User login
Mohs Micrographic Surgery During the COVID-19 Pandemic: Considering the Patient Perspective
Guidelines on Skin Cancer Surgeries During the COVID-19 Pandemic
At the start of the COVID-19 pandemic, the Centers for Disease Control and Prevention issued recommendations to decrease the spread of SARS-CoV-2 and optimize the use of personal protective equipment (PPE) for frontline workers.1 In the field of dermatologic surgery, the American College of Mohs Surgery, the National Comprehensive Cancer Network, the American Society for Dermatologic Surgery, and the American Academy of Dermatology made recommendations to postpone nonessential and nonurgent procedures.2-4 The initial guidelines of the American College of Mohs Surgery advised cancellation of all elective surgeries and deferred treatment of most cases of basal cell carcinoma for as long as 3 months; low-risk squamous cell carcinoma (SCC) and melanoma in situ treatment was deferred for as long as 2 or 3 months.3 Additional recommendations were made to reserve inpatient visits for suspicious lesions and high-risk cancers, postpone other nonessential and nonurgent appointments, and utilize telemedicine whenever possible.5
These recommendations led to great uncertainty and stress for patients and providers. Although numerous important variables, such as patient risk factors, severity of disease, availability of PPE and staff, and patient-to-provider transmission were considered when creating these guidelines, the patient’s experience likely was not a contributing factor.
COVID-19 Transmission During Mohs Surgery
There have been concerns that surgeons performing Mohs micrographic surgery (MMS) might be at an increased risk for COVID-19, given their close contact with high-risk sites (ie, nose, mouth) and cautery-generated aerosols; most of the estimated transmission risk associated with MMS has been based on head and neck surgery experience and publications.6-8 Tee and colleagues9 recently published their institution’s MMS COVID-19 preventive measures, which, to their knowledge, have prevented all intraoperative transmission of SARS-CoV-2, even in disease-positive patients. Currently, evidence is lacking to support a high risk for SARS-CoV-2 transmission during MMS when proper PPE and personal hygiene measures as well as strict infection control protocols—presurgical COVID-19 testing in high-risk cases, COVID-19 screening optimization, visitor restrictions, and appropriate disinfection between patients—are in place.
The Impact of Postponing Treatment on Patients
Although studies have focused on the effects of the COVID-19 pandemic on physicians practicing MMS,10 little is known about the effects of delays in skin cancer treatment on patients. A survey conducted in the United Kingdom investigating the patient’s perspective found that patients expressed worry and concern about the possibility that their MMS would be postponed and greatly appreciated continuation of treatment during the pandemic.11
Other medical specialties have reported their patient experiences during the pandemic. In a study examining patient perception of postponed surgical treatment of pelvic floor disorders due to COVID-19, nearly half of survey respondents were unhappy with the delay in receiving care. Furthermore, patients who reported being unhappy were more likely to report feelings of isolation and anxiety because their surgery was postponed.12 In another study involving patients with lung cancer, 9.1% (N=15) of patients postponed their treatment during the COVID-19 pandemic because of pandemic-related anxiety.13
With the goal of improving care at our institution, we conducted a brief institutional review board–approved survey to evaluate how postponing MMS treatment due to the COVID-19 pandemic affected patients. All MMS patients undergoing surgery in June 2020 and July 2020 (N=99) were asked to complete our voluntary and anonymous 23-question survey in person during their procedure. We obtained 88 responses (response rate, 89%). Twenty percent of surveyed patients (n=18) reported that their MMS had been postponed; 78% of those whose MMS was postponed (n=14) indicated some level of anxiety during the waiting period. It was unclear which patients had their treatment postponed based on national guidelines and which ones elected to postpone surgery.
Tips for Health Care Providers
Patient-provider communication highlighting specific skin cancer risk and the risk vs benefit of postponing treatment might reduce anxiety and stress during the waiting period.14 A study found that COVID-19 posed a bigger threat than most noninvasive skin cancers; therefore, the authors of that study concluded that treatment for most skin cancers could be safely postponed.15 Specifically, those authors recommended prioritizing treatment for Merkel cell carcinoma, invasive SCC, and melanoma with positive margins or macroscopic residual disease. They proposed that all other skin cancers, including basal cell carcinoma, SCC in situ, and melanoma with negative margins and no macroscopic residual disease, could be safely delayed for as long as 3 months.15
For patients with multiple risk factors for COVID-19–related morbidity or mortality, delaying skin cancer treatment likely has less risk than contracting the virus.15 This information should be communicated with patients. Investigation of specific patient concerns is warranted, and case-by-case evaluation of patients’ risk factors and skin cancer risk should be considered.
Based on the current, though limited, literature, delaying medical treatment can have a negative impact on the patient experience. Furthermore, proper precautions have been shown to limit intraoperative transmission of SARS-CoV-2 during MMS, but research is lacking. Practitioners should utilize shared decision-making and evaluate a given patient’s risk factors and concerns when deciding whether to postpone treatment. We encourage other institutions to evaluate the effects that delaying MMS has had on their patients, as further studies would improve understanding of patients’ experiences during a pandemic and potentially influence future dermatology guidelines.
- Center for Disease Control and Prevention. COVID-19. Accessed April 20, 2021. https://www.cdc.gov/coronavirus/2019-ncov/index.html
- American College of Mohs Surgery. Mohs surgery ambulatory protocol during COVID pandemic (version 6-3-20). June 4, 2020. Accessed April 20, 2021. http://staging.mohscollege.org/UserFiles/AM20/Member%20Alert/MohsSurgeryAmbulatoryProtocolDuringCOVIDPandemicFinal.pdf
- COVID-19 resources. National Comprehensive Cancer Network website. Accessed April 20, 2021. https://www.nccn.org/covid-19
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed April 10, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- Geskin LJ, Trager MH, Aasi SZ, et al. Perspectives on the recommendations for skin cancer management during the COVID-19 pandemic.J Am Acad Dermatol. 2020;83:295-296. doi:10.1016/j.jaad.2020.05.002
- Yuan JT, Jiang SIB. Urgent safety considerations for dermatologic surgeons in the COVID-19 pandemic. Dermatol Online J. 2020;26:1. Accessed April 20, 2021. http://escholarship.org/uc/item/2qr3w771
- Otolaryngologists may contract COVID-19 during surgery. ENTtoday. March 20, 2020. Accessed April 20, 2021. https://www.enttoday.org/article/otolaryngologists-may-contract-covid-19-during-surgery/
- Howard BE. High-risk aerosol-generating procedures in COVID-19: respiratory protective equipment considerations. Otolaryngol Head Neck Surg. 2020;163:98-103. doi:10.1177/0194599820927335
- Tee MW, Stewart C, Aliessa S, et al. Dermatological surgery during the COVID-19 pandemic: experience of a large academic center. J Am Acad Dermatol. 2021;84:1094-1096. doi:10.1016/j.jaad.2020.12.003
- Hooper J, Feng H. The impact of COVID-19 on micrographic surgery and dermatologic oncology fellows. Dermatol Surg. 2020;46:1762-1763. doi:10.1097/DSS.0000000000002766
- Nicholson P, Ali FR, Patalay R, et al. Patient perceptions of Mohs micrographic surgery during the COVID-19 pandemic and lessons for the next outbreak. Clin Exp Dermatol. 2021;46:179-180. doi:10.1111/ced.14423
- Mou T, Brown O, Gillingham A, et al. Patients’ perceptions on surgical care suspension for pelvic floor disorders during the COVID-19 pandemic. Female Pelvic Med Reconstr Surg. 2020;26:477-482. doi:10.1097/SPV.0000000000000918
- Fujita K, Ito T, Saito Z, et al. Impact of COVID-19 pandemic on lung cancer treatment scheduling. Thorac Cancer. 2020;11:2983-2986. doi:10.1111/1759-7714.13615
- Nikumb VB, Banerjee A, Kaur G, et al. Impact of doctor-patient communication on preoperative anxiety: study at industrial township, Pimpri, Pune. Ind Psychiatry J. 2009;18:19-21. doi:10.4103/0972-6748.57852
- Baumann BC, MacArthur KM, Brewer JD, et al. Management of primary skin cancer during a pandemic: multidisciplinary recommendations. Cancer. 2020;126:3900-3906. doi:10.1002/cncr.32969
Guidelines on Skin Cancer Surgeries During the COVID-19 Pandemic
At the start of the COVID-19 pandemic, the Centers for Disease Control and Prevention issued recommendations to decrease the spread of SARS-CoV-2 and optimize the use of personal protective equipment (PPE) for frontline workers.1 In the field of dermatologic surgery, the American College of Mohs Surgery, the National Comprehensive Cancer Network, the American Society for Dermatologic Surgery, and the American Academy of Dermatology made recommendations to postpone nonessential and nonurgent procedures.2-4 The initial guidelines of the American College of Mohs Surgery advised cancellation of all elective surgeries and deferred treatment of most cases of basal cell carcinoma for as long as 3 months; low-risk squamous cell carcinoma (SCC) and melanoma in situ treatment was deferred for as long as 2 or 3 months.3 Additional recommendations were made to reserve inpatient visits for suspicious lesions and high-risk cancers, postpone other nonessential and nonurgent appointments, and utilize telemedicine whenever possible.5
These recommendations led to great uncertainty and stress for patients and providers. Although numerous important variables, such as patient risk factors, severity of disease, availability of PPE and staff, and patient-to-provider transmission were considered when creating these guidelines, the patient’s experience likely was not a contributing factor.
COVID-19 Transmission During Mohs Surgery
There have been concerns that surgeons performing Mohs micrographic surgery (MMS) might be at an increased risk for COVID-19, given their close contact with high-risk sites (ie, nose, mouth) and cautery-generated aerosols; most of the estimated transmission risk associated with MMS has been based on head and neck surgery experience and publications.6-8 Tee and colleagues9 recently published their institution’s MMS COVID-19 preventive measures, which, to their knowledge, have prevented all intraoperative transmission of SARS-CoV-2, even in disease-positive patients. Currently, evidence is lacking to support a high risk for SARS-CoV-2 transmission during MMS when proper PPE and personal hygiene measures as well as strict infection control protocols—presurgical COVID-19 testing in high-risk cases, COVID-19 screening optimization, visitor restrictions, and appropriate disinfection between patients—are in place.
The Impact of Postponing Treatment on Patients
Although studies have focused on the effects of the COVID-19 pandemic on physicians practicing MMS,10 little is known about the effects of delays in skin cancer treatment on patients. A survey conducted in the United Kingdom investigating the patient’s perspective found that patients expressed worry and concern about the possibility that their MMS would be postponed and greatly appreciated continuation of treatment during the pandemic.11
Other medical specialties have reported their patient experiences during the pandemic. In a study examining patient perception of postponed surgical treatment of pelvic floor disorders due to COVID-19, nearly half of survey respondents were unhappy with the delay in receiving care. Furthermore, patients who reported being unhappy were more likely to report feelings of isolation and anxiety because their surgery was postponed.12 In another study involving patients with lung cancer, 9.1% (N=15) of patients postponed their treatment during the COVID-19 pandemic because of pandemic-related anxiety.13
With the goal of improving care at our institution, we conducted a brief institutional review board–approved survey to evaluate how postponing MMS treatment due to the COVID-19 pandemic affected patients. All MMS patients undergoing surgery in June 2020 and July 2020 (N=99) were asked to complete our voluntary and anonymous 23-question survey in person during their procedure. We obtained 88 responses (response rate, 89%). Twenty percent of surveyed patients (n=18) reported that their MMS had been postponed; 78% of those whose MMS was postponed (n=14) indicated some level of anxiety during the waiting period. It was unclear which patients had their treatment postponed based on national guidelines and which ones elected to postpone surgery.
Tips for Health Care Providers
Patient-provider communication highlighting specific skin cancer risk and the risk vs benefit of postponing treatment might reduce anxiety and stress during the waiting period.14 A study found that COVID-19 posed a bigger threat than most noninvasive skin cancers; therefore, the authors of that study concluded that treatment for most skin cancers could be safely postponed.15 Specifically, those authors recommended prioritizing treatment for Merkel cell carcinoma, invasive SCC, and melanoma with positive margins or macroscopic residual disease. They proposed that all other skin cancers, including basal cell carcinoma, SCC in situ, and melanoma with negative margins and no macroscopic residual disease, could be safely delayed for as long as 3 months.15
For patients with multiple risk factors for COVID-19–related morbidity or mortality, delaying skin cancer treatment likely has less risk than contracting the virus.15 This information should be communicated with patients. Investigation of specific patient concerns is warranted, and case-by-case evaluation of patients’ risk factors and skin cancer risk should be considered.
Based on the current, though limited, literature, delaying medical treatment can have a negative impact on the patient experience. Furthermore, proper precautions have been shown to limit intraoperative transmission of SARS-CoV-2 during MMS, but research is lacking. Practitioners should utilize shared decision-making and evaluate a given patient’s risk factors and concerns when deciding whether to postpone treatment. We encourage other institutions to evaluate the effects that delaying MMS has had on their patients, as further studies would improve understanding of patients’ experiences during a pandemic and potentially influence future dermatology guidelines.
Guidelines on Skin Cancer Surgeries During the COVID-19 Pandemic
At the start of the COVID-19 pandemic, the Centers for Disease Control and Prevention issued recommendations to decrease the spread of SARS-CoV-2 and optimize the use of personal protective equipment (PPE) for frontline workers.1 In the field of dermatologic surgery, the American College of Mohs Surgery, the National Comprehensive Cancer Network, the American Society for Dermatologic Surgery, and the American Academy of Dermatology made recommendations to postpone nonessential and nonurgent procedures.2-4 The initial guidelines of the American College of Mohs Surgery advised cancellation of all elective surgeries and deferred treatment of most cases of basal cell carcinoma for as long as 3 months; low-risk squamous cell carcinoma (SCC) and melanoma in situ treatment was deferred for as long as 2 or 3 months.3 Additional recommendations were made to reserve inpatient visits for suspicious lesions and high-risk cancers, postpone other nonessential and nonurgent appointments, and utilize telemedicine whenever possible.5
These recommendations led to great uncertainty and stress for patients and providers. Although numerous important variables, such as patient risk factors, severity of disease, availability of PPE and staff, and patient-to-provider transmission were considered when creating these guidelines, the patient’s experience likely was not a contributing factor.
COVID-19 Transmission During Mohs Surgery
There have been concerns that surgeons performing Mohs micrographic surgery (MMS) might be at an increased risk for COVID-19, given their close contact with high-risk sites (ie, nose, mouth) and cautery-generated aerosols; most of the estimated transmission risk associated with MMS has been based on head and neck surgery experience and publications.6-8 Tee and colleagues9 recently published their institution’s MMS COVID-19 preventive measures, which, to their knowledge, have prevented all intraoperative transmission of SARS-CoV-2, even in disease-positive patients. Currently, evidence is lacking to support a high risk for SARS-CoV-2 transmission during MMS when proper PPE and personal hygiene measures as well as strict infection control protocols—presurgical COVID-19 testing in high-risk cases, COVID-19 screening optimization, visitor restrictions, and appropriate disinfection between patients—are in place.
The Impact of Postponing Treatment on Patients
Although studies have focused on the effects of the COVID-19 pandemic on physicians practicing MMS,10 little is known about the effects of delays in skin cancer treatment on patients. A survey conducted in the United Kingdom investigating the patient’s perspective found that patients expressed worry and concern about the possibility that their MMS would be postponed and greatly appreciated continuation of treatment during the pandemic.11
Other medical specialties have reported their patient experiences during the pandemic. In a study examining patient perception of postponed surgical treatment of pelvic floor disorders due to COVID-19, nearly half of survey respondents were unhappy with the delay in receiving care. Furthermore, patients who reported being unhappy were more likely to report feelings of isolation and anxiety because their surgery was postponed.12 In another study involving patients with lung cancer, 9.1% (N=15) of patients postponed their treatment during the COVID-19 pandemic because of pandemic-related anxiety.13
With the goal of improving care at our institution, we conducted a brief institutional review board–approved survey to evaluate how postponing MMS treatment due to the COVID-19 pandemic affected patients. All MMS patients undergoing surgery in June 2020 and July 2020 (N=99) were asked to complete our voluntary and anonymous 23-question survey in person during their procedure. We obtained 88 responses (response rate, 89%). Twenty percent of surveyed patients (n=18) reported that their MMS had been postponed; 78% of those whose MMS was postponed (n=14) indicated some level of anxiety during the waiting period. It was unclear which patients had their treatment postponed based on national guidelines and which ones elected to postpone surgery.
Tips for Health Care Providers
Patient-provider communication highlighting specific skin cancer risk and the risk vs benefit of postponing treatment might reduce anxiety and stress during the waiting period.14 A study found that COVID-19 posed a bigger threat than most noninvasive skin cancers; therefore, the authors of that study concluded that treatment for most skin cancers could be safely postponed.15 Specifically, those authors recommended prioritizing treatment for Merkel cell carcinoma, invasive SCC, and melanoma with positive margins or macroscopic residual disease. They proposed that all other skin cancers, including basal cell carcinoma, SCC in situ, and melanoma with negative margins and no macroscopic residual disease, could be safely delayed for as long as 3 months.15
For patients with multiple risk factors for COVID-19–related morbidity or mortality, delaying skin cancer treatment likely has less risk than contracting the virus.15 This information should be communicated with patients. Investigation of specific patient concerns is warranted, and case-by-case evaluation of patients’ risk factors and skin cancer risk should be considered.
Based on the current, though limited, literature, delaying medical treatment can have a negative impact on the patient experience. Furthermore, proper precautions have been shown to limit intraoperative transmission of SARS-CoV-2 during MMS, but research is lacking. Practitioners should utilize shared decision-making and evaluate a given patient’s risk factors and concerns when deciding whether to postpone treatment. We encourage other institutions to evaluate the effects that delaying MMS has had on their patients, as further studies would improve understanding of patients’ experiences during a pandemic and potentially influence future dermatology guidelines.
- Center for Disease Control and Prevention. COVID-19. Accessed April 20, 2021. https://www.cdc.gov/coronavirus/2019-ncov/index.html
- American College of Mohs Surgery. Mohs surgery ambulatory protocol during COVID pandemic (version 6-3-20). June 4, 2020. Accessed April 20, 2021. http://staging.mohscollege.org/UserFiles/AM20/Member%20Alert/MohsSurgeryAmbulatoryProtocolDuringCOVIDPandemicFinal.pdf
- COVID-19 resources. National Comprehensive Cancer Network website. Accessed April 20, 2021. https://www.nccn.org/covid-19
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed April 10, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- Geskin LJ, Trager MH, Aasi SZ, et al. Perspectives on the recommendations for skin cancer management during the COVID-19 pandemic.J Am Acad Dermatol. 2020;83:295-296. doi:10.1016/j.jaad.2020.05.002
- Yuan JT, Jiang SIB. Urgent safety considerations for dermatologic surgeons in the COVID-19 pandemic. Dermatol Online J. 2020;26:1. Accessed April 20, 2021. http://escholarship.org/uc/item/2qr3w771
- Otolaryngologists may contract COVID-19 during surgery. ENTtoday. March 20, 2020. Accessed April 20, 2021. https://www.enttoday.org/article/otolaryngologists-may-contract-covid-19-during-surgery/
- Howard BE. High-risk aerosol-generating procedures in COVID-19: respiratory protective equipment considerations. Otolaryngol Head Neck Surg. 2020;163:98-103. doi:10.1177/0194599820927335
- Tee MW, Stewart C, Aliessa S, et al. Dermatological surgery during the COVID-19 pandemic: experience of a large academic center. J Am Acad Dermatol. 2021;84:1094-1096. doi:10.1016/j.jaad.2020.12.003
- Hooper J, Feng H. The impact of COVID-19 on micrographic surgery and dermatologic oncology fellows. Dermatol Surg. 2020;46:1762-1763. doi:10.1097/DSS.0000000000002766
- Nicholson P, Ali FR, Patalay R, et al. Patient perceptions of Mohs micrographic surgery during the COVID-19 pandemic and lessons for the next outbreak. Clin Exp Dermatol. 2021;46:179-180. doi:10.1111/ced.14423
- Mou T, Brown O, Gillingham A, et al. Patients’ perceptions on surgical care suspension for pelvic floor disorders during the COVID-19 pandemic. Female Pelvic Med Reconstr Surg. 2020;26:477-482. doi:10.1097/SPV.0000000000000918
- Fujita K, Ito T, Saito Z, et al. Impact of COVID-19 pandemic on lung cancer treatment scheduling. Thorac Cancer. 2020;11:2983-2986. doi:10.1111/1759-7714.13615
- Nikumb VB, Banerjee A, Kaur G, et al. Impact of doctor-patient communication on preoperative anxiety: study at industrial township, Pimpri, Pune. Ind Psychiatry J. 2009;18:19-21. doi:10.4103/0972-6748.57852
- Baumann BC, MacArthur KM, Brewer JD, et al. Management of primary skin cancer during a pandemic: multidisciplinary recommendations. Cancer. 2020;126:3900-3906. doi:10.1002/cncr.32969
- Center for Disease Control and Prevention. COVID-19. Accessed April 20, 2021. https://www.cdc.gov/coronavirus/2019-ncov/index.html
- American College of Mohs Surgery. Mohs surgery ambulatory protocol during COVID pandemic (version 6-3-20). June 4, 2020. Accessed April 20, 2021. http://staging.mohscollege.org/UserFiles/AM20/Member%20Alert/MohsSurgeryAmbulatoryProtocolDuringCOVIDPandemicFinal.pdf
- COVID-19 resources. National Comprehensive Cancer Network website. Accessed April 20, 2021. https://www.nccn.org/covid-19
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed April 10, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- Geskin LJ, Trager MH, Aasi SZ, et al. Perspectives on the recommendations for skin cancer management during the COVID-19 pandemic.J Am Acad Dermatol. 2020;83:295-296. doi:10.1016/j.jaad.2020.05.002
- Yuan JT, Jiang SIB. Urgent safety considerations for dermatologic surgeons in the COVID-19 pandemic. Dermatol Online J. 2020;26:1. Accessed April 20, 2021. http://escholarship.org/uc/item/2qr3w771
- Otolaryngologists may contract COVID-19 during surgery. ENTtoday. March 20, 2020. Accessed April 20, 2021. https://www.enttoday.org/article/otolaryngologists-may-contract-covid-19-during-surgery/
- Howard BE. High-risk aerosol-generating procedures in COVID-19: respiratory protective equipment considerations. Otolaryngol Head Neck Surg. 2020;163:98-103. doi:10.1177/0194599820927335
- Tee MW, Stewart C, Aliessa S, et al. Dermatological surgery during the COVID-19 pandemic: experience of a large academic center. J Am Acad Dermatol. 2021;84:1094-1096. doi:10.1016/j.jaad.2020.12.003
- Hooper J, Feng H. The impact of COVID-19 on micrographic surgery and dermatologic oncology fellows. Dermatol Surg. 2020;46:1762-1763. doi:10.1097/DSS.0000000000002766
- Nicholson P, Ali FR, Patalay R, et al. Patient perceptions of Mohs micrographic surgery during the COVID-19 pandemic and lessons for the next outbreak. Clin Exp Dermatol. 2021;46:179-180. doi:10.1111/ced.14423
- Mou T, Brown O, Gillingham A, et al. Patients’ perceptions on surgical care suspension for pelvic floor disorders during the COVID-19 pandemic. Female Pelvic Med Reconstr Surg. 2020;26:477-482. doi:10.1097/SPV.0000000000000918
- Fujita K, Ito T, Saito Z, et al. Impact of COVID-19 pandemic on lung cancer treatment scheduling. Thorac Cancer. 2020;11:2983-2986. doi:10.1111/1759-7714.13615
- Nikumb VB, Banerjee A, Kaur G, et al. Impact of doctor-patient communication on preoperative anxiety: study at industrial township, Pimpri, Pune. Ind Psychiatry J. 2009;18:19-21. doi:10.4103/0972-6748.57852
- Baumann BC, MacArthur KM, Brewer JD, et al. Management of primary skin cancer during a pandemic: multidisciplinary recommendations. Cancer. 2020;126:3900-3906. doi:10.1002/cncr.32969
Practice Points
- There is little evidence that supports a high risk for SARS-CoV-2 transmission during Mohs micrographic surgery when proper personal protective equipment and strict infection control protocols are in place.
- The effects of treatment delays due to COVID-19 on the patient experience have not been well studied, but the limited literature suggests a negative association.
- Shared decision-making and evaluation of individual patient risk factors and concerns should be considered when deciding whether to postpone skin cancer treatment.
Possible obesity effect detected in cancer death rates
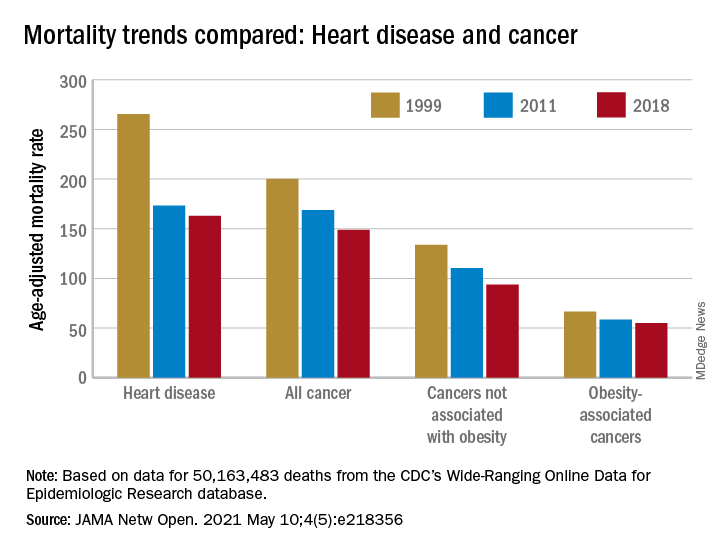
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
FROM JAMA NETWORK OPEN
Combination Therapy for Severe Asthma
Patients with severe asthma often experience symptoms and exacerbations that can interfere with daily life and further compromise lung function.
These patients often need combination therapy to achieve optimal control. This typically includes a low-dose inhaled corticosteroid (ICS) plus a long-acting beta-agonist (LABA).
For some patients, however, adherence to these therapies will not result in optimal outcomes.
Dr Monica Kraft, of the University of Arizona Health Sciences Center, discusses additional therapeutic options for these patients, which include increasing the dose of ICS or adding an oral corticosteroid such as prednisone or methylprednisolone.
When treatment-adherent patients are still unable to maintain control of their asthma symptoms, it may be optimal to move to biologic therapy.
There are currently five available biologics that work against IgE, IL-4/IL-13, IL-5, and IL-5R. Biomarker testing for blood eosinophils, exhaled nitric oxide, and serum IgE can help determine which biologic is best suited to each individual patient.
--
Robert and Irene Flinn Professor, Department of Medicine, Banner University Medical Center, North Campus; Chair, Department of Medicine, University of Arizona Health Sciences Center, Tucson, Arizona.
Monica Kraft, MD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: AstraZeneca; Genentech; Chiesi; Sanofi
Serve(d) as Chief Medical Officer for: RaeSedo, LLC
Received research grant from: National Institutes of Health; American Lung Association; Sanofi; AstraZeneca; Chiesi
received income in an amount equal to or greater than $250 from: AstraZeneca; Genentech; Chiesi; Sanof.
Patients with severe asthma often experience symptoms and exacerbations that can interfere with daily life and further compromise lung function.
These patients often need combination therapy to achieve optimal control. This typically includes a low-dose inhaled corticosteroid (ICS) plus a long-acting beta-agonist (LABA).
For some patients, however, adherence to these therapies will not result in optimal outcomes.
Dr Monica Kraft, of the University of Arizona Health Sciences Center, discusses additional therapeutic options for these patients, which include increasing the dose of ICS or adding an oral corticosteroid such as prednisone or methylprednisolone.
When treatment-adherent patients are still unable to maintain control of their asthma symptoms, it may be optimal to move to biologic therapy.
There are currently five available biologics that work against IgE, IL-4/IL-13, IL-5, and IL-5R. Biomarker testing for blood eosinophils, exhaled nitric oxide, and serum IgE can help determine which biologic is best suited to each individual patient.
--
Robert and Irene Flinn Professor, Department of Medicine, Banner University Medical Center, North Campus; Chair, Department of Medicine, University of Arizona Health Sciences Center, Tucson, Arizona.
Monica Kraft, MD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: AstraZeneca; Genentech; Chiesi; Sanofi
Serve(d) as Chief Medical Officer for: RaeSedo, LLC
Received research grant from: National Institutes of Health; American Lung Association; Sanofi; AstraZeneca; Chiesi
received income in an amount equal to or greater than $250 from: AstraZeneca; Genentech; Chiesi; Sanof.
Patients with severe asthma often experience symptoms and exacerbations that can interfere with daily life and further compromise lung function.
These patients often need combination therapy to achieve optimal control. This typically includes a low-dose inhaled corticosteroid (ICS) plus a long-acting beta-agonist (LABA).
For some patients, however, adherence to these therapies will not result in optimal outcomes.
Dr Monica Kraft, of the University of Arizona Health Sciences Center, discusses additional therapeutic options for these patients, which include increasing the dose of ICS or adding an oral corticosteroid such as prednisone or methylprednisolone.
When treatment-adherent patients are still unable to maintain control of their asthma symptoms, it may be optimal to move to biologic therapy.
There are currently five available biologics that work against IgE, IL-4/IL-13, IL-5, and IL-5R. Biomarker testing for blood eosinophils, exhaled nitric oxide, and serum IgE can help determine which biologic is best suited to each individual patient.
--
Robert and Irene Flinn Professor, Department of Medicine, Banner University Medical Center, North Campus; Chair, Department of Medicine, University of Arizona Health Sciences Center, Tucson, Arizona.
Monica Kraft, MD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: AstraZeneca; Genentech; Chiesi; Sanofi
Serve(d) as Chief Medical Officer for: RaeSedo, LLC
Received research grant from: National Institutes of Health; American Lung Association; Sanofi; AstraZeneca; Chiesi
received income in an amount equal to or greater than $250 from: AstraZeneca; Genentech; Chiesi; Sanof.
A simple new definition for ‘metabolically healthy obesity’?
Scientists have proposed a simple new definition for “metabolically healthy obesity” to identify individuals who do not have an increased risk of cardiovascular disease (CVD) death and total mortality.
The team – led by Anika Zembic, MPH, German Institute of Human Nutrition Potsdam-Rehbruecke, Nuthetal, Germany – performed an assessment of anthropometric and metabolic risk factors as well as mortality data from two cohorts that “yielded a simple definition to categorize participants with obesity as metabolically healthy or unhealthy.”
They defined “metabolically healthy” as systolic blood pressure <130 mm Hg and no use of blood pressure-lowering medication; waist-to-hip ratio <0.95 (in women) and <1.03 (in men); and no prevalent type 2 diabetes.
Based on this new definition, 42% of participants in the third U.S. National Health and Nutrition Examination Survey (NHANES-III) and 19% of participants in the UK Biobank study had metabolically healthy obesity and did not have an increased risk for CVD mortality and total mortality compared with individuals with metabolically healthy normal weight.
“People with a phenotype defined as metabolically unhealthy using this definition had significantly higher hazard ratios for [CVD] mortality and total mortality irrespective of body mass index category, and people with phenotypes defined as having metabolically healthy obesity displayed no increased risk,” the researchers noted in their article, published May 7 in JAMA Network Open.
“Our new definition may be important not only to stratify risk of mortality in people with obesity, but also in people with overweight and normal weight,” they concluded.
Thirty different definitions of ‘metabolically healthy obesity’
“To date, there is no universally accepted standard for defining [metabolically healthy obesity] and more than 30 different definitions have been used to operationalize the phenotypes in studies,” which may explain the “continued unresolved debate” about outcomes in patients with metabolically unhealthy obesity, Ayana K. April-Sanders, PhD, and Carlos J. Rodriguez, MD, MPH, from Albert Einstein College of Medicine, New York, wrote in an accompanying commentary.
The current study, they noted, suggests that waist-to-hip ratio is a better measure of central adiposity than waist circumference, and that the effect of dyslipidemia on CVD mortality may be weaker among individuals with obesity.
However, the findings may not be generalizable to other CVD outcomes, they cautioned.
And importantly, some individuals with metabolically healthy obesity will likely transition to unhealthy obesity over time due to weight gain, aging, and lack of physical activity.
Therefore, “the present study provides a prototype of how that definition can be derived, but more rigorous tests and evidence using similar techniques are needed, particularly in prospective studies,” according to Dr. April-Sanders and Dr. Rodriguez.
They call for more research to establish a standardized definition of metabolically healthy obesity and then, using that definition, to determine the prevalence of healthy and unhealthy obesity and identify factors that preserve healthy obesity.
Definition developed from NHANES cohort, validated in UK biobank
Ms. Zembic and colleagues explained that previous definitions for metabolically healthy obesity were mainly based on the absence of either metabolic syndrome or insulin resistance, but some individuals with obesity but without metabolic disease still have increased risks of CVD mortality and total mortality.
To develop a more precise definition of metabolically healthy obesity, the researchers analyzed data from 12,341 individuals in the United States who participated in NHANES-III, conducted between 1988 and 1994. The individuals were a mean age of 42 and 51% were women, and they were followed for an average of 14.5 years.
The researchers validated this definition using data from 374,079 individuals in the population-based UK Biobank cohort who were assessed in 2006 to 2010. Those individuals were a mean age of 56 and 55% were women, and they were followed for a mean of 7.8 years.
The combination of systolic blood pressure and waist-to-hip ratio had the strongest association with CVD mortality and total mortality, and the prevalence of type 2 diabetes was also associated with greater risk.
Regardless of BMI, all groups of metabolically unhealthy individuals had increased risks of CVD mortality and total mortality.
The study and some of the researchers were supported by grants from the German Federal Ministry of Education and Research.
A version of this article first appeared on Medscape.com.
Scientists have proposed a simple new definition for “metabolically healthy obesity” to identify individuals who do not have an increased risk of cardiovascular disease (CVD) death and total mortality.
The team – led by Anika Zembic, MPH, German Institute of Human Nutrition Potsdam-Rehbruecke, Nuthetal, Germany – performed an assessment of anthropometric and metabolic risk factors as well as mortality data from two cohorts that “yielded a simple definition to categorize participants with obesity as metabolically healthy or unhealthy.”
They defined “metabolically healthy” as systolic blood pressure <130 mm Hg and no use of blood pressure-lowering medication; waist-to-hip ratio <0.95 (in women) and <1.03 (in men); and no prevalent type 2 diabetes.
Based on this new definition, 42% of participants in the third U.S. National Health and Nutrition Examination Survey (NHANES-III) and 19% of participants in the UK Biobank study had metabolically healthy obesity and did not have an increased risk for CVD mortality and total mortality compared with individuals with metabolically healthy normal weight.
“People with a phenotype defined as metabolically unhealthy using this definition had significantly higher hazard ratios for [CVD] mortality and total mortality irrespective of body mass index category, and people with phenotypes defined as having metabolically healthy obesity displayed no increased risk,” the researchers noted in their article, published May 7 in JAMA Network Open.
“Our new definition may be important not only to stratify risk of mortality in people with obesity, but also in people with overweight and normal weight,” they concluded.
Thirty different definitions of ‘metabolically healthy obesity’
“To date, there is no universally accepted standard for defining [metabolically healthy obesity] and more than 30 different definitions have been used to operationalize the phenotypes in studies,” which may explain the “continued unresolved debate” about outcomes in patients with metabolically unhealthy obesity, Ayana K. April-Sanders, PhD, and Carlos J. Rodriguez, MD, MPH, from Albert Einstein College of Medicine, New York, wrote in an accompanying commentary.
The current study, they noted, suggests that waist-to-hip ratio is a better measure of central adiposity than waist circumference, and that the effect of dyslipidemia on CVD mortality may be weaker among individuals with obesity.
However, the findings may not be generalizable to other CVD outcomes, they cautioned.
And importantly, some individuals with metabolically healthy obesity will likely transition to unhealthy obesity over time due to weight gain, aging, and lack of physical activity.
Therefore, “the present study provides a prototype of how that definition can be derived, but more rigorous tests and evidence using similar techniques are needed, particularly in prospective studies,” according to Dr. April-Sanders and Dr. Rodriguez.
They call for more research to establish a standardized definition of metabolically healthy obesity and then, using that definition, to determine the prevalence of healthy and unhealthy obesity and identify factors that preserve healthy obesity.
Definition developed from NHANES cohort, validated in UK biobank
Ms. Zembic and colleagues explained that previous definitions for metabolically healthy obesity were mainly based on the absence of either metabolic syndrome or insulin resistance, but some individuals with obesity but without metabolic disease still have increased risks of CVD mortality and total mortality.
To develop a more precise definition of metabolically healthy obesity, the researchers analyzed data from 12,341 individuals in the United States who participated in NHANES-III, conducted between 1988 and 1994. The individuals were a mean age of 42 and 51% were women, and they were followed for an average of 14.5 years.
The researchers validated this definition using data from 374,079 individuals in the population-based UK Biobank cohort who were assessed in 2006 to 2010. Those individuals were a mean age of 56 and 55% were women, and they were followed for a mean of 7.8 years.
The combination of systolic blood pressure and waist-to-hip ratio had the strongest association with CVD mortality and total mortality, and the prevalence of type 2 diabetes was also associated with greater risk.
Regardless of BMI, all groups of metabolically unhealthy individuals had increased risks of CVD mortality and total mortality.
The study and some of the researchers were supported by grants from the German Federal Ministry of Education and Research.
A version of this article first appeared on Medscape.com.
Scientists have proposed a simple new definition for “metabolically healthy obesity” to identify individuals who do not have an increased risk of cardiovascular disease (CVD) death and total mortality.
The team – led by Anika Zembic, MPH, German Institute of Human Nutrition Potsdam-Rehbruecke, Nuthetal, Germany – performed an assessment of anthropometric and metabolic risk factors as well as mortality data from two cohorts that “yielded a simple definition to categorize participants with obesity as metabolically healthy or unhealthy.”
They defined “metabolically healthy” as systolic blood pressure <130 mm Hg and no use of blood pressure-lowering medication; waist-to-hip ratio <0.95 (in women) and <1.03 (in men); and no prevalent type 2 diabetes.
Based on this new definition, 42% of participants in the third U.S. National Health and Nutrition Examination Survey (NHANES-III) and 19% of participants in the UK Biobank study had metabolically healthy obesity and did not have an increased risk for CVD mortality and total mortality compared with individuals with metabolically healthy normal weight.
“People with a phenotype defined as metabolically unhealthy using this definition had significantly higher hazard ratios for [CVD] mortality and total mortality irrespective of body mass index category, and people with phenotypes defined as having metabolically healthy obesity displayed no increased risk,” the researchers noted in their article, published May 7 in JAMA Network Open.
“Our new definition may be important not only to stratify risk of mortality in people with obesity, but also in people with overweight and normal weight,” they concluded.
Thirty different definitions of ‘metabolically healthy obesity’
“To date, there is no universally accepted standard for defining [metabolically healthy obesity] and more than 30 different definitions have been used to operationalize the phenotypes in studies,” which may explain the “continued unresolved debate” about outcomes in patients with metabolically unhealthy obesity, Ayana K. April-Sanders, PhD, and Carlos J. Rodriguez, MD, MPH, from Albert Einstein College of Medicine, New York, wrote in an accompanying commentary.
The current study, they noted, suggests that waist-to-hip ratio is a better measure of central adiposity than waist circumference, and that the effect of dyslipidemia on CVD mortality may be weaker among individuals with obesity.
However, the findings may not be generalizable to other CVD outcomes, they cautioned.
And importantly, some individuals with metabolically healthy obesity will likely transition to unhealthy obesity over time due to weight gain, aging, and lack of physical activity.
Therefore, “the present study provides a prototype of how that definition can be derived, but more rigorous tests and evidence using similar techniques are needed, particularly in prospective studies,” according to Dr. April-Sanders and Dr. Rodriguez.
They call for more research to establish a standardized definition of metabolically healthy obesity and then, using that definition, to determine the prevalence of healthy and unhealthy obesity and identify factors that preserve healthy obesity.
Definition developed from NHANES cohort, validated in UK biobank
Ms. Zembic and colleagues explained that previous definitions for metabolically healthy obesity were mainly based on the absence of either metabolic syndrome or insulin resistance, but some individuals with obesity but without metabolic disease still have increased risks of CVD mortality and total mortality.
To develop a more precise definition of metabolically healthy obesity, the researchers analyzed data from 12,341 individuals in the United States who participated in NHANES-III, conducted between 1988 and 1994. The individuals were a mean age of 42 and 51% were women, and they were followed for an average of 14.5 years.
The researchers validated this definition using data from 374,079 individuals in the population-based UK Biobank cohort who were assessed in 2006 to 2010. Those individuals were a mean age of 56 and 55% were women, and they were followed for a mean of 7.8 years.
The combination of systolic blood pressure and waist-to-hip ratio had the strongest association with CVD mortality and total mortality, and the prevalence of type 2 diabetes was also associated with greater risk.
Regardless of BMI, all groups of metabolically unhealthy individuals had increased risks of CVD mortality and total mortality.
The study and some of the researchers were supported by grants from the German Federal Ministry of Education and Research.
A version of this article first appeared on Medscape.com.
Carbon monoxide diffusion with COPD declines more in women
Single breath diffusion capacity for carbon monoxide shows greater decline over time in COPD patients compared with controls, but declines significantly more in women compared with men, according to data from 602 adults with a history of smoking.
In previous studies, diffusion capacity for carbon monoxide (DLco) has been associated with decreased exercise capacity and poor health status in patients with COPD, but its association as a measure of disease progression has not been well studied, wrote Ciro Casanova, MD, of Hospital Universitario La Candelaria, Spain, and colleagues.
In a study published in the journal CHEST®, the researchers identified 506 adult smokers with COPD and 96 adult smoker controls without COPD. Lung function based on single breath DLco was measured each year for 5 years. The study population was part of the COPH History Assessment in SpaiN (CHAIN), an ongoing observational study of adults with COPD. COPD was defined as a history of at least 10 pack-years of smoking and a post-bronchodilator FEV1/FVC greater than 0.7 after 400 micrograms of albuterol, the researchers said.
During the 5-year period, the average overall annual decline in DLco was 1.34% in COPD patients, compared with .04% in non-COPD controls (P = .004). Among COPD patients, age, body mass index, FEV1%, and active smoking were not associated with longitudinal change in DLco values, the researchers said.
Notably, women with COPD at baseline had lower baseline DLco values compared with men (11.37%) and a significantly steeper decline in DLco (.89%) compared with men (P = .039). “Being a woman was the only factor that related to the annual rate of change in DLco,” the researchers said.
In a subgroup analysis, the researchers identified 305 COPD patients and 69 non-COPD controls who had at least 3 DLco measurements over the 5-year study period. In this group, 16.4% patients with COPD and 4.3% smokers without COPD showed significant yearly declines in DLco of –4.139% and –4.440%, respectively. Among COPD patients, significantly more women than men showed significant DLco declines (26% vs. 14%, P = .005). No significant differences were observed in mortality or hospitalizations per patient-year for COPD patients with and without DLco decline, the researchers said.
The study findings were limited by several factors including the lack of annual measurements of DLco among some patients, potential variability in the instruments used to measure DLco, and the absence of computerized tomography data for the chest, the researchers noted. However, the results support the value of the test for COPD progression when conducted at 3- to 4-year intervals, given the slow pace of the decline, they said. More research is needed, but “women seem to have a different susceptibility to cigarette smoke in the alveolar or pulmonary vascular domains,” they added.
DLco remains a valuable marker
The study is important because the usual longitudinal decline of diffusion capacity, an important physiological parameter in patients with COPD, was unknown, Juan P. de Torres, MD, of Queen’s University, Kingston, Ont., said in an interview.
“The finding of a different longitudinal decline of DLco in women was a surprise,” said Dr. de Torres, who was a coauthor on the study. “We knew from previous works from our group that COPD has a different clinical and prognostic behavior in women with COPD, but this specific finding is novel and important,” he said.
“These results provide information about the testing frequency (3-4 years) needed to use DLco as a marker of COPD progression in clinical practice,” Dr. de Torres added.
“What is the driving cause of this sex difference is unknown. We speculate that different causes of low DLco in COPD such as degree of emphysema, interstitial lung abnormalities, and pulmonary hypertension, may have a different prevalence and progression in women with COPD,” he said.
Looking ahead, “Large studies including an adequate sample of women with COPD is urgently needed because they will be the main face of COPD in the near future,” said Dr. de Torres. “Sex difference in their physiological characteristics, the reason to explain those differences and how they behave longitudinally is also urgently needed,” he added.
The study was supported in part by AstraZeneca and by the COPD research program of the Spanish Respiratory Society. The researchers and Dr. de Torres had no financial conflicts to disclose.
Single breath diffusion capacity for carbon monoxide shows greater decline over time in COPD patients compared with controls, but declines significantly more in women compared with men, according to data from 602 adults with a history of smoking.
In previous studies, diffusion capacity for carbon monoxide (DLco) has been associated with decreased exercise capacity and poor health status in patients with COPD, but its association as a measure of disease progression has not been well studied, wrote Ciro Casanova, MD, of Hospital Universitario La Candelaria, Spain, and colleagues.
In a study published in the journal CHEST®, the researchers identified 506 adult smokers with COPD and 96 adult smoker controls without COPD. Lung function based on single breath DLco was measured each year for 5 years. The study population was part of the COPH History Assessment in SpaiN (CHAIN), an ongoing observational study of adults with COPD. COPD was defined as a history of at least 10 pack-years of smoking and a post-bronchodilator FEV1/FVC greater than 0.7 after 400 micrograms of albuterol, the researchers said.
During the 5-year period, the average overall annual decline in DLco was 1.34% in COPD patients, compared with .04% in non-COPD controls (P = .004). Among COPD patients, age, body mass index, FEV1%, and active smoking were not associated with longitudinal change in DLco values, the researchers said.
Notably, women with COPD at baseline had lower baseline DLco values compared with men (11.37%) and a significantly steeper decline in DLco (.89%) compared with men (P = .039). “Being a woman was the only factor that related to the annual rate of change in DLco,” the researchers said.
In a subgroup analysis, the researchers identified 305 COPD patients and 69 non-COPD controls who had at least 3 DLco measurements over the 5-year study period. In this group, 16.4% patients with COPD and 4.3% smokers without COPD showed significant yearly declines in DLco of –4.139% and –4.440%, respectively. Among COPD patients, significantly more women than men showed significant DLco declines (26% vs. 14%, P = .005). No significant differences were observed in mortality or hospitalizations per patient-year for COPD patients with and without DLco decline, the researchers said.
The study findings were limited by several factors including the lack of annual measurements of DLco among some patients, potential variability in the instruments used to measure DLco, and the absence of computerized tomography data for the chest, the researchers noted. However, the results support the value of the test for COPD progression when conducted at 3- to 4-year intervals, given the slow pace of the decline, they said. More research is needed, but “women seem to have a different susceptibility to cigarette smoke in the alveolar or pulmonary vascular domains,” they added.
DLco remains a valuable marker
The study is important because the usual longitudinal decline of diffusion capacity, an important physiological parameter in patients with COPD, was unknown, Juan P. de Torres, MD, of Queen’s University, Kingston, Ont., said in an interview.
“The finding of a different longitudinal decline of DLco in women was a surprise,” said Dr. de Torres, who was a coauthor on the study. “We knew from previous works from our group that COPD has a different clinical and prognostic behavior in women with COPD, but this specific finding is novel and important,” he said.
“These results provide information about the testing frequency (3-4 years) needed to use DLco as a marker of COPD progression in clinical practice,” Dr. de Torres added.
“What is the driving cause of this sex difference is unknown. We speculate that different causes of low DLco in COPD such as degree of emphysema, interstitial lung abnormalities, and pulmonary hypertension, may have a different prevalence and progression in women with COPD,” he said.
Looking ahead, “Large studies including an adequate sample of women with COPD is urgently needed because they will be the main face of COPD in the near future,” said Dr. de Torres. “Sex difference in their physiological characteristics, the reason to explain those differences and how they behave longitudinally is also urgently needed,” he added.
The study was supported in part by AstraZeneca and by the COPD research program of the Spanish Respiratory Society. The researchers and Dr. de Torres had no financial conflicts to disclose.
Single breath diffusion capacity for carbon monoxide shows greater decline over time in COPD patients compared with controls, but declines significantly more in women compared with men, according to data from 602 adults with a history of smoking.
In previous studies, diffusion capacity for carbon monoxide (DLco) has been associated with decreased exercise capacity and poor health status in patients with COPD, but its association as a measure of disease progression has not been well studied, wrote Ciro Casanova, MD, of Hospital Universitario La Candelaria, Spain, and colleagues.
In a study published in the journal CHEST®, the researchers identified 506 adult smokers with COPD and 96 adult smoker controls without COPD. Lung function based on single breath DLco was measured each year for 5 years. The study population was part of the COPH History Assessment in SpaiN (CHAIN), an ongoing observational study of adults with COPD. COPD was defined as a history of at least 10 pack-years of smoking and a post-bronchodilator FEV1/FVC greater than 0.7 after 400 micrograms of albuterol, the researchers said.
During the 5-year period, the average overall annual decline in DLco was 1.34% in COPD patients, compared with .04% in non-COPD controls (P = .004). Among COPD patients, age, body mass index, FEV1%, and active smoking were not associated with longitudinal change in DLco values, the researchers said.
Notably, women with COPD at baseline had lower baseline DLco values compared with men (11.37%) and a significantly steeper decline in DLco (.89%) compared with men (P = .039). “Being a woman was the only factor that related to the annual rate of change in DLco,” the researchers said.
In a subgroup analysis, the researchers identified 305 COPD patients and 69 non-COPD controls who had at least 3 DLco measurements over the 5-year study period. In this group, 16.4% patients with COPD and 4.3% smokers without COPD showed significant yearly declines in DLco of –4.139% and –4.440%, respectively. Among COPD patients, significantly more women than men showed significant DLco declines (26% vs. 14%, P = .005). No significant differences were observed in mortality or hospitalizations per patient-year for COPD patients with and without DLco decline, the researchers said.
The study findings were limited by several factors including the lack of annual measurements of DLco among some patients, potential variability in the instruments used to measure DLco, and the absence of computerized tomography data for the chest, the researchers noted. However, the results support the value of the test for COPD progression when conducted at 3- to 4-year intervals, given the slow pace of the decline, they said. More research is needed, but “women seem to have a different susceptibility to cigarette smoke in the alveolar or pulmonary vascular domains,” they added.
DLco remains a valuable marker
The study is important because the usual longitudinal decline of diffusion capacity, an important physiological parameter in patients with COPD, was unknown, Juan P. de Torres, MD, of Queen’s University, Kingston, Ont., said in an interview.
“The finding of a different longitudinal decline of DLco in women was a surprise,” said Dr. de Torres, who was a coauthor on the study. “We knew from previous works from our group that COPD has a different clinical and prognostic behavior in women with COPD, but this specific finding is novel and important,” he said.
“These results provide information about the testing frequency (3-4 years) needed to use DLco as a marker of COPD progression in clinical practice,” Dr. de Torres added.
“What is the driving cause of this sex difference is unknown. We speculate that different causes of low DLco in COPD such as degree of emphysema, interstitial lung abnormalities, and pulmonary hypertension, may have a different prevalence and progression in women with COPD,” he said.
Looking ahead, “Large studies including an adequate sample of women with COPD is urgently needed because they will be the main face of COPD in the near future,” said Dr. de Torres. “Sex difference in their physiological characteristics, the reason to explain those differences and how they behave longitudinally is also urgently needed,” he added.
The study was supported in part by AstraZeneca and by the COPD research program of the Spanish Respiratory Society. The researchers and Dr. de Torres had no financial conflicts to disclose.
FROM CHEST
Novel hedgehog inhibitor strategies improve BCC outcomes
MD, a Mohs surgeon and chair of the department of dermatology at the Cleveland Clinic.

She and her colleagues have noticed an accelerated and durable response to hedgehog inhibitors after debulking and are studying cell signaling before and after debulking to better understand the issue.
Dr. Vidimos shared a remarkable case to illustrate the point during a clinical pearls talk at the annual meeting of the American College of Mohs Surgery.
An 82-year-old woman presented with a crusted, hemorrhagic, nodular basal cell carcinoma (BCC) that had overgrown over nearly her entire nose and left lower eyelid. A recurrence of a previous BCC, the tumor had been growing for a decade and had invaded her nasal bones but not the periorbital tissue.
An outside surgeon suggested a full rhinectomy and removal of the lower eyelid, but the woman refused.
Dr. Vidimos decided to treat her with vismodegib, but prior to doing so, she debulked the tumor to help with the pain and bleeding. She did not curette the portion of tumor extending through the ala into the nasal vestibule. “I let the vismodegib take care of that,” she said.
After 9 months, the tumor was virtually gone, with no recurrence after 3 years. Surgical debulking prior to hedgehog inhibition “reduces the tumor burden and may increase the efficacy and shorten the course of therapy,” Dr. Vidimos said.
The hedgehog inhibitors vismodegib (Erivedge) and sonidegib Odomzo are both approved for treating locally advanced BCC, with a complete response of 31% of locally advanced disease with vismodegib, according to one report.
But monotherapy is limited by intolerable side effects, most commonly muscle spasms, alopecia, and dysgeusia. To minimize the impact, Dr. Vidimos generally puts patients on treatment with Monday through Friday dosing and gives them the weekends off, a schedule she and her colleagues have reported works as well as daily dosing.
Still, many patients discontinue the drugs because of the side effects. Hedgehog inhibitors are also expensive and responses aren’t always durable. To increase efficacy and shorten the course of therapy, “we need alternative treatment strategies,” Dr. Vidimos said.
Up-front tumor debulking is one such strategy. Altered cell signaling pathways associated with tissue remodeling might improve response, and debulking may reduce the genetic heterogeneity of tumor cells, rendering remaining cells less resistant to hedgehog inhibition, she explained.
“It is exciting to see how tumor debulking may reduce tumor burden and heterogeneity, and thus lead to a durable response in extensive tumors,” said Vishal Patel, MD, assistant professor of dermatology and director of the cutaneous oncology program at George Washington University, Washington, who heard the presentation. “More investigation is needed to reproduce these results, but this approach may lead to improved outcomes with targeted therapies,” he said in an interview.
Combination therapy with other agents is another option, and there also seems to be a synergistic effect with radiation, with hedgehog inhibitors increasing cellular response to radiation therapy, Dr. Vidimos said.
Hedgehog inhibitors can also be used to shrink tumors before surgery. One small series found a 27% decrease in the area of the tumor after 3 to 6 months of preoperative vismodegib.
Dr. Vidimos shared another case to illustrate the point.
A 64-year-old woman fainted and presented to the ED with a hemoglobin of 3.2 mg/dL because of chronic blood loss from an ulcerated BCC on her upper back. The lesion measured 25 cm by 9 cm, and was 3.5 cm deep with no bone involvement. The woman was addicted to opioids by the time she presented.
She was started on vismodegib; the ulcer shrunk considerably after 6 months, and the woman underwent a resection. Only one small focus of BCC was found across 78 specimens submitted to Dr. Vidimos for Mohs reading.
Resection was followed by a muscle flap repair and radiation. At 5 and a half years, there is no evidence of disease; the only sign that the lesion had been there was a scar running along the woman’s upper spine.
The approach “was very successful for a very aggressive and worrisome tumor,” Dr. Vidimos said.
Dr. Vidimos did not have any relevant disclosures. Dr. Patel had no relevant disclosures.
MD, a Mohs surgeon and chair of the department of dermatology at the Cleveland Clinic.
She and her colleagues have noticed an accelerated and durable response to hedgehog inhibitors after debulking and are studying cell signaling before and after debulking to better understand the issue.
Dr. Vidimos shared a remarkable case to illustrate the point during a clinical pearls talk at the annual meeting of the American College of Mohs Surgery.
An 82-year-old woman presented with a crusted, hemorrhagic, nodular basal cell carcinoma (BCC) that had overgrown over nearly her entire nose and left lower eyelid. A recurrence of a previous BCC, the tumor had been growing for a decade and had invaded her nasal bones but not the periorbital tissue.
An outside surgeon suggested a full rhinectomy and removal of the lower eyelid, but the woman refused.
Dr. Vidimos decided to treat her with vismodegib, but prior to doing so, she debulked the tumor to help with the pain and bleeding. She did not curette the portion of tumor extending through the ala into the nasal vestibule. “I let the vismodegib take care of that,” she said.
After 9 months, the tumor was virtually gone, with no recurrence after 3 years. Surgical debulking prior to hedgehog inhibition “reduces the tumor burden and may increase the efficacy and shorten the course of therapy,” Dr. Vidimos said.
The hedgehog inhibitors vismodegib (Erivedge) and sonidegib Odomzo are both approved for treating locally advanced BCC, with a complete response of 31% of locally advanced disease with vismodegib, according to one report.
But monotherapy is limited by intolerable side effects, most commonly muscle spasms, alopecia, and dysgeusia. To minimize the impact, Dr. Vidimos generally puts patients on treatment with Monday through Friday dosing and gives them the weekends off, a schedule she and her colleagues have reported works as well as daily dosing.
Still, many patients discontinue the drugs because of the side effects. Hedgehog inhibitors are also expensive and responses aren’t always durable. To increase efficacy and shorten the course of therapy, “we need alternative treatment strategies,” Dr. Vidimos said.
Up-front tumor debulking is one such strategy. Altered cell signaling pathways associated with tissue remodeling might improve response, and debulking may reduce the genetic heterogeneity of tumor cells, rendering remaining cells less resistant to hedgehog inhibition, she explained.
“It is exciting to see how tumor debulking may reduce tumor burden and heterogeneity, and thus lead to a durable response in extensive tumors,” said Vishal Patel, MD, assistant professor of dermatology and director of the cutaneous oncology program at George Washington University, Washington, who heard the presentation. “More investigation is needed to reproduce these results, but this approach may lead to improved outcomes with targeted therapies,” he said in an interview.
Combination therapy with other agents is another option, and there also seems to be a synergistic effect with radiation, with hedgehog inhibitors increasing cellular response to radiation therapy, Dr. Vidimos said.
Hedgehog inhibitors can also be used to shrink tumors before surgery. One small series found a 27% decrease in the area of the tumor after 3 to 6 months of preoperative vismodegib.
Dr. Vidimos shared another case to illustrate the point.
A 64-year-old woman fainted and presented to the ED with a hemoglobin of 3.2 mg/dL because of chronic blood loss from an ulcerated BCC on her upper back. The lesion measured 25 cm by 9 cm, and was 3.5 cm deep with no bone involvement. The woman was addicted to opioids by the time she presented.
She was started on vismodegib; the ulcer shrunk considerably after 6 months, and the woman underwent a resection. Only one small focus of BCC was found across 78 specimens submitted to Dr. Vidimos for Mohs reading.
Resection was followed by a muscle flap repair and radiation. At 5 and a half years, there is no evidence of disease; the only sign that the lesion had been there was a scar running along the woman’s upper spine.
The approach “was very successful for a very aggressive and worrisome tumor,” Dr. Vidimos said.
Dr. Vidimos did not have any relevant disclosures. Dr. Patel had no relevant disclosures.
MD, a Mohs surgeon and chair of the department of dermatology at the Cleveland Clinic.
She and her colleagues have noticed an accelerated and durable response to hedgehog inhibitors after debulking and are studying cell signaling before and after debulking to better understand the issue.
Dr. Vidimos shared a remarkable case to illustrate the point during a clinical pearls talk at the annual meeting of the American College of Mohs Surgery.
An 82-year-old woman presented with a crusted, hemorrhagic, nodular basal cell carcinoma (BCC) that had overgrown over nearly her entire nose and left lower eyelid. A recurrence of a previous BCC, the tumor had been growing for a decade and had invaded her nasal bones but not the periorbital tissue.
An outside surgeon suggested a full rhinectomy and removal of the lower eyelid, but the woman refused.
Dr. Vidimos decided to treat her with vismodegib, but prior to doing so, she debulked the tumor to help with the pain and bleeding. She did not curette the portion of tumor extending through the ala into the nasal vestibule. “I let the vismodegib take care of that,” she said.
After 9 months, the tumor was virtually gone, with no recurrence after 3 years. Surgical debulking prior to hedgehog inhibition “reduces the tumor burden and may increase the efficacy and shorten the course of therapy,” Dr. Vidimos said.
The hedgehog inhibitors vismodegib (Erivedge) and sonidegib Odomzo are both approved for treating locally advanced BCC, with a complete response of 31% of locally advanced disease with vismodegib, according to one report.
But monotherapy is limited by intolerable side effects, most commonly muscle spasms, alopecia, and dysgeusia. To minimize the impact, Dr. Vidimos generally puts patients on treatment with Monday through Friday dosing and gives them the weekends off, a schedule she and her colleagues have reported works as well as daily dosing.
Still, many patients discontinue the drugs because of the side effects. Hedgehog inhibitors are also expensive and responses aren’t always durable. To increase efficacy and shorten the course of therapy, “we need alternative treatment strategies,” Dr. Vidimos said.
Up-front tumor debulking is one such strategy. Altered cell signaling pathways associated with tissue remodeling might improve response, and debulking may reduce the genetic heterogeneity of tumor cells, rendering remaining cells less resistant to hedgehog inhibition, she explained.
“It is exciting to see how tumor debulking may reduce tumor burden and heterogeneity, and thus lead to a durable response in extensive tumors,” said Vishal Patel, MD, assistant professor of dermatology and director of the cutaneous oncology program at George Washington University, Washington, who heard the presentation. “More investigation is needed to reproduce these results, but this approach may lead to improved outcomes with targeted therapies,” he said in an interview.
Combination therapy with other agents is another option, and there also seems to be a synergistic effect with radiation, with hedgehog inhibitors increasing cellular response to radiation therapy, Dr. Vidimos said.
Hedgehog inhibitors can also be used to shrink tumors before surgery. One small series found a 27% decrease in the area of the tumor after 3 to 6 months of preoperative vismodegib.
Dr. Vidimos shared another case to illustrate the point.
A 64-year-old woman fainted and presented to the ED with a hemoglobin of 3.2 mg/dL because of chronic blood loss from an ulcerated BCC on her upper back. The lesion measured 25 cm by 9 cm, and was 3.5 cm deep with no bone involvement. The woman was addicted to opioids by the time she presented.
She was started on vismodegib; the ulcer shrunk considerably after 6 months, and the woman underwent a resection. Only one small focus of BCC was found across 78 specimens submitted to Dr. Vidimos for Mohs reading.
Resection was followed by a muscle flap repair and radiation. At 5 and a half years, there is no evidence of disease; the only sign that the lesion had been there was a scar running along the woman’s upper spine.
The approach “was very successful for a very aggressive and worrisome tumor,” Dr. Vidimos said.
Dr. Vidimos did not have any relevant disclosures. Dr. Patel had no relevant disclosures.
FROM THE ACMS ANNUAL MEETING
New digital ADHD intervention tools are emerging
New digital tools are on the horizon to help patients with attention-deficit/hyperactivity disorder (ADHD) manage the condition.

Speakers at the World Congress on ADHD – Virtual Event described innovations aimed at improving medication compliance or reducing symptoms through the use of smartphone technology such as apps and text messaging, and video games. Some of these technologies have shown promising results in clinical trials, but the experts called for additional studies to further vet their efficacy.

Digital technologies have limitations and should be seen as adjunctive rather than standalone tools that can aid clinicians and educators, said Hannah Kirk, PhD, a psychology research fellow at Monash University’s Turner Institute for Brain and Mental Health in Clayton, Australia. Dr. Kirk joined three other speakers for the session: “ADHD in the digital age – From pitfalls to challenges.”
An explosion in technology
ADHD, the most common neurodevelopmental disorder, has global prevalence rates ranging from 5% to 7%, said Dr. Kirk. Digital technology and digital health “have been heralded as having enormous potential to improve early access and to improve the increasing demand in child support services,” she said.
The world has seen an explosion of digital technology innovation in the last decade, spurred on most recently by the COVID-19 pandemic. New demand exists for tools in educational and health care settings to provide information and support through websites, apps, SMS, video conferencing, and wearable devices, Dr. Kirk said.
Looking at the landscape of ADHD digital therapeutics, “there are probably tens of thousands of apps and other digital products to treat and manage conditions across the spectrum,” said Scott H. Kollins, PhD, MS, a clinical psychologist at Duke Health’s ADHD Clinic in Durham, N.C.

In general, few developers of these products have conducted rigorous, well-controlled trials, he noted.
Video game interventions
AKL-T01, a tool that pairs continuous fine motor tasks and perceptual reaction time tasks, went through several rounds of clinical trials to achieve federal approval as a digital therapeutic.
“This not just another video game,” said Dr. Kollins, who helped developed it. The tool’s adaptive algorithms adjust and monitor task difficulty based on performance, using a video game format and rewards to engage users.
Two phase 3 trials provided the basis for the Food and Drug Administration’s approval of AKL-T01, also known as EndeavorRx, in 2020. The first trial, published in The Lancet, randomized 348 children 1:1 to receive either the AKL-T01 treatment or a controlled intervention, which was a word game. Participating children aged 8-12 with a confirmed ADHD diagnosis were asked to play the game for about 25 minutes a day, 5 days a week over 4 weeks. The study excluded children who were taking medicine.
The researchers reported statistically significant improvements in attentional functioning in the AKL-T01 group as rated by test of variables of attention. The trial reported no serious adverse events, although one child in the AKL-T01 group withdrew from the study.
“As kids go through this treatment, it’s challenging and the difficulty levels increase, so it’s not surprising that kids get frustrated with that, or have emotional outbursts,” Dr. Kollins said. Those reactions suggest that the intervention was working, he added.
A follow-up study, published in npj Digital Medicine, broadened the scope. That study included children who had taken medication and extended the study period. Overall, 206 children aged 8-14 (130 on stimulants and 76 on no medication) played the game for 28 days, taking a pause for another 28 days, then reinitiating the treatment.
As in the first trial, AKL-T01 significantly improved ADHD-related impairment, a metric that continued to improve in the second round of treatment. Looking at secondary outcomes, the proportion of children deemed as clinical responders on the Impairment Rating Scale, 68.3% of all of the participants were responders by the end of the study on the ADHD ratings scale, meaning there was a greater than 30% improvement in symptoms. Upward of 50% of participants at the end of the second round of treatment showed substantial improvement in their ADHD ratings scale scores.
“This was really a substantial move ... the first-ever app-based video game approved by the FDA,” noted Dr. Kollins, who is affiliated with the Duke Clinical Research Institute. Some skeptics have called this a marketing ploy or have questioned the integrity of the FDA approval process.
“I would submit and argue that the rigor of the trial speaks for itself,” he said. “But it’s not surprising that there’s skepticism in the clinical community about something like this – a brand new treatment modality.”
In her own research, Dr. Kirk has studied game-based interventions aimed at assessing ADHD and improving cognitive training. In 2018, her team developed a touch screen game–based intervention for early evaluation of attention skills, using six activities. In a visual search task, children were asked to locate red lobsters on a screen that showed a variety of underwater creatures. In another selection attention task, children were asked to scan the screen for a particular target, such as a yellow star, and to indicate whether that target was absent or present on the screen. Other tasks assessed for sustained attention abilities and information processing speed.
She and her colleagues recruited 340 children aged 4-7 years to evaluate whether the tool produced consistent results over time, and compared favorably to existing measures of attention. None of the participants had been diagnosed with ADHD. To assess reliability, a subset of children completed another assessment 2 weeks after the first one. The study showed varying results according to activity. The visual search task had high test-retest reliability and the strongest validity, compared with the other tasks. The sustained attention tasks exhibited the weakest validity.
The next steps are to assess whether this tool is sensitive enough to detect differences between children with or without clinical attention difficulties such as ADHD, Dr. Kirk said.
Apps improve adherence
As some technologies focus on reducing symptoms through games, others seek to improve medication compliance through SMS and smartphone apps.
Studies have shown that medication can decrease incidence of smoking, mood disorders, traumatic brain injuries, car crashes, and educational outcomes. However, risk decreases only if compliance is good, said Joseph Biederman, MD. Right now, “there’s extremely poor adherence to stimulant medications in ADHD” across the world, said Dr. Biederman, chief of clinical and research programs in pediatric psychopharmacology and adult ADHD at Massachusetts General Hospital in Boston.
“This is a problem that’s driven by ADHD itself,” he continued. Prescribers don’t always have the time to educate the patient on medications, deal with misconceptions, or provide support for management of daily activities.
Text reminders may offer a solution. Partnering with a Canadian technology company, MEMOTEXT, Dr. Biederman and colleagues at Massachusetts General Hospital developed an SMS-based disease management intervention for ADHD.
The tool aims to manage work, home life, and social relationships by supporting the timely renewal of medications. It doesn’t just remind people to take their ADHD medication, it reminds them to take any other medication they need, and provides the reasons why it’s important to take these drugs. Through interactive questions, it also assesses the progress and knowledge of patients and families about ADHD.
Testing this app in pediatric settings, Dr. Biederman and colleagues published a study in the Journal of Psychopharmacology showing a dramatic increase in compliance – from 60% to 90%.
In another study, this one published in the Journal of Clinical Psychopharmacology, Dr. Biederman and colleagues found that compliance improved, from 35% to 70% in adults. The SMS program in these settings not only improved adherence, but it also reduced costs of ADHD-associated complications while adding beneficial support and value to patients, families, and prescribers, Dr. Biederman said.
Promising findings about the power of apps to increase ADHD medication adherence led Luis Augusto Rohde, MD, PhD, and colleagues to develop the FOCUS app in 2016, for use in his home country of Brazil. The app objectively monitors symptoms of ADHD and establishes cooperative relationships between the patient, their families, and caregivers, said Dr. Rohde, professor of child and adolescent psychiatry at the Federal University of Rio Grande do Sul’s department of psychiatry, Porto Alegre, Brazil.

FOCUS works through collaboration. Anyone involved in the patient’s care: teachers, family members, and health care professionals, can download the app. Through this shared connection with the patient, they can participate in weekly assessments of symptoms and adverse events. A task manager sends medication reminders to the patient, who can select activities to help monitor daily performance and customize rewards.
All of those features “make it much easier to plan and individualize treatments and discuss compliance and issues with the patient,” Dr. Rohde said.
FOCUS traffic ranges from 1,200 to 1,500 active users each week, offering a wealth of data to mine on compliance, behavior, and adverse events. An upcoming randomized clinical trial in three groups of patients will further explore FOCUS’s ability to increase adherence to treatment, Dr. Rohde said.
Digital tech pros and cons
The accessibility of digital technology to children living in remote areas is one of its biggest assets, Dr. Kirk said.
Digital technologies capture real time data, are easy to use, are suitable for young children with developmental disorders, have few adverse effects, and can be easily updated. However, there are some limitations, she added. Attitudes toward technology, time required to supervise their use, and funding to facilitate the use of such technology can hinder implementation. Given that digital technology is increasingly being used to collect sensitive medical data and assess clinical conditions, it’s crucial for these new technologies to be compliant with HIPAA requirements, Dr. Kirk said.
Developers need to be thoughtful and deliberate in how they design clinical evidence strategies for digital therapeutics for ADHD.
“There’s much work that needs to be done from a clinical, statistical, regulatory, and policy perspective, but this journey illustrates this can be done with ADHD and other mental health conditions.”
Dr. Kirk disclosed working previously for a small technology company in Melbourne that developed medical technologies for children. Dr. Kollins’ work has been supported by numerous U.S. agencies, including the National Institute of Mental Health. He has served as a consultant to numerous pharmaceutical companies tied to ADHD clinical psychopharmacology. Dr. Biederman has provided research support to Genentech, Headspace, Pfizer, Roche Translational & Clinical Research Center, and other pharmaceutical companies. Also, Dr. Biederman has a partnership with MEMOTEXT through Partners Healthcare Innovation. Dr. Rohde has received grant or research support from, and served as a consultant to, several companies, including Bial, Novartis, Pfizer, and Shire/Takeda. He has received authorship royalties from Oxford University Press and ArtMed, and travel grants from Shire.
New digital tools are on the horizon to help patients with attention-deficit/hyperactivity disorder (ADHD) manage the condition.
Speakers at the World Congress on ADHD – Virtual Event described innovations aimed at improving medication compliance or reducing symptoms through the use of smartphone technology such as apps and text messaging, and video games. Some of these technologies have shown promising results in clinical trials, but the experts called for additional studies to further vet their efficacy.
Digital technologies have limitations and should be seen as adjunctive rather than standalone tools that can aid clinicians and educators, said Hannah Kirk, PhD, a psychology research fellow at Monash University’s Turner Institute for Brain and Mental Health in Clayton, Australia. Dr. Kirk joined three other speakers for the session: “ADHD in the digital age – From pitfalls to challenges.”
An explosion in technology
ADHD, the most common neurodevelopmental disorder, has global prevalence rates ranging from 5% to 7%, said Dr. Kirk. Digital technology and digital health “have been heralded as having enormous potential to improve early access and to improve the increasing demand in child support services,” she said.
The world has seen an explosion of digital technology innovation in the last decade, spurred on most recently by the COVID-19 pandemic. New demand exists for tools in educational and health care settings to provide information and support through websites, apps, SMS, video conferencing, and wearable devices, Dr. Kirk said.
Looking at the landscape of ADHD digital therapeutics, “there are probably tens of thousands of apps and other digital products to treat and manage conditions across the spectrum,” said Scott H. Kollins, PhD, MS, a clinical psychologist at Duke Health’s ADHD Clinic in Durham, N.C.
In general, few developers of these products have conducted rigorous, well-controlled trials, he noted.
Video game interventions
AKL-T01, a tool that pairs continuous fine motor tasks and perceptual reaction time tasks, went through several rounds of clinical trials to achieve federal approval as a digital therapeutic.
“This not just another video game,” said Dr. Kollins, who helped developed it. The tool’s adaptive algorithms adjust and monitor task difficulty based on performance, using a video game format and rewards to engage users.
Two phase 3 trials provided the basis for the Food and Drug Administration’s approval of AKL-T01, also known as EndeavorRx, in 2020. The first trial, published in The Lancet, randomized 348 children 1:1 to receive either the AKL-T01 treatment or a controlled intervention, which was a word game. Participating children aged 8-12 with a confirmed ADHD diagnosis were asked to play the game for about 25 minutes a day, 5 days a week over 4 weeks. The study excluded children who were taking medicine.
The researchers reported statistically significant improvements in attentional functioning in the AKL-T01 group as rated by test of variables of attention. The trial reported no serious adverse events, although one child in the AKL-T01 group withdrew from the study.
“As kids go through this treatment, it’s challenging and the difficulty levels increase, so it’s not surprising that kids get frustrated with that, or have emotional outbursts,” Dr. Kollins said. Those reactions suggest that the intervention was working, he added.
A follow-up study, published in npj Digital Medicine, broadened the scope. That study included children who had taken medication and extended the study period. Overall, 206 children aged 8-14 (130 on stimulants and 76 on no medication) played the game for 28 days, taking a pause for another 28 days, then reinitiating the treatment.
As in the first trial, AKL-T01 significantly improved ADHD-related impairment, a metric that continued to improve in the second round of treatment. Looking at secondary outcomes, the proportion of children deemed as clinical responders on the Impairment Rating Scale, 68.3% of all of the participants were responders by the end of the study on the ADHD ratings scale, meaning there was a greater than 30% improvement in symptoms. Upward of 50% of participants at the end of the second round of treatment showed substantial improvement in their ADHD ratings scale scores.
“This was really a substantial move ... the first-ever app-based video game approved by the FDA,” noted Dr. Kollins, who is affiliated with the Duke Clinical Research Institute. Some skeptics have called this a marketing ploy or have questioned the integrity of the FDA approval process.
“I would submit and argue that the rigor of the trial speaks for itself,” he said. “But it’s not surprising that there’s skepticism in the clinical community about something like this – a brand new treatment modality.”
In her own research, Dr. Kirk has studied game-based interventions aimed at assessing ADHD and improving cognitive training. In 2018, her team developed a touch screen game–based intervention for early evaluation of attention skills, using six activities. In a visual search task, children were asked to locate red lobsters on a screen that showed a variety of underwater creatures. In another selection attention task, children were asked to scan the screen for a particular target, such as a yellow star, and to indicate whether that target was absent or present on the screen. Other tasks assessed for sustained attention abilities and information processing speed.
She and her colleagues recruited 340 children aged 4-7 years to evaluate whether the tool produced consistent results over time, and compared favorably to existing measures of attention. None of the participants had been diagnosed with ADHD. To assess reliability, a subset of children completed another assessment 2 weeks after the first one. The study showed varying results according to activity. The visual search task had high test-retest reliability and the strongest validity, compared with the other tasks. The sustained attention tasks exhibited the weakest validity.
The next steps are to assess whether this tool is sensitive enough to detect differences between children with or without clinical attention difficulties such as ADHD, Dr. Kirk said.
Apps improve adherence
As some technologies focus on reducing symptoms through games, others seek to improve medication compliance through SMS and smartphone apps.
Studies have shown that medication can decrease incidence of smoking, mood disorders, traumatic brain injuries, car crashes, and educational outcomes. However, risk decreases only if compliance is good, said Joseph Biederman, MD. Right now, “there’s extremely poor adherence to stimulant medications in ADHD” across the world, said Dr. Biederman, chief of clinical and research programs in pediatric psychopharmacology and adult ADHD at Massachusetts General Hospital in Boston.
“This is a problem that’s driven by ADHD itself,” he continued. Prescribers don’t always have the time to educate the patient on medications, deal with misconceptions, or provide support for management of daily activities.
Text reminders may offer a solution. Partnering with a Canadian technology company, MEMOTEXT, Dr. Biederman and colleagues at Massachusetts General Hospital developed an SMS-based disease management intervention for ADHD.
The tool aims to manage work, home life, and social relationships by supporting the timely renewal of medications. It doesn’t just remind people to take their ADHD medication, it reminds them to take any other medication they need, and provides the reasons why it’s important to take these drugs. Through interactive questions, it also assesses the progress and knowledge of patients and families about ADHD.
Testing this app in pediatric settings, Dr. Biederman and colleagues published a study in the Journal of Psychopharmacology showing a dramatic increase in compliance – from 60% to 90%.
In another study, this one published in the Journal of Clinical Psychopharmacology, Dr. Biederman and colleagues found that compliance improved, from 35% to 70% in adults. The SMS program in these settings not only improved adherence, but it also reduced costs of ADHD-associated complications while adding beneficial support and value to patients, families, and prescribers, Dr. Biederman said.
Promising findings about the power of apps to increase ADHD medication adherence led Luis Augusto Rohde, MD, PhD, and colleagues to develop the FOCUS app in 2016, for use in his home country of Brazil. The app objectively monitors symptoms of ADHD and establishes cooperative relationships between the patient, their families, and caregivers, said Dr. Rohde, professor of child and adolescent psychiatry at the Federal University of Rio Grande do Sul’s department of psychiatry, Porto Alegre, Brazil.
FOCUS works through collaboration. Anyone involved in the patient’s care: teachers, family members, and health care professionals, can download the app. Through this shared connection with the patient, they can participate in weekly assessments of symptoms and adverse events. A task manager sends medication reminders to the patient, who can select activities to help monitor daily performance and customize rewards.
All of those features “make it much easier to plan and individualize treatments and discuss compliance and issues with the patient,” Dr. Rohde said.
FOCUS traffic ranges from 1,200 to 1,500 active users each week, offering a wealth of data to mine on compliance, behavior, and adverse events. An upcoming randomized clinical trial in three groups of patients will further explore FOCUS’s ability to increase adherence to treatment, Dr. Rohde said.
Digital tech pros and cons
The accessibility of digital technology to children living in remote areas is one of its biggest assets, Dr. Kirk said.
Digital technologies capture real time data, are easy to use, are suitable for young children with developmental disorders, have few adverse effects, and can be easily updated. However, there are some limitations, she added. Attitudes toward technology, time required to supervise their use, and funding to facilitate the use of such technology can hinder implementation. Given that digital technology is increasingly being used to collect sensitive medical data and assess clinical conditions, it’s crucial for these new technologies to be compliant with HIPAA requirements, Dr. Kirk said.
Developers need to be thoughtful and deliberate in how they design clinical evidence strategies for digital therapeutics for ADHD.
“There’s much work that needs to be done from a clinical, statistical, regulatory, and policy perspective, but this journey illustrates this can be done with ADHD and other mental health conditions.”
Dr. Kirk disclosed working previously for a small technology company in Melbourne that developed medical technologies for children. Dr. Kollins’ work has been supported by numerous U.S. agencies, including the National Institute of Mental Health. He has served as a consultant to numerous pharmaceutical companies tied to ADHD clinical psychopharmacology. Dr. Biederman has provided research support to Genentech, Headspace, Pfizer, Roche Translational & Clinical Research Center, and other pharmaceutical companies. Also, Dr. Biederman has a partnership with MEMOTEXT through Partners Healthcare Innovation. Dr. Rohde has received grant or research support from, and served as a consultant to, several companies, including Bial, Novartis, Pfizer, and Shire/Takeda. He has received authorship royalties from Oxford University Press and ArtMed, and travel grants from Shire.
New digital tools are on the horizon to help patients with attention-deficit/hyperactivity disorder (ADHD) manage the condition.
Speakers at the World Congress on ADHD – Virtual Event described innovations aimed at improving medication compliance or reducing symptoms through the use of smartphone technology such as apps and text messaging, and video games. Some of these technologies have shown promising results in clinical trials, but the experts called for additional studies to further vet their efficacy.
Digital technologies have limitations and should be seen as adjunctive rather than standalone tools that can aid clinicians and educators, said Hannah Kirk, PhD, a psychology research fellow at Monash University’s Turner Institute for Brain and Mental Health in Clayton, Australia. Dr. Kirk joined three other speakers for the session: “ADHD in the digital age – From pitfalls to challenges.”
An explosion in technology
ADHD, the most common neurodevelopmental disorder, has global prevalence rates ranging from 5% to 7%, said Dr. Kirk. Digital technology and digital health “have been heralded as having enormous potential to improve early access and to improve the increasing demand in child support services,” she said.
The world has seen an explosion of digital technology innovation in the last decade, spurred on most recently by the COVID-19 pandemic. New demand exists for tools in educational and health care settings to provide information and support through websites, apps, SMS, video conferencing, and wearable devices, Dr. Kirk said.
Looking at the landscape of ADHD digital therapeutics, “there are probably tens of thousands of apps and other digital products to treat and manage conditions across the spectrum,” said Scott H. Kollins, PhD, MS, a clinical psychologist at Duke Health’s ADHD Clinic in Durham, N.C.
In general, few developers of these products have conducted rigorous, well-controlled trials, he noted.
Video game interventions
AKL-T01, a tool that pairs continuous fine motor tasks and perceptual reaction time tasks, went through several rounds of clinical trials to achieve federal approval as a digital therapeutic.
“This not just another video game,” said Dr. Kollins, who helped developed it. The tool’s adaptive algorithms adjust and monitor task difficulty based on performance, using a video game format and rewards to engage users.
Two phase 3 trials provided the basis for the Food and Drug Administration’s approval of AKL-T01, also known as EndeavorRx, in 2020. The first trial, published in The Lancet, randomized 348 children 1:1 to receive either the AKL-T01 treatment or a controlled intervention, which was a word game. Participating children aged 8-12 with a confirmed ADHD diagnosis were asked to play the game for about 25 minutes a day, 5 days a week over 4 weeks. The study excluded children who were taking medicine.
The researchers reported statistically significant improvements in attentional functioning in the AKL-T01 group as rated by test of variables of attention. The trial reported no serious adverse events, although one child in the AKL-T01 group withdrew from the study.
“As kids go through this treatment, it’s challenging and the difficulty levels increase, so it’s not surprising that kids get frustrated with that, or have emotional outbursts,” Dr. Kollins said. Those reactions suggest that the intervention was working, he added.
A follow-up study, published in npj Digital Medicine, broadened the scope. That study included children who had taken medication and extended the study period. Overall, 206 children aged 8-14 (130 on stimulants and 76 on no medication) played the game for 28 days, taking a pause for another 28 days, then reinitiating the treatment.
As in the first trial, AKL-T01 significantly improved ADHD-related impairment, a metric that continued to improve in the second round of treatment. Looking at secondary outcomes, the proportion of children deemed as clinical responders on the Impairment Rating Scale, 68.3% of all of the participants were responders by the end of the study on the ADHD ratings scale, meaning there was a greater than 30% improvement in symptoms. Upward of 50% of participants at the end of the second round of treatment showed substantial improvement in their ADHD ratings scale scores.
“This was really a substantial move ... the first-ever app-based video game approved by the FDA,” noted Dr. Kollins, who is affiliated with the Duke Clinical Research Institute. Some skeptics have called this a marketing ploy or have questioned the integrity of the FDA approval process.
“I would submit and argue that the rigor of the trial speaks for itself,” he said. “But it’s not surprising that there’s skepticism in the clinical community about something like this – a brand new treatment modality.”
In her own research, Dr. Kirk has studied game-based interventions aimed at assessing ADHD and improving cognitive training. In 2018, her team developed a touch screen game–based intervention for early evaluation of attention skills, using six activities. In a visual search task, children were asked to locate red lobsters on a screen that showed a variety of underwater creatures. In another selection attention task, children were asked to scan the screen for a particular target, such as a yellow star, and to indicate whether that target was absent or present on the screen. Other tasks assessed for sustained attention abilities and information processing speed.
She and her colleagues recruited 340 children aged 4-7 years to evaluate whether the tool produced consistent results over time, and compared favorably to existing measures of attention. None of the participants had been diagnosed with ADHD. To assess reliability, a subset of children completed another assessment 2 weeks after the first one. The study showed varying results according to activity. The visual search task had high test-retest reliability and the strongest validity, compared with the other tasks. The sustained attention tasks exhibited the weakest validity.
The next steps are to assess whether this tool is sensitive enough to detect differences between children with or without clinical attention difficulties such as ADHD, Dr. Kirk said.
Apps improve adherence
As some technologies focus on reducing symptoms through games, others seek to improve medication compliance through SMS and smartphone apps.
Studies have shown that medication can decrease incidence of smoking, mood disorders, traumatic brain injuries, car crashes, and educational outcomes. However, risk decreases only if compliance is good, said Joseph Biederman, MD. Right now, “there’s extremely poor adherence to stimulant medications in ADHD” across the world, said Dr. Biederman, chief of clinical and research programs in pediatric psychopharmacology and adult ADHD at Massachusetts General Hospital in Boston.
“This is a problem that’s driven by ADHD itself,” he continued. Prescribers don’t always have the time to educate the patient on medications, deal with misconceptions, or provide support for management of daily activities.
Text reminders may offer a solution. Partnering with a Canadian technology company, MEMOTEXT, Dr. Biederman and colleagues at Massachusetts General Hospital developed an SMS-based disease management intervention for ADHD.
The tool aims to manage work, home life, and social relationships by supporting the timely renewal of medications. It doesn’t just remind people to take their ADHD medication, it reminds them to take any other medication they need, and provides the reasons why it’s important to take these drugs. Through interactive questions, it also assesses the progress and knowledge of patients and families about ADHD.
Testing this app in pediatric settings, Dr. Biederman and colleagues published a study in the Journal of Psychopharmacology showing a dramatic increase in compliance – from 60% to 90%.
In another study, this one published in the Journal of Clinical Psychopharmacology, Dr. Biederman and colleagues found that compliance improved, from 35% to 70% in adults. The SMS program in these settings not only improved adherence, but it also reduced costs of ADHD-associated complications while adding beneficial support and value to patients, families, and prescribers, Dr. Biederman said.
Promising findings about the power of apps to increase ADHD medication adherence led Luis Augusto Rohde, MD, PhD, and colleagues to develop the FOCUS app in 2016, for use in his home country of Brazil. The app objectively monitors symptoms of ADHD and establishes cooperative relationships between the patient, their families, and caregivers, said Dr. Rohde, professor of child and adolescent psychiatry at the Federal University of Rio Grande do Sul’s department of psychiatry, Porto Alegre, Brazil.
FOCUS works through collaboration. Anyone involved in the patient’s care: teachers, family members, and health care professionals, can download the app. Through this shared connection with the patient, they can participate in weekly assessments of symptoms and adverse events. A task manager sends medication reminders to the patient, who can select activities to help monitor daily performance and customize rewards.
All of those features “make it much easier to plan and individualize treatments and discuss compliance and issues with the patient,” Dr. Rohde said.
FOCUS traffic ranges from 1,200 to 1,500 active users each week, offering a wealth of data to mine on compliance, behavior, and adverse events. An upcoming randomized clinical trial in three groups of patients will further explore FOCUS’s ability to increase adherence to treatment, Dr. Rohde said.
Digital tech pros and cons
The accessibility of digital technology to children living in remote areas is one of its biggest assets, Dr. Kirk said.
Digital technologies capture real time data, are easy to use, are suitable for young children with developmental disorders, have few adverse effects, and can be easily updated. However, there are some limitations, she added. Attitudes toward technology, time required to supervise their use, and funding to facilitate the use of such technology can hinder implementation. Given that digital technology is increasingly being used to collect sensitive medical data and assess clinical conditions, it’s crucial for these new technologies to be compliant with HIPAA requirements, Dr. Kirk said.
Developers need to be thoughtful and deliberate in how they design clinical evidence strategies for digital therapeutics for ADHD.
“There’s much work that needs to be done from a clinical, statistical, regulatory, and policy perspective, but this journey illustrates this can be done with ADHD and other mental health conditions.”
Dr. Kirk disclosed working previously for a small technology company in Melbourne that developed medical technologies for children. Dr. Kollins’ work has been supported by numerous U.S. agencies, including the National Institute of Mental Health. He has served as a consultant to numerous pharmaceutical companies tied to ADHD clinical psychopharmacology. Dr. Biederman has provided research support to Genentech, Headspace, Pfizer, Roche Translational & Clinical Research Center, and other pharmaceutical companies. Also, Dr. Biederman has a partnership with MEMOTEXT through Partners Healthcare Innovation. Dr. Rohde has received grant or research support from, and served as a consultant to, several companies, including Bial, Novartis, Pfizer, and Shire/Takeda. He has received authorship royalties from Oxford University Press and ArtMed, and travel grants from Shire.
FROM ADHD 2021
Once-nightly sodium oxybate agent effective in narcolepsy
, new research suggests. Top-line results from the phase 3 REST-ON trial released earlier this year showed that the agent known as FT218 (Avadel Pharmaceuticals) met all three of its coprimary efficacy endpoints at all three doses assessed (6 g, 7.5 g, and 9 g). Patients receiving the drug showed significantly greater improvements on the Maintenance of Wakefulness Test (MWT), the Clinical Global Impression of Improvement (CGI-I), and mean weekly attacks of cataplexy, compared with those who received placebo.
The new analyses, which focused on key secondary outcomes, showed that all three doses of the novel agent were associated with significant improvements in sleep quality, refreshing nature of sleep, sleep paralysis, disturbed nocturnal sleep, and scores on the Epworth Sleepiness Scale (ESS).
Principal investigator Michael J. Thorpy, MD, director of the Sleep-Wake Disorders Center at the Montefiore Medical Center, New York, said in a news release that the results represent “the promise of a potential new treatment strategy for physicians and patients.”
“I am particularly impressed by the consistency of results as early as 3 weeks with only a 6-g dose,” he added.
Dr. Thorpy, who is also a professor of neurology at the Albert Einstein College of Medicine, noted that the new formulation will be more convenient for patients. “The advantage of this medication is its once-nightly formulation, so patients don’t need to awaken during the night and can actually have a better night’s sleep,” he said.
Dr. Thorpy presented the study findings at the 2021 annual meeting of the American Academy of Neurology.
FT218 is currently under review by the U.S. Food and Drug Administration, which has set Oct. 15 as the Prescription Drug User Fee Act target date.
Forced awakening
Sodium oxybate was first approved by the FDA in 2002 to treat cataplexy in adults with narcolepsy and was expanded in 2005 to also treat excessive daytime sleepiness (EDS). That formulation is indicated for twice-nightly administration, with the second dose taken 2.5-4 hours after the first.
“The need for forced awakening to take the second dose ... may result in noncompliance, which may lead to reduced efficacy and/or mistimed doses,” the investigators noted.
FT218 is a modified-release version of sodium oxybate. A single 6-g dose of the investigational agent “has shown bioequivalent exposure to twice-nightly immediate-release [sodium oxybate] given as two 3-g doses,” wrote the researchers.
It also currently has Orphan Drug Designation from the FDA for the treatment of narcolepsy.
The randomized, double-blind, placebo-controlled, multicenter REST-ON study was conducted from November 2016 to March 2020 and included patients 16 years or older who had narcolepsy type 1 or type 2.
Patients received the active treatment (n = 107; mean age, 30.9 years; 64.5% women) or placebo (n = 105; mean age, 31.6 years; 71.4% women) according to a four-period forced uptitration dosing schedule of 4.5 g for 1 week, 6 g for 2 weeks, 7.5 g for 5 weeks, and 9 g for 5 weeks.
Secondary outcome measures included the ESS, sleep quality/refreshing nature of sleep on a visual analog scale, sleep paralysis and hypnagogic hallucinations on a sleep symptoms diary, disturbed nocturnal sleep on polysomnographic measures, and number of arousals as defined per the American Academy of Sleep Medicine Score Manual.
Reports of adverse events (AEs) were collected from time of informed consent until 7 days after the last dose received.
Improvement across doses
Results showed that, compared with placebo, improvement in disturbed nocturnal sleep from baseline was significantly greater for the active treatment at 6 g at week 3 (mean between-group difference, –11; P < .001), at 7.5 g at week 8 (mean difference, –17.7; P < .001), and at 9 g at week 13 (mean difference, –22.6; P < .001).
The mean difference between the three doses and placebo for reduction in number of arousals was –11.3 (P < .05), –19.4 (P < .001), and –23.7 (P < .001), respectively. And the 6 g at week 3, 7.5 g at week 8, and 9 g at week 13 doses showed significant (P < .001) improvements versus placebo on the ESS (mean difference, –2.1, –3.2, and –3.9, respectively).
All three doses also showed significant improvement in sleep quality and refreshing nature of sleep (P < .001 for all comparisons), as well as improvement of sleep paralysis (P = .04, P = .02, and P = .04, respectively).
There were no significant differences between FT218 and placebo for improvement in hypnagogic hallucinations. Dr. Thorpy noted that the number of patients with baseline hallucinations “was relatively small,” which may have led to this finding. “Had there been a much larger population with hallucinations, I suspect that we would have seen a statistically significant improvement there as well,” he said.
Generally well tolerated
The investigators noted that FT218 was “generally well tolerated, and the most common adverse reactions were well-known and established sodium oxybate adverse reactions.”
Treatment-related AEs that occurred in more than 2% of the patients receiving FT218 included nausea, dizziness, enuresis, headache, decreased appetite, and vomiting.
Seven serious AEs were reported, including five in those assigned to the active treatment. This included one case each of diabetes inadequate control, paresthesia, perirectal abscess, hypertension, and suicidal ideation. Only the case of suicidal ideation was considered to be a treatment-related AE.
The investigators noted that, although they have not yet delved into subgroup analysis to look for differences among sex, age, or race, they plan to do so in the future.
Overall, the results indicate that “FT218 is an effective agent not only for the major symptoms of sleepiness and cataplexy, but also the quality of sleep at night,” said Dr. Thorpy.
Asked whether he thinks the FDA will approve the drug, he said that it should be “straightforward” because it’s just a different formulation of an already-approved agent. “I very much expect there will not be any problems in this medication being approved,” Dr. Thorpy said.
Benefits ‘sleep architecture’
Commenting on the findings, Logan Schneider, MD, codirector of the Stanford/VA Alzheimer’s Center and clinical assistant professor at the Stanford Sleep Center, Redwood City, Calif., said that the investigators’ focus on these secondary outcomes “was really worthwhile.”
Dr. Schneider, who was not involved in the research, noted that, because the study only included patients with narcolepsy, the results can’t be extrapolated to groups who have other sleep disorders.
Still, “it is worthwhile now to expand beyond the two primary symptoms that are, in my consideration, life threatening: daytime sleepiness and cataplexy. We should also address more of the quality of life and other aspects of narcolepsy, including disturbed nocturnal sleep and sleep quality issues related to that,” he said.
“Being able to address those aspects and say, ‘I have a therapy that clearly helps the multidimensionality of our patients’ is very vindicating,” Dr. Schneider noted.
He was also impressed with the various measures the researchers used, rather than relying just on patient reports, “which are subject to recollection difficulties. This was a nice way to quantify possibly as a diagnostic marker the underlying disruption of sleep, as well as a possible treatment marker to show how well a therapy works.”
“It actually shows a beneficial effect on sleep architecture,” Dr. Schneider said.
The study was funded by Avadel Pharmaceuticals. Dr. Thorpy is a consultant/advisory board member for Avadel, Axsome, Balance Therapeutics, Eisai, Harmony Biosciences, Jazz Pharmaceuticals, NLS Pharmaceuticals, Suven Life Sciences, and Takeda Pharmaceutical. Dr. Schneider reports being an adviser and/or on the speakers’ bureau for similar drugs by Jazz Pharmaceuticals and Harmony Biosciences.
A version of this article first appeared on Medscape.com.
, new research suggests. Top-line results from the phase 3 REST-ON trial released earlier this year showed that the agent known as FT218 (Avadel Pharmaceuticals) met all three of its coprimary efficacy endpoints at all three doses assessed (6 g, 7.5 g, and 9 g). Patients receiving the drug showed significantly greater improvements on the Maintenance of Wakefulness Test (MWT), the Clinical Global Impression of Improvement (CGI-I), and mean weekly attacks of cataplexy, compared with those who received placebo.
The new analyses, which focused on key secondary outcomes, showed that all three doses of the novel agent were associated with significant improvements in sleep quality, refreshing nature of sleep, sleep paralysis, disturbed nocturnal sleep, and scores on the Epworth Sleepiness Scale (ESS).
Principal investigator Michael J. Thorpy, MD, director of the Sleep-Wake Disorders Center at the Montefiore Medical Center, New York, said in a news release that the results represent “the promise of a potential new treatment strategy for physicians and patients.”
“I am particularly impressed by the consistency of results as early as 3 weeks with only a 6-g dose,” he added.
Dr. Thorpy, who is also a professor of neurology at the Albert Einstein College of Medicine, noted that the new formulation will be more convenient for patients. “The advantage of this medication is its once-nightly formulation, so patients don’t need to awaken during the night and can actually have a better night’s sleep,” he said.
Dr. Thorpy presented the study findings at the 2021 annual meeting of the American Academy of Neurology.
FT218 is currently under review by the U.S. Food and Drug Administration, which has set Oct. 15 as the Prescription Drug User Fee Act target date.
Forced awakening
Sodium oxybate was first approved by the FDA in 2002 to treat cataplexy in adults with narcolepsy and was expanded in 2005 to also treat excessive daytime sleepiness (EDS). That formulation is indicated for twice-nightly administration, with the second dose taken 2.5-4 hours after the first.
“The need for forced awakening to take the second dose ... may result in noncompliance, which may lead to reduced efficacy and/or mistimed doses,” the investigators noted.
FT218 is a modified-release version of sodium oxybate. A single 6-g dose of the investigational agent “has shown bioequivalent exposure to twice-nightly immediate-release [sodium oxybate] given as two 3-g doses,” wrote the researchers.
It also currently has Orphan Drug Designation from the FDA for the treatment of narcolepsy.
The randomized, double-blind, placebo-controlled, multicenter REST-ON study was conducted from November 2016 to March 2020 and included patients 16 years or older who had narcolepsy type 1 or type 2.
Patients received the active treatment (n = 107; mean age, 30.9 years; 64.5% women) or placebo (n = 105; mean age, 31.6 years; 71.4% women) according to a four-period forced uptitration dosing schedule of 4.5 g for 1 week, 6 g for 2 weeks, 7.5 g for 5 weeks, and 9 g for 5 weeks.
Secondary outcome measures included the ESS, sleep quality/refreshing nature of sleep on a visual analog scale, sleep paralysis and hypnagogic hallucinations on a sleep symptoms diary, disturbed nocturnal sleep on polysomnographic measures, and number of arousals as defined per the American Academy of Sleep Medicine Score Manual.
Reports of adverse events (AEs) were collected from time of informed consent until 7 days after the last dose received.
Improvement across doses
Results showed that, compared with placebo, improvement in disturbed nocturnal sleep from baseline was significantly greater for the active treatment at 6 g at week 3 (mean between-group difference, –11; P < .001), at 7.5 g at week 8 (mean difference, –17.7; P < .001), and at 9 g at week 13 (mean difference, –22.6; P < .001).
The mean difference between the three doses and placebo for reduction in number of arousals was –11.3 (P < .05), –19.4 (P < .001), and –23.7 (P < .001), respectively. And the 6 g at week 3, 7.5 g at week 8, and 9 g at week 13 doses showed significant (P < .001) improvements versus placebo on the ESS (mean difference, –2.1, –3.2, and –3.9, respectively).
All three doses also showed significant improvement in sleep quality and refreshing nature of sleep (P < .001 for all comparisons), as well as improvement of sleep paralysis (P = .04, P = .02, and P = .04, respectively).
There were no significant differences between FT218 and placebo for improvement in hypnagogic hallucinations. Dr. Thorpy noted that the number of patients with baseline hallucinations “was relatively small,” which may have led to this finding. “Had there been a much larger population with hallucinations, I suspect that we would have seen a statistically significant improvement there as well,” he said.
Generally well tolerated
The investigators noted that FT218 was “generally well tolerated, and the most common adverse reactions were well-known and established sodium oxybate adverse reactions.”
Treatment-related AEs that occurred in more than 2% of the patients receiving FT218 included nausea, dizziness, enuresis, headache, decreased appetite, and vomiting.
Seven serious AEs were reported, including five in those assigned to the active treatment. This included one case each of diabetes inadequate control, paresthesia, perirectal abscess, hypertension, and suicidal ideation. Only the case of suicidal ideation was considered to be a treatment-related AE.
The investigators noted that, although they have not yet delved into subgroup analysis to look for differences among sex, age, or race, they plan to do so in the future.
Overall, the results indicate that “FT218 is an effective agent not only for the major symptoms of sleepiness and cataplexy, but also the quality of sleep at night,” said Dr. Thorpy.
Asked whether he thinks the FDA will approve the drug, he said that it should be “straightforward” because it’s just a different formulation of an already-approved agent. “I very much expect there will not be any problems in this medication being approved,” Dr. Thorpy said.
Benefits ‘sleep architecture’
Commenting on the findings, Logan Schneider, MD, codirector of the Stanford/VA Alzheimer’s Center and clinical assistant professor at the Stanford Sleep Center, Redwood City, Calif., said that the investigators’ focus on these secondary outcomes “was really worthwhile.”
Dr. Schneider, who was not involved in the research, noted that, because the study only included patients with narcolepsy, the results can’t be extrapolated to groups who have other sleep disorders.
Still, “it is worthwhile now to expand beyond the two primary symptoms that are, in my consideration, life threatening: daytime sleepiness and cataplexy. We should also address more of the quality of life and other aspects of narcolepsy, including disturbed nocturnal sleep and sleep quality issues related to that,” he said.
“Being able to address those aspects and say, ‘I have a therapy that clearly helps the multidimensionality of our patients’ is very vindicating,” Dr. Schneider noted.
He was also impressed with the various measures the researchers used, rather than relying just on patient reports, “which are subject to recollection difficulties. This was a nice way to quantify possibly as a diagnostic marker the underlying disruption of sleep, as well as a possible treatment marker to show how well a therapy works.”
“It actually shows a beneficial effect on sleep architecture,” Dr. Schneider said.
The study was funded by Avadel Pharmaceuticals. Dr. Thorpy is a consultant/advisory board member for Avadel, Axsome, Balance Therapeutics, Eisai, Harmony Biosciences, Jazz Pharmaceuticals, NLS Pharmaceuticals, Suven Life Sciences, and Takeda Pharmaceutical. Dr. Schneider reports being an adviser and/or on the speakers’ bureau for similar drugs by Jazz Pharmaceuticals and Harmony Biosciences.
A version of this article first appeared on Medscape.com.
, new research suggests. Top-line results from the phase 3 REST-ON trial released earlier this year showed that the agent known as FT218 (Avadel Pharmaceuticals) met all three of its coprimary efficacy endpoints at all three doses assessed (6 g, 7.5 g, and 9 g). Patients receiving the drug showed significantly greater improvements on the Maintenance of Wakefulness Test (MWT), the Clinical Global Impression of Improvement (CGI-I), and mean weekly attacks of cataplexy, compared with those who received placebo.
The new analyses, which focused on key secondary outcomes, showed that all three doses of the novel agent were associated with significant improvements in sleep quality, refreshing nature of sleep, sleep paralysis, disturbed nocturnal sleep, and scores on the Epworth Sleepiness Scale (ESS).
Principal investigator Michael J. Thorpy, MD, director of the Sleep-Wake Disorders Center at the Montefiore Medical Center, New York, said in a news release that the results represent “the promise of a potential new treatment strategy for physicians and patients.”
“I am particularly impressed by the consistency of results as early as 3 weeks with only a 6-g dose,” he added.
Dr. Thorpy, who is also a professor of neurology at the Albert Einstein College of Medicine, noted that the new formulation will be more convenient for patients. “The advantage of this medication is its once-nightly formulation, so patients don’t need to awaken during the night and can actually have a better night’s sleep,” he said.
Dr. Thorpy presented the study findings at the 2021 annual meeting of the American Academy of Neurology.
FT218 is currently under review by the U.S. Food and Drug Administration, which has set Oct. 15 as the Prescription Drug User Fee Act target date.
Forced awakening
Sodium oxybate was first approved by the FDA in 2002 to treat cataplexy in adults with narcolepsy and was expanded in 2005 to also treat excessive daytime sleepiness (EDS). That formulation is indicated for twice-nightly administration, with the second dose taken 2.5-4 hours after the first.
“The need for forced awakening to take the second dose ... may result in noncompliance, which may lead to reduced efficacy and/or mistimed doses,” the investigators noted.
FT218 is a modified-release version of sodium oxybate. A single 6-g dose of the investigational agent “has shown bioequivalent exposure to twice-nightly immediate-release [sodium oxybate] given as two 3-g doses,” wrote the researchers.
It also currently has Orphan Drug Designation from the FDA for the treatment of narcolepsy.
The randomized, double-blind, placebo-controlled, multicenter REST-ON study was conducted from November 2016 to March 2020 and included patients 16 years or older who had narcolepsy type 1 or type 2.
Patients received the active treatment (n = 107; mean age, 30.9 years; 64.5% women) or placebo (n = 105; mean age, 31.6 years; 71.4% women) according to a four-period forced uptitration dosing schedule of 4.5 g for 1 week, 6 g for 2 weeks, 7.5 g for 5 weeks, and 9 g for 5 weeks.
Secondary outcome measures included the ESS, sleep quality/refreshing nature of sleep on a visual analog scale, sleep paralysis and hypnagogic hallucinations on a sleep symptoms diary, disturbed nocturnal sleep on polysomnographic measures, and number of arousals as defined per the American Academy of Sleep Medicine Score Manual.
Reports of adverse events (AEs) were collected from time of informed consent until 7 days after the last dose received.
Improvement across doses
Results showed that, compared with placebo, improvement in disturbed nocturnal sleep from baseline was significantly greater for the active treatment at 6 g at week 3 (mean between-group difference, –11; P < .001), at 7.5 g at week 8 (mean difference, –17.7; P < .001), and at 9 g at week 13 (mean difference, –22.6; P < .001).
The mean difference between the three doses and placebo for reduction in number of arousals was –11.3 (P < .05), –19.4 (P < .001), and –23.7 (P < .001), respectively. And the 6 g at week 3, 7.5 g at week 8, and 9 g at week 13 doses showed significant (P < .001) improvements versus placebo on the ESS (mean difference, –2.1, –3.2, and –3.9, respectively).
All three doses also showed significant improvement in sleep quality and refreshing nature of sleep (P < .001 for all comparisons), as well as improvement of sleep paralysis (P = .04, P = .02, and P = .04, respectively).
There were no significant differences between FT218 and placebo for improvement in hypnagogic hallucinations. Dr. Thorpy noted that the number of patients with baseline hallucinations “was relatively small,” which may have led to this finding. “Had there been a much larger population with hallucinations, I suspect that we would have seen a statistically significant improvement there as well,” he said.
Generally well tolerated
The investigators noted that FT218 was “generally well tolerated, and the most common adverse reactions were well-known and established sodium oxybate adverse reactions.”
Treatment-related AEs that occurred in more than 2% of the patients receiving FT218 included nausea, dizziness, enuresis, headache, decreased appetite, and vomiting.
Seven serious AEs were reported, including five in those assigned to the active treatment. This included one case each of diabetes inadequate control, paresthesia, perirectal abscess, hypertension, and suicidal ideation. Only the case of suicidal ideation was considered to be a treatment-related AE.
The investigators noted that, although they have not yet delved into subgroup analysis to look for differences among sex, age, or race, they plan to do so in the future.
Overall, the results indicate that “FT218 is an effective agent not only for the major symptoms of sleepiness and cataplexy, but also the quality of sleep at night,” said Dr. Thorpy.
Asked whether he thinks the FDA will approve the drug, he said that it should be “straightforward” because it’s just a different formulation of an already-approved agent. “I very much expect there will not be any problems in this medication being approved,” Dr. Thorpy said.
Benefits ‘sleep architecture’
Commenting on the findings, Logan Schneider, MD, codirector of the Stanford/VA Alzheimer’s Center and clinical assistant professor at the Stanford Sleep Center, Redwood City, Calif., said that the investigators’ focus on these secondary outcomes “was really worthwhile.”
Dr. Schneider, who was not involved in the research, noted that, because the study only included patients with narcolepsy, the results can’t be extrapolated to groups who have other sleep disorders.
Still, “it is worthwhile now to expand beyond the two primary symptoms that are, in my consideration, life threatening: daytime sleepiness and cataplexy. We should also address more of the quality of life and other aspects of narcolepsy, including disturbed nocturnal sleep and sleep quality issues related to that,” he said.
“Being able to address those aspects and say, ‘I have a therapy that clearly helps the multidimensionality of our patients’ is very vindicating,” Dr. Schneider noted.
He was also impressed with the various measures the researchers used, rather than relying just on patient reports, “which are subject to recollection difficulties. This was a nice way to quantify possibly as a diagnostic marker the underlying disruption of sleep, as well as a possible treatment marker to show how well a therapy works.”
“It actually shows a beneficial effect on sleep architecture,” Dr. Schneider said.
The study was funded by Avadel Pharmaceuticals. Dr. Thorpy is a consultant/advisory board member for Avadel, Axsome, Balance Therapeutics, Eisai, Harmony Biosciences, Jazz Pharmaceuticals, NLS Pharmaceuticals, Suven Life Sciences, and Takeda Pharmaceutical. Dr. Schneider reports being an adviser and/or on the speakers’ bureau for similar drugs by Jazz Pharmaceuticals and Harmony Biosciences.
A version of this article first appeared on Medscape.com.
FROM AAN 2021
Motor abnormalities in children a harbinger of serious mental illness?
Motor problems in children may be a harbinger of serious mental illness, new research suggests.
Investigators found that motor abnormalities were twice as common among those who develop psychosis or depression, compared with their counterparts in the general population, suggesting that these abnormalities may help predict vulnerability and provide an opportunity for early intervention.
“We have learned there are motor signs that are measurable in adolescence [that are] more prevalent in these disorders,” said lead investigator Katherine S. F. Damme, PhD, adolescent development and preventive treatment program (ADAPT), Northwestern University, Chicago.
“This is just scratching the surface of motor signs, but they may have some transdiagnostic vulnerability across these psychopathologies” to which sensorimotor connectivity and motor behaviors “might provide additional insight,” Dr. Damme added.
The findings were presented at the Virtual Congress of the Schizophrenia International Research Society 2021.
A core symptom
There has been a lot of interest in the pathophysiology of psychosis and in detecting it early, said Dr. Damme. “It has devastating effects, and early intervention is of great importance,” she added.
However, previous research has typically focused on affect or cognition, rather than on motor signs, despite the fact that motor signs are a “core symptom of both psychosis and depression.”
The prevalence and presentation of motor signs in adolescence, which is a “critical time for identifying these risk markers” because of their proximity to the onset of psychosis, has been understudied, Dr. Damme said.
For their study, the investigators gathered motor function data from the Adolescent Brain Cognitive Development Study (ABCD), which included 10,835 children aged 9-11 years with broad demographic diversity from 21 sites across the United States.
Overall, 27.6% of the children were reported to have least one motor sign; approximately 3% were reported to have two or more motor signs.
The most common of these was dyscoordination, which was endorsed by 19.3% of participants. In addition, 8.8% were reported to have had experienced developmental motor delays, 1.5% had psychomotor agitation, and 0.3% had psychomotor retardation.
The investigators determined that 4.6% of participants met criteria for depression, 2.6% for a psychosis, and 1.8% for comorbid psychosis and depression.
Motor signs were much more common among children with depression, psychosis, or both than among those who did not have these conditions; 45.8% reported having at least one motor sign.
Developmental motor delays and dyscoordination occurred at about the same rate in both patients with depression and those with psychosis. Rates were higher among patients with both of these conditions than among those with either condition alone.
In contrast, psychomotor agitation was more common among patients with depression alone and among those with comorbid depression and psychosis than among patients with psychosis alone. The rate of psychomotor retardation was increased among patients with psychosis alone but was less common among patients with comorbidity than in the healthy control group.
Familial vulnerability
The investigators also assessed participants who had not been diagnosed with a mental illness but who had a family history of depression only (28.9%), a relative with psychosis-like experiences (0.6%), or a family history of both depression and psychosis experiences (1.8%).
Although the effect size was smaller, there was a higher rate of motor signs among participants with a family history of these conditions, Dr. Damme said. “Again, we see that it’s elevated across developmental motor delays and at a similar rate in people who have depression and psychosis.”
In addition, psychomotor agitation was linked to depression with psychosis and depression without it.
Sensorimotor connectivity network data for the cohort indicated there was no main effect of diagnosis on corticostriatal connectivity.
However, more depressive symptoms were related to less connectivity (P = .024). There was a similar finding for psychotic-like experiences. The total number of such experiences related to lower connectivity (P < .001).
During the postpresentation discussion, Ian Kelleher, MD, PhD, honorary clinical lecturer in psychiatry at the Royal College of Surgeons in Ireland, Dublin, said he was “surprised” by the finding that the rate of psychomotor retardation was lower among participants with psychosis and depression.
Dr. Damme noted that some of the motor sign item ratings came by way of a child interview and that some of these item ratings came from the adults in the children’s lives.
She added that she was not entirely sure whether asking an 8- to 11-year-old in a clinical interview whether they are experiencing motor signs “might be the best way to get at motor slowing.”
Subtle features
Commenting on the findings in an interview, Peter F. Liddle, MD, PhD, professor of psychiatry, at the University of Nottingham (England), noted that the “features we’re talking about are pretty subtle.
“What I’ve been wondering about for some time is whether we should be getting video recordings and using machine learning approaches to teach a computer to recognize normal movements vs abnormal movements, and particularly facial expression,” said Dr. Liddle, who was not involved with the research.
He called the current study “interesting” but noted several factors that affect the potential utility of the findings in predicting outcomes.
First, they “may not be very good for distinguishing schizophrenia from mood disorders; but if the question is simply determining which young person might go on to develop a significant mental disorder, then it may be useful,” Dr. Liddle said.
He endorsed the investigators’ conclusion that motor abnormalities may be a transdiagnostic marker. Beyond that, they may be “more useful as a predictor of the likely long-term severity, but that’s my own hypothesis based on my work,” he added.
Another question concerns the sensitivity of motor abnormalities as a predictive marker. With the rate of the abnormalities identified in those who developed psychosis and depression about double the rate in the overall population, “it sounds like those assessors were fairly sensitive. … but not all that specific,” said Dr. Liddle.
A third issue relates to treatment. “By the time people get sent to a psychiatrist for assessment for possible impending psychotic illness, they’ve often already had medication,” typically an antidepressant or antipsychotic.
“It’s very well established that dopamine-blocking antipsychotics produce hypokinesia and also dyskinesia,” which could then become a confounding factor, Dr. Liddle said.
The study was funded by grants from the National Institute of Mental Health. The study authors and Dr. Liddle have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Motor problems in children may be a harbinger of serious mental illness, new research suggests.
Investigators found that motor abnormalities were twice as common among those who develop psychosis or depression, compared with their counterparts in the general population, suggesting that these abnormalities may help predict vulnerability and provide an opportunity for early intervention.
“We have learned there are motor signs that are measurable in adolescence [that are] more prevalent in these disorders,” said lead investigator Katherine S. F. Damme, PhD, adolescent development and preventive treatment program (ADAPT), Northwestern University, Chicago.
“This is just scratching the surface of motor signs, but they may have some transdiagnostic vulnerability across these psychopathologies” to which sensorimotor connectivity and motor behaviors “might provide additional insight,” Dr. Damme added.
The findings were presented at the Virtual Congress of the Schizophrenia International Research Society 2021.
A core symptom
There has been a lot of interest in the pathophysiology of psychosis and in detecting it early, said Dr. Damme. “It has devastating effects, and early intervention is of great importance,” she added.
However, previous research has typically focused on affect or cognition, rather than on motor signs, despite the fact that motor signs are a “core symptom of both psychosis and depression.”
The prevalence and presentation of motor signs in adolescence, which is a “critical time for identifying these risk markers” because of their proximity to the onset of psychosis, has been understudied, Dr. Damme said.
For their study, the investigators gathered motor function data from the Adolescent Brain Cognitive Development Study (ABCD), which included 10,835 children aged 9-11 years with broad demographic diversity from 21 sites across the United States.
Overall, 27.6% of the children were reported to have least one motor sign; approximately 3% were reported to have two or more motor signs.
The most common of these was dyscoordination, which was endorsed by 19.3% of participants. In addition, 8.8% were reported to have had experienced developmental motor delays, 1.5% had psychomotor agitation, and 0.3% had psychomotor retardation.
The investigators determined that 4.6% of participants met criteria for depression, 2.6% for a psychosis, and 1.8% for comorbid psychosis and depression.
Motor signs were much more common among children with depression, psychosis, or both than among those who did not have these conditions; 45.8% reported having at least one motor sign.
Developmental motor delays and dyscoordination occurred at about the same rate in both patients with depression and those with psychosis. Rates were higher among patients with both of these conditions than among those with either condition alone.
In contrast, psychomotor agitation was more common among patients with depression alone and among those with comorbid depression and psychosis than among patients with psychosis alone. The rate of psychomotor retardation was increased among patients with psychosis alone but was less common among patients with comorbidity than in the healthy control group.
Familial vulnerability
The investigators also assessed participants who had not been diagnosed with a mental illness but who had a family history of depression only (28.9%), a relative with psychosis-like experiences (0.6%), or a family history of both depression and psychosis experiences (1.8%).
Although the effect size was smaller, there was a higher rate of motor signs among participants with a family history of these conditions, Dr. Damme said. “Again, we see that it’s elevated across developmental motor delays and at a similar rate in people who have depression and psychosis.”
In addition, psychomotor agitation was linked to depression with psychosis and depression without it.
Sensorimotor connectivity network data for the cohort indicated there was no main effect of diagnosis on corticostriatal connectivity.
However, more depressive symptoms were related to less connectivity (P = .024). There was a similar finding for psychotic-like experiences. The total number of such experiences related to lower connectivity (P < .001).
During the postpresentation discussion, Ian Kelleher, MD, PhD, honorary clinical lecturer in psychiatry at the Royal College of Surgeons in Ireland, Dublin, said he was “surprised” by the finding that the rate of psychomotor retardation was lower among participants with psychosis and depression.
Dr. Damme noted that some of the motor sign item ratings came by way of a child interview and that some of these item ratings came from the adults in the children’s lives.
She added that she was not entirely sure whether asking an 8- to 11-year-old in a clinical interview whether they are experiencing motor signs “might be the best way to get at motor slowing.”
Subtle features
Commenting on the findings in an interview, Peter F. Liddle, MD, PhD, professor of psychiatry, at the University of Nottingham (England), noted that the “features we’re talking about are pretty subtle.
“What I’ve been wondering about for some time is whether we should be getting video recordings and using machine learning approaches to teach a computer to recognize normal movements vs abnormal movements, and particularly facial expression,” said Dr. Liddle, who was not involved with the research.
He called the current study “interesting” but noted several factors that affect the potential utility of the findings in predicting outcomes.
First, they “may not be very good for distinguishing schizophrenia from mood disorders; but if the question is simply determining which young person might go on to develop a significant mental disorder, then it may be useful,” Dr. Liddle said.
He endorsed the investigators’ conclusion that motor abnormalities may be a transdiagnostic marker. Beyond that, they may be “more useful as a predictor of the likely long-term severity, but that’s my own hypothesis based on my work,” he added.
Another question concerns the sensitivity of motor abnormalities as a predictive marker. With the rate of the abnormalities identified in those who developed psychosis and depression about double the rate in the overall population, “it sounds like those assessors were fairly sensitive. … but not all that specific,” said Dr. Liddle.
A third issue relates to treatment. “By the time people get sent to a psychiatrist for assessment for possible impending psychotic illness, they’ve often already had medication,” typically an antidepressant or antipsychotic.
“It’s very well established that dopamine-blocking antipsychotics produce hypokinesia and also dyskinesia,” which could then become a confounding factor, Dr. Liddle said.
The study was funded by grants from the National Institute of Mental Health. The study authors and Dr. Liddle have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Motor problems in children may be a harbinger of serious mental illness, new research suggests.
Investigators found that motor abnormalities were twice as common among those who develop psychosis or depression, compared with their counterparts in the general population, suggesting that these abnormalities may help predict vulnerability and provide an opportunity for early intervention.
“We have learned there are motor signs that are measurable in adolescence [that are] more prevalent in these disorders,” said lead investigator Katherine S. F. Damme, PhD, adolescent development and preventive treatment program (ADAPT), Northwestern University, Chicago.
“This is just scratching the surface of motor signs, but they may have some transdiagnostic vulnerability across these psychopathologies” to which sensorimotor connectivity and motor behaviors “might provide additional insight,” Dr. Damme added.
The findings were presented at the Virtual Congress of the Schizophrenia International Research Society 2021.
A core symptom
There has been a lot of interest in the pathophysiology of psychosis and in detecting it early, said Dr. Damme. “It has devastating effects, and early intervention is of great importance,” she added.
However, previous research has typically focused on affect or cognition, rather than on motor signs, despite the fact that motor signs are a “core symptom of both psychosis and depression.”
The prevalence and presentation of motor signs in adolescence, which is a “critical time for identifying these risk markers” because of their proximity to the onset of psychosis, has been understudied, Dr. Damme said.
For their study, the investigators gathered motor function data from the Adolescent Brain Cognitive Development Study (ABCD), which included 10,835 children aged 9-11 years with broad demographic diversity from 21 sites across the United States.
Overall, 27.6% of the children were reported to have least one motor sign; approximately 3% were reported to have two or more motor signs.
The most common of these was dyscoordination, which was endorsed by 19.3% of participants. In addition, 8.8% were reported to have had experienced developmental motor delays, 1.5% had psychomotor agitation, and 0.3% had psychomotor retardation.
The investigators determined that 4.6% of participants met criteria for depression, 2.6% for a psychosis, and 1.8% for comorbid psychosis and depression.
Motor signs were much more common among children with depression, psychosis, or both than among those who did not have these conditions; 45.8% reported having at least one motor sign.
Developmental motor delays and dyscoordination occurred at about the same rate in both patients with depression and those with psychosis. Rates were higher among patients with both of these conditions than among those with either condition alone.
In contrast, psychomotor agitation was more common among patients with depression alone and among those with comorbid depression and psychosis than among patients with psychosis alone. The rate of psychomotor retardation was increased among patients with psychosis alone but was less common among patients with comorbidity than in the healthy control group.
Familial vulnerability
The investigators also assessed participants who had not been diagnosed with a mental illness but who had a family history of depression only (28.9%), a relative with psychosis-like experiences (0.6%), or a family history of both depression and psychosis experiences (1.8%).
Although the effect size was smaller, there was a higher rate of motor signs among participants with a family history of these conditions, Dr. Damme said. “Again, we see that it’s elevated across developmental motor delays and at a similar rate in people who have depression and psychosis.”
In addition, psychomotor agitation was linked to depression with psychosis and depression without it.
Sensorimotor connectivity network data for the cohort indicated there was no main effect of diagnosis on corticostriatal connectivity.
However, more depressive symptoms were related to less connectivity (P = .024). There was a similar finding for psychotic-like experiences. The total number of such experiences related to lower connectivity (P < .001).
During the postpresentation discussion, Ian Kelleher, MD, PhD, honorary clinical lecturer in psychiatry at the Royal College of Surgeons in Ireland, Dublin, said he was “surprised” by the finding that the rate of psychomotor retardation was lower among participants with psychosis and depression.
Dr. Damme noted that some of the motor sign item ratings came by way of a child interview and that some of these item ratings came from the adults in the children’s lives.
She added that she was not entirely sure whether asking an 8- to 11-year-old in a clinical interview whether they are experiencing motor signs “might be the best way to get at motor slowing.”
Subtle features
Commenting on the findings in an interview, Peter F. Liddle, MD, PhD, professor of psychiatry, at the University of Nottingham (England), noted that the “features we’re talking about are pretty subtle.
“What I’ve been wondering about for some time is whether we should be getting video recordings and using machine learning approaches to teach a computer to recognize normal movements vs abnormal movements, and particularly facial expression,” said Dr. Liddle, who was not involved with the research.
He called the current study “interesting” but noted several factors that affect the potential utility of the findings in predicting outcomes.
First, they “may not be very good for distinguishing schizophrenia from mood disorders; but if the question is simply determining which young person might go on to develop a significant mental disorder, then it may be useful,” Dr. Liddle said.
He endorsed the investigators’ conclusion that motor abnormalities may be a transdiagnostic marker. Beyond that, they may be “more useful as a predictor of the likely long-term severity, but that’s my own hypothesis based on my work,” he added.
Another question concerns the sensitivity of motor abnormalities as a predictive marker. With the rate of the abnormalities identified in those who developed psychosis and depression about double the rate in the overall population, “it sounds like those assessors were fairly sensitive. … but not all that specific,” said Dr. Liddle.
A third issue relates to treatment. “By the time people get sent to a psychiatrist for assessment for possible impending psychotic illness, they’ve often already had medication,” typically an antidepressant or antipsychotic.
“It’s very well established that dopamine-blocking antipsychotics produce hypokinesia and also dyskinesia,” which could then become a confounding factor, Dr. Liddle said.
The study was funded by grants from the National Institute of Mental Health. The study authors and Dr. Liddle have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.

Structural racism tied to psychosis risk in Black people
Social and economic disparities are linked to an increased risk for psychosis in Black and Latino communities, new research shows.

Results of a literature review of social and economic disparities in mental illness suggest that “structural racism” contributes to social and environmental conditions that affect psychosis risk.
“Black and Latino people suffer disproportionately from psychosis risk factors, at the neighborhood level and at the individual level, in large part as a result of structural racism,” study investigator Deidre M. Anglin, PhD, associate professor, department of psychology, City College of New York (N.Y.), told reporters attending a press briefing.
The social environment, which, for minorities, involves disadvantage and discrimination, may account for this increased psychosis risk, perhaps even more so than genetics, she said. Structural racism “is a critical public health threat,” Dr. Anglin added.
The findings were presented at the virtual American Psychiatric Association annual meeting and were simultaneously published online May 3 in The American Journal of Psychiatry.
Perpetual disadvantage
Dr. Anglin and colleagues examined U.S.-based evidence connecting characteristics of social environments with outcomes across the psychosis continuum – from psychotic experiences to schizophrenia.
Citing numerous studies, the researchers highlighted three key areas that reflect social and environmental conditions that may affect psychosis risk, and that disproportionately affect minorities. These were neighborhood factors, trauma in a U.S. context, and racial disparities during the prenatal and perinatal periods.
The data that were related to neighborhoods revealed “just how much racism has historically structured U.S. neighborhoods in ways that generationally perpetuate disadvantage for racially minoritized communities,” said Dr. Anglin.
“This happens through inequitable access to resources, such as health care, clean air, education, [and] employment, but also in terms of disproportionate exposure to environmental toxins and stressors,” she said.
These neighborhood factors are associated with cumulative stress that may be linked to heightened risk for psychosis, the investigators noted.
U.S. studies show that rates of adverse childhood experiences, such as abuse and emotional and physical neglect, are higher among racial and ethnic minorities.
Police victimization and gun violence disproportionately affect racial minorities and create what the investigators call “a unique type of collective trauma” in the United States. They note that Black men have a 1 in 1,000 chance of being victims of lethal force by police over their lifetimes. By comparison, White men have a 39 in 100,000 chance.
One study of a diverse sample from four large U.S. urban centers showed that those who self-reported different types of police victimization were more likely to report psychotic experiences. Another study showed that greater exposure to gun violence fatalities, regardless of police involvement, was positively associated with psychotic experiences.
Obstetric complications
A variety of obstetric complications, including infection, maternal inflammation, and stress, have been associated with increased risk for psychotic disorders in U.S. samples.
“What we saw emerge from the literature is that Black women in the U.S. are at substantially increased risk for many of these obstetrical complications compared to White women, and this is not necessarily explained by socioeconomic status,” said Dr. Anglin.
Neighborhood- and individual-level factors appear to affect the disparity in these outcomes. A recent study revealed that exposure to environmental contaminants such as air pollution is associated with higher rates of preterm birth and low birth weight differentially in Black mothers compared with other mothers, “possibly as a result of an interaction between prenatal stress and contaminants,” the investigators noted.
Research also indicates that Black women are more likely to have lower levels of cortisol during the second trimester of pregnancy compared with women of other racial and ethnic groups. Cortisol is essential for fetal growth. Evidence links lower cortisol levels in later stages of pregnancy with decreased fetal growth in individuals who develop schizophrenia.
, compared with White women of the same socioeconomic status.
Such findings “highlight a complex picture” involving maternal cortisol levels and other stress biomarkers, “potentially leading to poor birth outcomes and subsequent risk for psychotic disorders in adulthood,” the investigators noted.
The researchers call for the dismantling of structural racism and the social policies and norms it shapes. They also recommend changes in health care policy and in the approach to early intervention for psychosis among Black and other racially-minoritized groups.
“Altogether, the current evidence suggests the need to identify, address, and tackle the social determinants deeply ingrained in U.S. society, in tandem with empowering the most marginalized communities,” the researchers wrote.
“We recommend that the field of psychiatry devote considerably more effort to addressing structural racism and social determinants of psychosis in funding priorities, training, and intervention development,” they added.
Dr. Anglin suggests that mental health providers use what she called a “cultural formulation interview” that takes a person’s environmental and social context into consideration. Studies show that incorporating this into clinical practice helps reduce misdiagnosis of mental illness in Black populations, she said.
Call to action
Commenting on the findings in an interview, Ned H. Kalin, MD, editor of The American Journal of Psychiatry and professor and chair of the department of psychiatry, University of Wisconsin, Madison, said the study was well done and serves as a “call to action” to address the impact of structural racism on mental health issues and psychiatric diseases.
The article highlights the need for “collecting better data” on structural racism, said Dr. Kalin. “We know it’s a big issue, but we can’t even quantitate it, so we need some fundamental measures to use as a benchmark as we move forward, as we try to make change.”
He noted that racism “is so embedded in one’s experience and in our society that we sort of don’t even think about it as a trauma.”
In psychiatry, for example, trauma is often thought of as a loss or a traumatic event. “We don’t typically think of trauma as an experience that pervades one’s entire life,” but that needs to change, he said. “At the individual level and in the doctor’s office, being sensitive to and aware of these issues is absolutely critical.”
Dr. Anglin and Dr. Kalin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Social and economic disparities are linked to an increased risk for psychosis in Black and Latino communities, new research shows.
Results of a literature review of social and economic disparities in mental illness suggest that “structural racism” contributes to social and environmental conditions that affect psychosis risk.
“Black and Latino people suffer disproportionately from psychosis risk factors, at the neighborhood level and at the individual level, in large part as a result of structural racism,” study investigator Deidre M. Anglin, PhD, associate professor, department of psychology, City College of New York (N.Y.), told reporters attending a press briefing.
The social environment, which, for minorities, involves disadvantage and discrimination, may account for this increased psychosis risk, perhaps even more so than genetics, she said. Structural racism “is a critical public health threat,” Dr. Anglin added.
The findings were presented at the virtual American Psychiatric Association annual meeting and were simultaneously published online May 3 in The American Journal of Psychiatry.
Perpetual disadvantage
Dr. Anglin and colleagues examined U.S.-based evidence connecting characteristics of social environments with outcomes across the psychosis continuum – from psychotic experiences to schizophrenia.
Citing numerous studies, the researchers highlighted three key areas that reflect social and environmental conditions that may affect psychosis risk, and that disproportionately affect minorities. These were neighborhood factors, trauma in a U.S. context, and racial disparities during the prenatal and perinatal periods.
The data that were related to neighborhoods revealed “just how much racism has historically structured U.S. neighborhoods in ways that generationally perpetuate disadvantage for racially minoritized communities,” said Dr. Anglin.
“This happens through inequitable access to resources, such as health care, clean air, education, [and] employment, but also in terms of disproportionate exposure to environmental toxins and stressors,” she said.
These neighborhood factors are associated with cumulative stress that may be linked to heightened risk for psychosis, the investigators noted.
U.S. studies show that rates of adverse childhood experiences, such as abuse and emotional and physical neglect, are higher among racial and ethnic minorities.
Police victimization and gun violence disproportionately affect racial minorities and create what the investigators call “a unique type of collective trauma” in the United States. They note that Black men have a 1 in 1,000 chance of being victims of lethal force by police over their lifetimes. By comparison, White men have a 39 in 100,000 chance.
One study of a diverse sample from four large U.S. urban centers showed that those who self-reported different types of police victimization were more likely to report psychotic experiences. Another study showed that greater exposure to gun violence fatalities, regardless of police involvement, was positively associated with psychotic experiences.
Obstetric complications
A variety of obstetric complications, including infection, maternal inflammation, and stress, have been associated with increased risk for psychotic disorders in U.S. samples.
“What we saw emerge from the literature is that Black women in the U.S. are at substantially increased risk for many of these obstetrical complications compared to White women, and this is not necessarily explained by socioeconomic status,” said Dr. Anglin.
Neighborhood- and individual-level factors appear to affect the disparity in these outcomes. A recent study revealed that exposure to environmental contaminants such as air pollution is associated with higher rates of preterm birth and low birth weight differentially in Black mothers compared with other mothers, “possibly as a result of an interaction between prenatal stress and contaminants,” the investigators noted.
Research also indicates that Black women are more likely to have lower levels of cortisol during the second trimester of pregnancy compared with women of other racial and ethnic groups. Cortisol is essential for fetal growth. Evidence links lower cortisol levels in later stages of pregnancy with decreased fetal growth in individuals who develop schizophrenia.
, compared with White women of the same socioeconomic status.
Such findings “highlight a complex picture” involving maternal cortisol levels and other stress biomarkers, “potentially leading to poor birth outcomes and subsequent risk for psychotic disorders in adulthood,” the investigators noted.
The researchers call for the dismantling of structural racism and the social policies and norms it shapes. They also recommend changes in health care policy and in the approach to early intervention for psychosis among Black and other racially-minoritized groups.
“Altogether, the current evidence suggests the need to identify, address, and tackle the social determinants deeply ingrained in U.S. society, in tandem with empowering the most marginalized communities,” the researchers wrote.
“We recommend that the field of psychiatry devote considerably more effort to addressing structural racism and social determinants of psychosis in funding priorities, training, and intervention development,” they added.
Dr. Anglin suggests that mental health providers use what she called a “cultural formulation interview” that takes a person’s environmental and social context into consideration. Studies show that incorporating this into clinical practice helps reduce misdiagnosis of mental illness in Black populations, she said.
Call to action
Commenting on the findings in an interview, Ned H. Kalin, MD, editor of The American Journal of Psychiatry and professor and chair of the department of psychiatry, University of Wisconsin, Madison, said the study was well done and serves as a “call to action” to address the impact of structural racism on mental health issues and psychiatric diseases.
The article highlights the need for “collecting better data” on structural racism, said Dr. Kalin. “We know it’s a big issue, but we can’t even quantitate it, so we need some fundamental measures to use as a benchmark as we move forward, as we try to make change.”
He noted that racism “is so embedded in one’s experience and in our society that we sort of don’t even think about it as a trauma.”
In psychiatry, for example, trauma is often thought of as a loss or a traumatic event. “We don’t typically think of trauma as an experience that pervades one’s entire life,” but that needs to change, he said. “At the individual level and in the doctor’s office, being sensitive to and aware of these issues is absolutely critical.”
Dr. Anglin and Dr. Kalin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Social and economic disparities are linked to an increased risk for psychosis in Black and Latino communities, new research shows.
Results of a literature review of social and economic disparities in mental illness suggest that “structural racism” contributes to social and environmental conditions that affect psychosis risk.
“Black and Latino people suffer disproportionately from psychosis risk factors, at the neighborhood level and at the individual level, in large part as a result of structural racism,” study investigator Deidre M. Anglin, PhD, associate professor, department of psychology, City College of New York (N.Y.), told reporters attending a press briefing.
The social environment, which, for minorities, involves disadvantage and discrimination, may account for this increased psychosis risk, perhaps even more so than genetics, she said. Structural racism “is a critical public health threat,” Dr. Anglin added.
The findings were presented at the virtual American Psychiatric Association annual meeting and were simultaneously published online May 3 in The American Journal of Psychiatry.
Perpetual disadvantage
Dr. Anglin and colleagues examined U.S.-based evidence connecting characteristics of social environments with outcomes across the psychosis continuum – from psychotic experiences to schizophrenia.
Citing numerous studies, the researchers highlighted three key areas that reflect social and environmental conditions that may affect psychosis risk, and that disproportionately affect minorities. These were neighborhood factors, trauma in a U.S. context, and racial disparities during the prenatal and perinatal periods.
The data that were related to neighborhoods revealed “just how much racism has historically structured U.S. neighborhoods in ways that generationally perpetuate disadvantage for racially minoritized communities,” said Dr. Anglin.
“This happens through inequitable access to resources, such as health care, clean air, education, [and] employment, but also in terms of disproportionate exposure to environmental toxins and stressors,” she said.
These neighborhood factors are associated with cumulative stress that may be linked to heightened risk for psychosis, the investigators noted.
U.S. studies show that rates of adverse childhood experiences, such as abuse and emotional and physical neglect, are higher among racial and ethnic minorities.
Police victimization and gun violence disproportionately affect racial minorities and create what the investigators call “a unique type of collective trauma” in the United States. They note that Black men have a 1 in 1,000 chance of being victims of lethal force by police over their lifetimes. By comparison, White men have a 39 in 100,000 chance.
One study of a diverse sample from four large U.S. urban centers showed that those who self-reported different types of police victimization were more likely to report psychotic experiences. Another study showed that greater exposure to gun violence fatalities, regardless of police involvement, was positively associated with psychotic experiences.
Obstetric complications
A variety of obstetric complications, including infection, maternal inflammation, and stress, have been associated with increased risk for psychotic disorders in U.S. samples.
“What we saw emerge from the literature is that Black women in the U.S. are at substantially increased risk for many of these obstetrical complications compared to White women, and this is not necessarily explained by socioeconomic status,” said Dr. Anglin.
Neighborhood- and individual-level factors appear to affect the disparity in these outcomes. A recent study revealed that exposure to environmental contaminants such as air pollution is associated with higher rates of preterm birth and low birth weight differentially in Black mothers compared with other mothers, “possibly as a result of an interaction between prenatal stress and contaminants,” the investigators noted.
Research also indicates that Black women are more likely to have lower levels of cortisol during the second trimester of pregnancy compared with women of other racial and ethnic groups. Cortisol is essential for fetal growth. Evidence links lower cortisol levels in later stages of pregnancy with decreased fetal growth in individuals who develop schizophrenia.
, compared with White women of the same socioeconomic status.
Such findings “highlight a complex picture” involving maternal cortisol levels and other stress biomarkers, “potentially leading to poor birth outcomes and subsequent risk for psychotic disorders in adulthood,” the investigators noted.
The researchers call for the dismantling of structural racism and the social policies and norms it shapes. They also recommend changes in health care policy and in the approach to early intervention for psychosis among Black and other racially-minoritized groups.
“Altogether, the current evidence suggests the need to identify, address, and tackle the social determinants deeply ingrained in U.S. society, in tandem with empowering the most marginalized communities,” the researchers wrote.
“We recommend that the field of psychiatry devote considerably more effort to addressing structural racism and social determinants of psychosis in funding priorities, training, and intervention development,” they added.
Dr. Anglin suggests that mental health providers use what she called a “cultural formulation interview” that takes a person’s environmental and social context into consideration. Studies show that incorporating this into clinical practice helps reduce misdiagnosis of mental illness in Black populations, she said.
Call to action
Commenting on the findings in an interview, Ned H. Kalin, MD, editor of The American Journal of Psychiatry and professor and chair of the department of psychiatry, University of Wisconsin, Madison, said the study was well done and serves as a “call to action” to address the impact of structural racism on mental health issues and psychiatric diseases.
The article highlights the need for “collecting better data” on structural racism, said Dr. Kalin. “We know it’s a big issue, but we can’t even quantitate it, so we need some fundamental measures to use as a benchmark as we move forward, as we try to make change.”
He noted that racism “is so embedded in one’s experience and in our society that we sort of don’t even think about it as a trauma.”
In psychiatry, for example, trauma is often thought of as a loss or a traumatic event. “We don’t typically think of trauma as an experience that pervades one’s entire life,” but that needs to change, he said. “At the individual level and in the doctor’s office, being sensitive to and aware of these issues is absolutely critical.”
Dr. Anglin and Dr. Kalin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
