User login
Don’t bother with blood cultures for uncomplicated pediatric SSTIs
Blood cultures did not improve the assessment of children hospitalized with uncomplicated skin and soft tissue infections, based on data from a review of more than 500 children. The findings were published online Aug. 5 in Pediatrics.
Some current guidelines suggest obtaining blood cultures from children with skin and soft tissue infections (SSTIs) to help identify bacteremia and prevent sepsis, but the value of the test is unknown and evidence to support its use is limited, said Dr. Jay R. Malone of the University of Oklahoma, Oklahoma City, and colleagues.
The researchers compared 482 children with uncomplicated SSTIs and 98 children with complicated SSTIs (cSSTIs) who were admitted to a single hospital between Jan. 1, 2007, and Dec. 31, 2009, for cellulitis or abscesses. The average age of the children with SSTIs was 3 years, approximately half were male. The average age of the cSSTI children was significantly older (6 years) and included significantly more males (64%). Approximately half of the children in both groups had received at least one dose of antibiotics prior to hospital admission, and about one quarter of children in both groups presented with temperatures greater than 37.9 degrees Celsius.
Overall, none of the 482 children with uncomplicated SSTIs had positive blood cultures (although 3 were contaminated), compared with 10 positive cultures (12.5%) among 98 children with cSSTIs (Pediatrics 2013 Aug. 5 [doi: 10.1542/peds.2013-1384).
However, blood cultures were significantly more frequent for children with uncomplicated SSTIs compared to those with cSSTIs (94% vs. 82%), and those who had blood cultures were significantly more likely than were those who did not have cultures to have a C-reactive protein drawn (98% vs. 74%).
"This could be a result of a greater percentage of children with cSSTI being admitted to surgical services that may perform laboratory investigations less often than medical services," the researchers noted.
The most common infection sites for the uncomplicated SSTI group were the extremities (32%) and buttocks or perineum (27%), while the most common infection sites for the cSSTI group were the face or neck (39%) and extremities (24%).
Overall, the average length of hospital stay was 3 days for children with uncomplicated SSTIs, compared with 7 days for those with cSSTIs. However, the average length of hospital stay was almost a day longer for children with uncomplicated SSTIs who had blood cultures, compared with those who did not (.91 days; a significant difference).
The study was limited by several factors, including the retrospective design, the impact of antibiotics on the blood cultures, and the limited population of children who presented to an emergency department with SSTIs and were admitted to the hospital. Yet the results show that blood cultures in children with uncomplicated SSTIs yield a very low number of positive results, and do not appear to provide clinical value, the researchers said.
"Given the limited value of these tests, physicians might reasonably limit their use to children with complicated infections," they noted.
More research is needed on several fronts, including studies to define the criteria for hospitalizing children with SSTIs and to determine the risk of bacteremia in infants younger than 60 days, they added.
The researchers had no financial conflicts to disclose.
On Twitter @hsplete
Blood cultures did not improve the assessment of children hospitalized with uncomplicated skin and soft tissue infections, based on data from a review of more than 500 children. The findings were published online Aug. 5 in Pediatrics.
Some current guidelines suggest obtaining blood cultures from children with skin and soft tissue infections (SSTIs) to help identify bacteremia and prevent sepsis, but the value of the test is unknown and evidence to support its use is limited, said Dr. Jay R. Malone of the University of Oklahoma, Oklahoma City, and colleagues.
The researchers compared 482 children with uncomplicated SSTIs and 98 children with complicated SSTIs (cSSTIs) who were admitted to a single hospital between Jan. 1, 2007, and Dec. 31, 2009, for cellulitis or abscesses. The average age of the children with SSTIs was 3 years, approximately half were male. The average age of the cSSTI children was significantly older (6 years) and included significantly more males (64%). Approximately half of the children in both groups had received at least one dose of antibiotics prior to hospital admission, and about one quarter of children in both groups presented with temperatures greater than 37.9 degrees Celsius.
Overall, none of the 482 children with uncomplicated SSTIs had positive blood cultures (although 3 were contaminated), compared with 10 positive cultures (12.5%) among 98 children with cSSTIs (Pediatrics 2013 Aug. 5 [doi: 10.1542/peds.2013-1384).
However, blood cultures were significantly more frequent for children with uncomplicated SSTIs compared to those with cSSTIs (94% vs. 82%), and those who had blood cultures were significantly more likely than were those who did not have cultures to have a C-reactive protein drawn (98% vs. 74%).
"This could be a result of a greater percentage of children with cSSTI being admitted to surgical services that may perform laboratory investigations less often than medical services," the researchers noted.
The most common infection sites for the uncomplicated SSTI group were the extremities (32%) and buttocks or perineum (27%), while the most common infection sites for the cSSTI group were the face or neck (39%) and extremities (24%).
Overall, the average length of hospital stay was 3 days for children with uncomplicated SSTIs, compared with 7 days for those with cSSTIs. However, the average length of hospital stay was almost a day longer for children with uncomplicated SSTIs who had blood cultures, compared with those who did not (.91 days; a significant difference).
The study was limited by several factors, including the retrospective design, the impact of antibiotics on the blood cultures, and the limited population of children who presented to an emergency department with SSTIs and were admitted to the hospital. Yet the results show that blood cultures in children with uncomplicated SSTIs yield a very low number of positive results, and do not appear to provide clinical value, the researchers said.
"Given the limited value of these tests, physicians might reasonably limit their use to children with complicated infections," they noted.
More research is needed on several fronts, including studies to define the criteria for hospitalizing children with SSTIs and to determine the risk of bacteremia in infants younger than 60 days, they added.
The researchers had no financial conflicts to disclose.
On Twitter @hsplete
Blood cultures did not improve the assessment of children hospitalized with uncomplicated skin and soft tissue infections, based on data from a review of more than 500 children. The findings were published online Aug. 5 in Pediatrics.
Some current guidelines suggest obtaining blood cultures from children with skin and soft tissue infections (SSTIs) to help identify bacteremia and prevent sepsis, but the value of the test is unknown and evidence to support its use is limited, said Dr. Jay R. Malone of the University of Oklahoma, Oklahoma City, and colleagues.
The researchers compared 482 children with uncomplicated SSTIs and 98 children with complicated SSTIs (cSSTIs) who were admitted to a single hospital between Jan. 1, 2007, and Dec. 31, 2009, for cellulitis or abscesses. The average age of the children with SSTIs was 3 years, approximately half were male. The average age of the cSSTI children was significantly older (6 years) and included significantly more males (64%). Approximately half of the children in both groups had received at least one dose of antibiotics prior to hospital admission, and about one quarter of children in both groups presented with temperatures greater than 37.9 degrees Celsius.
Overall, none of the 482 children with uncomplicated SSTIs had positive blood cultures (although 3 were contaminated), compared with 10 positive cultures (12.5%) among 98 children with cSSTIs (Pediatrics 2013 Aug. 5 [doi: 10.1542/peds.2013-1384).
However, blood cultures were significantly more frequent for children with uncomplicated SSTIs compared to those with cSSTIs (94% vs. 82%), and those who had blood cultures were significantly more likely than were those who did not have cultures to have a C-reactive protein drawn (98% vs. 74%).
"This could be a result of a greater percentage of children with cSSTI being admitted to surgical services that may perform laboratory investigations less often than medical services," the researchers noted.
The most common infection sites for the uncomplicated SSTI group were the extremities (32%) and buttocks or perineum (27%), while the most common infection sites for the cSSTI group were the face or neck (39%) and extremities (24%).
Overall, the average length of hospital stay was 3 days for children with uncomplicated SSTIs, compared with 7 days for those with cSSTIs. However, the average length of hospital stay was almost a day longer for children with uncomplicated SSTIs who had blood cultures, compared with those who did not (.91 days; a significant difference).
The study was limited by several factors, including the retrospective design, the impact of antibiotics on the blood cultures, and the limited population of children who presented to an emergency department with SSTIs and were admitted to the hospital. Yet the results show that blood cultures in children with uncomplicated SSTIs yield a very low number of positive results, and do not appear to provide clinical value, the researchers said.
"Given the limited value of these tests, physicians might reasonably limit their use to children with complicated infections," they noted.
More research is needed on several fronts, including studies to define the criteria for hospitalizing children with SSTIs and to determine the risk of bacteremia in infants younger than 60 days, they added.
The researchers had no financial conflicts to disclose.
On Twitter @hsplete
FROM PEDIATRICS
Don’t bother with blood cultures for uncomplicated pediatric SSTIs
Blood cultures did not improve the assessment of children hospitalized with uncomplicated skin and soft tissue infections, based on data from a review of more than 500 children. The findings were published online Aug. 5 in Pediatrics.
Some current guidelines suggest obtaining blood cultures from children with skin and soft tissue infections (SSTIs) to help identify bacteremia and prevent sepsis, but the value of the test is unknown and evidence to support its use is limited, said Dr. Jay R. Malone of the University of Oklahoma, Oklahoma City, and colleagues.
The researchers compared 482 children with uncomplicated SSTIs and 98 children with complicated SSTIs (cSSTIs) who were admitted to a single hospital between Jan. 1, 2007, and Dec. 31, 2009, for cellulitis or abscesses. The average age of the children with SSTIs was 3 years, approximately half were male. The average age of the cSSTI children was significantly older (6 years) and included significantly more males (64%). Approximately half of the children in both groups had received at least one dose of antibiotics prior to hospital admission, and about one quarter of children in both groups presented with temperatures greater than 37.9 degrees Celsius.
Overall, none of the 482 children with uncomplicated SSTIs had positive blood cultures (although 3 were contaminated), compared with 10 positive cultures (12.5%) among 98 children with cSSTIs (Pediatrics 2013 Aug. 5 [doi: 10.1542/peds.2013-1384).
However, blood cultures were significantly more frequent for children with uncomplicated SSTIs compared to those with cSSTIs (94% vs. 82%), and those who had blood cultures were significantly more likely than were those who did not have cultures to have a C-reactive protein drawn (98% vs. 74%).
"This could be a result of a greater percentage of children with cSSTI being admitted to surgical services that may perform laboratory investigations less often than medical services," the researchers noted.
The most common infection sites for the uncomplicated SSTI group were the extremities (32%) and buttocks or perineum (27%), while the most common infection sites for the cSSTI group were the face or neck (39%) and extremities (24%).
Overall, the average length of hospital stay was 3 days for children with uncomplicated SSTIs, compared with 7 days for those with cSSTIs. However, the average length of hospital stay was almost a day longer for children with uncomplicated SSTIs who had blood cultures, compared with those who did not (.91 days; a significant difference).
The study was limited by several factors, including the retrospective design, the impact of antibiotics on the blood cultures, and the limited population of children who presented to an emergency department with SSTIs and were admitted to the hospital. Yet the results show that blood cultures in children with uncomplicated SSTIs yield a very low number of positive results, and do not appear to provide clinical value, the researchers said.
"Given the limited value of these tests, physicians might reasonably limit their use to children with complicated infections," they noted.
More research is needed on several fronts, including studies to define the criteria for hospitalizing children with SSTIs and to determine the risk of bacteremia in infants younger than 60 days, they added.
The researchers had no financial conflicts to disclose.
On Twitter @hsplete
Blood cultures did not improve the assessment of children hospitalized with uncomplicated skin and soft tissue infections, based on data from a review of more than 500 children. The findings were published online Aug. 5 in Pediatrics.
Some current guidelines suggest obtaining blood cultures from children with skin and soft tissue infections (SSTIs) to help identify bacteremia and prevent sepsis, but the value of the test is unknown and evidence to support its use is limited, said Dr. Jay R. Malone of the University of Oklahoma, Oklahoma City, and colleagues.
The researchers compared 482 children with uncomplicated SSTIs and 98 children with complicated SSTIs (cSSTIs) who were admitted to a single hospital between Jan. 1, 2007, and Dec. 31, 2009, for cellulitis or abscesses. The average age of the children with SSTIs was 3 years, approximately half were male. The average age of the cSSTI children was significantly older (6 years) and included significantly more males (64%). Approximately half of the children in both groups had received at least one dose of antibiotics prior to hospital admission, and about one quarter of children in both groups presented with temperatures greater than 37.9 degrees Celsius.
Overall, none of the 482 children with uncomplicated SSTIs had positive blood cultures (although 3 were contaminated), compared with 10 positive cultures (12.5%) among 98 children with cSSTIs (Pediatrics 2013 Aug. 5 [doi: 10.1542/peds.2013-1384).
However, blood cultures were significantly more frequent for children with uncomplicated SSTIs compared to those with cSSTIs (94% vs. 82%), and those who had blood cultures were significantly more likely than were those who did not have cultures to have a C-reactive protein drawn (98% vs. 74%).
"This could be a result of a greater percentage of children with cSSTI being admitted to surgical services that may perform laboratory investigations less often than medical services," the researchers noted.
The most common infection sites for the uncomplicated SSTI group were the extremities (32%) and buttocks or perineum (27%), while the most common infection sites for the cSSTI group were the face or neck (39%) and extremities (24%).
Overall, the average length of hospital stay was 3 days for children with uncomplicated SSTIs, compared with 7 days for those with cSSTIs. However, the average length of hospital stay was almost a day longer for children with uncomplicated SSTIs who had blood cultures, compared with those who did not (.91 days; a significant difference).
The study was limited by several factors, including the retrospective design, the impact of antibiotics on the blood cultures, and the limited population of children who presented to an emergency department with SSTIs and were admitted to the hospital. Yet the results show that blood cultures in children with uncomplicated SSTIs yield a very low number of positive results, and do not appear to provide clinical value, the researchers said.
"Given the limited value of these tests, physicians might reasonably limit their use to children with complicated infections," they noted.
More research is needed on several fronts, including studies to define the criteria for hospitalizing children with SSTIs and to determine the risk of bacteremia in infants younger than 60 days, they added.
The researchers had no financial conflicts to disclose.
On Twitter @hsplete
Blood cultures did not improve the assessment of children hospitalized with uncomplicated skin and soft tissue infections, based on data from a review of more than 500 children. The findings were published online Aug. 5 in Pediatrics.
Some current guidelines suggest obtaining blood cultures from children with skin and soft tissue infections (SSTIs) to help identify bacteremia and prevent sepsis, but the value of the test is unknown and evidence to support its use is limited, said Dr. Jay R. Malone of the University of Oklahoma, Oklahoma City, and colleagues.
The researchers compared 482 children with uncomplicated SSTIs and 98 children with complicated SSTIs (cSSTIs) who were admitted to a single hospital between Jan. 1, 2007, and Dec. 31, 2009, for cellulitis or abscesses. The average age of the children with SSTIs was 3 years, approximately half were male. The average age of the cSSTI children was significantly older (6 years) and included significantly more males (64%). Approximately half of the children in both groups had received at least one dose of antibiotics prior to hospital admission, and about one quarter of children in both groups presented with temperatures greater than 37.9 degrees Celsius.
Overall, none of the 482 children with uncomplicated SSTIs had positive blood cultures (although 3 were contaminated), compared with 10 positive cultures (12.5%) among 98 children with cSSTIs (Pediatrics 2013 Aug. 5 [doi: 10.1542/peds.2013-1384).
However, blood cultures were significantly more frequent for children with uncomplicated SSTIs compared to those with cSSTIs (94% vs. 82%), and those who had blood cultures were significantly more likely than were those who did not have cultures to have a C-reactive protein drawn (98% vs. 74%).
"This could be a result of a greater percentage of children with cSSTI being admitted to surgical services that may perform laboratory investigations less often than medical services," the researchers noted.
The most common infection sites for the uncomplicated SSTI group were the extremities (32%) and buttocks or perineum (27%), while the most common infection sites for the cSSTI group were the face or neck (39%) and extremities (24%).
Overall, the average length of hospital stay was 3 days for children with uncomplicated SSTIs, compared with 7 days for those with cSSTIs. However, the average length of hospital stay was almost a day longer for children with uncomplicated SSTIs who had blood cultures, compared with those who did not (.91 days; a significant difference).
The study was limited by several factors, including the retrospective design, the impact of antibiotics on the blood cultures, and the limited population of children who presented to an emergency department with SSTIs and were admitted to the hospital. Yet the results show that blood cultures in children with uncomplicated SSTIs yield a very low number of positive results, and do not appear to provide clinical value, the researchers said.
"Given the limited value of these tests, physicians might reasonably limit their use to children with complicated infections," they noted.
More research is needed on several fronts, including studies to define the criteria for hospitalizing children with SSTIs and to determine the risk of bacteremia in infants younger than 60 days, they added.
The researchers had no financial conflicts to disclose.
On Twitter @hsplete
FROM PEDIATRICS
Major finding: No positive blood cultures appeared in children hospitalized with uncomplicated skin and soft tissue infections, vs. 12.5% positive cultures in children with complicated SSTIs.
Data source: A retrospective study of the medical records of 482 children with uncomplicated SSTIs and 98 children with complicated SSTIs.
Disclosures: The researchers had no financial conflicts to disclose.
Make your scalp surgery seamless
WASHINGTON – To make scalp surgery seamless, remember what makes the scalp unique: hair and tension, Dr. Mark Welch said.
The scalp is "a bloodless plain," said Dr. Welch of the Skin Cancer Surgery Center in Bethesda, Md.
Also, the scalp is painless, so it’s possible to go beyond the field of anesthesia, he noted at the Atlantic Dermatological Conference.
To keep hair out of the surgical field, Dr. Welch uses a razor to shave the immediate area, and then tapes down the surrounding hair. "The surrounding hair will find its way into your surgery site and wound," he said. Alternatively, moistening the hair with saline or water can keep it away from the surgical field. Tubular bandaging also can be used to hold the hair away from the surgery site.
The tension on the scalp presents a unique surgical challenge, said Dr. Welch. "The scalp skin is holding the weight of the body; there’s lots of tension up there."
Dr. Welch said he starts with a temporary pulley stitch to decrease the distance across the wound, which allows easier placement of subcutaneous stitches. "Then the pulley stitch can come out," he said.
"One technique I use a lot is preplaced subcutaneous sutures," Dr. Welch said. "You leave yourself a tail long enough to tie, then go posterior to the first subcutaneous stitch, and then go back and tie the first stitch, then the second, then go to the external stitches."
Dr. Welch said he uses a running stitch for external stitches. "On the last external running stitch, go out and come back in on the same side, and angle it back slightly." This technique allows for a more perpendicular closing to the wound edge, he explained.
Dr. Welch cited one case of a large defect in a patient with skin cancer on the scalp. He opted for a pulley stitch with gel foam in the center, and some silver nitrate. The wound was essentially healed in 8 weeks, even without the defect being completely closed.
For scalp dressings, Dr. Welch said he often prefers a Xeroform gauze bolster, which he sews in place, "so we don’t have to use any tape." When the stitches come out after a week, flexible collodion can be used. "It hardens, and over the next 3 or 4 weeks of shampooing, it flakes off."
When using wraps, Dr. Welch recommends combining vertical and horizontal wraps to create tension and promote healing.
He said he had no financial conflicts to disclose.
WASHINGTON – To make scalp surgery seamless, remember what makes the scalp unique: hair and tension, Dr. Mark Welch said.
The scalp is "a bloodless plain," said Dr. Welch of the Skin Cancer Surgery Center in Bethesda, Md.
Also, the scalp is painless, so it’s possible to go beyond the field of anesthesia, he noted at the Atlantic Dermatological Conference.
To keep hair out of the surgical field, Dr. Welch uses a razor to shave the immediate area, and then tapes down the surrounding hair. "The surrounding hair will find its way into your surgery site and wound," he said. Alternatively, moistening the hair with saline or water can keep it away from the surgical field. Tubular bandaging also can be used to hold the hair away from the surgery site.
The tension on the scalp presents a unique surgical challenge, said Dr. Welch. "The scalp skin is holding the weight of the body; there’s lots of tension up there."
Dr. Welch said he starts with a temporary pulley stitch to decrease the distance across the wound, which allows easier placement of subcutaneous stitches. "Then the pulley stitch can come out," he said.
"One technique I use a lot is preplaced subcutaneous sutures," Dr. Welch said. "You leave yourself a tail long enough to tie, then go posterior to the first subcutaneous stitch, and then go back and tie the first stitch, then the second, then go to the external stitches."
Dr. Welch said he uses a running stitch for external stitches. "On the last external running stitch, go out and come back in on the same side, and angle it back slightly." This technique allows for a more perpendicular closing to the wound edge, he explained.
Dr. Welch cited one case of a large defect in a patient with skin cancer on the scalp. He opted for a pulley stitch with gel foam in the center, and some silver nitrate. The wound was essentially healed in 8 weeks, even without the defect being completely closed.
For scalp dressings, Dr. Welch said he often prefers a Xeroform gauze bolster, which he sews in place, "so we don’t have to use any tape." When the stitches come out after a week, flexible collodion can be used. "It hardens, and over the next 3 or 4 weeks of shampooing, it flakes off."
When using wraps, Dr. Welch recommends combining vertical and horizontal wraps to create tension and promote healing.
He said he had no financial conflicts to disclose.
WASHINGTON – To make scalp surgery seamless, remember what makes the scalp unique: hair and tension, Dr. Mark Welch said.
The scalp is "a bloodless plain," said Dr. Welch of the Skin Cancer Surgery Center in Bethesda, Md.
Also, the scalp is painless, so it’s possible to go beyond the field of anesthesia, he noted at the Atlantic Dermatological Conference.
To keep hair out of the surgical field, Dr. Welch uses a razor to shave the immediate area, and then tapes down the surrounding hair. "The surrounding hair will find its way into your surgery site and wound," he said. Alternatively, moistening the hair with saline or water can keep it away from the surgical field. Tubular bandaging also can be used to hold the hair away from the surgery site.
The tension on the scalp presents a unique surgical challenge, said Dr. Welch. "The scalp skin is holding the weight of the body; there’s lots of tension up there."
Dr. Welch said he starts with a temporary pulley stitch to decrease the distance across the wound, which allows easier placement of subcutaneous stitches. "Then the pulley stitch can come out," he said.
"One technique I use a lot is preplaced subcutaneous sutures," Dr. Welch said. "You leave yourself a tail long enough to tie, then go posterior to the first subcutaneous stitch, and then go back and tie the first stitch, then the second, then go to the external stitches."
Dr. Welch said he uses a running stitch for external stitches. "On the last external running stitch, go out and come back in on the same side, and angle it back slightly." This technique allows for a more perpendicular closing to the wound edge, he explained.
Dr. Welch cited one case of a large defect in a patient with skin cancer on the scalp. He opted for a pulley stitch with gel foam in the center, and some silver nitrate. The wound was essentially healed in 8 weeks, even without the defect being completely closed.
For scalp dressings, Dr. Welch said he often prefers a Xeroform gauze bolster, which he sews in place, "so we don’t have to use any tape." When the stitches come out after a week, flexible collodion can be used. "It hardens, and over the next 3 or 4 weeks of shampooing, it flakes off."
When using wraps, Dr. Welch recommends combining vertical and horizontal wraps to create tension and promote healing.
He said he had no financial conflicts to disclose.
EXPERT ANALYSIS FROM THE ATLANTIC DERMATOLOGICAL CONFERENCE
Nail surgery made simple
WASHINGTON – There’s a lot of anxiety about nail surgery, particularly nail biopsies, for both physicians and patients, according to Dr. Maral K. Skelsey.
The goals of successful nail surgery are threefold: avoid complications, reduce patient pain and anxiety, and optimize pathologic diagnosis, said Dr. Skelsey of Georgetown University Medical Center in Washington.
Because nail surgery is often performed to obtain a clinical diagnosis, a good specimen is needed to allow the dermatopathologist to make a diagnosis, she noted at the Atlantic Dermatological Conference.
Approach preoperative assessment for nail surgery as any other surgery, said Dr. Skelsey. Take a full history, including information about vascular impairment, arterial disease, latex allergies, and a history of anticoagulant use. "We don’t stop anticoagulants, usually," Dr. Skelsey noted, but she does assess the prothrombin time (PT/INR) within 1 week.
Also, don’t underestimate the value of an x-ray. "One thing I have found physicians don’t do often" is to x-ray to check for bony changes and any anatomic abnormalities, she said.
To help optimize nail surgery outcomes, Dr. Skelsey recommended the following preoperative instructions for patients: Remove nail polish, scrub the area with povidone-iodine twice daily for 3 days prior to surgery, bring open-toed shoes (for toenail surgeries), arrange for a ride home, and plan to elevate the hand or foot as much as possible for the first 48 hours following the procedure.
Also, it "will help reduce morbidity if you tell your patients ahead of time to reduce their exercise and activity" immediately after the procedure, she said.
The right tools "will make your nail surgery much more successful," Dr. Skelsey said. Her essential tools: a nail splitter, nail nipper, and nail elevator.
Allow the patient to recline with goggles and ear phones to reduce anxiety during the procedure, she said.
For anesthesia, "I always use a 30-gauge needle, injecting very slowly," she said. She prefers a wing block, injecting slowly at a 45-degree angle towards the bone. This injection also acts as a volumetric tourniquet.
When obtaining the specimen during nail surgery, "visualize the location of the pathology by reflecting the proximal nail fold with a suture of skin hook and full or partial nail avulsion," said Dr. Skelsey.
"You can use a punch biopsy for longitudinal melanonychia less than 3 mm," she noted, but for anything more than 3 mm, a transverse excision or shave biopsy with a tangential excision is needed.
After the biopsy, Dr. Skelsey said that she applies an absorbable gelatin sponge saturated in aluminum chloride.
"What’s very important is giving your dermatopathologist a good specimen," she said. Don’t forget to ink the margins and orient the specimen. "You don’t want to go through all this trouble and have someone tell you there is nothing there," she added. She also recommended using separate, labelled formalin jars for the nail plate, bed, and matrix.
Dr. Skelsey said that she had no financial conflicts to disclose.
WASHINGTON – There’s a lot of anxiety about nail surgery, particularly nail biopsies, for both physicians and patients, according to Dr. Maral K. Skelsey.
The goals of successful nail surgery are threefold: avoid complications, reduce patient pain and anxiety, and optimize pathologic diagnosis, said Dr. Skelsey of Georgetown University Medical Center in Washington.
Because nail surgery is often performed to obtain a clinical diagnosis, a good specimen is needed to allow the dermatopathologist to make a diagnosis, she noted at the Atlantic Dermatological Conference.
Approach preoperative assessment for nail surgery as any other surgery, said Dr. Skelsey. Take a full history, including information about vascular impairment, arterial disease, latex allergies, and a history of anticoagulant use. "We don’t stop anticoagulants, usually," Dr. Skelsey noted, but she does assess the prothrombin time (PT/INR) within 1 week.
Also, don’t underestimate the value of an x-ray. "One thing I have found physicians don’t do often" is to x-ray to check for bony changes and any anatomic abnormalities, she said.
To help optimize nail surgery outcomes, Dr. Skelsey recommended the following preoperative instructions for patients: Remove nail polish, scrub the area with povidone-iodine twice daily for 3 days prior to surgery, bring open-toed shoes (for toenail surgeries), arrange for a ride home, and plan to elevate the hand or foot as much as possible for the first 48 hours following the procedure.
Also, it "will help reduce morbidity if you tell your patients ahead of time to reduce their exercise and activity" immediately after the procedure, she said.
The right tools "will make your nail surgery much more successful," Dr. Skelsey said. Her essential tools: a nail splitter, nail nipper, and nail elevator.
Allow the patient to recline with goggles and ear phones to reduce anxiety during the procedure, she said.
For anesthesia, "I always use a 30-gauge needle, injecting very slowly," she said. She prefers a wing block, injecting slowly at a 45-degree angle towards the bone. This injection also acts as a volumetric tourniquet.
When obtaining the specimen during nail surgery, "visualize the location of the pathology by reflecting the proximal nail fold with a suture of skin hook and full or partial nail avulsion," said Dr. Skelsey.
"You can use a punch biopsy for longitudinal melanonychia less than 3 mm," she noted, but for anything more than 3 mm, a transverse excision or shave biopsy with a tangential excision is needed.
After the biopsy, Dr. Skelsey said that she applies an absorbable gelatin sponge saturated in aluminum chloride.
"What’s very important is giving your dermatopathologist a good specimen," she said. Don’t forget to ink the margins and orient the specimen. "You don’t want to go through all this trouble and have someone tell you there is nothing there," she added. She also recommended using separate, labelled formalin jars for the nail plate, bed, and matrix.
Dr. Skelsey said that she had no financial conflicts to disclose.
WASHINGTON – There’s a lot of anxiety about nail surgery, particularly nail biopsies, for both physicians and patients, according to Dr. Maral K. Skelsey.
The goals of successful nail surgery are threefold: avoid complications, reduce patient pain and anxiety, and optimize pathologic diagnosis, said Dr. Skelsey of Georgetown University Medical Center in Washington.
Because nail surgery is often performed to obtain a clinical diagnosis, a good specimen is needed to allow the dermatopathologist to make a diagnosis, she noted at the Atlantic Dermatological Conference.
Approach preoperative assessment for nail surgery as any other surgery, said Dr. Skelsey. Take a full history, including information about vascular impairment, arterial disease, latex allergies, and a history of anticoagulant use. "We don’t stop anticoagulants, usually," Dr. Skelsey noted, but she does assess the prothrombin time (PT/INR) within 1 week.
Also, don’t underestimate the value of an x-ray. "One thing I have found physicians don’t do often" is to x-ray to check for bony changes and any anatomic abnormalities, she said.
To help optimize nail surgery outcomes, Dr. Skelsey recommended the following preoperative instructions for patients: Remove nail polish, scrub the area with povidone-iodine twice daily for 3 days prior to surgery, bring open-toed shoes (for toenail surgeries), arrange for a ride home, and plan to elevate the hand or foot as much as possible for the first 48 hours following the procedure.
Also, it "will help reduce morbidity if you tell your patients ahead of time to reduce their exercise and activity" immediately after the procedure, she said.
The right tools "will make your nail surgery much more successful," Dr. Skelsey said. Her essential tools: a nail splitter, nail nipper, and nail elevator.
Allow the patient to recline with goggles and ear phones to reduce anxiety during the procedure, she said.
For anesthesia, "I always use a 30-gauge needle, injecting very slowly," she said. She prefers a wing block, injecting slowly at a 45-degree angle towards the bone. This injection also acts as a volumetric tourniquet.
When obtaining the specimen during nail surgery, "visualize the location of the pathology by reflecting the proximal nail fold with a suture of skin hook and full or partial nail avulsion," said Dr. Skelsey.
"You can use a punch biopsy for longitudinal melanonychia less than 3 mm," she noted, but for anything more than 3 mm, a transverse excision or shave biopsy with a tangential excision is needed.
After the biopsy, Dr. Skelsey said that she applies an absorbable gelatin sponge saturated in aluminum chloride.
"What’s very important is giving your dermatopathologist a good specimen," she said. Don’t forget to ink the margins and orient the specimen. "You don’t want to go through all this trouble and have someone tell you there is nothing there," she added. She also recommended using separate, labelled formalin jars for the nail plate, bed, and matrix.
Dr. Skelsey said that she had no financial conflicts to disclose.
EXPERT ANALYSIS FROM THE ATLANTIC DERMATOLOGICAL CONFERENCE
Congressional Skin Cancer Caucus launched
The Congressional Skin Cancer Caucus was approved as an official congressional member organization July 1 to support legislative activities and promote public awareness about skin cancer, the American Academy of Dermatology said in a statement.
The caucus is cosponsored by Rep. Jim Cooper (D-Tenn.), Rep. Carolyn Maloney (D-N.Y.), Rep. Peter Roskam (R-Ill.), and Rep. Charlie Dent (R-Pa.), and supported by the American College of Mohs Surgery and the AAD.
"As dermatologists on the front lines fighting skin cancer ... we are delighted to see this new caucus come to fruition," Dr. Dirk M. Elston, AAD president, said in a statement. "This bipartisan group has the potential to not only save lives but decrease skin cancer–related health care costs in the future."
Dr. Brent Moody, chairman of the public policy committee for the Mohs College, said in a statement, "The Mohs College, in partnership with the [AAD] and other advocates, including federal agencies, will work with the caucus to identify opportunities to further the mission of this new organization."
On Twitter @hsplete
The Congressional Skin Cancer Caucus was approved as an official congressional member organization July 1 to support legislative activities and promote public awareness about skin cancer, the American Academy of Dermatology said in a statement.
The caucus is cosponsored by Rep. Jim Cooper (D-Tenn.), Rep. Carolyn Maloney (D-N.Y.), Rep. Peter Roskam (R-Ill.), and Rep. Charlie Dent (R-Pa.), and supported by the American College of Mohs Surgery and the AAD.
"As dermatologists on the front lines fighting skin cancer ... we are delighted to see this new caucus come to fruition," Dr. Dirk M. Elston, AAD president, said in a statement. "This bipartisan group has the potential to not only save lives but decrease skin cancer–related health care costs in the future."
Dr. Brent Moody, chairman of the public policy committee for the Mohs College, said in a statement, "The Mohs College, in partnership with the [AAD] and other advocates, including federal agencies, will work with the caucus to identify opportunities to further the mission of this new organization."
On Twitter @hsplete
The Congressional Skin Cancer Caucus was approved as an official congressional member organization July 1 to support legislative activities and promote public awareness about skin cancer, the American Academy of Dermatology said in a statement.
The caucus is cosponsored by Rep. Jim Cooper (D-Tenn.), Rep. Carolyn Maloney (D-N.Y.), Rep. Peter Roskam (R-Ill.), and Rep. Charlie Dent (R-Pa.), and supported by the American College of Mohs Surgery and the AAD.
"As dermatologists on the front lines fighting skin cancer ... we are delighted to see this new caucus come to fruition," Dr. Dirk M. Elston, AAD president, said in a statement. "This bipartisan group has the potential to not only save lives but decrease skin cancer–related health care costs in the future."
Dr. Brent Moody, chairman of the public policy committee for the Mohs College, said in a statement, "The Mohs College, in partnership with the [AAD] and other advocates, including federal agencies, will work with the caucus to identify opportunities to further the mission of this new organization."
On Twitter @hsplete
Nano-antifungal shows promise as topical treatment
Nanotechnology may help control the fungal infections that can lead to mortality in burn patients, early research suggests.
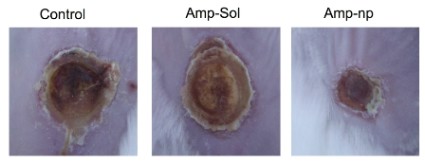
Nanoparticle encapsulated amphotericin b reduced fungal activity by 80%-95% compared with controls in a burn wound model. The findings were published online June 12 in Nanomedicine: Nanotechnology, Biology, and Medicine (doi:10.1016/j.nano.2013.06.002).
"Infection and sepsis persist as frequent causes of morbidity and mortality for burn victims due to extensive compromise of the skin and contiguous tissue that serve as a protective barrier against microbial invasion," wrote David A. Sanchez and his colleagues at the Albert Einstein College of Medicine, New York.
Currently available antifungals such as amphotericin b (AmB) are associated with liver toxicity at high doses, but the researchers proposed that encapsulating the drug would allow for topical use.
In this study, nanoparticle encapsulated AmB (AmB-np) significantly reduced fungal biofilm activity in a burn tissue model compared with untreated control areas over an exposure period of 24 hours, and a significant reduction in fungal activity compared with controls remained evident after 15 days of treatment. Fungal activity was measured via CFU assay to test for Candida spp strains including C. albicans, C. glabrata, and C. parapsilosis.
The researchers also compared AmB-np to solubilized AmB (AmB-sol) and found similar antifungal efficacy. The data substantiate the hypothesis "that encapsulated AmB is actively being liberated from the nanoparticles," they noted.
The burn tissue was assessed at 7 and 11 days from baseline wounding. AmB-np and AmB-sol were similarly effective and were associated with "decreased peripheral wound erythema, tissue induration and edema, and necrotic crusting in comparison to infected controls," the researchers said. However, histology data showed "more advanced re-epithelialization, organized dermal proliferation and appropriate/expected dermal remodeling as compared to the AmB-sol and untreated infected control," they added.
Toxicity concerns remain a controversy associated with nanoparticle application, the researchers noted. However, AmB-np showed no significant difference compared with nontreated and solubilized groups in an animal model. "Moreover, our histological studies show enhanced tissue healing in the AmB-np animals compared to the other groups," the researchers noted.
The findings were limited by the differences between a murine model and human skin, and by the absence of blank nanoparticles as controls. But the results suggest that AmB-np has clinical potential as a topical antifungal because of its "uncompromised antimycotic action" against multiple fungal strains, and its successful delivery in an in vivo burn wound model, the researchers said.
Mr. Sanchez and his colleagues had no financial conflicts to disclose.
On Twitter: @hsplete
Nanotechnology may help control the fungal infections that can lead to mortality in burn patients, early research suggests.
Nanoparticle encapsulated amphotericin b reduced fungal activity by 80%-95% compared with controls in a burn wound model. The findings were published online June 12 in Nanomedicine: Nanotechnology, Biology, and Medicine (doi:10.1016/j.nano.2013.06.002).
"Infection and sepsis persist as frequent causes of morbidity and mortality for burn victims due to extensive compromise of the skin and contiguous tissue that serve as a protective barrier against microbial invasion," wrote David A. Sanchez and his colleagues at the Albert Einstein College of Medicine, New York.
Currently available antifungals such as amphotericin b (AmB) are associated with liver toxicity at high doses, but the researchers proposed that encapsulating the drug would allow for topical use.
In this study, nanoparticle encapsulated AmB (AmB-np) significantly reduced fungal biofilm activity in a burn tissue model compared with untreated control areas over an exposure period of 24 hours, and a significant reduction in fungal activity compared with controls remained evident after 15 days of treatment. Fungal activity was measured via CFU assay to test for Candida spp strains including C. albicans, C. glabrata, and C. parapsilosis.
The researchers also compared AmB-np to solubilized AmB (AmB-sol) and found similar antifungal efficacy. The data substantiate the hypothesis "that encapsulated AmB is actively being liberated from the nanoparticles," they noted.
The burn tissue was assessed at 7 and 11 days from baseline wounding. AmB-np and AmB-sol were similarly effective and were associated with "decreased peripheral wound erythema, tissue induration and edema, and necrotic crusting in comparison to infected controls," the researchers said. However, histology data showed "more advanced re-epithelialization, organized dermal proliferation and appropriate/expected dermal remodeling as compared to the AmB-sol and untreated infected control," they added.
Toxicity concerns remain a controversy associated with nanoparticle application, the researchers noted. However, AmB-np showed no significant difference compared with nontreated and solubilized groups in an animal model. "Moreover, our histological studies show enhanced tissue healing in the AmB-np animals compared to the other groups," the researchers noted.
The findings were limited by the differences between a murine model and human skin, and by the absence of blank nanoparticles as controls. But the results suggest that AmB-np has clinical potential as a topical antifungal because of its "uncompromised antimycotic action" against multiple fungal strains, and its successful delivery in an in vivo burn wound model, the researchers said.
Mr. Sanchez and his colleagues had no financial conflicts to disclose.
On Twitter: @hsplete
Nanotechnology may help control the fungal infections that can lead to mortality in burn patients, early research suggests.
Nanoparticle encapsulated amphotericin b reduced fungal activity by 80%-95% compared with controls in a burn wound model. The findings were published online June 12 in Nanomedicine: Nanotechnology, Biology, and Medicine (doi:10.1016/j.nano.2013.06.002).
"Infection and sepsis persist as frequent causes of morbidity and mortality for burn victims due to extensive compromise of the skin and contiguous tissue that serve as a protective barrier against microbial invasion," wrote David A. Sanchez and his colleagues at the Albert Einstein College of Medicine, New York.
Currently available antifungals such as amphotericin b (AmB) are associated with liver toxicity at high doses, but the researchers proposed that encapsulating the drug would allow for topical use.
In this study, nanoparticle encapsulated AmB (AmB-np) significantly reduced fungal biofilm activity in a burn tissue model compared with untreated control areas over an exposure period of 24 hours, and a significant reduction in fungal activity compared with controls remained evident after 15 days of treatment. Fungal activity was measured via CFU assay to test for Candida spp strains including C. albicans, C. glabrata, and C. parapsilosis.
The researchers also compared AmB-np to solubilized AmB (AmB-sol) and found similar antifungal efficacy. The data substantiate the hypothesis "that encapsulated AmB is actively being liberated from the nanoparticles," they noted.
The burn tissue was assessed at 7 and 11 days from baseline wounding. AmB-np and AmB-sol were similarly effective and were associated with "decreased peripheral wound erythema, tissue induration and edema, and necrotic crusting in comparison to infected controls," the researchers said. However, histology data showed "more advanced re-epithelialization, organized dermal proliferation and appropriate/expected dermal remodeling as compared to the AmB-sol and untreated infected control," they added.
Toxicity concerns remain a controversy associated with nanoparticle application, the researchers noted. However, AmB-np showed no significant difference compared with nontreated and solubilized groups in an animal model. "Moreover, our histological studies show enhanced tissue healing in the AmB-np animals compared to the other groups," the researchers noted.
The findings were limited by the differences between a murine model and human skin, and by the absence of blank nanoparticles as controls. But the results suggest that AmB-np has clinical potential as a topical antifungal because of its "uncompromised antimycotic action" against multiple fungal strains, and its successful delivery in an in vivo burn wound model, the researchers said.
Mr. Sanchez and his colleagues had no financial conflicts to disclose.
On Twitter: @hsplete
FROM NANOMEDICINE: NANOTECHNOLOGY, BIOLOGY AND MEDICINE

Efinaconazole shows effectiveness against toenail fungus
A topical 10% efinaconazole solution was significantly more effective than was placebo against mild to moderate onychomycosis in a pair of randomized, controlled phase III studies comprising more than 1,000 patients.
Current topical therapies for distal lateral subungual onychomycosis (DLSO) are lacquer based, and require nail debridement and the removal of lacquer residue, said Dr. Boni Elewski of the University of Alabama, Birmingham, and her colleagues.
"Oral treatment is limited by drug interactions and risk of acute liver injury (requiring laboratory monitoring)," the researchers noted.

To test the efficacy of topical efinaconazole 10%, 1,655 adults with onychomycosis were randomized in two studies (study 1: 870 patients, study 2: 785 patients) at 118 sites in the United States, Canada, and Japan. In both studies, the mean area of target toenail involvement was approximately 36%, with an average of 2.8 affected nontarget toenails per patient. Demographic characteristics were not significantly different between the treatment and placebo groups in either study.
Overall, 18% and 15% of efinaconazole patients in study 1 and study 2, respectively, met the primary endpoint of complete cure at 52 weeks, compared with 3% and 6% of placebo patients, respectively. In addition, 55% and 53% of treatment patients in the two studies met the secondary endpoint of mycologic cure, compared with 7% of placebo patients in each study. Both complete cure and mycologic cure rates were in the range of cure rates achieved with oral therapies, the researchers noted.
The average age of the patients in studies 1 and 2 was 52 years and 51 years, respectively, and approximately 75% of the participants in both studies were men. Patients in each study were randomized to a topical solution of 10% efinaconazole or a placebo vehicle, self-applied at home once daily for 48 weeks. Patients were assessed at 12-week intervals during the study period, and reexamined at 52 weeks after a 4-week treatment-free period. The findings were published in the Journal of the American Academy of Dermatology (2013;68:600-8).
Overall, the rate of adverse events was similar between the drug and placebo groups. Efinaconazole was not associated with adverse events including redness, swelling, burning, itching, or vesiculation, and localized skin reactions were similar between the groups. A total of 235 patients discontinued the study early; the main reasons were patient request (98), lost to follow-up (78), and adverse events (33).
The study was limited by its specific patient population, which did not include children or those with severe disease, the researchers noted. Efinaconazole has not yet been studied in combination with oral antifungal treatment. But the findings suggest that topical efinaconazole is safe and effective, and "may be the first topical treatment for DLSO that can be considered a viable alternative to oral treatments," the researchers wrote.
Dr. Elewski has served as an adviser to Valeant Dermatology, a division of Valeant Pharmaceuticals, which funded the study and manufactures efinaconazole. Her coauthors disclosed that they were employees and stockholders of, and/or advisers and consultants to, several pharmaceutical companies, including Valeant.
On Twitter @hsplete
A topical 10% efinaconazole solution was significantly more effective than was placebo against mild to moderate onychomycosis in a pair of randomized, controlled phase III studies comprising more than 1,000 patients.
Current topical therapies for distal lateral subungual onychomycosis (DLSO) are lacquer based, and require nail debridement and the removal of lacquer residue, said Dr. Boni Elewski of the University of Alabama, Birmingham, and her colleagues.
"Oral treatment is limited by drug interactions and risk of acute liver injury (requiring laboratory monitoring)," the researchers noted.
To test the efficacy of topical efinaconazole 10%, 1,655 adults with onychomycosis were randomized in two studies (study 1: 870 patients, study 2: 785 patients) at 118 sites in the United States, Canada, and Japan. In both studies, the mean area of target toenail involvement was approximately 36%, with an average of 2.8 affected nontarget toenails per patient. Demographic characteristics were not significantly different between the treatment and placebo groups in either study.
Overall, 18% and 15% of efinaconazole patients in study 1 and study 2, respectively, met the primary endpoint of complete cure at 52 weeks, compared with 3% and 6% of placebo patients, respectively. In addition, 55% and 53% of treatment patients in the two studies met the secondary endpoint of mycologic cure, compared with 7% of placebo patients in each study. Both complete cure and mycologic cure rates were in the range of cure rates achieved with oral therapies, the researchers noted.
The average age of the patients in studies 1 and 2 was 52 years and 51 years, respectively, and approximately 75% of the participants in both studies were men. Patients in each study were randomized to a topical solution of 10% efinaconazole or a placebo vehicle, self-applied at home once daily for 48 weeks. Patients were assessed at 12-week intervals during the study period, and reexamined at 52 weeks after a 4-week treatment-free period. The findings were published in the Journal of the American Academy of Dermatology (2013;68:600-8).
Overall, the rate of adverse events was similar between the drug and placebo groups. Efinaconazole was not associated with adverse events including redness, swelling, burning, itching, or vesiculation, and localized skin reactions were similar between the groups. A total of 235 patients discontinued the study early; the main reasons were patient request (98), lost to follow-up (78), and adverse events (33).
The study was limited by its specific patient population, which did not include children or those with severe disease, the researchers noted. Efinaconazole has not yet been studied in combination with oral antifungal treatment. But the findings suggest that topical efinaconazole is safe and effective, and "may be the first topical treatment for DLSO that can be considered a viable alternative to oral treatments," the researchers wrote.
Dr. Elewski has served as an adviser to Valeant Dermatology, a division of Valeant Pharmaceuticals, which funded the study and manufactures efinaconazole. Her coauthors disclosed that they were employees and stockholders of, and/or advisers and consultants to, several pharmaceutical companies, including Valeant.
On Twitter @hsplete
A topical 10% efinaconazole solution was significantly more effective than was placebo against mild to moderate onychomycosis in a pair of randomized, controlled phase III studies comprising more than 1,000 patients.
Current topical therapies for distal lateral subungual onychomycosis (DLSO) are lacquer based, and require nail debridement and the removal of lacquer residue, said Dr. Boni Elewski of the University of Alabama, Birmingham, and her colleagues.
"Oral treatment is limited by drug interactions and risk of acute liver injury (requiring laboratory monitoring)," the researchers noted.
To test the efficacy of topical efinaconazole 10%, 1,655 adults with onychomycosis were randomized in two studies (study 1: 870 patients, study 2: 785 patients) at 118 sites in the United States, Canada, and Japan. In both studies, the mean area of target toenail involvement was approximately 36%, with an average of 2.8 affected nontarget toenails per patient. Demographic characteristics were not significantly different between the treatment and placebo groups in either study.
Overall, 18% and 15% of efinaconazole patients in study 1 and study 2, respectively, met the primary endpoint of complete cure at 52 weeks, compared with 3% and 6% of placebo patients, respectively. In addition, 55% and 53% of treatment patients in the two studies met the secondary endpoint of mycologic cure, compared with 7% of placebo patients in each study. Both complete cure and mycologic cure rates were in the range of cure rates achieved with oral therapies, the researchers noted.
The average age of the patients in studies 1 and 2 was 52 years and 51 years, respectively, and approximately 75% of the participants in both studies were men. Patients in each study were randomized to a topical solution of 10% efinaconazole or a placebo vehicle, self-applied at home once daily for 48 weeks. Patients were assessed at 12-week intervals during the study period, and reexamined at 52 weeks after a 4-week treatment-free period. The findings were published in the Journal of the American Academy of Dermatology (2013;68:600-8).
Overall, the rate of adverse events was similar between the drug and placebo groups. Efinaconazole was not associated with adverse events including redness, swelling, burning, itching, or vesiculation, and localized skin reactions were similar between the groups. A total of 235 patients discontinued the study early; the main reasons were patient request (98), lost to follow-up (78), and adverse events (33).
The study was limited by its specific patient population, which did not include children or those with severe disease, the researchers noted. Efinaconazole has not yet been studied in combination with oral antifungal treatment. But the findings suggest that topical efinaconazole is safe and effective, and "may be the first topical treatment for DLSO that can be considered a viable alternative to oral treatments," the researchers wrote.
Dr. Elewski has served as an adviser to Valeant Dermatology, a division of Valeant Pharmaceuticals, which funded the study and manufactures efinaconazole. Her coauthors disclosed that they were employees and stockholders of, and/or advisers and consultants to, several pharmaceutical companies, including Valeant.
On Twitter @hsplete
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Major finding: Topical efinaconazole 10% was significantly more effective against onychomycosis than was placebo in a pair of studies involving more than 1,000 patients.
Data source: Two multicenter, randomized, double-blind, placebo-controlled phase III studies of adults with onychomycosis.
Disclosures: Dr. Elewski has served as an adviser to Valeant Dermatology, a division of Valeant Pharmaceuticals, which funded the study and manufactures efinaconazole. Her coauthors disclosed that they were employees and stockholders of, or advisers and consultants to, several pharmaceutical companies, including Valeant.

Feet first for fungal diversity
DNA sequencing is helping researchers to get better acquainted with the fungi that inhabit the skin.
"By gaining a more complete awareness of the fungal and bacterial ecosystems, we can better address associated skin diseases, including skin conditions which can be related to cancer treatments," Dr. Heidi Kong, a dermatologist at the National Cancer Institute center for cancer research, said in a statement.
To provide a foundation for investigating fungal skin conditions, a research team from the NCI and the National Human Genome Research Institute examined fungi from 14 skin sites on 10 healthy adults.
"Fungal communities occupy complex niches, even on the human body," said Dr. Kong.
In fact, the feet are first when it comes to fungal diversity. Heels harbor approximately 80 genus-level types of fungi; researchers also identified 60 types in toenail swab samples and 40 types in samples from between the toes.
By contrast, the area inside the bend of the arms, the inside of the forearms, and the palms hosted 18-32 fungal genera each, while areas of the head and trunk, including the back, the back of the neck, inside and behind the ears, and between the eyebrows, contained just 2-10 types of fungi. Overall, Malassezia was the most popular genus, identified in 11 of the 14 body sites sampled.
"DNA sequence–based methods of identification enabled us to differentiate among species of fungi and to conclude that the diversity of fungi is highly dependent on the body site rather than the person," Dr. Kong said.
"Our study [Nature 2013 May 22 (doi:10.1038/nature12171)] focused on areas of the skin where we commonly find skin diseases that have been associated with fungi," she noted.
The researchers identified problems consistent with fungal infections, including heel scaling, toe web scaling, and toenail changes, in 20% of study participants.
Although individuals with heel site infections had common fungal communities at that site, those with toenail infections hosted a wide range of different fungal communities, the researchers noted.
In addition, they found "greater similarity in the fungal community structure on the left and right sides of the same person’s body compared to the same body parts on any two individuals," according to the press release. "Fungal communities also appear to be quite stable over time, with little change when tested on two separate occasions, up to 3 months apart."
On Twitter @hsplete
DNA sequencing is helping researchers to get better acquainted with the fungi that inhabit the skin.
"By gaining a more complete awareness of the fungal and bacterial ecosystems, we can better address associated skin diseases, including skin conditions which can be related to cancer treatments," Dr. Heidi Kong, a dermatologist at the National Cancer Institute center for cancer research, said in a statement.
To provide a foundation for investigating fungal skin conditions, a research team from the NCI and the National Human Genome Research Institute examined fungi from 14 skin sites on 10 healthy adults.
"Fungal communities occupy complex niches, even on the human body," said Dr. Kong.
In fact, the feet are first when it comes to fungal diversity. Heels harbor approximately 80 genus-level types of fungi; researchers also identified 60 types in toenail swab samples and 40 types in samples from between the toes.
By contrast, the area inside the bend of the arms, the inside of the forearms, and the palms hosted 18-32 fungal genera each, while areas of the head and trunk, including the back, the back of the neck, inside and behind the ears, and between the eyebrows, contained just 2-10 types of fungi. Overall, Malassezia was the most popular genus, identified in 11 of the 14 body sites sampled.
"DNA sequence–based methods of identification enabled us to differentiate among species of fungi and to conclude that the diversity of fungi is highly dependent on the body site rather than the person," Dr. Kong said.
"Our study [Nature 2013 May 22 (doi:10.1038/nature12171)] focused on areas of the skin where we commonly find skin diseases that have been associated with fungi," she noted.
The researchers identified problems consistent with fungal infections, including heel scaling, toe web scaling, and toenail changes, in 20% of study participants.
Although individuals with heel site infections had common fungal communities at that site, those with toenail infections hosted a wide range of different fungal communities, the researchers noted.
In addition, they found "greater similarity in the fungal community structure on the left and right sides of the same person’s body compared to the same body parts on any two individuals," according to the press release. "Fungal communities also appear to be quite stable over time, with little change when tested on two separate occasions, up to 3 months apart."
On Twitter @hsplete
DNA sequencing is helping researchers to get better acquainted with the fungi that inhabit the skin.
"By gaining a more complete awareness of the fungal and bacterial ecosystems, we can better address associated skin diseases, including skin conditions which can be related to cancer treatments," Dr. Heidi Kong, a dermatologist at the National Cancer Institute center for cancer research, said in a statement.
To provide a foundation for investigating fungal skin conditions, a research team from the NCI and the National Human Genome Research Institute examined fungi from 14 skin sites on 10 healthy adults.
"Fungal communities occupy complex niches, even on the human body," said Dr. Kong.
In fact, the feet are first when it comes to fungal diversity. Heels harbor approximately 80 genus-level types of fungi; researchers also identified 60 types in toenail swab samples and 40 types in samples from between the toes.
By contrast, the area inside the bend of the arms, the inside of the forearms, and the palms hosted 18-32 fungal genera each, while areas of the head and trunk, including the back, the back of the neck, inside and behind the ears, and between the eyebrows, contained just 2-10 types of fungi. Overall, Malassezia was the most popular genus, identified in 11 of the 14 body sites sampled.
"DNA sequence–based methods of identification enabled us to differentiate among species of fungi and to conclude that the diversity of fungi is highly dependent on the body site rather than the person," Dr. Kong said.
"Our study [Nature 2013 May 22 (doi:10.1038/nature12171)] focused on areas of the skin where we commonly find skin diseases that have been associated with fungi," she noted.
The researchers identified problems consistent with fungal infections, including heel scaling, toe web scaling, and toenail changes, in 20% of study participants.
Although individuals with heel site infections had common fungal communities at that site, those with toenail infections hosted a wide range of different fungal communities, the researchers noted.
In addition, they found "greater similarity in the fungal community structure on the left and right sides of the same person’s body compared to the same body parts on any two individuals," according to the press release. "Fungal communities also appear to be quite stable over time, with little change when tested on two separate occasions, up to 3 months apart."
On Twitter @hsplete
Daily sunscreen slowed skin aging in middle-aged adults
Daily sunscreen users were significantly less likely than discretionary sunscreen users to show signs of skin aging after 4.5 years, according to a study of young and middle-aged adults.
However, beta-carotene supplements appeared to have no effect on skin aging.

The findings from the randomized controlled trial were published online June 3 in Annals of Internal Medicine (2013;158:781-90).
"No known randomized studies in humans have evaluated the effect of sunscreen on surface changes associated with skin aging," wrote Maria Celia B. Hughes, MMedSci., of the Queensland Institute of Medical Research, Australia, and her colleagues.
The investigators used data from the Nambour (Australia) Skin Cancer Prevention Trial, in which 1,621 adults were studied from 1992 to 1996 to test the effect of sunscreen use or dietary supplements on skin cancer risk, photoaging, and actinic keratosis development.
To determine whether consistent, daily sunscreen use could prevent progression of skin aging, researchers randomized Nambour study participants under age 55 into four groups: daily use of broad-spectrum sunscreen plus 30 mg of beta-carotene; daily sunscreen use plus a placebo supplement; discretionary sunscreen use plus 30 mg of beta-carotene; and discretionary sunscreen use plus a placebo supplement.
The investigators focused on 903 adults younger than 55 to exclude the potential effects of growing old on participants’ skin aging.
Skin aging was assessed by comparing skin microtopography based on impressions taken of the backs of participants’ hands at baseline in 1992 and 4.5 years later in 1996. Assessors were blinded to the treatment groups.
"Most of the study participants were fair skinned, and more than 90% burned on acute sun exposure," the researchers noted. The groups were similar in terms of phenotype, sun exposure, and pretrial sunscreen use. All groups reported similar amounts of sun exposure during the study period; 78% of daily sunscreen users and 76% of discretionary sunscreen users reported being outdoors for less than 50% of their weekend time. In addition, the use of other sun protection measures, including seeking shade and wearing a hat, was similar among the groups.
By the end of the study, 77% of the daily sunscreen users applied sunscreen at least 3-4 days per week, vs. 33% of the discretionary users.
Overall, 58% of the participants in the current study met criteria for moderate photoaging at baseline in 1992, and 49% met those criteria in 1996. However, at the end of the 4.5-year period, daily sunscreen users were 24% less likely to show signs of skin aging than were discretionary users, a statistically significant difference.
When the odds of having a higher microtopography grade in 1996 than in 1992 were adjusted for sunburns and photoaging of the neck, the researchers noted, "only the daily sunscreen intervention group showed no detectable increase in microtopography grade."
No significant differences in skin aging were seen in participants randomized to beta-carotene vs. placebo.
The study was limited by several factors, including limited outcome data, which reduced the power to detect moderate treatment effects. In addition, the data were insufficient to rule out an effect of beta carotene on skin aging, the researchers noted.
However, "these results have important clinical implications," the researchers said. "A unit increase in microtopography significantly correlates with risk for actinic keratoses and skin cancer." Thus, the cosmetic benefits of reducing skin changes in middle age also may reduce cancer risk.
The National Health and Medical Research Council of Australia funded the study.
Daily sunscreen users were significantly less likely than discretionary sunscreen users to show signs of skin aging after 4.5 years, according to a study of young and middle-aged adults.
However, beta-carotene supplements appeared to have no effect on skin aging.
The findings from the randomized controlled trial were published online June 3 in Annals of Internal Medicine (2013;158:781-90).
"No known randomized studies in humans have evaluated the effect of sunscreen on surface changes associated with skin aging," wrote Maria Celia B. Hughes, MMedSci., of the Queensland Institute of Medical Research, Australia, and her colleagues.
The investigators used data from the Nambour (Australia) Skin Cancer Prevention Trial, in which 1,621 adults were studied from 1992 to 1996 to test the effect of sunscreen use or dietary supplements on skin cancer risk, photoaging, and actinic keratosis development.
To determine whether consistent, daily sunscreen use could prevent progression of skin aging, researchers randomized Nambour study participants under age 55 into four groups: daily use of broad-spectrum sunscreen plus 30 mg of beta-carotene; daily sunscreen use plus a placebo supplement; discretionary sunscreen use plus 30 mg of beta-carotene; and discretionary sunscreen use plus a placebo supplement.
The investigators focused on 903 adults younger than 55 to exclude the potential effects of growing old on participants’ skin aging.
Skin aging was assessed by comparing skin microtopography based on impressions taken of the backs of participants’ hands at baseline in 1992 and 4.5 years later in 1996. Assessors were blinded to the treatment groups.
"Most of the study participants were fair skinned, and more than 90% burned on acute sun exposure," the researchers noted. The groups were similar in terms of phenotype, sun exposure, and pretrial sunscreen use. All groups reported similar amounts of sun exposure during the study period; 78% of daily sunscreen users and 76% of discretionary sunscreen users reported being outdoors for less than 50% of their weekend time. In addition, the use of other sun protection measures, including seeking shade and wearing a hat, was similar among the groups.
By the end of the study, 77% of the daily sunscreen users applied sunscreen at least 3-4 days per week, vs. 33% of the discretionary users.
Overall, 58% of the participants in the current study met criteria for moderate photoaging at baseline in 1992, and 49% met those criteria in 1996. However, at the end of the 4.5-year period, daily sunscreen users were 24% less likely to show signs of skin aging than were discretionary users, a statistically significant difference.
When the odds of having a higher microtopography grade in 1996 than in 1992 were adjusted for sunburns and photoaging of the neck, the researchers noted, "only the daily sunscreen intervention group showed no detectable increase in microtopography grade."
No significant differences in skin aging were seen in participants randomized to beta-carotene vs. placebo.
The study was limited by several factors, including limited outcome data, which reduced the power to detect moderate treatment effects. In addition, the data were insufficient to rule out an effect of beta carotene on skin aging, the researchers noted.
However, "these results have important clinical implications," the researchers said. "A unit increase in microtopography significantly correlates with risk for actinic keratoses and skin cancer." Thus, the cosmetic benefits of reducing skin changes in middle age also may reduce cancer risk.
The National Health and Medical Research Council of Australia funded the study.
Daily sunscreen users were significantly less likely than discretionary sunscreen users to show signs of skin aging after 4.5 years, according to a study of young and middle-aged adults.
However, beta-carotene supplements appeared to have no effect on skin aging.
The findings from the randomized controlled trial were published online June 3 in Annals of Internal Medicine (2013;158:781-90).
"No known randomized studies in humans have evaluated the effect of sunscreen on surface changes associated with skin aging," wrote Maria Celia B. Hughes, MMedSci., of the Queensland Institute of Medical Research, Australia, and her colleagues.
The investigators used data from the Nambour (Australia) Skin Cancer Prevention Trial, in which 1,621 adults were studied from 1992 to 1996 to test the effect of sunscreen use or dietary supplements on skin cancer risk, photoaging, and actinic keratosis development.
To determine whether consistent, daily sunscreen use could prevent progression of skin aging, researchers randomized Nambour study participants under age 55 into four groups: daily use of broad-spectrum sunscreen plus 30 mg of beta-carotene; daily sunscreen use plus a placebo supplement; discretionary sunscreen use plus 30 mg of beta-carotene; and discretionary sunscreen use plus a placebo supplement.
The investigators focused on 903 adults younger than 55 to exclude the potential effects of growing old on participants’ skin aging.
Skin aging was assessed by comparing skin microtopography based on impressions taken of the backs of participants’ hands at baseline in 1992 and 4.5 years later in 1996. Assessors were blinded to the treatment groups.
"Most of the study participants were fair skinned, and more than 90% burned on acute sun exposure," the researchers noted. The groups were similar in terms of phenotype, sun exposure, and pretrial sunscreen use. All groups reported similar amounts of sun exposure during the study period; 78% of daily sunscreen users and 76% of discretionary sunscreen users reported being outdoors for less than 50% of their weekend time. In addition, the use of other sun protection measures, including seeking shade and wearing a hat, was similar among the groups.
By the end of the study, 77% of the daily sunscreen users applied sunscreen at least 3-4 days per week, vs. 33% of the discretionary users.
Overall, 58% of the participants in the current study met criteria for moderate photoaging at baseline in 1992, and 49% met those criteria in 1996. However, at the end of the 4.5-year period, daily sunscreen users were 24% less likely to show signs of skin aging than were discretionary users, a statistically significant difference.
When the odds of having a higher microtopography grade in 1996 than in 1992 were adjusted for sunburns and photoaging of the neck, the researchers noted, "only the daily sunscreen intervention group showed no detectable increase in microtopography grade."
No significant differences in skin aging were seen in participants randomized to beta-carotene vs. placebo.
The study was limited by several factors, including limited outcome data, which reduced the power to detect moderate treatment effects. In addition, the data were insufficient to rule out an effect of beta carotene on skin aging, the researchers noted.
However, "these results have important clinical implications," the researchers said. "A unit increase in microtopography significantly correlates with risk for actinic keratoses and skin cancer." Thus, the cosmetic benefits of reducing skin changes in middle age also may reduce cancer risk.
The National Health and Medical Research Council of Australia funded the study.
FROM ANNALS OF INTERNAL MEDICINE
Major finding: After 4.5 years, daily sunscreen users were 24% less likely to show signs of skin aging than were discretionary sunscreen users.
Data source: A randomized, controlled, community-based trial of 903 adults younger than 55 years.
Disclosures: The National Health and Medical Research Council of Australia funded the study.

Pulley stitch: A go-to for defects under tension
EDITOR'S NOTE: August 26, 2013: This article has been amended since it was first published to make it clear that Dr. Kelley Pagliai Redbord's description of the pulley stitch procedure was taken directly from an article published by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg.2011;37:1503-5). In her presentation, Dr. Redbord credited Dr. Yag-Howard and her article. However, this credit and attribution to Dr. Yag-Howard was not included in the article published.
WASHINGTON – The pulley stitch "is my go-to stitch for defects under tension," said Dr. Kelley Pagliai Redbord.
The pulley stitch allows for considerable reduction in the surface area of a large defect that can’t be closed by side-to-side stitches alone, making it an excellent choice for use on the scalp and legs, Dr. Redbord said at the Atlantic Dermatological Conference.
"When the tension across the wound is decreased, buried dermal sutures can be placed more easily and accurately," she said. "I use it a lot as an intraoperative tissue expander."
Dr. Redbord said that her description of the pulley stitch was taken from an article by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg. 2011; 37:1503-5).*
The pulley stitch can serve as a temporary suture that can be left in place or removed, said Dr. Redbord, a dermatologist in group practice in Rockville, Md.

The technique follows a far-near-near-far pattern, starting the stitch 8 mm from the wound edge (far), then bringing it to the opposite side just 4 mm from the wound edge (near). Dr. Redbord then reenters the stitch 4 mm from the wound edge on the initial side (near), and makes another pass to the opposite side 8 mm from the wound edge (far).
Multiple passes through the tissue create resistance that keeps the suture from slipping. "The loops of the stitch are placed at an oblique angle so that the inner and outer loops are offset and do not override each other," she noted. This technique minimizes potential skin damage from pressure necrosis caused by overriding loop sutures. The pulley stitch has a 2:1 mechanical advantage over an interrupted suture, and the additional friction of a second loop prevents the knot from slipping.
A modification of the pulley stitch is to loop the suture through an external loop on the opposite side of the incision, and pull across. "This new loop functions as a pulley and directs the tension away from the other strands," she said.
Another stitch with excellent eversion, in which the pulley stitch plays a key role, is the subcutaneous inverted cross mattress stitch (SICM). The SCIM is entirely subcutaneous, and combines the buried vertical mattress stitch and the buried pulley stitch.
The SCIM "uses the buried vertical mattress’s ability to evert wound edges and combines it with the pulley stitch’s ability to decrease tension at the wound edge," she said.
The four-step process is as follows:
• 1. Insert the needle into the dermis 3-5 mm lateral to the wound edge. Advance the needle into the upper reticular dermis, and then curve down to exit through the lower reticular dermis.
• 2. Insert the needle into the opposite edge of the wound at the lower reticular dermis and advance into the upper reticular dermis, then curve down and exit intradermally.
• 3. Insert the needle across the defect using an intradermal approach 1-2 mm lateral to the initial needle insertion point. Then, create a second buried vertical mattress stitch.
• 4. Pull the two stitches to close, which "creates a pulley effect with minimal recoil, and tie off," Dr. Redbord said.
"The pulley system locks the wound edges so that a knot can be tied without slipping," she added.
Dr. Redbord said she had no relevant financial disclosures.
EDITOR'S NOTE: August 26, 2013: This article has been amended since it was first published to make it clear that Dr. Kelley Pagliai Redbord's description of the pulley stitch procedure was taken directly from an article published by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg.2011;37:1503-5). In her presentation, Dr. Redbord credited Dr. Yag-Howard and her article. However, this credit and attribution to Dr. Yag-Howard was not included in the article published.
WASHINGTON – The pulley stitch "is my go-to stitch for defects under tension," said Dr. Kelley Pagliai Redbord.
The pulley stitch allows for considerable reduction in the surface area of a large defect that can’t be closed by side-to-side stitches alone, making it an excellent choice for use on the scalp and legs, Dr. Redbord said at the Atlantic Dermatological Conference.
"When the tension across the wound is decreased, buried dermal sutures can be placed more easily and accurately," she said. "I use it a lot as an intraoperative tissue expander."
Dr. Redbord said that her description of the pulley stitch was taken from an article by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg. 2011; 37:1503-5).*
The pulley stitch can serve as a temporary suture that can be left in place or removed, said Dr. Redbord, a dermatologist in group practice in Rockville, Md.
The technique follows a far-near-near-far pattern, starting the stitch 8 mm from the wound edge (far), then bringing it to the opposite side just 4 mm from the wound edge (near). Dr. Redbord then reenters the stitch 4 mm from the wound edge on the initial side (near), and makes another pass to the opposite side 8 mm from the wound edge (far).
Multiple passes through the tissue create resistance that keeps the suture from slipping. "The loops of the stitch are placed at an oblique angle so that the inner and outer loops are offset and do not override each other," she noted. This technique minimizes potential skin damage from pressure necrosis caused by overriding loop sutures. The pulley stitch has a 2:1 mechanical advantage over an interrupted suture, and the additional friction of a second loop prevents the knot from slipping.
A modification of the pulley stitch is to loop the suture through an external loop on the opposite side of the incision, and pull across. "This new loop functions as a pulley and directs the tension away from the other strands," she said.
Another stitch with excellent eversion, in which the pulley stitch plays a key role, is the subcutaneous inverted cross mattress stitch (SICM). The SCIM is entirely subcutaneous, and combines the buried vertical mattress stitch and the buried pulley stitch.
The SCIM "uses the buried vertical mattress’s ability to evert wound edges and combines it with the pulley stitch’s ability to decrease tension at the wound edge," she said.
The four-step process is as follows:
• 1. Insert the needle into the dermis 3-5 mm lateral to the wound edge. Advance the needle into the upper reticular dermis, and then curve down to exit through the lower reticular dermis.
• 2. Insert the needle into the opposite edge of the wound at the lower reticular dermis and advance into the upper reticular dermis, then curve down and exit intradermally.
• 3. Insert the needle across the defect using an intradermal approach 1-2 mm lateral to the initial needle insertion point. Then, create a second buried vertical mattress stitch.
• 4. Pull the two stitches to close, which "creates a pulley effect with minimal recoil, and tie off," Dr. Redbord said.
"The pulley system locks the wound edges so that a knot can be tied without slipping," she added.
Dr. Redbord said she had no relevant financial disclosures.
EDITOR'S NOTE: August 26, 2013: This article has been amended since it was first published to make it clear that Dr. Kelley Pagliai Redbord's description of the pulley stitch procedure was taken directly from an article published by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg.2011;37:1503-5). In her presentation, Dr. Redbord credited Dr. Yag-Howard and her article. However, this credit and attribution to Dr. Yag-Howard was not included in the article published.
WASHINGTON – The pulley stitch "is my go-to stitch for defects under tension," said Dr. Kelley Pagliai Redbord.
The pulley stitch allows for considerable reduction in the surface area of a large defect that can’t be closed by side-to-side stitches alone, making it an excellent choice for use on the scalp and legs, Dr. Redbord said at the Atlantic Dermatological Conference.
"When the tension across the wound is decreased, buried dermal sutures can be placed more easily and accurately," she said. "I use it a lot as an intraoperative tissue expander."
Dr. Redbord said that her description of the pulley stitch was taken from an article by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg. 2011; 37:1503-5).*
The pulley stitch can serve as a temporary suture that can be left in place or removed, said Dr. Redbord, a dermatologist in group practice in Rockville, Md.
The technique follows a far-near-near-far pattern, starting the stitch 8 mm from the wound edge (far), then bringing it to the opposite side just 4 mm from the wound edge (near). Dr. Redbord then reenters the stitch 4 mm from the wound edge on the initial side (near), and makes another pass to the opposite side 8 mm from the wound edge (far).
Multiple passes through the tissue create resistance that keeps the suture from slipping. "The loops of the stitch are placed at an oblique angle so that the inner and outer loops are offset and do not override each other," she noted. This technique minimizes potential skin damage from pressure necrosis caused by overriding loop sutures. The pulley stitch has a 2:1 mechanical advantage over an interrupted suture, and the additional friction of a second loop prevents the knot from slipping.
A modification of the pulley stitch is to loop the suture through an external loop on the opposite side of the incision, and pull across. "This new loop functions as a pulley and directs the tension away from the other strands," she said.
Another stitch with excellent eversion, in which the pulley stitch plays a key role, is the subcutaneous inverted cross mattress stitch (SICM). The SCIM is entirely subcutaneous, and combines the buried vertical mattress stitch and the buried pulley stitch.
The SCIM "uses the buried vertical mattress’s ability to evert wound edges and combines it with the pulley stitch’s ability to decrease tension at the wound edge," she said.
The four-step process is as follows:
• 1. Insert the needle into the dermis 3-5 mm lateral to the wound edge. Advance the needle into the upper reticular dermis, and then curve down to exit through the lower reticular dermis.
• 2. Insert the needle into the opposite edge of the wound at the lower reticular dermis and advance into the upper reticular dermis, then curve down and exit intradermally.
• 3. Insert the needle across the defect using an intradermal approach 1-2 mm lateral to the initial needle insertion point. Then, create a second buried vertical mattress stitch.
• 4. Pull the two stitches to close, which "creates a pulley effect with minimal recoil, and tie off," Dr. Redbord said.
"The pulley system locks the wound edges so that a knot can be tied without slipping," she added.
Dr. Redbord said she had no relevant financial disclosures.
EXPERT ANALYSIS FROM THE ATLANTIC DERMATOLOGICAL CONFERENCE
Major finding: Key numerical finding (e.g., number needed to treat to prevent one death/event; number lived or died as result of intervention). Maximum 10 words/1 sentence.
Data source: Include type of study (e.g., randomized, placebo controlled trial; retrospective case-control study). Include number in the study.
Disclosures: Sponsor of study, funding source, relevant disclosures. If author has no relevant disclosures, "Dr. X reported having no financial disclosures." If necessary, "Meeting Y did not require reports of financial disclosures." Check meeting website because many list disclosures. Written in sentence form.
