User login
Bundled Payment and Hospital Medicine, Pt. 2
Editor’s note: Second in a two-part series examining bundled payments and hospital medicine. In full disclosure, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
In part one of this series, we discussed the basics of the BPCI program. Now we will delve into specific roles and opportunities for hospitalists in bundled payment programs in general, and the BPCI program in particular.
The bundled payment model can be hard to explain. One example that might make it clearer is that of LASIK vision correction surgery, where a single bundled payment covers the fees of the ophthalmologist, the operating facility, and any other services (like optometry) and medications (like eye drops). Another example is the diagnosis-related group (DRG) payment for hospital care, in which all facility costs are bundled together into a single payment.
A simplistic way to differentiate bundled payment from accountable care organization (ACOs) is that the former is typically initiated by an acute medical or surgical event and concludes after a recovery period—often 30, 60, or 90 days. Conversely, the latter generally covers the care of individuals within a population over time, often focusing on the management of chronic conditions.
The Opportunity
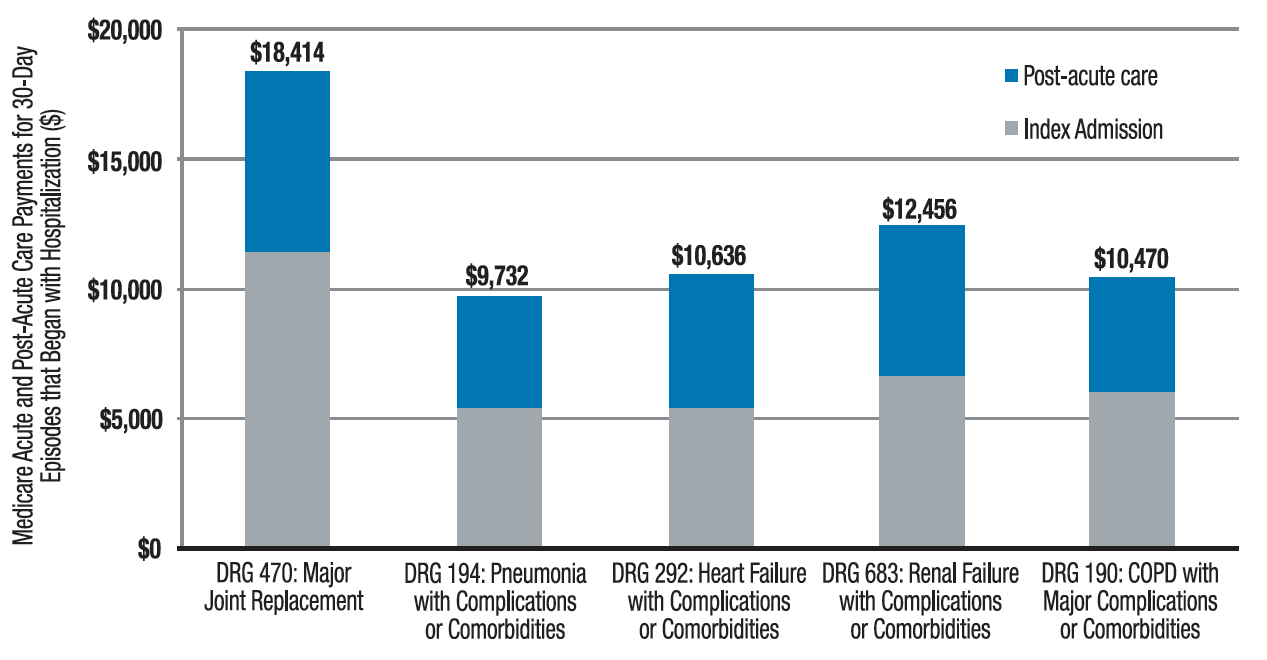
Two major opportunities for hospitalists to improve value (quality/cost) present themselves through the BPCI initiative. One is in post-acute facility utilization, and the other is in reducing readmissions. Figure 1 shows that for 30-day episodes starting with a hospitalization for five common conditions, payments for post-acute care are surprisingly close in amount to those for the preceding hospitalization.1
Much of the cost of post-acute care comes from skilled nursing facilities (SNFs) and, to a lesser degree, inpatient rehabilitation facilities. A broad range of research studies has demonstrated that inpatient care managed by hospitalists—compared with the traditional model—is associated with a decrease in inpatient costs; however, recent research indicates that the hospital cost savings generated by hospitalists are offset by more spending in the 30 days post discharge, specifically on more SNF care and increased readmissions.2 As another indicator that post-acute care needs a closer look, a 2013 Institute of Medicine report concluded that spending on post-acute care was responsible for the majority of Medicare’s overall regional variation in spending.1,3
Of course, success in a bundled payment model will also be derived from reducing costs in the hospital setting, such as those stemming from unnecessary or duplicative testing and imaging, injudicious use of consultants, and practices identified in programs such as Choosing Wisely.
How Your Practice Can Drive Bundled Payment Success
The aforementioned observations point to the need to improve the value of post-acute care by optimizing post-acute spending—driven mostly by SNF costs—and minimizing avoidable readmissions. I offer the following inpatient interventions to achieve these goals:
- Speak with patients early and often regarding expectations for recovery post discharge. When possible, set a goal of home discharge with the needed support.
- Write orders for early ambulation. Develop an early ambulation program with nursing and physical therapy.
- Address goals of care during the patient/family meeting. For appropriate patients with life-limiting illness, involve the palliative care service or equivalent and discuss the role of future aggressive interventions, including hospitalization, so that the course set is consistent with the patients’ goals and wishes.
- Lead the in-hospital team, instead of defaulting to others, like case management, in making an informed decision about ideal post-discharge location by factoring in caregiver availability, independence, and SNF needs. Marshal resources to enable a home recovery (i.e., home health evaluation), whether or not there is an intervening SNF stay. If patients go to a SNF, set expectations for length of stay in the facility.
- Adhere to best practices for care transitions, such as those in Project BOOST, including thorough medication reconciliation.
Beyond the Four Walls
As you aim for a high-value (high quality and affordable) discharge, your hospital medicine practice may consider new approaches to filling longstanding gaps in post-acute care. Forward-looking hospitalist groups have implemented the following approaches:
- Establish a post-discharge clinic where patients are seen after discharge, in the interim before they have an opportunity for primary care follow-up;
- Send teams to work in SNFs;
- Call patients after discharge to ensure they are following their plan of care;
- Leverage newer current procedural terminology (CPT) codes, like the Transitional Care Management or Chronic Care Management codes, to support your transitional care services;
- Provide home visits for high-risk patients; and
- Access waivers for G-codes for home visits and/or telemedicine outside of rural areas. These waivers exist under the BPCI initiative.
Shift from ‘Traditional’ Hospitalist to ‘Value’ Hospitalist
If some of the changes in practice needed to succeed in a bundled payment world seem daunting to you, it may be helpful to realize that with the challenge comes an opportunity. This opportunity for hospitalists parallels that of the early days of the specialty, when reducing length of stay created substantial support from hospital leaders and was a factor leading to the rapid growth in the number of hospitalists. In January, the U.S. Secretary of Health and Human Services set a goal to tie 50% of Medicare payments to ‘alternative payment models’ like bundled payments by 2018. In April, as part of the sustainable growth rate fix, Medicare announced it would create substantial new bonuses for physicians who have at least 25% of their revenue in such models.1
As healthcare policy aligns behind ‘alternative payment models,’ bundled payment programs are likely to be a potent driver of an evolving hospitalist specialty. Next-generation hospitalists will be asked to take a leadership role in addressing ‘value’ with responsibility for improving care coordination and affordability over an episode of illness.
Now may be the time to take to heart the words of computer scientist Alan Kay: “The best way to predict the future is to invent it.”

References
- Mechanic R. Post-acute care–the next frontier for controlling Medicare spending. N Engl J Med. 2014;370(8):692-694.
- Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-159.
- Newhouse JP, Garber AM. Geographic variation in Medicare services. N Engl J Med. 2013;368(16):1465-1468.
Editor’s note: Second in a two-part series examining bundled payments and hospital medicine. In full disclosure, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
In part one of this series, we discussed the basics of the BPCI program. Now we will delve into specific roles and opportunities for hospitalists in bundled payment programs in general, and the BPCI program in particular.
The bundled payment model can be hard to explain. One example that might make it clearer is that of LASIK vision correction surgery, where a single bundled payment covers the fees of the ophthalmologist, the operating facility, and any other services (like optometry) and medications (like eye drops). Another example is the diagnosis-related group (DRG) payment for hospital care, in which all facility costs are bundled together into a single payment.
A simplistic way to differentiate bundled payment from accountable care organization (ACOs) is that the former is typically initiated by an acute medical or surgical event and concludes after a recovery period—often 30, 60, or 90 days. Conversely, the latter generally covers the care of individuals within a population over time, often focusing on the management of chronic conditions.
The Opportunity
Two major opportunities for hospitalists to improve value (quality/cost) present themselves through the BPCI initiative. One is in post-acute facility utilization, and the other is in reducing readmissions. Figure 1 shows that for 30-day episodes starting with a hospitalization for five common conditions, payments for post-acute care are surprisingly close in amount to those for the preceding hospitalization.1
Much of the cost of post-acute care comes from skilled nursing facilities (SNFs) and, to a lesser degree, inpatient rehabilitation facilities. A broad range of research studies has demonstrated that inpatient care managed by hospitalists—compared with the traditional model—is associated with a decrease in inpatient costs; however, recent research indicates that the hospital cost savings generated by hospitalists are offset by more spending in the 30 days post discharge, specifically on more SNF care and increased readmissions.2 As another indicator that post-acute care needs a closer look, a 2013 Institute of Medicine report concluded that spending on post-acute care was responsible for the majority of Medicare’s overall regional variation in spending.1,3
Of course, success in a bundled payment model will also be derived from reducing costs in the hospital setting, such as those stemming from unnecessary or duplicative testing and imaging, injudicious use of consultants, and practices identified in programs such as Choosing Wisely.
How Your Practice Can Drive Bundled Payment Success
The aforementioned observations point to the need to improve the value of post-acute care by optimizing post-acute spending—driven mostly by SNF costs—and minimizing avoidable readmissions. I offer the following inpatient interventions to achieve these goals:
- Speak with patients early and often regarding expectations for recovery post discharge. When possible, set a goal of home discharge with the needed support.
- Write orders for early ambulation. Develop an early ambulation program with nursing and physical therapy.
- Address goals of care during the patient/family meeting. For appropriate patients with life-limiting illness, involve the palliative care service or equivalent and discuss the role of future aggressive interventions, including hospitalization, so that the course set is consistent with the patients’ goals and wishes.
- Lead the in-hospital team, instead of defaulting to others, like case management, in making an informed decision about ideal post-discharge location by factoring in caregiver availability, independence, and SNF needs. Marshal resources to enable a home recovery (i.e., home health evaluation), whether or not there is an intervening SNF stay. If patients go to a SNF, set expectations for length of stay in the facility.
- Adhere to best practices for care transitions, such as those in Project BOOST, including thorough medication reconciliation.
Beyond the Four Walls
As you aim for a high-value (high quality and affordable) discharge, your hospital medicine practice may consider new approaches to filling longstanding gaps in post-acute care. Forward-looking hospitalist groups have implemented the following approaches:
- Establish a post-discharge clinic where patients are seen after discharge, in the interim before they have an opportunity for primary care follow-up;
- Send teams to work in SNFs;
- Call patients after discharge to ensure they are following their plan of care;
- Leverage newer current procedural terminology (CPT) codes, like the Transitional Care Management or Chronic Care Management codes, to support your transitional care services;
- Provide home visits for high-risk patients; and
- Access waivers for G-codes for home visits and/or telemedicine outside of rural areas. These waivers exist under the BPCI initiative.
Shift from ‘Traditional’ Hospitalist to ‘Value’ Hospitalist
If some of the changes in practice needed to succeed in a bundled payment world seem daunting to you, it may be helpful to realize that with the challenge comes an opportunity. This opportunity for hospitalists parallels that of the early days of the specialty, when reducing length of stay created substantial support from hospital leaders and was a factor leading to the rapid growth in the number of hospitalists. In January, the U.S. Secretary of Health and Human Services set a goal to tie 50% of Medicare payments to ‘alternative payment models’ like bundled payments by 2018. In April, as part of the sustainable growth rate fix, Medicare announced it would create substantial new bonuses for physicians who have at least 25% of their revenue in such models.1
As healthcare policy aligns behind ‘alternative payment models,’ bundled payment programs are likely to be a potent driver of an evolving hospitalist specialty. Next-generation hospitalists will be asked to take a leadership role in addressing ‘value’ with responsibility for improving care coordination and affordability over an episode of illness.
Now may be the time to take to heart the words of computer scientist Alan Kay: “The best way to predict the future is to invent it.”
References
- Mechanic R. Post-acute care–the next frontier for controlling Medicare spending. N Engl J Med. 2014;370(8):692-694.
- Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-159.
- Newhouse JP, Garber AM. Geographic variation in Medicare services. N Engl J Med. 2013;368(16):1465-1468.
Editor’s note: Second in a two-part series examining bundled payments and hospital medicine. In full disclosure, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
In part one of this series, we discussed the basics of the BPCI program. Now we will delve into specific roles and opportunities for hospitalists in bundled payment programs in general, and the BPCI program in particular.
The bundled payment model can be hard to explain. One example that might make it clearer is that of LASIK vision correction surgery, where a single bundled payment covers the fees of the ophthalmologist, the operating facility, and any other services (like optometry) and medications (like eye drops). Another example is the diagnosis-related group (DRG) payment for hospital care, in which all facility costs are bundled together into a single payment.
A simplistic way to differentiate bundled payment from accountable care organization (ACOs) is that the former is typically initiated by an acute medical or surgical event and concludes after a recovery period—often 30, 60, or 90 days. Conversely, the latter generally covers the care of individuals within a population over time, often focusing on the management of chronic conditions.
The Opportunity
Two major opportunities for hospitalists to improve value (quality/cost) present themselves through the BPCI initiative. One is in post-acute facility utilization, and the other is in reducing readmissions. Figure 1 shows that for 30-day episodes starting with a hospitalization for five common conditions, payments for post-acute care are surprisingly close in amount to those for the preceding hospitalization.1
Much of the cost of post-acute care comes from skilled nursing facilities (SNFs) and, to a lesser degree, inpatient rehabilitation facilities. A broad range of research studies has demonstrated that inpatient care managed by hospitalists—compared with the traditional model—is associated with a decrease in inpatient costs; however, recent research indicates that the hospital cost savings generated by hospitalists are offset by more spending in the 30 days post discharge, specifically on more SNF care and increased readmissions.2 As another indicator that post-acute care needs a closer look, a 2013 Institute of Medicine report concluded that spending on post-acute care was responsible for the majority of Medicare’s overall regional variation in spending.1,3
Of course, success in a bundled payment model will also be derived from reducing costs in the hospital setting, such as those stemming from unnecessary or duplicative testing and imaging, injudicious use of consultants, and practices identified in programs such as Choosing Wisely.
How Your Practice Can Drive Bundled Payment Success
The aforementioned observations point to the need to improve the value of post-acute care by optimizing post-acute spending—driven mostly by SNF costs—and minimizing avoidable readmissions. I offer the following inpatient interventions to achieve these goals:
- Speak with patients early and often regarding expectations for recovery post discharge. When possible, set a goal of home discharge with the needed support.
- Write orders for early ambulation. Develop an early ambulation program with nursing and physical therapy.
- Address goals of care during the patient/family meeting. For appropriate patients with life-limiting illness, involve the palliative care service or equivalent and discuss the role of future aggressive interventions, including hospitalization, so that the course set is consistent with the patients’ goals and wishes.
- Lead the in-hospital team, instead of defaulting to others, like case management, in making an informed decision about ideal post-discharge location by factoring in caregiver availability, independence, and SNF needs. Marshal resources to enable a home recovery (i.e., home health evaluation), whether or not there is an intervening SNF stay. If patients go to a SNF, set expectations for length of stay in the facility.
- Adhere to best practices for care transitions, such as those in Project BOOST, including thorough medication reconciliation.
Beyond the Four Walls
As you aim for a high-value (high quality and affordable) discharge, your hospital medicine practice may consider new approaches to filling longstanding gaps in post-acute care. Forward-looking hospitalist groups have implemented the following approaches:
- Establish a post-discharge clinic where patients are seen after discharge, in the interim before they have an opportunity for primary care follow-up;
- Send teams to work in SNFs;
- Call patients after discharge to ensure they are following their plan of care;
- Leverage newer current procedural terminology (CPT) codes, like the Transitional Care Management or Chronic Care Management codes, to support your transitional care services;
- Provide home visits for high-risk patients; and
- Access waivers for G-codes for home visits and/or telemedicine outside of rural areas. These waivers exist under the BPCI initiative.
Shift from ‘Traditional’ Hospitalist to ‘Value’ Hospitalist
If some of the changes in practice needed to succeed in a bundled payment world seem daunting to you, it may be helpful to realize that with the challenge comes an opportunity. This opportunity for hospitalists parallels that of the early days of the specialty, when reducing length of stay created substantial support from hospital leaders and was a factor leading to the rapid growth in the number of hospitalists. In January, the U.S. Secretary of Health and Human Services set a goal to tie 50% of Medicare payments to ‘alternative payment models’ like bundled payments by 2018. In April, as part of the sustainable growth rate fix, Medicare announced it would create substantial new bonuses for physicians who have at least 25% of their revenue in such models.1
As healthcare policy aligns behind ‘alternative payment models,’ bundled payment programs are likely to be a potent driver of an evolving hospitalist specialty. Next-generation hospitalists will be asked to take a leadership role in addressing ‘value’ with responsibility for improving care coordination and affordability over an episode of illness.
Now may be the time to take to heart the words of computer scientist Alan Kay: “The best way to predict the future is to invent it.”
References
- Mechanic R. Post-acute care–the next frontier for controlling Medicare spending. N Engl J Med. 2014;370(8):692-694.
- Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-159.
- Newhouse JP, Garber AM. Geographic variation in Medicare services. N Engl J Med. 2013;368(16):1465-1468.
Changing the Paradigm: New Thoughts on Pathophysiology and Drugable Targets in Acne
Who is tired of the same old stuff when it comes to acne? Innovation in therapy has been stagnant with a flurry of “me too” reformulated fixed combinations. The only true advance has been in drug delivery, with new vehicles allowing for the solubilization of established drugs such as dapsone or the combination of incompatible actives such as benzoyl peroxide and a retinoid. Before we can welcome new drugs with open arms, we must first expand the construct of acne pathophysiology to identify more appropriate targets for said new drugs. In a recent article published online in the Journal of the American Academy of Dermatology in June, Metiko et al highlight this sentiment. Generations of dermatologists were taught the 3- to 4-step process (depending on the teacher) through which an acne lesion forms: (1) follicular epidermal hyperproliferation, (2) Propionibacterium acnes colonization, and (3) inflammation. However, the molecular underpinnings of this theory have been challenged for more than a decade, with research highlighting the presence of preclinical inflammation, most recently found to be mediated by IL-1ß through a specific inflammasome pathway, NLRP3 (NOD-like receptor family, pyrin domain containing 3). Maybe we are missing a bridge between this stellar basic science and the clinical dermatologist who contends that the pesky microcomedone is the acne instigator. This short but sweet letter once again calls this antiquated prose into question in a highly visible clinical dermatology journal.
In thinking of new pathways and targets, Gupta et al published an article online in Archives of Dermatological Research on May 19 on the role of peroxisome proliferator-activated receptors (PPARs) and PPAR agonists in the treatment of multiple dermatologic diseases. For our purposes, I will highlight the section on acne and will start at the end: More research is needed. Peroxisome proliferator-activated receptors are nuclear hormone receptors that regulate gene expression, cell growth and differentiation, apoptosis, inflammatory responses, and tumorigenesis after binding with specific ligands. With respect to acne specifically, PPARs influence 2 of the pathophysiologic factors—sebum production and inflammation—due to their effect on lipid deposition in the sebocytes and inhibition of proinflammatory gene expression and downregulation of inflammatory cytokines. It appears that activation or inhibition of specific PPAR subtypes can either increase or decrease sebum production or be pro- or anti-inflammatory. The tough part is which receptors to activate and which to inhibit. This review related to an interesting clinical study that evaluated oral zileuton 600 mg administered 4 times daily for 3 months for acne. Zileuton inhibits leukotriene B4 production, which, as it turns out, is a natural ligand for PPARα. The idea here is that this blockade would be anti-inflammatory and indirectly inhibit the sebum production via PPARα suppression. The pilot study was reported as successful, with a decrease in the papulopustular acne severity index in a time-dependent manner in subjects evaluated.
What’s the issue?
So, what’s the point of this long-winded, double-paper review? We need to expand our acne horizons. We need new bench-to-bedside approaches. Which is your favorite target?
Who is tired of the same old stuff when it comes to acne? Innovation in therapy has been stagnant with a flurry of “me too” reformulated fixed combinations. The only true advance has been in drug delivery, with new vehicles allowing for the solubilization of established drugs such as dapsone or the combination of incompatible actives such as benzoyl peroxide and a retinoid. Before we can welcome new drugs with open arms, we must first expand the construct of acne pathophysiology to identify more appropriate targets for said new drugs. In a recent article published online in the Journal of the American Academy of Dermatology in June, Metiko et al highlight this sentiment. Generations of dermatologists were taught the 3- to 4-step process (depending on the teacher) through which an acne lesion forms: (1) follicular epidermal hyperproliferation, (2) Propionibacterium acnes colonization, and (3) inflammation. However, the molecular underpinnings of this theory have been challenged for more than a decade, with research highlighting the presence of preclinical inflammation, most recently found to be mediated by IL-1ß through a specific inflammasome pathway, NLRP3 (NOD-like receptor family, pyrin domain containing 3). Maybe we are missing a bridge between this stellar basic science and the clinical dermatologist who contends that the pesky microcomedone is the acne instigator. This short but sweet letter once again calls this antiquated prose into question in a highly visible clinical dermatology journal.
In thinking of new pathways and targets, Gupta et al published an article online in Archives of Dermatological Research on May 19 on the role of peroxisome proliferator-activated receptors (PPARs) and PPAR agonists in the treatment of multiple dermatologic diseases. For our purposes, I will highlight the section on acne and will start at the end: More research is needed. Peroxisome proliferator-activated receptors are nuclear hormone receptors that regulate gene expression, cell growth and differentiation, apoptosis, inflammatory responses, and tumorigenesis after binding with specific ligands. With respect to acne specifically, PPARs influence 2 of the pathophysiologic factors—sebum production and inflammation—due to their effect on lipid deposition in the sebocytes and inhibition of proinflammatory gene expression and downregulation of inflammatory cytokines. It appears that activation or inhibition of specific PPAR subtypes can either increase or decrease sebum production or be pro- or anti-inflammatory. The tough part is which receptors to activate and which to inhibit. This review related to an interesting clinical study that evaluated oral zileuton 600 mg administered 4 times daily for 3 months for acne. Zileuton inhibits leukotriene B4 production, which, as it turns out, is a natural ligand for PPARα. The idea here is that this blockade would be anti-inflammatory and indirectly inhibit the sebum production via PPARα suppression. The pilot study was reported as successful, with a decrease in the papulopustular acne severity index in a time-dependent manner in subjects evaluated.
What’s the issue?
So, what’s the point of this long-winded, double-paper review? We need to expand our acne horizons. We need new bench-to-bedside approaches. Which is your favorite target?
Who is tired of the same old stuff when it comes to acne? Innovation in therapy has been stagnant with a flurry of “me too” reformulated fixed combinations. The only true advance has been in drug delivery, with new vehicles allowing for the solubilization of established drugs such as dapsone or the combination of incompatible actives such as benzoyl peroxide and a retinoid. Before we can welcome new drugs with open arms, we must first expand the construct of acne pathophysiology to identify more appropriate targets for said new drugs. In a recent article published online in the Journal of the American Academy of Dermatology in June, Metiko et al highlight this sentiment. Generations of dermatologists were taught the 3- to 4-step process (depending on the teacher) through which an acne lesion forms: (1) follicular epidermal hyperproliferation, (2) Propionibacterium acnes colonization, and (3) inflammation. However, the molecular underpinnings of this theory have been challenged for more than a decade, with research highlighting the presence of preclinical inflammation, most recently found to be mediated by IL-1ß through a specific inflammasome pathway, NLRP3 (NOD-like receptor family, pyrin domain containing 3). Maybe we are missing a bridge between this stellar basic science and the clinical dermatologist who contends that the pesky microcomedone is the acne instigator. This short but sweet letter once again calls this antiquated prose into question in a highly visible clinical dermatology journal.
In thinking of new pathways and targets, Gupta et al published an article online in Archives of Dermatological Research on May 19 on the role of peroxisome proliferator-activated receptors (PPARs) and PPAR agonists in the treatment of multiple dermatologic diseases. For our purposes, I will highlight the section on acne and will start at the end: More research is needed. Peroxisome proliferator-activated receptors are nuclear hormone receptors that regulate gene expression, cell growth and differentiation, apoptosis, inflammatory responses, and tumorigenesis after binding with specific ligands. With respect to acne specifically, PPARs influence 2 of the pathophysiologic factors—sebum production and inflammation—due to their effect on lipid deposition in the sebocytes and inhibition of proinflammatory gene expression and downregulation of inflammatory cytokines. It appears that activation or inhibition of specific PPAR subtypes can either increase or decrease sebum production or be pro- or anti-inflammatory. The tough part is which receptors to activate and which to inhibit. This review related to an interesting clinical study that evaluated oral zileuton 600 mg administered 4 times daily for 3 months for acne. Zileuton inhibits leukotriene B4 production, which, as it turns out, is a natural ligand for PPARα. The idea here is that this blockade would be anti-inflammatory and indirectly inhibit the sebum production via PPARα suppression. The pilot study was reported as successful, with a decrease in the papulopustular acne severity index in a time-dependent manner in subjects evaluated.
What’s the issue?
So, what’s the point of this long-winded, double-paper review? We need to expand our acne horizons. We need new bench-to-bedside approaches. Which is your favorite target?

Prenatal test can detect lymphoma in mothers

Photo by Graham Colm
GLASGOW—A non-invasive prenatal test (NIPT) used to identify chromosomal fetal disorders can detect maternal cancers before symptoms appear, a new study has shown.
Testing revealed chromosomal abnormalities in 3 women that bore a resemblance to abnormalities observed in cancers. And additional testing confirmed the women had cancer—Hodgkin lymphoma (HL), follicular lymphoma (FL), and ovarian carcinoma.
This research was presented at the European Human Genetics Conference 2015 and published simultaneously in JAMA Oncology.
Nathalie Brison, PhD, of University Hospitals Leuven in Belgium, and her colleagues conducted this research with the goal of improving the NIPT test. They wanted to overcome some of the technical problems that can cause the test to produce false-negative or false-positive results.
“Even though it is very reliable, we believed that we could make it even better, and, in doing so, we could also find other chromosomal abnormalities apart from the traditional trisomy syndromes—Down’s [trisomy 21], Edward’s [trisomy 18], and Patau [trisomy 13],” Dr Brison said.
“Using the new, adapted test in over 6000 pregnancies, and looking at other chromosomes, we identified 3 different genomic abnormalities in 3 women that could not be linked to either the maternal or fetal genomic profile. We realized that the abnormalities bore a resemblance to those found in cancer and referred the women to the oncology unit.”
Further examination, including whole-body MRI scanning and pathological and genetic investigations, revealed the presence of 3 different early stage cancers in the women: ovarian carcinoma, FL, and HL.
The researchers said that, without NIPT, these cancers likely would not have been detected until the women developed symptoms.
“Considering the bad prognosis of some cancers when detected later, and given that we know that it is both possible and safe to treat the disease during pregnancy, this is an important added advantage of NIPT,” said study author Joris Vermeesch, PhD, also of University Hospitals Leuven.
“During pregnancy, cancer-related symptoms may well be masked. Fatigue, nausea, abdominal pain, and vaginal blood loss are easily interpretable as a normal part of being pregnant. NIPT offers an opportunity for the accurate screening of high-risk women for cancer, allowing us to overcome the challenge of early diagnosis in pregnant women.”
Two of the 3 women diagnosed with cancer were treated. The woman with ovarian cancer was treated after delivery.
The woman with HL was treated during pregnancy and ultimately gave birth to a healthy girl. The woman with FL has indolent disease and may not require treatment for years, according to the researchers.
Follow-up investigations in the treated women showed that NIPT had the additional advantage of allowing for treatment monitoring. The researchers were able to see that chromosomal profiles became normal during and after chemotherapy.
Because NIPT involves looking at chromosomes other than 13, 18, and 21, the women taking part in this study were informed about the possibility of incidental findings.
“However, our study feeds into the ethical debate about whether or not to report incidental findings to patients and also has implications for the current political discussions concerning reimbursement and funding of NIPT by national healthcare systems,” Dr Vermeesch said.
The results also suggest that NIPT might enable the detection of pre-symptomatic cancers in the general population.
“We now know that it is possible to offer the accurate detection of chromosomally imbalanced cancers to the general population via minimally invasive screening methods,” Dr Brison said. “The normalization of the NIPT profile in these patients following treatment indicates that we can also measure response to treatment as early as after the first administration of chemotherapy.”
“Of course, larger-scale studies will be required to validate these results further, but we are confident that we have made an important step towards the possibility of wide-scale, effective, non-invasive cancer screening capable of detecting disease at an early stage.” ![]()
Photo by Graham Colm
GLASGOW—A non-invasive prenatal test (NIPT) used to identify chromosomal fetal disorders can detect maternal cancers before symptoms appear, a new study has shown.
Testing revealed chromosomal abnormalities in 3 women that bore a resemblance to abnormalities observed in cancers. And additional testing confirmed the women had cancer—Hodgkin lymphoma (HL), follicular lymphoma (FL), and ovarian carcinoma.
This research was presented at the European Human Genetics Conference 2015 and published simultaneously in JAMA Oncology.
Nathalie Brison, PhD, of University Hospitals Leuven in Belgium, and her colleagues conducted this research with the goal of improving the NIPT test. They wanted to overcome some of the technical problems that can cause the test to produce false-negative or false-positive results.
“Even though it is very reliable, we believed that we could make it even better, and, in doing so, we could also find other chromosomal abnormalities apart from the traditional trisomy syndromes—Down’s [trisomy 21], Edward’s [trisomy 18], and Patau [trisomy 13],” Dr Brison said.
“Using the new, adapted test in over 6000 pregnancies, and looking at other chromosomes, we identified 3 different genomic abnormalities in 3 women that could not be linked to either the maternal or fetal genomic profile. We realized that the abnormalities bore a resemblance to those found in cancer and referred the women to the oncology unit.”
Further examination, including whole-body MRI scanning and pathological and genetic investigations, revealed the presence of 3 different early stage cancers in the women: ovarian carcinoma, FL, and HL.
The researchers said that, without NIPT, these cancers likely would not have been detected until the women developed symptoms.
“Considering the bad prognosis of some cancers when detected later, and given that we know that it is both possible and safe to treat the disease during pregnancy, this is an important added advantage of NIPT,” said study author Joris Vermeesch, PhD, also of University Hospitals Leuven.
“During pregnancy, cancer-related symptoms may well be masked. Fatigue, nausea, abdominal pain, and vaginal blood loss are easily interpretable as a normal part of being pregnant. NIPT offers an opportunity for the accurate screening of high-risk women for cancer, allowing us to overcome the challenge of early diagnosis in pregnant women.”
Two of the 3 women diagnosed with cancer were treated. The woman with ovarian cancer was treated after delivery.
The woman with HL was treated during pregnancy and ultimately gave birth to a healthy girl. The woman with FL has indolent disease and may not require treatment for years, according to the researchers.
Follow-up investigations in the treated women showed that NIPT had the additional advantage of allowing for treatment monitoring. The researchers were able to see that chromosomal profiles became normal during and after chemotherapy.
Because NIPT involves looking at chromosomes other than 13, 18, and 21, the women taking part in this study were informed about the possibility of incidental findings.
“However, our study feeds into the ethical debate about whether or not to report incidental findings to patients and also has implications for the current political discussions concerning reimbursement and funding of NIPT by national healthcare systems,” Dr Vermeesch said.
The results also suggest that NIPT might enable the detection of pre-symptomatic cancers in the general population.
“We now know that it is possible to offer the accurate detection of chromosomally imbalanced cancers to the general population via minimally invasive screening methods,” Dr Brison said. “The normalization of the NIPT profile in these patients following treatment indicates that we can also measure response to treatment as early as after the first administration of chemotherapy.”
“Of course, larger-scale studies will be required to validate these results further, but we are confident that we have made an important step towards the possibility of wide-scale, effective, non-invasive cancer screening capable of detecting disease at an early stage.” ![]()
Photo by Graham Colm
GLASGOW—A non-invasive prenatal test (NIPT) used to identify chromosomal fetal disorders can detect maternal cancers before symptoms appear, a new study has shown.
Testing revealed chromosomal abnormalities in 3 women that bore a resemblance to abnormalities observed in cancers. And additional testing confirmed the women had cancer—Hodgkin lymphoma (HL), follicular lymphoma (FL), and ovarian carcinoma.
This research was presented at the European Human Genetics Conference 2015 and published simultaneously in JAMA Oncology.
Nathalie Brison, PhD, of University Hospitals Leuven in Belgium, and her colleagues conducted this research with the goal of improving the NIPT test. They wanted to overcome some of the technical problems that can cause the test to produce false-negative or false-positive results.
“Even though it is very reliable, we believed that we could make it even better, and, in doing so, we could also find other chromosomal abnormalities apart from the traditional trisomy syndromes—Down’s [trisomy 21], Edward’s [trisomy 18], and Patau [trisomy 13],” Dr Brison said.
“Using the new, adapted test in over 6000 pregnancies, and looking at other chromosomes, we identified 3 different genomic abnormalities in 3 women that could not be linked to either the maternal or fetal genomic profile. We realized that the abnormalities bore a resemblance to those found in cancer and referred the women to the oncology unit.”
Further examination, including whole-body MRI scanning and pathological and genetic investigations, revealed the presence of 3 different early stage cancers in the women: ovarian carcinoma, FL, and HL.
The researchers said that, without NIPT, these cancers likely would not have been detected until the women developed symptoms.
“Considering the bad prognosis of some cancers when detected later, and given that we know that it is both possible and safe to treat the disease during pregnancy, this is an important added advantage of NIPT,” said study author Joris Vermeesch, PhD, also of University Hospitals Leuven.
“During pregnancy, cancer-related symptoms may well be masked. Fatigue, nausea, abdominal pain, and vaginal blood loss are easily interpretable as a normal part of being pregnant. NIPT offers an opportunity for the accurate screening of high-risk women for cancer, allowing us to overcome the challenge of early diagnosis in pregnant women.”
Two of the 3 women diagnosed with cancer were treated. The woman with ovarian cancer was treated after delivery.
The woman with HL was treated during pregnancy and ultimately gave birth to a healthy girl. The woman with FL has indolent disease and may not require treatment for years, according to the researchers.
Follow-up investigations in the treated women showed that NIPT had the additional advantage of allowing for treatment monitoring. The researchers were able to see that chromosomal profiles became normal during and after chemotherapy.
Because NIPT involves looking at chromosomes other than 13, 18, and 21, the women taking part in this study were informed about the possibility of incidental findings.
“However, our study feeds into the ethical debate about whether or not to report incidental findings to patients and also has implications for the current political discussions concerning reimbursement and funding of NIPT by national healthcare systems,” Dr Vermeesch said.
The results also suggest that NIPT might enable the detection of pre-symptomatic cancers in the general population.
“We now know that it is possible to offer the accurate detection of chromosomally imbalanced cancers to the general population via minimally invasive screening methods,” Dr Brison said. “The normalization of the NIPT profile in these patients following treatment indicates that we can also measure response to treatment as early as after the first administration of chemotherapy.”
“Of course, larger-scale studies will be required to validate these results further, but we are confident that we have made an important step towards the possibility of wide-scale, effective, non-invasive cancer screening capable of detecting disease at an early stage.” ![]()
Host cell type may impact malaria treatment

Image by Peter H. Seeberger
A study published in PLOS Pathogens suggests the different metabolic states of reticulocytes and erythrocytes provide different growth conditions for the malaria parasites Plasmodium vivax and Plasmodium falciparum.
As P vivax grows exclusively in reticulocytes, and P falciparum grows primarily in erythrocytes, the research suggests drugs that work against one species might fail to be effective against the other.
Andrew Waters, PhD, of the University of Glasgow in the UK, and his colleagues set out to determine whether the 2 classes of host red blood cells offer different resources for parasite survival and whether these resources could influence antimalarial drug efficacy.
To do that, the team analyzed the metabolites present in reticulocytes and erythrocytes. They found that reticulocytes contain elevated levels of many metabolites that could potentially be scavenged by the invading and growing malaria parasite.
And there was a marked overlap in metabolic pathways observed in the reticulocyte and those predicted in the parasite. The researchers thought these common pathways might be uniquely dispensable to Plasmodium during its growth in reticulocytes but essential—and therefore a good drug target—for growth in erythrocytes.
To test this hypothesis, the team disrupted some of the overlapping pathways in P berghei, a species that causes malaria in mice and, similar to P vivax, has a strong preference for growth in reticulocytes.
They found the mutant P berghei strains could grow in mouse reticulocytes (utilizing the host’s metabolic products).
The researchers also compared the sensitivity of P berghei and P falciparum to a drug known to target one of the overlapping pathways, the pyrimidine biosynthesis inhibitor 5-fluoroorotate (5FOA).
They found that P berghei was considerably less sensitive to 5FOA than P falciparum. The IC50 value of 5FOA in vitro was almost 90-fold higher in P berghei than in P falciparum.
This was presumably because P berghei was able to scavenge the metabolites from their reticulocyte host environment, but no such external sources were available in the erythrocyte host cells invaded by P falciparum.
The researchers said their results indicate that reticulocytes provide a highly enriched host cell environment for Plasmodium parasites, and the availability of the reticulocyte metabolome might reduce or block the efficacy of antimalarial drugs that target parasite metabolism. ![]()
Image by Peter H. Seeberger
A study published in PLOS Pathogens suggests the different metabolic states of reticulocytes and erythrocytes provide different growth conditions for the malaria parasites Plasmodium vivax and Plasmodium falciparum.
As P vivax grows exclusively in reticulocytes, and P falciparum grows primarily in erythrocytes, the research suggests drugs that work against one species might fail to be effective against the other.
Andrew Waters, PhD, of the University of Glasgow in the UK, and his colleagues set out to determine whether the 2 classes of host red blood cells offer different resources for parasite survival and whether these resources could influence antimalarial drug efficacy.
To do that, the team analyzed the metabolites present in reticulocytes and erythrocytes. They found that reticulocytes contain elevated levels of many metabolites that could potentially be scavenged by the invading and growing malaria parasite.
And there was a marked overlap in metabolic pathways observed in the reticulocyte and those predicted in the parasite. The researchers thought these common pathways might be uniquely dispensable to Plasmodium during its growth in reticulocytes but essential—and therefore a good drug target—for growth in erythrocytes.
To test this hypothesis, the team disrupted some of the overlapping pathways in P berghei, a species that causes malaria in mice and, similar to P vivax, has a strong preference for growth in reticulocytes.
They found the mutant P berghei strains could grow in mouse reticulocytes (utilizing the host’s metabolic products).
The researchers also compared the sensitivity of P berghei and P falciparum to a drug known to target one of the overlapping pathways, the pyrimidine biosynthesis inhibitor 5-fluoroorotate (5FOA).
They found that P berghei was considerably less sensitive to 5FOA than P falciparum. The IC50 value of 5FOA in vitro was almost 90-fold higher in P berghei than in P falciparum.
This was presumably because P berghei was able to scavenge the metabolites from their reticulocyte host environment, but no such external sources were available in the erythrocyte host cells invaded by P falciparum.
The researchers said their results indicate that reticulocytes provide a highly enriched host cell environment for Plasmodium parasites, and the availability of the reticulocyte metabolome might reduce or block the efficacy of antimalarial drugs that target parasite metabolism. ![]()
Image by Peter H. Seeberger
A study published in PLOS Pathogens suggests the different metabolic states of reticulocytes and erythrocytes provide different growth conditions for the malaria parasites Plasmodium vivax and Plasmodium falciparum.
As P vivax grows exclusively in reticulocytes, and P falciparum grows primarily in erythrocytes, the research suggests drugs that work against one species might fail to be effective against the other.
Andrew Waters, PhD, of the University of Glasgow in the UK, and his colleagues set out to determine whether the 2 classes of host red blood cells offer different resources for parasite survival and whether these resources could influence antimalarial drug efficacy.
To do that, the team analyzed the metabolites present in reticulocytes and erythrocytes. They found that reticulocytes contain elevated levels of many metabolites that could potentially be scavenged by the invading and growing malaria parasite.
And there was a marked overlap in metabolic pathways observed in the reticulocyte and those predicted in the parasite. The researchers thought these common pathways might be uniquely dispensable to Plasmodium during its growth in reticulocytes but essential—and therefore a good drug target—for growth in erythrocytes.
To test this hypothesis, the team disrupted some of the overlapping pathways in P berghei, a species that causes malaria in mice and, similar to P vivax, has a strong preference for growth in reticulocytes.
They found the mutant P berghei strains could grow in mouse reticulocytes (utilizing the host’s metabolic products).
The researchers also compared the sensitivity of P berghei and P falciparum to a drug known to target one of the overlapping pathways, the pyrimidine biosynthesis inhibitor 5-fluoroorotate (5FOA).
They found that P berghei was considerably less sensitive to 5FOA than P falciparum. The IC50 value of 5FOA in vitro was almost 90-fold higher in P berghei than in P falciparum.
This was presumably because P berghei was able to scavenge the metabolites from their reticulocyte host environment, but no such external sources were available in the erythrocyte host cells invaded by P falciparum.
The researchers said their results indicate that reticulocytes provide a highly enriched host cell environment for Plasmodium parasites, and the availability of the reticulocyte metabolome might reduce or block the efficacy of antimalarial drugs that target parasite metabolism. ![]()
CMSC: Many menopausal and MS symptoms overlap
INDIANAPOLIS – About 50% of women with multiple sclerosis are postmenopausal, but objective data about the impact of menopause on the course of multiple sclerosis are lacking.
“We don’t know anything about the impact of menopause on the MS course; there is wide variability in patient-reported outcomes, but nothing written about comorbidities or symptom management,” Dr. Riley Bove, a neurologist at Brigham and Women’s Hospital, Boston, said at the annual meeting of the Consortium of Multiple Sclerosis Centers. “We’ve been working on this. A lot of it is unknown.”

She described menopause is “an opportunity for providers to tackle symptoms and improve well-being and discuss meaningful quality of life and priorities with patients. It can be a good time to talk about these things.”
In a study that Dr. Bove conducted with the online patient-powered research platform PatientsLikeMe, female MS patients were asked to describe the impact of menopause on their disease. Among the themes that emerged were an occasional perimenopausal onset of MS (“menopause and MS symptoms were pretty much simultaneous,” one 58-year-old respondent said); the effect of hot flashes on MS symptoms (“I confused the two, especially hot flashes,” said a 53-year-old woman); and worsening of MS-related disability after menopause, particularly surgical (“Before I stopped taking birth control pills I was working and able to walk and house clean , etc.,” a 53-year-old respondent said. “I had the surgery, and I started to progress toward being completely wheelchair bound.”)
When it comes to solid recommendations for how to manage MS symptoms that overlap with menopause, “we’re in an evidence-free zone,” Dr. Bove said. “Symptoms in MS are kind of like dominoes: You have difficulty sleeping and then your day is off, fatigue is up and your mood is off, and everything can spiral. In the clinic, perimenopausal women often say things like, ‘I feel like I’m falling apart’ or ‘something has to give’ or ‘I need a change.’ ”
Common overlapping symptoms include vasomotor manifestations such as hot flashes, cold flashes, vascular instability, and rapid heartbeat. “The leading mechanistic explanation for the vasomotor symptoms is that abrupt hormone deprivation will result in the loss of negative feedback over hypothalamic NA [noradrenaline] synthesis,” Dr. Bove explained. “The proximity of the hypothalamic thermoregulatory center to luteinizing hormone–releasing hormone-producing areas may also be involved.”
Sleep disturbances and insomnia in menopausal MS patients can impact fatigue and mood. Also, hot flashes can directly exacerbate the MS symptoms, fluctuating over the day or the week.
According to recommendations from the North American Menopause Society, estradiol is the most effective therapy for treating vasomotor symptoms. Other options include selective serotonin reuptake inhibitors (SSRIs) and selective noradrenergic reuptake inhibitors (SNRIs). “Probably the best studied SNRI is venlafaxine,” Dr. Bove said. “It seems to have modest effects on sleep quality and insomnia perimenopausally, as well as on hot flashes.”
Other alternatives include clonidine and gabapentin.
“If a patient wants to use [hormone therapy] for menopausal symptoms, it has to be an individualized approach,” Dr. Bove said. “You have to communicate with the primary care physician to understand what else is going on in this woman’s medical history. The current recommendations are to treat the symptoms with as low a dose as possible for as short a duration as possible. Our MS patients are also at risk for neurodegeneration, for brain volume loss, for cognitive decline, and for worsening function over time.”
With respect to cognition, observational studies have demonstrated that during a certain window of opportunity – defined as within 5 years of the last menstrual period – hormone therapy (HT) may have protective effects against Alzheimer’s disease and against cognitive decline in general. “Beyond this window of time, perhaps due to estrogen receptor down regulation, HT can be harmful, with an increased risk of stroke and dementia reported later on,” she said.
Against this, the Women’s Health Initiative Memory Study (WHIMS) looked at unopposed estrogen, and estrogen and progestin combination, compared with placebo. It found that in women who initiated HT at the age of 65 or older faced an increased risk of dementia from any cause, and of cognitive decline. “This study really put the kibosh on HT as a form of neuroprotection,” Dr. Bove said. “But perhaps it’s unfair to the many patients who are at risk for cognitive decline and neurodegeneration, because the WHIMS did not find an increased risk of adverse cognitive events in women in whom HT was started perimenopausally. Longitudinal, placebo-controlled trials of the effects of HT within the window of opportunity are required to either prove or refute the observational studies that already exist that suggest HT may be neuroprotective. This is an important point to discuss with patients.”
The impact of perimenopausal sleep disturbance on MS symptoms also is unknown. A practical approach to managing sleep disturbance in perimenopausal MS patients is to identify and assess the triggers. “If the bladder symptoms are the major trigger versus mood disturbances such as depression and anxiety, the intervention will be different,” she said. “Consider counseling and/or consultation with a sleep specialist.” Some patients may benefit from pharmacologic treatment to “get them over the hump and get them sleeping better for a little while, versus longer term management if they have a life history of insomnia,” she said. “If the problem is sleep management, you’ll need a drug with a longer half-life. Consider other comorbidities such as anxiety and restless leg syndrome.” Classes of medications to consider include benzodiazepines, nonbenzodiazepines, tricyclic antidepressants, SSRIs and SNRIs.
Mood symptoms commonly overlap in menopausal patients with MS, especially those related to depression and anxiety. “They may be underdiagnosed and undertreated,” Dr. Bove said. “It’s been shown that depression influences the perceived severity of other MS symptoms. Depression is a strong predictor of cognitive and sexual dysfunction, so our perimenopausal MS women have a vulnerability to more severe mood symptoms.” Managing mood symptoms “needs to be multifaceted” and may include psychotherapy to optimize coping abilities, antidepressants, support groups, fatigue and sleep optimization, and social work “to see how employment or financial stressors may be playing a role in a person’s mood.”
In addition, menopausal women may report changes in attention, executive function, multitasking, word finding difficulties, and memory problems, especially in the first year after the final menstrual period. “It’s known that about half of MS patients experience some degree of cognitive impairment,” she said. “Neurocognitive testing may help to identify particular areas of dysfunction that would be amenable to some kind of cognitive rehabilitation.”
Bladder symptoms also can impact postmenopausal patients, especially increasing bladder irritability and incontinence (stress and urge). In MS, “the baseline bladder dysfunction may be magnified,” Dr. Bove said. “If you’re trying to tease out whether the postmenopausal bladder symptoms are from menopause or MS, the MS relapses tend to have more urgency, frequency, and urge incontinence, and the presentation will be more acute. Urodynamic testing can be used to tease this out. The big lifestyle piece that urologists like to hone in on is that people in America drink too much fluid. A practical guideline is that after 3 p.m. just drink for thirst; don’t worry that everything will fall apart if you don’t get your eight glasses of water per day in. If you’re not thirsty, you probably don’t need it.”
While postmenopausal women face an increased risk for osteoporosis, that risk is magnified for MS patients because of the cumulative effect of steroid use – particularly for those who were diagnosed in the pre–disease-modifying-therapy era – being sedentary, and being deconditioned. “Other MS issues such as balance, vision problems, strength or cognitive impairments may all impact gait and compound the risk of falls,” Dr. Bove said. “Osteoporosis prevention and screening should be encouraged in these patients.”
Dr. Bove concluded her presentation by noting that in general, women with disabilities are less likely to be up to date on Pap tests, mammograms, and other important preventive screening tests. “The magnitude of disparities is greater for women with complex limitations,” she said. “Women with MS may have a lower cancer risk, but a larger tumor size at diagnosis.” For example, “is this because the patient is uncomfortable getting on an exam table to get a Pap smear, or is the physician not thinking about other aspects of the person’s life because the focus is on the MS?”
Dr. Bove disclosed that she has received funding from the National Multiple Sclerosis Society, the National Institutes of Health, and from the Harvard Clinical Investigator Training Program.
On Twitter @dougbrunk
INDIANAPOLIS – About 50% of women with multiple sclerosis are postmenopausal, but objective data about the impact of menopause on the course of multiple sclerosis are lacking.
“We don’t know anything about the impact of menopause on the MS course; there is wide variability in patient-reported outcomes, but nothing written about comorbidities or symptom management,” Dr. Riley Bove, a neurologist at Brigham and Women’s Hospital, Boston, said at the annual meeting of the Consortium of Multiple Sclerosis Centers. “We’ve been working on this. A lot of it is unknown.”
She described menopause is “an opportunity for providers to tackle symptoms and improve well-being and discuss meaningful quality of life and priorities with patients. It can be a good time to talk about these things.”
In a study that Dr. Bove conducted with the online patient-powered research platform PatientsLikeMe, female MS patients were asked to describe the impact of menopause on their disease. Among the themes that emerged were an occasional perimenopausal onset of MS (“menopause and MS symptoms were pretty much simultaneous,” one 58-year-old respondent said); the effect of hot flashes on MS symptoms (“I confused the two, especially hot flashes,” said a 53-year-old woman); and worsening of MS-related disability after menopause, particularly surgical (“Before I stopped taking birth control pills I was working and able to walk and house clean , etc.,” a 53-year-old respondent said. “I had the surgery, and I started to progress toward being completely wheelchair bound.”)
When it comes to solid recommendations for how to manage MS symptoms that overlap with menopause, “we’re in an evidence-free zone,” Dr. Bove said. “Symptoms in MS are kind of like dominoes: You have difficulty sleeping and then your day is off, fatigue is up and your mood is off, and everything can spiral. In the clinic, perimenopausal women often say things like, ‘I feel like I’m falling apart’ or ‘something has to give’ or ‘I need a change.’ ”
Common overlapping symptoms include vasomotor manifestations such as hot flashes, cold flashes, vascular instability, and rapid heartbeat. “The leading mechanistic explanation for the vasomotor symptoms is that abrupt hormone deprivation will result in the loss of negative feedback over hypothalamic NA [noradrenaline] synthesis,” Dr. Bove explained. “The proximity of the hypothalamic thermoregulatory center to luteinizing hormone–releasing hormone-producing areas may also be involved.”
Sleep disturbances and insomnia in menopausal MS patients can impact fatigue and mood. Also, hot flashes can directly exacerbate the MS symptoms, fluctuating over the day or the week.
According to recommendations from the North American Menopause Society, estradiol is the most effective therapy for treating vasomotor symptoms. Other options include selective serotonin reuptake inhibitors (SSRIs) and selective noradrenergic reuptake inhibitors (SNRIs). “Probably the best studied SNRI is venlafaxine,” Dr. Bove said. “It seems to have modest effects on sleep quality and insomnia perimenopausally, as well as on hot flashes.”
Other alternatives include clonidine and gabapentin.
“If a patient wants to use [hormone therapy] for menopausal symptoms, it has to be an individualized approach,” Dr. Bove said. “You have to communicate with the primary care physician to understand what else is going on in this woman’s medical history. The current recommendations are to treat the symptoms with as low a dose as possible for as short a duration as possible. Our MS patients are also at risk for neurodegeneration, for brain volume loss, for cognitive decline, and for worsening function over time.”
With respect to cognition, observational studies have demonstrated that during a certain window of opportunity – defined as within 5 years of the last menstrual period – hormone therapy (HT) may have protective effects against Alzheimer’s disease and against cognitive decline in general. “Beyond this window of time, perhaps due to estrogen receptor down regulation, HT can be harmful, with an increased risk of stroke and dementia reported later on,” she said.
Against this, the Women’s Health Initiative Memory Study (WHIMS) looked at unopposed estrogen, and estrogen and progestin combination, compared with placebo. It found that in women who initiated HT at the age of 65 or older faced an increased risk of dementia from any cause, and of cognitive decline. “This study really put the kibosh on HT as a form of neuroprotection,” Dr. Bove said. “But perhaps it’s unfair to the many patients who are at risk for cognitive decline and neurodegeneration, because the WHIMS did not find an increased risk of adverse cognitive events in women in whom HT was started perimenopausally. Longitudinal, placebo-controlled trials of the effects of HT within the window of opportunity are required to either prove or refute the observational studies that already exist that suggest HT may be neuroprotective. This is an important point to discuss with patients.”
The impact of perimenopausal sleep disturbance on MS symptoms also is unknown. A practical approach to managing sleep disturbance in perimenopausal MS patients is to identify and assess the triggers. “If the bladder symptoms are the major trigger versus mood disturbances such as depression and anxiety, the intervention will be different,” she said. “Consider counseling and/or consultation with a sleep specialist.” Some patients may benefit from pharmacologic treatment to “get them over the hump and get them sleeping better for a little while, versus longer term management if they have a life history of insomnia,” she said. “If the problem is sleep management, you’ll need a drug with a longer half-life. Consider other comorbidities such as anxiety and restless leg syndrome.” Classes of medications to consider include benzodiazepines, nonbenzodiazepines, tricyclic antidepressants, SSRIs and SNRIs.
Mood symptoms commonly overlap in menopausal patients with MS, especially those related to depression and anxiety. “They may be underdiagnosed and undertreated,” Dr. Bove said. “It’s been shown that depression influences the perceived severity of other MS symptoms. Depression is a strong predictor of cognitive and sexual dysfunction, so our perimenopausal MS women have a vulnerability to more severe mood symptoms.” Managing mood symptoms “needs to be multifaceted” and may include psychotherapy to optimize coping abilities, antidepressants, support groups, fatigue and sleep optimization, and social work “to see how employment or financial stressors may be playing a role in a person’s mood.”
In addition, menopausal women may report changes in attention, executive function, multitasking, word finding difficulties, and memory problems, especially in the first year after the final menstrual period. “It’s known that about half of MS patients experience some degree of cognitive impairment,” she said. “Neurocognitive testing may help to identify particular areas of dysfunction that would be amenable to some kind of cognitive rehabilitation.”
Bladder symptoms also can impact postmenopausal patients, especially increasing bladder irritability and incontinence (stress and urge). In MS, “the baseline bladder dysfunction may be magnified,” Dr. Bove said. “If you’re trying to tease out whether the postmenopausal bladder symptoms are from menopause or MS, the MS relapses tend to have more urgency, frequency, and urge incontinence, and the presentation will be more acute. Urodynamic testing can be used to tease this out. The big lifestyle piece that urologists like to hone in on is that people in America drink too much fluid. A practical guideline is that after 3 p.m. just drink for thirst; don’t worry that everything will fall apart if you don’t get your eight glasses of water per day in. If you’re not thirsty, you probably don’t need it.”
While postmenopausal women face an increased risk for osteoporosis, that risk is magnified for MS patients because of the cumulative effect of steroid use – particularly for those who were diagnosed in the pre–disease-modifying-therapy era – being sedentary, and being deconditioned. “Other MS issues such as balance, vision problems, strength or cognitive impairments may all impact gait and compound the risk of falls,” Dr. Bove said. “Osteoporosis prevention and screening should be encouraged in these patients.”
Dr. Bove concluded her presentation by noting that in general, women with disabilities are less likely to be up to date on Pap tests, mammograms, and other important preventive screening tests. “The magnitude of disparities is greater for women with complex limitations,” she said. “Women with MS may have a lower cancer risk, but a larger tumor size at diagnosis.” For example, “is this because the patient is uncomfortable getting on an exam table to get a Pap smear, or is the physician not thinking about other aspects of the person’s life because the focus is on the MS?”
Dr. Bove disclosed that she has received funding from the National Multiple Sclerosis Society, the National Institutes of Health, and from the Harvard Clinical Investigator Training Program.
On Twitter @dougbrunk
INDIANAPOLIS – About 50% of women with multiple sclerosis are postmenopausal, but objective data about the impact of menopause on the course of multiple sclerosis are lacking.
“We don’t know anything about the impact of menopause on the MS course; there is wide variability in patient-reported outcomes, but nothing written about comorbidities or symptom management,” Dr. Riley Bove, a neurologist at Brigham and Women’s Hospital, Boston, said at the annual meeting of the Consortium of Multiple Sclerosis Centers. “We’ve been working on this. A lot of it is unknown.”
She described menopause is “an opportunity for providers to tackle symptoms and improve well-being and discuss meaningful quality of life and priorities with patients. It can be a good time to talk about these things.”
In a study that Dr. Bove conducted with the online patient-powered research platform PatientsLikeMe, female MS patients were asked to describe the impact of menopause on their disease. Among the themes that emerged were an occasional perimenopausal onset of MS (“menopause and MS symptoms were pretty much simultaneous,” one 58-year-old respondent said); the effect of hot flashes on MS symptoms (“I confused the two, especially hot flashes,” said a 53-year-old woman); and worsening of MS-related disability after menopause, particularly surgical (“Before I stopped taking birth control pills I was working and able to walk and house clean , etc.,” a 53-year-old respondent said. “I had the surgery, and I started to progress toward being completely wheelchair bound.”)
When it comes to solid recommendations for how to manage MS symptoms that overlap with menopause, “we’re in an evidence-free zone,” Dr. Bove said. “Symptoms in MS are kind of like dominoes: You have difficulty sleeping and then your day is off, fatigue is up and your mood is off, and everything can spiral. In the clinic, perimenopausal women often say things like, ‘I feel like I’m falling apart’ or ‘something has to give’ or ‘I need a change.’ ”
Common overlapping symptoms include vasomotor manifestations such as hot flashes, cold flashes, vascular instability, and rapid heartbeat. “The leading mechanistic explanation for the vasomotor symptoms is that abrupt hormone deprivation will result in the loss of negative feedback over hypothalamic NA [noradrenaline] synthesis,” Dr. Bove explained. “The proximity of the hypothalamic thermoregulatory center to luteinizing hormone–releasing hormone-producing areas may also be involved.”
Sleep disturbances and insomnia in menopausal MS patients can impact fatigue and mood. Also, hot flashes can directly exacerbate the MS symptoms, fluctuating over the day or the week.
According to recommendations from the North American Menopause Society, estradiol is the most effective therapy for treating vasomotor symptoms. Other options include selective serotonin reuptake inhibitors (SSRIs) and selective noradrenergic reuptake inhibitors (SNRIs). “Probably the best studied SNRI is venlafaxine,” Dr. Bove said. “It seems to have modest effects on sleep quality and insomnia perimenopausally, as well as on hot flashes.”
Other alternatives include clonidine and gabapentin.
“If a patient wants to use [hormone therapy] for menopausal symptoms, it has to be an individualized approach,” Dr. Bove said. “You have to communicate with the primary care physician to understand what else is going on in this woman’s medical history. The current recommendations are to treat the symptoms with as low a dose as possible for as short a duration as possible. Our MS patients are also at risk for neurodegeneration, for brain volume loss, for cognitive decline, and for worsening function over time.”
With respect to cognition, observational studies have demonstrated that during a certain window of opportunity – defined as within 5 years of the last menstrual period – hormone therapy (HT) may have protective effects against Alzheimer’s disease and against cognitive decline in general. “Beyond this window of time, perhaps due to estrogen receptor down regulation, HT can be harmful, with an increased risk of stroke and dementia reported later on,” she said.
Against this, the Women’s Health Initiative Memory Study (WHIMS) looked at unopposed estrogen, and estrogen and progestin combination, compared with placebo. It found that in women who initiated HT at the age of 65 or older faced an increased risk of dementia from any cause, and of cognitive decline. “This study really put the kibosh on HT as a form of neuroprotection,” Dr. Bove said. “But perhaps it’s unfair to the many patients who are at risk for cognitive decline and neurodegeneration, because the WHIMS did not find an increased risk of adverse cognitive events in women in whom HT was started perimenopausally. Longitudinal, placebo-controlled trials of the effects of HT within the window of opportunity are required to either prove or refute the observational studies that already exist that suggest HT may be neuroprotective. This is an important point to discuss with patients.”
The impact of perimenopausal sleep disturbance on MS symptoms also is unknown. A practical approach to managing sleep disturbance in perimenopausal MS patients is to identify and assess the triggers. “If the bladder symptoms are the major trigger versus mood disturbances such as depression and anxiety, the intervention will be different,” she said. “Consider counseling and/or consultation with a sleep specialist.” Some patients may benefit from pharmacologic treatment to “get them over the hump and get them sleeping better for a little while, versus longer term management if they have a life history of insomnia,” she said. “If the problem is sleep management, you’ll need a drug with a longer half-life. Consider other comorbidities such as anxiety and restless leg syndrome.” Classes of medications to consider include benzodiazepines, nonbenzodiazepines, tricyclic antidepressants, SSRIs and SNRIs.
Mood symptoms commonly overlap in menopausal patients with MS, especially those related to depression and anxiety. “They may be underdiagnosed and undertreated,” Dr. Bove said. “It’s been shown that depression influences the perceived severity of other MS symptoms. Depression is a strong predictor of cognitive and sexual dysfunction, so our perimenopausal MS women have a vulnerability to more severe mood symptoms.” Managing mood symptoms “needs to be multifaceted” and may include psychotherapy to optimize coping abilities, antidepressants, support groups, fatigue and sleep optimization, and social work “to see how employment or financial stressors may be playing a role in a person’s mood.”
In addition, menopausal women may report changes in attention, executive function, multitasking, word finding difficulties, and memory problems, especially in the first year after the final menstrual period. “It’s known that about half of MS patients experience some degree of cognitive impairment,” she said. “Neurocognitive testing may help to identify particular areas of dysfunction that would be amenable to some kind of cognitive rehabilitation.”
Bladder symptoms also can impact postmenopausal patients, especially increasing bladder irritability and incontinence (stress and urge). In MS, “the baseline bladder dysfunction may be magnified,” Dr. Bove said. “If you’re trying to tease out whether the postmenopausal bladder symptoms are from menopause or MS, the MS relapses tend to have more urgency, frequency, and urge incontinence, and the presentation will be more acute. Urodynamic testing can be used to tease this out. The big lifestyle piece that urologists like to hone in on is that people in America drink too much fluid. A practical guideline is that after 3 p.m. just drink for thirst; don’t worry that everything will fall apart if you don’t get your eight glasses of water per day in. If you’re not thirsty, you probably don’t need it.”
While postmenopausal women face an increased risk for osteoporosis, that risk is magnified for MS patients because of the cumulative effect of steroid use – particularly for those who were diagnosed in the pre–disease-modifying-therapy era – being sedentary, and being deconditioned. “Other MS issues such as balance, vision problems, strength or cognitive impairments may all impact gait and compound the risk of falls,” Dr. Bove said. “Osteoporosis prevention and screening should be encouraged in these patients.”
Dr. Bove concluded her presentation by noting that in general, women with disabilities are less likely to be up to date on Pap tests, mammograms, and other important preventive screening tests. “The magnitude of disparities is greater for women with complex limitations,” she said. “Women with MS may have a lower cancer risk, but a larger tumor size at diagnosis.” For example, “is this because the patient is uncomfortable getting on an exam table to get a Pap smear, or is the physician not thinking about other aspects of the person’s life because the focus is on the MS?”
Dr. Bove disclosed that she has received funding from the National Multiple Sclerosis Society, the National Institutes of Health, and from the Harvard Clinical Investigator Training Program.
On Twitter @dougbrunk
EXPERT ANALYSIS AT THE CMSC ANNUAL MEETING

BCL-2 inhibitor shows potential for treating MM

to an attendee at ASCO 2015
© ASCO/Zach Boyden-Holmes
CHICAGO—A BCL-2 inhibitor that has shown activity in patients with chronic and acute leukemias could be a feasible treatment option for multiple myeloma (MM) too, according to research presented at the 2015 ASCO Annual Meeting.
In a pair of phase 1 studies, the drug, venetoclax, prompted responses in certain patients with relapsed or refractory MM, both when given alone and in combination with bortezomib and dexamethasone.
As monotherapy, venetoclax induced complete responses (CRs) in 2 patients with t(11;14), but the overall response rate (ORR) was low, and most patients discontinued treatment, largely due to progression.
Venetoclax in combination with bortezomib and dexamethasone prompted a response in nearly half of the patients studied, but more than half discontinued treatment. The combination produced a high ORR in patients who were bortezomib-naïve and bortezomib-sensitive, but there was no response among bortezomib-refractory patients.
“Multiple myeloma remains a high area of unmet medical need, and additional research to identify new therapies is important,” said investigator Cyrille Touzeau, MD, of the University of Nantes in France.
“The response rates shown in these studies suggest potential of venetoclax in this patient population and warrant further evaluation.”
Dr Touzeau and his colleagues presented these studies at ASCO as abstracts 8580 and 8576. Both studies were funded by AbbVie, the company developing venetoclax.
Venetoclax in combination
In a phase 1b study (abstract 8580*), the researchers evaluated venetoclax in combination with bortezomib and dexamethasone in 38 patients with relapsed or refractory MM.
The patients’ median age was 65 (range, 38-79). Five patients were t(11;14)-positive, 3 were t(4;14)-positive, 9 had del17p, and 19 had del13q. They had received a median of 5 prior lines of therapy (range, 1-15). Ten patients were bortezomib-refractory, 21 were lenalidomide-refractory, and 8 patients were refractory to both drugs.
The patients received venetoclax at doses ranging from 50 mg to 600 mg daily (with a 1-week lead-in period for the 50 mg cohort). On cycles 1-8, patients received dexamethasone (20 mg) and bortezomib (1.3 mg/m2) with venetoclax on days 1, 4, 8, and 11. They received dexamethasone (20 mg) with venetoclax on days 2, 5, 9, and 12.
On cycles 9-11, patients received dexamethasone (20 mg) and bortezomib (1.3 mg/m2) with venetoclax on days 1, 8, 15, and 22. Patients received venetoclax monotherapy for cycles 12 and beyond. They also received prophylaxis for tumor lysis syndrome.
Twenty-five patients (66%) discontinued treatment, 19 due to disease progression (including 4 deaths), 2 due to adverse events (AEs), 3 due to patient decision, and 1 due to withdrawn consent.
The ORR was 47% among the 36 evaluable patients, 83% for bortezomib-naïve patients (5/6), 60% for bortezomib-sensitive patients (12/20), and 0% for bortezomib-refractory patients (0/10).
Two patients had a stringent CR, 1 had a CR, 4 had a very good partial response, 10 had a partial response, and 2 had a minimal response. Six patients had stable disease, and 9 progressed.
The most common AEs—occurring in at least 20% of patients—were constipation (37%), diarrhea (32%), insomnia (32%), thrombocytopenia (29%), peripheral neuropathy (26%), asthenia (26%), dyspnea (26%), peripheral edema (24%), and anemia (21%).
Grade 3/4 AEs—occurring in at least 10% of patients—were thrombocytopenia (21%), anemia (13%), and dyspnea (11%). Serious AEs—each occurring in 5% of patients—were cardiac failure, pyrexia, sepsis, respiratory failure, pneumonia, and embolism.
Venetoclax as monotherapy
In a phase 1 study (abstract 8576*), researchers evaluated venetoclax as monotherapy in 29 patients with relapsed or refractory MM. Eleven patients were t(11;14)-positive, 2 were t(4;14)-positive, 4 had del17p, and 14 had del13q.
The patients’ median age was 66 (range, 42-79), and they had received a median of 6 prior therapies (range, 1-13). Fifteen patients were bortezomib-refractory, 12 were refractory to lenalidomide, and 10 patients were refractory to both drugs.
After a 2-week lead-in period, patients received venetoclax daily on a 21-day cycle, ranging from 300 mg to 1200 mg on a 3+3 design. They also received prophylaxis for tumor lysis syndrome. Patients who progressed during treatment were allowed to receive dexamethasone as well and continue the study.
Twenty-three patients (79%) discontinued treatment, 18 due to disease progression, 4 due to AEs, and 1 due to patient decision.
The ORR was 7% (n=2). Both patients achieved a CR, and both were t(11;14)-positive. One of the patients is in the 600 mg cohort and is still responding to treatment. The duration of response, thus far, is 2.1 months.
The other patient with a CR is in the 900 mg dose cohort. This patient is still responding as well, and the response duration, thus far, is 2.8 months.
Common AEs—occurring in at least 20% of patients—were diarrhea (41%), nausea (41%), fatigue (24%), vomiting (21%), asthenia (21%), and neutropenia (21%).
Grade 3/4 AEs—occurring in at least 10% of patients—were thrombocytopenia (24%), neutropenia (14%), and anemia (10%). Serious AEs—each occurring in 7% of patients—were pyrexia, malignant neoplasm progression, and cough.
Two patients had dose-limiting toxicities at the 600 mg dose of venetoclax. However, the researchers said the maximum tolerated dose was not reached, and the recommended phase 2 dose is 1200 mg. ![]()
*Information in the abstract differs from that presented at the meeting.
to an attendee at ASCO 2015
© ASCO/Zach Boyden-Holmes
CHICAGO—A BCL-2 inhibitor that has shown activity in patients with chronic and acute leukemias could be a feasible treatment option for multiple myeloma (MM) too, according to research presented at the 2015 ASCO Annual Meeting.
In a pair of phase 1 studies, the drug, venetoclax, prompted responses in certain patients with relapsed or refractory MM, both when given alone and in combination with bortezomib and dexamethasone.
As monotherapy, venetoclax induced complete responses (CRs) in 2 patients with t(11;14), but the overall response rate (ORR) was low, and most patients discontinued treatment, largely due to progression.
Venetoclax in combination with bortezomib and dexamethasone prompted a response in nearly half of the patients studied, but more than half discontinued treatment. The combination produced a high ORR in patients who were bortezomib-naïve and bortezomib-sensitive, but there was no response among bortezomib-refractory patients.
“Multiple myeloma remains a high area of unmet medical need, and additional research to identify new therapies is important,” said investigator Cyrille Touzeau, MD, of the University of Nantes in France.
“The response rates shown in these studies suggest potential of venetoclax in this patient population and warrant further evaluation.”
Dr Touzeau and his colleagues presented these studies at ASCO as abstracts 8580 and 8576. Both studies were funded by AbbVie, the company developing venetoclax.
Venetoclax in combination
In a phase 1b study (abstract 8580*), the researchers evaluated venetoclax in combination with bortezomib and dexamethasone in 38 patients with relapsed or refractory MM.
The patients’ median age was 65 (range, 38-79). Five patients were t(11;14)-positive, 3 were t(4;14)-positive, 9 had del17p, and 19 had del13q. They had received a median of 5 prior lines of therapy (range, 1-15). Ten patients were bortezomib-refractory, 21 were lenalidomide-refractory, and 8 patients were refractory to both drugs.
The patients received venetoclax at doses ranging from 50 mg to 600 mg daily (with a 1-week lead-in period for the 50 mg cohort). On cycles 1-8, patients received dexamethasone (20 mg) and bortezomib (1.3 mg/m2) with venetoclax on days 1, 4, 8, and 11. They received dexamethasone (20 mg) with venetoclax on days 2, 5, 9, and 12.
On cycles 9-11, patients received dexamethasone (20 mg) and bortezomib (1.3 mg/m2) with venetoclax on days 1, 8, 15, and 22. Patients received venetoclax monotherapy for cycles 12 and beyond. They also received prophylaxis for tumor lysis syndrome.
Twenty-five patients (66%) discontinued treatment, 19 due to disease progression (including 4 deaths), 2 due to adverse events (AEs), 3 due to patient decision, and 1 due to withdrawn consent.
The ORR was 47% among the 36 evaluable patients, 83% for bortezomib-naïve patients (5/6), 60% for bortezomib-sensitive patients (12/20), and 0% for bortezomib-refractory patients (0/10).
Two patients had a stringent CR, 1 had a CR, 4 had a very good partial response, 10 had a partial response, and 2 had a minimal response. Six patients had stable disease, and 9 progressed.
The most common AEs—occurring in at least 20% of patients—were constipation (37%), diarrhea (32%), insomnia (32%), thrombocytopenia (29%), peripheral neuropathy (26%), asthenia (26%), dyspnea (26%), peripheral edema (24%), and anemia (21%).
Grade 3/4 AEs—occurring in at least 10% of patients—were thrombocytopenia (21%), anemia (13%), and dyspnea (11%). Serious AEs—each occurring in 5% of patients—were cardiac failure, pyrexia, sepsis, respiratory failure, pneumonia, and embolism.
Venetoclax as monotherapy
In a phase 1 study (abstract 8576*), researchers evaluated venetoclax as monotherapy in 29 patients with relapsed or refractory MM. Eleven patients were t(11;14)-positive, 2 were t(4;14)-positive, 4 had del17p, and 14 had del13q.
The patients’ median age was 66 (range, 42-79), and they had received a median of 6 prior therapies (range, 1-13). Fifteen patients were bortezomib-refractory, 12 were refractory to lenalidomide, and 10 patients were refractory to both drugs.
After a 2-week lead-in period, patients received venetoclax daily on a 21-day cycle, ranging from 300 mg to 1200 mg on a 3+3 design. They also received prophylaxis for tumor lysis syndrome. Patients who progressed during treatment were allowed to receive dexamethasone as well and continue the study.
Twenty-three patients (79%) discontinued treatment, 18 due to disease progression, 4 due to AEs, and 1 due to patient decision.
The ORR was 7% (n=2). Both patients achieved a CR, and both were t(11;14)-positive. One of the patients is in the 600 mg cohort and is still responding to treatment. The duration of response, thus far, is 2.1 months.
The other patient with a CR is in the 900 mg dose cohort. This patient is still responding as well, and the response duration, thus far, is 2.8 months.
Common AEs—occurring in at least 20% of patients—were diarrhea (41%), nausea (41%), fatigue (24%), vomiting (21%), asthenia (21%), and neutropenia (21%).
Grade 3/4 AEs—occurring in at least 10% of patients—were thrombocytopenia (24%), neutropenia (14%), and anemia (10%). Serious AEs—each occurring in 7% of patients—were pyrexia, malignant neoplasm progression, and cough.
Two patients had dose-limiting toxicities at the 600 mg dose of venetoclax. However, the researchers said the maximum tolerated dose was not reached, and the recommended phase 2 dose is 1200 mg. ![]()
*Information in the abstract differs from that presented at the meeting.
to an attendee at ASCO 2015
© ASCO/Zach Boyden-Holmes
CHICAGO—A BCL-2 inhibitor that has shown activity in patients with chronic and acute leukemias could be a feasible treatment option for multiple myeloma (MM) too, according to research presented at the 2015 ASCO Annual Meeting.
In a pair of phase 1 studies, the drug, venetoclax, prompted responses in certain patients with relapsed or refractory MM, both when given alone and in combination with bortezomib and dexamethasone.
As monotherapy, venetoclax induced complete responses (CRs) in 2 patients with t(11;14), but the overall response rate (ORR) was low, and most patients discontinued treatment, largely due to progression.
Venetoclax in combination with bortezomib and dexamethasone prompted a response in nearly half of the patients studied, but more than half discontinued treatment. The combination produced a high ORR in patients who were bortezomib-naïve and bortezomib-sensitive, but there was no response among bortezomib-refractory patients.
“Multiple myeloma remains a high area of unmet medical need, and additional research to identify new therapies is important,” said investigator Cyrille Touzeau, MD, of the University of Nantes in France.
“The response rates shown in these studies suggest potential of venetoclax in this patient population and warrant further evaluation.”
Dr Touzeau and his colleagues presented these studies at ASCO as abstracts 8580 and 8576. Both studies were funded by AbbVie, the company developing venetoclax.
Venetoclax in combination
In a phase 1b study (abstract 8580*), the researchers evaluated venetoclax in combination with bortezomib and dexamethasone in 38 patients with relapsed or refractory MM.
The patients’ median age was 65 (range, 38-79). Five patients were t(11;14)-positive, 3 were t(4;14)-positive, 9 had del17p, and 19 had del13q. They had received a median of 5 prior lines of therapy (range, 1-15). Ten patients were bortezomib-refractory, 21 were lenalidomide-refractory, and 8 patients were refractory to both drugs.
The patients received venetoclax at doses ranging from 50 mg to 600 mg daily (with a 1-week lead-in period for the 50 mg cohort). On cycles 1-8, patients received dexamethasone (20 mg) and bortezomib (1.3 mg/m2) with venetoclax on days 1, 4, 8, and 11. They received dexamethasone (20 mg) with venetoclax on days 2, 5, 9, and 12.
On cycles 9-11, patients received dexamethasone (20 mg) and bortezomib (1.3 mg/m2) with venetoclax on days 1, 8, 15, and 22. Patients received venetoclax monotherapy for cycles 12 and beyond. They also received prophylaxis for tumor lysis syndrome.
Twenty-five patients (66%) discontinued treatment, 19 due to disease progression (including 4 deaths), 2 due to adverse events (AEs), 3 due to patient decision, and 1 due to withdrawn consent.
The ORR was 47% among the 36 evaluable patients, 83% for bortezomib-naïve patients (5/6), 60% for bortezomib-sensitive patients (12/20), and 0% for bortezomib-refractory patients (0/10).
Two patients had a stringent CR, 1 had a CR, 4 had a very good partial response, 10 had a partial response, and 2 had a minimal response. Six patients had stable disease, and 9 progressed.
The most common AEs—occurring in at least 20% of patients—were constipation (37%), diarrhea (32%), insomnia (32%), thrombocytopenia (29%), peripheral neuropathy (26%), asthenia (26%), dyspnea (26%), peripheral edema (24%), and anemia (21%).
Grade 3/4 AEs—occurring in at least 10% of patients—were thrombocytopenia (21%), anemia (13%), and dyspnea (11%). Serious AEs—each occurring in 5% of patients—were cardiac failure, pyrexia, sepsis, respiratory failure, pneumonia, and embolism.
Venetoclax as monotherapy
In a phase 1 study (abstract 8576*), researchers evaluated venetoclax as monotherapy in 29 patients with relapsed or refractory MM. Eleven patients were t(11;14)-positive, 2 were t(4;14)-positive, 4 had del17p, and 14 had del13q.
The patients’ median age was 66 (range, 42-79), and they had received a median of 6 prior therapies (range, 1-13). Fifteen patients were bortezomib-refractory, 12 were refractory to lenalidomide, and 10 patients were refractory to both drugs.
After a 2-week lead-in period, patients received venetoclax daily on a 21-day cycle, ranging from 300 mg to 1200 mg on a 3+3 design. They also received prophylaxis for tumor lysis syndrome. Patients who progressed during treatment were allowed to receive dexamethasone as well and continue the study.
Twenty-three patients (79%) discontinued treatment, 18 due to disease progression, 4 due to AEs, and 1 due to patient decision.
The ORR was 7% (n=2). Both patients achieved a CR, and both were t(11;14)-positive. One of the patients is in the 600 mg cohort and is still responding to treatment. The duration of response, thus far, is 2.1 months.
The other patient with a CR is in the 900 mg dose cohort. This patient is still responding as well, and the response duration, thus far, is 2.8 months.
Common AEs—occurring in at least 20% of patients—were diarrhea (41%), nausea (41%), fatigue (24%), vomiting (21%), asthenia (21%), and neutropenia (21%).
Grade 3/4 AEs—occurring in at least 10% of patients—were thrombocytopenia (24%), neutropenia (14%), and anemia (10%). Serious AEs—each occurring in 7% of patients—were pyrexia, malignant neoplasm progression, and cough.
Two patients had dose-limiting toxicities at the 600 mg dose of venetoclax. However, the researchers said the maximum tolerated dose was not reached, and the recommended phase 2 dose is 1200 mg. ![]()
*Information in the abstract differs from that presented at the meeting.
Effect of Dementia on Discharges
The aging of the US population has profound effects on all aspects of healthcare. By 2050, 80 million Americans will be over age 65 years, and the proportion of the population over 85 years is expanding at 6 times the rate of the general population.[1] This major shift in demographics poses significant challenges to hospitalists and others who provide acute care. The prevalence of dementia mirrors the trend of increasing life expectancy. Age is the most significant risk factor for dementia.[2] The prevalence of Alzheimer's disease increases at a predictable rate, about 5% per year after age 65 years. Half of the participants in the Berlin Aging Study were demented at age 95 years.[3] The care of persons with dementia deserves attention, careful consideration, and planning, as they present special needs while hospitalized affecting outcomes, cost, and discharge planning.
It is uncommon for those over age 70 years to be free of chronic conditions that frequently require treatment in hospitals. A study of community‐dwelling patients with mild Alzheimer's disease followed for 3 years found that two‐thirds of the participants required at least 1 hospitalization.[4] Significant risk factors for hospitalization included age and burden of co‐morbidity. Declines in global cognition, episodic memory, and executive function have been found in elderly patients after hospitalization controlling for severity of illness and preadmission cognitive status.[5] Furthermore, according to a review of Medicare data published by the Alzheimer's Association, hospital costs for treating any medical condition with coexisting dementia were over 3 times those of nondemented patients with the same condition.[6] The same study reported nursing home costs and home health provision to be 10.2 and 3.8 times the costs for nondemented recipients, respectively.
This study addresses 2 questions prompted by the observations above: What are the trends of dementia prevalence among patients admitted to hospitals for common acute medical conditions and which diagnoses impact substantially the likelihood of discharge to home? Awareness of the prevalence of dementia comorbidity with conditions that generate hospitalization can provide a stimulus for institutions to allocate appropriate resources to address the special needs of persons with cognitive impairment. Hospitalists and providers at all levels of care armed with this information can adapt their practices and interventions to influence outcomes and transitions in care.
METHODS
Basic Data and Design
We performed a retrospective cross‐sectional study[7] of hospitalized patients using the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), which contains annual hospital discharge data from a stratified, random sample of hospitals across the United States.[8] Data fields include diagnostic fields, procedure codes, age, sex, race, total charges, length of stay (LOS), admission source, and disposition status. The database for each year accessed contains hospital discharges accounting for 36,417,575 (2000) to 39,008,298 (2010) discharges per year. These databases for the years 2000 through 2012 allowed for examination of recent temporal trends in dementia, and assessment of dementia's association with discharge status after adjusting for relevant covariates.
Case Selection and Classification, and Data Elements
We defined dementia on the basis of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9) codes for dementia described by Quan et al.[9] (331.2, 290.* and 294.1) or Alzheimer's disease (ICD‐9 331.0). These ICD‐9 codes being present in any diagnosis field classified the hospitalization as having dementia as a comorbidity. All databases used in this study had Diagnosis Related Groups (DRGs) coding for version 18 and the similar DRG version 24. Both DRG versions were used to tabulate the frequency of dementia coding by DRG. Twelve medical DRGs that were among the 20 highest number of dementia coding diagnoses for each year were identified. Orthopedic DRGs, degenerative nervous system disorders, organic disturbances and mental retardation, psychoses, and rehabilitation DRGs were excluded from the study to focus on medical disorders without dementia as a component of the principal diagnosis. The DRGs for sepsis were also excluded, because significant change in the coding relating to mechanical ventilation duration were made on later DRG versions during the study period, making comparisons between different study years difficult. The DRGs chosen as inclusion criteria were 79 (respiratory infections and inflammations [noncommunity‐acquired pneumonia], 320 (kidney and urinary tract infections [UTI] age >17 years with complications or comorbidities [CC]), 141 (syncope and collapse with complications, comorbidities [syncope]), 14 (intracranial hemorrhage and stroke with infarction [stroke]), 89 (simple pneumonia and pleurisy age >17 years with CC [community‐acquired pneumonia)], 127 (heart failure and shock [CHF]), 88 (chronic obstructive pulmonary disease [COPD]), 138 cardiac arrhythmias and conduction disorders [arrhythmia]), 316 (kidney failure [AKI]), 182 (esophagitis/gastroenteritis age >17 years with CC [enteritis]), 174 (gastrointestinal hemorrhage with CC [GI bleed]), and 296 (nutritional and miscellaneous metabolic disorders [dehydration]). Only hospitalizations of patients aged 65 years were included, as geriatric patients were of primary interest.
The Charlson comorbidities as updated by Quan et al. (12 comordities)[10] were queried using published enhanced ICD‐9 algorithms.[9] Also tabulated were Alzheimer's disease (ICD‐9 331.0) and falls (E880E888).[11, 4] The primary reimbursement status coded as Medicaid or self‐pay was considered a field of interest, as it reflects socioeconomic status.[12] Medicare as the sole reimbursement source was also considered a field of interest, as this influences the hospital LOS requirement prior to reimbursable skilled nursing facilities (SNF) transfer.[13] Discharges were grouped into expired, discharge to home, transfers to SNF, and discharge to another acute‐care facility. Admission source from an SNF was identified.
Data Handling, Statistical Analysis, and Graphical Representation
The number of hospitalizations with dementia coding for each DRG was tabulated for each year. Negative binomial regression was performed using SAS for version 9.1 (SAS Institute, Cary, NC) for Windows (Microsoft Corp., Redmond, WA) to analyze time (year) effect for dementia in each DRG using the GENMOD procedure, taking into account the total number of hospitalizations for that DRG as the offset variable[14] as previously described.[15]
Most summary data generation and all logistic regression analyses were performed using SPSS for Windows version 13 (SPSS Inc., Chicago, IL). Multinomial logistic regression was performed to determine the degree to which dementia influenced the odds of being discharged home using SNF discharges as the reference group, with adjustment for other variables. The predictor variables included the updated Charlson comorbidities[10] and gender. As all patients chosen were age 65 years or older, this Charlson predictor variable was not part of the primary model. Expanded models added predictor variables: admission source from SNF, decade of age, calendar year, Medicaid or self‐pay status (socioeconomic status), Medicare alone status, and coding for a fall (E880E888). Model fit was examined.[16] Regression analyses were performed without race, an identifier missing in a significant number of discharges (14%28% per year).
RESULTS
General DRG Characteristics
The 12 DRG hospitalization dementia proportions are shown in Tables 1 and 2. The DRG hospitalizations studied constituted 29.8% of all hospitalizations in patients aged 65 years. The greatest number of hospitalizations was for DRG127 (CHF) and the least for DRG141 (syncope). The highest cumulative proportions of dementia codings (>13%) were associated with DRG79 (respiratory infections and inflammations [noncommunity‐acquired pneumonia)] and DRG320 (urinary tract infections age >17 years with CC [UTI]) (Table 2). The cumulative proportions (for all years) of dementia codings encompassing all years were between 5% and 11% in DRG141 (syncope), DRG89 (community‐acquired pneumonia), DRG316 (AKI), DRG174 (GI bleed), DRG296 (dehydration), and DRG14 (stroke). DRGs 88 (COPD), 182 (enteritis), 138 (arrhythmia), and 127 (CHF) had cumulative proportions >3% but <5%.
| DRG | Descriptor | Total No. | Median LOS | Discharge Dispositions (Dementia/Nondementia) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Dementia | No Dementia | Dementia | No Dementia | Home (%) | Transfer (%) | SNF (%) | Death (%) | ||
| |||||||||
| 79 | Noncommunity‐acquired pneumonia | 415,127 | 1,958,315 | 6 | 6 | 21.4/37.8 | 1.4/2.0 | 63.5/47.7 | 13.8/12.4 |
| 14 | Stroke | 379,725 | 4,089,142 | 5 | 4 | 26.1/39.6 | 1.8/3.2 | 63.0/46.8 | 9.1/10.5 |
| 320 | Urinary tract infection | 540,994 | 2,889,678 | 4 | 4 | 35.2/56.7 | 1.0/1.2 | 61.8/40.2 | 2.0/1.9 |
| 141 | Syncope | 173,325 | 1,705,651 | 3 | 3 | 58.8/77.6 | 1.1/1.9 | 39.7/20.1 | 0.4/0.4 |
| 296 | Dehydration | 341,681 | 2,894,380 | 4 | 3 | 35.1/63.5 | 1.0/1.5 | 59.8/31.4 | 4.1/3.6 |
| 316 | Acute kidney injury | 243,264 | 2,812,584 | 5 | 5 | 31.2/58.9 | 1.5/2.5 | 59.7/31.6 | 7.6/6.9 |
| 89 | Community‐acquired pneumonia | 591,555 | 6,530,468 | 5 | 4 | 32.7/66.0 | 1.3/1.8 | 58.2/27.5 | 7.8/4.7 |
| 182 | Enteritis | 167,677 | 3,430,585 | 4 | 3 | 51.7/81.5 | 1.1/1.4 | 45.4/15.9 | 1.7/1.2 |
| 88 | Chronic obstructive pulmonary disease | 183,486 | 5,654,875 | 4 | 4 | 49.8/80.6 | 1.1/1.3 | 46.9/16.4 | 2.3/1.7 |
| 127 | Congestive heart failure | 389,838 | 9,012,723 | 4 | 4 | 42.9/70.9 | 1.3/2.9 | 49.7/22.1 | 6.0/4.1 |
| 174 | Gastrointestinal bleeding | 233,665 | 3,482,551 | 4 | 4 | 38.6/74.5 | 1.4/2.2 | 55.7/20.4 | 4.3/2.9 |
| 138 | Arrhythmia | 162,629 | 3,279,538 | 4 | 3 | 46.6/78.0 | 2.9/4.9 | 47.2/14.7 | 3.3/2.4 |
| DRG | Descriptor | Yearly Admissions for Each DRG (Range) | Year Effect for Dementia |
|---|---|---|---|
| |||
| 79 | Noncommunity‐acquired pneumonia | 158,155(2012)198,048(2008) | Negative effect* |
| 320 | Urinary tract infection | 205,540(2000)325,294(2011) | NS |
| 296 | Dehydration | 194,920(2012)298,446(2002) | Negative effect |
| 141 | Syncope | 113,476(2000)164,017(2009) | NS |
| 14 | Stroke | 312,783(2007)391,845(2000) | NS |
| 89 | Community‐acquired pneumonia | 462,245(2014)640,114(2005) | Negative effect* |
| 316 | Acute kidney injury | 111,127(2000)351,942(2011) | Positive effect* |
| 174 | Gastrointestinal bleeding | 269,621(2010)302,099(2004) | Negative effect |
| 182 | Enteritis | 251,949(2000)308,570(2005) | Positive effect |
| 138 | Arrhythmia | 235,060(2000)309,481(2011) | NS |
| 127 | Congestive heart failure | 608,355(2012)789,423(2001) | Positive effect |
| 88 | Chronic obstructive pulmonary disease | 395,055(2004)505,824(2011) | Positive effect |
Patients hospitalized with dementia were older, had a higher proportion of females (range, 50.8%73.9% dementia; range, 46.9%69.8% nondementia), and had more falls (range, 1.5%14.6% dementia; range, 0.9%14.5% nondementia). The median LOS was 1 day greater for hospitalizations with dementia coding for DRGs 14 (stroke), 89 (community‐acquired pneumonia), 138 (arrhythmia), 182 (enteritis), and 296 (dehydration) (Table 1).
Temporal Characteristics
Using negative binomial regression, a significant positive time effect for dementia (ie, a greater proportion of dementia hospitalizations was noted with more recent years) was observed in DRGs 316 (AKI), 127 (CHF), 182 (enteritis), and 88 (COPD) (Table 2). Negative time effects (ie, a lower proportion of dementia hospitalizations was noted with more recent years) were noted for DRGs 79 (noncommunity‐acquired pneumonia), 89 (community‐acquired pneumonia), 174 (GI bleed), and296 (dehydration) (Table 2).
Multivariate Effects of Dementia on Discharge Disposition
Nominal regression, using the Charlson comorbidities/variables only, showed that the presence of dementia was associated with an adjusted odds ratio of <0.5 (0.180.46) for being discharged home for all DRGs (Table 3). For DRGs 174 (GI bleed), 88 (COPD), 182 (enteritis), 138 (arrhythmia), 127 (CHF), and 89 [community‐acquired pneumonia], the adjusted odds ratio was 0.18 to 0.24 (a 76% reduction in the adjusted likelihood for being discharged home). In contrast, DRGs 14 (stroke), 79 (noncommunity‐acquired pneumonia), and 320 (UTI) had adjusted odds ratios of 0.41 to 0.46 (a <60% reduction in the adjusted likelihood for being discharged home). Including additional covariates other than the Charlson criteria resulted in higher odds ratios and better model fits, but had the same dichotomy of dementia effect odds ratios (Table 3). The proportion of hospitalizations with disposition correctly predicted by the Charlson comorbidities alone ranged from 59.4% to 82.6% (Table 3). All models predicted a greater proportion of cases than expected by chance alone, with models also including non‐Charlson covariates showing modestly better fits (Table 3). Dementia had the lowest odds ratio associated with home discharge among all the Charlson comorbidities for all DRGs studied. Collinearity of predictor (independent) variables was demonstrated only in DRG 88 (COPD) and in DRG 127 (CHF) with the respective COPD and CHF Charlson variables. Removing these variables from the respective predictor models in those DRGs did not change the odds ratio associated with dementia (data not shown). Performing nominal regression excluding patients transferred to acute facilities slightly improved model fit but did not significantly change the odds ratios (data not shown).
| DRG | Dementia With Charlson Variables Only | Dementia Enhanced Model | |||||
|---|---|---|---|---|---|---|---|
| % Predicted | OR | 95% CI | % Predicted | OR | 95% CI | ||
| |||||||
| Noncommunity‐acquired pneumonia | 79 | 61.2 | 0.46 | 0.460.47 | 64.9 | 0.51 | 0.510.52 |
| Stroke | 14 | 61.9 | 0.46 | 0.460.47 | 65.5 | 0.55 | 0.540.55 |
| Urinary tract infection | 320 | 59.4 | 0.41 | 0.400.41 | 63.3 | 0.45 | 0.450.46 |
| Syncope | 141 | 79.4 | 0.34 | 0.340.34 | 80.2 | 0.39 | 0.380.39 |
| Dehydration | 296 | 66.5 | 0.31 | 0.310.31 | 68.5 | 0.36 | 0.360.37 |
| Acute kidney injury | 316 | 65.2 | 0.28 | 0.280.29 | 68.4 | 0.35 | 0.350.36 |
| Community‐acquired pneumonia | 89 | 70.1 | 0.24 | 0.240.24 | 72.1 | 0.30 | 0.300.30 |
| Enteritis | 182 | 82.3 | 0.22 | 0.210.22 | 83.2 | 0.28 | 0.270.28 |
| Chronic obstructive pulmonary disease | 88 | 82.2 | 0.21 | 0.210.22 | 82.9 | 0.29 | 0.280.29 |
| Congestive heart failure | 127 | 75.3 | 0.27 | 0.270.27 | 76.8 | 0.33 | 0.320.33 |
| Gastrointestinal bleeding | 174 | 77.2 | 0.18 | 0.180.19 | 78.8 | 0.23 | 0.230.23 |
| Arrhythmia | 138 | 82.6 | 0.18 | 0.180.18 | 83.6 | 0.24 | 0.230.24 |
DISCUSSION
We found that dementia diagnosis has a significant negative impact on the likelihood of discharge to home for all the common acute medical conditions prompting hospitalization. The magnitude of this association varied significantly among DRGs. We found that dementia comorbidity strongly predicts nonhome discharge locations for a number of chronic conditions such as CHF and COPD. These findings could help inpatient and outpatient providers better anticipate postacute‐care needs. In addition, the increases in dementia‐associated admissions for CHF and COPD highlight a need to understand how the growing dementia population may impact hospitals' public reporting (and penalties) of hospital readmissions or ambulatory care‐sensitive hospitalization.
The prevalence of dementia over time changed for particular DRGs. We found hospitalizations for CHF and COPD DRGs to have an increase in dementia proportions over time. CHF and COPD are conditions with a prevalence of dementia comorbidity among Medicare recipients of 16% to 17%.[17] These 2 diagnoses, as well as dementia, have been shown to have statistical predictor effects for acute ambulatory‐care sensitive hospitalizations.[18] Ambulatory care‐sensitive conditions[19] and nursing homesensitive avoidable conditions are proposed indicators/classifiers of hospitalizations that could have been avoided by care in their respective nonhospital settings.[20, 21] The increasing dementia proportion over time in both CHF and COPD DRGs suggests that dementia may increasingly contribute to avoidable hospitalizations. The decrease in dementia proportion over time was in conditions that could be characterized as acute conditions (community‐acquired pneumonia, noncommunity‐acquired pneumonia, dehydration, and GI bleed), whereas the conditions with increasing dementia over time included at least 2 chronic conditions, namely CHF and COPD. It is not known why AKI and enteritis should also be associated with increasing dementia over time. These patterns may reflect differences in management. For example, certain acute conditions in dementia patients may have been increasingly treated in the nonhospital setting, avoiding hospitalization.
Medically unnecessary hospitalizations have been the focus of initiatives by the Centers for Medicare & Medicaid Services, and include the readmission reduction program[22] and the recovery audit program's prepayment review demonstration.[23, 24] Several of the DRGs with stronger dementia effects on discharge disposition have been targets of these programs, including CHF, community‐acquired pneumonia, and COPD in the former, and GI bleed, enteritis, and syncope in the latter. The findings of the current study demonstrate that the presence of dementia strongly influences discharge disposition more in certain diagnostic categories. Although disease severity, care access, preventative measures, or provider behavior may have affected the outcomes, the findings raise the distinct possibility that dementia care could have driven admission patterns differentially. Increased awareness of the influence of dementia on hospitalizations and hospitalization discharges is important not only for clinicians but also for the payors, who may penalize (through denial of hospitalization reimbursement) acute‐care facilities motivated to provide support to dementia patients who are unable to receive adequate care in the community. Furthermore, related to this issue is the Medicare policy that disallows reimbursement for SNF transfer admissions unless preceded by a 3‐day acute‐care hospitalization.[25] Hospitals often face a dilemma of whether to admit patients and keep them hospitalized for the requisite period of time to allow for SNF care to be provided, or to deny this option to patients by discharging them sooner (or not admitting them at all).
Demented persons are frequent visitors to emergency departments, and often the impairment in fundamental activities of daily living is immediately apparent to the nurses and physicians caring for them. How does hospital staff come to grips with the potential conflict between duty to the patient and financial solvency of the institution? When dementia is the chief concern but not an acceptable indication for admission (eg, clinical indication for inpatient care[26]), a search for a reimbursable DRG may ensue, and this could contribute to the variability of dementia comorbidity's impact on hospital discharge disposition noted in this study.
This study has strengths in that the data are sampled in a manner that allows national estimates to be made. Although administrative data, such as the NIS, have limitations in coding accuracy/variability, important quality factors influencing relevant outcomes in the United States have been quantified using the NIS.[27] Because the data were deidentified and sampled rather than being complete, readmissions could not be assessed. Readmission is an important measure of the effectiveness of comprehensive geriatric care models[28] and patient‐centered care. It is possible that more readmissions for the same patient in the same year could have accounted for some of the trend findings. Furthermore, readmissions for the same patient in a given year could have impacted on the time‐related dementia prevalence calculations used. Changes in coding practices also could have impacted the dementia prevalence trends noted.
This study utilized comorbidities that have been typically used to characterize inpatient mortality.[10] The focus of this study, however, was not on mortality but on home discharge. The use of multinomial logistic regression instead of binomial logistic regression was based on the intention to examine home discharge using skilled nursing facility discharge as a reference but also incorporatingand accounting forother significant dispositions in the model such as death and other institutional transfers. Quan et al.[10] used the C statistic to describe and compare a mortality prediction model fit with the Charlson versus other comorbidity indices in national datasets. This statistic, however, is not used in multinomial logistic regression. Thus, it is difficult to compare the present modeling with the published models based on mortality (as a dichotomous outcome). The logistic regression models generally showed highly significant predictor effects for all predictor variables utilized (including dementia), but with a variable degree of correct prediction of disposition.
We originally hypothesized that hospitalized patients with dementia would require care in settings other than home at discharge, based on various key clinical and demographic factors, and that dementia comorbidity would display similar adjusted predictor effects for various common DRGs. Our findings of greater dementia‐associated odds ratios for particular DRGs suggest a more complex and variable dementia role in certain types of hospitalization, and that there are potential limitations in using Agency for Healthcare Research and Quality prevention quality indicators,[7, 26] developed for the purpose of tracking hospitalization data to assess quality and access to community‐based medical care.
Acknowledgements
The authors acknowledge the assistance of Suh Lee, BA, during the summer of 2012. This work was supported in part by an intramural grant from New York Medical College.
Disclosure: Nothing to report.
- Federal Interagency Forum on Aging‐Related Statistics. Older Americans 2012: key indicators of well‐being (older Americans 2012). Washington, DC: US Government Printing Office; 2012.
- Alzheimer's Organization. Risk factors. Available at: http://www.alz.org/alzheimers_disease_causes_risk_factors.asp Accessed February 15, 2015.
- Baltes PB, Mayer KV, eds. The Berlin Aging Study: aging from 70 to 100. Cambridge, United Kingdom: Cambridge University Press; 1999.
- , , , et al. Hospitalization in community‐dwelling persons with Alzheimer's disease: frequency and causes. Am Geriatr Soc. 2010;58:1542–1548.
- , , , , , . Cognitive decline after hospitalization in a community population of older persons. Neurology. 2012;78:950–956.
- Alzheimer's Association. Alzheimer's disease and chronic health conditions: the real challenge for 21st century Medicare. Alzheimer's Association website. Available at: https://www.alz.org/national/documents/report_chroniccare.pdf. Published 2003. Accessed February 15, 2015.
- , . An overview of clinical research: the lay of the land. Lancet. 2002;359:57–61.
- Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. HCUP databases. Available at: www.hcup-us.ahrq.gov/nisoverview.jsp. Modified December 11, 2013, Accessed May 31, 2015.
- , , , et al. Coding algorithms for defining comorbidities in ICD‐9‐CM and ICD‐10 administrative data. Med Care. 2005;43:1130–1139.
- , , , et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173:676–682.
- , . Falls, injuries due to falls, and the risk of admission to a nursing home. N Engl J Med. 1997;337:1279–1284.
- , , , . Insurance status and the transfer of hospitalized patients: an observational study. Ann Intern Med. 2014;160:81–90.
- Centers for Medicare 118:392–404.
- , , . Drug‐induced, dementia‐associated and non‐dementia, non‐drug delirium hospitalizations in the United States, 1998‐2005: an analysis of the national inpatient sample. Drugs Aging. 2010;27:51–61.
- , , , . Multiple discriminate analysis and logistic regression. In: Multivariate Data Analysis. 7th ed. Upper Saddle River, NJ: Prentice Hall; 2009.
- . A growing inpatient imperative: Alzheimer's disease. Hosp Health Netw. 2009;83:26, 28, 30.
- , , , , . The central role of comorbidity in predicting ambulatory care sensitive hospitalizations. Eur J Public Health. 2014;24(1):66–72.
- Agency for Healthcare Research and Quality. Prevention quality indicators technical specifications. Version 4.4. March 2012. Available at: http://www.qualityindicators.ahrq.gov/Archive/PQI_TechSpec_V44.aspx. Accessed September 1, 2012.
- , , , . Hospital transfers of nursing home residents with advanced dementia. J Am Geriatr Soc. 2012;60:905–909.
- , , , , . Potentially Avoidable Hospitalizations for Elderly Long‐stay Residents in Nursing Homes. Med Care. 2013;51(8):673–681.
- Centers for Medicare 15:592–601.
- , . Measurement of potentially preventable hospitalizations. white paper prepared for the long term quality alliance. Available at: http://www.ltqa.org/wp-content/themes/ltqaMain/custom/images//PreventableHospitalizations_021512_2.pdf. Published February 2012. Accessed August 6, 2013.
The aging of the US population has profound effects on all aspects of healthcare. By 2050, 80 million Americans will be over age 65 years, and the proportion of the population over 85 years is expanding at 6 times the rate of the general population.[1] This major shift in demographics poses significant challenges to hospitalists and others who provide acute care. The prevalence of dementia mirrors the trend of increasing life expectancy. Age is the most significant risk factor for dementia.[2] The prevalence of Alzheimer's disease increases at a predictable rate, about 5% per year after age 65 years. Half of the participants in the Berlin Aging Study were demented at age 95 years.[3] The care of persons with dementia deserves attention, careful consideration, and planning, as they present special needs while hospitalized affecting outcomes, cost, and discharge planning.
It is uncommon for those over age 70 years to be free of chronic conditions that frequently require treatment in hospitals. A study of community‐dwelling patients with mild Alzheimer's disease followed for 3 years found that two‐thirds of the participants required at least 1 hospitalization.[4] Significant risk factors for hospitalization included age and burden of co‐morbidity. Declines in global cognition, episodic memory, and executive function have been found in elderly patients after hospitalization controlling for severity of illness and preadmission cognitive status.[5] Furthermore, according to a review of Medicare data published by the Alzheimer's Association, hospital costs for treating any medical condition with coexisting dementia were over 3 times those of nondemented patients with the same condition.[6] The same study reported nursing home costs and home health provision to be 10.2 and 3.8 times the costs for nondemented recipients, respectively.
This study addresses 2 questions prompted by the observations above: What are the trends of dementia prevalence among patients admitted to hospitals for common acute medical conditions and which diagnoses impact substantially the likelihood of discharge to home? Awareness of the prevalence of dementia comorbidity with conditions that generate hospitalization can provide a stimulus for institutions to allocate appropriate resources to address the special needs of persons with cognitive impairment. Hospitalists and providers at all levels of care armed with this information can adapt their practices and interventions to influence outcomes and transitions in care.
METHODS
Basic Data and Design
We performed a retrospective cross‐sectional study[7] of hospitalized patients using the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), which contains annual hospital discharge data from a stratified, random sample of hospitals across the United States.[8] Data fields include diagnostic fields, procedure codes, age, sex, race, total charges, length of stay (LOS), admission source, and disposition status. The database for each year accessed contains hospital discharges accounting for 36,417,575 (2000) to 39,008,298 (2010) discharges per year. These databases for the years 2000 through 2012 allowed for examination of recent temporal trends in dementia, and assessment of dementia's association with discharge status after adjusting for relevant covariates.
Case Selection and Classification, and Data Elements
We defined dementia on the basis of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9) codes for dementia described by Quan et al.[9] (331.2, 290.* and 294.1) or Alzheimer's disease (ICD‐9 331.0). These ICD‐9 codes being present in any diagnosis field classified the hospitalization as having dementia as a comorbidity. All databases used in this study had Diagnosis Related Groups (DRGs) coding for version 18 and the similar DRG version 24. Both DRG versions were used to tabulate the frequency of dementia coding by DRG. Twelve medical DRGs that were among the 20 highest number of dementia coding diagnoses for each year were identified. Orthopedic DRGs, degenerative nervous system disorders, organic disturbances and mental retardation, psychoses, and rehabilitation DRGs were excluded from the study to focus on medical disorders without dementia as a component of the principal diagnosis. The DRGs for sepsis were also excluded, because significant change in the coding relating to mechanical ventilation duration were made on later DRG versions during the study period, making comparisons between different study years difficult. The DRGs chosen as inclusion criteria were 79 (respiratory infections and inflammations [noncommunity‐acquired pneumonia], 320 (kidney and urinary tract infections [UTI] age >17 years with complications or comorbidities [CC]), 141 (syncope and collapse with complications, comorbidities [syncope]), 14 (intracranial hemorrhage and stroke with infarction [stroke]), 89 (simple pneumonia and pleurisy age >17 years with CC [community‐acquired pneumonia)], 127 (heart failure and shock [CHF]), 88 (chronic obstructive pulmonary disease [COPD]), 138 cardiac arrhythmias and conduction disorders [arrhythmia]), 316 (kidney failure [AKI]), 182 (esophagitis/gastroenteritis age >17 years with CC [enteritis]), 174 (gastrointestinal hemorrhage with CC [GI bleed]), and 296 (nutritional and miscellaneous metabolic disorders [dehydration]). Only hospitalizations of patients aged 65 years were included, as geriatric patients were of primary interest.
The Charlson comorbidities as updated by Quan et al. (12 comordities)[10] were queried using published enhanced ICD‐9 algorithms.[9] Also tabulated were Alzheimer's disease (ICD‐9 331.0) and falls (E880E888).[11, 4] The primary reimbursement status coded as Medicaid or self‐pay was considered a field of interest, as it reflects socioeconomic status.[12] Medicare as the sole reimbursement source was also considered a field of interest, as this influences the hospital LOS requirement prior to reimbursable skilled nursing facilities (SNF) transfer.[13] Discharges were grouped into expired, discharge to home, transfers to SNF, and discharge to another acute‐care facility. Admission source from an SNF was identified.
Data Handling, Statistical Analysis, and Graphical Representation
The number of hospitalizations with dementia coding for each DRG was tabulated for each year. Negative binomial regression was performed using SAS for version 9.1 (SAS Institute, Cary, NC) for Windows (Microsoft Corp., Redmond, WA) to analyze time (year) effect for dementia in each DRG using the GENMOD procedure, taking into account the total number of hospitalizations for that DRG as the offset variable[14] as previously described.[15]
Most summary data generation and all logistic regression analyses were performed using SPSS for Windows version 13 (SPSS Inc., Chicago, IL). Multinomial logistic regression was performed to determine the degree to which dementia influenced the odds of being discharged home using SNF discharges as the reference group, with adjustment for other variables. The predictor variables included the updated Charlson comorbidities[10] and gender. As all patients chosen were age 65 years or older, this Charlson predictor variable was not part of the primary model. Expanded models added predictor variables: admission source from SNF, decade of age, calendar year, Medicaid or self‐pay status (socioeconomic status), Medicare alone status, and coding for a fall (E880E888). Model fit was examined.[16] Regression analyses were performed without race, an identifier missing in a significant number of discharges (14%28% per year).
RESULTS
General DRG Characteristics
The 12 DRG hospitalization dementia proportions are shown in Tables 1 and 2. The DRG hospitalizations studied constituted 29.8% of all hospitalizations in patients aged 65 years. The greatest number of hospitalizations was for DRG127 (CHF) and the least for DRG141 (syncope). The highest cumulative proportions of dementia codings (>13%) were associated with DRG79 (respiratory infections and inflammations [noncommunity‐acquired pneumonia)] and DRG320 (urinary tract infections age >17 years with CC [UTI]) (Table 2). The cumulative proportions (for all years) of dementia codings encompassing all years were between 5% and 11% in DRG141 (syncope), DRG89 (community‐acquired pneumonia), DRG316 (AKI), DRG174 (GI bleed), DRG296 (dehydration), and DRG14 (stroke). DRGs 88 (COPD), 182 (enteritis), 138 (arrhythmia), and 127 (CHF) had cumulative proportions >3% but <5%.
| DRG | Descriptor | Total No. | Median LOS | Discharge Dispositions (Dementia/Nondementia) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Dementia | No Dementia | Dementia | No Dementia | Home (%) | Transfer (%) | SNF (%) | Death (%) | ||
| |||||||||
| 79 | Noncommunity‐acquired pneumonia | 415,127 | 1,958,315 | 6 | 6 | 21.4/37.8 | 1.4/2.0 | 63.5/47.7 | 13.8/12.4 |
| 14 | Stroke | 379,725 | 4,089,142 | 5 | 4 | 26.1/39.6 | 1.8/3.2 | 63.0/46.8 | 9.1/10.5 |
| 320 | Urinary tract infection | 540,994 | 2,889,678 | 4 | 4 | 35.2/56.7 | 1.0/1.2 | 61.8/40.2 | 2.0/1.9 |
| 141 | Syncope | 173,325 | 1,705,651 | 3 | 3 | 58.8/77.6 | 1.1/1.9 | 39.7/20.1 | 0.4/0.4 |
| 296 | Dehydration | 341,681 | 2,894,380 | 4 | 3 | 35.1/63.5 | 1.0/1.5 | 59.8/31.4 | 4.1/3.6 |
| 316 | Acute kidney injury | 243,264 | 2,812,584 | 5 | 5 | 31.2/58.9 | 1.5/2.5 | 59.7/31.6 | 7.6/6.9 |
| 89 | Community‐acquired pneumonia | 591,555 | 6,530,468 | 5 | 4 | 32.7/66.0 | 1.3/1.8 | 58.2/27.5 | 7.8/4.7 |
| 182 | Enteritis | 167,677 | 3,430,585 | 4 | 3 | 51.7/81.5 | 1.1/1.4 | 45.4/15.9 | 1.7/1.2 |
| 88 | Chronic obstructive pulmonary disease | 183,486 | 5,654,875 | 4 | 4 | 49.8/80.6 | 1.1/1.3 | 46.9/16.4 | 2.3/1.7 |
| 127 | Congestive heart failure | 389,838 | 9,012,723 | 4 | 4 | 42.9/70.9 | 1.3/2.9 | 49.7/22.1 | 6.0/4.1 |
| 174 | Gastrointestinal bleeding | 233,665 | 3,482,551 | 4 | 4 | 38.6/74.5 | 1.4/2.2 | 55.7/20.4 | 4.3/2.9 |
| 138 | Arrhythmia | 162,629 | 3,279,538 | 4 | 3 | 46.6/78.0 | 2.9/4.9 | 47.2/14.7 | 3.3/2.4 |
| DRG | Descriptor | Yearly Admissions for Each DRG (Range) | Year Effect for Dementia |
|---|---|---|---|
| |||
| 79 | Noncommunity‐acquired pneumonia | 158,155(2012)198,048(2008) | Negative effect* |
| 320 | Urinary tract infection | 205,540(2000)325,294(2011) | NS |
| 296 | Dehydration | 194,920(2012)298,446(2002) | Negative effect |
| 141 | Syncope | 113,476(2000)164,017(2009) | NS |
| 14 | Stroke | 312,783(2007)391,845(2000) | NS |
| 89 | Community‐acquired pneumonia | 462,245(2014)640,114(2005) | Negative effect* |
| 316 | Acute kidney injury | 111,127(2000)351,942(2011) | Positive effect* |
| 174 | Gastrointestinal bleeding | 269,621(2010)302,099(2004) | Negative effect |
| 182 | Enteritis | 251,949(2000)308,570(2005) | Positive effect |
| 138 | Arrhythmia | 235,060(2000)309,481(2011) | NS |
| 127 | Congestive heart failure | 608,355(2012)789,423(2001) | Positive effect |
| 88 | Chronic obstructive pulmonary disease | 395,055(2004)505,824(2011) | Positive effect |
Patients hospitalized with dementia were older, had a higher proportion of females (range, 50.8%73.9% dementia; range, 46.9%69.8% nondementia), and had more falls (range, 1.5%14.6% dementia; range, 0.9%14.5% nondementia). The median LOS was 1 day greater for hospitalizations with dementia coding for DRGs 14 (stroke), 89 (community‐acquired pneumonia), 138 (arrhythmia), 182 (enteritis), and 296 (dehydration) (Table 1).
Temporal Characteristics
Using negative binomial regression, a significant positive time effect for dementia (ie, a greater proportion of dementia hospitalizations was noted with more recent years) was observed in DRGs 316 (AKI), 127 (CHF), 182 (enteritis), and 88 (COPD) (Table 2). Negative time effects (ie, a lower proportion of dementia hospitalizations was noted with more recent years) were noted for DRGs 79 (noncommunity‐acquired pneumonia), 89 (community‐acquired pneumonia), 174 (GI bleed), and296 (dehydration) (Table 2).
Multivariate Effects of Dementia on Discharge Disposition
Nominal regression, using the Charlson comorbidities/variables only, showed that the presence of dementia was associated with an adjusted odds ratio of <0.5 (0.180.46) for being discharged home for all DRGs (Table 3). For DRGs 174 (GI bleed), 88 (COPD), 182 (enteritis), 138 (arrhythmia), 127 (CHF), and 89 [community‐acquired pneumonia], the adjusted odds ratio was 0.18 to 0.24 (a 76% reduction in the adjusted likelihood for being discharged home). In contrast, DRGs 14 (stroke), 79 (noncommunity‐acquired pneumonia), and 320 (UTI) had adjusted odds ratios of 0.41 to 0.46 (a <60% reduction in the adjusted likelihood for being discharged home). Including additional covariates other than the Charlson criteria resulted in higher odds ratios and better model fits, but had the same dichotomy of dementia effect odds ratios (Table 3). The proportion of hospitalizations with disposition correctly predicted by the Charlson comorbidities alone ranged from 59.4% to 82.6% (Table 3). All models predicted a greater proportion of cases than expected by chance alone, with models also including non‐Charlson covariates showing modestly better fits (Table 3). Dementia had the lowest odds ratio associated with home discharge among all the Charlson comorbidities for all DRGs studied. Collinearity of predictor (independent) variables was demonstrated only in DRG 88 (COPD) and in DRG 127 (CHF) with the respective COPD and CHF Charlson variables. Removing these variables from the respective predictor models in those DRGs did not change the odds ratio associated with dementia (data not shown). Performing nominal regression excluding patients transferred to acute facilities slightly improved model fit but did not significantly change the odds ratios (data not shown).
| DRG | Dementia With Charlson Variables Only | Dementia Enhanced Model | |||||
|---|---|---|---|---|---|---|---|
| % Predicted | OR | 95% CI | % Predicted | OR | 95% CI | ||
| |||||||
| Noncommunity‐acquired pneumonia | 79 | 61.2 | 0.46 | 0.460.47 | 64.9 | 0.51 | 0.510.52 |
| Stroke | 14 | 61.9 | 0.46 | 0.460.47 | 65.5 | 0.55 | 0.540.55 |
| Urinary tract infection | 320 | 59.4 | 0.41 | 0.400.41 | 63.3 | 0.45 | 0.450.46 |
| Syncope | 141 | 79.4 | 0.34 | 0.340.34 | 80.2 | 0.39 | 0.380.39 |
| Dehydration | 296 | 66.5 | 0.31 | 0.310.31 | 68.5 | 0.36 | 0.360.37 |
| Acute kidney injury | 316 | 65.2 | 0.28 | 0.280.29 | 68.4 | 0.35 | 0.350.36 |
| Community‐acquired pneumonia | 89 | 70.1 | 0.24 | 0.240.24 | 72.1 | 0.30 | 0.300.30 |
| Enteritis | 182 | 82.3 | 0.22 | 0.210.22 | 83.2 | 0.28 | 0.270.28 |
| Chronic obstructive pulmonary disease | 88 | 82.2 | 0.21 | 0.210.22 | 82.9 | 0.29 | 0.280.29 |
| Congestive heart failure | 127 | 75.3 | 0.27 | 0.270.27 | 76.8 | 0.33 | 0.320.33 |
| Gastrointestinal bleeding | 174 | 77.2 | 0.18 | 0.180.19 | 78.8 | 0.23 | 0.230.23 |
| Arrhythmia | 138 | 82.6 | 0.18 | 0.180.18 | 83.6 | 0.24 | 0.230.24 |
DISCUSSION
We found that dementia diagnosis has a significant negative impact on the likelihood of discharge to home for all the common acute medical conditions prompting hospitalization. The magnitude of this association varied significantly among DRGs. We found that dementia comorbidity strongly predicts nonhome discharge locations for a number of chronic conditions such as CHF and COPD. These findings could help inpatient and outpatient providers better anticipate postacute‐care needs. In addition, the increases in dementia‐associated admissions for CHF and COPD highlight a need to understand how the growing dementia population may impact hospitals' public reporting (and penalties) of hospital readmissions or ambulatory care‐sensitive hospitalization.
The prevalence of dementia over time changed for particular DRGs. We found hospitalizations for CHF and COPD DRGs to have an increase in dementia proportions over time. CHF and COPD are conditions with a prevalence of dementia comorbidity among Medicare recipients of 16% to 17%.[17] These 2 diagnoses, as well as dementia, have been shown to have statistical predictor effects for acute ambulatory‐care sensitive hospitalizations.[18] Ambulatory care‐sensitive conditions[19] and nursing homesensitive avoidable conditions are proposed indicators/classifiers of hospitalizations that could have been avoided by care in their respective nonhospital settings.[20, 21] The increasing dementia proportion over time in both CHF and COPD DRGs suggests that dementia may increasingly contribute to avoidable hospitalizations. The decrease in dementia proportion over time was in conditions that could be characterized as acute conditions (community‐acquired pneumonia, noncommunity‐acquired pneumonia, dehydration, and GI bleed), whereas the conditions with increasing dementia over time included at least 2 chronic conditions, namely CHF and COPD. It is not known why AKI and enteritis should also be associated with increasing dementia over time. These patterns may reflect differences in management. For example, certain acute conditions in dementia patients may have been increasingly treated in the nonhospital setting, avoiding hospitalization.
Medically unnecessary hospitalizations have been the focus of initiatives by the Centers for Medicare & Medicaid Services, and include the readmission reduction program[22] and the recovery audit program's prepayment review demonstration.[23, 24] Several of the DRGs with stronger dementia effects on discharge disposition have been targets of these programs, including CHF, community‐acquired pneumonia, and COPD in the former, and GI bleed, enteritis, and syncope in the latter. The findings of the current study demonstrate that the presence of dementia strongly influences discharge disposition more in certain diagnostic categories. Although disease severity, care access, preventative measures, or provider behavior may have affected the outcomes, the findings raise the distinct possibility that dementia care could have driven admission patterns differentially. Increased awareness of the influence of dementia on hospitalizations and hospitalization discharges is important not only for clinicians but also for the payors, who may penalize (through denial of hospitalization reimbursement) acute‐care facilities motivated to provide support to dementia patients who are unable to receive adequate care in the community. Furthermore, related to this issue is the Medicare policy that disallows reimbursement for SNF transfer admissions unless preceded by a 3‐day acute‐care hospitalization.[25] Hospitals often face a dilemma of whether to admit patients and keep them hospitalized for the requisite period of time to allow for SNF care to be provided, or to deny this option to patients by discharging them sooner (or not admitting them at all).
Demented persons are frequent visitors to emergency departments, and often the impairment in fundamental activities of daily living is immediately apparent to the nurses and physicians caring for them. How does hospital staff come to grips with the potential conflict between duty to the patient and financial solvency of the institution? When dementia is the chief concern but not an acceptable indication for admission (eg, clinical indication for inpatient care[26]), a search for a reimbursable DRG may ensue, and this could contribute to the variability of dementia comorbidity's impact on hospital discharge disposition noted in this study.
This study has strengths in that the data are sampled in a manner that allows national estimates to be made. Although administrative data, such as the NIS, have limitations in coding accuracy/variability, important quality factors influencing relevant outcomes in the United States have been quantified using the NIS.[27] Because the data were deidentified and sampled rather than being complete, readmissions could not be assessed. Readmission is an important measure of the effectiveness of comprehensive geriatric care models[28] and patient‐centered care. It is possible that more readmissions for the same patient in the same year could have accounted for some of the trend findings. Furthermore, readmissions for the same patient in a given year could have impacted on the time‐related dementia prevalence calculations used. Changes in coding practices also could have impacted the dementia prevalence trends noted.
This study utilized comorbidities that have been typically used to characterize inpatient mortality.[10] The focus of this study, however, was not on mortality but on home discharge. The use of multinomial logistic regression instead of binomial logistic regression was based on the intention to examine home discharge using skilled nursing facility discharge as a reference but also incorporatingand accounting forother significant dispositions in the model such as death and other institutional transfers. Quan et al.[10] used the C statistic to describe and compare a mortality prediction model fit with the Charlson versus other comorbidity indices in national datasets. This statistic, however, is not used in multinomial logistic regression. Thus, it is difficult to compare the present modeling with the published models based on mortality (as a dichotomous outcome). The logistic regression models generally showed highly significant predictor effects for all predictor variables utilized (including dementia), but with a variable degree of correct prediction of disposition.
We originally hypothesized that hospitalized patients with dementia would require care in settings other than home at discharge, based on various key clinical and demographic factors, and that dementia comorbidity would display similar adjusted predictor effects for various common DRGs. Our findings of greater dementia‐associated odds ratios for particular DRGs suggest a more complex and variable dementia role in certain types of hospitalization, and that there are potential limitations in using Agency for Healthcare Research and Quality prevention quality indicators,[7, 26] developed for the purpose of tracking hospitalization data to assess quality and access to community‐based medical care.
Acknowledgements
The authors acknowledge the assistance of Suh Lee, BA, during the summer of 2012. This work was supported in part by an intramural grant from New York Medical College.
Disclosure: Nothing to report.
The aging of the US population has profound effects on all aspects of healthcare. By 2050, 80 million Americans will be over age 65 years, and the proportion of the population over 85 years is expanding at 6 times the rate of the general population.[1] This major shift in demographics poses significant challenges to hospitalists and others who provide acute care. The prevalence of dementia mirrors the trend of increasing life expectancy. Age is the most significant risk factor for dementia.[2] The prevalence of Alzheimer's disease increases at a predictable rate, about 5% per year after age 65 years. Half of the participants in the Berlin Aging Study were demented at age 95 years.[3] The care of persons with dementia deserves attention, careful consideration, and planning, as they present special needs while hospitalized affecting outcomes, cost, and discharge planning.
It is uncommon for those over age 70 years to be free of chronic conditions that frequently require treatment in hospitals. A study of community‐dwelling patients with mild Alzheimer's disease followed for 3 years found that two‐thirds of the participants required at least 1 hospitalization.[4] Significant risk factors for hospitalization included age and burden of co‐morbidity. Declines in global cognition, episodic memory, and executive function have been found in elderly patients after hospitalization controlling for severity of illness and preadmission cognitive status.[5] Furthermore, according to a review of Medicare data published by the Alzheimer's Association, hospital costs for treating any medical condition with coexisting dementia were over 3 times those of nondemented patients with the same condition.[6] The same study reported nursing home costs and home health provision to be 10.2 and 3.8 times the costs for nondemented recipients, respectively.
This study addresses 2 questions prompted by the observations above: What are the trends of dementia prevalence among patients admitted to hospitals for common acute medical conditions and which diagnoses impact substantially the likelihood of discharge to home? Awareness of the prevalence of dementia comorbidity with conditions that generate hospitalization can provide a stimulus for institutions to allocate appropriate resources to address the special needs of persons with cognitive impairment. Hospitalists and providers at all levels of care armed with this information can adapt their practices and interventions to influence outcomes and transitions in care.
METHODS
Basic Data and Design
We performed a retrospective cross‐sectional study[7] of hospitalized patients using the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), which contains annual hospital discharge data from a stratified, random sample of hospitals across the United States.[8] Data fields include diagnostic fields, procedure codes, age, sex, race, total charges, length of stay (LOS), admission source, and disposition status. The database for each year accessed contains hospital discharges accounting for 36,417,575 (2000) to 39,008,298 (2010) discharges per year. These databases for the years 2000 through 2012 allowed for examination of recent temporal trends in dementia, and assessment of dementia's association with discharge status after adjusting for relevant covariates.
Case Selection and Classification, and Data Elements
We defined dementia on the basis of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9) codes for dementia described by Quan et al.[9] (331.2, 290.* and 294.1) or Alzheimer's disease (ICD‐9 331.0). These ICD‐9 codes being present in any diagnosis field classified the hospitalization as having dementia as a comorbidity. All databases used in this study had Diagnosis Related Groups (DRGs) coding for version 18 and the similar DRG version 24. Both DRG versions were used to tabulate the frequency of dementia coding by DRG. Twelve medical DRGs that were among the 20 highest number of dementia coding diagnoses for each year were identified. Orthopedic DRGs, degenerative nervous system disorders, organic disturbances and mental retardation, psychoses, and rehabilitation DRGs were excluded from the study to focus on medical disorders without dementia as a component of the principal diagnosis. The DRGs for sepsis were also excluded, because significant change in the coding relating to mechanical ventilation duration were made on later DRG versions during the study period, making comparisons between different study years difficult. The DRGs chosen as inclusion criteria were 79 (respiratory infections and inflammations [noncommunity‐acquired pneumonia], 320 (kidney and urinary tract infections [UTI] age >17 years with complications or comorbidities [CC]), 141 (syncope and collapse with complications, comorbidities [syncope]), 14 (intracranial hemorrhage and stroke with infarction [stroke]), 89 (simple pneumonia and pleurisy age >17 years with CC [community‐acquired pneumonia)], 127 (heart failure and shock [CHF]), 88 (chronic obstructive pulmonary disease [COPD]), 138 cardiac arrhythmias and conduction disorders [arrhythmia]), 316 (kidney failure [AKI]), 182 (esophagitis/gastroenteritis age >17 years with CC [enteritis]), 174 (gastrointestinal hemorrhage with CC [GI bleed]), and 296 (nutritional and miscellaneous metabolic disorders [dehydration]). Only hospitalizations of patients aged 65 years were included, as geriatric patients were of primary interest.
The Charlson comorbidities as updated by Quan et al. (12 comordities)[10] were queried using published enhanced ICD‐9 algorithms.[9] Also tabulated were Alzheimer's disease (ICD‐9 331.0) and falls (E880E888).[11, 4] The primary reimbursement status coded as Medicaid or self‐pay was considered a field of interest, as it reflects socioeconomic status.[12] Medicare as the sole reimbursement source was also considered a field of interest, as this influences the hospital LOS requirement prior to reimbursable skilled nursing facilities (SNF) transfer.[13] Discharges were grouped into expired, discharge to home, transfers to SNF, and discharge to another acute‐care facility. Admission source from an SNF was identified.
Data Handling, Statistical Analysis, and Graphical Representation
The number of hospitalizations with dementia coding for each DRG was tabulated for each year. Negative binomial regression was performed using SAS for version 9.1 (SAS Institute, Cary, NC) for Windows (Microsoft Corp., Redmond, WA) to analyze time (year) effect for dementia in each DRG using the GENMOD procedure, taking into account the total number of hospitalizations for that DRG as the offset variable[14] as previously described.[15]
Most summary data generation and all logistic regression analyses were performed using SPSS for Windows version 13 (SPSS Inc., Chicago, IL). Multinomial logistic regression was performed to determine the degree to which dementia influenced the odds of being discharged home using SNF discharges as the reference group, with adjustment for other variables. The predictor variables included the updated Charlson comorbidities[10] and gender. As all patients chosen were age 65 years or older, this Charlson predictor variable was not part of the primary model. Expanded models added predictor variables: admission source from SNF, decade of age, calendar year, Medicaid or self‐pay status (socioeconomic status), Medicare alone status, and coding for a fall (E880E888). Model fit was examined.[16] Regression analyses were performed without race, an identifier missing in a significant number of discharges (14%28% per year).
RESULTS
General DRG Characteristics
The 12 DRG hospitalization dementia proportions are shown in Tables 1 and 2. The DRG hospitalizations studied constituted 29.8% of all hospitalizations in patients aged 65 years. The greatest number of hospitalizations was for DRG127 (CHF) and the least for DRG141 (syncope). The highest cumulative proportions of dementia codings (>13%) were associated with DRG79 (respiratory infections and inflammations [noncommunity‐acquired pneumonia)] and DRG320 (urinary tract infections age >17 years with CC [UTI]) (Table 2). The cumulative proportions (for all years) of dementia codings encompassing all years were between 5% and 11% in DRG141 (syncope), DRG89 (community‐acquired pneumonia), DRG316 (AKI), DRG174 (GI bleed), DRG296 (dehydration), and DRG14 (stroke). DRGs 88 (COPD), 182 (enteritis), 138 (arrhythmia), and 127 (CHF) had cumulative proportions >3% but <5%.
| DRG | Descriptor | Total No. | Median LOS | Discharge Dispositions (Dementia/Nondementia) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Dementia | No Dementia | Dementia | No Dementia | Home (%) | Transfer (%) | SNF (%) | Death (%) | ||
| |||||||||
| 79 | Noncommunity‐acquired pneumonia | 415,127 | 1,958,315 | 6 | 6 | 21.4/37.8 | 1.4/2.0 | 63.5/47.7 | 13.8/12.4 |
| 14 | Stroke | 379,725 | 4,089,142 | 5 | 4 | 26.1/39.6 | 1.8/3.2 | 63.0/46.8 | 9.1/10.5 |
| 320 | Urinary tract infection | 540,994 | 2,889,678 | 4 | 4 | 35.2/56.7 | 1.0/1.2 | 61.8/40.2 | 2.0/1.9 |
| 141 | Syncope | 173,325 | 1,705,651 | 3 | 3 | 58.8/77.6 | 1.1/1.9 | 39.7/20.1 | 0.4/0.4 |
| 296 | Dehydration | 341,681 | 2,894,380 | 4 | 3 | 35.1/63.5 | 1.0/1.5 | 59.8/31.4 | 4.1/3.6 |
| 316 | Acute kidney injury | 243,264 | 2,812,584 | 5 | 5 | 31.2/58.9 | 1.5/2.5 | 59.7/31.6 | 7.6/6.9 |
| 89 | Community‐acquired pneumonia | 591,555 | 6,530,468 | 5 | 4 | 32.7/66.0 | 1.3/1.8 | 58.2/27.5 | 7.8/4.7 |
| 182 | Enteritis | 167,677 | 3,430,585 | 4 | 3 | 51.7/81.5 | 1.1/1.4 | 45.4/15.9 | 1.7/1.2 |
| 88 | Chronic obstructive pulmonary disease | 183,486 | 5,654,875 | 4 | 4 | 49.8/80.6 | 1.1/1.3 | 46.9/16.4 | 2.3/1.7 |
| 127 | Congestive heart failure | 389,838 | 9,012,723 | 4 | 4 | 42.9/70.9 | 1.3/2.9 | 49.7/22.1 | 6.0/4.1 |
| 174 | Gastrointestinal bleeding | 233,665 | 3,482,551 | 4 | 4 | 38.6/74.5 | 1.4/2.2 | 55.7/20.4 | 4.3/2.9 |
| 138 | Arrhythmia | 162,629 | 3,279,538 | 4 | 3 | 46.6/78.0 | 2.9/4.9 | 47.2/14.7 | 3.3/2.4 |
| DRG | Descriptor | Yearly Admissions for Each DRG (Range) | Year Effect for Dementia |
|---|---|---|---|
| |||
| 79 | Noncommunity‐acquired pneumonia | 158,155(2012)198,048(2008) | Negative effect* |
| 320 | Urinary tract infection | 205,540(2000)325,294(2011) | NS |
| 296 | Dehydration | 194,920(2012)298,446(2002) | Negative effect |
| 141 | Syncope | 113,476(2000)164,017(2009) | NS |
| 14 | Stroke | 312,783(2007)391,845(2000) | NS |
| 89 | Community‐acquired pneumonia | 462,245(2014)640,114(2005) | Negative effect* |
| 316 | Acute kidney injury | 111,127(2000)351,942(2011) | Positive effect* |
| 174 | Gastrointestinal bleeding | 269,621(2010)302,099(2004) | Negative effect |
| 182 | Enteritis | 251,949(2000)308,570(2005) | Positive effect |
| 138 | Arrhythmia | 235,060(2000)309,481(2011) | NS |
| 127 | Congestive heart failure | 608,355(2012)789,423(2001) | Positive effect |
| 88 | Chronic obstructive pulmonary disease | 395,055(2004)505,824(2011) | Positive effect |
Patients hospitalized with dementia were older, had a higher proportion of females (range, 50.8%73.9% dementia; range, 46.9%69.8% nondementia), and had more falls (range, 1.5%14.6% dementia; range, 0.9%14.5% nondementia). The median LOS was 1 day greater for hospitalizations with dementia coding for DRGs 14 (stroke), 89 (community‐acquired pneumonia), 138 (arrhythmia), 182 (enteritis), and 296 (dehydration) (Table 1).
Temporal Characteristics
Using negative binomial regression, a significant positive time effect for dementia (ie, a greater proportion of dementia hospitalizations was noted with more recent years) was observed in DRGs 316 (AKI), 127 (CHF), 182 (enteritis), and 88 (COPD) (Table 2). Negative time effects (ie, a lower proportion of dementia hospitalizations was noted with more recent years) were noted for DRGs 79 (noncommunity‐acquired pneumonia), 89 (community‐acquired pneumonia), 174 (GI bleed), and296 (dehydration) (Table 2).
Multivariate Effects of Dementia on Discharge Disposition
Nominal regression, using the Charlson comorbidities/variables only, showed that the presence of dementia was associated with an adjusted odds ratio of <0.5 (0.180.46) for being discharged home for all DRGs (Table 3). For DRGs 174 (GI bleed), 88 (COPD), 182 (enteritis), 138 (arrhythmia), 127 (CHF), and 89 [community‐acquired pneumonia], the adjusted odds ratio was 0.18 to 0.24 (a 76% reduction in the adjusted likelihood for being discharged home). In contrast, DRGs 14 (stroke), 79 (noncommunity‐acquired pneumonia), and 320 (UTI) had adjusted odds ratios of 0.41 to 0.46 (a <60% reduction in the adjusted likelihood for being discharged home). Including additional covariates other than the Charlson criteria resulted in higher odds ratios and better model fits, but had the same dichotomy of dementia effect odds ratios (Table 3). The proportion of hospitalizations with disposition correctly predicted by the Charlson comorbidities alone ranged from 59.4% to 82.6% (Table 3). All models predicted a greater proportion of cases than expected by chance alone, with models also including non‐Charlson covariates showing modestly better fits (Table 3). Dementia had the lowest odds ratio associated with home discharge among all the Charlson comorbidities for all DRGs studied. Collinearity of predictor (independent) variables was demonstrated only in DRG 88 (COPD) and in DRG 127 (CHF) with the respective COPD and CHF Charlson variables. Removing these variables from the respective predictor models in those DRGs did not change the odds ratio associated with dementia (data not shown). Performing nominal regression excluding patients transferred to acute facilities slightly improved model fit but did not significantly change the odds ratios (data not shown).
| DRG | Dementia With Charlson Variables Only | Dementia Enhanced Model | |||||
|---|---|---|---|---|---|---|---|
| % Predicted | OR | 95% CI | % Predicted | OR | 95% CI | ||
| |||||||
| Noncommunity‐acquired pneumonia | 79 | 61.2 | 0.46 | 0.460.47 | 64.9 | 0.51 | 0.510.52 |
| Stroke | 14 | 61.9 | 0.46 | 0.460.47 | 65.5 | 0.55 | 0.540.55 |
| Urinary tract infection | 320 | 59.4 | 0.41 | 0.400.41 | 63.3 | 0.45 | 0.450.46 |
| Syncope | 141 | 79.4 | 0.34 | 0.340.34 | 80.2 | 0.39 | 0.380.39 |
| Dehydration | 296 | 66.5 | 0.31 | 0.310.31 | 68.5 | 0.36 | 0.360.37 |
| Acute kidney injury | 316 | 65.2 | 0.28 | 0.280.29 | 68.4 | 0.35 | 0.350.36 |
| Community‐acquired pneumonia | 89 | 70.1 | 0.24 | 0.240.24 | 72.1 | 0.30 | 0.300.30 |
| Enteritis | 182 | 82.3 | 0.22 | 0.210.22 | 83.2 | 0.28 | 0.270.28 |
| Chronic obstructive pulmonary disease | 88 | 82.2 | 0.21 | 0.210.22 | 82.9 | 0.29 | 0.280.29 |
| Congestive heart failure | 127 | 75.3 | 0.27 | 0.270.27 | 76.8 | 0.33 | 0.320.33 |
| Gastrointestinal bleeding | 174 | 77.2 | 0.18 | 0.180.19 | 78.8 | 0.23 | 0.230.23 |
| Arrhythmia | 138 | 82.6 | 0.18 | 0.180.18 | 83.6 | 0.24 | 0.230.24 |
DISCUSSION
We found that dementia diagnosis has a significant negative impact on the likelihood of discharge to home for all the common acute medical conditions prompting hospitalization. The magnitude of this association varied significantly among DRGs. We found that dementia comorbidity strongly predicts nonhome discharge locations for a number of chronic conditions such as CHF and COPD. These findings could help inpatient and outpatient providers better anticipate postacute‐care needs. In addition, the increases in dementia‐associated admissions for CHF and COPD highlight a need to understand how the growing dementia population may impact hospitals' public reporting (and penalties) of hospital readmissions or ambulatory care‐sensitive hospitalization.
The prevalence of dementia over time changed for particular DRGs. We found hospitalizations for CHF and COPD DRGs to have an increase in dementia proportions over time. CHF and COPD are conditions with a prevalence of dementia comorbidity among Medicare recipients of 16% to 17%.[17] These 2 diagnoses, as well as dementia, have been shown to have statistical predictor effects for acute ambulatory‐care sensitive hospitalizations.[18] Ambulatory care‐sensitive conditions[19] and nursing homesensitive avoidable conditions are proposed indicators/classifiers of hospitalizations that could have been avoided by care in their respective nonhospital settings.[20, 21] The increasing dementia proportion over time in both CHF and COPD DRGs suggests that dementia may increasingly contribute to avoidable hospitalizations. The decrease in dementia proportion over time was in conditions that could be characterized as acute conditions (community‐acquired pneumonia, noncommunity‐acquired pneumonia, dehydration, and GI bleed), whereas the conditions with increasing dementia over time included at least 2 chronic conditions, namely CHF and COPD. It is not known why AKI and enteritis should also be associated with increasing dementia over time. These patterns may reflect differences in management. For example, certain acute conditions in dementia patients may have been increasingly treated in the nonhospital setting, avoiding hospitalization.
Medically unnecessary hospitalizations have been the focus of initiatives by the Centers for Medicare & Medicaid Services, and include the readmission reduction program[22] and the recovery audit program's prepayment review demonstration.[23, 24] Several of the DRGs with stronger dementia effects on discharge disposition have been targets of these programs, including CHF, community‐acquired pneumonia, and COPD in the former, and GI bleed, enteritis, and syncope in the latter. The findings of the current study demonstrate that the presence of dementia strongly influences discharge disposition more in certain diagnostic categories. Although disease severity, care access, preventative measures, or provider behavior may have affected the outcomes, the findings raise the distinct possibility that dementia care could have driven admission patterns differentially. Increased awareness of the influence of dementia on hospitalizations and hospitalization discharges is important not only for clinicians but also for the payors, who may penalize (through denial of hospitalization reimbursement) acute‐care facilities motivated to provide support to dementia patients who are unable to receive adequate care in the community. Furthermore, related to this issue is the Medicare policy that disallows reimbursement for SNF transfer admissions unless preceded by a 3‐day acute‐care hospitalization.[25] Hospitals often face a dilemma of whether to admit patients and keep them hospitalized for the requisite period of time to allow for SNF care to be provided, or to deny this option to patients by discharging them sooner (or not admitting them at all).
Demented persons are frequent visitors to emergency departments, and often the impairment in fundamental activities of daily living is immediately apparent to the nurses and physicians caring for them. How does hospital staff come to grips with the potential conflict between duty to the patient and financial solvency of the institution? When dementia is the chief concern but not an acceptable indication for admission (eg, clinical indication for inpatient care[26]), a search for a reimbursable DRG may ensue, and this could contribute to the variability of dementia comorbidity's impact on hospital discharge disposition noted in this study.
This study has strengths in that the data are sampled in a manner that allows national estimates to be made. Although administrative data, such as the NIS, have limitations in coding accuracy/variability, important quality factors influencing relevant outcomes in the United States have been quantified using the NIS.[27] Because the data were deidentified and sampled rather than being complete, readmissions could not be assessed. Readmission is an important measure of the effectiveness of comprehensive geriatric care models[28] and patient‐centered care. It is possible that more readmissions for the same patient in the same year could have accounted for some of the trend findings. Furthermore, readmissions for the same patient in a given year could have impacted on the time‐related dementia prevalence calculations used. Changes in coding practices also could have impacted the dementia prevalence trends noted.
This study utilized comorbidities that have been typically used to characterize inpatient mortality.[10] The focus of this study, however, was not on mortality but on home discharge. The use of multinomial logistic regression instead of binomial logistic regression was based on the intention to examine home discharge using skilled nursing facility discharge as a reference but also incorporatingand accounting forother significant dispositions in the model such as death and other institutional transfers. Quan et al.[10] used the C statistic to describe and compare a mortality prediction model fit with the Charlson versus other comorbidity indices in national datasets. This statistic, however, is not used in multinomial logistic regression. Thus, it is difficult to compare the present modeling with the published models based on mortality (as a dichotomous outcome). The logistic regression models generally showed highly significant predictor effects for all predictor variables utilized (including dementia), but with a variable degree of correct prediction of disposition.
We originally hypothesized that hospitalized patients with dementia would require care in settings other than home at discharge, based on various key clinical and demographic factors, and that dementia comorbidity would display similar adjusted predictor effects for various common DRGs. Our findings of greater dementia‐associated odds ratios for particular DRGs suggest a more complex and variable dementia role in certain types of hospitalization, and that there are potential limitations in using Agency for Healthcare Research and Quality prevention quality indicators,[7, 26] developed for the purpose of tracking hospitalization data to assess quality and access to community‐based medical care.
Acknowledgements
The authors acknowledge the assistance of Suh Lee, BA, during the summer of 2012. This work was supported in part by an intramural grant from New York Medical College.
Disclosure: Nothing to report.
- Federal Interagency Forum on Aging‐Related Statistics. Older Americans 2012: key indicators of well‐being (older Americans 2012). Washington, DC: US Government Printing Office; 2012.
- Alzheimer's Organization. Risk factors. Available at: http://www.alz.org/alzheimers_disease_causes_risk_factors.asp Accessed February 15, 2015.
- Baltes PB, Mayer KV, eds. The Berlin Aging Study: aging from 70 to 100. Cambridge, United Kingdom: Cambridge University Press; 1999.
- , , , et al. Hospitalization in community‐dwelling persons with Alzheimer's disease: frequency and causes. Am Geriatr Soc. 2010;58:1542–1548.
- , , , , , . Cognitive decline after hospitalization in a community population of older persons. Neurology. 2012;78:950–956.
- Alzheimer's Association. Alzheimer's disease and chronic health conditions: the real challenge for 21st century Medicare. Alzheimer's Association website. Available at: https://www.alz.org/national/documents/report_chroniccare.pdf. Published 2003. Accessed February 15, 2015.
- , . An overview of clinical research: the lay of the land. Lancet. 2002;359:57–61.
- Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. HCUP databases. Available at: www.hcup-us.ahrq.gov/nisoverview.jsp. Modified December 11, 2013, Accessed May 31, 2015.
- , , , et al. Coding algorithms for defining comorbidities in ICD‐9‐CM and ICD‐10 administrative data. Med Care. 2005;43:1130–1139.
- , , , et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173:676–682.
- , . Falls, injuries due to falls, and the risk of admission to a nursing home. N Engl J Med. 1997;337:1279–1284.
- , , , . Insurance status and the transfer of hospitalized patients: an observational study. Ann Intern Med. 2014;160:81–90.
- Centers for Medicare 118:392–404.
- , , . Drug‐induced, dementia‐associated and non‐dementia, non‐drug delirium hospitalizations in the United States, 1998‐2005: an analysis of the national inpatient sample. Drugs Aging. 2010;27:51–61.
- , , , . Multiple discriminate analysis and logistic regression. In: Multivariate Data Analysis. 7th ed. Upper Saddle River, NJ: Prentice Hall; 2009.
- . A growing inpatient imperative: Alzheimer's disease. Hosp Health Netw. 2009;83:26, 28, 30.
- , , , , . The central role of comorbidity in predicting ambulatory care sensitive hospitalizations. Eur J Public Health. 2014;24(1):66–72.
- Agency for Healthcare Research and Quality. Prevention quality indicators technical specifications. Version 4.4. March 2012. Available at: http://www.qualityindicators.ahrq.gov/Archive/PQI_TechSpec_V44.aspx. Accessed September 1, 2012.
- , , , . Hospital transfers of nursing home residents with advanced dementia. J Am Geriatr Soc. 2012;60:905–909.
- , , , , . Potentially Avoidable Hospitalizations for Elderly Long‐stay Residents in Nursing Homes. Med Care. 2013;51(8):673–681.
- Centers for Medicare 15:592–601.
- , . Measurement of potentially preventable hospitalizations. white paper prepared for the long term quality alliance. Available at: http://www.ltqa.org/wp-content/themes/ltqaMain/custom/images//PreventableHospitalizations_021512_2.pdf. Published February 2012. Accessed August 6, 2013.
- Federal Interagency Forum on Aging‐Related Statistics. Older Americans 2012: key indicators of well‐being (older Americans 2012). Washington, DC: US Government Printing Office; 2012.
- Alzheimer's Organization. Risk factors. Available at: http://www.alz.org/alzheimers_disease_causes_risk_factors.asp Accessed February 15, 2015.
- Baltes PB, Mayer KV, eds. The Berlin Aging Study: aging from 70 to 100. Cambridge, United Kingdom: Cambridge University Press; 1999.
- , , , et al. Hospitalization in community‐dwelling persons with Alzheimer's disease: frequency and causes. Am Geriatr Soc. 2010;58:1542–1548.
- , , , , , . Cognitive decline after hospitalization in a community population of older persons. Neurology. 2012;78:950–956.
- Alzheimer's Association. Alzheimer's disease and chronic health conditions: the real challenge for 21st century Medicare. Alzheimer's Association website. Available at: https://www.alz.org/national/documents/report_chroniccare.pdf. Published 2003. Accessed February 15, 2015.
- , . An overview of clinical research: the lay of the land. Lancet. 2002;359:57–61.
- Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. HCUP databases. Available at: www.hcup-us.ahrq.gov/nisoverview.jsp. Modified December 11, 2013, Accessed May 31, 2015.
- , , , et al. Coding algorithms for defining comorbidities in ICD‐9‐CM and ICD‐10 administrative data. Med Care. 2005;43:1130–1139.
- , , , et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173:676–682.
- , . Falls, injuries due to falls, and the risk of admission to a nursing home. N Engl J Med. 1997;337:1279–1284.
- , , , . Insurance status and the transfer of hospitalized patients: an observational study. Ann Intern Med. 2014;160:81–90.
- Centers for Medicare 118:392–404.
- , , . Drug‐induced, dementia‐associated and non‐dementia, non‐drug delirium hospitalizations in the United States, 1998‐2005: an analysis of the national inpatient sample. Drugs Aging. 2010;27:51–61.
- , , , . Multiple discriminate analysis and logistic regression. In: Multivariate Data Analysis. 7th ed. Upper Saddle River, NJ: Prentice Hall; 2009.
- . A growing inpatient imperative: Alzheimer's disease. Hosp Health Netw. 2009;83:26, 28, 30.
- , , , , . The central role of comorbidity in predicting ambulatory care sensitive hospitalizations. Eur J Public Health. 2014;24(1):66–72.
- Agency for Healthcare Research and Quality. Prevention quality indicators technical specifications. Version 4.4. March 2012. Available at: http://www.qualityindicators.ahrq.gov/Archive/PQI_TechSpec_V44.aspx. Accessed September 1, 2012.
- , , , . Hospital transfers of nursing home residents with advanced dementia. J Am Geriatr Soc. 2012;60:905–909.
- , , , , . Potentially Avoidable Hospitalizations for Elderly Long‐stay Residents in Nursing Homes. Med Care. 2013;51(8):673–681.
- Centers for Medicare 15:592–601.
- , . Measurement of potentially preventable hospitalizations. white paper prepared for the long term quality alliance. Available at: http://www.ltqa.org/wp-content/themes/ltqaMain/custom/images//PreventableHospitalizations_021512_2.pdf. Published February 2012. Accessed August 6, 2013.
© 2015 Society of Hospital Medicine
Hospitalists and Palliative Care
In the inaugural issue of the Journal of Hospital Medicine, Diane Meier made a strong case for palliative care in hospitals[1] and I advocated for a close partnership between hospital medicine and palliative care.[2] Over the past decade, hospital medicine and palliative care have grown up together, like fraternal twins, driven by similar demographic trends and imperatives to improve value. In the early going, each sibling played to its strengths: hospital medicine to quality and palliative care to the patient experience. Today, with patient satisfaction a key metric for reimbursement, hospital medicine is focusing on patient experience and may learn from palliative care. Similarly, as palliative care has matured as a field, palliative care teams are being asked to demonstrate quality and may learn much from working with hospital medicine.
Increasingly, palliative care teams are focusing on quality improvement (QI) and collecting the data necessary to drive it.[3] In fact, there is sufficient interest in QI that 2 Web‐based, nationally available databases for collecting outcome data in palliative care have been established, the Palliative Care Quality Network (PCQN;
Although palliative care teams are engaging in QI, there is also the recognition that their efforts effect only those patients referred to their service and that they cannot meet all the need for palliative care in the hospital. Most palliative care teams are struggling to cope with the volume of consults, yet estimate that they are seeing fewer than half the patients who need to be seen.[6] True quality will require not only that palliative care teams improve the care they provide, but that each hospital and healthcare system adopt a population‐based approach to addressing palliative care needs. We will need to implement methods for identifying all patients with palliative care needs, not just the ones referred to palliative care teams, and create systems to meet those needs. Hospitalists and hospital medicine are critical partners in the effort to improve quality for the population of people with serious illness.
An essential aspect of this population‐based approach is recognizing that although some patients will have palliative care needs best addressed by a palliative care team of experts, others will have palliative care needs that can be met well by hospitalists, nurses, social workers, and chaplains who have the necessary skills to provide what has been called primary palliative care.[7] Working together, hospitalists and palliative care teams must develop screening tools integrated within the electronic health record (EHR) to identify patients with palliative care needs such as for completing an advance directive or pain management.[8] The Society of Hospital Medicine (SHM) has supported similar efforts focused on venous thromboembolism prophylaxis and transitions of care. Identifying palliative care issues proactively will ensure that they are not overlooked. In addition, there must be a system to address those needs. Hospitalists will play a key role in addressing primary palliative care needs. Many hospitalists through study, practice, and focus will develop expertise beyond primary palliative care and be able to address more complex patient needs. Our professional society, the SHM, could collaborate with the American Academy of Hospice and Palliative Medicine to develop a formal recognition for hospitalists who demonstrate skill and focus in palliative care as a way to ensure expertise, expand the cadre of physicians with palliative care skills, and encourage hospitalists to adopt this focus.
Finally, we will need to implement systems to collect key data on palliative care outcomes for all patients. For example, within the EHR we must be able to easily locate a goals of care discussion and its outcome as well as an advance directive. Furthermore, we should work to establish statewide and even national repositories of advance directives so that they are available when needed. Currently the PCQN and qdact collect such data on advance care planning and completion of advance directives, and can assess their impact on key patient outcomes. These organizations can collaborate on the solutions for measuring palliative care outcomes across a population. As an example, our palliative care team at UCSF is using PCQN data to drive a QI project focused on increasing the completion of Physician Orders for Life‐Sustaining Treatment forms for people seen by the palliative care team who are discharged and whose code status is anything other than full code. Our hospitalist group will adopt this QI project in the coming year based on recognition of its success and importance to the broader population of patients cared for by hospitalists. Such partnerships at the local and national level can improve quality in many dimensions of care including pain management and transitions. Addressing population‐based palliative care needs through a partnership between palliative care and hospital medicine will also allow us to answer many questions about the demographics of palliative care needs, the impact of various interventions for addressing needs on patient outcomes, and which patients need expert level palliative care among others.
Ten years ago I wrote that hospitalists and palliative care were a partnership for hope. Growing recognition of the benefits of palliative care, rising patient demand for palliative care, and an increasing focus on QI are quickly outstripping the ability of palliative care teams to provide that care on their own. To achieve the best patient care, that partnership must be more than hope. It must be a reality.
Disclosures
Dr. Pantilat's work is supported by grants from the Alafi Family Foundation, the Hellman Foundation, the UniHealth Foundation, the California HealthCare Foundation, the Archstone Foundation, and the Kettering Family Foundation. The author reports no conflicts of interest.
- . Palliative care in hospitals. J Hosp Med. 2006;1(1):21–28.
- . Palliative care and hospitalists: a partnership for hope. J Hosp Med. 2006;1(1):5–6.
- , , , et al. The quality imperative for palliative care. J Pain Symptom Manage. 2015;49(2):243–253.
- , , , . Foreword: quality improvement efforts: advancing the science of palliative care. J Pain Symptom Manage. 2011;42(5):649–651.
- , , , et al. Palliative Care Quality Network: toward quality improvement in palliative care. J Palliat Care. 2014;30(3):204–205.
- , , , , . Palliative care services in California hospitals: program prevalence and hospital characteristics. J Pain Symptom Manage. 2012;43(1):39–46.
- , . Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173–1175.
- , , , , . A rapid two‐stage screening protocol for palliative care in the emergency department: a quality improvement initiative. J Pain Symptom Manage. 2011;42(5):657–662.
In the inaugural issue of the Journal of Hospital Medicine, Diane Meier made a strong case for palliative care in hospitals[1] and I advocated for a close partnership between hospital medicine and palliative care.[2] Over the past decade, hospital medicine and palliative care have grown up together, like fraternal twins, driven by similar demographic trends and imperatives to improve value. In the early going, each sibling played to its strengths: hospital medicine to quality and palliative care to the patient experience. Today, with patient satisfaction a key metric for reimbursement, hospital medicine is focusing on patient experience and may learn from palliative care. Similarly, as palliative care has matured as a field, palliative care teams are being asked to demonstrate quality and may learn much from working with hospital medicine.
Increasingly, palliative care teams are focusing on quality improvement (QI) and collecting the data necessary to drive it.[3] In fact, there is sufficient interest in QI that 2 Web‐based, nationally available databases for collecting outcome data in palliative care have been established, the Palliative Care Quality Network (PCQN;
Although palliative care teams are engaging in QI, there is also the recognition that their efforts effect only those patients referred to their service and that they cannot meet all the need for palliative care in the hospital. Most palliative care teams are struggling to cope with the volume of consults, yet estimate that they are seeing fewer than half the patients who need to be seen.[6] True quality will require not only that palliative care teams improve the care they provide, but that each hospital and healthcare system adopt a population‐based approach to addressing palliative care needs. We will need to implement methods for identifying all patients with palliative care needs, not just the ones referred to palliative care teams, and create systems to meet those needs. Hospitalists and hospital medicine are critical partners in the effort to improve quality for the population of people with serious illness.
An essential aspect of this population‐based approach is recognizing that although some patients will have palliative care needs best addressed by a palliative care team of experts, others will have palliative care needs that can be met well by hospitalists, nurses, social workers, and chaplains who have the necessary skills to provide what has been called primary palliative care.[7] Working together, hospitalists and palliative care teams must develop screening tools integrated within the electronic health record (EHR) to identify patients with palliative care needs such as for completing an advance directive or pain management.[8] The Society of Hospital Medicine (SHM) has supported similar efforts focused on venous thromboembolism prophylaxis and transitions of care. Identifying palliative care issues proactively will ensure that they are not overlooked. In addition, there must be a system to address those needs. Hospitalists will play a key role in addressing primary palliative care needs. Many hospitalists through study, practice, and focus will develop expertise beyond primary palliative care and be able to address more complex patient needs. Our professional society, the SHM, could collaborate with the American Academy of Hospice and Palliative Medicine to develop a formal recognition for hospitalists who demonstrate skill and focus in palliative care as a way to ensure expertise, expand the cadre of physicians with palliative care skills, and encourage hospitalists to adopt this focus.
Finally, we will need to implement systems to collect key data on palliative care outcomes for all patients. For example, within the EHR we must be able to easily locate a goals of care discussion and its outcome as well as an advance directive. Furthermore, we should work to establish statewide and even national repositories of advance directives so that they are available when needed. Currently the PCQN and qdact collect such data on advance care planning and completion of advance directives, and can assess their impact on key patient outcomes. These organizations can collaborate on the solutions for measuring palliative care outcomes across a population. As an example, our palliative care team at UCSF is using PCQN data to drive a QI project focused on increasing the completion of Physician Orders for Life‐Sustaining Treatment forms for people seen by the palliative care team who are discharged and whose code status is anything other than full code. Our hospitalist group will adopt this QI project in the coming year based on recognition of its success and importance to the broader population of patients cared for by hospitalists. Such partnerships at the local and national level can improve quality in many dimensions of care including pain management and transitions. Addressing population‐based palliative care needs through a partnership between palliative care and hospital medicine will also allow us to answer many questions about the demographics of palliative care needs, the impact of various interventions for addressing needs on patient outcomes, and which patients need expert level palliative care among others.
Ten years ago I wrote that hospitalists and palliative care were a partnership for hope. Growing recognition of the benefits of palliative care, rising patient demand for palliative care, and an increasing focus on QI are quickly outstripping the ability of palliative care teams to provide that care on their own. To achieve the best patient care, that partnership must be more than hope. It must be a reality.
Disclosures
Dr. Pantilat's work is supported by grants from the Alafi Family Foundation, the Hellman Foundation, the UniHealth Foundation, the California HealthCare Foundation, the Archstone Foundation, and the Kettering Family Foundation. The author reports no conflicts of interest.
In the inaugural issue of the Journal of Hospital Medicine, Diane Meier made a strong case for palliative care in hospitals[1] and I advocated for a close partnership between hospital medicine and palliative care.[2] Over the past decade, hospital medicine and palliative care have grown up together, like fraternal twins, driven by similar demographic trends and imperatives to improve value. In the early going, each sibling played to its strengths: hospital medicine to quality and palliative care to the patient experience. Today, with patient satisfaction a key metric for reimbursement, hospital medicine is focusing on patient experience and may learn from palliative care. Similarly, as palliative care has matured as a field, palliative care teams are being asked to demonstrate quality and may learn much from working with hospital medicine.
Increasingly, palliative care teams are focusing on quality improvement (QI) and collecting the data necessary to drive it.[3] In fact, there is sufficient interest in QI that 2 Web‐based, nationally available databases for collecting outcome data in palliative care have been established, the Palliative Care Quality Network (PCQN;
Although palliative care teams are engaging in QI, there is also the recognition that their efforts effect only those patients referred to their service and that they cannot meet all the need for palliative care in the hospital. Most palliative care teams are struggling to cope with the volume of consults, yet estimate that they are seeing fewer than half the patients who need to be seen.[6] True quality will require not only that palliative care teams improve the care they provide, but that each hospital and healthcare system adopt a population‐based approach to addressing palliative care needs. We will need to implement methods for identifying all patients with palliative care needs, not just the ones referred to palliative care teams, and create systems to meet those needs. Hospitalists and hospital medicine are critical partners in the effort to improve quality for the population of people with serious illness.
An essential aspect of this population‐based approach is recognizing that although some patients will have palliative care needs best addressed by a palliative care team of experts, others will have palliative care needs that can be met well by hospitalists, nurses, social workers, and chaplains who have the necessary skills to provide what has been called primary palliative care.[7] Working together, hospitalists and palliative care teams must develop screening tools integrated within the electronic health record (EHR) to identify patients with palliative care needs such as for completing an advance directive or pain management.[8] The Society of Hospital Medicine (SHM) has supported similar efforts focused on venous thromboembolism prophylaxis and transitions of care. Identifying palliative care issues proactively will ensure that they are not overlooked. In addition, there must be a system to address those needs. Hospitalists will play a key role in addressing primary palliative care needs. Many hospitalists through study, practice, and focus will develop expertise beyond primary palliative care and be able to address more complex patient needs. Our professional society, the SHM, could collaborate with the American Academy of Hospice and Palliative Medicine to develop a formal recognition for hospitalists who demonstrate skill and focus in palliative care as a way to ensure expertise, expand the cadre of physicians with palliative care skills, and encourage hospitalists to adopt this focus.
Finally, we will need to implement systems to collect key data on palliative care outcomes for all patients. For example, within the EHR we must be able to easily locate a goals of care discussion and its outcome as well as an advance directive. Furthermore, we should work to establish statewide and even national repositories of advance directives so that they are available when needed. Currently the PCQN and qdact collect such data on advance care planning and completion of advance directives, and can assess their impact on key patient outcomes. These organizations can collaborate on the solutions for measuring palliative care outcomes across a population. As an example, our palliative care team at UCSF is using PCQN data to drive a QI project focused on increasing the completion of Physician Orders for Life‐Sustaining Treatment forms for people seen by the palliative care team who are discharged and whose code status is anything other than full code. Our hospitalist group will adopt this QI project in the coming year based on recognition of its success and importance to the broader population of patients cared for by hospitalists. Such partnerships at the local and national level can improve quality in many dimensions of care including pain management and transitions. Addressing population‐based palliative care needs through a partnership between palliative care and hospital medicine will also allow us to answer many questions about the demographics of palliative care needs, the impact of various interventions for addressing needs on patient outcomes, and which patients need expert level palliative care among others.
Ten years ago I wrote that hospitalists and palliative care were a partnership for hope. Growing recognition of the benefits of palliative care, rising patient demand for palliative care, and an increasing focus on QI are quickly outstripping the ability of palliative care teams to provide that care on their own. To achieve the best patient care, that partnership must be more than hope. It must be a reality.
Disclosures
Dr. Pantilat's work is supported by grants from the Alafi Family Foundation, the Hellman Foundation, the UniHealth Foundation, the California HealthCare Foundation, the Archstone Foundation, and the Kettering Family Foundation. The author reports no conflicts of interest.
- . Palliative care in hospitals. J Hosp Med. 2006;1(1):21–28.
- . Palliative care and hospitalists: a partnership for hope. J Hosp Med. 2006;1(1):5–6.
- , , , et al. The quality imperative for palliative care. J Pain Symptom Manage. 2015;49(2):243–253.
- , , , . Foreword: quality improvement efforts: advancing the science of palliative care. J Pain Symptom Manage. 2011;42(5):649–651.
- , , , et al. Palliative Care Quality Network: toward quality improvement in palliative care. J Palliat Care. 2014;30(3):204–205.
- , , , , . Palliative care services in California hospitals: program prevalence and hospital characteristics. J Pain Symptom Manage. 2012;43(1):39–46.
- , . Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173–1175.
- , , , , . A rapid two‐stage screening protocol for palliative care in the emergency department: a quality improvement initiative. J Pain Symptom Manage. 2011;42(5):657–662.
- . Palliative care in hospitals. J Hosp Med. 2006;1(1):21–28.
- . Palliative care and hospitalists: a partnership for hope. J Hosp Med. 2006;1(1):5–6.
- , , , et al. The quality imperative for palliative care. J Pain Symptom Manage. 2015;49(2):243–253.
- , , , . Foreword: quality improvement efforts: advancing the science of palliative care. J Pain Symptom Manage. 2011;42(5):649–651.
- , , , et al. Palliative Care Quality Network: toward quality improvement in palliative care. J Palliat Care. 2014;30(3):204–205.
- , , , , . Palliative care services in California hospitals: program prevalence and hospital characteristics. J Pain Symptom Manage. 2012;43(1):39–46.
- , . Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173–1175.
- , , , , . A rapid two‐stage screening protocol for palliative care in the emergency department: a quality improvement initiative. J Pain Symptom Manage. 2011;42(5):657–662.
CAR produces high CR rate in adults with rel/ref ALL

the 2015 ASCO Annual Meeting
© ASCO/Max Gersh
CHICAGO—A CD19-targeted chimeric antigen receptor (CAR) T-cell therapy can provide durable complete responses (CRs) or a bridge to allogeneic transplant in adults with relapsed or refractory acute lymphoblastic leukemia (ALL), updated results of a phase 1 study suggest.
The therapy, JCAR015, produced a CR rate of 87%, and 33% of these patients went on to transplant.
The median duration of response or relapse-free survival was 5.3 months. The median overall survival was 8.5 months.
Nearly a quarter of patients developed severe cytokine release syndrome (CRS), and nearly 30% experienced neurological toxicities. But researchers said these effects were largely treatable and reversible.
This study was temporarily placed on clinical hold last year, after 2 patients died from complications related to CRS. But the hold was soon lifted and enrollment and dosing criteria were changed in an attempt to prevent severe CRS.
Jae H. Park, MD, of Memorial Sloan Kettering Cancer Center in New York, presented updated results of this trial (NCT01044069) at the 2015 ASCO Annual Meeting (abstract 7010*). The study is sponsored by Memorial Sloan Kettering, but funding has also been provided by Juno Therapeutics, the company developing JCAR015.
Results from this trial have previously been reported in Science Translational Medicine (Davila et al 2014; Brentjens et al 2013), at AACR 2014, and at ASH 2014.
At ASCO, Dr Park presented results in 39 patients with relapsed/refractory, CD19+ ALL. All of them were evaluable for toxicity assessment, and 38 were evaluable for response with at least 1 month of follow-up.
There were 29 males, and the patients’ median age was 45 (range, 22-74). Thirty-three percent had Ph+ ALL, and 11% had the T315I mutation.
Forty-nine percent of patients had received 2 prior therapies, 23% had received 3, and 28% had received 4 or more. Thirty-six percent of patients had a prior allogeneic hematopoietic stem cell transplant (HSCT).
For this study, patients first underwent leukapheresis. While their T cells were being manufactured, they were allowed to receive salvage chemotherapy. Patients underwent repeat bone marrow biopsy to assess their disease status immediately prior to T-cell infusion.
Fifty-four percent of patients (n=21) had morphologic disease (>5% blasts in the bone marrow, median 52%) immediately prior to JCAR015 infusion, and the remaining patients (n=18) had minimal residual disease (MRD).
Two days after conditioning with cyclophosphamide, patients received an infusion of 1-3 x 106 CAR T cells/kg. At day 28, the researchers assessed patients’ disease with a repeat bone marrow biopsy.
Treatment results
The median follow-up was 5.6 months (1 to >38 months). Six patients had more than a year of follow-up.
The CR rate was 87% (33/38), and 81% of evaluable patients (26/32) were MRD-negative. The median time to CR was 23 days, and the median duration of response or relapse-free survival was 5.3 months.
“We examined the CR rates by different subgroup,” Dr Park noted. “We looked at whether patients had a pre-T-cell disease burden: morphologic disease vs minimal residual disease, whether they had an allogeneic bone marrow transplant prior to CAR T-cell infusion, their Ph+ status, age at infusion, and prior lines of therapy. And there was no [significant] difference between these groups for CRs and MRD-negative CR rate.”
At the time of presentation, 14 patients were disease-free, 10 of whom had not gone on to HSCT. In all, 11 patients went on to allogeneic HSCT.
Fourteen patients relapsed during follow-up, 3 after HSCT. Two of these patients had CD19-negative bone marrow blasts.
The median overall survival was 8.5 months in all patients and 10.8 months in patients who were MRD-negative. The median overall survival was 9.9 months in patients who underwent allogeneic HSCT and 8.5 months in patients who did not.
Dr Park said key adverse events were CRS—clinically manifested by fever, hypotension, and respiratory insufficiency—and neurological changes such as delirium, global encephalopathy, aphasia, and seizures.
Twenty-three percent of patients (n=9) developed severe CRS, 28% (n=11) had grade 3/4 neurotoxicity, and 8% (n=3) had grade 5 toxicity. The patients with grade 5 toxicities died of ventricular arrhythmia, sepsis, and an unknown cause (although this patient suffered a seizure).
The severity of CRS correlated with disease burden, and CRS was managed with an IL-6R inhibitor (n=4), a steroid (n=2), or both (n=9). Neurological symptoms were reversible and could occur independently of CRS, Dr Park said. ![]()
*Information in the abstract differs from that presented at the meeting.
the 2015 ASCO Annual Meeting
© ASCO/Max Gersh
CHICAGO—A CD19-targeted chimeric antigen receptor (CAR) T-cell therapy can provide durable complete responses (CRs) or a bridge to allogeneic transplant in adults with relapsed or refractory acute lymphoblastic leukemia (ALL), updated results of a phase 1 study suggest.
The therapy, JCAR015, produced a CR rate of 87%, and 33% of these patients went on to transplant.
The median duration of response or relapse-free survival was 5.3 months. The median overall survival was 8.5 months.
Nearly a quarter of patients developed severe cytokine release syndrome (CRS), and nearly 30% experienced neurological toxicities. But researchers said these effects were largely treatable and reversible.
This study was temporarily placed on clinical hold last year, after 2 patients died from complications related to CRS. But the hold was soon lifted and enrollment and dosing criteria were changed in an attempt to prevent severe CRS.
Jae H. Park, MD, of Memorial Sloan Kettering Cancer Center in New York, presented updated results of this trial (NCT01044069) at the 2015 ASCO Annual Meeting (abstract 7010*). The study is sponsored by Memorial Sloan Kettering, but funding has also been provided by Juno Therapeutics, the company developing JCAR015.
Results from this trial have previously been reported in Science Translational Medicine (Davila et al 2014; Brentjens et al 2013), at AACR 2014, and at ASH 2014.
At ASCO, Dr Park presented results in 39 patients with relapsed/refractory, CD19+ ALL. All of them were evaluable for toxicity assessment, and 38 were evaluable for response with at least 1 month of follow-up.
There were 29 males, and the patients’ median age was 45 (range, 22-74). Thirty-three percent had Ph+ ALL, and 11% had the T315I mutation.
Forty-nine percent of patients had received 2 prior therapies, 23% had received 3, and 28% had received 4 or more. Thirty-six percent of patients had a prior allogeneic hematopoietic stem cell transplant (HSCT).
For this study, patients first underwent leukapheresis. While their T cells were being manufactured, they were allowed to receive salvage chemotherapy. Patients underwent repeat bone marrow biopsy to assess their disease status immediately prior to T-cell infusion.
Fifty-four percent of patients (n=21) had morphologic disease (>5% blasts in the bone marrow, median 52%) immediately prior to JCAR015 infusion, and the remaining patients (n=18) had minimal residual disease (MRD).
Two days after conditioning with cyclophosphamide, patients received an infusion of 1-3 x 106 CAR T cells/kg. At day 28, the researchers assessed patients’ disease with a repeat bone marrow biopsy.
Treatment results
The median follow-up was 5.6 months (1 to >38 months). Six patients had more than a year of follow-up.
The CR rate was 87% (33/38), and 81% of evaluable patients (26/32) were MRD-negative. The median time to CR was 23 days, and the median duration of response or relapse-free survival was 5.3 months.
“We examined the CR rates by different subgroup,” Dr Park noted. “We looked at whether patients had a pre-T-cell disease burden: morphologic disease vs minimal residual disease, whether they had an allogeneic bone marrow transplant prior to CAR T-cell infusion, their Ph+ status, age at infusion, and prior lines of therapy. And there was no [significant] difference between these groups for CRs and MRD-negative CR rate.”
At the time of presentation, 14 patients were disease-free, 10 of whom had not gone on to HSCT. In all, 11 patients went on to allogeneic HSCT.
Fourteen patients relapsed during follow-up, 3 after HSCT. Two of these patients had CD19-negative bone marrow blasts.
The median overall survival was 8.5 months in all patients and 10.8 months in patients who were MRD-negative. The median overall survival was 9.9 months in patients who underwent allogeneic HSCT and 8.5 months in patients who did not.
Dr Park said key adverse events were CRS—clinically manifested by fever, hypotension, and respiratory insufficiency—and neurological changes such as delirium, global encephalopathy, aphasia, and seizures.
Twenty-three percent of patients (n=9) developed severe CRS, 28% (n=11) had grade 3/4 neurotoxicity, and 8% (n=3) had grade 5 toxicity. The patients with grade 5 toxicities died of ventricular arrhythmia, sepsis, and an unknown cause (although this patient suffered a seizure).
The severity of CRS correlated with disease burden, and CRS was managed with an IL-6R inhibitor (n=4), a steroid (n=2), or both (n=9). Neurological symptoms were reversible and could occur independently of CRS, Dr Park said. ![]()
*Information in the abstract differs from that presented at the meeting.
the 2015 ASCO Annual Meeting
© ASCO/Max Gersh
CHICAGO—A CD19-targeted chimeric antigen receptor (CAR) T-cell therapy can provide durable complete responses (CRs) or a bridge to allogeneic transplant in adults with relapsed or refractory acute lymphoblastic leukemia (ALL), updated results of a phase 1 study suggest.
The therapy, JCAR015, produced a CR rate of 87%, and 33% of these patients went on to transplant.
The median duration of response or relapse-free survival was 5.3 months. The median overall survival was 8.5 months.
Nearly a quarter of patients developed severe cytokine release syndrome (CRS), and nearly 30% experienced neurological toxicities. But researchers said these effects were largely treatable and reversible.
This study was temporarily placed on clinical hold last year, after 2 patients died from complications related to CRS. But the hold was soon lifted and enrollment and dosing criteria were changed in an attempt to prevent severe CRS.
Jae H. Park, MD, of Memorial Sloan Kettering Cancer Center in New York, presented updated results of this trial (NCT01044069) at the 2015 ASCO Annual Meeting (abstract 7010*). The study is sponsored by Memorial Sloan Kettering, but funding has also been provided by Juno Therapeutics, the company developing JCAR015.
Results from this trial have previously been reported in Science Translational Medicine (Davila et al 2014; Brentjens et al 2013), at AACR 2014, and at ASH 2014.
At ASCO, Dr Park presented results in 39 patients with relapsed/refractory, CD19+ ALL. All of them were evaluable for toxicity assessment, and 38 were evaluable for response with at least 1 month of follow-up.
There were 29 males, and the patients’ median age was 45 (range, 22-74). Thirty-three percent had Ph+ ALL, and 11% had the T315I mutation.
Forty-nine percent of patients had received 2 prior therapies, 23% had received 3, and 28% had received 4 or more. Thirty-six percent of patients had a prior allogeneic hematopoietic stem cell transplant (HSCT).
For this study, patients first underwent leukapheresis. While their T cells were being manufactured, they were allowed to receive salvage chemotherapy. Patients underwent repeat bone marrow biopsy to assess their disease status immediately prior to T-cell infusion.
Fifty-four percent of patients (n=21) had morphologic disease (>5% blasts in the bone marrow, median 52%) immediately prior to JCAR015 infusion, and the remaining patients (n=18) had minimal residual disease (MRD).
Two days after conditioning with cyclophosphamide, patients received an infusion of 1-3 x 106 CAR T cells/kg. At day 28, the researchers assessed patients’ disease with a repeat bone marrow biopsy.
Treatment results
The median follow-up was 5.6 months (1 to >38 months). Six patients had more than a year of follow-up.
The CR rate was 87% (33/38), and 81% of evaluable patients (26/32) were MRD-negative. The median time to CR was 23 days, and the median duration of response or relapse-free survival was 5.3 months.
“We examined the CR rates by different subgroup,” Dr Park noted. “We looked at whether patients had a pre-T-cell disease burden: morphologic disease vs minimal residual disease, whether they had an allogeneic bone marrow transplant prior to CAR T-cell infusion, their Ph+ status, age at infusion, and prior lines of therapy. And there was no [significant] difference between these groups for CRs and MRD-negative CR rate.”
At the time of presentation, 14 patients were disease-free, 10 of whom had not gone on to HSCT. In all, 11 patients went on to allogeneic HSCT.
Fourteen patients relapsed during follow-up, 3 after HSCT. Two of these patients had CD19-negative bone marrow blasts.
The median overall survival was 8.5 months in all patients and 10.8 months in patients who were MRD-negative. The median overall survival was 9.9 months in patients who underwent allogeneic HSCT and 8.5 months in patients who did not.
Dr Park said key adverse events were CRS—clinically manifested by fever, hypotension, and respiratory insufficiency—and neurological changes such as delirium, global encephalopathy, aphasia, and seizures.
Twenty-three percent of patients (n=9) developed severe CRS, 28% (n=11) had grade 3/4 neurotoxicity, and 8% (n=3) had grade 5 toxicity. The patients with grade 5 toxicities died of ventricular arrhythmia, sepsis, and an unknown cause (although this patient suffered a seizure).
The severity of CRS correlated with disease burden, and CRS was managed with an IL-6R inhibitor (n=4), a steroid (n=2), or both (n=9). Neurological symptoms were reversible and could occur independently of CRS, Dr Park said. ![]()
*Information in the abstract differs from that presented at the meeting.
Coffee Each Day Keeps the Melanoma Away

“An apple a day keeps the doctor away,” and coffee each day keeps the melanoma away. A recent analysis of data by Loftfield et al from a food frequency questionnaire published online on January 20 in the Journal of the National Cancer Institute demonstrated that caffeinated coffee intake was inversely associated with melanoma. Specifically, consuming 4 or more cups of caffeinated coffee each day was found to decrease the risk for melanoma by 20%.
The authors’ reference groups were derived from a National Institutes of Health–AARP prospective cohort diet and health study that commenced in 1995 to 1996 and concluded on December 31, 2006. They observed that the lower risk for melanoma was only associated with caffeinated coffee. Unexpectedly, they also observed that caffeinated coffee drinking only decreased the risk for melanoma but not melanoma in situ.
There is scientific evidence that coffee has a role in decreasing UVB-induced carcinogenesis. Caffeine (both orally and topically) inhibits UVB-induced carcinogenesis by absorbing UV radiation. Also, 5-O-caffeoylquinic acid (the major chlorogenic acid in coffee) and its metabolite caffeic acid inhibit cyclooxygenase 2 expression, which is overexpressed in human melanoma cells and in response to UVB exposure. In addition to caffeine, coffee also contains several bioactive compounds: diterpenes, polyphenols, and trigonelline. Topical diterpenes inhibit inflammation in epidermal cells. During coffee roasting, trigonelline generates nicotinic acid and nicotinamide, both of which are protective against UVB-induced skin carcinogenesis in mice and UVB-induced immunosuppression in both humans and mice.
What’s the issue?
According to an article in The Washington Post, the “apple” adage originated in the 1860s; the original phrase was “Eat an apple on going to bed, and you’ll keep the doctor from earning his bread,” which evolved to “An apple a day, no doctor to pay,” then “An apple a day sends the doctor away” before the current version was first used in 1922. As one who enjoys having a cup of caffeinated coffee next to my computer in the office or at home, I can easily welcome the prospect of a few additional cups each day to prevent melanoma. And, as advocates for a possible benefit to our patients’ better health, should we should provide complimentary caffeinated coffee in our office waiting rooms to encourage our dermatology patients to decrease their risk for developing melanoma?
“An apple a day keeps the doctor away,” and coffee each day keeps the melanoma away. A recent analysis of data by Loftfield et al from a food frequency questionnaire published online on January 20 in the Journal of the National Cancer Institute demonstrated that caffeinated coffee intake was inversely associated with melanoma. Specifically, consuming 4 or more cups of caffeinated coffee each day was found to decrease the risk for melanoma by 20%.
The authors’ reference groups were derived from a National Institutes of Health–AARP prospective cohort diet and health study that commenced in 1995 to 1996 and concluded on December 31, 2006. They observed that the lower risk for melanoma was only associated with caffeinated coffee. Unexpectedly, they also observed that caffeinated coffee drinking only decreased the risk for melanoma but not melanoma in situ.
There is scientific evidence that coffee has a role in decreasing UVB-induced carcinogenesis. Caffeine (both orally and topically) inhibits UVB-induced carcinogenesis by absorbing UV radiation. Also, 5-O-caffeoylquinic acid (the major chlorogenic acid in coffee) and its metabolite caffeic acid inhibit cyclooxygenase 2 expression, which is overexpressed in human melanoma cells and in response to UVB exposure. In addition to caffeine, coffee also contains several bioactive compounds: diterpenes, polyphenols, and trigonelline. Topical diterpenes inhibit inflammation in epidermal cells. During coffee roasting, trigonelline generates nicotinic acid and nicotinamide, both of which are protective against UVB-induced skin carcinogenesis in mice and UVB-induced immunosuppression in both humans and mice.
What’s the issue?
According to an article in The Washington Post, the “apple” adage originated in the 1860s; the original phrase was “Eat an apple on going to bed, and you’ll keep the doctor from earning his bread,” which evolved to “An apple a day, no doctor to pay,” then “An apple a day sends the doctor away” before the current version was first used in 1922. As one who enjoys having a cup of caffeinated coffee next to my computer in the office or at home, I can easily welcome the prospect of a few additional cups each day to prevent melanoma. And, as advocates for a possible benefit to our patients’ better health, should we should provide complimentary caffeinated coffee in our office waiting rooms to encourage our dermatology patients to decrease their risk for developing melanoma?
“An apple a day keeps the doctor away,” and coffee each day keeps the melanoma away. A recent analysis of data by Loftfield et al from a food frequency questionnaire published online on January 20 in the Journal of the National Cancer Institute demonstrated that caffeinated coffee intake was inversely associated with melanoma. Specifically, consuming 4 or more cups of caffeinated coffee each day was found to decrease the risk for melanoma by 20%.
The authors’ reference groups were derived from a National Institutes of Health–AARP prospective cohort diet and health study that commenced in 1995 to 1996 and concluded on December 31, 2006. They observed that the lower risk for melanoma was only associated with caffeinated coffee. Unexpectedly, they also observed that caffeinated coffee drinking only decreased the risk for melanoma but not melanoma in situ.
There is scientific evidence that coffee has a role in decreasing UVB-induced carcinogenesis. Caffeine (both orally and topically) inhibits UVB-induced carcinogenesis by absorbing UV radiation. Also, 5-O-caffeoylquinic acid (the major chlorogenic acid in coffee) and its metabolite caffeic acid inhibit cyclooxygenase 2 expression, which is overexpressed in human melanoma cells and in response to UVB exposure. In addition to caffeine, coffee also contains several bioactive compounds: diterpenes, polyphenols, and trigonelline. Topical diterpenes inhibit inflammation in epidermal cells. During coffee roasting, trigonelline generates nicotinic acid and nicotinamide, both of which are protective against UVB-induced skin carcinogenesis in mice and UVB-induced immunosuppression in both humans and mice.
What’s the issue?
According to an article in The Washington Post, the “apple” adage originated in the 1860s; the original phrase was “Eat an apple on going to bed, and you’ll keep the doctor from earning his bread,” which evolved to “An apple a day, no doctor to pay,” then “An apple a day sends the doctor away” before the current version was first used in 1922. As one who enjoys having a cup of caffeinated coffee next to my computer in the office or at home, I can easily welcome the prospect of a few additional cups each day to prevent melanoma. And, as advocates for a possible benefit to our patients’ better health, should we should provide complimentary caffeinated coffee in our office waiting rooms to encourage our dermatology patients to decrease their risk for developing melanoma?
