User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Gout too often treated only in emergency department
Only about one in three patients seen in the emergency department of an academic health system for acute gout had a follow-up visit that addressed this condition, Lesley Jackson, MD, of the University of Alabama at Birmingham, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network (G-CAN).
Dr. Jackson presented research done on patients seen within her university’s health system, looking at 72 patients seen in the ED between September 2021 and February 2022. Medications prescribed at discharge from the ED included corticosteroids (46 patients, or 64%), opioids (45 patients, 63%), NSAIDs (31 patients, 43%), and colchicine (23 patients, 32%).
Only 26 patients, or about 36%, had a subsequent outpatient visit in the UAB health system addressing gout, she said. Of 33 patients with any outpatient follow-up visit within the UAB system, 21 were within 1 month after the index ED visit, followed by 3 more prior to 3 months, and 9 more after 3 months.
The limitations of the study includes its collection of data from a single institution. But the results highlight the need for improved quality of care for gout, with too many people being treated for this condition primarily in the ED, she said.
In an email exchange arranged by the Arthritis Foundation, Herbert S. B. Baraf, MD, said he agreed that patients too often limit their treatment for gout to seeking care for acute attacks in the ED.
Because of competing demands, physicians working there are more to take a “Band-Aid” approach and not impress upon patients that gout is a lifelong condition that needs follow-up and monitoring, said Dr. Baraf, clinical professor of medicine at George Washington University, Washington, and an associate clinical professor at the University of Maryland, Baltimore. He retired from private practice in 2022.
“This problem is akin to the patient who has a hip fracture due to osteoporosis who gets a surgical repair but is never referred for osteoporotic management,” wrote Dr. Baraf, who is a former board member of the Arthritis Foundation.
He suggested viewing gout as a form of arthritis that has two components.
“The first, that which brings the patient to seek medical care, is the often exquisitely painful attack of pain and swelling in a joint or joints that comes on acutely,” he wrote. “Calming these attacks are the focus of the patient and the doctor, who does the evaluation as relief of pain and inflammation is the most pressing task at hand.”
But equally important is the second element, addressing the cause of these flare ups of arthritis, he wrote. Elevated uric acid leads to crystalline deposits of urate in the joints, particularly in the feet, ankles, knees, and hands. Over time, these deposits generate seemingly random flare ups of acute joint pain in one or more of these areas.
“Thus, when a patient presents to an emergency room with a first or second attack of gout, pain relief is the primary focus of the visit,” Dr. Baraf wrote. “But if over time that is the only focus, and the elevation of serum uric acid is not addressed, deposits will continue to mount and flare ups will occur with increasing frequency and severity.”
This study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Jackson has no relevant financial disclosures.
Only about one in three patients seen in the emergency department of an academic health system for acute gout had a follow-up visit that addressed this condition, Lesley Jackson, MD, of the University of Alabama at Birmingham, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network (G-CAN).
Dr. Jackson presented research done on patients seen within her university’s health system, looking at 72 patients seen in the ED between September 2021 and February 2022. Medications prescribed at discharge from the ED included corticosteroids (46 patients, or 64%), opioids (45 patients, 63%), NSAIDs (31 patients, 43%), and colchicine (23 patients, 32%).
Only 26 patients, or about 36%, had a subsequent outpatient visit in the UAB health system addressing gout, she said. Of 33 patients with any outpatient follow-up visit within the UAB system, 21 were within 1 month after the index ED visit, followed by 3 more prior to 3 months, and 9 more after 3 months.
The limitations of the study includes its collection of data from a single institution. But the results highlight the need for improved quality of care for gout, with too many people being treated for this condition primarily in the ED, she said.
In an email exchange arranged by the Arthritis Foundation, Herbert S. B. Baraf, MD, said he agreed that patients too often limit their treatment for gout to seeking care for acute attacks in the ED.
Because of competing demands, physicians working there are more to take a “Band-Aid” approach and not impress upon patients that gout is a lifelong condition that needs follow-up and monitoring, said Dr. Baraf, clinical professor of medicine at George Washington University, Washington, and an associate clinical professor at the University of Maryland, Baltimore. He retired from private practice in 2022.
“This problem is akin to the patient who has a hip fracture due to osteoporosis who gets a surgical repair but is never referred for osteoporotic management,” wrote Dr. Baraf, who is a former board member of the Arthritis Foundation.
He suggested viewing gout as a form of arthritis that has two components.
“The first, that which brings the patient to seek medical care, is the often exquisitely painful attack of pain and swelling in a joint or joints that comes on acutely,” he wrote. “Calming these attacks are the focus of the patient and the doctor, who does the evaluation as relief of pain and inflammation is the most pressing task at hand.”
But equally important is the second element, addressing the cause of these flare ups of arthritis, he wrote. Elevated uric acid leads to crystalline deposits of urate in the joints, particularly in the feet, ankles, knees, and hands. Over time, these deposits generate seemingly random flare ups of acute joint pain in one or more of these areas.
“Thus, when a patient presents to an emergency room with a first or second attack of gout, pain relief is the primary focus of the visit,” Dr. Baraf wrote. “But if over time that is the only focus, and the elevation of serum uric acid is not addressed, deposits will continue to mount and flare ups will occur with increasing frequency and severity.”
This study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Jackson has no relevant financial disclosures.
Only about one in three patients seen in the emergency department of an academic health system for acute gout had a follow-up visit that addressed this condition, Lesley Jackson, MD, of the University of Alabama at Birmingham, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network (G-CAN).
Dr. Jackson presented research done on patients seen within her university’s health system, looking at 72 patients seen in the ED between September 2021 and February 2022. Medications prescribed at discharge from the ED included corticosteroids (46 patients, or 64%), opioids (45 patients, 63%), NSAIDs (31 patients, 43%), and colchicine (23 patients, 32%).
Only 26 patients, or about 36%, had a subsequent outpatient visit in the UAB health system addressing gout, she said. Of 33 patients with any outpatient follow-up visit within the UAB system, 21 were within 1 month after the index ED visit, followed by 3 more prior to 3 months, and 9 more after 3 months.
The limitations of the study includes its collection of data from a single institution. But the results highlight the need for improved quality of care for gout, with too many people being treated for this condition primarily in the ED, she said.
In an email exchange arranged by the Arthritis Foundation, Herbert S. B. Baraf, MD, said he agreed that patients too often limit their treatment for gout to seeking care for acute attacks in the ED.
Because of competing demands, physicians working there are more to take a “Band-Aid” approach and not impress upon patients that gout is a lifelong condition that needs follow-up and monitoring, said Dr. Baraf, clinical professor of medicine at George Washington University, Washington, and an associate clinical professor at the University of Maryland, Baltimore. He retired from private practice in 2022.
“This problem is akin to the patient who has a hip fracture due to osteoporosis who gets a surgical repair but is never referred for osteoporotic management,” wrote Dr. Baraf, who is a former board member of the Arthritis Foundation.
He suggested viewing gout as a form of arthritis that has two components.
“The first, that which brings the patient to seek medical care, is the often exquisitely painful attack of pain and swelling in a joint or joints that comes on acutely,” he wrote. “Calming these attacks are the focus of the patient and the doctor, who does the evaluation as relief of pain and inflammation is the most pressing task at hand.”
But equally important is the second element, addressing the cause of these flare ups of arthritis, he wrote. Elevated uric acid leads to crystalline deposits of urate in the joints, particularly in the feet, ankles, knees, and hands. Over time, these deposits generate seemingly random flare ups of acute joint pain in one or more of these areas.
“Thus, when a patient presents to an emergency room with a first or second attack of gout, pain relief is the primary focus of the visit,” Dr. Baraf wrote. “But if over time that is the only focus, and the elevation of serum uric acid is not addressed, deposits will continue to mount and flare ups will occur with increasing frequency and severity.”
This study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Jackson has no relevant financial disclosures.
FROM G-CAN 2022
Mid-October flulike illness cases higher than past 5 years
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”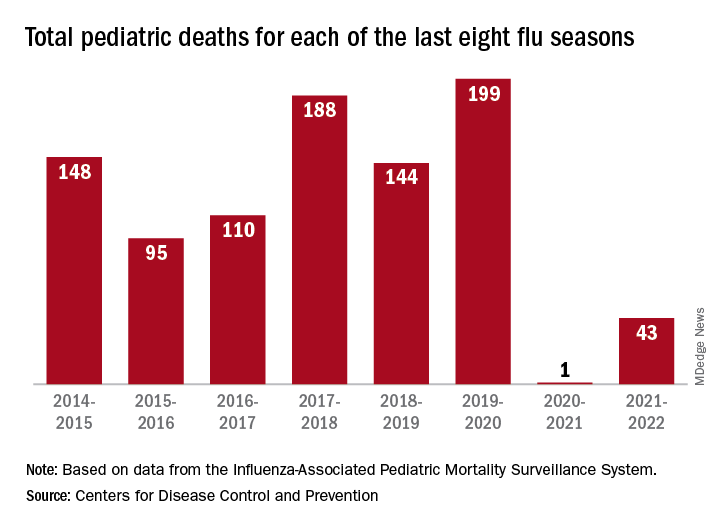
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Locked-in syndrome malpractice case ends with $75 million verdict against docs
The patient, Jonathan Buckelew, was taken to North Fulton Regional Hospital in Roswell, Ga., where imaging revealed that he had suffered a brain stem stroke.
The patient’s attorney, Laura Shamp, alleged in the legal complaint that a series of miscommunications and negligence by multiple providers delayed the diagnosis and treatment of the stroke until the next day, which led to catastrophic brain damage for the patient, who developed locked-in syndrome. The rare neurologic syndrome causes complete paralysis except for the muscles that control eye movements.
“Mr. Buckelew has expended millions of dollars for medical expenses for his care and he will need 24 hour a day care for the rest of his life,” his lawyer said in court documents.
Both physicians’ attorneys denied the claims and said their clients met the standard of care.
The jury attributed 60% fault to ED physician Matthew Womack, MD, and 40% to radiologist James Waldschmidt, MD.
Ms. Shamp alleged that Dr. Womack failed to inform the consulting neurologist of the chiropractic neck adjustment – a known stroke risk factor – and did not adequately communicate the results from CT angiography and lumbar puncture.
In addition, she said Dr. Womack failed to rule out a vertebral artery dissection and that Dr. Waldschmidt did not “[appreciate] an indisputable acute or subacute vertebral-basilar artery occlusion.”
Further allegations were levied against several other members of the patient’s care team, including the neurologist, a critical care physician, a physician assistant, and intensive care unit nurses, but they were not found liable by the jury.
The chiropractor, Michael Axt, DC, was named in the original complaint, but court documents filed earlier in 2022 requested that he be dismissed from the lawsuit, stating that he and the patient had reached an amicable resolution.
“This is a very large verdict,” James B. Edwards, JD, a medical malpractice attorney based in Texas who was not involved in the case, said in an interview. The diagnosis of locked-in syndrome likely contributed to the substantial monetary award.
“The more sympathetic the plaintiff and the situation, the greater risk of a verdict [against] the defendants,” Mr. Edwards said. “Cases that elicit significant and sometimes decisive sympathy include locked-in syndrome, permanent vegetative state, injury to the sexual or reproductive organs, burns, and blindness.”
The effectiveness and safety of chiropractic adjustments often come under fire. Although postmanipulation injuries are not common, they can have near-fatal consequences when they do occur.
In August, a healthy 28-year-old college student experienced four artery dissections after a chiropractic visit for low-back pain. She subsequently had a stroke and went into cardiac arrest. The patient survived but remains paralyzed.
Mr. Buckelew’s legal team said in a statement that his injuries would have been completely avoided had “the slew of health care providers ... acted according to the standard of care, caught and treated his stroke earlier, and communicated more effectively.”
On the day of the chiropractic adjustment, Ms. Shamp said Mr. Axt had documented that Mr. Buckelew’s primary complaints – neck pain, a headache, and bouts of blurred vision and ringing in the ears – began after exercise and had continued for several days.
In his closing statement, Dr. Womack’s attorney said the “chiropractor is solely responsible” for the patient’s injuries because he performed a manipulation despite the patient having a 2-week history of headaches.
Very few medical malpractice verdicts are appealed, though the sizable award in this suit may increase the likelihood that the defense will do so, Mr. Edwards said.
A version of this article first appeared on Medscape.com.
The patient, Jonathan Buckelew, was taken to North Fulton Regional Hospital in Roswell, Ga., where imaging revealed that he had suffered a brain stem stroke.
The patient’s attorney, Laura Shamp, alleged in the legal complaint that a series of miscommunications and negligence by multiple providers delayed the diagnosis and treatment of the stroke until the next day, which led to catastrophic brain damage for the patient, who developed locked-in syndrome. The rare neurologic syndrome causes complete paralysis except for the muscles that control eye movements.
“Mr. Buckelew has expended millions of dollars for medical expenses for his care and he will need 24 hour a day care for the rest of his life,” his lawyer said in court documents.
Both physicians’ attorneys denied the claims and said their clients met the standard of care.
The jury attributed 60% fault to ED physician Matthew Womack, MD, and 40% to radiologist James Waldschmidt, MD.
Ms. Shamp alleged that Dr. Womack failed to inform the consulting neurologist of the chiropractic neck adjustment – a known stroke risk factor – and did not adequately communicate the results from CT angiography and lumbar puncture.
In addition, she said Dr. Womack failed to rule out a vertebral artery dissection and that Dr. Waldschmidt did not “[appreciate] an indisputable acute or subacute vertebral-basilar artery occlusion.”
Further allegations were levied against several other members of the patient’s care team, including the neurologist, a critical care physician, a physician assistant, and intensive care unit nurses, but they were not found liable by the jury.
The chiropractor, Michael Axt, DC, was named in the original complaint, but court documents filed earlier in 2022 requested that he be dismissed from the lawsuit, stating that he and the patient had reached an amicable resolution.
“This is a very large verdict,” James B. Edwards, JD, a medical malpractice attorney based in Texas who was not involved in the case, said in an interview. The diagnosis of locked-in syndrome likely contributed to the substantial monetary award.
“The more sympathetic the plaintiff and the situation, the greater risk of a verdict [against] the defendants,” Mr. Edwards said. “Cases that elicit significant and sometimes decisive sympathy include locked-in syndrome, permanent vegetative state, injury to the sexual or reproductive organs, burns, and blindness.”
The effectiveness and safety of chiropractic adjustments often come under fire. Although postmanipulation injuries are not common, they can have near-fatal consequences when they do occur.
In August, a healthy 28-year-old college student experienced four artery dissections after a chiropractic visit for low-back pain. She subsequently had a stroke and went into cardiac arrest. The patient survived but remains paralyzed.
Mr. Buckelew’s legal team said in a statement that his injuries would have been completely avoided had “the slew of health care providers ... acted according to the standard of care, caught and treated his stroke earlier, and communicated more effectively.”
On the day of the chiropractic adjustment, Ms. Shamp said Mr. Axt had documented that Mr. Buckelew’s primary complaints – neck pain, a headache, and bouts of blurred vision and ringing in the ears – began after exercise and had continued for several days.
In his closing statement, Dr. Womack’s attorney said the “chiropractor is solely responsible” for the patient’s injuries because he performed a manipulation despite the patient having a 2-week history of headaches.
Very few medical malpractice verdicts are appealed, though the sizable award in this suit may increase the likelihood that the defense will do so, Mr. Edwards said.
A version of this article first appeared on Medscape.com.
The patient, Jonathan Buckelew, was taken to North Fulton Regional Hospital in Roswell, Ga., where imaging revealed that he had suffered a brain stem stroke.
The patient’s attorney, Laura Shamp, alleged in the legal complaint that a series of miscommunications and negligence by multiple providers delayed the diagnosis and treatment of the stroke until the next day, which led to catastrophic brain damage for the patient, who developed locked-in syndrome. The rare neurologic syndrome causes complete paralysis except for the muscles that control eye movements.
“Mr. Buckelew has expended millions of dollars for medical expenses for his care and he will need 24 hour a day care for the rest of his life,” his lawyer said in court documents.
Both physicians’ attorneys denied the claims and said their clients met the standard of care.
The jury attributed 60% fault to ED physician Matthew Womack, MD, and 40% to radiologist James Waldschmidt, MD.
Ms. Shamp alleged that Dr. Womack failed to inform the consulting neurologist of the chiropractic neck adjustment – a known stroke risk factor – and did not adequately communicate the results from CT angiography and lumbar puncture.
In addition, she said Dr. Womack failed to rule out a vertebral artery dissection and that Dr. Waldschmidt did not “[appreciate] an indisputable acute or subacute vertebral-basilar artery occlusion.”
Further allegations were levied against several other members of the patient’s care team, including the neurologist, a critical care physician, a physician assistant, and intensive care unit nurses, but they were not found liable by the jury.
The chiropractor, Michael Axt, DC, was named in the original complaint, but court documents filed earlier in 2022 requested that he be dismissed from the lawsuit, stating that he and the patient had reached an amicable resolution.
“This is a very large verdict,” James B. Edwards, JD, a medical malpractice attorney based in Texas who was not involved in the case, said in an interview. The diagnosis of locked-in syndrome likely contributed to the substantial monetary award.
“The more sympathetic the plaintiff and the situation, the greater risk of a verdict [against] the defendants,” Mr. Edwards said. “Cases that elicit significant and sometimes decisive sympathy include locked-in syndrome, permanent vegetative state, injury to the sexual or reproductive organs, burns, and blindness.”
The effectiveness and safety of chiropractic adjustments often come under fire. Although postmanipulation injuries are not common, they can have near-fatal consequences when they do occur.
In August, a healthy 28-year-old college student experienced four artery dissections after a chiropractic visit for low-back pain. She subsequently had a stroke and went into cardiac arrest. The patient survived but remains paralyzed.
Mr. Buckelew’s legal team said in a statement that his injuries would have been completely avoided had “the slew of health care providers ... acted according to the standard of care, caught and treated his stroke earlier, and communicated more effectively.”
On the day of the chiropractic adjustment, Ms. Shamp said Mr. Axt had documented that Mr. Buckelew’s primary complaints – neck pain, a headache, and bouts of blurred vision and ringing in the ears – began after exercise and had continued for several days.
In his closing statement, Dr. Womack’s attorney said the “chiropractor is solely responsible” for the patient’s injuries because he performed a manipulation despite the patient having a 2-week history of headaches.
Very few medical malpractice verdicts are appealed, though the sizable award in this suit may increase the likelihood that the defense will do so, Mr. Edwards said.
A version of this article first appeared on Medscape.com.
Medicare fines for high hospital readmissions drop, but nearly 2,300 facilities are still penalized
resulting in the lightest penalties since 2014.
The Hospital Readmissions Reduction Program has been a mainstay of Medicare’s hospital payment system since it began in 2012. Created by the Affordable Care Act, the program evaluates the frequency with which Medicare patients at most hospitals return within 30 days and lowers future payments to hospitals that had a greater-than-expected rate of return. Hospitals can lose up to 3% of each Medicare payment for a year.
The pandemic threw hospitals into turmoil, inundating them with COVID patients while forcing many to postpone elective surgeries for months. When the Centers for Medicare & Medicaid Services evaluated hospitals’ previous 3 years of readmissions, as it does annually, the government decided to exclude the first half of 2020 because of the chaos caused by the pandemic. CMS also excluded from its calculations Medicare patients who were readmitted with pneumonia across all three years because of the difficulty in distinguishing them from patients with COVID.
Akin Demehin, senior director of quality and patient safety policy at the American Hospital Association, said the changes were warranted. “The COVID pandemic did a lot of really unprecedented things to care patterns of hospitals,” he said.
After making those changes, CMS evaluated 2½ years of readmission cases for Medicare patients who’d had heart failure, heart attacks, chronic obstructive pulmonary disease, coronary artery bypass grafts, and knee and hip replacements. As a result of its analysis, CMS penalized 2,273 hospitals, the fewest since the fiscal year that ended in September 2014, a KHN analysis found.
The average payment reduction was 0.43%, also the lowest since 2014. The reductions will be applied to each Medicare payment to the affected hospitals from Oct. 1 to next September and cost them $320 million over that 12-month period.
Some hospitals will see their penalties greatly reduced from 2021. The penalty on St. Mary’s Hospital in Athens, Ga., is dropping from 2.54% to 0.06%. Saint Joseph East in Lexington, Ky., received the maximum penalty, 3%, in 2021; it will lose 0.78% as of Oct. 1. In Flemington, N.J., the penalty for Hunterdon Medical Center is dropping from 2.29% to 0.12%.
To limit penalties, many hospitals in recent years have instituted new strategies to keep former patients from needing a return visit. Robert Coates, MD, interim chief medical officer at Hunterdon Health, which owns Hunterdon Medical Center, said in a statement that the hospital set up a system to identify patients who visited the emergency room within 30 days of a hospital stay. Instead of readmitting them, Hunterdon helps them set up next-day appointments at a doctor’s office or home monitoring of their health. Hunterdon also calls all discharged patients to ensure they have filled their prescriptions and had a follow-up visit with a clinician within a week of leaving the hospital.
Jessica Satterfield, MD, director of quality and clinical excellence at St. Mary’s Health Care System, which operates St. Mary’s Hospital, said in a statement that the hospital identified patients at risk of readmission when they were first admitted and focused on making sure that their medications were correct and that they had follow-up visits. “We are proud that our efforts are bearing fruit in the form of greatly reduced penalties but, more importantly, as a reflection of the exceptional care our staff and medical staff provide to our patients,” Dr. Satterfield said.
Saint Joseph East did not respond to emails seeking comment.
Despite the changes, 43% of the nation’s 5,236 hospitals were penalized. Of the unpenalized, all but 770 were automatically exempted. The 2,193 exempted hospitals include those that specialize in children, psychiatric patients, or veterans. Rehabilitation and long-term care hospitals are also excluded from the program, as are critical access hospitals, which Medicare pays differently to help them stay open in areas with no other hospitals. The government also exempted Maryland hospitals because that state has a special payment arrangement with Medicare. Of the hospitals that Medicare assessed, 75% were penalized.
For the new fiscal year, Medicare also cited the pandemic in giving hospitals a reprieve from its other major quality-focused effort that assesses penalties: the Hospital-Acquired Condition Reduction Program. It slashes Medicare payments by 1% to the quarter of general hospitals with the highest rates of infections and other potentially preventable patient injuries. For the previous fiscal year, CMS punished 764 hospitals under that program. Those penalties – which would have cost hospitals an estimated $350 million in 2022 – will resume next fiscal year, with adjustments that better take COVID patients into account. CMS will also refine the readmissions penalty program to distinguish pneumonia patients from COVID patients.
“COVID has been a tremendously disruptive force for all aspects of health care, most certainly CMS’ quality measurement programs,” Mr. Demehin said. “It’s probably going to be a couple of volatile years for readmission penalties.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
resulting in the lightest penalties since 2014.
The Hospital Readmissions Reduction Program has been a mainstay of Medicare’s hospital payment system since it began in 2012. Created by the Affordable Care Act, the program evaluates the frequency with which Medicare patients at most hospitals return within 30 days and lowers future payments to hospitals that had a greater-than-expected rate of return. Hospitals can lose up to 3% of each Medicare payment for a year.
The pandemic threw hospitals into turmoil, inundating them with COVID patients while forcing many to postpone elective surgeries for months. When the Centers for Medicare & Medicaid Services evaluated hospitals’ previous 3 years of readmissions, as it does annually, the government decided to exclude the first half of 2020 because of the chaos caused by the pandemic. CMS also excluded from its calculations Medicare patients who were readmitted with pneumonia across all three years because of the difficulty in distinguishing them from patients with COVID.
Akin Demehin, senior director of quality and patient safety policy at the American Hospital Association, said the changes were warranted. “The COVID pandemic did a lot of really unprecedented things to care patterns of hospitals,” he said.
After making those changes, CMS evaluated 2½ years of readmission cases for Medicare patients who’d had heart failure, heart attacks, chronic obstructive pulmonary disease, coronary artery bypass grafts, and knee and hip replacements. As a result of its analysis, CMS penalized 2,273 hospitals, the fewest since the fiscal year that ended in September 2014, a KHN analysis found.
The average payment reduction was 0.43%, also the lowest since 2014. The reductions will be applied to each Medicare payment to the affected hospitals from Oct. 1 to next September and cost them $320 million over that 12-month period.
Some hospitals will see their penalties greatly reduced from 2021. The penalty on St. Mary’s Hospital in Athens, Ga., is dropping from 2.54% to 0.06%. Saint Joseph East in Lexington, Ky., received the maximum penalty, 3%, in 2021; it will lose 0.78% as of Oct. 1. In Flemington, N.J., the penalty for Hunterdon Medical Center is dropping from 2.29% to 0.12%.
To limit penalties, many hospitals in recent years have instituted new strategies to keep former patients from needing a return visit. Robert Coates, MD, interim chief medical officer at Hunterdon Health, which owns Hunterdon Medical Center, said in a statement that the hospital set up a system to identify patients who visited the emergency room within 30 days of a hospital stay. Instead of readmitting them, Hunterdon helps them set up next-day appointments at a doctor’s office or home monitoring of their health. Hunterdon also calls all discharged patients to ensure they have filled their prescriptions and had a follow-up visit with a clinician within a week of leaving the hospital.
Jessica Satterfield, MD, director of quality and clinical excellence at St. Mary’s Health Care System, which operates St. Mary’s Hospital, said in a statement that the hospital identified patients at risk of readmission when they were first admitted and focused on making sure that their medications were correct and that they had follow-up visits. “We are proud that our efforts are bearing fruit in the form of greatly reduced penalties but, more importantly, as a reflection of the exceptional care our staff and medical staff provide to our patients,” Dr. Satterfield said.
Saint Joseph East did not respond to emails seeking comment.
Despite the changes, 43% of the nation’s 5,236 hospitals were penalized. Of the unpenalized, all but 770 were automatically exempted. The 2,193 exempted hospitals include those that specialize in children, psychiatric patients, or veterans. Rehabilitation and long-term care hospitals are also excluded from the program, as are critical access hospitals, which Medicare pays differently to help them stay open in areas with no other hospitals. The government also exempted Maryland hospitals because that state has a special payment arrangement with Medicare. Of the hospitals that Medicare assessed, 75% were penalized.
For the new fiscal year, Medicare also cited the pandemic in giving hospitals a reprieve from its other major quality-focused effort that assesses penalties: the Hospital-Acquired Condition Reduction Program. It slashes Medicare payments by 1% to the quarter of general hospitals with the highest rates of infections and other potentially preventable patient injuries. For the previous fiscal year, CMS punished 764 hospitals under that program. Those penalties – which would have cost hospitals an estimated $350 million in 2022 – will resume next fiscal year, with adjustments that better take COVID patients into account. CMS will also refine the readmissions penalty program to distinguish pneumonia patients from COVID patients.
“COVID has been a tremendously disruptive force for all aspects of health care, most certainly CMS’ quality measurement programs,” Mr. Demehin said. “It’s probably going to be a couple of volatile years for readmission penalties.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
resulting in the lightest penalties since 2014.
The Hospital Readmissions Reduction Program has been a mainstay of Medicare’s hospital payment system since it began in 2012. Created by the Affordable Care Act, the program evaluates the frequency with which Medicare patients at most hospitals return within 30 days and lowers future payments to hospitals that had a greater-than-expected rate of return. Hospitals can lose up to 3% of each Medicare payment for a year.
The pandemic threw hospitals into turmoil, inundating them with COVID patients while forcing many to postpone elective surgeries for months. When the Centers for Medicare & Medicaid Services evaluated hospitals’ previous 3 years of readmissions, as it does annually, the government decided to exclude the first half of 2020 because of the chaos caused by the pandemic. CMS also excluded from its calculations Medicare patients who were readmitted with pneumonia across all three years because of the difficulty in distinguishing them from patients with COVID.
Akin Demehin, senior director of quality and patient safety policy at the American Hospital Association, said the changes were warranted. “The COVID pandemic did a lot of really unprecedented things to care patterns of hospitals,” he said.
After making those changes, CMS evaluated 2½ years of readmission cases for Medicare patients who’d had heart failure, heart attacks, chronic obstructive pulmonary disease, coronary artery bypass grafts, and knee and hip replacements. As a result of its analysis, CMS penalized 2,273 hospitals, the fewest since the fiscal year that ended in September 2014, a KHN analysis found.
The average payment reduction was 0.43%, also the lowest since 2014. The reductions will be applied to each Medicare payment to the affected hospitals from Oct. 1 to next September and cost them $320 million over that 12-month period.
Some hospitals will see their penalties greatly reduced from 2021. The penalty on St. Mary’s Hospital in Athens, Ga., is dropping from 2.54% to 0.06%. Saint Joseph East in Lexington, Ky., received the maximum penalty, 3%, in 2021; it will lose 0.78% as of Oct. 1. In Flemington, N.J., the penalty for Hunterdon Medical Center is dropping from 2.29% to 0.12%.
To limit penalties, many hospitals in recent years have instituted new strategies to keep former patients from needing a return visit. Robert Coates, MD, interim chief medical officer at Hunterdon Health, which owns Hunterdon Medical Center, said in a statement that the hospital set up a system to identify patients who visited the emergency room within 30 days of a hospital stay. Instead of readmitting them, Hunterdon helps them set up next-day appointments at a doctor’s office or home monitoring of their health. Hunterdon also calls all discharged patients to ensure they have filled their prescriptions and had a follow-up visit with a clinician within a week of leaving the hospital.
Jessica Satterfield, MD, director of quality and clinical excellence at St. Mary’s Health Care System, which operates St. Mary’s Hospital, said in a statement that the hospital identified patients at risk of readmission when they were first admitted and focused on making sure that their medications were correct and that they had follow-up visits. “We are proud that our efforts are bearing fruit in the form of greatly reduced penalties but, more importantly, as a reflection of the exceptional care our staff and medical staff provide to our patients,” Dr. Satterfield said.
Saint Joseph East did not respond to emails seeking comment.
Despite the changes, 43% of the nation’s 5,236 hospitals were penalized. Of the unpenalized, all but 770 were automatically exempted. The 2,193 exempted hospitals include those that specialize in children, psychiatric patients, or veterans. Rehabilitation and long-term care hospitals are also excluded from the program, as are critical access hospitals, which Medicare pays differently to help them stay open in areas with no other hospitals. The government also exempted Maryland hospitals because that state has a special payment arrangement with Medicare. Of the hospitals that Medicare assessed, 75% were penalized.
For the new fiscal year, Medicare also cited the pandemic in giving hospitals a reprieve from its other major quality-focused effort that assesses penalties: the Hospital-Acquired Condition Reduction Program. It slashes Medicare payments by 1% to the quarter of general hospitals with the highest rates of infections and other potentially preventable patient injuries. For the previous fiscal year, CMS punished 764 hospitals under that program. Those penalties – which would have cost hospitals an estimated $350 million in 2022 – will resume next fiscal year, with adjustments that better take COVID patients into account. CMS will also refine the readmissions penalty program to distinguish pneumonia patients from COVID patients.
“COVID has been a tremendously disruptive force for all aspects of health care, most certainly CMS’ quality measurement programs,” Mr. Demehin said. “It’s probably going to be a couple of volatile years for readmission penalties.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
‘Unappreciated’ ties between COVID and gut dysbiosis
(BSIs), new research suggests.
“Collectively, these results reveal an unappreciated link between SARS-CoV-2 infection, gut microbiome dysbiosis, and a severe complication of COVID-19, BSIs,” the study team reported in Nature Communications.
“Our findings suggest that coronavirus infection directly interferes with the healthy balance of microbes in the gut, further endangering patients in the process,” microbiologist and co–senior author Ken Cadwell, PhD, New York University, added in a news release. “Now that we have uncovered the source of this bacterial imbalance, physicians can better identify those coronavirus patients most at risk of a secondary bloodstream infection.”
In a mouse model, the researchers first demonstrated that the SARS-CoV-2 infection alone induces gut microbiome dysbiosis and gut epithelial cell alterations, which correlate with markers of gut barrier permeability.
Next, they analyzed the bacterial composition of stool samples from 96 adults hospitalized with COVID-19 in 2020 in New York and New Haven, Conn.
In line with their observations in mice, they found that the SARS-CoV-2 infection is associated with “severe microbiome injury,” characterized by the loss of gut microbiome diversity.
They also observed an increase in populations of several microbes known to include antibiotic-resistant species. An analysis of stool samples paired with blood cultures found that antibiotic-resistant bacteria in the gut migrated to the bloodstream in 20% of patients.
This migration could be caused by a combination of the immune-compromising effects of the viral infection and the antibiotic-driven depletion of commensal gut microbes, the researchers said.
However, COVID-19 patients are also uniquely exposed to other potential factors predisposing them to bacteremia, including immunosuppressive drugs, long hospital stays, and catheters, the investigators noted. The study is limited in its ability to investigate the individual effects of these factors.
“Our findings support a scenario in which gut-to-blood translocation of microorganisms following microbiome dysbiosis leads to dangerous BSIs during COVID-19, a complication seen in other immunocompromised patients, including patients with cancer, acute respiratory distress syndrome, and in ICU patients receiving probiotics,” the researchers wrote.
Investigating the underlying mechanism behind their observations could help inform “the judicious application of antibiotics and immunosuppressives in patients with respiratory viral infections and increase our resilience to pandemics,” they added.
Funding for the study was provided by the National Institutes of Health, the Yale School of Public Health, and numerous other sources. Dr. Cadwell has received research support from Pfizer, Takeda, Pacific Biosciences, Genentech, and AbbVie; consulted for or received an honoraria from PureTech Health, Genentech, and AbbVie; and is named as an inventor on US patent 10,722,600 and provisional patents 62/935,035 and 63/157,225.
A version of this article first appeared on Medscape.com.
(BSIs), new research suggests.
“Collectively, these results reveal an unappreciated link between SARS-CoV-2 infection, gut microbiome dysbiosis, and a severe complication of COVID-19, BSIs,” the study team reported in Nature Communications.
“Our findings suggest that coronavirus infection directly interferes with the healthy balance of microbes in the gut, further endangering patients in the process,” microbiologist and co–senior author Ken Cadwell, PhD, New York University, added in a news release. “Now that we have uncovered the source of this bacterial imbalance, physicians can better identify those coronavirus patients most at risk of a secondary bloodstream infection.”
In a mouse model, the researchers first demonstrated that the SARS-CoV-2 infection alone induces gut microbiome dysbiosis and gut epithelial cell alterations, which correlate with markers of gut barrier permeability.
Next, they analyzed the bacterial composition of stool samples from 96 adults hospitalized with COVID-19 in 2020 in New York and New Haven, Conn.
In line with their observations in mice, they found that the SARS-CoV-2 infection is associated with “severe microbiome injury,” characterized by the loss of gut microbiome diversity.
They also observed an increase in populations of several microbes known to include antibiotic-resistant species. An analysis of stool samples paired with blood cultures found that antibiotic-resistant bacteria in the gut migrated to the bloodstream in 20% of patients.
This migration could be caused by a combination of the immune-compromising effects of the viral infection and the antibiotic-driven depletion of commensal gut microbes, the researchers said.
However, COVID-19 patients are also uniquely exposed to other potential factors predisposing them to bacteremia, including immunosuppressive drugs, long hospital stays, and catheters, the investigators noted. The study is limited in its ability to investigate the individual effects of these factors.
“Our findings support a scenario in which gut-to-blood translocation of microorganisms following microbiome dysbiosis leads to dangerous BSIs during COVID-19, a complication seen in other immunocompromised patients, including patients with cancer, acute respiratory distress syndrome, and in ICU patients receiving probiotics,” the researchers wrote.
Investigating the underlying mechanism behind their observations could help inform “the judicious application of antibiotics and immunosuppressives in patients with respiratory viral infections and increase our resilience to pandemics,” they added.
Funding for the study was provided by the National Institutes of Health, the Yale School of Public Health, and numerous other sources. Dr. Cadwell has received research support from Pfizer, Takeda, Pacific Biosciences, Genentech, and AbbVie; consulted for or received an honoraria from PureTech Health, Genentech, and AbbVie; and is named as an inventor on US patent 10,722,600 and provisional patents 62/935,035 and 63/157,225.
A version of this article first appeared on Medscape.com.
(BSIs), new research suggests.
“Collectively, these results reveal an unappreciated link between SARS-CoV-2 infection, gut microbiome dysbiosis, and a severe complication of COVID-19, BSIs,” the study team reported in Nature Communications.
“Our findings suggest that coronavirus infection directly interferes with the healthy balance of microbes in the gut, further endangering patients in the process,” microbiologist and co–senior author Ken Cadwell, PhD, New York University, added in a news release. “Now that we have uncovered the source of this bacterial imbalance, physicians can better identify those coronavirus patients most at risk of a secondary bloodstream infection.”
In a mouse model, the researchers first demonstrated that the SARS-CoV-2 infection alone induces gut microbiome dysbiosis and gut epithelial cell alterations, which correlate with markers of gut barrier permeability.
Next, they analyzed the bacterial composition of stool samples from 96 adults hospitalized with COVID-19 in 2020 in New York and New Haven, Conn.
In line with their observations in mice, they found that the SARS-CoV-2 infection is associated with “severe microbiome injury,” characterized by the loss of gut microbiome diversity.
They also observed an increase in populations of several microbes known to include antibiotic-resistant species. An analysis of stool samples paired with blood cultures found that antibiotic-resistant bacteria in the gut migrated to the bloodstream in 20% of patients.
This migration could be caused by a combination of the immune-compromising effects of the viral infection and the antibiotic-driven depletion of commensal gut microbes, the researchers said.
However, COVID-19 patients are also uniquely exposed to other potential factors predisposing them to bacteremia, including immunosuppressive drugs, long hospital stays, and catheters, the investigators noted. The study is limited in its ability to investigate the individual effects of these factors.
“Our findings support a scenario in which gut-to-blood translocation of microorganisms following microbiome dysbiosis leads to dangerous BSIs during COVID-19, a complication seen in other immunocompromised patients, including patients with cancer, acute respiratory distress syndrome, and in ICU patients receiving probiotics,” the researchers wrote.
Investigating the underlying mechanism behind their observations could help inform “the judicious application of antibiotics and immunosuppressives in patients with respiratory viral infections and increase our resilience to pandemics,” they added.
Funding for the study was provided by the National Institutes of Health, the Yale School of Public Health, and numerous other sources. Dr. Cadwell has received research support from Pfizer, Takeda, Pacific Biosciences, Genentech, and AbbVie; consulted for or received an honoraria from PureTech Health, Genentech, and AbbVie; and is named as an inventor on US patent 10,722,600 and provisional patents 62/935,035 and 63/157,225.
A version of this article first appeared on Medscape.com.
FROM NATURE COMMUNICATIONS
Children and COVID: Weekly cases can’t sustain downward trend
New COVID-19 cases in children inched up in late October, just 1 week after dipping to their lowest level in more than a year, and some measures of pediatric emergency visits and hospital admissions rose as well.
There was an 8% increase in the number of cases for the week of Oct. 21-27, compared with the previous week, but this week’s total was still below 25,000, and the overall trend since the beginning of September is still one of decline, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.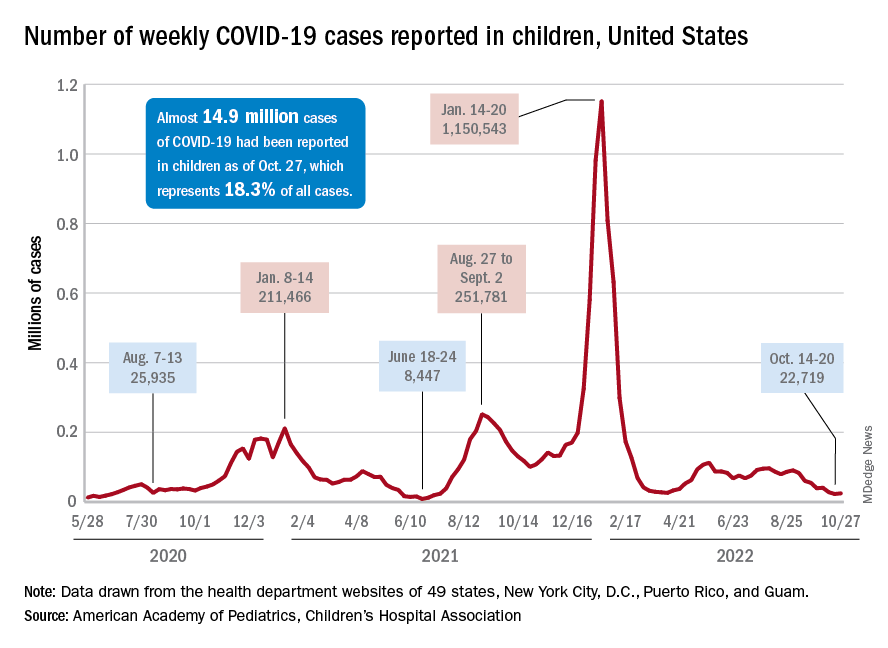
A similar increase can be seen for hospitalizations with confirmed COVID. The rate for children aged 0-17 years fell from 0.44 admissions per 100,000 population at the end of August to 0.16 per 100,000 on Oct. 23. Hospitalizations have since ticked up to 0.17 per 100,000, according to the Centers for Disease Control and Prevention.
Emergency department visits with diagnosed COVID among children aged 16-17 years, as a percentage of all ED visits, rose from 0.6% on Oct. 21 to 0.8% on Oct. 26. ED visits for 12- to 15-year-olds rose from 0.6% to 0.7% at about the same time, with both increases coming after declines that started in late August. No such increase has occurred yet among children aged 0-11 years, the CDC reported on its COVID Data Tracker.
One small milestone reached in the past week involved the proportion of all COVID cases that have occurred in children. The total number of child cases as of Oct. 27 was almost 14.9 million, which represents 18.3% of cases in all Americans, according to the AAP and CHA. That figure had been sitting at 18.4% since mid-August after reaching as high as 19.0% during the spring.
The CDC puts total COVID-related hospital admissions for children aged 0-17 at 163,588 since Aug. 1, 2020, which is 3.0% of all U.S. admissions. Total pediatric deaths number 1,843, or just about 0.2% of all COVID-related fatalities since the start of the pandemic, the CDC data show.
The latest vaccination figures show that 71.3% of children aged 12-17 years have received at least one dose, as have 38.8% of 5- to 11-year-olds, 8.4% of 2- to 4-year-olds, and 5.5% of those under age 2. Full vaccination by age group looks like this: 60.9% (12-17 years), 31.7% (5-11 years), 3.7% (2-4 years), and 2.1% (<2 years), the CDC reported. Almost 30% of children aged 12-17 have gotten a first booster dose, as have 16% of 5- to 11-year-olds.
New COVID-19 cases in children inched up in late October, just 1 week after dipping to their lowest level in more than a year, and some measures of pediatric emergency visits and hospital admissions rose as well.
There was an 8% increase in the number of cases for the week of Oct. 21-27, compared with the previous week, but this week’s total was still below 25,000, and the overall trend since the beginning of September is still one of decline, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
A similar increase can be seen for hospitalizations with confirmed COVID. The rate for children aged 0-17 years fell from 0.44 admissions per 100,000 population at the end of August to 0.16 per 100,000 on Oct. 23. Hospitalizations have since ticked up to 0.17 per 100,000, according to the Centers for Disease Control and Prevention.
Emergency department visits with diagnosed COVID among children aged 16-17 years, as a percentage of all ED visits, rose from 0.6% on Oct. 21 to 0.8% on Oct. 26. ED visits for 12- to 15-year-olds rose from 0.6% to 0.7% at about the same time, with both increases coming after declines that started in late August. No such increase has occurred yet among children aged 0-11 years, the CDC reported on its COVID Data Tracker.
One small milestone reached in the past week involved the proportion of all COVID cases that have occurred in children. The total number of child cases as of Oct. 27 was almost 14.9 million, which represents 18.3% of cases in all Americans, according to the AAP and CHA. That figure had been sitting at 18.4% since mid-August after reaching as high as 19.0% during the spring.
The CDC puts total COVID-related hospital admissions for children aged 0-17 at 163,588 since Aug. 1, 2020, which is 3.0% of all U.S. admissions. Total pediatric deaths number 1,843, or just about 0.2% of all COVID-related fatalities since the start of the pandemic, the CDC data show.
The latest vaccination figures show that 71.3% of children aged 12-17 years have received at least one dose, as have 38.8% of 5- to 11-year-olds, 8.4% of 2- to 4-year-olds, and 5.5% of those under age 2. Full vaccination by age group looks like this: 60.9% (12-17 years), 31.7% (5-11 years), 3.7% (2-4 years), and 2.1% (<2 years), the CDC reported. Almost 30% of children aged 12-17 have gotten a first booster dose, as have 16% of 5- to 11-year-olds.
New COVID-19 cases in children inched up in late October, just 1 week after dipping to their lowest level in more than a year, and some measures of pediatric emergency visits and hospital admissions rose as well.
There was an 8% increase in the number of cases for the week of Oct. 21-27, compared with the previous week, but this week’s total was still below 25,000, and the overall trend since the beginning of September is still one of decline, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
A similar increase can be seen for hospitalizations with confirmed COVID. The rate for children aged 0-17 years fell from 0.44 admissions per 100,000 population at the end of August to 0.16 per 100,000 on Oct. 23. Hospitalizations have since ticked up to 0.17 per 100,000, according to the Centers for Disease Control and Prevention.
Emergency department visits with diagnosed COVID among children aged 16-17 years, as a percentage of all ED visits, rose from 0.6% on Oct. 21 to 0.8% on Oct. 26. ED visits for 12- to 15-year-olds rose from 0.6% to 0.7% at about the same time, with both increases coming after declines that started in late August. No such increase has occurred yet among children aged 0-11 years, the CDC reported on its COVID Data Tracker.
One small milestone reached in the past week involved the proportion of all COVID cases that have occurred in children. The total number of child cases as of Oct. 27 was almost 14.9 million, which represents 18.3% of cases in all Americans, according to the AAP and CHA. That figure had been sitting at 18.4% since mid-August after reaching as high as 19.0% during the spring.
The CDC puts total COVID-related hospital admissions for children aged 0-17 at 163,588 since Aug. 1, 2020, which is 3.0% of all U.S. admissions. Total pediatric deaths number 1,843, or just about 0.2% of all COVID-related fatalities since the start of the pandemic, the CDC data show.
The latest vaccination figures show that 71.3% of children aged 12-17 years have received at least one dose, as have 38.8% of 5- to 11-year-olds, 8.4% of 2- to 4-year-olds, and 5.5% of those under age 2. Full vaccination by age group looks like this: 60.9% (12-17 years), 31.7% (5-11 years), 3.7% (2-4 years), and 2.1% (<2 years), the CDC reported. Almost 30% of children aged 12-17 have gotten a first booster dose, as have 16% of 5- to 11-year-olds.
Best anticoagulant for minimizing bleeding risk identified
A commonly prescribed direct oral anticoagulant (DOAC) has the lowest risk of bleeding, say researchers. Used to prevent strokes in those with atrial fibrillation (AFib), DOACs have recently become more common than warfarin, the previous standard treatment, as they do not require as much follow-up monitoring – which was “particularly valuable” during the COVID-19 pandemic – and have “less risk” of side effects, highlighted the authors of a new study, published in Annals of Internal Medicine.
However, the authors explained that, although current guidelines recommend using DOACs over warfarin in patients with AFib, “head-to-head trial data do not exist to guide the choice of DOAC.” So, they set out to try and fill this evidence gap by doing a large-scale comparison between all DOACs – apixaban, dabigatran, edoxaban, and rivaroxaban – in routine clinical practice.
Wallis Lau, PhD, University College London, and co–lead author, said: “Direct oral anticoagulants have been prescribed with increasing frequency worldwide in recent years, but evidence comparing them directly has been limited.”
One drug stood out
For the multinational population-based cohort study the researchers compared the efficacy and risk of side effects for the four most common DOACs. They reviewed data – from five standardized electronic health care databases that covered 221 million people in the United Kingdom, France, Germany, and the United States – of 527,226 patients who had been newly diagnosed with AFib between 2010 and 2019, and who had received a new DOAC prescription. The study included 281,320 apixaban users, 61,008 dabigatran users, 12,722 edoxaban users, and 172,176 rivaroxaban users.
Database-specific hazard ratios of ischemic stroke or systemic embolism, intracranial hemorrhage, gastrointestinal bleeding, and all-cause mortality between DOACs were estimated using a Cox regression model stratified by propensity score and pooled using a random-effects model.
In total, 9,530 ischemic stroke or systemic embolism events, 841 intercranial hemorrhage events, 8,319 gastrointestinal bleeding events, and 1,476 deaths were identified over the study follow-up. The researchers found that all four drugs were comparable on outcomes for ischemic stroke, intercranial hemorrhage, and all-cause mortality.
However, they identified a difference in the risk of gastrointestinal bleeding, which they highlighted “is one of the most common and concerning side effects of DOACs.”
“Apixaban stood out as having lower risk of gastrointestinal bleeding,” said the authors, with a 19%-28% lower risk when compared directly with each of the other three DOACs. Specifically, apixaban use was associated with lower risk for gastrointestinal bleeding than use of dabigatran (HR, 0.81; 95% confidence interval, 0.70-0.94), edoxaban (HR, 0.77; 95% CI, 0.66-0.91), or rivaroxaban (HR, 0.72; 95% CI, 0.66-0.79).
The researchers also highlighted that their findings held true when looking at data only from those aged over 80, and those with chronic kidney disease, two groups that are “often underrepresented” in clinical trials.
Apixaban may be preferable
The researchers concluded that, compared with dabigatran, edoxaban, and rivaroxaban.
“Our results indicate that apixaban may be preferable to other blood thinners because of the lower rate of gastrointestinal bleeding and similar rates of stroke, a finding that we hope will be supported by randomized controlled trials,” said Dr. Lau.
However, he emphasized that, “as with all medications, potential risks and benefits can differ between people, so considering the full spectrum of outcomes and side effects will still be necessary for each individual patient.”
The authors all declared no conflicting interests.
A version of this article first appeared on Medscape UK.
A commonly prescribed direct oral anticoagulant (DOAC) has the lowest risk of bleeding, say researchers. Used to prevent strokes in those with atrial fibrillation (AFib), DOACs have recently become more common than warfarin, the previous standard treatment, as they do not require as much follow-up monitoring – which was “particularly valuable” during the COVID-19 pandemic – and have “less risk” of side effects, highlighted the authors of a new study, published in Annals of Internal Medicine.
However, the authors explained that, although current guidelines recommend using DOACs over warfarin in patients with AFib, “head-to-head trial data do not exist to guide the choice of DOAC.” So, they set out to try and fill this evidence gap by doing a large-scale comparison between all DOACs – apixaban, dabigatran, edoxaban, and rivaroxaban – in routine clinical practice.
Wallis Lau, PhD, University College London, and co–lead author, said: “Direct oral anticoagulants have been prescribed with increasing frequency worldwide in recent years, but evidence comparing them directly has been limited.”
One drug stood out
For the multinational population-based cohort study the researchers compared the efficacy and risk of side effects for the four most common DOACs. They reviewed data – from five standardized electronic health care databases that covered 221 million people in the United Kingdom, France, Germany, and the United States – of 527,226 patients who had been newly diagnosed with AFib between 2010 and 2019, and who had received a new DOAC prescription. The study included 281,320 apixaban users, 61,008 dabigatran users, 12,722 edoxaban users, and 172,176 rivaroxaban users.
Database-specific hazard ratios of ischemic stroke or systemic embolism, intracranial hemorrhage, gastrointestinal bleeding, and all-cause mortality between DOACs were estimated using a Cox regression model stratified by propensity score and pooled using a random-effects model.
In total, 9,530 ischemic stroke or systemic embolism events, 841 intercranial hemorrhage events, 8,319 gastrointestinal bleeding events, and 1,476 deaths were identified over the study follow-up. The researchers found that all four drugs were comparable on outcomes for ischemic stroke, intercranial hemorrhage, and all-cause mortality.
However, they identified a difference in the risk of gastrointestinal bleeding, which they highlighted “is one of the most common and concerning side effects of DOACs.”
“Apixaban stood out as having lower risk of gastrointestinal bleeding,” said the authors, with a 19%-28% lower risk when compared directly with each of the other three DOACs. Specifically, apixaban use was associated with lower risk for gastrointestinal bleeding than use of dabigatran (HR, 0.81; 95% confidence interval, 0.70-0.94), edoxaban (HR, 0.77; 95% CI, 0.66-0.91), or rivaroxaban (HR, 0.72; 95% CI, 0.66-0.79).
The researchers also highlighted that their findings held true when looking at data only from those aged over 80, and those with chronic kidney disease, two groups that are “often underrepresented” in clinical trials.
Apixaban may be preferable
The researchers concluded that, compared with dabigatran, edoxaban, and rivaroxaban.
“Our results indicate that apixaban may be preferable to other blood thinners because of the lower rate of gastrointestinal bleeding and similar rates of stroke, a finding that we hope will be supported by randomized controlled trials,” said Dr. Lau.
However, he emphasized that, “as with all medications, potential risks and benefits can differ between people, so considering the full spectrum of outcomes and side effects will still be necessary for each individual patient.”
The authors all declared no conflicting interests.
A version of this article first appeared on Medscape UK.
A commonly prescribed direct oral anticoagulant (DOAC) has the lowest risk of bleeding, say researchers. Used to prevent strokes in those with atrial fibrillation (AFib), DOACs have recently become more common than warfarin, the previous standard treatment, as they do not require as much follow-up monitoring – which was “particularly valuable” during the COVID-19 pandemic – and have “less risk” of side effects, highlighted the authors of a new study, published in Annals of Internal Medicine.
However, the authors explained that, although current guidelines recommend using DOACs over warfarin in patients with AFib, “head-to-head trial data do not exist to guide the choice of DOAC.” So, they set out to try and fill this evidence gap by doing a large-scale comparison between all DOACs – apixaban, dabigatran, edoxaban, and rivaroxaban – in routine clinical practice.
Wallis Lau, PhD, University College London, and co–lead author, said: “Direct oral anticoagulants have been prescribed with increasing frequency worldwide in recent years, but evidence comparing them directly has been limited.”
One drug stood out
For the multinational population-based cohort study the researchers compared the efficacy and risk of side effects for the four most common DOACs. They reviewed data – from five standardized electronic health care databases that covered 221 million people in the United Kingdom, France, Germany, and the United States – of 527,226 patients who had been newly diagnosed with AFib between 2010 and 2019, and who had received a new DOAC prescription. The study included 281,320 apixaban users, 61,008 dabigatran users, 12,722 edoxaban users, and 172,176 rivaroxaban users.
Database-specific hazard ratios of ischemic stroke or systemic embolism, intracranial hemorrhage, gastrointestinal bleeding, and all-cause mortality between DOACs were estimated using a Cox regression model stratified by propensity score and pooled using a random-effects model.
In total, 9,530 ischemic stroke or systemic embolism events, 841 intercranial hemorrhage events, 8,319 gastrointestinal bleeding events, and 1,476 deaths were identified over the study follow-up. The researchers found that all four drugs were comparable on outcomes for ischemic stroke, intercranial hemorrhage, and all-cause mortality.
However, they identified a difference in the risk of gastrointestinal bleeding, which they highlighted “is one of the most common and concerning side effects of DOACs.”
“Apixaban stood out as having lower risk of gastrointestinal bleeding,” said the authors, with a 19%-28% lower risk when compared directly with each of the other three DOACs. Specifically, apixaban use was associated with lower risk for gastrointestinal bleeding than use of dabigatran (HR, 0.81; 95% confidence interval, 0.70-0.94), edoxaban (HR, 0.77; 95% CI, 0.66-0.91), or rivaroxaban (HR, 0.72; 95% CI, 0.66-0.79).
The researchers also highlighted that their findings held true when looking at data only from those aged over 80, and those with chronic kidney disease, two groups that are “often underrepresented” in clinical trials.
Apixaban may be preferable
The researchers concluded that, compared with dabigatran, edoxaban, and rivaroxaban.
“Our results indicate that apixaban may be preferable to other blood thinners because of the lower rate of gastrointestinal bleeding and similar rates of stroke, a finding that we hope will be supported by randomized controlled trials,” said Dr. Lau.
However, he emphasized that, “as with all medications, potential risks and benefits can differ between people, so considering the full spectrum of outcomes and side effects will still be necessary for each individual patient.”
The authors all declared no conflicting interests.
A version of this article first appeared on Medscape UK.
FROM ANNALS OF INTERNAL MEDICINE
Sexual assault–related visits to the ED are on the rise
Data from the Federal Bureau of Investigation show an increase in reported rapes and sexual assaults (SAs) since 2006, and studies of victims show an increased risk of conditions such as suicidal ideation, PTSD, depression, substance use, and chronic conditions, write Emily L. Vogt of the University of Michigan, Ann Arbor, and colleagues.
However, trends and disparities in ED use by adults seeking care following SA have not been explored, they said.
For a study that was published in JAMA Network Open, researchers reviewed data from the Nationwide Emergency Department Sample (NEDS), a large, nationally representative database managed by the Agency for Healthcare Research and Quality. The dataset consisted of 120 million to 143 million weighted ED visits reported annually from 2006 through 2016. The study population included adults aged 18-65 years who had made an ED visit that was recorded in the NEDS and that was coded as an SA. SA was defined using ICD-9 codes until the fourth quarter of 2015, at which time ICD-10 codes came into use.
Overall, the number of SA-related ED visits increased by 1,533.0% during the study period, from 3,607 in 2006 to 55,296 in 2019. The average annual percentage change was 23.0% (P < .001). The greatest increase occurred from 2015 to 2016, when annual visits increased from 17,709 to 47,732. This increase likely reflected the updated ICD-10 codes, in which there are categories for suspected adult rape, confirmed adult rape, and adult forced sexual exploitation, the researchers note.
Patients presenting to the ED after an SA were mainly women (91.5%). Individuals aged 18-25 years accounted for nearly half of the presentations. Individuals in the lowest and second-lowest income quartiles also were overrepresented.
Despite the increased presentation to EDs, admission rates for SA decreased, from 12.6% to 4.3%, the researchers note. Patients who were older and were insured through Medicaid were more likely to be admitted than persons of other demographic groups.
The researchers also found that increases in ED presentations outpaced increases in SA reports to law enforcement. They compared the ED trends with FBI-reported rapes/SAs from 2015 to 2019 and found increases of 7% and 22% during the times of ICD-9 and ICD-10 codes, respectively. However, in 2019, the number of SA survivors who sought ED care remained below the number who reported to law enforcement (55,296 vs. 139,815, as determined on the basis of revised SA definitions).
“Although the association between increased coding specificity and documentation of SA is still unclear, ICD-10 likely contributed to increased ED documentation of SA,” but the data show steady increases that are independent of the coding change, the researchers write.
The study findings were limited by several factors, including the potential for multiple representations of patients, coding errors associated with the NEDS database, and the reliance on voluntary reports in the NEDS and FBI datasets, the researchers note. The results were strengthened by the large, diverse sample size and by the inclusion of hospital admissions and crime data for comparison, they say.
“As few as 21% of survivors seek medical care after SA, meaning that the survivors captured in this study represent a fraction of total SA-related care need,” the researchers write. “Our finding that most SA ED visits are by young, female, and low-income survivors can inform policy changes to better support these individuals,” which could include the development of outpatient and longitudinal care settings to better serve these populations, they conclude.
Better understanding not only of the trends underlying SA reporting but also of the demographics of survivors who seek treatment and evaluation after SA is vital, said Robert Glatter, MD, in an interview.
“Being able to better understand how social and societal movements affect a patient’s comfort in reporting an SA is vital in tracking the numbers of people who seek care in the ED,” said Dr. Glatter, an emergency medicine physician at Lenox Hill Hospital at Northwell Health, New York, and also of Hofstra University, Hempstead, N.Y.
Dr. Glatter said he was not surprised by the significant increase in sexual assault presentations, especially in light of increased awareness and the influence of the #MeToo movement and other social justice movements over the past decade.
“While I believe that victims of sexual violence may now feel more empowered to report an assault, the volume of SA that go unreported remains a serious public health issue and concern” in the United States and globally, he emphasized.
A key message from the current study is that there is a need for investment in “compassionate and comprehensive care for all survivors of SA,” Dr. Glatter said. “This includes recognition of the extensive mental health consequences of SA that can lead to not only depression, PTSD, and anxiety but also to suicidal ideation and suicide. The longer-term medical effects become life altering, permeating families and future generations,” he emphasized.
“As a society, we must also place a strong emphasis on caring for all SA survivors, but particularly those who come from economically or socially disadvantaged backgrounds who are uninsured or underinsured,” Dr. Glatter said. Issues of race, gender identity, and sexual identity among SA survivors also must be taken into consideration, he added.
“We need to better understand how our health care system can provide more nuanced follow-up care and reporting for survivors in outpatient settings. … Making access easier, while ensuring confidentiality, will allow more survivors of SA to seek treatment and care,” he said. “We also need to understand how using forensic nurses in this capacity, and beyond the ED, can better serve minority and racially diverse communities” and to increase the recruitment and training of such specialized nurses to care for SA victims, Dr. Glatter noted.
The study was supported by internal funding from the University of Michigan and the department of obstetrics and gynecology. Corresponding author Erica C. Marsh, MD, has received personal fees from Myovant Sciences and Pfizer unrelated to the current study. Dr. Glatter has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Data from the Federal Bureau of Investigation show an increase in reported rapes and sexual assaults (SAs) since 2006, and studies of victims show an increased risk of conditions such as suicidal ideation, PTSD, depression, substance use, and chronic conditions, write Emily L. Vogt of the University of Michigan, Ann Arbor, and colleagues.
However, trends and disparities in ED use by adults seeking care following SA have not been explored, they said.
For a study that was published in JAMA Network Open, researchers reviewed data from the Nationwide Emergency Department Sample (NEDS), a large, nationally representative database managed by the Agency for Healthcare Research and Quality. The dataset consisted of 120 million to 143 million weighted ED visits reported annually from 2006 through 2016. The study population included adults aged 18-65 years who had made an ED visit that was recorded in the NEDS and that was coded as an SA. SA was defined using ICD-9 codes until the fourth quarter of 2015, at which time ICD-10 codes came into use.
Overall, the number of SA-related ED visits increased by 1,533.0% during the study period, from 3,607 in 2006 to 55,296 in 2019. The average annual percentage change was 23.0% (P < .001). The greatest increase occurred from 2015 to 2016, when annual visits increased from 17,709 to 47,732. This increase likely reflected the updated ICD-10 codes, in which there are categories for suspected adult rape, confirmed adult rape, and adult forced sexual exploitation, the researchers note.
Patients presenting to the ED after an SA were mainly women (91.5%). Individuals aged 18-25 years accounted for nearly half of the presentations. Individuals in the lowest and second-lowest income quartiles also were overrepresented.
Despite the increased presentation to EDs, admission rates for SA decreased, from 12.6% to 4.3%, the researchers note. Patients who were older and were insured through Medicaid were more likely to be admitted than persons of other demographic groups.
The researchers also found that increases in ED presentations outpaced increases in SA reports to law enforcement. They compared the ED trends with FBI-reported rapes/SAs from 2015 to 2019 and found increases of 7% and 22% during the times of ICD-9 and ICD-10 codes, respectively. However, in 2019, the number of SA survivors who sought ED care remained below the number who reported to law enforcement (55,296 vs. 139,815, as determined on the basis of revised SA definitions).
“Although the association between increased coding specificity and documentation of SA is still unclear, ICD-10 likely contributed to increased ED documentation of SA,” but the data show steady increases that are independent of the coding change, the researchers write.
The study findings were limited by several factors, including the potential for multiple representations of patients, coding errors associated with the NEDS database, and the reliance on voluntary reports in the NEDS and FBI datasets, the researchers note. The results were strengthened by the large, diverse sample size and by the inclusion of hospital admissions and crime data for comparison, they say.
“As few as 21% of survivors seek medical care after SA, meaning that the survivors captured in this study represent a fraction of total SA-related care need,” the researchers write. “Our finding that most SA ED visits are by young, female, and low-income survivors can inform policy changes to better support these individuals,” which could include the development of outpatient and longitudinal care settings to better serve these populations, they conclude.
Better understanding not only of the trends underlying SA reporting but also of the demographics of survivors who seek treatment and evaluation after SA is vital, said Robert Glatter, MD, in an interview.
“Being able to better understand how social and societal movements affect a patient’s comfort in reporting an SA is vital in tracking the numbers of people who seek care in the ED,” said Dr. Glatter, an emergency medicine physician at Lenox Hill Hospital at Northwell Health, New York, and also of Hofstra University, Hempstead, N.Y.
Dr. Glatter said he was not surprised by the significant increase in sexual assault presentations, especially in light of increased awareness and the influence of the #MeToo movement and other social justice movements over the past decade.
“While I believe that victims of sexual violence may now feel more empowered to report an assault, the volume of SA that go unreported remains a serious public health issue and concern” in the United States and globally, he emphasized.
A key message from the current study is that there is a need for investment in “compassionate and comprehensive care for all survivors of SA,” Dr. Glatter said. “This includes recognition of the extensive mental health consequences of SA that can lead to not only depression, PTSD, and anxiety but also to suicidal ideation and suicide. The longer-term medical effects become life altering, permeating families and future generations,” he emphasized.
“As a society, we must also place a strong emphasis on caring for all SA survivors, but particularly those who come from economically or socially disadvantaged backgrounds who are uninsured or underinsured,” Dr. Glatter said. Issues of race, gender identity, and sexual identity among SA survivors also must be taken into consideration, he added.
“We need to better understand how our health care system can provide more nuanced follow-up care and reporting for survivors in outpatient settings. … Making access easier, while ensuring confidentiality, will allow more survivors of SA to seek treatment and care,” he said. “We also need to understand how using forensic nurses in this capacity, and beyond the ED, can better serve minority and racially diverse communities” and to increase the recruitment and training of such specialized nurses to care for SA victims, Dr. Glatter noted.
The study was supported by internal funding from the University of Michigan and the department of obstetrics and gynecology. Corresponding author Erica C. Marsh, MD, has received personal fees from Myovant Sciences and Pfizer unrelated to the current study. Dr. Glatter has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Data from the Federal Bureau of Investigation show an increase in reported rapes and sexual assaults (SAs) since 2006, and studies of victims show an increased risk of conditions such as suicidal ideation, PTSD, depression, substance use, and chronic conditions, write Emily L. Vogt of the University of Michigan, Ann Arbor, and colleagues.
However, trends and disparities in ED use by adults seeking care following SA have not been explored, they said.
For a study that was published in JAMA Network Open, researchers reviewed data from the Nationwide Emergency Department Sample (NEDS), a large, nationally representative database managed by the Agency for Healthcare Research and Quality. The dataset consisted of 120 million to 143 million weighted ED visits reported annually from 2006 through 2016. The study population included adults aged 18-65 years who had made an ED visit that was recorded in the NEDS and that was coded as an SA. SA was defined using ICD-9 codes until the fourth quarter of 2015, at which time ICD-10 codes came into use.
Overall, the number of SA-related ED visits increased by 1,533.0% during the study period, from 3,607 in 2006 to 55,296 in 2019. The average annual percentage change was 23.0% (P < .001). The greatest increase occurred from 2015 to 2016, when annual visits increased from 17,709 to 47,732. This increase likely reflected the updated ICD-10 codes, in which there are categories for suspected adult rape, confirmed adult rape, and adult forced sexual exploitation, the researchers note.
Patients presenting to the ED after an SA were mainly women (91.5%). Individuals aged 18-25 years accounted for nearly half of the presentations. Individuals in the lowest and second-lowest income quartiles also were overrepresented.
Despite the increased presentation to EDs, admission rates for SA decreased, from 12.6% to 4.3%, the researchers note. Patients who were older and were insured through Medicaid were more likely to be admitted than persons of other demographic groups.
The researchers also found that increases in ED presentations outpaced increases in SA reports to law enforcement. They compared the ED trends with FBI-reported rapes/SAs from 2015 to 2019 and found increases of 7% and 22% during the times of ICD-9 and ICD-10 codes, respectively. However, in 2019, the number of SA survivors who sought ED care remained below the number who reported to law enforcement (55,296 vs. 139,815, as determined on the basis of revised SA definitions).
“Although the association between increased coding specificity and documentation of SA is still unclear, ICD-10 likely contributed to increased ED documentation of SA,” but the data show steady increases that are independent of the coding change, the researchers write.
The study findings were limited by several factors, including the potential for multiple representations of patients, coding errors associated with the NEDS database, and the reliance on voluntary reports in the NEDS and FBI datasets, the researchers note. The results were strengthened by the large, diverse sample size and by the inclusion of hospital admissions and crime data for comparison, they say.
“As few as 21% of survivors seek medical care after SA, meaning that the survivors captured in this study represent a fraction of total SA-related care need,” the researchers write. “Our finding that most SA ED visits are by young, female, and low-income survivors can inform policy changes to better support these individuals,” which could include the development of outpatient and longitudinal care settings to better serve these populations, they conclude.
Better understanding not only of the trends underlying SA reporting but also of the demographics of survivors who seek treatment and evaluation after SA is vital, said Robert Glatter, MD, in an interview.
“Being able to better understand how social and societal movements affect a patient’s comfort in reporting an SA is vital in tracking the numbers of people who seek care in the ED,” said Dr. Glatter, an emergency medicine physician at Lenox Hill Hospital at Northwell Health, New York, and also of Hofstra University, Hempstead, N.Y.
Dr. Glatter said he was not surprised by the significant increase in sexual assault presentations, especially in light of increased awareness and the influence of the #MeToo movement and other social justice movements over the past decade.
“While I believe that victims of sexual violence may now feel more empowered to report an assault, the volume of SA that go unreported remains a serious public health issue and concern” in the United States and globally, he emphasized.
A key message from the current study is that there is a need for investment in “compassionate and comprehensive care for all survivors of SA,” Dr. Glatter said. “This includes recognition of the extensive mental health consequences of SA that can lead to not only depression, PTSD, and anxiety but also to suicidal ideation and suicide. The longer-term medical effects become life altering, permeating families and future generations,” he emphasized.
“As a society, we must also place a strong emphasis on caring for all SA survivors, but particularly those who come from economically or socially disadvantaged backgrounds who are uninsured or underinsured,” Dr. Glatter said. Issues of race, gender identity, and sexual identity among SA survivors also must be taken into consideration, he added.
“We need to better understand how our health care system can provide more nuanced follow-up care and reporting for survivors in outpatient settings. … Making access easier, while ensuring confidentiality, will allow more survivors of SA to seek treatment and care,” he said. “We also need to understand how using forensic nurses in this capacity, and beyond the ED, can better serve minority and racially diverse communities” and to increase the recruitment and training of such specialized nurses to care for SA victims, Dr. Glatter noted.
The study was supported by internal funding from the University of Michigan and the department of obstetrics and gynecology. Corresponding author Erica C. Marsh, MD, has received personal fees from Myovant Sciences and Pfizer unrelated to the current study. Dr. Glatter has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Kidney function may help docs pick antiplatelet mix after stroke
Renal function should be considered when determining whether to pick ticagrelor-aspirin or clopidogrel-aspirin as the antiplatelet therapy for patients with minor stroke, according to new research.
The study, which was conducted in 202 centers in China and published in Annals of Internal Medicine, indicates that when patients had normal kidney function, ticagrelor-aspirin, compared with clopidogrel-aspirin, substantially reduced the risk for recurrent stroke within 90 days of follow-up.
However, this effect was not seen in patients with mildly, moderately or severely decreased kidney function.
Rates of severe or moderate bleeding did not differ substantially between the two treatments.
Results gleaned from CHANCE-2 data
The researchers, led by Anxin Wang, PhD, from Capital Medical University in Beijing, conducted a post hoc analysis of the CHANCE-2 (Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events-II) trial.
The trial included 6,378 patients who carried cytochrome P450 2C19 (CYP2C19) loss-of-function (LOF) alleles who had experienced a minor stroke or transient ischemic attack.
Patients received either ticagrelor-aspirin or clopidogrel-aspirin, and their renal function was measured by estimated glomerular filtration rate. The authors listed as a limitation that no data were available on the presence of albuminuria or proteinuria.
The researchers investigated what effect renal function had on the efficacy and safety of the therapies.
Differences in the therapies
Clopidogrel-aspirin is often recommended for preventing stroke. It can reduce thrombotic risk in patients with impaired kidney function, the authors noted. Ticagrelor can provide greater, faster, and more consistent P2Y12 inhibition than clopidogrel, and evidence shows it is effective in preventing stroke recurrence, particularly in people carrying CYP2C19 LOF alleles.
When people have reduced kidney function, clopidogrel may be harder to clear than ticagrelor and there may be increased plasma concentrations, so function is important to consider when choosing an antiplatelet therapy, the authors wrote.
Choice may come down to cost
Geoffrey Barnes, MD, MSc, associate professor of vascular and cardiovascular medicine at University of Michigan Medicine in Ann Arbor, said in an interview that there has been momentum toward ticagrelor as a more potent choice than clopidogrel not just in populations with minor stroke but for people with MI and coronary stents.
He said he found the results surprising and was intrigued that this paper suggests looking more skeptically at ticagrelor when kidney function is impaired.
Still, the choice may also come down to what the patient can afford at the pharmacy, he said.
“The reality is many patients still get clopidogrel either because that’s what their physicians have been prescribing for well over a decade or because of cost issues, and clopidogrel, for many patients, can be less expensive,” Dr. Barnes noted.
He said he would like to see more study in different populations as the prevalence of people carrying CYP2C19 allele differs by race and results might be different in a non-Asian population. That allele is thought to affect how clopidogrel is metabolized.
Study should spur more research
Nada El Husseini, MD, associate professor of neurology and Duke Telestroke Medical Director at Duke University Medical Center, Durham, N.C., said the study is hypothesis generating, but shouldn’t be thought of as the last word on the subject.
She pointed out some additional limitations of the study, including that it was a post hoc analysis. She explained that the question researchers asked in this study – about effect of kidney function on the safety and efficacy of the therapies – was not the focus of the original CHANCE-2 study, and, as such, the post hoc study may have been underpowered to answer the renal function question.
The authors acknowledged that limitation, noting that “the proportion of patients with severely decreased renal function was low.”
Among 6,378 patients, 4,050 (63.5%) had normal kidney function, 2,010 (31.5%) had mildly decreased function, and 318 (5.0%) had moderately to severely decreased function.
The study was funded by the Ministry of Science and Technology of the People’s Republic of China, the Beijing Municipal Science and Technology Commission, the Chinese Stroke Association, the National Science and Technology Major Project and the Beijing Municipal Administration of Hospitals Incubating Program). Salubris Pharmaceuticals contributed ticagrelor and, clopidogrel at no cost and with no restrictions. Dr. Wang reported no relevant financial relationships. Dr. Barnes and Dr. El Husseini reported no relevant financial relationships.
Renal function should be considered when determining whether to pick ticagrelor-aspirin or clopidogrel-aspirin as the antiplatelet therapy for patients with minor stroke, according to new research.
The study, which was conducted in 202 centers in China and published in Annals of Internal Medicine, indicates that when patients had normal kidney function, ticagrelor-aspirin, compared with clopidogrel-aspirin, substantially reduced the risk for recurrent stroke within 90 days of follow-up.
However, this effect was not seen in patients with mildly, moderately or severely decreased kidney function.
Rates of severe or moderate bleeding did not differ substantially between the two treatments.
Results gleaned from CHANCE-2 data
The researchers, led by Anxin Wang, PhD, from Capital Medical University in Beijing, conducted a post hoc analysis of the CHANCE-2 (Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events-II) trial.
The trial included 6,378 patients who carried cytochrome P450 2C19 (CYP2C19) loss-of-function (LOF) alleles who had experienced a minor stroke or transient ischemic attack.
Patients received either ticagrelor-aspirin or clopidogrel-aspirin, and their renal function was measured by estimated glomerular filtration rate. The authors listed as a limitation that no data were available on the presence of albuminuria or proteinuria.
The researchers investigated what effect renal function had on the efficacy and safety of the therapies.
Differences in the therapies
Clopidogrel-aspirin is often recommended for preventing stroke. It can reduce thrombotic risk in patients with impaired kidney function, the authors noted. Ticagrelor can provide greater, faster, and more consistent P2Y12 inhibition than clopidogrel, and evidence shows it is effective in preventing stroke recurrence, particularly in people carrying CYP2C19 LOF alleles.
When people have reduced kidney function, clopidogrel may be harder to clear than ticagrelor and there may be increased plasma concentrations, so function is important to consider when choosing an antiplatelet therapy, the authors wrote.
Choice may come down to cost
Geoffrey Barnes, MD, MSc, associate professor of vascular and cardiovascular medicine at University of Michigan Medicine in Ann Arbor, said in an interview that there has been momentum toward ticagrelor as a more potent choice than clopidogrel not just in populations with minor stroke but for people with MI and coronary stents.
He said he found the results surprising and was intrigued that this paper suggests looking more skeptically at ticagrelor when kidney function is impaired.
Still, the choice may also come down to what the patient can afford at the pharmacy, he said.
“The reality is many patients still get clopidogrel either because that’s what their physicians have been prescribing for well over a decade or because of cost issues, and clopidogrel, for many patients, can be less expensive,” Dr. Barnes noted.
He said he would like to see more study in different populations as the prevalence of people carrying CYP2C19 allele differs by race and results might be different in a non-Asian population. That allele is thought to affect how clopidogrel is metabolized.
Study should spur more research
Nada El Husseini, MD, associate professor of neurology and Duke Telestroke Medical Director at Duke University Medical Center, Durham, N.C., said the study is hypothesis generating, but shouldn’t be thought of as the last word on the subject.
She pointed out some additional limitations of the study, including that it was a post hoc analysis. She explained that the question researchers asked in this study – about effect of kidney function on the safety and efficacy of the therapies – was not the focus of the original CHANCE-2 study, and, as such, the post hoc study may have been underpowered to answer the renal function question.
The authors acknowledged that limitation, noting that “the proportion of patients with severely decreased renal function was low.”
Among 6,378 patients, 4,050 (63.5%) had normal kidney function, 2,010 (31.5%) had mildly decreased function, and 318 (5.0%) had moderately to severely decreased function.
The study was funded by the Ministry of Science and Technology of the People’s Republic of China, the Beijing Municipal Science and Technology Commission, the Chinese Stroke Association, the National Science and Technology Major Project and the Beijing Municipal Administration of Hospitals Incubating Program). Salubris Pharmaceuticals contributed ticagrelor and, clopidogrel at no cost and with no restrictions. Dr. Wang reported no relevant financial relationships. Dr. Barnes and Dr. El Husseini reported no relevant financial relationships.
Renal function should be considered when determining whether to pick ticagrelor-aspirin or clopidogrel-aspirin as the antiplatelet therapy for patients with minor stroke, according to new research.
The study, which was conducted in 202 centers in China and published in Annals of Internal Medicine, indicates that when patients had normal kidney function, ticagrelor-aspirin, compared with clopidogrel-aspirin, substantially reduced the risk for recurrent stroke within 90 days of follow-up.
However, this effect was not seen in patients with mildly, moderately or severely decreased kidney function.
Rates of severe or moderate bleeding did not differ substantially between the two treatments.
Results gleaned from CHANCE-2 data
The researchers, led by Anxin Wang, PhD, from Capital Medical University in Beijing, conducted a post hoc analysis of the CHANCE-2 (Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events-II) trial.
The trial included 6,378 patients who carried cytochrome P450 2C19 (CYP2C19) loss-of-function (LOF) alleles who had experienced a minor stroke or transient ischemic attack.
Patients received either ticagrelor-aspirin or clopidogrel-aspirin, and their renal function was measured by estimated glomerular filtration rate. The authors listed as a limitation that no data were available on the presence of albuminuria or proteinuria.
The researchers investigated what effect renal function had on the efficacy and safety of the therapies.
Differences in the therapies
Clopidogrel-aspirin is often recommended for preventing stroke. It can reduce thrombotic risk in patients with impaired kidney function, the authors noted. Ticagrelor can provide greater, faster, and more consistent P2Y12 inhibition than clopidogrel, and evidence shows it is effective in preventing stroke recurrence, particularly in people carrying CYP2C19 LOF alleles.
When people have reduced kidney function, clopidogrel may be harder to clear than ticagrelor and there may be increased plasma concentrations, so function is important to consider when choosing an antiplatelet therapy, the authors wrote.
Choice may come down to cost
Geoffrey Barnes, MD, MSc, associate professor of vascular and cardiovascular medicine at University of Michigan Medicine in Ann Arbor, said in an interview that there has been momentum toward ticagrelor as a more potent choice than clopidogrel not just in populations with minor stroke but for people with MI and coronary stents.
He said he found the results surprising and was intrigued that this paper suggests looking more skeptically at ticagrelor when kidney function is impaired.
Still, the choice may also come down to what the patient can afford at the pharmacy, he said.
“The reality is many patients still get clopidogrel either because that’s what their physicians have been prescribing for well over a decade or because of cost issues, and clopidogrel, for many patients, can be less expensive,” Dr. Barnes noted.
He said he would like to see more study in different populations as the prevalence of people carrying CYP2C19 allele differs by race and results might be different in a non-Asian population. That allele is thought to affect how clopidogrel is metabolized.
Study should spur more research
Nada El Husseini, MD, associate professor of neurology and Duke Telestroke Medical Director at Duke University Medical Center, Durham, N.C., said the study is hypothesis generating, but shouldn’t be thought of as the last word on the subject.
She pointed out some additional limitations of the study, including that it was a post hoc analysis. She explained that the question researchers asked in this study – about effect of kidney function on the safety and efficacy of the therapies – was not the focus of the original CHANCE-2 study, and, as such, the post hoc study may have been underpowered to answer the renal function question.
The authors acknowledged that limitation, noting that “the proportion of patients with severely decreased renal function was low.”
Among 6,378 patients, 4,050 (63.5%) had normal kidney function, 2,010 (31.5%) had mildly decreased function, and 318 (5.0%) had moderately to severely decreased function.
The study was funded by the Ministry of Science and Technology of the People’s Republic of China, the Beijing Municipal Science and Technology Commission, the Chinese Stroke Association, the National Science and Technology Major Project and the Beijing Municipal Administration of Hospitals Incubating Program). Salubris Pharmaceuticals contributed ticagrelor and, clopidogrel at no cost and with no restrictions. Dr. Wang reported no relevant financial relationships. Dr. Barnes and Dr. El Husseini reported no relevant financial relationships.
FROM ANNALS OF INTERNAL MEDICINE
Original COVID-19 vaccines fall short against Omicron subvariants for the immunocompromised
The effectiveness of up to three doses of COVID-19 vaccine was moderate overall and significantly lower among individuals with immunocompromising conditions, compared with the general population during the period of Omicron dominance, according to an analysis of data from more than 34,000 hospitalizations.
Previous studies have suggested lower COVID-19 vaccine effectiveness among immunocompromised individuals, compared with healthy individuals from the general population, but data from the period in which Omicron subvariants have been dominant are limited, wrote Amadea Britton, MD, of the Centers for Disease Control and Prevention’s COVID-19 Emergency Response Team, and colleagues.
The CDC currently recommends an expanded primary vaccine series of three doses of an mRNA vaccine, and the Advisory Committee on Immunization Practices has recommended a fourth dose with the new bivalent booster that contains elements of the Omicron variant, the researchers noted.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, the researchers identified 34,220 adults with immunocompromising conditions who were hospitalized for COVID-19–like illness between Dec. 16, 2021, and Aug. 20, 2022. These conditions included solid malignancy (40.5%), hematologic malignancy (14.6%), rheumatologic or inflammatory disorder (24.4%), other intrinsic immune condition or immunodeficiency (38.5%), or organ or stem cell transplant (8.6%). They used data from the CDC’s VISION Network, a multistate database. The data include spring and summer 2022, when the BA.4 and BA.5 Omicron subvariants dominated other strains, and adults with immunocompromising conditions were eligible for a total of four vaccine doses (two primary doses and two boosters). The median age of the study population was 69 years, and 25.7%, 41.7%, and 7.0% had received two, three, and four doses, respectively, of COVID-19 vaccine.
Overall, vaccine effectiveness (VE) among immunocompromised patients was 34% after two vaccine doses, increasing to 71% during days 7-89 after a third dose, then declining to 41% 90 days or more after that dose.
During the full Omicron period, VE was 36% for 14 or more days after dose two, 69% for 7-89 days after dose three, and 44% for 90 or more days after dose three.
When VE was stratified by sublineage period, VE was higher 7 or more days after dose three during the predominance of BA.1 (67%), compared with VE during the dominant periods of BA.2/BA.2.12.1 (32%) and BA.4/BA.5 (35%).
In the later periods when Omicron BA.2/BA.2.12.1 and BA.4/BA.5 variants dominated, and individuals who had received three doses of vaccine were eligible for a fourth, VE against these variants was 32% 90 or more days after dose three and 43% 7 or more days after dose four.
VE was lowest among individuals with potentially more severe immunocompromising conditions, notably solid organ or stem cell transplants, the researchers wrote in their discussion.
The study findings were limited by several factors including the use of ICD-9 and -10 discharge diagnosis codes for immunocompromising conditions, potential confounding in VE models, lack of data on outpatient treatments such as nirmatelvir/ritonavir (Paxlovid), and lack of COVID-19 genomic sequencing data that may have affected which sublineage was identified, the researchers noted.
However, “this study confirms that even with boosters, immunocompromised adults, because of their weakened immune systems, are still at high risk of moderate to severe COVID,” said coauthor Brian Dixon, PhD, of the Regenstrief Institute and Indiana University Richard M. Fairbanks School of Public Health, Indianapolis, in a press release about the study.
“Given the incomplete protection against hospitalization afforded by monovalent COVID-19 vaccines, persons with immunocompromising conditions might benefit from updated bivalent vaccine booster doses that target recently circulating Omicron sublineages, in line with ACIP [Advisory Committee on Immunization Practices] recommendations,” the researchers concluded in the study.
The study was funded by the CDC. The researchers had no financial conflicts to disclose. The VISION Network is a collaboration between the CDC, the Regenstrief Institute, and seven health care systems across the United States: Columbia University Irving Medical Center (New York), HealthPartners (Wisconsin), Intermountain Healthcare (Utah), Kaiser Permanente Northern California, Kaiser Permanente Northwest (Washington State), the University of Colorado, and Paso Del Norte Health Information Exchange (Texas).
The effectiveness of up to three doses of COVID-19 vaccine was moderate overall and significantly lower among individuals with immunocompromising conditions, compared with the general population during the period of Omicron dominance, according to an analysis of data from more than 34,000 hospitalizations.
Previous studies have suggested lower COVID-19 vaccine effectiveness among immunocompromised individuals, compared with healthy individuals from the general population, but data from the period in which Omicron subvariants have been dominant are limited, wrote Amadea Britton, MD, of the Centers for Disease Control and Prevention’s COVID-19 Emergency Response Team, and colleagues.
The CDC currently recommends an expanded primary vaccine series of three doses of an mRNA vaccine, and the Advisory Committee on Immunization Practices has recommended a fourth dose with the new bivalent booster that contains elements of the Omicron variant, the researchers noted.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, the researchers identified 34,220 adults with immunocompromising conditions who were hospitalized for COVID-19–like illness between Dec. 16, 2021, and Aug. 20, 2022. These conditions included solid malignancy (40.5%), hematologic malignancy (14.6%), rheumatologic or inflammatory disorder (24.4%), other intrinsic immune condition or immunodeficiency (38.5%), or organ or stem cell transplant (8.6%). They used data from the CDC’s VISION Network, a multistate database. The data include spring and summer 2022, when the BA.4 and BA.5 Omicron subvariants dominated other strains, and adults with immunocompromising conditions were eligible for a total of four vaccine doses (two primary doses and two boosters). The median age of the study population was 69 years, and 25.7%, 41.7%, and 7.0% had received two, three, and four doses, respectively, of COVID-19 vaccine.
Overall, vaccine effectiveness (VE) among immunocompromised patients was 34% after two vaccine doses, increasing to 71% during days 7-89 after a third dose, then declining to 41% 90 days or more after that dose.
During the full Omicron period, VE was 36% for 14 or more days after dose two, 69% for 7-89 days after dose three, and 44% for 90 or more days after dose three.
When VE was stratified by sublineage period, VE was higher 7 or more days after dose three during the predominance of BA.1 (67%), compared with VE during the dominant periods of BA.2/BA.2.12.1 (32%) and BA.4/BA.5 (35%).
In the later periods when Omicron BA.2/BA.2.12.1 and BA.4/BA.5 variants dominated, and individuals who had received three doses of vaccine were eligible for a fourth, VE against these variants was 32% 90 or more days after dose three and 43% 7 or more days after dose four.
VE was lowest among individuals with potentially more severe immunocompromising conditions, notably solid organ or stem cell transplants, the researchers wrote in their discussion.
The study findings were limited by several factors including the use of ICD-9 and -10 discharge diagnosis codes for immunocompromising conditions, potential confounding in VE models, lack of data on outpatient treatments such as nirmatelvir/ritonavir (Paxlovid), and lack of COVID-19 genomic sequencing data that may have affected which sublineage was identified, the researchers noted.
However, “this study confirms that even with boosters, immunocompromised adults, because of their weakened immune systems, are still at high risk of moderate to severe COVID,” said coauthor Brian Dixon, PhD, of the Regenstrief Institute and Indiana University Richard M. Fairbanks School of Public Health, Indianapolis, in a press release about the study.
“Given the incomplete protection against hospitalization afforded by monovalent COVID-19 vaccines, persons with immunocompromising conditions might benefit from updated bivalent vaccine booster doses that target recently circulating Omicron sublineages, in line with ACIP [Advisory Committee on Immunization Practices] recommendations,” the researchers concluded in the study.
The study was funded by the CDC. The researchers had no financial conflicts to disclose. The VISION Network is a collaboration between the CDC, the Regenstrief Institute, and seven health care systems across the United States: Columbia University Irving Medical Center (New York), HealthPartners (Wisconsin), Intermountain Healthcare (Utah), Kaiser Permanente Northern California, Kaiser Permanente Northwest (Washington State), the University of Colorado, and Paso Del Norte Health Information Exchange (Texas).
The effectiveness of up to three doses of COVID-19 vaccine was moderate overall and significantly lower among individuals with immunocompromising conditions, compared with the general population during the period of Omicron dominance, according to an analysis of data from more than 34,000 hospitalizations.
Previous studies have suggested lower COVID-19 vaccine effectiveness among immunocompromised individuals, compared with healthy individuals from the general population, but data from the period in which Omicron subvariants have been dominant are limited, wrote Amadea Britton, MD, of the Centers for Disease Control and Prevention’s COVID-19 Emergency Response Team, and colleagues.
The CDC currently recommends an expanded primary vaccine series of three doses of an mRNA vaccine, and the Advisory Committee on Immunization Practices has recommended a fourth dose with the new bivalent booster that contains elements of the Omicron variant, the researchers noted.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, the researchers identified 34,220 adults with immunocompromising conditions who were hospitalized for COVID-19–like illness between Dec. 16, 2021, and Aug. 20, 2022. These conditions included solid malignancy (40.5%), hematologic malignancy (14.6%), rheumatologic or inflammatory disorder (24.4%), other intrinsic immune condition or immunodeficiency (38.5%), or organ or stem cell transplant (8.6%). They used data from the CDC’s VISION Network, a multistate database. The data include spring and summer 2022, when the BA.4 and BA.5 Omicron subvariants dominated other strains, and adults with immunocompromising conditions were eligible for a total of four vaccine doses (two primary doses and two boosters). The median age of the study population was 69 years, and 25.7%, 41.7%, and 7.0% had received two, three, and four doses, respectively, of COVID-19 vaccine.
Overall, vaccine effectiveness (VE) among immunocompromised patients was 34% after two vaccine doses, increasing to 71% during days 7-89 after a third dose, then declining to 41% 90 days or more after that dose.
During the full Omicron period, VE was 36% for 14 or more days after dose two, 69% for 7-89 days after dose three, and 44% for 90 or more days after dose three.
When VE was stratified by sublineage period, VE was higher 7 or more days after dose three during the predominance of BA.1 (67%), compared with VE during the dominant periods of BA.2/BA.2.12.1 (32%) and BA.4/BA.5 (35%).
In the later periods when Omicron BA.2/BA.2.12.1 and BA.4/BA.5 variants dominated, and individuals who had received three doses of vaccine were eligible for a fourth, VE against these variants was 32% 90 or more days after dose three and 43% 7 or more days after dose four.
VE was lowest among individuals with potentially more severe immunocompromising conditions, notably solid organ or stem cell transplants, the researchers wrote in their discussion.
The study findings were limited by several factors including the use of ICD-9 and -10 discharge diagnosis codes for immunocompromising conditions, potential confounding in VE models, lack of data on outpatient treatments such as nirmatelvir/ritonavir (Paxlovid), and lack of COVID-19 genomic sequencing data that may have affected which sublineage was identified, the researchers noted.
However, “this study confirms that even with boosters, immunocompromised adults, because of their weakened immune systems, are still at high risk of moderate to severe COVID,” said coauthor Brian Dixon, PhD, of the Regenstrief Institute and Indiana University Richard M. Fairbanks School of Public Health, Indianapolis, in a press release about the study.
“Given the incomplete protection against hospitalization afforded by monovalent COVID-19 vaccines, persons with immunocompromising conditions might benefit from updated bivalent vaccine booster doses that target recently circulating Omicron sublineages, in line with ACIP [Advisory Committee on Immunization Practices] recommendations,” the researchers concluded in the study.
The study was funded by the CDC. The researchers had no financial conflicts to disclose. The VISION Network is a collaboration between the CDC, the Regenstrief Institute, and seven health care systems across the United States: Columbia University Irving Medical Center (New York), HealthPartners (Wisconsin), Intermountain Healthcare (Utah), Kaiser Permanente Northern California, Kaiser Permanente Northwest (Washington State), the University of Colorado, and Paso Del Norte Health Information Exchange (Texas).
FROM MMWR