User login
Should you continue to participate in Medicare?
Since writing about the new MACRA bureaucracy, and the Morton’s Choice facing private practitioners between Scylla (the Merit-based Incentive Payment System) and Charybdis (the still largely undefined Alternate Payment Models), a question I’ve been hearing with increasing frequency is whether it wouldn’t be better to simply opt out of Medicare participation entirely.
It is easy to see why more and more physicians are asking that question. Although the incoming administration has promised significant (but largely unspecified) changes to the health care system – as I wrote last month – reimbursements continue to decrease, onerous regulations continue to increase, and there is no evidence to suggest that either of those trends will change anytime soon. That leaves many physicians wondering whether their continued participation with Medicare (and Medicaid, for those who accept it) is ultimately worth it.

It is difficult to assign a firm answer to the basic question of whether or not opting out is a good idea. As usual, it will depend upon your unique circumstances, as well as the size and composition of your practice. This is not a decision to make lightly, or hastily – particularly if a significant percentage of your patients have federal or state health care coverage.
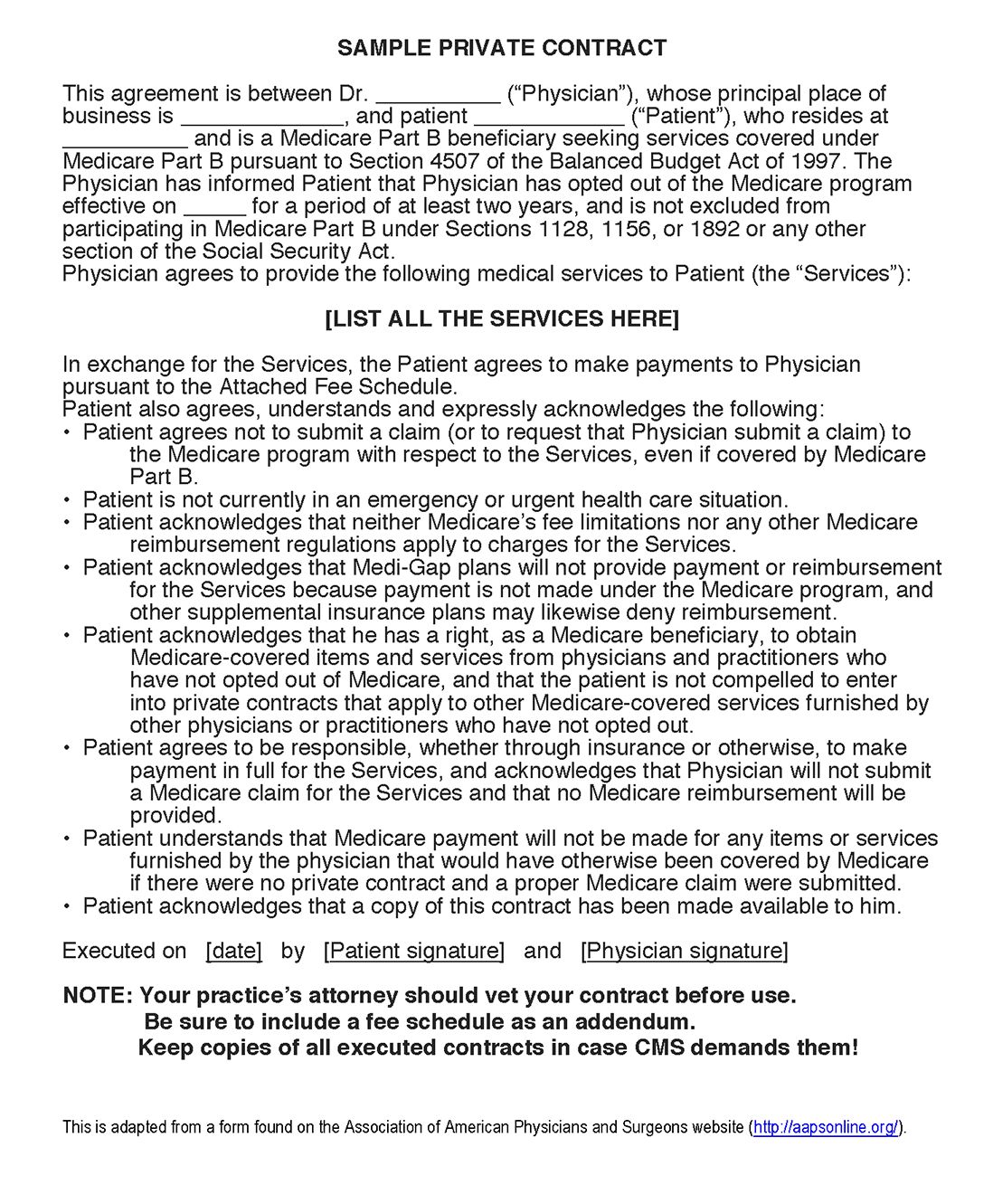
You will need to carefully consider the pros and cons involved, beginning with the fact that once you pull the trigger, there’s no going back for at least 2 years. (If you are opting out for the very first time, you do have 90 days to change your mind and opt back in.) And you must create a physician-patient agreement covering your treatment and billing guidelines, and make sure all of your Medicare/Medicaid patients sign it.
The obvious benefit of opting out is the freedom to do and bill what and how you wish. Once liberated from CMS compliance restrictions, you can spend your time treating patients, rather than catering to and being controlled by the government. The physician-patient relationship regains its proper priority; you can work directly with your patients in structuring their care plans and pursuing the best treatment options. Physicians with small, relatively young patient populations often find the prospect of charting their own course particularly attractive.
Not only that, but some commercial carriers require Medicare participation in order to maintain credentialing with them. So if you opt out of federal and state participation, you will also need to opt out of commercial plans with that requirement. Hospital admitting privileges may also be contingent on Medicare participation; be sure to check your hospitals’ bylaws.
Another challenge is pushback from patients. While few patients like dealing with insurance claims, fewer still are willing to pay for their care themselves. When drafting a physician-patient agreement, it must be made very clear that you are not going to bill Medicare or Medicaid for services rendered, and that patients cannot do so either. Inevitably, a substantial percentage of your Medicare/Medicaid-covered patients will choose to switch to a participating physician.
If you do decide to opt out, here is how you do it:
1. Notify your patients that you will be opting out by a specific date, which should be the first day of a calendar quarter.
2. File an affidavit (available at CMS.gov) with your local Medicare carrier at least 30 days before your opt-out date.
3. Draft and post a fee schedule.
4. Draft a private contract to be signed by all Medicare beneficiaries, covering all services that would normally be covered by Medicare. Be sure to run it past your attorney.
5. Install procedures to ensure that your office never files a Medicare claim, and never provides information to enable a patient to file a Medicare claim. The two exceptions – for emergency care, and for covered services that Medicare would deem unnecessary – should be used sparingly, and with caution.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Since writing about the new MACRA bureaucracy, and the Morton’s Choice facing private practitioners between Scylla (the Merit-based Incentive Payment System) and Charybdis (the still largely undefined Alternate Payment Models), a question I’ve been hearing with increasing frequency is whether it wouldn’t be better to simply opt out of Medicare participation entirely.
It is easy to see why more and more physicians are asking that question. Although the incoming administration has promised significant (but largely unspecified) changes to the health care system – as I wrote last month – reimbursements continue to decrease, onerous regulations continue to increase, and there is no evidence to suggest that either of those trends will change anytime soon. That leaves many physicians wondering whether their continued participation with Medicare (and Medicaid, for those who accept it) is ultimately worth it.
It is difficult to assign a firm answer to the basic question of whether or not opting out is a good idea. As usual, it will depend upon your unique circumstances, as well as the size and composition of your practice. This is not a decision to make lightly, or hastily – particularly if a significant percentage of your patients have federal or state health care coverage.
You will need to carefully consider the pros and cons involved, beginning with the fact that once you pull the trigger, there’s no going back for at least 2 years. (If you are opting out for the very first time, you do have 90 days to change your mind and opt back in.) And you must create a physician-patient agreement covering your treatment and billing guidelines, and make sure all of your Medicare/Medicaid patients sign it.
The obvious benefit of opting out is the freedom to do and bill what and how you wish. Once liberated from CMS compliance restrictions, you can spend your time treating patients, rather than catering to and being controlled by the government. The physician-patient relationship regains its proper priority; you can work directly with your patients in structuring their care plans and pursuing the best treatment options. Physicians with small, relatively young patient populations often find the prospect of charting their own course particularly attractive.
Not only that, but some commercial carriers require Medicare participation in order to maintain credentialing with them. So if you opt out of federal and state participation, you will also need to opt out of commercial plans with that requirement. Hospital admitting privileges may also be contingent on Medicare participation; be sure to check your hospitals’ bylaws.
Another challenge is pushback from patients. While few patients like dealing with insurance claims, fewer still are willing to pay for their care themselves. When drafting a physician-patient agreement, it must be made very clear that you are not going to bill Medicare or Medicaid for services rendered, and that patients cannot do so either. Inevitably, a substantial percentage of your Medicare/Medicaid-covered patients will choose to switch to a participating physician.
If you do decide to opt out, here is how you do it:
1. Notify your patients that you will be opting out by a specific date, which should be the first day of a calendar quarter.
2. File an affidavit (available at CMS.gov) with your local Medicare carrier at least 30 days before your opt-out date.
3. Draft and post a fee schedule.
4. Draft a private contract to be signed by all Medicare beneficiaries, covering all services that would normally be covered by Medicare. Be sure to run it past your attorney.
5. Install procedures to ensure that your office never files a Medicare claim, and never provides information to enable a patient to file a Medicare claim. The two exceptions – for emergency care, and for covered services that Medicare would deem unnecessary – should be used sparingly, and with caution.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Since writing about the new MACRA bureaucracy, and the Morton’s Choice facing private practitioners between Scylla (the Merit-based Incentive Payment System) and Charybdis (the still largely undefined Alternate Payment Models), a question I’ve been hearing with increasing frequency is whether it wouldn’t be better to simply opt out of Medicare participation entirely.
It is easy to see why more and more physicians are asking that question. Although the incoming administration has promised significant (but largely unspecified) changes to the health care system – as I wrote last month – reimbursements continue to decrease, onerous regulations continue to increase, and there is no evidence to suggest that either of those trends will change anytime soon. That leaves many physicians wondering whether their continued participation with Medicare (and Medicaid, for those who accept it) is ultimately worth it.
It is difficult to assign a firm answer to the basic question of whether or not opting out is a good idea. As usual, it will depend upon your unique circumstances, as well as the size and composition of your practice. This is not a decision to make lightly, or hastily – particularly if a significant percentage of your patients have federal or state health care coverage.
You will need to carefully consider the pros and cons involved, beginning with the fact that once you pull the trigger, there’s no going back for at least 2 years. (If you are opting out for the very first time, you do have 90 days to change your mind and opt back in.) And you must create a physician-patient agreement covering your treatment and billing guidelines, and make sure all of your Medicare/Medicaid patients sign it.
The obvious benefit of opting out is the freedom to do and bill what and how you wish. Once liberated from CMS compliance restrictions, you can spend your time treating patients, rather than catering to and being controlled by the government. The physician-patient relationship regains its proper priority; you can work directly with your patients in structuring their care plans and pursuing the best treatment options. Physicians with small, relatively young patient populations often find the prospect of charting their own course particularly attractive.
Not only that, but some commercial carriers require Medicare participation in order to maintain credentialing with them. So if you opt out of federal and state participation, you will also need to opt out of commercial plans with that requirement. Hospital admitting privileges may also be contingent on Medicare participation; be sure to check your hospitals’ bylaws.
Another challenge is pushback from patients. While few patients like dealing with insurance claims, fewer still are willing to pay for their care themselves. When drafting a physician-patient agreement, it must be made very clear that you are not going to bill Medicare or Medicaid for services rendered, and that patients cannot do so either. Inevitably, a substantial percentage of your Medicare/Medicaid-covered patients will choose to switch to a participating physician.
If you do decide to opt out, here is how you do it:
1. Notify your patients that you will be opting out by a specific date, which should be the first day of a calendar quarter.
2. File an affidavit (available at CMS.gov) with your local Medicare carrier at least 30 days before your opt-out date.
3. Draft and post a fee schedule.
4. Draft a private contract to be signed by all Medicare beneficiaries, covering all services that would normally be covered by Medicare. Be sure to run it past your attorney.
5. Install procedures to ensure that your office never files a Medicare claim, and never provides information to enable a patient to file a Medicare claim. The two exceptions – for emergency care, and for covered services that Medicare would deem unnecessary – should be used sparingly, and with caution.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

FDA approves rucaparib for BRCA-positive advanced ovarian cancer
The Food and Drug Administration has granted accelerated approval to rucaparib for the treatment of women with advanced ovarian cancer who have been treated with two or more chemotherapies and whose tumors have a germline or somatic BRCA gene mutation. The FDA also approved the FoundationFocus CDxBRCA companion diagnostic for use with rucaparib to detect BRCA1 and BRCA2 gene mutations in the tumor tissue.
Approval of rucaparib (Rubraca), a poly ADP-ribose polymerase (PARP) inhibitor, was based on an objective response rate (ORR) of 54%, and a median duration of response of 9.2 months, in a pooled analysis of two, single-arm clinical trials, the FDA said in a statement.
All 106 patients in the two trials had BRCA-mutated advanced ovarian cancer and had been treated with two or more chemotherapy regimens. They received rucaparib 600 mg orally twice daily. BRCA gene mutations were confirmed in 96% of participants with available tumor tissue using the FoundationFocus CDxBRCA companion diagnostic. ORR was similar for patients with a BRCA1 gene mutation or BRCA2 gene mutation.![]()
Patients should be monitored for hematologic toxicity at baseline and monthly thereafter, and use of rucaparib should be discontinued if MDS/AML is confirmed, the FDA said on its website.
Rucaparib is marketed by Clovis Oncology. The FoundationFocus CDxBRCA companion diagnostic is marketed by Foundation Medicine.
[email protected]
On Twitter @nikolaideslaura
The Food and Drug Administration has granted accelerated approval to rucaparib for the treatment of women with advanced ovarian cancer who have been treated with two or more chemotherapies and whose tumors have a germline or somatic BRCA gene mutation. The FDA also approved the FoundationFocus CDxBRCA companion diagnostic for use with rucaparib to detect BRCA1 and BRCA2 gene mutations in the tumor tissue.
Approval of rucaparib (Rubraca), a poly ADP-ribose polymerase (PARP) inhibitor, was based on an objective response rate (ORR) of 54%, and a median duration of response of 9.2 months, in a pooled analysis of two, single-arm clinical trials, the FDA said in a statement.
All 106 patients in the two trials had BRCA-mutated advanced ovarian cancer and had been treated with two or more chemotherapy regimens. They received rucaparib 600 mg orally twice daily. BRCA gene mutations were confirmed in 96% of participants with available tumor tissue using the FoundationFocus CDxBRCA companion diagnostic. ORR was similar for patients with a BRCA1 gene mutation or BRCA2 gene mutation.![]()
Patients should be monitored for hematologic toxicity at baseline and monthly thereafter, and use of rucaparib should be discontinued if MDS/AML is confirmed, the FDA said on its website.
Rucaparib is marketed by Clovis Oncology. The FoundationFocus CDxBRCA companion diagnostic is marketed by Foundation Medicine.
[email protected]
On Twitter @nikolaideslaura
The Food and Drug Administration has granted accelerated approval to rucaparib for the treatment of women with advanced ovarian cancer who have been treated with two or more chemotherapies and whose tumors have a germline or somatic BRCA gene mutation. The FDA also approved the FoundationFocus CDxBRCA companion diagnostic for use with rucaparib to detect BRCA1 and BRCA2 gene mutations in the tumor tissue.
Approval of rucaparib (Rubraca), a poly ADP-ribose polymerase (PARP) inhibitor, was based on an objective response rate (ORR) of 54%, and a median duration of response of 9.2 months, in a pooled analysis of two, single-arm clinical trials, the FDA said in a statement.
All 106 patients in the two trials had BRCA-mutated advanced ovarian cancer and had been treated with two or more chemotherapy regimens. They received rucaparib 600 mg orally twice daily. BRCA gene mutations were confirmed in 96% of participants with available tumor tissue using the FoundationFocus CDxBRCA companion diagnostic. ORR was similar for patients with a BRCA1 gene mutation or BRCA2 gene mutation.![]()
Patients should be monitored for hematologic toxicity at baseline and monthly thereafter, and use of rucaparib should be discontinued if MDS/AML is confirmed, the FDA said on its website.
Rucaparib is marketed by Clovis Oncology. The FoundationFocus CDxBRCA companion diagnostic is marketed by Foundation Medicine.
[email protected]
On Twitter @nikolaideslaura
SLND after neoadjuvant chemo is feasible, but more study needed
SAN ANTONIO – Sentinel lymph node detection after neoadjuvant chemotherapy (NAC) is a safe and feasible strategy for preventing unnecessary systematic lymphadenectomy in patients with operable breast cancer and no clinical signs of cancer in the axillary lymph nodes prior to NAC, according to findings from the French prospective multicenter GANEA 2 trial.
However, further study is needed to assess the clinical impact of the 12% false negative rate associated with sentinel lymph node detection (SLND) in the current study, according to Jean-Marc Classe, MD, who reported the findings at the San Antonio Breast Cancer Symposium.
SLND was feasible in that it was achieved in 570 of 590 women (97%) with large operable breast tumors and negative findings on axillary sonography with fine needle cytology who were enrolled in the study, said Dr. Classe of Institut Cancerologie de l’Ouest Rene Gauducheau, Nantes, France.
Cancer cells were detected by SLND in 139 subjects after NAC and surgery, and all of those patients underwent axillary lymph node dissection. Another 418 had no sentinel node involvement after NAC and surgery, and had adequate follow-up; among those, overall 3-year survival was 97.8% and 3-year disease-free survival was 94.8%,
“In this group of patients ... we found only one axillary relapse,” he said.
These rates are comparable to historical survival rates among those without axillary involvement who undergo axillary lymph node dissection rather than sentinel lymph node detection, and the findings suggest that women with no clinical signs of axillary involvement could be spared systematic lymphadenectomy, he said.
“The standard surgical treatment after neoadjuvant chemotherapy is breast cancer surgery and lymphadenectomy level 1 and 2, but since the [National Surgical Adjuvant Breast and Bowel Project] B-27 trial, we all know that after neoadjuvant chemotherapy there are not any involved nodes in 50%-58% of patients,” he said, adding that about half of all lymphadenectomies in these patients are therefore unnecessary.
That percentage increases to more than 70% in “the very specific situation of patients treated for HER2+ breast cancer with cytologically proved axillary metastases after neoadjuvant chemotherapy,” he said.
“So we know that there is a place for sentinel lymph node biopsy after neoadjuvant chemotherapy in order to avoid unnecessary lymphadenectomy,” he said.
However, the high false negative rate associated with SLND in this and in prior studies, including the first GANEA trial, remains a concern. In fact, the most recent guidelines stated that the proof was too weak to strongly recommend sentinel lymph node biopsy after NAC, he noted.
The GANEA 2 trial was performed in response to a call in those guidelines for additional studies to assess the long-term risks of this strategy.
Study subjects included patients with FIGO stage T1-T3 infiltrating breast cancer who were enrolled from 15 French institutions between July 2010 and February 2014. Those with inflammatory cancer, local relapse, contraindications for NAC, or interrupted NAC due to progressive disease were excluded.
Follow-up included a medical visit with clinical assessment every 6 months and annual mammography.
The findings suggest that in patients with no proof of node involvement before treatment, SLND “seems to be safe within the limits of the short-term follow-up of this study,” Dr. Classe said, noting that given the concerns about the false negative rate and the uncertainty about the clinical impact of that, this approach “is not proved to be a safe procedure outside of trials.”
The strategy will be further evaluated, with a focus on eliminating false negative results, in the GANEA 3 trial, he said.
Dr. Classe reported having no disclosures.
SAN ANTONIO – Sentinel lymph node detection after neoadjuvant chemotherapy (NAC) is a safe and feasible strategy for preventing unnecessary systematic lymphadenectomy in patients with operable breast cancer and no clinical signs of cancer in the axillary lymph nodes prior to NAC, according to findings from the French prospective multicenter GANEA 2 trial.
However, further study is needed to assess the clinical impact of the 12% false negative rate associated with sentinel lymph node detection (SLND) in the current study, according to Jean-Marc Classe, MD, who reported the findings at the San Antonio Breast Cancer Symposium.
SLND was feasible in that it was achieved in 570 of 590 women (97%) with large operable breast tumors and negative findings on axillary sonography with fine needle cytology who were enrolled in the study, said Dr. Classe of Institut Cancerologie de l’Ouest Rene Gauducheau, Nantes, France.
Cancer cells were detected by SLND in 139 subjects after NAC and surgery, and all of those patients underwent axillary lymph node dissection. Another 418 had no sentinel node involvement after NAC and surgery, and had adequate follow-up; among those, overall 3-year survival was 97.8% and 3-year disease-free survival was 94.8%,
“In this group of patients ... we found only one axillary relapse,” he said.
These rates are comparable to historical survival rates among those without axillary involvement who undergo axillary lymph node dissection rather than sentinel lymph node detection, and the findings suggest that women with no clinical signs of axillary involvement could be spared systematic lymphadenectomy, he said.
“The standard surgical treatment after neoadjuvant chemotherapy is breast cancer surgery and lymphadenectomy level 1 and 2, but since the [National Surgical Adjuvant Breast and Bowel Project] B-27 trial, we all know that after neoadjuvant chemotherapy there are not any involved nodes in 50%-58% of patients,” he said, adding that about half of all lymphadenectomies in these patients are therefore unnecessary.
That percentage increases to more than 70% in “the very specific situation of patients treated for HER2+ breast cancer with cytologically proved axillary metastases after neoadjuvant chemotherapy,” he said.
“So we know that there is a place for sentinel lymph node biopsy after neoadjuvant chemotherapy in order to avoid unnecessary lymphadenectomy,” he said.
However, the high false negative rate associated with SLND in this and in prior studies, including the first GANEA trial, remains a concern. In fact, the most recent guidelines stated that the proof was too weak to strongly recommend sentinel lymph node biopsy after NAC, he noted.
The GANEA 2 trial was performed in response to a call in those guidelines for additional studies to assess the long-term risks of this strategy.
Study subjects included patients with FIGO stage T1-T3 infiltrating breast cancer who were enrolled from 15 French institutions between July 2010 and February 2014. Those with inflammatory cancer, local relapse, contraindications for NAC, or interrupted NAC due to progressive disease were excluded.
Follow-up included a medical visit with clinical assessment every 6 months and annual mammography.
The findings suggest that in patients with no proof of node involvement before treatment, SLND “seems to be safe within the limits of the short-term follow-up of this study,” Dr. Classe said, noting that given the concerns about the false negative rate and the uncertainty about the clinical impact of that, this approach “is not proved to be a safe procedure outside of trials.”
The strategy will be further evaluated, with a focus on eliminating false negative results, in the GANEA 3 trial, he said.
Dr. Classe reported having no disclosures.
SAN ANTONIO – Sentinel lymph node detection after neoadjuvant chemotherapy (NAC) is a safe and feasible strategy for preventing unnecessary systematic lymphadenectomy in patients with operable breast cancer and no clinical signs of cancer in the axillary lymph nodes prior to NAC, according to findings from the French prospective multicenter GANEA 2 trial.
However, further study is needed to assess the clinical impact of the 12% false negative rate associated with sentinel lymph node detection (SLND) in the current study, according to Jean-Marc Classe, MD, who reported the findings at the San Antonio Breast Cancer Symposium.
SLND was feasible in that it was achieved in 570 of 590 women (97%) with large operable breast tumors and negative findings on axillary sonography with fine needle cytology who were enrolled in the study, said Dr. Classe of Institut Cancerologie de l’Ouest Rene Gauducheau, Nantes, France.
Cancer cells were detected by SLND in 139 subjects after NAC and surgery, and all of those patients underwent axillary lymph node dissection. Another 418 had no sentinel node involvement after NAC and surgery, and had adequate follow-up; among those, overall 3-year survival was 97.8% and 3-year disease-free survival was 94.8%,
“In this group of patients ... we found only one axillary relapse,” he said.
These rates are comparable to historical survival rates among those without axillary involvement who undergo axillary lymph node dissection rather than sentinel lymph node detection, and the findings suggest that women with no clinical signs of axillary involvement could be spared systematic lymphadenectomy, he said.
“The standard surgical treatment after neoadjuvant chemotherapy is breast cancer surgery and lymphadenectomy level 1 and 2, but since the [National Surgical Adjuvant Breast and Bowel Project] B-27 trial, we all know that after neoadjuvant chemotherapy there are not any involved nodes in 50%-58% of patients,” he said, adding that about half of all lymphadenectomies in these patients are therefore unnecessary.
That percentage increases to more than 70% in “the very specific situation of patients treated for HER2+ breast cancer with cytologically proved axillary metastases after neoadjuvant chemotherapy,” he said.
“So we know that there is a place for sentinel lymph node biopsy after neoadjuvant chemotherapy in order to avoid unnecessary lymphadenectomy,” he said.
However, the high false negative rate associated with SLND in this and in prior studies, including the first GANEA trial, remains a concern. In fact, the most recent guidelines stated that the proof was too weak to strongly recommend sentinel lymph node biopsy after NAC, he noted.
The GANEA 2 trial was performed in response to a call in those guidelines for additional studies to assess the long-term risks of this strategy.
Study subjects included patients with FIGO stage T1-T3 infiltrating breast cancer who were enrolled from 15 French institutions between July 2010 and February 2014. Those with inflammatory cancer, local relapse, contraindications for NAC, or interrupted NAC due to progressive disease were excluded.
Follow-up included a medical visit with clinical assessment every 6 months and annual mammography.
The findings suggest that in patients with no proof of node involvement before treatment, SLND “seems to be safe within the limits of the short-term follow-up of this study,” Dr. Classe said, noting that given the concerns about the false negative rate and the uncertainty about the clinical impact of that, this approach “is not proved to be a safe procedure outside of trials.”
The strategy will be further evaluated, with a focus on eliminating false negative results, in the GANEA 3 trial, he said.
Dr. Classe reported having no disclosures.
AT SABCS 2016
Key clinical point:
Major finding: Overall 3-year survival was 97.8% and 3-year disease-free survival was 94.8% in 418 breast cancer patients who had no sentinel node involvement after NAC and surgery.
Data source: The prospective multicenter GANEA 2 trial of 590 patients.
Disclosures: Dr. Classe reported having no disclosures.
Latest CDC data: Opioid deaths still rising
Opioid-related deaths continue to rise in the United States, with a 16% increase between 2014 and 2015 driven largely by overdoses of illegally manufactured fentanyl and heroin, according to a report released Dec. 16 by the Centers for Disease Control and Prevention.
CDC investigators analyzed drug-related mortality for 2010 through 2015 in a national statistics database for all 50 states and the District of Columbia, as well as drug-related deaths by subcategories of drugs in 28 states for 2014 through 2015. They found that the rapidly evolving opioid epidemic has not only continued but worsened in many ways, across all demographics and geographical regions of the country, said Rose A. Rudd, MSPH, of the CDC’s National Center for Injury Prevention and Control in Atlanta, and her associates (MMWR. 2016 Dec 16;65:1-8).![]()
• Mortality from drug overdoses rose significantly over the 5-year study period, from 12.3 per 100,000 in 2010 to 16.3 per 100,000 in 2015. It rose in 30 states and in the District of Columbia, stayed stable in 19 states, and initially decreased but then rose again in 2 states (Florida and South Carolina).
• During the last year for which data are complete (2015), deaths from drug overdoses rose by approximately 12%, “signifying a continuing trend since 1999.”
• Sixty-three percent of the 52,404 deaths from drug overdoses in 2015 involved an opioid.
• The age-adjusted opioid-related death rate rose by 16% during the last year, from 9.0 per 100,000 in 2014 to 10.4 per 100,000 in 2015.
• These significant increases were driven by a rise in deaths from synthetic opioids other than methadone – chiefly illicitly manufactured fentanyl and heroin, which rose by 72.2% and 20.6%, respectively.
• In contrast, death rates tied to natural or semisynthetic opioids increased by only 2.6%, while those tied to methadone decreased by 9.1%.
Dr. Rudd and her associates cited several limitations. One is that some drug overdose death certificates did not identify specific drugs. Another is that heroin and morphine are metabolized similarly, which means that some heroin deaths might have been misclassified. Also, it could be problematic to generalize the findings, because the “state-specific analyses of opioid deaths are restricted to 28 states.”
“The ongoing epidemic of opioid deaths requires intense attention and action,” Dr. Rudd and her associates wrote. “Intensifying efforts to distribute naloxone (an antidote to reverse an opioid overdose), enhancing access to treatment ... and implementing harm reduction services are urgently needed.”
The study was conducted by the CDC.
Opioid-related deaths continue to rise in the United States, with a 16% increase between 2014 and 2015 driven largely by overdoses of illegally manufactured fentanyl and heroin, according to a report released Dec. 16 by the Centers for Disease Control and Prevention.
CDC investigators analyzed drug-related mortality for 2010 through 2015 in a national statistics database for all 50 states and the District of Columbia, as well as drug-related deaths by subcategories of drugs in 28 states for 2014 through 2015. They found that the rapidly evolving opioid epidemic has not only continued but worsened in many ways, across all demographics and geographical regions of the country, said Rose A. Rudd, MSPH, of the CDC’s National Center for Injury Prevention and Control in Atlanta, and her associates (MMWR. 2016 Dec 16;65:1-8).![]()
• Mortality from drug overdoses rose significantly over the 5-year study period, from 12.3 per 100,000 in 2010 to 16.3 per 100,000 in 2015. It rose in 30 states and in the District of Columbia, stayed stable in 19 states, and initially decreased but then rose again in 2 states (Florida and South Carolina).
• During the last year for which data are complete (2015), deaths from drug overdoses rose by approximately 12%, “signifying a continuing trend since 1999.”
• Sixty-three percent of the 52,404 deaths from drug overdoses in 2015 involved an opioid.
• The age-adjusted opioid-related death rate rose by 16% during the last year, from 9.0 per 100,000 in 2014 to 10.4 per 100,000 in 2015.
• These significant increases were driven by a rise in deaths from synthetic opioids other than methadone – chiefly illicitly manufactured fentanyl and heroin, which rose by 72.2% and 20.6%, respectively.
• In contrast, death rates tied to natural or semisynthetic opioids increased by only 2.6%, while those tied to methadone decreased by 9.1%.
Dr. Rudd and her associates cited several limitations. One is that some drug overdose death certificates did not identify specific drugs. Another is that heroin and morphine are metabolized similarly, which means that some heroin deaths might have been misclassified. Also, it could be problematic to generalize the findings, because the “state-specific analyses of opioid deaths are restricted to 28 states.”
“The ongoing epidemic of opioid deaths requires intense attention and action,” Dr. Rudd and her associates wrote. “Intensifying efforts to distribute naloxone (an antidote to reverse an opioid overdose), enhancing access to treatment ... and implementing harm reduction services are urgently needed.”
The study was conducted by the CDC.
Opioid-related deaths continue to rise in the United States, with a 16% increase between 2014 and 2015 driven largely by overdoses of illegally manufactured fentanyl and heroin, according to a report released Dec. 16 by the Centers for Disease Control and Prevention.
CDC investigators analyzed drug-related mortality for 2010 through 2015 in a national statistics database for all 50 states and the District of Columbia, as well as drug-related deaths by subcategories of drugs in 28 states for 2014 through 2015. They found that the rapidly evolving opioid epidemic has not only continued but worsened in many ways, across all demographics and geographical regions of the country, said Rose A. Rudd, MSPH, of the CDC’s National Center for Injury Prevention and Control in Atlanta, and her associates (MMWR. 2016 Dec 16;65:1-8).![]()
• Mortality from drug overdoses rose significantly over the 5-year study period, from 12.3 per 100,000 in 2010 to 16.3 per 100,000 in 2015. It rose in 30 states and in the District of Columbia, stayed stable in 19 states, and initially decreased but then rose again in 2 states (Florida and South Carolina).
• During the last year for which data are complete (2015), deaths from drug overdoses rose by approximately 12%, “signifying a continuing trend since 1999.”
• Sixty-three percent of the 52,404 deaths from drug overdoses in 2015 involved an opioid.
• The age-adjusted opioid-related death rate rose by 16% during the last year, from 9.0 per 100,000 in 2014 to 10.4 per 100,000 in 2015.
• These significant increases were driven by a rise in deaths from synthetic opioids other than methadone – chiefly illicitly manufactured fentanyl and heroin, which rose by 72.2% and 20.6%, respectively.
• In contrast, death rates tied to natural or semisynthetic opioids increased by only 2.6%, while those tied to methadone decreased by 9.1%.
Dr. Rudd and her associates cited several limitations. One is that some drug overdose death certificates did not identify specific drugs. Another is that heroin and morphine are metabolized similarly, which means that some heroin deaths might have been misclassified. Also, it could be problematic to generalize the findings, because the “state-specific analyses of opioid deaths are restricted to 28 states.”
“The ongoing epidemic of opioid deaths requires intense attention and action,” Dr. Rudd and her associates wrote. “Intensifying efforts to distribute naloxone (an antidote to reverse an opioid overdose), enhancing access to treatment ... and implementing harm reduction services are urgently needed.”
The study was conducted by the CDC.
FROM MMWR
Key clinical point: The most recent Centers for Disease Control and Prevention data show that opioid-related deaths continue to rise, with a 16% increase from 2014 to 2015, which was driven largely by overdoses of illegally manufactured fentanyl and heroin.
Major finding: Sixty-three percent of the 52,404 deaths from drug overdoses in 2015 involved opioid overdoses.
Data source: Analysis of drug-related mortality data from 2010 to 2015 in the National Vital Statistics System for all 50 states and the District of Columbia, plus an analysis of drug-related deaths by subcategories of drugs in 28 states from 2014 to 2015.
Disclosures: The study was conducted by the CDC.
PCI or CABG in the high-risk patient
The recent report from the SYNTAX trials should give pause to our interventionalist colleagues embarking on multiple angioplasty and stenting procedures in patients with complex coronary anatomy.
SYNTAX randomized 1,800 patients with left main or triple-vessel coronary artery disease to either percutaneous coronary intervention (PCI) with the TAXUS drug-eluting stent or coronary artery bypass grafting (CABG) after being judged by a heart team as being in equipoise in regard to the appropriateness of either procedure (Eur Heart J. 2011;32;2125-34). The findings of several previous analyses have trended toward benefit for CABG, but none as clearly as SYNTAX. The original study was reported 6 years ago (Lancet 2013 Feb;381:629-38) and indicated that CABG was superior to PCI in patients with complex lesions. The most recent 5-year data of that study (J Am Coll Cardiol. 2016 Jan:67;42-55) indicates that cardiac mortality in the CABG patients is superior to that in the PCI group (5.3% vs. 9.6%, respectively), and the follow-up data provide more in-depth analysis in addition to the mechanism of death. Most importantly, the recent 5-year data clarify the reasons PCI fails to measure up to the results of CABG in patients with complex coronary artery disease.

One of the overriding predictors of increased mortality with PCI is the increased complexity of anatomy. The higher SYNTAX score was related to incomplete revascularization using PCI, compared with CABG. The presence of concomitant peripheral and carotid vascular disease, in addition to a left ventricular ejection fraction of less than 30%, favored the CABG group. Multiple stents and stent thrombosis were also issues leading to the increased mortality in the PCI group. The main cause of death was recurrent myocardial infarction, which occurred more frequently in the PCI patients and was associated with incomplete revascularization.
The data in the SYNTAX follow-up is not new, but do reinforce what has been reported in previous meta-analyses. This study does, however, emphasize the importance of recurrent infarction as a cause of death in these patients with complex anatomy. It is possible that new stent technology and coronary flow assessment at the time of intervention could have improved the outcome of this comparison and improved the long-term patency of the stented vessels. PCI is an evolving technology heavily affected by the experience of the operator. CABG surgery has also changed, and its associated mortality and morbidity have also changed and improved. It is clear that this population raises important questions in which the operators need to individualize their decision based on trials like SYNTAX.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The recent report from the SYNTAX trials should give pause to our interventionalist colleagues embarking on multiple angioplasty and stenting procedures in patients with complex coronary anatomy.
SYNTAX randomized 1,800 patients with left main or triple-vessel coronary artery disease to either percutaneous coronary intervention (PCI) with the TAXUS drug-eluting stent or coronary artery bypass grafting (CABG) after being judged by a heart team as being in equipoise in regard to the appropriateness of either procedure (Eur Heart J. 2011;32;2125-34). The findings of several previous analyses have trended toward benefit for CABG, but none as clearly as SYNTAX. The original study was reported 6 years ago (Lancet 2013 Feb;381:629-38) and indicated that CABG was superior to PCI in patients with complex lesions. The most recent 5-year data of that study (J Am Coll Cardiol. 2016 Jan:67;42-55) indicates that cardiac mortality in the CABG patients is superior to that in the PCI group (5.3% vs. 9.6%, respectively), and the follow-up data provide more in-depth analysis in addition to the mechanism of death. Most importantly, the recent 5-year data clarify the reasons PCI fails to measure up to the results of CABG in patients with complex coronary artery disease.
One of the overriding predictors of increased mortality with PCI is the increased complexity of anatomy. The higher SYNTAX score was related to incomplete revascularization using PCI, compared with CABG. The presence of concomitant peripheral and carotid vascular disease, in addition to a left ventricular ejection fraction of less than 30%, favored the CABG group. Multiple stents and stent thrombosis were also issues leading to the increased mortality in the PCI group. The main cause of death was recurrent myocardial infarction, which occurred more frequently in the PCI patients and was associated with incomplete revascularization.
The data in the SYNTAX follow-up is not new, but do reinforce what has been reported in previous meta-analyses. This study does, however, emphasize the importance of recurrent infarction as a cause of death in these patients with complex anatomy. It is possible that new stent technology and coronary flow assessment at the time of intervention could have improved the outcome of this comparison and improved the long-term patency of the stented vessels. PCI is an evolving technology heavily affected by the experience of the operator. CABG surgery has also changed, and its associated mortality and morbidity have also changed and improved. It is clear that this population raises important questions in which the operators need to individualize their decision based on trials like SYNTAX.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The recent report from the SYNTAX trials should give pause to our interventionalist colleagues embarking on multiple angioplasty and stenting procedures in patients with complex coronary anatomy.
SYNTAX randomized 1,800 patients with left main or triple-vessel coronary artery disease to either percutaneous coronary intervention (PCI) with the TAXUS drug-eluting stent or coronary artery bypass grafting (CABG) after being judged by a heart team as being in equipoise in regard to the appropriateness of either procedure (Eur Heart J. 2011;32;2125-34). The findings of several previous analyses have trended toward benefit for CABG, but none as clearly as SYNTAX. The original study was reported 6 years ago (Lancet 2013 Feb;381:629-38) and indicated that CABG was superior to PCI in patients with complex lesions. The most recent 5-year data of that study (J Am Coll Cardiol. 2016 Jan:67;42-55) indicates that cardiac mortality in the CABG patients is superior to that in the PCI group (5.3% vs. 9.6%, respectively), and the follow-up data provide more in-depth analysis in addition to the mechanism of death. Most importantly, the recent 5-year data clarify the reasons PCI fails to measure up to the results of CABG in patients with complex coronary artery disease.
One of the overriding predictors of increased mortality with PCI is the increased complexity of anatomy. The higher SYNTAX score was related to incomplete revascularization using PCI, compared with CABG. The presence of concomitant peripheral and carotid vascular disease, in addition to a left ventricular ejection fraction of less than 30%, favored the CABG group. Multiple stents and stent thrombosis were also issues leading to the increased mortality in the PCI group. The main cause of death was recurrent myocardial infarction, which occurred more frequently in the PCI patients and was associated with incomplete revascularization.
The data in the SYNTAX follow-up is not new, but do reinforce what has been reported in previous meta-analyses. This study does, however, emphasize the importance of recurrent infarction as a cause of death in these patients with complex anatomy. It is possible that new stent technology and coronary flow assessment at the time of intervention could have improved the outcome of this comparison and improved the long-term patency of the stented vessels. PCI is an evolving technology heavily affected by the experience of the operator. CABG surgery has also changed, and its associated mortality and morbidity have also changed and improved. It is clear that this population raises important questions in which the operators need to individualize their decision based on trials like SYNTAX.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Entresto cuts LV mass in hypertensive patients
NEW ORLEANS – Hypertensive patients without heart failure treated with the heart failure formulation sacubitril plus valsartan had a significantly greater drop in their left ventricular mass than did patients treated with olmesartan in a randomized trial with 114 patients.
Treatment with sacubitril plus valsartan for both 3 and 12 months led to roughly twice as much reduction in left ventricular (LV) mass as did treatment with olmesartan, and this difference persisted after adjustment for between-group differences in blood pressure reduction, Roland E. Schmieder, MD, reported at the American Heart Association Scientific Sessions.

During clinical development of sacubitril plus valsartan (Entresto), the company that owns this compound, Novartis, ran a few small studies using the formulation to treat hypertension, but eventually those studies stopped, he said in an interview. “I hope this pushes development of other neprilysin inhibitor formulations for their blood pressure effects. I think this finding helps us understand why sacubitril plus valsartan was so effective for treating heart failure.” (N Engl J Med. 2014 Sep 11;371[11]:933-1004.)
The study enrolled patients with mild or moderate hypertension; the average blood pressure of enrolled patients was 155/92 mm Hg. They averaged 60 years of age, two-thirds were men, and their average LV mass index at baseline was 72 g/m2. The study excluded patients with heart failure. Patients randomized to receive sacubitril plus valsartan began on a dose of 200 mg/day, and after 2 weeks this rose to 400 mg/day, the maximum recommended dosage in the labeling. Patients randomized to olmesartan began on 20 mg/day, and after 2 weeks their dosage increased to 40 mg/day. Patients in both arms were also eligible to receive amlodipine for additional blood pressure lowering if deemed necessary by the treating physician.
The sacubitril plus valsartan group patients had an average cut in systolic blood pressure of about 26 mm Hg, both 3 and 12 months after the start of treatment. Patients in the olmesartan arm had decreases of 23 mm Hg and 21 mm Hg, respectively, at the two follow-up times. These between-group differences were statistically significant, Dr. Schmieder said.
Measurement of LV mass index using MRI scans showed an average reduction of LV mass index, compared with baseline of 6.4 g/m2 and 6.8 g/m2 after 3 and 12 months of treatment with sacubitril plus valsartan, and average reductions from baseline of 2.3 g/m2 and 3.5 g/m2 at the two follow-up examinations for patients treated with olmesartan. These statistically significant differences remained after adjustment for degree of blood pressure reduction at 3 and 12 months.
Additional measurements showed no between-group differences in aortic distensibility, but central pulse pressure also showed a significantly greater reduction with sacubitril plus valsartan, compared with olmesartan.
The trial was investigator initiated and received funding from Novartis. Dr. Schmieder has received honoraria from Novartis and also from AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, and Servier.
[email protected]
On Twitter @mitchelzoler
This study produced very interesting and convincing data. The results suggested that treating hypertension with sacubitril plus valsartan produced a significant, incremental improvement in left ventricular mass beyond the formulation’s blood pressure effect. This could potentially have importance when treating patients with hypertension and left ventricular hypertrophy.
Olmesartan was a fair comparator to use. It arguably is the most potent angiotensin receptor blocker for reducing blood pressure. However, in routine practice we generally combine an angiotensin receptor blocker with a diuretic to get maximum blood pressure lowering. In addition, it is not new to show that blood pressure lowering reduces left ventricular size.

These data are too limited and the cost for prescribing sacubitril plus valsartan is so high, compared with most other antihypertensive drugs, that I would like to see additional study results documenting this effect before I’d be willing to prescribe sacubitril plus valsartan to patients with hypertension but no heart failure.
Dan J. Fintel, MD , a cardiologist and professor of medicine at Northwestern University in Chicago, made these comments in an interview. He has been a speaker on behalf of AstraZeneca, BMS, Daiichi Sankyo, Janssen, Merck, and Pfizer.
This study produced very interesting and convincing data. The results suggested that treating hypertension with sacubitril plus valsartan produced a significant, incremental improvement in left ventricular mass beyond the formulation’s blood pressure effect. This could potentially have importance when treating patients with hypertension and left ventricular hypertrophy.
Olmesartan was a fair comparator to use. It arguably is the most potent angiotensin receptor blocker for reducing blood pressure. However, in routine practice we generally combine an angiotensin receptor blocker with a diuretic to get maximum blood pressure lowering. In addition, it is not new to show that blood pressure lowering reduces left ventricular size.
These data are too limited and the cost for prescribing sacubitril plus valsartan is so high, compared with most other antihypertensive drugs, that I would like to see additional study results documenting this effect before I’d be willing to prescribe sacubitril plus valsartan to patients with hypertension but no heart failure.
Dan J. Fintel, MD , a cardiologist and professor of medicine at Northwestern University in Chicago, made these comments in an interview. He has been a speaker on behalf of AstraZeneca, BMS, Daiichi Sankyo, Janssen, Merck, and Pfizer.
This study produced very interesting and convincing data. The results suggested that treating hypertension with sacubitril plus valsartan produced a significant, incremental improvement in left ventricular mass beyond the formulation’s blood pressure effect. This could potentially have importance when treating patients with hypertension and left ventricular hypertrophy.
Olmesartan was a fair comparator to use. It arguably is the most potent angiotensin receptor blocker for reducing blood pressure. However, in routine practice we generally combine an angiotensin receptor blocker with a diuretic to get maximum blood pressure lowering. In addition, it is not new to show that blood pressure lowering reduces left ventricular size.
These data are too limited and the cost for prescribing sacubitril plus valsartan is so high, compared with most other antihypertensive drugs, that I would like to see additional study results documenting this effect before I’d be willing to prescribe sacubitril plus valsartan to patients with hypertension but no heart failure.
Dan J. Fintel, MD , a cardiologist and professor of medicine at Northwestern University in Chicago, made these comments in an interview. He has been a speaker on behalf of AstraZeneca, BMS, Daiichi Sankyo, Janssen, Merck, and Pfizer.
NEW ORLEANS – Hypertensive patients without heart failure treated with the heart failure formulation sacubitril plus valsartan had a significantly greater drop in their left ventricular mass than did patients treated with olmesartan in a randomized trial with 114 patients.
Treatment with sacubitril plus valsartan for both 3 and 12 months led to roughly twice as much reduction in left ventricular (LV) mass as did treatment with olmesartan, and this difference persisted after adjustment for between-group differences in blood pressure reduction, Roland E. Schmieder, MD, reported at the American Heart Association Scientific Sessions.
During clinical development of sacubitril plus valsartan (Entresto), the company that owns this compound, Novartis, ran a few small studies using the formulation to treat hypertension, but eventually those studies stopped, he said in an interview. “I hope this pushes development of other neprilysin inhibitor formulations for their blood pressure effects. I think this finding helps us understand why sacubitril plus valsartan was so effective for treating heart failure.” (N Engl J Med. 2014 Sep 11;371[11]:933-1004.)
The study enrolled patients with mild or moderate hypertension; the average blood pressure of enrolled patients was 155/92 mm Hg. They averaged 60 years of age, two-thirds were men, and their average LV mass index at baseline was 72 g/m2. The study excluded patients with heart failure. Patients randomized to receive sacubitril plus valsartan began on a dose of 200 mg/day, and after 2 weeks this rose to 400 mg/day, the maximum recommended dosage in the labeling. Patients randomized to olmesartan began on 20 mg/day, and after 2 weeks their dosage increased to 40 mg/day. Patients in both arms were also eligible to receive amlodipine for additional blood pressure lowering if deemed necessary by the treating physician.
The sacubitril plus valsartan group patients had an average cut in systolic blood pressure of about 26 mm Hg, both 3 and 12 months after the start of treatment. Patients in the olmesartan arm had decreases of 23 mm Hg and 21 mm Hg, respectively, at the two follow-up times. These between-group differences were statistically significant, Dr. Schmieder said.
Measurement of LV mass index using MRI scans showed an average reduction of LV mass index, compared with baseline of 6.4 g/m2 and 6.8 g/m2 after 3 and 12 months of treatment with sacubitril plus valsartan, and average reductions from baseline of 2.3 g/m2 and 3.5 g/m2 at the two follow-up examinations for patients treated with olmesartan. These statistically significant differences remained after adjustment for degree of blood pressure reduction at 3 and 12 months.
Additional measurements showed no between-group differences in aortic distensibility, but central pulse pressure also showed a significantly greater reduction with sacubitril plus valsartan, compared with olmesartan.
The trial was investigator initiated and received funding from Novartis. Dr. Schmieder has received honoraria from Novartis and also from AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, and Servier.
[email protected]
On Twitter @mitchelzoler
NEW ORLEANS – Hypertensive patients without heart failure treated with the heart failure formulation sacubitril plus valsartan had a significantly greater drop in their left ventricular mass than did patients treated with olmesartan in a randomized trial with 114 patients.
Treatment with sacubitril plus valsartan for both 3 and 12 months led to roughly twice as much reduction in left ventricular (LV) mass as did treatment with olmesartan, and this difference persisted after adjustment for between-group differences in blood pressure reduction, Roland E. Schmieder, MD, reported at the American Heart Association Scientific Sessions.
During clinical development of sacubitril plus valsartan (Entresto), the company that owns this compound, Novartis, ran a few small studies using the formulation to treat hypertension, but eventually those studies stopped, he said in an interview. “I hope this pushes development of other neprilysin inhibitor formulations for their blood pressure effects. I think this finding helps us understand why sacubitril plus valsartan was so effective for treating heart failure.” (N Engl J Med. 2014 Sep 11;371[11]:933-1004.)
The study enrolled patients with mild or moderate hypertension; the average blood pressure of enrolled patients was 155/92 mm Hg. They averaged 60 years of age, two-thirds were men, and their average LV mass index at baseline was 72 g/m2. The study excluded patients with heart failure. Patients randomized to receive sacubitril plus valsartan began on a dose of 200 mg/day, and after 2 weeks this rose to 400 mg/day, the maximum recommended dosage in the labeling. Patients randomized to olmesartan began on 20 mg/day, and after 2 weeks their dosage increased to 40 mg/day. Patients in both arms were also eligible to receive amlodipine for additional blood pressure lowering if deemed necessary by the treating physician.
The sacubitril plus valsartan group patients had an average cut in systolic blood pressure of about 26 mm Hg, both 3 and 12 months after the start of treatment. Patients in the olmesartan arm had decreases of 23 mm Hg and 21 mm Hg, respectively, at the two follow-up times. These between-group differences were statistically significant, Dr. Schmieder said.
Measurement of LV mass index using MRI scans showed an average reduction of LV mass index, compared with baseline of 6.4 g/m2 and 6.8 g/m2 after 3 and 12 months of treatment with sacubitril plus valsartan, and average reductions from baseline of 2.3 g/m2 and 3.5 g/m2 at the two follow-up examinations for patients treated with olmesartan. These statistically significant differences remained after adjustment for degree of blood pressure reduction at 3 and 12 months.
Additional measurements showed no between-group differences in aortic distensibility, but central pulse pressure also showed a significantly greater reduction with sacubitril plus valsartan, compared with olmesartan.
The trial was investigator initiated and received funding from Novartis. Dr. Schmieder has received honoraria from Novartis and also from AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, and Servier.
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: .
Major finding: After 1 year, average left ventricular mass index fell 6.8 g/m2 from baseline with sacubitril/valsartan and 3.5 g/m2 with olmesartan.
Data source: A multicenter, randomized trial with 114 patients with mild or moderate hypertension.
Disclosures: The trial was investigator initiated and received funding from Novartis, the company that markets sacubitril plus valsartan (Entresto). Dr. Schmieder has received honoraria from Novartis and also from AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, and Servier.
Curricular milestones in rheumatology: Is granular better?
A new curricular “road map” attempts to lay out precisely what rheumatology fellows are expected to be able to know and do at different time points in their training.
The 80 “curricular milestones” for rheumatology, developed under the direction of the Accreditation Council for Graduate Medical Education, are meant to complement the 23 internal medicine subspecialty reporting milestones already mandated by the ACGME for use in trainee evaluation.
Unlike the reporting milestones, which came into use in 2014, the curricular milestones are not compulsory. Instead they “offer a guide so that trainees and the people teaching them know what’s expected of them,” said Lisa Criscione-Schreiber, MD, of Duke University, Durham, N.C., the lead author of a recent article in Arthritis Care & Research describing the new milestones (Arthritis Care Res. 2016 Nov 11. doi: 10.1002/acr.23151).

While the reporting milestones are designed to target broader competencies, the curricular milestones are highly granular. For example, a rheumatology fellow at 12 months is expected to be able to “perform compensated polarized microscopy to examine and interpret synovial fluid,” according to one milestone; before 24 months of training, he or she is expected to be able to teach others to do the same.
Authors of an accompanying editorial (Arthritis Care Res. 2016 Nov 11. doi: 10.1002/acr.23150) by Richard Panush, MD, of the University of Southern California in Los Angeles, Eric Hsieh, MD, also of USC, and Nortin Hadler, MD, of the University of North Carolina at Chapel Hill, praised the curricular milestones as meticulous and well conceived, but questioned their complexity and the broader push toward rubric-based training, particularly in the absence of evidence showing it to be superior to established methods.

Ultimately, Dr. Panush acknowledged in an interview, the move to milestones – including the curricular milestones – may prove worthwhile. But it simply “isn’t as sufficiently grounded in science as we would have liked for such a major departure from everything we have done, and with all that implementing the change would imply: the time, the manpower, the cost,” he said.
A leap of faith?
Dr. Criscione-Schreiber, who is Duke’s rheumatology program director, acknowledged that the milestones’ value and utility remain to be determined. “We’re not sure it’s the best way, but it’s a try,” she said. “We’re all in an era of continuous quality improvement in which you change something then test whether it works. The ACGME is collecting data about all this – if they find out it’s burdensome, they have assured program directors that they will change it.”
But Dr. Brown conceded that the editorialists’ concerns were valid. “The ACGME has been the main organization describing parameters by which we train doctors, and it is relatively unopposed. We’ve seen a proliferation of the rubric-based approach, and we are adopting these [curricular milestones] without scientific evidence. I commend the editorial authors in saying we need to find ways to measure this to see if it does improve, but if we wait for that evidence before we move forward, we’ll never get past square one.”
Observation and feedback
A key goal of the milestones is to encourage direct observation of trainees. Dr. Panush and his colleagues, in their editorial, argue that “a wise and astute clinician educator ... can judge when trainees are ready to function independently and have learned how to keep learning and changing without needing menus of evaluations or detailed instruments.”
Dr. Criscione-Schreiber said there’s traditionally been less direct observation in rheumatology training than people would like to think. “It used to be more like what we call the piano analogy. You send them into a room for an hour alone with a piano and some sheet music and they come out saying ‘I can play the piano.’ And you believe them.”
Dr. Brown, meanwhile, compared traditional training approaches to what he called the teabag model. The trainee “was the teabag steeping in the hot water of an academic medical center, and the major criteria for finishing was time,” he said. “I think all of us would recognize that this doesn’t take into consideration different environments, different learning styles and rates of learning.”

Using the milestones
Dr. Panush, in an interview, noted that the implementation of rubric-based education in internal medicine training came with a host of problems resulting in published critiques. He cited a recent article by Ronald Witteles, MD, and Abraham Verghese, MD, both of Stanford (Calif.) University, that criticized the reporting milestones as onerous to implement in large internal medicine programs, leading to excess administrative work and box-ticking (JAMA Intern Med. 2016;176[11]:1599-1600).
But rheumatology fellowship programs, which are generally small, may be less likely to find the curricular milestones burdensome, their champions say. The success of these milestones depends, in large part, on how people choose to integrate them into their training programs.
“The milestones appear a little daunting because they’re new,” Dr. Bolster said, cautioning that they are not designed to be foisted wholesale on trainees. Used judiciously, she said, the curricular milestones can help identify areas of strength and weakness and foster dialogue. “What I do is select a few of them, a couple of times a year, to go over with each fellow,” she said. “I also recommend them for fellows to use as self-reflection, so that they may determine where they are in terms of training.”
Details vs. the big picture
Anne Bass, MD, the rheumatology program director at the Hospital for Special Surgery in New York, who did not take part in either the curricular milestones writing committee or the editorial, said they could be used piecemeal, helping program directors to design portions of their curriculum, or to provide feedback and remediation by pointing out areas of trainee weakness.

But Dr. Bass also said, echoing a concern of the editorialists, that she felt that the milestones’ emphasis on highly specific strengths and weaknesses risked “losing the forest for the trees.”
A trainee who appears weak in one knowledge area is likely to have broader shortcomings, she said.
“If you’re somebody who gets the basic facts, you’re able to interview the patient, do the physical exam, and collect the information, but you’re not really able to apply it yet – that’s probably something global to that trainee that will apply with other areas as well,” not just the milestone you’re measuring, Dr. Bass said.
“The whole point about milestones is it’s showing you where along the continuum you are. But the continuum goes from data collection and description to application, testing, management, teaching – that’s kind of the spectrum, and that development is generally across the board. It’s not usually specific to one area.”
Training rheumatologists like pilots
The authors of the milestones say they’re responding to a sense widely shared in the rheumatology community that training must adapt to the needs of a changing field.
“Medicine is not the same as it was 10 or even 5 years ago, and certainly not as it was 20 years ago. A physician who is going to practice 10 years from now will require a different skill set,” Dr. Criscione-Schreiber said.
This, of course, includes many skills not directly related to patient care but rather successful functioning within current systems of health care delivery.
Dr. Criscione-Schreiber said that amid a coming shortage of rheumatologists, the next generation must be prepared to lead teams.
“We’re going to have clinics with nurses doing much of the education, and a whole team of people taking care of patients, if we have any hope of caring for the population in the U.S. that needs rheumatologists. It’s different from training a one-on-one doctor who sits in the room with a patient for 25 minutes,” she said.
Dr. Brown said he views the milestones effort, whether it proves successful or not, as an attempt to train in a way that ensures all future rheumatologists share the same core skills.
“People ask us all the time which doctor should they see for this or that condition, because they want to see someone really good,” Dr. Brown said. “Contrast that to the last time you got on an airplane. Did you ask a friend which pilot you should fly with? No, because you trusted that the pilot was competent, and had all requisite training, to safely pilot the plane. We want medicine to have many of those qualities and characteristics.”
Human beings are more complicated than airplanes, Dr. Brown acknowledged. “So it’s not perfectly analogous. But if we can more granularly describe training, and what it is we want to achieve, we’d all benefit – to the point where we can confidently tell you to see the rheumatologist trained in an accredited program who’s nearest your home.”
A new curricular “road map” attempts to lay out precisely what rheumatology fellows are expected to be able to know and do at different time points in their training.
The 80 “curricular milestones” for rheumatology, developed under the direction of the Accreditation Council for Graduate Medical Education, are meant to complement the 23 internal medicine subspecialty reporting milestones already mandated by the ACGME for use in trainee evaluation.
Unlike the reporting milestones, which came into use in 2014, the curricular milestones are not compulsory. Instead they “offer a guide so that trainees and the people teaching them know what’s expected of them,” said Lisa Criscione-Schreiber, MD, of Duke University, Durham, N.C., the lead author of a recent article in Arthritis Care & Research describing the new milestones (Arthritis Care Res. 2016 Nov 11. doi: 10.1002/acr.23151).
While the reporting milestones are designed to target broader competencies, the curricular milestones are highly granular. For example, a rheumatology fellow at 12 months is expected to be able to “perform compensated polarized microscopy to examine and interpret synovial fluid,” according to one milestone; before 24 months of training, he or she is expected to be able to teach others to do the same.
Authors of an accompanying editorial (Arthritis Care Res. 2016 Nov 11. doi: 10.1002/acr.23150) by Richard Panush, MD, of the University of Southern California in Los Angeles, Eric Hsieh, MD, also of USC, and Nortin Hadler, MD, of the University of North Carolina at Chapel Hill, praised the curricular milestones as meticulous and well conceived, but questioned their complexity and the broader push toward rubric-based training, particularly in the absence of evidence showing it to be superior to established methods.
Ultimately, Dr. Panush acknowledged in an interview, the move to milestones – including the curricular milestones – may prove worthwhile. But it simply “isn’t as sufficiently grounded in science as we would have liked for such a major departure from everything we have done, and with all that implementing the change would imply: the time, the manpower, the cost,” he said.
A leap of faith?
Dr. Criscione-Schreiber, who is Duke’s rheumatology program director, acknowledged that the milestones’ value and utility remain to be determined. “We’re not sure it’s the best way, but it’s a try,” she said. “We’re all in an era of continuous quality improvement in which you change something then test whether it works. The ACGME is collecting data about all this – if they find out it’s burdensome, they have assured program directors that they will change it.”
But Dr. Brown conceded that the editorialists’ concerns were valid. “The ACGME has been the main organization describing parameters by which we train doctors, and it is relatively unopposed. We’ve seen a proliferation of the rubric-based approach, and we are adopting these [curricular milestones] without scientific evidence. I commend the editorial authors in saying we need to find ways to measure this to see if it does improve, but if we wait for that evidence before we move forward, we’ll never get past square one.”
Observation and feedback
A key goal of the milestones is to encourage direct observation of trainees. Dr. Panush and his colleagues, in their editorial, argue that “a wise and astute clinician educator ... can judge when trainees are ready to function independently and have learned how to keep learning and changing without needing menus of evaluations or detailed instruments.”
Dr. Criscione-Schreiber said there’s traditionally been less direct observation in rheumatology training than people would like to think. “It used to be more like what we call the piano analogy. You send them into a room for an hour alone with a piano and some sheet music and they come out saying ‘I can play the piano.’ And you believe them.”
Dr. Brown, meanwhile, compared traditional training approaches to what he called the teabag model. The trainee “was the teabag steeping in the hot water of an academic medical center, and the major criteria for finishing was time,” he said. “I think all of us would recognize that this doesn’t take into consideration different environments, different learning styles and rates of learning.”
Using the milestones
Dr. Panush, in an interview, noted that the implementation of rubric-based education in internal medicine training came with a host of problems resulting in published critiques. He cited a recent article by Ronald Witteles, MD, and Abraham Verghese, MD, both of Stanford (Calif.) University, that criticized the reporting milestones as onerous to implement in large internal medicine programs, leading to excess administrative work and box-ticking (JAMA Intern Med. 2016;176[11]:1599-1600).
But rheumatology fellowship programs, which are generally small, may be less likely to find the curricular milestones burdensome, their champions say. The success of these milestones depends, in large part, on how people choose to integrate them into their training programs.
“The milestones appear a little daunting because they’re new,” Dr. Bolster said, cautioning that they are not designed to be foisted wholesale on trainees. Used judiciously, she said, the curricular milestones can help identify areas of strength and weakness and foster dialogue. “What I do is select a few of them, a couple of times a year, to go over with each fellow,” she said. “I also recommend them for fellows to use as self-reflection, so that they may determine where they are in terms of training.”
Details vs. the big picture
Anne Bass, MD, the rheumatology program director at the Hospital for Special Surgery in New York, who did not take part in either the curricular milestones writing committee or the editorial, said they could be used piecemeal, helping program directors to design portions of their curriculum, or to provide feedback and remediation by pointing out areas of trainee weakness.
But Dr. Bass also said, echoing a concern of the editorialists, that she felt that the milestones’ emphasis on highly specific strengths and weaknesses risked “losing the forest for the trees.”
A trainee who appears weak in one knowledge area is likely to have broader shortcomings, she said.
“If you’re somebody who gets the basic facts, you’re able to interview the patient, do the physical exam, and collect the information, but you’re not really able to apply it yet – that’s probably something global to that trainee that will apply with other areas as well,” not just the milestone you’re measuring, Dr. Bass said.
“The whole point about milestones is it’s showing you where along the continuum you are. But the continuum goes from data collection and description to application, testing, management, teaching – that’s kind of the spectrum, and that development is generally across the board. It’s not usually specific to one area.”
Training rheumatologists like pilots
The authors of the milestones say they’re responding to a sense widely shared in the rheumatology community that training must adapt to the needs of a changing field.
“Medicine is not the same as it was 10 or even 5 years ago, and certainly not as it was 20 years ago. A physician who is going to practice 10 years from now will require a different skill set,” Dr. Criscione-Schreiber said.
This, of course, includes many skills not directly related to patient care but rather successful functioning within current systems of health care delivery.
Dr. Criscione-Schreiber said that amid a coming shortage of rheumatologists, the next generation must be prepared to lead teams.
“We’re going to have clinics with nurses doing much of the education, and a whole team of people taking care of patients, if we have any hope of caring for the population in the U.S. that needs rheumatologists. It’s different from training a one-on-one doctor who sits in the room with a patient for 25 minutes,” she said.
Dr. Brown said he views the milestones effort, whether it proves successful or not, as an attempt to train in a way that ensures all future rheumatologists share the same core skills.
“People ask us all the time which doctor should they see for this or that condition, because they want to see someone really good,” Dr. Brown said. “Contrast that to the last time you got on an airplane. Did you ask a friend which pilot you should fly with? No, because you trusted that the pilot was competent, and had all requisite training, to safely pilot the plane. We want medicine to have many of those qualities and characteristics.”
Human beings are more complicated than airplanes, Dr. Brown acknowledged. “So it’s not perfectly analogous. But if we can more granularly describe training, and what it is we want to achieve, we’d all benefit – to the point where we can confidently tell you to see the rheumatologist trained in an accredited program who’s nearest your home.”
A new curricular “road map” attempts to lay out precisely what rheumatology fellows are expected to be able to know and do at different time points in their training.
The 80 “curricular milestones” for rheumatology, developed under the direction of the Accreditation Council for Graduate Medical Education, are meant to complement the 23 internal medicine subspecialty reporting milestones already mandated by the ACGME for use in trainee evaluation.
Unlike the reporting milestones, which came into use in 2014, the curricular milestones are not compulsory. Instead they “offer a guide so that trainees and the people teaching them know what’s expected of them,” said Lisa Criscione-Schreiber, MD, of Duke University, Durham, N.C., the lead author of a recent article in Arthritis Care & Research describing the new milestones (Arthritis Care Res. 2016 Nov 11. doi: 10.1002/acr.23151).
While the reporting milestones are designed to target broader competencies, the curricular milestones are highly granular. For example, a rheumatology fellow at 12 months is expected to be able to “perform compensated polarized microscopy to examine and interpret synovial fluid,” according to one milestone; before 24 months of training, he or she is expected to be able to teach others to do the same.
Authors of an accompanying editorial (Arthritis Care Res. 2016 Nov 11. doi: 10.1002/acr.23150) by Richard Panush, MD, of the University of Southern California in Los Angeles, Eric Hsieh, MD, also of USC, and Nortin Hadler, MD, of the University of North Carolina at Chapel Hill, praised the curricular milestones as meticulous and well conceived, but questioned their complexity and the broader push toward rubric-based training, particularly in the absence of evidence showing it to be superior to established methods.
Ultimately, Dr. Panush acknowledged in an interview, the move to milestones – including the curricular milestones – may prove worthwhile. But it simply “isn’t as sufficiently grounded in science as we would have liked for such a major departure from everything we have done, and with all that implementing the change would imply: the time, the manpower, the cost,” he said.
A leap of faith?
Dr. Criscione-Schreiber, who is Duke’s rheumatology program director, acknowledged that the milestones’ value and utility remain to be determined. “We’re not sure it’s the best way, but it’s a try,” she said. “We’re all in an era of continuous quality improvement in which you change something then test whether it works. The ACGME is collecting data about all this – if they find out it’s burdensome, they have assured program directors that they will change it.”
But Dr. Brown conceded that the editorialists’ concerns were valid. “The ACGME has been the main organization describing parameters by which we train doctors, and it is relatively unopposed. We’ve seen a proliferation of the rubric-based approach, and we are adopting these [curricular milestones] without scientific evidence. I commend the editorial authors in saying we need to find ways to measure this to see if it does improve, but if we wait for that evidence before we move forward, we’ll never get past square one.”
Observation and feedback
A key goal of the milestones is to encourage direct observation of trainees. Dr. Panush and his colleagues, in their editorial, argue that “a wise and astute clinician educator ... can judge when trainees are ready to function independently and have learned how to keep learning and changing without needing menus of evaluations or detailed instruments.”
Dr. Criscione-Schreiber said there’s traditionally been less direct observation in rheumatology training than people would like to think. “It used to be more like what we call the piano analogy. You send them into a room for an hour alone with a piano and some sheet music and they come out saying ‘I can play the piano.’ And you believe them.”
Dr. Brown, meanwhile, compared traditional training approaches to what he called the teabag model. The trainee “was the teabag steeping in the hot water of an academic medical center, and the major criteria for finishing was time,” he said. “I think all of us would recognize that this doesn’t take into consideration different environments, different learning styles and rates of learning.”
Using the milestones
Dr. Panush, in an interview, noted that the implementation of rubric-based education in internal medicine training came with a host of problems resulting in published critiques. He cited a recent article by Ronald Witteles, MD, and Abraham Verghese, MD, both of Stanford (Calif.) University, that criticized the reporting milestones as onerous to implement in large internal medicine programs, leading to excess administrative work and box-ticking (JAMA Intern Med. 2016;176[11]:1599-1600).
But rheumatology fellowship programs, which are generally small, may be less likely to find the curricular milestones burdensome, their champions say. The success of these milestones depends, in large part, on how people choose to integrate them into their training programs.
“The milestones appear a little daunting because they’re new,” Dr. Bolster said, cautioning that they are not designed to be foisted wholesale on trainees. Used judiciously, she said, the curricular milestones can help identify areas of strength and weakness and foster dialogue. “What I do is select a few of them, a couple of times a year, to go over with each fellow,” she said. “I also recommend them for fellows to use as self-reflection, so that they may determine where they are in terms of training.”
Details vs. the big picture
Anne Bass, MD, the rheumatology program director at the Hospital for Special Surgery in New York, who did not take part in either the curricular milestones writing committee or the editorial, said they could be used piecemeal, helping program directors to design portions of their curriculum, or to provide feedback and remediation by pointing out areas of trainee weakness.
But Dr. Bass also said, echoing a concern of the editorialists, that she felt that the milestones’ emphasis on highly specific strengths and weaknesses risked “losing the forest for the trees.”
A trainee who appears weak in one knowledge area is likely to have broader shortcomings, she said.
“If you’re somebody who gets the basic facts, you’re able to interview the patient, do the physical exam, and collect the information, but you’re not really able to apply it yet – that’s probably something global to that trainee that will apply with other areas as well,” not just the milestone you’re measuring, Dr. Bass said.
“The whole point about milestones is it’s showing you where along the continuum you are. But the continuum goes from data collection and description to application, testing, management, teaching – that’s kind of the spectrum, and that development is generally across the board. It’s not usually specific to one area.”
Training rheumatologists like pilots
The authors of the milestones say they’re responding to a sense widely shared in the rheumatology community that training must adapt to the needs of a changing field.
“Medicine is not the same as it was 10 or even 5 years ago, and certainly not as it was 20 years ago. A physician who is going to practice 10 years from now will require a different skill set,” Dr. Criscione-Schreiber said.
This, of course, includes many skills not directly related to patient care but rather successful functioning within current systems of health care delivery.
Dr. Criscione-Schreiber said that amid a coming shortage of rheumatologists, the next generation must be prepared to lead teams.
“We’re going to have clinics with nurses doing much of the education, and a whole team of people taking care of patients, if we have any hope of caring for the population in the U.S. that needs rheumatologists. It’s different from training a one-on-one doctor who sits in the room with a patient for 25 minutes,” she said.
Dr. Brown said he views the milestones effort, whether it proves successful or not, as an attempt to train in a way that ensures all future rheumatologists share the same core skills.
“People ask us all the time which doctor should they see for this or that condition, because they want to see someone really good,” Dr. Brown said. “Contrast that to the last time you got on an airplane. Did you ask a friend which pilot you should fly with? No, because you trusted that the pilot was competent, and had all requisite training, to safely pilot the plane. We want medicine to have many of those qualities and characteristics.”
Human beings are more complicated than airplanes, Dr. Brown acknowledged. “So it’s not perfectly analogous. But if we can more granularly describe training, and what it is we want to achieve, we’d all benefit – to the point where we can confidently tell you to see the rheumatologist trained in an accredited program who’s nearest your home.”
FROM ARTHRITIS CARE & RESEARCH
Addressing sexuality, gender identity issues is key to positive outcomes
A while ago, I gave a talk on LGBT health to a group of primary care pediatricians. Although I was glad that they invited me to speak, I also sensed some discomfort in the audience. At the end of the lecture, many pediatricians told me that they were uncomfortable with bringing up the topic of sexuality and gender identity with their patients, and others wanted guidance on how to ask questions on sexuality and gender identity.
There are many barriers for primary pediatricians in addressing sexuality and gender identity concerns in their patients. First, pediatricians often will have up to 15 minutes for a visit, so they will have little time to address a complex issue. Second, primary care pediatricians may have known many of their patients since birth, and asking questions on sexuality and gender can feel awkward. Finally, many pediatricians may be working in more conservative areas in the country where asking questions on sexuality and gender identity may be controversial.

Although a very important topic, there is not much empirical evidence on how to ask questions on sexuality and gender appropriately, and most of these recommendations are based on my own experience working with LGBT youth. Regardless, I hope these pointers will help the primary care pediatrician address the needs of LGBT youth efficiently and with sensitivity.
Tip No. 1: The environment counts
I cannot overstate how important it is to make your clinic a welcoming place for LGBT youth. Having various signs and stickers – like rainbow flags or the Human Rights Campaign sticker – will signal to LGBT youth that they are safe in your clinic. Creating a safe and welcoming environment is important because many people in the LGBT community have experienced rejection and discrimination from their primary care doctors.1 Making your clinic a safe space will make it easier and efficient for patients to ask questions about sexuality and gender identity (see Dr. Gaya Chelvakumar’s column “Creating safe spaces for LGBTQ youth, families in health care settings” at pediatricnews.com).
Tip No. 2: Consider the context
Most likely, many presenting complaints – such as colds or sports injuries – of your adolescent patients will not involve sexual orientation or gender identity. There are exceptions. If you suspect an STD, then the risk for certain infections, such as HIV2 or gonorrhea of the anus or of the pharynx3 are higher in gay young men. For the latter, your screening method would be different (that is, obtaining a pharyngeal swab or an anal swab instead of a urine sample). Also, because many LGBT youth have higher rates of mental health problems compared with heterosexual youth,4 you may want to ask questions about sexuality or gender identity to patients complaining of depressive or anxiety symptoms. This is especially important for transgender youth, because the implementation of pubertal blockers or cross-sex hormones can be therapeutic.5 To prevent or reduce many of these health problems, asking about sexuality and gender identity is a good idea during the well visit, when you may have more time.
Tip No. 3: Not all developmental stages are considered equal
Adolescence is a period of rapid and phasic growth. Formation of an identity is one of the major psychosocial tasks for adolescence,6 and sexuality and gender are important identities. In general, in early adolescence identity becomes an issue as the teenager gains autonomy from parents. I typically start asking questions about sexuality and gender when the patient is 11 or 12, because many children may not understand sexuality and gender identity at a younger age. At these ages, I ask these questions with the parents in the room, then I ask them confidentially on subsequent well visits. This approach serves two purposes: it will prepare the adolescent for these complex and thought-provoking questions in future encounters, and it gives the parents an idea of the type of questions you will ask the children when they are old enough for the confidential visit, helping parents feel more comfortable in stepping out of the room during this time.
Tip No. 4: Keep it confidential
Many adolescents are reluctant to see a doctor, even if they are sick. The primary reason adolescents do not seek care is the fear that the provider will tell their parents about their illness.7 Although this should be applicable to all of your adolescent patients, you should make an extra effort to explicitly state to LGBT patients that the clinic visit is confidential (with the exception of risk of suicide, homicide, or child abuse). This is important for LGBT youth who are not out to their parents and may be in danger if they do come out.8
Tip No. 5: Normalize, normalize, normalize
Because of the stigma and discrimination surrounding sexual orientation and gender identity, many LGBT youth will be reluctant to disclose their sexual orientation or gender identity to their health care providers. At the same time, heterosexual youth may think that you’re asking them questions about sexuality or gender identity because you suspect them to be a member of the LGBT community. To avoid this awkward situation, many pediatricians do not ask these questions at all. A good remedy for this is to preface your questions about sexual orientation or gender identity by saying that you ask these questions to all your patients – that way no one feels singled out.
Tip No. 6: Ask for permission
As previously mentioned, members of the LGBT community may experience discrimination from their health care providers after disclosing to them their sexual orientation or gender identity.1 This rejection can be traumatizing for LGBT youth, making them reluctant to discuss any issues related to sexual orientation or gender identity with any medical provider. As part of the trauma-informed approach, asking for permission before delving into issues related to sexual orientation and gender identity will give LGBT patients a sense of control, especially in an environment where there is a significant power differential.
Tip No. 7: Treat this as a skill
Despite the pressures for primary care pediatricians to maintain an efficient and effective clinical practice, many strive to learn new skills to provide the best care for their patients. Asking questions about sexuality and gender identity should be one of those skills. As with any skill, it will feel unnatural at first, and it will require practice. Mastering this skill, however, will help you address the health needs of this vulnerable population.
Asking questions about sexuality and gender identity is difficult for the primary care pediatrician. Hopefully, these tips can help you develop this important skill. It will also help you reach out to a population that is wary of the health care system.
References
1. J Am Board Fam Med. 2016;29(1):156-60.
2. https://www.cdc.gov/hiv/group/msm/index.html.
3. https://www.cdc.gov/std/tg2015/default.htm.
4. J Adolesc Health. 2011;49(2):115-23.
5. Nat Rev Endocrinol. 2011;7(8):466-72.
6. Neinstein LS. Adolescent health care: a practical guide. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2008.
7. J Adolesc Health. 2007;40(3):218-26.
8. Am J Orthopsychiatry. 1998;68(3):361-71.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center and a postdoctoral fellow in the department of pediatrics at the University of Pittsburgh. Email him at [email protected].
A while ago, I gave a talk on LGBT health to a group of primary care pediatricians. Although I was glad that they invited me to speak, I also sensed some discomfort in the audience. At the end of the lecture, many pediatricians told me that they were uncomfortable with bringing up the topic of sexuality and gender identity with their patients, and others wanted guidance on how to ask questions on sexuality and gender identity.
There are many barriers for primary pediatricians in addressing sexuality and gender identity concerns in their patients. First, pediatricians often will have up to 15 minutes for a visit, so they will have little time to address a complex issue. Second, primary care pediatricians may have known many of their patients since birth, and asking questions on sexuality and gender can feel awkward. Finally, many pediatricians may be working in more conservative areas in the country where asking questions on sexuality and gender identity may be controversial.
Although a very important topic, there is not much empirical evidence on how to ask questions on sexuality and gender appropriately, and most of these recommendations are based on my own experience working with LGBT youth. Regardless, I hope these pointers will help the primary care pediatrician address the needs of LGBT youth efficiently and with sensitivity.
Tip No. 1: The environment counts
I cannot overstate how important it is to make your clinic a welcoming place for LGBT youth. Having various signs and stickers – like rainbow flags or the Human Rights Campaign sticker – will signal to LGBT youth that they are safe in your clinic. Creating a safe and welcoming environment is important because many people in the LGBT community have experienced rejection and discrimination from their primary care doctors.1 Making your clinic a safe space will make it easier and efficient for patients to ask questions about sexuality and gender identity (see Dr. Gaya Chelvakumar’s column “Creating safe spaces for LGBTQ youth, families in health care settings” at pediatricnews.com).
Tip No. 2: Consider the context
Most likely, many presenting complaints – such as colds or sports injuries – of your adolescent patients will not involve sexual orientation or gender identity. There are exceptions. If you suspect an STD, then the risk for certain infections, such as HIV2 or gonorrhea of the anus or of the pharynx3 are higher in gay young men. For the latter, your screening method would be different (that is, obtaining a pharyngeal swab or an anal swab instead of a urine sample). Also, because many LGBT youth have higher rates of mental health problems compared with heterosexual youth,4 you may want to ask questions about sexuality or gender identity to patients complaining of depressive or anxiety symptoms. This is especially important for transgender youth, because the implementation of pubertal blockers or cross-sex hormones can be therapeutic.5 To prevent or reduce many of these health problems, asking about sexuality and gender identity is a good idea during the well visit, when you may have more time.
Tip No. 3: Not all developmental stages are considered equal
Adolescence is a period of rapid and phasic growth. Formation of an identity is one of the major psychosocial tasks for adolescence,6 and sexuality and gender are important identities. In general, in early adolescence identity becomes an issue as the teenager gains autonomy from parents. I typically start asking questions about sexuality and gender when the patient is 11 or 12, because many children may not understand sexuality and gender identity at a younger age. At these ages, I ask these questions with the parents in the room, then I ask them confidentially on subsequent well visits. This approach serves two purposes: it will prepare the adolescent for these complex and thought-provoking questions in future encounters, and it gives the parents an idea of the type of questions you will ask the children when they are old enough for the confidential visit, helping parents feel more comfortable in stepping out of the room during this time.
Tip No. 4: Keep it confidential
Many adolescents are reluctant to see a doctor, even if they are sick. The primary reason adolescents do not seek care is the fear that the provider will tell their parents about their illness.7 Although this should be applicable to all of your adolescent patients, you should make an extra effort to explicitly state to LGBT patients that the clinic visit is confidential (with the exception of risk of suicide, homicide, or child abuse). This is important for LGBT youth who are not out to their parents and may be in danger if they do come out.8
Tip No. 5: Normalize, normalize, normalize
Because of the stigma and discrimination surrounding sexual orientation and gender identity, many LGBT youth will be reluctant to disclose their sexual orientation or gender identity to their health care providers. At the same time, heterosexual youth may think that you’re asking them questions about sexuality or gender identity because you suspect them to be a member of the LGBT community. To avoid this awkward situation, many pediatricians do not ask these questions at all. A good remedy for this is to preface your questions about sexual orientation or gender identity by saying that you ask these questions to all your patients – that way no one feels singled out.
Tip No. 6: Ask for permission
As previously mentioned, members of the LGBT community may experience discrimination from their health care providers after disclosing to them their sexual orientation or gender identity.1 This rejection can be traumatizing for LGBT youth, making them reluctant to discuss any issues related to sexual orientation or gender identity with any medical provider. As part of the trauma-informed approach, asking for permission before delving into issues related to sexual orientation and gender identity will give LGBT patients a sense of control, especially in an environment where there is a significant power differential.
Tip No. 7: Treat this as a skill
Despite the pressures for primary care pediatricians to maintain an efficient and effective clinical practice, many strive to learn new skills to provide the best care for their patients. Asking questions about sexuality and gender identity should be one of those skills. As with any skill, it will feel unnatural at first, and it will require practice. Mastering this skill, however, will help you address the health needs of this vulnerable population.
Asking questions about sexuality and gender identity is difficult for the primary care pediatrician. Hopefully, these tips can help you develop this important skill. It will also help you reach out to a population that is wary of the health care system.
References
1. J Am Board Fam Med. 2016;29(1):156-60.
2. https://www.cdc.gov/hiv/group/msm/index.html.
3. https://www.cdc.gov/std/tg2015/default.htm.
4. J Adolesc Health. 2011;49(2):115-23.
5. Nat Rev Endocrinol. 2011;7(8):466-72.
6. Neinstein LS. Adolescent health care: a practical guide. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2008.
7. J Adolesc Health. 2007;40(3):218-26.
8. Am J Orthopsychiatry. 1998;68(3):361-71.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center and a postdoctoral fellow in the department of pediatrics at the University of Pittsburgh. Email him at [email protected].
A while ago, I gave a talk on LGBT health to a group of primary care pediatricians. Although I was glad that they invited me to speak, I also sensed some discomfort in the audience. At the end of the lecture, many pediatricians told me that they were uncomfortable with bringing up the topic of sexuality and gender identity with their patients, and others wanted guidance on how to ask questions on sexuality and gender identity.
There are many barriers for primary pediatricians in addressing sexuality and gender identity concerns in their patients. First, pediatricians often will have up to 15 minutes for a visit, so they will have little time to address a complex issue. Second, primary care pediatricians may have known many of their patients since birth, and asking questions on sexuality and gender can feel awkward. Finally, many pediatricians may be working in more conservative areas in the country where asking questions on sexuality and gender identity may be controversial.
Although a very important topic, there is not much empirical evidence on how to ask questions on sexuality and gender appropriately, and most of these recommendations are based on my own experience working with LGBT youth. Regardless, I hope these pointers will help the primary care pediatrician address the needs of LGBT youth efficiently and with sensitivity.
Tip No. 1: The environment counts
I cannot overstate how important it is to make your clinic a welcoming place for LGBT youth. Having various signs and stickers – like rainbow flags or the Human Rights Campaign sticker – will signal to LGBT youth that they are safe in your clinic. Creating a safe and welcoming environment is important because many people in the LGBT community have experienced rejection and discrimination from their primary care doctors.1 Making your clinic a safe space will make it easier and efficient for patients to ask questions about sexuality and gender identity (see Dr. Gaya Chelvakumar’s column “Creating safe spaces for LGBTQ youth, families in health care settings” at pediatricnews.com).
Tip No. 2: Consider the context
Most likely, many presenting complaints – such as colds or sports injuries – of your adolescent patients will not involve sexual orientation or gender identity. There are exceptions. If you suspect an STD, then the risk for certain infections, such as HIV2 or gonorrhea of the anus or of the pharynx3 are higher in gay young men. For the latter, your screening method would be different (that is, obtaining a pharyngeal swab or an anal swab instead of a urine sample). Also, because many LGBT youth have higher rates of mental health problems compared with heterosexual youth,4 you may want to ask questions about sexuality or gender identity to patients complaining of depressive or anxiety symptoms. This is especially important for transgender youth, because the implementation of pubertal blockers or cross-sex hormones can be therapeutic.5 To prevent or reduce many of these health problems, asking about sexuality and gender identity is a good idea during the well visit, when you may have more time.
Tip No. 3: Not all developmental stages are considered equal
Adolescence is a period of rapid and phasic growth. Formation of an identity is one of the major psychosocial tasks for adolescence,6 and sexuality and gender are important identities. In general, in early adolescence identity becomes an issue as the teenager gains autonomy from parents. I typically start asking questions about sexuality and gender when the patient is 11 or 12, because many children may not understand sexuality and gender identity at a younger age. At these ages, I ask these questions with the parents in the room, then I ask them confidentially on subsequent well visits. This approach serves two purposes: it will prepare the adolescent for these complex and thought-provoking questions in future encounters, and it gives the parents an idea of the type of questions you will ask the children when they are old enough for the confidential visit, helping parents feel more comfortable in stepping out of the room during this time.
Tip No. 4: Keep it confidential
Many adolescents are reluctant to see a doctor, even if they are sick. The primary reason adolescents do not seek care is the fear that the provider will tell their parents about their illness.7 Although this should be applicable to all of your adolescent patients, you should make an extra effort to explicitly state to LGBT patients that the clinic visit is confidential (with the exception of risk of suicide, homicide, or child abuse). This is important for LGBT youth who are not out to their parents and may be in danger if they do come out.8
Tip No. 5: Normalize, normalize, normalize
Because of the stigma and discrimination surrounding sexual orientation and gender identity, many LGBT youth will be reluctant to disclose their sexual orientation or gender identity to their health care providers. At the same time, heterosexual youth may think that you’re asking them questions about sexuality or gender identity because you suspect them to be a member of the LGBT community. To avoid this awkward situation, many pediatricians do not ask these questions at all. A good remedy for this is to preface your questions about sexual orientation or gender identity by saying that you ask these questions to all your patients – that way no one feels singled out.
Tip No. 6: Ask for permission
As previously mentioned, members of the LGBT community may experience discrimination from their health care providers after disclosing to them their sexual orientation or gender identity.1 This rejection can be traumatizing for LGBT youth, making them reluctant to discuss any issues related to sexual orientation or gender identity with any medical provider. As part of the trauma-informed approach, asking for permission before delving into issues related to sexual orientation and gender identity will give LGBT patients a sense of control, especially in an environment where there is a significant power differential.
Tip No. 7: Treat this as a skill
Despite the pressures for primary care pediatricians to maintain an efficient and effective clinical practice, many strive to learn new skills to provide the best care for their patients. Asking questions about sexuality and gender identity should be one of those skills. As with any skill, it will feel unnatural at first, and it will require practice. Mastering this skill, however, will help you address the health needs of this vulnerable population.
Asking questions about sexuality and gender identity is difficult for the primary care pediatrician. Hopefully, these tips can help you develop this important skill. It will also help you reach out to a population that is wary of the health care system.
References
1. J Am Board Fam Med. 2016;29(1):156-60.
2. https://www.cdc.gov/hiv/group/msm/index.html.
3. https://www.cdc.gov/std/tg2015/default.htm.
4. J Adolesc Health. 2011;49(2):115-23.
5. Nat Rev Endocrinol. 2011;7(8):466-72.
6. Neinstein LS. Adolescent health care: a practical guide. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2008.
7. J Adolesc Health. 2007;40(3):218-26.
8. Am J Orthopsychiatry. 1998;68(3):361-71.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center and a postdoctoral fellow in the department of pediatrics at the University of Pittsburgh. Email him at [email protected].
A Multimodal Strategy to Manage Pain in an In-Patient and Out-Patient Total Joint Program: What Do You Need to Know?
Contents
Opioid-Sparing Pain Control in Outpatient Total Joint Arthroplasty
John W. Barrington, MD
Addressing the Opioid Epidemic With Multimodal Pain Management
Michael A. Kelly, MD
Comprehensive Care for Joint Replacement (CJR) Bundle Expense in Perioperative Pain Management
Susan D. Bear, PharmD, BCPS
The Role of Liposomal Bupivacaine in Value-Based Care
Richard Iorio, MD
Contents
Opioid-Sparing Pain Control in Outpatient Total Joint Arthroplasty
John W. Barrington, MD
Addressing the Opioid Epidemic With Multimodal Pain Management
Michael A. Kelly, MD
Comprehensive Care for Joint Replacement (CJR) Bundle Expense in Perioperative Pain Management
Susan D. Bear, PharmD, BCPS
The Role of Liposomal Bupivacaine in Value-Based Care
Richard Iorio, MD
Contents
Opioid-Sparing Pain Control in Outpatient Total Joint Arthroplasty
John W. Barrington, MD
Addressing the Opioid Epidemic With Multimodal Pain Management
Michael A. Kelly, MD
Comprehensive Care for Joint Replacement (CJR) Bundle Expense in Perioperative Pain Management
Susan D. Bear, PharmD, BCPS
The Role of Liposomal Bupivacaine in Value-Based Care
Richard Iorio, MD

Oral pomalidomide effective against Kaposi’s sarcoma
Oral pomalidomide, a derivative of thalidomide with immunomodulatory, antiangiogenic, and antiproliferative properties, proved to be well tolerated and effective against Kaposi’s sarcoma (KS) in a small phase I/II study, investigators reported in the Journal of Clinical Oncology.
There is a substantial need for oral therapies for KS, which often recurs and requires treatment, at least intermittently, for years. Existing treatments are cytotoxic agents, such as anthracyclines that are poorly tolerated and unsuitable for long-term use, said Mark N. Polizzotto, MD, of the National Cancer Institute, Bethesda, Md., and his associates.
They examined the tolerability and efficacy of pomalidomide against KS in a single-center, open-label trial involving 21 men and 1 transgender woman who had at least five evaluable cutaneous lesions. Fifteen of these participants had HIV infection. All of the patients were heavily pretreated with antiretrovirals and other agents, including thalidomide or lenalidomide, and most (17) had advanced KS with tumor-associated edema. The study participants received 5-mg oral pomalidomide once daily for 21 days in 28-day cycles for up to 12 cycles.
Sixteen patients showed an objective tumor response (overall response rate, 73%), including four who achieved a complete response (ORR, 18%). All 7 of the participants who didn’t have HIV showed an objective tumor response (ORR, 100%), as did 9 of the 15 HIV-infected participants (ORR, 60%). Three more participants, including one who was nonadeherent and lost to follow-up, achieved a partial tumor response.
Tumor responses included a decrease in the number of lesions and a decrease in the number of nodular lesions, as well as complete flattening of lesions, resolution of edema, and improvement in appearance. “The latter is particularly important because visible KS is a major source of stigma,” Dr. Polizzotto and his associates said (J Clin Oncol. 2016 Oct 3;34[34]:4125-32).
Two patients reported substantial subjective improvement in foot pain and appearance; one said he was pleased to be able to resume wearing closed shoes, the investigators noted. Treatment response generally was rapid, often commencing before the first follow-up at 4 weeks.
Pomalidomide was generally well tolerated. Adverse effects were frequent but mild and self-limiting, and they included neutropenia, constipation, anemia, fatigue, and rash. No patients required hospitalization, and there were no thromboembolic events. Three study participants developed malignancies after treatment: an Epstein-Barr-virus–associated Hodgkin lymphoma 1 year after the trial, a primary effusion lymphoma 15 months after, and a squamous-cell skin carcinoma. These probably reflect the patients’ underlying immunodeficiency, but the possibility that pomalidomide could contribute to malignancies in this high-risk population should be carefully explored in future studies, the investigators said.
“In resource-rich regions, pomalidomide may be of particular use in HIV-uninfected patients, in patients who have received substantial cumulative doses of anthracyclines, and in patients with less extensive but symptomatic disease for whom avoidance of cytotoxic chemotherapy would be beneficial. In resource-limited regions, there is an urgent need for effective and tolerable oral agents; with appropriate safeguards and monitoring, pomalidomide could address this,” Dr. Polizzotto and his associates wrote.
“Confirmatory studies of pomalidomide, alone and in combination with cytotoxic chemotherapy, are planned, including in sub-Saharan Africa,” they added.
Oral pomalidomide, a derivative of thalidomide with immunomodulatory, antiangiogenic, and antiproliferative properties, proved to be well tolerated and effective against Kaposi’s sarcoma (KS) in a small phase I/II study, investigators reported in the Journal of Clinical Oncology.
There is a substantial need for oral therapies for KS, which often recurs and requires treatment, at least intermittently, for years. Existing treatments are cytotoxic agents, such as anthracyclines that are poorly tolerated and unsuitable for long-term use, said Mark N. Polizzotto, MD, of the National Cancer Institute, Bethesda, Md., and his associates.
They examined the tolerability and efficacy of pomalidomide against KS in a single-center, open-label trial involving 21 men and 1 transgender woman who had at least five evaluable cutaneous lesions. Fifteen of these participants had HIV infection. All of the patients were heavily pretreated with antiretrovirals and other agents, including thalidomide or lenalidomide, and most (17) had advanced KS with tumor-associated edema. The study participants received 5-mg oral pomalidomide once daily for 21 days in 28-day cycles for up to 12 cycles.
Sixteen patients showed an objective tumor response (overall response rate, 73%), including four who achieved a complete response (ORR, 18%). All 7 of the participants who didn’t have HIV showed an objective tumor response (ORR, 100%), as did 9 of the 15 HIV-infected participants (ORR, 60%). Three more participants, including one who was nonadeherent and lost to follow-up, achieved a partial tumor response.
Tumor responses included a decrease in the number of lesions and a decrease in the number of nodular lesions, as well as complete flattening of lesions, resolution of edema, and improvement in appearance. “The latter is particularly important because visible KS is a major source of stigma,” Dr. Polizzotto and his associates said (J Clin Oncol. 2016 Oct 3;34[34]:4125-32).
Two patients reported substantial subjective improvement in foot pain and appearance; one said he was pleased to be able to resume wearing closed shoes, the investigators noted. Treatment response generally was rapid, often commencing before the first follow-up at 4 weeks.
Pomalidomide was generally well tolerated. Adverse effects were frequent but mild and self-limiting, and they included neutropenia, constipation, anemia, fatigue, and rash. No patients required hospitalization, and there were no thromboembolic events. Three study participants developed malignancies after treatment: an Epstein-Barr-virus–associated Hodgkin lymphoma 1 year after the trial, a primary effusion lymphoma 15 months after, and a squamous-cell skin carcinoma. These probably reflect the patients’ underlying immunodeficiency, but the possibility that pomalidomide could contribute to malignancies in this high-risk population should be carefully explored in future studies, the investigators said.
“In resource-rich regions, pomalidomide may be of particular use in HIV-uninfected patients, in patients who have received substantial cumulative doses of anthracyclines, and in patients with less extensive but symptomatic disease for whom avoidance of cytotoxic chemotherapy would be beneficial. In resource-limited regions, there is an urgent need for effective and tolerable oral agents; with appropriate safeguards and monitoring, pomalidomide could address this,” Dr. Polizzotto and his associates wrote.
“Confirmatory studies of pomalidomide, alone and in combination with cytotoxic chemotherapy, are planned, including in sub-Saharan Africa,” they added.
Oral pomalidomide, a derivative of thalidomide with immunomodulatory, antiangiogenic, and antiproliferative properties, proved to be well tolerated and effective against Kaposi’s sarcoma (KS) in a small phase I/II study, investigators reported in the Journal of Clinical Oncology.
There is a substantial need for oral therapies for KS, which often recurs and requires treatment, at least intermittently, for years. Existing treatments are cytotoxic agents, such as anthracyclines that are poorly tolerated and unsuitable for long-term use, said Mark N. Polizzotto, MD, of the National Cancer Institute, Bethesda, Md., and his associates.
They examined the tolerability and efficacy of pomalidomide against KS in a single-center, open-label trial involving 21 men and 1 transgender woman who had at least five evaluable cutaneous lesions. Fifteen of these participants had HIV infection. All of the patients were heavily pretreated with antiretrovirals and other agents, including thalidomide or lenalidomide, and most (17) had advanced KS with tumor-associated edema. The study participants received 5-mg oral pomalidomide once daily for 21 days in 28-day cycles for up to 12 cycles.
Sixteen patients showed an objective tumor response (overall response rate, 73%), including four who achieved a complete response (ORR, 18%). All 7 of the participants who didn’t have HIV showed an objective tumor response (ORR, 100%), as did 9 of the 15 HIV-infected participants (ORR, 60%). Three more participants, including one who was nonadeherent and lost to follow-up, achieved a partial tumor response.
Tumor responses included a decrease in the number of lesions and a decrease in the number of nodular lesions, as well as complete flattening of lesions, resolution of edema, and improvement in appearance. “The latter is particularly important because visible KS is a major source of stigma,” Dr. Polizzotto and his associates said (J Clin Oncol. 2016 Oct 3;34[34]:4125-32).
Two patients reported substantial subjective improvement in foot pain and appearance; one said he was pleased to be able to resume wearing closed shoes, the investigators noted. Treatment response generally was rapid, often commencing before the first follow-up at 4 weeks.
Pomalidomide was generally well tolerated. Adverse effects were frequent but mild and self-limiting, and they included neutropenia, constipation, anemia, fatigue, and rash. No patients required hospitalization, and there were no thromboembolic events. Three study participants developed malignancies after treatment: an Epstein-Barr-virus–associated Hodgkin lymphoma 1 year after the trial, a primary effusion lymphoma 15 months after, and a squamous-cell skin carcinoma. These probably reflect the patients’ underlying immunodeficiency, but the possibility that pomalidomide could contribute to malignancies in this high-risk population should be carefully explored in future studies, the investigators said.
“In resource-rich regions, pomalidomide may be of particular use in HIV-uninfected patients, in patients who have received substantial cumulative doses of anthracyclines, and in patients with less extensive but symptomatic disease for whom avoidance of cytotoxic chemotherapy would be beneficial. In resource-limited regions, there is an urgent need for effective and tolerable oral agents; with appropriate safeguards and monitoring, pomalidomide could address this,” Dr. Polizzotto and his associates wrote.
“Confirmatory studies of pomalidomide, alone and in combination with cytotoxic chemotherapy, are planned, including in sub-Saharan Africa,” they added.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Oral pomalidomide, a derivative of thalidomide with immunomodulatory, antiangiogenic, and antiproliferative properties, proved to be well tolerated and effective against Kaposi’s sarcoma in a small phase I/II study.
Major finding: All 7 of the participants who didn’t have HIV showed an objective tumor response with pomalidomide (ORR, 100%), as did 9 of the 15 HIV-infected participants (ORR, 60%).
Data source: A single-center open-label phase I/II study involving 22 adults with KS, including 15 who had HIV infection.
Disclosures: This study was supported by the National Institutes of Health, the National Cancer Institute, Celgene, and the National Institute of Allergy and Infectious Diseases. Dr. Polizzotto and some of his associates reported that their institutions received research funding from Celgene; one of his associates also reported ties to Ovid, Trek, PTC, Avila, Semorex, and Sorrento.