User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Schizophrenia and HIV: missed opportunities for care
“People don’t think about schizophrenia when they think about HIV,” Christina Mangurian, MD, professor of clinical psychiatry and vice chair for diversity and health equity at the University of California, San Francisco (UCSF), told this news organization.

The problem is complicated. According to the Centers for Disease Control and Prevention and National Institutes of Health, roughly 6% of people with serious mental illness are living with HIV, a rate that is about 10 times higher than the general U.S. population (0.4%). However, findings from a study by Dr. Mangurian and her team, published online in the journal AIDS, demonstrated that half of Medicaid patients with schizophrenia and HIV admitted to inpatient units in New York State were not coded as such upon discharge.
These data raise the question: , lack of social support, and under-recognition by practitioners that a problem even exists?
Lost in the care continuum
Dr. Mangurian and her research team examined documentation of pre-existing HIV/AIDS diagnoses and absence of ICD-9-CM HIV/AIDS coding at psychiatric discharge among 14,602 adults (aged 18-64 years) admitted to hospital inpatient units in New York State between Jan. 1, 2012, and Dec. 31, 2013. HIV diagnoses were defined as recent (within 30 days of admission) or distant (within 30-366 days of admission), and first admission was used as the index in people with multiple hospitalizations.
People living with HIV comprised 5.1% (741) of the overall dataset; 34% were diagnosed with schizophrenia and 27.9% with bipolar disorders. Overall, 54.5% were male and 50.7% were non-Hispanic Black. Furthermore, 58.3% were discharged without HIV/AIDS ICD-9 coding, reinforcing the likelihood that they were lost in the care continuum.
Dr. Mangurian explained that this break in the chain of care upon discharge can have an important impact on efforts to break the cycle of HIV transmission.
“There’s data that people with serious mental illnesses like schizophrenia are less likely to have sex, but when they do they’re more likely to engage in risky sexual behaviors, including sex for money [and] unprotected sex with partners who use injection drugs or who have HIV,” she said.
Although the majority of patients – both with and without prior HIV diagnoses – were older, adjusted models demonstrated that people aged 18-24 years had more than twice the odds of having their HIV/AIDS undocumented at discharge, compared with older adults aged 55-64 years (adjusted odds ratio, 2.37; P = .038), as were those aged 25-34 years (aOR, 2.17; P = .003). Individuals with more distant HIV diagnoses had three times the odds for an undocumented HIV/AIDS discharge, compared with more recent diagnoses (aOR, 3.25; P < .001).
Additional factors contributing to the lack of ICD-9 discharge coding included shorter lengths of stay (0-3 days vs. 15-30 days; aOR, 0.03; P = .01) and fewer HIV claims for HIV/AIDS services before hospitalization (1-2 vs. 3-9; aOR, 0.34; P < .01). Hospitals serving medium or high levels of Medicaid patients were also less likely to document HIV/AIDS before discharge (medium aOR, 1.69, P = .01; high aOR, 1.71, P = .03).
The study is not without limitations. For example, the 10-year-old dataset might not entirely reflect more recent structural or systemic changes for improving HIV detection on inpatient psychiatric units. Moreover, there was no comparator group without psychiatric inpatient admission.
Still, “[if these patients] didn’t have a discharge diagnosis, then it’s possible that they were not managed for their HIV, or their HIV was not addressed while they were in the hospital,” Sarah Andrews, MD, assistant professor of psychiatry and behavioral sciences and AIDS psychiatrist at Johns Hopkins School of Medicine, Baltimore, explained.
Dr. Andrews, who was not involved in the study, noted that this omission is significant. “A psychiatric admission or medical admission in general is a great opportunity to further manage and treat comorbidities. When we have a patient who comes in with HIV and they haven’t been on an antiviral prior to admission, we try to get infectious disease to give us recommendations of what to start, what labs to draw, to help them re-establish care,” she said.
Severe mental health an HIV disparity
Despite the burden of HIV among patient populations with serious mental health issues and data suggesting that these populations are over-represented among new HIV infections, the study findings point to an important missed opportunity for meeting several key outcomes on the HIV/AIDS care continuum, especially linkage to and retention in care.
The challenge is multifactorial.
In an earlier publication appearing in April 2021 in The Lancet HIV, Dr. Mangurian and colleagues explore a concept known as the “purview paradox,” which refers to a practitioner’s belief about who should be responsible for offering patients a particular intervention.
Structural and systemic issues also abound, as psychiatry records are often kept separate from the rest of the medical system due to insurer billing issues. “The true integration of all psychiatric and medical care has to happen to make sure that all of our patients receive the care that they deserve,” explained Dr. Mangurian.
Dr. Andrews agrees. “HIV care, as well as psychiatry, case management, pharmacy ... putting them together really helps decrease the risk of falling through the cracks and being able to refer appropriately for mental health,” she said.
Aside from changing practitioner attitudes and awareness and changing systems to include the wrap-around care model, current guidelines also need to reflect the role that patients with HIV and psychiatric comorbidities play in HIV transmission. Dr. Andrews and Dr. Mangurian agree: Routine screening in psychiatric inpatient units might be a good start.
The study was independently supported. Dr. Mangurian has reported grant funding from Genentech Charitable Foundation. Dr. Andrews has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“People don’t think about schizophrenia when they think about HIV,” Christina Mangurian, MD, professor of clinical psychiatry and vice chair for diversity and health equity at the University of California, San Francisco (UCSF), told this news organization.
The problem is complicated. According to the Centers for Disease Control and Prevention and National Institutes of Health, roughly 6% of people with serious mental illness are living with HIV, a rate that is about 10 times higher than the general U.S. population (0.4%). However, findings from a study by Dr. Mangurian and her team, published online in the journal AIDS, demonstrated that half of Medicaid patients with schizophrenia and HIV admitted to inpatient units in New York State were not coded as such upon discharge.
These data raise the question: , lack of social support, and under-recognition by practitioners that a problem even exists?
Lost in the care continuum
Dr. Mangurian and her research team examined documentation of pre-existing HIV/AIDS diagnoses and absence of ICD-9-CM HIV/AIDS coding at psychiatric discharge among 14,602 adults (aged 18-64 years) admitted to hospital inpatient units in New York State between Jan. 1, 2012, and Dec. 31, 2013. HIV diagnoses were defined as recent (within 30 days of admission) or distant (within 30-366 days of admission), and first admission was used as the index in people with multiple hospitalizations.
People living with HIV comprised 5.1% (741) of the overall dataset; 34% were diagnosed with schizophrenia and 27.9% with bipolar disorders. Overall, 54.5% were male and 50.7% were non-Hispanic Black. Furthermore, 58.3% were discharged without HIV/AIDS ICD-9 coding, reinforcing the likelihood that they were lost in the care continuum.
Dr. Mangurian explained that this break in the chain of care upon discharge can have an important impact on efforts to break the cycle of HIV transmission.
“There’s data that people with serious mental illnesses like schizophrenia are less likely to have sex, but when they do they’re more likely to engage in risky sexual behaviors, including sex for money [and] unprotected sex with partners who use injection drugs or who have HIV,” she said.
Although the majority of patients – both with and without prior HIV diagnoses – were older, adjusted models demonstrated that people aged 18-24 years had more than twice the odds of having their HIV/AIDS undocumented at discharge, compared with older adults aged 55-64 years (adjusted odds ratio, 2.37; P = .038), as were those aged 25-34 years (aOR, 2.17; P = .003). Individuals with more distant HIV diagnoses had three times the odds for an undocumented HIV/AIDS discharge, compared with more recent diagnoses (aOR, 3.25; P < .001).
Additional factors contributing to the lack of ICD-9 discharge coding included shorter lengths of stay (0-3 days vs. 15-30 days; aOR, 0.03; P = .01) and fewer HIV claims for HIV/AIDS services before hospitalization (1-2 vs. 3-9; aOR, 0.34; P < .01). Hospitals serving medium or high levels of Medicaid patients were also less likely to document HIV/AIDS before discharge (medium aOR, 1.69, P = .01; high aOR, 1.71, P = .03).
The study is not without limitations. For example, the 10-year-old dataset might not entirely reflect more recent structural or systemic changes for improving HIV detection on inpatient psychiatric units. Moreover, there was no comparator group without psychiatric inpatient admission.
Still, “[if these patients] didn’t have a discharge diagnosis, then it’s possible that they were not managed for their HIV, or their HIV was not addressed while they were in the hospital,” Sarah Andrews, MD, assistant professor of psychiatry and behavioral sciences and AIDS psychiatrist at Johns Hopkins School of Medicine, Baltimore, explained.
Dr. Andrews, who was not involved in the study, noted that this omission is significant. “A psychiatric admission or medical admission in general is a great opportunity to further manage and treat comorbidities. When we have a patient who comes in with HIV and they haven’t been on an antiviral prior to admission, we try to get infectious disease to give us recommendations of what to start, what labs to draw, to help them re-establish care,” she said.
Severe mental health an HIV disparity
Despite the burden of HIV among patient populations with serious mental health issues and data suggesting that these populations are over-represented among new HIV infections, the study findings point to an important missed opportunity for meeting several key outcomes on the HIV/AIDS care continuum, especially linkage to and retention in care.
The challenge is multifactorial.
In an earlier publication appearing in April 2021 in The Lancet HIV, Dr. Mangurian and colleagues explore a concept known as the “purview paradox,” which refers to a practitioner’s belief about who should be responsible for offering patients a particular intervention.
Structural and systemic issues also abound, as psychiatry records are often kept separate from the rest of the medical system due to insurer billing issues. “The true integration of all psychiatric and medical care has to happen to make sure that all of our patients receive the care that they deserve,” explained Dr. Mangurian.
Dr. Andrews agrees. “HIV care, as well as psychiatry, case management, pharmacy ... putting them together really helps decrease the risk of falling through the cracks and being able to refer appropriately for mental health,” she said.
Aside from changing practitioner attitudes and awareness and changing systems to include the wrap-around care model, current guidelines also need to reflect the role that patients with HIV and psychiatric comorbidities play in HIV transmission. Dr. Andrews and Dr. Mangurian agree: Routine screening in psychiatric inpatient units might be a good start.
The study was independently supported. Dr. Mangurian has reported grant funding from Genentech Charitable Foundation. Dr. Andrews has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“People don’t think about schizophrenia when they think about HIV,” Christina Mangurian, MD, professor of clinical psychiatry and vice chair for diversity and health equity at the University of California, San Francisco (UCSF), told this news organization.
The problem is complicated. According to the Centers for Disease Control and Prevention and National Institutes of Health, roughly 6% of people with serious mental illness are living with HIV, a rate that is about 10 times higher than the general U.S. population (0.4%). However, findings from a study by Dr. Mangurian and her team, published online in the journal AIDS, demonstrated that half of Medicaid patients with schizophrenia and HIV admitted to inpatient units in New York State were not coded as such upon discharge.
These data raise the question: , lack of social support, and under-recognition by practitioners that a problem even exists?
Lost in the care continuum
Dr. Mangurian and her research team examined documentation of pre-existing HIV/AIDS diagnoses and absence of ICD-9-CM HIV/AIDS coding at psychiatric discharge among 14,602 adults (aged 18-64 years) admitted to hospital inpatient units in New York State between Jan. 1, 2012, and Dec. 31, 2013. HIV diagnoses were defined as recent (within 30 days of admission) or distant (within 30-366 days of admission), and first admission was used as the index in people with multiple hospitalizations.
People living with HIV comprised 5.1% (741) of the overall dataset; 34% were diagnosed with schizophrenia and 27.9% with bipolar disorders. Overall, 54.5% were male and 50.7% were non-Hispanic Black. Furthermore, 58.3% were discharged without HIV/AIDS ICD-9 coding, reinforcing the likelihood that they were lost in the care continuum.
Dr. Mangurian explained that this break in the chain of care upon discharge can have an important impact on efforts to break the cycle of HIV transmission.
“There’s data that people with serious mental illnesses like schizophrenia are less likely to have sex, but when they do they’re more likely to engage in risky sexual behaviors, including sex for money [and] unprotected sex with partners who use injection drugs or who have HIV,” she said.
Although the majority of patients – both with and without prior HIV diagnoses – were older, adjusted models demonstrated that people aged 18-24 years had more than twice the odds of having their HIV/AIDS undocumented at discharge, compared with older adults aged 55-64 years (adjusted odds ratio, 2.37; P = .038), as were those aged 25-34 years (aOR, 2.17; P = .003). Individuals with more distant HIV diagnoses had three times the odds for an undocumented HIV/AIDS discharge, compared with more recent diagnoses (aOR, 3.25; P < .001).
Additional factors contributing to the lack of ICD-9 discharge coding included shorter lengths of stay (0-3 days vs. 15-30 days; aOR, 0.03; P = .01) and fewer HIV claims for HIV/AIDS services before hospitalization (1-2 vs. 3-9; aOR, 0.34; P < .01). Hospitals serving medium or high levels of Medicaid patients were also less likely to document HIV/AIDS before discharge (medium aOR, 1.69, P = .01; high aOR, 1.71, P = .03).
The study is not without limitations. For example, the 10-year-old dataset might not entirely reflect more recent structural or systemic changes for improving HIV detection on inpatient psychiatric units. Moreover, there was no comparator group without psychiatric inpatient admission.
Still, “[if these patients] didn’t have a discharge diagnosis, then it’s possible that they were not managed for their HIV, or their HIV was not addressed while they were in the hospital,” Sarah Andrews, MD, assistant professor of psychiatry and behavioral sciences and AIDS psychiatrist at Johns Hopkins School of Medicine, Baltimore, explained.
Dr. Andrews, who was not involved in the study, noted that this omission is significant. “A psychiatric admission or medical admission in general is a great opportunity to further manage and treat comorbidities. When we have a patient who comes in with HIV and they haven’t been on an antiviral prior to admission, we try to get infectious disease to give us recommendations of what to start, what labs to draw, to help them re-establish care,” she said.
Severe mental health an HIV disparity
Despite the burden of HIV among patient populations with serious mental health issues and data suggesting that these populations are over-represented among new HIV infections, the study findings point to an important missed opportunity for meeting several key outcomes on the HIV/AIDS care continuum, especially linkage to and retention in care.
The challenge is multifactorial.
In an earlier publication appearing in April 2021 in The Lancet HIV, Dr. Mangurian and colleagues explore a concept known as the “purview paradox,” which refers to a practitioner’s belief about who should be responsible for offering patients a particular intervention.
Structural and systemic issues also abound, as psychiatry records are often kept separate from the rest of the medical system due to insurer billing issues. “The true integration of all psychiatric and medical care has to happen to make sure that all of our patients receive the care that they deserve,” explained Dr. Mangurian.
Dr. Andrews agrees. “HIV care, as well as psychiatry, case management, pharmacy ... putting them together really helps decrease the risk of falling through the cracks and being able to refer appropriately for mental health,” she said.
Aside from changing practitioner attitudes and awareness and changing systems to include the wrap-around care model, current guidelines also need to reflect the role that patients with HIV and psychiatric comorbidities play in HIV transmission. Dr. Andrews and Dr. Mangurian agree: Routine screening in psychiatric inpatient units might be a good start.
The study was independently supported. Dr. Mangurian has reported grant funding from Genentech Charitable Foundation. Dr. Andrews has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and COVID: Decline in new cases reaches 7th week
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.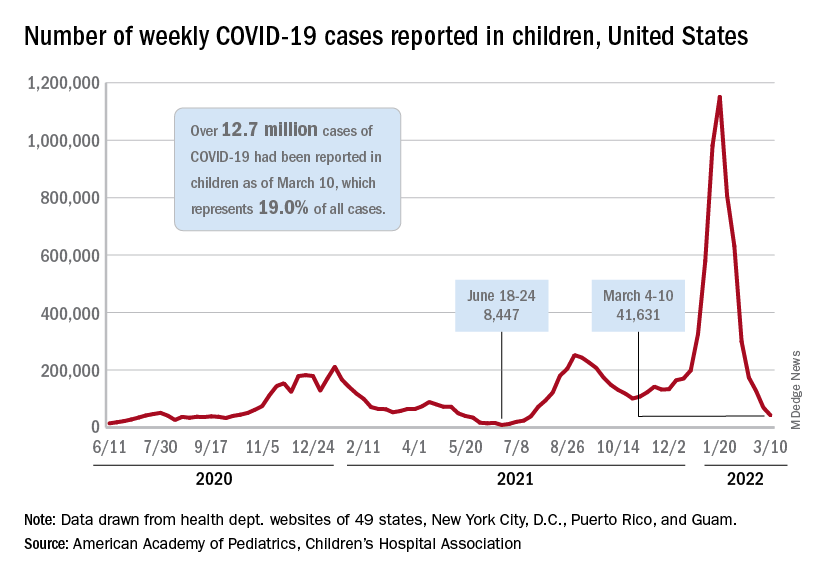
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
Air trapping common in patients with long COVID
, according to a prospective study that compared 100 COVID-19 survivors who had persistent symptoms and 106 healthy control persons.
“Something is going on in the distal airways related to either inflammation or fibrosis that is giving us a signal of air trapping,” noted senior author Alejandro P. Comellas, MD, in a press release. The study was stimulated by reports from University of Iowa clinicians noting that many patients with initial SARS-CoV-2 infection who were either hospitalized or were treated in the ambulatory setting later reported shortness of breath and other respiratory symptoms indicative of chronic lung disease.
Study results
Investigators classified patients (mean age, 48 years; 66 women) with post-acute sequelae of COVID-19 according to whether they were ambulatory (67%), hospitalized (17%), or required treatment in the intensive care unit (16%). They then compared CT findings of patients who had COVID-19 and persistent symptoms with those of a healthy control group.
COVID-19 severity did not affect the percentage of cases of lung with air trapping among these patients. Air trapping occurred at rates of 25.4% among ambulatory patients, 34.6% in hospitalized patients, and in 27.3% of those requiring intensive care (P = .10). The percentage of lungs affected by air trapping in ambulatory participants was sharply and significantly higher than in healthy controls (25.4% vs. 7.2%; P < .001). Also, air trapping persisted; it was still present in 8 of 9 participants who underwent imaging more than 200 days post diagnosis.
Qualitative analysis of chest CT images showed that the most common imaging abnormality was air trapping (58%); ground glass opacities (GGOs) were found in 51% (46/91), note Dr. Comellas and coauthors. This suggests ongoing lung inflammation, edema, or fibrosis. These symptoms are often observed during acute COVID-19, frequently in an organizing pneumonia pattern, and have been shown to persist for months after infection in survivors of severe disease. The mean percentage of total lung classified as having regional GGOs on chest CT scans was 13.2% and 28.7%, respectively, in the hospitalized and ICU groups, both very much higher than in the ambulatory group, at 3.7% (P < .001 for both). Among healthy controls, the GGO rate on chest CT was only 0.06% (P < .001).
In addition, air trapping correlated with the ratio of residual volume to total lung capacity (r = 0.6; P < .001) but not with spirometry results. In fact, the investigators did not observe airflow obstruction by spirometry in any group, suggesting that air trapping in these patients involves only small rather than large airways and that these small airways contribute little to total airway resistance. Only when a large percentage, perhaps 75% or more, of all small airways are obstructed will spirometry pick up small airways disease, the authors observe.
Continuing disease
The findings taken together suggest that functional small airways disease and air trapping are a consequence of SARS-CoV-2 infection, according to Dr. Comellas. “If a portion of patients continues to have small airways disease, then we need to think about the mechanisms behind it,” he said. “It could be something related to inflammation that’s reversible, or it may be something related to a scar that is irreversible, and then we need to look at ways to prevent further progression of the disease.” Furthermore, “studies aimed at determining the natural history of functional small airways disease in patients with post-acute sequelae of COVID-19 and the biological mechanisms that underlie these findings are urgently needed to identify therapeutic and preventative interventions,” Dr. Comellas, professor of internal medicine at Carver College of Medicine, University of Iowa, Iowa City, concluded.
The study limitations, the authors state, include the fact that theirs was a single-center study that enrolled participants infected early during the COVID-19 pandemic and did not include patients with Delta or Omicron variants, thus limiting the generalizability of the findings.
The study was published in Radiology.
The reported findings “indicate a long-term impact on bronchiolar obstruction,” states Brett M. Elicker, MD, professor of clinical radiology, University of California, San Francisco, in an accompanying editorial . Because collagen may be absorbed for months after an acute insult, it is not entirely clear whether the abnormalities seen in the current study will be permanent. He said further, “the presence of ground glass opacity and/or fibrosis on CT were most common in the patients admitted to the ICU and likely correspond to post-organizing pneumonia and/or post-diffuse alveolar damage fibrosis.”
Dr. Elicker also pointed out that organizing pneumonia is especially common among patients with COVID-19 and is usually highly steroid-responsive. The opacities improve or resolve with treatment, but sometimes residual fibrosis occurs. “Longer-term studies assessing the clinical and imaging manifestations 1-2 years after the initial infection are needed to fully ascertain the permanent manifestations of post-COVID fibrosis.”
The study was supported by grants from the National Institutes of Health. The authors and Dr. Elicker have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a prospective study that compared 100 COVID-19 survivors who had persistent symptoms and 106 healthy control persons.
“Something is going on in the distal airways related to either inflammation or fibrosis that is giving us a signal of air trapping,” noted senior author Alejandro P. Comellas, MD, in a press release. The study was stimulated by reports from University of Iowa clinicians noting that many patients with initial SARS-CoV-2 infection who were either hospitalized or were treated in the ambulatory setting later reported shortness of breath and other respiratory symptoms indicative of chronic lung disease.
Study results
Investigators classified patients (mean age, 48 years; 66 women) with post-acute sequelae of COVID-19 according to whether they were ambulatory (67%), hospitalized (17%), or required treatment in the intensive care unit (16%). They then compared CT findings of patients who had COVID-19 and persistent symptoms with those of a healthy control group.
COVID-19 severity did not affect the percentage of cases of lung with air trapping among these patients. Air trapping occurred at rates of 25.4% among ambulatory patients, 34.6% in hospitalized patients, and in 27.3% of those requiring intensive care (P = .10). The percentage of lungs affected by air trapping in ambulatory participants was sharply and significantly higher than in healthy controls (25.4% vs. 7.2%; P < .001). Also, air trapping persisted; it was still present in 8 of 9 participants who underwent imaging more than 200 days post diagnosis.
Qualitative analysis of chest CT images showed that the most common imaging abnormality was air trapping (58%); ground glass opacities (GGOs) were found in 51% (46/91), note Dr. Comellas and coauthors. This suggests ongoing lung inflammation, edema, or fibrosis. These symptoms are often observed during acute COVID-19, frequently in an organizing pneumonia pattern, and have been shown to persist for months after infection in survivors of severe disease. The mean percentage of total lung classified as having regional GGOs on chest CT scans was 13.2% and 28.7%, respectively, in the hospitalized and ICU groups, both very much higher than in the ambulatory group, at 3.7% (P < .001 for both). Among healthy controls, the GGO rate on chest CT was only 0.06% (P < .001).
In addition, air trapping correlated with the ratio of residual volume to total lung capacity (r = 0.6; P < .001) but not with spirometry results. In fact, the investigators did not observe airflow obstruction by spirometry in any group, suggesting that air trapping in these patients involves only small rather than large airways and that these small airways contribute little to total airway resistance. Only when a large percentage, perhaps 75% or more, of all small airways are obstructed will spirometry pick up small airways disease, the authors observe.
Continuing disease
The findings taken together suggest that functional small airways disease and air trapping are a consequence of SARS-CoV-2 infection, according to Dr. Comellas. “If a portion of patients continues to have small airways disease, then we need to think about the mechanisms behind it,” he said. “It could be something related to inflammation that’s reversible, or it may be something related to a scar that is irreversible, and then we need to look at ways to prevent further progression of the disease.” Furthermore, “studies aimed at determining the natural history of functional small airways disease in patients with post-acute sequelae of COVID-19 and the biological mechanisms that underlie these findings are urgently needed to identify therapeutic and preventative interventions,” Dr. Comellas, professor of internal medicine at Carver College of Medicine, University of Iowa, Iowa City, concluded.
The study limitations, the authors state, include the fact that theirs was a single-center study that enrolled participants infected early during the COVID-19 pandemic and did not include patients with Delta or Omicron variants, thus limiting the generalizability of the findings.
The study was published in Radiology.
The reported findings “indicate a long-term impact on bronchiolar obstruction,” states Brett M. Elicker, MD, professor of clinical radiology, University of California, San Francisco, in an accompanying editorial . Because collagen may be absorbed for months after an acute insult, it is not entirely clear whether the abnormalities seen in the current study will be permanent. He said further, “the presence of ground glass opacity and/or fibrosis on CT were most common in the patients admitted to the ICU and likely correspond to post-organizing pneumonia and/or post-diffuse alveolar damage fibrosis.”
Dr. Elicker also pointed out that organizing pneumonia is especially common among patients with COVID-19 and is usually highly steroid-responsive. The opacities improve or resolve with treatment, but sometimes residual fibrosis occurs. “Longer-term studies assessing the clinical and imaging manifestations 1-2 years after the initial infection are needed to fully ascertain the permanent manifestations of post-COVID fibrosis.”
The study was supported by grants from the National Institutes of Health. The authors and Dr. Elicker have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a prospective study that compared 100 COVID-19 survivors who had persistent symptoms and 106 healthy control persons.
“Something is going on in the distal airways related to either inflammation or fibrosis that is giving us a signal of air trapping,” noted senior author Alejandro P. Comellas, MD, in a press release. The study was stimulated by reports from University of Iowa clinicians noting that many patients with initial SARS-CoV-2 infection who were either hospitalized or were treated in the ambulatory setting later reported shortness of breath and other respiratory symptoms indicative of chronic lung disease.
Study results
Investigators classified patients (mean age, 48 years; 66 women) with post-acute sequelae of COVID-19 according to whether they were ambulatory (67%), hospitalized (17%), or required treatment in the intensive care unit (16%). They then compared CT findings of patients who had COVID-19 and persistent symptoms with those of a healthy control group.
COVID-19 severity did not affect the percentage of cases of lung with air trapping among these patients. Air trapping occurred at rates of 25.4% among ambulatory patients, 34.6% in hospitalized patients, and in 27.3% of those requiring intensive care (P = .10). The percentage of lungs affected by air trapping in ambulatory participants was sharply and significantly higher than in healthy controls (25.4% vs. 7.2%; P < .001). Also, air trapping persisted; it was still present in 8 of 9 participants who underwent imaging more than 200 days post diagnosis.
Qualitative analysis of chest CT images showed that the most common imaging abnormality was air trapping (58%); ground glass opacities (GGOs) were found in 51% (46/91), note Dr. Comellas and coauthors. This suggests ongoing lung inflammation, edema, or fibrosis. These symptoms are often observed during acute COVID-19, frequently in an organizing pneumonia pattern, and have been shown to persist for months after infection in survivors of severe disease. The mean percentage of total lung classified as having regional GGOs on chest CT scans was 13.2% and 28.7%, respectively, in the hospitalized and ICU groups, both very much higher than in the ambulatory group, at 3.7% (P < .001 for both). Among healthy controls, the GGO rate on chest CT was only 0.06% (P < .001).
In addition, air trapping correlated with the ratio of residual volume to total lung capacity (r = 0.6; P < .001) but not with spirometry results. In fact, the investigators did not observe airflow obstruction by spirometry in any group, suggesting that air trapping in these patients involves only small rather than large airways and that these small airways contribute little to total airway resistance. Only when a large percentage, perhaps 75% or more, of all small airways are obstructed will spirometry pick up small airways disease, the authors observe.
Continuing disease
The findings taken together suggest that functional small airways disease and air trapping are a consequence of SARS-CoV-2 infection, according to Dr. Comellas. “If a portion of patients continues to have small airways disease, then we need to think about the mechanisms behind it,” he said. “It could be something related to inflammation that’s reversible, or it may be something related to a scar that is irreversible, and then we need to look at ways to prevent further progression of the disease.” Furthermore, “studies aimed at determining the natural history of functional small airways disease in patients with post-acute sequelae of COVID-19 and the biological mechanisms that underlie these findings are urgently needed to identify therapeutic and preventative interventions,” Dr. Comellas, professor of internal medicine at Carver College of Medicine, University of Iowa, Iowa City, concluded.
The study limitations, the authors state, include the fact that theirs was a single-center study that enrolled participants infected early during the COVID-19 pandemic and did not include patients with Delta or Omicron variants, thus limiting the generalizability of the findings.
The study was published in Radiology.
The reported findings “indicate a long-term impact on bronchiolar obstruction,” states Brett M. Elicker, MD, professor of clinical radiology, University of California, San Francisco, in an accompanying editorial . Because collagen may be absorbed for months after an acute insult, it is not entirely clear whether the abnormalities seen in the current study will be permanent. He said further, “the presence of ground glass opacity and/or fibrosis on CT were most common in the patients admitted to the ICU and likely correspond to post-organizing pneumonia and/or post-diffuse alveolar damage fibrosis.”
Dr. Elicker also pointed out that organizing pneumonia is especially common among patients with COVID-19 and is usually highly steroid-responsive. The opacities improve or resolve with treatment, but sometimes residual fibrosis occurs. “Longer-term studies assessing the clinical and imaging manifestations 1-2 years after the initial infection are needed to fully ascertain the permanent manifestations of post-COVID fibrosis.”
The study was supported by grants from the National Institutes of Health. The authors and Dr. Elicker have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM RADIOLOGY
‘Overwhelming’ need to study COVID vaccine–associated tinnitus
It’s now known that tinnitus may be an unexpected side effect of SARS-CoV-2 vaccination, and there is an urgent need to understand the precise mechanisms and best treatment for vaccine-associated tinnitus, researchers say.
As of mid-September 2021, 12,247 cases of tinnitus, or ringing in the ears, following COVID-19 vaccination had been reported to the Vaccine Adverse Event Reporting System of the U.S. Centers for Disease Control and Prevention.
“Despite several cases of tinnitus being reported following SARS-CoV-2 vaccination, the precise pathophysiology is still not clear,” write Syed Hassan Ahmed, 3rd-year MBBS student, Dow University of Health Sciences, Karachi, Pakistan, and coauthors.
The researchers review what is known and unknown about SARS-CoV-2 vaccine-associated tinnitus in an article published online Feb. 11 in Annals of Medicine and Surgery.
Molecular mimicry?
The researchers say cross-reactivity between anti-spike SARS-CoV-2 antibodies and otologic antigens is one possibility, based on the mechanisms behind other COVID-19 vaccine–induced disorders and the phenomenon of molecular mimicry.
“The heptapeptide resemblance between coronavirus spike glycoprotein and numerous human proteins further supports molecular mimicry as a potential mechanism behind such vaccine-induced disorders,” they write.
Anti-spike antibodies may react with antigens anywhere along the auditory pathway and fuel an inflammatory reaction, they point out.
“Therefore, understanding the phenomenon of cross-reactivity and molecular mimicry may be helpful in postulating potential treatment behind not only tinnitus but also the rare events of vaccination associated hearing loss and other otologic manifestations,” the authors say.
Genetic predispositions and associated conditions may also play a significant role in determining whether an individual develops vaccine-induced tinnitus.
Stress and anxiety following COVID vaccination may also play a role, inasmuch as anxiety-related adverse events following vaccination have been reported. Vaccine-related anxiety as a potential cause of tinnitus developing after vaccination needs to be explored, they write.
Jury out on best management
How best to manage COVID vaccine-associated tinnitus also remains unclear, but it starts with a well-established diagnosis, the authors say.
A well-focused and detailed history and examination are essential, with particular emphasis placed on preexisting health conditions, specifically, autoimmune diseases, such as Hashimoto thyroiditis; otologic conditions, such as sensorineural hearing loss; glaucoma; and psychological well-being. According to the review, patients often present with a history of one or more of these disorders.
“However, any such association has not yet been established and requires further investigation to be concluded as potential risk factors for vaccine-induced tinnitus,” they caution.
Routine cranial nerve examination, otoscopy, Weber test, and Rinne test, which are used for tinnitus diagnosis in general, may be helpful for confirmation of vaccine-associated tinnitus.
Owing to the significant association between tinnitus and hearing impairment, audiology should also performed, the authors say.
Although treatments for non–vaccine-induced tinnitus vary significantly, corticosteroids are the top treatment choice for SARS-CoV-2 vaccine-induced tinnitus reported in the literature.
Trials of other drug and nondrug interventions that may uniquely help with vaccine-associated tinnitus are urgently needed, the authors say.
Summing up, the reviewers say, “Although the incidence of COVID-19 vaccine-associated tinnitus is rare, there is an overwhelming need to discern the precise pathophysiology and clinical management as a better understanding of adverse events may help in encountering vaccine hesitancy and hence fostering the COVID-19 global vaccination program.
“Despite the incidence of adverse events, the benefits of the SARS-CoV-2 vaccine in reducing hospitalization and deaths continue to outweigh the rare ramifications,” they conclude.
The research had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It’s now known that tinnitus may be an unexpected side effect of SARS-CoV-2 vaccination, and there is an urgent need to understand the precise mechanisms and best treatment for vaccine-associated tinnitus, researchers say.
As of mid-September 2021, 12,247 cases of tinnitus, or ringing in the ears, following COVID-19 vaccination had been reported to the Vaccine Adverse Event Reporting System of the U.S. Centers for Disease Control and Prevention.
“Despite several cases of tinnitus being reported following SARS-CoV-2 vaccination, the precise pathophysiology is still not clear,” write Syed Hassan Ahmed, 3rd-year MBBS student, Dow University of Health Sciences, Karachi, Pakistan, and coauthors.
The researchers review what is known and unknown about SARS-CoV-2 vaccine-associated tinnitus in an article published online Feb. 11 in Annals of Medicine and Surgery.
Molecular mimicry?
The researchers say cross-reactivity between anti-spike SARS-CoV-2 antibodies and otologic antigens is one possibility, based on the mechanisms behind other COVID-19 vaccine–induced disorders and the phenomenon of molecular mimicry.
“The heptapeptide resemblance between coronavirus spike glycoprotein and numerous human proteins further supports molecular mimicry as a potential mechanism behind such vaccine-induced disorders,” they write.
Anti-spike antibodies may react with antigens anywhere along the auditory pathway and fuel an inflammatory reaction, they point out.
“Therefore, understanding the phenomenon of cross-reactivity and molecular mimicry may be helpful in postulating potential treatment behind not only tinnitus but also the rare events of vaccination associated hearing loss and other otologic manifestations,” the authors say.
Genetic predispositions and associated conditions may also play a significant role in determining whether an individual develops vaccine-induced tinnitus.
Stress and anxiety following COVID vaccination may also play a role, inasmuch as anxiety-related adverse events following vaccination have been reported. Vaccine-related anxiety as a potential cause of tinnitus developing after vaccination needs to be explored, they write.
Jury out on best management
How best to manage COVID vaccine-associated tinnitus also remains unclear, but it starts with a well-established diagnosis, the authors say.
A well-focused and detailed history and examination are essential, with particular emphasis placed on preexisting health conditions, specifically, autoimmune diseases, such as Hashimoto thyroiditis; otologic conditions, such as sensorineural hearing loss; glaucoma; and psychological well-being. According to the review, patients often present with a history of one or more of these disorders.
“However, any such association has not yet been established and requires further investigation to be concluded as potential risk factors for vaccine-induced tinnitus,” they caution.
Routine cranial nerve examination, otoscopy, Weber test, and Rinne test, which are used for tinnitus diagnosis in general, may be helpful for confirmation of vaccine-associated tinnitus.
Owing to the significant association between tinnitus and hearing impairment, audiology should also performed, the authors say.
Although treatments for non–vaccine-induced tinnitus vary significantly, corticosteroids are the top treatment choice for SARS-CoV-2 vaccine-induced tinnitus reported in the literature.
Trials of other drug and nondrug interventions that may uniquely help with vaccine-associated tinnitus are urgently needed, the authors say.
Summing up, the reviewers say, “Although the incidence of COVID-19 vaccine-associated tinnitus is rare, there is an overwhelming need to discern the precise pathophysiology and clinical management as a better understanding of adverse events may help in encountering vaccine hesitancy and hence fostering the COVID-19 global vaccination program.
“Despite the incidence of adverse events, the benefits of the SARS-CoV-2 vaccine in reducing hospitalization and deaths continue to outweigh the rare ramifications,” they conclude.
The research had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It’s now known that tinnitus may be an unexpected side effect of SARS-CoV-2 vaccination, and there is an urgent need to understand the precise mechanisms and best treatment for vaccine-associated tinnitus, researchers say.
As of mid-September 2021, 12,247 cases of tinnitus, or ringing in the ears, following COVID-19 vaccination had been reported to the Vaccine Adverse Event Reporting System of the U.S. Centers for Disease Control and Prevention.
“Despite several cases of tinnitus being reported following SARS-CoV-2 vaccination, the precise pathophysiology is still not clear,” write Syed Hassan Ahmed, 3rd-year MBBS student, Dow University of Health Sciences, Karachi, Pakistan, and coauthors.
The researchers review what is known and unknown about SARS-CoV-2 vaccine-associated tinnitus in an article published online Feb. 11 in Annals of Medicine and Surgery.
Molecular mimicry?
The researchers say cross-reactivity between anti-spike SARS-CoV-2 antibodies and otologic antigens is one possibility, based on the mechanisms behind other COVID-19 vaccine–induced disorders and the phenomenon of molecular mimicry.
“The heptapeptide resemblance between coronavirus spike glycoprotein and numerous human proteins further supports molecular mimicry as a potential mechanism behind such vaccine-induced disorders,” they write.
Anti-spike antibodies may react with antigens anywhere along the auditory pathway and fuel an inflammatory reaction, they point out.
“Therefore, understanding the phenomenon of cross-reactivity and molecular mimicry may be helpful in postulating potential treatment behind not only tinnitus but also the rare events of vaccination associated hearing loss and other otologic manifestations,” the authors say.
Genetic predispositions and associated conditions may also play a significant role in determining whether an individual develops vaccine-induced tinnitus.
Stress and anxiety following COVID vaccination may also play a role, inasmuch as anxiety-related adverse events following vaccination have been reported. Vaccine-related anxiety as a potential cause of tinnitus developing after vaccination needs to be explored, they write.
Jury out on best management
How best to manage COVID vaccine-associated tinnitus also remains unclear, but it starts with a well-established diagnosis, the authors say.
A well-focused and detailed history and examination are essential, with particular emphasis placed on preexisting health conditions, specifically, autoimmune diseases, such as Hashimoto thyroiditis; otologic conditions, such as sensorineural hearing loss; glaucoma; and psychological well-being. According to the review, patients often present with a history of one or more of these disorders.
“However, any such association has not yet been established and requires further investigation to be concluded as potential risk factors for vaccine-induced tinnitus,” they caution.
Routine cranial nerve examination, otoscopy, Weber test, and Rinne test, which are used for tinnitus diagnosis in general, may be helpful for confirmation of vaccine-associated tinnitus.
Owing to the significant association between tinnitus and hearing impairment, audiology should also performed, the authors say.
Although treatments for non–vaccine-induced tinnitus vary significantly, corticosteroids are the top treatment choice for SARS-CoV-2 vaccine-induced tinnitus reported in the literature.
Trials of other drug and nondrug interventions that may uniquely help with vaccine-associated tinnitus are urgently needed, the authors say.
Summing up, the reviewers say, “Although the incidence of COVID-19 vaccine-associated tinnitus is rare, there is an overwhelming need to discern the precise pathophysiology and clinical management as a better understanding of adverse events may help in encountering vaccine hesitancy and hence fostering the COVID-19 global vaccination program.
“Despite the incidence of adverse events, the benefits of the SARS-CoV-2 vaccine in reducing hospitalization and deaths continue to outweigh the rare ramifications,” they conclude.
The research had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF MEDICINE AND SURGERY
Biden administration’s new test-to-treat program pits pharmacists against physicians
The Biden administration’s new test-to-treat program is simple on the surface: if you feel like you may have COVID-19, go to a pharmacy, get tested, and, if positive, get treated with an antiviral medication on the spot.
One large physicians’ group is concerned that the program leaves doctors on the margins, and may put patients at risk if there are adverse effects from the medications. Pharmacists groups, on the other hand, say the program is too restrictive, according to an article by the research group Advisory Board.
Recently, the White House announced that more than 1,000 pharmacy clinics across the United States had registered to participate in the initiative, according to CNN. Ordering of the drugs is underway in many of these clinics, a White House official told the network.
Besides retail clinics in chain pharmacies, the antivirals will also be available in community health centers, long-term-care facilities, and Veterans Health Administration clinics, according to a statement from the U.S. Department of Health and Human Services.
The two antiviral pills authorized by the U.S. Food and Drug Administration include Pfizer’s Paxlovid, for people 12 and older, and Merck’s molnupiravir, for adults. Either drug has to be taken within 5 days after symptoms appear to be effective in preventing serious illness.
The need for speed is a major reason why the government chose to work with retail clinics that are more accessible than most primary care offices. However, the American Medical Association (AMA), the National Community Pharmacists Association (NCPA), and the American Pharmacists Association (APhA) have publicly criticized the administration’s approach.
The pharmacists’ groups are concerned that the program is limited only to pharmacies with clinics on site, thus restricting the number of pharmacies qualified to participate. Fourteen pharmacy groups, including the NCPA and the APhA, have also sent a letter to the Biden administration urging it to remove barriers to pharmacies ordering the medications.
The groups also want permission as “clinically trained medication experts” to prescribe the drugs and ensure their safe use.
The AMA on March 4 took issue with the prescribing component, saying that “the pharmacy-based clinic component of the test-to-treat plan flouts patient safety and risks significant negative health outcomes.”
In the AMA’s view, prescribing Paxlovid without a patient’s physician being present poses a risk for adverse drug interactions, as neither the nurse practitioners in retail clinics nor the pharmacists who dispense the drug have full knowledge of a patient›s medical history.
The next day, the AMA released another statement, saying it was reassured by comments from administration officials “that patients who have access to a regular source of care should contact their physician shortly after testing positive for COVID-19 to assess their treatment options.”
“Traditional doctor-only approach”
Having patients call their doctors after testing positive for COVID in a pharmacy “strikes me as unnecessary in the vast majority of cases, and it will delay treatment,” Robert Wachter, MD, professor and chair of the department of medicine at the University of California San Francisco, said in an interview. “In this case, it seems like the AMA is taking a very traditional doctor-only approach. And the world has changed. It’s much more of a team sport than an individual sport, the way it was years ago.”
Dr. Wachter said he has the utmost respect for pharmacists’ ability to screen prescriptions for adverse drug interactions. “We’re required to do medication reconciliation when patients see us,” he says. “And in many hospitals, we delegate that to pharmacists. They’re at least as good at it if not better than physicians are.”
While it’s essential to know what other medications a patient is taking, he noted, pharmacies have computer records of all the prescriptions they’ve filled for patients. In addition, pharmacies have access to complete medication histories through Surescripts, the company that enables electronic prescribing transactions between prescribers and pharmacies.
Drug interactions “not trivial”
Preeti Malani, MD, the chief health officer and a professor of medicine in the division of infectious diseases at the University of Michigan in Ann Arbor, told this news organization that the potential interactions between Paxlovid and some other medications are “not trivial.”
However, she said, “The really dangerous drugs are the ones for people who have had organ transplants and the like. Those aren’t individuals who are going to shop at a pharmacy.”
Besides the antirejection drugs, Dr. Wachter said, there can be serious interactions with cholesterol-lowering medications. If a person is taking Lipitor, for instance, “Someone would have to make the decision on whether it’s ok for me to stop it for a while, or to lower the dose. But I trust the pharmacist to do that as well as anybody.”
Except for these potential drug interactions with Paxlovid, the antiviral medications are “quite safe,” he said, adding that being able to treat people who test positive for COVID-19 right away is a big advantage of the test-to-treat program, considering how difficult it is for many people to get access to a doctor. That delay could mean that the antivirals are not prescribed and taken until they are no longer effective.
Both Dr. Wachter and Dr. Malani said that the widespread distribution of pharmacies and their extended hours are other big pluses, especially for people who can’t easily leave work or travel far to visit a physician.
Dr. Malani cautioned that there are still kinks to work out in the test-to-treat program. It will be a while before the retail clinics all have the antiviral drugs, and many pharmacies don’t have clinics on site.
Still, she said people can still go to their physicians to be tested, and presumably those doctors can also write antiviral prescriptions. But it’s not clear where the antivirals will be available in the near term.
“Right now, we’re playing catch-up,” Dr. Malani said. “But pharmacies are an important piece of the puzzle.”
Looking at the big picture, she said, “We know that neither vaccination nor natural infection provides long lasting immunity, and so there will be a role for antivirals in order to make this a manageable illness. And when you’re talking about millions of cases, as we were having a few months ago, the health system can’t field all those patients. So we do need a system where I can go to a pharmacy and get a test and treatment.”
A version of this article first appeared on Medscape.com.
The Biden administration’s new test-to-treat program is simple on the surface: if you feel like you may have COVID-19, go to a pharmacy, get tested, and, if positive, get treated with an antiviral medication on the spot.
One large physicians’ group is concerned that the program leaves doctors on the margins, and may put patients at risk if there are adverse effects from the medications. Pharmacists groups, on the other hand, say the program is too restrictive, according to an article by the research group Advisory Board.
Recently, the White House announced that more than 1,000 pharmacy clinics across the United States had registered to participate in the initiative, according to CNN. Ordering of the drugs is underway in many of these clinics, a White House official told the network.
Besides retail clinics in chain pharmacies, the antivirals will also be available in community health centers, long-term-care facilities, and Veterans Health Administration clinics, according to a statement from the U.S. Department of Health and Human Services.
The two antiviral pills authorized by the U.S. Food and Drug Administration include Pfizer’s Paxlovid, for people 12 and older, and Merck’s molnupiravir, for adults. Either drug has to be taken within 5 days after symptoms appear to be effective in preventing serious illness.
The need for speed is a major reason why the government chose to work with retail clinics that are more accessible than most primary care offices. However, the American Medical Association (AMA), the National Community Pharmacists Association (NCPA), and the American Pharmacists Association (APhA) have publicly criticized the administration’s approach.
The pharmacists’ groups are concerned that the program is limited only to pharmacies with clinics on site, thus restricting the number of pharmacies qualified to participate. Fourteen pharmacy groups, including the NCPA and the APhA, have also sent a letter to the Biden administration urging it to remove barriers to pharmacies ordering the medications.
The groups also want permission as “clinically trained medication experts” to prescribe the drugs and ensure their safe use.
The AMA on March 4 took issue with the prescribing component, saying that “the pharmacy-based clinic component of the test-to-treat plan flouts patient safety and risks significant negative health outcomes.”
In the AMA’s view, prescribing Paxlovid without a patient’s physician being present poses a risk for adverse drug interactions, as neither the nurse practitioners in retail clinics nor the pharmacists who dispense the drug have full knowledge of a patient›s medical history.
The next day, the AMA released another statement, saying it was reassured by comments from administration officials “that patients who have access to a regular source of care should contact their physician shortly after testing positive for COVID-19 to assess their treatment options.”
“Traditional doctor-only approach”
Having patients call their doctors after testing positive for COVID in a pharmacy “strikes me as unnecessary in the vast majority of cases, and it will delay treatment,” Robert Wachter, MD, professor and chair of the department of medicine at the University of California San Francisco, said in an interview. “In this case, it seems like the AMA is taking a very traditional doctor-only approach. And the world has changed. It’s much more of a team sport than an individual sport, the way it was years ago.”
Dr. Wachter said he has the utmost respect for pharmacists’ ability to screen prescriptions for adverse drug interactions. “We’re required to do medication reconciliation when patients see us,” he says. “And in many hospitals, we delegate that to pharmacists. They’re at least as good at it if not better than physicians are.”
While it’s essential to know what other medications a patient is taking, he noted, pharmacies have computer records of all the prescriptions they’ve filled for patients. In addition, pharmacies have access to complete medication histories through Surescripts, the company that enables electronic prescribing transactions between prescribers and pharmacies.
Drug interactions “not trivial”
Preeti Malani, MD, the chief health officer and a professor of medicine in the division of infectious diseases at the University of Michigan in Ann Arbor, told this news organization that the potential interactions between Paxlovid and some other medications are “not trivial.”
However, she said, “The really dangerous drugs are the ones for people who have had organ transplants and the like. Those aren’t individuals who are going to shop at a pharmacy.”
Besides the antirejection drugs, Dr. Wachter said, there can be serious interactions with cholesterol-lowering medications. If a person is taking Lipitor, for instance, “Someone would have to make the decision on whether it’s ok for me to stop it for a while, or to lower the dose. But I trust the pharmacist to do that as well as anybody.”
Except for these potential drug interactions with Paxlovid, the antiviral medications are “quite safe,” he said, adding that being able to treat people who test positive for COVID-19 right away is a big advantage of the test-to-treat program, considering how difficult it is for many people to get access to a doctor. That delay could mean that the antivirals are not prescribed and taken until they are no longer effective.
Both Dr. Wachter and Dr. Malani said that the widespread distribution of pharmacies and their extended hours are other big pluses, especially for people who can’t easily leave work or travel far to visit a physician.
Dr. Malani cautioned that there are still kinks to work out in the test-to-treat program. It will be a while before the retail clinics all have the antiviral drugs, and many pharmacies don’t have clinics on site.
Still, she said people can still go to their physicians to be tested, and presumably those doctors can also write antiviral prescriptions. But it’s not clear where the antivirals will be available in the near term.
“Right now, we’re playing catch-up,” Dr. Malani said. “But pharmacies are an important piece of the puzzle.”
Looking at the big picture, she said, “We know that neither vaccination nor natural infection provides long lasting immunity, and so there will be a role for antivirals in order to make this a manageable illness. And when you’re talking about millions of cases, as we were having a few months ago, the health system can’t field all those patients. So we do need a system where I can go to a pharmacy and get a test and treatment.”
A version of this article first appeared on Medscape.com.
The Biden administration’s new test-to-treat program is simple on the surface: if you feel like you may have COVID-19, go to a pharmacy, get tested, and, if positive, get treated with an antiviral medication on the spot.
One large physicians’ group is concerned that the program leaves doctors on the margins, and may put patients at risk if there are adverse effects from the medications. Pharmacists groups, on the other hand, say the program is too restrictive, according to an article by the research group Advisory Board.
Recently, the White House announced that more than 1,000 pharmacy clinics across the United States had registered to participate in the initiative, according to CNN. Ordering of the drugs is underway in many of these clinics, a White House official told the network.
Besides retail clinics in chain pharmacies, the antivirals will also be available in community health centers, long-term-care facilities, and Veterans Health Administration clinics, according to a statement from the U.S. Department of Health and Human Services.
The two antiviral pills authorized by the U.S. Food and Drug Administration include Pfizer’s Paxlovid, for people 12 and older, and Merck’s molnupiravir, for adults. Either drug has to be taken within 5 days after symptoms appear to be effective in preventing serious illness.
The need for speed is a major reason why the government chose to work with retail clinics that are more accessible than most primary care offices. However, the American Medical Association (AMA), the National Community Pharmacists Association (NCPA), and the American Pharmacists Association (APhA) have publicly criticized the administration’s approach.
The pharmacists’ groups are concerned that the program is limited only to pharmacies with clinics on site, thus restricting the number of pharmacies qualified to participate. Fourteen pharmacy groups, including the NCPA and the APhA, have also sent a letter to the Biden administration urging it to remove barriers to pharmacies ordering the medications.
The groups also want permission as “clinically trained medication experts” to prescribe the drugs and ensure their safe use.
The AMA on March 4 took issue with the prescribing component, saying that “the pharmacy-based clinic component of the test-to-treat plan flouts patient safety and risks significant negative health outcomes.”
In the AMA’s view, prescribing Paxlovid without a patient’s physician being present poses a risk for adverse drug interactions, as neither the nurse practitioners in retail clinics nor the pharmacists who dispense the drug have full knowledge of a patient›s medical history.
The next day, the AMA released another statement, saying it was reassured by comments from administration officials “that patients who have access to a regular source of care should contact their physician shortly after testing positive for COVID-19 to assess their treatment options.”
“Traditional doctor-only approach”
Having patients call their doctors after testing positive for COVID in a pharmacy “strikes me as unnecessary in the vast majority of cases, and it will delay treatment,” Robert Wachter, MD, professor and chair of the department of medicine at the University of California San Francisco, said in an interview. “In this case, it seems like the AMA is taking a very traditional doctor-only approach. And the world has changed. It’s much more of a team sport than an individual sport, the way it was years ago.”
Dr. Wachter said he has the utmost respect for pharmacists’ ability to screen prescriptions for adverse drug interactions. “We’re required to do medication reconciliation when patients see us,” he says. “And in many hospitals, we delegate that to pharmacists. They’re at least as good at it if not better than physicians are.”
While it’s essential to know what other medications a patient is taking, he noted, pharmacies have computer records of all the prescriptions they’ve filled for patients. In addition, pharmacies have access to complete medication histories through Surescripts, the company that enables electronic prescribing transactions between prescribers and pharmacies.
Drug interactions “not trivial”
Preeti Malani, MD, the chief health officer and a professor of medicine in the division of infectious diseases at the University of Michigan in Ann Arbor, told this news organization that the potential interactions between Paxlovid and some other medications are “not trivial.”
However, she said, “The really dangerous drugs are the ones for people who have had organ transplants and the like. Those aren’t individuals who are going to shop at a pharmacy.”
Besides the antirejection drugs, Dr. Wachter said, there can be serious interactions with cholesterol-lowering medications. If a person is taking Lipitor, for instance, “Someone would have to make the decision on whether it’s ok for me to stop it for a while, or to lower the dose. But I trust the pharmacist to do that as well as anybody.”
Except for these potential drug interactions with Paxlovid, the antiviral medications are “quite safe,” he said, adding that being able to treat people who test positive for COVID-19 right away is a big advantage of the test-to-treat program, considering how difficult it is for many people to get access to a doctor. That delay could mean that the antivirals are not prescribed and taken until they are no longer effective.
Both Dr. Wachter and Dr. Malani said that the widespread distribution of pharmacies and their extended hours are other big pluses, especially for people who can’t easily leave work or travel far to visit a physician.
Dr. Malani cautioned that there are still kinks to work out in the test-to-treat program. It will be a while before the retail clinics all have the antiviral drugs, and many pharmacies don’t have clinics on site.
Still, she said people can still go to their physicians to be tested, and presumably those doctors can also write antiviral prescriptions. But it’s not clear where the antivirals will be available in the near term.
“Right now, we’re playing catch-up,” Dr. Malani said. “But pharmacies are an important piece of the puzzle.”
Looking at the big picture, she said, “We know that neither vaccination nor natural infection provides long lasting immunity, and so there will be a role for antivirals in order to make this a manageable illness. And when you’re talking about millions of cases, as we were having a few months ago, the health system can’t field all those patients. So we do need a system where I can go to a pharmacy and get a test and treatment.”
A version of this article first appeared on Medscape.com.
Pharma should stop doing business in Russia, says ethicist
Should pharmaceutical companies continue to do business in Russia, running ongoing clinical trials, starting new ones, or continuing to sell their products there?
Some argue that medicine and science must not get enmeshed in politics, staying above the fray to protect their independence and credibility. Other defenders of business-as-usual say the pharmaceutical industry deals in health and aids the vulnerable. Humanitarianism requires continued interaction with Russia.
I think both arguments fail.
We are fighting a war with Russia. It is a war of economic strangulation, social isolation, and pushing Russia as hard as we can to become a pariah state so that internal pressure on Putin will cause him to rethink his cruel, unjustified invasion or the Russian people to replace him. This pressure must be harsh and it must happen quickly. Why?
Having failed to rapidly defeat the Ukrainian army in the war’s first weeks, Russian commanders are now resorting to the horrible barbarism they used in previous wars in Chechnya and Syria: flattening cities, attacking civilians, killing children with massive and indiscriminate firepower.
To mention one recent horror among many, Russian shelling destroyed a maternity hospital in Mariupol. Ukraine’s president, Volodymyr Zelensky, in bemoaning the Russians for their continuing series of war crimes called on the world to act.
“Mariupol. Direct Strike of Russian troops at the maternity hospital,” he wrote in a Twitter post. “People, children are under the wreckage. Atrocity! How much longer will the world be an accomplice ignoring terror?”
The Russian government’s response: “It is not the first time we have seen pathetic outcries concerning the so-called atrocities,” said Minister of Foreign Affairs Sergei Lavrov, claiming the hospital was being used as a base by an “ultra-radical” Ukrainian battalion.
Health and its preservation are key parts of the aim of medicine and science. There is no way that medicine and science can ignore what war does to health, what attacks on hospitals do to the sick and those who serve them there, the psychological toll that intentional terrorism takes on civilians and their defenders, and what the destruction of infrastructure means for the long-term well-being of Ukrainians.
There can be no collusion with war criminals. There can be no denial of the inextricable link between medicine, science, and politics. Medicine and science are controlled by political forces; their use for good or evil is driven by political considerations, and each doctor, scientist, and scientific society must take a stand when politics corrodes the underlying aims of research and healing.
How far does noncooperation with Russia go? Very, very far. All research, both ongoing and new, must cease immediately. Whatever can be done to minimize harm to existing subjects in a short period of time ought to be done, but that is it.
Similarly, no sale of medicines or therapies ought to be occurring, be they life-saving or consumer products. Putin will see to it that such shipments go to the military or are sold on the black market for revenue, and there is nothing pharma companies can do to stop that.
The Russian people need to be pinched not only by the loss of cheeseburgers and boutique coffee but by products they use to maintain their well-being. War is cruel that way, but if you tolerate a government that is bombing and shelling a peaceful neighbor to oblivion, then pharma must ensure that efforts to make Putin and his kleptocratic goons feel the wrath of their fellow citizens.
Given the realities of nuclear Armageddon, the civilized world must fight obvious barbarity as best it can with sanctions, financial assaults, property seizures, and forgoing commerce, including important raw materials and health products. War, even in a fiscal form, is not without terrible costs; but achieving a rapid, just resolution against tyranny permits no exceptions for pharma or any other business if it is a war that must be fought.
Dr. Caplan is director of the division of medical ethics at New York University. He has consulted with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
Should pharmaceutical companies continue to do business in Russia, running ongoing clinical trials, starting new ones, or continuing to sell their products there?
Some argue that medicine and science must not get enmeshed in politics, staying above the fray to protect their independence and credibility. Other defenders of business-as-usual say the pharmaceutical industry deals in health and aids the vulnerable. Humanitarianism requires continued interaction with Russia.
I think both arguments fail.
We are fighting a war with Russia. It is a war of economic strangulation, social isolation, and pushing Russia as hard as we can to become a pariah state so that internal pressure on Putin will cause him to rethink his cruel, unjustified invasion or the Russian people to replace him. This pressure must be harsh and it must happen quickly. Why?
Having failed to rapidly defeat the Ukrainian army in the war’s first weeks, Russian commanders are now resorting to the horrible barbarism they used in previous wars in Chechnya and Syria: flattening cities, attacking civilians, killing children with massive and indiscriminate firepower.
To mention one recent horror among many, Russian shelling destroyed a maternity hospital in Mariupol. Ukraine’s president, Volodymyr Zelensky, in bemoaning the Russians for their continuing series of war crimes called on the world to act.
“Mariupol. Direct Strike of Russian troops at the maternity hospital,” he wrote in a Twitter post. “People, children are under the wreckage. Atrocity! How much longer will the world be an accomplice ignoring terror?”
The Russian government’s response: “It is not the first time we have seen pathetic outcries concerning the so-called atrocities,” said Minister of Foreign Affairs Sergei Lavrov, claiming the hospital was being used as a base by an “ultra-radical” Ukrainian battalion.
Health and its preservation are key parts of the aim of medicine and science. There is no way that medicine and science can ignore what war does to health, what attacks on hospitals do to the sick and those who serve them there, the psychological toll that intentional terrorism takes on civilians and their defenders, and what the destruction of infrastructure means for the long-term well-being of Ukrainians.
There can be no collusion with war criminals. There can be no denial of the inextricable link between medicine, science, and politics. Medicine and science are controlled by political forces; their use for good or evil is driven by political considerations, and each doctor, scientist, and scientific society must take a stand when politics corrodes the underlying aims of research and healing.
How far does noncooperation with Russia go? Very, very far. All research, both ongoing and new, must cease immediately. Whatever can be done to minimize harm to existing subjects in a short period of time ought to be done, but that is it.
Similarly, no sale of medicines or therapies ought to be occurring, be they life-saving or consumer products. Putin will see to it that such shipments go to the military or are sold on the black market for revenue, and there is nothing pharma companies can do to stop that.
The Russian people need to be pinched not only by the loss of cheeseburgers and boutique coffee but by products they use to maintain their well-being. War is cruel that way, but if you tolerate a government that is bombing and shelling a peaceful neighbor to oblivion, then pharma must ensure that efforts to make Putin and his kleptocratic goons feel the wrath of their fellow citizens.
Given the realities of nuclear Armageddon, the civilized world must fight obvious barbarity as best it can with sanctions, financial assaults, property seizures, and forgoing commerce, including important raw materials and health products. War, even in a fiscal form, is not without terrible costs; but achieving a rapid, just resolution against tyranny permits no exceptions for pharma or any other business if it is a war that must be fought.
Dr. Caplan is director of the division of medical ethics at New York University. He has consulted with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
Should pharmaceutical companies continue to do business in Russia, running ongoing clinical trials, starting new ones, or continuing to sell their products there?
Some argue that medicine and science must not get enmeshed in politics, staying above the fray to protect their independence and credibility. Other defenders of business-as-usual say the pharmaceutical industry deals in health and aids the vulnerable. Humanitarianism requires continued interaction with Russia.
I think both arguments fail.
We are fighting a war with Russia. It is a war of economic strangulation, social isolation, and pushing Russia as hard as we can to become a pariah state so that internal pressure on Putin will cause him to rethink his cruel, unjustified invasion or the Russian people to replace him. This pressure must be harsh and it must happen quickly. Why?
Having failed to rapidly defeat the Ukrainian army in the war’s first weeks, Russian commanders are now resorting to the horrible barbarism they used in previous wars in Chechnya and Syria: flattening cities, attacking civilians, killing children with massive and indiscriminate firepower.
To mention one recent horror among many, Russian shelling destroyed a maternity hospital in Mariupol. Ukraine’s president, Volodymyr Zelensky, in bemoaning the Russians for their continuing series of war crimes called on the world to act.
“Mariupol. Direct Strike of Russian troops at the maternity hospital,” he wrote in a Twitter post. “People, children are under the wreckage. Atrocity! How much longer will the world be an accomplice ignoring terror?”
The Russian government’s response: “It is not the first time we have seen pathetic outcries concerning the so-called atrocities,” said Minister of Foreign Affairs Sergei Lavrov, claiming the hospital was being used as a base by an “ultra-radical” Ukrainian battalion.
Health and its preservation are key parts of the aim of medicine and science. There is no way that medicine and science can ignore what war does to health, what attacks on hospitals do to the sick and those who serve them there, the psychological toll that intentional terrorism takes on civilians and their defenders, and what the destruction of infrastructure means for the long-term well-being of Ukrainians.
There can be no collusion with war criminals. There can be no denial of the inextricable link between medicine, science, and politics. Medicine and science are controlled by political forces; their use for good or evil is driven by political considerations, and each doctor, scientist, and scientific society must take a stand when politics corrodes the underlying aims of research and healing.
How far does noncooperation with Russia go? Very, very far. All research, both ongoing and new, must cease immediately. Whatever can be done to minimize harm to existing subjects in a short period of time ought to be done, but that is it.
Similarly, no sale of medicines or therapies ought to be occurring, be they life-saving or consumer products. Putin will see to it that such shipments go to the military or are sold on the black market for revenue, and there is nothing pharma companies can do to stop that.
The Russian people need to be pinched not only by the loss of cheeseburgers and boutique coffee but by products they use to maintain their well-being. War is cruel that way, but if you tolerate a government that is bombing and shelling a peaceful neighbor to oblivion, then pharma must ensure that efforts to make Putin and his kleptocratic goons feel the wrath of their fellow citizens.
Given the realities of nuclear Armageddon, the civilized world must fight obvious barbarity as best it can with sanctions, financial assaults, property seizures, and forgoing commerce, including important raw materials and health products. War, even in a fiscal form, is not without terrible costs; but achieving a rapid, just resolution against tyranny permits no exceptions for pharma or any other business if it is a war that must be fought.
Dr. Caplan is director of the division of medical ethics at New York University. He has consulted with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.

Which companies aren’t exiting Russia? Big pharma
Even as the war in Ukraine has prompted an exodus of international companies — from fast-food chains and oil producers to luxury retailers — from Russia,
Airlines, automakers, banks, and technology giants — at least 320 companies by one count — are among the businesses curtailing operations or making high-profile exits from Russia as its invasion of Ukraine intensifies. McDonald’s, Starbucks, and Coca-Cola announced a pause in sales recently.
But drugmakers, medical device manufacturers, and health care companies, which are exempted from U.S. and European sanctions, said Russians need access to medicines and medical equipment and contend that international humanitarian law requires they keep supply chains open.
“As a health care company, we have an important purpose, which is why at this time we continue to serve people in all countries in which we operate who depend on us for essential products, some life-sustaining,” said Scott Stoffel, divisional vice president for Illinois-based Abbott Laboratories, which manufactures and sells medicines in Russia for oncology, women’s health, pancreatic insufficiency, and liver health.
Johnson & Johnson — which has corporate offices in Moscow, Novosibirsk, St. Petersburg, and Yekaterinburg — said in a statement, “We remain committed to providing essential health products to those in need in Ukraine, Russia, and the region, in compliance with current sanctions and while adapting to the rapidly changing situation on the ground.”
The reluctance of drugmakers to pause operations in Russia is being met with a growing chorus of criticism.
Pharmaceutical companies that say they must continue to manufacture drugs in Russia for humanitarian reasons are “being misguided at best, cynical in the medium case, and outright deplorably misleading and deceptive,” said Jeffrey Sonnenfeld, DBA, a professor at the Yale School of Management who is tracking which companies have curtailed operations in Russia. He noted that banks and technology companies also provide essential services.
“Russians are put in a tragic position of unearned suffering. If we continue to make life palatable for them, then we are continuing to support the regime,” Dr. Sonnenfeld said. “These drug companies will be seen as complicit with the most vicious operation on the planet. Instead of protecting life, they are going to be seen as destroying life. The goal here is to show that Putin is not in control of all sectors of the economy.”
U.S. pharmaceutical and medical companies have operated in Russia for decades, and many ramped up operations after Russia invaded and annexed Crimea in 2014, navigating the fraught relationship between the United States and Russia amid sanctions. In 2010, Vladimir Putin, then Russian prime minister, announced an ambitious national plan for the Russian pharmaceutical industry that would be a pillar in his efforts to reestablish his country as an influential superpower and wean the country off Western pharmaceutical imports. Under the plan, called “Pharma-2020” and “Pharma-2030,” the government required Western pharmaceutical companies eager to sell to Russia’s growing middle class to locate production inside the country.
Pfizer, Johnson & Johnson, Novartis, and Abbott are among the drugmakers that manufacture pharmaceutical drugs at facilities in St. Petersburg and elsewhere in the country and typically sell those drugs as branded generics or under Russian brands.
Pfizer’s CEO, Albert Bourla, said on CBS that the giant drugmaker is not going to make further investments in Russia, but that it will not cut ties with Russia, as multinational companies in other industries are doing.
Pharmaceutical manufacturing plants in Kaluga, a major manufacturing center for Volkswagen and Volvo southwest of Moscow, have been funded through a partnership between Rusnano, a state-owned venture that promotes the development of high-tech enterprises, and U.S. venture capital firms.
Russia also has sought to position itself as an attractive research market, offering an inexpensive and lax regulatory environment for clinical drug trials. Last year, Pfizer conducted in Russia clinical trials of Paxlovid, its experimental antiviral pill to treat covid-19. Before the invasion began in late February, 3,072 trials were underway in Russia and 503 were underway in Ukraine, according to BioWorld, a reporting hub focused on drug development that features data from Cortellis.
AstraZeneca is the top sponsor of clinical trials in Russia, with 49 trials, followed by a subsidiary of Merck, with 48 trials.
So far, drugmakers’ response to the Ukraine invasion has largely centered on public pledges to donate essential medicines and vaccines to Ukrainian patients and refugees. They’ve also made general comments about the need to keep open the supply of medicines flowing within Russia.
Abbott has pledged $2 million to support humanitarian efforts in Ukraine, and Pfizer, based in New York, said it has supplied $1 million in humanitarian grants. Swiss drug maker Novartis said it was expanding humanitarian efforts in Ukraine and working to “ensure the continued supply of our medicines in Ukraine.”
But no major pharmaceutical or medical device maker has announced plans to shutter manufacturing plants or halt sales inside Russia.
In an open letter, hundreds of leaders of mainly smaller biotechnology companies have called on industry members to cease business activities in Russia, including “investment in Russian companies and new investment within the borders of Russia,” and to halt trade and collaboration with Russian companies, except for supplying food and medicines. How many of the signatories have business operations in Russia was unclear.
Ulrich Neumann, director for market access at Janssen, a Johnson & Johnson company, was among those who signed the letter, but whether he was speaking for the company was unclear. In its own statement posted on social media, the company said it’s “committed to providing access to our essential medical products in the countries where we operate, in compliance with current international sanctions.”
GlaxoSmithKline, headquartered in the United Kingdom, said in a statement that it’s stopping all advertising in Russia and will not enter into contracts that “directly support the Russian administration or military.” But the company said that as a “supplier of needed medicines, vaccines and everyday health products, we have a responsibility to do all we can to make them available. For this reason, we will continue to supply our products to the people of Russia, while we can.”
Nell Minow, vice chair of ValueEdge Advisors, an investment consulting firm, noted that drug companies have been treated differently than other industries during previous global conflicts. For example, some corporate ethicists advised against pharmaceutical companies’ total divestment from South Africa’s apartheid regime to ensure essential medicines flowed to the country.
“There is a difference between a hamburger and a pill,” Mr. Minow said. Companies should strongly condemn Russia’s actions, she said, but unless the United States enters directly into a war with Russia, companies that make essential medicines and health care products should continue to operate. Before U.S. involvement in World War II, she added, there were “some American companies that did business with Germany until the last minute.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. KHN senior correspondent Arthur Allen contributed to this article.
Even as the war in Ukraine has prompted an exodus of international companies — from fast-food chains and oil producers to luxury retailers — from Russia,
Airlines, automakers, banks, and technology giants — at least 320 companies by one count — are among the businesses curtailing operations or making high-profile exits from Russia as its invasion of Ukraine intensifies. McDonald’s, Starbucks, and Coca-Cola announced a pause in sales recently.
But drugmakers, medical device manufacturers, and health care companies, which are exempted from U.S. and European sanctions, said Russians need access to medicines and medical equipment and contend that international humanitarian law requires they keep supply chains open.
“As a health care company, we have an important purpose, which is why at this time we continue to serve people in all countries in which we operate who depend on us for essential products, some life-sustaining,” said Scott Stoffel, divisional vice president for Illinois-based Abbott Laboratories, which manufactures and sells medicines in Russia for oncology, women’s health, pancreatic insufficiency, and liver health.
Johnson & Johnson — which has corporate offices in Moscow, Novosibirsk, St. Petersburg, and Yekaterinburg — said in a statement, “We remain committed to providing essential health products to those in need in Ukraine, Russia, and the region, in compliance with current sanctions and while adapting to the rapidly changing situation on the ground.”
The reluctance of drugmakers to pause operations in Russia is being met with a growing chorus of criticism.
Pharmaceutical companies that say they must continue to manufacture drugs in Russia for humanitarian reasons are “being misguided at best, cynical in the medium case, and outright deplorably misleading and deceptive,” said Jeffrey Sonnenfeld, DBA, a professor at the Yale School of Management who is tracking which companies have curtailed operations in Russia. He noted that banks and technology companies also provide essential services.
“Russians are put in a tragic position of unearned suffering. If we continue to make life palatable for them, then we are continuing to support the regime,” Dr. Sonnenfeld said. “These drug companies will be seen as complicit with the most vicious operation on the planet. Instead of protecting life, they are going to be seen as destroying life. The goal here is to show that Putin is not in control of all sectors of the economy.”
U.S. pharmaceutical and medical companies have operated in Russia for decades, and many ramped up operations after Russia invaded and annexed Crimea in 2014, navigating the fraught relationship between the United States and Russia amid sanctions. In 2010, Vladimir Putin, then Russian prime minister, announced an ambitious national plan for the Russian pharmaceutical industry that would be a pillar in his efforts to reestablish his country as an influential superpower and wean the country off Western pharmaceutical imports. Under the plan, called “Pharma-2020” and “Pharma-2030,” the government required Western pharmaceutical companies eager to sell to Russia’s growing middle class to locate production inside the country.
Pfizer, Johnson & Johnson, Novartis, and Abbott are among the drugmakers that manufacture pharmaceutical drugs at facilities in St. Petersburg and elsewhere in the country and typically sell those drugs as branded generics or under Russian brands.
Pfizer’s CEO, Albert Bourla, said on CBS that the giant drugmaker is not going to make further investments in Russia, but that it will not cut ties with Russia, as multinational companies in other industries are doing.
Pharmaceutical manufacturing plants in Kaluga, a major manufacturing center for Volkswagen and Volvo southwest of Moscow, have been funded through a partnership between Rusnano, a state-owned venture that promotes the development of high-tech enterprises, and U.S. venture capital firms.
Russia also has sought to position itself as an attractive research market, offering an inexpensive and lax regulatory environment for clinical drug trials. Last year, Pfizer conducted in Russia clinical trials of Paxlovid, its experimental antiviral pill to treat covid-19. Before the invasion began in late February, 3,072 trials were underway in Russia and 503 were underway in Ukraine, according to BioWorld, a reporting hub focused on drug development that features data from Cortellis.
AstraZeneca is the top sponsor of clinical trials in Russia, with 49 trials, followed by a subsidiary of Merck, with 48 trials.
So far, drugmakers’ response to the Ukraine invasion has largely centered on public pledges to donate essential medicines and vaccines to Ukrainian patients and refugees. They’ve also made general comments about the need to keep open the supply of medicines flowing within Russia.
Abbott has pledged $2 million to support humanitarian efforts in Ukraine, and Pfizer, based in New York, said it has supplied $1 million in humanitarian grants. Swiss drug maker Novartis said it was expanding humanitarian efforts in Ukraine and working to “ensure the continued supply of our medicines in Ukraine.”
But no major pharmaceutical or medical device maker has announced plans to shutter manufacturing plants or halt sales inside Russia.
In an open letter, hundreds of leaders of mainly smaller biotechnology companies have called on industry members to cease business activities in Russia, including “investment in Russian companies and new investment within the borders of Russia,” and to halt trade and collaboration with Russian companies, except for supplying food and medicines. How many of the signatories have business operations in Russia was unclear.
Ulrich Neumann, director for market access at Janssen, a Johnson & Johnson company, was among those who signed the letter, but whether he was speaking for the company was unclear. In its own statement posted on social media, the company said it’s “committed to providing access to our essential medical products in the countries where we operate, in compliance with current international sanctions.”
GlaxoSmithKline, headquartered in the United Kingdom, said in a statement that it’s stopping all advertising in Russia and will not enter into contracts that “directly support the Russian administration or military.” But the company said that as a “supplier of needed medicines, vaccines and everyday health products, we have a responsibility to do all we can to make them available. For this reason, we will continue to supply our products to the people of Russia, while we can.”
Nell Minow, vice chair of ValueEdge Advisors, an investment consulting firm, noted that drug companies have been treated differently than other industries during previous global conflicts. For example, some corporate ethicists advised against pharmaceutical companies’ total divestment from South Africa’s apartheid regime to ensure essential medicines flowed to the country.
“There is a difference between a hamburger and a pill,” Mr. Minow said. Companies should strongly condemn Russia’s actions, she said, but unless the United States enters directly into a war with Russia, companies that make essential medicines and health care products should continue to operate. Before U.S. involvement in World War II, she added, there were “some American companies that did business with Germany until the last minute.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. KHN senior correspondent Arthur Allen contributed to this article.
Even as the war in Ukraine has prompted an exodus of international companies — from fast-food chains and oil producers to luxury retailers — from Russia,
Airlines, automakers, banks, and technology giants — at least 320 companies by one count — are among the businesses curtailing operations or making high-profile exits from Russia as its invasion of Ukraine intensifies. McDonald’s, Starbucks, and Coca-Cola announced a pause in sales recently.
But drugmakers, medical device manufacturers, and health care companies, which are exempted from U.S. and European sanctions, said Russians need access to medicines and medical equipment and contend that international humanitarian law requires they keep supply chains open.
“As a health care company, we have an important purpose, which is why at this time we continue to serve people in all countries in which we operate who depend on us for essential products, some life-sustaining,” said Scott Stoffel, divisional vice president for Illinois-based Abbott Laboratories, which manufactures and sells medicines in Russia for oncology, women’s health, pancreatic insufficiency, and liver health.
Johnson & Johnson — which has corporate offices in Moscow, Novosibirsk, St. Petersburg, and Yekaterinburg — said in a statement, “We remain committed to providing essential health products to those in need in Ukraine, Russia, and the region, in compliance with current sanctions and while adapting to the rapidly changing situation on the ground.”
The reluctance of drugmakers to pause operations in Russia is being met with a growing chorus of criticism.
Pharmaceutical companies that say they must continue to manufacture drugs in Russia for humanitarian reasons are “being misguided at best, cynical in the medium case, and outright deplorably misleading and deceptive,” said Jeffrey Sonnenfeld, DBA, a professor at the Yale School of Management who is tracking which companies have curtailed operations in Russia. He noted that banks and technology companies also provide essential services.
“Russians are put in a tragic position of unearned suffering. If we continue to make life palatable for them, then we are continuing to support the regime,” Dr. Sonnenfeld said. “These drug companies will be seen as complicit with the most vicious operation on the planet. Instead of protecting life, they are going to be seen as destroying life. The goal here is to show that Putin is not in control of all sectors of the economy.”
U.S. pharmaceutical and medical companies have operated in Russia for decades, and many ramped up operations after Russia invaded and annexed Crimea in 2014, navigating the fraught relationship between the United States and Russia amid sanctions. In 2010, Vladimir Putin, then Russian prime minister, announced an ambitious national plan for the Russian pharmaceutical industry that would be a pillar in his efforts to reestablish his country as an influential superpower and wean the country off Western pharmaceutical imports. Under the plan, called “Pharma-2020” and “Pharma-2030,” the government required Western pharmaceutical companies eager to sell to Russia’s growing middle class to locate production inside the country.
Pfizer, Johnson & Johnson, Novartis, and Abbott are among the drugmakers that manufacture pharmaceutical drugs at facilities in St. Petersburg and elsewhere in the country and typically sell those drugs as branded generics or under Russian brands.
Pfizer’s CEO, Albert Bourla, said on CBS that the giant drugmaker is not going to make further investments in Russia, but that it will not cut ties with Russia, as multinational companies in other industries are doing.
Pharmaceutical manufacturing plants in Kaluga, a major manufacturing center for Volkswagen and Volvo southwest of Moscow, have been funded through a partnership between Rusnano, a state-owned venture that promotes the development of high-tech enterprises, and U.S. venture capital firms.
Russia also has sought to position itself as an attractive research market, offering an inexpensive and lax regulatory environment for clinical drug trials. Last year, Pfizer conducted in Russia clinical trials of Paxlovid, its experimental antiviral pill to treat covid-19. Before the invasion began in late February, 3,072 trials were underway in Russia and 503 were underway in Ukraine, according to BioWorld, a reporting hub focused on drug development that features data from Cortellis.
AstraZeneca is the top sponsor of clinical trials in Russia, with 49 trials, followed by a subsidiary of Merck, with 48 trials.
So far, drugmakers’ response to the Ukraine invasion has largely centered on public pledges to donate essential medicines and vaccines to Ukrainian patients and refugees. They’ve also made general comments about the need to keep open the supply of medicines flowing within Russia.
Abbott has pledged $2 million to support humanitarian efforts in Ukraine, and Pfizer, based in New York, said it has supplied $1 million in humanitarian grants. Swiss drug maker Novartis said it was expanding humanitarian efforts in Ukraine and working to “ensure the continued supply of our medicines in Ukraine.”
But no major pharmaceutical or medical device maker has announced plans to shutter manufacturing plants or halt sales inside Russia.
In an open letter, hundreds of leaders of mainly smaller biotechnology companies have called on industry members to cease business activities in Russia, including “investment in Russian companies and new investment within the borders of Russia,” and to halt trade and collaboration with Russian companies, except for supplying food and medicines. How many of the signatories have business operations in Russia was unclear.
Ulrich Neumann, director for market access at Janssen, a Johnson & Johnson company, was among those who signed the letter, but whether he was speaking for the company was unclear. In its own statement posted on social media, the company said it’s “committed to providing access to our essential medical products in the countries where we operate, in compliance with current international sanctions.”
GlaxoSmithKline, headquartered in the United Kingdom, said in a statement that it’s stopping all advertising in Russia and will not enter into contracts that “directly support the Russian administration or military.” But the company said that as a “supplier of needed medicines, vaccines and everyday health products, we have a responsibility to do all we can to make them available. For this reason, we will continue to supply our products to the people of Russia, while we can.”
Nell Minow, vice chair of ValueEdge Advisors, an investment consulting firm, noted that drug companies have been treated differently than other industries during previous global conflicts. For example, some corporate ethicists advised against pharmaceutical companies’ total divestment from South Africa’s apartheid regime to ensure essential medicines flowed to the country.
“There is a difference between a hamburger and a pill,” Mr. Minow said. Companies should strongly condemn Russia’s actions, she said, but unless the United States enters directly into a war with Russia, companies that make essential medicines and health care products should continue to operate. Before U.S. involvement in World War II, she added, there were “some American companies that did business with Germany until the last minute.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. KHN senior correspondent Arthur Allen contributed to this article.
MSM have higher CD4 counts at HIV diagnosis than heterosexuals
according to an analysis of more than 300,000 people living with HIV globally.
“It was quite a startling finding for us, because it’s now telling everybody, ‘Look, if you have MSM [men who have sex with men] coming into your clinic, expect CD4 counts at diagnosis to be higher than if the person got the infection as a heterosexual,’” Narendra Dixit, PhD, senior fellow at the Indian Institute of Science’s Centre for Biosystems Science and Engineering, Bangalore, India, said in an interview.
And that means, he said, that the pattern may appear in local clinics.
“If they find that there are differences in the CD4 counts between heterosexuals and MSMs, they should not be surprised anymore,” he said.
Dr. Dixit proposed that the reason for this may be that the viruses transmitted among heterosexuals are more virulent, but the study didn’t provide evidence of that.
Immune health at HIV diagnosis
In this study, which was published online March 10 in PLOS Pathogens, Dr. Dixit and colleague Anathu James, PhD, a data scientist and an epidemiologist at the Indian Institute of Science, culled data from 337,119 people captured in studies in the United Kingdom, the United States, Europe, Australia, and China. For all participants, CD4 counts were drawn at the time of diagnosis and before starting HIV treatment. Dr. Dixit and Dr. James then divided the studies by HIV transmission group – gay and bisexual men versus heterosexuals – and then averaged CD4 counts in each study.
Then they created a mathematical model to estimate how quickly each group might progress to an AIDS-defining illness, given those initial CD4 counts.
What they found was that the mean CD4 count was consistently higher in the gay and bisexual males than in the heterosexuals, no matter where they lived. For instance, mean CD4 counts at diagnosis were a mean of 437 cells/mm3 among gay and bisexual men in one European cohort, compared to a mean of 307 among heterosexuals. In the U.S. data, the mean CD4 count for gay and bisexual men was 390, compared to 314 among heterosexuals. In China, the same held true: Gay men had a mean CD4 count of 368 cells/mm3; heterosexuals had a mean CD4 count of 270.
This remained true when they only looked at people between the ages of 13 and 29 years in the United States or whether they were younger than 40 in Europe and Australia. In Europe and Australia, though, heterosexual women younger than 40 had higher CD4 counts than either straight or gay men. But this difference did not reach statistical significance, and gay men had higher CD4 counts overall when the investigators didn’t segregate the data by age group.
“We were stunned,” Dr. Dixit told this news organization. “People never thought there could be a difference in the CD4 counts just because the mode of transmission is different – or, in this case, because the risk groups are different.”
There was no difference, though, in viral load at diagnosis.
In their mathematical model on progression to AIDS, the investigators estimated that these lower CD4 counts at diagnosis would lead to a progression to AIDS that was 19% higher for straight people than for gay and bisexual men. What this implies for practice is less clear. Right now, Dr. Dixit hopes the data will be used to conduct molecular analysis of HIV strains in heterosexuals and gay and bisexual men to see if the HIV circulating in straight communities is different – and perhaps more virulent – than the HIV circulating among gay and bisexual men. Previous research has suggested that CD4 counts can be used as a proxy for virulence.
Dr. Dixit’s mathematical model follows recent news of a highly virulent strain of HIV that’s been present in the Netherlands for decades. “More virulent” in that case meant that it was more highly transmissible and led to higher viral loads and a quicker decline of the immune CD4 cells. So when news of Dr. Dixit’s study went out, it was accompanied by a press release stating as fact that “HIV-1 infections are more virulent when transmitted through penile-vaginal intercourse.” The study’s title states that HIV is “more virulent” in heterosexuals.
But this study doesn’t actually show that, said virology researcher Timothy Henrich, MD, associate professor of medicine at the University of California, San Francisco, in an interview. In the Netherlands study, investigators took the additional step of analyzing HIV genomes. But this was not done in the recent PLOS Pathogens study.
“This was essentially a large meta-analysis of multiple large cohorts across many different countries,” said Dr. Henrich, who was not involved in the study. “There was no in-depth sequence analysis to say, ‘Oh yeah, this is because of a difference in the viruses that are being transmitted.’ If I were reviewing this paper, I probably would have said, ‘This is an interesting observation, but please don’t go overboard in your conclusions.’”
The study made Dr. Henrich want to know more. For instance, what method did each study use to determine CD4 counts? Did they control for the length of time since acquisition? Dr. Henrich said that if they didn’t differentiate between acute infection and chronic infection, he wasn’t sure what conclusions could be drawn from the data. Dr. Dixit told this news organization that they used the plateau level – the point after acute infection when CD4 counts settle into a consistent level. But it’s unclear how far from HIV acquisition each of the people in these studies was.
What Dr. Henrich does know, he said, is that big data are going to continue to change how we think about and investigate HIV transmission and virulence and what it could mean for clinical practice. The National Institutes of Health, for instance, will soon require all researchers receiving their funding to make their raw data publicly available soon after publication.
“We’re going to see a lot more of these large studies going forward,” he said. And if molecular analyses bear out Dr. Dixit’s conclusion – which he called “a big if” – “maybe we could use this study as a way” to do this work in the future.
The study was funded by DBT Network and the Wellcome Trust India Alliance Senior Fellowship. Dr. Dixit has disclosed no relevant financial relationships. Dr. Henrich is conducting studies funded in whole or in part by Merck and Gilead Sciences.
A version of this article first appeared on Medscape.com.
according to an analysis of more than 300,000 people living with HIV globally.
“It was quite a startling finding for us, because it’s now telling everybody, ‘Look, if you have MSM [men who have sex with men] coming into your clinic, expect CD4 counts at diagnosis to be higher than if the person got the infection as a heterosexual,’” Narendra Dixit, PhD, senior fellow at the Indian Institute of Science’s Centre for Biosystems Science and Engineering, Bangalore, India, said in an interview.
And that means, he said, that the pattern may appear in local clinics.
“If they find that there are differences in the CD4 counts between heterosexuals and MSMs, they should not be surprised anymore,” he said.
Dr. Dixit proposed that the reason for this may be that the viruses transmitted among heterosexuals are more virulent, but the study didn’t provide evidence of that.
Immune health at HIV diagnosis
In this study, which was published online March 10 in PLOS Pathogens, Dr. Dixit and colleague Anathu James, PhD, a data scientist and an epidemiologist at the Indian Institute of Science, culled data from 337,119 people captured in studies in the United Kingdom, the United States, Europe, Australia, and China. For all participants, CD4 counts were drawn at the time of diagnosis and before starting HIV treatment. Dr. Dixit and Dr. James then divided the studies by HIV transmission group – gay and bisexual men versus heterosexuals – and then averaged CD4 counts in each study.
Then they created a mathematical model to estimate how quickly each group might progress to an AIDS-defining illness, given those initial CD4 counts.
What they found was that the mean CD4 count was consistently higher in the gay and bisexual males than in the heterosexuals, no matter where they lived. For instance, mean CD4 counts at diagnosis were a mean of 437 cells/mm3 among gay and bisexual men in one European cohort, compared to a mean of 307 among heterosexuals. In the U.S. data, the mean CD4 count for gay and bisexual men was 390, compared to 314 among heterosexuals. In China, the same held true: Gay men had a mean CD4 count of 368 cells/mm3; heterosexuals had a mean CD4 count of 270.
This remained true when they only looked at people between the ages of 13 and 29 years in the United States or whether they were younger than 40 in Europe and Australia. In Europe and Australia, though, heterosexual women younger than 40 had higher CD4 counts than either straight or gay men. But this difference did not reach statistical significance, and gay men had higher CD4 counts overall when the investigators didn’t segregate the data by age group.
“We were stunned,” Dr. Dixit told this news organization. “People never thought there could be a difference in the CD4 counts just because the mode of transmission is different – or, in this case, because the risk groups are different.”
There was no difference, though, in viral load at diagnosis.
In their mathematical model on progression to AIDS, the investigators estimated that these lower CD4 counts at diagnosis would lead to a progression to AIDS that was 19% higher for straight people than for gay and bisexual men. What this implies for practice is less clear. Right now, Dr. Dixit hopes the data will be used to conduct molecular analysis of HIV strains in heterosexuals and gay and bisexual men to see if the HIV circulating in straight communities is different – and perhaps more virulent – than the HIV circulating among gay and bisexual men. Previous research has suggested that CD4 counts can be used as a proxy for virulence.
Dr. Dixit’s mathematical model follows recent news of a highly virulent strain of HIV that’s been present in the Netherlands for decades. “More virulent” in that case meant that it was more highly transmissible and led to higher viral loads and a quicker decline of the immune CD4 cells. So when news of Dr. Dixit’s study went out, it was accompanied by a press release stating as fact that “HIV-1 infections are more virulent when transmitted through penile-vaginal intercourse.” The study’s title states that HIV is “more virulent” in heterosexuals.
But this study doesn’t actually show that, said virology researcher Timothy Henrich, MD, associate professor of medicine at the University of California, San Francisco, in an interview. In the Netherlands study, investigators took the additional step of analyzing HIV genomes. But this was not done in the recent PLOS Pathogens study.
“This was essentially a large meta-analysis of multiple large cohorts across many different countries,” said Dr. Henrich, who was not involved in the study. “There was no in-depth sequence analysis to say, ‘Oh yeah, this is because of a difference in the viruses that are being transmitted.’ If I were reviewing this paper, I probably would have said, ‘This is an interesting observation, but please don’t go overboard in your conclusions.’”
The study made Dr. Henrich want to know more. For instance, what method did each study use to determine CD4 counts? Did they control for the length of time since acquisition? Dr. Henrich said that if they didn’t differentiate between acute infection and chronic infection, he wasn’t sure what conclusions could be drawn from the data. Dr. Dixit told this news organization that they used the plateau level – the point after acute infection when CD4 counts settle into a consistent level. But it’s unclear how far from HIV acquisition each of the people in these studies was.
What Dr. Henrich does know, he said, is that big data are going to continue to change how we think about and investigate HIV transmission and virulence and what it could mean for clinical practice. The National Institutes of Health, for instance, will soon require all researchers receiving their funding to make their raw data publicly available soon after publication.
“We’re going to see a lot more of these large studies going forward,” he said. And if molecular analyses bear out Dr. Dixit’s conclusion – which he called “a big if” – “maybe we could use this study as a way” to do this work in the future.
The study was funded by DBT Network and the Wellcome Trust India Alliance Senior Fellowship. Dr. Dixit has disclosed no relevant financial relationships. Dr. Henrich is conducting studies funded in whole or in part by Merck and Gilead Sciences.
A version of this article first appeared on Medscape.com.
according to an analysis of more than 300,000 people living with HIV globally.
“It was quite a startling finding for us, because it’s now telling everybody, ‘Look, if you have MSM [men who have sex with men] coming into your clinic, expect CD4 counts at diagnosis to be higher than if the person got the infection as a heterosexual,’” Narendra Dixit, PhD, senior fellow at the Indian Institute of Science’s Centre for Biosystems Science and Engineering, Bangalore, India, said in an interview.
And that means, he said, that the pattern may appear in local clinics.
“If they find that there are differences in the CD4 counts between heterosexuals and MSMs, they should not be surprised anymore,” he said.
Dr. Dixit proposed that the reason for this may be that the viruses transmitted among heterosexuals are more virulent, but the study didn’t provide evidence of that.
Immune health at HIV diagnosis
In this study, which was published online March 10 in PLOS Pathogens, Dr. Dixit and colleague Anathu James, PhD, a data scientist and an epidemiologist at the Indian Institute of Science, culled data from 337,119 people captured in studies in the United Kingdom, the United States, Europe, Australia, and China. For all participants, CD4 counts were drawn at the time of diagnosis and before starting HIV treatment. Dr. Dixit and Dr. James then divided the studies by HIV transmission group – gay and bisexual men versus heterosexuals – and then averaged CD4 counts in each study.
Then they created a mathematical model to estimate how quickly each group might progress to an AIDS-defining illness, given those initial CD4 counts.
What they found was that the mean CD4 count was consistently higher in the gay and bisexual males than in the heterosexuals, no matter where they lived. For instance, mean CD4 counts at diagnosis were a mean of 437 cells/mm3 among gay and bisexual men in one European cohort, compared to a mean of 307 among heterosexuals. In the U.S. data, the mean CD4 count for gay and bisexual men was 390, compared to 314 among heterosexuals. In China, the same held true: Gay men had a mean CD4 count of 368 cells/mm3; heterosexuals had a mean CD4 count of 270.
This remained true when they only looked at people between the ages of 13 and 29 years in the United States or whether they were younger than 40 in Europe and Australia. In Europe and Australia, though, heterosexual women younger than 40 had higher CD4 counts than either straight or gay men. But this difference did not reach statistical significance, and gay men had higher CD4 counts overall when the investigators didn’t segregate the data by age group.
“We were stunned,” Dr. Dixit told this news organization. “People never thought there could be a difference in the CD4 counts just because the mode of transmission is different – or, in this case, because the risk groups are different.”
There was no difference, though, in viral load at diagnosis.
In their mathematical model on progression to AIDS, the investigators estimated that these lower CD4 counts at diagnosis would lead to a progression to AIDS that was 19% higher for straight people than for gay and bisexual men. What this implies for practice is less clear. Right now, Dr. Dixit hopes the data will be used to conduct molecular analysis of HIV strains in heterosexuals and gay and bisexual men to see if the HIV circulating in straight communities is different – and perhaps more virulent – than the HIV circulating among gay and bisexual men. Previous research has suggested that CD4 counts can be used as a proxy for virulence.
Dr. Dixit’s mathematical model follows recent news of a highly virulent strain of HIV that’s been present in the Netherlands for decades. “More virulent” in that case meant that it was more highly transmissible and led to higher viral loads and a quicker decline of the immune CD4 cells. So when news of Dr. Dixit’s study went out, it was accompanied by a press release stating as fact that “HIV-1 infections are more virulent when transmitted through penile-vaginal intercourse.” The study’s title states that HIV is “more virulent” in heterosexuals.
But this study doesn’t actually show that, said virology researcher Timothy Henrich, MD, associate professor of medicine at the University of California, San Francisco, in an interview. In the Netherlands study, investigators took the additional step of analyzing HIV genomes. But this was not done in the recent PLOS Pathogens study.
“This was essentially a large meta-analysis of multiple large cohorts across many different countries,” said Dr. Henrich, who was not involved in the study. “There was no in-depth sequence analysis to say, ‘Oh yeah, this is because of a difference in the viruses that are being transmitted.’ If I were reviewing this paper, I probably would have said, ‘This is an interesting observation, but please don’t go overboard in your conclusions.’”
The study made Dr. Henrich want to know more. For instance, what method did each study use to determine CD4 counts? Did they control for the length of time since acquisition? Dr. Henrich said that if they didn’t differentiate between acute infection and chronic infection, he wasn’t sure what conclusions could be drawn from the data. Dr. Dixit told this news organization that they used the plateau level – the point after acute infection when CD4 counts settle into a consistent level. But it’s unclear how far from HIV acquisition each of the people in these studies was.
What Dr. Henrich does know, he said, is that big data are going to continue to change how we think about and investigate HIV transmission and virulence and what it could mean for clinical practice. The National Institutes of Health, for instance, will soon require all researchers receiving their funding to make their raw data publicly available soon after publication.
“We’re going to see a lot more of these large studies going forward,” he said. And if molecular analyses bear out Dr. Dixit’s conclusion – which he called “a big if” – “maybe we could use this study as a way” to do this work in the future.
The study was funded by DBT Network and the Wellcome Trust India Alliance Senior Fellowship. Dr. Dixit has disclosed no relevant financial relationships. Dr. Henrich is conducting studies funded in whole or in part by Merck and Gilead Sciences.
A version of this article first appeared on Medscape.com.
FROM PLOS PATHOGENS
Antiseptic as good as antibiotics for preventing recurrent UTI
The antiseptic methenamine hippurate (MH) is known to sterilize urine and has been suggested to be of use in preventing urinary tract infections (UTIs), but firm evidence has so far been lacking. Now researchers led by clinicians and scientists from Newcastle-upon-Tyne, England, have provided the ALTAR trial (Alternative to Prophylactic Antibiotics for the Treatment of Recurrent UTIs in Women).
Daily low-dose antibiotics as recommended by current guidelines for prophylactic treatment of recurrent UTI have been linked to antibiotic resistance. Using MH as an alternative could play an important role in helping to tackle the global problem of increasing antibiotic resistance, the team said.
Study details
They recruited 240 women aged 18 or over with recurrent UTIs requiring prophylactic treatment from eight secondary care urology and urogynecology centers in the United Kingdom from June 2016 to June 2018. Women were randomized to receive MH or daily low-dose antibiotics for 12 months, with follow up for a further 6 months beyond that.
Before trial entry the women had experienced an average of more than six UTI episodes per year. During the 12-month treatment period, in the modified intention-to-treat population, there were 90 symptomatic, antibiotic-treated UTI episodes reported over 101 person-years of follow-up in the antibiotic group, and 141 episodes over 102 person-years in the MH group.
This yielded a UTI rate of 0.89 episodes per person-year in the antibiotic group, compared with 1.38 in the MH group, an absolute difference of 0.49 episodes per person-year. In the 6-month posttreatment follow-up period, the UTI incidence rate was 1.19 episodes per person-year in the antibiotic prophylaxis group versus 1.72 in the MH group, an absolute difference of 0.53.
Before the trial, a patient and public involvement group had predefined the noninferiority margin as one episode of UTI per person-year. The small difference between the two groups was less than this, confirming noninferiority of MH to antibiotic prophylaxis in this setting. This finding was consistent across the modified intention-to-treat, strict intention-to-treat, per protocol, and modified per protocol (post hoc) analyses.
Thus the ALTAR results showed that MH was no worse than antibiotics at preventing UTIs, and MH was also associated with reduced antibiotic consumption.
The vast majority of participants were over 90% adherent with the allocated treatment. Patient satisfaction was generally high and rates of adverse events and adverse reactions generally low, and both were comparable between treatment groups. Adverse reactions were reported by 34/142 (24%) in the antibiotic group and 35/127 (28%) in the MH group, and most reactions were mild. In the antibiotic group there were two serious adverse reactions (severe abdominal pain and raised alanine transaminase), whereas six participants in the MH group reported an episode of febrile UTI and four were admitted to hospital because of UTI.
Substantial global health care problem
At least 50% and up to 80% of all women have at least one acute UTI in their lifetime, most often uncomplicated acute cystitis. About a quarter of them go on to suffer recurrent infection, defined as three or more repeat infections in the past year, or two infections in the preceding 6 months. Frequent recurrences thus represent “a substantial global health care problem,” the authors say.
Guidelines from the United Kingdom, Europe, and the United States acknowledge the need for preventive strategies and strongly recommend the use of daily, low-dose antibiotics as standard prophylactic treatment. However, the United Kingdom’s antimicrobial resistance strategy recommends a “strong focus on infection prevention,” and aims to reduce antimicrobial use in humans by 15% before 2024.
“To achieve that, exploration of nonantibiotic preventive treatments in common conditions such as UTI is essential,” the team said.
MH is one such nonantibiotic treatment. It is bactericidal and works by denaturing bacterial proteins and nucleic acids. Although previous Cochrane systematic reviews had concluded that it could be effective for preventing UTI, further large trials were needed.
“This trial adds to the evidence base for the use of MH for prophylactic treatment in adult women with recurrent UTI. Although the MH group had a 55% higher rate of UTI episodes than the antibiotics group, the absolute difference was just 0.49 UTI episodes per year, which has limited clinical consequence,” the team concluded.
Results could ‘support a change in practice’
In older patients, particularly, the risks of long-term antibiotic prophylaxis might outweigh the benefits, and the authors said that their results “could support a change in practice in terms of preventive treatments for recurrent UTI and provide patients and clinicians with a credible alternative to daily antibiotics, giving them the confidence to pursue strategies that avoid long-term antibiotic use.”
They acknowledged limitations of the study, including that treatment allocation was not masked, crossover between arms was allowed, and differences in antibiotics prescribed may have affected the results. In addition, data regarding long-term safety of MH are scarce.
However, they said that the trial accurately represented the broad range of women with recurrent UTI, and that its results “might encourage patients and clinicians to consider MH as a first line treatment for UTI prevention in women.”
In a linked editorial, scientists from the Institute for Evidence-Based Healthcare at Bond University in Queensland, Australia, commented: “Although the results need cautious interpretation, they align with others, and this new research increases the confidence with which MH can be offered as an option to women needing prophylaxis against recurrent urinary tract infection.”
References
Harding C et al. Alternative to prophylactic antibiotics for the treatment of recurrent urinary tract infections in women: multicentre, open label, randomised, noninferiority trial. BMJ 2022 Mar 9;376:e068229.
Hoffmann TC et al. Methenamine hippurate for recurrent urinary tract infections. BMJ 2022 Mar 9;376:o533.
A version of this article first appeared on Medscape.co.uk.
The antiseptic methenamine hippurate (MH) is known to sterilize urine and has been suggested to be of use in preventing urinary tract infections (UTIs), but firm evidence has so far been lacking. Now researchers led by clinicians and scientists from Newcastle-upon-Tyne, England, have provided the ALTAR trial (Alternative to Prophylactic Antibiotics for the Treatment of Recurrent UTIs in Women).
Daily low-dose antibiotics as recommended by current guidelines for prophylactic treatment of recurrent UTI have been linked to antibiotic resistance. Using MH as an alternative could play an important role in helping to tackle the global problem of increasing antibiotic resistance, the team said.
Study details
They recruited 240 women aged 18 or over with recurrent UTIs requiring prophylactic treatment from eight secondary care urology and urogynecology centers in the United Kingdom from June 2016 to June 2018. Women were randomized to receive MH or daily low-dose antibiotics for 12 months, with follow up for a further 6 months beyond that.
Before trial entry the women had experienced an average of more than six UTI episodes per year. During the 12-month treatment period, in the modified intention-to-treat population, there were 90 symptomatic, antibiotic-treated UTI episodes reported over 101 person-years of follow-up in the antibiotic group, and 141 episodes over 102 person-years in the MH group.
This yielded a UTI rate of 0.89 episodes per person-year in the antibiotic group, compared with 1.38 in the MH group, an absolute difference of 0.49 episodes per person-year. In the 6-month posttreatment follow-up period, the UTI incidence rate was 1.19 episodes per person-year in the antibiotic prophylaxis group versus 1.72 in the MH group, an absolute difference of 0.53.
Before the trial, a patient and public involvement group had predefined the noninferiority margin as one episode of UTI per person-year. The small difference between the two groups was less than this, confirming noninferiority of MH to antibiotic prophylaxis in this setting. This finding was consistent across the modified intention-to-treat, strict intention-to-treat, per protocol, and modified per protocol (post hoc) analyses.
Thus the ALTAR results showed that MH was no worse than antibiotics at preventing UTIs, and MH was also associated with reduced antibiotic consumption.
The vast majority of participants were over 90% adherent with the allocated treatment. Patient satisfaction was generally high and rates of adverse events and adverse reactions generally low, and both were comparable between treatment groups. Adverse reactions were reported by 34/142 (24%) in the antibiotic group and 35/127 (28%) in the MH group, and most reactions were mild. In the antibiotic group there were two serious adverse reactions (severe abdominal pain and raised alanine transaminase), whereas six participants in the MH group reported an episode of febrile UTI and four were admitted to hospital because of UTI.
Substantial global health care problem
At least 50% and up to 80% of all women have at least one acute UTI in their lifetime, most often uncomplicated acute cystitis. About a quarter of them go on to suffer recurrent infection, defined as three or more repeat infections in the past year, or two infections in the preceding 6 months. Frequent recurrences thus represent “a substantial global health care problem,” the authors say.
Guidelines from the United Kingdom, Europe, and the United States acknowledge the need for preventive strategies and strongly recommend the use of daily, low-dose antibiotics as standard prophylactic treatment. However, the United Kingdom’s antimicrobial resistance strategy recommends a “strong focus on infection prevention,” and aims to reduce antimicrobial use in humans by 15% before 2024.
“To achieve that, exploration of nonantibiotic preventive treatments in common conditions such as UTI is essential,” the team said.
MH is one such nonantibiotic treatment. It is bactericidal and works by denaturing bacterial proteins and nucleic acids. Although previous Cochrane systematic reviews had concluded that it could be effective for preventing UTI, further large trials were needed.
“This trial adds to the evidence base for the use of MH for prophylactic treatment in adult women with recurrent UTI. Although the MH group had a 55% higher rate of UTI episodes than the antibiotics group, the absolute difference was just 0.49 UTI episodes per year, which has limited clinical consequence,” the team concluded.
Results could ‘support a change in practice’
In older patients, particularly, the risks of long-term antibiotic prophylaxis might outweigh the benefits, and the authors said that their results “could support a change in practice in terms of preventive treatments for recurrent UTI and provide patients and clinicians with a credible alternative to daily antibiotics, giving them the confidence to pursue strategies that avoid long-term antibiotic use.”
They acknowledged limitations of the study, including that treatment allocation was not masked, crossover between arms was allowed, and differences in antibiotics prescribed may have affected the results. In addition, data regarding long-term safety of MH are scarce.
However, they said that the trial accurately represented the broad range of women with recurrent UTI, and that its results “might encourage patients and clinicians to consider MH as a first line treatment for UTI prevention in women.”
In a linked editorial, scientists from the Institute for Evidence-Based Healthcare at Bond University in Queensland, Australia, commented: “Although the results need cautious interpretation, they align with others, and this new research increases the confidence with which MH can be offered as an option to women needing prophylaxis against recurrent urinary tract infection.”
References
Harding C et al. Alternative to prophylactic antibiotics for the treatment of recurrent urinary tract infections in women: multicentre, open label, randomised, noninferiority trial. BMJ 2022 Mar 9;376:e068229.
Hoffmann TC et al. Methenamine hippurate for recurrent urinary tract infections. BMJ 2022 Mar 9;376:o533.
A version of this article first appeared on Medscape.co.uk.
The antiseptic methenamine hippurate (MH) is known to sterilize urine and has been suggested to be of use in preventing urinary tract infections (UTIs), but firm evidence has so far been lacking. Now researchers led by clinicians and scientists from Newcastle-upon-Tyne, England, have provided the ALTAR trial (Alternative to Prophylactic Antibiotics for the Treatment of Recurrent UTIs in Women).
Daily low-dose antibiotics as recommended by current guidelines for prophylactic treatment of recurrent UTI have been linked to antibiotic resistance. Using MH as an alternative could play an important role in helping to tackle the global problem of increasing antibiotic resistance, the team said.
Study details
They recruited 240 women aged 18 or over with recurrent UTIs requiring prophylactic treatment from eight secondary care urology and urogynecology centers in the United Kingdom from June 2016 to June 2018. Women were randomized to receive MH or daily low-dose antibiotics for 12 months, with follow up for a further 6 months beyond that.
Before trial entry the women had experienced an average of more than six UTI episodes per year. During the 12-month treatment period, in the modified intention-to-treat population, there were 90 symptomatic, antibiotic-treated UTI episodes reported over 101 person-years of follow-up in the antibiotic group, and 141 episodes over 102 person-years in the MH group.
This yielded a UTI rate of 0.89 episodes per person-year in the antibiotic group, compared with 1.38 in the MH group, an absolute difference of 0.49 episodes per person-year. In the 6-month posttreatment follow-up period, the UTI incidence rate was 1.19 episodes per person-year in the antibiotic prophylaxis group versus 1.72 in the MH group, an absolute difference of 0.53.
Before the trial, a patient and public involvement group had predefined the noninferiority margin as one episode of UTI per person-year. The small difference between the two groups was less than this, confirming noninferiority of MH to antibiotic prophylaxis in this setting. This finding was consistent across the modified intention-to-treat, strict intention-to-treat, per protocol, and modified per protocol (post hoc) analyses.
Thus the ALTAR results showed that MH was no worse than antibiotics at preventing UTIs, and MH was also associated with reduced antibiotic consumption.
The vast majority of participants were over 90% adherent with the allocated treatment. Patient satisfaction was generally high and rates of adverse events and adverse reactions generally low, and both were comparable between treatment groups. Adverse reactions were reported by 34/142 (24%) in the antibiotic group and 35/127 (28%) in the MH group, and most reactions were mild. In the antibiotic group there were two serious adverse reactions (severe abdominal pain and raised alanine transaminase), whereas six participants in the MH group reported an episode of febrile UTI and four were admitted to hospital because of UTI.
Substantial global health care problem
At least 50% and up to 80% of all women have at least one acute UTI in their lifetime, most often uncomplicated acute cystitis. About a quarter of them go on to suffer recurrent infection, defined as three or more repeat infections in the past year, or two infections in the preceding 6 months. Frequent recurrences thus represent “a substantial global health care problem,” the authors say.
Guidelines from the United Kingdom, Europe, and the United States acknowledge the need for preventive strategies and strongly recommend the use of daily, low-dose antibiotics as standard prophylactic treatment. However, the United Kingdom’s antimicrobial resistance strategy recommends a “strong focus on infection prevention,” and aims to reduce antimicrobial use in humans by 15% before 2024.
“To achieve that, exploration of nonantibiotic preventive treatments in common conditions such as UTI is essential,” the team said.
MH is one such nonantibiotic treatment. It is bactericidal and works by denaturing bacterial proteins and nucleic acids. Although previous Cochrane systematic reviews had concluded that it could be effective for preventing UTI, further large trials were needed.
“This trial adds to the evidence base for the use of MH for prophylactic treatment in adult women with recurrent UTI. Although the MH group had a 55% higher rate of UTI episodes than the antibiotics group, the absolute difference was just 0.49 UTI episodes per year, which has limited clinical consequence,” the team concluded.
Results could ‘support a change in practice’
In older patients, particularly, the risks of long-term antibiotic prophylaxis might outweigh the benefits, and the authors said that their results “could support a change in practice in terms of preventive treatments for recurrent UTI and provide patients and clinicians with a credible alternative to daily antibiotics, giving them the confidence to pursue strategies that avoid long-term antibiotic use.”
They acknowledged limitations of the study, including that treatment allocation was not masked, crossover between arms was allowed, and differences in antibiotics prescribed may have affected the results. In addition, data regarding long-term safety of MH are scarce.
However, they said that the trial accurately represented the broad range of women with recurrent UTI, and that its results “might encourage patients and clinicians to consider MH as a first line treatment for UTI prevention in women.”
In a linked editorial, scientists from the Institute for Evidence-Based Healthcare at Bond University in Queensland, Australia, commented: “Although the results need cautious interpretation, they align with others, and this new research increases the confidence with which MH can be offered as an option to women needing prophylaxis against recurrent urinary tract infection.”
References
Harding C et al. Alternative to prophylactic antibiotics for the treatment of recurrent urinary tract infections in women: multicentre, open label, randomised, noninferiority trial. BMJ 2022 Mar 9;376:e068229.
Hoffmann TC et al. Methenamine hippurate for recurrent urinary tract infections. BMJ 2022 Mar 9;376:o533.
A version of this article first appeared on Medscape.co.uk.
COVID-19 often more severe with congenital heart defects
Adults with a congenital heart defect (CHD) are at increased risk for serious illness and death when hospitalized with COVID-19, making vaccination and other preventive measures even important in this population, say researchers with the Centers for Disease Control and Prevention.
“We found that hospitalized patients with heart defects are up to twice as likely to have critical outcomes of COVID-19 illness (admission to the intensive care unit, use of a ventilator to help with breathing, or death) compared to hospitalized COVID-19 patients without heart defects,” Karrie Downing, MPH, epidemiologist, with the CDC’s National Center on Birth Defects and Developmental Disabilities, said in an interview.
“Additionally, we learned that people with hearts defects who were older or who also had other conditions like heart failure, pulmonary hypertension, Down syndrome, diabetes, or obesity were the most likely to have critical COVID-19 illness, but children and adults with heart defects without these other conditions were still at increased risk,” Ms. Downing said.
The message for health care providers is clear: “Encourage your patients with heart defects to get vaccinated and discuss with your patients the need for other preventive measures to avoid infection that may progress to severe COVID-19 illness,” Ms. Downing added.
The study was published online March 7, 2022, in Circulation.
The researchers analyzed data on 235,638 patients hospitalized with COVID-19 between March 2020 and January 2021, including 421 (0.2%) with CHD. Most CHD patients were older than 30 years (73%) and 61% were men, with 55% non-Hispanic white, 19% Hispanic and 16% non-Hispanic Black.
Overall, 68% of CHD patients had at least one comorbidity, as did 59% of patients without CHD.
Rates of ICU admission were higher in the CHD group (54% vs. 43%), as were rates of invasive mechanical ventilation (24% vs. 15%) and in-hospital death (11% vs. 7%).
After accounting for patient characteristics, ICU admission, invasive mechanical ventilation and death were more prevalent among COVID-19 patients with rather than without CHD, with adjusted prevalence ratios of 1.4, 1.8 and 2.0, respectively.
When stratified by high-risk characteristics, prevalence estimates for ICU admission, invasive mechanical ventilation and death remained higher among patients with COVID-19 and CHD across nearly all strata, including younger age groups and those without heart failure, pulmonary hypertension, Down syndrome, diabetes, or obesity, the researchers reported.
Ms. Downing said more work is needed to identify why the clinical course of COVID-19 disease results in admission to the ICU, the need for a ventilator, or death for some hospitalized patients with CHD and not for others.
“There could be a number of social, environmental, economic, medical, and genetic factors playing a role. But staying up to date with COVID-19 vaccines and following preventive measures for COVID-19 are effective ways to reduce the risk of severe illness from COVID-19,” Ms. Downing said.
The study had no specific funding. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
Adults with a congenital heart defect (CHD) are at increased risk for serious illness and death when hospitalized with COVID-19, making vaccination and other preventive measures even important in this population, say researchers with the Centers for Disease Control and Prevention.
“We found that hospitalized patients with heart defects are up to twice as likely to have critical outcomes of COVID-19 illness (admission to the intensive care unit, use of a ventilator to help with breathing, or death) compared to hospitalized COVID-19 patients without heart defects,” Karrie Downing, MPH, epidemiologist, with the CDC’s National Center on Birth Defects and Developmental Disabilities, said in an interview.
“Additionally, we learned that people with hearts defects who were older or who also had other conditions like heart failure, pulmonary hypertension, Down syndrome, diabetes, or obesity were the most likely to have critical COVID-19 illness, but children and adults with heart defects without these other conditions were still at increased risk,” Ms. Downing said.
The message for health care providers is clear: “Encourage your patients with heart defects to get vaccinated and discuss with your patients the need for other preventive measures to avoid infection that may progress to severe COVID-19 illness,” Ms. Downing added.
The study was published online March 7, 2022, in Circulation.
The researchers analyzed data on 235,638 patients hospitalized with COVID-19 between March 2020 and January 2021, including 421 (0.2%) with CHD. Most CHD patients were older than 30 years (73%) and 61% were men, with 55% non-Hispanic white, 19% Hispanic and 16% non-Hispanic Black.
Overall, 68% of CHD patients had at least one comorbidity, as did 59% of patients without CHD.
Rates of ICU admission were higher in the CHD group (54% vs. 43%), as were rates of invasive mechanical ventilation (24% vs. 15%) and in-hospital death (11% vs. 7%).
After accounting for patient characteristics, ICU admission, invasive mechanical ventilation and death were more prevalent among COVID-19 patients with rather than without CHD, with adjusted prevalence ratios of 1.4, 1.8 and 2.0, respectively.
When stratified by high-risk characteristics, prevalence estimates for ICU admission, invasive mechanical ventilation and death remained higher among patients with COVID-19 and CHD across nearly all strata, including younger age groups and those without heart failure, pulmonary hypertension, Down syndrome, diabetes, or obesity, the researchers reported.
Ms. Downing said more work is needed to identify why the clinical course of COVID-19 disease results in admission to the ICU, the need for a ventilator, or death for some hospitalized patients with CHD and not for others.
“There could be a number of social, environmental, economic, medical, and genetic factors playing a role. But staying up to date with COVID-19 vaccines and following preventive measures for COVID-19 are effective ways to reduce the risk of severe illness from COVID-19,” Ms. Downing said.
The study had no specific funding. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
Adults with a congenital heart defect (CHD) are at increased risk for serious illness and death when hospitalized with COVID-19, making vaccination and other preventive measures even important in this population, say researchers with the Centers for Disease Control and Prevention.
“We found that hospitalized patients with heart defects are up to twice as likely to have critical outcomes of COVID-19 illness (admission to the intensive care unit, use of a ventilator to help with breathing, or death) compared to hospitalized COVID-19 patients without heart defects,” Karrie Downing, MPH, epidemiologist, with the CDC’s National Center on Birth Defects and Developmental Disabilities, said in an interview.
“Additionally, we learned that people with hearts defects who were older or who also had other conditions like heart failure, pulmonary hypertension, Down syndrome, diabetes, or obesity were the most likely to have critical COVID-19 illness, but children and adults with heart defects without these other conditions were still at increased risk,” Ms. Downing said.
The message for health care providers is clear: “Encourage your patients with heart defects to get vaccinated and discuss with your patients the need for other preventive measures to avoid infection that may progress to severe COVID-19 illness,” Ms. Downing added.
The study was published online March 7, 2022, in Circulation.
The researchers analyzed data on 235,638 patients hospitalized with COVID-19 between March 2020 and January 2021, including 421 (0.2%) with CHD. Most CHD patients were older than 30 years (73%) and 61% were men, with 55% non-Hispanic white, 19% Hispanic and 16% non-Hispanic Black.
Overall, 68% of CHD patients had at least one comorbidity, as did 59% of patients without CHD.
Rates of ICU admission were higher in the CHD group (54% vs. 43%), as were rates of invasive mechanical ventilation (24% vs. 15%) and in-hospital death (11% vs. 7%).
After accounting for patient characteristics, ICU admission, invasive mechanical ventilation and death were more prevalent among COVID-19 patients with rather than without CHD, with adjusted prevalence ratios of 1.4, 1.8 and 2.0, respectively.
When stratified by high-risk characteristics, prevalence estimates for ICU admission, invasive mechanical ventilation and death remained higher among patients with COVID-19 and CHD across nearly all strata, including younger age groups and those without heart failure, pulmonary hypertension, Down syndrome, diabetes, or obesity, the researchers reported.
Ms. Downing said more work is needed to identify why the clinical course of COVID-19 disease results in admission to the ICU, the need for a ventilator, or death for some hospitalized patients with CHD and not for others.
“There could be a number of social, environmental, economic, medical, and genetic factors playing a role. But staying up to date with COVID-19 vaccines and following preventive measures for COVID-19 are effective ways to reduce the risk of severe illness from COVID-19,” Ms. Downing said.
The study had no specific funding. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION