User login
Standard Triple Therapy for H. Pylori Lowest Ranked among 14 Treatment Regimens
Clinical question: How do current Helicobacter pylori treatments compare in efficacy and tolerance?
Background: Efficacy of standard “triple therapy” for H. pylori (proton pump inhibitor plus clarithromycin and amoxicillin or metronidazole) is declining due to the development of antibiotic resistance. Different medication combinations and/or time courses are currently used, but comparative effectiveness of these treatments has not been evaluated comprehensively.
Study design: Systematic review and network meta-analysis.
Setting: Cochrane Library, PubMed, and Embase databases.
Synopsis: One hundred forty-three RCTs evaluating a total of 14 treatments for H. pylori were identified. Network meta-analysis was performed to rank order treatments for efficacy (eradication rate of H. pylori) and tolerance (adverse event occurrence rate). Seven days of “concomitant treatment” (proton pump inhibitor plus three antibiotics) ranked the highest in efficacy (eradication rate 0.94; 95% confidence interval [CI] 0.89-0.98), though this treatment group comprised a very small proportion of overall participants and studies and may be subject to bias. Seven days of standard “triple therapy” ranked the lowest in efficacy (eradication rate 0.73; 95% CI 0.71-0.75).
Of note, subgroup analysis showed variation in efficacy rankings by geographic location, suggesting that findings may not be universally applicable. Only two treatments showed significantly different adverse event occurrence rates compared to standard “triple therapy,” indicating overall similar tolerance for most treatments.
Bottom line: Several treatment regimens may be more effective than standard H. pylori “triple therapy” and equally well tolerated.
Citation: Li BZ, Threapleton DE, Wang JY, et al. Comparative effectiveness and tolerance of treatments for Helicobacter pylori: systematic review and network meta-analysis. BMJ. 2015;351:h4052.
Clinical question: How do current Helicobacter pylori treatments compare in efficacy and tolerance?
Background: Efficacy of standard “triple therapy” for H. pylori (proton pump inhibitor plus clarithromycin and amoxicillin or metronidazole) is declining due to the development of antibiotic resistance. Different medication combinations and/or time courses are currently used, but comparative effectiveness of these treatments has not been evaluated comprehensively.
Study design: Systematic review and network meta-analysis.
Setting: Cochrane Library, PubMed, and Embase databases.
Synopsis: One hundred forty-three RCTs evaluating a total of 14 treatments for H. pylori were identified. Network meta-analysis was performed to rank order treatments for efficacy (eradication rate of H. pylori) and tolerance (adverse event occurrence rate). Seven days of “concomitant treatment” (proton pump inhibitor plus three antibiotics) ranked the highest in efficacy (eradication rate 0.94; 95% confidence interval [CI] 0.89-0.98), though this treatment group comprised a very small proportion of overall participants and studies and may be subject to bias. Seven days of standard “triple therapy” ranked the lowest in efficacy (eradication rate 0.73; 95% CI 0.71-0.75).
Of note, subgroup analysis showed variation in efficacy rankings by geographic location, suggesting that findings may not be universally applicable. Only two treatments showed significantly different adverse event occurrence rates compared to standard “triple therapy,” indicating overall similar tolerance for most treatments.
Bottom line: Several treatment regimens may be more effective than standard H. pylori “triple therapy” and equally well tolerated.
Citation: Li BZ, Threapleton DE, Wang JY, et al. Comparative effectiveness and tolerance of treatments for Helicobacter pylori: systematic review and network meta-analysis. BMJ. 2015;351:h4052.
Clinical question: How do current Helicobacter pylori treatments compare in efficacy and tolerance?
Background: Efficacy of standard “triple therapy” for H. pylori (proton pump inhibitor plus clarithromycin and amoxicillin or metronidazole) is declining due to the development of antibiotic resistance. Different medication combinations and/or time courses are currently used, but comparative effectiveness of these treatments has not been evaluated comprehensively.
Study design: Systematic review and network meta-analysis.
Setting: Cochrane Library, PubMed, and Embase databases.
Synopsis: One hundred forty-three RCTs evaluating a total of 14 treatments for H. pylori were identified. Network meta-analysis was performed to rank order treatments for efficacy (eradication rate of H. pylori) and tolerance (adverse event occurrence rate). Seven days of “concomitant treatment” (proton pump inhibitor plus three antibiotics) ranked the highest in efficacy (eradication rate 0.94; 95% confidence interval [CI] 0.89-0.98), though this treatment group comprised a very small proportion of overall participants and studies and may be subject to bias. Seven days of standard “triple therapy” ranked the lowest in efficacy (eradication rate 0.73; 95% CI 0.71-0.75).
Of note, subgroup analysis showed variation in efficacy rankings by geographic location, suggesting that findings may not be universally applicable. Only two treatments showed significantly different adverse event occurrence rates compared to standard “triple therapy,” indicating overall similar tolerance for most treatments.
Bottom line: Several treatment regimens may be more effective than standard H. pylori “triple therapy” and equally well tolerated.
Citation: Li BZ, Threapleton DE, Wang JY, et al. Comparative effectiveness and tolerance of treatments for Helicobacter pylori: systematic review and network meta-analysis. BMJ. 2015;351:h4052.
Social Isolation, Polypharmacy Predict Medication Noncompliance Post-Discharge in Cardiac Patients
Clinical question: What are predictors of primary medication nonadherence after discharge?
Background: Primary nonadherence occurs when a patient receives a prescription at hospital discharge but does not fill it. Predictors of post-discharge primary nonadherence could serve as useful targets to guide adherence interventions.
Study design: RCT, secondary analysis.
Setting: Two tertiary care, U.S. academic hospitals.
Synopsis: Using the Pharmacist Intervention for Low Literacy in Cardiovascular Disease (PILL-CVD) study database, investigators conducted a secondary analysis of adults hospitalized for acute coronary syndrome or acute decompensated heart failure who received pharmacist-assisted medication reconciliation, discharge counseling, low-literacy adherence aids, and a follow-up phone call. The prevalence of primary nonadherence one to four days post-discharge was 9.4% among 341 patients. In subsequent multivariate analysis, significant factors for noncompliance were living alone (odds ratio 2.2, 95% CI 1.01-4.8, P=0.047) and more than 10 total discharge medications (odds ratio 2.3, 95% CI 1.05-4.98, P=0.036).
Limitations to this study include biases from patient-reported outcomes, lack of patient copayment data, and limited characterization of discharge medication type.
Bottom line: Among patients hospitalized for cardiac events, social isolation and polypharmacy predict primary medication nonadherence to discharge medications despite intensive pharmacist counseling.
Citation: Wooldridge K, Schnipper JL, Goggins K, Dittus RS, Kripalani S. Refractory primary medication nonadherence: prevalence and predictors after pharmacist counseling at hospital discharge [published online ahead of print August 21, 2015]. J Hosp Med. doi: 10.1002/jhm.2446.
Clinical question: What are predictors of primary medication nonadherence after discharge?
Background: Primary nonadherence occurs when a patient receives a prescription at hospital discharge but does not fill it. Predictors of post-discharge primary nonadherence could serve as useful targets to guide adherence interventions.
Study design: RCT, secondary analysis.
Setting: Two tertiary care, U.S. academic hospitals.
Synopsis: Using the Pharmacist Intervention for Low Literacy in Cardiovascular Disease (PILL-CVD) study database, investigators conducted a secondary analysis of adults hospitalized for acute coronary syndrome or acute decompensated heart failure who received pharmacist-assisted medication reconciliation, discharge counseling, low-literacy adherence aids, and a follow-up phone call. The prevalence of primary nonadherence one to four days post-discharge was 9.4% among 341 patients. In subsequent multivariate analysis, significant factors for noncompliance were living alone (odds ratio 2.2, 95% CI 1.01-4.8, P=0.047) and more than 10 total discharge medications (odds ratio 2.3, 95% CI 1.05-4.98, P=0.036).
Limitations to this study include biases from patient-reported outcomes, lack of patient copayment data, and limited characterization of discharge medication type.
Bottom line: Among patients hospitalized for cardiac events, social isolation and polypharmacy predict primary medication nonadherence to discharge medications despite intensive pharmacist counseling.
Citation: Wooldridge K, Schnipper JL, Goggins K, Dittus RS, Kripalani S. Refractory primary medication nonadherence: prevalence and predictors after pharmacist counseling at hospital discharge [published online ahead of print August 21, 2015]. J Hosp Med. doi: 10.1002/jhm.2446.
Clinical question: What are predictors of primary medication nonadherence after discharge?
Background: Primary nonadherence occurs when a patient receives a prescription at hospital discharge but does not fill it. Predictors of post-discharge primary nonadherence could serve as useful targets to guide adherence interventions.
Study design: RCT, secondary analysis.
Setting: Two tertiary care, U.S. academic hospitals.
Synopsis: Using the Pharmacist Intervention for Low Literacy in Cardiovascular Disease (PILL-CVD) study database, investigators conducted a secondary analysis of adults hospitalized for acute coronary syndrome or acute decompensated heart failure who received pharmacist-assisted medication reconciliation, discharge counseling, low-literacy adherence aids, and a follow-up phone call. The prevalence of primary nonadherence one to four days post-discharge was 9.4% among 341 patients. In subsequent multivariate analysis, significant factors for noncompliance were living alone (odds ratio 2.2, 95% CI 1.01-4.8, P=0.047) and more than 10 total discharge medications (odds ratio 2.3, 95% CI 1.05-4.98, P=0.036).
Limitations to this study include biases from patient-reported outcomes, lack of patient copayment data, and limited characterization of discharge medication type.
Bottom line: Among patients hospitalized for cardiac events, social isolation and polypharmacy predict primary medication nonadherence to discharge medications despite intensive pharmacist counseling.
Citation: Wooldridge K, Schnipper JL, Goggins K, Dittus RS, Kripalani S. Refractory primary medication nonadherence: prevalence and predictors after pharmacist counseling at hospital discharge [published online ahead of print August 21, 2015]. J Hosp Med. doi: 10.1002/jhm.2446.
Inpatient Navigators Reduce Length of Stay without Increasing Readmissions
Clinical question: Does a patient navigator (PN) who facilitates communication between patients and providers impact hospital length of stay (LOS) and readmissions?
Background: Increasing complexity of hospitalization challenges the safety of care transitions. There are few studies about the effectiveness of innovations targeting both communication and transitional care planning.
Study design: Retrospective, cohort study.
Setting: Single academic health center in Canada, 2010-2014.
Synopsis: PNs, dedicated team-based facilitators not responsible for clinical care, served as liaisons between patients and providers on general medicine teams. They rounded with medical teams, tracked action items, expedited tests and consults, and proactively served as direct primary contacts for patients/families during and after hospitalization. PNs had no specified prior training; they underwent on-the-job training with regular feedback.
Researchers matched 7,841 hospitalizations (5,628 with PN; 2,213 without) by case mix, age, and resource intensity. LOS and 30-day readmissions were primary outcomes. Hospitalizations with PNs were 21% shorter (1.3 days; 6.2 v 7.5 days, P<0.001) than those without PNs.
There were no differences in 30-day readmission rates (13.1 v 13.8%, P=0.48). In this single center study in Canada, the impact of PN salaries (the only program cost) relative to savings is unknown.
Bottom line: Inpatient navigators streamline communication and decrease LOS without increasing readmissions. Additional cost-benefit analyses are needed.
Citation: Kwan JL, Morgan MW, Stewart TE, Bell CM. Impact of an innovative patient navigator program on length of stay and 30-day readmission [published online ahead of print August 10, 2015]. J Hosp Med. doi: 10.1002/jhm.2442.
Clinical question: Does a patient navigator (PN) who facilitates communication between patients and providers impact hospital length of stay (LOS) and readmissions?
Background: Increasing complexity of hospitalization challenges the safety of care transitions. There are few studies about the effectiveness of innovations targeting both communication and transitional care planning.
Study design: Retrospective, cohort study.
Setting: Single academic health center in Canada, 2010-2014.
Synopsis: PNs, dedicated team-based facilitators not responsible for clinical care, served as liaisons between patients and providers on general medicine teams. They rounded with medical teams, tracked action items, expedited tests and consults, and proactively served as direct primary contacts for patients/families during and after hospitalization. PNs had no specified prior training; they underwent on-the-job training with regular feedback.
Researchers matched 7,841 hospitalizations (5,628 with PN; 2,213 without) by case mix, age, and resource intensity. LOS and 30-day readmissions were primary outcomes. Hospitalizations with PNs were 21% shorter (1.3 days; 6.2 v 7.5 days, P<0.001) than those without PNs.
There were no differences in 30-day readmission rates (13.1 v 13.8%, P=0.48). In this single center study in Canada, the impact of PN salaries (the only program cost) relative to savings is unknown.
Bottom line: Inpatient navigators streamline communication and decrease LOS without increasing readmissions. Additional cost-benefit analyses are needed.
Citation: Kwan JL, Morgan MW, Stewart TE, Bell CM. Impact of an innovative patient navigator program on length of stay and 30-day readmission [published online ahead of print August 10, 2015]. J Hosp Med. doi: 10.1002/jhm.2442.
Clinical question: Does a patient navigator (PN) who facilitates communication between patients and providers impact hospital length of stay (LOS) and readmissions?
Background: Increasing complexity of hospitalization challenges the safety of care transitions. There are few studies about the effectiveness of innovations targeting both communication and transitional care planning.
Study design: Retrospective, cohort study.
Setting: Single academic health center in Canada, 2010-2014.
Synopsis: PNs, dedicated team-based facilitators not responsible for clinical care, served as liaisons between patients and providers on general medicine teams. They rounded with medical teams, tracked action items, expedited tests and consults, and proactively served as direct primary contacts for patients/families during and after hospitalization. PNs had no specified prior training; they underwent on-the-job training with regular feedback.
Researchers matched 7,841 hospitalizations (5,628 with PN; 2,213 without) by case mix, age, and resource intensity. LOS and 30-day readmissions were primary outcomes. Hospitalizations with PNs were 21% shorter (1.3 days; 6.2 v 7.5 days, P<0.001) than those without PNs.
There were no differences in 30-day readmission rates (13.1 v 13.8%, P=0.48). In this single center study in Canada, the impact of PN salaries (the only program cost) relative to savings is unknown.
Bottom line: Inpatient navigators streamline communication and decrease LOS without increasing readmissions. Additional cost-benefit analyses are needed.
Citation: Kwan JL, Morgan MW, Stewart TE, Bell CM. Impact of an innovative patient navigator program on length of stay and 30-day readmission [published online ahead of print August 10, 2015]. J Hosp Med. doi: 10.1002/jhm.2442.
Dexamethasone Potential Therapy for Asthma Exacerbations in Pediatric Inpatients
Clinical question: In children hospitalized in a non-ICU setting with asthma exacerbation, how effective is dexamethasone compared to prednisone/prednisolone?
Background: Asthma is the second most common reason for hospital admission in childhood.1 National guidelines recommend treatment with systemic corticosteroids in addition to beta-agonists.2 Traditionally, prednisone/prednisolone has been used for asthma exacerbations, but multiple recent studies in ED settings have shown equal efficacy with dexamethasone for mild to moderate exacerbations. Benefits of dexamethasone use include a longer half-life (so single dose or two-day courses can be used), good enteral absorption, general palatability, less emesis, and better adherence. To this point, no studies have compared dexamethasone with prednisone/prednisolone therapy in hospitalized children.
Study design: Multicenter, retrospective cohort study.
Setting: Freestanding, tertiary care children’s hospitals.
Synopsis: The authors used the PHIS (Pediatric Health Information System) database, which includes clinical and billing data from 42 children’s hospitals, to compare children who received dexamethasone to those who were treated with prednisone/prednisolone therapy for asthma exacerbations in the inpatient setting. Patients were included if they were aged four to 17 years, were hospitalized between January 2007 and December 2012 with ICD-9 code for a principal diagnosis of asthma, and received either dexamethasone or prednisone/prednisolone.
Exclusion criteria included:
- Management in the ICU at the time of admission;
- All patient refined diagnosis related groups (APR-DRG) severity level moderate or extreme;
- Complex chronic conditions;
- Secondary diagnosis other than asthma requiring steroids, or treatment with racemic epinephrine;
- Only the first admission was included out of multiple hospitalizations within a 30-day period; and/or
- Patient was treated with both dexamethasone and prednisone/prednisolone.
The primary outcome evaluated was length of stay (LOS); secondary outcomes included readmissions, cost, and transfer to ICU during hospitalization. The authors compared the overall groups, then performed 1:1 propensity score matching to address residual confounding; this statistical technique closely matches patient characteristics between cohorts.
Overall, there were 40,257 hospitalizations, with 1,166 children (2.9%) receiving dexamethasone and 39,091 (97.1%) receiving prednisone/prednisolone. The use of dexamethasone varied greatly between hospitals (35/42 hospitals used dexamethasone, with rates ranging from 0.047% to 77.4%).
In the post-match cohort, 1,284 patients were evaluated, 642 in each group. In this cohort, patients with dexamethasone had significantly shorter LOS (67.4% had LOS less than one day vs. 59.5% in the prednisone/prednisolone group; 6.7% of dexamethasone patients had LOS of more than three days vs. 12% of prednisone/prednisolone patients). Costs were lower for the dexamethasone group, both for the index admission and for episode admission (defined as index admission plus seven-day readmissions). There was no difference in readmissions between the groups, and no patients in this cohort were transferred to the ICU.
There are several limitations to this study. Dexamethasone use varied widely among participating hospitals. The data source did not permit access to dosing, duration, or compliance with therapy and could not compare albuterol use between groups. The findings may not be generalizable to all populations, because it excluded patients with high severity and medical complexity and only evaluated tertiary care children’s hospitals.
Bottom line: Dexamethasone is a potential alternative therapy for asthma exacerbations in the inpatient setting. Further studies are needed to evaluate effectiveness, including dosing, frequency, and duration.
Citation: Parikh K, Hall M, Mittal V, et al. Comparative effectiveness of dexamethasone versus prednisone in children hospitalized with asthma. J Pediatr. 2015;167(3):639-644.

References
- Yu H, Wier LM, Elixhauser A. Hospital stays for children, 2009. HCUP statistical brief #118. Agency for Healthcare Research and Quality. August 2011. Accessed November 1, 2015.
- National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma–Summary Report 2007. Accessed November 1, 2015.
Clinical question: In children hospitalized in a non-ICU setting with asthma exacerbation, how effective is dexamethasone compared to prednisone/prednisolone?
Background: Asthma is the second most common reason for hospital admission in childhood.1 National guidelines recommend treatment with systemic corticosteroids in addition to beta-agonists.2 Traditionally, prednisone/prednisolone has been used for asthma exacerbations, but multiple recent studies in ED settings have shown equal efficacy with dexamethasone for mild to moderate exacerbations. Benefits of dexamethasone use include a longer half-life (so single dose or two-day courses can be used), good enteral absorption, general palatability, less emesis, and better adherence. To this point, no studies have compared dexamethasone with prednisone/prednisolone therapy in hospitalized children.
Study design: Multicenter, retrospective cohort study.
Setting: Freestanding, tertiary care children’s hospitals.
Synopsis: The authors used the PHIS (Pediatric Health Information System) database, which includes clinical and billing data from 42 children’s hospitals, to compare children who received dexamethasone to those who were treated with prednisone/prednisolone therapy for asthma exacerbations in the inpatient setting. Patients were included if they were aged four to 17 years, were hospitalized between January 2007 and December 2012 with ICD-9 code for a principal diagnosis of asthma, and received either dexamethasone or prednisone/prednisolone.
Exclusion criteria included:
- Management in the ICU at the time of admission;
- All patient refined diagnosis related groups (APR-DRG) severity level moderate or extreme;
- Complex chronic conditions;
- Secondary diagnosis other than asthma requiring steroids, or treatment with racemic epinephrine;
- Only the first admission was included out of multiple hospitalizations within a 30-day period; and/or
- Patient was treated with both dexamethasone and prednisone/prednisolone.
The primary outcome evaluated was length of stay (LOS); secondary outcomes included readmissions, cost, and transfer to ICU during hospitalization. The authors compared the overall groups, then performed 1:1 propensity score matching to address residual confounding; this statistical technique closely matches patient characteristics between cohorts.
Overall, there were 40,257 hospitalizations, with 1,166 children (2.9%) receiving dexamethasone and 39,091 (97.1%) receiving prednisone/prednisolone. The use of dexamethasone varied greatly between hospitals (35/42 hospitals used dexamethasone, with rates ranging from 0.047% to 77.4%).
In the post-match cohort, 1,284 patients were evaluated, 642 in each group. In this cohort, patients with dexamethasone had significantly shorter LOS (67.4% had LOS less than one day vs. 59.5% in the prednisone/prednisolone group; 6.7% of dexamethasone patients had LOS of more than three days vs. 12% of prednisone/prednisolone patients). Costs were lower for the dexamethasone group, both for the index admission and for episode admission (defined as index admission plus seven-day readmissions). There was no difference in readmissions between the groups, and no patients in this cohort were transferred to the ICU.
There are several limitations to this study. Dexamethasone use varied widely among participating hospitals. The data source did not permit access to dosing, duration, or compliance with therapy and could not compare albuterol use between groups. The findings may not be generalizable to all populations, because it excluded patients with high severity and medical complexity and only evaluated tertiary care children’s hospitals.
Bottom line: Dexamethasone is a potential alternative therapy for asthma exacerbations in the inpatient setting. Further studies are needed to evaluate effectiveness, including dosing, frequency, and duration.
Citation: Parikh K, Hall M, Mittal V, et al. Comparative effectiveness of dexamethasone versus prednisone in children hospitalized with asthma. J Pediatr. 2015;167(3):639-644.
References
- Yu H, Wier LM, Elixhauser A. Hospital stays for children, 2009. HCUP statistical brief #118. Agency for Healthcare Research and Quality. August 2011. Accessed November 1, 2015.
- National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma–Summary Report 2007. Accessed November 1, 2015.
Clinical question: In children hospitalized in a non-ICU setting with asthma exacerbation, how effective is dexamethasone compared to prednisone/prednisolone?
Background: Asthma is the second most common reason for hospital admission in childhood.1 National guidelines recommend treatment with systemic corticosteroids in addition to beta-agonists.2 Traditionally, prednisone/prednisolone has been used for asthma exacerbations, but multiple recent studies in ED settings have shown equal efficacy with dexamethasone for mild to moderate exacerbations. Benefits of dexamethasone use include a longer half-life (so single dose or two-day courses can be used), good enteral absorption, general palatability, less emesis, and better adherence. To this point, no studies have compared dexamethasone with prednisone/prednisolone therapy in hospitalized children.
Study design: Multicenter, retrospective cohort study.
Setting: Freestanding, tertiary care children’s hospitals.
Synopsis: The authors used the PHIS (Pediatric Health Information System) database, which includes clinical and billing data from 42 children’s hospitals, to compare children who received dexamethasone to those who were treated with prednisone/prednisolone therapy for asthma exacerbations in the inpatient setting. Patients were included if they were aged four to 17 years, were hospitalized between January 2007 and December 2012 with ICD-9 code for a principal diagnosis of asthma, and received either dexamethasone or prednisone/prednisolone.
Exclusion criteria included:
- Management in the ICU at the time of admission;
- All patient refined diagnosis related groups (APR-DRG) severity level moderate or extreme;
- Complex chronic conditions;
- Secondary diagnosis other than asthma requiring steroids, or treatment with racemic epinephrine;
- Only the first admission was included out of multiple hospitalizations within a 30-day period; and/or
- Patient was treated with both dexamethasone and prednisone/prednisolone.
The primary outcome evaluated was length of stay (LOS); secondary outcomes included readmissions, cost, and transfer to ICU during hospitalization. The authors compared the overall groups, then performed 1:1 propensity score matching to address residual confounding; this statistical technique closely matches patient characteristics between cohorts.
Overall, there were 40,257 hospitalizations, with 1,166 children (2.9%) receiving dexamethasone and 39,091 (97.1%) receiving prednisone/prednisolone. The use of dexamethasone varied greatly between hospitals (35/42 hospitals used dexamethasone, with rates ranging from 0.047% to 77.4%).
In the post-match cohort, 1,284 patients were evaluated, 642 in each group. In this cohort, patients with dexamethasone had significantly shorter LOS (67.4% had LOS less than one day vs. 59.5% in the prednisone/prednisolone group; 6.7% of dexamethasone patients had LOS of more than three days vs. 12% of prednisone/prednisolone patients). Costs were lower for the dexamethasone group, both for the index admission and for episode admission (defined as index admission plus seven-day readmissions). There was no difference in readmissions between the groups, and no patients in this cohort were transferred to the ICU.
There are several limitations to this study. Dexamethasone use varied widely among participating hospitals. The data source did not permit access to dosing, duration, or compliance with therapy and could not compare albuterol use between groups. The findings may not be generalizable to all populations, because it excluded patients with high severity and medical complexity and only evaluated tertiary care children’s hospitals.
Bottom line: Dexamethasone is a potential alternative therapy for asthma exacerbations in the inpatient setting. Further studies are needed to evaluate effectiveness, including dosing, frequency, and duration.
Citation: Parikh K, Hall M, Mittal V, et al. Comparative effectiveness of dexamethasone versus prednisone in children hospitalized with asthma. J Pediatr. 2015;167(3):639-644.
References
- Yu H, Wier LM, Elixhauser A. Hospital stays for children, 2009. HCUP statistical brief #118. Agency for Healthcare Research and Quality. August 2011. Accessed November 1, 2015.
- National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma–Summary Report 2007. Accessed November 1, 2015.
What Are the Strategies for Secondary Stroke Prevention after Transient Ischemic Attack?
Case
Mr. G is an 80-year-old man with a pacemaker, peripheral artery disease, atrial fibrillation (AF) on warfarin, and tachy-brady syndrome. He presented after experiencing episodes in which he was unable to speak and had weakness on his right side. He had a normal neurological exam upon arrival to the ED, and his blood pressure was 160/80 mm Hg.
Overview
Transient ischemic attacks (TIAs) are brief interruptions in brain perfusion that do not result in permanent neurologic damage. Up to half a million TIAs occur each year in the U.S., and they account for one third of acute cerebrovascular disease.1 While the term suggests that TIAs are benign, they are in fact an important warning sign of impending stroke and are essentially analogous to unstable angina. Some 10% of TIAs convert to full strokes within 90 days, but growing evidence suggests appropriate interventions can decrease this risk to 3%.2
Unfortunately, the symptoms of TIA have usually resolved by the time patients arrive at the hospital, which makes them challenging to diagnose. This article provides a summary of how to diagnose TIA accurately, using a focused history informed by cerebrovascular localization; how to triage, evaluate, and risk stratify patients; and how to implement preventative strategies.
Review of the Data
Classically, TIAs are defined as lasting less than 24 hours; however, 24 hours is an arbitrary number, and most TIAs last less than one hour.1 Furthermore, this definition has evolved with advances in neuroimaging that reveal that up to 50% of classically defined TIAs have evidence of infarct on MRI.1 There is no absolute temporal cut-off after which infarct is always seen on MRI, but longer duration of symptoms correlates with a higher likelihood of infarct. To reconcile these observations, a recently proposed definition stipulates that a true TIA lasts no more than one hour and does not show evidence of infarct on MRI.3
The causes of TIA are identical to those for ischemic stroke. Cerebral ischemia can result from an embolus, arterial thrombosis, or hypoperfusion due to arterial stenosis. Emboli can be cardiac, most commonly due to AF, or non-cardiac, stemming from a ruptured atherosclerotic plaque in the aortic arch, the carotid or vertebral artery, or an intracranial vessel. Atherosclerotic disease in the carotid arteries or intracranial vessels can also lead to thrombosis and occlusion or flow-related TIAs as a result of severe stenosis.
Risk factors for TIA mirror those for heart disease. Non-modifiable risk factors include older age, black race, male sex, and family history of stroke. Modifiable factors include hypertension, hyperlipidemia, tobacco smoking, diabetes, and AF.4
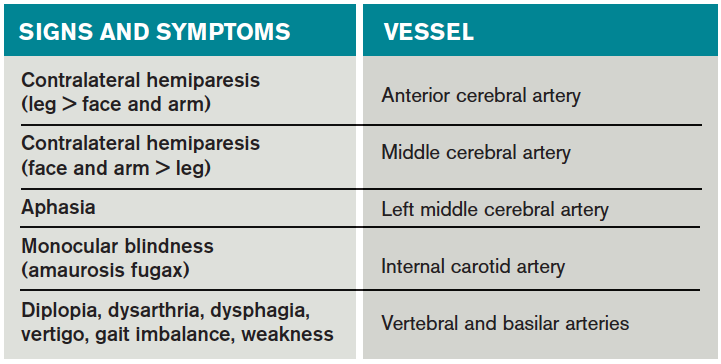
Most of the time, patients’ symptoms will have resolved by the time they are evaluated by a physician. Therefore, the diagnosis of TIA relies almost exclusively on the patient history. Eliciting a good history helps physicians determine whether the episode of transient neurologic dysfunction was caused by cerebral ischemia, as opposed to another mechanism, such as migraine or seizure. This calls for a basic understanding of cerebrovascular anatomy (see Table 1).
Types of Ischemia
Anterior cerebral artery ischemia causes contralateral leg weakness because it supplies the medial frontal and parietal lobes, where the legs in the sensorimotor homunculus are represented. Middle cerebral artery (MCA) ischemia causes contralateral face and arm weakness out of proportion to leg weakness. Ischemia in Broca’s area of the brain, which is supplied by the left MCA, may also cause expressive aphasia. Transient monocular blindness is a TIA of the retina due to atheroemboli originating from the internal carotid artery. Vertebrobasilar TIA is less common than anterior circulation TIA and manifests with brainstem symptoms that include diplopia, dysarthria, dysphagia, vertigo, gait imbalance, and weakness. In general, language and motor symptoms are more specific for cerebral ischemia and therefore more worrisome for TIA than sensory symptoms.5
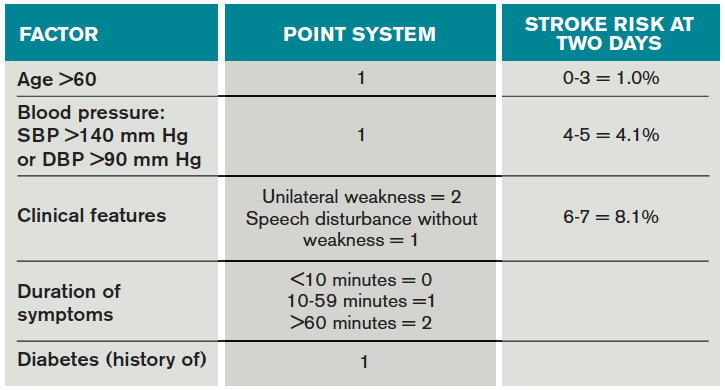
Once a clinical diagnosis of TIA is made, an ABCD2 score (age, blood pressure, clinical features, duration of TIA, presence of diabetes) can be used to predict the short-term risk of subsequent stroke (see Table 2).6,7 A general rule of thumb is to admit patients who present within 72 hours of the event and have an ABCD2 score of three or higher for observation, work-up, and initiation of secondary prevention.1
Although only a small percentage of patients with TIA will have a stroke during the period of observation in the hospital, this approach may be cost effective based on the assumption that hospitalized patients are more likely to receive intravenous tissue plasminogen activator.8 The decision should also be guided by clinical judgment. It is reasonable to admit a patient whose diagnostic workup cannot be rapidly completed.1
The workup for TIA includes routine labs, EKG with cardiac monitoring, and brain imaging. Labs are useful to evaluate for other mimics of TIA such as hyponatremia and glucose abnormalities. In addition, risk factors such as hyperlipidemia and diabetes should be evaluated with fasting lipid panel and blood glucose. The purpose of EKG and telemetry is to identify MI and capture paroxysmal AF. The goal of imaging is to ascertain the presence of vascular disease and to exclude a non-ischemic etiology. While less likely to cause transient neurologic symptoms, a hemorrhagic event must be ruled out, as it would trigger a different management pathway.
Imaging for TIA
There are two primary modes of brain imaging: computed tomography (CT) and MRI. Most patients who are suspected to have had a TIA undergo CT scan, and an infarct is seen about 20% of the time.1 The presence of an infarct usually correlates with the duration of symptoms and has prognostic value. In one study, a new infarct was associated with four times higher risk of stroke in the subsequent 90 days.9 Diffusion-weighted imaging, an MR-based technique, is the preferred modality when it is available because of its higher sensitivity and specificity for identifying acute lesions.1 In an international and multicenter study, incorporating imaging data increased the discriminatory power of stroke prediction.10
Extracranial imaging is mandatory to rule out carotid stenosis as a potential etiology of TIA. The least invasive modality is ultrasound, which can detect carotid stenosis with a sensitivity and specificity approaching 80%.1 While both the intra- and extracranial vasculature can be concurrently assessed using MR- or CT-angiography (CTA), this is not usually necessary in the acute setting, because only detecting carotid stenosis will result in a management change.1
Carotid endarterectomy is standard for symptomatic patients with greater than 70% stenosis and is a consideration for symptomatic patients with greater than 50% stenosis if it is the most probable explanation for the ischemic event.11 Despite a comprehensive workup, about 50% of TIA cases remain cryptogenic.12 In some of these patients, AF can be detected using extended ambulatory cardiac monitoring.12
The goal of admitting high-risk patients is to expedite workup and initiate therapy. Two studies have shown that immediate initiation of preventative treatment significantly reduces the risk of stroke by as much as 80%.13,14 Unless there is a specific indication for anticoagulation, all TIA patients should be started on an antiplatelet agent such as aspirin or clopidogrel. A large randomized trial conducted in China and published in 2013 demonstrated that dual antiplatelet therapy with aspirin and clopidogrel for 21 days, followed by clopidogrel monotherapy, reduced the risk of stroke compared to aspirin monotherapy. An international multicenter trial designed to test the efficacy of short-term dual antiplatelet therapy is ongoing, and if the benefit of this approach is confirmed, this will likely become the standard of care. Evidence-based indications for anticoagulation after TIA are restricted to AF and mural thrombus in the setting of recent MI. Patients with implanted mechanical devices, including left ventricular assist devices and metal heart valves, should also receive anticoagulation.15
Risk factors should also be targeted in every case. Hypertension should be treated with a goal of lower than 140/90 mm Hg (or 130/80 mm Hg in diabetics and those with renal disease). Studies have shown that patients who are discharged with a blood pressure lower than 140/90 mm Hg are more likely to maintain this blood pressure at one-year follow-up.16 The choice of medication is less well studied, but drugs that act on the renin-angiotensin-aldosterone system and thiazides are generally preferred.15 Treatment with a statin is recommended after cerebrovascular ischemic events, with a goal LDL under 100. This reduces risk of secondary stroke by about 20%.17
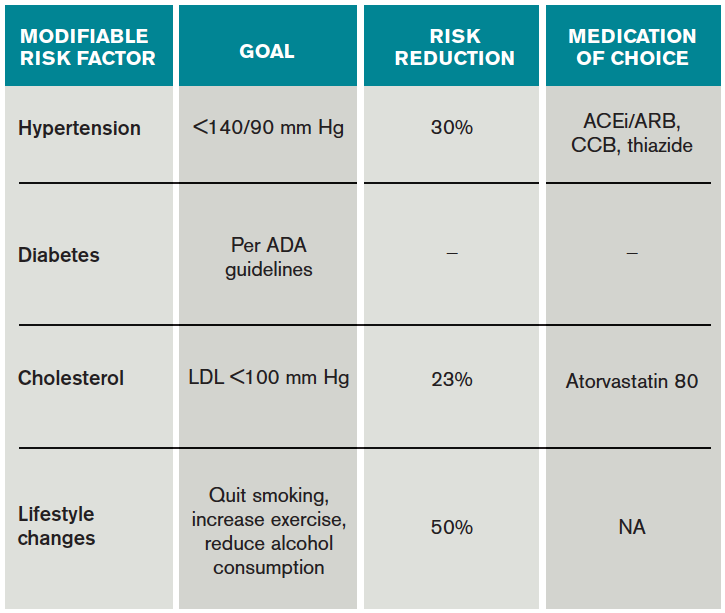
At discharge, it is also important to counsel patients on their role in preventing strokes. As with many diseases, making lifestyle changes is key to stroke prevention. Encourage smoking cessation and an increase in physical activity, and discourage heavy alcohol use. The association between smoking and the risk for first stroke is well established. Moderate to high-intensity exercise can reduce secondary stroke risk by as much as 50%18 (see Table 3). While light alcohol consumption can be protective against strokes, heavy use is strongly discouraged. Emerging data suggest obstructive sleep apnea (OSA) may be another modifiable risk factor for stroke and TIA, so screening for potential OSA and referral may be needed.15
Back to the Case
When Mr. G arrived at the ED, his symptoms had resolved. Based on the history of expressive aphasia and right-sided weakness, he most likely had a TIA in the left MCA territory. Hemorrhage was ruled out with a non-contrast head CT. His pacemaker precluded obtaining an MRI. CTA revealed diffuse atherosclerotic disease without evidence of carotid stenosis. His ABCD2 score was six given his age, blood pressure, weakness, and symptom duration, and he was admitted for an expedited workup. His sodium and glucose were within normal limits. His hemoglobin A1c was 6.5%, his LDL was 120, and his international normalized ratio (INR) was therapeutic at 2.1. His TIA may have been due to AF, despite a therapeutic INR, because warfarin does not fully eliminate the stroke risk. It might also have been caused by intracranial atherosclerosis.
Two days later, the patient was discharged on atorvastatin at 80 mg, and his lisinopril was increased for blood pressure control. For his age group, A1c of 6.5% was acceptable, and he was not initiated on glycemic control.
Bottom Line
TIAs are diagnosed based on patient history. Urgent initiation of secondary prevention is important to reduce the short-term risk of stroke and should be implemented by the time of discharge from the hospital.
Dr. Zeng is a hospitalist in the department of internal medicine at Vanderbilt University Medical Center in Nashville, and Dr. Douglas is associate professor in the department of neurology at the University of California at San Francisco.
References
- Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276-2293.
- Sundararajan V, Thrift AG, Phan TG, Choi PM, Clissold B, Srikanth VK. Trends over time in the risk of stroke after an incident transient ischemic attack. Stroke. 2014;45(11):3214-3218.
- Albers GW, Caplan LR, Easton JD, et al. Transient ischemic attack–proposal for a new definition. N Engl J Med. 2002;347(21):1713-1716.
- Grysiewicz RA, Thomas K, Pandey DK. Epidemiology of ischemic and hemorrhagic stroke: incidence, prevalence, mortality, and risk factors. Neurol Clin. 2008;26(4):871-895, vii.
- Johnston SC, Sidney S, Bernstein AL, Gress DR. A comparison of risk factors for recurrent TIA and stroke in patients diagnosed with TIA. Neurology. 2003;60(2):280-285.
- Tsivgoulis G, Stamboulis E, Sharma VK, et al. Multicenter external validation of the ABCD2 score in triaging TIA patients. Neurology. 2010;74(17):1351-1357.
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
- Nguyen-Huynh MN, Johnston SC. Is hospitalization after TIA cost-effective on the basis of treatment with tPA? Neurology. 2005;65(11):1799-1801.
- Douglas VC, Johnston CM, Elkins J, Sidney S, Gress DR, Johnston SC. Head computed tomography findings predict short-term stroke risk after transient ischemic attack. Stroke. 2003;34(12):2894-2898.
- Giles MF, Albers GW, Amarenco P, et al. Addition of brain infarction to the ABCD2 Score (ABCD2I): a collaborative analysis of unpublished data on 4574 patients. Stroke. 2010;41(9):1907-1913.
- Lanzino G, Rabinstein AA, Brown RD Jr. Treatment of carotid artery stenosis: medical therapy, surgery, or stenting? Mayo Clin Proc. 2009;84(4):362-387; quiz 367-368.
- Gladstone DJ, Spring M, Dorian P, et al. Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med. 2014;370(26):2467-2477.
- Lavallée PC, Meseguer E, Abboud H, et al. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6(11):953-960.
- Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370(9596):1432-1442.
- Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160-2236.
- Roumie CL, Zillich AJ, Bravata DM, et al. Hypertension treatment intensification among stroke survivors with uncontrolled blood pressure. Stroke. 2015;46(2):465-470.
- Amarenco P, Bogousslavsky J, Callahan A, et al. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- Lennon O, Galvin R, Smith K, Doody C, Blake C. Lifestyle interventions for secondary disease prevention in stroke and transient ischaemic attack: a systematic review. Eur J Prev Cardiol. 2014;21(8):1026-1039.
Case
Mr. G is an 80-year-old man with a pacemaker, peripheral artery disease, atrial fibrillation (AF) on warfarin, and tachy-brady syndrome. He presented after experiencing episodes in which he was unable to speak and had weakness on his right side. He had a normal neurological exam upon arrival to the ED, and his blood pressure was 160/80 mm Hg.
Overview
Transient ischemic attacks (TIAs) are brief interruptions in brain perfusion that do not result in permanent neurologic damage. Up to half a million TIAs occur each year in the U.S., and they account for one third of acute cerebrovascular disease.1 While the term suggests that TIAs are benign, they are in fact an important warning sign of impending stroke and are essentially analogous to unstable angina. Some 10% of TIAs convert to full strokes within 90 days, but growing evidence suggests appropriate interventions can decrease this risk to 3%.2
Unfortunately, the symptoms of TIA have usually resolved by the time patients arrive at the hospital, which makes them challenging to diagnose. This article provides a summary of how to diagnose TIA accurately, using a focused history informed by cerebrovascular localization; how to triage, evaluate, and risk stratify patients; and how to implement preventative strategies.
Review of the Data
Classically, TIAs are defined as lasting less than 24 hours; however, 24 hours is an arbitrary number, and most TIAs last less than one hour.1 Furthermore, this definition has evolved with advances in neuroimaging that reveal that up to 50% of classically defined TIAs have evidence of infarct on MRI.1 There is no absolute temporal cut-off after which infarct is always seen on MRI, but longer duration of symptoms correlates with a higher likelihood of infarct. To reconcile these observations, a recently proposed definition stipulates that a true TIA lasts no more than one hour and does not show evidence of infarct on MRI.3
The causes of TIA are identical to those for ischemic stroke. Cerebral ischemia can result from an embolus, arterial thrombosis, or hypoperfusion due to arterial stenosis. Emboli can be cardiac, most commonly due to AF, or non-cardiac, stemming from a ruptured atherosclerotic plaque in the aortic arch, the carotid or vertebral artery, or an intracranial vessel. Atherosclerotic disease in the carotid arteries or intracranial vessels can also lead to thrombosis and occlusion or flow-related TIAs as a result of severe stenosis.
Risk factors for TIA mirror those for heart disease. Non-modifiable risk factors include older age, black race, male sex, and family history of stroke. Modifiable factors include hypertension, hyperlipidemia, tobacco smoking, diabetes, and AF.4
Most of the time, patients’ symptoms will have resolved by the time they are evaluated by a physician. Therefore, the diagnosis of TIA relies almost exclusively on the patient history. Eliciting a good history helps physicians determine whether the episode of transient neurologic dysfunction was caused by cerebral ischemia, as opposed to another mechanism, such as migraine or seizure. This calls for a basic understanding of cerebrovascular anatomy (see Table 1).
Types of Ischemia
Anterior cerebral artery ischemia causes contralateral leg weakness because it supplies the medial frontal and parietal lobes, where the legs in the sensorimotor homunculus are represented. Middle cerebral artery (MCA) ischemia causes contralateral face and arm weakness out of proportion to leg weakness. Ischemia in Broca’s area of the brain, which is supplied by the left MCA, may also cause expressive aphasia. Transient monocular blindness is a TIA of the retina due to atheroemboli originating from the internal carotid artery. Vertebrobasilar TIA is less common than anterior circulation TIA and manifests with brainstem symptoms that include diplopia, dysarthria, dysphagia, vertigo, gait imbalance, and weakness. In general, language and motor symptoms are more specific for cerebral ischemia and therefore more worrisome for TIA than sensory symptoms.5
Once a clinical diagnosis of TIA is made, an ABCD2 score (age, blood pressure, clinical features, duration of TIA, presence of diabetes) can be used to predict the short-term risk of subsequent stroke (see Table 2).6,7 A general rule of thumb is to admit patients who present within 72 hours of the event and have an ABCD2 score of three or higher for observation, work-up, and initiation of secondary prevention.1
Although only a small percentage of patients with TIA will have a stroke during the period of observation in the hospital, this approach may be cost effective based on the assumption that hospitalized patients are more likely to receive intravenous tissue plasminogen activator.8 The decision should also be guided by clinical judgment. It is reasonable to admit a patient whose diagnostic workup cannot be rapidly completed.1
The workup for TIA includes routine labs, EKG with cardiac monitoring, and brain imaging. Labs are useful to evaluate for other mimics of TIA such as hyponatremia and glucose abnormalities. In addition, risk factors such as hyperlipidemia and diabetes should be evaluated with fasting lipid panel and blood glucose. The purpose of EKG and telemetry is to identify MI and capture paroxysmal AF. The goal of imaging is to ascertain the presence of vascular disease and to exclude a non-ischemic etiology. While less likely to cause transient neurologic symptoms, a hemorrhagic event must be ruled out, as it would trigger a different management pathway.
Imaging for TIA
There are two primary modes of brain imaging: computed tomography (CT) and MRI. Most patients who are suspected to have had a TIA undergo CT scan, and an infarct is seen about 20% of the time.1 The presence of an infarct usually correlates with the duration of symptoms and has prognostic value. In one study, a new infarct was associated with four times higher risk of stroke in the subsequent 90 days.9 Diffusion-weighted imaging, an MR-based technique, is the preferred modality when it is available because of its higher sensitivity and specificity for identifying acute lesions.1 In an international and multicenter study, incorporating imaging data increased the discriminatory power of stroke prediction.10
Extracranial imaging is mandatory to rule out carotid stenosis as a potential etiology of TIA. The least invasive modality is ultrasound, which can detect carotid stenosis with a sensitivity and specificity approaching 80%.1 While both the intra- and extracranial vasculature can be concurrently assessed using MR- or CT-angiography (CTA), this is not usually necessary in the acute setting, because only detecting carotid stenosis will result in a management change.1
Carotid endarterectomy is standard for symptomatic patients with greater than 70% stenosis and is a consideration for symptomatic patients with greater than 50% stenosis if it is the most probable explanation for the ischemic event.11 Despite a comprehensive workup, about 50% of TIA cases remain cryptogenic.12 In some of these patients, AF can be detected using extended ambulatory cardiac monitoring.12
The goal of admitting high-risk patients is to expedite workup and initiate therapy. Two studies have shown that immediate initiation of preventative treatment significantly reduces the risk of stroke by as much as 80%.13,14 Unless there is a specific indication for anticoagulation, all TIA patients should be started on an antiplatelet agent such as aspirin or clopidogrel. A large randomized trial conducted in China and published in 2013 demonstrated that dual antiplatelet therapy with aspirin and clopidogrel for 21 days, followed by clopidogrel monotherapy, reduced the risk of stroke compared to aspirin monotherapy. An international multicenter trial designed to test the efficacy of short-term dual antiplatelet therapy is ongoing, and if the benefit of this approach is confirmed, this will likely become the standard of care. Evidence-based indications for anticoagulation after TIA are restricted to AF and mural thrombus in the setting of recent MI. Patients with implanted mechanical devices, including left ventricular assist devices and metal heart valves, should also receive anticoagulation.15
Risk factors should also be targeted in every case. Hypertension should be treated with a goal of lower than 140/90 mm Hg (or 130/80 mm Hg in diabetics and those with renal disease). Studies have shown that patients who are discharged with a blood pressure lower than 140/90 mm Hg are more likely to maintain this blood pressure at one-year follow-up.16 The choice of medication is less well studied, but drugs that act on the renin-angiotensin-aldosterone system and thiazides are generally preferred.15 Treatment with a statin is recommended after cerebrovascular ischemic events, with a goal LDL under 100. This reduces risk of secondary stroke by about 20%.17
At discharge, it is also important to counsel patients on their role in preventing strokes. As with many diseases, making lifestyle changes is key to stroke prevention. Encourage smoking cessation and an increase in physical activity, and discourage heavy alcohol use. The association between smoking and the risk for first stroke is well established. Moderate to high-intensity exercise can reduce secondary stroke risk by as much as 50%18 (see Table 3). While light alcohol consumption can be protective against strokes, heavy use is strongly discouraged. Emerging data suggest obstructive sleep apnea (OSA) may be another modifiable risk factor for stroke and TIA, so screening for potential OSA and referral may be needed.15
Back to the Case
When Mr. G arrived at the ED, his symptoms had resolved. Based on the history of expressive aphasia and right-sided weakness, he most likely had a TIA in the left MCA territory. Hemorrhage was ruled out with a non-contrast head CT. His pacemaker precluded obtaining an MRI. CTA revealed diffuse atherosclerotic disease without evidence of carotid stenosis. His ABCD2 score was six given his age, blood pressure, weakness, and symptom duration, and he was admitted for an expedited workup. His sodium and glucose were within normal limits. His hemoglobin A1c was 6.5%, his LDL was 120, and his international normalized ratio (INR) was therapeutic at 2.1. His TIA may have been due to AF, despite a therapeutic INR, because warfarin does not fully eliminate the stroke risk. It might also have been caused by intracranial atherosclerosis.
Two days later, the patient was discharged on atorvastatin at 80 mg, and his lisinopril was increased for blood pressure control. For his age group, A1c of 6.5% was acceptable, and he was not initiated on glycemic control.
Bottom Line
TIAs are diagnosed based on patient history. Urgent initiation of secondary prevention is important to reduce the short-term risk of stroke and should be implemented by the time of discharge from the hospital.
Dr. Zeng is a hospitalist in the department of internal medicine at Vanderbilt University Medical Center in Nashville, and Dr. Douglas is associate professor in the department of neurology at the University of California at San Francisco.
References
- Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276-2293.
- Sundararajan V, Thrift AG, Phan TG, Choi PM, Clissold B, Srikanth VK. Trends over time in the risk of stroke after an incident transient ischemic attack. Stroke. 2014;45(11):3214-3218.
- Albers GW, Caplan LR, Easton JD, et al. Transient ischemic attack–proposal for a new definition. N Engl J Med. 2002;347(21):1713-1716.
- Grysiewicz RA, Thomas K, Pandey DK. Epidemiology of ischemic and hemorrhagic stroke: incidence, prevalence, mortality, and risk factors. Neurol Clin. 2008;26(4):871-895, vii.
- Johnston SC, Sidney S, Bernstein AL, Gress DR. A comparison of risk factors for recurrent TIA and stroke in patients diagnosed with TIA. Neurology. 2003;60(2):280-285.
- Tsivgoulis G, Stamboulis E, Sharma VK, et al. Multicenter external validation of the ABCD2 score in triaging TIA patients. Neurology. 2010;74(17):1351-1357.
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
- Nguyen-Huynh MN, Johnston SC. Is hospitalization after TIA cost-effective on the basis of treatment with tPA? Neurology. 2005;65(11):1799-1801.
- Douglas VC, Johnston CM, Elkins J, Sidney S, Gress DR, Johnston SC. Head computed tomography findings predict short-term stroke risk after transient ischemic attack. Stroke. 2003;34(12):2894-2898.
- Giles MF, Albers GW, Amarenco P, et al. Addition of brain infarction to the ABCD2 Score (ABCD2I): a collaborative analysis of unpublished data on 4574 patients. Stroke. 2010;41(9):1907-1913.
- Lanzino G, Rabinstein AA, Brown RD Jr. Treatment of carotid artery stenosis: medical therapy, surgery, or stenting? Mayo Clin Proc. 2009;84(4):362-387; quiz 367-368.
- Gladstone DJ, Spring M, Dorian P, et al. Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med. 2014;370(26):2467-2477.
- Lavallée PC, Meseguer E, Abboud H, et al. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6(11):953-960.
- Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370(9596):1432-1442.
- Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160-2236.
- Roumie CL, Zillich AJ, Bravata DM, et al. Hypertension treatment intensification among stroke survivors with uncontrolled blood pressure. Stroke. 2015;46(2):465-470.
- Amarenco P, Bogousslavsky J, Callahan A, et al. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- Lennon O, Galvin R, Smith K, Doody C, Blake C. Lifestyle interventions for secondary disease prevention in stroke and transient ischaemic attack: a systematic review. Eur J Prev Cardiol. 2014;21(8):1026-1039.
Case
Mr. G is an 80-year-old man with a pacemaker, peripheral artery disease, atrial fibrillation (AF) on warfarin, and tachy-brady syndrome. He presented after experiencing episodes in which he was unable to speak and had weakness on his right side. He had a normal neurological exam upon arrival to the ED, and his blood pressure was 160/80 mm Hg.
Overview
Transient ischemic attacks (TIAs) are brief interruptions in brain perfusion that do not result in permanent neurologic damage. Up to half a million TIAs occur each year in the U.S., and they account for one third of acute cerebrovascular disease.1 While the term suggests that TIAs are benign, they are in fact an important warning sign of impending stroke and are essentially analogous to unstable angina. Some 10% of TIAs convert to full strokes within 90 days, but growing evidence suggests appropriate interventions can decrease this risk to 3%.2
Unfortunately, the symptoms of TIA have usually resolved by the time patients arrive at the hospital, which makes them challenging to diagnose. This article provides a summary of how to diagnose TIA accurately, using a focused history informed by cerebrovascular localization; how to triage, evaluate, and risk stratify patients; and how to implement preventative strategies.
Review of the Data
Classically, TIAs are defined as lasting less than 24 hours; however, 24 hours is an arbitrary number, and most TIAs last less than one hour.1 Furthermore, this definition has evolved with advances in neuroimaging that reveal that up to 50% of classically defined TIAs have evidence of infarct on MRI.1 There is no absolute temporal cut-off after which infarct is always seen on MRI, but longer duration of symptoms correlates with a higher likelihood of infarct. To reconcile these observations, a recently proposed definition stipulates that a true TIA lasts no more than one hour and does not show evidence of infarct on MRI.3
The causes of TIA are identical to those for ischemic stroke. Cerebral ischemia can result from an embolus, arterial thrombosis, or hypoperfusion due to arterial stenosis. Emboli can be cardiac, most commonly due to AF, or non-cardiac, stemming from a ruptured atherosclerotic plaque in the aortic arch, the carotid or vertebral artery, or an intracranial vessel. Atherosclerotic disease in the carotid arteries or intracranial vessels can also lead to thrombosis and occlusion or flow-related TIAs as a result of severe stenosis.
Risk factors for TIA mirror those for heart disease. Non-modifiable risk factors include older age, black race, male sex, and family history of stroke. Modifiable factors include hypertension, hyperlipidemia, tobacco smoking, diabetes, and AF.4
Most of the time, patients’ symptoms will have resolved by the time they are evaluated by a physician. Therefore, the diagnosis of TIA relies almost exclusively on the patient history. Eliciting a good history helps physicians determine whether the episode of transient neurologic dysfunction was caused by cerebral ischemia, as opposed to another mechanism, such as migraine or seizure. This calls for a basic understanding of cerebrovascular anatomy (see Table 1).
Types of Ischemia
Anterior cerebral artery ischemia causes contralateral leg weakness because it supplies the medial frontal and parietal lobes, where the legs in the sensorimotor homunculus are represented. Middle cerebral artery (MCA) ischemia causes contralateral face and arm weakness out of proportion to leg weakness. Ischemia in Broca’s area of the brain, which is supplied by the left MCA, may also cause expressive aphasia. Transient monocular blindness is a TIA of the retina due to atheroemboli originating from the internal carotid artery. Vertebrobasilar TIA is less common than anterior circulation TIA and manifests with brainstem symptoms that include diplopia, dysarthria, dysphagia, vertigo, gait imbalance, and weakness. In general, language and motor symptoms are more specific for cerebral ischemia and therefore more worrisome for TIA than sensory symptoms.5
Once a clinical diagnosis of TIA is made, an ABCD2 score (age, blood pressure, clinical features, duration of TIA, presence of diabetes) can be used to predict the short-term risk of subsequent stroke (see Table 2).6,7 A general rule of thumb is to admit patients who present within 72 hours of the event and have an ABCD2 score of three or higher for observation, work-up, and initiation of secondary prevention.1
Although only a small percentage of patients with TIA will have a stroke during the period of observation in the hospital, this approach may be cost effective based on the assumption that hospitalized patients are more likely to receive intravenous tissue plasminogen activator.8 The decision should also be guided by clinical judgment. It is reasonable to admit a patient whose diagnostic workup cannot be rapidly completed.1
The workup for TIA includes routine labs, EKG with cardiac monitoring, and brain imaging. Labs are useful to evaluate for other mimics of TIA such as hyponatremia and glucose abnormalities. In addition, risk factors such as hyperlipidemia and diabetes should be evaluated with fasting lipid panel and blood glucose. The purpose of EKG and telemetry is to identify MI and capture paroxysmal AF. The goal of imaging is to ascertain the presence of vascular disease and to exclude a non-ischemic etiology. While less likely to cause transient neurologic symptoms, a hemorrhagic event must be ruled out, as it would trigger a different management pathway.
Imaging for TIA
There are two primary modes of brain imaging: computed tomography (CT) and MRI. Most patients who are suspected to have had a TIA undergo CT scan, and an infarct is seen about 20% of the time.1 The presence of an infarct usually correlates with the duration of symptoms and has prognostic value. In one study, a new infarct was associated with four times higher risk of stroke in the subsequent 90 days.9 Diffusion-weighted imaging, an MR-based technique, is the preferred modality when it is available because of its higher sensitivity and specificity for identifying acute lesions.1 In an international and multicenter study, incorporating imaging data increased the discriminatory power of stroke prediction.10
Extracranial imaging is mandatory to rule out carotid stenosis as a potential etiology of TIA. The least invasive modality is ultrasound, which can detect carotid stenosis with a sensitivity and specificity approaching 80%.1 While both the intra- and extracranial vasculature can be concurrently assessed using MR- or CT-angiography (CTA), this is not usually necessary in the acute setting, because only detecting carotid stenosis will result in a management change.1
Carotid endarterectomy is standard for symptomatic patients with greater than 70% stenosis and is a consideration for symptomatic patients with greater than 50% stenosis if it is the most probable explanation for the ischemic event.11 Despite a comprehensive workup, about 50% of TIA cases remain cryptogenic.12 In some of these patients, AF can be detected using extended ambulatory cardiac monitoring.12
The goal of admitting high-risk patients is to expedite workup and initiate therapy. Two studies have shown that immediate initiation of preventative treatment significantly reduces the risk of stroke by as much as 80%.13,14 Unless there is a specific indication for anticoagulation, all TIA patients should be started on an antiplatelet agent such as aspirin or clopidogrel. A large randomized trial conducted in China and published in 2013 demonstrated that dual antiplatelet therapy with aspirin and clopidogrel for 21 days, followed by clopidogrel monotherapy, reduced the risk of stroke compared to aspirin monotherapy. An international multicenter trial designed to test the efficacy of short-term dual antiplatelet therapy is ongoing, and if the benefit of this approach is confirmed, this will likely become the standard of care. Evidence-based indications for anticoagulation after TIA are restricted to AF and mural thrombus in the setting of recent MI. Patients with implanted mechanical devices, including left ventricular assist devices and metal heart valves, should also receive anticoagulation.15
Risk factors should also be targeted in every case. Hypertension should be treated with a goal of lower than 140/90 mm Hg (or 130/80 mm Hg in diabetics and those with renal disease). Studies have shown that patients who are discharged with a blood pressure lower than 140/90 mm Hg are more likely to maintain this blood pressure at one-year follow-up.16 The choice of medication is less well studied, but drugs that act on the renin-angiotensin-aldosterone system and thiazides are generally preferred.15 Treatment with a statin is recommended after cerebrovascular ischemic events, with a goal LDL under 100. This reduces risk of secondary stroke by about 20%.17
At discharge, it is also important to counsel patients on their role in preventing strokes. As with many diseases, making lifestyle changes is key to stroke prevention. Encourage smoking cessation and an increase in physical activity, and discourage heavy alcohol use. The association between smoking and the risk for first stroke is well established. Moderate to high-intensity exercise can reduce secondary stroke risk by as much as 50%18 (see Table 3). While light alcohol consumption can be protective against strokes, heavy use is strongly discouraged. Emerging data suggest obstructive sleep apnea (OSA) may be another modifiable risk factor for stroke and TIA, so screening for potential OSA and referral may be needed.15
Back to the Case
When Mr. G arrived at the ED, his symptoms had resolved. Based on the history of expressive aphasia and right-sided weakness, he most likely had a TIA in the left MCA territory. Hemorrhage was ruled out with a non-contrast head CT. His pacemaker precluded obtaining an MRI. CTA revealed diffuse atherosclerotic disease without evidence of carotid stenosis. His ABCD2 score was six given his age, blood pressure, weakness, and symptom duration, and he was admitted for an expedited workup. His sodium and glucose were within normal limits. His hemoglobin A1c was 6.5%, his LDL was 120, and his international normalized ratio (INR) was therapeutic at 2.1. His TIA may have been due to AF, despite a therapeutic INR, because warfarin does not fully eliminate the stroke risk. It might also have been caused by intracranial atherosclerosis.
Two days later, the patient was discharged on atorvastatin at 80 mg, and his lisinopril was increased for blood pressure control. For his age group, A1c of 6.5% was acceptable, and he was not initiated on glycemic control.
Bottom Line
TIAs are diagnosed based on patient history. Urgent initiation of secondary prevention is important to reduce the short-term risk of stroke and should be implemented by the time of discharge from the hospital.
Dr. Zeng is a hospitalist in the department of internal medicine at Vanderbilt University Medical Center in Nashville, and Dr. Douglas is associate professor in the department of neurology at the University of California at San Francisco.
References
- Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276-2293.
- Sundararajan V, Thrift AG, Phan TG, Choi PM, Clissold B, Srikanth VK. Trends over time in the risk of stroke after an incident transient ischemic attack. Stroke. 2014;45(11):3214-3218.
- Albers GW, Caplan LR, Easton JD, et al. Transient ischemic attack–proposal for a new definition. N Engl J Med. 2002;347(21):1713-1716.
- Grysiewicz RA, Thomas K, Pandey DK. Epidemiology of ischemic and hemorrhagic stroke: incidence, prevalence, mortality, and risk factors. Neurol Clin. 2008;26(4):871-895, vii.
- Johnston SC, Sidney S, Bernstein AL, Gress DR. A comparison of risk factors for recurrent TIA and stroke in patients diagnosed with TIA. Neurology. 2003;60(2):280-285.
- Tsivgoulis G, Stamboulis E, Sharma VK, et al. Multicenter external validation of the ABCD2 score in triaging TIA patients. Neurology. 2010;74(17):1351-1357.
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
- Nguyen-Huynh MN, Johnston SC. Is hospitalization after TIA cost-effective on the basis of treatment with tPA? Neurology. 2005;65(11):1799-1801.
- Douglas VC, Johnston CM, Elkins J, Sidney S, Gress DR, Johnston SC. Head computed tomography findings predict short-term stroke risk after transient ischemic attack. Stroke. 2003;34(12):2894-2898.
- Giles MF, Albers GW, Amarenco P, et al. Addition of brain infarction to the ABCD2 Score (ABCD2I): a collaborative analysis of unpublished data on 4574 patients. Stroke. 2010;41(9):1907-1913.
- Lanzino G, Rabinstein AA, Brown RD Jr. Treatment of carotid artery stenosis: medical therapy, surgery, or stenting? Mayo Clin Proc. 2009;84(4):362-387; quiz 367-368.
- Gladstone DJ, Spring M, Dorian P, et al. Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med. 2014;370(26):2467-2477.
- Lavallée PC, Meseguer E, Abboud H, et al. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6(11):953-960.
- Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370(9596):1432-1442.
- Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160-2236.
- Roumie CL, Zillich AJ, Bravata DM, et al. Hypertension treatment intensification among stroke survivors with uncontrolled blood pressure. Stroke. 2015;46(2):465-470.
- Amarenco P, Bogousslavsky J, Callahan A, et al. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- Lennon O, Galvin R, Smith K, Doody C, Blake C. Lifestyle interventions for secondary disease prevention in stroke and transient ischaemic attack: a systematic review. Eur J Prev Cardiol. 2014;21(8):1026-1039.
Radiofrequency volumetric thermal ablation for symptomatic uterine fibroids
In 2002, Dr. Bruce B. Lee first described a laparoscopic technique to ablate symptomatic uterine fibroids utilizing radiofrequency under ultrasound guidance. Since this time, several papers have documented the procedure’s feasibility and efficacy, including reduction in menstrual blood loss, fibroid volume decrease, and improvement in quality of life.
In a randomized, prospective, single-center, longitudinal study that compared laparoscopic radiofrequency volumetric thermal ablation (RFVTA) of fibroids with laparoscopic myomectomy, Dr. Sara Y. Brucker and her colleagues concluded that RFVTA resulted in the treatment of more fibroids, a significantly shorter hospital stay, and less intraoperative blood loss than did laparoscopic myomectomy (Int J Gynaecol Obstet. 2014 Jun;125[3]:261-5).

More recently, in the literature and at the 2015 American Association of Gynecologic Laparoscopists (AAGL) Global Congress in November, viable, full-term pregnancies have been reported in patients previously treated for symptomatic fibroids via RFVTA (J Reprod Med. 2015 May-Jun;60[5-6]:194-8).
The system for performing RFVTA of symptomatic fibroids – the Acessa System (Halt Medical) – has continued to improve. Earlier this year, Dr. Donald I. Galen described the use of electromagnetic image guidance, which has been cleared by the Food and Drug Administration and incorporated into the Acessa Guidance System. Dr. Galen’s feasibility study showed that the guidance system enhances the ultrasonic image of Acessa’s handpiece to facilitate accurate tip placement during the targeting and ablation of uterine fibroids (Biomed Eng Online. 2015 Oct 15;14:90).
In this edition of the Master Class in Gynecologic Surgery, Dr. Jay M. Berman discusses the use of RFVTA for the treatment of symptomatic uterine fibroids. Dr. Berman is interim chairman of Wayne State University’s department of obstetrics and gynecology and interim specialist in chief for obstetrics and gynecology at the Detroit Medical Center. He served as a principal investigator of the pivotal trial of Acessa and has reported on reproductive outcomes. Dr. Berman has long been interested in alternatives to hysterectomy for fibroid management and has incorporated RFVTA into his armamentarium of therapies.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, and a past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller reported that he is a consultant for Halt Medical Inc., which developed the Acessa System.
In 2002, Dr. Bruce B. Lee first described a laparoscopic technique to ablate symptomatic uterine fibroids utilizing radiofrequency under ultrasound guidance. Since this time, several papers have documented the procedure’s feasibility and efficacy, including reduction in menstrual blood loss, fibroid volume decrease, and improvement in quality of life.
In a randomized, prospective, single-center, longitudinal study that compared laparoscopic radiofrequency volumetric thermal ablation (RFVTA) of fibroids with laparoscopic myomectomy, Dr. Sara Y. Brucker and her colleagues concluded that RFVTA resulted in the treatment of more fibroids, a significantly shorter hospital stay, and less intraoperative blood loss than did laparoscopic myomectomy (Int J Gynaecol Obstet. 2014 Jun;125[3]:261-5).
More recently, in the literature and at the 2015 American Association of Gynecologic Laparoscopists (AAGL) Global Congress in November, viable, full-term pregnancies have been reported in patients previously treated for symptomatic fibroids via RFVTA (J Reprod Med. 2015 May-Jun;60[5-6]:194-8).
The system for performing RFVTA of symptomatic fibroids – the Acessa System (Halt Medical) – has continued to improve. Earlier this year, Dr. Donald I. Galen described the use of electromagnetic image guidance, which has been cleared by the Food and Drug Administration and incorporated into the Acessa Guidance System. Dr. Galen’s feasibility study showed that the guidance system enhances the ultrasonic image of Acessa’s handpiece to facilitate accurate tip placement during the targeting and ablation of uterine fibroids (Biomed Eng Online. 2015 Oct 15;14:90).
In this edition of the Master Class in Gynecologic Surgery, Dr. Jay M. Berman discusses the use of RFVTA for the treatment of symptomatic uterine fibroids. Dr. Berman is interim chairman of Wayne State University’s department of obstetrics and gynecology and interim specialist in chief for obstetrics and gynecology at the Detroit Medical Center. He served as a principal investigator of the pivotal trial of Acessa and has reported on reproductive outcomes. Dr. Berman has long been interested in alternatives to hysterectomy for fibroid management and has incorporated RFVTA into his armamentarium of therapies.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, and a past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller reported that he is a consultant for Halt Medical Inc., which developed the Acessa System.
In 2002, Dr. Bruce B. Lee first described a laparoscopic technique to ablate symptomatic uterine fibroids utilizing radiofrequency under ultrasound guidance. Since this time, several papers have documented the procedure’s feasibility and efficacy, including reduction in menstrual blood loss, fibroid volume decrease, and improvement in quality of life.
In a randomized, prospective, single-center, longitudinal study that compared laparoscopic radiofrequency volumetric thermal ablation (RFVTA) of fibroids with laparoscopic myomectomy, Dr. Sara Y. Brucker and her colleagues concluded that RFVTA resulted in the treatment of more fibroids, a significantly shorter hospital stay, and less intraoperative blood loss than did laparoscopic myomectomy (Int J Gynaecol Obstet. 2014 Jun;125[3]:261-5).
More recently, in the literature and at the 2015 American Association of Gynecologic Laparoscopists (AAGL) Global Congress in November, viable, full-term pregnancies have been reported in patients previously treated for symptomatic fibroids via RFVTA (J Reprod Med. 2015 May-Jun;60[5-6]:194-8).
The system for performing RFVTA of symptomatic fibroids – the Acessa System (Halt Medical) – has continued to improve. Earlier this year, Dr. Donald I. Galen described the use of electromagnetic image guidance, which has been cleared by the Food and Drug Administration and incorporated into the Acessa Guidance System. Dr. Galen’s feasibility study showed that the guidance system enhances the ultrasonic image of Acessa’s handpiece to facilitate accurate tip placement during the targeting and ablation of uterine fibroids (Biomed Eng Online. 2015 Oct 15;14:90).
In this edition of the Master Class in Gynecologic Surgery, Dr. Jay M. Berman discusses the use of RFVTA for the treatment of symptomatic uterine fibroids. Dr. Berman is interim chairman of Wayne State University’s department of obstetrics and gynecology and interim specialist in chief for obstetrics and gynecology at the Detroit Medical Center. He served as a principal investigator of the pivotal trial of Acessa and has reported on reproductive outcomes. Dr. Berman has long been interested in alternatives to hysterectomy for fibroid management and has incorporated RFVTA into his armamentarium of therapies.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, and a past president of the AAGL and the International Society for Gynecologic Endoscopy (ISGE). He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/Society of Reproductive Surgery fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller reported that he is a consultant for Halt Medical Inc., which developed the Acessa System.

RFVTA system offers alternative to myomectomy
Uterine myomas cause heavy menstrual bleeding and other clinically significant symptoms in 35%-50% of affected women and have been shown to be the leading indication for hysterectomy in the United States among women aged 35-54 years.
Research has shown that a significant number of women who undergo hysterectomy for treatment of fibroids later regret the loss of their uterus and have other concerns and complications. Other options for therapy include various pharmacologic treatments, a progestin-releasing intrauterine device, uterine artery embolization, endometrial ablation, MRI-guided focused ultrasound surgery, and myomectomy performed laparoscopically, robotically, or hysteroscopically.
Myomectomy seems largely to preserve fertility, but rates of recurrence and additional procedures for bleeding and myoma symptoms are still high – upward of 30% in some studies. Overall, we need other more efficacious and minimally invasive options.

Radiofrequency volumetric thermal ablation (RFVTA) achieved through the Acessa System (Halt Medical) has been the newest addition to our armamentarium for treatment of symptomatic fibroids. It is suitable for every type of fibroid except for type 0 pedunculated intracavitary fibroids and type 7 pedunculated subserosal fibroids, which is significant because deep intramural fibroids have been difficult to target and treat by other methods.
Three-year outcome data show sustained improvements in fibroid symptoms and quality of life, with an incidence of recurrences and additional procedures – approximately 11% – that appears to be substantially lower than for other uterine-sparing fibroid treatments. In addition, while the technology is not indicated for women seeking future childbearing, successful pregnancies are being reported, suggesting that full-term pregnancies – and vaginal delivery in some cases – may be possible after RFVTA.
The principles
Radiofrequency ablation has been used for years in the treatment of liver and kidney tumors. The basic concept is that volumetric thermal ablation results in coagulative necrosis.
The Acessa System, approved by the Food and Drug Administration in late 2012, was designed to treat fibroids, which have much firmer tissue than the tissues being targeted in other radiofrequency ablation procedures. It uses a specially designed intrauterine ultrasound probe and radiofrequency probe, and it combines three fundamental gynecologic skills: Laparoscopy using two trocars and requiring no special suturing skills; ultrasound using a laparoscopic ultrasound probe to scan and manipulate; and probe placement under laparoscopic ultrasound guidance.
Specifically, the system allows for percutaneous, laparoscopic ultrasound–guided radiofrequency ablation of fibroids with a disposable 3.4-mm handpiece coupled to a dual-function radiofrequency generator. The handpiece contains a retractable array of electrodes, so that the fibroid may be ablated with one electrode or with the deployed electrode array.
The generator controls and monitors the ablation with real-time feedback from thermocouples. It monitors and displays the temperature at each needle tip, the average temperature of the array, and the return temperatures on two dispersive electrode pads that are placed on the anterior thighs. The electrode pads are designed to reduce the incidence of pad burns, which are a complication with other radiofrequency ablation devices. The system will automatically stop treatment if either of the pad thermocouples registers a skin temperature greater than 40° C (JSLS. 2014 Apr-Jun;18[2]:182-90).
The outcomes
Laparoscopic ultrasound–guided RFVTA has been studied in five prospective trials, including one multicenter international trial of 135 premenopausal women – the pivotal trial for FDA clearance – in which 104 women were followed for 3 years and found to have prolonged symptom relief and improved quality of life.
At baseline, the women had symptomatic uterine myomas and moderate to severe heavy menstrual bleeding measured by alkaline hematin analysis of returned sanitary products. Their mean symptom severity scores on the Uterine Fibroid Symptom and Quality-of-Life Questionnaire (UFS-QOL) decreased significantly from baseline to 3 months and changed little after that, for a total change of –32.6 over the study period.
The cumulative repeat intervention rate at 3 years was 11%, with 14 of the 135 participants having repeat interventions to treat bleeding and myoma symptoms. Seven of these women were found to have adenomyosis (J Minim Invasive Gynecol. 2014 Sep-Oct;21[5]:767-74).
The surprisingly low reintervention rates may stem from the benefits of direct contact imaging of the uterus. A comparison of images from the pivotal trial has shown that intraoperative ultrasound detected more than twice as many fibroids as did preoperative transvaginal ultrasound, and about one-third more than preoperative MRIs (J Minim Invasive Gynecol. 2013 Nov-Dec;20[6]:770-4).
Interestingly, four women became pregnant over the study’s 3-year follow-up, despite the inclusion requirement that women desire uterine conservation but not future childbearing.
We have followed reproductive outcomes in women after RFVTA of symptomatic fibroids in other studies as well. In our most recent analysis, presented in November at the 2015 American Association of Gynecologic Laparoscopists Global Congress, we identified 10 pregnancies among participants of the five prospective trials.
Of 232 women enrolled in premarket RFVTA studies – trials in which completing childbearing and continuing contraception were requirements – six conceived at 3.5-15 months post ablation. The number of myomas treated ranged from one to seven and included multiple types and dimensions. Five of these six women delivered full-term healthy babies – one by vaginal delivery and four by cesarean section. The sixth patient had a spontaneous abortion in the first trimester.
Of 43 women who participated in two randomized clinical trials undertaken after FDA clearance, four conceived at 4-23.5 months post ablation. Three of these women had uneventful, full-term pregnancies with vaginal births. The fourth had a cesarean section at 38 weeks.
Considering the theoretical advantages of the Acessa procedure – that it is less damaging to healthy myometrium – and the outcomes reported thus far, it appears likely that Acessa will be preferable to myomectomy. Early results from an ongoing 5-year German study that randomized 50 women to RFVTA or laparoscopic myomectomy show that RFVTA resulted in the treatment of more fibroids and involved a significantly shorter hospital stay and post-operative recovery (Int J Gynaecol Obstet. 2014 Jun;125[3]:261-5).
The technique
The patient is pretreated with a nonsteroidal anti-inflammatory agent and prophylactic antibiotic. She is placed in a supine position with arms tucked, and a single-toothed tenaculum is placed on the cervix from 12 to 6 o’clock, without any instrument for manipulation of the uterus. The system’s dispersive electrode pads are placed symmetrically just above the patella on the anterior thighs; asymmetrical placement could potentially increase the risk of a pad burn.
Two standard laparoscopic ports are placed. A 5-mm trocar for the camera and video laparoscope is placed through the umbilicus or at a supraumbilical or left upper–quadrant level, depending on the patient’s anatomy, her surgical history, and the size of the uterus. A thorough visual inspection of the abdomen should be performed to look for unsuspected findings.
A 10-mm trocar is then placed at the level of the top of the fundus for the intra-abdominal ultrasound probe. Laparoscopic ultrasound is used to survey the entire uterus, map the fibroids, and plan an approach. Once the fibroid to be treated first is identified, the ability to stabilize the uterus accordingly is assessed, and the dimensions of the fibroid are taken. The dimensions will be used by the surgeon with a volume algorithm to calculate the length of ablation time based on the size of the fibroid and electrode deployment.
Under ultrasound guidance, the Acessa radiofrequency ablation handpiece is inserted percutaneously at 12, 3, 6, or 9 o’clock relative to the ultrasound trocar, based on the location of the target fibroid. The uterus must be stabilized, with the handpiece and ultrasound probe parallel and in plane. The handpiece is then inserted 1 cm into the target fibroid through the uterine serosal surface, utilizing a combination of laparoscopic and ultrasound views. Care must be taken to use gentle rotation and minimal downward pressure as the tip of the handpiece is quite sharp.
The location of the tip is confirmed by laparoscopic ultrasound, and the 7-needle electrode array can then be deployed to the ablation site. All three dimensions of the fibroid should be viewed for placement and deployment of the electrodes. Care is taken to avoid large blood vessels and ensure that the electrodes are confined within the fibroid and within the uterus.
Radiofrequency ablation is carried out with a low-voltage, high-frequency alternating current. The radiofrequency waves heat the tissue to an average temperature of 95° C for a length of time determined by a treatment algorithm. The wattage automatically adjusts to maintain the treatment temperature for the calculated duration of ablation.
Small fibroids can be treated in a manual mode without deployment of the electrode array at a current output of 15 W.
At the conclusion of the ablation, the electrodes are withdrawn into the handpiece, the generator is changed to coagulation mode, and the handpiece is slowly withdrawn under ultrasound visualization. The tract is simultaneously coagulated. A bit of additional coagulation is facilitated by pausing at the serosal surface.
Additional fibroids can be ablated through another insertion of the handpiece, either through the same tract or through a new tract.
Larger fibroids may require multiple ablations. The maximum size of ablation is about 5 cm, so it is important to plan the treatment of larger fibroids. This can be accomplished by carefully scanning large fibroids and visualizing the number of overlapping ablations needed to treat the entire volume. I ask my assistant to record the size and location of each ablation; I find this helpful both for organizing the treatment of large fibroids and for dictating the operative report.
It is important to appreciate that treatment of one area can make it difficult to visualize nearby fibroids with ultrasound. The effect dissipates in about 30-45 minutes. It is one reason why having a fibroid map prior to treatment is so important.
Once all fibroids are treated, a final inspection is performed. We usually use a suction irrigator to clean out whatever small amounts of blood are present, and the laparoscopic and port sites are closed in standard fashion.
Patients are seen 1 week postoperatively and are instructed to call in cases of pain, fever, bleeding, or chills. Most patients require only NSAIDs for pain relief and return to work in 2-7 days.
Many patients experience a slightly heavier than normal first menses after treatment. Pelvic rest is recommended for 3 weeks as a precaution, and avoidance of intrauterine procedures is advised because the uterus will be soft and thus may be easily perforated. Patients who have had type 1, type 2, or type 2-5 fibroids ablated may experience drainage for several weeks as the fibroid tissue is reabsorbed.
Dr. Berman is interim chairman of Wayne State University’s department of obstetrics and gynecology and interim specialist-in-chief for obstetrics and gynecology at the Detroit Medical Center. He was a principal investigator of the 3-year outcome study of Acessa sponsored by Halt Medical. He is a consultant for Halt Medical and directs physician training in the use of Acessa.
Uterine myomas cause heavy menstrual bleeding and other clinically significant symptoms in 35%-50% of affected women and have been shown to be the leading indication for hysterectomy in the United States among women aged 35-54 years.
Research has shown that a significant number of women who undergo hysterectomy for treatment of fibroids later regret the loss of their uterus and have other concerns and complications. Other options for therapy include various pharmacologic treatments, a progestin-releasing intrauterine device, uterine artery embolization, endometrial ablation, MRI-guided focused ultrasound surgery, and myomectomy performed laparoscopically, robotically, or hysteroscopically.
Myomectomy seems largely to preserve fertility, but rates of recurrence and additional procedures for bleeding and myoma symptoms are still high – upward of 30% in some studies. Overall, we need other more efficacious and minimally invasive options.
Radiofrequency volumetric thermal ablation (RFVTA) achieved through the Acessa System (Halt Medical) has been the newest addition to our armamentarium for treatment of symptomatic fibroids. It is suitable for every type of fibroid except for type 0 pedunculated intracavitary fibroids and type 7 pedunculated subserosal fibroids, which is significant because deep intramural fibroids have been difficult to target and treat by other methods.
Three-year outcome data show sustained improvements in fibroid symptoms and quality of life, with an incidence of recurrences and additional procedures – approximately 11% – that appears to be substantially lower than for other uterine-sparing fibroid treatments. In addition, while the technology is not indicated for women seeking future childbearing, successful pregnancies are being reported, suggesting that full-term pregnancies – and vaginal delivery in some cases – may be possible after RFVTA.
The principles
Radiofrequency ablation has been used for years in the treatment of liver and kidney tumors. The basic concept is that volumetric thermal ablation results in coagulative necrosis.
The Acessa System, approved by the Food and Drug Administration in late 2012, was designed to treat fibroids, which have much firmer tissue than the tissues being targeted in other radiofrequency ablation procedures. It uses a specially designed intrauterine ultrasound probe and radiofrequency probe, and it combines three fundamental gynecologic skills: Laparoscopy using two trocars and requiring no special suturing skills; ultrasound using a laparoscopic ultrasound probe to scan and manipulate; and probe placement under laparoscopic ultrasound guidance.
Specifically, the system allows for percutaneous, laparoscopic ultrasound–guided radiofrequency ablation of fibroids with a disposable 3.4-mm handpiece coupled to a dual-function radiofrequency generator. The handpiece contains a retractable array of electrodes, so that the fibroid may be ablated with one electrode or with the deployed electrode array.
The generator controls and monitors the ablation with real-time feedback from thermocouples. It monitors and displays the temperature at each needle tip, the average temperature of the array, and the return temperatures on two dispersive electrode pads that are placed on the anterior thighs. The electrode pads are designed to reduce the incidence of pad burns, which are a complication with other radiofrequency ablation devices. The system will automatically stop treatment if either of the pad thermocouples registers a skin temperature greater than 40° C (JSLS. 2014 Apr-Jun;18[2]:182-90).
The outcomes
Laparoscopic ultrasound–guided RFVTA has been studied in five prospective trials, including one multicenter international trial of 135 premenopausal women – the pivotal trial for FDA clearance – in which 104 women were followed for 3 years and found to have prolonged symptom relief and improved quality of life.
At baseline, the women had symptomatic uterine myomas and moderate to severe heavy menstrual bleeding measured by alkaline hematin analysis of returned sanitary products. Their mean symptom severity scores on the Uterine Fibroid Symptom and Quality-of-Life Questionnaire (UFS-QOL) decreased significantly from baseline to 3 months and changed little after that, for a total change of –32.6 over the study period.
The cumulative repeat intervention rate at 3 years was 11%, with 14 of the 135 participants having repeat interventions to treat bleeding and myoma symptoms. Seven of these women were found to have adenomyosis (J Minim Invasive Gynecol. 2014 Sep-Oct;21[5]:767-74).
The surprisingly low reintervention rates may stem from the benefits of direct contact imaging of the uterus. A comparison of images from the pivotal trial has shown that intraoperative ultrasound detected more than twice as many fibroids as did preoperative transvaginal ultrasound, and about one-third more than preoperative MRIs (J Minim Invasive Gynecol. 2013 Nov-Dec;20[6]:770-4).
Interestingly, four women became pregnant over the study’s 3-year follow-up, despite the inclusion requirement that women desire uterine conservation but not future childbearing.
We have followed reproductive outcomes in women after RFVTA of symptomatic fibroids in other studies as well. In our most recent analysis, presented in November at the 2015 American Association of Gynecologic Laparoscopists Global Congress, we identified 10 pregnancies among participants of the five prospective trials.
Of 232 women enrolled in premarket RFVTA studies – trials in which completing childbearing and continuing contraception were requirements – six conceived at 3.5-15 months post ablation. The number of myomas treated ranged from one to seven and included multiple types and dimensions. Five of these six women delivered full-term healthy babies – one by vaginal delivery and four by cesarean section. The sixth patient had a spontaneous abortion in the first trimester.
Of 43 women who participated in two randomized clinical trials undertaken after FDA clearance, four conceived at 4-23.5 months post ablation. Three of these women had uneventful, full-term pregnancies with vaginal births. The fourth had a cesarean section at 38 weeks.
Considering the theoretical advantages of the Acessa procedure – that it is less damaging to healthy myometrium – and the outcomes reported thus far, it appears likely that Acessa will be preferable to myomectomy. Early results from an ongoing 5-year German study that randomized 50 women to RFVTA or laparoscopic myomectomy show that RFVTA resulted in the treatment of more fibroids and involved a significantly shorter hospital stay and post-operative recovery (Int J Gynaecol Obstet. 2014 Jun;125[3]:261-5).
The technique
The patient is pretreated with a nonsteroidal anti-inflammatory agent and prophylactic antibiotic. She is placed in a supine position with arms tucked, and a single-toothed tenaculum is placed on the cervix from 12 to 6 o’clock, without any instrument for manipulation of the uterus. The system’s dispersive electrode pads are placed symmetrically just above the patella on the anterior thighs; asymmetrical placement could potentially increase the risk of a pad burn.
Two standard laparoscopic ports are placed. A 5-mm trocar for the camera and video laparoscope is placed through the umbilicus or at a supraumbilical or left upper–quadrant level, depending on the patient’s anatomy, her surgical history, and the size of the uterus. A thorough visual inspection of the abdomen should be performed to look for unsuspected findings.
A 10-mm trocar is then placed at the level of the top of the fundus for the intra-abdominal ultrasound probe. Laparoscopic ultrasound is used to survey the entire uterus, map the fibroids, and plan an approach. Once the fibroid to be treated first is identified, the ability to stabilize the uterus accordingly is assessed, and the dimensions of the fibroid are taken. The dimensions will be used by the surgeon with a volume algorithm to calculate the length of ablation time based on the size of the fibroid and electrode deployment.
Under ultrasound guidance, the Acessa radiofrequency ablation handpiece is inserted percutaneously at 12, 3, 6, or 9 o’clock relative to the ultrasound trocar, based on the location of the target fibroid. The uterus must be stabilized, with the handpiece and ultrasound probe parallel and in plane. The handpiece is then inserted 1 cm into the target fibroid through the uterine serosal surface, utilizing a combination of laparoscopic and ultrasound views. Care must be taken to use gentle rotation and minimal downward pressure as the tip of the handpiece is quite sharp.
The location of the tip is confirmed by laparoscopic ultrasound, and the 7-needle electrode array can then be deployed to the ablation site. All three dimensions of the fibroid should be viewed for placement and deployment of the electrodes. Care is taken to avoid large blood vessels and ensure that the electrodes are confined within the fibroid and within the uterus.
Radiofrequency ablation is carried out with a low-voltage, high-frequency alternating current. The radiofrequency waves heat the tissue to an average temperature of 95° C for a length of time determined by a treatment algorithm. The wattage automatically adjusts to maintain the treatment temperature for the calculated duration of ablation.
Small fibroids can be treated in a manual mode without deployment of the electrode array at a current output of 15 W.
At the conclusion of the ablation, the electrodes are withdrawn into the handpiece, the generator is changed to coagulation mode, and the handpiece is slowly withdrawn under ultrasound visualization. The tract is simultaneously coagulated. A bit of additional coagulation is facilitated by pausing at the serosal surface.
Additional fibroids can be ablated through another insertion of the handpiece, either through the same tract or through a new tract.
Larger fibroids may require multiple ablations. The maximum size of ablation is about 5 cm, so it is important to plan the treatment of larger fibroids. This can be accomplished by carefully scanning large fibroids and visualizing the number of overlapping ablations needed to treat the entire volume. I ask my assistant to record the size and location of each ablation; I find this helpful both for organizing the treatment of large fibroids and for dictating the operative report.
It is important to appreciate that treatment of one area can make it difficult to visualize nearby fibroids with ultrasound. The effect dissipates in about 30-45 minutes. It is one reason why having a fibroid map prior to treatment is so important.
Once all fibroids are treated, a final inspection is performed. We usually use a suction irrigator to clean out whatever small amounts of blood are present, and the laparoscopic and port sites are closed in standard fashion.
Patients are seen 1 week postoperatively and are instructed to call in cases of pain, fever, bleeding, or chills. Most patients require only NSAIDs for pain relief and return to work in 2-7 days.
Many patients experience a slightly heavier than normal first menses after treatment. Pelvic rest is recommended for 3 weeks as a precaution, and avoidance of intrauterine procedures is advised because the uterus will be soft and thus may be easily perforated. Patients who have had type 1, type 2, or type 2-5 fibroids ablated may experience drainage for several weeks as the fibroid tissue is reabsorbed.
Dr. Berman is interim chairman of Wayne State University’s department of obstetrics and gynecology and interim specialist-in-chief for obstetrics and gynecology at the Detroit Medical Center. He was a principal investigator of the 3-year outcome study of Acessa sponsored by Halt Medical. He is a consultant for Halt Medical and directs physician training in the use of Acessa.
Uterine myomas cause heavy menstrual bleeding and other clinically significant symptoms in 35%-50% of affected women and have been shown to be the leading indication for hysterectomy in the United States among women aged 35-54 years.
Research has shown that a significant number of women who undergo hysterectomy for treatment of fibroids later regret the loss of their uterus and have other concerns and complications. Other options for therapy include various pharmacologic treatments, a progestin-releasing intrauterine device, uterine artery embolization, endometrial ablation, MRI-guided focused ultrasound surgery, and myomectomy performed laparoscopically, robotically, or hysteroscopically.
Myomectomy seems largely to preserve fertility, but rates of recurrence and additional procedures for bleeding and myoma symptoms are still high – upward of 30% in some studies. Overall, we need other more efficacious and minimally invasive options.
Radiofrequency volumetric thermal ablation (RFVTA) achieved through the Acessa System (Halt Medical) has been the newest addition to our armamentarium for treatment of symptomatic fibroids. It is suitable for every type of fibroid except for type 0 pedunculated intracavitary fibroids and type 7 pedunculated subserosal fibroids, which is significant because deep intramural fibroids have been difficult to target and treat by other methods.
Three-year outcome data show sustained improvements in fibroid symptoms and quality of life, with an incidence of recurrences and additional procedures – approximately 11% – that appears to be substantially lower than for other uterine-sparing fibroid treatments. In addition, while the technology is not indicated for women seeking future childbearing, successful pregnancies are being reported, suggesting that full-term pregnancies – and vaginal delivery in some cases – may be possible after RFVTA.
The principles
Radiofrequency ablation has been used for years in the treatment of liver and kidney tumors. The basic concept is that volumetric thermal ablation results in coagulative necrosis.
The Acessa System, approved by the Food and Drug Administration in late 2012, was designed to treat fibroids, which have much firmer tissue than the tissues being targeted in other radiofrequency ablation procedures. It uses a specially designed intrauterine ultrasound probe and radiofrequency probe, and it combines three fundamental gynecologic skills: Laparoscopy using two trocars and requiring no special suturing skills; ultrasound using a laparoscopic ultrasound probe to scan and manipulate; and probe placement under laparoscopic ultrasound guidance.
Specifically, the system allows for percutaneous, laparoscopic ultrasound–guided radiofrequency ablation of fibroids with a disposable 3.4-mm handpiece coupled to a dual-function radiofrequency generator. The handpiece contains a retractable array of electrodes, so that the fibroid may be ablated with one electrode or with the deployed electrode array.
The generator controls and monitors the ablation with real-time feedback from thermocouples. It monitors and displays the temperature at each needle tip, the average temperature of the array, and the return temperatures on two dispersive electrode pads that are placed on the anterior thighs. The electrode pads are designed to reduce the incidence of pad burns, which are a complication with other radiofrequency ablation devices. The system will automatically stop treatment if either of the pad thermocouples registers a skin temperature greater than 40° C (JSLS. 2014 Apr-Jun;18[2]:182-90).
The outcomes
Laparoscopic ultrasound–guided RFVTA has been studied in five prospective trials, including one multicenter international trial of 135 premenopausal women – the pivotal trial for FDA clearance – in which 104 women were followed for 3 years and found to have prolonged symptom relief and improved quality of life.
At baseline, the women had symptomatic uterine myomas and moderate to severe heavy menstrual bleeding measured by alkaline hematin analysis of returned sanitary products. Their mean symptom severity scores on the Uterine Fibroid Symptom and Quality-of-Life Questionnaire (UFS-QOL) decreased significantly from baseline to 3 months and changed little after that, for a total change of –32.6 over the study period.
The cumulative repeat intervention rate at 3 years was 11%, with 14 of the 135 participants having repeat interventions to treat bleeding and myoma symptoms. Seven of these women were found to have adenomyosis (J Minim Invasive Gynecol. 2014 Sep-Oct;21[5]:767-74).
The surprisingly low reintervention rates may stem from the benefits of direct contact imaging of the uterus. A comparison of images from the pivotal trial has shown that intraoperative ultrasound detected more than twice as many fibroids as did preoperative transvaginal ultrasound, and about one-third more than preoperative MRIs (J Minim Invasive Gynecol. 2013 Nov-Dec;20[6]:770-4).
Interestingly, four women became pregnant over the study’s 3-year follow-up, despite the inclusion requirement that women desire uterine conservation but not future childbearing.
We have followed reproductive outcomes in women after RFVTA of symptomatic fibroids in other studies as well. In our most recent analysis, presented in November at the 2015 American Association of Gynecologic Laparoscopists Global Congress, we identified 10 pregnancies among participants of the five prospective trials.
Of 232 women enrolled in premarket RFVTA studies – trials in which completing childbearing and continuing contraception were requirements – six conceived at 3.5-15 months post ablation. The number of myomas treated ranged from one to seven and included multiple types and dimensions. Five of these six women delivered full-term healthy babies – one by vaginal delivery and four by cesarean section. The sixth patient had a spontaneous abortion in the first trimester.
Of 43 women who participated in two randomized clinical trials undertaken after FDA clearance, four conceived at 4-23.5 months post ablation. Three of these women had uneventful, full-term pregnancies with vaginal births. The fourth had a cesarean section at 38 weeks.
Considering the theoretical advantages of the Acessa procedure – that it is less damaging to healthy myometrium – and the outcomes reported thus far, it appears likely that Acessa will be preferable to myomectomy. Early results from an ongoing 5-year German study that randomized 50 women to RFVTA or laparoscopic myomectomy show that RFVTA resulted in the treatment of more fibroids and involved a significantly shorter hospital stay and post-operative recovery (Int J Gynaecol Obstet. 2014 Jun;125[3]:261-5).
The technique
The patient is pretreated with a nonsteroidal anti-inflammatory agent and prophylactic antibiotic. She is placed in a supine position with arms tucked, and a single-toothed tenaculum is placed on the cervix from 12 to 6 o’clock, without any instrument for manipulation of the uterus. The system’s dispersive electrode pads are placed symmetrically just above the patella on the anterior thighs; asymmetrical placement could potentially increase the risk of a pad burn.
Two standard laparoscopic ports are placed. A 5-mm trocar for the camera and video laparoscope is placed through the umbilicus or at a supraumbilical or left upper–quadrant level, depending on the patient’s anatomy, her surgical history, and the size of the uterus. A thorough visual inspection of the abdomen should be performed to look for unsuspected findings.
A 10-mm trocar is then placed at the level of the top of the fundus for the intra-abdominal ultrasound probe. Laparoscopic ultrasound is used to survey the entire uterus, map the fibroids, and plan an approach. Once the fibroid to be treated first is identified, the ability to stabilize the uterus accordingly is assessed, and the dimensions of the fibroid are taken. The dimensions will be used by the surgeon with a volume algorithm to calculate the length of ablation time based on the size of the fibroid and electrode deployment.
Under ultrasound guidance, the Acessa radiofrequency ablation handpiece is inserted percutaneously at 12, 3, 6, or 9 o’clock relative to the ultrasound trocar, based on the location of the target fibroid. The uterus must be stabilized, with the handpiece and ultrasound probe parallel and in plane. The handpiece is then inserted 1 cm into the target fibroid through the uterine serosal surface, utilizing a combination of laparoscopic and ultrasound views. Care must be taken to use gentle rotation and minimal downward pressure as the tip of the handpiece is quite sharp.
The location of the tip is confirmed by laparoscopic ultrasound, and the 7-needle electrode array can then be deployed to the ablation site. All three dimensions of the fibroid should be viewed for placement and deployment of the electrodes. Care is taken to avoid large blood vessels and ensure that the electrodes are confined within the fibroid and within the uterus.
Radiofrequency ablation is carried out with a low-voltage, high-frequency alternating current. The radiofrequency waves heat the tissue to an average temperature of 95° C for a length of time determined by a treatment algorithm. The wattage automatically adjusts to maintain the treatment temperature for the calculated duration of ablation.
Small fibroids can be treated in a manual mode without deployment of the electrode array at a current output of 15 W.
At the conclusion of the ablation, the electrodes are withdrawn into the handpiece, the generator is changed to coagulation mode, and the handpiece is slowly withdrawn under ultrasound visualization. The tract is simultaneously coagulated. A bit of additional coagulation is facilitated by pausing at the serosal surface.
Additional fibroids can be ablated through another insertion of the handpiece, either through the same tract or through a new tract.
Larger fibroids may require multiple ablations. The maximum size of ablation is about 5 cm, so it is important to plan the treatment of larger fibroids. This can be accomplished by carefully scanning large fibroids and visualizing the number of overlapping ablations needed to treat the entire volume. I ask my assistant to record the size and location of each ablation; I find this helpful both for organizing the treatment of large fibroids and for dictating the operative report.
It is important to appreciate that treatment of one area can make it difficult to visualize nearby fibroids with ultrasound. The effect dissipates in about 30-45 minutes. It is one reason why having a fibroid map prior to treatment is so important.
Once all fibroids are treated, a final inspection is performed. We usually use a suction irrigator to clean out whatever small amounts of blood are present, and the laparoscopic and port sites are closed in standard fashion.
Patients are seen 1 week postoperatively and are instructed to call in cases of pain, fever, bleeding, or chills. Most patients require only NSAIDs for pain relief and return to work in 2-7 days.
Many patients experience a slightly heavier than normal first menses after treatment. Pelvic rest is recommended for 3 weeks as a precaution, and avoidance of intrauterine procedures is advised because the uterus will be soft and thus may be easily perforated. Patients who have had type 1, type 2, or type 2-5 fibroids ablated may experience drainage for several weeks as the fibroid tissue is reabsorbed.
Dr. Berman is interim chairman of Wayne State University’s department of obstetrics and gynecology and interim specialist-in-chief for obstetrics and gynecology at the Detroit Medical Center. He was a principal investigator of the 3-year outcome study of Acessa sponsored by Halt Medical. He is a consultant for Halt Medical and directs physician training in the use of Acessa.

New insight into blood vessel formation

Image by Louis Heiser
and Robert Ackland
Research published in Cell Reports has provided new insight into cellular movement during angiogenesis.
Blood vessel growth was previously thought to occur in the direction of the vessel tip, stretching in a manner that left the lead cells behind.
However, recent studies have suggested that both tip cells and trailing cells move at different speeds and in different directions, changing positions to extend the blood vessel into the surrounding matrix.
With the current study, researchers wanted to determine how to gain control of the complex cellular motion involved in angiogenesis. They approached the problem using a combination of biology, mathematical models, and computer simulations.
“We watched the movement of the vascular endothelial cells in real time, created a mathematical model of the movement, and then performed simulations on a computer,” said Koichi Nishiyama, MD, PhD, of Kumamoto University in Japan.
“We found that we could reproduce blood vessel growth and the motion of the entire cellular structure by using only very simple cell-autonomous mechanisms. The mechanisms, such as speed and direction of movement, of every single cell change stochastically. It’s really interesting.”
Dr Nishiyama and his colleagues attempted to increase the accuracy of their simulation by adding a new rule to the mathematical model. This rule reduced the movement of cells at the tip of the blood vessel as the distance between tip cells and subsequent cells increased.
The researchers also conducted an experiment using actual cells to confirm whether the predicted cellular movement of the simulation was a feasible biological phenomenon.
They performed an operation to widen the distance between the tip cells and subsequent cells using a laser. The results showed that the forward movement of the tip cells was stopped in the same manner predicted by the simulations.
“We found that complex cell motility, such as that seen during blood vessel growth, is a process in which coexisting cells successfully control themselves spontaneously and move in a coordinated manner through the influence of adjacent cells,” Dr Nishiyama said.
“The ability to directly control this phenomenon was made apparent in our study. These results will add to the understanding of the formation of not only blood vessels but also various tissues and the fundamental mechanisms of the origins of the organism.” ![]()
Image by Louis Heiser
and Robert Ackland
Research published in Cell Reports has provided new insight into cellular movement during angiogenesis.
Blood vessel growth was previously thought to occur in the direction of the vessel tip, stretching in a manner that left the lead cells behind.
However, recent studies have suggested that both tip cells and trailing cells move at different speeds and in different directions, changing positions to extend the blood vessel into the surrounding matrix.
With the current study, researchers wanted to determine how to gain control of the complex cellular motion involved in angiogenesis. They approached the problem using a combination of biology, mathematical models, and computer simulations.
“We watched the movement of the vascular endothelial cells in real time, created a mathematical model of the movement, and then performed simulations on a computer,” said Koichi Nishiyama, MD, PhD, of Kumamoto University in Japan.
“We found that we could reproduce blood vessel growth and the motion of the entire cellular structure by using only very simple cell-autonomous mechanisms. The mechanisms, such as speed and direction of movement, of every single cell change stochastically. It’s really interesting.”
Dr Nishiyama and his colleagues attempted to increase the accuracy of their simulation by adding a new rule to the mathematical model. This rule reduced the movement of cells at the tip of the blood vessel as the distance between tip cells and subsequent cells increased.
The researchers also conducted an experiment using actual cells to confirm whether the predicted cellular movement of the simulation was a feasible biological phenomenon.
They performed an operation to widen the distance between the tip cells and subsequent cells using a laser. The results showed that the forward movement of the tip cells was stopped in the same manner predicted by the simulations.
“We found that complex cell motility, such as that seen during blood vessel growth, is a process in which coexisting cells successfully control themselves spontaneously and move in a coordinated manner through the influence of adjacent cells,” Dr Nishiyama said.
“The ability to directly control this phenomenon was made apparent in our study. These results will add to the understanding of the formation of not only blood vessels but also various tissues and the fundamental mechanisms of the origins of the organism.” ![]()
Image by Louis Heiser
and Robert Ackland
Research published in Cell Reports has provided new insight into cellular movement during angiogenesis.
Blood vessel growth was previously thought to occur in the direction of the vessel tip, stretching in a manner that left the lead cells behind.
However, recent studies have suggested that both tip cells and trailing cells move at different speeds and in different directions, changing positions to extend the blood vessel into the surrounding matrix.
With the current study, researchers wanted to determine how to gain control of the complex cellular motion involved in angiogenesis. They approached the problem using a combination of biology, mathematical models, and computer simulations.
“We watched the movement of the vascular endothelial cells in real time, created a mathematical model of the movement, and then performed simulations on a computer,” said Koichi Nishiyama, MD, PhD, of Kumamoto University in Japan.
“We found that we could reproduce blood vessel growth and the motion of the entire cellular structure by using only very simple cell-autonomous mechanisms. The mechanisms, such as speed and direction of movement, of every single cell change stochastically. It’s really interesting.”
Dr Nishiyama and his colleagues attempted to increase the accuracy of their simulation by adding a new rule to the mathematical model. This rule reduced the movement of cells at the tip of the blood vessel as the distance between tip cells and subsequent cells increased.
The researchers also conducted an experiment using actual cells to confirm whether the predicted cellular movement of the simulation was a feasible biological phenomenon.
They performed an operation to widen the distance between the tip cells and subsequent cells using a laser. The results showed that the forward movement of the tip cells was stopped in the same manner predicted by the simulations.
“We found that complex cell motility, such as that seen during blood vessel growth, is a process in which coexisting cells successfully control themselves spontaneously and move in a coordinated manner through the influence of adjacent cells,” Dr Nishiyama said.
“The ability to directly control this phenomenon was made apparent in our study. These results will add to the understanding of the formation of not only blood vessels but also various tissues and the fundamental mechanisms of the origins of the organism.” ![]()
AURKA inhibitors could prevent GVHD

Photo by Einar Fredriksen
A gene expression profiling study has suggested the aurora kinase A (AURKA) pathway may drive graft-vs-host disease (GVHD).
This indicates that AURKA inhibitors, which are readily available in the clinic, might prove useful as GVHD prophylaxis.
Scott Furlan, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues conducted this research and reported the results in Science Translational Medicine.
The researchers compared the transcriptome of T cells from monkeys with acute GVHD, both treated and untreated for the complication, to healthy controls.
Specifically, the team measured the expression profiles of CD3+ T cells from 5 cohorts of rhesus macaques:
- Allogeneic transplant recipients receiving no GHVD prophylaxis
- Allogeneic transplant recipients receiving sirolimus monotherapy
- Allogeneic transplant recipients receiving tacrolimus-methotrexate
- Autologous transplant recipients
- Healthy controls.
This comparison revealed pathways that were abnormally activated during GVHD in allogeneic transplant recipients receiving no prophylaxis. This included pathways involved in immune signaling, T-cell proliferation, and cell-cycle progression.
Within these pathways were potentially druggable targets that had never before been linked to GVHD.
The researchers said the most notable pathway was AURKA, which controls cell-cycle progression as well cell growth, differentiation, and survival.
When they analyzed tissue samples from transplant patients, the team found that T cells highly expressed AURKA during GVHD.
And in a mouse model of GVHD, a drug targeting AURKA (MLN8237) reduced the severity of GVHD and improved survival. The median survival time was 22.5 days in vehicle-treated controls and 40.5 days in mice that received MLN8237 (P<0.0001).
The researchers said these results suggest that AURKA inhibitors, many of which are commercially available or currently being tested in clinical trials, might help prevent GVHD. ![]()
Photo by Einar Fredriksen
A gene expression profiling study has suggested the aurora kinase A (AURKA) pathway may drive graft-vs-host disease (GVHD).
This indicates that AURKA inhibitors, which are readily available in the clinic, might prove useful as GVHD prophylaxis.
Scott Furlan, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues conducted this research and reported the results in Science Translational Medicine.
The researchers compared the transcriptome of T cells from monkeys with acute GVHD, both treated and untreated for the complication, to healthy controls.
Specifically, the team measured the expression profiles of CD3+ T cells from 5 cohorts of rhesus macaques:
- Allogeneic transplant recipients receiving no GHVD prophylaxis
- Allogeneic transplant recipients receiving sirolimus monotherapy
- Allogeneic transplant recipients receiving tacrolimus-methotrexate
- Autologous transplant recipients
- Healthy controls.
This comparison revealed pathways that were abnormally activated during GVHD in allogeneic transplant recipients receiving no prophylaxis. This included pathways involved in immune signaling, T-cell proliferation, and cell-cycle progression.
Within these pathways were potentially druggable targets that had never before been linked to GVHD.
The researchers said the most notable pathway was AURKA, which controls cell-cycle progression as well cell growth, differentiation, and survival.
When they analyzed tissue samples from transplant patients, the team found that T cells highly expressed AURKA during GVHD.
And in a mouse model of GVHD, a drug targeting AURKA (MLN8237) reduced the severity of GVHD and improved survival. The median survival time was 22.5 days in vehicle-treated controls and 40.5 days in mice that received MLN8237 (P<0.0001).
The researchers said these results suggest that AURKA inhibitors, many of which are commercially available or currently being tested in clinical trials, might help prevent GVHD. ![]()
Photo by Einar Fredriksen
A gene expression profiling study has suggested the aurora kinase A (AURKA) pathway may drive graft-vs-host disease (GVHD).
This indicates that AURKA inhibitors, which are readily available in the clinic, might prove useful as GVHD prophylaxis.
Scott Furlan, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues conducted this research and reported the results in Science Translational Medicine.
The researchers compared the transcriptome of T cells from monkeys with acute GVHD, both treated and untreated for the complication, to healthy controls.
Specifically, the team measured the expression profiles of CD3+ T cells from 5 cohorts of rhesus macaques:
- Allogeneic transplant recipients receiving no GHVD prophylaxis
- Allogeneic transplant recipients receiving sirolimus monotherapy
- Allogeneic transplant recipients receiving tacrolimus-methotrexate
- Autologous transplant recipients
- Healthy controls.
This comparison revealed pathways that were abnormally activated during GVHD in allogeneic transplant recipients receiving no prophylaxis. This included pathways involved in immune signaling, T-cell proliferation, and cell-cycle progression.
Within these pathways were potentially druggable targets that had never before been linked to GVHD.
The researchers said the most notable pathway was AURKA, which controls cell-cycle progression as well cell growth, differentiation, and survival.
When they analyzed tissue samples from transplant patients, the team found that T cells highly expressed AURKA during GVHD.
And in a mouse model of GVHD, a drug targeting AURKA (MLN8237) reduced the severity of GVHD and improved survival. The median survival time was 22.5 days in vehicle-treated controls and 40.5 days in mice that received MLN8237 (P<0.0001).
The researchers said these results suggest that AURKA inhibitors, many of which are commercially available or currently being tested in clinical trials, might help prevent GVHD. ![]()
FDA approves elotuzumab for MM

Photo courtesy of
Bristol-Myers Squibb
The US Food and Drug Administration (FDA) has approved elotuzumab (Empliciti) for use in combination with lenalidomide and dexamethasone to treat multiple myeloma (MM) patients who have received 1 to 3 prior therapies.
Elotuzumab is an immunostimulatory antibody that specifically targets signaling lymphocyte activation molecule family member 7 (SLAMF7), a cell-surface glycoprotein that is expressed on myeloma cells independent of cytogenetic abnormalities.
Elotuzumab is the first immunostimulatory antibody approved for MM.
Bristol-Myers Squibb said it expects to begin shipping elotuzumab this week. The drug will be available for injection for intravenous use in 300 mg and 400 mg vials.
Elotuzumab is currently under review by the European Medicines Agency and has been granted accelerated assessment.
The FDA previously granted elotuzumab breakthrough therapy designation, orphan drug designation, and priority review.
Bristol-Myers Squibb and AbbVie are co-developing elotuzumab, with Bristol-Myers Squibb solely responsible for commercial activities. For more details on the drug, see the full prescribing information.
ELOQUENT-2 trial
The FDA’s approval of elotuzumab is primarily based on data from the phase 3 ELOQUENT-2 trial, which were presented at ASCO 2015 and published in NEJM.
The trial included 646 MM patients who had received 1 to 3 prior therapies. Baseline patient demographics and disease characteristics were well balanced between treatment arms.
Patients were randomized 1:1 to receive either elotuzumab at 10 mg/kg in combination with lenalidomide and dexamethasone (len-dex) or len-dex alone in 4-week cycles until disease progression or unacceptable toxicity.
The minimum follow-up for all study subjects was 24 months. The co-primary endpoints were progression-free survival (PFS) and overall response rate.
The overall response rate was 78.5% in the elotuzumab arm and 65.5% in the len-dex arm (P=0.0002).
The median PFS was 19.4 months in the elotuzumab arm and 14.9 months in the len-dex arm (P=0.0004). At 1 year, the PFS was 68% in the elotuzumab arm and 57% in the len-dex arm. At 2 years, the PFS was 41% and 27%, respectively.
Serious adverse events occurred in 65.4% of patients in the elotuzumab arm and 56.5% in the len-dex arm. The most frequent serious adverse events in each arm, respectively, were pneumonia (15.4% vs 11%), pyrexia (6.9% vs 4.7%), respiratory tract infection (3.1% vs 1.3%), anemia (2.8% vs 1.9%), pulmonary embolism (3.1% vs 2.5%), and acute renal failure (2.5% vs 1.9%).
The most common adverse events in the elotuzumab arm and len-dex arm, respectively, were fatigue (61.6% vs 51.7%), diarrhea (46.9% vs 36.0%), pyrexia (37.4% vs 24.6%), constipation (35.5% vs 27.1%), cough (34.3% vs 18.9%), peripheral neuropathy (26.7% vs 20.8%), nasopharyngitis (24.5% vs 19.2%), upper respiratory tract infection (22.6% vs 17.4%), decreased appetite (20.8% vs 12.6%), and pneumonia (20.1% vs 14.2%). ![]()
Photo courtesy of
Bristol-Myers Squibb
The US Food and Drug Administration (FDA) has approved elotuzumab (Empliciti) for use in combination with lenalidomide and dexamethasone to treat multiple myeloma (MM) patients who have received 1 to 3 prior therapies.
Elotuzumab is an immunostimulatory antibody that specifically targets signaling lymphocyte activation molecule family member 7 (SLAMF7), a cell-surface glycoprotein that is expressed on myeloma cells independent of cytogenetic abnormalities.
Elotuzumab is the first immunostimulatory antibody approved for MM.
Bristol-Myers Squibb said it expects to begin shipping elotuzumab this week. The drug will be available for injection for intravenous use in 300 mg and 400 mg vials.
Elotuzumab is currently under review by the European Medicines Agency and has been granted accelerated assessment.
The FDA previously granted elotuzumab breakthrough therapy designation, orphan drug designation, and priority review.
Bristol-Myers Squibb and AbbVie are co-developing elotuzumab, with Bristol-Myers Squibb solely responsible for commercial activities. For more details on the drug, see the full prescribing information.
ELOQUENT-2 trial
The FDA’s approval of elotuzumab is primarily based on data from the phase 3 ELOQUENT-2 trial, which were presented at ASCO 2015 and published in NEJM.
The trial included 646 MM patients who had received 1 to 3 prior therapies. Baseline patient demographics and disease characteristics were well balanced between treatment arms.
Patients were randomized 1:1 to receive either elotuzumab at 10 mg/kg in combination with lenalidomide and dexamethasone (len-dex) or len-dex alone in 4-week cycles until disease progression or unacceptable toxicity.
The minimum follow-up for all study subjects was 24 months. The co-primary endpoints were progression-free survival (PFS) and overall response rate.
The overall response rate was 78.5% in the elotuzumab arm and 65.5% in the len-dex arm (P=0.0002).
The median PFS was 19.4 months in the elotuzumab arm and 14.9 months in the len-dex arm (P=0.0004). At 1 year, the PFS was 68% in the elotuzumab arm and 57% in the len-dex arm. At 2 years, the PFS was 41% and 27%, respectively.
Serious adverse events occurred in 65.4% of patients in the elotuzumab arm and 56.5% in the len-dex arm. The most frequent serious adverse events in each arm, respectively, were pneumonia (15.4% vs 11%), pyrexia (6.9% vs 4.7%), respiratory tract infection (3.1% vs 1.3%), anemia (2.8% vs 1.9%), pulmonary embolism (3.1% vs 2.5%), and acute renal failure (2.5% vs 1.9%).
The most common adverse events in the elotuzumab arm and len-dex arm, respectively, were fatigue (61.6% vs 51.7%), diarrhea (46.9% vs 36.0%), pyrexia (37.4% vs 24.6%), constipation (35.5% vs 27.1%), cough (34.3% vs 18.9%), peripheral neuropathy (26.7% vs 20.8%), nasopharyngitis (24.5% vs 19.2%), upper respiratory tract infection (22.6% vs 17.4%), decreased appetite (20.8% vs 12.6%), and pneumonia (20.1% vs 14.2%). ![]()
Photo courtesy of
Bristol-Myers Squibb
The US Food and Drug Administration (FDA) has approved elotuzumab (Empliciti) for use in combination with lenalidomide and dexamethasone to treat multiple myeloma (MM) patients who have received 1 to 3 prior therapies.
Elotuzumab is an immunostimulatory antibody that specifically targets signaling lymphocyte activation molecule family member 7 (SLAMF7), a cell-surface glycoprotein that is expressed on myeloma cells independent of cytogenetic abnormalities.
Elotuzumab is the first immunostimulatory antibody approved for MM.
Bristol-Myers Squibb said it expects to begin shipping elotuzumab this week. The drug will be available for injection for intravenous use in 300 mg and 400 mg vials.
Elotuzumab is currently under review by the European Medicines Agency and has been granted accelerated assessment.
The FDA previously granted elotuzumab breakthrough therapy designation, orphan drug designation, and priority review.
Bristol-Myers Squibb and AbbVie are co-developing elotuzumab, with Bristol-Myers Squibb solely responsible for commercial activities. For more details on the drug, see the full prescribing information.
ELOQUENT-2 trial
The FDA’s approval of elotuzumab is primarily based on data from the phase 3 ELOQUENT-2 trial, which were presented at ASCO 2015 and published in NEJM.
The trial included 646 MM patients who had received 1 to 3 prior therapies. Baseline patient demographics and disease characteristics were well balanced between treatment arms.
Patients were randomized 1:1 to receive either elotuzumab at 10 mg/kg in combination with lenalidomide and dexamethasone (len-dex) or len-dex alone in 4-week cycles until disease progression or unacceptable toxicity.
The minimum follow-up for all study subjects was 24 months. The co-primary endpoints were progression-free survival (PFS) and overall response rate.
The overall response rate was 78.5% in the elotuzumab arm and 65.5% in the len-dex arm (P=0.0002).
The median PFS was 19.4 months in the elotuzumab arm and 14.9 months in the len-dex arm (P=0.0004). At 1 year, the PFS was 68% in the elotuzumab arm and 57% in the len-dex arm. At 2 years, the PFS was 41% and 27%, respectively.
Serious adverse events occurred in 65.4% of patients in the elotuzumab arm and 56.5% in the len-dex arm. The most frequent serious adverse events in each arm, respectively, were pneumonia (15.4% vs 11%), pyrexia (6.9% vs 4.7%), respiratory tract infection (3.1% vs 1.3%), anemia (2.8% vs 1.9%), pulmonary embolism (3.1% vs 2.5%), and acute renal failure (2.5% vs 1.9%).
The most common adverse events in the elotuzumab arm and len-dex arm, respectively, were fatigue (61.6% vs 51.7%), diarrhea (46.9% vs 36.0%), pyrexia (37.4% vs 24.6%), constipation (35.5% vs 27.1%), cough (34.3% vs 18.9%), peripheral neuropathy (26.7% vs 20.8%), nasopharyngitis (24.5% vs 19.2%), upper respiratory tract infection (22.6% vs 17.4%), decreased appetite (20.8% vs 12.6%), and pneumonia (20.1% vs 14.2%). ![]()