User login
Misinterpretation is a science, not an art
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?

Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.

A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.

We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?
Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.
A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.
We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?
Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.
A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.
We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
For older adults, smelling the roses may be more difficult
Young and old alike are affected – more than 80%-90% of those diagnosed with the virus, according to some estimates. While most people recover in a few months, 16% take half a year or longer to do so, research has found. According to new estimates, up to 1.6 million Americans have chronic olfactory dysfunction due to COVID-19.
Seniors are especially vulnerable, experts suggest. “We know that many older adults have a compromised sense of smell to begin with. Add to that the insult of COVID, and it made these problems worse,” said Dr. Jayant Pinto, professor of surgery and a specialist in sinus and nasal diseases at the University of Chicago Medical Center.
Recent data highlight the interaction between COVID-19, advanced age, and loss of smell. When Italian researchers evaluated 101 patients who’d been hospitalized for mild to moderate COVID-19, 50 showed objective signs of smell impairment 6 months later. Those 65 or older were nearly twice as likely to be impaired; those 75 or older were more than 2½ times as likely.
Most people aren’t aware of the extent to which smell can be diminished in later life. More than half of 65- to 80-year-olds have some degree of smell loss, or olfactory dysfunction, as it’s known in the scientific literature. That rises to as high as 80% for those even older. People affected often report concerns about safety, less enjoyment eating, and an impaired quality of life.
But because the ability to detect, identify, and discriminate among odors declines gradually, most older adults – up to 75% of those with some degree of olfactory dysfunction – don’t realize they’re affected.
A host of factors are believed to contribute to age-related smell loss, including a reduction in the number of olfactory sensory neurons in the nose, which are essential for detecting odors; changes in stem cells that replenish these neurons every few months; atrophy of the processing center for smell in the brain, called the olfactory bulb; and the shrinkage of brain centers closely connected with the olfactory bulb, such as the hippocampus, a region central to learning and memory.
Also, environmental toxic substances such as air pollution play a part, research shows. “Olfactory neurons in your nose are basically little pieces of your brain hanging out in the outside world,” and exposure to them over time damages those neurons and the tissues that support them, explained Pamela Dalton, PhD, a principal investigator at the Monell Chemical Senses Center, a smell and taste research institute in Philadelphia.
Still, the complex workings of the olfactory system have not been mapped in detail yet, and much remains unknown, said Dr. Sandeep Robert Datta, professor of neurobiology at Harvard Medical School, Boston.
“We tend to think of our sense of smell as primarily aesthetic,” he said. “What’s very clear is that it’s far more important. The olfactory system plays a key role in maintaining our emotional well-being and connecting us with the world.”
Dr. Datta experienced this after having a bone marrow transplant followed by chemotherapy years ago. Unable to smell or taste food, he said, he felt “very disoriented” in his environment.
Common consequences of smell loss include a loss of appetite (without smell, taste is deeply compromised), difficulty monitoring personal hygiene, depression, and an inability to detect noxious fumes. In older adults, this can lead to weight loss, malnutrition, frailty, inadequate personal care, and accidents caused by gas leaks or fires.
Jerome Pisano, 75, of Bloomington, Ill., has been living with smell loss for 5 years. Repeated tests and consultations with physicians haven’t pinpointed a reason for this ailment, and sometimes he feels “hopeless,” he admitted.
Before he became smell-impaired, Mr. Pisano was certified as a wine specialist. He has an 800-bottle wine cellar. “I can’t appreciate that as much as I’d like. I miss the smell of cut grass. Flowers. My wife’s cooking,” he said. “It certainly does decrease my quality of life.”
Smell loss is also associated in various research studies with a higher risk of death for older adults. One study, authored by Dr. Pinto and colleagues, found that older adults with olfactory dysfunction were nearly three times as likely to die over a period of 5 years as were seniors whose sense of smell remained intact.
“Our sense of smell signals how our nervous system is doing and how well our brain is doing overall,” Dr. Pinto said. According to a review published earlier this year, 90% of people with early-stage Parkinson’s disease and more than 80% of people with Alzheimer’s disease have olfactory dysfunction – a symptom that can precede other symptoms by many years.
There is no treatment for smell loss associated with neurological illness or head trauma, but if someone has persistent sinus problems or allergies that cause congestion, an over-the-counter antihistamine or nasal steroid spray can help. Usually, smell returns in a few weeks.
For smell loss following a viral infection, the picture is less clear. It’s not known, yet, which viruses are associated with olfactory dysfunction, why they damage smell, and what trajectory recovery takes. COVID-19 may help shine a light on this since it has inspired a wave of research on olfaction loss around the world.
“What characteristics make people more vulnerable to a persistent loss of smell after a virus? We don’t know that, but I think we will because that research is underway and we’ve never had a cohort [of people with smell loss] this large to study,” said Dr. Dalton, of the Monell center.
Some experts recommend smell training, noting evidence of efficacy and no indication of harm. This involves sniffing four distinct scents (often eucalyptus, lemon, rose, and cloves) twice a day for 30 seconds each, usually for 4 weeks. Sometimes the practice is combined with pictures of the items being smelled, a form of visual reinforcement.
The theory is that “practice, practice, practice” will stimulate the olfactory system, said Charles Greer, PhD, professor of neurosurgery and neuroscience at Yale University, New Haven, Conn. Although scientific support isn’t well established, he said, he often recommends that people who think their smell is declining “get a shelf full of spices and smell them on a regular basis.”
Richard Doty, PhD, director of the University of Pennsylvania’s Smell and Taste Center, remains skeptical. He’s writing a review of smell training and notes that 20%-30% of people with viral infections and smell loss recover in a relatively short time, whether or not they pursue this therapy.
“The main thing we recommend is avoid polluted environments and get your full complement of vitamins,” since several vitamins play an important role in maintaining the olfactory system, he said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Young and old alike are affected – more than 80%-90% of those diagnosed with the virus, according to some estimates. While most people recover in a few months, 16% take half a year or longer to do so, research has found. According to new estimates, up to 1.6 million Americans have chronic olfactory dysfunction due to COVID-19.
Seniors are especially vulnerable, experts suggest. “We know that many older adults have a compromised sense of smell to begin with. Add to that the insult of COVID, and it made these problems worse,” said Dr. Jayant Pinto, professor of surgery and a specialist in sinus and nasal diseases at the University of Chicago Medical Center.
Recent data highlight the interaction between COVID-19, advanced age, and loss of smell. When Italian researchers evaluated 101 patients who’d been hospitalized for mild to moderate COVID-19, 50 showed objective signs of smell impairment 6 months later. Those 65 or older were nearly twice as likely to be impaired; those 75 or older were more than 2½ times as likely.
Most people aren’t aware of the extent to which smell can be diminished in later life. More than half of 65- to 80-year-olds have some degree of smell loss, or olfactory dysfunction, as it’s known in the scientific literature. That rises to as high as 80% for those even older. People affected often report concerns about safety, less enjoyment eating, and an impaired quality of life.
But because the ability to detect, identify, and discriminate among odors declines gradually, most older adults – up to 75% of those with some degree of olfactory dysfunction – don’t realize they’re affected.
A host of factors are believed to contribute to age-related smell loss, including a reduction in the number of olfactory sensory neurons in the nose, which are essential for detecting odors; changes in stem cells that replenish these neurons every few months; atrophy of the processing center for smell in the brain, called the olfactory bulb; and the shrinkage of brain centers closely connected with the olfactory bulb, such as the hippocampus, a region central to learning and memory.
Also, environmental toxic substances such as air pollution play a part, research shows. “Olfactory neurons in your nose are basically little pieces of your brain hanging out in the outside world,” and exposure to them over time damages those neurons and the tissues that support them, explained Pamela Dalton, PhD, a principal investigator at the Monell Chemical Senses Center, a smell and taste research institute in Philadelphia.
Still, the complex workings of the olfactory system have not been mapped in detail yet, and much remains unknown, said Dr. Sandeep Robert Datta, professor of neurobiology at Harvard Medical School, Boston.
“We tend to think of our sense of smell as primarily aesthetic,” he said. “What’s very clear is that it’s far more important. The olfactory system plays a key role in maintaining our emotional well-being and connecting us with the world.”
Dr. Datta experienced this after having a bone marrow transplant followed by chemotherapy years ago. Unable to smell or taste food, he said, he felt “very disoriented” in his environment.
Common consequences of smell loss include a loss of appetite (without smell, taste is deeply compromised), difficulty monitoring personal hygiene, depression, and an inability to detect noxious fumes. In older adults, this can lead to weight loss, malnutrition, frailty, inadequate personal care, and accidents caused by gas leaks or fires.
Jerome Pisano, 75, of Bloomington, Ill., has been living with smell loss for 5 years. Repeated tests and consultations with physicians haven’t pinpointed a reason for this ailment, and sometimes he feels “hopeless,” he admitted.
Before he became smell-impaired, Mr. Pisano was certified as a wine specialist. He has an 800-bottle wine cellar. “I can’t appreciate that as much as I’d like. I miss the smell of cut grass. Flowers. My wife’s cooking,” he said. “It certainly does decrease my quality of life.”
Smell loss is also associated in various research studies with a higher risk of death for older adults. One study, authored by Dr. Pinto and colleagues, found that older adults with olfactory dysfunction were nearly three times as likely to die over a period of 5 years as were seniors whose sense of smell remained intact.
“Our sense of smell signals how our nervous system is doing and how well our brain is doing overall,” Dr. Pinto said. According to a review published earlier this year, 90% of people with early-stage Parkinson’s disease and more than 80% of people with Alzheimer’s disease have olfactory dysfunction – a symptom that can precede other symptoms by many years.
There is no treatment for smell loss associated with neurological illness or head trauma, but if someone has persistent sinus problems or allergies that cause congestion, an over-the-counter antihistamine or nasal steroid spray can help. Usually, smell returns in a few weeks.
For smell loss following a viral infection, the picture is less clear. It’s not known, yet, which viruses are associated with olfactory dysfunction, why they damage smell, and what trajectory recovery takes. COVID-19 may help shine a light on this since it has inspired a wave of research on olfaction loss around the world.
“What characteristics make people more vulnerable to a persistent loss of smell after a virus? We don’t know that, but I think we will because that research is underway and we’ve never had a cohort [of people with smell loss] this large to study,” said Dr. Dalton, of the Monell center.
Some experts recommend smell training, noting evidence of efficacy and no indication of harm. This involves sniffing four distinct scents (often eucalyptus, lemon, rose, and cloves) twice a day for 30 seconds each, usually for 4 weeks. Sometimes the practice is combined with pictures of the items being smelled, a form of visual reinforcement.
The theory is that “practice, practice, practice” will stimulate the olfactory system, said Charles Greer, PhD, professor of neurosurgery and neuroscience at Yale University, New Haven, Conn. Although scientific support isn’t well established, he said, he often recommends that people who think their smell is declining “get a shelf full of spices and smell them on a regular basis.”
Richard Doty, PhD, director of the University of Pennsylvania’s Smell and Taste Center, remains skeptical. He’s writing a review of smell training and notes that 20%-30% of people with viral infections and smell loss recover in a relatively short time, whether or not they pursue this therapy.
“The main thing we recommend is avoid polluted environments and get your full complement of vitamins,” since several vitamins play an important role in maintaining the olfactory system, he said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Young and old alike are affected – more than 80%-90% of those diagnosed with the virus, according to some estimates. While most people recover in a few months, 16% take half a year or longer to do so, research has found. According to new estimates, up to 1.6 million Americans have chronic olfactory dysfunction due to COVID-19.
Seniors are especially vulnerable, experts suggest. “We know that many older adults have a compromised sense of smell to begin with. Add to that the insult of COVID, and it made these problems worse,” said Dr. Jayant Pinto, professor of surgery and a specialist in sinus and nasal diseases at the University of Chicago Medical Center.
Recent data highlight the interaction between COVID-19, advanced age, and loss of smell. When Italian researchers evaluated 101 patients who’d been hospitalized for mild to moderate COVID-19, 50 showed objective signs of smell impairment 6 months later. Those 65 or older were nearly twice as likely to be impaired; those 75 or older were more than 2½ times as likely.
Most people aren’t aware of the extent to which smell can be diminished in later life. More than half of 65- to 80-year-olds have some degree of smell loss, or olfactory dysfunction, as it’s known in the scientific literature. That rises to as high as 80% for those even older. People affected often report concerns about safety, less enjoyment eating, and an impaired quality of life.
But because the ability to detect, identify, and discriminate among odors declines gradually, most older adults – up to 75% of those with some degree of olfactory dysfunction – don’t realize they’re affected.
A host of factors are believed to contribute to age-related smell loss, including a reduction in the number of olfactory sensory neurons in the nose, which are essential for detecting odors; changes in stem cells that replenish these neurons every few months; atrophy of the processing center for smell in the brain, called the olfactory bulb; and the shrinkage of brain centers closely connected with the olfactory bulb, such as the hippocampus, a region central to learning and memory.
Also, environmental toxic substances such as air pollution play a part, research shows. “Olfactory neurons in your nose are basically little pieces of your brain hanging out in the outside world,” and exposure to them over time damages those neurons and the tissues that support them, explained Pamela Dalton, PhD, a principal investigator at the Monell Chemical Senses Center, a smell and taste research institute in Philadelphia.
Still, the complex workings of the olfactory system have not been mapped in detail yet, and much remains unknown, said Dr. Sandeep Robert Datta, professor of neurobiology at Harvard Medical School, Boston.
“We tend to think of our sense of smell as primarily aesthetic,” he said. “What’s very clear is that it’s far more important. The olfactory system plays a key role in maintaining our emotional well-being and connecting us with the world.”
Dr. Datta experienced this after having a bone marrow transplant followed by chemotherapy years ago. Unable to smell or taste food, he said, he felt “very disoriented” in his environment.
Common consequences of smell loss include a loss of appetite (without smell, taste is deeply compromised), difficulty monitoring personal hygiene, depression, and an inability to detect noxious fumes. In older adults, this can lead to weight loss, malnutrition, frailty, inadequate personal care, and accidents caused by gas leaks or fires.
Jerome Pisano, 75, of Bloomington, Ill., has been living with smell loss for 5 years. Repeated tests and consultations with physicians haven’t pinpointed a reason for this ailment, and sometimes he feels “hopeless,” he admitted.
Before he became smell-impaired, Mr. Pisano was certified as a wine specialist. He has an 800-bottle wine cellar. “I can’t appreciate that as much as I’d like. I miss the smell of cut grass. Flowers. My wife’s cooking,” he said. “It certainly does decrease my quality of life.”
Smell loss is also associated in various research studies with a higher risk of death for older adults. One study, authored by Dr. Pinto and colleagues, found that older adults with olfactory dysfunction were nearly three times as likely to die over a period of 5 years as were seniors whose sense of smell remained intact.
“Our sense of smell signals how our nervous system is doing and how well our brain is doing overall,” Dr. Pinto said. According to a review published earlier this year, 90% of people with early-stage Parkinson’s disease and more than 80% of people with Alzheimer’s disease have olfactory dysfunction – a symptom that can precede other symptoms by many years.
There is no treatment for smell loss associated with neurological illness or head trauma, but if someone has persistent sinus problems or allergies that cause congestion, an over-the-counter antihistamine or nasal steroid spray can help. Usually, smell returns in a few weeks.
For smell loss following a viral infection, the picture is less clear. It’s not known, yet, which viruses are associated with olfactory dysfunction, why they damage smell, and what trajectory recovery takes. COVID-19 may help shine a light on this since it has inspired a wave of research on olfaction loss around the world.
“What characteristics make people more vulnerable to a persistent loss of smell after a virus? We don’t know that, but I think we will because that research is underway and we’ve never had a cohort [of people with smell loss] this large to study,” said Dr. Dalton, of the Monell center.
Some experts recommend smell training, noting evidence of efficacy and no indication of harm. This involves sniffing four distinct scents (often eucalyptus, lemon, rose, and cloves) twice a day for 30 seconds each, usually for 4 weeks. Sometimes the practice is combined with pictures of the items being smelled, a form of visual reinforcement.
The theory is that “practice, practice, practice” will stimulate the olfactory system, said Charles Greer, PhD, professor of neurosurgery and neuroscience at Yale University, New Haven, Conn. Although scientific support isn’t well established, he said, he often recommends that people who think their smell is declining “get a shelf full of spices and smell them on a regular basis.”
Richard Doty, PhD, director of the University of Pennsylvania’s Smell and Taste Center, remains skeptical. He’s writing a review of smell training and notes that 20%-30% of people with viral infections and smell loss recover in a relatively short time, whether or not they pursue this therapy.
“The main thing we recommend is avoid polluted environments and get your full complement of vitamins,” since several vitamins play an important role in maintaining the olfactory system, he said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Rhinosinusitis without nasal polyps lowers QoL in COPD
Concomitant rhinosinusitis without nasal polyps (RSsNP) in patients with chronic obstructive pulmonary disease (COPD) is associated with a poorer, disease-specific, health-related quality of life (HRQoL), a Norwegian study is showing.
“Chronic rhinosinusitis has an impact on patients’ HRQoL,” lead author Marte Rystad Øie, Trondheim (Norway) University Hospital, said in an interview.
“We found that RSsNP in COPD was associated with more psychological issues, higher COPD symptom burden, and overall COPD-related HRQoL after adjusting for lung function, so RSsNP does have clinical relevance and [our findings] support previous studies that have suggested that rhinosinusitis should be recognized as a comorbidity in COPD,” she emphasized.
The study was published in the Nov. 1 issue of Respiratory Medicine.
Study sample
The study sample consisted of 90 patients with COPD and 93 control subjects, all age 40-80 years. “Generic HRQoL was measured with the Norwegian version of the SF-36v2 Health Survey Standard questionnaire,” the authors wrote, and responses were compared between patients with COPD and controls as well as between subgroups of patients who had COPD both with and without RSsNP.
Disease-specific HRQoL was assessed by the Sinonasal Outcome Test-22 (SNOT-22); the St. Georges Respiratory Questionnaire (SGRQ), and the COPD Assessment Test (CAT), and responses were again compared between patients who had COPD with and without RSsNP. In the COPD group, “severe” and “very severe” airflow obstruction was present in 56.5% of patients with RSsNP compared with 38.6% of patients without RSsNP, as Ms. Øie reported.
Furthermore, total SNOT-22 along with psychological subscale scores were both significantly higher in patients who had COPD with RSsNP than those without RSsNP. Among those with RSsNP, the mean value of the total SNOT-22 score was 36.8 whereas the mean value of the psychological subscale score was 22.6. Comparable mean values among patients who had COPD without RSsNP were 9.5 and 6.5, respectively (P < .05).
Total scores on the SGRQ were again significantly greater in patients who had COPD with RSsNP at a mean of 43.3 compared with a mean of 34 in those without RSsNP, investigators observe. Similarly, scores for the symptom and activity domains again on the SGRQ were significantly greater for patients who had COPD with RSsNP than those without nasal polyps. As for the total CAT score, once again it was significantly higher in patients who had COPD with RSsNP at a mean of 18.8 compared with a mean of 13.5 in those without RSsNP (P < .05).
Indeed, patients with RSsNP were four times more likely to have CAT scores indicating the condition was having a high or very high impact on their HRQoL compared with patients without RSsNP (P < .001). As the authors pointed out, having a high impact on HRQoL translates into patients having to stop their desired activities and having no good days in the week.
“This suggests that having RSsNP substantially adds to the activity limitation experienced by patients with COPD,” they emphasized. The authors also found that RSsNP was significantly associated with poorer physical functioning after adjusting for COPD as reflected by SF-36v2 findings, again suggesting that patients who had COPD with concomitant RSsNP have an additional limitation in activity and a heavier symptom burden.
As Ms. Øie explained, rhinosinusitis has two clinical phenotypes: that with nasal polyps and that without nasal polyps, the latter being twice as prevalent. In fact, rhinosinusitis with nasal polyps is associated with asthma, as she pointed out. Given, however, that rhinosinusitis without polyps is amenable to treatment with daily use of nasal steroids, it is possible to reduce the burden of symptoms and psychological stress associated with RSsNP in COPD.
Limitations of the study include the fact that investigators did not assess patients for the presence of any comorbidities that could contribute to poorer HRQoL in this patient population.
The study was funded by Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Concomitant rhinosinusitis without nasal polyps (RSsNP) in patients with chronic obstructive pulmonary disease (COPD) is associated with a poorer, disease-specific, health-related quality of life (HRQoL), a Norwegian study is showing.
“Chronic rhinosinusitis has an impact on patients’ HRQoL,” lead author Marte Rystad Øie, Trondheim (Norway) University Hospital, said in an interview.
“We found that RSsNP in COPD was associated with more psychological issues, higher COPD symptom burden, and overall COPD-related HRQoL after adjusting for lung function, so RSsNP does have clinical relevance and [our findings] support previous studies that have suggested that rhinosinusitis should be recognized as a comorbidity in COPD,” she emphasized.
The study was published in the Nov. 1 issue of Respiratory Medicine.
Study sample
The study sample consisted of 90 patients with COPD and 93 control subjects, all age 40-80 years. “Generic HRQoL was measured with the Norwegian version of the SF-36v2 Health Survey Standard questionnaire,” the authors wrote, and responses were compared between patients with COPD and controls as well as between subgroups of patients who had COPD both with and without RSsNP.
Disease-specific HRQoL was assessed by the Sinonasal Outcome Test-22 (SNOT-22); the St. Georges Respiratory Questionnaire (SGRQ), and the COPD Assessment Test (CAT), and responses were again compared between patients who had COPD with and without RSsNP. In the COPD group, “severe” and “very severe” airflow obstruction was present in 56.5% of patients with RSsNP compared with 38.6% of patients without RSsNP, as Ms. Øie reported.
Furthermore, total SNOT-22 along with psychological subscale scores were both significantly higher in patients who had COPD with RSsNP than those without RSsNP. Among those with RSsNP, the mean value of the total SNOT-22 score was 36.8 whereas the mean value of the psychological subscale score was 22.6. Comparable mean values among patients who had COPD without RSsNP were 9.5 and 6.5, respectively (P < .05).
Total scores on the SGRQ were again significantly greater in patients who had COPD with RSsNP at a mean of 43.3 compared with a mean of 34 in those without RSsNP, investigators observe. Similarly, scores for the symptom and activity domains again on the SGRQ were significantly greater for patients who had COPD with RSsNP than those without nasal polyps. As for the total CAT score, once again it was significantly higher in patients who had COPD with RSsNP at a mean of 18.8 compared with a mean of 13.5 in those without RSsNP (P < .05).
Indeed, patients with RSsNP were four times more likely to have CAT scores indicating the condition was having a high or very high impact on their HRQoL compared with patients without RSsNP (P < .001). As the authors pointed out, having a high impact on HRQoL translates into patients having to stop their desired activities and having no good days in the week.
“This suggests that having RSsNP substantially adds to the activity limitation experienced by patients with COPD,” they emphasized. The authors also found that RSsNP was significantly associated with poorer physical functioning after adjusting for COPD as reflected by SF-36v2 findings, again suggesting that patients who had COPD with concomitant RSsNP have an additional limitation in activity and a heavier symptom burden.
As Ms. Øie explained, rhinosinusitis has two clinical phenotypes: that with nasal polyps and that without nasal polyps, the latter being twice as prevalent. In fact, rhinosinusitis with nasal polyps is associated with asthma, as she pointed out. Given, however, that rhinosinusitis without polyps is amenable to treatment with daily use of nasal steroids, it is possible to reduce the burden of symptoms and psychological stress associated with RSsNP in COPD.
Limitations of the study include the fact that investigators did not assess patients for the presence of any comorbidities that could contribute to poorer HRQoL in this patient population.
The study was funded by Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Concomitant rhinosinusitis without nasal polyps (RSsNP) in patients with chronic obstructive pulmonary disease (COPD) is associated with a poorer, disease-specific, health-related quality of life (HRQoL), a Norwegian study is showing.
“Chronic rhinosinusitis has an impact on patients’ HRQoL,” lead author Marte Rystad Øie, Trondheim (Norway) University Hospital, said in an interview.
“We found that RSsNP in COPD was associated with more psychological issues, higher COPD symptom burden, and overall COPD-related HRQoL after adjusting for lung function, so RSsNP does have clinical relevance and [our findings] support previous studies that have suggested that rhinosinusitis should be recognized as a comorbidity in COPD,” she emphasized.
The study was published in the Nov. 1 issue of Respiratory Medicine.
Study sample
The study sample consisted of 90 patients with COPD and 93 control subjects, all age 40-80 years. “Generic HRQoL was measured with the Norwegian version of the SF-36v2 Health Survey Standard questionnaire,” the authors wrote, and responses were compared between patients with COPD and controls as well as between subgroups of patients who had COPD both with and without RSsNP.
Disease-specific HRQoL was assessed by the Sinonasal Outcome Test-22 (SNOT-22); the St. Georges Respiratory Questionnaire (SGRQ), and the COPD Assessment Test (CAT), and responses were again compared between patients who had COPD with and without RSsNP. In the COPD group, “severe” and “very severe” airflow obstruction was present in 56.5% of patients with RSsNP compared with 38.6% of patients without RSsNP, as Ms. Øie reported.
Furthermore, total SNOT-22 along with psychological subscale scores were both significantly higher in patients who had COPD with RSsNP than those without RSsNP. Among those with RSsNP, the mean value of the total SNOT-22 score was 36.8 whereas the mean value of the psychological subscale score was 22.6. Comparable mean values among patients who had COPD without RSsNP were 9.5 and 6.5, respectively (P < .05).
Total scores on the SGRQ were again significantly greater in patients who had COPD with RSsNP at a mean of 43.3 compared with a mean of 34 in those without RSsNP, investigators observe. Similarly, scores for the symptom and activity domains again on the SGRQ were significantly greater for patients who had COPD with RSsNP than those without nasal polyps. As for the total CAT score, once again it was significantly higher in patients who had COPD with RSsNP at a mean of 18.8 compared with a mean of 13.5 in those without RSsNP (P < .05).
Indeed, patients with RSsNP were four times more likely to have CAT scores indicating the condition was having a high or very high impact on their HRQoL compared with patients without RSsNP (P < .001). As the authors pointed out, having a high impact on HRQoL translates into patients having to stop their desired activities and having no good days in the week.
“This suggests that having RSsNP substantially adds to the activity limitation experienced by patients with COPD,” they emphasized. The authors also found that RSsNP was significantly associated with poorer physical functioning after adjusting for COPD as reflected by SF-36v2 findings, again suggesting that patients who had COPD with concomitant RSsNP have an additional limitation in activity and a heavier symptom burden.
As Ms. Øie explained, rhinosinusitis has two clinical phenotypes: that with nasal polyps and that without nasal polyps, the latter being twice as prevalent. In fact, rhinosinusitis with nasal polyps is associated with asthma, as she pointed out. Given, however, that rhinosinusitis without polyps is amenable to treatment with daily use of nasal steroids, it is possible to reduce the burden of symptoms and psychological stress associated with RSsNP in COPD.
Limitations of the study include the fact that investigators did not assess patients for the presence of any comorbidities that could contribute to poorer HRQoL in this patient population.
The study was funded by Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA authorizes COVID boosters for all U.S. adults
“Authorizing the use of a single booster dose of either the Moderna or Pfizer-BioNTech COVID-19 vaccine for individuals 18 years of age and older helps to provide continued protection against COVID-19, including the serious consequences that can occur, such as hospitalization and death,” said acting FDA Commissioner Janet Woodcock, MD, in an FDA press statement.
The Center for Disease Control and Prevention’s Advisory Committee on Immunization Practices will meet on Nov. 19 to review the science supporting a more widespread need for booster doses, and is expected to vote on official recommendations for their use in the United States. The CDC director must then sign off on the panel’s recommendations.
“As soon as the FDA reviews those data and provides an authorization, we at CDC will act swiftly,” Rochelle P. Walensky, MD, MPH, said at a recent White House briefing.
Several states – including Louisiana, Maine, and Colorado – have already authorized boosters for all adults as cases rise in Europe and across the Western and Northeastern regions of the United States.
FDA officials said they hoped that widening eligibility for boosters would cut down on confusion for people and hopefully speed uptake of the shots.
“Streamlining the eligibility criteria and making booster doses available to all individuals 18 years of age and older will also help to eliminate confusion about who may receive a booster dose and ensure booster doses are available to all who may need one,” said Peter Marks, MD, PhD, who heads the FDA’s Center for Biologics Evaluation and Research.
A version of this article first appeared on WebMD.com.
“Authorizing the use of a single booster dose of either the Moderna or Pfizer-BioNTech COVID-19 vaccine for individuals 18 years of age and older helps to provide continued protection against COVID-19, including the serious consequences that can occur, such as hospitalization and death,” said acting FDA Commissioner Janet Woodcock, MD, in an FDA press statement.
The Center for Disease Control and Prevention’s Advisory Committee on Immunization Practices will meet on Nov. 19 to review the science supporting a more widespread need for booster doses, and is expected to vote on official recommendations for their use in the United States. The CDC director must then sign off on the panel’s recommendations.
“As soon as the FDA reviews those data and provides an authorization, we at CDC will act swiftly,” Rochelle P. Walensky, MD, MPH, said at a recent White House briefing.
Several states – including Louisiana, Maine, and Colorado – have already authorized boosters for all adults as cases rise in Europe and across the Western and Northeastern regions of the United States.
FDA officials said they hoped that widening eligibility for boosters would cut down on confusion for people and hopefully speed uptake of the shots.
“Streamlining the eligibility criteria and making booster doses available to all individuals 18 years of age and older will also help to eliminate confusion about who may receive a booster dose and ensure booster doses are available to all who may need one,” said Peter Marks, MD, PhD, who heads the FDA’s Center for Biologics Evaluation and Research.
A version of this article first appeared on WebMD.com.
“Authorizing the use of a single booster dose of either the Moderna or Pfizer-BioNTech COVID-19 vaccine for individuals 18 years of age and older helps to provide continued protection against COVID-19, including the serious consequences that can occur, such as hospitalization and death,” said acting FDA Commissioner Janet Woodcock, MD, in an FDA press statement.
The Center for Disease Control and Prevention’s Advisory Committee on Immunization Practices will meet on Nov. 19 to review the science supporting a more widespread need for booster doses, and is expected to vote on official recommendations for their use in the United States. The CDC director must then sign off on the panel’s recommendations.
“As soon as the FDA reviews those data and provides an authorization, we at CDC will act swiftly,” Rochelle P. Walensky, MD, MPH, said at a recent White House briefing.
Several states – including Louisiana, Maine, and Colorado – have already authorized boosters for all adults as cases rise in Europe and across the Western and Northeastern regions of the United States.
FDA officials said they hoped that widening eligibility for boosters would cut down on confusion for people and hopefully speed uptake of the shots.
“Streamlining the eligibility criteria and making booster doses available to all individuals 18 years of age and older will also help to eliminate confusion about who may receive a booster dose and ensure booster doses are available to all who may need one,” said Peter Marks, MD, PhD, who heads the FDA’s Center for Biologics Evaluation and Research.
A version of this article first appeared on WebMD.com.
Mask-wearing cuts new COVID-19 cases by 53%, study says
Social distancing and handwashing were also effective at lowering the number of cases, but wearing masks was the most effective tool against the coronavirus.
“Personal and social measures, including handwashing, mask wearing, and physical distancing are effective at reducing the incidence of COVID-19,” the study authors wrote.
The research team, which included public health and infectious disease specialists in Australia, China, and the U.K., evaluated 72 studies of COVID-19 precautions during the pandemic. They later looked at eight studies that focused on handwashing, mask wearing, and physical distancing.
Among six studies that looked at mask wearing, the researchers found a 53% reduction in COVID-19 cases. In the broader analysis with additional studies, wearing a mask reduced coronavirus transmission, cases, and deaths.
In one study across 200 countries, mandatory mask wearing resulted in nearly 46% fewer negative outcomes from COVID-19. In another study in the U.S., coronavirus transmission was reduced 29% in states where masks were mandatory.
But the research team couldn’t analyze the impact of the type of face mask used, the frequency of mask wearing, or the overall compliance with wearing face masks.
Among five studies that looked at physical distancing, the researchers found a 25% reduction in the rate of COVID-19. A study in the U.S. showed a 12% decrease in coronavirus transmission, while another study in Iran reported a reduction in COVID-19 mortality.
Handwashing interventions also suggested a substantial reduction of COVID-19 cases up to 53%, the researchers wrote. But in adjusted models, the results weren’t statistically significant due to the small number of studies included.
Other studies found significant decreases related to other public health measures, such as quarantines, broad lockdowns, border closures, school closures, business closures, and travel restrictions. Still, the research team couldn’t analyze the overall effectiveness of these measures due to the different ways the studies were conducted.
The study lines up with other research conducted so far during the pandemic, the research team wrote, which indicates that wearing masks and physical distancing can reduce transmission, cases, and deaths.
That said, more studies are needed, particularly now that vaccinations are available and contagious coronavirus variants have become prevalent.
“Further research is needed to assess the effectiveness of public health measures after adequate vaccination coverage has been achieved,” they wrote.
“It is likely that further control of the COVID-19 pandemic depends not only on high vaccination coverage and its effectiveness but also on ongoing adherence to effective and sustainable public health measures,” they concluded.
A version of this article first appeared on WebMD.com.
Social distancing and handwashing were also effective at lowering the number of cases, but wearing masks was the most effective tool against the coronavirus.
“Personal and social measures, including handwashing, mask wearing, and physical distancing are effective at reducing the incidence of COVID-19,” the study authors wrote.
The research team, which included public health and infectious disease specialists in Australia, China, and the U.K., evaluated 72 studies of COVID-19 precautions during the pandemic. They later looked at eight studies that focused on handwashing, mask wearing, and physical distancing.
Among six studies that looked at mask wearing, the researchers found a 53% reduction in COVID-19 cases. In the broader analysis with additional studies, wearing a mask reduced coronavirus transmission, cases, and deaths.
In one study across 200 countries, mandatory mask wearing resulted in nearly 46% fewer negative outcomes from COVID-19. In another study in the U.S., coronavirus transmission was reduced 29% in states where masks were mandatory.
But the research team couldn’t analyze the impact of the type of face mask used, the frequency of mask wearing, or the overall compliance with wearing face masks.
Among five studies that looked at physical distancing, the researchers found a 25% reduction in the rate of COVID-19. A study in the U.S. showed a 12% decrease in coronavirus transmission, while another study in Iran reported a reduction in COVID-19 mortality.
Handwashing interventions also suggested a substantial reduction of COVID-19 cases up to 53%, the researchers wrote. But in adjusted models, the results weren’t statistically significant due to the small number of studies included.
Other studies found significant decreases related to other public health measures, such as quarantines, broad lockdowns, border closures, school closures, business closures, and travel restrictions. Still, the research team couldn’t analyze the overall effectiveness of these measures due to the different ways the studies were conducted.
The study lines up with other research conducted so far during the pandemic, the research team wrote, which indicates that wearing masks and physical distancing can reduce transmission, cases, and deaths.
That said, more studies are needed, particularly now that vaccinations are available and contagious coronavirus variants have become prevalent.
“Further research is needed to assess the effectiveness of public health measures after adequate vaccination coverage has been achieved,” they wrote.
“It is likely that further control of the COVID-19 pandemic depends not only on high vaccination coverage and its effectiveness but also on ongoing adherence to effective and sustainable public health measures,” they concluded.
A version of this article first appeared on WebMD.com.
Social distancing and handwashing were also effective at lowering the number of cases, but wearing masks was the most effective tool against the coronavirus.
“Personal and social measures, including handwashing, mask wearing, and physical distancing are effective at reducing the incidence of COVID-19,” the study authors wrote.
The research team, which included public health and infectious disease specialists in Australia, China, and the U.K., evaluated 72 studies of COVID-19 precautions during the pandemic. They later looked at eight studies that focused on handwashing, mask wearing, and physical distancing.
Among six studies that looked at mask wearing, the researchers found a 53% reduction in COVID-19 cases. In the broader analysis with additional studies, wearing a mask reduced coronavirus transmission, cases, and deaths.
In one study across 200 countries, mandatory mask wearing resulted in nearly 46% fewer negative outcomes from COVID-19. In another study in the U.S., coronavirus transmission was reduced 29% in states where masks were mandatory.
But the research team couldn’t analyze the impact of the type of face mask used, the frequency of mask wearing, or the overall compliance with wearing face masks.
Among five studies that looked at physical distancing, the researchers found a 25% reduction in the rate of COVID-19. A study in the U.S. showed a 12% decrease in coronavirus transmission, while another study in Iran reported a reduction in COVID-19 mortality.
Handwashing interventions also suggested a substantial reduction of COVID-19 cases up to 53%, the researchers wrote. But in adjusted models, the results weren’t statistically significant due to the small number of studies included.
Other studies found significant decreases related to other public health measures, such as quarantines, broad lockdowns, border closures, school closures, business closures, and travel restrictions. Still, the research team couldn’t analyze the overall effectiveness of these measures due to the different ways the studies were conducted.
The study lines up with other research conducted so far during the pandemic, the research team wrote, which indicates that wearing masks and physical distancing can reduce transmission, cases, and deaths.
That said, more studies are needed, particularly now that vaccinations are available and contagious coronavirus variants have become prevalent.
“Further research is needed to assess the effectiveness of public health measures after adequate vaccination coverage has been achieved,” they wrote.
“It is likely that further control of the COVID-19 pandemic depends not only on high vaccination coverage and its effectiveness but also on ongoing adherence to effective and sustainable public health measures,” they concluded.
A version of this article first appeared on WebMD.com.
FROM THE BMJ
Text-based COVID monitoring system could reduce deaths, relieve ED in winter surge
COVID Watch, a text message–based remote monitoring program developed by the University of Pennsylvania Health System, was associated with a 68% reduction in the risk of death, compared with those who received usual care. This was the main finding of a paper published in the Annals of Internal Medicine.
The investigators also determined that patients who enrolled in the program were more likely to seek care in the ED and when they did, they came in on average 2 days sooner than those who received usual care.
“When our clinical team designed COVID Watch the goal was to facilitate hospital care for patients who require it, while supporting access to care for patients who can safely remain at home,” study author M. Kit Delgado, MD, MS, an assistant professor of emergency medicine and epidemiology at Penn Presbyterian Medical Center in Philadelphia, said in an interview.
Researchers had initially hoped COVID Watch would relieve pressure on EDs, Dr. Delgado said.
Significantly lower mortality seen among COVID Watch group
For the study, Dr. Delgado and colleagues enrolled 3,488 patients in COVID Watch and 4,377 in the usual care group to compare outcomes at 30 and 60 days.
“We didn’t include patients who were diagnosed with COVID in the ER or hospital, so this is a lower-risk cohort of patients who test positive in outpatient settings,” Dr. Delgado noted. “Outpatients who received usual care and COVID Watch both had relatively low mortality, but it was significantly lower in those who were in COVID Watch.”
The researchers found that 3 patients in the COVID Watch group died within 30 days of their enrollment, compared with 12 in the control group. At 60 days after enrollment, 5 people within COVID Watch died, compared with 16 not using the system. More than one-third of the deaths in the usual care group occurred outside the hospital, compared with zero deaths among those in COVID Watch.
More than half of program participants were Black or Latino
The messaging system also reduced mortality rates among “all major racial and ethnic subgroups,” the researchers said, with more than 50% of the patients enrolled in COVID Watch having been Black or Latino.
“This is important because Black and Hispanic communities have experienced higher exposure and infection rates, decreased access to care, and have had higher mortality rates,” Dr. Delgado said. “Therefore, the results imply that this type of program could play a role in decreasing disparities in COVID outcomes if scaled more broadly.”
Outside expert: COVID Watch bring new approach to digital health monitoring
The study not only highlights the efficacy and sustainment of the COVID Watch program, but it sheds light on the possibility of using text message monitoring systems on other chronic disease conditions, said Jamie Faro, PhD, who was not involved in the study.
“It brings a new approach to health monitoring using digital means, which may lessen the burden on health care providers and be more cost effective than usual care approaches,” said Dr. Faro, who is assistant professor at the department of population and quantitative health sciences at the University of Massachusetts, Worcester. “Text messaging, which is used by over 80% of Americans, can allow us to reach a large percentage of the population for remote health care monitoring.”
Researchers of the current study said the findings “reveal a model for outpatient health system management of patients with COVID-19 and possibly other conditions where the early detection of clinical declines is critical.” Dr. Faro said that COVID Watch can have a measurable impact on an outcome that is truly life or death. However, it would be critical to understand how to reach those who either “were not offered or refused to take part in the program.”
The authors of the paper and Dr. Faro had no disclosures.
COVID Watch, a text message–based remote monitoring program developed by the University of Pennsylvania Health System, was associated with a 68% reduction in the risk of death, compared with those who received usual care. This was the main finding of a paper published in the Annals of Internal Medicine.
The investigators also determined that patients who enrolled in the program were more likely to seek care in the ED and when they did, they came in on average 2 days sooner than those who received usual care.
“When our clinical team designed COVID Watch the goal was to facilitate hospital care for patients who require it, while supporting access to care for patients who can safely remain at home,” study author M. Kit Delgado, MD, MS, an assistant professor of emergency medicine and epidemiology at Penn Presbyterian Medical Center in Philadelphia, said in an interview.
Researchers had initially hoped COVID Watch would relieve pressure on EDs, Dr. Delgado said.
Significantly lower mortality seen among COVID Watch group
For the study, Dr. Delgado and colleagues enrolled 3,488 patients in COVID Watch and 4,377 in the usual care group to compare outcomes at 30 and 60 days.
“We didn’t include patients who were diagnosed with COVID in the ER or hospital, so this is a lower-risk cohort of patients who test positive in outpatient settings,” Dr. Delgado noted. “Outpatients who received usual care and COVID Watch both had relatively low mortality, but it was significantly lower in those who were in COVID Watch.”
The researchers found that 3 patients in the COVID Watch group died within 30 days of their enrollment, compared with 12 in the control group. At 60 days after enrollment, 5 people within COVID Watch died, compared with 16 not using the system. More than one-third of the deaths in the usual care group occurred outside the hospital, compared with zero deaths among those in COVID Watch.
More than half of program participants were Black or Latino
The messaging system also reduced mortality rates among “all major racial and ethnic subgroups,” the researchers said, with more than 50% of the patients enrolled in COVID Watch having been Black or Latino.
“This is important because Black and Hispanic communities have experienced higher exposure and infection rates, decreased access to care, and have had higher mortality rates,” Dr. Delgado said. “Therefore, the results imply that this type of program could play a role in decreasing disparities in COVID outcomes if scaled more broadly.”
Outside expert: COVID Watch bring new approach to digital health monitoring
The study not only highlights the efficacy and sustainment of the COVID Watch program, but it sheds light on the possibility of using text message monitoring systems on other chronic disease conditions, said Jamie Faro, PhD, who was not involved in the study.
“It brings a new approach to health monitoring using digital means, which may lessen the burden on health care providers and be more cost effective than usual care approaches,” said Dr. Faro, who is assistant professor at the department of population and quantitative health sciences at the University of Massachusetts, Worcester. “Text messaging, which is used by over 80% of Americans, can allow us to reach a large percentage of the population for remote health care monitoring.”
Researchers of the current study said the findings “reveal a model for outpatient health system management of patients with COVID-19 and possibly other conditions where the early detection of clinical declines is critical.” Dr. Faro said that COVID Watch can have a measurable impact on an outcome that is truly life or death. However, it would be critical to understand how to reach those who either “were not offered or refused to take part in the program.”
The authors of the paper and Dr. Faro had no disclosures.
COVID Watch, a text message–based remote monitoring program developed by the University of Pennsylvania Health System, was associated with a 68% reduction in the risk of death, compared with those who received usual care. This was the main finding of a paper published in the Annals of Internal Medicine.
The investigators also determined that patients who enrolled in the program were more likely to seek care in the ED and when they did, they came in on average 2 days sooner than those who received usual care.
“When our clinical team designed COVID Watch the goal was to facilitate hospital care for patients who require it, while supporting access to care for patients who can safely remain at home,” study author M. Kit Delgado, MD, MS, an assistant professor of emergency medicine and epidemiology at Penn Presbyterian Medical Center in Philadelphia, said in an interview.
Researchers had initially hoped COVID Watch would relieve pressure on EDs, Dr. Delgado said.
Significantly lower mortality seen among COVID Watch group
For the study, Dr. Delgado and colleagues enrolled 3,488 patients in COVID Watch and 4,377 in the usual care group to compare outcomes at 30 and 60 days.
“We didn’t include patients who were diagnosed with COVID in the ER or hospital, so this is a lower-risk cohort of patients who test positive in outpatient settings,” Dr. Delgado noted. “Outpatients who received usual care and COVID Watch both had relatively low mortality, but it was significantly lower in those who were in COVID Watch.”
The researchers found that 3 patients in the COVID Watch group died within 30 days of their enrollment, compared with 12 in the control group. At 60 days after enrollment, 5 people within COVID Watch died, compared with 16 not using the system. More than one-third of the deaths in the usual care group occurred outside the hospital, compared with zero deaths among those in COVID Watch.
More than half of program participants were Black or Latino
The messaging system also reduced mortality rates among “all major racial and ethnic subgroups,” the researchers said, with more than 50% of the patients enrolled in COVID Watch having been Black or Latino.
“This is important because Black and Hispanic communities have experienced higher exposure and infection rates, decreased access to care, and have had higher mortality rates,” Dr. Delgado said. “Therefore, the results imply that this type of program could play a role in decreasing disparities in COVID outcomes if scaled more broadly.”
Outside expert: COVID Watch bring new approach to digital health monitoring
The study not only highlights the efficacy and sustainment of the COVID Watch program, but it sheds light on the possibility of using text message monitoring systems on other chronic disease conditions, said Jamie Faro, PhD, who was not involved in the study.
“It brings a new approach to health monitoring using digital means, which may lessen the burden on health care providers and be more cost effective than usual care approaches,” said Dr. Faro, who is assistant professor at the department of population and quantitative health sciences at the University of Massachusetts, Worcester. “Text messaging, which is used by over 80% of Americans, can allow us to reach a large percentage of the population for remote health care monitoring.”
Researchers of the current study said the findings “reveal a model for outpatient health system management of patients with COVID-19 and possibly other conditions where the early detection of clinical declines is critical.” Dr. Faro said that COVID Watch can have a measurable impact on an outcome that is truly life or death. However, it would be critical to understand how to reach those who either “were not offered or refused to take part in the program.”
The authors of the paper and Dr. Faro had no disclosures.
FROM ANNALS OF INTERNAL MEDICINE
Comparing pulmonary embolism mortality risk scores
Background: Though most PEs do not have significant complications, 15% may be associated with risk of death or hemodynamic compromise. Retrospectively derived risk scores are used to risk-stratify patients and guide acute treatment strategies. It is unclear how well existing risk scores estimate mortality outcomes in patients with acute PE.

Study design: Multicenter cohort study.
Setting: Eight hospitals participating in Pulmonary Embolism Response Team (PERT) consortium registry.
Synopsis: The study included 416 patients with radiographically confirmed acute PE, baseline data for risk calculations, and PERT consultation to consider advanced therapies. Four risk scores (PESI, simplified PESI, BOVA, and European Society of Cardiology) were calculated for each patient independently of clinical care. Patients were assigned into lower- and higher-risk groups. All-cause mortality was assessed on days 7 and 30. The discrimination of each risk score was measured using area under the curve (AUC). Seven-day mortality ranged 1.3%-3.1% in the lower-risk group, and 7%-16.3% in the high-risk group. Thirty-day mortality in the low-risk group ranged 2.6%-10.2% and 14.4%-26.3% in the high-risk group. PE risk scores have only moderate discrimination for mortality at 7 days (AUC range, 0.616-0.666) and less discrimination at 30 days (AUC range, 0.550-0.694) with little association among the risk scores. Limitations include failure to capture all presenting PEs and inability to differentiate between all-cause and specific PE-related mortality.
Bottom line: While helpful in predicting shorter-term mortality, acute PE risk scores are not highly accurate at predicting longer-term mortality and should be integrated with broad clinical information when making management decisions.
Citation: Barnes GD et al. Comparison of 4 acute pulmonary embolism mortality risk scores in patients evaluated by pulmonary embolism response teams. JAMA Netw Open. 2020 Aug 3;3(8):e2010779. doi:
Dr. Korovaichuk is a hospitalist at Northwestern Memorial Hospital and assistant professor of medicine, Feinberg School of Medicine, both in Chicago.
Background: Though most PEs do not have significant complications, 15% may be associated with risk of death or hemodynamic compromise. Retrospectively derived risk scores are used to risk-stratify patients and guide acute treatment strategies. It is unclear how well existing risk scores estimate mortality outcomes in patients with acute PE.
Study design: Multicenter cohort study.
Setting: Eight hospitals participating in Pulmonary Embolism Response Team (PERT) consortium registry.
Synopsis: The study included 416 patients with radiographically confirmed acute PE, baseline data for risk calculations, and PERT consultation to consider advanced therapies. Four risk scores (PESI, simplified PESI, BOVA, and European Society of Cardiology) were calculated for each patient independently of clinical care. Patients were assigned into lower- and higher-risk groups. All-cause mortality was assessed on days 7 and 30. The discrimination of each risk score was measured using area under the curve (AUC). Seven-day mortality ranged 1.3%-3.1% in the lower-risk group, and 7%-16.3% in the high-risk group. Thirty-day mortality in the low-risk group ranged 2.6%-10.2% and 14.4%-26.3% in the high-risk group. PE risk scores have only moderate discrimination for mortality at 7 days (AUC range, 0.616-0.666) and less discrimination at 30 days (AUC range, 0.550-0.694) with little association among the risk scores. Limitations include failure to capture all presenting PEs and inability to differentiate between all-cause and specific PE-related mortality.
Bottom line: While helpful in predicting shorter-term mortality, acute PE risk scores are not highly accurate at predicting longer-term mortality and should be integrated with broad clinical information when making management decisions.
Citation: Barnes GD et al. Comparison of 4 acute pulmonary embolism mortality risk scores in patients evaluated by pulmonary embolism response teams. JAMA Netw Open. 2020 Aug 3;3(8):e2010779. doi:
Dr. Korovaichuk is a hospitalist at Northwestern Memorial Hospital and assistant professor of medicine, Feinberg School of Medicine, both in Chicago.
Background: Though most PEs do not have significant complications, 15% may be associated with risk of death or hemodynamic compromise. Retrospectively derived risk scores are used to risk-stratify patients and guide acute treatment strategies. It is unclear how well existing risk scores estimate mortality outcomes in patients with acute PE.
Study design: Multicenter cohort study.
Setting: Eight hospitals participating in Pulmonary Embolism Response Team (PERT) consortium registry.
Synopsis: The study included 416 patients with radiographically confirmed acute PE, baseline data for risk calculations, and PERT consultation to consider advanced therapies. Four risk scores (PESI, simplified PESI, BOVA, and European Society of Cardiology) were calculated for each patient independently of clinical care. Patients were assigned into lower- and higher-risk groups. All-cause mortality was assessed on days 7 and 30. The discrimination of each risk score was measured using area under the curve (AUC). Seven-day mortality ranged 1.3%-3.1% in the lower-risk group, and 7%-16.3% in the high-risk group. Thirty-day mortality in the low-risk group ranged 2.6%-10.2% and 14.4%-26.3% in the high-risk group. PE risk scores have only moderate discrimination for mortality at 7 days (AUC range, 0.616-0.666) and less discrimination at 30 days (AUC range, 0.550-0.694) with little association among the risk scores. Limitations include failure to capture all presenting PEs and inability to differentiate between all-cause and specific PE-related mortality.
Bottom line: While helpful in predicting shorter-term mortality, acute PE risk scores are not highly accurate at predicting longer-term mortality and should be integrated with broad clinical information when making management decisions.
Citation: Barnes GD et al. Comparison of 4 acute pulmonary embolism mortality risk scores in patients evaluated by pulmonary embolism response teams. JAMA Netw Open. 2020 Aug 3;3(8):e2010779. doi:
Dr. Korovaichuk is a hospitalist at Northwestern Memorial Hospital and assistant professor of medicine, Feinberg School of Medicine, both in Chicago.
Pulmonary rehabilitation: Similar benefit in both IPF and COPD patients
Patients with idiopathic pulmonary fibrosis (IPF) complete and respond to pulmonary rehabilitation at rates similar to patients with chronic obstructive pulmonary disease (COPD), according to results of a real-world study. The findings reported in an article published in the journal CHEST® reinforce pulmonary rehabilitation’s benefits for this population.
A progressive decline in respiratory and physical function characterizes IPF, with median survival from diagnosis of 3-5 years, according to Claire Nolan, PhD, of Harefield Hospital, Middlesex, England, and colleagues. The effects of pharmacologic therapies on IPF on symptom burden and quality of life are modest, although lung function decline may be slowed. Supporting evidence for pulmonary rehabilitation benefit in IPF is more modest than it is for COPD, for which exercise capacity, dyspnea, and health-related quality of life improvement have been demonstrated.
“We did not design a randomized, controlled trial,” Dr. Nolan said in an interview, “as it was considered unethical by the local ethics committee to withhold pulmonary rehabilitation based on clinical guidance in the United Kingdom.” She pointed out that initial pulmonary rehabilitation trials in COPD included an intervention (pulmonary rehabilitation) and a control (standard medical care) arm.
The study aims were to compare the effects of pulmonary rehabilitation with real-world data between IPF and COPD with respect to magnitude of effect and survival. The authors’ hypothesis was that IPF patients would have a blunted response to pulmonary rehabilitation with reduced completion rates, compared with a matched COPD group, and with increased mortality.
Study details
Investigators use propensity score matching of 163 IPF patients with a control group of 163 patients with COPD referred to pulmonary rehabilitation. Completion rates, responses, and survival status were recorded for 1-year following pulmonary rehabilitation discharge. The 8-week outpatient program was composed of two supervised exercise and education sessions with additional unsupervised home-based exercise each week.
While spirometry data, as expected, showed a higher proportion of IPF patients using supplemental oxygen, pulmonary rehabilitation completion rates were similar for both groups (IPF, 69%; COPD, 63%; P = .24) and there was no between group difference in the number of sessions attended (P = .39). Medical Research Council (muscle strength) (MRC), incremental shuttle walk test (ISW), and Chronic Respiratory Questionnaire total score (CRQ-T) improved significantly in both groups, again with no significant difference between groups.
Over the study course, there was progressive, significant worsening of forced vital capacity percentage, predicted, prescription supplemental oxygen, resting peripheral oxygen saturation, exercise capacity, health-related quality of life and pulmonary rehabilitation adherence across groups of responders (n = 63; 38%), nonresponders (n = 50; 31%) and noncompleters (n = 50; 31%). Among the IPF patients, 6 died before completing pulmonary rehabilitation, with 42 (27%) dying during follow-up.
Benefits of rehabilitation
Multivariable analyses showed that noncompletion and nonresponse were associated with significantly higher risk of all-cause mortality at 1-year. Also, time to all-cause mortality was shorter (P = .001) for noncompleters and nonresponders, compared with completers. A trend toward higher completion rates in the IPF group, compared with the COPD group, may be explained, the researchers explained, by fewer hospitalizations over the prior 12 months in the IPF group.
“Although many programs are designed for people with COPD,” Dr. Nolan and colleagues concluded, “our study demonstrates that people with IPF have similar clinical benefits and completion rates to those with COPD. These data reinforce the importance of referral to and engagement in pulmonary rehabilitation amongst the IPF population.”
These findings, Dr. Nolan emphasized, emerged from a single center, and validation in other settings is needed.
This study was funded by a National Institute for Health Research Doctoral Research Fellowship (2014-07-089) and a Medical Research Council New Investigator Research Grant (98576).
Patients with idiopathic pulmonary fibrosis (IPF) complete and respond to pulmonary rehabilitation at rates similar to patients with chronic obstructive pulmonary disease (COPD), according to results of a real-world study. The findings reported in an article published in the journal CHEST® reinforce pulmonary rehabilitation’s benefits for this population.
A progressive decline in respiratory and physical function characterizes IPF, with median survival from diagnosis of 3-5 years, according to Claire Nolan, PhD, of Harefield Hospital, Middlesex, England, and colleagues. The effects of pharmacologic therapies on IPF on symptom burden and quality of life are modest, although lung function decline may be slowed. Supporting evidence for pulmonary rehabilitation benefit in IPF is more modest than it is for COPD, for which exercise capacity, dyspnea, and health-related quality of life improvement have been demonstrated.
“We did not design a randomized, controlled trial,” Dr. Nolan said in an interview, “as it was considered unethical by the local ethics committee to withhold pulmonary rehabilitation based on clinical guidance in the United Kingdom.” She pointed out that initial pulmonary rehabilitation trials in COPD included an intervention (pulmonary rehabilitation) and a control (standard medical care) arm.
The study aims were to compare the effects of pulmonary rehabilitation with real-world data between IPF and COPD with respect to magnitude of effect and survival. The authors’ hypothesis was that IPF patients would have a blunted response to pulmonary rehabilitation with reduced completion rates, compared with a matched COPD group, and with increased mortality.
Study details
Investigators use propensity score matching of 163 IPF patients with a control group of 163 patients with COPD referred to pulmonary rehabilitation. Completion rates, responses, and survival status were recorded for 1-year following pulmonary rehabilitation discharge. The 8-week outpatient program was composed of two supervised exercise and education sessions with additional unsupervised home-based exercise each week.
While spirometry data, as expected, showed a higher proportion of IPF patients using supplemental oxygen, pulmonary rehabilitation completion rates were similar for both groups (IPF, 69%; COPD, 63%; P = .24) and there was no between group difference in the number of sessions attended (P = .39). Medical Research Council (muscle strength) (MRC), incremental shuttle walk test (ISW), and Chronic Respiratory Questionnaire total score (CRQ-T) improved significantly in both groups, again with no significant difference between groups.
Over the study course, there was progressive, significant worsening of forced vital capacity percentage, predicted, prescription supplemental oxygen, resting peripheral oxygen saturation, exercise capacity, health-related quality of life and pulmonary rehabilitation adherence across groups of responders (n = 63; 38%), nonresponders (n = 50; 31%) and noncompleters (n = 50; 31%). Among the IPF patients, 6 died before completing pulmonary rehabilitation, with 42 (27%) dying during follow-up.
Benefits of rehabilitation
Multivariable analyses showed that noncompletion and nonresponse were associated with significantly higher risk of all-cause mortality at 1-year. Also, time to all-cause mortality was shorter (P = .001) for noncompleters and nonresponders, compared with completers. A trend toward higher completion rates in the IPF group, compared with the COPD group, may be explained, the researchers explained, by fewer hospitalizations over the prior 12 months in the IPF group.
“Although many programs are designed for people with COPD,” Dr. Nolan and colleagues concluded, “our study demonstrates that people with IPF have similar clinical benefits and completion rates to those with COPD. These data reinforce the importance of referral to and engagement in pulmonary rehabilitation amongst the IPF population.”
These findings, Dr. Nolan emphasized, emerged from a single center, and validation in other settings is needed.
This study was funded by a National Institute for Health Research Doctoral Research Fellowship (2014-07-089) and a Medical Research Council New Investigator Research Grant (98576).
Patients with idiopathic pulmonary fibrosis (IPF) complete and respond to pulmonary rehabilitation at rates similar to patients with chronic obstructive pulmonary disease (COPD), according to results of a real-world study. The findings reported in an article published in the journal CHEST® reinforce pulmonary rehabilitation’s benefits for this population.
A progressive decline in respiratory and physical function characterizes IPF, with median survival from diagnosis of 3-5 years, according to Claire Nolan, PhD, of Harefield Hospital, Middlesex, England, and colleagues. The effects of pharmacologic therapies on IPF on symptom burden and quality of life are modest, although lung function decline may be slowed. Supporting evidence for pulmonary rehabilitation benefit in IPF is more modest than it is for COPD, for which exercise capacity, dyspnea, and health-related quality of life improvement have been demonstrated.
“We did not design a randomized, controlled trial,” Dr. Nolan said in an interview, “as it was considered unethical by the local ethics committee to withhold pulmonary rehabilitation based on clinical guidance in the United Kingdom.” She pointed out that initial pulmonary rehabilitation trials in COPD included an intervention (pulmonary rehabilitation) and a control (standard medical care) arm.
The study aims were to compare the effects of pulmonary rehabilitation with real-world data between IPF and COPD with respect to magnitude of effect and survival. The authors’ hypothesis was that IPF patients would have a blunted response to pulmonary rehabilitation with reduced completion rates, compared with a matched COPD group, and with increased mortality.
Study details
Investigators use propensity score matching of 163 IPF patients with a control group of 163 patients with COPD referred to pulmonary rehabilitation. Completion rates, responses, and survival status were recorded for 1-year following pulmonary rehabilitation discharge. The 8-week outpatient program was composed of two supervised exercise and education sessions with additional unsupervised home-based exercise each week.
While spirometry data, as expected, showed a higher proportion of IPF patients using supplemental oxygen, pulmonary rehabilitation completion rates were similar for both groups (IPF, 69%; COPD, 63%; P = .24) and there was no between group difference in the number of sessions attended (P = .39). Medical Research Council (muscle strength) (MRC), incremental shuttle walk test (ISW), and Chronic Respiratory Questionnaire total score (CRQ-T) improved significantly in both groups, again with no significant difference between groups.
Over the study course, there was progressive, significant worsening of forced vital capacity percentage, predicted, prescription supplemental oxygen, resting peripheral oxygen saturation, exercise capacity, health-related quality of life and pulmonary rehabilitation adherence across groups of responders (n = 63; 38%), nonresponders (n = 50; 31%) and noncompleters (n = 50; 31%). Among the IPF patients, 6 died before completing pulmonary rehabilitation, with 42 (27%) dying during follow-up.
Benefits of rehabilitation
Multivariable analyses showed that noncompletion and nonresponse were associated with significantly higher risk of all-cause mortality at 1-year. Also, time to all-cause mortality was shorter (P = .001) for noncompleters and nonresponders, compared with completers. A trend toward higher completion rates in the IPF group, compared with the COPD group, may be explained, the researchers explained, by fewer hospitalizations over the prior 12 months in the IPF group.
“Although many programs are designed for people with COPD,” Dr. Nolan and colleagues concluded, “our study demonstrates that people with IPF have similar clinical benefits and completion rates to those with COPD. These data reinforce the importance of referral to and engagement in pulmonary rehabilitation amongst the IPF population.”
These findings, Dr. Nolan emphasized, emerged from a single center, and validation in other settings is needed.
This study was funded by a National Institute for Health Research Doctoral Research Fellowship (2014-07-089) and a Medical Research Council New Investigator Research Grant (98576).
FROM THE JOURNAL CHEST®
Long QT and Cardiac Arrest After Symptomatic Improvement of Pulmonary Edema
A case of extreme QT prolongation induced following symptomatic resolution of acute pulmonary edema is both relatively unknown and poorly understood.
Abnormalities in the T-wave morphology of an electrocardiogram (ECG) are classically attributed to ischemic cardiac disease. However, these changes can be seen in a variety of other etiologies, including noncardiac pathology, which should be considered whenever reviewing an ECG: central nervous system disease, including stroke and subarachnoid hemorrhage; hypothermia; pulmonary disease, such as pulmonary embolism or chronic obstructive pulmonary disease; myopericarditis; drug effects; and electrolyte abnormalities.
Prolongation of the QT interval, on the other hand, can be precipitated by medications, metabolic derangements, or genetic phenotypes. The QT interval is measured from the beginning of the QRS complex to the termination of the T wave and represents the total time for ventricular depolarization and repolarization. The QT interval must be corrected based on the patient’s heart rate, known as the QTc. As the QTc interval lengthens, there is increased risk of R-on-T phenomena, which may result in Torsades de Pointes (TdP). Typical features of TdP include an antecedent prolonged QTc, cyclic polymorphic ventricular tachycardia on the surface ECG, and either a short-lived spontaneously terminating course or degeneration into ventricular fibrillation (VF) and sudden cardiac death.1 These dysrhythmias become more likely as the QTc interval exceeds 500 msec.2
The combination of new-onset global T-wave inversions with prolongation of the QT interval has been reported in only a few limited conditions. Some known causes of these QT T changes include cardiac ischemia, status epilepticus, pheochromocytoma, and acute cocaine intoxication.3 One uncommon and rarely reported cause of extreme QT prolongation and T-wave inversion is acute pulmonary edema. The ECG findings are not present on initial patient presentation; rather the dynamic changes occur after resolution of the pulmonary symptoms. Despite significant ECG changes, all prior reported cases describe ECG normalization without significant morbidity.4,5 We report a case of extreme QT prolongation following acute pulmonary edema that resulted in cardiac arrest secondary to VF.
Case Presentation
A 72-year-old male with medical history of combined systolic and diastolic heart failure, ischemic cardiomyopathy, coronary artery disease, cerebral vascular accident, hypertension, hyperlipidemia, type 2 diabetes mellitus, and tobacco dependence presented to the emergency department (ED) by emergency medical services after awaking with acute onset of dyspnea and diaphoresis. On arrival at the ED, the patient was noted to be in respiratory distress (ie, unable to speak single words) and was extremely diaphoretic. His initial vital signs included blood pressure, 186/113 mm Hg, heart rate, 104 beats per minute, respiratory rate, 40 breaths per minute, and temperature, 36.4 °C. The patient was quickly placed on bilevel positive airway pressure and given sublingual nitroglycerin followed by transdermal nitroglycerin with a single dose of 40 mg IV furosemide, which improved his respiratory status. A chest X-ray was consistent with pulmonary edema, and his brain natriuretic peptide was 1654 pg/mL. An ECG demonstrated new T-wave inversions, and his troponin increased from 0.04 to 0.24 ng/mL during his ED stay (Figure 1). He was started on a heparin infusion and admitted to the hospital for hypertensive emergency with presumed acute decompensated heart failure and non-ST-elevated myocardial infarction.
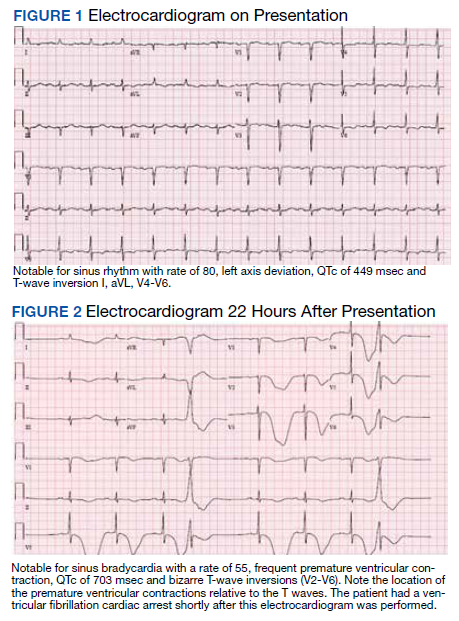
Throughout the patient’s first night, the troponin level started to down-trend after peaking at 0.24 ng/mL, and his oxygen requirements decreased allowing transition to nasal cannula. However, his repeat ECGs demonstrated significant T-wave abnormalities, new premature ventricular contractions, bradycardia, and a prolonging QTc interval to 703 msec (Figure 2). At this time, the patient’s electrolytes were normal, specifically a potassium level of 4.4 mEq/L, calcium 8.8 mg/dL, magnesium 2.0 mg/dL, and phosphorus 2.6 mg/dL. Given the worsening ECG changes, a computed tomography scan of his head was ordered to rule out intracranial pathology. While in the scanner, the patient went into pulseless VF, prompting defibrillation with 200 J. In addition, he was given 75 mg IV lidocaine, 2 g IV magnesium, and 1 ampule of both calcium chloride and sodium bicarbonate. With treatment, he had return of spontaneous circulation and was taken promptly to cardiac catheterization. The catheterization showed no significant obstructive coronary artery disease, and no interventions were performed. The patient was transferred to the cardiac intensive care unit for continued care.
During his course in the intensive care unit, the patient’s potassium and magnesium levels were maintained at high-normal levels. The patient was started on a dobutamine infusion to increase his heart rate and attempt to decrease his QTc. The patient also underwent cardiac magnetic resonance imaging (MRI) to evaluate for possible myocarditis, which showed no evidence of acute inflammation. Echocardiogram demonstrated an ejection fraction of 40% and global hypokinesis but no specific regional abnormalities and no change from prior echocardiogram performed 1 year earlier. Over the course of 3 days, his ECG normalized and his QTc shortened to 477 msec. Genetic testing was performed and did not reveal any mutations associated with long QT syndrome. Ultimately, an automated internal cardiac defibrillator (AICD) was placed, and the patient was discharged home.
Over the 2 years since his initial event, the patient has not experienced recurrent VF and his AICD has not fired. The patient continues to have ED presentations for heart-failure symptoms, though he has been stable from an electrophysiologic standpoint and his QTc remains less than 500 msec.
Discussion
Prolongation of the QT interval as a result of deep, global T-wave inversions after resolution of acute pulmonary edema has been minimally reported.4,5 This phenomenon has been described in the cardiology literature but has not been discussed in the emergency medicine literature and bears consideration in this case.4,5 As noted, an extensive evaluation did not reveal another cause of QTc prolongation. The patient had normal electrolytes and temperature, his neurologic examination and computed tomography were not remarkable. The patient had no obstructive coronary artery disease on catheterization, no evidence of acute myocarditis on cardiac MRI, no prescribed medications associated with QT prolongation, and no evidence of genetic mutations associated with QT prolongation on testing. The minimal troponin elevation was felt to represent a type II myocardial infarction related to ischemia due to supply-demand mismatch rather than acute plaque rupture.
Littmann published a case series of 9 cases of delayed onset T-wave inversion and extreme QTc prolongation in the 24 to 48 hours following treatment and symptomatic improvement in acute pulmonary edema.4 In each of his patients, an ischemic cardiac insult was ruled out as the etiology of the pulmonary edema by laboratory assessment, echocardiography, and left heart catheterization.All of the patients in this case series recovered without incident and with normalization of the QTc interval.4 Similarly, in our patient, significant QT T changes occurred approximately 22 hours after presentation and with resolution of symptoms of pulmonary edema. Pascale and colleagues also published a series of 3 patients developing similar ECG patterns following a hypertensive crisis with resolution of ECG findings and without any morbidity.5 In contrast, our patient experienced significant morbidity secondary to the extreme QTc prolongation.
Conclusions
We believe this is the first reported case of excessive prolongation of the QTc with VF arrest secondary to resolution of acute pulmonary edema. The pattern observed in our patient follows the patterns outlined in the previous case series—patients present with acute pulmonary edema and hypertensive crisis but develop significant ECG abnormalities about 24 hours after the resolution of the high catecholamine state. Our patient did have a history of prior cardiac insult, given the QTc changes developed acutely, with frequent premature ventricular contractions, and the cardiac arrest occurred at maximal QTc prolongation, yet after resolution of the high catecholamine state, the treatment team felt there was likely an uncaptured and short-lived episode of TdP that degenerated into VF. This theory is further supported by the lack of recurrent VF episodes, confirmed by AICD interrogation, after normalization of the QTc in our patient.
1. Passman R, Kadish A. Polymorphic ventricular tachycardia, long Q-T syndrome, and torsades de pointes. Med Clin North Am. 2001;85(2):321-341. doi:10.1016/s0025-7125(05)70318-7
2. Kallergis EM, Goudis CA, Simantirakis EN, Kochiadakis GE, Vardas PE. Mechanisms, risk factors, and management of acquired long QT syndrome: a comprehensive review. ScientificWorldJournal. 2012;2012:212178. doi:10.1100/2012/212178
3. Miller MA, Elmariah S, Fischer A. Giant T-wave inversions and extreme QT prolongation. Circ Arrhythm Electrophysiol. 2009;2(6):e42-e43. doi:10.1161/CIRCEP.108.825729
4. Littmann L. Large T wave inversion and QT prolongation associated with pulmonary edema: a report of nine cases. J Am Coll Cardiol. 1999;34(4):1106-1110. doi:10.1016/s0735-1097(99)00311-3
5. Pascale P, Quartenoud B, Stauffer JC. Isolated large inverted T wave in pulmonary edema due to hypertensive crisis: a novel electrocardiographic phenomenon mimicking ischemia?. Clin Res Cardiol. 2007;96(5):288-294. doi:10.1007/s00392-007-0504-1
A case of extreme QT prolongation induced following symptomatic resolution of acute pulmonary edema is both relatively unknown and poorly understood.
A case of extreme QT prolongation induced following symptomatic resolution of acute pulmonary edema is both relatively unknown and poorly understood.
Abnormalities in the T-wave morphology of an electrocardiogram (ECG) are classically attributed to ischemic cardiac disease. However, these changes can be seen in a variety of other etiologies, including noncardiac pathology, which should be considered whenever reviewing an ECG: central nervous system disease, including stroke and subarachnoid hemorrhage; hypothermia; pulmonary disease, such as pulmonary embolism or chronic obstructive pulmonary disease; myopericarditis; drug effects; and electrolyte abnormalities.
Prolongation of the QT interval, on the other hand, can be precipitated by medications, metabolic derangements, or genetic phenotypes. The QT interval is measured from the beginning of the QRS complex to the termination of the T wave and represents the total time for ventricular depolarization and repolarization. The QT interval must be corrected based on the patient’s heart rate, known as the QTc. As the QTc interval lengthens, there is increased risk of R-on-T phenomena, which may result in Torsades de Pointes (TdP). Typical features of TdP include an antecedent prolonged QTc, cyclic polymorphic ventricular tachycardia on the surface ECG, and either a short-lived spontaneously terminating course or degeneration into ventricular fibrillation (VF) and sudden cardiac death.1 These dysrhythmias become more likely as the QTc interval exceeds 500 msec.2
The combination of new-onset global T-wave inversions with prolongation of the QT interval has been reported in only a few limited conditions. Some known causes of these QT T changes include cardiac ischemia, status epilepticus, pheochromocytoma, and acute cocaine intoxication.3 One uncommon and rarely reported cause of extreme QT prolongation and T-wave inversion is acute pulmonary edema. The ECG findings are not present on initial patient presentation; rather the dynamic changes occur after resolution of the pulmonary symptoms. Despite significant ECG changes, all prior reported cases describe ECG normalization without significant morbidity.4,5 We report a case of extreme QT prolongation following acute pulmonary edema that resulted in cardiac arrest secondary to VF.
Case Presentation
A 72-year-old male with medical history of combined systolic and diastolic heart failure, ischemic cardiomyopathy, coronary artery disease, cerebral vascular accident, hypertension, hyperlipidemia, type 2 diabetes mellitus, and tobacco dependence presented to the emergency department (ED) by emergency medical services after awaking with acute onset of dyspnea and diaphoresis. On arrival at the ED, the patient was noted to be in respiratory distress (ie, unable to speak single words) and was extremely diaphoretic. His initial vital signs included blood pressure, 186/113 mm Hg, heart rate, 104 beats per minute, respiratory rate, 40 breaths per minute, and temperature, 36.4 °C. The patient was quickly placed on bilevel positive airway pressure and given sublingual nitroglycerin followed by transdermal nitroglycerin with a single dose of 40 mg IV furosemide, which improved his respiratory status. A chest X-ray was consistent with pulmonary edema, and his brain natriuretic peptide was 1654 pg/mL. An ECG demonstrated new T-wave inversions, and his troponin increased from 0.04 to 0.24 ng/mL during his ED stay (Figure 1). He was started on a heparin infusion and admitted to the hospital for hypertensive emergency with presumed acute decompensated heart failure and non-ST-elevated myocardial infarction.
Throughout the patient’s first night, the troponin level started to down-trend after peaking at 0.24 ng/mL, and his oxygen requirements decreased allowing transition to nasal cannula. However, his repeat ECGs demonstrated significant T-wave abnormalities, new premature ventricular contractions, bradycardia, and a prolonging QTc interval to 703 msec (Figure 2). At this time, the patient’s electrolytes were normal, specifically a potassium level of 4.4 mEq/L, calcium 8.8 mg/dL, magnesium 2.0 mg/dL, and phosphorus 2.6 mg/dL. Given the worsening ECG changes, a computed tomography scan of his head was ordered to rule out intracranial pathology. While in the scanner, the patient went into pulseless VF, prompting defibrillation with 200 J. In addition, he was given 75 mg IV lidocaine, 2 g IV magnesium, and 1 ampule of both calcium chloride and sodium bicarbonate. With treatment, he had return of spontaneous circulation and was taken promptly to cardiac catheterization. The catheterization showed no significant obstructive coronary artery disease, and no interventions were performed. The patient was transferred to the cardiac intensive care unit for continued care.
During his course in the intensive care unit, the patient’s potassium and magnesium levels were maintained at high-normal levels. The patient was started on a dobutamine infusion to increase his heart rate and attempt to decrease his QTc. The patient also underwent cardiac magnetic resonance imaging (MRI) to evaluate for possible myocarditis, which showed no evidence of acute inflammation. Echocardiogram demonstrated an ejection fraction of 40% and global hypokinesis but no specific regional abnormalities and no change from prior echocardiogram performed 1 year earlier. Over the course of 3 days, his ECG normalized and his QTc shortened to 477 msec. Genetic testing was performed and did not reveal any mutations associated with long QT syndrome. Ultimately, an automated internal cardiac defibrillator (AICD) was placed, and the patient was discharged home.
Over the 2 years since his initial event, the patient has not experienced recurrent VF and his AICD has not fired. The patient continues to have ED presentations for heart-failure symptoms, though he has been stable from an electrophysiologic standpoint and his QTc remains less than 500 msec.
Discussion
Prolongation of the QT interval as a result of deep, global T-wave inversions after resolution of acute pulmonary edema has been minimally reported.4,5 This phenomenon has been described in the cardiology literature but has not been discussed in the emergency medicine literature and bears consideration in this case.4,5 As noted, an extensive evaluation did not reveal another cause of QTc prolongation. The patient had normal electrolytes and temperature, his neurologic examination and computed tomography were not remarkable. The patient had no obstructive coronary artery disease on catheterization, no evidence of acute myocarditis on cardiac MRI, no prescribed medications associated with QT prolongation, and no evidence of genetic mutations associated with QT prolongation on testing. The minimal troponin elevation was felt to represent a type II myocardial infarction related to ischemia due to supply-demand mismatch rather than acute plaque rupture.
Littmann published a case series of 9 cases of delayed onset T-wave inversion and extreme QTc prolongation in the 24 to 48 hours following treatment and symptomatic improvement in acute pulmonary edema.4 In each of his patients, an ischemic cardiac insult was ruled out as the etiology of the pulmonary edema by laboratory assessment, echocardiography, and left heart catheterization.All of the patients in this case series recovered without incident and with normalization of the QTc interval.4 Similarly, in our patient, significant QT T changes occurred approximately 22 hours after presentation and with resolution of symptoms of pulmonary edema. Pascale and colleagues also published a series of 3 patients developing similar ECG patterns following a hypertensive crisis with resolution of ECG findings and without any morbidity.5 In contrast, our patient experienced significant morbidity secondary to the extreme QTc prolongation.
Conclusions
We believe this is the first reported case of excessive prolongation of the QTc with VF arrest secondary to resolution of acute pulmonary edema. The pattern observed in our patient follows the patterns outlined in the previous case series—patients present with acute pulmonary edema and hypertensive crisis but develop significant ECG abnormalities about 24 hours after the resolution of the high catecholamine state. Our patient did have a history of prior cardiac insult, given the QTc changes developed acutely, with frequent premature ventricular contractions, and the cardiac arrest occurred at maximal QTc prolongation, yet after resolution of the high catecholamine state, the treatment team felt there was likely an uncaptured and short-lived episode of TdP that degenerated into VF. This theory is further supported by the lack of recurrent VF episodes, confirmed by AICD interrogation, after normalization of the QTc in our patient.
Abnormalities in the T-wave morphology of an electrocardiogram (ECG) are classically attributed to ischemic cardiac disease. However, these changes can be seen in a variety of other etiologies, including noncardiac pathology, which should be considered whenever reviewing an ECG: central nervous system disease, including stroke and subarachnoid hemorrhage; hypothermia; pulmonary disease, such as pulmonary embolism or chronic obstructive pulmonary disease; myopericarditis; drug effects; and electrolyte abnormalities.
Prolongation of the QT interval, on the other hand, can be precipitated by medications, metabolic derangements, or genetic phenotypes. The QT interval is measured from the beginning of the QRS complex to the termination of the T wave and represents the total time for ventricular depolarization and repolarization. The QT interval must be corrected based on the patient’s heart rate, known as the QTc. As the QTc interval lengthens, there is increased risk of R-on-T phenomena, which may result in Torsades de Pointes (TdP). Typical features of TdP include an antecedent prolonged QTc, cyclic polymorphic ventricular tachycardia on the surface ECG, and either a short-lived spontaneously terminating course or degeneration into ventricular fibrillation (VF) and sudden cardiac death.1 These dysrhythmias become more likely as the QTc interval exceeds 500 msec.2
The combination of new-onset global T-wave inversions with prolongation of the QT interval has been reported in only a few limited conditions. Some known causes of these QT T changes include cardiac ischemia, status epilepticus, pheochromocytoma, and acute cocaine intoxication.3 One uncommon and rarely reported cause of extreme QT prolongation and T-wave inversion is acute pulmonary edema. The ECG findings are not present on initial patient presentation; rather the dynamic changes occur after resolution of the pulmonary symptoms. Despite significant ECG changes, all prior reported cases describe ECG normalization without significant morbidity.4,5 We report a case of extreme QT prolongation following acute pulmonary edema that resulted in cardiac arrest secondary to VF.
Case Presentation
A 72-year-old male with medical history of combined systolic and diastolic heart failure, ischemic cardiomyopathy, coronary artery disease, cerebral vascular accident, hypertension, hyperlipidemia, type 2 diabetes mellitus, and tobacco dependence presented to the emergency department (ED) by emergency medical services after awaking with acute onset of dyspnea and diaphoresis. On arrival at the ED, the patient was noted to be in respiratory distress (ie, unable to speak single words) and was extremely diaphoretic. His initial vital signs included blood pressure, 186/113 mm Hg, heart rate, 104 beats per minute, respiratory rate, 40 breaths per minute, and temperature, 36.4 °C. The patient was quickly placed on bilevel positive airway pressure and given sublingual nitroglycerin followed by transdermal nitroglycerin with a single dose of 40 mg IV furosemide, which improved his respiratory status. A chest X-ray was consistent with pulmonary edema, and his brain natriuretic peptide was 1654 pg/mL. An ECG demonstrated new T-wave inversions, and his troponin increased from 0.04 to 0.24 ng/mL during his ED stay (Figure 1). He was started on a heparin infusion and admitted to the hospital for hypertensive emergency with presumed acute decompensated heart failure and non-ST-elevated myocardial infarction.
Throughout the patient’s first night, the troponin level started to down-trend after peaking at 0.24 ng/mL, and his oxygen requirements decreased allowing transition to nasal cannula. However, his repeat ECGs demonstrated significant T-wave abnormalities, new premature ventricular contractions, bradycardia, and a prolonging QTc interval to 703 msec (Figure 2). At this time, the patient’s electrolytes were normal, specifically a potassium level of 4.4 mEq/L, calcium 8.8 mg/dL, magnesium 2.0 mg/dL, and phosphorus 2.6 mg/dL. Given the worsening ECG changes, a computed tomography scan of his head was ordered to rule out intracranial pathology. While in the scanner, the patient went into pulseless VF, prompting defibrillation with 200 J. In addition, he was given 75 mg IV lidocaine, 2 g IV magnesium, and 1 ampule of both calcium chloride and sodium bicarbonate. With treatment, he had return of spontaneous circulation and was taken promptly to cardiac catheterization. The catheterization showed no significant obstructive coronary artery disease, and no interventions were performed. The patient was transferred to the cardiac intensive care unit for continued care.
During his course in the intensive care unit, the patient’s potassium and magnesium levels were maintained at high-normal levels. The patient was started on a dobutamine infusion to increase his heart rate and attempt to decrease his QTc. The patient also underwent cardiac magnetic resonance imaging (MRI) to evaluate for possible myocarditis, which showed no evidence of acute inflammation. Echocardiogram demonstrated an ejection fraction of 40% and global hypokinesis but no specific regional abnormalities and no change from prior echocardiogram performed 1 year earlier. Over the course of 3 days, his ECG normalized and his QTc shortened to 477 msec. Genetic testing was performed and did not reveal any mutations associated with long QT syndrome. Ultimately, an automated internal cardiac defibrillator (AICD) was placed, and the patient was discharged home.
Over the 2 years since his initial event, the patient has not experienced recurrent VF and his AICD has not fired. The patient continues to have ED presentations for heart-failure symptoms, though he has been stable from an electrophysiologic standpoint and his QTc remains less than 500 msec.
Discussion
Prolongation of the QT interval as a result of deep, global T-wave inversions after resolution of acute pulmonary edema has been minimally reported.4,5 This phenomenon has been described in the cardiology literature but has not been discussed in the emergency medicine literature and bears consideration in this case.4,5 As noted, an extensive evaluation did not reveal another cause of QTc prolongation. The patient had normal electrolytes and temperature, his neurologic examination and computed tomography were not remarkable. The patient had no obstructive coronary artery disease on catheterization, no evidence of acute myocarditis on cardiac MRI, no prescribed medications associated with QT prolongation, and no evidence of genetic mutations associated with QT prolongation on testing. The minimal troponin elevation was felt to represent a type II myocardial infarction related to ischemia due to supply-demand mismatch rather than acute plaque rupture.
Littmann published a case series of 9 cases of delayed onset T-wave inversion and extreme QTc prolongation in the 24 to 48 hours following treatment and symptomatic improvement in acute pulmonary edema.4 In each of his patients, an ischemic cardiac insult was ruled out as the etiology of the pulmonary edema by laboratory assessment, echocardiography, and left heart catheterization.All of the patients in this case series recovered without incident and with normalization of the QTc interval.4 Similarly, in our patient, significant QT T changes occurred approximately 22 hours after presentation and with resolution of symptoms of pulmonary edema. Pascale and colleagues also published a series of 3 patients developing similar ECG patterns following a hypertensive crisis with resolution of ECG findings and without any morbidity.5 In contrast, our patient experienced significant morbidity secondary to the extreme QTc prolongation.
Conclusions
We believe this is the first reported case of excessive prolongation of the QTc with VF arrest secondary to resolution of acute pulmonary edema. The pattern observed in our patient follows the patterns outlined in the previous case series—patients present with acute pulmonary edema and hypertensive crisis but develop significant ECG abnormalities about 24 hours after the resolution of the high catecholamine state. Our patient did have a history of prior cardiac insult, given the QTc changes developed acutely, with frequent premature ventricular contractions, and the cardiac arrest occurred at maximal QTc prolongation, yet after resolution of the high catecholamine state, the treatment team felt there was likely an uncaptured and short-lived episode of TdP that degenerated into VF. This theory is further supported by the lack of recurrent VF episodes, confirmed by AICD interrogation, after normalization of the QTc in our patient.
1. Passman R, Kadish A. Polymorphic ventricular tachycardia, long Q-T syndrome, and torsades de pointes. Med Clin North Am. 2001;85(2):321-341. doi:10.1016/s0025-7125(05)70318-7
2. Kallergis EM, Goudis CA, Simantirakis EN, Kochiadakis GE, Vardas PE. Mechanisms, risk factors, and management of acquired long QT syndrome: a comprehensive review. ScientificWorldJournal. 2012;2012:212178. doi:10.1100/2012/212178
3. Miller MA, Elmariah S, Fischer A. Giant T-wave inversions and extreme QT prolongation. Circ Arrhythm Electrophysiol. 2009;2(6):e42-e43. doi:10.1161/CIRCEP.108.825729
4. Littmann L. Large T wave inversion and QT prolongation associated with pulmonary edema: a report of nine cases. J Am Coll Cardiol. 1999;34(4):1106-1110. doi:10.1016/s0735-1097(99)00311-3
5. Pascale P, Quartenoud B, Stauffer JC. Isolated large inverted T wave in pulmonary edema due to hypertensive crisis: a novel electrocardiographic phenomenon mimicking ischemia?. Clin Res Cardiol. 2007;96(5):288-294. doi:10.1007/s00392-007-0504-1
1. Passman R, Kadish A. Polymorphic ventricular tachycardia, long Q-T syndrome, and torsades de pointes. Med Clin North Am. 2001;85(2):321-341. doi:10.1016/s0025-7125(05)70318-7
2. Kallergis EM, Goudis CA, Simantirakis EN, Kochiadakis GE, Vardas PE. Mechanisms, risk factors, and management of acquired long QT syndrome: a comprehensive review. ScientificWorldJournal. 2012;2012:212178. doi:10.1100/2012/212178
3. Miller MA, Elmariah S, Fischer A. Giant T-wave inversions and extreme QT prolongation. Circ Arrhythm Electrophysiol. 2009;2(6):e42-e43. doi:10.1161/CIRCEP.108.825729
4. Littmann L. Large T wave inversion and QT prolongation associated with pulmonary edema: a report of nine cases. J Am Coll Cardiol. 1999;34(4):1106-1110. doi:10.1016/s0735-1097(99)00311-3
5. Pascale P, Quartenoud B, Stauffer JC. Isolated large inverted T wave in pulmonary edema due to hypertensive crisis: a novel electrocardiographic phenomenon mimicking ischemia?. Clin Res Cardiol. 2007;96(5):288-294. doi:10.1007/s00392-007-0504-1
Genomic classifier is one piece of the ILD diagnosis puzzle
Although genomic testing is useful when an interstitial lung disease diagnosis is uncertain, the testing results themselves aren’t sufficient to make the diagnosis, Daniel Dilling, MD, FCCP, said in a presentation at the annual meeting of the American College of Chest Physicians, which was held virtually.

The genomic classifier (Envisia, Veracyte) helps differentiate idiopathic pulmonary fibrosis (IPF) by detecting usual interstitial pneumonia (UIP), the hallmark pattern of this interstitial lung disease.
However, UIP is just one piece of the larger diagnostic puzzle, according to Dr. Dilling, professor of medicine in the interstitial lung disease program at Loyola University Medical Center in Maywood, Ill.
“Remember, it’s just a pattern, and not a diagnosis of IPF,” Dr. Dilling said in his presentation.
Genomic classifier results correlate well with both histologic and radiographic UIP pattern, studies show.
However, Dr. Dilling said the value of the genomic classifier is not in isolation.
“We don’t use this in a vacuum,” he said. “It increases our confidence and consensus, but it has to be incorporated into a multidisciplinary discussion group.”
Part of the diagnostic pathway
Dr. Dilling said the genomic classifier should be considered part of a diagnostic pathway in uncertain cases, particularly when the risk of surgical lung biopsy is high.
Current clinical practice guidelines recommend surgical lung biopsy for histopathologic diagnosis when clinical and radiologic findings are not definitive for IPF, the speaker said.
However, surgical lung biopsy carries some risk, and sometimes it can’t be done, he added.
In his presentation, Dr. Dilling cited a systematic review and meta-analysis of 23 studies looking at surgical lung biopsy for the diagnosis of interstitial lung diseases.
The postoperative mortality rate was 3.6% in that meta-analysis, published in 2015 in the Journal of Thoracic and Cardiovascular Surgery.
“The final decision regarding whether or not to perform a [surgical lung biopsy] must be based on the balance between benefits to establish a secure diagnosis and the potential risks,” authors wrote at the time.
Mortality risk is higher in immunocompromised and acutely ill patient populations, according to Dr. Dilling, who added that as many of 19% of patients will have complications from surgical lung biopsy.
Genomic classifier studies
In a proof-of-principle study, published in 2017 in the Annals of the American Thoracic Society, authors described how they used machine learning to train an algorithm to distinguish UIP from non-UIP pattern in tissue obtained by transbronchial biopsy (TBB).
The top-performing algorithm distinguished UIP from non-UIP conditions in single TBB samples with specificity of 86% and sensitivity of 63%, according to investigators, who said at the time that independent validation would be needed before the genomic classifier could be applied in clinical settings.
In a prospective validation study, published in 2019 in The Lancet Respiratory Medicine, the genomic classifier identified UIP in TBB samples from 49 patients with a specificity of 88% and sensitivity of 70%.
Excluding patients with definite or probable UIP as shown on high-resolution computed tomography, results show that the classifier had a sensitivity of 76%, specificity of 88%, and positive predictive value of 81%.
“The performance of the test is good, even in that scenario,” Dr. Dilling said.
Real-world results
Dr. Dilling also highlighted a “real-world” study, published earlier in 2021, demonstrating that UIP pattern recognized by a genomic classifier had encouraging sensitivity and specificity when combined with high-resolution CT and clinical factors.
That study included 96 patients who had both diagnostic lung pathology and a transbronchial lung biopsy for molecular testing with the classifier.
The classifier had a sensitivity of 60.3% and a specificity of 92.1% for histology-proven UIP pattern, investigators said in their report, which appears in the American Journal of Respiratory and Critical Care Medicine.
Local radiologists identified UIP with a sensitivity of 34.0% and specificity of 96.9%. But adding genomic classifier testing to local radiology testing increased the diagnostic yield, investigators said, with a sensitivity of 79.2% and specificity of 90.6%.
“This might suggest that the implementation of this into a local [multidisciplinary discussion] with your local radiology expertise might really improve your recognition of UIP,” Dr. Dilling said.
Dr. Dilling reported disclosures related to Bellerophon, Boehringer Ingelheim, Genentech, Nitto Denko, and Lung Bioengineering.
Although genomic testing is useful when an interstitial lung disease diagnosis is uncertain, the testing results themselves aren’t sufficient to make the diagnosis, Daniel Dilling, MD, FCCP, said in a presentation at the annual meeting of the American College of Chest Physicians, which was held virtually.
The genomic classifier (Envisia, Veracyte) helps differentiate idiopathic pulmonary fibrosis (IPF) by detecting usual interstitial pneumonia (UIP), the hallmark pattern of this interstitial lung disease.
However, UIP is just one piece of the larger diagnostic puzzle, according to Dr. Dilling, professor of medicine in the interstitial lung disease program at Loyola University Medical Center in Maywood, Ill.
“Remember, it’s just a pattern, and not a diagnosis of IPF,” Dr. Dilling said in his presentation.
Genomic classifier results correlate well with both histologic and radiographic UIP pattern, studies show.
However, Dr. Dilling said the value of the genomic classifier is not in isolation.
“We don’t use this in a vacuum,” he said. “It increases our confidence and consensus, but it has to be incorporated into a multidisciplinary discussion group.”
Part of the diagnostic pathway
Dr. Dilling said the genomic classifier should be considered part of a diagnostic pathway in uncertain cases, particularly when the risk of surgical lung biopsy is high.
Current clinical practice guidelines recommend surgical lung biopsy for histopathologic diagnosis when clinical and radiologic findings are not definitive for IPF, the speaker said.
However, surgical lung biopsy carries some risk, and sometimes it can’t be done, he added.
In his presentation, Dr. Dilling cited a systematic review and meta-analysis of 23 studies looking at surgical lung biopsy for the diagnosis of interstitial lung diseases.
The postoperative mortality rate was 3.6% in that meta-analysis, published in 2015 in the Journal of Thoracic and Cardiovascular Surgery.
“The final decision regarding whether or not to perform a [surgical lung biopsy] must be based on the balance between benefits to establish a secure diagnosis and the potential risks,” authors wrote at the time.
Mortality risk is higher in immunocompromised and acutely ill patient populations, according to Dr. Dilling, who added that as many of 19% of patients will have complications from surgical lung biopsy.
Genomic classifier studies
In a proof-of-principle study, published in 2017 in the Annals of the American Thoracic Society, authors described how they used machine learning to train an algorithm to distinguish UIP from non-UIP pattern in tissue obtained by transbronchial biopsy (TBB).
The top-performing algorithm distinguished UIP from non-UIP conditions in single TBB samples with specificity of 86% and sensitivity of 63%, according to investigators, who said at the time that independent validation would be needed before the genomic classifier could be applied in clinical settings.
In a prospective validation study, published in 2019 in The Lancet Respiratory Medicine, the genomic classifier identified UIP in TBB samples from 49 patients with a specificity of 88% and sensitivity of 70%.
Excluding patients with definite or probable UIP as shown on high-resolution computed tomography, results show that the classifier had a sensitivity of 76%, specificity of 88%, and positive predictive value of 81%.
“The performance of the test is good, even in that scenario,” Dr. Dilling said.
Real-world results
Dr. Dilling also highlighted a “real-world” study, published earlier in 2021, demonstrating that UIP pattern recognized by a genomic classifier had encouraging sensitivity and specificity when combined with high-resolution CT and clinical factors.
That study included 96 patients who had both diagnostic lung pathology and a transbronchial lung biopsy for molecular testing with the classifier.
The classifier had a sensitivity of 60.3% and a specificity of 92.1% for histology-proven UIP pattern, investigators said in their report, which appears in the American Journal of Respiratory and Critical Care Medicine.
Local radiologists identified UIP with a sensitivity of 34.0% and specificity of 96.9%. But adding genomic classifier testing to local radiology testing increased the diagnostic yield, investigators said, with a sensitivity of 79.2% and specificity of 90.6%.
“This might suggest that the implementation of this into a local [multidisciplinary discussion] with your local radiology expertise might really improve your recognition of UIP,” Dr. Dilling said.
Dr. Dilling reported disclosures related to Bellerophon, Boehringer Ingelheim, Genentech, Nitto Denko, and Lung Bioengineering.
Although genomic testing is useful when an interstitial lung disease diagnosis is uncertain, the testing results themselves aren’t sufficient to make the diagnosis, Daniel Dilling, MD, FCCP, said in a presentation at the annual meeting of the American College of Chest Physicians, which was held virtually.
The genomic classifier (Envisia, Veracyte) helps differentiate idiopathic pulmonary fibrosis (IPF) by detecting usual interstitial pneumonia (UIP), the hallmark pattern of this interstitial lung disease.
However, UIP is just one piece of the larger diagnostic puzzle, according to Dr. Dilling, professor of medicine in the interstitial lung disease program at Loyola University Medical Center in Maywood, Ill.
“Remember, it’s just a pattern, and not a diagnosis of IPF,” Dr. Dilling said in his presentation.
Genomic classifier results correlate well with both histologic and radiographic UIP pattern, studies show.
However, Dr. Dilling said the value of the genomic classifier is not in isolation.
“We don’t use this in a vacuum,” he said. “It increases our confidence and consensus, but it has to be incorporated into a multidisciplinary discussion group.”
Part of the diagnostic pathway
Dr. Dilling said the genomic classifier should be considered part of a diagnostic pathway in uncertain cases, particularly when the risk of surgical lung biopsy is high.
Current clinical practice guidelines recommend surgical lung biopsy for histopathologic diagnosis when clinical and radiologic findings are not definitive for IPF, the speaker said.
However, surgical lung biopsy carries some risk, and sometimes it can’t be done, he added.
In his presentation, Dr. Dilling cited a systematic review and meta-analysis of 23 studies looking at surgical lung biopsy for the diagnosis of interstitial lung diseases.
The postoperative mortality rate was 3.6% in that meta-analysis, published in 2015 in the Journal of Thoracic and Cardiovascular Surgery.
“The final decision regarding whether or not to perform a [surgical lung biopsy] must be based on the balance between benefits to establish a secure diagnosis and the potential risks,” authors wrote at the time.
Mortality risk is higher in immunocompromised and acutely ill patient populations, according to Dr. Dilling, who added that as many of 19% of patients will have complications from surgical lung biopsy.
Genomic classifier studies
In a proof-of-principle study, published in 2017 in the Annals of the American Thoracic Society, authors described how they used machine learning to train an algorithm to distinguish UIP from non-UIP pattern in tissue obtained by transbronchial biopsy (TBB).
The top-performing algorithm distinguished UIP from non-UIP conditions in single TBB samples with specificity of 86% and sensitivity of 63%, according to investigators, who said at the time that independent validation would be needed before the genomic classifier could be applied in clinical settings.
In a prospective validation study, published in 2019 in The Lancet Respiratory Medicine, the genomic classifier identified UIP in TBB samples from 49 patients with a specificity of 88% and sensitivity of 70%.
Excluding patients with definite or probable UIP as shown on high-resolution computed tomography, results show that the classifier had a sensitivity of 76%, specificity of 88%, and positive predictive value of 81%.
“The performance of the test is good, even in that scenario,” Dr. Dilling said.
Real-world results
Dr. Dilling also highlighted a “real-world” study, published earlier in 2021, demonstrating that UIP pattern recognized by a genomic classifier had encouraging sensitivity and specificity when combined with high-resolution CT and clinical factors.
That study included 96 patients who had both diagnostic lung pathology and a transbronchial lung biopsy for molecular testing with the classifier.
The classifier had a sensitivity of 60.3% and a specificity of 92.1% for histology-proven UIP pattern, investigators said in their report, which appears in the American Journal of Respiratory and Critical Care Medicine.
Local radiologists identified UIP with a sensitivity of 34.0% and specificity of 96.9%. But adding genomic classifier testing to local radiology testing increased the diagnostic yield, investigators said, with a sensitivity of 79.2% and specificity of 90.6%.
“This might suggest that the implementation of this into a local [multidisciplinary discussion] with your local radiology expertise might really improve your recognition of UIP,” Dr. Dilling said.
Dr. Dilling reported disclosures related to Bellerophon, Boehringer Ingelheim, Genentech, Nitto Denko, and Lung Bioengineering.
FROM CHEST 2021