User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

SHM Chapter innovations: A provider exchange program
The SHM Annual Conference is more than an educational event. It also provides an opportunity to collaborate, network and create innovative ideas to improve the quality of inpatient care.

During the 2019 Annual Conference (HM19) – the last “in-person” Annual Conference before the COVID pandemic – SHM chapter leaders from the New Mexico chapter (Krystle Apodaca) and the Wiregrass chapter (Amith Skandhan), which covers the counties of Southern Alabama and the Panhandle of Florida, met during a networking event.
As we talked, we realized the unique differences and similarities our practice settings shared. We debated the role of clinician wellbeing, quality of medical education, and faculty development on individual hospital medicine group (HMG) practice styles.
Clinician well-being is the prerequisite to the Triple Aim of improving the health of populations, enhancing the patient experience, and reducing the cost of care. Engagement in local SHM chapter activities promotes the efficiency of practice, a culture of wellness, and personal resilience. Each HMG faces similar challenges but approaches to solving them vary. Professional challenges can affect the well-being of individual clinicians. During our discussion we realized that an interinstitutional exchange programs could provide a platform to exchange ideas and establish mentors.
The quality of medical education is directly linked to the quality of faculty development. Improving the quality of medical education requires a multifaceted approach by highly developed faculty. The complex factors affecting medical education and faculty development are further complicated by geographic location, patient characteristics, and professional growth opportunities.
Overcoming these obstacles requires an innovative and collaborative approach. Although faculty exchanges are common in academic medicine, they are not commonly attempted with HMGs. Hospitalists are responsible for a significant part of inpatient training for residents, medical students, and nurse practitioners/physician assistants (NPs/PAs) but their faculty training can vary based on location.
As a young specialty, hospital medicine is still evolving and incorporating NPs/PAs and physician hospitalists in varied practice models. Each HMG addresses common obstacles differently based on their culture and practice styles. As chapter leaders we determined that an exchange program would afford the opportunity for visiting faculty members to experience these differences.
We shared the idea of a chapter-level exchange with SHM’s Chapter Development Committee and obtained chapter development funds to execute the event. We also requested that an SHM national board member visit during the exchange to provide insight and feedback. We researched the characteristics of individual academic HMGs and structured a faculty exchange involving physicians and NPs/PAs. During the exchange program planning, the visiting faculty itinerary was tailored to a well-planned agenda for one week, with separate tracks for physicians and NPs/PAs, giving increased access to their individual peer practice styles. Additionally, the visiting faculty had meetings and discussions with the HMG and hospital leadership, to specifically address the visiting faculty’s institutional challenges.
The overall goal of the exchange program was to promote cross-institutional collaboration, increase engagement, improve medical education through faculty development and improve the quality of care. The focus of the exchange program was to share ideas and innovation, and learn the approaches to unique challenges at each institution. Out of this also grew collaboration and mentoring opportunities.
SHM’s New Mexico chapter is based in Albuquerque, a city in the desert Southwest with an ethnically diverse population of 545,000, The chapter leadership works at the University of New Mexico (UNM), a 553-bed medical center. UNM has a well-established internal medicine residency program, an academic hospitalist program, and an NP/PA fellowship program embedded within the hospital medicine department. At the time of the exchange, the HMG at UNM has 26 physicians and 9 NP/PA’s.
The SHM Wiregrass chapter is located in Dothan, Ala., a town of 80,000 near the Gulf of Mexico. Chapter leadership works at Southeast Health, a tertiary care facility with 420 beds, an affiliated medical school, and an internal medicine residency program. At the time of the exchange, the HMG at SEH has 28 physicians and 5 NP/PA’s.
These are two similarly sized hospital medicine programs, located in different geographic regions, and serving different populations. SHM board member Howard Epstein, MD, SFHM, vice president and chief medical officer of Presbyterian Healthcare Services in Albuquerque, participated on behalf of the Society when SEH faculty visited UNM. Kris Rehm, MD, SFHM, a pediatric hospitalist and the vice chair of outreach medicine at Vanderbilt University Medical Center, Nashville, came to Dothan during the faculty visit by UNM.
Two SEH faculty members, a physician and an NP, visited the University of New Mexico Hospital for one week. They participated as observers, rounding with the teams and meeting the UNM HMG leadership. The focus of the discussions included faculty education, a curriculum for quality improvement, and ways to address practice challenges. The SEH faculty also presented a QI project from their institution, and established collaborative relationships.
During the second part of the exchange, three UNM faculty members, including one physician and two NPs, visited SEH for one week. During the visit, they observed NP/PA hospitalist team models, discussed innovations, established mentoring relationships with leadership, and discussed QI projects at SEH. Additionally, the visiting UNM faculty participated in Women In Medicine events and participated as judges for a poster competition. They also had an opportunity to explore the rural landscape and visit the beach.
The evaluation process after the exchanges involved interviews, a survey, and the establishment of shared QI projects in mutual areas of challenge. The survey provided feedback, lessons learned from the exchange, and areas to be improved. Collaborative QI projects currently underway as a result of the exchange include paging etiquette, quality of sleep for hospitalized patients, and onboarding of NPs/PAs in HMGs.
This innovation changed our thinking as medical educators by addressing faculty development and medical education via clinician well-being. The physician and NP/PA Faculty Exchange program was an essential and meaningful innovation that resulted in increased SHM member engagement, crossinstitutional collaboration, networking, and mentorship.
This event created opportunities for faculty collaboration and expanded the professional network of participating institutions. The costs of the exchange were minimal given support from SHM. We believe that once the COVID pandemic has ended, this initiative has the potential to expand facilitated exchanges nationally and internationally, enhance faculty development, and improve medical education.
Dr. Apodaca is assistant professor and nurse practitioner hospitalist at the University of New Mexico. She serves as codirector of the UNM APP Hospital Medicine Fellowship and director of the APP Hospital Medicine Team. Dr. Skandhan is a hospitalist and member of the Core Faculty for the Internal Medicine Residency Program at Southeast Health (SEH), Dothan Ala., and an assistant professor at the Alabama College of Osteopathic Medicine. He serves as the medical director/physician liaison for the Clinical Documentation Program at SEH and also as the director for physician integration for Southeast Health Statera Network, an Accountable Care Organization.
The SHM Annual Conference is more than an educational event. It also provides an opportunity to collaborate, network and create innovative ideas to improve the quality of inpatient care.
During the 2019 Annual Conference (HM19) – the last “in-person” Annual Conference before the COVID pandemic – SHM chapter leaders from the New Mexico chapter (Krystle Apodaca) and the Wiregrass chapter (Amith Skandhan), which covers the counties of Southern Alabama and the Panhandle of Florida, met during a networking event.
As we talked, we realized the unique differences and similarities our practice settings shared. We debated the role of clinician wellbeing, quality of medical education, and faculty development on individual hospital medicine group (HMG) practice styles.
Clinician well-being is the prerequisite to the Triple Aim of improving the health of populations, enhancing the patient experience, and reducing the cost of care. Engagement in local SHM chapter activities promotes the efficiency of practice, a culture of wellness, and personal resilience. Each HMG faces similar challenges but approaches to solving them vary. Professional challenges can affect the well-being of individual clinicians. During our discussion we realized that an interinstitutional exchange programs could provide a platform to exchange ideas and establish mentors.
The quality of medical education is directly linked to the quality of faculty development. Improving the quality of medical education requires a multifaceted approach by highly developed faculty. The complex factors affecting medical education and faculty development are further complicated by geographic location, patient characteristics, and professional growth opportunities.
Overcoming these obstacles requires an innovative and collaborative approach. Although faculty exchanges are common in academic medicine, they are not commonly attempted with HMGs. Hospitalists are responsible for a significant part of inpatient training for residents, medical students, and nurse practitioners/physician assistants (NPs/PAs) but their faculty training can vary based on location.
As a young specialty, hospital medicine is still evolving and incorporating NPs/PAs and physician hospitalists in varied practice models. Each HMG addresses common obstacles differently based on their culture and practice styles. As chapter leaders we determined that an exchange program would afford the opportunity for visiting faculty members to experience these differences.
We shared the idea of a chapter-level exchange with SHM’s Chapter Development Committee and obtained chapter development funds to execute the event. We also requested that an SHM national board member visit during the exchange to provide insight and feedback. We researched the characteristics of individual academic HMGs and structured a faculty exchange involving physicians and NPs/PAs. During the exchange program planning, the visiting faculty itinerary was tailored to a well-planned agenda for one week, with separate tracks for physicians and NPs/PAs, giving increased access to their individual peer practice styles. Additionally, the visiting faculty had meetings and discussions with the HMG and hospital leadership, to specifically address the visiting faculty’s institutional challenges.
The overall goal of the exchange program was to promote cross-institutional collaboration, increase engagement, improve medical education through faculty development and improve the quality of care. The focus of the exchange program was to share ideas and innovation, and learn the approaches to unique challenges at each institution. Out of this also grew collaboration and mentoring opportunities.
SHM’s New Mexico chapter is based in Albuquerque, a city in the desert Southwest with an ethnically diverse population of 545,000, The chapter leadership works at the University of New Mexico (UNM), a 553-bed medical center. UNM has a well-established internal medicine residency program, an academic hospitalist program, and an NP/PA fellowship program embedded within the hospital medicine department. At the time of the exchange, the HMG at UNM has 26 physicians and 9 NP/PA’s.
The SHM Wiregrass chapter is located in Dothan, Ala., a town of 80,000 near the Gulf of Mexico. Chapter leadership works at Southeast Health, a tertiary care facility with 420 beds, an affiliated medical school, and an internal medicine residency program. At the time of the exchange, the HMG at SEH has 28 physicians and 5 NP/PA’s.
These are two similarly sized hospital medicine programs, located in different geographic regions, and serving different populations. SHM board member Howard Epstein, MD, SFHM, vice president and chief medical officer of Presbyterian Healthcare Services in Albuquerque, participated on behalf of the Society when SEH faculty visited UNM. Kris Rehm, MD, SFHM, a pediatric hospitalist and the vice chair of outreach medicine at Vanderbilt University Medical Center, Nashville, came to Dothan during the faculty visit by UNM.
Two SEH faculty members, a physician and an NP, visited the University of New Mexico Hospital for one week. They participated as observers, rounding with the teams and meeting the UNM HMG leadership. The focus of the discussions included faculty education, a curriculum for quality improvement, and ways to address practice challenges. The SEH faculty also presented a QI project from their institution, and established collaborative relationships.
During the second part of the exchange, three UNM faculty members, including one physician and two NPs, visited SEH for one week. During the visit, they observed NP/PA hospitalist team models, discussed innovations, established mentoring relationships with leadership, and discussed QI projects at SEH. Additionally, the visiting UNM faculty participated in Women In Medicine events and participated as judges for a poster competition. They also had an opportunity to explore the rural landscape and visit the beach.
The evaluation process after the exchanges involved interviews, a survey, and the establishment of shared QI projects in mutual areas of challenge. The survey provided feedback, lessons learned from the exchange, and areas to be improved. Collaborative QI projects currently underway as a result of the exchange include paging etiquette, quality of sleep for hospitalized patients, and onboarding of NPs/PAs in HMGs.
This innovation changed our thinking as medical educators by addressing faculty development and medical education via clinician well-being. The physician and NP/PA Faculty Exchange program was an essential and meaningful innovation that resulted in increased SHM member engagement, crossinstitutional collaboration, networking, and mentorship.
This event created opportunities for faculty collaboration and expanded the professional network of participating institutions. The costs of the exchange were minimal given support from SHM. We believe that once the COVID pandemic has ended, this initiative has the potential to expand facilitated exchanges nationally and internationally, enhance faculty development, and improve medical education.
Dr. Apodaca is assistant professor and nurse practitioner hospitalist at the University of New Mexico. She serves as codirector of the UNM APP Hospital Medicine Fellowship and director of the APP Hospital Medicine Team. Dr. Skandhan is a hospitalist and member of the Core Faculty for the Internal Medicine Residency Program at Southeast Health (SEH), Dothan Ala., and an assistant professor at the Alabama College of Osteopathic Medicine. He serves as the medical director/physician liaison for the Clinical Documentation Program at SEH and also as the director for physician integration for Southeast Health Statera Network, an Accountable Care Organization.
The SHM Annual Conference is more than an educational event. It also provides an opportunity to collaborate, network and create innovative ideas to improve the quality of inpatient care.
During the 2019 Annual Conference (HM19) – the last “in-person” Annual Conference before the COVID pandemic – SHM chapter leaders from the New Mexico chapter (Krystle Apodaca) and the Wiregrass chapter (Amith Skandhan), which covers the counties of Southern Alabama and the Panhandle of Florida, met during a networking event.
As we talked, we realized the unique differences and similarities our practice settings shared. We debated the role of clinician wellbeing, quality of medical education, and faculty development on individual hospital medicine group (HMG) practice styles.
Clinician well-being is the prerequisite to the Triple Aim of improving the health of populations, enhancing the patient experience, and reducing the cost of care. Engagement in local SHM chapter activities promotes the efficiency of practice, a culture of wellness, and personal resilience. Each HMG faces similar challenges but approaches to solving them vary. Professional challenges can affect the well-being of individual clinicians. During our discussion we realized that an interinstitutional exchange programs could provide a platform to exchange ideas and establish mentors.
The quality of medical education is directly linked to the quality of faculty development. Improving the quality of medical education requires a multifaceted approach by highly developed faculty. The complex factors affecting medical education and faculty development are further complicated by geographic location, patient characteristics, and professional growth opportunities.
Overcoming these obstacles requires an innovative and collaborative approach. Although faculty exchanges are common in academic medicine, they are not commonly attempted with HMGs. Hospitalists are responsible for a significant part of inpatient training for residents, medical students, and nurse practitioners/physician assistants (NPs/PAs) but their faculty training can vary based on location.
As a young specialty, hospital medicine is still evolving and incorporating NPs/PAs and physician hospitalists in varied practice models. Each HMG addresses common obstacles differently based on their culture and practice styles. As chapter leaders we determined that an exchange program would afford the opportunity for visiting faculty members to experience these differences.
We shared the idea of a chapter-level exchange with SHM’s Chapter Development Committee and obtained chapter development funds to execute the event. We also requested that an SHM national board member visit during the exchange to provide insight and feedback. We researched the characteristics of individual academic HMGs and structured a faculty exchange involving physicians and NPs/PAs. During the exchange program planning, the visiting faculty itinerary was tailored to a well-planned agenda for one week, with separate tracks for physicians and NPs/PAs, giving increased access to their individual peer practice styles. Additionally, the visiting faculty had meetings and discussions with the HMG and hospital leadership, to specifically address the visiting faculty’s institutional challenges.
The overall goal of the exchange program was to promote cross-institutional collaboration, increase engagement, improve medical education through faculty development and improve the quality of care. The focus of the exchange program was to share ideas and innovation, and learn the approaches to unique challenges at each institution. Out of this also grew collaboration and mentoring opportunities.
SHM’s New Mexico chapter is based in Albuquerque, a city in the desert Southwest with an ethnically diverse population of 545,000, The chapter leadership works at the University of New Mexico (UNM), a 553-bed medical center. UNM has a well-established internal medicine residency program, an academic hospitalist program, and an NP/PA fellowship program embedded within the hospital medicine department. At the time of the exchange, the HMG at UNM has 26 physicians and 9 NP/PA’s.
The SHM Wiregrass chapter is located in Dothan, Ala., a town of 80,000 near the Gulf of Mexico. Chapter leadership works at Southeast Health, a tertiary care facility with 420 beds, an affiliated medical school, and an internal medicine residency program. At the time of the exchange, the HMG at SEH has 28 physicians and 5 NP/PA’s.
These are two similarly sized hospital medicine programs, located in different geographic regions, and serving different populations. SHM board member Howard Epstein, MD, SFHM, vice president and chief medical officer of Presbyterian Healthcare Services in Albuquerque, participated on behalf of the Society when SEH faculty visited UNM. Kris Rehm, MD, SFHM, a pediatric hospitalist and the vice chair of outreach medicine at Vanderbilt University Medical Center, Nashville, came to Dothan during the faculty visit by UNM.
Two SEH faculty members, a physician and an NP, visited the University of New Mexico Hospital for one week. They participated as observers, rounding with the teams and meeting the UNM HMG leadership. The focus of the discussions included faculty education, a curriculum for quality improvement, and ways to address practice challenges. The SEH faculty also presented a QI project from their institution, and established collaborative relationships.
During the second part of the exchange, three UNM faculty members, including one physician and two NPs, visited SEH for one week. During the visit, they observed NP/PA hospitalist team models, discussed innovations, established mentoring relationships with leadership, and discussed QI projects at SEH. Additionally, the visiting UNM faculty participated in Women In Medicine events and participated as judges for a poster competition. They also had an opportunity to explore the rural landscape and visit the beach.
The evaluation process after the exchanges involved interviews, a survey, and the establishment of shared QI projects in mutual areas of challenge. The survey provided feedback, lessons learned from the exchange, and areas to be improved. Collaborative QI projects currently underway as a result of the exchange include paging etiquette, quality of sleep for hospitalized patients, and onboarding of NPs/PAs in HMGs.
This innovation changed our thinking as medical educators by addressing faculty development and medical education via clinician well-being. The physician and NP/PA Faculty Exchange program was an essential and meaningful innovation that resulted in increased SHM member engagement, crossinstitutional collaboration, networking, and mentorship.
This event created opportunities for faculty collaboration and expanded the professional network of participating institutions. The costs of the exchange were minimal given support from SHM. We believe that once the COVID pandemic has ended, this initiative has the potential to expand facilitated exchanges nationally and internationally, enhance faculty development, and improve medical education.
Dr. Apodaca is assistant professor and nurse practitioner hospitalist at the University of New Mexico. She serves as codirector of the UNM APP Hospital Medicine Fellowship and director of the APP Hospital Medicine Team. Dr. Skandhan is a hospitalist and member of the Core Faculty for the Internal Medicine Residency Program at Southeast Health (SEH), Dothan Ala., and an assistant professor at the Alabama College of Osteopathic Medicine. He serves as the medical director/physician liaison for the Clinical Documentation Program at SEH and also as the director for physician integration for Southeast Health Statera Network, an Accountable Care Organization.
C. difficile linked to surgery risk in pediatric Crohn’s
In pediatric Crohn’s disease, a Clostridioides difficile infection detected within the first year after diagnosis is associated with a shorter time to first bowel resection surgery, according to a study that included both a retrospective and prospective analysis. The researchers also found evidence that changes in methionine biosynthesis and depletion of beneficial bacteria may contribute to risk of surgery.
C. difficile infection (CDI) disproportionately affects individuals with inflammatory bowel disease (IBD). Pediatric IBD patients have a 34% risk of recurrent CDI infection, compared with 7.5% in the general population. Previous research found that adults with ulcerative colitis and CDI are at more risk of colectomy, but the finding has not been replicated in children.
In a study published in Inflammatory Bowel Diseases, researchers led by Jennifer Hellmann and Lee Denson of the University of Cincinnati conducted a single-center retrospective analysis of 75 pediatric Crohn’s disease patients. They also conducted a prospective study of 70 pediatric Crohn’s disease patients, using shotgun metagenome sequencing to examine the relationship between microbiota composition and C. difficile carriage or surgery history.
Nineteen percent of patients tested positive for C. difficile. Use of antibiotics was associated with C. difficile (odds ratio, 7.9; P = .02). Of patients who underwent C. difficile testing in the first year, 23 went on to have surgery: 21% who were C. difficile negative required surgery, compared with 67% of those who were positive (hazard ratio, 4.4; P = .0003). The mean time to surgery was 527 days for C. difficile–positive patients and 1,268 days for those who were negative.
A multivariate regression analysis on 54 patients with complete data sets showed that the presence of C. difficile was associated with increased risk of surgery (OR, 16.2; P = .0006). When the analysis was run on all 73 patients, using null value for missing data, the results were similar (OR, 9.17; P = .008).
Shotgun sequencing found that 47 of 114 bacterial species that were associated with the presence of C. difficile were also associated with prior surgery for Crohn’s disease. Species included some that may play a role in mucosal homeostasis, such as Bifidobacterium breve and several Alistipes and Ruminococcus species. That suggests that a reduction in the numbers of these taxa may be associated with C. difficile presence and surgical risk.
The researchers also found that methionine synthesis pathways were depressed in C. difficile–positive and surgery patients. Methionine may bolster antioxidant capacity and improve villus morphology. IBD patients with dysbiosis and those experiencing Crohn’s disease exacerbations have been shown to have decreased methionine pathway activity, suggesting methionine biosynthesis changes have clinical relevance.
The study was funded by the National Institutes of Health.
SOURCE: Hellmann J et al. Inflamm Bowel Dis. 2020. doi: 10.1093/ibd/izz263.
In pediatric Crohn’s disease, a Clostridioides difficile infection detected within the first year after diagnosis is associated with a shorter time to first bowel resection surgery, according to a study that included both a retrospective and prospective analysis. The researchers also found evidence that changes in methionine biosynthesis and depletion of beneficial bacteria may contribute to risk of surgery.
C. difficile infection (CDI) disproportionately affects individuals with inflammatory bowel disease (IBD). Pediatric IBD patients have a 34% risk of recurrent CDI infection, compared with 7.5% in the general population. Previous research found that adults with ulcerative colitis and CDI are at more risk of colectomy, but the finding has not been replicated in children.
In a study published in Inflammatory Bowel Diseases, researchers led by Jennifer Hellmann and Lee Denson of the University of Cincinnati conducted a single-center retrospective analysis of 75 pediatric Crohn’s disease patients. They also conducted a prospective study of 70 pediatric Crohn’s disease patients, using shotgun metagenome sequencing to examine the relationship between microbiota composition and C. difficile carriage or surgery history.
Nineteen percent of patients tested positive for C. difficile. Use of antibiotics was associated with C. difficile (odds ratio, 7.9; P = .02). Of patients who underwent C. difficile testing in the first year, 23 went on to have surgery: 21% who were C. difficile negative required surgery, compared with 67% of those who were positive (hazard ratio, 4.4; P = .0003). The mean time to surgery was 527 days for C. difficile–positive patients and 1,268 days for those who were negative.
A multivariate regression analysis on 54 patients with complete data sets showed that the presence of C. difficile was associated with increased risk of surgery (OR, 16.2; P = .0006). When the analysis was run on all 73 patients, using null value for missing data, the results were similar (OR, 9.17; P = .008).
Shotgun sequencing found that 47 of 114 bacterial species that were associated with the presence of C. difficile were also associated with prior surgery for Crohn’s disease. Species included some that may play a role in mucosal homeostasis, such as Bifidobacterium breve and several Alistipes and Ruminococcus species. That suggests that a reduction in the numbers of these taxa may be associated with C. difficile presence and surgical risk.
The researchers also found that methionine synthesis pathways were depressed in C. difficile–positive and surgery patients. Methionine may bolster antioxidant capacity and improve villus morphology. IBD patients with dysbiosis and those experiencing Crohn’s disease exacerbations have been shown to have decreased methionine pathway activity, suggesting methionine biosynthesis changes have clinical relevance.
The study was funded by the National Institutes of Health.
SOURCE: Hellmann J et al. Inflamm Bowel Dis. 2020. doi: 10.1093/ibd/izz263.
In pediatric Crohn’s disease, a Clostridioides difficile infection detected within the first year after diagnosis is associated with a shorter time to first bowel resection surgery, according to a study that included both a retrospective and prospective analysis. The researchers also found evidence that changes in methionine biosynthesis and depletion of beneficial bacteria may contribute to risk of surgery.
C. difficile infection (CDI) disproportionately affects individuals with inflammatory bowel disease (IBD). Pediatric IBD patients have a 34% risk of recurrent CDI infection, compared with 7.5% in the general population. Previous research found that adults with ulcerative colitis and CDI are at more risk of colectomy, but the finding has not been replicated in children.
In a study published in Inflammatory Bowel Diseases, researchers led by Jennifer Hellmann and Lee Denson of the University of Cincinnati conducted a single-center retrospective analysis of 75 pediatric Crohn’s disease patients. They also conducted a prospective study of 70 pediatric Crohn’s disease patients, using shotgun metagenome sequencing to examine the relationship between microbiota composition and C. difficile carriage or surgery history.
Nineteen percent of patients tested positive for C. difficile. Use of antibiotics was associated with C. difficile (odds ratio, 7.9; P = .02). Of patients who underwent C. difficile testing in the first year, 23 went on to have surgery: 21% who were C. difficile negative required surgery, compared with 67% of those who were positive (hazard ratio, 4.4; P = .0003). The mean time to surgery was 527 days for C. difficile–positive patients and 1,268 days for those who were negative.
A multivariate regression analysis on 54 patients with complete data sets showed that the presence of C. difficile was associated with increased risk of surgery (OR, 16.2; P = .0006). When the analysis was run on all 73 patients, using null value for missing data, the results were similar (OR, 9.17; P = .008).
Shotgun sequencing found that 47 of 114 bacterial species that were associated with the presence of C. difficile were also associated with prior surgery for Crohn’s disease. Species included some that may play a role in mucosal homeostasis, such as Bifidobacterium breve and several Alistipes and Ruminococcus species. That suggests that a reduction in the numbers of these taxa may be associated with C. difficile presence and surgical risk.
The researchers also found that methionine synthesis pathways were depressed in C. difficile–positive and surgery patients. Methionine may bolster antioxidant capacity and improve villus morphology. IBD patients with dysbiosis and those experiencing Crohn’s disease exacerbations have been shown to have decreased methionine pathway activity, suggesting methionine biosynthesis changes have clinical relevance.
The study was funded by the National Institutes of Health.
SOURCE: Hellmann J et al. Inflamm Bowel Dis. 2020. doi: 10.1093/ibd/izz263.
Fecal transplant linked to reduced C. difficile mortality
Vancomycin followed by fecal microbiota transplant (FMT) was associated with reduced Clostridioides difficile (C. diff)-related mortality in patients hospitalized with refractory severe or fulminant C. diff infection (CDI) at a single center. The improvements came after Indiana University implemented an FMT option in 2013.
About 8% of C. diff patients develop severe or fulminant CDI (SFCDI), which can lead to toxic colon and multiorgan failure. Surgery is the current recommended treatment for these patients if they are refractory to vancomycin, but 30-day mortality is above 40%. FMT is recommended for recurrent CDI, and it achieves cure rates greater than 80%, along with fewer relapses compared with anti-CDI antibiotic therapy.
FMT has been shown to be effective for SFCDI, with a 91% cure rate for serious CDI and 66% for fulminant CDI.
In the study published in the September issue of Clinical Gastroenterology and Hepatology, researchers led by Yao-Wen Cheng, MD, and Monika Fischer, MD, of Indiana University, assessed the effect of FMT on SFCDI after their institution adopted it as a treatment protocol for SFCDI. Patients could receive FMT if there was evidence that their SFCDI was refractory, or if they had two or more CDI recurrences. The treatment includes oral vancomycin and pseudomembrane-driven sequential FMT.
Two hundred five patients were admitted before FMT implementation, 225 after. Fifty patients received FMT because of refractory SFCDI. A median of two FMTs was conducted per patient. 21 other patients received FMT for nonrefractory SFCDI or other conditions, including 18 patients with multiple recurrent CDI.
Thirty-day CDI-related mortality dropped after FMT implementation (4.4% versus 10.2%; P =.02). This was true in both the fulminant subset (9.1% versus 21.3%; P =.015) and the refractory group (12.1% versus 43.2%; P < .001).
The researchers used segmented logistic regression to determine if the improved outcomes could be due to nontreatment factors that varied over time, and found that the difference in CDI-related mortality was eliminated except for refractory SFCDI patients (odds of mortality after FMT implementation, 0.09; P =.023). There was no significant difference between those receiving non-CDI antibiotics (4.8%) and those who did not (6.9%; P =.75).
FMT was associated with lower frequency of CDI-related colectomy overall (2.7% versus 6.8%; P =.041), as well as in the fulminant (5.5% versus 15.7%; P =.017) and refractory subgroups (7.6% versus 31.8%; P =.001).
The findings follow another study that showed improved 3-month mortality for FMT among patients hospitalized with severe CDI (12.1% versus 42.2%; P < .003).
The results underscore the utility of FMT for SFCDI, and suggest it might have the most benefit in refractory SFCDI. The authors believe that FMT should be an alternative to colectomy when first-line anti-CDI antibiotics are partially or completely ineffective. In the absence of FMT, patients who go on to fail vancomycin or fidaxomicin will likely continue to be managed medically, with up to 80% mortality, or through salvage colectomy, with postsurgical morality rates of 30-40%.
Although a randomized trial could answer the question of FMT efficacy more definitively, it is unlikely to be conducted for ethical reasons.
“Further investigation is required to clearly define FMT’s role and timing in the clinical course of severe and fulminant CDI. However, our study suggests that FMT should be offered to patients with severe and fulminant CDI who do not respond to a 5-day course of anti-CDI antibiotics and may be considered in lieu of or before colectomy,” the researchers wrote.
No source of funding was disclosed.
SOURCE: Cheng YW et al. Clin Gastroenterol Hepatol. 2020;18:2234-43. doi: 10.1016/j.cgh.2019.12.029.
Vancomycin followed by fecal microbiota transplant (FMT) was associated with reduced Clostridioides difficile (C. diff)-related mortality in patients hospitalized with refractory severe or fulminant C. diff infection (CDI) at a single center. The improvements came after Indiana University implemented an FMT option in 2013.
About 8% of C. diff patients develop severe or fulminant CDI (SFCDI), which can lead to toxic colon and multiorgan failure. Surgery is the current recommended treatment for these patients if they are refractory to vancomycin, but 30-day mortality is above 40%. FMT is recommended for recurrent CDI, and it achieves cure rates greater than 80%, along with fewer relapses compared with anti-CDI antibiotic therapy.
FMT has been shown to be effective for SFCDI, with a 91% cure rate for serious CDI and 66% for fulminant CDI.
In the study published in the September issue of Clinical Gastroenterology and Hepatology, researchers led by Yao-Wen Cheng, MD, and Monika Fischer, MD, of Indiana University, assessed the effect of FMT on SFCDI after their institution adopted it as a treatment protocol for SFCDI. Patients could receive FMT if there was evidence that their SFCDI was refractory, or if they had two or more CDI recurrences. The treatment includes oral vancomycin and pseudomembrane-driven sequential FMT.
Two hundred five patients were admitted before FMT implementation, 225 after. Fifty patients received FMT because of refractory SFCDI. A median of two FMTs was conducted per patient. 21 other patients received FMT for nonrefractory SFCDI or other conditions, including 18 patients with multiple recurrent CDI.
Thirty-day CDI-related mortality dropped after FMT implementation (4.4% versus 10.2%; P =.02). This was true in both the fulminant subset (9.1% versus 21.3%; P =.015) and the refractory group (12.1% versus 43.2%; P < .001).
The researchers used segmented logistic regression to determine if the improved outcomes could be due to nontreatment factors that varied over time, and found that the difference in CDI-related mortality was eliminated except for refractory SFCDI patients (odds of mortality after FMT implementation, 0.09; P =.023). There was no significant difference between those receiving non-CDI antibiotics (4.8%) and those who did not (6.9%; P =.75).
FMT was associated with lower frequency of CDI-related colectomy overall (2.7% versus 6.8%; P =.041), as well as in the fulminant (5.5% versus 15.7%; P =.017) and refractory subgroups (7.6% versus 31.8%; P =.001).
The findings follow another study that showed improved 3-month mortality for FMT among patients hospitalized with severe CDI (12.1% versus 42.2%; P < .003).
The results underscore the utility of FMT for SFCDI, and suggest it might have the most benefit in refractory SFCDI. The authors believe that FMT should be an alternative to colectomy when first-line anti-CDI antibiotics are partially or completely ineffective. In the absence of FMT, patients who go on to fail vancomycin or fidaxomicin will likely continue to be managed medically, with up to 80% mortality, or through salvage colectomy, with postsurgical morality rates of 30-40%.
Although a randomized trial could answer the question of FMT efficacy more definitively, it is unlikely to be conducted for ethical reasons.
“Further investigation is required to clearly define FMT’s role and timing in the clinical course of severe and fulminant CDI. However, our study suggests that FMT should be offered to patients with severe and fulminant CDI who do not respond to a 5-day course of anti-CDI antibiotics and may be considered in lieu of or before colectomy,” the researchers wrote.
No source of funding was disclosed.
SOURCE: Cheng YW et al. Clin Gastroenterol Hepatol. 2020;18:2234-43. doi: 10.1016/j.cgh.2019.12.029.
Vancomycin followed by fecal microbiota transplant (FMT) was associated with reduced Clostridioides difficile (C. diff)-related mortality in patients hospitalized with refractory severe or fulminant C. diff infection (CDI) at a single center. The improvements came after Indiana University implemented an FMT option in 2013.
About 8% of C. diff patients develop severe or fulminant CDI (SFCDI), which can lead to toxic colon and multiorgan failure. Surgery is the current recommended treatment for these patients if they are refractory to vancomycin, but 30-day mortality is above 40%. FMT is recommended for recurrent CDI, and it achieves cure rates greater than 80%, along with fewer relapses compared with anti-CDI antibiotic therapy.
FMT has been shown to be effective for SFCDI, with a 91% cure rate for serious CDI and 66% for fulminant CDI.
In the study published in the September issue of Clinical Gastroenterology and Hepatology, researchers led by Yao-Wen Cheng, MD, and Monika Fischer, MD, of Indiana University, assessed the effect of FMT on SFCDI after their institution adopted it as a treatment protocol for SFCDI. Patients could receive FMT if there was evidence that their SFCDI was refractory, or if they had two or more CDI recurrences. The treatment includes oral vancomycin and pseudomembrane-driven sequential FMT.
Two hundred five patients were admitted before FMT implementation, 225 after. Fifty patients received FMT because of refractory SFCDI. A median of two FMTs was conducted per patient. 21 other patients received FMT for nonrefractory SFCDI or other conditions, including 18 patients with multiple recurrent CDI.
Thirty-day CDI-related mortality dropped after FMT implementation (4.4% versus 10.2%; P =.02). This was true in both the fulminant subset (9.1% versus 21.3%; P =.015) and the refractory group (12.1% versus 43.2%; P < .001).
The researchers used segmented logistic regression to determine if the improved outcomes could be due to nontreatment factors that varied over time, and found that the difference in CDI-related mortality was eliminated except for refractory SFCDI patients (odds of mortality after FMT implementation, 0.09; P =.023). There was no significant difference between those receiving non-CDI antibiotics (4.8%) and those who did not (6.9%; P =.75).
FMT was associated with lower frequency of CDI-related colectomy overall (2.7% versus 6.8%; P =.041), as well as in the fulminant (5.5% versus 15.7%; P =.017) and refractory subgroups (7.6% versus 31.8%; P =.001).
The findings follow another study that showed improved 3-month mortality for FMT among patients hospitalized with severe CDI (12.1% versus 42.2%; P < .003).
The results underscore the utility of FMT for SFCDI, and suggest it might have the most benefit in refractory SFCDI. The authors believe that FMT should be an alternative to colectomy when first-line anti-CDI antibiotics are partially or completely ineffective. In the absence of FMT, patients who go on to fail vancomycin or fidaxomicin will likely continue to be managed medically, with up to 80% mortality, or through salvage colectomy, with postsurgical morality rates of 30-40%.
Although a randomized trial could answer the question of FMT efficacy more definitively, it is unlikely to be conducted for ethical reasons.
“Further investigation is required to clearly define FMT’s role and timing in the clinical course of severe and fulminant CDI. However, our study suggests that FMT should be offered to patients with severe and fulminant CDI who do not respond to a 5-day course of anti-CDI antibiotics and may be considered in lieu of or before colectomy,” the researchers wrote.
No source of funding was disclosed.
SOURCE: Cheng YW et al. Clin Gastroenterol Hepatol. 2020;18:2234-43. doi: 10.1016/j.cgh.2019.12.029.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Medicine and the meritocracy
Addressing systemic bias, gender inequity and discrimination
There are many challenges facing modern medicine today. Recent events have highlighted important issues affecting our society as a whole – systemic racism, sexism, and implicit bias. In medicine, we have seen a renewed focus on health equity, health disparities and the implicit systemic bias that affect those who work in the field. It is truly troubling that it has taken the continued loss of black lives to police brutality and a pandemic for this conversation to happen at every level in society.

Systemic bias is present throughout corporate America, and it is no different within the physician workforce. Overall, there has been gradual interest in promoting and teaching diversity. Institutions have been slowly creating policies and administrative positions focused on inclusion and diversity over the last decade. So has diversity training objectively increased representation and advancement of women and minority groups? Do traditionally marginalized groups have better access to health? And are women and people of color (POC) represented equally in leadership positions in medicine?
Clearly, the answers are not straightforward.
Diving into the data
A guilty pleasure of mine is to assess how diverse and inclusive an institution is by looking at the wall of pictures recognizing top leadership in hospitals. Despite women accounting for 47.9% of graduates from medical school in 2018-2019, I still see very few women or POC elevated to this level. Of the total women graduates, 22.6% were Asian, 8% were Black and 5.4% were Hispanic.
Being of Indian descent, I am a woman of color (albeit one who may not be as profoundly affected by racism in medicine as my less represented colleagues). It is especially rare for me to see someone I can identify with in the ranks of top leadership. I find encouragement in seeing any woman on any leadership board because to me, it means that there is hope. The literature seems to support this degree of disparity as well. For example, a recent analysis shows that presidential leadership in medical societies are predominantly held by men (82.6% male vs. 17.4% female). Other datasets demonstrate that only 15% of deans and interim deans are women and AAMC’s report shows that women account for only 18% of all department chairs.
Growing up, my parents fueled my interest to pursue medicine. They described it as a noble profession that rewarded true merit and dedication to the cause. However, those that have been traditionally elevated in medicine are men. If merit knows no gender, why does a gender gap exist? If merit is blind to race, why are minorities so poorly represented in the workforce (much less in leadership)? My view of the wall leaves me wondering about the role of both sexism and racism in medicine.
These visual representations of the medical culture reinforce the acceptable norms and values – white and masculine – in medicine. The feminist movement over the last several decades has increased awareness about the need for equality of the sexes. However, it was not until the concept of intersectionality was introduced by Black feminist Professor Kimberle Crenshaw, that feminism become a more inclusive term. Professor Crenshaw’s paper details how every individual has intersecting factors – race, gender, sexual identity, socioeconomic status – that create the sum of their experience be it privilege, oppression, or discrimination.
For example, a White woman has privileges that a woman of color does not. Among non-white women, race and sexual identity are confounding factors – a Black woman, a Black LGBTQ woman, and an Asian woman, for example, will not experience discrimination in the same way. The farther you deviate from the accepted norms and values, the harder it is for you to obtain support and achieve recognition.
Addressing the patriarchal structure and systemic bias in medicine
Why do patriarchal structures still exist in medicine? How do we resolve systemic bias? Addressing them in isolation – race or gender or sexual identity – is unlikely to create long-lasting change. For change to occur, organizations and individuals need to be intrinsically motivated. Creating awareness and challenging the status quo is the first step.
Over the last decade, implicit bias training and diversity training have become mandatory in various industries and states. Diversity training has grown to be a multi-billion-dollar industry that corporate America has embraced over the last several years. And yet, research shows that mandating such training may not be the most effective. To get results, organizations need to implement programs that “spark engagement, increase contact between different groups and draw on people’s desire to look good to others.”
Historically, the medical curriculum has not included a discourse on feminist theories and the advancement of women in medicine. Cultural competency training is typically offered on an annual basis once we are in the workforce, but in my experience, it focuses more on our interactions with patients and other health care colleagues, and less with regards to our physician peers and leadership. Is this enough to change deep rooted beliefs and traditions?
We can take our cue from non-medical organizations and consider changing this culture of no culture in medicine – introducing diversity task forces that hold departments accountable for recruiting and promoting women and minorities; employing diversity managers; voluntary training; cross-training to increase contact among different groups and mentoring programs that match senior leadership to women and POC. While some medical institutions have implemented some of these principles, changing century-old traditions will require embracing concepts of organizational change and every available effective tool.
Committing to change
Change is especially hard when the target outcome is not accurately quantifiable – even if you can measure attitudes, values, and beliefs, these are subject to reporting bias and tokenism. At the organizational level, change management involves employing a systematic approach to change organizational values, goals, policies, and processes.
Individual change, self-reflection, and personal growth are key components in changing culture. Reflexivity is being aware of your own values, norms, position, and power – an important concept to understand and apply in our everyday interactions. Believing that one’s class, gender, race and sexual orientation are irrelevant to their practice of medicine would not foster the change that we direly need in medicine. Rather, identifying how your own values and professional identity are shaped by your medical training, your organization and the broader cultural context are critically important to developing a greater empathic sense to motivate systemic change.
There has been valuable discussion on bottom-up changes to ensure women and POC have support, encouragement and a pathway to advance in an organization. Some of these include policy and process changes including providing flexible working conditions for women and sponsorship of women and minorities to help them navigate the barriers and microaggressions they encounter at work. While technical (policy) changes form the foundation for any organizational change, it is important to remember that the people side of change – the resistance that you encounter for any change effort in an organization – is equally important to address at the organizational level. A top-down approach is also vital to ensure that change is permanent in an organization and does not end when the individuals responsible for the change leave the organization.
Lewin’s three-stage change management model provides a framework for structural and organizational change in hospital systems. The three-stages of this model are: unfreezing, changing, and refreezing. Unfreezing is the process of determining what needs to change and obtaining leadership support. The actual change process involves getting people on board, empowering them to change and communicating with them frequently. Refreezing cements this change into the organization’s culture by providing support and training to sustain changes. Research has shown that Lewin’s change management model has applicability in the hospital setting.
Industry research in change management methodologies in the business sector has identified sponsorship by CEOs/senior management of an organization and having a structured implementation model for change management as two important factors for ensuring that change efforts are successful and sustainable.
This can be extrapolated to health care organizations – top leadership committed to changing the status quo should solidify organizational commitment by incorporating new attainable and measurable goals into their vision for the organization. Designing a phased implementation of change management methodologies should follow an open discussion to identify an organization’s weaknesses, strengths, capacity, and readiness for change. Lastly, helping busy professionals adapt to change requires innovative and continuous improvement strategies using formal, systematic tools for organization-wide strategic deployment.
Without a concrete commitment at the organizational level, programs such as diversity training may end up being band-aids on wounds that run deep.
I believe that the combination of both individual and organizational commitment to change systemic bias in medicine can be quite powerful. One without the other will fail to permanently change the system. The work to true equality – regardless of the intersecting factors of discrimination – starts with a commitment to change. We may all have different opportunities because of the inequality that is apparent in our systems today, but if we unite around the goal of a bias-free, merit-based equality, it gives us the strength we need to overcome challenges that we once thought insurmountable.
Each one of us is a leader in our own right. Speaking up for those with less power or opportunity than us and supporting talent and hard work solidifies medicine as a meritocracy. Even if the magnitude of change that we fight for may not be realized during our time in medical practice, our commitment to eradicate sexism, racism and discrimination will shape the future of medicine.
Just as our children are a legacy that we leave behind, our work in correcting bias in medicine will pave the path for a better future for the doctors of tomorrow. After all, when I think that my young daughter will be affected by what I do or do not do to address the discrimination, there is no better motivation for me to break down every barrier for her success.
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany Medical College in Albany, NY. This article first appeared on The Hospital Leader, the official blog of SHM.
Addressing systemic bias, gender inequity and discrimination
Addressing systemic bias, gender inequity and discrimination
There are many challenges facing modern medicine today. Recent events have highlighted important issues affecting our society as a whole – systemic racism, sexism, and implicit bias. In medicine, we have seen a renewed focus on health equity, health disparities and the implicit systemic bias that affect those who work in the field. It is truly troubling that it has taken the continued loss of black lives to police brutality and a pandemic for this conversation to happen at every level in society.
Systemic bias is present throughout corporate America, and it is no different within the physician workforce. Overall, there has been gradual interest in promoting and teaching diversity. Institutions have been slowly creating policies and administrative positions focused on inclusion and diversity over the last decade. So has diversity training objectively increased representation and advancement of women and minority groups? Do traditionally marginalized groups have better access to health? And are women and people of color (POC) represented equally in leadership positions in medicine?
Clearly, the answers are not straightforward.
Diving into the data
A guilty pleasure of mine is to assess how diverse and inclusive an institution is by looking at the wall of pictures recognizing top leadership in hospitals. Despite women accounting for 47.9% of graduates from medical school in 2018-2019, I still see very few women or POC elevated to this level. Of the total women graduates, 22.6% were Asian, 8% were Black and 5.4% were Hispanic.
Being of Indian descent, I am a woman of color (albeit one who may not be as profoundly affected by racism in medicine as my less represented colleagues). It is especially rare for me to see someone I can identify with in the ranks of top leadership. I find encouragement in seeing any woman on any leadership board because to me, it means that there is hope. The literature seems to support this degree of disparity as well. For example, a recent analysis shows that presidential leadership in medical societies are predominantly held by men (82.6% male vs. 17.4% female). Other datasets demonstrate that only 15% of deans and interim deans are women and AAMC’s report shows that women account for only 18% of all department chairs.
Growing up, my parents fueled my interest to pursue medicine. They described it as a noble profession that rewarded true merit and dedication to the cause. However, those that have been traditionally elevated in medicine are men. If merit knows no gender, why does a gender gap exist? If merit is blind to race, why are minorities so poorly represented in the workforce (much less in leadership)? My view of the wall leaves me wondering about the role of both sexism and racism in medicine.
These visual representations of the medical culture reinforce the acceptable norms and values – white and masculine – in medicine. The feminist movement over the last several decades has increased awareness about the need for equality of the sexes. However, it was not until the concept of intersectionality was introduced by Black feminist Professor Kimberle Crenshaw, that feminism become a more inclusive term. Professor Crenshaw’s paper details how every individual has intersecting factors – race, gender, sexual identity, socioeconomic status – that create the sum of their experience be it privilege, oppression, or discrimination.
For example, a White woman has privileges that a woman of color does not. Among non-white women, race and sexual identity are confounding factors – a Black woman, a Black LGBTQ woman, and an Asian woman, for example, will not experience discrimination in the same way. The farther you deviate from the accepted norms and values, the harder it is for you to obtain support and achieve recognition.
Addressing the patriarchal structure and systemic bias in medicine
Why do patriarchal structures still exist in medicine? How do we resolve systemic bias? Addressing them in isolation – race or gender or sexual identity – is unlikely to create long-lasting change. For change to occur, organizations and individuals need to be intrinsically motivated. Creating awareness and challenging the status quo is the first step.
Over the last decade, implicit bias training and diversity training have become mandatory in various industries and states. Diversity training has grown to be a multi-billion-dollar industry that corporate America has embraced over the last several years. And yet, research shows that mandating such training may not be the most effective. To get results, organizations need to implement programs that “spark engagement, increase contact between different groups and draw on people’s desire to look good to others.”
Historically, the medical curriculum has not included a discourse on feminist theories and the advancement of women in medicine. Cultural competency training is typically offered on an annual basis once we are in the workforce, but in my experience, it focuses more on our interactions with patients and other health care colleagues, and less with regards to our physician peers and leadership. Is this enough to change deep rooted beliefs and traditions?
We can take our cue from non-medical organizations and consider changing this culture of no culture in medicine – introducing diversity task forces that hold departments accountable for recruiting and promoting women and minorities; employing diversity managers; voluntary training; cross-training to increase contact among different groups and mentoring programs that match senior leadership to women and POC. While some medical institutions have implemented some of these principles, changing century-old traditions will require embracing concepts of organizational change and every available effective tool.
Committing to change
Change is especially hard when the target outcome is not accurately quantifiable – even if you can measure attitudes, values, and beliefs, these are subject to reporting bias and tokenism. At the organizational level, change management involves employing a systematic approach to change organizational values, goals, policies, and processes.
Individual change, self-reflection, and personal growth are key components in changing culture. Reflexivity is being aware of your own values, norms, position, and power – an important concept to understand and apply in our everyday interactions. Believing that one’s class, gender, race and sexual orientation are irrelevant to their practice of medicine would not foster the change that we direly need in medicine. Rather, identifying how your own values and professional identity are shaped by your medical training, your organization and the broader cultural context are critically important to developing a greater empathic sense to motivate systemic change.
There has been valuable discussion on bottom-up changes to ensure women and POC have support, encouragement and a pathway to advance in an organization. Some of these include policy and process changes including providing flexible working conditions for women and sponsorship of women and minorities to help them navigate the barriers and microaggressions they encounter at work. While technical (policy) changes form the foundation for any organizational change, it is important to remember that the people side of change – the resistance that you encounter for any change effort in an organization – is equally important to address at the organizational level. A top-down approach is also vital to ensure that change is permanent in an organization and does not end when the individuals responsible for the change leave the organization.
Lewin’s three-stage change management model provides a framework for structural and organizational change in hospital systems. The three-stages of this model are: unfreezing, changing, and refreezing. Unfreezing is the process of determining what needs to change and obtaining leadership support. The actual change process involves getting people on board, empowering them to change and communicating with them frequently. Refreezing cements this change into the organization’s culture by providing support and training to sustain changes. Research has shown that Lewin’s change management model has applicability in the hospital setting.
Industry research in change management methodologies in the business sector has identified sponsorship by CEOs/senior management of an organization and having a structured implementation model for change management as two important factors for ensuring that change efforts are successful and sustainable.
This can be extrapolated to health care organizations – top leadership committed to changing the status quo should solidify organizational commitment by incorporating new attainable and measurable goals into their vision for the organization. Designing a phased implementation of change management methodologies should follow an open discussion to identify an organization’s weaknesses, strengths, capacity, and readiness for change. Lastly, helping busy professionals adapt to change requires innovative and continuous improvement strategies using formal, systematic tools for organization-wide strategic deployment.
Without a concrete commitment at the organizational level, programs such as diversity training may end up being band-aids on wounds that run deep.
I believe that the combination of both individual and organizational commitment to change systemic bias in medicine can be quite powerful. One without the other will fail to permanently change the system. The work to true equality – regardless of the intersecting factors of discrimination – starts with a commitment to change. We may all have different opportunities because of the inequality that is apparent in our systems today, but if we unite around the goal of a bias-free, merit-based equality, it gives us the strength we need to overcome challenges that we once thought insurmountable.
Each one of us is a leader in our own right. Speaking up for those with less power or opportunity than us and supporting talent and hard work solidifies medicine as a meritocracy. Even if the magnitude of change that we fight for may not be realized during our time in medical practice, our commitment to eradicate sexism, racism and discrimination will shape the future of medicine.
Just as our children are a legacy that we leave behind, our work in correcting bias in medicine will pave the path for a better future for the doctors of tomorrow. After all, when I think that my young daughter will be affected by what I do or do not do to address the discrimination, there is no better motivation for me to break down every barrier for her success.
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany Medical College in Albany, NY. This article first appeared on The Hospital Leader, the official blog of SHM.
There are many challenges facing modern medicine today. Recent events have highlighted important issues affecting our society as a whole – systemic racism, sexism, and implicit bias. In medicine, we have seen a renewed focus on health equity, health disparities and the implicit systemic bias that affect those who work in the field. It is truly troubling that it has taken the continued loss of black lives to police brutality and a pandemic for this conversation to happen at every level in society.
Systemic bias is present throughout corporate America, and it is no different within the physician workforce. Overall, there has been gradual interest in promoting and teaching diversity. Institutions have been slowly creating policies and administrative positions focused on inclusion and diversity over the last decade. So has diversity training objectively increased representation and advancement of women and minority groups? Do traditionally marginalized groups have better access to health? And are women and people of color (POC) represented equally in leadership positions in medicine?
Clearly, the answers are not straightforward.
Diving into the data
A guilty pleasure of mine is to assess how diverse and inclusive an institution is by looking at the wall of pictures recognizing top leadership in hospitals. Despite women accounting for 47.9% of graduates from medical school in 2018-2019, I still see very few women or POC elevated to this level. Of the total women graduates, 22.6% were Asian, 8% were Black and 5.4% were Hispanic.
Being of Indian descent, I am a woman of color (albeit one who may not be as profoundly affected by racism in medicine as my less represented colleagues). It is especially rare for me to see someone I can identify with in the ranks of top leadership. I find encouragement in seeing any woman on any leadership board because to me, it means that there is hope. The literature seems to support this degree of disparity as well. For example, a recent analysis shows that presidential leadership in medical societies are predominantly held by men (82.6% male vs. 17.4% female). Other datasets demonstrate that only 15% of deans and interim deans are women and AAMC’s report shows that women account for only 18% of all department chairs.
Growing up, my parents fueled my interest to pursue medicine. They described it as a noble profession that rewarded true merit and dedication to the cause. However, those that have been traditionally elevated in medicine are men. If merit knows no gender, why does a gender gap exist? If merit is blind to race, why are minorities so poorly represented in the workforce (much less in leadership)? My view of the wall leaves me wondering about the role of both sexism and racism in medicine.
These visual representations of the medical culture reinforce the acceptable norms and values – white and masculine – in medicine. The feminist movement over the last several decades has increased awareness about the need for equality of the sexes. However, it was not until the concept of intersectionality was introduced by Black feminist Professor Kimberle Crenshaw, that feminism become a more inclusive term. Professor Crenshaw’s paper details how every individual has intersecting factors – race, gender, sexual identity, socioeconomic status – that create the sum of their experience be it privilege, oppression, or discrimination.
For example, a White woman has privileges that a woman of color does not. Among non-white women, race and sexual identity are confounding factors – a Black woman, a Black LGBTQ woman, and an Asian woman, for example, will not experience discrimination in the same way. The farther you deviate from the accepted norms and values, the harder it is for you to obtain support and achieve recognition.
Addressing the patriarchal structure and systemic bias in medicine
Why do patriarchal structures still exist in medicine? How do we resolve systemic bias? Addressing them in isolation – race or gender or sexual identity – is unlikely to create long-lasting change. For change to occur, organizations and individuals need to be intrinsically motivated. Creating awareness and challenging the status quo is the first step.
Over the last decade, implicit bias training and diversity training have become mandatory in various industries and states. Diversity training has grown to be a multi-billion-dollar industry that corporate America has embraced over the last several years. And yet, research shows that mandating such training may not be the most effective. To get results, organizations need to implement programs that “spark engagement, increase contact between different groups and draw on people’s desire to look good to others.”
Historically, the medical curriculum has not included a discourse on feminist theories and the advancement of women in medicine. Cultural competency training is typically offered on an annual basis once we are in the workforce, but in my experience, it focuses more on our interactions with patients and other health care colleagues, and less with regards to our physician peers and leadership. Is this enough to change deep rooted beliefs and traditions?
We can take our cue from non-medical organizations and consider changing this culture of no culture in medicine – introducing diversity task forces that hold departments accountable for recruiting and promoting women and minorities; employing diversity managers; voluntary training; cross-training to increase contact among different groups and mentoring programs that match senior leadership to women and POC. While some medical institutions have implemented some of these principles, changing century-old traditions will require embracing concepts of organizational change and every available effective tool.
Committing to change
Change is especially hard when the target outcome is not accurately quantifiable – even if you can measure attitudes, values, and beliefs, these are subject to reporting bias and tokenism. At the organizational level, change management involves employing a systematic approach to change organizational values, goals, policies, and processes.
Individual change, self-reflection, and personal growth are key components in changing culture. Reflexivity is being aware of your own values, norms, position, and power – an important concept to understand and apply in our everyday interactions. Believing that one’s class, gender, race and sexual orientation are irrelevant to their practice of medicine would not foster the change that we direly need in medicine. Rather, identifying how your own values and professional identity are shaped by your medical training, your organization and the broader cultural context are critically important to developing a greater empathic sense to motivate systemic change.
There has been valuable discussion on bottom-up changes to ensure women and POC have support, encouragement and a pathway to advance in an organization. Some of these include policy and process changes including providing flexible working conditions for women and sponsorship of women and minorities to help them navigate the barriers and microaggressions they encounter at work. While technical (policy) changes form the foundation for any organizational change, it is important to remember that the people side of change – the resistance that you encounter for any change effort in an organization – is equally important to address at the organizational level. A top-down approach is also vital to ensure that change is permanent in an organization and does not end when the individuals responsible for the change leave the organization.
Lewin’s three-stage change management model provides a framework for structural and organizational change in hospital systems. The three-stages of this model are: unfreezing, changing, and refreezing. Unfreezing is the process of determining what needs to change and obtaining leadership support. The actual change process involves getting people on board, empowering them to change and communicating with them frequently. Refreezing cements this change into the organization’s culture by providing support and training to sustain changes. Research has shown that Lewin’s change management model has applicability in the hospital setting.
Industry research in change management methodologies in the business sector has identified sponsorship by CEOs/senior management of an organization and having a structured implementation model for change management as two important factors for ensuring that change efforts are successful and sustainable.
This can be extrapolated to health care organizations – top leadership committed to changing the status quo should solidify organizational commitment by incorporating new attainable and measurable goals into their vision for the organization. Designing a phased implementation of change management methodologies should follow an open discussion to identify an organization’s weaknesses, strengths, capacity, and readiness for change. Lastly, helping busy professionals adapt to change requires innovative and continuous improvement strategies using formal, systematic tools for organization-wide strategic deployment.
Without a concrete commitment at the organizational level, programs such as diversity training may end up being band-aids on wounds that run deep.
I believe that the combination of both individual and organizational commitment to change systemic bias in medicine can be quite powerful. One without the other will fail to permanently change the system. The work to true equality – regardless of the intersecting factors of discrimination – starts with a commitment to change. We may all have different opportunities because of the inequality that is apparent in our systems today, but if we unite around the goal of a bias-free, merit-based equality, it gives us the strength we need to overcome challenges that we once thought insurmountable.
Each one of us is a leader in our own right. Speaking up for those with less power or opportunity than us and supporting talent and hard work solidifies medicine as a meritocracy. Even if the magnitude of change that we fight for may not be realized during our time in medical practice, our commitment to eradicate sexism, racism and discrimination will shape the future of medicine.
Just as our children are a legacy that we leave behind, our work in correcting bias in medicine will pave the path for a better future for the doctors of tomorrow. After all, when I think that my young daughter will be affected by what I do or do not do to address the discrimination, there is no better motivation for me to break down every barrier for her success.
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany Medical College in Albany, NY. This article first appeared on The Hospital Leader, the official blog of SHM.
What’s in a number? 697,633 children with COVID-19
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
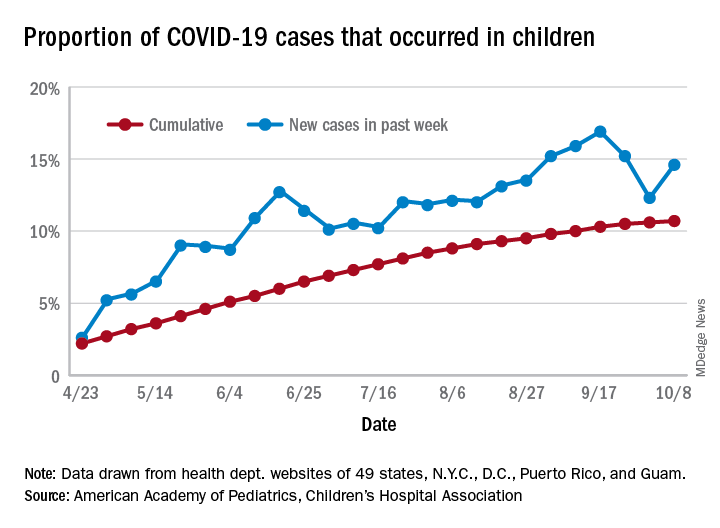
For the week, 14.6% of all COVID-19 cases reported in the United States occurred in children, after 2 consecutive weeks of declines that saw the proportion drop from 16.9% to 12.3%. The cumulative rate of child cases for the entire pandemic is 10.7%, with total child cases in the United States now up to 697,633 and cases among all ages at just over 6.5 million, the AAP and the CHA said Oct. 12 in their weekly COVID-19 report.
Nationally, there were 927 cases reported per 100,000 children as of Oct. 8, with rates at the state level varying from 176 per 100,000 in Vermont to 2,221 per 100,000 in North Dakota. Two other states were over 2,000 cases per 100,000 children: Tennessee (2,155) and South Carolina (2,116), based on data from the health departments of 49 states (New York does not report age distribution), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
Severe illness continues to be rare in children, and national (25 states and New York City) hospitalization rates dropped in the last week. The proportion of hospitalizations occurring in children slipped from a pandemic high of 1.8% the previous week to 1.7% during the week of Oct. 8, and the rate of hospitalizations for children with COVID-19 was down to 1.4% from 1.6% the week before and 1.9% on Sept. 3, the AAP and the CHA said.
Mortality data from 42 states and New York City also show a decline. For the third consecutive week, children represented just 0.06% of all COVID-19 deaths in the United States, down from a high of 0.07% on Sept. 17. Only 0.02% of all cases in children have resulted in death, and that figure has been dropping since early June, when it reached 0.06%, according to the AAP/CHA report. As of Oct. 8, there have been 115 total deaths reported in children.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
For the week, 14.6% of all COVID-19 cases reported in the United States occurred in children, after 2 consecutive weeks of declines that saw the proportion drop from 16.9% to 12.3%. The cumulative rate of child cases for the entire pandemic is 10.7%, with total child cases in the United States now up to 697,633 and cases among all ages at just over 6.5 million, the AAP and the CHA said Oct. 12 in their weekly COVID-19 report.
Nationally, there were 927 cases reported per 100,000 children as of Oct. 8, with rates at the state level varying from 176 per 100,000 in Vermont to 2,221 per 100,000 in North Dakota. Two other states were over 2,000 cases per 100,000 children: Tennessee (2,155) and South Carolina (2,116), based on data from the health departments of 49 states (New York does not report age distribution), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
Severe illness continues to be rare in children, and national (25 states and New York City) hospitalization rates dropped in the last week. The proportion of hospitalizations occurring in children slipped from a pandemic high of 1.8% the previous week to 1.7% during the week of Oct. 8, and the rate of hospitalizations for children with COVID-19 was down to 1.4% from 1.6% the week before and 1.9% on Sept. 3, the AAP and the CHA said.
Mortality data from 42 states and New York City also show a decline. For the third consecutive week, children represented just 0.06% of all COVID-19 deaths in the United States, down from a high of 0.07% on Sept. 17. Only 0.02% of all cases in children have resulted in death, and that figure has been dropping since early June, when it reached 0.06%, according to the AAP/CHA report. As of Oct. 8, there have been 115 total deaths reported in children.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
For the week, 14.6% of all COVID-19 cases reported in the United States occurred in children, after 2 consecutive weeks of declines that saw the proportion drop from 16.9% to 12.3%. The cumulative rate of child cases for the entire pandemic is 10.7%, with total child cases in the United States now up to 697,633 and cases among all ages at just over 6.5 million, the AAP and the CHA said Oct. 12 in their weekly COVID-19 report.
Nationally, there were 927 cases reported per 100,000 children as of Oct. 8, with rates at the state level varying from 176 per 100,000 in Vermont to 2,221 per 100,000 in North Dakota. Two other states were over 2,000 cases per 100,000 children: Tennessee (2,155) and South Carolina (2,116), based on data from the health departments of 49 states (New York does not report age distribution), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
Severe illness continues to be rare in children, and national (25 states and New York City) hospitalization rates dropped in the last week. The proportion of hospitalizations occurring in children slipped from a pandemic high of 1.8% the previous week to 1.7% during the week of Oct. 8, and the rate of hospitalizations for children with COVID-19 was down to 1.4% from 1.6% the week before and 1.9% on Sept. 3, the AAP and the CHA said.
Mortality data from 42 states and New York City also show a decline. For the third consecutive week, children represented just 0.06% of all COVID-19 deaths in the United States, down from a high of 0.07% on Sept. 17. Only 0.02% of all cases in children have resulted in death, and that figure has been dropping since early June, when it reached 0.06%, according to the AAP/CHA report. As of Oct. 8, there have been 115 total deaths reported in children.
Flu vaccine significantly cuts pediatric hospitalizations
Unlike previous studies focused on vaccine effectiveness (VE) in ambulatory care office visits, Angela P. Campbell, MD, MPH, and associates have uncovered evidence of the overall benefit influenza vaccines play in reducing hospitalizations and emergency department visits in pediatric influenza patients.

“Our data provide important VE estimates against severe influenza in children,” the researchers noted in Pediatrics, adding that the findings “provide important evidence supporting the annual recommendation that all children 6 months and older should receive influenza vaccination.”
Dr. Campbell and colleagues collected ongoing surveillance data from the New Vaccine Surveillance Network (NVSN), which is a network of pediatric hospitals across seven cities, including Kansas City, Mo.; Rochester, N.Y.; Cincinnati; Pittsburgh; Nashville, Tenn.; Houston; and Seattle. The influenza season encompassed the period Nov. 7, 2018 to June 21, 2019.
A total of 2,748 hospitalized children and 2,676 children who had completed ED visits that did not lead to hospitalization were included. Once those under 6 months were excluded, 1,792 hospitalized children were included in the VE analysis; of these, 226 (13%) tested positive for influenza infection, including 211 (93%) with influenza A viruses and 15 (7%) with influenza B viruses. Fully 1,611 of the patients (90%), had verified vaccine status, while 181 (10%) had solely parental reported vaccine status. The researchers reported 88 (5%) of the patients received mechanical ventilation and 7 (<1%) died.
Most noteworthy, They further estimated a significant reduction in hospitalizations linked to A(H3N2) and A(H1N1)pdm09 viruses, even in the presence of circulating A(H3N2) viruses that differed from the A(H3N2) vaccine component.
Studies from other countries during the same time period showed that while “significant protection against influenza-associated ambulatory care visits and hospitalizations among children infected with A(H1N1)pdm09 viruses” was observed, the same could not be said for protection against A(H3N2) viruses, which varied among pediatric outpatients in the United States (24%), in England (17% outpatient; 31% inpatient), Europe (46%), and Canada (48%). They explained that such variation in vaccine protection is multifactorial, and includes virus-, host-, and environment-related factors. They also noted that regional variations in circulating viruses, host factors including age, imprinting, and previous vaccination could explain the study’s finding of vaccine protection against both A(H1N1)pdm09 and A(H3N2) viruses.
When comparing VE estimates between ED visits and hospitalizations, the researchers observed one significant difference, that “hospitalized children likely represent more medically complex patients, with 58% having underlying medical conditions and 38% reporting at lease one hospitalization in the past year, compared with 28% and 14% respectively, among ED participants.”
Strengths of the study included the prospective multisite enrollment that provided data across diverse locations and representation from pediatric hospitalizations and ED care, which were not previously strongly represented in the literature. The single-season study with small sample size was considered a limitation, as was the inability to evaluate full and partial vaccine status. Vaccine data also were limited for many of the ED patients observed.
Dr. Campbell and colleagues did caution that while they consider their test-negative design optimal for evaluating both hospitalized and ED patients, they feel their results should not be “interpreted as VE against influenza-associated ambulatory care visits or infections that are not medically attended.”
In a separate interview, Michael E. Pichichero, MD, director of the Rochester General Hospital Research Institute and a clinical professor of pediatrics at the University of Rochester (N.Y.), observed: “There are really no surprises here. A well done contemporary study confirms again the benefits of annual influenza vaccinations for children. Viral coinfections involving SARS-CoV-2 and influenza have been reported from Australia to cause heightened illnesses. That observation provides further impetus for parents to have their children receive influenza vaccinations.”
The researchers cited multiple sources of financial support for their ongoing work, including Sanofi, Quidel, Moderna, Karius, GlaxoSmithKline, Merck, AstraZeneca, and Pfizer. Funding for this study was supported by the Centers for Disease Control and Prevention. Dr. Pichichero said he had no relevant financial disclosures.
SOURCE: Campbell AP et al. Pediatrics. 2020. doi: 10.1542/peds.2020-1368.
Unlike previous studies focused on vaccine effectiveness (VE) in ambulatory care office visits, Angela P. Campbell, MD, MPH, and associates have uncovered evidence of the overall benefit influenza vaccines play in reducing hospitalizations and emergency department visits in pediatric influenza patients.
“Our data provide important VE estimates against severe influenza in children,” the researchers noted in Pediatrics, adding that the findings “provide important evidence supporting the annual recommendation that all children 6 months and older should receive influenza vaccination.”
Dr. Campbell and colleagues collected ongoing surveillance data from the New Vaccine Surveillance Network (NVSN), which is a network of pediatric hospitals across seven cities, including Kansas City, Mo.; Rochester, N.Y.; Cincinnati; Pittsburgh; Nashville, Tenn.; Houston; and Seattle. The influenza season encompassed the period Nov. 7, 2018 to June 21, 2019.
A total of 2,748 hospitalized children and 2,676 children who had completed ED visits that did not lead to hospitalization were included. Once those under 6 months were excluded, 1,792 hospitalized children were included in the VE analysis; of these, 226 (13%) tested positive for influenza infection, including 211 (93%) with influenza A viruses and 15 (7%) with influenza B viruses. Fully 1,611 of the patients (90%), had verified vaccine status, while 181 (10%) had solely parental reported vaccine status. The researchers reported 88 (5%) of the patients received mechanical ventilation and 7 (<1%) died.
Most noteworthy, They further estimated a significant reduction in hospitalizations linked to A(H3N2) and A(H1N1)pdm09 viruses, even in the presence of circulating A(H3N2) viruses that differed from the A(H3N2) vaccine component.
Studies from other countries during the same time period showed that while “significant protection against influenza-associated ambulatory care visits and hospitalizations among children infected with A(H1N1)pdm09 viruses” was observed, the same could not be said for protection against A(H3N2) viruses, which varied among pediatric outpatients in the United States (24%), in England (17% outpatient; 31% inpatient), Europe (46%), and Canada (48%). They explained that such variation in vaccine protection is multifactorial, and includes virus-, host-, and environment-related factors. They also noted that regional variations in circulating viruses, host factors including age, imprinting, and previous vaccination could explain the study’s finding of vaccine protection against both A(H1N1)pdm09 and A(H3N2) viruses.
When comparing VE estimates between ED visits and hospitalizations, the researchers observed one significant difference, that “hospitalized children likely represent more medically complex patients, with 58% having underlying medical conditions and 38% reporting at lease one hospitalization in the past year, compared with 28% and 14% respectively, among ED participants.”
Strengths of the study included the prospective multisite enrollment that provided data across diverse locations and representation from pediatric hospitalizations and ED care, which were not previously strongly represented in the literature. The single-season study with small sample size was considered a limitation, as was the inability to evaluate full and partial vaccine status. Vaccine data also were limited for many of the ED patients observed.
Dr. Campbell and colleagues did caution that while they consider their test-negative design optimal for evaluating both hospitalized and ED patients, they feel their results should not be “interpreted as VE against influenza-associated ambulatory care visits or infections that are not medically attended.”
In a separate interview, Michael E. Pichichero, MD, director of the Rochester General Hospital Research Institute and a clinical professor of pediatrics at the University of Rochester (N.Y.), observed: “There are really no surprises here. A well done contemporary study confirms again the benefits of annual influenza vaccinations for children. Viral coinfections involving SARS-CoV-2 and influenza have been reported from Australia to cause heightened illnesses. That observation provides further impetus for parents to have their children receive influenza vaccinations.”
The researchers cited multiple sources of financial support for their ongoing work, including Sanofi, Quidel, Moderna, Karius, GlaxoSmithKline, Merck, AstraZeneca, and Pfizer. Funding for this study was supported by the Centers for Disease Control and Prevention. Dr. Pichichero said he had no relevant financial disclosures.
SOURCE: Campbell AP et al. Pediatrics. 2020. doi: 10.1542/peds.2020-1368.
Unlike previous studies focused on vaccine effectiveness (VE) in ambulatory care office visits, Angela P. Campbell, MD, MPH, and associates have uncovered evidence of the overall benefit influenza vaccines play in reducing hospitalizations and emergency department visits in pediatric influenza patients.
“Our data provide important VE estimates against severe influenza in children,” the researchers noted in Pediatrics, adding that the findings “provide important evidence supporting the annual recommendation that all children 6 months and older should receive influenza vaccination.”
Dr. Campbell and colleagues collected ongoing surveillance data from the New Vaccine Surveillance Network (NVSN), which is a network of pediatric hospitals across seven cities, including Kansas City, Mo.; Rochester, N.Y.; Cincinnati; Pittsburgh; Nashville, Tenn.; Houston; and Seattle. The influenza season encompassed the period Nov. 7, 2018 to June 21, 2019.
A total of 2,748 hospitalized children and 2,676 children who had completed ED visits that did not lead to hospitalization were included. Once those under 6 months were excluded, 1,792 hospitalized children were included in the VE analysis; of these, 226 (13%) tested positive for influenza infection, including 211 (93%) with influenza A viruses and 15 (7%) with influenza B viruses. Fully 1,611 of the patients (90%), had verified vaccine status, while 181 (10%) had solely parental reported vaccine status. The researchers reported 88 (5%) of the patients received mechanical ventilation and 7 (<1%) died.
Most noteworthy, They further estimated a significant reduction in hospitalizations linked to A(H3N2) and A(H1N1)pdm09 viruses, even in the presence of circulating A(H3N2) viruses that differed from the A(H3N2) vaccine component.
Studies from other countries during the same time period showed that while “significant protection against influenza-associated ambulatory care visits and hospitalizations among children infected with A(H1N1)pdm09 viruses” was observed, the same could not be said for protection against A(H3N2) viruses, which varied among pediatric outpatients in the United States (24%), in England (17% outpatient; 31% inpatient), Europe (46%), and Canada (48%). They explained that such variation in vaccine protection is multifactorial, and includes virus-, host-, and environment-related factors. They also noted that regional variations in circulating viruses, host factors including age, imprinting, and previous vaccination could explain the study’s finding of vaccine protection against both A(H1N1)pdm09 and A(H3N2) viruses.
When comparing VE estimates between ED visits and hospitalizations, the researchers observed one significant difference, that “hospitalized children likely represent more medically complex patients, with 58% having underlying medical conditions and 38% reporting at lease one hospitalization in the past year, compared with 28% and 14% respectively, among ED participants.”
Strengths of the study included the prospective multisite enrollment that provided data across diverse locations and representation from pediatric hospitalizations and ED care, which were not previously strongly represented in the literature. The single-season study with small sample size was considered a limitation, as was the inability to evaluate full and partial vaccine status. Vaccine data also were limited for many of the ED patients observed.
Dr. Campbell and colleagues did caution that while they consider their test-negative design optimal for evaluating both hospitalized and ED patients, they feel their results should not be “interpreted as VE against influenza-associated ambulatory care visits or infections that are not medically attended.”
In a separate interview, Michael E. Pichichero, MD, director of the Rochester General Hospital Research Institute and a clinical professor of pediatrics at the University of Rochester (N.Y.), observed: “There are really no surprises here. A well done contemporary study confirms again the benefits of annual influenza vaccinations for children. Viral coinfections involving SARS-CoV-2 and influenza have been reported from Australia to cause heightened illnesses. That observation provides further impetus for parents to have their children receive influenza vaccinations.”
The researchers cited multiple sources of financial support for their ongoing work, including Sanofi, Quidel, Moderna, Karius, GlaxoSmithKline, Merck, AstraZeneca, and Pfizer. Funding for this study was supported by the Centers for Disease Control and Prevention. Dr. Pichichero said he had no relevant financial disclosures.
SOURCE: Campbell AP et al. Pediatrics. 2020. doi: 10.1542/peds.2020-1368.
FROM PEDIATRICS
COVID-19 pandemic amplifies uncertainty for immigrant hospitalists
H1-B visa program needs improvement
Statistics tell the tale of immigrants in the American health care workforce in broad strokes. In an interview, though, one hospitalist shared the particulars of his professional and personal journey since arriving in the United States from India 15 years ago.

Mihir Patel, MD, MPH, FHM, came to the United States in 2005 to complete a Master’s in Public Health. Fifteen years later, he is still waiting for the green card that signifies U.S. permanent residency status. The paperwork for the application, he said, was completed in 2012. Since then, he’s been renewing his H-1B visa every three years, and he has no expectation that anything will change soon.
“If you are from India, which has a significant backlog of green cards – up to 50 years…you just wait forever,” he said. “Many people even die waiting for their green card to arrive.”
Arriving on a student visa, Dr. Patel completed his MPH in 2008 and began an internal medicine residency that same year, holding a J-1 visa for the 3 years of his US residency program.
“Post-residency, I started working in a rural hospital in an underserved area of northeast Tennessee as a hospitalist,” thus completing the 3 years of service in a rural underserved area that’s a requirement for J-1 visa holders, said Dr. Patel. “I loved this rural community hospital so much that I ended up staying there for 6 years. During my work at this rural hospital, I was able to enjoy the autonomy of managing a small ICU, doing both critical care procedures and management of intubated critical patients while working as a hospitalist,” he said. Dr. Patel served as chief of staff at the hospital for two years, and also served on the board of directors for his 400-physician medical group.
“I was a proud member of this rural community – Rogersville,” said Dr. Patel. Although he and his wife, who was completing her hospitalist residency, lived in Johnson City, Tenn., “I did not mind driving 120 miles round trip every day to go to my small-town hospital for 6 years,” he said.
Spending this time in rural Tennessee allowed Dr. Patel to finish the requirements necessary for the Physician National Interest Waiver and submit his application for permanent residency. The waiver, though, doesn’t give him priority status in the waiting list for permanent residency status.
After a stint in northern California to be closer to extended family, the pull of “beautiful northeast Tennesse and the rural community” was too strong, so Dr. Patel and his family moved back to Johnson City in 2018.

Now, Dr. Patel is a hospitalist at Ballad Health System in Johnson City. He is the corporate director of Ballad’s telemedicine program and is now also the medical director of the COVID-19 Strike Team. He co-founded and is president of the Blue Ridge Chapter of the Society of Hospital Medicine. Under another H-1B visa, Dr. Patel works part-time from home as a telehospitalist, covering six hospitals in 4 different states.
Even in ordinary circumstances, the H-1B visa comes with constraints. Although Dr. Patel’s 6-year old daughter was born in the U.S. and is a citizen, Dr. Patel and his wife have to reapply for their visas every 3 years. “If we travel outside the U.S., we have to get our visas stamped. We cannot change jobs easily due to fear of visa denial, especially with the recent political environment,” said Dr. Patel. “It feels like we are essential health care workers but non-essential immigrants.”
Having recently completed a physician executive MBA program, Dr. Patel said he’d like to start a business of his own using Lean health care principles and telemedicine to improve rural health care. “But while on an H-1B I cannot do anything outside my sponsored employment,” he said.
Ideally, health care organizations would have high flexibility in how and where staff are deployed when a surge of COVID-19 patients hits. Dr. Patel made the point that visa restrictions can make this much harder: “During this COVID crisis, this restriction can cause significant negative impact for small rural hospitals, where local physicians are quarantined and available physicians are on a visa who cannot legally work outside their primary facilities – even though they are willing to work,” he said. “One cannot even work using telemedicine in the same health system, if that is not specifically mentioned during H-1B petition filling. More than 15,000 physicians who are struck by the green card backlog are in the same situation all over U.S.,” he added.
These constraints, though, pale before the consequences of a worst-case pandemic scenario for an immigrant family, where the physician – the primary visa-holder – becomes disabled or dies. In this case, dependent family members must self-deport. “In addition, there would not be any disability or Social Security benefits for the physician or dependents, as they are not citizens or green card holders and they cannot legally stay in the US,” noted Dr. Patel. “Any hospitalist working during the COVID-19 pandemic can have this fate due to our high exposure risk.”
Reauthorizing the H1-B visa program
SHM has been advocating to improve the H1-B visa system for years, Dr. Patel said, The Fairness for High Skilled Immigrants Act passed the U.S. House of Representatives with bipartisan support, and the Society is advocating for its passage in the Senate.

The Fairness for High-Skilled Immigrants Act (S. 386) simplifies the employment-based immigration system by removing per-country caps, converting the employment-based immigration system into a “first-come, first serve” system that does not discriminate on country of origin. The act will also help alleviate the decades-long green card and permanent residency application backlogs.
Dr. Patel emphasized the importance of action by Congress to reauthorize the physician visa waiver program and expediting physician permanent residency. “This is a crisis and we are all physicians who are ready to serve, regardless of our country of origin. Please let us help this great nation by giving us freedom from visa restrictions and providing security for our families.
“During wartime, all frontline soldiers are naturalized and given citizenship by presidential mandate; this is more than war and we are not asking for citizenship – but at least give us a green card which we have already satisfied all requirements for. If not now, then when?” he asked.
H1-B visa program needs improvement
H1-B visa program needs improvement
Statistics tell the tale of immigrants in the American health care workforce in broad strokes. In an interview, though, one hospitalist shared the particulars of his professional and personal journey since arriving in the United States from India 15 years ago.
Mihir Patel, MD, MPH, FHM, came to the United States in 2005 to complete a Master’s in Public Health. Fifteen years later, he is still waiting for the green card that signifies U.S. permanent residency status. The paperwork for the application, he said, was completed in 2012. Since then, he’s been renewing his H-1B visa every three years, and he has no expectation that anything will change soon.
“If you are from India, which has a significant backlog of green cards – up to 50 years…you just wait forever,” he said. “Many people even die waiting for their green card to arrive.”
Arriving on a student visa, Dr. Patel completed his MPH in 2008 and began an internal medicine residency that same year, holding a J-1 visa for the 3 years of his US residency program.
“Post-residency, I started working in a rural hospital in an underserved area of northeast Tennessee as a hospitalist,” thus completing the 3 years of service in a rural underserved area that’s a requirement for J-1 visa holders, said Dr. Patel. “I loved this rural community hospital so much that I ended up staying there for 6 years. During my work at this rural hospital, I was able to enjoy the autonomy of managing a small ICU, doing both critical care procedures and management of intubated critical patients while working as a hospitalist,” he said. Dr. Patel served as chief of staff at the hospital for two years, and also served on the board of directors for his 400-physician medical group.
“I was a proud member of this rural community – Rogersville,” said Dr. Patel. Although he and his wife, who was completing her hospitalist residency, lived in Johnson City, Tenn., “I did not mind driving 120 miles round trip every day to go to my small-town hospital for 6 years,” he said.
Spending this time in rural Tennessee allowed Dr. Patel to finish the requirements necessary for the Physician National Interest Waiver and submit his application for permanent residency. The waiver, though, doesn’t give him priority status in the waiting list for permanent residency status.
After a stint in northern California to be closer to extended family, the pull of “beautiful northeast Tennesse and the rural community” was too strong, so Dr. Patel and his family moved back to Johnson City in 2018.
Now, Dr. Patel is a hospitalist at Ballad Health System in Johnson City. He is the corporate director of Ballad’s telemedicine program and is now also the medical director of the COVID-19 Strike Team. He co-founded and is president of the Blue Ridge Chapter of the Society of Hospital Medicine. Under another H-1B visa, Dr. Patel works part-time from home as a telehospitalist, covering six hospitals in 4 different states.
Even in ordinary circumstances, the H-1B visa comes with constraints. Although Dr. Patel’s 6-year old daughter was born in the U.S. and is a citizen, Dr. Patel and his wife have to reapply for their visas every 3 years. “If we travel outside the U.S., we have to get our visas stamped. We cannot change jobs easily due to fear of visa denial, especially with the recent political environment,” said Dr. Patel. “It feels like we are essential health care workers but non-essential immigrants.”
Having recently completed a physician executive MBA program, Dr. Patel said he’d like to start a business of his own using Lean health care principles and telemedicine to improve rural health care. “But while on an H-1B I cannot do anything outside my sponsored employment,” he said.
Ideally, health care organizations would have high flexibility in how and where staff are deployed when a surge of COVID-19 patients hits. Dr. Patel made the point that visa restrictions can make this much harder: “During this COVID crisis, this restriction can cause significant negative impact for small rural hospitals, where local physicians are quarantined and available physicians are on a visa who cannot legally work outside their primary facilities – even though they are willing to work,” he said. “One cannot even work using telemedicine in the same health system, if that is not specifically mentioned during H-1B petition filling. More than 15,000 physicians who are struck by the green card backlog are in the same situation all over U.S.,” he added.
These constraints, though, pale before the consequences of a worst-case pandemic scenario for an immigrant family, where the physician – the primary visa-holder – becomes disabled or dies. In this case, dependent family members must self-deport. “In addition, there would not be any disability or Social Security benefits for the physician or dependents, as they are not citizens or green card holders and they cannot legally stay in the US,” noted Dr. Patel. “Any hospitalist working during the COVID-19 pandemic can have this fate due to our high exposure risk.”
Reauthorizing the H1-B visa program
SHM has been advocating to improve the H1-B visa system for years, Dr. Patel said, The Fairness for High Skilled Immigrants Act passed the U.S. House of Representatives with bipartisan support, and the Society is advocating for its passage in the Senate.
The Fairness for High-Skilled Immigrants Act (S. 386) simplifies the employment-based immigration system by removing per-country caps, converting the employment-based immigration system into a “first-come, first serve” system that does not discriminate on country of origin. The act will also help alleviate the decades-long green card and permanent residency application backlogs.
Dr. Patel emphasized the importance of action by Congress to reauthorize the physician visa waiver program and expediting physician permanent residency. “This is a crisis and we are all physicians who are ready to serve, regardless of our country of origin. Please let us help this great nation by giving us freedom from visa restrictions and providing security for our families.
“During wartime, all frontline soldiers are naturalized and given citizenship by presidential mandate; this is more than war and we are not asking for citizenship – but at least give us a green card which we have already satisfied all requirements for. If not now, then when?” he asked.
Statistics tell the tale of immigrants in the American health care workforce in broad strokes. In an interview, though, one hospitalist shared the particulars of his professional and personal journey since arriving in the United States from India 15 years ago.
Mihir Patel, MD, MPH, FHM, came to the United States in 2005 to complete a Master’s in Public Health. Fifteen years later, he is still waiting for the green card that signifies U.S. permanent residency status. The paperwork for the application, he said, was completed in 2012. Since then, he’s been renewing his H-1B visa every three years, and he has no expectation that anything will change soon.
“If you are from India, which has a significant backlog of green cards – up to 50 years…you just wait forever,” he said. “Many people even die waiting for their green card to arrive.”
Arriving on a student visa, Dr. Patel completed his MPH in 2008 and began an internal medicine residency that same year, holding a J-1 visa for the 3 years of his US residency program.
“Post-residency, I started working in a rural hospital in an underserved area of northeast Tennessee as a hospitalist,” thus completing the 3 years of service in a rural underserved area that’s a requirement for J-1 visa holders, said Dr. Patel. “I loved this rural community hospital so much that I ended up staying there for 6 years. During my work at this rural hospital, I was able to enjoy the autonomy of managing a small ICU, doing both critical care procedures and management of intubated critical patients while working as a hospitalist,” he said. Dr. Patel served as chief of staff at the hospital for two years, and also served on the board of directors for his 400-physician medical group.
“I was a proud member of this rural community – Rogersville,” said Dr. Patel. Although he and his wife, who was completing her hospitalist residency, lived in Johnson City, Tenn., “I did not mind driving 120 miles round trip every day to go to my small-town hospital for 6 years,” he said.
Spending this time in rural Tennessee allowed Dr. Patel to finish the requirements necessary for the Physician National Interest Waiver and submit his application for permanent residency. The waiver, though, doesn’t give him priority status in the waiting list for permanent residency status.
After a stint in northern California to be closer to extended family, the pull of “beautiful northeast Tennesse and the rural community” was too strong, so Dr. Patel and his family moved back to Johnson City in 2018.
Now, Dr. Patel is a hospitalist at Ballad Health System in Johnson City. He is the corporate director of Ballad’s telemedicine program and is now also the medical director of the COVID-19 Strike Team. He co-founded and is president of the Blue Ridge Chapter of the Society of Hospital Medicine. Under another H-1B visa, Dr. Patel works part-time from home as a telehospitalist, covering six hospitals in 4 different states.
Even in ordinary circumstances, the H-1B visa comes with constraints. Although Dr. Patel’s 6-year old daughter was born in the U.S. and is a citizen, Dr. Patel and his wife have to reapply for their visas every 3 years. “If we travel outside the U.S., we have to get our visas stamped. We cannot change jobs easily due to fear of visa denial, especially with the recent political environment,” said Dr. Patel. “It feels like we are essential health care workers but non-essential immigrants.”
Having recently completed a physician executive MBA program, Dr. Patel said he’d like to start a business of his own using Lean health care principles and telemedicine to improve rural health care. “But while on an H-1B I cannot do anything outside my sponsored employment,” he said.
Ideally, health care organizations would have high flexibility in how and where staff are deployed when a surge of COVID-19 patients hits. Dr. Patel made the point that visa restrictions can make this much harder: “During this COVID crisis, this restriction can cause significant negative impact for small rural hospitals, where local physicians are quarantined and available physicians are on a visa who cannot legally work outside their primary facilities – even though they are willing to work,” he said. “One cannot even work using telemedicine in the same health system, if that is not specifically mentioned during H-1B petition filling. More than 15,000 physicians who are struck by the green card backlog are in the same situation all over U.S.,” he added.
These constraints, though, pale before the consequences of a worst-case pandemic scenario for an immigrant family, where the physician – the primary visa-holder – becomes disabled or dies. In this case, dependent family members must self-deport. “In addition, there would not be any disability or Social Security benefits for the physician or dependents, as they are not citizens or green card holders and they cannot legally stay in the US,” noted Dr. Patel. “Any hospitalist working during the COVID-19 pandemic can have this fate due to our high exposure risk.”
Reauthorizing the H1-B visa program
SHM has been advocating to improve the H1-B visa system for years, Dr. Patel said, The Fairness for High Skilled Immigrants Act passed the U.S. House of Representatives with bipartisan support, and the Society is advocating for its passage in the Senate.
The Fairness for High-Skilled Immigrants Act (S. 386) simplifies the employment-based immigration system by removing per-country caps, converting the employment-based immigration system into a “first-come, first serve” system that does not discriminate on country of origin. The act will also help alleviate the decades-long green card and permanent residency application backlogs.
Dr. Patel emphasized the importance of action by Congress to reauthorize the physician visa waiver program and expediting physician permanent residency. “This is a crisis and we are all physicians who are ready to serve, regardless of our country of origin. Please let us help this great nation by giving us freedom from visa restrictions and providing security for our families.
“During wartime, all frontline soldiers are naturalized and given citizenship by presidential mandate; this is more than war and we are not asking for citizenship – but at least give us a green card which we have already satisfied all requirements for. If not now, then when?” he asked.
‘Profound human toll’ in excess deaths from COVID-19 calculated in two studies
However, additional deaths could be indirectly related because people avoided emergency care during the pandemic, new research shows.
Deaths linked to COVID-19 varied by state and phase of the pandemic, as reported in a study from researchers at Virginia Commonwealth University and Yale University that was published online October 12 in JAMA.
Another study published online simultaneously in JAMA took more of an international perspective. Investigators from the University of Pennsylvania and Harvard University found that in America there were more excess deaths and there was higher all-cause mortality during the pandemic than in 18 other countries.
Although the ongoing number of deaths attributable to COVID-19 continues to garner attention, there can be a lag of weeks or months in how long it takes some public health agencies to update their figures.
“For the public at large, the take-home message is twofold: that the number of deaths caused by the pandemic exceeds publicly reported COVID-19 death counts by 20% and that states that reopened or lifted restrictions early suffered a protracted surge in excess deaths that extended into the summer,” lead author of the US-focused study, Steven H. Woolf, MD, MPH, told Medscape Medical News.
The take-away for physicians is in the bigger picture – it is likely that the COVID-19 pandemic is responsible for deaths from other conditions as well. “Surges in COVID-19 were accompanied by an increase in deaths attributed to other causes, such as heart disease and Alzheimer’s disease and dementia,” said Woolf, director emeritus and senior adviser at the Center on Society and Health and professor in the Department of Family Medicine and Population Health at the Virginia Commonwealth University School of Medicine in Richmond, Virginia.
The investigators identified 225,530 excess US deaths in the 5 months from March to July. They report that 67% were directly attributable to COVID-19.
Deaths linked to COVID-19 included those in which the disease was listed as an underlying or contributing cause. US total death rates are “remarkably consistent” year after year, and the investigators calculated a 20% overall jump in mortality.
The study included data from the National Center for Health Statistics and the US Census Bureau for 48 states and the District of Columbia. Connecticut and North Carolina were excluded because of missing data.
Woolf and colleagues also found statistically higher rates of deaths from two other causes, heart disease and Alzheimer’s disease/dementia.
Altered states
New York, New Jersey, Massachusetts, Louisiana, Arizona, Mississippi, Maryland, Delaware, Rhode Island, and Michigan had the highest per capita excess death rates. Three states experienced the shortest epidemics during the study period: New York, New Jersey, and Massachusetts.
Some lessons could be learned by looking at how individual states managed large numbers of people with COVID-19. “Although we suspected that states that reopened early might have put themselves at risk of a pandemic surge, the consistency with which that occurred and the devastating numbers of deaths they suffered was a surprise,” Woolf said.
“The goal of our study is not to look in the rearview mirror and lament what happened months ago but to learn the lesson going forward: Our country will be unable to take control of this pandemic without more robust efforts to control community spread,” Woolf said. “Our study found that states that did this well, such as New York and New Jersey, experienced large surges but bent the curve and were back to baseline in less than 10 weeks.
“If we could do this as a country, countless lives could be saved.”
A global perspective
The United States experienced high mortality linked to COVID-19, as well as high all-cause mortality, compared with 18 other countries, as reported in the study by University of Pennsylvania and Harvard University researchers.
The United States ranked third, with 72 deaths per 100,000 people, among countries with moderate or high mortality. Although perhaps not surprising given the state of SARS-CoV-2 infection across the United States, a question remains as to what extent the relatively high mortality rate is linked to early outbreaks vs “poor long-term response,” the researchers note.
Alyssa Bilinski, MSc, and lead author Ezekiel J. Emanuel, MD, PhD, chair of the Department of Medical Ethics and Health Policy at the University of Pennsylvania Perelman School of Medicine in Philadelphia, calculated the difference in COVID-19 deaths among countries through Sept. 19, 2020. On this date, the United States reported a total 198,589 COVID-19 deaths.
They calculated that, if the US death rates were similar to those in Australia, the United States would have experienced 187,661 fewer COVID-19 deaths. If similar to those of Canada, there would have been 117,622 fewer deaths in the United States.
The US death rate was lower than six other countries with high COVID-19 mortality in the early spring, including Belgium, Spain, and the United Kingdom. However, after May 10, the per capita mortality rate in the United States exceeded the others.
Between May 10 and Sept. 19, the death rate in Italy was 9.1 per 100,000, vs 36.9 per 100,000.
“After the first peak in early spring, US death rates from COVID-19 and from all causes remained higher than even countries with high COVID-19 mortality,” the researchers note. “This may have been a result of several factors, including weak public health infrastructure and a decentralized, inconsistent US response to the pandemic.”
“Mortifying and motivating”
Woolf and colleagues estimate that more than 225,000 excess deaths occurred in recent months; this represents a 20% increase over expected deaths, note Harvey V. Fineberg, MD, PhD, of the Gordon and Betty Moore Foundation, in an accompanying editorial in JAMA.
“Importantly, a condition such as COVID-19 can contribute both directly and indirectly to excess mortality,” he writes.
Although the direct contribution to the mortality rates by those infected is straightforward, “the indirect contribution may relate to circumstances or choices due to the COVID-19 pandemic: for example, a patient who develops symptoms of a stroke is too concerned about COVID-19 to go to the emergency department, and a potentially reversible condition becomes fatal.”
Fineberg notes that “a general indication of the death toll from COVID-19 and the excess deaths related to the pandemic, as presented by Woolf et al, are sufficiently mortifying and motivating.”
“Profound human toll”
“The importance of the estimate by Woolf et al – which suggests that for the entirety of 2020, more than 400,000 excess deaths will occur – cannot be overstated, because it accounts for what could be declines in some causes of death, like motor vehicle crashes, but increases in others, like myocardial infarction,” write Howard Bauchner, MD, editor in chief of JAMA, and Phil B. Fontanarosa, MD, MBA, executive editor of JAMA, in another accompanying editorial.
“These deaths reflect a true measure of the human cost of the Great Pandemic of 2020,” they add.
The study from Emanuel and Bilinski was notable for calculating the excess COVID-19 and all-cause mortality to Sept. 2020, they note. “After the initial peak in early spring, US death rates from COVID-19 and from all causes remained higher than rates in countries with high COVID-19 mortality.”
“Few people will forget the Great Pandemic of 2020, where and how they lived, how it substantially changed their lives, and for many, the profound human toll it has taken,” Bauchner and Fontanarosa write.
The study by Woolf and colleagues was supported by National Center for Advancing Translational Sciences, the National Institute on Aging, and the National Institute of Allergy and Infectious Diseases. The study by Bilinski and Emanuel was partially funded by the Colton Foundation. Woolf, Emanuel, Fineberg, Bauchner, and Fontanarosa have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
However, additional deaths could be indirectly related because people avoided emergency care during the pandemic, new research shows.
Deaths linked to COVID-19 varied by state and phase of the pandemic, as reported in a study from researchers at Virginia Commonwealth University and Yale University that was published online October 12 in JAMA.
Another study published online simultaneously in JAMA took more of an international perspective. Investigators from the University of Pennsylvania and Harvard University found that in America there were more excess deaths and there was higher all-cause mortality during the pandemic than in 18 other countries.
Although the ongoing number of deaths attributable to COVID-19 continues to garner attention, there can be a lag of weeks or months in how long it takes some public health agencies to update their figures.
“For the public at large, the take-home message is twofold: that the number of deaths caused by the pandemic exceeds publicly reported COVID-19 death counts by 20% and that states that reopened or lifted restrictions early suffered a protracted surge in excess deaths that extended into the summer,” lead author of the US-focused study, Steven H. Woolf, MD, MPH, told Medscape Medical News.
The take-away for physicians is in the bigger picture – it is likely that the COVID-19 pandemic is responsible for deaths from other conditions as well. “Surges in COVID-19 were accompanied by an increase in deaths attributed to other causes, such as heart disease and Alzheimer’s disease and dementia,” said Woolf, director emeritus and senior adviser at the Center on Society and Health and professor in the Department of Family Medicine and Population Health at the Virginia Commonwealth University School of Medicine in Richmond, Virginia.
The investigators identified 225,530 excess US deaths in the 5 months from March to July. They report that 67% were directly attributable to COVID-19.
Deaths linked to COVID-19 included those in which the disease was listed as an underlying or contributing cause. US total death rates are “remarkably consistent” year after year, and the investigators calculated a 20% overall jump in mortality.
The study included data from the National Center for Health Statistics and the US Census Bureau for 48 states and the District of Columbia. Connecticut and North Carolina were excluded because of missing data.
Woolf and colleagues also found statistically higher rates of deaths from two other causes, heart disease and Alzheimer’s disease/dementia.
Altered states
New York, New Jersey, Massachusetts, Louisiana, Arizona, Mississippi, Maryland, Delaware, Rhode Island, and Michigan had the highest per capita excess death rates. Three states experienced the shortest epidemics during the study period: New York, New Jersey, and Massachusetts.
Some lessons could be learned by looking at how individual states managed large numbers of people with COVID-19. “Although we suspected that states that reopened early might have put themselves at risk of a pandemic surge, the consistency with which that occurred and the devastating numbers of deaths they suffered was a surprise,” Woolf said.
“The goal of our study is not to look in the rearview mirror and lament what happened months ago but to learn the lesson going forward: Our country will be unable to take control of this pandemic without more robust efforts to control community spread,” Woolf said. “Our study found that states that did this well, such as New York and New Jersey, experienced large surges but bent the curve and were back to baseline in less than 10 weeks.
“If we could do this as a country, countless lives could be saved.”
A global perspective
The United States experienced high mortality linked to COVID-19, as well as high all-cause mortality, compared with 18 other countries, as reported in the study by University of Pennsylvania and Harvard University researchers.
The United States ranked third, with 72 deaths per 100,000 people, among countries with moderate or high mortality. Although perhaps not surprising given the state of SARS-CoV-2 infection across the United States, a question remains as to what extent the relatively high mortality rate is linked to early outbreaks vs “poor long-term response,” the researchers note.
Alyssa Bilinski, MSc, and lead author Ezekiel J. Emanuel, MD, PhD, chair of the Department of Medical Ethics and Health Policy at the University of Pennsylvania Perelman School of Medicine in Philadelphia, calculated the difference in COVID-19 deaths among countries through Sept. 19, 2020. On this date, the United States reported a total 198,589 COVID-19 deaths.
They calculated that, if the US death rates were similar to those in Australia, the United States would have experienced 187,661 fewer COVID-19 deaths. If similar to those of Canada, there would have been 117,622 fewer deaths in the United States.
The US death rate was lower than six other countries with high COVID-19 mortality in the early spring, including Belgium, Spain, and the United Kingdom. However, after May 10, the per capita mortality rate in the United States exceeded the others.
Between May 10 and Sept. 19, the death rate in Italy was 9.1 per 100,000, vs 36.9 per 100,000.
“After the first peak in early spring, US death rates from COVID-19 and from all causes remained higher than even countries with high COVID-19 mortality,” the researchers note. “This may have been a result of several factors, including weak public health infrastructure and a decentralized, inconsistent US response to the pandemic.”
“Mortifying and motivating”
Woolf and colleagues estimate that more than 225,000 excess deaths occurred in recent months; this represents a 20% increase over expected deaths, note Harvey V. Fineberg, MD, PhD, of the Gordon and Betty Moore Foundation, in an accompanying editorial in JAMA.
“Importantly, a condition such as COVID-19 can contribute both directly and indirectly to excess mortality,” he writes.
Although the direct contribution to the mortality rates by those infected is straightforward, “the indirect contribution may relate to circumstances or choices due to the COVID-19 pandemic: for example, a patient who develops symptoms of a stroke is too concerned about COVID-19 to go to the emergency department, and a potentially reversible condition becomes fatal.”
Fineberg notes that “a general indication of the death toll from COVID-19 and the excess deaths related to the pandemic, as presented by Woolf et al, are sufficiently mortifying and motivating.”
“Profound human toll”
“The importance of the estimate by Woolf et al – which suggests that for the entirety of 2020, more than 400,000 excess deaths will occur – cannot be overstated, because it accounts for what could be declines in some causes of death, like motor vehicle crashes, but increases in others, like myocardial infarction,” write Howard Bauchner, MD, editor in chief of JAMA, and Phil B. Fontanarosa, MD, MBA, executive editor of JAMA, in another accompanying editorial.
“These deaths reflect a true measure of the human cost of the Great Pandemic of 2020,” they add.
The study from Emanuel and Bilinski was notable for calculating the excess COVID-19 and all-cause mortality to Sept. 2020, they note. “After the initial peak in early spring, US death rates from COVID-19 and from all causes remained higher than rates in countries with high COVID-19 mortality.”
“Few people will forget the Great Pandemic of 2020, where and how they lived, how it substantially changed their lives, and for many, the profound human toll it has taken,” Bauchner and Fontanarosa write.
The study by Woolf and colleagues was supported by National Center for Advancing Translational Sciences, the National Institute on Aging, and the National Institute of Allergy and Infectious Diseases. The study by Bilinski and Emanuel was partially funded by the Colton Foundation. Woolf, Emanuel, Fineberg, Bauchner, and Fontanarosa have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
However, additional deaths could be indirectly related because people avoided emergency care during the pandemic, new research shows.
Deaths linked to COVID-19 varied by state and phase of the pandemic, as reported in a study from researchers at Virginia Commonwealth University and Yale University that was published online October 12 in JAMA.
Another study published online simultaneously in JAMA took more of an international perspective. Investigators from the University of Pennsylvania and Harvard University found that in America there were more excess deaths and there was higher all-cause mortality during the pandemic than in 18 other countries.
Although the ongoing number of deaths attributable to COVID-19 continues to garner attention, there can be a lag of weeks or months in how long it takes some public health agencies to update their figures.
“For the public at large, the take-home message is twofold: that the number of deaths caused by the pandemic exceeds publicly reported COVID-19 death counts by 20% and that states that reopened or lifted restrictions early suffered a protracted surge in excess deaths that extended into the summer,” lead author of the US-focused study, Steven H. Woolf, MD, MPH, told Medscape Medical News.
The take-away for physicians is in the bigger picture – it is likely that the COVID-19 pandemic is responsible for deaths from other conditions as well. “Surges in COVID-19 were accompanied by an increase in deaths attributed to other causes, such as heart disease and Alzheimer’s disease and dementia,” said Woolf, director emeritus and senior adviser at the Center on Society and Health and professor in the Department of Family Medicine and Population Health at the Virginia Commonwealth University School of Medicine in Richmond, Virginia.
The investigators identified 225,530 excess US deaths in the 5 months from March to July. They report that 67% were directly attributable to COVID-19.
Deaths linked to COVID-19 included those in which the disease was listed as an underlying or contributing cause. US total death rates are “remarkably consistent” year after year, and the investigators calculated a 20% overall jump in mortality.
The study included data from the National Center for Health Statistics and the US Census Bureau for 48 states and the District of Columbia. Connecticut and North Carolina were excluded because of missing data.
Woolf and colleagues also found statistically higher rates of deaths from two other causes, heart disease and Alzheimer’s disease/dementia.
Altered states
New York, New Jersey, Massachusetts, Louisiana, Arizona, Mississippi, Maryland, Delaware, Rhode Island, and Michigan had the highest per capita excess death rates. Three states experienced the shortest epidemics during the study period: New York, New Jersey, and Massachusetts.
Some lessons could be learned by looking at how individual states managed large numbers of people with COVID-19. “Although we suspected that states that reopened early might have put themselves at risk of a pandemic surge, the consistency with which that occurred and the devastating numbers of deaths they suffered was a surprise,” Woolf said.
“The goal of our study is not to look in the rearview mirror and lament what happened months ago but to learn the lesson going forward: Our country will be unable to take control of this pandemic without more robust efforts to control community spread,” Woolf said. “Our study found that states that did this well, such as New York and New Jersey, experienced large surges but bent the curve and were back to baseline in less than 10 weeks.
“If we could do this as a country, countless lives could be saved.”
A global perspective
The United States experienced high mortality linked to COVID-19, as well as high all-cause mortality, compared with 18 other countries, as reported in the study by University of Pennsylvania and Harvard University researchers.
The United States ranked third, with 72 deaths per 100,000 people, among countries with moderate or high mortality. Although perhaps not surprising given the state of SARS-CoV-2 infection across the United States, a question remains as to what extent the relatively high mortality rate is linked to early outbreaks vs “poor long-term response,” the researchers note.
Alyssa Bilinski, MSc, and lead author Ezekiel J. Emanuel, MD, PhD, chair of the Department of Medical Ethics and Health Policy at the University of Pennsylvania Perelman School of Medicine in Philadelphia, calculated the difference in COVID-19 deaths among countries through Sept. 19, 2020. On this date, the United States reported a total 198,589 COVID-19 deaths.
They calculated that, if the US death rates were similar to those in Australia, the United States would have experienced 187,661 fewer COVID-19 deaths. If similar to those of Canada, there would have been 117,622 fewer deaths in the United States.
The US death rate was lower than six other countries with high COVID-19 mortality in the early spring, including Belgium, Spain, and the United Kingdom. However, after May 10, the per capita mortality rate in the United States exceeded the others.
Between May 10 and Sept. 19, the death rate in Italy was 9.1 per 100,000, vs 36.9 per 100,000.
“After the first peak in early spring, US death rates from COVID-19 and from all causes remained higher than even countries with high COVID-19 mortality,” the researchers note. “This may have been a result of several factors, including weak public health infrastructure and a decentralized, inconsistent US response to the pandemic.”
“Mortifying and motivating”
Woolf and colleagues estimate that more than 225,000 excess deaths occurred in recent months; this represents a 20% increase over expected deaths, note Harvey V. Fineberg, MD, PhD, of the Gordon and Betty Moore Foundation, in an accompanying editorial in JAMA.
“Importantly, a condition such as COVID-19 can contribute both directly and indirectly to excess mortality,” he writes.
Although the direct contribution to the mortality rates by those infected is straightforward, “the indirect contribution may relate to circumstances or choices due to the COVID-19 pandemic: for example, a patient who develops symptoms of a stroke is too concerned about COVID-19 to go to the emergency department, and a potentially reversible condition becomes fatal.”
Fineberg notes that “a general indication of the death toll from COVID-19 and the excess deaths related to the pandemic, as presented by Woolf et al, are sufficiently mortifying and motivating.”
“Profound human toll”
“The importance of the estimate by Woolf et al – which suggests that for the entirety of 2020, more than 400,000 excess deaths will occur – cannot be overstated, because it accounts for what could be declines in some causes of death, like motor vehicle crashes, but increases in others, like myocardial infarction,” write Howard Bauchner, MD, editor in chief of JAMA, and Phil B. Fontanarosa, MD, MBA, executive editor of JAMA, in another accompanying editorial.
“These deaths reflect a true measure of the human cost of the Great Pandemic of 2020,” they add.
The study from Emanuel and Bilinski was notable for calculating the excess COVID-19 and all-cause mortality to Sept. 2020, they note. “After the initial peak in early spring, US death rates from COVID-19 and from all causes remained higher than rates in countries with high COVID-19 mortality.”
“Few people will forget the Great Pandemic of 2020, where and how they lived, how it substantially changed their lives, and for many, the profound human toll it has taken,” Bauchner and Fontanarosa write.
The study by Woolf and colleagues was supported by National Center for Advancing Translational Sciences, the National Institute on Aging, and the National Institute of Allergy and Infectious Diseases. The study by Bilinski and Emanuel was partially funded by the Colton Foundation. Woolf, Emanuel, Fineberg, Bauchner, and Fontanarosa have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Fourteen-day sports hiatus recommended for children after COVID-19
Children should not return to sports for 14 days after exposure to COVID-19, and those with moderate symptoms should undergo an electrocardiogram before returning, according to the American Academy of Pediatrics.
said Susannah Briskin, MD, a pediatric sports medicine specialist at Rainbow Babies and Children’s Hospital in Cleveland.
“There has been emerging evidence about cases of myocarditis occurring in athletes, including athletes who are asymptomatic with COVID-19,” she said in an interview.
The update aligns the AAP recommendations with those from the American College of Cardiologists, she added.
Recent imaging studies have turned up signs of myocarditis in athletes recovering from mild or asymptomatic cases of COVID-19 and have prompted calls for clearer guidelines about imaging studies and return to play.
Viral myocarditis poses a risk to athletes because it can lead to potentially fatal arrhythmias, Dr. Briskin said.
Although children benefit from participating in sports, these activities also put them at risk of contracting COVID-19 and spreading it to others, the guidance noted.
To balance the risks and benefits, the academy proposed guidelines that vary depending on the severity of the presentation.
In the first category are patients with a severe presentation (hypotension, arrhythmias, need for intubation or extracorporeal membrane oxygenation support, kidney or cardiac failure) or with multisystem inflammatory syndrome. Clinicians should treat these patients as though they have myocarditis. Patients should be restricted from engaging in sports and other exercise for 3-6 months, the guidance stated.
The primary care physician and “appropriate pediatric medical subspecialist, preferably in consultation with a pediatric cardiologist,” should clear them before they return to activities. In examining patients for return to play, clinicians should focus on cardiac symptoms, including chest pain, shortness of breath, fatigue, palpitations, or syncope, the guidance said.
In another category are patients with cardiac symptoms, those with concerning findings on examination, and those with moderate symptoms of COVID-19, including prolonged fever. These patients should undergo an ECG and possibly be referred to a pediatric cardiologist, the guidelines said. These symptoms must be absent for at least 14 days before these patients can return to sports, and the athletes should obtain clearance from their primary care physicians before they resume.
In a third category are patients who have been infected with SARS-CoV-2 or who have had close contact with someone who was infected but who have not themselves experienced symptoms. These athletes should refrain from sports for at least 14 days, the guidelines said.
Children who don’t fall into any of these categories should not be tested for the virus or antibodies to it before participation in sports, the academy said.
The guidelines don’t vary depending on the sport. But the academy has issued separate guidance for parents and guardians to help them evaluate the risk for COVID-19 transmission by sport.
Athletes participating in “sports that have greater amount of contact time or proximity to people would be at higher risk for contracting COVID-19,” Dr. Briskin said. “But I think that’s all fairly common sense, given the recommendations for non–sport-related activity just in terms of social distancing and masking.”
The new guidance called on sports organizers to minimize contact by, for example, modifying drills and conditioning. It recommended that athletes wear masks except during vigorous exercise or when participating in water sports, as well as in other circumstances in which the mask could become a safety hazard.
They also recommended using handwashing stations or hand sanitizer, avoiding contact with shared surfaces, and avoiding small rooms and areas with poor ventilation.
Dr. Briskin disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Children should not return to sports for 14 days after exposure to COVID-19, and those with moderate symptoms should undergo an electrocardiogram before returning, according to the American Academy of Pediatrics.
said Susannah Briskin, MD, a pediatric sports medicine specialist at Rainbow Babies and Children’s Hospital in Cleveland.
“There has been emerging evidence about cases of myocarditis occurring in athletes, including athletes who are asymptomatic with COVID-19,” she said in an interview.
The update aligns the AAP recommendations with those from the American College of Cardiologists, she added.
Recent imaging studies have turned up signs of myocarditis in athletes recovering from mild or asymptomatic cases of COVID-19 and have prompted calls for clearer guidelines about imaging studies and return to play.
Viral myocarditis poses a risk to athletes because it can lead to potentially fatal arrhythmias, Dr. Briskin said.
Although children benefit from participating in sports, these activities also put them at risk of contracting COVID-19 and spreading it to others, the guidance noted.
To balance the risks and benefits, the academy proposed guidelines that vary depending on the severity of the presentation.
In the first category are patients with a severe presentation (hypotension, arrhythmias, need for intubation or extracorporeal membrane oxygenation support, kidney or cardiac failure) or with multisystem inflammatory syndrome. Clinicians should treat these patients as though they have myocarditis. Patients should be restricted from engaging in sports and other exercise for 3-6 months, the guidance stated.
The primary care physician and “appropriate pediatric medical subspecialist, preferably in consultation with a pediatric cardiologist,” should clear them before they return to activities. In examining patients for return to play, clinicians should focus on cardiac symptoms, including chest pain, shortness of breath, fatigue, palpitations, or syncope, the guidance said.
In another category are patients with cardiac symptoms, those with concerning findings on examination, and those with moderate symptoms of COVID-19, including prolonged fever. These patients should undergo an ECG and possibly be referred to a pediatric cardiologist, the guidelines said. These symptoms must be absent for at least 14 days before these patients can return to sports, and the athletes should obtain clearance from their primary care physicians before they resume.
In a third category are patients who have been infected with SARS-CoV-2 or who have had close contact with someone who was infected but who have not themselves experienced symptoms. These athletes should refrain from sports for at least 14 days, the guidelines said.
Children who don’t fall into any of these categories should not be tested for the virus or antibodies to it before participation in sports, the academy said.
The guidelines don’t vary depending on the sport. But the academy has issued separate guidance for parents and guardians to help them evaluate the risk for COVID-19 transmission by sport.
Athletes participating in “sports that have greater amount of contact time or proximity to people would be at higher risk for contracting COVID-19,” Dr. Briskin said. “But I think that’s all fairly common sense, given the recommendations for non–sport-related activity just in terms of social distancing and masking.”
The new guidance called on sports organizers to minimize contact by, for example, modifying drills and conditioning. It recommended that athletes wear masks except during vigorous exercise or when participating in water sports, as well as in other circumstances in which the mask could become a safety hazard.
They also recommended using handwashing stations or hand sanitizer, avoiding contact with shared surfaces, and avoiding small rooms and areas with poor ventilation.
Dr. Briskin disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Children should not return to sports for 14 days after exposure to COVID-19, and those with moderate symptoms should undergo an electrocardiogram before returning, according to the American Academy of Pediatrics.
said Susannah Briskin, MD, a pediatric sports medicine specialist at Rainbow Babies and Children’s Hospital in Cleveland.
“There has been emerging evidence about cases of myocarditis occurring in athletes, including athletes who are asymptomatic with COVID-19,” she said in an interview.
The update aligns the AAP recommendations with those from the American College of Cardiologists, she added.
Recent imaging studies have turned up signs of myocarditis in athletes recovering from mild or asymptomatic cases of COVID-19 and have prompted calls for clearer guidelines about imaging studies and return to play.
Viral myocarditis poses a risk to athletes because it can lead to potentially fatal arrhythmias, Dr. Briskin said.
Although children benefit from participating in sports, these activities also put them at risk of contracting COVID-19 and spreading it to others, the guidance noted.
To balance the risks and benefits, the academy proposed guidelines that vary depending on the severity of the presentation.
In the first category are patients with a severe presentation (hypotension, arrhythmias, need for intubation or extracorporeal membrane oxygenation support, kidney or cardiac failure) or with multisystem inflammatory syndrome. Clinicians should treat these patients as though they have myocarditis. Patients should be restricted from engaging in sports and other exercise for 3-6 months, the guidance stated.
The primary care physician and “appropriate pediatric medical subspecialist, preferably in consultation with a pediatric cardiologist,” should clear them before they return to activities. In examining patients for return to play, clinicians should focus on cardiac symptoms, including chest pain, shortness of breath, fatigue, palpitations, or syncope, the guidance said.
In another category are patients with cardiac symptoms, those with concerning findings on examination, and those with moderate symptoms of COVID-19, including prolonged fever. These patients should undergo an ECG and possibly be referred to a pediatric cardiologist, the guidelines said. These symptoms must be absent for at least 14 days before these patients can return to sports, and the athletes should obtain clearance from their primary care physicians before they resume.
In a third category are patients who have been infected with SARS-CoV-2 or who have had close contact with someone who was infected but who have not themselves experienced symptoms. These athletes should refrain from sports for at least 14 days, the guidelines said.
Children who don’t fall into any of these categories should not be tested for the virus or antibodies to it before participation in sports, the academy said.
The guidelines don’t vary depending on the sport. But the academy has issued separate guidance for parents and guardians to help them evaluate the risk for COVID-19 transmission by sport.
Athletes participating in “sports that have greater amount of contact time or proximity to people would be at higher risk for contracting COVID-19,” Dr. Briskin said. “But I think that’s all fairly common sense, given the recommendations for non–sport-related activity just in terms of social distancing and masking.”
The new guidance called on sports organizers to minimize contact by, for example, modifying drills and conditioning. It recommended that athletes wear masks except during vigorous exercise or when participating in water sports, as well as in other circumstances in which the mask could become a safety hazard.
They also recommended using handwashing stations or hand sanitizer, avoiding contact with shared surfaces, and avoiding small rooms and areas with poor ventilation.
Dr. Briskin disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Hospital leadership lessons in the era of COVID-19
The year 2020 has brought the COVID-19 pandemic and civil unrest and protests, which have resulted in unprecedented health care challenges to hospitals and clinics. The daunting prospect of a fall influenza season has hospital staff and administrators looking ahead to still greater challenges.

This year of crisis has put even greater emphasis on leadership in hospitals, as patients, clinicians, and staff look for direction in the face of uncertainty and stress. But hospital leaders often arrive at their positions unprepared for their roles, according to Leonard Marcus, PhD, director of the Program for Health Care Negotiation and Conflict Resolution at Harvard T.H. Chan School of Public Health, Boston.
“Many times what happens in medicine is that someone with the greatest technical skills or greatest clinical skills emerges to be leader of a department, or a group, or a hospital, without having really paid attention to how they can build their leadership skills,” Dr. Marcus said during the 2020 Society of Hospital Medicine Leadership Virtual Seminar, held online Sept. 16-17.
Over 2 days, Dr. Marcus discussed the complex environments faced by hospital leaders, and some of the tools and strategies that can be used to maintain calm, problem-solve, and chart a course ahead.
He emphasized that hospitals and medical systems are complex, nonlinear organizations, which could be swept up by change in the form of mergers, financial policies, patient surges due to local emergencies, or pandemics.
“Complexity has to be central to how you think about leadership. If you think you can control everything, that doesn’t work that well,” said Dr. Marcus.
Most think of leadership as hierarchical, with a boss on top and underlings below, though this is starting to change. Dr. Marcus suggested a different view. Instead of just “leading down” to those who report to them, leaders should consider “leading up” to their own bosses or oversight committees, and across to other departments or even beyond to interlinked organizations such as nursing homes.
“Being able to build that connectivity not only within your hospital, but beyond your hospital, lets you see the chain that goes through the experience of any patient. You are looking at the problem from a much wider lens. We call this meta-leadership,” Dr. Marcus said.
A key focus of meta-leadership is to create a culture where individuals are working together to help one another succeed. Leadership in hospitals is often dominated by egos, with individual leaders battling one another in a win-lose effort, and this gets in the way of incorporating different perspectives into problem-solving.
Dr. Marcus used an example from previous seminars in which he instructed participants to arm wrestle the person sitting next to them. The goal was to attain as many pins as possible in 30 seconds. About half would fight as hard as they could, and achieve a few victories. The other half worked cooperatively, letting one person win, then the other, so that they could have 30 or 40 wins each. Dr. Marcus told the story of a young nurse who was paired up with a much stronger surgeon. She let him win twice, and when he asked her why she wasn’t resisting, she took his arm and placed it in a winning position, then a losing position, and then a winning position again, and he instantly understood that the cooperative approach could be more effective. Why didn’t she just tell him? She told Dr. Marcus that she knew he wouldn’t take instruction, so she let him win and then demonstrated an alternative. “We nurses learned how to do that a long time ago,” she told Dr. Marcus.
The idea is collaborative problem-solving. “How do you orient people looking to you for leadership so that we’re in this together and we can accomplish a whole lot more in 30 seconds if we’re working together instead of always battling one another? If we’re always battling one another, we’re putting all of our effort into the contest,” said Dr. Marcus. This sort of approach is all the more important when facing the complexity experienced by hospital systems, especially during crises such as COVID-19.
A critical element of meta-leadership is emotional intelligence, which includes elements such as self-awareness, self-regulation, empathy, determining motivation of yourself and others, and the social skills to portray yourself as caring, open, and interested.
Emotional intelligence also can help recognize when you’ve entered survival mode in reaction to a crisis or incident, or something as simple as losing your car keys – what Dr. Marcus terms “going to the basement.” Responses revolve around freeze, fight, or flight. It’s helpful in the wake of a car accident, but not when trying to make managerial decisions or respond to a complex situation. It’s vital for leaders to quickly get themselves out of the basement, said Dr. Marcus, and that they help other members of the team get out as well.
He recommended protocols designed in advance, both to recognize when you’re in the basement, and to lift yourself out. Dr. Marcus uses a trigger script, telling himself “I can do this,” and then when he’s working with other people, “we can do this.” He also speaks slowly, measuring every word. Whatever you do, “it has to be a pivot you do to get yourself out of the basement,” he said. It can be helpful to predict the kinds of situations that send you “to the basement” to help recognize it when it has happened.
It’s very important not to lead, negotiate, or make important decisions while in the basement, according to Dr. Marcus. If one thinks about some of the things they’ve said to others while under duress, they are often some of the statements they regret most.
Practical leadership skills
On the second day of the Leadership Seminar, Dr. Marcus moved his focus to using leadership skills and techniques. One important technique is to incorporate multiple perspectives. He gave the example of an opaque cube with a cone inside it, with a window on the side and one on top. Viewers from the side see the cone in profile, and see it as a triangle. Viewers from the top see an aerial perspective that looks like the circular base of the cone. The two groups could argue about what’s inside the cube, but they can only identify the object if they work together.
“When dealing with complex reality, you oftentimes find there are different people with different perspectives on a problem. They may have different experiences of what the problem is, and what often happens is that people get into an adversarial fight. Looking at the problem from different perspectives actually allows a much richer and more comprehensive view,” said Dr. Marcus.
The metaphor comes from a study of the tragic events at the Twin Towers in Manhattan on Sept. 11, 2001. The New York Fire Department had a command center at the base of the building, while the police had a helicopter flying around the buildings. The helicopter could see the steel girders beginning to melt and predicted a collapse, and therefore ordered their personnel out of the buildings. But they were unable to convey that information to the firefighters, who continued to send personnel into the buildings. In all, 343 firefighters lost their lives. The police force lost 32.
To best understand a problem, a key element is the “unknown knowns.” That is, information that is available, that someone has, but is unknown to you. It takes some imagination to conceive of what “unknown knowns” might be out there, but it’s worth the effort to identify possible knowledge sources. It’s vital to seek out this information, because a common leadership mistake is to assume you know something when you really don’t.
“In many ways what you’re doing is looking for obstacles. It could be you don’t have access to the information, that it’s beyond some sort of curtain you need to overcome, or it could be people in your own department who have the information and they’re not sharing it with you,” Dr. Marcus said.
He outlined a tool called the POP-DOC loop, which is a 6-step exercise designed to analyze problems and implement solutions. Step 1 is Perceiving the situation, determining knowns and unknowns, and incorporating multiple perspectives, emotions, and politics. Step 2 is to Orient oneself: examine patterns and how they may replicate themselves as long as conditions don’t change. For example, during COVID-19, physicians have begun to learn how the virus transmits and how it affects the immune system. Step 3, based on those patterns is to make Predictions. With COVID-19, it’s predictable that people who assemble without wearing masks are vulnerable to transmission. Step 4 is to use the predictions to begin to make Decisions. Step 5 is to begin Operationalizing those decisions, and step 6 is to Communicate those decisions effectively.
Dr. Marcus emphasized that POP-DOC is not a one-time exercise. Once decisions have been made and implemented, if they aren’t having the planned effect, it’s important to incorporate the results of those actions and start right back at the beginning of the POP-DOC loop.
“The POP side of the loop is perceiving, analysis. You get out of the basement and understand the situation that surrounds you. On the DOC side, you lead down, lead up, lead across and lead beyond. You’re bringing people into the action to get things done,” Dr. Marcus said.
Another tool Dr. Marcus described, aimed at problem-solving and negotiation, is the “Walk in the Woods.” The idea is to bring two parties together to help each other succeed. The first step is Self-Interest, where both parties articulate their objectives, perspectives, and fears. The second step, Enlarged Interests, requires each party to list their points of agreement, and only then should they focus on and list their points of disagreement. During conflict, people tend to focus on their disagreements. The parties often find that they agree on more than they realize, and this can frame the disagreements as more manageable. The third step, Enlightened Interest, is a free thinking period where both parties come up with potential solutions that had not been previously considered. In step 4, Aligned Interests, the parties discuss some of those ideas that can be explored further.
The Walk in the Woods is applicable to a wide range of situations, and negotiation is central to being a leader. “Being a clinician is all about negotiating – with patients, family members, with other clinicians, with the institution,” Dr. Marcus said. “We all want the patient to have the best possible care, and in the course of those conversations if we can better understand people, have empathy, and if there are new ideas or ways we can individualize our care, let’s do it, and then at the end of the day combine our motivations so that we’re providing the best possible care.”
In the end, meta-leadership is about creating a culture where individuals strive to help each other succeed, said Dr. Marcus. “That’s the essence: involving people, making them part of the solution, and if it’s a solution they’ve created together, everyone wants to make that solution a success.”
For more information, see the book “You’re It,” coauthored by Dr. Marcus, and available on Amazon for $16.99 in hardback, or $3.99 in Kindle format.
The year 2020 has brought the COVID-19 pandemic and civil unrest and protests, which have resulted in unprecedented health care challenges to hospitals and clinics. The daunting prospect of a fall influenza season has hospital staff and administrators looking ahead to still greater challenges.
This year of crisis has put even greater emphasis on leadership in hospitals, as patients, clinicians, and staff look for direction in the face of uncertainty and stress. But hospital leaders often arrive at their positions unprepared for their roles, according to Leonard Marcus, PhD, director of the Program for Health Care Negotiation and Conflict Resolution at Harvard T.H. Chan School of Public Health, Boston.
“Many times what happens in medicine is that someone with the greatest technical skills or greatest clinical skills emerges to be leader of a department, or a group, or a hospital, without having really paid attention to how they can build their leadership skills,” Dr. Marcus said during the 2020 Society of Hospital Medicine Leadership Virtual Seminar, held online Sept. 16-17.
Over 2 days, Dr. Marcus discussed the complex environments faced by hospital leaders, and some of the tools and strategies that can be used to maintain calm, problem-solve, and chart a course ahead.
He emphasized that hospitals and medical systems are complex, nonlinear organizations, which could be swept up by change in the form of mergers, financial policies, patient surges due to local emergencies, or pandemics.
“Complexity has to be central to how you think about leadership. If you think you can control everything, that doesn’t work that well,” said Dr. Marcus.
Most think of leadership as hierarchical, with a boss on top and underlings below, though this is starting to change. Dr. Marcus suggested a different view. Instead of just “leading down” to those who report to them, leaders should consider “leading up” to their own bosses or oversight committees, and across to other departments or even beyond to interlinked organizations such as nursing homes.
“Being able to build that connectivity not only within your hospital, but beyond your hospital, lets you see the chain that goes through the experience of any patient. You are looking at the problem from a much wider lens. We call this meta-leadership,” Dr. Marcus said.
A key focus of meta-leadership is to create a culture where individuals are working together to help one another succeed. Leadership in hospitals is often dominated by egos, with individual leaders battling one another in a win-lose effort, and this gets in the way of incorporating different perspectives into problem-solving.
Dr. Marcus used an example from previous seminars in which he instructed participants to arm wrestle the person sitting next to them. The goal was to attain as many pins as possible in 30 seconds. About half would fight as hard as they could, and achieve a few victories. The other half worked cooperatively, letting one person win, then the other, so that they could have 30 or 40 wins each. Dr. Marcus told the story of a young nurse who was paired up with a much stronger surgeon. She let him win twice, and when he asked her why she wasn’t resisting, she took his arm and placed it in a winning position, then a losing position, and then a winning position again, and he instantly understood that the cooperative approach could be more effective. Why didn’t she just tell him? She told Dr. Marcus that she knew he wouldn’t take instruction, so she let him win and then demonstrated an alternative. “We nurses learned how to do that a long time ago,” she told Dr. Marcus.
The idea is collaborative problem-solving. “How do you orient people looking to you for leadership so that we’re in this together and we can accomplish a whole lot more in 30 seconds if we’re working together instead of always battling one another? If we’re always battling one another, we’re putting all of our effort into the contest,” said Dr. Marcus. This sort of approach is all the more important when facing the complexity experienced by hospital systems, especially during crises such as COVID-19.
A critical element of meta-leadership is emotional intelligence, which includes elements such as self-awareness, self-regulation, empathy, determining motivation of yourself and others, and the social skills to portray yourself as caring, open, and interested.
Emotional intelligence also can help recognize when you’ve entered survival mode in reaction to a crisis or incident, or something as simple as losing your car keys – what Dr. Marcus terms “going to the basement.” Responses revolve around freeze, fight, or flight. It’s helpful in the wake of a car accident, but not when trying to make managerial decisions or respond to a complex situation. It’s vital for leaders to quickly get themselves out of the basement, said Dr. Marcus, and that they help other members of the team get out as well.
He recommended protocols designed in advance, both to recognize when you’re in the basement, and to lift yourself out. Dr. Marcus uses a trigger script, telling himself “I can do this,” and then when he’s working with other people, “we can do this.” He also speaks slowly, measuring every word. Whatever you do, “it has to be a pivot you do to get yourself out of the basement,” he said. It can be helpful to predict the kinds of situations that send you “to the basement” to help recognize it when it has happened.
It’s very important not to lead, negotiate, or make important decisions while in the basement, according to Dr. Marcus. If one thinks about some of the things they’ve said to others while under duress, they are often some of the statements they regret most.
Practical leadership skills
On the second day of the Leadership Seminar, Dr. Marcus moved his focus to using leadership skills and techniques. One important technique is to incorporate multiple perspectives. He gave the example of an opaque cube with a cone inside it, with a window on the side and one on top. Viewers from the side see the cone in profile, and see it as a triangle. Viewers from the top see an aerial perspective that looks like the circular base of the cone. The two groups could argue about what’s inside the cube, but they can only identify the object if they work together.
“When dealing with complex reality, you oftentimes find there are different people with different perspectives on a problem. They may have different experiences of what the problem is, and what often happens is that people get into an adversarial fight. Looking at the problem from different perspectives actually allows a much richer and more comprehensive view,” said Dr. Marcus.
The metaphor comes from a study of the tragic events at the Twin Towers in Manhattan on Sept. 11, 2001. The New York Fire Department had a command center at the base of the building, while the police had a helicopter flying around the buildings. The helicopter could see the steel girders beginning to melt and predicted a collapse, and therefore ordered their personnel out of the buildings. But they were unable to convey that information to the firefighters, who continued to send personnel into the buildings. In all, 343 firefighters lost their lives. The police force lost 32.
To best understand a problem, a key element is the “unknown knowns.” That is, information that is available, that someone has, but is unknown to you. It takes some imagination to conceive of what “unknown knowns” might be out there, but it’s worth the effort to identify possible knowledge sources. It’s vital to seek out this information, because a common leadership mistake is to assume you know something when you really don’t.
“In many ways what you’re doing is looking for obstacles. It could be you don’t have access to the information, that it’s beyond some sort of curtain you need to overcome, or it could be people in your own department who have the information and they’re not sharing it with you,” Dr. Marcus said.
He outlined a tool called the POP-DOC loop, which is a 6-step exercise designed to analyze problems and implement solutions. Step 1 is Perceiving the situation, determining knowns and unknowns, and incorporating multiple perspectives, emotions, and politics. Step 2 is to Orient oneself: examine patterns and how they may replicate themselves as long as conditions don’t change. For example, during COVID-19, physicians have begun to learn how the virus transmits and how it affects the immune system. Step 3, based on those patterns is to make Predictions. With COVID-19, it’s predictable that people who assemble without wearing masks are vulnerable to transmission. Step 4 is to use the predictions to begin to make Decisions. Step 5 is to begin Operationalizing those decisions, and step 6 is to Communicate those decisions effectively.
Dr. Marcus emphasized that POP-DOC is not a one-time exercise. Once decisions have been made and implemented, if they aren’t having the planned effect, it’s important to incorporate the results of those actions and start right back at the beginning of the POP-DOC loop.
“The POP side of the loop is perceiving, analysis. You get out of the basement and understand the situation that surrounds you. On the DOC side, you lead down, lead up, lead across and lead beyond. You’re bringing people into the action to get things done,” Dr. Marcus said.
Another tool Dr. Marcus described, aimed at problem-solving and negotiation, is the “Walk in the Woods.” The idea is to bring two parties together to help each other succeed. The first step is Self-Interest, where both parties articulate their objectives, perspectives, and fears. The second step, Enlarged Interests, requires each party to list their points of agreement, and only then should they focus on and list their points of disagreement. During conflict, people tend to focus on their disagreements. The parties often find that they agree on more than they realize, and this can frame the disagreements as more manageable. The third step, Enlightened Interest, is a free thinking period where both parties come up with potential solutions that had not been previously considered. In step 4, Aligned Interests, the parties discuss some of those ideas that can be explored further.
The Walk in the Woods is applicable to a wide range of situations, and negotiation is central to being a leader. “Being a clinician is all about negotiating – with patients, family members, with other clinicians, with the institution,” Dr. Marcus said. “We all want the patient to have the best possible care, and in the course of those conversations if we can better understand people, have empathy, and if there are new ideas or ways we can individualize our care, let’s do it, and then at the end of the day combine our motivations so that we’re providing the best possible care.”
In the end, meta-leadership is about creating a culture where individuals strive to help each other succeed, said Dr. Marcus. “That’s the essence: involving people, making them part of the solution, and if it’s a solution they’ve created together, everyone wants to make that solution a success.”
For more information, see the book “You’re It,” coauthored by Dr. Marcus, and available on Amazon for $16.99 in hardback, or $3.99 in Kindle format.
The year 2020 has brought the COVID-19 pandemic and civil unrest and protests, which have resulted in unprecedented health care challenges to hospitals and clinics. The daunting prospect of a fall influenza season has hospital staff and administrators looking ahead to still greater challenges.
This year of crisis has put even greater emphasis on leadership in hospitals, as patients, clinicians, and staff look for direction in the face of uncertainty and stress. But hospital leaders often arrive at their positions unprepared for their roles, according to Leonard Marcus, PhD, director of the Program for Health Care Negotiation and Conflict Resolution at Harvard T.H. Chan School of Public Health, Boston.
“Many times what happens in medicine is that someone with the greatest technical skills or greatest clinical skills emerges to be leader of a department, or a group, or a hospital, without having really paid attention to how they can build their leadership skills,” Dr. Marcus said during the 2020 Society of Hospital Medicine Leadership Virtual Seminar, held online Sept. 16-17.
Over 2 days, Dr. Marcus discussed the complex environments faced by hospital leaders, and some of the tools and strategies that can be used to maintain calm, problem-solve, and chart a course ahead.
He emphasized that hospitals and medical systems are complex, nonlinear organizations, which could be swept up by change in the form of mergers, financial policies, patient surges due to local emergencies, or pandemics.
“Complexity has to be central to how you think about leadership. If you think you can control everything, that doesn’t work that well,” said Dr. Marcus.
Most think of leadership as hierarchical, with a boss on top and underlings below, though this is starting to change. Dr. Marcus suggested a different view. Instead of just “leading down” to those who report to them, leaders should consider “leading up” to their own bosses or oversight committees, and across to other departments or even beyond to interlinked organizations such as nursing homes.
“Being able to build that connectivity not only within your hospital, but beyond your hospital, lets you see the chain that goes through the experience of any patient. You are looking at the problem from a much wider lens. We call this meta-leadership,” Dr. Marcus said.
A key focus of meta-leadership is to create a culture where individuals are working together to help one another succeed. Leadership in hospitals is often dominated by egos, with individual leaders battling one another in a win-lose effort, and this gets in the way of incorporating different perspectives into problem-solving.
Dr. Marcus used an example from previous seminars in which he instructed participants to arm wrestle the person sitting next to them. The goal was to attain as many pins as possible in 30 seconds. About half would fight as hard as they could, and achieve a few victories. The other half worked cooperatively, letting one person win, then the other, so that they could have 30 or 40 wins each. Dr. Marcus told the story of a young nurse who was paired up with a much stronger surgeon. She let him win twice, and when he asked her why she wasn’t resisting, she took his arm and placed it in a winning position, then a losing position, and then a winning position again, and he instantly understood that the cooperative approach could be more effective. Why didn’t she just tell him? She told Dr. Marcus that she knew he wouldn’t take instruction, so she let him win and then demonstrated an alternative. “We nurses learned how to do that a long time ago,” she told Dr. Marcus.
The idea is collaborative problem-solving. “How do you orient people looking to you for leadership so that we’re in this together and we can accomplish a whole lot more in 30 seconds if we’re working together instead of always battling one another? If we’re always battling one another, we’re putting all of our effort into the contest,” said Dr. Marcus. This sort of approach is all the more important when facing the complexity experienced by hospital systems, especially during crises such as COVID-19.
A critical element of meta-leadership is emotional intelligence, which includes elements such as self-awareness, self-regulation, empathy, determining motivation of yourself and others, and the social skills to portray yourself as caring, open, and interested.
Emotional intelligence also can help recognize when you’ve entered survival mode in reaction to a crisis or incident, or something as simple as losing your car keys – what Dr. Marcus terms “going to the basement.” Responses revolve around freeze, fight, or flight. It’s helpful in the wake of a car accident, but not when trying to make managerial decisions or respond to a complex situation. It’s vital for leaders to quickly get themselves out of the basement, said Dr. Marcus, and that they help other members of the team get out as well.
He recommended protocols designed in advance, both to recognize when you’re in the basement, and to lift yourself out. Dr. Marcus uses a trigger script, telling himself “I can do this,” and then when he’s working with other people, “we can do this.” He also speaks slowly, measuring every word. Whatever you do, “it has to be a pivot you do to get yourself out of the basement,” he said. It can be helpful to predict the kinds of situations that send you “to the basement” to help recognize it when it has happened.
It’s very important not to lead, negotiate, or make important decisions while in the basement, according to Dr. Marcus. If one thinks about some of the things they’ve said to others while under duress, they are often some of the statements they regret most.
Practical leadership skills
On the second day of the Leadership Seminar, Dr. Marcus moved his focus to using leadership skills and techniques. One important technique is to incorporate multiple perspectives. He gave the example of an opaque cube with a cone inside it, with a window on the side and one on top. Viewers from the side see the cone in profile, and see it as a triangle. Viewers from the top see an aerial perspective that looks like the circular base of the cone. The two groups could argue about what’s inside the cube, but they can only identify the object if they work together.
“When dealing with complex reality, you oftentimes find there are different people with different perspectives on a problem. They may have different experiences of what the problem is, and what often happens is that people get into an adversarial fight. Looking at the problem from different perspectives actually allows a much richer and more comprehensive view,” said Dr. Marcus.
The metaphor comes from a study of the tragic events at the Twin Towers in Manhattan on Sept. 11, 2001. The New York Fire Department had a command center at the base of the building, while the police had a helicopter flying around the buildings. The helicopter could see the steel girders beginning to melt and predicted a collapse, and therefore ordered their personnel out of the buildings. But they were unable to convey that information to the firefighters, who continued to send personnel into the buildings. In all, 343 firefighters lost their lives. The police force lost 32.
To best understand a problem, a key element is the “unknown knowns.” That is, information that is available, that someone has, but is unknown to you. It takes some imagination to conceive of what “unknown knowns” might be out there, but it’s worth the effort to identify possible knowledge sources. It’s vital to seek out this information, because a common leadership mistake is to assume you know something when you really don’t.
“In many ways what you’re doing is looking for obstacles. It could be you don’t have access to the information, that it’s beyond some sort of curtain you need to overcome, or it could be people in your own department who have the information and they’re not sharing it with you,” Dr. Marcus said.
He outlined a tool called the POP-DOC loop, which is a 6-step exercise designed to analyze problems and implement solutions. Step 1 is Perceiving the situation, determining knowns and unknowns, and incorporating multiple perspectives, emotions, and politics. Step 2 is to Orient oneself: examine patterns and how they may replicate themselves as long as conditions don’t change. For example, during COVID-19, physicians have begun to learn how the virus transmits and how it affects the immune system. Step 3, based on those patterns is to make Predictions. With COVID-19, it’s predictable that people who assemble without wearing masks are vulnerable to transmission. Step 4 is to use the predictions to begin to make Decisions. Step 5 is to begin Operationalizing those decisions, and step 6 is to Communicate those decisions effectively.
Dr. Marcus emphasized that POP-DOC is not a one-time exercise. Once decisions have been made and implemented, if they aren’t having the planned effect, it’s important to incorporate the results of those actions and start right back at the beginning of the POP-DOC loop.
“The POP side of the loop is perceiving, analysis. You get out of the basement and understand the situation that surrounds you. On the DOC side, you lead down, lead up, lead across and lead beyond. You’re bringing people into the action to get things done,” Dr. Marcus said.
Another tool Dr. Marcus described, aimed at problem-solving and negotiation, is the “Walk in the Woods.” The idea is to bring two parties together to help each other succeed. The first step is Self-Interest, where both parties articulate their objectives, perspectives, and fears. The second step, Enlarged Interests, requires each party to list their points of agreement, and only then should they focus on and list their points of disagreement. During conflict, people tend to focus on their disagreements. The parties often find that they agree on more than they realize, and this can frame the disagreements as more manageable. The third step, Enlightened Interest, is a free thinking period where both parties come up with potential solutions that had not been previously considered. In step 4, Aligned Interests, the parties discuss some of those ideas that can be explored further.
The Walk in the Woods is applicable to a wide range of situations, and negotiation is central to being a leader. “Being a clinician is all about negotiating – with patients, family members, with other clinicians, with the institution,” Dr. Marcus said. “We all want the patient to have the best possible care, and in the course of those conversations if we can better understand people, have empathy, and if there are new ideas or ways we can individualize our care, let’s do it, and then at the end of the day combine our motivations so that we’re providing the best possible care.”
In the end, meta-leadership is about creating a culture where individuals strive to help each other succeed, said Dr. Marcus. “That’s the essence: involving people, making them part of the solution, and if it’s a solution they’ve created together, everyone wants to make that solution a success.”
For more information, see the book “You’re It,” coauthored by Dr. Marcus, and available on Amazon for $16.99 in hardback, or $3.99 in Kindle format.
FROM THE SHM LEADERSHIP SEMINAR