User login
Should magnesium be used for COPD exacerbations?
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are a major driver of disease-related morbidity. Their prevention and treatment are a focus of COPD management. Antibiotics, corticosteroids, and nebulized bronchodilators are all given to patients with AECOPD, and while the supporting data aren’t perfect, there’s little debate surrounding their use. These medications are well known to most physicians; we’re comfortable with their efficacy and aware of their side effects. They are nothing if not familiar.
What about magnesium (Mg), though? Apparently, in the emergency room (ER) it is part of the standard AECOPD cocktail. I would argue that Mg is familiar to most too; every internal medicine trainee in the United States is taught to infuse 2 g of Mg intravenously for any inpatient (ICU or otherwise) with a serum level <2.0 mg/dL. In fact, “electrolyte protocols” are part of the order sets at most hospitals where I’ve worked. Mg is infused reflexively when it drops below certain levels.
I’m less familiar with using Mg in the setting of an AECOPD, though. A recent online post by an academic ER physician (Richard Pescatore, DO) urged caution in this setting. He argues that too many in the ER are embracing the “Dutch Hypothesis” and treating asthma and COPD as the same disease. Dr. Pescatore believes that Mg works for asthma exacerbations because asthma is a disease of smooth muscle and large airways, while COPD is not. COPD, he says, is a disease of the small airways, largely resulting from parenchymal distortions due to emphysema. Therefore, Mg, which is thought to act on the smooth muscle surrounding the large airways, won’t be beneficial for AECOPD and may even cause harm.
Data are lacking
What data exist for using Mg for AECOPD? The best randomized controlled trial (RCT) I could find was published in 1995 and is cited in the reader’s rebuttal. The trial found a significant improvement in peak expiratory flow rate (PEFR) with Mg and a nonsignificant reduction in hospitalizations.
A poorly done systematic review of RCTs using Mg for AECOPD was published in 2014, and in 2020 the Agency for Healthcare Research and Quality (AHRQ) included Mg in its well-executed meta-analysis of pharmacologic treatments for AECOPD. Data across the four to five Mg RCTs included in each of the reviews (study inclusion criteria were slightly different) could not be combined. All RCTs were small, and only soft outcomes like PEFR and forced expiratory volume in 1 second (FEV1) seemed to improve with Mg. No adverse events were noted, but this should be interpreted with caution given that many studies did not report on adverse events at all.
A small RCT published this year (after both systematic reviews were completed) showed that using intravenous magnesium sulfate had no significant effect on FEV1, vital signs, or symptoms.
In summary, the data aren’t great. Mg doesn’t show up at all as a treatment option in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Report on COPD, and the authors of the AHRQ review concluded that large, high-quality RCTs are needed to assess the impact of Mg in AECOPD. Although I didn’t do an extensive review of Mg for asthma exacerbations, it’s not clear that the data here are much better. Mg gets an honorable mention (add for severe exacerbations when there’s inadequate response to standard treatments) in both the 2007 National Heart, Lung, and Blood Institute (NHLBI) guideline and the 2019 Global Initiative for Asthma (GINA) guide. The 2020 update to the 2007 NHLBI guideline is more targeted in its review and does not cover Mg as a treatment option. On the basis of my anecdotal clinical experience and on networking with airway experts, I do think Mg is used more often for asthma than for AECOPD.
Final thoughts on using Mg for AECOPD
All that being said, is it reasonable to use Mg for AECOPD? I think so. I’d stick to using it for severe cases where conventional treatments have failed, just like the NHLBI and GINA advise for asthma. I’d also limit it to 2-3 g, which is the dosing range employed by several of the existing AECOPD RCTs. The assertion that Mg may be harmful in AECOPD because COPD affects the small airways, and asthma does not, is misguided. Both affect the small airways. Furthermore, none of our inhaled therapies reach the small airways, so one can’t argue against using Mg because it only targets larger airways without abandoning albuterol and ipratropium as well. I don’t think anyone would advise that. Given what we now know about asthma and COPD phenotypes and asthma-COPD overlap, I’d caution against pedantic theories about response to therapies.
Aaron B. Holley, MD, is an associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He has received research grants from Fisher-Paykel and has received payments from the American College of Chest Physicians.
A version of this article first appeared on Medscape.com.
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are a major driver of disease-related morbidity. Their prevention and treatment are a focus of COPD management. Antibiotics, corticosteroids, and nebulized bronchodilators are all given to patients with AECOPD, and while the supporting data aren’t perfect, there’s little debate surrounding their use. These medications are well known to most physicians; we’re comfortable with their efficacy and aware of their side effects. They are nothing if not familiar.
What about magnesium (Mg), though? Apparently, in the emergency room (ER) it is part of the standard AECOPD cocktail. I would argue that Mg is familiar to most too; every internal medicine trainee in the United States is taught to infuse 2 g of Mg intravenously for any inpatient (ICU or otherwise) with a serum level <2.0 mg/dL. In fact, “electrolyte protocols” are part of the order sets at most hospitals where I’ve worked. Mg is infused reflexively when it drops below certain levels.
I’m less familiar with using Mg in the setting of an AECOPD, though. A recent online post by an academic ER physician (Richard Pescatore, DO) urged caution in this setting. He argues that too many in the ER are embracing the “Dutch Hypothesis” and treating asthma and COPD as the same disease. Dr. Pescatore believes that Mg works for asthma exacerbations because asthma is a disease of smooth muscle and large airways, while COPD is not. COPD, he says, is a disease of the small airways, largely resulting from parenchymal distortions due to emphysema. Therefore, Mg, which is thought to act on the smooth muscle surrounding the large airways, won’t be beneficial for AECOPD and may even cause harm.
Data are lacking
What data exist for using Mg for AECOPD? The best randomized controlled trial (RCT) I could find was published in 1995 and is cited in the reader’s rebuttal. The trial found a significant improvement in peak expiratory flow rate (PEFR) with Mg and a nonsignificant reduction in hospitalizations.
A poorly done systematic review of RCTs using Mg for AECOPD was published in 2014, and in 2020 the Agency for Healthcare Research and Quality (AHRQ) included Mg in its well-executed meta-analysis of pharmacologic treatments for AECOPD. Data across the four to five Mg RCTs included in each of the reviews (study inclusion criteria were slightly different) could not be combined. All RCTs were small, and only soft outcomes like PEFR and forced expiratory volume in 1 second (FEV1) seemed to improve with Mg. No adverse events were noted, but this should be interpreted with caution given that many studies did not report on adverse events at all.
A small RCT published this year (after both systematic reviews were completed) showed that using intravenous magnesium sulfate had no significant effect on FEV1, vital signs, or symptoms.
In summary, the data aren’t great. Mg doesn’t show up at all as a treatment option in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Report on COPD, and the authors of the AHRQ review concluded that large, high-quality RCTs are needed to assess the impact of Mg in AECOPD. Although I didn’t do an extensive review of Mg for asthma exacerbations, it’s not clear that the data here are much better. Mg gets an honorable mention (add for severe exacerbations when there’s inadequate response to standard treatments) in both the 2007 National Heart, Lung, and Blood Institute (NHLBI) guideline and the 2019 Global Initiative for Asthma (GINA) guide. The 2020 update to the 2007 NHLBI guideline is more targeted in its review and does not cover Mg as a treatment option. On the basis of my anecdotal clinical experience and on networking with airway experts, I do think Mg is used more often for asthma than for AECOPD.
Final thoughts on using Mg for AECOPD
All that being said, is it reasonable to use Mg for AECOPD? I think so. I’d stick to using it for severe cases where conventional treatments have failed, just like the NHLBI and GINA advise for asthma. I’d also limit it to 2-3 g, which is the dosing range employed by several of the existing AECOPD RCTs. The assertion that Mg may be harmful in AECOPD because COPD affects the small airways, and asthma does not, is misguided. Both affect the small airways. Furthermore, none of our inhaled therapies reach the small airways, so one can’t argue against using Mg because it only targets larger airways without abandoning albuterol and ipratropium as well. I don’t think anyone would advise that. Given what we now know about asthma and COPD phenotypes and asthma-COPD overlap, I’d caution against pedantic theories about response to therapies.
Aaron B. Holley, MD, is an associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He has received research grants from Fisher-Paykel and has received payments from the American College of Chest Physicians.
A version of this article first appeared on Medscape.com.
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are a major driver of disease-related morbidity. Their prevention and treatment are a focus of COPD management. Antibiotics, corticosteroids, and nebulized bronchodilators are all given to patients with AECOPD, and while the supporting data aren’t perfect, there’s little debate surrounding their use. These medications are well known to most physicians; we’re comfortable with their efficacy and aware of their side effects. They are nothing if not familiar.
What about magnesium (Mg), though? Apparently, in the emergency room (ER) it is part of the standard AECOPD cocktail. I would argue that Mg is familiar to most too; every internal medicine trainee in the United States is taught to infuse 2 g of Mg intravenously for any inpatient (ICU or otherwise) with a serum level <2.0 mg/dL. In fact, “electrolyte protocols” are part of the order sets at most hospitals where I’ve worked. Mg is infused reflexively when it drops below certain levels.
I’m less familiar with using Mg in the setting of an AECOPD, though. A recent online post by an academic ER physician (Richard Pescatore, DO) urged caution in this setting. He argues that too many in the ER are embracing the “Dutch Hypothesis” and treating asthma and COPD as the same disease. Dr. Pescatore believes that Mg works for asthma exacerbations because asthma is a disease of smooth muscle and large airways, while COPD is not. COPD, he says, is a disease of the small airways, largely resulting from parenchymal distortions due to emphysema. Therefore, Mg, which is thought to act on the smooth muscle surrounding the large airways, won’t be beneficial for AECOPD and may even cause harm.
Data are lacking
What data exist for using Mg for AECOPD? The best randomized controlled trial (RCT) I could find was published in 1995 and is cited in the reader’s rebuttal. The trial found a significant improvement in peak expiratory flow rate (PEFR) with Mg and a nonsignificant reduction in hospitalizations.
A poorly done systematic review of RCTs using Mg for AECOPD was published in 2014, and in 2020 the Agency for Healthcare Research and Quality (AHRQ) included Mg in its well-executed meta-analysis of pharmacologic treatments for AECOPD. Data across the four to five Mg RCTs included in each of the reviews (study inclusion criteria were slightly different) could not be combined. All RCTs were small, and only soft outcomes like PEFR and forced expiratory volume in 1 second (FEV1) seemed to improve with Mg. No adverse events were noted, but this should be interpreted with caution given that many studies did not report on adverse events at all.
A small RCT published this year (after both systematic reviews were completed) showed that using intravenous magnesium sulfate had no significant effect on FEV1, vital signs, or symptoms.
In summary, the data aren’t great. Mg doesn’t show up at all as a treatment option in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Report on COPD, and the authors of the AHRQ review concluded that large, high-quality RCTs are needed to assess the impact of Mg in AECOPD. Although I didn’t do an extensive review of Mg for asthma exacerbations, it’s not clear that the data here are much better. Mg gets an honorable mention (add for severe exacerbations when there’s inadequate response to standard treatments) in both the 2007 National Heart, Lung, and Blood Institute (NHLBI) guideline and the 2019 Global Initiative for Asthma (GINA) guide. The 2020 update to the 2007 NHLBI guideline is more targeted in its review and does not cover Mg as a treatment option. On the basis of my anecdotal clinical experience and on networking with airway experts, I do think Mg is used more often for asthma than for AECOPD.
Final thoughts on using Mg for AECOPD
All that being said, is it reasonable to use Mg for AECOPD? I think so. I’d stick to using it for severe cases where conventional treatments have failed, just like the NHLBI and GINA advise for asthma. I’d also limit it to 2-3 g, which is the dosing range employed by several of the existing AECOPD RCTs. The assertion that Mg may be harmful in AECOPD because COPD affects the small airways, and asthma does not, is misguided. Both affect the small airways. Furthermore, none of our inhaled therapies reach the small airways, so one can’t argue against using Mg because it only targets larger airways without abandoning albuterol and ipratropium as well. I don’t think anyone would advise that. Given what we now know about asthma and COPD phenotypes and asthma-COPD overlap, I’d caution against pedantic theories about response to therapies.
Aaron B. Holley, MD, is an associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He has received research grants from Fisher-Paykel and has received payments from the American College of Chest Physicians.
A version of this article first appeared on Medscape.com.
Tranexamic acid fails to prevent ICH growth: TRAIGE trial results
(ICH), a new study shows.
In the randomized controlled trial, the rate of hematoma expansion was 40.4% among patients who received tranexamic acid and 41.5% among those who received placebo. The degree of disability at 90 days also did not differ between treatment arms.
“Our work has once again shown that tranexamic acid is safe in spontaneous ICH,” said Jingyi Liu, MD, a physician in the neurocritical care unit at Beijing Tiantan Hospital, Capital Medical University, Beijing. “Larger studies with more specified population are needed to further assess safety and efficacy of tranexamic acid in patients with ICH.”
The findings of the TRAIGE study were presented at the virtual European Stroke Organization Conference (ESOC) 2021. They were also published online June 28 in Stroke and Vascular Neurology.
Imaging-based patient selection
ICH is often fatal and entails a high risk for disability, the researchers wrote. Approximately 40% of patients with ICH die within a month of onset, and about two-thirds of patients do not achieve long-term functional independence.
Intracerebral hematoma expansion is predictive of poor clinical outcome in ICH. Data indicate that tranexamic acid, an antifibrinolytic agent, reduces hematoma expansion. But evidence of a clinical benefit of tranexamic acid has been elusive, they noted.
This lack of observed benefit may result from the inappropriate selection of research participants. The emergence of imaging biomarkers may help address this potential problem. In recent years, the blend sign and the black hole sign on noncontrast CT, as well as the spot sign on CT angiography, have been associated with higher risk for hematoma expansion and worse clinical outcome, the researchers wrote.
Between January 2015 and March 2020, the investigators enrolled consecutive patients with acute primary spontaneous ICH into their prospective study. Eligible patients presented at any of 10 stroke centers in China. They had the spot sign, blend sign, or black hole sign at admission and were able to receive treatment within 8 hours of onset.
The investigators randomly assigned patients in equal groups to receive placebo (0.9% NaCl) or tranexamic acid. Patients and study investigators were blinded to treatment assignment. Treatment was administered as an intravenous infusion over 8 hours.
The study’s primary endpoint was intracerebral hematoma expansion by 24 hours after start of treatment. Expansion was defined as an increase of > 6 mL or a growth of > 33% from baseline. Secondary endpoints included poor clinical outcome, defined as a Modified Rankin Scale (mRS) score of 4-6, and all-cause mortality, both at 90 days.
No differences in disability
The investigators enrolled 171 patients in their study; 24-hour CT images were available for 169 of them. Follow-up data at 90 days were available for 164 patients. The mean age of the patients was 55.9 years, and 72.5% of participants were men. At baseline, the mean ICH volume was 23.7 mL, and the median hematoma volume was 19.8 mL.
All patients received treatment within 8 hours. Hematoma expansion occurred in 40.9% of patients overall; 34.9% had a poor clinical outcome.
The investigators found no significant difference between treatment arms in the rate of hematoma expansion. This outcome occurred in 40.4% of the tranexamic acid group and 41.5% of the placebo group (odds ratio, 0.96; P = .89).
In addition, the researchers found no significant difference in the distribution of mRS scores at day 90 (P = .70). The rate of all-cause mortality at 90 days was lower in the tranexamic acid group (8.1%) than in the control group (10.0%), but this difference was not statistically significant (P = .71).
Potential clotting risk
One reason for the lack of observed benefit with tranexamic acid may be an inappropriate sample size, said Dr. Liu. Patient recruitment was difficult, especially in centers that used the spot sign as an inclusion criterion.
“We think a positive result could be seen in a substantially larger sample size,” said Dr. Liu. “Furthermore, we infer from our subgroup analysis that a more specified patient selection and shorter treatment window may be required for better effect.”
In some of their subgroup analyses, the researchers found a trend toward an increased effect in patients with moderate-size hematoma who received treatment in an earlier window. “That could be the targeted population for future studies,” said Dr. Liu. “We are working on further analysis of the population and possibly international collaboration.”
But tranexamic acid also entails risks, said Louis R. Caplan, MD, professor of neurology at Harvard Medical School, Boston, who provided independent commentary on the findings. “Tranexamic acid works on the thrombolytic system, so it increases clotting, and it does have a risk in people who are older and have risk factors for coronary disease and pulmonary embolism.”
As in ischemic stroke, time to treatment is a crucial consideration. Patients with ICH may receive treatment within 5 or 6 hours of onset, but most hemorrhages have reached their maximum size at that point. “The number of people that you can actually help by reducing the size is small,” said Dr. Caplan. “And then reducing the size in most hemorrhages doesn’t make any clinical difference.”
Stereotactic drainage, in which fluid is physically removed, is more likely to lead to long-term improvement for some patients with hemorrhage than limiting expansion, said Dr. Caplan. “That seems to be a more promising therapy,” he added.
The study was supported by the National Key R&D program of China, the National Natural Science Foundation of China, and the Beijing Science and Technology Commission. Dr. Liu and Dr. Caplan have disclosed no relevant financial relationshps.
A version of this article first appeared on Medscape.com.
(ICH), a new study shows.
In the randomized controlled trial, the rate of hematoma expansion was 40.4% among patients who received tranexamic acid and 41.5% among those who received placebo. The degree of disability at 90 days also did not differ between treatment arms.
“Our work has once again shown that tranexamic acid is safe in spontaneous ICH,” said Jingyi Liu, MD, a physician in the neurocritical care unit at Beijing Tiantan Hospital, Capital Medical University, Beijing. “Larger studies with more specified population are needed to further assess safety and efficacy of tranexamic acid in patients with ICH.”
The findings of the TRAIGE study were presented at the virtual European Stroke Organization Conference (ESOC) 2021. They were also published online June 28 in Stroke and Vascular Neurology.
Imaging-based patient selection
ICH is often fatal and entails a high risk for disability, the researchers wrote. Approximately 40% of patients with ICH die within a month of onset, and about two-thirds of patients do not achieve long-term functional independence.
Intracerebral hematoma expansion is predictive of poor clinical outcome in ICH. Data indicate that tranexamic acid, an antifibrinolytic agent, reduces hematoma expansion. But evidence of a clinical benefit of tranexamic acid has been elusive, they noted.
This lack of observed benefit may result from the inappropriate selection of research participants. The emergence of imaging biomarkers may help address this potential problem. In recent years, the blend sign and the black hole sign on noncontrast CT, as well as the spot sign on CT angiography, have been associated with higher risk for hematoma expansion and worse clinical outcome, the researchers wrote.
Between January 2015 and March 2020, the investigators enrolled consecutive patients with acute primary spontaneous ICH into their prospective study. Eligible patients presented at any of 10 stroke centers in China. They had the spot sign, blend sign, or black hole sign at admission and were able to receive treatment within 8 hours of onset.
The investigators randomly assigned patients in equal groups to receive placebo (0.9% NaCl) or tranexamic acid. Patients and study investigators were blinded to treatment assignment. Treatment was administered as an intravenous infusion over 8 hours.
The study’s primary endpoint was intracerebral hematoma expansion by 24 hours after start of treatment. Expansion was defined as an increase of > 6 mL or a growth of > 33% from baseline. Secondary endpoints included poor clinical outcome, defined as a Modified Rankin Scale (mRS) score of 4-6, and all-cause mortality, both at 90 days.
No differences in disability
The investigators enrolled 171 patients in their study; 24-hour CT images were available for 169 of them. Follow-up data at 90 days were available for 164 patients. The mean age of the patients was 55.9 years, and 72.5% of participants were men. At baseline, the mean ICH volume was 23.7 mL, and the median hematoma volume was 19.8 mL.
All patients received treatment within 8 hours. Hematoma expansion occurred in 40.9% of patients overall; 34.9% had a poor clinical outcome.
The investigators found no significant difference between treatment arms in the rate of hematoma expansion. This outcome occurred in 40.4% of the tranexamic acid group and 41.5% of the placebo group (odds ratio, 0.96; P = .89).
In addition, the researchers found no significant difference in the distribution of mRS scores at day 90 (P = .70). The rate of all-cause mortality at 90 days was lower in the tranexamic acid group (8.1%) than in the control group (10.0%), but this difference was not statistically significant (P = .71).
Potential clotting risk
One reason for the lack of observed benefit with tranexamic acid may be an inappropriate sample size, said Dr. Liu. Patient recruitment was difficult, especially in centers that used the spot sign as an inclusion criterion.
“We think a positive result could be seen in a substantially larger sample size,” said Dr. Liu. “Furthermore, we infer from our subgroup analysis that a more specified patient selection and shorter treatment window may be required for better effect.”
In some of their subgroup analyses, the researchers found a trend toward an increased effect in patients with moderate-size hematoma who received treatment in an earlier window. “That could be the targeted population for future studies,” said Dr. Liu. “We are working on further analysis of the population and possibly international collaboration.”
But tranexamic acid also entails risks, said Louis R. Caplan, MD, professor of neurology at Harvard Medical School, Boston, who provided independent commentary on the findings. “Tranexamic acid works on the thrombolytic system, so it increases clotting, and it does have a risk in people who are older and have risk factors for coronary disease and pulmonary embolism.”
As in ischemic stroke, time to treatment is a crucial consideration. Patients with ICH may receive treatment within 5 or 6 hours of onset, but most hemorrhages have reached their maximum size at that point. “The number of people that you can actually help by reducing the size is small,” said Dr. Caplan. “And then reducing the size in most hemorrhages doesn’t make any clinical difference.”
Stereotactic drainage, in which fluid is physically removed, is more likely to lead to long-term improvement for some patients with hemorrhage than limiting expansion, said Dr. Caplan. “That seems to be a more promising therapy,” he added.
The study was supported by the National Key R&D program of China, the National Natural Science Foundation of China, and the Beijing Science and Technology Commission. Dr. Liu and Dr. Caplan have disclosed no relevant financial relationshps.
A version of this article first appeared on Medscape.com.
(ICH), a new study shows.
In the randomized controlled trial, the rate of hematoma expansion was 40.4% among patients who received tranexamic acid and 41.5% among those who received placebo. The degree of disability at 90 days also did not differ between treatment arms.
“Our work has once again shown that tranexamic acid is safe in spontaneous ICH,” said Jingyi Liu, MD, a physician in the neurocritical care unit at Beijing Tiantan Hospital, Capital Medical University, Beijing. “Larger studies with more specified population are needed to further assess safety and efficacy of tranexamic acid in patients with ICH.”
The findings of the TRAIGE study were presented at the virtual European Stroke Organization Conference (ESOC) 2021. They were also published online June 28 in Stroke and Vascular Neurology.
Imaging-based patient selection
ICH is often fatal and entails a high risk for disability, the researchers wrote. Approximately 40% of patients with ICH die within a month of onset, and about two-thirds of patients do not achieve long-term functional independence.
Intracerebral hematoma expansion is predictive of poor clinical outcome in ICH. Data indicate that tranexamic acid, an antifibrinolytic agent, reduces hematoma expansion. But evidence of a clinical benefit of tranexamic acid has been elusive, they noted.
This lack of observed benefit may result from the inappropriate selection of research participants. The emergence of imaging biomarkers may help address this potential problem. In recent years, the blend sign and the black hole sign on noncontrast CT, as well as the spot sign on CT angiography, have been associated with higher risk for hematoma expansion and worse clinical outcome, the researchers wrote.
Between January 2015 and March 2020, the investigators enrolled consecutive patients with acute primary spontaneous ICH into their prospective study. Eligible patients presented at any of 10 stroke centers in China. They had the spot sign, blend sign, or black hole sign at admission and were able to receive treatment within 8 hours of onset.
The investigators randomly assigned patients in equal groups to receive placebo (0.9% NaCl) or tranexamic acid. Patients and study investigators were blinded to treatment assignment. Treatment was administered as an intravenous infusion over 8 hours.
The study’s primary endpoint was intracerebral hematoma expansion by 24 hours after start of treatment. Expansion was defined as an increase of > 6 mL or a growth of > 33% from baseline. Secondary endpoints included poor clinical outcome, defined as a Modified Rankin Scale (mRS) score of 4-6, and all-cause mortality, both at 90 days.
No differences in disability
The investigators enrolled 171 patients in their study; 24-hour CT images were available for 169 of them. Follow-up data at 90 days were available for 164 patients. The mean age of the patients was 55.9 years, and 72.5% of participants were men. At baseline, the mean ICH volume was 23.7 mL, and the median hematoma volume was 19.8 mL.
All patients received treatment within 8 hours. Hematoma expansion occurred in 40.9% of patients overall; 34.9% had a poor clinical outcome.
The investigators found no significant difference between treatment arms in the rate of hematoma expansion. This outcome occurred in 40.4% of the tranexamic acid group and 41.5% of the placebo group (odds ratio, 0.96; P = .89).
In addition, the researchers found no significant difference in the distribution of mRS scores at day 90 (P = .70). The rate of all-cause mortality at 90 days was lower in the tranexamic acid group (8.1%) than in the control group (10.0%), but this difference was not statistically significant (P = .71).
Potential clotting risk
One reason for the lack of observed benefit with tranexamic acid may be an inappropriate sample size, said Dr. Liu. Patient recruitment was difficult, especially in centers that used the spot sign as an inclusion criterion.
“We think a positive result could be seen in a substantially larger sample size,” said Dr. Liu. “Furthermore, we infer from our subgroup analysis that a more specified patient selection and shorter treatment window may be required for better effect.”
In some of their subgroup analyses, the researchers found a trend toward an increased effect in patients with moderate-size hematoma who received treatment in an earlier window. “That could be the targeted population for future studies,” said Dr. Liu. “We are working on further analysis of the population and possibly international collaboration.”
But tranexamic acid also entails risks, said Louis R. Caplan, MD, professor of neurology at Harvard Medical School, Boston, who provided independent commentary on the findings. “Tranexamic acid works on the thrombolytic system, so it increases clotting, and it does have a risk in people who are older and have risk factors for coronary disease and pulmonary embolism.”
As in ischemic stroke, time to treatment is a crucial consideration. Patients with ICH may receive treatment within 5 or 6 hours of onset, but most hemorrhages have reached their maximum size at that point. “The number of people that you can actually help by reducing the size is small,” said Dr. Caplan. “And then reducing the size in most hemorrhages doesn’t make any clinical difference.”
Stereotactic drainage, in which fluid is physically removed, is more likely to lead to long-term improvement for some patients with hemorrhage than limiting expansion, said Dr. Caplan. “That seems to be a more promising therapy,” he added.
The study was supported by the National Key R&D program of China, the National Natural Science Foundation of China, and the Beijing Science and Technology Commission. Dr. Liu and Dr. Caplan have disclosed no relevant financial relationshps.
A version of this article first appeared on Medscape.com.
FROM ESOC 2021
When should patients with kidney disease receive nephrology referral?
And combining the two methods – predicted kidney failure risk with lab values – will lead to better patient outcomes by pinpointing CKD patients who most need specialty care, said study author Vishal Duggal, MD, who was a postdoctoral fellow in medical informatics at the Veterans Affairs Palo Alto (Calif.) Health Care System while conducting the research.
“We hope this can provide guidance to primary care physicians and nephrologists to give context for their decision-making,” Dr. Duggal told this news organization.
The VA is the largest provider of CKD care in the United States, developing clinical practice guidelines for CKD management that include suggested indications for nephrology referral based on laboratory values. Laboratory values that are typically used to guide referral include estimated glomerular filtration rate (eGFR) and its rate of decline per year, as well as heavy proteinuria in patients with and without diabetes.
Dr. Duggal and colleagues – who published their findings in the American Journal of Kidney Diseases – conducted a retrospective analysis of nearly 400,000 veterans with CKD over a yearlong period to determine if referral volume would change if it was based on the estimated risk for kidney failure, rather than solely using laboratory values.
They also estimated the potential volume of nephrology referrals based on a combination of both estimated risk for kidney failure and laboratory data.
Kidney failure risk was calculated using an electronic clinical decision support tool, called Kidney Failure Risk Equation incorporating age, eGFR, gender, and urine albumin-to-creatinine ratio.
Targeting fewer patients to specialty care
Among all participants with CKD not already receiving nephrology care, more than 150,000 (41.5%) had a urine albumin or protein measurement leading to computable risk for end-stage kidney disease.
More than 66,200 patients met actual laboratory indications for referral but had not previously seen a nephrologist. Among these patients, 11,752 (17.7%) were referred to nephrology in the following year, and all had a median 2-year predicted risk for kidney failure of 1.5%.
Referred patients were more likely to meet several potential referral criteria, especially eGFR less than 30 mL/min per 1.73 m2 and heavy proteinuria. Those with heavy proteinuria with diabetes, or the eGFR indication, had the highest predicted risk for kidney failure at 2 years, at 10% and 7.1% respectively.
Boosting referral volume can be problematic if patients aren’t prioritized by need, Dr. Duggal said, noting that many reasons explain why fewer than one in five CKD patients meeting lab indications for referral aren’t actually referred.
This can include patient preference, he noted: “Kidney disease is a disease of aging, and some patients don’t want to see a specialist or escalate their care.”
“Also, not everyone who has CKD is recommended to see a nephrologist, since primary care physicians do manage a lot of CKD as well.”
Basing referral on predicted kidney failure risk alone, a 2-year risk threshold of at least 1%, would identify a comparable number of patients (n = 72,948) as laboratory-based criteria, the team found, although they note that the patients identified using the KFRE tool would be at higher risk than those identified by lab values alone.
But when they combined the two – a minimum kidney failure risk of at least 1% over 2 years being applied to all new patients meeting lab-based referral indications, those pinpointed for nephrology referral dropped by 42.3%, from 66,276 to an estimated 38,229 patients.
“The current guidelines that just incorporate lab values identify a significant number of patients who are at low risk of developing end-stage kidney disease (ESKD), so incorporating kidney failure risk into current guidelines would target fewer patients to get to specialty care,” Dr. Duggal explained.
KFRE tool can be found online
Dr. Duggal emphasized that his findings do not change nephrology referral guidelines, but said physicians can find the KFRE tool online and use it to supplement their decision-making about a patient’s care.
“Further incorporating this [kidney failure] risk into referral practices might highlight a patient at extremely high risk who would benefit more from an interdisciplinary care team,” he said.
This could include, for example, a nutritionist to help the patient modify his or her diet. “Getting that kind of teaching process in place for a patient might be highly valuable,” he added.
Dr. Duggal disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
And combining the two methods – predicted kidney failure risk with lab values – will lead to better patient outcomes by pinpointing CKD patients who most need specialty care, said study author Vishal Duggal, MD, who was a postdoctoral fellow in medical informatics at the Veterans Affairs Palo Alto (Calif.) Health Care System while conducting the research.
“We hope this can provide guidance to primary care physicians and nephrologists to give context for their decision-making,” Dr. Duggal told this news organization.
The VA is the largest provider of CKD care in the United States, developing clinical practice guidelines for CKD management that include suggested indications for nephrology referral based on laboratory values. Laboratory values that are typically used to guide referral include estimated glomerular filtration rate (eGFR) and its rate of decline per year, as well as heavy proteinuria in patients with and without diabetes.
Dr. Duggal and colleagues – who published their findings in the American Journal of Kidney Diseases – conducted a retrospective analysis of nearly 400,000 veterans with CKD over a yearlong period to determine if referral volume would change if it was based on the estimated risk for kidney failure, rather than solely using laboratory values.
They also estimated the potential volume of nephrology referrals based on a combination of both estimated risk for kidney failure and laboratory data.
Kidney failure risk was calculated using an electronic clinical decision support tool, called Kidney Failure Risk Equation incorporating age, eGFR, gender, and urine albumin-to-creatinine ratio.
Targeting fewer patients to specialty care
Among all participants with CKD not already receiving nephrology care, more than 150,000 (41.5%) had a urine albumin or protein measurement leading to computable risk for end-stage kidney disease.
More than 66,200 patients met actual laboratory indications for referral but had not previously seen a nephrologist. Among these patients, 11,752 (17.7%) were referred to nephrology in the following year, and all had a median 2-year predicted risk for kidney failure of 1.5%.
Referred patients were more likely to meet several potential referral criteria, especially eGFR less than 30 mL/min per 1.73 m2 and heavy proteinuria. Those with heavy proteinuria with diabetes, or the eGFR indication, had the highest predicted risk for kidney failure at 2 years, at 10% and 7.1% respectively.
Boosting referral volume can be problematic if patients aren’t prioritized by need, Dr. Duggal said, noting that many reasons explain why fewer than one in five CKD patients meeting lab indications for referral aren’t actually referred.
This can include patient preference, he noted: “Kidney disease is a disease of aging, and some patients don’t want to see a specialist or escalate their care.”
“Also, not everyone who has CKD is recommended to see a nephrologist, since primary care physicians do manage a lot of CKD as well.”
Basing referral on predicted kidney failure risk alone, a 2-year risk threshold of at least 1%, would identify a comparable number of patients (n = 72,948) as laboratory-based criteria, the team found, although they note that the patients identified using the KFRE tool would be at higher risk than those identified by lab values alone.
But when they combined the two – a minimum kidney failure risk of at least 1% over 2 years being applied to all new patients meeting lab-based referral indications, those pinpointed for nephrology referral dropped by 42.3%, from 66,276 to an estimated 38,229 patients.
“The current guidelines that just incorporate lab values identify a significant number of patients who are at low risk of developing end-stage kidney disease (ESKD), so incorporating kidney failure risk into current guidelines would target fewer patients to get to specialty care,” Dr. Duggal explained.
KFRE tool can be found online
Dr. Duggal emphasized that his findings do not change nephrology referral guidelines, but said physicians can find the KFRE tool online and use it to supplement their decision-making about a patient’s care.
“Further incorporating this [kidney failure] risk into referral practices might highlight a patient at extremely high risk who would benefit more from an interdisciplinary care team,” he said.
This could include, for example, a nutritionist to help the patient modify his or her diet. “Getting that kind of teaching process in place for a patient might be highly valuable,” he added.
Dr. Duggal disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
And combining the two methods – predicted kidney failure risk with lab values – will lead to better patient outcomes by pinpointing CKD patients who most need specialty care, said study author Vishal Duggal, MD, who was a postdoctoral fellow in medical informatics at the Veterans Affairs Palo Alto (Calif.) Health Care System while conducting the research.
“We hope this can provide guidance to primary care physicians and nephrologists to give context for their decision-making,” Dr. Duggal told this news organization.
The VA is the largest provider of CKD care in the United States, developing clinical practice guidelines for CKD management that include suggested indications for nephrology referral based on laboratory values. Laboratory values that are typically used to guide referral include estimated glomerular filtration rate (eGFR) and its rate of decline per year, as well as heavy proteinuria in patients with and without diabetes.
Dr. Duggal and colleagues – who published their findings in the American Journal of Kidney Diseases – conducted a retrospective analysis of nearly 400,000 veterans with CKD over a yearlong period to determine if referral volume would change if it was based on the estimated risk for kidney failure, rather than solely using laboratory values.
They also estimated the potential volume of nephrology referrals based on a combination of both estimated risk for kidney failure and laboratory data.
Kidney failure risk was calculated using an electronic clinical decision support tool, called Kidney Failure Risk Equation incorporating age, eGFR, gender, and urine albumin-to-creatinine ratio.
Targeting fewer patients to specialty care
Among all participants with CKD not already receiving nephrology care, more than 150,000 (41.5%) had a urine albumin or protein measurement leading to computable risk for end-stage kidney disease.
More than 66,200 patients met actual laboratory indications for referral but had not previously seen a nephrologist. Among these patients, 11,752 (17.7%) were referred to nephrology in the following year, and all had a median 2-year predicted risk for kidney failure of 1.5%.
Referred patients were more likely to meet several potential referral criteria, especially eGFR less than 30 mL/min per 1.73 m2 and heavy proteinuria. Those with heavy proteinuria with diabetes, or the eGFR indication, had the highest predicted risk for kidney failure at 2 years, at 10% and 7.1% respectively.
Boosting referral volume can be problematic if patients aren’t prioritized by need, Dr. Duggal said, noting that many reasons explain why fewer than one in five CKD patients meeting lab indications for referral aren’t actually referred.
This can include patient preference, he noted: “Kidney disease is a disease of aging, and some patients don’t want to see a specialist or escalate their care.”
“Also, not everyone who has CKD is recommended to see a nephrologist, since primary care physicians do manage a lot of CKD as well.”
Basing referral on predicted kidney failure risk alone, a 2-year risk threshold of at least 1%, would identify a comparable number of patients (n = 72,948) as laboratory-based criteria, the team found, although they note that the patients identified using the KFRE tool would be at higher risk than those identified by lab values alone.
But when they combined the two – a minimum kidney failure risk of at least 1% over 2 years being applied to all new patients meeting lab-based referral indications, those pinpointed for nephrology referral dropped by 42.3%, from 66,276 to an estimated 38,229 patients.
“The current guidelines that just incorporate lab values identify a significant number of patients who are at low risk of developing end-stage kidney disease (ESKD), so incorporating kidney failure risk into current guidelines would target fewer patients to get to specialty care,” Dr. Duggal explained.
KFRE tool can be found online
Dr. Duggal emphasized that his findings do not change nephrology referral guidelines, but said physicians can find the KFRE tool online and use it to supplement their decision-making about a patient’s care.
“Further incorporating this [kidney failure] risk into referral practices might highlight a patient at extremely high risk who would benefit more from an interdisciplinary care team,” he said.
This could include, for example, a nutritionist to help the patient modify his or her diet. “Getting that kind of teaching process in place for a patient might be highly valuable,” he added.
Dr. Duggal disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New European guidelines on CVD prevention
The new guidelines were published online Aug. 30 in the European Heart Journal to coincide with presentation at the European Stroke Congress (ESOC) 2021.
They were developed by an ESOC task force in collaboration with 12 medical societies and with special contribution of the European Association of Preventive Cardiology.
“A chief goal of the task force was to create a single CVD prevention guideline for everyone – for primary care, for hospital care, for guiding clinical practice – so one guideline for all,” said cochair of the guideline committee Frank Visseren, MD, PhD, University Medical Center Utrecht, Netherlands. “We also wanted to make a more personalized CVD prevention guideline, instead of a one-size-fits-all. In clinical practice, people are very, very different, and we really want to have a more individualized prevention guideline,” said Dr. Visseren, as well as provide “more room for shared decision-making.”
Prevention at the individual and population levels
The new guidelines also give more attention to CVD prevention in older persons. “Many of our patients are over 70 years old and we really want to have more detail, more guidance on older persons,” said Dr. Visseren.
The guideline is divided into two sections. One section covers CVD prevention at the individual level in apparently healthy people, in patients with established CVD, and in those with diabetes, familial hypercholesterolemia, or chronic kidney disease.
The other section covers CVD prevention at the population level, including public health policy, interventions, and the environment, including putting in place measures to reduce air pollution, use of fossil fuels, and limiting carbon dioxide emissions.
Targets for blood lipids, blood pressure, and glycemic control in diabetes remain in line with recent ESC guidelines on dyslipidemias, hypertension, or diabetes.
However, the guidelines introduce a new stepwise treatment-intensification approach to achieve these targets, with consideration of CVD risk, treatment benefit of risk factors, risk modifiers, comorbidities, and patient preferences.
The 2021 CVD prevention guidelines also embrace the recently published Systemic Coronary Risk Estimation 2 (SCORE2) and Systemic Coronary Risk Estimation 2-Older Persons (SCORE2-OP) algorithms. “The algorithms we are using are a bit old and we want to have more updated risk prediction, because that’s the starting point of CVD prevention,” Dr. Visseren said.
The guidelines also introduce age-specific risk thresholds for risk factor treatments in apparently healthy people and provide estimation of lifetime CVD risk and treatment benefit. This will allow clinicians to have “an informed discussion with patients on lifetime risk and potential treatment benefits,” Dr. Visseren said.
For the first time, the guidelines recommend smoking cessation regardless of whether it leads to weight gain, as weight gain does not lessen the benefits of cessation.
Regarding exercise, adults of all ages should aim for at least 150-300 minutes a week of moderate, or 75-150 minutes a week of vigorous, aerobic physical activity. The guidelines recommend reducing sedentary time and engaging in at least light activity throughout the day.
Regarding nutrition, the guidelines advise adopting a Mediterranean or similar diet; restricting alcohol intake to a maximum of 100 g per week (a standard drink is 8-14 g); eating fish, preferably fatty fish, at least once a week; and restricting consumption of meat, particularly processed meat.
Also for the first time, the guidelines state that bariatric surgery should be considered for obese individuals at elevated risk of CVD when a healthy diet and exercise fail to lead to weight loss that is maintained.
They note that individuals with mental disorders need additional attention and support to improve adherence to lifestyle changes and drug treatment.
They advise consideration of referring patients with heart disease and significant stress and anxiety to psychotherapeutic stress management to reduce stress symptoms and improve CV outcomes.
Potential cost issues that could be considered when implementing the guidelines are also reviewed.
Dr. Visseren acknowledged and thanked the task force members for continuing their work on the guidelines over the 2 “challenging” years.
Setting the bar lower?
Discussant for the guideline presentation, Diederick Grobbee, MD, University Medical Center Utrecht, who was not involved in drafting the guidelines, said he does have one conflict of interest, which is a “passion for prevention.” From that perspective, he said the guideline panel “should be applauded; the once-every-5-year issuing of the prevention guidelines is a major event.”
Dr. Grobbee noted that the working group “really tried to follow their ambitions and goals, in a way making the guidelines simpler, or perhaps setting the bar not initially as high as we used to do, which may, in fact, sometimes scare off physicians and patients alike.”
“We’ve had prevention guidelines for quite some time now, yet looking at what is accomplished in practice is sobering,” said Dr. Grobbee. Introducing a stepwise approach is “really appealing,” he added.
A version of this article first appeared on Medscape.com.
The new guidelines were published online Aug. 30 in the European Heart Journal to coincide with presentation at the European Stroke Congress (ESOC) 2021.
They were developed by an ESOC task force in collaboration with 12 medical societies and with special contribution of the European Association of Preventive Cardiology.
“A chief goal of the task force was to create a single CVD prevention guideline for everyone – for primary care, for hospital care, for guiding clinical practice – so one guideline for all,” said cochair of the guideline committee Frank Visseren, MD, PhD, University Medical Center Utrecht, Netherlands. “We also wanted to make a more personalized CVD prevention guideline, instead of a one-size-fits-all. In clinical practice, people are very, very different, and we really want to have a more individualized prevention guideline,” said Dr. Visseren, as well as provide “more room for shared decision-making.”
Prevention at the individual and population levels
The new guidelines also give more attention to CVD prevention in older persons. “Many of our patients are over 70 years old and we really want to have more detail, more guidance on older persons,” said Dr. Visseren.
The guideline is divided into two sections. One section covers CVD prevention at the individual level in apparently healthy people, in patients with established CVD, and in those with diabetes, familial hypercholesterolemia, or chronic kidney disease.
The other section covers CVD prevention at the population level, including public health policy, interventions, and the environment, including putting in place measures to reduce air pollution, use of fossil fuels, and limiting carbon dioxide emissions.
Targets for blood lipids, blood pressure, and glycemic control in diabetes remain in line with recent ESC guidelines on dyslipidemias, hypertension, or diabetes.
However, the guidelines introduce a new stepwise treatment-intensification approach to achieve these targets, with consideration of CVD risk, treatment benefit of risk factors, risk modifiers, comorbidities, and patient preferences.
The 2021 CVD prevention guidelines also embrace the recently published Systemic Coronary Risk Estimation 2 (SCORE2) and Systemic Coronary Risk Estimation 2-Older Persons (SCORE2-OP) algorithms. “The algorithms we are using are a bit old and we want to have more updated risk prediction, because that’s the starting point of CVD prevention,” Dr. Visseren said.
The guidelines also introduce age-specific risk thresholds for risk factor treatments in apparently healthy people and provide estimation of lifetime CVD risk and treatment benefit. This will allow clinicians to have “an informed discussion with patients on lifetime risk and potential treatment benefits,” Dr. Visseren said.
For the first time, the guidelines recommend smoking cessation regardless of whether it leads to weight gain, as weight gain does not lessen the benefits of cessation.
Regarding exercise, adults of all ages should aim for at least 150-300 minutes a week of moderate, or 75-150 minutes a week of vigorous, aerobic physical activity. The guidelines recommend reducing sedentary time and engaging in at least light activity throughout the day.
Regarding nutrition, the guidelines advise adopting a Mediterranean or similar diet; restricting alcohol intake to a maximum of 100 g per week (a standard drink is 8-14 g); eating fish, preferably fatty fish, at least once a week; and restricting consumption of meat, particularly processed meat.
Also for the first time, the guidelines state that bariatric surgery should be considered for obese individuals at elevated risk of CVD when a healthy diet and exercise fail to lead to weight loss that is maintained.
They note that individuals with mental disorders need additional attention and support to improve adherence to lifestyle changes and drug treatment.
They advise consideration of referring patients with heart disease and significant stress and anxiety to psychotherapeutic stress management to reduce stress symptoms and improve CV outcomes.
Potential cost issues that could be considered when implementing the guidelines are also reviewed.
Dr. Visseren acknowledged and thanked the task force members for continuing their work on the guidelines over the 2 “challenging” years.
Setting the bar lower?
Discussant for the guideline presentation, Diederick Grobbee, MD, University Medical Center Utrecht, who was not involved in drafting the guidelines, said he does have one conflict of interest, which is a “passion for prevention.” From that perspective, he said the guideline panel “should be applauded; the once-every-5-year issuing of the prevention guidelines is a major event.”
Dr. Grobbee noted that the working group “really tried to follow their ambitions and goals, in a way making the guidelines simpler, or perhaps setting the bar not initially as high as we used to do, which may, in fact, sometimes scare off physicians and patients alike.”
“We’ve had prevention guidelines for quite some time now, yet looking at what is accomplished in practice is sobering,” said Dr. Grobbee. Introducing a stepwise approach is “really appealing,” he added.
A version of this article first appeared on Medscape.com.
The new guidelines were published online Aug. 30 in the European Heart Journal to coincide with presentation at the European Stroke Congress (ESOC) 2021.
They were developed by an ESOC task force in collaboration with 12 medical societies and with special contribution of the European Association of Preventive Cardiology.
“A chief goal of the task force was to create a single CVD prevention guideline for everyone – for primary care, for hospital care, for guiding clinical practice – so one guideline for all,” said cochair of the guideline committee Frank Visseren, MD, PhD, University Medical Center Utrecht, Netherlands. “We also wanted to make a more personalized CVD prevention guideline, instead of a one-size-fits-all. In clinical practice, people are very, very different, and we really want to have a more individualized prevention guideline,” said Dr. Visseren, as well as provide “more room for shared decision-making.”
Prevention at the individual and population levels
The new guidelines also give more attention to CVD prevention in older persons. “Many of our patients are over 70 years old and we really want to have more detail, more guidance on older persons,” said Dr. Visseren.
The guideline is divided into two sections. One section covers CVD prevention at the individual level in apparently healthy people, in patients with established CVD, and in those with diabetes, familial hypercholesterolemia, or chronic kidney disease.
The other section covers CVD prevention at the population level, including public health policy, interventions, and the environment, including putting in place measures to reduce air pollution, use of fossil fuels, and limiting carbon dioxide emissions.
Targets for blood lipids, blood pressure, and glycemic control in diabetes remain in line with recent ESC guidelines on dyslipidemias, hypertension, or diabetes.
However, the guidelines introduce a new stepwise treatment-intensification approach to achieve these targets, with consideration of CVD risk, treatment benefit of risk factors, risk modifiers, comorbidities, and patient preferences.
The 2021 CVD prevention guidelines also embrace the recently published Systemic Coronary Risk Estimation 2 (SCORE2) and Systemic Coronary Risk Estimation 2-Older Persons (SCORE2-OP) algorithms. “The algorithms we are using are a bit old and we want to have more updated risk prediction, because that’s the starting point of CVD prevention,” Dr. Visseren said.
The guidelines also introduce age-specific risk thresholds for risk factor treatments in apparently healthy people and provide estimation of lifetime CVD risk and treatment benefit. This will allow clinicians to have “an informed discussion with patients on lifetime risk and potential treatment benefits,” Dr. Visseren said.
For the first time, the guidelines recommend smoking cessation regardless of whether it leads to weight gain, as weight gain does not lessen the benefits of cessation.
Regarding exercise, adults of all ages should aim for at least 150-300 minutes a week of moderate, or 75-150 minutes a week of vigorous, aerobic physical activity. The guidelines recommend reducing sedentary time and engaging in at least light activity throughout the day.
Regarding nutrition, the guidelines advise adopting a Mediterranean or similar diet; restricting alcohol intake to a maximum of 100 g per week (a standard drink is 8-14 g); eating fish, preferably fatty fish, at least once a week; and restricting consumption of meat, particularly processed meat.
Also for the first time, the guidelines state that bariatric surgery should be considered for obese individuals at elevated risk of CVD when a healthy diet and exercise fail to lead to weight loss that is maintained.
They note that individuals with mental disorders need additional attention and support to improve adherence to lifestyle changes and drug treatment.
They advise consideration of referring patients with heart disease and significant stress and anxiety to psychotherapeutic stress management to reduce stress symptoms and improve CV outcomes.
Potential cost issues that could be considered when implementing the guidelines are also reviewed.
Dr. Visseren acknowledged and thanked the task force members for continuing their work on the guidelines over the 2 “challenging” years.
Setting the bar lower?
Discussant for the guideline presentation, Diederick Grobbee, MD, University Medical Center Utrecht, who was not involved in drafting the guidelines, said he does have one conflict of interest, which is a “passion for prevention.” From that perspective, he said the guideline panel “should be applauded; the once-every-5-year issuing of the prevention guidelines is a major event.”
Dr. Grobbee noted that the working group “really tried to follow their ambitions and goals, in a way making the guidelines simpler, or perhaps setting the bar not initially as high as we used to do, which may, in fact, sometimes scare off physicians and patients alike.”
“We’ve had prevention guidelines for quite some time now, yet looking at what is accomplished in practice is sobering,” said Dr. Grobbee. Introducing a stepwise approach is “really appealing,” he added.
A version of this article first appeared on Medscape.com.
FROM ESC 2021
Toward ‘superhuman cognition’: The future of brain-computer interfaces
The brain is inarguably the most complex and mysterious organ in the human body.
As the epicenter of intelligence, mastermind of movement, and song for our senses, the brain is more than a 3-lb organ encased in shell and fluid. Rather, it is the crown jewel that defines the self and, broadly, humanity.
For decades now, researchers have been exploring the potential for connecting our own astounding biological “computer” with actual physical mainframes. These so-called “brain-computer interfaces” (BCIs) are showing promise in treating an array of conditions, including paralysis, deafness, stroke, and even psychiatric disorders.
Among the big players in this area of research is billionaire entrepreneur Elon Musk, who in 2016 founded Neuralink. The company’s short-term mission is to develop a brain-to-machine interface to help people with neurologic conditions (for example, Parkinson’s disease). The long-term mission is to steer humanity into the era of “superhuman cognition.”
But first, some neuroscience 101.
Neurons are specialized cells that transmit and receive information. The basic structure of a neuron includes the dendrite, soma, and axon. The dendrite is the signal receiver. The soma is the cell body that is connected to the dendrites and serves as a structure to pass signals. The axon, also known as the nerve fiber, transmits the signal away from the soma.
Neurons communicate with each other at the synapse (for example, axon-dendrite connection). Neurons send information to each other through action potentials. An action potential may be defined as an electric impulse that transmits down the axon, causing the release of neurotransmitters, which may consequently either inhibit or excite the next neuron (leading to the initiation of another action potential).
So how will the company and other BCI companies tap into this evolutionarily ancient system to develop an implant that will obtain and decode information output from the brain?
The Neuralink implant is composed of three parts: The Link, neural threads, and the charger.
A robotic system, controlled by a neurosurgeon, will place an implant into the brain. The Link is the central component. It processes and transmits neural signals. The micron-scale neural threads are connected to the Link and other areas of the brain. The threads also contain electrodes, which are responsible for detecting neural signals. The charger ensures the battery is charged via wireless connection.
The invasive nature of this implant allows for precise readouts of electric outputs from the brain – unlike noninvasive devices, which are less sensitive and specific. Additionally, owing to its small size, engineers and neurosurgeons can implant the device in very specific brain regions as well as customize electrode distribution.
The Neuralink implant would be paired with an application via Bluetooth connection. The goal is to enable someone with the implant to control their device or computer by simply thinking. The application offers several exercises to help guide and train individuals on how to use the implant for its intended purpose. , as well as partake in creative activities such as photography.
Existing text and speech synthesis technology are already underway. For example, Synchron, a BCI platform company, is investigating the use of Stentrode for people with severe paralysis. This neuroprosthesis was designed to help people associate thought with movement through Bluetooth technology (for example, texting, emailing, shopping, online banking). Preliminary results from a study in which the device was used for patients with amyotrophic lateral sclerosis showed improvements in functional independence via direct thinking.
Software intended to enable high-performance handwriting utilizing BCI technology is being developed by Francis R. Willett, PhD, at Stanford (Calif.) University. The technology has also shown promise.
“We’ve learned that the brain retains its ability to prescribe fine movements a full decade after the body has lost its ability to execute those movements,” says Dr. Willett, who recently reported on results from a BCI study of handwriting conversion in an individual with full-body paralysis. Through a recurrent neural networking decoding approach, the BrainGate study participant was able to type 90 characters per minute – with an impressive 94.1% raw accuracy – using thoughts alone.
Although not a fully implantable brain device, this percutaneous implant has also been studied of its capacity to restore arm function among individuals who suffered from chronic stroke. Preliminary results from the Cortimo trials, led by Mijail D. Serruya, MD, an assistant professor at Thomas Jefferson University, Philadelphia, have been positive. Researchers implanted microelectrode arrays to decode brain signals and power motor function in a participant who had experienced a stroke 2 years earlier. The participant was able to use a powered arm brace on their paralyzed arm.
Neuralink recently released a video demonstrating the use of the interface in a monkey named Pager as it played a game with a joystick. Company researchers inserted a 1024-Electrode neural recording and data transmission device called the N1 Link into the left and right motor cortices. Using the implant, neural activity was sent to a decoder algorithm. Throughout the process, the decoder algorithm was refined and calibrated. After a few minutes, Pager was able to control the cursor on the screen using his mind instead of the joystick.
Mr. Musk hopes to develop Neuralink further to change not only the way we treat neurological disorders but also the way we interact with ourselves and our environment. It’s a lofty goal to be sure, but one that doesn’t seem outside the realm of possibility in the near future.
Known unknowns: The ethical dilemmas
One major conundrum facing the future of BCI technology is that researchers don’t fully understand the science regarding how brain signaling, artificial intelligence (AI) software, and prostheses interact. Although offloading computations improves the predictive nature of AI algorithms, there are concerns of identity and personal agency.
How do we know that an action is truly the result of one’s own thinking or, rather, the outcome of AI software? In this context, the autocorrect function while typing can be incredibly useful when we’re in a pinch for time, when we’re using one hand to type, or because of ease. However, it’s also easy to create and send out unintended or inappropriate messages.
These algorithms are designed to learn from our behavior and anticipate our next move. However, a question arises as to whether we are the authors of our own thoughts or whether we are simply the device that delivers messages under the control of external forces.
“People may question whether new personality changes they experience are truly representative of themselves or whether they are now a product of the implant (e.g., ‘Is that really me?’; ‘Have I grown as a person, or is it the technology?’). This then raises questions about agency and who we are as people,” says Kerry Bowman, PhD, a clinical bioethicist and assistant professor at the Temerty Faculty of Medicine of the University of Toronto.
It’s important to have safeguards in place to ensure the privacy of our thoughts. In an age where data is currency, it’s crucial to establish boundaries to preserve our autonomy and prevent exploitation (for example, by private companies or hackers). Although Neuralink and BCIs generally are certainly pushing the boundaries of neural engineering in profound ways, it’s important to note the biological and ethical implications of this technology.
As Dr. Bowman points out, “throughout the entire human story, under the worst of human circumstances, such as captivity and torture, the one safe ground and place for all people has been the privacy of one’s own mind. No one could ever interfere, take away, or be aware of those thoughts. However, this technology challenges one’s own privacy – that this technology (and, by extension, a company) could be aware of those thoughts.”
A version of this article first appeared on Medscape.com.
The brain is inarguably the most complex and mysterious organ in the human body.
As the epicenter of intelligence, mastermind of movement, and song for our senses, the brain is more than a 3-lb organ encased in shell and fluid. Rather, it is the crown jewel that defines the self and, broadly, humanity.
For decades now, researchers have been exploring the potential for connecting our own astounding biological “computer” with actual physical mainframes. These so-called “brain-computer interfaces” (BCIs) are showing promise in treating an array of conditions, including paralysis, deafness, stroke, and even psychiatric disorders.
Among the big players in this area of research is billionaire entrepreneur Elon Musk, who in 2016 founded Neuralink. The company’s short-term mission is to develop a brain-to-machine interface to help people with neurologic conditions (for example, Parkinson’s disease). The long-term mission is to steer humanity into the era of “superhuman cognition.”
But first, some neuroscience 101.
Neurons are specialized cells that transmit and receive information. The basic structure of a neuron includes the dendrite, soma, and axon. The dendrite is the signal receiver. The soma is the cell body that is connected to the dendrites and serves as a structure to pass signals. The axon, also known as the nerve fiber, transmits the signal away from the soma.
Neurons communicate with each other at the synapse (for example, axon-dendrite connection). Neurons send information to each other through action potentials. An action potential may be defined as an electric impulse that transmits down the axon, causing the release of neurotransmitters, which may consequently either inhibit or excite the next neuron (leading to the initiation of another action potential).
So how will the company and other BCI companies tap into this evolutionarily ancient system to develop an implant that will obtain and decode information output from the brain?
The Neuralink implant is composed of three parts: The Link, neural threads, and the charger.
A robotic system, controlled by a neurosurgeon, will place an implant into the brain. The Link is the central component. It processes and transmits neural signals. The micron-scale neural threads are connected to the Link and other areas of the brain. The threads also contain electrodes, which are responsible for detecting neural signals. The charger ensures the battery is charged via wireless connection.
The invasive nature of this implant allows for precise readouts of electric outputs from the brain – unlike noninvasive devices, which are less sensitive and specific. Additionally, owing to its small size, engineers and neurosurgeons can implant the device in very specific brain regions as well as customize electrode distribution.
The Neuralink implant would be paired with an application via Bluetooth connection. The goal is to enable someone with the implant to control their device or computer by simply thinking. The application offers several exercises to help guide and train individuals on how to use the implant for its intended purpose. , as well as partake in creative activities such as photography.
Existing text and speech synthesis technology are already underway. For example, Synchron, a BCI platform company, is investigating the use of Stentrode for people with severe paralysis. This neuroprosthesis was designed to help people associate thought with movement through Bluetooth technology (for example, texting, emailing, shopping, online banking). Preliminary results from a study in which the device was used for patients with amyotrophic lateral sclerosis showed improvements in functional independence via direct thinking.
Software intended to enable high-performance handwriting utilizing BCI technology is being developed by Francis R. Willett, PhD, at Stanford (Calif.) University. The technology has also shown promise.
“We’ve learned that the brain retains its ability to prescribe fine movements a full decade after the body has lost its ability to execute those movements,” says Dr. Willett, who recently reported on results from a BCI study of handwriting conversion in an individual with full-body paralysis. Through a recurrent neural networking decoding approach, the BrainGate study participant was able to type 90 characters per minute – with an impressive 94.1% raw accuracy – using thoughts alone.
Although not a fully implantable brain device, this percutaneous implant has also been studied of its capacity to restore arm function among individuals who suffered from chronic stroke. Preliminary results from the Cortimo trials, led by Mijail D. Serruya, MD, an assistant professor at Thomas Jefferson University, Philadelphia, have been positive. Researchers implanted microelectrode arrays to decode brain signals and power motor function in a participant who had experienced a stroke 2 years earlier. The participant was able to use a powered arm brace on their paralyzed arm.
Neuralink recently released a video demonstrating the use of the interface in a monkey named Pager as it played a game with a joystick. Company researchers inserted a 1024-Electrode neural recording and data transmission device called the N1 Link into the left and right motor cortices. Using the implant, neural activity was sent to a decoder algorithm. Throughout the process, the decoder algorithm was refined and calibrated. After a few minutes, Pager was able to control the cursor on the screen using his mind instead of the joystick.
Mr. Musk hopes to develop Neuralink further to change not only the way we treat neurological disorders but also the way we interact with ourselves and our environment. It’s a lofty goal to be sure, but one that doesn’t seem outside the realm of possibility in the near future.
Known unknowns: The ethical dilemmas
One major conundrum facing the future of BCI technology is that researchers don’t fully understand the science regarding how brain signaling, artificial intelligence (AI) software, and prostheses interact. Although offloading computations improves the predictive nature of AI algorithms, there are concerns of identity and personal agency.
How do we know that an action is truly the result of one’s own thinking or, rather, the outcome of AI software? In this context, the autocorrect function while typing can be incredibly useful when we’re in a pinch for time, when we’re using one hand to type, or because of ease. However, it’s also easy to create and send out unintended or inappropriate messages.
These algorithms are designed to learn from our behavior and anticipate our next move. However, a question arises as to whether we are the authors of our own thoughts or whether we are simply the device that delivers messages under the control of external forces.
“People may question whether new personality changes they experience are truly representative of themselves or whether they are now a product of the implant (e.g., ‘Is that really me?’; ‘Have I grown as a person, or is it the technology?’). This then raises questions about agency and who we are as people,” says Kerry Bowman, PhD, a clinical bioethicist and assistant professor at the Temerty Faculty of Medicine of the University of Toronto.
It’s important to have safeguards in place to ensure the privacy of our thoughts. In an age where data is currency, it’s crucial to establish boundaries to preserve our autonomy and prevent exploitation (for example, by private companies or hackers). Although Neuralink and BCIs generally are certainly pushing the boundaries of neural engineering in profound ways, it’s important to note the biological and ethical implications of this technology.
As Dr. Bowman points out, “throughout the entire human story, under the worst of human circumstances, such as captivity and torture, the one safe ground and place for all people has been the privacy of one’s own mind. No one could ever interfere, take away, or be aware of those thoughts. However, this technology challenges one’s own privacy – that this technology (and, by extension, a company) could be aware of those thoughts.”
A version of this article first appeared on Medscape.com.
The brain is inarguably the most complex and mysterious organ in the human body.
As the epicenter of intelligence, mastermind of movement, and song for our senses, the brain is more than a 3-lb organ encased in shell and fluid. Rather, it is the crown jewel that defines the self and, broadly, humanity.
For decades now, researchers have been exploring the potential for connecting our own astounding biological “computer” with actual physical mainframes. These so-called “brain-computer interfaces” (BCIs) are showing promise in treating an array of conditions, including paralysis, deafness, stroke, and even psychiatric disorders.
Among the big players in this area of research is billionaire entrepreneur Elon Musk, who in 2016 founded Neuralink. The company’s short-term mission is to develop a brain-to-machine interface to help people with neurologic conditions (for example, Parkinson’s disease). The long-term mission is to steer humanity into the era of “superhuman cognition.”
But first, some neuroscience 101.
Neurons are specialized cells that transmit and receive information. The basic structure of a neuron includes the dendrite, soma, and axon. The dendrite is the signal receiver. The soma is the cell body that is connected to the dendrites and serves as a structure to pass signals. The axon, also known as the nerve fiber, transmits the signal away from the soma.
Neurons communicate with each other at the synapse (for example, axon-dendrite connection). Neurons send information to each other through action potentials. An action potential may be defined as an electric impulse that transmits down the axon, causing the release of neurotransmitters, which may consequently either inhibit or excite the next neuron (leading to the initiation of another action potential).
So how will the company and other BCI companies tap into this evolutionarily ancient system to develop an implant that will obtain and decode information output from the brain?
The Neuralink implant is composed of three parts: The Link, neural threads, and the charger.
A robotic system, controlled by a neurosurgeon, will place an implant into the brain. The Link is the central component. It processes and transmits neural signals. The micron-scale neural threads are connected to the Link and other areas of the brain. The threads also contain electrodes, which are responsible for detecting neural signals. The charger ensures the battery is charged via wireless connection.
The invasive nature of this implant allows for precise readouts of electric outputs from the brain – unlike noninvasive devices, which are less sensitive and specific. Additionally, owing to its small size, engineers and neurosurgeons can implant the device in very specific brain regions as well as customize electrode distribution.
The Neuralink implant would be paired with an application via Bluetooth connection. The goal is to enable someone with the implant to control their device or computer by simply thinking. The application offers several exercises to help guide and train individuals on how to use the implant for its intended purpose. , as well as partake in creative activities such as photography.
Existing text and speech synthesis technology are already underway. For example, Synchron, a BCI platform company, is investigating the use of Stentrode for people with severe paralysis. This neuroprosthesis was designed to help people associate thought with movement through Bluetooth technology (for example, texting, emailing, shopping, online banking). Preliminary results from a study in which the device was used for patients with amyotrophic lateral sclerosis showed improvements in functional independence via direct thinking.
Software intended to enable high-performance handwriting utilizing BCI technology is being developed by Francis R. Willett, PhD, at Stanford (Calif.) University. The technology has also shown promise.
“We’ve learned that the brain retains its ability to prescribe fine movements a full decade after the body has lost its ability to execute those movements,” says Dr. Willett, who recently reported on results from a BCI study of handwriting conversion in an individual with full-body paralysis. Through a recurrent neural networking decoding approach, the BrainGate study participant was able to type 90 characters per minute – with an impressive 94.1% raw accuracy – using thoughts alone.
Although not a fully implantable brain device, this percutaneous implant has also been studied of its capacity to restore arm function among individuals who suffered from chronic stroke. Preliminary results from the Cortimo trials, led by Mijail D. Serruya, MD, an assistant professor at Thomas Jefferson University, Philadelphia, have been positive. Researchers implanted microelectrode arrays to decode brain signals and power motor function in a participant who had experienced a stroke 2 years earlier. The participant was able to use a powered arm brace on their paralyzed arm.
Neuralink recently released a video demonstrating the use of the interface in a monkey named Pager as it played a game with a joystick. Company researchers inserted a 1024-Electrode neural recording and data transmission device called the N1 Link into the left and right motor cortices. Using the implant, neural activity was sent to a decoder algorithm. Throughout the process, the decoder algorithm was refined and calibrated. After a few minutes, Pager was able to control the cursor on the screen using his mind instead of the joystick.
Mr. Musk hopes to develop Neuralink further to change not only the way we treat neurological disorders but also the way we interact with ourselves and our environment. It’s a lofty goal to be sure, but one that doesn’t seem outside the realm of possibility in the near future.
Known unknowns: The ethical dilemmas
One major conundrum facing the future of BCI technology is that researchers don’t fully understand the science regarding how brain signaling, artificial intelligence (AI) software, and prostheses interact. Although offloading computations improves the predictive nature of AI algorithms, there are concerns of identity and personal agency.
How do we know that an action is truly the result of one’s own thinking or, rather, the outcome of AI software? In this context, the autocorrect function while typing can be incredibly useful when we’re in a pinch for time, when we’re using one hand to type, or because of ease. However, it’s also easy to create and send out unintended or inappropriate messages.
These algorithms are designed to learn from our behavior and anticipate our next move. However, a question arises as to whether we are the authors of our own thoughts or whether we are simply the device that delivers messages under the control of external forces.
“People may question whether new personality changes they experience are truly representative of themselves or whether they are now a product of the implant (e.g., ‘Is that really me?’; ‘Have I grown as a person, or is it the technology?’). This then raises questions about agency and who we are as people,” says Kerry Bowman, PhD, a clinical bioethicist and assistant professor at the Temerty Faculty of Medicine of the University of Toronto.
It’s important to have safeguards in place to ensure the privacy of our thoughts. In an age where data is currency, it’s crucial to establish boundaries to preserve our autonomy and prevent exploitation (for example, by private companies or hackers). Although Neuralink and BCIs generally are certainly pushing the boundaries of neural engineering in profound ways, it’s important to note the biological and ethical implications of this technology.
As Dr. Bowman points out, “throughout the entire human story, under the worst of human circumstances, such as captivity and torture, the one safe ground and place for all people has been the privacy of one’s own mind. No one could ever interfere, take away, or be aware of those thoughts. However, this technology challenges one’s own privacy – that this technology (and, by extension, a company) could be aware of those thoughts.”
A version of this article first appeared on Medscape.com.
Hospitalists address patient experience during the pandemic
Adopt strategies to communicate with compassion
A patient’s lived experience of being in the hospital is shaped by a variety of factors, according to Minesh Patel, MD, Mid-Atlantic regional medical director for the Tacoma, Wash.–based hospitalist performance company Sound Physicians. Some – but not all – of these factors are captured in the “patient experience” questions on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that is sent to randomly selected patients shortly after their discharge from the hospital.

In March 2020, the COVID-19 pandemic caused hospitals to institute quarantining measures and “no visitor” policies as doctors and other hospital staff donned masks, visors, and other emotionally distancing personal protective equipment (PPE). All of these factors impacted patients’ experience as well as their hospitals’ HCAHPS scores, Dr. Patel said. And since these policies applied to all hospitalized patients, a patient did not need to have COVID-19 to experience many of the same restrictions imposed by the pandemic.
“A lot of the care hospitalists provide involves touch, sitting down and looking at the patient eye to eye, on the same level,” said Dr. Patel, a practicing hospitalist at Frederick (Md.) Health Hospital. “That had to take a back seat to infection control.”
Meanwhile, lengths of stay were longer for COVID-19 patients, who were often very sick and alone in their hospital rooms for prolonged periods, sometimes on mechanical ventilation, isolated without the support of their families. Health care providers tried to minimize time spent at the bedside because of viral exposure risks. Nobody really knew how to treat patients’ severe respiratory distress, especially at first. “So we basically threw the kitchen sink at it, following the evolving CDC guidelines, and hoped it would work,” he explained.
“When we saw our patient experience scores plummeting across the division, we said, ‘This is not good.’ We could see that we weren’t spending as much time at the bedside, and our patients were lonely and scared.” There was also greater fragmentation of care, all of which impacted patients’ experience in partnering hospitals.
Dr. Patel and his team spearheaded a number of processes across their partner hospitals to help patients and their families get the information they needed and understand what was happening during their treatment. “At that moment, real-time feedback was essential,” he explained. “We implemented the TED protocol – Teach back, Empathy and ‘Double-backing,’ which means spending a shorter visit on morning rounds but going back to the patient’s bedside for a second daily visit at the end of the shift, thereby establishing a second touch point.” Teach back is a strategy of asking patients to repeat back in their own words what they understood the doctor to be saying about their care.
The group developed ID buttons – called “Suttons” or Sound Buttons – with a larger picture of the doctor’s smiling face pinned to their medical gowns. The hospitalists started scheduling Zoom calls with families from the ICU rooms of COVID-19 patients. “We employ clinical performance nurses as collaborative influencers. They visit patients’ bedsides and work with staff on improving patient experience,” Dr. Patel said. “And we printed thank-you cards with the doctor’s name, photo, and an individualized message for their patients.” Together these measures measurably improved patient experience scores across partnering hospitals.
What is patient experience?
Evaluated by the Agency for Healthcare Research and Quality and endorsed by the National Quality Forum, HCAHPS hospital quality surveys ask patients (or their family members, who may be the ones completing the survey) 29 well-tested questions about the recent hospital stay and how they experienced it. Nineteen of those questions explore critical aspects of the patient’s experience in areas such as communication, responsiveness of staff, information about their diagnosis, medications, and discharge – and if they would recommend the hospital to others.
Surveys can be done by mail, phone, or interactive voice recognition and are offered in seven different languages. They can be administered by the hospital itself or by an approved survey vendor. They are sent between 48 hours and 6 weeks after the patient’s hospital discharge.
Nationwide results from HCAHPS survey have been published since 2008 in a searchable, comparable format on the consumer-focused government website Hospital Compare. The data have been used in a value-based incentive purchasing program since 2012. Hospital Compare also incorporates measures of quality such as mortality, readmission, and hospital-acquired infection rates as well as process measures such as how well facilities provide recommended care.
Starting in 2016, overall hospital quality has been encapsulated in a Star rating, which summarizes a variety of measures across seven areas of quality into a single number from one to five for each hospital. One of those seven areas is patient experience.
Hospitals may choose to ask additional questions of their own along with the HCAHPS survey, to gather additional, actionable quality data for internal purposes. Internal surveys with results closer to real time, instead of the months-to-years lag in posting HCAHPS scores, enable the hospital to respond to issues that emerge.
It’s not just the scores
“A lot of leaders in the hospital business will tell you ‘It’s not about the scores,’ ” Dr. Patel related. “But you need scores to tell how your practice is doing. It’s a testament to the kind of care you are providing as a hospital medicine program. These are important questions: Did your doctor listen to you, communicate in ways you understood, and treat you with courtesy?” Scores are scores, he said, but more importantly, are patients getting the information they need? Do they understand what’s going on in their care?
“You have to look at the scores and ask, what can we do differently to impact patient experience? What are we doing wrong? What can we do better? If the scores as a collective experience of hospitalized patients are plummeting, it must mean they’re not feeling good about the care they are receiving, and not recognizing what we’re trying to do for them.”
Declining HCAHPS scores last year could easily be explained by what was going on with COVID-19, Dr. Patel said. “But we want our patient experience to be seamless. We have to put ourselves in the patient’s shoes. For them, it’s about whether they felt they were treated well or not. We had to reinvent ourselves and find new ways to compensate for the limitations imposed by the pandemic,” he said.
“We also recognized that our No. 1 job as a group is to take care of our doctors, so that they can take care of their patients. We provided quarantine pay, implemented a buddy system for doctors, used CME dollars to pay for COVID education and, if they felt ill, we said they needed to stay home, while we paid their shift anyway,” he said. “When you do that kind of thing and engage them in your mission, frontline hospitalists can help to improve quality of care, decrease costs, and increase patient safety.”
A sacred encounter
For Sarah Richards, MD, a hospitalist with Nebraska Medicine in Omaha, what happens in the hospital room between the hospitalist and the patient is a sacred encounter. “It’s about relationship and trust,” she said, noting that it’s hard to capture all of that in survey data. It might be better expressed in words: “ ‘How are things going for you?’ To me, that’s the real patient experience. When I talk with physicians about patient experience, I start with why this matters. We know, for example, that when patients trust us, they are more likely to engage with their care and adhere to the treatment plan.”

Dr. Richards said standard hospital quality surveys can be a blunt tool. The HCAHPS survey, conducted around a week after the hospitalization, has a low response rate, and returns are not representative of the demographic served in the hospital. “The inpatient data are not always helpful, but this is what we have to work with. One choice hospitals have is for the leadership to choose not to use the data for individual bonuses, recognition, or discipline, since the questions ask patients about the care they received collectively from all of their doctors,” she said.
But as hospitalists have worked longer shifts under more stress while wearing PPE – which makes it harder to communicate with their patients – there is a dynamic that has emerged, which deserves more study. “I think doctors gave it their all in the pandemic. I’m a hospitalist, and people told me I’m a hero. But did that change my impact at work (on patient experience)?” she said.
Dr. Richards sits on SHM’s Patient Experience Special Interest Group (SIG), which was tasked with providing tools to help mitigate the effects of the pandemic. These include a fact sheet, “Communication Tips for 5 Common Conundrums in the COVID-19 Pandemic”, and a downloadable pocket card called “The 5 Rs of Cultural Humility.”
Also on the SIG is Mark Rudolph, MD, SFHM, Sound Physicians’ chief experience officer, whose job title reflects a growing, systematic attention to patient experience in U.S. hospitals. “Most clinicians are familiar with the surveys and the results of those surveys,” he told The Hospitalist. “People in our field can get frustrated with the surveys, and have a lot to say about the quality of the scores themselves – what is actually being measured. Is the patient upset because the coffee was cold, or due to a bad clinical experience? Is it about the care they received from the hospitalist, or the physical setting of the hospital?”
Doing the right thing
To be a patient hospitalized with an acute illness is a form of suffering, Dr. Rudolph said. “We know patient experience in the hospital since March of 2020 has been frightening and horrible. These people are as sick as can be. Everything about the experience is horrible. Every effort you can make to reduce that suffering is important. If you are a patient in the hospital and don’t know what’s happening to you, that’s terrifying.”

He encourages hospitalists to look beyond the scores or the idea that they are just trying to improve their scores. “Look instead at the actual content of the questions around communication with doctors. The competencies addressed in the survey questions – listening and explaining things clearly, for example – are effective guides for patient experience improvement efforts. You can be confident you’re doing the right thing for the patient by focusing on these skills, even if you don’t see immediate changes in survey scores.”
Hospitals that did not allow visitors had worse clinical outcomes and worse patient experience ratings, and recent research confirms that when family visitors are not allowed, outcomes are worse in areas such as patient ratings of medical staff responsiveness, fall rates, and sepsis rates.1 “None of that should be surprising. Not having family present just ups the ante. Any hospital patients could benefit from an advocate sitting next to them, helping them to the bathroom, and keeping them from falling out of bed,” Dr. Rudolph said.
“In the past year, we have placed a premium on communicating with these patients with kindness and compassion, to help them understand what’s happening to them,” he said. Out of necessity, hospitals have had to rejigger their processes, which has led to more efficient and better care, although the jury is still out on whether that will persist post pandemic.
Communicating with compassion
Swati Mehta, MD, a hospitalist at Sequoia Hospital in Redwood City, Calif., and director of quality performance and patient experience at Vituity, a physician-owned and -led multispecialty partnership, said COVID-19 was a wake-up call for hospitalists. There have been successful models for enhancing hospitalized patients’ experience, but it took the challenges of COVID-19 for many hospitalists to adopt them.

“Early in 2020, our data analysis showed emerging positive trends, reflecting our patients’ appreciation for what doctors were doing in the crisis and awareness of the challenges they faced. But after that uptick, global measures and national data showed drops for health care organizations and providers. Patients’ expectations were not being met. We needed to respond and meet patients where they were at. We needed to do things differently,” she said.
Keeping patients well informed and treating them with respect are paramount – and more important than ever – as reflected in Dr. Mehta’s “6H” model to promote a human connection between doctors and patients.2 As chair of SHM’s Patient Experience SIG, she led the creation of COVID-19–specific communication tips for hospitalists based on the 6H model. “I’m very committed to treating patients with compassion,” she said.
For Vituity, those approaches included making greater use of the hospital at home model for patients who reported to the emergency department but met certain criteria for discharge. They would be sent home with daily nursing visits and 24-hour virtual access to hospitalists. Vituity hospitalists also worked more closely with emergency departments to provide emergency psychiatric interventions for anxious patients, and with primary care physicians. Patient care navigators helped to enhance transitions of care. In addition, their hospitalist team added personalized pictures over their gowns so patients could see the hospitalists’ faces despite PPE.
Another Vituity innovation was virtual rounding, with iPads in the patient’s room and the physician in another room. “I did telerounds at our Redwood City hospital with patients with COVID who were very lonely, anxious, and afraid because they couldn’t have family visitors,” Dr. Mehta said. Telerounds offered greater protection and safety for both providers and patients, reduced the need for PPE, and improved collaboration with the nursing team, primary care providers, and families.
A recent perspective published in the New England Journal of Medicine suggests that the Zoom family conference may offer distinct advantages over in-person family conferences.3 It allows for greater participation by primary care clinicians who knew the patient before the current hospitalization and thus might have important contributions to discharge plans.
The pandemic stimulated many hospitals to take a closer look at all areas of their service delivery, Dr. Rudolph concluded. “We’ve made big changes with a lot of fearlessness in a short amount of time, which is not typical for hospitals. We showed that the pace of innovation can be faster if we lower the threshold of risk.”
References
1. Silvera GA et al. The influence of COVID-19 visitation restrictions on patient experience and safety outcomes: A critical role for subjective advocates. Patient Experience Journal. 8(1) doi: 10.35680/2372-0247.1596.
2. Mehta S. How to truly connect with your patients: Introducing the ‘6H model.’ The Hospitalist. 2020 Aug 14.
3. Lee TH. Zoom family meeting. N Engl J Med. 2021 Apr 29;384(17):1586-7.
Adopt strategies to communicate with compassion
Adopt strategies to communicate with compassion
A patient’s lived experience of being in the hospital is shaped by a variety of factors, according to Minesh Patel, MD, Mid-Atlantic regional medical director for the Tacoma, Wash.–based hospitalist performance company Sound Physicians. Some – but not all – of these factors are captured in the “patient experience” questions on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that is sent to randomly selected patients shortly after their discharge from the hospital.
In March 2020, the COVID-19 pandemic caused hospitals to institute quarantining measures and “no visitor” policies as doctors and other hospital staff donned masks, visors, and other emotionally distancing personal protective equipment (PPE). All of these factors impacted patients’ experience as well as their hospitals’ HCAHPS scores, Dr. Patel said. And since these policies applied to all hospitalized patients, a patient did not need to have COVID-19 to experience many of the same restrictions imposed by the pandemic.
“A lot of the care hospitalists provide involves touch, sitting down and looking at the patient eye to eye, on the same level,” said Dr. Patel, a practicing hospitalist at Frederick (Md.) Health Hospital. “That had to take a back seat to infection control.”
Meanwhile, lengths of stay were longer for COVID-19 patients, who were often very sick and alone in their hospital rooms for prolonged periods, sometimes on mechanical ventilation, isolated without the support of their families. Health care providers tried to minimize time spent at the bedside because of viral exposure risks. Nobody really knew how to treat patients’ severe respiratory distress, especially at first. “So we basically threw the kitchen sink at it, following the evolving CDC guidelines, and hoped it would work,” he explained.
“When we saw our patient experience scores plummeting across the division, we said, ‘This is not good.’ We could see that we weren’t spending as much time at the bedside, and our patients were lonely and scared.” There was also greater fragmentation of care, all of which impacted patients’ experience in partnering hospitals.
Dr. Patel and his team spearheaded a number of processes across their partner hospitals to help patients and their families get the information they needed and understand what was happening during their treatment. “At that moment, real-time feedback was essential,” he explained. “We implemented the TED protocol – Teach back, Empathy and ‘Double-backing,’ which means spending a shorter visit on morning rounds but going back to the patient’s bedside for a second daily visit at the end of the shift, thereby establishing a second touch point.” Teach back is a strategy of asking patients to repeat back in their own words what they understood the doctor to be saying about their care.
The group developed ID buttons – called “Suttons” or Sound Buttons – with a larger picture of the doctor’s smiling face pinned to their medical gowns. The hospitalists started scheduling Zoom calls with families from the ICU rooms of COVID-19 patients. “We employ clinical performance nurses as collaborative influencers. They visit patients’ bedsides and work with staff on improving patient experience,” Dr. Patel said. “And we printed thank-you cards with the doctor’s name, photo, and an individualized message for their patients.” Together these measures measurably improved patient experience scores across partnering hospitals.
What is patient experience?
Evaluated by the Agency for Healthcare Research and Quality and endorsed by the National Quality Forum, HCAHPS hospital quality surveys ask patients (or their family members, who may be the ones completing the survey) 29 well-tested questions about the recent hospital stay and how they experienced it. Nineteen of those questions explore critical aspects of the patient’s experience in areas such as communication, responsiveness of staff, information about their diagnosis, medications, and discharge – and if they would recommend the hospital to others.
Surveys can be done by mail, phone, or interactive voice recognition and are offered in seven different languages. They can be administered by the hospital itself or by an approved survey vendor. They are sent between 48 hours and 6 weeks after the patient’s hospital discharge.
Nationwide results from HCAHPS survey have been published since 2008 in a searchable, comparable format on the consumer-focused government website Hospital Compare. The data have been used in a value-based incentive purchasing program since 2012. Hospital Compare also incorporates measures of quality such as mortality, readmission, and hospital-acquired infection rates as well as process measures such as how well facilities provide recommended care.
Starting in 2016, overall hospital quality has been encapsulated in a Star rating, which summarizes a variety of measures across seven areas of quality into a single number from one to five for each hospital. One of those seven areas is patient experience.
Hospitals may choose to ask additional questions of their own along with the HCAHPS survey, to gather additional, actionable quality data for internal purposes. Internal surveys with results closer to real time, instead of the months-to-years lag in posting HCAHPS scores, enable the hospital to respond to issues that emerge.
It’s not just the scores
“A lot of leaders in the hospital business will tell you ‘It’s not about the scores,’ ” Dr. Patel related. “But you need scores to tell how your practice is doing. It’s a testament to the kind of care you are providing as a hospital medicine program. These are important questions: Did your doctor listen to you, communicate in ways you understood, and treat you with courtesy?” Scores are scores, he said, but more importantly, are patients getting the information they need? Do they understand what’s going on in their care?
“You have to look at the scores and ask, what can we do differently to impact patient experience? What are we doing wrong? What can we do better? If the scores as a collective experience of hospitalized patients are plummeting, it must mean they’re not feeling good about the care they are receiving, and not recognizing what we’re trying to do for them.”
Declining HCAHPS scores last year could easily be explained by what was going on with COVID-19, Dr. Patel said. “But we want our patient experience to be seamless. We have to put ourselves in the patient’s shoes. For them, it’s about whether they felt they were treated well or not. We had to reinvent ourselves and find new ways to compensate for the limitations imposed by the pandemic,” he said.
“We also recognized that our No. 1 job as a group is to take care of our doctors, so that they can take care of their patients. We provided quarantine pay, implemented a buddy system for doctors, used CME dollars to pay for COVID education and, if they felt ill, we said they needed to stay home, while we paid their shift anyway,” he said. “When you do that kind of thing and engage them in your mission, frontline hospitalists can help to improve quality of care, decrease costs, and increase patient safety.”
A sacred encounter
For Sarah Richards, MD, a hospitalist with Nebraska Medicine in Omaha, what happens in the hospital room between the hospitalist and the patient is a sacred encounter. “It’s about relationship and trust,” she said, noting that it’s hard to capture all of that in survey data. It might be better expressed in words: “ ‘How are things going for you?’ To me, that’s the real patient experience. When I talk with physicians about patient experience, I start with why this matters. We know, for example, that when patients trust us, they are more likely to engage with their care and adhere to the treatment plan.”
Dr. Richards said standard hospital quality surveys can be a blunt tool. The HCAHPS survey, conducted around a week after the hospitalization, has a low response rate, and returns are not representative of the demographic served in the hospital. “The inpatient data are not always helpful, but this is what we have to work with. One choice hospitals have is for the leadership to choose not to use the data for individual bonuses, recognition, or discipline, since the questions ask patients about the care they received collectively from all of their doctors,” she said.
But as hospitalists have worked longer shifts under more stress while wearing PPE – which makes it harder to communicate with their patients – there is a dynamic that has emerged, which deserves more study. “I think doctors gave it their all in the pandemic. I’m a hospitalist, and people told me I’m a hero. But did that change my impact at work (on patient experience)?” she said.
Dr. Richards sits on SHM’s Patient Experience Special Interest Group (SIG), which was tasked with providing tools to help mitigate the effects of the pandemic. These include a fact sheet, “Communication Tips for 5 Common Conundrums in the COVID-19 Pandemic”, and a downloadable pocket card called “The 5 Rs of Cultural Humility.”
Also on the SIG is Mark Rudolph, MD, SFHM, Sound Physicians’ chief experience officer, whose job title reflects a growing, systematic attention to patient experience in U.S. hospitals. “Most clinicians are familiar with the surveys and the results of those surveys,” he told The Hospitalist. “People in our field can get frustrated with the surveys, and have a lot to say about the quality of the scores themselves – what is actually being measured. Is the patient upset because the coffee was cold, or due to a bad clinical experience? Is it about the care they received from the hospitalist, or the physical setting of the hospital?”
Doing the right thing
To be a patient hospitalized with an acute illness is a form of suffering, Dr. Rudolph said. “We know patient experience in the hospital since March of 2020 has been frightening and horrible. These people are as sick as can be. Everything about the experience is horrible. Every effort you can make to reduce that suffering is important. If you are a patient in the hospital and don’t know what’s happening to you, that’s terrifying.”
He encourages hospitalists to look beyond the scores or the idea that they are just trying to improve their scores. “Look instead at the actual content of the questions around communication with doctors. The competencies addressed in the survey questions – listening and explaining things clearly, for example – are effective guides for patient experience improvement efforts. You can be confident you’re doing the right thing for the patient by focusing on these skills, even if you don’t see immediate changes in survey scores.”
Hospitals that did not allow visitors had worse clinical outcomes and worse patient experience ratings, and recent research confirms that when family visitors are not allowed, outcomes are worse in areas such as patient ratings of medical staff responsiveness, fall rates, and sepsis rates.1 “None of that should be surprising. Not having family present just ups the ante. Any hospital patients could benefit from an advocate sitting next to them, helping them to the bathroom, and keeping them from falling out of bed,” Dr. Rudolph said.
“In the past year, we have placed a premium on communicating with these patients with kindness and compassion, to help them understand what’s happening to them,” he said. Out of necessity, hospitals have had to rejigger their processes, which has led to more efficient and better care, although the jury is still out on whether that will persist post pandemic.
Communicating with compassion
Swati Mehta, MD, a hospitalist at Sequoia Hospital in Redwood City, Calif., and director of quality performance and patient experience at Vituity, a physician-owned and -led multispecialty partnership, said COVID-19 was a wake-up call for hospitalists. There have been successful models for enhancing hospitalized patients’ experience, but it took the challenges of COVID-19 for many hospitalists to adopt them.
“Early in 2020, our data analysis showed emerging positive trends, reflecting our patients’ appreciation for what doctors were doing in the crisis and awareness of the challenges they faced. But after that uptick, global measures and national data showed drops for health care organizations and providers. Patients’ expectations were not being met. We needed to respond and meet patients where they were at. We needed to do things differently,” she said.
Keeping patients well informed and treating them with respect are paramount – and more important than ever – as reflected in Dr. Mehta’s “6H” model to promote a human connection between doctors and patients.2 As chair of SHM’s Patient Experience SIG, she led the creation of COVID-19–specific communication tips for hospitalists based on the 6H model. “I’m very committed to treating patients with compassion,” she said.
For Vituity, those approaches included making greater use of the hospital at home model for patients who reported to the emergency department but met certain criteria for discharge. They would be sent home with daily nursing visits and 24-hour virtual access to hospitalists. Vituity hospitalists also worked more closely with emergency departments to provide emergency psychiatric interventions for anxious patients, and with primary care physicians. Patient care navigators helped to enhance transitions of care. In addition, their hospitalist team added personalized pictures over their gowns so patients could see the hospitalists’ faces despite PPE.
Another Vituity innovation was virtual rounding, with iPads in the patient’s room and the physician in another room. “I did telerounds at our Redwood City hospital with patients with COVID who were very lonely, anxious, and afraid because they couldn’t have family visitors,” Dr. Mehta said. Telerounds offered greater protection and safety for both providers and patients, reduced the need for PPE, and improved collaboration with the nursing team, primary care providers, and families.
A recent perspective published in the New England Journal of Medicine suggests that the Zoom family conference may offer distinct advantages over in-person family conferences.3 It allows for greater participation by primary care clinicians who knew the patient before the current hospitalization and thus might have important contributions to discharge plans.
The pandemic stimulated many hospitals to take a closer look at all areas of their service delivery, Dr. Rudolph concluded. “We’ve made big changes with a lot of fearlessness in a short amount of time, which is not typical for hospitals. We showed that the pace of innovation can be faster if we lower the threshold of risk.”
References
1. Silvera GA et al. The influence of COVID-19 visitation restrictions on patient experience and safety outcomes: A critical role for subjective advocates. Patient Experience Journal. 8(1) doi: 10.35680/2372-0247.1596.
2. Mehta S. How to truly connect with your patients: Introducing the ‘6H model.’ The Hospitalist. 2020 Aug 14.
3. Lee TH. Zoom family meeting. N Engl J Med. 2021 Apr 29;384(17):1586-7.
A patient’s lived experience of being in the hospital is shaped by a variety of factors, according to Minesh Patel, MD, Mid-Atlantic regional medical director for the Tacoma, Wash.–based hospitalist performance company Sound Physicians. Some – but not all – of these factors are captured in the “patient experience” questions on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that is sent to randomly selected patients shortly after their discharge from the hospital.
In March 2020, the COVID-19 pandemic caused hospitals to institute quarantining measures and “no visitor” policies as doctors and other hospital staff donned masks, visors, and other emotionally distancing personal protective equipment (PPE). All of these factors impacted patients’ experience as well as their hospitals’ HCAHPS scores, Dr. Patel said. And since these policies applied to all hospitalized patients, a patient did not need to have COVID-19 to experience many of the same restrictions imposed by the pandemic.
“A lot of the care hospitalists provide involves touch, sitting down and looking at the patient eye to eye, on the same level,” said Dr. Patel, a practicing hospitalist at Frederick (Md.) Health Hospital. “That had to take a back seat to infection control.”
Meanwhile, lengths of stay were longer for COVID-19 patients, who were often very sick and alone in their hospital rooms for prolonged periods, sometimes on mechanical ventilation, isolated without the support of their families. Health care providers tried to minimize time spent at the bedside because of viral exposure risks. Nobody really knew how to treat patients’ severe respiratory distress, especially at first. “So we basically threw the kitchen sink at it, following the evolving CDC guidelines, and hoped it would work,” he explained.
“When we saw our patient experience scores plummeting across the division, we said, ‘This is not good.’ We could see that we weren’t spending as much time at the bedside, and our patients were lonely and scared.” There was also greater fragmentation of care, all of which impacted patients’ experience in partnering hospitals.
Dr. Patel and his team spearheaded a number of processes across their partner hospitals to help patients and their families get the information they needed and understand what was happening during their treatment. “At that moment, real-time feedback was essential,” he explained. “We implemented the TED protocol – Teach back, Empathy and ‘Double-backing,’ which means spending a shorter visit on morning rounds but going back to the patient’s bedside for a second daily visit at the end of the shift, thereby establishing a second touch point.” Teach back is a strategy of asking patients to repeat back in their own words what they understood the doctor to be saying about their care.
The group developed ID buttons – called “Suttons” or Sound Buttons – with a larger picture of the doctor’s smiling face pinned to their medical gowns. The hospitalists started scheduling Zoom calls with families from the ICU rooms of COVID-19 patients. “We employ clinical performance nurses as collaborative influencers. They visit patients’ bedsides and work with staff on improving patient experience,” Dr. Patel said. “And we printed thank-you cards with the doctor’s name, photo, and an individualized message for their patients.” Together these measures measurably improved patient experience scores across partnering hospitals.
What is patient experience?
Evaluated by the Agency for Healthcare Research and Quality and endorsed by the National Quality Forum, HCAHPS hospital quality surveys ask patients (or their family members, who may be the ones completing the survey) 29 well-tested questions about the recent hospital stay and how they experienced it. Nineteen of those questions explore critical aspects of the patient’s experience in areas such as communication, responsiveness of staff, information about their diagnosis, medications, and discharge – and if they would recommend the hospital to others.
Surveys can be done by mail, phone, or interactive voice recognition and are offered in seven different languages. They can be administered by the hospital itself or by an approved survey vendor. They are sent between 48 hours and 6 weeks after the patient’s hospital discharge.
Nationwide results from HCAHPS survey have been published since 2008 in a searchable, comparable format on the consumer-focused government website Hospital Compare. The data have been used in a value-based incentive purchasing program since 2012. Hospital Compare also incorporates measures of quality such as mortality, readmission, and hospital-acquired infection rates as well as process measures such as how well facilities provide recommended care.
Starting in 2016, overall hospital quality has been encapsulated in a Star rating, which summarizes a variety of measures across seven areas of quality into a single number from one to five for each hospital. One of those seven areas is patient experience.
Hospitals may choose to ask additional questions of their own along with the HCAHPS survey, to gather additional, actionable quality data for internal purposes. Internal surveys with results closer to real time, instead of the months-to-years lag in posting HCAHPS scores, enable the hospital to respond to issues that emerge.
It’s not just the scores
“A lot of leaders in the hospital business will tell you ‘It’s not about the scores,’ ” Dr. Patel related. “But you need scores to tell how your practice is doing. It’s a testament to the kind of care you are providing as a hospital medicine program. These are important questions: Did your doctor listen to you, communicate in ways you understood, and treat you with courtesy?” Scores are scores, he said, but more importantly, are patients getting the information they need? Do they understand what’s going on in their care?
“You have to look at the scores and ask, what can we do differently to impact patient experience? What are we doing wrong? What can we do better? If the scores as a collective experience of hospitalized patients are plummeting, it must mean they’re not feeling good about the care they are receiving, and not recognizing what we’re trying to do for them.”
Declining HCAHPS scores last year could easily be explained by what was going on with COVID-19, Dr. Patel said. “But we want our patient experience to be seamless. We have to put ourselves in the patient’s shoes. For them, it’s about whether they felt they were treated well or not. We had to reinvent ourselves and find new ways to compensate for the limitations imposed by the pandemic,” he said.
“We also recognized that our No. 1 job as a group is to take care of our doctors, so that they can take care of their patients. We provided quarantine pay, implemented a buddy system for doctors, used CME dollars to pay for COVID education and, if they felt ill, we said they needed to stay home, while we paid their shift anyway,” he said. “When you do that kind of thing and engage them in your mission, frontline hospitalists can help to improve quality of care, decrease costs, and increase patient safety.”
A sacred encounter
For Sarah Richards, MD, a hospitalist with Nebraska Medicine in Omaha, what happens in the hospital room between the hospitalist and the patient is a sacred encounter. “It’s about relationship and trust,” she said, noting that it’s hard to capture all of that in survey data. It might be better expressed in words: “ ‘How are things going for you?’ To me, that’s the real patient experience. When I talk with physicians about patient experience, I start with why this matters. We know, for example, that when patients trust us, they are more likely to engage with their care and adhere to the treatment plan.”
Dr. Richards said standard hospital quality surveys can be a blunt tool. The HCAHPS survey, conducted around a week after the hospitalization, has a low response rate, and returns are not representative of the demographic served in the hospital. “The inpatient data are not always helpful, but this is what we have to work with. One choice hospitals have is for the leadership to choose not to use the data for individual bonuses, recognition, or discipline, since the questions ask patients about the care they received collectively from all of their doctors,” she said.
But as hospitalists have worked longer shifts under more stress while wearing PPE – which makes it harder to communicate with their patients – there is a dynamic that has emerged, which deserves more study. “I think doctors gave it their all in the pandemic. I’m a hospitalist, and people told me I’m a hero. But did that change my impact at work (on patient experience)?” she said.
Dr. Richards sits on SHM’s Patient Experience Special Interest Group (SIG), which was tasked with providing tools to help mitigate the effects of the pandemic. These include a fact sheet, “Communication Tips for 5 Common Conundrums in the COVID-19 Pandemic”, and a downloadable pocket card called “The 5 Rs of Cultural Humility.”
Also on the SIG is Mark Rudolph, MD, SFHM, Sound Physicians’ chief experience officer, whose job title reflects a growing, systematic attention to patient experience in U.S. hospitals. “Most clinicians are familiar with the surveys and the results of those surveys,” he told The Hospitalist. “People in our field can get frustrated with the surveys, and have a lot to say about the quality of the scores themselves – what is actually being measured. Is the patient upset because the coffee was cold, or due to a bad clinical experience? Is it about the care they received from the hospitalist, or the physical setting of the hospital?”
Doing the right thing
To be a patient hospitalized with an acute illness is a form of suffering, Dr. Rudolph said. “We know patient experience in the hospital since March of 2020 has been frightening and horrible. These people are as sick as can be. Everything about the experience is horrible. Every effort you can make to reduce that suffering is important. If you are a patient in the hospital and don’t know what’s happening to you, that’s terrifying.”
He encourages hospitalists to look beyond the scores or the idea that they are just trying to improve their scores. “Look instead at the actual content of the questions around communication with doctors. The competencies addressed in the survey questions – listening and explaining things clearly, for example – are effective guides for patient experience improvement efforts. You can be confident you’re doing the right thing for the patient by focusing on these skills, even if you don’t see immediate changes in survey scores.”
Hospitals that did not allow visitors had worse clinical outcomes and worse patient experience ratings, and recent research confirms that when family visitors are not allowed, outcomes are worse in areas such as patient ratings of medical staff responsiveness, fall rates, and sepsis rates.1 “None of that should be surprising. Not having family present just ups the ante. Any hospital patients could benefit from an advocate sitting next to them, helping them to the bathroom, and keeping them from falling out of bed,” Dr. Rudolph said.
“In the past year, we have placed a premium on communicating with these patients with kindness and compassion, to help them understand what’s happening to them,” he said. Out of necessity, hospitals have had to rejigger their processes, which has led to more efficient and better care, although the jury is still out on whether that will persist post pandemic.
Communicating with compassion
Swati Mehta, MD, a hospitalist at Sequoia Hospital in Redwood City, Calif., and director of quality performance and patient experience at Vituity, a physician-owned and -led multispecialty partnership, said COVID-19 was a wake-up call for hospitalists. There have been successful models for enhancing hospitalized patients’ experience, but it took the challenges of COVID-19 for many hospitalists to adopt them.
“Early in 2020, our data analysis showed emerging positive trends, reflecting our patients’ appreciation for what doctors were doing in the crisis and awareness of the challenges they faced. But after that uptick, global measures and national data showed drops for health care organizations and providers. Patients’ expectations were not being met. We needed to respond and meet patients where they were at. We needed to do things differently,” she said.
Keeping patients well informed and treating them with respect are paramount – and more important than ever – as reflected in Dr. Mehta’s “6H” model to promote a human connection between doctors and patients.2 As chair of SHM’s Patient Experience SIG, she led the creation of COVID-19–specific communication tips for hospitalists based on the 6H model. “I’m very committed to treating patients with compassion,” she said.
For Vituity, those approaches included making greater use of the hospital at home model for patients who reported to the emergency department but met certain criteria for discharge. They would be sent home with daily nursing visits and 24-hour virtual access to hospitalists. Vituity hospitalists also worked more closely with emergency departments to provide emergency psychiatric interventions for anxious patients, and with primary care physicians. Patient care navigators helped to enhance transitions of care. In addition, their hospitalist team added personalized pictures over their gowns so patients could see the hospitalists’ faces despite PPE.
Another Vituity innovation was virtual rounding, with iPads in the patient’s room and the physician in another room. “I did telerounds at our Redwood City hospital with patients with COVID who were very lonely, anxious, and afraid because they couldn’t have family visitors,” Dr. Mehta said. Telerounds offered greater protection and safety for both providers and patients, reduced the need for PPE, and improved collaboration with the nursing team, primary care providers, and families.
A recent perspective published in the New England Journal of Medicine suggests that the Zoom family conference may offer distinct advantages over in-person family conferences.3 It allows for greater participation by primary care clinicians who knew the patient before the current hospitalization and thus might have important contributions to discharge plans.
The pandemic stimulated many hospitals to take a closer look at all areas of their service delivery, Dr. Rudolph concluded. “We’ve made big changes with a lot of fearlessness in a short amount of time, which is not typical for hospitals. We showed that the pace of innovation can be faster if we lower the threshold of risk.”
References
1. Silvera GA et al. The influence of COVID-19 visitation restrictions on patient experience and safety outcomes: A critical role for subjective advocates. Patient Experience Journal. 8(1) doi: 10.35680/2372-0247.1596.
2. Mehta S. How to truly connect with your patients: Introducing the ‘6H model.’ The Hospitalist. 2020 Aug 14.
3. Lee TH. Zoom family meeting. N Engl J Med. 2021 Apr 29;384(17):1586-7.
Teleintegrated versus telereferral care for complex psychiatric disorders
Two models for treating patients with complex psychiatric disorders in primary care are equally effective, new research suggests.

Results from a pragmatic, randomized comparative effectiveness study involving more than 1,000 patients showed that both integrated telepsychiatry collaborative care (TCC) and telepsychiatry/telepsychology enhanced referral (TER) provided “significantly and substantially” improved clinical outcomes, researchers noted.
However, the referral model required substantially more mental health specialist time than does the integrated model.
Therefore, ,” lead author John Fortney, PhD, department of psychiatry and behavioral sciences, University of Washington, Seattle, told this news organization.
The findings were published online Aug. 25 in JAMA Psychiatry.
Clinically meaningful improvement
The Study to Promote Innovation in Rural Integrated Telepsychiatry (SPIRIT) trial included 1,004 adults with untreated posttraumatic stress disorder and/or bipolar disorder. The participants were from 24 primary care clinics in rural and underserved areas in which there were no on-site psychiatrists or psychologists.
In SPIRIT, 508 patients were randomly allocated to TCC, and 496 were assigned to TER.
With TCC, an on-site behavioral health care manager and an off-site telepsychiatrist consultant support the primary care clinician in prescribing medications. With TER, an off-site telepsychiatrist prescribes medication, and an off-site telepsychologist delivers therapy.
The primary outcome was mental health functioning at 12 months, as measured by the Veterans RAND 12-item Health Survey Mental Component Summary (MCS) score. MSC scores range from 0 to 100.
Baseline MCS scores for the study participants were two standard deviations below the national average. The mean MCS scores were 39.7 and 41.2 in the TCC and TER groups, respectively.
There was no significant difference between TCC and TER in 12-month MCS score (beta = 1.0; 95% confidence interval, –0.8 to 2.8; P = .28). In addition, no significant differences in treatment effects were identified.
Patients in both groups experienced “large and clinically meaningful” improvements in MCS scores from baseline to 12 months (Cohen d = 0.81 and 0.90 for TCC and TER, respectively), the researchers report.
‘Bit of a surprise’
The comparative effectiveness of both models in this study was “a bit of a surprise,” Dr. Fortney noted.
“We hypothesized that TCC would have better outcomes than TER because we thought patients would be more likely to engage in treatment,” he said.
In collaborative care, the familiar primary care practitioner is the prescriber. The local care manager’s job is to keep patients engaged in care, said Dr. Fortney.
“However, because the medical school telemental health providers were privileged and credentialed to practice in the primary care clinic, the referral process to the telepsychiatrist and telepsychologist was much more successful than it usually is. So engagement was the same in both groups, and thus outcomes were equally as good,” Dr. Fortney said.
He noted that the referral model is used more than the collaborative care model “because it is similar to the more traditional approach to managing complex psychiatric disorders. I would say this is true both before and after COVID-19, but more so after.”
From a health care system perspective, “clinical leadership should implement whichever approach is most sustainable,” the investigators concluded.
Good news for clinics
Commenting on the study, Adam C. Powell, PhD, president of Payer+Provider Syndicate, said the “similar efficacy” of teleintegrated care and telereferral care for delivering behavioral health services in primary care is “good news for clinics,” because it suggests that clinicians may pick between the two modes of delivery and achieve similar outcomes.
“The resources available within a clinic may determine which of these approaches is most viable. The teleintegrated care approach requires the clinic to have more extensive resources locally,” Dr. Powell noted.
However, he pointed out that the study did not report relative costs of the two approaches, which may also be a factor in determining which one clinics choose to implement.
“Overall, the study shows that advances in telemedicine are making it possible for patients to access telepsychiatry and to achieve improvements in their mental health. Given the lack of access that many patients face, telepsychiatry offers one potential solution,” Dr. Powell concluded.
The SPIRIT study was funded by a grant from the Patient-Centered Outcomes Research Institute. Dr. Fortney and Dr. Powell have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Two models for treating patients with complex psychiatric disorders in primary care are equally effective, new research suggests.
Results from a pragmatic, randomized comparative effectiveness study involving more than 1,000 patients showed that both integrated telepsychiatry collaborative care (TCC) and telepsychiatry/telepsychology enhanced referral (TER) provided “significantly and substantially” improved clinical outcomes, researchers noted.
However, the referral model required substantially more mental health specialist time than does the integrated model.
Therefore, ,” lead author John Fortney, PhD, department of psychiatry and behavioral sciences, University of Washington, Seattle, told this news organization.
The findings were published online Aug. 25 in JAMA Psychiatry.
Clinically meaningful improvement
The Study to Promote Innovation in Rural Integrated Telepsychiatry (SPIRIT) trial included 1,004 adults with untreated posttraumatic stress disorder and/or bipolar disorder. The participants were from 24 primary care clinics in rural and underserved areas in which there were no on-site psychiatrists or psychologists.
In SPIRIT, 508 patients were randomly allocated to TCC, and 496 were assigned to TER.
With TCC, an on-site behavioral health care manager and an off-site telepsychiatrist consultant support the primary care clinician in prescribing medications. With TER, an off-site telepsychiatrist prescribes medication, and an off-site telepsychologist delivers therapy.
The primary outcome was mental health functioning at 12 months, as measured by the Veterans RAND 12-item Health Survey Mental Component Summary (MCS) score. MSC scores range from 0 to 100.
Baseline MCS scores for the study participants were two standard deviations below the national average. The mean MCS scores were 39.7 and 41.2 in the TCC and TER groups, respectively.
There was no significant difference between TCC and TER in 12-month MCS score (beta = 1.0; 95% confidence interval, –0.8 to 2.8; P = .28). In addition, no significant differences in treatment effects were identified.
Patients in both groups experienced “large and clinically meaningful” improvements in MCS scores from baseline to 12 months (Cohen d = 0.81 and 0.90 for TCC and TER, respectively), the researchers report.
‘Bit of a surprise’
The comparative effectiveness of both models in this study was “a bit of a surprise,” Dr. Fortney noted.
“We hypothesized that TCC would have better outcomes than TER because we thought patients would be more likely to engage in treatment,” he said.
In collaborative care, the familiar primary care practitioner is the prescriber. The local care manager’s job is to keep patients engaged in care, said Dr. Fortney.
“However, because the medical school telemental health providers were privileged and credentialed to practice in the primary care clinic, the referral process to the telepsychiatrist and telepsychologist was much more successful than it usually is. So engagement was the same in both groups, and thus outcomes were equally as good,” Dr. Fortney said.
He noted that the referral model is used more than the collaborative care model “because it is similar to the more traditional approach to managing complex psychiatric disorders. I would say this is true both before and after COVID-19, but more so after.”
From a health care system perspective, “clinical leadership should implement whichever approach is most sustainable,” the investigators concluded.
Good news for clinics
Commenting on the study, Adam C. Powell, PhD, president of Payer+Provider Syndicate, said the “similar efficacy” of teleintegrated care and telereferral care for delivering behavioral health services in primary care is “good news for clinics,” because it suggests that clinicians may pick between the two modes of delivery and achieve similar outcomes.
“The resources available within a clinic may determine which of these approaches is most viable. The teleintegrated care approach requires the clinic to have more extensive resources locally,” Dr. Powell noted.
However, he pointed out that the study did not report relative costs of the two approaches, which may also be a factor in determining which one clinics choose to implement.
“Overall, the study shows that advances in telemedicine are making it possible for patients to access telepsychiatry and to achieve improvements in their mental health. Given the lack of access that many patients face, telepsychiatry offers one potential solution,” Dr. Powell concluded.
The SPIRIT study was funded by a grant from the Patient-Centered Outcomes Research Institute. Dr. Fortney and Dr. Powell have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Two models for treating patients with complex psychiatric disorders in primary care are equally effective, new research suggests.
Results from a pragmatic, randomized comparative effectiveness study involving more than 1,000 patients showed that both integrated telepsychiatry collaborative care (TCC) and telepsychiatry/telepsychology enhanced referral (TER) provided “significantly and substantially” improved clinical outcomes, researchers noted.
However, the referral model required substantially more mental health specialist time than does the integrated model.
Therefore, ,” lead author John Fortney, PhD, department of psychiatry and behavioral sciences, University of Washington, Seattle, told this news organization.
The findings were published online Aug. 25 in JAMA Psychiatry.
Clinically meaningful improvement
The Study to Promote Innovation in Rural Integrated Telepsychiatry (SPIRIT) trial included 1,004 adults with untreated posttraumatic stress disorder and/or bipolar disorder. The participants were from 24 primary care clinics in rural and underserved areas in which there were no on-site psychiatrists or psychologists.
In SPIRIT, 508 patients were randomly allocated to TCC, and 496 were assigned to TER.
With TCC, an on-site behavioral health care manager and an off-site telepsychiatrist consultant support the primary care clinician in prescribing medications. With TER, an off-site telepsychiatrist prescribes medication, and an off-site telepsychologist delivers therapy.
The primary outcome was mental health functioning at 12 months, as measured by the Veterans RAND 12-item Health Survey Mental Component Summary (MCS) score. MSC scores range from 0 to 100.
Baseline MCS scores for the study participants were two standard deviations below the national average. The mean MCS scores were 39.7 and 41.2 in the TCC and TER groups, respectively.
There was no significant difference between TCC and TER in 12-month MCS score (beta = 1.0; 95% confidence interval, –0.8 to 2.8; P = .28). In addition, no significant differences in treatment effects were identified.
Patients in both groups experienced “large and clinically meaningful” improvements in MCS scores from baseline to 12 months (Cohen d = 0.81 and 0.90 for TCC and TER, respectively), the researchers report.
‘Bit of a surprise’
The comparative effectiveness of both models in this study was “a bit of a surprise,” Dr. Fortney noted.
“We hypothesized that TCC would have better outcomes than TER because we thought patients would be more likely to engage in treatment,” he said.
In collaborative care, the familiar primary care practitioner is the prescriber. The local care manager’s job is to keep patients engaged in care, said Dr. Fortney.
“However, because the medical school telemental health providers were privileged and credentialed to practice in the primary care clinic, the referral process to the telepsychiatrist and telepsychologist was much more successful than it usually is. So engagement was the same in both groups, and thus outcomes were equally as good,” Dr. Fortney said.
He noted that the referral model is used more than the collaborative care model “because it is similar to the more traditional approach to managing complex psychiatric disorders. I would say this is true both before and after COVID-19, but more so after.”
From a health care system perspective, “clinical leadership should implement whichever approach is most sustainable,” the investigators concluded.
Good news for clinics
Commenting on the study, Adam C. Powell, PhD, president of Payer+Provider Syndicate, said the “similar efficacy” of teleintegrated care and telereferral care for delivering behavioral health services in primary care is “good news for clinics,” because it suggests that clinicians may pick between the two modes of delivery and achieve similar outcomes.
“The resources available within a clinic may determine which of these approaches is most viable. The teleintegrated care approach requires the clinic to have more extensive resources locally,” Dr. Powell noted.
However, he pointed out that the study did not report relative costs of the two approaches, which may also be a factor in determining which one clinics choose to implement.
“Overall, the study shows that advances in telemedicine are making it possible for patients to access telepsychiatry and to achieve improvements in their mental health. Given the lack of access that many patients face, telepsychiatry offers one potential solution,” Dr. Powell concluded.
The SPIRIT study was funded by a grant from the Patient-Centered Outcomes Research Institute. Dr. Fortney and Dr. Powell have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antiviral Therapy Improves Hepatocellular Cancer Survival
Hepatocellular cancer (HCC) is the most common type of hepatic cancers, accounting for 65% of all hepatic cancers.1 Among all cancers, HCC is one of the fastest growing causes of death in the United States, and the rate of new HCC cases are on the rise over several decades.2 There are many risk factors leading to HCC, including alcohol use, obesity, and smoking. Infection with hepatitis C virus (HCV) poses a significant risk.1
The pathogenesis of HCV-induced carcinogenesis is mediated by a unique host-induced immunologic response. Viral replication induces production of inflammatory factors, such as tumor necrosis factor (TNF-α), interferon (IFN), and oxidative stress on hepatocytes, resulting in cell injury, death, and regeneration. Repetitive cycles of cellular death and regeneration induce fibrosis, which may lead to cirrhosis.3 Hence, early treatment of HCV infection and achieving sustained virologic response (SVR) may lead to decreased incidence and mortality associated with HCC.
Treatment of HCV infection has become more effective with the development of direct-acting antivirals (DAAs) leading to SVR in > 90% of patients compared with 40 to 50% with IFN-based treatment.4,5 DAAs have been proved safe and highly effective in eradicating HCV infection even in patients with advanced liver disease with decompensated cirrhosis.6 Although achieving SVR indicates a complete cure from chronic HCV infection, several studies have shown subsequent risk of developing HCC persists even after successful HCV treatment.7-9 Some studies show that using DAAs to achieve SVR in patients with HCV infection leads to a decreased relative risk of HCC development compared with patients who do not receive treatment.10-12 But data on HCC risk following DAA-induced SVR vs IFN-induced SVR are somewhat conflicting.
Much of the information regarding the association between SVR and HCC has been gleaned from large data banks without accounting for individual patient characteristics that can be obtained through full chart review. Due to small sample sizes in many chart review studies, the impact that SVR from DAA therapy has on the progression and severity of HCC is not entirely clear. The aim of our study is to evaluate the effect of HCV treatment and SVR status on overall survival (OS) in patients with HCC. Second, we aim to compare survival benefits, if any exist, among the 2 major HCV treatment modalities (IFN vs DAA).
Methods
We performed a retrospective review of patients at Memphis Veterans Affairs Medical Center (VAMC) in Tennessee to determine whether treatment for HCV infection in general, and achieving SVR in particular, makes a difference in progression, recurrence, or OS among patients with HCV infection who develop HCC. We identified 111 patients with a diagnosis of both HCV and new or recurrent HCC lesions from November 2008 to March 2019 (Table 1). We divided these patients based on their HCV treatment status, SVR status, and treatment types (IFN vs DAA).
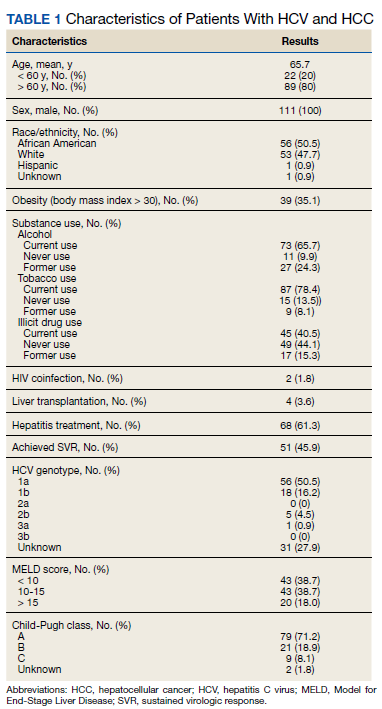
The inclusion criteria were patients aged > 18 years treated at the Memphis VAMC who have HCV infection and developed HCC. Exclusion criteria were patients who developed HCC from other causes such as alcoholic steatohepatitis, hepatitis B virus infection, hemochromatosis, patients without HCV infection, and patients who were not established at the Memphis VAMC. This protocol was approved by the Memphis VAMC Institutional Review Board.
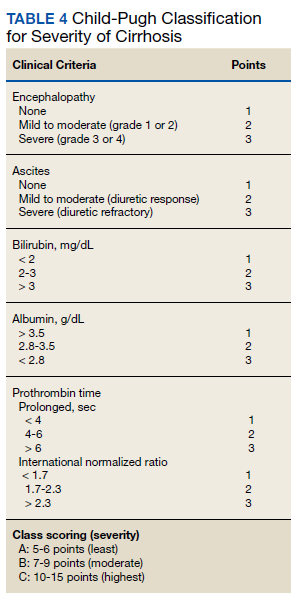
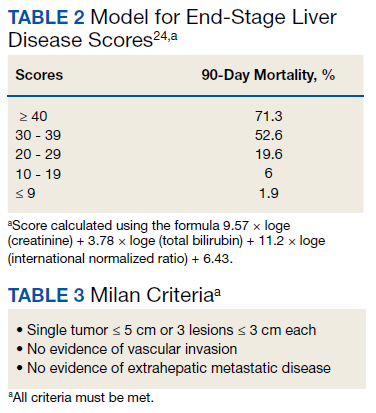
HCC diagnosis was determined using International Classification of Diseases codes (9th revision: 155 and 155.2; 10th revision: CD 22 and 22.9). We also used records of multidisciplinary gastrointestinal malignancy tumor conferences to identify patient who had been diagnosed and treated for HCV infection. We identified patients who were treated with DAA vs IFN as well as patients who had achieved SVR (classified as having negative HCV RNA tests at the end of DAA treatment). We were unable to evaluate Barcelona Clinic Liver Cancer staging since this required documented performance status that was not available in many patient records. We selected cases consistent with both treatment for HCV infection and subsequent development of HCC. Patient data included age; OS time; HIV status HCV genotype; time and status of progression to HCC; type and duration of treatment; and alcohol, tobacco, and drug use. Disease status was measured using the Model for End-Stage Liver Disease (MELD) score (Table 2), Milan criteria (Table 3), and Child-Pugh score (Table 4).
Statistical Analysis
OS was measured from the date of HCC diagnosis to the date of death or last follow-up. Progression-free survival (PFS) was defined from the date of HCC treatment initiation to the date of first HCC recurrence. We compared survival data for the SVR and non-SVR subgroups, the HCV treatment vs non-HCV treatment subgroups, and the IFN therapy vs DAA therapy subgroups, using the Kaplan-Meier method. The differences between subgroups were assessed using a log-rank test. Multivariate analysis using Cox proportional hazards regression model was used to identify factors that had significant impact on OS. Those factors included age; race; alcohol, tobacco, and illicit drug use; SVR status; HCV treatment status; IFN-based regimen vs DAA; MELD, and Child-Pugh scores. The results were expressed as hazard ratios (HRs) and 95% CI. Calculations were made using Statistical Analysis SAS and IBM SPSS software.
Results
The study included 111 patients. The mean age was 65.7 years; all were male and half of were Black patients. The gender imbalance was due to the predominantly male patient population at Memphis VAMC. Among 111 patients with HCV infection and HCC, 68 patients were treated for HCV infection and had significantly improved OS and PFS compared with the nontreatment group. The median 5-year OS was 44.6 months (95% CI, 966-3202) in the treated HCV infection group compared with 15.1 months in the untreated HCV infection group with a Wilcoxon P = .0005 (Figure 1). Similarly, patients treated for HCV infection had a significantly better 5-year PFS of 15.3 months (95% CI, 294-726) compared with the nontreatment group 9.5 months (95% CI, 205-405) with a Wilcoxon P = .04 (Figure 2).
Among 68 patients treated for HCV infection, 51 achieved SVR, and 34 achieved SVR after the diagnosis of HCC. Patients who achieved SVR had an improved 5-year OS when compared with patients who did not achieve SVR (median 65.8 months [95% CI, 1222-NA] vs 15.7 months [95% CI, 242-853], Wilcoxon P < .001) (Figure 3). Similarly, patients with SVR had improved 5-year PFS when compared with the non-SVR group (median 20.5 months [95% CI, 431-914] vs 8.9 months [95% CI, 191-340], Wilcoxon P = .007 (Figure 4). Achievement of SVR after HCC diagnosis suggests a significantly improved OS (HR 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI, 0.23-1.82, P = .41)
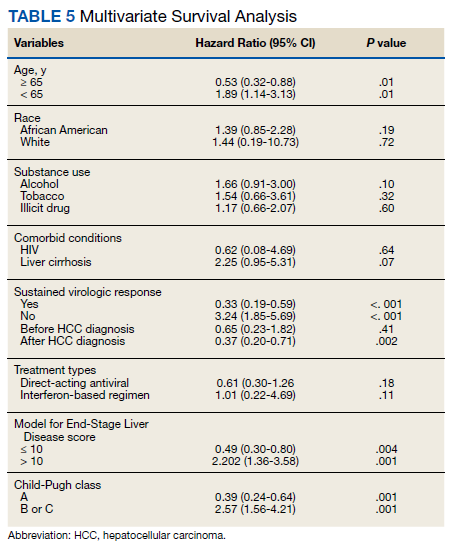
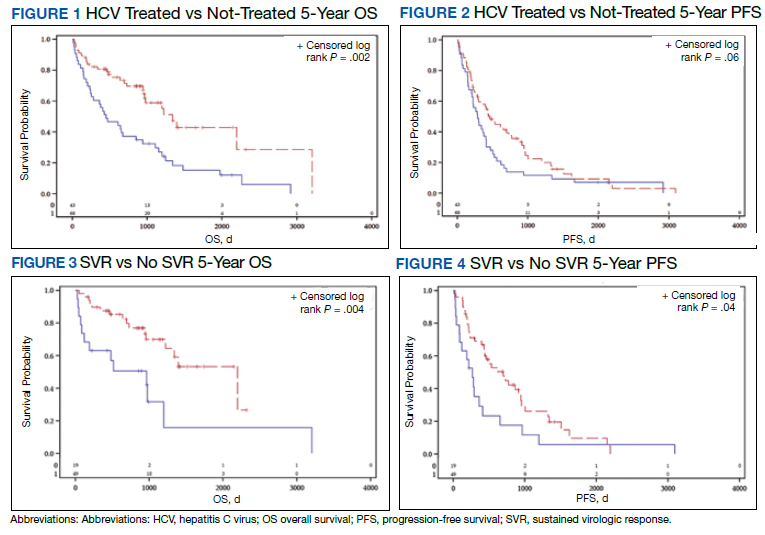
Multivariate Cox regression was used to determine factors with significant survival impact. Advanced age at diagnosis (aged ≥ 65 years) (HR, 0.53; 95% CI, 0.320-0.880; P = .01), SVR status (HR, 0.33; 95% CI, 0.190-0.587; P < .001), achieving SVR after HCC diagnosis (HR, 0.37; 95% CI, 0.20-0.71; P = .002), low MELD score (< 10) (HR, 0.49; 95% CI, 0.30-0.80; P = .004) and low Child-Pugh score (class A) (HR, 0.39; 95% CI, 0.24-0.64; P = .001) have a significant positive impact on OS. Survival was not significantly influenced by race, tobacco, drug use, HIV or cirrhosis status, or HCV treatment type. In addition, higher Child-Pugh class (B or C), higher MELD score (> 10), and younger age at diagnosis (< 65 years) have a negative impact on survival outcome (Table 5).
Discussion
The survival benefit of HCV eradication and achieving SVR status has been well established in patients with HCC.13 In a retrospective cohort study of 250 patients with HCV infection who had received curative treatment for HCC, multivariate analysis demonstrated that achieving SVR is an independent predictor of OS.14 The 3-year and 5-year OS rates were 97% and 94% for the SVR group, and 91% and 60% for the non‐SVR group, respectively (P < .001). Similarly, according to Sou and colleagues, of 122 patients with HCV-related HCC, patients with SVR had longer OS than patients with no SVR (P = .04).15 One of the hypotheses that could explain the survival benefit in patients who achieved SVR is the effect of achieving SVR in reducing persistent liver inflammation and associated liver mortality, and therefore lowering risks of complication in patients with HCC.16 In our study, multivariate analysis shows that achieving SVR is associated with significant improved OS (HR, 0.33). In contrast, patients with HCC who have not achieved SVR are associated with worse survival (HR, 3.24). This finding supports early treatment of HCV to obtain SVR in HCV-related patients with HCC, even after development of HCC.
Among 68 patients treated for HCV infection, 45 patients were treated after HCC diagnosis, and 34 patients achieved SVR after HCC diagnosis. The average time between HCV infection treatment after HCC diagnosis was 6 months. Our data suggested that achievement of SVR after HCC diagnosis suggests an improved OS (HR, 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI,0.23-1.82; P = .41). This lack of statistical significance is likely due to small sample size of patients achieving SVR prior to HCC diagnosis. Our results are consistent with the findings regarding the efficacy and timing of DAA treatment in patients with active HCC. According to Singal and colleagues, achieving SVR after DAA therapy may result in improved liver function and facilitate additional HCC-directed therapy, which potentially improves survival.17-19
Nagaoki and colleagues found that there was no significant difference in OS in patients with HCC between the DAA and IFN groups. According to the study, the 3-year and 5-year OS rates were 96% and 96% for DAA patients and 93% and 73% for IFN patients, respectively (P = .16).14 This finding is consistent with the results of our study. HCV treatment type (IFN vs DAA) was not found to be associated with either OS or PFS time, regardless of time period.
A higher MELD score (> 10) and a higher Child-Pugh class (B or C) score are associated with worse survival outcome regardless of SVR status. While patients with a low MELD score (≤ 10) have a better survival rate (HR 0.49), a higher MELD score has a significantly higher HR and therefore worse survival outcomes (HR, 2.20). Similarly, patients with Child-Pugh A (HR, 0.39) have a better survival outcome compared with those patients with Child-Pugh class B or C (HR, 2.57). This finding is consistent with results of multiple studies indicating that advanced liver disease, as measured by a high MELD score and Child-Pugh class score, can be used to predict the survival outcome in patients with HCV-related HCC.20-22
Unlike other studies that look at a single prognostic variable, our study evaluated prognostic impacts of multiple variables (age, SVR status, the order of SVR in relation to HCC development, HCV treatment type, MELD score and Child-Pugh class) in patients with HCC. The study included patients treated for HCV after development of HCC along with other multiple variables leading to OS benefit. It is one of the only studies in the United States that compared 5-year OS and PFS among patients with HCC treated for HCV and achieved SVR. The studies by Nagaoki and colleagues and Sou and colleagues were conducted in Japan, and some of their subset analyses were univariate. Among our study population of veterans, 50% were African American patients, suggesting that they may have similar OS benefit when compared to White patients with HCC and HCV treatment.
Limitations
Our findings were limited in that our study population is too small to conduct further subset analysis that would allow statistical significance of those subsets, such as the suggested benefit of SVR in patients who presented with HCC after antiviral therapy. Another limitation is the all-male population, likely a result of the older veteran population at the Memphis VAMC. The mean age at diagnosis was 65 years, which is slightly higher than the general population. Compared to the SEER database, HCC is most frequently diagnosed among people aged 55 to 64 years.23 The age difference was likely due to our aging veteran population.
Further studies are needed to determine the significance of SVR on HCC recurrence and treatment. Immunotherapy is now first-line treatment for patients with local advanced HCC. All the immunotherapy studies excluded patients with active HCV infection. Hence, we need more data on HCV treatment timing among patients scheduled to start treatment with immunotherapy.
Conclusions
In a population of older veterans, treatment of HCV infection leads to OS benefit among patients with HCC. In addition, patients with HCV infection who achieve SVR have an OS benefit over patients unable to achieve SVR. The type of treatment, DAA vs IFN-based regimen, did not show significant survival benefit.
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1. Published 2017 May 29. doi:10.4103/jcar.JCar_9_16
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi:10.3322/caac.21492
3. Farazi PA, DePinho RA. Hepatocellular carcinoma pathogenesis: from genes to environment. Nat Rev Cancer. 2006;6(9):674-687. doi:10.1038/nrc1934
4. Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for hepatitis c virus infection: a systematic review. Ann Intern Med. 2017;166(9):637-648. doi:10.7326/M16-2575
5. Kouris G, Hydery T, Greenwood BC, et al. Effectiveness of Ledipasvir/Sofosbuvir and predictors of treatment failure in members with hepatitis C genotype 1 infection: a retrospective cohort study in a medicaid population. J Manag Care Spec Pharm. 2018;24(7):591-597. doi:10.18553/jmcp.2018.24.7.591
6. Jacobson IM, Lawitz E, Kwo PY, et al. Safety and efficacy of elbasvir/grazoprevir in patients with hepatitis c virus infection and compensated cirrhosis: an integrated analysis. Gastroenterology. 2017;152(6):1372-1382.e2. doi:10.1053/j.gastro.2017.01.050
7. Nahon P, Layese R, Bourcier V, et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology. 2018;155(5):1436-1450.e6. doi:10.1053/j.gastro.2018.07.01510.
8. Innes H, Barclay ST, Hayes PC, et al. The risk of hepatocellular carcinoma in cirrhotic patients with hepatitis C and sustained viral response: role of the treatment regimen. J Hepatol. 2018;68(4):646-654. doi:10.1016/j.jhep.2017.10.033
9. Romano A, Angeli P, Piovesan S, et al. Newly diagnosed hepatocellular carcinoma in patients with advanced hepatitis C treated with DAAs: a prospective population study. J Hepatol. 2018;69(2):345-352. doi:10.1016/j.jhep.2018.03.009
10. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017;153(4):996-1005.e1. doi:10.1053/j.gastro.2017.06.0122
11. Singh S, Nautiyal A, Loke YK. Oral direct-acting antivirals and the incidence or recurrence of hepatocellular carcinoma: a systematic review and meta-analysis. Frontline Gastroenterol. 2018;9(4):262-270. doi:10.1136/flgastro-2018-101017
12. Kuftinec G, Loehfelm T, Corwin M, et al. De novo hepatocellular carcinoma occurrence in hepatitis C cirrhotics treated with direct-acting antiviral agents. Hepat Oncol. 2018;5(1):HEP06. Published 2018 Jul 25. doi:10.2217/hep-2018-00033
13. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158(5 Pt 1):329-337. doi:10.7326/0003-4819-158-5-201303050-00005
14. Nagaoki Y, Imamura M, Nishida Y, et al. The impact of interferon-free direct-acting antivirals on clinical outcome after curative treatment for hepatitis C virus-associated hepatocellular carcinoma: comparison with interferon-based therapy. J Med Virol. 2019;91(4):650-658. doi:10.1002/jmv.25352
15. Sou FM, Wu CK, Chang KC, et al. Clinical characteristics and prognosis of HCC occurrence after antiviral therapy for HCV patients between sustained and non-sustained responders. J Formos Med Assoc. 2019;118(1 Pt 3):504-513. doi:10.1016/j.jfma.2018.10.017
16. Roche B, Coilly A, Duclos-Vallee JC, Samuel D. The impact of treatment of hepatitis C with DAAs on the occurrence of HCC. Liver Int. 2018;38(suppl 1):139-145. doi:10.1111/liv.13659
17. Singal AG, Lim JK, Kanwal F. AGA clinical practice update on interaction between oral direct-acting antivirals for chronic hepatitis C infection and hepatocellular carcinoma: expert review. Gastroenterology. 2019;156(8):2149-2157. doi:10.1053/j.gastro.2019.02.046
18. Toyoda H, Kumada T, Hayashi K, et al. Characteristics and prognosis of hepatocellular carcinoma detected in sustained responders to interferon therapy for chronic hepatitis C. Cancer Detect Prev. 2003;27(6):498-502. doi:10.1016/j.cdp.2003.09.00719. Okamura Y, Sugiura T, Ito T, et al. The achievement of a sustained virological response either before or after hepatectomy improves the prognosis of patients with primary hepatitis C virus-related hepatocellular carcinoma. Ann Surg Oncol. 2019; 26(13):4566-4575. doi:10.1245/s10434-019-07911-w
20. Wray CJ, Harvin JA, Silberfein EJ, Ko TC, Kao LS. Pilot prognostic model of extremely poor survival among high-risk hepatocellular carcinoma patients. Cancer. 2012;118(24):6118-6125. doi:10.1002/cncr.27649
21. Kim JH, Kim JH, Choi JH, et al. Value of the model for end-stage liver disease for predicting survival in hepatocellular carcinoma patients treated with transarterial chemoembolization. Scand J Gastroenterol. 2009;44(3):346-357. doi:10.1080/00365520802530838
22. Vogeler M, Mohr I, Pfeiffenberger J, et al. Applicability of scoring systems predicting outcome of transarterial chemoembolization for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2020;146(4):1033-1050. doi:10.1007/s00432-020-03135-8
23. National Institutes of Health, Surveillance, Epidemiology, and End Results. Cancer stat facts: cancer of the liver and intrahepatic bile duct. Accessed July 15, 2021. https://seer.cancer.gov/statfacts/html/livibd.html
24. Singal AK, Kamath PS. Model for End-stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
Hepatocellular cancer (HCC) is the most common type of hepatic cancers, accounting for 65% of all hepatic cancers.1 Among all cancers, HCC is one of the fastest growing causes of death in the United States, and the rate of new HCC cases are on the rise over several decades.2 There are many risk factors leading to HCC, including alcohol use, obesity, and smoking. Infection with hepatitis C virus (HCV) poses a significant risk.1
The pathogenesis of HCV-induced carcinogenesis is mediated by a unique host-induced immunologic response. Viral replication induces production of inflammatory factors, such as tumor necrosis factor (TNF-α), interferon (IFN), and oxidative stress on hepatocytes, resulting in cell injury, death, and regeneration. Repetitive cycles of cellular death and regeneration induce fibrosis, which may lead to cirrhosis.3 Hence, early treatment of HCV infection and achieving sustained virologic response (SVR) may lead to decreased incidence and mortality associated with HCC.
Treatment of HCV infection has become more effective with the development of direct-acting antivirals (DAAs) leading to SVR in > 90% of patients compared with 40 to 50% with IFN-based treatment.4,5 DAAs have been proved safe and highly effective in eradicating HCV infection even in patients with advanced liver disease with decompensated cirrhosis.6 Although achieving SVR indicates a complete cure from chronic HCV infection, several studies have shown subsequent risk of developing HCC persists even after successful HCV treatment.7-9 Some studies show that using DAAs to achieve SVR in patients with HCV infection leads to a decreased relative risk of HCC development compared with patients who do not receive treatment.10-12 But data on HCC risk following DAA-induced SVR vs IFN-induced SVR are somewhat conflicting.
Much of the information regarding the association between SVR and HCC has been gleaned from large data banks without accounting for individual patient characteristics that can be obtained through full chart review. Due to small sample sizes in many chart review studies, the impact that SVR from DAA therapy has on the progression and severity of HCC is not entirely clear. The aim of our study is to evaluate the effect of HCV treatment and SVR status on overall survival (OS) in patients with HCC. Second, we aim to compare survival benefits, if any exist, among the 2 major HCV treatment modalities (IFN vs DAA).
Methods
We performed a retrospective review of patients at Memphis Veterans Affairs Medical Center (VAMC) in Tennessee to determine whether treatment for HCV infection in general, and achieving SVR in particular, makes a difference in progression, recurrence, or OS among patients with HCV infection who develop HCC. We identified 111 patients with a diagnosis of both HCV and new or recurrent HCC lesions from November 2008 to March 2019 (Table 1). We divided these patients based on their HCV treatment status, SVR status, and treatment types (IFN vs DAA).
The inclusion criteria were patients aged > 18 years treated at the Memphis VAMC who have HCV infection and developed HCC. Exclusion criteria were patients who developed HCC from other causes such as alcoholic steatohepatitis, hepatitis B virus infection, hemochromatosis, patients without HCV infection, and patients who were not established at the Memphis VAMC. This protocol was approved by the Memphis VAMC Institutional Review Board.
HCC diagnosis was determined using International Classification of Diseases codes (9th revision: 155 and 155.2; 10th revision: CD 22 and 22.9). We also used records of multidisciplinary gastrointestinal malignancy tumor conferences to identify patient who had been diagnosed and treated for HCV infection. We identified patients who were treated with DAA vs IFN as well as patients who had achieved SVR (classified as having negative HCV RNA tests at the end of DAA treatment). We were unable to evaluate Barcelona Clinic Liver Cancer staging since this required documented performance status that was not available in many patient records. We selected cases consistent with both treatment for HCV infection and subsequent development of HCC. Patient data included age; OS time; HIV status HCV genotype; time and status of progression to HCC; type and duration of treatment; and alcohol, tobacco, and drug use. Disease status was measured using the Model for End-Stage Liver Disease (MELD) score (Table 2), Milan criteria (Table 3), and Child-Pugh score (Table 4).
Statistical Analysis
OS was measured from the date of HCC diagnosis to the date of death or last follow-up. Progression-free survival (PFS) was defined from the date of HCC treatment initiation to the date of first HCC recurrence. We compared survival data for the SVR and non-SVR subgroups, the HCV treatment vs non-HCV treatment subgroups, and the IFN therapy vs DAA therapy subgroups, using the Kaplan-Meier method. The differences between subgroups were assessed using a log-rank test. Multivariate analysis using Cox proportional hazards regression model was used to identify factors that had significant impact on OS. Those factors included age; race; alcohol, tobacco, and illicit drug use; SVR status; HCV treatment status; IFN-based regimen vs DAA; MELD, and Child-Pugh scores. The results were expressed as hazard ratios (HRs) and 95% CI. Calculations were made using Statistical Analysis SAS and IBM SPSS software.
Results
The study included 111 patients. The mean age was 65.7 years; all were male and half of were Black patients. The gender imbalance was due to the predominantly male patient population at Memphis VAMC. Among 111 patients with HCV infection and HCC, 68 patients were treated for HCV infection and had significantly improved OS and PFS compared with the nontreatment group. The median 5-year OS was 44.6 months (95% CI, 966-3202) in the treated HCV infection group compared with 15.1 months in the untreated HCV infection group with a Wilcoxon P = .0005 (Figure 1). Similarly, patients treated for HCV infection had a significantly better 5-year PFS of 15.3 months (95% CI, 294-726) compared with the nontreatment group 9.5 months (95% CI, 205-405) with a Wilcoxon P = .04 (Figure 2).
Among 68 patients treated for HCV infection, 51 achieved SVR, and 34 achieved SVR after the diagnosis of HCC. Patients who achieved SVR had an improved 5-year OS when compared with patients who did not achieve SVR (median 65.8 months [95% CI, 1222-NA] vs 15.7 months [95% CI, 242-853], Wilcoxon P < .001) (Figure 3). Similarly, patients with SVR had improved 5-year PFS when compared with the non-SVR group (median 20.5 months [95% CI, 431-914] vs 8.9 months [95% CI, 191-340], Wilcoxon P = .007 (Figure 4). Achievement of SVR after HCC diagnosis suggests a significantly improved OS (HR 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI, 0.23-1.82, P = .41)
Multivariate Cox regression was used to determine factors with significant survival impact. Advanced age at diagnosis (aged ≥ 65 years) (HR, 0.53; 95% CI, 0.320-0.880; P = .01), SVR status (HR, 0.33; 95% CI, 0.190-0.587; P < .001), achieving SVR after HCC diagnosis (HR, 0.37; 95% CI, 0.20-0.71; P = .002), low MELD score (< 10) (HR, 0.49; 95% CI, 0.30-0.80; P = .004) and low Child-Pugh score (class A) (HR, 0.39; 95% CI, 0.24-0.64; P = .001) have a significant positive impact on OS. Survival was not significantly influenced by race, tobacco, drug use, HIV or cirrhosis status, or HCV treatment type. In addition, higher Child-Pugh class (B or C), higher MELD score (> 10), and younger age at diagnosis (< 65 years) have a negative impact on survival outcome (Table 5).
Discussion
The survival benefit of HCV eradication and achieving SVR status has been well established in patients with HCC.13 In a retrospective cohort study of 250 patients with HCV infection who had received curative treatment for HCC, multivariate analysis demonstrated that achieving SVR is an independent predictor of OS.14 The 3-year and 5-year OS rates were 97% and 94% for the SVR group, and 91% and 60% for the non‐SVR group, respectively (P < .001). Similarly, according to Sou and colleagues, of 122 patients with HCV-related HCC, patients with SVR had longer OS than patients with no SVR (P = .04).15 One of the hypotheses that could explain the survival benefit in patients who achieved SVR is the effect of achieving SVR in reducing persistent liver inflammation and associated liver mortality, and therefore lowering risks of complication in patients with HCC.16 In our study, multivariate analysis shows that achieving SVR is associated with significant improved OS (HR, 0.33). In contrast, patients with HCC who have not achieved SVR are associated with worse survival (HR, 3.24). This finding supports early treatment of HCV to obtain SVR in HCV-related patients with HCC, even after development of HCC.
Among 68 patients treated for HCV infection, 45 patients were treated after HCC diagnosis, and 34 patients achieved SVR after HCC diagnosis. The average time between HCV infection treatment after HCC diagnosis was 6 months. Our data suggested that achievement of SVR after HCC diagnosis suggests an improved OS (HR, 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI,0.23-1.82; P = .41). This lack of statistical significance is likely due to small sample size of patients achieving SVR prior to HCC diagnosis. Our results are consistent with the findings regarding the efficacy and timing of DAA treatment in patients with active HCC. According to Singal and colleagues, achieving SVR after DAA therapy may result in improved liver function and facilitate additional HCC-directed therapy, which potentially improves survival.17-19
Nagaoki and colleagues found that there was no significant difference in OS in patients with HCC between the DAA and IFN groups. According to the study, the 3-year and 5-year OS rates were 96% and 96% for DAA patients and 93% and 73% for IFN patients, respectively (P = .16).14 This finding is consistent with the results of our study. HCV treatment type (IFN vs DAA) was not found to be associated with either OS or PFS time, regardless of time period.
A higher MELD score (> 10) and a higher Child-Pugh class (B or C) score are associated with worse survival outcome regardless of SVR status. While patients with a low MELD score (≤ 10) have a better survival rate (HR 0.49), a higher MELD score has a significantly higher HR and therefore worse survival outcomes (HR, 2.20). Similarly, patients with Child-Pugh A (HR, 0.39) have a better survival outcome compared with those patients with Child-Pugh class B or C (HR, 2.57). This finding is consistent with results of multiple studies indicating that advanced liver disease, as measured by a high MELD score and Child-Pugh class score, can be used to predict the survival outcome in patients with HCV-related HCC.20-22
Unlike other studies that look at a single prognostic variable, our study evaluated prognostic impacts of multiple variables (age, SVR status, the order of SVR in relation to HCC development, HCV treatment type, MELD score and Child-Pugh class) in patients with HCC. The study included patients treated for HCV after development of HCC along with other multiple variables leading to OS benefit. It is one of the only studies in the United States that compared 5-year OS and PFS among patients with HCC treated for HCV and achieved SVR. The studies by Nagaoki and colleagues and Sou and colleagues were conducted in Japan, and some of their subset analyses were univariate. Among our study population of veterans, 50% were African American patients, suggesting that they may have similar OS benefit when compared to White patients with HCC and HCV treatment.
Limitations
Our findings were limited in that our study population is too small to conduct further subset analysis that would allow statistical significance of those subsets, such as the suggested benefit of SVR in patients who presented with HCC after antiviral therapy. Another limitation is the all-male population, likely a result of the older veteran population at the Memphis VAMC. The mean age at diagnosis was 65 years, which is slightly higher than the general population. Compared to the SEER database, HCC is most frequently diagnosed among people aged 55 to 64 years.23 The age difference was likely due to our aging veteran population.
Further studies are needed to determine the significance of SVR on HCC recurrence and treatment. Immunotherapy is now first-line treatment for patients with local advanced HCC. All the immunotherapy studies excluded patients with active HCV infection. Hence, we need more data on HCV treatment timing among patients scheduled to start treatment with immunotherapy.
Conclusions
In a population of older veterans, treatment of HCV infection leads to OS benefit among patients with HCC. In addition, patients with HCV infection who achieve SVR have an OS benefit over patients unable to achieve SVR. The type of treatment, DAA vs IFN-based regimen, did not show significant survival benefit.
Hepatocellular cancer (HCC) is the most common type of hepatic cancers, accounting for 65% of all hepatic cancers.1 Among all cancers, HCC is one of the fastest growing causes of death in the United States, and the rate of new HCC cases are on the rise over several decades.2 There are many risk factors leading to HCC, including alcohol use, obesity, and smoking. Infection with hepatitis C virus (HCV) poses a significant risk.1
The pathogenesis of HCV-induced carcinogenesis is mediated by a unique host-induced immunologic response. Viral replication induces production of inflammatory factors, such as tumor necrosis factor (TNF-α), interferon (IFN), and oxidative stress on hepatocytes, resulting in cell injury, death, and regeneration. Repetitive cycles of cellular death and regeneration induce fibrosis, which may lead to cirrhosis.3 Hence, early treatment of HCV infection and achieving sustained virologic response (SVR) may lead to decreased incidence and mortality associated with HCC.
Treatment of HCV infection has become more effective with the development of direct-acting antivirals (DAAs) leading to SVR in > 90% of patients compared with 40 to 50% with IFN-based treatment.4,5 DAAs have been proved safe and highly effective in eradicating HCV infection even in patients with advanced liver disease with decompensated cirrhosis.6 Although achieving SVR indicates a complete cure from chronic HCV infection, several studies have shown subsequent risk of developing HCC persists even after successful HCV treatment.7-9 Some studies show that using DAAs to achieve SVR in patients with HCV infection leads to a decreased relative risk of HCC development compared with patients who do not receive treatment.10-12 But data on HCC risk following DAA-induced SVR vs IFN-induced SVR are somewhat conflicting.
Much of the information regarding the association between SVR and HCC has been gleaned from large data banks without accounting for individual patient characteristics that can be obtained through full chart review. Due to small sample sizes in many chart review studies, the impact that SVR from DAA therapy has on the progression and severity of HCC is not entirely clear. The aim of our study is to evaluate the effect of HCV treatment and SVR status on overall survival (OS) in patients with HCC. Second, we aim to compare survival benefits, if any exist, among the 2 major HCV treatment modalities (IFN vs DAA).
Methods
We performed a retrospective review of patients at Memphis Veterans Affairs Medical Center (VAMC) in Tennessee to determine whether treatment for HCV infection in general, and achieving SVR in particular, makes a difference in progression, recurrence, or OS among patients with HCV infection who develop HCC. We identified 111 patients with a diagnosis of both HCV and new or recurrent HCC lesions from November 2008 to March 2019 (Table 1). We divided these patients based on their HCV treatment status, SVR status, and treatment types (IFN vs DAA).
The inclusion criteria were patients aged > 18 years treated at the Memphis VAMC who have HCV infection and developed HCC. Exclusion criteria were patients who developed HCC from other causes such as alcoholic steatohepatitis, hepatitis B virus infection, hemochromatosis, patients without HCV infection, and patients who were not established at the Memphis VAMC. This protocol was approved by the Memphis VAMC Institutional Review Board.
HCC diagnosis was determined using International Classification of Diseases codes (9th revision: 155 and 155.2; 10th revision: CD 22 and 22.9). We also used records of multidisciplinary gastrointestinal malignancy tumor conferences to identify patient who had been diagnosed and treated for HCV infection. We identified patients who were treated with DAA vs IFN as well as patients who had achieved SVR (classified as having negative HCV RNA tests at the end of DAA treatment). We were unable to evaluate Barcelona Clinic Liver Cancer staging since this required documented performance status that was not available in many patient records. We selected cases consistent with both treatment for HCV infection and subsequent development of HCC. Patient data included age; OS time; HIV status HCV genotype; time and status of progression to HCC; type and duration of treatment; and alcohol, tobacco, and drug use. Disease status was measured using the Model for End-Stage Liver Disease (MELD) score (Table 2), Milan criteria (Table 3), and Child-Pugh score (Table 4).
Statistical Analysis
OS was measured from the date of HCC diagnosis to the date of death or last follow-up. Progression-free survival (PFS) was defined from the date of HCC treatment initiation to the date of first HCC recurrence. We compared survival data for the SVR and non-SVR subgroups, the HCV treatment vs non-HCV treatment subgroups, and the IFN therapy vs DAA therapy subgroups, using the Kaplan-Meier method. The differences between subgroups were assessed using a log-rank test. Multivariate analysis using Cox proportional hazards regression model was used to identify factors that had significant impact on OS. Those factors included age; race; alcohol, tobacco, and illicit drug use; SVR status; HCV treatment status; IFN-based regimen vs DAA; MELD, and Child-Pugh scores. The results were expressed as hazard ratios (HRs) and 95% CI. Calculations were made using Statistical Analysis SAS and IBM SPSS software.
Results
The study included 111 patients. The mean age was 65.7 years; all were male and half of were Black patients. The gender imbalance was due to the predominantly male patient population at Memphis VAMC. Among 111 patients with HCV infection and HCC, 68 patients were treated for HCV infection and had significantly improved OS and PFS compared with the nontreatment group. The median 5-year OS was 44.6 months (95% CI, 966-3202) in the treated HCV infection group compared with 15.1 months in the untreated HCV infection group with a Wilcoxon P = .0005 (Figure 1). Similarly, patients treated for HCV infection had a significantly better 5-year PFS of 15.3 months (95% CI, 294-726) compared with the nontreatment group 9.5 months (95% CI, 205-405) with a Wilcoxon P = .04 (Figure 2).
Among 68 patients treated for HCV infection, 51 achieved SVR, and 34 achieved SVR after the diagnosis of HCC. Patients who achieved SVR had an improved 5-year OS when compared with patients who did not achieve SVR (median 65.8 months [95% CI, 1222-NA] vs 15.7 months [95% CI, 242-853], Wilcoxon P < .001) (Figure 3). Similarly, patients with SVR had improved 5-year PFS when compared with the non-SVR group (median 20.5 months [95% CI, 431-914] vs 8.9 months [95% CI, 191-340], Wilcoxon P = .007 (Figure 4). Achievement of SVR after HCC diagnosis suggests a significantly improved OS (HR 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI, 0.23-1.82, P = .41)
Multivariate Cox regression was used to determine factors with significant survival impact. Advanced age at diagnosis (aged ≥ 65 years) (HR, 0.53; 95% CI, 0.320-0.880; P = .01), SVR status (HR, 0.33; 95% CI, 0.190-0.587; P < .001), achieving SVR after HCC diagnosis (HR, 0.37; 95% CI, 0.20-0.71; P = .002), low MELD score (< 10) (HR, 0.49; 95% CI, 0.30-0.80; P = .004) and low Child-Pugh score (class A) (HR, 0.39; 95% CI, 0.24-0.64; P = .001) have a significant positive impact on OS. Survival was not significantly influenced by race, tobacco, drug use, HIV or cirrhosis status, or HCV treatment type. In addition, higher Child-Pugh class (B or C), higher MELD score (> 10), and younger age at diagnosis (< 65 years) have a negative impact on survival outcome (Table 5).
Discussion
The survival benefit of HCV eradication and achieving SVR status has been well established in patients with HCC.13 In a retrospective cohort study of 250 patients with HCV infection who had received curative treatment for HCC, multivariate analysis demonstrated that achieving SVR is an independent predictor of OS.14 The 3-year and 5-year OS rates were 97% and 94% for the SVR group, and 91% and 60% for the non‐SVR group, respectively (P < .001). Similarly, according to Sou and colleagues, of 122 patients with HCV-related HCC, patients with SVR had longer OS than patients with no SVR (P = .04).15 One of the hypotheses that could explain the survival benefit in patients who achieved SVR is the effect of achieving SVR in reducing persistent liver inflammation and associated liver mortality, and therefore lowering risks of complication in patients with HCC.16 In our study, multivariate analysis shows that achieving SVR is associated with significant improved OS (HR, 0.33). In contrast, patients with HCC who have not achieved SVR are associated with worse survival (HR, 3.24). This finding supports early treatment of HCV to obtain SVR in HCV-related patients with HCC, even after development of HCC.
Among 68 patients treated for HCV infection, 45 patients were treated after HCC diagnosis, and 34 patients achieved SVR after HCC diagnosis. The average time between HCV infection treatment after HCC diagnosis was 6 months. Our data suggested that achievement of SVR after HCC diagnosis suggests an improved OS (HR, 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI,0.23-1.82; P = .41). This lack of statistical significance is likely due to small sample size of patients achieving SVR prior to HCC diagnosis. Our results are consistent with the findings regarding the efficacy and timing of DAA treatment in patients with active HCC. According to Singal and colleagues, achieving SVR after DAA therapy may result in improved liver function and facilitate additional HCC-directed therapy, which potentially improves survival.17-19
Nagaoki and colleagues found that there was no significant difference in OS in patients with HCC between the DAA and IFN groups. According to the study, the 3-year and 5-year OS rates were 96% and 96% for DAA patients and 93% and 73% for IFN patients, respectively (P = .16).14 This finding is consistent with the results of our study. HCV treatment type (IFN vs DAA) was not found to be associated with either OS or PFS time, regardless of time period.
A higher MELD score (> 10) and a higher Child-Pugh class (B or C) score are associated with worse survival outcome regardless of SVR status. While patients with a low MELD score (≤ 10) have a better survival rate (HR 0.49), a higher MELD score has a significantly higher HR and therefore worse survival outcomes (HR, 2.20). Similarly, patients with Child-Pugh A (HR, 0.39) have a better survival outcome compared with those patients with Child-Pugh class B or C (HR, 2.57). This finding is consistent with results of multiple studies indicating that advanced liver disease, as measured by a high MELD score and Child-Pugh class score, can be used to predict the survival outcome in patients with HCV-related HCC.20-22
Unlike other studies that look at a single prognostic variable, our study evaluated prognostic impacts of multiple variables (age, SVR status, the order of SVR in relation to HCC development, HCV treatment type, MELD score and Child-Pugh class) in patients with HCC. The study included patients treated for HCV after development of HCC along with other multiple variables leading to OS benefit. It is one of the only studies in the United States that compared 5-year OS and PFS among patients with HCC treated for HCV and achieved SVR. The studies by Nagaoki and colleagues and Sou and colleagues were conducted in Japan, and some of their subset analyses were univariate. Among our study population of veterans, 50% were African American patients, suggesting that they may have similar OS benefit when compared to White patients with HCC and HCV treatment.
Limitations
Our findings were limited in that our study population is too small to conduct further subset analysis that would allow statistical significance of those subsets, such as the suggested benefit of SVR in patients who presented with HCC after antiviral therapy. Another limitation is the all-male population, likely a result of the older veteran population at the Memphis VAMC. The mean age at diagnosis was 65 years, which is slightly higher than the general population. Compared to the SEER database, HCC is most frequently diagnosed among people aged 55 to 64 years.23 The age difference was likely due to our aging veteran population.
Further studies are needed to determine the significance of SVR on HCC recurrence and treatment. Immunotherapy is now first-line treatment for patients with local advanced HCC. All the immunotherapy studies excluded patients with active HCV infection. Hence, we need more data on HCV treatment timing among patients scheduled to start treatment with immunotherapy.
Conclusions
In a population of older veterans, treatment of HCV infection leads to OS benefit among patients with HCC. In addition, patients with HCV infection who achieve SVR have an OS benefit over patients unable to achieve SVR. The type of treatment, DAA vs IFN-based regimen, did not show significant survival benefit.
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1. Published 2017 May 29. doi:10.4103/jcar.JCar_9_16
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi:10.3322/caac.21492
3. Farazi PA, DePinho RA. Hepatocellular carcinoma pathogenesis: from genes to environment. Nat Rev Cancer. 2006;6(9):674-687. doi:10.1038/nrc1934
4. Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for hepatitis c virus infection: a systematic review. Ann Intern Med. 2017;166(9):637-648. doi:10.7326/M16-2575
5. Kouris G, Hydery T, Greenwood BC, et al. Effectiveness of Ledipasvir/Sofosbuvir and predictors of treatment failure in members with hepatitis C genotype 1 infection: a retrospective cohort study in a medicaid population. J Manag Care Spec Pharm. 2018;24(7):591-597. doi:10.18553/jmcp.2018.24.7.591
6. Jacobson IM, Lawitz E, Kwo PY, et al. Safety and efficacy of elbasvir/grazoprevir in patients with hepatitis c virus infection and compensated cirrhosis: an integrated analysis. Gastroenterology. 2017;152(6):1372-1382.e2. doi:10.1053/j.gastro.2017.01.050
7. Nahon P, Layese R, Bourcier V, et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology. 2018;155(5):1436-1450.e6. doi:10.1053/j.gastro.2018.07.01510.
8. Innes H, Barclay ST, Hayes PC, et al. The risk of hepatocellular carcinoma in cirrhotic patients with hepatitis C and sustained viral response: role of the treatment regimen. J Hepatol. 2018;68(4):646-654. doi:10.1016/j.jhep.2017.10.033
9. Romano A, Angeli P, Piovesan S, et al. Newly diagnosed hepatocellular carcinoma in patients with advanced hepatitis C treated with DAAs: a prospective population study. J Hepatol. 2018;69(2):345-352. doi:10.1016/j.jhep.2018.03.009
10. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017;153(4):996-1005.e1. doi:10.1053/j.gastro.2017.06.0122
11. Singh S, Nautiyal A, Loke YK. Oral direct-acting antivirals and the incidence or recurrence of hepatocellular carcinoma: a systematic review and meta-analysis. Frontline Gastroenterol. 2018;9(4):262-270. doi:10.1136/flgastro-2018-101017
12. Kuftinec G, Loehfelm T, Corwin M, et al. De novo hepatocellular carcinoma occurrence in hepatitis C cirrhotics treated with direct-acting antiviral agents. Hepat Oncol. 2018;5(1):HEP06. Published 2018 Jul 25. doi:10.2217/hep-2018-00033
13. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158(5 Pt 1):329-337. doi:10.7326/0003-4819-158-5-201303050-00005
14. Nagaoki Y, Imamura M, Nishida Y, et al. The impact of interferon-free direct-acting antivirals on clinical outcome after curative treatment for hepatitis C virus-associated hepatocellular carcinoma: comparison with interferon-based therapy. J Med Virol. 2019;91(4):650-658. doi:10.1002/jmv.25352
15. Sou FM, Wu CK, Chang KC, et al. Clinical characteristics and prognosis of HCC occurrence after antiviral therapy for HCV patients between sustained and non-sustained responders. J Formos Med Assoc. 2019;118(1 Pt 3):504-513. doi:10.1016/j.jfma.2018.10.017
16. Roche B, Coilly A, Duclos-Vallee JC, Samuel D. The impact of treatment of hepatitis C with DAAs on the occurrence of HCC. Liver Int. 2018;38(suppl 1):139-145. doi:10.1111/liv.13659
17. Singal AG, Lim JK, Kanwal F. AGA clinical practice update on interaction between oral direct-acting antivirals for chronic hepatitis C infection and hepatocellular carcinoma: expert review. Gastroenterology. 2019;156(8):2149-2157. doi:10.1053/j.gastro.2019.02.046
18. Toyoda H, Kumada T, Hayashi K, et al. Characteristics and prognosis of hepatocellular carcinoma detected in sustained responders to interferon therapy for chronic hepatitis C. Cancer Detect Prev. 2003;27(6):498-502. doi:10.1016/j.cdp.2003.09.00719. Okamura Y, Sugiura T, Ito T, et al. The achievement of a sustained virological response either before or after hepatectomy improves the prognosis of patients with primary hepatitis C virus-related hepatocellular carcinoma. Ann Surg Oncol. 2019; 26(13):4566-4575. doi:10.1245/s10434-019-07911-w
20. Wray CJ, Harvin JA, Silberfein EJ, Ko TC, Kao LS. Pilot prognostic model of extremely poor survival among high-risk hepatocellular carcinoma patients. Cancer. 2012;118(24):6118-6125. doi:10.1002/cncr.27649
21. Kim JH, Kim JH, Choi JH, et al. Value of the model for end-stage liver disease for predicting survival in hepatocellular carcinoma patients treated with transarterial chemoembolization. Scand J Gastroenterol. 2009;44(3):346-357. doi:10.1080/00365520802530838
22. Vogeler M, Mohr I, Pfeiffenberger J, et al. Applicability of scoring systems predicting outcome of transarterial chemoembolization for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2020;146(4):1033-1050. doi:10.1007/s00432-020-03135-8
23. National Institutes of Health, Surveillance, Epidemiology, and End Results. Cancer stat facts: cancer of the liver and intrahepatic bile duct. Accessed July 15, 2021. https://seer.cancer.gov/statfacts/html/livibd.html
24. Singal AK, Kamath PS. Model for End-stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1. Published 2017 May 29. doi:10.4103/jcar.JCar_9_16
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi:10.3322/caac.21492
3. Farazi PA, DePinho RA. Hepatocellular carcinoma pathogenesis: from genes to environment. Nat Rev Cancer. 2006;6(9):674-687. doi:10.1038/nrc1934
4. Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for hepatitis c virus infection: a systematic review. Ann Intern Med. 2017;166(9):637-648. doi:10.7326/M16-2575
5. Kouris G, Hydery T, Greenwood BC, et al. Effectiveness of Ledipasvir/Sofosbuvir and predictors of treatment failure in members with hepatitis C genotype 1 infection: a retrospective cohort study in a medicaid population. J Manag Care Spec Pharm. 2018;24(7):591-597. doi:10.18553/jmcp.2018.24.7.591
6. Jacobson IM, Lawitz E, Kwo PY, et al. Safety and efficacy of elbasvir/grazoprevir in patients with hepatitis c virus infection and compensated cirrhosis: an integrated analysis. Gastroenterology. 2017;152(6):1372-1382.e2. doi:10.1053/j.gastro.2017.01.050
7. Nahon P, Layese R, Bourcier V, et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology. 2018;155(5):1436-1450.e6. doi:10.1053/j.gastro.2018.07.01510.
8. Innes H, Barclay ST, Hayes PC, et al. The risk of hepatocellular carcinoma in cirrhotic patients with hepatitis C and sustained viral response: role of the treatment regimen. J Hepatol. 2018;68(4):646-654. doi:10.1016/j.jhep.2017.10.033
9. Romano A, Angeli P, Piovesan S, et al. Newly diagnosed hepatocellular carcinoma in patients with advanced hepatitis C treated with DAAs: a prospective population study. J Hepatol. 2018;69(2):345-352. doi:10.1016/j.jhep.2018.03.009
10. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017;153(4):996-1005.e1. doi:10.1053/j.gastro.2017.06.0122
11. Singh S, Nautiyal A, Loke YK. Oral direct-acting antivirals and the incidence or recurrence of hepatocellular carcinoma: a systematic review and meta-analysis. Frontline Gastroenterol. 2018;9(4):262-270. doi:10.1136/flgastro-2018-101017
12. Kuftinec G, Loehfelm T, Corwin M, et al. De novo hepatocellular carcinoma occurrence in hepatitis C cirrhotics treated with direct-acting antiviral agents. Hepat Oncol. 2018;5(1):HEP06. Published 2018 Jul 25. doi:10.2217/hep-2018-00033
13. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158(5 Pt 1):329-337. doi:10.7326/0003-4819-158-5-201303050-00005
14. Nagaoki Y, Imamura M, Nishida Y, et al. The impact of interferon-free direct-acting antivirals on clinical outcome after curative treatment for hepatitis C virus-associated hepatocellular carcinoma: comparison with interferon-based therapy. J Med Virol. 2019;91(4):650-658. doi:10.1002/jmv.25352
15. Sou FM, Wu CK, Chang KC, et al. Clinical characteristics and prognosis of HCC occurrence after antiviral therapy for HCV patients between sustained and non-sustained responders. J Formos Med Assoc. 2019;118(1 Pt 3):504-513. doi:10.1016/j.jfma.2018.10.017
16. Roche B, Coilly A, Duclos-Vallee JC, Samuel D. The impact of treatment of hepatitis C with DAAs on the occurrence of HCC. Liver Int. 2018;38(suppl 1):139-145. doi:10.1111/liv.13659
17. Singal AG, Lim JK, Kanwal F. AGA clinical practice update on interaction between oral direct-acting antivirals for chronic hepatitis C infection and hepatocellular carcinoma: expert review. Gastroenterology. 2019;156(8):2149-2157. doi:10.1053/j.gastro.2019.02.046
18. Toyoda H, Kumada T, Hayashi K, et al. Characteristics and prognosis of hepatocellular carcinoma detected in sustained responders to interferon therapy for chronic hepatitis C. Cancer Detect Prev. 2003;27(6):498-502. doi:10.1016/j.cdp.2003.09.00719. Okamura Y, Sugiura T, Ito T, et al. The achievement of a sustained virological response either before or after hepatectomy improves the prognosis of patients with primary hepatitis C virus-related hepatocellular carcinoma. Ann Surg Oncol. 2019; 26(13):4566-4575. doi:10.1245/s10434-019-07911-w
20. Wray CJ, Harvin JA, Silberfein EJ, Ko TC, Kao LS. Pilot prognostic model of extremely poor survival among high-risk hepatocellular carcinoma patients. Cancer. 2012;118(24):6118-6125. doi:10.1002/cncr.27649
21. Kim JH, Kim JH, Choi JH, et al. Value of the model for end-stage liver disease for predicting survival in hepatocellular carcinoma patients treated with transarterial chemoembolization. Scand J Gastroenterol. 2009;44(3):346-357. doi:10.1080/00365520802530838
22. Vogeler M, Mohr I, Pfeiffenberger J, et al. Applicability of scoring systems predicting outcome of transarterial chemoembolization for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2020;146(4):1033-1050. doi:10.1007/s00432-020-03135-8
23. National Institutes of Health, Surveillance, Epidemiology, and End Results. Cancer stat facts: cancer of the liver and intrahepatic bile duct. Accessed July 15, 2021. https://seer.cancer.gov/statfacts/html/livibd.html
24. Singal AK, Kamath PS. Model for End-stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
United Healthcare settles claims it violated mental health parity
The nation’s largest health care insurer has agreed to pay $16 million in restitution and penalties to consumers, the federal government, and the state of New York to settle complaints that it illegally limited outpatient psychotherapy.

The settlement resolves a joint U.S. Department of Labor and New York Attorney General investigation and lawsuit that found that United Healthcare and United Behavioral Health (UBH) had, since at least 2013, violated the federal Mental Health Parity and Addiction Equity Act of 2008.
United Healthcare and UBH are fighting similar claims in Wit v United Behavioral Health, which is currently on appeal at the U.S. Court of Appeals for the Ninth Circuit. If that complaint is decided against UBH, the insurer might have to reprocess more than 67,000 claims.
The joint New York–federal investigation determined that United Healthcare reduced reimbursement rates for out-of-network mental health services and denied payment for many services using its Algorithms for Effective Reporting and Treatment (ALERT) utilization review program.
All outpatient psychotherapy was subjected to review; by comparison, only a handful of medical and surgical services were. That violated parity laws, the New York Attorney General’s office said in a statement.
“United’s denial of these vital services was both unlawful and dangerous,” New York Attorney General Letitia James said in the statement.
“Protecting access to mental health and substance disorder treatment is a priority for the Department of Labor and something I believe in strongly as a person in long-term recovery,” U.S. Secretary of Labor Marty Walsh said in another statement.
Mr. Walsh added that the settlement “provides compensation for many people who were denied full benefits and equitable treatment.”
‘Investigations change behavior’
Commenting for this news organization, Joe Parks, MD, medical director of the National Council for Mental Wellbeing, applauded the settlement.
“These kinds of investigations change behavior, and people get better coverage,” Dr. Parks said.
He also applauded New York, saying that it “has been one of the more assertive states in expecting companies to comply with parity requirements. They should be emulated by other states.”
Dr. Parks noted that a 2019 U.S. Government Accountability Office report showed that only 20 states routinely conducted parity compliance reviews.
A spokesperson for the American Psychiatric Association said it was notable that the Department of Labor focused on three issues that it had not publicly investigated before.
These were payment parity, the use of algorithms in mental health to identify practitioners and patients who use more health care than expected of the “average” person, and requiring disclosure of how the insurer set rates, guidelines, and medical necessity standards.
The American Psychological Association’s chief of psychological practice, Jared L. Skillings, PhD, said the group was gratified that the Department of Labor and New York took complaints seriously and that it “is encouraged that United Behavioral Health and United Healthcare have agreed to change their unfair procedures regarding reimbursement and denial of psychological care.”
The association “will monitor implementation of the settlement with high hopes for fair treatment for patients with mental health needs,” Dr. Skillings said in an interview.
Across-the-board cuts for therapy
The investigation found that United Healthcare reduced the allowable reimbursement amount for all nonphysicians across the board for psychotherapy – by 25% for PhD-level psychologists and by 35% for all MA-level therapists.
The company’s ALERT system used arbitrary thresholds to trigger utilization review, which “often led to denials of coverage when providers could not justify continued treatment after 20 sessions,” said the New York attorney general.
Beneficiaries had to figure out how to pay for continuing services or abruptly end necessary treatment.
United Healthcare agreed to stop reducing reimbursement and to not employ a similar policy in New York for at least 2 years. It will stop using ALERT and stop issuing denials for psychotherapy through at least 2023.
In addition, “We are committed to ensuring all our members have access to care and to reimbursing providers consistent with the terms of the member’s health plan and state and federal rules,” United Healthcare said.
Dr. Parks noted that United Healthcare had stopped using ALERT long before the settlement and was instead employing Level of Care Utilization System for Psychiatric and Addiction Services (LOCUS) and American Society of Addiction Medicine criteria, which he called “a good step forward.”
‘Meaningful’ payout
United Healthcare will pay $14.3 million in restitution to consumers, including $9 million to 20,000 New Yorkers who received denials of or reductions in reimbursement. The company will also pay more than $2 million in penalties, with $1.3 million going to New York.
The insurer has annual revenues of some $250 billion.
“It’s not a large amount of money in United’s overall business operation,” said Dr. Parks.
However, “It certainly could be a meaningful amount of money for the individuals that didn’t get coverage that paid out of pocket,” he added.
A version of this article first appeared on Medscape.com.
The nation’s largest health care insurer has agreed to pay $16 million in restitution and penalties to consumers, the federal government, and the state of New York to settle complaints that it illegally limited outpatient psychotherapy.
The settlement resolves a joint U.S. Department of Labor and New York Attorney General investigation and lawsuit that found that United Healthcare and United Behavioral Health (UBH) had, since at least 2013, violated the federal Mental Health Parity and Addiction Equity Act of 2008.
United Healthcare and UBH are fighting similar claims in Wit v United Behavioral Health, which is currently on appeal at the U.S. Court of Appeals for the Ninth Circuit. If that complaint is decided against UBH, the insurer might have to reprocess more than 67,000 claims.
The joint New York–federal investigation determined that United Healthcare reduced reimbursement rates for out-of-network mental health services and denied payment for many services using its Algorithms for Effective Reporting and Treatment (ALERT) utilization review program.
All outpatient psychotherapy was subjected to review; by comparison, only a handful of medical and surgical services were. That violated parity laws, the New York Attorney General’s office said in a statement.
“United’s denial of these vital services was both unlawful and dangerous,” New York Attorney General Letitia James said in the statement.
“Protecting access to mental health and substance disorder treatment is a priority for the Department of Labor and something I believe in strongly as a person in long-term recovery,” U.S. Secretary of Labor Marty Walsh said in another statement.
Mr. Walsh added that the settlement “provides compensation for many people who were denied full benefits and equitable treatment.”
‘Investigations change behavior’
Commenting for this news organization, Joe Parks, MD, medical director of the National Council for Mental Wellbeing, applauded the settlement.
“These kinds of investigations change behavior, and people get better coverage,” Dr. Parks said.
He also applauded New York, saying that it “has been one of the more assertive states in expecting companies to comply with parity requirements. They should be emulated by other states.”
Dr. Parks noted that a 2019 U.S. Government Accountability Office report showed that only 20 states routinely conducted parity compliance reviews.
A spokesperson for the American Psychiatric Association said it was notable that the Department of Labor focused on three issues that it had not publicly investigated before.
These were payment parity, the use of algorithms in mental health to identify practitioners and patients who use more health care than expected of the “average” person, and requiring disclosure of how the insurer set rates, guidelines, and medical necessity standards.
The American Psychological Association’s chief of psychological practice, Jared L. Skillings, PhD, said the group was gratified that the Department of Labor and New York took complaints seriously and that it “is encouraged that United Behavioral Health and United Healthcare have agreed to change their unfair procedures regarding reimbursement and denial of psychological care.”
The association “will monitor implementation of the settlement with high hopes for fair treatment for patients with mental health needs,” Dr. Skillings said in an interview.
Across-the-board cuts for therapy
The investigation found that United Healthcare reduced the allowable reimbursement amount for all nonphysicians across the board for psychotherapy – by 25% for PhD-level psychologists and by 35% for all MA-level therapists.
The company’s ALERT system used arbitrary thresholds to trigger utilization review, which “often led to denials of coverage when providers could not justify continued treatment after 20 sessions,” said the New York attorney general.
Beneficiaries had to figure out how to pay for continuing services or abruptly end necessary treatment.
United Healthcare agreed to stop reducing reimbursement and to not employ a similar policy in New York for at least 2 years. It will stop using ALERT and stop issuing denials for psychotherapy through at least 2023.
In addition, “We are committed to ensuring all our members have access to care and to reimbursing providers consistent with the terms of the member’s health plan and state and federal rules,” United Healthcare said.
Dr. Parks noted that United Healthcare had stopped using ALERT long before the settlement and was instead employing Level of Care Utilization System for Psychiatric and Addiction Services (LOCUS) and American Society of Addiction Medicine criteria, which he called “a good step forward.”
‘Meaningful’ payout
United Healthcare will pay $14.3 million in restitution to consumers, including $9 million to 20,000 New Yorkers who received denials of or reductions in reimbursement. The company will also pay more than $2 million in penalties, with $1.3 million going to New York.
The insurer has annual revenues of some $250 billion.
“It’s not a large amount of money in United’s overall business operation,” said Dr. Parks.
However, “It certainly could be a meaningful amount of money for the individuals that didn’t get coverage that paid out of pocket,” he added.
A version of this article first appeared on Medscape.com.
The nation’s largest health care insurer has agreed to pay $16 million in restitution and penalties to consumers, the federal government, and the state of New York to settle complaints that it illegally limited outpatient psychotherapy.
The settlement resolves a joint U.S. Department of Labor and New York Attorney General investigation and lawsuit that found that United Healthcare and United Behavioral Health (UBH) had, since at least 2013, violated the federal Mental Health Parity and Addiction Equity Act of 2008.
United Healthcare and UBH are fighting similar claims in Wit v United Behavioral Health, which is currently on appeal at the U.S. Court of Appeals for the Ninth Circuit. If that complaint is decided against UBH, the insurer might have to reprocess more than 67,000 claims.
The joint New York–federal investigation determined that United Healthcare reduced reimbursement rates for out-of-network mental health services and denied payment for many services using its Algorithms for Effective Reporting and Treatment (ALERT) utilization review program.
All outpatient psychotherapy was subjected to review; by comparison, only a handful of medical and surgical services were. That violated parity laws, the New York Attorney General’s office said in a statement.
“United’s denial of these vital services was both unlawful and dangerous,” New York Attorney General Letitia James said in the statement.
“Protecting access to mental health and substance disorder treatment is a priority for the Department of Labor and something I believe in strongly as a person in long-term recovery,” U.S. Secretary of Labor Marty Walsh said in another statement.
Mr. Walsh added that the settlement “provides compensation for many people who were denied full benefits and equitable treatment.”
‘Investigations change behavior’
Commenting for this news organization, Joe Parks, MD, medical director of the National Council for Mental Wellbeing, applauded the settlement.
“These kinds of investigations change behavior, and people get better coverage,” Dr. Parks said.
He also applauded New York, saying that it “has been one of the more assertive states in expecting companies to comply with parity requirements. They should be emulated by other states.”
Dr. Parks noted that a 2019 U.S. Government Accountability Office report showed that only 20 states routinely conducted parity compliance reviews.
A spokesperson for the American Psychiatric Association said it was notable that the Department of Labor focused on three issues that it had not publicly investigated before.
These were payment parity, the use of algorithms in mental health to identify practitioners and patients who use more health care than expected of the “average” person, and requiring disclosure of how the insurer set rates, guidelines, and medical necessity standards.
The American Psychological Association’s chief of psychological practice, Jared L. Skillings, PhD, said the group was gratified that the Department of Labor and New York took complaints seriously and that it “is encouraged that United Behavioral Health and United Healthcare have agreed to change their unfair procedures regarding reimbursement and denial of psychological care.”
The association “will monitor implementation of the settlement with high hopes for fair treatment for patients with mental health needs,” Dr. Skillings said in an interview.
Across-the-board cuts for therapy
The investigation found that United Healthcare reduced the allowable reimbursement amount for all nonphysicians across the board for psychotherapy – by 25% for PhD-level psychologists and by 35% for all MA-level therapists.
The company’s ALERT system used arbitrary thresholds to trigger utilization review, which “often led to denials of coverage when providers could not justify continued treatment after 20 sessions,” said the New York attorney general.
Beneficiaries had to figure out how to pay for continuing services or abruptly end necessary treatment.
United Healthcare agreed to stop reducing reimbursement and to not employ a similar policy in New York for at least 2 years. It will stop using ALERT and stop issuing denials for psychotherapy through at least 2023.
In addition, “We are committed to ensuring all our members have access to care and to reimbursing providers consistent with the terms of the member’s health plan and state and federal rules,” United Healthcare said.
Dr. Parks noted that United Healthcare had stopped using ALERT long before the settlement and was instead employing Level of Care Utilization System for Psychiatric and Addiction Services (LOCUS) and American Society of Addiction Medicine criteria, which he called “a good step forward.”
‘Meaningful’ payout
United Healthcare will pay $14.3 million in restitution to consumers, including $9 million to 20,000 New Yorkers who received denials of or reductions in reimbursement. The company will also pay more than $2 million in penalties, with $1.3 million going to New York.
The insurer has annual revenues of some $250 billion.
“It’s not a large amount of money in United’s overall business operation,” said Dr. Parks.
However, “It certainly could be a meaningful amount of money for the individuals that didn’t get coverage that paid out of pocket,” he added.
A version of this article first appeared on Medscape.com.
FDA approves first once-weekly growth hormone for children
The U.S. Food and Drug Administration has approved lonapegsomatropin (Skytrofa, Ascendis Pharma), the first weekly subcutaneous injectable growth hormone for children with growth hormone deficiency (GHD).
The approval was based on the findings of the 52-week, phase 3 heiGHt trial in 161 treatment-naive pediatric patients with GHD, which was recently published in the Journal of Clinical Endocrinology & Metabolism.
Since 1987, the standard treatment for pediatric GHD, in which the pituitary gland does not produce enough growth hormone, has been a daily injection of somatropin (recombinant DNA human growth hormone).
“I am excited to be able to reduce the number of shots for some children requiring growth hormone therapy” with this new dosing option, Bradley S. Miller, MD, PhD, who was not involved with the research, said in an email.
“I am hopeful that a once-weekly growth hormone option will improve adherence to growth hormone therapy, leading to improved growth and metabolic outcomes,” added Dr. Miller, professor and division director, pediatric endocrinology, at the University of Minnesota Masonic Children’s Hospital, Minneapolis.
Lonapegsomatropin is approved for the treatment of pediatric patients age 1 year and older who weigh at least 11.5 kg (25.4 pounds) and have short stature due to inadequate secretion of endogenous growth hormone, according to the prescribing information.
The drug molecule consists of a prodrug of somatropin that is inactive when it is bound to a proprietary TransCon (transient conjugation) inert carrier using a TransCon linker. The three-part molecule breaks apart after injection, exposing the active somatropin that is slowly released.
The heiGHt trial demonstrated noninferiority of lonapegsomatropin to somatropin daily injections. Children who received weekly lonapegsomatropin grew 11.2 cm (4.4 inches) per year, whereas those who received an equivalent total dose of somatropin daily injections grew 10.3 cm (4.1 inches) per year.
Safety outcomes – the ratio of bone age to chronologic age, adverse events, tolerability, and immunogenicity – were similar in both groups.
Anticipated uptake, other drugs on horizon
Lonapegsomatropin is expected to be available shortly in the United States along with a suite of patient support programs, according to a company press release.
“The impact of the approval of lonapegsomatropin on clinical practice will depend upon its availability, coverage by insurance providers, and patient/provider comfort with using a new product,” Dr. Miller said.
For most pediatric endocrinologists, daily growth hormone has been available their entire careers, so he expects it will take some time for the pediatric endocrinology community to be comfortable prescribing long-acting growth hormone (LAGH), the name given to the once-weekly products.
In the meantime, an FDA decision on another once-weekly growth hormone, somatrogon (OPKO Health/Pfizer) for children with GHD is expected very soon, in October 2021.
And a weekly injectable somapacitan (Sogroya, Novo Nordisk), approved by the FDA in September last year for adults with GHD, is also being studied in children, with estimated study completion in 2024.
“Approval of more LAGH molecules, approval of LAGH for more indications, real-world evidence of safety, efficacy, and improved adherence, and personal experience with LAGH will all likely lead to increased LAGH use over time,” Dr. Miller speculated.
“Over the long-term, I expect insurance providers will cover LAGH products,” he surmised, “but that the price will be similar to or slightly higher than daily growth hormone.”
However, if improved adherence with LAGH is demonstrated and associated with better treatment outcomes, the price of LAGH will likely increase and use of daily growth hormone will decrease, he predicts.
Paul Saenger, MD, who was not involved with the research, believes “all three long-acting growth hormone drugs will eventually be approved for GHD in children.”
“The price will be the same or may be at most 10% more than daily growth hormone replacement,” Dr. Saenger, a pediatric endocrinologist and clinical assistant professor at NYU Long Island School of Medicine, New York, said in an email.
However, daily subcutaneous injections will still be warranted for certain children with GHD, Dr. Miller noted.
“Daily growth hormone may be better than LAGH for a small number of children who have severe GHD associated with hypoglycemia,” he said. “The low levels of growth hormone at the end of the weekly interval of LAGH may allow hypoglycemia to occur in this population.”
Phase 3 trial in 161 treatment-naive children with GHD
The heiGHt trial randomized treatment-naive prepubertal children with GHD 2:1 to weekly lonapegsomatropin or daily somatropin (Genotropin, Pfizer) at 73 sites in 15 countries.
The children were a mean age of 8.5 years (range, 3.2-13.1 years), 82% were boys, and 94% were White.
There were no reported serious adverse events or discontinuations related to lonapegsomatropin.
The most common adverse reactions in ≥5% of these pediatric patients were viral infection (15%), pyrexia (15%), cough (11%), nausea and vomiting (11%), hemorrhage (7%), diarrhea (6%), abdominal pain (6%), and arthralgia and arthritis (6%).
Both study groups reported low incidences of transient, non-neutralizing anti-hGH binding antibodies and no cases of persistent antibodies.
Trial limitations include the fact the study was not blinded (as patients received a weekly or daily injection) and drug doses were fixed at 0.24 mg human growth hormone/kg/week, although in real-world clinical practice, doses may be titrated.
Lonapegsomatropin has been studied in more than 300 children with GHD in the phase 3 program in the heiGHt trial (treatment-naive patients), fliGHt trial (treatment-experienced patients), and enliGHten trial (an ongoing long-term extension trial that includes some patients who have been taking lonapegsomatropin for more than 4 years).
The study was sponsored by Ascendis Pharma. Some of the phase 3 study authors are company employees.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has approved lonapegsomatropin (Skytrofa, Ascendis Pharma), the first weekly subcutaneous injectable growth hormone for children with growth hormone deficiency (GHD).
The approval was based on the findings of the 52-week, phase 3 heiGHt trial in 161 treatment-naive pediatric patients with GHD, which was recently published in the Journal of Clinical Endocrinology & Metabolism.
Since 1987, the standard treatment for pediatric GHD, in which the pituitary gland does not produce enough growth hormone, has been a daily injection of somatropin (recombinant DNA human growth hormone).
“I am excited to be able to reduce the number of shots for some children requiring growth hormone therapy” with this new dosing option, Bradley S. Miller, MD, PhD, who was not involved with the research, said in an email.
“I am hopeful that a once-weekly growth hormone option will improve adherence to growth hormone therapy, leading to improved growth and metabolic outcomes,” added Dr. Miller, professor and division director, pediatric endocrinology, at the University of Minnesota Masonic Children’s Hospital, Minneapolis.
Lonapegsomatropin is approved for the treatment of pediatric patients age 1 year and older who weigh at least 11.5 kg (25.4 pounds) and have short stature due to inadequate secretion of endogenous growth hormone, according to the prescribing information.
The drug molecule consists of a prodrug of somatropin that is inactive when it is bound to a proprietary TransCon (transient conjugation) inert carrier using a TransCon linker. The three-part molecule breaks apart after injection, exposing the active somatropin that is slowly released.
The heiGHt trial demonstrated noninferiority of lonapegsomatropin to somatropin daily injections. Children who received weekly lonapegsomatropin grew 11.2 cm (4.4 inches) per year, whereas those who received an equivalent total dose of somatropin daily injections grew 10.3 cm (4.1 inches) per year.
Safety outcomes – the ratio of bone age to chronologic age, adverse events, tolerability, and immunogenicity – were similar in both groups.
Anticipated uptake, other drugs on horizon
Lonapegsomatropin is expected to be available shortly in the United States along with a suite of patient support programs, according to a company press release.
“The impact of the approval of lonapegsomatropin on clinical practice will depend upon its availability, coverage by insurance providers, and patient/provider comfort with using a new product,” Dr. Miller said.
For most pediatric endocrinologists, daily growth hormone has been available their entire careers, so he expects it will take some time for the pediatric endocrinology community to be comfortable prescribing long-acting growth hormone (LAGH), the name given to the once-weekly products.
In the meantime, an FDA decision on another once-weekly growth hormone, somatrogon (OPKO Health/Pfizer) for children with GHD is expected very soon, in October 2021.
And a weekly injectable somapacitan (Sogroya, Novo Nordisk), approved by the FDA in September last year for adults with GHD, is also being studied in children, with estimated study completion in 2024.
“Approval of more LAGH molecules, approval of LAGH for more indications, real-world evidence of safety, efficacy, and improved adherence, and personal experience with LAGH will all likely lead to increased LAGH use over time,” Dr. Miller speculated.
“Over the long-term, I expect insurance providers will cover LAGH products,” he surmised, “but that the price will be similar to or slightly higher than daily growth hormone.”
However, if improved adherence with LAGH is demonstrated and associated with better treatment outcomes, the price of LAGH will likely increase and use of daily growth hormone will decrease, he predicts.
Paul Saenger, MD, who was not involved with the research, believes “all three long-acting growth hormone drugs will eventually be approved for GHD in children.”
“The price will be the same or may be at most 10% more than daily growth hormone replacement,” Dr. Saenger, a pediatric endocrinologist and clinical assistant professor at NYU Long Island School of Medicine, New York, said in an email.
However, daily subcutaneous injections will still be warranted for certain children with GHD, Dr. Miller noted.
“Daily growth hormone may be better than LAGH for a small number of children who have severe GHD associated with hypoglycemia,” he said. “The low levels of growth hormone at the end of the weekly interval of LAGH may allow hypoglycemia to occur in this population.”
Phase 3 trial in 161 treatment-naive children with GHD
The heiGHt trial randomized treatment-naive prepubertal children with GHD 2:1 to weekly lonapegsomatropin or daily somatropin (Genotropin, Pfizer) at 73 sites in 15 countries.
The children were a mean age of 8.5 years (range, 3.2-13.1 years), 82% were boys, and 94% were White.
There were no reported serious adverse events or discontinuations related to lonapegsomatropin.
The most common adverse reactions in ≥5% of these pediatric patients were viral infection (15%), pyrexia (15%), cough (11%), nausea and vomiting (11%), hemorrhage (7%), diarrhea (6%), abdominal pain (6%), and arthralgia and arthritis (6%).
Both study groups reported low incidences of transient, non-neutralizing anti-hGH binding antibodies and no cases of persistent antibodies.
Trial limitations include the fact the study was not blinded (as patients received a weekly or daily injection) and drug doses were fixed at 0.24 mg human growth hormone/kg/week, although in real-world clinical practice, doses may be titrated.
Lonapegsomatropin has been studied in more than 300 children with GHD in the phase 3 program in the heiGHt trial (treatment-naive patients), fliGHt trial (treatment-experienced patients), and enliGHten trial (an ongoing long-term extension trial that includes some patients who have been taking lonapegsomatropin for more than 4 years).
The study was sponsored by Ascendis Pharma. Some of the phase 3 study authors are company employees.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has approved lonapegsomatropin (Skytrofa, Ascendis Pharma), the first weekly subcutaneous injectable growth hormone for children with growth hormone deficiency (GHD).
The approval was based on the findings of the 52-week, phase 3 heiGHt trial in 161 treatment-naive pediatric patients with GHD, which was recently published in the Journal of Clinical Endocrinology & Metabolism.
Since 1987, the standard treatment for pediatric GHD, in which the pituitary gland does not produce enough growth hormone, has been a daily injection of somatropin (recombinant DNA human growth hormone).
“I am excited to be able to reduce the number of shots for some children requiring growth hormone therapy” with this new dosing option, Bradley S. Miller, MD, PhD, who was not involved with the research, said in an email.
“I am hopeful that a once-weekly growth hormone option will improve adherence to growth hormone therapy, leading to improved growth and metabolic outcomes,” added Dr. Miller, professor and division director, pediatric endocrinology, at the University of Minnesota Masonic Children’s Hospital, Minneapolis.
Lonapegsomatropin is approved for the treatment of pediatric patients age 1 year and older who weigh at least 11.5 kg (25.4 pounds) and have short stature due to inadequate secretion of endogenous growth hormone, according to the prescribing information.
The drug molecule consists of a prodrug of somatropin that is inactive when it is bound to a proprietary TransCon (transient conjugation) inert carrier using a TransCon linker. The three-part molecule breaks apart after injection, exposing the active somatropin that is slowly released.
The heiGHt trial demonstrated noninferiority of lonapegsomatropin to somatropin daily injections. Children who received weekly lonapegsomatropin grew 11.2 cm (4.4 inches) per year, whereas those who received an equivalent total dose of somatropin daily injections grew 10.3 cm (4.1 inches) per year.
Safety outcomes – the ratio of bone age to chronologic age, adverse events, tolerability, and immunogenicity – were similar in both groups.
Anticipated uptake, other drugs on horizon
Lonapegsomatropin is expected to be available shortly in the United States along with a suite of patient support programs, according to a company press release.
“The impact of the approval of lonapegsomatropin on clinical practice will depend upon its availability, coverage by insurance providers, and patient/provider comfort with using a new product,” Dr. Miller said.
For most pediatric endocrinologists, daily growth hormone has been available their entire careers, so he expects it will take some time for the pediatric endocrinology community to be comfortable prescribing long-acting growth hormone (LAGH), the name given to the once-weekly products.
In the meantime, an FDA decision on another once-weekly growth hormone, somatrogon (OPKO Health/Pfizer) for children with GHD is expected very soon, in October 2021.
And a weekly injectable somapacitan (Sogroya, Novo Nordisk), approved by the FDA in September last year for adults with GHD, is also being studied in children, with estimated study completion in 2024.
“Approval of more LAGH molecules, approval of LAGH for more indications, real-world evidence of safety, efficacy, and improved adherence, and personal experience with LAGH will all likely lead to increased LAGH use over time,” Dr. Miller speculated.
“Over the long-term, I expect insurance providers will cover LAGH products,” he surmised, “but that the price will be similar to or slightly higher than daily growth hormone.”
However, if improved adherence with LAGH is demonstrated and associated with better treatment outcomes, the price of LAGH will likely increase and use of daily growth hormone will decrease, he predicts.
Paul Saenger, MD, who was not involved with the research, believes “all three long-acting growth hormone drugs will eventually be approved for GHD in children.”
“The price will be the same or may be at most 10% more than daily growth hormone replacement,” Dr. Saenger, a pediatric endocrinologist and clinical assistant professor at NYU Long Island School of Medicine, New York, said in an email.
However, daily subcutaneous injections will still be warranted for certain children with GHD, Dr. Miller noted.
“Daily growth hormone may be better than LAGH for a small number of children who have severe GHD associated with hypoglycemia,” he said. “The low levels of growth hormone at the end of the weekly interval of LAGH may allow hypoglycemia to occur in this population.”
Phase 3 trial in 161 treatment-naive children with GHD
The heiGHt trial randomized treatment-naive prepubertal children with GHD 2:1 to weekly lonapegsomatropin or daily somatropin (Genotropin, Pfizer) at 73 sites in 15 countries.
The children were a mean age of 8.5 years (range, 3.2-13.1 years), 82% were boys, and 94% were White.
There were no reported serious adverse events or discontinuations related to lonapegsomatropin.
The most common adverse reactions in ≥5% of these pediatric patients were viral infection (15%), pyrexia (15%), cough (11%), nausea and vomiting (11%), hemorrhage (7%), diarrhea (6%), abdominal pain (6%), and arthralgia and arthritis (6%).
Both study groups reported low incidences of transient, non-neutralizing anti-hGH binding antibodies and no cases of persistent antibodies.
Trial limitations include the fact the study was not blinded (as patients received a weekly or daily injection) and drug doses were fixed at 0.24 mg human growth hormone/kg/week, although in real-world clinical practice, doses may be titrated.
Lonapegsomatropin has been studied in more than 300 children with GHD in the phase 3 program in the heiGHt trial (treatment-naive patients), fliGHt trial (treatment-experienced patients), and enliGHten trial (an ongoing long-term extension trial that includes some patients who have been taking lonapegsomatropin for more than 4 years).
The study was sponsored by Ascendis Pharma. Some of the phase 3 study authors are company employees.
A version of this article first appeared on Medscape.com.