User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

Quick Byte: Trauma care
Innovating quickly
The U.S. military has completely transformed trauma care over the past 17 years, and that success offers lessons for civilian medicine.

In the civilian world, it takes an average of 17 years for a new discovery to change medical practice, but the military has developed or significantly expanded more than 27 major innovations, such as redesigned tourniquets and new transport procedures, in about a decade. As a result, the death rate from battlefield wounds has decreased by half.
Reference
Kellermann A et al. How the US military reinvented trauma care and what this means for US medicine. Health Aff. 2018 Jul 3. doi: 10.1377/hblog20180628.431867.
Innovating quickly
Innovating quickly
The U.S. military has completely transformed trauma care over the past 17 years, and that success offers lessons for civilian medicine.
In the civilian world, it takes an average of 17 years for a new discovery to change medical practice, but the military has developed or significantly expanded more than 27 major innovations, such as redesigned tourniquets and new transport procedures, in about a decade. As a result, the death rate from battlefield wounds has decreased by half.
Reference
Kellermann A et al. How the US military reinvented trauma care and what this means for US medicine. Health Aff. 2018 Jul 3. doi: 10.1377/hblog20180628.431867.
The U.S. military has completely transformed trauma care over the past 17 years, and that success offers lessons for civilian medicine.
In the civilian world, it takes an average of 17 years for a new discovery to change medical practice, but the military has developed or significantly expanded more than 27 major innovations, such as redesigned tourniquets and new transport procedures, in about a decade. As a result, the death rate from battlefield wounds has decreased by half.
Reference
Kellermann A et al. How the US military reinvented trauma care and what this means for US medicine. Health Aff. 2018 Jul 3. doi: 10.1377/hblog20180628.431867.
Intensive blood pressure lowering may not reduce risk of recurrent stroke
HONOLULU – according to research presented at the International Stroke Conference sponsored by the American Heart Association.
Combined with data from previous trials, these results support a target systolic blood pressure of less than 130 mm Hg and a diastolic blood pressure of less than 80 mm Hg for secondary stroke prevention, said Kazuo Kitagawa, MD, PhD.
Lowering blood pressure reduces the risk of recurrent stroke, but investigators have not identified the best target blood pressure for this indication. The Secondary Prevention of Small Subcortical Strokes Trial (SPS3) examined the efficacy of intensive blood pressure treatment for secondary stroke prevention. The investigators randomized more than 3,000 patients with recent lacunar stroke to intensive or standard blood pressure treatment. Intensive treatment (a target systolic blood pressure of less than 130 mm Hg) conferred a nonsignificant reduction of the risk of recurrent stroke. A 2018 meta-analysis of SPS3 and two smaller randomized controlled trials also showed that intensive treatment did not significantly reduce the risk of recurrent stroke.
A new multicenter trial
Dr. Kitagawa, of Tokyo Women’s Medical University, and colleagues conducted a new trial to evaluate whether intensive blood pressure reduction significantly reduced the risk of recurrent stroke, compared with standard treatment (a systolic target of less than 140 mm Hg and a diastolic target of less than 90 mm Hg). Between 2010 and 2016, they enrolled patients with a history of stroke within the previous 3 years at 140 hospitals in Japan. Participants were randomized to standard blood pressure treatment or intensive blood pressure treatment (defined in this study as a systolic target of less than 120 mm Hg and a diastolic target of less than 80 mm Hg). The primary end point was recurrent stroke.
Both treatment regimens were based on stepwise multidrug rationing. Step 1 was an angiotensin II receptor blockade (ARB), step 2 was the addition of diuretics, step 3 was the addition of calcium channel blockers, step 4 was an increase of the ARB, step 5 was increase of the calcium channel blocker, and step 6 was the addition of spironolactone.
This trial was stopped at the end of 2016 because of slow recruitment and funding cessation. Investigators randomized 1,280 patients out of a planned 2,000. Seventeen patients were excluded from analysis. At baseline, participants’ mean age was 67 years, and mean systolic blood pressure was 145 mm Hg. The qualifying event was ischemic stroke for 85% of patients and intracerebral hemorrhage for 15%. Mean follow-up duration was 3.9 years.
Intensive treatment reduced blood pressure
At 1 year, the mean systolic blood pressure was 132.0 mm Hg in the standard-treatment group and 123.7 mm Hg in the intensive-treatment group. Mean diastolic blood pressure was 77.5 mm Hg in the standard-treatment group and 72.8 mm Hg in the intensive-treatment group. The investigators observed a significant difference in blood pressure between the groups throughout the study period.
The annual rate of stroke recurrence was 2.26% in the standard-treatment group and 1.65% in the intensive-treatment group. Intensive treatment tended to reduce stroke recurrence (hazard ratio, 0.73), but the result was not statistically significant. “The nonsignificant finding might be due to early termination or the modest difference in blood pressure level [between groups],” said Dr. Kitagawa.
Subgroup analyses did not indicate any interaction between treatment group and age, sex, qualifying event, mean systolic blood pressure at baseline, or diabetes. The rate of ischemic stroke was similar between the two groups, but the rate of intracerebral hemorrhage was lower in the intensive treatment group than in the standard treatment group. The rate of serious adverse events was similar between treatment groups.
When Dr. Kitagawa and colleagues pooled their data with those examined in the 2018 meta-analysis, they found that intensive treatment significantly reduced the risk of recurrent stroke (hazard ratio, 0.68), compared with standard treatment.
This study was sponsored by Biomedis International.
SOURCE: Kitagawa K et al. ISC 2019, Abstract LB10.
HONOLULU – according to research presented at the International Stroke Conference sponsored by the American Heart Association.
Combined with data from previous trials, these results support a target systolic blood pressure of less than 130 mm Hg and a diastolic blood pressure of less than 80 mm Hg for secondary stroke prevention, said Kazuo Kitagawa, MD, PhD.
Lowering blood pressure reduces the risk of recurrent stroke, but investigators have not identified the best target blood pressure for this indication. The Secondary Prevention of Small Subcortical Strokes Trial (SPS3) examined the efficacy of intensive blood pressure treatment for secondary stroke prevention. The investigators randomized more than 3,000 patients with recent lacunar stroke to intensive or standard blood pressure treatment. Intensive treatment (a target systolic blood pressure of less than 130 mm Hg) conferred a nonsignificant reduction of the risk of recurrent stroke. A 2018 meta-analysis of SPS3 and two smaller randomized controlled trials also showed that intensive treatment did not significantly reduce the risk of recurrent stroke.
A new multicenter trial
Dr. Kitagawa, of Tokyo Women’s Medical University, and colleagues conducted a new trial to evaluate whether intensive blood pressure reduction significantly reduced the risk of recurrent stroke, compared with standard treatment (a systolic target of less than 140 mm Hg and a diastolic target of less than 90 mm Hg). Between 2010 and 2016, they enrolled patients with a history of stroke within the previous 3 years at 140 hospitals in Japan. Participants were randomized to standard blood pressure treatment or intensive blood pressure treatment (defined in this study as a systolic target of less than 120 mm Hg and a diastolic target of less than 80 mm Hg). The primary end point was recurrent stroke.
Both treatment regimens were based on stepwise multidrug rationing. Step 1 was an angiotensin II receptor blockade (ARB), step 2 was the addition of diuretics, step 3 was the addition of calcium channel blockers, step 4 was an increase of the ARB, step 5 was increase of the calcium channel blocker, and step 6 was the addition of spironolactone.
This trial was stopped at the end of 2016 because of slow recruitment and funding cessation. Investigators randomized 1,280 patients out of a planned 2,000. Seventeen patients were excluded from analysis. At baseline, participants’ mean age was 67 years, and mean systolic blood pressure was 145 mm Hg. The qualifying event was ischemic stroke for 85% of patients and intracerebral hemorrhage for 15%. Mean follow-up duration was 3.9 years.
Intensive treatment reduced blood pressure
At 1 year, the mean systolic blood pressure was 132.0 mm Hg in the standard-treatment group and 123.7 mm Hg in the intensive-treatment group. Mean diastolic blood pressure was 77.5 mm Hg in the standard-treatment group and 72.8 mm Hg in the intensive-treatment group. The investigators observed a significant difference in blood pressure between the groups throughout the study period.
The annual rate of stroke recurrence was 2.26% in the standard-treatment group and 1.65% in the intensive-treatment group. Intensive treatment tended to reduce stroke recurrence (hazard ratio, 0.73), but the result was not statistically significant. “The nonsignificant finding might be due to early termination or the modest difference in blood pressure level [between groups],” said Dr. Kitagawa.
Subgroup analyses did not indicate any interaction between treatment group and age, sex, qualifying event, mean systolic blood pressure at baseline, or diabetes. The rate of ischemic stroke was similar between the two groups, but the rate of intracerebral hemorrhage was lower in the intensive treatment group than in the standard treatment group. The rate of serious adverse events was similar between treatment groups.
When Dr. Kitagawa and colleagues pooled their data with those examined in the 2018 meta-analysis, they found that intensive treatment significantly reduced the risk of recurrent stroke (hazard ratio, 0.68), compared with standard treatment.
This study was sponsored by Biomedis International.
SOURCE: Kitagawa K et al. ISC 2019, Abstract LB10.
HONOLULU – according to research presented at the International Stroke Conference sponsored by the American Heart Association.
Combined with data from previous trials, these results support a target systolic blood pressure of less than 130 mm Hg and a diastolic blood pressure of less than 80 mm Hg for secondary stroke prevention, said Kazuo Kitagawa, MD, PhD.
Lowering blood pressure reduces the risk of recurrent stroke, but investigators have not identified the best target blood pressure for this indication. The Secondary Prevention of Small Subcortical Strokes Trial (SPS3) examined the efficacy of intensive blood pressure treatment for secondary stroke prevention. The investigators randomized more than 3,000 patients with recent lacunar stroke to intensive or standard blood pressure treatment. Intensive treatment (a target systolic blood pressure of less than 130 mm Hg) conferred a nonsignificant reduction of the risk of recurrent stroke. A 2018 meta-analysis of SPS3 and two smaller randomized controlled trials also showed that intensive treatment did not significantly reduce the risk of recurrent stroke.
A new multicenter trial
Dr. Kitagawa, of Tokyo Women’s Medical University, and colleagues conducted a new trial to evaluate whether intensive blood pressure reduction significantly reduced the risk of recurrent stroke, compared with standard treatment (a systolic target of less than 140 mm Hg and a diastolic target of less than 90 mm Hg). Between 2010 and 2016, they enrolled patients with a history of stroke within the previous 3 years at 140 hospitals in Japan. Participants were randomized to standard blood pressure treatment or intensive blood pressure treatment (defined in this study as a systolic target of less than 120 mm Hg and a diastolic target of less than 80 mm Hg). The primary end point was recurrent stroke.
Both treatment regimens were based on stepwise multidrug rationing. Step 1 was an angiotensin II receptor blockade (ARB), step 2 was the addition of diuretics, step 3 was the addition of calcium channel blockers, step 4 was an increase of the ARB, step 5 was increase of the calcium channel blocker, and step 6 was the addition of spironolactone.
This trial was stopped at the end of 2016 because of slow recruitment and funding cessation. Investigators randomized 1,280 patients out of a planned 2,000. Seventeen patients were excluded from analysis. At baseline, participants’ mean age was 67 years, and mean systolic blood pressure was 145 mm Hg. The qualifying event was ischemic stroke for 85% of patients and intracerebral hemorrhage for 15%. Mean follow-up duration was 3.9 years.
Intensive treatment reduced blood pressure
At 1 year, the mean systolic blood pressure was 132.0 mm Hg in the standard-treatment group and 123.7 mm Hg in the intensive-treatment group. Mean diastolic blood pressure was 77.5 mm Hg in the standard-treatment group and 72.8 mm Hg in the intensive-treatment group. The investigators observed a significant difference in blood pressure between the groups throughout the study period.
The annual rate of stroke recurrence was 2.26% in the standard-treatment group and 1.65% in the intensive-treatment group. Intensive treatment tended to reduce stroke recurrence (hazard ratio, 0.73), but the result was not statistically significant. “The nonsignificant finding might be due to early termination or the modest difference in blood pressure level [between groups],” said Dr. Kitagawa.
Subgroup analyses did not indicate any interaction between treatment group and age, sex, qualifying event, mean systolic blood pressure at baseline, or diabetes. The rate of ischemic stroke was similar between the two groups, but the rate of intracerebral hemorrhage was lower in the intensive treatment group than in the standard treatment group. The rate of serious adverse events was similar between treatment groups.
When Dr. Kitagawa and colleagues pooled their data with those examined in the 2018 meta-analysis, they found that intensive treatment significantly reduced the risk of recurrent stroke (hazard ratio, 0.68), compared with standard treatment.
This study was sponsored by Biomedis International.
SOURCE: Kitagawa K et al. ISC 2019, Abstract LB10.
REPORTING FROM ISC 2019
Improving research dissemination among hospitalists
Social media a great platform
Medical journals and societies are trying to figure out ways to use social media to connect with hospitalists and others interested in their subject matter, says Charlie Wray, DO, MS, lead author of a paper proposing a way they can do that: implementing a journal-sponsored club on Twitter.

“At the Journal of Hospital Medicine (JHM), we noticed that there was a large community of hospitalists on Twitter who were looking for a community to engage in hospital medicine topics,” Dr. Wray said. “We created #JHMChat to bring the hospital medicine community together on a regular basis to talk about pertinent research, medical education philosophies, and value-based care interventions. Our ultimate goal was to increase engagement, networking, and communication among this community, while highlighting the work that is being published in JHM.”
A study of #JHMChat showed that social media is a great platform for large organizations to reach out, connect, and create a community around, he added. “We were very surprised by both the Twitter metrics (i.e., number of participants and overall impressions), which showed very large dissemination numbers, in addition to the external dissemination metrics (i.e., page views and altmetrics scores), which showed that each chat basically corresponded to a release of a new issue. This could be informative to other journals as they look for ways to increase their web traffic or disseminate their work to their respective audiences.”
Dr. Wray hopes the study alerts hospitalists to the fact that there is a large and ever-growing community available within social media.
“Second, we know that careers in hospital medicine can be tough, regardless of whether you’re at a community hospital or a large academic center. Knowing that there is a community with which you can connect to is both comforting and reassuring.”
Reference
Wray C et al. The adoption of an online journal club to improve research dissemination and social media engagement among hospitalists. J Hosp Med. 2018 Nov;13(11):764-9.
Social media a great platform
Social media a great platform
Medical journals and societies are trying to figure out ways to use social media to connect with hospitalists and others interested in their subject matter, says Charlie Wray, DO, MS, lead author of a paper proposing a way they can do that: implementing a journal-sponsored club on Twitter.
“At the Journal of Hospital Medicine (JHM), we noticed that there was a large community of hospitalists on Twitter who were looking for a community to engage in hospital medicine topics,” Dr. Wray said. “We created #JHMChat to bring the hospital medicine community together on a regular basis to talk about pertinent research, medical education philosophies, and value-based care interventions. Our ultimate goal was to increase engagement, networking, and communication among this community, while highlighting the work that is being published in JHM.”
A study of #JHMChat showed that social media is a great platform for large organizations to reach out, connect, and create a community around, he added. “We were very surprised by both the Twitter metrics (i.e., number of participants and overall impressions), which showed very large dissemination numbers, in addition to the external dissemination metrics (i.e., page views and altmetrics scores), which showed that each chat basically corresponded to a release of a new issue. This could be informative to other journals as they look for ways to increase their web traffic or disseminate their work to their respective audiences.”
Dr. Wray hopes the study alerts hospitalists to the fact that there is a large and ever-growing community available within social media.
“Second, we know that careers in hospital medicine can be tough, regardless of whether you’re at a community hospital or a large academic center. Knowing that there is a community with which you can connect to is both comforting and reassuring.”
Reference
Wray C et al. The adoption of an online journal club to improve research dissemination and social media engagement among hospitalists. J Hosp Med. 2018 Nov;13(11):764-9.
Medical journals and societies are trying to figure out ways to use social media to connect with hospitalists and others interested in their subject matter, says Charlie Wray, DO, MS, lead author of a paper proposing a way they can do that: implementing a journal-sponsored club on Twitter.
“At the Journal of Hospital Medicine (JHM), we noticed that there was a large community of hospitalists on Twitter who were looking for a community to engage in hospital medicine topics,” Dr. Wray said. “We created #JHMChat to bring the hospital medicine community together on a regular basis to talk about pertinent research, medical education philosophies, and value-based care interventions. Our ultimate goal was to increase engagement, networking, and communication among this community, while highlighting the work that is being published in JHM.”
A study of #JHMChat showed that social media is a great platform for large organizations to reach out, connect, and create a community around, he added. “We were very surprised by both the Twitter metrics (i.e., number of participants and overall impressions), which showed very large dissemination numbers, in addition to the external dissemination metrics (i.e., page views and altmetrics scores), which showed that each chat basically corresponded to a release of a new issue. This could be informative to other journals as they look for ways to increase their web traffic or disseminate their work to their respective audiences.”
Dr. Wray hopes the study alerts hospitalists to the fact that there is a large and ever-growing community available within social media.
“Second, we know that careers in hospital medicine can be tough, regardless of whether you’re at a community hospital or a large academic center. Knowing that there is a community with which you can connect to is both comforting and reassuring.”
Reference
Wray C et al. The adoption of an online journal club to improve research dissemination and social media engagement among hospitalists. J Hosp Med. 2018 Nov;13(11):764-9.
Andexanet alfa effectively reverses factor Xa inhibition
HONOLULU – according to a study presented at the International Stroke Conference sponsored by the American Heart Association. The medication is associated with a low rate of mortality resulting from intracerebral hemorrhage (ICH), compared with the general population of patients with ICH receiving anticoagulation.

Factor Xa inhibitors such as apixaban and rivaroxaban effectively prevent thromboembolic events but may cause or exacerbate acute major bleeding. Andexanet alfa, a modified, recombinant, inactive form of human factor Xa, was developed and approved as a reversal agent for factor Xa inhibitors. In a 2015 study, andexanet rapidly and safely reversed anti–factor Xa activity in large cohorts of patients without bleeding.
A single-cohort study
Truman John Milling Jr., MD, an emergency medicine physician at Dell Seton Medical Center at the University of Texas in Austin, and his colleagues conducted the Andexanet Alfa, a Novel Antidote to the Anticoagulation Effects of Factor Xa Inhibitors (ANNEXA-4) study to evaluate the drug’s safety and efficacy in patients with acute major bleeding associated with treatment with a factor Xa inhibitor. For participants to be eligible, their bleeding had to be life threatening with signs of hemodynamic compromise, be associated with a decrease in hemoglobin level of at least 2 g/dL, or occur in a critical organ such as the brain. An independent academic committee determined whether patients met these criteria.
The trial’s primary efficacy outcomes were change from baseline in anti–factor Xa activity and the percentage of patients with excellent or good hemostatic efficacy at 12 hours. The primary safety endpoints were death, thrombotic events, and the development of neutralizing antibodies to andexanet or to native factor X and factor Xa. The efficacy population included patients with major bleeding and baseline anti–factor Xa activity of at least 75 ng/mL. The safety population included all patients who received a dose of andexanet. The independent committee adjudicated the efficacy and safety outcomes.
Hemostasis was sustained for 12 hours
The investigators enrolled 352 participants into the study, all of whom received andexanet and were followed for at least 30 days or until death. The population’s mean age was 77 years. “These were older and sicker patients with a significant amount of comorbid disease,” said Dr. Milling. The primary indication for anticoagulation was atrial fibrillation in 80% of patients. The primary site of bleeding was intracranial in 64% of patients and gastrointestinal in 26% of patients. The remaining 10% of patients had bleeding affecting other areas (such as pericardial or intramuscular bleeding).
The investigators included 254 patients in the efficacy population. At the end of the administration of the andexanet bolus, the median value for anti–factor Xa activity decreased by 92% among participants receiving apixaban, 92% among participants receiving rivaroxaban, and 75% among patients receiving enoxaparin. Among patients receiving apixaban, the median value for anti–factor Xa activity was decreased by 32% at 4 hours, 34% at 8 hours, and 38% at 12 hours. Among patients receiving rivaroxaban, the median value for anti–factor Xa activity was decreased by 42% at 4 hours, 48% at 8 hours, and 62% at 12 hours.
Dr. Milling and his colleagues assessed hemostatic efficacy in 249 patients. Of this group, 82% achieved good or excellent hemostasis. Among participants with good or excellent hemostasis, 84% had excellent results, and 16% had good results. Subanalysis by factor Xa inhibitor, type of bleed, age, and dose of andexanet did not alter the findings significantly.
To determine whether hemostasis had been sustained sufficiently to prevent clinical deterioration, the investigators examined 71 patients with ICH and a single-compartment bleed. From 1 hour to 12 hours, one patient’s outcome changed from excellent/good to poor/none, and one patient’s outcome changed from excellent to good. For the majority of these patients, however, good hemostasis was sustained from 1 to 12 hours.
The rate of thromboembolic events was 9.7%, which is in the expected range for this population, said Dr. Milling. These events were distributed evenly among the 4 weeks of the study. Stroke and deep vein thrombosis accounted for most of these events, and pulmonary emboli and heart attacks occurred as well. “Once we restarted oral anticoagulation ... there were no more thrombotic events,” said Dr. Milling. No patient developed neutralizing antibodies to factor X or factor Xa, nor did any patient develop neutralizing antibodies to andexanet.
The overall mortality rate was 13.9%. The rate of mortality resulting from ICH was 15%, and the rate of mortality resulting from gastrointestinal bleeding was 11%. These results are impressive, considering that patients had received anticoagulants, said Dr. Milling.
Portola Pharmaceuticals, the maker of andexanet alfa, funded the study. Dr. Milling reported receiving funding and honoraria from the Population Health Research Institute at McMasters University, Janssen, CSL Behring, and Octapharma. He also received a small research payment from Portola Pharmaceuticals. Several of the investigators reported receiving funding from Portola Pharmaceuticals.
SOURCE: Milling TJ et al. ISC 2019, Abstract LB7.
HONOLULU – according to a study presented at the International Stroke Conference sponsored by the American Heart Association. The medication is associated with a low rate of mortality resulting from intracerebral hemorrhage (ICH), compared with the general population of patients with ICH receiving anticoagulation.
Factor Xa inhibitors such as apixaban and rivaroxaban effectively prevent thromboembolic events but may cause or exacerbate acute major bleeding. Andexanet alfa, a modified, recombinant, inactive form of human factor Xa, was developed and approved as a reversal agent for factor Xa inhibitors. In a 2015 study, andexanet rapidly and safely reversed anti–factor Xa activity in large cohorts of patients without bleeding.
A single-cohort study
Truman John Milling Jr., MD, an emergency medicine physician at Dell Seton Medical Center at the University of Texas in Austin, and his colleagues conducted the Andexanet Alfa, a Novel Antidote to the Anticoagulation Effects of Factor Xa Inhibitors (ANNEXA-4) study to evaluate the drug’s safety and efficacy in patients with acute major bleeding associated with treatment with a factor Xa inhibitor. For participants to be eligible, their bleeding had to be life threatening with signs of hemodynamic compromise, be associated with a decrease in hemoglobin level of at least 2 g/dL, or occur in a critical organ such as the brain. An independent academic committee determined whether patients met these criteria.
The trial’s primary efficacy outcomes were change from baseline in anti–factor Xa activity and the percentage of patients with excellent or good hemostatic efficacy at 12 hours. The primary safety endpoints were death, thrombotic events, and the development of neutralizing antibodies to andexanet or to native factor X and factor Xa. The efficacy population included patients with major bleeding and baseline anti–factor Xa activity of at least 75 ng/mL. The safety population included all patients who received a dose of andexanet. The independent committee adjudicated the efficacy and safety outcomes.
Hemostasis was sustained for 12 hours
The investigators enrolled 352 participants into the study, all of whom received andexanet and were followed for at least 30 days or until death. The population’s mean age was 77 years. “These were older and sicker patients with a significant amount of comorbid disease,” said Dr. Milling. The primary indication for anticoagulation was atrial fibrillation in 80% of patients. The primary site of bleeding was intracranial in 64% of patients and gastrointestinal in 26% of patients. The remaining 10% of patients had bleeding affecting other areas (such as pericardial or intramuscular bleeding).
The investigators included 254 patients in the efficacy population. At the end of the administration of the andexanet bolus, the median value for anti–factor Xa activity decreased by 92% among participants receiving apixaban, 92% among participants receiving rivaroxaban, and 75% among patients receiving enoxaparin. Among patients receiving apixaban, the median value for anti–factor Xa activity was decreased by 32% at 4 hours, 34% at 8 hours, and 38% at 12 hours. Among patients receiving rivaroxaban, the median value for anti–factor Xa activity was decreased by 42% at 4 hours, 48% at 8 hours, and 62% at 12 hours.
Dr. Milling and his colleagues assessed hemostatic efficacy in 249 patients. Of this group, 82% achieved good or excellent hemostasis. Among participants with good or excellent hemostasis, 84% had excellent results, and 16% had good results. Subanalysis by factor Xa inhibitor, type of bleed, age, and dose of andexanet did not alter the findings significantly.
To determine whether hemostasis had been sustained sufficiently to prevent clinical deterioration, the investigators examined 71 patients with ICH and a single-compartment bleed. From 1 hour to 12 hours, one patient’s outcome changed from excellent/good to poor/none, and one patient’s outcome changed from excellent to good. For the majority of these patients, however, good hemostasis was sustained from 1 to 12 hours.
The rate of thromboembolic events was 9.7%, which is in the expected range for this population, said Dr. Milling. These events were distributed evenly among the 4 weeks of the study. Stroke and deep vein thrombosis accounted for most of these events, and pulmonary emboli and heart attacks occurred as well. “Once we restarted oral anticoagulation ... there were no more thrombotic events,” said Dr. Milling. No patient developed neutralizing antibodies to factor X or factor Xa, nor did any patient develop neutralizing antibodies to andexanet.
The overall mortality rate was 13.9%. The rate of mortality resulting from ICH was 15%, and the rate of mortality resulting from gastrointestinal bleeding was 11%. These results are impressive, considering that patients had received anticoagulants, said Dr. Milling.
Portola Pharmaceuticals, the maker of andexanet alfa, funded the study. Dr. Milling reported receiving funding and honoraria from the Population Health Research Institute at McMasters University, Janssen, CSL Behring, and Octapharma. He also received a small research payment from Portola Pharmaceuticals. Several of the investigators reported receiving funding from Portola Pharmaceuticals.
SOURCE: Milling TJ et al. ISC 2019, Abstract LB7.
HONOLULU – according to a study presented at the International Stroke Conference sponsored by the American Heart Association. The medication is associated with a low rate of mortality resulting from intracerebral hemorrhage (ICH), compared with the general population of patients with ICH receiving anticoagulation.
Factor Xa inhibitors such as apixaban and rivaroxaban effectively prevent thromboembolic events but may cause or exacerbate acute major bleeding. Andexanet alfa, a modified, recombinant, inactive form of human factor Xa, was developed and approved as a reversal agent for factor Xa inhibitors. In a 2015 study, andexanet rapidly and safely reversed anti–factor Xa activity in large cohorts of patients without bleeding.
A single-cohort study
Truman John Milling Jr., MD, an emergency medicine physician at Dell Seton Medical Center at the University of Texas in Austin, and his colleagues conducted the Andexanet Alfa, a Novel Antidote to the Anticoagulation Effects of Factor Xa Inhibitors (ANNEXA-4) study to evaluate the drug’s safety and efficacy in patients with acute major bleeding associated with treatment with a factor Xa inhibitor. For participants to be eligible, their bleeding had to be life threatening with signs of hemodynamic compromise, be associated with a decrease in hemoglobin level of at least 2 g/dL, or occur in a critical organ such as the brain. An independent academic committee determined whether patients met these criteria.
The trial’s primary efficacy outcomes were change from baseline in anti–factor Xa activity and the percentage of patients with excellent or good hemostatic efficacy at 12 hours. The primary safety endpoints were death, thrombotic events, and the development of neutralizing antibodies to andexanet or to native factor X and factor Xa. The efficacy population included patients with major bleeding and baseline anti–factor Xa activity of at least 75 ng/mL. The safety population included all patients who received a dose of andexanet. The independent committee adjudicated the efficacy and safety outcomes.
Hemostasis was sustained for 12 hours
The investigators enrolled 352 participants into the study, all of whom received andexanet and were followed for at least 30 days or until death. The population’s mean age was 77 years. “These were older and sicker patients with a significant amount of comorbid disease,” said Dr. Milling. The primary indication for anticoagulation was atrial fibrillation in 80% of patients. The primary site of bleeding was intracranial in 64% of patients and gastrointestinal in 26% of patients. The remaining 10% of patients had bleeding affecting other areas (such as pericardial or intramuscular bleeding).
The investigators included 254 patients in the efficacy population. At the end of the administration of the andexanet bolus, the median value for anti–factor Xa activity decreased by 92% among participants receiving apixaban, 92% among participants receiving rivaroxaban, and 75% among patients receiving enoxaparin. Among patients receiving apixaban, the median value for anti–factor Xa activity was decreased by 32% at 4 hours, 34% at 8 hours, and 38% at 12 hours. Among patients receiving rivaroxaban, the median value for anti–factor Xa activity was decreased by 42% at 4 hours, 48% at 8 hours, and 62% at 12 hours.
Dr. Milling and his colleagues assessed hemostatic efficacy in 249 patients. Of this group, 82% achieved good or excellent hemostasis. Among participants with good or excellent hemostasis, 84% had excellent results, and 16% had good results. Subanalysis by factor Xa inhibitor, type of bleed, age, and dose of andexanet did not alter the findings significantly.
To determine whether hemostasis had been sustained sufficiently to prevent clinical deterioration, the investigators examined 71 patients with ICH and a single-compartment bleed. From 1 hour to 12 hours, one patient’s outcome changed from excellent/good to poor/none, and one patient’s outcome changed from excellent to good. For the majority of these patients, however, good hemostasis was sustained from 1 to 12 hours.
The rate of thromboembolic events was 9.7%, which is in the expected range for this population, said Dr. Milling. These events were distributed evenly among the 4 weeks of the study. Stroke and deep vein thrombosis accounted for most of these events, and pulmonary emboli and heart attacks occurred as well. “Once we restarted oral anticoagulation ... there were no more thrombotic events,” said Dr. Milling. No patient developed neutralizing antibodies to factor X or factor Xa, nor did any patient develop neutralizing antibodies to andexanet.
The overall mortality rate was 13.9%. The rate of mortality resulting from ICH was 15%, and the rate of mortality resulting from gastrointestinal bleeding was 11%. These results are impressive, considering that patients had received anticoagulants, said Dr. Milling.
Portola Pharmaceuticals, the maker of andexanet alfa, funded the study. Dr. Milling reported receiving funding and honoraria from the Population Health Research Institute at McMasters University, Janssen, CSL Behring, and Octapharma. He also received a small research payment from Portola Pharmaceuticals. Several of the investigators reported receiving funding from Portola Pharmaceuticals.
SOURCE: Milling TJ et al. ISC 2019, Abstract LB7.
REPORTING FROM ISC 2019
Is a telehospitalist service right for you and your group?
Telemedicine “ripe for adoption” by hospitalists
For medical inpatients, the advent of virtual care began decades ago with telephones and the ability of physicians to give “verbal orders” while outside the hospital. It evolved into widespread adoption of pagers and is now ubiquitous through smart phones, texting, and HIPPA-compliant applications. In the past few years, inpatient telemedicine programs have been developed and studied including tele-ICU, telestroke, and now the telehospitalist.

Telemedicine is not new and has seen rapid adoption in the outpatient setting over the past decade,1 especially since the passing of telemedicine parity laws in 35 states to support equal reimbursement with face-to-face visits.2 In addition, 24 states have joined the Interstate Medical Licensure Compact (IMLC).3 This voluntary program provides an expedited pathway to licensure for qualified physicians who practice in multiple states. The goal is to increase access to care for patients in underserved and rural areas and to allow easier consultation through telemedicine. Combined, these two federal initiatives have lowered two major barriers to entry for telemedicine: reimbursement and credentialing.
Only a handful of papers have been published on the telehospitalist model with one of the first in 2007 in The Hospitalist reporting on the intersection between tele-ICU and telehospitalist care.4 More recent work describes the implementation of a telehospitalist program between a large university hospitalist program and a rural, critical access hospital.5 A key goal of this program, developed by Dr. Ethan Kuperman and colleagues at the University of Iowa, was to keep patients at the critical access hospital that previously would have been transferred. This has obvious benefits for patients, the critical access hospital, and the local community. It also benefited the tertiary care referral center, which was dealing with high occupancy rates. Keeping lower acuity patients at the critical access hospital helps maintain access for more complex patients at the referral center. This same principle has applied to the use of the tele-ICU where lower acuity ICU patients could remain in the small, rural ICU, and only those patients who the intensivist believes would benefit from a higher level of care in a tertiary center would be transferred.
As this study and others have shown, telemedicine is ripe for adoption by hospitalists. The bigger question is how should it fit into the current model of hospital medicine? There are several different applications we are familiar with and each has unique considerations. The first model, as applied in the Kuperman paper, is for a larger hospitalist program to provide a telehospitalist service to a smaller, unaffiliated hospital (for example, critical access hospitals) that employs nurse practitioners or physician assistants on site but can’t recruit or retain full-time hospitalist coverage. In this collaborative model of care, the local provider performs the physical exam but provides care under the guidance and supervision of a hospital medicine specialist. This is expected to improve outcomes and bring the benefits of hospital medicine, including improved outcomes and decreased hospital spending, to smaller communities.6 In this model, the critical access hospital pays a fee for the service and retains the billing to third party payers.

A variation on that model would provide telehospitalist services to other hospitals within an existing health care network (such as Kaiser Permanente, Intermountain Healthcare, government hospitals) that have different financial models with incentives to collaborate. The Veterans Health Administration is embarking on a pilot through the VA Office of Rural Health to provide a telehospitalist service to small rural VA hospitals using the consultative model during the day with a nurse practitioner at the local site and physician backup from the emergency department. Although existing night cross-coverage will be maintained by a physician on call, this telehospitalist service may also evolve into providing cross-coverage on nights and weekends.
A third would be like a locum tenens model in which telehospitalist services are contracted for short periods of time when coverage is needed for vacations or staff shortages. A fourth model of telehospitalist care would be to international areas in need of hospitalist expertise, like a medical mission model but without the expense or time required to travel. Other models will likely evolve based on the demand for services, supply of hospitalists, changes in regulations, and reimbursement.
Another important consideration is how this will evolve for the practicing hospitalist. Will we have dedicated virtual hospitalists, akin to the “nocturnist” who covers nights and weekends? Or will working on the telehospitalist service be in the rotation of duties like many programs have with teaching and “nonteaching” services, medical consultation, and even transition clinics and emergency department triage responsibilities? It could serve as a lower-intensity service that can be staffed during office-based time that would include scholarly work, quality improvement, and administrative duties. If financially viable, it could be mutually beneficial for both the provider and recipient sides of telehospitalist care.
For any of these models to work, technical aspects must be ironed-out. It is indispensable for the provider to have remote access to the electronic health record for data review, documentation, and placing orders if needed. Adequate broadband for effective video connection, accompanied by the appropriate HIPPA-compliant software and hardware must be in place. Although highly specialized hardware has been developed, including remote stethoscopes and otoscopes, the key component is a good camera and video screen on each end of the interaction. Based upon prior experience with telemedicine programs, establishment of trusting relationships with the receiving hospital staff, physicians, and nurse practitioners is also critical. Optimally, the telehospitalist would have an opportunity to travel to the remote site to meet with the local care team and learn about the local resources and community. Many other operational and logistical issues need to be considered and will be supported by the Society of Hospital Medicine through publications, online resources, and national and regional meeting educational content on telehospitalist programs.
As hospital medicine adopts the telehospitalist model, it brings with it important considerations. First, is how we embrace the concept of the medical virtualist, a term used to describe physicians who spend the majority or all of their time caring for patients using a virtual medium.7 We find it difficult to imagine spending all or the majority of our time as a virtual hospitalist, but years ago many could not imagine someone being a full-time hospitalist or nocturnist. Some individuals will see this as a career opportunity that allows them to work as a hospitalist regardless of where they live or where the hospital is located. That has obvious advantages for both career choice and the provision of hospital medicine expertise to low-resourced or low-volume settings, such as rural or international locations and nights and weekends.
Second, the telehospitalist model will require professional standards, training, reimbursement and coding adjustments, hardware and software development, and managing patient expectations for care.
Lastly, hospitals, health care systems, hospitalist groups, and even individual hospitalists will have to determine how best to take advantage of this innovative model of care to provide the highest possible quality, in a cost-efficient manner, that supports professional satisfaction and development.
Dr. Kaboli and Dr. Gutierrez are based at the Center for Access and Delivery Research and Evaluation (CADRE) at the Iowa City VA Healthcare System, the Veterans Rural Health Resource Center-Iowa City, VA Office of Rural Health, and the department of internal medicine, University of Iowa, both in Iowa City.
References
1. Barnett ML et al. Trends in telemedicine use in a large commercially insured population, 2005-2017. JAMA. 2018;320(20):2147-9.
2. American Telemedicine Association State Policy Resource Center. 2018; http://www.americantelemed.org/main/policy-page/state-policy-resource-center. Accessed 2018 Dec 14.
3. Interstate Medical Licensure Compact 2018; https://imlcc.org/. Accessed 2018 Dec 14.
4. Hengehold D. The telehospitalist. The Hospitalist. 2007;7(July). https://www.the-hospitalist.org/hospitalist/article/123381/telehospitalist. Accessed 2018 Dec 14.
5. Kuperman EF et al. The virtual hospitalist: A single-site implementation bringing hospitalist coverage to critical access hospitals. J Hosp Med. 2018;13(11):759-63.
6. Peterson MC. A systematic review of outcomes and quality measures in adult patients cared for by hospitalists vs nonhospitalists. Mayo Clinic proceedings. 2009;84(3):248-54.
7. Nochomovitz M, Sharma R. Is it time for a new medical specialty?: The medical virtualist. JAMA. 2018;319(5):437-8.
Telemedicine “ripe for adoption” by hospitalists
Telemedicine “ripe for adoption” by hospitalists
For medical inpatients, the advent of virtual care began decades ago with telephones and the ability of physicians to give “verbal orders” while outside the hospital. It evolved into widespread adoption of pagers and is now ubiquitous through smart phones, texting, and HIPPA-compliant applications. In the past few years, inpatient telemedicine programs have been developed and studied including tele-ICU, telestroke, and now the telehospitalist.
Telemedicine is not new and has seen rapid adoption in the outpatient setting over the past decade,1 especially since the passing of telemedicine parity laws in 35 states to support equal reimbursement with face-to-face visits.2 In addition, 24 states have joined the Interstate Medical Licensure Compact (IMLC).3 This voluntary program provides an expedited pathway to licensure for qualified physicians who practice in multiple states. The goal is to increase access to care for patients in underserved and rural areas and to allow easier consultation through telemedicine. Combined, these two federal initiatives have lowered two major barriers to entry for telemedicine: reimbursement and credentialing.
Only a handful of papers have been published on the telehospitalist model with one of the first in 2007 in The Hospitalist reporting on the intersection between tele-ICU and telehospitalist care.4 More recent work describes the implementation of a telehospitalist program between a large university hospitalist program and a rural, critical access hospital.5 A key goal of this program, developed by Dr. Ethan Kuperman and colleagues at the University of Iowa, was to keep patients at the critical access hospital that previously would have been transferred. This has obvious benefits for patients, the critical access hospital, and the local community. It also benefited the tertiary care referral center, which was dealing with high occupancy rates. Keeping lower acuity patients at the critical access hospital helps maintain access for more complex patients at the referral center. This same principle has applied to the use of the tele-ICU where lower acuity ICU patients could remain in the small, rural ICU, and only those patients who the intensivist believes would benefit from a higher level of care in a tertiary center would be transferred.
As this study and others have shown, telemedicine is ripe for adoption by hospitalists. The bigger question is how should it fit into the current model of hospital medicine? There are several different applications we are familiar with and each has unique considerations. The first model, as applied in the Kuperman paper, is for a larger hospitalist program to provide a telehospitalist service to a smaller, unaffiliated hospital (for example, critical access hospitals) that employs nurse practitioners or physician assistants on site but can’t recruit or retain full-time hospitalist coverage. In this collaborative model of care, the local provider performs the physical exam but provides care under the guidance and supervision of a hospital medicine specialist. This is expected to improve outcomes and bring the benefits of hospital medicine, including improved outcomes and decreased hospital spending, to smaller communities.6 In this model, the critical access hospital pays a fee for the service and retains the billing to third party payers.
A variation on that model would provide telehospitalist services to other hospitals within an existing health care network (such as Kaiser Permanente, Intermountain Healthcare, government hospitals) that have different financial models with incentives to collaborate. The Veterans Health Administration is embarking on a pilot through the VA Office of Rural Health to provide a telehospitalist service to small rural VA hospitals using the consultative model during the day with a nurse practitioner at the local site and physician backup from the emergency department. Although existing night cross-coverage will be maintained by a physician on call, this telehospitalist service may also evolve into providing cross-coverage on nights and weekends.
A third would be like a locum tenens model in which telehospitalist services are contracted for short periods of time when coverage is needed for vacations or staff shortages. A fourth model of telehospitalist care would be to international areas in need of hospitalist expertise, like a medical mission model but without the expense or time required to travel. Other models will likely evolve based on the demand for services, supply of hospitalists, changes in regulations, and reimbursement.
Another important consideration is how this will evolve for the practicing hospitalist. Will we have dedicated virtual hospitalists, akin to the “nocturnist” who covers nights and weekends? Or will working on the telehospitalist service be in the rotation of duties like many programs have with teaching and “nonteaching” services, medical consultation, and even transition clinics and emergency department triage responsibilities? It could serve as a lower-intensity service that can be staffed during office-based time that would include scholarly work, quality improvement, and administrative duties. If financially viable, it could be mutually beneficial for both the provider and recipient sides of telehospitalist care.
For any of these models to work, technical aspects must be ironed-out. It is indispensable for the provider to have remote access to the electronic health record for data review, documentation, and placing orders if needed. Adequate broadband for effective video connection, accompanied by the appropriate HIPPA-compliant software and hardware must be in place. Although highly specialized hardware has been developed, including remote stethoscopes and otoscopes, the key component is a good camera and video screen on each end of the interaction. Based upon prior experience with telemedicine programs, establishment of trusting relationships with the receiving hospital staff, physicians, and nurse practitioners is also critical. Optimally, the telehospitalist would have an opportunity to travel to the remote site to meet with the local care team and learn about the local resources and community. Many other operational and logistical issues need to be considered and will be supported by the Society of Hospital Medicine through publications, online resources, and national and regional meeting educational content on telehospitalist programs.
As hospital medicine adopts the telehospitalist model, it brings with it important considerations. First, is how we embrace the concept of the medical virtualist, a term used to describe physicians who spend the majority or all of their time caring for patients using a virtual medium.7 We find it difficult to imagine spending all or the majority of our time as a virtual hospitalist, but years ago many could not imagine someone being a full-time hospitalist or nocturnist. Some individuals will see this as a career opportunity that allows them to work as a hospitalist regardless of where they live or where the hospital is located. That has obvious advantages for both career choice and the provision of hospital medicine expertise to low-resourced or low-volume settings, such as rural or international locations and nights and weekends.
Second, the telehospitalist model will require professional standards, training, reimbursement and coding adjustments, hardware and software development, and managing patient expectations for care.
Lastly, hospitals, health care systems, hospitalist groups, and even individual hospitalists will have to determine how best to take advantage of this innovative model of care to provide the highest possible quality, in a cost-efficient manner, that supports professional satisfaction and development.
Dr. Kaboli and Dr. Gutierrez are based at the Center for Access and Delivery Research and Evaluation (CADRE) at the Iowa City VA Healthcare System, the Veterans Rural Health Resource Center-Iowa City, VA Office of Rural Health, and the department of internal medicine, University of Iowa, both in Iowa City.
References
1. Barnett ML et al. Trends in telemedicine use in a large commercially insured population, 2005-2017. JAMA. 2018;320(20):2147-9.
2. American Telemedicine Association State Policy Resource Center. 2018; http://www.americantelemed.org/main/policy-page/state-policy-resource-center. Accessed 2018 Dec 14.
3. Interstate Medical Licensure Compact 2018; https://imlcc.org/. Accessed 2018 Dec 14.
4. Hengehold D. The telehospitalist. The Hospitalist. 2007;7(July). https://www.the-hospitalist.org/hospitalist/article/123381/telehospitalist. Accessed 2018 Dec 14.
5. Kuperman EF et al. The virtual hospitalist: A single-site implementation bringing hospitalist coverage to critical access hospitals. J Hosp Med. 2018;13(11):759-63.
6. Peterson MC. A systematic review of outcomes and quality measures in adult patients cared for by hospitalists vs nonhospitalists. Mayo Clinic proceedings. 2009;84(3):248-54.
7. Nochomovitz M, Sharma R. Is it time for a new medical specialty?: The medical virtualist. JAMA. 2018;319(5):437-8.
For medical inpatients, the advent of virtual care began decades ago with telephones and the ability of physicians to give “verbal orders” while outside the hospital. It evolved into widespread adoption of pagers and is now ubiquitous through smart phones, texting, and HIPPA-compliant applications. In the past few years, inpatient telemedicine programs have been developed and studied including tele-ICU, telestroke, and now the telehospitalist.
Telemedicine is not new and has seen rapid adoption in the outpatient setting over the past decade,1 especially since the passing of telemedicine parity laws in 35 states to support equal reimbursement with face-to-face visits.2 In addition, 24 states have joined the Interstate Medical Licensure Compact (IMLC).3 This voluntary program provides an expedited pathway to licensure for qualified physicians who practice in multiple states. The goal is to increase access to care for patients in underserved and rural areas and to allow easier consultation through telemedicine. Combined, these two federal initiatives have lowered two major barriers to entry for telemedicine: reimbursement and credentialing.
Only a handful of papers have been published on the telehospitalist model with one of the first in 2007 in The Hospitalist reporting on the intersection between tele-ICU and telehospitalist care.4 More recent work describes the implementation of a telehospitalist program between a large university hospitalist program and a rural, critical access hospital.5 A key goal of this program, developed by Dr. Ethan Kuperman and colleagues at the University of Iowa, was to keep patients at the critical access hospital that previously would have been transferred. This has obvious benefits for patients, the critical access hospital, and the local community. It also benefited the tertiary care referral center, which was dealing with high occupancy rates. Keeping lower acuity patients at the critical access hospital helps maintain access for more complex patients at the referral center. This same principle has applied to the use of the tele-ICU where lower acuity ICU patients could remain in the small, rural ICU, and only those patients who the intensivist believes would benefit from a higher level of care in a tertiary center would be transferred.
As this study and others have shown, telemedicine is ripe for adoption by hospitalists. The bigger question is how should it fit into the current model of hospital medicine? There are several different applications we are familiar with and each has unique considerations. The first model, as applied in the Kuperman paper, is for a larger hospitalist program to provide a telehospitalist service to a smaller, unaffiliated hospital (for example, critical access hospitals) that employs nurse practitioners or physician assistants on site but can’t recruit or retain full-time hospitalist coverage. In this collaborative model of care, the local provider performs the physical exam but provides care under the guidance and supervision of a hospital medicine specialist. This is expected to improve outcomes and bring the benefits of hospital medicine, including improved outcomes and decreased hospital spending, to smaller communities.6 In this model, the critical access hospital pays a fee for the service and retains the billing to third party payers.
A variation on that model would provide telehospitalist services to other hospitals within an existing health care network (such as Kaiser Permanente, Intermountain Healthcare, government hospitals) that have different financial models with incentives to collaborate. The Veterans Health Administration is embarking on a pilot through the VA Office of Rural Health to provide a telehospitalist service to small rural VA hospitals using the consultative model during the day with a nurse practitioner at the local site and physician backup from the emergency department. Although existing night cross-coverage will be maintained by a physician on call, this telehospitalist service may also evolve into providing cross-coverage on nights and weekends.
A third would be like a locum tenens model in which telehospitalist services are contracted for short periods of time when coverage is needed for vacations or staff shortages. A fourth model of telehospitalist care would be to international areas in need of hospitalist expertise, like a medical mission model but without the expense or time required to travel. Other models will likely evolve based on the demand for services, supply of hospitalists, changes in regulations, and reimbursement.
Another important consideration is how this will evolve for the practicing hospitalist. Will we have dedicated virtual hospitalists, akin to the “nocturnist” who covers nights and weekends? Or will working on the telehospitalist service be in the rotation of duties like many programs have with teaching and “nonteaching” services, medical consultation, and even transition clinics and emergency department triage responsibilities? It could serve as a lower-intensity service that can be staffed during office-based time that would include scholarly work, quality improvement, and administrative duties. If financially viable, it could be mutually beneficial for both the provider and recipient sides of telehospitalist care.
For any of these models to work, technical aspects must be ironed-out. It is indispensable for the provider to have remote access to the electronic health record for data review, documentation, and placing orders if needed. Adequate broadband for effective video connection, accompanied by the appropriate HIPPA-compliant software and hardware must be in place. Although highly specialized hardware has been developed, including remote stethoscopes and otoscopes, the key component is a good camera and video screen on each end of the interaction. Based upon prior experience with telemedicine programs, establishment of trusting relationships with the receiving hospital staff, physicians, and nurse practitioners is also critical. Optimally, the telehospitalist would have an opportunity to travel to the remote site to meet with the local care team and learn about the local resources and community. Many other operational and logistical issues need to be considered and will be supported by the Society of Hospital Medicine through publications, online resources, and national and regional meeting educational content on telehospitalist programs.
As hospital medicine adopts the telehospitalist model, it brings with it important considerations. First, is how we embrace the concept of the medical virtualist, a term used to describe physicians who spend the majority or all of their time caring for patients using a virtual medium.7 We find it difficult to imagine spending all or the majority of our time as a virtual hospitalist, but years ago many could not imagine someone being a full-time hospitalist or nocturnist. Some individuals will see this as a career opportunity that allows them to work as a hospitalist regardless of where they live or where the hospital is located. That has obvious advantages for both career choice and the provision of hospital medicine expertise to low-resourced or low-volume settings, such as rural or international locations and nights and weekends.
Second, the telehospitalist model will require professional standards, training, reimbursement and coding adjustments, hardware and software development, and managing patient expectations for care.
Lastly, hospitals, health care systems, hospitalist groups, and even individual hospitalists will have to determine how best to take advantage of this innovative model of care to provide the highest possible quality, in a cost-efficient manner, that supports professional satisfaction and development.
Dr. Kaboli and Dr. Gutierrez are based at the Center for Access and Delivery Research and Evaluation (CADRE) at the Iowa City VA Healthcare System, the Veterans Rural Health Resource Center-Iowa City, VA Office of Rural Health, and the department of internal medicine, University of Iowa, both in Iowa City.
References
1. Barnett ML et al. Trends in telemedicine use in a large commercially insured population, 2005-2017. JAMA. 2018;320(20):2147-9.
2. American Telemedicine Association State Policy Resource Center. 2018; http://www.americantelemed.org/main/policy-page/state-policy-resource-center. Accessed 2018 Dec 14.
3. Interstate Medical Licensure Compact 2018; https://imlcc.org/. Accessed 2018 Dec 14.
4. Hengehold D. The telehospitalist. The Hospitalist. 2007;7(July). https://www.the-hospitalist.org/hospitalist/article/123381/telehospitalist. Accessed 2018 Dec 14.
5. Kuperman EF et al. The virtual hospitalist: A single-site implementation bringing hospitalist coverage to critical access hospitals. J Hosp Med. 2018;13(11):759-63.
6. Peterson MC. A systematic review of outcomes and quality measures in adult patients cared for by hospitalists vs nonhospitalists. Mayo Clinic proceedings. 2009;84(3):248-54.
7. Nochomovitz M, Sharma R. Is it time for a new medical specialty?: The medical virtualist. JAMA. 2018;319(5):437-8.
The power of policy at HM19
Mini-track features CMS insights
Due to the steadily growing interest of SHM members in health care policy and advocacy issues, the 2019 Annual Conference will include a mini-track dedicated to policy issues.

To be held on Monday, March 25th at HM19 in Orlando, the health care policy mini-track will update conference attendees on some of the Washington developments that affect hospitalists, said Josh Boswell, director of government relations at SHM.
“Many of the policy developments in D.C. are directly impacting our members’ practices,” he said. “A couple of years ago, it was decided to add a specific track at the annual conference to cover some of these policy issues, and we’ve generally had positive feedback on the sessions.”
This year, the mini-track will consist of two separate sessions, held back to back. “Both sessions are designed to give attendees an entrée into health policy and explain developments that are happening right now in Washington that impact their practice,” said Joshua Lapps, government relations manager at SHM.
The first session – “CMS Policy Update: An Overview of Meaningful Measures and the Quality Payment Program” – will take place from 2:00 to 3:30 p.m., and will feature Reena Duseja, MD, MS, the acting director for Quality Measurement and Value-Based Incentives Group in the Centers for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services. Dr. Duseja oversees the development of measures and analyses for a variety of CMS quality reporting and value-based purchasing programs. She is also an emergency medicine physician and was an associate professor at the University of California, San Francisco, in the department of emergency medicine, where she led quality improvement activities.

“The session with Dr. Duseja will be an inside look into the approach that CMS is taking for quality measurement and pay-for-performance programs, specifically looking at the quality payment program which came out of the Medicare Access and Chip Reauthorization Act,” Mr. Lapps said. “It will be a high-level discussion about how the programs affect hospitalists, and how hospitalists participate in the programs. It’s also a chance for attendees to hear some of the thinking inside CMS.”
Dr. Duseja is also hoping to get feedback from HM19 attendees. “She wants the session to be educational for our members, as well as an opportunity for her to learn from hospitalists,” Mr. Lapps said.
According to Dr. Duseja, her presentation will provide attendees with an overview of the Quality Payment Program under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), specifically highlighting policy changes from 2018 to 2019 to the Merit-based Incentive Payment System (MIPS) and Meaningful Measures Initiative. Attendees will learn more about CMS’s approach to quality and quality measurement, as well as the future of quality reporting programs.
Following Dr. Duseja’s presentation, the second mini-track session will take place from 3:40 to 4:25 p.m. It will focus more intently on the processes around health care policy making.
“We heard from our members who attended this mini-track at the past two annual conferences that they would like us to explain how policy making works: the play-by-play in D.C. on how we get to where we are,” Mr. Boswell said.
The second session will feature a presentation by Jennifer Bell, founding partner at Chamber Hill Strategies, who represents SHM in Washington. “Jennifer will be discussing how Washington works, the policy process and the pressure points at which SHM and its members can exert influence,” Mr. Lapps said.
Attendees can expect to learn a lot from either session, Mr. Lapps said. “Attendees will learn about the basic contours of the Quality Payment Program that Medicare oversees, and some of the specific new elements of that program this year that were designed with hospitalists in mind. For example, Dr. Duseja will be talking about a facility-based reporting option under the Merit-Based Incentive Payment System. I think our members should gain a concrete understanding of some of the new directions that CMS is heading this year. Overall, they’ll have a better sense of the vision behind quality measures and quality measurement. This is a really exciting opportunity to hear from someone who is both a clinician and works on policy at CMS.”
The policy mini-track offers hospitalists a chance to get a look “behind the curtain” at policy making from someone who is helping to write the rules.
“Attendees will gain insight on where they fit in these programs – and also have the opportunity to tell Dr. Duseja if they don’t feel these programs are a good fit for them,” Mr. Boswell said. “Oftentimes these programs are not structured ideally for hospitalists. So, hearing directly from hospitalists who are experiencing problems would be extraordinarily helpful to a CMS official. I think attendees should view the policy track not only as an opportunity to learn from CMS, but as an opportunity to educate CMS about our issues.”
Mini-track features CMS insights
Mini-track features CMS insights
Due to the steadily growing interest of SHM members in health care policy and advocacy issues, the 2019 Annual Conference will include a mini-track dedicated to policy issues.
To be held on Monday, March 25th at HM19 in Orlando, the health care policy mini-track will update conference attendees on some of the Washington developments that affect hospitalists, said Josh Boswell, director of government relations at SHM.
“Many of the policy developments in D.C. are directly impacting our members’ practices,” he said. “A couple of years ago, it was decided to add a specific track at the annual conference to cover some of these policy issues, and we’ve generally had positive feedback on the sessions.”
This year, the mini-track will consist of two separate sessions, held back to back. “Both sessions are designed to give attendees an entrée into health policy and explain developments that are happening right now in Washington that impact their practice,” said Joshua Lapps, government relations manager at SHM.
The first session – “CMS Policy Update: An Overview of Meaningful Measures and the Quality Payment Program” – will take place from 2:00 to 3:30 p.m., and will feature Reena Duseja, MD, MS, the acting director for Quality Measurement and Value-Based Incentives Group in the Centers for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services. Dr. Duseja oversees the development of measures and analyses for a variety of CMS quality reporting and value-based purchasing programs. She is also an emergency medicine physician and was an associate professor at the University of California, San Francisco, in the department of emergency medicine, where she led quality improvement activities.
“The session with Dr. Duseja will be an inside look into the approach that CMS is taking for quality measurement and pay-for-performance programs, specifically looking at the quality payment program which came out of the Medicare Access and Chip Reauthorization Act,” Mr. Lapps said. “It will be a high-level discussion about how the programs affect hospitalists, and how hospitalists participate in the programs. It’s also a chance for attendees to hear some of the thinking inside CMS.”
Dr. Duseja is also hoping to get feedback from HM19 attendees. “She wants the session to be educational for our members, as well as an opportunity for her to learn from hospitalists,” Mr. Lapps said.
According to Dr. Duseja, her presentation will provide attendees with an overview of the Quality Payment Program under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), specifically highlighting policy changes from 2018 to 2019 to the Merit-based Incentive Payment System (MIPS) and Meaningful Measures Initiative. Attendees will learn more about CMS’s approach to quality and quality measurement, as well as the future of quality reporting programs.
Following Dr. Duseja’s presentation, the second mini-track session will take place from 3:40 to 4:25 p.m. It will focus more intently on the processes around health care policy making.
“We heard from our members who attended this mini-track at the past two annual conferences that they would like us to explain how policy making works: the play-by-play in D.C. on how we get to where we are,” Mr. Boswell said.
The second session will feature a presentation by Jennifer Bell, founding partner at Chamber Hill Strategies, who represents SHM in Washington. “Jennifer will be discussing how Washington works, the policy process and the pressure points at which SHM and its members can exert influence,” Mr. Lapps said.
Attendees can expect to learn a lot from either session, Mr. Lapps said. “Attendees will learn about the basic contours of the Quality Payment Program that Medicare oversees, and some of the specific new elements of that program this year that were designed with hospitalists in mind. For example, Dr. Duseja will be talking about a facility-based reporting option under the Merit-Based Incentive Payment System. I think our members should gain a concrete understanding of some of the new directions that CMS is heading this year. Overall, they’ll have a better sense of the vision behind quality measures and quality measurement. This is a really exciting opportunity to hear from someone who is both a clinician and works on policy at CMS.”
The policy mini-track offers hospitalists a chance to get a look “behind the curtain” at policy making from someone who is helping to write the rules.
“Attendees will gain insight on where they fit in these programs – and also have the opportunity to tell Dr. Duseja if they don’t feel these programs are a good fit for them,” Mr. Boswell said. “Oftentimes these programs are not structured ideally for hospitalists. So, hearing directly from hospitalists who are experiencing problems would be extraordinarily helpful to a CMS official. I think attendees should view the policy track not only as an opportunity to learn from CMS, but as an opportunity to educate CMS about our issues.”
Due to the steadily growing interest of SHM members in health care policy and advocacy issues, the 2019 Annual Conference will include a mini-track dedicated to policy issues.
To be held on Monday, March 25th at HM19 in Orlando, the health care policy mini-track will update conference attendees on some of the Washington developments that affect hospitalists, said Josh Boswell, director of government relations at SHM.
“Many of the policy developments in D.C. are directly impacting our members’ practices,” he said. “A couple of years ago, it was decided to add a specific track at the annual conference to cover some of these policy issues, and we’ve generally had positive feedback on the sessions.”
This year, the mini-track will consist of two separate sessions, held back to back. “Both sessions are designed to give attendees an entrée into health policy and explain developments that are happening right now in Washington that impact their practice,” said Joshua Lapps, government relations manager at SHM.
The first session – “CMS Policy Update: An Overview of Meaningful Measures and the Quality Payment Program” – will take place from 2:00 to 3:30 p.m., and will feature Reena Duseja, MD, MS, the acting director for Quality Measurement and Value-Based Incentives Group in the Centers for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services. Dr. Duseja oversees the development of measures and analyses for a variety of CMS quality reporting and value-based purchasing programs. She is also an emergency medicine physician and was an associate professor at the University of California, San Francisco, in the department of emergency medicine, where she led quality improvement activities.
“The session with Dr. Duseja will be an inside look into the approach that CMS is taking for quality measurement and pay-for-performance programs, specifically looking at the quality payment program which came out of the Medicare Access and Chip Reauthorization Act,” Mr. Lapps said. “It will be a high-level discussion about how the programs affect hospitalists, and how hospitalists participate in the programs. It’s also a chance for attendees to hear some of the thinking inside CMS.”
Dr. Duseja is also hoping to get feedback from HM19 attendees. “She wants the session to be educational for our members, as well as an opportunity for her to learn from hospitalists,” Mr. Lapps said.
According to Dr. Duseja, her presentation will provide attendees with an overview of the Quality Payment Program under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), specifically highlighting policy changes from 2018 to 2019 to the Merit-based Incentive Payment System (MIPS) and Meaningful Measures Initiative. Attendees will learn more about CMS’s approach to quality and quality measurement, as well as the future of quality reporting programs.
Following Dr. Duseja’s presentation, the second mini-track session will take place from 3:40 to 4:25 p.m. It will focus more intently on the processes around health care policy making.
“We heard from our members who attended this mini-track at the past two annual conferences that they would like us to explain how policy making works: the play-by-play in D.C. on how we get to where we are,” Mr. Boswell said.
The second session will feature a presentation by Jennifer Bell, founding partner at Chamber Hill Strategies, who represents SHM in Washington. “Jennifer will be discussing how Washington works, the policy process and the pressure points at which SHM and its members can exert influence,” Mr. Lapps said.
Attendees can expect to learn a lot from either session, Mr. Lapps said. “Attendees will learn about the basic contours of the Quality Payment Program that Medicare oversees, and some of the specific new elements of that program this year that were designed with hospitalists in mind. For example, Dr. Duseja will be talking about a facility-based reporting option under the Merit-Based Incentive Payment System. I think our members should gain a concrete understanding of some of the new directions that CMS is heading this year. Overall, they’ll have a better sense of the vision behind quality measures and quality measurement. This is a really exciting opportunity to hear from someone who is both a clinician and works on policy at CMS.”
The policy mini-track offers hospitalists a chance to get a look “behind the curtain” at policy making from someone who is helping to write the rules.
“Attendees will gain insight on where they fit in these programs – and also have the opportunity to tell Dr. Duseja if they don’t feel these programs are a good fit for them,” Mr. Boswell said. “Oftentimes these programs are not structured ideally for hospitalists. So, hearing directly from hospitalists who are experiencing problems would be extraordinarily helpful to a CMS official. I think attendees should view the policy track not only as an opportunity to learn from CMS, but as an opportunity to educate CMS about our issues.”

Journal of Hospital Medicine launches new clinical guidelines series
The Journal of Hospital Medicine, the official peer-reviewed journal of the Society of Hospital Medicine, has launched its second new series this year, entitled Clinical Guideline Highlights for the Hospitalist. Alongside the new Leadership and Professional Development series, this addition plays a large role in the vision for the future of the journal, spearheaded by new editor in chief, Samir Shah, MD, MSCE, MHM.

“As a new deputy editor for reviews and perspectives, I’m thrilled to help execute Dr. Shah’s vision for a series of articles that aims to facilitate the rapid translation of the latest evidence-based guidelines into hospitalist practice,” said Erin Shaughnessy, MD. “My coeditor, Dr. Read Pierce, and I envision these reviews as tools to enable busy clinicians to quickly understand the latest research and apply it to practice.”
The March issue of JHM features an introduction to the series as well as the first two articles, “The Use of Intravenous Fluids in the Hospitalized Adult” and “Maintenance Intravenous Fluids in Infants and Children.” The introduction provides details on the formatting of the series and discusses a second format that will be introduced in 2019 called Progress Notes, which will be shorter than JHM’s traditional review format. Progress Notes will accept two types or articles, clinical and methodological, and will focus on diagnostics, therapeutics, or risk assessment and prevention of a clinical problem relevant to hospitalists.
“National guidelines and society position statements are important in informing care standards but can be time consuming to read, and only a small portion may be pertinent to the practice of hospital medicine,” Dr. Shah said. “Our Clinical Guideline Highlights for the Hospitalist series, under the leadership of Dr. Shaughnessy and Dr. Pierce, will distill the key elements of national guidelines with a focus on recommendations that are most relevant to the practicing hospitalist. Authors include a brief critique to ensure hospitalists understand the strength of evidence behind the guideline when making decisions.”
Along with this series comes another new feature for the journal, Hospital Medicine: The Year in Review. This annual feature “concisely compiles and critiques the top articles in both adult and pediatric hospital medicine in the past year” and “will serve as a written corollary to the popular ‘Updates in Hospital Medicine’ presentation at the SHM Annual Conference.”
With so many updates, “JHM’s overarching commitment remains unchanged: support clinicians, leaders, and scholars in our field in their pursuit of delivering evidence-based, high-value clinical care.” The journal will continue to accept traditional, long-form review on topics relevant to hospitalists.
Visit www.journalofhospitalmedicine.com for the Clinical Guideline Highlights for the Hospitalist series and additional research.
The Journal of Hospital Medicine, the official peer-reviewed journal of the Society of Hospital Medicine, has launched its second new series this year, entitled Clinical Guideline Highlights for the Hospitalist. Alongside the new Leadership and Professional Development series, this addition plays a large role in the vision for the future of the journal, spearheaded by new editor in chief, Samir Shah, MD, MSCE, MHM.
“As a new deputy editor for reviews and perspectives, I’m thrilled to help execute Dr. Shah’s vision for a series of articles that aims to facilitate the rapid translation of the latest evidence-based guidelines into hospitalist practice,” said Erin Shaughnessy, MD. “My coeditor, Dr. Read Pierce, and I envision these reviews as tools to enable busy clinicians to quickly understand the latest research and apply it to practice.”
The March issue of JHM features an introduction to the series as well as the first two articles, “The Use of Intravenous Fluids in the Hospitalized Adult” and “Maintenance Intravenous Fluids in Infants and Children.” The introduction provides details on the formatting of the series and discusses a second format that will be introduced in 2019 called Progress Notes, which will be shorter than JHM’s traditional review format. Progress Notes will accept two types or articles, clinical and methodological, and will focus on diagnostics, therapeutics, or risk assessment and prevention of a clinical problem relevant to hospitalists.
“National guidelines and society position statements are important in informing care standards but can be time consuming to read, and only a small portion may be pertinent to the practice of hospital medicine,” Dr. Shah said. “Our Clinical Guideline Highlights for the Hospitalist series, under the leadership of Dr. Shaughnessy and Dr. Pierce, will distill the key elements of national guidelines with a focus on recommendations that are most relevant to the practicing hospitalist. Authors include a brief critique to ensure hospitalists understand the strength of evidence behind the guideline when making decisions.”
Along with this series comes another new feature for the journal, Hospital Medicine: The Year in Review. This annual feature “concisely compiles and critiques the top articles in both adult and pediatric hospital medicine in the past year” and “will serve as a written corollary to the popular ‘Updates in Hospital Medicine’ presentation at the SHM Annual Conference.”
With so many updates, “JHM’s overarching commitment remains unchanged: support clinicians, leaders, and scholars in our field in their pursuit of delivering evidence-based, high-value clinical care.” The journal will continue to accept traditional, long-form review on topics relevant to hospitalists.
Visit www.journalofhospitalmedicine.com for the Clinical Guideline Highlights for the Hospitalist series and additional research.
The Journal of Hospital Medicine, the official peer-reviewed journal of the Society of Hospital Medicine, has launched its second new series this year, entitled Clinical Guideline Highlights for the Hospitalist. Alongside the new Leadership and Professional Development series, this addition plays a large role in the vision for the future of the journal, spearheaded by new editor in chief, Samir Shah, MD, MSCE, MHM.
“As a new deputy editor for reviews and perspectives, I’m thrilled to help execute Dr. Shah’s vision for a series of articles that aims to facilitate the rapid translation of the latest evidence-based guidelines into hospitalist practice,” said Erin Shaughnessy, MD. “My coeditor, Dr. Read Pierce, and I envision these reviews as tools to enable busy clinicians to quickly understand the latest research and apply it to practice.”
The March issue of JHM features an introduction to the series as well as the first two articles, “The Use of Intravenous Fluids in the Hospitalized Adult” and “Maintenance Intravenous Fluids in Infants and Children.” The introduction provides details on the formatting of the series and discusses a second format that will be introduced in 2019 called Progress Notes, which will be shorter than JHM’s traditional review format. Progress Notes will accept two types or articles, clinical and methodological, and will focus on diagnostics, therapeutics, or risk assessment and prevention of a clinical problem relevant to hospitalists.
“National guidelines and society position statements are important in informing care standards but can be time consuming to read, and only a small portion may be pertinent to the practice of hospital medicine,” Dr. Shah said. “Our Clinical Guideline Highlights for the Hospitalist series, under the leadership of Dr. Shaughnessy and Dr. Pierce, will distill the key elements of national guidelines with a focus on recommendations that are most relevant to the practicing hospitalist. Authors include a brief critique to ensure hospitalists understand the strength of evidence behind the guideline when making decisions.”
Along with this series comes another new feature for the journal, Hospital Medicine: The Year in Review. This annual feature “concisely compiles and critiques the top articles in both adult and pediatric hospital medicine in the past year” and “will serve as a written corollary to the popular ‘Updates in Hospital Medicine’ presentation at the SHM Annual Conference.”
With so many updates, “JHM’s overarching commitment remains unchanged: support clinicians, leaders, and scholars in our field in their pursuit of delivering evidence-based, high-value clinical care.” The journal will continue to accept traditional, long-form review on topics relevant to hospitalists.
Visit www.journalofhospitalmedicine.com for the Clinical Guideline Highlights for the Hospitalist series and additional research.
Learning from the history of hospitals
Storytelling can inform medical practice
Every year the Society of Hospital Medicine’s Annual Conference Committee examines prior attendee surveys, reviews the content presented the preceding year, and asks itself what new areas of learning are needed by hospitalists, said Dustin Smith, MD, SFHM, hospitalist and associate professor of medicine at Emory University School of Medicine in Atlanta, and HM19 course director.
“The conference’s schedule-at-a-glance of content can be overwhelming, so we have tried to use distinct educational tracks to provide focus and clarity for conference attendees,” he said. “Every year there are a few areas where questions often come up about complex clinical situations where established medical guidelines aren’t much help.”
As a result, for HM19 an educational mini-track called “Between the Guidelines” was developed to gather up several of these areas of clinical complexity where what’s available in established clinical practice guidelines doesn’t offer clear answers, Dr. Smith said. These include controversies around antithrombotic therapy in patients with major bleeds, and a debate on controversial aspects of guidelines to direct inpatient care.
Another planned session, “The History of Hospitals via Arts and Stories,” fits nicely into this mini-track, Dr. Smith noted.
“It’s a history lesson you can’t glean from medical guidelines, which maybe points us toward what to incorporate and what not to repeat from across the history of hospitals,” he said. “That could help us better appreciate the work hospitalists are doing today and into the future.”

Jordan Messler, MD, a hospitalist with the Morton Plant Hospitalist group in Clearwater, Fla., will lead the session and thinks that modern physicians can learn a lot from both the history of medicine and the evolution of hospitals, starting with the ancient Greek physician, Galen (129-200 AD), who directed the celebrated Asclepeion or hospital in Pergamon (present-day Bergama, Turkey). Dr. Messler said this ancient hospital’s treatment of disease also addressed the senses, the emotions, and the spirit – an early prototype for whole-person care – with an emphasis on self-therapy through rest, relaxation, exercise, and the promotion of healthy lifestyles.1
A different perspective on hospitals
“People used to travel to Pergamon for healing at the Asclepeion, next to the amphitheater, where plays and music were presented, and to be outdoors in the natural elements. Now we’re seeing hospitals being built with healing gardens, and a new emphasis on how artwork and music and environmental design can assist in healing,” Dr. Messler said.
Dr. Messler explained that his “History of Hospitals” presentation will also survey the advent of more recent hospitals in France in the 18th century, pioneering work done at Johns Hopkins Hospital in Baltimore and Bellevue Hospital in New York, and the influence on the modern hospital of nursing pioneer Florence Nightingale (1820-1910). Dr. Messler said she helped improve hospitals in her day, which still influences their modern design, and fundamentally changed the role of nursing in hospitals, introducing professional training standards for nurses.

He also noted that the portico of the beautiful 15th century Hospital of the Innocents in Florence, Italy, the first organic creation of Filippo Brunelleschi (1377-1446), marks the birth of Renaissance architecture in Florence. The Hospital of Santa Maria Nuova, founded in 1288, is the oldest hospital still active in Florence.
Part of the goal for this new annual conference session is to take a break from more clinically focused presentations, and to think about the hospital from a different perspective, Dr. Messler said. His session will emphasize the power of stories and storytelling to inform and inspire medical practice.
“This is not something that can be applied clinically the next day, but lessons from the past can inform the design of hospitals and how we manage patients,” he said. “We need to ask ourselves, ‘How can we analyze hospital history to inform what we do today?’ ”
References
“Asclepeion.” Wikipedia. Accessed Jan. 28, 2019: https://en.wikipedia.org/wiki/Asclepeion.
Storytelling can inform medical practice
Storytelling can inform medical practice
Every year the Society of Hospital Medicine’s Annual Conference Committee examines prior attendee surveys, reviews the content presented the preceding year, and asks itself what new areas of learning are needed by hospitalists, said Dustin Smith, MD, SFHM, hospitalist and associate professor of medicine at Emory University School of Medicine in Atlanta, and HM19 course director.
“The conference’s schedule-at-a-glance of content can be overwhelming, so we have tried to use distinct educational tracks to provide focus and clarity for conference attendees,” he said. “Every year there are a few areas where questions often come up about complex clinical situations where established medical guidelines aren’t much help.”
As a result, for HM19 an educational mini-track called “Between the Guidelines” was developed to gather up several of these areas of clinical complexity where what’s available in established clinical practice guidelines doesn’t offer clear answers, Dr. Smith said. These include controversies around antithrombotic therapy in patients with major bleeds, and a debate on controversial aspects of guidelines to direct inpatient care.
Another planned session, “The History of Hospitals via Arts and Stories,” fits nicely into this mini-track, Dr. Smith noted.
“It’s a history lesson you can’t glean from medical guidelines, which maybe points us toward what to incorporate and what not to repeat from across the history of hospitals,” he said. “That could help us better appreciate the work hospitalists are doing today and into the future.”
Jordan Messler, MD, a hospitalist with the Morton Plant Hospitalist group in Clearwater, Fla., will lead the session and thinks that modern physicians can learn a lot from both the history of medicine and the evolution of hospitals, starting with the ancient Greek physician, Galen (129-200 AD), who directed the celebrated Asclepeion or hospital in Pergamon (present-day Bergama, Turkey). Dr. Messler said this ancient hospital’s treatment of disease also addressed the senses, the emotions, and the spirit – an early prototype for whole-person care – with an emphasis on self-therapy through rest, relaxation, exercise, and the promotion of healthy lifestyles.1
A different perspective on hospitals
“People used to travel to Pergamon for healing at the Asclepeion, next to the amphitheater, where plays and music were presented, and to be outdoors in the natural elements. Now we’re seeing hospitals being built with healing gardens, and a new emphasis on how artwork and music and environmental design can assist in healing,” Dr. Messler said.
Dr. Messler explained that his “History of Hospitals” presentation will also survey the advent of more recent hospitals in France in the 18th century, pioneering work done at Johns Hopkins Hospital in Baltimore and Bellevue Hospital in New York, and the influence on the modern hospital of nursing pioneer Florence Nightingale (1820-1910). Dr. Messler said she helped improve hospitals in her day, which still influences their modern design, and fundamentally changed the role of nursing in hospitals, introducing professional training standards for nurses.
He also noted that the portico of the beautiful 15th century Hospital of the Innocents in Florence, Italy, the first organic creation of Filippo Brunelleschi (1377-1446), marks the birth of Renaissance architecture in Florence. The Hospital of Santa Maria Nuova, founded in 1288, is the oldest hospital still active in Florence.
Part of the goal for this new annual conference session is to take a break from more clinically focused presentations, and to think about the hospital from a different perspective, Dr. Messler said. His session will emphasize the power of stories and storytelling to inform and inspire medical practice.
“This is not something that can be applied clinically the next day, but lessons from the past can inform the design of hospitals and how we manage patients,” he said. “We need to ask ourselves, ‘How can we analyze hospital history to inform what we do today?’ ”
References
“Asclepeion.” Wikipedia. Accessed Jan. 28, 2019: https://en.wikipedia.org/wiki/Asclepeion.
Every year the Society of Hospital Medicine’s Annual Conference Committee examines prior attendee surveys, reviews the content presented the preceding year, and asks itself what new areas of learning are needed by hospitalists, said Dustin Smith, MD, SFHM, hospitalist and associate professor of medicine at Emory University School of Medicine in Atlanta, and HM19 course director.
“The conference’s schedule-at-a-glance of content can be overwhelming, so we have tried to use distinct educational tracks to provide focus and clarity for conference attendees,” he said. “Every year there are a few areas where questions often come up about complex clinical situations where established medical guidelines aren’t much help.”
As a result, for HM19 an educational mini-track called “Between the Guidelines” was developed to gather up several of these areas of clinical complexity where what’s available in established clinical practice guidelines doesn’t offer clear answers, Dr. Smith said. These include controversies around antithrombotic therapy in patients with major bleeds, and a debate on controversial aspects of guidelines to direct inpatient care.
Another planned session, “The History of Hospitals via Arts and Stories,” fits nicely into this mini-track, Dr. Smith noted.
“It’s a history lesson you can’t glean from medical guidelines, which maybe points us toward what to incorporate and what not to repeat from across the history of hospitals,” he said. “That could help us better appreciate the work hospitalists are doing today and into the future.”
Jordan Messler, MD, a hospitalist with the Morton Plant Hospitalist group in Clearwater, Fla., will lead the session and thinks that modern physicians can learn a lot from both the history of medicine and the evolution of hospitals, starting with the ancient Greek physician, Galen (129-200 AD), who directed the celebrated Asclepeion or hospital in Pergamon (present-day Bergama, Turkey). Dr. Messler said this ancient hospital’s treatment of disease also addressed the senses, the emotions, and the spirit – an early prototype for whole-person care – with an emphasis on self-therapy through rest, relaxation, exercise, and the promotion of healthy lifestyles.1
A different perspective on hospitals
“People used to travel to Pergamon for healing at the Asclepeion, next to the amphitheater, where plays and music were presented, and to be outdoors in the natural elements. Now we’re seeing hospitals being built with healing gardens, and a new emphasis on how artwork and music and environmental design can assist in healing,” Dr. Messler said.
Dr. Messler explained that his “History of Hospitals” presentation will also survey the advent of more recent hospitals in France in the 18th century, pioneering work done at Johns Hopkins Hospital in Baltimore and Bellevue Hospital in New York, and the influence on the modern hospital of nursing pioneer Florence Nightingale (1820-1910). Dr. Messler said she helped improve hospitals in her day, which still influences their modern design, and fundamentally changed the role of nursing in hospitals, introducing professional training standards for nurses.
He also noted that the portico of the beautiful 15th century Hospital of the Innocents in Florence, Italy, the first organic creation of Filippo Brunelleschi (1377-1446), marks the birth of Renaissance architecture in Florence. The Hospital of Santa Maria Nuova, founded in 1288, is the oldest hospital still active in Florence.
Part of the goal for this new annual conference session is to take a break from more clinically focused presentations, and to think about the hospital from a different perspective, Dr. Messler said. His session will emphasize the power of stories and storytelling to inform and inspire medical practice.
“This is not something that can be applied clinically the next day, but lessons from the past can inform the design of hospitals and how we manage patients,” he said. “We need to ask ourselves, ‘How can we analyze hospital history to inform what we do today?’ ”
References
“Asclepeion.” Wikipedia. Accessed Jan. 28, 2019: https://en.wikipedia.org/wiki/Asclepeion.
Advance care planning codes not being used
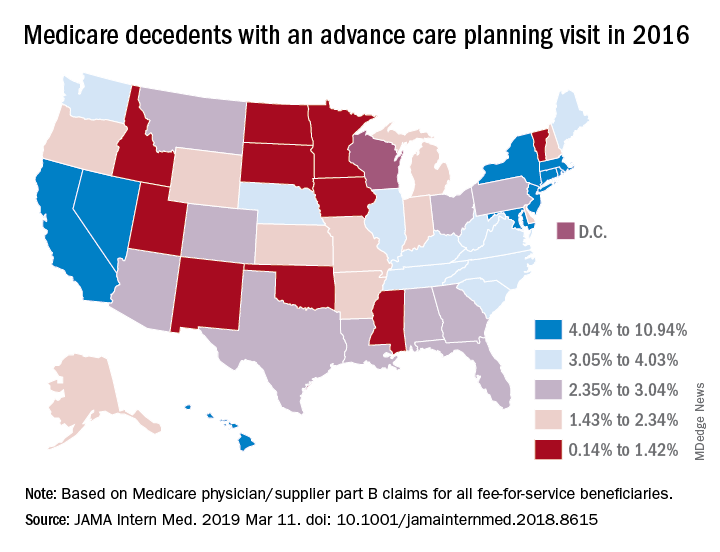
Starting in 2016, the Centers for Medicare & Medicaid Services began paying physicians for advance care planning discussions with the approval of two new codes: 99497 and 99498. The codes pay about $86 for the first 30 minutes of a face-to-face conversation with a patient, family member, and/or surrogate and about $75 for additional sessions. Services can be furnished in both inpatient and ambulatory settings, and payment is not limited to particular physician specialties.
In 2016, health care professionals in New England (Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont) billed Medicare 26,522 times for the advance care planning (ACP) codes for a total of 24,536 patients, which represented less than 1% of Medicare beneficiaries in New England at the time, according to Kimberly Pelland, MPH, of Healthcentric Advisors, Providence, R.I., and her colleagues. Most claims were billed in the office, followed by in nursing homes, and in hospitals; 40% of conversations occurred during an annual wellness visit (JAMA Intern Med. 2019 March 11. doi:10.1001/jamainternmed.2018.8107).
Internists billed Medicare the most for ACP claims (65%), followed by family physicians (22%) gerontologists (5%), and oncologist/hematologists (0.3%), according to the analysis based on 2016 Medicare claims data and Census Bureau data. A greater proportion of patients with ACP claims were female, aged 85 years or older, enrolled in hospice, and died in the study year. Patients had higher odds of having an ACP claim if they were older and had lower income, and if they had cancer, heart failure, stroke, chronic kidney disease, or dementia. Male patients who were Asian, black, and Hispanic had lower chances of having an ACP claim.
In a related study, Emmanuelle Belanger, PhD, of Brown University, Providence, R.I., and her colleagues examined national Medicare data from 2016 to the third quarter of 2017. Across the United States, 2% of Medicare patients aged 65 years and older received advance care planning services that were billed under the ACP codes (JAMA Intern Med. 2019 March 11. doi: 10.1001/jamainternmed.2018.8615). Visits billed under the ACP codes increased from 538,275 to 633,214 during the same time period. Claim rates were higher among patients who died within the study period, reaching 3% in 2016 and 6% in 2017. The percentage of decedents with an ACP billed visit varied strongly across states, with states such as North Dakota, South Dakota, and Wyoming having the fewest ACP visits billed and states such as California and Nevada having the most. ACP billed visits increased in all settings in 2017, but primarily in hospitals and nursing homes. Nationally, internists billed the codes most (48%), followed by family physicians (28%).

While the two studies indicate low usage of the ACP codes, many physicians are discussing advance care planning with their patients, said Mary M. Newman, MD, an internist based in Lutherville, Md., and former American College of Physicians adviser to the American Medical Association Relative Scale Value Update Committee (RUC).
“What cannot be captured by tracking under Medicare claims data are those shorter conversations that we have frequently,” Dr. Newman said in an interview. “If we have a short conversation about advance care planning, it gets folded into our evaluation and management visit. It’s not going to be separately billed.”
At the same time, some patients are not ready to discuss end-of-life options and decline the discussions when asked, Dr. Newman said. Particularly for healthier patients, end of life care is not a primary focus, she noted.
“Not everybody’s ready to have an advance care planning [discussion] that lasts 16-45 minutes,” she said. “Many people over age 65 are not ready to deal with advance care planning in their day-to-day lives, and it may not be what they wish to discuss. I offer the option to patients and some say, ‘Yes, I’d love to,’ and others decline or postpone.”
Low usage of the ACP codes may be associated with lack of awareness, uncertainty about appropriate code use, or associated billing that is not part of the standard workflow, Ankita Mehta, MD, of Mount Sinai in New York wrote an editorial accompanying the studies (JAMA Intern Med. 2019 March 11. doi:10.1001/jamainternmed.2018.8105).
“Regardless, the low rates of utilization of ACP codes is alarming and highlights the need to create strategies to integrate ACP discussions into standard practice and build ACP documentation and billing in clinical workflow,” Dr. Mehta said.
Dr. Newman agreed that more education among physicians is needed.
“The amount of education clinicians have received varies tremendously across the geography of the country,” she said. “I think the codes are going to be slowly adopted. The challenge to us is to make sure we’re all better educated on palliative care as people age and get sick and that we are sensitive to our patients explicit and implicit needs for these discussions.”
Starting in 2016, the Centers for Medicare & Medicaid Services began paying physicians for advance care planning discussions with the approval of two new codes: 99497 and 99498. The codes pay about $86 for the first 30 minutes of a face-to-face conversation with a patient, family member, and/or surrogate and about $75 for additional sessions. Services can be furnished in both inpatient and ambulatory settings, and payment is not limited to particular physician specialties.
In 2016, health care professionals in New England (Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont) billed Medicare 26,522 times for the advance care planning (ACP) codes for a total of 24,536 patients, which represented less than 1% of Medicare beneficiaries in New England at the time, according to Kimberly Pelland, MPH, of Healthcentric Advisors, Providence, R.I., and her colleagues. Most claims were billed in the office, followed by in nursing homes, and in hospitals; 40% of conversations occurred during an annual wellness visit (JAMA Intern Med. 2019 March 11. doi:10.1001/jamainternmed.2018.8107).
Internists billed Medicare the most for ACP claims (65%), followed by family physicians (22%) gerontologists (5%), and oncologist/hematologists (0.3%), according to the analysis based on 2016 Medicare claims data and Census Bureau data. A greater proportion of patients with ACP claims were female, aged 85 years or older, enrolled in hospice, and died in the study year. Patients had higher odds of having an ACP claim if they were older and had lower income, and if they had cancer, heart failure, stroke, chronic kidney disease, or dementia. Male patients who were Asian, black, and Hispanic had lower chances of having an ACP claim.
In a related study, Emmanuelle Belanger, PhD, of Brown University, Providence, R.I., and her colleagues examined national Medicare data from 2016 to the third quarter of 2017. Across the United States, 2% of Medicare patients aged 65 years and older received advance care planning services that were billed under the ACP codes (JAMA Intern Med. 2019 March 11. doi: 10.1001/jamainternmed.2018.8615). Visits billed under the ACP codes increased from 538,275 to 633,214 during the same time period. Claim rates were higher among patients who died within the study period, reaching 3% in 2016 and 6% in 2017. The percentage of decedents with an ACP billed visit varied strongly across states, with states such as North Dakota, South Dakota, and Wyoming having the fewest ACP visits billed and states such as California and Nevada having the most. ACP billed visits increased in all settings in 2017, but primarily in hospitals and nursing homes. Nationally, internists billed the codes most (48%), followed by family physicians (28%).
While the two studies indicate low usage of the ACP codes, many physicians are discussing advance care planning with their patients, said Mary M. Newman, MD, an internist based in Lutherville, Md., and former American College of Physicians adviser to the American Medical Association Relative Scale Value Update Committee (RUC).
“What cannot be captured by tracking under Medicare claims data are those shorter conversations that we have frequently,” Dr. Newman said in an interview. “If we have a short conversation about advance care planning, it gets folded into our evaluation and management visit. It’s not going to be separately billed.”
At the same time, some patients are not ready to discuss end-of-life options and decline the discussions when asked, Dr. Newman said. Particularly for healthier patients, end of life care is not a primary focus, she noted.
“Not everybody’s ready to have an advance care planning [discussion] that lasts 16-45 minutes,” she said. “Many people over age 65 are not ready to deal with advance care planning in their day-to-day lives, and it may not be what they wish to discuss. I offer the option to patients and some say, ‘Yes, I’d love to,’ and others decline or postpone.”
Low usage of the ACP codes may be associated with lack of awareness, uncertainty about appropriate code use, or associated billing that is not part of the standard workflow, Ankita Mehta, MD, of Mount Sinai in New York wrote an editorial accompanying the studies (JAMA Intern Med. 2019 March 11. doi:10.1001/jamainternmed.2018.8105).
“Regardless, the low rates of utilization of ACP codes is alarming and highlights the need to create strategies to integrate ACP discussions into standard practice and build ACP documentation and billing in clinical workflow,” Dr. Mehta said.
Dr. Newman agreed that more education among physicians is needed.
“The amount of education clinicians have received varies tremendously across the geography of the country,” she said. “I think the codes are going to be slowly adopted. The challenge to us is to make sure we’re all better educated on palliative care as people age and get sick and that we are sensitive to our patients explicit and implicit needs for these discussions.”
Starting in 2016, the Centers for Medicare & Medicaid Services began paying physicians for advance care planning discussions with the approval of two new codes: 99497 and 99498. The codes pay about $86 for the first 30 minutes of a face-to-face conversation with a patient, family member, and/or surrogate and about $75 for additional sessions. Services can be furnished in both inpatient and ambulatory settings, and payment is not limited to particular physician specialties.
In 2016, health care professionals in New England (Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont) billed Medicare 26,522 times for the advance care planning (ACP) codes for a total of 24,536 patients, which represented less than 1% of Medicare beneficiaries in New England at the time, according to Kimberly Pelland, MPH, of Healthcentric Advisors, Providence, R.I., and her colleagues. Most claims were billed in the office, followed by in nursing homes, and in hospitals; 40% of conversations occurred during an annual wellness visit (JAMA Intern Med. 2019 March 11. doi:10.1001/jamainternmed.2018.8107).
Internists billed Medicare the most for ACP claims (65%), followed by family physicians (22%) gerontologists (5%), and oncologist/hematologists (0.3%), according to the analysis based on 2016 Medicare claims data and Census Bureau data. A greater proportion of patients with ACP claims were female, aged 85 years or older, enrolled in hospice, and died in the study year. Patients had higher odds of having an ACP claim if they were older and had lower income, and if they had cancer, heart failure, stroke, chronic kidney disease, or dementia. Male patients who were Asian, black, and Hispanic had lower chances of having an ACP claim.
In a related study, Emmanuelle Belanger, PhD, of Brown University, Providence, R.I., and her colleagues examined national Medicare data from 2016 to the third quarter of 2017. Across the United States, 2% of Medicare patients aged 65 years and older received advance care planning services that were billed under the ACP codes (JAMA Intern Med. 2019 March 11. doi: 10.1001/jamainternmed.2018.8615). Visits billed under the ACP codes increased from 538,275 to 633,214 during the same time period. Claim rates were higher among patients who died within the study period, reaching 3% in 2016 and 6% in 2017. The percentage of decedents with an ACP billed visit varied strongly across states, with states such as North Dakota, South Dakota, and Wyoming having the fewest ACP visits billed and states such as California and Nevada having the most. ACP billed visits increased in all settings in 2017, but primarily in hospitals and nursing homes. Nationally, internists billed the codes most (48%), followed by family physicians (28%).
While the two studies indicate low usage of the ACP codes, many physicians are discussing advance care planning with their patients, said Mary M. Newman, MD, an internist based in Lutherville, Md., and former American College of Physicians adviser to the American Medical Association Relative Scale Value Update Committee (RUC).
“What cannot be captured by tracking under Medicare claims data are those shorter conversations that we have frequently,” Dr. Newman said in an interview. “If we have a short conversation about advance care planning, it gets folded into our evaluation and management visit. It’s not going to be separately billed.”
At the same time, some patients are not ready to discuss end-of-life options and decline the discussions when asked, Dr. Newman said. Particularly for healthier patients, end of life care is not a primary focus, she noted.
“Not everybody’s ready to have an advance care planning [discussion] that lasts 16-45 minutes,” she said. “Many people over age 65 are not ready to deal with advance care planning in their day-to-day lives, and it may not be what they wish to discuss. I offer the option to patients and some say, ‘Yes, I’d love to,’ and others decline or postpone.”
Low usage of the ACP codes may be associated with lack of awareness, uncertainty about appropriate code use, or associated billing that is not part of the standard workflow, Ankita Mehta, MD, of Mount Sinai in New York wrote an editorial accompanying the studies (JAMA Intern Med. 2019 March 11. doi:10.1001/jamainternmed.2018.8105).
“Regardless, the low rates of utilization of ACP codes is alarming and highlights the need to create strategies to integrate ACP discussions into standard practice and build ACP documentation and billing in clinical workflow,” Dr. Mehta said.
Dr. Newman agreed that more education among physicians is needed.
“The amount of education clinicians have received varies tremendously across the geography of the country,” she said. “I think the codes are going to be slowly adopted. The challenge to us is to make sure we’re all better educated on palliative care as people age and get sick and that we are sensitive to our patients explicit and implicit needs for these discussions.”
Heart failure remains a common, costly concern
Heart failure remains one of the deadliest chronic medical conditions, with 5-year mortality rates approaching 50%, and is the most common diagnosis for adults aged 65 years and older who are admitted to the hospital, according to Albert J. Hicks III, MD.

Dr. Hicks, a cardiologist at Baylor Scott & White Health in Temple, Tex., will discuss the latest challenges and hottest topics surrounding heart failure in the “Updates in Heart Failure” session on Monday, at HM19.
The growth of an aging population in the United States further emphasizes the importance of heart failure as a topic of interest to clinicians, Dr. Hicks said in an interview. He noted that heart failure is the highest medical expenditure for Medicare, and estimates suggest the condition will cost the U.S. health care system $30 billion by the year 2030, he said. With these numbers in mind, the timing of referring patients to an advanced heart failure team is a key issue.
But the timing of referral for advanced care is just one of the hot topics on the agenda for the “Updates in Heart Failure” session, Dr. Hicks said. Other topics include heart failure epidemiology (incidence, prevalence, morbidity, mortality, and disparities); economics of heart failure (burden of care on the U.S. health care system); heart failure hospitalizations and readmissions (risk factors, comorbidities, patient compliance issues); pathophysiology (why heart failure is so deadly); signs and symptoms of heart failure (how to recognize them); treatment of stage C heart failure, with a review of old and new drugs and devices; and treatment of stage D heart failure, including palliative care, mechanical circulatory support, and heart transplantation.
Dr. Hicks’ primary goal for the session is to “increase awareness of the high mortality associated with a heart failure diagnosis,” he said. He also hopes to educate hospitalists about the latest medications, devices, and resources for heart failure patients and to give them the tools and knowledge to help reduce morbidity and mortality in their heart failure patients.
Session attendees also will benefit from Dr. Hicks’ practical advice on identifying warning signs that indicate a heart failure patient may need a medical assist device or a heart transplant and on encouraging early referral of heart failure patients to advanced heart failure specialists before irreversible end-organ damage occurs.
Dr. Hicks hypothesized that the high mortality associated with a heart failure diagnosis, hospital readmission, and late referral will generate the liveliest discussion because issues of costs and resources continue to evolve.
His take-home message: “Early recognition and referral of heart failure patients to a heart failure cardiologist can improve patient costs, morbidity, and survival.
Dr. Hicks had no relevant financial conflicts to disclose.
Updates in Heart Failure
Monday, 2:00-2:40 p.m.
Woodrow Wilson
Heart failure remains one of the deadliest chronic medical conditions, with 5-year mortality rates approaching 50%, and is the most common diagnosis for adults aged 65 years and older who are admitted to the hospital, according to Albert J. Hicks III, MD.
Dr. Hicks, a cardiologist at Baylor Scott & White Health in Temple, Tex., will discuss the latest challenges and hottest topics surrounding heart failure in the “Updates in Heart Failure” session on Monday, at HM19.
The growth of an aging population in the United States further emphasizes the importance of heart failure as a topic of interest to clinicians, Dr. Hicks said in an interview. He noted that heart failure is the highest medical expenditure for Medicare, and estimates suggest the condition will cost the U.S. health care system $30 billion by the year 2030, he said. With these numbers in mind, the timing of referring patients to an advanced heart failure team is a key issue.
But the timing of referral for advanced care is just one of the hot topics on the agenda for the “Updates in Heart Failure” session, Dr. Hicks said. Other topics include heart failure epidemiology (incidence, prevalence, morbidity, mortality, and disparities); economics of heart failure (burden of care on the U.S. health care system); heart failure hospitalizations and readmissions (risk factors, comorbidities, patient compliance issues); pathophysiology (why heart failure is so deadly); signs and symptoms of heart failure (how to recognize them); treatment of stage C heart failure, with a review of old and new drugs and devices; and treatment of stage D heart failure, including palliative care, mechanical circulatory support, and heart transplantation.
Dr. Hicks’ primary goal for the session is to “increase awareness of the high mortality associated with a heart failure diagnosis,” he said. He also hopes to educate hospitalists about the latest medications, devices, and resources for heart failure patients and to give them the tools and knowledge to help reduce morbidity and mortality in their heart failure patients.
Session attendees also will benefit from Dr. Hicks’ practical advice on identifying warning signs that indicate a heart failure patient may need a medical assist device or a heart transplant and on encouraging early referral of heart failure patients to advanced heart failure specialists before irreversible end-organ damage occurs.
Dr. Hicks hypothesized that the high mortality associated with a heart failure diagnosis, hospital readmission, and late referral will generate the liveliest discussion because issues of costs and resources continue to evolve.
His take-home message: “Early recognition and referral of heart failure patients to a heart failure cardiologist can improve patient costs, morbidity, and survival.
Dr. Hicks had no relevant financial conflicts to disclose.
Updates in Heart Failure
Monday, 2:00-2:40 p.m.
Woodrow Wilson
Heart failure remains one of the deadliest chronic medical conditions, with 5-year mortality rates approaching 50%, and is the most common diagnosis for adults aged 65 years and older who are admitted to the hospital, according to Albert J. Hicks III, MD.
Dr. Hicks, a cardiologist at Baylor Scott & White Health in Temple, Tex., will discuss the latest challenges and hottest topics surrounding heart failure in the “Updates in Heart Failure” session on Monday, at HM19.
The growth of an aging population in the United States further emphasizes the importance of heart failure as a topic of interest to clinicians, Dr. Hicks said in an interview. He noted that heart failure is the highest medical expenditure for Medicare, and estimates suggest the condition will cost the U.S. health care system $30 billion by the year 2030, he said. With these numbers in mind, the timing of referring patients to an advanced heart failure team is a key issue.
But the timing of referral for advanced care is just one of the hot topics on the agenda for the “Updates in Heart Failure” session, Dr. Hicks said. Other topics include heart failure epidemiology (incidence, prevalence, morbidity, mortality, and disparities); economics of heart failure (burden of care on the U.S. health care system); heart failure hospitalizations and readmissions (risk factors, comorbidities, patient compliance issues); pathophysiology (why heart failure is so deadly); signs and symptoms of heart failure (how to recognize them); treatment of stage C heart failure, with a review of old and new drugs and devices; and treatment of stage D heart failure, including palliative care, mechanical circulatory support, and heart transplantation.
Dr. Hicks’ primary goal for the session is to “increase awareness of the high mortality associated with a heart failure diagnosis,” he said. He also hopes to educate hospitalists about the latest medications, devices, and resources for heart failure patients and to give them the tools and knowledge to help reduce morbidity and mortality in their heart failure patients.
Session attendees also will benefit from Dr. Hicks’ practical advice on identifying warning signs that indicate a heart failure patient may need a medical assist device or a heart transplant and on encouraging early referral of heart failure patients to advanced heart failure specialists before irreversible end-organ damage occurs.
Dr. Hicks hypothesized that the high mortality associated with a heart failure diagnosis, hospital readmission, and late referral will generate the liveliest discussion because issues of costs and resources continue to evolve.
His take-home message: “Early recognition and referral of heart failure patients to a heart failure cardiologist can improve patient costs, morbidity, and survival.
Dr. Hicks had no relevant financial conflicts to disclose.
Updates in Heart Failure
Monday, 2:00-2:40 p.m.
Woodrow Wilson