User login
Official Newspaper of the American College of Surgeons
Less aggressive anticoagulation appears safe after high-risk aortic valve replacement
MINNEAPOLIS – High-risk patients receiving the On-X mechanical aortic valve can be safely managed with less aggressive anticoagulation than currently recommended, interim results of the PROACT trial suggest.*
The lower target international normalized ratio (INR) in the trial resulted in a decline of more than 50% in bleeding events and did not increase the risk of thromboembolism, reported Dr. John Puskas, international principal investigator for PROACT (Prospective Randomized On-X Anticoagulation Clinical Trial) and associate chief of cardiothoracic surgery at Emory University in Atlanta.

"This aortic bileaflet mechanical valve may be safely managed in these select patients at an INR of 1.5 to 2.0, with daily low-dose aspirin," he said at the annual meeting of the American Association for Thoracic Surgery.
Current American College of Cardiology and American Heart Association guidelines recommend that warfarin be dosed to achieve an INR of 2.0 to 3.0 after implantation of a bileaflet mechanical valve, and that once-daily aspirin 75-100 mg be added for all patients with mechanical heart valves.
Dr. Puskas and his associates analyzed data from 375 high-risk patients randomly assigned to lower-dose warfarin (INR 1.5-2.0) or to continue standard-dose warfarin (INR 2.0-3.0), 3 months after implantation with the On-X bileaflet mechanical heart valve. All patients received aspirin 81 mg daily. INR was adjusted by rigorous home self-monitoring, with an average of 9 days between readings and at least 96% compliance.
High-risk patients included those with chronic atrial fibrillation, left ventricular ejection fraction less than 30%, ventricular aneurysm, left atrium diameter greater than 50 mm, prior neurological events, on estrogen replacement therapy, hypercoagulability, or inadequate platelet response to aspirin or clopidogrel (Plavix). There were 185 patients in the experimental, test arm and 190 in the control arm. After randomization, 11 test patients had a neurological event (5 strokes, 6 transient ischemic attacks) and crossed over to the control group, per protocol.
After an average follow-up of 3.82 years, patients managed with a lower target INR had a significant benefit compared with controls with respect to number of major bleeding events (10 vs. 25, respectively), minor bleeds (8 vs. 25), total bleeds (18 vs. 50), and all bleeding and thrombus (38 vs. 64), Dr. Puskas said. The corresponding rate ratios (RRs) were 0.45, 0.36, 0.40, and 0.66.
There was no difference between groups in the composite primary endpoint of major bleed, stroke, transient ischemic attack, thromboembolic events and thrombosis (30 events vs. 39 events; RR, 0.86; P = .54), he said.
Specifically, hemorrhagic stroke occurred in 1 test patient and 2 controls (RR, 0.56) and ischemic stroke in 5 patients in each group (RR, 1.12), he said.
Valve-related mortality was also similar in the test and control groups (5 deaths vs. 4 deaths), as was total mortality (10 vs. 11), Dr. Puskas said.
Invited discussant Dr. A. Pieter Kappetein, a member of the RE-ALIGN trial steering committee and professor of thoracic surgery at Erasmus Medical Center in Rotterdam, the Netherlands, said the number of patients in the analysis was extremely low and questioned the validity of combining bleeding and thromboembolic events in the primary endpoint.
"In this study, you mix the efficacy endpoint with the safety endpoints," he said, observing that they move in opposite directions.
In light of such large-scale trials as ARISTOTLE and RELY, he asked whether PROACT should be considered a pilot trial and whether a new trial, designed with roughly 8,000 patients, should be performed that would also include newer anticoagulation agents to adequately evaluate reduced anticoagulation in mechanical valves.
"Is it not potentially dangerous if we do not know what the increase is for thrombosis and follow your conclusions?" he added.
Dr. Puskas said he shared Dr. Kappetein’s concern about the noninferiority design of the trial and that it was a topic of great discussion with the Food and Drug Administration (FDA). He also agreed that thrombotic events and bleeding events move in the opposite direction.
"What we are really looking for is to determine the sweet spot where those two curves intersect," he said. "While it is theoretically and intellectually correct to say that thrombosis is the efficacy issue and hemorrhage is the safety issue, we are obliged to combine those for two reasons.
"The first is practical; no company will sponsor an 8,000-patient trial, and second, this is, in fact, a trade-off in the minds of patients and clinicians. So, it is a relevant clinical endpoint – the unholy composite, if you will – of thrombosis and hemorrhage."
Finally, a member of the audience asked whether the results would hold up with standard management because universal point-of-care home testing is not the "real world" in the United States.
Dr. Puskas replied that it is in Scandinavia and other parts of the world, and admonished American clinicians, including himself, "to catch up to what should be standard of care." He noted that, based on the roughly 53,000 INR readings in PROACT, controlling INR within your range was more important in terms of adverse events, particularly hemorrhagic events, than what arm patients were assigned to.
"Home monitoring is available, it’s not high tech and it’s much easier for patients," he said. "To be perfectly blunt, there’s really no excuse for us not using it uniformly in America. Quite frankly, it is a conflict of interest between local caregivers and their patients’ well-being.
"There is a small revenue stream to cardiology offices and primary care doctors running Coumadin clinics, and that is keeping us in the system that we have now rather than home monitoring through bigger, centralized Coumadin clinics."
Dr. Puskas did not report data on PROACT’s low-risk arm managed with clopidogrel 75 mg/day plus aspirin 325 mg/day, or a third arm managed on warfarin at an INR of 2.0-2.5 plus aspirin 81 mg/day. The low-risk data will not be available for at least one more year, although the investigators are in discussion with the FDA about a possible interim analysis, he said in an interview.
The evaluable high-risk patients were 79% male, 93% were in sinus rhythm preoperatively, and concomitant procedures included coronary artery bypass grafting in 27%, aortic aneurysm repair in 14%, and other procedures in 25%. Their average age was 55 years.
Life Technologies sponsored the study. Dr. Puskas reported having no financial relationship with Life Technologies.
Correction, 6/18/2013: An earlier version of this article stated that the On-X aortic valve is investigational. This was a misstatement. The valve itself has been approved in the United States since 2001. The PROACT trial applications of lowered INR and an aspirin/Plavix regimen are not approved.
MINNEAPOLIS – High-risk patients receiving the On-X mechanical aortic valve can be safely managed with less aggressive anticoagulation than currently recommended, interim results of the PROACT trial suggest.*
The lower target international normalized ratio (INR) in the trial resulted in a decline of more than 50% in bleeding events and did not increase the risk of thromboembolism, reported Dr. John Puskas, international principal investigator for PROACT (Prospective Randomized On-X Anticoagulation Clinical Trial) and associate chief of cardiothoracic surgery at Emory University in Atlanta.
"This aortic bileaflet mechanical valve may be safely managed in these select patients at an INR of 1.5 to 2.0, with daily low-dose aspirin," he said at the annual meeting of the American Association for Thoracic Surgery.
Current American College of Cardiology and American Heart Association guidelines recommend that warfarin be dosed to achieve an INR of 2.0 to 3.0 after implantation of a bileaflet mechanical valve, and that once-daily aspirin 75-100 mg be added for all patients with mechanical heart valves.
Dr. Puskas and his associates analyzed data from 375 high-risk patients randomly assigned to lower-dose warfarin (INR 1.5-2.0) or to continue standard-dose warfarin (INR 2.0-3.0), 3 months after implantation with the On-X bileaflet mechanical heart valve. All patients received aspirin 81 mg daily. INR was adjusted by rigorous home self-monitoring, with an average of 9 days between readings and at least 96% compliance.
High-risk patients included those with chronic atrial fibrillation, left ventricular ejection fraction less than 30%, ventricular aneurysm, left atrium diameter greater than 50 mm, prior neurological events, on estrogen replacement therapy, hypercoagulability, or inadequate platelet response to aspirin or clopidogrel (Plavix). There were 185 patients in the experimental, test arm and 190 in the control arm. After randomization, 11 test patients had a neurological event (5 strokes, 6 transient ischemic attacks) and crossed over to the control group, per protocol.
After an average follow-up of 3.82 years, patients managed with a lower target INR had a significant benefit compared with controls with respect to number of major bleeding events (10 vs. 25, respectively), minor bleeds (8 vs. 25), total bleeds (18 vs. 50), and all bleeding and thrombus (38 vs. 64), Dr. Puskas said. The corresponding rate ratios (RRs) were 0.45, 0.36, 0.40, and 0.66.
There was no difference between groups in the composite primary endpoint of major bleed, stroke, transient ischemic attack, thromboembolic events and thrombosis (30 events vs. 39 events; RR, 0.86; P = .54), he said.
Specifically, hemorrhagic stroke occurred in 1 test patient and 2 controls (RR, 0.56) and ischemic stroke in 5 patients in each group (RR, 1.12), he said.
Valve-related mortality was also similar in the test and control groups (5 deaths vs. 4 deaths), as was total mortality (10 vs. 11), Dr. Puskas said.
Invited discussant Dr. A. Pieter Kappetein, a member of the RE-ALIGN trial steering committee and professor of thoracic surgery at Erasmus Medical Center in Rotterdam, the Netherlands, said the number of patients in the analysis was extremely low and questioned the validity of combining bleeding and thromboembolic events in the primary endpoint.
"In this study, you mix the efficacy endpoint with the safety endpoints," he said, observing that they move in opposite directions.
In light of such large-scale trials as ARISTOTLE and RELY, he asked whether PROACT should be considered a pilot trial and whether a new trial, designed with roughly 8,000 patients, should be performed that would also include newer anticoagulation agents to adequately evaluate reduced anticoagulation in mechanical valves.
"Is it not potentially dangerous if we do not know what the increase is for thrombosis and follow your conclusions?" he added.
Dr. Puskas said he shared Dr. Kappetein’s concern about the noninferiority design of the trial and that it was a topic of great discussion with the Food and Drug Administration (FDA). He also agreed that thrombotic events and bleeding events move in the opposite direction.
"What we are really looking for is to determine the sweet spot where those two curves intersect," he said. "While it is theoretically and intellectually correct to say that thrombosis is the efficacy issue and hemorrhage is the safety issue, we are obliged to combine those for two reasons.
"The first is practical; no company will sponsor an 8,000-patient trial, and second, this is, in fact, a trade-off in the minds of patients and clinicians. So, it is a relevant clinical endpoint – the unholy composite, if you will – of thrombosis and hemorrhage."
Finally, a member of the audience asked whether the results would hold up with standard management because universal point-of-care home testing is not the "real world" in the United States.
Dr. Puskas replied that it is in Scandinavia and other parts of the world, and admonished American clinicians, including himself, "to catch up to what should be standard of care." He noted that, based on the roughly 53,000 INR readings in PROACT, controlling INR within your range was more important in terms of adverse events, particularly hemorrhagic events, than what arm patients were assigned to.
"Home monitoring is available, it’s not high tech and it’s much easier for patients," he said. "To be perfectly blunt, there’s really no excuse for us not using it uniformly in America. Quite frankly, it is a conflict of interest between local caregivers and their patients’ well-being.
"There is a small revenue stream to cardiology offices and primary care doctors running Coumadin clinics, and that is keeping us in the system that we have now rather than home monitoring through bigger, centralized Coumadin clinics."
Dr. Puskas did not report data on PROACT’s low-risk arm managed with clopidogrel 75 mg/day plus aspirin 325 mg/day, or a third arm managed on warfarin at an INR of 2.0-2.5 plus aspirin 81 mg/day. The low-risk data will not be available for at least one more year, although the investigators are in discussion with the FDA about a possible interim analysis, he said in an interview.
The evaluable high-risk patients were 79% male, 93% were in sinus rhythm preoperatively, and concomitant procedures included coronary artery bypass grafting in 27%, aortic aneurysm repair in 14%, and other procedures in 25%. Their average age was 55 years.
Life Technologies sponsored the study. Dr. Puskas reported having no financial relationship with Life Technologies.
Correction, 6/18/2013: An earlier version of this article stated that the On-X aortic valve is investigational. This was a misstatement. The valve itself has been approved in the United States since 2001. The PROACT trial applications of lowered INR and an aspirin/Plavix regimen are not approved.
MINNEAPOLIS – High-risk patients receiving the On-X mechanical aortic valve can be safely managed with less aggressive anticoagulation than currently recommended, interim results of the PROACT trial suggest.*
The lower target international normalized ratio (INR) in the trial resulted in a decline of more than 50% in bleeding events and did not increase the risk of thromboembolism, reported Dr. John Puskas, international principal investigator for PROACT (Prospective Randomized On-X Anticoagulation Clinical Trial) and associate chief of cardiothoracic surgery at Emory University in Atlanta.
"This aortic bileaflet mechanical valve may be safely managed in these select patients at an INR of 1.5 to 2.0, with daily low-dose aspirin," he said at the annual meeting of the American Association for Thoracic Surgery.
Current American College of Cardiology and American Heart Association guidelines recommend that warfarin be dosed to achieve an INR of 2.0 to 3.0 after implantation of a bileaflet mechanical valve, and that once-daily aspirin 75-100 mg be added for all patients with mechanical heart valves.
Dr. Puskas and his associates analyzed data from 375 high-risk patients randomly assigned to lower-dose warfarin (INR 1.5-2.0) or to continue standard-dose warfarin (INR 2.0-3.0), 3 months after implantation with the On-X bileaflet mechanical heart valve. All patients received aspirin 81 mg daily. INR was adjusted by rigorous home self-monitoring, with an average of 9 days between readings and at least 96% compliance.
High-risk patients included those with chronic atrial fibrillation, left ventricular ejection fraction less than 30%, ventricular aneurysm, left atrium diameter greater than 50 mm, prior neurological events, on estrogen replacement therapy, hypercoagulability, or inadequate platelet response to aspirin or clopidogrel (Plavix). There were 185 patients in the experimental, test arm and 190 in the control arm. After randomization, 11 test patients had a neurological event (5 strokes, 6 transient ischemic attacks) and crossed over to the control group, per protocol.
After an average follow-up of 3.82 years, patients managed with a lower target INR had a significant benefit compared with controls with respect to number of major bleeding events (10 vs. 25, respectively), minor bleeds (8 vs. 25), total bleeds (18 vs. 50), and all bleeding and thrombus (38 vs. 64), Dr. Puskas said. The corresponding rate ratios (RRs) were 0.45, 0.36, 0.40, and 0.66.
There was no difference between groups in the composite primary endpoint of major bleed, stroke, transient ischemic attack, thromboembolic events and thrombosis (30 events vs. 39 events; RR, 0.86; P = .54), he said.
Specifically, hemorrhagic stroke occurred in 1 test patient and 2 controls (RR, 0.56) and ischemic stroke in 5 patients in each group (RR, 1.12), he said.
Valve-related mortality was also similar in the test and control groups (5 deaths vs. 4 deaths), as was total mortality (10 vs. 11), Dr. Puskas said.
Invited discussant Dr. A. Pieter Kappetein, a member of the RE-ALIGN trial steering committee and professor of thoracic surgery at Erasmus Medical Center in Rotterdam, the Netherlands, said the number of patients in the analysis was extremely low and questioned the validity of combining bleeding and thromboembolic events in the primary endpoint.
"In this study, you mix the efficacy endpoint with the safety endpoints," he said, observing that they move in opposite directions.
In light of such large-scale trials as ARISTOTLE and RELY, he asked whether PROACT should be considered a pilot trial and whether a new trial, designed with roughly 8,000 patients, should be performed that would also include newer anticoagulation agents to adequately evaluate reduced anticoagulation in mechanical valves.
"Is it not potentially dangerous if we do not know what the increase is for thrombosis and follow your conclusions?" he added.
Dr. Puskas said he shared Dr. Kappetein’s concern about the noninferiority design of the trial and that it was a topic of great discussion with the Food and Drug Administration (FDA). He also agreed that thrombotic events and bleeding events move in the opposite direction.
"What we are really looking for is to determine the sweet spot where those two curves intersect," he said. "While it is theoretically and intellectually correct to say that thrombosis is the efficacy issue and hemorrhage is the safety issue, we are obliged to combine those for two reasons.
"The first is practical; no company will sponsor an 8,000-patient trial, and second, this is, in fact, a trade-off in the minds of patients and clinicians. So, it is a relevant clinical endpoint – the unholy composite, if you will – of thrombosis and hemorrhage."
Finally, a member of the audience asked whether the results would hold up with standard management because universal point-of-care home testing is not the "real world" in the United States.
Dr. Puskas replied that it is in Scandinavia and other parts of the world, and admonished American clinicians, including himself, "to catch up to what should be standard of care." He noted that, based on the roughly 53,000 INR readings in PROACT, controlling INR within your range was more important in terms of adverse events, particularly hemorrhagic events, than what arm patients were assigned to.
"Home monitoring is available, it’s not high tech and it’s much easier for patients," he said. "To be perfectly blunt, there’s really no excuse for us not using it uniformly in America. Quite frankly, it is a conflict of interest between local caregivers and their patients’ well-being.
"There is a small revenue stream to cardiology offices and primary care doctors running Coumadin clinics, and that is keeping us in the system that we have now rather than home monitoring through bigger, centralized Coumadin clinics."
Dr. Puskas did not report data on PROACT’s low-risk arm managed with clopidogrel 75 mg/day plus aspirin 325 mg/day, or a third arm managed on warfarin at an INR of 2.0-2.5 plus aspirin 81 mg/day. The low-risk data will not be available for at least one more year, although the investigators are in discussion with the FDA about a possible interim analysis, he said in an interview.
The evaluable high-risk patients were 79% male, 93% were in sinus rhythm preoperatively, and concomitant procedures included coronary artery bypass grafting in 27%, aortic aneurysm repair in 14%, and other procedures in 25%. Their average age was 55 years.
Life Technologies sponsored the study. Dr. Puskas reported having no financial relationship with Life Technologies.
Correction, 6/18/2013: An earlier version of this article stated that the On-X aortic valve is investigational. This was a misstatement. The valve itself has been approved in the United States since 2001. The PROACT trial applications of lowered INR and an aspirin/Plavix regimen are not approved.
AT THE AATS ANNUAL MEETING
Major finding: The composite primary endpoint of major bleed, stroke, transient ischemic attack, thromboembolic events, and thrombosis occurred in 30 patients managed with less aggressive anticoagulation and in 39 managed with standard warfarin anticoagulation (rate ratio, 0.86; P = .54).
Data source: Interim analysis of 375 high-risk aortic valve replacement patients in the Prospective Randomized On-X Anticoagulation Trial.
Disclosures: Life Technologies sponsored the study. Dr. Puskas reported having no financial relationship with Life Technologies.

Genetic tests gauge breast-cancer recurrence risk
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.

But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.

All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.

|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.
But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.
All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.
But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.
All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
AT IMPAKT 2013 BREAST CANCER CONFERENCE
Major finding: Low-risk patients by the PAM50 test had 97.6% 15-year disease-free survival compared with 82.5% in high-risk patients.
Data source: A retrospective analysis of 1,478 women enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial.
Disclosures: Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.

Preop walking speed predicts postop morbidity
INDIANAPOLIS – Slower walking speed on the timed-up-and-go test in elderly patients scheduled for surgery is a significantly better forecaster of postoperative complications and 1-year mortality than are the considerably more complex patient risk calculators currently considered standard of care, Dr. Thomas N. Robinson reported at the annual meeting of the American Surgical Association.
"I think what walking speed reflects is global reduced physiologic reserve. It’s frailty. And by definition, an individual who’s frail will have adverse health care outcomes," explained Dr. Robinson, a general surgeon at the University of Colorado, Denver.

Use of preoperative walking speed to assess postoperative risk is a paradigm shift, he noted. Current surgical risk assessment strategies rely upon math-heavy patient risk calculators which evaluate single end-organ dysfunction, in some cases summing up the individual scores for heart, lung, liver, and other organ dysfunction in an attempt to define chronic disease burden. But in older patients, this approach is less effective than a simple frailty assessment based upon mobility: that is, walking speed, he continued.
Surgeons in the Veterans Affairs health care system use a risk calculator that involves input of 24 variables. Hitting the "compute risk" button then produces the patient’s estimated 30-day morbidity and mortality risks.
Dr. Robinson presented a prospective study in which the VA tool was compared to the timed-up-and-go (TUG) test in 272 patients aged older than 65 years who were followed for a minimum of 1 year after elective surgery. To see how the two tests performed across surgical specialties, the investigators included 174 patients with a cardiac operation and 98 who had colorectal surgery.
In the TUG test, a clinician starts a stopwatch as the patient rises from a chair, walks 10 feet, returns, and sits back down. The patient is instructed to walk at his or her normal pace and is free to use a walking aid. Dr. Robinson chose to study the TUG rather than a simple 5-meter gait speed test because he considers TUG more relevant to surgical patients.
"TUG combines lower extremity strength to stand up in addition to walking speed. And if you think about somebody who needs to make the transition from hospital to home, lower extremity strength is important," he said.
The investigators categorized a TUG time of 10 seconds or less as fast, 11-14 seconds as intermediate, and 15 seconds or longer as slow. Of note, the subjects’ TUG times were unrelated to common comorbid conditions in the elderly, including stroke, diabetes, heart failure, and hypertension.
In contrast, walking speed was strongly associated with classic indicators of frailty. For example, impaired cognition was present in 3% of subjects with a fast TUG time, 41% of those with an intermediate time, and 92% of slow performers. Another frailty indicator – a history of falling within the past 6 months – was present in 7% of the fast group, 21% of intermediate TUG walkers, and 85% of those with a TUG speed of 15 seconds or more.
In the cardiac surgery group, one or more postsurgical complications occurred in 11% of the 53 patients in the fast group, 25% of 88 patients with an intermediate TUG time, and 52% of 33 individuals in the slow group. The 1-year mortality rates were 2%, 3%, and 12%, respectively.
Similarly, in the colorectal surgery group, the complication rate was 12% among 30 fast walkers, 29% of 42 patients in the intermediate group, and 77% of 26 patients in the slow group. The 1-year mortality rates were 3%, 10%, and 31%, respectively.
The investigators judged comparative test performance in predicting postoperative morbidity and mortality on the basis of the receiver operating characteristic area under the curve, which was 77% with the TUG test compared to 55% with the VA risk calculator in the colorectal surgery patients. In the cardiac surgery group, the figures were 68% for TUG and 55% with the risk calculator.
Geriatricians typically measure TUG in seconds as a continuous variable. Dr. Robinson and coworkers decided the test would be more useful for surgeons if they created the three discrete categories of fast, intermediate, and slow.
Discussant Dr. Michael E. Zenilman praised the investigators for what he called "an outstanding study," and one that’s particularly welcome right now, as the wave of aging baby boomers swells.
"As we take care of more elderly patients, it’s important that we develop tools like this to quickly and objectively assess risk. The tools that we have now, such as the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) models and the VA risk calculator, are for me just too complicated," said Dr. Zenilman of Johns Hopkins University, Baltimore. Dr. Zenilman is the university’s vice chair and regional director of surgery for the Washington area. Noting that TUG, Mini-Mental Status scores, history of falling, and serum albumin levels all have been shown to serve as proxies for frailty, he asked Dr. Robinson to predict which one he thinks will win out as a postoperative risk predictor.
Dr. Robinson replied that TUG is a good frailty assessment tool for now, but he and others are trying to develop something better. The American College of Surgeons geriatric task force is collaborating with the NSQIP to identify variables present in patients’ charts that correlate with global frailty and can serve as reliable predictors of postoperative risk.
He reported having no financial conflicts.
INDIANAPOLIS – Slower walking speed on the timed-up-and-go test in elderly patients scheduled for surgery is a significantly better forecaster of postoperative complications and 1-year mortality than are the considerably more complex patient risk calculators currently considered standard of care, Dr. Thomas N. Robinson reported at the annual meeting of the American Surgical Association.
"I think what walking speed reflects is global reduced physiologic reserve. It’s frailty. And by definition, an individual who’s frail will have adverse health care outcomes," explained Dr. Robinson, a general surgeon at the University of Colorado, Denver.
Use of preoperative walking speed to assess postoperative risk is a paradigm shift, he noted. Current surgical risk assessment strategies rely upon math-heavy patient risk calculators which evaluate single end-organ dysfunction, in some cases summing up the individual scores for heart, lung, liver, and other organ dysfunction in an attempt to define chronic disease burden. But in older patients, this approach is less effective than a simple frailty assessment based upon mobility: that is, walking speed, he continued.
Surgeons in the Veterans Affairs health care system use a risk calculator that involves input of 24 variables. Hitting the "compute risk" button then produces the patient’s estimated 30-day morbidity and mortality risks.
Dr. Robinson presented a prospective study in which the VA tool was compared to the timed-up-and-go (TUG) test in 272 patients aged older than 65 years who were followed for a minimum of 1 year after elective surgery. To see how the two tests performed across surgical specialties, the investigators included 174 patients with a cardiac operation and 98 who had colorectal surgery.
In the TUG test, a clinician starts a stopwatch as the patient rises from a chair, walks 10 feet, returns, and sits back down. The patient is instructed to walk at his or her normal pace and is free to use a walking aid. Dr. Robinson chose to study the TUG rather than a simple 5-meter gait speed test because he considers TUG more relevant to surgical patients.
"TUG combines lower extremity strength to stand up in addition to walking speed. And if you think about somebody who needs to make the transition from hospital to home, lower extremity strength is important," he said.
The investigators categorized a TUG time of 10 seconds or less as fast, 11-14 seconds as intermediate, and 15 seconds or longer as slow. Of note, the subjects’ TUG times were unrelated to common comorbid conditions in the elderly, including stroke, diabetes, heart failure, and hypertension.
In contrast, walking speed was strongly associated with classic indicators of frailty. For example, impaired cognition was present in 3% of subjects with a fast TUG time, 41% of those with an intermediate time, and 92% of slow performers. Another frailty indicator – a history of falling within the past 6 months – was present in 7% of the fast group, 21% of intermediate TUG walkers, and 85% of those with a TUG speed of 15 seconds or more.
In the cardiac surgery group, one or more postsurgical complications occurred in 11% of the 53 patients in the fast group, 25% of 88 patients with an intermediate TUG time, and 52% of 33 individuals in the slow group. The 1-year mortality rates were 2%, 3%, and 12%, respectively.
Similarly, in the colorectal surgery group, the complication rate was 12% among 30 fast walkers, 29% of 42 patients in the intermediate group, and 77% of 26 patients in the slow group. The 1-year mortality rates were 3%, 10%, and 31%, respectively.
The investigators judged comparative test performance in predicting postoperative morbidity and mortality on the basis of the receiver operating characteristic area under the curve, which was 77% with the TUG test compared to 55% with the VA risk calculator in the colorectal surgery patients. In the cardiac surgery group, the figures were 68% for TUG and 55% with the risk calculator.
Geriatricians typically measure TUG in seconds as a continuous variable. Dr. Robinson and coworkers decided the test would be more useful for surgeons if they created the three discrete categories of fast, intermediate, and slow.
Discussant Dr. Michael E. Zenilman praised the investigators for what he called "an outstanding study," and one that’s particularly welcome right now, as the wave of aging baby boomers swells.
"As we take care of more elderly patients, it’s important that we develop tools like this to quickly and objectively assess risk. The tools that we have now, such as the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) models and the VA risk calculator, are for me just too complicated," said Dr. Zenilman of Johns Hopkins University, Baltimore. Dr. Zenilman is the university’s vice chair and regional director of surgery for the Washington area. Noting that TUG, Mini-Mental Status scores, history of falling, and serum albumin levels all have been shown to serve as proxies for frailty, he asked Dr. Robinson to predict which one he thinks will win out as a postoperative risk predictor.
Dr. Robinson replied that TUG is a good frailty assessment tool for now, but he and others are trying to develop something better. The American College of Surgeons geriatric task force is collaborating with the NSQIP to identify variables present in patients’ charts that correlate with global frailty and can serve as reliable predictors of postoperative risk.
He reported having no financial conflicts.
INDIANAPOLIS – Slower walking speed on the timed-up-and-go test in elderly patients scheduled for surgery is a significantly better forecaster of postoperative complications and 1-year mortality than are the considerably more complex patient risk calculators currently considered standard of care, Dr. Thomas N. Robinson reported at the annual meeting of the American Surgical Association.
"I think what walking speed reflects is global reduced physiologic reserve. It’s frailty. And by definition, an individual who’s frail will have adverse health care outcomes," explained Dr. Robinson, a general surgeon at the University of Colorado, Denver.
Use of preoperative walking speed to assess postoperative risk is a paradigm shift, he noted. Current surgical risk assessment strategies rely upon math-heavy patient risk calculators which evaluate single end-organ dysfunction, in some cases summing up the individual scores for heart, lung, liver, and other organ dysfunction in an attempt to define chronic disease burden. But in older patients, this approach is less effective than a simple frailty assessment based upon mobility: that is, walking speed, he continued.
Surgeons in the Veterans Affairs health care system use a risk calculator that involves input of 24 variables. Hitting the "compute risk" button then produces the patient’s estimated 30-day morbidity and mortality risks.
Dr. Robinson presented a prospective study in which the VA tool was compared to the timed-up-and-go (TUG) test in 272 patients aged older than 65 years who were followed for a minimum of 1 year after elective surgery. To see how the two tests performed across surgical specialties, the investigators included 174 patients with a cardiac operation and 98 who had colorectal surgery.
In the TUG test, a clinician starts a stopwatch as the patient rises from a chair, walks 10 feet, returns, and sits back down. The patient is instructed to walk at his or her normal pace and is free to use a walking aid. Dr. Robinson chose to study the TUG rather than a simple 5-meter gait speed test because he considers TUG more relevant to surgical patients.
"TUG combines lower extremity strength to stand up in addition to walking speed. And if you think about somebody who needs to make the transition from hospital to home, lower extremity strength is important," he said.
The investigators categorized a TUG time of 10 seconds or less as fast, 11-14 seconds as intermediate, and 15 seconds or longer as slow. Of note, the subjects’ TUG times were unrelated to common comorbid conditions in the elderly, including stroke, diabetes, heart failure, and hypertension.
In contrast, walking speed was strongly associated with classic indicators of frailty. For example, impaired cognition was present in 3% of subjects with a fast TUG time, 41% of those with an intermediate time, and 92% of slow performers. Another frailty indicator – a history of falling within the past 6 months – was present in 7% of the fast group, 21% of intermediate TUG walkers, and 85% of those with a TUG speed of 15 seconds or more.
In the cardiac surgery group, one or more postsurgical complications occurred in 11% of the 53 patients in the fast group, 25% of 88 patients with an intermediate TUG time, and 52% of 33 individuals in the slow group. The 1-year mortality rates were 2%, 3%, and 12%, respectively.
Similarly, in the colorectal surgery group, the complication rate was 12% among 30 fast walkers, 29% of 42 patients in the intermediate group, and 77% of 26 patients in the slow group. The 1-year mortality rates were 3%, 10%, and 31%, respectively.
The investigators judged comparative test performance in predicting postoperative morbidity and mortality on the basis of the receiver operating characteristic area under the curve, which was 77% with the TUG test compared to 55% with the VA risk calculator in the colorectal surgery patients. In the cardiac surgery group, the figures were 68% for TUG and 55% with the risk calculator.
Geriatricians typically measure TUG in seconds as a continuous variable. Dr. Robinson and coworkers decided the test would be more useful for surgeons if they created the three discrete categories of fast, intermediate, and slow.
Discussant Dr. Michael E. Zenilman praised the investigators for what he called "an outstanding study," and one that’s particularly welcome right now, as the wave of aging baby boomers swells.
"As we take care of more elderly patients, it’s important that we develop tools like this to quickly and objectively assess risk. The tools that we have now, such as the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) models and the VA risk calculator, are for me just too complicated," said Dr. Zenilman of Johns Hopkins University, Baltimore. Dr. Zenilman is the university’s vice chair and regional director of surgery for the Washington area. Noting that TUG, Mini-Mental Status scores, history of falling, and serum albumin levels all have been shown to serve as proxies for frailty, he asked Dr. Robinson to predict which one he thinks will win out as a postoperative risk predictor.
Dr. Robinson replied that TUG is a good frailty assessment tool for now, but he and others are trying to develop something better. The American College of Surgeons geriatric task force is collaborating with the NSQIP to identify variables present in patients’ charts that correlate with global frailty and can serve as reliable predictors of postoperative risk.
He reported having no financial conflicts.
AT THE ASA ANNUAL MEETING
Major Finding. One-year mortality rates for fast, intermediate, and slow cardiac patients were 2%, 3%, and 12%, respectively. In the colorectal surgery group, the 1-year mortality rates were 3%, 10%, and 31%, respectively.
Data Source: A prospective cohort study of postsurgical complications and 1-year mortality in 98 elderly patients undergoing elective colorectal surgery and 174 with elective cardiac surgery. All underwent a preoperative timed-up-and-go test as well as assessment via the Veterans Affairs surgical risk calculator.
Disclosures: The study presenter reported having no conflicts of interest.

Most ovarian cysts in adolescents resolve
SAN DIEGO – Most ovarian cysts in adolescents will resolve, but those greater than 100 mL in size are the most predictive of ovarian pathology and need for surgical intervention.
The findings, presented during a poster session at the annual meeting of the North American Society for Pediatric and Adolescent Gynecology, come from a study of 78 adolescent females at Children’s Mercy Hospital, Kansas City, who were given a diagnostic ICD-9 code consistent with ovarian cyst or mass between 2004 and 2012.
"There is insufficient documentation that most cysts will either decrease in size or resolve, but clear criteria for conservative management in this group has not been described," researchers led by Dr. Crystal Meacham wrote in the poster. "When indicated, laparoscopic intervention of ovarian cysts in adolescents has been well studied and is the preferred surgical approach."
In an effort to determine predictive characteristics that would aid in safe observation and expectant management versus the need for surgical intervention, Dr. Meacham and her associates limited their analysis to adolescents with ovarian cysts greater than or equal to 3 cm in largest diameter on imaging. They recorded cyst volume at initial presentation and follow-up imaging was recorded. Cysts were categorized into three groups based on size: small (0-49 mL), medium (50-100 mL), and large (greater than 100 mL).
The average cyst volume at initial imaging was 62.17 mL, while the average volume at follow-up imaging was 25.81 mL, a reduction that reached statistical significance (P is less than .0001). Of the 78 cysts, 61 (90%) resolved and 17 did not. The researchers found that cysts in the large-volume category were most likely to persist and require surgical intervention.
"Level of cyst complexity is not a predictive characteristic for ovarian cyst resolution nor an indication for surgical management," they wrote. "The pathology most consistent with cysts of the large-volume category, and thus requiring surgery, is serous cystadenoma. Large cyst volume is most predictive of ovarian pathology and need for surgical intervention."
The researchers had no relevant financial disclosures.
SAN DIEGO – Most ovarian cysts in adolescents will resolve, but those greater than 100 mL in size are the most predictive of ovarian pathology and need for surgical intervention.
The findings, presented during a poster session at the annual meeting of the North American Society for Pediatric and Adolescent Gynecology, come from a study of 78 adolescent females at Children’s Mercy Hospital, Kansas City, who were given a diagnostic ICD-9 code consistent with ovarian cyst or mass between 2004 and 2012.
"There is insufficient documentation that most cysts will either decrease in size or resolve, but clear criteria for conservative management in this group has not been described," researchers led by Dr. Crystal Meacham wrote in the poster. "When indicated, laparoscopic intervention of ovarian cysts in adolescents has been well studied and is the preferred surgical approach."
In an effort to determine predictive characteristics that would aid in safe observation and expectant management versus the need for surgical intervention, Dr. Meacham and her associates limited their analysis to adolescents with ovarian cysts greater than or equal to 3 cm in largest diameter on imaging. They recorded cyst volume at initial presentation and follow-up imaging was recorded. Cysts were categorized into three groups based on size: small (0-49 mL), medium (50-100 mL), and large (greater than 100 mL).
The average cyst volume at initial imaging was 62.17 mL, while the average volume at follow-up imaging was 25.81 mL, a reduction that reached statistical significance (P is less than .0001). Of the 78 cysts, 61 (90%) resolved and 17 did not. The researchers found that cysts in the large-volume category were most likely to persist and require surgical intervention.
"Level of cyst complexity is not a predictive characteristic for ovarian cyst resolution nor an indication for surgical management," they wrote. "The pathology most consistent with cysts of the large-volume category, and thus requiring surgery, is serous cystadenoma. Large cyst volume is most predictive of ovarian pathology and need for surgical intervention."
The researchers had no relevant financial disclosures.
SAN DIEGO – Most ovarian cysts in adolescents will resolve, but those greater than 100 mL in size are the most predictive of ovarian pathology and need for surgical intervention.
The findings, presented during a poster session at the annual meeting of the North American Society for Pediatric and Adolescent Gynecology, come from a study of 78 adolescent females at Children’s Mercy Hospital, Kansas City, who were given a diagnostic ICD-9 code consistent with ovarian cyst or mass between 2004 and 2012.
"There is insufficient documentation that most cysts will either decrease in size or resolve, but clear criteria for conservative management in this group has not been described," researchers led by Dr. Crystal Meacham wrote in the poster. "When indicated, laparoscopic intervention of ovarian cysts in adolescents has been well studied and is the preferred surgical approach."
In an effort to determine predictive characteristics that would aid in safe observation and expectant management versus the need for surgical intervention, Dr. Meacham and her associates limited their analysis to adolescents with ovarian cysts greater than or equal to 3 cm in largest diameter on imaging. They recorded cyst volume at initial presentation and follow-up imaging was recorded. Cysts were categorized into three groups based on size: small (0-49 mL), medium (50-100 mL), and large (greater than 100 mL).
The average cyst volume at initial imaging was 62.17 mL, while the average volume at follow-up imaging was 25.81 mL, a reduction that reached statistical significance (P is less than .0001). Of the 78 cysts, 61 (90%) resolved and 17 did not. The researchers found that cysts in the large-volume category were most likely to persist and require surgical intervention.
"Level of cyst complexity is not a predictive characteristic for ovarian cyst resolution nor an indication for surgical management," they wrote. "The pathology most consistent with cysts of the large-volume category, and thus requiring surgery, is serous cystadenoma. Large cyst volume is most predictive of ovarian pathology and need for surgical intervention."
The researchers had no relevant financial disclosures.
AT THE NASPAG ANNUAL MEETING
Major finding: Of the 78 cysts, 61 (90%) resolved and 17 did not.
Data source: A study of 78 adolescent females at Children’s Mercy Hospital, Kansas City, who were given a diagnostic ICD-9 code consistent with ovarian cyst or mass between 2004 and 2012.
Disclosures: The researchers had no relevant financial disclosures.
Forecast warns of urologist shortage
SAN DIEGO – The number of urologists practicing in the United States is expected to decrease by 29% between 2009 and 2025, according to a new analysis.
"It’s one thing if the demand for urologists is going up and the supply is stable, but to have the demand go up and the supply almost falling off of a cliff is worrisome," Dr. Raj S. Pruthi said in an interview at the annual meeting of the American Urological Association. "The people who will be hardest hit by this are ones who already struggle with access: those who live in rural communities."

Dr. Pruthi and his colleagues used stock and flow models, starting with the supply of urologists in 2009. They added new entrants from the graduate medical education (GME) pipeline and subtracted attrition from training and from the workforce due to retirement or breaks from practice. The forecast model estimates a 29% head count reduction and a 25% decrease in the full-time equivalent (FTE) supply of urologists between 2009 and 2025. The projected decrease is more than four times greater than the Health Resources and Services Administration’s Physician Supply Model, which estimated a 7% decrease over the same time period.
Dr. Pruthi warned that none of the proposed changes to GME (recommendations from the Council of Graduate Medical Education’s 16th report or a recent proposal to Congress) will increase GME enough to offset the projected decline in head count. "GME funding has been capped since 1996," he said. "We’re setting forth a recipe for a very big problem that we’re going to have for future generations in terms of who’s going to take care of" a rapidly aging population.
As the Affordable Health Care Act takes shape, "one thing that’s not been considered adequately is physician supply," added Dr. Pruthi, chief of urologic surgery at the University of North Carolina at Chapel Hill. "Are there enough of us to help care for the population? That needs to be part of the calculus. We need to do efficient, appropriate care. We need to cut health care costs, but we have to remember our physician supply."
The shrinking number of urologists could affect mortality rates, as research has demonstrated an association between a higher density of urologists in a defined area and lower mortality from prostate, bladder, and kidney cancer. "As supply contracts, rural areas are likely to have an even greater loss of urologic surgeons since these areas have a higher percentage of surgeons closer to retirement age than urban areas," the researchers noted in their abstract. "The result may decrease access to screening, medical and surgical treatment for urologic conditions."
Dr. Pruthi acknowledged that the ability to predict physician demand is an imprecise science. However, "there is indirect data to suggest that our demand isn’t going to go away. It’s only going to go up with that rising incidence and with the rising number of aging baby boomers. Second, we don’t know the appropriate ratio of supply and demand. If you have limited supply, you have limited access. Is our culture accepting of that? Some of these limitations to access may have health consequences."
He and his associates plan to conduct more detailed work on the projection model, including the impact of increasing numbers of women entering the urology field. "About 5% of urologists are female, but in current residency matching the numbers are about 25% female," he said. "What impact will that have? We don’t know yet."
Dr. Pruthi said that he had no relevant financial conflicts to disclose.
SAN DIEGO – The number of urologists practicing in the United States is expected to decrease by 29% between 2009 and 2025, according to a new analysis.
"It’s one thing if the demand for urologists is going up and the supply is stable, but to have the demand go up and the supply almost falling off of a cliff is worrisome," Dr. Raj S. Pruthi said in an interview at the annual meeting of the American Urological Association. "The people who will be hardest hit by this are ones who already struggle with access: those who live in rural communities."
Dr. Pruthi and his colleagues used stock and flow models, starting with the supply of urologists in 2009. They added new entrants from the graduate medical education (GME) pipeline and subtracted attrition from training and from the workforce due to retirement or breaks from practice. The forecast model estimates a 29% head count reduction and a 25% decrease in the full-time equivalent (FTE) supply of urologists between 2009 and 2025. The projected decrease is more than four times greater than the Health Resources and Services Administration’s Physician Supply Model, which estimated a 7% decrease over the same time period.
Dr. Pruthi warned that none of the proposed changes to GME (recommendations from the Council of Graduate Medical Education’s 16th report or a recent proposal to Congress) will increase GME enough to offset the projected decline in head count. "GME funding has been capped since 1996," he said. "We’re setting forth a recipe for a very big problem that we’re going to have for future generations in terms of who’s going to take care of" a rapidly aging population.
As the Affordable Health Care Act takes shape, "one thing that’s not been considered adequately is physician supply," added Dr. Pruthi, chief of urologic surgery at the University of North Carolina at Chapel Hill. "Are there enough of us to help care for the population? That needs to be part of the calculus. We need to do efficient, appropriate care. We need to cut health care costs, but we have to remember our physician supply."
The shrinking number of urologists could affect mortality rates, as research has demonstrated an association between a higher density of urologists in a defined area and lower mortality from prostate, bladder, and kidney cancer. "As supply contracts, rural areas are likely to have an even greater loss of urologic surgeons since these areas have a higher percentage of surgeons closer to retirement age than urban areas," the researchers noted in their abstract. "The result may decrease access to screening, medical and surgical treatment for urologic conditions."
Dr. Pruthi acknowledged that the ability to predict physician demand is an imprecise science. However, "there is indirect data to suggest that our demand isn’t going to go away. It’s only going to go up with that rising incidence and with the rising number of aging baby boomers. Second, we don’t know the appropriate ratio of supply and demand. If you have limited supply, you have limited access. Is our culture accepting of that? Some of these limitations to access may have health consequences."
He and his associates plan to conduct more detailed work on the projection model, including the impact of increasing numbers of women entering the urology field. "About 5% of urologists are female, but in current residency matching the numbers are about 25% female," he said. "What impact will that have? We don’t know yet."
Dr. Pruthi said that he had no relevant financial conflicts to disclose.
SAN DIEGO – The number of urologists practicing in the United States is expected to decrease by 29% between 2009 and 2025, according to a new analysis.
"It’s one thing if the demand for urologists is going up and the supply is stable, but to have the demand go up and the supply almost falling off of a cliff is worrisome," Dr. Raj S. Pruthi said in an interview at the annual meeting of the American Urological Association. "The people who will be hardest hit by this are ones who already struggle with access: those who live in rural communities."
Dr. Pruthi and his colleagues used stock and flow models, starting with the supply of urologists in 2009. They added new entrants from the graduate medical education (GME) pipeline and subtracted attrition from training and from the workforce due to retirement or breaks from practice. The forecast model estimates a 29% head count reduction and a 25% decrease in the full-time equivalent (FTE) supply of urologists between 2009 and 2025. The projected decrease is more than four times greater than the Health Resources and Services Administration’s Physician Supply Model, which estimated a 7% decrease over the same time period.
Dr. Pruthi warned that none of the proposed changes to GME (recommendations from the Council of Graduate Medical Education’s 16th report or a recent proposal to Congress) will increase GME enough to offset the projected decline in head count. "GME funding has been capped since 1996," he said. "We’re setting forth a recipe for a very big problem that we’re going to have for future generations in terms of who’s going to take care of" a rapidly aging population.
As the Affordable Health Care Act takes shape, "one thing that’s not been considered adequately is physician supply," added Dr. Pruthi, chief of urologic surgery at the University of North Carolina at Chapel Hill. "Are there enough of us to help care for the population? That needs to be part of the calculus. We need to do efficient, appropriate care. We need to cut health care costs, but we have to remember our physician supply."
The shrinking number of urologists could affect mortality rates, as research has demonstrated an association between a higher density of urologists in a defined area and lower mortality from prostate, bladder, and kidney cancer. "As supply contracts, rural areas are likely to have an even greater loss of urologic surgeons since these areas have a higher percentage of surgeons closer to retirement age than urban areas," the researchers noted in their abstract. "The result may decrease access to screening, medical and surgical treatment for urologic conditions."
Dr. Pruthi acknowledged that the ability to predict physician demand is an imprecise science. However, "there is indirect data to suggest that our demand isn’t going to go away. It’s only going to go up with that rising incidence and with the rising number of aging baby boomers. Second, we don’t know the appropriate ratio of supply and demand. If you have limited supply, you have limited access. Is our culture accepting of that? Some of these limitations to access may have health consequences."
He and his associates plan to conduct more detailed work on the projection model, including the impact of increasing numbers of women entering the urology field. "About 5% of urologists are female, but in current residency matching the numbers are about 25% female," he said. "What impact will that have? We don’t know yet."
Dr. Pruthi said that he had no relevant financial conflicts to disclose.
AT THE AUA ANNUAL MEETING
Major finding: The forecast model estimates a 29% head count reduction and a 25% decrease in the full-time equivalent (FTE) supply of urologists between 2009 and 2025.
Data source: An analysis that used stock and flow models, starting with the supply of urologists in 2009.
Disclosures: Dr. Pruthi said that he had no relevant disclosures.

Early surgery for adhesive bowel obstruction can save lives
INDIANAPOLIS – Patients requiring surgery for adhesive small bowel obstruction have markedly lower major morbidity and mortality rates if they’re operated on within 24 hours of hospital admission, according to an analysis of a large national database.
This finding is at odds with the conventional wisdom.
Both the World Society of Emergency Surgery and the Eastern Association for the Surgery of Trauma recommend in published guidelines an initial 3-5 days of nonoperative management to give the obstruction a chance to resolve on its own, Dr. Pedro G. Teixeira noted in presenting the study findings at the annual meeting of the American Surgical Association.

He and his coinvestigators identified 4,163 patients in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database for 2005-2010 who underwent emergency laparotomy for adhesive bowel obstruction. Thirty-day mortality was 3% in those operated upon within 24 hours of hospital admission. It rose in stepwise fashion thereafter: 4% mortality with surgery at 24-48 hours, 7% with surgery at 48-72 hours, and 9% a threefold increase – when surgery was delayed beyond 72 hours, according to Dr. Teixeira of the University of Southern California, Los Angeles.
Similarly, the incidence of systemic infectious complications, including pneumonia, urinary tract infections, and sepsis, climbed from 12% with early operation to 17% when surgery occurred at 24-48 hours, 21% at 48-72 hours, and 24% thereafter.
In a multivariate analysis adjusted for baseline comorbidities and other potential confounding variables, surgery delayed for 24 hours or more after admission was associated with a highly significant 58% increased risk of mortality, a 33% increase in surgical site infections, a 36% greater risk of pneumonia, and a 47% increased risk of septic shock, he continued.
Discussant Gregory J. Jurkovich commented that this study challenges current dogma and harkens back to a century-old adage that has since been cast aside, namely, "Never let the sun set on a bowel obstruction."
The trouble is, however, that having a low threshold for surgery within 24 hours would subject a massive number of patients to an unnecessary operation.
An analysis of Nationwide Inpatient Sample data for 2009 by other investigators concluded that bowel obstruction resolved on its own within 3 days in 60% of patients and within 5 days in 80%. Fewer than 20% of the patients who presented with adhesive small bowel obstruction without evidence of ischemia underwent surgery, noted Dr. Jurkovich, director of surgery at Denver Health Medical Center and professor of trauma surgery and vice chairman of the department of surgery at the University of Colorado at Denver.
Dr. Teixeira concurred that bowel obstruction will resolve on its own in most patients. The challenge for surgeons in light of his study findings, he stressed, is to expedite the identification of those patients who will fail the period of nonoperative management. The best tool for that, in his view, is a CT scan of the abdomen and pelvis with water-soluble contrast.
At the University of Southern California, he explained, a patient who presents with adhesive bowel obstruction without evidence of ischemia undergoes the CT scan and is admitted to the surgical observation unit for close monitoring.
"At our institution, failure to demonstrate contrast progression through the colon within 24 hours would be a very strong indication for surgical exploration," according to Dr. Teixeira.
He reported having no financial conflicts.
The study by Dr. Teixeira is intriguing in
that it suggests a return to practice patterns from a prior era.
|
| Dr. Chad Whelan |
The study does report increased risk in
complications including mortality with delays in surgery for small bowel
obstructions, even with risk adjustment. However, this is not a controlled
trial which limits our ability to reach definitive conclusions from it. Still,
hospitalists often are the primary physicians for patients admitted for small
bowel obstructions and should be aware of these findings so that they can
ensure that they have early surgical involvement.
Chad Whelan, M.D., is associate chief medical officer for
performance improvement and innovation and an associate professor of medicine
at the University
of Chicago Medical Center.
The study by Dr. Teixeira is intriguing in
that it suggests a return to practice patterns from a prior era.
|
|
| Dr. Chad Whelan |
The study does report increased risk in
complications including mortality with delays in surgery for small bowel
obstructions, even with risk adjustment. However, this is not a controlled
trial which limits our ability to reach definitive conclusions from it. Still,
hospitalists often are the primary physicians for patients admitted for small
bowel obstructions and should be aware of these findings so that they can
ensure that they have early surgical involvement.
Chad Whelan, M.D., is associate chief medical officer for
performance improvement and innovation and an associate professor of medicine
at the University
of Chicago Medical Center.
The study by Dr. Teixeira is intriguing in
that it suggests a return to practice patterns from a prior era.
|
|
| Dr. Chad Whelan |
The study does report increased risk in
complications including mortality with delays in surgery for small bowel
obstructions, even with risk adjustment. However, this is not a controlled
trial which limits our ability to reach definitive conclusions from it. Still,
hospitalists often are the primary physicians for patients admitted for small
bowel obstructions and should be aware of these findings so that they can
ensure that they have early surgical involvement.
Chad Whelan, M.D., is associate chief medical officer for
performance improvement and innovation and an associate professor of medicine
at the University
of Chicago Medical Center.
INDIANAPOLIS – Patients requiring surgery for adhesive small bowel obstruction have markedly lower major morbidity and mortality rates if they’re operated on within 24 hours of hospital admission, according to an analysis of a large national database.
This finding is at odds with the conventional wisdom.
Both the World Society of Emergency Surgery and the Eastern Association for the Surgery of Trauma recommend in published guidelines an initial 3-5 days of nonoperative management to give the obstruction a chance to resolve on its own, Dr. Pedro G. Teixeira noted in presenting the study findings at the annual meeting of the American Surgical Association.
He and his coinvestigators identified 4,163 patients in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database for 2005-2010 who underwent emergency laparotomy for adhesive bowel obstruction. Thirty-day mortality was 3% in those operated upon within 24 hours of hospital admission. It rose in stepwise fashion thereafter: 4% mortality with surgery at 24-48 hours, 7% with surgery at 48-72 hours, and 9% a threefold increase – when surgery was delayed beyond 72 hours, according to Dr. Teixeira of the University of Southern California, Los Angeles.
Similarly, the incidence of systemic infectious complications, including pneumonia, urinary tract infections, and sepsis, climbed from 12% with early operation to 17% when surgery occurred at 24-48 hours, 21% at 48-72 hours, and 24% thereafter.
In a multivariate analysis adjusted for baseline comorbidities and other potential confounding variables, surgery delayed for 24 hours or more after admission was associated with a highly significant 58% increased risk of mortality, a 33% increase in surgical site infections, a 36% greater risk of pneumonia, and a 47% increased risk of septic shock, he continued.
Discussant Gregory J. Jurkovich commented that this study challenges current dogma and harkens back to a century-old adage that has since been cast aside, namely, "Never let the sun set on a bowel obstruction."
The trouble is, however, that having a low threshold for surgery within 24 hours would subject a massive number of patients to an unnecessary operation.
An analysis of Nationwide Inpatient Sample data for 2009 by other investigators concluded that bowel obstruction resolved on its own within 3 days in 60% of patients and within 5 days in 80%. Fewer than 20% of the patients who presented with adhesive small bowel obstruction without evidence of ischemia underwent surgery, noted Dr. Jurkovich, director of surgery at Denver Health Medical Center and professor of trauma surgery and vice chairman of the department of surgery at the University of Colorado at Denver.
Dr. Teixeira concurred that bowel obstruction will resolve on its own in most patients. The challenge for surgeons in light of his study findings, he stressed, is to expedite the identification of those patients who will fail the period of nonoperative management. The best tool for that, in his view, is a CT scan of the abdomen and pelvis with water-soluble contrast.
At the University of Southern California, he explained, a patient who presents with adhesive bowel obstruction without evidence of ischemia undergoes the CT scan and is admitted to the surgical observation unit for close monitoring.
"At our institution, failure to demonstrate contrast progression through the colon within 24 hours would be a very strong indication for surgical exploration," according to Dr. Teixeira.
He reported having no financial conflicts.
INDIANAPOLIS – Patients requiring surgery for adhesive small bowel obstruction have markedly lower major morbidity and mortality rates if they’re operated on within 24 hours of hospital admission, according to an analysis of a large national database.
This finding is at odds with the conventional wisdom.
Both the World Society of Emergency Surgery and the Eastern Association for the Surgery of Trauma recommend in published guidelines an initial 3-5 days of nonoperative management to give the obstruction a chance to resolve on its own, Dr. Pedro G. Teixeira noted in presenting the study findings at the annual meeting of the American Surgical Association.
He and his coinvestigators identified 4,163 patients in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database for 2005-2010 who underwent emergency laparotomy for adhesive bowel obstruction. Thirty-day mortality was 3% in those operated upon within 24 hours of hospital admission. It rose in stepwise fashion thereafter: 4% mortality with surgery at 24-48 hours, 7% with surgery at 48-72 hours, and 9% a threefold increase – when surgery was delayed beyond 72 hours, according to Dr. Teixeira of the University of Southern California, Los Angeles.
Similarly, the incidence of systemic infectious complications, including pneumonia, urinary tract infections, and sepsis, climbed from 12% with early operation to 17% when surgery occurred at 24-48 hours, 21% at 48-72 hours, and 24% thereafter.
In a multivariate analysis adjusted for baseline comorbidities and other potential confounding variables, surgery delayed for 24 hours or more after admission was associated with a highly significant 58% increased risk of mortality, a 33% increase in surgical site infections, a 36% greater risk of pneumonia, and a 47% increased risk of septic shock, he continued.
Discussant Gregory J. Jurkovich commented that this study challenges current dogma and harkens back to a century-old adage that has since been cast aside, namely, "Never let the sun set on a bowel obstruction."
The trouble is, however, that having a low threshold for surgery within 24 hours would subject a massive number of patients to an unnecessary operation.
An analysis of Nationwide Inpatient Sample data for 2009 by other investigators concluded that bowel obstruction resolved on its own within 3 days in 60% of patients and within 5 days in 80%. Fewer than 20% of the patients who presented with adhesive small bowel obstruction without evidence of ischemia underwent surgery, noted Dr. Jurkovich, director of surgery at Denver Health Medical Center and professor of trauma surgery and vice chairman of the department of surgery at the University of Colorado at Denver.
Dr. Teixeira concurred that bowel obstruction will resolve on its own in most patients. The challenge for surgeons in light of his study findings, he stressed, is to expedite the identification of those patients who will fail the period of nonoperative management. The best tool for that, in his view, is a CT scan of the abdomen and pelvis with water-soluble contrast.
At the University of Southern California, he explained, a patient who presents with adhesive bowel obstruction without evidence of ischemia undergoes the CT scan and is admitted to the surgical observation unit for close monitoring.
"At our institution, failure to demonstrate contrast progression through the colon within 24 hours would be a very strong indication for surgical exploration," according to Dr. Teixeira.
He reported having no financial conflicts.
AT THE ASA ANNUAL MEETING
Major Finding: Surgery for adhesive small bowel obstruction had a 30-day mortality rate of 3% if performed within 24 hours of hospital admission, rising stepwise to 9% when the operation was delayed beyond 72 hours.
Data Source: This was a retrospective analysis of 4,163 patients in the American College of Surgeons National Quality Improvement Program database for 2005-2010 who underwent emergency laparotomy for adhesive bowel obstruction.
Disclosures: The presenter reported having no conflicts of interest.

Mesh, native tissue for prolapse repair yield similar 3-year outcomes
CHARLESTON, S.C. – Cure rates and patient satisfaction following vaginal prolapse repair were high at 3-year follow-up regardless of whether vaginal mesh or native tissue was used for the repair, according to findings from a prospective randomized trial.
The findings raise questions about the long-term value of vaginal mesh repairs because subjects treated with mesh had more complications without experiencing benefit beyond that observed in the native tissue repair patients, Dr. Robert E. Gutman reported at the annual meeting of the Society of Gynecologic Surgeons.

Of 65 women who were enrolled in the trial before enrollment was halted because of a 15.6% mesh exposure rate, 51 – including 25 in the mesh group and 26 in the no mesh group – had quality of life data available for the planned 3-year final analysis, and 41 had 2- or 3-year pelvic organ prolapse quantification (POP-Q) examination information available.
No differences were noted between the groups with respect to POP-Q stage or individual POP-Q points at 3 years, and the majority in both the mesh and no mesh groups (90% and 86%, respectively) improved in stage from baseline, said Dr. Gutman of MedStar Washington Hospital Center and of the department of obstetrics and gynecology and urology at Georgetown University, both in Washington.
Furthermore, no differences were seen between the groups with respect to symptomatic improvement as assessed by the Pelvic Floor Distress Inventory (PFDI), the Pelvic Floor Impact Questionnaire (PFIQ), and the Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire (PISQ), including subscale scores. Also, cure rates – using a variety of definitions for cure – did not differ between the groups.
For example, based on a POP-Q stage of 1 or less as a definition of cure, 45% and 43% of those in the mesh and no mesh groups, respectively, were cured. When no prolapse beyond the hymen was used as a definition, 85% and 71% were cured When absence of bulge symptoms (a "no" answer to item 3 on the PFDI) was used as a definition, 92% and 81% were cured. The differences between the groups for these and other definitions – including a rating of very much better or much better on the Patient Global Impression of Improvement Index (PGI-I), having no prolapse reoperation, and composite outcomes using various combinations of these definitions – were not statistically significant, Dr. Gutman said.
Of note, no new mesh exposures occurred between the previously reported 1-year analysis (three cases required surgical excision before 1 year) and the 3-year analysis. The only prolapse reoperation after 1 year was in a woman who also had a reoperation prior to the 1-year analysis, he said at the meeting, which was jointly sponsored by the American College of Surgeons.
Also of note, the anatomic cure rate was lowest for the anterior compartment, and this did not differ between the mesh and no mesh groups.
Patients included in the study were women with stage 2-4 prolapse who were randomized to the mesh or no mesh group at baseline. Three-month and 1-year outcomes were previously reported.
Although the study is underpowered because of the early halting of enrollment, and is limited by the substantial number of patients lost to follow-up, it also has several strengths, including the long-term follow-up, multicenter design, and robust definitions of cure.
Therefore, the findings of a similar cure rate in the mesh and no mesh groups, excellent quality of life improvements in both groups, a mesh exposure rate of 15.6%, and a finding of only one new mesh exposure between 1- and 3-year follow-up, suggest that a "balanced approach is really required for vaginal mesh repairs, including a thorough patient consent," Dr. Gutman concluded.
He reported having no relevant financial disclosures.
CHARLESTON, S.C. – Cure rates and patient satisfaction following vaginal prolapse repair were high at 3-year follow-up regardless of whether vaginal mesh or native tissue was used for the repair, according to findings from a prospective randomized trial.
The findings raise questions about the long-term value of vaginal mesh repairs because subjects treated with mesh had more complications without experiencing benefit beyond that observed in the native tissue repair patients, Dr. Robert E. Gutman reported at the annual meeting of the Society of Gynecologic Surgeons.
Of 65 women who were enrolled in the trial before enrollment was halted because of a 15.6% mesh exposure rate, 51 – including 25 in the mesh group and 26 in the no mesh group – had quality of life data available for the planned 3-year final analysis, and 41 had 2- or 3-year pelvic organ prolapse quantification (POP-Q) examination information available.
No differences were noted between the groups with respect to POP-Q stage or individual POP-Q points at 3 years, and the majority in both the mesh and no mesh groups (90% and 86%, respectively) improved in stage from baseline, said Dr. Gutman of MedStar Washington Hospital Center and of the department of obstetrics and gynecology and urology at Georgetown University, both in Washington.
Furthermore, no differences were seen between the groups with respect to symptomatic improvement as assessed by the Pelvic Floor Distress Inventory (PFDI), the Pelvic Floor Impact Questionnaire (PFIQ), and the Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire (PISQ), including subscale scores. Also, cure rates – using a variety of definitions for cure – did not differ between the groups.
For example, based on a POP-Q stage of 1 or less as a definition of cure, 45% and 43% of those in the mesh and no mesh groups, respectively, were cured. When no prolapse beyond the hymen was used as a definition, 85% and 71% were cured When absence of bulge symptoms (a "no" answer to item 3 on the PFDI) was used as a definition, 92% and 81% were cured. The differences between the groups for these and other definitions – including a rating of very much better or much better on the Patient Global Impression of Improvement Index (PGI-I), having no prolapse reoperation, and composite outcomes using various combinations of these definitions – were not statistically significant, Dr. Gutman said.
Of note, no new mesh exposures occurred between the previously reported 1-year analysis (three cases required surgical excision before 1 year) and the 3-year analysis. The only prolapse reoperation after 1 year was in a woman who also had a reoperation prior to the 1-year analysis, he said at the meeting, which was jointly sponsored by the American College of Surgeons.
Also of note, the anatomic cure rate was lowest for the anterior compartment, and this did not differ between the mesh and no mesh groups.
Patients included in the study were women with stage 2-4 prolapse who were randomized to the mesh or no mesh group at baseline. Three-month and 1-year outcomes were previously reported.
Although the study is underpowered because of the early halting of enrollment, and is limited by the substantial number of patients lost to follow-up, it also has several strengths, including the long-term follow-up, multicenter design, and robust definitions of cure.
Therefore, the findings of a similar cure rate in the mesh and no mesh groups, excellent quality of life improvements in both groups, a mesh exposure rate of 15.6%, and a finding of only one new mesh exposure between 1- and 3-year follow-up, suggest that a "balanced approach is really required for vaginal mesh repairs, including a thorough patient consent," Dr. Gutman concluded.
He reported having no relevant financial disclosures.
CHARLESTON, S.C. – Cure rates and patient satisfaction following vaginal prolapse repair were high at 3-year follow-up regardless of whether vaginal mesh or native tissue was used for the repair, according to findings from a prospective randomized trial.
The findings raise questions about the long-term value of vaginal mesh repairs because subjects treated with mesh had more complications without experiencing benefit beyond that observed in the native tissue repair patients, Dr. Robert E. Gutman reported at the annual meeting of the Society of Gynecologic Surgeons.
Of 65 women who were enrolled in the trial before enrollment was halted because of a 15.6% mesh exposure rate, 51 – including 25 in the mesh group and 26 in the no mesh group – had quality of life data available for the planned 3-year final analysis, and 41 had 2- or 3-year pelvic organ prolapse quantification (POP-Q) examination information available.
No differences were noted between the groups with respect to POP-Q stage or individual POP-Q points at 3 years, and the majority in both the mesh and no mesh groups (90% and 86%, respectively) improved in stage from baseline, said Dr. Gutman of MedStar Washington Hospital Center and of the department of obstetrics and gynecology and urology at Georgetown University, both in Washington.
Furthermore, no differences were seen between the groups with respect to symptomatic improvement as assessed by the Pelvic Floor Distress Inventory (PFDI), the Pelvic Floor Impact Questionnaire (PFIQ), and the Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire (PISQ), including subscale scores. Also, cure rates – using a variety of definitions for cure – did not differ between the groups.
For example, based on a POP-Q stage of 1 or less as a definition of cure, 45% and 43% of those in the mesh and no mesh groups, respectively, were cured. When no prolapse beyond the hymen was used as a definition, 85% and 71% were cured When absence of bulge symptoms (a "no" answer to item 3 on the PFDI) was used as a definition, 92% and 81% were cured. The differences between the groups for these and other definitions – including a rating of very much better or much better on the Patient Global Impression of Improvement Index (PGI-I), having no prolapse reoperation, and composite outcomes using various combinations of these definitions – were not statistically significant, Dr. Gutman said.
Of note, no new mesh exposures occurred between the previously reported 1-year analysis (three cases required surgical excision before 1 year) and the 3-year analysis. The only prolapse reoperation after 1 year was in a woman who also had a reoperation prior to the 1-year analysis, he said at the meeting, which was jointly sponsored by the American College of Surgeons.
Also of note, the anatomic cure rate was lowest for the anterior compartment, and this did not differ between the mesh and no mesh groups.
Patients included in the study were women with stage 2-4 prolapse who were randomized to the mesh or no mesh group at baseline. Three-month and 1-year outcomes were previously reported.
Although the study is underpowered because of the early halting of enrollment, and is limited by the substantial number of patients lost to follow-up, it also has several strengths, including the long-term follow-up, multicenter design, and robust definitions of cure.
Therefore, the findings of a similar cure rate in the mesh and no mesh groups, excellent quality of life improvements in both groups, a mesh exposure rate of 15.6%, and a finding of only one new mesh exposure between 1- and 3-year follow-up, suggest that a "balanced approach is really required for vaginal mesh repairs, including a thorough patient consent," Dr. Gutman concluded.
He reported having no relevant financial disclosures.
AT THE SGS ANNUAL MEETING
Major finding: Ninety percent of mesh patients improved in prolapse stage from baseline, vs. 86% of no mesh patients.
Data source: A randomized controlled study of 65 patients.
Disclosures: Dr. Gutman reported having no relevant financial disclosures.

Retropubic midurethral sling bests mini-sling for SUI
CHARLESTON, S.C. – Single-incision mini-slings for the treatment of stress urinary incontinence are associated with higher failure and reoperation rates than are retropubic midurethral slings, according to findings from a survey and review of medical records of more than 200 patients.
At a mean follow-up of 21 months, 71 of 93 (76%) women who underwent a single-incision mini-sling procedure reported treatment failure, defined as overall incontinence, compared with 70 of 109 (64%) women who underwent a retropubic midurethral sling procedure, Dr. Annetta M. Madsen reported at the annual meeting of the Society of Gynecologic Surgeons.
After adjustment for body mass index and follow-up time, which differed between the groups, the odds ratio for treatment failure in the mini-sling vs. retropubic midurethral sling group was 1.84, which trended toward statistical significance, said Dr. Madsen of the Mayo Clinic, Rochester, Minn.
The secondary outcomes of postoperative stress-specific incontinence occurred in 47% and 29% of the mini-sling and retropubic midurethral sling groups, respectively. This difference did reach statistical significance (adjusted odds ratio, 2.4). There was no significant difference between the groups with respect to de novo urge.
As for other secondary endpoints, the mini-sling group had significantly reduced odds of reporting global improvement and patient satisfaction, and significantly increased odds of surgery for recurrent or persistent stress urinary incontinence (SUI), compared with the retropubic midurethral sling group, but the retropubic midurethral sling group had a higher reoperation rate for mesh erosion, Dr. Madsen said.
There was no difference in urethrolysis between the groups.
Study participants were women with a mean age of 60 years with SUI or stress-predominant mixed urinary incontinence, who underwent a sling procedure between January, 2008, and December, 2009. Treatment failure was defined by a score of greater than 0 on the International Consultation on Incontinence Questionnaire, an affirmative response to questions about stress incontinence on the questionnaire, or a need for a repeat anti-incontinence procedure.
The mini-sling and retropubic midurethral sling groups were similar with respect to most demographics – with the exception of BMI and duration of follow-up, and also were similar with respect to baseline urodynamics, Dr. Madsen noted.
Although retropubic and transobturator midurethral slings have been shown to have similar efficacy, it has remained unknown how single-incision mini-slings compare with these types of slings, she said.
These findings suggest that the retropubic midurethral sling is associated with higher risk of mesh exposure and reoperation for mesh complications, but with lower rates of stress-specific incontinence, higher global impression of improvement and patient satisfaction, and similar rates of overall urethrolysis and reoperation rates for any indication, Dr. Madsen concluded.
She reported having no disclosures. The meeting was jointly sponsored by the American College of Surgeons.
CHARLESTON, S.C. – Single-incision mini-slings for the treatment of stress urinary incontinence are associated with higher failure and reoperation rates than are retropubic midurethral slings, according to findings from a survey and review of medical records of more than 200 patients.
At a mean follow-up of 21 months, 71 of 93 (76%) women who underwent a single-incision mini-sling procedure reported treatment failure, defined as overall incontinence, compared with 70 of 109 (64%) women who underwent a retropubic midurethral sling procedure, Dr. Annetta M. Madsen reported at the annual meeting of the Society of Gynecologic Surgeons.
After adjustment for body mass index and follow-up time, which differed between the groups, the odds ratio for treatment failure in the mini-sling vs. retropubic midurethral sling group was 1.84, which trended toward statistical significance, said Dr. Madsen of the Mayo Clinic, Rochester, Minn.
The secondary outcomes of postoperative stress-specific incontinence occurred in 47% and 29% of the mini-sling and retropubic midurethral sling groups, respectively. This difference did reach statistical significance (adjusted odds ratio, 2.4). There was no significant difference between the groups with respect to de novo urge.
As for other secondary endpoints, the mini-sling group had significantly reduced odds of reporting global improvement and patient satisfaction, and significantly increased odds of surgery for recurrent or persistent stress urinary incontinence (SUI), compared with the retropubic midurethral sling group, but the retropubic midurethral sling group had a higher reoperation rate for mesh erosion, Dr. Madsen said.
There was no difference in urethrolysis between the groups.
Study participants were women with a mean age of 60 years with SUI or stress-predominant mixed urinary incontinence, who underwent a sling procedure between January, 2008, and December, 2009. Treatment failure was defined by a score of greater than 0 on the International Consultation on Incontinence Questionnaire, an affirmative response to questions about stress incontinence on the questionnaire, or a need for a repeat anti-incontinence procedure.
The mini-sling and retropubic midurethral sling groups were similar with respect to most demographics – with the exception of BMI and duration of follow-up, and also were similar with respect to baseline urodynamics, Dr. Madsen noted.
Although retropubic and transobturator midurethral slings have been shown to have similar efficacy, it has remained unknown how single-incision mini-slings compare with these types of slings, she said.
These findings suggest that the retropubic midurethral sling is associated with higher risk of mesh exposure and reoperation for mesh complications, but with lower rates of stress-specific incontinence, higher global impression of improvement and patient satisfaction, and similar rates of overall urethrolysis and reoperation rates for any indication, Dr. Madsen concluded.
She reported having no disclosures. The meeting was jointly sponsored by the American College of Surgeons.
CHARLESTON, S.C. – Single-incision mini-slings for the treatment of stress urinary incontinence are associated with higher failure and reoperation rates than are retropubic midurethral slings, according to findings from a survey and review of medical records of more than 200 patients.
At a mean follow-up of 21 months, 71 of 93 (76%) women who underwent a single-incision mini-sling procedure reported treatment failure, defined as overall incontinence, compared with 70 of 109 (64%) women who underwent a retropubic midurethral sling procedure, Dr. Annetta M. Madsen reported at the annual meeting of the Society of Gynecologic Surgeons.
After adjustment for body mass index and follow-up time, which differed between the groups, the odds ratio for treatment failure in the mini-sling vs. retropubic midurethral sling group was 1.84, which trended toward statistical significance, said Dr. Madsen of the Mayo Clinic, Rochester, Minn.
The secondary outcomes of postoperative stress-specific incontinence occurred in 47% and 29% of the mini-sling and retropubic midurethral sling groups, respectively. This difference did reach statistical significance (adjusted odds ratio, 2.4). There was no significant difference between the groups with respect to de novo urge.
As for other secondary endpoints, the mini-sling group had significantly reduced odds of reporting global improvement and patient satisfaction, and significantly increased odds of surgery for recurrent or persistent stress urinary incontinence (SUI), compared with the retropubic midurethral sling group, but the retropubic midurethral sling group had a higher reoperation rate for mesh erosion, Dr. Madsen said.
There was no difference in urethrolysis between the groups.
Study participants were women with a mean age of 60 years with SUI or stress-predominant mixed urinary incontinence, who underwent a sling procedure between January, 2008, and December, 2009. Treatment failure was defined by a score of greater than 0 on the International Consultation on Incontinence Questionnaire, an affirmative response to questions about stress incontinence on the questionnaire, or a need for a repeat anti-incontinence procedure.
The mini-sling and retropubic midurethral sling groups were similar with respect to most demographics – with the exception of BMI and duration of follow-up, and also were similar with respect to baseline urodynamics, Dr. Madsen noted.
Although retropubic and transobturator midurethral slings have been shown to have similar efficacy, it has remained unknown how single-incision mini-slings compare with these types of slings, she said.
These findings suggest that the retropubic midurethral sling is associated with higher risk of mesh exposure and reoperation for mesh complications, but with lower rates of stress-specific incontinence, higher global impression of improvement and patient satisfaction, and similar rates of overall urethrolysis and reoperation rates for any indication, Dr. Madsen concluded.
She reported having no disclosures. The meeting was jointly sponsored by the American College of Surgeons.
AT THE SGS ANNUAL MEETING
Major finding: Overall incontinence and stress-specific incontinence were more likely with mini-sling vs. retropubic midurethral sling procedures (odds ratios, 1.84, 2.4, respectively).
Data source: A historical cohort study of 202 women with stress urinary incontinence.
Disclosures: Dr. Madsen reported having no disclosures. The meeting was jointly sponsored by the American College of Surgeons.
Esophagectomy cases rising steadily
INDIANAPOLIS – Transthoracic esophagectomy for esophageal cancer provides significantly lower in-hospital mortality and major morbidity rates than does transhiatal esophagectomy, according to an analysis of a large multiyear national database.
Further, in-hospital outcomes of esophagectomy didn’t differ significantly between high-volume centers – in this study, defined as those doing 10 or more cases per year – and low-volume centers, Dr. Mehraneh D. Jafari reported at the annual meeting of the American Surgical Association.

That finding was met with skepticism, and discussants were quick to argue that study limitations make it difficult to draw any meaningful conclusions from the data. For one thing, speakers contended that defining a high-volume center based upon an institutional threshold of 10 or more cases per year sets the bar far too low given that a single dedicated esophageal surgery specialist might easily perform 50 or more esophagectomies annually.
Dr. Jafari presented an analysis of 11,473 transthoracic and 3,717 transhiatal esophagectomies performed for esophageal cancer. The data came from the Nationwide Inpatient Sample (NIS) during 2001-2010. The NIS records data on in-hospital outcomes for a nationally representative sample composed of roughly 20% of the country’s hospital discharges each year.
The number of esophagectomies rose steadily by an average of 4% annually during the study years, reflecting the substantial national increase in cases of esophageal cancer. The growing case count, expected to reach an estimated 18,000 cases of esophageal cancer nationwide in 2013, has been attributed to rising rates of gastroesophageal reflux disease, Barrett’s esophagus, and obesity. Transthoracic esophagectomy, used in 76% of cases, remained the preferred operative strategy throughout the study years.
In-hospital outcomes were markedly better in patients who had transthoracic esophagectomy. After adjustment for potential confounding variables in a multivariate analysis, transhiatal esophagectomy recipients had a 67% increased risk of in-hospital mortality and a 39% greater risk of serious complications, including a 37% increased risk of pulmonary complications. However, anastomotic leak rates were similar with both operations, according to Dr. Jafari of the University of California, Irvine.
Of note, the referral rate to high-volume esophagectomy centers climbed steadily over time, rising from 22% of all cases in 2001 to 58% in 2010.

The 35 high-volume centers performed an average of 16 cases per year. In contrast, the 484 low-volume centers averaged 2 cases per year. In-hospital mortality among the 9,386 patients treated in low-volume centers averaged 7.6% compared with 4.3% for patients in high-volume centers. Overall in-hospital serious morbidity rates were greater in the low-volume centers as well: 47% versus 41%. While these raw differences were statistically significant, a risk-adjusted multivariate analysis found no significant outcome differences between low- and high-volume centers.
Discussant Dr. Michael J. Zinner noted that in an earlier study he and his coworkers showed that an institutional threshold of roughly 30 esophagectomies per year is required to discriminate between low- and high-volume centers in terms of in-hospital mortality. So why define high-volume centers as those doing a mere 10 cases per year? asked Dr. Zinner, chairman of the department of surgery at Brigham and Women’s Hospital and professor of surgery at Harvard Medical School, Boston.
"The problem here is if you establish 30 cases per year as the threshold for a high-volume center, I can tell you there are probably less than 20 centers in the whole U.S. capable of doing that volume. That’s a real issue, because then how are patients who live in a remote region going to get care at one of those centers?" replied Dr. Jafari’s senior coauthor Dr. Ninh T. Nguyen, professor and vice-chair of surgery at UC Irvine.
"I think instead we should try to lift all boats: develop a national esophageal center network to identify the qualities reflective of better outcomes in the high-volume centers and introduce those factors at low-volume centers. This way we’re not impeding access to care for our patients," he continued.
Dr. Nguyen said that in-hospital surgical morbidity rates in the NIS need to be taken with a grain of salt, as the accuracy of coding for complications is "rather low." The development of minimally invasive techniques for intrathoracic anastomosis has transformed transthoracic esophagectomy into a procedure with an improved complication profile.
"I switched to transthoracic esophagectomy 5 years ago. One reason was development of the minimally invasive approach. As a result, we’re not scared of a chest anastomosis like we used to be. When patients undergoing transthoracic esophagectomy with thoracotomy had a leak in the chest they had a very high risk for mortality. That’s not the case anymore. We have not observed any mortality associated with a leak in the chest for many, many years now," he said.
The investigators reported having no conflicts of interest.
Dr. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
I have major problems with this study, stemming from inherent limitations in the Nationwide Inpatient Sample. It’s an administrative database set up chiefly to track costs, utilization, and length of stay. It contains no information at all on key clinical outcomes such as 30- and 90-day mortality, discharge disposition, or 30-day readmission rates.

|
|
In addition, the accuracy of the quoted in-hospital morbidity rates is suspect, probably because data entry isn’t performed by trained researchers. For example, the 8% incidence of renal failure in esophagectomy patients cited in this study sounds too high to be right.
And there’s another major problem with this database: The superior outcomes reported for transthoracic esophagectomy recipients in this study fly in the face of earlier, well-conducted meta-analyses that reached the opposite conclusion. The most likely explanation for the discordant findings lies in the fact that the NIS doesn’t show whether a transthoracic esophagectomy was performed via open thoracotomy in the old-school manner or with an intrathoracic anastomosis created using contemporary minimally invasive techniques which, while complex, have been associated with better outcomes.
Dr. James D. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
I have major problems with this study, stemming from inherent limitations in the Nationwide Inpatient Sample. It’s an administrative database set up chiefly to track costs, utilization, and length of stay. It contains no information at all on key clinical outcomes such as 30- and 90-day mortality, discharge disposition, or 30-day readmission rates.
|
|
|
In addition, the accuracy of the quoted in-hospital morbidity rates is suspect, probably because data entry isn’t performed by trained researchers. For example, the 8% incidence of renal failure in esophagectomy patients cited in this study sounds too high to be right.
And there’s another major problem with this database: The superior outcomes reported for transthoracic esophagectomy recipients in this study fly in the face of earlier, well-conducted meta-analyses that reached the opposite conclusion. The most likely explanation for the discordant findings lies in the fact that the NIS doesn’t show whether a transthoracic esophagectomy was performed via open thoracotomy in the old-school manner or with an intrathoracic anastomosis created using contemporary minimally invasive techniques which, while complex, have been associated with better outcomes.
Dr. James D. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
I have major problems with this study, stemming from inherent limitations in the Nationwide Inpatient Sample. It’s an administrative database set up chiefly to track costs, utilization, and length of stay. It contains no information at all on key clinical outcomes such as 30- and 90-day mortality, discharge disposition, or 30-day readmission rates.
|
|
|
In addition, the accuracy of the quoted in-hospital morbidity rates is suspect, probably because data entry isn’t performed by trained researchers. For example, the 8% incidence of renal failure in esophagectomy patients cited in this study sounds too high to be right.
And there’s another major problem with this database: The superior outcomes reported for transthoracic esophagectomy recipients in this study fly in the face of earlier, well-conducted meta-analyses that reached the opposite conclusion. The most likely explanation for the discordant findings lies in the fact that the NIS doesn’t show whether a transthoracic esophagectomy was performed via open thoracotomy in the old-school manner or with an intrathoracic anastomosis created using contemporary minimally invasive techniques which, while complex, have been associated with better outcomes.
Dr. James D. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
INDIANAPOLIS – Transthoracic esophagectomy for esophageal cancer provides significantly lower in-hospital mortality and major morbidity rates than does transhiatal esophagectomy, according to an analysis of a large multiyear national database.
Further, in-hospital outcomes of esophagectomy didn’t differ significantly between high-volume centers – in this study, defined as those doing 10 or more cases per year – and low-volume centers, Dr. Mehraneh D. Jafari reported at the annual meeting of the American Surgical Association.
That finding was met with skepticism, and discussants were quick to argue that study limitations make it difficult to draw any meaningful conclusions from the data. For one thing, speakers contended that defining a high-volume center based upon an institutional threshold of 10 or more cases per year sets the bar far too low given that a single dedicated esophageal surgery specialist might easily perform 50 or more esophagectomies annually.
Dr. Jafari presented an analysis of 11,473 transthoracic and 3,717 transhiatal esophagectomies performed for esophageal cancer. The data came from the Nationwide Inpatient Sample (NIS) during 2001-2010. The NIS records data on in-hospital outcomes for a nationally representative sample composed of roughly 20% of the country’s hospital discharges each year.
The number of esophagectomies rose steadily by an average of 4% annually during the study years, reflecting the substantial national increase in cases of esophageal cancer. The growing case count, expected to reach an estimated 18,000 cases of esophageal cancer nationwide in 2013, has been attributed to rising rates of gastroesophageal reflux disease, Barrett’s esophagus, and obesity. Transthoracic esophagectomy, used in 76% of cases, remained the preferred operative strategy throughout the study years.
In-hospital outcomes were markedly better in patients who had transthoracic esophagectomy. After adjustment for potential confounding variables in a multivariate analysis, transhiatal esophagectomy recipients had a 67% increased risk of in-hospital mortality and a 39% greater risk of serious complications, including a 37% increased risk of pulmonary complications. However, anastomotic leak rates were similar with both operations, according to Dr. Jafari of the University of California, Irvine.
Of note, the referral rate to high-volume esophagectomy centers climbed steadily over time, rising from 22% of all cases in 2001 to 58% in 2010.
The 35 high-volume centers performed an average of 16 cases per year. In contrast, the 484 low-volume centers averaged 2 cases per year. In-hospital mortality among the 9,386 patients treated in low-volume centers averaged 7.6% compared with 4.3% for patients in high-volume centers. Overall in-hospital serious morbidity rates were greater in the low-volume centers as well: 47% versus 41%. While these raw differences were statistically significant, a risk-adjusted multivariate analysis found no significant outcome differences between low- and high-volume centers.
Discussant Dr. Michael J. Zinner noted that in an earlier study he and his coworkers showed that an institutional threshold of roughly 30 esophagectomies per year is required to discriminate between low- and high-volume centers in terms of in-hospital mortality. So why define high-volume centers as those doing a mere 10 cases per year? asked Dr. Zinner, chairman of the department of surgery at Brigham and Women’s Hospital and professor of surgery at Harvard Medical School, Boston.
"The problem here is if you establish 30 cases per year as the threshold for a high-volume center, I can tell you there are probably less than 20 centers in the whole U.S. capable of doing that volume. That’s a real issue, because then how are patients who live in a remote region going to get care at one of those centers?" replied Dr. Jafari’s senior coauthor Dr. Ninh T. Nguyen, professor and vice-chair of surgery at UC Irvine.
"I think instead we should try to lift all boats: develop a national esophageal center network to identify the qualities reflective of better outcomes in the high-volume centers and introduce those factors at low-volume centers. This way we’re not impeding access to care for our patients," he continued.
Dr. Nguyen said that in-hospital surgical morbidity rates in the NIS need to be taken with a grain of salt, as the accuracy of coding for complications is "rather low." The development of minimally invasive techniques for intrathoracic anastomosis has transformed transthoracic esophagectomy into a procedure with an improved complication profile.
"I switched to transthoracic esophagectomy 5 years ago. One reason was development of the minimally invasive approach. As a result, we’re not scared of a chest anastomosis like we used to be. When patients undergoing transthoracic esophagectomy with thoracotomy had a leak in the chest they had a very high risk for mortality. That’s not the case anymore. We have not observed any mortality associated with a leak in the chest for many, many years now," he said.
The investigators reported having no conflicts of interest.
Dr. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
INDIANAPOLIS – Transthoracic esophagectomy for esophageal cancer provides significantly lower in-hospital mortality and major morbidity rates than does transhiatal esophagectomy, according to an analysis of a large multiyear national database.
Further, in-hospital outcomes of esophagectomy didn’t differ significantly between high-volume centers – in this study, defined as those doing 10 or more cases per year – and low-volume centers, Dr. Mehraneh D. Jafari reported at the annual meeting of the American Surgical Association.
That finding was met with skepticism, and discussants were quick to argue that study limitations make it difficult to draw any meaningful conclusions from the data. For one thing, speakers contended that defining a high-volume center based upon an institutional threshold of 10 or more cases per year sets the bar far too low given that a single dedicated esophageal surgery specialist might easily perform 50 or more esophagectomies annually.
Dr. Jafari presented an analysis of 11,473 transthoracic and 3,717 transhiatal esophagectomies performed for esophageal cancer. The data came from the Nationwide Inpatient Sample (NIS) during 2001-2010. The NIS records data on in-hospital outcomes for a nationally representative sample composed of roughly 20% of the country’s hospital discharges each year.
The number of esophagectomies rose steadily by an average of 4% annually during the study years, reflecting the substantial national increase in cases of esophageal cancer. The growing case count, expected to reach an estimated 18,000 cases of esophageal cancer nationwide in 2013, has been attributed to rising rates of gastroesophageal reflux disease, Barrett’s esophagus, and obesity. Transthoracic esophagectomy, used in 76% of cases, remained the preferred operative strategy throughout the study years.
In-hospital outcomes were markedly better in patients who had transthoracic esophagectomy. After adjustment for potential confounding variables in a multivariate analysis, transhiatal esophagectomy recipients had a 67% increased risk of in-hospital mortality and a 39% greater risk of serious complications, including a 37% increased risk of pulmonary complications. However, anastomotic leak rates were similar with both operations, according to Dr. Jafari of the University of California, Irvine.
Of note, the referral rate to high-volume esophagectomy centers climbed steadily over time, rising from 22% of all cases in 2001 to 58% in 2010.
The 35 high-volume centers performed an average of 16 cases per year. In contrast, the 484 low-volume centers averaged 2 cases per year. In-hospital mortality among the 9,386 patients treated in low-volume centers averaged 7.6% compared with 4.3% for patients in high-volume centers. Overall in-hospital serious morbidity rates were greater in the low-volume centers as well: 47% versus 41%. While these raw differences were statistically significant, a risk-adjusted multivariate analysis found no significant outcome differences between low- and high-volume centers.
Discussant Dr. Michael J. Zinner noted that in an earlier study he and his coworkers showed that an institutional threshold of roughly 30 esophagectomies per year is required to discriminate between low- and high-volume centers in terms of in-hospital mortality. So why define high-volume centers as those doing a mere 10 cases per year? asked Dr. Zinner, chairman of the department of surgery at Brigham and Women’s Hospital and professor of surgery at Harvard Medical School, Boston.
"The problem here is if you establish 30 cases per year as the threshold for a high-volume center, I can tell you there are probably less than 20 centers in the whole U.S. capable of doing that volume. That’s a real issue, because then how are patients who live in a remote region going to get care at one of those centers?" replied Dr. Jafari’s senior coauthor Dr. Ninh T. Nguyen, professor and vice-chair of surgery at UC Irvine.
"I think instead we should try to lift all boats: develop a national esophageal center network to identify the qualities reflective of better outcomes in the high-volume centers and introduce those factors at low-volume centers. This way we’re not impeding access to care for our patients," he continued.
Dr. Nguyen said that in-hospital surgical morbidity rates in the NIS need to be taken with a grain of salt, as the accuracy of coding for complications is "rather low." The development of minimally invasive techniques for intrathoracic anastomosis has transformed transthoracic esophagectomy into a procedure with an improved complication profile.
"I switched to transthoracic esophagectomy 5 years ago. One reason was development of the minimally invasive approach. As a result, we’re not scared of a chest anastomosis like we used to be. When patients undergoing transthoracic esophagectomy with thoracotomy had a leak in the chest they had a very high risk for mortality. That’s not the case anymore. We have not observed any mortality associated with a leak in the chest for many, many years now," he said.
The investigators reported having no conflicts of interest.
Dr. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
AT THE ASA ANNUAL MEETING
Major finding: In-hospital mortality occurred nationally in 5.8% of esophageal cancer patients who underwent transthoracic esophagectomy compared with 8.3% of transhiatal esophagectomy recipients.
Data source: A retrospective study of more than 15,000 patients who underwent esophagectomy for esophageal cancer during 2001-2010 and were Included in the Nationwide Inpatient Sample, a database sponsored by the Agency for Healthcare Research and Quality.
Disclosures: The study presenters reported having no financial conflicts.
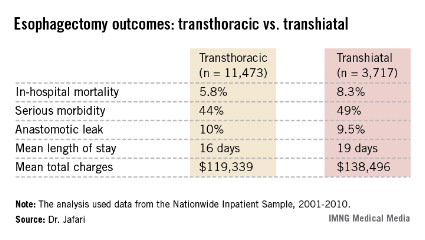
Checking up on advance care planning - and charting, too
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
