User login
ASCO: Trial highlights cognitive toll of adjuvant whole-brain radiation
CHICAGO – Patients with limited brain metastases treated with radiosurgery have a higher risk of cognitive decline if they then undergo whole-brain radiation therapy, researchers reported at the annual meeting of the American Society of Clinical Oncology.
The phase III North Central Cancer Treatment Group (NCCTG)/Alliance trial also found that although whole-brain radiation therapy (WBRT) roughly halved the likelihood of progression in the brain, it did not prolong survival. And quality of life was worse with its use as well.

“We recommend initial treatment with stereotactic radiation alone and close monitoring in order to better preserve cognitive function, and then reserving whole-brain radiation until the time of symptomatic progression,” senior study author Dr. Jan C. Buckner, professor of oncology at the Mayo Clinic, Rochester, Minnesota, said in a press briefing.
He ticked off a list of alternative approaches for avoiding cognitive problems in general for patients with brain tumors: “If at all possible, use either no radiation, low-dose radiation, hippocampal-sparing radiation, or a combination of radiation and memantine as a way to reduce the risk of cognitive decline because essentially, the brain does not like to be radiated.”
ASCO expert Dr. Brian Michael Alexander said, “This scenario is a pretty complex one, and one that I take a lot of time talking to my patients about.” The disconnect between local control and survival with whole-brain radiation may be due to the availability of very good salvage therapies when brain metastases recur (so that recurrence is irrelevant) or a situation wherein progressive disease outside the brain is driving mortality, he proposed.

“If [the latter] is more of the answer, then … the population of patients who are unlikely to have deaths from progression of disease outside the brain may be the only place where you find a benefit for whole-brain radiation therapy,” according to Dr. Alexander, who is also Disease Center Leader of Radiation Oncology and a physician with the Center for Neuro-Oncology at the Dana-Farber Cancer Institute, and an assistant professor of Radiation Oncology at Harvard Medical School, both in Boston.
Given the totality of data today on the risks and benefits of this therapy, “I think the burden of proof is now switched, to say, can we prove that whole-brain radiation therapy is beneficial in a subset of patients?” he maintained, adding that the calculus may be changing with better systemic therapies, such as targeted agents for lung cancer, that may reduce brain metastases.
In their National Institutes of Health–funded trial, Dr. Buckner and colleagues studied 213 adults who had one to three cerebral metastases measuring up to 3 cm in diameter. They were randomly assigned to receive radiosurgery alone or radiosurgery followed by WBRT. Cognitive progression, the trial’s primary endpoint, was assessed with a battery of tests.
With a median follow-up of 7.2 months, the 3-month rate of cognitive progression, defined as a decline of greater than one standard deviation from baseline in any of the six tests used, was 92% in the WBRT group and 64% in the control group (P = .0007). Specifically, the former were more likely to experience declines in immediate recall (30% vs. 8%), delayed recall (51% vs. 20%), and verbal fluency (19% vs. 2%).
The overall difference in cognitive decline persisted at 6 months and there was additionally a trend at 12 months among the small subset of patients still alive. The WBRT group also had significantly worse scores for patient-reported quality of life.
The 3-month rate of failure in the central nervous system was lower for the patients given WBRT (6% vs. 25%, P less than .0001), but overall survival did not differ significantly between groups, either in the entire population or in subgroups. “In spite of imaging evidence of disease control, there was no overall impact on survival in these patients as they died of other causes,” reported Dr. Buckner.
In the session where the results were presented, invited discussant Dr. Andrew B. Lassman, the John Harris Associate Professor of Neurology and the Chief of Neuro-oncology at Columbia University Medical Center, New York, said, “I think there are other interpretations [of the findings] when placing this study in the context of other trials for brain metastases.”
“First, whole-brain radiotherapy does increase survival in the appropriate context. Second, deferring whole-brain radiotherapy leads to more rapid and more numerous recurrences of brain metastases, which also cause neurocognitive injury,” he elaborated. “Accordingly, whole-brain radiotherapy should be used in selected cases when brain metastases are a life-limiting site of disease. This is a form of precision medicine.”
Adequate assessment of any survival benefit of this therapy requires appropriate patient selection, Dr. Lassman maintained. Therefore, ongoing analysis of the trial’s results according to patients’ graded prognostic assessment (GPA) scores are eagerly awaited.
“Whole-brain radiotherapy remains a useful tool in the appropriate context that should not be discarded, but it is a crude tool with significant toxicities that is now over 60 years old. Refinements and new approaches are needed and in development,” he concluded.
Dr. Buckner disclosed that he has a consulting or advisory role with Merck Serono and is provided with travel, accommodations, and expenses by Genentech/Roche. The trial was funded by the National Institutes of Health.
CHICAGO – Patients with limited brain metastases treated with radiosurgery have a higher risk of cognitive decline if they then undergo whole-brain radiation therapy, researchers reported at the annual meeting of the American Society of Clinical Oncology.
The phase III North Central Cancer Treatment Group (NCCTG)/Alliance trial also found that although whole-brain radiation therapy (WBRT) roughly halved the likelihood of progression in the brain, it did not prolong survival. And quality of life was worse with its use as well.
“We recommend initial treatment with stereotactic radiation alone and close monitoring in order to better preserve cognitive function, and then reserving whole-brain radiation until the time of symptomatic progression,” senior study author Dr. Jan C. Buckner, professor of oncology at the Mayo Clinic, Rochester, Minnesota, said in a press briefing.
He ticked off a list of alternative approaches for avoiding cognitive problems in general for patients with brain tumors: “If at all possible, use either no radiation, low-dose radiation, hippocampal-sparing radiation, or a combination of radiation and memantine as a way to reduce the risk of cognitive decline because essentially, the brain does not like to be radiated.”
ASCO expert Dr. Brian Michael Alexander said, “This scenario is a pretty complex one, and one that I take a lot of time talking to my patients about.” The disconnect between local control and survival with whole-brain radiation may be due to the availability of very good salvage therapies when brain metastases recur (so that recurrence is irrelevant) or a situation wherein progressive disease outside the brain is driving mortality, he proposed.
“If [the latter] is more of the answer, then … the population of patients who are unlikely to have deaths from progression of disease outside the brain may be the only place where you find a benefit for whole-brain radiation therapy,” according to Dr. Alexander, who is also Disease Center Leader of Radiation Oncology and a physician with the Center for Neuro-Oncology at the Dana-Farber Cancer Institute, and an assistant professor of Radiation Oncology at Harvard Medical School, both in Boston.
Given the totality of data today on the risks and benefits of this therapy, “I think the burden of proof is now switched, to say, can we prove that whole-brain radiation therapy is beneficial in a subset of patients?” he maintained, adding that the calculus may be changing with better systemic therapies, such as targeted agents for lung cancer, that may reduce brain metastases.
In their National Institutes of Health–funded trial, Dr. Buckner and colleagues studied 213 adults who had one to three cerebral metastases measuring up to 3 cm in diameter. They were randomly assigned to receive radiosurgery alone or radiosurgery followed by WBRT. Cognitive progression, the trial’s primary endpoint, was assessed with a battery of tests.
With a median follow-up of 7.2 months, the 3-month rate of cognitive progression, defined as a decline of greater than one standard deviation from baseline in any of the six tests used, was 92% in the WBRT group and 64% in the control group (P = .0007). Specifically, the former were more likely to experience declines in immediate recall (30% vs. 8%), delayed recall (51% vs. 20%), and verbal fluency (19% vs. 2%).
The overall difference in cognitive decline persisted at 6 months and there was additionally a trend at 12 months among the small subset of patients still alive. The WBRT group also had significantly worse scores for patient-reported quality of life.
The 3-month rate of failure in the central nervous system was lower for the patients given WBRT (6% vs. 25%, P less than .0001), but overall survival did not differ significantly between groups, either in the entire population or in subgroups. “In spite of imaging evidence of disease control, there was no overall impact on survival in these patients as they died of other causes,” reported Dr. Buckner.
In the session where the results were presented, invited discussant Dr. Andrew B. Lassman, the John Harris Associate Professor of Neurology and the Chief of Neuro-oncology at Columbia University Medical Center, New York, said, “I think there are other interpretations [of the findings] when placing this study in the context of other trials for brain metastases.”
“First, whole-brain radiotherapy does increase survival in the appropriate context. Second, deferring whole-brain radiotherapy leads to more rapid and more numerous recurrences of brain metastases, which also cause neurocognitive injury,” he elaborated. “Accordingly, whole-brain radiotherapy should be used in selected cases when brain metastases are a life-limiting site of disease. This is a form of precision medicine.”
Adequate assessment of any survival benefit of this therapy requires appropriate patient selection, Dr. Lassman maintained. Therefore, ongoing analysis of the trial’s results according to patients’ graded prognostic assessment (GPA) scores are eagerly awaited.
“Whole-brain radiotherapy remains a useful tool in the appropriate context that should not be discarded, but it is a crude tool with significant toxicities that is now over 60 years old. Refinements and new approaches are needed and in development,” he concluded.
Dr. Buckner disclosed that he has a consulting or advisory role with Merck Serono and is provided with travel, accommodations, and expenses by Genentech/Roche. The trial was funded by the National Institutes of Health.
CHICAGO – Patients with limited brain metastases treated with radiosurgery have a higher risk of cognitive decline if they then undergo whole-brain radiation therapy, researchers reported at the annual meeting of the American Society of Clinical Oncology.
The phase III North Central Cancer Treatment Group (NCCTG)/Alliance trial also found that although whole-brain radiation therapy (WBRT) roughly halved the likelihood of progression in the brain, it did not prolong survival. And quality of life was worse with its use as well.
“We recommend initial treatment with stereotactic radiation alone and close monitoring in order to better preserve cognitive function, and then reserving whole-brain radiation until the time of symptomatic progression,” senior study author Dr. Jan C. Buckner, professor of oncology at the Mayo Clinic, Rochester, Minnesota, said in a press briefing.
He ticked off a list of alternative approaches for avoiding cognitive problems in general for patients with brain tumors: “If at all possible, use either no radiation, low-dose radiation, hippocampal-sparing radiation, or a combination of radiation and memantine as a way to reduce the risk of cognitive decline because essentially, the brain does not like to be radiated.”
ASCO expert Dr. Brian Michael Alexander said, “This scenario is a pretty complex one, and one that I take a lot of time talking to my patients about.” The disconnect between local control and survival with whole-brain radiation may be due to the availability of very good salvage therapies when brain metastases recur (so that recurrence is irrelevant) or a situation wherein progressive disease outside the brain is driving mortality, he proposed.
“If [the latter] is more of the answer, then … the population of patients who are unlikely to have deaths from progression of disease outside the brain may be the only place where you find a benefit for whole-brain radiation therapy,” according to Dr. Alexander, who is also Disease Center Leader of Radiation Oncology and a physician with the Center for Neuro-Oncology at the Dana-Farber Cancer Institute, and an assistant professor of Radiation Oncology at Harvard Medical School, both in Boston.
Given the totality of data today on the risks and benefits of this therapy, “I think the burden of proof is now switched, to say, can we prove that whole-brain radiation therapy is beneficial in a subset of patients?” he maintained, adding that the calculus may be changing with better systemic therapies, such as targeted agents for lung cancer, that may reduce brain metastases.
In their National Institutes of Health–funded trial, Dr. Buckner and colleagues studied 213 adults who had one to three cerebral metastases measuring up to 3 cm in diameter. They were randomly assigned to receive radiosurgery alone or radiosurgery followed by WBRT. Cognitive progression, the trial’s primary endpoint, was assessed with a battery of tests.
With a median follow-up of 7.2 months, the 3-month rate of cognitive progression, defined as a decline of greater than one standard deviation from baseline in any of the six tests used, was 92% in the WBRT group and 64% in the control group (P = .0007). Specifically, the former were more likely to experience declines in immediate recall (30% vs. 8%), delayed recall (51% vs. 20%), and verbal fluency (19% vs. 2%).
The overall difference in cognitive decline persisted at 6 months and there was additionally a trend at 12 months among the small subset of patients still alive. The WBRT group also had significantly worse scores for patient-reported quality of life.
The 3-month rate of failure in the central nervous system was lower for the patients given WBRT (6% vs. 25%, P less than .0001), but overall survival did not differ significantly between groups, either in the entire population or in subgroups. “In spite of imaging evidence of disease control, there was no overall impact on survival in these patients as they died of other causes,” reported Dr. Buckner.
In the session where the results were presented, invited discussant Dr. Andrew B. Lassman, the John Harris Associate Professor of Neurology and the Chief of Neuro-oncology at Columbia University Medical Center, New York, said, “I think there are other interpretations [of the findings] when placing this study in the context of other trials for brain metastases.”
“First, whole-brain radiotherapy does increase survival in the appropriate context. Second, deferring whole-brain radiotherapy leads to more rapid and more numerous recurrences of brain metastases, which also cause neurocognitive injury,” he elaborated. “Accordingly, whole-brain radiotherapy should be used in selected cases when brain metastases are a life-limiting site of disease. This is a form of precision medicine.”
Adequate assessment of any survival benefit of this therapy requires appropriate patient selection, Dr. Lassman maintained. Therefore, ongoing analysis of the trial’s results according to patients’ graded prognostic assessment (GPA) scores are eagerly awaited.
“Whole-brain radiotherapy remains a useful tool in the appropriate context that should not be discarded, but it is a crude tool with significant toxicities that is now over 60 years old. Refinements and new approaches are needed and in development,” he concluded.
Dr. Buckner disclosed that he has a consulting or advisory role with Merck Serono and is provided with travel, accommodations, and expenses by Genentech/Roche. The trial was funded by the National Institutes of Health.
AT THE ASCO ANNUAL MEETING 2015
Key clinical point: Adding whole-brain radiation after radiosurgery increases the risk of cognitive decline in patients with limited brain metastases.
Major finding: Patients were more likely to experience cognitive decline if they received WBRT after radiosurgery vs. radiosurgery alone (92% vs. 64%).
Data source: A randomized phase III trial among 213 patients with one to three small brain metastases.
Disclosures: Dr. Buckner disclosed that he has a consulting or advisory role with Merck Serono and is provided with travel, accommodations, and expenses by Genentech/Roche. The trial was funded by the National Institutes of Health.

Drug prolongs PFS in indolent, refractory NHL

the 2015 ASCO Annual Meeting
CHICAGO—Adding obinutuzumab to treatment with bendamustine improves progression-free survival (PFS) in patients with rituximab-refractory, indolent non-Hodgkin lymphoma (NHL), interim results of the phase 3 GADOLIN trial suggest.
Study investigators said patients who received obinutuzumab and bendamustine followed by obinutuzumab maintenance had roughly double the PFS of patients who received bendamustine alone.
There was no significant difference between the treatment groups with regard to response rates or overall survival (OS), but the investigators said longer follow-up is needed to determine if obinutuzumab confers a benefit in OS.
This trial was stopped before its protocol-specified final analysis because of the PFS benefit observed in the obinutuzumab arm.
Laurie Sehn, MD, of the BC Cancer Agency in Vancouver, Canada, presented these results at the 2015 ASCO Annual Meeting (abstract LBA8502). Genentech Inc. and F. Hoffmann-La Roche Ltd. funded this research.
The trial included 413 patients with rituximab-refractory NHL, including follicular lymphoma (FL), marginal zone lymphoma (MZL), small lymphocytic lymphoma (SLL), and Waldenstrom’s macroglobulinemia (WM).
The patients were randomized to receive bendamustine alone (120 mg/m2/day on days 1 and 2 for up to six 28-day cycles) or a combination of bendamustine (90 mg/m2/day on days 1 and 2 for up to six 28-day cycles) plus obinutuzumab (1000 mg on days 1, 8, and 15 for cycle 1, followed by 1 dose for up to six 28-day cycles), followed by obinutuzumab maintenance (1000 mg every 2 months for 2 years or until progression).
Dr Sehn said there were no significant differences in baseline characteristics between the treatment arms. Patients in both arms had received a median of 2 prior treatments, and the median time from last treatment was about 4 months.
Of the 194 patients randomized to treatment in the obinutuzumab-bendamustine (OB) arm, 79.9% had FL, 13.9% had MZL, and 6.2% had SLL. Of the 202 patients randomized to the bendamustine-alone (control) arm, 82.2% had FL, 9.4% had MZL, 7.9% had SLL, and 0.5% had WM.
Ultimately, 156 patients completed induction in the OB arm, as did 129 patients in the control arm. Thirty-six patients completed maintenance with obinutuzumab, and 46 were still receiving maintenance at the time of analysis.
Safety results
Dr Sehn said there were no unexpected safety signals among patients in the OB arm.
About 99% of patients in the OB arm experienced at least 1 adverse event (AE), as did 98% of patients in the control arm. Severe AEs occurred in 38.1% and 32.8% of patients, respectively, and grade 3/4 AEs occurred in 67% and 62.1%, respectively.
AEs leading to treatment withdrawal occurred in 18% and 15.7% of patients, respectively. And AEs leading to death occurred in 6.2% and 6.1%, respectively.
Grade 3/4 AEs that occurred in at least 2% of patients in the OB and control arms, respectively, were neutropenia (33% vs 26.3%), thrombocytopenia (10.8% vs 16.2%), infusion-related reactions (10.8% vs 5.6%), anemia (7.7% vs 10.1%), febrile neutropenia (4.6% vs 3.5%), nausea (1% vs 3%), fatigue (1.5% vs 2.5%), diarrhea (1% vs 2.5%), and vomiting (2.1% vs 1%).
Response and survival
According to an independent radiology facility, 69.2% of patients in the OB arm had responded to treatment at the end of induction, as had 63% of the control arm. The best overall response by the 12-month mark was 78.7% and 76.6%, respectively.
The median follow-up was 21 months. At that point, the median PFS had not been reached in the OB arm but was 14.9 months in the control arm (P<0.0001), according to the independent radiology facility.
According to investigators, the median PFS was 29.2 months and 14 months, respectively (P<0.0001).
The median OS has not been reached in either arm (P=0.4017). Thirty-four patients (18%) in the OB arm died, as did 41 (20%) in the control arm.
Dr Sehn said longer follow-up is needed to determine the potential OS benefit associated with obinutuzumab, but the PFS benefit of OB is clinically meaningful.
“The fact that this new approach doubled average remission time marks a major step forward for our patients,” she said. “Obinutuzumab may offer patients the chance to stay well for a significantly longer period of time, putting off the need for additional chemotherapy.” ![]()
the 2015 ASCO Annual Meeting
CHICAGO—Adding obinutuzumab to treatment with bendamustine improves progression-free survival (PFS) in patients with rituximab-refractory, indolent non-Hodgkin lymphoma (NHL), interim results of the phase 3 GADOLIN trial suggest.
Study investigators said patients who received obinutuzumab and bendamustine followed by obinutuzumab maintenance had roughly double the PFS of patients who received bendamustine alone.
There was no significant difference between the treatment groups with regard to response rates or overall survival (OS), but the investigators said longer follow-up is needed to determine if obinutuzumab confers a benefit in OS.
This trial was stopped before its protocol-specified final analysis because of the PFS benefit observed in the obinutuzumab arm.
Laurie Sehn, MD, of the BC Cancer Agency in Vancouver, Canada, presented these results at the 2015 ASCO Annual Meeting (abstract LBA8502). Genentech Inc. and F. Hoffmann-La Roche Ltd. funded this research.
The trial included 413 patients with rituximab-refractory NHL, including follicular lymphoma (FL), marginal zone lymphoma (MZL), small lymphocytic lymphoma (SLL), and Waldenstrom’s macroglobulinemia (WM).
The patients were randomized to receive bendamustine alone (120 mg/m2/day on days 1 and 2 for up to six 28-day cycles) or a combination of bendamustine (90 mg/m2/day on days 1 and 2 for up to six 28-day cycles) plus obinutuzumab (1000 mg on days 1, 8, and 15 for cycle 1, followed by 1 dose for up to six 28-day cycles), followed by obinutuzumab maintenance (1000 mg every 2 months for 2 years or until progression).
Dr Sehn said there were no significant differences in baseline characteristics between the treatment arms. Patients in both arms had received a median of 2 prior treatments, and the median time from last treatment was about 4 months.
Of the 194 patients randomized to treatment in the obinutuzumab-bendamustine (OB) arm, 79.9% had FL, 13.9% had MZL, and 6.2% had SLL. Of the 202 patients randomized to the bendamustine-alone (control) arm, 82.2% had FL, 9.4% had MZL, 7.9% had SLL, and 0.5% had WM.
Ultimately, 156 patients completed induction in the OB arm, as did 129 patients in the control arm. Thirty-six patients completed maintenance with obinutuzumab, and 46 were still receiving maintenance at the time of analysis.
Safety results
Dr Sehn said there were no unexpected safety signals among patients in the OB arm.
About 99% of patients in the OB arm experienced at least 1 adverse event (AE), as did 98% of patients in the control arm. Severe AEs occurred in 38.1% and 32.8% of patients, respectively, and grade 3/4 AEs occurred in 67% and 62.1%, respectively.
AEs leading to treatment withdrawal occurred in 18% and 15.7% of patients, respectively. And AEs leading to death occurred in 6.2% and 6.1%, respectively.
Grade 3/4 AEs that occurred in at least 2% of patients in the OB and control arms, respectively, were neutropenia (33% vs 26.3%), thrombocytopenia (10.8% vs 16.2%), infusion-related reactions (10.8% vs 5.6%), anemia (7.7% vs 10.1%), febrile neutropenia (4.6% vs 3.5%), nausea (1% vs 3%), fatigue (1.5% vs 2.5%), diarrhea (1% vs 2.5%), and vomiting (2.1% vs 1%).
Response and survival
According to an independent radiology facility, 69.2% of patients in the OB arm had responded to treatment at the end of induction, as had 63% of the control arm. The best overall response by the 12-month mark was 78.7% and 76.6%, respectively.
The median follow-up was 21 months. At that point, the median PFS had not been reached in the OB arm but was 14.9 months in the control arm (P<0.0001), according to the independent radiology facility.
According to investigators, the median PFS was 29.2 months and 14 months, respectively (P<0.0001).
The median OS has not been reached in either arm (P=0.4017). Thirty-four patients (18%) in the OB arm died, as did 41 (20%) in the control arm.
Dr Sehn said longer follow-up is needed to determine the potential OS benefit associated with obinutuzumab, but the PFS benefit of OB is clinically meaningful.
“The fact that this new approach doubled average remission time marks a major step forward for our patients,” she said. “Obinutuzumab may offer patients the chance to stay well for a significantly longer period of time, putting off the need for additional chemotherapy.” ![]()
the 2015 ASCO Annual Meeting
CHICAGO—Adding obinutuzumab to treatment with bendamustine improves progression-free survival (PFS) in patients with rituximab-refractory, indolent non-Hodgkin lymphoma (NHL), interim results of the phase 3 GADOLIN trial suggest.
Study investigators said patients who received obinutuzumab and bendamustine followed by obinutuzumab maintenance had roughly double the PFS of patients who received bendamustine alone.
There was no significant difference between the treatment groups with regard to response rates or overall survival (OS), but the investigators said longer follow-up is needed to determine if obinutuzumab confers a benefit in OS.
This trial was stopped before its protocol-specified final analysis because of the PFS benefit observed in the obinutuzumab arm.
Laurie Sehn, MD, of the BC Cancer Agency in Vancouver, Canada, presented these results at the 2015 ASCO Annual Meeting (abstract LBA8502). Genentech Inc. and F. Hoffmann-La Roche Ltd. funded this research.
The trial included 413 patients with rituximab-refractory NHL, including follicular lymphoma (FL), marginal zone lymphoma (MZL), small lymphocytic lymphoma (SLL), and Waldenstrom’s macroglobulinemia (WM).
The patients were randomized to receive bendamustine alone (120 mg/m2/day on days 1 and 2 for up to six 28-day cycles) or a combination of bendamustine (90 mg/m2/day on days 1 and 2 for up to six 28-day cycles) plus obinutuzumab (1000 mg on days 1, 8, and 15 for cycle 1, followed by 1 dose for up to six 28-day cycles), followed by obinutuzumab maintenance (1000 mg every 2 months for 2 years or until progression).
Dr Sehn said there were no significant differences in baseline characteristics between the treatment arms. Patients in both arms had received a median of 2 prior treatments, and the median time from last treatment was about 4 months.
Of the 194 patients randomized to treatment in the obinutuzumab-bendamustine (OB) arm, 79.9% had FL, 13.9% had MZL, and 6.2% had SLL. Of the 202 patients randomized to the bendamustine-alone (control) arm, 82.2% had FL, 9.4% had MZL, 7.9% had SLL, and 0.5% had WM.
Ultimately, 156 patients completed induction in the OB arm, as did 129 patients in the control arm. Thirty-six patients completed maintenance with obinutuzumab, and 46 were still receiving maintenance at the time of analysis.
Safety results
Dr Sehn said there were no unexpected safety signals among patients in the OB arm.
About 99% of patients in the OB arm experienced at least 1 adverse event (AE), as did 98% of patients in the control arm. Severe AEs occurred in 38.1% and 32.8% of patients, respectively, and grade 3/4 AEs occurred in 67% and 62.1%, respectively.
AEs leading to treatment withdrawal occurred in 18% and 15.7% of patients, respectively. And AEs leading to death occurred in 6.2% and 6.1%, respectively.
Grade 3/4 AEs that occurred in at least 2% of patients in the OB and control arms, respectively, were neutropenia (33% vs 26.3%), thrombocytopenia (10.8% vs 16.2%), infusion-related reactions (10.8% vs 5.6%), anemia (7.7% vs 10.1%), febrile neutropenia (4.6% vs 3.5%), nausea (1% vs 3%), fatigue (1.5% vs 2.5%), diarrhea (1% vs 2.5%), and vomiting (2.1% vs 1%).
Response and survival
According to an independent radiology facility, 69.2% of patients in the OB arm had responded to treatment at the end of induction, as had 63% of the control arm. The best overall response by the 12-month mark was 78.7% and 76.6%, respectively.
The median follow-up was 21 months. At that point, the median PFS had not been reached in the OB arm but was 14.9 months in the control arm (P<0.0001), according to the independent radiology facility.
According to investigators, the median PFS was 29.2 months and 14 months, respectively (P<0.0001).
The median OS has not been reached in either arm (P=0.4017). Thirty-four patients (18%) in the OB arm died, as did 41 (20%) in the control arm.
Dr Sehn said longer follow-up is needed to determine the potential OS benefit associated with obinutuzumab, but the PFS benefit of OB is clinically meaningful.
“The fact that this new approach doubled average remission time marks a major step forward for our patients,” she said. “Obinutuzumab may offer patients the chance to stay well for a significantly longer period of time, putting off the need for additional chemotherapy.” ![]()
Breastfeeding may lower risk of ALL

Photo by Petr Kratochvil
Breastfeeding a child may reduce his risk of developing acute lymphoblastic leukemia (ALL) but perhaps not acute myeloid leukemia (AML), according to a review published in JAMA Pediatrics.
Researchers found that breastfeeding a child for 6 months or longer was associated with a 19% lower risk of childhood leukemia, compared with no
breastfeeding or breastfeeding for a shorter period of time.
And children who were breastfed for any amount of time had an 11% lower risk of childhood leukemia than children who were never breastfed.
However, when the researchers analyzed studies of ALL and AML separately, they found that breastfeeding was not associated with a significantly lower risk of AML.
Efrat L. Amitay, PhD, and Lital Keinan-Boker, MD, PhD, of the University of Haifa in Israel, conducted this research.
In a review of 18 studies, the pair found that breastfeeding a child for 6 months or longer was associated with a significantly lower risk of childhood leukemia, compared with no breastfeeding or breastfeeding for a shorter period of time (odds ratio [OR]=0.81).
And a separate analysis of 15 studies showed that children who were breastfed for any amount of time had a lower risk of childhood leukemia than children who were never breastfed (OR=0.89).
The researchers also conducted meta-analyses of AML studies and ALL studies separately—11 ALL and 6 AML studies. And they found a significant inverse association between breastfeeding for 6 months or more and ALL risk (OR=0.82) but no significant association for AML risk (OR=0.74).
The researchers said several biological mechanisms may explain the association between breastfeeding and a reduced risk of childhood leukemia. However, more high-quality studies are needed to clarify those mechanisms. ![]()
Photo by Petr Kratochvil
Breastfeeding a child may reduce his risk of developing acute lymphoblastic leukemia (ALL) but perhaps not acute myeloid leukemia (AML), according to a review published in JAMA Pediatrics.
Researchers found that breastfeeding a child for 6 months or longer was associated with a 19% lower risk of childhood leukemia, compared with no
breastfeeding or breastfeeding for a shorter period of time.
And children who were breastfed for any amount of time had an 11% lower risk of childhood leukemia than children who were never breastfed.
However, when the researchers analyzed studies of ALL and AML separately, they found that breastfeeding was not associated with a significantly lower risk of AML.
Efrat L. Amitay, PhD, and Lital Keinan-Boker, MD, PhD, of the University of Haifa in Israel, conducted this research.
In a review of 18 studies, the pair found that breastfeeding a child for 6 months or longer was associated with a significantly lower risk of childhood leukemia, compared with no breastfeeding or breastfeeding for a shorter period of time (odds ratio [OR]=0.81).
And a separate analysis of 15 studies showed that children who were breastfed for any amount of time had a lower risk of childhood leukemia than children who were never breastfed (OR=0.89).
The researchers also conducted meta-analyses of AML studies and ALL studies separately—11 ALL and 6 AML studies. And they found a significant inverse association between breastfeeding for 6 months or more and ALL risk (OR=0.82) but no significant association for AML risk (OR=0.74).
The researchers said several biological mechanisms may explain the association between breastfeeding and a reduced risk of childhood leukemia. However, more high-quality studies are needed to clarify those mechanisms. ![]()
Photo by Petr Kratochvil
Breastfeeding a child may reduce his risk of developing acute lymphoblastic leukemia (ALL) but perhaps not acute myeloid leukemia (AML), according to a review published in JAMA Pediatrics.
Researchers found that breastfeeding a child for 6 months or longer was associated with a 19% lower risk of childhood leukemia, compared with no
breastfeeding or breastfeeding for a shorter period of time.
And children who were breastfed for any amount of time had an 11% lower risk of childhood leukemia than children who were never breastfed.
However, when the researchers analyzed studies of ALL and AML separately, they found that breastfeeding was not associated with a significantly lower risk of AML.
Efrat L. Amitay, PhD, and Lital Keinan-Boker, MD, PhD, of the University of Haifa in Israel, conducted this research.
In a review of 18 studies, the pair found that breastfeeding a child for 6 months or longer was associated with a significantly lower risk of childhood leukemia, compared with no breastfeeding or breastfeeding for a shorter period of time (odds ratio [OR]=0.81).
And a separate analysis of 15 studies showed that children who were breastfed for any amount of time had a lower risk of childhood leukemia than children who were never breastfed (OR=0.89).
The researchers also conducted meta-analyses of AML studies and ALL studies separately—11 ALL and 6 AML studies. And they found a significant inverse association between breastfeeding for 6 months or more and ALL risk (OR=0.82) but no significant association for AML risk (OR=0.74).
The researchers said several biological mechanisms may explain the association between breastfeeding and a reduced risk of childhood leukemia. However, more high-quality studies are needed to clarify those mechanisms. ![]()
Newer anticoagulants may not be best for elderly, study shows
A meta-analysis of 92,816 people taking anticoagulants has shown that the risk of gastrointestinal (GI) bleeding related to the newer oral anticoagulants dabigatran and rivaroxaban is similar to that for warfarin.
But for patients older than 65, the risk of GI bleeding increases. By age 76, the risk may be 3 to 5 times higher when taking the newer anticoagulants compared to warfarin.
These findings were published in BMJ.
“The new anticoagulants have really been popular with patients who have previously only had one choice of oral anticoagulant,” said study author Neena S. Abraham, MD, of the Mayo Clinic in Scottsdale, Arizona.
“However, they may not be the right choice for everyone. Our findings definitely point toward important age-related risk that merit consideration when doctors are making treatment recommendations.”
Dr Abraham and her colleagues compared the risk of GI bleeding with newer anticoagulants and warfarin using national data available on privately insured patients and Medicare Advantage enrollees from the Optum Labs Data Warehouse.
Data on apixaban were not included in the study because there were too few patients prescribed apixaban in the dataset during the period of observation, from November 1, 2010, to September 30, 2013.
The cohort included 8578 (9.2%) patients on dabigatran, 16,253 (17.5%) on rivaroxaban, and 67,985 (73.2%) on warfarin. Patients were 18 years of age or older.
The researchers found that, among atrial fibrillation (AF) patients older than 75, the risk of GI bleeding was higher than with warfarin. The hazard ratios (HRs) were 2.49 (95% confidence interval [CI] 1.61 to 3.83) and 1.62 (95% CI 1.02 to 2.58), respectively.
However, among older patients without AF, the risk of GI bleeding was comparable with dabigatran and warfarin. The HRs were 1.56 (95% CI 0.42 to 5.80) and 2.73 (95% CI 0.83 to 8.94), respectively.
Older AF patients taking rivaroxaban had an increased risk of GI bleeding compared to patients taking warfarin. The HRs were 2.91 (95% CI 1.65 to 4.81) and 2.05 (95% CI 1.17 to 3.59), respectively.
And older patients without AF had an increased risk of GI bleeding with rivaroxaban compared to warfarin. The HRs were 4.58 (95% CI 2.40 to 8.72) and 4.40 (95% CI 2.43 to 7.96), respectively.
The researchers also found that, for those patients under 65, the newer agents seemed to confer a lower risk of GI bleeding than warfarin. ![]()
A meta-analysis of 92,816 people taking anticoagulants has shown that the risk of gastrointestinal (GI) bleeding related to the newer oral anticoagulants dabigatran and rivaroxaban is similar to that for warfarin.
But for patients older than 65, the risk of GI bleeding increases. By age 76, the risk may be 3 to 5 times higher when taking the newer anticoagulants compared to warfarin.
These findings were published in BMJ.
“The new anticoagulants have really been popular with patients who have previously only had one choice of oral anticoagulant,” said study author Neena S. Abraham, MD, of the Mayo Clinic in Scottsdale, Arizona.
“However, they may not be the right choice for everyone. Our findings definitely point toward important age-related risk that merit consideration when doctors are making treatment recommendations.”
Dr Abraham and her colleagues compared the risk of GI bleeding with newer anticoagulants and warfarin using national data available on privately insured patients and Medicare Advantage enrollees from the Optum Labs Data Warehouse.
Data on apixaban were not included in the study because there were too few patients prescribed apixaban in the dataset during the period of observation, from November 1, 2010, to September 30, 2013.
The cohort included 8578 (9.2%) patients on dabigatran, 16,253 (17.5%) on rivaroxaban, and 67,985 (73.2%) on warfarin. Patients were 18 years of age or older.
The researchers found that, among atrial fibrillation (AF) patients older than 75, the risk of GI bleeding was higher than with warfarin. The hazard ratios (HRs) were 2.49 (95% confidence interval [CI] 1.61 to 3.83) and 1.62 (95% CI 1.02 to 2.58), respectively.
However, among older patients without AF, the risk of GI bleeding was comparable with dabigatran and warfarin. The HRs were 1.56 (95% CI 0.42 to 5.80) and 2.73 (95% CI 0.83 to 8.94), respectively.
Older AF patients taking rivaroxaban had an increased risk of GI bleeding compared to patients taking warfarin. The HRs were 2.91 (95% CI 1.65 to 4.81) and 2.05 (95% CI 1.17 to 3.59), respectively.
And older patients without AF had an increased risk of GI bleeding with rivaroxaban compared to warfarin. The HRs were 4.58 (95% CI 2.40 to 8.72) and 4.40 (95% CI 2.43 to 7.96), respectively.
The researchers also found that, for those patients under 65, the newer agents seemed to confer a lower risk of GI bleeding than warfarin. ![]()
A meta-analysis of 92,816 people taking anticoagulants has shown that the risk of gastrointestinal (GI) bleeding related to the newer oral anticoagulants dabigatran and rivaroxaban is similar to that for warfarin.
But for patients older than 65, the risk of GI bleeding increases. By age 76, the risk may be 3 to 5 times higher when taking the newer anticoagulants compared to warfarin.
These findings were published in BMJ.
“The new anticoagulants have really been popular with patients who have previously only had one choice of oral anticoagulant,” said study author Neena S. Abraham, MD, of the Mayo Clinic in Scottsdale, Arizona.
“However, they may not be the right choice for everyone. Our findings definitely point toward important age-related risk that merit consideration when doctors are making treatment recommendations.”
Dr Abraham and her colleagues compared the risk of GI bleeding with newer anticoagulants and warfarin using national data available on privately insured patients and Medicare Advantage enrollees from the Optum Labs Data Warehouse.
Data on apixaban were not included in the study because there were too few patients prescribed apixaban in the dataset during the period of observation, from November 1, 2010, to September 30, 2013.
The cohort included 8578 (9.2%) patients on dabigatran, 16,253 (17.5%) on rivaroxaban, and 67,985 (73.2%) on warfarin. Patients were 18 years of age or older.
The researchers found that, among atrial fibrillation (AF) patients older than 75, the risk of GI bleeding was higher than with warfarin. The hazard ratios (HRs) were 2.49 (95% confidence interval [CI] 1.61 to 3.83) and 1.62 (95% CI 1.02 to 2.58), respectively.
However, among older patients without AF, the risk of GI bleeding was comparable with dabigatran and warfarin. The HRs were 1.56 (95% CI 0.42 to 5.80) and 2.73 (95% CI 0.83 to 8.94), respectively.
Older AF patients taking rivaroxaban had an increased risk of GI bleeding compared to patients taking warfarin. The HRs were 2.91 (95% CI 1.65 to 4.81) and 2.05 (95% CI 1.17 to 3.59), respectively.
And older patients without AF had an increased risk of GI bleeding with rivaroxaban compared to warfarin. The HRs were 4.58 (95% CI 2.40 to 8.72) and 4.40 (95% CI 2.43 to 7.96), respectively.
The researchers also found that, for those patients under 65, the newer agents seemed to confer a lower risk of GI bleeding than warfarin. ![]()
Hole in Jaw Has Drained Fluid for 20 Years
ANSWER
The correct answer is all of the above (choice “d”). The patient’s actual diagnosis, sinus tract of odontogenic origin (choice “a”), will be discussed further.
Branchial cleft cyst (choice “b”) is always in the differential for neck masses, and squamous cell carcinoma (choice “c”) should always be considered in cases of nonhealing lesions—although 20 years is an unlikely timeframe for that diagnosis! Additional differential possibilities include thyroglossal duct cyst and pyogenic granuloma.
DISCUSSION
Sinus tracts of odontogenic origin, also called dentocutaneous sinus tracts, are primarily caused by periapical abscesses. As the purulent material accumulates in the confined space around the apical area, pressure increases; this sets in motion a tunneling process that terminates in an outlet, often inside the mouth but also (often enough) on the skin.
In the latter instance, known as extraoral sinus, the opening forms along the chin or submental area. In 80% of cases, the source is the mandibular teeth.
Dermocutaneous sinuses of maxillary origin, though not unknown, are decidedly unusual. They can drain anywhere on the maxilla, including around the nose. In edentulous patients, retained tooth fragments or segments of apical abscesses can act as the nidus for this process.
When a draining sinus manifests more acutely or occurs in a patient from a high-risk area (eg, Mexico or Central America), other diagnoses must be considered. These include scrofula, in which regional nymph nodes, infected by Mycobacterium tuberculosis or atypical mycobacterial organism, break down and drain. The indolent nature and chronicity of this patient’s problem effectively ruled out this diagnosis.
Culture of the fluid draining from the abscess would reveal a number of organisms (mostly of the strep family) but would not show the actual causative bacteria, since they are typically anaerobic. Biopsy of the surrounding tissue is occasionally necessary, when squamous cell carcinoma or other neoplastic process is suspected.
TREATMENT
The patient was advised to see a dentist, who will likely obtain a panoramic radiograph of her teeth, with particular attention to the affected area.
If an abscess is identified, as expected, treatment would entail root canal or extraction. The sinus tract would then heal rather quickly.
Antibiotics would be of limited use without elimination of the pocket. However, when patients complain of discomfort or outright pain, antibiotics (eg, penicillin V potassium or amoxicillin/clavulanate) can help to reduce the inflammation and offer some relief.
ANSWER
The correct answer is all of the above (choice “d”). The patient’s actual diagnosis, sinus tract of odontogenic origin (choice “a”), will be discussed further.
Branchial cleft cyst (choice “b”) is always in the differential for neck masses, and squamous cell carcinoma (choice “c”) should always be considered in cases of nonhealing lesions—although 20 years is an unlikely timeframe for that diagnosis! Additional differential possibilities include thyroglossal duct cyst and pyogenic granuloma.
DISCUSSION
Sinus tracts of odontogenic origin, also called dentocutaneous sinus tracts, are primarily caused by periapical abscesses. As the purulent material accumulates in the confined space around the apical area, pressure increases; this sets in motion a tunneling process that terminates in an outlet, often inside the mouth but also (often enough) on the skin.
In the latter instance, known as extraoral sinus, the opening forms along the chin or submental area. In 80% of cases, the source is the mandibular teeth.
Dermocutaneous sinuses of maxillary origin, though not unknown, are decidedly unusual. They can drain anywhere on the maxilla, including around the nose. In edentulous patients, retained tooth fragments or segments of apical abscesses can act as the nidus for this process.
When a draining sinus manifests more acutely or occurs in a patient from a high-risk area (eg, Mexico or Central America), other diagnoses must be considered. These include scrofula, in which regional nymph nodes, infected by Mycobacterium tuberculosis or atypical mycobacterial organism, break down and drain. The indolent nature and chronicity of this patient’s problem effectively ruled out this diagnosis.
Culture of the fluid draining from the abscess would reveal a number of organisms (mostly of the strep family) but would not show the actual causative bacteria, since they are typically anaerobic. Biopsy of the surrounding tissue is occasionally necessary, when squamous cell carcinoma or other neoplastic process is suspected.
TREATMENT
The patient was advised to see a dentist, who will likely obtain a panoramic radiograph of her teeth, with particular attention to the affected area.
If an abscess is identified, as expected, treatment would entail root canal or extraction. The sinus tract would then heal rather quickly.
Antibiotics would be of limited use without elimination of the pocket. However, when patients complain of discomfort or outright pain, antibiotics (eg, penicillin V potassium or amoxicillin/clavulanate) can help to reduce the inflammation and offer some relief.
ANSWER
The correct answer is all of the above (choice “d”). The patient’s actual diagnosis, sinus tract of odontogenic origin (choice “a”), will be discussed further.
Branchial cleft cyst (choice “b”) is always in the differential for neck masses, and squamous cell carcinoma (choice “c”) should always be considered in cases of nonhealing lesions—although 20 years is an unlikely timeframe for that diagnosis! Additional differential possibilities include thyroglossal duct cyst and pyogenic granuloma.
DISCUSSION
Sinus tracts of odontogenic origin, also called dentocutaneous sinus tracts, are primarily caused by periapical abscesses. As the purulent material accumulates in the confined space around the apical area, pressure increases; this sets in motion a tunneling process that terminates in an outlet, often inside the mouth but also (often enough) on the skin.
In the latter instance, known as extraoral sinus, the opening forms along the chin or submental area. In 80% of cases, the source is the mandibular teeth.
Dermocutaneous sinuses of maxillary origin, though not unknown, are decidedly unusual. They can drain anywhere on the maxilla, including around the nose. In edentulous patients, retained tooth fragments or segments of apical abscesses can act as the nidus for this process.
When a draining sinus manifests more acutely or occurs in a patient from a high-risk area (eg, Mexico or Central America), other diagnoses must be considered. These include scrofula, in which regional nymph nodes, infected by Mycobacterium tuberculosis or atypical mycobacterial organism, break down and drain. The indolent nature and chronicity of this patient’s problem effectively ruled out this diagnosis.
Culture of the fluid draining from the abscess would reveal a number of organisms (mostly of the strep family) but would not show the actual causative bacteria, since they are typically anaerobic. Biopsy of the surrounding tissue is occasionally necessary, when squamous cell carcinoma or other neoplastic process is suspected.
TREATMENT
The patient was advised to see a dentist, who will likely obtain a panoramic radiograph of her teeth, with particular attention to the affected area.
If an abscess is identified, as expected, treatment would entail root canal or extraction. The sinus tract would then heal rather quickly.
Antibiotics would be of limited use without elimination of the pocket. However, when patients complain of discomfort or outright pain, antibiotics (eg, penicillin V potassium or amoxicillin/clavulanate) can help to reduce the inflammation and offer some relief.

A 74-year-old woman is referred to dermatology by the primary care provider at her nursing home. She has a small hole on her left jaw that has drained foul-smelling material for more than 20 years. Although the site has never been painful, it occasionally swells and becomes slightly sensitive before slowly returning to its usual small size over a period of weeks. The patient is in generally poor health, with early dementia, chronic congestive heart failure, and diabetes. All her teeth were removed almost 30 years ago. She is afebrile and in no acute distress. On the submental aspect of her left jaw, there is a round, 6-cm area of skin that is retracted and fixed around a centrally placed sinus opening (measuring about 2 to 3 mm). A scant amount of purulent-looking fluid can be expressed from the spot. The area is faintly pink, but there is no evidence of increased warmth or tenderness on palpation.

Weighing the Options for Obesity Meds
In June 2013, the American Medical Association classified obesity as a disease. Since then, several medical societies have published guidelines to help clinicians improve care of affected patients. One avenue is, of course, pharmacologic treatment.
Until recently, there was only one FDA-approved medication for chronic weight loss on the market: orlistat, which was approved in 1999. (Phentermine and diethylpropion are only indicated for short-term use). After a long hiatus, the FDA approved two additional agents (phentermine/topiramate and lorcaserin)in 2012 and another two (liraglutide and bupropion/naltrexone) in 2014.
While clinicians appreciate having options for managing their patients’ conditions, in this case, many are overwhelmed by the choices. Most health care providers have not received formal training in obesity management. This column will attempt to fill the information gap in terms of what agents are available and what factors should be assessed before prescribing any of them.
Proviso: Experts claim obesity is a chronic disease, similar to hypertension, and should be managed as such. Although not discussed here, the most important aspect of weight loss and maintenance is lifestyle intervention (diet, exercise, and behavioral modification). It should be emphasized that no medication works by itself; all should be used as an adjunct tool to reinforce adherence to lifestyle changes.1 Furthermore, patients may be disappointed to learn that without these changes, the weight may return when they cease medication use.
CASE Deb, age 61, presents to your office for routine follow-up. She has a history of type 2 diabetes, dyslipidemia, hypertension, atrial fibrillation, depression, and chronic back pain due to a herniated disc. Her medications include insulin glargine, glyburide, pioglitazone, atorvastatin, metoprolol, paroxetine, and acetaminophen/hydrocodone.
Her vital signs include a blood pressure of 143/91 mm Hg and a pulse of 93 beats/min. She has a BMI of 37 and a waist circumference of 35 in.
Deb, concerned about her weight, would like to discuss weight-loss options. She has tried three different commercial programs; each time, she was able to lose 30 to 50 lb in three to six months but regained the weight once she stopped the program. She reports excessive appetite as the main reason for her rebound weight gain. Her exercise is limited due to her back pain.
She recently tried OTC orlistat but could not tolerate it due to flatulence and fecal urgency. She reports an incident in which she couldn’t reach the bathroom in time.
Continue for Discussion >>
DISCUSSION
The Endocrine Society’s recommended approaches to obesity management include diet, exercise, and behavioral modification for patients with a BMI ≥ 25. The addition of pharmacotherapy can be considered for those with a BMI ≥ 30 or with a BMI ≥ 27 and one or more weight-related comorbidities (eg, diabetes, dyslipidemia, hypertension). This matches the FDA-approved product labeling for chronic weight-loss medications. Bariatric surgery should be considered for patients with a BMI ≥ 40 or with a BMI ≥ 35 and at least one weight-related comorbidity.
Orlistat
Orlistat is available OTC in a 60-mg thrice-daily form. A higher dosage (120 mg tid) is available via prescription. Orlistat decreases fat absorption in the gastrointestinal (GI) tract by inhibiting GI lipase. Average weight loss with orlistat is 3% at first and second year, and, when compared with placebo, 2.4% greater at four years.2
Orlistat should be prescribed with a multivitamin due to decreased absorption of fat-soluble vitamins. It is contraindicated in patients with malabsorption syndrome and gallbladder disease (> 2% incidence3). It can increase cyclosporine exposure, and rare cases of liver failure have been reported. The most common adverse effect is related to steatorrhea. Of the available options, orlistat is the only medication that has no effect on neurohormonal regulation in appetite control and metabolic rate, which may be a limiting factor.
CASE POINT Due to Deb’s intolerance of and embarrassment with GI adverse effects, she requests an alternative medication.
Lorcaserin
Lorcaserin is a selective serotonin 2C receptor agonist that reduces appetite by affecting anorexigenic pro-opiomelanocortin (POMC) neurons in the hypothalamus. Of note, lorcaserin “selects” the 2C receptor instead of 2A and 2B; 2B receptors are found in both aortic and mitral valves, which may explain the association between fenfluramine/phentermine (commonly known as “fen/phen” and withdrawn from the market in 1997) and possible cardiac valvulopathy. (Fenfluramine is an amphetamine derivative that nonselectively stimulates serotonin release and inhibits reuptake.)
Lorcaserin comes in a 10-mg twice-daily dosage. In studies, patients taking lorcaserin had an average weight loss of 3.3% more than those taking placebo at one year; weight loss was maintained through the second year for those who continued on medication. However, those who stopped the medication at one year had regained their weight by the two-year mark.4
It is recommended that the medication be discontinued if patients don’t achieve a loss of more than 5% of body weight by 12 weeks.
In a study that enrolled diabetic patients, lorcaserin also demonstrated a 0.9% reduction in A1C, which is similar to or even better than some oral antidiabetic medications.4 However, since the manufacturer was not planning for an antidiabetic indication, A1C was only a secondary endpoint. The reduction is most likely due to decreased caloric intake and weight loss.
The most common adverse effects of lorcaserin include headache, dizziness, and fatigue. The discontinuation rate due to intolerance was 8.6%, compared to 6.7% with placebo.5
Although this was not observed in clinical studies, co-administration of lorcaserin (a serotonin receptor agonist) with other serotonergic or antidopaminergic agents can theoretically cause serotonin syndrome or neuroleptic malignant syndrome–like reactions. Caution is therefore advisable when prescribing these agents. The package insert carries a warning for cardiac valvulopathy due to fen/phen’s history and a lack of long-term cardiovascular safety data.
CASE POINT Deb is taking paroxetine (an SSRI) for her depression. Since you are concerned about serotonin syndrome, you decide to keep exploring options. Checking the package insert for phentermine/topiramate, you learn that it does not have a potential adverse reaction related to co-administration with SSRIs.
Phentermine/Topiramate
Phentermine, a sympathomimetic medication, was approved for short-term (12-week) use for weight loss in the 1960s. Topiramate, an antiseizure and migraine prophylactic medication, enhances appetite suppression—although the exact mechanism of action is unknown.1
Four once-daily doses are available: 3.75/23 mg, 7.5/46 mg, 11.25/69 mg, and 15/92 mg. Dosing starts with 3.75/23 mg for two weeks, then increases to 7.5/46 mg. If a loss of 5% or more of body weight is achieved, the patient can continue the dosage; if not, it can be increased to 11.25/69 mg for two weeks and then to 15/92 mg. The average weight loss for mid and maximum dose was 6.6% and 8.6% greater than placebo at one year.5
Commonly reported adverse effects include paraesthesia, dysgeusia (distortion of sense of taste), dizziness, insomnia, constipation, and dry mouth. Due to phentermine’s sympathomimetic action, mild increases in heart rate and blood pressure were reported. The Endocrine Society recommends against the use of phentermine in patients with uncontrolled hypertension and a history of heart disease.1
Weight loss is generally not recommended during pregnancy, and all weight loss medications are classified as category X for pregnancy. Strict caution is advised with this particular agent, as topiramate has known teratogenicity and therefore comes with a Risk Evaluation Mitigation Strategy. Patients must be advised to use appropriate contraception while taking topiramate, and a pregnancy test should be performed before medication commencement and monthly thereafter.
Abrupt cessation of topiramate can cause seizure. When taking the 15/92-mg dosage, the patient should reduce to one tablet every other day for at least one week before discontinuation.
CASE POINT Deb’s blood pressure is still not at goal. This, along with her history of atrial fibrillation and high pulse, prompts you to consider another option.
Bupropion/Naltrexone
Bupropion, a widely used antidepressant, inhibits the uptake of norepinephrine and dopamine and thereby blocks the reward pathway that various foods can induce. Naltrexone, an opioid antagonist, blocks the opioid pathway and can be helpful in enhancing weight loss.
This combination comes in an 8/90-mg tablet. The suggested titration regimen is to start with one tablet per day and increase by one tablet every week, up to the maximum dosage of two tablets twice a day. Average weight loss was 3.1% greater than placebo at one year with the maximum dosage. An A1C reduction of 0.6% was seen in diabetic patients.6 It is recommended to stop the medication and seek an alternative treatment option if > 5% loss of body weight is not achieved by 12 weeks.
GI adverse effects (eg, nausea and vomiting) are common; these can be reduced with a slower titration regimen or by prescribing a maximum of one tablet twice daily (instead of two). Every antidepressant carries suicidal risk, and caution is advised with their use. Bupropion can also lower the seizure threshold, and it is contraindicated for patients with seizure disorder. It is also contraindicated in patients who are undergoing abrupt cessation of alcohol, benzodiazepines, or barbiturates. It can increase pulse and blood pressure during early titration; regular blood pressure monitoring is warranted.
CASE POINT Due to Deb’s opioid usage and uncontrolled hypertension, you discuss a final option that was recently approved for weight loss.
Liraglutide
This glucagon-like peptide-1 (GLP1) receptor agonist affects the brain to suppress/control appetite, slows down gastric emptying, and induces early satiety. A 3-mg dosage was approved in December 2014, but 0.6-, 1.2-, and 1.8-mg dosages have been available since 2010 for patients with type 2 diabetes.
Average weight loss was 4.5% greater than placebo at one year.7 If < 4% weight loss is achieved by 16 weeks, consider using an alternative agent.
The most common adverse effect is GI upset, which could be related to the mechanism of action (slower gastric emptying). Although self-reported GI upset was high (39%), the actual discontinuation rate was low (2.9% for nausea, 1.7% for vomiting, and 1.4% for diarrhea).3
This adverse effect could, in certain contexts, be considered “wanted,” since it discourages overeating or eating too quickly. My clinical pearl is to tell patients taking liraglutide that they are “trapped” and have to eat smaller portions and eat more slowly or they will be more prone to GI effects. With this strategy, we can encourage portion control and responsibility for behavior. (Please note that this is my experience with the diabetic dosage of liraglutide; I do not have any clinical experience with the obesity dosage, which was not clinically available at the time of writing.)
Both branded versions of liraglutide carry a black-box warning for thyroid C-cell tumors, which were observed in rodents but unproven in humans. The medication is contraindicated in patients with medullary thyroid cancer or with multiple endocrine neoplasia 2 syndrome. Increased rates of acute pancreatitis, cholecystitis, and cholelithiasis were seen in studies, and caution is advised.
Continue for A Word About Meds That Cause Weight Gain >>
A WORD ABOUT MEDS THAT CAUSE WEIGHT GAIN
The Endocrine Society has published a list of medications that can influence weight gain, along with suggestions for alternative agents that are either weight neutral or promote weight loss.
Note that our case patient, Deb, is taking insulin, a sulfonylurea (glyburide), and thiazolidinedione (pioglitazone) for diabetes—all of which can promote weight gain. Guidelines suggest choosing metformin, DPP4 inhibitors, GLP1 agonists, amylin analog, and SGLT2 inhibitors instead when weight gain is a major concern.1
Guidelines also suggest using ACE inhibitors, angiotensin receptor blockers, and calcium channel blockers instead of β-blockers as firstline antihypertensive therapy for diabetic patients.1 Adequate blood pressure and lipid control are imperative in diabetes management.
CASE POINT Deb would need better hypertension control before she considers weight-loss medication. Since she is also taking paroxetine, which among SSRIs is associated with greatest weight gain, a changed to fluoxetine or sertraline should be considered.2
Next page: Conclusion >>
CONCLUSION
There are now five medications approved by the FDA for chronic weight loss, with more to come. Agents with different mechanisms of action give us options to help obese patients and hopefully reduce and prevent obesity-related complications. It is important for clinicians to be competent in managing obesity, especially since we live in an era in which the disease is considered pandemic.
REFERENCES
1. Apovian CM, Aronne LJ, Bessesen DH, et al; Endocrine Society. Pharmacological management of obesity: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015;100(2):342-362.
2. Xenical [package insert]. South San Francisco, CA: Genentech USA, Inc; 2012.
3. Fujioka K. Safety and tolerability of medications approved for chronic weight management. Obesity (Silver Spring). 2015;22 (suppl 1):S7-S11.
4. Belviq [package insert]. Woodcliff Lake, NJ: Eisai Inc; 2015.
5. Qsymia [package insert]. Mountain View, CA: Vivus, Inc; 2013.
6. Contrave [package insert]. Deerfield, IL: Takeda USA, Inc; 2014.
7. Saxenda [package insert]. Plainsboro, NJ: Novo Nordisk; 2014.
Clinician Reviews in partnership with![]()
Ji Hyun Chun practices with Optum Medical Partners: Endocrinology in Orange County, California. The author has no financial relationships to disclose.
Clinician Reviews in partnership with![]()
Ji Hyun Chun practices with Optum Medical Partners: Endocrinology in Orange County, California. The author has no financial relationships to disclose.
Clinician Reviews in partnership with![]()
Ji Hyun Chun practices with Optum Medical Partners: Endocrinology in Orange County, California. The author has no financial relationships to disclose.
In June 2013, the American Medical Association classified obesity as a disease. Since then, several medical societies have published guidelines to help clinicians improve care of affected patients. One avenue is, of course, pharmacologic treatment.
Until recently, there was only one FDA-approved medication for chronic weight loss on the market: orlistat, which was approved in 1999. (Phentermine and diethylpropion are only indicated for short-term use). After a long hiatus, the FDA approved two additional agents (phentermine/topiramate and lorcaserin)in 2012 and another two (liraglutide and bupropion/naltrexone) in 2014.
While clinicians appreciate having options for managing their patients’ conditions, in this case, many are overwhelmed by the choices. Most health care providers have not received formal training in obesity management. This column will attempt to fill the information gap in terms of what agents are available and what factors should be assessed before prescribing any of them.
Proviso: Experts claim obesity is a chronic disease, similar to hypertension, and should be managed as such. Although not discussed here, the most important aspect of weight loss and maintenance is lifestyle intervention (diet, exercise, and behavioral modification). It should be emphasized that no medication works by itself; all should be used as an adjunct tool to reinforce adherence to lifestyle changes.1 Furthermore, patients may be disappointed to learn that without these changes, the weight may return when they cease medication use.
CASE Deb, age 61, presents to your office for routine follow-up. She has a history of type 2 diabetes, dyslipidemia, hypertension, atrial fibrillation, depression, and chronic back pain due to a herniated disc. Her medications include insulin glargine, glyburide, pioglitazone, atorvastatin, metoprolol, paroxetine, and acetaminophen/hydrocodone.
Her vital signs include a blood pressure of 143/91 mm Hg and a pulse of 93 beats/min. She has a BMI of 37 and a waist circumference of 35 in.
Deb, concerned about her weight, would like to discuss weight-loss options. She has tried three different commercial programs; each time, she was able to lose 30 to 50 lb in three to six months but regained the weight once she stopped the program. She reports excessive appetite as the main reason for her rebound weight gain. Her exercise is limited due to her back pain.
She recently tried OTC orlistat but could not tolerate it due to flatulence and fecal urgency. She reports an incident in which she couldn’t reach the bathroom in time.
Continue for Discussion >>
DISCUSSION
The Endocrine Society’s recommended approaches to obesity management include diet, exercise, and behavioral modification for patients with a BMI ≥ 25. The addition of pharmacotherapy can be considered for those with a BMI ≥ 30 or with a BMI ≥ 27 and one or more weight-related comorbidities (eg, diabetes, dyslipidemia, hypertension). This matches the FDA-approved product labeling for chronic weight-loss medications. Bariatric surgery should be considered for patients with a BMI ≥ 40 or with a BMI ≥ 35 and at least one weight-related comorbidity.
Orlistat
Orlistat is available OTC in a 60-mg thrice-daily form. A higher dosage (120 mg tid) is available via prescription. Orlistat decreases fat absorption in the gastrointestinal (GI) tract by inhibiting GI lipase. Average weight loss with orlistat is 3% at first and second year, and, when compared with placebo, 2.4% greater at four years.2
Orlistat should be prescribed with a multivitamin due to decreased absorption of fat-soluble vitamins. It is contraindicated in patients with malabsorption syndrome and gallbladder disease (> 2% incidence3). It can increase cyclosporine exposure, and rare cases of liver failure have been reported. The most common adverse effect is related to steatorrhea. Of the available options, orlistat is the only medication that has no effect on neurohormonal regulation in appetite control and metabolic rate, which may be a limiting factor.
CASE POINT Due to Deb’s intolerance of and embarrassment with GI adverse effects, she requests an alternative medication.
Lorcaserin
Lorcaserin is a selective serotonin 2C receptor agonist that reduces appetite by affecting anorexigenic pro-opiomelanocortin (POMC) neurons in the hypothalamus. Of note, lorcaserin “selects” the 2C receptor instead of 2A and 2B; 2B receptors are found in both aortic and mitral valves, which may explain the association between fenfluramine/phentermine (commonly known as “fen/phen” and withdrawn from the market in 1997) and possible cardiac valvulopathy. (Fenfluramine is an amphetamine derivative that nonselectively stimulates serotonin release and inhibits reuptake.)
Lorcaserin comes in a 10-mg twice-daily dosage. In studies, patients taking lorcaserin had an average weight loss of 3.3% more than those taking placebo at one year; weight loss was maintained through the second year for those who continued on medication. However, those who stopped the medication at one year had regained their weight by the two-year mark.4
It is recommended that the medication be discontinued if patients don’t achieve a loss of more than 5% of body weight by 12 weeks.
In a study that enrolled diabetic patients, lorcaserin also demonstrated a 0.9% reduction in A1C, which is similar to or even better than some oral antidiabetic medications.4 However, since the manufacturer was not planning for an antidiabetic indication, A1C was only a secondary endpoint. The reduction is most likely due to decreased caloric intake and weight loss.
The most common adverse effects of lorcaserin include headache, dizziness, and fatigue. The discontinuation rate due to intolerance was 8.6%, compared to 6.7% with placebo.5
Although this was not observed in clinical studies, co-administration of lorcaserin (a serotonin receptor agonist) with other serotonergic or antidopaminergic agents can theoretically cause serotonin syndrome or neuroleptic malignant syndrome–like reactions. Caution is therefore advisable when prescribing these agents. The package insert carries a warning for cardiac valvulopathy due to fen/phen’s history and a lack of long-term cardiovascular safety data.
CASE POINT Deb is taking paroxetine (an SSRI) for her depression. Since you are concerned about serotonin syndrome, you decide to keep exploring options. Checking the package insert for phentermine/topiramate, you learn that it does not have a potential adverse reaction related to co-administration with SSRIs.
Phentermine/Topiramate
Phentermine, a sympathomimetic medication, was approved for short-term (12-week) use for weight loss in the 1960s. Topiramate, an antiseizure and migraine prophylactic medication, enhances appetite suppression—although the exact mechanism of action is unknown.1
Four once-daily doses are available: 3.75/23 mg, 7.5/46 mg, 11.25/69 mg, and 15/92 mg. Dosing starts with 3.75/23 mg for two weeks, then increases to 7.5/46 mg. If a loss of 5% or more of body weight is achieved, the patient can continue the dosage; if not, it can be increased to 11.25/69 mg for two weeks and then to 15/92 mg. The average weight loss for mid and maximum dose was 6.6% and 8.6% greater than placebo at one year.5
Commonly reported adverse effects include paraesthesia, dysgeusia (distortion of sense of taste), dizziness, insomnia, constipation, and dry mouth. Due to phentermine’s sympathomimetic action, mild increases in heart rate and blood pressure were reported. The Endocrine Society recommends against the use of phentermine in patients with uncontrolled hypertension and a history of heart disease.1
Weight loss is generally not recommended during pregnancy, and all weight loss medications are classified as category X for pregnancy. Strict caution is advised with this particular agent, as topiramate has known teratogenicity and therefore comes with a Risk Evaluation Mitigation Strategy. Patients must be advised to use appropriate contraception while taking topiramate, and a pregnancy test should be performed before medication commencement and monthly thereafter.
Abrupt cessation of topiramate can cause seizure. When taking the 15/92-mg dosage, the patient should reduce to one tablet every other day for at least one week before discontinuation.
CASE POINT Deb’s blood pressure is still not at goal. This, along with her history of atrial fibrillation and high pulse, prompts you to consider another option.
Bupropion/Naltrexone
Bupropion, a widely used antidepressant, inhibits the uptake of norepinephrine and dopamine and thereby blocks the reward pathway that various foods can induce. Naltrexone, an opioid antagonist, blocks the opioid pathway and can be helpful in enhancing weight loss.
This combination comes in an 8/90-mg tablet. The suggested titration regimen is to start with one tablet per day and increase by one tablet every week, up to the maximum dosage of two tablets twice a day. Average weight loss was 3.1% greater than placebo at one year with the maximum dosage. An A1C reduction of 0.6% was seen in diabetic patients.6 It is recommended to stop the medication and seek an alternative treatment option if > 5% loss of body weight is not achieved by 12 weeks.
GI adverse effects (eg, nausea and vomiting) are common; these can be reduced with a slower titration regimen or by prescribing a maximum of one tablet twice daily (instead of two). Every antidepressant carries suicidal risk, and caution is advised with their use. Bupropion can also lower the seizure threshold, and it is contraindicated for patients with seizure disorder. It is also contraindicated in patients who are undergoing abrupt cessation of alcohol, benzodiazepines, or barbiturates. It can increase pulse and blood pressure during early titration; regular blood pressure monitoring is warranted.
CASE POINT Due to Deb’s opioid usage and uncontrolled hypertension, you discuss a final option that was recently approved for weight loss.
Liraglutide
This glucagon-like peptide-1 (GLP1) receptor agonist affects the brain to suppress/control appetite, slows down gastric emptying, and induces early satiety. A 3-mg dosage was approved in December 2014, but 0.6-, 1.2-, and 1.8-mg dosages have been available since 2010 for patients with type 2 diabetes.
Average weight loss was 4.5% greater than placebo at one year.7 If < 4% weight loss is achieved by 16 weeks, consider using an alternative agent.
The most common adverse effect is GI upset, which could be related to the mechanism of action (slower gastric emptying). Although self-reported GI upset was high (39%), the actual discontinuation rate was low (2.9% for nausea, 1.7% for vomiting, and 1.4% for diarrhea).3
This adverse effect could, in certain contexts, be considered “wanted,” since it discourages overeating or eating too quickly. My clinical pearl is to tell patients taking liraglutide that they are “trapped” and have to eat smaller portions and eat more slowly or they will be more prone to GI effects. With this strategy, we can encourage portion control and responsibility for behavior. (Please note that this is my experience with the diabetic dosage of liraglutide; I do not have any clinical experience with the obesity dosage, which was not clinically available at the time of writing.)
Both branded versions of liraglutide carry a black-box warning for thyroid C-cell tumors, which were observed in rodents but unproven in humans. The medication is contraindicated in patients with medullary thyroid cancer or with multiple endocrine neoplasia 2 syndrome. Increased rates of acute pancreatitis, cholecystitis, and cholelithiasis were seen in studies, and caution is advised.
Continue for A Word About Meds That Cause Weight Gain >>
A WORD ABOUT MEDS THAT CAUSE WEIGHT GAIN
The Endocrine Society has published a list of medications that can influence weight gain, along with suggestions for alternative agents that are either weight neutral or promote weight loss.
Note that our case patient, Deb, is taking insulin, a sulfonylurea (glyburide), and thiazolidinedione (pioglitazone) for diabetes—all of which can promote weight gain. Guidelines suggest choosing metformin, DPP4 inhibitors, GLP1 agonists, amylin analog, and SGLT2 inhibitors instead when weight gain is a major concern.1
Guidelines also suggest using ACE inhibitors, angiotensin receptor blockers, and calcium channel blockers instead of β-blockers as firstline antihypertensive therapy for diabetic patients.1 Adequate blood pressure and lipid control are imperative in diabetes management.
CASE POINT Deb would need better hypertension control before she considers weight-loss medication. Since she is also taking paroxetine, which among SSRIs is associated with greatest weight gain, a changed to fluoxetine or sertraline should be considered.2
Next page: Conclusion >>
CONCLUSION
There are now five medications approved by the FDA for chronic weight loss, with more to come. Agents with different mechanisms of action give us options to help obese patients and hopefully reduce and prevent obesity-related complications. It is important for clinicians to be competent in managing obesity, especially since we live in an era in which the disease is considered pandemic.
REFERENCES
1. Apovian CM, Aronne LJ, Bessesen DH, et al; Endocrine Society. Pharmacological management of obesity: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015;100(2):342-362.
2. Xenical [package insert]. South San Francisco, CA: Genentech USA, Inc; 2012.
3. Fujioka K. Safety and tolerability of medications approved for chronic weight management. Obesity (Silver Spring). 2015;22 (suppl 1):S7-S11.
4. Belviq [package insert]. Woodcliff Lake, NJ: Eisai Inc; 2015.
5. Qsymia [package insert]. Mountain View, CA: Vivus, Inc; 2013.
6. Contrave [package insert]. Deerfield, IL: Takeda USA, Inc; 2014.
7. Saxenda [package insert]. Plainsboro, NJ: Novo Nordisk; 2014.
In June 2013, the American Medical Association classified obesity as a disease. Since then, several medical societies have published guidelines to help clinicians improve care of affected patients. One avenue is, of course, pharmacologic treatment.
Until recently, there was only one FDA-approved medication for chronic weight loss on the market: orlistat, which was approved in 1999. (Phentermine and diethylpropion are only indicated for short-term use). After a long hiatus, the FDA approved two additional agents (phentermine/topiramate and lorcaserin)in 2012 and another two (liraglutide and bupropion/naltrexone) in 2014.
While clinicians appreciate having options for managing their patients’ conditions, in this case, many are overwhelmed by the choices. Most health care providers have not received formal training in obesity management. This column will attempt to fill the information gap in terms of what agents are available and what factors should be assessed before prescribing any of them.
Proviso: Experts claim obesity is a chronic disease, similar to hypertension, and should be managed as such. Although not discussed here, the most important aspect of weight loss and maintenance is lifestyle intervention (diet, exercise, and behavioral modification). It should be emphasized that no medication works by itself; all should be used as an adjunct tool to reinforce adherence to lifestyle changes.1 Furthermore, patients may be disappointed to learn that without these changes, the weight may return when they cease medication use.
CASE Deb, age 61, presents to your office for routine follow-up. She has a history of type 2 diabetes, dyslipidemia, hypertension, atrial fibrillation, depression, and chronic back pain due to a herniated disc. Her medications include insulin glargine, glyburide, pioglitazone, atorvastatin, metoprolol, paroxetine, and acetaminophen/hydrocodone.
Her vital signs include a blood pressure of 143/91 mm Hg and a pulse of 93 beats/min. She has a BMI of 37 and a waist circumference of 35 in.
Deb, concerned about her weight, would like to discuss weight-loss options. She has tried three different commercial programs; each time, she was able to lose 30 to 50 lb in three to six months but regained the weight once she stopped the program. She reports excessive appetite as the main reason for her rebound weight gain. Her exercise is limited due to her back pain.
She recently tried OTC orlistat but could not tolerate it due to flatulence and fecal urgency. She reports an incident in which she couldn’t reach the bathroom in time.
Continue for Discussion >>
DISCUSSION
The Endocrine Society’s recommended approaches to obesity management include diet, exercise, and behavioral modification for patients with a BMI ≥ 25. The addition of pharmacotherapy can be considered for those with a BMI ≥ 30 or with a BMI ≥ 27 and one or more weight-related comorbidities (eg, diabetes, dyslipidemia, hypertension). This matches the FDA-approved product labeling for chronic weight-loss medications. Bariatric surgery should be considered for patients with a BMI ≥ 40 or with a BMI ≥ 35 and at least one weight-related comorbidity.
Orlistat
Orlistat is available OTC in a 60-mg thrice-daily form. A higher dosage (120 mg tid) is available via prescription. Orlistat decreases fat absorption in the gastrointestinal (GI) tract by inhibiting GI lipase. Average weight loss with orlistat is 3% at first and second year, and, when compared with placebo, 2.4% greater at four years.2
Orlistat should be prescribed with a multivitamin due to decreased absorption of fat-soluble vitamins. It is contraindicated in patients with malabsorption syndrome and gallbladder disease (> 2% incidence3). It can increase cyclosporine exposure, and rare cases of liver failure have been reported. The most common adverse effect is related to steatorrhea. Of the available options, orlistat is the only medication that has no effect on neurohormonal regulation in appetite control and metabolic rate, which may be a limiting factor.
CASE POINT Due to Deb’s intolerance of and embarrassment with GI adverse effects, she requests an alternative medication.
Lorcaserin
Lorcaserin is a selective serotonin 2C receptor agonist that reduces appetite by affecting anorexigenic pro-opiomelanocortin (POMC) neurons in the hypothalamus. Of note, lorcaserin “selects” the 2C receptor instead of 2A and 2B; 2B receptors are found in both aortic and mitral valves, which may explain the association between fenfluramine/phentermine (commonly known as “fen/phen” and withdrawn from the market in 1997) and possible cardiac valvulopathy. (Fenfluramine is an amphetamine derivative that nonselectively stimulates serotonin release and inhibits reuptake.)
Lorcaserin comes in a 10-mg twice-daily dosage. In studies, patients taking lorcaserin had an average weight loss of 3.3% more than those taking placebo at one year; weight loss was maintained through the second year for those who continued on medication. However, those who stopped the medication at one year had regained their weight by the two-year mark.4
It is recommended that the medication be discontinued if patients don’t achieve a loss of more than 5% of body weight by 12 weeks.
In a study that enrolled diabetic patients, lorcaserin also demonstrated a 0.9% reduction in A1C, which is similar to or even better than some oral antidiabetic medications.4 However, since the manufacturer was not planning for an antidiabetic indication, A1C was only a secondary endpoint. The reduction is most likely due to decreased caloric intake and weight loss.
The most common adverse effects of lorcaserin include headache, dizziness, and fatigue. The discontinuation rate due to intolerance was 8.6%, compared to 6.7% with placebo.5
Although this was not observed in clinical studies, co-administration of lorcaserin (a serotonin receptor agonist) with other serotonergic or antidopaminergic agents can theoretically cause serotonin syndrome or neuroleptic malignant syndrome–like reactions. Caution is therefore advisable when prescribing these agents. The package insert carries a warning for cardiac valvulopathy due to fen/phen’s history and a lack of long-term cardiovascular safety data.
CASE POINT Deb is taking paroxetine (an SSRI) for her depression. Since you are concerned about serotonin syndrome, you decide to keep exploring options. Checking the package insert for phentermine/topiramate, you learn that it does not have a potential adverse reaction related to co-administration with SSRIs.
Phentermine/Topiramate
Phentermine, a sympathomimetic medication, was approved for short-term (12-week) use for weight loss in the 1960s. Topiramate, an antiseizure and migraine prophylactic medication, enhances appetite suppression—although the exact mechanism of action is unknown.1
Four once-daily doses are available: 3.75/23 mg, 7.5/46 mg, 11.25/69 mg, and 15/92 mg. Dosing starts with 3.75/23 mg for two weeks, then increases to 7.5/46 mg. If a loss of 5% or more of body weight is achieved, the patient can continue the dosage; if not, it can be increased to 11.25/69 mg for two weeks and then to 15/92 mg. The average weight loss for mid and maximum dose was 6.6% and 8.6% greater than placebo at one year.5
Commonly reported adverse effects include paraesthesia, dysgeusia (distortion of sense of taste), dizziness, insomnia, constipation, and dry mouth. Due to phentermine’s sympathomimetic action, mild increases in heart rate and blood pressure were reported. The Endocrine Society recommends against the use of phentermine in patients with uncontrolled hypertension and a history of heart disease.1
Weight loss is generally not recommended during pregnancy, and all weight loss medications are classified as category X for pregnancy. Strict caution is advised with this particular agent, as topiramate has known teratogenicity and therefore comes with a Risk Evaluation Mitigation Strategy. Patients must be advised to use appropriate contraception while taking topiramate, and a pregnancy test should be performed before medication commencement and monthly thereafter.
Abrupt cessation of topiramate can cause seizure. When taking the 15/92-mg dosage, the patient should reduce to one tablet every other day for at least one week before discontinuation.
CASE POINT Deb’s blood pressure is still not at goal. This, along with her history of atrial fibrillation and high pulse, prompts you to consider another option.
Bupropion/Naltrexone
Bupropion, a widely used antidepressant, inhibits the uptake of norepinephrine and dopamine and thereby blocks the reward pathway that various foods can induce. Naltrexone, an opioid antagonist, blocks the opioid pathway and can be helpful in enhancing weight loss.
This combination comes in an 8/90-mg tablet. The suggested titration regimen is to start with one tablet per day and increase by one tablet every week, up to the maximum dosage of two tablets twice a day. Average weight loss was 3.1% greater than placebo at one year with the maximum dosage. An A1C reduction of 0.6% was seen in diabetic patients.6 It is recommended to stop the medication and seek an alternative treatment option if > 5% loss of body weight is not achieved by 12 weeks.
GI adverse effects (eg, nausea and vomiting) are common; these can be reduced with a slower titration regimen or by prescribing a maximum of one tablet twice daily (instead of two). Every antidepressant carries suicidal risk, and caution is advised with their use. Bupropion can also lower the seizure threshold, and it is contraindicated for patients with seizure disorder. It is also contraindicated in patients who are undergoing abrupt cessation of alcohol, benzodiazepines, or barbiturates. It can increase pulse and blood pressure during early titration; regular blood pressure monitoring is warranted.
CASE POINT Due to Deb’s opioid usage and uncontrolled hypertension, you discuss a final option that was recently approved for weight loss.
Liraglutide
This glucagon-like peptide-1 (GLP1) receptor agonist affects the brain to suppress/control appetite, slows down gastric emptying, and induces early satiety. A 3-mg dosage was approved in December 2014, but 0.6-, 1.2-, and 1.8-mg dosages have been available since 2010 for patients with type 2 diabetes.
Average weight loss was 4.5% greater than placebo at one year.7 If < 4% weight loss is achieved by 16 weeks, consider using an alternative agent.
The most common adverse effect is GI upset, which could be related to the mechanism of action (slower gastric emptying). Although self-reported GI upset was high (39%), the actual discontinuation rate was low (2.9% for nausea, 1.7% for vomiting, and 1.4% for diarrhea).3
This adverse effect could, in certain contexts, be considered “wanted,” since it discourages overeating or eating too quickly. My clinical pearl is to tell patients taking liraglutide that they are “trapped” and have to eat smaller portions and eat more slowly or they will be more prone to GI effects. With this strategy, we can encourage portion control and responsibility for behavior. (Please note that this is my experience with the diabetic dosage of liraglutide; I do not have any clinical experience with the obesity dosage, which was not clinically available at the time of writing.)
Both branded versions of liraglutide carry a black-box warning for thyroid C-cell tumors, which were observed in rodents but unproven in humans. The medication is contraindicated in patients with medullary thyroid cancer or with multiple endocrine neoplasia 2 syndrome. Increased rates of acute pancreatitis, cholecystitis, and cholelithiasis were seen in studies, and caution is advised.
Continue for A Word About Meds That Cause Weight Gain >>
A WORD ABOUT MEDS THAT CAUSE WEIGHT GAIN
The Endocrine Society has published a list of medications that can influence weight gain, along with suggestions for alternative agents that are either weight neutral or promote weight loss.
Note that our case patient, Deb, is taking insulin, a sulfonylurea (glyburide), and thiazolidinedione (pioglitazone) for diabetes—all of which can promote weight gain. Guidelines suggest choosing metformin, DPP4 inhibitors, GLP1 agonists, amylin analog, and SGLT2 inhibitors instead when weight gain is a major concern.1
Guidelines also suggest using ACE inhibitors, angiotensin receptor blockers, and calcium channel blockers instead of β-blockers as firstline antihypertensive therapy for diabetic patients.1 Adequate blood pressure and lipid control are imperative in diabetes management.
CASE POINT Deb would need better hypertension control before she considers weight-loss medication. Since she is also taking paroxetine, which among SSRIs is associated with greatest weight gain, a changed to fluoxetine or sertraline should be considered.2
Next page: Conclusion >>
CONCLUSION
There are now five medications approved by the FDA for chronic weight loss, with more to come. Agents with different mechanisms of action give us options to help obese patients and hopefully reduce and prevent obesity-related complications. It is important for clinicians to be competent in managing obesity, especially since we live in an era in which the disease is considered pandemic.
REFERENCES
1. Apovian CM, Aronne LJ, Bessesen DH, et al; Endocrine Society. Pharmacological management of obesity: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015;100(2):342-362.
2. Xenical [package insert]. South San Francisco, CA: Genentech USA, Inc; 2012.
3. Fujioka K. Safety and tolerability of medications approved for chronic weight management. Obesity (Silver Spring). 2015;22 (suppl 1):S7-S11.
4. Belviq [package insert]. Woodcliff Lake, NJ: Eisai Inc; 2015.
5. Qsymia [package insert]. Mountain View, CA: Vivus, Inc; 2013.
6. Contrave [package insert]. Deerfield, IL: Takeda USA, Inc; 2014.
7. Saxenda [package insert]. Plainsboro, NJ: Novo Nordisk; 2014.
Woman Complains of Knee Pain Following Fight

ANSWER
The radiograph shows a small calcification along the medial aspect of the medial collateral ligament. This finding is known as a Pellegrini-Stieda lesion. While it certainly could represent a small avulsion fracture, the lack of joint fluid and soft-tissue swelling makes this diagnosis less likely. The patient was treated symptomatically with anti-inflammatory medications.
ANSWER
The radiograph shows a small calcification along the medial aspect of the medial collateral ligament. This finding is known as a Pellegrini-Stieda lesion. While it certainly could represent a small avulsion fracture, the lack of joint fluid and soft-tissue swelling makes this diagnosis less likely. The patient was treated symptomatically with anti-inflammatory medications.
ANSWER
The radiograph shows a small calcification along the medial aspect of the medial collateral ligament. This finding is known as a Pellegrini-Stieda lesion. While it certainly could represent a small avulsion fracture, the lack of joint fluid and soft-tissue swelling makes this diagnosis less likely. The patient was treated symptomatically with anti-inflammatory medications.
A 35-year-old woman presents for evaluation of left knee pain secondary to an assault. She says she was involved in a fight and was struck multiple times throughout her whole body. She states she is “sore all over,” but her knee bothers her the most, as it is difficult and painful to bear weight. The patient’s medical history is unremarkable. Physical exam shows a young female who is uncomfortable but in no obvious distress. Her vital signs are normal. You note bruises throughout her body. Inspection of her left knee shows no obvious deformity or swelling. There is some mild bruising and pain present to palpation. She has limited flexion and extension secondary to pain. However, the joint itself appears stable. Radiographs of the knee are obtained. What is your impression?
Neighbor Finds Man on Knees, Vomiting
ANSWER
The correct interpretation of this ECG includes atrial fibrillation and ST- and T-wave changes consistent with a central nervous system hemorrhage, as well as a markedly prolonged QT interval.
The most common ECG alterations seen in cases of acute subarachnoid hemorrhage include repolarization abnormalities due to imbalance of autonomic cardiovascular control. While ST depression is more common in patients with poor outcomes, it is not predictive.
ANSWER
The correct interpretation of this ECG includes atrial fibrillation and ST- and T-wave changes consistent with a central nervous system hemorrhage, as well as a markedly prolonged QT interval.
The most common ECG alterations seen in cases of acute subarachnoid hemorrhage include repolarization abnormalities due to imbalance of autonomic cardiovascular control. While ST depression is more common in patients with poor outcomes, it is not predictive.
ANSWER
The correct interpretation of this ECG includes atrial fibrillation and ST- and T-wave changes consistent with a central nervous system hemorrhage, as well as a markedly prolonged QT interval.
The most common ECG alterations seen in cases of acute subarachnoid hemorrhage include repolarization abnormalities due to imbalance of autonomic cardiovascular control. While ST depression is more common in patients with poor outcomes, it is not predictive.
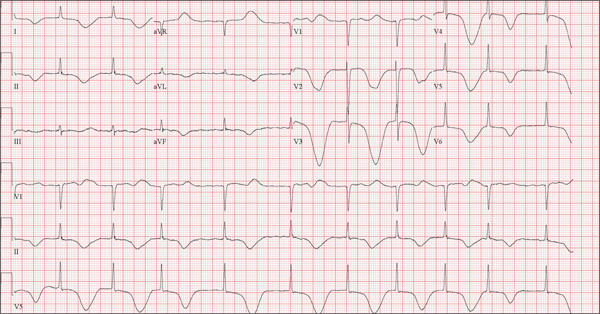
A 68-year-old man was found on his knees, vomiting, in his backyard by a neighbor early this morning. When asked if he was OK, the patient responded that he suddenly felt nauseated and had a headache. The neighbor helped him to his feet and, noticing that his left leg and arm were weak, called 911. During that time, the neighbor observed slurred speech. As they waited for the ambulance to arrive, the patient was able to say that this was the worst headache he’d ever had. When the paramedics arrived, they recorded a blood pressure of 198/120 mm Hg, consistent in both arms. Medical history is remarkable for hypertension, paroxysmal atrial fibrillation, adult-onset diabetes, and nephrolithiasis. Surgical history is remarkable for appendectomy, cholecystectomy, and lithotripsy. The patient is a retired civil engineer who lives at home alone. His wife died three years ago of complications from uterine cancer. He has one adult son who is in excellent health but lives on the opposite coast. The patient has never smoked and drinks approximately one six-pack of beer per month. Current medications include hydrochlorothiazide, metformin, and rivaroxaban. He is allergic to sulfa-containing medications. A complete review of systems is not obtained, given the patient’s slurred speech and progressive aphasia. He is able to nod yes or no to specific questions, and no significant symptoms or findings are identified. At the hospital, the patient is agitated and in apparent distress, with severe headache and aphasia. Vital signs include a blood pressure of 180/110 mm Hg; pulse, 60 beats/min; respiratory rate, 14 breaths/min; and temperature, 98.4°F. The O2 saturation is 96.4% on room air. Pertinent physical findings include aphasia, oculomotor nerve palsy, nuchal rigidity, and findings of a left-sided (right hemispheric) progressive hemiparesis. The remainder of the physical examination is noncontributory. Samples are drawn for laboratory testing, and an ECG is obtained prior to the patient’s transfer to radiology for CT of the head. The ECG findings include a ventricular rate of 62 beats/min; QRS duration, 88 ms; QT/QTc interval, 718/728 ms; P axis, not measured; R axis, 35°; and T axis, 209°. What is your interpretation of this ECG?
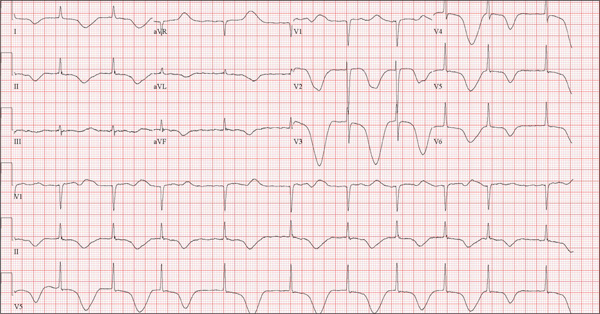
Healthcare Industry Agents of Change Promote Responsible Spending
1 Caring Wisely Program
http://healthvalue.ucsf.edu/caring-wisely
- Started in 2012 within the division of hospital medicine at the University of California, San Francisco (UCSF), the program sponsored or collaborated on six high-value care projects within its first year. “We don’t shy away from the fact that part of what we do is address cost, but it is about making sure that we’ve got the right mindset and right frame, which is that we’re going to improve quality while decreasing costs and keeping it really patient centered,” says Christopher Moriates, MD, program director and an assistant clinical professor.
- Beyond its successful Nebs No More After 24 project, Caring Wisely helped hospital pharmacists and the UCSF Medication Outcomes Center develop and implement an evidence-based initiative to cut inappropriate stress ulcer prophylaxis in intensive care unit patients. After its first month, the program had cut unnecessary use of the medication from 19% to 6.6%.
2 Choosing Wisely Program
- Launched in 2012 as an initiative of the ABIM Foundation and based on a pilot project by the National Physicians Alliance, Choosing Wisely was designed to encourage more proactive conversations between providers and patients. The goal is to help patients choose care that is both evidence-based and necessary, while minimizing harm and avoiding duplication of tests or procedures.
- Since its debut, the program has gathered nearly 60 specialty society lists of “Five Things Physicians and Patients Should Question,” including two lists compiled by SHM for adult and pediatric hospital medicine. As a complement, Consumer Reports and many of the specialty societies have collaborated on 75 patient-friendly reports that dispense advice about whether a test, treatment, or procedure is really needed.
3 Costs of Care
- Founded in 2009 by Neel Shah, MD, an assistant professor at Harvard Medical School, the nonprofit got its start by collecting stories from patients and physicians about unnecessary or inflated healthcare costs. “It had a manifesto about what the role of physicians ought to be and thinking about healthcare costs, and that message actually really resonated with a lot of people,” Dr. Shah says. “That basic message that we decide what goes on the bill, patients have to pay for it, and yet we don’t know what it’s costing them—that just seemed crazy and we heard from a lot of people, both from patients with whom that message resonated and physicians who were like, ‘Yeah.’”
- In 2010, the organizers hosted their first essay contest and ended up receiving more than 300 entries; several were subsequently included as case reports in a report on healthcare waste by the Institute of Medicine. The nonprofit, supported by the ABIM Foundation and other institutions, has since led to an educational venture called the Teaching Value Project, a textbook titled Understanding Value-Based Care (McGraw-Hill), and a “Costs of Care” iPhone app—all designed to help clinicians make high-value clinical decisions and increase price transparency.
4 The Do No Harm Project
http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/
GIM/education/DoNoHarmProject/Pages/Welcome.aspx
- Launched in 2012 at the University of Colorado by Brandon Combs, MD, and Tanner Caverly, MD, MPH, the project is aimed at medical trainees. Starting with the internal medicine program, the physicians asked medical residents to reflect on a patient who had suffered an adverse consequence from medical overuse. “This was reasonable care that was nevertheless unneeded or unwanted by a fully informed patient,” Dr. Combs says. “So this isn’t errors or malpractice; this is the stuff that flies under the radar, the stuff that people might miss.”
- The project uses clinical vignettes written by medical trainees (including those found in the “Teachable Moments” section of JAMA Internal Medicine) to improve the recognition of potential harm from overuse and to spur a culture change. In 2013, the Teaching Value and Choosing Wisely Competition, jointly sponsored by Costs of Care and the ABIM Foundation, recognized the project as one of its Innovations award winners; so far, five internal medicine and emergency medicine programs around the country have adopted the model.
5 I-CARE
- The Interactive Cost-Awareness Resident Exercise (I-CARE) was launched in 2011 by Yale hospitalist Robert Fogerty, MD, MPH, and colleagues. The friendly competition among medical students, interns, residents, and attending physicians uses a traditional morning report structure and charge data. At these conferences, the providers compete to come up with the correct diagnosis using the fewest resources possible. In 2013, the Teaching Value and Choosing Wisely competition, jointly sponsored by Costs of Care and the ABIM Foundation, recognized I-CARE as one of its Innovations award winners.
- “Physicians tend not to have a lot of business training,” Dr. Fogerty says. “They don’t have a lot of financial training. They don’t have a lot of economics background, and when you tell them that healthcare expense is 18% of GDP [gross domestic product], they don’t really know what that means. When you tell them that that would be in the top 10 of world economies, now they’re starting to get a picture of it. And when you tell them that that CAT scan you just ordered is going to cost your patient $1,200, that’s an eye-opening number that they can understand. So I think the purpose behind I-CARE was to take this seemingly insurmountable problem and to begin to digest it into small enough bits of information that allowed this problem to be accessible to the trainees.”
6 Providers for Responsible Ordering (PRO)
www.providersforresponsibleordering.org
- The organization launched in 2009 with a mission to “promote high-value care and create a culture that minimizes unnecessary or potentially-harmful diagnostic tests and interventions.” By the end of 2014, five chapters had been established and more than 150 providers had signed the PRO pledge that asks signatories, in part, “to provide my patients with all of the care that they need and none that they do not, thereby protecting them from unnecessary diagnostic tests and treatments.”
- “Our model is simple and yet powerful. It’s a grass-roots effort that any interested provider can join, and it builds on a peer-to-peer approach of establishment of chapters that solve local problems and reporting of those solutions back to the national group,” says Anthony Accurso, MD, PRO faculty director at Johns Hopkins Bayview Medical Center in Baltimore.
1 Caring Wisely Program
http://healthvalue.ucsf.edu/caring-wisely
- Started in 2012 within the division of hospital medicine at the University of California, San Francisco (UCSF), the program sponsored or collaborated on six high-value care projects within its first year. “We don’t shy away from the fact that part of what we do is address cost, but it is about making sure that we’ve got the right mindset and right frame, which is that we’re going to improve quality while decreasing costs and keeping it really patient centered,” says Christopher Moriates, MD, program director and an assistant clinical professor.
- Beyond its successful Nebs No More After 24 project, Caring Wisely helped hospital pharmacists and the UCSF Medication Outcomes Center develop and implement an evidence-based initiative to cut inappropriate stress ulcer prophylaxis in intensive care unit patients. After its first month, the program had cut unnecessary use of the medication from 19% to 6.6%.
2 Choosing Wisely Program
- Launched in 2012 as an initiative of the ABIM Foundation and based on a pilot project by the National Physicians Alliance, Choosing Wisely was designed to encourage more proactive conversations between providers and patients. The goal is to help patients choose care that is both evidence-based and necessary, while minimizing harm and avoiding duplication of tests or procedures.
- Since its debut, the program has gathered nearly 60 specialty society lists of “Five Things Physicians and Patients Should Question,” including two lists compiled by SHM for adult and pediatric hospital medicine. As a complement, Consumer Reports and many of the specialty societies have collaborated on 75 patient-friendly reports that dispense advice about whether a test, treatment, or procedure is really needed.
3 Costs of Care
- Founded in 2009 by Neel Shah, MD, an assistant professor at Harvard Medical School, the nonprofit got its start by collecting stories from patients and physicians about unnecessary or inflated healthcare costs. “It had a manifesto about what the role of physicians ought to be and thinking about healthcare costs, and that message actually really resonated with a lot of people,” Dr. Shah says. “That basic message that we decide what goes on the bill, patients have to pay for it, and yet we don’t know what it’s costing them—that just seemed crazy and we heard from a lot of people, both from patients with whom that message resonated and physicians who were like, ‘Yeah.’”
- In 2010, the organizers hosted their first essay contest and ended up receiving more than 300 entries; several were subsequently included as case reports in a report on healthcare waste by the Institute of Medicine. The nonprofit, supported by the ABIM Foundation and other institutions, has since led to an educational venture called the Teaching Value Project, a textbook titled Understanding Value-Based Care (McGraw-Hill), and a “Costs of Care” iPhone app—all designed to help clinicians make high-value clinical decisions and increase price transparency.
4 The Do No Harm Project
http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/
GIM/education/DoNoHarmProject/Pages/Welcome.aspx
- Launched in 2012 at the University of Colorado by Brandon Combs, MD, and Tanner Caverly, MD, MPH, the project is aimed at medical trainees. Starting with the internal medicine program, the physicians asked medical residents to reflect on a patient who had suffered an adverse consequence from medical overuse. “This was reasonable care that was nevertheless unneeded or unwanted by a fully informed patient,” Dr. Combs says. “So this isn’t errors or malpractice; this is the stuff that flies under the radar, the stuff that people might miss.”
- The project uses clinical vignettes written by medical trainees (including those found in the “Teachable Moments” section of JAMA Internal Medicine) to improve the recognition of potential harm from overuse and to spur a culture change. In 2013, the Teaching Value and Choosing Wisely Competition, jointly sponsored by Costs of Care and the ABIM Foundation, recognized the project as one of its Innovations award winners; so far, five internal medicine and emergency medicine programs around the country have adopted the model.
5 I-CARE
- The Interactive Cost-Awareness Resident Exercise (I-CARE) was launched in 2011 by Yale hospitalist Robert Fogerty, MD, MPH, and colleagues. The friendly competition among medical students, interns, residents, and attending physicians uses a traditional morning report structure and charge data. At these conferences, the providers compete to come up with the correct diagnosis using the fewest resources possible. In 2013, the Teaching Value and Choosing Wisely competition, jointly sponsored by Costs of Care and the ABIM Foundation, recognized I-CARE as one of its Innovations award winners.
- “Physicians tend not to have a lot of business training,” Dr. Fogerty says. “They don’t have a lot of financial training. They don’t have a lot of economics background, and when you tell them that healthcare expense is 18% of GDP [gross domestic product], they don’t really know what that means. When you tell them that that would be in the top 10 of world economies, now they’re starting to get a picture of it. And when you tell them that that CAT scan you just ordered is going to cost your patient $1,200, that’s an eye-opening number that they can understand. So I think the purpose behind I-CARE was to take this seemingly insurmountable problem and to begin to digest it into small enough bits of information that allowed this problem to be accessible to the trainees.”
6 Providers for Responsible Ordering (PRO)
www.providersforresponsibleordering.org
- The organization launched in 2009 with a mission to “promote high-value care and create a culture that minimizes unnecessary or potentially-harmful diagnostic tests and interventions.” By the end of 2014, five chapters had been established and more than 150 providers had signed the PRO pledge that asks signatories, in part, “to provide my patients with all of the care that they need and none that they do not, thereby protecting them from unnecessary diagnostic tests and treatments.”
- “Our model is simple and yet powerful. It’s a grass-roots effort that any interested provider can join, and it builds on a peer-to-peer approach of establishment of chapters that solve local problems and reporting of those solutions back to the national group,” says Anthony Accurso, MD, PRO faculty director at Johns Hopkins Bayview Medical Center in Baltimore.
1 Caring Wisely Program
http://healthvalue.ucsf.edu/caring-wisely
- Started in 2012 within the division of hospital medicine at the University of California, San Francisco (UCSF), the program sponsored or collaborated on six high-value care projects within its first year. “We don’t shy away from the fact that part of what we do is address cost, but it is about making sure that we’ve got the right mindset and right frame, which is that we’re going to improve quality while decreasing costs and keeping it really patient centered,” says Christopher Moriates, MD, program director and an assistant clinical professor.
- Beyond its successful Nebs No More After 24 project, Caring Wisely helped hospital pharmacists and the UCSF Medication Outcomes Center develop and implement an evidence-based initiative to cut inappropriate stress ulcer prophylaxis in intensive care unit patients. After its first month, the program had cut unnecessary use of the medication from 19% to 6.6%.
2 Choosing Wisely Program
- Launched in 2012 as an initiative of the ABIM Foundation and based on a pilot project by the National Physicians Alliance, Choosing Wisely was designed to encourage more proactive conversations between providers and patients. The goal is to help patients choose care that is both evidence-based and necessary, while minimizing harm and avoiding duplication of tests or procedures.
- Since its debut, the program has gathered nearly 60 specialty society lists of “Five Things Physicians and Patients Should Question,” including two lists compiled by SHM for adult and pediatric hospital medicine. As a complement, Consumer Reports and many of the specialty societies have collaborated on 75 patient-friendly reports that dispense advice about whether a test, treatment, or procedure is really needed.
3 Costs of Care
- Founded in 2009 by Neel Shah, MD, an assistant professor at Harvard Medical School, the nonprofit got its start by collecting stories from patients and physicians about unnecessary or inflated healthcare costs. “It had a manifesto about what the role of physicians ought to be and thinking about healthcare costs, and that message actually really resonated with a lot of people,” Dr. Shah says. “That basic message that we decide what goes on the bill, patients have to pay for it, and yet we don’t know what it’s costing them—that just seemed crazy and we heard from a lot of people, both from patients with whom that message resonated and physicians who were like, ‘Yeah.’”
- In 2010, the organizers hosted their first essay contest and ended up receiving more than 300 entries; several were subsequently included as case reports in a report on healthcare waste by the Institute of Medicine. The nonprofit, supported by the ABIM Foundation and other institutions, has since led to an educational venture called the Teaching Value Project, a textbook titled Understanding Value-Based Care (McGraw-Hill), and a “Costs of Care” iPhone app—all designed to help clinicians make high-value clinical decisions and increase price transparency.
4 The Do No Harm Project
http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/
GIM/education/DoNoHarmProject/Pages/Welcome.aspx
- Launched in 2012 at the University of Colorado by Brandon Combs, MD, and Tanner Caverly, MD, MPH, the project is aimed at medical trainees. Starting with the internal medicine program, the physicians asked medical residents to reflect on a patient who had suffered an adverse consequence from medical overuse. “This was reasonable care that was nevertheless unneeded or unwanted by a fully informed patient,” Dr. Combs says. “So this isn’t errors or malpractice; this is the stuff that flies under the radar, the stuff that people might miss.”
- The project uses clinical vignettes written by medical trainees (including those found in the “Teachable Moments” section of JAMA Internal Medicine) to improve the recognition of potential harm from overuse and to spur a culture change. In 2013, the Teaching Value and Choosing Wisely Competition, jointly sponsored by Costs of Care and the ABIM Foundation, recognized the project as one of its Innovations award winners; so far, five internal medicine and emergency medicine programs around the country have adopted the model.
5 I-CARE
- The Interactive Cost-Awareness Resident Exercise (I-CARE) was launched in 2011 by Yale hospitalist Robert Fogerty, MD, MPH, and colleagues. The friendly competition among medical students, interns, residents, and attending physicians uses a traditional morning report structure and charge data. At these conferences, the providers compete to come up with the correct diagnosis using the fewest resources possible. In 2013, the Teaching Value and Choosing Wisely competition, jointly sponsored by Costs of Care and the ABIM Foundation, recognized I-CARE as one of its Innovations award winners.
- “Physicians tend not to have a lot of business training,” Dr. Fogerty says. “They don’t have a lot of financial training. They don’t have a lot of economics background, and when you tell them that healthcare expense is 18% of GDP [gross domestic product], they don’t really know what that means. When you tell them that that would be in the top 10 of world economies, now they’re starting to get a picture of it. And when you tell them that that CAT scan you just ordered is going to cost your patient $1,200, that’s an eye-opening number that they can understand. So I think the purpose behind I-CARE was to take this seemingly insurmountable problem and to begin to digest it into small enough bits of information that allowed this problem to be accessible to the trainees.”
6 Providers for Responsible Ordering (PRO)
www.providersforresponsibleordering.org
- The organization launched in 2009 with a mission to “promote high-value care and create a culture that minimizes unnecessary or potentially-harmful diagnostic tests and interventions.” By the end of 2014, five chapters had been established and more than 150 providers had signed the PRO pledge that asks signatories, in part, “to provide my patients with all of the care that they need and none that they do not, thereby protecting them from unnecessary diagnostic tests and treatments.”
- “Our model is simple and yet powerful. It’s a grass-roots effort that any interested provider can join, and it builds on a peer-to-peer approach of establishment of chapters that solve local problems and reporting of those solutions back to the national group,” says Anthony Accurso, MD, PRO faculty director at Johns Hopkins Bayview Medical Center in Baltimore.
Practical Approaches in the Management of Bipolar Depression: Overcoming Challenges and Avoiding Pitfalls
In the past 2 decades, the burden of care for psychiatric complaints in primary care—including bipolar depression—has increased considerably. The prevalence of bipolar disorder (BPD) in primary care has been recently estimated to range up to 4.3%, and in studies with broader definitions of the disorder or in populations with higher-than-usual psychiatric disorders, the prevalence has been reported to be up to 11.4%. Even though BPD is seen commonly in primary care, there are still profound disparities in the delivery of care, including underdiagnosis, misdiagnosis, and inappropriate treatments. There is abundant evidence that BPD can be successfully managed in the primary care setting when adequate physician education, collaborative care teams, and patient education are employed. Efficacious and well-tolerated pharmacologic treatments for BPD are available, and evidence-based pharmacotherapy can be optimally managed by the primary care provider. In this supplement, experts in BPD discuss the recognition and management of bipolar depression and associated comorbidities in the primary care setting.
In the past 2 decades, the burden of care for psychiatric complaints in primary care—including bipolar depression—has increased considerably. The prevalence of bipolar disorder (BPD) in primary care has been recently estimated to range up to 4.3%, and in studies with broader definitions of the disorder or in populations with higher-than-usual psychiatric disorders, the prevalence has been reported to be up to 11.4%. Even though BPD is seen commonly in primary care, there are still profound disparities in the delivery of care, including underdiagnosis, misdiagnosis, and inappropriate treatments. There is abundant evidence that BPD can be successfully managed in the primary care setting when adequate physician education, collaborative care teams, and patient education are employed. Efficacious and well-tolerated pharmacologic treatments for BPD are available, and evidence-based pharmacotherapy can be optimally managed by the primary care provider. In this supplement, experts in BPD discuss the recognition and management of bipolar depression and associated comorbidities in the primary care setting.
In the past 2 decades, the burden of care for psychiatric complaints in primary care—including bipolar depression—has increased considerably. The prevalence of bipolar disorder (BPD) in primary care has been recently estimated to range up to 4.3%, and in studies with broader definitions of the disorder or in populations with higher-than-usual psychiatric disorders, the prevalence has been reported to be up to 11.4%. Even though BPD is seen commonly in primary care, there are still profound disparities in the delivery of care, including underdiagnosis, misdiagnosis, and inappropriate treatments. There is abundant evidence that BPD can be successfully managed in the primary care setting when adequate physician education, collaborative care teams, and patient education are employed. Efficacious and well-tolerated pharmacologic treatments for BPD are available, and evidence-based pharmacotherapy can be optimally managed by the primary care provider. In this supplement, experts in BPD discuss the recognition and management of bipolar depression and associated comorbidities in the primary care setting.
