User login
‘Don’t say gay’: The politicization of gender-diverse youth
The past several weeks have been rather tumultuous for LGBTQ Americans, particularly transgender youth. The Texas attorney general penned a legal opinion stating that hormone therapy and puberty blockers for transgender youth constitute “child abuse” under Texas law. Following the statement, Texas governor Greg Abbott swiftly issued a directive to protective services to launch investigations into families providing such services to their children. Almost simultaneously, the Florida Senate approved the Parental Rights in Education bill (dubbed the “Don’t Say Gay” bill by opponents), which limits how sexual orientation and gender identity are taught in the classroom.
Despite the benefits of gender-affirming care for gender-diverse youth, 22 states have introduced legislation that bans the provision of gender-affirming medical care under the age of 18, even with the consent of parents or legal guardians.1 Unfortunately, gender-diverse youth are more likely than are their cisgender peers to experience poverty, homelessness, depression, suicide, and violence.1 As a result of ongoing stigma, many gender-diverse patients are hesitant to seek out professional medical care, which includes mental health care, routine health care, and gender-affirming therapies. The positive effects of gender-affirming care for transgender youth are clear, and life saving for many. Gender-affirming medical interventions improve social and mental health outcomes, such as decreased suicidal ideation, depression, and improved peer relations that last until adulthood.1

As with all aspects in medicine, providers and families of gender-diverse youth need to balance the four ethical principles that guide decision-making and informed consent. For practitioners working with the pediatric/adolescent populations, the age at which pediatric or adolescent patients can truly provide consent or assent is still not determined.2 This presents a unique set of challenges in the realm of gender-affirming care particularly when children/adolescents and their parents have differing perspectives on proposed treatment plans. For example, when discussing fertility preservation, a 16-year-old patient is much more likely to understand implications of future fertility than a 9-year-old patient. Furthermore, providers must find the delicate balance between maximizing treatment benefits (beneficence) while minimizing harm (nonmaleficence), while also discussing the uncertainty about the long-term risks of gender-affirming treatments.2 The final obligation for health care providers is ensuring all patients have equitable access to care (justice) – which is why we must all oppose legislation that criminalizes treatment for gender-diverse youth, regardless of our individual opinions on gender-affirming care for patients.
Opponents of gender-affirming care for transgender youth often cite concern about permanent effects or psychological distress if a child begins gender-affirming therapy and then chooses to discontinue. While the medical community should be, and is alarmed about patients who detransition, the solution to limiting the number of patients who experience regret or detransition is most certainly not criminalizing or universally banning gender-affirming care for all patients.3 Experts in transgender medicine and surgery (some of whom are transgender themselves) have expressed apprehension regarding the evaluation of gender-diverse children and youth. The concern is not whether gender-diverse youth should receive gender-affirming treatments, but rather they questioned the assessments made by providers who may be less fully qualified to deliver treatment and who deviate from well-established standards of care.4 The logical solution would be to further improve upon the current standards of care, ensure providers have appropriate training, and to expand multidisciplinary models of gender-affirming centers for youth.
If politicians were truly worried about the welfare of gender-diverse children, there would be a shift in the allocation of funds or resources to improve research endeavors and establish effective multidisciplinary clinics to meet the needs of this marginalized patient population. While the medical community should carefully examine gender-affirming care in transgender youth, criminalizing care is unconscionable. Our community needs more evidence-based research, providers, and centers, not politics.
The LGBTQ community and providers are rightfully fearful of the repercussions of such legislation. And the politicians and supporters of such bills should be equally apprehensive of the negative consequences this legislation will have on the mental health of transgender youth.
While the model for gender-affirming medicine and surgery needs continual assessment to ensure all patients, regardless of age and goals of transition, are receiving evidence-based, quality care, these discussions and subsequent decision-making should occur among medical professionals, not among politicians and the lay press.4
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Hughes LD et al. ‘These laws will be devastating’: Provider perspectives on legislation banning gender-affirming care for transgender adolescents. J Adol Health;2021;69:976-82.
2. Kimberly LL et al. Ethical issues in gender-affirming care for youth. Pediatrics. Pediatrics;018;142(6)e20181537.
3. Ashley F. Psychol Sexual Orient Gender Divers. APA PsycNet. 2021.
4. Ault A. Transgender docs warn about gender-affirmative care for youth. WebMD. 2021 Nov. Accessed March 14, 2022.
The past several weeks have been rather tumultuous for LGBTQ Americans, particularly transgender youth. The Texas attorney general penned a legal opinion stating that hormone therapy and puberty blockers for transgender youth constitute “child abuse” under Texas law. Following the statement, Texas governor Greg Abbott swiftly issued a directive to protective services to launch investigations into families providing such services to their children. Almost simultaneously, the Florida Senate approved the Parental Rights in Education bill (dubbed the “Don’t Say Gay” bill by opponents), which limits how sexual orientation and gender identity are taught in the classroom.
Despite the benefits of gender-affirming care for gender-diverse youth, 22 states have introduced legislation that bans the provision of gender-affirming medical care under the age of 18, even with the consent of parents or legal guardians.1 Unfortunately, gender-diverse youth are more likely than are their cisgender peers to experience poverty, homelessness, depression, suicide, and violence.1 As a result of ongoing stigma, many gender-diverse patients are hesitant to seek out professional medical care, which includes mental health care, routine health care, and gender-affirming therapies. The positive effects of gender-affirming care for transgender youth are clear, and life saving for many. Gender-affirming medical interventions improve social and mental health outcomes, such as decreased suicidal ideation, depression, and improved peer relations that last until adulthood.1
As with all aspects in medicine, providers and families of gender-diverse youth need to balance the four ethical principles that guide decision-making and informed consent. For practitioners working with the pediatric/adolescent populations, the age at which pediatric or adolescent patients can truly provide consent or assent is still not determined.2 This presents a unique set of challenges in the realm of gender-affirming care particularly when children/adolescents and their parents have differing perspectives on proposed treatment plans. For example, when discussing fertility preservation, a 16-year-old patient is much more likely to understand implications of future fertility than a 9-year-old patient. Furthermore, providers must find the delicate balance between maximizing treatment benefits (beneficence) while minimizing harm (nonmaleficence), while also discussing the uncertainty about the long-term risks of gender-affirming treatments.2 The final obligation for health care providers is ensuring all patients have equitable access to care (justice) – which is why we must all oppose legislation that criminalizes treatment for gender-diverse youth, regardless of our individual opinions on gender-affirming care for patients.
Opponents of gender-affirming care for transgender youth often cite concern about permanent effects or psychological distress if a child begins gender-affirming therapy and then chooses to discontinue. While the medical community should be, and is alarmed about patients who detransition, the solution to limiting the number of patients who experience regret or detransition is most certainly not criminalizing or universally banning gender-affirming care for all patients.3 Experts in transgender medicine and surgery (some of whom are transgender themselves) have expressed apprehension regarding the evaluation of gender-diverse children and youth. The concern is not whether gender-diverse youth should receive gender-affirming treatments, but rather they questioned the assessments made by providers who may be less fully qualified to deliver treatment and who deviate from well-established standards of care.4 The logical solution would be to further improve upon the current standards of care, ensure providers have appropriate training, and to expand multidisciplinary models of gender-affirming centers for youth.
If politicians were truly worried about the welfare of gender-diverse children, there would be a shift in the allocation of funds or resources to improve research endeavors and establish effective multidisciplinary clinics to meet the needs of this marginalized patient population. While the medical community should carefully examine gender-affirming care in transgender youth, criminalizing care is unconscionable. Our community needs more evidence-based research, providers, and centers, not politics.
The LGBTQ community and providers are rightfully fearful of the repercussions of such legislation. And the politicians and supporters of such bills should be equally apprehensive of the negative consequences this legislation will have on the mental health of transgender youth.
While the model for gender-affirming medicine and surgery needs continual assessment to ensure all patients, regardless of age and goals of transition, are receiving evidence-based, quality care, these discussions and subsequent decision-making should occur among medical professionals, not among politicians and the lay press.4
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Hughes LD et al. ‘These laws will be devastating’: Provider perspectives on legislation banning gender-affirming care for transgender adolescents. J Adol Health;2021;69:976-82.
2. Kimberly LL et al. Ethical issues in gender-affirming care for youth. Pediatrics. Pediatrics;018;142(6)e20181537.
3. Ashley F. Psychol Sexual Orient Gender Divers. APA PsycNet. 2021.
4. Ault A. Transgender docs warn about gender-affirmative care for youth. WebMD. 2021 Nov. Accessed March 14, 2022.
The past several weeks have been rather tumultuous for LGBTQ Americans, particularly transgender youth. The Texas attorney general penned a legal opinion stating that hormone therapy and puberty blockers for transgender youth constitute “child abuse” under Texas law. Following the statement, Texas governor Greg Abbott swiftly issued a directive to protective services to launch investigations into families providing such services to their children. Almost simultaneously, the Florida Senate approved the Parental Rights in Education bill (dubbed the “Don’t Say Gay” bill by opponents), which limits how sexual orientation and gender identity are taught in the classroom.
Despite the benefits of gender-affirming care for gender-diverse youth, 22 states have introduced legislation that bans the provision of gender-affirming medical care under the age of 18, even with the consent of parents or legal guardians.1 Unfortunately, gender-diverse youth are more likely than are their cisgender peers to experience poverty, homelessness, depression, suicide, and violence.1 As a result of ongoing stigma, many gender-diverse patients are hesitant to seek out professional medical care, which includes mental health care, routine health care, and gender-affirming therapies. The positive effects of gender-affirming care for transgender youth are clear, and life saving for many. Gender-affirming medical interventions improve social and mental health outcomes, such as decreased suicidal ideation, depression, and improved peer relations that last until adulthood.1
As with all aspects in medicine, providers and families of gender-diverse youth need to balance the four ethical principles that guide decision-making and informed consent. For practitioners working with the pediatric/adolescent populations, the age at which pediatric or adolescent patients can truly provide consent or assent is still not determined.2 This presents a unique set of challenges in the realm of gender-affirming care particularly when children/adolescents and their parents have differing perspectives on proposed treatment plans. For example, when discussing fertility preservation, a 16-year-old patient is much more likely to understand implications of future fertility than a 9-year-old patient. Furthermore, providers must find the delicate balance between maximizing treatment benefits (beneficence) while minimizing harm (nonmaleficence), while also discussing the uncertainty about the long-term risks of gender-affirming treatments.2 The final obligation for health care providers is ensuring all patients have equitable access to care (justice) – which is why we must all oppose legislation that criminalizes treatment for gender-diverse youth, regardless of our individual opinions on gender-affirming care for patients.
Opponents of gender-affirming care for transgender youth often cite concern about permanent effects or psychological distress if a child begins gender-affirming therapy and then chooses to discontinue. While the medical community should be, and is alarmed about patients who detransition, the solution to limiting the number of patients who experience regret or detransition is most certainly not criminalizing or universally banning gender-affirming care for all patients.3 Experts in transgender medicine and surgery (some of whom are transgender themselves) have expressed apprehension regarding the evaluation of gender-diverse children and youth. The concern is not whether gender-diverse youth should receive gender-affirming treatments, but rather they questioned the assessments made by providers who may be less fully qualified to deliver treatment and who deviate from well-established standards of care.4 The logical solution would be to further improve upon the current standards of care, ensure providers have appropriate training, and to expand multidisciplinary models of gender-affirming centers for youth.
If politicians were truly worried about the welfare of gender-diverse children, there would be a shift in the allocation of funds or resources to improve research endeavors and establish effective multidisciplinary clinics to meet the needs of this marginalized patient population. While the medical community should carefully examine gender-affirming care in transgender youth, criminalizing care is unconscionable. Our community needs more evidence-based research, providers, and centers, not politics.
The LGBTQ community and providers are rightfully fearful of the repercussions of such legislation. And the politicians and supporters of such bills should be equally apprehensive of the negative consequences this legislation will have on the mental health of transgender youth.
While the model for gender-affirming medicine and surgery needs continual assessment to ensure all patients, regardless of age and goals of transition, are receiving evidence-based, quality care, these discussions and subsequent decision-making should occur among medical professionals, not among politicians and the lay press.4
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Hughes LD et al. ‘These laws will be devastating’: Provider perspectives on legislation banning gender-affirming care for transgender adolescents. J Adol Health;2021;69:976-82.
2. Kimberly LL et al. Ethical issues in gender-affirming care for youth. Pediatrics. Pediatrics;018;142(6)e20181537.
3. Ashley F. Psychol Sexual Orient Gender Divers. APA PsycNet. 2021.
4. Ault A. Transgender docs warn about gender-affirmative care for youth. WebMD. 2021 Nov. Accessed March 14, 2022.
Doctors have failed them, say those with transgender regret
In a unique Zoom conference,
The forum was convened on what was dubbed #DetransitionAwarenessDay by Genspect, a parent-based organization that seeks to put the brakes on medical transitions for children and adolescents. The group has doubts about the gender-affirming care model supported by the World Professional Association for Transgender Health, the American Medical Association, the American Academy of Pediatrics, and other medical groups.
“Affirmative” medical care is defined as treatment with puberty blockers and cross-sex hormones for those with gender dysphoria to transition to the opposite sex and is often followed by gender reassignment surgery. However, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed for those under aged 18, in particular, with several countries pulling back on medical treatment and instead emphasizing psychotherapy first.
The purpose of the second annual Genspect meeting was to shed light on the experiences of individuals who have detransitioned – those that identified as transgender and transitioned, but then decided to end their medical transition. People logged on from all over the United States, Canada, New Zealand, Australia, the United Kingdom, Germany, Spain, Chile, and Brazil, among other countries.
“This is a minority within a minority,” said Genspect advisor Stella O’Malley, adding that the first meeting in 2021 was held because “too many people were dismissing the stories of the detransitioners.” Ms. O’Malley is a psychotherapist, a clinical advisor to the Society for Evidence-Based Gender Medicine, and a founding member of the International Association of Therapists for Desisters and Detransitioners.
“It’s become blindingly obvious over the last year that ... ‘detrans’ is a huge part of the trans phenomenon,” said Ms. O’Malley, adding that detransitioners have been “undermined and dismissed.”
Laura Edwards-Leeper, PhD (@DrLauraEL), a prominent gender therapist who has recently expressed concern regarding adequate gatekeeping when treating youth with gender dysphoria, agreed.
She tweeted: “You simply can’t call yourself a legit gender provider if you don’t believe that detransitioners exist. As part of the informed consent process for transitioning, it is unethical to not discuss this possibility with young people.” Dr. Edwards-Leeper is professor emeritus at Pacific University in Hillsboro, Ore.
Speakers in the forum largely offered experiences, not data. They pointed out that there has been little to no study of detransition, but all testified that it was less rare than it has been portrayed by the transgender community.
Struggles with going back
“There are so many reasons why people detransition,” said Sinead Watson, aged 30, a Genspect advisor who transitioned from female to male, starting in 2015, and who decided to detransition in 2019. Citing a study by Lisa Littman, MD, MPH, published in 2021, Ms. Watson said the most common reasons for detransitioning were realizing that gender dysphoria was caused by other issues; internal homophobia; and the unbearable nature of transphobia.
Ms. Watson said the hardest part of detransitioning was admitting to herself that her transition had been a mistake. “It’s embarrassing and you feel ashamed and guilty,” she said, adding that it may mean losing friends who now regard you as a “bigot, while you’re also dealing with transition regret.”
“It’s a living hell, especially when none of your therapists or counselors will listen to you,” she said. “Detransitioning isn’t fun.”
Carol (@sourpatches2077) said she knew for a year that her transition had been a mistake.
“The biggest part was I couldn’t tell my family,” said Carol, who identifies as a lesbian. “I put them through so much. It seems ridiculous to go: ‘Oops, I made this huge [expletive] mistake,’ ” she said, describing the moment she did tell them as “devastating.”
Grace (@hormonehangover) said she remembers finally hitting a moment of “undeniability” some years after transitioning. “I accept it, I’ve ruined my life, this is wrong,” she remembers thinking. “It was devastating, but I couldn’t deny it anymore.”
Don’t trust therapists
People experiencing feelings of unease “need a therapist who will listen to them,” said Ms. Watson. When she first detransitioned, her therapists treated her badly. “They just didn’t want to speak about detransition,” she said, adding that “it was like a kick in the stomach.”
Ms. Watson said she’d like to see more training about detransition, but also on “preventative techniques,” adding that many people transition who should not. “I don’t want more detransitioners – I want less.
“In order for that to happen, we need to treat people with gender dysphoria properly,” said Ms. Watson, adding that the affirmative model is “disgusting, and that’s what needs to change.”
“I would tell somebody to not go to a therapist,” said Carol. Identifying as a butch lesbian, she felt like her therapists had pushed her into transitioning to male. “The No. 1 thing not understood by the mental health professionals is that the vast majority of homosexuals were gender-nonconforming children.” She added that this is especially true of butch lesbians.
Therapists – and doctors – also need to acknowledge both the trauma of transition and detransition, she said.
Kaiser, where she had transitioned, offered her breast reconstruction. Carol said it felt demeaning. “Like you’re Mr. Potatohead: ‘Here, we can just ... put on some new parts and you’re good to go.’ ”
“Doctors are concretizing transient obsessions,” said Helena Kerschner (@lacroicsz), quoting a chatroom user.
Ms. Kerschner gave a presentation on “fandom”: becoming obsessed with a movie, book, TV show, musician, or celebrity, spending every waking hour chatting online or writing fan fiction, or attempting to interact with the celebrity online. It’s a fantasy-dominated world and “the vast majority” of participants are teenage girls who are “identifying as trans,” in part, because they are fed a community-reinforced message that it’s better to be a boy.
Therapists and physicians who help them transition “are harming them for life based on something they would have grown out of or overcome without the permanent damage,” Ms. Kerschner added.
Doctors ‘gaslighting’ people into believing that transition is the answer
A pervasive theme during the webinar was that many people are being misdiagnosed with gender dysphoria, which may not be resolved by medical transition.
Allie, a 22-year-old who stopped taking testosterone after 1½ years, said she initially started the transition to male when she gave up trying to figure out why she could not identify with, or befriend, women, and after a childhood and adolescence spent mostly in the company of boys and being more interested in traditionally male activities.
She endured sexual abuse as a teenager and her parents divorced while she was in high school. Allie also had multiple suicide attempts and many incidents of self-harm. When she decided to transition, at age 18, she went to a private clinic and received cross-sex hormones within a few months of her first and only 30-minute consultation. “There was no explorative therapy,” she said, adding that she was never given a formal diagnosis of gender dysphoria.
For the first year, she said she was “over the freaking moon” because she felt like it was the answer. But things started to unravel while she attended university, and she attempted suicide attempt at age 20. A social worker at the school identified her symptoms – which had been the same since childhood – as autism. She then decided to cease her transition.
Another detransitioner, Laura Becker, said it took 5 years after her transition to recognize that she had undiagnosed PTSD from emotional and psychiatric abuse. Despite a history of substance abuse, self-harm, suicidal ideation, and other mental health issues, she was given testosterone and had a double mastectomy at age 20. She became fixated on gay men, which devolved into a methamphetamine- and crack-fueled relationship with a man she met on the gay dating platform Grindr.
“No one around me knew any better or knew how to help, including the medical professionals who performed the mastectomy and who casually signed off and administered my medical transition,” she said.
Once she was aware of her PTSD she started to detransition, which itself was traumatic, said Laura.
Limpida, aged 24, said he felt pushed into transitioning after seeking help at a Planned Parenthood clinic. He identified as trans at age 15 and spent years attempting to be a woman socially, but every step made him feel more miserable, he said. When he went to the clinic at age 21 to get estrogen, he said he felt like the staff was dismissive of his mental health concerns – including that he was suicidal, had substance abuse, and was severely depressed. He was told he was the “perfect candidate” for transitioning.
A year later, he said he felt worse. The nurse suggested he seek out surgery. After Limpida researched what was involved, he decided to detransition. He has since received an autism diagnosis.
Robin, also aged 24, said the idea of surgery had helped push him into detransitioning, which began in 2020 after 4 years of estrogen. He said he had always been gender nonconforming and knew he was gay at an early age. He believes that gender-nonconforming people are “gaslighted” into thinking that transitioning is the answer.
Lack of evidence-based, informed consent
Michelle Alleva, who stopped identifying as transgender in 2020 but had ceased testosterone 4 years earlier because of side effects, cited what she called a lack of evidence base for the effectiveness and safety of medical transitions.
“You need to have a really, really good evidence base in place if you’re going straight to an invasive treatment that is going to cause permanent changes to your body,” she said.
Access to medical transition used to involve more “gatekeeping” through mental health evaluations and other interventions, she said, but there has been a shift from treating what was considered a psychiatric issue to essentially affirming an identity.
“This shift was activist driven, not evidence based,” she emphasized.
Most studies showing satisfaction with transition only involve a few years of follow-up, she said. She added that the longest follow-up study of transition, published in 2011 and spanning 30 years, showed that the suicide rate 10-15 years post surgery was 20 times higher than the general population.
Studies of regret were primarily conducted before the rapid increase in the number of trans-identifying individuals, she said, which makes it hard to draw conclusions about pediatric transition. Getting estimates on this population is difficult because so many who detransition do not tell their clinicians, and many studies have short follow-up times or a high loss to follow-up.
Ms. Alleva also took issue with the notion that physicians were offering true informed consent, noting that it’s not possible to know if someone is psychologically sound if they haven’t had a thorough mental health evaluation and that there are so many unknowns with medical transition, including that many of the therapies are not approved for the uses being employed.
With regret on the rise, “we need professionals that are prepared for detransitioners,” said Ms. Alleva. “Some of us have lost trust in health care professionals as a result of our experience.”
“It’s a huge feeling of institutional betrayal,” said Grace.
A version of this article first appeared on Medscape.com.
In a unique Zoom conference,
The forum was convened on what was dubbed #DetransitionAwarenessDay by Genspect, a parent-based organization that seeks to put the brakes on medical transitions for children and adolescents. The group has doubts about the gender-affirming care model supported by the World Professional Association for Transgender Health, the American Medical Association, the American Academy of Pediatrics, and other medical groups.
“Affirmative” medical care is defined as treatment with puberty blockers and cross-sex hormones for those with gender dysphoria to transition to the opposite sex and is often followed by gender reassignment surgery. However, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed for those under aged 18, in particular, with several countries pulling back on medical treatment and instead emphasizing psychotherapy first.
The purpose of the second annual Genspect meeting was to shed light on the experiences of individuals who have detransitioned – those that identified as transgender and transitioned, but then decided to end their medical transition. People logged on from all over the United States, Canada, New Zealand, Australia, the United Kingdom, Germany, Spain, Chile, and Brazil, among other countries.
“This is a minority within a minority,” said Genspect advisor Stella O’Malley, adding that the first meeting in 2021 was held because “too many people were dismissing the stories of the detransitioners.” Ms. O’Malley is a psychotherapist, a clinical advisor to the Society for Evidence-Based Gender Medicine, and a founding member of the International Association of Therapists for Desisters and Detransitioners.
“It’s become blindingly obvious over the last year that ... ‘detrans’ is a huge part of the trans phenomenon,” said Ms. O’Malley, adding that detransitioners have been “undermined and dismissed.”
Laura Edwards-Leeper, PhD (@DrLauraEL), a prominent gender therapist who has recently expressed concern regarding adequate gatekeeping when treating youth with gender dysphoria, agreed.
She tweeted: “You simply can’t call yourself a legit gender provider if you don’t believe that detransitioners exist. As part of the informed consent process for transitioning, it is unethical to not discuss this possibility with young people.” Dr. Edwards-Leeper is professor emeritus at Pacific University in Hillsboro, Ore.
Speakers in the forum largely offered experiences, not data. They pointed out that there has been little to no study of detransition, but all testified that it was less rare than it has been portrayed by the transgender community.
Struggles with going back
“There are so many reasons why people detransition,” said Sinead Watson, aged 30, a Genspect advisor who transitioned from female to male, starting in 2015, and who decided to detransition in 2019. Citing a study by Lisa Littman, MD, MPH, published in 2021, Ms. Watson said the most common reasons for detransitioning were realizing that gender dysphoria was caused by other issues; internal homophobia; and the unbearable nature of transphobia.
Ms. Watson said the hardest part of detransitioning was admitting to herself that her transition had been a mistake. “It’s embarrassing and you feel ashamed and guilty,” she said, adding that it may mean losing friends who now regard you as a “bigot, while you’re also dealing with transition regret.”
“It’s a living hell, especially when none of your therapists or counselors will listen to you,” she said. “Detransitioning isn’t fun.”
Carol (@sourpatches2077) said she knew for a year that her transition had been a mistake.
“The biggest part was I couldn’t tell my family,” said Carol, who identifies as a lesbian. “I put them through so much. It seems ridiculous to go: ‘Oops, I made this huge [expletive] mistake,’ ” she said, describing the moment she did tell them as “devastating.”
Grace (@hormonehangover) said she remembers finally hitting a moment of “undeniability” some years after transitioning. “I accept it, I’ve ruined my life, this is wrong,” she remembers thinking. “It was devastating, but I couldn’t deny it anymore.”
Don’t trust therapists
People experiencing feelings of unease “need a therapist who will listen to them,” said Ms. Watson. When she first detransitioned, her therapists treated her badly. “They just didn’t want to speak about detransition,” she said, adding that “it was like a kick in the stomach.”
Ms. Watson said she’d like to see more training about detransition, but also on “preventative techniques,” adding that many people transition who should not. “I don’t want more detransitioners – I want less.
“In order for that to happen, we need to treat people with gender dysphoria properly,” said Ms. Watson, adding that the affirmative model is “disgusting, and that’s what needs to change.”
“I would tell somebody to not go to a therapist,” said Carol. Identifying as a butch lesbian, she felt like her therapists had pushed her into transitioning to male. “The No. 1 thing not understood by the mental health professionals is that the vast majority of homosexuals were gender-nonconforming children.” She added that this is especially true of butch lesbians.
Therapists – and doctors – also need to acknowledge both the trauma of transition and detransition, she said.
Kaiser, where she had transitioned, offered her breast reconstruction. Carol said it felt demeaning. “Like you’re Mr. Potatohead: ‘Here, we can just ... put on some new parts and you’re good to go.’ ”
“Doctors are concretizing transient obsessions,” said Helena Kerschner (@lacroicsz), quoting a chatroom user.
Ms. Kerschner gave a presentation on “fandom”: becoming obsessed with a movie, book, TV show, musician, or celebrity, spending every waking hour chatting online or writing fan fiction, or attempting to interact with the celebrity online. It’s a fantasy-dominated world and “the vast majority” of participants are teenage girls who are “identifying as trans,” in part, because they are fed a community-reinforced message that it’s better to be a boy.
Therapists and physicians who help them transition “are harming them for life based on something they would have grown out of or overcome without the permanent damage,” Ms. Kerschner added.
Doctors ‘gaslighting’ people into believing that transition is the answer
A pervasive theme during the webinar was that many people are being misdiagnosed with gender dysphoria, which may not be resolved by medical transition.
Allie, a 22-year-old who stopped taking testosterone after 1½ years, said she initially started the transition to male when she gave up trying to figure out why she could not identify with, or befriend, women, and after a childhood and adolescence spent mostly in the company of boys and being more interested in traditionally male activities.
She endured sexual abuse as a teenager and her parents divorced while she was in high school. Allie also had multiple suicide attempts and many incidents of self-harm. When she decided to transition, at age 18, she went to a private clinic and received cross-sex hormones within a few months of her first and only 30-minute consultation. “There was no explorative therapy,” she said, adding that she was never given a formal diagnosis of gender dysphoria.
For the first year, she said she was “over the freaking moon” because she felt like it was the answer. But things started to unravel while she attended university, and she attempted suicide attempt at age 20. A social worker at the school identified her symptoms – which had been the same since childhood – as autism. She then decided to cease her transition.
Another detransitioner, Laura Becker, said it took 5 years after her transition to recognize that she had undiagnosed PTSD from emotional and psychiatric abuse. Despite a history of substance abuse, self-harm, suicidal ideation, and other mental health issues, she was given testosterone and had a double mastectomy at age 20. She became fixated on gay men, which devolved into a methamphetamine- and crack-fueled relationship with a man she met on the gay dating platform Grindr.
“No one around me knew any better or knew how to help, including the medical professionals who performed the mastectomy and who casually signed off and administered my medical transition,” she said.
Once she was aware of her PTSD she started to detransition, which itself was traumatic, said Laura.
Limpida, aged 24, said he felt pushed into transitioning after seeking help at a Planned Parenthood clinic. He identified as trans at age 15 and spent years attempting to be a woman socially, but every step made him feel more miserable, he said. When he went to the clinic at age 21 to get estrogen, he said he felt like the staff was dismissive of his mental health concerns – including that he was suicidal, had substance abuse, and was severely depressed. He was told he was the “perfect candidate” for transitioning.
A year later, he said he felt worse. The nurse suggested he seek out surgery. After Limpida researched what was involved, he decided to detransition. He has since received an autism diagnosis.
Robin, also aged 24, said the idea of surgery had helped push him into detransitioning, which began in 2020 after 4 years of estrogen. He said he had always been gender nonconforming and knew he was gay at an early age. He believes that gender-nonconforming people are “gaslighted” into thinking that transitioning is the answer.
Lack of evidence-based, informed consent
Michelle Alleva, who stopped identifying as transgender in 2020 but had ceased testosterone 4 years earlier because of side effects, cited what she called a lack of evidence base for the effectiveness and safety of medical transitions.
“You need to have a really, really good evidence base in place if you’re going straight to an invasive treatment that is going to cause permanent changes to your body,” she said.
Access to medical transition used to involve more “gatekeeping” through mental health evaluations and other interventions, she said, but there has been a shift from treating what was considered a psychiatric issue to essentially affirming an identity.
“This shift was activist driven, not evidence based,” she emphasized.
Most studies showing satisfaction with transition only involve a few years of follow-up, she said. She added that the longest follow-up study of transition, published in 2011 and spanning 30 years, showed that the suicide rate 10-15 years post surgery was 20 times higher than the general population.
Studies of regret were primarily conducted before the rapid increase in the number of trans-identifying individuals, she said, which makes it hard to draw conclusions about pediatric transition. Getting estimates on this population is difficult because so many who detransition do not tell their clinicians, and many studies have short follow-up times or a high loss to follow-up.
Ms. Alleva also took issue with the notion that physicians were offering true informed consent, noting that it’s not possible to know if someone is psychologically sound if they haven’t had a thorough mental health evaluation and that there are so many unknowns with medical transition, including that many of the therapies are not approved for the uses being employed.
With regret on the rise, “we need professionals that are prepared for detransitioners,” said Ms. Alleva. “Some of us have lost trust in health care professionals as a result of our experience.”
“It’s a huge feeling of institutional betrayal,” said Grace.
A version of this article first appeared on Medscape.com.
In a unique Zoom conference,
The forum was convened on what was dubbed #DetransitionAwarenessDay by Genspect, a parent-based organization that seeks to put the brakes on medical transitions for children and adolescents. The group has doubts about the gender-affirming care model supported by the World Professional Association for Transgender Health, the American Medical Association, the American Academy of Pediatrics, and other medical groups.
“Affirmative” medical care is defined as treatment with puberty blockers and cross-sex hormones for those with gender dysphoria to transition to the opposite sex and is often followed by gender reassignment surgery. However, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed for those under aged 18, in particular, with several countries pulling back on medical treatment and instead emphasizing psychotherapy first.
The purpose of the second annual Genspect meeting was to shed light on the experiences of individuals who have detransitioned – those that identified as transgender and transitioned, but then decided to end their medical transition. People logged on from all over the United States, Canada, New Zealand, Australia, the United Kingdom, Germany, Spain, Chile, and Brazil, among other countries.
“This is a minority within a minority,” said Genspect advisor Stella O’Malley, adding that the first meeting in 2021 was held because “too many people were dismissing the stories of the detransitioners.” Ms. O’Malley is a psychotherapist, a clinical advisor to the Society for Evidence-Based Gender Medicine, and a founding member of the International Association of Therapists for Desisters and Detransitioners.
“It’s become blindingly obvious over the last year that ... ‘detrans’ is a huge part of the trans phenomenon,” said Ms. O’Malley, adding that detransitioners have been “undermined and dismissed.”
Laura Edwards-Leeper, PhD (@DrLauraEL), a prominent gender therapist who has recently expressed concern regarding adequate gatekeeping when treating youth with gender dysphoria, agreed.
She tweeted: “You simply can’t call yourself a legit gender provider if you don’t believe that detransitioners exist. As part of the informed consent process for transitioning, it is unethical to not discuss this possibility with young people.” Dr. Edwards-Leeper is professor emeritus at Pacific University in Hillsboro, Ore.
Speakers in the forum largely offered experiences, not data. They pointed out that there has been little to no study of detransition, but all testified that it was less rare than it has been portrayed by the transgender community.
Struggles with going back
“There are so many reasons why people detransition,” said Sinead Watson, aged 30, a Genspect advisor who transitioned from female to male, starting in 2015, and who decided to detransition in 2019. Citing a study by Lisa Littman, MD, MPH, published in 2021, Ms. Watson said the most common reasons for detransitioning were realizing that gender dysphoria was caused by other issues; internal homophobia; and the unbearable nature of transphobia.
Ms. Watson said the hardest part of detransitioning was admitting to herself that her transition had been a mistake. “It’s embarrassing and you feel ashamed and guilty,” she said, adding that it may mean losing friends who now regard you as a “bigot, while you’re also dealing with transition regret.”
“It’s a living hell, especially when none of your therapists or counselors will listen to you,” she said. “Detransitioning isn’t fun.”
Carol (@sourpatches2077) said she knew for a year that her transition had been a mistake.
“The biggest part was I couldn’t tell my family,” said Carol, who identifies as a lesbian. “I put them through so much. It seems ridiculous to go: ‘Oops, I made this huge [expletive] mistake,’ ” she said, describing the moment she did tell them as “devastating.”
Grace (@hormonehangover) said she remembers finally hitting a moment of “undeniability” some years after transitioning. “I accept it, I’ve ruined my life, this is wrong,” she remembers thinking. “It was devastating, but I couldn’t deny it anymore.”
Don’t trust therapists
People experiencing feelings of unease “need a therapist who will listen to them,” said Ms. Watson. When she first detransitioned, her therapists treated her badly. “They just didn’t want to speak about detransition,” she said, adding that “it was like a kick in the stomach.”
Ms. Watson said she’d like to see more training about detransition, but also on “preventative techniques,” adding that many people transition who should not. “I don’t want more detransitioners – I want less.
“In order for that to happen, we need to treat people with gender dysphoria properly,” said Ms. Watson, adding that the affirmative model is “disgusting, and that’s what needs to change.”
“I would tell somebody to not go to a therapist,” said Carol. Identifying as a butch lesbian, she felt like her therapists had pushed her into transitioning to male. “The No. 1 thing not understood by the mental health professionals is that the vast majority of homosexuals were gender-nonconforming children.” She added that this is especially true of butch lesbians.
Therapists – and doctors – also need to acknowledge both the trauma of transition and detransition, she said.
Kaiser, where she had transitioned, offered her breast reconstruction. Carol said it felt demeaning. “Like you’re Mr. Potatohead: ‘Here, we can just ... put on some new parts and you’re good to go.’ ”
“Doctors are concretizing transient obsessions,” said Helena Kerschner (@lacroicsz), quoting a chatroom user.
Ms. Kerschner gave a presentation on “fandom”: becoming obsessed with a movie, book, TV show, musician, or celebrity, spending every waking hour chatting online or writing fan fiction, or attempting to interact with the celebrity online. It’s a fantasy-dominated world and “the vast majority” of participants are teenage girls who are “identifying as trans,” in part, because they are fed a community-reinforced message that it’s better to be a boy.
Therapists and physicians who help them transition “are harming them for life based on something they would have grown out of or overcome without the permanent damage,” Ms. Kerschner added.
Doctors ‘gaslighting’ people into believing that transition is the answer
A pervasive theme during the webinar was that many people are being misdiagnosed with gender dysphoria, which may not be resolved by medical transition.
Allie, a 22-year-old who stopped taking testosterone after 1½ years, said she initially started the transition to male when she gave up trying to figure out why she could not identify with, or befriend, women, and after a childhood and adolescence spent mostly in the company of boys and being more interested in traditionally male activities.
She endured sexual abuse as a teenager and her parents divorced while she was in high school. Allie also had multiple suicide attempts and many incidents of self-harm. When she decided to transition, at age 18, she went to a private clinic and received cross-sex hormones within a few months of her first and only 30-minute consultation. “There was no explorative therapy,” she said, adding that she was never given a formal diagnosis of gender dysphoria.
For the first year, she said she was “over the freaking moon” because she felt like it was the answer. But things started to unravel while she attended university, and she attempted suicide attempt at age 20. A social worker at the school identified her symptoms – which had been the same since childhood – as autism. She then decided to cease her transition.
Another detransitioner, Laura Becker, said it took 5 years after her transition to recognize that she had undiagnosed PTSD from emotional and psychiatric abuse. Despite a history of substance abuse, self-harm, suicidal ideation, and other mental health issues, she was given testosterone and had a double mastectomy at age 20. She became fixated on gay men, which devolved into a methamphetamine- and crack-fueled relationship with a man she met on the gay dating platform Grindr.
“No one around me knew any better or knew how to help, including the medical professionals who performed the mastectomy and who casually signed off and administered my medical transition,” she said.
Once she was aware of her PTSD she started to detransition, which itself was traumatic, said Laura.
Limpida, aged 24, said he felt pushed into transitioning after seeking help at a Planned Parenthood clinic. He identified as trans at age 15 and spent years attempting to be a woman socially, but every step made him feel more miserable, he said. When he went to the clinic at age 21 to get estrogen, he said he felt like the staff was dismissive of his mental health concerns – including that he was suicidal, had substance abuse, and was severely depressed. He was told he was the “perfect candidate” for transitioning.
A year later, he said he felt worse. The nurse suggested he seek out surgery. After Limpida researched what was involved, he decided to detransition. He has since received an autism diagnosis.
Robin, also aged 24, said the idea of surgery had helped push him into detransitioning, which began in 2020 after 4 years of estrogen. He said he had always been gender nonconforming and knew he was gay at an early age. He believes that gender-nonconforming people are “gaslighted” into thinking that transitioning is the answer.
Lack of evidence-based, informed consent
Michelle Alleva, who stopped identifying as transgender in 2020 but had ceased testosterone 4 years earlier because of side effects, cited what she called a lack of evidence base for the effectiveness and safety of medical transitions.
“You need to have a really, really good evidence base in place if you’re going straight to an invasive treatment that is going to cause permanent changes to your body,” she said.
Access to medical transition used to involve more “gatekeeping” through mental health evaluations and other interventions, she said, but there has been a shift from treating what was considered a psychiatric issue to essentially affirming an identity.
“This shift was activist driven, not evidence based,” she emphasized.
Most studies showing satisfaction with transition only involve a few years of follow-up, she said. She added that the longest follow-up study of transition, published in 2011 and spanning 30 years, showed that the suicide rate 10-15 years post surgery was 20 times higher than the general population.
Studies of regret were primarily conducted before the rapid increase in the number of trans-identifying individuals, she said, which makes it hard to draw conclusions about pediatric transition. Getting estimates on this population is difficult because so many who detransition do not tell their clinicians, and many studies have short follow-up times or a high loss to follow-up.
Ms. Alleva also took issue with the notion that physicians were offering true informed consent, noting that it’s not possible to know if someone is psychologically sound if they haven’t had a thorough mental health evaluation and that there are so many unknowns with medical transition, including that many of the therapies are not approved for the uses being employed.
With regret on the rise, “we need professionals that are prepared for detransitioners,” said Ms. Alleva. “Some of us have lost trust in health care professionals as a result of our experience.”
“It’s a huge feeling of institutional betrayal,” said Grace.
A version of this article first appeared on Medscape.com.
Debate heats up on how best to treat gender-questioning kids
The past week has seen heated debate about the complex issue of how to best treat children with gender dysphoria, with further developments in a number of U.S. states and in Sweden.
In the U.S., more states have moved to prevent the use of any medical treatment, such as puberty blockers or cross-sex hormones, in kids younger than the age of 18, most recently in a state Senate vote in Alabama last week, and in Texas, where Governor Greg Abbott is said to have ordered state agencies to investigate reports of gender-transition procedures on children as “child abuse.”
At least one parent has, because of this, established a crowdfunding page to try to raise money to move away from Texas, fearful of being accused of child abuse if their child with gender dysphoria receives hormone therapy. And a countersuit has been filed there by the ACLU of Texas and Lambda Legal, a civil rights organization, on behalf of one parent said to be under investigation.
But on the flip side, parents living in more liberal states – where children under the age of 18 can often get hormones to transition without parental consent – are considering moving out of them to protect their children. These parents are concerned that their kids do not know enough about the side effects of puberty blockers, or lifetime use of cross-sex hormones and its implications, to be able to make properly informed decisions at such a young age.
Meanwhile, Sweden has further tightened its restrictions on medical therapy to treat gender-questioning kids, with a recent announcement from its National Board of Health and Welfare (NBHW), on Feb. 22, urging restraint in hormone treatment of minors with gender dysphoria following a review by the agency there that assesses health technologies, the SBU.
Based on the review results, the NBHW’s overall conclusion is that the risks of puberty blocking and cross-sex hormone treatment for those under 18 currently outweigh the possible benefits for the group as a whole. The agency now says hormone treatment should only be offered in exceptional cases outside the framework of research, and principally, only in adolescents with childhood-onset gender dysphoria, as opposed to those who develop it during puberty, or in their teens, as is the case with most teenagers currently presenting.
At the same time, gender-affirming hormone treatment for adolescents who identify as transgender or nonbinary is associated with changes in depression and suicidality, according to a new U.S. survey published Feb. 25 in JAMA Network Health.
However, experts who spoke to this news organization were critical of the study, noting it was small, conducted in just 104 youth who were an average age of 15.8 years and of whom only 63% completed the survey at the final timepoint, just 1 year after starting therapy. In addition, there was no control group, among other limitations.
“The most worrying thing is that they haven’t described the pros and cons of the treatment that they are researching. We know that there are risks inherent in using gender-affirming medicine, as with all medications,” Anna Hutchinson, DClinPsych, of the Integrated Psychology Clinic, London, told this news organization.
“For example, when people with gender dysphoria use cross-sex hormones, there is a burden of treatment that can last a lifetime, both for those who benefit from the treatment and those who detransition or regret later on,” said Dr. Hutchinson, who has extensive experience of working with young people with issues related to sexuality or gender.
“This isn’t mentioned at all, which makes the paper appear quite biased towards using one approach for managing gender dysphoria and related distress, whilst not acknowledging any risks of doing so or considering alternatives,” she noted.
Why were some treated with hormones while others weren’t?
The newly published survey is by PhD student Diana M. Tordoff, MPH, of the Department of Epidemiology, University of Washington, Seattle, and colleagues. Published alongside was an invited commentary by Brett Dolotina, BS, of Massachusetts General Hospital, Boston, and Jack L. Turban, MD, MHS, of Stanford (Calif.) University.
The study was conducted at an urban multidisciplinary gender clinic in Seattle among transgender and nonbinary adolescents and young adults seeking gender-affirming care from August 2017 to June 2018. Data were analyzed from August 2020 to November 2021.
Participating in the study were 104 youths aged 13-20 years (mean age, 15.8 years), 63 transmasculine (born female) individuals (60.6%), 27 transfeminine (born male) individuals (26.0%), 10 nonbinary or gender-fluid individuals (9.6%), and four youths who responded, “I don’t know,” or did not respond to the gender-identity question (3.8%).
At baseline, 59 individuals (56.7%) had moderate-to-severe depression, 52 individuals (50.0%) had moderate-to-severe anxiety, and 45 individuals (43.3%) reported self-harm or suicidal thoughts.
By the end of the study, 69 youths (66.3%) had received puberty blockers, cross-sex hormones (testosterone for girls transitioning to male and estrogen for boys transitioning to female), or both interventions, while 35 youths had not received either intervention (33.7%).
After adjustment for temporal trends and potential confounders, there were a 60% lower odds of depression (adjusted odds ratio, 0.40; 95% confidence interval, 0.17-0.95) and 73% lower odds of suicidality (aOR, 0.27; 95% CI, 0.11-0.65) among youths who had initiated puberty blockers or cross-sex hormones.
There was no association between these treatments and anxiety, however (aOR, 1.01; 95% CI, 0.41-2.51).
Dr. Hutchinson points out that nonbinary and gender fluid “are not diagnostic or clinical terms,” adding, “there is no information about how the groups were chosen or if any of them met the criteria for gender dysphoria. It seems strange to not have measured gender dysphoria, both before and after interventions, in a group of children presenting with gender dysphoria.”
She adds: “I am questioning why ‘gender-affirming’ medicine appears to be being used here as a specific intervention for depression and suicidality? [That] wouldn’t usually be the first reason to commence these particular treatments. Why didn’t they provide therapy or antidepressant medication to this group of young people, as is routine for managing mood and/or suicidality in all other patient cohorts?”
In their commentary, Mr. Dolotina and Dr. Turban observe: “The rate of suicidality among the Tordoff et al. sample after receiving gender-affirming care was still much higher than national rates of suicidality among youth in the U.S., denoting that ... other mental health determinants must be addressed ... including gender minority stress.”
Small study, no control group, large loss to follow-up
Dr. Hutchinson also criticizes the small sample size of just 104 youth and “large loss to follow-up, whereby only 65 of those 104 [youth] completed the final survey in a short time [1 year].” This could indicate “that only the most satisfied kids stayed the course,” she suggests.
And importantly, the findings on depression and suicidality rely on the experience of only five people in the no-treatment group at 12 months, she points out.
Also, as the authors themselves acknowledge, they didn’t control for other psychiatric medicines that the participants might have been taking at baseline.
“It’s important to know more about all of this in order to draw accurate conclusions about what works, or does not, for whom,” noted Dr. Hutchinson.
Most patients, too, she notes, were females-to-males taking testosterone. Therefore, the finding that they experienced a reduction in depression might simply reflect the widely reported antidepressant effects of testosterone.
Also expressing concern about the small sample size and “lack of a control group” is Michelle Mackness, MC, a Canadian counselor in private practice who has experience working with gender-questioning individuals, detransitioners, and those experiencing complications related to their transition.
“Tordoff et al.’s assertion that there is a ‘robust evidence base’ supporting pediatric transition seems out-of-step with recent global developments in care policies and protocols for gender-questioning youth,” she points out.
“Neither the study authors or commentators acknowledge, let alone address, the fact that Finland, the U.K., and Sweden have recently determined that the evidence allegedly supporting medical interventions for pediatric transition is ‘inconclusive’,” she adds.
Asked to respond, Ms. Tordoff did not directly address this question. Rather, she reiterated to this news organization: “We found that receipt of puberty blockers and gender-affirming hormones was associated with a 60% lower odds of depression and a 73% lower odds of suicidal thoughts by the end of our study follow-up. We conducted extensive sensitivity analyses, which support the robustness of our study findings.”
She added: “These results are consistent with other recently published prospective cohort studies (please see citations provided within the manuscript).”
Parents may move states
It is this concern about the lifetime burden of treatment involved with transitioning that gives some parents of children with gender dysphoria pause for thought, especially those who live in more liberal U.S. states.
Indeed, two of America’s leading psychologists who work in this field, including one who is transgender herself, told this news organization in November they are now concerned about a lack of adequate psychological evaluations of youth with gender dysphoria before any medical treatment is considered.
So while one parent, Violet A., last week established a GoFundMe page for her child, entitled, “Help Us Move Isa to Safety,” stating she needed to move from Texas due to Governor Abbott’s pronouncements there “to a state that won’t consider me an abuser when I seek medical care for my trans child and potentially remove her from my custody,” some parents feel the need instead to move from more liberal states.
Some tell their stories anonymously, as they don’t want to risk causing their gender-questioning children further distress, as detailed on the Genspect website.
A version of this article first appeared on Medscape.com.
The past week has seen heated debate about the complex issue of how to best treat children with gender dysphoria, with further developments in a number of U.S. states and in Sweden.
In the U.S., more states have moved to prevent the use of any medical treatment, such as puberty blockers or cross-sex hormones, in kids younger than the age of 18, most recently in a state Senate vote in Alabama last week, and in Texas, where Governor Greg Abbott is said to have ordered state agencies to investigate reports of gender-transition procedures on children as “child abuse.”
At least one parent has, because of this, established a crowdfunding page to try to raise money to move away from Texas, fearful of being accused of child abuse if their child with gender dysphoria receives hormone therapy. And a countersuit has been filed there by the ACLU of Texas and Lambda Legal, a civil rights organization, on behalf of one parent said to be under investigation.
But on the flip side, parents living in more liberal states – where children under the age of 18 can often get hormones to transition without parental consent – are considering moving out of them to protect their children. These parents are concerned that their kids do not know enough about the side effects of puberty blockers, or lifetime use of cross-sex hormones and its implications, to be able to make properly informed decisions at such a young age.
Meanwhile, Sweden has further tightened its restrictions on medical therapy to treat gender-questioning kids, with a recent announcement from its National Board of Health and Welfare (NBHW), on Feb. 22, urging restraint in hormone treatment of minors with gender dysphoria following a review by the agency there that assesses health technologies, the SBU.
Based on the review results, the NBHW’s overall conclusion is that the risks of puberty blocking and cross-sex hormone treatment for those under 18 currently outweigh the possible benefits for the group as a whole. The agency now says hormone treatment should only be offered in exceptional cases outside the framework of research, and principally, only in adolescents with childhood-onset gender dysphoria, as opposed to those who develop it during puberty, or in their teens, as is the case with most teenagers currently presenting.
At the same time, gender-affirming hormone treatment for adolescents who identify as transgender or nonbinary is associated with changes in depression and suicidality, according to a new U.S. survey published Feb. 25 in JAMA Network Health.
However, experts who spoke to this news organization were critical of the study, noting it was small, conducted in just 104 youth who were an average age of 15.8 years and of whom only 63% completed the survey at the final timepoint, just 1 year after starting therapy. In addition, there was no control group, among other limitations.
“The most worrying thing is that they haven’t described the pros and cons of the treatment that they are researching. We know that there are risks inherent in using gender-affirming medicine, as with all medications,” Anna Hutchinson, DClinPsych, of the Integrated Psychology Clinic, London, told this news organization.
“For example, when people with gender dysphoria use cross-sex hormones, there is a burden of treatment that can last a lifetime, both for those who benefit from the treatment and those who detransition or regret later on,” said Dr. Hutchinson, who has extensive experience of working with young people with issues related to sexuality or gender.
“This isn’t mentioned at all, which makes the paper appear quite biased towards using one approach for managing gender dysphoria and related distress, whilst not acknowledging any risks of doing so or considering alternatives,” she noted.
Why were some treated with hormones while others weren’t?
The newly published survey is by PhD student Diana M. Tordoff, MPH, of the Department of Epidemiology, University of Washington, Seattle, and colleagues. Published alongside was an invited commentary by Brett Dolotina, BS, of Massachusetts General Hospital, Boston, and Jack L. Turban, MD, MHS, of Stanford (Calif.) University.
The study was conducted at an urban multidisciplinary gender clinic in Seattle among transgender and nonbinary adolescents and young adults seeking gender-affirming care from August 2017 to June 2018. Data were analyzed from August 2020 to November 2021.
Participating in the study were 104 youths aged 13-20 years (mean age, 15.8 years), 63 transmasculine (born female) individuals (60.6%), 27 transfeminine (born male) individuals (26.0%), 10 nonbinary or gender-fluid individuals (9.6%), and four youths who responded, “I don’t know,” or did not respond to the gender-identity question (3.8%).
At baseline, 59 individuals (56.7%) had moderate-to-severe depression, 52 individuals (50.0%) had moderate-to-severe anxiety, and 45 individuals (43.3%) reported self-harm or suicidal thoughts.
By the end of the study, 69 youths (66.3%) had received puberty blockers, cross-sex hormones (testosterone for girls transitioning to male and estrogen for boys transitioning to female), or both interventions, while 35 youths had not received either intervention (33.7%).
After adjustment for temporal trends and potential confounders, there were a 60% lower odds of depression (adjusted odds ratio, 0.40; 95% confidence interval, 0.17-0.95) and 73% lower odds of suicidality (aOR, 0.27; 95% CI, 0.11-0.65) among youths who had initiated puberty blockers or cross-sex hormones.
There was no association between these treatments and anxiety, however (aOR, 1.01; 95% CI, 0.41-2.51).
Dr. Hutchinson points out that nonbinary and gender fluid “are not diagnostic or clinical terms,” adding, “there is no information about how the groups were chosen or if any of them met the criteria for gender dysphoria. It seems strange to not have measured gender dysphoria, both before and after interventions, in a group of children presenting with gender dysphoria.”
She adds: “I am questioning why ‘gender-affirming’ medicine appears to be being used here as a specific intervention for depression and suicidality? [That] wouldn’t usually be the first reason to commence these particular treatments. Why didn’t they provide therapy or antidepressant medication to this group of young people, as is routine for managing mood and/or suicidality in all other patient cohorts?”
In their commentary, Mr. Dolotina and Dr. Turban observe: “The rate of suicidality among the Tordoff et al. sample after receiving gender-affirming care was still much higher than national rates of suicidality among youth in the U.S., denoting that ... other mental health determinants must be addressed ... including gender minority stress.”
Small study, no control group, large loss to follow-up
Dr. Hutchinson also criticizes the small sample size of just 104 youth and “large loss to follow-up, whereby only 65 of those 104 [youth] completed the final survey in a short time [1 year].” This could indicate “that only the most satisfied kids stayed the course,” she suggests.
And importantly, the findings on depression and suicidality rely on the experience of only five people in the no-treatment group at 12 months, she points out.
Also, as the authors themselves acknowledge, they didn’t control for other psychiatric medicines that the participants might have been taking at baseline.
“It’s important to know more about all of this in order to draw accurate conclusions about what works, or does not, for whom,” noted Dr. Hutchinson.
Most patients, too, she notes, were females-to-males taking testosterone. Therefore, the finding that they experienced a reduction in depression might simply reflect the widely reported antidepressant effects of testosterone.
Also expressing concern about the small sample size and “lack of a control group” is Michelle Mackness, MC, a Canadian counselor in private practice who has experience working with gender-questioning individuals, detransitioners, and those experiencing complications related to their transition.
“Tordoff et al.’s assertion that there is a ‘robust evidence base’ supporting pediatric transition seems out-of-step with recent global developments in care policies and protocols for gender-questioning youth,” she points out.
“Neither the study authors or commentators acknowledge, let alone address, the fact that Finland, the U.K., and Sweden have recently determined that the evidence allegedly supporting medical interventions for pediatric transition is ‘inconclusive’,” she adds.
Asked to respond, Ms. Tordoff did not directly address this question. Rather, she reiterated to this news organization: “We found that receipt of puberty blockers and gender-affirming hormones was associated with a 60% lower odds of depression and a 73% lower odds of suicidal thoughts by the end of our study follow-up. We conducted extensive sensitivity analyses, which support the robustness of our study findings.”
She added: “These results are consistent with other recently published prospective cohort studies (please see citations provided within the manuscript).”
Parents may move states
It is this concern about the lifetime burden of treatment involved with transitioning that gives some parents of children with gender dysphoria pause for thought, especially those who live in more liberal U.S. states.
Indeed, two of America’s leading psychologists who work in this field, including one who is transgender herself, told this news organization in November they are now concerned about a lack of adequate psychological evaluations of youth with gender dysphoria before any medical treatment is considered.
So while one parent, Violet A., last week established a GoFundMe page for her child, entitled, “Help Us Move Isa to Safety,” stating she needed to move from Texas due to Governor Abbott’s pronouncements there “to a state that won’t consider me an abuser when I seek medical care for my trans child and potentially remove her from my custody,” some parents feel the need instead to move from more liberal states.
Some tell their stories anonymously, as they don’t want to risk causing their gender-questioning children further distress, as detailed on the Genspect website.
A version of this article first appeared on Medscape.com.
The past week has seen heated debate about the complex issue of how to best treat children with gender dysphoria, with further developments in a number of U.S. states and in Sweden.
In the U.S., more states have moved to prevent the use of any medical treatment, such as puberty blockers or cross-sex hormones, in kids younger than the age of 18, most recently in a state Senate vote in Alabama last week, and in Texas, where Governor Greg Abbott is said to have ordered state agencies to investigate reports of gender-transition procedures on children as “child abuse.”
At least one parent has, because of this, established a crowdfunding page to try to raise money to move away from Texas, fearful of being accused of child abuse if their child with gender dysphoria receives hormone therapy. And a countersuit has been filed there by the ACLU of Texas and Lambda Legal, a civil rights organization, on behalf of one parent said to be under investigation.
But on the flip side, parents living in more liberal states – where children under the age of 18 can often get hormones to transition without parental consent – are considering moving out of them to protect their children. These parents are concerned that their kids do not know enough about the side effects of puberty blockers, or lifetime use of cross-sex hormones and its implications, to be able to make properly informed decisions at such a young age.
Meanwhile, Sweden has further tightened its restrictions on medical therapy to treat gender-questioning kids, with a recent announcement from its National Board of Health and Welfare (NBHW), on Feb. 22, urging restraint in hormone treatment of minors with gender dysphoria following a review by the agency there that assesses health technologies, the SBU.
Based on the review results, the NBHW’s overall conclusion is that the risks of puberty blocking and cross-sex hormone treatment for those under 18 currently outweigh the possible benefits for the group as a whole. The agency now says hormone treatment should only be offered in exceptional cases outside the framework of research, and principally, only in adolescents with childhood-onset gender dysphoria, as opposed to those who develop it during puberty, or in their teens, as is the case with most teenagers currently presenting.
At the same time, gender-affirming hormone treatment for adolescents who identify as transgender or nonbinary is associated with changes in depression and suicidality, according to a new U.S. survey published Feb. 25 in JAMA Network Health.
However, experts who spoke to this news organization were critical of the study, noting it was small, conducted in just 104 youth who were an average age of 15.8 years and of whom only 63% completed the survey at the final timepoint, just 1 year after starting therapy. In addition, there was no control group, among other limitations.
“The most worrying thing is that they haven’t described the pros and cons of the treatment that they are researching. We know that there are risks inherent in using gender-affirming medicine, as with all medications,” Anna Hutchinson, DClinPsych, of the Integrated Psychology Clinic, London, told this news organization.
“For example, when people with gender dysphoria use cross-sex hormones, there is a burden of treatment that can last a lifetime, both for those who benefit from the treatment and those who detransition or regret later on,” said Dr. Hutchinson, who has extensive experience of working with young people with issues related to sexuality or gender.
“This isn’t mentioned at all, which makes the paper appear quite biased towards using one approach for managing gender dysphoria and related distress, whilst not acknowledging any risks of doing so or considering alternatives,” she noted.
Why were some treated with hormones while others weren’t?
The newly published survey is by PhD student Diana M. Tordoff, MPH, of the Department of Epidemiology, University of Washington, Seattle, and colleagues. Published alongside was an invited commentary by Brett Dolotina, BS, of Massachusetts General Hospital, Boston, and Jack L. Turban, MD, MHS, of Stanford (Calif.) University.
The study was conducted at an urban multidisciplinary gender clinic in Seattle among transgender and nonbinary adolescents and young adults seeking gender-affirming care from August 2017 to June 2018. Data were analyzed from August 2020 to November 2021.
Participating in the study were 104 youths aged 13-20 years (mean age, 15.8 years), 63 transmasculine (born female) individuals (60.6%), 27 transfeminine (born male) individuals (26.0%), 10 nonbinary or gender-fluid individuals (9.6%), and four youths who responded, “I don’t know,” or did not respond to the gender-identity question (3.8%).
At baseline, 59 individuals (56.7%) had moderate-to-severe depression, 52 individuals (50.0%) had moderate-to-severe anxiety, and 45 individuals (43.3%) reported self-harm or suicidal thoughts.
By the end of the study, 69 youths (66.3%) had received puberty blockers, cross-sex hormones (testosterone for girls transitioning to male and estrogen for boys transitioning to female), or both interventions, while 35 youths had not received either intervention (33.7%).
After adjustment for temporal trends and potential confounders, there were a 60% lower odds of depression (adjusted odds ratio, 0.40; 95% confidence interval, 0.17-0.95) and 73% lower odds of suicidality (aOR, 0.27; 95% CI, 0.11-0.65) among youths who had initiated puberty blockers or cross-sex hormones.
There was no association between these treatments and anxiety, however (aOR, 1.01; 95% CI, 0.41-2.51).
Dr. Hutchinson points out that nonbinary and gender fluid “are not diagnostic or clinical terms,” adding, “there is no information about how the groups were chosen or if any of them met the criteria for gender dysphoria. It seems strange to not have measured gender dysphoria, both before and after interventions, in a group of children presenting with gender dysphoria.”
She adds: “I am questioning why ‘gender-affirming’ medicine appears to be being used here as a specific intervention for depression and suicidality? [That] wouldn’t usually be the first reason to commence these particular treatments. Why didn’t they provide therapy or antidepressant medication to this group of young people, as is routine for managing mood and/or suicidality in all other patient cohorts?”
In their commentary, Mr. Dolotina and Dr. Turban observe: “The rate of suicidality among the Tordoff et al. sample after receiving gender-affirming care was still much higher than national rates of suicidality among youth in the U.S., denoting that ... other mental health determinants must be addressed ... including gender minority stress.”
Small study, no control group, large loss to follow-up
Dr. Hutchinson also criticizes the small sample size of just 104 youth and “large loss to follow-up, whereby only 65 of those 104 [youth] completed the final survey in a short time [1 year].” This could indicate “that only the most satisfied kids stayed the course,” she suggests.
And importantly, the findings on depression and suicidality rely on the experience of only five people in the no-treatment group at 12 months, she points out.
Also, as the authors themselves acknowledge, they didn’t control for other psychiatric medicines that the participants might have been taking at baseline.
“It’s important to know more about all of this in order to draw accurate conclusions about what works, or does not, for whom,” noted Dr. Hutchinson.
Most patients, too, she notes, were females-to-males taking testosterone. Therefore, the finding that they experienced a reduction in depression might simply reflect the widely reported antidepressant effects of testosterone.
Also expressing concern about the small sample size and “lack of a control group” is Michelle Mackness, MC, a Canadian counselor in private practice who has experience working with gender-questioning individuals, detransitioners, and those experiencing complications related to their transition.
“Tordoff et al.’s assertion that there is a ‘robust evidence base’ supporting pediatric transition seems out-of-step with recent global developments in care policies and protocols for gender-questioning youth,” she points out.
“Neither the study authors or commentators acknowledge, let alone address, the fact that Finland, the U.K., and Sweden have recently determined that the evidence allegedly supporting medical interventions for pediatric transition is ‘inconclusive’,” she adds.
Asked to respond, Ms. Tordoff did not directly address this question. Rather, she reiterated to this news organization: “We found that receipt of puberty blockers and gender-affirming hormones was associated with a 60% lower odds of depression and a 73% lower odds of suicidal thoughts by the end of our study follow-up. We conducted extensive sensitivity analyses, which support the robustness of our study findings.”
She added: “These results are consistent with other recently published prospective cohort studies (please see citations provided within the manuscript).”
Parents may move states
It is this concern about the lifetime burden of treatment involved with transitioning that gives some parents of children with gender dysphoria pause for thought, especially those who live in more liberal U.S. states.
Indeed, two of America’s leading psychologists who work in this field, including one who is transgender herself, told this news organization in November they are now concerned about a lack of adequate psychological evaluations of youth with gender dysphoria before any medical treatment is considered.
So while one parent, Violet A., last week established a GoFundMe page for her child, entitled, “Help Us Move Isa to Safety,” stating she needed to move from Texas due to Governor Abbott’s pronouncements there “to a state that won’t consider me an abuser when I seek medical care for my trans child and potentially remove her from my custody,” some parents feel the need instead to move from more liberal states.
Some tell their stories anonymously, as they don’t want to risk causing their gender-questioning children further distress, as detailed on the Genspect website.
A version of this article first appeared on Medscape.com.
Obstetrical care for gender diverse patients: A summary from the SMFM annual meeting
The purpose of this commentary is to provide a brief summary of discussions centering around reproductive health experiences and obstetrical care for gender-diverse patients from the recent Society of Maternal & Fetal Medicine meeting. Two presentations featured patient perspectives combined with physician lectures to provide a comprehensive outlook on unique reproductive care needs for this growing population.
One of the speakers, Trystan Reese, is a transgender activist, educator, and transgender male who chose to carry his own pregnancy and subsequently delivered his son in 2017. During the summit, he described many barriers that he faced during his pregnancy and offered providers suggestions on how to improve the care for members of the gender-diverse community seeking to start a family.
We often think of conception and pregnancy as experiences unique to one gender. This is simply not the case. In discussing preconceptual care and pregnancy, it is paramount for providers to make the distinction between gender identity and natal sex. Gender identity is an internal sense of self in relation to natal sex. Depending on this intrinsic feeling, people may identify as cisgender, transgender, or as a gender outside of the standard binary. Natal sex describes biologic characteristics such as chromosomal makeup, reproductive anatomy, and secondary sexual changes. In keeping these distinctions in mind, pregnancy is therefore exclusive to a person’s natal sex, not gender identity. One of the biggest challenges in caring for transgender patients who desire pregnancy, is the psychological distress related to the gendered notions surrounding this experience.1
There are many ways in which patients encounter unintentional marginalization within the medical system. For example, many electronic medical record systems don’t allow for pronouns or give error messages if the patient’s gender identity is different from their sex assigned at birth. Patients who attend prenatal appointments or birth classes are given documents that center around cisgender women and heterosexual relationships. The labor and delivery wards themselves typically include language such as “maternity,” and birth certificates have distinct “mother” and “father” denotations.1 Insurance coverage for prenatal care and delivery can be problematic if a patient who is assigned female at birth has changed their gender marker to “male” on their insurance card.
Many of these roadblocks can be ameliorated by utilizing more inclusive terminology. Terms such as “maternal” can be replaced with “pregnant patients, parent, or patients giving birth.” Names of maternity wards can be altered to perinatal units, which is more inclusive and more descriptive of the wide variety of patients that may experience childbirth and parenthood.1 Introducing “you-centered” language can also be helpful. Instead of saying “women may find ...” providers can try saying “patients may find ...” or “individuals may find.”1
Most of the medical and obstetrical care of gender-diverse patients is routine. Prenatal labs, aneuploidy screening, ultrasounds, and fetal surveillance do not differ between transgender and cisgender patients. However, the experience of pregnancy itself can significantly heighten feelings of dysphoria as it inherently leads to patients confronting aspects of their biological sex.2 Because of the teratogenic nature of testosterone, patients are required to stop taking testosterone prior to conception and for the duration of pregnancy. This can also heighten dysphoria and lead to increased rates of anxiety and depression.3
Many transgender patients can safely achieve a normal vaginal birth.4 A small survey of 41 people demonstrated that more transgender men who had taken testosterone were delivered by cesarean section (36% vs. 19%).3 Staff training is an important aspect of caring for a transgender patient in labor to ensure that all members of the labor unit are cognizant of appropriate name and pronoun usage. Another interesting, although unsurprising, fact is that many transgender gestational parents chose a community-based (out-of-hospital) birth according to a 2014 study.1 This is predominantly because of the discrimination patients face when delivering within a hospital setting.
Postpartum depression screening should be conducted prior to patients leaving the hospital and individualized during postpartum appointments. Reinitiation of testosterone can occur 4-6 weeks after delivery.1
While pregnancy can pose some unique challenges to gender-diverse individuals, these intricacies are not insurmountable. The result of pregnancy, regardless of one’s gender identity, is the same – parenthood. One patient’s description of his experience was particularly poignant: “Pregnancy and childbirth were very male experiences for me. When I birthed my children, I was born into fatherhood.”1 It is up to all providers to modify clinical settings, as well as our patient interactions and use of language, if we are to provide inclusion in obstetrics.1,5
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Brandt JS et al. “Understanding intersections: Care for transgender and gender diverse patient populations.” SMFM 2022 annual meeting. 2022 Feb 2.
2. Hoffkling A et al. BMC Pregnancy Childbirth. 2017 Nov 8;17(Suppl 2):332.
3. Light AD et al. Obstet Gynecol. 2014;124:1120-7.
4. Moseson H et al. Int J Transgend Health. 2021 Nov 17;22(1-2):30-41.
5. Brandt JS et al. Obstetrical care for trans*person, in “Trans*gynecology: Managing transgender patients in obstetrics and gynecology practice.” (Cambridge, England: Cambridge University Press, 2022).
The purpose of this commentary is to provide a brief summary of discussions centering around reproductive health experiences and obstetrical care for gender-diverse patients from the recent Society of Maternal & Fetal Medicine meeting. Two presentations featured patient perspectives combined with physician lectures to provide a comprehensive outlook on unique reproductive care needs for this growing population.
One of the speakers, Trystan Reese, is a transgender activist, educator, and transgender male who chose to carry his own pregnancy and subsequently delivered his son in 2017. During the summit, he described many barriers that he faced during his pregnancy and offered providers suggestions on how to improve the care for members of the gender-diverse community seeking to start a family.
We often think of conception and pregnancy as experiences unique to one gender. This is simply not the case. In discussing preconceptual care and pregnancy, it is paramount for providers to make the distinction between gender identity and natal sex. Gender identity is an internal sense of self in relation to natal sex. Depending on this intrinsic feeling, people may identify as cisgender, transgender, or as a gender outside of the standard binary. Natal sex describes biologic characteristics such as chromosomal makeup, reproductive anatomy, and secondary sexual changes. In keeping these distinctions in mind, pregnancy is therefore exclusive to a person’s natal sex, not gender identity. One of the biggest challenges in caring for transgender patients who desire pregnancy, is the psychological distress related to the gendered notions surrounding this experience.1
There are many ways in which patients encounter unintentional marginalization within the medical system. For example, many electronic medical record systems don’t allow for pronouns or give error messages if the patient’s gender identity is different from their sex assigned at birth. Patients who attend prenatal appointments or birth classes are given documents that center around cisgender women and heterosexual relationships. The labor and delivery wards themselves typically include language such as “maternity,” and birth certificates have distinct “mother” and “father” denotations.1 Insurance coverage for prenatal care and delivery can be problematic if a patient who is assigned female at birth has changed their gender marker to “male” on their insurance card.
Many of these roadblocks can be ameliorated by utilizing more inclusive terminology. Terms such as “maternal” can be replaced with “pregnant patients, parent, or patients giving birth.” Names of maternity wards can be altered to perinatal units, which is more inclusive and more descriptive of the wide variety of patients that may experience childbirth and parenthood.1 Introducing “you-centered” language can also be helpful. Instead of saying “women may find ...” providers can try saying “patients may find ...” or “individuals may find.”1
Most of the medical and obstetrical care of gender-diverse patients is routine. Prenatal labs, aneuploidy screening, ultrasounds, and fetal surveillance do not differ between transgender and cisgender patients. However, the experience of pregnancy itself can significantly heighten feelings of dysphoria as it inherently leads to patients confronting aspects of their biological sex.2 Because of the teratogenic nature of testosterone, patients are required to stop taking testosterone prior to conception and for the duration of pregnancy. This can also heighten dysphoria and lead to increased rates of anxiety and depression.3
Many transgender patients can safely achieve a normal vaginal birth.4 A small survey of 41 people demonstrated that more transgender men who had taken testosterone were delivered by cesarean section (36% vs. 19%).3 Staff training is an important aspect of caring for a transgender patient in labor to ensure that all members of the labor unit are cognizant of appropriate name and pronoun usage. Another interesting, although unsurprising, fact is that many transgender gestational parents chose a community-based (out-of-hospital) birth according to a 2014 study.1 This is predominantly because of the discrimination patients face when delivering within a hospital setting.
Postpartum depression screening should be conducted prior to patients leaving the hospital and individualized during postpartum appointments. Reinitiation of testosterone can occur 4-6 weeks after delivery.1
While pregnancy can pose some unique challenges to gender-diverse individuals, these intricacies are not insurmountable. The result of pregnancy, regardless of one’s gender identity, is the same – parenthood. One patient’s description of his experience was particularly poignant: “Pregnancy and childbirth were very male experiences for me. When I birthed my children, I was born into fatherhood.”1 It is up to all providers to modify clinical settings, as well as our patient interactions and use of language, if we are to provide inclusion in obstetrics.1,5
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Brandt JS et al. “Understanding intersections: Care for transgender and gender diverse patient populations.” SMFM 2022 annual meeting. 2022 Feb 2.
2. Hoffkling A et al. BMC Pregnancy Childbirth. 2017 Nov 8;17(Suppl 2):332.
3. Light AD et al. Obstet Gynecol. 2014;124:1120-7.
4. Moseson H et al. Int J Transgend Health. 2021 Nov 17;22(1-2):30-41.
5. Brandt JS et al. Obstetrical care for trans*person, in “Trans*gynecology: Managing transgender patients in obstetrics and gynecology practice.” (Cambridge, England: Cambridge University Press, 2022).
The purpose of this commentary is to provide a brief summary of discussions centering around reproductive health experiences and obstetrical care for gender-diverse patients from the recent Society of Maternal & Fetal Medicine meeting. Two presentations featured patient perspectives combined with physician lectures to provide a comprehensive outlook on unique reproductive care needs for this growing population.
One of the speakers, Trystan Reese, is a transgender activist, educator, and transgender male who chose to carry his own pregnancy and subsequently delivered his son in 2017. During the summit, he described many barriers that he faced during his pregnancy and offered providers suggestions on how to improve the care for members of the gender-diverse community seeking to start a family.
We often think of conception and pregnancy as experiences unique to one gender. This is simply not the case. In discussing preconceptual care and pregnancy, it is paramount for providers to make the distinction between gender identity and natal sex. Gender identity is an internal sense of self in relation to natal sex. Depending on this intrinsic feeling, people may identify as cisgender, transgender, or as a gender outside of the standard binary. Natal sex describes biologic characteristics such as chromosomal makeup, reproductive anatomy, and secondary sexual changes. In keeping these distinctions in mind, pregnancy is therefore exclusive to a person’s natal sex, not gender identity. One of the biggest challenges in caring for transgender patients who desire pregnancy, is the psychological distress related to the gendered notions surrounding this experience.1
There are many ways in which patients encounter unintentional marginalization within the medical system. For example, many electronic medical record systems don’t allow for pronouns or give error messages if the patient’s gender identity is different from their sex assigned at birth. Patients who attend prenatal appointments or birth classes are given documents that center around cisgender women and heterosexual relationships. The labor and delivery wards themselves typically include language such as “maternity,” and birth certificates have distinct “mother” and “father” denotations.1 Insurance coverage for prenatal care and delivery can be problematic if a patient who is assigned female at birth has changed their gender marker to “male” on their insurance card.
Many of these roadblocks can be ameliorated by utilizing more inclusive terminology. Terms such as “maternal” can be replaced with “pregnant patients, parent, or patients giving birth.” Names of maternity wards can be altered to perinatal units, which is more inclusive and more descriptive of the wide variety of patients that may experience childbirth and parenthood.1 Introducing “you-centered” language can also be helpful. Instead of saying “women may find ...” providers can try saying “patients may find ...” or “individuals may find.”1
Most of the medical and obstetrical care of gender-diverse patients is routine. Prenatal labs, aneuploidy screening, ultrasounds, and fetal surveillance do not differ between transgender and cisgender patients. However, the experience of pregnancy itself can significantly heighten feelings of dysphoria as it inherently leads to patients confronting aspects of their biological sex.2 Because of the teratogenic nature of testosterone, patients are required to stop taking testosterone prior to conception and for the duration of pregnancy. This can also heighten dysphoria and lead to increased rates of anxiety and depression.3
Many transgender patients can safely achieve a normal vaginal birth.4 A small survey of 41 people demonstrated that more transgender men who had taken testosterone were delivered by cesarean section (36% vs. 19%).3 Staff training is an important aspect of caring for a transgender patient in labor to ensure that all members of the labor unit are cognizant of appropriate name and pronoun usage. Another interesting, although unsurprising, fact is that many transgender gestational parents chose a community-based (out-of-hospital) birth according to a 2014 study.1 This is predominantly because of the discrimination patients face when delivering within a hospital setting.
Postpartum depression screening should be conducted prior to patients leaving the hospital and individualized during postpartum appointments. Reinitiation of testosterone can occur 4-6 weeks after delivery.1
While pregnancy can pose some unique challenges to gender-diverse individuals, these intricacies are not insurmountable. The result of pregnancy, regardless of one’s gender identity, is the same – parenthood. One patient’s description of his experience was particularly poignant: “Pregnancy and childbirth were very male experiences for me. When I birthed my children, I was born into fatherhood.”1 It is up to all providers to modify clinical settings, as well as our patient interactions and use of language, if we are to provide inclusion in obstetrics.1,5
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Brandt JS et al. “Understanding intersections: Care for transgender and gender diverse patient populations.” SMFM 2022 annual meeting. 2022 Feb 2.
2. Hoffkling A et al. BMC Pregnancy Childbirth. 2017 Nov 8;17(Suppl 2):332.
3. Light AD et al. Obstet Gynecol. 2014;124:1120-7.
4. Moseson H et al. Int J Transgend Health. 2021 Nov 17;22(1-2):30-41.
5. Brandt JS et al. Obstetrical care for trans*person, in “Trans*gynecology: Managing transgender patients in obstetrics and gynecology practice.” (Cambridge, England: Cambridge University Press, 2022).
Proposed insurance policy ignites debate over transgender health care
A new proposed insurance rule to limit discrimination in health plans has ignited a debate over transgender health care.
The policy, known as the Notice of Benefit and Payment Parameters, is part of the Biden administration’s proposal for 2023 for government health insurance exchanges. The rule would require health plans to ensure their benefit designs and implementation don’t discriminate based on sexual orientation, gender identity, age, sociodemographic factors, or other conditions.
The Obama administration first implemented the standard, but the Trump administration removed “sexual orientation” and “gender identity” from the antidiscrimination language in 2020. The Biden proposal would restore protections for those categories.
“We believe such amendments are warranted in light of the existing trends in health care discrimination and are necessary to better address barriers to health equity for LGBTQI+ individuals,” the Department of Health and Human Services wrote in the proposed rule.
The Biden administration, Democratic lawmakers, and advocacy groups have noted that the rule is vital for LGBTQ consumers to access care. But some private insurance companies have said the policy could drive up costs and that the language about what constitutes discrimination is too vague. Conservative groups have also argued that no clinical evidence supports covering care that affirms gender identity, such as hormone blockers or surgery.
Under the proposed rule, an insurer in the government health exchanges wouldn’t be classified as providing “essential health benefits” under federal law if discrimination was found, Roll Call reported. State regulators would be required to enforce the proposal.
The Department of Health and Human Services and the Centers for Medicare and Medicaid Services listed examples of presumptive discrimination that would be banned, such as limiting gender-affirmative care within a health plan. Several state health plains either don’t address coverage or limit coverage for specific services for transgender people, Roll Call reported.
Health benefit plans wouldn’t have to cover every possible health care service, Katie Keith, a researcher at Georgetown University’s Center on Health Insurance Reforms, wrote in an article for Health Affairs. However, an insurer can’t have a different policy or restricted plans for transgender people over patients whose gender identity and sexual orientation match their birth gender.
The proposed rule has sparked a flurry of reactions in recent weeks. America’s Health Insurance Plans, a trade association for health insurance companies, said the nondiscrimination framework is overly broad and limits insurers’ abilities to design plans with controlled costs.
The rule “could create a slippery slope of eliminating benefit limits that are based on clinical evidence, support value-based care, and ensure affordable premiums,” the group wrote in a response letter.
Some conservative groups have pushed back against the coverage requirements as well. The Family Research Council and the Heritage Foundation have questioned the benefits or validity of gender-affirmative care, according to Roll Call.
On the other hand, the HIV+ Hepatitis Policy Initiative said the new rule could help patients who have long faced coverage issues. For instance, some insurers put HIV drugs on the highest-cost plan tiers, which can lead to major expenses for patients.
“It’s not just HIV. It’s other [chronic disease] patients, too,” Carl Schmid, executive director of the patient advocacy group, told Roll Call.
Other insurers, such as the Alliance of Community Health Plans, have said that the updated rule doesn’t give insurers enough time to implement changes. Under the proposal, insurers would have 60 days from final publication to ensure that plans meet the nondiscrimination framework. The group has suggested an effective date of 2024 or later, rather than 2023.
At the same time, some insurance groups have said they’re ready for the change now. The Association for Community Affiliated Plans, which represents small nonprofit plans, said many of its member health plans have already committed resources to ensure all patients can access services, including gender-affirming services or gender identity support for LGBTQ patients.
“We find that their forward-thinking work is – and should be – increasingly the norm,” Margaret Murray, the association’s CEO, wrote in a response letter.
Comments on the proposed rule were due Jan. 27. Now the proposal will wind through the annual approval process.
A version of this article first appeared on WebMD.com.
A new proposed insurance rule to limit discrimination in health plans has ignited a debate over transgender health care.
The policy, known as the Notice of Benefit and Payment Parameters, is part of the Biden administration’s proposal for 2023 for government health insurance exchanges. The rule would require health plans to ensure their benefit designs and implementation don’t discriminate based on sexual orientation, gender identity, age, sociodemographic factors, or other conditions.
The Obama administration first implemented the standard, but the Trump administration removed “sexual orientation” and “gender identity” from the antidiscrimination language in 2020. The Biden proposal would restore protections for those categories.
“We believe such amendments are warranted in light of the existing trends in health care discrimination and are necessary to better address barriers to health equity for LGBTQI+ individuals,” the Department of Health and Human Services wrote in the proposed rule.
The Biden administration, Democratic lawmakers, and advocacy groups have noted that the rule is vital for LGBTQ consumers to access care. But some private insurance companies have said the policy could drive up costs and that the language about what constitutes discrimination is too vague. Conservative groups have also argued that no clinical evidence supports covering care that affirms gender identity, such as hormone blockers or surgery.
Under the proposed rule, an insurer in the government health exchanges wouldn’t be classified as providing “essential health benefits” under federal law if discrimination was found, Roll Call reported. State regulators would be required to enforce the proposal.
The Department of Health and Human Services and the Centers for Medicare and Medicaid Services listed examples of presumptive discrimination that would be banned, such as limiting gender-affirmative care within a health plan. Several state health plains either don’t address coverage or limit coverage for specific services for transgender people, Roll Call reported.
Health benefit plans wouldn’t have to cover every possible health care service, Katie Keith, a researcher at Georgetown University’s Center on Health Insurance Reforms, wrote in an article for Health Affairs. However, an insurer can’t have a different policy or restricted plans for transgender people over patients whose gender identity and sexual orientation match their birth gender.
The proposed rule has sparked a flurry of reactions in recent weeks. America’s Health Insurance Plans, a trade association for health insurance companies, said the nondiscrimination framework is overly broad and limits insurers’ abilities to design plans with controlled costs.
The rule “could create a slippery slope of eliminating benefit limits that are based on clinical evidence, support value-based care, and ensure affordable premiums,” the group wrote in a response letter.
Some conservative groups have pushed back against the coverage requirements as well. The Family Research Council and the Heritage Foundation have questioned the benefits or validity of gender-affirmative care, according to Roll Call.
On the other hand, the HIV+ Hepatitis Policy Initiative said the new rule could help patients who have long faced coverage issues. For instance, some insurers put HIV drugs on the highest-cost plan tiers, which can lead to major expenses for patients.
“It’s not just HIV. It’s other [chronic disease] patients, too,” Carl Schmid, executive director of the patient advocacy group, told Roll Call.
Other insurers, such as the Alliance of Community Health Plans, have said that the updated rule doesn’t give insurers enough time to implement changes. Under the proposal, insurers would have 60 days from final publication to ensure that plans meet the nondiscrimination framework. The group has suggested an effective date of 2024 or later, rather than 2023.
At the same time, some insurance groups have said they’re ready for the change now. The Association for Community Affiliated Plans, which represents small nonprofit plans, said many of its member health plans have already committed resources to ensure all patients can access services, including gender-affirming services or gender identity support for LGBTQ patients.
“We find that their forward-thinking work is – and should be – increasingly the norm,” Margaret Murray, the association’s CEO, wrote in a response letter.
Comments on the proposed rule were due Jan. 27. Now the proposal will wind through the annual approval process.
A version of this article first appeared on WebMD.com.
A new proposed insurance rule to limit discrimination in health plans has ignited a debate over transgender health care.
The policy, known as the Notice of Benefit and Payment Parameters, is part of the Biden administration’s proposal for 2023 for government health insurance exchanges. The rule would require health plans to ensure their benefit designs and implementation don’t discriminate based on sexual orientation, gender identity, age, sociodemographic factors, or other conditions.
The Obama administration first implemented the standard, but the Trump administration removed “sexual orientation” and “gender identity” from the antidiscrimination language in 2020. The Biden proposal would restore protections for those categories.
“We believe such amendments are warranted in light of the existing trends in health care discrimination and are necessary to better address barriers to health equity for LGBTQI+ individuals,” the Department of Health and Human Services wrote in the proposed rule.
The Biden administration, Democratic lawmakers, and advocacy groups have noted that the rule is vital for LGBTQ consumers to access care. But some private insurance companies have said the policy could drive up costs and that the language about what constitutes discrimination is too vague. Conservative groups have also argued that no clinical evidence supports covering care that affirms gender identity, such as hormone blockers or surgery.
Under the proposed rule, an insurer in the government health exchanges wouldn’t be classified as providing “essential health benefits” under federal law if discrimination was found, Roll Call reported. State regulators would be required to enforce the proposal.
The Department of Health and Human Services and the Centers for Medicare and Medicaid Services listed examples of presumptive discrimination that would be banned, such as limiting gender-affirmative care within a health plan. Several state health plains either don’t address coverage or limit coverage for specific services for transgender people, Roll Call reported.
Health benefit plans wouldn’t have to cover every possible health care service, Katie Keith, a researcher at Georgetown University’s Center on Health Insurance Reforms, wrote in an article for Health Affairs. However, an insurer can’t have a different policy or restricted plans for transgender people over patients whose gender identity and sexual orientation match their birth gender.
The proposed rule has sparked a flurry of reactions in recent weeks. America’s Health Insurance Plans, a trade association for health insurance companies, said the nondiscrimination framework is overly broad and limits insurers’ abilities to design plans with controlled costs.
The rule “could create a slippery slope of eliminating benefit limits that are based on clinical evidence, support value-based care, and ensure affordable premiums,” the group wrote in a response letter.
Some conservative groups have pushed back against the coverage requirements as well. The Family Research Council and the Heritage Foundation have questioned the benefits or validity of gender-affirmative care, according to Roll Call.
On the other hand, the HIV+ Hepatitis Policy Initiative said the new rule could help patients who have long faced coverage issues. For instance, some insurers put HIV drugs on the highest-cost plan tiers, which can lead to major expenses for patients.
“It’s not just HIV. It’s other [chronic disease] patients, too,” Carl Schmid, executive director of the patient advocacy group, told Roll Call.
Other insurers, such as the Alliance of Community Health Plans, have said that the updated rule doesn’t give insurers enough time to implement changes. Under the proposal, insurers would have 60 days from final publication to ensure that plans meet the nondiscrimination framework. The group has suggested an effective date of 2024 or later, rather than 2023.
At the same time, some insurance groups have said they’re ready for the change now. The Association for Community Affiliated Plans, which represents small nonprofit plans, said many of its member health plans have already committed resources to ensure all patients can access services, including gender-affirming services or gender identity support for LGBTQ patients.
“We find that their forward-thinking work is – and should be – increasingly the norm,” Margaret Murray, the association’s CEO, wrote in a response letter.
Comments on the proposed rule were due Jan. 27. Now the proposal will wind through the annual approval process.
A version of this article first appeared on WebMD.com.
LGBTQ parents fare worse giving birth
Members of the LGBTQ community who give birth appear to have a greater risk of hypertensive disorders of pregnancy and postpartum hemorrhage, according to new research presented at the annual meeting sponsored by the Society for Maternal-Fetal Medicine.
“Our study found that birthing patients in likely sexual and gender minority partnerships experienced disparities in clinical outcomes,” Stephanie Leonard, PhD, an epidemiology and biostatistics instructor at the Stanford (Calif.) University division of maternal-fetal medicine and obstetrics, told attendees at the meeting. The disparities are likely because of various social determinants and possibly higher use of assisted reproductive technology (ART). The findings establish “how these are significant disparities that have been largely overlooked and set the groundwork for doing further research on maybe ways that we can improve the inclusivity of obstetric care.”
Jenny Mei, MD, a maternal-fetal medicine fellow at the University of California, Los Angeles, who attended the presentation but was not involved in the research, said the findings were “overall unfortunate but not surprising given the existing studies looking at LGBTQ patients and their poorer health outcomes, largely due to lack of access to health care and discrimination in the health care setting.”
Dr. Leonard described the societal, interpersonal, and individual factors that can contribute to health disparities among gender and sexual minority patients.
“At the societal level, there are expectations of what it means to be pregnant, to give birth, and to be a parent. At the community level, there’s the clinical care environment, and at the interpersonal level, there’s an obstetrician’s relationship with the patient,” Dr. Leonard said. “At the individual level, most notably is minority stress, the biological effects of the chronic experience of discrimination.”
It has historically been difficult to collect data on this patient population, but a change in the design of the California birth certificate made it possible to gather more data than previously possible. The updated California birth certificate, issued in 2016, allows the parent not giving birth to check off whether they are the child’s mother, father, parent, or “not specified” instead of defaulting to “father.” In addition, the parent giving birth can select mother, father, parent or not specified instead of being “mother” by default.
The researchers classified sexual and gender minority (SGM) partnerships as those in which the parent giving birth was identified as the father and those where both parents were identified as mothers. Non-SGM minority partnerships were those in which the birthing parent was identified as the mother and the nonbirthing parent was identified as the father.
The population-based cohort study included data from all live birth hospitalizations from 2016-2019 in California, whose annual births represent one in eight babies born each year in the United States. The population of SGM patients different significantly from the non-SGM population in nearly every demographic and clinical factor except rates of pre-existing diabetes. For example, 42% of the SGM birthing patients were age 35 or older, compared with 23% of the non-SGM patients.
SGM patients were more likely to be born in the United States, were more likely to be White, and were less likely to be Asian or Hispanic. SGM patients had higher education levels and were more likely to have private insurance. They were also more likely to be nulliparous and have chronic hypertension. Average body mass index for SGM patients was 33 kg/m2, compared with 30 for non-SGM patients. SGM patients were also much more likely to have multifetal gestation: 7.1% of SGM patients versus 1.5% of non-SGM patients.
In terms of clinical outcomes, 14% of SGM patients had hypertensive disorders of pregnancy, compared with 8% of non-SGM patients. Before adjustment for potential confounders, SGM patients were also twice as likely to have postpartum hemorrhage (8% vs. 4% in non-SGM patients) and postterm birth at 42-44 weeks (0.6% vs 0.3% in non-SGM patients).
“Having increased postterm birth is a matter of declining induction of labor, as it is recommended to have an induction by 41 weeks of gestation in general,” Dr. Mei said in an interview. “It is also possible this patient cohort faces more barriers in access to care and possible discrimination as sexual/gender minority patients.”
Rates of severe preeclampsia, induction of labor, cesarean delivery, preterm birth, low birth weight, and a low Apgar score were also higher among SGM patients, but these associations were no longer significant after adjustment for age, education, payment method, parity, prepregnancy weight, comorbidities, and multifetal gestation. The difference in hypertensive disorders of pregnancy, postpartum hemorrhage, and postterm birth remained statistically significant after adjustment.
Past research has shown that only about a third of cisgender female same-sex marriages used ART, so the disparities cannot be completely explained by ART use, Dr. Leonard said.
“I think the main drivers are structural disparities,” Dr. Leonard said. “Every obstetric clinic is focused in a way that’s about mother-father, and many people who don’t feel like they fit into that paradigm feel excluded and disengage with health care.”
Elliott Main, MD, a clinical professor of obstetrics and gynecology at Stanford University and coauthor of the study noted that discrimination and stigma likely play a substantial role in the disparities.
“Sexual and/or gender minority people face this discrimination at structural and interpersonal levels on a regular basis, which can lead to chronic stress and its harmful physical effects as well as lower-quality health care,” Dr. Main said in an interview.
Another coauthor, Juno Obedin-Maliver, MD, an assistant professor of obstetrics and gynecology at Stanford, emphasized how much room for improvement exists in care for SGM obstetric patients.
“We hope that this study brings needed attention to the disparities in perinatal health experienced by sexual and/or gender minority people,” Dr. Obedin-Maliver said. “There is much we can do to better understand the family building goals of sexual and/or gender minority people and help those to be achieved with healthy outcomes for parents and their children.”
One limitation of the study is that it’s possible to misclassify individuals using the birth certificate data, and not everyone may be comfortable selecting the box that accurately represents their identity, particularly if they aren’t “out” or fear discrimination or stigma, so the population may underrepresent the actual numbers of sexual and gender minority individuals giving birth. Dr. Mei added that it would be helpful to see data on neonatal ICU admissions and use of ART.
It’s difficult to say how generalizable the findings are, Dr. Mei said. “It is possible the findings would be more exaggerated in the rest of the country outside of California, if we assume there is potentially lower health access and more stigma.” The fact that California offers different gender options for the birthing and nonbirthing parent is, by itself, an indication of a potentially more accepting social environment than might be found in other states.
”The take-home message is that this patient population is higher risk, likely partially due to baseline increased risk factors, such as older maternal age and likely use of ART, and partially due to possible lack of health access and stigma,” Dr. Mei said. “Health care providers should be notably cognizant of these increased risks, particularly in the psychosocial context and make efforts to reduce those burdens as much as possible.”
The research was funded by the Stanford Maternal and Child Health Research Institute. Dr. Obedin-Maliver has consulted for Sage Therapeutics, Ibis Reproductive Health, and Hims. Dr. Mei and the other authors had no disclosures.
Members of the LGBTQ community who give birth appear to have a greater risk of hypertensive disorders of pregnancy and postpartum hemorrhage, according to new research presented at the annual meeting sponsored by the Society for Maternal-Fetal Medicine.
“Our study found that birthing patients in likely sexual and gender minority partnerships experienced disparities in clinical outcomes,” Stephanie Leonard, PhD, an epidemiology and biostatistics instructor at the Stanford (Calif.) University division of maternal-fetal medicine and obstetrics, told attendees at the meeting. The disparities are likely because of various social determinants and possibly higher use of assisted reproductive technology (ART). The findings establish “how these are significant disparities that have been largely overlooked and set the groundwork for doing further research on maybe ways that we can improve the inclusivity of obstetric care.”
Jenny Mei, MD, a maternal-fetal medicine fellow at the University of California, Los Angeles, who attended the presentation but was not involved in the research, said the findings were “overall unfortunate but not surprising given the existing studies looking at LGBTQ patients and their poorer health outcomes, largely due to lack of access to health care and discrimination in the health care setting.”
Dr. Leonard described the societal, interpersonal, and individual factors that can contribute to health disparities among gender and sexual minority patients.
“At the societal level, there are expectations of what it means to be pregnant, to give birth, and to be a parent. At the community level, there’s the clinical care environment, and at the interpersonal level, there’s an obstetrician’s relationship with the patient,” Dr. Leonard said. “At the individual level, most notably is minority stress, the biological effects of the chronic experience of discrimination.”
It has historically been difficult to collect data on this patient population, but a change in the design of the California birth certificate made it possible to gather more data than previously possible. The updated California birth certificate, issued in 2016, allows the parent not giving birth to check off whether they are the child’s mother, father, parent, or “not specified” instead of defaulting to “father.” In addition, the parent giving birth can select mother, father, parent or not specified instead of being “mother” by default.
The researchers classified sexual and gender minority (SGM) partnerships as those in which the parent giving birth was identified as the father and those where both parents were identified as mothers. Non-SGM minority partnerships were those in which the birthing parent was identified as the mother and the nonbirthing parent was identified as the father.
The population-based cohort study included data from all live birth hospitalizations from 2016-2019 in California, whose annual births represent one in eight babies born each year in the United States. The population of SGM patients different significantly from the non-SGM population in nearly every demographic and clinical factor except rates of pre-existing diabetes. For example, 42% of the SGM birthing patients were age 35 or older, compared with 23% of the non-SGM patients.
SGM patients were more likely to be born in the United States, were more likely to be White, and were less likely to be Asian or Hispanic. SGM patients had higher education levels and were more likely to have private insurance. They were also more likely to be nulliparous and have chronic hypertension. Average body mass index for SGM patients was 33 kg/m2, compared with 30 for non-SGM patients. SGM patients were also much more likely to have multifetal gestation: 7.1% of SGM patients versus 1.5% of non-SGM patients.
In terms of clinical outcomes, 14% of SGM patients had hypertensive disorders of pregnancy, compared with 8% of non-SGM patients. Before adjustment for potential confounders, SGM patients were also twice as likely to have postpartum hemorrhage (8% vs. 4% in non-SGM patients) and postterm birth at 42-44 weeks (0.6% vs 0.3% in non-SGM patients).
“Having increased postterm birth is a matter of declining induction of labor, as it is recommended to have an induction by 41 weeks of gestation in general,” Dr. Mei said in an interview. “It is also possible this patient cohort faces more barriers in access to care and possible discrimination as sexual/gender minority patients.”
Rates of severe preeclampsia, induction of labor, cesarean delivery, preterm birth, low birth weight, and a low Apgar score were also higher among SGM patients, but these associations were no longer significant after adjustment for age, education, payment method, parity, prepregnancy weight, comorbidities, and multifetal gestation. The difference in hypertensive disorders of pregnancy, postpartum hemorrhage, and postterm birth remained statistically significant after adjustment.
Past research has shown that only about a third of cisgender female same-sex marriages used ART, so the disparities cannot be completely explained by ART use, Dr. Leonard said.
“I think the main drivers are structural disparities,” Dr. Leonard said. “Every obstetric clinic is focused in a way that’s about mother-father, and many people who don’t feel like they fit into that paradigm feel excluded and disengage with health care.”
Elliott Main, MD, a clinical professor of obstetrics and gynecology at Stanford University and coauthor of the study noted that discrimination and stigma likely play a substantial role in the disparities.
“Sexual and/or gender minority people face this discrimination at structural and interpersonal levels on a regular basis, which can lead to chronic stress and its harmful physical effects as well as lower-quality health care,” Dr. Main said in an interview.
Another coauthor, Juno Obedin-Maliver, MD, an assistant professor of obstetrics and gynecology at Stanford, emphasized how much room for improvement exists in care for SGM obstetric patients.
“We hope that this study brings needed attention to the disparities in perinatal health experienced by sexual and/or gender minority people,” Dr. Obedin-Maliver said. “There is much we can do to better understand the family building goals of sexual and/or gender minority people and help those to be achieved with healthy outcomes for parents and their children.”
One limitation of the study is that it’s possible to misclassify individuals using the birth certificate data, and not everyone may be comfortable selecting the box that accurately represents their identity, particularly if they aren’t “out” or fear discrimination or stigma, so the population may underrepresent the actual numbers of sexual and gender minority individuals giving birth. Dr. Mei added that it would be helpful to see data on neonatal ICU admissions and use of ART.
It’s difficult to say how generalizable the findings are, Dr. Mei said. “It is possible the findings would be more exaggerated in the rest of the country outside of California, if we assume there is potentially lower health access and more stigma.” The fact that California offers different gender options for the birthing and nonbirthing parent is, by itself, an indication of a potentially more accepting social environment than might be found in other states.
”The take-home message is that this patient population is higher risk, likely partially due to baseline increased risk factors, such as older maternal age and likely use of ART, and partially due to possible lack of health access and stigma,” Dr. Mei said. “Health care providers should be notably cognizant of these increased risks, particularly in the psychosocial context and make efforts to reduce those burdens as much as possible.”
The research was funded by the Stanford Maternal and Child Health Research Institute. Dr. Obedin-Maliver has consulted for Sage Therapeutics, Ibis Reproductive Health, and Hims. Dr. Mei and the other authors had no disclosures.
Members of the LGBTQ community who give birth appear to have a greater risk of hypertensive disorders of pregnancy and postpartum hemorrhage, according to new research presented at the annual meeting sponsored by the Society for Maternal-Fetal Medicine.
“Our study found that birthing patients in likely sexual and gender minority partnerships experienced disparities in clinical outcomes,” Stephanie Leonard, PhD, an epidemiology and biostatistics instructor at the Stanford (Calif.) University division of maternal-fetal medicine and obstetrics, told attendees at the meeting. The disparities are likely because of various social determinants and possibly higher use of assisted reproductive technology (ART). The findings establish “how these are significant disparities that have been largely overlooked and set the groundwork for doing further research on maybe ways that we can improve the inclusivity of obstetric care.”
Jenny Mei, MD, a maternal-fetal medicine fellow at the University of California, Los Angeles, who attended the presentation but was not involved in the research, said the findings were “overall unfortunate but not surprising given the existing studies looking at LGBTQ patients and their poorer health outcomes, largely due to lack of access to health care and discrimination in the health care setting.”
Dr. Leonard described the societal, interpersonal, and individual factors that can contribute to health disparities among gender and sexual minority patients.
“At the societal level, there are expectations of what it means to be pregnant, to give birth, and to be a parent. At the community level, there’s the clinical care environment, and at the interpersonal level, there’s an obstetrician’s relationship with the patient,” Dr. Leonard said. “At the individual level, most notably is minority stress, the biological effects of the chronic experience of discrimination.”
It has historically been difficult to collect data on this patient population, but a change in the design of the California birth certificate made it possible to gather more data than previously possible. The updated California birth certificate, issued in 2016, allows the parent not giving birth to check off whether they are the child’s mother, father, parent, or “not specified” instead of defaulting to “father.” In addition, the parent giving birth can select mother, father, parent or not specified instead of being “mother” by default.
The researchers classified sexual and gender minority (SGM) partnerships as those in which the parent giving birth was identified as the father and those where both parents were identified as mothers. Non-SGM minority partnerships were those in which the birthing parent was identified as the mother and the nonbirthing parent was identified as the father.
The population-based cohort study included data from all live birth hospitalizations from 2016-2019 in California, whose annual births represent one in eight babies born each year in the United States. The population of SGM patients different significantly from the non-SGM population in nearly every demographic and clinical factor except rates of pre-existing diabetes. For example, 42% of the SGM birthing patients were age 35 or older, compared with 23% of the non-SGM patients.
SGM patients were more likely to be born in the United States, were more likely to be White, and were less likely to be Asian or Hispanic. SGM patients had higher education levels and were more likely to have private insurance. They were also more likely to be nulliparous and have chronic hypertension. Average body mass index for SGM patients was 33 kg/m2, compared with 30 for non-SGM patients. SGM patients were also much more likely to have multifetal gestation: 7.1% of SGM patients versus 1.5% of non-SGM patients.
In terms of clinical outcomes, 14% of SGM patients had hypertensive disorders of pregnancy, compared with 8% of non-SGM patients. Before adjustment for potential confounders, SGM patients were also twice as likely to have postpartum hemorrhage (8% vs. 4% in non-SGM patients) and postterm birth at 42-44 weeks (0.6% vs 0.3% in non-SGM patients).
“Having increased postterm birth is a matter of declining induction of labor, as it is recommended to have an induction by 41 weeks of gestation in general,” Dr. Mei said in an interview. “It is also possible this patient cohort faces more barriers in access to care and possible discrimination as sexual/gender minority patients.”
Rates of severe preeclampsia, induction of labor, cesarean delivery, preterm birth, low birth weight, and a low Apgar score were also higher among SGM patients, but these associations were no longer significant after adjustment for age, education, payment method, parity, prepregnancy weight, comorbidities, and multifetal gestation. The difference in hypertensive disorders of pregnancy, postpartum hemorrhage, and postterm birth remained statistically significant after adjustment.
Past research has shown that only about a third of cisgender female same-sex marriages used ART, so the disparities cannot be completely explained by ART use, Dr. Leonard said.
“I think the main drivers are structural disparities,” Dr. Leonard said. “Every obstetric clinic is focused in a way that’s about mother-father, and many people who don’t feel like they fit into that paradigm feel excluded and disengage with health care.”
Elliott Main, MD, a clinical professor of obstetrics and gynecology at Stanford University and coauthor of the study noted that discrimination and stigma likely play a substantial role in the disparities.
“Sexual and/or gender minority people face this discrimination at structural and interpersonal levels on a regular basis, which can lead to chronic stress and its harmful physical effects as well as lower-quality health care,” Dr. Main said in an interview.
Another coauthor, Juno Obedin-Maliver, MD, an assistant professor of obstetrics and gynecology at Stanford, emphasized how much room for improvement exists in care for SGM obstetric patients.
“We hope that this study brings needed attention to the disparities in perinatal health experienced by sexual and/or gender minority people,” Dr. Obedin-Maliver said. “There is much we can do to better understand the family building goals of sexual and/or gender minority people and help those to be achieved with healthy outcomes for parents and their children.”
One limitation of the study is that it’s possible to misclassify individuals using the birth certificate data, and not everyone may be comfortable selecting the box that accurately represents their identity, particularly if they aren’t “out” or fear discrimination or stigma, so the population may underrepresent the actual numbers of sexual and gender minority individuals giving birth. Dr. Mei added that it would be helpful to see data on neonatal ICU admissions and use of ART.
It’s difficult to say how generalizable the findings are, Dr. Mei said. “It is possible the findings would be more exaggerated in the rest of the country outside of California, if we assume there is potentially lower health access and more stigma.” The fact that California offers different gender options for the birthing and nonbirthing parent is, by itself, an indication of a potentially more accepting social environment than might be found in other states.
”The take-home message is that this patient population is higher risk, likely partially due to baseline increased risk factors, such as older maternal age and likely use of ART, and partially due to possible lack of health access and stigma,” Dr. Mei said. “Health care providers should be notably cognizant of these increased risks, particularly in the psychosocial context and make efforts to reduce those burdens as much as possible.”
The research was funded by the Stanford Maternal and Child Health Research Institute. Dr. Obedin-Maliver has consulted for Sage Therapeutics, Ibis Reproductive Health, and Hims. Dr. Mei and the other authors had no disclosures.
FROM THE PREGNANCY MEETING
Referrals to gender clinics in Sweden drop after media coverage
Media coverage of transgender health care judged to be “negative” was associated with a drop of around 30% in referral rates to gender identity clinics in Sweden among young people under age 19, a new study indicates.
Malin Indremo, MS, from the department of neuroscience, Uppsala (Sweden) University, and colleagues explored the effect of the documentaries, “The Trans Train and Teenage Girls,” which they explain was a “Swedish public service television show” representing “investigative journalism.” The two-part documentary series was aired in Sweden in April 2019 and October 2019, respectively, and is now available in English on YouTube.
In their article, published online in JAMA Network Open, the authors said they consider “The Trans Train” programs to be “negative” media coverage because the “documentaries addressed the distinct increase among adolescents referred to gender identity clinics in recent years. Two young adults who regretted their transition and parents of transgender individuals who questioned the clinics’ assessments of their children were interviewed, and concerns were raised about whether gender-confirming treatments are based on sufficient scientific evidence.”
The programs, they suggest, may have influenced and jeopardized young transgender individuals’ access to transgender-specific health care.
Stella O’Malley, a U.K.-based psychotherapist specializing in transgender care and executive director of Genspect, an international organization that provides support to the parents of young people who are questioning their gender, expressed her disappointment with the study’s conclusions.
“I’m really surprised and disappointed that the researchers believe that negative coverage is the reason for a drop in referrals when it is more accurate to say that the information provided by ‘The Trans Train’ documentaries was concerning and suggests that further critical analysis and a review needs to be carried out on the clinics in question,” she said in an interview.
Ms. O’Malley herself made a documentary for Channel 4 in the United Kingdom, broadcast in 2018, called: “Trans Kids: It’s Time to Talk.”
Rapidly increasing numbers of youth, especially girls, question gender
As Ms. Indremo and coauthors explained – and as has been widely reported by this news organization – “the number of referrals to gender identity clinics have rapidly increased worldwide” in recent years, and this “has been especially prominent in adolescents and young adults.”
In addition, they acknowledged, “there has been a shift in gender ratio, with a preponderance toward individuals who were assigned female at birth (AFAB).”
This was the topic of “The Trans Train” programs, and in fact, following their broadcast, Ms. Indremo and colleagues noted that “an intense debate in national media [in Sweden] arose from the documentaries.”
Their research aimed to explore the association between both “positive” and “negative” media coverage and the number of referrals to gender identity clinics for young people (under aged 19) respectively. Data from the six gender clinics in Sweden were included between January 2017 and December 2019.
In the period studied, the clinics received 1,784 referrals, including 613 referrals in 2017, 663 referrals in 2018, and 508 referrals in 2019.
From the age-specific data that included 1,674 referrals, 359 individuals (21.4%) were younger than 13 years and 1,315 individuals (78.6%) were aged 13-18 years. From the assigned sex-specific data that included 1,435 referrals, 1,034 individuals (72.1%) were AFAB and 401 individuals (27.9%) were assigned male at birth (AMAB). Information on sex assigned at birth was lacking from one clinic, which was excluded from the analysis.
When they examined data for the 3 months following the airing of the first part of “The Trans Train” documentary series (in April 2019), they found that referrals to gender clinics fell by 25.4% overall, compared with the 3 months before part 1 was screened. Specifically, they fell by 25.3% for young people aged 13-18 years and by 32.2% for those born female.
In the extended analyses of 6 months following part 1, a decrease of total referrals by 30.7% was observed, while referrals for AFAB individuals decreased by 37.4% and referrals for individuals aged 13-18 years decreased by 27.7%. A decrease of referrals by 41.7% for children aged younger than 13 years was observed in the 6-month analysis, as well as a decrease of 8.2% among AMAB individuals.
“The Trans Train” documentaries, Ms. Indremo and colleagues said, “were criticized for being negatively biased and giving an oversimplified picture of transgender health care.”
Did the nature of the trans train documentaries influence referrals?
In an invited commentary published in JAMA Network Open, Ken C. Pang, PhD, from the Murdoch Children’s Research Institute, Melbourne, and colleagues noted: “Although the mechanisms underlying this decrease [in referrals] were not formally explored in their study, the authors reasonably speculated that both parents and referring health professionals may have been less likely to support a child or adolescent’s attendance at a specialist pediatric gender clinic following the documentaries.”
Dr. Pang and colleagues went on to say it is “the ... responsibility of media organizations in ensuring that stories depicting health care for transgender and gender diverse (TGD) young people are fair, balanced, nuanced, and accurate.”
Often, media reports have “fallen short of these standards and lacked the voices of TGD young people who have benefited from gender-affirming care or the perspectives of health professionals with expertise in providing such care,” they added.
“For example, some [media reports] have suggested that the growing number of referrals to such clinics is not owing to greater awareness of gender diversity and empowerment of TGD young people but is instead being driven by other factors such as peer influence, while others have warned that the use of gender-affirming hormonal interventions in TGD young people represents an undue risk,” they continue.
Ms. Indremo and colleagues didn’t see any drop-in referrals after the second part of the series, aired in October 2019, but they say this was likely because referrals were “already lowered” by the airing of the first part of the documentaries.
Nor did they see an increase in referrals following what they say was a “positive” media event in the form of a story about a professional Swedish handball player who announced the decision to quit his career to seek care for gender dysphoria.
“One may assume that a single news event is not significant enough to influence referral counts,” they suggested, noting also that Sweden represents “a society where there is already a relatively high level of awareness of gender identity issues.”
“Our results point to a differential association of media attention depending on the tone of the media content,” they observed.
Dr. Pang and coauthors noted it would be “helpful to examine whether similar media coverage in other countries has been associated with similar decreases in referral numbers and whether particular types of media stories are more prone to having this association.”
Parents and doctors debate treatment of gender dysphoria
In Sweden, custodians’ permission as well as custodians’ help is needed for minors to access care for gender dysphoria, said Ms. Indremo and coauthors. “It is possible that the content of the documentaries contributed to a higher custodian barrier to having their children referred for assessment, believing it may not be in the best interest of their child. This would highly impact young transgender individuals’ possibilities to access care.”
They also acknowledge that health care practitioners who refer young people to specialist clinics might also have been influenced by the documentaries, noting “some commentators argued that all treatments for gender dysphoria be stopped, and that ‘all health care given at the gender identity clinics was an experiment lacking scientific basis.’ ”
In April 2021, Angela Sämfjord, MD, child and adolescent psychiatrist at Sahlgrenska University Hospital, Gothenburg, Sweden, who started a child and adolescent clinic – the Lundstrom Gender Clinic – told this news organization she had reevaluated her approach even prior to “The Trans Train” documentaries and had resigned in 2018 because of her own fears about the lack of evidence for hormonal and surgical treatments of youth with gender dysphoria.
Following the debate that ensued after the airing of “The Trans Train” programs, the Swedish National Board of Health and Welfare published new recommendations in March 2021, which reflected a significant change in direction for the evaluation of gender dysphoria in minors, emphasizing the requirement for a thorough mental health assessment.
And in May 2021, Karolinska Children’s Hospital, which houses one of the leading gender identity clinics in Sweden, announced it would stop the routine medical treatment of children with gender dysphoria under the age of 18, which meant a total ban on the prescribing of puberty blockers and cross-sex hormones to minors. Such treatment could henceforth only be carried out within the setting of a clinical trial approved by the EPM (Ethical Review Agency/Swedish Institutional Review Board), it said.
The remaining five gender identity clinics in Sweden decided upon their own rules, but in general, they have become much more cautious regarding medical treatment of minors within the past year. Also, there is a desire in Sweden to reduce the number of gender identity clinics for minors from the current six to perhaps a maximum of three nationwide.
However, neither Ms. Indremo and colleagues nor Dr. Pang and colleagues mentioned the subsequent change to the Swedish NBHW recommendations on evaluation of gender dysphoria in minors in JAMA articles.
New NBHW recommendations about medical treatment of gender dysphoria with puberty blockers and cross-sex hormones for minors were due to be issued in 2021 but have been delayed.
Debate in other countries
Sweden is not alone in discussing this issue. In 2020, Finland became the first country in the world to issue new guidelines that concluded there is a lack of quality evidence to support the use of hormonal interventions in adolescents with gender dysphoria.
This issue has been hotly debated in the United Kingdom – not least with the Keira Bell court case and two National Institute for Health and Clinical Excellence evidence reviews concluding there is a lack of data to support the use of puberty-blocking agents and “cross-sex” hormones in youth with gender dysphoria.
And a number of U.S. states are attempting to outlaw the medical and surgical treatment of gender dysphoria in minors. Even health care professionals who have been treating young people with gender dysphoria for years – some of whom are transgender themselves – have started to speak out and are questioning what they call “sloppy care” given to many such youth.
Indeed, a recent survey shows that detransitioners – individuals who suffer from gender dysphoria, transition to the opposite sex but then regret their decision and detransition – are getting short shrift when it comes to care, with over half of the 100 surveyed saying they feel they did not receive adequate evaluation from a doctor or mental health professional before starting to transition.
And new draft standards of care for treating people with gender dysphoria by the World Professional Association for Transgender Health have drawn criticism from experts.
‘First do no harm’
In their conclusion, Dr. Pang and coauthors said that, with respect to the media coverage of young people with gender dysphoria, “who are, after all, one of the most vulnerable subgroups within our society, perhaps our media should recall one of the core tenets of health care and ensure their stories ‘first, do no harm.’”
However, in a commentary recently published in Child and Adolescent Mental Health, Alison Clayton, MBBS, from the University of Melbourne, and coauthors again pointed out that evidence reviews of the use of puberty blockers in young people with gender dysphoria show “there is very low certainty of the benefits of puberty blockers, an unknown risk of harm, and there is need for more rigorous research.”
“The clinically prudent thing to do, if we aim to ‘first, do no harm,’ is to proceed with extreme caution, especially given the rapidly rising case numbers and novel gender dysphoria presentations,” Clayton and colleagues concluded.
Ms. Indremo and coauthors reported no relevant financial relationships. Dr. Pang reported being a member of the Australian Professional Association for Trans Health and its research committee. One commentary coauthor has reported being a member of WPATH.
A version of this article first appeared on Medscape.com.
Media coverage of transgender health care judged to be “negative” was associated with a drop of around 30% in referral rates to gender identity clinics in Sweden among young people under age 19, a new study indicates.
Malin Indremo, MS, from the department of neuroscience, Uppsala (Sweden) University, and colleagues explored the effect of the documentaries, “The Trans Train and Teenage Girls,” which they explain was a “Swedish public service television show” representing “investigative journalism.” The two-part documentary series was aired in Sweden in April 2019 and October 2019, respectively, and is now available in English on YouTube.
In their article, published online in JAMA Network Open, the authors said they consider “The Trans Train” programs to be “negative” media coverage because the “documentaries addressed the distinct increase among adolescents referred to gender identity clinics in recent years. Two young adults who regretted their transition and parents of transgender individuals who questioned the clinics’ assessments of their children were interviewed, and concerns were raised about whether gender-confirming treatments are based on sufficient scientific evidence.”
The programs, they suggest, may have influenced and jeopardized young transgender individuals’ access to transgender-specific health care.
Stella O’Malley, a U.K.-based psychotherapist specializing in transgender care and executive director of Genspect, an international organization that provides support to the parents of young people who are questioning their gender, expressed her disappointment with the study’s conclusions.
“I’m really surprised and disappointed that the researchers believe that negative coverage is the reason for a drop in referrals when it is more accurate to say that the information provided by ‘The Trans Train’ documentaries was concerning and suggests that further critical analysis and a review needs to be carried out on the clinics in question,” she said in an interview.
Ms. O’Malley herself made a documentary for Channel 4 in the United Kingdom, broadcast in 2018, called: “Trans Kids: It’s Time to Talk.”
Rapidly increasing numbers of youth, especially girls, question gender
As Ms. Indremo and coauthors explained – and as has been widely reported by this news organization – “the number of referrals to gender identity clinics have rapidly increased worldwide” in recent years, and this “has been especially prominent in adolescents and young adults.”
In addition, they acknowledged, “there has been a shift in gender ratio, with a preponderance toward individuals who were assigned female at birth (AFAB).”
This was the topic of “The Trans Train” programs, and in fact, following their broadcast, Ms. Indremo and colleagues noted that “an intense debate in national media [in Sweden] arose from the documentaries.”
Their research aimed to explore the association between both “positive” and “negative” media coverage and the number of referrals to gender identity clinics for young people (under aged 19) respectively. Data from the six gender clinics in Sweden were included between January 2017 and December 2019.
In the period studied, the clinics received 1,784 referrals, including 613 referrals in 2017, 663 referrals in 2018, and 508 referrals in 2019.
From the age-specific data that included 1,674 referrals, 359 individuals (21.4%) were younger than 13 years and 1,315 individuals (78.6%) were aged 13-18 years. From the assigned sex-specific data that included 1,435 referrals, 1,034 individuals (72.1%) were AFAB and 401 individuals (27.9%) were assigned male at birth (AMAB). Information on sex assigned at birth was lacking from one clinic, which was excluded from the analysis.
When they examined data for the 3 months following the airing of the first part of “The Trans Train” documentary series (in April 2019), they found that referrals to gender clinics fell by 25.4% overall, compared with the 3 months before part 1 was screened. Specifically, they fell by 25.3% for young people aged 13-18 years and by 32.2% for those born female.
In the extended analyses of 6 months following part 1, a decrease of total referrals by 30.7% was observed, while referrals for AFAB individuals decreased by 37.4% and referrals for individuals aged 13-18 years decreased by 27.7%. A decrease of referrals by 41.7% for children aged younger than 13 years was observed in the 6-month analysis, as well as a decrease of 8.2% among AMAB individuals.
“The Trans Train” documentaries, Ms. Indremo and colleagues said, “were criticized for being negatively biased and giving an oversimplified picture of transgender health care.”
Did the nature of the trans train documentaries influence referrals?
In an invited commentary published in JAMA Network Open, Ken C. Pang, PhD, from the Murdoch Children’s Research Institute, Melbourne, and colleagues noted: “Although the mechanisms underlying this decrease [in referrals] were not formally explored in their study, the authors reasonably speculated that both parents and referring health professionals may have been less likely to support a child or adolescent’s attendance at a specialist pediatric gender clinic following the documentaries.”
Dr. Pang and colleagues went on to say it is “the ... responsibility of media organizations in ensuring that stories depicting health care for transgender and gender diverse (TGD) young people are fair, balanced, nuanced, and accurate.”
Often, media reports have “fallen short of these standards and lacked the voices of TGD young people who have benefited from gender-affirming care or the perspectives of health professionals with expertise in providing such care,” they added.
“For example, some [media reports] have suggested that the growing number of referrals to such clinics is not owing to greater awareness of gender diversity and empowerment of TGD young people but is instead being driven by other factors such as peer influence, while others have warned that the use of gender-affirming hormonal interventions in TGD young people represents an undue risk,” they continue.
Ms. Indremo and colleagues didn’t see any drop-in referrals after the second part of the series, aired in October 2019, but they say this was likely because referrals were “already lowered” by the airing of the first part of the documentaries.
Nor did they see an increase in referrals following what they say was a “positive” media event in the form of a story about a professional Swedish handball player who announced the decision to quit his career to seek care for gender dysphoria.
“One may assume that a single news event is not significant enough to influence referral counts,” they suggested, noting also that Sweden represents “a society where there is already a relatively high level of awareness of gender identity issues.”
“Our results point to a differential association of media attention depending on the tone of the media content,” they observed.
Dr. Pang and coauthors noted it would be “helpful to examine whether similar media coverage in other countries has been associated with similar decreases in referral numbers and whether particular types of media stories are more prone to having this association.”
Parents and doctors debate treatment of gender dysphoria
In Sweden, custodians’ permission as well as custodians’ help is needed for minors to access care for gender dysphoria, said Ms. Indremo and coauthors. “It is possible that the content of the documentaries contributed to a higher custodian barrier to having their children referred for assessment, believing it may not be in the best interest of their child. This would highly impact young transgender individuals’ possibilities to access care.”
They also acknowledge that health care practitioners who refer young people to specialist clinics might also have been influenced by the documentaries, noting “some commentators argued that all treatments for gender dysphoria be stopped, and that ‘all health care given at the gender identity clinics was an experiment lacking scientific basis.’ ”
In April 2021, Angela Sämfjord, MD, child and adolescent psychiatrist at Sahlgrenska University Hospital, Gothenburg, Sweden, who started a child and adolescent clinic – the Lundstrom Gender Clinic – told this news organization she had reevaluated her approach even prior to “The Trans Train” documentaries and had resigned in 2018 because of her own fears about the lack of evidence for hormonal and surgical treatments of youth with gender dysphoria.
Following the debate that ensued after the airing of “The Trans Train” programs, the Swedish National Board of Health and Welfare published new recommendations in March 2021, which reflected a significant change in direction for the evaluation of gender dysphoria in minors, emphasizing the requirement for a thorough mental health assessment.
And in May 2021, Karolinska Children’s Hospital, which houses one of the leading gender identity clinics in Sweden, announced it would stop the routine medical treatment of children with gender dysphoria under the age of 18, which meant a total ban on the prescribing of puberty blockers and cross-sex hormones to minors. Such treatment could henceforth only be carried out within the setting of a clinical trial approved by the EPM (Ethical Review Agency/Swedish Institutional Review Board), it said.
The remaining five gender identity clinics in Sweden decided upon their own rules, but in general, they have become much more cautious regarding medical treatment of minors within the past year. Also, there is a desire in Sweden to reduce the number of gender identity clinics for minors from the current six to perhaps a maximum of three nationwide.
However, neither Ms. Indremo and colleagues nor Dr. Pang and colleagues mentioned the subsequent change to the Swedish NBHW recommendations on evaluation of gender dysphoria in minors in JAMA articles.
New NBHW recommendations about medical treatment of gender dysphoria with puberty blockers and cross-sex hormones for minors were due to be issued in 2021 but have been delayed.
Debate in other countries
Sweden is not alone in discussing this issue. In 2020, Finland became the first country in the world to issue new guidelines that concluded there is a lack of quality evidence to support the use of hormonal interventions in adolescents with gender dysphoria.
This issue has been hotly debated in the United Kingdom – not least with the Keira Bell court case and two National Institute for Health and Clinical Excellence evidence reviews concluding there is a lack of data to support the use of puberty-blocking agents and “cross-sex” hormones in youth with gender dysphoria.
And a number of U.S. states are attempting to outlaw the medical and surgical treatment of gender dysphoria in minors. Even health care professionals who have been treating young people with gender dysphoria for years – some of whom are transgender themselves – have started to speak out and are questioning what they call “sloppy care” given to many such youth.
Indeed, a recent survey shows that detransitioners – individuals who suffer from gender dysphoria, transition to the opposite sex but then regret their decision and detransition – are getting short shrift when it comes to care, with over half of the 100 surveyed saying they feel they did not receive adequate evaluation from a doctor or mental health professional before starting to transition.
And new draft standards of care for treating people with gender dysphoria by the World Professional Association for Transgender Health have drawn criticism from experts.
‘First do no harm’
In their conclusion, Dr. Pang and coauthors said that, with respect to the media coverage of young people with gender dysphoria, “who are, after all, one of the most vulnerable subgroups within our society, perhaps our media should recall one of the core tenets of health care and ensure their stories ‘first, do no harm.’”
However, in a commentary recently published in Child and Adolescent Mental Health, Alison Clayton, MBBS, from the University of Melbourne, and coauthors again pointed out that evidence reviews of the use of puberty blockers in young people with gender dysphoria show “there is very low certainty of the benefits of puberty blockers, an unknown risk of harm, and there is need for more rigorous research.”
“The clinically prudent thing to do, if we aim to ‘first, do no harm,’ is to proceed with extreme caution, especially given the rapidly rising case numbers and novel gender dysphoria presentations,” Clayton and colleagues concluded.
Ms. Indremo and coauthors reported no relevant financial relationships. Dr. Pang reported being a member of the Australian Professional Association for Trans Health and its research committee. One commentary coauthor has reported being a member of WPATH.
A version of this article first appeared on Medscape.com.
Media coverage of transgender health care judged to be “negative” was associated with a drop of around 30% in referral rates to gender identity clinics in Sweden among young people under age 19, a new study indicates.
Malin Indremo, MS, from the department of neuroscience, Uppsala (Sweden) University, and colleagues explored the effect of the documentaries, “The Trans Train and Teenage Girls,” which they explain was a “Swedish public service television show” representing “investigative journalism.” The two-part documentary series was aired in Sweden in April 2019 and October 2019, respectively, and is now available in English on YouTube.
In their article, published online in JAMA Network Open, the authors said they consider “The Trans Train” programs to be “negative” media coverage because the “documentaries addressed the distinct increase among adolescents referred to gender identity clinics in recent years. Two young adults who regretted their transition and parents of transgender individuals who questioned the clinics’ assessments of their children were interviewed, and concerns were raised about whether gender-confirming treatments are based on sufficient scientific evidence.”
The programs, they suggest, may have influenced and jeopardized young transgender individuals’ access to transgender-specific health care.
Stella O’Malley, a U.K.-based psychotherapist specializing in transgender care and executive director of Genspect, an international organization that provides support to the parents of young people who are questioning their gender, expressed her disappointment with the study’s conclusions.
“I’m really surprised and disappointed that the researchers believe that negative coverage is the reason for a drop in referrals when it is more accurate to say that the information provided by ‘The Trans Train’ documentaries was concerning and suggests that further critical analysis and a review needs to be carried out on the clinics in question,” she said in an interview.
Ms. O’Malley herself made a documentary for Channel 4 in the United Kingdom, broadcast in 2018, called: “Trans Kids: It’s Time to Talk.”
Rapidly increasing numbers of youth, especially girls, question gender
As Ms. Indremo and coauthors explained – and as has been widely reported by this news organization – “the number of referrals to gender identity clinics have rapidly increased worldwide” in recent years, and this “has been especially prominent in adolescents and young adults.”
In addition, they acknowledged, “there has been a shift in gender ratio, with a preponderance toward individuals who were assigned female at birth (AFAB).”
This was the topic of “The Trans Train” programs, and in fact, following their broadcast, Ms. Indremo and colleagues noted that “an intense debate in national media [in Sweden] arose from the documentaries.”
Their research aimed to explore the association between both “positive” and “negative” media coverage and the number of referrals to gender identity clinics for young people (under aged 19) respectively. Data from the six gender clinics in Sweden were included between January 2017 and December 2019.
In the period studied, the clinics received 1,784 referrals, including 613 referrals in 2017, 663 referrals in 2018, and 508 referrals in 2019.
From the age-specific data that included 1,674 referrals, 359 individuals (21.4%) were younger than 13 years and 1,315 individuals (78.6%) were aged 13-18 years. From the assigned sex-specific data that included 1,435 referrals, 1,034 individuals (72.1%) were AFAB and 401 individuals (27.9%) were assigned male at birth (AMAB). Information on sex assigned at birth was lacking from one clinic, which was excluded from the analysis.
When they examined data for the 3 months following the airing of the first part of “The Trans Train” documentary series (in April 2019), they found that referrals to gender clinics fell by 25.4% overall, compared with the 3 months before part 1 was screened. Specifically, they fell by 25.3% for young people aged 13-18 years and by 32.2% for those born female.
In the extended analyses of 6 months following part 1, a decrease of total referrals by 30.7% was observed, while referrals for AFAB individuals decreased by 37.4% and referrals for individuals aged 13-18 years decreased by 27.7%. A decrease of referrals by 41.7% for children aged younger than 13 years was observed in the 6-month analysis, as well as a decrease of 8.2% among AMAB individuals.
“The Trans Train” documentaries, Ms. Indremo and colleagues said, “were criticized for being negatively biased and giving an oversimplified picture of transgender health care.”
Did the nature of the trans train documentaries influence referrals?
In an invited commentary published in JAMA Network Open, Ken C. Pang, PhD, from the Murdoch Children’s Research Institute, Melbourne, and colleagues noted: “Although the mechanisms underlying this decrease [in referrals] were not formally explored in their study, the authors reasonably speculated that both parents and referring health professionals may have been less likely to support a child or adolescent’s attendance at a specialist pediatric gender clinic following the documentaries.”
Dr. Pang and colleagues went on to say it is “the ... responsibility of media organizations in ensuring that stories depicting health care for transgender and gender diverse (TGD) young people are fair, balanced, nuanced, and accurate.”
Often, media reports have “fallen short of these standards and lacked the voices of TGD young people who have benefited from gender-affirming care or the perspectives of health professionals with expertise in providing such care,” they added.
“For example, some [media reports] have suggested that the growing number of referrals to such clinics is not owing to greater awareness of gender diversity and empowerment of TGD young people but is instead being driven by other factors such as peer influence, while others have warned that the use of gender-affirming hormonal interventions in TGD young people represents an undue risk,” they continue.
Ms. Indremo and colleagues didn’t see any drop-in referrals after the second part of the series, aired in October 2019, but they say this was likely because referrals were “already lowered” by the airing of the first part of the documentaries.
Nor did they see an increase in referrals following what they say was a “positive” media event in the form of a story about a professional Swedish handball player who announced the decision to quit his career to seek care for gender dysphoria.
“One may assume that a single news event is not significant enough to influence referral counts,” they suggested, noting also that Sweden represents “a society where there is already a relatively high level of awareness of gender identity issues.”
“Our results point to a differential association of media attention depending on the tone of the media content,” they observed.
Dr. Pang and coauthors noted it would be “helpful to examine whether similar media coverage in other countries has been associated with similar decreases in referral numbers and whether particular types of media stories are more prone to having this association.”
Parents and doctors debate treatment of gender dysphoria
In Sweden, custodians’ permission as well as custodians’ help is needed for minors to access care for gender dysphoria, said Ms. Indremo and coauthors. “It is possible that the content of the documentaries contributed to a higher custodian barrier to having their children referred for assessment, believing it may not be in the best interest of their child. This would highly impact young transgender individuals’ possibilities to access care.”
They also acknowledge that health care practitioners who refer young people to specialist clinics might also have been influenced by the documentaries, noting “some commentators argued that all treatments for gender dysphoria be stopped, and that ‘all health care given at the gender identity clinics was an experiment lacking scientific basis.’ ”
In April 2021, Angela Sämfjord, MD, child and adolescent psychiatrist at Sahlgrenska University Hospital, Gothenburg, Sweden, who started a child and adolescent clinic – the Lundstrom Gender Clinic – told this news organization she had reevaluated her approach even prior to “The Trans Train” documentaries and had resigned in 2018 because of her own fears about the lack of evidence for hormonal and surgical treatments of youth with gender dysphoria.
Following the debate that ensued after the airing of “The Trans Train” programs, the Swedish National Board of Health and Welfare published new recommendations in March 2021, which reflected a significant change in direction for the evaluation of gender dysphoria in minors, emphasizing the requirement for a thorough mental health assessment.
And in May 2021, Karolinska Children’s Hospital, which houses one of the leading gender identity clinics in Sweden, announced it would stop the routine medical treatment of children with gender dysphoria under the age of 18, which meant a total ban on the prescribing of puberty blockers and cross-sex hormones to minors. Such treatment could henceforth only be carried out within the setting of a clinical trial approved by the EPM (Ethical Review Agency/Swedish Institutional Review Board), it said.
The remaining five gender identity clinics in Sweden decided upon their own rules, but in general, they have become much more cautious regarding medical treatment of minors within the past year. Also, there is a desire in Sweden to reduce the number of gender identity clinics for minors from the current six to perhaps a maximum of three nationwide.
However, neither Ms. Indremo and colleagues nor Dr. Pang and colleagues mentioned the subsequent change to the Swedish NBHW recommendations on evaluation of gender dysphoria in minors in JAMA articles.
New NBHW recommendations about medical treatment of gender dysphoria with puberty blockers and cross-sex hormones for minors were due to be issued in 2021 but have been delayed.
Debate in other countries
Sweden is not alone in discussing this issue. In 2020, Finland became the first country in the world to issue new guidelines that concluded there is a lack of quality evidence to support the use of hormonal interventions in adolescents with gender dysphoria.
This issue has been hotly debated in the United Kingdom – not least with the Keira Bell court case and two National Institute for Health and Clinical Excellence evidence reviews concluding there is a lack of data to support the use of puberty-blocking agents and “cross-sex” hormones in youth with gender dysphoria.
And a number of U.S. states are attempting to outlaw the medical and surgical treatment of gender dysphoria in minors. Even health care professionals who have been treating young people with gender dysphoria for years – some of whom are transgender themselves – have started to speak out and are questioning what they call “sloppy care” given to many such youth.
Indeed, a recent survey shows that detransitioners – individuals who suffer from gender dysphoria, transition to the opposite sex but then regret their decision and detransition – are getting short shrift when it comes to care, with over half of the 100 surveyed saying they feel they did not receive adequate evaluation from a doctor or mental health professional before starting to transition.
And new draft standards of care for treating people with gender dysphoria by the World Professional Association for Transgender Health have drawn criticism from experts.
‘First do no harm’
In their conclusion, Dr. Pang and coauthors said that, with respect to the media coverage of young people with gender dysphoria, “who are, after all, one of the most vulnerable subgroups within our society, perhaps our media should recall one of the core tenets of health care and ensure their stories ‘first, do no harm.’”
However, in a commentary recently published in Child and Adolescent Mental Health, Alison Clayton, MBBS, from the University of Melbourne, and coauthors again pointed out that evidence reviews of the use of puberty blockers in young people with gender dysphoria show “there is very low certainty of the benefits of puberty blockers, an unknown risk of harm, and there is need for more rigorous research.”
“The clinically prudent thing to do, if we aim to ‘first, do no harm,’ is to proceed with extreme caution, especially given the rapidly rising case numbers and novel gender dysphoria presentations,” Clayton and colleagues concluded.
Ms. Indremo and coauthors reported no relevant financial relationships. Dr. Pang reported being a member of the Australian Professional Association for Trans Health and its research committee. One commentary coauthor has reported being a member of WPATH.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Hormone therapy in transgender teens linked to better adult mental health
In another salvo in the heated debate over treatment for kids who believe they’re transgender, a study published in PLoS One suggests that transgender adults who received hormone therapy as teenagers are mentally healthier in a pair of ways than those who didn’t.
The study, which only looks at transgender adults, doesn’t confirm that hormone therapy in childhood is a beneficial treatment. Still, “we found that for all age groups, access to [adolescent] gender-affirming hormone initiation was associated with lower odds of past-year suicidal ideation and past-month severe psychological distress measured in adulthood,” said lead author Jack Turban, MD, chief fellow in child and adolescent psychiatry at Stanford (Calif.) University, in an interview. “We also found better mental-health outcomes for those who started gender-affirming hormones as adolescents when compared to those who didn’t start them until they were adults.”
The use of hormone treatment and puberty blockers by transgender teens is extremely controversial. Critics say the treatments are harmful and unnecessary, and Republican politicians are trying to ban their use in some states. Last spring, Arkansas became the first state to ban the treatments. The law is on hold amid a legal challenge.
The researchers launched the study to gain more insight into the impact of hormone therapy on children. “There have been several longitudinal studies showing that mental health improves following gender-affirming medical care for transgender youth, but there has been less research looking at the relationship between when these medications are started and adult mental health outcomes,” Dr. Turban said. “This is the first study to look at various ages of initiation of gender-affirming hormones and compare outcomes between those who started gender-affirming hormones during adolescence and those who did not start them until adulthood.”
For the new study, the authors analyzed the findings of the 2015 U.S. Transgender Survey of 27,715 adults and focused on 21,598 who said they’d wanted hormone therapy (40% aged 18-24, 83% White, 35% transgender male, 41% transgender female, with the rest using other terms such as “queer” or “nonbinary” to describe themselves).
Of these subjects, 41.0% never received hormone therapy, 0.6% underwent therapy in early adolescence, 1.7% received it in late adolescence, and 56.8% got it as adults.
The researchers made various adjustments for confounders – age, partnership status, employment status, K-12 harassment, and experience of gender identity conversion efforts. Those who received hormone therapy had lower odds of past-year suicidal ideation vs. those who didn’t: adjusted odds ratio, 0.4; 95% confidence interval, 0.2-0.6; P < .0001 for therapy that occurred from age 14 to 15, aOR, 0.5; 95% CI, 0.4-0.7; P < .0001, for therapy that occurred from age 16 to 17, and aOR, 0.8; 95% CI, 0.7-0.8; P < .0001 for therapy that occurred in adulthood.
However, there was no statistically significant link between hormone therapy and past-year suicidal ideation with a plan or past-year suicide attempt.
The study also found lower rates of past-month severe psychological distress: aOR. 0.3; 95% CI, 0.2-0.4; P < .0001 for therapy from age 14 to 15, aOR, 0.3; 95% CI, 0.3-0.4; P < .0001 for therapy from age 16 to 17, and aOR, 0.6 (95% CI, 0.5-0.6; P < .0001) for therapy in adulthood.
There was no statistically significant link between hormone therapy and past-month binge drinking or lifetime illicit drug use.
“The findings indicate that clinicians caring for adolescents need to be properly trained in gender-affirming medical care, including hormone therapy, in order to help promote good mental health outcomes for transgender people. Comprehensive training in gender-affirming care is currently not part of standard medical education curricula,” said study coauthor Alex Keuroghlian, MD, MPH, director of the National LGBTQIA+ Health Education Center at the Fenway Institute and associate professor of psychiatry at Harvard Medical School, Boston, in an interview.
The study has limitations. The survey population doesn’t include anyone who committed suicide, nor does it include people who had gender dysphoria as children but didn’t go on to identify as transgender as adults. It is also retrospective. “There is a general consensus that, given the data we have so far, it would be unethical to conduct a randomized controlled trial in this space,” said study lead author Dr. Turban.
Several critics of hormone therapy in teens support a psychotherapy-based approach to gender dysphoria that considers whether other factors are at play than transgender orientation. They’ve united to attack research based on the 2015 transgender survey. In a 2021 report in Archives of Sexual Behavior, they called it “a highly skewed sample” and objected to “a conflation of ethical nonaffirmative psychotherapy with conversion therapy.”
In an interview, one of the critics – developmental psychologist and retired University of Sydney professor Dianna Kenny, PhD – said the new study’s “serious problem of recall bias” about hormone therapy in the survey is “insurmountable.” The survey, she said, also fails to explore why participants who wanted hormone therapy didn’t get it.
Dr. Kenny, who believes all hormone therapy in teens with gender dysphoria outside of clinical trials is inappropriate, also pointed out that hormone therapy has many side effects. She added that young people with gender dysphoria often “realize through a process of cognitive and psychosocial maturation that they were not ‘genuinely’ trans but suffering from other conditions that needed treatment – e.g., internalized homophobia, trauma, including sexual abuse, attention-deficit/hyperactivity disorder, autism spectrum disorder, etc.”
No specific funding is reported, although two of the authors report receiving various grants, fellowship and research funding. Dr. Turban discloses textbook royalties from Springer Nature and expert witness payments from the ACLU. Dr. Keuroghlian discloses textbook royalties from McGraw Hill. Dr. Kenny reports no disclosures.
In another salvo in the heated debate over treatment for kids who believe they’re transgender, a study published in PLoS One suggests that transgender adults who received hormone therapy as teenagers are mentally healthier in a pair of ways than those who didn’t.
The study, which only looks at transgender adults, doesn’t confirm that hormone therapy in childhood is a beneficial treatment. Still, “we found that for all age groups, access to [adolescent] gender-affirming hormone initiation was associated with lower odds of past-year suicidal ideation and past-month severe psychological distress measured in adulthood,” said lead author Jack Turban, MD, chief fellow in child and adolescent psychiatry at Stanford (Calif.) University, in an interview. “We also found better mental-health outcomes for those who started gender-affirming hormones as adolescents when compared to those who didn’t start them until they were adults.”
The use of hormone treatment and puberty blockers by transgender teens is extremely controversial. Critics say the treatments are harmful and unnecessary, and Republican politicians are trying to ban their use in some states. Last spring, Arkansas became the first state to ban the treatments. The law is on hold amid a legal challenge.
The researchers launched the study to gain more insight into the impact of hormone therapy on children. “There have been several longitudinal studies showing that mental health improves following gender-affirming medical care for transgender youth, but there has been less research looking at the relationship between when these medications are started and adult mental health outcomes,” Dr. Turban said. “This is the first study to look at various ages of initiation of gender-affirming hormones and compare outcomes between those who started gender-affirming hormones during adolescence and those who did not start them until adulthood.”
For the new study, the authors analyzed the findings of the 2015 U.S. Transgender Survey of 27,715 adults and focused on 21,598 who said they’d wanted hormone therapy (40% aged 18-24, 83% White, 35% transgender male, 41% transgender female, with the rest using other terms such as “queer” or “nonbinary” to describe themselves).
Of these subjects, 41.0% never received hormone therapy, 0.6% underwent therapy in early adolescence, 1.7% received it in late adolescence, and 56.8% got it as adults.
The researchers made various adjustments for confounders – age, partnership status, employment status, K-12 harassment, and experience of gender identity conversion efforts. Those who received hormone therapy had lower odds of past-year suicidal ideation vs. those who didn’t: adjusted odds ratio, 0.4; 95% confidence interval, 0.2-0.6; P < .0001 for therapy that occurred from age 14 to 15, aOR, 0.5; 95% CI, 0.4-0.7; P < .0001, for therapy that occurred from age 16 to 17, and aOR, 0.8; 95% CI, 0.7-0.8; P < .0001 for therapy that occurred in adulthood.
However, there was no statistically significant link between hormone therapy and past-year suicidal ideation with a plan or past-year suicide attempt.
The study also found lower rates of past-month severe psychological distress: aOR. 0.3; 95% CI, 0.2-0.4; P < .0001 for therapy from age 14 to 15, aOR, 0.3; 95% CI, 0.3-0.4; P < .0001 for therapy from age 16 to 17, and aOR, 0.6 (95% CI, 0.5-0.6; P < .0001) for therapy in adulthood.
There was no statistically significant link between hormone therapy and past-month binge drinking or lifetime illicit drug use.
“The findings indicate that clinicians caring for adolescents need to be properly trained in gender-affirming medical care, including hormone therapy, in order to help promote good mental health outcomes for transgender people. Comprehensive training in gender-affirming care is currently not part of standard medical education curricula,” said study coauthor Alex Keuroghlian, MD, MPH, director of the National LGBTQIA+ Health Education Center at the Fenway Institute and associate professor of psychiatry at Harvard Medical School, Boston, in an interview.
The study has limitations. The survey population doesn’t include anyone who committed suicide, nor does it include people who had gender dysphoria as children but didn’t go on to identify as transgender as adults. It is also retrospective. “There is a general consensus that, given the data we have so far, it would be unethical to conduct a randomized controlled trial in this space,” said study lead author Dr. Turban.
Several critics of hormone therapy in teens support a psychotherapy-based approach to gender dysphoria that considers whether other factors are at play than transgender orientation. They’ve united to attack research based on the 2015 transgender survey. In a 2021 report in Archives of Sexual Behavior, they called it “a highly skewed sample” and objected to “a conflation of ethical nonaffirmative psychotherapy with conversion therapy.”
In an interview, one of the critics – developmental psychologist and retired University of Sydney professor Dianna Kenny, PhD – said the new study’s “serious problem of recall bias” about hormone therapy in the survey is “insurmountable.” The survey, she said, also fails to explore why participants who wanted hormone therapy didn’t get it.
Dr. Kenny, who believes all hormone therapy in teens with gender dysphoria outside of clinical trials is inappropriate, also pointed out that hormone therapy has many side effects. She added that young people with gender dysphoria often “realize through a process of cognitive and psychosocial maturation that they were not ‘genuinely’ trans but suffering from other conditions that needed treatment – e.g., internalized homophobia, trauma, including sexual abuse, attention-deficit/hyperactivity disorder, autism spectrum disorder, etc.”
No specific funding is reported, although two of the authors report receiving various grants, fellowship and research funding. Dr. Turban discloses textbook royalties from Springer Nature and expert witness payments from the ACLU. Dr. Keuroghlian discloses textbook royalties from McGraw Hill. Dr. Kenny reports no disclosures.
In another salvo in the heated debate over treatment for kids who believe they’re transgender, a study published in PLoS One suggests that transgender adults who received hormone therapy as teenagers are mentally healthier in a pair of ways than those who didn’t.
The study, which only looks at transgender adults, doesn’t confirm that hormone therapy in childhood is a beneficial treatment. Still, “we found that for all age groups, access to [adolescent] gender-affirming hormone initiation was associated with lower odds of past-year suicidal ideation and past-month severe psychological distress measured in adulthood,” said lead author Jack Turban, MD, chief fellow in child and adolescent psychiatry at Stanford (Calif.) University, in an interview. “We also found better mental-health outcomes for those who started gender-affirming hormones as adolescents when compared to those who didn’t start them until they were adults.”
The use of hormone treatment and puberty blockers by transgender teens is extremely controversial. Critics say the treatments are harmful and unnecessary, and Republican politicians are trying to ban their use in some states. Last spring, Arkansas became the first state to ban the treatments. The law is on hold amid a legal challenge.
The researchers launched the study to gain more insight into the impact of hormone therapy on children. “There have been several longitudinal studies showing that mental health improves following gender-affirming medical care for transgender youth, but there has been less research looking at the relationship between when these medications are started and adult mental health outcomes,” Dr. Turban said. “This is the first study to look at various ages of initiation of gender-affirming hormones and compare outcomes between those who started gender-affirming hormones during adolescence and those who did not start them until adulthood.”
For the new study, the authors analyzed the findings of the 2015 U.S. Transgender Survey of 27,715 adults and focused on 21,598 who said they’d wanted hormone therapy (40% aged 18-24, 83% White, 35% transgender male, 41% transgender female, with the rest using other terms such as “queer” or “nonbinary” to describe themselves).
Of these subjects, 41.0% never received hormone therapy, 0.6% underwent therapy in early adolescence, 1.7% received it in late adolescence, and 56.8% got it as adults.
The researchers made various adjustments for confounders – age, partnership status, employment status, K-12 harassment, and experience of gender identity conversion efforts. Those who received hormone therapy had lower odds of past-year suicidal ideation vs. those who didn’t: adjusted odds ratio, 0.4; 95% confidence interval, 0.2-0.6; P < .0001 for therapy that occurred from age 14 to 15, aOR, 0.5; 95% CI, 0.4-0.7; P < .0001, for therapy that occurred from age 16 to 17, and aOR, 0.8; 95% CI, 0.7-0.8; P < .0001 for therapy that occurred in adulthood.
However, there was no statistically significant link between hormone therapy and past-year suicidal ideation with a plan or past-year suicide attempt.
The study also found lower rates of past-month severe psychological distress: aOR. 0.3; 95% CI, 0.2-0.4; P < .0001 for therapy from age 14 to 15, aOR, 0.3; 95% CI, 0.3-0.4; P < .0001 for therapy from age 16 to 17, and aOR, 0.6 (95% CI, 0.5-0.6; P < .0001) for therapy in adulthood.
There was no statistically significant link between hormone therapy and past-month binge drinking or lifetime illicit drug use.
“The findings indicate that clinicians caring for adolescents need to be properly trained in gender-affirming medical care, including hormone therapy, in order to help promote good mental health outcomes for transgender people. Comprehensive training in gender-affirming care is currently not part of standard medical education curricula,” said study coauthor Alex Keuroghlian, MD, MPH, director of the National LGBTQIA+ Health Education Center at the Fenway Institute and associate professor of psychiatry at Harvard Medical School, Boston, in an interview.
The study has limitations. The survey population doesn’t include anyone who committed suicide, nor does it include people who had gender dysphoria as children but didn’t go on to identify as transgender as adults. It is also retrospective. “There is a general consensus that, given the data we have so far, it would be unethical to conduct a randomized controlled trial in this space,” said study lead author Dr. Turban.
Several critics of hormone therapy in teens support a psychotherapy-based approach to gender dysphoria that considers whether other factors are at play than transgender orientation. They’ve united to attack research based on the 2015 transgender survey. In a 2021 report in Archives of Sexual Behavior, they called it “a highly skewed sample” and objected to “a conflation of ethical nonaffirmative psychotherapy with conversion therapy.”
In an interview, one of the critics – developmental psychologist and retired University of Sydney professor Dianna Kenny, PhD – said the new study’s “serious problem of recall bias” about hormone therapy in the survey is “insurmountable.” The survey, she said, also fails to explore why participants who wanted hormone therapy didn’t get it.
Dr. Kenny, who believes all hormone therapy in teens with gender dysphoria outside of clinical trials is inappropriate, also pointed out that hormone therapy has many side effects. She added that young people with gender dysphoria often “realize through a process of cognitive and psychosocial maturation that they were not ‘genuinely’ trans but suffering from other conditions that needed treatment – e.g., internalized homophobia, trauma, including sexual abuse, attention-deficit/hyperactivity disorder, autism spectrum disorder, etc.”
No specific funding is reported, although two of the authors report receiving various grants, fellowship and research funding. Dr. Turban discloses textbook royalties from Springer Nature and expert witness payments from the ACLU. Dr. Keuroghlian discloses textbook royalties from McGraw Hill. Dr. Kenny reports no disclosures.
FROM PLOS ONE
Detransition, baby: Examining factors leading to ‘detransitioning’ and regret in the transgender community
Over the holiday season I had the pleasure of finally reading the national bestseller, Detransition, Baby. On the surface, the story depicts the complex relationships between Reese, a transgender woman who strongly desires a family, her ex-wife, Ames – a transgender woman who detransitioned to live as a cisgender man – and Ames’ cisgender female partner, who is unexpectedly pregnant with his child. The story delves much deeper than the relationships between these characters, as it exceptionally articulates many of the emotional intricacies of the transgender experience and addresses one of the most taboo topics in the transgender community – detransitioning and regret.
The terms “transition” and “detransition” have fallen out of favor in the vernacular of the transgender population as they incorrectly imply that gender identity is contingent upon gender-affirmation processes.1,2 More importantly, the terms “detransition” and regret are not synonymous. Conflating these terms has undermined the intrinsic nature of gender identity, which has resulted in political and legal consequences seeking to limit or outright ban care for transgender patients.
As a gender-affirming surgeon, one of the most common questions I get asked is the rate of regret patients have after their surgeries. While I have no issue answering the question when it is presented, I do not hesitate to point out some of the problematic subtext inherent in such inquiries. Within the line of questioning, many often comment, “It’s so permanent,” “I can’t believe people can do this to their bodies,” or “How sure are patients before undergoing these surgeries?” While these comments and queries can be downright offensive, they seem to stem from the difficulty people have comprehending gender dysphoria and the painstaking steps people take to affirm their identity. The implication of these comments also reveals a more deep-seated issue – general distrust of individual bodily autonomy, personal identity, and choice.
For the obstetrician-gynecologist, understanding the concept of autonomous, patient-centered decision-making should be second nature, as we face a similar line of interrogation when discussing abortion, contraception, and pregnancy. No other field faces this level of scrutiny when it comes to defending a patient’s bodily autonomy. For example, given the history of reproductive injustice with tubal ligation procedures, the American College of Obstetricians and Gynecologists has issued clear guidelines regarding counseling of women while acknowledging the tenuous history of these procedures with minority subgroups. According to their committee opinion, ethical counseling for such a permanent procedure involves understanding the content of information presented to the patient, how that information is conveyed, and self-reflection on the part of the provider.3 The approach to counseling and understanding gender-affirming care is no different.
I want to be clear that regret after gender-affirming surgery is rare, occurring in 0%-3.8% of patients.4-6 In a separate study, 91% of patients expressed significant improvement in quality of life after surgery.7 However, what is disheartening about patients who experience surgical regret is that it originates from continued difficulty from the transition process itself and ongoing discrimination – even though the patient’s physical characteristics match their gender identity.4-6 Similarly, in another survey which examined 17,151 participants who had pursued gender affirmation (broadly defined), approximately 2,242 (13.1%) reported a history of detransition.2 Among these adults, the vast majority (82.5%), cited external factors such as school harassment, sexual violence, family pressure, and social stigma as reasons for detransitioning.2 Other associated factors included male sex assigned at birth, nonbinary gender identity, bisexual orientation, and having an unsupportive family.2
When Ames is explaining his “detransition” to his cisfemale partner, he states: “I got sick of living as trans …[sic]… I am trans, but I don’t need to do trans.”8 While there is still more research needed to further understand detransitioning and surgical regret, these few studies demonstrate a heart-breaking reality – in many aspects of our society it is still extremely difficult to live as a transgender person.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa. She did not report any disclosures.
References
1. National LGBTQIA+ Health Education Center, A program of the Fenway Institute: LGBTQIA+ glossary of terms for health care teams. 2020. Available at www.lgbtqiahealtheducation.org/wp-content/uploads/2020/10/Glossary-2020.08.30.pdf. Accessed Dec. 30, 2021.
2. Turban JL et al. LGBT Health 2021;8(4):273-80.
3. Sterilization of women: Ethical issues and considerations. Committee Opinion No. 695. American College of Obstetricians and Gynecologists. Obstet Gynecol 2017;129:e109-16.
4. Ruppin U, Pfafflin F. Arch Sex Behav. 2015;44:1321-9.
5. Lawrence AA. Arch Sex Behav. 2003;32:299-315.
6. Landen M et al. Acta Psychiatr Scand. 1998;97:284-9.
7. Papdopulos NA et al. J Sex Med. 2017;14(5):721-30.
8. Peters T. Detransition, Baby. New York: Penguin Random House, 2021.
Over the holiday season I had the pleasure of finally reading the national bestseller, Detransition, Baby. On the surface, the story depicts the complex relationships between Reese, a transgender woman who strongly desires a family, her ex-wife, Ames – a transgender woman who detransitioned to live as a cisgender man – and Ames’ cisgender female partner, who is unexpectedly pregnant with his child. The story delves much deeper than the relationships between these characters, as it exceptionally articulates many of the emotional intricacies of the transgender experience and addresses one of the most taboo topics in the transgender community – detransitioning and regret.
The terms “transition” and “detransition” have fallen out of favor in the vernacular of the transgender population as they incorrectly imply that gender identity is contingent upon gender-affirmation processes.1,2 More importantly, the terms “detransition” and regret are not synonymous. Conflating these terms has undermined the intrinsic nature of gender identity, which has resulted in political and legal consequences seeking to limit or outright ban care for transgender patients.
As a gender-affirming surgeon, one of the most common questions I get asked is the rate of regret patients have after their surgeries. While I have no issue answering the question when it is presented, I do not hesitate to point out some of the problematic subtext inherent in such inquiries. Within the line of questioning, many often comment, “It’s so permanent,” “I can’t believe people can do this to their bodies,” or “How sure are patients before undergoing these surgeries?” While these comments and queries can be downright offensive, they seem to stem from the difficulty people have comprehending gender dysphoria and the painstaking steps people take to affirm their identity. The implication of these comments also reveals a more deep-seated issue – general distrust of individual bodily autonomy, personal identity, and choice.
For the obstetrician-gynecologist, understanding the concept of autonomous, patient-centered decision-making should be second nature, as we face a similar line of interrogation when discussing abortion, contraception, and pregnancy. No other field faces this level of scrutiny when it comes to defending a patient’s bodily autonomy. For example, given the history of reproductive injustice with tubal ligation procedures, the American College of Obstetricians and Gynecologists has issued clear guidelines regarding counseling of women while acknowledging the tenuous history of these procedures with minority subgroups. According to their committee opinion, ethical counseling for such a permanent procedure involves understanding the content of information presented to the patient, how that information is conveyed, and self-reflection on the part of the provider.3 The approach to counseling and understanding gender-affirming care is no different.
I want to be clear that regret after gender-affirming surgery is rare, occurring in 0%-3.8% of patients.4-6 In a separate study, 91% of patients expressed significant improvement in quality of life after surgery.7 However, what is disheartening about patients who experience surgical regret is that it originates from continued difficulty from the transition process itself and ongoing discrimination – even though the patient’s physical characteristics match their gender identity.4-6 Similarly, in another survey which examined 17,151 participants who had pursued gender affirmation (broadly defined), approximately 2,242 (13.1%) reported a history of detransition.2 Among these adults, the vast majority (82.5%), cited external factors such as school harassment, sexual violence, family pressure, and social stigma as reasons for detransitioning.2 Other associated factors included male sex assigned at birth, nonbinary gender identity, bisexual orientation, and having an unsupportive family.2
When Ames is explaining his “detransition” to his cisfemale partner, he states: “I got sick of living as trans …[sic]… I am trans, but I don’t need to do trans.”8 While there is still more research needed to further understand detransitioning and surgical regret, these few studies demonstrate a heart-breaking reality – in many aspects of our society it is still extremely difficult to live as a transgender person.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa. She did not report any disclosures.
References
1. National LGBTQIA+ Health Education Center, A program of the Fenway Institute: LGBTQIA+ glossary of terms for health care teams. 2020. Available at www.lgbtqiahealtheducation.org/wp-content/uploads/2020/10/Glossary-2020.08.30.pdf. Accessed Dec. 30, 2021.
2. Turban JL et al. LGBT Health 2021;8(4):273-80.
3. Sterilization of women: Ethical issues and considerations. Committee Opinion No. 695. American College of Obstetricians and Gynecologists. Obstet Gynecol 2017;129:e109-16.
4. Ruppin U, Pfafflin F. Arch Sex Behav. 2015;44:1321-9.
5. Lawrence AA. Arch Sex Behav. 2003;32:299-315.
6. Landen M et al. Acta Psychiatr Scand. 1998;97:284-9.
7. Papdopulos NA et al. J Sex Med. 2017;14(5):721-30.
8. Peters T. Detransition, Baby. New York: Penguin Random House, 2021.
Over the holiday season I had the pleasure of finally reading the national bestseller, Detransition, Baby. On the surface, the story depicts the complex relationships between Reese, a transgender woman who strongly desires a family, her ex-wife, Ames – a transgender woman who detransitioned to live as a cisgender man – and Ames’ cisgender female partner, who is unexpectedly pregnant with his child. The story delves much deeper than the relationships between these characters, as it exceptionally articulates many of the emotional intricacies of the transgender experience and addresses one of the most taboo topics in the transgender community – detransitioning and regret.
The terms “transition” and “detransition” have fallen out of favor in the vernacular of the transgender population as they incorrectly imply that gender identity is contingent upon gender-affirmation processes.1,2 More importantly, the terms “detransition” and regret are not synonymous. Conflating these terms has undermined the intrinsic nature of gender identity, which has resulted in political and legal consequences seeking to limit or outright ban care for transgender patients.
As a gender-affirming surgeon, one of the most common questions I get asked is the rate of regret patients have after their surgeries. While I have no issue answering the question when it is presented, I do not hesitate to point out some of the problematic subtext inherent in such inquiries. Within the line of questioning, many often comment, “It’s so permanent,” “I can’t believe people can do this to their bodies,” or “How sure are patients before undergoing these surgeries?” While these comments and queries can be downright offensive, they seem to stem from the difficulty people have comprehending gender dysphoria and the painstaking steps people take to affirm their identity. The implication of these comments also reveals a more deep-seated issue – general distrust of individual bodily autonomy, personal identity, and choice.
For the obstetrician-gynecologist, understanding the concept of autonomous, patient-centered decision-making should be second nature, as we face a similar line of interrogation when discussing abortion, contraception, and pregnancy. No other field faces this level of scrutiny when it comes to defending a patient’s bodily autonomy. For example, given the history of reproductive injustice with tubal ligation procedures, the American College of Obstetricians and Gynecologists has issued clear guidelines regarding counseling of women while acknowledging the tenuous history of these procedures with minority subgroups. According to their committee opinion, ethical counseling for such a permanent procedure involves understanding the content of information presented to the patient, how that information is conveyed, and self-reflection on the part of the provider.3 The approach to counseling and understanding gender-affirming care is no different.
I want to be clear that regret after gender-affirming surgery is rare, occurring in 0%-3.8% of patients.4-6 In a separate study, 91% of patients expressed significant improvement in quality of life after surgery.7 However, what is disheartening about patients who experience surgical regret is that it originates from continued difficulty from the transition process itself and ongoing discrimination – even though the patient’s physical characteristics match their gender identity.4-6 Similarly, in another survey which examined 17,151 participants who had pursued gender affirmation (broadly defined), approximately 2,242 (13.1%) reported a history of detransition.2 Among these adults, the vast majority (82.5%), cited external factors such as school harassment, sexual violence, family pressure, and social stigma as reasons for detransitioning.2 Other associated factors included male sex assigned at birth, nonbinary gender identity, bisexual orientation, and having an unsupportive family.2
When Ames is explaining his “detransition” to his cisfemale partner, he states: “I got sick of living as trans …[sic]… I am trans, but I don’t need to do trans.”8 While there is still more research needed to further understand detransitioning and surgical regret, these few studies demonstrate a heart-breaking reality – in many aspects of our society it is still extremely difficult to live as a transgender person.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa. She did not report any disclosures.
References
1. National LGBTQIA+ Health Education Center, A program of the Fenway Institute: LGBTQIA+ glossary of terms for health care teams. 2020. Available at www.lgbtqiahealtheducation.org/wp-content/uploads/2020/10/Glossary-2020.08.30.pdf. Accessed Dec. 30, 2021.
2. Turban JL et al. LGBT Health 2021;8(4):273-80.
3. Sterilization of women: Ethical issues and considerations. Committee Opinion No. 695. American College of Obstetricians and Gynecologists. Obstet Gynecol 2017;129:e109-16.
4. Ruppin U, Pfafflin F. Arch Sex Behav. 2015;44:1321-9.
5. Lawrence AA. Arch Sex Behav. 2003;32:299-315.
6. Landen M et al. Acta Psychiatr Scand. 1998;97:284-9.
7. Papdopulos NA et al. J Sex Med. 2017;14(5):721-30.
8. Peters T. Detransition, Baby. New York: Penguin Random House, 2021.
Changing terminology in LGBTQ+ spaces: How to keep up with the lingo
For those of us who see adolescent patients on a regular basis, it seems that they use new vocabulary almost every day. While you may not need to know what “lit” means, you probably do need to understand terms used to describe your patients’ identities. At times it feels like we, as providers, have to be on TikTok to keep up with our patients, and while this may be an amusing way to educate ourselves, a judicious Google search can be much more helpful. The interesting part about LGBTQ+ terminology is that it stems from the community and thus is frequently updated to reflect our evolving understanding of gender, sexuality, and identity. That being said, it can make it difficult for those who are not plugged in to the community to keep up to date. While we have learned in medicine to use accurate terminology and appropriate three-letter acronyms (or “TLAs” as one of my residents referenced them when I was a medical student) to describe medical conditions, the LGBTQ+ community has its own set of terms and acronyms. These new words may seem daunting, but they are often based in Latin roots or prefixes such as a-, demi-, poly-, and pan-, which may be familiar to those of us who use plenty of other Latin-based terms in medicine and our everyday lives. By paying attention to how people define and use terminology, we can better recognize their true identities and become better providers.
The first, and perhaps most important, piece of advice is to maintain cultural humility. Know when to admit you don’t recognize a term and politely ask the definition. For example, the first time I heard the term “demiboy” I said “I’m not familiar with that word. Can you explain what it means to you?” Phrasing the question as such is also helpful in that it gives the individuals a chance to really define their identity. In addition, some words may be used differently by various individuals and by asking what the word means to them, you can have a better understanding of how they are using the terminology. In this particular instance, the patient felt more masculine, but not 100%, partway between agender (meaning having no gender identity) and being “all male.” By embracing cultural humility, we place the patients in the role of expert on their own identity and orientation. According to Maria Ruud, DNP, of the University of Minnesota, Minneapolis, cultural humility is the “ongoing self-reflection and education …[seeking] to gain an awareness of their own assumptions and biases that may contribute to health disparities.”1

Another reason it is important to keep up on the language is that some adolescents, particularly younger adolescents, may not be using the terminology correctly. It can be very helpful to know the difference between polyamorous and pansexual when a 12-year-old describes themselves as polyamorous (having consenting, nonmonogamous relationships) but provides the definition for pansexual (being attracted to all gender identities). Yes, this has happened to me, and yes, my resident was appropriately confused. Correcting someone else’s vocabulary can be tricky and even inappropriate or condescending; therefore, tread cautiously. It may be appropriate, however, to correct colleagues’ or even patients’ family members’ language if they are using terms that may be hurtful to your patients. I do not allow slurs in my clinic, and when parents are using incorrect pronouns on purpose, I will often let them know that it is my job to respect their child’s identity where it is in the moment and that they have asked me to use specific pronouns, so I will continue to refer to their child with those pronouns. Reflecting the language of the patient can be a powerful statement providing them with the autonomy that they deserve as burgeoning adults navigating the complicated journey of identity.
As providers who often have to defend ourselves against “Dr. Google,” we may be leery of just searching randomly for the definition of a new word and hoping a site is credible. One site that I have used repeatedly is www.itspronouncedmetrosexual.com by Sam Killermann,2 a gender and sexuality educator.
Mr. Killermann has also produced an E-book that is regularly updated to reflect changing terminology, which can be obtained for a small donation. As Mr. Killermann explains, “New language can be intimidating, and the language of gender and sexuality is often that.”3 In reality, the definitions aren’t scary and often the words can describe something you already know exists but didn’t recognize had a specific term. Not everyone can know every term and its definition; in fact, many members of the LGBTQ+ community don’t know or even understand every term. Below is a shortened list with some of the more common terms you may encounter; however, individuals may use them differently so it is never out of place to clarify your understanding of the term’s definition.
With these resources, along with cultural humility and reflection of others’ language, we can all start to have more meaningful conversations with our patients around their identity and relationships with others.
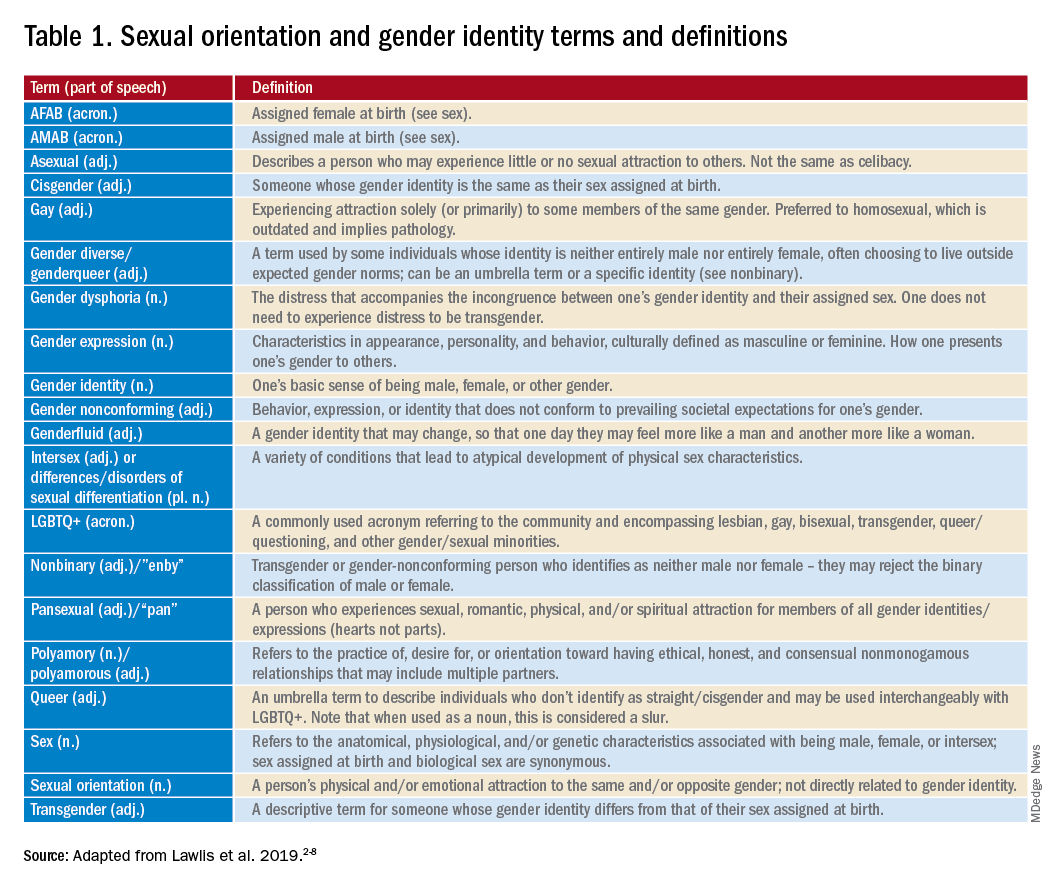
Dr. Lawlis is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures. Email her at [email protected].
References
1. Ruud M. Nursing for women’s health. 2018;22(3):255-63.
2. Killermann S. It’s Pronounced Metrosexual. 2020.
3. Killermann S. Defining LGBTQ+: A guide to gender and sexuality terminology. 2019, Feb 25.
4. The Joint Commission. Advancing effective communication, cultural competence, and patient- and family-centered care for the lesbian, gay, bisexual, and transgender (LGBT) community: A field guide. Oak Brook, Ill. 2011.
5. LGBT health disparities. American Psychiatric Association Public Interest Government Relations Office. 2013 May.
6. Lawlis S et al. Health services for LGBTQ+ patients. Psychiatr Ann. 2019;49(10):426-35.
7. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
8. Center of Excellence for Transgender Health, department of family and community medicine, UCSF. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2016 Jun 17.
For those of us who see adolescent patients on a regular basis, it seems that they use new vocabulary almost every day. While you may not need to know what “lit” means, you probably do need to understand terms used to describe your patients’ identities. At times it feels like we, as providers, have to be on TikTok to keep up with our patients, and while this may be an amusing way to educate ourselves, a judicious Google search can be much more helpful. The interesting part about LGBTQ+ terminology is that it stems from the community and thus is frequently updated to reflect our evolving understanding of gender, sexuality, and identity. That being said, it can make it difficult for those who are not plugged in to the community to keep up to date. While we have learned in medicine to use accurate terminology and appropriate three-letter acronyms (or “TLAs” as one of my residents referenced them when I was a medical student) to describe medical conditions, the LGBTQ+ community has its own set of terms and acronyms. These new words may seem daunting, but they are often based in Latin roots or prefixes such as a-, demi-, poly-, and pan-, which may be familiar to those of us who use plenty of other Latin-based terms in medicine and our everyday lives. By paying attention to how people define and use terminology, we can better recognize their true identities and become better providers.
The first, and perhaps most important, piece of advice is to maintain cultural humility. Know when to admit you don’t recognize a term and politely ask the definition. For example, the first time I heard the term “demiboy” I said “I’m not familiar with that word. Can you explain what it means to you?” Phrasing the question as such is also helpful in that it gives the individuals a chance to really define their identity. In addition, some words may be used differently by various individuals and by asking what the word means to them, you can have a better understanding of how they are using the terminology. In this particular instance, the patient felt more masculine, but not 100%, partway between agender (meaning having no gender identity) and being “all male.” By embracing cultural humility, we place the patients in the role of expert on their own identity and orientation. According to Maria Ruud, DNP, of the University of Minnesota, Minneapolis, cultural humility is the “ongoing self-reflection and education …[seeking] to gain an awareness of their own assumptions and biases that may contribute to health disparities.”1
Another reason it is important to keep up on the language is that some adolescents, particularly younger adolescents, may not be using the terminology correctly. It can be very helpful to know the difference between polyamorous and pansexual when a 12-year-old describes themselves as polyamorous (having consenting, nonmonogamous relationships) but provides the definition for pansexual (being attracted to all gender identities). Yes, this has happened to me, and yes, my resident was appropriately confused. Correcting someone else’s vocabulary can be tricky and even inappropriate or condescending; therefore, tread cautiously. It may be appropriate, however, to correct colleagues’ or even patients’ family members’ language if they are using terms that may be hurtful to your patients. I do not allow slurs in my clinic, and when parents are using incorrect pronouns on purpose, I will often let them know that it is my job to respect their child’s identity where it is in the moment and that they have asked me to use specific pronouns, so I will continue to refer to their child with those pronouns. Reflecting the language of the patient can be a powerful statement providing them with the autonomy that they deserve as burgeoning adults navigating the complicated journey of identity.
As providers who often have to defend ourselves against “Dr. Google,” we may be leery of just searching randomly for the definition of a new word and hoping a site is credible. One site that I have used repeatedly is www.itspronouncedmetrosexual.com by Sam Killermann,2 a gender and sexuality educator.
Mr. Killermann has also produced an E-book that is regularly updated to reflect changing terminology, which can be obtained for a small donation. As Mr. Killermann explains, “New language can be intimidating, and the language of gender and sexuality is often that.”3 In reality, the definitions aren’t scary and often the words can describe something you already know exists but didn’t recognize had a specific term. Not everyone can know every term and its definition; in fact, many members of the LGBTQ+ community don’t know or even understand every term. Below is a shortened list with some of the more common terms you may encounter; however, individuals may use them differently so it is never out of place to clarify your understanding of the term’s definition.
With these resources, along with cultural humility and reflection of others’ language, we can all start to have more meaningful conversations with our patients around their identity and relationships with others.
Dr. Lawlis is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures. Email her at [email protected].
References
1. Ruud M. Nursing for women’s health. 2018;22(3):255-63.
2. Killermann S. It’s Pronounced Metrosexual. 2020.
3. Killermann S. Defining LGBTQ+: A guide to gender and sexuality terminology. 2019, Feb 25.
4. The Joint Commission. Advancing effective communication, cultural competence, and patient- and family-centered care for the lesbian, gay, bisexual, and transgender (LGBT) community: A field guide. Oak Brook, Ill. 2011.
5. LGBT health disparities. American Psychiatric Association Public Interest Government Relations Office. 2013 May.
6. Lawlis S et al. Health services for LGBTQ+ patients. Psychiatr Ann. 2019;49(10):426-35.
7. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
8. Center of Excellence for Transgender Health, department of family and community medicine, UCSF. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2016 Jun 17.
For those of us who see adolescent patients on a regular basis, it seems that they use new vocabulary almost every day. While you may not need to know what “lit” means, you probably do need to understand terms used to describe your patients’ identities. At times it feels like we, as providers, have to be on TikTok to keep up with our patients, and while this may be an amusing way to educate ourselves, a judicious Google search can be much more helpful. The interesting part about LGBTQ+ terminology is that it stems from the community and thus is frequently updated to reflect our evolving understanding of gender, sexuality, and identity. That being said, it can make it difficult for those who are not plugged in to the community to keep up to date. While we have learned in medicine to use accurate terminology and appropriate three-letter acronyms (or “TLAs” as one of my residents referenced them when I was a medical student) to describe medical conditions, the LGBTQ+ community has its own set of terms and acronyms. These new words may seem daunting, but they are often based in Latin roots or prefixes such as a-, demi-, poly-, and pan-, which may be familiar to those of us who use plenty of other Latin-based terms in medicine and our everyday lives. By paying attention to how people define and use terminology, we can better recognize their true identities and become better providers.
The first, and perhaps most important, piece of advice is to maintain cultural humility. Know when to admit you don’t recognize a term and politely ask the definition. For example, the first time I heard the term “demiboy” I said “I’m not familiar with that word. Can you explain what it means to you?” Phrasing the question as such is also helpful in that it gives the individuals a chance to really define their identity. In addition, some words may be used differently by various individuals and by asking what the word means to them, you can have a better understanding of how they are using the terminology. In this particular instance, the patient felt more masculine, but not 100%, partway between agender (meaning having no gender identity) and being “all male.” By embracing cultural humility, we place the patients in the role of expert on their own identity and orientation. According to Maria Ruud, DNP, of the University of Minnesota, Minneapolis, cultural humility is the “ongoing self-reflection and education …[seeking] to gain an awareness of their own assumptions and biases that may contribute to health disparities.”1
Another reason it is important to keep up on the language is that some adolescents, particularly younger adolescents, may not be using the terminology correctly. It can be very helpful to know the difference between polyamorous and pansexual when a 12-year-old describes themselves as polyamorous (having consenting, nonmonogamous relationships) but provides the definition for pansexual (being attracted to all gender identities). Yes, this has happened to me, and yes, my resident was appropriately confused. Correcting someone else’s vocabulary can be tricky and even inappropriate or condescending; therefore, tread cautiously. It may be appropriate, however, to correct colleagues’ or even patients’ family members’ language if they are using terms that may be hurtful to your patients. I do not allow slurs in my clinic, and when parents are using incorrect pronouns on purpose, I will often let them know that it is my job to respect their child’s identity where it is in the moment and that they have asked me to use specific pronouns, so I will continue to refer to their child with those pronouns. Reflecting the language of the patient can be a powerful statement providing them with the autonomy that they deserve as burgeoning adults navigating the complicated journey of identity.
As providers who often have to defend ourselves against “Dr. Google,” we may be leery of just searching randomly for the definition of a new word and hoping a site is credible. One site that I have used repeatedly is www.itspronouncedmetrosexual.com by Sam Killermann,2 a gender and sexuality educator.
Mr. Killermann has also produced an E-book that is regularly updated to reflect changing terminology, which can be obtained for a small donation. As Mr. Killermann explains, “New language can be intimidating, and the language of gender and sexuality is often that.”3 In reality, the definitions aren’t scary and often the words can describe something you already know exists but didn’t recognize had a specific term. Not everyone can know every term and its definition; in fact, many members of the LGBTQ+ community don’t know or even understand every term. Below is a shortened list with some of the more common terms you may encounter; however, individuals may use them differently so it is never out of place to clarify your understanding of the term’s definition.
With these resources, along with cultural humility and reflection of others’ language, we can all start to have more meaningful conversations with our patients around their identity and relationships with others.
Dr. Lawlis is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures. Email her at [email protected].
References
1. Ruud M. Nursing for women’s health. 2018;22(3):255-63.
2. Killermann S. It’s Pronounced Metrosexual. 2020.
3. Killermann S. Defining LGBTQ+: A guide to gender and sexuality terminology. 2019, Feb 25.
4. The Joint Commission. Advancing effective communication, cultural competence, and patient- and family-centered care for the lesbian, gay, bisexual, and transgender (LGBT) community: A field guide. Oak Brook, Ill. 2011.
5. LGBT health disparities. American Psychiatric Association Public Interest Government Relations Office. 2013 May.
6. Lawlis S et al. Health services for LGBTQ+ patients. Psychiatr Ann. 2019;49(10):426-35.
7. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
8. Center of Excellence for Transgender Health, department of family and community medicine, UCSF. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2016 Jun 17.