User login
Treatment of Ampicillin-Resistant Enterococcus faecium Urinary Tract Infections
Enterococcus species account for about 110,000 urinary tract infections (UTIs) annually in the U.S.1 The most common species isolated are Enterococcus faecalis and Enterococcus faecium (E faecium). Amoxicillin is the drug of choice for the treatment of enterococcal UTIs. Second-line therapies include vancomycin and nitrofurantoin. Alternative therapies include daptomycin and linezolid; however, these newer agents ideally would be reserved for more serious infections to preserve activity.2
Increased E faecium resistance to ampicillin and vancomycin has limited the therapeutic options. The results of a study by Zhanel and colleagues assessed the prevalence of resistant enterococcal urine isolates in North America.3 Of the 658 E faecium urine isolates, about 96% were resistant to ampicillin and 94% were resistant to vancoymcin.3 Nitrofurantoin has much lower resistance rates; however, its use is contraindicated in patients with a creatinine clearance (CrCl) < 60 mL/min.4 Data supporting the contraindication are limited, but the results of a study by Oplinger and Andrews suggested that using nitrofurantoin in patients with a CrCl ≥ 40 mL/min may be safe and effective.5 A therapeutic dilemma may occur when resistant E faecium UTIs are encountered and viable treatment options are limited due to intolerances, administration difficulties, lack of susceptibility data, or cost.
Related: Antimicrobial Stewardship in an Outpatient Parenteral Antibiotic Therapy Program
Based on the current Clinical and Laboratory Standards Institute standard, Enterococcus species with a minimal inhibitory concentration (MIC) ≥ 16 μg/mL are considered ampicillin resistant. Microbiology laboratories use the same breakpoint regardless of the site of infection.6 Amoxicillin concentrates in the urine; therefore, urinary concentrations are much higher than serum concentrations. The mean serum peak concentration after a single dose of oral amoxicillin 500 mg is 7.6 μg/mL.7 After a single dose of oral amoxicillin 500 mg, the average concentration in pooled urine collected over 6 hours was 1,100 μg/mL.8
In 2002, Williamson and colleagues analyzed 30 ampicillin- resistant E faecium urine isolates. Reported MICs were 128 μg/mL (30%), 256 μg/mL (60%), and 512 μg/mL (10%).9 A more recent retrospective analysis analyzed 234 ampicillin-resistant E faecium urine isolates. The MIC ranged from 32 to 1,024 μg/mL, with a median MIC of 256 μg/mL. Only 5 isolates had an MIC value > 1,000 μg/mL, but each of these isolates was within 1 dilution of 512 μg/mL.10 Because penicillins exhibit time-dependent killing, an optimal response will occur as long as the urine concentration is above the MIC for at least 50% of the dosing interval.11 Therefore, therapeutic doses of amoxicillin are expected to produce urine concentrations that exceed the MIC of resistant E faecium urine isolates. The purpose of this study was to determine if amoxicillin was a viable treatment option for ampicillin-resistant E faecium UTIs based on this in vitro theory.
Methods
Veterans aged ≥ 18 years with a positive urine culture for ampicillin- resistant E faecium who received antibiotic therapy for cystitis at the Jesse Brown VA Medical Center (JBVAMC) from January 1, 2005, through June 22, 2010, were evaluated in this retrospective cohort study. Exclusion criteria were the presence of any other organisms in the initial urine culture, prostatic involvement, and the presence of E faecium in a blood culture. Subjects treated with multiple antibiotics concurrently and with sequential treatment of different antibiotics with no evaluation of efficacy between courses were also excluded.
Related: Urologist Workforce Variation Across the VHA
All included subjects were evaluated for resolution of symptoms; improvement in leukocyte esterase count and white blood cell (WBC) count from urine analysis (UA); and eradication of E faecium from a repeat urine culture. The response to treatment was classified as cure, presumed cure, or failure. The criteria for cure were based on the following: resolution of symptoms if present at baseline; repeat UA indicating improvement from the initial positive UA (if obtained); and eradication of E faecium in a repeat urine culture (if obtained).
At least 1 of the aforementioned criteria must have been met to be classified as cure. If more than 1 of the aforementioned criteria was present, then each one must have been met to be classified as cure. To be evaluated for presumed cure, the subject must have had symptoms at baseline. No documentation of ongoing symptoms in subjects who had an appropriate follow-up but did not have a repeat UA or urine culture indicated presumed cure. Persistence or worsening of pretreatment symptoms, a repeat UA without improvement from the initial positive UA, or a repeat urine culture demonstrating continued presence of E faecium indicated failure. The primary endpoint for the study was to determine whether amoxicillin was effective for the management of ampicillin-resistant E faecium UTIs. This study was conducted in compliance with the University of Illinois at Chicago Institutional Review Board and JBVAMC Human Subjects Research Committee requirements.
Results
This study included 20 positive urine cultures for ampicillin-resistant E faecium in 19 subjects. Nine cases were treated with amoxicillin, and 11 cases were treated with nitrofurantoin. At baseline, the mean age was 75 years, mean duration of therapy was 14 days, and all the subjects were male. The baseline characteristics of the 2 groups were similar with the exception of an older population, shorter duration of therapy, and increased incidence of chronic kidney disease in the amoxicillin treatment group, P = .02, .03, and .01, respectively.
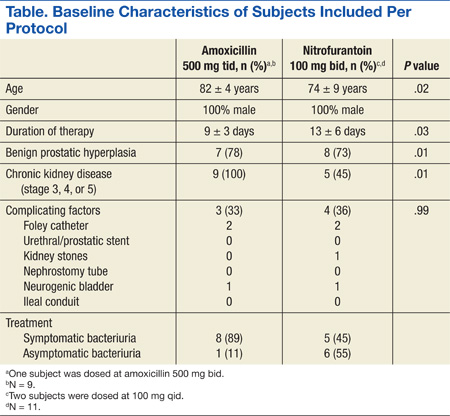
Symptoms were documented in 8 of 9 (89%) cases at the time of the positive culture in the amoxicillin treatment group and 5 of 11 (45%) cases in the nitrofurantoin treatment group (Table). The asymptomatic amoxicillin treatment group case and 5 of the 6 nitrofurantoin treatment group asymptomatic cases received treatment prior to a urologic procedure in accordance with the Infectious Diseases Society of America (IDSA) guidelines for the treatment of asymptomatic bacteriuria. The urologic procedures included transurethral resection of a bladder tumor, cystoscopy, urethral dilation, cystometrogram, and transurethral resection of the prostate. One asymptomatic subject in the nitrofurantoin group did not have any documentation to support an appropriate indication for treatment. All positive cultures were > 100,000 colonies/mL except for 1 culture in the nitrofurantoin treatment group, which was 45,000 colonies/mL, but because the subject was symptomatic, treatment was administered and a repeat urine culture was negative.
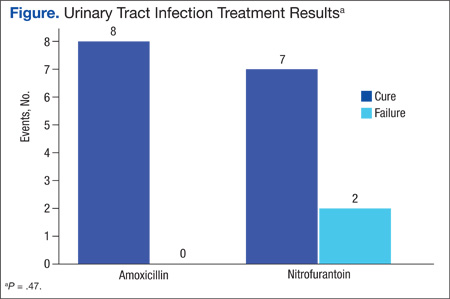
There were 8 cases classified as cure, 1 presumed cure, and no failures in the amoxicillin group. In the nitrofurantoin group, 7 cases were classified as cure, 1 presumed cure, and 3 failures. The presumed cures were excluded from the statistical analysis due to inability to ensure these cases were truly cured. Also excluded from the statistical analysis was one of the failures in the nitrofurantoin group, because the subject was asymptomatic with no known indication for treatment. This left 8 cases classified as cure and no failures in the amoxicillin group compared with 7 cases classified as cure and 2 failures in the nitrofurantoin group, P = .47 (Figure). Statistical analysis was performed using the Fisher exact test.
Discussion
There was no statistically significant difference between amoxicillin and nitrofurantoin for the treatment of ampicillin-resistant E faecium UTIs. There were no failures in the amoxicillin group despite all isolates displaying resistance based on current breakpoints, supporting the theory that higher urine concentrations of amoxicillin may overcome the MIC of resistant isolates.
Related: Novel Therapy for Treating Complicated UTIs
Of the 11 cases treated with nitrofurantoin, 3 were classified failures. The first failure in the nitrofurantoin group was an asymptomatic subject who did not have a repeat urine culture but had a repeat UA, which showed a persistent elevation in WBC and leukocyte esterase count. This subject was removed from the statistical analysis, as treatment was not indicated per IDSA guidelines. No reason could be identified for the second failure, as a repeat culture demonstrated continued presence of E faecium. Chronic kidney disease (CKD) contributed to the third failure in the nitrofurantoin treatment group; the subject’s CrCl was about 17 mL/min. After treatment, the subject had a repeat urine culture, which indicated the continued presence of E faecium. The subject was later successfully treated with amoxicillin. Both cultures in the same subject were included in the final analysis per protocol, as the subject had an adequate evaluation of efficacy between courses. Four additional cases with CKD were treated with nitrofurantoin; however, their CrCl ranged from 40 to 55 mL/min, and all were classified cure or presumed cure.
Limitations
There were several limitations to this study. Due to the strict inclusion and exclusion criteria, a limited number of subjects were evaluated. Given that this was a retrospective study, it is possible that symptoms were reported by a subject but not appropriately documented. Another significant limitation of this trial was that MICs were not determined due to the retrospective nature of the study. External validity was also limited due to a predominately elderly and male population. Safety data regarding different therapies were not collected, as this study evaluated only the efficacy of therapies.
Conclusion
Although this was a very small retrospective analysis, to the authors knowledge this is the first clinical study supporting the in vitro theory that amoxicillin (500 mg every 8 hours) may overcome the MIC of resistant isolates due to achievement of higher urinary concentrations. Because this was a small retrospective analysis, more prospective evidence is needed to confirm these results.
Acknowledgements
Heather Kim, biostatistician, University of Illinois at Chicago. CCTS Support: UL1RR029879.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Huycke MM, Sahm DF, Gilmore MS. Multiple-drug resistant enterococci: the nature of the problem and an agenda for the future. Emerg Infect Dis. 1998;4(2):239-249.
2. Heintz BH, Halilovic J, Christensen CL. Vancomycin -resistant enterococcal urinary tract infections. Pharmacotherapy. 2010;30(11):1136-1149.
3. Zhanel GG, Laing NM, Nichol KA, et al; NAVRESS Group. Antibiotic activity against urinary tract infection (UTI) isolates of vancomycin-resistant enterococci (VRE): results from the 2002 North American Vancomycin Resistant Enterococci Susceptibility Study (NAVRESS). J Antimicrob Chemother. 2003;52(3):382-388.
4. Macrobid [package insert]. Pine Brook, NJ: Almatica Pharma; 2013.
5. Oplinger M, Andrews CO. Nitrofurantoin contraindicated in patients with a creatinine clearance below 60 mL/min: looking for the evidence. Ann Pharmacother. 2013;47(1):106-111.
6. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute; 2007.
7. Gordon RC, Regamey C, Kirby WM. Comparative clinical pharmacology of amoxicillin and ampicillin administered orally. Antimicrob Agents Chemother. 1972;1(6):504-507.
8. Sutherland R, Croydon EA, Rolinson GN. Amoxycillin: a new semi-synthetic penicillin. Br Med J. 1972;3(5817):13-16.
9. Williamson JC, Craft DW, Butts JD, Raasch RH. In vitro assessment of urinary isolates of ampicillin-resistant enterococci. Ann Pharmacother. 2002;36(2):246-250.
10. Dumkow LE, Perri MB, Zervos M. Time to stop using alternatives to ampicillin for enterococcal UTIs? In-vitro susceptibility trends for enterococcus urinary isolates over a one-year period in Detroit. Poster presented at: 53rd Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC); September 10-13, 2013; Denver, CO.
11. Quintiliani R. Using pharmacodynamics and pharmacokinetics concepts to optimize treatment of infectious diseases. Infect Med. 2004;21(5):219-232.
Enterococcus species account for about 110,000 urinary tract infections (UTIs) annually in the U.S.1 The most common species isolated are Enterococcus faecalis and Enterococcus faecium (E faecium). Amoxicillin is the drug of choice for the treatment of enterococcal UTIs. Second-line therapies include vancomycin and nitrofurantoin. Alternative therapies include daptomycin and linezolid; however, these newer agents ideally would be reserved for more serious infections to preserve activity.2
Increased E faecium resistance to ampicillin and vancomycin has limited the therapeutic options. The results of a study by Zhanel and colleagues assessed the prevalence of resistant enterococcal urine isolates in North America.3 Of the 658 E faecium urine isolates, about 96% were resistant to ampicillin and 94% were resistant to vancoymcin.3 Nitrofurantoin has much lower resistance rates; however, its use is contraindicated in patients with a creatinine clearance (CrCl) < 60 mL/min.4 Data supporting the contraindication are limited, but the results of a study by Oplinger and Andrews suggested that using nitrofurantoin in patients with a CrCl ≥ 40 mL/min may be safe and effective.5 A therapeutic dilemma may occur when resistant E faecium UTIs are encountered and viable treatment options are limited due to intolerances, administration difficulties, lack of susceptibility data, or cost.
Related: Antimicrobial Stewardship in an Outpatient Parenteral Antibiotic Therapy Program
Based on the current Clinical and Laboratory Standards Institute standard, Enterococcus species with a minimal inhibitory concentration (MIC) ≥ 16 μg/mL are considered ampicillin resistant. Microbiology laboratories use the same breakpoint regardless of the site of infection.6 Amoxicillin concentrates in the urine; therefore, urinary concentrations are much higher than serum concentrations. The mean serum peak concentration after a single dose of oral amoxicillin 500 mg is 7.6 μg/mL.7 After a single dose of oral amoxicillin 500 mg, the average concentration in pooled urine collected over 6 hours was 1,100 μg/mL.8
In 2002, Williamson and colleagues analyzed 30 ampicillin- resistant E faecium urine isolates. Reported MICs were 128 μg/mL (30%), 256 μg/mL (60%), and 512 μg/mL (10%).9 A more recent retrospective analysis analyzed 234 ampicillin-resistant E faecium urine isolates. The MIC ranged from 32 to 1,024 μg/mL, with a median MIC of 256 μg/mL. Only 5 isolates had an MIC value > 1,000 μg/mL, but each of these isolates was within 1 dilution of 512 μg/mL.10 Because penicillins exhibit time-dependent killing, an optimal response will occur as long as the urine concentration is above the MIC for at least 50% of the dosing interval.11 Therefore, therapeutic doses of amoxicillin are expected to produce urine concentrations that exceed the MIC of resistant E faecium urine isolates. The purpose of this study was to determine if amoxicillin was a viable treatment option for ampicillin-resistant E faecium UTIs based on this in vitro theory.
Methods
Veterans aged ≥ 18 years with a positive urine culture for ampicillin- resistant E faecium who received antibiotic therapy for cystitis at the Jesse Brown VA Medical Center (JBVAMC) from January 1, 2005, through June 22, 2010, were evaluated in this retrospective cohort study. Exclusion criteria were the presence of any other organisms in the initial urine culture, prostatic involvement, and the presence of E faecium in a blood culture. Subjects treated with multiple antibiotics concurrently and with sequential treatment of different antibiotics with no evaluation of efficacy between courses were also excluded.
Related: Urologist Workforce Variation Across the VHA
All included subjects were evaluated for resolution of symptoms; improvement in leukocyte esterase count and white blood cell (WBC) count from urine analysis (UA); and eradication of E faecium from a repeat urine culture. The response to treatment was classified as cure, presumed cure, or failure. The criteria for cure were based on the following: resolution of symptoms if present at baseline; repeat UA indicating improvement from the initial positive UA (if obtained); and eradication of E faecium in a repeat urine culture (if obtained).
At least 1 of the aforementioned criteria must have been met to be classified as cure. If more than 1 of the aforementioned criteria was present, then each one must have been met to be classified as cure. To be evaluated for presumed cure, the subject must have had symptoms at baseline. No documentation of ongoing symptoms in subjects who had an appropriate follow-up but did not have a repeat UA or urine culture indicated presumed cure. Persistence or worsening of pretreatment symptoms, a repeat UA without improvement from the initial positive UA, or a repeat urine culture demonstrating continued presence of E faecium indicated failure. The primary endpoint for the study was to determine whether amoxicillin was effective for the management of ampicillin-resistant E faecium UTIs. This study was conducted in compliance with the University of Illinois at Chicago Institutional Review Board and JBVAMC Human Subjects Research Committee requirements.
Results
This study included 20 positive urine cultures for ampicillin-resistant E faecium in 19 subjects. Nine cases were treated with amoxicillin, and 11 cases were treated with nitrofurantoin. At baseline, the mean age was 75 years, mean duration of therapy was 14 days, and all the subjects were male. The baseline characteristics of the 2 groups were similar with the exception of an older population, shorter duration of therapy, and increased incidence of chronic kidney disease in the amoxicillin treatment group, P = .02, .03, and .01, respectively.
Symptoms were documented in 8 of 9 (89%) cases at the time of the positive culture in the amoxicillin treatment group and 5 of 11 (45%) cases in the nitrofurantoin treatment group (Table). The asymptomatic amoxicillin treatment group case and 5 of the 6 nitrofurantoin treatment group asymptomatic cases received treatment prior to a urologic procedure in accordance with the Infectious Diseases Society of America (IDSA) guidelines for the treatment of asymptomatic bacteriuria. The urologic procedures included transurethral resection of a bladder tumor, cystoscopy, urethral dilation, cystometrogram, and transurethral resection of the prostate. One asymptomatic subject in the nitrofurantoin group did not have any documentation to support an appropriate indication for treatment. All positive cultures were > 100,000 colonies/mL except for 1 culture in the nitrofurantoin treatment group, which was 45,000 colonies/mL, but because the subject was symptomatic, treatment was administered and a repeat urine culture was negative.
There were 8 cases classified as cure, 1 presumed cure, and no failures in the amoxicillin group. In the nitrofurantoin group, 7 cases were classified as cure, 1 presumed cure, and 3 failures. The presumed cures were excluded from the statistical analysis due to inability to ensure these cases were truly cured. Also excluded from the statistical analysis was one of the failures in the nitrofurantoin group, because the subject was asymptomatic with no known indication for treatment. This left 8 cases classified as cure and no failures in the amoxicillin group compared with 7 cases classified as cure and 2 failures in the nitrofurantoin group, P = .47 (Figure). Statistical analysis was performed using the Fisher exact test.
Discussion
There was no statistically significant difference between amoxicillin and nitrofurantoin for the treatment of ampicillin-resistant E faecium UTIs. There were no failures in the amoxicillin group despite all isolates displaying resistance based on current breakpoints, supporting the theory that higher urine concentrations of amoxicillin may overcome the MIC of resistant isolates.
Related: Novel Therapy for Treating Complicated UTIs
Of the 11 cases treated with nitrofurantoin, 3 were classified failures. The first failure in the nitrofurantoin group was an asymptomatic subject who did not have a repeat urine culture but had a repeat UA, which showed a persistent elevation in WBC and leukocyte esterase count. This subject was removed from the statistical analysis, as treatment was not indicated per IDSA guidelines. No reason could be identified for the second failure, as a repeat culture demonstrated continued presence of E faecium. Chronic kidney disease (CKD) contributed to the third failure in the nitrofurantoin treatment group; the subject’s CrCl was about 17 mL/min. After treatment, the subject had a repeat urine culture, which indicated the continued presence of E faecium. The subject was later successfully treated with amoxicillin. Both cultures in the same subject were included in the final analysis per protocol, as the subject had an adequate evaluation of efficacy between courses. Four additional cases with CKD were treated with nitrofurantoin; however, their CrCl ranged from 40 to 55 mL/min, and all were classified cure or presumed cure.
Limitations
There were several limitations to this study. Due to the strict inclusion and exclusion criteria, a limited number of subjects were evaluated. Given that this was a retrospective study, it is possible that symptoms were reported by a subject but not appropriately documented. Another significant limitation of this trial was that MICs were not determined due to the retrospective nature of the study. External validity was also limited due to a predominately elderly and male population. Safety data regarding different therapies were not collected, as this study evaluated only the efficacy of therapies.
Conclusion
Although this was a very small retrospective analysis, to the authors knowledge this is the first clinical study supporting the in vitro theory that amoxicillin (500 mg every 8 hours) may overcome the MIC of resistant isolates due to achievement of higher urinary concentrations. Because this was a small retrospective analysis, more prospective evidence is needed to confirm these results.
Acknowledgements
Heather Kim, biostatistician, University of Illinois at Chicago. CCTS Support: UL1RR029879.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Enterococcus species account for about 110,000 urinary tract infections (UTIs) annually in the U.S.1 The most common species isolated are Enterococcus faecalis and Enterococcus faecium (E faecium). Amoxicillin is the drug of choice for the treatment of enterococcal UTIs. Second-line therapies include vancomycin and nitrofurantoin. Alternative therapies include daptomycin and linezolid; however, these newer agents ideally would be reserved for more serious infections to preserve activity.2
Increased E faecium resistance to ampicillin and vancomycin has limited the therapeutic options. The results of a study by Zhanel and colleagues assessed the prevalence of resistant enterococcal urine isolates in North America.3 Of the 658 E faecium urine isolates, about 96% were resistant to ampicillin and 94% were resistant to vancoymcin.3 Nitrofurantoin has much lower resistance rates; however, its use is contraindicated in patients with a creatinine clearance (CrCl) < 60 mL/min.4 Data supporting the contraindication are limited, but the results of a study by Oplinger and Andrews suggested that using nitrofurantoin in patients with a CrCl ≥ 40 mL/min may be safe and effective.5 A therapeutic dilemma may occur when resistant E faecium UTIs are encountered and viable treatment options are limited due to intolerances, administration difficulties, lack of susceptibility data, or cost.
Related: Antimicrobial Stewardship in an Outpatient Parenteral Antibiotic Therapy Program
Based on the current Clinical and Laboratory Standards Institute standard, Enterococcus species with a minimal inhibitory concentration (MIC) ≥ 16 μg/mL are considered ampicillin resistant. Microbiology laboratories use the same breakpoint regardless of the site of infection.6 Amoxicillin concentrates in the urine; therefore, urinary concentrations are much higher than serum concentrations. The mean serum peak concentration after a single dose of oral amoxicillin 500 mg is 7.6 μg/mL.7 After a single dose of oral amoxicillin 500 mg, the average concentration in pooled urine collected over 6 hours was 1,100 μg/mL.8
In 2002, Williamson and colleagues analyzed 30 ampicillin- resistant E faecium urine isolates. Reported MICs were 128 μg/mL (30%), 256 μg/mL (60%), and 512 μg/mL (10%).9 A more recent retrospective analysis analyzed 234 ampicillin-resistant E faecium urine isolates. The MIC ranged from 32 to 1,024 μg/mL, with a median MIC of 256 μg/mL. Only 5 isolates had an MIC value > 1,000 μg/mL, but each of these isolates was within 1 dilution of 512 μg/mL.10 Because penicillins exhibit time-dependent killing, an optimal response will occur as long as the urine concentration is above the MIC for at least 50% of the dosing interval.11 Therefore, therapeutic doses of amoxicillin are expected to produce urine concentrations that exceed the MIC of resistant E faecium urine isolates. The purpose of this study was to determine if amoxicillin was a viable treatment option for ampicillin-resistant E faecium UTIs based on this in vitro theory.
Methods
Veterans aged ≥ 18 years with a positive urine culture for ampicillin- resistant E faecium who received antibiotic therapy for cystitis at the Jesse Brown VA Medical Center (JBVAMC) from January 1, 2005, through June 22, 2010, were evaluated in this retrospective cohort study. Exclusion criteria were the presence of any other organisms in the initial urine culture, prostatic involvement, and the presence of E faecium in a blood culture. Subjects treated with multiple antibiotics concurrently and with sequential treatment of different antibiotics with no evaluation of efficacy between courses were also excluded.
Related: Urologist Workforce Variation Across the VHA
All included subjects were evaluated for resolution of symptoms; improvement in leukocyte esterase count and white blood cell (WBC) count from urine analysis (UA); and eradication of E faecium from a repeat urine culture. The response to treatment was classified as cure, presumed cure, or failure. The criteria for cure were based on the following: resolution of symptoms if present at baseline; repeat UA indicating improvement from the initial positive UA (if obtained); and eradication of E faecium in a repeat urine culture (if obtained).
At least 1 of the aforementioned criteria must have been met to be classified as cure. If more than 1 of the aforementioned criteria was present, then each one must have been met to be classified as cure. To be evaluated for presumed cure, the subject must have had symptoms at baseline. No documentation of ongoing symptoms in subjects who had an appropriate follow-up but did not have a repeat UA or urine culture indicated presumed cure. Persistence or worsening of pretreatment symptoms, a repeat UA without improvement from the initial positive UA, or a repeat urine culture demonstrating continued presence of E faecium indicated failure. The primary endpoint for the study was to determine whether amoxicillin was effective for the management of ampicillin-resistant E faecium UTIs. This study was conducted in compliance with the University of Illinois at Chicago Institutional Review Board and JBVAMC Human Subjects Research Committee requirements.
Results
This study included 20 positive urine cultures for ampicillin-resistant E faecium in 19 subjects. Nine cases were treated with amoxicillin, and 11 cases were treated with nitrofurantoin. At baseline, the mean age was 75 years, mean duration of therapy was 14 days, and all the subjects were male. The baseline characteristics of the 2 groups were similar with the exception of an older population, shorter duration of therapy, and increased incidence of chronic kidney disease in the amoxicillin treatment group, P = .02, .03, and .01, respectively.
Symptoms were documented in 8 of 9 (89%) cases at the time of the positive culture in the amoxicillin treatment group and 5 of 11 (45%) cases in the nitrofurantoin treatment group (Table). The asymptomatic amoxicillin treatment group case and 5 of the 6 nitrofurantoin treatment group asymptomatic cases received treatment prior to a urologic procedure in accordance with the Infectious Diseases Society of America (IDSA) guidelines for the treatment of asymptomatic bacteriuria. The urologic procedures included transurethral resection of a bladder tumor, cystoscopy, urethral dilation, cystometrogram, and transurethral resection of the prostate. One asymptomatic subject in the nitrofurantoin group did not have any documentation to support an appropriate indication for treatment. All positive cultures were > 100,000 colonies/mL except for 1 culture in the nitrofurantoin treatment group, which was 45,000 colonies/mL, but because the subject was symptomatic, treatment was administered and a repeat urine culture was negative.
There were 8 cases classified as cure, 1 presumed cure, and no failures in the amoxicillin group. In the nitrofurantoin group, 7 cases were classified as cure, 1 presumed cure, and 3 failures. The presumed cures were excluded from the statistical analysis due to inability to ensure these cases were truly cured. Also excluded from the statistical analysis was one of the failures in the nitrofurantoin group, because the subject was asymptomatic with no known indication for treatment. This left 8 cases classified as cure and no failures in the amoxicillin group compared with 7 cases classified as cure and 2 failures in the nitrofurantoin group, P = .47 (Figure). Statistical analysis was performed using the Fisher exact test.
Discussion
There was no statistically significant difference between amoxicillin and nitrofurantoin for the treatment of ampicillin-resistant E faecium UTIs. There were no failures in the amoxicillin group despite all isolates displaying resistance based on current breakpoints, supporting the theory that higher urine concentrations of amoxicillin may overcome the MIC of resistant isolates.
Related: Novel Therapy for Treating Complicated UTIs
Of the 11 cases treated with nitrofurantoin, 3 were classified failures. The first failure in the nitrofurantoin group was an asymptomatic subject who did not have a repeat urine culture but had a repeat UA, which showed a persistent elevation in WBC and leukocyte esterase count. This subject was removed from the statistical analysis, as treatment was not indicated per IDSA guidelines. No reason could be identified for the second failure, as a repeat culture demonstrated continued presence of E faecium. Chronic kidney disease (CKD) contributed to the third failure in the nitrofurantoin treatment group; the subject’s CrCl was about 17 mL/min. After treatment, the subject had a repeat urine culture, which indicated the continued presence of E faecium. The subject was later successfully treated with amoxicillin. Both cultures in the same subject were included in the final analysis per protocol, as the subject had an adequate evaluation of efficacy between courses. Four additional cases with CKD were treated with nitrofurantoin; however, their CrCl ranged from 40 to 55 mL/min, and all were classified cure or presumed cure.
Limitations
There were several limitations to this study. Due to the strict inclusion and exclusion criteria, a limited number of subjects were evaluated. Given that this was a retrospective study, it is possible that symptoms were reported by a subject but not appropriately documented. Another significant limitation of this trial was that MICs were not determined due to the retrospective nature of the study. External validity was also limited due to a predominately elderly and male population. Safety data regarding different therapies were not collected, as this study evaluated only the efficacy of therapies.
Conclusion
Although this was a very small retrospective analysis, to the authors knowledge this is the first clinical study supporting the in vitro theory that amoxicillin (500 mg every 8 hours) may overcome the MIC of resistant isolates due to achievement of higher urinary concentrations. Because this was a small retrospective analysis, more prospective evidence is needed to confirm these results.
Acknowledgements
Heather Kim, biostatistician, University of Illinois at Chicago. CCTS Support: UL1RR029879.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Huycke MM, Sahm DF, Gilmore MS. Multiple-drug resistant enterococci: the nature of the problem and an agenda for the future. Emerg Infect Dis. 1998;4(2):239-249.
2. Heintz BH, Halilovic J, Christensen CL. Vancomycin -resistant enterococcal urinary tract infections. Pharmacotherapy. 2010;30(11):1136-1149.
3. Zhanel GG, Laing NM, Nichol KA, et al; NAVRESS Group. Antibiotic activity against urinary tract infection (UTI) isolates of vancomycin-resistant enterococci (VRE): results from the 2002 North American Vancomycin Resistant Enterococci Susceptibility Study (NAVRESS). J Antimicrob Chemother. 2003;52(3):382-388.
4. Macrobid [package insert]. Pine Brook, NJ: Almatica Pharma; 2013.
5. Oplinger M, Andrews CO. Nitrofurantoin contraindicated in patients with a creatinine clearance below 60 mL/min: looking for the evidence. Ann Pharmacother. 2013;47(1):106-111.
6. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute; 2007.
7. Gordon RC, Regamey C, Kirby WM. Comparative clinical pharmacology of amoxicillin and ampicillin administered orally. Antimicrob Agents Chemother. 1972;1(6):504-507.
8. Sutherland R, Croydon EA, Rolinson GN. Amoxycillin: a new semi-synthetic penicillin. Br Med J. 1972;3(5817):13-16.
9. Williamson JC, Craft DW, Butts JD, Raasch RH. In vitro assessment of urinary isolates of ampicillin-resistant enterococci. Ann Pharmacother. 2002;36(2):246-250.
10. Dumkow LE, Perri MB, Zervos M. Time to stop using alternatives to ampicillin for enterococcal UTIs? In-vitro susceptibility trends for enterococcus urinary isolates over a one-year period in Detroit. Poster presented at: 53rd Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC); September 10-13, 2013; Denver, CO.
11. Quintiliani R. Using pharmacodynamics and pharmacokinetics concepts to optimize treatment of infectious diseases. Infect Med. 2004;21(5):219-232.
1. Huycke MM, Sahm DF, Gilmore MS. Multiple-drug resistant enterococci: the nature of the problem and an agenda for the future. Emerg Infect Dis. 1998;4(2):239-249.
2. Heintz BH, Halilovic J, Christensen CL. Vancomycin -resistant enterococcal urinary tract infections. Pharmacotherapy. 2010;30(11):1136-1149.
3. Zhanel GG, Laing NM, Nichol KA, et al; NAVRESS Group. Antibiotic activity against urinary tract infection (UTI) isolates of vancomycin-resistant enterococci (VRE): results from the 2002 North American Vancomycin Resistant Enterococci Susceptibility Study (NAVRESS). J Antimicrob Chemother. 2003;52(3):382-388.
4. Macrobid [package insert]. Pine Brook, NJ: Almatica Pharma; 2013.
5. Oplinger M, Andrews CO. Nitrofurantoin contraindicated in patients with a creatinine clearance below 60 mL/min: looking for the evidence. Ann Pharmacother. 2013;47(1):106-111.
6. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute; 2007.
7. Gordon RC, Regamey C, Kirby WM. Comparative clinical pharmacology of amoxicillin and ampicillin administered orally. Antimicrob Agents Chemother. 1972;1(6):504-507.
8. Sutherland R, Croydon EA, Rolinson GN. Amoxycillin: a new semi-synthetic penicillin. Br Med J. 1972;3(5817):13-16.
9. Williamson JC, Craft DW, Butts JD, Raasch RH. In vitro assessment of urinary isolates of ampicillin-resistant enterococci. Ann Pharmacother. 2002;36(2):246-250.
10. Dumkow LE, Perri MB, Zervos M. Time to stop using alternatives to ampicillin for enterococcal UTIs? In-vitro susceptibility trends for enterococcus urinary isolates over a one-year period in Detroit. Poster presented at: 53rd Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC); September 10-13, 2013; Denver, CO.
11. Quintiliani R. Using pharmacodynamics and pharmacokinetics concepts to optimize treatment of infectious diseases. Infect Med. 2004;21(5):219-232.
Assay could guide therapy for MM, other cancers

showing multiple myeloma
Researchers say they have created a microenvironment in a dish that can be used to anticipate a multiple myeloma (MM) patient’s response to treatment.
The team developed an assay that involves co-culturing MM cells with their surrounding nontumor cells, all from the same patient, in a microscale petri dish.
The researchers then treated the tumor cells with bortezomib, and, after 3 days, they could determine whether the drug was effective or not.
The team described this research in Integrative Biology.
They compared the results of their ex vivo tests with the success or failure rates of actual MM patients who received bortezomib, and 100% of the ex vivo test results matched the patients’ results.
The researchers therefore believe this assay could save many MM patients the psychological stress of having to try multiple drugs until they find the most effective one. The assay could reduce clinicians’ need for this trial-and-error approach while lowering the cost of treatment, the team said.
Study author Chorom Pak, PhD, of the University of Toronto in Ontario, Canada, has founded a service-based company called Lynx Biosciences based on these findings. Now, she and her colleagues are planning to conduct a prospective trial in which they will use the ex vivo tests to identify responsive and nonresponsive patients.
The researchers believe this work could have wide-ranging implications for the treatment of MM and other malignancies, but their work is far from over.
“This is only one type of cancer, one particular drug, and we’re a long way from implementing this and helping patients in a widespread way,” said study author David Beebe, PhD, of the University of Wisconsin Carbone Cancer Center in Madison.
“But it’s happening. This is an exciting time in this area, and we’re definitely going to see more of this.” ![]()
showing multiple myeloma
Researchers say they have created a microenvironment in a dish that can be used to anticipate a multiple myeloma (MM) patient’s response to treatment.
The team developed an assay that involves co-culturing MM cells with their surrounding nontumor cells, all from the same patient, in a microscale petri dish.
The researchers then treated the tumor cells with bortezomib, and, after 3 days, they could determine whether the drug was effective or not.
The team described this research in Integrative Biology.
They compared the results of their ex vivo tests with the success or failure rates of actual MM patients who received bortezomib, and 100% of the ex vivo test results matched the patients’ results.
The researchers therefore believe this assay could save many MM patients the psychological stress of having to try multiple drugs until they find the most effective one. The assay could reduce clinicians’ need for this trial-and-error approach while lowering the cost of treatment, the team said.
Study author Chorom Pak, PhD, of the University of Toronto in Ontario, Canada, has founded a service-based company called Lynx Biosciences based on these findings. Now, she and her colleagues are planning to conduct a prospective trial in which they will use the ex vivo tests to identify responsive and nonresponsive patients.
The researchers believe this work could have wide-ranging implications for the treatment of MM and other malignancies, but their work is far from over.
“This is only one type of cancer, one particular drug, and we’re a long way from implementing this and helping patients in a widespread way,” said study author David Beebe, PhD, of the University of Wisconsin Carbone Cancer Center in Madison.
“But it’s happening. This is an exciting time in this area, and we’re definitely going to see more of this.” ![]()
showing multiple myeloma
Researchers say they have created a microenvironment in a dish that can be used to anticipate a multiple myeloma (MM) patient’s response to treatment.
The team developed an assay that involves co-culturing MM cells with their surrounding nontumor cells, all from the same patient, in a microscale petri dish.
The researchers then treated the tumor cells with bortezomib, and, after 3 days, they could determine whether the drug was effective or not.
The team described this research in Integrative Biology.
They compared the results of their ex vivo tests with the success or failure rates of actual MM patients who received bortezomib, and 100% of the ex vivo test results matched the patients’ results.
The researchers therefore believe this assay could save many MM patients the psychological stress of having to try multiple drugs until they find the most effective one. The assay could reduce clinicians’ need for this trial-and-error approach while lowering the cost of treatment, the team said.
Study author Chorom Pak, PhD, of the University of Toronto in Ontario, Canada, has founded a service-based company called Lynx Biosciences based on these findings. Now, she and her colleagues are planning to conduct a prospective trial in which they will use the ex vivo tests to identify responsive and nonresponsive patients.
The researchers believe this work could have wide-ranging implications for the treatment of MM and other malignancies, but their work is far from over.
“This is only one type of cancer, one particular drug, and we’re a long way from implementing this and helping patients in a widespread way,” said study author David Beebe, PhD, of the University of Wisconsin Carbone Cancer Center in Madison.
“But it’s happening. This is an exciting time in this area, and we’re definitely going to see more of this.” ![]()
New trial design accounts for patient behavior

Photo by Esther Dyson
New research suggests patient behavior can have a serious impact on the effectiveness of a treatment, and procedures used in double-blind randomized controlled trials (DBRCTs) may not allow researchers to assess the effects of behavior on treatment.
To solve this problem, a group of investigators has proposed a new trial design, called a two-by-two trial, that can account for behavior-treatment interactions.
They described this design in PLOS ONE.
Study rationale
The study authors pointed out that patient behaviors can directly relate to a trial. For example, a patient who believes in the drug might religiously stick to his or her treatment regimen, while someone more skeptical might skip a few doses.
Alternatively, patient behaviors may relate to how the person acts in general, such as preferences in diet, exercise, and social engagement. And in the design of today’s standard trials, these behaviors are not accounted for, said author Erik Snowberg, PhD, of the California Institute of Technology in Pasadena.
He noted that DBRCTs typically assign patients to an experimental group that receives the new treatment and a control group that does not. As the trial is double-blinded, neither the subjects nor their doctors know who falls into which group.
However, patients do know their probability of getting the treatment, and that 50% likelihood of getting the new treatment might not be enough to encourage a patient to change behaviors that could influence the efficacy of the drug, Dr Snowberg said.
For example, if a subject wants to lose weight and knows he has a high probability—a 70% chance—of being in the experimental group for a new weight loss drug, he may be more likely to take the drug as directed and to make other healthy lifestyle choices that can contribute to weight loss. As a result, he might lose more weight, boosting the apparent effectiveness of the drug.
However, if the subject knows he only has a 30% chance of being in the experimental group, he might be less motivated to both take the drug as directed and to make those other changes. As a result, he might lose less weight—even if he is in the treatment group—and the same drug would seem less effective.
“Most medical research just wants to know if a drug will work or not,” Dr Snowberg said. “We wanted to go a step further, designing new trials that would take into account the way people behave. As social scientists, we naturally turned to the mathematical tools of formal social science to do this.”
New trial design
Dr Snowberg and his colleagues found that, with the two-by-two trial, they can tease out the effects of behavior and the interaction of behavior and treatment, as well as the effects of treatment alone. The new trial design, which still randomizes treatment, also randomizes the probability of treatment, which can change a patient’s behavior.
In a two-by-two trial, instead of patients first being assigned to either the experimental or control groups, they are randomly assigned to either a “high probability of treatment” group or a “low probability of treatment” group.
The patients in the high probability group are then randomized to either the treatment or the control group, giving them a 70% chance of receiving the treatment. Patients in the low probability group are also randomized to treatment or control, and their likelihood of receiving the treatment is 30%. The patients are then informed of their probability of treatment.
By randomizing both the treatment and the probability of treatment, researchers can quantify the effects of treatment, the effects of behavior, and the effects of the interaction between treatment and behavior, Dr Snowberg said. And determining each is essential for understanding the overall efficacy of treatment.
“It’s a very small change to the design of the trial, but it’s important,” he said. “The effect of a treatment has these two constituent parts: pure treatment effect and the treatment-behavior interaction. Standard blind trials just randomize the likelihood of treatment, so you can’t see this interaction. Although you can’t just tell someone to randomize their behavior, we found a way that you can randomize the probability that a patient will get something that will change their behavior.”
Testing the design
Because it is difficult to implement new trial design changes in active trials, Dr Snowberg and his colleagues wanted to first test their idea with a meta-analysis of data from previous clinical trials. They devised a new mathematical formula that can be used to analyze DBRCT data.
The formula teases out the health outcomes resulting from treatment alone as well as outcomes resulting from an interaction between treatment and behavior.
The investigators used the formula to analyze 6 DBRCTs evaluating the antidepressants imipramine (a tricyclic antidepressant also known as Tofranil) and paroxetine (a selective serotonin reuptake inhibitor sold as Paxil).
First, the researchers wanted to see if there was evidence that patients behave differently when they have a high probability of treatment and when they have a low probability of treatment.
The trials recorded how many patients dropped out of the study, so this was the behavior Dr Snowberg and his colleagues analyzed. They found that, in trials where patients happened to have a relatively high probability of treatment—near 70%—the dropout rate was significantly lower than in trials where patients had a lower probability of treatment—around 50%.
Although the team did not have any specific behaviors to analyze, other than dropping out of the study, they also wanted to determine if behavior in general could have added to the effect of the treatments.
Using their statistical techniques, the investigators found that imipramine seemed to have a pure treatment effect but no effect from the interaction between treatment and behavior. That is, the drug seemed to work fine, regardless of any behavioral differences that may have been present.
The researchers also found that paroxetine seemed to have no effect from the treatment alone or behavior alone. However, an interaction between the treatment and behavior did effectively decrease depression.
Because this study was conducted in the past, the investigators could not determine which specific behavior was responsible for the interaction, but with the mathematical formula, they were able to tell that this behavior was necessary for the drug to be effective.
In their paper, Dr Snowberg and his colleagues speculate how a situation like this might come about.
“Maybe there is a drug, for instance, that makes people feel better in social situations, and if you’re in the high probability group, then maybe you’d be more willing to go out to parties to see if the drug helps you talk to people,” Dr Snowberg explained.
“Your behavior drives you to go to the party, and once you’re at the party, the drug helps you feel comfortable talking to people. That would be an example of an interaction effect. You couldn’t get that if people just took this drug alone at home.”
Although this specific example is just speculation, Dr Snowberg said the researchers’ actual results reveal that some behavior or set of behaviors interact with paroxetine to effectively treat depression. And, without this behavior, the drug appears to be ineffective.
“Normally, what you get when you run a standard blind trial is some sort of mishmash of the treatment effect and the treatment-behavior interaction effect,” Dr Snowberg said. “But knowing the full interaction effect is important.”
“Our work indicates that clinical trials underestimate the efficacy of a drug where behavior matters. It may be the case that 50% probability isn’t high enough for people to change any of their behaviors, especially if it’s a really uncertain new treatment. Then, it’s just going to look like the drug doesn’t work, and that isn’t the case.”
Because the meta-analysis supported the team’s hypothesis—that the interaction between treatment and behavior can have an effect on health outcomes—the next step is incorporating these new ideas into an active clinical trial.
Dr Snowberg said the best fit would be a drug trial for a condition, such as a mental health disorder or an addiction, that is known to be associated with behavior. At the very least, he hopes these results will lead the medical research community to a conversation about ways to improve the DBRCT. ![]()
Photo by Esther Dyson
New research suggests patient behavior can have a serious impact on the effectiveness of a treatment, and procedures used in double-blind randomized controlled trials (DBRCTs) may not allow researchers to assess the effects of behavior on treatment.
To solve this problem, a group of investigators has proposed a new trial design, called a two-by-two trial, that can account for behavior-treatment interactions.
They described this design in PLOS ONE.
Study rationale
The study authors pointed out that patient behaviors can directly relate to a trial. For example, a patient who believes in the drug might religiously stick to his or her treatment regimen, while someone more skeptical might skip a few doses.
Alternatively, patient behaviors may relate to how the person acts in general, such as preferences in diet, exercise, and social engagement. And in the design of today’s standard trials, these behaviors are not accounted for, said author Erik Snowberg, PhD, of the California Institute of Technology in Pasadena.
He noted that DBRCTs typically assign patients to an experimental group that receives the new treatment and a control group that does not. As the trial is double-blinded, neither the subjects nor their doctors know who falls into which group.
However, patients do know their probability of getting the treatment, and that 50% likelihood of getting the new treatment might not be enough to encourage a patient to change behaviors that could influence the efficacy of the drug, Dr Snowberg said.
For example, if a subject wants to lose weight and knows he has a high probability—a 70% chance—of being in the experimental group for a new weight loss drug, he may be more likely to take the drug as directed and to make other healthy lifestyle choices that can contribute to weight loss. As a result, he might lose more weight, boosting the apparent effectiveness of the drug.
However, if the subject knows he only has a 30% chance of being in the experimental group, he might be less motivated to both take the drug as directed and to make those other changes. As a result, he might lose less weight—even if he is in the treatment group—and the same drug would seem less effective.
“Most medical research just wants to know if a drug will work or not,” Dr Snowberg said. “We wanted to go a step further, designing new trials that would take into account the way people behave. As social scientists, we naturally turned to the mathematical tools of formal social science to do this.”
New trial design
Dr Snowberg and his colleagues found that, with the two-by-two trial, they can tease out the effects of behavior and the interaction of behavior and treatment, as well as the effects of treatment alone. The new trial design, which still randomizes treatment, also randomizes the probability of treatment, which can change a patient’s behavior.
In a two-by-two trial, instead of patients first being assigned to either the experimental or control groups, they are randomly assigned to either a “high probability of treatment” group or a “low probability of treatment” group.
The patients in the high probability group are then randomized to either the treatment or the control group, giving them a 70% chance of receiving the treatment. Patients in the low probability group are also randomized to treatment or control, and their likelihood of receiving the treatment is 30%. The patients are then informed of their probability of treatment.
By randomizing both the treatment and the probability of treatment, researchers can quantify the effects of treatment, the effects of behavior, and the effects of the interaction between treatment and behavior, Dr Snowberg said. And determining each is essential for understanding the overall efficacy of treatment.
“It’s a very small change to the design of the trial, but it’s important,” he said. “The effect of a treatment has these two constituent parts: pure treatment effect and the treatment-behavior interaction. Standard blind trials just randomize the likelihood of treatment, so you can’t see this interaction. Although you can’t just tell someone to randomize their behavior, we found a way that you can randomize the probability that a patient will get something that will change their behavior.”
Testing the design
Because it is difficult to implement new trial design changes in active trials, Dr Snowberg and his colleagues wanted to first test their idea with a meta-analysis of data from previous clinical trials. They devised a new mathematical formula that can be used to analyze DBRCT data.
The formula teases out the health outcomes resulting from treatment alone as well as outcomes resulting from an interaction between treatment and behavior.
The investigators used the formula to analyze 6 DBRCTs evaluating the antidepressants imipramine (a tricyclic antidepressant also known as Tofranil) and paroxetine (a selective serotonin reuptake inhibitor sold as Paxil).
First, the researchers wanted to see if there was evidence that patients behave differently when they have a high probability of treatment and when they have a low probability of treatment.
The trials recorded how many patients dropped out of the study, so this was the behavior Dr Snowberg and his colleagues analyzed. They found that, in trials where patients happened to have a relatively high probability of treatment—near 70%—the dropout rate was significantly lower than in trials where patients had a lower probability of treatment—around 50%.
Although the team did not have any specific behaviors to analyze, other than dropping out of the study, they also wanted to determine if behavior in general could have added to the effect of the treatments.
Using their statistical techniques, the investigators found that imipramine seemed to have a pure treatment effect but no effect from the interaction between treatment and behavior. That is, the drug seemed to work fine, regardless of any behavioral differences that may have been present.
The researchers also found that paroxetine seemed to have no effect from the treatment alone or behavior alone. However, an interaction between the treatment and behavior did effectively decrease depression.
Because this study was conducted in the past, the investigators could not determine which specific behavior was responsible for the interaction, but with the mathematical formula, they were able to tell that this behavior was necessary for the drug to be effective.
In their paper, Dr Snowberg and his colleagues speculate how a situation like this might come about.
“Maybe there is a drug, for instance, that makes people feel better in social situations, and if you’re in the high probability group, then maybe you’d be more willing to go out to parties to see if the drug helps you talk to people,” Dr Snowberg explained.
“Your behavior drives you to go to the party, and once you’re at the party, the drug helps you feel comfortable talking to people. That would be an example of an interaction effect. You couldn’t get that if people just took this drug alone at home.”
Although this specific example is just speculation, Dr Snowberg said the researchers’ actual results reveal that some behavior or set of behaviors interact with paroxetine to effectively treat depression. And, without this behavior, the drug appears to be ineffective.
“Normally, what you get when you run a standard blind trial is some sort of mishmash of the treatment effect and the treatment-behavior interaction effect,” Dr Snowberg said. “But knowing the full interaction effect is important.”
“Our work indicates that clinical trials underestimate the efficacy of a drug where behavior matters. It may be the case that 50% probability isn’t high enough for people to change any of their behaviors, especially if it’s a really uncertain new treatment. Then, it’s just going to look like the drug doesn’t work, and that isn’t the case.”
Because the meta-analysis supported the team’s hypothesis—that the interaction between treatment and behavior can have an effect on health outcomes—the next step is incorporating these new ideas into an active clinical trial.
Dr Snowberg said the best fit would be a drug trial for a condition, such as a mental health disorder or an addiction, that is known to be associated with behavior. At the very least, he hopes these results will lead the medical research community to a conversation about ways to improve the DBRCT. ![]()
Photo by Esther Dyson
New research suggests patient behavior can have a serious impact on the effectiveness of a treatment, and procedures used in double-blind randomized controlled trials (DBRCTs) may not allow researchers to assess the effects of behavior on treatment.
To solve this problem, a group of investigators has proposed a new trial design, called a two-by-two trial, that can account for behavior-treatment interactions.
They described this design in PLOS ONE.
Study rationale
The study authors pointed out that patient behaviors can directly relate to a trial. For example, a patient who believes in the drug might religiously stick to his or her treatment regimen, while someone more skeptical might skip a few doses.
Alternatively, patient behaviors may relate to how the person acts in general, such as preferences in diet, exercise, and social engagement. And in the design of today’s standard trials, these behaviors are not accounted for, said author Erik Snowberg, PhD, of the California Institute of Technology in Pasadena.
He noted that DBRCTs typically assign patients to an experimental group that receives the new treatment and a control group that does not. As the trial is double-blinded, neither the subjects nor their doctors know who falls into which group.
However, patients do know their probability of getting the treatment, and that 50% likelihood of getting the new treatment might not be enough to encourage a patient to change behaviors that could influence the efficacy of the drug, Dr Snowberg said.
For example, if a subject wants to lose weight and knows he has a high probability—a 70% chance—of being in the experimental group for a new weight loss drug, he may be more likely to take the drug as directed and to make other healthy lifestyle choices that can contribute to weight loss. As a result, he might lose more weight, boosting the apparent effectiveness of the drug.
However, if the subject knows he only has a 30% chance of being in the experimental group, he might be less motivated to both take the drug as directed and to make those other changes. As a result, he might lose less weight—even if he is in the treatment group—and the same drug would seem less effective.
“Most medical research just wants to know if a drug will work or not,” Dr Snowberg said. “We wanted to go a step further, designing new trials that would take into account the way people behave. As social scientists, we naturally turned to the mathematical tools of formal social science to do this.”
New trial design
Dr Snowberg and his colleagues found that, with the two-by-two trial, they can tease out the effects of behavior and the interaction of behavior and treatment, as well as the effects of treatment alone. The new trial design, which still randomizes treatment, also randomizes the probability of treatment, which can change a patient’s behavior.
In a two-by-two trial, instead of patients first being assigned to either the experimental or control groups, they are randomly assigned to either a “high probability of treatment” group or a “low probability of treatment” group.
The patients in the high probability group are then randomized to either the treatment or the control group, giving them a 70% chance of receiving the treatment. Patients in the low probability group are also randomized to treatment or control, and their likelihood of receiving the treatment is 30%. The patients are then informed of their probability of treatment.
By randomizing both the treatment and the probability of treatment, researchers can quantify the effects of treatment, the effects of behavior, and the effects of the interaction between treatment and behavior, Dr Snowberg said. And determining each is essential for understanding the overall efficacy of treatment.
“It’s a very small change to the design of the trial, but it’s important,” he said. “The effect of a treatment has these two constituent parts: pure treatment effect and the treatment-behavior interaction. Standard blind trials just randomize the likelihood of treatment, so you can’t see this interaction. Although you can’t just tell someone to randomize their behavior, we found a way that you can randomize the probability that a patient will get something that will change their behavior.”
Testing the design
Because it is difficult to implement new trial design changes in active trials, Dr Snowberg and his colleagues wanted to first test their idea with a meta-analysis of data from previous clinical trials. They devised a new mathematical formula that can be used to analyze DBRCT data.
The formula teases out the health outcomes resulting from treatment alone as well as outcomes resulting from an interaction between treatment and behavior.
The investigators used the formula to analyze 6 DBRCTs evaluating the antidepressants imipramine (a tricyclic antidepressant also known as Tofranil) and paroxetine (a selective serotonin reuptake inhibitor sold as Paxil).
First, the researchers wanted to see if there was evidence that patients behave differently when they have a high probability of treatment and when they have a low probability of treatment.
The trials recorded how many patients dropped out of the study, so this was the behavior Dr Snowberg and his colleagues analyzed. They found that, in trials where patients happened to have a relatively high probability of treatment—near 70%—the dropout rate was significantly lower than in trials where patients had a lower probability of treatment—around 50%.
Although the team did not have any specific behaviors to analyze, other than dropping out of the study, they also wanted to determine if behavior in general could have added to the effect of the treatments.
Using their statistical techniques, the investigators found that imipramine seemed to have a pure treatment effect but no effect from the interaction between treatment and behavior. That is, the drug seemed to work fine, regardless of any behavioral differences that may have been present.
The researchers also found that paroxetine seemed to have no effect from the treatment alone or behavior alone. However, an interaction between the treatment and behavior did effectively decrease depression.
Because this study was conducted in the past, the investigators could not determine which specific behavior was responsible for the interaction, but with the mathematical formula, they were able to tell that this behavior was necessary for the drug to be effective.
In their paper, Dr Snowberg and his colleagues speculate how a situation like this might come about.
“Maybe there is a drug, for instance, that makes people feel better in social situations, and if you’re in the high probability group, then maybe you’d be more willing to go out to parties to see if the drug helps you talk to people,” Dr Snowberg explained.
“Your behavior drives you to go to the party, and once you’re at the party, the drug helps you feel comfortable talking to people. That would be an example of an interaction effect. You couldn’t get that if people just took this drug alone at home.”
Although this specific example is just speculation, Dr Snowberg said the researchers’ actual results reveal that some behavior or set of behaviors interact with paroxetine to effectively treat depression. And, without this behavior, the drug appears to be ineffective.
“Normally, what you get when you run a standard blind trial is some sort of mishmash of the treatment effect and the treatment-behavior interaction effect,” Dr Snowberg said. “But knowing the full interaction effect is important.”
“Our work indicates that clinical trials underestimate the efficacy of a drug where behavior matters. It may be the case that 50% probability isn’t high enough for people to change any of their behaviors, especially if it’s a really uncertain new treatment. Then, it’s just going to look like the drug doesn’t work, and that isn’t the case.”
Because the meta-analysis supported the team’s hypothesis—that the interaction between treatment and behavior can have an effect on health outcomes—the next step is incorporating these new ideas into an active clinical trial.
Dr Snowberg said the best fit would be a drug trial for a condition, such as a mental health disorder or an addiction, that is known to be associated with behavior. At the very least, he hopes these results will lead the medical research community to a conversation about ways to improve the DBRCT. ![]()
Program helped reduce VTE in trauma patients

Photo by Piotr Bodzek
Data from a statewide quality collaborative helped the University of Michigan Trauma Service reduce its annual rate of venous thromboembolism (VTE), according to an article published in the Journal of the American College of Surgeons.
The data suggested that changing first-line VTE prophylaxis from unfractionated heparin to enoxaparin would decrease the incidence of VTE, and it did. The annual VTE incidence fell from about 36 cases to about 14.
Researchers said this study should not be interpreted as a head-to-head comparison of unfractionated heparin and enoxaparin as VTE prophylaxis in trauma patients. Instead, it should be seen as a model of how hospitals and physicians can use quality improvement data in a real-world setting.
Existing medical evidence has shown that both heparin and enoxaparin can be effective in preventing VTE, depending on factors such as how the agents are dosed and administered.
“Based on our data, the enoxaparin regimen was more effective than heparin,” said study author David A. Machado-Aranda, MD, of the University of Michigan in Ann Arbor.
“Now, this result could be different in another institution, another collaborative, another geographical area, or another patient population based on the circumstances encountered.”
Dr Machado-Aranda and his colleagues participate in the Michigan Trauma Quality Improvement Program (MTQIP), a statewide program of 27 ACS Level 1 and 2 trauma centers.
The program showed the researchers that the rate of VTE was higher for the University of Michigan Trauma Service than the collaborative average.
A closer look at the data revealed that VTE rates among trauma patients who received unfractionated heparin were twice as high as rates for patients who received enoxaparin.
After the University of Michigan Trauma Service switched from using unfractionated heparin to enoxaparin as first-line VTE prophylaxis, the rate of VTE dropped from 6.2% to 2.6%.
“What we’ve done is to use the collaborative as our ‘mission control’ to see where we’re heading and what our trajectory is,” Dr Machado-Aranda said. “Once we saw ourselves deviating from a favorable trajectory, we used the data derived from the collaborative to investigate our problem.”
“We also accessed many different resources to review best practices, receive suggestions from other collaborative participants, and perform root-cause analysis. An action plan was formulated, approved, and implemented to get our trauma service off of an unfavorable trajectory for VTE complications.”
Dr Machado-Aranda noted that the trauma team encountered some challenges in changing the protocol for VTE prophylaxis. Hospital administration and other departments were concerned about the higher cost of enoxaparin.
In the end, “the increased costs of using enoxaparin were more than offset by savings generated by reducing the rate of venous thromboembolism complications,” he said.
The trauma surgeons also found they had to review the data with the neurosurgeons and orthopedic surgeons on staff to understand and alleviate their concerns about enoxaparin and potential higher rates of bleeding complications.
The neurosurgical group had previously published a study that showed higher rates of intracranial bleeding in patients undergoing brain tumor surgery who received enoxaparin rather than sequential compression devices alone.
“These results became extrapolated into the trauma setting, and it took us some time convincing our neurosurgeons to consider changing their practice for trauma patients,” Dr Machado-Aranda said. ![]()
Photo by Piotr Bodzek
Data from a statewide quality collaborative helped the University of Michigan Trauma Service reduce its annual rate of venous thromboembolism (VTE), according to an article published in the Journal of the American College of Surgeons.
The data suggested that changing first-line VTE prophylaxis from unfractionated heparin to enoxaparin would decrease the incidence of VTE, and it did. The annual VTE incidence fell from about 36 cases to about 14.
Researchers said this study should not be interpreted as a head-to-head comparison of unfractionated heparin and enoxaparin as VTE prophylaxis in trauma patients. Instead, it should be seen as a model of how hospitals and physicians can use quality improvement data in a real-world setting.
Existing medical evidence has shown that both heparin and enoxaparin can be effective in preventing VTE, depending on factors such as how the agents are dosed and administered.
“Based on our data, the enoxaparin regimen was more effective than heparin,” said study author David A. Machado-Aranda, MD, of the University of Michigan in Ann Arbor.
“Now, this result could be different in another institution, another collaborative, another geographical area, or another patient population based on the circumstances encountered.”
Dr Machado-Aranda and his colleagues participate in the Michigan Trauma Quality Improvement Program (MTQIP), a statewide program of 27 ACS Level 1 and 2 trauma centers.
The program showed the researchers that the rate of VTE was higher for the University of Michigan Trauma Service than the collaborative average.
A closer look at the data revealed that VTE rates among trauma patients who received unfractionated heparin were twice as high as rates for patients who received enoxaparin.
After the University of Michigan Trauma Service switched from using unfractionated heparin to enoxaparin as first-line VTE prophylaxis, the rate of VTE dropped from 6.2% to 2.6%.
“What we’ve done is to use the collaborative as our ‘mission control’ to see where we’re heading and what our trajectory is,” Dr Machado-Aranda said. “Once we saw ourselves deviating from a favorable trajectory, we used the data derived from the collaborative to investigate our problem.”
“We also accessed many different resources to review best practices, receive suggestions from other collaborative participants, and perform root-cause analysis. An action plan was formulated, approved, and implemented to get our trauma service off of an unfavorable trajectory for VTE complications.”
Dr Machado-Aranda noted that the trauma team encountered some challenges in changing the protocol for VTE prophylaxis. Hospital administration and other departments were concerned about the higher cost of enoxaparin.
In the end, “the increased costs of using enoxaparin were more than offset by savings generated by reducing the rate of venous thromboembolism complications,” he said.
The trauma surgeons also found they had to review the data with the neurosurgeons and orthopedic surgeons on staff to understand and alleviate their concerns about enoxaparin and potential higher rates of bleeding complications.
The neurosurgical group had previously published a study that showed higher rates of intracranial bleeding in patients undergoing brain tumor surgery who received enoxaparin rather than sequential compression devices alone.
“These results became extrapolated into the trauma setting, and it took us some time convincing our neurosurgeons to consider changing their practice for trauma patients,” Dr Machado-Aranda said. ![]()
Photo by Piotr Bodzek
Data from a statewide quality collaborative helped the University of Michigan Trauma Service reduce its annual rate of venous thromboembolism (VTE), according to an article published in the Journal of the American College of Surgeons.
The data suggested that changing first-line VTE prophylaxis from unfractionated heparin to enoxaparin would decrease the incidence of VTE, and it did. The annual VTE incidence fell from about 36 cases to about 14.
Researchers said this study should not be interpreted as a head-to-head comparison of unfractionated heparin and enoxaparin as VTE prophylaxis in trauma patients. Instead, it should be seen as a model of how hospitals and physicians can use quality improvement data in a real-world setting.
Existing medical evidence has shown that both heparin and enoxaparin can be effective in preventing VTE, depending on factors such as how the agents are dosed and administered.
“Based on our data, the enoxaparin regimen was more effective than heparin,” said study author David A. Machado-Aranda, MD, of the University of Michigan in Ann Arbor.
“Now, this result could be different in another institution, another collaborative, another geographical area, or another patient population based on the circumstances encountered.”
Dr Machado-Aranda and his colleagues participate in the Michigan Trauma Quality Improvement Program (MTQIP), a statewide program of 27 ACS Level 1 and 2 trauma centers.
The program showed the researchers that the rate of VTE was higher for the University of Michigan Trauma Service than the collaborative average.
A closer look at the data revealed that VTE rates among trauma patients who received unfractionated heparin were twice as high as rates for patients who received enoxaparin.
After the University of Michigan Trauma Service switched from using unfractionated heparin to enoxaparin as first-line VTE prophylaxis, the rate of VTE dropped from 6.2% to 2.6%.
“What we’ve done is to use the collaborative as our ‘mission control’ to see where we’re heading and what our trajectory is,” Dr Machado-Aranda said. “Once we saw ourselves deviating from a favorable trajectory, we used the data derived from the collaborative to investigate our problem.”
“We also accessed many different resources to review best practices, receive suggestions from other collaborative participants, and perform root-cause analysis. An action plan was formulated, approved, and implemented to get our trauma service off of an unfavorable trajectory for VTE complications.”
Dr Machado-Aranda noted that the trauma team encountered some challenges in changing the protocol for VTE prophylaxis. Hospital administration and other departments were concerned about the higher cost of enoxaparin.
In the end, “the increased costs of using enoxaparin were more than offset by savings generated by reducing the rate of venous thromboembolism complications,” he said.
The trauma surgeons also found they had to review the data with the neurosurgeons and orthopedic surgeons on staff to understand and alleviate their concerns about enoxaparin and potential higher rates of bleeding complications.
The neurosurgical group had previously published a study that showed higher rates of intracranial bleeding in patients undergoing brain tumor surgery who received enoxaparin rather than sequential compression devices alone.
“These results became extrapolated into the trauma setting, and it took us some time convincing our neurosurgeons to consider changing their practice for trauma patients,” Dr Machado-Aranda said. ![]()
HRS: Blacks show higher A fib–stroke risk than whites do
BOSTON – Black people with new-onset atrial fibrillation have a 60% increased risk for stroke compared with white people who have incident atrial fibrillation when not maintained on an appropriate anticlotting regimen, according to prospectively collected data from more than 56,000 subjects at a U.S. center.
But in the subgroup of new-onset atrial fibrillation (AF) patients who received appropriate treatment with aspirin or an anticoagulant, the stroke rates among white and blacks equalized. The analysis showed that 46% of the more than 3,000 people who developed AF during follow-up received aspirin if their CHA2DS2-VASc score was less than 2, or anticoagulation with warfarin or a new oral anticoagulant if their score was 2 or greater, Dr. Parin J. Patel said at the annual scientific sessions of the Heart Rhythm Society.

The majority of the followed cohort with incident atrial fibrillation did not receive this treatment, and in the total group, the relative rate of stroke among blacks exceeded that of whites by a statistically significant 60% in an analysis that adjusted for several demographic and clinical features. The excess of strokes occurred at about the same rate in black women compared with white women, and in black men compared with white men, reported Dr. Patel, an electrophysiologist at the University of Pennsylvania in Philadelphia.
The implication is that because their stroke risk is greater, blacks with AF should especially receive appropriate stroke prophylaxis and AF therapy, he said. The overall findings also highlight the substantial stroke risk faced by all AF patients.
The data came from the University of Pennsylvania Atrial Fibrillation-Free study of 91,274 people who underwent an ECG examination in the University of Pennsylvania health system during 2004-2009 along with an index clinical encounter within 30 days. Excluding patients with a prevalent AF or other arrhythmia, prevalent stroke, or incomplete data left 56,835 AF- and stroke-free people to follow for incident AF, which occurred in 3,891 patients. At the time of AF diagnosis, the average age of patients was 63 years; more than a third had hypertension; a fifth had diabetes; and a fifth had heart failure. One-third of the incident-AF group was black, 58% were white, and the remainder were from other demographic groups.
Dr. Patel and his associates defined an AF-related stroke as any that occurred within 6 months before AF diagnosis or anytime after, which occurred in 645 (17%) of the incident-AF patients. The more than 50,000 AF-free people followed in the study had a total of 3,001 strokes not related to AF during follow-up, which meant that 18% of all strokes in the entire cohort were AF related.
Among the 645 AF-related strokes, roughly half occurred during the 6 months before AF diagnosis, and the other half following AF diagnosis. An analysis that focused exclusively on strokes that occurred after AF diagnosis showed that this subset of AF-associated strokes also occurred significantly more often in blacks than in whites.
Dr. Patel had no disclosures.
On Twitter @mitchelzoler
BOSTON – Black people with new-onset atrial fibrillation have a 60% increased risk for stroke compared with white people who have incident atrial fibrillation when not maintained on an appropriate anticlotting regimen, according to prospectively collected data from more than 56,000 subjects at a U.S. center.
But in the subgroup of new-onset atrial fibrillation (AF) patients who received appropriate treatment with aspirin or an anticoagulant, the stroke rates among white and blacks equalized. The analysis showed that 46% of the more than 3,000 people who developed AF during follow-up received aspirin if their CHA2DS2-VASc score was less than 2, or anticoagulation with warfarin or a new oral anticoagulant if their score was 2 or greater, Dr. Parin J. Patel said at the annual scientific sessions of the Heart Rhythm Society.
The majority of the followed cohort with incident atrial fibrillation did not receive this treatment, and in the total group, the relative rate of stroke among blacks exceeded that of whites by a statistically significant 60% in an analysis that adjusted for several demographic and clinical features. The excess of strokes occurred at about the same rate in black women compared with white women, and in black men compared with white men, reported Dr. Patel, an electrophysiologist at the University of Pennsylvania in Philadelphia.
The implication is that because their stroke risk is greater, blacks with AF should especially receive appropriate stroke prophylaxis and AF therapy, he said. The overall findings also highlight the substantial stroke risk faced by all AF patients.
The data came from the University of Pennsylvania Atrial Fibrillation-Free study of 91,274 people who underwent an ECG examination in the University of Pennsylvania health system during 2004-2009 along with an index clinical encounter within 30 days. Excluding patients with a prevalent AF or other arrhythmia, prevalent stroke, or incomplete data left 56,835 AF- and stroke-free people to follow for incident AF, which occurred in 3,891 patients. At the time of AF diagnosis, the average age of patients was 63 years; more than a third had hypertension; a fifth had diabetes; and a fifth had heart failure. One-third of the incident-AF group was black, 58% were white, and the remainder were from other demographic groups.
Dr. Patel and his associates defined an AF-related stroke as any that occurred within 6 months before AF diagnosis or anytime after, which occurred in 645 (17%) of the incident-AF patients. The more than 50,000 AF-free people followed in the study had a total of 3,001 strokes not related to AF during follow-up, which meant that 18% of all strokes in the entire cohort were AF related.
Among the 645 AF-related strokes, roughly half occurred during the 6 months before AF diagnosis, and the other half following AF diagnosis. An analysis that focused exclusively on strokes that occurred after AF diagnosis showed that this subset of AF-associated strokes also occurred significantly more often in blacks than in whites.
Dr. Patel had no disclosures.
On Twitter @mitchelzoler
BOSTON – Black people with new-onset atrial fibrillation have a 60% increased risk for stroke compared with white people who have incident atrial fibrillation when not maintained on an appropriate anticlotting regimen, according to prospectively collected data from more than 56,000 subjects at a U.S. center.
But in the subgroup of new-onset atrial fibrillation (AF) patients who received appropriate treatment with aspirin or an anticoagulant, the stroke rates among white and blacks equalized. The analysis showed that 46% of the more than 3,000 people who developed AF during follow-up received aspirin if their CHA2DS2-VASc score was less than 2, or anticoagulation with warfarin or a new oral anticoagulant if their score was 2 or greater, Dr. Parin J. Patel said at the annual scientific sessions of the Heart Rhythm Society.
The majority of the followed cohort with incident atrial fibrillation did not receive this treatment, and in the total group, the relative rate of stroke among blacks exceeded that of whites by a statistically significant 60% in an analysis that adjusted for several demographic and clinical features. The excess of strokes occurred at about the same rate in black women compared with white women, and in black men compared with white men, reported Dr. Patel, an electrophysiologist at the University of Pennsylvania in Philadelphia.
The implication is that because their stroke risk is greater, blacks with AF should especially receive appropriate stroke prophylaxis and AF therapy, he said. The overall findings also highlight the substantial stroke risk faced by all AF patients.
The data came from the University of Pennsylvania Atrial Fibrillation-Free study of 91,274 people who underwent an ECG examination in the University of Pennsylvania health system during 2004-2009 along with an index clinical encounter within 30 days. Excluding patients with a prevalent AF or other arrhythmia, prevalent stroke, or incomplete data left 56,835 AF- and stroke-free people to follow for incident AF, which occurred in 3,891 patients. At the time of AF diagnosis, the average age of patients was 63 years; more than a third had hypertension; a fifth had diabetes; and a fifth had heart failure. One-third of the incident-AF group was black, 58% were white, and the remainder were from other demographic groups.
Dr. Patel and his associates defined an AF-related stroke as any that occurred within 6 months before AF diagnosis or anytime after, which occurred in 645 (17%) of the incident-AF patients. The more than 50,000 AF-free people followed in the study had a total of 3,001 strokes not related to AF during follow-up, which meant that 18% of all strokes in the entire cohort were AF related.
Among the 645 AF-related strokes, roughly half occurred during the 6 months before AF diagnosis, and the other half following AF diagnosis. An analysis that focused exclusively on strokes that occurred after AF diagnosis showed that this subset of AF-associated strokes also occurred significantly more often in blacks than in whites.
Dr. Patel had no disclosures.
On Twitter @mitchelzoler
AT HEART RHYTHM 2015
Key clinical point: Strokes associated with newly diagnosed atrial fibrillation were significantly more common in African American patients than in white patients.
Major finding: The rate of atrial fibrillation–associated stroke was 60% higher in black patients than in white patients.
Data source: A review of prospectively-collected data from 56,835 people who underwent a baseline ECG at one U.S. center during 2004-2009.
Disclosures: Dr. Patel had no disclosures.

Listen Now: Hospital Medicine Intersects with Global Patient Safety
Dr. Phuoc Le of the University of California at San Francisco and Dr. Bijay Achariya of Mass General Hospital in Boston, both practicing global hospitalists, share their perspectives on the US hospitalist movement, how it intersects with the global patient safety movement, and the opportunities presented for hospitalists with a global perspective to make a difference for patients everywhere.
Dr. Phuoc Le of the University of California at San Francisco and Dr. Bijay Achariya of Mass General Hospital in Boston, both practicing global hospitalists, share their perspectives on the US hospitalist movement, how it intersects with the global patient safety movement, and the opportunities presented for hospitalists with a global perspective to make a difference for patients everywhere.
Dr. Phuoc Le of the University of California at San Francisco and Dr. Bijay Achariya of Mass General Hospital in Boston, both practicing global hospitalists, share their perspectives on the US hospitalist movement, how it intersects with the global patient safety movement, and the opportunities presented for hospitalists with a global perspective to make a difference for patients everywhere.
Q&A with the FDA: Implementing the Pregnancy and Lactation Labeling Rule
On June 30, pharmaceutical and biological manufacturers will begin implementing the Food and Drug Administration’s revised rules for pregnancy and lactation drug labeling. The Pregnancy and Lactation Labeling Rule (PLLR) amends the Physician Labeling Rule (PLR, issued in 2006) and new labels aimed at providing clearer and more accurate information on drug risks will gradually roll out over the next 5 years.
The new rule – several years in the making – replaces pregnancy categories A, B, C, D, and X with short, integrated summaries that provide physicians with more information for discussing with patients the risks and benefits of a medication. The summaries will be brief and easy to read, and will contain evidence-based information that specifically addresses drug risks for women during pregnancy and lactation, as well as for men and women of reproductive potential. Under the PLLR, the pregnancy subsection of the risk summary will include for the first time information for any drug that has a pregnancy exposure registry.
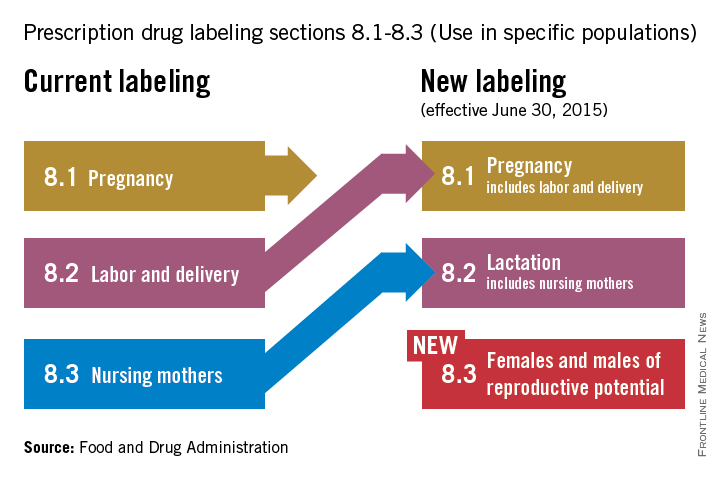
Dr. John Whyte, director of Professional Affairs and Stakeholder Engagment (PASE) at the FDA Center for Drug Evaluation and Research, answers questions about the new rule from Ob.Gyn. News journalists and our Drugs, Pregnancy & Lactation columnists.
Question: Instead of the traditional letter categories, prescribers will now have to read the pregnancy and lactation subsections of the labeling. What can the agency do to ensure prescribers are reading all of the new contextual information in the drug label?
Answer: The agency has initiated outreach efforts to help prescribers become familiar with the new information in labeling. The most important information is now under a new heading called Risk Summary. This narrative summary replaces the pregnancy letter categories with a summary of information that is known about a product. The new labeling rule explains, based on available information, the potential benefits and risks for the mother, the fetus, and the breastfeeding child. The decision to replace the pregnancy letter categories with the summary paragraph was reached after extensive consultation with experts and stakeholders who were concerned that the traditional letter categories were overly simplistic.

Q: PLLR praises the value of pregnancy exposure registries and mandates that if a registry exists for an approved product, then the label must include the registry’s website address. There is no requirement, however, that industry actually fund these registries. Why did the agency stop short of requiring companies to provide ongoing support for pregnancy exposure registries?
A: FDA has the authority to require the establishment of pregnancy registries when there is a safety concern that would benefit from the collection of data in a postapproval study, or when a particular product will be used by a large number of females of reproductive age. However, FDA does not have the authority to require companies to fund existing pregnancy exposure registries.
Q: How does the FDA plan to review all of the summary statements of available data regarding reproductive safety considering the breadth of drugs in various therapeutic areas that will need to be reviewed?
A: All labeling changes, including the changes required by the PLLR, must be submitted to the FDA for review and approval. Changes to the Pregnancy and Lactation subsections of labeling have been integrated into standard labeling review processes. In addition, the Division of Pediatric and Maternal Health, in the Office of New Drugs, works with the primary review divisions to help coordinate PLLR review processes.
Q: Are the manufacturers of generic drugs expected to “piggyback” the label for a branded molecule with respect to the pregnancy label?
A: Generic drug products (Abbreviated New Drug Applications) are required by regulation to have the “same” labeling as the reference drug listed. When the labeling is revised for the referenced drug, generic drug manufacturers also are required to update their labeling.
Q: In the new system, how will labeling stay up to date when important new data are published on a drug sometimes two to three times a year?
A: When new information becomes available that causes the labeling to be inaccurate, false, or misleading, drug manufacturers are required by regulation to update labeling.
Q: The rule is phased in over time. Drugs already on the market are given more time to switch to the new system. How long will physicians need to deal simultaneously with the old and the new formats?
A: There have been two labeling formats in use for some time as products approved prior to 2001 are not required to conform to either PLLR or PLR. The agency encourages manufacturers to voluntarily convert labeling of older products into PLR format. However, products approved prior to 2001 will be required to remove the pregnancy letter category by June 30, 2018, (3 years after the implementation of the PLLR).
Q: Does the FDA have any plans to address labeling for over-the-counter products in terms of their impact on pregnancy, lactation, and reproductive potential?
A: The PLLR does not apply to over-the-counter products. However, the agency is continually reviewing the safety of products used over the counter, including impacts on pregnancy, lactation, and reproductive potential.
Q: How does the FDA plan to assess over time the usefulness of the new labeling for prescribers and patients and make revisions?
A: The draft guidance was issued concurrently with PLLR. Based on the comments received from the public on the draft, as well as learning from the initial revisions of labeling, the guidance will be revised as needed. Guidance statements issued by FDA are regularly reviewed and revised as needed.
Dr. Whyte, a board-certified internist, is the director of Professional Affairs and Stakeholder Engagement at the FDA. Do you have other questions about the PLLR? Send them to [email protected].
On June 30, pharmaceutical and biological manufacturers will begin implementing the Food and Drug Administration’s revised rules for pregnancy and lactation drug labeling. The Pregnancy and Lactation Labeling Rule (PLLR) amends the Physician Labeling Rule (PLR, issued in 2006) and new labels aimed at providing clearer and more accurate information on drug risks will gradually roll out over the next 5 years.
The new rule – several years in the making – replaces pregnancy categories A, B, C, D, and X with short, integrated summaries that provide physicians with more information for discussing with patients the risks and benefits of a medication. The summaries will be brief and easy to read, and will contain evidence-based information that specifically addresses drug risks for women during pregnancy and lactation, as well as for men and women of reproductive potential. Under the PLLR, the pregnancy subsection of the risk summary will include for the first time information for any drug that has a pregnancy exposure registry.
Dr. John Whyte, director of Professional Affairs and Stakeholder Engagment (PASE) at the FDA Center for Drug Evaluation and Research, answers questions about the new rule from Ob.Gyn. News journalists and our Drugs, Pregnancy & Lactation columnists.
Question: Instead of the traditional letter categories, prescribers will now have to read the pregnancy and lactation subsections of the labeling. What can the agency do to ensure prescribers are reading all of the new contextual information in the drug label?
Answer: The agency has initiated outreach efforts to help prescribers become familiar with the new information in labeling. The most important information is now under a new heading called Risk Summary. This narrative summary replaces the pregnancy letter categories with a summary of information that is known about a product. The new labeling rule explains, based on available information, the potential benefits and risks for the mother, the fetus, and the breastfeeding child. The decision to replace the pregnancy letter categories with the summary paragraph was reached after extensive consultation with experts and stakeholders who were concerned that the traditional letter categories were overly simplistic.
Q: PLLR praises the value of pregnancy exposure registries and mandates that if a registry exists for an approved product, then the label must include the registry’s website address. There is no requirement, however, that industry actually fund these registries. Why did the agency stop short of requiring companies to provide ongoing support for pregnancy exposure registries?
A: FDA has the authority to require the establishment of pregnancy registries when there is a safety concern that would benefit from the collection of data in a postapproval study, or when a particular product will be used by a large number of females of reproductive age. However, FDA does not have the authority to require companies to fund existing pregnancy exposure registries.
Q: How does the FDA plan to review all of the summary statements of available data regarding reproductive safety considering the breadth of drugs in various therapeutic areas that will need to be reviewed?
A: All labeling changes, including the changes required by the PLLR, must be submitted to the FDA for review and approval. Changes to the Pregnancy and Lactation subsections of labeling have been integrated into standard labeling review processes. In addition, the Division of Pediatric and Maternal Health, in the Office of New Drugs, works with the primary review divisions to help coordinate PLLR review processes.
Q: Are the manufacturers of generic drugs expected to “piggyback” the label for a branded molecule with respect to the pregnancy label?
A: Generic drug products (Abbreviated New Drug Applications) are required by regulation to have the “same” labeling as the reference drug listed. When the labeling is revised for the referenced drug, generic drug manufacturers also are required to update their labeling.
Q: In the new system, how will labeling stay up to date when important new data are published on a drug sometimes two to three times a year?
A: When new information becomes available that causes the labeling to be inaccurate, false, or misleading, drug manufacturers are required by regulation to update labeling.
Q: The rule is phased in over time. Drugs already on the market are given more time to switch to the new system. How long will physicians need to deal simultaneously with the old and the new formats?
A: There have been two labeling formats in use for some time as products approved prior to 2001 are not required to conform to either PLLR or PLR. The agency encourages manufacturers to voluntarily convert labeling of older products into PLR format. However, products approved prior to 2001 will be required to remove the pregnancy letter category by June 30, 2018, (3 years after the implementation of the PLLR).
Q: Does the FDA have any plans to address labeling for over-the-counter products in terms of their impact on pregnancy, lactation, and reproductive potential?
A: The PLLR does not apply to over-the-counter products. However, the agency is continually reviewing the safety of products used over the counter, including impacts on pregnancy, lactation, and reproductive potential.
Q: How does the FDA plan to assess over time the usefulness of the new labeling for prescribers and patients and make revisions?
A: The draft guidance was issued concurrently with PLLR. Based on the comments received from the public on the draft, as well as learning from the initial revisions of labeling, the guidance will be revised as needed. Guidance statements issued by FDA are regularly reviewed and revised as needed.
Dr. Whyte, a board-certified internist, is the director of Professional Affairs and Stakeholder Engagement at the FDA. Do you have other questions about the PLLR? Send them to [email protected].
On June 30, pharmaceutical and biological manufacturers will begin implementing the Food and Drug Administration’s revised rules for pregnancy and lactation drug labeling. The Pregnancy and Lactation Labeling Rule (PLLR) amends the Physician Labeling Rule (PLR, issued in 2006) and new labels aimed at providing clearer and more accurate information on drug risks will gradually roll out over the next 5 years.
The new rule – several years in the making – replaces pregnancy categories A, B, C, D, and X with short, integrated summaries that provide physicians with more information for discussing with patients the risks and benefits of a medication. The summaries will be brief and easy to read, and will contain evidence-based information that specifically addresses drug risks for women during pregnancy and lactation, as well as for men and women of reproductive potential. Under the PLLR, the pregnancy subsection of the risk summary will include for the first time information for any drug that has a pregnancy exposure registry.
Dr. John Whyte, director of Professional Affairs and Stakeholder Engagment (PASE) at the FDA Center for Drug Evaluation and Research, answers questions about the new rule from Ob.Gyn. News journalists and our Drugs, Pregnancy & Lactation columnists.
Question: Instead of the traditional letter categories, prescribers will now have to read the pregnancy and lactation subsections of the labeling. What can the agency do to ensure prescribers are reading all of the new contextual information in the drug label?
Answer: The agency has initiated outreach efforts to help prescribers become familiar with the new information in labeling. The most important information is now under a new heading called Risk Summary. This narrative summary replaces the pregnancy letter categories with a summary of information that is known about a product. The new labeling rule explains, based on available information, the potential benefits and risks for the mother, the fetus, and the breastfeeding child. The decision to replace the pregnancy letter categories with the summary paragraph was reached after extensive consultation with experts and stakeholders who were concerned that the traditional letter categories were overly simplistic.
Q: PLLR praises the value of pregnancy exposure registries and mandates that if a registry exists for an approved product, then the label must include the registry’s website address. There is no requirement, however, that industry actually fund these registries. Why did the agency stop short of requiring companies to provide ongoing support for pregnancy exposure registries?
A: FDA has the authority to require the establishment of pregnancy registries when there is a safety concern that would benefit from the collection of data in a postapproval study, or when a particular product will be used by a large number of females of reproductive age. However, FDA does not have the authority to require companies to fund existing pregnancy exposure registries.
Q: How does the FDA plan to review all of the summary statements of available data regarding reproductive safety considering the breadth of drugs in various therapeutic areas that will need to be reviewed?
A: All labeling changes, including the changes required by the PLLR, must be submitted to the FDA for review and approval. Changes to the Pregnancy and Lactation subsections of labeling have been integrated into standard labeling review processes. In addition, the Division of Pediatric and Maternal Health, in the Office of New Drugs, works with the primary review divisions to help coordinate PLLR review processes.
Q: Are the manufacturers of generic drugs expected to “piggyback” the label for a branded molecule with respect to the pregnancy label?
A: Generic drug products (Abbreviated New Drug Applications) are required by regulation to have the “same” labeling as the reference drug listed. When the labeling is revised for the referenced drug, generic drug manufacturers also are required to update their labeling.
Q: In the new system, how will labeling stay up to date when important new data are published on a drug sometimes two to three times a year?
A: When new information becomes available that causes the labeling to be inaccurate, false, or misleading, drug manufacturers are required by regulation to update labeling.
Q: The rule is phased in over time. Drugs already on the market are given more time to switch to the new system. How long will physicians need to deal simultaneously with the old and the new formats?
A: There have been two labeling formats in use for some time as products approved prior to 2001 are not required to conform to either PLLR or PLR. The agency encourages manufacturers to voluntarily convert labeling of older products into PLR format. However, products approved prior to 2001 will be required to remove the pregnancy letter category by June 30, 2018, (3 years after the implementation of the PLLR).
Q: Does the FDA have any plans to address labeling for over-the-counter products in terms of their impact on pregnancy, lactation, and reproductive potential?
A: The PLLR does not apply to over-the-counter products. However, the agency is continually reviewing the safety of products used over the counter, including impacts on pregnancy, lactation, and reproductive potential.
Q: How does the FDA plan to assess over time the usefulness of the new labeling for prescribers and patients and make revisions?
A: The draft guidance was issued concurrently with PLLR. Based on the comments received from the public on the draft, as well as learning from the initial revisions of labeling, the guidance will be revised as needed. Guidance statements issued by FDA are regularly reviewed and revised as needed.
Dr. Whyte, a board-certified internist, is the director of Professional Affairs and Stakeholder Engagement at the FDA. Do you have other questions about the PLLR? Send them to [email protected].
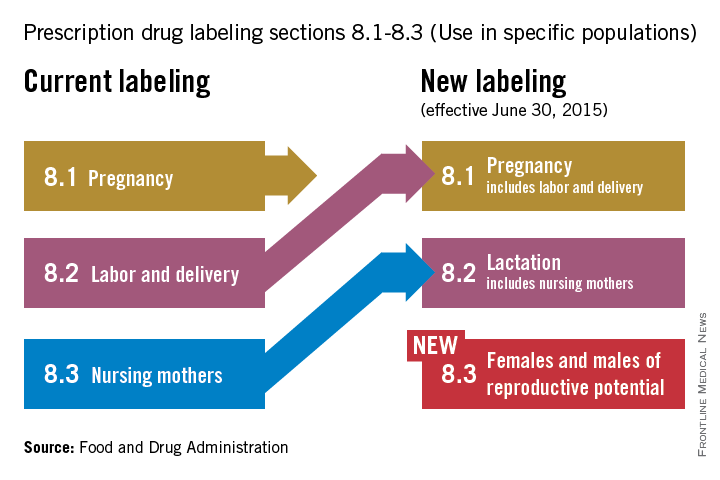
Addressing unmet contraception needs in patients with cancer
Approximately 740,000 women are diagnosed with cancer every year in the United States, and because of improved screening, diagnosis, and treatment, women of reproductive age have an 80%-90% 5-year survival rate. The most common cancers in reproductive age women include breast, thyroid, melanoma, colorectal, and cervical cancers. Fertility intention is a critical topic to discuss with reproductive-age cancer patients. Women with cancer often have unmet contraception needs during and following cancer treatment. Providing women with a desired, effective form of contraception that is appropriate with regard to the cancer is critical.
Multiple studies have demonstrated that pregnancy prevention is not adequately addressed in cancer patients. On the one hand, many patients believe they are no longer fertile because of a combination of the illness and the cancer treatment, and on the other hand, many providers may not be adequately trained to offer their patients the full range of contraceptive options (Am. J. Obstet. Gynecol. 2009;201:191.e1-4). One study demonstrated that discussions around fecundity and contraception are occurring about 50% of the time (J. Natl. Cancer. Inst. Monogr. 2005:98-100).

In response, the American Society for Reproductive Medicine has issued guidelines regarding fertility planning in cancer patients (Fertil. Steril. 2005;83:1622-8). While every patient’s circumstance is unique, recommendations are for patients to avoid pregnancy for at least 1 year beyond the completion of medical and surgical treatment of cancer. For those cancers that are hormone mediated, recommendations are to wait 2-5 years before attempting to conceive (J. Obstet. Gynaecol. Can. 2002;24:164-80; J. Gen. Intern. Med. 2009; 24: S401-6).
Unless patients are educated about and offered the most effective forms of contraception, they are at risk of unintended pregnancy, which may result in severe consequences, as patients may be on teratogenic medications or dealing with comorbid conditions originating from cancer and cancer treatment (Contraception 2012;86:191-8).
Cancer treatments have variable impact on subsequent fertility (with the obvious exception of surgical removal of gynecologic organs resulting in sterilization). With all nonsurgical cancer treatments, the potential for subsequent fertility depends on the chemotherapeutic agents, the duration of treatment, or use of pelvic radiation. As in patients without cancer, age is inversely related to subsequent fertility. Reviews of the literature have shown that fecundability decreases by 10%-50% post chemotherapy.
Clinicians caring for these women may find it challenging to assess future fertility. Some chemotherapies induce amenorrhea, but spontaneous return of menstruation and ovarian function is possible in younger women. Traditional diagnostic tests to assess fertility, including serum FSH (follicle stimulating hormone) and/or AMH (anti-Müllerian hormone), may help in predicting future fertility. These tests can be used both in patients who desire to pursue pregnancy and in those desiring to avoid pregnancy as menstrual status may not accurately predict fertility.
Contraception counseling should begin by informing women of the most effective forms of contraception (Obstet. Gynecol. 2011;118:184-96). It is important to consider the option of sterilization, especially when this desire predated the cancer diagnosis. In patients who are in a monogamous relationship with a male partner, vasectomy should be encouraged as a safe and effective alternative. When a woman is considering sterilization, she needs to be counseled as to the risk of regret, which is higher in younger women. Sterilization should not be performed if the consent or decision-making process is rushed by the cancer treatment.
As cancer screening, diagnosis, and treatment continue to improve, more reproductive-age women will be living longer with a need for effective contraception. In the next edition of Gynecologic Oncology Consult, I will review the safety and efficacy of specific contraceptive methods in patients with cancer.
Dr. Zerden is a family planning fellow in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. His research interests include postpartum contraception, methods of female sterilization, and family planning health services integration. He reported having no financial disclosures.
Approximately 740,000 women are diagnosed with cancer every year in the United States, and because of improved screening, diagnosis, and treatment, women of reproductive age have an 80%-90% 5-year survival rate. The most common cancers in reproductive age women include breast, thyroid, melanoma, colorectal, and cervical cancers. Fertility intention is a critical topic to discuss with reproductive-age cancer patients. Women with cancer often have unmet contraception needs during and following cancer treatment. Providing women with a desired, effective form of contraception that is appropriate with regard to the cancer is critical.
Multiple studies have demonstrated that pregnancy prevention is not adequately addressed in cancer patients. On the one hand, many patients believe they are no longer fertile because of a combination of the illness and the cancer treatment, and on the other hand, many providers may not be adequately trained to offer their patients the full range of contraceptive options (Am. J. Obstet. Gynecol. 2009;201:191.e1-4). One study demonstrated that discussions around fecundity and contraception are occurring about 50% of the time (J. Natl. Cancer. Inst. Monogr. 2005:98-100).
In response, the American Society for Reproductive Medicine has issued guidelines regarding fertility planning in cancer patients (Fertil. Steril. 2005;83:1622-8). While every patient’s circumstance is unique, recommendations are for patients to avoid pregnancy for at least 1 year beyond the completion of medical and surgical treatment of cancer. For those cancers that are hormone mediated, recommendations are to wait 2-5 years before attempting to conceive (J. Obstet. Gynaecol. Can. 2002;24:164-80; J. Gen. Intern. Med. 2009; 24: S401-6).
Unless patients are educated about and offered the most effective forms of contraception, they are at risk of unintended pregnancy, which may result in severe consequences, as patients may be on teratogenic medications or dealing with comorbid conditions originating from cancer and cancer treatment (Contraception 2012;86:191-8).
Cancer treatments have variable impact on subsequent fertility (with the obvious exception of surgical removal of gynecologic organs resulting in sterilization). With all nonsurgical cancer treatments, the potential for subsequent fertility depends on the chemotherapeutic agents, the duration of treatment, or use of pelvic radiation. As in patients without cancer, age is inversely related to subsequent fertility. Reviews of the literature have shown that fecundability decreases by 10%-50% post chemotherapy.
Clinicians caring for these women may find it challenging to assess future fertility. Some chemotherapies induce amenorrhea, but spontaneous return of menstruation and ovarian function is possible in younger women. Traditional diagnostic tests to assess fertility, including serum FSH (follicle stimulating hormone) and/or AMH (anti-Müllerian hormone), may help in predicting future fertility. These tests can be used both in patients who desire to pursue pregnancy and in those desiring to avoid pregnancy as menstrual status may not accurately predict fertility.
Contraception counseling should begin by informing women of the most effective forms of contraception (Obstet. Gynecol. 2011;118:184-96). It is important to consider the option of sterilization, especially when this desire predated the cancer diagnosis. In patients who are in a monogamous relationship with a male partner, vasectomy should be encouraged as a safe and effective alternative. When a woman is considering sterilization, she needs to be counseled as to the risk of regret, which is higher in younger women. Sterilization should not be performed if the consent or decision-making process is rushed by the cancer treatment.
As cancer screening, diagnosis, and treatment continue to improve, more reproductive-age women will be living longer with a need for effective contraception. In the next edition of Gynecologic Oncology Consult, I will review the safety and efficacy of specific contraceptive methods in patients with cancer.
Dr. Zerden is a family planning fellow in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. His research interests include postpartum contraception, methods of female sterilization, and family planning health services integration. He reported having no financial disclosures.
Approximately 740,000 women are diagnosed with cancer every year in the United States, and because of improved screening, diagnosis, and treatment, women of reproductive age have an 80%-90% 5-year survival rate. The most common cancers in reproductive age women include breast, thyroid, melanoma, colorectal, and cervical cancers. Fertility intention is a critical topic to discuss with reproductive-age cancer patients. Women with cancer often have unmet contraception needs during and following cancer treatment. Providing women with a desired, effective form of contraception that is appropriate with regard to the cancer is critical.
Multiple studies have demonstrated that pregnancy prevention is not adequately addressed in cancer patients. On the one hand, many patients believe they are no longer fertile because of a combination of the illness and the cancer treatment, and on the other hand, many providers may not be adequately trained to offer their patients the full range of contraceptive options (Am. J. Obstet. Gynecol. 2009;201:191.e1-4). One study demonstrated that discussions around fecundity and contraception are occurring about 50% of the time (J. Natl. Cancer. Inst. Monogr. 2005:98-100).
In response, the American Society for Reproductive Medicine has issued guidelines regarding fertility planning in cancer patients (Fertil. Steril. 2005;83:1622-8). While every patient’s circumstance is unique, recommendations are for patients to avoid pregnancy for at least 1 year beyond the completion of medical and surgical treatment of cancer. For those cancers that are hormone mediated, recommendations are to wait 2-5 years before attempting to conceive (J. Obstet. Gynaecol. Can. 2002;24:164-80; J. Gen. Intern. Med. 2009; 24: S401-6).
Unless patients are educated about and offered the most effective forms of contraception, they are at risk of unintended pregnancy, which may result in severe consequences, as patients may be on teratogenic medications or dealing with comorbid conditions originating from cancer and cancer treatment (Contraception 2012;86:191-8).
Cancer treatments have variable impact on subsequent fertility (with the obvious exception of surgical removal of gynecologic organs resulting in sterilization). With all nonsurgical cancer treatments, the potential for subsequent fertility depends on the chemotherapeutic agents, the duration of treatment, or use of pelvic radiation. As in patients without cancer, age is inversely related to subsequent fertility. Reviews of the literature have shown that fecundability decreases by 10%-50% post chemotherapy.
Clinicians caring for these women may find it challenging to assess future fertility. Some chemotherapies induce amenorrhea, but spontaneous return of menstruation and ovarian function is possible in younger women. Traditional diagnostic tests to assess fertility, including serum FSH (follicle stimulating hormone) and/or AMH (anti-Müllerian hormone), may help in predicting future fertility. These tests can be used both in patients who desire to pursue pregnancy and in those desiring to avoid pregnancy as menstrual status may not accurately predict fertility.
Contraception counseling should begin by informing women of the most effective forms of contraception (Obstet. Gynecol. 2011;118:184-96). It is important to consider the option of sterilization, especially when this desire predated the cancer diagnosis. In patients who are in a monogamous relationship with a male partner, vasectomy should be encouraged as a safe and effective alternative. When a woman is considering sterilization, she needs to be counseled as to the risk of regret, which is higher in younger women. Sterilization should not be performed if the consent or decision-making process is rushed by the cancer treatment.
As cancer screening, diagnosis, and treatment continue to improve, more reproductive-age women will be living longer with a need for effective contraception. In the next edition of Gynecologic Oncology Consult, I will review the safety and efficacy of specific contraceptive methods in patients with cancer.
Dr. Zerden is a family planning fellow in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. His research interests include postpartum contraception, methods of female sterilization, and family planning health services integration. He reported having no financial disclosures.

VIDEO: Assessment tool rapidly screens lupus cognition
ROME – The Montreal Cognitive Assessment provides a quick and easy-to-use screening tool to identify patients with systemic lupus erythematosus with cognitive impairment, Dr. Zahi Touma reported in a poster at the European Congress of Rheumatology.
In a consecutive series of 78 patients screened with the Montreal Cognitive Assessment (MoCA), the free, single-page test, which can be administered in about 10 minutes, showed a sensitivity of 69% and specificity of 68%, compared with the current standard, the Hopkins Verbal Learning Test-Revised, said Dr. Touma, a rheumatologist at the University of Toronto.
Other easy-to-use and quick screening tools, such as the Mini-Mental State Examination, had substantially worse performance in the study. He and his associates found a sensitivity of 21% and specificity of 91% using the Mini-Mental State exam. For screening, higher sensitivity is desirable so that fewer patients with potential cognitive impairment are missed, he noted.
“Ease of use and time needed for assessment as well as appropriate psychometric properties make the MoCA the preferential screening test for cognitive impairment in patients with SLE,” Dr. Touma said in his poster.
Cognitive impairment is very common among patients with systemic lupus erythematosus (SLE). In this study, Dr Touma found a 47% prevalence using MoCA. Cognitive impairment, however, often goes unidentified in SLE patients, likely because of lack of awareness among rheumatologists as well as the absence of a quick and easily administered screening tool, he said in a video interview.
Dr. Touma said he hopes that the apparent efficacy of an easy-to-use screening tool like MoCA will help boost appreciation for the high prevalence of cognitive impairment in SLE patients. He suggested that clinicians screen for cognitive impairment as soon as SLE is diagnosed and that they perform follow-up screening during subsequent patient encounters with SLE patients who initially present without cognitive impairment.
Dr. Touma had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
ROME – The Montreal Cognitive Assessment provides a quick and easy-to-use screening tool to identify patients with systemic lupus erythematosus with cognitive impairment, Dr. Zahi Touma reported in a poster at the European Congress of Rheumatology.
In a consecutive series of 78 patients screened with the Montreal Cognitive Assessment (MoCA), the free, single-page test, which can be administered in about 10 minutes, showed a sensitivity of 69% and specificity of 68%, compared with the current standard, the Hopkins Verbal Learning Test-Revised, said Dr. Touma, a rheumatologist at the University of Toronto.
Other easy-to-use and quick screening tools, such as the Mini-Mental State Examination, had substantially worse performance in the study. He and his associates found a sensitivity of 21% and specificity of 91% using the Mini-Mental State exam. For screening, higher sensitivity is desirable so that fewer patients with potential cognitive impairment are missed, he noted.
“Ease of use and time needed for assessment as well as appropriate psychometric properties make the MoCA the preferential screening test for cognitive impairment in patients with SLE,” Dr. Touma said in his poster.
Cognitive impairment is very common among patients with systemic lupus erythematosus (SLE). In this study, Dr Touma found a 47% prevalence using MoCA. Cognitive impairment, however, often goes unidentified in SLE patients, likely because of lack of awareness among rheumatologists as well as the absence of a quick and easily administered screening tool, he said in a video interview.
Dr. Touma said he hopes that the apparent efficacy of an easy-to-use screening tool like MoCA will help boost appreciation for the high prevalence of cognitive impairment in SLE patients. He suggested that clinicians screen for cognitive impairment as soon as SLE is diagnosed and that they perform follow-up screening during subsequent patient encounters with SLE patients who initially present without cognitive impairment.
Dr. Touma had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
ROME – The Montreal Cognitive Assessment provides a quick and easy-to-use screening tool to identify patients with systemic lupus erythematosus with cognitive impairment, Dr. Zahi Touma reported in a poster at the European Congress of Rheumatology.
In a consecutive series of 78 patients screened with the Montreal Cognitive Assessment (MoCA), the free, single-page test, which can be administered in about 10 minutes, showed a sensitivity of 69% and specificity of 68%, compared with the current standard, the Hopkins Verbal Learning Test-Revised, said Dr. Touma, a rheumatologist at the University of Toronto.
Other easy-to-use and quick screening tools, such as the Mini-Mental State Examination, had substantially worse performance in the study. He and his associates found a sensitivity of 21% and specificity of 91% using the Mini-Mental State exam. For screening, higher sensitivity is desirable so that fewer patients with potential cognitive impairment are missed, he noted.
“Ease of use and time needed for assessment as well as appropriate psychometric properties make the MoCA the preferential screening test for cognitive impairment in patients with SLE,” Dr. Touma said in his poster.
Cognitive impairment is very common among patients with systemic lupus erythematosus (SLE). In this study, Dr Touma found a 47% prevalence using MoCA. Cognitive impairment, however, often goes unidentified in SLE patients, likely because of lack of awareness among rheumatologists as well as the absence of a quick and easily administered screening tool, he said in a video interview.
Dr. Touma said he hopes that the apparent efficacy of an easy-to-use screening tool like MoCA will help boost appreciation for the high prevalence of cognitive impairment in SLE patients. He suggested that clinicians screen for cognitive impairment as soon as SLE is diagnosed and that they perform follow-up screening during subsequent patient encounters with SLE patients who initially present without cognitive impairment.
Dr. Touma had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
AT THE EULAR 2015 CONGRESS
Product News: 06 2015
Intensive Eye Treatment
Niadyne, Incorporated, introduces the NIA24 Intensive Eye Treatment, a dual-phase, predosed, multiaction eye mask to reduce the look of fine lines, wrinkles, and dark circles. The treatment begins with the aesthetician combining the predosed treatment base with the activating powder just prior to use. Once combined, the activated components are applied around the eye area. The Intensive Eye Treatment contains Pro-Niacin to help stimulate skin barrier repair, improve cell turnover, and energize skin. Haloxyl tripeptide complex decreases the red and blue color of dark circles under the eyes and acts as an anti-inflammatory agent. Lumispheres skin brightener diminishes the appearance of fine lines. Other ingredients firm and tighten skin, while reducing undereye bags and puffiness. The Intensive Eye Treatment is a professional treatment that is available exclusively through physicians. For more information, visit www.nia24.com/professional-treatments/.
Kybella Injection
Kythera Biopharmaceuticals announces US Food and Drug Administration approval of Kybella (deoxycholic acid), also known as ATX-101, a nonsurgical treatment indicated for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults. Kybella is administered by injections into the fat under the chin, which causes destruction of fat cells. Once destroyed, those cells cannot store or accumulate fat. Each in-office treatment session is typically 15 to 20 minutes, and up to 6 treatments may be administered. Many patients experience visible results in 2 to 4 treatments. Once the aesthetic response is achieved, re-treatment is not expected. Kybella physician training programs will be initiated in late summer. For more information, visit www.mykybella.com.
Sun Shield Broad Spectrum Matte Sunscreen Lotion
Obagi Medical Products, Inc, a division of Valeant Pharmaceuticals North America LLC, introduces the Sun Shield Broad Spectrum Matte SPF 50 Sunscreen Lotion. It combines UVB absorption and UVA protection with a completely sheer application. It contains 10.5% zinc oxide and 7.5% octinoxate. The Sun Shield Broad Spectrum Matte Sunscreen Lotion is ideal for use on all skin types and is physician dispensed. For more information, visit www.obagi.com.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at [email protected].
Intensive Eye Treatment
Niadyne, Incorporated, introduces the NIA24 Intensive Eye Treatment, a dual-phase, predosed, multiaction eye mask to reduce the look of fine lines, wrinkles, and dark circles. The treatment begins with the aesthetician combining the predosed treatment base with the activating powder just prior to use. Once combined, the activated components are applied around the eye area. The Intensive Eye Treatment contains Pro-Niacin to help stimulate skin barrier repair, improve cell turnover, and energize skin. Haloxyl tripeptide complex decreases the red and blue color of dark circles under the eyes and acts as an anti-inflammatory agent. Lumispheres skin brightener diminishes the appearance of fine lines. Other ingredients firm and tighten skin, while reducing undereye bags and puffiness. The Intensive Eye Treatment is a professional treatment that is available exclusively through physicians. For more information, visit www.nia24.com/professional-treatments/.
Kybella Injection
Kythera Biopharmaceuticals announces US Food and Drug Administration approval of Kybella (deoxycholic acid), also known as ATX-101, a nonsurgical treatment indicated for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults. Kybella is administered by injections into the fat under the chin, which causes destruction of fat cells. Once destroyed, those cells cannot store or accumulate fat. Each in-office treatment session is typically 15 to 20 minutes, and up to 6 treatments may be administered. Many patients experience visible results in 2 to 4 treatments. Once the aesthetic response is achieved, re-treatment is not expected. Kybella physician training programs will be initiated in late summer. For more information, visit www.mykybella.com.
Sun Shield Broad Spectrum Matte Sunscreen Lotion
Obagi Medical Products, Inc, a division of Valeant Pharmaceuticals North America LLC, introduces the Sun Shield Broad Spectrum Matte SPF 50 Sunscreen Lotion. It combines UVB absorption and UVA protection with a completely sheer application. It contains 10.5% zinc oxide and 7.5% octinoxate. The Sun Shield Broad Spectrum Matte Sunscreen Lotion is ideal for use on all skin types and is physician dispensed. For more information, visit www.obagi.com.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at [email protected].
Intensive Eye Treatment
Niadyne, Incorporated, introduces the NIA24 Intensive Eye Treatment, a dual-phase, predosed, multiaction eye mask to reduce the look of fine lines, wrinkles, and dark circles. The treatment begins with the aesthetician combining the predosed treatment base with the activating powder just prior to use. Once combined, the activated components are applied around the eye area. The Intensive Eye Treatment contains Pro-Niacin to help stimulate skin barrier repair, improve cell turnover, and energize skin. Haloxyl tripeptide complex decreases the red and blue color of dark circles under the eyes and acts as an anti-inflammatory agent. Lumispheres skin brightener diminishes the appearance of fine lines. Other ingredients firm and tighten skin, while reducing undereye bags and puffiness. The Intensive Eye Treatment is a professional treatment that is available exclusively through physicians. For more information, visit www.nia24.com/professional-treatments/.
Kybella Injection
Kythera Biopharmaceuticals announces US Food and Drug Administration approval of Kybella (deoxycholic acid), also known as ATX-101, a nonsurgical treatment indicated for improvement in the appearance of moderate to severe convexity or fullness associated with submental fat in adults. Kybella is administered by injections into the fat under the chin, which causes destruction of fat cells. Once destroyed, those cells cannot store or accumulate fat. Each in-office treatment session is typically 15 to 20 minutes, and up to 6 treatments may be administered. Many patients experience visible results in 2 to 4 treatments. Once the aesthetic response is achieved, re-treatment is not expected. Kybella physician training programs will be initiated in late summer. For more information, visit www.mykybella.com.
Sun Shield Broad Spectrum Matte Sunscreen Lotion
Obagi Medical Products, Inc, a division of Valeant Pharmaceuticals North America LLC, introduces the Sun Shield Broad Spectrum Matte SPF 50 Sunscreen Lotion. It combines UVB absorption and UVA protection with a completely sheer application. It contains 10.5% zinc oxide and 7.5% octinoxate. The Sun Shield Broad Spectrum Matte Sunscreen Lotion is ideal for use on all skin types and is physician dispensed. For more information, visit www.obagi.com.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at [email protected].

{kind=link}