User login
Try exposure therapy, SSRIs for PTSD
LAS VEGAS– There is no cure for posttraumatic stress disorder, but helping its sufferers reduce symptoms, improve resistance, and achieve a better quality of life is possible.
“We have no idea what the best treatments are for PTSD,” Dr. Charles B. Nemeroff, the Leonard M. Miller Professor, and chairman of the department of psychiatry and behavioral sciences at the University of Miami, told an audience at the annual psychopharmacology update held by the Nevada Psychiatric Association.

Whether to rely upon psychosocial or pharmacologic interventions, or a combination of the two, to help shift PTSD from a debilitating condition into a manageable, chronic one, it is important to understand PTSD as a brain disease. “To accurately treat PTSD, consider it within a neurobiological context,” Dr. Nemeroff said. “Ordinarily, the brain is evolved to deal with stress, but it can be compromised.”
In chronic PTSD, brain studies have shown a noted shrinkage in the hippocampus, contributing to memory impairment, similar to the reduced hippocampal volume in child-abuse victims. Additionally, cortical function in the brain is affected in PTSD, creating difficulty with exercising judgment and good decision making.
“One way to think about PTSD is that the cortex is unable to reign in the limbic system,” Dr. Nemeroff said. “The hippocampus is impaired, the amygdala is hyperactive, and there is a tremendous emotional drive, so the ‘thinking’ part of the brain can’t [overcome] the emotional, reptilian brain.”
The result is that a person remains stuck in a hyperaroused state. “We know that the neurobiological basis for PTSD involves a prolonged, vigilant response to stress [involving] a multitude of brain circuits ... and of course the sympathetic nervous system and the pituitary and adrenal systems,” Dr. Nemeroff said.
Beyond brain changes, a genetic predisposition to PTSD accounts for a third of all cases, while an additional one-third are attributable to additional biological risk factors, according to Dr. Nemeroff (Nature 2011;470:492-7).
Just as with all anxiety-related disorders, women are more PTSD susceptible than are men. One of the “few things everybody agrees on,” Dr. Nemeroff said, is that early-life trauma such as neglect or abuse is a definite risk factor for PTSD, in part because early-life stress is thought to permanently program the brain regions involved in stress- and anxiety-mediation. Add to that, any adult level trauma, and they two “synergize. The more adult trauma coupled with early childhood abuse or neglect, the higher the level of PTSD.”
Meanwhile, poor social support, especially after the occurrence of a traumatic event, is a traditional prognosticator of poor recovery from PTSD, as are a family history of mood disorders, lower I.Q. and education, and experiencing other stressors the year before or after a traumatic event.
Dr. Nemeroff said that although the goals of treatment are reduced core symptoms, improved quality of life and function, strength, and resilience against subsequent stress, “the sad fact of the matter is that we don’t have a clue what the best treatment is, because we have no predictors of treatment response for PTSD.”
The most common treatments for PTSD are selective serotonin reuptake inhibitors (SSRIs), although the best data available suggest that prolonged imaginal exposure therapy is the most effective, Dr. Nemeroff said. It can be provided either virtually or in person, and includes breathing techniques, psychoeducation, and cognitive therapy. The Institute of Medicine gives exposure therapy its highest rating for scientific evidence, said Dr. Nemeroff, who is a board member of the institute.
Pharmacologic treatments approved by the Food and Drug Administration for PTSD treatment include sertraline and paroxetine, although other antidepressants can be prescribed off-label to some effect.
With sertraline, there is a “pretty low bar” of efficacy, according to Dr. Nemeroff, since only a 30% improvement in symptoms was recorded in 60% of study participants for FDA approval. It’s important to remember the treatment-response in PTSD is much slower than in major depression, Dr. Nemeroff said. “It can take as much as 9 months, so don’t give up.”
Combining sertraline with prolonged exposure therapy is even more effective, he said (J. Trauma Stress 2006;19:625-38). Meanwhile, other data show what paroxetine alone performed better than placebo, but the data are mixed for the drug in combination with prolonged exposure therapy (Am. J. Psychiatry 2012;169:80-8), (J. Clin. Psychiatry 2008;69:400-5), (J. Clin. Neurosci. 2008;62:646-52), and (Am. J. Psychiatry 2001;158:1982-8).
Dr. Nemeroff said lately, he has been treating PTSD patients with venlafaxine 450 mg, which is much higher than the usual dose of about 220 mg, with “considerably good results” (Arch. Gen. Psychiatry 2006;63:1158-65).
Improvements in memory and hippocampal volume generally are found with SSRI treatments, as well as reductions in symptom severity, according to Dr. Nemeroff.
For PTSD patients who are struggling with insomnia and other sleep-related problems, Dr. Nemeroff said prazosin has been “phenomenal,” especially in reducing nightmares (Am. J. Psychiatry 2013;170:1003-10).
One drug class to avoid using with PTSD patients is benzodiazepines, he said. “Every study has shown that benzodiazepines in PTSD do not work, and they come with a high rate of substance abuse in this population.”
*Dr. Nemeroff disclosed that he receives research and grant support from the National Institutes of Health. He also serves as a consultant for several companies, including Xhale, Takeda, SK Pharma, Shire, Roche, Lilly, Allergan, Mitsubishi Tanabe Pharma Development America, Taisho Pharmaceutical, Lundbeck, Prismic Pharmaceuticals, and Clintara LLC. He is a stockholder in Xhale, Celgene, Seattle Genetics, Abbvie, Titan Pharmaceuticals, and OPKO Health.
In addition, he holds financial/proprietary interest in patents for method/devices for the transdermal delivery of lithium and for a method of assessing antidepressant drug therapy.
*Correction, 4/10/2015: An earlier version of this story misstated Dr. Nemeroff's disclosures.
On Twitter @whitneymcknight
LAS VEGAS– There is no cure for posttraumatic stress disorder, but helping its sufferers reduce symptoms, improve resistance, and achieve a better quality of life is possible.
“We have no idea what the best treatments are for PTSD,” Dr. Charles B. Nemeroff, the Leonard M. Miller Professor, and chairman of the department of psychiatry and behavioral sciences at the University of Miami, told an audience at the annual psychopharmacology update held by the Nevada Psychiatric Association.
Whether to rely upon psychosocial or pharmacologic interventions, or a combination of the two, to help shift PTSD from a debilitating condition into a manageable, chronic one, it is important to understand PTSD as a brain disease. “To accurately treat PTSD, consider it within a neurobiological context,” Dr. Nemeroff said. “Ordinarily, the brain is evolved to deal with stress, but it can be compromised.”
In chronic PTSD, brain studies have shown a noted shrinkage in the hippocampus, contributing to memory impairment, similar to the reduced hippocampal volume in child-abuse victims. Additionally, cortical function in the brain is affected in PTSD, creating difficulty with exercising judgment and good decision making.
“One way to think about PTSD is that the cortex is unable to reign in the limbic system,” Dr. Nemeroff said. “The hippocampus is impaired, the amygdala is hyperactive, and there is a tremendous emotional drive, so the ‘thinking’ part of the brain can’t [overcome] the emotional, reptilian brain.”
The result is that a person remains stuck in a hyperaroused state. “We know that the neurobiological basis for PTSD involves a prolonged, vigilant response to stress [involving] a multitude of brain circuits ... and of course the sympathetic nervous system and the pituitary and adrenal systems,” Dr. Nemeroff said.
Beyond brain changes, a genetic predisposition to PTSD accounts for a third of all cases, while an additional one-third are attributable to additional biological risk factors, according to Dr. Nemeroff (Nature 2011;470:492-7).
Just as with all anxiety-related disorders, women are more PTSD susceptible than are men. One of the “few things everybody agrees on,” Dr. Nemeroff said, is that early-life trauma such as neglect or abuse is a definite risk factor for PTSD, in part because early-life stress is thought to permanently program the brain regions involved in stress- and anxiety-mediation. Add to that, any adult level trauma, and they two “synergize. The more adult trauma coupled with early childhood abuse or neglect, the higher the level of PTSD.”
Meanwhile, poor social support, especially after the occurrence of a traumatic event, is a traditional prognosticator of poor recovery from PTSD, as are a family history of mood disorders, lower I.Q. and education, and experiencing other stressors the year before or after a traumatic event.
Dr. Nemeroff said that although the goals of treatment are reduced core symptoms, improved quality of life and function, strength, and resilience against subsequent stress, “the sad fact of the matter is that we don’t have a clue what the best treatment is, because we have no predictors of treatment response for PTSD.”
The most common treatments for PTSD are selective serotonin reuptake inhibitors (SSRIs), although the best data available suggest that prolonged imaginal exposure therapy is the most effective, Dr. Nemeroff said. It can be provided either virtually or in person, and includes breathing techniques, psychoeducation, and cognitive therapy. The Institute of Medicine gives exposure therapy its highest rating for scientific evidence, said Dr. Nemeroff, who is a board member of the institute.
Pharmacologic treatments approved by the Food and Drug Administration for PTSD treatment include sertraline and paroxetine, although other antidepressants can be prescribed off-label to some effect.
With sertraline, there is a “pretty low bar” of efficacy, according to Dr. Nemeroff, since only a 30% improvement in symptoms was recorded in 60% of study participants for FDA approval. It’s important to remember the treatment-response in PTSD is much slower than in major depression, Dr. Nemeroff said. “It can take as much as 9 months, so don’t give up.”
Combining sertraline with prolonged exposure therapy is even more effective, he said (J. Trauma Stress 2006;19:625-38). Meanwhile, other data show what paroxetine alone performed better than placebo, but the data are mixed for the drug in combination with prolonged exposure therapy (Am. J. Psychiatry 2012;169:80-8), (J. Clin. Psychiatry 2008;69:400-5), (J. Clin. Neurosci. 2008;62:646-52), and (Am. J. Psychiatry 2001;158:1982-8).
Dr. Nemeroff said lately, he has been treating PTSD patients with venlafaxine 450 mg, which is much higher than the usual dose of about 220 mg, with “considerably good results” (Arch. Gen. Psychiatry 2006;63:1158-65).
Improvements in memory and hippocampal volume generally are found with SSRI treatments, as well as reductions in symptom severity, according to Dr. Nemeroff.
For PTSD patients who are struggling with insomnia and other sleep-related problems, Dr. Nemeroff said prazosin has been “phenomenal,” especially in reducing nightmares (Am. J. Psychiatry 2013;170:1003-10).
One drug class to avoid using with PTSD patients is benzodiazepines, he said. “Every study has shown that benzodiazepines in PTSD do not work, and they come with a high rate of substance abuse in this population.”
*Dr. Nemeroff disclosed that he receives research and grant support from the National Institutes of Health. He also serves as a consultant for several companies, including Xhale, Takeda, SK Pharma, Shire, Roche, Lilly, Allergan, Mitsubishi Tanabe Pharma Development America, Taisho Pharmaceutical, Lundbeck, Prismic Pharmaceuticals, and Clintara LLC. He is a stockholder in Xhale, Celgene, Seattle Genetics, Abbvie, Titan Pharmaceuticals, and OPKO Health.
In addition, he holds financial/proprietary interest in patents for method/devices for the transdermal delivery of lithium and for a method of assessing antidepressant drug therapy.
*Correction, 4/10/2015: An earlier version of this story misstated Dr. Nemeroff's disclosures.
On Twitter @whitneymcknight
LAS VEGAS– There is no cure for posttraumatic stress disorder, but helping its sufferers reduce symptoms, improve resistance, and achieve a better quality of life is possible.
“We have no idea what the best treatments are for PTSD,” Dr. Charles B. Nemeroff, the Leonard M. Miller Professor, and chairman of the department of psychiatry and behavioral sciences at the University of Miami, told an audience at the annual psychopharmacology update held by the Nevada Psychiatric Association.
Whether to rely upon psychosocial or pharmacologic interventions, or a combination of the two, to help shift PTSD from a debilitating condition into a manageable, chronic one, it is important to understand PTSD as a brain disease. “To accurately treat PTSD, consider it within a neurobiological context,” Dr. Nemeroff said. “Ordinarily, the brain is evolved to deal with stress, but it can be compromised.”
In chronic PTSD, brain studies have shown a noted shrinkage in the hippocampus, contributing to memory impairment, similar to the reduced hippocampal volume in child-abuse victims. Additionally, cortical function in the brain is affected in PTSD, creating difficulty with exercising judgment and good decision making.
“One way to think about PTSD is that the cortex is unable to reign in the limbic system,” Dr. Nemeroff said. “The hippocampus is impaired, the amygdala is hyperactive, and there is a tremendous emotional drive, so the ‘thinking’ part of the brain can’t [overcome] the emotional, reptilian brain.”
The result is that a person remains stuck in a hyperaroused state. “We know that the neurobiological basis for PTSD involves a prolonged, vigilant response to stress [involving] a multitude of brain circuits ... and of course the sympathetic nervous system and the pituitary and adrenal systems,” Dr. Nemeroff said.
Beyond brain changes, a genetic predisposition to PTSD accounts for a third of all cases, while an additional one-third are attributable to additional biological risk factors, according to Dr. Nemeroff (Nature 2011;470:492-7).
Just as with all anxiety-related disorders, women are more PTSD susceptible than are men. One of the “few things everybody agrees on,” Dr. Nemeroff said, is that early-life trauma such as neglect or abuse is a definite risk factor for PTSD, in part because early-life stress is thought to permanently program the brain regions involved in stress- and anxiety-mediation. Add to that, any adult level trauma, and they two “synergize. The more adult trauma coupled with early childhood abuse or neglect, the higher the level of PTSD.”
Meanwhile, poor social support, especially after the occurrence of a traumatic event, is a traditional prognosticator of poor recovery from PTSD, as are a family history of mood disorders, lower I.Q. and education, and experiencing other stressors the year before or after a traumatic event.
Dr. Nemeroff said that although the goals of treatment are reduced core symptoms, improved quality of life and function, strength, and resilience against subsequent stress, “the sad fact of the matter is that we don’t have a clue what the best treatment is, because we have no predictors of treatment response for PTSD.”
The most common treatments for PTSD are selective serotonin reuptake inhibitors (SSRIs), although the best data available suggest that prolonged imaginal exposure therapy is the most effective, Dr. Nemeroff said. It can be provided either virtually or in person, and includes breathing techniques, psychoeducation, and cognitive therapy. The Institute of Medicine gives exposure therapy its highest rating for scientific evidence, said Dr. Nemeroff, who is a board member of the institute.
Pharmacologic treatments approved by the Food and Drug Administration for PTSD treatment include sertraline and paroxetine, although other antidepressants can be prescribed off-label to some effect.
With sertraline, there is a “pretty low bar” of efficacy, according to Dr. Nemeroff, since only a 30% improvement in symptoms was recorded in 60% of study participants for FDA approval. It’s important to remember the treatment-response in PTSD is much slower than in major depression, Dr. Nemeroff said. “It can take as much as 9 months, so don’t give up.”
Combining sertraline with prolonged exposure therapy is even more effective, he said (J. Trauma Stress 2006;19:625-38). Meanwhile, other data show what paroxetine alone performed better than placebo, but the data are mixed for the drug in combination with prolonged exposure therapy (Am. J. Psychiatry 2012;169:80-8), (J. Clin. Psychiatry 2008;69:400-5), (J. Clin. Neurosci. 2008;62:646-52), and (Am. J. Psychiatry 2001;158:1982-8).
Dr. Nemeroff said lately, he has been treating PTSD patients with venlafaxine 450 mg, which is much higher than the usual dose of about 220 mg, with “considerably good results” (Arch. Gen. Psychiatry 2006;63:1158-65).
Improvements in memory and hippocampal volume generally are found with SSRI treatments, as well as reductions in symptom severity, according to Dr. Nemeroff.
For PTSD patients who are struggling with insomnia and other sleep-related problems, Dr. Nemeroff said prazosin has been “phenomenal,” especially in reducing nightmares (Am. J. Psychiatry 2013;170:1003-10).
One drug class to avoid using with PTSD patients is benzodiazepines, he said. “Every study has shown that benzodiazepines in PTSD do not work, and they come with a high rate of substance abuse in this population.”
*Dr. Nemeroff disclosed that he receives research and grant support from the National Institutes of Health. He also serves as a consultant for several companies, including Xhale, Takeda, SK Pharma, Shire, Roche, Lilly, Allergan, Mitsubishi Tanabe Pharma Development America, Taisho Pharmaceutical, Lundbeck, Prismic Pharmaceuticals, and Clintara LLC. He is a stockholder in Xhale, Celgene, Seattle Genetics, Abbvie, Titan Pharmaceuticals, and OPKO Health.
In addition, he holds financial/proprietary interest in patents for method/devices for the transdermal delivery of lithium and for a method of assessing antidepressant drug therapy.
*Correction, 4/10/2015: An earlier version of this story misstated Dr. Nemeroff's disclosures.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE NPA PSYCHOPHARMOCOLOGY UPDATE

Scalp Hyperkeratosis in Children With Skin of Color: Diagnostic and Therapeutic Considerations
Scalp hyperkeratosis (scaling or flaking) is a common symptom in childhood and is typified by fine to thick hyperkeratosis of the scalp with or without underlying erythema. The causes of scalp hyperkeratosis in childhood vary based on the demographics of the population. In a population where approximately half of the pediatric patients were white, scaling of the scalp was more common in patients with seborrheic dermatitis and/or atopic dermatitis (AD) who were aged 0 to 2 years, and tinea capitis was only noted in children who were black.1 In children with skin of color, scalp hyperkeratosis has been noted as a marker of tinea capitis, especially in patients aged 3 to 11 years,2,3 and the level of suspicion should consistently remain high for this age group. In another study of an all-black population of schoolchildren aged 5 to 13 years (N=224), 3% demonstrated signs and symptoms of tinea capitis and 14% were found to be asymptomatic carriers.4 Although generally benign in nature, scalp hyperkeratosis can be associated with systemic illnesses such as juvenile dermatomyositis and Langerhans cell histiocytosis.5 This article addresses the diagnosis and treatment of scalp hyperkeratosis in children with skin of color, focusing on differences in exposure to contagious cases, hairstyling practices, and biological factors that may impact the disease process.
CAUSES OF SCALP HYPERKERATOSIS IN CHILDHOOD
Scalp hyperkeratosis in childhood usually is caused by common benign conditions, but some level of suspicion should be maintained for more severe etiologic conditions such as Langerhans cell histiocytosis and collagen vascular diseases (eg, juvenile dermatomyositis).6 Langerhans cell histiocytosis of the scalp might be obscured by background pigmentation in black children.
Scalp scaling can be a minor criterion in the diagnosis of AD. Atopic dermatitis should be suspected in Asian children with scalp scaling. Although one study in Bangladesh revealed scalp involvement in only 5.2% of pediatric patients with AD,7 a study in China reported an incidence rate as high as 49.7% (with a similarly high incidence of eyelid dermatitis).8 Children with AD also may have dry hair.9 Atopic dermatitis of the scalp is typified by itching, fine hyperkeratosis, and notably eczematous scalp lesions ranging from excoriated or oozing erythematous plaques to lichenification with hair miniaturization, primarily from scratch-induced breakage.10 The latter finding often is noted in black adolescent girls with long-term moderate to severe AD (personal observation).
Seborrheic dermatitis is a hypersensitivity response to yeast colonization of the scalp with Malassezia species. The infantile form is extremely common (also known as cradle cap). Characteristically, greasy yellow hyperkeratosis in fine to thick sheets is noted on the scalp in children younger than 2 years, especially infants, often with involvement of skin folds. One study noted that seborrheic dermatitis occurs in 6% of school-aged children as opposed to 19% of children younger than 2 years.1 Severe seborrheic dermatitis in infancy may be a prelude to AD, with the incidence being 3 times higher in children with prior seborrheic dermatitis.11 In teenagers, seborrheic dermatitis often accompanies acne onset in the early pubertal years.12
Psoriasis is an autoimmune inflammatory dermatosis that most commonly affects white children. In childhood, pityriasis amiantacea, psoriasiform scalp hyperkeratosis, is more common than in adulthood, with thick, stuck-on scales bound to the hairs. This variant is uncommon in Hispanic and Asian children and is almost never seen in black children but has been reported in cohorts of Turkish children.13 In a series of 85 Egyptian children with pityriasis amiantacea, diagnosis of scalp psoriasis was made in 35.3%, eczematous dermatitis in 34.2%, and tinea capitis in 12.9%.14 Consequently, a high degree of suspicion for tinea capitis should be held if pityriasis amiantacea is found in children with skin of color.15,16
Tinea capitis is a dermatophyte infection of the scalp, hair, and surrounding skin. The presence of tinea capitis on the scalp is associated with environmental exposure to dermatophytes (eg, school, household).4,17 The infection is largely caused by Trichophyton tonsurans in the United States, which causes a seborrheic appearance and less commonly alopecia (black dot or thinning), plaques with scale, or kerion. The presence of cervical lymph nodes and/or alopecia increases the chances of tinea being the diagnosis. Potassium hydroxide preparation and fungal culture can be performed to corroborate the diagnosis.1-3 Other etiologies of scalp hyperkeratosis such as juvenile pityriasis rubra pilaris and lice are extremely uncommon in black children, but lice may be seen in Hispanic and Asian girls with long straight hair who attend school. Discoid lupus is more common in children with skin of color but is rare overall. When noted, accompanying mottled dyspigmentation and scarring alopecia are noted in addition to a high risk for developing systemic lupus erythematosus. Biopsy and screening for systemic lupus are necessary, as the risk for progression from discoid lupus to systemic disease is 26% over 3 years.18
THE BIOLOGY OF HAIR IN CHILDREN WITH SKIN OF COLOR
To some extent, the biology of hair impacts the occurrence, appearance, and treatment of scalp hyperkeratosis in children with skin of color. First, it is important to remember that follicular density is lower in black patients as compared to Asian patients with a consequently lower hair count overall, which results in the easy appearance of hair loss, particularly at the margins of the scalp.19,20 Second, the shape of the hair follicle differs among races and ethnicities. Asian patients have round hair shafts coming from straight follicles, which allows for greater natural hair hydration, resulting in somewhat less aggressive scalp disease. Hispanic patients may have similarly straight hair or may have elliptical or curled shafts, the latter being noted in black patients. Furthermore, a curled hair shaft results in poor flow of sebum across the hair, resulting in greater scalp xerosis, more susceptibility to traction alopecia, and ultimately a greater risk for infections.20-23 Finally, the scalp is continuous with the face and neck, and Asian patients have greater sensitivity to skin care products in these areas, resulting in difficulty of treatment in this patient population and the need for use of gentle products.
HAIR CARE PRACTICES IN CHILDREN WITH SKIN OF COLOR
Hair care in patients with skin of color can be costly, difficult, and potentially damaging, with 99% of black girls reporting pomade or oil usage. Costly and complex hair care practices begin in childhood for patients with skin of color. In a series of 201 surveyed black girls with a mean age of 9.8 years, 80% had used hot combs and 42% used relaxers.24 Traction styles were common with 81% using ponytails, 67% braids, and 49% cornrows in the last 12 months. These styles are thought to affect hair health, particularly through induction of traction-related damage, folliculitis, and alopecia. Furthermore, chemical relaxers, hot combs, blowouts, and hair setting may be introduced during childhood.24 These practices appear to disturb the integrity of the hair follicle, leaving it more susceptible to irritation and infection.
Hair care in the pediatric population often is complicated by the fact that multiple children are being styled in tandem, either at home or in a salon, resulting in shared equipment and fomite spread. Even just proximity to a case of tinea capitis in the household will increase risk for tinea capitis. Furthermore, it is quite commonplace for black patients to use pomades and shampoos that contain antifungals, especially selenium sulfide, which makes it difficult to obtain accurate culture results. In India, use of mustard oil also has been linked to increased risk for tinea capitis.25
Other issues related to hair care include frequent dry scalp in patients with skin of color due to poor sebum distribution along the hair shaft. As a result, frequent washing may exacerbate scalp xerosis and further irritate seborrheic dermatitis and/or AD.
DIAGNOSTIC CONSIDERATIONS FOR SCALP HYPERKERATOSIS IN CHILDHOOD
Dermatologists should have a greater level of suspicion for tinea capitis in black and Hispanic children compared to white children. The index of suspicion should be high given that antifungal shampoos and pomades may minimize the clinical appearance. Although trends in overall incidence in the United States suggest tinea capitis is becoming less common, there still is a stronger representation of the disease in black patients.26 A study of positive fungal cultures from one clinic in Mississippi (N=1220) showed that two-thirds of patients were children younger than 13 years; 87% of patients with positive cultures for dermatophytes were black.27 The endothrix type of tinea capitis caused by T tonsurans often presents with a seborrheic appearance, and fungal culture is warranted in all pediatric patients with skin of color who have scalp hyperkeratosis. Asian children can be regarded with a lower level of suspicion for tinea capitis, similar to white patients in the United States. Variation in incidence of tinea capitis does exist worldwide and the practitioner may need to address these issues in patients who travel or are recent immigrants.
When identifying tinea capitis infections in children with skin of color, physicians should consider the patient’s personal and family history, comorbid skin disorders, dermoscopy, microscopy and fungal staining, and fungal culture (Figure).
A paradigm for the diagnosis of scalp hyperkeratosis in children with skin of color.
Personal and Family History
The first diagnostic consideration is the patient’s personal and family history. A history of AD, asthma, or allergies will support but not confirm the diagnosis of AD. Prior tinea capitis infections and household contacts with tinea infections support the presence of tinea capitis.17 Recent implementation of anti–tumor necrosis factor a inhibitor therapy in a psoriatic child can flare scalp disease, mimicking tinea capitis.28 The patient’s guardians should be queried about potential infectious contacts, whether they themselves have signs of scalp disease or tinea corporis (ringworm) or whether they have a pet with problematic fur. Physicians also should query patients and their guardians about recent use of topical antifungal shampoos, pomades, creams (both over-the-counter [OTC] and prescription), and/or oral antifungals. When these agents are used, there is a possibility that fungal examinations may be negative in the presence of true infection with tinea capitis. Traction alopecia, often preceded by fine scale, is more likely to present in patients who wear their hair in cornrows, while seborrheic dermatitis may be associated with hair extensions, reduced frequency of washing (61% of black girls surveyed wash every 2 weeks), and/or reduced usage of hair oils in black girls.24 Knowledge of the patient’s personal hair care history, such as use of pomades; frequency and method of washing/drying hair; types of hair care products used daily to wash and style hair; use of chemical relaxers; or recent hairstyling with cornrows, braids, or hair extensions, also is essential to the diagnosis of tinea capitis. Usage of traction-related styling practices in patients with chemically relaxed hair can enhance the risk for traction alopecia.29
Comorbid Skin Disorders
The patient also should be examined for comorbid skin disorders, including tinea corporis, alopecia (particularly in the areas of hyperkeratosis), and the presence of nuchal lymphadenopathy. For each extra clinical finding, the chances of a final diagnosis of tinea capitis rises, allowing for empiric diagnosis to be made that can be confirmed by a variety of tests.1-3
Dermoscopy
Next, the patient should undergo dermoscopic evaluation. On dermoscopy, tinea capitis typically presents with broken hairs, black dots on the scalp, comma-shaped hairs, and short corkscrew hairs, all of which should clear with therapy.30-33 Dermoscopic findings of AD would reveal underlying xerosis and prominent vasculature due to inflammation, and alopecia areata would present with yellow dots at the orifices of the hair follicles, exclamation point hairs, and vellus hairs.34,35 Traction alopecia may be noted by retained hairs along the hairline, which is known as the fringe sign.36
Microscopy and Fungal Staining
Microscopic preparations can be performed to identify tinea capitis using fungal stains of slide-based specimens. Breakage of short hairs onto the slide and/or cotton swab is a soft sign corroborating endothrix infection of the hairs. Potassium hydroxide can enhance visualization of the hyperkeratotic scalp, but for most black patients, use of antifungal agents reduces fungal hyphae and spores in the areas of hyperkeratosis and may limit the utility of examining the skin microscopically. Assessment of the broken hairs obtained by gentle friction with one glass slide and catching the scales onto another glass slide may yield the best results in the evaluation of tinea capitis (a technique taught to me by Robin Hornung, MD, Everett, Washington). Hairs obtained in this manner often are fragile and break due to endothrix infection replacing and weakening the shaft of the hairs. In the United States, fungal samples usually are obtained with cotton swabs, but a recent study suggested that brushing is superior to scraping to obtain samples; the combination of sampling techniques may improve the yield of a culture.37 Because topical agents are unable to enter the hair cortex, the hair shaft is the most likely to show fungal spores under the microscope when antifungal shampoos or pomades are used. Other testing methods such as Swartz-Lamkins or calcofluor white staining can be used on similar scrapings. Biopsy and periodic acid–Schiff staining of thick scales or crust can help differentiate tinea capitis from pityriasis amiantacea when the crust is too thick to be softened via potassium hydroxide preparation.38
Fungal Culture
Fungal culture onto media that contains nutrients for dermatophyte growth can be used for 4 purposes in tinea capitis: (1) to confirm infection, (2) to identify species of infection, (3) to confirm mycological cure when difficulty in clearance of disease has been noted, and (4) to obtain a specimen for sensitivity screening regarding antifungals when necessary, an uncommon but occasionally useful test in individuals with disease that has failed treatment with 1 or more antifungals.27
THERAPY FOR SCALP HYPERKERATOSIS IN CHILDREN WITH SKIN OF COLOR
In patients with scalp hyperkeratosis, it is important to address the specific cause of the disease. Therapy for scalp hyperkeratosis in children with skin of color includes altered hair care practices, use of OTC and prescription agents, and containment of fomites in the case of infections. Biopsy of atypical scalp hyperkeratosis cases is needed to diagnose rare etiologies such as discoid lupus or Langerhans cell histiocytosis. For individuals with systemic disease including Langerhans cell histiocytosis, which is generally accompanied by nodes and plaques in the inguinal region or other intertriginous sites, immediate hematology and oncology workup is required.39 For collagen vascular diseases such as lupus or dermatomyositis, appropriate referral to rheumatology and systemic therapy is warranted.
Altered Hair Care Practices
The use of prophylactic ketoconazole 1% shampoo may not reduce the risk for recurrence of tinea capitis over standard good hygiene, removal of fomites, and adherence to prescribed therapy.40 Use of selenium sulfide has been shown to effectively reduce contagion risk.41
Fragrance- and dye-free shampoos can be helpful in providing gentle cleansing of the scalp, which is especially important in Asian patients who have greater facial and eyelid sensitivity. Free-and-clear shampoos can be used alternatively with shampoos containing selenium sulfide or sulfur to eliminate comorbid seborrhea. Black patients should be advised to shampoo and condition their hair once weekly, and Asian and Hispanic patients should shampoo and condition 2 to 3 times weekly to remove scale and potentially reduce risk for tinea acquisition.42 Children with straight hair should shampoo with increased frequency in the summer to manually remove sweat-induced macerated hyperkeratosis. Conditioners also should be used consistently after shampooing to enhance hair health.
Use of OTC and Prescription Agents
Atopic Dermatitis
Topical corticosteroid agents can be used in increasing strengths to treat AD of the scalp in children with skin of color, from OTC scalp products containing hydrocortisone 1% to prescription-based agents. Hydration of the hair also is needed to counteract reduced water content.43 Due to the innate xerosis of the scalp in black patients and atopic patients, the use of oil-based or lotion products may provide the most hydration for patients with scalp disease.44 Alcohol-based agents, either drops or foams, may enhance xerosis and should be used sparingly.
Seborrheic Dermatitis
Alternating treatment with medicated shampoos containing selenium sulfide and ketoconazole can aid in the removal of seborrhea. Pomades including borage seed oil–based agents can be massaged into the scalp,45 particularly for treatment of infantile seborrhea, and should not necessarily be washed off daily in dark-skinned patients. Additional focused application of topical corticosteroids to the scalp also is helpful. Due to innate scalp xerosis in black children, therapy should be similar to AD.
Psoriasis
In the setting of pityriasis amiantacea, albeit rare in children with skin of color, oil-based agents can soften hyperkeratosis for removal. Sterile mineral oil or commercially available scalp preparations of peanut oil with fluocinolone or mineral oil with glycerin can aid in the removal of scales without harming the hair, but usage must be age appropriate. The addition of focused application of age-appropriate topical corticosteroids for areas of severe hyperkeratosis can aid in clearance of the lesions.44 Recently, a stable combination of calcipo-triene 0.005%–betamethasone dipropionate 0.064% has been approved in the United States for the therapy of scalp psoriasis in adolescents.46
Tinea Capitis
Antifungal shampoos including selenium sulfide will reduce contagion risk when used by both the patient and his/her family members. Frequency of shampooing is similar to that described for AD. Between shampooing, pomades with selenium sulfide can be applied to the scalp to enhance overall clearance.
Oral antifungals are the basis of treatment and use of griseofulvin is the gold standard. Terbinafine has been approved by the US Food and Drug Administration for treatment of tinea capitis; for children weighing less than 25 kg the dosage is 125 mg daily, for 25 to 35 kg the dosage is 187.5 mg daily, and for more than 35 kg the dosage is 250 mg daily. Shorter therapeutic courses may be required, making it a good second-line agent. Laboratory screening in children prior to therapy is not always performed but should be done in cases where fatty liver might be suspected.47 Monitoring liver function tests is best when exceeding 3 months of usage or shifting from one antifungal to another.3
Containment of Fomites
There are several procedures that should be followed to contain scalp infection in children with skin of color. First, all objects that come into contact with the scalp (eg, hats, hoods, brushes, pillowcases) should be washed with hot water or replaced weekly. Sharing these objects with friends or family should be strongly discouraged. Patients and their family members also should be instructed to use medicated (eg, selenium sulfide) shampoos and conditioners. Finally, patients are advised to avoid use of shared classroom garments or mats for sleeping.
LONG-TERM SEQUELAE OF SCALP HYPERKERATOSIS
Long-term sequelae of scalp hyperkeratosis often are discounted in children, but the disease can have lasting and damaging effects on the scalp. Sequelae include discomfort from chronicity and psychological distress. In particular, years of scalp pruritus can promote lichenification of the scalp and miniaturization of the hair follicles. Furthermore, itching due to sweating can limit participation in sports. Finally, tinea capitis is thought to be a risk factor for central centrifugal cicatricial alopecia (or can occur comorbidly with central centrifugal cicatricial alopecia causing severe pruritus), a chronic scarring hair loss that is seen primarily in black adult females.48 Erythema nodosum also has been reported as an associated finding in the case of kerion.49 One study reported associated findings that included thyroid cancer in individuals irradiated for tinea capitis in the 1950s.50
Conclusion
Scalp hyperkeratosis in children with skin of color, especially black patients, is more likely to be associated with tinea capitis and is more challenging to treat due to innate scalp xerosis in black patients and increased sensitivity of facial skin in Asian children. Ultimately, institution of therapy when needed and good scalp and hair care may prevent long-term sequelae.
1. Williams JV, Eichenfield LF, Burke BL, et al. Prevalence of scalp scaling in prepubertal children. Pediatrics. 2005;115:e1-e6.
2. Coley MK, Bhanusali DG, Silverberg JI, et al. Scalp hyperkeratosis and alopecia in children of color. J Drugs Dermatol. 2011;10:511-516.
3. Bhanusali D, Coley M, Silverberg JI, et al. Treatment outcomes for tinea capitis in a skin of color population. J Drugs Dermatol. 2012;11:852-856.
4. Williams JV, Honig PJ, McGinley KJ, et al. Semiquantitative study of tinea capitis and the asymptomatic carrier state in inner-city school children. Pediatrics. 1995;96:265-267.
5. McDonald LL, Smith ML. Diagnostic dilemmas in pediatric/adolescent dermatology: scaly scalp. J Pediatr Health Care. 1998;12:80-84.
6. Peloro TM, Miller OF 3rd, Hahn TF, et al. Juvenile dermatomyositis: a retrospective review of a 30-year experience. J Am Acad Dermatol. 2001;45:28-34.
7. Wahab MA, Rahman MH, Khondker L, et al. Minor criteria for atopic dermatitis in children. Mymensingh Med J. 2011;20:419-424.
8. Shi M, Zhang H, Chen X, et al. Clinical features of atopic dermatitis in a hospital-based setting in China. J Eur Acad Dermatol Venereol [published online ahead of print January 9, 2011]. 2011;25:1206-1212.
9. Kim KS, Shin MK, Kim JH, et al. Effects of atopic dermatitis on the morphology and water content of scalp hair. Microsc Res Tech. 2012;75:620-625.
10. Sabin BR, Peters N, Peters AT. Chapter 20: atopic dermatitis. Allergy Asthma Proc. 2012;33:S67-S69.
11. Alexopoulos A, Kakourou T, Orfanou I, et al. Retrospective analysis of the relationship between infantile seborrheic dermatitis and atopic dermatitis [published online ahead of print November 13, 2013]. Pediatr Dermatol. 2014;31:125-130.
12. Elish D, Silverberg NB. Infantile seborrheic dermatitis. Cutis. 2006;77:297-300.
13. Sarifakioglu E, Yilmaz AE, Gorpelioglu C, et al. Prevalence of scalp disorders and hair loss in children. Cutis. 2012;90:225-229.
14. Abdel-Hamid IA, Agha SA, Moustafa YM, et al. Pityriasis amiantacea: a clinical and etiopathologic study of 85 patients. Int J Dermatol. 2003;42:260-264.
15. Oostveen AM, Jong EM, Evers AW, et al. Reliability, responsiveness and validity of Scalpdex in children with scalp psoriasis: the Dutch study. Acta Derm Venereol. 2014;94:198-202.
16. Silverberg NB. Atlas of Pediatric Cutaneous Biodiversity: Comparative Dermatologic Atlas of Pediatric Skin of All Colors. New York, NY: Springer; 2012.
17. Sharma V, Silverberg NB, Howard R, et al. Do hair care practices affect the acquisition of tinea capitis? a case-control study. Arch Pediatr Adolesc Med. 2001;155:818-821.
18. Moises-Alfaro C, Berrón-Pérez R, Carrasco-Daza D, et al. Discoid lupus erythematosus in children: clinical, histopathologic, and follow-up features in 27 cases. Pediatr Dermatol. 2003;20:103-107.
19. Ramos-e-Silva M. Ethnic hair and skin: what is the state of the science? Chicago, Illinois—September 29-30, 2001. Clin Dermatol. 2002;20:321-324.
20. Heath CR, McMichael AJ. Biology of hair follicle. In: Kelly AP, Taylor SC, eds. Dermatology for Skin of Color. New York, NY: McGraw Hill; 2009:105-109.
21. Khumalo NP. African hair morphology: macrostructure to ultrastructure. Int J Dermatol. 2005;44(suppl 1):10-12.
22. Thibaut S, Bernard BA. The biology of hair shape. Int J Dermatol. 2005;44(suppl 1):2-3.
23. Taylor SC. Skin of color: biology, structure, function, and implications for dermatologic disease. J Am Acad Dermatol. 2002;46(suppl 2):S41-S62.
24. Rucker Wright D, Gathers R, Kapke A, et al. Hair care practices and their association with scalp and hair disorders in African American girls. J Am Acad Dermatol. 2011;64:253-262.
25. Kumar V, Sharma RC, Chander R. Clinicomycological study of tinea capitis. Indian J Dermatol Venereol Leprol. 1996;62:207-209.
26. Mirmirani P, Tucker LY. Epidemiologic trends in pediatric tinea capitis: a population-based study from Kaiser Permanente Northern California [published online ahead of print October 2, 2013]. J Am Acad Dermatol. 2013;69:916-921.
27. Chapman JC, Daniel CR 3rd, Daniel JG, et al. Tinea capitis caused by dermatophytes: a 15-year retrospective study from a Mississippi Dermatology Clinic. Cutis. 2011;88:230-233.
28. Perman MJ, Lovell DJ, Denson LA, et al. Five cases of anti-tumor necrosis factor alpha-induced psoriasis presenting with severe scalp involvement in children. Pediatr Dermatol. 2012;29:454-459.
29. Khumalo NP, Jessop S, Gumedze F, et al. Determinants of marginal traction alopecia in African girls and women. J Am Acad Dermatol. 2008;59:432-438.
30. Vazquez-Lopez F, Palacios-Garcia L, Argenziano G. Dermoscopic corkscrew hairs dissolve after successful therapy of Trichophyton violaceum tinea capitis: a case report. Australas J Dermatol. 2012;53:118-119.
31. Pinheiro AM, Lobato LA, Varella TC. Dermoscopy findings in tinea capitis: case report and literature review. An Bras Dermatol. 2012;87:313-314.
32. Mapelli ET, Gualandri L, Cerri A, et al. Comma hairs in tinea capitis: a useful dermatoscopic sign for diagnosis of tinea capitis. Pediatr Dermatol. 2012;29:223-224.
33. Hughes R, Chiaverini C, Bahadoran P, et al. Corkscrew hair: a new dermoscopic sign for diagnosis of tinea capitis in black children. Arch Dermatol. 2011;147:355-356.
34. Ekiz O, Sen BB, Rifaiog˘lu EN, et al. Trichoscopy in paediatric patients with tinea capitis: a useful method to differentiate from alopecia areata [published online ahead of print August 24, 2013]. J Eur Acad Dermatol Venereol. 2014;28:1255-1258.
35. Lencastre A, Tosti A. Role of trichoscopy in children’s scalp and hair disorders [published online ahead of print Aug 13, 2013]. Pediatr Dermatol. 2013;30:674-682.
36. Samrao A, Price VH, Zedek D, et al. The “fringe sign”—a useful clinical finding in traction alopecia of the marginal hair line. Dermatol Online J. 2011;17:1.
37. Nasir S, Ralph N, O’Neill C, et al. Trends in tinea capitis in an Irish pediatric population and a comparison of scalp brushings versus scalp scrapings as methods of investigation [published online ahead of print February 22, 2013]. Pediatr Dermatol. 2014;31:622-623.
38. Alvarez MS, Silverberg NB. Tinea capitis. Cutis. 2006;78:189-196.
39. Simko SJ, Garmezy B, Abhyankar H, et al. Differentiating skin-limited and multisystem Langerhans cell histiocytosis. J Pediatr. 2014;165:990-996.
40. Bookstaver PB, Watson HJ, Winters SD, et al. Prophylactic ketoconazole shampoo for tinea capitis in a high-risk pediatric population. J Pediatr Pharmacol Ther. 2011;16:199-203.
41. Allen HB, Honig PJ, Leyden JJ, et al. Selenium sulfide: adjunctive therapy for tinea capitis. Pediatrics. 1982;69:81-83.
42. Crawford K, Hernandez C. A review of hair care products for black individuals. Cutis. 2014;93:289-293.
43. Kim KS, Shin MK, Kim JH, et al. Effects of atopic dermatitis on the morphology and water content of scalp hair [published online ahead of print November 7, 2011]. Microsc Res Tech. 2012;75:620-625.
44. Kapila S, Hong E, Fischer G. A comparative study of childhood psoriasis and atopic dermatitis and greater understanding of the overlapping condition, psoriasis-dermatitis. Australas J Dermatol. 2012;53:98-105.
45. Tollesson A, Frithz A. Borage oil, an effective new treatment for infantile seborrhoeic dermatitis. Br J Dermatol. 1993;129:95.
46. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriol plus betamethasone dipropionate gel in the treatment of scalp psoriasis in adolescents 12-17 years of age [published online ahead of print October 22, 2014]. Br J Dermatol. 2014;171:1470-1477.
47. Singer C, Stancu P, Coşoveanu S, et al. Non-alcoholic fatty liver disease in children. Curr Health Sci J. 2014;40:170-176.
48. Chiang C, Price V, Mirmirani P. Central centrifugal cicatricial alopecia: superimposed tinea capitis as the etiology of chronic scalp pruritus. Dermatol Online J. 2008;14:3.
49. Morrone A, Calcaterra R, Valenzano M, et al. Erythema nodosum induced by kerion celsi of the scalp in a woman. Mycoses. 2011;54:e237-e239.
50. Boaventura P, Pereira D, Celestino R, et al. Genetic alterations in thyroid tumors from patients irradiated in childhood for tinea capitis treatment. Eur J Endocrinol. 2013;169:673-679.
Scalp hyperkeratosis (scaling or flaking) is a common symptom in childhood and is typified by fine to thick hyperkeratosis of the scalp with or without underlying erythema. The causes of scalp hyperkeratosis in childhood vary based on the demographics of the population. In a population where approximately half of the pediatric patients were white, scaling of the scalp was more common in patients with seborrheic dermatitis and/or atopic dermatitis (AD) who were aged 0 to 2 years, and tinea capitis was only noted in children who were black.1 In children with skin of color, scalp hyperkeratosis has been noted as a marker of tinea capitis, especially in patients aged 3 to 11 years,2,3 and the level of suspicion should consistently remain high for this age group. In another study of an all-black population of schoolchildren aged 5 to 13 years (N=224), 3% demonstrated signs and symptoms of tinea capitis and 14% were found to be asymptomatic carriers.4 Although generally benign in nature, scalp hyperkeratosis can be associated with systemic illnesses such as juvenile dermatomyositis and Langerhans cell histiocytosis.5 This article addresses the diagnosis and treatment of scalp hyperkeratosis in children with skin of color, focusing on differences in exposure to contagious cases, hairstyling practices, and biological factors that may impact the disease process.
CAUSES OF SCALP HYPERKERATOSIS IN CHILDHOOD
Scalp hyperkeratosis in childhood usually is caused by common benign conditions, but some level of suspicion should be maintained for more severe etiologic conditions such as Langerhans cell histiocytosis and collagen vascular diseases (eg, juvenile dermatomyositis).6 Langerhans cell histiocytosis of the scalp might be obscured by background pigmentation in black children.
Scalp scaling can be a minor criterion in the diagnosis of AD. Atopic dermatitis should be suspected in Asian children with scalp scaling. Although one study in Bangladesh revealed scalp involvement in only 5.2% of pediatric patients with AD,7 a study in China reported an incidence rate as high as 49.7% (with a similarly high incidence of eyelid dermatitis).8 Children with AD also may have dry hair.9 Atopic dermatitis of the scalp is typified by itching, fine hyperkeratosis, and notably eczematous scalp lesions ranging from excoriated or oozing erythematous plaques to lichenification with hair miniaturization, primarily from scratch-induced breakage.10 The latter finding often is noted in black adolescent girls with long-term moderate to severe AD (personal observation).
Seborrheic dermatitis is a hypersensitivity response to yeast colonization of the scalp with Malassezia species. The infantile form is extremely common (also known as cradle cap). Characteristically, greasy yellow hyperkeratosis in fine to thick sheets is noted on the scalp in children younger than 2 years, especially infants, often with involvement of skin folds. One study noted that seborrheic dermatitis occurs in 6% of school-aged children as opposed to 19% of children younger than 2 years.1 Severe seborrheic dermatitis in infancy may be a prelude to AD, with the incidence being 3 times higher in children with prior seborrheic dermatitis.11 In teenagers, seborrheic dermatitis often accompanies acne onset in the early pubertal years.12
Psoriasis is an autoimmune inflammatory dermatosis that most commonly affects white children. In childhood, pityriasis amiantacea, psoriasiform scalp hyperkeratosis, is more common than in adulthood, with thick, stuck-on scales bound to the hairs. This variant is uncommon in Hispanic and Asian children and is almost never seen in black children but has been reported in cohorts of Turkish children.13 In a series of 85 Egyptian children with pityriasis amiantacea, diagnosis of scalp psoriasis was made in 35.3%, eczematous dermatitis in 34.2%, and tinea capitis in 12.9%.14 Consequently, a high degree of suspicion for tinea capitis should be held if pityriasis amiantacea is found in children with skin of color.15,16
Tinea capitis is a dermatophyte infection of the scalp, hair, and surrounding skin. The presence of tinea capitis on the scalp is associated with environmental exposure to dermatophytes (eg, school, household).4,17 The infection is largely caused by Trichophyton tonsurans in the United States, which causes a seborrheic appearance and less commonly alopecia (black dot or thinning), plaques with scale, or kerion. The presence of cervical lymph nodes and/or alopecia increases the chances of tinea being the diagnosis. Potassium hydroxide preparation and fungal culture can be performed to corroborate the diagnosis.1-3 Other etiologies of scalp hyperkeratosis such as juvenile pityriasis rubra pilaris and lice are extremely uncommon in black children, but lice may be seen in Hispanic and Asian girls with long straight hair who attend school. Discoid lupus is more common in children with skin of color but is rare overall. When noted, accompanying mottled dyspigmentation and scarring alopecia are noted in addition to a high risk for developing systemic lupus erythematosus. Biopsy and screening for systemic lupus are necessary, as the risk for progression from discoid lupus to systemic disease is 26% over 3 years.18
THE BIOLOGY OF HAIR IN CHILDREN WITH SKIN OF COLOR
To some extent, the biology of hair impacts the occurrence, appearance, and treatment of scalp hyperkeratosis in children with skin of color. First, it is important to remember that follicular density is lower in black patients as compared to Asian patients with a consequently lower hair count overall, which results in the easy appearance of hair loss, particularly at the margins of the scalp.19,20 Second, the shape of the hair follicle differs among races and ethnicities. Asian patients have round hair shafts coming from straight follicles, which allows for greater natural hair hydration, resulting in somewhat less aggressive scalp disease. Hispanic patients may have similarly straight hair or may have elliptical or curled shafts, the latter being noted in black patients. Furthermore, a curled hair shaft results in poor flow of sebum across the hair, resulting in greater scalp xerosis, more susceptibility to traction alopecia, and ultimately a greater risk for infections.20-23 Finally, the scalp is continuous with the face and neck, and Asian patients have greater sensitivity to skin care products in these areas, resulting in difficulty of treatment in this patient population and the need for use of gentle products.
HAIR CARE PRACTICES IN CHILDREN WITH SKIN OF COLOR
Hair care in patients with skin of color can be costly, difficult, and potentially damaging, with 99% of black girls reporting pomade or oil usage. Costly and complex hair care practices begin in childhood for patients with skin of color. In a series of 201 surveyed black girls with a mean age of 9.8 years, 80% had used hot combs and 42% used relaxers.24 Traction styles were common with 81% using ponytails, 67% braids, and 49% cornrows in the last 12 months. These styles are thought to affect hair health, particularly through induction of traction-related damage, folliculitis, and alopecia. Furthermore, chemical relaxers, hot combs, blowouts, and hair setting may be introduced during childhood.24 These practices appear to disturb the integrity of the hair follicle, leaving it more susceptible to irritation and infection.
Hair care in the pediatric population often is complicated by the fact that multiple children are being styled in tandem, either at home or in a salon, resulting in shared equipment and fomite spread. Even just proximity to a case of tinea capitis in the household will increase risk for tinea capitis. Furthermore, it is quite commonplace for black patients to use pomades and shampoos that contain antifungals, especially selenium sulfide, which makes it difficult to obtain accurate culture results. In India, use of mustard oil also has been linked to increased risk for tinea capitis.25
Other issues related to hair care include frequent dry scalp in patients with skin of color due to poor sebum distribution along the hair shaft. As a result, frequent washing may exacerbate scalp xerosis and further irritate seborrheic dermatitis and/or AD.
DIAGNOSTIC CONSIDERATIONS FOR SCALP HYPERKERATOSIS IN CHILDHOOD
Dermatologists should have a greater level of suspicion for tinea capitis in black and Hispanic children compared to white children. The index of suspicion should be high given that antifungal shampoos and pomades may minimize the clinical appearance. Although trends in overall incidence in the United States suggest tinea capitis is becoming less common, there still is a stronger representation of the disease in black patients.26 A study of positive fungal cultures from one clinic in Mississippi (N=1220) showed that two-thirds of patients were children younger than 13 years; 87% of patients with positive cultures for dermatophytes were black.27 The endothrix type of tinea capitis caused by T tonsurans often presents with a seborrheic appearance, and fungal culture is warranted in all pediatric patients with skin of color who have scalp hyperkeratosis. Asian children can be regarded with a lower level of suspicion for tinea capitis, similar to white patients in the United States. Variation in incidence of tinea capitis does exist worldwide and the practitioner may need to address these issues in patients who travel or are recent immigrants.
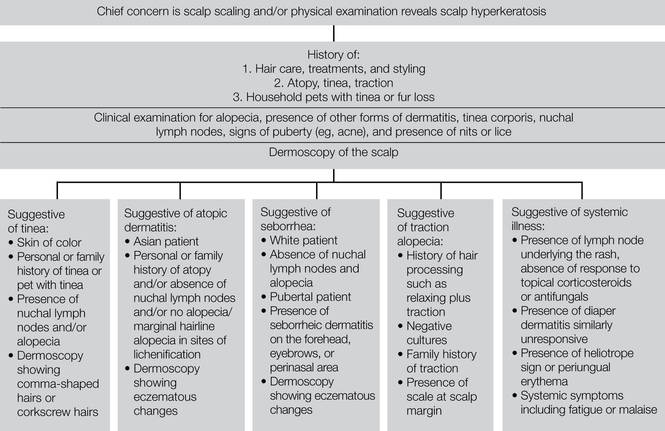
When identifying tinea capitis infections in children with skin of color, physicians should consider the patient’s personal and family history, comorbid skin disorders, dermoscopy, microscopy and fungal staining, and fungal culture (Figure).
A paradigm for the diagnosis of scalp hyperkeratosis in children with skin of color.
Personal and Family History
The first diagnostic consideration is the patient’s personal and family history. A history of AD, asthma, or allergies will support but not confirm the diagnosis of AD. Prior tinea capitis infections and household contacts with tinea infections support the presence of tinea capitis.17 Recent implementation of anti–tumor necrosis factor a inhibitor therapy in a psoriatic child can flare scalp disease, mimicking tinea capitis.28 The patient’s guardians should be queried about potential infectious contacts, whether they themselves have signs of scalp disease or tinea corporis (ringworm) or whether they have a pet with problematic fur. Physicians also should query patients and their guardians about recent use of topical antifungal shampoos, pomades, creams (both over-the-counter [OTC] and prescription), and/or oral antifungals. When these agents are used, there is a possibility that fungal examinations may be negative in the presence of true infection with tinea capitis. Traction alopecia, often preceded by fine scale, is more likely to present in patients who wear their hair in cornrows, while seborrheic dermatitis may be associated with hair extensions, reduced frequency of washing (61% of black girls surveyed wash every 2 weeks), and/or reduced usage of hair oils in black girls.24 Knowledge of the patient’s personal hair care history, such as use of pomades; frequency and method of washing/drying hair; types of hair care products used daily to wash and style hair; use of chemical relaxers; or recent hairstyling with cornrows, braids, or hair extensions, also is essential to the diagnosis of tinea capitis. Usage of traction-related styling practices in patients with chemically relaxed hair can enhance the risk for traction alopecia.29
Comorbid Skin Disorders
The patient also should be examined for comorbid skin disorders, including tinea corporis, alopecia (particularly in the areas of hyperkeratosis), and the presence of nuchal lymphadenopathy. For each extra clinical finding, the chances of a final diagnosis of tinea capitis rises, allowing for empiric diagnosis to be made that can be confirmed by a variety of tests.1-3
Dermoscopy
Next, the patient should undergo dermoscopic evaluation. On dermoscopy, tinea capitis typically presents with broken hairs, black dots on the scalp, comma-shaped hairs, and short corkscrew hairs, all of which should clear with therapy.30-33 Dermoscopic findings of AD would reveal underlying xerosis and prominent vasculature due to inflammation, and alopecia areata would present with yellow dots at the orifices of the hair follicles, exclamation point hairs, and vellus hairs.34,35 Traction alopecia may be noted by retained hairs along the hairline, which is known as the fringe sign.36
Microscopy and Fungal Staining
Microscopic preparations can be performed to identify tinea capitis using fungal stains of slide-based specimens. Breakage of short hairs onto the slide and/or cotton swab is a soft sign corroborating endothrix infection of the hairs. Potassium hydroxide can enhance visualization of the hyperkeratotic scalp, but for most black patients, use of antifungal agents reduces fungal hyphae and spores in the areas of hyperkeratosis and may limit the utility of examining the skin microscopically. Assessment of the broken hairs obtained by gentle friction with one glass slide and catching the scales onto another glass slide may yield the best results in the evaluation of tinea capitis (a technique taught to me by Robin Hornung, MD, Everett, Washington). Hairs obtained in this manner often are fragile and break due to endothrix infection replacing and weakening the shaft of the hairs. In the United States, fungal samples usually are obtained with cotton swabs, but a recent study suggested that brushing is superior to scraping to obtain samples; the combination of sampling techniques may improve the yield of a culture.37 Because topical agents are unable to enter the hair cortex, the hair shaft is the most likely to show fungal spores under the microscope when antifungal shampoos or pomades are used. Other testing methods such as Swartz-Lamkins or calcofluor white staining can be used on similar scrapings. Biopsy and periodic acid–Schiff staining of thick scales or crust can help differentiate tinea capitis from pityriasis amiantacea when the crust is too thick to be softened via potassium hydroxide preparation.38
Fungal Culture
Fungal culture onto media that contains nutrients for dermatophyte growth can be used for 4 purposes in tinea capitis: (1) to confirm infection, (2) to identify species of infection, (3) to confirm mycological cure when difficulty in clearance of disease has been noted, and (4) to obtain a specimen for sensitivity screening regarding antifungals when necessary, an uncommon but occasionally useful test in individuals with disease that has failed treatment with 1 or more antifungals.27
THERAPY FOR SCALP HYPERKERATOSIS IN CHILDREN WITH SKIN OF COLOR
In patients with scalp hyperkeratosis, it is important to address the specific cause of the disease. Therapy for scalp hyperkeratosis in children with skin of color includes altered hair care practices, use of OTC and prescription agents, and containment of fomites in the case of infections. Biopsy of atypical scalp hyperkeratosis cases is needed to diagnose rare etiologies such as discoid lupus or Langerhans cell histiocytosis. For individuals with systemic disease including Langerhans cell histiocytosis, which is generally accompanied by nodes and plaques in the inguinal region or other intertriginous sites, immediate hematology and oncology workup is required.39 For collagen vascular diseases such as lupus or dermatomyositis, appropriate referral to rheumatology and systemic therapy is warranted.
Altered Hair Care Practices
The use of prophylactic ketoconazole 1% shampoo may not reduce the risk for recurrence of tinea capitis over standard good hygiene, removal of fomites, and adherence to prescribed therapy.40 Use of selenium sulfide has been shown to effectively reduce contagion risk.41
Fragrance- and dye-free shampoos can be helpful in providing gentle cleansing of the scalp, which is especially important in Asian patients who have greater facial and eyelid sensitivity. Free-and-clear shampoos can be used alternatively with shampoos containing selenium sulfide or sulfur to eliminate comorbid seborrhea. Black patients should be advised to shampoo and condition their hair once weekly, and Asian and Hispanic patients should shampoo and condition 2 to 3 times weekly to remove scale and potentially reduce risk for tinea acquisition.42 Children with straight hair should shampoo with increased frequency in the summer to manually remove sweat-induced macerated hyperkeratosis. Conditioners also should be used consistently after shampooing to enhance hair health.
Use of OTC and Prescription Agents
Atopic Dermatitis
Topical corticosteroid agents can be used in increasing strengths to treat AD of the scalp in children with skin of color, from OTC scalp products containing hydrocortisone 1% to prescription-based agents. Hydration of the hair also is needed to counteract reduced water content.43 Due to the innate xerosis of the scalp in black patients and atopic patients, the use of oil-based or lotion products may provide the most hydration for patients with scalp disease.44 Alcohol-based agents, either drops or foams, may enhance xerosis and should be used sparingly.
Seborrheic Dermatitis
Alternating treatment with medicated shampoos containing selenium sulfide and ketoconazole can aid in the removal of seborrhea. Pomades including borage seed oil–based agents can be massaged into the scalp,45 particularly for treatment of infantile seborrhea, and should not necessarily be washed off daily in dark-skinned patients. Additional focused application of topical corticosteroids to the scalp also is helpful. Due to innate scalp xerosis in black children, therapy should be similar to AD.
Psoriasis
In the setting of pityriasis amiantacea, albeit rare in children with skin of color, oil-based agents can soften hyperkeratosis for removal. Sterile mineral oil or commercially available scalp preparations of peanut oil with fluocinolone or mineral oil with glycerin can aid in the removal of scales without harming the hair, but usage must be age appropriate. The addition of focused application of age-appropriate topical corticosteroids for areas of severe hyperkeratosis can aid in clearance of the lesions.44 Recently, a stable combination of calcipo-triene 0.005%–betamethasone dipropionate 0.064% has been approved in the United States for the therapy of scalp psoriasis in adolescents.46
Tinea Capitis
Antifungal shampoos including selenium sulfide will reduce contagion risk when used by both the patient and his/her family members. Frequency of shampooing is similar to that described for AD. Between shampooing, pomades with selenium sulfide can be applied to the scalp to enhance overall clearance.
Oral antifungals are the basis of treatment and use of griseofulvin is the gold standard. Terbinafine has been approved by the US Food and Drug Administration for treatment of tinea capitis; for children weighing less than 25 kg the dosage is 125 mg daily, for 25 to 35 kg the dosage is 187.5 mg daily, and for more than 35 kg the dosage is 250 mg daily. Shorter therapeutic courses may be required, making it a good second-line agent. Laboratory screening in children prior to therapy is not always performed but should be done in cases where fatty liver might be suspected.47 Monitoring liver function tests is best when exceeding 3 months of usage or shifting from one antifungal to another.3
Containment of Fomites
There are several procedures that should be followed to contain scalp infection in children with skin of color. First, all objects that come into contact with the scalp (eg, hats, hoods, brushes, pillowcases) should be washed with hot water or replaced weekly. Sharing these objects with friends or family should be strongly discouraged. Patients and their family members also should be instructed to use medicated (eg, selenium sulfide) shampoos and conditioners. Finally, patients are advised to avoid use of shared classroom garments or mats for sleeping.
LONG-TERM SEQUELAE OF SCALP HYPERKERATOSIS
Long-term sequelae of scalp hyperkeratosis often are discounted in children, but the disease can have lasting and damaging effects on the scalp. Sequelae include discomfort from chronicity and psychological distress. In particular, years of scalp pruritus can promote lichenification of the scalp and miniaturization of the hair follicles. Furthermore, itching due to sweating can limit participation in sports. Finally, tinea capitis is thought to be a risk factor for central centrifugal cicatricial alopecia (or can occur comorbidly with central centrifugal cicatricial alopecia causing severe pruritus), a chronic scarring hair loss that is seen primarily in black adult females.48 Erythema nodosum also has been reported as an associated finding in the case of kerion.49 One study reported associated findings that included thyroid cancer in individuals irradiated for tinea capitis in the 1950s.50
Conclusion
Scalp hyperkeratosis in children with skin of color, especially black patients, is more likely to be associated with tinea capitis and is more challenging to treat due to innate scalp xerosis in black patients and increased sensitivity of facial skin in Asian children. Ultimately, institution of therapy when needed and good scalp and hair care may prevent long-term sequelae.
Scalp hyperkeratosis (scaling or flaking) is a common symptom in childhood and is typified by fine to thick hyperkeratosis of the scalp with or without underlying erythema. The causes of scalp hyperkeratosis in childhood vary based on the demographics of the population. In a population where approximately half of the pediatric patients were white, scaling of the scalp was more common in patients with seborrheic dermatitis and/or atopic dermatitis (AD) who were aged 0 to 2 years, and tinea capitis was only noted in children who were black.1 In children with skin of color, scalp hyperkeratosis has been noted as a marker of tinea capitis, especially in patients aged 3 to 11 years,2,3 and the level of suspicion should consistently remain high for this age group. In another study of an all-black population of schoolchildren aged 5 to 13 years (N=224), 3% demonstrated signs and symptoms of tinea capitis and 14% were found to be asymptomatic carriers.4 Although generally benign in nature, scalp hyperkeratosis can be associated with systemic illnesses such as juvenile dermatomyositis and Langerhans cell histiocytosis.5 This article addresses the diagnosis and treatment of scalp hyperkeratosis in children with skin of color, focusing on differences in exposure to contagious cases, hairstyling practices, and biological factors that may impact the disease process.
CAUSES OF SCALP HYPERKERATOSIS IN CHILDHOOD
Scalp hyperkeratosis in childhood usually is caused by common benign conditions, but some level of suspicion should be maintained for more severe etiologic conditions such as Langerhans cell histiocytosis and collagen vascular diseases (eg, juvenile dermatomyositis).6 Langerhans cell histiocytosis of the scalp might be obscured by background pigmentation in black children.
Scalp scaling can be a minor criterion in the diagnosis of AD. Atopic dermatitis should be suspected in Asian children with scalp scaling. Although one study in Bangladesh revealed scalp involvement in only 5.2% of pediatric patients with AD,7 a study in China reported an incidence rate as high as 49.7% (with a similarly high incidence of eyelid dermatitis).8 Children with AD also may have dry hair.9 Atopic dermatitis of the scalp is typified by itching, fine hyperkeratosis, and notably eczematous scalp lesions ranging from excoriated or oozing erythematous plaques to lichenification with hair miniaturization, primarily from scratch-induced breakage.10 The latter finding often is noted in black adolescent girls with long-term moderate to severe AD (personal observation).
Seborrheic dermatitis is a hypersensitivity response to yeast colonization of the scalp with Malassezia species. The infantile form is extremely common (also known as cradle cap). Characteristically, greasy yellow hyperkeratosis in fine to thick sheets is noted on the scalp in children younger than 2 years, especially infants, often with involvement of skin folds. One study noted that seborrheic dermatitis occurs in 6% of school-aged children as opposed to 19% of children younger than 2 years.1 Severe seborrheic dermatitis in infancy may be a prelude to AD, with the incidence being 3 times higher in children with prior seborrheic dermatitis.11 In teenagers, seborrheic dermatitis often accompanies acne onset in the early pubertal years.12
Psoriasis is an autoimmune inflammatory dermatosis that most commonly affects white children. In childhood, pityriasis amiantacea, psoriasiform scalp hyperkeratosis, is more common than in adulthood, with thick, stuck-on scales bound to the hairs. This variant is uncommon in Hispanic and Asian children and is almost never seen in black children but has been reported in cohorts of Turkish children.13 In a series of 85 Egyptian children with pityriasis amiantacea, diagnosis of scalp psoriasis was made in 35.3%, eczematous dermatitis in 34.2%, and tinea capitis in 12.9%.14 Consequently, a high degree of suspicion for tinea capitis should be held if pityriasis amiantacea is found in children with skin of color.15,16
Tinea capitis is a dermatophyte infection of the scalp, hair, and surrounding skin. The presence of tinea capitis on the scalp is associated with environmental exposure to dermatophytes (eg, school, household).4,17 The infection is largely caused by Trichophyton tonsurans in the United States, which causes a seborrheic appearance and less commonly alopecia (black dot or thinning), plaques with scale, or kerion. The presence of cervical lymph nodes and/or alopecia increases the chances of tinea being the diagnosis. Potassium hydroxide preparation and fungal culture can be performed to corroborate the diagnosis.1-3 Other etiologies of scalp hyperkeratosis such as juvenile pityriasis rubra pilaris and lice are extremely uncommon in black children, but lice may be seen in Hispanic and Asian girls with long straight hair who attend school. Discoid lupus is more common in children with skin of color but is rare overall. When noted, accompanying mottled dyspigmentation and scarring alopecia are noted in addition to a high risk for developing systemic lupus erythematosus. Biopsy and screening for systemic lupus are necessary, as the risk for progression from discoid lupus to systemic disease is 26% over 3 years.18
THE BIOLOGY OF HAIR IN CHILDREN WITH SKIN OF COLOR
To some extent, the biology of hair impacts the occurrence, appearance, and treatment of scalp hyperkeratosis in children with skin of color. First, it is important to remember that follicular density is lower in black patients as compared to Asian patients with a consequently lower hair count overall, which results in the easy appearance of hair loss, particularly at the margins of the scalp.19,20 Second, the shape of the hair follicle differs among races and ethnicities. Asian patients have round hair shafts coming from straight follicles, which allows for greater natural hair hydration, resulting in somewhat less aggressive scalp disease. Hispanic patients may have similarly straight hair or may have elliptical or curled shafts, the latter being noted in black patients. Furthermore, a curled hair shaft results in poor flow of sebum across the hair, resulting in greater scalp xerosis, more susceptibility to traction alopecia, and ultimately a greater risk for infections.20-23 Finally, the scalp is continuous with the face and neck, and Asian patients have greater sensitivity to skin care products in these areas, resulting in difficulty of treatment in this patient population and the need for use of gentle products.
HAIR CARE PRACTICES IN CHILDREN WITH SKIN OF COLOR
Hair care in patients with skin of color can be costly, difficult, and potentially damaging, with 99% of black girls reporting pomade or oil usage. Costly and complex hair care practices begin in childhood for patients with skin of color. In a series of 201 surveyed black girls with a mean age of 9.8 years, 80% had used hot combs and 42% used relaxers.24 Traction styles were common with 81% using ponytails, 67% braids, and 49% cornrows in the last 12 months. These styles are thought to affect hair health, particularly through induction of traction-related damage, folliculitis, and alopecia. Furthermore, chemical relaxers, hot combs, blowouts, and hair setting may be introduced during childhood.24 These practices appear to disturb the integrity of the hair follicle, leaving it more susceptible to irritation and infection.
Hair care in the pediatric population often is complicated by the fact that multiple children are being styled in tandem, either at home or in a salon, resulting in shared equipment and fomite spread. Even just proximity to a case of tinea capitis in the household will increase risk for tinea capitis. Furthermore, it is quite commonplace for black patients to use pomades and shampoos that contain antifungals, especially selenium sulfide, which makes it difficult to obtain accurate culture results. In India, use of mustard oil also has been linked to increased risk for tinea capitis.25
Other issues related to hair care include frequent dry scalp in patients with skin of color due to poor sebum distribution along the hair shaft. As a result, frequent washing may exacerbate scalp xerosis and further irritate seborrheic dermatitis and/or AD.
DIAGNOSTIC CONSIDERATIONS FOR SCALP HYPERKERATOSIS IN CHILDHOOD
Dermatologists should have a greater level of suspicion for tinea capitis in black and Hispanic children compared to white children. The index of suspicion should be high given that antifungal shampoos and pomades may minimize the clinical appearance. Although trends in overall incidence in the United States suggest tinea capitis is becoming less common, there still is a stronger representation of the disease in black patients.26 A study of positive fungal cultures from one clinic in Mississippi (N=1220) showed that two-thirds of patients were children younger than 13 years; 87% of patients with positive cultures for dermatophytes were black.27 The endothrix type of tinea capitis caused by T tonsurans often presents with a seborrheic appearance, and fungal culture is warranted in all pediatric patients with skin of color who have scalp hyperkeratosis. Asian children can be regarded with a lower level of suspicion for tinea capitis, similar to white patients in the United States. Variation in incidence of tinea capitis does exist worldwide and the practitioner may need to address these issues in patients who travel or are recent immigrants.
When identifying tinea capitis infections in children with skin of color, physicians should consider the patient’s personal and family history, comorbid skin disorders, dermoscopy, microscopy and fungal staining, and fungal culture (Figure).
A paradigm for the diagnosis of scalp hyperkeratosis in children with skin of color.
Personal and Family History
The first diagnostic consideration is the patient’s personal and family history. A history of AD, asthma, or allergies will support but not confirm the diagnosis of AD. Prior tinea capitis infections and household contacts with tinea infections support the presence of tinea capitis.17 Recent implementation of anti–tumor necrosis factor a inhibitor therapy in a psoriatic child can flare scalp disease, mimicking tinea capitis.28 The patient’s guardians should be queried about potential infectious contacts, whether they themselves have signs of scalp disease or tinea corporis (ringworm) or whether they have a pet with problematic fur. Physicians also should query patients and their guardians about recent use of topical antifungal shampoos, pomades, creams (both over-the-counter [OTC] and prescription), and/or oral antifungals. When these agents are used, there is a possibility that fungal examinations may be negative in the presence of true infection with tinea capitis. Traction alopecia, often preceded by fine scale, is more likely to present in patients who wear their hair in cornrows, while seborrheic dermatitis may be associated with hair extensions, reduced frequency of washing (61% of black girls surveyed wash every 2 weeks), and/or reduced usage of hair oils in black girls.24 Knowledge of the patient’s personal hair care history, such as use of pomades; frequency and method of washing/drying hair; types of hair care products used daily to wash and style hair; use of chemical relaxers; or recent hairstyling with cornrows, braids, or hair extensions, also is essential to the diagnosis of tinea capitis. Usage of traction-related styling practices in patients with chemically relaxed hair can enhance the risk for traction alopecia.29
Comorbid Skin Disorders
The patient also should be examined for comorbid skin disorders, including tinea corporis, alopecia (particularly in the areas of hyperkeratosis), and the presence of nuchal lymphadenopathy. For each extra clinical finding, the chances of a final diagnosis of tinea capitis rises, allowing for empiric diagnosis to be made that can be confirmed by a variety of tests.1-3
Dermoscopy
Next, the patient should undergo dermoscopic evaluation. On dermoscopy, tinea capitis typically presents with broken hairs, black dots on the scalp, comma-shaped hairs, and short corkscrew hairs, all of which should clear with therapy.30-33 Dermoscopic findings of AD would reveal underlying xerosis and prominent vasculature due to inflammation, and alopecia areata would present with yellow dots at the orifices of the hair follicles, exclamation point hairs, and vellus hairs.34,35 Traction alopecia may be noted by retained hairs along the hairline, which is known as the fringe sign.36
Microscopy and Fungal Staining
Microscopic preparations can be performed to identify tinea capitis using fungal stains of slide-based specimens. Breakage of short hairs onto the slide and/or cotton swab is a soft sign corroborating endothrix infection of the hairs. Potassium hydroxide can enhance visualization of the hyperkeratotic scalp, but for most black patients, use of antifungal agents reduces fungal hyphae and spores in the areas of hyperkeratosis and may limit the utility of examining the skin microscopically. Assessment of the broken hairs obtained by gentle friction with one glass slide and catching the scales onto another glass slide may yield the best results in the evaluation of tinea capitis (a technique taught to me by Robin Hornung, MD, Everett, Washington). Hairs obtained in this manner often are fragile and break due to endothrix infection replacing and weakening the shaft of the hairs. In the United States, fungal samples usually are obtained with cotton swabs, but a recent study suggested that brushing is superior to scraping to obtain samples; the combination of sampling techniques may improve the yield of a culture.37 Because topical agents are unable to enter the hair cortex, the hair shaft is the most likely to show fungal spores under the microscope when antifungal shampoos or pomades are used. Other testing methods such as Swartz-Lamkins or calcofluor white staining can be used on similar scrapings. Biopsy and periodic acid–Schiff staining of thick scales or crust can help differentiate tinea capitis from pityriasis amiantacea when the crust is too thick to be softened via potassium hydroxide preparation.38
Fungal Culture
Fungal culture onto media that contains nutrients for dermatophyte growth can be used for 4 purposes in tinea capitis: (1) to confirm infection, (2) to identify species of infection, (3) to confirm mycological cure when difficulty in clearance of disease has been noted, and (4) to obtain a specimen for sensitivity screening regarding antifungals when necessary, an uncommon but occasionally useful test in individuals with disease that has failed treatment with 1 or more antifungals.27
THERAPY FOR SCALP HYPERKERATOSIS IN CHILDREN WITH SKIN OF COLOR
In patients with scalp hyperkeratosis, it is important to address the specific cause of the disease. Therapy for scalp hyperkeratosis in children with skin of color includes altered hair care practices, use of OTC and prescription agents, and containment of fomites in the case of infections. Biopsy of atypical scalp hyperkeratosis cases is needed to diagnose rare etiologies such as discoid lupus or Langerhans cell histiocytosis. For individuals with systemic disease including Langerhans cell histiocytosis, which is generally accompanied by nodes and plaques in the inguinal region or other intertriginous sites, immediate hematology and oncology workup is required.39 For collagen vascular diseases such as lupus or dermatomyositis, appropriate referral to rheumatology and systemic therapy is warranted.
Altered Hair Care Practices
The use of prophylactic ketoconazole 1% shampoo may not reduce the risk for recurrence of tinea capitis over standard good hygiene, removal of fomites, and adherence to prescribed therapy.40 Use of selenium sulfide has been shown to effectively reduce contagion risk.41
Fragrance- and dye-free shampoos can be helpful in providing gentle cleansing of the scalp, which is especially important in Asian patients who have greater facial and eyelid sensitivity. Free-and-clear shampoos can be used alternatively with shampoos containing selenium sulfide or sulfur to eliminate comorbid seborrhea. Black patients should be advised to shampoo and condition their hair once weekly, and Asian and Hispanic patients should shampoo and condition 2 to 3 times weekly to remove scale and potentially reduce risk for tinea acquisition.42 Children with straight hair should shampoo with increased frequency in the summer to manually remove sweat-induced macerated hyperkeratosis. Conditioners also should be used consistently after shampooing to enhance hair health.
Use of OTC and Prescription Agents
Atopic Dermatitis
Topical corticosteroid agents can be used in increasing strengths to treat AD of the scalp in children with skin of color, from OTC scalp products containing hydrocortisone 1% to prescription-based agents. Hydration of the hair also is needed to counteract reduced water content.43 Due to the innate xerosis of the scalp in black patients and atopic patients, the use of oil-based or lotion products may provide the most hydration for patients with scalp disease.44 Alcohol-based agents, either drops or foams, may enhance xerosis and should be used sparingly.
Seborrheic Dermatitis
Alternating treatment with medicated shampoos containing selenium sulfide and ketoconazole can aid in the removal of seborrhea. Pomades including borage seed oil–based agents can be massaged into the scalp,45 particularly for treatment of infantile seborrhea, and should not necessarily be washed off daily in dark-skinned patients. Additional focused application of topical corticosteroids to the scalp also is helpful. Due to innate scalp xerosis in black children, therapy should be similar to AD.
Psoriasis
In the setting of pityriasis amiantacea, albeit rare in children with skin of color, oil-based agents can soften hyperkeratosis for removal. Sterile mineral oil or commercially available scalp preparations of peanut oil with fluocinolone or mineral oil with glycerin can aid in the removal of scales without harming the hair, but usage must be age appropriate. The addition of focused application of age-appropriate topical corticosteroids for areas of severe hyperkeratosis can aid in clearance of the lesions.44 Recently, a stable combination of calcipo-triene 0.005%–betamethasone dipropionate 0.064% has been approved in the United States for the therapy of scalp psoriasis in adolescents.46
Tinea Capitis
Antifungal shampoos including selenium sulfide will reduce contagion risk when used by both the patient and his/her family members. Frequency of shampooing is similar to that described for AD. Between shampooing, pomades with selenium sulfide can be applied to the scalp to enhance overall clearance.
Oral antifungals are the basis of treatment and use of griseofulvin is the gold standard. Terbinafine has been approved by the US Food and Drug Administration for treatment of tinea capitis; for children weighing less than 25 kg the dosage is 125 mg daily, for 25 to 35 kg the dosage is 187.5 mg daily, and for more than 35 kg the dosage is 250 mg daily. Shorter therapeutic courses may be required, making it a good second-line agent. Laboratory screening in children prior to therapy is not always performed but should be done in cases where fatty liver might be suspected.47 Monitoring liver function tests is best when exceeding 3 months of usage or shifting from one antifungal to another.3
Containment of Fomites
There are several procedures that should be followed to contain scalp infection in children with skin of color. First, all objects that come into contact with the scalp (eg, hats, hoods, brushes, pillowcases) should be washed with hot water or replaced weekly. Sharing these objects with friends or family should be strongly discouraged. Patients and their family members also should be instructed to use medicated (eg, selenium sulfide) shampoos and conditioners. Finally, patients are advised to avoid use of shared classroom garments or mats for sleeping.
LONG-TERM SEQUELAE OF SCALP HYPERKERATOSIS
Long-term sequelae of scalp hyperkeratosis often are discounted in children, but the disease can have lasting and damaging effects on the scalp. Sequelae include discomfort from chronicity and psychological distress. In particular, years of scalp pruritus can promote lichenification of the scalp and miniaturization of the hair follicles. Furthermore, itching due to sweating can limit participation in sports. Finally, tinea capitis is thought to be a risk factor for central centrifugal cicatricial alopecia (or can occur comorbidly with central centrifugal cicatricial alopecia causing severe pruritus), a chronic scarring hair loss that is seen primarily in black adult females.48 Erythema nodosum also has been reported as an associated finding in the case of kerion.49 One study reported associated findings that included thyroid cancer in individuals irradiated for tinea capitis in the 1950s.50
Conclusion
Scalp hyperkeratosis in children with skin of color, especially black patients, is more likely to be associated with tinea capitis and is more challenging to treat due to innate scalp xerosis in black patients and increased sensitivity of facial skin in Asian children. Ultimately, institution of therapy when needed and good scalp and hair care may prevent long-term sequelae.
1. Williams JV, Eichenfield LF, Burke BL, et al. Prevalence of scalp scaling in prepubertal children. Pediatrics. 2005;115:e1-e6.
2. Coley MK, Bhanusali DG, Silverberg JI, et al. Scalp hyperkeratosis and alopecia in children of color. J Drugs Dermatol. 2011;10:511-516.
3. Bhanusali D, Coley M, Silverberg JI, et al. Treatment outcomes for tinea capitis in a skin of color population. J Drugs Dermatol. 2012;11:852-856.
4. Williams JV, Honig PJ, McGinley KJ, et al. Semiquantitative study of tinea capitis and the asymptomatic carrier state in inner-city school children. Pediatrics. 1995;96:265-267.
5. McDonald LL, Smith ML. Diagnostic dilemmas in pediatric/adolescent dermatology: scaly scalp. J Pediatr Health Care. 1998;12:80-84.
6. Peloro TM, Miller OF 3rd, Hahn TF, et al. Juvenile dermatomyositis: a retrospective review of a 30-year experience. J Am Acad Dermatol. 2001;45:28-34.
7. Wahab MA, Rahman MH, Khondker L, et al. Minor criteria for atopic dermatitis in children. Mymensingh Med J. 2011;20:419-424.
8. Shi M, Zhang H, Chen X, et al. Clinical features of atopic dermatitis in a hospital-based setting in China. J Eur Acad Dermatol Venereol [published online ahead of print January 9, 2011]. 2011;25:1206-1212.
9. Kim KS, Shin MK, Kim JH, et al. Effects of atopic dermatitis on the morphology and water content of scalp hair. Microsc Res Tech. 2012;75:620-625.
10. Sabin BR, Peters N, Peters AT. Chapter 20: atopic dermatitis. Allergy Asthma Proc. 2012;33:S67-S69.
11. Alexopoulos A, Kakourou T, Orfanou I, et al. Retrospective analysis of the relationship between infantile seborrheic dermatitis and atopic dermatitis [published online ahead of print November 13, 2013]. Pediatr Dermatol. 2014;31:125-130.
12. Elish D, Silverberg NB. Infantile seborrheic dermatitis. Cutis. 2006;77:297-300.
13. Sarifakioglu E, Yilmaz AE, Gorpelioglu C, et al. Prevalence of scalp disorders and hair loss in children. Cutis. 2012;90:225-229.
14. Abdel-Hamid IA, Agha SA, Moustafa YM, et al. Pityriasis amiantacea: a clinical and etiopathologic study of 85 patients. Int J Dermatol. 2003;42:260-264.
15. Oostveen AM, Jong EM, Evers AW, et al. Reliability, responsiveness and validity of Scalpdex in children with scalp psoriasis: the Dutch study. Acta Derm Venereol. 2014;94:198-202.
16. Silverberg NB. Atlas of Pediatric Cutaneous Biodiversity: Comparative Dermatologic Atlas of Pediatric Skin of All Colors. New York, NY: Springer; 2012.
17. Sharma V, Silverberg NB, Howard R, et al. Do hair care practices affect the acquisition of tinea capitis? a case-control study. Arch Pediatr Adolesc Med. 2001;155:818-821.
18. Moises-Alfaro C, Berrón-Pérez R, Carrasco-Daza D, et al. Discoid lupus erythematosus in children: clinical, histopathologic, and follow-up features in 27 cases. Pediatr Dermatol. 2003;20:103-107.
19. Ramos-e-Silva M. Ethnic hair and skin: what is the state of the science? Chicago, Illinois—September 29-30, 2001. Clin Dermatol. 2002;20:321-324.
20. Heath CR, McMichael AJ. Biology of hair follicle. In: Kelly AP, Taylor SC, eds. Dermatology for Skin of Color. New York, NY: McGraw Hill; 2009:105-109.
21. Khumalo NP. African hair morphology: macrostructure to ultrastructure. Int J Dermatol. 2005;44(suppl 1):10-12.
22. Thibaut S, Bernard BA. The biology of hair shape. Int J Dermatol. 2005;44(suppl 1):2-3.
23. Taylor SC. Skin of color: biology, structure, function, and implications for dermatologic disease. J Am Acad Dermatol. 2002;46(suppl 2):S41-S62.
24. Rucker Wright D, Gathers R, Kapke A, et al. Hair care practices and their association with scalp and hair disorders in African American girls. J Am Acad Dermatol. 2011;64:253-262.
25. Kumar V, Sharma RC, Chander R. Clinicomycological study of tinea capitis. Indian J Dermatol Venereol Leprol. 1996;62:207-209.
26. Mirmirani P, Tucker LY. Epidemiologic trends in pediatric tinea capitis: a population-based study from Kaiser Permanente Northern California [published online ahead of print October 2, 2013]. J Am Acad Dermatol. 2013;69:916-921.
27. Chapman JC, Daniel CR 3rd, Daniel JG, et al. Tinea capitis caused by dermatophytes: a 15-year retrospective study from a Mississippi Dermatology Clinic. Cutis. 2011;88:230-233.
28. Perman MJ, Lovell DJ, Denson LA, et al. Five cases of anti-tumor necrosis factor alpha-induced psoriasis presenting with severe scalp involvement in children. Pediatr Dermatol. 2012;29:454-459.
29. Khumalo NP, Jessop S, Gumedze F, et al. Determinants of marginal traction alopecia in African girls and women. J Am Acad Dermatol. 2008;59:432-438.
30. Vazquez-Lopez F, Palacios-Garcia L, Argenziano G. Dermoscopic corkscrew hairs dissolve after successful therapy of Trichophyton violaceum tinea capitis: a case report. Australas J Dermatol. 2012;53:118-119.
31. Pinheiro AM, Lobato LA, Varella TC. Dermoscopy findings in tinea capitis: case report and literature review. An Bras Dermatol. 2012;87:313-314.
32. Mapelli ET, Gualandri L, Cerri A, et al. Comma hairs in tinea capitis: a useful dermatoscopic sign for diagnosis of tinea capitis. Pediatr Dermatol. 2012;29:223-224.
33. Hughes R, Chiaverini C, Bahadoran P, et al. Corkscrew hair: a new dermoscopic sign for diagnosis of tinea capitis in black children. Arch Dermatol. 2011;147:355-356.
34. Ekiz O, Sen BB, Rifaiog˘lu EN, et al. Trichoscopy in paediatric patients with tinea capitis: a useful method to differentiate from alopecia areata [published online ahead of print August 24, 2013]. J Eur Acad Dermatol Venereol. 2014;28:1255-1258.
35. Lencastre A, Tosti A. Role of trichoscopy in children’s scalp and hair disorders [published online ahead of print Aug 13, 2013]. Pediatr Dermatol. 2013;30:674-682.
36. Samrao A, Price VH, Zedek D, et al. The “fringe sign”—a useful clinical finding in traction alopecia of the marginal hair line. Dermatol Online J. 2011;17:1.
37. Nasir S, Ralph N, O’Neill C, et al. Trends in tinea capitis in an Irish pediatric population and a comparison of scalp brushings versus scalp scrapings as methods of investigation [published online ahead of print February 22, 2013]. Pediatr Dermatol. 2014;31:622-623.
38. Alvarez MS, Silverberg NB. Tinea capitis. Cutis. 2006;78:189-196.
39. Simko SJ, Garmezy B, Abhyankar H, et al. Differentiating skin-limited and multisystem Langerhans cell histiocytosis. J Pediatr. 2014;165:990-996.
40. Bookstaver PB, Watson HJ, Winters SD, et al. Prophylactic ketoconazole shampoo for tinea capitis in a high-risk pediatric population. J Pediatr Pharmacol Ther. 2011;16:199-203.
41. Allen HB, Honig PJ, Leyden JJ, et al. Selenium sulfide: adjunctive therapy for tinea capitis. Pediatrics. 1982;69:81-83.
42. Crawford K, Hernandez C. A review of hair care products for black individuals. Cutis. 2014;93:289-293.
43. Kim KS, Shin MK, Kim JH, et al. Effects of atopic dermatitis on the morphology and water content of scalp hair [published online ahead of print November 7, 2011]. Microsc Res Tech. 2012;75:620-625.
44. Kapila S, Hong E, Fischer G. A comparative study of childhood psoriasis and atopic dermatitis and greater understanding of the overlapping condition, psoriasis-dermatitis. Australas J Dermatol. 2012;53:98-105.
45. Tollesson A, Frithz A. Borage oil, an effective new treatment for infantile seborrhoeic dermatitis. Br J Dermatol. 1993;129:95.
46. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriol plus betamethasone dipropionate gel in the treatment of scalp psoriasis in adolescents 12-17 years of age [published online ahead of print October 22, 2014]. Br J Dermatol. 2014;171:1470-1477.
47. Singer C, Stancu P, Coşoveanu S, et al. Non-alcoholic fatty liver disease in children. Curr Health Sci J. 2014;40:170-176.
48. Chiang C, Price V, Mirmirani P. Central centrifugal cicatricial alopecia: superimposed tinea capitis as the etiology of chronic scalp pruritus. Dermatol Online J. 2008;14:3.
49. Morrone A, Calcaterra R, Valenzano M, et al. Erythema nodosum induced by kerion celsi of the scalp in a woman. Mycoses. 2011;54:e237-e239.
50. Boaventura P, Pereira D, Celestino R, et al. Genetic alterations in thyroid tumors from patients irradiated in childhood for tinea capitis treatment. Eur J Endocrinol. 2013;169:673-679.
1. Williams JV, Eichenfield LF, Burke BL, et al. Prevalence of scalp scaling in prepubertal children. Pediatrics. 2005;115:e1-e6.
2. Coley MK, Bhanusali DG, Silverberg JI, et al. Scalp hyperkeratosis and alopecia in children of color. J Drugs Dermatol. 2011;10:511-516.
3. Bhanusali D, Coley M, Silverberg JI, et al. Treatment outcomes for tinea capitis in a skin of color population. J Drugs Dermatol. 2012;11:852-856.
4. Williams JV, Honig PJ, McGinley KJ, et al. Semiquantitative study of tinea capitis and the asymptomatic carrier state in inner-city school children. Pediatrics. 1995;96:265-267.
5. McDonald LL, Smith ML. Diagnostic dilemmas in pediatric/adolescent dermatology: scaly scalp. J Pediatr Health Care. 1998;12:80-84.
6. Peloro TM, Miller OF 3rd, Hahn TF, et al. Juvenile dermatomyositis: a retrospective review of a 30-year experience. J Am Acad Dermatol. 2001;45:28-34.
7. Wahab MA, Rahman MH, Khondker L, et al. Minor criteria for atopic dermatitis in children. Mymensingh Med J. 2011;20:419-424.
8. Shi M, Zhang H, Chen X, et al. Clinical features of atopic dermatitis in a hospital-based setting in China. J Eur Acad Dermatol Venereol [published online ahead of print January 9, 2011]. 2011;25:1206-1212.
9. Kim KS, Shin MK, Kim JH, et al. Effects of atopic dermatitis on the morphology and water content of scalp hair. Microsc Res Tech. 2012;75:620-625.
10. Sabin BR, Peters N, Peters AT. Chapter 20: atopic dermatitis. Allergy Asthma Proc. 2012;33:S67-S69.
11. Alexopoulos A, Kakourou T, Orfanou I, et al. Retrospective analysis of the relationship between infantile seborrheic dermatitis and atopic dermatitis [published online ahead of print November 13, 2013]. Pediatr Dermatol. 2014;31:125-130.
12. Elish D, Silverberg NB. Infantile seborrheic dermatitis. Cutis. 2006;77:297-300.
13. Sarifakioglu E, Yilmaz AE, Gorpelioglu C, et al. Prevalence of scalp disorders and hair loss in children. Cutis. 2012;90:225-229.
14. Abdel-Hamid IA, Agha SA, Moustafa YM, et al. Pityriasis amiantacea: a clinical and etiopathologic study of 85 patients. Int J Dermatol. 2003;42:260-264.
15. Oostveen AM, Jong EM, Evers AW, et al. Reliability, responsiveness and validity of Scalpdex in children with scalp psoriasis: the Dutch study. Acta Derm Venereol. 2014;94:198-202.
16. Silverberg NB. Atlas of Pediatric Cutaneous Biodiversity: Comparative Dermatologic Atlas of Pediatric Skin of All Colors. New York, NY: Springer; 2012.
17. Sharma V, Silverberg NB, Howard R, et al. Do hair care practices affect the acquisition of tinea capitis? a case-control study. Arch Pediatr Adolesc Med. 2001;155:818-821.
18. Moises-Alfaro C, Berrón-Pérez R, Carrasco-Daza D, et al. Discoid lupus erythematosus in children: clinical, histopathologic, and follow-up features in 27 cases. Pediatr Dermatol. 2003;20:103-107.
19. Ramos-e-Silva M. Ethnic hair and skin: what is the state of the science? Chicago, Illinois—September 29-30, 2001. Clin Dermatol. 2002;20:321-324.
20. Heath CR, McMichael AJ. Biology of hair follicle. In: Kelly AP, Taylor SC, eds. Dermatology for Skin of Color. New York, NY: McGraw Hill; 2009:105-109.
21. Khumalo NP. African hair morphology: macrostructure to ultrastructure. Int J Dermatol. 2005;44(suppl 1):10-12.
22. Thibaut S, Bernard BA. The biology of hair shape. Int J Dermatol. 2005;44(suppl 1):2-3.
23. Taylor SC. Skin of color: biology, structure, function, and implications for dermatologic disease. J Am Acad Dermatol. 2002;46(suppl 2):S41-S62.
24. Rucker Wright D, Gathers R, Kapke A, et al. Hair care practices and their association with scalp and hair disorders in African American girls. J Am Acad Dermatol. 2011;64:253-262.
25. Kumar V, Sharma RC, Chander R. Clinicomycological study of tinea capitis. Indian J Dermatol Venereol Leprol. 1996;62:207-209.
26. Mirmirani P, Tucker LY. Epidemiologic trends in pediatric tinea capitis: a population-based study from Kaiser Permanente Northern California [published online ahead of print October 2, 2013]. J Am Acad Dermatol. 2013;69:916-921.
27. Chapman JC, Daniel CR 3rd, Daniel JG, et al. Tinea capitis caused by dermatophytes: a 15-year retrospective study from a Mississippi Dermatology Clinic. Cutis. 2011;88:230-233.
28. Perman MJ, Lovell DJ, Denson LA, et al. Five cases of anti-tumor necrosis factor alpha-induced psoriasis presenting with severe scalp involvement in children. Pediatr Dermatol. 2012;29:454-459.
29. Khumalo NP, Jessop S, Gumedze F, et al. Determinants of marginal traction alopecia in African girls and women. J Am Acad Dermatol. 2008;59:432-438.
30. Vazquez-Lopez F, Palacios-Garcia L, Argenziano G. Dermoscopic corkscrew hairs dissolve after successful therapy of Trichophyton violaceum tinea capitis: a case report. Australas J Dermatol. 2012;53:118-119.
31. Pinheiro AM, Lobato LA, Varella TC. Dermoscopy findings in tinea capitis: case report and literature review. An Bras Dermatol. 2012;87:313-314.
32. Mapelli ET, Gualandri L, Cerri A, et al. Comma hairs in tinea capitis: a useful dermatoscopic sign for diagnosis of tinea capitis. Pediatr Dermatol. 2012;29:223-224.
33. Hughes R, Chiaverini C, Bahadoran P, et al. Corkscrew hair: a new dermoscopic sign for diagnosis of tinea capitis in black children. Arch Dermatol. 2011;147:355-356.
34. Ekiz O, Sen BB, Rifaiog˘lu EN, et al. Trichoscopy in paediatric patients with tinea capitis: a useful method to differentiate from alopecia areata [published online ahead of print August 24, 2013]. J Eur Acad Dermatol Venereol. 2014;28:1255-1258.
35. Lencastre A, Tosti A. Role of trichoscopy in children’s scalp and hair disorders [published online ahead of print Aug 13, 2013]. Pediatr Dermatol. 2013;30:674-682.
36. Samrao A, Price VH, Zedek D, et al. The “fringe sign”—a useful clinical finding in traction alopecia of the marginal hair line. Dermatol Online J. 2011;17:1.
37. Nasir S, Ralph N, O’Neill C, et al. Trends in tinea capitis in an Irish pediatric population and a comparison of scalp brushings versus scalp scrapings as methods of investigation [published online ahead of print February 22, 2013]. Pediatr Dermatol. 2014;31:622-623.
38. Alvarez MS, Silverberg NB. Tinea capitis. Cutis. 2006;78:189-196.
39. Simko SJ, Garmezy B, Abhyankar H, et al. Differentiating skin-limited and multisystem Langerhans cell histiocytosis. J Pediatr. 2014;165:990-996.
40. Bookstaver PB, Watson HJ, Winters SD, et al. Prophylactic ketoconazole shampoo for tinea capitis in a high-risk pediatric population. J Pediatr Pharmacol Ther. 2011;16:199-203.
41. Allen HB, Honig PJ, Leyden JJ, et al. Selenium sulfide: adjunctive therapy for tinea capitis. Pediatrics. 1982;69:81-83.
42. Crawford K, Hernandez C. A review of hair care products for black individuals. Cutis. 2014;93:289-293.
43. Kim KS, Shin MK, Kim JH, et al. Effects of atopic dermatitis on the morphology and water content of scalp hair [published online ahead of print November 7, 2011]. Microsc Res Tech. 2012;75:620-625.
44. Kapila S, Hong E, Fischer G. A comparative study of childhood psoriasis and atopic dermatitis and greater understanding of the overlapping condition, psoriasis-dermatitis. Australas J Dermatol. 2012;53:98-105.
45. Tollesson A, Frithz A. Borage oil, an effective new treatment for infantile seborrhoeic dermatitis. Br J Dermatol. 1993;129:95.
46. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriol plus betamethasone dipropionate gel in the treatment of scalp psoriasis in adolescents 12-17 years of age [published online ahead of print October 22, 2014]. Br J Dermatol. 2014;171:1470-1477.
47. Singer C, Stancu P, Coşoveanu S, et al. Non-alcoholic fatty liver disease in children. Curr Health Sci J. 2014;40:170-176.
48. Chiang C, Price V, Mirmirani P. Central centrifugal cicatricial alopecia: superimposed tinea capitis as the etiology of chronic scalp pruritus. Dermatol Online J. 2008;14:3.
49. Morrone A, Calcaterra R, Valenzano M, et al. Erythema nodosum induced by kerion celsi of the scalp in a woman. Mycoses. 2011;54:e237-e239.
50. Boaventura P, Pereira D, Celestino R, et al. Genetic alterations in thyroid tumors from patients irradiated in childhood for tinea capitis treatment. Eur J Endocrinol. 2013;169:673-679.
Practice Points
- Scalp hyperkeratosis is a common finding in children, especially those with skin of color.
- Fungal culture may be helpful in the diagnosis of scalp hyperkeratosis in children of any age but should be performed in patients aged 3 to 11 years with skin of color.
- Therapy of scalp disease in children with skin of color should be adjusted based on hair type and disease features.
HM15 Session Analysis: The Physician-Administrator Management Dyad
Hm15 Presenters: Chuck Ainsworth, MD, MCC,; Dan Virnich, MD, MBA; Roberta Himebaugh, MBA, SFHM; Robert Hickling, MHA; Sendil Krishnan, MD
Summation: The presenters, a group of physicians and administrators for hospital medicine groups, explored three dyad models. These three models were:
- Office of the Executive, where there is one senior executive and a junior executive;
- Coordinated Co-Leadership, where each of the two co-leaders has separate direct reports; and
- Integrated Co-Leadership, where there are two co-leaders and the staff report to the co-leader team.
The discussion ensued to outline the benefit of a dyad leadership model, which can lead to growth and success in advancing the commitment to patient care. The group also emphasized the importance of providing leadership training and education to optimize the dyad leadership model. Bringing together physician and administrator dyads enables an organization to have complimentary expertise to advance hospital medicine programs into the next era.
Hm15 Presenters: Chuck Ainsworth, MD, MCC,; Dan Virnich, MD, MBA; Roberta Himebaugh, MBA, SFHM; Robert Hickling, MHA; Sendil Krishnan, MD
Summation: The presenters, a group of physicians and administrators for hospital medicine groups, explored three dyad models. These three models were:
- Office of the Executive, where there is one senior executive and a junior executive;
- Coordinated Co-Leadership, where each of the two co-leaders has separate direct reports; and
- Integrated Co-Leadership, where there are two co-leaders and the staff report to the co-leader team.
The discussion ensued to outline the benefit of a dyad leadership model, which can lead to growth and success in advancing the commitment to patient care. The group also emphasized the importance of providing leadership training and education to optimize the dyad leadership model. Bringing together physician and administrator dyads enables an organization to have complimentary expertise to advance hospital medicine programs into the next era.
Hm15 Presenters: Chuck Ainsworth, MD, MCC,; Dan Virnich, MD, MBA; Roberta Himebaugh, MBA, SFHM; Robert Hickling, MHA; Sendil Krishnan, MD
Summation: The presenters, a group of physicians and administrators for hospital medicine groups, explored three dyad models. These three models were:
- Office of the Executive, where there is one senior executive and a junior executive;
- Coordinated Co-Leadership, where each of the two co-leaders has separate direct reports; and
- Integrated Co-Leadership, where there are two co-leaders and the staff report to the co-leader team.
The discussion ensued to outline the benefit of a dyad leadership model, which can lead to growth and success in advancing the commitment to patient care. The group also emphasized the importance of providing leadership training and education to optimize the dyad leadership model. Bringing together physician and administrator dyads enables an organization to have complimentary expertise to advance hospital medicine programs into the next era.
HM15 Session Analysis: Innovative Hospitalist Staffing Models
HM15 Presenters: John Nelson, MD, MHM; Daniel Hanson, MD, FHM; Darren Thomas, MD
Summation: The presenters, from three entirely different geographic regions across the U.S., walked the audience through several different innovative hospitalist staffing models, from staffing in a multi-hospital system to integrating of advanced practice clinicians to deploying staggered staffing techniques to match the patient demand and enhance continuity of care.
Many multi-hospital systems are challenged to consider creative solutions on how to meet individual hospital staffing needs, while also creating staffing efficiencies across the system, such as cross coverage at night and back-up staffing solutions for increased patient volumes and unexpected staffing vacancies.
Examples to enhance patient continuity were presented throughout, such as pairing together a hospitalist from one week to a hospitalist from an alternate week to care for the same patients.
Similarly, the experts provided a compelling case to consider pairing hospitalist providers with patients, and referring physicians longitudinally across multiple admissions.
Key Takeaways:
1. Patients Come First - consider patient alignment, or continuity, in determing provider scheduling options.
2. Multi-hospital Systems - establish the onboarding parameters needed for providers to be successful in covering more than one hospital and how to build into your scheduling model.
3. Integrate the Care Team - ensure the roles of the integrated provider team (e.g., physicians and advanced practice clinicians) are clearly understood when developing the schedule.
4. Know Your Numbers - clearly understand the workload demands to properly balance the scheduling needs before establishing the schedule.
5. Regular Review - regularly review all of these areas and revise your schedule based on the changing landscape of demands on your hospital medicine group.
HM15 Presenters: John Nelson, MD, MHM; Daniel Hanson, MD, FHM; Darren Thomas, MD
Summation: The presenters, from three entirely different geographic regions across the U.S., walked the audience through several different innovative hospitalist staffing models, from staffing in a multi-hospital system to integrating of advanced practice clinicians to deploying staggered staffing techniques to match the patient demand and enhance continuity of care.
Many multi-hospital systems are challenged to consider creative solutions on how to meet individual hospital staffing needs, while also creating staffing efficiencies across the system, such as cross coverage at night and back-up staffing solutions for increased patient volumes and unexpected staffing vacancies.
Examples to enhance patient continuity were presented throughout, such as pairing together a hospitalist from one week to a hospitalist from an alternate week to care for the same patients.
Similarly, the experts provided a compelling case to consider pairing hospitalist providers with patients, and referring physicians longitudinally across multiple admissions.
Key Takeaways:
1. Patients Come First - consider patient alignment, or continuity, in determing provider scheduling options.
2. Multi-hospital Systems - establish the onboarding parameters needed for providers to be successful in covering more than one hospital and how to build into your scheduling model.
3. Integrate the Care Team - ensure the roles of the integrated provider team (e.g., physicians and advanced practice clinicians) are clearly understood when developing the schedule.
4. Know Your Numbers - clearly understand the workload demands to properly balance the scheduling needs before establishing the schedule.
5. Regular Review - regularly review all of these areas and revise your schedule based on the changing landscape of demands on your hospital medicine group.
HM15 Presenters: John Nelson, MD, MHM; Daniel Hanson, MD, FHM; Darren Thomas, MD
Summation: The presenters, from three entirely different geographic regions across the U.S., walked the audience through several different innovative hospitalist staffing models, from staffing in a multi-hospital system to integrating of advanced practice clinicians to deploying staggered staffing techniques to match the patient demand and enhance continuity of care.
Many multi-hospital systems are challenged to consider creative solutions on how to meet individual hospital staffing needs, while also creating staffing efficiencies across the system, such as cross coverage at night and back-up staffing solutions for increased patient volumes and unexpected staffing vacancies.
Examples to enhance patient continuity were presented throughout, such as pairing together a hospitalist from one week to a hospitalist from an alternate week to care for the same patients.
Similarly, the experts provided a compelling case to consider pairing hospitalist providers with patients, and referring physicians longitudinally across multiple admissions.
Key Takeaways:
1. Patients Come First - consider patient alignment, or continuity, in determing provider scheduling options.
2. Multi-hospital Systems - establish the onboarding parameters needed for providers to be successful in covering more than one hospital and how to build into your scheduling model.
3. Integrate the Care Team - ensure the roles of the integrated provider team (e.g., physicians and advanced practice clinicians) are clearly understood when developing the schedule.
4. Know Your Numbers - clearly understand the workload demands to properly balance the scheduling needs before establishing the schedule.
5. Regular Review - regularly review all of these areas and revise your schedule based on the changing landscape of demands on your hospital medicine group.
A look at top upcoming clinical trials in electrophysiology
SAN DIEGO – How to prevent sudden arrhythmic death in vulnerable but currently unprotected populations is being addressed by ongoing studies that variously evaluate a pharmacologic, an implanted device-based, or a wearable solution, according to Dr. Bruce D. Lindsay.
Dr. Lindsay, head of the cardiac electrophysiology and pacing section at the Cleveland Clinic, presented an overview of selected major ongoing clinical trials in electrophysiology at the annual meeting of the American College of Cardiology. He focused on five hot topics: prevention of sudden death, atrial fibrillation (AF) ablation, prevention of implantable device-related infections, device-based treatment of heart failure, and leadless pacing systems.
Preventing sudden death
Ongoing phase III trials are evaluating the safety, tolerability, and efficacy of an oral Gilead drug known for now as GS-6615. The drug, a selective late sodium current inhibitor, is designed to shorten the corrected QTc interval in patients with several forms of long QT syndrome.
A different approach is being studied in REFINE-ICD (Risk Estimation Following Infarction Noninvasive Evaluation – ICD Efficacy), a 1,400-subject trial recruiting patients who’ve had an acute MI within the previous year, have abnormal findings on 24-hour Holter monitoring, and have moderate left ventricular dysfunction as defined by an ejection fraction of 35%-50%. The trial will assess whether prophylactic placement of an implantable cardioverter-defibrillator (ICD) guided by noninvasive risk assessment based on heart rate turbulence and T-wave alternans analysis will reduce mortality in MI survivors.
“This is a group that’s at lower risk than current ICD recipients, but because it’s such a large group they account for a lot of sudden deaths,” the cardiologist said.

Another phase III trial currently recruiting participants is a 1,900-patient postmarketing study aimed at defining which patients benefit from using the LifeVest wearable defibrillator during the first 3 months following an acute MI resulting in ventricular dysfunction.
AF ablation
The most important ongoing study in this field, in Dr. Lindsay’s view, is CABANA (Catheter Ablation Versus Anti-Arrhythmic Drug Therapy for Atrial Fibrillation Trial). This National Institutes of Health–sponsored study is aimed at showing whether ablation is superior to rate or rhythm control drug therapy in terms of all-cause mortality, disabling stroke, serious bleeding, and/or cardiac arrest. Secondary endpoints include cost, quality of life, hospitalization rates, and the relationship of left atrial size to progression of AF and its contribution to morbidity and mortality.
A promising, innovative ablation strategy known as focal impulse and rotor ablation for paroxysmal AF is under evaluation in the German REAFFIRM (Randomized Evaluation of Atrial Fibrillation Treatment With Focal Impulse and Rotor Modulation Guided Procedures). A similar U.S. study known as FIRMAT-PAF (Focal Impulse and Rotor Modulation Ablation Trial for Treatment of Paroxysmal Atrial Fibrillation) had to be abandoned, however, because of its inability to recruit patients.
New ablation technologies are also being introduced. Three pivotal trials totaling roughly 1,500 patients are evaluating the Biosense Webster nMARQ multielectrode irrigated catheter for paroxysmal AF in the reMARQable trial; a Medtronic phased radiofrequency ablation catheter for persistent AF in the VICTORY AF study; and a CardioFocus endoscopic ablation catheter for paroxysmal AF.
Preventing cardiac implantable device infections
WRAP-IT (the World-Wide Randomized Antibiotic Envelope Infection Trial) is currently enrolling 7,000 patients at 225 sites. This is a Merck-sponsored randomized, prospective, single-blind postmarketing study examining the ability of a proprietary mesh envelope to reduce major infections and costs in the 12 months following device generator replacement, upgrade, or revision, or new implantation of a cardiac resynchronization device. The Tyrx mesh envelope releases minocycline and rifampin for at least 7 days, then eventually becomes fully absorbed.
“Device infection is a huge problem in our field,” Dr. Lindsay noted. “This envelope may have important implications at large, or it may prove to be especially useful in people at high risk for infection.”
Heart failure
Vagal nerve stimulation via an implantable system is one of the hottest areas in the field of heart failure, the electrophysiologist said. Two major trials are ongoing: the Sorin-sponsored VANGUARD (Vagal Nerve Stimulation: Safeguarding Heart Failure Patients) trial, and INNOVATE HF (Increase of Vagal Tone in CHF), sponsored by Biocontrol Medical.
Leadless pacing
St. Jude’s Nanostim and Medtronic’s Micra are very small leadless devices implanted in the right ventricular apex via minimally invasive techniques. Both devices are investigational in the United States, although the Nanostim is approved in Europe. Clinical interest is enormous because lead-related problems have always been the Achilles’ heel of pacemaker therapy. While the Nanostim and Micra can be utilized only for single right ventricular pacing in VVI or VVIR mode, Dr. Lindsay said further advances, including leadless dual-chamber sensing and pacing and biventricular pacing, are likely.
He reported serving as a consultant to Biosense Webster, Boston Scientific, and Medtronic.
SAN DIEGO – How to prevent sudden arrhythmic death in vulnerable but currently unprotected populations is being addressed by ongoing studies that variously evaluate a pharmacologic, an implanted device-based, or a wearable solution, according to Dr. Bruce D. Lindsay.
Dr. Lindsay, head of the cardiac electrophysiology and pacing section at the Cleveland Clinic, presented an overview of selected major ongoing clinical trials in electrophysiology at the annual meeting of the American College of Cardiology. He focused on five hot topics: prevention of sudden death, atrial fibrillation (AF) ablation, prevention of implantable device-related infections, device-based treatment of heart failure, and leadless pacing systems.
Preventing sudden death
Ongoing phase III trials are evaluating the safety, tolerability, and efficacy of an oral Gilead drug known for now as GS-6615. The drug, a selective late sodium current inhibitor, is designed to shorten the corrected QTc interval in patients with several forms of long QT syndrome.
A different approach is being studied in REFINE-ICD (Risk Estimation Following Infarction Noninvasive Evaluation – ICD Efficacy), a 1,400-subject trial recruiting patients who’ve had an acute MI within the previous year, have abnormal findings on 24-hour Holter monitoring, and have moderate left ventricular dysfunction as defined by an ejection fraction of 35%-50%. The trial will assess whether prophylactic placement of an implantable cardioverter-defibrillator (ICD) guided by noninvasive risk assessment based on heart rate turbulence and T-wave alternans analysis will reduce mortality in MI survivors.
“This is a group that’s at lower risk than current ICD recipients, but because it’s such a large group they account for a lot of sudden deaths,” the cardiologist said.
Another phase III trial currently recruiting participants is a 1,900-patient postmarketing study aimed at defining which patients benefit from using the LifeVest wearable defibrillator during the first 3 months following an acute MI resulting in ventricular dysfunction.
AF ablation
The most important ongoing study in this field, in Dr. Lindsay’s view, is CABANA (Catheter Ablation Versus Anti-Arrhythmic Drug Therapy for Atrial Fibrillation Trial). This National Institutes of Health–sponsored study is aimed at showing whether ablation is superior to rate or rhythm control drug therapy in terms of all-cause mortality, disabling stroke, serious bleeding, and/or cardiac arrest. Secondary endpoints include cost, quality of life, hospitalization rates, and the relationship of left atrial size to progression of AF and its contribution to morbidity and mortality.
A promising, innovative ablation strategy known as focal impulse and rotor ablation for paroxysmal AF is under evaluation in the German REAFFIRM (Randomized Evaluation of Atrial Fibrillation Treatment With Focal Impulse and Rotor Modulation Guided Procedures). A similar U.S. study known as FIRMAT-PAF (Focal Impulse and Rotor Modulation Ablation Trial for Treatment of Paroxysmal Atrial Fibrillation) had to be abandoned, however, because of its inability to recruit patients.
New ablation technologies are also being introduced. Three pivotal trials totaling roughly 1,500 patients are evaluating the Biosense Webster nMARQ multielectrode irrigated catheter for paroxysmal AF in the reMARQable trial; a Medtronic phased radiofrequency ablation catheter for persistent AF in the VICTORY AF study; and a CardioFocus endoscopic ablation catheter for paroxysmal AF.
Preventing cardiac implantable device infections
WRAP-IT (the World-Wide Randomized Antibiotic Envelope Infection Trial) is currently enrolling 7,000 patients at 225 sites. This is a Merck-sponsored randomized, prospective, single-blind postmarketing study examining the ability of a proprietary mesh envelope to reduce major infections and costs in the 12 months following device generator replacement, upgrade, or revision, or new implantation of a cardiac resynchronization device. The Tyrx mesh envelope releases minocycline and rifampin for at least 7 days, then eventually becomes fully absorbed.
“Device infection is a huge problem in our field,” Dr. Lindsay noted. “This envelope may have important implications at large, or it may prove to be especially useful in people at high risk for infection.”
Heart failure
Vagal nerve stimulation via an implantable system is one of the hottest areas in the field of heart failure, the electrophysiologist said. Two major trials are ongoing: the Sorin-sponsored VANGUARD (Vagal Nerve Stimulation: Safeguarding Heart Failure Patients) trial, and INNOVATE HF (Increase of Vagal Tone in CHF), sponsored by Biocontrol Medical.
Leadless pacing
St. Jude’s Nanostim and Medtronic’s Micra are very small leadless devices implanted in the right ventricular apex via minimally invasive techniques. Both devices are investigational in the United States, although the Nanostim is approved in Europe. Clinical interest is enormous because lead-related problems have always been the Achilles’ heel of pacemaker therapy. While the Nanostim and Micra can be utilized only for single right ventricular pacing in VVI or VVIR mode, Dr. Lindsay said further advances, including leadless dual-chamber sensing and pacing and biventricular pacing, are likely.
He reported serving as a consultant to Biosense Webster, Boston Scientific, and Medtronic.
SAN DIEGO – How to prevent sudden arrhythmic death in vulnerable but currently unprotected populations is being addressed by ongoing studies that variously evaluate a pharmacologic, an implanted device-based, or a wearable solution, according to Dr. Bruce D. Lindsay.
Dr. Lindsay, head of the cardiac electrophysiology and pacing section at the Cleveland Clinic, presented an overview of selected major ongoing clinical trials in electrophysiology at the annual meeting of the American College of Cardiology. He focused on five hot topics: prevention of sudden death, atrial fibrillation (AF) ablation, prevention of implantable device-related infections, device-based treatment of heart failure, and leadless pacing systems.
Preventing sudden death
Ongoing phase III trials are evaluating the safety, tolerability, and efficacy of an oral Gilead drug known for now as GS-6615. The drug, a selective late sodium current inhibitor, is designed to shorten the corrected QTc interval in patients with several forms of long QT syndrome.
A different approach is being studied in REFINE-ICD (Risk Estimation Following Infarction Noninvasive Evaluation – ICD Efficacy), a 1,400-subject trial recruiting patients who’ve had an acute MI within the previous year, have abnormal findings on 24-hour Holter monitoring, and have moderate left ventricular dysfunction as defined by an ejection fraction of 35%-50%. The trial will assess whether prophylactic placement of an implantable cardioverter-defibrillator (ICD) guided by noninvasive risk assessment based on heart rate turbulence and T-wave alternans analysis will reduce mortality in MI survivors.
“This is a group that’s at lower risk than current ICD recipients, but because it’s such a large group they account for a lot of sudden deaths,” the cardiologist said.
Another phase III trial currently recruiting participants is a 1,900-patient postmarketing study aimed at defining which patients benefit from using the LifeVest wearable defibrillator during the first 3 months following an acute MI resulting in ventricular dysfunction.
AF ablation
The most important ongoing study in this field, in Dr. Lindsay’s view, is CABANA (Catheter Ablation Versus Anti-Arrhythmic Drug Therapy for Atrial Fibrillation Trial). This National Institutes of Health–sponsored study is aimed at showing whether ablation is superior to rate or rhythm control drug therapy in terms of all-cause mortality, disabling stroke, serious bleeding, and/or cardiac arrest. Secondary endpoints include cost, quality of life, hospitalization rates, and the relationship of left atrial size to progression of AF and its contribution to morbidity and mortality.
A promising, innovative ablation strategy known as focal impulse and rotor ablation for paroxysmal AF is under evaluation in the German REAFFIRM (Randomized Evaluation of Atrial Fibrillation Treatment With Focal Impulse and Rotor Modulation Guided Procedures). A similar U.S. study known as FIRMAT-PAF (Focal Impulse and Rotor Modulation Ablation Trial for Treatment of Paroxysmal Atrial Fibrillation) had to be abandoned, however, because of its inability to recruit patients.
New ablation technologies are also being introduced. Three pivotal trials totaling roughly 1,500 patients are evaluating the Biosense Webster nMARQ multielectrode irrigated catheter for paroxysmal AF in the reMARQable trial; a Medtronic phased radiofrequency ablation catheter for persistent AF in the VICTORY AF study; and a CardioFocus endoscopic ablation catheter for paroxysmal AF.
Preventing cardiac implantable device infections
WRAP-IT (the World-Wide Randomized Antibiotic Envelope Infection Trial) is currently enrolling 7,000 patients at 225 sites. This is a Merck-sponsored randomized, prospective, single-blind postmarketing study examining the ability of a proprietary mesh envelope to reduce major infections and costs in the 12 months following device generator replacement, upgrade, or revision, or new implantation of a cardiac resynchronization device. The Tyrx mesh envelope releases minocycline and rifampin for at least 7 days, then eventually becomes fully absorbed.
“Device infection is a huge problem in our field,” Dr. Lindsay noted. “This envelope may have important implications at large, or it may prove to be especially useful in people at high risk for infection.”
Heart failure
Vagal nerve stimulation via an implantable system is one of the hottest areas in the field of heart failure, the electrophysiologist said. Two major trials are ongoing: the Sorin-sponsored VANGUARD (Vagal Nerve Stimulation: Safeguarding Heart Failure Patients) trial, and INNOVATE HF (Increase of Vagal Tone in CHF), sponsored by Biocontrol Medical.
Leadless pacing
St. Jude’s Nanostim and Medtronic’s Micra are very small leadless devices implanted in the right ventricular apex via minimally invasive techniques. Both devices are investigational in the United States, although the Nanostim is approved in Europe. Clinical interest is enormous because lead-related problems have always been the Achilles’ heel of pacemaker therapy. While the Nanostim and Micra can be utilized only for single right ventricular pacing in VVI or VVIR mode, Dr. Lindsay said further advances, including leadless dual-chamber sensing and pacing and biventricular pacing, are likely.
He reported serving as a consultant to Biosense Webster, Boston Scientific, and Medtronic.
EXPERT ANALYSIS FROM ACC 15

Form of catheter-directed thrombolysis cured patients of submassive PEs
Ultrasound-accelerated catheter-directed thrombolysis (USAT) was successful at treating acute submassive pulmonary embolisms, according to a retrospective study.
Acute pulmonary hypertension and right ventricular dysfunction (RVD), on average, became significantly less severe in all of the study’s 45 participants. Specifically, main pulmonary artery pressure decreased to 31.1 mm Hg from 49.8 mm Hg. The improvement in RVD was demonstrated by a decreased right ventricle-to-left-ventricle ratio to 0.93 from 1.59.
Although no complications occurred as a result of catheter placement, six complications resulted from other causes. Those complications included four minor venous access-site hemorrhagic complications and two major bleeding complications: a flank hematoma and an arm hematoma.
“USAT is a safe and efficacious method of treatment of submassive PE to reduce acute pulmonary hypertension and RVD. Future studies should be aimed at examining the long-term effect of USAT on mortality, exercise tolerance, and pulmonary hypertension,” wrote Dr. Sandeep Bagla of the Inova Alexandria (Va.) Hospital and his colleagues.
Find the full study in the Journal of Vascular and Interventional Radiology (doi:10.1016/j.jvir.2014.12.017).
Ultrasound-accelerated catheter-directed thrombolysis (USAT) was successful at treating acute submassive pulmonary embolisms, according to a retrospective study.
Acute pulmonary hypertension and right ventricular dysfunction (RVD), on average, became significantly less severe in all of the study’s 45 participants. Specifically, main pulmonary artery pressure decreased to 31.1 mm Hg from 49.8 mm Hg. The improvement in RVD was demonstrated by a decreased right ventricle-to-left-ventricle ratio to 0.93 from 1.59.
Although no complications occurred as a result of catheter placement, six complications resulted from other causes. Those complications included four minor venous access-site hemorrhagic complications and two major bleeding complications: a flank hematoma and an arm hematoma.
“USAT is a safe and efficacious method of treatment of submassive PE to reduce acute pulmonary hypertension and RVD. Future studies should be aimed at examining the long-term effect of USAT on mortality, exercise tolerance, and pulmonary hypertension,” wrote Dr. Sandeep Bagla of the Inova Alexandria (Va.) Hospital and his colleagues.
Find the full study in the Journal of Vascular and Interventional Radiology (doi:10.1016/j.jvir.2014.12.017).
Ultrasound-accelerated catheter-directed thrombolysis (USAT) was successful at treating acute submassive pulmonary embolisms, according to a retrospective study.
Acute pulmonary hypertension and right ventricular dysfunction (RVD), on average, became significantly less severe in all of the study’s 45 participants. Specifically, main pulmonary artery pressure decreased to 31.1 mm Hg from 49.8 mm Hg. The improvement in RVD was demonstrated by a decreased right ventricle-to-left-ventricle ratio to 0.93 from 1.59.
Although no complications occurred as a result of catheter placement, six complications resulted from other causes. Those complications included four minor venous access-site hemorrhagic complications and two major bleeding complications: a flank hematoma and an arm hematoma.
“USAT is a safe and efficacious method of treatment of submassive PE to reduce acute pulmonary hypertension and RVD. Future studies should be aimed at examining the long-term effect of USAT on mortality, exercise tolerance, and pulmonary hypertension,” wrote Dr. Sandeep Bagla of the Inova Alexandria (Va.) Hospital and his colleagues.
Find the full study in the Journal of Vascular and Interventional Radiology (doi:10.1016/j.jvir.2014.12.017).
Two genes identified as VTE risk loci
A meta-analysis has identified two genes as susceptibility loci for venous thromboembolism, according to Marine Germain of the Institute for Cardiometabolism and Nutrition, Paris, and associates.
The identified risk loci were TSPAN15 and SLC44A2, with the odds ratios for VTE at 1.31 and 1.21, respectively. The most significant single-nucleotide polymorphism for the TSPAN15 loci was the intronic rs78707713; for SLC44A2, the most significant SNP was the nonsynonymous rs2288904, with ORs of 1.42 and 1.28, respectively. Although these associations are not strong, statistical evidence was much more convincing in the discovery and replication stages, the researchers reported.
“The identified VTE-associated SNPs map to genes that are not in conventional pathways to thrombosis that have marked most of the genetic associations to date, suggesting that these genetic variants represent novel biological pathways leading to VTE,” the investigators wrote.
Find the full study in the American Journal of Human Genetics (2015 April 2 [doi:10.1016/j.ajhg.2015.01.019]).
A meta-analysis has identified two genes as susceptibility loci for venous thromboembolism, according to Marine Germain of the Institute for Cardiometabolism and Nutrition, Paris, and associates.
The identified risk loci were TSPAN15 and SLC44A2, with the odds ratios for VTE at 1.31 and 1.21, respectively. The most significant single-nucleotide polymorphism for the TSPAN15 loci was the intronic rs78707713; for SLC44A2, the most significant SNP was the nonsynonymous rs2288904, with ORs of 1.42 and 1.28, respectively. Although these associations are not strong, statistical evidence was much more convincing in the discovery and replication stages, the researchers reported.
“The identified VTE-associated SNPs map to genes that are not in conventional pathways to thrombosis that have marked most of the genetic associations to date, suggesting that these genetic variants represent novel biological pathways leading to VTE,” the investigators wrote.
Find the full study in the American Journal of Human Genetics (2015 April 2 [doi:10.1016/j.ajhg.2015.01.019]).
A meta-analysis has identified two genes as susceptibility loci for venous thromboembolism, according to Marine Germain of the Institute for Cardiometabolism and Nutrition, Paris, and associates.
The identified risk loci were TSPAN15 and SLC44A2, with the odds ratios for VTE at 1.31 and 1.21, respectively. The most significant single-nucleotide polymorphism for the TSPAN15 loci was the intronic rs78707713; for SLC44A2, the most significant SNP was the nonsynonymous rs2288904, with ORs of 1.42 and 1.28, respectively. Although these associations are not strong, statistical evidence was much more convincing in the discovery and replication stages, the researchers reported.
“The identified VTE-associated SNPs map to genes that are not in conventional pathways to thrombosis that have marked most of the genetic associations to date, suggesting that these genetic variants represent novel biological pathways leading to VTE,” the investigators wrote.
Find the full study in the American Journal of Human Genetics (2015 April 2 [doi:10.1016/j.ajhg.2015.01.019]).
Study: More DVTs than expected in patients who had varicose vein surgeries
A retrospective study of patients who underwent varicose vein surgeries with a tourniquet found a greater incidence of deep vein thromboses (DVTs) than previous studies.
Within the first 3 postoperative days, 113 (7.7%) of the 1,461 patients had DVTs. The researchers also found that DVTs occurred significantly more often in patients with gastrocnemius vein dilation (GVD). A total of 410 (28%) of the study’s participants had GVTs, and the incidence of DVTs was significantly greater in individuals with GVD compared to those without such a symptom. GVD had a higher predictive power for postoperative DVT than did all of the other risk factors examined in univariate and multivariate analyses.
The vast majority of the DVTs diagnosed were isolated distal. While 94 patients suffered from this kind of DVT, the remaining 19 DVTs were proximal. According to Dr. Chen Kai of Wenzhou (China) Medical University, and colleagues, proximal DVTs were nearly always asymptomatic and a larger percentage of them took more time to disappear than did the distal DVTs. Within 6 months following anticoagulant therapy, 94.3% of the distal DVTs exhibited thrombus resolution and 55.6% of the proximal DVTs were thrombus free. None of the study’s participants had died because of DVT or pulmonary embolus during the 6 months following their surgeries.
This study’s “present data reflect a higher incidence of postoperative DVT than previous studies, and we also identify GVD as a significant risk factor. Larger prospective studies will be needed to evaluate this issue precisely and to understand the clinical relevance of these results,” wrote the researchers.Find the full study in Thombosis Research (doi: 10.1016/j.thromres.2015.03.008).
A retrospective study of patients who underwent varicose vein surgeries with a tourniquet found a greater incidence of deep vein thromboses (DVTs) than previous studies.
Within the first 3 postoperative days, 113 (7.7%) of the 1,461 patients had DVTs. The researchers also found that DVTs occurred significantly more often in patients with gastrocnemius vein dilation (GVD). A total of 410 (28%) of the study’s participants had GVTs, and the incidence of DVTs was significantly greater in individuals with GVD compared to those without such a symptom. GVD had a higher predictive power for postoperative DVT than did all of the other risk factors examined in univariate and multivariate analyses.
The vast majority of the DVTs diagnosed were isolated distal. While 94 patients suffered from this kind of DVT, the remaining 19 DVTs were proximal. According to Dr. Chen Kai of Wenzhou (China) Medical University, and colleagues, proximal DVTs were nearly always asymptomatic and a larger percentage of them took more time to disappear than did the distal DVTs. Within 6 months following anticoagulant therapy, 94.3% of the distal DVTs exhibited thrombus resolution and 55.6% of the proximal DVTs were thrombus free. None of the study’s participants had died because of DVT or pulmonary embolus during the 6 months following their surgeries.
This study’s “present data reflect a higher incidence of postoperative DVT than previous studies, and we also identify GVD as a significant risk factor. Larger prospective studies will be needed to evaluate this issue precisely and to understand the clinical relevance of these results,” wrote the researchers.Find the full study in Thombosis Research (doi: 10.1016/j.thromres.2015.03.008).
A retrospective study of patients who underwent varicose vein surgeries with a tourniquet found a greater incidence of deep vein thromboses (DVTs) than previous studies.
Within the first 3 postoperative days, 113 (7.7%) of the 1,461 patients had DVTs. The researchers also found that DVTs occurred significantly more often in patients with gastrocnemius vein dilation (GVD). A total of 410 (28%) of the study’s participants had GVTs, and the incidence of DVTs was significantly greater in individuals with GVD compared to those without such a symptom. GVD had a higher predictive power for postoperative DVT than did all of the other risk factors examined in univariate and multivariate analyses.
The vast majority of the DVTs diagnosed were isolated distal. While 94 patients suffered from this kind of DVT, the remaining 19 DVTs were proximal. According to Dr. Chen Kai of Wenzhou (China) Medical University, and colleagues, proximal DVTs were nearly always asymptomatic and a larger percentage of them took more time to disappear than did the distal DVTs. Within 6 months following anticoagulant therapy, 94.3% of the distal DVTs exhibited thrombus resolution and 55.6% of the proximal DVTs were thrombus free. None of the study’s participants had died because of DVT or pulmonary embolus during the 6 months following their surgeries.
This study’s “present data reflect a higher incidence of postoperative DVT than previous studies, and we also identify GVD as a significant risk factor. Larger prospective studies will be needed to evaluate this issue precisely and to understand the clinical relevance of these results,” wrote the researchers.Find the full study in Thombosis Research (doi: 10.1016/j.thromres.2015.03.008).
Are you a victim of the cognitive load theory?
My job recently changed to include some administrative responsibilities, so having done purely clinical work for my entire career as a physician, I thought it wise to begin broadening my horizons to learn how to best meet the new challenges ahead of me. Fortunately, not only was the Hospital Medicine 2015 conference just an hour’s drive away, it occurred just when I needed it most, within days of my taking on a new role.
Naturally, I opted for the Practice Management track this year since I will need a different skill set than I currently have. In the first session, called Case Studies in Improving Patient Experience, I learned about a patient named John, who had developed typical ischemic chest pain during a weekly tennis game with his wife. His doctors did everything right, or so they thought. They exceeded the national guidelines for each quality measure, including the time it took them to revascularize his blocked artery. John had no significant residual damage and within 2 weeks was back on the tennis courts.

But there had been a huge disconnect. His doctors practiced excellent medicine, yet John was displeased with his care. The hospital team had not communicated well with John during his hospital stay. A great success story seen through the eyes of his medical team was a great failure as seen through the eyes of John and his wife. The hospital team’s lack of communication trumped the fact that they had played a huge role in saving John’s life.
As a matter of fact, John and his wife were so distraught over their experience that they went to the hospital administration to express their concerns about how poorly they had been treated.
This story also was aired as part of a segment on National Public Radio. Some of the comments of listeners echoed the sentiments we hear often, such as “doctors don’t know how to communicate with patients” and “doctors don’t care.” While the former statement may be true in many cases, the latter couldn’t be further from the truth. We do care. Why else would we sacrifice so much of our lives to help others? There are certainly other careers that pay more than medicine, especially considering all the time and financial investment that go into becoming a physician.
So why is it that as intelligent as we are as a group, we often fall short of meeting the communication goals that are so important to our patients? Some believe – and I am one of them – that most physicians are examples of the cognitive load theory. Our brains are simply overloaded. This theory, developed by psychologist John Sweller in the 1980s, refers to the total amount of mental effort used in one’s working memory.
There are three types of cognitive load: intrinsic, extraneous, and germane. Intrinsic cognitive load refers to how much effort goes into a particular topic, and in the field of medicine, the complexity of the information we deal with is very high, as is our intrinsic load.
Extraneous cognitive load refers to how this information is presented to us. When the pager is incessantly beeping, a line of nurses is waiting to ask a question, you desperately need to get to the ED to admit a potential stroke patient, and you eye a family member anxiously pacing the hallway and waiting for a chance to speak with you, your brain is bombarded with a variety of complex issues coming in all directions. In short, your extraneous load is through the roof.
The germane cognitive load refers to the work you put into processing information and creating a permanent store of that knowledge, creating a schema, so to speak. For instance, after much experience, it has become relatively simple to classify a patient as having heart failure if he presents with bilateral leg edema, progressive shortness of breath, and crackles on exam.
Experience helps us with our germane cognitive load and sometimes we have little control over our intrinisic load, but there are many potential opportunities to organize our extraneous cognitive load into chunks that flow more seamlessly, make our workday run more smoothly, and free up mental energy and time to deal effectively with other important issues. We all have our personal preferences for how we like our workday to flow. Chances are, with a little creativity, we can have a significant impact on our own extraneous loads.
Getting back to John, he is just one of many patients who feel emotionally neglected, not respected, or not kept up to date regarding their statuses. Considering his doctors, they were probably overwhelmed with the load they were carrying; the responsibility for a life is something only medical professionals can fully grasp. I know there have been times when I too felt simply overwhelmed and unable to do every single thing that would have been good, but not crucial, to the goal of curing the patient. Had I managed my intrinisic load better, perhaps I would have been better equipped to spend more time talking to patients and their family members. I suspect I am not alone.
My job recently changed to include some administrative responsibilities, so having done purely clinical work for my entire career as a physician, I thought it wise to begin broadening my horizons to learn how to best meet the new challenges ahead of me. Fortunately, not only was the Hospital Medicine 2015 conference just an hour’s drive away, it occurred just when I needed it most, within days of my taking on a new role.
Naturally, I opted for the Practice Management track this year since I will need a different skill set than I currently have. In the first session, called Case Studies in Improving Patient Experience, I learned about a patient named John, who had developed typical ischemic chest pain during a weekly tennis game with his wife. His doctors did everything right, or so they thought. They exceeded the national guidelines for each quality measure, including the time it took them to revascularize his blocked artery. John had no significant residual damage and within 2 weeks was back on the tennis courts.
But there had been a huge disconnect. His doctors practiced excellent medicine, yet John was displeased with his care. The hospital team had not communicated well with John during his hospital stay. A great success story seen through the eyes of his medical team was a great failure as seen through the eyes of John and his wife. The hospital team’s lack of communication trumped the fact that they had played a huge role in saving John’s life.
As a matter of fact, John and his wife were so distraught over their experience that they went to the hospital administration to express their concerns about how poorly they had been treated.
This story also was aired as part of a segment on National Public Radio. Some of the comments of listeners echoed the sentiments we hear often, such as “doctors don’t know how to communicate with patients” and “doctors don’t care.” While the former statement may be true in many cases, the latter couldn’t be further from the truth. We do care. Why else would we sacrifice so much of our lives to help others? There are certainly other careers that pay more than medicine, especially considering all the time and financial investment that go into becoming a physician.
So why is it that as intelligent as we are as a group, we often fall short of meeting the communication goals that are so important to our patients? Some believe – and I am one of them – that most physicians are examples of the cognitive load theory. Our brains are simply overloaded. This theory, developed by psychologist John Sweller in the 1980s, refers to the total amount of mental effort used in one’s working memory.
There are three types of cognitive load: intrinsic, extraneous, and germane. Intrinsic cognitive load refers to how much effort goes into a particular topic, and in the field of medicine, the complexity of the information we deal with is very high, as is our intrinsic load.
Extraneous cognitive load refers to how this information is presented to us. When the pager is incessantly beeping, a line of nurses is waiting to ask a question, you desperately need to get to the ED to admit a potential stroke patient, and you eye a family member anxiously pacing the hallway and waiting for a chance to speak with you, your brain is bombarded with a variety of complex issues coming in all directions. In short, your extraneous load is through the roof.
The germane cognitive load refers to the work you put into processing information and creating a permanent store of that knowledge, creating a schema, so to speak. For instance, after much experience, it has become relatively simple to classify a patient as having heart failure if he presents with bilateral leg edema, progressive shortness of breath, and crackles on exam.
Experience helps us with our germane cognitive load and sometimes we have little control over our intrinisic load, but there are many potential opportunities to organize our extraneous cognitive load into chunks that flow more seamlessly, make our workday run more smoothly, and free up mental energy and time to deal effectively with other important issues. We all have our personal preferences for how we like our workday to flow. Chances are, with a little creativity, we can have a significant impact on our own extraneous loads.
Getting back to John, he is just one of many patients who feel emotionally neglected, not respected, or not kept up to date regarding their statuses. Considering his doctors, they were probably overwhelmed with the load they were carrying; the responsibility for a life is something only medical professionals can fully grasp. I know there have been times when I too felt simply overwhelmed and unable to do every single thing that would have been good, but not crucial, to the goal of curing the patient. Had I managed my intrinisic load better, perhaps I would have been better equipped to spend more time talking to patients and their family members. I suspect I am not alone.
My job recently changed to include some administrative responsibilities, so having done purely clinical work for my entire career as a physician, I thought it wise to begin broadening my horizons to learn how to best meet the new challenges ahead of me. Fortunately, not only was the Hospital Medicine 2015 conference just an hour’s drive away, it occurred just when I needed it most, within days of my taking on a new role.
Naturally, I opted for the Practice Management track this year since I will need a different skill set than I currently have. In the first session, called Case Studies in Improving Patient Experience, I learned about a patient named John, who had developed typical ischemic chest pain during a weekly tennis game with his wife. His doctors did everything right, or so they thought. They exceeded the national guidelines for each quality measure, including the time it took them to revascularize his blocked artery. John had no significant residual damage and within 2 weeks was back on the tennis courts.
But there had been a huge disconnect. His doctors practiced excellent medicine, yet John was displeased with his care. The hospital team had not communicated well with John during his hospital stay. A great success story seen through the eyes of his medical team was a great failure as seen through the eyes of John and his wife. The hospital team’s lack of communication trumped the fact that they had played a huge role in saving John’s life.
As a matter of fact, John and his wife were so distraught over their experience that they went to the hospital administration to express their concerns about how poorly they had been treated.
This story also was aired as part of a segment on National Public Radio. Some of the comments of listeners echoed the sentiments we hear often, such as “doctors don’t know how to communicate with patients” and “doctors don’t care.” While the former statement may be true in many cases, the latter couldn’t be further from the truth. We do care. Why else would we sacrifice so much of our lives to help others? There are certainly other careers that pay more than medicine, especially considering all the time and financial investment that go into becoming a physician.
So why is it that as intelligent as we are as a group, we often fall short of meeting the communication goals that are so important to our patients? Some believe – and I am one of them – that most physicians are examples of the cognitive load theory. Our brains are simply overloaded. This theory, developed by psychologist John Sweller in the 1980s, refers to the total amount of mental effort used in one’s working memory.
There are three types of cognitive load: intrinsic, extraneous, and germane. Intrinsic cognitive load refers to how much effort goes into a particular topic, and in the field of medicine, the complexity of the information we deal with is very high, as is our intrinsic load.
Extraneous cognitive load refers to how this information is presented to us. When the pager is incessantly beeping, a line of nurses is waiting to ask a question, you desperately need to get to the ED to admit a potential stroke patient, and you eye a family member anxiously pacing the hallway and waiting for a chance to speak with you, your brain is bombarded with a variety of complex issues coming in all directions. In short, your extraneous load is through the roof.
The germane cognitive load refers to the work you put into processing information and creating a permanent store of that knowledge, creating a schema, so to speak. For instance, after much experience, it has become relatively simple to classify a patient as having heart failure if he presents with bilateral leg edema, progressive shortness of breath, and crackles on exam.
Experience helps us with our germane cognitive load and sometimes we have little control over our intrinisic load, but there are many potential opportunities to organize our extraneous cognitive load into chunks that flow more seamlessly, make our workday run more smoothly, and free up mental energy and time to deal effectively with other important issues. We all have our personal preferences for how we like our workday to flow. Chances are, with a little creativity, we can have a significant impact on our own extraneous loads.
Getting back to John, he is just one of many patients who feel emotionally neglected, not respected, or not kept up to date regarding their statuses. Considering his doctors, they were probably overwhelmed with the load they were carrying; the responsibility for a life is something only medical professionals can fully grasp. I know there have been times when I too felt simply overwhelmed and unable to do every single thing that would have been good, but not crucial, to the goal of curing the patient. Had I managed my intrinisic load better, perhaps I would have been better equipped to spend more time talking to patients and their family members. I suspect I am not alone.

VTE with transient risk factors is being overtreated
After a first episode of venous thromboembolism, more than 40% of patients with transient risk factors underwent anticoagulation therapy for 12 months or longer – a duration at least four times longer than the period recommended in guidelines, said authors of a large prospective cohort study.
Patients with VTE associated with surgery had about a 0.7% risk/patient-year of recurrence after 3 months of anticoagulation therapy. Patients with transient nonsurgical risk factors had about a 4% risk/patient-year of VTE recurrence.
Further, these patients were more likely to have major bleeding events than recurrent VTEs and were more likely to die of a fatal bleed than from a recurrent pulmonary embolism. Additionally, 38% of major bleeds among patients with transient risk factors occurred during the first 3 months of anticoagulation therapy.
“Our data suggest that in real life, physicians appear to be more concerned about the risk of recurrent VTE after discontinuing therapy than about the risk of bleeding,” said Dr. Walter Ageno at the University of Insubria in Varese, Italy, and his associates. “Clinicians base their treatment decisions on individual risk stratification, taking into account the location of VTE and the presence of additional risk factors for recurrence and bleeding. However, before adequately validated clinical prediction rules become available, this approach may expose a substantial proportion of patients, in particular those with VTE secondary to transient risk factors, to a possibly unnecessary risk of bleeding.”
The American College of Chest Physicians recommends 3 months of anticoagulation therapy for patients with VTE secondary to surgery or a transient, nonsurgical risk factor, and extended (possibly indefinite) anticoagulation for patients with unprovoked VTE or VTE caused by cancer. To look at real-world practice, the researchers carried out a prospective cohort study of 6,944 VTE patients in Italy, Spain, and Belgium. In all, 32% of patients had transient risk factors, 41% had unprovoked VTE, and 27% had cancer (Thrombosis Res. 2015;135:666-72). After excluding patients who died within a year after VTE, 42% of patients with transient risk factors such as recent surgery, pregnancy, or prolonged travel were treated with anticoagulants for more than 12 months, the researchers reported. Significant predictors of extended anticoagulation treatment including being older than 65 years old, having chronic heart failure, pulmonary embolism at presentation, and recurrent VTE during anticoagulation, the researchers also reported. Patients who weighed less than 75 kg, had anemia, or had transient risk factors for VTE were less likely to undergo prolonged treatment than were other patients.
“There is still uncertainty among experts on the optimal duration of secondary prevention of VTE,” concluded the investigators. “This decision should be taken by balancing the risk of recurrence after stopping treatment with the risk of bleeding if treatment is continued.”
Adequately validated clinical prediction rules are needed to make those decisions, the researchers said. Until such tools are validated, a substantial proportion of patients with transiet and secondary risk factors for VTE may be exposed to a possibly unnecessary risk of bleeding, they concluded.
Sanofi Spain and Bayer Pharma AG funded the study. The investigators reported having no relevant conflicts of interest.
After a first episode of venous thromboembolism, more than 40% of patients with transient risk factors underwent anticoagulation therapy for 12 months or longer – a duration at least four times longer than the period recommended in guidelines, said authors of a large prospective cohort study.
Patients with VTE associated with surgery had about a 0.7% risk/patient-year of recurrence after 3 months of anticoagulation therapy. Patients with transient nonsurgical risk factors had about a 4% risk/patient-year of VTE recurrence.
Further, these patients were more likely to have major bleeding events than recurrent VTEs and were more likely to die of a fatal bleed than from a recurrent pulmonary embolism. Additionally, 38% of major bleeds among patients with transient risk factors occurred during the first 3 months of anticoagulation therapy.
“Our data suggest that in real life, physicians appear to be more concerned about the risk of recurrent VTE after discontinuing therapy than about the risk of bleeding,” said Dr. Walter Ageno at the University of Insubria in Varese, Italy, and his associates. “Clinicians base their treatment decisions on individual risk stratification, taking into account the location of VTE and the presence of additional risk factors for recurrence and bleeding. However, before adequately validated clinical prediction rules become available, this approach may expose a substantial proportion of patients, in particular those with VTE secondary to transient risk factors, to a possibly unnecessary risk of bleeding.”
The American College of Chest Physicians recommends 3 months of anticoagulation therapy for patients with VTE secondary to surgery or a transient, nonsurgical risk factor, and extended (possibly indefinite) anticoagulation for patients with unprovoked VTE or VTE caused by cancer. To look at real-world practice, the researchers carried out a prospective cohort study of 6,944 VTE patients in Italy, Spain, and Belgium. In all, 32% of patients had transient risk factors, 41% had unprovoked VTE, and 27% had cancer (Thrombosis Res. 2015;135:666-72). After excluding patients who died within a year after VTE, 42% of patients with transient risk factors such as recent surgery, pregnancy, or prolonged travel were treated with anticoagulants for more than 12 months, the researchers reported. Significant predictors of extended anticoagulation treatment including being older than 65 years old, having chronic heart failure, pulmonary embolism at presentation, and recurrent VTE during anticoagulation, the researchers also reported. Patients who weighed less than 75 kg, had anemia, or had transient risk factors for VTE were less likely to undergo prolonged treatment than were other patients.
“There is still uncertainty among experts on the optimal duration of secondary prevention of VTE,” concluded the investigators. “This decision should be taken by balancing the risk of recurrence after stopping treatment with the risk of bleeding if treatment is continued.”
Adequately validated clinical prediction rules are needed to make those decisions, the researchers said. Until such tools are validated, a substantial proportion of patients with transiet and secondary risk factors for VTE may be exposed to a possibly unnecessary risk of bleeding, they concluded.
Sanofi Spain and Bayer Pharma AG funded the study. The investigators reported having no relevant conflicts of interest.
After a first episode of venous thromboembolism, more than 40% of patients with transient risk factors underwent anticoagulation therapy for 12 months or longer – a duration at least four times longer than the period recommended in guidelines, said authors of a large prospective cohort study.
Patients with VTE associated with surgery had about a 0.7% risk/patient-year of recurrence after 3 months of anticoagulation therapy. Patients with transient nonsurgical risk factors had about a 4% risk/patient-year of VTE recurrence.
Further, these patients were more likely to have major bleeding events than recurrent VTEs and were more likely to die of a fatal bleed than from a recurrent pulmonary embolism. Additionally, 38% of major bleeds among patients with transient risk factors occurred during the first 3 months of anticoagulation therapy.
“Our data suggest that in real life, physicians appear to be more concerned about the risk of recurrent VTE after discontinuing therapy than about the risk of bleeding,” said Dr. Walter Ageno at the University of Insubria in Varese, Italy, and his associates. “Clinicians base their treatment decisions on individual risk stratification, taking into account the location of VTE and the presence of additional risk factors for recurrence and bleeding. However, before adequately validated clinical prediction rules become available, this approach may expose a substantial proportion of patients, in particular those with VTE secondary to transient risk factors, to a possibly unnecessary risk of bleeding.”
The American College of Chest Physicians recommends 3 months of anticoagulation therapy for patients with VTE secondary to surgery or a transient, nonsurgical risk factor, and extended (possibly indefinite) anticoagulation for patients with unprovoked VTE or VTE caused by cancer. To look at real-world practice, the researchers carried out a prospective cohort study of 6,944 VTE patients in Italy, Spain, and Belgium. In all, 32% of patients had transient risk factors, 41% had unprovoked VTE, and 27% had cancer (Thrombosis Res. 2015;135:666-72). After excluding patients who died within a year after VTE, 42% of patients with transient risk factors such as recent surgery, pregnancy, or prolonged travel were treated with anticoagulants for more than 12 months, the researchers reported. Significant predictors of extended anticoagulation treatment including being older than 65 years old, having chronic heart failure, pulmonary embolism at presentation, and recurrent VTE during anticoagulation, the researchers also reported. Patients who weighed less than 75 kg, had anemia, or had transient risk factors for VTE were less likely to undergo prolonged treatment than were other patients.
“There is still uncertainty among experts on the optimal duration of secondary prevention of VTE,” concluded the investigators. “This decision should be taken by balancing the risk of recurrence after stopping treatment with the risk of bleeding if treatment is continued.”
Adequately validated clinical prediction rules are needed to make those decisions, the researchers said. Until such tools are validated, a substantial proportion of patients with transiet and secondary risk factors for VTE may be exposed to a possibly unnecessary risk of bleeding, they concluded.
Sanofi Spain and Bayer Pharma AG funded the study. The investigators reported having no relevant conflicts of interest.
FROM THROMBOSIS RESEARCH
Key clinical point: After venous thromboembolism, patients with transient or removable risk factors for VTE often underwent unneeded, prolonged anticoagulation therapy.
Major finding: Of patients with transient VTE risk factors, 42% underwent anticoagulation therapy for 12 months or longer.
Data source: Prospective cohort study of 6,944 patients with VTE.
Disclosures: Sanofi Spain and Bayer Pharma AG funded the study. The investigators reported having no relevant conflicts of interest.