User login
Trichoepithelioma and Spiradenoma Collision Tumor
The coexistence of more than one cutaneous adnexal neoplasm in a single biopsy specimen is unusual and is most frequently recognized in the context of a nevus sebaceous or Brooke-Spiegler syndrome, an autosomal-dominant inherited disease characterized by cutaneous adnexal neoplasms, most commonly cylindromas and trichoepitheliomas.1-3 Brooke-Spiegler syndrome is caused by germline mutations in the cylindromatosis gene, CYLD, located on band 16q12; it functions as a tumor suppressor gene and has regulatory roles in development, immunity, and inflammation.1 Weyers et al3 first recognized the tendency for adnexal collision tumors to present in patients with Brooke-Spiegler syndrome; they reported a patient with Brooke-Spiegler syndrome with spiradenomas found in the immediate vicinity of trichoepitheliomas and in continuity with hair follicles.
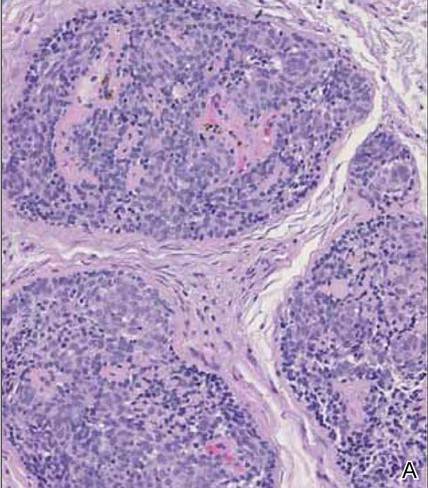
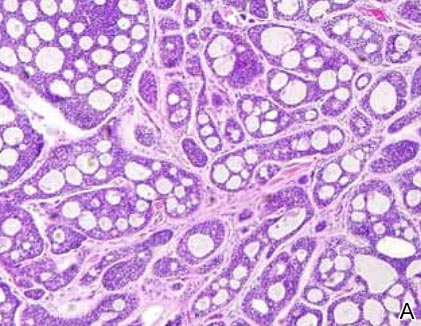
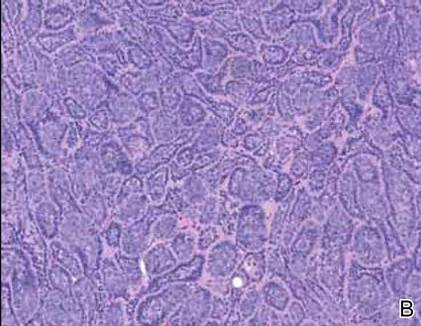
Spiradenomas are composed of large, sharply demarcated, rounded nodules of basaloid cells with little cytoplasm (Figure 1).4 The basaloid nodules may demonstrate a trabecular architecture, and on close inspection 2 cell types—paler cells with more cytoplasm and darker cells with less cytoplasm—are distinguishable (Figure 2A). Lymphocytes often are scattered within the tumor nodules and/or stroma. In Brooke-Spiegler syndrome, collision tumors containing a spiradenomatous component in collision with trichoepithelioma are not uncommon.1 Spiradenomas in Brooke-Spiegler syndrome have been reported to contain sebaceous differentiation or foci with an adenoid cystic carcinoma (ACC)–like pattern and are known to occur as hybrid lesions of spiradenoma and cylindroma or trichoepithelioma (as in this case).
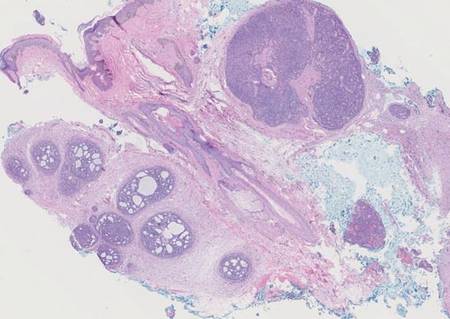
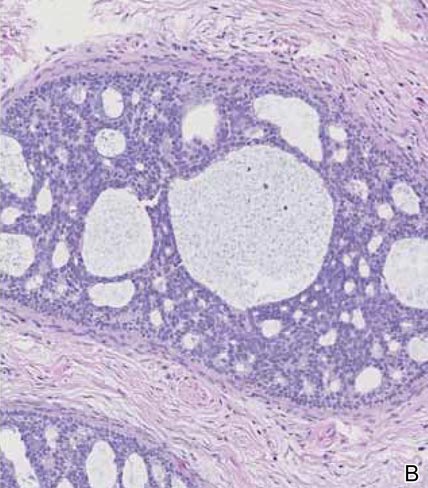
In this case, 2 distinct neoplasms (spiradenoma and trichoepithelioma) are apparent, side by side, with an intervening hair follicle (Figure 1). Trichoepitheliomas, also known as cribriform trichoblastomas,5 are characterized by lobules of basaloid cells resembling basal cell carcinoma surrounded by a fibroblast-rich stroma. They often contain fingerlike projections and adopt a cribriform morphology within the tumor lobules (Figure 2B).4 Numerous horn cysts may be present, but their absence does not preclude the diagnosis. Mucin may be present within the cribriform tumor islands (Figure 2B) but not in the stroma. Characteristically, trichoepitheliomas are distinctly negative for CK7 (Figure 3), and unlike spiradenomas, they lack a myoepithelial component.6 This staining pattern in combination with the tumor’s proximity to an adjacent hair follicle makes a diagnosis of trichoepithelioma and spiradenoma collision tumor most likely and supports a clinical suspicion for Brooke-Spiegler syndrome.
|
Although spiradenomas sometimes contain cystic cavities (microcystic change), they typically are filled with finely granular eosinophilic material, not mucin, that is diastase resistant and periodic acid–Schiff positive (Figure 4).7 Spiradenomas classically stain positive with CK7 (Figure 3), epithelial membrane antigen, and carcinoembryonic antigen, and have a substantial myoepithelial component, as evidenced by the myoepithelial component staining with p63, S-100, and smooth muscle actin (SMA).7-9 The distinct lack of staining with CK7 and SMA in the tumor on the left in Figure 3 confirms that these tumors are of different lineage, rather than representing cystic change within a spiradenoma.

| 
|
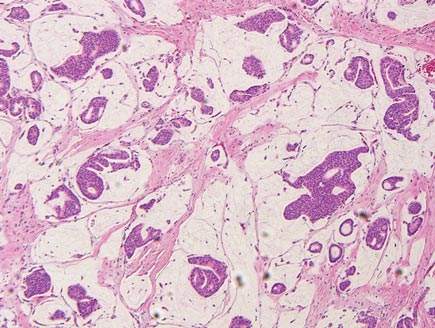
Adenoid cystic carcinoma is a rare neoplasm that may occur in a primary cutaneous form, as a direct extension from an underlying salivary gland neoplasm, or rarely as a focal pattern within spiradenomas occurring both sporadically or in the context of Brooke-Spiegler syndrome.2,7 The tumor is composed of variably sized cribriform islands of basaloid to pink cells concentrically arranged around glandlike spaces filled with mucin (Figure 5A). In contrast to trichoepithelioma, ACC occurs in the mid to deep dermis, often extending into subcutaneous fat with an infiltrative border, and is not often found in close proximity to hair follicles.7 Characteristically, hyaline basement membrane–like material that is periodic acid–Schiff positive is found between the tumor cells and also surrounding the individual lobules. Immunohistochemically, ACC has a myoepithelial component that stains positive with SMA, S-100, and p63; additionally, the tumor cells express low- and high-molecular-weight keratin and demonstrate variable epithelial membrane antigen positivity.10 In the current case, the superficial location, close association with a hair follicle, and lack of staining with both CK7 (Figure 3) and SMA (not shown) make ACC arising within a spiradenoma a less likely diagnosis.
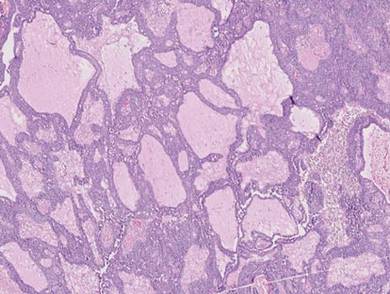
Cylindromas are composed of basaloid islands interconnected in a jigsaw puzzle configuration (Figure 5B).4 Similar to spiradenomas, they also are composed of 2 cell populations. Characteristically, the tumor islands are outlined by a hyalinized eosinophilic basement membrane. Hyalinized droplets of basement membrane zone material also may be noted in the islands. Unlike spiradenomas, they lack both intratumoral lymphocytes and a trabecular growth pattern. Although spiradenocylindromas (cylindroma and spiradenoma collision tumors) are perhaps the most common collision tumor associated with Brooke-Spiegler syndrome, there is no evidence suggesting the presence of a cylindroma in the current case.
|
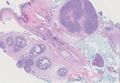
Primary cutaneous mucinous carcinoma is a rare neoplasm with a predilection for the eyelids; lesions occurring outside of this facial distribution, particularly of the breast, warrant a workup for metastatic disease.7 It typically occurs in the deeper dermis with involvement of the subcutaneous fat and is characterized by delicate fibrous septa enveloping large lakes of mucin, which contain islands of tumor cells (Figure 6). It has not been reported in association with spiradenomas. In addition, the tumor cells typically are CK7 positive.
1. Kazakov DV, Soukup R, Mukensnabl P, et al. Brooke-Spiegler syndrome: report of a case with combined lesions containing cylindromatous, spiradenomatous, trichoblastomatous, and sebaceous differentiation. Am J Dermatopathol. 2005;27:27-33.
2. Petersson F, Kutzner H, Spagnolo DV, et al. Adenoid cystic carcinoma-like pattern in spiradenoma and spiradenocylindroma: a rare feature in sporadic neoplasms and those associated with Brooke-Spiegler syndrome. Am J Dermatopathol. 2009;31:642-648.
3. Weyers W, Nilles M, Eckert F, et al. Spiradenomas in Brooke-Spiegler syndrome. Am J Dermatopathol. 1993;15:156-161.
4. Elston DM, Ferringer T. Dermatopathology. Edinburgh, Scotland: Elsevier Saunders; 2009.
5. Ackerman AB, de Viragh PA, Chongchitnant N. Neoplasms with Follicular Differentiation. Philadelphia, PA: Lea & Febiger; 1993.
6. Yamamoto O, Asahi M. Cytokeratin expression in trichoblastic fibroma (small nodular type trichoblastoma), trichoepithelioma and basal cell carcinoma. Br J Dermatol. 1999;140:8-16.
7. Calonje JE, Brenn T, Lazar AJ, et al. McKee’s Pathology of the Skin with Clinical Correlations. 4th ed. St Louis, MO: Elsevier Saunders; 2012.
8. Meybehm M, Fischer HP. Spiradenoma and dermal cylindroma: comparative immunohistochemical analysis and histogenetic considerations. Am J Dermatopathol. 1997;19:154-161.
9. Kurokawa I, Nishimura K, Tarumi C, et al. Eccrinespiradenoma: co-expression of cytokeratin and smooth muscle actin suggesting differentiation toward myoepithelial cells. J Eur Acad Dermatol Venereol. 2007;21:121-123.
10. Thompson LD, Penner C, Ho NJ, et al. Sinonasal tract and nasopharyngeal adenoid cystic carcinoma: a clinicopathologic and immunophenotypic study of 86 cases. Head Neck Pathol. 2014;8:88-109.
The coexistence of more than one cutaneous adnexal neoplasm in a single biopsy specimen is unusual and is most frequently recognized in the context of a nevus sebaceous or Brooke-Spiegler syndrome, an autosomal-dominant inherited disease characterized by cutaneous adnexal neoplasms, most commonly cylindromas and trichoepitheliomas.1-3 Brooke-Spiegler syndrome is caused by germline mutations in the cylindromatosis gene, CYLD, located on band 16q12; it functions as a tumor suppressor gene and has regulatory roles in development, immunity, and inflammation.1 Weyers et al3 first recognized the tendency for adnexal collision tumors to present in patients with Brooke-Spiegler syndrome; they reported a patient with Brooke-Spiegler syndrome with spiradenomas found in the immediate vicinity of trichoepitheliomas and in continuity with hair follicles.
Spiradenomas are composed of large, sharply demarcated, rounded nodules of basaloid cells with little cytoplasm (Figure 1).4 The basaloid nodules may demonstrate a trabecular architecture, and on close inspection 2 cell types—paler cells with more cytoplasm and darker cells with less cytoplasm—are distinguishable (Figure 2A). Lymphocytes often are scattered within the tumor nodules and/or stroma. In Brooke-Spiegler syndrome, collision tumors containing a spiradenomatous component in collision with trichoepithelioma are not uncommon.1 Spiradenomas in Brooke-Spiegler syndrome have been reported to contain sebaceous differentiation or foci with an adenoid cystic carcinoma (ACC)–like pattern and are known to occur as hybrid lesions of spiradenoma and cylindroma or trichoepithelioma (as in this case).
In this case, 2 distinct neoplasms (spiradenoma and trichoepithelioma) are apparent, side by side, with an intervening hair follicle (Figure 1). Trichoepitheliomas, also known as cribriform trichoblastomas,5 are characterized by lobules of basaloid cells resembling basal cell carcinoma surrounded by a fibroblast-rich stroma. They often contain fingerlike projections and adopt a cribriform morphology within the tumor lobules (Figure 2B).4 Numerous horn cysts may be present, but their absence does not preclude the diagnosis. Mucin may be present within the cribriform tumor islands (Figure 2B) but not in the stroma. Characteristically, trichoepitheliomas are distinctly negative for CK7 (Figure 3), and unlike spiradenomas, they lack a myoepithelial component.6 This staining pattern in combination with the tumor’s proximity to an adjacent hair follicle makes a diagnosis of trichoepithelioma and spiradenoma collision tumor most likely and supports a clinical suspicion for Brooke-Spiegler syndrome.
|
|
Although spiradenomas sometimes contain cystic cavities (microcystic change), they typically are filled with finely granular eosinophilic material, not mucin, that is diastase resistant and periodic acid–Schiff positive (Figure 4).7 Spiradenomas classically stain positive with CK7 (Figure 3), epithelial membrane antigen, and carcinoembryonic antigen, and have a substantial myoepithelial component, as evidenced by the myoepithelial component staining with p63, S-100, and smooth muscle actin (SMA).7-9 The distinct lack of staining with CK7 and SMA in the tumor on the left in Figure 3 confirms that these tumors are of different lineage, rather than representing cystic change within a spiradenoma.
|
|
|
Adenoid cystic carcinoma is a rare neoplasm that may occur in a primary cutaneous form, as a direct extension from an underlying salivary gland neoplasm, or rarely as a focal pattern within spiradenomas occurring both sporadically or in the context of Brooke-Spiegler syndrome.2,7 The tumor is composed of variably sized cribriform islands of basaloid to pink cells concentrically arranged around glandlike spaces filled with mucin (Figure 5A). In contrast to trichoepithelioma, ACC occurs in the mid to deep dermis, often extending into subcutaneous fat with an infiltrative border, and is not often found in close proximity to hair follicles.7 Characteristically, hyaline basement membrane–like material that is periodic acid–Schiff positive is found between the tumor cells and also surrounding the individual lobules. Immunohistochemically, ACC has a myoepithelial component that stains positive with SMA, S-100, and p63; additionally, the tumor cells express low- and high-molecular-weight keratin and demonstrate variable epithelial membrane antigen positivity.10 In the current case, the superficial location, close association with a hair follicle, and lack of staining with both CK7 (Figure 3) and SMA (not shown) make ACC arising within a spiradenoma a less likely diagnosis.
Cylindromas are composed of basaloid islands interconnected in a jigsaw puzzle configuration (Figure 5B).4 Similar to spiradenomas, they also are composed of 2 cell populations. Characteristically, the tumor islands are outlined by a hyalinized eosinophilic basement membrane. Hyalinized droplets of basement membrane zone material also may be noted in the islands. Unlike spiradenomas, they lack both intratumoral lymphocytes and a trabecular growth pattern. Although spiradenocylindromas (cylindroma and spiradenoma collision tumors) are perhaps the most common collision tumor associated with Brooke-Spiegler syndrome, there is no evidence suggesting the presence of a cylindroma in the current case.
|
|
Primary cutaneous mucinous carcinoma is a rare neoplasm with a predilection for the eyelids; lesions occurring outside of this facial distribution, particularly of the breast, warrant a workup for metastatic disease.7 It typically occurs in the deeper dermis with involvement of the subcutaneous fat and is characterized by delicate fibrous septa enveloping large lakes of mucin, which contain islands of tumor cells (Figure 6). It has not been reported in association with spiradenomas. In addition, the tumor cells typically are CK7 positive.
The coexistence of more than one cutaneous adnexal neoplasm in a single biopsy specimen is unusual and is most frequently recognized in the context of a nevus sebaceous or Brooke-Spiegler syndrome, an autosomal-dominant inherited disease characterized by cutaneous adnexal neoplasms, most commonly cylindromas and trichoepitheliomas.1-3 Brooke-Spiegler syndrome is caused by germline mutations in the cylindromatosis gene, CYLD, located on band 16q12; it functions as a tumor suppressor gene and has regulatory roles in development, immunity, and inflammation.1 Weyers et al3 first recognized the tendency for adnexal collision tumors to present in patients with Brooke-Spiegler syndrome; they reported a patient with Brooke-Spiegler syndrome with spiradenomas found in the immediate vicinity of trichoepitheliomas and in continuity with hair follicles.
Spiradenomas are composed of large, sharply demarcated, rounded nodules of basaloid cells with little cytoplasm (Figure 1).4 The basaloid nodules may demonstrate a trabecular architecture, and on close inspection 2 cell types—paler cells with more cytoplasm and darker cells with less cytoplasm—are distinguishable (Figure 2A). Lymphocytes often are scattered within the tumor nodules and/or stroma. In Brooke-Spiegler syndrome, collision tumors containing a spiradenomatous component in collision with trichoepithelioma are not uncommon.1 Spiradenomas in Brooke-Spiegler syndrome have been reported to contain sebaceous differentiation or foci with an adenoid cystic carcinoma (ACC)–like pattern and are known to occur as hybrid lesions of spiradenoma and cylindroma or trichoepithelioma (as in this case).
In this case, 2 distinct neoplasms (spiradenoma and trichoepithelioma) are apparent, side by side, with an intervening hair follicle (Figure 1). Trichoepitheliomas, also known as cribriform trichoblastomas,5 are characterized by lobules of basaloid cells resembling basal cell carcinoma surrounded by a fibroblast-rich stroma. They often contain fingerlike projections and adopt a cribriform morphology within the tumor lobules (Figure 2B).4 Numerous horn cysts may be present, but their absence does not preclude the diagnosis. Mucin may be present within the cribriform tumor islands (Figure 2B) but not in the stroma. Characteristically, trichoepitheliomas are distinctly negative for CK7 (Figure 3), and unlike spiradenomas, they lack a myoepithelial component.6 This staining pattern in combination with the tumor’s proximity to an adjacent hair follicle makes a diagnosis of trichoepithelioma and spiradenoma collision tumor most likely and supports a clinical suspicion for Brooke-Spiegler syndrome.
|
|
Although spiradenomas sometimes contain cystic cavities (microcystic change), they typically are filled with finely granular eosinophilic material, not mucin, that is diastase resistant and periodic acid–Schiff positive (Figure 4).7 Spiradenomas classically stain positive with CK7 (Figure 3), epithelial membrane antigen, and carcinoembryonic antigen, and have a substantial myoepithelial component, as evidenced by the myoepithelial component staining with p63, S-100, and smooth muscle actin (SMA).7-9 The distinct lack of staining with CK7 and SMA in the tumor on the left in Figure 3 confirms that these tumors are of different lineage, rather than representing cystic change within a spiradenoma.
|
|
|
Adenoid cystic carcinoma is a rare neoplasm that may occur in a primary cutaneous form, as a direct extension from an underlying salivary gland neoplasm, or rarely as a focal pattern within spiradenomas occurring both sporadically or in the context of Brooke-Spiegler syndrome.2,7 The tumor is composed of variably sized cribriform islands of basaloid to pink cells concentrically arranged around glandlike spaces filled with mucin (Figure 5A). In contrast to trichoepithelioma, ACC occurs in the mid to deep dermis, often extending into subcutaneous fat with an infiltrative border, and is not often found in close proximity to hair follicles.7 Characteristically, hyaline basement membrane–like material that is periodic acid–Schiff positive is found between the tumor cells and also surrounding the individual lobules. Immunohistochemically, ACC has a myoepithelial component that stains positive with SMA, S-100, and p63; additionally, the tumor cells express low- and high-molecular-weight keratin and demonstrate variable epithelial membrane antigen positivity.10 In the current case, the superficial location, close association with a hair follicle, and lack of staining with both CK7 (Figure 3) and SMA (not shown) make ACC arising within a spiradenoma a less likely diagnosis.
Cylindromas are composed of basaloid islands interconnected in a jigsaw puzzle configuration (Figure 5B).4 Similar to spiradenomas, they also are composed of 2 cell populations. Characteristically, the tumor islands are outlined by a hyalinized eosinophilic basement membrane. Hyalinized droplets of basement membrane zone material also may be noted in the islands. Unlike spiradenomas, they lack both intratumoral lymphocytes and a trabecular growth pattern. Although spiradenocylindromas (cylindroma and spiradenoma collision tumors) are perhaps the most common collision tumor associated with Brooke-Spiegler syndrome, there is no evidence suggesting the presence of a cylindroma in the current case.
|
|
Primary cutaneous mucinous carcinoma is a rare neoplasm with a predilection for the eyelids; lesions occurring outside of this facial distribution, particularly of the breast, warrant a workup for metastatic disease.7 It typically occurs in the deeper dermis with involvement of the subcutaneous fat and is characterized by delicate fibrous septa enveloping large lakes of mucin, which contain islands of tumor cells (Figure 6). It has not been reported in association with spiradenomas. In addition, the tumor cells typically are CK7 positive.
1. Kazakov DV, Soukup R, Mukensnabl P, et al. Brooke-Spiegler syndrome: report of a case with combined lesions containing cylindromatous, spiradenomatous, trichoblastomatous, and sebaceous differentiation. Am J Dermatopathol. 2005;27:27-33.
2. Petersson F, Kutzner H, Spagnolo DV, et al. Adenoid cystic carcinoma-like pattern in spiradenoma and spiradenocylindroma: a rare feature in sporadic neoplasms and those associated with Brooke-Spiegler syndrome. Am J Dermatopathol. 2009;31:642-648.
3. Weyers W, Nilles M, Eckert F, et al. Spiradenomas in Brooke-Spiegler syndrome. Am J Dermatopathol. 1993;15:156-161.
4. Elston DM, Ferringer T. Dermatopathology. Edinburgh, Scotland: Elsevier Saunders; 2009.
5. Ackerman AB, de Viragh PA, Chongchitnant N. Neoplasms with Follicular Differentiation. Philadelphia, PA: Lea & Febiger; 1993.
6. Yamamoto O, Asahi M. Cytokeratin expression in trichoblastic fibroma (small nodular type trichoblastoma), trichoepithelioma and basal cell carcinoma. Br J Dermatol. 1999;140:8-16.
7. Calonje JE, Brenn T, Lazar AJ, et al. McKee’s Pathology of the Skin with Clinical Correlations. 4th ed. St Louis, MO: Elsevier Saunders; 2012.
8. Meybehm M, Fischer HP. Spiradenoma and dermal cylindroma: comparative immunohistochemical analysis and histogenetic considerations. Am J Dermatopathol. 1997;19:154-161.
9. Kurokawa I, Nishimura K, Tarumi C, et al. Eccrinespiradenoma: co-expression of cytokeratin and smooth muscle actin suggesting differentiation toward myoepithelial cells. J Eur Acad Dermatol Venereol. 2007;21:121-123.
10. Thompson LD, Penner C, Ho NJ, et al. Sinonasal tract and nasopharyngeal adenoid cystic carcinoma: a clinicopathologic and immunophenotypic study of 86 cases. Head Neck Pathol. 2014;8:88-109.
1. Kazakov DV, Soukup R, Mukensnabl P, et al. Brooke-Spiegler syndrome: report of a case with combined lesions containing cylindromatous, spiradenomatous, trichoblastomatous, and sebaceous differentiation. Am J Dermatopathol. 2005;27:27-33.
2. Petersson F, Kutzner H, Spagnolo DV, et al. Adenoid cystic carcinoma-like pattern in spiradenoma and spiradenocylindroma: a rare feature in sporadic neoplasms and those associated with Brooke-Spiegler syndrome. Am J Dermatopathol. 2009;31:642-648.
3. Weyers W, Nilles M, Eckert F, et al. Spiradenomas in Brooke-Spiegler syndrome. Am J Dermatopathol. 1993;15:156-161.
4. Elston DM, Ferringer T. Dermatopathology. Edinburgh, Scotland: Elsevier Saunders; 2009.
5. Ackerman AB, de Viragh PA, Chongchitnant N. Neoplasms with Follicular Differentiation. Philadelphia, PA: Lea & Febiger; 1993.
6. Yamamoto O, Asahi M. Cytokeratin expression in trichoblastic fibroma (small nodular type trichoblastoma), trichoepithelioma and basal cell carcinoma. Br J Dermatol. 1999;140:8-16.
7. Calonje JE, Brenn T, Lazar AJ, et al. McKee’s Pathology of the Skin with Clinical Correlations. 4th ed. St Louis, MO: Elsevier Saunders; 2012.
8. Meybehm M, Fischer HP. Spiradenoma and dermal cylindroma: comparative immunohistochemical analysis and histogenetic considerations. Am J Dermatopathol. 1997;19:154-161.
9. Kurokawa I, Nishimura K, Tarumi C, et al. Eccrinespiradenoma: co-expression of cytokeratin and smooth muscle actin suggesting differentiation toward myoepithelial cells. J Eur Acad Dermatol Venereol. 2007;21:121-123.
10. Thompson LD, Penner C, Ho NJ, et al. Sinonasal tract and nasopharyngeal adenoid cystic carcinoma: a clinicopathologic and immunophenotypic study of 86 cases. Head Neck Pathol. 2014;8:88-109.
Lateral neck dissection morbidity high, but transient
CHICAGO – Lateral neck dissection for thyroid cancer is associated with significant early postoperative morbidity of 20%, even in the hands of experienced endocrine surgeons at a high-volume medical center.
Among 99 procedures, 20 patients had 26 complications, including surgical site infection in 10, chyle leak in 7, spinal accessory nerve dysfunction in 7, and seroma in 2.

Long-term complications were rare, however, occurring in just one patient with a spinal accessory nerve injury, Dr. Jason A. Glenn said at the annual meeting of the Central Surgical Association.
Using a prospectively collected thyroid database, the investigators reviewed 96 patients who underwent lateral neck dissection (LND) for suspicion of initial or recurrent lateral neck metastases by one of four experienced endocrine surgeons at the Medical College of Wisconsin in Milwaukee.
Three patients had reoperations during the study period of February 2009 and June 2014, resulting in 99 procedures and 198 lateral necks evaluated preoperatively. Most patients were women (73%) and their median age was 45 years.
LND was performed on 127 necks and metastatic disease was confirmed in 111 (87%). This included all 82 patients who had positive preoperative fine needle aspiration (FNA), 25 of 37 patients operated on without FNA, and 4 of 8 patients with a negative or nondiagnostic FNA, Dr. Glenn said.
The median number of lymph nodes excised was 22 (range 1-122), with a median of 3 (range 0-39) malignant nodes per lateral neck.
“FNA is an important adjunct in the preoperative evaluation, especially when it returns a positive result,” he said. “However, when FNA is negative, not available, or not performed, you really must consider the entire clinical picture, as 64% of these patients were found to have lymph node metastases in our study.”
Surgical drains were placed in 94% of the 127 lateral neck dissections and remained in place for a median of 6 days. The median length of stay was 1 day.
There was no association between drain duration and surgical site infection, although chyle leak was associated with a significantly longer median drain duration (12 days vs. 6 days; P value < .01), Dr. Glenn said.
Two of the seven patients with chyle leak, defined by drain output that was milky white and/or exceeded 1,000 cc in 24 hours, underwent reoperation with ligation of the cervical thoracic duct and fibrin sealant application. Both leaks resolved and patients were discharge on postoperative day 2.
“Surgical drains allow for early leak recognition and monitoring of leak resolution,” he said. “Most of these complications were diagnosed and managed on an outpatient basis, highlighting the importance of continuity of care between the inpatient and outpatient setting for the treatment of thyroid cancer.”
Discussant Janice L. Pasieka, head of general surgery and a clinical professor of surgery and oncology at the University of Calgary (Alberta), said the retrospective review is a very valuable contribution to the literature because of its comprehensive follow-up.
“Today, most patients with this type of procedure are discharged within the 23 hours, and as such, complications such as nerve palsies, chyle leaks, and surgical site infections are not apparent for the majority of patients during their hospital stay,” Dr. Pasieka said. “Many times, the true incidences are lost unless the patient re-presents to the health care system, thus introducing your bias of only those significant enough to require intervention.”
Dr. Glenn and his coauthors reported no financial disclosures.
CHICAGO – Lateral neck dissection for thyroid cancer is associated with significant early postoperative morbidity of 20%, even in the hands of experienced endocrine surgeons at a high-volume medical center.
Among 99 procedures, 20 patients had 26 complications, including surgical site infection in 10, chyle leak in 7, spinal accessory nerve dysfunction in 7, and seroma in 2.
Long-term complications were rare, however, occurring in just one patient with a spinal accessory nerve injury, Dr. Jason A. Glenn said at the annual meeting of the Central Surgical Association.
Using a prospectively collected thyroid database, the investigators reviewed 96 patients who underwent lateral neck dissection (LND) for suspicion of initial or recurrent lateral neck metastases by one of four experienced endocrine surgeons at the Medical College of Wisconsin in Milwaukee.
Three patients had reoperations during the study period of February 2009 and June 2014, resulting in 99 procedures and 198 lateral necks evaluated preoperatively. Most patients were women (73%) and their median age was 45 years.
LND was performed on 127 necks and metastatic disease was confirmed in 111 (87%). This included all 82 patients who had positive preoperative fine needle aspiration (FNA), 25 of 37 patients operated on without FNA, and 4 of 8 patients with a negative or nondiagnostic FNA, Dr. Glenn said.
The median number of lymph nodes excised was 22 (range 1-122), with a median of 3 (range 0-39) malignant nodes per lateral neck.
“FNA is an important adjunct in the preoperative evaluation, especially when it returns a positive result,” he said. “However, when FNA is negative, not available, or not performed, you really must consider the entire clinical picture, as 64% of these patients were found to have lymph node metastases in our study.”
Surgical drains were placed in 94% of the 127 lateral neck dissections and remained in place for a median of 6 days. The median length of stay was 1 day.
There was no association between drain duration and surgical site infection, although chyle leak was associated with a significantly longer median drain duration (12 days vs. 6 days; P value < .01), Dr. Glenn said.
Two of the seven patients with chyle leak, defined by drain output that was milky white and/or exceeded 1,000 cc in 24 hours, underwent reoperation with ligation of the cervical thoracic duct and fibrin sealant application. Both leaks resolved and patients were discharge on postoperative day 2.
“Surgical drains allow for early leak recognition and monitoring of leak resolution,” he said. “Most of these complications were diagnosed and managed on an outpatient basis, highlighting the importance of continuity of care between the inpatient and outpatient setting for the treatment of thyroid cancer.”
Discussant Janice L. Pasieka, head of general surgery and a clinical professor of surgery and oncology at the University of Calgary (Alberta), said the retrospective review is a very valuable contribution to the literature because of its comprehensive follow-up.
“Today, most patients with this type of procedure are discharged within the 23 hours, and as such, complications such as nerve palsies, chyle leaks, and surgical site infections are not apparent for the majority of patients during their hospital stay,” Dr. Pasieka said. “Many times, the true incidences are lost unless the patient re-presents to the health care system, thus introducing your bias of only those significant enough to require intervention.”
Dr. Glenn and his coauthors reported no financial disclosures.
CHICAGO – Lateral neck dissection for thyroid cancer is associated with significant early postoperative morbidity of 20%, even in the hands of experienced endocrine surgeons at a high-volume medical center.
Among 99 procedures, 20 patients had 26 complications, including surgical site infection in 10, chyle leak in 7, spinal accessory nerve dysfunction in 7, and seroma in 2.
Long-term complications were rare, however, occurring in just one patient with a spinal accessory nerve injury, Dr. Jason A. Glenn said at the annual meeting of the Central Surgical Association.
Using a prospectively collected thyroid database, the investigators reviewed 96 patients who underwent lateral neck dissection (LND) for suspicion of initial or recurrent lateral neck metastases by one of four experienced endocrine surgeons at the Medical College of Wisconsin in Milwaukee.
Three patients had reoperations during the study period of February 2009 and June 2014, resulting in 99 procedures and 198 lateral necks evaluated preoperatively. Most patients were women (73%) and their median age was 45 years.
LND was performed on 127 necks and metastatic disease was confirmed in 111 (87%). This included all 82 patients who had positive preoperative fine needle aspiration (FNA), 25 of 37 patients operated on without FNA, and 4 of 8 patients with a negative or nondiagnostic FNA, Dr. Glenn said.
The median number of lymph nodes excised was 22 (range 1-122), with a median of 3 (range 0-39) malignant nodes per lateral neck.
“FNA is an important adjunct in the preoperative evaluation, especially when it returns a positive result,” he said. “However, when FNA is negative, not available, or not performed, you really must consider the entire clinical picture, as 64% of these patients were found to have lymph node metastases in our study.”
Surgical drains were placed in 94% of the 127 lateral neck dissections and remained in place for a median of 6 days. The median length of stay was 1 day.
There was no association between drain duration and surgical site infection, although chyle leak was associated with a significantly longer median drain duration (12 days vs. 6 days; P value < .01), Dr. Glenn said.
Two of the seven patients with chyle leak, defined by drain output that was milky white and/or exceeded 1,000 cc in 24 hours, underwent reoperation with ligation of the cervical thoracic duct and fibrin sealant application. Both leaks resolved and patients were discharge on postoperative day 2.
“Surgical drains allow for early leak recognition and monitoring of leak resolution,” he said. “Most of these complications were diagnosed and managed on an outpatient basis, highlighting the importance of continuity of care between the inpatient and outpatient setting for the treatment of thyroid cancer.”
Discussant Janice L. Pasieka, head of general surgery and a clinical professor of surgery and oncology at the University of Calgary (Alberta), said the retrospective review is a very valuable contribution to the literature because of its comprehensive follow-up.
“Today, most patients with this type of procedure are discharged within the 23 hours, and as such, complications such as nerve palsies, chyle leaks, and surgical site infections are not apparent for the majority of patients during their hospital stay,” Dr. Pasieka said. “Many times, the true incidences are lost unless the patient re-presents to the health care system, thus introducing your bias of only those significant enough to require intervention.”
Dr. Glenn and his coauthors reported no financial disclosures.
AT THE ANNUAL MEETING OF THE CENTRAL SURGICAL ASSOCIATION
Key clinical point: Lateral neck dissections for thyroid cancer are associated with high early morbidity but few long-term complications.
Major finding: The overall complication rate was 20%, however, most were transient.
Data source: Retrospective observational series of 96 patients undergoing lateral neck dissection.
Disclosures: Dr. Glenn and his coauthors reported no financial disclosures.

A Ripple Effect of Groin Skin Issues
For several months, a 60-year-old woman has had a rash on the right side of her groin, which her primary care provider diagnosed as a “probable yeast infection.” The patient was given a prescription for nystatin cream; when this did not help, she was prescribed a combination clotrimazole/betamethasone cream. Initial signs of improvement prompted her to continue application daily.
However, although the original rash cleared, other skin changes occurred in the area. These alarmed the patient’s primary care provider, who observed them during a follow-up exam. In response, the patient requested a referral to dermatology.

EXAMINATION
The entire right crural area is bright red and shiny. Multiple blood vessels are seen coursing over the surface of the area. There is no edema, increased warmth, or tenderness on palpation.
Punch biopsy shows marked epidermal atrophy and fails to show any evidence of cellular atypia.
What is the diagnosis?
DISCUSSION
When the patient was advised to stop using the combination cream, the “new” problem resolved quickly and her skin returned to normal. Although the source of the original rash remains unknown, what is clear is that the prescribed steroid induced marked atrophy. This then became “the problem.”
The groin is particularly susceptible to these types of changes. Why? Three reasons are occlusion, thin skin, and hydration. Read on for further explanation!
Occlusion, intentional or not, is known to potentiate the effects of topical steroids. The nature of intertriginous skin (skin folds) is that it effectively occludes the medicated skin, magnifying positive and negative effects. This means that the steroid works better and faster, but it also makes atrophy more likely (and equally quick to develop). When steroids are used for sufficient duration in susceptible areas—groin, axillae, under the breasts—focal areas of epidermis can wither totally, leaving an actual hole in the skin through which subcutaneous fat can be seen.
Furthermore, intertriginous skin is inherently thin (as are eyelids, neck skin, and the face). As a result, it takes less time for these changes to develop. The groin is especially prone to this problem because well-hydrated skin facilitates better penetration of the steroid.
This situation would likely have been avoided if the patient had used the prescribed product for only a week or two. A better option might have been a prescription for a weaker steroid (eg, hydocortisone 2.5%), although even that can be problematic if the medication is used for an extended period.
Though not quite as effective, topical NSAID preparations (calcineurin inhibitors such as pimecrolimus and tacrolimus) cause no such problems. They can help to reduce steroid use—for example, the patient can apply the steroid every third day and the calcineurin inhibitor on the other days.
The vehicle (the base in which the steroid is mixed) matters as well. Steroid ointments are inherently “self-occlusive,” especially in intertriginous areas—a fact that calls for increased caution in their use.
The atrophic look seen in this patient’s groin could have had other causes, such as T-cell or B-cell lymphoma. These were effectively ruled out by the biopsy.
TAKE-HOME LEARNING POINTS
• Epidermal atrophy is especially common on intertriginous skin (skin folds).
• The stronger the steroid (classes 1 through 7, with 1 being the strongest), the faster the atrophy occurs.
• Occlusion—caused by opposing skin folds or by other material (eg, socks, plastic wrap)—potentiates the positive and negative effects of topical steroids.
• Thin, moist skin allows better penetration by topical steroids, making them work better but also making atrophy more likely.
• Calcineurin inhibitors (eg, tacrolimus or pimecrolimus) have no such adverse effects and can help to reduce overuse of topical steroids in susceptible areas.
For several months, a 60-year-old woman has had a rash on the right side of her groin, which her primary care provider diagnosed as a “probable yeast infection.” The patient was given a prescription for nystatin cream; when this did not help, she was prescribed a combination clotrimazole/betamethasone cream. Initial signs of improvement prompted her to continue application daily.
However, although the original rash cleared, other skin changes occurred in the area. These alarmed the patient’s primary care provider, who observed them during a follow-up exam. In response, the patient requested a referral to dermatology.
EXAMINATION
The entire right crural area is bright red and shiny. Multiple blood vessels are seen coursing over the surface of the area. There is no edema, increased warmth, or tenderness on palpation.
Punch biopsy shows marked epidermal atrophy and fails to show any evidence of cellular atypia.
What is the diagnosis?
DISCUSSION
When the patient was advised to stop using the combination cream, the “new” problem resolved quickly and her skin returned to normal. Although the source of the original rash remains unknown, what is clear is that the prescribed steroid induced marked atrophy. This then became “the problem.”
The groin is particularly susceptible to these types of changes. Why? Three reasons are occlusion, thin skin, and hydration. Read on for further explanation!
Occlusion, intentional or not, is known to potentiate the effects of topical steroids. The nature of intertriginous skin (skin folds) is that it effectively occludes the medicated skin, magnifying positive and negative effects. This means that the steroid works better and faster, but it also makes atrophy more likely (and equally quick to develop). When steroids are used for sufficient duration in susceptible areas—groin, axillae, under the breasts—focal areas of epidermis can wither totally, leaving an actual hole in the skin through which subcutaneous fat can be seen.
Furthermore, intertriginous skin is inherently thin (as are eyelids, neck skin, and the face). As a result, it takes less time for these changes to develop. The groin is especially prone to this problem because well-hydrated skin facilitates better penetration of the steroid.
This situation would likely have been avoided if the patient had used the prescribed product for only a week or two. A better option might have been a prescription for a weaker steroid (eg, hydocortisone 2.5%), although even that can be problematic if the medication is used for an extended period.
Though not quite as effective, topical NSAID preparations (calcineurin inhibitors such as pimecrolimus and tacrolimus) cause no such problems. They can help to reduce steroid use—for example, the patient can apply the steroid every third day and the calcineurin inhibitor on the other days.
The vehicle (the base in which the steroid is mixed) matters as well. Steroid ointments are inherently “self-occlusive,” especially in intertriginous areas—a fact that calls for increased caution in their use.
The atrophic look seen in this patient’s groin could have had other causes, such as T-cell or B-cell lymphoma. These were effectively ruled out by the biopsy.
TAKE-HOME LEARNING POINTS
• Epidermal atrophy is especially common on intertriginous skin (skin folds).
• The stronger the steroid (classes 1 through 7, with 1 being the strongest), the faster the atrophy occurs.
• Occlusion—caused by opposing skin folds or by other material (eg, socks, plastic wrap)—potentiates the positive and negative effects of topical steroids.
• Thin, moist skin allows better penetration by topical steroids, making them work better but also making atrophy more likely.
• Calcineurin inhibitors (eg, tacrolimus or pimecrolimus) have no such adverse effects and can help to reduce overuse of topical steroids in susceptible areas.
For several months, a 60-year-old woman has had a rash on the right side of her groin, which her primary care provider diagnosed as a “probable yeast infection.” The patient was given a prescription for nystatin cream; when this did not help, she was prescribed a combination clotrimazole/betamethasone cream. Initial signs of improvement prompted her to continue application daily.
However, although the original rash cleared, other skin changes occurred in the area. These alarmed the patient’s primary care provider, who observed them during a follow-up exam. In response, the patient requested a referral to dermatology.
EXAMINATION
The entire right crural area is bright red and shiny. Multiple blood vessels are seen coursing over the surface of the area. There is no edema, increased warmth, or tenderness on palpation.
Punch biopsy shows marked epidermal atrophy and fails to show any evidence of cellular atypia.
What is the diagnosis?
DISCUSSION
When the patient was advised to stop using the combination cream, the “new” problem resolved quickly and her skin returned to normal. Although the source of the original rash remains unknown, what is clear is that the prescribed steroid induced marked atrophy. This then became “the problem.”
The groin is particularly susceptible to these types of changes. Why? Three reasons are occlusion, thin skin, and hydration. Read on for further explanation!
Occlusion, intentional or not, is known to potentiate the effects of topical steroids. The nature of intertriginous skin (skin folds) is that it effectively occludes the medicated skin, magnifying positive and negative effects. This means that the steroid works better and faster, but it also makes atrophy more likely (and equally quick to develop). When steroids are used for sufficient duration in susceptible areas—groin, axillae, under the breasts—focal areas of epidermis can wither totally, leaving an actual hole in the skin through which subcutaneous fat can be seen.
Furthermore, intertriginous skin is inherently thin (as are eyelids, neck skin, and the face). As a result, it takes less time for these changes to develop. The groin is especially prone to this problem because well-hydrated skin facilitates better penetration of the steroid.
This situation would likely have been avoided if the patient had used the prescribed product for only a week or two. A better option might have been a prescription for a weaker steroid (eg, hydocortisone 2.5%), although even that can be problematic if the medication is used for an extended period.
Though not quite as effective, topical NSAID preparations (calcineurin inhibitors such as pimecrolimus and tacrolimus) cause no such problems. They can help to reduce steroid use—for example, the patient can apply the steroid every third day and the calcineurin inhibitor on the other days.
The vehicle (the base in which the steroid is mixed) matters as well. Steroid ointments are inherently “self-occlusive,” especially in intertriginous areas—a fact that calls for increased caution in their use.
The atrophic look seen in this patient’s groin could have had other causes, such as T-cell or B-cell lymphoma. These were effectively ruled out by the biopsy.
TAKE-HOME LEARNING POINTS
• Epidermal atrophy is especially common on intertriginous skin (skin folds).
• The stronger the steroid (classes 1 through 7, with 1 being the strongest), the faster the atrophy occurs.
• Occlusion—caused by opposing skin folds or by other material (eg, socks, plastic wrap)—potentiates the positive and negative effects of topical steroids.
• Thin, moist skin allows better penetration by topical steroids, making them work better but also making atrophy more likely.
• Calcineurin inhibitors (eg, tacrolimus or pimecrolimus) have no such adverse effects and can help to reduce overuse of topical steroids in susceptible areas.

Point/Counterpoint: Covered stent grafts vs. drug-eluting stents for treating long superficial femoral artery occlusions
Well, at least one thing is for sure – we would not have been having this discussion a mere 10 years ago.
I remained sheepishly silent for most of my early career as well-intentioned invasive and noninvasive specialists criticized the state of evidence supporting the legitimacy of endovascular interventions as a competitive strategy to manage infrainguinal peripheral arterial disease. Good data from well-controlled randomized clinical trials were not available to make a case for endovascular therapies.

Over the recent decade and a half, however, a number of contributing factors have influenced thinking and what we now consider standard of care for symptomatic disease of the superficial femoral artery (SFA). The proposal of an “endovascular first” interventional approach has evolved to a consensually agreed upon management strategy by all interested disciplines.
This did not occur on a whim. Rather, out of the shadows of relative ignorance there slowly emerged a welcomed accumulation of a large number of publications that detail the outcomes of a wide variety of randomized trials with a range of endovascular devices. This has allowed us to enter an era where valid comparisons between interventional therapies is not only possible, but allows us to more appropriately offer care to vascular patients with more nuanced strategies. These are strategies that recognize subtleties between subgroups of individuals stratified on the basis of patient demographics and lesion characteristics in a way not appreciated prior to the recent spate of endovascular device studies.
Thus, thanks to the dedication and hard work of many, we are now at a stage where we can have meaningful dialogues on a variety of endovascular topics, such as the one at hand, and proponents can argue their perspectives armed with objective evidence to support their positions. In this discussion regarding covered stent grafts and drug-eluting stents, we wish we had even more data.
Specifically, we are missing direct head-to-head comparisons between the two devices in patients with long SFA lesions. So, what do we know?
Here are some fundamental facts: The most commonly used covered stent graft for management of femoropopliteal occlusive disease is the Viabahn endoprosthesis (W. L. Gore and Associates, Flagstaff, Ariz.). The prosthesis is composed of a self-expanding nitinol stent framework and expanded polytetrafluoroethylene (ePTFE) graft with its surface lined with a coating of covalently bound heparin (Propaten bioactive surface).The only approved drug-eluting stent with significant safety and effectiveness data available is the Zilver PTX paclitaxel-eluting, self-expanding nitinol stent (Cook Medical Inc., Bloomington, Ind.).
Now in terms of the proposition, we need to discuss the meaning of the word “long” with reference to the SFA. Just what do we consider a long SFA lesion? I think all of us could agree that an arterial stenosis or occlusion of 6 cm or less is short. Lesions between 5 cm or 6 cm to 10 cm or 12 cm in length are moderately long, and disease greater than 10 cm or 12 cm is commonly characterized as long. Segments of disease greater than 20 cm long are typically considered very long or extremely long lesions from an endovascular interventional perspective.
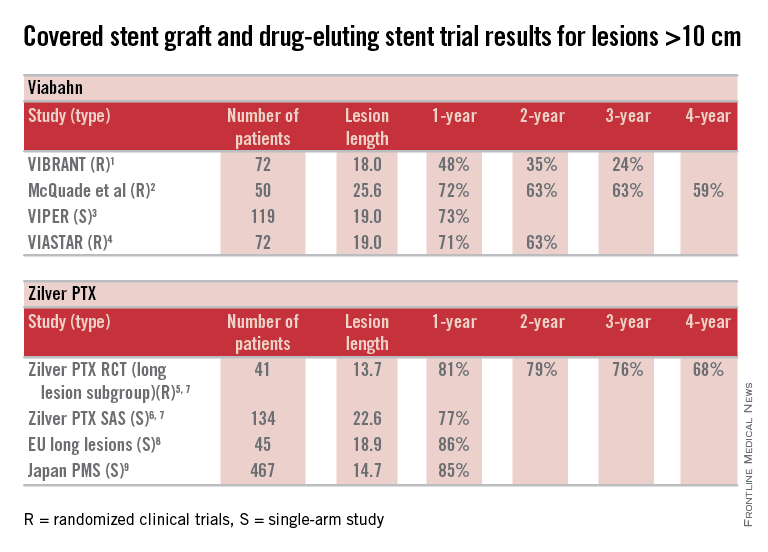
So, how can currently available trial outcomes help us? Below, I have compiled a table that includes most of the recent clinical trial data for Viabahn and Zilver PTX in patients with long SFA occlusive disease.
OK, what can we honestly say about these data besides recognizing that we are at risk when we make any conclusions based upon cross-trial comparisons? Such an accounting of results is fraught with problems, but what we can say is that the table grossly confirms the current consensus that both devices enhance the standard of care for long lesions over traditional balloon angioplasty (PTA) and bare metal stent technologies.
Beyond this, however, it is accepted that patency results with Viabahn are lesion-length immune – that is, outcomes in long and extremely long segments of disease are not very different from the patency achieved in short lesions. This is clearly different than what is traditionally found for interventions with PTA or bare metal stents. There is not enough controlled data for extremely long lesions to reach a conclusion on drug-eluting stents; however, there is an initial suggestion that they behave in a manner more similar to stent grafts than traditional devices.
Grossly, the table suggests that the midterm and available greater than 1-year patency results with Viabahn and Zilver PTX are relatively comparable. What about the price of the device? What role does it play in our selection of the current most cost-effective endovascular strategy for long SFA lesions?
In my institution Viabahn is more expensive than Zilver PTX with a relative cost premium of about 30%-50% depending on the treatment length. Of course, when treating long TASC C and D lesions any up-front difference in the costs of the devices used initially is more than made up for by any relative reduction in subsequent reinterventions.
So, there you have it. Look at the table as simply a current snapshot. In the future, we will benefit from additional trials and comparisons, not to mention better endovascular technologies to address symptomatic long SFA lesions.
Dr. Dake is the Thelma and Henry Doelger Professor of Cardiovascular Surgery at the Stanford (Calif.) School of Medicine. He disclosed that he is a member of the Peripheral Scientific Advisory Board: Abbott Vascular Member, is on the Aortic Medical Advisory Board: W. L. Gore, is a consultant for Cook Medical, Medtronic, and Surmodics Research, and receives grants/clinical trial support from W. L. Gore, Medtronic, and Novate.
References for table
1. J. Vasc. Surg. 2013;58:386-95.
2. J. Vasc. Surg. 2010;52:584-90.
3. J. Vasc. Interv. Radiol. 2013;24:165-73.
4. Cardiovasc. Interv. Radiol. 2015;38:25-32.
5. Circ. Cardiovasc. Interv. 2011;4:495-504.
6. J. Am. Coll. Cardiol. 2013;61:2417-27.
7. J. Endovasc. Ther. 2011;18:613-23.
8. Zeller T. Oral presentations. 2014.
9. Yokoi H. Oral presentations. 2014.
There remains a continued debate among investigators as to the best modality for treatment of stenosis/occlusion of the SFA especially with the recent advent of drug-eluting technology. However, I suggest that for long lesions over 15 cm only covered stent grafts continue to outperform the competition.

If we review the numerous studies available on treatment of SFA disease, the Viabahn-covered stent device (W. L. Gore & Associates, Flagstaff, Ariz.) is by far the most studied modality. There are currently 22 independent studies available providing data on 1,473 limbs. Several of these reports are multicenter studies and many of them are prospective randomized trials. Two of the most recent are the VIPER (J. Vasc. Intervent. Radiol. 2013;24:165-73) and VIASTAR study (JACC 2013;62:1320-27).
The VIPER study prospectively enrolled 119 patients (72 with TASC II C/D disease; mean lesion length 190 mm). Primary patency was reported at 73% at 1 year but in patients with less than 20% oversizing, as is recommended by the IFU, patency as high as 88% was noted. Additionally, there was no difference in patency in smaller-diameter vessels (5 mm) versus larger-diameter vessels (6-7 mm).
In a head-to-head randomized controlled trial of Viabahn to bare metal stents (BMS), the VIASTAR study enrolled 141 patients (72 in covered stent arm; mean lesion length 190 mm). On a per protocol evaluation, the patency at 1 year was 78% and 71% on an intention-to-treat evaluation with a patency of 70% and 63% respectively at 2 years. There was no statistical difference between the two evaluations on intention to treat vs. per protocol but there was clear superiority demonstrated against BMS.
Furthermore, in a prospective, randomized, head-to-head comparison of Viabahn to prosthetic above knee femoral popliteal bypass, it was shown that there was no difference in primary or secondary patency between the two groups out to 4 years follow-up (J. Vasc. Surg. 2010;52:584-91). This included an average lesion length of 25.6 cm with a primary and secondary patency of 59% and 74% in the Viabahn group and 58% and 71% in the surgery group. When compared to a large meta-analysis for femoral popliteal bypass outcomes reported on by Bates and AbuRahma in 2004 (J. Endovasc. Ther. 2004;11[suppl. II]:II-107–27), the patency for the surgical arm with prosthetic bypass in the above Viabahn study was similar at 4 years to the 38 peer-reviewed articles Bates et al. reviewed with over 4,000 limbs. The reported primary and secondary patency at 4 years for prosthetic femoral above knee popliteal bypass was 51% and 61%, respectively in his review. Although the above Viabahn study was not powered to formally demonstrate noninferiority to surgical bypass with prosthetic, it did strongly suggest and show just that.
How do we put these data together with the Zilver data and how do we decide what is best for our patients? Some operators have expressed concern over a perceived risk for a “higher rate of amputation” or “a worse Rutherford level of ischemia on presentation” if patients with the Viabahn stent graft occlude post procedure. Commonly, this results from extrapolation of prior studies looking at results of occlusion with an ePTFE bypass. In fact, review of peer-reviewed data reveal none of the prospective studies outlined above, or those currently available, demonstrate that either of these perceptions are true and there are no published prospective data that support these fears either. In the studies listed above as well as all current prospective studies available evaluating Viabahn usage, the highest rate of amputation reported was 5% by Fisher in 2006 with all of the remaining studies reporting an amputation rate of 2% or less (when reported). Moreover, it has not been demonstrated that patients with this device present with an increased level of ischemia secondary to sudden occlusion.
There is one report used to argue against the use of the Viabahn stent graft (J. Vasc. Surg. 2008;47:967-74). This study evaluated prospectively 109 patients (71 for claudication; 38 for critical limb ischemia) treated for SFA occlusive disease (mean lesion length 15.7 cm). Only 19 of the 109 patients (17%) were treated with Viabahn (17 for claudication; 2 for critical limb ischemia). The remaining limbs were treated with various other BMS devices (n=10). The authors concluded that patients initially treated with Viabahn who presented back with occlusion had a higher chance of presenting with acute symptoms (i.e., a worse Rutherford score). The lesion length treated in the Viabahn group, however, was nearly twice as long as all the other stent platforms combined (25.4 cm vs. 13.7 cm) and there was a higher level of tibial artery deterioration with thrombosis of the BMS group, compared with the Viabahn group (7.7% vs. 5.3%). The number of Viabahn patients presenting with acute thrombosis was not defined. With the small number of limbs treated in the Viabahn group, the conclusions expressed cannot be statistically supported.
What about the in-vogue DES device?
Dr. Dake and his colleagues recently presented 5-year data on the Zilver DES platform at VIVA 2014. He reported a primary patency at 5 years of 66.4% showing superiority to angioplasty alone as well as angioplasty with provisional stenting. This study enrolled 479 patients into the randomization arm and also had a registry arm that although often included in reporting of patency, does not stand up to the scrutiny of peer review. Even though there were some patients with longer lesions, the randomized arm mean lesion length was only 66 mm, which does not compare to the published longer mean lesion length of the Viabahn device. Bosiers et al. (J. Cardiovasc. Surg. 2013 54:115-222) reviewed 135 patients treated with the Zilver device (a subgroup derived from the 787 patients enrolled in the registry data of the Zilver trial) with a mean lesion length of 226 mm. They reported 77.6% primary patency but only at 1 year. Again, however, this is registry derived data and does not have the scientific validity of a randomized trial.
So what can I conclude from these experiences? We know today that covered stent grafts have been widely used and reported on, including by Dr. Dake himself (Radiology 2000 October;217:95-104) and all appear to have had similar conclusions.
The mean lesion length treated in these studies of Viabahn is often longer than 15 cm and nearly all studies report primary patency outcomes. Zilver supporters on the other hand are prone to quote TLR which is an inferior endpoint (as recently noted in an editorial by Dr. Russell Samson (Vasc. Spec. 2015;11:2). Costs of both devices are an issue but may vary by region and institution. However, Viabahn does have the advantage of longer devices, compared with the Zilver (15 and 25 cm vs. 10 cm) so fewer devices may be required to treat long lesions. Although short lesions may be better addressed with BMS or DES, for longer SFA lesions over 12-15 cm there are very few truly comparable data that argue against the use of Viabahn.
Dr. Gable is chief of vascular and endovascular surgery at The Heart Hospital Baylor Plano (Tex.). He is also an associate medical editor for Vascular Specialist. He disclosed that he is a consultant, speaker, and receives research support from W. L. Gore and Medtronic.
Well, at least one thing is for sure – we would not have been having this discussion a mere 10 years ago.
I remained sheepishly silent for most of my early career as well-intentioned invasive and noninvasive specialists criticized the state of evidence supporting the legitimacy of endovascular interventions as a competitive strategy to manage infrainguinal peripheral arterial disease. Good data from well-controlled randomized clinical trials were not available to make a case for endovascular therapies.
Over the recent decade and a half, however, a number of contributing factors have influenced thinking and what we now consider standard of care for symptomatic disease of the superficial femoral artery (SFA). The proposal of an “endovascular first” interventional approach has evolved to a consensually agreed upon management strategy by all interested disciplines.
This did not occur on a whim. Rather, out of the shadows of relative ignorance there slowly emerged a welcomed accumulation of a large number of publications that detail the outcomes of a wide variety of randomized trials with a range of endovascular devices. This has allowed us to enter an era where valid comparisons between interventional therapies is not only possible, but allows us to more appropriately offer care to vascular patients with more nuanced strategies. These are strategies that recognize subtleties between subgroups of individuals stratified on the basis of patient demographics and lesion characteristics in a way not appreciated prior to the recent spate of endovascular device studies.
Thus, thanks to the dedication and hard work of many, we are now at a stage where we can have meaningful dialogues on a variety of endovascular topics, such as the one at hand, and proponents can argue their perspectives armed with objective evidence to support their positions. In this discussion regarding covered stent grafts and drug-eluting stents, we wish we had even more data.
Specifically, we are missing direct head-to-head comparisons between the two devices in patients with long SFA lesions. So, what do we know?
Here are some fundamental facts: The most commonly used covered stent graft for management of femoropopliteal occlusive disease is the Viabahn endoprosthesis (W. L. Gore and Associates, Flagstaff, Ariz.). The prosthesis is composed of a self-expanding nitinol stent framework and expanded polytetrafluoroethylene (ePTFE) graft with its surface lined with a coating of covalently bound heparin (Propaten bioactive surface).The only approved drug-eluting stent with significant safety and effectiveness data available is the Zilver PTX paclitaxel-eluting, self-expanding nitinol stent (Cook Medical Inc., Bloomington, Ind.).
Now in terms of the proposition, we need to discuss the meaning of the word “long” with reference to the SFA. Just what do we consider a long SFA lesion? I think all of us could agree that an arterial stenosis or occlusion of 6 cm or less is short. Lesions between 5 cm or 6 cm to 10 cm or 12 cm in length are moderately long, and disease greater than 10 cm or 12 cm is commonly characterized as long. Segments of disease greater than 20 cm long are typically considered very long or extremely long lesions from an endovascular interventional perspective.
So, how can currently available trial outcomes help us? Below, I have compiled a table that includes most of the recent clinical trial data for Viabahn and Zilver PTX in patients with long SFA occlusive disease.
OK, what can we honestly say about these data besides recognizing that we are at risk when we make any conclusions based upon cross-trial comparisons? Such an accounting of results is fraught with problems, but what we can say is that the table grossly confirms the current consensus that both devices enhance the standard of care for long lesions over traditional balloon angioplasty (PTA) and bare metal stent technologies.
Beyond this, however, it is accepted that patency results with Viabahn are lesion-length immune – that is, outcomes in long and extremely long segments of disease are not very different from the patency achieved in short lesions. This is clearly different than what is traditionally found for interventions with PTA or bare metal stents. There is not enough controlled data for extremely long lesions to reach a conclusion on drug-eluting stents; however, there is an initial suggestion that they behave in a manner more similar to stent grafts than traditional devices.
Grossly, the table suggests that the midterm and available greater than 1-year patency results with Viabahn and Zilver PTX are relatively comparable. What about the price of the device? What role does it play in our selection of the current most cost-effective endovascular strategy for long SFA lesions?
In my institution Viabahn is more expensive than Zilver PTX with a relative cost premium of about 30%-50% depending on the treatment length. Of course, when treating long TASC C and D lesions any up-front difference in the costs of the devices used initially is more than made up for by any relative reduction in subsequent reinterventions.
So, there you have it. Look at the table as simply a current snapshot. In the future, we will benefit from additional trials and comparisons, not to mention better endovascular technologies to address symptomatic long SFA lesions.
Dr. Dake is the Thelma and Henry Doelger Professor of Cardiovascular Surgery at the Stanford (Calif.) School of Medicine. He disclosed that he is a member of the Peripheral Scientific Advisory Board: Abbott Vascular Member, is on the Aortic Medical Advisory Board: W. L. Gore, is a consultant for Cook Medical, Medtronic, and Surmodics Research, and receives grants/clinical trial support from W. L. Gore, Medtronic, and Novate.
References for table
1. J. Vasc. Surg. 2013;58:386-95.
2. J. Vasc. Surg. 2010;52:584-90.
3. J. Vasc. Interv. Radiol. 2013;24:165-73.
4. Cardiovasc. Interv. Radiol. 2015;38:25-32.
5. Circ. Cardiovasc. Interv. 2011;4:495-504.
6. J. Am. Coll. Cardiol. 2013;61:2417-27.
7. J. Endovasc. Ther. 2011;18:613-23.
8. Zeller T. Oral presentations. 2014.
9. Yokoi H. Oral presentations. 2014.
There remains a continued debate among investigators as to the best modality for treatment of stenosis/occlusion of the SFA especially with the recent advent of drug-eluting technology. However, I suggest that for long lesions over 15 cm only covered stent grafts continue to outperform the competition.
If we review the numerous studies available on treatment of SFA disease, the Viabahn-covered stent device (W. L. Gore & Associates, Flagstaff, Ariz.) is by far the most studied modality. There are currently 22 independent studies available providing data on 1,473 limbs. Several of these reports are multicenter studies and many of them are prospective randomized trials. Two of the most recent are the VIPER (J. Vasc. Intervent. Radiol. 2013;24:165-73) and VIASTAR study (JACC 2013;62:1320-27).
The VIPER study prospectively enrolled 119 patients (72 with TASC II C/D disease; mean lesion length 190 mm). Primary patency was reported at 73% at 1 year but in patients with less than 20% oversizing, as is recommended by the IFU, patency as high as 88% was noted. Additionally, there was no difference in patency in smaller-diameter vessels (5 mm) versus larger-diameter vessels (6-7 mm).
In a head-to-head randomized controlled trial of Viabahn to bare metal stents (BMS), the VIASTAR study enrolled 141 patients (72 in covered stent arm; mean lesion length 190 mm). On a per protocol evaluation, the patency at 1 year was 78% and 71% on an intention-to-treat evaluation with a patency of 70% and 63% respectively at 2 years. There was no statistical difference between the two evaluations on intention to treat vs. per protocol but there was clear superiority demonstrated against BMS.
Furthermore, in a prospective, randomized, head-to-head comparison of Viabahn to prosthetic above knee femoral popliteal bypass, it was shown that there was no difference in primary or secondary patency between the two groups out to 4 years follow-up (J. Vasc. Surg. 2010;52:584-91). This included an average lesion length of 25.6 cm with a primary and secondary patency of 59% and 74% in the Viabahn group and 58% and 71% in the surgery group. When compared to a large meta-analysis for femoral popliteal bypass outcomes reported on by Bates and AbuRahma in 2004 (J. Endovasc. Ther. 2004;11[suppl. II]:II-107–27), the patency for the surgical arm with prosthetic bypass in the above Viabahn study was similar at 4 years to the 38 peer-reviewed articles Bates et al. reviewed with over 4,000 limbs. The reported primary and secondary patency at 4 years for prosthetic femoral above knee popliteal bypass was 51% and 61%, respectively in his review. Although the above Viabahn study was not powered to formally demonstrate noninferiority to surgical bypass with prosthetic, it did strongly suggest and show just that.
How do we put these data together with the Zilver data and how do we decide what is best for our patients? Some operators have expressed concern over a perceived risk for a “higher rate of amputation” or “a worse Rutherford level of ischemia on presentation” if patients with the Viabahn stent graft occlude post procedure. Commonly, this results from extrapolation of prior studies looking at results of occlusion with an ePTFE bypass. In fact, review of peer-reviewed data reveal none of the prospective studies outlined above, or those currently available, demonstrate that either of these perceptions are true and there are no published prospective data that support these fears either. In the studies listed above as well as all current prospective studies available evaluating Viabahn usage, the highest rate of amputation reported was 5% by Fisher in 2006 with all of the remaining studies reporting an amputation rate of 2% or less (when reported). Moreover, it has not been demonstrated that patients with this device present with an increased level of ischemia secondary to sudden occlusion.
There is one report used to argue against the use of the Viabahn stent graft (J. Vasc. Surg. 2008;47:967-74). This study evaluated prospectively 109 patients (71 for claudication; 38 for critical limb ischemia) treated for SFA occlusive disease (mean lesion length 15.7 cm). Only 19 of the 109 patients (17%) were treated with Viabahn (17 for claudication; 2 for critical limb ischemia). The remaining limbs were treated with various other BMS devices (n=10). The authors concluded that patients initially treated with Viabahn who presented back with occlusion had a higher chance of presenting with acute symptoms (i.e., a worse Rutherford score). The lesion length treated in the Viabahn group, however, was nearly twice as long as all the other stent platforms combined (25.4 cm vs. 13.7 cm) and there was a higher level of tibial artery deterioration with thrombosis of the BMS group, compared with the Viabahn group (7.7% vs. 5.3%). The number of Viabahn patients presenting with acute thrombosis was not defined. With the small number of limbs treated in the Viabahn group, the conclusions expressed cannot be statistically supported.
What about the in-vogue DES device?
Dr. Dake and his colleagues recently presented 5-year data on the Zilver DES platform at VIVA 2014. He reported a primary patency at 5 years of 66.4% showing superiority to angioplasty alone as well as angioplasty with provisional stenting. This study enrolled 479 patients into the randomization arm and also had a registry arm that although often included in reporting of patency, does not stand up to the scrutiny of peer review. Even though there were some patients with longer lesions, the randomized arm mean lesion length was only 66 mm, which does not compare to the published longer mean lesion length of the Viabahn device. Bosiers et al. (J. Cardiovasc. Surg. 2013 54:115-222) reviewed 135 patients treated with the Zilver device (a subgroup derived from the 787 patients enrolled in the registry data of the Zilver trial) with a mean lesion length of 226 mm. They reported 77.6% primary patency but only at 1 year. Again, however, this is registry derived data and does not have the scientific validity of a randomized trial.
So what can I conclude from these experiences? We know today that covered stent grafts have been widely used and reported on, including by Dr. Dake himself (Radiology 2000 October;217:95-104) and all appear to have had similar conclusions.
The mean lesion length treated in these studies of Viabahn is often longer than 15 cm and nearly all studies report primary patency outcomes. Zilver supporters on the other hand are prone to quote TLR which is an inferior endpoint (as recently noted in an editorial by Dr. Russell Samson (Vasc. Spec. 2015;11:2). Costs of both devices are an issue but may vary by region and institution. However, Viabahn does have the advantage of longer devices, compared with the Zilver (15 and 25 cm vs. 10 cm) so fewer devices may be required to treat long lesions. Although short lesions may be better addressed with BMS or DES, for longer SFA lesions over 12-15 cm there are very few truly comparable data that argue against the use of Viabahn.
Dr. Gable is chief of vascular and endovascular surgery at The Heart Hospital Baylor Plano (Tex.). He is also an associate medical editor for Vascular Specialist. He disclosed that he is a consultant, speaker, and receives research support from W. L. Gore and Medtronic.
Well, at least one thing is for sure – we would not have been having this discussion a mere 10 years ago.
I remained sheepishly silent for most of my early career as well-intentioned invasive and noninvasive specialists criticized the state of evidence supporting the legitimacy of endovascular interventions as a competitive strategy to manage infrainguinal peripheral arterial disease. Good data from well-controlled randomized clinical trials were not available to make a case for endovascular therapies.
Over the recent decade and a half, however, a number of contributing factors have influenced thinking and what we now consider standard of care for symptomatic disease of the superficial femoral artery (SFA). The proposal of an “endovascular first” interventional approach has evolved to a consensually agreed upon management strategy by all interested disciplines.
This did not occur on a whim. Rather, out of the shadows of relative ignorance there slowly emerged a welcomed accumulation of a large number of publications that detail the outcomes of a wide variety of randomized trials with a range of endovascular devices. This has allowed us to enter an era where valid comparisons between interventional therapies is not only possible, but allows us to more appropriately offer care to vascular patients with more nuanced strategies. These are strategies that recognize subtleties between subgroups of individuals stratified on the basis of patient demographics and lesion characteristics in a way not appreciated prior to the recent spate of endovascular device studies.
Thus, thanks to the dedication and hard work of many, we are now at a stage where we can have meaningful dialogues on a variety of endovascular topics, such as the one at hand, and proponents can argue their perspectives armed with objective evidence to support their positions. In this discussion regarding covered stent grafts and drug-eluting stents, we wish we had even more data.
Specifically, we are missing direct head-to-head comparisons between the two devices in patients with long SFA lesions. So, what do we know?
Here are some fundamental facts: The most commonly used covered stent graft for management of femoropopliteal occlusive disease is the Viabahn endoprosthesis (W. L. Gore and Associates, Flagstaff, Ariz.). The prosthesis is composed of a self-expanding nitinol stent framework and expanded polytetrafluoroethylene (ePTFE) graft with its surface lined with a coating of covalently bound heparin (Propaten bioactive surface).The only approved drug-eluting stent with significant safety and effectiveness data available is the Zilver PTX paclitaxel-eluting, self-expanding nitinol stent (Cook Medical Inc., Bloomington, Ind.).
Now in terms of the proposition, we need to discuss the meaning of the word “long” with reference to the SFA. Just what do we consider a long SFA lesion? I think all of us could agree that an arterial stenosis or occlusion of 6 cm or less is short. Lesions between 5 cm or 6 cm to 10 cm or 12 cm in length are moderately long, and disease greater than 10 cm or 12 cm is commonly characterized as long. Segments of disease greater than 20 cm long are typically considered very long or extremely long lesions from an endovascular interventional perspective.
So, how can currently available trial outcomes help us? Below, I have compiled a table that includes most of the recent clinical trial data for Viabahn and Zilver PTX in patients with long SFA occlusive disease.
OK, what can we honestly say about these data besides recognizing that we are at risk when we make any conclusions based upon cross-trial comparisons? Such an accounting of results is fraught with problems, but what we can say is that the table grossly confirms the current consensus that both devices enhance the standard of care for long lesions over traditional balloon angioplasty (PTA) and bare metal stent technologies.
Beyond this, however, it is accepted that patency results with Viabahn are lesion-length immune – that is, outcomes in long and extremely long segments of disease are not very different from the patency achieved in short lesions. This is clearly different than what is traditionally found for interventions with PTA or bare metal stents. There is not enough controlled data for extremely long lesions to reach a conclusion on drug-eluting stents; however, there is an initial suggestion that they behave in a manner more similar to stent grafts than traditional devices.
Grossly, the table suggests that the midterm and available greater than 1-year patency results with Viabahn and Zilver PTX are relatively comparable. What about the price of the device? What role does it play in our selection of the current most cost-effective endovascular strategy for long SFA lesions?
In my institution Viabahn is more expensive than Zilver PTX with a relative cost premium of about 30%-50% depending on the treatment length. Of course, when treating long TASC C and D lesions any up-front difference in the costs of the devices used initially is more than made up for by any relative reduction in subsequent reinterventions.
So, there you have it. Look at the table as simply a current snapshot. In the future, we will benefit from additional trials and comparisons, not to mention better endovascular technologies to address symptomatic long SFA lesions.
Dr. Dake is the Thelma and Henry Doelger Professor of Cardiovascular Surgery at the Stanford (Calif.) School of Medicine. He disclosed that he is a member of the Peripheral Scientific Advisory Board: Abbott Vascular Member, is on the Aortic Medical Advisory Board: W. L. Gore, is a consultant for Cook Medical, Medtronic, and Surmodics Research, and receives grants/clinical trial support from W. L. Gore, Medtronic, and Novate.
References for table
1. J. Vasc. Surg. 2013;58:386-95.
2. J. Vasc. Surg. 2010;52:584-90.
3. J. Vasc. Interv. Radiol. 2013;24:165-73.
4. Cardiovasc. Interv. Radiol. 2015;38:25-32.
5. Circ. Cardiovasc. Interv. 2011;4:495-504.
6. J. Am. Coll. Cardiol. 2013;61:2417-27.
7. J. Endovasc. Ther. 2011;18:613-23.
8. Zeller T. Oral presentations. 2014.
9. Yokoi H. Oral presentations. 2014.
There remains a continued debate among investigators as to the best modality for treatment of stenosis/occlusion of the SFA especially with the recent advent of drug-eluting technology. However, I suggest that for long lesions over 15 cm only covered stent grafts continue to outperform the competition.
If we review the numerous studies available on treatment of SFA disease, the Viabahn-covered stent device (W. L. Gore & Associates, Flagstaff, Ariz.) is by far the most studied modality. There are currently 22 independent studies available providing data on 1,473 limbs. Several of these reports are multicenter studies and many of them are prospective randomized trials. Two of the most recent are the VIPER (J. Vasc. Intervent. Radiol. 2013;24:165-73) and VIASTAR study (JACC 2013;62:1320-27).
The VIPER study prospectively enrolled 119 patients (72 with TASC II C/D disease; mean lesion length 190 mm). Primary patency was reported at 73% at 1 year but in patients with less than 20% oversizing, as is recommended by the IFU, patency as high as 88% was noted. Additionally, there was no difference in patency in smaller-diameter vessels (5 mm) versus larger-diameter vessels (6-7 mm).
In a head-to-head randomized controlled trial of Viabahn to bare metal stents (BMS), the VIASTAR study enrolled 141 patients (72 in covered stent arm; mean lesion length 190 mm). On a per protocol evaluation, the patency at 1 year was 78% and 71% on an intention-to-treat evaluation with a patency of 70% and 63% respectively at 2 years. There was no statistical difference between the two evaluations on intention to treat vs. per protocol but there was clear superiority demonstrated against BMS.
Furthermore, in a prospective, randomized, head-to-head comparison of Viabahn to prosthetic above knee femoral popliteal bypass, it was shown that there was no difference in primary or secondary patency between the two groups out to 4 years follow-up (J. Vasc. Surg. 2010;52:584-91). This included an average lesion length of 25.6 cm with a primary and secondary patency of 59% and 74% in the Viabahn group and 58% and 71% in the surgery group. When compared to a large meta-analysis for femoral popliteal bypass outcomes reported on by Bates and AbuRahma in 2004 (J. Endovasc. Ther. 2004;11[suppl. II]:II-107–27), the patency for the surgical arm with prosthetic bypass in the above Viabahn study was similar at 4 years to the 38 peer-reviewed articles Bates et al. reviewed with over 4,000 limbs. The reported primary and secondary patency at 4 years for prosthetic femoral above knee popliteal bypass was 51% and 61%, respectively in his review. Although the above Viabahn study was not powered to formally demonstrate noninferiority to surgical bypass with prosthetic, it did strongly suggest and show just that.
How do we put these data together with the Zilver data and how do we decide what is best for our patients? Some operators have expressed concern over a perceived risk for a “higher rate of amputation” or “a worse Rutherford level of ischemia on presentation” if patients with the Viabahn stent graft occlude post procedure. Commonly, this results from extrapolation of prior studies looking at results of occlusion with an ePTFE bypass. In fact, review of peer-reviewed data reveal none of the prospective studies outlined above, or those currently available, demonstrate that either of these perceptions are true and there are no published prospective data that support these fears either. In the studies listed above as well as all current prospective studies available evaluating Viabahn usage, the highest rate of amputation reported was 5% by Fisher in 2006 with all of the remaining studies reporting an amputation rate of 2% or less (when reported). Moreover, it has not been demonstrated that patients with this device present with an increased level of ischemia secondary to sudden occlusion.
There is one report used to argue against the use of the Viabahn stent graft (J. Vasc. Surg. 2008;47:967-74). This study evaluated prospectively 109 patients (71 for claudication; 38 for critical limb ischemia) treated for SFA occlusive disease (mean lesion length 15.7 cm). Only 19 of the 109 patients (17%) were treated with Viabahn (17 for claudication; 2 for critical limb ischemia). The remaining limbs were treated with various other BMS devices (n=10). The authors concluded that patients initially treated with Viabahn who presented back with occlusion had a higher chance of presenting with acute symptoms (i.e., a worse Rutherford score). The lesion length treated in the Viabahn group, however, was nearly twice as long as all the other stent platforms combined (25.4 cm vs. 13.7 cm) and there was a higher level of tibial artery deterioration with thrombosis of the BMS group, compared with the Viabahn group (7.7% vs. 5.3%). The number of Viabahn patients presenting with acute thrombosis was not defined. With the small number of limbs treated in the Viabahn group, the conclusions expressed cannot be statistically supported.
What about the in-vogue DES device?
Dr. Dake and his colleagues recently presented 5-year data on the Zilver DES platform at VIVA 2014. He reported a primary patency at 5 years of 66.4% showing superiority to angioplasty alone as well as angioplasty with provisional stenting. This study enrolled 479 patients into the randomization arm and also had a registry arm that although often included in reporting of patency, does not stand up to the scrutiny of peer review. Even though there were some patients with longer lesions, the randomized arm mean lesion length was only 66 mm, which does not compare to the published longer mean lesion length of the Viabahn device. Bosiers et al. (J. Cardiovasc. Surg. 2013 54:115-222) reviewed 135 patients treated with the Zilver device (a subgroup derived from the 787 patients enrolled in the registry data of the Zilver trial) with a mean lesion length of 226 mm. They reported 77.6% primary patency but only at 1 year. Again, however, this is registry derived data and does not have the scientific validity of a randomized trial.
So what can I conclude from these experiences? We know today that covered stent grafts have been widely used and reported on, including by Dr. Dake himself (Radiology 2000 October;217:95-104) and all appear to have had similar conclusions.
The mean lesion length treated in these studies of Viabahn is often longer than 15 cm and nearly all studies report primary patency outcomes. Zilver supporters on the other hand are prone to quote TLR which is an inferior endpoint (as recently noted in an editorial by Dr. Russell Samson (Vasc. Spec. 2015;11:2). Costs of both devices are an issue but may vary by region and institution. However, Viabahn does have the advantage of longer devices, compared with the Zilver (15 and 25 cm vs. 10 cm) so fewer devices may be required to treat long lesions. Although short lesions may be better addressed with BMS or DES, for longer SFA lesions over 12-15 cm there are very few truly comparable data that argue against the use of Viabahn.
Dr. Gable is chief of vascular and endovascular surgery at The Heart Hospital Baylor Plano (Tex.). He is also an associate medical editor for Vascular Specialist. He disclosed that he is a consultant, speaker, and receives research support from W. L. Gore and Medtronic.

Hospital Management of Patients Presenting with ALTE: An Evidence-Based Approach
In a presentation on guidelines for ALTE, Jack Percelay, SHM representative to the AAP Subcommittee, provided further insight to the work that has been done for the clinical entity known as apparent life-threatening events (ALTE) since a consensus statement was put forward by the NIH in 1986. The original statement emphasized 4 possible features to constitute ALTE: apnea, color change, change in tone or gagging. The imprecise nature of the definition, along with both provider and caretaker anxiety related to the diagnosis, have lead to a cascade of diagnostic testing and treatments for what is a symptom complex, not a disease.
Subsequent work in the field has clarified that an ALTE is not a risk factor for SIDS. Of the myriad of etiologies that can cause an ALTE, many will have a readily identifiable etiology that a good history and physical exam will diagnose. Most other diseases, if not diagnosed at initial presentation, will become apparent subsequently without any significant consequences (for example epilepsy). Two diagnoses, which if missed, may have significant consequences include child abuse and a cardiac arrhythmia.
In an effort to synthesize new data along with expert opinion, the American Academy of Pediatrics has convened a Subcommittee on the Guideline for ALTE, lead by Joel Tieder, to develop a new practice guideline. This guideline is still in development with certain areas not ready for broad dissemination. The highlight of the new guideline will be a proposal for a name change for ALTEs. Dr Percelay reports the proposed new name would be BRUE (pronounced “brew”), Brief Resolved Unexplained Event. He anticipates further information to be published that will offer a framework to specify which infants to consider at low risk of recurrence versus higher risk for significant pathology. For those infants identified as low risk, the guideline will offer specific evaluation and treatment recommendations. An anticipated key point of the new guideline will be that a careful history and physical is the cornerstone of the initial evaluation and that in the absence of specific historical or exam findings, diagnostic testing of well-appearing infants is of low value.
In a presentation on guidelines for ALTE, Jack Percelay, SHM representative to the AAP Subcommittee, provided further insight to the work that has been done for the clinical entity known as apparent life-threatening events (ALTE) since a consensus statement was put forward by the NIH in 1986. The original statement emphasized 4 possible features to constitute ALTE: apnea, color change, change in tone or gagging. The imprecise nature of the definition, along with both provider and caretaker anxiety related to the diagnosis, have lead to a cascade of diagnostic testing and treatments for what is a symptom complex, not a disease.
Subsequent work in the field has clarified that an ALTE is not a risk factor for SIDS. Of the myriad of etiologies that can cause an ALTE, many will have a readily identifiable etiology that a good history and physical exam will diagnose. Most other diseases, if not diagnosed at initial presentation, will become apparent subsequently without any significant consequences (for example epilepsy). Two diagnoses, which if missed, may have significant consequences include child abuse and a cardiac arrhythmia.
In an effort to synthesize new data along with expert opinion, the American Academy of Pediatrics has convened a Subcommittee on the Guideline for ALTE, lead by Joel Tieder, to develop a new practice guideline. This guideline is still in development with certain areas not ready for broad dissemination. The highlight of the new guideline will be a proposal for a name change for ALTEs. Dr Percelay reports the proposed new name would be BRUE (pronounced “brew”), Brief Resolved Unexplained Event. He anticipates further information to be published that will offer a framework to specify which infants to consider at low risk of recurrence versus higher risk for significant pathology. For those infants identified as low risk, the guideline will offer specific evaluation and treatment recommendations. An anticipated key point of the new guideline will be that a careful history and physical is the cornerstone of the initial evaluation and that in the absence of specific historical or exam findings, diagnostic testing of well-appearing infants is of low value.
In a presentation on guidelines for ALTE, Jack Percelay, SHM representative to the AAP Subcommittee, provided further insight to the work that has been done for the clinical entity known as apparent life-threatening events (ALTE) since a consensus statement was put forward by the NIH in 1986. The original statement emphasized 4 possible features to constitute ALTE: apnea, color change, change in tone or gagging. The imprecise nature of the definition, along with both provider and caretaker anxiety related to the diagnosis, have lead to a cascade of diagnostic testing and treatments for what is a symptom complex, not a disease.
Subsequent work in the field has clarified that an ALTE is not a risk factor for SIDS. Of the myriad of etiologies that can cause an ALTE, many will have a readily identifiable etiology that a good history and physical exam will diagnose. Most other diseases, if not diagnosed at initial presentation, will become apparent subsequently without any significant consequences (for example epilepsy). Two diagnoses, which if missed, may have significant consequences include child abuse and a cardiac arrhythmia.
In an effort to synthesize new data along with expert opinion, the American Academy of Pediatrics has convened a Subcommittee on the Guideline for ALTE, lead by Joel Tieder, to develop a new practice guideline. This guideline is still in development with certain areas not ready for broad dissemination. The highlight of the new guideline will be a proposal for a name change for ALTEs. Dr Percelay reports the proposed new name would be BRUE (pronounced “brew”), Brief Resolved Unexplained Event. He anticipates further information to be published that will offer a framework to specify which infants to consider at low risk of recurrence versus higher risk for significant pathology. For those infants identified as low risk, the guideline will offer specific evaluation and treatment recommendations. An anticipated key point of the new guideline will be that a careful history and physical is the cornerstone of the initial evaluation and that in the absence of specific historical or exam findings, diagnostic testing of well-appearing infants is of low value.
Inhibitor gets orphan designation for DLBCL

The US Food and Drug Administration (FDA) has granted orphan drug designation to CUDC-907 for the treatment of diffuse large B-cell lymphoma (DLBCL).
CUDC-907 is an oral, dual inhibitor of histone deacetylase and phosphoinositide 3-kinase enzymes. It is currently under investigation in phase 1 trials in patients with relapsed or refractory lymphomas, multiple myeloma, and advanced/relapsed solid tumors.
The FDA grants orphan status to products intended for treating diseases that affect fewer than 200,000 people in the US. Orphan designation qualifies the drug’s developer—in this case, Curis, Inc.—with incentives such as tax credits for qualified trials, the ability to apply for annual grant funding, and 7 years of market exclusivity once the drug is approved.
Phase 1 data
At the 2013 ASH Annual Meeting, researchers presented interim data from a phase 1, dose-escalation trial of CUDC-907 in patients with advanced lymphoma or multiple myeloma.
Thirteen patients had received CUDC-907 on either once-daily (QD) or twice-weekly (BIW) schedules at doses of 30 mg QD (n=7), 60 mg QD (n=3), or 60 mg BIW (n=3).
Dose-limiting toxicities (DLTs) of grade 3 diarrhea and grade 4 hyperglycemia were reported in 1 patient at the 60 mg QD dose. The most frequent grade 3 or 4 adverse events reported in 2 or more patients included thrombocytopenia, diarrhea, and neutropenia. Tolerability limited the ability to further dose escalate using the QD schedule.
No DLTs or dose interruptions were reported for patients enrolled on the BIW schedule. So dose escalation is ongoing with the BIW schedule as well as a separate, thrice-weekly treatment schedule.
Of the 13 patients treated, 11 were evaluable for response. One patient with mixed follicular lymphoma/DLBCL achieved a partial response, with a 70% reduction in a single target lesion observed at the 30 mg QD dose level.
Seven other patients met criteria for stable disease, including 4 with stable disease lasting at least 4 cycles of treatment.
Following the ASH presentation, Curis reported additional data from a subset of patients that suggest CUDC-907 has antitumor activity in patients with DLBCL.
For the November 10, 2014, data cutoff period, 8 patients with DLBCL were evaluable. One of these patients had a complete response, 2 had a partial response (tumor shrinkage greater than 50%), and 4 had tumor shrinkage ranging from 5% to 46%.
The dose-escalation stage of the trial is nearing completion, and Curis expects to present full data this year. Curis has also initiated an expansion cohort to further evaluate CUDC-907 in patients with DLBCL or multiple myeloma at the recommended phase 2 dose. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to CUDC-907 for the treatment of diffuse large B-cell lymphoma (DLBCL).
CUDC-907 is an oral, dual inhibitor of histone deacetylase and phosphoinositide 3-kinase enzymes. It is currently under investigation in phase 1 trials in patients with relapsed or refractory lymphomas, multiple myeloma, and advanced/relapsed solid tumors.
The FDA grants orphan status to products intended for treating diseases that affect fewer than 200,000 people in the US. Orphan designation qualifies the drug’s developer—in this case, Curis, Inc.—with incentives such as tax credits for qualified trials, the ability to apply for annual grant funding, and 7 years of market exclusivity once the drug is approved.
Phase 1 data
At the 2013 ASH Annual Meeting, researchers presented interim data from a phase 1, dose-escalation trial of CUDC-907 in patients with advanced lymphoma or multiple myeloma.
Thirteen patients had received CUDC-907 on either once-daily (QD) or twice-weekly (BIW) schedules at doses of 30 mg QD (n=7), 60 mg QD (n=3), or 60 mg BIW (n=3).
Dose-limiting toxicities (DLTs) of grade 3 diarrhea and grade 4 hyperglycemia were reported in 1 patient at the 60 mg QD dose. The most frequent grade 3 or 4 adverse events reported in 2 or more patients included thrombocytopenia, diarrhea, and neutropenia. Tolerability limited the ability to further dose escalate using the QD schedule.
No DLTs or dose interruptions were reported for patients enrolled on the BIW schedule. So dose escalation is ongoing with the BIW schedule as well as a separate, thrice-weekly treatment schedule.
Of the 13 patients treated, 11 were evaluable for response. One patient with mixed follicular lymphoma/DLBCL achieved a partial response, with a 70% reduction in a single target lesion observed at the 30 mg QD dose level.
Seven other patients met criteria for stable disease, including 4 with stable disease lasting at least 4 cycles of treatment.
Following the ASH presentation, Curis reported additional data from a subset of patients that suggest CUDC-907 has antitumor activity in patients with DLBCL.
For the November 10, 2014, data cutoff period, 8 patients with DLBCL were evaluable. One of these patients had a complete response, 2 had a partial response (tumor shrinkage greater than 50%), and 4 had tumor shrinkage ranging from 5% to 46%.
The dose-escalation stage of the trial is nearing completion, and Curis expects to present full data this year. Curis has also initiated an expansion cohort to further evaluate CUDC-907 in patients with DLBCL or multiple myeloma at the recommended phase 2 dose. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to CUDC-907 for the treatment of diffuse large B-cell lymphoma (DLBCL).
CUDC-907 is an oral, dual inhibitor of histone deacetylase and phosphoinositide 3-kinase enzymes. It is currently under investigation in phase 1 trials in patients with relapsed or refractory lymphomas, multiple myeloma, and advanced/relapsed solid tumors.
The FDA grants orphan status to products intended for treating diseases that affect fewer than 200,000 people in the US. Orphan designation qualifies the drug’s developer—in this case, Curis, Inc.—with incentives such as tax credits for qualified trials, the ability to apply for annual grant funding, and 7 years of market exclusivity once the drug is approved.
Phase 1 data
At the 2013 ASH Annual Meeting, researchers presented interim data from a phase 1, dose-escalation trial of CUDC-907 in patients with advanced lymphoma or multiple myeloma.
Thirteen patients had received CUDC-907 on either once-daily (QD) or twice-weekly (BIW) schedules at doses of 30 mg QD (n=7), 60 mg QD (n=3), or 60 mg BIW (n=3).
Dose-limiting toxicities (DLTs) of grade 3 diarrhea and grade 4 hyperglycemia were reported in 1 patient at the 60 mg QD dose. The most frequent grade 3 or 4 adverse events reported in 2 or more patients included thrombocytopenia, diarrhea, and neutropenia. Tolerability limited the ability to further dose escalate using the QD schedule.
No DLTs or dose interruptions were reported for patients enrolled on the BIW schedule. So dose escalation is ongoing with the BIW schedule as well as a separate, thrice-weekly treatment schedule.
Of the 13 patients treated, 11 were evaluable for response. One patient with mixed follicular lymphoma/DLBCL achieved a partial response, with a 70% reduction in a single target lesion observed at the 30 mg QD dose level.
Seven other patients met criteria for stable disease, including 4 with stable disease lasting at least 4 cycles of treatment.
Following the ASH presentation, Curis reported additional data from a subset of patients that suggest CUDC-907 has antitumor activity in patients with DLBCL.
For the November 10, 2014, data cutoff period, 8 patients with DLBCL were evaluable. One of these patients had a complete response, 2 had a partial response (tumor shrinkage greater than 50%), and 4 had tumor shrinkage ranging from 5% to 46%.
The dose-escalation stage of the trial is nearing completion, and Curis expects to present full data this year. Curis has also initiated an expansion cohort to further evaluate CUDC-907 in patients with DLBCL or multiple myeloma at the recommended phase 2 dose. ![]()
Blood products can transmit food allergies
![]()
In rare cases, children can develop allergies to previously tolerated foods after receiving blood products via transfusion, according to a case study published in Canadian Medical Association Journal.
“It is very unusual to identify someone who experienced passive transfer of allergy from blood products,” said study author Julia Upton, MD, of The Hospital for Sick Children in Toronto, Ontario, Canada.
“Importantly, this condition has an excellent prognosis and typically resolves within a few months.”
Dr Upton and her colleagues found that blood donors who have food allergies can transfer immunoglobulin E, an antibody that reacts against allergens, from blood products such as platelets, although this is rare.
The researchers said it is important for parents and physicians to be aware of this event in case children have anaphylactic reactions after receiving blood products, particularly after eating peanuts, tree nuts, and fish, foods they could previously consume without reaction.
These reactions—with symptoms such as facial swelling, throat discomfort, or sudden fatigue—should be treated immediately at an emergency department.
When there is passive transfer of allergies after blood transfusion, physicians should follow up with the family after a few months to decide the timing of careful reintroduction of the temporary allergens into a child’s diet.
Physicians should report suspected cases of passive transfer of allergies to the hospital’s transfusion service to investigate the cause and ensure the safety of the country’s blood supply. ![]()
![]()
In rare cases, children can develop allergies to previously tolerated foods after receiving blood products via transfusion, according to a case study published in Canadian Medical Association Journal.
“It is very unusual to identify someone who experienced passive transfer of allergy from blood products,” said study author Julia Upton, MD, of The Hospital for Sick Children in Toronto, Ontario, Canada.
“Importantly, this condition has an excellent prognosis and typically resolves within a few months.”
Dr Upton and her colleagues found that blood donors who have food allergies can transfer immunoglobulin E, an antibody that reacts against allergens, from blood products such as platelets, although this is rare.
The researchers said it is important for parents and physicians to be aware of this event in case children have anaphylactic reactions after receiving blood products, particularly after eating peanuts, tree nuts, and fish, foods they could previously consume without reaction.
These reactions—with symptoms such as facial swelling, throat discomfort, or sudden fatigue—should be treated immediately at an emergency department.
When there is passive transfer of allergies after blood transfusion, physicians should follow up with the family after a few months to decide the timing of careful reintroduction of the temporary allergens into a child’s diet.
Physicians should report suspected cases of passive transfer of allergies to the hospital’s transfusion service to investigate the cause and ensure the safety of the country’s blood supply. ![]()
![]()
In rare cases, children can develop allergies to previously tolerated foods after receiving blood products via transfusion, according to a case study published in Canadian Medical Association Journal.
“It is very unusual to identify someone who experienced passive transfer of allergy from blood products,” said study author Julia Upton, MD, of The Hospital for Sick Children in Toronto, Ontario, Canada.
“Importantly, this condition has an excellent prognosis and typically resolves within a few months.”
Dr Upton and her colleagues found that blood donors who have food allergies can transfer immunoglobulin E, an antibody that reacts against allergens, from blood products such as platelets, although this is rare.
The researchers said it is important for parents and physicians to be aware of this event in case children have anaphylactic reactions after receiving blood products, particularly after eating peanuts, tree nuts, and fish, foods they could previously consume without reaction.
These reactions—with symptoms such as facial swelling, throat discomfort, or sudden fatigue—should be treated immediately at an emergency department.
When there is passive transfer of allergies after blood transfusion, physicians should follow up with the family after a few months to decide the timing of careful reintroduction of the temporary allergens into a child’s diet.
Physicians should report suspected cases of passive transfer of allergies to the hospital’s transfusion service to investigate the cause and ensure the safety of the country’s blood supply. ![]()
SHM, IPC Healthcare Launch Hospitalist-Focused, Post–Acute-Care Educational Program
Hospitalists practicing in post–acute-care facilities have a new resource via an SHM partnership.
The society and IPC Healthcare of North Hollywood, Calif., debuted at the "Primer for Hospitalists on Skilled Nursing Facilities" at 2015 annual meeting.
The educational program, housed at SHM's Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post–acute-care facilities. Lessons are grouped into five sections and two modules, with a focus on skilled-nursing facilities (SNFs), the most common post–acute-care settings.
"The types of resources that are available are different, and that's not only in terms of staff, but the availability of specialists, the availability of testing capabilities," says Joseph Miller, SHM's senior vice president for practice management.
"If you need to work with a cardiologist for a particular patient…how do you engage them?" Miller adds. "You're not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?"
Miller says that some 30% of hospitalist groups are practicing in post-acute settings, with the number only expected to rise. That's why SHM partnered with IPC to adapt and supplement that firm's post–acute-care program.
In addition, the rise of bundled payments and other reimbursement plans that include the post-discharge period also make now the right time for SHM to help provide educational resources, he adds.
Miller compared hospitalists to football quarterbacks, coordinating patient care as part of a team. Historically their focus has only been on care within the four walls of the hospital. But this is changing.
“Discharging a patient is like throwing a football pass," Miller says. “Today you don’t pay much attention to the receiver—whether he catches the ball or not. In the future, hospitalists will need to be concerned with completing the pass and scoring a touchdown.”
Visit our website for more on post-acute care.
Hospitalists practicing in post–acute-care facilities have a new resource via an SHM partnership.
The society and IPC Healthcare of North Hollywood, Calif., debuted at the "Primer for Hospitalists on Skilled Nursing Facilities" at 2015 annual meeting.
The educational program, housed at SHM's Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post–acute-care facilities. Lessons are grouped into five sections and two modules, with a focus on skilled-nursing facilities (SNFs), the most common post–acute-care settings.
"The types of resources that are available are different, and that's not only in terms of staff, but the availability of specialists, the availability of testing capabilities," says Joseph Miller, SHM's senior vice president for practice management.
"If you need to work with a cardiologist for a particular patient…how do you engage them?" Miller adds. "You're not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?"
Miller says that some 30% of hospitalist groups are practicing in post-acute settings, with the number only expected to rise. That's why SHM partnered with IPC to adapt and supplement that firm's post–acute-care program.
In addition, the rise of bundled payments and other reimbursement plans that include the post-discharge period also make now the right time for SHM to help provide educational resources, he adds.
Miller compared hospitalists to football quarterbacks, coordinating patient care as part of a team. Historically their focus has only been on care within the four walls of the hospital. But this is changing.
“Discharging a patient is like throwing a football pass," Miller says. “Today you don’t pay much attention to the receiver—whether he catches the ball or not. In the future, hospitalists will need to be concerned with completing the pass and scoring a touchdown.”
Visit our website for more on post-acute care.
Hospitalists practicing in post–acute-care facilities have a new resource via an SHM partnership.
The society and IPC Healthcare of North Hollywood, Calif., debuted at the "Primer for Hospitalists on Skilled Nursing Facilities" at 2015 annual meeting.
The educational program, housed at SHM's Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post–acute-care facilities. Lessons are grouped into five sections and two modules, with a focus on skilled-nursing facilities (SNFs), the most common post–acute-care settings.
"The types of resources that are available are different, and that's not only in terms of staff, but the availability of specialists, the availability of testing capabilities," says Joseph Miller, SHM's senior vice president for practice management.
"If you need to work with a cardiologist for a particular patient…how do you engage them?" Miller adds. "You're not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?"
Miller says that some 30% of hospitalist groups are practicing in post-acute settings, with the number only expected to rise. That's why SHM partnered with IPC to adapt and supplement that firm's post–acute-care program.
In addition, the rise of bundled payments and other reimbursement plans that include the post-discharge period also make now the right time for SHM to help provide educational resources, he adds.
Miller compared hospitalists to football quarterbacks, coordinating patient care as part of a team. Historically their focus has only been on care within the four walls of the hospital. But this is changing.
“Discharging a patient is like throwing a football pass," Miller says. “Today you don’t pay much attention to the receiver—whether he catches the ball or not. In the future, hospitalists will need to be concerned with completing the pass and scoring a touchdown.”
Visit our website for more on post-acute care.
Disparities in National Hospital Ratings Systems Produce No Clear Winners, Losers
A recent study found different approaches used by four popular hospital ratings systems resulted in disagreement about the ranking of many U.S. hospitals.
"Only 10% of hospitals that were rated as a high performer on one of the systems were rated as a high performer on another rating system," says lead author John Matthew Austin, MS, PhD, assistant professor of anesthesiology and critical care medicine at Johns Hopkins University School of Medicine in Baltimore. "There was no one hospital that was rated as a high performer on all four."
The study, which appeared in Health Affairs, looked at the hospital ratings systems of U.S. News, Healthgrades, The Leapfrog Group, and Consumer Reports, and found none took the same approach to assessing hospital quality. Of the 83 hospitals rated by all four systems, none were universally recognized as either a high performer or a low performer.
"I think the impact, or the influence, on consumers is that these conflicting ratings could generate confusion," Dr. Austin says. "Depending on which rating system you look at, it may give you a different answer on which hospital or where you should seek care. If you look at these four rating systems in a community, you may actually wind up being directed to four different hospitals."
David Pressel, MD, PhD, medical director of inpatient care at Alfred I. duPont Hospital for Children in Wilmington, Del., emphasized the difficulty of defining quality.
"Measuring quality is really difficult and hard, and people, physicians, and hospitals struggle with this," he explains. "I think it's very important that people recognize in rating systems there’s always going to be a top 10% or top 50% and a bottom 10% or 50%, and what's really important is not if you're in the top or bottom but what the scatter of the data is. If the scatter of the data is very narrow, they may not be providing much worse care than the top hospitals. I think that is lost on the public."
Dr. Austin's study identified varying missions and methodologies for each ratings system.
"U.S. News' Best Hospitals is actually intending to identify the best medical centers for the most complicated cases," Dr. Austin says. "The Leapfrog Hospital Safety Score has a very laser focus on patient safety, so freedom from harm, things like errors, infections."
Dr. Austin also noticed that some rating systems were more descriptive about their methods than others.
"Some of the ratings are much more transparent in what they share, in terms of how hospitals are rated, and others are less clear," he notes. "Healthgrades lists the top 100 hospitals. They're supposedly looking at hospital outcomes, but they don't publicly make their methodology available in terms of their risk-adjustment levels."
The rating systems also communicated their ratings differently. Leapfrog issues letter grades A–F; Consumer Reports and U.S. News issue scores from 0–100; and Healthgrades identifies the top 50 and top 100 hospitals but doesn’t rank hospitals, and hospitals that are not in the top 100 are not rated at all.
The study authors outlined possible improvements to eliminate some of these disparities, including reaching out to the sponsoring organizations and encouraging them to be more transparent about their ratings to allow for easier patient interpretation.
"Patients should understand what's being measured," Dr. Austin says. "Hospitals should be able to duplicate their ratings, so full transparency of the measures themselves, of the methodologies, is really important. We feel like these are a great start, but we definitely have some issues that still need to be resolved around measurements. We need better standardized measures."
Visit our website for more information on hospital ratings.
A recent study found different approaches used by four popular hospital ratings systems resulted in disagreement about the ranking of many U.S. hospitals.
"Only 10% of hospitals that were rated as a high performer on one of the systems were rated as a high performer on another rating system," says lead author John Matthew Austin, MS, PhD, assistant professor of anesthesiology and critical care medicine at Johns Hopkins University School of Medicine in Baltimore. "There was no one hospital that was rated as a high performer on all four."
The study, which appeared in Health Affairs, looked at the hospital ratings systems of U.S. News, Healthgrades, The Leapfrog Group, and Consumer Reports, and found none took the same approach to assessing hospital quality. Of the 83 hospitals rated by all four systems, none were universally recognized as either a high performer or a low performer.
"I think the impact, or the influence, on consumers is that these conflicting ratings could generate confusion," Dr. Austin says. "Depending on which rating system you look at, it may give you a different answer on which hospital or where you should seek care. If you look at these four rating systems in a community, you may actually wind up being directed to four different hospitals."
David Pressel, MD, PhD, medical director of inpatient care at Alfred I. duPont Hospital for Children in Wilmington, Del., emphasized the difficulty of defining quality.
"Measuring quality is really difficult and hard, and people, physicians, and hospitals struggle with this," he explains. "I think it's very important that people recognize in rating systems there’s always going to be a top 10% or top 50% and a bottom 10% or 50%, and what's really important is not if you're in the top or bottom but what the scatter of the data is. If the scatter of the data is very narrow, they may not be providing much worse care than the top hospitals. I think that is lost on the public."
Dr. Austin's study identified varying missions and methodologies for each ratings system.
"U.S. News' Best Hospitals is actually intending to identify the best medical centers for the most complicated cases," Dr. Austin says. "The Leapfrog Hospital Safety Score has a very laser focus on patient safety, so freedom from harm, things like errors, infections."
Dr. Austin also noticed that some rating systems were more descriptive about their methods than others.
"Some of the ratings are much more transparent in what they share, in terms of how hospitals are rated, and others are less clear," he notes. "Healthgrades lists the top 100 hospitals. They're supposedly looking at hospital outcomes, but they don't publicly make their methodology available in terms of their risk-adjustment levels."
The rating systems also communicated their ratings differently. Leapfrog issues letter grades A–F; Consumer Reports and U.S. News issue scores from 0–100; and Healthgrades identifies the top 50 and top 100 hospitals but doesn’t rank hospitals, and hospitals that are not in the top 100 are not rated at all.
The study authors outlined possible improvements to eliminate some of these disparities, including reaching out to the sponsoring organizations and encouraging them to be more transparent about their ratings to allow for easier patient interpretation.
"Patients should understand what's being measured," Dr. Austin says. "Hospitals should be able to duplicate their ratings, so full transparency of the measures themselves, of the methodologies, is really important. We feel like these are a great start, but we definitely have some issues that still need to be resolved around measurements. We need better standardized measures."
Visit our website for more information on hospital ratings.
A recent study found different approaches used by four popular hospital ratings systems resulted in disagreement about the ranking of many U.S. hospitals.
"Only 10% of hospitals that were rated as a high performer on one of the systems were rated as a high performer on another rating system," says lead author John Matthew Austin, MS, PhD, assistant professor of anesthesiology and critical care medicine at Johns Hopkins University School of Medicine in Baltimore. "There was no one hospital that was rated as a high performer on all four."
The study, which appeared in Health Affairs, looked at the hospital ratings systems of U.S. News, Healthgrades, The Leapfrog Group, and Consumer Reports, and found none took the same approach to assessing hospital quality. Of the 83 hospitals rated by all four systems, none were universally recognized as either a high performer or a low performer.
"I think the impact, or the influence, on consumers is that these conflicting ratings could generate confusion," Dr. Austin says. "Depending on which rating system you look at, it may give you a different answer on which hospital or where you should seek care. If you look at these four rating systems in a community, you may actually wind up being directed to four different hospitals."
David Pressel, MD, PhD, medical director of inpatient care at Alfred I. duPont Hospital for Children in Wilmington, Del., emphasized the difficulty of defining quality.
"Measuring quality is really difficult and hard, and people, physicians, and hospitals struggle with this," he explains. "I think it's very important that people recognize in rating systems there’s always going to be a top 10% or top 50% and a bottom 10% or 50%, and what's really important is not if you're in the top or bottom but what the scatter of the data is. If the scatter of the data is very narrow, they may not be providing much worse care than the top hospitals. I think that is lost on the public."
Dr. Austin's study identified varying missions and methodologies for each ratings system.
"U.S. News' Best Hospitals is actually intending to identify the best medical centers for the most complicated cases," Dr. Austin says. "The Leapfrog Hospital Safety Score has a very laser focus on patient safety, so freedom from harm, things like errors, infections."
Dr. Austin also noticed that some rating systems were more descriptive about their methods than others.
"Some of the ratings are much more transparent in what they share, in terms of how hospitals are rated, and others are less clear," he notes. "Healthgrades lists the top 100 hospitals. They're supposedly looking at hospital outcomes, but they don't publicly make their methodology available in terms of their risk-adjustment levels."
The rating systems also communicated their ratings differently. Leapfrog issues letter grades A–F; Consumer Reports and U.S. News issue scores from 0–100; and Healthgrades identifies the top 50 and top 100 hospitals but doesn’t rank hospitals, and hospitals that are not in the top 100 are not rated at all.
The study authors outlined possible improvements to eliminate some of these disparities, including reaching out to the sponsoring organizations and encouraging them to be more transparent about their ratings to allow for easier patient interpretation.
"Patients should understand what's being measured," Dr. Austin says. "Hospitals should be able to duplicate their ratings, so full transparency of the measures themselves, of the methodologies, is really important. We feel like these are a great start, but we definitely have some issues that still need to be resolved around measurements. We need better standardized measures."
Visit our website for more information on hospital ratings.
Practice Question Answers: Allergic Contact Dermatitis, Part 3
1. Which of the following is an amide-type anesthetic?
a. benzocaine
b. cocaine
c. lidocaine
d. procaine
e. tetracaine
2. A patient is referred for patch testing for suspected allergic contact dermatitis and is found to have positivity to hydrocortisone butyrate. The patient should try to avoid all of the following, except:
a. desonide
b. desoximetasone
c. fluocinolone
d. fluocinonide
e. triamcinolone
3. A patient with a documented contact allergy to neomycin sulfate should avoid all of the following medications, except:
a. bacitracin
b. gentamicin
c. kanamycin
d. mupirocin
e. streptomycin
4. Imidazolidinyl urea can cross-react with all of the following, except:
a. diazolidinyl urea
b. DMDM hydantoin
c. para-aminobenzoic acid
d. quaternium-15
e. tris(hydroxymethyl)nitromethane
5. Mercaptobenzothiazole can coreact with all of the following, except:
a. carbamates
b. dibenzothiazyl disulfide
c. mercapto mix
d. methyldibromo glutaronitrile
e. thiurams
1. Which of the following is an amide-type anesthetic?
a. benzocaine
b. cocaine
c. lidocaine
d. procaine
e. tetracaine
2. A patient is referred for patch testing for suspected allergic contact dermatitis and is found to have positivity to hydrocortisone butyrate. The patient should try to avoid all of the following, except:
a. desonide
b. desoximetasone
c. fluocinolone
d. fluocinonide
e. triamcinolone
3. A patient with a documented contact allergy to neomycin sulfate should avoid all of the following medications, except:
a. bacitracin
b. gentamicin
c. kanamycin
d. mupirocin
e. streptomycin
4. Imidazolidinyl urea can cross-react with all of the following, except:
a. diazolidinyl urea
b. DMDM hydantoin
c. para-aminobenzoic acid
d. quaternium-15
e. tris(hydroxymethyl)nitromethane
5. Mercaptobenzothiazole can coreact with all of the following, except:
a. carbamates
b. dibenzothiazyl disulfide
c. mercapto mix
d. methyldibromo glutaronitrile
e. thiurams
1. Which of the following is an amide-type anesthetic?
a. benzocaine
b. cocaine
c. lidocaine
d. procaine
e. tetracaine
2. A patient is referred for patch testing for suspected allergic contact dermatitis and is found to have positivity to hydrocortisone butyrate. The patient should try to avoid all of the following, except:
a. desonide
b. desoximetasone
c. fluocinolone
d. fluocinonide
e. triamcinolone
3. A patient with a documented contact allergy to neomycin sulfate should avoid all of the following medications, except:
a. bacitracin
b. gentamicin
c. kanamycin
d. mupirocin
e. streptomycin
4. Imidazolidinyl urea can cross-react with all of the following, except:
a. diazolidinyl urea
b. DMDM hydantoin
c. para-aminobenzoic acid
d. quaternium-15
e. tris(hydroxymethyl)nitromethane
5. Mercaptobenzothiazole can coreact with all of the following, except:
a. carbamates
b. dibenzothiazyl disulfide
c. mercapto mix
d. methyldibromo glutaronitrile
e. thiurams