User login
M. Alexander Otto began his reporting career early in 1999 covering the pharmaceutical industry for a national pharmacists' magazine and freelancing for the Washington Post and other newspapers. He then joined BNA, now part of Bloomberg News, covering health law and the protection of people and animals in medical research. Alex next worked for the McClatchy Company. Based on his work, Alex won a year-long Knight Science Journalism Fellowship to MIT in 2008-2009. He joined the company shortly thereafter. Alex has a newspaper journalism degree from Syracuse (N.Y.) University and a master's degree in medical science -- a physician assistant degree -- from George Washington University. Alex is based in Seattle.
Cardiologists underrecognize angina about half the time
Angina is underrecognized by cardiologists in clinic visits, compared with assessments made by the patients themselves, suggesting that a standard screening tool be used to improve accuracy.
Researchers conducted a survey of 1,257 patients and their 155 doctors at 25 cardiology outpatient practices in 19 states. All patients had documented coronary artery disease and completed the Seattle Angina Questionnaire (SAQ) before their office visits to assess angina symptoms and frequency. Right after they left, their cardiologists estimated and recorded their idea of how often their patients had heart pain and what their symptoms were.

Patient and physician estimates didn’t match: 411 patients (33%) reported at least one bout of angina in the previous month, but their physicians estimated a frequency of 14% (173 patients). Heart failure patients were more than three times as likely to have their angina underestimated, and patients who reported a single bout of angina per month were about 70% less likely than those who reported daily or weekly attacks.
Years in practice and the number of angina patients in the case load didn’t seem to make a difference. Patient demographics, atypical symptoms, and comorbidities besides heart failure didn’t either. “Some physicians were much better at recognizing the frequency of patients’ angina,” said lead investigator Suzanne Arnold, MD, a cardiologist at Saint Luke’s Mid America Heart Institute in Kansas City, Mo., and her associates.
“Evaluation of angina is subject to limitations inherent in history taking, including pre-existing biases and time constraints on the part of physicians and patients. ... Under-recognition of angina by physicians may result in under treatment with revascularization or medications that could improve patients’ quality of life,” and it wastes healthcare dollars, they said.
The team concluded that angina needs to be assessed directly from patients with a standardized survey like the Seattle Angina Questionnaire (SAQ). “We still routinely depend solely on an unstructured interview instead of directly asking patients using standardized assessments,” the investigators noted. “A more systematic approach is needed for eliciting a history and assessing angina in patients with coronary artery disease to appropriately guide further testing and treatment. ... The use of a validated, patient-centered tool for eliciting patients’ angina, such as the SAQ, should be tested in routine clinical care to see if it improves angina recognition, treatment, and outcomes,” the study team said (Circ Cardiovasc Qual Outcomes. 2016 AUG 16;doi: 10.1161/CIRCOUTCOMES.116.002781).
Patients in the study were, on average, 69 years old, and the majority were white men. About 40% reported previous myocardial infarctions, and more than half were stented. Well over three quarters were on beta-blockers for angina.
The senior investigator, John Spertus, MD, holds a copyright on the SAQ used in the study. Gilead Sciences funded the work. Investigators reported ties to Gilead, Abbvie, Genentech, Glumetrics, Maquet, Sanofi, AstraZeneca, Edwards Life Sciences, Roche, St. Jude Medical, Regeneron, Lilly, and ZS Pharma.
Angina is underrecognized by cardiologists in clinic visits, compared with assessments made by the patients themselves, suggesting that a standard screening tool be used to improve accuracy.
Researchers conducted a survey of 1,257 patients and their 155 doctors at 25 cardiology outpatient practices in 19 states. All patients had documented coronary artery disease and completed the Seattle Angina Questionnaire (SAQ) before their office visits to assess angina symptoms and frequency. Right after they left, their cardiologists estimated and recorded their idea of how often their patients had heart pain and what their symptoms were.
Patient and physician estimates didn’t match: 411 patients (33%) reported at least one bout of angina in the previous month, but their physicians estimated a frequency of 14% (173 patients). Heart failure patients were more than three times as likely to have their angina underestimated, and patients who reported a single bout of angina per month were about 70% less likely than those who reported daily or weekly attacks.
Years in practice and the number of angina patients in the case load didn’t seem to make a difference. Patient demographics, atypical symptoms, and comorbidities besides heart failure didn’t either. “Some physicians were much better at recognizing the frequency of patients’ angina,” said lead investigator Suzanne Arnold, MD, a cardiologist at Saint Luke’s Mid America Heart Institute in Kansas City, Mo., and her associates.
“Evaluation of angina is subject to limitations inherent in history taking, including pre-existing biases and time constraints on the part of physicians and patients. ... Under-recognition of angina by physicians may result in under treatment with revascularization or medications that could improve patients’ quality of life,” and it wastes healthcare dollars, they said.
The team concluded that angina needs to be assessed directly from patients with a standardized survey like the Seattle Angina Questionnaire (SAQ). “We still routinely depend solely on an unstructured interview instead of directly asking patients using standardized assessments,” the investigators noted. “A more systematic approach is needed for eliciting a history and assessing angina in patients with coronary artery disease to appropriately guide further testing and treatment. ... The use of a validated, patient-centered tool for eliciting patients’ angina, such as the SAQ, should be tested in routine clinical care to see if it improves angina recognition, treatment, and outcomes,” the study team said (Circ Cardiovasc Qual Outcomes. 2016 AUG 16;doi: 10.1161/CIRCOUTCOMES.116.002781).
Patients in the study were, on average, 69 years old, and the majority were white men. About 40% reported previous myocardial infarctions, and more than half were stented. Well over three quarters were on beta-blockers for angina.
The senior investigator, John Spertus, MD, holds a copyright on the SAQ used in the study. Gilead Sciences funded the work. Investigators reported ties to Gilead, Abbvie, Genentech, Glumetrics, Maquet, Sanofi, AstraZeneca, Edwards Life Sciences, Roche, St. Jude Medical, Regeneron, Lilly, and ZS Pharma.
Angina is underrecognized by cardiologists in clinic visits, compared with assessments made by the patients themselves, suggesting that a standard screening tool be used to improve accuracy.
Researchers conducted a survey of 1,257 patients and their 155 doctors at 25 cardiology outpatient practices in 19 states. All patients had documented coronary artery disease and completed the Seattle Angina Questionnaire (SAQ) before their office visits to assess angina symptoms and frequency. Right after they left, their cardiologists estimated and recorded their idea of how often their patients had heart pain and what their symptoms were.
Patient and physician estimates didn’t match: 411 patients (33%) reported at least one bout of angina in the previous month, but their physicians estimated a frequency of 14% (173 patients). Heart failure patients were more than three times as likely to have their angina underestimated, and patients who reported a single bout of angina per month were about 70% less likely than those who reported daily or weekly attacks.
Years in practice and the number of angina patients in the case load didn’t seem to make a difference. Patient demographics, atypical symptoms, and comorbidities besides heart failure didn’t either. “Some physicians were much better at recognizing the frequency of patients’ angina,” said lead investigator Suzanne Arnold, MD, a cardiologist at Saint Luke’s Mid America Heart Institute in Kansas City, Mo., and her associates.
“Evaluation of angina is subject to limitations inherent in history taking, including pre-existing biases and time constraints on the part of physicians and patients. ... Under-recognition of angina by physicians may result in under treatment with revascularization or medications that could improve patients’ quality of life,” and it wastes healthcare dollars, they said.
The team concluded that angina needs to be assessed directly from patients with a standardized survey like the Seattle Angina Questionnaire (SAQ). “We still routinely depend solely on an unstructured interview instead of directly asking patients using standardized assessments,” the investigators noted. “A more systematic approach is needed for eliciting a history and assessing angina in patients with coronary artery disease to appropriately guide further testing and treatment. ... The use of a validated, patient-centered tool for eliciting patients’ angina, such as the SAQ, should be tested in routine clinical care to see if it improves angina recognition, treatment, and outcomes,” the study team said (Circ Cardiovasc Qual Outcomes. 2016 AUG 16;doi: 10.1161/CIRCOUTCOMES.116.002781).
Patients in the study were, on average, 69 years old, and the majority were white men. About 40% reported previous myocardial infarctions, and more than half were stented. Well over three quarters were on beta-blockers for angina.
The senior investigator, John Spertus, MD, holds a copyright on the SAQ used in the study. Gilead Sciences funded the work. Investigators reported ties to Gilead, Abbvie, Genentech, Glumetrics, Maquet, Sanofi, AstraZeneca, Edwards Life Sciences, Roche, St. Jude Medical, Regeneron, Lilly, and ZS Pharma.
FROM CIRCULATION CARDIOVASCULAR QUALITY AND OUTCOMES
Key clinical point: Cardiologists miss angina nearly half of the time.
Major finding: Patient and physician estimates don’t match up; 411 patients (33%) reported at least one bout of angina in the previous month, but their physicians estimated a frequency of 14% (173 patients).
Data source: A survey of 1,257 patients and their 155 doctors at 25 cardiology outpatient practices in 19 states.
Disclosures: The senior investigator, John Spertus, MD, holds a copyright on the Seattle Angina Questionnaire used in the study. Gilead Sciences funded the work. Investigators reported ties to Gilead, Abbvie, Genentech, Glumetrics, Maquet, Sanofi, AstraZeneca, Edwards Life Sciences, Roche, St. Jude Medical, Regeneron, Lilly, and ZS Pharma.

Post-TORS neck dissections extend hospital stay
SEATTLE – Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later, according to a review of 441 patients by Stony Brook (N.Y.) University.
The average hospital length of stay (LOS) was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as transoral robotic surgery (TORS). The 92 patients (20.9%) who had staged procedures - neck dissections and TORS about a month apart, with TORS usually done first - stayed in the hospital an average of 8 days (P less than .0001). After risk adjustment, LOS was 43% shorter for concurrent dissections.
Cardiac arrhythmias were also more common in staged patients, perhaps because they had general anesthesia twice in a short period or maybe because staged patients were more likely to be obese (18.5% vs. 7.5%; P less than .01).
However, there were no statistically significant outcome differences otherwise, and the investigators concluded that “concurrent and staged procedures are equally safe. It is therefore reasonable to allow operator preference and patient factors to determine surgical logistics.”
Neck dissection timing has been controversial since the advent of TORS several years ago, when surgeons and administrators realized they could fit more cases into the schedule by doing neck dissections, which can take a few hours, at a different time.
Proponents of the staged approach argue, among other things, that it reduces the risk of fistulas and tracheotomies, and allows surgeons a second go at positive margins. Advocates of concurrent procedures counter that fistulas, if found, can be repaired right away, and that same-time surgery saves money, allows for earlier adjuvant therapy, and cuts anesthesia risks.
There hasn’t been much data to settle the debate, and no one has compared LOS before, so it was “important” to look into the matter, lead investigator Catherine Frenkel, MD, a Stony Brook general surgery resident, said at the American Head and Neck Society International Conference on Head and Neck Cancer.
German investigators also recently concluded that it’s pretty much a draw between concurrent and staged dissections. In a study of 41 TORS cases, “the timing of neck dissection did not make a significant difference in the outcomes. We suggest, therefore, that aspiring and established TORS teams do not restrict their appropriate indications due to robotic slot and theatre time constraints, but perform each indicated TORS case as soon as possible within their given systems, even if the neck dissections cannot be done on the same day,” they said (Eur J Surg Oncol. 2015 Jun;41[6]:773-8).
In addition to obese patients, those who had tongue or tonsil lesions were more likely to be staged in the Stony Brook analysis. About half of the surgeons in the study stuck solely to concurrent procedures, while a handful opted for the staged approach, and the rest did both. Perhaps not surprisingly, high-volume surgeons – those who did five or more TORS cases per year – were more likely to stage.
Almost two-thirds of patients had at least one complication, most commonly renal failure, heart problems, extended ventilation, and surgical errors, which included accidental punctures, postop fistulas, hemorrhages, and wound complications. A total of 13% of patients had at least one postop readmission. Apart from arrhythmias, there were no statistically significant differences in complication or 30-day readmission rates between concurrent and staged patients. High-volume surgeons were less likely to have complications.
Postop bleeding was another common problem, and more likely with staged surgeries (12% vs. 7%). Concurrent procedures had a slightly higher rate of new tracheotomies and gastrostomies, but again the differences were not statistically significant, even with pedicle and free-flap reconstruction. There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
SEATTLE – Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later, according to a review of 441 patients by Stony Brook (N.Y.) University.
The average hospital length of stay (LOS) was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as transoral robotic surgery (TORS). The 92 patients (20.9%) who had staged procedures - neck dissections and TORS about a month apart, with TORS usually done first - stayed in the hospital an average of 8 days (P less than .0001). After risk adjustment, LOS was 43% shorter for concurrent dissections.
Cardiac arrhythmias were also more common in staged patients, perhaps because they had general anesthesia twice in a short period or maybe because staged patients were more likely to be obese (18.5% vs. 7.5%; P less than .01).
However, there were no statistically significant outcome differences otherwise, and the investigators concluded that “concurrent and staged procedures are equally safe. It is therefore reasonable to allow operator preference and patient factors to determine surgical logistics.”
Neck dissection timing has been controversial since the advent of TORS several years ago, when surgeons and administrators realized they could fit more cases into the schedule by doing neck dissections, which can take a few hours, at a different time.
Proponents of the staged approach argue, among other things, that it reduces the risk of fistulas and tracheotomies, and allows surgeons a second go at positive margins. Advocates of concurrent procedures counter that fistulas, if found, can be repaired right away, and that same-time surgery saves money, allows for earlier adjuvant therapy, and cuts anesthesia risks.
There hasn’t been much data to settle the debate, and no one has compared LOS before, so it was “important” to look into the matter, lead investigator Catherine Frenkel, MD, a Stony Brook general surgery resident, said at the American Head and Neck Society International Conference on Head and Neck Cancer.
German investigators also recently concluded that it’s pretty much a draw between concurrent and staged dissections. In a study of 41 TORS cases, “the timing of neck dissection did not make a significant difference in the outcomes. We suggest, therefore, that aspiring and established TORS teams do not restrict their appropriate indications due to robotic slot and theatre time constraints, but perform each indicated TORS case as soon as possible within their given systems, even if the neck dissections cannot be done on the same day,” they said (Eur J Surg Oncol. 2015 Jun;41[6]:773-8).
In addition to obese patients, those who had tongue or tonsil lesions were more likely to be staged in the Stony Brook analysis. About half of the surgeons in the study stuck solely to concurrent procedures, while a handful opted for the staged approach, and the rest did both. Perhaps not surprisingly, high-volume surgeons – those who did five or more TORS cases per year – were more likely to stage.
Almost two-thirds of patients had at least one complication, most commonly renal failure, heart problems, extended ventilation, and surgical errors, which included accidental punctures, postop fistulas, hemorrhages, and wound complications. A total of 13% of patients had at least one postop readmission. Apart from arrhythmias, there were no statistically significant differences in complication or 30-day readmission rates between concurrent and staged patients. High-volume surgeons were less likely to have complications.
Postop bleeding was another common problem, and more likely with staged surgeries (12% vs. 7%). Concurrent procedures had a slightly higher rate of new tracheotomies and gastrostomies, but again the differences were not statistically significant, even with pedicle and free-flap reconstruction. There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
SEATTLE – Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later, according to a review of 441 patients by Stony Brook (N.Y.) University.
The average hospital length of stay (LOS) was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as transoral robotic surgery (TORS). The 92 patients (20.9%) who had staged procedures - neck dissections and TORS about a month apart, with TORS usually done first - stayed in the hospital an average of 8 days (P less than .0001). After risk adjustment, LOS was 43% shorter for concurrent dissections.
Cardiac arrhythmias were also more common in staged patients, perhaps because they had general anesthesia twice in a short period or maybe because staged patients were more likely to be obese (18.5% vs. 7.5%; P less than .01).
However, there were no statistically significant outcome differences otherwise, and the investigators concluded that “concurrent and staged procedures are equally safe. It is therefore reasonable to allow operator preference and patient factors to determine surgical logistics.”
Neck dissection timing has been controversial since the advent of TORS several years ago, when surgeons and administrators realized they could fit more cases into the schedule by doing neck dissections, which can take a few hours, at a different time.
Proponents of the staged approach argue, among other things, that it reduces the risk of fistulas and tracheotomies, and allows surgeons a second go at positive margins. Advocates of concurrent procedures counter that fistulas, if found, can be repaired right away, and that same-time surgery saves money, allows for earlier adjuvant therapy, and cuts anesthesia risks.
There hasn’t been much data to settle the debate, and no one has compared LOS before, so it was “important” to look into the matter, lead investigator Catherine Frenkel, MD, a Stony Brook general surgery resident, said at the American Head and Neck Society International Conference on Head and Neck Cancer.
German investigators also recently concluded that it’s pretty much a draw between concurrent and staged dissections. In a study of 41 TORS cases, “the timing of neck dissection did not make a significant difference in the outcomes. We suggest, therefore, that aspiring and established TORS teams do not restrict their appropriate indications due to robotic slot and theatre time constraints, but perform each indicated TORS case as soon as possible within their given systems, even if the neck dissections cannot be done on the same day,” they said (Eur J Surg Oncol. 2015 Jun;41[6]:773-8).
In addition to obese patients, those who had tongue or tonsil lesions were more likely to be staged in the Stony Brook analysis. About half of the surgeons in the study stuck solely to concurrent procedures, while a handful opted for the staged approach, and the rest did both. Perhaps not surprisingly, high-volume surgeons – those who did five or more TORS cases per year – were more likely to stage.
Almost two-thirds of patients had at least one complication, most commonly renal failure, heart problems, extended ventilation, and surgical errors, which included accidental punctures, postop fistulas, hemorrhages, and wound complications. A total of 13% of patients had at least one postop readmission. Apart from arrhythmias, there were no statistically significant differences in complication or 30-day readmission rates between concurrent and staged patients. High-volume surgeons were less likely to have complications.
Postop bleeding was another common problem, and more likely with staged surgeries (12% vs. 7%). Concurrent procedures had a slightly higher rate of new tracheotomies and gastrostomies, but again the differences were not statistically significant, even with pedicle and free-flap reconstruction. There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
AT THE INTERNATIONAL CONFERENCE ON HEAD AND NECK CANCER
Key clinical point: Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later.
Major finding: The average hospital length of stay was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as TORS. The 92 patients (20.9%) who had staged procedures – neck dissections and TORS about a month apart, with TORS usually done first – stayed in the hospital an average of 8 days (P less than .0001).
Data source: Review of 441 TORS patients.
Disclosures: There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
Preop G-tubes save money in head and neck cancer resections
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.

Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.
Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.
Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
AT AHNS 2016
Key clinical point: It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after.
Major finding: At 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postop group, a savings of $9,248 per patient.
Data source: Review of 184 patients.
Disclosures: There was no outside funding for the work, and the presenter had no disclosures.

Intraoperative nerve stimulation reduces risk of shoulder pain from neck dissection
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.

After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.
After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.
After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
AT AHNS 2016
Key clinical point: Direct, intraoperative electrical stimulation of the spinal accessory nerve reduces shoulder pain and dysfunction from oncologic neck dissection.
Major finding: At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Score, while the controls lost a mean of 29.4 points.
Data source: Randomized trial with 41 patients.
Disclosures: There was no outside funding for the work. The presenter had no disclosures; a co-investigator was a Medtronic consultant.

Skip SNL biopsy for desmoplastic melanoma
SEATTLE – Sentinel lymph node biopsy in patients with head or neck desmoplastic melanoma is positive only 6% of the time, and it doesn’t change the risk of recurrence.
Although sentinel lymph node biopsy (SLNB) is routine in more common forms of cutaneous melanoma, findings from a retrospective case-control study suggest that it’s “not really necessary” for desmoplastic melanoma (DM) of the head or neck, said lead investigator Dylan Roden, MD, of the department of otolaryngology, New York University. General surgeons have pretty much come to that conclusion for DM elsewhere on the body, but it hasn’t been shown before for neck and head lesions, he said.

DM, an invasive form of melanoma in which malignant cells are surrounded by fibrous tissue, accounts for maybe 2% of cutaneous melanomas, with half or so presenting on the head or neck. The reason SLNB is of less use than with other melanomas is that DM “doesn’t often spread through the lymphatics. It’s not that patients won’t ever have metastases, but maybe it will be through the blood. Removing a lymph node won’t necessarily” detect it, Dr. Roden said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Forgoing SLNB has the added benefit of shaving an hour and a half or more off surgery, which is important since DM patients tend to be older, he added.
The NYU team matched 32 of their cases with 60 controls with more common superficial spreading or nodular melanoma of the head and neck, based on age, gender, ulceration status, and tumor stage. Mean tumor thickness in both groups was more than 4 mm.
SLNB was performed in 16 DM patients (50%) and 36 control patients (60%); it was positive in one DM patient (6.3%) versus 8 of 28 controls with reported results (28.6%).
Eleven DM patients (34%) had a recurrence, which was less frequent then in controls, where 33 patients (55%) had a recurrence (P = .05). “SNLB did not change the risk of overall or regional recurrence” in DM, Dr. Roden said.
Recurrence was more than twice as likely in control patients (odds ratio, 2.33; P = .06). Meanwhile, recurrence in DM was linked to perineural invasion (P = .02), but not ulceration status (P = .12) or mitoses (P = .40).
DM patients also had better 5-year overall survival (79% versus 62%) and disease-free survival (70% versus 42%; P for both = .06). In general, DM “has a more favorable prognosis,” Dr. Roden said.
Cases and controls were in their mid-60s, on average, and most were men. Ulceration was present in about a quarter of patients. Mitosis was more common in superficial spreading and nodular patients (92% versus 53%; P less than .001), while perineural invasion was more common in DM (40% versus 7%; P less than.001).
Although outcomes were more favorable for DM, previous studies have found a higher rate of sentinel lymph node metastases – above 20% – for DM lesions with mixed, rather than pure, pathology. The 6.3% positive SLNB rate at NYU is more in line with what’s been reported before for pure lesions. The team plans to look into the matter.
There was no outside funding for the work, and Dr. Roden had no disclosures.
SEATTLE – Sentinel lymph node biopsy in patients with head or neck desmoplastic melanoma is positive only 6% of the time, and it doesn’t change the risk of recurrence.
Although sentinel lymph node biopsy (SLNB) is routine in more common forms of cutaneous melanoma, findings from a retrospective case-control study suggest that it’s “not really necessary” for desmoplastic melanoma (DM) of the head or neck, said lead investigator Dylan Roden, MD, of the department of otolaryngology, New York University. General surgeons have pretty much come to that conclusion for DM elsewhere on the body, but it hasn’t been shown before for neck and head lesions, he said.
DM, an invasive form of melanoma in which malignant cells are surrounded by fibrous tissue, accounts for maybe 2% of cutaneous melanomas, with half or so presenting on the head or neck. The reason SLNB is of less use than with other melanomas is that DM “doesn’t often spread through the lymphatics. It’s not that patients won’t ever have metastases, but maybe it will be through the blood. Removing a lymph node won’t necessarily” detect it, Dr. Roden said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Forgoing SLNB has the added benefit of shaving an hour and a half or more off surgery, which is important since DM patients tend to be older, he added.
The NYU team matched 32 of their cases with 60 controls with more common superficial spreading or nodular melanoma of the head and neck, based on age, gender, ulceration status, and tumor stage. Mean tumor thickness in both groups was more than 4 mm.
SLNB was performed in 16 DM patients (50%) and 36 control patients (60%); it was positive in one DM patient (6.3%) versus 8 of 28 controls with reported results (28.6%).
Eleven DM patients (34%) had a recurrence, which was less frequent then in controls, where 33 patients (55%) had a recurrence (P = .05). “SNLB did not change the risk of overall or regional recurrence” in DM, Dr. Roden said.
Recurrence was more than twice as likely in control patients (odds ratio, 2.33; P = .06). Meanwhile, recurrence in DM was linked to perineural invasion (P = .02), but not ulceration status (P = .12) or mitoses (P = .40).
DM patients also had better 5-year overall survival (79% versus 62%) and disease-free survival (70% versus 42%; P for both = .06). In general, DM “has a more favorable prognosis,” Dr. Roden said.
Cases and controls were in their mid-60s, on average, and most were men. Ulceration was present in about a quarter of patients. Mitosis was more common in superficial spreading and nodular patients (92% versus 53%; P less than .001), while perineural invasion was more common in DM (40% versus 7%; P less than.001).
Although outcomes were more favorable for DM, previous studies have found a higher rate of sentinel lymph node metastases – above 20% – for DM lesions with mixed, rather than pure, pathology. The 6.3% positive SLNB rate at NYU is more in line with what’s been reported before for pure lesions. The team plans to look into the matter.
There was no outside funding for the work, and Dr. Roden had no disclosures.
SEATTLE – Sentinel lymph node biopsy in patients with head or neck desmoplastic melanoma is positive only 6% of the time, and it doesn’t change the risk of recurrence.
Although sentinel lymph node biopsy (SLNB) is routine in more common forms of cutaneous melanoma, findings from a retrospective case-control study suggest that it’s “not really necessary” for desmoplastic melanoma (DM) of the head or neck, said lead investigator Dylan Roden, MD, of the department of otolaryngology, New York University. General surgeons have pretty much come to that conclusion for DM elsewhere on the body, but it hasn’t been shown before for neck and head lesions, he said.
DM, an invasive form of melanoma in which malignant cells are surrounded by fibrous tissue, accounts for maybe 2% of cutaneous melanomas, with half or so presenting on the head or neck. The reason SLNB is of less use than with other melanomas is that DM “doesn’t often spread through the lymphatics. It’s not that patients won’t ever have metastases, but maybe it will be through the blood. Removing a lymph node won’t necessarily” detect it, Dr. Roden said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Forgoing SLNB has the added benefit of shaving an hour and a half or more off surgery, which is important since DM patients tend to be older, he added.
The NYU team matched 32 of their cases with 60 controls with more common superficial spreading or nodular melanoma of the head and neck, based on age, gender, ulceration status, and tumor stage. Mean tumor thickness in both groups was more than 4 mm.
SLNB was performed in 16 DM patients (50%) and 36 control patients (60%); it was positive in one DM patient (6.3%) versus 8 of 28 controls with reported results (28.6%).
Eleven DM patients (34%) had a recurrence, which was less frequent then in controls, where 33 patients (55%) had a recurrence (P = .05). “SNLB did not change the risk of overall or regional recurrence” in DM, Dr. Roden said.
Recurrence was more than twice as likely in control patients (odds ratio, 2.33; P = .06). Meanwhile, recurrence in DM was linked to perineural invasion (P = .02), but not ulceration status (P = .12) or mitoses (P = .40).
DM patients also had better 5-year overall survival (79% versus 62%) and disease-free survival (70% versus 42%; P for both = .06). In general, DM “has a more favorable prognosis,” Dr. Roden said.
Cases and controls were in their mid-60s, on average, and most were men. Ulceration was present in about a quarter of patients. Mitosis was more common in superficial spreading and nodular patients (92% versus 53%; P less than .001), while perineural invasion was more common in DM (40% versus 7%; P less than.001).
Although outcomes were more favorable for DM, previous studies have found a higher rate of sentinel lymph node metastases – above 20% – for DM lesions with mixed, rather than pure, pathology. The 6.3% positive SLNB rate at NYU is more in line with what’s been reported before for pure lesions. The team plans to look into the matter.
There was no outside funding for the work, and Dr. Roden had no disclosures.
AT AHNS 2016
Key clinical point: Sentinel lymph node biopsy in patients with head or neck desmoplastic melanoma is positive only 6% of the time, and it doesn’t change the risk of recurrence.
Major finding: SLNB was performed in 16 DM patients (50%) and 36 control patients (60%); it was positive in one DM patient (6.3%) versus 8 of 28 controls with reported results (28.6%).
Data source: Retrospective case-control study with 92 patients
Disclosures: There was no outside funding for the work, and the presenter had no disclosures.

Testosterone might counteract chemotherapy heart damage
SEATTLE – Adjunct testosterone improved short-term cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial from the University of Texas Medical Branch, Galveston.
The finding suggests that testosterone might counteract the cardiotoxic effects of chemotherapy, reducing “the incidence of chemotherapy-induced remodeling. It might also have rehabilitation implications and make patients better surgical candidates. Further investigation is warranted,” said investigator Albert Chamberlain, MD, an endocrine research fellow at the university. Although the results were positive, follow-up was short; years-long data are needed to know if testosterone really protects the heart from chemotherapy damage.

Dr. Chamberlain’s team looked into the issue because “many current chemotherapy drug classes have cardiotoxicity that progresses subclinically for a long time” before problems emerge. “Testosterone is known to cause vasodilation in both large and resistance arteries,” which might help prevent damage. “With that in mind, we decided to” investigate testosterone’s impact on cardiac performance during chemotherapy, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Five women and one man were randomized to weekly intramuscular 100 mg testosterone injections for 7 weeks; six men and four women were randomized to placebo injections. They were all recently diagnosed with stage IIIB, IV, or recurrent head and neck cancer, or cervical cancer, and were undergoing concomitant standard-of-care chemotherapy or chemoradiation. Cardiac function was measured blindly by transthoracic echocardiogram at baseline and the end of the study.
The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011). Heart rate, arterial pressure, end-diastolic volume, and end-systolic volume remained unchanged in both groups, so the improved systolic function was attributed to reduced vascular resistance in the testosterone group (–26.5% versus +3.9% in the placebo group, P = 0.001).
Systolic improvements remained as cardiac index increased 27.6% in the testosterone group versus 2.8% in the placebo group. Testosterone didn’t seem to have any negative impacts on diastolic function. A placebo patient had a stroke, but there were no other adverse events in the study.
Although improved stroke volume is likely due to the reduced afterload, “increased contractility cannot be eliminated as a potential contributing factor. End diastolic volume remained unchanged in both groups, [suggesting] that preload is unlikely to be the mechanism for increased stroke volume,” Dr. Chamberlain said.
This study was funded by the National Cancer Institute. Dr. Chamberlain reported having no relevant disclosures.

|
Dr. Benjamin Judson |
The data are promising but preliminary for a problem we see a lot, chemotherapy-induced cardiotoxicity that presents years after treatment. We have to be really careful before we give testosterone to anyone who is under active treatment for cancer, because I don’t think we really know if it’s safe.
Benjamin Judson, MD, is an associate professor of otolaryngologic surgery at Yale Medical School in New Haven, Conn. He moderated Dr. Chamberlain’s talk and was not involved in the study.
|
|
Dr. Benjamin Judson |
The data are promising but preliminary for a problem we see a lot, chemotherapy-induced cardiotoxicity that presents years after treatment. We have to be really careful before we give testosterone to anyone who is under active treatment for cancer, because I don’t think we really know if it’s safe.
Benjamin Judson, MD, is an associate professor of otolaryngologic surgery at Yale Medical School in New Haven, Conn. He moderated Dr. Chamberlain’s talk and was not involved in the study.
|
|
Dr. Benjamin Judson |
The data are promising but preliminary for a problem we see a lot, chemotherapy-induced cardiotoxicity that presents years after treatment. We have to be really careful before we give testosterone to anyone who is under active treatment for cancer, because I don’t think we really know if it’s safe.
Benjamin Judson, MD, is an associate professor of otolaryngologic surgery at Yale Medical School in New Haven, Conn. He moderated Dr. Chamberlain’s talk and was not involved in the study.
SEATTLE – Adjunct testosterone improved short-term cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial from the University of Texas Medical Branch, Galveston.
The finding suggests that testosterone might counteract the cardiotoxic effects of chemotherapy, reducing “the incidence of chemotherapy-induced remodeling. It might also have rehabilitation implications and make patients better surgical candidates. Further investigation is warranted,” said investigator Albert Chamberlain, MD, an endocrine research fellow at the university. Although the results were positive, follow-up was short; years-long data are needed to know if testosterone really protects the heart from chemotherapy damage.
Dr. Chamberlain’s team looked into the issue because “many current chemotherapy drug classes have cardiotoxicity that progresses subclinically for a long time” before problems emerge. “Testosterone is known to cause vasodilation in both large and resistance arteries,” which might help prevent damage. “With that in mind, we decided to” investigate testosterone’s impact on cardiac performance during chemotherapy, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Five women and one man were randomized to weekly intramuscular 100 mg testosterone injections for 7 weeks; six men and four women were randomized to placebo injections. They were all recently diagnosed with stage IIIB, IV, or recurrent head and neck cancer, or cervical cancer, and were undergoing concomitant standard-of-care chemotherapy or chemoradiation. Cardiac function was measured blindly by transthoracic echocardiogram at baseline and the end of the study.
The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011). Heart rate, arterial pressure, end-diastolic volume, and end-systolic volume remained unchanged in both groups, so the improved systolic function was attributed to reduced vascular resistance in the testosterone group (–26.5% versus +3.9% in the placebo group, P = 0.001).
Systolic improvements remained as cardiac index increased 27.6% in the testosterone group versus 2.8% in the placebo group. Testosterone didn’t seem to have any negative impacts on diastolic function. A placebo patient had a stroke, but there were no other adverse events in the study.
Although improved stroke volume is likely due to the reduced afterload, “increased contractility cannot be eliminated as a potential contributing factor. End diastolic volume remained unchanged in both groups, [suggesting] that preload is unlikely to be the mechanism for increased stroke volume,” Dr. Chamberlain said.
This study was funded by the National Cancer Institute. Dr. Chamberlain reported having no relevant disclosures.
SEATTLE – Adjunct testosterone improved short-term cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial from the University of Texas Medical Branch, Galveston.
The finding suggests that testosterone might counteract the cardiotoxic effects of chemotherapy, reducing “the incidence of chemotherapy-induced remodeling. It might also have rehabilitation implications and make patients better surgical candidates. Further investigation is warranted,” said investigator Albert Chamberlain, MD, an endocrine research fellow at the university. Although the results were positive, follow-up was short; years-long data are needed to know if testosterone really protects the heart from chemotherapy damage.
Dr. Chamberlain’s team looked into the issue because “many current chemotherapy drug classes have cardiotoxicity that progresses subclinically for a long time” before problems emerge. “Testosterone is known to cause vasodilation in both large and resistance arteries,” which might help prevent damage. “With that in mind, we decided to” investigate testosterone’s impact on cardiac performance during chemotherapy, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Five women and one man were randomized to weekly intramuscular 100 mg testosterone injections for 7 weeks; six men and four women were randomized to placebo injections. They were all recently diagnosed with stage IIIB, IV, or recurrent head and neck cancer, or cervical cancer, and were undergoing concomitant standard-of-care chemotherapy or chemoradiation. Cardiac function was measured blindly by transthoracic echocardiogram at baseline and the end of the study.
The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011). Heart rate, arterial pressure, end-diastolic volume, and end-systolic volume remained unchanged in both groups, so the improved systolic function was attributed to reduced vascular resistance in the testosterone group (–26.5% versus +3.9% in the placebo group, P = 0.001).
Systolic improvements remained as cardiac index increased 27.6% in the testosterone group versus 2.8% in the placebo group. Testosterone didn’t seem to have any negative impacts on diastolic function. A placebo patient had a stroke, but there were no other adverse events in the study.
Although improved stroke volume is likely due to the reduced afterload, “increased contractility cannot be eliminated as a potential contributing factor. End diastolic volume remained unchanged in both groups, [suggesting] that preload is unlikely to be the mechanism for increased stroke volume,” Dr. Chamberlain said.
This study was funded by the National Cancer Institute. Dr. Chamberlain reported having no relevant disclosures.
AT AHNS 2016
Key clinical point: Adjunct testosterone improved cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial.
Major finding: The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011), but there was no years-long follow-up to show lasting cardiac benefit.
Data source: Randomized trial with 16 patients.
Disclosures: The National Cancer Institute funded the work. The lead investigator had no disclosures.

A few 20-shot sessions might be enough for deoxycholic acid
NEWPORT BEACH, CALIF. – It’s unclear how well deoxycholic acid (Kybella) will work in the clinic because doctors and patients are generally opting for fewer injections and fewer treatment sessions than were evaluated in phase III studies, according to Lawrence Bass, MD.
The fat cytolytic was approved in 2015 for shrinking double chins, with up to six 50-injection sessions. In trials, patients tended to get more than 40 shots in their first two sessions and more than 30 in subsequent sessions. At that dosing, 40.5% of patients in one trial and 46% in another lost at least 10% of their submental volume on MRI, according to Food and Drug Administration review documents.

However, at the Summit in Aesthetic Medicine, Dr. Bass, a plastic surgeon in New York City, said that, in clinical practice, patients are typically being treated with 20 injections for two or three sessions – partly because of cost. “This product costs $300 for each 2 mL vial, which means in a typical 20-injection treatment, you use $600 of material,” he noted. An average treatment session in Manhattan costs patients about $1,500. In other parts of the country, sessions are probably around $1,200 each, he added.
Also, the necks of patients enrolled in trials “had to be pretty big, but the necks we are probably going to treat with this are the smaller and medium ones. The big ones are just going to do liposuction or something else,” he said. Given all the variables, “we don’t know how well the study experience is going to match clinical experience.”
Dr. Bass treated his first postapproval patient, a 52-year-old woman, with two 20-injection treatment sessions 2 months apart. “The fat definitely cleaned out” and her skin looked a bit tighter, but it’s tough to know if her skin truly tightened or simply draped flatter, he said.
FDA labeling notes that “the safe and effective use of Kybella for the treatment of subcutaneous fat outside the submental region has not been established and is not recommended,” but this advice is unlikely to keep doctors from trying it in off-label areas.
One issue is that “almost every other area is a whole lot bigger” than a double chin, Dr. Bass said. Treating a tummy with 50 injections six to eight times, for example, would cost patients $12,000-$15,000, which is “a whole lot more than lipo,” he added.
Also, administering more than 50 injections at a time for a larger area is not possible because of toxicity. Trying to get around that limit and cut costs by diluting deoxycholic acid or spacing the injections farther apart doesn’t seem to be an option, since phase II testing showed a loss of efficacy with that approach.
Dr. Bass tried deoxycholic acid on a woman with leftover tummy bulges following liposuction. After two 40-injection sessions, “there was still a little shape there, so I don’t think I’ll be doing that again,” he said at the meeting, which is held by Global Academy for Medical Education. Global Academy and this news organization are owned the same company.
Gynecomastia, meanwhile, would probably require too many shots, and the jowl, another potential target, is too close to the marginal mandibular branch of the facial nerve, “so you are not supposed to inject there,” Dr. Bass said. Diluted deoxycholic acid might be an option for bulging periorbital fat, “but I am going to let somebody who is braver than me try that for a while before I go there.”
Dr. Bass is an investigator and speaker for Cynosure, an investigator for Endo Pharmaceuticals and Neothetics, and an advisor to Merz. He participated in phase III testing of deoxycholic acid.
The indication approved for deoxycholic acid is “for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults.”
NEWPORT BEACH, CALIF. – It’s unclear how well deoxycholic acid (Kybella) will work in the clinic because doctors and patients are generally opting for fewer injections and fewer treatment sessions than were evaluated in phase III studies, according to Lawrence Bass, MD.
The fat cytolytic was approved in 2015 for shrinking double chins, with up to six 50-injection sessions. In trials, patients tended to get more than 40 shots in their first two sessions and more than 30 in subsequent sessions. At that dosing, 40.5% of patients in one trial and 46% in another lost at least 10% of their submental volume on MRI, according to Food and Drug Administration review documents.
However, at the Summit in Aesthetic Medicine, Dr. Bass, a plastic surgeon in New York City, said that, in clinical practice, patients are typically being treated with 20 injections for two or three sessions – partly because of cost. “This product costs $300 for each 2 mL vial, which means in a typical 20-injection treatment, you use $600 of material,” he noted. An average treatment session in Manhattan costs patients about $1,500. In other parts of the country, sessions are probably around $1,200 each, he added.
Also, the necks of patients enrolled in trials “had to be pretty big, but the necks we are probably going to treat with this are the smaller and medium ones. The big ones are just going to do liposuction or something else,” he said. Given all the variables, “we don’t know how well the study experience is going to match clinical experience.”
Dr. Bass treated his first postapproval patient, a 52-year-old woman, with two 20-injection treatment sessions 2 months apart. “The fat definitely cleaned out” and her skin looked a bit tighter, but it’s tough to know if her skin truly tightened or simply draped flatter, he said.
FDA labeling notes that “the safe and effective use of Kybella for the treatment of subcutaneous fat outside the submental region has not been established and is not recommended,” but this advice is unlikely to keep doctors from trying it in off-label areas.
One issue is that “almost every other area is a whole lot bigger” than a double chin, Dr. Bass said. Treating a tummy with 50 injections six to eight times, for example, would cost patients $12,000-$15,000, which is “a whole lot more than lipo,” he added.
Also, administering more than 50 injections at a time for a larger area is not possible because of toxicity. Trying to get around that limit and cut costs by diluting deoxycholic acid or spacing the injections farther apart doesn’t seem to be an option, since phase II testing showed a loss of efficacy with that approach.
Dr. Bass tried deoxycholic acid on a woman with leftover tummy bulges following liposuction. After two 40-injection sessions, “there was still a little shape there, so I don’t think I’ll be doing that again,” he said at the meeting, which is held by Global Academy for Medical Education. Global Academy and this news organization are owned the same company.
Gynecomastia, meanwhile, would probably require too many shots, and the jowl, another potential target, is too close to the marginal mandibular branch of the facial nerve, “so you are not supposed to inject there,” Dr. Bass said. Diluted deoxycholic acid might be an option for bulging periorbital fat, “but I am going to let somebody who is braver than me try that for a while before I go there.”
Dr. Bass is an investigator and speaker for Cynosure, an investigator for Endo Pharmaceuticals and Neothetics, and an advisor to Merz. He participated in phase III testing of deoxycholic acid.
The indication approved for deoxycholic acid is “for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults.”
NEWPORT BEACH, CALIF. – It’s unclear how well deoxycholic acid (Kybella) will work in the clinic because doctors and patients are generally opting for fewer injections and fewer treatment sessions than were evaluated in phase III studies, according to Lawrence Bass, MD.
The fat cytolytic was approved in 2015 for shrinking double chins, with up to six 50-injection sessions. In trials, patients tended to get more than 40 shots in their first two sessions and more than 30 in subsequent sessions. At that dosing, 40.5% of patients in one trial and 46% in another lost at least 10% of their submental volume on MRI, according to Food and Drug Administration review documents.
However, at the Summit in Aesthetic Medicine, Dr. Bass, a plastic surgeon in New York City, said that, in clinical practice, patients are typically being treated with 20 injections for two or three sessions – partly because of cost. “This product costs $300 for each 2 mL vial, which means in a typical 20-injection treatment, you use $600 of material,” he noted. An average treatment session in Manhattan costs patients about $1,500. In other parts of the country, sessions are probably around $1,200 each, he added.
Also, the necks of patients enrolled in trials “had to be pretty big, but the necks we are probably going to treat with this are the smaller and medium ones. The big ones are just going to do liposuction or something else,” he said. Given all the variables, “we don’t know how well the study experience is going to match clinical experience.”
Dr. Bass treated his first postapproval patient, a 52-year-old woman, with two 20-injection treatment sessions 2 months apart. “The fat definitely cleaned out” and her skin looked a bit tighter, but it’s tough to know if her skin truly tightened or simply draped flatter, he said.
FDA labeling notes that “the safe and effective use of Kybella for the treatment of subcutaneous fat outside the submental region has not been established and is not recommended,” but this advice is unlikely to keep doctors from trying it in off-label areas.
One issue is that “almost every other area is a whole lot bigger” than a double chin, Dr. Bass said. Treating a tummy with 50 injections six to eight times, for example, would cost patients $12,000-$15,000, which is “a whole lot more than lipo,” he added.
Also, administering more than 50 injections at a time for a larger area is not possible because of toxicity. Trying to get around that limit and cut costs by diluting deoxycholic acid or spacing the injections farther apart doesn’t seem to be an option, since phase II testing showed a loss of efficacy with that approach.
Dr. Bass tried deoxycholic acid on a woman with leftover tummy bulges following liposuction. After two 40-injection sessions, “there was still a little shape there, so I don’t think I’ll be doing that again,” he said at the meeting, which is held by Global Academy for Medical Education. Global Academy and this news organization are owned the same company.
Gynecomastia, meanwhile, would probably require too many shots, and the jowl, another potential target, is too close to the marginal mandibular branch of the facial nerve, “so you are not supposed to inject there,” Dr. Bass said. Diluted deoxycholic acid might be an option for bulging periorbital fat, “but I am going to let somebody who is braver than me try that for a while before I go there.”
Dr. Bass is an investigator and speaker for Cynosure, an investigator for Endo Pharmaceuticals and Neothetics, and an advisor to Merz. He participated in phase III testing of deoxycholic acid.
The indication approved for deoxycholic acid is “for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults.”
EXPERT ANALYSIS FROM THE SUMMIT IN AESTHETIC MEDICINE

New IDSA aspergillosis guidelines endorse galactomannan for diagnosis
New aspergillosis guidelines from the Infectious Diseases Society of America recommend serum and bronchoalveolar lavage galactomannan as a marker for the diagnosis of invasive Aspergillus in adult and pediatric patients who have hematologic malignancies or have undergone hematopoietic stem cell transplants.
Serial monitoring of serum galactomannan (GM) is also useful to monitor disease progression, therapeutic response, and prognosis in hematologic malignancy and hematopoietic stem cell transplant (HSCT) patients who have elevated baseline GM (Clin Infect Dis. 2016 Jun 29. doi: 10.1093/cid/ciw326).
Serum beta-D-glucan assays also are recommended for diagnosing invasive Aspergillus (IA) in high-risk hematologic malignancy and allogeneic HSCT patients, although these tests are not very specific for the infection.
The advice illustrates the Society’s emphasis on early diagnosis in its new guidelines, which supplant the group’s 2008 guidance. There are almost 100 recommendations covering – in depth – the management of invasive, allergic, and chronic Aspergillus infections in all their manifestations. It’s a step-by-step, how-to manual for handling the problem.

“Aspergillosis mortality rates have decreased significantly in recent years, but there is still significant mortality from the infection, and we have a ways to go. We felt that early diagnosis was key, which is why it’s such an important part of these guidelines,” said lead author Thomas Patterson, MD, chief of the Division of Infectious Diseases at the University of Texas Health Science Center, San Antonio. He highlighted the most important developments in a recent interview.
“We know a lot more since 2008 about the benefits of using biomarkers like GM in bronchoalveolar lavage samples, which could be highly useful for diagnosis. However, biomarkers have not been as well validated for biologic response and are not recommended” in most cases for monitoring how well patients are doing. Also, “biomarkers are not as useful in solid organ transplants; we discuss that” in the guidelines, Dr. Patterson said.
The society came out against routine polymerase chain reaction (PCR) testing of blood samples for diagnosis. Although there has been a lot of work on the technique, the evidence isn’t strong enough yet to establish overall clinical benefit, but there is emerging evidence for the diagnostic use of PCR in conjunction with radiologic findings.
For treatment, voriconazole remains the go-to drug, but the guidelines make room for more recently approved therapies. “We now have isavuconazole, which may be better tolerated,” but it’s recommended only as an alternative to voriconazole because evidence comes mostly from a single clinical trial, he said.
Posaconazole extended-release tablets are strongly recommended as prophylaxis based on high-quality evidence from studies in neutropenic patients. Posaconazole extended-release tablets result in significantly higher antifungal blood levels than those seen with voriconazole, and “it certainly has been useful in some patients”; however, posaconazole is not approved for primary therapy in the United States, Dr. Patterson said.
A large clinical trial that tested voriconazole plus an echinocandin against voriconazole alone found that in patients diagnosed using serum galactomannan – especially those with hematologic malignancies – outcomes were better with the combination. “The panel felt combinations could be considered in some patients” but didn’t recommend them for routine use because [again,] there’s not strong evidence,” he said.
For now, it seems that higher-risk patients with hematologic malignancies and those with more widespread disease might be the ones who benefit most from combination therapy.
“We also discussed allergic and saprophytic diseases. We know that some patients with allergic bronchopulmonary aspergillosis will respond to antifungal therapy, and perhaps reduce their need for steroids, so that’s now part of the suggestions, as well,” he said.
The IDSA funded the work. Dr. Patterson receives research funding from Astellas, Merck, and Revolution Medicines, and has been an adviser to numerous drug companies.
New aspergillosis guidelines from the Infectious Diseases Society of America recommend serum and bronchoalveolar lavage galactomannan as a marker for the diagnosis of invasive Aspergillus in adult and pediatric patients who have hematologic malignancies or have undergone hematopoietic stem cell transplants.
Serial monitoring of serum galactomannan (GM) is also useful to monitor disease progression, therapeutic response, and prognosis in hematologic malignancy and hematopoietic stem cell transplant (HSCT) patients who have elevated baseline GM (Clin Infect Dis. 2016 Jun 29. doi: 10.1093/cid/ciw326).
Serum beta-D-glucan assays also are recommended for diagnosing invasive Aspergillus (IA) in high-risk hematologic malignancy and allogeneic HSCT patients, although these tests are not very specific for the infection.
The advice illustrates the Society’s emphasis on early diagnosis in its new guidelines, which supplant the group’s 2008 guidance. There are almost 100 recommendations covering – in depth – the management of invasive, allergic, and chronic Aspergillus infections in all their manifestations. It’s a step-by-step, how-to manual for handling the problem.
“Aspergillosis mortality rates have decreased significantly in recent years, but there is still significant mortality from the infection, and we have a ways to go. We felt that early diagnosis was key, which is why it’s such an important part of these guidelines,” said lead author Thomas Patterson, MD, chief of the Division of Infectious Diseases at the University of Texas Health Science Center, San Antonio. He highlighted the most important developments in a recent interview.
“We know a lot more since 2008 about the benefits of using biomarkers like GM in bronchoalveolar lavage samples, which could be highly useful for diagnosis. However, biomarkers have not been as well validated for biologic response and are not recommended” in most cases for monitoring how well patients are doing. Also, “biomarkers are not as useful in solid organ transplants; we discuss that” in the guidelines, Dr. Patterson said.
The society came out against routine polymerase chain reaction (PCR) testing of blood samples for diagnosis. Although there has been a lot of work on the technique, the evidence isn’t strong enough yet to establish overall clinical benefit, but there is emerging evidence for the diagnostic use of PCR in conjunction with radiologic findings.
For treatment, voriconazole remains the go-to drug, but the guidelines make room for more recently approved therapies. “We now have isavuconazole, which may be better tolerated,” but it’s recommended only as an alternative to voriconazole because evidence comes mostly from a single clinical trial, he said.
Posaconazole extended-release tablets are strongly recommended as prophylaxis based on high-quality evidence from studies in neutropenic patients. Posaconazole extended-release tablets result in significantly higher antifungal blood levels than those seen with voriconazole, and “it certainly has been useful in some patients”; however, posaconazole is not approved for primary therapy in the United States, Dr. Patterson said.
A large clinical trial that tested voriconazole plus an echinocandin against voriconazole alone found that in patients diagnosed using serum galactomannan – especially those with hematologic malignancies – outcomes were better with the combination. “The panel felt combinations could be considered in some patients” but didn’t recommend them for routine use because [again,] there’s not strong evidence,” he said.
For now, it seems that higher-risk patients with hematologic malignancies and those with more widespread disease might be the ones who benefit most from combination therapy.
“We also discussed allergic and saprophytic diseases. We know that some patients with allergic bronchopulmonary aspergillosis will respond to antifungal therapy, and perhaps reduce their need for steroids, so that’s now part of the suggestions, as well,” he said.
The IDSA funded the work. Dr. Patterson receives research funding from Astellas, Merck, and Revolution Medicines, and has been an adviser to numerous drug companies.
New aspergillosis guidelines from the Infectious Diseases Society of America recommend serum and bronchoalveolar lavage galactomannan as a marker for the diagnosis of invasive Aspergillus in adult and pediatric patients who have hematologic malignancies or have undergone hematopoietic stem cell transplants.
Serial monitoring of serum galactomannan (GM) is also useful to monitor disease progression, therapeutic response, and prognosis in hematologic malignancy and hematopoietic stem cell transplant (HSCT) patients who have elevated baseline GM (Clin Infect Dis. 2016 Jun 29. doi: 10.1093/cid/ciw326).
Serum beta-D-glucan assays also are recommended for diagnosing invasive Aspergillus (IA) in high-risk hematologic malignancy and allogeneic HSCT patients, although these tests are not very specific for the infection.
The advice illustrates the Society’s emphasis on early diagnosis in its new guidelines, which supplant the group’s 2008 guidance. There are almost 100 recommendations covering – in depth – the management of invasive, allergic, and chronic Aspergillus infections in all their manifestations. It’s a step-by-step, how-to manual for handling the problem.
“Aspergillosis mortality rates have decreased significantly in recent years, but there is still significant mortality from the infection, and we have a ways to go. We felt that early diagnosis was key, which is why it’s such an important part of these guidelines,” said lead author Thomas Patterson, MD, chief of the Division of Infectious Diseases at the University of Texas Health Science Center, San Antonio. He highlighted the most important developments in a recent interview.
“We know a lot more since 2008 about the benefits of using biomarkers like GM in bronchoalveolar lavage samples, which could be highly useful for diagnosis. However, biomarkers have not been as well validated for biologic response and are not recommended” in most cases for monitoring how well patients are doing. Also, “biomarkers are not as useful in solid organ transplants; we discuss that” in the guidelines, Dr. Patterson said.
The society came out against routine polymerase chain reaction (PCR) testing of blood samples for diagnosis. Although there has been a lot of work on the technique, the evidence isn’t strong enough yet to establish overall clinical benefit, but there is emerging evidence for the diagnostic use of PCR in conjunction with radiologic findings.
For treatment, voriconazole remains the go-to drug, but the guidelines make room for more recently approved therapies. “We now have isavuconazole, which may be better tolerated,” but it’s recommended only as an alternative to voriconazole because evidence comes mostly from a single clinical trial, he said.
Posaconazole extended-release tablets are strongly recommended as prophylaxis based on high-quality evidence from studies in neutropenic patients. Posaconazole extended-release tablets result in significantly higher antifungal blood levels than those seen with voriconazole, and “it certainly has been useful in some patients”; however, posaconazole is not approved for primary therapy in the United States, Dr. Patterson said.
A large clinical trial that tested voriconazole plus an echinocandin against voriconazole alone found that in patients diagnosed using serum galactomannan – especially those with hematologic malignancies – outcomes were better with the combination. “The panel felt combinations could be considered in some patients” but didn’t recommend them for routine use because [again,] there’s not strong evidence,” he said.
For now, it seems that higher-risk patients with hematologic malignancies and those with more widespread disease might be the ones who benefit most from combination therapy.
“We also discussed allergic and saprophytic diseases. We know that some patients with allergic bronchopulmonary aspergillosis will respond to antifungal therapy, and perhaps reduce their need for steroids, so that’s now part of the suggestions, as well,” he said.
The IDSA funded the work. Dr. Patterson receives research funding from Astellas, Merck, and Revolution Medicines, and has been an adviser to numerous drug companies.
FROM CLINICAL INFECTIOUS DISEASES

Common surgeries linked to chronic opioid use among opioid-naive patients
Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories, according to an insurance claims analysis from Stanford (Calif.) University.
The researchers reviewed opioid prescribing in the first postop year – excluding the first 90 days – for 641,941 patients and compared that information with opioid prescribing for 18,011,137 adult patients who did not have surgery. None of the subjects had filled an opioid prescription in the previous year (JAMA Intern Med. 2016 Jul 11. doi: 10.1001/jamainternmed.2016.3298).
Chronic opioid use, defined as filling at least 120 days of opioid prescriptions within the first year of surgery, ranged up to 1.41% for total knee replacement, versus 0.136% in the nonsurgical controls. After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; total hip replacement and simple mastectomy almost threefold; and laparoscopic cholecystectomy and open appendectomy almost twofold. Cesarean delivery increased the risk of chronic use by 28%.
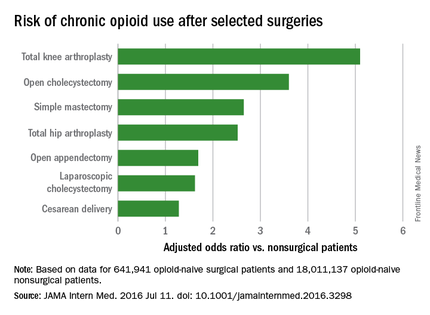
With the exception of knee and hip replacements, “these procedures are not indicated to relieve pain and are not thought to place patients at risk for long-term pain ... Our results suggest that primary care clinicians and surgeons should monitor opioid use closely in the postsurgical period,” wrote Eric C. Sun, MD, PhD, of the department of anesthesiology, perioperative and pain medicine at Stanford (Calif.) University, and his colleagues.
Preoperative antidepressants and benzodiazepines carried about the same risk of chronic use as alcohol abuse (odds ratio 1.83; P less than .001), while drug abuse history increased the risk even more (OR 3.15; P less than .001). Male sex, age over 50 years, and history of depression were also associated with chronic use on multivariate analysis. Meanwhile, transurethral prostatectomy, laparoscopic appendectomy, functional endoscopic sinus surgery, and cataract surgery did not increase chronic use risk.
“Surgical patients, particularly those at higher risk for chronic opioid use, may benefit from techniques to reduce the risk such as multimodal analgesia and regional anesthesia, particularly in light of literature suggesting that these interventions may improve other perioperative outcomes ... Patients may also benefit from other preoperative and postoperative interventions, such as evidence-based psychobehavioral pain management skills,” the investigators said.
It wasn’t clear until now that even opioid-naive patients are at risk for opioid problems after surgery. Stanford’s investigation is not the first to link surgery and opioid abuse, but previous studies tended to focus on patients with preexisting use and more painful operations.
The study included prescriptions for oral and patch fentanyl, hydrocodone, oral hydromorphone, methadone, morphine, oxymorphone, and oxycodone. Hydrocodone cough remedies and acetaminophen/codeine analgesics were excluded.
Nonsurgical patients tended to be younger than their surgical peers (mean 42 vs. 44 years) and more likely to be male (49% vs. 26%).
The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories, according to an insurance claims analysis from Stanford (Calif.) University.
The researchers reviewed opioid prescribing in the first postop year – excluding the first 90 days – for 641,941 patients and compared that information with opioid prescribing for 18,011,137 adult patients who did not have surgery. None of the subjects had filled an opioid prescription in the previous year (JAMA Intern Med. 2016 Jul 11. doi: 10.1001/jamainternmed.2016.3298).
Chronic opioid use, defined as filling at least 120 days of opioid prescriptions within the first year of surgery, ranged up to 1.41% for total knee replacement, versus 0.136% in the nonsurgical controls. After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; total hip replacement and simple mastectomy almost threefold; and laparoscopic cholecystectomy and open appendectomy almost twofold. Cesarean delivery increased the risk of chronic use by 28%.
With the exception of knee and hip replacements, “these procedures are not indicated to relieve pain and are not thought to place patients at risk for long-term pain ... Our results suggest that primary care clinicians and surgeons should monitor opioid use closely in the postsurgical period,” wrote Eric C. Sun, MD, PhD, of the department of anesthesiology, perioperative and pain medicine at Stanford (Calif.) University, and his colleagues.
Preoperative antidepressants and benzodiazepines carried about the same risk of chronic use as alcohol abuse (odds ratio 1.83; P less than .001), while drug abuse history increased the risk even more (OR 3.15; P less than .001). Male sex, age over 50 years, and history of depression were also associated with chronic use on multivariate analysis. Meanwhile, transurethral prostatectomy, laparoscopic appendectomy, functional endoscopic sinus surgery, and cataract surgery did not increase chronic use risk.
“Surgical patients, particularly those at higher risk for chronic opioid use, may benefit from techniques to reduce the risk such as multimodal analgesia and regional anesthesia, particularly in light of literature suggesting that these interventions may improve other perioperative outcomes ... Patients may also benefit from other preoperative and postoperative interventions, such as evidence-based psychobehavioral pain management skills,” the investigators said.
It wasn’t clear until now that even opioid-naive patients are at risk for opioid problems after surgery. Stanford’s investigation is not the first to link surgery and opioid abuse, but previous studies tended to focus on patients with preexisting use and more painful operations.
The study included prescriptions for oral and patch fentanyl, hydrocodone, oral hydromorphone, methadone, morphine, oxymorphone, and oxycodone. Hydrocodone cough remedies and acetaminophen/codeine analgesics were excluded.
Nonsurgical patients tended to be younger than their surgical peers (mean 42 vs. 44 years) and more likely to be male (49% vs. 26%).
The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories, according to an insurance claims analysis from Stanford (Calif.) University.
The researchers reviewed opioid prescribing in the first postop year – excluding the first 90 days – for 641,941 patients and compared that information with opioid prescribing for 18,011,137 adult patients who did not have surgery. None of the subjects had filled an opioid prescription in the previous year (JAMA Intern Med. 2016 Jul 11. doi: 10.1001/jamainternmed.2016.3298).
Chronic opioid use, defined as filling at least 120 days of opioid prescriptions within the first year of surgery, ranged up to 1.41% for total knee replacement, versus 0.136% in the nonsurgical controls. After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; total hip replacement and simple mastectomy almost threefold; and laparoscopic cholecystectomy and open appendectomy almost twofold. Cesarean delivery increased the risk of chronic use by 28%.
With the exception of knee and hip replacements, “these procedures are not indicated to relieve pain and are not thought to place patients at risk for long-term pain ... Our results suggest that primary care clinicians and surgeons should monitor opioid use closely in the postsurgical period,” wrote Eric C. Sun, MD, PhD, of the department of anesthesiology, perioperative and pain medicine at Stanford (Calif.) University, and his colleagues.
Preoperative antidepressants and benzodiazepines carried about the same risk of chronic use as alcohol abuse (odds ratio 1.83; P less than .001), while drug abuse history increased the risk even more (OR 3.15; P less than .001). Male sex, age over 50 years, and history of depression were also associated with chronic use on multivariate analysis. Meanwhile, transurethral prostatectomy, laparoscopic appendectomy, functional endoscopic sinus surgery, and cataract surgery did not increase chronic use risk.
“Surgical patients, particularly those at higher risk for chronic opioid use, may benefit from techniques to reduce the risk such as multimodal analgesia and regional anesthesia, particularly in light of literature suggesting that these interventions may improve other perioperative outcomes ... Patients may also benefit from other preoperative and postoperative interventions, such as evidence-based psychobehavioral pain management skills,” the investigators said.
It wasn’t clear until now that even opioid-naive patients are at risk for opioid problems after surgery. Stanford’s investigation is not the first to link surgery and opioid abuse, but previous studies tended to focus on patients with preexisting use and more painful operations.
The study included prescriptions for oral and patch fentanyl, hydrocodone, oral hydromorphone, methadone, morphine, oxymorphone, and oxycodone. Hydrocodone cough remedies and acetaminophen/codeine analgesics were excluded.
Nonsurgical patients tended to be younger than their surgical peers (mean 42 vs. 44 years) and more likely to be male (49% vs. 26%).
The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
FROM JAMA INTERNAL MEDICINE
Key clinical point: Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially among those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories.
Major finding: After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; and total hip replacement and simple mastectomy almost threefold.
Data source: Insurance claims of more than 18 million people.
Disclosures: The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
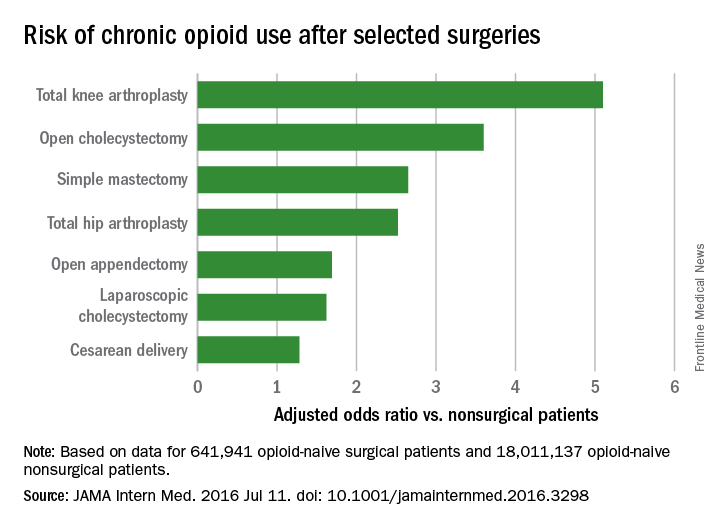
Blood Aspergillus RNA a promising biomarker for invasive aspergillosis
Elevated Aspergillus RNA blood levels after 4-6 weeks of antifungal treatment predict poor response at week 12 in patients with proven or probable invasive aspergillosis, according to results of a small observational study of 41 evaluable patients.
The investigators are working to address the need for reliable biomarkers of early invasive aspergillosis (IA) treatment response. Standard clinical and radiological criteria are somewhat subjective, and serial biopsies and bronchoalveolar lavage are often impractical, reported Yanan Zhao, PhD, of the New Jersey Medical School–Rutgers Biomedical and Health Sciences, Newark, and her associates.
Study participants’ blood was checked for serum galactomannan (GM), 1, 3-beta-D-glucan (BG), and Aspergillus RNA within 24 hours of starting antifungal therapy, then twice per week during the first 2 weeks, then once during weeks 4, 6, and 12, the investigators reported (Med Mycol. 2016 Jun 22. pii: myw043).
Ribosomal Aspergillus RNA – like GM and BG, a marker of fungal load – was measured by nucleic acid sequence-based amplification (NASBA), a robust isothermal amplification technique more sensitive than polymerase chain reaction due largely “to increased starting target numbers (RNA versus DNA) and more robust amplification.” Although NASBA has been used before to diagnose IA, using it to monitor treatment “is still in its infancy,” the authors noted.
Eleven of 14 patients who did not respond to treatment at 12 weeks (79%) had Aspergillus RNA in their blood after 4 weeks of treatment, and 12 (86%) were positive at 6 weeks.
Among patients who did respond at 12 weeks, 11 of 27 (41%) had RNA in their blood at 4 weeks, and 14 (52%) at 6 weeks. The findings were statistically significant.
There was no correlation between Aspergillus RNA and serum GM levels in terms of outcomes, but the kinetics of circulating Aspergillus RNA correlated with BG in some patients, with an excellent match in three.
Serum GM responds fairly soon if treatment is working. Aspergillus RNA, however, responds more slowly, like BG. “This may explain ... the correlation between Aspergillus RNA and BG ... Therefore, the combination of Aspergillus RNA and BG might be useful to assess therapeutic response, particularly in GM negative cases,” the investigators said.
This work was funded by Merck. Four investigators are current or former employees.
Elevated Aspergillus RNA blood levels after 4-6 weeks of antifungal treatment predict poor response at week 12 in patients with proven or probable invasive aspergillosis, according to results of a small observational study of 41 evaluable patients.
The investigators are working to address the need for reliable biomarkers of early invasive aspergillosis (IA) treatment response. Standard clinical and radiological criteria are somewhat subjective, and serial biopsies and bronchoalveolar lavage are often impractical, reported Yanan Zhao, PhD, of the New Jersey Medical School–Rutgers Biomedical and Health Sciences, Newark, and her associates.
Study participants’ blood was checked for serum galactomannan (GM), 1, 3-beta-D-glucan (BG), and Aspergillus RNA within 24 hours of starting antifungal therapy, then twice per week during the first 2 weeks, then once during weeks 4, 6, and 12, the investigators reported (Med Mycol. 2016 Jun 22. pii: myw043).
Ribosomal Aspergillus RNA – like GM and BG, a marker of fungal load – was measured by nucleic acid sequence-based amplification (NASBA), a robust isothermal amplification technique more sensitive than polymerase chain reaction due largely “to increased starting target numbers (RNA versus DNA) and more robust amplification.” Although NASBA has been used before to diagnose IA, using it to monitor treatment “is still in its infancy,” the authors noted.
Eleven of 14 patients who did not respond to treatment at 12 weeks (79%) had Aspergillus RNA in their blood after 4 weeks of treatment, and 12 (86%) were positive at 6 weeks.
Among patients who did respond at 12 weeks, 11 of 27 (41%) had RNA in their blood at 4 weeks, and 14 (52%) at 6 weeks. The findings were statistically significant.
There was no correlation between Aspergillus RNA and serum GM levels in terms of outcomes, but the kinetics of circulating Aspergillus RNA correlated with BG in some patients, with an excellent match in three.
Serum GM responds fairly soon if treatment is working. Aspergillus RNA, however, responds more slowly, like BG. “This may explain ... the correlation between Aspergillus RNA and BG ... Therefore, the combination of Aspergillus RNA and BG might be useful to assess therapeutic response, particularly in GM negative cases,” the investigators said.
This work was funded by Merck. Four investigators are current or former employees.
Elevated Aspergillus RNA blood levels after 4-6 weeks of antifungal treatment predict poor response at week 12 in patients with proven or probable invasive aspergillosis, according to results of a small observational study of 41 evaluable patients.
The investigators are working to address the need for reliable biomarkers of early invasive aspergillosis (IA) treatment response. Standard clinical and radiological criteria are somewhat subjective, and serial biopsies and bronchoalveolar lavage are often impractical, reported Yanan Zhao, PhD, of the New Jersey Medical School–Rutgers Biomedical and Health Sciences, Newark, and her associates.
Study participants’ blood was checked for serum galactomannan (GM), 1, 3-beta-D-glucan (BG), and Aspergillus RNA within 24 hours of starting antifungal therapy, then twice per week during the first 2 weeks, then once during weeks 4, 6, and 12, the investigators reported (Med Mycol. 2016 Jun 22. pii: myw043).
Ribosomal Aspergillus RNA – like GM and BG, a marker of fungal load – was measured by nucleic acid sequence-based amplification (NASBA), a robust isothermal amplification technique more sensitive than polymerase chain reaction due largely “to increased starting target numbers (RNA versus DNA) and more robust amplification.” Although NASBA has been used before to diagnose IA, using it to monitor treatment “is still in its infancy,” the authors noted.
Eleven of 14 patients who did not respond to treatment at 12 weeks (79%) had Aspergillus RNA in their blood after 4 weeks of treatment, and 12 (86%) were positive at 6 weeks.
Among patients who did respond at 12 weeks, 11 of 27 (41%) had RNA in their blood at 4 weeks, and 14 (52%) at 6 weeks. The findings were statistically significant.
There was no correlation between Aspergillus RNA and serum GM levels in terms of outcomes, but the kinetics of circulating Aspergillus RNA correlated with BG in some patients, with an excellent match in three.
Serum GM responds fairly soon if treatment is working. Aspergillus RNA, however, responds more slowly, like BG. “This may explain ... the correlation between Aspergillus RNA and BG ... Therefore, the combination of Aspergillus RNA and BG might be useful to assess therapeutic response, particularly in GM negative cases,” the investigators said.
This work was funded by Merck. Four investigators are current or former employees.
FROM MEDICAL MYCOLOGY
Key clinical point: Elevated Aspergillus RNA blood levels during the first 4-6 weeks of antifungal treatment predicts poor response at week 12.
Major finding: Eleven of 14 patients who did not respond to antifungals at 12 weeks (79%) had Aspergillus RNA in their blood after 4 weeks of treatment, versus 11 of 27 (41%) who did respond (P = .046).
Data source: Small observational study of patients with proven or probable invasive aspergillosis.
Disclosures: This work was funded by Merck. Four investigators are current or former employees.