User login
The hunger game
How do you feel about hunger? Do you trust in its power? Having written one book on picky eating based solely on my mother’s wisdom, supplemented with a scanty amount of Internet-based research, I have spent and continue to spend a good bit of time thinking about hunger.
I have concluded that it is a very powerful force and that when a child gets hungry enough, he will eat, even foods that he has previously rejected. It is that assumption that is at the core of my advice to parents of picky eaters. I suspect that many of you share that same philosophy and recommend a strategy that is heavy on patience. Of course the problem lies in getting parents to adopt that attitude and accept the fact that if they just present a healthy diet and step back, hunger will eventually win, and the child will eat.

However, the devil is in the details. Have the parents set rules that will prevent the child from overdrinking? Have they really stopped talking about what the child, and everyone else in the family, is or isn’t eating? Are the parents setting good examples with their own eating habits and comments about food?
Because 99% of my patient population have been healthy, I have always felt comfortable relying on the power of hunger to win the battle over picky eating. If properly managed, none of my patients was going to die or suffer permanent consequences from picky eating. However, I have always wondered whether hunger could be leveraged to safely manage selective eating in children with serious health problems. I have a suspicion that it would succeed, but luckily I have never been presented with a case to test my hunch.
I recently read a very personal account written by the mother of a child with severe congenital cardiac disease that supports my gut feeling that when carefully monitored, starvation can be an effective strategy in managing selective eating (“When Your Baby Won’t Eat,” by Virginia Sole-Smith, The New York Times Magazine, Feb. 4, 2016). Three surgeries in the first few months of life necessitated that the child be fed by gavage. Attempts at breastfeeding failed, as it often does in situations like this. Struggles with gavage tube placement at home became such an emotionally traumatic ordeal that eventually a gastrostomy tube was placed when the child was 6 months old.
The family was led to believe that an important window in the child’s oral development had closed as a result of interventions necessitated by the child’s cardiac malformations. Although she was neurologically and physically capable of eating, getting her to do so was going to require long-term behavior modification, and there was no guarantee that this approach would completely undo what bad luck and prior management strategies had created. She might never relate to food as a normal child does.
After several attempts at behavior management using one-to-one reinforcement, this mother began to do some research. She discovered that of the nearly 30 feeding programs in children’s hospitals and private clinics, almost all use variations of a similar behavior modification strategy that had not worked for her daughter. As she observed: “This behavioral model presumes that children who don’t eat need external motivation.”
Eventually, the family found help in one of the few feeding programs in the United States that has adopted a dramatically different “child-centered” approach in which “therapists believe that all children have some internal motivation to eat, as well as an innate ability to effectively self-regulate their intake.” The solution to this child’s problem didn’t occur overnight. It began by exposing the child to a variety of foods in situations free of attempts to get her to eat – no coercion or rewards, regardless of how subtle they might have seemed. Once the child was experimenting with food, her tube feedings were gradually decreased in volume and caloric content. And, voila! Hunger won and the child began meeting her total nutritional needs by eating, in some cases with gusto.
Of course I was easy to convince because the results confirmed my hunch. But, do you believe that hunger can and should be used as the centerpiece in the management of selective eating, even in cases well beyond the parameters of garden variety picky eating? Are you willing to play the hunger game along with me?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
How do you feel about hunger? Do you trust in its power? Having written one book on picky eating based solely on my mother’s wisdom, supplemented with a scanty amount of Internet-based research, I have spent and continue to spend a good bit of time thinking about hunger.
I have concluded that it is a very powerful force and that when a child gets hungry enough, he will eat, even foods that he has previously rejected. It is that assumption that is at the core of my advice to parents of picky eaters. I suspect that many of you share that same philosophy and recommend a strategy that is heavy on patience. Of course the problem lies in getting parents to adopt that attitude and accept the fact that if they just present a healthy diet and step back, hunger will eventually win, and the child will eat.
However, the devil is in the details. Have the parents set rules that will prevent the child from overdrinking? Have they really stopped talking about what the child, and everyone else in the family, is or isn’t eating? Are the parents setting good examples with their own eating habits and comments about food?
Because 99% of my patient population have been healthy, I have always felt comfortable relying on the power of hunger to win the battle over picky eating. If properly managed, none of my patients was going to die or suffer permanent consequences from picky eating. However, I have always wondered whether hunger could be leveraged to safely manage selective eating in children with serious health problems. I have a suspicion that it would succeed, but luckily I have never been presented with a case to test my hunch.
I recently read a very personal account written by the mother of a child with severe congenital cardiac disease that supports my gut feeling that when carefully monitored, starvation can be an effective strategy in managing selective eating (“When Your Baby Won’t Eat,” by Virginia Sole-Smith, The New York Times Magazine, Feb. 4, 2016). Three surgeries in the first few months of life necessitated that the child be fed by gavage. Attempts at breastfeeding failed, as it often does in situations like this. Struggles with gavage tube placement at home became such an emotionally traumatic ordeal that eventually a gastrostomy tube was placed when the child was 6 months old.
The family was led to believe that an important window in the child’s oral development had closed as a result of interventions necessitated by the child’s cardiac malformations. Although she was neurologically and physically capable of eating, getting her to do so was going to require long-term behavior modification, and there was no guarantee that this approach would completely undo what bad luck and prior management strategies had created. She might never relate to food as a normal child does.
After several attempts at behavior management using one-to-one reinforcement, this mother began to do some research. She discovered that of the nearly 30 feeding programs in children’s hospitals and private clinics, almost all use variations of a similar behavior modification strategy that had not worked for her daughter. As she observed: “This behavioral model presumes that children who don’t eat need external motivation.”
Eventually, the family found help in one of the few feeding programs in the United States that has adopted a dramatically different “child-centered” approach in which “therapists believe that all children have some internal motivation to eat, as well as an innate ability to effectively self-regulate their intake.” The solution to this child’s problem didn’t occur overnight. It began by exposing the child to a variety of foods in situations free of attempts to get her to eat – no coercion or rewards, regardless of how subtle they might have seemed. Once the child was experimenting with food, her tube feedings were gradually decreased in volume and caloric content. And, voila! Hunger won and the child began meeting her total nutritional needs by eating, in some cases with gusto.
Of course I was easy to convince because the results confirmed my hunch. But, do you believe that hunger can and should be used as the centerpiece in the management of selective eating, even in cases well beyond the parameters of garden variety picky eating? Are you willing to play the hunger game along with me?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
How do you feel about hunger? Do you trust in its power? Having written one book on picky eating based solely on my mother’s wisdom, supplemented with a scanty amount of Internet-based research, I have spent and continue to spend a good bit of time thinking about hunger.
I have concluded that it is a very powerful force and that when a child gets hungry enough, he will eat, even foods that he has previously rejected. It is that assumption that is at the core of my advice to parents of picky eaters. I suspect that many of you share that same philosophy and recommend a strategy that is heavy on patience. Of course the problem lies in getting parents to adopt that attitude and accept the fact that if they just present a healthy diet and step back, hunger will eventually win, and the child will eat.
However, the devil is in the details. Have the parents set rules that will prevent the child from overdrinking? Have they really stopped talking about what the child, and everyone else in the family, is or isn’t eating? Are the parents setting good examples with their own eating habits and comments about food?
Because 99% of my patient population have been healthy, I have always felt comfortable relying on the power of hunger to win the battle over picky eating. If properly managed, none of my patients was going to die or suffer permanent consequences from picky eating. However, I have always wondered whether hunger could be leveraged to safely manage selective eating in children with serious health problems. I have a suspicion that it would succeed, but luckily I have never been presented with a case to test my hunch.
I recently read a very personal account written by the mother of a child with severe congenital cardiac disease that supports my gut feeling that when carefully monitored, starvation can be an effective strategy in managing selective eating (“When Your Baby Won’t Eat,” by Virginia Sole-Smith, The New York Times Magazine, Feb. 4, 2016). Three surgeries in the first few months of life necessitated that the child be fed by gavage. Attempts at breastfeeding failed, as it often does in situations like this. Struggles with gavage tube placement at home became such an emotionally traumatic ordeal that eventually a gastrostomy tube was placed when the child was 6 months old.
The family was led to believe that an important window in the child’s oral development had closed as a result of interventions necessitated by the child’s cardiac malformations. Although she was neurologically and physically capable of eating, getting her to do so was going to require long-term behavior modification, and there was no guarantee that this approach would completely undo what bad luck and prior management strategies had created. She might never relate to food as a normal child does.
After several attempts at behavior management using one-to-one reinforcement, this mother began to do some research. She discovered that of the nearly 30 feeding programs in children’s hospitals and private clinics, almost all use variations of a similar behavior modification strategy that had not worked for her daughter. As she observed: “This behavioral model presumes that children who don’t eat need external motivation.”
Eventually, the family found help in one of the few feeding programs in the United States that has adopted a dramatically different “child-centered” approach in which “therapists believe that all children have some internal motivation to eat, as well as an innate ability to effectively self-regulate their intake.” The solution to this child’s problem didn’t occur overnight. It began by exposing the child to a variety of foods in situations free of attempts to get her to eat – no coercion or rewards, regardless of how subtle they might have seemed. Once the child was experimenting with food, her tube feedings were gradually decreased in volume and caloric content. And, voila! Hunger won and the child began meeting her total nutritional needs by eating, in some cases with gusto.
Of course I was easy to convince because the results confirmed my hunch. But, do you believe that hunger can and should be used as the centerpiece in the management of selective eating, even in cases well beyond the parameters of garden variety picky eating? Are you willing to play the hunger game along with me?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

ISC: Thrombectomy shown highly cost-effective for stroke
LOS ANGELES – Endovascular thrombectomy is not only clinically the best option for many patients with acute, ischemic strokes involving a proximal occlusion in a large cerebral artery; it’s also highly cost effective, based on follow-up analyses of two of the five randomized trials published in 2015 that collectively established thrombectomy as standard of care for these patients.
Thrombectomy plus administration of intravenous tissue plasminogen activator (TPA), compared with TPA only, “is highly cost effective and economically dominant with lower long-term cost and better outcomes,” Theresa I. Shireman, Ph.D., said at the International Stroke Conference.

And in an independent analysis of data from a totally different trial, endovascular thrombectomy on average reduced patients’ acute length of hospitalization, improved their survival and quality of life, and was cost saving when compared with treatment with intravenous TPA only, which had previously been the standard of care, Dr. Bruce C.V. Campbell reported at the meeting.
The analysis presented by Dr. Shireman used data collected in the SWIFT-PRIME trial, which randomized 196 patients at centers in the United States and Europe to treatment with either intravenous TPA plus endovascular thrombectomy or TPA alone. Average total costs during the index hospitalization ran to roughly $46,000 in the combined-treatment arm and about $29,000 in the TPA-only arm, a difference largely driven by a roughly $15,000 average incremental cost for the thrombectomy procedure, said Dr. Shireman, professor of health services research at Brown University in Providence, R.I.
However, the cost-effectiveness of thrombectomy began to kick in soon after. During the 90 days following index hospitalization, patients who underwent thrombectomy had substantial average reductions in their need for inpatient rehabilitation, time spent in skilled nursing facilities, and in outpatient rehabilitation. Overall, total medical costs during the first 90 days post discharge ran on average close to $5,000 less per patient following thrombectomy. In addition, based on their health status after 90 days, patients treated with thrombectomy were projected to have a greater than 1.7-year average life expectancy than those randomized to TPA only, with a projected net gain of 1.74 quality-adjusted life years (QALY) per patient and with a projected average decrease of roughly $23,000 in total lifetime medical costs.

Based on this average increase in QALYs and decreased long-term cost, adding thrombectomy to TPA for routine treatment of the types of patients enrolled in SWIFT-PRIME was economically dominant, Dr. Shireman said at the meeting sponsored by the American Heart Association. She also projected that despite the higher upfront cost for adding thrombectomy to treatment, the eventual savings in long-term care meant that thrombectomy began producing a net saving once patients survived for more than 22 months following their index hospitalization.
Dr. Campbell reported very similar findings in his analysis of data collected from the EXTEND-IA trial, which randomized 70 patients at 10 centers in Australia and New Zealand. During the first 90 days of treatment, including the index hospitalization, treatment with thrombectomy plus TPA saved an average of roughly $4,000 U.S.per patient, compared with TPA only, even though the average incremental cost for adding thrombectomy was nearly $11,000 U.S. The overall increased total 90-day costs with TPA only was largely driven by a substantially longer time spent hospitalized among the TPA-only patients, compared with those treated with thrombectomy plus TPA, said Dr. Campbell, a neurologist and head of hyperacute stroke at Royal Melbourne Hospital.
In addition, adding thrombectomy resulted in a projected average 4-year increase in life expectancy, and an average gain of about 3 QALYs per patient. Thrombectomy “is an incredibly powerful procedure, not just in terms of clinical response but also in terms of economics,” he concluded. Even when judged by the worst-case scenario of the analysis, “there is a 100% probability that the cost-effectiveness per QALY is less than $10,000 U.S., which is incredible value,” Dr. Campbell said.
SWIFT-PRIME was sponsored by Covidien/Medtronic. EXTEND-IA received partial funding through an unrestricted grant from Covidien/Medtronic. Dr. Shireman and Dr. Campbell had no personal disclosures.
On Twitter @mitchelzoler
LOS ANGELES – Endovascular thrombectomy is not only clinically the best option for many patients with acute, ischemic strokes involving a proximal occlusion in a large cerebral artery; it’s also highly cost effective, based on follow-up analyses of two of the five randomized trials published in 2015 that collectively established thrombectomy as standard of care for these patients.
Thrombectomy plus administration of intravenous tissue plasminogen activator (TPA), compared with TPA only, “is highly cost effective and economically dominant with lower long-term cost and better outcomes,” Theresa I. Shireman, Ph.D., said at the International Stroke Conference.
And in an independent analysis of data from a totally different trial, endovascular thrombectomy on average reduced patients’ acute length of hospitalization, improved their survival and quality of life, and was cost saving when compared with treatment with intravenous TPA only, which had previously been the standard of care, Dr. Bruce C.V. Campbell reported at the meeting.
The analysis presented by Dr. Shireman used data collected in the SWIFT-PRIME trial, which randomized 196 patients at centers in the United States and Europe to treatment with either intravenous TPA plus endovascular thrombectomy or TPA alone. Average total costs during the index hospitalization ran to roughly $46,000 in the combined-treatment arm and about $29,000 in the TPA-only arm, a difference largely driven by a roughly $15,000 average incremental cost for the thrombectomy procedure, said Dr. Shireman, professor of health services research at Brown University in Providence, R.I.
However, the cost-effectiveness of thrombectomy began to kick in soon after. During the 90 days following index hospitalization, patients who underwent thrombectomy had substantial average reductions in their need for inpatient rehabilitation, time spent in skilled nursing facilities, and in outpatient rehabilitation. Overall, total medical costs during the first 90 days post discharge ran on average close to $5,000 less per patient following thrombectomy. In addition, based on their health status after 90 days, patients treated with thrombectomy were projected to have a greater than 1.7-year average life expectancy than those randomized to TPA only, with a projected net gain of 1.74 quality-adjusted life years (QALY) per patient and with a projected average decrease of roughly $23,000 in total lifetime medical costs.
Based on this average increase in QALYs and decreased long-term cost, adding thrombectomy to TPA for routine treatment of the types of patients enrolled in SWIFT-PRIME was economically dominant, Dr. Shireman said at the meeting sponsored by the American Heart Association. She also projected that despite the higher upfront cost for adding thrombectomy to treatment, the eventual savings in long-term care meant that thrombectomy began producing a net saving once patients survived for more than 22 months following their index hospitalization.
Dr. Campbell reported very similar findings in his analysis of data collected from the EXTEND-IA trial, which randomized 70 patients at 10 centers in Australia and New Zealand. During the first 90 days of treatment, including the index hospitalization, treatment with thrombectomy plus TPA saved an average of roughly $4,000 U.S.per patient, compared with TPA only, even though the average incremental cost for adding thrombectomy was nearly $11,000 U.S. The overall increased total 90-day costs with TPA only was largely driven by a substantially longer time spent hospitalized among the TPA-only patients, compared with those treated with thrombectomy plus TPA, said Dr. Campbell, a neurologist and head of hyperacute stroke at Royal Melbourne Hospital.
In addition, adding thrombectomy resulted in a projected average 4-year increase in life expectancy, and an average gain of about 3 QALYs per patient. Thrombectomy “is an incredibly powerful procedure, not just in terms of clinical response but also in terms of economics,” he concluded. Even when judged by the worst-case scenario of the analysis, “there is a 100% probability that the cost-effectiveness per QALY is less than $10,000 U.S., which is incredible value,” Dr. Campbell said.
SWIFT-PRIME was sponsored by Covidien/Medtronic. EXTEND-IA received partial funding through an unrestricted grant from Covidien/Medtronic. Dr. Shireman and Dr. Campbell had no personal disclosures.
On Twitter @mitchelzoler
LOS ANGELES – Endovascular thrombectomy is not only clinically the best option for many patients with acute, ischemic strokes involving a proximal occlusion in a large cerebral artery; it’s also highly cost effective, based on follow-up analyses of two of the five randomized trials published in 2015 that collectively established thrombectomy as standard of care for these patients.
Thrombectomy plus administration of intravenous tissue plasminogen activator (TPA), compared with TPA only, “is highly cost effective and economically dominant with lower long-term cost and better outcomes,” Theresa I. Shireman, Ph.D., said at the International Stroke Conference.
And in an independent analysis of data from a totally different trial, endovascular thrombectomy on average reduced patients’ acute length of hospitalization, improved their survival and quality of life, and was cost saving when compared with treatment with intravenous TPA only, which had previously been the standard of care, Dr. Bruce C.V. Campbell reported at the meeting.
The analysis presented by Dr. Shireman used data collected in the SWIFT-PRIME trial, which randomized 196 patients at centers in the United States and Europe to treatment with either intravenous TPA plus endovascular thrombectomy or TPA alone. Average total costs during the index hospitalization ran to roughly $46,000 in the combined-treatment arm and about $29,000 in the TPA-only arm, a difference largely driven by a roughly $15,000 average incremental cost for the thrombectomy procedure, said Dr. Shireman, professor of health services research at Brown University in Providence, R.I.
However, the cost-effectiveness of thrombectomy began to kick in soon after. During the 90 days following index hospitalization, patients who underwent thrombectomy had substantial average reductions in their need for inpatient rehabilitation, time spent in skilled nursing facilities, and in outpatient rehabilitation. Overall, total medical costs during the first 90 days post discharge ran on average close to $5,000 less per patient following thrombectomy. In addition, based on their health status after 90 days, patients treated with thrombectomy were projected to have a greater than 1.7-year average life expectancy than those randomized to TPA only, with a projected net gain of 1.74 quality-adjusted life years (QALY) per patient and with a projected average decrease of roughly $23,000 in total lifetime medical costs.
Based on this average increase in QALYs and decreased long-term cost, adding thrombectomy to TPA for routine treatment of the types of patients enrolled in SWIFT-PRIME was economically dominant, Dr. Shireman said at the meeting sponsored by the American Heart Association. She also projected that despite the higher upfront cost for adding thrombectomy to treatment, the eventual savings in long-term care meant that thrombectomy began producing a net saving once patients survived for more than 22 months following their index hospitalization.
Dr. Campbell reported very similar findings in his analysis of data collected from the EXTEND-IA trial, which randomized 70 patients at 10 centers in Australia and New Zealand. During the first 90 days of treatment, including the index hospitalization, treatment with thrombectomy plus TPA saved an average of roughly $4,000 U.S.per patient, compared with TPA only, even though the average incremental cost for adding thrombectomy was nearly $11,000 U.S. The overall increased total 90-day costs with TPA only was largely driven by a substantially longer time spent hospitalized among the TPA-only patients, compared with those treated with thrombectomy plus TPA, said Dr. Campbell, a neurologist and head of hyperacute stroke at Royal Melbourne Hospital.
In addition, adding thrombectomy resulted in a projected average 4-year increase in life expectancy, and an average gain of about 3 QALYs per patient. Thrombectomy “is an incredibly powerful procedure, not just in terms of clinical response but also in terms of economics,” he concluded. Even when judged by the worst-case scenario of the analysis, “there is a 100% probability that the cost-effectiveness per QALY is less than $10,000 U.S., which is incredible value,” Dr. Campbell said.
SWIFT-PRIME was sponsored by Covidien/Medtronic. EXTEND-IA received partial funding through an unrestricted grant from Covidien/Medtronic. Dr. Shireman and Dr. Campbell had no personal disclosures.
On Twitter @mitchelzoler
AT THE INTERNATIONAL STROKE CONFERENCE
Key clinical point: Adding endovascular thrombectomy to TPA treatment for selected patients with acute, ischemic stroke proved highly cost effective on the basis of data collected in two independent randomized trials.
Major finding: In SWIFT-PRIME, thrombectomy saved a projected average of $23,000 in lifetime health care costs and added 1.74 QALYs.
Data source: SWIFT-PRIME, an international, multicenter, randomized trial that enrolled 196 patients.
Disclosures: SWIFT-PRIME was sponsored by Covidien/Medtronic. EXTEND-IA received partial funding through an unrestricted grant from Covidien/Medtronic. Dr. Shireman and Dr. Campbell had no personal disclosures.

The Great Masquerader
1. Several weeks ago, this 56-year-old man noticed numerous asymptomatic round macules and papules on his palms and soles, many with scaly peripheral margins. Similar lesions are noted on the penile corona and glans. There is a faint but definite morbiliform, blanchable pink rash covering most of the patient’s trunk, taking on a “shawl” distribution across the shoulders. The patient is exclusively homosexual and recently engaged in high-risk sexual activity.

| 
|
Diagnosis: It would be hard to imagine a more classic example of secondary syphilis than was seen in this case, occurring in a patient so obviously at risk. But it’s only “obvious” if you’re ready and aware of how syphilis manifests. It also helps if you understand how common it is and who’s likely to get it.
TAKE-HOME LEARNING POINTS
• Palmar and plantar rashes are unusual and should prompt the examiner to expand the history and physical.
• Secondary syphilis, though uncommon, is far from rare, especially among gay men engaging in high-risk sexual behavior.
• It’s common for the patient to deny the appearance of the chancre of primary syphilis, and such a lesion would be long gone by the time those of secondary syphilis manifest.
• Conditions involving the skin should be seen by a dermatology provider, regardless of location. This includes diseases of the skin, hair, nails, oral mucosa, genitals, feet, or palms. One potential exception is the eye itself, though most diseases “of the eye” are, in reality, diseases of the periocular skin—and belong with a dermatology provider.
For more information on this case, see “When There’s More to the Story ….” Clin Rev. 2013;12;2013(12):W2.
For the next photograph, proceed to the next page >>
2. First appearing a month ago, this rash was first confined to the patient’s abdomen and subsequently spread. The blanchable, erythematous papules and nodules are fairly dense, uniformly covering most of his skin but sparing face and soles. Two 7-mm scaly brown nodules are seen on his right palm. There are no palpable nodes in the usual locations. More than 10 years ago, the patient was diagnosed with HIV, which is well controlled with medication. Homosexually active, he denies having any new contacts.

Diagnosis: This case presents a fairly typical clinical picture of secondary syphilis—a diagnosis that requires confirmation with syphilis serology: rapid plasma reagin (RPR) or Venereal Disease Research Laboratory (VDRL) testing. The latter measures antibodies to the lipids formed by the host against lipids formed on the treponemal cell surface.
In this case, the diagnosis had to be confirmed by more specific treponemal tests, usually conducted by the local health department, to which positive results must be reported. If further testing confirms the diagnosis (as expected), the patient will be treated by the health department. Investigators will question him, attempting to determine the source of the infection and thereby quell an outbreak.
For more information on this case, see “Unusual Cause for Asymptomatic Rash.” Clin Rev. 2013;23(9):W6.
For the next photograph, proceed to the next page >>
3. A 43-year-old man presented with a rapidly enlarging ulcerated nodule on the right ankle with a necrotic and crusted center. He also had multiple red-brown papules on the trunk and extremities. Some of these lesions had central erosions, while others had surface scale. He was known to be HIV positive but had no lymphadenopathy.

Diagnosis: Lues maligna is used to describe a rare noduloulcerative form of secondary syphilis.1 It was first described in 18592 and has been associated with other disorders such as diabetes mellitus3 and chronic alcoholism.4 Patients usually are gravely ill and develop polymorphic ulcerating lesions. Facial and scalp involvement are common, but patients typically do not have palmoplantar involvement in conventional presentations of secondary syphilis.
…The patient’s rapid plasma reagin titer at the time of the fourth biopsy was 1:256, and appropriate treatment with penicillin resulted in complete clearance of the lesions in 3 to 4 weeks.
For more information on this case, see “Rapidly Enlarging Noduloulcerative Lesions.” Cutis. 2014;94(3):E20-E22.
Photograph and case description courtesy of Cutis. 2014;94(3):E20-E22.
Related article
Man, 54, With Delusions and Seizures
2011;21(4):20, 22, 24
1. Several weeks ago, this 56-year-old man noticed numerous asymptomatic round macules and papules on his palms and soles, many with scaly peripheral margins. Similar lesions are noted on the penile corona and glans. There is a faint but definite morbiliform, blanchable pink rash covering most of the patient’s trunk, taking on a “shawl” distribution across the shoulders. The patient is exclusively homosexual and recently engaged in high-risk sexual activity.
|
|
|
Diagnosis: It would be hard to imagine a more classic example of secondary syphilis than was seen in this case, occurring in a patient so obviously at risk. But it’s only “obvious” if you’re ready and aware of how syphilis manifests. It also helps if you understand how common it is and who’s likely to get it.
TAKE-HOME LEARNING POINTS
• Palmar and plantar rashes are unusual and should prompt the examiner to expand the history and physical.
• Secondary syphilis, though uncommon, is far from rare, especially among gay men engaging in high-risk sexual behavior.
• It’s common for the patient to deny the appearance of the chancre of primary syphilis, and such a lesion would be long gone by the time those of secondary syphilis manifest.
• Conditions involving the skin should be seen by a dermatology provider, regardless of location. This includes diseases of the skin, hair, nails, oral mucosa, genitals, feet, or palms. One potential exception is the eye itself, though most diseases “of the eye” are, in reality, diseases of the periocular skin—and belong with a dermatology provider.
For more information on this case, see “When There’s More to the Story ….” Clin Rev. 2013;12;2013(12):W2.
For the next photograph, proceed to the next page >>
2. First appearing a month ago, this rash was first confined to the patient’s abdomen and subsequently spread. The blanchable, erythematous papules and nodules are fairly dense, uniformly covering most of his skin but sparing face and soles. Two 7-mm scaly brown nodules are seen on his right palm. There are no palpable nodes in the usual locations. More than 10 years ago, the patient was diagnosed with HIV, which is well controlled with medication. Homosexually active, he denies having any new contacts.
Diagnosis: This case presents a fairly typical clinical picture of secondary syphilis—a diagnosis that requires confirmation with syphilis serology: rapid plasma reagin (RPR) or Venereal Disease Research Laboratory (VDRL) testing. The latter measures antibodies to the lipids formed by the host against lipids formed on the treponemal cell surface.
In this case, the diagnosis had to be confirmed by more specific treponemal tests, usually conducted by the local health department, to which positive results must be reported. If further testing confirms the diagnosis (as expected), the patient will be treated by the health department. Investigators will question him, attempting to determine the source of the infection and thereby quell an outbreak.
For more information on this case, see “Unusual Cause for Asymptomatic Rash.” Clin Rev. 2013;23(9):W6.
For the next photograph, proceed to the next page >>
3. A 43-year-old man presented with a rapidly enlarging ulcerated nodule on the right ankle with a necrotic and crusted center. He also had multiple red-brown papules on the trunk and extremities. Some of these lesions had central erosions, while others had surface scale. He was known to be HIV positive but had no lymphadenopathy.
Diagnosis: Lues maligna is used to describe a rare noduloulcerative form of secondary syphilis.1 It was first described in 18592 and has been associated with other disorders such as diabetes mellitus3 and chronic alcoholism.4 Patients usually are gravely ill and develop polymorphic ulcerating lesions. Facial and scalp involvement are common, but patients typically do not have palmoplantar involvement in conventional presentations of secondary syphilis.
…The patient’s rapid plasma reagin titer at the time of the fourth biopsy was 1:256, and appropriate treatment with penicillin resulted in complete clearance of the lesions in 3 to 4 weeks.
For more information on this case, see “Rapidly Enlarging Noduloulcerative Lesions.” Cutis. 2014;94(3):E20-E22.
Photograph and case description courtesy of Cutis. 2014;94(3):E20-E22.
Related article
Man, 54, With Delusions and Seizures
2011;21(4):20, 22, 24
1. Several weeks ago, this 56-year-old man noticed numerous asymptomatic round macules and papules on his palms and soles, many with scaly peripheral margins. Similar lesions are noted on the penile corona and glans. There is a faint but definite morbiliform, blanchable pink rash covering most of the patient’s trunk, taking on a “shawl” distribution across the shoulders. The patient is exclusively homosexual and recently engaged in high-risk sexual activity.
|
|
|
Diagnosis: It would be hard to imagine a more classic example of secondary syphilis than was seen in this case, occurring in a patient so obviously at risk. But it’s only “obvious” if you’re ready and aware of how syphilis manifests. It also helps if you understand how common it is and who’s likely to get it.
TAKE-HOME LEARNING POINTS
• Palmar and plantar rashes are unusual and should prompt the examiner to expand the history and physical.
• Secondary syphilis, though uncommon, is far from rare, especially among gay men engaging in high-risk sexual behavior.
• It’s common for the patient to deny the appearance of the chancre of primary syphilis, and such a lesion would be long gone by the time those of secondary syphilis manifest.
• Conditions involving the skin should be seen by a dermatology provider, regardless of location. This includes diseases of the skin, hair, nails, oral mucosa, genitals, feet, or palms. One potential exception is the eye itself, though most diseases “of the eye” are, in reality, diseases of the periocular skin—and belong with a dermatology provider.
For more information on this case, see “When There’s More to the Story ….” Clin Rev. 2013;12;2013(12):W2.
For the next photograph, proceed to the next page >>
2. First appearing a month ago, this rash was first confined to the patient’s abdomen and subsequently spread. The blanchable, erythematous papules and nodules are fairly dense, uniformly covering most of his skin but sparing face and soles. Two 7-mm scaly brown nodules are seen on his right palm. There are no palpable nodes in the usual locations. More than 10 years ago, the patient was diagnosed with HIV, which is well controlled with medication. Homosexually active, he denies having any new contacts.
Diagnosis: This case presents a fairly typical clinical picture of secondary syphilis—a diagnosis that requires confirmation with syphilis serology: rapid plasma reagin (RPR) or Venereal Disease Research Laboratory (VDRL) testing. The latter measures antibodies to the lipids formed by the host against lipids formed on the treponemal cell surface.
In this case, the diagnosis had to be confirmed by more specific treponemal tests, usually conducted by the local health department, to which positive results must be reported. If further testing confirms the diagnosis (as expected), the patient will be treated by the health department. Investigators will question him, attempting to determine the source of the infection and thereby quell an outbreak.
For more information on this case, see “Unusual Cause for Asymptomatic Rash.” Clin Rev. 2013;23(9):W6.
For the next photograph, proceed to the next page >>
3. A 43-year-old man presented with a rapidly enlarging ulcerated nodule on the right ankle with a necrotic and crusted center. He also had multiple red-brown papules on the trunk and extremities. Some of these lesions had central erosions, while others had surface scale. He was known to be HIV positive but had no lymphadenopathy.
Diagnosis: Lues maligna is used to describe a rare noduloulcerative form of secondary syphilis.1 It was first described in 18592 and has been associated with other disorders such as diabetes mellitus3 and chronic alcoholism.4 Patients usually are gravely ill and develop polymorphic ulcerating lesions. Facial and scalp involvement are common, but patients typically do not have palmoplantar involvement in conventional presentations of secondary syphilis.
…The patient’s rapid plasma reagin titer at the time of the fourth biopsy was 1:256, and appropriate treatment with penicillin resulted in complete clearance of the lesions in 3 to 4 weeks.
For more information on this case, see “Rapidly Enlarging Noduloulcerative Lesions.” Cutis. 2014;94(3):E20-E22.
Photograph and case description courtesy of Cutis. 2014;94(3):E20-E22.
Related article
Man, 54, With Delusions and Seizures
2011;21(4):20, 22, 24
Opicapone May Reduce Off Time for Patients With Parkinson’s Disease
Administering 50 mg of opicapone as an adjunct to levodopa treatment decreases the amount of off time by approximately 61 minutes, compared with placebo, for patients with Parkinson’s disease and end-of-dose motor fluctuations, according to research published in the February issue of Lancet Neurology. Data indicate that the drug is safe, well tolerated, and noninferior to entacapone for this indication.
Opicapone is “the only once-daily catechol-O-methyltransferase (COMT) inhibitor to provide a mean reduction in time in the off state that is clinically relevant,” said Joaquim J. Ferreira, MD, Professor of Neurology and Clinical Pharmacology at the University of Lisbon, and colleagues. Administering the drug once daily could simplify a patient’s drug regimen by permitting the physician to decrease the total daily levodopa dose, increase the dosing interval, and reduce the number of intakes, thereby maximizing the benefit of therapy, he added.
Comparing Opicapone, Entacapone, and Placebo
The half-life of oral levodopa is between 60 and 90 minutes and is linked with end-of-dose motor fluctuations. COMT inhibitors increase the plasma elimination half-life of levodopa and decrease peak–trough variations. Entacapone, a COMT inhibitor, provides moderate reductions in daily off time, but needs to be administered with each dose of levodopa. Neurologists thus have sought a more effective COMT inhibitor that can be used easily in clinical practice.
Dr. Ferreira and colleagues assessed the safety and efficacy of opicapone as an adjunct to levodopa, compared with placebo and entacapone, in patients with Parkinson’s disease and motor fluctuations. Eligible participants had had a clinical diagnosis of Parkinson’s disease for at least three years, a Hoehn and Yahr stage of 1 to 3 during the on state, and at least one year of clinical improvement with levodopa treatment. People who had used entacapone previously, had significant dyskinesia disability, or had severe or unpredictable off periods were excluded from the study.
Equal groups of patients were computer randomized to once-daily opicapone (5 mg, 25 mg, or 50 mg), placebo, or 200 mg of entacapone with every levodopa intake. The participants and investigators were blinded to treatment allocation throughout the study. Opicapone capsules and entacapone tablets were overencapsulated to maintain blinding.
Doses of study drugs were given concomitantly with each levodopa intake. Patients in the opicapone groups received placebo for the daytime doses and active treatment for the bedtime dose. Patients in the entacapone group took the active treatment during the day and placebo as the bedtime dose. Investigators assessed participants at screening, baseline, and at five subsequent time points.
The study’s primary end point was the change from baseline to the end of study treatment in absolute off time, as assessed by daily patient diaries. Secondary end points included the change from baseline to the end of study treatment in the proportion of patients who had at least a one-hour reduction in absolute off time and the change from baseline to the end of study treatment in the proportion of patients who had at least a one-hour increase in absolute total on time.
For statistical analysis, population sets were defined as the full analysis set, which included all randomly assigned patients who took at least one dose of study drug and had at least one assessment of time in the off state after baseline; the per-protocol set, which included all patients in the full analysis set who did not have any major protocol deviations; and the safety set, which included all patients who received at least one dose of study drug.
Opicapone Was Noninferior to Entacapone
The researchers enrolled 600 patients, of whom 121 received placebo, 122 received 200 mg of entacapone, 122 received 5 mg of opicapone, 119 received 25 mg of opicapone, and 116 received 50 mg of opicapone. The full analysis included 590 patients, and the per-protocol analysis included 537 patients. In all, 542 patients completed the study. Patient demographics, baseline Parkinson’s disease characteristics, and treatment history did not differ between the treatment groups in the safety analysis.
In the full analysis, the adjusted mean change from baseline in absolute off time was –116.8 minutes in the opicapone 50 mg group, compared with –96.3 minutes in the entacapone group, –91.3 minutes in the opicapone 5 mg group, –85.9 minutes in the opicapone 25 mg group, and –56.0 minutes in the placebo group. The per-protocol analysis yielded similar results.
The investigators only tested the 50-mg dose of opicapone for noninferiority of absolute off time. This treatment was superior to placebo and noninferior to entacapone. The researchers found no significant differences between placebo and opicapone 5 mg or opicapone 25 mg. Entacapone was superior to placebo.
Compared with placebo, the proportion of patients with a reduction in off time of at least one hour was significantly higher in patient who received 25 mg or 50 mg of opicapone, and the proportion of patients with an increase in on time of at least one hour was significantly higher in patients who received 50 mg of opicapone. No significant differences were noted in off and on state rates for entacapone versus placebo. Results for the other secondary end points supported those of the primary analysis.
Adverse Events Were Uncommon
The percentage of patients who discontinued because of treatment-emergent adverse events was low and similar across the treatment groups. The most common treatment-emergent adverse events leading to discontinuation were diarrhea, visual hallucinations, and dyskinesia. Dyskinesia was the most frequently reported treatment-emergent adverse event possibly related to the study drug, and the highest incidence occurred in the opicapone groups. Approximately 80% of treatment-emergent dyskinesias occurred in patients in all groups who already had dyskinesia at baseline. The incidence of serious treatment-emergent adverse events was low (ie, 7% or less) in all groups, and 35% of these events were judged to be unrelated to the study drug.
“The beneficial effects of opicapone 50 mg at reducing the time in the off state were accompanied by a corresponding increase in time in the on state without troublesome dyskinesia, whereas the duration of time in the on state with troublesome dyskinesia did not change,” said Dr. Ferreira. The study results “suggest an overall positive risk-to-benefit ratio for the use of opicapone in patients with Parkinson’s disease with end-of-dose motor fluctuations,” he added. Results of the authors’ open-label extension study will be published in the future.
—Erik Greb
Suggested Reading
Ferreira JJ, Lees A, Rocha JF, et al. Opicapone as an adjunct to levodopa in patients with Parkinson’s disease and end-of-dose motor fluctuations: a randomised, double-blind, controlled trial. Lancet Neurol. 2016;15(2):154-165.
Administering 50 mg of opicapone as an adjunct to levodopa treatment decreases the amount of off time by approximately 61 minutes, compared with placebo, for patients with Parkinson’s disease and end-of-dose motor fluctuations, according to research published in the February issue of Lancet Neurology. Data indicate that the drug is safe, well tolerated, and noninferior to entacapone for this indication.
Opicapone is “the only once-daily catechol-O-methyltransferase (COMT) inhibitor to provide a mean reduction in time in the off state that is clinically relevant,” said Joaquim J. Ferreira, MD, Professor of Neurology and Clinical Pharmacology at the University of Lisbon, and colleagues. Administering the drug once daily could simplify a patient’s drug regimen by permitting the physician to decrease the total daily levodopa dose, increase the dosing interval, and reduce the number of intakes, thereby maximizing the benefit of therapy, he added.
Comparing Opicapone, Entacapone, and Placebo
The half-life of oral levodopa is between 60 and 90 minutes and is linked with end-of-dose motor fluctuations. COMT inhibitors increase the plasma elimination half-life of levodopa and decrease peak–trough variations. Entacapone, a COMT inhibitor, provides moderate reductions in daily off time, but needs to be administered with each dose of levodopa. Neurologists thus have sought a more effective COMT inhibitor that can be used easily in clinical practice.
Dr. Ferreira and colleagues assessed the safety and efficacy of opicapone as an adjunct to levodopa, compared with placebo and entacapone, in patients with Parkinson’s disease and motor fluctuations. Eligible participants had had a clinical diagnosis of Parkinson’s disease for at least three years, a Hoehn and Yahr stage of 1 to 3 during the on state, and at least one year of clinical improvement with levodopa treatment. People who had used entacapone previously, had significant dyskinesia disability, or had severe or unpredictable off periods were excluded from the study.
Equal groups of patients were computer randomized to once-daily opicapone (5 mg, 25 mg, or 50 mg), placebo, or 200 mg of entacapone with every levodopa intake. The participants and investigators were blinded to treatment allocation throughout the study. Opicapone capsules and entacapone tablets were overencapsulated to maintain blinding.
Doses of study drugs were given concomitantly with each levodopa intake. Patients in the opicapone groups received placebo for the daytime doses and active treatment for the bedtime dose. Patients in the entacapone group took the active treatment during the day and placebo as the bedtime dose. Investigators assessed participants at screening, baseline, and at five subsequent time points.
The study’s primary end point was the change from baseline to the end of study treatment in absolute off time, as assessed by daily patient diaries. Secondary end points included the change from baseline to the end of study treatment in the proportion of patients who had at least a one-hour reduction in absolute off time and the change from baseline to the end of study treatment in the proportion of patients who had at least a one-hour increase in absolute total on time.
For statistical analysis, population sets were defined as the full analysis set, which included all randomly assigned patients who took at least one dose of study drug and had at least one assessment of time in the off state after baseline; the per-protocol set, which included all patients in the full analysis set who did not have any major protocol deviations; and the safety set, which included all patients who received at least one dose of study drug.
Opicapone Was Noninferior to Entacapone
The researchers enrolled 600 patients, of whom 121 received placebo, 122 received 200 mg of entacapone, 122 received 5 mg of opicapone, 119 received 25 mg of opicapone, and 116 received 50 mg of opicapone. The full analysis included 590 patients, and the per-protocol analysis included 537 patients. In all, 542 patients completed the study. Patient demographics, baseline Parkinson’s disease characteristics, and treatment history did not differ between the treatment groups in the safety analysis.
In the full analysis, the adjusted mean change from baseline in absolute off time was –116.8 minutes in the opicapone 50 mg group, compared with –96.3 minutes in the entacapone group, –91.3 minutes in the opicapone 5 mg group, –85.9 minutes in the opicapone 25 mg group, and –56.0 minutes in the placebo group. The per-protocol analysis yielded similar results.
The investigators only tested the 50-mg dose of opicapone for noninferiority of absolute off time. This treatment was superior to placebo and noninferior to entacapone. The researchers found no significant differences between placebo and opicapone 5 mg or opicapone 25 mg. Entacapone was superior to placebo.
Compared with placebo, the proportion of patients with a reduction in off time of at least one hour was significantly higher in patient who received 25 mg or 50 mg of opicapone, and the proportion of patients with an increase in on time of at least one hour was significantly higher in patients who received 50 mg of opicapone. No significant differences were noted in off and on state rates for entacapone versus placebo. Results for the other secondary end points supported those of the primary analysis.
Adverse Events Were Uncommon
The percentage of patients who discontinued because of treatment-emergent adverse events was low and similar across the treatment groups. The most common treatment-emergent adverse events leading to discontinuation were diarrhea, visual hallucinations, and dyskinesia. Dyskinesia was the most frequently reported treatment-emergent adverse event possibly related to the study drug, and the highest incidence occurred in the opicapone groups. Approximately 80% of treatment-emergent dyskinesias occurred in patients in all groups who already had dyskinesia at baseline. The incidence of serious treatment-emergent adverse events was low (ie, 7% or less) in all groups, and 35% of these events were judged to be unrelated to the study drug.
“The beneficial effects of opicapone 50 mg at reducing the time in the off state were accompanied by a corresponding increase in time in the on state without troublesome dyskinesia, whereas the duration of time in the on state with troublesome dyskinesia did not change,” said Dr. Ferreira. The study results “suggest an overall positive risk-to-benefit ratio for the use of opicapone in patients with Parkinson’s disease with end-of-dose motor fluctuations,” he added. Results of the authors’ open-label extension study will be published in the future.
—Erik Greb
Administering 50 mg of opicapone as an adjunct to levodopa treatment decreases the amount of off time by approximately 61 minutes, compared with placebo, for patients with Parkinson’s disease and end-of-dose motor fluctuations, according to research published in the February issue of Lancet Neurology. Data indicate that the drug is safe, well tolerated, and noninferior to entacapone for this indication.
Opicapone is “the only once-daily catechol-O-methyltransferase (COMT) inhibitor to provide a mean reduction in time in the off state that is clinically relevant,” said Joaquim J. Ferreira, MD, Professor of Neurology and Clinical Pharmacology at the University of Lisbon, and colleagues. Administering the drug once daily could simplify a patient’s drug regimen by permitting the physician to decrease the total daily levodopa dose, increase the dosing interval, and reduce the number of intakes, thereby maximizing the benefit of therapy, he added.
Comparing Opicapone, Entacapone, and Placebo
The half-life of oral levodopa is between 60 and 90 minutes and is linked with end-of-dose motor fluctuations. COMT inhibitors increase the plasma elimination half-life of levodopa and decrease peak–trough variations. Entacapone, a COMT inhibitor, provides moderate reductions in daily off time, but needs to be administered with each dose of levodopa. Neurologists thus have sought a more effective COMT inhibitor that can be used easily in clinical practice.
Dr. Ferreira and colleagues assessed the safety and efficacy of opicapone as an adjunct to levodopa, compared with placebo and entacapone, in patients with Parkinson’s disease and motor fluctuations. Eligible participants had had a clinical diagnosis of Parkinson’s disease for at least three years, a Hoehn and Yahr stage of 1 to 3 during the on state, and at least one year of clinical improvement with levodopa treatment. People who had used entacapone previously, had significant dyskinesia disability, or had severe or unpredictable off periods were excluded from the study.
Equal groups of patients were computer randomized to once-daily opicapone (5 mg, 25 mg, or 50 mg), placebo, or 200 mg of entacapone with every levodopa intake. The participants and investigators were blinded to treatment allocation throughout the study. Opicapone capsules and entacapone tablets were overencapsulated to maintain blinding.
Doses of study drugs were given concomitantly with each levodopa intake. Patients in the opicapone groups received placebo for the daytime doses and active treatment for the bedtime dose. Patients in the entacapone group took the active treatment during the day and placebo as the bedtime dose. Investigators assessed participants at screening, baseline, and at five subsequent time points.
The study’s primary end point was the change from baseline to the end of study treatment in absolute off time, as assessed by daily patient diaries. Secondary end points included the change from baseline to the end of study treatment in the proportion of patients who had at least a one-hour reduction in absolute off time and the change from baseline to the end of study treatment in the proportion of patients who had at least a one-hour increase in absolute total on time.
For statistical analysis, population sets were defined as the full analysis set, which included all randomly assigned patients who took at least one dose of study drug and had at least one assessment of time in the off state after baseline; the per-protocol set, which included all patients in the full analysis set who did not have any major protocol deviations; and the safety set, which included all patients who received at least one dose of study drug.
Opicapone Was Noninferior to Entacapone
The researchers enrolled 600 patients, of whom 121 received placebo, 122 received 200 mg of entacapone, 122 received 5 mg of opicapone, 119 received 25 mg of opicapone, and 116 received 50 mg of opicapone. The full analysis included 590 patients, and the per-protocol analysis included 537 patients. In all, 542 patients completed the study. Patient demographics, baseline Parkinson’s disease characteristics, and treatment history did not differ between the treatment groups in the safety analysis.
In the full analysis, the adjusted mean change from baseline in absolute off time was –116.8 minutes in the opicapone 50 mg group, compared with –96.3 minutes in the entacapone group, –91.3 minutes in the opicapone 5 mg group, –85.9 minutes in the opicapone 25 mg group, and –56.0 minutes in the placebo group. The per-protocol analysis yielded similar results.
The investigators only tested the 50-mg dose of opicapone for noninferiority of absolute off time. This treatment was superior to placebo and noninferior to entacapone. The researchers found no significant differences between placebo and opicapone 5 mg or opicapone 25 mg. Entacapone was superior to placebo.
Compared with placebo, the proportion of patients with a reduction in off time of at least one hour was significantly higher in patient who received 25 mg or 50 mg of opicapone, and the proportion of patients with an increase in on time of at least one hour was significantly higher in patients who received 50 mg of opicapone. No significant differences were noted in off and on state rates for entacapone versus placebo. Results for the other secondary end points supported those of the primary analysis.
Adverse Events Were Uncommon
The percentage of patients who discontinued because of treatment-emergent adverse events was low and similar across the treatment groups. The most common treatment-emergent adverse events leading to discontinuation were diarrhea, visual hallucinations, and dyskinesia. Dyskinesia was the most frequently reported treatment-emergent adverse event possibly related to the study drug, and the highest incidence occurred in the opicapone groups. Approximately 80% of treatment-emergent dyskinesias occurred in patients in all groups who already had dyskinesia at baseline. The incidence of serious treatment-emergent adverse events was low (ie, 7% or less) in all groups, and 35% of these events were judged to be unrelated to the study drug.
“The beneficial effects of opicapone 50 mg at reducing the time in the off state were accompanied by a corresponding increase in time in the on state without troublesome dyskinesia, whereas the duration of time in the on state with troublesome dyskinesia did not change,” said Dr. Ferreira. The study results “suggest an overall positive risk-to-benefit ratio for the use of opicapone in patients with Parkinson’s disease with end-of-dose motor fluctuations,” he added. Results of the authors’ open-label extension study will be published in the future.
—Erik Greb
Suggested Reading
Ferreira JJ, Lees A, Rocha JF, et al. Opicapone as an adjunct to levodopa in patients with Parkinson’s disease and end-of-dose motor fluctuations: a randomised, double-blind, controlled trial. Lancet Neurol. 2016;15(2):154-165.
Suggested Reading
Ferreira JJ, Lees A, Rocha JF, et al. Opicapone as an adjunct to levodopa in patients with Parkinson’s disease and end-of-dose motor fluctuations: a randomised, double-blind, controlled trial. Lancet Neurol. 2016;15(2):154-165.
BRAIN Initiative Could Advance the Field of Neuromodulation
LAS VEGAS—Through various programs, the BRAIN Initiative seeks to fund research in 2016 that could advance the field of neuromodulation, according to a lecture given at the 19th Annual Meeting of the North American Neuromodulation Society. These investigations could affect the treatment of epilepsy, headache, Parkinson’s disease, or other neurologic disorders.
The BRAIN Initiative has two main objectives, said Stephanie Fertig, MBA, Director of Small Business Programs at the National Institute of Neurological Disorders and Stroke. The first is to foster the development of new technologies for mapping connections in the brain and discovering patterns of neural activity. The second goal is to use these new technologies, as well as existing technologies, to further neurologists’ understanding of how the neural circuit affects the function of the healthy or diseased brain. The initiative, which President Obama introduced in 2013, is a collaboration between federal agencies, including the National Science Foundation and NIH, private foundations, universities, and industry. Information on the BRAIN Initiative can be found online at www.braininitiative.nih.gov.
Researchers Invited to Apply for Funding
Several of the BRAIN Initiative’s programs are intended to promote the identification, development, and optimization of new technologies and approaches for large-scale recording and modulation in the nervous system. The goal is to foster research that will add to scientific understanding of the dynamic signaling in the nervous system, said Ms. Fertig. One program seeks applications to study new and untested ideas for recording and modulating technology, including ideas in the initial stages of conceptualization. Other programs aim to further proof-of-concept testing for such technology, as well as to enable the optimization of the technology with feedback from the user community.
Another of the initiative’s programs is intended to fund nonclinical and clinical studies that will help advance invasive recording or stimulating devices that could, in turn, treat CNS disorders and improve understanding of the human brain. Researchers will receive support for the implementation of clinical prototype devices, nonclinical safety and efficacy testing, design verification and validation activities, and pursuit of regulatory approval for a small clinical study. The program will consider clinical studies of acute or short-term procedures that entail nonsignificant risk (as determined by an Institutional Review Board), as well as those that entail a significant risk and require an Investigational Device Exemption (IDE) from the FDA. The BRAIN Initiative provides two options for researchers interested in funding for invasive devices, said Ms. Fertig. “One is if you need to do some nonclinical work before you get your IDE and then move into the clinic. That’s the phase translational to clinical research track. Then there’s the direct-to-clinical research program,” which is appropriate for investigators who do not need to perform nonclinical work and are ready for a clinical study.
Public–Private Partnership Program
The BRAIN Initiative also created a Public–Private Partnership Program to facilitate collaboration between clinical investigators and manufacturers of invasive recording or stimulating devices. This program is intended to promote clinical research and foster partnerships between clinical researchers and the developers of “next-generation implantable stimulating–recording devices,” said Ms. Fertig. Data about the safety and utility of such devices can be costly to obtain, but the Public–Private Partnership Program will enable researchers to use existing manufacturers’ safety data. To date, six device manufacturers (ie, Medtronic, Boston Scientific, Blackrock, NeuroPace, NeuroNexus, and Second Sight) have signed a memorandum of understanding with NIH to provide support and information on materials (eg, devices and software). The information will guide investigators who want to pursue specific agreements with manufacturers for the submission of research proposals to NIH. Furthermore, NIH has created templates of collaborative research agreements and confidential disclosure agreements to quicken the legal and administrative process for establishing partnerships between manufacturers and academic research institutions.
Funding Supports Device-Related Research
The BRAIN Initiative already has funded various studies that could lead to new invasive treatments for various neurologic disorders. Leigh R. Hochberg, MD, PhD, Director of the Neurotechnology Trials Unit at Massachusetts General Hospital in Boston, and associates received NIH support for the development of the BrainGate device. Dr. Hochberg created BrainGate, a brain implant system, to allow patients with quadriplegia to control external devices such as prosthetic arms by thought alone. Dr. Hochberg’s BRAIN project is to develop BrainGate into a fully implanted medical treatment system without external components. The goal is to enable patients to use the device independently on an ongoing basis.
In addition, Gregory A. Worrell, MD, PhD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and colleagues received funding to study wireless devices that measure brain activity, predict seizure onset, and deliver therapeutic stimulation to mitigate seizures. Dr. Worrell’s group initially plans to conduct a preclinical study to test one such device in dogs with epilepsy. If the device is successful, the group will perform a pilot clinical trial in patients with epilepsy.
Finally, Nicholas D. Schiff, MD, Jerold B. Katz Professor of Neurology and Neuroscience at Weill Cornell Medical College in New York, and colleagues received support for their efforts to develop device therapy for cognitive impairment associated with traumatic brain injury. They are focusing on a device that delivers deep brain stimulation to the thalamus, which they hypothesize may restore the disrupted circuit function that underlies the cognitive disability.
—Erik Greb
Suggested Reading
Brinkmann BH, Patterson EE, Vite C, et al. Forecasting seizures using intracranial EEG measures and SVM in naturally occurring canine epilepsy. PLoS One. 2015;10(8):e0133900.
Gummadavelli A, Motelow JE, Smith N, et al. Thalamic stimulation to improve level of consciousness after seizures: evaluation of electrophysiology and behavior. Epilepsia. 2015;56(1):114-124.
Hochberg LR, Bacher D, Jarosiewicz B, et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature. 2012;485(7398):372-375.
LAS VEGAS—Through various programs, the BRAIN Initiative seeks to fund research in 2016 that could advance the field of neuromodulation, according to a lecture given at the 19th Annual Meeting of the North American Neuromodulation Society. These investigations could affect the treatment of epilepsy, headache, Parkinson’s disease, or other neurologic disorders.
The BRAIN Initiative has two main objectives, said Stephanie Fertig, MBA, Director of Small Business Programs at the National Institute of Neurological Disorders and Stroke. The first is to foster the development of new technologies for mapping connections in the brain and discovering patterns of neural activity. The second goal is to use these new technologies, as well as existing technologies, to further neurologists’ understanding of how the neural circuit affects the function of the healthy or diseased brain. The initiative, which President Obama introduced in 2013, is a collaboration between federal agencies, including the National Science Foundation and NIH, private foundations, universities, and industry. Information on the BRAIN Initiative can be found online at www.braininitiative.nih.gov.
Researchers Invited to Apply for Funding
Several of the BRAIN Initiative’s programs are intended to promote the identification, development, and optimization of new technologies and approaches for large-scale recording and modulation in the nervous system. The goal is to foster research that will add to scientific understanding of the dynamic signaling in the nervous system, said Ms. Fertig. One program seeks applications to study new and untested ideas for recording and modulating technology, including ideas in the initial stages of conceptualization. Other programs aim to further proof-of-concept testing for such technology, as well as to enable the optimization of the technology with feedback from the user community.
Another of the initiative’s programs is intended to fund nonclinical and clinical studies that will help advance invasive recording or stimulating devices that could, in turn, treat CNS disorders and improve understanding of the human brain. Researchers will receive support for the implementation of clinical prototype devices, nonclinical safety and efficacy testing, design verification and validation activities, and pursuit of regulatory approval for a small clinical study. The program will consider clinical studies of acute or short-term procedures that entail nonsignificant risk (as determined by an Institutional Review Board), as well as those that entail a significant risk and require an Investigational Device Exemption (IDE) from the FDA. The BRAIN Initiative provides two options for researchers interested in funding for invasive devices, said Ms. Fertig. “One is if you need to do some nonclinical work before you get your IDE and then move into the clinic. That’s the phase translational to clinical research track. Then there’s the direct-to-clinical research program,” which is appropriate for investigators who do not need to perform nonclinical work and are ready for a clinical study.
Public–Private Partnership Program
The BRAIN Initiative also created a Public–Private Partnership Program to facilitate collaboration between clinical investigators and manufacturers of invasive recording or stimulating devices. This program is intended to promote clinical research and foster partnerships between clinical researchers and the developers of “next-generation implantable stimulating–recording devices,” said Ms. Fertig. Data about the safety and utility of such devices can be costly to obtain, but the Public–Private Partnership Program will enable researchers to use existing manufacturers’ safety data. To date, six device manufacturers (ie, Medtronic, Boston Scientific, Blackrock, NeuroPace, NeuroNexus, and Second Sight) have signed a memorandum of understanding with NIH to provide support and information on materials (eg, devices and software). The information will guide investigators who want to pursue specific agreements with manufacturers for the submission of research proposals to NIH. Furthermore, NIH has created templates of collaborative research agreements and confidential disclosure agreements to quicken the legal and administrative process for establishing partnerships between manufacturers and academic research institutions.
Funding Supports Device-Related Research
The BRAIN Initiative already has funded various studies that could lead to new invasive treatments for various neurologic disorders. Leigh R. Hochberg, MD, PhD, Director of the Neurotechnology Trials Unit at Massachusetts General Hospital in Boston, and associates received NIH support for the development of the BrainGate device. Dr. Hochberg created BrainGate, a brain implant system, to allow patients with quadriplegia to control external devices such as prosthetic arms by thought alone. Dr. Hochberg’s BRAIN project is to develop BrainGate into a fully implanted medical treatment system without external components. The goal is to enable patients to use the device independently on an ongoing basis.
In addition, Gregory A. Worrell, MD, PhD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and colleagues received funding to study wireless devices that measure brain activity, predict seizure onset, and deliver therapeutic stimulation to mitigate seizures. Dr. Worrell’s group initially plans to conduct a preclinical study to test one such device in dogs with epilepsy. If the device is successful, the group will perform a pilot clinical trial in patients with epilepsy.
Finally, Nicholas D. Schiff, MD, Jerold B. Katz Professor of Neurology and Neuroscience at Weill Cornell Medical College in New York, and colleagues received support for their efforts to develop device therapy for cognitive impairment associated with traumatic brain injury. They are focusing on a device that delivers deep brain stimulation to the thalamus, which they hypothesize may restore the disrupted circuit function that underlies the cognitive disability.
—Erik Greb
LAS VEGAS—Through various programs, the BRAIN Initiative seeks to fund research in 2016 that could advance the field of neuromodulation, according to a lecture given at the 19th Annual Meeting of the North American Neuromodulation Society. These investigations could affect the treatment of epilepsy, headache, Parkinson’s disease, or other neurologic disorders.
The BRAIN Initiative has two main objectives, said Stephanie Fertig, MBA, Director of Small Business Programs at the National Institute of Neurological Disorders and Stroke. The first is to foster the development of new technologies for mapping connections in the brain and discovering patterns of neural activity. The second goal is to use these new technologies, as well as existing technologies, to further neurologists’ understanding of how the neural circuit affects the function of the healthy or diseased brain. The initiative, which President Obama introduced in 2013, is a collaboration between federal agencies, including the National Science Foundation and NIH, private foundations, universities, and industry. Information on the BRAIN Initiative can be found online at www.braininitiative.nih.gov.
Researchers Invited to Apply for Funding
Several of the BRAIN Initiative’s programs are intended to promote the identification, development, and optimization of new technologies and approaches for large-scale recording and modulation in the nervous system. The goal is to foster research that will add to scientific understanding of the dynamic signaling in the nervous system, said Ms. Fertig. One program seeks applications to study new and untested ideas for recording and modulating technology, including ideas in the initial stages of conceptualization. Other programs aim to further proof-of-concept testing for such technology, as well as to enable the optimization of the technology with feedback from the user community.
Another of the initiative’s programs is intended to fund nonclinical and clinical studies that will help advance invasive recording or stimulating devices that could, in turn, treat CNS disorders and improve understanding of the human brain. Researchers will receive support for the implementation of clinical prototype devices, nonclinical safety and efficacy testing, design verification and validation activities, and pursuit of regulatory approval for a small clinical study. The program will consider clinical studies of acute or short-term procedures that entail nonsignificant risk (as determined by an Institutional Review Board), as well as those that entail a significant risk and require an Investigational Device Exemption (IDE) from the FDA. The BRAIN Initiative provides two options for researchers interested in funding for invasive devices, said Ms. Fertig. “One is if you need to do some nonclinical work before you get your IDE and then move into the clinic. That’s the phase translational to clinical research track. Then there’s the direct-to-clinical research program,” which is appropriate for investigators who do not need to perform nonclinical work and are ready for a clinical study.
Public–Private Partnership Program
The BRAIN Initiative also created a Public–Private Partnership Program to facilitate collaboration between clinical investigators and manufacturers of invasive recording or stimulating devices. This program is intended to promote clinical research and foster partnerships between clinical researchers and the developers of “next-generation implantable stimulating–recording devices,” said Ms. Fertig. Data about the safety and utility of such devices can be costly to obtain, but the Public–Private Partnership Program will enable researchers to use existing manufacturers’ safety data. To date, six device manufacturers (ie, Medtronic, Boston Scientific, Blackrock, NeuroPace, NeuroNexus, and Second Sight) have signed a memorandum of understanding with NIH to provide support and information on materials (eg, devices and software). The information will guide investigators who want to pursue specific agreements with manufacturers for the submission of research proposals to NIH. Furthermore, NIH has created templates of collaborative research agreements and confidential disclosure agreements to quicken the legal and administrative process for establishing partnerships between manufacturers and academic research institutions.
Funding Supports Device-Related Research
The BRAIN Initiative already has funded various studies that could lead to new invasive treatments for various neurologic disorders. Leigh R. Hochberg, MD, PhD, Director of the Neurotechnology Trials Unit at Massachusetts General Hospital in Boston, and associates received NIH support for the development of the BrainGate device. Dr. Hochberg created BrainGate, a brain implant system, to allow patients with quadriplegia to control external devices such as prosthetic arms by thought alone. Dr. Hochberg’s BRAIN project is to develop BrainGate into a fully implanted medical treatment system without external components. The goal is to enable patients to use the device independently on an ongoing basis.
In addition, Gregory A. Worrell, MD, PhD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and colleagues received funding to study wireless devices that measure brain activity, predict seizure onset, and deliver therapeutic stimulation to mitigate seizures. Dr. Worrell’s group initially plans to conduct a preclinical study to test one such device in dogs with epilepsy. If the device is successful, the group will perform a pilot clinical trial in patients with epilepsy.
Finally, Nicholas D. Schiff, MD, Jerold B. Katz Professor of Neurology and Neuroscience at Weill Cornell Medical College in New York, and colleagues received support for their efforts to develop device therapy for cognitive impairment associated with traumatic brain injury. They are focusing on a device that delivers deep brain stimulation to the thalamus, which they hypothesize may restore the disrupted circuit function that underlies the cognitive disability.
—Erik Greb
Suggested Reading
Brinkmann BH, Patterson EE, Vite C, et al. Forecasting seizures using intracranial EEG measures and SVM in naturally occurring canine epilepsy. PLoS One. 2015;10(8):e0133900.
Gummadavelli A, Motelow JE, Smith N, et al. Thalamic stimulation to improve level of consciousness after seizures: evaluation of electrophysiology and behavior. Epilepsia. 2015;56(1):114-124.
Hochberg LR, Bacher D, Jarosiewicz B, et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature. 2012;485(7398):372-375.
Suggested Reading
Brinkmann BH, Patterson EE, Vite C, et al. Forecasting seizures using intracranial EEG measures and SVM in naturally occurring canine epilepsy. PLoS One. 2015;10(8):e0133900.
Gummadavelli A, Motelow JE, Smith N, et al. Thalamic stimulation to improve level of consciousness after seizures: evaluation of electrophysiology and behavior. Epilepsia. 2015;56(1):114-124.
Hochberg LR, Bacher D, Jarosiewicz B, et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature. 2012;485(7398):372-375.
VIDEO: A better way to treat large intraventricular hemorrhages
LOS ANGELES – For intraventricular hemorrhages of at least 20 mL, alteplase (Activase – Genentech) delivered directly into the clot by external ventricular drain almost doubles the odds of achieving a modified Rankin Score of 0-3 by 6 months.
More clot is removed – and patients with large intraventricular hemorrhages (IVHs) do better – with more vigorous alteplase dosing and when more than one drain is used.
The findings come from the Clot Lysis Evaluation of Accelerated Resolution (CLEAR III) trial, which randomized 249 IVH patients to 1 mg alteplase every 8 hours for up to 12 doses, and 251 to saline on the same schedule, delivered by external ventricular drain. The intervention didn’t make much difference with small hemorrhages.
In a video interview at the International Stroke Conference, investigator Dr. Issam Awad, a professor of surgery and neurology and director of neurovascular surgery at the University of Chicago, explained how to do the technique correctly for larger clots, and the expected benefits.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LOS ANGELES – For intraventricular hemorrhages of at least 20 mL, alteplase (Activase – Genentech) delivered directly into the clot by external ventricular drain almost doubles the odds of achieving a modified Rankin Score of 0-3 by 6 months.
More clot is removed – and patients with large intraventricular hemorrhages (IVHs) do better – with more vigorous alteplase dosing and when more than one drain is used.
The findings come from the Clot Lysis Evaluation of Accelerated Resolution (CLEAR III) trial, which randomized 249 IVH patients to 1 mg alteplase every 8 hours for up to 12 doses, and 251 to saline on the same schedule, delivered by external ventricular drain. The intervention didn’t make much difference with small hemorrhages.
In a video interview at the International Stroke Conference, investigator Dr. Issam Awad, a professor of surgery and neurology and director of neurovascular surgery at the University of Chicago, explained how to do the technique correctly for larger clots, and the expected benefits.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LOS ANGELES – For intraventricular hemorrhages of at least 20 mL, alteplase (Activase – Genentech) delivered directly into the clot by external ventricular drain almost doubles the odds of achieving a modified Rankin Score of 0-3 by 6 months.
More clot is removed – and patients with large intraventricular hemorrhages (IVHs) do better – with more vigorous alteplase dosing and when more than one drain is used.
The findings come from the Clot Lysis Evaluation of Accelerated Resolution (CLEAR III) trial, which randomized 249 IVH patients to 1 mg alteplase every 8 hours for up to 12 doses, and 251 to saline on the same schedule, delivered by external ventricular drain. The intervention didn’t make much difference with small hemorrhages.
In a video interview at the International Stroke Conference, investigator Dr. Issam Awad, a professor of surgery and neurology and director of neurovascular surgery at the University of Chicago, explained how to do the technique correctly for larger clots, and the expected benefits.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE INTERNATIONAL STROKE CONFERENCE

VIDEO: Intracranial warfarin bleeds smaller with prothrombin complex instead of FFP
LOS ANGELES – The international normalized ratio fell to 1.2 or less within 3 hours among 18 of 27 (67%) patients who received four-factor prothrombin complex concentrate (octaplex [Octapharma]) for warfarin-related intracranial hemorrhages, but only 2 of 23 (9%) who received fresh frozen plasma, according to a randomized trial from Germany.
Hematoma expansion was reduced by 16.9 mL (P = .026) at 3 hours and 16.4 mL (P = .018) at 24 hours in the prothrombin complex concentrate (PCC) group.
All the patients presented within 12 hours of symptom onset with an INR of at least 2; they received fresh frozen plasma (FFP) or four-factor PCC within an hour of their cerebral CT. There were eight deaths in the FFP group, including five due to hematoma expansion. The five deaths in the PCC group occurred after day 5, and one was thought to be because of hematoma expansion. Patients were 76 years old, on average, and the majority were men; both groups received vitamin K.
The findings make a case for PCC at a time when it’s unclear how best to handle warfarin-related intracranial bleeds, and whether the extra cost of PCC is worth it. Investigator Dr. Thorsten Steiner, a professor of neurology at the University of Heidelberg (Germany), addressed the relevant issues, including PCC safety, in a video interview at the International Stroke Conference sponsored by the American Heart Association. The investigator-initiated trial was funded by Octapharma, and Dr. Steiner reported receiving a research grant from the company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LOS ANGELES – The international normalized ratio fell to 1.2 or less within 3 hours among 18 of 27 (67%) patients who received four-factor prothrombin complex concentrate (octaplex [Octapharma]) for warfarin-related intracranial hemorrhages, but only 2 of 23 (9%) who received fresh frozen plasma, according to a randomized trial from Germany.
Hematoma expansion was reduced by 16.9 mL (P = .026) at 3 hours and 16.4 mL (P = .018) at 24 hours in the prothrombin complex concentrate (PCC) group.
All the patients presented within 12 hours of symptom onset with an INR of at least 2; they received fresh frozen plasma (FFP) or four-factor PCC within an hour of their cerebral CT. There were eight deaths in the FFP group, including five due to hematoma expansion. The five deaths in the PCC group occurred after day 5, and one was thought to be because of hematoma expansion. Patients were 76 years old, on average, and the majority were men; both groups received vitamin K.
The findings make a case for PCC at a time when it’s unclear how best to handle warfarin-related intracranial bleeds, and whether the extra cost of PCC is worth it. Investigator Dr. Thorsten Steiner, a professor of neurology at the University of Heidelberg (Germany), addressed the relevant issues, including PCC safety, in a video interview at the International Stroke Conference sponsored by the American Heart Association. The investigator-initiated trial was funded by Octapharma, and Dr. Steiner reported receiving a research grant from the company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LOS ANGELES – The international normalized ratio fell to 1.2 or less within 3 hours among 18 of 27 (67%) patients who received four-factor prothrombin complex concentrate (octaplex [Octapharma]) for warfarin-related intracranial hemorrhages, but only 2 of 23 (9%) who received fresh frozen plasma, according to a randomized trial from Germany.
Hematoma expansion was reduced by 16.9 mL (P = .026) at 3 hours and 16.4 mL (P = .018) at 24 hours in the prothrombin complex concentrate (PCC) group.
All the patients presented within 12 hours of symptom onset with an INR of at least 2; they received fresh frozen plasma (FFP) or four-factor PCC within an hour of their cerebral CT. There were eight deaths in the FFP group, including five due to hematoma expansion. The five deaths in the PCC group occurred after day 5, and one was thought to be because of hematoma expansion. Patients were 76 years old, on average, and the majority were men; both groups received vitamin K.
The findings make a case for PCC at a time when it’s unclear how best to handle warfarin-related intracranial bleeds, and whether the extra cost of PCC is worth it. Investigator Dr. Thorsten Steiner, a professor of neurology at the University of Heidelberg (Germany), addressed the relevant issues, including PCC safety, in a video interview at the International Stroke Conference sponsored by the American Heart Association. The investigator-initiated trial was funded by Octapharma, and Dr. Steiner reported receiving a research grant from the company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE INTERNATIONAL STROKE CONFERENCE

Natalizumab May Increase Risk of JCV Seroconversion
Patients with multiple sclerosis (MS) who receive natalizumab may have as much as a 10-fold greater risk of seroconversion to John Cunningham virus (JCV)-positive status, according to a study published online January 27 in Neurology Neuroimmunology & Neuroinflammation.
“An increase in the levels of anti-JCV antibodies could signify an increased risk of progressive multifocal leukoencephalopathy (PML),” said the study’s senior author, Heinz Wiendl, MD, Professor of Neurology at the University of Münster in Germany.
Dr. Wiendl and colleagues performed a longitudinal analysis of 525 German patients with MS and 711 French patients with MS, all of whom were treated with natalizumab, to assess whether the therapy influenced JCV seroconversion or JCV index value (ie, the level of anti-JCV antibody titers). An independent contractor processed and analyzed sera samples with the second-generation enzyme-linked immunosorbent assay kit STRATIFY JCV DxSelect.
Seroconversion and Increasing Index Value
Of the 525 German patients, 296 (56.4%) were JCV-negative throughout the observation period, and 171 were JCV-positive (32.6%). Forty-three patients changed from being JCV-negative to JCV-positive (8.2%), and 15 patients changed from being JCV-positive to JCV-negative (2.9%). When the authors used JCV serostatus to determine seroconversion, the longitudinal assessment started out with 339 initially JCV-negative patients. The serostatus of 43 of these initially JCV-negative patients changed to JCV-positive, which is a rate of 12.7% in 14.8 months (10.3% per year).
Of the 711 French patients, 243 initially were JCV-negative. The serostatus of 20 (8.2%) of these latter patients changed to JCV-positive in their first year of treatment, and 21 (8.6%) of the patients became JCV-positive in their second year of treatment. In all, the serostatus of 41 of 243 patients (16.9%) changed to JCV-positive in the first two years of natalizumab treatment (8.5% per year).
In addition, JCV index values changed in 525 patients during the observation period. The proportion of patients with an index value less than 0.4 was reduced by 20 patients (ie, from 65.1% to 61.3%), and the group of patients with low risk (ie, values between 0.4 and 0.9) was reduced by one patient to 7.8%. The patient groups with medium (ie, 0.9–1.5) and high risk (ie, greater than 1.5) increased by seven patients from 4.6% to 5.9% and by 14 patients from 22.3% to 25%, respectively.Furthermore, 161 of 201 JCV-positive patients (80%) had stable JCV index values over time. The remaining 40 patients (20%) had fluctuations of more than 30% in 14.8 months. Six of these patients (3%) had decreasing index values, and 34 (17%) had increasing index values (mean, 200.8%). Overall, the index value of all JCV-positive patients increased by an average of 15.9% in 14.8 months (12.9% per year).
Increased Index May Not Indicate Imminent PML
The high rate of seroconversion that the investigators observed “clearly supports the facilitation by treatment with natalizumab,” said Dr. Wiendl. “Our observed seroconversion of 8% to 10% per year and the rise in seroprevalence of 5% to 6% in 15 to 24 months is at least eight to 10 times as much as would be expected by age.” The study results imply that not every patient with MS is susceptible to JCV seroconversion by treatment, but natalizumab might facilitate seroconversion in patients who are susceptible.
No research has examined the influence of other MS treatments on JCV index values, and the investigators thus cannot be certain that natalizumab treatment caused the increase in index values observed in the study. But because there was no correlation between age and index value in JCV-positive patients, it is valid to speculate that natalizumab treatment induces rising JCV index values.
“If the hypothesis that treatment with natalizumab is associated with enhanced JCV seroconversion and higher index values is proven, it would also be important to determine whether cessation of natalizumab therapy (or perhaps prolonged infusion intervals) could lead to lower JCV index values as well,” Dr. Wiendl continued. The association “does not diminish [natalizumab’s] clinical efficacy, but calls for more elaborate strategies for PML risk stratification according to current scientific developments, also regarding patients with prior use of immunosuppressants, where the JCV index is not helpful.
“It is important that people with MS taking natalizumab speak with their doctor before making any changes to their treatment,” Dr. Wiendl added. “Still, this study shows anti-JCV antibodies may serve as a useful biomarker…. The results of this study underscore the need for frequent monitoring of anti-JCV antibodies in people who are being treated with natalizumab for MS.”
JCV serology, however, should not be the only PML risk biomarker to stratify patients treated with natalizumab, said Dr. Wiendl. Neurologists should explore and potentially apply additional biomarkers such as CD62L in peripheral blood or IgM bands in CSF. Together, all of these biomarkers may provide more accurate information about patients’ PML risk and help reduce the incidence of PML.
The investigators’ data extend earlier paired, longitudinal studies in various countries of patients treated with natalizumab who had similarly high rates of conversion and a rise in titers, said Adil Javed, MD, PhD, Associate Professor of Neurology, and Anthony T. Reder, MD, Professor of Neurology, both at the University of Chicago, in an accompanying editorial. Although the JCV index appears to be a valid serum marker of risk for PML, “risk is relative,” they said. “Despite a higher JCV replication state, an increase in JCV-antibody index does not necessarily mean that PML infection is imminent…. Schwab et al extend growing observations that JCV-antibody index values need to be monitored and that seroconversion or rising JCV-antibody titers alter the risk of PML in patients treated with natalizumab.”
—Erik Greb
Suggested Reading
Schwab N, Schneider-Hohendorf T, Pignolet B, et al. Therapy with natalizumab is associated with high JCV seroconversion and rising JCV index values. Neurol Neuroimmunol Neuroinflamm. 2016;3(1):e195.
Javed A, Reder AT. Rising JCV-Ab index during natalizumab therapy for MS: Inauspicious for a highly efficacious drug. Neurol Neuroimmunol Neuroinflamm. 2016;3(1):e199.
Patients with multiple sclerosis (MS) who receive natalizumab may have as much as a 10-fold greater risk of seroconversion to John Cunningham virus (JCV)-positive status, according to a study published online January 27 in Neurology Neuroimmunology & Neuroinflammation.
“An increase in the levels of anti-JCV antibodies could signify an increased risk of progressive multifocal leukoencephalopathy (PML),” said the study’s senior author, Heinz Wiendl, MD, Professor of Neurology at the University of Münster in Germany.
Dr. Wiendl and colleagues performed a longitudinal analysis of 525 German patients with MS and 711 French patients with MS, all of whom were treated with natalizumab, to assess whether the therapy influenced JCV seroconversion or JCV index value (ie, the level of anti-JCV antibody titers). An independent contractor processed and analyzed sera samples with the second-generation enzyme-linked immunosorbent assay kit STRATIFY JCV DxSelect.
Seroconversion and Increasing Index Value
Of the 525 German patients, 296 (56.4%) were JCV-negative throughout the observation period, and 171 were JCV-positive (32.6%). Forty-three patients changed from being JCV-negative to JCV-positive (8.2%), and 15 patients changed from being JCV-positive to JCV-negative (2.9%). When the authors used JCV serostatus to determine seroconversion, the longitudinal assessment started out with 339 initially JCV-negative patients. The serostatus of 43 of these initially JCV-negative patients changed to JCV-positive, which is a rate of 12.7% in 14.8 months (10.3% per year).
Of the 711 French patients, 243 initially were JCV-negative. The serostatus of 20 (8.2%) of these latter patients changed to JCV-positive in their first year of treatment, and 21 (8.6%) of the patients became JCV-positive in their second year of treatment. In all, the serostatus of 41 of 243 patients (16.9%) changed to JCV-positive in the first two years of natalizumab treatment (8.5% per year).
In addition, JCV index values changed in 525 patients during the observation period. The proportion of patients with an index value less than 0.4 was reduced by 20 patients (ie, from 65.1% to 61.3%), and the group of patients with low risk (ie, values between 0.4 and 0.9) was reduced by one patient to 7.8%. The patient groups with medium (ie, 0.9–1.5) and high risk (ie, greater than 1.5) increased by seven patients from 4.6% to 5.9% and by 14 patients from 22.3% to 25%, respectively.Furthermore, 161 of 201 JCV-positive patients (80%) had stable JCV index values over time. The remaining 40 patients (20%) had fluctuations of more than 30% in 14.8 months. Six of these patients (3%) had decreasing index values, and 34 (17%) had increasing index values (mean, 200.8%). Overall, the index value of all JCV-positive patients increased by an average of 15.9% in 14.8 months (12.9% per year).
Increased Index May Not Indicate Imminent PML
The high rate of seroconversion that the investigators observed “clearly supports the facilitation by treatment with natalizumab,” said Dr. Wiendl. “Our observed seroconversion of 8% to 10% per year and the rise in seroprevalence of 5% to 6% in 15 to 24 months is at least eight to 10 times as much as would be expected by age.” The study results imply that not every patient with MS is susceptible to JCV seroconversion by treatment, but natalizumab might facilitate seroconversion in patients who are susceptible.
No research has examined the influence of other MS treatments on JCV index values, and the investigators thus cannot be certain that natalizumab treatment caused the increase in index values observed in the study. But because there was no correlation between age and index value in JCV-positive patients, it is valid to speculate that natalizumab treatment induces rising JCV index values.
“If the hypothesis that treatment with natalizumab is associated with enhanced JCV seroconversion and higher index values is proven, it would also be important to determine whether cessation of natalizumab therapy (or perhaps prolonged infusion intervals) could lead to lower JCV index values as well,” Dr. Wiendl continued. The association “does not diminish [natalizumab’s] clinical efficacy, but calls for more elaborate strategies for PML risk stratification according to current scientific developments, also regarding patients with prior use of immunosuppressants, where the JCV index is not helpful.
“It is important that people with MS taking natalizumab speak with their doctor before making any changes to their treatment,” Dr. Wiendl added. “Still, this study shows anti-JCV antibodies may serve as a useful biomarker…. The results of this study underscore the need for frequent monitoring of anti-JCV antibodies in people who are being treated with natalizumab for MS.”
JCV serology, however, should not be the only PML risk biomarker to stratify patients treated with natalizumab, said Dr. Wiendl. Neurologists should explore and potentially apply additional biomarkers such as CD62L in peripheral blood or IgM bands in CSF. Together, all of these biomarkers may provide more accurate information about patients’ PML risk and help reduce the incidence of PML.
The investigators’ data extend earlier paired, longitudinal studies in various countries of patients treated with natalizumab who had similarly high rates of conversion and a rise in titers, said Adil Javed, MD, PhD, Associate Professor of Neurology, and Anthony T. Reder, MD, Professor of Neurology, both at the University of Chicago, in an accompanying editorial. Although the JCV index appears to be a valid serum marker of risk for PML, “risk is relative,” they said. “Despite a higher JCV replication state, an increase in JCV-antibody index does not necessarily mean that PML infection is imminent…. Schwab et al extend growing observations that JCV-antibody index values need to be monitored and that seroconversion or rising JCV-antibody titers alter the risk of PML in patients treated with natalizumab.”
—Erik Greb
Patients with multiple sclerosis (MS) who receive natalizumab may have as much as a 10-fold greater risk of seroconversion to John Cunningham virus (JCV)-positive status, according to a study published online January 27 in Neurology Neuroimmunology & Neuroinflammation.
“An increase in the levels of anti-JCV antibodies could signify an increased risk of progressive multifocal leukoencephalopathy (PML),” said the study’s senior author, Heinz Wiendl, MD, Professor of Neurology at the University of Münster in Germany.
Dr. Wiendl and colleagues performed a longitudinal analysis of 525 German patients with MS and 711 French patients with MS, all of whom were treated with natalizumab, to assess whether the therapy influenced JCV seroconversion or JCV index value (ie, the level of anti-JCV antibody titers). An independent contractor processed and analyzed sera samples with the second-generation enzyme-linked immunosorbent assay kit STRATIFY JCV DxSelect.
Seroconversion and Increasing Index Value
Of the 525 German patients, 296 (56.4%) were JCV-negative throughout the observation period, and 171 were JCV-positive (32.6%). Forty-three patients changed from being JCV-negative to JCV-positive (8.2%), and 15 patients changed from being JCV-positive to JCV-negative (2.9%). When the authors used JCV serostatus to determine seroconversion, the longitudinal assessment started out with 339 initially JCV-negative patients. The serostatus of 43 of these initially JCV-negative patients changed to JCV-positive, which is a rate of 12.7% in 14.8 months (10.3% per year).
Of the 711 French patients, 243 initially were JCV-negative. The serostatus of 20 (8.2%) of these latter patients changed to JCV-positive in their first year of treatment, and 21 (8.6%) of the patients became JCV-positive in their second year of treatment. In all, the serostatus of 41 of 243 patients (16.9%) changed to JCV-positive in the first two years of natalizumab treatment (8.5% per year).
In addition, JCV index values changed in 525 patients during the observation period. The proportion of patients with an index value less than 0.4 was reduced by 20 patients (ie, from 65.1% to 61.3%), and the group of patients with low risk (ie, values between 0.4 and 0.9) was reduced by one patient to 7.8%. The patient groups with medium (ie, 0.9–1.5) and high risk (ie, greater than 1.5) increased by seven patients from 4.6% to 5.9% and by 14 patients from 22.3% to 25%, respectively.Furthermore, 161 of 201 JCV-positive patients (80%) had stable JCV index values over time. The remaining 40 patients (20%) had fluctuations of more than 30% in 14.8 months. Six of these patients (3%) had decreasing index values, and 34 (17%) had increasing index values (mean, 200.8%). Overall, the index value of all JCV-positive patients increased by an average of 15.9% in 14.8 months (12.9% per year).
Increased Index May Not Indicate Imminent PML
The high rate of seroconversion that the investigators observed “clearly supports the facilitation by treatment with natalizumab,” said Dr. Wiendl. “Our observed seroconversion of 8% to 10% per year and the rise in seroprevalence of 5% to 6% in 15 to 24 months is at least eight to 10 times as much as would be expected by age.” The study results imply that not every patient with MS is susceptible to JCV seroconversion by treatment, but natalizumab might facilitate seroconversion in patients who are susceptible.
No research has examined the influence of other MS treatments on JCV index values, and the investigators thus cannot be certain that natalizumab treatment caused the increase in index values observed in the study. But because there was no correlation between age and index value in JCV-positive patients, it is valid to speculate that natalizumab treatment induces rising JCV index values.
“If the hypothesis that treatment with natalizumab is associated with enhanced JCV seroconversion and higher index values is proven, it would also be important to determine whether cessation of natalizumab therapy (or perhaps prolonged infusion intervals) could lead to lower JCV index values as well,” Dr. Wiendl continued. The association “does not diminish [natalizumab’s] clinical efficacy, but calls for more elaborate strategies for PML risk stratification according to current scientific developments, also regarding patients with prior use of immunosuppressants, where the JCV index is not helpful.
“It is important that people with MS taking natalizumab speak with their doctor before making any changes to their treatment,” Dr. Wiendl added. “Still, this study shows anti-JCV antibodies may serve as a useful biomarker…. The results of this study underscore the need for frequent monitoring of anti-JCV antibodies in people who are being treated with natalizumab for MS.”
JCV serology, however, should not be the only PML risk biomarker to stratify patients treated with natalizumab, said Dr. Wiendl. Neurologists should explore and potentially apply additional biomarkers such as CD62L in peripheral blood or IgM bands in CSF. Together, all of these biomarkers may provide more accurate information about patients’ PML risk and help reduce the incidence of PML.
The investigators’ data extend earlier paired, longitudinal studies in various countries of patients treated with natalizumab who had similarly high rates of conversion and a rise in titers, said Adil Javed, MD, PhD, Associate Professor of Neurology, and Anthony T. Reder, MD, Professor of Neurology, both at the University of Chicago, in an accompanying editorial. Although the JCV index appears to be a valid serum marker of risk for PML, “risk is relative,” they said. “Despite a higher JCV replication state, an increase in JCV-antibody index does not necessarily mean that PML infection is imminent…. Schwab et al extend growing observations that JCV-antibody index values need to be monitored and that seroconversion or rising JCV-antibody titers alter the risk of PML in patients treated with natalizumab.”
—Erik Greb
Suggested Reading
Schwab N, Schneider-Hohendorf T, Pignolet B, et al. Therapy with natalizumab is associated with high JCV seroconversion and rising JCV index values. Neurol Neuroimmunol Neuroinflamm. 2016;3(1):e195.
Javed A, Reder AT. Rising JCV-Ab index during natalizumab therapy for MS: Inauspicious for a highly efficacious drug. Neurol Neuroimmunol Neuroinflamm. 2016;3(1):e199.
Suggested Reading
Schwab N, Schneider-Hohendorf T, Pignolet B, et al. Therapy with natalizumab is associated with high JCV seroconversion and rising JCV index values. Neurol Neuroimmunol Neuroinflamm. 2016;3(1):e195.
Javed A, Reder AT. Rising JCV-Ab index during natalizumab therapy for MS: Inauspicious for a highly efficacious drug. Neurol Neuroimmunol Neuroinflamm. 2016;3(1):e199.
Key Elements of Critical Care
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.

Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1

Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
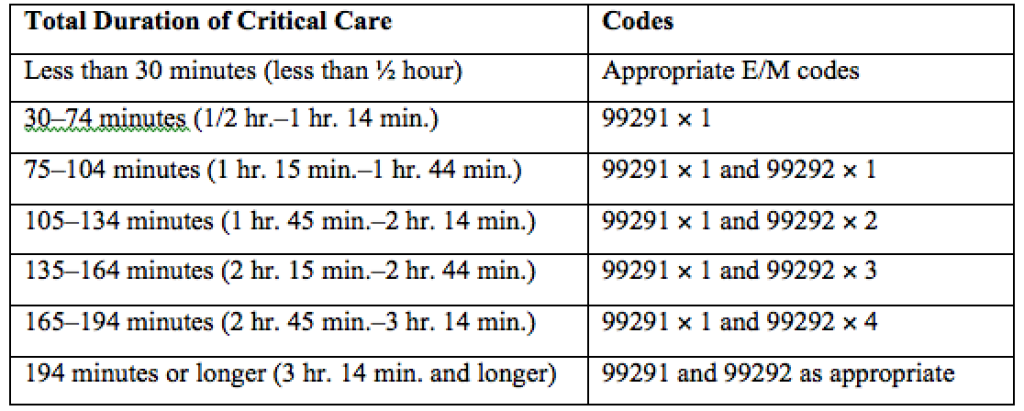
Pre-labor cesarean delivery linked to ALL

Photo by Nina Matthews
Researchers have found a potential correlation between pre-labor cesarean delivery (PLCD) and acute lymphoblastic leukemia (ALL).
The team analyzed data from 13 studies and found a 23% increase in the risk of ALL in children born by PLCD.
However, there was no link between PLCD and acute myeloid leukemia (AML), and there was no correlation between emergency cesareans and ALL or AML.
Erin Marcotte, PhD, of the University of Minnesota, and her colleagues reported these results in The Lancet Haematology.
The researchers analyzed data from the Childhood Leukemia International Consortium. They looked at 33,571 subjects overall, including 23,351 control subjects, 8780 cases of ALL, and 1332 cases of AML.
The analyses were controlled for a number of outside factors, including breastfeeding, parental education levels, and ethnicity.
“Our goal was to determine if there was an association between cesarean deliveries and ALL [and] to identify potential new targets for research into cancer prevention if there is a correlation,” Dr Marcotte said.
“While the link between overall cesarean delivery and childhood leukemia was not statistically significant, it was notable to find an association between pre-labor cesarean delivery and ALL.”
The data suggested AML was not associated with cesarean delivery. The odds ratios (ORs) were 0.99 for all cesarean deliveries, 0.83 for PLCD, and 1.05 for emergency cesarean delivery.
The ORs for ALL were 1.06 overall, 1.02 for emergency cesarean delivery, and 1.23 (P=0.018) for PLCD.
The reason for the increased risk of ALL with PLCD is not known. The researchers said several mechanisms may be at play, including the stress response in the fetus caused by labor and the colonization of microbiota a newborn experiences during a vaginal delivery that is missed during a cesarean birth.
“The most plausible explanation for the association between ALL and pre-labor cesarean delivery is in the cortisol, or stress-related, mechanism,” Dr Marcotte said. “Because ALL is not associated with all cesarean deliveries, it seems less likely the microbiota colonization is a significant factor in this phenomenon. We believe further investigation into this cortisol-mechanism link is warranted due to these findings.”
The researchers said the strength of association in these findings is comparable to other studies looking at cesarean delivery rates and other childhood outcomes, including Type I diabetes and asthma. They believe further investigation into this study’s findings is needed, utilizing more detailed and reliable delivery information.
“This association deserves a closer look to better determine what’s behind the link,” said Logan Spector, PhD, of the University of Minnesota.
“Cortisol exposure is plausible since similar compounds are used to treat ALL. We also know that some are born with cells that are on the path to becoming leukemia. Thus, our working hypothesis is that cortisol exposure at birth may eliminate these pre-leukemic cells.” ![]()
Photo by Nina Matthews
Researchers have found a potential correlation between pre-labor cesarean delivery (PLCD) and acute lymphoblastic leukemia (ALL).
The team analyzed data from 13 studies and found a 23% increase in the risk of ALL in children born by PLCD.
However, there was no link between PLCD and acute myeloid leukemia (AML), and there was no correlation between emergency cesareans and ALL or AML.
Erin Marcotte, PhD, of the University of Minnesota, and her colleagues reported these results in The Lancet Haematology.
The researchers analyzed data from the Childhood Leukemia International Consortium. They looked at 33,571 subjects overall, including 23,351 control subjects, 8780 cases of ALL, and 1332 cases of AML.
The analyses were controlled for a number of outside factors, including breastfeeding, parental education levels, and ethnicity.
“Our goal was to determine if there was an association between cesarean deliveries and ALL [and] to identify potential new targets for research into cancer prevention if there is a correlation,” Dr Marcotte said.
“While the link between overall cesarean delivery and childhood leukemia was not statistically significant, it was notable to find an association between pre-labor cesarean delivery and ALL.”
The data suggested AML was not associated with cesarean delivery. The odds ratios (ORs) were 0.99 for all cesarean deliveries, 0.83 for PLCD, and 1.05 for emergency cesarean delivery.
The ORs for ALL were 1.06 overall, 1.02 for emergency cesarean delivery, and 1.23 (P=0.018) for PLCD.
The reason for the increased risk of ALL with PLCD is not known. The researchers said several mechanisms may be at play, including the stress response in the fetus caused by labor and the colonization of microbiota a newborn experiences during a vaginal delivery that is missed during a cesarean birth.
“The most plausible explanation for the association between ALL and pre-labor cesarean delivery is in the cortisol, or stress-related, mechanism,” Dr Marcotte said. “Because ALL is not associated with all cesarean deliveries, it seems less likely the microbiota colonization is a significant factor in this phenomenon. We believe further investigation into this cortisol-mechanism link is warranted due to these findings.”
The researchers said the strength of association in these findings is comparable to other studies looking at cesarean delivery rates and other childhood outcomes, including Type I diabetes and asthma. They believe further investigation into this study’s findings is needed, utilizing more detailed and reliable delivery information.
“This association deserves a closer look to better determine what’s behind the link,” said Logan Spector, PhD, of the University of Minnesota.
“Cortisol exposure is plausible since similar compounds are used to treat ALL. We also know that some are born with cells that are on the path to becoming leukemia. Thus, our working hypothesis is that cortisol exposure at birth may eliminate these pre-leukemic cells.” ![]()
Photo by Nina Matthews
Researchers have found a potential correlation between pre-labor cesarean delivery (PLCD) and acute lymphoblastic leukemia (ALL).
The team analyzed data from 13 studies and found a 23% increase in the risk of ALL in children born by PLCD.
However, there was no link between PLCD and acute myeloid leukemia (AML), and there was no correlation between emergency cesareans and ALL or AML.
Erin Marcotte, PhD, of the University of Minnesota, and her colleagues reported these results in The Lancet Haematology.
The researchers analyzed data from the Childhood Leukemia International Consortium. They looked at 33,571 subjects overall, including 23,351 control subjects, 8780 cases of ALL, and 1332 cases of AML.
The analyses were controlled for a number of outside factors, including breastfeeding, parental education levels, and ethnicity.
“Our goal was to determine if there was an association between cesarean deliveries and ALL [and] to identify potential new targets for research into cancer prevention if there is a correlation,” Dr Marcotte said.
“While the link between overall cesarean delivery and childhood leukemia was not statistically significant, it was notable to find an association between pre-labor cesarean delivery and ALL.”
The data suggested AML was not associated with cesarean delivery. The odds ratios (ORs) were 0.99 for all cesarean deliveries, 0.83 for PLCD, and 1.05 for emergency cesarean delivery.
The ORs for ALL were 1.06 overall, 1.02 for emergency cesarean delivery, and 1.23 (P=0.018) for PLCD.
The reason for the increased risk of ALL with PLCD is not known. The researchers said several mechanisms may be at play, including the stress response in the fetus caused by labor and the colonization of microbiota a newborn experiences during a vaginal delivery that is missed during a cesarean birth.
“The most plausible explanation for the association between ALL and pre-labor cesarean delivery is in the cortisol, or stress-related, mechanism,” Dr Marcotte said. “Because ALL is not associated with all cesarean deliveries, it seems less likely the microbiota colonization is a significant factor in this phenomenon. We believe further investigation into this cortisol-mechanism link is warranted due to these findings.”
The researchers said the strength of association in these findings is comparable to other studies looking at cesarean delivery rates and other childhood outcomes, including Type I diabetes and asthma. They believe further investigation into this study’s findings is needed, utilizing more detailed and reliable delivery information.
“This association deserves a closer look to better determine what’s behind the link,” said Logan Spector, PhD, of the University of Minnesota.
“Cortisol exposure is plausible since similar compounds are used to treat ALL. We also know that some are born with cells that are on the path to becoming leukemia. Thus, our working hypothesis is that cortisol exposure at birth may eliminate these pre-leukemic cells.” ![]()