User login
FDA updates clobazam label to reflect risk of severe skin reactions
The antiseizure medication clobazam can cause potentially severe skin reactions that may lead to injury and death, and the drug label has been changed to reflect this information, according to a statement issued by the Food and Drug Administration on Dec. 3.
The FDA has approved changes to the Warnings and Precautions section of the medication label and the patient Medication Guide to describe the possible reactions: Stevens-Johnson syndrome and toxic epidermal necrolysis. These reactions can occur at any time while a patient is taking clobazam (Onfi), but the risk is greatest during the first 8 weeks of treatment or when the patient has discontinued and then resumed use of the drug, the FDA said.
The label change is based in part on the results of an FDA case series of 20 patients (6 U.S. patients, including 5 children, and 14 foreign patients), in which all cases of Stevens-Johnson syndrome and toxic epidermal necrolysis associated with clobazam resulted in hospitalization; in addition, one case resulted in blindness, and another resulted in death.
"Patients should not stop taking Onfi without first talking to their health care professionals," according to the agency’s statement. "Stopping Onfi suddenly can cause serious withdrawal problems, such as seizures that will not stop, hallucinations (hearing or seeing things that are not real), shaking, nervousness, and stomach or muscle cramps."
The FDA advised health professionals to consider clobazam as a cause in patients with possible drug-induced skin reactions, and to discontinue the drug at the first sign of rash, "unless it is clearly not drug related."
Health professionals should inform patients taking clobazam, a benzodiazepine used to manage seizures in children with severe epilepsy (Lennox-Gastaut syndrome) in combination with other antiepileptic medications, to seek medical attention immediately if they develop a rash, skin blistering or peeling, hives, or sores in the mouth.
"Serious skin reactions have not generally been associated with other benzodiazepines," the FDA noted.
Since clobazam was approved in October 2011 and through September 2013, the FDA says that approximately 31,000 patients received a dispensed prescription for the drug from U.S. outpatient retail pharmacies, which account for the majority of all clobazam bottle sales. The agency also noted that clobazam has been marketed outside the United States for about 40 years under various brand names for the treatment of anxiety and seizures.
To view the complete safety announcement online, visit the FDA's website.
The antiseizure medication clobazam can cause potentially severe skin reactions that may lead to injury and death, and the drug label has been changed to reflect this information, according to a statement issued by the Food and Drug Administration on Dec. 3.
The FDA has approved changes to the Warnings and Precautions section of the medication label and the patient Medication Guide to describe the possible reactions: Stevens-Johnson syndrome and toxic epidermal necrolysis. These reactions can occur at any time while a patient is taking clobazam (Onfi), but the risk is greatest during the first 8 weeks of treatment or when the patient has discontinued and then resumed use of the drug, the FDA said.
The label change is based in part on the results of an FDA case series of 20 patients (6 U.S. patients, including 5 children, and 14 foreign patients), in which all cases of Stevens-Johnson syndrome and toxic epidermal necrolysis associated with clobazam resulted in hospitalization; in addition, one case resulted in blindness, and another resulted in death.
"Patients should not stop taking Onfi without first talking to their health care professionals," according to the agency’s statement. "Stopping Onfi suddenly can cause serious withdrawal problems, such as seizures that will not stop, hallucinations (hearing or seeing things that are not real), shaking, nervousness, and stomach or muscle cramps."
The FDA advised health professionals to consider clobazam as a cause in patients with possible drug-induced skin reactions, and to discontinue the drug at the first sign of rash, "unless it is clearly not drug related."
Health professionals should inform patients taking clobazam, a benzodiazepine used to manage seizures in children with severe epilepsy (Lennox-Gastaut syndrome) in combination with other antiepileptic medications, to seek medical attention immediately if they develop a rash, skin blistering or peeling, hives, or sores in the mouth.
"Serious skin reactions have not generally been associated with other benzodiazepines," the FDA noted.
Since clobazam was approved in October 2011 and through September 2013, the FDA says that approximately 31,000 patients received a dispensed prescription for the drug from U.S. outpatient retail pharmacies, which account for the majority of all clobazam bottle sales. The agency also noted that clobazam has been marketed outside the United States for about 40 years under various brand names for the treatment of anxiety and seizures.
To view the complete safety announcement online, visit the FDA's website.
The antiseizure medication clobazam can cause potentially severe skin reactions that may lead to injury and death, and the drug label has been changed to reflect this information, according to a statement issued by the Food and Drug Administration on Dec. 3.
The FDA has approved changes to the Warnings and Precautions section of the medication label and the patient Medication Guide to describe the possible reactions: Stevens-Johnson syndrome and toxic epidermal necrolysis. These reactions can occur at any time while a patient is taking clobazam (Onfi), but the risk is greatest during the first 8 weeks of treatment or when the patient has discontinued and then resumed use of the drug, the FDA said.
The label change is based in part on the results of an FDA case series of 20 patients (6 U.S. patients, including 5 children, and 14 foreign patients), in which all cases of Stevens-Johnson syndrome and toxic epidermal necrolysis associated with clobazam resulted in hospitalization; in addition, one case resulted in blindness, and another resulted in death.
"Patients should not stop taking Onfi without first talking to their health care professionals," according to the agency’s statement. "Stopping Onfi suddenly can cause serious withdrawal problems, such as seizures that will not stop, hallucinations (hearing or seeing things that are not real), shaking, nervousness, and stomach or muscle cramps."
The FDA advised health professionals to consider clobazam as a cause in patients with possible drug-induced skin reactions, and to discontinue the drug at the first sign of rash, "unless it is clearly not drug related."
Health professionals should inform patients taking clobazam, a benzodiazepine used to manage seizures in children with severe epilepsy (Lennox-Gastaut syndrome) in combination with other antiepileptic medications, to seek medical attention immediately if they develop a rash, skin blistering or peeling, hives, or sores in the mouth.
"Serious skin reactions have not generally been associated with other benzodiazepines," the FDA noted.
Since clobazam was approved in October 2011 and through September 2013, the FDA says that approximately 31,000 patients received a dispensed prescription for the drug from U.S. outpatient retail pharmacies, which account for the majority of all clobazam bottle sales. The agency also noted that clobazam has been marketed outside the United States for about 40 years under various brand names for the treatment of anxiety and seizures.
To view the complete safety announcement online, visit the FDA's website.
Impact of psoriasis on sexual activity
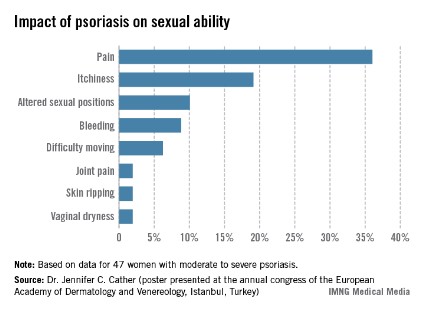
One third of a group of women with psoriasis reported that the pain associated with their condition interfered with their sexual activity, according to findings from a survey presented by Dr. Jennifer C. Cather.
Based on responses from a survey of 60 women with moderate to severe psoriasis, the specific complaints that were the most common ways in which psoriasis interfered with sexual activity were itchiness (19%), the need to adjust sexual position (10%), and bleeding (9%), Dr. Cather reported at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. The survey was part of an effort to determine the impact of psoriasis on women’s sexual activity, desires, and relationships.
The data were previously presented in a poster at the annual congress of the European Academy of Dermatology and Venereology (Istanbul.
SDEF and this news organization are owned by Frontline Medical Communications. Dr. Cather disclosed that she is a consultant, speaker, or researcher for AbbVie, Novartis, Leo, Janssen, Amgen, Celgene, Merck, and Pfizer.

One third of a group of women with psoriasis reported that the pain associated with their condition interfered with their sexual activity, according to findings from a survey presented by Dr. Jennifer C. Cather.
Based on responses from a survey of 60 women with moderate to severe psoriasis, the specific complaints that were the most common ways in which psoriasis interfered with sexual activity were itchiness (19%), the need to adjust sexual position (10%), and bleeding (9%), Dr. Cather reported at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. The survey was part of an effort to determine the impact of psoriasis on women’s sexual activity, desires, and relationships.
The data were previously presented in a poster at the annual congress of the European Academy of Dermatology and Venereology (Istanbul.
SDEF and this news organization are owned by Frontline Medical Communications. Dr. Cather disclosed that she is a consultant, speaker, or researcher for AbbVie, Novartis, Leo, Janssen, Amgen, Celgene, Merck, and Pfizer.
One third of a group of women with psoriasis reported that the pain associated with their condition interfered with their sexual activity, according to findings from a survey presented by Dr. Jennifer C. Cather.
Based on responses from a survey of 60 women with moderate to severe psoriasis, the specific complaints that were the most common ways in which psoriasis interfered with sexual activity were itchiness (19%), the need to adjust sexual position (10%), and bleeding (9%), Dr. Cather reported at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. The survey was part of an effort to determine the impact of psoriasis on women’s sexual activity, desires, and relationships.
The data were previously presented in a poster at the annual congress of the European Academy of Dermatology and Venereology (Istanbul.
SDEF and this news organization are owned by Frontline Medical Communications. Dr. Cather disclosed that she is a consultant, speaker, or researcher for AbbVie, Novartis, Leo, Janssen, Amgen, Celgene, Merck, and Pfizer.
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR
Patient Education on Heart Failure Risk is Crucial in Psoriasis
As evidence supporting an association between psoriasis and cardiovascular disease continues to mount, dermatologists may be the first line of defense in lowering heart failure risk.
"The increased risk of cardiovascular disease for patients with psoriasis may be of a similar magnitude as other well-described CV risk factors, such as uncontrolled hypertension," said Dr. Bruce E. Strober of the University of Connecticut, Farmington. "Further, epidemiological studies show that psoriasis patients have a shortened life expectancy, likely as a result of their experience with CV comorbitidies."
Patient education is essential, he noted at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. "At the very least, dermatologists should alert patients of the link between psoriasis and CV disease, and remind these patients of the necessity of having a primary care physician who monitors conventional risk factors of CV disease. Patients should be reminded that psoriasis is ‘systemic disease of inflammation’ that creates risks beyond the skin and may shorten life expectancy."
"Dermatologists who care for moderate to severe psoriasis patients should measure blood pressure and draw baseline blood tests assessing for abnormalities of cholesterol, triglycerides, kidney function, liver function, and blood glucose. Abnormalities should prompt an appropriate referral to a primary care physician," he noted.
In a population-based Dutch study presented at the annual congress of the European Society of Cardiology in September, adults with mild psoriasis developed 4.02 cases of new-onset heart failure per 1,000 person-years of follow-up, compared with 4.50/1,000 person-years in patients with severe psoriasis; both of which were significantly higher than the rate of 2.27/1,000 person-years in the general population.
Data from a 2006 study found that diabetes, hypertension, hyperlipidemia, and obesity were more prevalent in psoriasis patients, when compared with controls (J. Am. Acad. Dermatol. 2006;55:829-35). Diabetes and obesity were significantly more prevalent in patients with severe psoriasis, compared with patients with mild psoriasis.
Although the reasons for the increased cardiovascular risk in psoriasis patients remain unknown, possible causes include the use of dyslipidemic therapies, including corticosteroids, acitretin, and cyclosporine, as well as uncontrolled inflammation that could lead to endothelial dysfunction and dyslipidemia, said Dr. Strober. The prevalence of other associated and/or independent risk factors including obesity, hypertension, smoking, and alcohol misuse in psoriasis patients, also could play a role.
Dr. Strober disclosed relationships with multiple pharmaceutical companies including Abbott, Amgen, Janssen, Pfizer, Novartis, and Celgene. SDEF and this news organization are owned by Frontline Medical Communications.
As evidence supporting an association between psoriasis and cardiovascular disease continues to mount, dermatologists may be the first line of defense in lowering heart failure risk.
"The increased risk of cardiovascular disease for patients with psoriasis may be of a similar magnitude as other well-described CV risk factors, such as uncontrolled hypertension," said Dr. Bruce E. Strober of the University of Connecticut, Farmington. "Further, epidemiological studies show that psoriasis patients have a shortened life expectancy, likely as a result of their experience with CV comorbitidies."
Patient education is essential, he noted at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. "At the very least, dermatologists should alert patients of the link between psoriasis and CV disease, and remind these patients of the necessity of having a primary care physician who monitors conventional risk factors of CV disease. Patients should be reminded that psoriasis is ‘systemic disease of inflammation’ that creates risks beyond the skin and may shorten life expectancy."
"Dermatologists who care for moderate to severe psoriasis patients should measure blood pressure and draw baseline blood tests assessing for abnormalities of cholesterol, triglycerides, kidney function, liver function, and blood glucose. Abnormalities should prompt an appropriate referral to a primary care physician," he noted.
In a population-based Dutch study presented at the annual congress of the European Society of Cardiology in September, adults with mild psoriasis developed 4.02 cases of new-onset heart failure per 1,000 person-years of follow-up, compared with 4.50/1,000 person-years in patients with severe psoriasis; both of which were significantly higher than the rate of 2.27/1,000 person-years in the general population.
Data from a 2006 study found that diabetes, hypertension, hyperlipidemia, and obesity were more prevalent in psoriasis patients, when compared with controls (J. Am. Acad. Dermatol. 2006;55:829-35). Diabetes and obesity were significantly more prevalent in patients with severe psoriasis, compared with patients with mild psoriasis.
Although the reasons for the increased cardiovascular risk in psoriasis patients remain unknown, possible causes include the use of dyslipidemic therapies, including corticosteroids, acitretin, and cyclosporine, as well as uncontrolled inflammation that could lead to endothelial dysfunction and dyslipidemia, said Dr. Strober. The prevalence of other associated and/or independent risk factors including obesity, hypertension, smoking, and alcohol misuse in psoriasis patients, also could play a role.
Dr. Strober disclosed relationships with multiple pharmaceutical companies including Abbott, Amgen, Janssen, Pfizer, Novartis, and Celgene. SDEF and this news organization are owned by Frontline Medical Communications.
As evidence supporting an association between psoriasis and cardiovascular disease continues to mount, dermatologists may be the first line of defense in lowering heart failure risk.
"The increased risk of cardiovascular disease for patients with psoriasis may be of a similar magnitude as other well-described CV risk factors, such as uncontrolled hypertension," said Dr. Bruce E. Strober of the University of Connecticut, Farmington. "Further, epidemiological studies show that psoriasis patients have a shortened life expectancy, likely as a result of their experience with CV comorbitidies."
Patient education is essential, he noted at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. "At the very least, dermatologists should alert patients of the link between psoriasis and CV disease, and remind these patients of the necessity of having a primary care physician who monitors conventional risk factors of CV disease. Patients should be reminded that psoriasis is ‘systemic disease of inflammation’ that creates risks beyond the skin and may shorten life expectancy."
"Dermatologists who care for moderate to severe psoriasis patients should measure blood pressure and draw baseline blood tests assessing for abnormalities of cholesterol, triglycerides, kidney function, liver function, and blood glucose. Abnormalities should prompt an appropriate referral to a primary care physician," he noted.
In a population-based Dutch study presented at the annual congress of the European Society of Cardiology in September, adults with mild psoriasis developed 4.02 cases of new-onset heart failure per 1,000 person-years of follow-up, compared with 4.50/1,000 person-years in patients with severe psoriasis; both of which were significantly higher than the rate of 2.27/1,000 person-years in the general population.
Data from a 2006 study found that diabetes, hypertension, hyperlipidemia, and obesity were more prevalent in psoriasis patients, when compared with controls (J. Am. Acad. Dermatol. 2006;55:829-35). Diabetes and obesity were significantly more prevalent in patients with severe psoriasis, compared with patients with mild psoriasis.
Although the reasons for the increased cardiovascular risk in psoriasis patients remain unknown, possible causes include the use of dyslipidemic therapies, including corticosteroids, acitretin, and cyclosporine, as well as uncontrolled inflammation that could lead to endothelial dysfunction and dyslipidemia, said Dr. Strober. The prevalence of other associated and/or independent risk factors including obesity, hypertension, smoking, and alcohol misuse in psoriasis patients, also could play a role.
Dr. Strober disclosed relationships with multiple pharmaceutical companies including Abbott, Amgen, Janssen, Pfizer, Novartis, and Celgene. SDEF and this news organization are owned by Frontline Medical Communications.
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Patient education on heart failure risk is crucial in psoriasis
As evidence supporting an association between psoriasis and cardiovascular disease continues to mount, dermatologists may be the first line of defense in lowering heart failure risk.
"The increased risk of cardiovascular disease for patients with psoriasis may be of a similar magnitude as other well-described CV risk factors, such as uncontrolled hypertension," said Dr. Bruce E. Strober of the University of Connecticut, Farmington. "Further, epidemiological studies show that psoriasis patients have a shortened life expectancy, likely as a result of their experience with CV comorbitidies."

Patient education is essential, he noted at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. "At the very least, dermatologists should alert patients of the link between psoriasis and CV disease, and remind these patients of the necessity of having a primary care physician who monitors conventional risk factors of CV disease. Patients should be reminded that psoriasis is ‘systemic disease of inflammation’ that creates risks beyond the skin and may shorten life expectancy."
"Dermatologists who care for moderate to severe psoriasis patients should measure blood pressure and draw baseline blood tests assessing for abnormalities of cholesterol, triglycerides, kidney function, liver function, and blood glucose. Abnormalities should prompt an appropriate referral to a primary care physician," he noted.
In a population-based Dutch study presented at the annual congress of the European Society of Cardiology in September, adults with mild psoriasis developed 4.02 cases of new-onset heart failure per 1,000 person-years of follow-up, compared with 4.50/1,000 person-years in patients with severe psoriasis; both of which were significantly higher than the rate of 2.27/1,000 person-years in the general population.
Data from a 2006 study found that diabetes, hypertension, hyperlipidemia, and obesity were more prevalent in psoriasis patients, when compared with controls (J. Am. Acad. Dermatol. 2006;55:829-35). Diabetes and obesity were significantly more prevalent in patients with severe psoriasis, compared with patients with mild psoriasis.
Although the reasons for the increased cardiovascular risk in psoriasis patients remain unknown, possible causes include the use of dyslipidemic therapies, including corticosteroids, acitretin, and cyclosporine, as well as uncontrolled inflammation that could lead to endothelial dysfunction and dyslipidemia, said Dr. Strober. The prevalence of other associated and/or independent risk factors including obesity, hypertension, smoking, and alcohol misuse in psoriasis patients, also could play a role.
Dr. Strober disclosed relationships with multiple pharmaceutical companies including Abbott, Amgen, Janssen, Pfizer, Novartis, and Celgene. SDEF and this news organization are owned by Frontline Medical Communications.
As evidence supporting an association between psoriasis and cardiovascular disease continues to mount, dermatologists may be the first line of defense in lowering heart failure risk.
"The increased risk of cardiovascular disease for patients with psoriasis may be of a similar magnitude as other well-described CV risk factors, such as uncontrolled hypertension," said Dr. Bruce E. Strober of the University of Connecticut, Farmington. "Further, epidemiological studies show that psoriasis patients have a shortened life expectancy, likely as a result of their experience with CV comorbitidies."
Patient education is essential, he noted at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. "At the very least, dermatologists should alert patients of the link between psoriasis and CV disease, and remind these patients of the necessity of having a primary care physician who monitors conventional risk factors of CV disease. Patients should be reminded that psoriasis is ‘systemic disease of inflammation’ that creates risks beyond the skin and may shorten life expectancy."
"Dermatologists who care for moderate to severe psoriasis patients should measure blood pressure and draw baseline blood tests assessing for abnormalities of cholesterol, triglycerides, kidney function, liver function, and blood glucose. Abnormalities should prompt an appropriate referral to a primary care physician," he noted.
In a population-based Dutch study presented at the annual congress of the European Society of Cardiology in September, adults with mild psoriasis developed 4.02 cases of new-onset heart failure per 1,000 person-years of follow-up, compared with 4.50/1,000 person-years in patients with severe psoriasis; both of which were significantly higher than the rate of 2.27/1,000 person-years in the general population.
Data from a 2006 study found that diabetes, hypertension, hyperlipidemia, and obesity were more prevalent in psoriasis patients, when compared with controls (J. Am. Acad. Dermatol. 2006;55:829-35). Diabetes and obesity were significantly more prevalent in patients with severe psoriasis, compared with patients with mild psoriasis.
Although the reasons for the increased cardiovascular risk in psoriasis patients remain unknown, possible causes include the use of dyslipidemic therapies, including corticosteroids, acitretin, and cyclosporine, as well as uncontrolled inflammation that could lead to endothelial dysfunction and dyslipidemia, said Dr. Strober. The prevalence of other associated and/or independent risk factors including obesity, hypertension, smoking, and alcohol misuse in psoriasis patients, also could play a role.
Dr. Strober disclosed relationships with multiple pharmaceutical companies including Abbott, Amgen, Janssen, Pfizer, Novartis, and Celgene. SDEF and this news organization are owned by Frontline Medical Communications.
As evidence supporting an association between psoriasis and cardiovascular disease continues to mount, dermatologists may be the first line of defense in lowering heart failure risk.
"The increased risk of cardiovascular disease for patients with psoriasis may be of a similar magnitude as other well-described CV risk factors, such as uncontrolled hypertension," said Dr. Bruce E. Strober of the University of Connecticut, Farmington. "Further, epidemiological studies show that psoriasis patients have a shortened life expectancy, likely as a result of their experience with CV comorbitidies."
Patient education is essential, he noted at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. "At the very least, dermatologists should alert patients of the link between psoriasis and CV disease, and remind these patients of the necessity of having a primary care physician who monitors conventional risk factors of CV disease. Patients should be reminded that psoriasis is ‘systemic disease of inflammation’ that creates risks beyond the skin and may shorten life expectancy."
"Dermatologists who care for moderate to severe psoriasis patients should measure blood pressure and draw baseline blood tests assessing for abnormalities of cholesterol, triglycerides, kidney function, liver function, and blood glucose. Abnormalities should prompt an appropriate referral to a primary care physician," he noted.
In a population-based Dutch study presented at the annual congress of the European Society of Cardiology in September, adults with mild psoriasis developed 4.02 cases of new-onset heart failure per 1,000 person-years of follow-up, compared with 4.50/1,000 person-years in patients with severe psoriasis; both of which were significantly higher than the rate of 2.27/1,000 person-years in the general population.
Data from a 2006 study found that diabetes, hypertension, hyperlipidemia, and obesity were more prevalent in psoriasis patients, when compared with controls (J. Am. Acad. Dermatol. 2006;55:829-35). Diabetes and obesity were significantly more prevalent in patients with severe psoriasis, compared with patients with mild psoriasis.
Although the reasons for the increased cardiovascular risk in psoriasis patients remain unknown, possible causes include the use of dyslipidemic therapies, including corticosteroids, acitretin, and cyclosporine, as well as uncontrolled inflammation that could lead to endothelial dysfunction and dyslipidemia, said Dr. Strober. The prevalence of other associated and/or independent risk factors including obesity, hypertension, smoking, and alcohol misuse in psoriasis patients, also could play a role.
Dr. Strober disclosed relationships with multiple pharmaceutical companies including Abbott, Amgen, Janssen, Pfizer, Novartis, and Celgene. SDEF and this news organization are owned by Frontline Medical Communications.
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Don't Brush Off Topical Therapies for Psoriasis
Biologics and systemic therapies command much of the spotlight for treating psoriasis, but topical therapy remains an effective option for many psoriasis patients, according to Dr. Linda Stein Gold.
In fact, up to 80% of psoriasis patients can be adequately treated with topical therapy (N. Engl. J. Med. 2005;352:1899-912), said Dr. Stein Gold at the Skin Disease Education Foundation’s (SDEF’s) annual Las Vegas dermatology seminar.
She offered several principles to help clinicians make the most of topical therapies by troubleshooting potential problems.
• Check the amount. One gram of most topical psoriasis products covers 4% of body surface area per application, so a 60-gram tube should treat 4% of body surface area for a month, said Dr. Stein Gold, citing guidelines developed by Dr. Alan Menter and his colleagues and approved by the American Academy of Dermatology in 2009.
• Don’t miss corticosteroid allergies. "We are missing this," said Dr. Stein Gold, director of dermatology research at Henry Ford Hospital in Detroit. Suspect a possible allergy if a patient returns with a worsening rash after using hydrocortisone, for example. Data have shown that between 0.2% and 5% of all dermatitis patients have a steroid allergy. "Allergy to the active molecule or to the vehicle should be suspected in all patients who don’t respond as expected to topical steroids," she noted.
• Visit (or revisit) vitamin D. Another plus for topical therapy is the usefulness of topical vitamin D for tricky areas, such as the forehead, armpit, groin, and the area behind the ears. Data from a randomized trial of 75 patients found calcitriol ointment to be significantly more effective against target lesions and better tolerated by patients than calcipotriene ointment (Br. J. Dermatol. 2003;148:326-33).
• Don’t forget coal tar. Simple, but effective, coal tar is a proven safe topical psoriasis treatment and is available in several vehicles, including solution and foam. Data from a study of more than 13,000 patients with psoriasis and eczema found that coal tar was safe, and that it did not increase the risk for skin cancer (J. Invest. Dermatol. 2010;130:953-61).
The future of topical psoriasis therapy is not static, said Dr. Stein Gold. New molecules – notably topical Janus kinase inhibitors and phosphodiesterase-4 inhibitors – are currently being explored in clinical trials.
Dr. Stein Gold disclosed relationships with Leo, Medicis, and other companies. SDEF and this news organization are owned by Frontline Medical Communications.
Biologics and systemic therapies command much of the spotlight for treating psoriasis, but topical therapy remains an effective option for many psoriasis patients, according to Dr. Linda Stein Gold.
In fact, up to 80% of psoriasis patients can be adequately treated with topical therapy (N. Engl. J. Med. 2005;352:1899-912), said Dr. Stein Gold at the Skin Disease Education Foundation’s (SDEF’s) annual Las Vegas dermatology seminar.
She offered several principles to help clinicians make the most of topical therapies by troubleshooting potential problems.
• Check the amount. One gram of most topical psoriasis products covers 4% of body surface area per application, so a 60-gram tube should treat 4% of body surface area for a month, said Dr. Stein Gold, citing guidelines developed by Dr. Alan Menter and his colleagues and approved by the American Academy of Dermatology in 2009.
• Don’t miss corticosteroid allergies. "We are missing this," said Dr. Stein Gold, director of dermatology research at Henry Ford Hospital in Detroit. Suspect a possible allergy if a patient returns with a worsening rash after using hydrocortisone, for example. Data have shown that between 0.2% and 5% of all dermatitis patients have a steroid allergy. "Allergy to the active molecule or to the vehicle should be suspected in all patients who don’t respond as expected to topical steroids," she noted.
• Visit (or revisit) vitamin D. Another plus for topical therapy is the usefulness of topical vitamin D for tricky areas, such as the forehead, armpit, groin, and the area behind the ears. Data from a randomized trial of 75 patients found calcitriol ointment to be significantly more effective against target lesions and better tolerated by patients than calcipotriene ointment (Br. J. Dermatol. 2003;148:326-33).
• Don’t forget coal tar. Simple, but effective, coal tar is a proven safe topical psoriasis treatment and is available in several vehicles, including solution and foam. Data from a study of more than 13,000 patients with psoriasis and eczema found that coal tar was safe, and that it did not increase the risk for skin cancer (J. Invest. Dermatol. 2010;130:953-61).
The future of topical psoriasis therapy is not static, said Dr. Stein Gold. New molecules – notably topical Janus kinase inhibitors and phosphodiesterase-4 inhibitors – are currently being explored in clinical trials.
Dr. Stein Gold disclosed relationships with Leo, Medicis, and other companies. SDEF and this news organization are owned by Frontline Medical Communications.
Biologics and systemic therapies command much of the spotlight for treating psoriasis, but topical therapy remains an effective option for many psoriasis patients, according to Dr. Linda Stein Gold.
In fact, up to 80% of psoriasis patients can be adequately treated with topical therapy (N. Engl. J. Med. 2005;352:1899-912), said Dr. Stein Gold at the Skin Disease Education Foundation’s (SDEF’s) annual Las Vegas dermatology seminar.
She offered several principles to help clinicians make the most of topical therapies by troubleshooting potential problems.
• Check the amount. One gram of most topical psoriasis products covers 4% of body surface area per application, so a 60-gram tube should treat 4% of body surface area for a month, said Dr. Stein Gold, citing guidelines developed by Dr. Alan Menter and his colleagues and approved by the American Academy of Dermatology in 2009.
• Don’t miss corticosteroid allergies. "We are missing this," said Dr. Stein Gold, director of dermatology research at Henry Ford Hospital in Detroit. Suspect a possible allergy if a patient returns with a worsening rash after using hydrocortisone, for example. Data have shown that between 0.2% and 5% of all dermatitis patients have a steroid allergy. "Allergy to the active molecule or to the vehicle should be suspected in all patients who don’t respond as expected to topical steroids," she noted.
• Visit (or revisit) vitamin D. Another plus for topical therapy is the usefulness of topical vitamin D for tricky areas, such as the forehead, armpit, groin, and the area behind the ears. Data from a randomized trial of 75 patients found calcitriol ointment to be significantly more effective against target lesions and better tolerated by patients than calcipotriene ointment (Br. J. Dermatol. 2003;148:326-33).
• Don’t forget coal tar. Simple, but effective, coal tar is a proven safe topical psoriasis treatment and is available in several vehicles, including solution and foam. Data from a study of more than 13,000 patients with psoriasis and eczema found that coal tar was safe, and that it did not increase the risk for skin cancer (J. Invest. Dermatol. 2010;130:953-61).
The future of topical psoriasis therapy is not static, said Dr. Stein Gold. New molecules – notably topical Janus kinase inhibitors and phosphodiesterase-4 inhibitors – are currently being explored in clinical trials.
Dr. Stein Gold disclosed relationships with Leo, Medicis, and other companies. SDEF and this news organization are owned by Frontline Medical Communications.
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Don’t brush off topical therapies for psoriasis
Biologics and systemic therapies command much of the spotlight for treating psoriasis, but topical therapy remains an effective option for many psoriasis patients, according to Dr. Linda Stein Gold.
In fact, up to 80% of psoriasis patients can be adequately treated with topical therapy (N. Engl. J. Med. 2005;352:1899-912), said Dr. Stein Gold at the Skin Disease Education Foundation’s (SDEF’s) annual Las Vegas dermatology seminar.

She offered several principles to help clinicians make the most of topical therapies by troubleshooting potential problems.
• Check the amount. One gram of most topical psoriasis products covers 4% of body surface area per application, so a 60-gram tube should treat 4% of body surface area for a month, said Dr. Stein Gold, citing guidelines developed by Dr. Alan Menter and his colleagues and approved by the American Academy of Dermatology in 2009.
• Don’t miss corticosteroid allergies. "We are missing this," said Dr. Stein Gold, director of dermatology research at Henry Ford Hospital in Detroit. Suspect a possible allergy if a patient returns with a worsening rash after using hydrocortisone, for example. Data have shown that between 0.2% and 5% of all dermatitis patients have a steroid allergy. "Allergy to the active molecule or to the vehicle should be suspected in all patients who don’t respond as expected to topical steroids," she noted.
• Visit (or revisit) vitamin D. Another plus for topical therapy is the usefulness of topical vitamin D for tricky areas, such as the forehead, armpit, groin, and the area behind the ears. Data from a randomized trial of 75 patients found calcitriol ointment to be significantly more effective against target lesions and better tolerated by patients than calcipotriene ointment (Br. J. Dermatol. 2003;148:326-33).
• Don’t forget coal tar. Simple, but effective, coal tar is a proven safe topical psoriasis treatment and is available in several vehicles, including solution and foam. Data from a study of more than 13,000 patients with psoriasis and eczema found that coal tar was safe, and that it did not increase the risk for skin cancer (J. Invest. Dermatol. 2010;130:953-61).
The future of topical psoriasis therapy is not static, said Dr. Stein Gold. New molecules – notably topical Janus kinase inhibitors and phosphodiesterase-4 inhibitors – are currently being explored in clinical trials.
Dr. Stein Gold disclosed relationships with Leo, Medicis, and other companies. SDEF and this news organization are owned by Frontline Medical Communications.
Biologics and systemic therapies command much of the spotlight for treating psoriasis, but topical therapy remains an effective option for many psoriasis patients, according to Dr. Linda Stein Gold.
In fact, up to 80% of psoriasis patients can be adequately treated with topical therapy (N. Engl. J. Med. 2005;352:1899-912), said Dr. Stein Gold at the Skin Disease Education Foundation’s (SDEF’s) annual Las Vegas dermatology seminar.
She offered several principles to help clinicians make the most of topical therapies by troubleshooting potential problems.
• Check the amount. One gram of most topical psoriasis products covers 4% of body surface area per application, so a 60-gram tube should treat 4% of body surface area for a month, said Dr. Stein Gold, citing guidelines developed by Dr. Alan Menter and his colleagues and approved by the American Academy of Dermatology in 2009.
• Don’t miss corticosteroid allergies. "We are missing this," said Dr. Stein Gold, director of dermatology research at Henry Ford Hospital in Detroit. Suspect a possible allergy if a patient returns with a worsening rash after using hydrocortisone, for example. Data have shown that between 0.2% and 5% of all dermatitis patients have a steroid allergy. "Allergy to the active molecule or to the vehicle should be suspected in all patients who don’t respond as expected to topical steroids," she noted.
• Visit (or revisit) vitamin D. Another plus for topical therapy is the usefulness of topical vitamin D for tricky areas, such as the forehead, armpit, groin, and the area behind the ears. Data from a randomized trial of 75 patients found calcitriol ointment to be significantly more effective against target lesions and better tolerated by patients than calcipotriene ointment (Br. J. Dermatol. 2003;148:326-33).
• Don’t forget coal tar. Simple, but effective, coal tar is a proven safe topical psoriasis treatment and is available in several vehicles, including solution and foam. Data from a study of more than 13,000 patients with psoriasis and eczema found that coal tar was safe, and that it did not increase the risk for skin cancer (J. Invest. Dermatol. 2010;130:953-61).
The future of topical psoriasis therapy is not static, said Dr. Stein Gold. New molecules – notably topical Janus kinase inhibitors and phosphodiesterase-4 inhibitors – are currently being explored in clinical trials.
Dr. Stein Gold disclosed relationships with Leo, Medicis, and other companies. SDEF and this news organization are owned by Frontline Medical Communications.
Biologics and systemic therapies command much of the spotlight for treating psoriasis, but topical therapy remains an effective option for many psoriasis patients, according to Dr. Linda Stein Gold.
In fact, up to 80% of psoriasis patients can be adequately treated with topical therapy (N. Engl. J. Med. 2005;352:1899-912), said Dr. Stein Gold at the Skin Disease Education Foundation’s (SDEF’s) annual Las Vegas dermatology seminar.
She offered several principles to help clinicians make the most of topical therapies by troubleshooting potential problems.
• Check the amount. One gram of most topical psoriasis products covers 4% of body surface area per application, so a 60-gram tube should treat 4% of body surface area for a month, said Dr. Stein Gold, citing guidelines developed by Dr. Alan Menter and his colleagues and approved by the American Academy of Dermatology in 2009.
• Don’t miss corticosteroid allergies. "We are missing this," said Dr. Stein Gold, director of dermatology research at Henry Ford Hospital in Detroit. Suspect a possible allergy if a patient returns with a worsening rash after using hydrocortisone, for example. Data have shown that between 0.2% and 5% of all dermatitis patients have a steroid allergy. "Allergy to the active molecule or to the vehicle should be suspected in all patients who don’t respond as expected to topical steroids," she noted.
• Visit (or revisit) vitamin D. Another plus for topical therapy is the usefulness of topical vitamin D for tricky areas, such as the forehead, armpit, groin, and the area behind the ears. Data from a randomized trial of 75 patients found calcitriol ointment to be significantly more effective against target lesions and better tolerated by patients than calcipotriene ointment (Br. J. Dermatol. 2003;148:326-33).
• Don’t forget coal tar. Simple, but effective, coal tar is a proven safe topical psoriasis treatment and is available in several vehicles, including solution and foam. Data from a study of more than 13,000 patients with psoriasis and eczema found that coal tar was safe, and that it did not increase the risk for skin cancer (J. Invest. Dermatol. 2010;130:953-61).
The future of topical psoriasis therapy is not static, said Dr. Stein Gold. New molecules – notably topical Janus kinase inhibitors and phosphodiesterase-4 inhibitors – are currently being explored in clinical trials.
Dr. Stein Gold disclosed relationships with Leo, Medicis, and other companies. SDEF and this news organization are owned by Frontline Medical Communications.
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Flu outlook 2013-2014: Don’t hesitate. Vaccinate!
WASHINGTON – Vaccination against the flu is on an upswing in the United States, with more than half of eligible children receiving the vaccine last year, but it’s important to keep the momentum going and encourage early vaccination this season, according to a panel of health care professionals.
"Don’t hesitate, vaccinate," said Dr. Howard K. Koh, assistant secretary for health at the U.S. Department for Health and Human Services. Dr. Koh was one of several health officials, who spoke today at a press conference sponsored by the National Foundation for Infectious Diseases (NFID).

This year, an ample supply and multiple choices of vaccines should make it easy for health care providers to get vaccinated themselves and promote vaccination for their patients, said Dr. Koh. The Affordable Care Act provides coverage of all recommended vaccines, including flu vaccine, he noted. The flu is "predictably unpredictable" and hit hard and early last year, so there is no reason to delay vaccination, he said.
Flu vaccination for children aged 6 months to 17 years reached an all-time high of 57% last year, a 5% increase from the previous year, said Dr. Anne Schuchat, assistant surgeon general and director of the Centers for Disease Control and Prevention’s National Center for Immunization and Respiratory Diseases. Flu vaccination is now recommended for everyone, and even the historically vaccination-resistant 18-49-year-old age group showed an increase to 31% last year, up 2.5% from the 2010-2011 season, which is encouraging, Dr. Schuchat said.
Approximately 135 million influenza vaccine doses are expected to be available in locations including doctors’ offices, hospitals, pharmacies, and workplaces, said Dr. William Schaffner, immediate past president of the NFID and an infectious disease specialist at Vanderbilt University Hospital in Nashville, Tenn.
This year’s options include not only the trivalent vaccine but also a quadrivalent option that is designed to provide immunity to two types of A and two types of B influenza strains. The quadrivalent vaccine is available as a standard intramuscular shot and as a nasal spray. The trivalent vaccine is available in five variations: a standard intramuscular shot, an egg-free shot, a transdermal shot (smaller needles, for the needle-phobic), a high-dose vaccine specifically for adults aged 65 years and older, and a cell-culture vaccine (for adults aged 18 years and older). Additional details for health care professionals about the different types of vaccines and this year’s flu outlook are available on the CDC’s seasonal flu website.
Overall, 72% of health care personnel were vaccinated against the flu last year, including 92% of physicians, based on data from an Internet survey, Physician assistants, nurses, nurse practitioners, and pharmacists had vaccination rates greater than 80%, while nonclinical health care personnel, such as housekeeping and food service staff, came in at 65%.
In addition to keeping their patients safe by getting vaccinated themselves, clinicians can boost flu vaccination rates for their patients by discussing the benefits with them, said Dr. Schuchat. For example, data show that pregnant women are significantly more likely to be vaccinated against the flu if their doctor recommends the vaccine and makes it available in the office, she said.
Several online tools related to the flu and flu vaccination are available this season via vaccines.gov. The tools can be used by consumers as well as clinicians, and include an interactive map that tracks vaccination patterns in communities and a vaccine finder that allows users to type in their zip code and identify places close to home where the flu vaccine is available.
On Twitter @hsplete
WASHINGTON – Vaccination against the flu is on an upswing in the United States, with more than half of eligible children receiving the vaccine last year, but it’s important to keep the momentum going and encourage early vaccination this season, according to a panel of health care professionals.
"Don’t hesitate, vaccinate," said Dr. Howard K. Koh, assistant secretary for health at the U.S. Department for Health and Human Services. Dr. Koh was one of several health officials, who spoke today at a press conference sponsored by the National Foundation for Infectious Diseases (NFID).
This year, an ample supply and multiple choices of vaccines should make it easy for health care providers to get vaccinated themselves and promote vaccination for their patients, said Dr. Koh. The Affordable Care Act provides coverage of all recommended vaccines, including flu vaccine, he noted. The flu is "predictably unpredictable" and hit hard and early last year, so there is no reason to delay vaccination, he said.
Flu vaccination for children aged 6 months to 17 years reached an all-time high of 57% last year, a 5% increase from the previous year, said Dr. Anne Schuchat, assistant surgeon general and director of the Centers for Disease Control and Prevention’s National Center for Immunization and Respiratory Diseases. Flu vaccination is now recommended for everyone, and even the historically vaccination-resistant 18-49-year-old age group showed an increase to 31% last year, up 2.5% from the 2010-2011 season, which is encouraging, Dr. Schuchat said.
Approximately 135 million influenza vaccine doses are expected to be available in locations including doctors’ offices, hospitals, pharmacies, and workplaces, said Dr. William Schaffner, immediate past president of the NFID and an infectious disease specialist at Vanderbilt University Hospital in Nashville, Tenn.
This year’s options include not only the trivalent vaccine but also a quadrivalent option that is designed to provide immunity to two types of A and two types of B influenza strains. The quadrivalent vaccine is available as a standard intramuscular shot and as a nasal spray. The trivalent vaccine is available in five variations: a standard intramuscular shot, an egg-free shot, a transdermal shot (smaller needles, for the needle-phobic), a high-dose vaccine specifically for adults aged 65 years and older, and a cell-culture vaccine (for adults aged 18 years and older). Additional details for health care professionals about the different types of vaccines and this year’s flu outlook are available on the CDC’s seasonal flu website.
Overall, 72% of health care personnel were vaccinated against the flu last year, including 92% of physicians, based on data from an Internet survey, Physician assistants, nurses, nurse practitioners, and pharmacists had vaccination rates greater than 80%, while nonclinical health care personnel, such as housekeeping and food service staff, came in at 65%.
In addition to keeping their patients safe by getting vaccinated themselves, clinicians can boost flu vaccination rates for their patients by discussing the benefits with them, said Dr. Schuchat. For example, data show that pregnant women are significantly more likely to be vaccinated against the flu if their doctor recommends the vaccine and makes it available in the office, she said.
Several online tools related to the flu and flu vaccination are available this season via vaccines.gov. The tools can be used by consumers as well as clinicians, and include an interactive map that tracks vaccination patterns in communities and a vaccine finder that allows users to type in their zip code and identify places close to home where the flu vaccine is available.
On Twitter @hsplete
WASHINGTON – Vaccination against the flu is on an upswing in the United States, with more than half of eligible children receiving the vaccine last year, but it’s important to keep the momentum going and encourage early vaccination this season, according to a panel of health care professionals.
"Don’t hesitate, vaccinate," said Dr. Howard K. Koh, assistant secretary for health at the U.S. Department for Health and Human Services. Dr. Koh was one of several health officials, who spoke today at a press conference sponsored by the National Foundation for Infectious Diseases (NFID).
This year, an ample supply and multiple choices of vaccines should make it easy for health care providers to get vaccinated themselves and promote vaccination for their patients, said Dr. Koh. The Affordable Care Act provides coverage of all recommended vaccines, including flu vaccine, he noted. The flu is "predictably unpredictable" and hit hard and early last year, so there is no reason to delay vaccination, he said.
Flu vaccination for children aged 6 months to 17 years reached an all-time high of 57% last year, a 5% increase from the previous year, said Dr. Anne Schuchat, assistant surgeon general and director of the Centers for Disease Control and Prevention’s National Center for Immunization and Respiratory Diseases. Flu vaccination is now recommended for everyone, and even the historically vaccination-resistant 18-49-year-old age group showed an increase to 31% last year, up 2.5% from the 2010-2011 season, which is encouraging, Dr. Schuchat said.
Approximately 135 million influenza vaccine doses are expected to be available in locations including doctors’ offices, hospitals, pharmacies, and workplaces, said Dr. William Schaffner, immediate past president of the NFID and an infectious disease specialist at Vanderbilt University Hospital in Nashville, Tenn.
This year’s options include not only the trivalent vaccine but also a quadrivalent option that is designed to provide immunity to two types of A and two types of B influenza strains. The quadrivalent vaccine is available as a standard intramuscular shot and as a nasal spray. The trivalent vaccine is available in five variations: a standard intramuscular shot, an egg-free shot, a transdermal shot (smaller needles, for the needle-phobic), a high-dose vaccine specifically for adults aged 65 years and older, and a cell-culture vaccine (for adults aged 18 years and older). Additional details for health care professionals about the different types of vaccines and this year’s flu outlook are available on the CDC’s seasonal flu website.
Overall, 72% of health care personnel were vaccinated against the flu last year, including 92% of physicians, based on data from an Internet survey, Physician assistants, nurses, nurse practitioners, and pharmacists had vaccination rates greater than 80%, while nonclinical health care personnel, such as housekeeping and food service staff, came in at 65%.
In addition to keeping their patients safe by getting vaccinated themselves, clinicians can boost flu vaccination rates for their patients by discussing the benefits with them, said Dr. Schuchat. For example, data show that pregnant women are significantly more likely to be vaccinated against the flu if their doctor recommends the vaccine and makes it available in the office, she said.
Several online tools related to the flu and flu vaccination are available this season via vaccines.gov. The tools can be used by consumers as well as clinicians, and include an interactive map that tracks vaccination patterns in communities and a vaccine finder that allows users to type in their zip code and identify places close to home where the flu vaccine is available.
On Twitter @hsplete
AT THE NFID ANNUAL INFLUENZA PRESS CONFERENCE

Fewer than 1% of doctors mention sunscreen to patients
Physicians miss 99.9% of their opportunities to counsel patients about use of sunscreen, and dermatologists pass up 98% of those teaching moments, based on data from approximately 18 billion patient visits recorded between January 1989 and December 2010. The findings were published online on Sept. 4 in JAMA Dermatology.
Despite the rising incidence of skin cancer and recommendations from medical organizations that clinicians counsel patients about sun-protective behaviors, "sun-protection counseling ranks among the lowest topics of primary prevention discussed between physicians and patients," said Dr. Kristie Akamine of Wake Forest University in Winston-Salem, N.C., and her colleagues.
To identify trends in sunscreen recommendations by different specialties, the researchers reviewed data from the National Ambulatory Medical Care Survey (NAMCS), an ongoing survey conducted by the National Center for Health Statistics (JAMA Dermatol. 2013 Sept. 4 [doi:10.1001/jamadermatol.2013.4741]).

Overall, sunscreen was recommended at only 12.9 million of 18.3 billion patient visits (0.07%). Most of the appointments at which sunscreen was recommended were visits to a dermatologist (86%), followed by visits to family physicians or general practitioners (10%), pediatricians (1.4%), other specialists (1.4%), and internists (1.1%).
Although dermatologists were the most frequent recommenders of sunscreen, the mention of sunscreen was recorded at only 1.6% of all dermatology visits and 11% of visits associated with a diagnosis of skin cancer, the researchers said. Of note, dermatologists recommended use of sunscreen to skin cancer patients less frequently than did general/family physicians (11% vs. 56%), they added.
Overall, sunscreen was least often recommended for children younger than 10 years; by contrast, patients in their 70s were most likely to receive a recommendation for sunscreen use.
In addition, white patients were nine times more likely than black patients to receive a recommendation for sunscreen use.
Across all specialties, patients with a diagnosis of actinic keratosis accounted for 21% of the visits at which sunscreen was recommended.
The study was limited by several factors, including the cross-sectional nature of the data, which included both new and follow-up visits, and the lack of information about whether sunscreen was discussed at an earlier visit or not documented by the physician on the survey report, Dr. Akamine and her associates noted.
The results, however, suggest that sunscreen use recommendation is less frequent than advised by multiple medical organizations. "The high incidence and morbidity of skin cancer can be greatly reduced with the implementation of sun-protection behaviors, which patients should be counseled about at outpatient visits," the researchers said.
Lead author Dr. Akamine had no financial conflicts to disclose. Corresponding author Dr. Steven Feldman disclosed financial relationships with multiple pharmaceutical companies, but this study was not sponsored by a pharmaceutical company.
On Twitter @hsplete
Physicians miss 99.9% of their opportunities to counsel patients about use of sunscreen, and dermatologists pass up 98% of those teaching moments, based on data from approximately 18 billion patient visits recorded between January 1989 and December 2010. The findings were published online on Sept. 4 in JAMA Dermatology.
Despite the rising incidence of skin cancer and recommendations from medical organizations that clinicians counsel patients about sun-protective behaviors, "sun-protection counseling ranks among the lowest topics of primary prevention discussed between physicians and patients," said Dr. Kristie Akamine of Wake Forest University in Winston-Salem, N.C., and her colleagues.
To identify trends in sunscreen recommendations by different specialties, the researchers reviewed data from the National Ambulatory Medical Care Survey (NAMCS), an ongoing survey conducted by the National Center for Health Statistics (JAMA Dermatol. 2013 Sept. 4 [doi:10.1001/jamadermatol.2013.4741]).
Overall, sunscreen was recommended at only 12.9 million of 18.3 billion patient visits (0.07%). Most of the appointments at which sunscreen was recommended were visits to a dermatologist (86%), followed by visits to family physicians or general practitioners (10%), pediatricians (1.4%), other specialists (1.4%), and internists (1.1%).
Although dermatologists were the most frequent recommenders of sunscreen, the mention of sunscreen was recorded at only 1.6% of all dermatology visits and 11% of visits associated with a diagnosis of skin cancer, the researchers said. Of note, dermatologists recommended use of sunscreen to skin cancer patients less frequently than did general/family physicians (11% vs. 56%), they added.
Overall, sunscreen was least often recommended for children younger than 10 years; by contrast, patients in their 70s were most likely to receive a recommendation for sunscreen use.
In addition, white patients were nine times more likely than black patients to receive a recommendation for sunscreen use.
Across all specialties, patients with a diagnosis of actinic keratosis accounted for 21% of the visits at which sunscreen was recommended.
The study was limited by several factors, including the cross-sectional nature of the data, which included both new and follow-up visits, and the lack of information about whether sunscreen was discussed at an earlier visit or not documented by the physician on the survey report, Dr. Akamine and her associates noted.
The results, however, suggest that sunscreen use recommendation is less frequent than advised by multiple medical organizations. "The high incidence and morbidity of skin cancer can be greatly reduced with the implementation of sun-protection behaviors, which patients should be counseled about at outpatient visits," the researchers said.
Lead author Dr. Akamine had no financial conflicts to disclose. Corresponding author Dr. Steven Feldman disclosed financial relationships with multiple pharmaceutical companies, but this study was not sponsored by a pharmaceutical company.
On Twitter @hsplete
Physicians miss 99.9% of their opportunities to counsel patients about use of sunscreen, and dermatologists pass up 98% of those teaching moments, based on data from approximately 18 billion patient visits recorded between January 1989 and December 2010. The findings were published online on Sept. 4 in JAMA Dermatology.
Despite the rising incidence of skin cancer and recommendations from medical organizations that clinicians counsel patients about sun-protective behaviors, "sun-protection counseling ranks among the lowest topics of primary prevention discussed between physicians and patients," said Dr. Kristie Akamine of Wake Forest University in Winston-Salem, N.C., and her colleagues.
To identify trends in sunscreen recommendations by different specialties, the researchers reviewed data from the National Ambulatory Medical Care Survey (NAMCS), an ongoing survey conducted by the National Center for Health Statistics (JAMA Dermatol. 2013 Sept. 4 [doi:10.1001/jamadermatol.2013.4741]).
Overall, sunscreen was recommended at only 12.9 million of 18.3 billion patient visits (0.07%). Most of the appointments at which sunscreen was recommended were visits to a dermatologist (86%), followed by visits to family physicians or general practitioners (10%), pediatricians (1.4%), other specialists (1.4%), and internists (1.1%).
Although dermatologists were the most frequent recommenders of sunscreen, the mention of sunscreen was recorded at only 1.6% of all dermatology visits and 11% of visits associated with a diagnosis of skin cancer, the researchers said. Of note, dermatologists recommended use of sunscreen to skin cancer patients less frequently than did general/family physicians (11% vs. 56%), they added.
Overall, sunscreen was least often recommended for children younger than 10 years; by contrast, patients in their 70s were most likely to receive a recommendation for sunscreen use.
In addition, white patients were nine times more likely than black patients to receive a recommendation for sunscreen use.
Across all specialties, patients with a diagnosis of actinic keratosis accounted for 21% of the visits at which sunscreen was recommended.
The study was limited by several factors, including the cross-sectional nature of the data, which included both new and follow-up visits, and the lack of information about whether sunscreen was discussed at an earlier visit or not documented by the physician on the survey report, Dr. Akamine and her associates noted.
The results, however, suggest that sunscreen use recommendation is less frequent than advised by multiple medical organizations. "The high incidence and morbidity of skin cancer can be greatly reduced with the implementation of sun-protection behaviors, which patients should be counseled about at outpatient visits," the researchers said.
Lead author Dr. Akamine had no financial conflicts to disclose. Corresponding author Dr. Steven Feldman disclosed financial relationships with multiple pharmaceutical companies, but this study was not sponsored by a pharmaceutical company.
On Twitter @hsplete
FROM JAMA DERMATOLOGY
Major Finding: Overall, physicians recommended sunscreen at 12.9 million of 18.3 billion patient visits (0.07%).
Data Source: The National Ambulatory Medical Care Survey, an ongoing survey conducted by the National Center for Health Statistics.
Disclosures: Lead author Dr. Akamine had no financial conflicts to disclose. Corresponding author Dr. Steven Feldman disclosed financial relationships with multiple pharmaceutical companies, but this study was not sponsored by a pharmaceutical company.

Debunking Sun Protection Myths
Fair-skinned people are known to be at higher risk for skin cancer and other problems associated with too much exposure to the sun. But people with skin of color are also vulnerable to the harmful effects of ultraviolet rays emitted by both the sun and indoor tanning beds, said Dr. Adam Friedman, director of dermatologic research, division of dermatology, Montefiore Medical Center in New York.
"Darker skin has more reactive melanocytes, or pigment-making cells, and has more and stronger melanosomes, which are small packets that contain skin pigment, both of which provide some inherent protection against UV rays but not enough, he said. "This unique biological difference in darker skin causes the harmful effects of UV exposure to occur more slowly in people of color, and the effects require more direct sun exposure. But the damage does happen, from cosmetic problems such as premature aging of the skin to serious conditions such as skin cancer."
"There are three major misconceptions that I encounter with my patients in the Bronx," Dr. Friedman said.
• Darker skin makes one immune to the harmful effects of the sun.
• There is no risk of exposure on cloudy days.
• One needs to get vitamin D via sun exposure.
"All three are completely false, and ultimately they perpetuate and result in improper skin protection," he noted.
"Skin cancer is rarer in people with skin of color, but it does occur and can be extremely serious when diagnosis is delayed," Dr. Friedman said. For example, melanoma, the most deadly form of skin cancer, is more than 20 times more common in whites than in African Americans, but people with darker skin are at greater risk of late diagnosis with advanced, thicker melanomas and lower survival rates. In fact, the overall 5-year melanoma survival rate for African Americans is only 77%, versus 91% for Caucasians, he said.
"I advise all of my patients to routinely check their own skin for any changes in appearance, and to see a dermatologist annually for a full body exam," Dr. Friedman emphasized.
Traditional sunscreens, especially those containing mineral-based agents such as titanium dioxide and zinc oxide, do not blend well when used on darker skin. The resulting chalky appearance is unacceptable to many patients, Dr. Friedman said. Fortunately, new formulations are changing that.
The newer sunscreens combine several agents to both decrease the concentration needed of each and allow for a synergistic effect between them, "ultimately offering a better sunscreen formula that can blend well into any skin type," said Dr. Friedman. Patients should look for products containing micronized or nanosized zinc oxide or titanium dioxide, which do not scatter light in the visible spectrum (to which older versions of these products owe their chalky appearance) but are highly effective at blocking UV radiation, he advised. Products that combine these mineral agents with multiple chemical blockers such as ecamsule, avobenzone, and cinoxate are particularly effective and cosmetically acceptable. Patients may be most likely to use sunscreens that utilize vehicles that enhance dispersal of these ingredients to limit clumping and phase separation, such as talc and Bentone gel.
In addition, pH stabilizers such as dimethicone are important, as the skin acidity in skin of color is lower and needs to be maintained to prevent degradation of skin adhesion proteins. Dr. Friedman recommends that his skin of color patients use SPF 30 broad-spectrum sunscreen, generously applied, and lip balm with an SPF of at least 30.
Dr. Friedman often hears from patients that they avoid sunscreen because it prevents them from getting vitamin D from the sun, which they believe is the best source. "You can enjoy the best of both worlds – use sunscreen when you spend time outdoors and take a vitamin D supplement, which is a very effective way to get adequate daily intake," he said. He advises his patients to remain vigilant about how much sun exposure they get. "Sunscreen alone is not enough to protect you from skin cancer, especially between the hours of 10:00 a.m. and 2:00 p.m. I encourage all of my patients to seek shade during that time of day and wear hats, sunglasses, and protective clothing if possible," he said.
Dr. Friedman had no financial conflicts to disclose.
[email protected]
On Twitter @hsplete
Fair-skinned people are known to be at higher risk for skin cancer and other problems associated with too much exposure to the sun. But people with skin of color are also vulnerable to the harmful effects of ultraviolet rays emitted by both the sun and indoor tanning beds, said Dr. Adam Friedman, director of dermatologic research, division of dermatology, Montefiore Medical Center in New York.
"Darker skin has more reactive melanocytes, or pigment-making cells, and has more and stronger melanosomes, which are small packets that contain skin pigment, both of which provide some inherent protection against UV rays but not enough, he said. "This unique biological difference in darker skin causes the harmful effects of UV exposure to occur more slowly in people of color, and the effects require more direct sun exposure. But the damage does happen, from cosmetic problems such as premature aging of the skin to serious conditions such as skin cancer."
"There are three major misconceptions that I encounter with my patients in the Bronx," Dr. Friedman said.
• Darker skin makes one immune to the harmful effects of the sun.
• There is no risk of exposure on cloudy days.
• One needs to get vitamin D via sun exposure.
"All three are completely false, and ultimately they perpetuate and result in improper skin protection," he noted.
"Skin cancer is rarer in people with skin of color, but it does occur and can be extremely serious when diagnosis is delayed," Dr. Friedman said. For example, melanoma, the most deadly form of skin cancer, is more than 20 times more common in whites than in African Americans, but people with darker skin are at greater risk of late diagnosis with advanced, thicker melanomas and lower survival rates. In fact, the overall 5-year melanoma survival rate for African Americans is only 77%, versus 91% for Caucasians, he said.
"I advise all of my patients to routinely check their own skin for any changes in appearance, and to see a dermatologist annually for a full body exam," Dr. Friedman emphasized.
Traditional sunscreens, especially those containing mineral-based agents such as titanium dioxide and zinc oxide, do not blend well when used on darker skin. The resulting chalky appearance is unacceptable to many patients, Dr. Friedman said. Fortunately, new formulations are changing that.
The newer sunscreens combine several agents to both decrease the concentration needed of each and allow for a synergistic effect between them, "ultimately offering a better sunscreen formula that can blend well into any skin type," said Dr. Friedman. Patients should look for products containing micronized or nanosized zinc oxide or titanium dioxide, which do not scatter light in the visible spectrum (to which older versions of these products owe their chalky appearance) but are highly effective at blocking UV radiation, he advised. Products that combine these mineral agents with multiple chemical blockers such as ecamsule, avobenzone, and cinoxate are particularly effective and cosmetically acceptable. Patients may be most likely to use sunscreens that utilize vehicles that enhance dispersal of these ingredients to limit clumping and phase separation, such as talc and Bentone gel.
In addition, pH stabilizers such as dimethicone are important, as the skin acidity in skin of color is lower and needs to be maintained to prevent degradation of skin adhesion proteins. Dr. Friedman recommends that his skin of color patients use SPF 30 broad-spectrum sunscreen, generously applied, and lip balm with an SPF of at least 30.
Dr. Friedman often hears from patients that they avoid sunscreen because it prevents them from getting vitamin D from the sun, which they believe is the best source. "You can enjoy the best of both worlds – use sunscreen when you spend time outdoors and take a vitamin D supplement, which is a very effective way to get adequate daily intake," he said. He advises his patients to remain vigilant about how much sun exposure they get. "Sunscreen alone is not enough to protect you from skin cancer, especially between the hours of 10:00 a.m. and 2:00 p.m. I encourage all of my patients to seek shade during that time of day and wear hats, sunglasses, and protective clothing if possible," he said.
Dr. Friedman had no financial conflicts to disclose.
[email protected]
On Twitter @hsplete
Fair-skinned people are known to be at higher risk for skin cancer and other problems associated with too much exposure to the sun. But people with skin of color are also vulnerable to the harmful effects of ultraviolet rays emitted by both the sun and indoor tanning beds, said Dr. Adam Friedman, director of dermatologic research, division of dermatology, Montefiore Medical Center in New York.
"Darker skin has more reactive melanocytes, or pigment-making cells, and has more and stronger melanosomes, which are small packets that contain skin pigment, both of which provide some inherent protection against UV rays but not enough, he said. "This unique biological difference in darker skin causes the harmful effects of UV exposure to occur more slowly in people of color, and the effects require more direct sun exposure. But the damage does happen, from cosmetic problems such as premature aging of the skin to serious conditions such as skin cancer."
"There are three major misconceptions that I encounter with my patients in the Bronx," Dr. Friedman said.
• Darker skin makes one immune to the harmful effects of the sun.
• There is no risk of exposure on cloudy days.
• One needs to get vitamin D via sun exposure.
"All three are completely false, and ultimately they perpetuate and result in improper skin protection," he noted.
"Skin cancer is rarer in people with skin of color, but it does occur and can be extremely serious when diagnosis is delayed," Dr. Friedman said. For example, melanoma, the most deadly form of skin cancer, is more than 20 times more common in whites than in African Americans, but people with darker skin are at greater risk of late diagnosis with advanced, thicker melanomas and lower survival rates. In fact, the overall 5-year melanoma survival rate for African Americans is only 77%, versus 91% for Caucasians, he said.
"I advise all of my patients to routinely check their own skin for any changes in appearance, and to see a dermatologist annually for a full body exam," Dr. Friedman emphasized.
Traditional sunscreens, especially those containing mineral-based agents such as titanium dioxide and zinc oxide, do not blend well when used on darker skin. The resulting chalky appearance is unacceptable to many patients, Dr. Friedman said. Fortunately, new formulations are changing that.
The newer sunscreens combine several agents to both decrease the concentration needed of each and allow for a synergistic effect between them, "ultimately offering a better sunscreen formula that can blend well into any skin type," said Dr. Friedman. Patients should look for products containing micronized or nanosized zinc oxide or titanium dioxide, which do not scatter light in the visible spectrum (to which older versions of these products owe their chalky appearance) but are highly effective at blocking UV radiation, he advised. Products that combine these mineral agents with multiple chemical blockers such as ecamsule, avobenzone, and cinoxate are particularly effective and cosmetically acceptable. Patients may be most likely to use sunscreens that utilize vehicles that enhance dispersal of these ingredients to limit clumping and phase separation, such as talc and Bentone gel.
In addition, pH stabilizers such as dimethicone are important, as the skin acidity in skin of color is lower and needs to be maintained to prevent degradation of skin adhesion proteins. Dr. Friedman recommends that his skin of color patients use SPF 30 broad-spectrum sunscreen, generously applied, and lip balm with an SPF of at least 30.
Dr. Friedman often hears from patients that they avoid sunscreen because it prevents them from getting vitamin D from the sun, which they believe is the best source. "You can enjoy the best of both worlds – use sunscreen when you spend time outdoors and take a vitamin D supplement, which is a very effective way to get adequate daily intake," he said. He advises his patients to remain vigilant about how much sun exposure they get. "Sunscreen alone is not enough to protect you from skin cancer, especially between the hours of 10:00 a.m. and 2:00 p.m. I encourage all of my patients to seek shade during that time of day and wear hats, sunglasses, and protective clothing if possible," he said.
Dr. Friedman had no financial conflicts to disclose.
[email protected]
On Twitter @hsplete
EXPERT ANALYSIS FROM THE SKIN OF COLOR SEMINAR SERIES
Debunking sun protection myths for skin of color patients
Fair-skinned people are known to be at higher risk for skin cancer and other problems associated with too much exposure to the sun. But people with skin of color are also vulnerable to the harmful effects of ultraviolet rays emitted by both the sun and indoor tanning beds, said Dr. Adam Friedman, director of dermatologic research, division of dermatology, Montefiore Medical Center in New York.
"Darker skin has more reactive melanocytes, or pigment-making cells, and has more and stronger melanosomes, which are small packets that contain skin pigment, both of which provide some inherent protection against UV rays but not enough, he said. "This unique biological difference in darker skin causes the harmful effects of UV exposure to occur more slowly in people of color, and the effects require more direct sun exposure. But the damage does happen, from cosmetic problems such as premature aging of the skin to serious conditions such as skin cancer."
"There are three major misconceptions that I encounter with my patients in the Bronx," Dr. Friedman said.
• Darker skin makes one immune to the harmful effects of the sun.
• There is no risk of exposure on cloudy days.
• One needs to get vitamin D via sun exposure.
"All three are completely false, and ultimately they perpetuate and result in improper skin protection," he noted.
"Skin cancer is rarer in people with skin of color, but it does occur and can be extremely serious when diagnosis is delayed," Dr. Friedman said. For example, melanoma, the most deadly form of skin cancer, is more than 20 times more common in whites than in African Americans, but people with darker skin are at greater risk of late diagnosis with advanced, thicker melanomas and lower survival rates. In fact, the overall 5-year melanoma survival rate for African Americans is only 77%, versus 91% for Caucasians, he said.
"I advise all of my patients to routinely check their own skin for any changes in appearance, and to see a dermatologist annually for a full body exam," Dr. Friedman emphasized.
Traditional sunscreens, especially those containing mineral-based agents such as titanium dioxide and zinc oxide, do not blend well when used on darker skin. The resulting chalky appearance is unacceptable to many patients, Dr. Friedman said. Fortunately, new formulations are changing that.
The newer sunscreens combine several agents to both decrease the concentration needed of each and allow for a synergistic effect between them, "ultimately offering a better sunscreen formula that can blend well into any skin type," said Dr. Friedman. Patients should look for products containing micronized or nanosized zinc oxide or titanium dioxide, which do not scatter light in the visible spectrum (to which older versions of these products owe their chalky appearance) but are highly effective at blocking UV radiation, he advised. Products that combine these mineral agents with multiple chemical blockers such as ecamsule, avobenzone, and cinoxate are particularly effective and cosmetically acceptable. Patients may be most likely to use sunscreens that utilize vehicles that enhance dispersal of these ingredients to limit clumping and phase separation, such as talc and Bentone gel.
In addition, pH stabilizers such as dimethicone are important, as the skin acidity in skin of color is lower and needs to be maintained to prevent degradation of skin adhesion proteins. Dr. Friedman recommends that his skin of color patients use SPF 30 broad-spectrum sunscreen, generously applied, and lip balm with an SPF of at least 30.
Dr. Friedman often hears from patients that they avoid sunscreen because it prevents them from getting vitamin D from the sun, which they believe is the best source. "You can enjoy the best of both worlds – use sunscreen when you spend time outdoors and take a vitamin D supplement, which is a very effective way to get adequate daily intake," he said. He advises his patients to remain vigilant about how much sun exposure they get. "Sunscreen alone is not enough to protect you from skin cancer, especially between the hours of 10:00 a.m. and 2:00 p.m. I encourage all of my patients to seek shade during that time of day and wear hats, sunglasses, and protective clothing if possible," he said.
Dr. Friedman had no financial conflicts to disclose.
[email protected]
On Twitter @hsplete
Fair-skinned people are known to be at higher risk for skin cancer and other problems associated with too much exposure to the sun. But people with skin of color are also vulnerable to the harmful effects of ultraviolet rays emitted by both the sun and indoor tanning beds, said Dr. Adam Friedman, director of dermatologic research, division of dermatology, Montefiore Medical Center in New York.
"Darker skin has more reactive melanocytes, or pigment-making cells, and has more and stronger melanosomes, which are small packets that contain skin pigment, both of which provide some inherent protection against UV rays but not enough, he said. "This unique biological difference in darker skin causes the harmful effects of UV exposure to occur more slowly in people of color, and the effects require more direct sun exposure. But the damage does happen, from cosmetic problems such as premature aging of the skin to serious conditions such as skin cancer."
"There are three major misconceptions that I encounter with my patients in the Bronx," Dr. Friedman said.
• Darker skin makes one immune to the harmful effects of the sun.
• There is no risk of exposure on cloudy days.
• One needs to get vitamin D via sun exposure.
"All three are completely false, and ultimately they perpetuate and result in improper skin protection," he noted.
"Skin cancer is rarer in people with skin of color, but it does occur and can be extremely serious when diagnosis is delayed," Dr. Friedman said. For example, melanoma, the most deadly form of skin cancer, is more than 20 times more common in whites than in African Americans, but people with darker skin are at greater risk of late diagnosis with advanced, thicker melanomas and lower survival rates. In fact, the overall 5-year melanoma survival rate for African Americans is only 77%, versus 91% for Caucasians, he said.
"I advise all of my patients to routinely check their own skin for any changes in appearance, and to see a dermatologist annually for a full body exam," Dr. Friedman emphasized.
Traditional sunscreens, especially those containing mineral-based agents such as titanium dioxide and zinc oxide, do not blend well when used on darker skin. The resulting chalky appearance is unacceptable to many patients, Dr. Friedman said. Fortunately, new formulations are changing that.
The newer sunscreens combine several agents to both decrease the concentration needed of each and allow for a synergistic effect between them, "ultimately offering a better sunscreen formula that can blend well into any skin type," said Dr. Friedman. Patients should look for products containing micronized or nanosized zinc oxide or titanium dioxide, which do not scatter light in the visible spectrum (to which older versions of these products owe their chalky appearance) but are highly effective at blocking UV radiation, he advised. Products that combine these mineral agents with multiple chemical blockers such as ecamsule, avobenzone, and cinoxate are particularly effective and cosmetically acceptable. Patients may be most likely to use sunscreens that utilize vehicles that enhance dispersal of these ingredients to limit clumping and phase separation, such as talc and Bentone gel.
In addition, pH stabilizers such as dimethicone are important, as the skin acidity in skin of color is lower and needs to be maintained to prevent degradation of skin adhesion proteins. Dr. Friedman recommends that his skin of color patients use SPF 30 broad-spectrum sunscreen, generously applied, and lip balm with an SPF of at least 30.
Dr. Friedman often hears from patients that they avoid sunscreen because it prevents them from getting vitamin D from the sun, which they believe is the best source. "You can enjoy the best of both worlds – use sunscreen when you spend time outdoors and take a vitamin D supplement, which is a very effective way to get adequate daily intake," he said. He advises his patients to remain vigilant about how much sun exposure they get. "Sunscreen alone is not enough to protect you from skin cancer, especially between the hours of 10:00 a.m. and 2:00 p.m. I encourage all of my patients to seek shade during that time of day and wear hats, sunglasses, and protective clothing if possible," he said.
Dr. Friedman had no financial conflicts to disclose.
[email protected]
On Twitter @hsplete
Fair-skinned people are known to be at higher risk for skin cancer and other problems associated with too much exposure to the sun. But people with skin of color are also vulnerable to the harmful effects of ultraviolet rays emitted by both the sun and indoor tanning beds, said Dr. Adam Friedman, director of dermatologic research, division of dermatology, Montefiore Medical Center in New York.
"Darker skin has more reactive melanocytes, or pigment-making cells, and has more and stronger melanosomes, which are small packets that contain skin pigment, both of which provide some inherent protection against UV rays but not enough, he said. "This unique biological difference in darker skin causes the harmful effects of UV exposure to occur more slowly in people of color, and the effects require more direct sun exposure. But the damage does happen, from cosmetic problems such as premature aging of the skin to serious conditions such as skin cancer."
"There are three major misconceptions that I encounter with my patients in the Bronx," Dr. Friedman said.
• Darker skin makes one immune to the harmful effects of the sun.
• There is no risk of exposure on cloudy days.
• One needs to get vitamin D via sun exposure.
"All three are completely false, and ultimately they perpetuate and result in improper skin protection," he noted.
"Skin cancer is rarer in people with skin of color, but it does occur and can be extremely serious when diagnosis is delayed," Dr. Friedman said. For example, melanoma, the most deadly form of skin cancer, is more than 20 times more common in whites than in African Americans, but people with darker skin are at greater risk of late diagnosis with advanced, thicker melanomas and lower survival rates. In fact, the overall 5-year melanoma survival rate for African Americans is only 77%, versus 91% for Caucasians, he said.
"I advise all of my patients to routinely check their own skin for any changes in appearance, and to see a dermatologist annually for a full body exam," Dr. Friedman emphasized.
Traditional sunscreens, especially those containing mineral-based agents such as titanium dioxide and zinc oxide, do not blend well when used on darker skin. The resulting chalky appearance is unacceptable to many patients, Dr. Friedman said. Fortunately, new formulations are changing that.
The newer sunscreens combine several agents to both decrease the concentration needed of each and allow for a synergistic effect between them, "ultimately offering a better sunscreen formula that can blend well into any skin type," said Dr. Friedman. Patients should look for products containing micronized or nanosized zinc oxide or titanium dioxide, which do not scatter light in the visible spectrum (to which older versions of these products owe their chalky appearance) but are highly effective at blocking UV radiation, he advised. Products that combine these mineral agents with multiple chemical blockers such as ecamsule, avobenzone, and cinoxate are particularly effective and cosmetically acceptable. Patients may be most likely to use sunscreens that utilize vehicles that enhance dispersal of these ingredients to limit clumping and phase separation, such as talc and Bentone gel.
In addition, pH stabilizers such as dimethicone are important, as the skin acidity in skin of color is lower and needs to be maintained to prevent degradation of skin adhesion proteins. Dr. Friedman recommends that his skin of color patients use SPF 30 broad-spectrum sunscreen, generously applied, and lip balm with an SPF of at least 30.
Dr. Friedman often hears from patients that they avoid sunscreen because it prevents them from getting vitamin D from the sun, which they believe is the best source. "You can enjoy the best of both worlds – use sunscreen when you spend time outdoors and take a vitamin D supplement, which is a very effective way to get adequate daily intake," he said. He advises his patients to remain vigilant about how much sun exposure they get. "Sunscreen alone is not enough to protect you from skin cancer, especially between the hours of 10:00 a.m. and 2:00 p.m. I encourage all of my patients to seek shade during that time of day and wear hats, sunglasses, and protective clothing if possible," he said.
Dr. Friedman had no financial conflicts to disclose.
[email protected]
On Twitter @hsplete
EXPERT ANALYSIS FROM THE SKIN OF COLOR SEMINAR SERIES