User login
Intervention Helps Transition From Postpartum Care to PCP Engagement
, according to study results published in JAMA Network Open. The intervention bundle includes default scheduling of postpartum primary care appointments and tailored reminders and messaging.
Researchers, led by Mark A. Clapp, MD, MPH, with Massachusetts General Hospital in Boston, highlighted a care transition gap common after a woman gives birth. More than 30% of pregnant people have at least one chronic condition and nearly 20% develop gestational diabetes or pregnancy-related hypertension, which increases the risk of future chronic disease, the authors write. They are closely monitored for these conditions during pregnancy, but many face barriers in transitioning to engagement with primary care.
Scheduling appointments, difficulty in finding information, and insurance or billing issues can impede access to care. In this study, the primary outcome measure was whether women completed a primary care visit for routine or chronic condition care within 4 months of delivery.
Intervention vs Control Group
The intervention included an introduction message talking about the importance of a primary care visit and notification that a staff member would be scheduling an appointment on the patients’ behalf within a 4-month window of the estimated due date (EDD). Patients could opt out or ask for specific scheduling. If a patient had already seen their primary care physician (PCP) for an annual visit within the year, they were scheduled for an annual visit when they were next eligible, even if outside the 4-month study follow-up.
For those who did not opt out and had appointments scheduled for them, reminders were sent about 1 month after the EDD and 1 week before the scheduled appointment through the EHR patient portal. Salient labeling of the message was used to describe the visit. For those for whom an appointment could not be scheduled, similar reminders were sent on the importance of primary care follow-up, urging patients to contact their primary care office directly to schedule. Reminders included evidence-based, best-practice wording including that “the appointment had been reserved for them.”
Patients in the control group received one message within 2 weeks of the EDD with a generic recommendation for primary care follow-up after delivery.
Researchers found that 40% of the intervention group (95% confidence interval (CI), 33.1%-47.4%) and 22% of the control group (95% CI, 6.4%-28.8%), completed a primary care visit within 4 months. “[T]he intervention increased PCP visit completion by 18.7 percentage points (95% CI, 9.1-28.2 percentage points),” they write. Those who received the intervention also had fewer postpartum readmissions (1.7% vs 5.8%) and were more likely to have had these services from a PCP: blood pressure screening (42.8% vs 28.3%); weight assessment (42.8% vs 27.7%); and depression screening (32.8% vs 16.8%).
Meghan Bellerose, MPH, with the Department of Health Services, Policy, and Practice at Brown University School of Public Health in Providence, Rhode Island, described in an accompanying editorial the “postpartum cliff.”
“Health system engagement plummets soon after childbirth in the US,” she writes. “Under current care practices, obstetric clinicians deliver a single postpartum visit within 12 weeks of delivery, after which patients are responsible for navigating the transition to primary care on their own.”
The intervention Dr. Clapp and colleagues propose could help increase the benefit of state and federal policies aimed at increasing care continuity after delivery, she writes. She pointed to the American Rescue Plan Act of 2021, in which states were given the option to provide 12 months of continuous Medicaid coverage to low-income postpartum women, up from the previous 2 months of coverage. By early May of 2024, 46 states had chosen the longer coverage.
Without a better bridge between postpartum and primary care, she notes, “we will not see the full value of extended Medicaid coverage.”
“The findings of Clapp et al. suggest that a relatively low-resource, scalable intervention including default scheduling of postpartum-to-primary care appointments and salient messaging could increase the use of primary care in the postpartum year to extend the effects of this policy.”
Still, Only 40% Used Primary Care
She noted, however, that despite the finding that the intervention in this study nearly doubled the percentage of primary care visits in 4 months, primary care use still was only 40%. Study staff were not able to schedule an appointment for 24% of the intervention group within a year, even though participants identified a PCP at enrollment. Reasons for that included the patient already having used their yearly primary care visit; patients needing to restart care with their primary care clinician or choose a new clinician; and study staff being unable to reach primary care offices for scheduling.
Clearly, “there is more work to be done to remove administrative barriers to care after delivery,” she writes.
Dr. Clapp reports holding equity from the Delfina Care Scientific Advisory Board outside the submitted work. Coauthor Dr. Ganguli reports grants from the National Institute on Aging, Commonwealth Fund, and Arnold Ventures, and personal fees from FPrime outside the submitted work. Dr. Cohen reports grants from the National Academy of Medicine and the National Academy on Aging during the conduct of the study. The study was funded by the National Institute on Aging via the Massachusetts Institute of Technology Roybal Center for Translational Research to Improve Health Care for the Aging and the National Bureau of Economic Research Roybal Center for Behavior Change in Health. Editorialist Meghan Bellerose reported no relevant financial disclosures.
, according to study results published in JAMA Network Open. The intervention bundle includes default scheduling of postpartum primary care appointments and tailored reminders and messaging.
Researchers, led by Mark A. Clapp, MD, MPH, with Massachusetts General Hospital in Boston, highlighted a care transition gap common after a woman gives birth. More than 30% of pregnant people have at least one chronic condition and nearly 20% develop gestational diabetes or pregnancy-related hypertension, which increases the risk of future chronic disease, the authors write. They are closely monitored for these conditions during pregnancy, but many face barriers in transitioning to engagement with primary care.
Scheduling appointments, difficulty in finding information, and insurance or billing issues can impede access to care. In this study, the primary outcome measure was whether women completed a primary care visit for routine or chronic condition care within 4 months of delivery.
Intervention vs Control Group
The intervention included an introduction message talking about the importance of a primary care visit and notification that a staff member would be scheduling an appointment on the patients’ behalf within a 4-month window of the estimated due date (EDD). Patients could opt out or ask for specific scheduling. If a patient had already seen their primary care physician (PCP) for an annual visit within the year, they were scheduled for an annual visit when they were next eligible, even if outside the 4-month study follow-up.
For those who did not opt out and had appointments scheduled for them, reminders were sent about 1 month after the EDD and 1 week before the scheduled appointment through the EHR patient portal. Salient labeling of the message was used to describe the visit. For those for whom an appointment could not be scheduled, similar reminders were sent on the importance of primary care follow-up, urging patients to contact their primary care office directly to schedule. Reminders included evidence-based, best-practice wording including that “the appointment had been reserved for them.”
Patients in the control group received one message within 2 weeks of the EDD with a generic recommendation for primary care follow-up after delivery.
Researchers found that 40% of the intervention group (95% confidence interval (CI), 33.1%-47.4%) and 22% of the control group (95% CI, 6.4%-28.8%), completed a primary care visit within 4 months. “[T]he intervention increased PCP visit completion by 18.7 percentage points (95% CI, 9.1-28.2 percentage points),” they write. Those who received the intervention also had fewer postpartum readmissions (1.7% vs 5.8%) and were more likely to have had these services from a PCP: blood pressure screening (42.8% vs 28.3%); weight assessment (42.8% vs 27.7%); and depression screening (32.8% vs 16.8%).
Meghan Bellerose, MPH, with the Department of Health Services, Policy, and Practice at Brown University School of Public Health in Providence, Rhode Island, described in an accompanying editorial the “postpartum cliff.”
“Health system engagement plummets soon after childbirth in the US,” she writes. “Under current care practices, obstetric clinicians deliver a single postpartum visit within 12 weeks of delivery, after which patients are responsible for navigating the transition to primary care on their own.”
The intervention Dr. Clapp and colleagues propose could help increase the benefit of state and federal policies aimed at increasing care continuity after delivery, she writes. She pointed to the American Rescue Plan Act of 2021, in which states were given the option to provide 12 months of continuous Medicaid coverage to low-income postpartum women, up from the previous 2 months of coverage. By early May of 2024, 46 states had chosen the longer coverage.
Without a better bridge between postpartum and primary care, she notes, “we will not see the full value of extended Medicaid coverage.”
“The findings of Clapp et al. suggest that a relatively low-resource, scalable intervention including default scheduling of postpartum-to-primary care appointments and salient messaging could increase the use of primary care in the postpartum year to extend the effects of this policy.”
Still, Only 40% Used Primary Care
She noted, however, that despite the finding that the intervention in this study nearly doubled the percentage of primary care visits in 4 months, primary care use still was only 40%. Study staff were not able to schedule an appointment for 24% of the intervention group within a year, even though participants identified a PCP at enrollment. Reasons for that included the patient already having used their yearly primary care visit; patients needing to restart care with their primary care clinician or choose a new clinician; and study staff being unable to reach primary care offices for scheduling.
Clearly, “there is more work to be done to remove administrative barriers to care after delivery,” she writes.
Dr. Clapp reports holding equity from the Delfina Care Scientific Advisory Board outside the submitted work. Coauthor Dr. Ganguli reports grants from the National Institute on Aging, Commonwealth Fund, and Arnold Ventures, and personal fees from FPrime outside the submitted work. Dr. Cohen reports grants from the National Academy of Medicine and the National Academy on Aging during the conduct of the study. The study was funded by the National Institute on Aging via the Massachusetts Institute of Technology Roybal Center for Translational Research to Improve Health Care for the Aging and the National Bureau of Economic Research Roybal Center for Behavior Change in Health. Editorialist Meghan Bellerose reported no relevant financial disclosures.
, according to study results published in JAMA Network Open. The intervention bundle includes default scheduling of postpartum primary care appointments and tailored reminders and messaging.
Researchers, led by Mark A. Clapp, MD, MPH, with Massachusetts General Hospital in Boston, highlighted a care transition gap common after a woman gives birth. More than 30% of pregnant people have at least one chronic condition and nearly 20% develop gestational diabetes or pregnancy-related hypertension, which increases the risk of future chronic disease, the authors write. They are closely monitored for these conditions during pregnancy, but many face barriers in transitioning to engagement with primary care.
Scheduling appointments, difficulty in finding information, and insurance or billing issues can impede access to care. In this study, the primary outcome measure was whether women completed a primary care visit for routine or chronic condition care within 4 months of delivery.
Intervention vs Control Group
The intervention included an introduction message talking about the importance of a primary care visit and notification that a staff member would be scheduling an appointment on the patients’ behalf within a 4-month window of the estimated due date (EDD). Patients could opt out or ask for specific scheduling. If a patient had already seen their primary care physician (PCP) for an annual visit within the year, they were scheduled for an annual visit when they were next eligible, even if outside the 4-month study follow-up.
For those who did not opt out and had appointments scheduled for them, reminders were sent about 1 month after the EDD and 1 week before the scheduled appointment through the EHR patient portal. Salient labeling of the message was used to describe the visit. For those for whom an appointment could not be scheduled, similar reminders were sent on the importance of primary care follow-up, urging patients to contact their primary care office directly to schedule. Reminders included evidence-based, best-practice wording including that “the appointment had been reserved for them.”
Patients in the control group received one message within 2 weeks of the EDD with a generic recommendation for primary care follow-up after delivery.
Researchers found that 40% of the intervention group (95% confidence interval (CI), 33.1%-47.4%) and 22% of the control group (95% CI, 6.4%-28.8%), completed a primary care visit within 4 months. “[T]he intervention increased PCP visit completion by 18.7 percentage points (95% CI, 9.1-28.2 percentage points),” they write. Those who received the intervention also had fewer postpartum readmissions (1.7% vs 5.8%) and were more likely to have had these services from a PCP: blood pressure screening (42.8% vs 28.3%); weight assessment (42.8% vs 27.7%); and depression screening (32.8% vs 16.8%).
Meghan Bellerose, MPH, with the Department of Health Services, Policy, and Practice at Brown University School of Public Health in Providence, Rhode Island, described in an accompanying editorial the “postpartum cliff.”
“Health system engagement plummets soon after childbirth in the US,” she writes. “Under current care practices, obstetric clinicians deliver a single postpartum visit within 12 weeks of delivery, after which patients are responsible for navigating the transition to primary care on their own.”
The intervention Dr. Clapp and colleagues propose could help increase the benefit of state and federal policies aimed at increasing care continuity after delivery, she writes. She pointed to the American Rescue Plan Act of 2021, in which states were given the option to provide 12 months of continuous Medicaid coverage to low-income postpartum women, up from the previous 2 months of coverage. By early May of 2024, 46 states had chosen the longer coverage.
Without a better bridge between postpartum and primary care, she notes, “we will not see the full value of extended Medicaid coverage.”
“The findings of Clapp et al. suggest that a relatively low-resource, scalable intervention including default scheduling of postpartum-to-primary care appointments and salient messaging could increase the use of primary care in the postpartum year to extend the effects of this policy.”
Still, Only 40% Used Primary Care
She noted, however, that despite the finding that the intervention in this study nearly doubled the percentage of primary care visits in 4 months, primary care use still was only 40%. Study staff were not able to schedule an appointment for 24% of the intervention group within a year, even though participants identified a PCP at enrollment. Reasons for that included the patient already having used their yearly primary care visit; patients needing to restart care with their primary care clinician or choose a new clinician; and study staff being unable to reach primary care offices for scheduling.
Clearly, “there is more work to be done to remove administrative barriers to care after delivery,” she writes.
Dr. Clapp reports holding equity from the Delfina Care Scientific Advisory Board outside the submitted work. Coauthor Dr. Ganguli reports grants from the National Institute on Aging, Commonwealth Fund, and Arnold Ventures, and personal fees from FPrime outside the submitted work. Dr. Cohen reports grants from the National Academy of Medicine and the National Academy on Aging during the conduct of the study. The study was funded by the National Institute on Aging via the Massachusetts Institute of Technology Roybal Center for Translational Research to Improve Health Care for the Aging and the National Bureau of Economic Research Roybal Center for Behavior Change in Health. Editorialist Meghan Bellerose reported no relevant financial disclosures.
FROM JAMA NETWORK OPEN
New ACOG Guidance Advises Clinicians on Cannabis Use for Gynecologic Pain
An increasing proportion of people are using cannabis products for pain, including that associated with gynecologic conditions, according to new guidance from the American College of Obstetricians and Gynecologists. The organization published its first guidance in July on the use of cannabis products for gynecologic pain.
“Many of our patients are using these products and many of our members are getting questions from their patients asking whether they should be using them,” Kimberly Gecsi, MD, a professor of ob.gyn. at Medical College of Wisconsin and Froedtert Health in Milwaukee, Wisconsin, and one of the document’s coauthors, said in an interview.* “We want ACOG members to walk away with some understanding that their patients are using these products, what the different products are, and the current state of the science so they can guide their patients about the potential advantages as well as the potential risks.”
Use of cannabis in the past month in the United States rose 38.2% between 2015 and 2019, according to the National Survey on Drug Use and Health. Other research using data from that survey found that US use of cannabis for medicinal purposes more than doubled, from 1.2% to 2.5% between 2013-2014 and 2019-2020, and use in states where it was legalized increased fourfold. Though little data exist on its use for gynecologic pain, at least one peer-reviewed online survey found that 61% of those who had never used it and 90% of those who had ever used it were willing to consider its use for gynecologic pain.
In assessing the current evidence, the researchers excluded studies looking at use of cannabis to manage symptoms related to cancer, obstetrics, or gynecologic malignancy. Of the remaining evidence, however, “there just isn’t enough data on gynecologic pain to really have tipped the scale toward a recommendation,” Dr. Gecsi said.
The consensus recommendations therefore state that current data are not sufficient to recommend or discourage use of cannabis products to treat pain linked to gynecologic conditions. Yet the potential for benefit suggests that “if they are already using these products, there’s no need to discourage them, especially if the patients feel they are getting some benefit from them,” Dr. Gecsi said.
The guidance also highlights the importance of clinicians being aware that their patients may be using these products and being prepared to discuss with them the limited data available as well as the theoretical benefits and potential negative effects for adult patients. In adolescent patients, however, the increased risk of negative cognitive effects and psychotic conditions currently appears to outweigh the theoretical benefits. Use of cannabis products in teens should therefore not be recommended until more data is available on the short-term and long-term effects of its use on adolescent brain development, the authors wrote.
Josephine Urbina, MD, MAS, an assistant professor of ob.gyn. and reproductive sciences at the University of California, San Francisco, said that the guidance confirms what most ob.gyns. suspected regarding the lack of data to support or refute the use of cannabis.
“Patients usually see cannabis as a last resort to control their pain,” Dr. Urbina added. “It seems that this decision to start using cannabis isn’t one that’s taken lightly, and they’re usually at their wits’ end. Some patients use cannabis as an adjunct so that they don’t have to rely on stronger pain medications like opioids, which we all know have a proven track record for being addicting.”
The ACOG guidance notes limited survey data suggesting that cannabis may help reduce patients’ use of opioids for pain relief, though there’s not enough data to confirm this potential benefit. The authors also highlight the limited data suggesting that PEA-transpolydatin may be effective for relieving pain related to primary dysmenorrhea, endometriosis, and chronic pelvic pain, but, again, there’s not yet enough data to formally recommend its use.
Current treatments for pain from gynecologic conditions depend on the cause of the pain, Dr. Gecsi said. One of the more common causes of pain, for example, is endometriosis, which can be treated with medications, including hormonal ones, or with surgery.
Other first-line treatments for pain, can include nonsteroidal anti-inflammatory drug and, for more complex cases, gonadotropin-releasing hormone agonists, antidepressants, and anticonvulsants. “Nonpharmacological treatments like physical therapy, acupuncture, cognitive-behavioral therapy and lifestyle changes, including diet and exercise, can also be beneficial,” Dr. Urbina added.
The new guidance also attempts to clarify the confusing legal landscape associated with cannabis use. In addition to the patchwork of state laws, federal distinctions in cannabis legality have been shifting in recent years. The 2018 Farm Bill defined any product with 0.3% or less tetrahydrocannabinol (THC) as hemp, which is now legal and commercially available in all states. That change introduced a wide range of topical and edible cannabidiol products to the market, even in states where marijuana is otherwise still illegal.
Products with a THC concentration greater than 0.3%, however, remain classified as a Schedule I drug, though the Justice Department proposed a rule in May to change that classification to Schedule III, which includes drugs such as ketamine, anabolic steroids, testosterone, and Tylenol with codeine. The guidance also includes a box of definitions for different types of cannabis products and differences in bioavailability, time to onset of effects, and duration of effects for different routes of exposure.
Kiran Kavipurapu, DO, JD, MPH, an assistant clinical professor and ob.gyn. residency program director at the University of California, Los Angeles, said the increasing availability and legalization of cannabis has meant that more patients are coming to their doctors’ offices having already tried it for medicinal purposes.
“Cannabis use discussions are often initiated by patients who are either inquiring about its benefits or because they have already tried it and want a physician to weigh in,” Dr. Kavipurapu said in an interview. “Over the past 5 years or so, this has become an increasingly common topic along with discussion of herbal or naturopathic remedies to supplement treatment of gynecologic conditions.”
Yet stigma about its use can lead patients to feel hesitant about bringing it up, Dr. Kavipurapu added. “I think it is necessary for clinicians to create a safe environment for patients to discuss their use of any and all therapies or supplements so their physician can assess for potential drug interactions or other harmful effects,” he said.
Dr. Gecsi agreed that this need to reassure patients was an important aspect of ACOG’s new guidance. Clinicians “should make sure that they strive to always foster a relationship with their patients where their patients can feel safe sharing their use and other things going on in their lives without feeling like they’re going to get in trouble,. Our job is not to put our patients at risk for any kind of legal or criminal problems.”
Meanwhile, the legal restrictions on cannabis remain a substantial barrier to the additional research that’s needed to make more informed recommendations about its use to patients, Dr. Gecsi said. But the inadequate amount of research goes beyond the challenges of studying cannabis in particular, Dr. Urbina noted.
“The paucity of research in women’s health, particularly in the realm of sexual and reproductive health care, underscores the urgent need to prioritize this topic in order to ensure comprehensive and equitable healthcare for women,” Dr. Urbina said. Underrepresentation of women’s health issues in clinical studies has led to knowledge gaps and “suboptimal treatment options for conditions unique to or more prevalent among women,” and it’s another reason for the lack of robust data on cannabis use for gynecologic-related pain.
“Prioritizing research in women’s health is essential to developing effective interventions, understanding gender-specific responses to treatments, and addressing the complex interplay of biological, social, and psychological factors affecting women’s well-being,” Dr. Urbina said. “Furthermore, advancing reproductive health research supports women’s reproductive autonomy, empowering them with the knowledge and resources to make informed decisions about their bodies and lives. By investing in robust, inclusive research, we can close existing gaps, improve health outcomes, and promote gender equity in healthcare — something that has been long overdue in this country.”
The guidance did not use external funding. Dr. Gecsi, Dr. Urbina, and Dr. Kavipurapu had no disclosures.
*This story was corrected on July 25, 2024.
An increasing proportion of people are using cannabis products for pain, including that associated with gynecologic conditions, according to new guidance from the American College of Obstetricians and Gynecologists. The organization published its first guidance in July on the use of cannabis products for gynecologic pain.
“Many of our patients are using these products and many of our members are getting questions from their patients asking whether they should be using them,” Kimberly Gecsi, MD, a professor of ob.gyn. at Medical College of Wisconsin and Froedtert Health in Milwaukee, Wisconsin, and one of the document’s coauthors, said in an interview.* “We want ACOG members to walk away with some understanding that their patients are using these products, what the different products are, and the current state of the science so they can guide their patients about the potential advantages as well as the potential risks.”
Use of cannabis in the past month in the United States rose 38.2% between 2015 and 2019, according to the National Survey on Drug Use and Health. Other research using data from that survey found that US use of cannabis for medicinal purposes more than doubled, from 1.2% to 2.5% between 2013-2014 and 2019-2020, and use in states where it was legalized increased fourfold. Though little data exist on its use for gynecologic pain, at least one peer-reviewed online survey found that 61% of those who had never used it and 90% of those who had ever used it were willing to consider its use for gynecologic pain.
In assessing the current evidence, the researchers excluded studies looking at use of cannabis to manage symptoms related to cancer, obstetrics, or gynecologic malignancy. Of the remaining evidence, however, “there just isn’t enough data on gynecologic pain to really have tipped the scale toward a recommendation,” Dr. Gecsi said.
The consensus recommendations therefore state that current data are not sufficient to recommend or discourage use of cannabis products to treat pain linked to gynecologic conditions. Yet the potential for benefit suggests that “if they are already using these products, there’s no need to discourage them, especially if the patients feel they are getting some benefit from them,” Dr. Gecsi said.
The guidance also highlights the importance of clinicians being aware that their patients may be using these products and being prepared to discuss with them the limited data available as well as the theoretical benefits and potential negative effects for adult patients. In adolescent patients, however, the increased risk of negative cognitive effects and psychotic conditions currently appears to outweigh the theoretical benefits. Use of cannabis products in teens should therefore not be recommended until more data is available on the short-term and long-term effects of its use on adolescent brain development, the authors wrote.
Josephine Urbina, MD, MAS, an assistant professor of ob.gyn. and reproductive sciences at the University of California, San Francisco, said that the guidance confirms what most ob.gyns. suspected regarding the lack of data to support or refute the use of cannabis.
“Patients usually see cannabis as a last resort to control their pain,” Dr. Urbina added. “It seems that this decision to start using cannabis isn’t one that’s taken lightly, and they’re usually at their wits’ end. Some patients use cannabis as an adjunct so that they don’t have to rely on stronger pain medications like opioids, which we all know have a proven track record for being addicting.”
The ACOG guidance notes limited survey data suggesting that cannabis may help reduce patients’ use of opioids for pain relief, though there’s not enough data to confirm this potential benefit. The authors also highlight the limited data suggesting that PEA-transpolydatin may be effective for relieving pain related to primary dysmenorrhea, endometriosis, and chronic pelvic pain, but, again, there’s not yet enough data to formally recommend its use.
Current treatments for pain from gynecologic conditions depend on the cause of the pain, Dr. Gecsi said. One of the more common causes of pain, for example, is endometriosis, which can be treated with medications, including hormonal ones, or with surgery.
Other first-line treatments for pain, can include nonsteroidal anti-inflammatory drug and, for more complex cases, gonadotropin-releasing hormone agonists, antidepressants, and anticonvulsants. “Nonpharmacological treatments like physical therapy, acupuncture, cognitive-behavioral therapy and lifestyle changes, including diet and exercise, can also be beneficial,” Dr. Urbina added.
The new guidance also attempts to clarify the confusing legal landscape associated with cannabis use. In addition to the patchwork of state laws, federal distinctions in cannabis legality have been shifting in recent years. The 2018 Farm Bill defined any product with 0.3% or less tetrahydrocannabinol (THC) as hemp, which is now legal and commercially available in all states. That change introduced a wide range of topical and edible cannabidiol products to the market, even in states where marijuana is otherwise still illegal.
Products with a THC concentration greater than 0.3%, however, remain classified as a Schedule I drug, though the Justice Department proposed a rule in May to change that classification to Schedule III, which includes drugs such as ketamine, anabolic steroids, testosterone, and Tylenol with codeine. The guidance also includes a box of definitions for different types of cannabis products and differences in bioavailability, time to onset of effects, and duration of effects for different routes of exposure.
Kiran Kavipurapu, DO, JD, MPH, an assistant clinical professor and ob.gyn. residency program director at the University of California, Los Angeles, said the increasing availability and legalization of cannabis has meant that more patients are coming to their doctors’ offices having already tried it for medicinal purposes.
“Cannabis use discussions are often initiated by patients who are either inquiring about its benefits or because they have already tried it and want a physician to weigh in,” Dr. Kavipurapu said in an interview. “Over the past 5 years or so, this has become an increasingly common topic along with discussion of herbal or naturopathic remedies to supplement treatment of gynecologic conditions.”
Yet stigma about its use can lead patients to feel hesitant about bringing it up, Dr. Kavipurapu added. “I think it is necessary for clinicians to create a safe environment for patients to discuss their use of any and all therapies or supplements so their physician can assess for potential drug interactions or other harmful effects,” he said.
Dr. Gecsi agreed that this need to reassure patients was an important aspect of ACOG’s new guidance. Clinicians “should make sure that they strive to always foster a relationship with their patients where their patients can feel safe sharing their use and other things going on in their lives without feeling like they’re going to get in trouble,. Our job is not to put our patients at risk for any kind of legal or criminal problems.”
Meanwhile, the legal restrictions on cannabis remain a substantial barrier to the additional research that’s needed to make more informed recommendations about its use to patients, Dr. Gecsi said. But the inadequate amount of research goes beyond the challenges of studying cannabis in particular, Dr. Urbina noted.
“The paucity of research in women’s health, particularly in the realm of sexual and reproductive health care, underscores the urgent need to prioritize this topic in order to ensure comprehensive and equitable healthcare for women,” Dr. Urbina said. Underrepresentation of women’s health issues in clinical studies has led to knowledge gaps and “suboptimal treatment options for conditions unique to or more prevalent among women,” and it’s another reason for the lack of robust data on cannabis use for gynecologic-related pain.
“Prioritizing research in women’s health is essential to developing effective interventions, understanding gender-specific responses to treatments, and addressing the complex interplay of biological, social, and psychological factors affecting women’s well-being,” Dr. Urbina said. “Furthermore, advancing reproductive health research supports women’s reproductive autonomy, empowering them with the knowledge and resources to make informed decisions about their bodies and lives. By investing in robust, inclusive research, we can close existing gaps, improve health outcomes, and promote gender equity in healthcare — something that has been long overdue in this country.”
The guidance did not use external funding. Dr. Gecsi, Dr. Urbina, and Dr. Kavipurapu had no disclosures.
*This story was corrected on July 25, 2024.
An increasing proportion of people are using cannabis products for pain, including that associated with gynecologic conditions, according to new guidance from the American College of Obstetricians and Gynecologists. The organization published its first guidance in July on the use of cannabis products for gynecologic pain.
“Many of our patients are using these products and many of our members are getting questions from their patients asking whether they should be using them,” Kimberly Gecsi, MD, a professor of ob.gyn. at Medical College of Wisconsin and Froedtert Health in Milwaukee, Wisconsin, and one of the document’s coauthors, said in an interview.* “We want ACOG members to walk away with some understanding that their patients are using these products, what the different products are, and the current state of the science so they can guide their patients about the potential advantages as well as the potential risks.”
Use of cannabis in the past month in the United States rose 38.2% between 2015 and 2019, according to the National Survey on Drug Use and Health. Other research using data from that survey found that US use of cannabis for medicinal purposes more than doubled, from 1.2% to 2.5% between 2013-2014 and 2019-2020, and use in states where it was legalized increased fourfold. Though little data exist on its use for gynecologic pain, at least one peer-reviewed online survey found that 61% of those who had never used it and 90% of those who had ever used it were willing to consider its use for gynecologic pain.
In assessing the current evidence, the researchers excluded studies looking at use of cannabis to manage symptoms related to cancer, obstetrics, or gynecologic malignancy. Of the remaining evidence, however, “there just isn’t enough data on gynecologic pain to really have tipped the scale toward a recommendation,” Dr. Gecsi said.
The consensus recommendations therefore state that current data are not sufficient to recommend or discourage use of cannabis products to treat pain linked to gynecologic conditions. Yet the potential for benefit suggests that “if they are already using these products, there’s no need to discourage them, especially if the patients feel they are getting some benefit from them,” Dr. Gecsi said.
The guidance also highlights the importance of clinicians being aware that their patients may be using these products and being prepared to discuss with them the limited data available as well as the theoretical benefits and potential negative effects for adult patients. In adolescent patients, however, the increased risk of negative cognitive effects and psychotic conditions currently appears to outweigh the theoretical benefits. Use of cannabis products in teens should therefore not be recommended until more data is available on the short-term and long-term effects of its use on adolescent brain development, the authors wrote.
Josephine Urbina, MD, MAS, an assistant professor of ob.gyn. and reproductive sciences at the University of California, San Francisco, said that the guidance confirms what most ob.gyns. suspected regarding the lack of data to support or refute the use of cannabis.
“Patients usually see cannabis as a last resort to control their pain,” Dr. Urbina added. “It seems that this decision to start using cannabis isn’t one that’s taken lightly, and they’re usually at their wits’ end. Some patients use cannabis as an adjunct so that they don’t have to rely on stronger pain medications like opioids, which we all know have a proven track record for being addicting.”
The ACOG guidance notes limited survey data suggesting that cannabis may help reduce patients’ use of opioids for pain relief, though there’s not enough data to confirm this potential benefit. The authors also highlight the limited data suggesting that PEA-transpolydatin may be effective for relieving pain related to primary dysmenorrhea, endometriosis, and chronic pelvic pain, but, again, there’s not yet enough data to formally recommend its use.
Current treatments for pain from gynecologic conditions depend on the cause of the pain, Dr. Gecsi said. One of the more common causes of pain, for example, is endometriosis, which can be treated with medications, including hormonal ones, or with surgery.
Other first-line treatments for pain, can include nonsteroidal anti-inflammatory drug and, for more complex cases, gonadotropin-releasing hormone agonists, antidepressants, and anticonvulsants. “Nonpharmacological treatments like physical therapy, acupuncture, cognitive-behavioral therapy and lifestyle changes, including diet and exercise, can also be beneficial,” Dr. Urbina added.
The new guidance also attempts to clarify the confusing legal landscape associated with cannabis use. In addition to the patchwork of state laws, federal distinctions in cannabis legality have been shifting in recent years. The 2018 Farm Bill defined any product with 0.3% or less tetrahydrocannabinol (THC) as hemp, which is now legal and commercially available in all states. That change introduced a wide range of topical and edible cannabidiol products to the market, even in states where marijuana is otherwise still illegal.
Products with a THC concentration greater than 0.3%, however, remain classified as a Schedule I drug, though the Justice Department proposed a rule in May to change that classification to Schedule III, which includes drugs such as ketamine, anabolic steroids, testosterone, and Tylenol with codeine. The guidance also includes a box of definitions for different types of cannabis products and differences in bioavailability, time to onset of effects, and duration of effects for different routes of exposure.
Kiran Kavipurapu, DO, JD, MPH, an assistant clinical professor and ob.gyn. residency program director at the University of California, Los Angeles, said the increasing availability and legalization of cannabis has meant that more patients are coming to their doctors’ offices having already tried it for medicinal purposes.
“Cannabis use discussions are often initiated by patients who are either inquiring about its benefits or because they have already tried it and want a physician to weigh in,” Dr. Kavipurapu said in an interview. “Over the past 5 years or so, this has become an increasingly common topic along with discussion of herbal or naturopathic remedies to supplement treatment of gynecologic conditions.”
Yet stigma about its use can lead patients to feel hesitant about bringing it up, Dr. Kavipurapu added. “I think it is necessary for clinicians to create a safe environment for patients to discuss their use of any and all therapies or supplements so their physician can assess for potential drug interactions or other harmful effects,” he said.
Dr. Gecsi agreed that this need to reassure patients was an important aspect of ACOG’s new guidance. Clinicians “should make sure that they strive to always foster a relationship with their patients where their patients can feel safe sharing their use and other things going on in their lives without feeling like they’re going to get in trouble,. Our job is not to put our patients at risk for any kind of legal or criminal problems.”
Meanwhile, the legal restrictions on cannabis remain a substantial barrier to the additional research that’s needed to make more informed recommendations about its use to patients, Dr. Gecsi said. But the inadequate amount of research goes beyond the challenges of studying cannabis in particular, Dr. Urbina noted.
“The paucity of research in women’s health, particularly in the realm of sexual and reproductive health care, underscores the urgent need to prioritize this topic in order to ensure comprehensive and equitable healthcare for women,” Dr. Urbina said. Underrepresentation of women’s health issues in clinical studies has led to knowledge gaps and “suboptimal treatment options for conditions unique to or more prevalent among women,” and it’s another reason for the lack of robust data on cannabis use for gynecologic-related pain.
“Prioritizing research in women’s health is essential to developing effective interventions, understanding gender-specific responses to treatments, and addressing the complex interplay of biological, social, and psychological factors affecting women’s well-being,” Dr. Urbina said. “Furthermore, advancing reproductive health research supports women’s reproductive autonomy, empowering them with the knowledge and resources to make informed decisions about their bodies and lives. By investing in robust, inclusive research, we can close existing gaps, improve health outcomes, and promote gender equity in healthcare — something that has been long overdue in this country.”
The guidance did not use external funding. Dr. Gecsi, Dr. Urbina, and Dr. Kavipurapu had no disclosures.
*This story was corrected on July 25, 2024.
Could an EHR Nudge Reduce Unnecessary Biopsies?
Participating surgeons noted that the reminder system added minimal friction to their workflow, as it did not require additional clicks or actions on the day of the patient visit, reported lead author Neil Carleton, PhD, of UPMC Hillman Cancer Center, Pittsburgh, and colleagues in JAMA Surgery (JAMA Surg. 2024 Jul 17. doi: 10.1001/jamasurg.2024.2407).
This effort to reduce the rate of SLNB stems from the Choosing Wisely campaign, which recommends against axillary staging in women 70 years and older with early-stage, clinically node-negative (cN0), hormone receptor–positive (HR+) breast cancer, the investigators said.
“These recommendations were developed because axillary staging did not impact survival, and rates of SLN positivity were low because of the tumor’s biological phenotype,” they wrote. “Even in older patients with tumors that exhibit concerning clinicopathologic features, limited nodal involvement does not often alter receipt of chemotherapy independently from genomic testing. Despite these recommendations, most women still receive axillary surgery.”
How Did the Nudge System Aim to Reduce the Rate of SLNB?
The nudge intervention involved adding a new column to the Epic schedule view, which flagged eligible patients during their first outpatient surgical consultation. The flag appeared as a caution sign or red clipboard icon. When surgeons hovered over the icon, a text box appeared, reminding them to consider omitting SLNB after a detailed review of core biopsy pathology and ultrasonographic imaging.
The intervention was evaluated at eight outpatient clinics within an integrated healthcare system that included seven breast surgical oncologists.
The study began with a 12-month preintervention period to serve as a control, during which time SLNB rate was determined via 194 patients in the target demographic. SLNB rate was again collected during the 12-month intervention period, which involved 193 patients meeting enrollment criteria. Between these periods, the investigators conducted a brief session lasting less than 30 minutes to introduce the surgeons to the rationale and design of the nudge column.
How Effective Was the Nudge System?
The intervention reduced the SLNB rate from 46.9% to 23.8%, representing a 49.3% decrease in use of SLNB. Efficacy was further supported by a significant reduction in SLNB according to an interrupted time series model (adjusted odds ratio, 0.26; 95% confidence interval, 0.07 to 0.90; P = .03). Extended follow-up showed that this effect was durable beyond the intervention period, with a 6-month mean reduction in SLNB of 15.6%.
Omission of SLNB led to higher rates of pathological node positivity during the intervention period (15.2% vs 8.8%), with all positive cases staged as pN1. Adjuvant therapy recommendations were similar between groups and driven by genomic testing, not nodal status. The intervention period also saw a decrease in referrals for lymphedema evaluation (3.6% vs. 6.2%).
How Might the Nudge System Be Implemented in Other Practices?
Although the SLNB nudge system was effective in the present study, likelihood of uptake among practices could vary widely, according to Anne M. Wallace, MD, professor of clinical surgery at UC San Diego Health and director of the Moores Comprehensive Breast Health Program.
On a fundamental level, not all centers use Epic software, which could present issues with compatibility, Dr. Wallace said in an interview. More importantly, she added, many institutions already have EHR-based alerts and reminders in place, so it is not always feasible to add a new nudge for every possible clinical scenario.
“Already there are so many little icons that we have to go through now when we close a note,” she said. “That’s why electronic medical records are becoming one of the leading stressors in medicine.”
This presents a more complex challenge, Dr. Wallace said, particularly as potentially practice-changing data are becoming available, and physicians may not have time to learn about them and integrate them into routine practice. She suggested that the present system may be most appropriate for oncologists in solo practice, or in small group practices where it is more challenging to have routine conversations about changing standards of care.
What Are the Risks of Using the Nudge System?
One of those conversations may surround the validity of the recommendation implemented in the present study.
Although the Society of Surgical Oncology recommends against SLNB in the described demographic, other experts, including Dr. Wallace, take a more nuanced view of the decision.
She noted that some patients with a chronological age of 70 may have a lower biological age, casting doubt on the legitimacy of the age threshold, and those near the threshold may wish to make the decision about staging for themselves.
Beyond these concerns, Dr. Wallace described two potential risks involved in forgoing SLNB.
First, there’s the potential for underestimating the tumor’s severity, she said, as this could mean a trip back to the operating room. A tumor initially thought to be low-grade might later be found to be high-grade, necessitating further surgery. Some patients might refuse additional surgery, leaving the more aggressive tumor untreated.
Second, the nudge system could complicate radiation treatment decisions, Dr. Wallace said. Without full nodal status, some radiation oncologists might push for additional radiation therapy, which incurs a greater treatment burden than SNLB.
What Are Some Alternatives to the Nudge System?
After discussing the strengths and weaknesses of the present EHR-based nudge system, and others like it, Dr. Wallace returned to the importance of ongoing communication among colleagues managing complex cases.
At UC San Diego Health, where oncologists meet weekly for a 2-hour breast cancer conference, “we nudge each other,” she said.
This study was supported by the Shear Family Foundation, UPMC eRecord Ambulatory Decision Support and Analytics, UPMC Hillman Cancer Center Biostatistics Facility, and National Institutes of Health. The investigators disclosed relationships with Pfizer, Amgen, the Lewin Group, and Milestone Pennsylvania, and others.
Participating surgeons noted that the reminder system added minimal friction to their workflow, as it did not require additional clicks or actions on the day of the patient visit, reported lead author Neil Carleton, PhD, of UPMC Hillman Cancer Center, Pittsburgh, and colleagues in JAMA Surgery (JAMA Surg. 2024 Jul 17. doi: 10.1001/jamasurg.2024.2407).
This effort to reduce the rate of SLNB stems from the Choosing Wisely campaign, which recommends against axillary staging in women 70 years and older with early-stage, clinically node-negative (cN0), hormone receptor–positive (HR+) breast cancer, the investigators said.
“These recommendations were developed because axillary staging did not impact survival, and rates of SLN positivity were low because of the tumor’s biological phenotype,” they wrote. “Even in older patients with tumors that exhibit concerning clinicopathologic features, limited nodal involvement does not often alter receipt of chemotherapy independently from genomic testing. Despite these recommendations, most women still receive axillary surgery.”
How Did the Nudge System Aim to Reduce the Rate of SLNB?
The nudge intervention involved adding a new column to the Epic schedule view, which flagged eligible patients during their first outpatient surgical consultation. The flag appeared as a caution sign or red clipboard icon. When surgeons hovered over the icon, a text box appeared, reminding them to consider omitting SLNB after a detailed review of core biopsy pathology and ultrasonographic imaging.
The intervention was evaluated at eight outpatient clinics within an integrated healthcare system that included seven breast surgical oncologists.
The study began with a 12-month preintervention period to serve as a control, during which time SLNB rate was determined via 194 patients in the target demographic. SLNB rate was again collected during the 12-month intervention period, which involved 193 patients meeting enrollment criteria. Between these periods, the investigators conducted a brief session lasting less than 30 minutes to introduce the surgeons to the rationale and design of the nudge column.
How Effective Was the Nudge System?
The intervention reduced the SLNB rate from 46.9% to 23.8%, representing a 49.3% decrease in use of SLNB. Efficacy was further supported by a significant reduction in SLNB according to an interrupted time series model (adjusted odds ratio, 0.26; 95% confidence interval, 0.07 to 0.90; P = .03). Extended follow-up showed that this effect was durable beyond the intervention period, with a 6-month mean reduction in SLNB of 15.6%.
Omission of SLNB led to higher rates of pathological node positivity during the intervention period (15.2% vs 8.8%), with all positive cases staged as pN1. Adjuvant therapy recommendations were similar between groups and driven by genomic testing, not nodal status. The intervention period also saw a decrease in referrals for lymphedema evaluation (3.6% vs. 6.2%).
How Might the Nudge System Be Implemented in Other Practices?
Although the SLNB nudge system was effective in the present study, likelihood of uptake among practices could vary widely, according to Anne M. Wallace, MD, professor of clinical surgery at UC San Diego Health and director of the Moores Comprehensive Breast Health Program.
On a fundamental level, not all centers use Epic software, which could present issues with compatibility, Dr. Wallace said in an interview. More importantly, she added, many institutions already have EHR-based alerts and reminders in place, so it is not always feasible to add a new nudge for every possible clinical scenario.
“Already there are so many little icons that we have to go through now when we close a note,” she said. “That’s why electronic medical records are becoming one of the leading stressors in medicine.”
This presents a more complex challenge, Dr. Wallace said, particularly as potentially practice-changing data are becoming available, and physicians may not have time to learn about them and integrate them into routine practice. She suggested that the present system may be most appropriate for oncologists in solo practice, or in small group practices where it is more challenging to have routine conversations about changing standards of care.
What Are the Risks of Using the Nudge System?
One of those conversations may surround the validity of the recommendation implemented in the present study.
Although the Society of Surgical Oncology recommends against SLNB in the described demographic, other experts, including Dr. Wallace, take a more nuanced view of the decision.
She noted that some patients with a chronological age of 70 may have a lower biological age, casting doubt on the legitimacy of the age threshold, and those near the threshold may wish to make the decision about staging for themselves.
Beyond these concerns, Dr. Wallace described two potential risks involved in forgoing SLNB.
First, there’s the potential for underestimating the tumor’s severity, she said, as this could mean a trip back to the operating room. A tumor initially thought to be low-grade might later be found to be high-grade, necessitating further surgery. Some patients might refuse additional surgery, leaving the more aggressive tumor untreated.
Second, the nudge system could complicate radiation treatment decisions, Dr. Wallace said. Without full nodal status, some radiation oncologists might push for additional radiation therapy, which incurs a greater treatment burden than SNLB.
What Are Some Alternatives to the Nudge System?
After discussing the strengths and weaknesses of the present EHR-based nudge system, and others like it, Dr. Wallace returned to the importance of ongoing communication among colleagues managing complex cases.
At UC San Diego Health, where oncologists meet weekly for a 2-hour breast cancer conference, “we nudge each other,” she said.
This study was supported by the Shear Family Foundation, UPMC eRecord Ambulatory Decision Support and Analytics, UPMC Hillman Cancer Center Biostatistics Facility, and National Institutes of Health. The investigators disclosed relationships with Pfizer, Amgen, the Lewin Group, and Milestone Pennsylvania, and others.
Participating surgeons noted that the reminder system added minimal friction to their workflow, as it did not require additional clicks or actions on the day of the patient visit, reported lead author Neil Carleton, PhD, of UPMC Hillman Cancer Center, Pittsburgh, and colleagues in JAMA Surgery (JAMA Surg. 2024 Jul 17. doi: 10.1001/jamasurg.2024.2407).
This effort to reduce the rate of SLNB stems from the Choosing Wisely campaign, which recommends against axillary staging in women 70 years and older with early-stage, clinically node-negative (cN0), hormone receptor–positive (HR+) breast cancer, the investigators said.
“These recommendations were developed because axillary staging did not impact survival, and rates of SLN positivity were low because of the tumor’s biological phenotype,” they wrote. “Even in older patients with tumors that exhibit concerning clinicopathologic features, limited nodal involvement does not often alter receipt of chemotherapy independently from genomic testing. Despite these recommendations, most women still receive axillary surgery.”
How Did the Nudge System Aim to Reduce the Rate of SLNB?
The nudge intervention involved adding a new column to the Epic schedule view, which flagged eligible patients during their first outpatient surgical consultation. The flag appeared as a caution sign or red clipboard icon. When surgeons hovered over the icon, a text box appeared, reminding them to consider omitting SLNB after a detailed review of core biopsy pathology and ultrasonographic imaging.
The intervention was evaluated at eight outpatient clinics within an integrated healthcare system that included seven breast surgical oncologists.
The study began with a 12-month preintervention period to serve as a control, during which time SLNB rate was determined via 194 patients in the target demographic. SLNB rate was again collected during the 12-month intervention period, which involved 193 patients meeting enrollment criteria. Between these periods, the investigators conducted a brief session lasting less than 30 minutes to introduce the surgeons to the rationale and design of the nudge column.
How Effective Was the Nudge System?
The intervention reduced the SLNB rate from 46.9% to 23.8%, representing a 49.3% decrease in use of SLNB. Efficacy was further supported by a significant reduction in SLNB according to an interrupted time series model (adjusted odds ratio, 0.26; 95% confidence interval, 0.07 to 0.90; P = .03). Extended follow-up showed that this effect was durable beyond the intervention period, with a 6-month mean reduction in SLNB of 15.6%.
Omission of SLNB led to higher rates of pathological node positivity during the intervention period (15.2% vs 8.8%), with all positive cases staged as pN1. Adjuvant therapy recommendations were similar between groups and driven by genomic testing, not nodal status. The intervention period also saw a decrease in referrals for lymphedema evaluation (3.6% vs. 6.2%).
How Might the Nudge System Be Implemented in Other Practices?
Although the SLNB nudge system was effective in the present study, likelihood of uptake among practices could vary widely, according to Anne M. Wallace, MD, professor of clinical surgery at UC San Diego Health and director of the Moores Comprehensive Breast Health Program.
On a fundamental level, not all centers use Epic software, which could present issues with compatibility, Dr. Wallace said in an interview. More importantly, she added, many institutions already have EHR-based alerts and reminders in place, so it is not always feasible to add a new nudge for every possible clinical scenario.
“Already there are so many little icons that we have to go through now when we close a note,” she said. “That’s why electronic medical records are becoming one of the leading stressors in medicine.”
This presents a more complex challenge, Dr. Wallace said, particularly as potentially practice-changing data are becoming available, and physicians may not have time to learn about them and integrate them into routine practice. She suggested that the present system may be most appropriate for oncologists in solo practice, or in small group practices where it is more challenging to have routine conversations about changing standards of care.
What Are the Risks of Using the Nudge System?
One of those conversations may surround the validity of the recommendation implemented in the present study.
Although the Society of Surgical Oncology recommends against SLNB in the described demographic, other experts, including Dr. Wallace, take a more nuanced view of the decision.
She noted that some patients with a chronological age of 70 may have a lower biological age, casting doubt on the legitimacy of the age threshold, and those near the threshold may wish to make the decision about staging for themselves.
Beyond these concerns, Dr. Wallace described two potential risks involved in forgoing SLNB.
First, there’s the potential for underestimating the tumor’s severity, she said, as this could mean a trip back to the operating room. A tumor initially thought to be low-grade might later be found to be high-grade, necessitating further surgery. Some patients might refuse additional surgery, leaving the more aggressive tumor untreated.
Second, the nudge system could complicate radiation treatment decisions, Dr. Wallace said. Without full nodal status, some radiation oncologists might push for additional radiation therapy, which incurs a greater treatment burden than SNLB.
What Are Some Alternatives to the Nudge System?
After discussing the strengths and weaknesses of the present EHR-based nudge system, and others like it, Dr. Wallace returned to the importance of ongoing communication among colleagues managing complex cases.
At UC San Diego Health, where oncologists meet weekly for a 2-hour breast cancer conference, “we nudge each other,” she said.
This study was supported by the Shear Family Foundation, UPMC eRecord Ambulatory Decision Support and Analytics, UPMC Hillman Cancer Center Biostatistics Facility, and National Institutes of Health. The investigators disclosed relationships with Pfizer, Amgen, the Lewin Group, and Milestone Pennsylvania, and others.
FROM JAMA SURGERY
Rural Hospitals Built During Baby Boom Now Face Baby Bust
Rural regions like the one surrounding a southern Iowa town used to have a lot more babies and many more places to give birth to them.
At least 41 Iowa hospitals have shuttered their labor and delivery units since 2000. Those facilities, representing about a third of all Iowa hospitals, are located mostly in rural areas where birth numbers have plummeted. In some Iowa counties, annual numbers of births have fallen by three quarters since the height of the baby boom in the 1950s and 1960s, when many rural hospitals were built or expanded, state and federal records show.
Similar trends are playing out nationwide, as hospitals struggle to maintain staff and facilities to safely handle dwindling numbers of births. More than half of rural US hospitals now lack the service.
“People just aren’t having as many kids,” said Addie Comegys, who lives in southern Iowa and has regularly traveled 45 minutes each way for prenatal checkups at Oskaloosa’s hospital this summer. Her mother had six children, starting in the 1980s, when big families didn’t seem so rare.
“Now, if you have three kids, people are like, ‘Oh my gosh, are you ever going to stop?’ ” said Ms. Comegys, 29, who is expecting her second child in late August.
These days, many Americans choose to have small families or no children at all. Modern birth control methods help make such decisions stick. The trend is amplified in small towns when young adults move away, taking any childbearing potential with them.
Hospital leaders who close obstetrics units often cite declining birth numbers, along with staffing challenges and financial losses. The closures can be a particular challenge for pregnant women who lack the reliable transportation and flexible schedules needed to travel long distances for prenatal care and birthing services.
The baby boom peaked in 1957, when about 4.3 million children were born in the United States. The annual number of births dropped below 3.7 million by 2022, even though the overall US population nearly doubled over that same period.
West Virginia has seen the steepest decline in births, a 62% drop in those 65 years, according to federal data. Iowa’s births dropped 43% over that period. Of the state’s 99 counties, just four — all urban or suburban — recorded more births.
Births have increased in only 13 states since 1957. Most of them, such as Arizona, California, Florida, and Nevada, are places that have attracted waves of newcomers from other states and countries. But even those states have had obstetrics units close in rural areas.
In Iowa, Oskaloosa’s hospital has bucked the trend and kept its labor and delivery unit open, partly by pulling in patients from 14 other counties. Last year, the hospital even managed the rare feat of recruiting two obstetrician-gynecologists to expand its services.
The publicly owned hospital, called Mahaska Health, expects to deliver 250 babies this year, up from about 160 in previous years, CEO Kevin DeRonde said.
“It’s an essential service, and we needed to keep it going and grow it,” Mr. DeRonde said.
Many of the US hospitals that are now dropping obstetrics units were built or expanded in the mid-1900s, when America went on a rural-hospital building spree, thanks to federal funding from the Hill-Burton Act.
“It was an amazing program,” said Brock Slabach, chief operations officer for the National Rural Health Association. “Basically, if you were a county that wanted a hospital, they gave you the money.”
Mr. Slabach said that in addition to declining birth numbers, obstetrics units are experiencing a drop in occupancy because most patients go home after a night or two. In the past, patients typically spent several days in the hospital after giving birth.
Dwindling caseloads can raise safety concerns for obstetrics units.
A study published in JAMA in 2023 found that women were more likely to suffer serious complications if they gave birth in rural hospitals that handled 110 or fewer births a year. The authors said they didn’t support closing low-volume units because that could lead more women to have complications related to traveling for care. Instead, they recommended improving training and coordination among rural health providers.
Stephanie Radke, MD, a University of Iowa obstetrics and gynecology professor who studies access to birthing services, said it is almost inevitable that when rural birth numbers plunge, some obstetrics units will close. “We talk about that as a bad event, but we don’t really talk about why it happens,” she said.
Dr. Radke said maintaining a set number of obstetrics units is less important than ensuring good care for pregnant women and their babies. It’s difficult to maintain quality of care when the staff doesn’t consistently practice deliveries, she said, but it is hard to define that line. “What is realistic?” she said. “I don’t think a unit should be open that only delivers 50 babies a year.”
In some cases, she said, hospitals near each other have consolidated obstetrics units, pooling their resources into one program that has enough staffers and handles sufficient cases. “You’re not always really creating a care desert when that happens,” she said.
The decline in births has accelerated in many areas in recent years. Kenneth Johnson, a sociology professor and demographer at the University of New Hampshire, said it is understandable that many rural hospitals have closed obstetrics units. “I’m actually surprised some of them have lasted as long as they have,” he said.
Dr. Johnson said rural areas that have seen the steepest population declines tend to be far from cities and lack recreational attractions, such as mountains or large bodies of water. Some have avoided population losses by attracting immigrant workers, who tend to have larger families in the first generation or two after they move to the United States, he said.
Katy B. Kozhimannil, a University of Minnesota health policy professor who studies rural issues, said declining birth numbers and obstetric unit closures can create a vicious cycle. Fewer babies being born in a region can lead a birthing unit to shutter. Then the loss of such a unit can discourage young people from moving to the area, driving birth numbers even lower.
In many regions, people with private insurance, flexible schedules, and reliable transportation choose to travel to larger hospitals for their prenatal care and to give birth, Dr. Kozhimannil said. That leaves rural hospitals with a larger proportion of patients on Medicaid, a public program that pays about half what private insurance pays for the same services, she said.
Iowa ranks near the bottom of all states for obstetrician-gynecologists per capita. But Oskaloosa’s hospital hit the jackpot last year, when it recruited Taylar Swartz Summers, DO, and Garth Summers, DO, a married couple who both recently finished their obstetrics training. Dr. Swartz Summers grew up in the area, and she wanted to return to serve women there.
She hopes the number of obstetrics units will level off after the wave of closures. “It’s not even just for delivery, but we need access just to women’s healthcare in general,” she said. “I would love to see women’s healthcare be at the forefront of our government’s mind.”
Dr. Swartz Summers noted that the state has only one obstetrics training program, which is at the University of Iowa. She said she and her husband plan to help spark interest in rural obstetrics by hosting University of Iowa residency rotations at the Oskaloosa hospital.
Ms. Comegys, a patient of Dr. Swartz Summer’s, could have chosen a hospital birthing center closer to her home, but she wasn’t confident in its quality. Other hospitals in her region had shuttered their obstetrics units. She is grateful to have a flexible job, a reliable car, and a supportive family, so she can travel to Oskaloosa for checkups and to give birth there. She knows many other women are not so lucky, and she worries other obstetrics units are at risk.
“It’s sad, but I could see more closing,” she said.
A version of this article first appeared on Medscape.com.
Rural regions like the one surrounding a southern Iowa town used to have a lot more babies and many more places to give birth to them.
At least 41 Iowa hospitals have shuttered their labor and delivery units since 2000. Those facilities, representing about a third of all Iowa hospitals, are located mostly in rural areas where birth numbers have plummeted. In some Iowa counties, annual numbers of births have fallen by three quarters since the height of the baby boom in the 1950s and 1960s, when many rural hospitals were built or expanded, state and federal records show.
Similar trends are playing out nationwide, as hospitals struggle to maintain staff and facilities to safely handle dwindling numbers of births. More than half of rural US hospitals now lack the service.
“People just aren’t having as many kids,” said Addie Comegys, who lives in southern Iowa and has regularly traveled 45 minutes each way for prenatal checkups at Oskaloosa’s hospital this summer. Her mother had six children, starting in the 1980s, when big families didn’t seem so rare.
“Now, if you have three kids, people are like, ‘Oh my gosh, are you ever going to stop?’ ” said Ms. Comegys, 29, who is expecting her second child in late August.
These days, many Americans choose to have small families or no children at all. Modern birth control methods help make such decisions stick. The trend is amplified in small towns when young adults move away, taking any childbearing potential with them.
Hospital leaders who close obstetrics units often cite declining birth numbers, along with staffing challenges and financial losses. The closures can be a particular challenge for pregnant women who lack the reliable transportation and flexible schedules needed to travel long distances for prenatal care and birthing services.
The baby boom peaked in 1957, when about 4.3 million children were born in the United States. The annual number of births dropped below 3.7 million by 2022, even though the overall US population nearly doubled over that same period.
West Virginia has seen the steepest decline in births, a 62% drop in those 65 years, according to federal data. Iowa’s births dropped 43% over that period. Of the state’s 99 counties, just four — all urban or suburban — recorded more births.
Births have increased in only 13 states since 1957. Most of them, such as Arizona, California, Florida, and Nevada, are places that have attracted waves of newcomers from other states and countries. But even those states have had obstetrics units close in rural areas.
In Iowa, Oskaloosa’s hospital has bucked the trend and kept its labor and delivery unit open, partly by pulling in patients from 14 other counties. Last year, the hospital even managed the rare feat of recruiting two obstetrician-gynecologists to expand its services.
The publicly owned hospital, called Mahaska Health, expects to deliver 250 babies this year, up from about 160 in previous years, CEO Kevin DeRonde said.
“It’s an essential service, and we needed to keep it going and grow it,” Mr. DeRonde said.
Many of the US hospitals that are now dropping obstetrics units were built or expanded in the mid-1900s, when America went on a rural-hospital building spree, thanks to federal funding from the Hill-Burton Act.
“It was an amazing program,” said Brock Slabach, chief operations officer for the National Rural Health Association. “Basically, if you were a county that wanted a hospital, they gave you the money.”
Mr. Slabach said that in addition to declining birth numbers, obstetrics units are experiencing a drop in occupancy because most patients go home after a night or two. In the past, patients typically spent several days in the hospital after giving birth.
Dwindling caseloads can raise safety concerns for obstetrics units.
A study published in JAMA in 2023 found that women were more likely to suffer serious complications if they gave birth in rural hospitals that handled 110 or fewer births a year. The authors said they didn’t support closing low-volume units because that could lead more women to have complications related to traveling for care. Instead, they recommended improving training and coordination among rural health providers.
Stephanie Radke, MD, a University of Iowa obstetrics and gynecology professor who studies access to birthing services, said it is almost inevitable that when rural birth numbers plunge, some obstetrics units will close. “We talk about that as a bad event, but we don’t really talk about why it happens,” she said.
Dr. Radke said maintaining a set number of obstetrics units is less important than ensuring good care for pregnant women and their babies. It’s difficult to maintain quality of care when the staff doesn’t consistently practice deliveries, she said, but it is hard to define that line. “What is realistic?” she said. “I don’t think a unit should be open that only delivers 50 babies a year.”
In some cases, she said, hospitals near each other have consolidated obstetrics units, pooling their resources into one program that has enough staffers and handles sufficient cases. “You’re not always really creating a care desert when that happens,” she said.
The decline in births has accelerated in many areas in recent years. Kenneth Johnson, a sociology professor and demographer at the University of New Hampshire, said it is understandable that many rural hospitals have closed obstetrics units. “I’m actually surprised some of them have lasted as long as they have,” he said.
Dr. Johnson said rural areas that have seen the steepest population declines tend to be far from cities and lack recreational attractions, such as mountains or large bodies of water. Some have avoided population losses by attracting immigrant workers, who tend to have larger families in the first generation or two after they move to the United States, he said.
Katy B. Kozhimannil, a University of Minnesota health policy professor who studies rural issues, said declining birth numbers and obstetric unit closures can create a vicious cycle. Fewer babies being born in a region can lead a birthing unit to shutter. Then the loss of such a unit can discourage young people from moving to the area, driving birth numbers even lower.
In many regions, people with private insurance, flexible schedules, and reliable transportation choose to travel to larger hospitals for their prenatal care and to give birth, Dr. Kozhimannil said. That leaves rural hospitals with a larger proportion of patients on Medicaid, a public program that pays about half what private insurance pays for the same services, she said.
Iowa ranks near the bottom of all states for obstetrician-gynecologists per capita. But Oskaloosa’s hospital hit the jackpot last year, when it recruited Taylar Swartz Summers, DO, and Garth Summers, DO, a married couple who both recently finished their obstetrics training. Dr. Swartz Summers grew up in the area, and she wanted to return to serve women there.
She hopes the number of obstetrics units will level off after the wave of closures. “It’s not even just for delivery, but we need access just to women’s healthcare in general,” she said. “I would love to see women’s healthcare be at the forefront of our government’s mind.”
Dr. Swartz Summers noted that the state has only one obstetrics training program, which is at the University of Iowa. She said she and her husband plan to help spark interest in rural obstetrics by hosting University of Iowa residency rotations at the Oskaloosa hospital.
Ms. Comegys, a patient of Dr. Swartz Summer’s, could have chosen a hospital birthing center closer to her home, but she wasn’t confident in its quality. Other hospitals in her region had shuttered their obstetrics units. She is grateful to have a flexible job, a reliable car, and a supportive family, so she can travel to Oskaloosa for checkups and to give birth there. She knows many other women are not so lucky, and she worries other obstetrics units are at risk.
“It’s sad, but I could see more closing,” she said.
A version of this article first appeared on Medscape.com.
Rural regions like the one surrounding a southern Iowa town used to have a lot more babies and many more places to give birth to them.
At least 41 Iowa hospitals have shuttered their labor and delivery units since 2000. Those facilities, representing about a third of all Iowa hospitals, are located mostly in rural areas where birth numbers have plummeted. In some Iowa counties, annual numbers of births have fallen by three quarters since the height of the baby boom in the 1950s and 1960s, when many rural hospitals were built or expanded, state and federal records show.
Similar trends are playing out nationwide, as hospitals struggle to maintain staff and facilities to safely handle dwindling numbers of births. More than half of rural US hospitals now lack the service.
“People just aren’t having as many kids,” said Addie Comegys, who lives in southern Iowa and has regularly traveled 45 minutes each way for prenatal checkups at Oskaloosa’s hospital this summer. Her mother had six children, starting in the 1980s, when big families didn’t seem so rare.
“Now, if you have three kids, people are like, ‘Oh my gosh, are you ever going to stop?’ ” said Ms. Comegys, 29, who is expecting her second child in late August.
These days, many Americans choose to have small families or no children at all. Modern birth control methods help make such decisions stick. The trend is amplified in small towns when young adults move away, taking any childbearing potential with them.
Hospital leaders who close obstetrics units often cite declining birth numbers, along with staffing challenges and financial losses. The closures can be a particular challenge for pregnant women who lack the reliable transportation and flexible schedules needed to travel long distances for prenatal care and birthing services.
The baby boom peaked in 1957, when about 4.3 million children were born in the United States. The annual number of births dropped below 3.7 million by 2022, even though the overall US population nearly doubled over that same period.
West Virginia has seen the steepest decline in births, a 62% drop in those 65 years, according to federal data. Iowa’s births dropped 43% over that period. Of the state’s 99 counties, just four — all urban or suburban — recorded more births.
Births have increased in only 13 states since 1957. Most of them, such as Arizona, California, Florida, and Nevada, are places that have attracted waves of newcomers from other states and countries. But even those states have had obstetrics units close in rural areas.
In Iowa, Oskaloosa’s hospital has bucked the trend and kept its labor and delivery unit open, partly by pulling in patients from 14 other counties. Last year, the hospital even managed the rare feat of recruiting two obstetrician-gynecologists to expand its services.
The publicly owned hospital, called Mahaska Health, expects to deliver 250 babies this year, up from about 160 in previous years, CEO Kevin DeRonde said.
“It’s an essential service, and we needed to keep it going and grow it,” Mr. DeRonde said.
Many of the US hospitals that are now dropping obstetrics units were built or expanded in the mid-1900s, when America went on a rural-hospital building spree, thanks to federal funding from the Hill-Burton Act.
“It was an amazing program,” said Brock Slabach, chief operations officer for the National Rural Health Association. “Basically, if you were a county that wanted a hospital, they gave you the money.”
Mr. Slabach said that in addition to declining birth numbers, obstetrics units are experiencing a drop in occupancy because most patients go home after a night or two. In the past, patients typically spent several days in the hospital after giving birth.
Dwindling caseloads can raise safety concerns for obstetrics units.
A study published in JAMA in 2023 found that women were more likely to suffer serious complications if they gave birth in rural hospitals that handled 110 or fewer births a year. The authors said they didn’t support closing low-volume units because that could lead more women to have complications related to traveling for care. Instead, they recommended improving training and coordination among rural health providers.
Stephanie Radke, MD, a University of Iowa obstetrics and gynecology professor who studies access to birthing services, said it is almost inevitable that when rural birth numbers plunge, some obstetrics units will close. “We talk about that as a bad event, but we don’t really talk about why it happens,” she said.
Dr. Radke said maintaining a set number of obstetrics units is less important than ensuring good care for pregnant women and their babies. It’s difficult to maintain quality of care when the staff doesn’t consistently practice deliveries, she said, but it is hard to define that line. “What is realistic?” she said. “I don’t think a unit should be open that only delivers 50 babies a year.”
In some cases, she said, hospitals near each other have consolidated obstetrics units, pooling their resources into one program that has enough staffers and handles sufficient cases. “You’re not always really creating a care desert when that happens,” she said.
The decline in births has accelerated in many areas in recent years. Kenneth Johnson, a sociology professor and demographer at the University of New Hampshire, said it is understandable that many rural hospitals have closed obstetrics units. “I’m actually surprised some of them have lasted as long as they have,” he said.
Dr. Johnson said rural areas that have seen the steepest population declines tend to be far from cities and lack recreational attractions, such as mountains or large bodies of water. Some have avoided population losses by attracting immigrant workers, who tend to have larger families in the first generation or two after they move to the United States, he said.
Katy B. Kozhimannil, a University of Minnesota health policy professor who studies rural issues, said declining birth numbers and obstetric unit closures can create a vicious cycle. Fewer babies being born in a region can lead a birthing unit to shutter. Then the loss of such a unit can discourage young people from moving to the area, driving birth numbers even lower.
In many regions, people with private insurance, flexible schedules, and reliable transportation choose to travel to larger hospitals for their prenatal care and to give birth, Dr. Kozhimannil said. That leaves rural hospitals with a larger proportion of patients on Medicaid, a public program that pays about half what private insurance pays for the same services, she said.
Iowa ranks near the bottom of all states for obstetrician-gynecologists per capita. But Oskaloosa’s hospital hit the jackpot last year, when it recruited Taylar Swartz Summers, DO, and Garth Summers, DO, a married couple who both recently finished their obstetrics training. Dr. Swartz Summers grew up in the area, and she wanted to return to serve women there.
She hopes the number of obstetrics units will level off after the wave of closures. “It’s not even just for delivery, but we need access just to women’s healthcare in general,” she said. “I would love to see women’s healthcare be at the forefront of our government’s mind.”
Dr. Swartz Summers noted that the state has only one obstetrics training program, which is at the University of Iowa. She said she and her husband plan to help spark interest in rural obstetrics by hosting University of Iowa residency rotations at the Oskaloosa hospital.
Ms. Comegys, a patient of Dr. Swartz Summer’s, could have chosen a hospital birthing center closer to her home, but she wasn’t confident in its quality. Other hospitals in her region had shuttered their obstetrics units. She is grateful to have a flexible job, a reliable car, and a supportive family, so she can travel to Oskaloosa for checkups and to give birth there. She knows many other women are not so lucky, and she worries other obstetrics units are at risk.
“It’s sad, but I could see more closing,” she said.
A version of this article first appeared on Medscape.com.
Almost 10% of Infected Pregnant People Develop Long COVID
Almost 1 in 10 pregnant people infected with COVID-19 end up developing long COVID, according to a study published in Obstetrics & Gynecology.
Researchers at University of Utah Health looked at the medical records of more than 1500 people who got COVID-19 while pregnant and checked their self-reported symptoms at least 6 months after infection, according to a news release from the school.
The scientists discovered that 9.3% of those people reported long COVID symptoms, such as fatigue and issues in their gut.
To make sure those long COVID symptoms were not actually symptoms of pregnancy, the research team did a second analysis of people who reported symptoms more than 12 weeks after giving birth. The risk of long COVID was about the same as in the first analysis.
“It was surprising to me that the prevalence was that high,” Torri D. Metz, MD, vice chair for research of obstetrics and gynecology at the school and co-leader of the study, said in the release. “This is something that does continue to affect otherwise reasonably healthy and young populations.”
The school said this is the first study to look at long COVID risks in pregnant people. Previous research found other dangers for pregnant people who get COVID, such as a higher chance of hospitalization or death, or complications such as preterm birth.
In the general population, research shows that 10%-20% of people who get COVID develop long COVID.
Dr. Metz said healthcare providers need to remain alert about long COVID, including in pregnant people.
“We need to have this on our radar as we’re seeing patients. It’s something we really don’t want to miss. And we want to get people referred to appropriate specialists who treat long COVID,” she said.
A version of this article first appeared on WebMD.com.
Almost 1 in 10 pregnant people infected with COVID-19 end up developing long COVID, according to a study published in Obstetrics & Gynecology.
Researchers at University of Utah Health looked at the medical records of more than 1500 people who got COVID-19 while pregnant and checked their self-reported symptoms at least 6 months after infection, according to a news release from the school.
The scientists discovered that 9.3% of those people reported long COVID symptoms, such as fatigue and issues in their gut.
To make sure those long COVID symptoms were not actually symptoms of pregnancy, the research team did a second analysis of people who reported symptoms more than 12 weeks after giving birth. The risk of long COVID was about the same as in the first analysis.
“It was surprising to me that the prevalence was that high,” Torri D. Metz, MD, vice chair for research of obstetrics and gynecology at the school and co-leader of the study, said in the release. “This is something that does continue to affect otherwise reasonably healthy and young populations.”
The school said this is the first study to look at long COVID risks in pregnant people. Previous research found other dangers for pregnant people who get COVID, such as a higher chance of hospitalization or death, or complications such as preterm birth.
In the general population, research shows that 10%-20% of people who get COVID develop long COVID.
Dr. Metz said healthcare providers need to remain alert about long COVID, including in pregnant people.
“We need to have this on our radar as we’re seeing patients. It’s something we really don’t want to miss. And we want to get people referred to appropriate specialists who treat long COVID,” she said.
A version of this article first appeared on WebMD.com.
Almost 1 in 10 pregnant people infected with COVID-19 end up developing long COVID, according to a study published in Obstetrics & Gynecology.
Researchers at University of Utah Health looked at the medical records of more than 1500 people who got COVID-19 while pregnant and checked their self-reported symptoms at least 6 months after infection, according to a news release from the school.
The scientists discovered that 9.3% of those people reported long COVID symptoms, such as fatigue and issues in their gut.
To make sure those long COVID symptoms were not actually symptoms of pregnancy, the research team did a second analysis of people who reported symptoms more than 12 weeks after giving birth. The risk of long COVID was about the same as in the first analysis.
“It was surprising to me that the prevalence was that high,” Torri D. Metz, MD, vice chair for research of obstetrics and gynecology at the school and co-leader of the study, said in the release. “This is something that does continue to affect otherwise reasonably healthy and young populations.”
The school said this is the first study to look at long COVID risks in pregnant people. Previous research found other dangers for pregnant people who get COVID, such as a higher chance of hospitalization or death, or complications such as preterm birth.
In the general population, research shows that 10%-20% of people who get COVID develop long COVID.
Dr. Metz said healthcare providers need to remain alert about long COVID, including in pregnant people.
“We need to have this on our radar as we’re seeing patients. It’s something we really don’t want to miss. And we want to get people referred to appropriate specialists who treat long COVID,” she said.
A version of this article first appeared on WebMD.com.
FROM OBSTETRICS & GYNECOLOGY
Endometriosis, Especially Severe Types, Boosts Ovarian Cancer Risk
Ovarian cancer risk was higher in women with endometriosis overall and markedly increased in those with severe forms, a large population-based cohort study found.
The findings, published in JAMA, suggest these women may benefit from counseling on ovarian cancer risk and prevention and potentially from targeted screening, according to a group led by Mollie E. Barnard, ScD, of the Huntsman Cancer Institute at the University of Utah in Salt Lake City.
While the absolute increase in number of cases was small, endometriosis patients overall had a more than fourfold higher risk for any type of ovarian cancer. Those with more severe forms, such as ovarian endometriomas or deep infiltrating endometriosis, had a nearly 10-fold higher risk of any type of ovarian cancer. In addition, those with more severe endometriosis had a 19-fold higher risk of type 1 (slow-growing) ovarian cancer and almost three times the risk of the more aggressive type 2.
“Given the rarity of ovarian cancer, the excess risk was relatively small, with 10-20 additional cases per 10,000 women. Nevertheless, women with endometriosis, notably the more severe subtypes, may be an important population for targeted cancer screening and prevention studies,” said corresponding author Karen C. Schliep, PhD, MSPH, associate professor in the university’s Division of Public Health.
Prior studies have shown modest associations between endometriosis and ovarian cancer, Dr. Schliep said in an interview. A 2021 systematic review and meta-analysis found endometriosis conferred nearly double the risk of ovarian cancer, although associations varied by ovarian cancer histotype. Few studies have been large enough to assess associations between endometriosis types — including superficial or peritoneal endometriosis vs ovarian endometriomas or deep infiltrating endometriosis and ovarian cancer histotypes such as low-grade serous, endometrioid, clear cell, and mucinous carcinomas (type 1), and the most aggressive and lethal form, high-grade serous type 2, she said in an interview. “Our large health administrative database of over 11 million individuals with linked electronic health and cancer registry data allowed us to answer this as yet poorly studied research question.”
Study Details
Drawing on Utah electronic health records from 1992 to 2019, the investigators matched 78,893 women with endometriosis in a 1:5 ratio to unaffected women. Cases were categorized as superficial endometriosis, ovarian endometriomas, deep infiltrating endometriosis, or other, and the types of endometriosis were matched to ovarian cancer histotypes.
The mean age of patients at first endometriosis diagnosis was 36 and the mean follow-up was 12 years. Compared with controls, endometriosis patients were more likely to be nulliparous (31% vs 24%) and to have had a hysterectomy (39% vs 6%) during follow-up.
There were 596 reported cases of ovarian cancer in the cohort. Those with incident endometriosis were 4.2 times more likely to develop ovarian cancer (95% CI, 3.59-4.91), 7.48 times more likely to develop type 1 ovarian cancer (95% CI, 5.80-9.65), and 2.70 times more likely to develop type 2 ovarian cancer (95% CI, 2.09-3.49) compared with those without endometriosis.
The magnitudes of these associations varied by endometriosis subtype. Individuals diagnosed with deep infiltrating endometriosis and/or ovarian endometriomas had 9.66 times the risk of ovarian cancer vs individuals without endometriosis (95% CI, 7.77-12.00). “Women with, compared to without, more severe endometriosis had a 19-fold higher risk of type 1 ovarian cancer, including endometrioid, clear cell, mucinous, and low-grade serous,” Dr. Schliep said, with associated risk highest for malignant subtypes such as clear cell and endometrioid carcinoma (adjusted hazard ratios, 11.15 and 7.96, respectively.
According to Dr. Schliep, physicians should encourage endometriosis patients to be aware of but not worry about ovarian cancer risk because the likelihood of developing it remains low. For their part, patients can reduce their risk of cancer through a balanced diet with low intake of alcohol, regular exercise, a healthy weight, and abstention from smoking.
Her message for researchers is as follows: “We need more studies that explore how different types of endometriosis impact different types of ovarian cancer risk. These studies will guide improved ovarian cancer screening and prevention strategies among women with severe endometriosis, with or without other important ovarian cancer risk factors such as BRCA 1/2 variations.”
An accompanying editorial called the Utah study “eloquent” and noted its distinguishing contribution of observing associations between subtypes of endometriosis with overall risk for ovarian cancer as well as histologic subtypes of epithelial ovarian cancer.
Nevertheless, Michael T. McHale, MD, of the Department of Obstetrics, Gynecology, and Reproductive Sciences at Moores Cancer Center, UC San Diego Health, University of California, expressed some methodological concerns. Although the authors attempted to control for key confounders, he noted, the dataset could not provide details on the medical management of endometriosis, such as oral contraceptives or gonadotropin-releasing hormone agonists. “Additionally, there is a possibility that women in the control cohort could have had undiagnosed endometriosis,” he wrote.
Furthermore, making clinical recommendations from these reported observations, particularly with respect to deep infiltrating endometriosis, would require a clear and consistent definition of this type in the dataset over the entire study interval from 1992 to 2019 and for the state of Utah, which the authors did not provide.
“Despite this potential challenge, the increased risk associated with deep infiltrating and/or ovarian endometriosis was clearly significant,” Dr. McHale wrote.
And although the absolute number of ovarian cancers is limited, in his view, the increased risk is sufficiently significant to advise women who have completed childbearing or have alternative fertility options to consider “more definitive surgery.”
This study was supported by multiple not-for-profit agencies, including the National Cancer Institute, the University of Utah, the National Center for Research Resources, the Utah Department of Health and Human Services, the Utah Cancer Registry, the US Centers for Disease Control and Prevention, the Huntsman Cancer Foundation, the National Institutes of Health, and Doris Duke Foundation. Dr. Barnard reported grants from the National Cancer Institute during the conduct of the study and personal fees from Epi Excellence LLC outside the submitted work. Other coauthors reported similar funding from nonprofit agencies or private research organizations. Dr Schliep disclosed no competing interests. Dr McHale reported educational consulting for Eisai Training outside the submitted work.
Ovarian cancer risk was higher in women with endometriosis overall and markedly increased in those with severe forms, a large population-based cohort study found.
The findings, published in JAMA, suggest these women may benefit from counseling on ovarian cancer risk and prevention and potentially from targeted screening, according to a group led by Mollie E. Barnard, ScD, of the Huntsman Cancer Institute at the University of Utah in Salt Lake City.
While the absolute increase in number of cases was small, endometriosis patients overall had a more than fourfold higher risk for any type of ovarian cancer. Those with more severe forms, such as ovarian endometriomas or deep infiltrating endometriosis, had a nearly 10-fold higher risk of any type of ovarian cancer. In addition, those with more severe endometriosis had a 19-fold higher risk of type 1 (slow-growing) ovarian cancer and almost three times the risk of the more aggressive type 2.
“Given the rarity of ovarian cancer, the excess risk was relatively small, with 10-20 additional cases per 10,000 women. Nevertheless, women with endometriosis, notably the more severe subtypes, may be an important population for targeted cancer screening and prevention studies,” said corresponding author Karen C. Schliep, PhD, MSPH, associate professor in the university’s Division of Public Health.
Prior studies have shown modest associations between endometriosis and ovarian cancer, Dr. Schliep said in an interview. A 2021 systematic review and meta-analysis found endometriosis conferred nearly double the risk of ovarian cancer, although associations varied by ovarian cancer histotype. Few studies have been large enough to assess associations between endometriosis types — including superficial or peritoneal endometriosis vs ovarian endometriomas or deep infiltrating endometriosis and ovarian cancer histotypes such as low-grade serous, endometrioid, clear cell, and mucinous carcinomas (type 1), and the most aggressive and lethal form, high-grade serous type 2, she said in an interview. “Our large health administrative database of over 11 million individuals with linked electronic health and cancer registry data allowed us to answer this as yet poorly studied research question.”
Study Details
Drawing on Utah electronic health records from 1992 to 2019, the investigators matched 78,893 women with endometriosis in a 1:5 ratio to unaffected women. Cases were categorized as superficial endometriosis, ovarian endometriomas, deep infiltrating endometriosis, or other, and the types of endometriosis were matched to ovarian cancer histotypes.
The mean age of patients at first endometriosis diagnosis was 36 and the mean follow-up was 12 years. Compared with controls, endometriosis patients were more likely to be nulliparous (31% vs 24%) and to have had a hysterectomy (39% vs 6%) during follow-up.
There were 596 reported cases of ovarian cancer in the cohort. Those with incident endometriosis were 4.2 times more likely to develop ovarian cancer (95% CI, 3.59-4.91), 7.48 times more likely to develop type 1 ovarian cancer (95% CI, 5.80-9.65), and 2.70 times more likely to develop type 2 ovarian cancer (95% CI, 2.09-3.49) compared with those without endometriosis.
The magnitudes of these associations varied by endometriosis subtype. Individuals diagnosed with deep infiltrating endometriosis and/or ovarian endometriomas had 9.66 times the risk of ovarian cancer vs individuals without endometriosis (95% CI, 7.77-12.00). “Women with, compared to without, more severe endometriosis had a 19-fold higher risk of type 1 ovarian cancer, including endometrioid, clear cell, mucinous, and low-grade serous,” Dr. Schliep said, with associated risk highest for malignant subtypes such as clear cell and endometrioid carcinoma (adjusted hazard ratios, 11.15 and 7.96, respectively.
According to Dr. Schliep, physicians should encourage endometriosis patients to be aware of but not worry about ovarian cancer risk because the likelihood of developing it remains low. For their part, patients can reduce their risk of cancer through a balanced diet with low intake of alcohol, regular exercise, a healthy weight, and abstention from smoking.
Her message for researchers is as follows: “We need more studies that explore how different types of endometriosis impact different types of ovarian cancer risk. These studies will guide improved ovarian cancer screening and prevention strategies among women with severe endometriosis, with or without other important ovarian cancer risk factors such as BRCA 1/2 variations.”
An accompanying editorial called the Utah study “eloquent” and noted its distinguishing contribution of observing associations between subtypes of endometriosis with overall risk for ovarian cancer as well as histologic subtypes of epithelial ovarian cancer.
Nevertheless, Michael T. McHale, MD, of the Department of Obstetrics, Gynecology, and Reproductive Sciences at Moores Cancer Center, UC San Diego Health, University of California, expressed some methodological concerns. Although the authors attempted to control for key confounders, he noted, the dataset could not provide details on the medical management of endometriosis, such as oral contraceptives or gonadotropin-releasing hormone agonists. “Additionally, there is a possibility that women in the control cohort could have had undiagnosed endometriosis,” he wrote.
Furthermore, making clinical recommendations from these reported observations, particularly with respect to deep infiltrating endometriosis, would require a clear and consistent definition of this type in the dataset over the entire study interval from 1992 to 2019 and for the state of Utah, which the authors did not provide.
“Despite this potential challenge, the increased risk associated with deep infiltrating and/or ovarian endometriosis was clearly significant,” Dr. McHale wrote.
And although the absolute number of ovarian cancers is limited, in his view, the increased risk is sufficiently significant to advise women who have completed childbearing or have alternative fertility options to consider “more definitive surgery.”
This study was supported by multiple not-for-profit agencies, including the National Cancer Institute, the University of Utah, the National Center for Research Resources, the Utah Department of Health and Human Services, the Utah Cancer Registry, the US Centers for Disease Control and Prevention, the Huntsman Cancer Foundation, the National Institutes of Health, and Doris Duke Foundation. Dr. Barnard reported grants from the National Cancer Institute during the conduct of the study and personal fees from Epi Excellence LLC outside the submitted work. Other coauthors reported similar funding from nonprofit agencies or private research organizations. Dr Schliep disclosed no competing interests. Dr McHale reported educational consulting for Eisai Training outside the submitted work.
Ovarian cancer risk was higher in women with endometriosis overall and markedly increased in those with severe forms, a large population-based cohort study found.
The findings, published in JAMA, suggest these women may benefit from counseling on ovarian cancer risk and prevention and potentially from targeted screening, according to a group led by Mollie E. Barnard, ScD, of the Huntsman Cancer Institute at the University of Utah in Salt Lake City.
While the absolute increase in number of cases was small, endometriosis patients overall had a more than fourfold higher risk for any type of ovarian cancer. Those with more severe forms, such as ovarian endometriomas or deep infiltrating endometriosis, had a nearly 10-fold higher risk of any type of ovarian cancer. In addition, those with more severe endometriosis had a 19-fold higher risk of type 1 (slow-growing) ovarian cancer and almost three times the risk of the more aggressive type 2.
“Given the rarity of ovarian cancer, the excess risk was relatively small, with 10-20 additional cases per 10,000 women. Nevertheless, women with endometriosis, notably the more severe subtypes, may be an important population for targeted cancer screening and prevention studies,” said corresponding author Karen C. Schliep, PhD, MSPH, associate professor in the university’s Division of Public Health.
Prior studies have shown modest associations between endometriosis and ovarian cancer, Dr. Schliep said in an interview. A 2021 systematic review and meta-analysis found endometriosis conferred nearly double the risk of ovarian cancer, although associations varied by ovarian cancer histotype. Few studies have been large enough to assess associations between endometriosis types — including superficial or peritoneal endometriosis vs ovarian endometriomas or deep infiltrating endometriosis and ovarian cancer histotypes such as low-grade serous, endometrioid, clear cell, and mucinous carcinomas (type 1), and the most aggressive and lethal form, high-grade serous type 2, she said in an interview. “Our large health administrative database of over 11 million individuals with linked electronic health and cancer registry data allowed us to answer this as yet poorly studied research question.”
Study Details
Drawing on Utah electronic health records from 1992 to 2019, the investigators matched 78,893 women with endometriosis in a 1:5 ratio to unaffected women. Cases were categorized as superficial endometriosis, ovarian endometriomas, deep infiltrating endometriosis, or other, and the types of endometriosis were matched to ovarian cancer histotypes.
The mean age of patients at first endometriosis diagnosis was 36 and the mean follow-up was 12 years. Compared with controls, endometriosis patients were more likely to be nulliparous (31% vs 24%) and to have had a hysterectomy (39% vs 6%) during follow-up.
There were 596 reported cases of ovarian cancer in the cohort. Those with incident endometriosis were 4.2 times more likely to develop ovarian cancer (95% CI, 3.59-4.91), 7.48 times more likely to develop type 1 ovarian cancer (95% CI, 5.80-9.65), and 2.70 times more likely to develop type 2 ovarian cancer (95% CI, 2.09-3.49) compared with those without endometriosis.
The magnitudes of these associations varied by endometriosis subtype. Individuals diagnosed with deep infiltrating endometriosis and/or ovarian endometriomas had 9.66 times the risk of ovarian cancer vs individuals without endometriosis (95% CI, 7.77-12.00). “Women with, compared to without, more severe endometriosis had a 19-fold higher risk of type 1 ovarian cancer, including endometrioid, clear cell, mucinous, and low-grade serous,” Dr. Schliep said, with associated risk highest for malignant subtypes such as clear cell and endometrioid carcinoma (adjusted hazard ratios, 11.15 and 7.96, respectively.
According to Dr. Schliep, physicians should encourage endometriosis patients to be aware of but not worry about ovarian cancer risk because the likelihood of developing it remains low. For their part, patients can reduce their risk of cancer through a balanced diet with low intake of alcohol, regular exercise, a healthy weight, and abstention from smoking.
Her message for researchers is as follows: “We need more studies that explore how different types of endometriosis impact different types of ovarian cancer risk. These studies will guide improved ovarian cancer screening and prevention strategies among women with severe endometriosis, with or without other important ovarian cancer risk factors such as BRCA 1/2 variations.”
An accompanying editorial called the Utah study “eloquent” and noted its distinguishing contribution of observing associations between subtypes of endometriosis with overall risk for ovarian cancer as well as histologic subtypes of epithelial ovarian cancer.
Nevertheless, Michael T. McHale, MD, of the Department of Obstetrics, Gynecology, and Reproductive Sciences at Moores Cancer Center, UC San Diego Health, University of California, expressed some methodological concerns. Although the authors attempted to control for key confounders, he noted, the dataset could not provide details on the medical management of endometriosis, such as oral contraceptives or gonadotropin-releasing hormone agonists. “Additionally, there is a possibility that women in the control cohort could have had undiagnosed endometriosis,” he wrote.
Furthermore, making clinical recommendations from these reported observations, particularly with respect to deep infiltrating endometriosis, would require a clear and consistent definition of this type in the dataset over the entire study interval from 1992 to 2019 and for the state of Utah, which the authors did not provide.
“Despite this potential challenge, the increased risk associated with deep infiltrating and/or ovarian endometriosis was clearly significant,” Dr. McHale wrote.
And although the absolute number of ovarian cancers is limited, in his view, the increased risk is sufficiently significant to advise women who have completed childbearing or have alternative fertility options to consider “more definitive surgery.”
This study was supported by multiple not-for-profit agencies, including the National Cancer Institute, the University of Utah, the National Center for Research Resources, the Utah Department of Health and Human Services, the Utah Cancer Registry, the US Centers for Disease Control and Prevention, the Huntsman Cancer Foundation, the National Institutes of Health, and Doris Duke Foundation. Dr. Barnard reported grants from the National Cancer Institute during the conduct of the study and personal fees from Epi Excellence LLC outside the submitted work. Other coauthors reported similar funding from nonprofit agencies or private research organizations. Dr Schliep disclosed no competing interests. Dr McHale reported educational consulting for Eisai Training outside the submitted work.
FROM JAMA
Meet the Pregnancy Challenges of Women With Chronic Conditions
Preconception and prenatal care are more complicated in women with chronic health conditions but attention to disease management and promoting the adoption of a healthier lifestyle can improve outcomes for mothers and infants, according to a growing body of research.
The latest version of the International Federation of Gynecology and Obstetrics Preconception Checklist, published in the International Journal of Gynecology & Obstetrics, highlights preexisting chronic medical conditions such as diabetes, lupus, and obesity as key factors to address in preconception care through disease management. A growing number of studies support the impact of these strategies on short- and long-term outcomes for mothers and babies, according to the authors.
Meet Glycemic Control Goals Prior to Pregnancy
“Women with diabetes can have healthy pregnancies but need to prepare for pregnancy in advance,” Ellen W. Seely, MD, professor of medicine at Harvard Medical School and director of clinical research in the endocrinology, diabetes, and hypertension division of Brigham and Women’s Hospital, Boston, said in an interview.
“If glucose levels are running high in the first trimester, this is associated with an increased risk of birth defects, some of which are very serious,” said Dr. Seely. Getting glucose levels under control reduces the risk of birth defects in women with diabetes close to that of the general population, she said.
The American Diabetes Association has set a goal for women to attain an HbA1c of less than 6.5% before conception, Dr. Seely said. “In addition, some women with diabetes may be on medications that should be changed to another class prior to pregnancy,” she noted. Women with type 1 or type 2 diabetes often have hypertension as well, but ACE inhibitors are associated with an increased risk of fetal renal damage that can result in neonatal death; therefore, these medications should be stopped prior to pregnancy, Dr. Seely emphasized.
“If a woman with type 2 diabetes is on medications other than insulin, recommendations from the ADA are to change to insulin prior to pregnancy, since we have the most data on the safety profile of insulin use in pregnancy,” she said.
To help women with diabetes improve glycemic control prior to pregnancy, Dr. Seely recommends home glucose monitoring, with checks of glucose four times a day, fasting, and 2 hours after each meal, and adjustment of insulin accordingly.
A healthy diet and physical activity remain important components of glycemic control as well. A barrier to proper preconception and prenatal care for women with diabetes is not knowing that a pregnancy should be planned, Dr. Seely said. Discussions about pregnancy should start at puberty for women with diabetes, according to the ADA, and the topic should be raised yearly so women can optimize their health and adjust medications prior to conception.
Although studies of drugs have been done to inform preconception care for women with diabetes, research is lacking in several areas, notably the safety of GLP-1 agonists in pregnancy, said Dr. Seely. “This class of drug is commonly used in type 2 diabetes and the current recommendation is to stop these agents 2 months prior to conception,” she said.
Conceive in Times of Lupus Remission
Advance planning also is important for a healthy pregnancy in women with systemic lupus erythematosus (SLE), Sayna Norouzi, MD, director of the glomerular disease clinic and polycystic kidney disease clinic of Loma Linda University Medical Center, California, said in an interview.
“Lupus mostly affects women of childbearing age and can create many challenges during pregnancy,” said Dr. Norouzi, the corresponding author of a recent review on managing lupus nephritis during pregnancy.
“Women with lupus face an increased risk of pregnancy complications such as preeclampsia, problems with fetal growth, stillbirth, and premature birth, and these risks increase based on factors such as disease activity, certain antibodies in the body, and other baseline existing conditions such as high blood pressure,” she said.
“It can be difficult to distinguish between a lupus flare and pregnancy-related issues, so proper management is important,” she noted. The Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Syndrome and Systemic Lupus Erythematosus (PROMISSE) study findings indicated a lupus nephritis relapse rate of 7.8% of patients in complete remission and 21% of those in partial remission during pregnancy, said Dr. Norouzi. “Current evidence has shown that SLE patients without lupus nephritis flare in the preconception period have a small risk of relapse during pregnancy,” she said.
Before and during pregnancy, women with lupus should work with their treating physicians to adjust medications for safety, watch for signs of flare, and aim to conceive during a period of lupus remission.
Preconception care for women with lupus nephritis involves a careful review of the medications used to control the disease and protect the kidneys and other organs, said Dr. Norouzi.
“Adjustments,” she said, “should be personalized, taking into account the mother’s health and the safety of the baby. Managing the disease actively during pregnancy may require changes to the treatment plan while minimizing risks,” she noted. However, changing medications can cause challenges for patients, as medications that are safer for pregnancy may lead to new symptoms and side effects, and patients will need to work closely with their healthcare providers to overcome new issues that arise, she added.
Preconception lifestyle changes such as increasing exercise and adopting a healthier diet can help with blood pressure control for kidney disease patients, said Dr. Norouzi.
In the review article, Dr. Norouzi and colleagues noted that preconception counseling for patients with lupus should address common comorbidities such as hypertension, diabetes, obesity, and dyslipidemia, and the risk for immediate and long-term cardiovascular complications.
Benefits of Preconception Obesity Care Extend to Infants
Current guidelines from the American College of Obstetricians and Gynecologists and the Institute of Medicine advise lifestyle interventions to reduce excessive weight gain during pregnancy and reduce the risk of inflammation, oxidative stress, insulin resistance, and lipotoxicity that can promote complications in the mother and fetus during pregnancy.
In addition, a growing number of studies suggest that women with obesity who make healthy lifestyle changes prior to conception can reduce obesity-associated risks to their infants.
Adults born to women with obesity are at increased risk of cardiovascular disease and early signs of heart remodeling are identifiable in newborns, Samuel J. Burden, PhD, a research associate in the department of women and children’s health, Kings’ College, London, said in an interview. “It is therefore important to investigate whether intervening either before or during pregnancy by promoting a healthy lifestyle can reduce this adverse impact on the heart and blood vessels,” he said.
In a recent study published in the International Journal of Obesity, Dr. Burden and colleagues examined data from eight studies based on data from five randomized, controlled trials including children of mothers with obesity who engaged in healthy lifestyle interventions of improved diet and increased physical activity prior to and during pregnancy. The study population included children ranging in age from less than 2 months to 3-7 years.
Lifestyle interventions for mothers both before conception and during pregnancy were associated with significant changes in cardiac remodeling in the children, notably reduced interventricular septal wall thickness. Additionally, five studies of cardiac systolic function and three studies of diastolic function showed improvement in blood pressure in children of mothers who took part in the interventions.
Dr. Burden acknowledged that lifestyle changes in women with obesity before conception and during pregnancy can be challenging, but should be encouraged. “During pregnancy, it may also seem unnatural to increase daily physical activity or change the way you are eating.” He emphasized that patients should consult their physicians and follow an established program. More randomized, controlled trials are needed from the preconception period to examine whether the health benefits are greater if the intervention begins prior to pregnancy, said Dr. Burden. However, “the current findings indeed indicate that women with obesity who lead a healthy lifestyle before and during their pregnancy can reduce the degree of unhealthy heart remodeling in their children,” he said.
Dr. Seely, Dr. Norouzi, and Dr. Burden had no financial conflicts to disclose.
Preconception and prenatal care are more complicated in women with chronic health conditions but attention to disease management and promoting the adoption of a healthier lifestyle can improve outcomes for mothers and infants, according to a growing body of research.
The latest version of the International Federation of Gynecology and Obstetrics Preconception Checklist, published in the International Journal of Gynecology & Obstetrics, highlights preexisting chronic medical conditions such as diabetes, lupus, and obesity as key factors to address in preconception care through disease management. A growing number of studies support the impact of these strategies on short- and long-term outcomes for mothers and babies, according to the authors.
Meet Glycemic Control Goals Prior to Pregnancy
“Women with diabetes can have healthy pregnancies but need to prepare for pregnancy in advance,” Ellen W. Seely, MD, professor of medicine at Harvard Medical School and director of clinical research in the endocrinology, diabetes, and hypertension division of Brigham and Women’s Hospital, Boston, said in an interview.
“If glucose levels are running high in the first trimester, this is associated with an increased risk of birth defects, some of which are very serious,” said Dr. Seely. Getting glucose levels under control reduces the risk of birth defects in women with diabetes close to that of the general population, she said.
The American Diabetes Association has set a goal for women to attain an HbA1c of less than 6.5% before conception, Dr. Seely said. “In addition, some women with diabetes may be on medications that should be changed to another class prior to pregnancy,” she noted. Women with type 1 or type 2 diabetes often have hypertension as well, but ACE inhibitors are associated with an increased risk of fetal renal damage that can result in neonatal death; therefore, these medications should be stopped prior to pregnancy, Dr. Seely emphasized.
“If a woman with type 2 diabetes is on medications other than insulin, recommendations from the ADA are to change to insulin prior to pregnancy, since we have the most data on the safety profile of insulin use in pregnancy,” she said.
To help women with diabetes improve glycemic control prior to pregnancy, Dr. Seely recommends home glucose monitoring, with checks of glucose four times a day, fasting, and 2 hours after each meal, and adjustment of insulin accordingly.
A healthy diet and physical activity remain important components of glycemic control as well. A barrier to proper preconception and prenatal care for women with diabetes is not knowing that a pregnancy should be planned, Dr. Seely said. Discussions about pregnancy should start at puberty for women with diabetes, according to the ADA, and the topic should be raised yearly so women can optimize their health and adjust medications prior to conception.
Although studies of drugs have been done to inform preconception care for women with diabetes, research is lacking in several areas, notably the safety of GLP-1 agonists in pregnancy, said Dr. Seely. “This class of drug is commonly used in type 2 diabetes and the current recommendation is to stop these agents 2 months prior to conception,” she said.
Conceive in Times of Lupus Remission
Advance planning also is important for a healthy pregnancy in women with systemic lupus erythematosus (SLE), Sayna Norouzi, MD, director of the glomerular disease clinic and polycystic kidney disease clinic of Loma Linda University Medical Center, California, said in an interview.
“Lupus mostly affects women of childbearing age and can create many challenges during pregnancy,” said Dr. Norouzi, the corresponding author of a recent review on managing lupus nephritis during pregnancy.
“Women with lupus face an increased risk of pregnancy complications such as preeclampsia, problems with fetal growth, stillbirth, and premature birth, and these risks increase based on factors such as disease activity, certain antibodies in the body, and other baseline existing conditions such as high blood pressure,” she said.
“It can be difficult to distinguish between a lupus flare and pregnancy-related issues, so proper management is important,” she noted. The Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Syndrome and Systemic Lupus Erythematosus (PROMISSE) study findings indicated a lupus nephritis relapse rate of 7.8% of patients in complete remission and 21% of those in partial remission during pregnancy, said Dr. Norouzi. “Current evidence has shown that SLE patients without lupus nephritis flare in the preconception period have a small risk of relapse during pregnancy,” she said.
Before and during pregnancy, women with lupus should work with their treating physicians to adjust medications for safety, watch for signs of flare, and aim to conceive during a period of lupus remission.
Preconception care for women with lupus nephritis involves a careful review of the medications used to control the disease and protect the kidneys and other organs, said Dr. Norouzi.
“Adjustments,” she said, “should be personalized, taking into account the mother’s health and the safety of the baby. Managing the disease actively during pregnancy may require changes to the treatment plan while minimizing risks,” she noted. However, changing medications can cause challenges for patients, as medications that are safer for pregnancy may lead to new symptoms and side effects, and patients will need to work closely with their healthcare providers to overcome new issues that arise, she added.
Preconception lifestyle changes such as increasing exercise and adopting a healthier diet can help with blood pressure control for kidney disease patients, said Dr. Norouzi.
In the review article, Dr. Norouzi and colleagues noted that preconception counseling for patients with lupus should address common comorbidities such as hypertension, diabetes, obesity, and dyslipidemia, and the risk for immediate and long-term cardiovascular complications.
Benefits of Preconception Obesity Care Extend to Infants
Current guidelines from the American College of Obstetricians and Gynecologists and the Institute of Medicine advise lifestyle interventions to reduce excessive weight gain during pregnancy and reduce the risk of inflammation, oxidative stress, insulin resistance, and lipotoxicity that can promote complications in the mother and fetus during pregnancy.
In addition, a growing number of studies suggest that women with obesity who make healthy lifestyle changes prior to conception can reduce obesity-associated risks to their infants.
Adults born to women with obesity are at increased risk of cardiovascular disease and early signs of heart remodeling are identifiable in newborns, Samuel J. Burden, PhD, a research associate in the department of women and children’s health, Kings’ College, London, said in an interview. “It is therefore important to investigate whether intervening either before or during pregnancy by promoting a healthy lifestyle can reduce this adverse impact on the heart and blood vessels,” he said.
In a recent study published in the International Journal of Obesity, Dr. Burden and colleagues examined data from eight studies based on data from five randomized, controlled trials including children of mothers with obesity who engaged in healthy lifestyle interventions of improved diet and increased physical activity prior to and during pregnancy. The study population included children ranging in age from less than 2 months to 3-7 years.
Lifestyle interventions for mothers both before conception and during pregnancy were associated with significant changes in cardiac remodeling in the children, notably reduced interventricular septal wall thickness. Additionally, five studies of cardiac systolic function and three studies of diastolic function showed improvement in blood pressure in children of mothers who took part in the interventions.
Dr. Burden acknowledged that lifestyle changes in women with obesity before conception and during pregnancy can be challenging, but should be encouraged. “During pregnancy, it may also seem unnatural to increase daily physical activity or change the way you are eating.” He emphasized that patients should consult their physicians and follow an established program. More randomized, controlled trials are needed from the preconception period to examine whether the health benefits are greater if the intervention begins prior to pregnancy, said Dr. Burden. However, “the current findings indeed indicate that women with obesity who lead a healthy lifestyle before and during their pregnancy can reduce the degree of unhealthy heart remodeling in their children,” he said.
Dr. Seely, Dr. Norouzi, and Dr. Burden had no financial conflicts to disclose.
Preconception and prenatal care are more complicated in women with chronic health conditions but attention to disease management and promoting the adoption of a healthier lifestyle can improve outcomes for mothers and infants, according to a growing body of research.
The latest version of the International Federation of Gynecology and Obstetrics Preconception Checklist, published in the International Journal of Gynecology & Obstetrics, highlights preexisting chronic medical conditions such as diabetes, lupus, and obesity as key factors to address in preconception care through disease management. A growing number of studies support the impact of these strategies on short- and long-term outcomes for mothers and babies, according to the authors.
Meet Glycemic Control Goals Prior to Pregnancy
“Women with diabetes can have healthy pregnancies but need to prepare for pregnancy in advance,” Ellen W. Seely, MD, professor of medicine at Harvard Medical School and director of clinical research in the endocrinology, diabetes, and hypertension division of Brigham and Women’s Hospital, Boston, said in an interview.
“If glucose levels are running high in the first trimester, this is associated with an increased risk of birth defects, some of which are very serious,” said Dr. Seely. Getting glucose levels under control reduces the risk of birth defects in women with diabetes close to that of the general population, she said.
The American Diabetes Association has set a goal for women to attain an HbA1c of less than 6.5% before conception, Dr. Seely said. “In addition, some women with diabetes may be on medications that should be changed to another class prior to pregnancy,” she noted. Women with type 1 or type 2 diabetes often have hypertension as well, but ACE inhibitors are associated with an increased risk of fetal renal damage that can result in neonatal death; therefore, these medications should be stopped prior to pregnancy, Dr. Seely emphasized.
“If a woman with type 2 diabetes is on medications other than insulin, recommendations from the ADA are to change to insulin prior to pregnancy, since we have the most data on the safety profile of insulin use in pregnancy,” she said.
To help women with diabetes improve glycemic control prior to pregnancy, Dr. Seely recommends home glucose monitoring, with checks of glucose four times a day, fasting, and 2 hours after each meal, and adjustment of insulin accordingly.
A healthy diet and physical activity remain important components of glycemic control as well. A barrier to proper preconception and prenatal care for women with diabetes is not knowing that a pregnancy should be planned, Dr. Seely said. Discussions about pregnancy should start at puberty for women with diabetes, according to the ADA, and the topic should be raised yearly so women can optimize their health and adjust medications prior to conception.
Although studies of drugs have been done to inform preconception care for women with diabetes, research is lacking in several areas, notably the safety of GLP-1 agonists in pregnancy, said Dr. Seely. “This class of drug is commonly used in type 2 diabetes and the current recommendation is to stop these agents 2 months prior to conception,” she said.
Conceive in Times of Lupus Remission
Advance planning also is important for a healthy pregnancy in women with systemic lupus erythematosus (SLE), Sayna Norouzi, MD, director of the glomerular disease clinic and polycystic kidney disease clinic of Loma Linda University Medical Center, California, said in an interview.
“Lupus mostly affects women of childbearing age and can create many challenges during pregnancy,” said Dr. Norouzi, the corresponding author of a recent review on managing lupus nephritis during pregnancy.
“Women with lupus face an increased risk of pregnancy complications such as preeclampsia, problems with fetal growth, stillbirth, and premature birth, and these risks increase based on factors such as disease activity, certain antibodies in the body, and other baseline existing conditions such as high blood pressure,” she said.
“It can be difficult to distinguish between a lupus flare and pregnancy-related issues, so proper management is important,” she noted. The Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Syndrome and Systemic Lupus Erythematosus (PROMISSE) study findings indicated a lupus nephritis relapse rate of 7.8% of patients in complete remission and 21% of those in partial remission during pregnancy, said Dr. Norouzi. “Current evidence has shown that SLE patients without lupus nephritis flare in the preconception period have a small risk of relapse during pregnancy,” she said.
Before and during pregnancy, women with lupus should work with their treating physicians to adjust medications for safety, watch for signs of flare, and aim to conceive during a period of lupus remission.
Preconception care for women with lupus nephritis involves a careful review of the medications used to control the disease and protect the kidneys and other organs, said Dr. Norouzi.
“Adjustments,” she said, “should be personalized, taking into account the mother’s health and the safety of the baby. Managing the disease actively during pregnancy may require changes to the treatment plan while minimizing risks,” she noted. However, changing medications can cause challenges for patients, as medications that are safer for pregnancy may lead to new symptoms and side effects, and patients will need to work closely with their healthcare providers to overcome new issues that arise, she added.
Preconception lifestyle changes such as increasing exercise and adopting a healthier diet can help with blood pressure control for kidney disease patients, said Dr. Norouzi.
In the review article, Dr. Norouzi and colleagues noted that preconception counseling for patients with lupus should address common comorbidities such as hypertension, diabetes, obesity, and dyslipidemia, and the risk for immediate and long-term cardiovascular complications.
Benefits of Preconception Obesity Care Extend to Infants
Current guidelines from the American College of Obstetricians and Gynecologists and the Institute of Medicine advise lifestyle interventions to reduce excessive weight gain during pregnancy and reduce the risk of inflammation, oxidative stress, insulin resistance, and lipotoxicity that can promote complications in the mother and fetus during pregnancy.
In addition, a growing number of studies suggest that women with obesity who make healthy lifestyle changes prior to conception can reduce obesity-associated risks to their infants.
Adults born to women with obesity are at increased risk of cardiovascular disease and early signs of heart remodeling are identifiable in newborns, Samuel J. Burden, PhD, a research associate in the department of women and children’s health, Kings’ College, London, said in an interview. “It is therefore important to investigate whether intervening either before or during pregnancy by promoting a healthy lifestyle can reduce this adverse impact on the heart and blood vessels,” he said.
In a recent study published in the International Journal of Obesity, Dr. Burden and colleagues examined data from eight studies based on data from five randomized, controlled trials including children of mothers with obesity who engaged in healthy lifestyle interventions of improved diet and increased physical activity prior to and during pregnancy. The study population included children ranging in age from less than 2 months to 3-7 years.
Lifestyle interventions for mothers both before conception and during pregnancy were associated with significant changes in cardiac remodeling in the children, notably reduced interventricular septal wall thickness. Additionally, five studies of cardiac systolic function and three studies of diastolic function showed improvement in blood pressure in children of mothers who took part in the interventions.
Dr. Burden acknowledged that lifestyle changes in women with obesity before conception and during pregnancy can be challenging, but should be encouraged. “During pregnancy, it may also seem unnatural to increase daily physical activity or change the way you are eating.” He emphasized that patients should consult their physicians and follow an established program. More randomized, controlled trials are needed from the preconception period to examine whether the health benefits are greater if the intervention begins prior to pregnancy, said Dr. Burden. However, “the current findings indeed indicate that women with obesity who lead a healthy lifestyle before and during their pregnancy can reduce the degree of unhealthy heart remodeling in their children,” he said.
Dr. Seely, Dr. Norouzi, and Dr. Burden had no financial conflicts to disclose.
Few Women Know Uterine Fibroid Risk, Treatment Options
Most women (72%) are not aware they are at risk for developing uterine fibroids, though up to 77% of women will develop them in their lifetime, results of a new survey indicate.
Data from The Harris Poll, conducted on behalf of the Society of Interventional Radiology, also found that 17% of women mistakenly think a hysterectomy is the only treatment option, including more than one in four women (27%) who are between the ages of 18 and 34. Results were shared in a press release. The survey included 1,122 US women, some who have been diagnosed with uterine fibroids.
Fibroids may not cause symptoms for some, but some women may have heavy, prolonged, debilitating bleeding. Some women experience pelvic pain, a diminished sex life, and declining energy. However, the growths do not spread to other body regions and typically are not dangerous.
Hysterectomy Is Only One Option
Among the women in the survey who had been diagnosed with fibroids, 53% were presented the option of hysterectomy and 20% were told about other, less-invasive options, including over-the-counter NSAIDs (19%); uterine fibroid embolization (UFE) (17%); oral contraceptives (17%); and endometrial ablation (17%).
“Women need to be informed about the complete range of options available for treating their uterine fibroids, not just the surgical options as is most commonly done by gynecologists,” John C. Lipman, MD, founder and medical director of the Atlanta Fibroid Center in Smyrna, Georgia, said in the press release.
The survey also found that:
- More than half of women ages 18-34 (56%) and women ages 35-44 (51%) were either not familiar with uterine fibroids or never heard of them.
- Awareness was particularly low among Hispanic women, as 50% of Hispanic women say they’ve never heard of or aren’t familiar with the condition, compared with 37% of Black women who answered that way.
- More than one third (36%) of Black women and 22% of Hispanic women mistakenly think they are not at risk for developing fibroids, yet research has shown that uterine fibroids are three times more common in Black women and two times more common in Hispanic women than in White women.
For this study, the full sample data is accurate to within +/– 3.2 percentage points using a 95% confidence level. The data are part of the report “The Fibroid Fix: What Women Need to Know,” published on July 9 by the Society of Interventional Radiology.
Linda Fan, MD, chief of gynecology at Yale University in New Haven, Connecticut, said she is not surprised by those numbers. She says many patients are referred to her department who have not been given the full array of medical options for their fibroids or have not had thorough discussions with their providers, such as whether they want to preserve their fertility, or how they feel about an incision, undergoing anesthesia, or having their uterus removed.
Sometimes the hysterectomy choice is clear, she said — for instance, if there are indications of the rare cancer leiomyosarcoma, or if a postmenopausal woman has rapid growth of fibroids or heavy bleeding. Fibroids should not start growing after menopause, she said.
Additional options include radiofrequency ablation, performed while a patient is under anesthesia, by laparoscopy or hysteroscopy. The procedure uses ultrasound to watch a probe as it shrinks the fibroids with heat.
Currently, if a woman wants large fibroids removed and wants to keep her fertility options open, Dr. Fan says, myomectomy or medication are best “because we have the most information or data on (those options).”
When treating patients who don’t prioritize fertility, she said, UFE is a good option that doesn’t need incisions or anesthesia. But patients sometimes require a lot of pain medication afterward, Dr. Fan said. With radiofrequency ablation, specifically the Acessa and Sonata procedures, she said, “patients don’t experience a lot of pain after the procedure because the shrinking happens when they’re asleep under anesthesia.”
Uterine Fibroid Embolization a Nonsurgical Option
The report describes how UFE works but the Harris Poll showed that 60% of women who have heard of UFE did not hear about it first from a healthcare provider.
“UFE is a nonsurgical treatment, performed by interventional radiologists, that has been proven to significantly reduce heavy menstrual bleeding, relieve uterine pain, and improve energy levels,” the authors write. “Through a tiny incision in the wrist or thigh, a catheter is guided via imaging to the vessels leading to the fibroids. Through this catheter, small clear particles are injected to block the blood flow leading to the fibroids causing them to shrink and disappear.”
After UFE, most women leave the hospital the day of or the day after treatment, according to the report authors, who add that many patients also report they can resume normal activity in about 2 weeks, more quickly than with surgical treatments.
In some cases, watchful waiting will be the best option, the report notes, and that may require repeated checkups and scans.
Dr. Lipman is an adviser on The Fibroid Fix report.
Most women (72%) are not aware they are at risk for developing uterine fibroids, though up to 77% of women will develop them in their lifetime, results of a new survey indicate.
Data from The Harris Poll, conducted on behalf of the Society of Interventional Radiology, also found that 17% of women mistakenly think a hysterectomy is the only treatment option, including more than one in four women (27%) who are between the ages of 18 and 34. Results were shared in a press release. The survey included 1,122 US women, some who have been diagnosed with uterine fibroids.
Fibroids may not cause symptoms for some, but some women may have heavy, prolonged, debilitating bleeding. Some women experience pelvic pain, a diminished sex life, and declining energy. However, the growths do not spread to other body regions and typically are not dangerous.
Hysterectomy Is Only One Option
Among the women in the survey who had been diagnosed with fibroids, 53% were presented the option of hysterectomy and 20% were told about other, less-invasive options, including over-the-counter NSAIDs (19%); uterine fibroid embolization (UFE) (17%); oral contraceptives (17%); and endometrial ablation (17%).
“Women need to be informed about the complete range of options available for treating their uterine fibroids, not just the surgical options as is most commonly done by gynecologists,” John C. Lipman, MD, founder and medical director of the Atlanta Fibroid Center in Smyrna, Georgia, said in the press release.
The survey also found that:
- More than half of women ages 18-34 (56%) and women ages 35-44 (51%) were either not familiar with uterine fibroids or never heard of them.
- Awareness was particularly low among Hispanic women, as 50% of Hispanic women say they’ve never heard of or aren’t familiar with the condition, compared with 37% of Black women who answered that way.
- More than one third (36%) of Black women and 22% of Hispanic women mistakenly think they are not at risk for developing fibroids, yet research has shown that uterine fibroids are three times more common in Black women and two times more common in Hispanic women than in White women.
For this study, the full sample data is accurate to within +/– 3.2 percentage points using a 95% confidence level. The data are part of the report “The Fibroid Fix: What Women Need to Know,” published on July 9 by the Society of Interventional Radiology.
Linda Fan, MD, chief of gynecology at Yale University in New Haven, Connecticut, said she is not surprised by those numbers. She says many patients are referred to her department who have not been given the full array of medical options for their fibroids or have not had thorough discussions with their providers, such as whether they want to preserve their fertility, or how they feel about an incision, undergoing anesthesia, or having their uterus removed.
Sometimes the hysterectomy choice is clear, she said — for instance, if there are indications of the rare cancer leiomyosarcoma, or if a postmenopausal woman has rapid growth of fibroids or heavy bleeding. Fibroids should not start growing after menopause, she said.
Additional options include radiofrequency ablation, performed while a patient is under anesthesia, by laparoscopy or hysteroscopy. The procedure uses ultrasound to watch a probe as it shrinks the fibroids with heat.
Currently, if a woman wants large fibroids removed and wants to keep her fertility options open, Dr. Fan says, myomectomy or medication are best “because we have the most information or data on (those options).”
When treating patients who don’t prioritize fertility, she said, UFE is a good option that doesn’t need incisions or anesthesia. But patients sometimes require a lot of pain medication afterward, Dr. Fan said. With radiofrequency ablation, specifically the Acessa and Sonata procedures, she said, “patients don’t experience a lot of pain after the procedure because the shrinking happens when they’re asleep under anesthesia.”
Uterine Fibroid Embolization a Nonsurgical Option
The report describes how UFE works but the Harris Poll showed that 60% of women who have heard of UFE did not hear about it first from a healthcare provider.
“UFE is a nonsurgical treatment, performed by interventional radiologists, that has been proven to significantly reduce heavy menstrual bleeding, relieve uterine pain, and improve energy levels,” the authors write. “Through a tiny incision in the wrist or thigh, a catheter is guided via imaging to the vessels leading to the fibroids. Through this catheter, small clear particles are injected to block the blood flow leading to the fibroids causing them to shrink and disappear.”
After UFE, most women leave the hospital the day of or the day after treatment, according to the report authors, who add that many patients also report they can resume normal activity in about 2 weeks, more quickly than with surgical treatments.
In some cases, watchful waiting will be the best option, the report notes, and that may require repeated checkups and scans.
Dr. Lipman is an adviser on The Fibroid Fix report.
Most women (72%) are not aware they are at risk for developing uterine fibroids, though up to 77% of women will develop them in their lifetime, results of a new survey indicate.
Data from The Harris Poll, conducted on behalf of the Society of Interventional Radiology, also found that 17% of women mistakenly think a hysterectomy is the only treatment option, including more than one in four women (27%) who are between the ages of 18 and 34. Results were shared in a press release. The survey included 1,122 US women, some who have been diagnosed with uterine fibroids.
Fibroids may not cause symptoms for some, but some women may have heavy, prolonged, debilitating bleeding. Some women experience pelvic pain, a diminished sex life, and declining energy. However, the growths do not spread to other body regions and typically are not dangerous.
Hysterectomy Is Only One Option
Among the women in the survey who had been diagnosed with fibroids, 53% were presented the option of hysterectomy and 20% were told about other, less-invasive options, including over-the-counter NSAIDs (19%); uterine fibroid embolization (UFE) (17%); oral contraceptives (17%); and endometrial ablation (17%).
“Women need to be informed about the complete range of options available for treating their uterine fibroids, not just the surgical options as is most commonly done by gynecologists,” John C. Lipman, MD, founder and medical director of the Atlanta Fibroid Center in Smyrna, Georgia, said in the press release.
The survey also found that:
- More than half of women ages 18-34 (56%) and women ages 35-44 (51%) were either not familiar with uterine fibroids or never heard of them.
- Awareness was particularly low among Hispanic women, as 50% of Hispanic women say they’ve never heard of or aren’t familiar with the condition, compared with 37% of Black women who answered that way.
- More than one third (36%) of Black women and 22% of Hispanic women mistakenly think they are not at risk for developing fibroids, yet research has shown that uterine fibroids are three times more common in Black women and two times more common in Hispanic women than in White women.
For this study, the full sample data is accurate to within +/– 3.2 percentage points using a 95% confidence level. The data are part of the report “The Fibroid Fix: What Women Need to Know,” published on July 9 by the Society of Interventional Radiology.
Linda Fan, MD, chief of gynecology at Yale University in New Haven, Connecticut, said she is not surprised by those numbers. She says many patients are referred to her department who have not been given the full array of medical options for their fibroids or have not had thorough discussions with their providers, such as whether they want to preserve their fertility, or how they feel about an incision, undergoing anesthesia, or having their uterus removed.
Sometimes the hysterectomy choice is clear, she said — for instance, if there are indications of the rare cancer leiomyosarcoma, or if a postmenopausal woman has rapid growth of fibroids or heavy bleeding. Fibroids should not start growing after menopause, she said.
Additional options include radiofrequency ablation, performed while a patient is under anesthesia, by laparoscopy or hysteroscopy. The procedure uses ultrasound to watch a probe as it shrinks the fibroids with heat.
Currently, if a woman wants large fibroids removed and wants to keep her fertility options open, Dr. Fan says, myomectomy or medication are best “because we have the most information or data on (those options).”
When treating patients who don’t prioritize fertility, she said, UFE is a good option that doesn’t need incisions or anesthesia. But patients sometimes require a lot of pain medication afterward, Dr. Fan said. With radiofrequency ablation, specifically the Acessa and Sonata procedures, she said, “patients don’t experience a lot of pain after the procedure because the shrinking happens when they’re asleep under anesthesia.”
Uterine Fibroid Embolization a Nonsurgical Option
The report describes how UFE works but the Harris Poll showed that 60% of women who have heard of UFE did not hear about it first from a healthcare provider.
“UFE is a nonsurgical treatment, performed by interventional radiologists, that has been proven to significantly reduce heavy menstrual bleeding, relieve uterine pain, and improve energy levels,” the authors write. “Through a tiny incision in the wrist or thigh, a catheter is guided via imaging to the vessels leading to the fibroids. Through this catheter, small clear particles are injected to block the blood flow leading to the fibroids causing them to shrink and disappear.”
After UFE, most women leave the hospital the day of or the day after treatment, according to the report authors, who add that many patients also report they can resume normal activity in about 2 weeks, more quickly than with surgical treatments.
In some cases, watchful waiting will be the best option, the report notes, and that may require repeated checkups and scans.
Dr. Lipman is an adviser on The Fibroid Fix report.
Managing Cancer in Pregnancy: Improvements and Considerations
Introduction: Tremendous Progress on Cancer Extends to Cancer in Pregnancy
The biomedical research enterprise that took shape in the United States after World War II has had numerous positive effects, including significant progress made during the past 75-plus years in the diagnosis, prevention, and treatment of cancer.
President Franklin D. Roosevelt’s 1944 request of Dr. Vannevar Bush, director of the then Office of Scientific Research and Development, to organize a program that would advance and apply scientific knowledge for times of peace — just as it been advanced and applied in times of war — culminated in a historic report, Science – The Endless Frontier. Presented in 1945 to President Harry S. Truman, this report helped fuel decades of broad, bold, and coordinated government-sponsored biomedical research aimed at addressing disease and improving the health of the American people (National Science Foundation, 1945).
Discoveries made from research in basic and translational sciences deepened our knowledge of the cellular and molecular underpinnings of cancer, leading to advances in chemotherapy, radiotherapy, and other treatment approaches as well as continual refinements in their application. Similarly, our diagnostic armamentarium has significantly improved.

As a result, we have reduced both the incidence and mortality of cancer. Today, some cancers can be prevented. Others can be reversed or put in remission. Granted, progress has been variable, with some cancers such as ovarian cancer still having relatively low survival rates. Much more needs to be done. Overall, however, the positive effects of the U.S. biomedical research enterprise on cancer are evident. According to the National Cancer Institute’s most recent report on the status of cancer, death rates from cancer fell 1.9% per year on average in females from 2015 to 2019 (Cancer. 2022 Oct 22. doi: 10.1002/cncr.34479).
It is not only patients whose cancer occurs outside of pregnancy who have benefited. When treatment is appropriately selected and timing considerations are made, patients whose cancer is diagnosed during pregnancy — and their children — can have good outcomes.
To explain how the management of cancer in pregnancy has improved, we have invited Gautam G. Rao, MD, gynecologic oncologist and associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, to write this installment of the Master Class in Obstetrics. As Dr. Rao explains, radiation is not as dangerous to the fetus as once thought, and the safety of many chemotherapeutic regimens in pregnancy has been documented. Obstetricians can and should counsel patients, he explains, about the likelihood of good maternal and fetal outcomes.
E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Managing Cancer in Pregnancy
Cancer can cause fear and distress for any patient, but when cancer is diagnosed during pregnancy, an expectant mother fears not only for her own health but for the health of her unborn child. Fortunately, ob.gyn.s and multidisciplinary teams have good reason to reassure patients about the likelihood of good outcomes.
Cancer treatment in pregnancy has improved with advancements in imaging and chemotherapy, and while maternal and fetal outcomes of prenatal cancer treatment are not well reported, evidence acquired in recent years from case series and retrospective studies shows that most imaging studies and procedural diagnostic tests – and many treatments – can be performed safely in pregnancy.

Decades ago, we avoided CT scans during pregnancy because of concerns about radiation exposure to the fetus, leaving some patients without an accurate staging of their cancer. Today, we have evidence that a CT scan is generally safe in pregnancy. Similarly, the safety of many chemotherapeutic regimens in pregnancy has been documented in recent decades,and the use of chemotherapy during pregnancy has increased progressively. Radiation is also commonly utilized in the management of cancers that may occur during pregnancy, such as breast cancer.1
Considerations of timing are often central to decision-making; chemotherapy and radiotherapy are generally avoided in the first trimester to prevent structural fetal anomalies, for instance, and delaying cancer treatment is often warranted when the patient is a few weeks away from delivery. On occasion, iatrogenic preterm birth is considered when the risks to the mother of delaying a necessary cancer treatment outweigh the risks to the fetus of prematurity.1
Pregnancy termination is rarely indicated, however, and information gathered over the past 2 decades suggests that fetal and placental metastases are rare.1 There is broad agreement that prenatal treatment of cancer in pregnancy should adhere as much as possible to protocols and guidelines for nonpregnant patients and that treatment delays driven by fear of fetal anomalies and miscarriage are unnecessary.
Cancer Incidence, Use of Diagnostic Imaging
Data on the incidence of cancer in pregnancy comes from population-based cancer registries, and unfortunately, these data are not standardized and are often incomplete. Many studies include cancer diagnosed up to 1 year after pregnancy, and some include preinvasive disease. Estimates therefore vary considerably (see Table 1 for a sampling of estimates incidences.)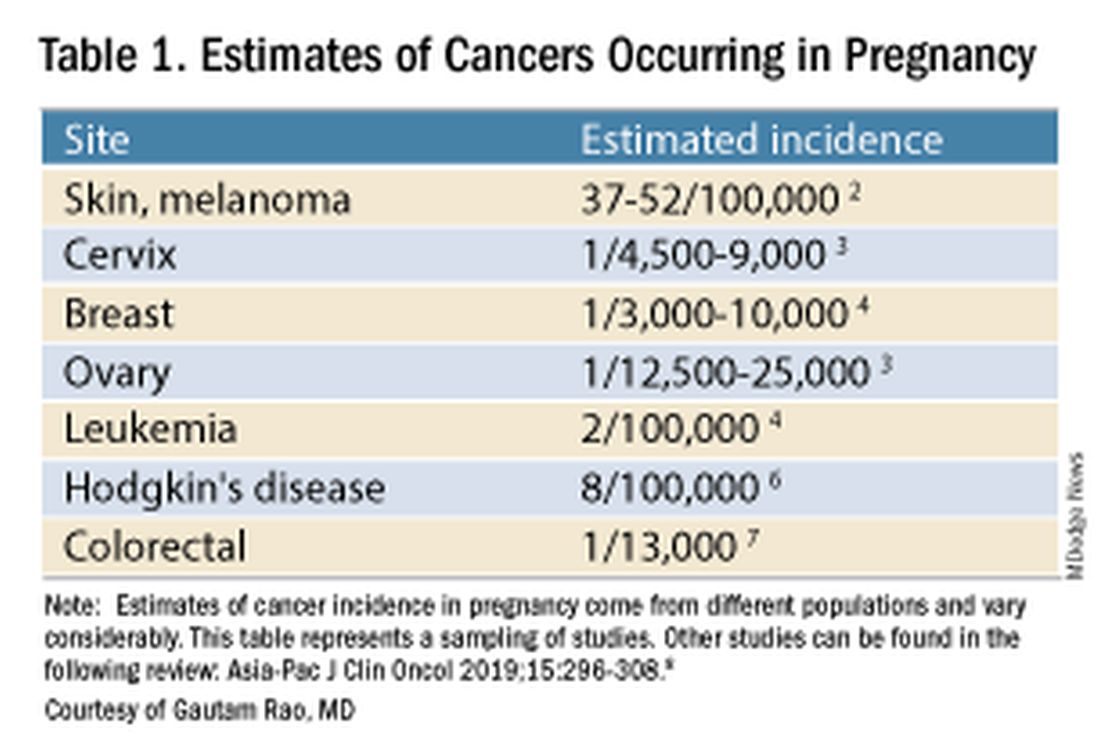
It has been reported, and often cited in the literature, that invasive malignancy complicates one in 1,000 pregnancies and that the incidence of cancer in pregnancy (invasive and noninvasive malignancies) has been rising over time.8 Increasing maternal age is believed to be playing a role in this rise; as women delay childbearing, they enter the age range in which some cancers become more common. Additionally, improvements in screening and diagnostics have led to earlier cancer detection. The incidence of ovarian neoplasms found during pregnancy has increased, for instance, with the routine use of diagnostic ultrasound in pregnancy.1
Among the studies showing an increased incidence of pregnancy-associated cancer is a population-based study in Australia, which found that from 1994 to 2007 the crude incidence of pregnancy-associated cancer increased from 112.3 to 191.5 per 100,000 pregnancies (P < .001).9 A cohort study in the United States documented an increase in incidence from 75.0 per 100,000 pregnancies in 2002 to 138.5 per 100,000 pregnancies in 2012.10
Overall, the literature shows us that the skin, cervix, and breast are also common sites for malignancy during pregnancy.1 According to a 2022 review, breast cancer during pregnancy is less often hormone receptor–positive and more frequently triple negative compared with age-matched controls.11 The frequencies of other pregnancy-associated cancers appear overall to be similar to that of cancer occurring in all women across their reproductive years.1
Too often, diagnosis is delayed because cancer symptoms can be masked by or can mimic normal physiological changes in pregnancy. For instance, breast cancer can be difficult to diagnose during pregnancy and lactation due to anatomic changes in the breast parenchyma. Several studies published in the 1990s showed that breast cancer presents at a more advanced stage in pregnant patients than in nonpregnant patients because of this delay.1 Skin changes suggestive of melanoma can be attributed to hyperpigmentation of pregnancy, for instance. Several observational studies have suggested that thicker melanomas found in pregnancy may be because of delayed diagnosis.8
It is important that we thoroughly investigate signs and symptoms suggestive of a malignancy and not automatically attribute these symptoms to the pregnancy itself. Cervical biopsy of a mass or lesion suspicious for cervical cancer can be done safely during pregnancy and should not be delayed or deferred.
Fetal radiation exposure from radiologic examinations has long been a concern, but we know today that while the imaging modality should be chosen to minimize fetal radiation exposure, CT scans and even PET scans should be performed if these exams are deemed best for evaluation. Embryonic exposure to a dose of less than 50 mGy is rarely if at all associated with fetal malformations or miscarriage and a radiation dose of 100 mGy may be considered a floor for consideration of therapeutic termination of pregnancy.1,8
CT exams are associated with a fetal dose far less than 50 mGy (see Table 2 for radiation doses).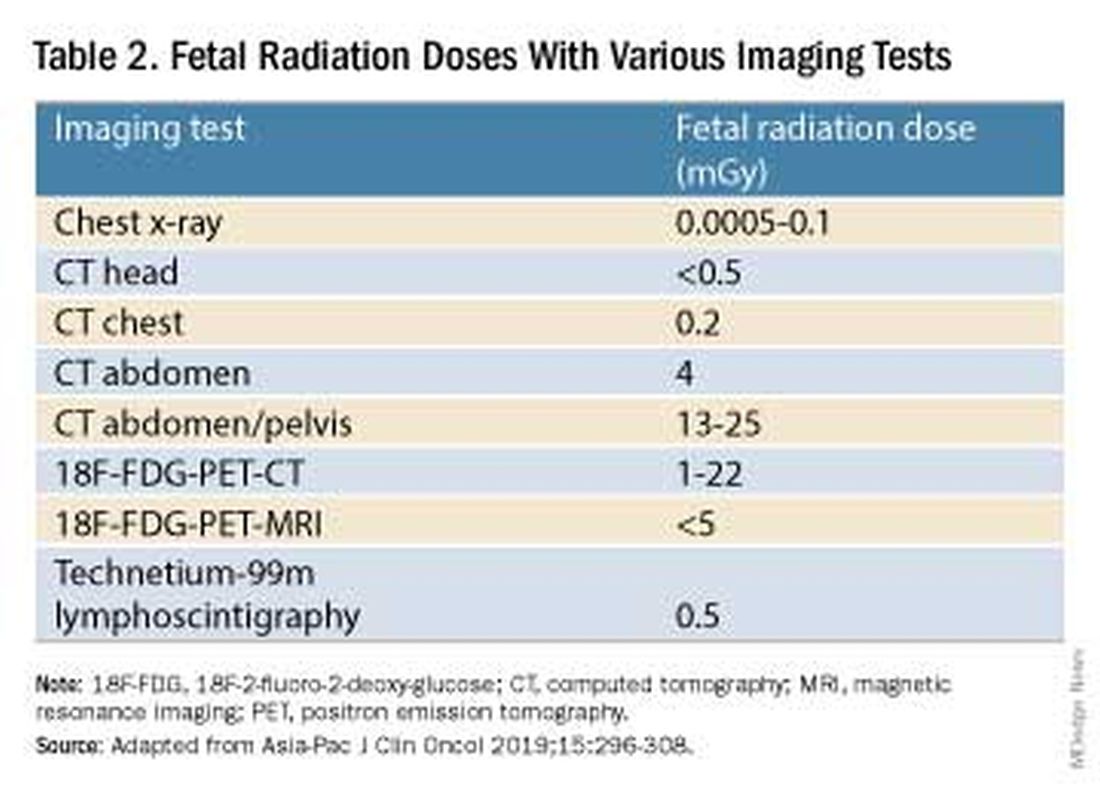
Magnetic resonance imaging with a magnet strength of 3 Tesla or less in any trimester is not associated with an increased risk of harm to the fetus or in early childhood, but the contrast agent gadolinium should be avoided in pregnancy as it has been associated with an increased risk of stillbirth, neonatal death, and childhood inflammatory, rheumatologic, and infiltrative skin lesions.1,8,12
Chemotherapy, Surgery, and Radiation in Pregnancy
The management of cancer during pregnancy requires a multidisciplinary team including medical, gynecologic, or radiation oncologists, and maternal-fetal medicine specialists (Figure 1). Prematurity and low birth weight are frequent complications for fetuses exposed to chemotherapy, although there is some uncertainty as to whether the treatment is causative. However, congenital anomalies no longer are a major concern, provided that drugs are appropriately selected and that fetal exposure occurs during the second or third trimester.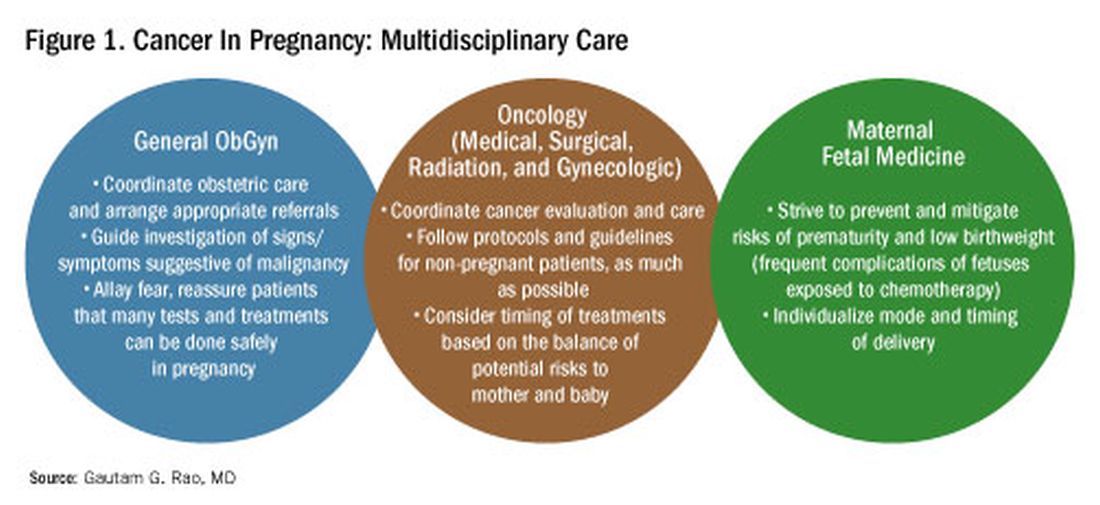
For instance, alkylating agents including cisplatin (an important drug in the management of gynecologic malignancies) have been associated with congenital anomalies in the first trimester but not in the second and third trimesters, and a variety of antimetabolites — excluding methotrexate and aminopterin — similarly have been shown to be relatively safe when used after the first trimester.1
Small studies have shown no long-term effects of chemotherapy exposure on postnatal growth and long-term neurologic/neurocognitive function,1 but this is an area that needs more research.
Also in need of investigation is the safety of newer agents in pregnancy. Data are limited on the use of new targeted treatments, monoclonal antibodies, and immunotherapies in pregnancy and their effects on the fetus, with current knowledge coming mainly from single case reports.13
Until more is learned — a challenge given that pregnant women are generally excluded from clinical trials — management teams are generally postponing use of these therapies until after delivery. Considering the pace of new developments revolutionizing cancer treatment, this topic will likely get more complex and confusing before we begin acquiring sufficient knowledge.
The timing of surgery for malignancy in pregnancy is similarly based on the balance of maternal and fetal risks, including the risk of maternal disease progression, the risk of preterm delivery, and the prevention of fetal metastases. In general, the safest time is the second trimester.
Maternal surgery in the third trimester may be associated with a risk of premature labor and altered uteroplacental perfusion. A 2005 systematic review of 12,452 women who underwent nonobstetric surgery during pregnancy provides some reassurance, however; compared with the general obstetric population, there was no increase in the rate of miscarriage or major birth defects.14
Radiotherapy used to be contraindicated in pregnancy but many experts today believe it can be safely utilized provided the uterus is out of field and is protected from scattered radiation. The head, neck, and breast, for instance, can be treated with newer radiotherapies, including stereotactic ablative radiation therapy.8 Patients with advanced cervical cancer often receive chemotherapy during pregnancy to slow metastatic growth followed by definitive treatment with postpartum radiation or surgery.
More research is needed, but available data on maternal outcomes are encouraging. For instance, there appear to be no significant differences in short- and long-term complications or survival between women who are pregnant and nonpregnant when treated for invasive cervical cancer.8 Similarly, while earlier studies of breast cancer diagnosed during pregnancy suggested a poor prognosis, data now show similar prognoses for pregnant and nonpregnant patients when controlled for stage.1
Dr. Rao is a gynecologic oncologist and associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. He reported no relevant disclosures.
References
1. Rao GG. Chapter 42. Clinical Obstetrics: The Fetus & Mother, 4th ed. Reece EA et al. (eds): 2021.
2. Bannister-Tyrrell M et al. Aust N Z J Obstet Gynaecol. 2014;55:116-122.
3. Oehler MK et al. Aust N Z J Obstet Gynaecol. 2003;43(6):414-420.
4. Ruiz R et al. Breast. 2017;35:136-141. doi: 10.1016/j.breast.2017.07.008.
5. Nolan S et al. Am J Obstet Gynecol. 2019;220(1):S480. doi: 10.1016/j.ajog.2018.11.752.
6. El-Messidi A et al. J Perinat Med. 2015;43(6):683-688. doi: 10.1515/jpm-2014-0133.
7. Pellino G et al. Eur J Gastroenterol Hepatol. 2017;29(7):743-753. doi: 10.1097/MEG.0000000000000863.
8. Eastwood-Wilshere N et al. Asia-Pac J Clin Oncol. 2019;15:296-308.
9. Lee YY et al. BJOG. 2012;119(13):1572-1582.
10. Cottreau CM et al. J Womens Health (Larchmt). 2019 Feb;28(2):250-257.
11. Boere I et al. Best Pract Res Clin Obstet Gynaecol. 2022;82:46-59.
12. Ray JG et al. JAMA 2016;316(9):952-961.
13. Schwab R et al. Cancers. (Basel) 2021;13(12):3048.
14. Cohen-Kerem et al. Am J Surg. 2005;190(3):467-473.
Introduction: Tremendous Progress on Cancer Extends to Cancer in Pregnancy
The biomedical research enterprise that took shape in the United States after World War II has had numerous positive effects, including significant progress made during the past 75-plus years in the diagnosis, prevention, and treatment of cancer.
President Franklin D. Roosevelt’s 1944 request of Dr. Vannevar Bush, director of the then Office of Scientific Research and Development, to organize a program that would advance and apply scientific knowledge for times of peace — just as it been advanced and applied in times of war — culminated in a historic report, Science – The Endless Frontier. Presented in 1945 to President Harry S. Truman, this report helped fuel decades of broad, bold, and coordinated government-sponsored biomedical research aimed at addressing disease and improving the health of the American people (National Science Foundation, 1945).
Discoveries made from research in basic and translational sciences deepened our knowledge of the cellular and molecular underpinnings of cancer, leading to advances in chemotherapy, radiotherapy, and other treatment approaches as well as continual refinements in their application. Similarly, our diagnostic armamentarium has significantly improved.
As a result, we have reduced both the incidence and mortality of cancer. Today, some cancers can be prevented. Others can be reversed or put in remission. Granted, progress has been variable, with some cancers such as ovarian cancer still having relatively low survival rates. Much more needs to be done. Overall, however, the positive effects of the U.S. biomedical research enterprise on cancer are evident. According to the National Cancer Institute’s most recent report on the status of cancer, death rates from cancer fell 1.9% per year on average in females from 2015 to 2019 (Cancer. 2022 Oct 22. doi: 10.1002/cncr.34479).
It is not only patients whose cancer occurs outside of pregnancy who have benefited. When treatment is appropriately selected and timing considerations are made, patients whose cancer is diagnosed during pregnancy — and their children — can have good outcomes.
To explain how the management of cancer in pregnancy has improved, we have invited Gautam G. Rao, MD, gynecologic oncologist and associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, to write this installment of the Master Class in Obstetrics. As Dr. Rao explains, radiation is not as dangerous to the fetus as once thought, and the safety of many chemotherapeutic regimens in pregnancy has been documented. Obstetricians can and should counsel patients, he explains, about the likelihood of good maternal and fetal outcomes.
E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Managing Cancer in Pregnancy
Cancer can cause fear and distress for any patient, but when cancer is diagnosed during pregnancy, an expectant mother fears not only for her own health but for the health of her unborn child. Fortunately, ob.gyn.s and multidisciplinary teams have good reason to reassure patients about the likelihood of good outcomes.
Cancer treatment in pregnancy has improved with advancements in imaging and chemotherapy, and while maternal and fetal outcomes of prenatal cancer treatment are not well reported, evidence acquired in recent years from case series and retrospective studies shows that most imaging studies and procedural diagnostic tests – and many treatments – can be performed safely in pregnancy.
Decades ago, we avoided CT scans during pregnancy because of concerns about radiation exposure to the fetus, leaving some patients without an accurate staging of their cancer. Today, we have evidence that a CT scan is generally safe in pregnancy. Similarly, the safety of many chemotherapeutic regimens in pregnancy has been documented in recent decades,and the use of chemotherapy during pregnancy has increased progressively. Radiation is also commonly utilized in the management of cancers that may occur during pregnancy, such as breast cancer.1
Considerations of timing are often central to decision-making; chemotherapy and radiotherapy are generally avoided in the first trimester to prevent structural fetal anomalies, for instance, and delaying cancer treatment is often warranted when the patient is a few weeks away from delivery. On occasion, iatrogenic preterm birth is considered when the risks to the mother of delaying a necessary cancer treatment outweigh the risks to the fetus of prematurity.1
Pregnancy termination is rarely indicated, however, and information gathered over the past 2 decades suggests that fetal and placental metastases are rare.1 There is broad agreement that prenatal treatment of cancer in pregnancy should adhere as much as possible to protocols and guidelines for nonpregnant patients and that treatment delays driven by fear of fetal anomalies and miscarriage are unnecessary.
Cancer Incidence, Use of Diagnostic Imaging
Data on the incidence of cancer in pregnancy comes from population-based cancer registries, and unfortunately, these data are not standardized and are often incomplete. Many studies include cancer diagnosed up to 1 year after pregnancy, and some include preinvasive disease. Estimates therefore vary considerably (see Table 1 for a sampling of estimates incidences.)
It has been reported, and often cited in the literature, that invasive malignancy complicates one in 1,000 pregnancies and that the incidence of cancer in pregnancy (invasive and noninvasive malignancies) has been rising over time.8 Increasing maternal age is believed to be playing a role in this rise; as women delay childbearing, they enter the age range in which some cancers become more common. Additionally, improvements in screening and diagnostics have led to earlier cancer detection. The incidence of ovarian neoplasms found during pregnancy has increased, for instance, with the routine use of diagnostic ultrasound in pregnancy.1
Among the studies showing an increased incidence of pregnancy-associated cancer is a population-based study in Australia, which found that from 1994 to 2007 the crude incidence of pregnancy-associated cancer increased from 112.3 to 191.5 per 100,000 pregnancies (P < .001).9 A cohort study in the United States documented an increase in incidence from 75.0 per 100,000 pregnancies in 2002 to 138.5 per 100,000 pregnancies in 2012.10
Overall, the literature shows us that the skin, cervix, and breast are also common sites for malignancy during pregnancy.1 According to a 2022 review, breast cancer during pregnancy is less often hormone receptor–positive and more frequently triple negative compared with age-matched controls.11 The frequencies of other pregnancy-associated cancers appear overall to be similar to that of cancer occurring in all women across their reproductive years.1
Too often, diagnosis is delayed because cancer symptoms can be masked by or can mimic normal physiological changes in pregnancy. For instance, breast cancer can be difficult to diagnose during pregnancy and lactation due to anatomic changes in the breast parenchyma. Several studies published in the 1990s showed that breast cancer presents at a more advanced stage in pregnant patients than in nonpregnant patients because of this delay.1 Skin changes suggestive of melanoma can be attributed to hyperpigmentation of pregnancy, for instance. Several observational studies have suggested that thicker melanomas found in pregnancy may be because of delayed diagnosis.8
It is important that we thoroughly investigate signs and symptoms suggestive of a malignancy and not automatically attribute these symptoms to the pregnancy itself. Cervical biopsy of a mass or lesion suspicious for cervical cancer can be done safely during pregnancy and should not be delayed or deferred.
Fetal radiation exposure from radiologic examinations has long been a concern, but we know today that while the imaging modality should be chosen to minimize fetal radiation exposure, CT scans and even PET scans should be performed if these exams are deemed best for evaluation. Embryonic exposure to a dose of less than 50 mGy is rarely if at all associated with fetal malformations or miscarriage and a radiation dose of 100 mGy may be considered a floor for consideration of therapeutic termination of pregnancy.1,8
CT exams are associated with a fetal dose far less than 50 mGy (see Table 2 for radiation doses).
Magnetic resonance imaging with a magnet strength of 3 Tesla or less in any trimester is not associated with an increased risk of harm to the fetus or in early childhood, but the contrast agent gadolinium should be avoided in pregnancy as it has been associated with an increased risk of stillbirth, neonatal death, and childhood inflammatory, rheumatologic, and infiltrative skin lesions.1,8,12
Chemotherapy, Surgery, and Radiation in Pregnancy
The management of cancer during pregnancy requires a multidisciplinary team including medical, gynecologic, or radiation oncologists, and maternal-fetal medicine specialists (Figure 1). Prematurity and low birth weight are frequent complications for fetuses exposed to chemotherapy, although there is some uncertainty as to whether the treatment is causative. However, congenital anomalies no longer are a major concern, provided that drugs are appropriately selected and that fetal exposure occurs during the second or third trimester.
For instance, alkylating agents including cisplatin (an important drug in the management of gynecologic malignancies) have been associated with congenital anomalies in the first trimester but not in the second and third trimesters, and a variety of antimetabolites — excluding methotrexate and aminopterin — similarly have been shown to be relatively safe when used after the first trimester.1
Small studies have shown no long-term effects of chemotherapy exposure on postnatal growth and long-term neurologic/neurocognitive function,1 but this is an area that needs more research.
Also in need of investigation is the safety of newer agents in pregnancy. Data are limited on the use of new targeted treatments, monoclonal antibodies, and immunotherapies in pregnancy and their effects on the fetus, with current knowledge coming mainly from single case reports.13
Until more is learned — a challenge given that pregnant women are generally excluded from clinical trials — management teams are generally postponing use of these therapies until after delivery. Considering the pace of new developments revolutionizing cancer treatment, this topic will likely get more complex and confusing before we begin acquiring sufficient knowledge.
The timing of surgery for malignancy in pregnancy is similarly based on the balance of maternal and fetal risks, including the risk of maternal disease progression, the risk of preterm delivery, and the prevention of fetal metastases. In general, the safest time is the second trimester.
Maternal surgery in the third trimester may be associated with a risk of premature labor and altered uteroplacental perfusion. A 2005 systematic review of 12,452 women who underwent nonobstetric surgery during pregnancy provides some reassurance, however; compared with the general obstetric population, there was no increase in the rate of miscarriage or major birth defects.14
Radiotherapy used to be contraindicated in pregnancy but many experts today believe it can be safely utilized provided the uterus is out of field and is protected from scattered radiation. The head, neck, and breast, for instance, can be treated with newer radiotherapies, including stereotactic ablative radiation therapy.8 Patients with advanced cervical cancer often receive chemotherapy during pregnancy to slow metastatic growth followed by definitive treatment with postpartum radiation or surgery.
More research is needed, but available data on maternal outcomes are encouraging. For instance, there appear to be no significant differences in short- and long-term complications or survival between women who are pregnant and nonpregnant when treated for invasive cervical cancer.8 Similarly, while earlier studies of breast cancer diagnosed during pregnancy suggested a poor prognosis, data now show similar prognoses for pregnant and nonpregnant patients when controlled for stage.1
Dr. Rao is a gynecologic oncologist and associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. He reported no relevant disclosures.
References
1. Rao GG. Chapter 42. Clinical Obstetrics: The Fetus & Mother, 4th ed. Reece EA et al. (eds): 2021.
2. Bannister-Tyrrell M et al. Aust N Z J Obstet Gynaecol. 2014;55:116-122.
3. Oehler MK et al. Aust N Z J Obstet Gynaecol. 2003;43(6):414-420.
4. Ruiz R et al. Breast. 2017;35:136-141. doi: 10.1016/j.breast.2017.07.008.
5. Nolan S et al. Am J Obstet Gynecol. 2019;220(1):S480. doi: 10.1016/j.ajog.2018.11.752.
6. El-Messidi A et al. J Perinat Med. 2015;43(6):683-688. doi: 10.1515/jpm-2014-0133.
7. Pellino G et al. Eur J Gastroenterol Hepatol. 2017;29(7):743-753. doi: 10.1097/MEG.0000000000000863.
8. Eastwood-Wilshere N et al. Asia-Pac J Clin Oncol. 2019;15:296-308.
9. Lee YY et al. BJOG. 2012;119(13):1572-1582.
10. Cottreau CM et al. J Womens Health (Larchmt). 2019 Feb;28(2):250-257.
11. Boere I et al. Best Pract Res Clin Obstet Gynaecol. 2022;82:46-59.
12. Ray JG et al. JAMA 2016;316(9):952-961.
13. Schwab R et al. Cancers. (Basel) 2021;13(12):3048.
14. Cohen-Kerem et al. Am J Surg. 2005;190(3):467-473.
Introduction: Tremendous Progress on Cancer Extends to Cancer in Pregnancy
The biomedical research enterprise that took shape in the United States after World War II has had numerous positive effects, including significant progress made during the past 75-plus years in the diagnosis, prevention, and treatment of cancer.
President Franklin D. Roosevelt’s 1944 request of Dr. Vannevar Bush, director of the then Office of Scientific Research and Development, to organize a program that would advance and apply scientific knowledge for times of peace — just as it been advanced and applied in times of war — culminated in a historic report, Science – The Endless Frontier. Presented in 1945 to President Harry S. Truman, this report helped fuel decades of broad, bold, and coordinated government-sponsored biomedical research aimed at addressing disease and improving the health of the American people (National Science Foundation, 1945).
Discoveries made from research in basic and translational sciences deepened our knowledge of the cellular and molecular underpinnings of cancer, leading to advances in chemotherapy, radiotherapy, and other treatment approaches as well as continual refinements in their application. Similarly, our diagnostic armamentarium has significantly improved.
As a result, we have reduced both the incidence and mortality of cancer. Today, some cancers can be prevented. Others can be reversed or put in remission. Granted, progress has been variable, with some cancers such as ovarian cancer still having relatively low survival rates. Much more needs to be done. Overall, however, the positive effects of the U.S. biomedical research enterprise on cancer are evident. According to the National Cancer Institute’s most recent report on the status of cancer, death rates from cancer fell 1.9% per year on average in females from 2015 to 2019 (Cancer. 2022 Oct 22. doi: 10.1002/cncr.34479).
It is not only patients whose cancer occurs outside of pregnancy who have benefited. When treatment is appropriately selected and timing considerations are made, patients whose cancer is diagnosed during pregnancy — and their children — can have good outcomes.
To explain how the management of cancer in pregnancy has improved, we have invited Gautam G. Rao, MD, gynecologic oncologist and associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, to write this installment of the Master Class in Obstetrics. As Dr. Rao explains, radiation is not as dangerous to the fetus as once thought, and the safety of many chemotherapeutic regimens in pregnancy has been documented. Obstetricians can and should counsel patients, he explains, about the likelihood of good maternal and fetal outcomes.
E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Managing Cancer in Pregnancy
Cancer can cause fear and distress for any patient, but when cancer is diagnosed during pregnancy, an expectant mother fears not only for her own health but for the health of her unborn child. Fortunately, ob.gyn.s and multidisciplinary teams have good reason to reassure patients about the likelihood of good outcomes.
Cancer treatment in pregnancy has improved with advancements in imaging and chemotherapy, and while maternal and fetal outcomes of prenatal cancer treatment are not well reported, evidence acquired in recent years from case series and retrospective studies shows that most imaging studies and procedural diagnostic tests – and many treatments – can be performed safely in pregnancy.
Decades ago, we avoided CT scans during pregnancy because of concerns about radiation exposure to the fetus, leaving some patients without an accurate staging of their cancer. Today, we have evidence that a CT scan is generally safe in pregnancy. Similarly, the safety of many chemotherapeutic regimens in pregnancy has been documented in recent decades,and the use of chemotherapy during pregnancy has increased progressively. Radiation is also commonly utilized in the management of cancers that may occur during pregnancy, such as breast cancer.1
Considerations of timing are often central to decision-making; chemotherapy and radiotherapy are generally avoided in the first trimester to prevent structural fetal anomalies, for instance, and delaying cancer treatment is often warranted when the patient is a few weeks away from delivery. On occasion, iatrogenic preterm birth is considered when the risks to the mother of delaying a necessary cancer treatment outweigh the risks to the fetus of prematurity.1
Pregnancy termination is rarely indicated, however, and information gathered over the past 2 decades suggests that fetal and placental metastases are rare.1 There is broad agreement that prenatal treatment of cancer in pregnancy should adhere as much as possible to protocols and guidelines for nonpregnant patients and that treatment delays driven by fear of fetal anomalies and miscarriage are unnecessary.
Cancer Incidence, Use of Diagnostic Imaging
Data on the incidence of cancer in pregnancy comes from population-based cancer registries, and unfortunately, these data are not standardized and are often incomplete. Many studies include cancer diagnosed up to 1 year after pregnancy, and some include preinvasive disease. Estimates therefore vary considerably (see Table 1 for a sampling of estimates incidences.)
It has been reported, and often cited in the literature, that invasive malignancy complicates one in 1,000 pregnancies and that the incidence of cancer in pregnancy (invasive and noninvasive malignancies) has been rising over time.8 Increasing maternal age is believed to be playing a role in this rise; as women delay childbearing, they enter the age range in which some cancers become more common. Additionally, improvements in screening and diagnostics have led to earlier cancer detection. The incidence of ovarian neoplasms found during pregnancy has increased, for instance, with the routine use of diagnostic ultrasound in pregnancy.1
Among the studies showing an increased incidence of pregnancy-associated cancer is a population-based study in Australia, which found that from 1994 to 2007 the crude incidence of pregnancy-associated cancer increased from 112.3 to 191.5 per 100,000 pregnancies (P < .001).9 A cohort study in the United States documented an increase in incidence from 75.0 per 100,000 pregnancies in 2002 to 138.5 per 100,000 pregnancies in 2012.10
Overall, the literature shows us that the skin, cervix, and breast are also common sites for malignancy during pregnancy.1 According to a 2022 review, breast cancer during pregnancy is less often hormone receptor–positive and more frequently triple negative compared with age-matched controls.11 The frequencies of other pregnancy-associated cancers appear overall to be similar to that of cancer occurring in all women across their reproductive years.1
Too often, diagnosis is delayed because cancer symptoms can be masked by or can mimic normal physiological changes in pregnancy. For instance, breast cancer can be difficult to diagnose during pregnancy and lactation due to anatomic changes in the breast parenchyma. Several studies published in the 1990s showed that breast cancer presents at a more advanced stage in pregnant patients than in nonpregnant patients because of this delay.1 Skin changes suggestive of melanoma can be attributed to hyperpigmentation of pregnancy, for instance. Several observational studies have suggested that thicker melanomas found in pregnancy may be because of delayed diagnosis.8
It is important that we thoroughly investigate signs and symptoms suggestive of a malignancy and not automatically attribute these symptoms to the pregnancy itself. Cervical biopsy of a mass or lesion suspicious for cervical cancer can be done safely during pregnancy and should not be delayed or deferred.
Fetal radiation exposure from radiologic examinations has long been a concern, but we know today that while the imaging modality should be chosen to minimize fetal radiation exposure, CT scans and even PET scans should be performed if these exams are deemed best for evaluation. Embryonic exposure to a dose of less than 50 mGy is rarely if at all associated with fetal malformations or miscarriage and a radiation dose of 100 mGy may be considered a floor for consideration of therapeutic termination of pregnancy.1,8
CT exams are associated with a fetal dose far less than 50 mGy (see Table 2 for radiation doses).
Magnetic resonance imaging with a magnet strength of 3 Tesla or less in any trimester is not associated with an increased risk of harm to the fetus or in early childhood, but the contrast agent gadolinium should be avoided in pregnancy as it has been associated with an increased risk of stillbirth, neonatal death, and childhood inflammatory, rheumatologic, and infiltrative skin lesions.1,8,12
Chemotherapy, Surgery, and Radiation in Pregnancy
The management of cancer during pregnancy requires a multidisciplinary team including medical, gynecologic, or radiation oncologists, and maternal-fetal medicine specialists (Figure 1). Prematurity and low birth weight are frequent complications for fetuses exposed to chemotherapy, although there is some uncertainty as to whether the treatment is causative. However, congenital anomalies no longer are a major concern, provided that drugs are appropriately selected and that fetal exposure occurs during the second or third trimester.
For instance, alkylating agents including cisplatin (an important drug in the management of gynecologic malignancies) have been associated with congenital anomalies in the first trimester but not in the second and third trimesters, and a variety of antimetabolites — excluding methotrexate and aminopterin — similarly have been shown to be relatively safe when used after the first trimester.1
Small studies have shown no long-term effects of chemotherapy exposure on postnatal growth and long-term neurologic/neurocognitive function,1 but this is an area that needs more research.
Also in need of investigation is the safety of newer agents in pregnancy. Data are limited on the use of new targeted treatments, monoclonal antibodies, and immunotherapies in pregnancy and their effects on the fetus, with current knowledge coming mainly from single case reports.13
Until more is learned — a challenge given that pregnant women are generally excluded from clinical trials — management teams are generally postponing use of these therapies until after delivery. Considering the pace of new developments revolutionizing cancer treatment, this topic will likely get more complex and confusing before we begin acquiring sufficient knowledge.
The timing of surgery for malignancy in pregnancy is similarly based on the balance of maternal and fetal risks, including the risk of maternal disease progression, the risk of preterm delivery, and the prevention of fetal metastases. In general, the safest time is the second trimester.
Maternal surgery in the third trimester may be associated with a risk of premature labor and altered uteroplacental perfusion. A 2005 systematic review of 12,452 women who underwent nonobstetric surgery during pregnancy provides some reassurance, however; compared with the general obstetric population, there was no increase in the rate of miscarriage or major birth defects.14
Radiotherapy used to be contraindicated in pregnancy but many experts today believe it can be safely utilized provided the uterus is out of field and is protected from scattered radiation. The head, neck, and breast, for instance, can be treated with newer radiotherapies, including stereotactic ablative radiation therapy.8 Patients with advanced cervical cancer often receive chemotherapy during pregnancy to slow metastatic growth followed by definitive treatment with postpartum radiation or surgery.
More research is needed, but available data on maternal outcomes are encouraging. For instance, there appear to be no significant differences in short- and long-term complications or survival between women who are pregnant and nonpregnant when treated for invasive cervical cancer.8 Similarly, while earlier studies of breast cancer diagnosed during pregnancy suggested a poor prognosis, data now show similar prognoses for pregnant and nonpregnant patients when controlled for stage.1
Dr. Rao is a gynecologic oncologist and associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. He reported no relevant disclosures.
References
1. Rao GG. Chapter 42. Clinical Obstetrics: The Fetus & Mother, 4th ed. Reece EA et al. (eds): 2021.
2. Bannister-Tyrrell M et al. Aust N Z J Obstet Gynaecol. 2014;55:116-122.
3. Oehler MK et al. Aust N Z J Obstet Gynaecol. 2003;43(6):414-420.
4. Ruiz R et al. Breast. 2017;35:136-141. doi: 10.1016/j.breast.2017.07.008.
5. Nolan S et al. Am J Obstet Gynecol. 2019;220(1):S480. doi: 10.1016/j.ajog.2018.11.752.
6. El-Messidi A et al. J Perinat Med. 2015;43(6):683-688. doi: 10.1515/jpm-2014-0133.
7. Pellino G et al. Eur J Gastroenterol Hepatol. 2017;29(7):743-753. doi: 10.1097/MEG.0000000000000863.
8. Eastwood-Wilshere N et al. Asia-Pac J Clin Oncol. 2019;15:296-308.
9. Lee YY et al. BJOG. 2012;119(13):1572-1582.
10. Cottreau CM et al. J Womens Health (Larchmt). 2019 Feb;28(2):250-257.
11. Boere I et al. Best Pract Res Clin Obstet Gynaecol. 2022;82:46-59.
12. Ray JG et al. JAMA 2016;316(9):952-961.
13. Schwab R et al. Cancers. (Basel) 2021;13(12):3048.
14. Cohen-Kerem et al. Am J Surg. 2005;190(3):467-473.
Good Vibrations: Help Patients Help Themselves to Better Sex
This transcript has been edited for clarity.
Rachel S. Rubin, MD: Hi, everybody. Welcome back to another episode of Sex Matters. I am Dr Rachel Rubin. I’m a urologist and sexual medicine specialist in the Washington, DC, area, and I am thrilled to bring you this next guest. This is someone I am a huge fan of. I have been following her research for decades now, and we are so blessed to have her: Debby Herbenick. Why don’t you introduce yourself and tell people all about your research?
Debby Herbenick, PhD: I’m a professor at the Indiana University School of Public Health, and I’ve been a sexuality researcher and educator for about 25 years. I’ve studied issues related to women’s orgasm, vibrator use, how people feel about their genitals, and how that impacts whether or not they are comfortable seeking healthcare. Most recently, I’ve been looking at emerging sexual practices.
Dr. Rubin: You can’t be in sexual medicine without knowing Dr. Herbenick’s work. It is just instrumental to our knowledge about what people are actually doing, what people care about, and what’s happening out there. Probably not a day goes by that I don’t quote your research on how women experience sexual pleasure, how women orgasm. Can you talk briefly about that research?
Dr. Herbenick: The key is really variety. People need to feel comfortable with the way that they experience their bodies and their own paths to pleasure, and feel supported in being able to explore in that way.
Dr. Rubin: And what are some resources? What I often quote is that everyone thinks, because of Hollywood and pornography, that women orgasm from vaginal penetration alone, which of course we know physiologically doesn’t make sense. The numbers are staggering. People often go to their doctor and say: “I’m not normal. I can’t orgasm from penetration. Is there something wrong with me?”
Dr. Herbenick: Most women are not orgasming from vaginal intercourse alone. Many have added direct clitoral stimulation. Others prefer to receive oral sex. Some are having orgasms with a vibrator or other kinds of sex toys. And for some, it’s not just the behavior, right? It’s having the behavior in a certain amount of intimacy or connection with a partner, so really focusing on that as well.
Dr. Rubin: Your data show that more than 50% of women have used vibration in the past. I tell my male patients as well that the penis and the clitoris are the same. The penis likes vibration too, but many have never tried it. As a clinician, being able to encourage patients to use these devices and tools is really important. Your data help us show that this is an important aspect of pleasure.
Dr. Herbenick: I’m always glad to hear they’re helpful. And, of course, our research really focused on vibrators, but it’s been so interesting to see the sexual enhancement products change over the years. And now we have all these air pressure toys, too, which are especially useful for people who really can’t take or don’t prefer direct contact with their clitoris or other genital parts.
Dr. Rubin: I tell my patients all the time that the sex devices that we use today are not the same things from back in the day. There are so many high technological advances in this space that are really wonderful tools for me as a doctor, that I can really help my patients understand and use just to have more fun.
Dr. Herbenick: Absolutely.
Dr. Rubin: Very few of us are sexual medicine–trained physicians who feel confident and comfortable talking about sexual health issues. How can they find you or follow you?
Dr. Herbenick: I’m on social media as Debby Herbenick. I’m also on our website at Indiana University, the Center for Sexual Health Promotion.
Dr. Rubin: Thank you so much for joining us today.
Rachel S. Rubin, MD, is assistant clinical professor, Department of Urology, Georgetown University, Washington, DC, and in private practice in North Bethesda, Maryland. She disclosed financial relationships with Sprout, Maternal Medical, Absorption Pharmaceuticals, GSK, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: Hi, everybody. Welcome back to another episode of Sex Matters. I am Dr Rachel Rubin. I’m a urologist and sexual medicine specialist in the Washington, DC, area, and I am thrilled to bring you this next guest. This is someone I am a huge fan of. I have been following her research for decades now, and we are so blessed to have her: Debby Herbenick. Why don’t you introduce yourself and tell people all about your research?
Debby Herbenick, PhD: I’m a professor at the Indiana University School of Public Health, and I’ve been a sexuality researcher and educator for about 25 years. I’ve studied issues related to women’s orgasm, vibrator use, how people feel about their genitals, and how that impacts whether or not they are comfortable seeking healthcare. Most recently, I’ve been looking at emerging sexual practices.
Dr. Rubin: You can’t be in sexual medicine without knowing Dr. Herbenick’s work. It is just instrumental to our knowledge about what people are actually doing, what people care about, and what’s happening out there. Probably not a day goes by that I don’t quote your research on how women experience sexual pleasure, how women orgasm. Can you talk briefly about that research?
Dr. Herbenick: The key is really variety. People need to feel comfortable with the way that they experience their bodies and their own paths to pleasure, and feel supported in being able to explore in that way.
Dr. Rubin: And what are some resources? What I often quote is that everyone thinks, because of Hollywood and pornography, that women orgasm from vaginal penetration alone, which of course we know physiologically doesn’t make sense. The numbers are staggering. People often go to their doctor and say: “I’m not normal. I can’t orgasm from penetration. Is there something wrong with me?”
Dr. Herbenick: Most women are not orgasming from vaginal intercourse alone. Many have added direct clitoral stimulation. Others prefer to receive oral sex. Some are having orgasms with a vibrator or other kinds of sex toys. And for some, it’s not just the behavior, right? It’s having the behavior in a certain amount of intimacy or connection with a partner, so really focusing on that as well.
Dr. Rubin: Your data show that more than 50% of women have used vibration in the past. I tell my male patients as well that the penis and the clitoris are the same. The penis likes vibration too, but many have never tried it. As a clinician, being able to encourage patients to use these devices and tools is really important. Your data help us show that this is an important aspect of pleasure.
Dr. Herbenick: I’m always glad to hear they’re helpful. And, of course, our research really focused on vibrators, but it’s been so interesting to see the sexual enhancement products change over the years. And now we have all these air pressure toys, too, which are especially useful for people who really can’t take or don’t prefer direct contact with their clitoris or other genital parts.
Dr. Rubin: I tell my patients all the time that the sex devices that we use today are not the same things from back in the day. There are so many high technological advances in this space that are really wonderful tools for me as a doctor, that I can really help my patients understand and use just to have more fun.
Dr. Herbenick: Absolutely.
Dr. Rubin: Very few of us are sexual medicine–trained physicians who feel confident and comfortable talking about sexual health issues. How can they find you or follow you?
Dr. Herbenick: I’m on social media as Debby Herbenick. I’m also on our website at Indiana University, the Center for Sexual Health Promotion.
Dr. Rubin: Thank you so much for joining us today.
Rachel S. Rubin, MD, is assistant clinical professor, Department of Urology, Georgetown University, Washington, DC, and in private practice in North Bethesda, Maryland. She disclosed financial relationships with Sprout, Maternal Medical, Absorption Pharmaceuticals, GSK, and Endo.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: Hi, everybody. Welcome back to another episode of Sex Matters. I am Dr Rachel Rubin. I’m a urologist and sexual medicine specialist in the Washington, DC, area, and I am thrilled to bring you this next guest. This is someone I am a huge fan of. I have been following her research for decades now, and we are so blessed to have her: Debby Herbenick. Why don’t you introduce yourself and tell people all about your research?
Debby Herbenick, PhD: I’m a professor at the Indiana University School of Public Health, and I’ve been a sexuality researcher and educator for about 25 years. I’ve studied issues related to women’s orgasm, vibrator use, how people feel about their genitals, and how that impacts whether or not they are comfortable seeking healthcare. Most recently, I’ve been looking at emerging sexual practices.
Dr. Rubin: You can’t be in sexual medicine without knowing Dr. Herbenick’s work. It is just instrumental to our knowledge about what people are actually doing, what people care about, and what’s happening out there. Probably not a day goes by that I don’t quote your research on how women experience sexual pleasure, how women orgasm. Can you talk briefly about that research?
Dr. Herbenick: The key is really variety. People need to feel comfortable with the way that they experience their bodies and their own paths to pleasure, and feel supported in being able to explore in that way.
Dr. Rubin: And what are some resources? What I often quote is that everyone thinks, because of Hollywood and pornography, that women orgasm from vaginal penetration alone, which of course we know physiologically doesn’t make sense. The numbers are staggering. People often go to their doctor and say: “I’m not normal. I can’t orgasm from penetration. Is there something wrong with me?”
Dr. Herbenick: Most women are not orgasming from vaginal intercourse alone. Many have added direct clitoral stimulation. Others prefer to receive oral sex. Some are having orgasms with a vibrator or other kinds of sex toys. And for some, it’s not just the behavior, right? It’s having the behavior in a certain amount of intimacy or connection with a partner, so really focusing on that as well.
Dr. Rubin: Your data show that more than 50% of women have used vibration in the past. I tell my male patients as well that the penis and the clitoris are the same. The penis likes vibration too, but many have never tried it. As a clinician, being able to encourage patients to use these devices and tools is really important. Your data help us show that this is an important aspect of pleasure.
Dr. Herbenick: I’m always glad to hear they’re helpful. And, of course, our research really focused on vibrators, but it’s been so interesting to see the sexual enhancement products change over the years. And now we have all these air pressure toys, too, which are especially useful for people who really can’t take or don’t prefer direct contact with their clitoris or other genital parts.
Dr. Rubin: I tell my patients all the time that the sex devices that we use today are not the same things from back in the day. There are so many high technological advances in this space that are really wonderful tools for me as a doctor, that I can really help my patients understand and use just to have more fun.
Dr. Herbenick: Absolutely.
Dr. Rubin: Very few of us are sexual medicine–trained physicians who feel confident and comfortable talking about sexual health issues. How can they find you or follow you?
Dr. Herbenick: I’m on social media as Debby Herbenick. I’m also on our website at Indiana University, the Center for Sexual Health Promotion.
Dr. Rubin: Thank you so much for joining us today.
Rachel S. Rubin, MD, is assistant clinical professor, Department of Urology, Georgetown University, Washington, DC, and in private practice in North Bethesda, Maryland. She disclosed financial relationships with Sprout, Maternal Medical, Absorption Pharmaceuticals, GSK, and Endo.
A version of this article first appeared on Medscape.com.