User login
Rising microbiome investigator: Ting-Chin David Shen, MD, PhD
We spoke with Dr. Shen, instructor of medicine at the University of Pennsylvania and the recipient of the AGA Research Foundation’s 2016 Microbiome Junior Investigator Award, to learn about his passion for gut microbiome research.
How would you sum up your research in one sentence?
My research examines the metabolic interactions between the gut microbiota and the mammalian host, with a particular emphasis on amino acid metabolism and nitrogen flux via the bacterial enzyme urease.
What impact do you hope your research will have on patients?
My hope is that by better understanding the biological mechanisms by which the gut microbiota impacts host metabolism, we can modulate its effects to treat a variety of conditions and diseases including hepatic encephalopathy, inborn errors of metabolism, obesity, malnutrition, etc.
What inspired you to focus your research career on the gut microbiome?
My clinical experience as a gastroenterologist inspired my interest in metabolic and nutritional research. When I learned of the impact that the gut microbiota has on host metabolism, it created an entirely different perspective for me in terms of thinking about how to treat metabolic and nutritional disorders. There are tremendous opportunities in modifying our gut microbiota in concert with dietary interventions in order to modulate our metabolism.
What recent publication from your lab best represents your work, if anyone wants to learn more?
The following work examined how the use of a defined bacterial consortium without urease activity can reduce colonic ammonia level upon inoculation into the gut and ameliorate morbidity and mortality in a murine model of liver disease: Shen T.D., Albenberg L.A., Bittinger K., et al, Engineering the gut microbiota to treat hyperammonemia. J Clin Invest. 2015 Jul 1;125(7):2841-50. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4563680/.
We spoke with Dr. Shen, instructor of medicine at the University of Pennsylvania and the recipient of the AGA Research Foundation’s 2016 Microbiome Junior Investigator Award, to learn about his passion for gut microbiome research.
How would you sum up your research in one sentence?
My research examines the metabolic interactions between the gut microbiota and the mammalian host, with a particular emphasis on amino acid metabolism and nitrogen flux via the bacterial enzyme urease.
What impact do you hope your research will have on patients?
My hope is that by better understanding the biological mechanisms by which the gut microbiota impacts host metabolism, we can modulate its effects to treat a variety of conditions and diseases including hepatic encephalopathy, inborn errors of metabolism, obesity, malnutrition, etc.
What inspired you to focus your research career on the gut microbiome?
My clinical experience as a gastroenterologist inspired my interest in metabolic and nutritional research. When I learned of the impact that the gut microbiota has on host metabolism, it created an entirely different perspective for me in terms of thinking about how to treat metabolic and nutritional disorders. There are tremendous opportunities in modifying our gut microbiota in concert with dietary interventions in order to modulate our metabolism.
What recent publication from your lab best represents your work, if anyone wants to learn more?
The following work examined how the use of a defined bacterial consortium without urease activity can reduce colonic ammonia level upon inoculation into the gut and ameliorate morbidity and mortality in a murine model of liver disease: Shen T.D., Albenberg L.A., Bittinger K., et al, Engineering the gut microbiota to treat hyperammonemia. J Clin Invest. 2015 Jul 1;125(7):2841-50. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4563680/.
We spoke with Dr. Shen, instructor of medicine at the University of Pennsylvania and the recipient of the AGA Research Foundation’s 2016 Microbiome Junior Investigator Award, to learn about his passion for gut microbiome research.
How would you sum up your research in one sentence?
My research examines the metabolic interactions between the gut microbiota and the mammalian host, with a particular emphasis on amino acid metabolism and nitrogen flux via the bacterial enzyme urease.
What impact do you hope your research will have on patients?
My hope is that by better understanding the biological mechanisms by which the gut microbiota impacts host metabolism, we can modulate its effects to treat a variety of conditions and diseases including hepatic encephalopathy, inborn errors of metabolism, obesity, malnutrition, etc.
What inspired you to focus your research career on the gut microbiome?
My clinical experience as a gastroenterologist inspired my interest in metabolic and nutritional research. When I learned of the impact that the gut microbiota has on host metabolism, it created an entirely different perspective for me in terms of thinking about how to treat metabolic and nutritional disorders. There are tremendous opportunities in modifying our gut microbiota in concert with dietary interventions in order to modulate our metabolism.
What recent publication from your lab best represents your work, if anyone wants to learn more?
The following work examined how the use of a defined bacterial consortium without urease activity can reduce colonic ammonia level upon inoculation into the gut and ameliorate morbidity and mortality in a murine model of liver disease: Shen T.D., Albenberg L.A., Bittinger K., et al, Engineering the gut microbiota to treat hyperammonemia. J Clin Invest. 2015 Jul 1;125(7):2841-50. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4563680/.
Red flag raised on CMS indication-based formulary policy
Physician groups are expressing concerns regarding a new policy that will allow indication-based formulary design in the Medicare Part D prescription drug benefit.

The Centers for Medicare & Medicaid Services announced the new policy in an Aug. 29 memo to Part D plan sponsors.
According to a fact sheet issued by CMS on the same day, indication-based formulary design “is a formulary management tool that allows health plans to tailor on-formulary coverage of drugs predicated on specific indications.”
Current Part D policy requires plan sponsors to cover all Food and Drug Administration–approved indications for each drug that is on a plan formulary. Sponsors can begin to implement the new indication-based formulary design policy for plans issued in 2020.
The memo notes that, if a Part D plan sponsor chooses to opt into this policy, “it must ensure that there is another therapeutically similar drug on formulary for the nonformulary indication. For example, if a tumor necrosis factor (TNF) blocker is FDA-approved for both Crohn’s disease and plaque psoriasis, but the Part D plan will include it on formulary for plaque psoriasis only, the plan must ensure that there is another TNF blocker on formulary that will be covered for Crohn’s disease.”
Beneficiaries can use the exceptions process to get coverage for a drug that has an indication not on the formulary.

“By allowing Medicare’s prescription drug plans to cover the best drug for each patient condition, plans will have more negotiating power with drug companies, which will result in lower prices for Medicare beneficiaries,” CMS Administrator Seema Verma said in a statement.
However, physician groups should be concerned about the definition of “best drug.” Is this definition based upon efficacy, results of clinical trials, clinical effectiveness research, or just cost? Will there be transparenecy surrounding rebates?
The “proposed changes will exacerbate many of the access issues patients currently face with plan usage of existing utilization management practices, such as step therapy,” the American College of Rheumatology said in a statement. “Unlike step therapy, which often delays effective treatments, this proposal would go even further and allow plans to remove therapies from the formulary altogether, leaving patients completely unable to access treatments that doctors and patients choose together. ... We also have concerns on what this would mean for work being done on compendia inclusion to secure off-label drug coverage if plans don’t have to cover all FDA-approved indications.”
A similar situation exists in patients with inflammatory bowel disease in which step therapy has largely been replaced by risk assessments. The AGA Crohn’s and UC Care Pathways are based on this principle.

Under the plan, Medicare patients will face increased challenges as they navigate health plans to make sure that their needed drug is on their selected formulary, which can change based on what health conditions they have,” AMA President Barbara McAneny, MD, said in a statement. Dr. McAneny added that it will be even more difficult for physicians who are working with patients to get them on the best medicines covered by the patient’s formulary.
“Physicians already lack ready access to accurate formulary information – preferred/tier status, on/off formulary, PA [prior authorization] and step therapy requirements – at the point of care in their EHRs,” she said. “These transparency problems will expand by an order of magnitude by the complications this change introduces.”
Physician groups are expressing concerns regarding a new policy that will allow indication-based formulary design in the Medicare Part D prescription drug benefit.
The Centers for Medicare & Medicaid Services announced the new policy in an Aug. 29 memo to Part D plan sponsors.
According to a fact sheet issued by CMS on the same day, indication-based formulary design “is a formulary management tool that allows health plans to tailor on-formulary coverage of drugs predicated on specific indications.”
Current Part D policy requires plan sponsors to cover all Food and Drug Administration–approved indications for each drug that is on a plan formulary. Sponsors can begin to implement the new indication-based formulary design policy for plans issued in 2020.
The memo notes that, if a Part D plan sponsor chooses to opt into this policy, “it must ensure that there is another therapeutically similar drug on formulary for the nonformulary indication. For example, if a tumor necrosis factor (TNF) blocker is FDA-approved for both Crohn’s disease and plaque psoriasis, but the Part D plan will include it on formulary for plaque psoriasis only, the plan must ensure that there is another TNF blocker on formulary that will be covered for Crohn’s disease.”
Beneficiaries can use the exceptions process to get coverage for a drug that has an indication not on the formulary.
“By allowing Medicare’s prescription drug plans to cover the best drug for each patient condition, plans will have more negotiating power with drug companies, which will result in lower prices for Medicare beneficiaries,” CMS Administrator Seema Verma said in a statement.
However, physician groups should be concerned about the definition of “best drug.” Is this definition based upon efficacy, results of clinical trials, clinical effectiveness research, or just cost? Will there be transparenecy surrounding rebates?
The “proposed changes will exacerbate many of the access issues patients currently face with plan usage of existing utilization management practices, such as step therapy,” the American College of Rheumatology said in a statement. “Unlike step therapy, which often delays effective treatments, this proposal would go even further and allow plans to remove therapies from the formulary altogether, leaving patients completely unable to access treatments that doctors and patients choose together. ... We also have concerns on what this would mean for work being done on compendia inclusion to secure off-label drug coverage if plans don’t have to cover all FDA-approved indications.”
A similar situation exists in patients with inflammatory bowel disease in which step therapy has largely been replaced by risk assessments. The AGA Crohn’s and UC Care Pathways are based on this principle.
Under the plan, Medicare patients will face increased challenges as they navigate health plans to make sure that their needed drug is on their selected formulary, which can change based on what health conditions they have,” AMA President Barbara McAneny, MD, said in a statement. Dr. McAneny added that it will be even more difficult for physicians who are working with patients to get them on the best medicines covered by the patient’s formulary.
“Physicians already lack ready access to accurate formulary information – preferred/tier status, on/off formulary, PA [prior authorization] and step therapy requirements – at the point of care in their EHRs,” she said. “These transparency problems will expand by an order of magnitude by the complications this change introduces.”
Physician groups are expressing concerns regarding a new policy that will allow indication-based formulary design in the Medicare Part D prescription drug benefit.
The Centers for Medicare & Medicaid Services announced the new policy in an Aug. 29 memo to Part D plan sponsors.
According to a fact sheet issued by CMS on the same day, indication-based formulary design “is a formulary management tool that allows health plans to tailor on-formulary coverage of drugs predicated on specific indications.”
Current Part D policy requires plan sponsors to cover all Food and Drug Administration–approved indications for each drug that is on a plan formulary. Sponsors can begin to implement the new indication-based formulary design policy for plans issued in 2020.
The memo notes that, if a Part D plan sponsor chooses to opt into this policy, “it must ensure that there is another therapeutically similar drug on formulary for the nonformulary indication. For example, if a tumor necrosis factor (TNF) blocker is FDA-approved for both Crohn’s disease and plaque psoriasis, but the Part D plan will include it on formulary for plaque psoriasis only, the plan must ensure that there is another TNF blocker on formulary that will be covered for Crohn’s disease.”
Beneficiaries can use the exceptions process to get coverage for a drug that has an indication not on the formulary.
“By allowing Medicare’s prescription drug plans to cover the best drug for each patient condition, plans will have more negotiating power with drug companies, which will result in lower prices for Medicare beneficiaries,” CMS Administrator Seema Verma said in a statement.
However, physician groups should be concerned about the definition of “best drug.” Is this definition based upon efficacy, results of clinical trials, clinical effectiveness research, or just cost? Will there be transparenecy surrounding rebates?
The “proposed changes will exacerbate many of the access issues patients currently face with plan usage of existing utilization management practices, such as step therapy,” the American College of Rheumatology said in a statement. “Unlike step therapy, which often delays effective treatments, this proposal would go even further and allow plans to remove therapies from the formulary altogether, leaving patients completely unable to access treatments that doctors and patients choose together. ... We also have concerns on what this would mean for work being done on compendia inclusion to secure off-label drug coverage if plans don’t have to cover all FDA-approved indications.”
A similar situation exists in patients with inflammatory bowel disease in which step therapy has largely been replaced by risk assessments. The AGA Crohn’s and UC Care Pathways are based on this principle.
Under the plan, Medicare patients will face increased challenges as they navigate health plans to make sure that their needed drug is on their selected formulary, which can change based on what health conditions they have,” AMA President Barbara McAneny, MD, said in a statement. Dr. McAneny added that it will be even more difficult for physicians who are working with patients to get them on the best medicines covered by the patient’s formulary.
“Physicians already lack ready access to accurate formulary information – preferred/tier status, on/off formulary, PA [prior authorization] and step therapy requirements – at the point of care in their EHRs,” she said. “These transparency problems will expand by an order of magnitude by the complications this change introduces.”
Treating cannabinoid hyperemesis syndrome
Incidence may increase as marijuana use rises
Case
WS is a 54-year-old African American male with a medical history of diabetes mellitus type 2, hypertension, obstructive sleep apnea, and gastroparesis. He has multiple admissions for intractable nausea, vomiting, and abdominal pain believed to be from diabetic gastroparesis despite a normal gastric-emptying study. Endoscopy done in prior admission showed duodenitis, gastritis, and esophagitis, and colonoscopy revealed diverticulosis. He had a negative gastric-emptying study of 6% retention at 4 hrs. His last hemoglobin A1c was 5 and his glucose has been well controlled. He is hospitalized again for intractable abdominal pain, nausea, and vomiting. His examination was unremarkable except for dry mucosa and epigastric tenderness. His labs were also insignificant except for prerenal azotemia. Upon further questioning he admitted to significant marijuana use, and his symptoms transiently improved with a hot shower in the hospital. He was diagnosed with cannabinoid hyperemesis syndrome (CHS) and admitted for further management.
Background
In the United States, 9 states and the District of Columbia have legalized recreational marijuana use, and 29 states and DC have legalized medical marijuana. Marijuana use is likely to rise, and with it may arise an increasing incidence of CHS.
The exact prevalence of CHS is not known. Diagnosis is often delayed as there is no reliable diagnostic test. A high index of suspicion is needed for prompt diagnosis.
CHS was first described in 2004 in South Australia and since then many case reports have been published. Marijuana has both proemetic and antiemetic effects. Unlike its antiemetic effect, the pathophysiology of the proemetic effect of marijuana is not well understood.

Key clinical features
CHS typically has three phases. Initially patients present with prodromal symptoms of abdominal discomfort and nausea. There is no emesis at this early phase. Patients are still able to tolerate a liquid diet in this prodromal phase.
This is followed by a more active phase of intractable vomiting, which is relieved by hot showers or baths. Most patients take compulsively long hot showers or baths many times a day. Also, they develop diaphoresis, restlessness, agitation, and weight loss.
The active phase is followed by a recovery phase when symptoms resolve and patients return to baseline, only to have it recur if marijuana use continues.
Diagnostic approach and management
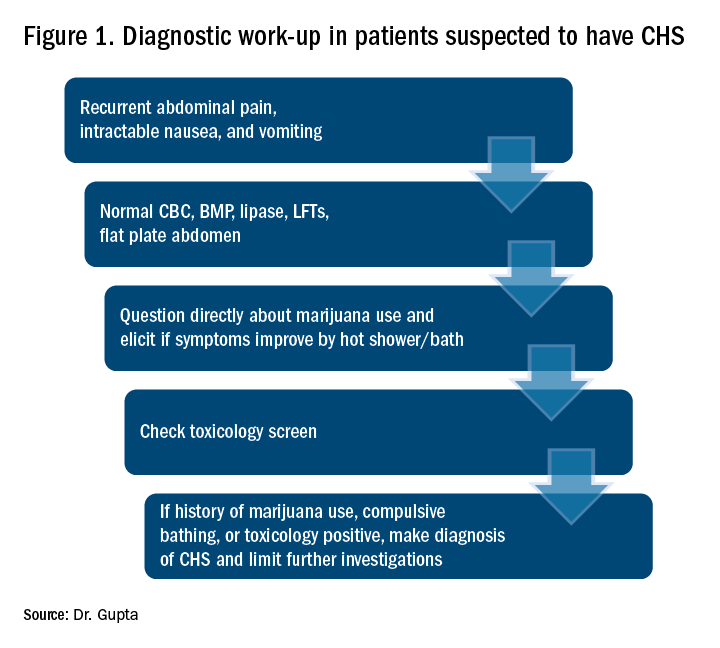
CHS should be suspected in patients coming in with recurrent symptoms of abdominal pain, nausea and vomiting, and who have normal CBC, basic metabolic panel, lipase, and liver function tests. Patients should be directly questioned about marijuana use and whether symptoms are relieved with hot showers. A toxicology screen should be done. For patients with marijuana use and compulsive hot showers, further work up of their symptoms (e.g., upper endoscopy, abdominal ultrasound, and/or nuclear medicine emptying study) should be avoided. Figure 1 shows the suggested work-up.
The differential diagnosis for recurrent abdominal pain, nausea, and vomiting is chronic pancreatitis, gastroparesis, severe gastritis, medication adverse effects (especially GLP1 receptor agonists), cyclic vomiting syndrome, psychogenic vomiting, and (with the rise of narcotic abuse) narcotic bowel syndrome.
Our patient had a history of diabetes with an HbA1c at goal and a normal nuclear medicine gastric-emptying study (6% retention at 4 hours). He was also on liraglutide, but his symptoms predated this medicine use.
The mainstay of treatment for CHS is supportive therapy with intravenous fluids and antiemetics like 5-HT3-receptor antagonists (ondansetron); D2-receptor antagonists (metoclopramide); and H1-receptor antagonists (diphenhydramine). The effectiveness of these agents is limited, which is also a clue for the diagnosis of CHS. If traditional agents fail in controlling the symptoms, haloperidol can be tried, but it has been used with limited success. Our patient did not respond to traditional antiemetics, but responded well to a small dose of lorazepam. Even though a benzodiazepine is not the mainstay of treatment, it may be tried if other agents fail. Acid-suppression therapy with a proton pump inhibitor should be used as esophagogastroduodenoscopy (EGD) usually reveals mild gastritis and esophagitis, as in our patient. Narcotic use should be avoided for management of abdominal pain.
Patients should be counseled against marijuana use. This may be difficult if marijuana is being used as an appetite stimulant or for treatment of chemotherapy-induced nausea and vomiting. If willing, patients should be referred to a substance abuse rehabilitation center.
Back to the case
In this case, after a diagnosis of CHS was made, the patient was counseled against marijuana use. His abdominal pain and intractable vomiting did not improve with conservative management of n.p.o status, prochlorperazine, metoclopramide, and ondansetron. He was given a trial of low-dose lorazepam with significant improvement in his symptoms. He was counseled extensively against marijuana use and discharged. A follow-up phone call at 3 months showed continued abstinence and no recurrence of symptoms.
Dr. Gupta is a hospitalist at Yale New Haven Health and Bridgeport (Conn.) Hospital.
References
1. Bajgoric S et al. Cannabinoid hyperemesis syndrome: A guide for the practising clinician. BMJ Case Rep. 2015. doi: 10.1136/bcr-2015-210246.
2. Batke M et al. The cannabis hyperemesis syndrome characterized by persistent nausea and vomiting, abdominal pain, and compulsive bathing associated with chronic marijuana use: A report of eight cases in the united states. Dig Dis Sci. 2010 Nov;55(11):3113-9.
3. Iacopetti CL et al. Cannabinoid hyperemesis syndrome: a case report and review of pathophysiology. Clin Med Res. 2014 Sep;12(1-2):65-7.
4. Hickey JL et al. Haloperidol for treatment of cannabinoid hyperemesis syndrome. Am J Emerg Med. 2013 Jun. 31(6):1003.e5-6. Epub 2013 Apr 10.
Key points
Suspect CHS for patients with recurrent abdominal pain, nausea, and vomiting with negative initial work-up.
- Ask directly about marijuana use.
- Ask whether symptoms are relieved with hot shower/ bath.
- Send a toxicology screen.
- Make a diagnosis of CHS if:
1. Positive marijuana use.
2. Symptom improvement with hot baths or
3. Toxicology positive for marijuana.
- Manage conservatively with hydration and antiemetics.
- Suspect CHS if traditional antiemetics are not providing relief .
- If traditional antiemetics fail, trial of haloperidol or low-dose benzodiazepines.
- Avoid narcotics.
- Avoid unnecessary investigations.
- Counsel patients against marijuana use and refer to substance abuse center if patient agrees.
Incidence may increase as marijuana use rises
Incidence may increase as marijuana use rises
Case
WS is a 54-year-old African American male with a medical history of diabetes mellitus type 2, hypertension, obstructive sleep apnea, and gastroparesis. He has multiple admissions for intractable nausea, vomiting, and abdominal pain believed to be from diabetic gastroparesis despite a normal gastric-emptying study. Endoscopy done in prior admission showed duodenitis, gastritis, and esophagitis, and colonoscopy revealed diverticulosis. He had a negative gastric-emptying study of 6% retention at 4 hrs. His last hemoglobin A1c was 5 and his glucose has been well controlled. He is hospitalized again for intractable abdominal pain, nausea, and vomiting. His examination was unremarkable except for dry mucosa and epigastric tenderness. His labs were also insignificant except for prerenal azotemia. Upon further questioning he admitted to significant marijuana use, and his symptoms transiently improved with a hot shower in the hospital. He was diagnosed with cannabinoid hyperemesis syndrome (CHS) and admitted for further management.
Background
In the United States, 9 states and the District of Columbia have legalized recreational marijuana use, and 29 states and DC have legalized medical marijuana. Marijuana use is likely to rise, and with it may arise an increasing incidence of CHS.
The exact prevalence of CHS is not known. Diagnosis is often delayed as there is no reliable diagnostic test. A high index of suspicion is needed for prompt diagnosis.
CHS was first described in 2004 in South Australia and since then many case reports have been published. Marijuana has both proemetic and antiemetic effects. Unlike its antiemetic effect, the pathophysiology of the proemetic effect of marijuana is not well understood.
Key clinical features
CHS typically has three phases. Initially patients present with prodromal symptoms of abdominal discomfort and nausea. There is no emesis at this early phase. Patients are still able to tolerate a liquid diet in this prodromal phase.
This is followed by a more active phase of intractable vomiting, which is relieved by hot showers or baths. Most patients take compulsively long hot showers or baths many times a day. Also, they develop diaphoresis, restlessness, agitation, and weight loss.
The active phase is followed by a recovery phase when symptoms resolve and patients return to baseline, only to have it recur if marijuana use continues.
Diagnostic approach and management
CHS should be suspected in patients coming in with recurrent symptoms of abdominal pain, nausea and vomiting, and who have normal CBC, basic metabolic panel, lipase, and liver function tests. Patients should be directly questioned about marijuana use and whether symptoms are relieved with hot showers. A toxicology screen should be done. For patients with marijuana use and compulsive hot showers, further work up of their symptoms (e.g., upper endoscopy, abdominal ultrasound, and/or nuclear medicine emptying study) should be avoided. Figure 1 shows the suggested work-up.
The differential diagnosis for recurrent abdominal pain, nausea, and vomiting is chronic pancreatitis, gastroparesis, severe gastritis, medication adverse effects (especially GLP1 receptor agonists), cyclic vomiting syndrome, psychogenic vomiting, and (with the rise of narcotic abuse) narcotic bowel syndrome.
Our patient had a history of diabetes with an HbA1c at goal and a normal nuclear medicine gastric-emptying study (6% retention at 4 hours). He was also on liraglutide, but his symptoms predated this medicine use.
The mainstay of treatment for CHS is supportive therapy with intravenous fluids and antiemetics like 5-HT3-receptor antagonists (ondansetron); D2-receptor antagonists (metoclopramide); and H1-receptor antagonists (diphenhydramine). The effectiveness of these agents is limited, which is also a clue for the diagnosis of CHS. If traditional agents fail in controlling the symptoms, haloperidol can be tried, but it has been used with limited success. Our patient did not respond to traditional antiemetics, but responded well to a small dose of lorazepam. Even though a benzodiazepine is not the mainstay of treatment, it may be tried if other agents fail. Acid-suppression therapy with a proton pump inhibitor should be used as esophagogastroduodenoscopy (EGD) usually reveals mild gastritis and esophagitis, as in our patient. Narcotic use should be avoided for management of abdominal pain.
Patients should be counseled against marijuana use. This may be difficult if marijuana is being used as an appetite stimulant or for treatment of chemotherapy-induced nausea and vomiting. If willing, patients should be referred to a substance abuse rehabilitation center.
Back to the case
In this case, after a diagnosis of CHS was made, the patient was counseled against marijuana use. His abdominal pain and intractable vomiting did not improve with conservative management of n.p.o status, prochlorperazine, metoclopramide, and ondansetron. He was given a trial of low-dose lorazepam with significant improvement in his symptoms. He was counseled extensively against marijuana use and discharged. A follow-up phone call at 3 months showed continued abstinence and no recurrence of symptoms.
Dr. Gupta is a hospitalist at Yale New Haven Health and Bridgeport (Conn.) Hospital.
References
1. Bajgoric S et al. Cannabinoid hyperemesis syndrome: A guide for the practising clinician. BMJ Case Rep. 2015. doi: 10.1136/bcr-2015-210246.
2. Batke M et al. The cannabis hyperemesis syndrome characterized by persistent nausea and vomiting, abdominal pain, and compulsive bathing associated with chronic marijuana use: A report of eight cases in the united states. Dig Dis Sci. 2010 Nov;55(11):3113-9.
3. Iacopetti CL et al. Cannabinoid hyperemesis syndrome: a case report and review of pathophysiology. Clin Med Res. 2014 Sep;12(1-2):65-7.
4. Hickey JL et al. Haloperidol for treatment of cannabinoid hyperemesis syndrome. Am J Emerg Med. 2013 Jun. 31(6):1003.e5-6. Epub 2013 Apr 10.
Key points
Suspect CHS for patients with recurrent abdominal pain, nausea, and vomiting with negative initial work-up.
- Ask directly about marijuana use.
- Ask whether symptoms are relieved with hot shower/ bath.
- Send a toxicology screen.
- Make a diagnosis of CHS if:
1. Positive marijuana use.
2. Symptom improvement with hot baths or
3. Toxicology positive for marijuana.
- Manage conservatively with hydration and antiemetics.
- Suspect CHS if traditional antiemetics are not providing relief .
- If traditional antiemetics fail, trial of haloperidol or low-dose benzodiazepines.
- Avoid narcotics.
- Avoid unnecessary investigations.
- Counsel patients against marijuana use and refer to substance abuse center if patient agrees.
Case
WS is a 54-year-old African American male with a medical history of diabetes mellitus type 2, hypertension, obstructive sleep apnea, and gastroparesis. He has multiple admissions for intractable nausea, vomiting, and abdominal pain believed to be from diabetic gastroparesis despite a normal gastric-emptying study. Endoscopy done in prior admission showed duodenitis, gastritis, and esophagitis, and colonoscopy revealed diverticulosis. He had a negative gastric-emptying study of 6% retention at 4 hrs. His last hemoglobin A1c was 5 and his glucose has been well controlled. He is hospitalized again for intractable abdominal pain, nausea, and vomiting. His examination was unremarkable except for dry mucosa and epigastric tenderness. His labs were also insignificant except for prerenal azotemia. Upon further questioning he admitted to significant marijuana use, and his symptoms transiently improved with a hot shower in the hospital. He was diagnosed with cannabinoid hyperemesis syndrome (CHS) and admitted for further management.
Background
In the United States, 9 states and the District of Columbia have legalized recreational marijuana use, and 29 states and DC have legalized medical marijuana. Marijuana use is likely to rise, and with it may arise an increasing incidence of CHS.
The exact prevalence of CHS is not known. Diagnosis is often delayed as there is no reliable diagnostic test. A high index of suspicion is needed for prompt diagnosis.
CHS was first described in 2004 in South Australia and since then many case reports have been published. Marijuana has both proemetic and antiemetic effects. Unlike its antiemetic effect, the pathophysiology of the proemetic effect of marijuana is not well understood.
Key clinical features
CHS typically has three phases. Initially patients present with prodromal symptoms of abdominal discomfort and nausea. There is no emesis at this early phase. Patients are still able to tolerate a liquid diet in this prodromal phase.
This is followed by a more active phase of intractable vomiting, which is relieved by hot showers or baths. Most patients take compulsively long hot showers or baths many times a day. Also, they develop diaphoresis, restlessness, agitation, and weight loss.
The active phase is followed by a recovery phase when symptoms resolve and patients return to baseline, only to have it recur if marijuana use continues.
Diagnostic approach and management
CHS should be suspected in patients coming in with recurrent symptoms of abdominal pain, nausea and vomiting, and who have normal CBC, basic metabolic panel, lipase, and liver function tests. Patients should be directly questioned about marijuana use and whether symptoms are relieved with hot showers. A toxicology screen should be done. For patients with marijuana use and compulsive hot showers, further work up of their symptoms (e.g., upper endoscopy, abdominal ultrasound, and/or nuclear medicine emptying study) should be avoided. Figure 1 shows the suggested work-up.
The differential diagnosis for recurrent abdominal pain, nausea, and vomiting is chronic pancreatitis, gastroparesis, severe gastritis, medication adverse effects (especially GLP1 receptor agonists), cyclic vomiting syndrome, psychogenic vomiting, and (with the rise of narcotic abuse) narcotic bowel syndrome.
Our patient had a history of diabetes with an HbA1c at goal and a normal nuclear medicine gastric-emptying study (6% retention at 4 hours). He was also on liraglutide, but his symptoms predated this medicine use.
The mainstay of treatment for CHS is supportive therapy with intravenous fluids and antiemetics like 5-HT3-receptor antagonists (ondansetron); D2-receptor antagonists (metoclopramide); and H1-receptor antagonists (diphenhydramine). The effectiveness of these agents is limited, which is also a clue for the diagnosis of CHS. If traditional agents fail in controlling the symptoms, haloperidol can be tried, but it has been used with limited success. Our patient did not respond to traditional antiemetics, but responded well to a small dose of lorazepam. Even though a benzodiazepine is not the mainstay of treatment, it may be tried if other agents fail. Acid-suppression therapy with a proton pump inhibitor should be used as esophagogastroduodenoscopy (EGD) usually reveals mild gastritis and esophagitis, as in our patient. Narcotic use should be avoided for management of abdominal pain.
Patients should be counseled against marijuana use. This may be difficult if marijuana is being used as an appetite stimulant or for treatment of chemotherapy-induced nausea and vomiting. If willing, patients should be referred to a substance abuse rehabilitation center.
Back to the case
In this case, after a diagnosis of CHS was made, the patient was counseled against marijuana use. His abdominal pain and intractable vomiting did not improve with conservative management of n.p.o status, prochlorperazine, metoclopramide, and ondansetron. He was given a trial of low-dose lorazepam with significant improvement in his symptoms. He was counseled extensively against marijuana use and discharged. A follow-up phone call at 3 months showed continued abstinence and no recurrence of symptoms.
Dr. Gupta is a hospitalist at Yale New Haven Health and Bridgeport (Conn.) Hospital.
References
1. Bajgoric S et al. Cannabinoid hyperemesis syndrome: A guide for the practising clinician. BMJ Case Rep. 2015. doi: 10.1136/bcr-2015-210246.
2. Batke M et al. The cannabis hyperemesis syndrome characterized by persistent nausea and vomiting, abdominal pain, and compulsive bathing associated with chronic marijuana use: A report of eight cases in the united states. Dig Dis Sci. 2010 Nov;55(11):3113-9.
3. Iacopetti CL et al. Cannabinoid hyperemesis syndrome: a case report and review of pathophysiology. Clin Med Res. 2014 Sep;12(1-2):65-7.
4. Hickey JL et al. Haloperidol for treatment of cannabinoid hyperemesis syndrome. Am J Emerg Med. 2013 Jun. 31(6):1003.e5-6. Epub 2013 Apr 10.
Key points
Suspect CHS for patients with recurrent abdominal pain, nausea, and vomiting with negative initial work-up.
- Ask directly about marijuana use.
- Ask whether symptoms are relieved with hot shower/ bath.
- Send a toxicology screen.
- Make a diagnosis of CHS if:
1. Positive marijuana use.
2. Symptom improvement with hot baths or
3. Toxicology positive for marijuana.
- Manage conservatively with hydration and antiemetics.
- Suspect CHS if traditional antiemetics are not providing relief .
- If traditional antiemetics fail, trial of haloperidol or low-dose benzodiazepines.
- Avoid narcotics.
- Avoid unnecessary investigations.
- Counsel patients against marijuana use and refer to substance abuse center if patient agrees.

FDA Approves Galcanezumab for Migraine Prevention
The treatment is the third anti-CGRP antibody to receive regulatory approval.
ROCKVILLE, MD—The FDA has approved galcanezumab-gnlm (Emgality) for the preventive treatment of migraine in adults. Eli Lilly and Company manufactures the therapy. Emgality is the third calcitonin gene-related peptide (CGRP) antagonist to receive regulatory approval.
The approval is based on the results of three phase III clinical trials: EVOLVE-1, EVOLVE-2, and REGAIN. EVOLVE-1 and EVOLVE-2 were six-month, double-blind, placebo-controlled studies that included adults with episodic migraine. REGAIN was a three-month, double-blind, placebo-controlled study of adults with chronic migraine. The primary end point of all three trials was mean change from baseline in the number of monthly headache days.
In all trials, patients received either placebo, 120 mg of galcanezumab-gnlm after an initial loading dose of 240 mg, or 240 mg of galcanezumab-gnlm. In EVOLVE-1 and EVOLVE-2, people who received galcanezumab-gnlm had significantly fewer headache days per month than people who received placebo, and those who received galcanezumab-gnlm were also more likely to achieve a 50%, 75%, and 100% reduction in headache days.
In REGAIN, patients who received galcanezumab-gnlm experienced fewer monthly headache days than those who received placebo and were more likely to achieve a 50% reduction in headache days. There was no difference between groups in the likelihood of achieving a 75% or 100% reduction.
The recommended dosage, according to the label, is a monthly, 120-mg subcutaneous injection with an initial loading dose of 240 mg. The most common adverse event associated with galcanezumab-gnlm is injection-site reaction.
Galcanezumab-gnlm is under final review by the European Commission for approval in Europe.
—Lucas Franki
The treatment is the third anti-CGRP antibody to receive regulatory approval.
The treatment is the third anti-CGRP antibody to receive regulatory approval.
ROCKVILLE, MD—The FDA has approved galcanezumab-gnlm (Emgality) for the preventive treatment of migraine in adults. Eli Lilly and Company manufactures the therapy. Emgality is the third calcitonin gene-related peptide (CGRP) antagonist to receive regulatory approval.
The approval is based on the results of three phase III clinical trials: EVOLVE-1, EVOLVE-2, and REGAIN. EVOLVE-1 and EVOLVE-2 were six-month, double-blind, placebo-controlled studies that included adults with episodic migraine. REGAIN was a three-month, double-blind, placebo-controlled study of adults with chronic migraine. The primary end point of all three trials was mean change from baseline in the number of monthly headache days.
In all trials, patients received either placebo, 120 mg of galcanezumab-gnlm after an initial loading dose of 240 mg, or 240 mg of galcanezumab-gnlm. In EVOLVE-1 and EVOLVE-2, people who received galcanezumab-gnlm had significantly fewer headache days per month than people who received placebo, and those who received galcanezumab-gnlm were also more likely to achieve a 50%, 75%, and 100% reduction in headache days.
In REGAIN, patients who received galcanezumab-gnlm experienced fewer monthly headache days than those who received placebo and were more likely to achieve a 50% reduction in headache days. There was no difference between groups in the likelihood of achieving a 75% or 100% reduction.
The recommended dosage, according to the label, is a monthly, 120-mg subcutaneous injection with an initial loading dose of 240 mg. The most common adverse event associated with galcanezumab-gnlm is injection-site reaction.
Galcanezumab-gnlm is under final review by the European Commission for approval in Europe.
—Lucas Franki
ROCKVILLE, MD—The FDA has approved galcanezumab-gnlm (Emgality) for the preventive treatment of migraine in adults. Eli Lilly and Company manufactures the therapy. Emgality is the third calcitonin gene-related peptide (CGRP) antagonist to receive regulatory approval.
The approval is based on the results of three phase III clinical trials: EVOLVE-1, EVOLVE-2, and REGAIN. EVOLVE-1 and EVOLVE-2 were six-month, double-blind, placebo-controlled studies that included adults with episodic migraine. REGAIN was a three-month, double-blind, placebo-controlled study of adults with chronic migraine. The primary end point of all three trials was mean change from baseline in the number of monthly headache days.
In all trials, patients received either placebo, 120 mg of galcanezumab-gnlm after an initial loading dose of 240 mg, or 240 mg of galcanezumab-gnlm. In EVOLVE-1 and EVOLVE-2, people who received galcanezumab-gnlm had significantly fewer headache days per month than people who received placebo, and those who received galcanezumab-gnlm were also more likely to achieve a 50%, 75%, and 100% reduction in headache days.
In REGAIN, patients who received galcanezumab-gnlm experienced fewer monthly headache days than those who received placebo and were more likely to achieve a 50% reduction in headache days. There was no difference between groups in the likelihood of achieving a 75% or 100% reduction.
The recommended dosage, according to the label, is a monthly, 120-mg subcutaneous injection with an initial loading dose of 240 mg. The most common adverse event associated with galcanezumab-gnlm is injection-site reaction.
Galcanezumab-gnlm is under final review by the European Commission for approval in Europe.
—Lucas Franki
New MS Subtype Shows Absence of Cerebral White Matter Demyelination
A new subtype of multiple sclerosis (MS) called myelocortical MS is characterized by demyelination only in the spinal cord and cerebral cortex and not in the cerebral white matter, according to a study published online ahead of print August 21 in Lancet Neurology. The findings are based on an examination of the brains and spinal cords of 100 patients who died of MS.
Bruce D. Trapp, PhD, the Morris R. and Ruth V. Graham Endowed Chair in Biomedical Research at the Lerner Research Institute at the Cleveland Clinic in Ohio, and his coauthors said that while the demyelination of cerebral white matter is a pathologic hallmark of MS, previous research has found that only around half of cerebral T2-weighted hyperintense white matter lesions are demyelinated, and these lesions account for less than a third of variance in the rate of brain atrophy.
“In the absence of specific MRI metrics for demyelination, the relationship between cerebral white-matter demyelination and neurodegeneration remains speculative,” they said.

In this study, researchers scanned the brains with MRI before autopsy, then took centimeter-thick hemispheric slices to study the white-matter lesions. They identified 12 individuals as having what they describe as myelocortical MS, characterized by the absence of areas of cerebral white-matter discoloration indicative of demyelinated lesions.
The authors then compared these individuals with 12 individuals with typical MS matched by age, sex, MRI protocol, MS disease subtype, disease duration, and Expanded Disability Status Scale score.
Not Typical MS
They found that while individuals with myelocortical MS did not have demyelinated lesions in the cerebral white matter, they had areas of demyelinated lesions in the cerebral cortex similar to those of individuals with typical MS (median 4.45% vs 9.74%, respectively). However, the individuals with myelocortical MS had a significantly smaller area of spinal cord demyelination (median 3.81% vs 13.81%).
Individuals with myelocortical MS also had significantly lower mean cortical neuronal densities, compared with healthy control brains, in layer III, layer V, and layer VI. But individuals with typical MS only had a lower cortical neuronal density in layer V when compared with controls.
Dr. Trapp and colleagues also saw that in typical MS, neuronal density decreased as the area of brain white-matter demyelination increased. However, this negative linear correlation was not seen in myelocortical MS.
On MRI, researchers were still able to see abnormalities in the cerebral white matter in individuals with myelocortical MS, in T2-weighted, T1-weighted, and magnetization transfer ratios (MTR) images. They also found similar total T2-weighted and T1-weighted lesion volumes in individuals with myelocortical MS and those with typical MS, although individuals with typical MS had significantly greater MTR lesion volumes.
The Hallmarks of Myelocortical MS
“We propose that myelocortical MS is characterized by spinal cord demyelination, subpial cortical demyelination, and an absence of cerebral white-matter demyelination,” Dr. Trapp and colleagues wrote. “Our findings indicate that abnormal cerebral white-matter T2-T1-MTR regions of interest are not always demyelinated, and this pathologic evidence suggests that cerebral white-matter demyelination and cortical neuronal degeneration can be independent events in myelocortical MS.”
The authors acknowledged that one limitation of their study may have been selection bias, as all the patients in the study died from complications of advanced MS. They suggested that it was therefore not appropriate to conclude that the prevalence of myelocortical MS seen in their sample would be similar across the entire MS population, nor were the findings likely to apply to pateints with earlier stage disease.
The study received funding from the NIH and the National MS Society. One author is an employee of Renovo Neural, and three authors are employees of Biogen. One author declared a pending patent related to automated lesion segmentation from MRI images, and four authors declared funding, fees, and nonfinancial support from pharmaceutical companies.
—Bianca Nogrady
Suggested Reading
Trapp BD, Vignos M, Dudman J, et al. Cortical neuronal densities and cerebral white matter demyelination in multiple sclerosis: a retrospective study. Lancet Neurol. 2018 Aug 21 [Epub ahead of print].
A new subtype of multiple sclerosis (MS) called myelocortical MS is characterized by demyelination only in the spinal cord and cerebral cortex and not in the cerebral white matter, according to a study published online ahead of print August 21 in Lancet Neurology. The findings are based on an examination of the brains and spinal cords of 100 patients who died of MS.
Bruce D. Trapp, PhD, the Morris R. and Ruth V. Graham Endowed Chair in Biomedical Research at the Lerner Research Institute at the Cleveland Clinic in Ohio, and his coauthors said that while the demyelination of cerebral white matter is a pathologic hallmark of MS, previous research has found that only around half of cerebral T2-weighted hyperintense white matter lesions are demyelinated, and these lesions account for less than a third of variance in the rate of brain atrophy.
“In the absence of specific MRI metrics for demyelination, the relationship between cerebral white-matter demyelination and neurodegeneration remains speculative,” they said.
In this study, researchers scanned the brains with MRI before autopsy, then took centimeter-thick hemispheric slices to study the white-matter lesions. They identified 12 individuals as having what they describe as myelocortical MS, characterized by the absence of areas of cerebral white-matter discoloration indicative of demyelinated lesions.
The authors then compared these individuals with 12 individuals with typical MS matched by age, sex, MRI protocol, MS disease subtype, disease duration, and Expanded Disability Status Scale score.
Not Typical MS
They found that while individuals with myelocortical MS did not have demyelinated lesions in the cerebral white matter, they had areas of demyelinated lesions in the cerebral cortex similar to those of individuals with typical MS (median 4.45% vs 9.74%, respectively). However, the individuals with myelocortical MS had a significantly smaller area of spinal cord demyelination (median 3.81% vs 13.81%).
Individuals with myelocortical MS also had significantly lower mean cortical neuronal densities, compared with healthy control brains, in layer III, layer V, and layer VI. But individuals with typical MS only had a lower cortical neuronal density in layer V when compared with controls.
Dr. Trapp and colleagues also saw that in typical MS, neuronal density decreased as the area of brain white-matter demyelination increased. However, this negative linear correlation was not seen in myelocortical MS.
On MRI, researchers were still able to see abnormalities in the cerebral white matter in individuals with myelocortical MS, in T2-weighted, T1-weighted, and magnetization transfer ratios (MTR) images. They also found similar total T2-weighted and T1-weighted lesion volumes in individuals with myelocortical MS and those with typical MS, although individuals with typical MS had significantly greater MTR lesion volumes.
The Hallmarks of Myelocortical MS
“We propose that myelocortical MS is characterized by spinal cord demyelination, subpial cortical demyelination, and an absence of cerebral white-matter demyelination,” Dr. Trapp and colleagues wrote. “Our findings indicate that abnormal cerebral white-matter T2-T1-MTR regions of interest are not always demyelinated, and this pathologic evidence suggests that cerebral white-matter demyelination and cortical neuronal degeneration can be independent events in myelocortical MS.”
The authors acknowledged that one limitation of their study may have been selection bias, as all the patients in the study died from complications of advanced MS. They suggested that it was therefore not appropriate to conclude that the prevalence of myelocortical MS seen in their sample would be similar across the entire MS population, nor were the findings likely to apply to pateints with earlier stage disease.
The study received funding from the NIH and the National MS Society. One author is an employee of Renovo Neural, and three authors are employees of Biogen. One author declared a pending patent related to automated lesion segmentation from MRI images, and four authors declared funding, fees, and nonfinancial support from pharmaceutical companies.
—Bianca Nogrady
Suggested Reading
Trapp BD, Vignos M, Dudman J, et al. Cortical neuronal densities and cerebral white matter demyelination in multiple sclerosis: a retrospective study. Lancet Neurol. 2018 Aug 21 [Epub ahead of print].
A new subtype of multiple sclerosis (MS) called myelocortical MS is characterized by demyelination only in the spinal cord and cerebral cortex and not in the cerebral white matter, according to a study published online ahead of print August 21 in Lancet Neurology. The findings are based on an examination of the brains and spinal cords of 100 patients who died of MS.
Bruce D. Trapp, PhD, the Morris R. and Ruth V. Graham Endowed Chair in Biomedical Research at the Lerner Research Institute at the Cleveland Clinic in Ohio, and his coauthors said that while the demyelination of cerebral white matter is a pathologic hallmark of MS, previous research has found that only around half of cerebral T2-weighted hyperintense white matter lesions are demyelinated, and these lesions account for less than a third of variance in the rate of brain atrophy.
“In the absence of specific MRI metrics for demyelination, the relationship between cerebral white-matter demyelination and neurodegeneration remains speculative,” they said.
In this study, researchers scanned the brains with MRI before autopsy, then took centimeter-thick hemispheric slices to study the white-matter lesions. They identified 12 individuals as having what they describe as myelocortical MS, characterized by the absence of areas of cerebral white-matter discoloration indicative of demyelinated lesions.
The authors then compared these individuals with 12 individuals with typical MS matched by age, sex, MRI protocol, MS disease subtype, disease duration, and Expanded Disability Status Scale score.
Not Typical MS
They found that while individuals with myelocortical MS did not have demyelinated lesions in the cerebral white matter, they had areas of demyelinated lesions in the cerebral cortex similar to those of individuals with typical MS (median 4.45% vs 9.74%, respectively). However, the individuals with myelocortical MS had a significantly smaller area of spinal cord demyelination (median 3.81% vs 13.81%).
Individuals with myelocortical MS also had significantly lower mean cortical neuronal densities, compared with healthy control brains, in layer III, layer V, and layer VI. But individuals with typical MS only had a lower cortical neuronal density in layer V when compared with controls.
Dr. Trapp and colleagues also saw that in typical MS, neuronal density decreased as the area of brain white-matter demyelination increased. However, this negative linear correlation was not seen in myelocortical MS.
On MRI, researchers were still able to see abnormalities in the cerebral white matter in individuals with myelocortical MS, in T2-weighted, T1-weighted, and magnetization transfer ratios (MTR) images. They also found similar total T2-weighted and T1-weighted lesion volumes in individuals with myelocortical MS and those with typical MS, although individuals with typical MS had significantly greater MTR lesion volumes.
The Hallmarks of Myelocortical MS
“We propose that myelocortical MS is characterized by spinal cord demyelination, subpial cortical demyelination, and an absence of cerebral white-matter demyelination,” Dr. Trapp and colleagues wrote. “Our findings indicate that abnormal cerebral white-matter T2-T1-MTR regions of interest are not always demyelinated, and this pathologic evidence suggests that cerebral white-matter demyelination and cortical neuronal degeneration can be independent events in myelocortical MS.”
The authors acknowledged that one limitation of their study may have been selection bias, as all the patients in the study died from complications of advanced MS. They suggested that it was therefore not appropriate to conclude that the prevalence of myelocortical MS seen in their sample would be similar across the entire MS population, nor were the findings likely to apply to pateints with earlier stage disease.
The study received funding from the NIH and the National MS Society. One author is an employee of Renovo Neural, and three authors are employees of Biogen. One author declared a pending patent related to automated lesion segmentation from MRI images, and four authors declared funding, fees, and nonfinancial support from pharmaceutical companies.
—Bianca Nogrady
Suggested Reading
Trapp BD, Vignos M, Dudman J, et al. Cortical neuronal densities and cerebral white matter demyelination in multiple sclerosis: a retrospective study. Lancet Neurol. 2018 Aug 21 [Epub ahead of print].
U.S. obesity continues to advance
The prevalence of adult obesity was at or above 35% for seven states in 2017, which is up from five states in 2016 and no states in 2012, according to the Centers for Disease Control and Prevention.
Iowa and Oklahoma, the two newest states with prevalences at or exceeding 35%, joined Alabama, Arkansas, Louisiana, Mississippi, and West Virginia, which has the country’s highest rate of adult obesity at 38.1%. Colorado’s 22.6% rate is the lowest prevalence among all states. The District of Columbia and Hawaii also have prevalences under 25%; previously, Massachusetts also was in this group, but its prevalence went up to 25.9% last year, the CDC reported.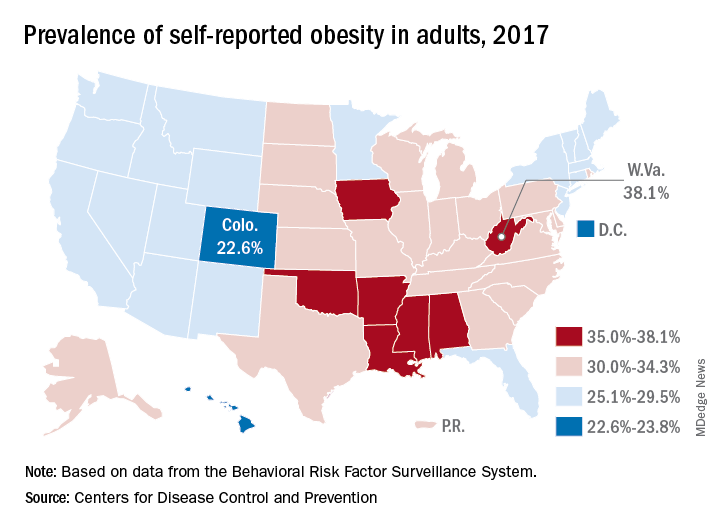
Regional disparities in self-reported adult obesity put the South (32.4%) and the Midwest (32.3%) well ahead of the Northeast (27.7%) and the West (26.1%) in 2017. Racial and ethnic disparities also were seen, with large gaps between blacks, who had a prevalence of 39%, and Hispanics (32.4%) and whites (29.3%). Obesity prevalence was 35% or higher among black adults in 31 states and D.C., while this was true among Hispanics in eight states and among whites in one (West Virginia), although the prevalence was at or above 35% for multiple racial groups in some of these states, the CDC reported based on data from the Behavioral Risk Factor Surveillance System.
“Obesity costs the United States health care system over $147 billion a year [and] research has shown that obesity affects work productivity and military readiness,” the CDC said in a written statement. “To protect the health of the next generation, support for healthy behaviors such as healthy eating, better sleep, stress management, and physical activity should start early and expand to reach Americans across the lifespan in the communities where they live, learn, work, and play.”
The AGA Obesity Practice Guide provides physicians with a comprehensive, multi-disciplinary process to guide and personalize innovative obesity care for safe and effective weight management. Learn more at http://ow.ly/p1Fh30lOXYD
The prevalence of adult obesity was at or above 35% for seven states in 2017, which is up from five states in 2016 and no states in 2012, according to the Centers for Disease Control and Prevention.
Iowa and Oklahoma, the two newest states with prevalences at or exceeding 35%, joined Alabama, Arkansas, Louisiana, Mississippi, and West Virginia, which has the country’s highest rate of adult obesity at 38.1%. Colorado’s 22.6% rate is the lowest prevalence among all states. The District of Columbia and Hawaii also have prevalences under 25%; previously, Massachusetts also was in this group, but its prevalence went up to 25.9% last year, the CDC reported.
Regional disparities in self-reported adult obesity put the South (32.4%) and the Midwest (32.3%) well ahead of the Northeast (27.7%) and the West (26.1%) in 2017. Racial and ethnic disparities also were seen, with large gaps between blacks, who had a prevalence of 39%, and Hispanics (32.4%) and whites (29.3%). Obesity prevalence was 35% or higher among black adults in 31 states and D.C., while this was true among Hispanics in eight states and among whites in one (West Virginia), although the prevalence was at or above 35% for multiple racial groups in some of these states, the CDC reported based on data from the Behavioral Risk Factor Surveillance System.
“Obesity costs the United States health care system over $147 billion a year [and] research has shown that obesity affects work productivity and military readiness,” the CDC said in a written statement. “To protect the health of the next generation, support for healthy behaviors such as healthy eating, better sleep, stress management, and physical activity should start early and expand to reach Americans across the lifespan in the communities where they live, learn, work, and play.”
The AGA Obesity Practice Guide provides physicians with a comprehensive, multi-disciplinary process to guide and personalize innovative obesity care for safe and effective weight management. Learn more at http://ow.ly/p1Fh30lOXYD
The prevalence of adult obesity was at or above 35% for seven states in 2017, which is up from five states in 2016 and no states in 2012, according to the Centers for Disease Control and Prevention.
Iowa and Oklahoma, the two newest states with prevalences at or exceeding 35%, joined Alabama, Arkansas, Louisiana, Mississippi, and West Virginia, which has the country’s highest rate of adult obesity at 38.1%. Colorado’s 22.6% rate is the lowest prevalence among all states. The District of Columbia and Hawaii also have prevalences under 25%; previously, Massachusetts also was in this group, but its prevalence went up to 25.9% last year, the CDC reported.
Regional disparities in self-reported adult obesity put the South (32.4%) and the Midwest (32.3%) well ahead of the Northeast (27.7%) and the West (26.1%) in 2017. Racial and ethnic disparities also were seen, with large gaps between blacks, who had a prevalence of 39%, and Hispanics (32.4%) and whites (29.3%). Obesity prevalence was 35% or higher among black adults in 31 states and D.C., while this was true among Hispanics in eight states and among whites in one (West Virginia), although the prevalence was at or above 35% for multiple racial groups in some of these states, the CDC reported based on data from the Behavioral Risk Factor Surveillance System.
“Obesity costs the United States health care system over $147 billion a year [and] research has shown that obesity affects work productivity and military readiness,” the CDC said in a written statement. “To protect the health of the next generation, support for healthy behaviors such as healthy eating, better sleep, stress management, and physical activity should start early and expand to reach Americans across the lifespan in the communities where they live, learn, work, and play.”
The AGA Obesity Practice Guide provides physicians with a comprehensive, multi-disciplinary process to guide and personalize innovative obesity care for safe and effective weight management. Learn more at http://ow.ly/p1Fh30lOXYD
Autologous fecal transplant restores microbiota after allo-HSCT
For patients who undergo allogeneic hematopoietic stem cell transplant (allo-HSCT) with intensive antibiotics, a subsequent autologous fecal transplant (auto-FMT) can restore intestinal microbiota, a recent study found.
Loss of normal gut bacteria after allo-HSCT and antibiotics is a common occurrence and known risk factor for graft-versus-host disease (GVHD) and intestinal infection.
“Overall, patients who lose gut microbiota diversity at the time of hematopoietic stem cell engraftment have higher rates of transplant-related death,” reported Ying Taur, MD, of the Memorial Sloan Kettering Cancer Center in New York, and his colleagues. “We explored whether the microbiota could be restored in allo-HSCT patients through the use of auto-FMT.”
Allo-HSCT patients are immune suppressed for months after engraftment, so safety concerns led the investigators to use auto-FMT rather than a fecal transplant from another individual. The complex population of viruses, fungi, archaea, bacteria, and protozoa that inhabit the human gut remains poorly understood, as does the infectious potential of a heterologous fecal donor.
“Despite remarkable advances in recent years, current technologies are incapable of comprehensively determining fecal composition,” the authors wrote in Science Translational Medicine.
The study involved 25 patients undergoing allo-HSCT with intensive antibiotic therapy. Prior to engraftment, fecal samples were collected from all patients and analyzed for composition and diversity, measured by inverse Simpson index.
Samples were then frozen and stored. Fecal analysis also was performed after engraftment, and again after the auto-FMT time point. Auto-FMT was performed in 14 patients; 11 patients served as controls and did not receive treatment. Patients were followed for 1 year.
The investigators found that all of the patients who underwent auto-FMT recovered their pre–allo-HSCT microbiota composition and diversity, compared with none of the controls (P less than .0001). Further analysis showed that auto-FMT increased diversity (inverse Simpson index) by 64%, compared with 38% in controls.
“We have demonstrated the potential of auto-FMT as a clinical intervention to restore intestinal microbiota diversity to levels deemed safe in patients, thereby reversing the disruptive effects of broad-spectrum antibiotic treatment for patients undergoing allo-HSCT transplant,” the investigators concluded.
Study funding was provided by the Leonard Tow Foundation and the Memorial Sloan Kettering’s Center for Microbes, Inflammation, and Cancer. The authors reported financial relationships with Merck, AbbVie, Nektar Therapeutics, Novartis, and others.
SOURCE: Taur Y et al. Sci Transl Med. 2018 Sep 26. doi: 10.1126/scitranslmed.aap9489.
For patients who undergo allogeneic hematopoietic stem cell transplant (allo-HSCT) with intensive antibiotics, a subsequent autologous fecal transplant (auto-FMT) can restore intestinal microbiota, a recent study found.
Loss of normal gut bacteria after allo-HSCT and antibiotics is a common occurrence and known risk factor for graft-versus-host disease (GVHD) and intestinal infection.
“Overall, patients who lose gut microbiota diversity at the time of hematopoietic stem cell engraftment have higher rates of transplant-related death,” reported Ying Taur, MD, of the Memorial Sloan Kettering Cancer Center in New York, and his colleagues. “We explored whether the microbiota could be restored in allo-HSCT patients through the use of auto-FMT.”
Allo-HSCT patients are immune suppressed for months after engraftment, so safety concerns led the investigators to use auto-FMT rather than a fecal transplant from another individual. The complex population of viruses, fungi, archaea, bacteria, and protozoa that inhabit the human gut remains poorly understood, as does the infectious potential of a heterologous fecal donor.
“Despite remarkable advances in recent years, current technologies are incapable of comprehensively determining fecal composition,” the authors wrote in Science Translational Medicine.
The study involved 25 patients undergoing allo-HSCT with intensive antibiotic therapy. Prior to engraftment, fecal samples were collected from all patients and analyzed for composition and diversity, measured by inverse Simpson index.
Samples were then frozen and stored. Fecal analysis also was performed after engraftment, and again after the auto-FMT time point. Auto-FMT was performed in 14 patients; 11 patients served as controls and did not receive treatment. Patients were followed for 1 year.
The investigators found that all of the patients who underwent auto-FMT recovered their pre–allo-HSCT microbiota composition and diversity, compared with none of the controls (P less than .0001). Further analysis showed that auto-FMT increased diversity (inverse Simpson index) by 64%, compared with 38% in controls.
“We have demonstrated the potential of auto-FMT as a clinical intervention to restore intestinal microbiota diversity to levels deemed safe in patients, thereby reversing the disruptive effects of broad-spectrum antibiotic treatment for patients undergoing allo-HSCT transplant,” the investigators concluded.
Study funding was provided by the Leonard Tow Foundation and the Memorial Sloan Kettering’s Center for Microbes, Inflammation, and Cancer. The authors reported financial relationships with Merck, AbbVie, Nektar Therapeutics, Novartis, and others.
SOURCE: Taur Y et al. Sci Transl Med. 2018 Sep 26. doi: 10.1126/scitranslmed.aap9489.
For patients who undergo allogeneic hematopoietic stem cell transplant (allo-HSCT) with intensive antibiotics, a subsequent autologous fecal transplant (auto-FMT) can restore intestinal microbiota, a recent study found.
Loss of normal gut bacteria after allo-HSCT and antibiotics is a common occurrence and known risk factor for graft-versus-host disease (GVHD) and intestinal infection.
“Overall, patients who lose gut microbiota diversity at the time of hematopoietic stem cell engraftment have higher rates of transplant-related death,” reported Ying Taur, MD, of the Memorial Sloan Kettering Cancer Center in New York, and his colleagues. “We explored whether the microbiota could be restored in allo-HSCT patients through the use of auto-FMT.”
Allo-HSCT patients are immune suppressed for months after engraftment, so safety concerns led the investigators to use auto-FMT rather than a fecal transplant from another individual. The complex population of viruses, fungi, archaea, bacteria, and protozoa that inhabit the human gut remains poorly understood, as does the infectious potential of a heterologous fecal donor.
“Despite remarkable advances in recent years, current technologies are incapable of comprehensively determining fecal composition,” the authors wrote in Science Translational Medicine.
The study involved 25 patients undergoing allo-HSCT with intensive antibiotic therapy. Prior to engraftment, fecal samples were collected from all patients and analyzed for composition and diversity, measured by inverse Simpson index.
Samples were then frozen and stored. Fecal analysis also was performed after engraftment, and again after the auto-FMT time point. Auto-FMT was performed in 14 patients; 11 patients served as controls and did not receive treatment. Patients were followed for 1 year.
The investigators found that all of the patients who underwent auto-FMT recovered their pre–allo-HSCT microbiota composition and diversity, compared with none of the controls (P less than .0001). Further analysis showed that auto-FMT increased diversity (inverse Simpson index) by 64%, compared with 38% in controls.
“We have demonstrated the potential of auto-FMT as a clinical intervention to restore intestinal microbiota diversity to levels deemed safe in patients, thereby reversing the disruptive effects of broad-spectrum antibiotic treatment for patients undergoing allo-HSCT transplant,” the investigators concluded.
Study funding was provided by the Leonard Tow Foundation and the Memorial Sloan Kettering’s Center for Microbes, Inflammation, and Cancer. The authors reported financial relationships with Merck, AbbVie, Nektar Therapeutics, Novartis, and others.
SOURCE: Taur Y et al. Sci Transl Med. 2018 Sep 26. doi: 10.1126/scitranslmed.aap9489.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point:
Major finding: All patients who received auto-FMT regained pre–allo-HSCT microbiota composition and diversity (P less than .0001).
Study details: An open-label study involving 25 allo-HSCT patients that compared auto-FMT with no treatment.
Disclosures: Study funding was provided by the Leonard Tow Foundation and the Memorial Sloan Kettering’s Center for Microbes, Inflammation, and Cancer. The authors reported disclosures related Merck, AbbVie, Nektar Therapeutics, Novartis, and others.
Source: Taur Y et al. Sci Transl Med. 2018 Sep 26. doi: 10.1126/scitranslmed.aap9489.
New and Noteworthy Information—October 2018
CPAP After Stroke May Improve Function
Treating sleep apnea after a stroke or transient ischemic attack (TIA) may improve speech impairment, neurologic symptoms, walking, and physical function, according to a study published August 15 in the Journal of the American Heart Association. To examine whether continuous positive airway pressure (CPAP) improves clinical outcomes among patients with stroke or TIA who have obstructive sleep apnea, researchers analyzed data from a trial that included 252 patients with stroke or TIA. Participants were randomized to intervention groups that received polysomnography soon after the stroke or TIA or to a control group. Among the 81 patients in the intervention groups with sleep apnea, more than 70% used CPAP during approximately one year of follow-up. In intention-to-treat analyses, changes in NIH Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scores were similar across groups. In as-treated analyses among patients with sleep apnea, CPAP use was associated with improved NIHSS and mRS scores. In addition, 59% of intervention patients with sleep apnea had a final NIHSS score of 0 or 1 versus 38% of controls with sleep apnea.
Bravata DM, Sico J, Fragoso CAV, et al. Diagnosing and treating sleep apnea in patients with acute cerebrovascular disease. J Am Heart Assoc. 2018;7:e008841.
Intervention Reduces Cognitive Decline in Blacks With MCI
Among black patients with mild cognitive impairment (MCI), a behavioral intervention that aims to increase social, cognitive, and physical activity reduces the risk of memory decline, compared with supportive therapy, according to a study published online ahead of print September 10 in JAMA Neurology. Between June 2011 and October 2014, researchers enrolled 221 black participants with MCI (mean age, 75.8; 79% women) into a clinical trial. Participants were randomized to behavioral activation or supportive therapy (ie, an attention control treatment). The primary outcome was a decline of six or more recalled words on the total recall score of the Hopkins Verbal Learning Test-Revised at six, 12, 18, and 24 months. The two-year incidence of memory decline was lower in the behavioral activation group than in the supportive therapy group (1.2% vs 9.3%). Behavioral activation reduced the risk of cognitive decline by 88%, compared with supportive therapy.
Rovner BW, Casten RJ, Hegel MT, Leiby B. Preventing cognitive decline in black individuals with mild cognitive impairment: a randomized clinical trial. JAMA Neurol. 2018 Sep 10 [Epub ahead of print].
Medical Marijuana May Treat Nerve Pain
Among patients with neuropathic pain, sublingual tetrahydrocannabinol (THC) significantly reduces pain versus placebo, according to a randomized, double-blind study published online ahead of print September 5 in Neurology. The trial included 15 men with chronic radicular nerve pain (average age, 33). Before and one hour after treatment with THC or placebo oil, participants rated their pain levels on a scale from zero to 100. At least one week later, they received the other treatment. The average pain level before treatment was 53. After taking THC, participants’ average pain level was 35, compared with an average pain level of 43 after taking placebo. Functional MRI showed that the drug’s analgesic effect correlated with reduced functional connectivity between brain areas involved in emotion and pain processing.
Weizman L, Dayan L, Brill S, et al. Cannabis analgesia in chronic neuropathic pain is associated with altered brain connectivity. Neurology. 2018 Sep 5 [Epub ahead of print].
For Which Clots Is t-PA Most Effective?
In patients with acute ischemic stroke, a more distal thrombus location, greater thrombus permeability, and longer time to assessment of recanalization are associated with recanalization of an arterial occlusion after administration of IV alteplase, according to a study published in the September 11 issue of JAMA. This multicenter prospective cohort study included 575 patients with acute ischemic stroke and intracranial arterial occlusion demonstrated on CT angiogram (CTA). In all, 275 participants received IV alteplase, 195 participants received IV alteplase plus endovascular thrombectomy, 48 participants received endovascular thrombectomy, and 57 participants received conservative treatment. Median time from baseline CTA to recanalization assessment was 158 minutes. Successful recanalization occurred at an unadjusted rate of 27.3%, including in 30.4% of patients who received IV alteplase and 13.3% who did not.
Menon BK, Al-Ajlan FS, Najm M, et al. Association of clinical, imaging, and thrombus characteristics with recanalization of visible intracranial occlusion in patients with acute ischemic stroke. JAMA. 2018;320(10):1017-1026.
FDA Approves Ajovy for Adults With Migraine
The FDA has approved Ajovy (fremanezumab-vfrm), a calcitonin gene-related peptide (CGRP) antagonist, for the preventive treatment of migraine in adults. Dosing options include 225 mg monthly administered as one subcutaneous injection or 675 mg quarterly administered as three subcutaneous injections. The injections can be administered by a healthcare professional or by a patient or caregiver. The treatment was evaluated in two phase III, placebo-controlled clinical trials that enrolled patients with migraine. The trials examined the therapy as a stand-alone preventive treatment and in combination with oral preventive treatments. Patients experienced a reduction in monthly migraine days during a 12-week period. The most common adverse reactions were injection site reactions. Ajovy is a humanized monoclonal antibody that binds to CGRP ligand and blocks its binding to the receptor. Teva Pharmaceutical Industries, which markets Ajovy, is headquartered in Jerusalem.
Is Daytime Sleepiness Associated With an Alzheimer’s Disease Biomarker?
Excessive daytime sleepiness (EDS) is associated with more than 2.5 times the odds of β-amyloid (Aβ) deposition an average of 15.7 years later, according to a study published online ahead of print September 5 in Sleep. Researchers studied 124 participants in the Baltimore Longitudinal Study of Aging Neuroimaging Substudy who completed self-reported measures of EDS and napping at baseline and underwent 11C-Pittsburgh compound B-PET scans of the brain an average of 15.7 years later. Participants’ mean age was 60.1 at baseline; 24.4% had EDS, and 28.5% napped. In unadjusted analyses, compared with participants without EDS, people with EDS had more than three times the odds of being Aβ+ (ie, having a cortical distribution volume ratio of greater than 1.06) at follow-up. After adjusting for age, sex, education, and BMI, the odds ratio was 2.75.
Spira AP, An Y, Wu MN, et al. Excessive daytime sleepiness and napping in cognitively normal adults: associations with subsequent amyloid deposition measured by PiB PET. Sleep. 2018 Sep 5 [Epub ahead of print].
Sepsis Heightens Risk of Stroke and Heart Attack
Patients recovering from sepsis have a greater risk of myocardial infarction or stroke in the first four weeks after hospital discharge, compared with population and hospital controls, according to a study published September 10 in the Canadian Medical Association Journal. This retrospective population-based cohort study included 42,316 patients with sepsis identified from the National Health Insurance Research Database in Taiwan. In all, 831 patients with sepsis had a stroke and 184 had a myocardial infarction within 180 days of discharge from the hospital. Compared with population controls, the risk was highest in the first seven days after discharge (hazard ratio, 4.78). Compared with hospital controls, the risk was attenuated but remained elevated before day 36 after discharge (hazard ratio, 1.32).
Lai CC, Lee MG, Lee WC, et al. Susceptible period for cardiovascular complications in patients recovering from sepsis. CMAJ. 2018;190(36):E1062-E1069.
Ten-Year Risk Factors for Dementia
Age, sex, and APOE genotype identify high-risk groups for Alzheimer’s disease and dementia, according to a study published September 4 in the Canadian Medical Association Journal. The study looked at data from 104,537 people in Copenhagen. Participants completed a questionnaire and underwent physical examination and blood sampling at baseline. The researchers obtained diagnoses of dementia and cerebrovascular disease from the Danish National Patient Registry through November 10, 2014. The absolute 10-year risk of Alzheimer’s disease among 3,017 people who were carriers of the APOE ε44 genotype was 7% for women and 6% for men ages 60 to 69, 16% for women and 12% for men ages 70 to 79, and 24% for women and 19% for men ages 80 and older.
Rasmussen KL, Tybjærg-Hansen A, Nordestgaard BG, Frikke-Schmidt R. Absolute 10-year risk of dementia by age, sex and APOE genotype: a population-based cohort study. CMAJ. 2018;190(35):E1033-E1041.
Is Job Stress Associated With Parkinson’s Disease Risk?
Occupational stress may increase Parkinson’s disease risk, according to a study published online ahead of print August 25 in Movement Disorders. Researchers conducted a population-based cohort study of 2,544,748 Swedes whose occupations had been reported in censuses. They identified incident Parkinson’s disease cases using Swedish national health registers and analyzed the data using Cox regression with age as the underlying time scale, adjusting for sex, education, and chronic obstructive pulmonary disease as a proxy for smoking. During a mean follow-up of 21.3 years, 21,544 incident Parkinson’s disease cases were identified. High job demands were associated with increased risk of Parkinson’s disease among men, most evidently in men with high levels of education. High levels of job control were associated with increased risk among people with low levels of education, and this association was stronger in women.
Sieurin J, Andel R, Tillander A, et al. Occupational stress and risk for Parkinson’s disease: a nationwide cohort study. Mov Disord. 2018 Aug 25 [Epub ahead of print].
FDA Approves Tiglutik for ALS
The FDA has approved Tiglutik (riluzole) oral suspension for the treatment of amyotrophic lateral sclerosis (ALS). Tiglutik is a thickened liquid taken twice daily by oral syringe. The approval of Tiglutik is based on bioavailability studies comparing oral riluzole tablets to Tiglutik oral suspension. The most common side effects of Tiglutik are consistent with the established clinical profile of riluzole and include oral hypoesthesia, asthenia, nausea, decreased lung function, hypertension, and abdominal pain. The recommended dosage is 50 mg/10 mL. The drug should be taken at least one hour before or two hours after a meal. In clinical studies, riluzole modulated glutamate neurotransmission by inhibiting glutamate release and postsynaptic glutamate receptor signaling. ITF Pharma, which markets the drug, is headquartered in Berwyn, Pennsylvania.
—Kimberly Williams
CPAP After Stroke May Improve Function
Treating sleep apnea after a stroke or transient ischemic attack (TIA) may improve speech impairment, neurologic symptoms, walking, and physical function, according to a study published August 15 in the Journal of the American Heart Association. To examine whether continuous positive airway pressure (CPAP) improves clinical outcomes among patients with stroke or TIA who have obstructive sleep apnea, researchers analyzed data from a trial that included 252 patients with stroke or TIA. Participants were randomized to intervention groups that received polysomnography soon after the stroke or TIA or to a control group. Among the 81 patients in the intervention groups with sleep apnea, more than 70% used CPAP during approximately one year of follow-up. In intention-to-treat analyses, changes in NIH Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scores were similar across groups. In as-treated analyses among patients with sleep apnea, CPAP use was associated with improved NIHSS and mRS scores. In addition, 59% of intervention patients with sleep apnea had a final NIHSS score of 0 or 1 versus 38% of controls with sleep apnea.
Bravata DM, Sico J, Fragoso CAV, et al. Diagnosing and treating sleep apnea in patients with acute cerebrovascular disease. J Am Heart Assoc. 2018;7:e008841.
Intervention Reduces Cognitive Decline in Blacks With MCI
Among black patients with mild cognitive impairment (MCI), a behavioral intervention that aims to increase social, cognitive, and physical activity reduces the risk of memory decline, compared with supportive therapy, according to a study published online ahead of print September 10 in JAMA Neurology. Between June 2011 and October 2014, researchers enrolled 221 black participants with MCI (mean age, 75.8; 79% women) into a clinical trial. Participants were randomized to behavioral activation or supportive therapy (ie, an attention control treatment). The primary outcome was a decline of six or more recalled words on the total recall score of the Hopkins Verbal Learning Test-Revised at six, 12, 18, and 24 months. The two-year incidence of memory decline was lower in the behavioral activation group than in the supportive therapy group (1.2% vs 9.3%). Behavioral activation reduced the risk of cognitive decline by 88%, compared with supportive therapy.
Rovner BW, Casten RJ, Hegel MT, Leiby B. Preventing cognitive decline in black individuals with mild cognitive impairment: a randomized clinical trial. JAMA Neurol. 2018 Sep 10 [Epub ahead of print].
Medical Marijuana May Treat Nerve Pain
Among patients with neuropathic pain, sublingual tetrahydrocannabinol (THC) significantly reduces pain versus placebo, according to a randomized, double-blind study published online ahead of print September 5 in Neurology. The trial included 15 men with chronic radicular nerve pain (average age, 33). Before and one hour after treatment with THC or placebo oil, participants rated their pain levels on a scale from zero to 100. At least one week later, they received the other treatment. The average pain level before treatment was 53. After taking THC, participants’ average pain level was 35, compared with an average pain level of 43 after taking placebo. Functional MRI showed that the drug’s analgesic effect correlated with reduced functional connectivity between brain areas involved in emotion and pain processing.
Weizman L, Dayan L, Brill S, et al. Cannabis analgesia in chronic neuropathic pain is associated with altered brain connectivity. Neurology. 2018 Sep 5 [Epub ahead of print].
For Which Clots Is t-PA Most Effective?
In patients with acute ischemic stroke, a more distal thrombus location, greater thrombus permeability, and longer time to assessment of recanalization are associated with recanalization of an arterial occlusion after administration of IV alteplase, according to a study published in the September 11 issue of JAMA. This multicenter prospective cohort study included 575 patients with acute ischemic stroke and intracranial arterial occlusion demonstrated on CT angiogram (CTA). In all, 275 participants received IV alteplase, 195 participants received IV alteplase plus endovascular thrombectomy, 48 participants received endovascular thrombectomy, and 57 participants received conservative treatment. Median time from baseline CTA to recanalization assessment was 158 minutes. Successful recanalization occurred at an unadjusted rate of 27.3%, including in 30.4% of patients who received IV alteplase and 13.3% who did not.
Menon BK, Al-Ajlan FS, Najm M, et al. Association of clinical, imaging, and thrombus characteristics with recanalization of visible intracranial occlusion in patients with acute ischemic stroke. JAMA. 2018;320(10):1017-1026.
FDA Approves Ajovy for Adults With Migraine
The FDA has approved Ajovy (fremanezumab-vfrm), a calcitonin gene-related peptide (CGRP) antagonist, for the preventive treatment of migraine in adults. Dosing options include 225 mg monthly administered as one subcutaneous injection or 675 mg quarterly administered as three subcutaneous injections. The injections can be administered by a healthcare professional or by a patient or caregiver. The treatment was evaluated in two phase III, placebo-controlled clinical trials that enrolled patients with migraine. The trials examined the therapy as a stand-alone preventive treatment and in combination with oral preventive treatments. Patients experienced a reduction in monthly migraine days during a 12-week period. The most common adverse reactions were injection site reactions. Ajovy is a humanized monoclonal antibody that binds to CGRP ligand and blocks its binding to the receptor. Teva Pharmaceutical Industries, which markets Ajovy, is headquartered in Jerusalem.
Is Daytime Sleepiness Associated With an Alzheimer’s Disease Biomarker?
Excessive daytime sleepiness (EDS) is associated with more than 2.5 times the odds of β-amyloid (Aβ) deposition an average of 15.7 years later, according to a study published online ahead of print September 5 in Sleep. Researchers studied 124 participants in the Baltimore Longitudinal Study of Aging Neuroimaging Substudy who completed self-reported measures of EDS and napping at baseline and underwent 11C-Pittsburgh compound B-PET scans of the brain an average of 15.7 years later. Participants’ mean age was 60.1 at baseline; 24.4% had EDS, and 28.5% napped. In unadjusted analyses, compared with participants without EDS, people with EDS had more than three times the odds of being Aβ+ (ie, having a cortical distribution volume ratio of greater than 1.06) at follow-up. After adjusting for age, sex, education, and BMI, the odds ratio was 2.75.
Spira AP, An Y, Wu MN, et al. Excessive daytime sleepiness and napping in cognitively normal adults: associations with subsequent amyloid deposition measured by PiB PET. Sleep. 2018 Sep 5 [Epub ahead of print].
Sepsis Heightens Risk of Stroke and Heart Attack
Patients recovering from sepsis have a greater risk of myocardial infarction or stroke in the first four weeks after hospital discharge, compared with population and hospital controls, according to a study published September 10 in the Canadian Medical Association Journal. This retrospective population-based cohort study included 42,316 patients with sepsis identified from the National Health Insurance Research Database in Taiwan. In all, 831 patients with sepsis had a stroke and 184 had a myocardial infarction within 180 days of discharge from the hospital. Compared with population controls, the risk was highest in the first seven days after discharge (hazard ratio, 4.78). Compared with hospital controls, the risk was attenuated but remained elevated before day 36 after discharge (hazard ratio, 1.32).
Lai CC, Lee MG, Lee WC, et al. Susceptible period for cardiovascular complications in patients recovering from sepsis. CMAJ. 2018;190(36):E1062-E1069.
Ten-Year Risk Factors for Dementia
Age, sex, and APOE genotype identify high-risk groups for Alzheimer’s disease and dementia, according to a study published September 4 in the Canadian Medical Association Journal. The study looked at data from 104,537 people in Copenhagen. Participants completed a questionnaire and underwent physical examination and blood sampling at baseline. The researchers obtained diagnoses of dementia and cerebrovascular disease from the Danish National Patient Registry through November 10, 2014. The absolute 10-year risk of Alzheimer’s disease among 3,017 people who were carriers of the APOE ε44 genotype was 7% for women and 6% for men ages 60 to 69, 16% for women and 12% for men ages 70 to 79, and 24% for women and 19% for men ages 80 and older.
Rasmussen KL, Tybjærg-Hansen A, Nordestgaard BG, Frikke-Schmidt R. Absolute 10-year risk of dementia by age, sex and APOE genotype: a population-based cohort study. CMAJ. 2018;190(35):E1033-E1041.
Is Job Stress Associated With Parkinson’s Disease Risk?
Occupational stress may increase Parkinson’s disease risk, according to a study published online ahead of print August 25 in Movement Disorders. Researchers conducted a population-based cohort study of 2,544,748 Swedes whose occupations had been reported in censuses. They identified incident Parkinson’s disease cases using Swedish national health registers and analyzed the data using Cox regression with age as the underlying time scale, adjusting for sex, education, and chronic obstructive pulmonary disease as a proxy for smoking. During a mean follow-up of 21.3 years, 21,544 incident Parkinson’s disease cases were identified. High job demands were associated with increased risk of Parkinson’s disease among men, most evidently in men with high levels of education. High levels of job control were associated with increased risk among people with low levels of education, and this association was stronger in women.
Sieurin J, Andel R, Tillander A, et al. Occupational stress and risk for Parkinson’s disease: a nationwide cohort study. Mov Disord. 2018 Aug 25 [Epub ahead of print].
FDA Approves Tiglutik for ALS
The FDA has approved Tiglutik (riluzole) oral suspension for the treatment of amyotrophic lateral sclerosis (ALS). Tiglutik is a thickened liquid taken twice daily by oral syringe. The approval of Tiglutik is based on bioavailability studies comparing oral riluzole tablets to Tiglutik oral suspension. The most common side effects of Tiglutik are consistent with the established clinical profile of riluzole and include oral hypoesthesia, asthenia, nausea, decreased lung function, hypertension, and abdominal pain. The recommended dosage is 50 mg/10 mL. The drug should be taken at least one hour before or two hours after a meal. In clinical studies, riluzole modulated glutamate neurotransmission by inhibiting glutamate release and postsynaptic glutamate receptor signaling. ITF Pharma, which markets the drug, is headquartered in Berwyn, Pennsylvania.
—Kimberly Williams
CPAP After Stroke May Improve Function
Treating sleep apnea after a stroke or transient ischemic attack (TIA) may improve speech impairment, neurologic symptoms, walking, and physical function, according to a study published August 15 in the Journal of the American Heart Association. To examine whether continuous positive airway pressure (CPAP) improves clinical outcomes among patients with stroke or TIA who have obstructive sleep apnea, researchers analyzed data from a trial that included 252 patients with stroke or TIA. Participants were randomized to intervention groups that received polysomnography soon after the stroke or TIA or to a control group. Among the 81 patients in the intervention groups with sleep apnea, more than 70% used CPAP during approximately one year of follow-up. In intention-to-treat analyses, changes in NIH Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scores were similar across groups. In as-treated analyses among patients with sleep apnea, CPAP use was associated with improved NIHSS and mRS scores. In addition, 59% of intervention patients with sleep apnea had a final NIHSS score of 0 or 1 versus 38% of controls with sleep apnea.
Bravata DM, Sico J, Fragoso CAV, et al. Diagnosing and treating sleep apnea in patients with acute cerebrovascular disease. J Am Heart Assoc. 2018;7:e008841.
Intervention Reduces Cognitive Decline in Blacks With MCI
Among black patients with mild cognitive impairment (MCI), a behavioral intervention that aims to increase social, cognitive, and physical activity reduces the risk of memory decline, compared with supportive therapy, according to a study published online ahead of print September 10 in JAMA Neurology. Between June 2011 and October 2014, researchers enrolled 221 black participants with MCI (mean age, 75.8; 79% women) into a clinical trial. Participants were randomized to behavioral activation or supportive therapy (ie, an attention control treatment). The primary outcome was a decline of six or more recalled words on the total recall score of the Hopkins Verbal Learning Test-Revised at six, 12, 18, and 24 months. The two-year incidence of memory decline was lower in the behavioral activation group than in the supportive therapy group (1.2% vs 9.3%). Behavioral activation reduced the risk of cognitive decline by 88%, compared with supportive therapy.
Rovner BW, Casten RJ, Hegel MT, Leiby B. Preventing cognitive decline in black individuals with mild cognitive impairment: a randomized clinical trial. JAMA Neurol. 2018 Sep 10 [Epub ahead of print].
Medical Marijuana May Treat Nerve Pain
Among patients with neuropathic pain, sublingual tetrahydrocannabinol (THC) significantly reduces pain versus placebo, according to a randomized, double-blind study published online ahead of print September 5 in Neurology. The trial included 15 men with chronic radicular nerve pain (average age, 33). Before and one hour after treatment with THC or placebo oil, participants rated their pain levels on a scale from zero to 100. At least one week later, they received the other treatment. The average pain level before treatment was 53. After taking THC, participants’ average pain level was 35, compared with an average pain level of 43 after taking placebo. Functional MRI showed that the drug’s analgesic effect correlated with reduced functional connectivity between brain areas involved in emotion and pain processing.
Weizman L, Dayan L, Brill S, et al. Cannabis analgesia in chronic neuropathic pain is associated with altered brain connectivity. Neurology. 2018 Sep 5 [Epub ahead of print].
For Which Clots Is t-PA Most Effective?
In patients with acute ischemic stroke, a more distal thrombus location, greater thrombus permeability, and longer time to assessment of recanalization are associated with recanalization of an arterial occlusion after administration of IV alteplase, according to a study published in the September 11 issue of JAMA. This multicenter prospective cohort study included 575 patients with acute ischemic stroke and intracranial arterial occlusion demonstrated on CT angiogram (CTA). In all, 275 participants received IV alteplase, 195 participants received IV alteplase plus endovascular thrombectomy, 48 participants received endovascular thrombectomy, and 57 participants received conservative treatment. Median time from baseline CTA to recanalization assessment was 158 minutes. Successful recanalization occurred at an unadjusted rate of 27.3%, including in 30.4% of patients who received IV alteplase and 13.3% who did not.
Menon BK, Al-Ajlan FS, Najm M, et al. Association of clinical, imaging, and thrombus characteristics with recanalization of visible intracranial occlusion in patients with acute ischemic stroke. JAMA. 2018;320(10):1017-1026.
FDA Approves Ajovy for Adults With Migraine
The FDA has approved Ajovy (fremanezumab-vfrm), a calcitonin gene-related peptide (CGRP) antagonist, for the preventive treatment of migraine in adults. Dosing options include 225 mg monthly administered as one subcutaneous injection or 675 mg quarterly administered as three subcutaneous injections. The injections can be administered by a healthcare professional or by a patient or caregiver. The treatment was evaluated in two phase III, placebo-controlled clinical trials that enrolled patients with migraine. The trials examined the therapy as a stand-alone preventive treatment and in combination with oral preventive treatments. Patients experienced a reduction in monthly migraine days during a 12-week period. The most common adverse reactions were injection site reactions. Ajovy is a humanized monoclonal antibody that binds to CGRP ligand and blocks its binding to the receptor. Teva Pharmaceutical Industries, which markets Ajovy, is headquartered in Jerusalem.
Is Daytime Sleepiness Associated With an Alzheimer’s Disease Biomarker?
Excessive daytime sleepiness (EDS) is associated with more than 2.5 times the odds of β-amyloid (Aβ) deposition an average of 15.7 years later, according to a study published online ahead of print September 5 in Sleep. Researchers studied 124 participants in the Baltimore Longitudinal Study of Aging Neuroimaging Substudy who completed self-reported measures of EDS and napping at baseline and underwent 11C-Pittsburgh compound B-PET scans of the brain an average of 15.7 years later. Participants’ mean age was 60.1 at baseline; 24.4% had EDS, and 28.5% napped. In unadjusted analyses, compared with participants without EDS, people with EDS had more than three times the odds of being Aβ+ (ie, having a cortical distribution volume ratio of greater than 1.06) at follow-up. After adjusting for age, sex, education, and BMI, the odds ratio was 2.75.
Spira AP, An Y, Wu MN, et al. Excessive daytime sleepiness and napping in cognitively normal adults: associations with subsequent amyloid deposition measured by PiB PET. Sleep. 2018 Sep 5 [Epub ahead of print].
Sepsis Heightens Risk of Stroke and Heart Attack
Patients recovering from sepsis have a greater risk of myocardial infarction or stroke in the first four weeks after hospital discharge, compared with population and hospital controls, according to a study published September 10 in the Canadian Medical Association Journal. This retrospective population-based cohort study included 42,316 patients with sepsis identified from the National Health Insurance Research Database in Taiwan. In all, 831 patients with sepsis had a stroke and 184 had a myocardial infarction within 180 days of discharge from the hospital. Compared with population controls, the risk was highest in the first seven days after discharge (hazard ratio, 4.78). Compared with hospital controls, the risk was attenuated but remained elevated before day 36 after discharge (hazard ratio, 1.32).
Lai CC, Lee MG, Lee WC, et al. Susceptible period for cardiovascular complications in patients recovering from sepsis. CMAJ. 2018;190(36):E1062-E1069.
Ten-Year Risk Factors for Dementia
Age, sex, and APOE genotype identify high-risk groups for Alzheimer’s disease and dementia, according to a study published September 4 in the Canadian Medical Association Journal. The study looked at data from 104,537 people in Copenhagen. Participants completed a questionnaire and underwent physical examination and blood sampling at baseline. The researchers obtained diagnoses of dementia and cerebrovascular disease from the Danish National Patient Registry through November 10, 2014. The absolute 10-year risk of Alzheimer’s disease among 3,017 people who were carriers of the APOE ε44 genotype was 7% for women and 6% for men ages 60 to 69, 16% for women and 12% for men ages 70 to 79, and 24% for women and 19% for men ages 80 and older.
Rasmussen KL, Tybjærg-Hansen A, Nordestgaard BG, Frikke-Schmidt R. Absolute 10-year risk of dementia by age, sex and APOE genotype: a population-based cohort study. CMAJ. 2018;190(35):E1033-E1041.
Is Job Stress Associated With Parkinson’s Disease Risk?
Occupational stress may increase Parkinson’s disease risk, according to a study published online ahead of print August 25 in Movement Disorders. Researchers conducted a population-based cohort study of 2,544,748 Swedes whose occupations had been reported in censuses. They identified incident Parkinson’s disease cases using Swedish national health registers and analyzed the data using Cox regression with age as the underlying time scale, adjusting for sex, education, and chronic obstructive pulmonary disease as a proxy for smoking. During a mean follow-up of 21.3 years, 21,544 incident Parkinson’s disease cases were identified. High job demands were associated with increased risk of Parkinson’s disease among men, most evidently in men with high levels of education. High levels of job control were associated with increased risk among people with low levels of education, and this association was stronger in women.
Sieurin J, Andel R, Tillander A, et al. Occupational stress and risk for Parkinson’s disease: a nationwide cohort study. Mov Disord. 2018 Aug 25 [Epub ahead of print].
FDA Approves Tiglutik for ALS
The FDA has approved Tiglutik (riluzole) oral suspension for the treatment of amyotrophic lateral sclerosis (ALS). Tiglutik is a thickened liquid taken twice daily by oral syringe. The approval of Tiglutik is based on bioavailability studies comparing oral riluzole tablets to Tiglutik oral suspension. The most common side effects of Tiglutik are consistent with the established clinical profile of riluzole and include oral hypoesthesia, asthenia, nausea, decreased lung function, hypertension, and abdominal pain. The recommended dosage is 50 mg/10 mL. The drug should be taken at least one hour before or two hours after a meal. In clinical studies, riluzole modulated glutamate neurotransmission by inhibiting glutamate release and postsynaptic glutamate receptor signaling. ITF Pharma, which markets the drug, is headquartered in Berwyn, Pennsylvania.
—Kimberly Williams

Endogenous retroviruses may unlock new immunotherapy targets
Future epigenetic drugs could activate human endogenous retroviruses (HERVs) in cancer cells to enable immunotherapy, investigators suggest.
Activated HERVs may sensitize cancer cells or serve as novel tumor-associated antigenic targets, reported Anders Steenholdt Attermann, PhD, of the department of micro- and nanotechnology at the Technical University of Denmark in Kongens Lyngby, and colleagues.
A remarkable 8% of the human genome is composed of HERVs.
“They are remnants of retroviral germline infections that resulted in chromosomal integration into all the cells of the progeny, but their viral replication is defective in the present-day human genome,” the authors wrote in Annals of Oncology.
The therapeutic potential for these remnants is complex, as is their relationship with the immune system and neoplasia. Studies dating back to 2002 have found unique associations between HERVs and various types of cancer, including renal cell carcinoma, melanoma, gastrointestinal cancer, colorectal cancer, and breast cancer.
“Early data point towards distinct features for the expression profiles of different HERVs,” the authors wrote, “but these characteristics remain to be fully elucidated. There may be substantial differences in their biological effects, potential roles in immune sensitization, and ability to form an antigen reservoir.”
HERVs may be activated by cancer or epigenetic drugs. While certain cancers may activate particular HERVs into targetable antigens, other cancer-activated HERVs actually shield tumors from the immune system. Still other HERVs require epigenetic drugs for activation, such as DNA methyltransferase inhibitors. These drugs could transform HERVs into “intrinsic adjuvants” or novel antigens; either of which may improve the efficacy of existing immunotherapies like checkpoint inhibitors.
To leverage HERVs for immunotherapy, a better understanding of immune tolerance is needed. Some research suggests that since HERVs share similarities with exogenous viruses, tolerance to HERVs must be incomplete to allow for immune responses to exogenous viruses. In contrast, incomplete tolerance would conceivably lead to autoimmune disease.
“Hence, peripheral tolerance and ignorance mechanisms may play prominent roles in the control of HERV-specific T-cell recognition in healthy individuals,” the authors wrote. “Understanding the differences in HERV expression in the thymus and peripheral tissues would be of great importance for the use of HERVs as immunotherapeutic targets.”
When more clearly understood, HERVs may feature in emerging combination therapies.
“The combination of epigenetic drugs and immunotherapy is exciting for future cancer therapy,” the authors wrote, “especially for cancer types with low mutational burden that respond poorly to immunotherapy or cancer types with poor responses to immune checkpoint inhibitor treatment.”
It appears that the authors’ excitement is shared – almost 50 clinical trials are currently studying epigenetic drug/immunotherapy combinations.
Study funding was provided by the Lundbeck Foundation Fellowship, the European Research Council, the stand-up-to-cancer (SU2C) epigenetic dream team, and StG 677268 NextDART.
SOURCE: Attermann et al. Ann Oncol. 2018 Sep 18. doi: 10.1093/annonc/mdy413.
Future epigenetic drugs could activate human endogenous retroviruses (HERVs) in cancer cells to enable immunotherapy, investigators suggest.
Activated HERVs may sensitize cancer cells or serve as novel tumor-associated antigenic targets, reported Anders Steenholdt Attermann, PhD, of the department of micro- and nanotechnology at the Technical University of Denmark in Kongens Lyngby, and colleagues.
A remarkable 8% of the human genome is composed of HERVs.
“They are remnants of retroviral germline infections that resulted in chromosomal integration into all the cells of the progeny, but their viral replication is defective in the present-day human genome,” the authors wrote in Annals of Oncology.
The therapeutic potential for these remnants is complex, as is their relationship with the immune system and neoplasia. Studies dating back to 2002 have found unique associations between HERVs and various types of cancer, including renal cell carcinoma, melanoma, gastrointestinal cancer, colorectal cancer, and breast cancer.
“Early data point towards distinct features for the expression profiles of different HERVs,” the authors wrote, “but these characteristics remain to be fully elucidated. There may be substantial differences in their biological effects, potential roles in immune sensitization, and ability to form an antigen reservoir.”
HERVs may be activated by cancer or epigenetic drugs. While certain cancers may activate particular HERVs into targetable antigens, other cancer-activated HERVs actually shield tumors from the immune system. Still other HERVs require epigenetic drugs for activation, such as DNA methyltransferase inhibitors. These drugs could transform HERVs into “intrinsic adjuvants” or novel antigens; either of which may improve the efficacy of existing immunotherapies like checkpoint inhibitors.
To leverage HERVs for immunotherapy, a better understanding of immune tolerance is needed. Some research suggests that since HERVs share similarities with exogenous viruses, tolerance to HERVs must be incomplete to allow for immune responses to exogenous viruses. In contrast, incomplete tolerance would conceivably lead to autoimmune disease.
“Hence, peripheral tolerance and ignorance mechanisms may play prominent roles in the control of HERV-specific T-cell recognition in healthy individuals,” the authors wrote. “Understanding the differences in HERV expression in the thymus and peripheral tissues would be of great importance for the use of HERVs as immunotherapeutic targets.”
When more clearly understood, HERVs may feature in emerging combination therapies.
“The combination of epigenetic drugs and immunotherapy is exciting for future cancer therapy,” the authors wrote, “especially for cancer types with low mutational burden that respond poorly to immunotherapy or cancer types with poor responses to immune checkpoint inhibitor treatment.”
It appears that the authors’ excitement is shared – almost 50 clinical trials are currently studying epigenetic drug/immunotherapy combinations.
Study funding was provided by the Lundbeck Foundation Fellowship, the European Research Council, the stand-up-to-cancer (SU2C) epigenetic dream team, and StG 677268 NextDART.
SOURCE: Attermann et al. Ann Oncol. 2018 Sep 18. doi: 10.1093/annonc/mdy413.
Future epigenetic drugs could activate human endogenous retroviruses (HERVs) in cancer cells to enable immunotherapy, investigators suggest.
Activated HERVs may sensitize cancer cells or serve as novel tumor-associated antigenic targets, reported Anders Steenholdt Attermann, PhD, of the department of micro- and nanotechnology at the Technical University of Denmark in Kongens Lyngby, and colleagues.
A remarkable 8% of the human genome is composed of HERVs.
“They are remnants of retroviral germline infections that resulted in chromosomal integration into all the cells of the progeny, but their viral replication is defective in the present-day human genome,” the authors wrote in Annals of Oncology.
The therapeutic potential for these remnants is complex, as is their relationship with the immune system and neoplasia. Studies dating back to 2002 have found unique associations between HERVs and various types of cancer, including renal cell carcinoma, melanoma, gastrointestinal cancer, colorectal cancer, and breast cancer.
“Early data point towards distinct features for the expression profiles of different HERVs,” the authors wrote, “but these characteristics remain to be fully elucidated. There may be substantial differences in their biological effects, potential roles in immune sensitization, and ability to form an antigen reservoir.”
HERVs may be activated by cancer or epigenetic drugs. While certain cancers may activate particular HERVs into targetable antigens, other cancer-activated HERVs actually shield tumors from the immune system. Still other HERVs require epigenetic drugs for activation, such as DNA methyltransferase inhibitors. These drugs could transform HERVs into “intrinsic adjuvants” or novel antigens; either of which may improve the efficacy of existing immunotherapies like checkpoint inhibitors.
To leverage HERVs for immunotherapy, a better understanding of immune tolerance is needed. Some research suggests that since HERVs share similarities with exogenous viruses, tolerance to HERVs must be incomplete to allow for immune responses to exogenous viruses. In contrast, incomplete tolerance would conceivably lead to autoimmune disease.
“Hence, peripheral tolerance and ignorance mechanisms may play prominent roles in the control of HERV-specific T-cell recognition in healthy individuals,” the authors wrote. “Understanding the differences in HERV expression in the thymus and peripheral tissues would be of great importance for the use of HERVs as immunotherapeutic targets.”
When more clearly understood, HERVs may feature in emerging combination therapies.
“The combination of epigenetic drugs and immunotherapy is exciting for future cancer therapy,” the authors wrote, “especially for cancer types with low mutational burden that respond poorly to immunotherapy or cancer types with poor responses to immune checkpoint inhibitor treatment.”
It appears that the authors’ excitement is shared – almost 50 clinical trials are currently studying epigenetic drug/immunotherapy combinations.
Study funding was provided by the Lundbeck Foundation Fellowship, the European Research Council, the stand-up-to-cancer (SU2C) epigenetic dream team, and StG 677268 NextDART.
SOURCE: Attermann et al. Ann Oncol. 2018 Sep 18. doi: 10.1093/annonc/mdy413.
FROM ANNALS OF ONCOLOGY
Key clinical point: Future epigenetic drugs may activate human endogenous retroviruses (HERVs) in cancer cells to enable immunotherapeutic targeting.
Major finding: Almost 50 clinical trials are currently investigating combinations of immunotherapies and epigenetic drugs.
Study details: A review article covering HERVs and their relationship with epigenetic drugs and immunotherapy.
Disclosures: Study funding was provided by the Lundbeck Foundation Fellowship, the European Research Council, the stand-up-to-cancer (SU2C) epigenetic dream team, and StG 677268 NextDART. No conflicts of interest were reported.
Source: Attermann et al. Ann Oncol. 2018 Sep 18. doi: 10.1093/annonc/mdy413.
Value-based care news abounds at ACEP18
The answer is none.
The question (for $1,000, Alex) is how many of the dozens of proposals to create physician-focused alternative payment models (APMs) have been approved under the new federal Quality Payment Program?
However, ACEP’s submission, entitled the Acute Unscheduled Care Model (AUCM): Enhancing Appropriate Admissions, seems to have gotten close to a nod when federal health care leaders showed up at a recent meeting on the model.
Reviewers from the Physician-Focused Payment Model Technical Advisory Committee “thought that we met all 10 criteria for models that the secretary put forth for evaluating physician-focused payment models,” Jeffrey Davis, ACEP director of regulatory affairs, said in an interview, adding that the attendance at the meeting of Alex Azar, secretary of Health & Human Serviecs, and Seema Verma, administrator of the Centers for Medicare & Medicaid Services, was a positive development.
To read our full story, check out the link below.
Key sessions at ACEP18 on QPP, MACRA, APMs, and MIPS include:
MO-058 Goodbye SGR! Hello MACRA and MIPS
Monday, Oct. 1 | 1:30 PM
TU-131 FAST FACTS: Reimbursement Topics for the Practicing Emergency Physician
Tuesday, Oct. 2 | 10:00 AM
TU-187 Alternative Payment Models: The New Reimbursement Frontier
Tuesday, Oct. 2 | 4:00 PM
The answer is none.
The question (for $1,000, Alex) is how many of the dozens of proposals to create physician-focused alternative payment models (APMs) have been approved under the new federal Quality Payment Program?
However, ACEP’s submission, entitled the Acute Unscheduled Care Model (AUCM): Enhancing Appropriate Admissions, seems to have gotten close to a nod when federal health care leaders showed up at a recent meeting on the model.
Reviewers from the Physician-Focused Payment Model Technical Advisory Committee “thought that we met all 10 criteria for models that the secretary put forth for evaluating physician-focused payment models,” Jeffrey Davis, ACEP director of regulatory affairs, said in an interview, adding that the attendance at the meeting of Alex Azar, secretary of Health & Human Serviecs, and Seema Verma, administrator of the Centers for Medicare & Medicaid Services, was a positive development.
To read our full story, check out the link below.
Key sessions at ACEP18 on QPP, MACRA, APMs, and MIPS include:
MO-058 Goodbye SGR! Hello MACRA and MIPS
Monday, Oct. 1 | 1:30 PM
TU-131 FAST FACTS: Reimbursement Topics for the Practicing Emergency Physician
Tuesday, Oct. 2 | 10:00 AM
TU-187 Alternative Payment Models: The New Reimbursement Frontier
Tuesday, Oct. 2 | 4:00 PM
The answer is none.
The question (for $1,000, Alex) is how many of the dozens of proposals to create physician-focused alternative payment models (APMs) have been approved under the new federal Quality Payment Program?
However, ACEP’s submission, entitled the Acute Unscheduled Care Model (AUCM): Enhancing Appropriate Admissions, seems to have gotten close to a nod when federal health care leaders showed up at a recent meeting on the model.
Reviewers from the Physician-Focused Payment Model Technical Advisory Committee “thought that we met all 10 criteria for models that the secretary put forth for evaluating physician-focused payment models,” Jeffrey Davis, ACEP director of regulatory affairs, said in an interview, adding that the attendance at the meeting of Alex Azar, secretary of Health & Human Serviecs, and Seema Verma, administrator of the Centers for Medicare & Medicaid Services, was a positive development.
To read our full story, check out the link below.
Key sessions at ACEP18 on QPP, MACRA, APMs, and MIPS include:
MO-058 Goodbye SGR! Hello MACRA and MIPS
Monday, Oct. 1 | 1:30 PM
TU-131 FAST FACTS: Reimbursement Topics for the Practicing Emergency Physician
Tuesday, Oct. 2 | 10:00 AM
TU-187 Alternative Payment Models: The New Reimbursement Frontier
Tuesday, Oct. 2 | 4:00 PM
REPORTING FROM ACEP18