User login
Cardiovascular events in U.S. RA patients fall to non-RA level
MADRID – U.S. patients with rheumatoid arthritis stopped having an excess of cardiovascular disease events during the 2000s.
During both the 1980s and 1990s, patients with rheumatoid arthritis (RA) residing in a 27-county region in southeastern Minnesota and northwestern Wisconsin had cardiovascular disease event rates that were more than twice the rates in similar adults without RA, but that changed during the 2000s, Elena Myasoedova, MD, said in a poster she presented at the European Congress of Rheumatology. During 2000-2009, RA patients enrolled in the Rochester (Minn.) Epidemiology Project had an incidence of cardiovascular disease events at a rate that was 12% lower, compared with matched adults without RA who were also enrolled in the same regional database, reported Dr. Myasoedova, a rheumatologist at the Mayo Clinic in Rochester, and her associates.
“We hypothesize that improved management of RA, including implementation of a treat-to-target strategy and the introduction of biological drugs could have influenced this, as well as increased awareness of and improved prevention of cardiovascular disease,” Dr. Myasoedova said in an interview. The findings “give us a hint that tight control of RA disease activity is also likely to help cardiovascular disease burden.”
She and her associates identified 906 people enrolled in the Rochester Epidemiology Project who had incident RA based on the 1987 criteria of the American College of Rheumatology and matched them by age, sex, and index year with 905 people in the registry without RA. These cohorts included roughly 200 people from each subgroup tracked during the 1980s, 300 from each subgroup tracked during the 1990s, and about 400 in each subgroup tracked during the 2000s. They averaged about 56 years old, and about two-thirds were women.
During the 1980s, the cumulative incidence of nonfatal MI, nonfatal stroke, or cardiovascular disease (CVD) death was 2.11-fold more common among the RA patients than in the matched controls without RA, and during the 1990s this ratio showed a 2.13-fold excess of CVD events among the RA patients. The between-group differences in both decades were statistically significant. During the 2000s, the RA patients actually had a nominally lower rate of CVD events, at 0.88 times the rate of the controls, a difference that was not statistically significant.
Dr. Myasoedova and her associates had previously reported a similar finding in an analysis that used a smaller number of people and focused exclusively on rates of CVD (J Rheumatol. 2017 Jun;44[6]:732-9).
A few factors limit the generalizability of the finding, Dr. Myasoedova cautioned. First, the population studied was about 90% white. Also, people in the Rochester Epidemiology Project receive their medical care from clinicians at the Mayo Clinic or an affiliated hospital in the region covered by the Project.
“These data are from a large, tertiary care center,” and so the findings are most directly applicable to patients who receive medical care in a similar setting that provides guideline-directed management of both RA and CVD risk.
A long-standing hypothesis is that CVD has an inflammatory component. These data support that concept by suggesting that when inflammatory disease is well controlled in RA patients, their CVD risk drops, Dr. Myasoedova said. “CVD has been seen as the number one comorbidity for RA patients, and it remains that way, but it’s very reassuring that the CVD rate has improved. It shows we’re doing something right.”
The study received no commercial funding. Dr. Myasoedova had no relevant disclosures.
SOURCE: Myasoedova E et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):1024-5. Abstract FRI0654. DOI: 10.1136/annrheumdis-2019-eular.4996.
MADRID – U.S. patients with rheumatoid arthritis stopped having an excess of cardiovascular disease events during the 2000s.
During both the 1980s and 1990s, patients with rheumatoid arthritis (RA) residing in a 27-county region in southeastern Minnesota and northwestern Wisconsin had cardiovascular disease event rates that were more than twice the rates in similar adults without RA, but that changed during the 2000s, Elena Myasoedova, MD, said in a poster she presented at the European Congress of Rheumatology. During 2000-2009, RA patients enrolled in the Rochester (Minn.) Epidemiology Project had an incidence of cardiovascular disease events at a rate that was 12% lower, compared with matched adults without RA who were also enrolled in the same regional database, reported Dr. Myasoedova, a rheumatologist at the Mayo Clinic in Rochester, and her associates.
“We hypothesize that improved management of RA, including implementation of a treat-to-target strategy and the introduction of biological drugs could have influenced this, as well as increased awareness of and improved prevention of cardiovascular disease,” Dr. Myasoedova said in an interview. The findings “give us a hint that tight control of RA disease activity is also likely to help cardiovascular disease burden.”
She and her associates identified 906 people enrolled in the Rochester Epidemiology Project who had incident RA based on the 1987 criteria of the American College of Rheumatology and matched them by age, sex, and index year with 905 people in the registry without RA. These cohorts included roughly 200 people from each subgroup tracked during the 1980s, 300 from each subgroup tracked during the 1990s, and about 400 in each subgroup tracked during the 2000s. They averaged about 56 years old, and about two-thirds were women.
During the 1980s, the cumulative incidence of nonfatal MI, nonfatal stroke, or cardiovascular disease (CVD) death was 2.11-fold more common among the RA patients than in the matched controls without RA, and during the 1990s this ratio showed a 2.13-fold excess of CVD events among the RA patients. The between-group differences in both decades were statistically significant. During the 2000s, the RA patients actually had a nominally lower rate of CVD events, at 0.88 times the rate of the controls, a difference that was not statistically significant.
Dr. Myasoedova and her associates had previously reported a similar finding in an analysis that used a smaller number of people and focused exclusively on rates of CVD (J Rheumatol. 2017 Jun;44[6]:732-9).
A few factors limit the generalizability of the finding, Dr. Myasoedova cautioned. First, the population studied was about 90% white. Also, people in the Rochester Epidemiology Project receive their medical care from clinicians at the Mayo Clinic or an affiliated hospital in the region covered by the Project.
“These data are from a large, tertiary care center,” and so the findings are most directly applicable to patients who receive medical care in a similar setting that provides guideline-directed management of both RA and CVD risk.
A long-standing hypothesis is that CVD has an inflammatory component. These data support that concept by suggesting that when inflammatory disease is well controlled in RA patients, their CVD risk drops, Dr. Myasoedova said. “CVD has been seen as the number one comorbidity for RA patients, and it remains that way, but it’s very reassuring that the CVD rate has improved. It shows we’re doing something right.”
The study received no commercial funding. Dr. Myasoedova had no relevant disclosures.
SOURCE: Myasoedova E et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):1024-5. Abstract FRI0654. DOI: 10.1136/annrheumdis-2019-eular.4996.
MADRID – U.S. patients with rheumatoid arthritis stopped having an excess of cardiovascular disease events during the 2000s.
During both the 1980s and 1990s, patients with rheumatoid arthritis (RA) residing in a 27-county region in southeastern Minnesota and northwestern Wisconsin had cardiovascular disease event rates that were more than twice the rates in similar adults without RA, but that changed during the 2000s, Elena Myasoedova, MD, said in a poster she presented at the European Congress of Rheumatology. During 2000-2009, RA patients enrolled in the Rochester (Minn.) Epidemiology Project had an incidence of cardiovascular disease events at a rate that was 12% lower, compared with matched adults without RA who were also enrolled in the same regional database, reported Dr. Myasoedova, a rheumatologist at the Mayo Clinic in Rochester, and her associates.
“We hypothesize that improved management of RA, including implementation of a treat-to-target strategy and the introduction of biological drugs could have influenced this, as well as increased awareness of and improved prevention of cardiovascular disease,” Dr. Myasoedova said in an interview. The findings “give us a hint that tight control of RA disease activity is also likely to help cardiovascular disease burden.”
She and her associates identified 906 people enrolled in the Rochester Epidemiology Project who had incident RA based on the 1987 criteria of the American College of Rheumatology and matched them by age, sex, and index year with 905 people in the registry without RA. These cohorts included roughly 200 people from each subgroup tracked during the 1980s, 300 from each subgroup tracked during the 1990s, and about 400 in each subgroup tracked during the 2000s. They averaged about 56 years old, and about two-thirds were women.
During the 1980s, the cumulative incidence of nonfatal MI, nonfatal stroke, or cardiovascular disease (CVD) death was 2.11-fold more common among the RA patients than in the matched controls without RA, and during the 1990s this ratio showed a 2.13-fold excess of CVD events among the RA patients. The between-group differences in both decades were statistically significant. During the 2000s, the RA patients actually had a nominally lower rate of CVD events, at 0.88 times the rate of the controls, a difference that was not statistically significant.
Dr. Myasoedova and her associates had previously reported a similar finding in an analysis that used a smaller number of people and focused exclusively on rates of CVD (J Rheumatol. 2017 Jun;44[6]:732-9).
A few factors limit the generalizability of the finding, Dr. Myasoedova cautioned. First, the population studied was about 90% white. Also, people in the Rochester Epidemiology Project receive their medical care from clinicians at the Mayo Clinic or an affiliated hospital in the region covered by the Project.
“These data are from a large, tertiary care center,” and so the findings are most directly applicable to patients who receive medical care in a similar setting that provides guideline-directed management of both RA and CVD risk.
A long-standing hypothesis is that CVD has an inflammatory component. These data support that concept by suggesting that when inflammatory disease is well controlled in RA patients, their CVD risk drops, Dr. Myasoedova said. “CVD has been seen as the number one comorbidity for RA patients, and it remains that way, but it’s very reassuring that the CVD rate has improved. It shows we’re doing something right.”
The study received no commercial funding. Dr. Myasoedova had no relevant disclosures.
SOURCE: Myasoedova E et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):1024-5. Abstract FRI0654. DOI: 10.1136/annrheumdis-2019-eular.4996.
REPORTING FROM EULAR 2019 CONGRESS

Lowering hyperuricemia improved endothelial function but failed as an antihypertensive
MADRID – Using allopurinol to reduce hyperuricemia in young adults with prehypertension or stage 1 hypertension failed to significantly lower blood pressure but succeeded in significantly improving endothelial function as measured by increased flow-mediated arterial dilation in a single-center crossover study with 82 participants.
The finding of improved endothelial function suggests that reducing hyperuricemia may be a new way to manage hypertension or prevent progression to stage 1 hypertension, improve cardiovascular health, and ultimately cut cardiovascular events, Angelo L. Gaffo, MD, said at the European Congress of Rheumatology. The results indicated that the BP-lowering effect of allopurinol treatment was strongest in people who entered the study with the highest serum urate levels, greater than 6.5 mg/dL, an indication that the next step in developing this approach should be targeting it to people with serum urate levels in this range, said Dr. Gaffo, a rheumatologist at the University of Alabama at Birmingham.
“It’s just a matter of finding the right population to see the blood pressure reduction effect,” Dr. Gaffo said in an interview.
He and his associates designed the SURPHER (Serum Urate Reduction to Prevent Hypertension) study to assess the impact of allopurinol treatment in people aged 18-40 years with prehypertension or stage 1 hypertension as defined by U.S. BP standards at the time they launched the study in 2016 (Contemp Clin Trials. 2016 Sep;50:238-44). Enrolled participants had to be nonsmokers; have an estimated glomerular filtration rate of greater than 60 mL/min per 1.73 m2; have a serum urate level of at least 5.0 mg/dL in men and at least 4.0 mg/dL in women; and be without diabetes, antihypertensive medications, prior urate-lowering treatment, or a history of gout. The 99 people who started the study averaged 28 years old, nearly two-thirds were men, 40% were African Americans, and 52% were white. The participants’ average body mass index was nearly 31 kg/m2, and their average BP was 127/81 mm Hg. Average serum urate levels were 6.4 mg/dL in men and 4.9 mg/dL in women. Participants received 300 mg/day allopurinol or placebo, and after 4 weeks crossed to the alternate regimen, with 82 people completing the full protocol. While on allopurinol, serum urate levels fell by an average of 1.3 mg/dL, a statistically significant drop; on placebo, the levels showed no significant change from baseline.
The primary endpoint was the change in BP on allopurinol treatment, which overall showed no statistically significant difference, compared with when participants received placebo. The results also showed no significant impact of allopurinol treatment, compared with placebo, in serum levels of high-sensitivity C-reactive protein, a measure of inflammation. However, for the secondary endpoint of change in endothelial function as measured by a change in flow-mediated dilation (FMD), the results showed a statistically significant effect of allopurinol treatment. While on allopurinol, average FMD increased from 10.3% at baseline to 14.5% on the drug, a 41% relative increase, while on placebo the average FMD rate showed a slight reduction. Allopurinol treatment was safe and well tolerated during the study.
The results also showed that among people with a baseline serum urate level of greater than 6.5 mg/dL (15 of the 82 study completers) systolic BP fell by an average of about 5 mm Hg.
The results suggested that the concept of reducing hyperuricemia in people with early-stage hypertension or prehypertension might be viable for people with higher serum urate levels than most of those enrolled in SURPHER, Dr. Gaffo said. He noted that prior study results in obese adolescents showed that treating hyperuricemia was able to produce a meaningful BP reduction (Hypertension. 2012 Nov;60[5]:1148-56).
SURPHER received no commercial funding. Dr. Gaffo has received research funding from Amgen and AstraZeneca.
MADRID – Using allopurinol to reduce hyperuricemia in young adults with prehypertension or stage 1 hypertension failed to significantly lower blood pressure but succeeded in significantly improving endothelial function as measured by increased flow-mediated arterial dilation in a single-center crossover study with 82 participants.
The finding of improved endothelial function suggests that reducing hyperuricemia may be a new way to manage hypertension or prevent progression to stage 1 hypertension, improve cardiovascular health, and ultimately cut cardiovascular events, Angelo L. Gaffo, MD, said at the European Congress of Rheumatology. The results indicated that the BP-lowering effect of allopurinol treatment was strongest in people who entered the study with the highest serum urate levels, greater than 6.5 mg/dL, an indication that the next step in developing this approach should be targeting it to people with serum urate levels in this range, said Dr. Gaffo, a rheumatologist at the University of Alabama at Birmingham.
“It’s just a matter of finding the right population to see the blood pressure reduction effect,” Dr. Gaffo said in an interview.
He and his associates designed the SURPHER (Serum Urate Reduction to Prevent Hypertension) study to assess the impact of allopurinol treatment in people aged 18-40 years with prehypertension or stage 1 hypertension as defined by U.S. BP standards at the time they launched the study in 2016 (Contemp Clin Trials. 2016 Sep;50:238-44). Enrolled participants had to be nonsmokers; have an estimated glomerular filtration rate of greater than 60 mL/min per 1.73 m2; have a serum urate level of at least 5.0 mg/dL in men and at least 4.0 mg/dL in women; and be without diabetes, antihypertensive medications, prior urate-lowering treatment, or a history of gout. The 99 people who started the study averaged 28 years old, nearly two-thirds were men, 40% were African Americans, and 52% were white. The participants’ average body mass index was nearly 31 kg/m2, and their average BP was 127/81 mm Hg. Average serum urate levels were 6.4 mg/dL in men and 4.9 mg/dL in women. Participants received 300 mg/day allopurinol or placebo, and after 4 weeks crossed to the alternate regimen, with 82 people completing the full protocol. While on allopurinol, serum urate levels fell by an average of 1.3 mg/dL, a statistically significant drop; on placebo, the levels showed no significant change from baseline.
The primary endpoint was the change in BP on allopurinol treatment, which overall showed no statistically significant difference, compared with when participants received placebo. The results also showed no significant impact of allopurinol treatment, compared with placebo, in serum levels of high-sensitivity C-reactive protein, a measure of inflammation. However, for the secondary endpoint of change in endothelial function as measured by a change in flow-mediated dilation (FMD), the results showed a statistically significant effect of allopurinol treatment. While on allopurinol, average FMD increased from 10.3% at baseline to 14.5% on the drug, a 41% relative increase, while on placebo the average FMD rate showed a slight reduction. Allopurinol treatment was safe and well tolerated during the study.
The results also showed that among people with a baseline serum urate level of greater than 6.5 mg/dL (15 of the 82 study completers) systolic BP fell by an average of about 5 mm Hg.
The results suggested that the concept of reducing hyperuricemia in people with early-stage hypertension or prehypertension might be viable for people with higher serum urate levels than most of those enrolled in SURPHER, Dr. Gaffo said. He noted that prior study results in obese adolescents showed that treating hyperuricemia was able to produce a meaningful BP reduction (Hypertension. 2012 Nov;60[5]:1148-56).
SURPHER received no commercial funding. Dr. Gaffo has received research funding from Amgen and AstraZeneca.
MADRID – Using allopurinol to reduce hyperuricemia in young adults with prehypertension or stage 1 hypertension failed to significantly lower blood pressure but succeeded in significantly improving endothelial function as measured by increased flow-mediated arterial dilation in a single-center crossover study with 82 participants.
The finding of improved endothelial function suggests that reducing hyperuricemia may be a new way to manage hypertension or prevent progression to stage 1 hypertension, improve cardiovascular health, and ultimately cut cardiovascular events, Angelo L. Gaffo, MD, said at the European Congress of Rheumatology. The results indicated that the BP-lowering effect of allopurinol treatment was strongest in people who entered the study with the highest serum urate levels, greater than 6.5 mg/dL, an indication that the next step in developing this approach should be targeting it to people with serum urate levels in this range, said Dr. Gaffo, a rheumatologist at the University of Alabama at Birmingham.
“It’s just a matter of finding the right population to see the blood pressure reduction effect,” Dr. Gaffo said in an interview.
He and his associates designed the SURPHER (Serum Urate Reduction to Prevent Hypertension) study to assess the impact of allopurinol treatment in people aged 18-40 years with prehypertension or stage 1 hypertension as defined by U.S. BP standards at the time they launched the study in 2016 (Contemp Clin Trials. 2016 Sep;50:238-44). Enrolled participants had to be nonsmokers; have an estimated glomerular filtration rate of greater than 60 mL/min per 1.73 m2; have a serum urate level of at least 5.0 mg/dL in men and at least 4.0 mg/dL in women; and be without diabetes, antihypertensive medications, prior urate-lowering treatment, or a history of gout. The 99 people who started the study averaged 28 years old, nearly two-thirds were men, 40% were African Americans, and 52% were white. The participants’ average body mass index was nearly 31 kg/m2, and their average BP was 127/81 mm Hg. Average serum urate levels were 6.4 mg/dL in men and 4.9 mg/dL in women. Participants received 300 mg/day allopurinol or placebo, and after 4 weeks crossed to the alternate regimen, with 82 people completing the full protocol. While on allopurinol, serum urate levels fell by an average of 1.3 mg/dL, a statistically significant drop; on placebo, the levels showed no significant change from baseline.
The primary endpoint was the change in BP on allopurinol treatment, which overall showed no statistically significant difference, compared with when participants received placebo. The results also showed no significant impact of allopurinol treatment, compared with placebo, in serum levels of high-sensitivity C-reactive protein, a measure of inflammation. However, for the secondary endpoint of change in endothelial function as measured by a change in flow-mediated dilation (FMD), the results showed a statistically significant effect of allopurinol treatment. While on allopurinol, average FMD increased from 10.3% at baseline to 14.5% on the drug, a 41% relative increase, while on placebo the average FMD rate showed a slight reduction. Allopurinol treatment was safe and well tolerated during the study.
The results also showed that among people with a baseline serum urate level of greater than 6.5 mg/dL (15 of the 82 study completers) systolic BP fell by an average of about 5 mm Hg.
The results suggested that the concept of reducing hyperuricemia in people with early-stage hypertension or prehypertension might be viable for people with higher serum urate levels than most of those enrolled in SURPHER, Dr. Gaffo said. He noted that prior study results in obese adolescents showed that treating hyperuricemia was able to produce a meaningful BP reduction (Hypertension. 2012 Nov;60[5]:1148-56).
SURPHER received no commercial funding. Dr. Gaffo has received research funding from Amgen and AstraZeneca.
REPORTING FROM EULAR 2019 CONGRESS

Patients with CAPS still improving on long-term canakinumab
MADRID – An observational study that includes adults and children with cryopyrin-associated periodic syndromes and related diseases has provided real-world evidence that clinical improvement accrues on canakinumab (Ilaris) years after treatment was initiated, according to Norbert Blank, MD, of the division of rheumatology at the University of Heidelberg (Germany).
Summarizing data he presented at the European Congress of Rheumatology, Dr. Blank explained in an interview that the observational study has accrued more than 50 patients so far, with the goal of reaching 300 patients with cryopyrin-associated periodic syndromes and related rare diseases that have responded to anti–interleukin-1 therapy, such as Muckle-Wells syndrome, familial cold autoinflammatory syndrome, and familial Mediterranean fever.
Most of the patients participating in the observational study, called RELIANCE, were already on canakinumab at the time of enrollment, often for several years. Yet in follow-up so far – which exceeds 1 year for some of the participants – improvement from the time of entry has been seen for some outcomes, such as activity level, according to Dr. Blank.
Canakinumab has been well tolerated with no new or unexpected adverse events emerging in the follow-up so far. Although these data remain limited, Dr. Blank considers them reassuring.
With detailed characterization of these rare diseases at baseline, observational studies like RELIANCE provide valuable real-world data about disease presentation, according to Dr. Blank. He believes that further follow-up will provide a rich source of information about disease course in response to anti-IL-1 therapy, which is being individualized according to response.
MADRID – An observational study that includes adults and children with cryopyrin-associated periodic syndromes and related diseases has provided real-world evidence that clinical improvement accrues on canakinumab (Ilaris) years after treatment was initiated, according to Norbert Blank, MD, of the division of rheumatology at the University of Heidelberg (Germany).
Summarizing data he presented at the European Congress of Rheumatology, Dr. Blank explained in an interview that the observational study has accrued more than 50 patients so far, with the goal of reaching 300 patients with cryopyrin-associated periodic syndromes and related rare diseases that have responded to anti–interleukin-1 therapy, such as Muckle-Wells syndrome, familial cold autoinflammatory syndrome, and familial Mediterranean fever.
Most of the patients participating in the observational study, called RELIANCE, were already on canakinumab at the time of enrollment, often for several years. Yet in follow-up so far – which exceeds 1 year for some of the participants – improvement from the time of entry has been seen for some outcomes, such as activity level, according to Dr. Blank.
Canakinumab has been well tolerated with no new or unexpected adverse events emerging in the follow-up so far. Although these data remain limited, Dr. Blank considers them reassuring.
With detailed characterization of these rare diseases at baseline, observational studies like RELIANCE provide valuable real-world data about disease presentation, according to Dr. Blank. He believes that further follow-up will provide a rich source of information about disease course in response to anti-IL-1 therapy, which is being individualized according to response.
MADRID – An observational study that includes adults and children with cryopyrin-associated periodic syndromes and related diseases has provided real-world evidence that clinical improvement accrues on canakinumab (Ilaris) years after treatment was initiated, according to Norbert Blank, MD, of the division of rheumatology at the University of Heidelberg (Germany).
Summarizing data he presented at the European Congress of Rheumatology, Dr. Blank explained in an interview that the observational study has accrued more than 50 patients so far, with the goal of reaching 300 patients with cryopyrin-associated periodic syndromes and related rare diseases that have responded to anti–interleukin-1 therapy, such as Muckle-Wells syndrome, familial cold autoinflammatory syndrome, and familial Mediterranean fever.
Most of the patients participating in the observational study, called RELIANCE, were already on canakinumab at the time of enrollment, often for several years. Yet in follow-up so far – which exceeds 1 year for some of the participants – improvement from the time of entry has been seen for some outcomes, such as activity level, according to Dr. Blank.
Canakinumab has been well tolerated with no new or unexpected adverse events emerging in the follow-up so far. Although these data remain limited, Dr. Blank considers them reassuring.
With detailed characterization of these rare diseases at baseline, observational studies like RELIANCE provide valuable real-world data about disease presentation, according to Dr. Blank. He believes that further follow-up will provide a rich source of information about disease course in response to anti-IL-1 therapy, which is being individualized according to response.
REPORTING FROM EULAR 2019 CONGRESS
Psychiatry residents not getting training in treating chronic pain
SAN FRANCISCO –
Given the unique role of psychiatrists in helping chronic pain patients with coping strategies and managing comorbid psychiatric illness, this void is concerning, said Ali Ahsan Ali, MD, a resident psychiatrist at the Micah School of Medicine at Mount Sinai/Elmhurst Hospital Center in New York, in an interview at the annual meeting of the American Psychiatric Association.
In a video interview, Dr. Ali spoke with Ahmar M. Butt, MD, about how and why Dr. Ali and his colleagues conducted the survey of all 221 U.S. psychiatry residency programs in January 2019. They also discuss the implications of these trends for patients, particularly in light of the country’s opioid crisis.
Dr. Ali had no disclosures. Dr. Butt is board certified in general psychiatry, child and adolescent psychiatry, and preventive medicine, with a subspecialty in addiction medicine. Dr. Butt is interim program director of the psychiatry residency program at Broadlawns UnityPointe Health, Des Moines, Iowa. He had no disclosures.
SAN FRANCISCO –
Given the unique role of psychiatrists in helping chronic pain patients with coping strategies and managing comorbid psychiatric illness, this void is concerning, said Ali Ahsan Ali, MD, a resident psychiatrist at the Micah School of Medicine at Mount Sinai/Elmhurst Hospital Center in New York, in an interview at the annual meeting of the American Psychiatric Association.
In a video interview, Dr. Ali spoke with Ahmar M. Butt, MD, about how and why Dr. Ali and his colleagues conducted the survey of all 221 U.S. psychiatry residency programs in January 2019. They also discuss the implications of these trends for patients, particularly in light of the country’s opioid crisis.
Dr. Ali had no disclosures. Dr. Butt is board certified in general psychiatry, child and adolescent psychiatry, and preventive medicine, with a subspecialty in addiction medicine. Dr. Butt is interim program director of the psychiatry residency program at Broadlawns UnityPointe Health, Des Moines, Iowa. He had no disclosures.
SAN FRANCISCO –
Given the unique role of psychiatrists in helping chronic pain patients with coping strategies and managing comorbid psychiatric illness, this void is concerning, said Ali Ahsan Ali, MD, a resident psychiatrist at the Micah School of Medicine at Mount Sinai/Elmhurst Hospital Center in New York, in an interview at the annual meeting of the American Psychiatric Association.
In a video interview, Dr. Ali spoke with Ahmar M. Butt, MD, about how and why Dr. Ali and his colleagues conducted the survey of all 221 U.S. psychiatry residency programs in January 2019. They also discuss the implications of these trends for patients, particularly in light of the country’s opioid crisis.
Dr. Ali had no disclosures. Dr. Butt is board certified in general psychiatry, child and adolescent psychiatry, and preventive medicine, with a subspecialty in addiction medicine. Dr. Butt is interim program director of the psychiatry residency program at Broadlawns UnityPointe Health, Des Moines, Iowa. He had no disclosures.
REPORTING FROM APA 2019

Patient selection important for osteoarthritis structural and symptom endpoints
MADRID – To achieve positive trials with new agents in osteoarthritis, patient selection should be considered in the context of the primary endpoints, according to Philip G. Conaghan, MBBS, PhD, chair of musculoskeletal medicine at the University of Leeds (England).
In an interview, Dr. Conaghan explained that the issue has arisen with emerging agents that are designed for structural improvements with the expectation that symptom improvements will follow. Recapping a presentation he made at the European Congress of Rheumatology, he cautioned that the key aspects of trial design for these novel agents, including patient and endpoint selection, are particularly challenging.
As an example, Dr. Conaghan referred to the experience so far with the ongoing phase 2 FORWARD trial with sprifermin, a recombinant form of human fibroblast growth factor. In this study, sprifermin has already shown promise for growing cartilage, but the benefit accrues slowly, and there is no symptomatic improvement early in the course of treatment.
Based on the experience with FORWARD, much has been learned about a potential tension between structural and symptomatic endpoints in osteoarthritis, according to Dr. Conaghan. For one, it appears to be important to select patients most likely to achieve measurable structural improvements quickly to achieve a positive result in a reasonable period of time.
For another, it may be necessary to select symptom endpoints that reflect structural change while cautioning patients about the potential for a long delay before a clinical benefit is experienced.
In osteoarthritis, clinical benefit has been traditionally captured with relief of pain. Although an improvement in joint structure might be the best way to produce this result, this has to be proved. Reasonable and achievable endpoints are needed for emerging drugs with the potential to rebuild the joint not just to control pain, he said.
SOURCE: Gühring H et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):70-1. Abstract OP0010. doi: 10.1136/annrheumdis-2019-eular.1216.
MADRID – To achieve positive trials with new agents in osteoarthritis, patient selection should be considered in the context of the primary endpoints, according to Philip G. Conaghan, MBBS, PhD, chair of musculoskeletal medicine at the University of Leeds (England).
In an interview, Dr. Conaghan explained that the issue has arisen with emerging agents that are designed for structural improvements with the expectation that symptom improvements will follow. Recapping a presentation he made at the European Congress of Rheumatology, he cautioned that the key aspects of trial design for these novel agents, including patient and endpoint selection, are particularly challenging.
As an example, Dr. Conaghan referred to the experience so far with the ongoing phase 2 FORWARD trial with sprifermin, a recombinant form of human fibroblast growth factor. In this study, sprifermin has already shown promise for growing cartilage, but the benefit accrues slowly, and there is no symptomatic improvement early in the course of treatment.
Based on the experience with FORWARD, much has been learned about a potential tension between structural and symptomatic endpoints in osteoarthritis, according to Dr. Conaghan. For one, it appears to be important to select patients most likely to achieve measurable structural improvements quickly to achieve a positive result in a reasonable period of time.
For another, it may be necessary to select symptom endpoints that reflect structural change while cautioning patients about the potential for a long delay before a clinical benefit is experienced.
In osteoarthritis, clinical benefit has been traditionally captured with relief of pain. Although an improvement in joint structure might be the best way to produce this result, this has to be proved. Reasonable and achievable endpoints are needed for emerging drugs with the potential to rebuild the joint not just to control pain, he said.
SOURCE: Gühring H et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):70-1. Abstract OP0010. doi: 10.1136/annrheumdis-2019-eular.1216.
MADRID – To achieve positive trials with new agents in osteoarthritis, patient selection should be considered in the context of the primary endpoints, according to Philip G. Conaghan, MBBS, PhD, chair of musculoskeletal medicine at the University of Leeds (England).
In an interview, Dr. Conaghan explained that the issue has arisen with emerging agents that are designed for structural improvements with the expectation that symptom improvements will follow. Recapping a presentation he made at the European Congress of Rheumatology, he cautioned that the key aspects of trial design for these novel agents, including patient and endpoint selection, are particularly challenging.
As an example, Dr. Conaghan referred to the experience so far with the ongoing phase 2 FORWARD trial with sprifermin, a recombinant form of human fibroblast growth factor. In this study, sprifermin has already shown promise for growing cartilage, but the benefit accrues slowly, and there is no symptomatic improvement early in the course of treatment.
Based on the experience with FORWARD, much has been learned about a potential tension between structural and symptomatic endpoints in osteoarthritis, according to Dr. Conaghan. For one, it appears to be important to select patients most likely to achieve measurable structural improvements quickly to achieve a positive result in a reasonable period of time.
For another, it may be necessary to select symptom endpoints that reflect structural change while cautioning patients about the potential for a long delay before a clinical benefit is experienced.
In osteoarthritis, clinical benefit has been traditionally captured with relief of pain. Although an improvement in joint structure might be the best way to produce this result, this has to be proved. Reasonable and achievable endpoints are needed for emerging drugs with the potential to rebuild the joint not just to control pain, he said.
SOURCE: Gühring H et al. Ann Rheum Dis. Jun 2019;78(Suppl 2):70-1. Abstract OP0010. doi: 10.1136/annrheumdis-2019-eular.1216.
REPORTING FROM EULAR 2019 CONGRESS

Treat-to-target slowly emerging in axial spondyloarthritis
MADRID – Treating patients with axial spondyloarthritis (axSpA) until a specific target is reached is an emerging concept that has gained a lot of traction in the past few years, Pedro Machado, MD, said at the European Congress of Rheumatology.

“The availability of biologic therapies has improved the clinical outcomes for our patients with axial spondyloarthritis and targeting clinical remission or inactive disease is now an achievable treatment goal in clinical practice,” he observed. “This has trigged the question: Is there a role for ‘treat-to-target’ in axial spondyloarthritis?”
Dr. Machado, an honorary consultant in rheumatology and muscle diseases at University College Hospital and the National Hospital for Neurology and Neurosurgery in London, took a critical look at the treat-to-target approach during a clinical science session at the meeting, organized by the European League Against Rheumatism (EULAR).
The concept of treat-to-target is not new, he acknowledged, having been imported from other chronic conditions where there is a very specific target to achieve – such as lowering glycated hemoglobin in diabetes or hypertension or hyperlipidemia in cardiovascular disease.
“The concept involves changing or escalating therapy according to a predefined target under the assumption that this may lead to a better outcome compared to what we call ‘routine care,’ ” Dr. Machado explained.
Treat-to-target is not only well established in nonrheumatic diseases but also has proved to work in patients with rheumatoid arthritis and psoriatic arthritis with evidence from the TICORA (Tight Control of Rheumatoid Arthritis) and TICOPA (Tight Control in Psoriatic Arthritis) trials.
Whether the approach can also work in axSpA is open to debate, and one of the main arguments against using a treat-to-target in axSpA asks, what exactly is the target? While there is no firm agreement yet, Dr. Machado observed that achieving either clinical remission or inactive disease would be the most likely target.
It could be argued this is already being done to some degree, but “we need to be more ambitious,” Dr. Machado said. Indeed, current Assessment of Spondyloarthritis International Society/EULAR recommendations for the treatment of axSpA (Ann Rheum Dis. 2017;76[6]:978–91) note when patients with high disease activity despite sufficient standard treatment should be escalated to treatment with a biologic disease-modifying antirheumatic drug (bDMARD). High disease activity was defined as an Ankylosing Spondylitis Disease Activity Score (ASDAS) of 2.1 or more or a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) score of 4 or more.
Another argument against using the approach concerns the evidence base. There are no prospective, randomized trials supporting the use of treat-to-target over routine care. However, there is a lot of observational evidence, Dr. Machado said in an interview. Such studies have shown that achieving inactive disease may improve structural outcomes and stop the development of radiographic damage of the spine. Importantly, these observational studies also show that achieving inactive disease may also help to improve patients’ functional outcomes and quality of life.
Evidence backing a treat-to-target approach in axSpA from a randomized, controlled trial may currently be lacking, but the TiCOSPA (Tight Control in Spondyloarthritis) trial is in progress and should help change that, Dr. Machado said.
“The missing bit is a randomized trial, but I would say that the observational evidence is almost enough to advocate a treat-to-target strategy in axial spondyloarthritis.” This was also the view of an international task force that recently published recommendations and overarching principles for a treat-target strategy in spondyloarthritis, including axSpA (Ann Rheum Dis. 2018;77:3-17).
Of course, a treat-to-target approach may not be without its pitfalls. There are a limited number of drugs currently that could be used to “hit the target” of disease activity, Dr. Machado said in his presentation. The approach might also lead to ‘overtreatment,’ and more treatment is not always better as it could not only lead to more adverse events, but it also may mean the approach is not cost-effective.
Depending on the TiCOSPA study results, which are expected next year, Dr. Machado said that “the feasibility and cost-effectiveness of such a strategy in clinical practice also needs to be tested.”
MADRID – Treating patients with axial spondyloarthritis (axSpA) until a specific target is reached is an emerging concept that has gained a lot of traction in the past few years, Pedro Machado, MD, said at the European Congress of Rheumatology.
“The availability of biologic therapies has improved the clinical outcomes for our patients with axial spondyloarthritis and targeting clinical remission or inactive disease is now an achievable treatment goal in clinical practice,” he observed. “This has trigged the question: Is there a role for ‘treat-to-target’ in axial spondyloarthritis?”
Dr. Machado, an honorary consultant in rheumatology and muscle diseases at University College Hospital and the National Hospital for Neurology and Neurosurgery in London, took a critical look at the treat-to-target approach during a clinical science session at the meeting, organized by the European League Against Rheumatism (EULAR).
The concept of treat-to-target is not new, he acknowledged, having been imported from other chronic conditions where there is a very specific target to achieve – such as lowering glycated hemoglobin in diabetes or hypertension or hyperlipidemia in cardiovascular disease.
“The concept involves changing or escalating therapy according to a predefined target under the assumption that this may lead to a better outcome compared to what we call ‘routine care,’ ” Dr. Machado explained.
Treat-to-target is not only well established in nonrheumatic diseases but also has proved to work in patients with rheumatoid arthritis and psoriatic arthritis with evidence from the TICORA (Tight Control of Rheumatoid Arthritis) and TICOPA (Tight Control in Psoriatic Arthritis) trials.
Whether the approach can also work in axSpA is open to debate, and one of the main arguments against using a treat-to-target in axSpA asks, what exactly is the target? While there is no firm agreement yet, Dr. Machado observed that achieving either clinical remission or inactive disease would be the most likely target.
It could be argued this is already being done to some degree, but “we need to be more ambitious,” Dr. Machado said. Indeed, current Assessment of Spondyloarthritis International Society/EULAR recommendations for the treatment of axSpA (Ann Rheum Dis. 2017;76[6]:978–91) note when patients with high disease activity despite sufficient standard treatment should be escalated to treatment with a biologic disease-modifying antirheumatic drug (bDMARD). High disease activity was defined as an Ankylosing Spondylitis Disease Activity Score (ASDAS) of 2.1 or more or a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) score of 4 or more.
Another argument against using the approach concerns the evidence base. There are no prospective, randomized trials supporting the use of treat-to-target over routine care. However, there is a lot of observational evidence, Dr. Machado said in an interview. Such studies have shown that achieving inactive disease may improve structural outcomes and stop the development of radiographic damage of the spine. Importantly, these observational studies also show that achieving inactive disease may also help to improve patients’ functional outcomes and quality of life.
Evidence backing a treat-to-target approach in axSpA from a randomized, controlled trial may currently be lacking, but the TiCOSPA (Tight Control in Spondyloarthritis) trial is in progress and should help change that, Dr. Machado said.
“The missing bit is a randomized trial, but I would say that the observational evidence is almost enough to advocate a treat-to-target strategy in axial spondyloarthritis.” This was also the view of an international task force that recently published recommendations and overarching principles for a treat-target strategy in spondyloarthritis, including axSpA (Ann Rheum Dis. 2018;77:3-17).
Of course, a treat-to-target approach may not be without its pitfalls. There are a limited number of drugs currently that could be used to “hit the target” of disease activity, Dr. Machado said in his presentation. The approach might also lead to ‘overtreatment,’ and more treatment is not always better as it could not only lead to more adverse events, but it also may mean the approach is not cost-effective.
Depending on the TiCOSPA study results, which are expected next year, Dr. Machado said that “the feasibility and cost-effectiveness of such a strategy in clinical practice also needs to be tested.”
MADRID – Treating patients with axial spondyloarthritis (axSpA) until a specific target is reached is an emerging concept that has gained a lot of traction in the past few years, Pedro Machado, MD, said at the European Congress of Rheumatology.
“The availability of biologic therapies has improved the clinical outcomes for our patients with axial spondyloarthritis and targeting clinical remission or inactive disease is now an achievable treatment goal in clinical practice,” he observed. “This has trigged the question: Is there a role for ‘treat-to-target’ in axial spondyloarthritis?”
Dr. Machado, an honorary consultant in rheumatology and muscle diseases at University College Hospital and the National Hospital for Neurology and Neurosurgery in London, took a critical look at the treat-to-target approach during a clinical science session at the meeting, organized by the European League Against Rheumatism (EULAR).
The concept of treat-to-target is not new, he acknowledged, having been imported from other chronic conditions where there is a very specific target to achieve – such as lowering glycated hemoglobin in diabetes or hypertension or hyperlipidemia in cardiovascular disease.
“The concept involves changing or escalating therapy according to a predefined target under the assumption that this may lead to a better outcome compared to what we call ‘routine care,’ ” Dr. Machado explained.
Treat-to-target is not only well established in nonrheumatic diseases but also has proved to work in patients with rheumatoid arthritis and psoriatic arthritis with evidence from the TICORA (Tight Control of Rheumatoid Arthritis) and TICOPA (Tight Control in Psoriatic Arthritis) trials.
Whether the approach can also work in axSpA is open to debate, and one of the main arguments against using a treat-to-target in axSpA asks, what exactly is the target? While there is no firm agreement yet, Dr. Machado observed that achieving either clinical remission or inactive disease would be the most likely target.
It could be argued this is already being done to some degree, but “we need to be more ambitious,” Dr. Machado said. Indeed, current Assessment of Spondyloarthritis International Society/EULAR recommendations for the treatment of axSpA (Ann Rheum Dis. 2017;76[6]:978–91) note when patients with high disease activity despite sufficient standard treatment should be escalated to treatment with a biologic disease-modifying antirheumatic drug (bDMARD). High disease activity was defined as an Ankylosing Spondylitis Disease Activity Score (ASDAS) of 2.1 or more or a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) score of 4 or more.
Another argument against using the approach concerns the evidence base. There are no prospective, randomized trials supporting the use of treat-to-target over routine care. However, there is a lot of observational evidence, Dr. Machado said in an interview. Such studies have shown that achieving inactive disease may improve structural outcomes and stop the development of radiographic damage of the spine. Importantly, these observational studies also show that achieving inactive disease may also help to improve patients’ functional outcomes and quality of life.
Evidence backing a treat-to-target approach in axSpA from a randomized, controlled trial may currently be lacking, but the TiCOSPA (Tight Control in Spondyloarthritis) trial is in progress and should help change that, Dr. Machado said.
“The missing bit is a randomized trial, but I would say that the observational evidence is almost enough to advocate a treat-to-target strategy in axial spondyloarthritis.” This was also the view of an international task force that recently published recommendations and overarching principles for a treat-target strategy in spondyloarthritis, including axSpA (Ann Rheum Dis. 2018;77:3-17).
Of course, a treat-to-target approach may not be without its pitfalls. There are a limited number of drugs currently that could be used to “hit the target” of disease activity, Dr. Machado said in his presentation. The approach might also lead to ‘overtreatment,’ and more treatment is not always better as it could not only lead to more adverse events, but it also may mean the approach is not cost-effective.
Depending on the TiCOSPA study results, which are expected next year, Dr. Machado said that “the feasibility and cost-effectiveness of such a strategy in clinical practice also needs to be tested.”
EXPERT analysis FROM THE EULAR 2019 Congress

Psychiatrists discuss work on climate change
SAN FRANCISCO –

“We can find reasons to hope even in dark times,” Dr. Van Susteren said. “We understand science. We have all the tools ... this is what we do for a living. We warn about behaviors that are going hurt us now and are going to be even worse down the road.”
In a video discussion, Dr. Van Susteren spoke with David A. Pollack, MD, about the accomplishments of the Climate Psychiatry Alliance, an organization they helped launch more than 2 years ago that warns the medical profession and the public about risks of climate change and the impact of climate disruption on mental health. One victory, for example, was getting the APA to vote to divest from fossil fuels.
Dr. Van Susteren and Dr. Pollack also discuss steps psychiatrists can take as individuals to provide care for patients suffering from the effects of climate change – such as prescribing “park therapy.” In their offices, physicians can look toward emerging solutions such as My Green Doctor and Health Care Without Harm, Dr. Pollack said.
Dr. Van Susteren has a private psychiatry private practice in Washington and has no disclosures. Dr. Pollack is affiliated with Oregon Health & Science University in Portland. He has no disclosures.
SAN FRANCISCO –
“We can find reasons to hope even in dark times,” Dr. Van Susteren said. “We understand science. We have all the tools ... this is what we do for a living. We warn about behaviors that are going hurt us now and are going to be even worse down the road.”
In a video discussion, Dr. Van Susteren spoke with David A. Pollack, MD, about the accomplishments of the Climate Psychiatry Alliance, an organization they helped launch more than 2 years ago that warns the medical profession and the public about risks of climate change and the impact of climate disruption on mental health. One victory, for example, was getting the APA to vote to divest from fossil fuels.
Dr. Van Susteren and Dr. Pollack also discuss steps psychiatrists can take as individuals to provide care for patients suffering from the effects of climate change – such as prescribing “park therapy.” In their offices, physicians can look toward emerging solutions such as My Green Doctor and Health Care Without Harm, Dr. Pollack said.
Dr. Van Susteren has a private psychiatry private practice in Washington and has no disclosures. Dr. Pollack is affiliated with Oregon Health & Science University in Portland. He has no disclosures.
SAN FRANCISCO –
“We can find reasons to hope even in dark times,” Dr. Van Susteren said. “We understand science. We have all the tools ... this is what we do for a living. We warn about behaviors that are going hurt us now and are going to be even worse down the road.”
In a video discussion, Dr. Van Susteren spoke with David A. Pollack, MD, about the accomplishments of the Climate Psychiatry Alliance, an organization they helped launch more than 2 years ago that warns the medical profession and the public about risks of climate change and the impact of climate disruption on mental health. One victory, for example, was getting the APA to vote to divest from fossil fuels.
Dr. Van Susteren and Dr. Pollack also discuss steps psychiatrists can take as individuals to provide care for patients suffering from the effects of climate change – such as prescribing “park therapy.” In their offices, physicians can look toward emerging solutions such as My Green Doctor and Health Care Without Harm, Dr. Pollack said.
Dr. Van Susteren has a private psychiatry private practice in Washington and has no disclosures. Dr. Pollack is affiliated with Oregon Health & Science University in Portland. He has no disclosures.
REPORTING FROM APA 2019

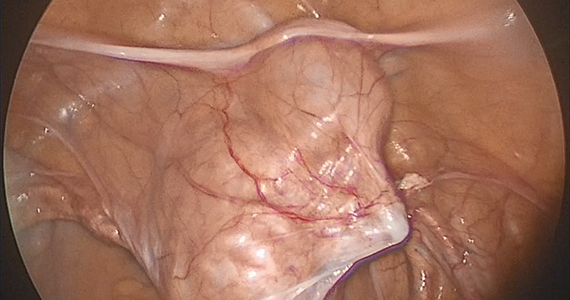
Novel method to demarcate bladder dissection during posthysterectomy sacrocolpopexy
![]()

Additional videos from SGS are available here, including these recent offerings:
• Instructional video for fourth-degree obstetric laceration repair using modified beef tongue model
• The art of manipulation: Simplifying hysterectomy by preparing the learner
• Vaginal and bilateral thigh removal of a transobturator sling
![]()
Additional videos from SGS are available here, including these recent offerings:
• Instructional video for fourth-degree obstetric laceration repair using modified beef tongue model
• The art of manipulation: Simplifying hysterectomy by preparing the learner
• Vaginal and bilateral thigh removal of a transobturator sling
![]()
Additional videos from SGS are available here, including these recent offerings:
• Instructional video for fourth-degree obstetric laceration repair using modified beef tongue model
• The art of manipulation: Simplifying hysterectomy by preparing the learner
• Vaginal and bilateral thigh removal of a transobturator sling
More liberal criteria could greatly expand clinical trial participation
CHICAGO – Fewer than 1 in 20 adults with cancer enroll in clinical trials, and even when cancer patients are willing to participate in a trial, they are often excluded because of comorbidities, prior therapies, or a host of other factors that could confound results.
But as a team of investigators shows in a proof-of-concept study, more generous exclusion criteria in some trials could nearly double the number of participants. Using retrospective, deidentified electronic health record data from the American Society of Clinical Oncology CancerLinQ Discovery database, R. Donald Harvey, PharmD and colleagues found that when they applied broader inclusion criteria for patients with advanced non–small cell lung cancer (NSCLC), the number of patients who would be eligible for clinical trials nearly doubled from 5,495 to 10,349.
In this video interview from the ASCO annual meeting, Dr. Harvey of the Winship Cancer Institute of Emory University in Atlanta discusses collaborations between the oncology community, federal agencies, and the pharmaceutical industry that could improve clinical trials by safely increasing sample sizes.
The study received funding from ASCO. Dr. Harvey disclosed consulting or advisory roles with and institutional research funding from multiple entities.
CHICAGO – Fewer than 1 in 20 adults with cancer enroll in clinical trials, and even when cancer patients are willing to participate in a trial, they are often excluded because of comorbidities, prior therapies, or a host of other factors that could confound results.
But as a team of investigators shows in a proof-of-concept study, more generous exclusion criteria in some trials could nearly double the number of participants. Using retrospective, deidentified electronic health record data from the American Society of Clinical Oncology CancerLinQ Discovery database, R. Donald Harvey, PharmD and colleagues found that when they applied broader inclusion criteria for patients with advanced non–small cell lung cancer (NSCLC), the number of patients who would be eligible for clinical trials nearly doubled from 5,495 to 10,349.
In this video interview from the ASCO annual meeting, Dr. Harvey of the Winship Cancer Institute of Emory University in Atlanta discusses collaborations between the oncology community, federal agencies, and the pharmaceutical industry that could improve clinical trials by safely increasing sample sizes.
The study received funding from ASCO. Dr. Harvey disclosed consulting or advisory roles with and institutional research funding from multiple entities.
CHICAGO – Fewer than 1 in 20 adults with cancer enroll in clinical trials, and even when cancer patients are willing to participate in a trial, they are often excluded because of comorbidities, prior therapies, or a host of other factors that could confound results.
But as a team of investigators shows in a proof-of-concept study, more generous exclusion criteria in some trials could nearly double the number of participants. Using retrospective, deidentified electronic health record data from the American Society of Clinical Oncology CancerLinQ Discovery database, R. Donald Harvey, PharmD and colleagues found that when they applied broader inclusion criteria for patients with advanced non–small cell lung cancer (NSCLC), the number of patients who would be eligible for clinical trials nearly doubled from 5,495 to 10,349.
In this video interview from the ASCO annual meeting, Dr. Harvey of the Winship Cancer Institute of Emory University in Atlanta discusses collaborations between the oncology community, federal agencies, and the pharmaceutical industry that could improve clinical trials by safely increasing sample sizes.
The study received funding from ASCO. Dr. Harvey disclosed consulting or advisory roles with and institutional research funding from multiple entities.
REPORTING FROM ASCO 2019

Steady advances made since recognition of neuromyelitis optica 20 years ago
SEATTLE – At the annual meeting of the Consortium of Multiple Sclerosis Centers, Brian Weinshenker, MD, professor of neurology at the Mayo Clinic in Rochester, Minn., summarized some of the milestones in the timeline of NMO research.
These milestones include the 2004 identification of NMO-IgG, an autoantibody marker of NMO that distinguishes it from multiple sclerosis; the 2005 discovery that the antibody was reactive to aquaporin 4, the dominant CNS water channel and an astrocyte protein; further characterizations of NMO manifestations; the revised international panel diagnostic criteria in 2015; and the current phase 3 trials of three potential treatments for NMO – eculizumab, inebilizumab, and satralizumab.
Dr. Weinshenker reported the following disclosures: receiving royalties from the RSR Group, Oxford University, Hospices Civils de Lyon, and MVZ Labor PD Dr. Volkmann und Kollegen for a patent of NMO-IgG as a diagnostic test for NMO and related disorders; serving as an adjudication committee member for clinical trials in NMO being conducted by MedImmune and Alexion; and consulting for Chugai regarding a clinical trial for NMO.
SEATTLE – At the annual meeting of the Consortium of Multiple Sclerosis Centers, Brian Weinshenker, MD, professor of neurology at the Mayo Clinic in Rochester, Minn., summarized some of the milestones in the timeline of NMO research.
These milestones include the 2004 identification of NMO-IgG, an autoantibody marker of NMO that distinguishes it from multiple sclerosis; the 2005 discovery that the antibody was reactive to aquaporin 4, the dominant CNS water channel and an astrocyte protein; further characterizations of NMO manifestations; the revised international panel diagnostic criteria in 2015; and the current phase 3 trials of three potential treatments for NMO – eculizumab, inebilizumab, and satralizumab.
Dr. Weinshenker reported the following disclosures: receiving royalties from the RSR Group, Oxford University, Hospices Civils de Lyon, and MVZ Labor PD Dr. Volkmann und Kollegen for a patent of NMO-IgG as a diagnostic test for NMO and related disorders; serving as an adjudication committee member for clinical trials in NMO being conducted by MedImmune and Alexion; and consulting for Chugai regarding a clinical trial for NMO.
SEATTLE – At the annual meeting of the Consortium of Multiple Sclerosis Centers, Brian Weinshenker, MD, professor of neurology at the Mayo Clinic in Rochester, Minn., summarized some of the milestones in the timeline of NMO research.
These milestones include the 2004 identification of NMO-IgG, an autoantibody marker of NMO that distinguishes it from multiple sclerosis; the 2005 discovery that the antibody was reactive to aquaporin 4, the dominant CNS water channel and an astrocyte protein; further characterizations of NMO manifestations; the revised international panel diagnostic criteria in 2015; and the current phase 3 trials of three potential treatments for NMO – eculizumab, inebilizumab, and satralizumab.
Dr. Weinshenker reported the following disclosures: receiving royalties from the RSR Group, Oxford University, Hospices Civils de Lyon, and MVZ Labor PD Dr. Volkmann und Kollegen for a patent of NMO-IgG as a diagnostic test for NMO and related disorders; serving as an adjudication committee member for clinical trials in NMO being conducted by MedImmune and Alexion; and consulting for Chugai regarding a clinical trial for NMO.
EXPERT ANALYSIS FROM CMSC 2019
