 4.7% from 2017-2019. The effect was even greater among those vaccinated prior to sexual debut; for those patients, the incidence of the four vaccine types dropped from 8.8% to 1.7% over the course of the study. Declines over time also occurred for anal types HPV-31 (adjusted odds ratio [aOR] = 0.76) and HPV-45 (aOR = 0.77). Those vaccinated prior to any sexual intercourse had 19% lower odds of infection per year with a vaccine-covered HPV type.
“We were really excited to see that the types targeted by the vaccines were considerably lower over time in our population,” Dr. Schlecht told this news organization. “This is an important observation, since most of these types are the most worrisome for cervical cancer.”
They were surprised, however, to see overall HPV prevalence increase over time, particularly with the high-risk HPV types that were not covered by the quadrivalent vaccine.
Prevalence of cervical high-risk types not in the vaccine increased from 25.1% from 2008-2010 to 30.5% from 2017-2019. Odds of detection of high-risk HPV types not covered by the vaccine increased 8% each year, particularly for HPV-56 and HPV-68; anal HPV types increased 11% each year. Neither age nor recent number of sexual partners affected the findings.
“The underlying mechanisms for the observed increased detection of specific non-vaccine HPV types over time are not yet clear.”
“We hope this doesn’t translate into some increase in cervical neoplasia that is unanticipated,” Dr. Schlecht said. He noted that the attributable risks for cancer associated with nonvaccine high-risk HPV types remain low. “Theoretical concerns are one thing; actual data is what drives the show,” he said.
The research was funded by the National Institutes of Health and the Icahn School of Medicine at Mount Sinai, New York. Dr. Schlecht has served on advisory boards for Merck, GlaxoSmithKline (GSK), and PDS Biotechnology. One author previously served on a GSK advisory board, and another worked with Merck on an early vaccine trial. Dr. Ault has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nearly 1 in 5 parents put off care for their kids in pandemic
Many families delayed much-needed health care for their children out of fears that they may be exposed to SARS-CoV-2, according to data from the Urban Institute April 2021 Health Reform Monitoring Survey.
Data from 9,067 adults aged 18 to 64 years indicate that nearly 1 in 5 parents delayed or did not get care for their children in the past 12 months because of fear of exposure to the virus.
“It’s not surprising given the timing of the survey – April 2021 – when many people couldn’t get a vaccine yet and were reporting delayed care because of concerns about exposure during the past 30 days,” study author Dulce Gonzalez, BA, a research associate in the Health Policy Center at the Urban Institute, said in an interview.
In a previous survey that the Urban Institute conducted in September 2020, 28.8% of parents reported delaying or forgoing one or more types of health care for their children because of virus concerns or health care practitioner service limits.
These concerns still affect parents’ decision making when it comes to their child’s health. Nearly 1 in 10 parents reported that they had skipped doctor’s appointments for their children in the past 30 days. More than 1 in 10 adults forwent their own health care in the past month for the same reason.
“I think it’s important for parents to understand that health care workers and health care facilities are equipped to prevent infections from spreading,” Mundeep Kainth, DO, MPH, who was not involved in the study, told this news organization. “COVID-19 is not the first infection that we’ve seen in the medical setting, and we definitely are well aware of how it can spread and have been taking many precautions.”
The most common type of delayed or forgone care was dental care (5.3%), followed by well-child visits (4.0%) and general or specialist visits (3.2%). About 3% of parents said their child had missed out on immunizations. Nearly 6% of parents said their child had missed out on multiple types of care.
One reason dental care is the most commonly skipped type of care is because people might not consider dental care to be as urgent as other types of care, Ms. Gonzalez said. However, oral health can affect a person’s overall wellness.
Dr. Kainth, an infection disease specialist at Cohen Children’s Medical Center, New Hyde Park, New York, said the lack of immunization because of COVID-19 can have adverse health effects on children and could possibly lead to outbreaks in schools and day care settings. In the Urban Institute’s 2020 survey, 18.5% of parents said putting off their child’s health care worsened their child’s health, and 15.6% said it limited their children’s ability to go to school or day care.
“We are already concerned that we will have pockets of [vaccine-preventable] infections that we normally did not see before in communities where they are not vaccinating their children at high enough numbers,” Dr. Kainth said. “It is a little concerning that there’s probably a lot of catch up to be done for particular vaccines that are specifically for those entering day care and school.”
The current survey also found that parents with incomes below 250% of the federal poverty level were more likely than those with higher incomes to have put off care for their children in the past 30 days. More than 12% of families living in poverty put off care for their children, compared with 6.5% of those with higher incomes. They were also more likely to delay or forgo multiple types of care, at 8.1% versus 3.3%. Parents with lower family incomes were also more likely to report that their children had unmet needs for dental care, checkups, or other preventive care.
“We know that lower-income parents could be more exposed to costs they might not be able to afford if they were to get sick,” Ms. Gonzalez said. “Low-income adults have been disproportionately affected by job loss during the pandemic. They are also more likely to live in communities that have faced the largest health impacts of COVID-19.”
“There’s also advantages to the pediatrician visit that are not just about providing care but also providing guidance and advice to families and parents who are maybe struggling with certain issues that are above and beyond just the medical advice,” Dr. Kainth explained.
“That is probably the most tragic part of hearing that parents and kids are not going to the well visits, because that’s where families get a lot of support. And I think at this time, we probably need that more than ever,” she continued.
The authors said the findings highlight the importance of increasing rates of COVID-19 vaccinations among eligible adolescents and encouraging vaccinations for children younger than 12 when they become eligible, not only to protect them from COVID-19 but also to help families feel comfortable obtaining care.
The study was funded by the Robert Wood Johnson Foundation. The authors and Dr. Kainth have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many families delayed much-needed health care for their children out of fears that they may be exposed to SARS-CoV-2, according to data from the Urban Institute April 2021 Health Reform Monitoring Survey.
Data from 9,067 adults aged 18 to 64 years indicate that nearly 1 in 5 parents delayed or did not get care for their children in the past 12 months because of fear of exposure to the virus.
“It’s not surprising given the timing of the survey – April 2021 – when many people couldn’t get a vaccine yet and were reporting delayed care because of concerns about exposure during the past 30 days,” study author Dulce Gonzalez, BA, a research associate in the Health Policy Center at the Urban Institute, said in an interview.
In a previous survey that the Urban Institute conducted in September 2020, 28.8% of parents reported delaying or forgoing one or more types of health care for their children because of virus concerns or health care practitioner service limits.
These concerns still affect parents’ decision making when it comes to their child’s health. Nearly 1 in 10 parents reported that they had skipped doctor’s appointments for their children in the past 30 days. More than 1 in 10 adults forwent their own health care in the past month for the same reason.
“I think it’s important for parents to understand that health care workers and health care facilities are equipped to prevent infections from spreading,” Mundeep Kainth, DO, MPH, who was not involved in the study, told this news organization. “COVID-19 is not the first infection that we’ve seen in the medical setting, and we definitely are well aware of how it can spread and have been taking many precautions.”
The most common type of delayed or forgone care was dental care (5.3%), followed by well-child visits (4.0%) and general or specialist visits (3.2%). About 3% of parents said their child had missed out on immunizations. Nearly 6% of parents said their child had missed out on multiple types of care.
One reason dental care is the most commonly skipped type of care is because people might not consider dental care to be as urgent as other types of care, Ms. Gonzalez said. However, oral health can affect a person’s overall wellness.
Dr. Kainth, an infection disease specialist at Cohen Children’s Medical Center, New Hyde Park, New York, said the lack of immunization because of COVID-19 can have adverse health effects on children and could possibly lead to outbreaks in schools and day care settings. In the Urban Institute’s 2020 survey, 18.5% of parents said putting off their child’s health care worsened their child’s health, and 15.6% said it limited their children’s ability to go to school or day care.
“We are already concerned that we will have pockets of [vaccine-preventable] infections that we normally did not see before in communities where they are not vaccinating their children at high enough numbers,” Dr. Kainth said. “It is a little concerning that there’s probably a lot of catch up to be done for particular vaccines that are specifically for those entering day care and school.”
The current survey also found that parents with incomes below 250% of the federal poverty level were more likely than those with higher incomes to have put off care for their children in the past 30 days. More than 12% of families living in poverty put off care for their children, compared with 6.5% of those with higher incomes. They were also more likely to delay or forgo multiple types of care, at 8.1% versus 3.3%. Parents with lower family incomes were also more likely to report that their children had unmet needs for dental care, checkups, or other preventive care.
“We know that lower-income parents could be more exposed to costs they might not be able to afford if they were to get sick,” Ms. Gonzalez said. “Low-income adults have been disproportionately affected by job loss during the pandemic. They are also more likely to live in communities that have faced the largest health impacts of COVID-19.”
“There’s also advantages to the pediatrician visit that are not just about providing care but also providing guidance and advice to families and parents who are maybe struggling with certain issues that are above and beyond just the medical advice,” Dr. Kainth explained.
“That is probably the most tragic part of hearing that parents and kids are not going to the well visits, because that’s where families get a lot of support. And I think at this time, we probably need that more than ever,” she continued.
The authors said the findings highlight the importance of increasing rates of COVID-19 vaccinations among eligible adolescents and encouraging vaccinations for children younger than 12 when they become eligible, not only to protect them from COVID-19 but also to help families feel comfortable obtaining care.
The study was funded by the Robert Wood Johnson Foundation. The authors and Dr. Kainth have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many families delayed much-needed health care for their children out of fears that they may be exposed to SARS-CoV-2, according to data from the Urban Institute April 2021 Health Reform Monitoring Survey.
Data from 9,067 adults aged 18 to 64 years indicate that nearly 1 in 5 parents delayed or did not get care for their children in the past 12 months because of fear of exposure to the virus.
“It’s not surprising given the timing of the survey – April 2021 – when many people couldn’t get a vaccine yet and were reporting delayed care because of concerns about exposure during the past 30 days,” study author Dulce Gonzalez, BA, a research associate in the Health Policy Center at the Urban Institute, said in an interview.
In a previous survey that the Urban Institute conducted in September 2020, 28.8% of parents reported delaying or forgoing one or more types of health care for their children because of virus concerns or health care practitioner service limits.
These concerns still affect parents’ decision making when it comes to their child’s health. Nearly 1 in 10 parents reported that they had skipped doctor’s appointments for their children in the past 30 days. More than 1 in 10 adults forwent their own health care in the past month for the same reason.
“I think it’s important for parents to understand that health care workers and health care facilities are equipped to prevent infections from spreading,” Mundeep Kainth, DO, MPH, who was not involved in the study, told this news organization. “COVID-19 is not the first infection that we’ve seen in the medical setting, and we definitely are well aware of how it can spread and have been taking many precautions.”
The most common type of delayed or forgone care was dental care (5.3%), followed by well-child visits (4.0%) and general or specialist visits (3.2%). About 3% of parents said their child had missed out on immunizations. Nearly 6% of parents said their child had missed out on multiple types of care.
One reason dental care is the most commonly skipped type of care is because people might not consider dental care to be as urgent as other types of care, Ms. Gonzalez said. However, oral health can affect a person’s overall wellness.
Dr. Kainth, an infection disease specialist at Cohen Children’s Medical Center, New Hyde Park, New York, said the lack of immunization because of COVID-19 can have adverse health effects on children and could possibly lead to outbreaks in schools and day care settings. In the Urban Institute’s 2020 survey, 18.5% of parents said putting off their child’s health care worsened their child’s health, and 15.6% said it limited their children’s ability to go to school or day care.
“We are already concerned that we will have pockets of [vaccine-preventable] infections that we normally did not see before in communities where they are not vaccinating their children at high enough numbers,” Dr. Kainth said. “It is a little concerning that there’s probably a lot of catch up to be done for particular vaccines that are specifically for those entering day care and school.”
The current survey also found that parents with incomes below 250% of the federal poverty level were more likely than those with higher incomes to have put off care for their children in the past 30 days. More than 12% of families living in poverty put off care for their children, compared with 6.5% of those with higher incomes. They were also more likely to delay or forgo multiple types of care, at 8.1% versus 3.3%. Parents with lower family incomes were also more likely to report that their children had unmet needs for dental care, checkups, or other preventive care.
“We know that lower-income parents could be more exposed to costs they might not be able to afford if they were to get sick,” Ms. Gonzalez said. “Low-income adults have been disproportionately affected by job loss during the pandemic. They are also more likely to live in communities that have faced the largest health impacts of COVID-19.”
“There’s also advantages to the pediatrician visit that are not just about providing care but also providing guidance and advice to families and parents who are maybe struggling with certain issues that are above and beyond just the medical advice,” Dr. Kainth explained.
“That is probably the most tragic part of hearing that parents and kids are not going to the well visits, because that’s where families get a lot of support. And I think at this time, we probably need that more than ever,” she continued.
The authors said the findings highlight the importance of increasing rates of COVID-19 vaccinations among eligible adolescents and encouraging vaccinations for children younger than 12 when they become eligible, not only to protect them from COVID-19 but also to help families feel comfortable obtaining care.
The study was funded by the Robert Wood Johnson Foundation. The authors and Dr. Kainth have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
To be, or not to be? More counseling needed for gender dysphoria
Clinicians should not blindly accept a person’s self-diagnosis as transgender and desire to medically transition without closer inspection; rather, they should make a distinction between ‘acceptance’ and conducting an in-depth, respectful, and collaborative exploration of an individual’s claims about what they believe will best promote their well-being.
These are the conclusions of two experts in ethics and clinical psychology in an extended essay published in the Journal of Medical Ethics.
“It’s not about making life harder for people who wish to transition but about improving care for all people who identify as transgender,” lead author Alessandra Lemma, DClin Psych, visiting professor in the psychoanalysis unit at University College London, said in an interview.
She stressed that the argument is neither for nor against medical transitioning per se.
“It’s an invitation to think about how the medical and mental health care communities can best support anyone considering a transition, whether they eventually pursue that course of action or not. The provision of psychotherapy, irrespective of whether the individual medically transitions or not, makes for a better outcome either way,” said Dr. Lemma, who cares for adolescents as well as adults with gender dysphoria in her private practice in London.
Reflective space has been eroded in gender identity services for the young
There has been an exponential increase in the number of adolescents who identify as transgender in Western countries in recent years. This news organization has covered the debate in detail, which has intensified worldwide in the last 12 months, regarding how best to treat youth with gender dysphoria.
This has “raised concern about how the laudable aims of gender affirmative care may be ushering children and young people too quickly into medical transitioning,” generally defined as treatment with puberty blockers in minors followed by cross-sex hormones to transition to the opposite sex, “leading subsequently to a wish to detransition with all the attendant physical and psychological complications,” wrote Dr. Lemma and her coauthor, Julian Savulescu, MD, professor of practical ethics, University of Oxford (England).
While the United Kingdom and other countries such as Finland have tightened regulations regarding the treatment of minors, “these medical interventions continue to be provided in many other countries,” they noted.
Such affirmative care has recently been interpreted by “influential sections of the transgender community” as forbidding “’questioning’ of any kind of the person’s stated gender and what will help them,” the essayists stated.
But Dr. Lemma noted that, for teenagers, this is typically a time to “try on” different identities and ways of presenting oneself to the world.
“All this requires a reflective space during the decision-making process, and this has been eroded in many gender identity services for young people especially, with a massive pressure on services.”
Family issues, trauma, and comorbid conditions can all influence people too, she noted, adding that what may be happening unconsciously may be driving the decision to modify the body.
“I cannot see that it would be harmful to anyone to have the opportunity to really think about what they are doing before making decisions about medical interventions,” she asserted.
Decision to transition must be judged to be autonomous
Dr. Lemma noted that even in those instances where medical transitioning, on balance, is the best option, it’s important to acknowledge that the process has a psychological impact.
“What matters is that in facing a major life-changing decision, an individual has the opportunity to understand the developmental and social experiences that drive their experience of gender dysphoria such that the decisions they make about medical transitioning can be said to be taken more autonomously,” she and Dr. Savulescu wrote.
And for those people who opt for full gender reassignment surgery, they are the first to say, “I don’t think I could have got through this as well as I have without psychological support,” Dr. Lemma remarked.
Ultimately, what’s important is to ensure the protection of those individuals whose needs will most likely not be met by medical transitioning, while not making it impossible for those who are suffering to get the care they need in order to transition, she concluded.
Until 2016, Dr. Lemma was professor of psychological therapies at the Tavistock and Portman NHS Foundation Trust and Essex University. During that time she worked with adult transgender individuals at the Portman clinic but not at the Gender Identity Service at the Tavistock clinic. Currently, she works in private practice with transgender individuals at the Queen Anne Street Practice, London. Dr. Savulescu has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Clinicians should not blindly accept a person’s self-diagnosis as transgender and desire to medically transition without closer inspection; rather, they should make a distinction between ‘acceptance’ and conducting an in-depth, respectful, and collaborative exploration of an individual’s claims about what they believe will best promote their well-being.
These are the conclusions of two experts in ethics and clinical psychology in an extended essay published in the Journal of Medical Ethics.
“It’s not about making life harder for people who wish to transition but about improving care for all people who identify as transgender,” lead author Alessandra Lemma, DClin Psych, visiting professor in the psychoanalysis unit at University College London, said in an interview.
She stressed that the argument is neither for nor against medical transitioning per se.
“It’s an invitation to think about how the medical and mental health care communities can best support anyone considering a transition, whether they eventually pursue that course of action or not. The provision of psychotherapy, irrespective of whether the individual medically transitions or not, makes for a better outcome either way,” said Dr. Lemma, who cares for adolescents as well as adults with gender dysphoria in her private practice in London.
Reflective space has been eroded in gender identity services for the young
There has been an exponential increase in the number of adolescents who identify as transgender in Western countries in recent years. This news organization has covered the debate in detail, which has intensified worldwide in the last 12 months, regarding how best to treat youth with gender dysphoria.
This has “raised concern about how the laudable aims of gender affirmative care may be ushering children and young people too quickly into medical transitioning,” generally defined as treatment with puberty blockers in minors followed by cross-sex hormones to transition to the opposite sex, “leading subsequently to a wish to detransition with all the attendant physical and psychological complications,” wrote Dr. Lemma and her coauthor, Julian Savulescu, MD, professor of practical ethics, University of Oxford (England).
While the United Kingdom and other countries such as Finland have tightened regulations regarding the treatment of minors, “these medical interventions continue to be provided in many other countries,” they noted.
Such affirmative care has recently been interpreted by “influential sections of the transgender community” as forbidding “’questioning’ of any kind of the person’s stated gender and what will help them,” the essayists stated.
But Dr. Lemma noted that, for teenagers, this is typically a time to “try on” different identities and ways of presenting oneself to the world.
“All this requires a reflective space during the decision-making process, and this has been eroded in many gender identity services for young people especially, with a massive pressure on services.”
Family issues, trauma, and comorbid conditions can all influence people too, she noted, adding that what may be happening unconsciously may be driving the decision to modify the body.
“I cannot see that it would be harmful to anyone to have the opportunity to really think about what they are doing before making decisions about medical interventions,” she asserted.
Decision to transition must be judged to be autonomous
Dr. Lemma noted that even in those instances where medical transitioning, on balance, is the best option, it’s important to acknowledge that the process has a psychological impact.
“What matters is that in facing a major life-changing decision, an individual has the opportunity to understand the developmental and social experiences that drive their experience of gender dysphoria such that the decisions they make about medical transitioning can be said to be taken more autonomously,” she and Dr. Savulescu wrote.
And for those people who opt for full gender reassignment surgery, they are the first to say, “I don’t think I could have got through this as well as I have without psychological support,” Dr. Lemma remarked.
Ultimately, what’s important is to ensure the protection of those individuals whose needs will most likely not be met by medical transitioning, while not making it impossible for those who are suffering to get the care they need in order to transition, she concluded.
Until 2016, Dr. Lemma was professor of psychological therapies at the Tavistock and Portman NHS Foundation Trust and Essex University. During that time she worked with adult transgender individuals at the Portman clinic but not at the Gender Identity Service at the Tavistock clinic. Currently, she works in private practice with transgender individuals at the Queen Anne Street Practice, London. Dr. Savulescu has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Clinicians should not blindly accept a person’s self-diagnosis as transgender and desire to medically transition without closer inspection; rather, they should make a distinction between ‘acceptance’ and conducting an in-depth, respectful, and collaborative exploration of an individual’s claims about what they believe will best promote their well-being.
These are the conclusions of two experts in ethics and clinical psychology in an extended essay published in the Journal of Medical Ethics.
“It’s not about making life harder for people who wish to transition but about improving care for all people who identify as transgender,” lead author Alessandra Lemma, DClin Psych, visiting professor in the psychoanalysis unit at University College London, said in an interview.
She stressed that the argument is neither for nor against medical transitioning per se.
“It’s an invitation to think about how the medical and mental health care communities can best support anyone considering a transition, whether they eventually pursue that course of action or not. The provision of psychotherapy, irrespective of whether the individual medically transitions or not, makes for a better outcome either way,” said Dr. Lemma, who cares for adolescents as well as adults with gender dysphoria in her private practice in London.
Reflective space has been eroded in gender identity services for the young
There has been an exponential increase in the number of adolescents who identify as transgender in Western countries in recent years. This news organization has covered the debate in detail, which has intensified worldwide in the last 12 months, regarding how best to treat youth with gender dysphoria.
This has “raised concern about how the laudable aims of gender affirmative care may be ushering children and young people too quickly into medical transitioning,” generally defined as treatment with puberty blockers in minors followed by cross-sex hormones to transition to the opposite sex, “leading subsequently to a wish to detransition with all the attendant physical and psychological complications,” wrote Dr. Lemma and her coauthor, Julian Savulescu, MD, professor of practical ethics, University of Oxford (England).
While the United Kingdom and other countries such as Finland have tightened regulations regarding the treatment of minors, “these medical interventions continue to be provided in many other countries,” they noted.
Such affirmative care has recently been interpreted by “influential sections of the transgender community” as forbidding “’questioning’ of any kind of the person’s stated gender and what will help them,” the essayists stated.
But Dr. Lemma noted that, for teenagers, this is typically a time to “try on” different identities and ways of presenting oneself to the world.
“All this requires a reflective space during the decision-making process, and this has been eroded in many gender identity services for young people especially, with a massive pressure on services.”
Family issues, trauma, and comorbid conditions can all influence people too, she noted, adding that what may be happening unconsciously may be driving the decision to modify the body.
“I cannot see that it would be harmful to anyone to have the opportunity to really think about what they are doing before making decisions about medical interventions,” she asserted.
Decision to transition must be judged to be autonomous
Dr. Lemma noted that even in those instances where medical transitioning, on balance, is the best option, it’s important to acknowledge that the process has a psychological impact.
“What matters is that in facing a major life-changing decision, an individual has the opportunity to understand the developmental and social experiences that drive their experience of gender dysphoria such that the decisions they make about medical transitioning can be said to be taken more autonomously,” she and Dr. Savulescu wrote.
And for those people who opt for full gender reassignment surgery, they are the first to say, “I don’t think I could have got through this as well as I have without psychological support,” Dr. Lemma remarked.
Ultimately, what’s important is to ensure the protection of those individuals whose needs will most likely not be met by medical transitioning, while not making it impossible for those who are suffering to get the care they need in order to transition, she concluded.
Until 2016, Dr. Lemma was professor of psychological therapies at the Tavistock and Portman NHS Foundation Trust and Essex University. During that time she worked with adult transgender individuals at the Portman clinic but not at the Gender Identity Service at the Tavistock clinic. Currently, she works in private practice with transgender individuals at the Queen Anne Street Practice, London. Dr. Savulescu has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.