User login
Quick antibiotic delivery reduces intensive care needs

Photo by Logan Tuttle
Time is of the essence when delivering antibiotics to pediatric cancer patients who present with fever and neutropenia, a new study suggests.
Patients who received antibiotics within 60 minutes of hospital admission were significantly less likely to require intensive care than patients who received antibiotics outside of an hour.
Children who received antibiotics faster also had a lower mortality rate, but the difference between the 2 groups was not statistically significant.
Joanne Hilden, MD, of Children’s Hospital Colorado in Aurora, and her colleagues detailed these results in Pediatric Blood & Cancer.
Dr Hilden noted that administering antibiotics within 60 minutes of a patient’s admission can be difficult, but she and her colleagues were able to adopt policies that sped up the process at their institution.
“We’re talking about kids who have gone home after chemotherapy and then a parent calls the hospital reporting a fever,” Dr Hilden said. “The question is, can we get the patient back to the hospital, then get a white cell count, and get antibiotics on board when needed all within an hour of their arrival?”
“It’s a huge challenge. This study shows that it’s important we make it happen. There’s less intensive care and fewer fatalities for kids who get antibiotics sooner.”
To determine the impact of timely antibiotic administration, Dr Hilden and her colleagues initially analyzed 116 children with hematologic and solid tumor malignancies who developed fever and neutropenia.
But the team found no significant differences in outcomes whether patients received antibiotics within or outside of the 60-minute window.
So the researchers extended the time period of their study and expanded the cohort to 220 patients.
This time, only the need for intensive care unit (ICU)-level care was significantly different between the 2 groups, with 12.6% of patients who received antibiotics within 60 minutes requiring ICU-level care, compared to 29.9% of patients who received antibiotics outside of an hour (P=0.003).
The researchers also found differences between the 2 groups with regard to the mean length of hospital stay (6.9 days vs 5.7 days), the mean duration of fever (3 days vs 2 days), the need for imaging workup (5.2% vs 9.1%), the incidence of bacteremia (13% vs 15.4%), and mortality rate (3.9% vs 0.7%). But none of these differences were statistically significant.
Still, Dr Hilden and her colleagues said it was important to reduce the time to antibiotic delivery at their institution, which took an average of 150 minutes when this study began. By instituting new policies, the team found they could deliver antibiotics in less than 60 minutes nearly 100% of the time.
To do this, hospital staff began prescribing antibiotics upon a pediatric cancer patient’s arrival, holding that order, and then allowing antibiotics to be delivered immediately after learning the results of neutrophil count testing. This eliminated the need to find a prescriber once the patient’s white blood cell count was known.
The researchers also found they could cut the time needed to determine a patient’s neutrophil count. Traditionally, determining neutropenia requires a full white blood cell count, followed by a differential by a human technician. But human verification reverses the machine results in less than 0.5% of cases.
The team discovered that the benefit of speed obtained by eliminating human verification outweighed the risk of administering unneeded antibiotics in very few cases. Depending on preliminary rather than technician-verified results of white cell counts reduced the time of testing from 45 minutes to 20.
The researchers also instituted changes to clinic flow procedures, such as notifying the full care team as soon as a family was advised to come into the hospital.
“Another thing we show is that just increasing the awareness of how important it is to get antibiotics on board quickly in these cases speeds delivery,” Dr Hilden said.
This knowledge and the aforementioned interventions allowed the researchers to reduce the time to antibiotic delivery to a median of 46 minutes.
“Only 11% of pediatric cancer patients with fever and neutropenia have serious complications,” Dr Hilden noted. “That’s low, but we can make it 0%, and this study shows that getting antibiotics onboard quickly goes a long way toward that goal.” ![]()
Photo by Logan Tuttle
Time is of the essence when delivering antibiotics to pediatric cancer patients who present with fever and neutropenia, a new study suggests.
Patients who received antibiotics within 60 minutes of hospital admission were significantly less likely to require intensive care than patients who received antibiotics outside of an hour.
Children who received antibiotics faster also had a lower mortality rate, but the difference between the 2 groups was not statistically significant.
Joanne Hilden, MD, of Children’s Hospital Colorado in Aurora, and her colleagues detailed these results in Pediatric Blood & Cancer.
Dr Hilden noted that administering antibiotics within 60 minutes of a patient’s admission can be difficult, but she and her colleagues were able to adopt policies that sped up the process at their institution.
“We’re talking about kids who have gone home after chemotherapy and then a parent calls the hospital reporting a fever,” Dr Hilden said. “The question is, can we get the patient back to the hospital, then get a white cell count, and get antibiotics on board when needed all within an hour of their arrival?”
“It’s a huge challenge. This study shows that it’s important we make it happen. There’s less intensive care and fewer fatalities for kids who get antibiotics sooner.”
To determine the impact of timely antibiotic administration, Dr Hilden and her colleagues initially analyzed 116 children with hematologic and solid tumor malignancies who developed fever and neutropenia.
But the team found no significant differences in outcomes whether patients received antibiotics within or outside of the 60-minute window.
So the researchers extended the time period of their study and expanded the cohort to 220 patients.
This time, only the need for intensive care unit (ICU)-level care was significantly different between the 2 groups, with 12.6% of patients who received antibiotics within 60 minutes requiring ICU-level care, compared to 29.9% of patients who received antibiotics outside of an hour (P=0.003).
The researchers also found differences between the 2 groups with regard to the mean length of hospital stay (6.9 days vs 5.7 days), the mean duration of fever (3 days vs 2 days), the need for imaging workup (5.2% vs 9.1%), the incidence of bacteremia (13% vs 15.4%), and mortality rate (3.9% vs 0.7%). But none of these differences were statistically significant.
Still, Dr Hilden and her colleagues said it was important to reduce the time to antibiotic delivery at their institution, which took an average of 150 minutes when this study began. By instituting new policies, the team found they could deliver antibiotics in less than 60 minutes nearly 100% of the time.
To do this, hospital staff began prescribing antibiotics upon a pediatric cancer patient’s arrival, holding that order, and then allowing antibiotics to be delivered immediately after learning the results of neutrophil count testing. This eliminated the need to find a prescriber once the patient’s white blood cell count was known.
The researchers also found they could cut the time needed to determine a patient’s neutrophil count. Traditionally, determining neutropenia requires a full white blood cell count, followed by a differential by a human technician. But human verification reverses the machine results in less than 0.5% of cases.
The team discovered that the benefit of speed obtained by eliminating human verification outweighed the risk of administering unneeded antibiotics in very few cases. Depending on preliminary rather than technician-verified results of white cell counts reduced the time of testing from 45 minutes to 20.
The researchers also instituted changes to clinic flow procedures, such as notifying the full care team as soon as a family was advised to come into the hospital.
“Another thing we show is that just increasing the awareness of how important it is to get antibiotics on board quickly in these cases speeds delivery,” Dr Hilden said.
This knowledge and the aforementioned interventions allowed the researchers to reduce the time to antibiotic delivery to a median of 46 minutes.
“Only 11% of pediatric cancer patients with fever and neutropenia have serious complications,” Dr Hilden noted. “That’s low, but we can make it 0%, and this study shows that getting antibiotics onboard quickly goes a long way toward that goal.” ![]()
Photo by Logan Tuttle
Time is of the essence when delivering antibiotics to pediatric cancer patients who present with fever and neutropenia, a new study suggests.
Patients who received antibiotics within 60 minutes of hospital admission were significantly less likely to require intensive care than patients who received antibiotics outside of an hour.
Children who received antibiotics faster also had a lower mortality rate, but the difference between the 2 groups was not statistically significant.
Joanne Hilden, MD, of Children’s Hospital Colorado in Aurora, and her colleagues detailed these results in Pediatric Blood & Cancer.
Dr Hilden noted that administering antibiotics within 60 minutes of a patient’s admission can be difficult, but she and her colleagues were able to adopt policies that sped up the process at their institution.
“We’re talking about kids who have gone home after chemotherapy and then a parent calls the hospital reporting a fever,” Dr Hilden said. “The question is, can we get the patient back to the hospital, then get a white cell count, and get antibiotics on board when needed all within an hour of their arrival?”
“It’s a huge challenge. This study shows that it’s important we make it happen. There’s less intensive care and fewer fatalities for kids who get antibiotics sooner.”
To determine the impact of timely antibiotic administration, Dr Hilden and her colleagues initially analyzed 116 children with hematologic and solid tumor malignancies who developed fever and neutropenia.
But the team found no significant differences in outcomes whether patients received antibiotics within or outside of the 60-minute window.
So the researchers extended the time period of their study and expanded the cohort to 220 patients.
This time, only the need for intensive care unit (ICU)-level care was significantly different between the 2 groups, with 12.6% of patients who received antibiotics within 60 minutes requiring ICU-level care, compared to 29.9% of patients who received antibiotics outside of an hour (P=0.003).
The researchers also found differences between the 2 groups with regard to the mean length of hospital stay (6.9 days vs 5.7 days), the mean duration of fever (3 days vs 2 days), the need for imaging workup (5.2% vs 9.1%), the incidence of bacteremia (13% vs 15.4%), and mortality rate (3.9% vs 0.7%). But none of these differences were statistically significant.
Still, Dr Hilden and her colleagues said it was important to reduce the time to antibiotic delivery at their institution, which took an average of 150 minutes when this study began. By instituting new policies, the team found they could deliver antibiotics in less than 60 minutes nearly 100% of the time.
To do this, hospital staff began prescribing antibiotics upon a pediatric cancer patient’s arrival, holding that order, and then allowing antibiotics to be delivered immediately after learning the results of neutrophil count testing. This eliminated the need to find a prescriber once the patient’s white blood cell count was known.
The researchers also found they could cut the time needed to determine a patient’s neutrophil count. Traditionally, determining neutropenia requires a full white blood cell count, followed by a differential by a human technician. But human verification reverses the machine results in less than 0.5% of cases.
The team discovered that the benefit of speed obtained by eliminating human verification outweighed the risk of administering unneeded antibiotics in very few cases. Depending on preliminary rather than technician-verified results of white cell counts reduced the time of testing from 45 minutes to 20.
The researchers also instituted changes to clinic flow procedures, such as notifying the full care team as soon as a family was advised to come into the hospital.
“Another thing we show is that just increasing the awareness of how important it is to get antibiotics on board quickly in these cases speeds delivery,” Dr Hilden said.
This knowledge and the aforementioned interventions allowed the researchers to reduce the time to antibiotic delivery to a median of 46 minutes.
“Only 11% of pediatric cancer patients with fever and neutropenia have serious complications,” Dr Hilden noted. “That’s low, but we can make it 0%, and this study shows that getting antibiotics onboard quickly goes a long way toward that goal.” ![]()
Managing anticoagulant-related bleeding in the brain

Photo courtesy of NIH
A retrospective study has revealed insights that may help physicians manage patients with anticoagulant-associated intracerebral hemorrhage.
Attaining an international normalized ratio (INR) below 1.3 and systolic blood pressure below 160 mm Hg, both within 4 hours of hospital admission, were associated with lower rates of hematoma enlargement.
And resuming anticoagulant therapy conferred a lower risk of ischemic events without increasing bleeding complications.
Hagen B. Huttner, MD, of the University of Erlangen-Nuremberg in Erlangen, Germany, and his colleagues published these findings in JAMA.
The investigators noted that, among all types of stroke, there is a substantial lack of data about how to manage oral-anticoagulant-related intracranial hemorrhage. Two of the most pressing questions are how to prevent hematoma enlargement and how to manage anticoagulation in the long-term.
There is a consensus that elevated INR levels should be reversed to minimize hematoma enlargement, but the mode of reversal, timing, and extent of INR reversal are unclear. And valid data on the safety and clinical benefit of resuming oral anticoagulant use have not been established.
So Dr Huttner and his colleagues conducted their study to gain some insight. They looked at patients treated at 19 German tertiary care centers from 2006 to 2012, assessing long-term functional outcomes in 1176 patients, hematoma enlargement in 853 patients, and anticoagulant resumption in 719 patients.
Thirty-six percent of patients experienced hematoma enlargement. Patients were less likely to experience enlargement if they had achieved INR levels below 1.3 within 4 hours of hospital admission. Enlargement occurred in 19.8% of these patients, compared to 41.5% of other patients (P<0.001).
Patients were also less likely to have hematoma enlargement if their systolic blood pressure was lower than 160 mm Hg at 4 hours after admission. Enlargement occurred in 33.1% of these patients and 52.4% of other patients (P<0.001).
Patients who had both of these favorable factors had even lower rates of hematoma enlargement than patients with higher INR and blood pressure levels—18.1% and 44.2%, respectively (P<0.001). And having both favorable factors conferred a lower rate of in-hospital mortality as well—13.5% and 20.7%, respectively (P=0.03).
About 24% of patients resumed oral anticoagulant therapy. Those who did had fewer ischemic complications than their peers—5.2% and 15%, respectively (P<0.001). But there was no significant difference between the groups with regard to hemorrhagic complications—8.1% and 6.6%, respectively (P=0.48).
The investigators concluded that, although this study has revealed clinically valuable associations, the results must be replicated in prospective studies. ![]()
Photo courtesy of NIH
A retrospective study has revealed insights that may help physicians manage patients with anticoagulant-associated intracerebral hemorrhage.
Attaining an international normalized ratio (INR) below 1.3 and systolic blood pressure below 160 mm Hg, both within 4 hours of hospital admission, were associated with lower rates of hematoma enlargement.
And resuming anticoagulant therapy conferred a lower risk of ischemic events without increasing bleeding complications.
Hagen B. Huttner, MD, of the University of Erlangen-Nuremberg in Erlangen, Germany, and his colleagues published these findings in JAMA.
The investigators noted that, among all types of stroke, there is a substantial lack of data about how to manage oral-anticoagulant-related intracranial hemorrhage. Two of the most pressing questions are how to prevent hematoma enlargement and how to manage anticoagulation in the long-term.
There is a consensus that elevated INR levels should be reversed to minimize hematoma enlargement, but the mode of reversal, timing, and extent of INR reversal are unclear. And valid data on the safety and clinical benefit of resuming oral anticoagulant use have not been established.
So Dr Huttner and his colleagues conducted their study to gain some insight. They looked at patients treated at 19 German tertiary care centers from 2006 to 2012, assessing long-term functional outcomes in 1176 patients, hematoma enlargement in 853 patients, and anticoagulant resumption in 719 patients.
Thirty-six percent of patients experienced hematoma enlargement. Patients were less likely to experience enlargement if they had achieved INR levels below 1.3 within 4 hours of hospital admission. Enlargement occurred in 19.8% of these patients, compared to 41.5% of other patients (P<0.001).
Patients were also less likely to have hematoma enlargement if their systolic blood pressure was lower than 160 mm Hg at 4 hours after admission. Enlargement occurred in 33.1% of these patients and 52.4% of other patients (P<0.001).
Patients who had both of these favorable factors had even lower rates of hematoma enlargement than patients with higher INR and blood pressure levels—18.1% and 44.2%, respectively (P<0.001). And having both favorable factors conferred a lower rate of in-hospital mortality as well—13.5% and 20.7%, respectively (P=0.03).
About 24% of patients resumed oral anticoagulant therapy. Those who did had fewer ischemic complications than their peers—5.2% and 15%, respectively (P<0.001). But there was no significant difference between the groups with regard to hemorrhagic complications—8.1% and 6.6%, respectively (P=0.48).
The investigators concluded that, although this study has revealed clinically valuable associations, the results must be replicated in prospective studies. ![]()
Photo courtesy of NIH
A retrospective study has revealed insights that may help physicians manage patients with anticoagulant-associated intracerebral hemorrhage.
Attaining an international normalized ratio (INR) below 1.3 and systolic blood pressure below 160 mm Hg, both within 4 hours of hospital admission, were associated with lower rates of hematoma enlargement.
And resuming anticoagulant therapy conferred a lower risk of ischemic events without increasing bleeding complications.
Hagen B. Huttner, MD, of the University of Erlangen-Nuremberg in Erlangen, Germany, and his colleagues published these findings in JAMA.
The investigators noted that, among all types of stroke, there is a substantial lack of data about how to manage oral-anticoagulant-related intracranial hemorrhage. Two of the most pressing questions are how to prevent hematoma enlargement and how to manage anticoagulation in the long-term.
There is a consensus that elevated INR levels should be reversed to minimize hematoma enlargement, but the mode of reversal, timing, and extent of INR reversal are unclear. And valid data on the safety and clinical benefit of resuming oral anticoagulant use have not been established.
So Dr Huttner and his colleagues conducted their study to gain some insight. They looked at patients treated at 19 German tertiary care centers from 2006 to 2012, assessing long-term functional outcomes in 1176 patients, hematoma enlargement in 853 patients, and anticoagulant resumption in 719 patients.
Thirty-six percent of patients experienced hematoma enlargement. Patients were less likely to experience enlargement if they had achieved INR levels below 1.3 within 4 hours of hospital admission. Enlargement occurred in 19.8% of these patients, compared to 41.5% of other patients (P<0.001).
Patients were also less likely to have hematoma enlargement if their systolic blood pressure was lower than 160 mm Hg at 4 hours after admission. Enlargement occurred in 33.1% of these patients and 52.4% of other patients (P<0.001).
Patients who had both of these favorable factors had even lower rates of hematoma enlargement than patients with higher INR and blood pressure levels—18.1% and 44.2%, respectively (P<0.001). And having both favorable factors conferred a lower rate of in-hospital mortality as well—13.5% and 20.7%, respectively (P=0.03).
About 24% of patients resumed oral anticoagulant therapy. Those who did had fewer ischemic complications than their peers—5.2% and 15%, respectively (P<0.001). But there was no significant difference between the groups with regard to hemorrhagic complications—8.1% and 6.6%, respectively (P=0.48).
The investigators concluded that, although this study has revealed clinically valuable associations, the results must be replicated in prospective studies. ![]()
Team uses 3D printing to create drug carrier

Photo by Aaron Logan
Researchers have used a 3D printer to create a carrier that allows for local and sustained delivery of the immunosuppressive drug cyclosporine A (CsA) after cell transplantation.
The carrier is a combination of microspheres and hydrogel. In murine experiments, it delivered a local, sustained load of CsA in an amount that eliminated the need for additional drugs to treat immune rejection.
The researchers described these results in Cell Transplantation.
“Our objective was to show the feasibility of using a subcutaneous, 3D-printed drug delivery system to achieve local and sustained CsA release and to investigate the local immunosuppressive effects of the CsA after cell transplantation,” said study author Dong-Woo Cho, PhD, of the Pohang University of Science and Technology in Korea.
“The improved load-bearing capacity of the combined microsphere and hydrogel system, and its ability to maintain its integrity and shape during the implantation period, helped to deliver a sustained CsA release, preventing the acceleration of the secretion of cytokines related to immune rejection.”
The researchers noted that CsA improves the success rate of transplants, but systemic administration requires high doses that can have severe side effects. The benefit of a carrier is that it provides local drug delivery.
Other research groups have attempted CsA delivery via either microspheres or hydrogels, but most encountered serious problems, such as embolisms or organ damage due to migration of the microspheres from the injection site.
In addition, weak mechanical properties in some delivery systems caused premature dissolution and placed limitations on drug load quantity.
However, Dr Cho’s group said their carrier’s improved structure and load-bearing capacity allowed for sustained release of CsA at the desired site.
Their carrier is a hybrid of a CsA-poly (lactic-co-glycolic) acid microsphere-loaded hydrogel and a polymeric framework, which ensures the carrier can endure external force under physiological conditions.
In in vitro experiments with the carrier, the researchers observed decreased expression of cytokines, which are secreted by spleen cells activated by Concanavalin A and are related to immune rejection.
The team also implanted in mice drug carriers seeded with xenogeneic cells, and they observed significant suppression of T-cell-mediated rejection for 4 weeks.
The researchers believe this study could help overcome existing cell transplantation limitations caused by systemic immunosuppression. They said their carrier could be a promising solution for treating a range of diseases that require cell-based therapy. ![]()
Photo by Aaron Logan
Researchers have used a 3D printer to create a carrier that allows for local and sustained delivery of the immunosuppressive drug cyclosporine A (CsA) after cell transplantation.
The carrier is a combination of microspheres and hydrogel. In murine experiments, it delivered a local, sustained load of CsA in an amount that eliminated the need for additional drugs to treat immune rejection.
The researchers described these results in Cell Transplantation.
“Our objective was to show the feasibility of using a subcutaneous, 3D-printed drug delivery system to achieve local and sustained CsA release and to investigate the local immunosuppressive effects of the CsA after cell transplantation,” said study author Dong-Woo Cho, PhD, of the Pohang University of Science and Technology in Korea.
“The improved load-bearing capacity of the combined microsphere and hydrogel system, and its ability to maintain its integrity and shape during the implantation period, helped to deliver a sustained CsA release, preventing the acceleration of the secretion of cytokines related to immune rejection.”
The researchers noted that CsA improves the success rate of transplants, but systemic administration requires high doses that can have severe side effects. The benefit of a carrier is that it provides local drug delivery.
Other research groups have attempted CsA delivery via either microspheres or hydrogels, but most encountered serious problems, such as embolisms or organ damage due to migration of the microspheres from the injection site.
In addition, weak mechanical properties in some delivery systems caused premature dissolution and placed limitations on drug load quantity.
However, Dr Cho’s group said their carrier’s improved structure and load-bearing capacity allowed for sustained release of CsA at the desired site.
Their carrier is a hybrid of a CsA-poly (lactic-co-glycolic) acid microsphere-loaded hydrogel and a polymeric framework, which ensures the carrier can endure external force under physiological conditions.
In in vitro experiments with the carrier, the researchers observed decreased expression of cytokines, which are secreted by spleen cells activated by Concanavalin A and are related to immune rejection.
The team also implanted in mice drug carriers seeded with xenogeneic cells, and they observed significant suppression of T-cell-mediated rejection for 4 weeks.
The researchers believe this study could help overcome existing cell transplantation limitations caused by systemic immunosuppression. They said their carrier could be a promising solution for treating a range of diseases that require cell-based therapy. ![]()
Photo by Aaron Logan
Researchers have used a 3D printer to create a carrier that allows for local and sustained delivery of the immunosuppressive drug cyclosporine A (CsA) after cell transplantation.
The carrier is a combination of microspheres and hydrogel. In murine experiments, it delivered a local, sustained load of CsA in an amount that eliminated the need for additional drugs to treat immune rejection.
The researchers described these results in Cell Transplantation.
“Our objective was to show the feasibility of using a subcutaneous, 3D-printed drug delivery system to achieve local and sustained CsA release and to investigate the local immunosuppressive effects of the CsA after cell transplantation,” said study author Dong-Woo Cho, PhD, of the Pohang University of Science and Technology in Korea.
“The improved load-bearing capacity of the combined microsphere and hydrogel system, and its ability to maintain its integrity and shape during the implantation period, helped to deliver a sustained CsA release, preventing the acceleration of the secretion of cytokines related to immune rejection.”
The researchers noted that CsA improves the success rate of transplants, but systemic administration requires high doses that can have severe side effects. The benefit of a carrier is that it provides local drug delivery.
Other research groups have attempted CsA delivery via either microspheres or hydrogels, but most encountered serious problems, such as embolisms or organ damage due to migration of the microspheres from the injection site.
In addition, weak mechanical properties in some delivery systems caused premature dissolution and placed limitations on drug load quantity.
However, Dr Cho’s group said their carrier’s improved structure and load-bearing capacity allowed for sustained release of CsA at the desired site.
Their carrier is a hybrid of a CsA-poly (lactic-co-glycolic) acid microsphere-loaded hydrogel and a polymeric framework, which ensures the carrier can endure external force under physiological conditions.
In in vitro experiments with the carrier, the researchers observed decreased expression of cytokines, which are secreted by spleen cells activated by Concanavalin A and are related to immune rejection.
The team also implanted in mice drug carriers seeded with xenogeneic cells, and they observed significant suppression of T-cell-mediated rejection for 4 weeks.
The researchers believe this study could help overcome existing cell transplantation limitations caused by systemic immunosuppression. They said their carrier could be a promising solution for treating a range of diseases that require cell-based therapy. ![]()
Skiing accident claims life of leukemia expert

Photo courtesy of RPCI
Meir Wetzler, MD, Chief of the Leukemia Section at the Roswell Park Cancer Institute (RPCI) in Buffalo, New York, has died at the age of 60.
Dr Wetzler passed away on February 23, in a Denver, Colorado, hospital a little more than 2 weeks after a skiing accident.
He was nationally prominent in his field and served on the Chronic Myelogenous Leukemia (CML) Treatment Committee of the National Comprehensive Cancer Network, helping set the standard of care for CML patients.
Originally from Israel, Dr Wetzler earned his medical degree at Hebrew University’s Hadassah Medical School in Jerusalem and did his residency in internal medicine at Kaplan Hospital in Rehovot before coming to the US.
From 1988 to 1992, he served 2 fellowships—in clinical immunology/biologic therapy and medical oncology—at MD Anderson Cancer Center in Houston, Texas. He joined the Leukemia Division of RPCI in 1994.
Dr Wetzler’s colleagues said he worked tirelessly with cooperative groups and pharmaceutical companies to attract new trials to RPCI for the benefit of his patients.
“He gave a piece of himself in everything he did, from his research to his care for patients to his interactions with his team of colleagues,” said Kara Eaton-Weaver, RPCI’s Executive Director of the Patient and Family Experience. “Meir was a transformational leader who built a culture of empathy, compassion, integrity, and innovation.”
“He was like a father,” said Linda Lutgen-Dunckley, a pathology resource technician at RPCI. “Everybody was part of a team, and nobody was less important than he was. He felt everybody played their part on the team.”
Dr Wetzler is survived by his wife, Chana, and their 4 children: Mor, Shira, Adam, and Modi.
The Dr Meir Wetzler Memorial Fund for Leukemia Research has been established to benefit leukemia research. A portion of the donations will be used to plant a tree in his memory in RPCI’s Kaminski Park & Gardens. To donate directly, visit giving.roswellpark.org/wetzler.
To send a personal message to Dr Wetzler’s family, direct it to Jamie Genovese at Roswell Park Cancer Institute, Department of Medicine, Elm and Carlton Streets, Buffalo, NY 14263. Messages can also be dropped off at RPCI’s Leukemia Center. ![]()
Photo courtesy of RPCI
Meir Wetzler, MD, Chief of the Leukemia Section at the Roswell Park Cancer Institute (RPCI) in Buffalo, New York, has died at the age of 60.
Dr Wetzler passed away on February 23, in a Denver, Colorado, hospital a little more than 2 weeks after a skiing accident.
He was nationally prominent in his field and served on the Chronic Myelogenous Leukemia (CML) Treatment Committee of the National Comprehensive Cancer Network, helping set the standard of care for CML patients.
Originally from Israel, Dr Wetzler earned his medical degree at Hebrew University’s Hadassah Medical School in Jerusalem and did his residency in internal medicine at Kaplan Hospital in Rehovot before coming to the US.
From 1988 to 1992, he served 2 fellowships—in clinical immunology/biologic therapy and medical oncology—at MD Anderson Cancer Center in Houston, Texas. He joined the Leukemia Division of RPCI in 1994.
Dr Wetzler’s colleagues said he worked tirelessly with cooperative groups and pharmaceutical companies to attract new trials to RPCI for the benefit of his patients.
“He gave a piece of himself in everything he did, from his research to his care for patients to his interactions with his team of colleagues,” said Kara Eaton-Weaver, RPCI’s Executive Director of the Patient and Family Experience. “Meir was a transformational leader who built a culture of empathy, compassion, integrity, and innovation.”
“He was like a father,” said Linda Lutgen-Dunckley, a pathology resource technician at RPCI. “Everybody was part of a team, and nobody was less important than he was. He felt everybody played their part on the team.”
Dr Wetzler is survived by his wife, Chana, and their 4 children: Mor, Shira, Adam, and Modi.
The Dr Meir Wetzler Memorial Fund for Leukemia Research has been established to benefit leukemia research. A portion of the donations will be used to plant a tree in his memory in RPCI’s Kaminski Park & Gardens. To donate directly, visit giving.roswellpark.org/wetzler.
To send a personal message to Dr Wetzler’s family, direct it to Jamie Genovese at Roswell Park Cancer Institute, Department of Medicine, Elm and Carlton Streets, Buffalo, NY 14263. Messages can also be dropped off at RPCI’s Leukemia Center. ![]()
Photo courtesy of RPCI
Meir Wetzler, MD, Chief of the Leukemia Section at the Roswell Park Cancer Institute (RPCI) in Buffalo, New York, has died at the age of 60.
Dr Wetzler passed away on February 23, in a Denver, Colorado, hospital a little more than 2 weeks after a skiing accident.
He was nationally prominent in his field and served on the Chronic Myelogenous Leukemia (CML) Treatment Committee of the National Comprehensive Cancer Network, helping set the standard of care for CML patients.
Originally from Israel, Dr Wetzler earned his medical degree at Hebrew University’s Hadassah Medical School in Jerusalem and did his residency in internal medicine at Kaplan Hospital in Rehovot before coming to the US.
From 1988 to 1992, he served 2 fellowships—in clinical immunology/biologic therapy and medical oncology—at MD Anderson Cancer Center in Houston, Texas. He joined the Leukemia Division of RPCI in 1994.
Dr Wetzler’s colleagues said he worked tirelessly with cooperative groups and pharmaceutical companies to attract new trials to RPCI for the benefit of his patients.
“He gave a piece of himself in everything he did, from his research to his care for patients to his interactions with his team of colleagues,” said Kara Eaton-Weaver, RPCI’s Executive Director of the Patient and Family Experience. “Meir was a transformational leader who built a culture of empathy, compassion, integrity, and innovation.”
“He was like a father,” said Linda Lutgen-Dunckley, a pathology resource technician at RPCI. “Everybody was part of a team, and nobody was less important than he was. He felt everybody played their part on the team.”
Dr Wetzler is survived by his wife, Chana, and their 4 children: Mor, Shira, Adam, and Modi.
The Dr Meir Wetzler Memorial Fund for Leukemia Research has been established to benefit leukemia research. A portion of the donations will be used to plant a tree in his memory in RPCI’s Kaminski Park & Gardens. To donate directly, visit giving.roswellpark.org/wetzler.
To send a personal message to Dr Wetzler’s family, direct it to Jamie Genovese at Roswell Park Cancer Institute, Department of Medicine, Elm and Carlton Streets, Buffalo, NY 14263. Messages can also be dropped off at RPCI’s Leukemia Center. ![]()
Ob.gyns. can help end the HIV epidemic
Despite staggering scientific and medical advances, the HIV epidemic in the United States has not changed significantly over the past decade. The estimated incidence of HIV infection has remained stable overall, with between 45,000 and 55,000 new HIV infections diagnosed per year.
This is disheartening because, even without a vaccine, I believe we have the tools today to drive the epidemic down to zero. First of all, we know how to effectively diagnose and treat the infection, and we have evidence that antiretroviral treatment is an effective prevention tool. Secondly, advances in chemoprophylaxis have made pre-exposure prophylaxis a reality.

Ob.gyns. played a central role in one of the greatest successes of the use of antiretroviral drugs: the virtual elimination of mother-to-child transmission of HIV in the United States. Now, by fully utilizing the tools available today, ob.gyns. can play a critical role in ending the epidemic in the United States and beyond.
Tools for diagnosis and treatment
We have so many missed opportunities in fighting the HIV epidemic.
This is evident in data compiled for a model called the “HIV Care Continuum,” or HIV “Cascade of Care.” The model captures the sequential stages of HIV care from diagnosis to suppression of the virus. It was developed in 2011 by Dr. Edward Gardner, an infectious disease/HIV expert at Denver Public Health, and has since been used at the federal, state, and local levels to help identify gaps in HIV services.
Not too long ago, diagnosis was the biggest problem in reducing the public health burden of HIV. Today, the biggest problem is linking and keeping individuals in care. According to the latest analysis by the U.S. Centers for Disease Control and Prevention of the HIV Care Continuum, of the 1.2 million people estimated to be living with HIV in America in 2011, approximately 86% were diagnosed, but only 40% were linked to and stayed in care, 37% were prescribed antiretroviral therapy (ART), and 30% had achieved viral suppression.
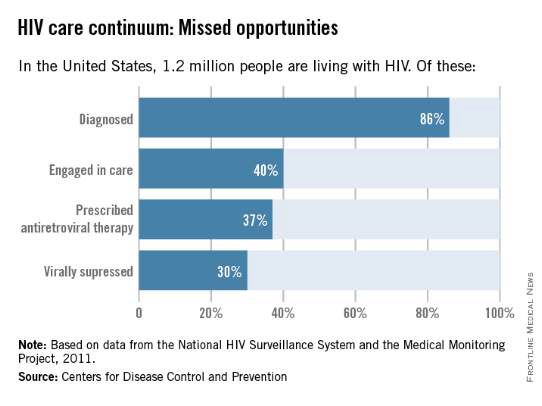
Only 30% of Americans living with HIV infection today are effectively treated, according to these data, even though we have the drugs and drug regimens available to treat everyone effectively.
Other analyses have included an additional stage of being initially linked to care (rather than being linked to care and retained in care). This presentation of the cascade, or continuum, further illuminates the progressive drop-off and that shows why an effective, sustained linkage to care is a critical component to ending the HIV epidemic.
One of these studies – an analysis published in 2013 – showed that approximately 82% of people were diagnosed, 66% were linked to care, 37% were retained in care, 33% were prescribed antiretroviral therapy, and 25% had a suppressed viral load of 200 copies/mL or less (JAMA. Intern. Med. 2013;173:1337-44).
With regard to women specifically, the CDC estimates that one in four people living with HIV infection are women, and that only about half of the women who are diagnosed with the infection are staying in care. Even fewer – 4 in 10 – have viral suppression, according to the CDC.
Expanding the management of HIV in the primary care setting could move us closer to ensuring that everyone in the United States who is infected with HIV is aware of the infection, is committed to treatment, and is virologically suppressed.
Like other primary care physicians, ob.gyns often have some degree of long-term continuity with patients – or the ability to create such continuity – that can be helpful for ensuring treatment compliance.
Ob.gyns also have valuable contact with adolescents, who fare worse throughout the cascade and are significantly more likely than older individuals to have unknown infections. An analysis published in 2014 of data for youth ages 13-29 shows that only 40% of HIV-infected youth were aware of their diagnosis and that an estimated 6% or less of HIV-infected youth were virally suppressed (AIDS. Patient. Care. STDS. 2014;28:128-135).
HIV testing should occur much more frequently than a decade ago, given the move in 2006 by the CDC from targeted risk-based testing to routine opt-out testing for all patients aged 13-64.
Treatment, moreover, has become much simpler in many respects. We have available to us more than 30 different drugs for individualizing therapy and providing treatment that allows patients to live a natural lifetime.
While such a large array of options may require those ob.gyns. who see only a few HIV-infected patients a year to work in consultation with an expert, many of the regimens require only a single, once-a-day pill. And while there was much debate as recently as five years ago about when to start treatment, there now is consensus that treatment should be started immediately after diagnosis (even in pregnant women), rather than waiting for the immune system to show signs of decline.
In fact, there is growing evidence that early treatment is key for both the infected individual and for individuals at risk. In the HIV Prevention Trials Network 052 study of discordant couples, for instance, early antiretroviral therapy in an infected partner not only reduced the number of clinical events; it almost completely blocked sexual transmission of the virus to an HIV-negative partner (N. Engl. J. Med. 2011;365:493-505).
The 052 study was a landmark “treatment as prevention” study. Other research has similarly shown that when the viral load of HIV-infected individuals is significantly reduced, their infectivity is reduced. And on a larger scale, research has shown that when we do this on a population basis, achieving widespread and continual treatment success, we can significantly impact the epidemic. This has been the case with the population of intravenous drug users in Vancouver, where the community viral load was significantly reduced by successful treatment that prevented new infections in this once-high-risk population.
Emerging data suggests that early diagnosis and treatment will likely also impact the likelihood of infected individuals achieving “functional cure.” The issue of functional cure – of achieving viral loads that are so low that drug therapy is no longer needed – has been receiving increasing attention in recent years, with the most promising findings reported thus far involving early treatment.
Tools for preexposure prophylaxis
For many years, we fit HIV care neatly into either the treatment or prevention category. More recently, we have come to appreciate that treatment is prevention, that a comprehensive prevention strategy must include treatment of infected individuals.
On the purely prevention side, it is important to continue educating women about safe sex behaviors. Most new HIV infections in women (84%) result from heterosexual contact, according to the CDC. For those who remain at risk of acquiring HIV despite education and counseling (eg., individuals who continue to engage in high-risk behaviors, or who have an HIV-positive partner), pre-exposure prophylaxis (PrEP) is now a safe and effective tool for preventing transmission. Patients deemed to be at high risk of acquiring HIV need to be made aware of this option.
PrEP originally was recommended only for gay or bisexual men, but in May 2014, the CDC recommended it for all individuals at risk and released the first comprehensive clinical practice guidelines for the prevention tool (www.cdc.gov/hiv/pdf/guidelines/PrEPguidelines2014.pdf).
The PrEP medication, Truvada, is a combination of two drugs (tenovovir and emtricitabine) that, when taken daily on a consistent basis, significantly reduces the risk of getting HIV infection. Several large national and international studies have documented risk reductions of 73% to 92% when the medication was taken every day or almost every day. It is clearly within the purview of any ob.gyn to prescribe, monitor, and manage such prevention therapy.
The availability and relative ease of such a tool, along with advances in treatment and knowledge gained from the HIV Care Continuum, should re-energize ob.gyns. to up the ante in efforts to end the epidemic.
Experience in our clinical program that provides care and treatment to patients in the Baltimore-Washington area has taught us that we do much better when we integrate HIV care within primary care. It’s much more likely that patients will “stay close” with their ob.gyn than to another specialist.
Certainly, HIV infection has its “hot spots” and areas of much lower prevalence, but regardless of where we reside, we must continue to appreciate that the epidemic has had a significant impact on women and that this will persist unless we can all better utilize our available tools, such as early diagnosis and effective treatment that are linked long-term with other primary care physicians.
For women, ob.gyns represent a great resource for our nation to make progress toward President Obama’s National HIV Strategy.
Dr. Redfield reported that he has no disclosures relevant to this Master Class.
Despite staggering scientific and medical advances, the HIV epidemic in the United States has not changed significantly over the past decade. The estimated incidence of HIV infection has remained stable overall, with between 45,000 and 55,000 new HIV infections diagnosed per year.
This is disheartening because, even without a vaccine, I believe we have the tools today to drive the epidemic down to zero. First of all, we know how to effectively diagnose and treat the infection, and we have evidence that antiretroviral treatment is an effective prevention tool. Secondly, advances in chemoprophylaxis have made pre-exposure prophylaxis a reality.
Ob.gyns. played a central role in one of the greatest successes of the use of antiretroviral drugs: the virtual elimination of mother-to-child transmission of HIV in the United States. Now, by fully utilizing the tools available today, ob.gyns. can play a critical role in ending the epidemic in the United States and beyond.
Tools for diagnosis and treatment
We have so many missed opportunities in fighting the HIV epidemic.
This is evident in data compiled for a model called the “HIV Care Continuum,” or HIV “Cascade of Care.” The model captures the sequential stages of HIV care from diagnosis to suppression of the virus. It was developed in 2011 by Dr. Edward Gardner, an infectious disease/HIV expert at Denver Public Health, and has since been used at the federal, state, and local levels to help identify gaps in HIV services.
Not too long ago, diagnosis was the biggest problem in reducing the public health burden of HIV. Today, the biggest problem is linking and keeping individuals in care. According to the latest analysis by the U.S. Centers for Disease Control and Prevention of the HIV Care Continuum, of the 1.2 million people estimated to be living with HIV in America in 2011, approximately 86% were diagnosed, but only 40% were linked to and stayed in care, 37% were prescribed antiretroviral therapy (ART), and 30% had achieved viral suppression.
Only 30% of Americans living with HIV infection today are effectively treated, according to these data, even though we have the drugs and drug regimens available to treat everyone effectively.
Other analyses have included an additional stage of being initially linked to care (rather than being linked to care and retained in care). This presentation of the cascade, or continuum, further illuminates the progressive drop-off and that shows why an effective, sustained linkage to care is a critical component to ending the HIV epidemic.
One of these studies – an analysis published in 2013 – showed that approximately 82% of people were diagnosed, 66% were linked to care, 37% were retained in care, 33% were prescribed antiretroviral therapy, and 25% had a suppressed viral load of 200 copies/mL or less (JAMA. Intern. Med. 2013;173:1337-44).
With regard to women specifically, the CDC estimates that one in four people living with HIV infection are women, and that only about half of the women who are diagnosed with the infection are staying in care. Even fewer – 4 in 10 – have viral suppression, according to the CDC.
Expanding the management of HIV in the primary care setting could move us closer to ensuring that everyone in the United States who is infected with HIV is aware of the infection, is committed to treatment, and is virologically suppressed.
Like other primary care physicians, ob.gyns often have some degree of long-term continuity with patients – or the ability to create such continuity – that can be helpful for ensuring treatment compliance.
Ob.gyns also have valuable contact with adolescents, who fare worse throughout the cascade and are significantly more likely than older individuals to have unknown infections. An analysis published in 2014 of data for youth ages 13-29 shows that only 40% of HIV-infected youth were aware of their diagnosis and that an estimated 6% or less of HIV-infected youth were virally suppressed (AIDS. Patient. Care. STDS. 2014;28:128-135).
HIV testing should occur much more frequently than a decade ago, given the move in 2006 by the CDC from targeted risk-based testing to routine opt-out testing for all patients aged 13-64.
Treatment, moreover, has become much simpler in many respects. We have available to us more than 30 different drugs for individualizing therapy and providing treatment that allows patients to live a natural lifetime.
While such a large array of options may require those ob.gyns. who see only a few HIV-infected patients a year to work in consultation with an expert, many of the regimens require only a single, once-a-day pill. And while there was much debate as recently as five years ago about when to start treatment, there now is consensus that treatment should be started immediately after diagnosis (even in pregnant women), rather than waiting for the immune system to show signs of decline.
In fact, there is growing evidence that early treatment is key for both the infected individual and for individuals at risk. In the HIV Prevention Trials Network 052 study of discordant couples, for instance, early antiretroviral therapy in an infected partner not only reduced the number of clinical events; it almost completely blocked sexual transmission of the virus to an HIV-negative partner (N. Engl. J. Med. 2011;365:493-505).
The 052 study was a landmark “treatment as prevention” study. Other research has similarly shown that when the viral load of HIV-infected individuals is significantly reduced, their infectivity is reduced. And on a larger scale, research has shown that when we do this on a population basis, achieving widespread and continual treatment success, we can significantly impact the epidemic. This has been the case with the population of intravenous drug users in Vancouver, where the community viral load was significantly reduced by successful treatment that prevented new infections in this once-high-risk population.
Emerging data suggests that early diagnosis and treatment will likely also impact the likelihood of infected individuals achieving “functional cure.” The issue of functional cure – of achieving viral loads that are so low that drug therapy is no longer needed – has been receiving increasing attention in recent years, with the most promising findings reported thus far involving early treatment.
Tools for preexposure prophylaxis
For many years, we fit HIV care neatly into either the treatment or prevention category. More recently, we have come to appreciate that treatment is prevention, that a comprehensive prevention strategy must include treatment of infected individuals.
On the purely prevention side, it is important to continue educating women about safe sex behaviors. Most new HIV infections in women (84%) result from heterosexual contact, according to the CDC. For those who remain at risk of acquiring HIV despite education and counseling (eg., individuals who continue to engage in high-risk behaviors, or who have an HIV-positive partner), pre-exposure prophylaxis (PrEP) is now a safe and effective tool for preventing transmission. Patients deemed to be at high risk of acquiring HIV need to be made aware of this option.
PrEP originally was recommended only for gay or bisexual men, but in May 2014, the CDC recommended it for all individuals at risk and released the first comprehensive clinical practice guidelines for the prevention tool (www.cdc.gov/hiv/pdf/guidelines/PrEPguidelines2014.pdf).
The PrEP medication, Truvada, is a combination of two drugs (tenovovir and emtricitabine) that, when taken daily on a consistent basis, significantly reduces the risk of getting HIV infection. Several large national and international studies have documented risk reductions of 73% to 92% when the medication was taken every day or almost every day. It is clearly within the purview of any ob.gyn to prescribe, monitor, and manage such prevention therapy.
The availability and relative ease of such a tool, along with advances in treatment and knowledge gained from the HIV Care Continuum, should re-energize ob.gyns. to up the ante in efforts to end the epidemic.
Experience in our clinical program that provides care and treatment to patients in the Baltimore-Washington area has taught us that we do much better when we integrate HIV care within primary care. It’s much more likely that patients will “stay close” with their ob.gyn than to another specialist.
Certainly, HIV infection has its “hot spots” and areas of much lower prevalence, but regardless of where we reside, we must continue to appreciate that the epidemic has had a significant impact on women and that this will persist unless we can all better utilize our available tools, such as early diagnosis and effective treatment that are linked long-term with other primary care physicians.
For women, ob.gyns represent a great resource for our nation to make progress toward President Obama’s National HIV Strategy.
Dr. Redfield reported that he has no disclosures relevant to this Master Class.
Despite staggering scientific and medical advances, the HIV epidemic in the United States has not changed significantly over the past decade. The estimated incidence of HIV infection has remained stable overall, with between 45,000 and 55,000 new HIV infections diagnosed per year.
This is disheartening because, even without a vaccine, I believe we have the tools today to drive the epidemic down to zero. First of all, we know how to effectively diagnose and treat the infection, and we have evidence that antiretroviral treatment is an effective prevention tool. Secondly, advances in chemoprophylaxis have made pre-exposure prophylaxis a reality.
Ob.gyns. played a central role in one of the greatest successes of the use of antiretroviral drugs: the virtual elimination of mother-to-child transmission of HIV in the United States. Now, by fully utilizing the tools available today, ob.gyns. can play a critical role in ending the epidemic in the United States and beyond.
Tools for diagnosis and treatment
We have so many missed opportunities in fighting the HIV epidemic.
This is evident in data compiled for a model called the “HIV Care Continuum,” or HIV “Cascade of Care.” The model captures the sequential stages of HIV care from diagnosis to suppression of the virus. It was developed in 2011 by Dr. Edward Gardner, an infectious disease/HIV expert at Denver Public Health, and has since been used at the federal, state, and local levels to help identify gaps in HIV services.
Not too long ago, diagnosis was the biggest problem in reducing the public health burden of HIV. Today, the biggest problem is linking and keeping individuals in care. According to the latest analysis by the U.S. Centers for Disease Control and Prevention of the HIV Care Continuum, of the 1.2 million people estimated to be living with HIV in America in 2011, approximately 86% were diagnosed, but only 40% were linked to and stayed in care, 37% were prescribed antiretroviral therapy (ART), and 30% had achieved viral suppression.
Only 30% of Americans living with HIV infection today are effectively treated, according to these data, even though we have the drugs and drug regimens available to treat everyone effectively.
Other analyses have included an additional stage of being initially linked to care (rather than being linked to care and retained in care). This presentation of the cascade, or continuum, further illuminates the progressive drop-off and that shows why an effective, sustained linkage to care is a critical component to ending the HIV epidemic.
One of these studies – an analysis published in 2013 – showed that approximately 82% of people were diagnosed, 66% were linked to care, 37% were retained in care, 33% were prescribed antiretroviral therapy, and 25% had a suppressed viral load of 200 copies/mL or less (JAMA. Intern. Med. 2013;173:1337-44).
With regard to women specifically, the CDC estimates that one in four people living with HIV infection are women, and that only about half of the women who are diagnosed with the infection are staying in care. Even fewer – 4 in 10 – have viral suppression, according to the CDC.
Expanding the management of HIV in the primary care setting could move us closer to ensuring that everyone in the United States who is infected with HIV is aware of the infection, is committed to treatment, and is virologically suppressed.
Like other primary care physicians, ob.gyns often have some degree of long-term continuity with patients – or the ability to create such continuity – that can be helpful for ensuring treatment compliance.
Ob.gyns also have valuable contact with adolescents, who fare worse throughout the cascade and are significantly more likely than older individuals to have unknown infections. An analysis published in 2014 of data for youth ages 13-29 shows that only 40% of HIV-infected youth were aware of their diagnosis and that an estimated 6% or less of HIV-infected youth were virally suppressed (AIDS. Patient. Care. STDS. 2014;28:128-135).
HIV testing should occur much more frequently than a decade ago, given the move in 2006 by the CDC from targeted risk-based testing to routine opt-out testing for all patients aged 13-64.
Treatment, moreover, has become much simpler in many respects. We have available to us more than 30 different drugs for individualizing therapy and providing treatment that allows patients to live a natural lifetime.
While such a large array of options may require those ob.gyns. who see only a few HIV-infected patients a year to work in consultation with an expert, many of the regimens require only a single, once-a-day pill. And while there was much debate as recently as five years ago about when to start treatment, there now is consensus that treatment should be started immediately after diagnosis (even in pregnant women), rather than waiting for the immune system to show signs of decline.
In fact, there is growing evidence that early treatment is key for both the infected individual and for individuals at risk. In the HIV Prevention Trials Network 052 study of discordant couples, for instance, early antiretroviral therapy in an infected partner not only reduced the number of clinical events; it almost completely blocked sexual transmission of the virus to an HIV-negative partner (N. Engl. J. Med. 2011;365:493-505).
The 052 study was a landmark “treatment as prevention” study. Other research has similarly shown that when the viral load of HIV-infected individuals is significantly reduced, their infectivity is reduced. And on a larger scale, research has shown that when we do this on a population basis, achieving widespread and continual treatment success, we can significantly impact the epidemic. This has been the case with the population of intravenous drug users in Vancouver, where the community viral load was significantly reduced by successful treatment that prevented new infections in this once-high-risk population.
Emerging data suggests that early diagnosis and treatment will likely also impact the likelihood of infected individuals achieving “functional cure.” The issue of functional cure – of achieving viral loads that are so low that drug therapy is no longer needed – has been receiving increasing attention in recent years, with the most promising findings reported thus far involving early treatment.
Tools for preexposure prophylaxis
For many years, we fit HIV care neatly into either the treatment or prevention category. More recently, we have come to appreciate that treatment is prevention, that a comprehensive prevention strategy must include treatment of infected individuals.
On the purely prevention side, it is important to continue educating women about safe sex behaviors. Most new HIV infections in women (84%) result from heterosexual contact, according to the CDC. For those who remain at risk of acquiring HIV despite education and counseling (eg., individuals who continue to engage in high-risk behaviors, or who have an HIV-positive partner), pre-exposure prophylaxis (PrEP) is now a safe and effective tool for preventing transmission. Patients deemed to be at high risk of acquiring HIV need to be made aware of this option.
PrEP originally was recommended only for gay or bisexual men, but in May 2014, the CDC recommended it for all individuals at risk and released the first comprehensive clinical practice guidelines for the prevention tool (www.cdc.gov/hiv/pdf/guidelines/PrEPguidelines2014.pdf).
The PrEP medication, Truvada, is a combination of two drugs (tenovovir and emtricitabine) that, when taken daily on a consistent basis, significantly reduces the risk of getting HIV infection. Several large national and international studies have documented risk reductions of 73% to 92% when the medication was taken every day or almost every day. It is clearly within the purview of any ob.gyn to prescribe, monitor, and manage such prevention therapy.
The availability and relative ease of such a tool, along with advances in treatment and knowledge gained from the HIV Care Continuum, should re-energize ob.gyns. to up the ante in efforts to end the epidemic.
Experience in our clinical program that provides care and treatment to patients in the Baltimore-Washington area has taught us that we do much better when we integrate HIV care within primary care. It’s much more likely that patients will “stay close” with their ob.gyn than to another specialist.
Certainly, HIV infection has its “hot spots” and areas of much lower prevalence, but regardless of where we reside, we must continue to appreciate that the epidemic has had a significant impact on women and that this will persist unless we can all better utilize our available tools, such as early diagnosis and effective treatment that are linked long-term with other primary care physicians.
For women, ob.gyns represent a great resource for our nation to make progress toward President Obama’s National HIV Strategy.
Dr. Redfield reported that he has no disclosures relevant to this Master Class.

HIV treatment adherence still a challenge
It’s hard to believe that it was 30 years ago that HIV was discovered as the cause of AIDS by Dr. Robert Gallo and Dr. Luc Montagnier. Since then, the medical community has focused on preventing and eradicating the virus and its transmission. Despite the advent of highly efficacious antiretroviral therapy, and education efforts to prevent transmission, the disease continues to cause significant morbidity and mortality.
Surveillance data from the Centers for Disease Control and Prevention have indicated that screening and prevention efforts led to a decline in perinatally acquired HIV and AIDS by 80% and 93%, respectively. However, we still have far to go.

The CDC estimated that in 2010 more than 1 million people over age 13 were living with HIV, and approximately 50,000 new cases of HIV occur each year in the United States.
President Obama’s National HIV/AIDS Strategy for the United States, released in 2010, set ambitious goals for eradicating the disease in our country. We can only hope to achieve the President’s aims if the fight against the disease is taken up by all health care professionals, on multiple fronts, and throughout the many stages of a patient’s health.
In a 2011 Master Class, we addressed the importance of ob.gyns. testing nonpregnant women for HIV, as well as employing HIV prevention strategies to keep our female patients healthy, and prevent potential mother-to-baby transmission of the virus. Although transmission has decreased significantly, helping patients follow their treatment regimens remains a major barrier to eradicating the disease.
Ob.gyns. may be the only physicians who many women see throughout their lives. Therefore, we have a unique opportunity to educate our patients about seeking appropriate care and the need for adhering to treatment regimens.
Our guest author this month is Dr. Robert R. Redfield Jr., a distinguished professor in the department of medicine at the University of Maryland, Baltimore, and associate director of the university’s Institute of Human Virology, with clinical and research programs in virtually all countries in the continent of Africa. Dr. Redfield will discuss the role that physicians can play in terms of linking patients to care as a means of treating those with HIV and reducing the burden of disease. Dr. Redfield’s expertise in the area of novel therapeutics for the treatment of the virus, and his clinical experience in treating patients, provides a unique perspective into this important public health issue.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].
It’s hard to believe that it was 30 years ago that HIV was discovered as the cause of AIDS by Dr. Robert Gallo and Dr. Luc Montagnier. Since then, the medical community has focused on preventing and eradicating the virus and its transmission. Despite the advent of highly efficacious antiretroviral therapy, and education efforts to prevent transmission, the disease continues to cause significant morbidity and mortality.
Surveillance data from the Centers for Disease Control and Prevention have indicated that screening and prevention efforts led to a decline in perinatally acquired HIV and AIDS by 80% and 93%, respectively. However, we still have far to go.
The CDC estimated that in 2010 more than 1 million people over age 13 were living with HIV, and approximately 50,000 new cases of HIV occur each year in the United States.
President Obama’s National HIV/AIDS Strategy for the United States, released in 2010, set ambitious goals for eradicating the disease in our country. We can only hope to achieve the President’s aims if the fight against the disease is taken up by all health care professionals, on multiple fronts, and throughout the many stages of a patient’s health.
In a 2011 Master Class, we addressed the importance of ob.gyns. testing nonpregnant women for HIV, as well as employing HIV prevention strategies to keep our female patients healthy, and prevent potential mother-to-baby transmission of the virus. Although transmission has decreased significantly, helping patients follow their treatment regimens remains a major barrier to eradicating the disease.
Ob.gyns. may be the only physicians who many women see throughout their lives. Therefore, we have a unique opportunity to educate our patients about seeking appropriate care and the need for adhering to treatment regimens.
Our guest author this month is Dr. Robert R. Redfield Jr., a distinguished professor in the department of medicine at the University of Maryland, Baltimore, and associate director of the university’s Institute of Human Virology, with clinical and research programs in virtually all countries in the continent of Africa. Dr. Redfield will discuss the role that physicians can play in terms of linking patients to care as a means of treating those with HIV and reducing the burden of disease. Dr. Redfield’s expertise in the area of novel therapeutics for the treatment of the virus, and his clinical experience in treating patients, provides a unique perspective into this important public health issue.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].
It’s hard to believe that it was 30 years ago that HIV was discovered as the cause of AIDS by Dr. Robert Gallo and Dr. Luc Montagnier. Since then, the medical community has focused on preventing and eradicating the virus and its transmission. Despite the advent of highly efficacious antiretroviral therapy, and education efforts to prevent transmission, the disease continues to cause significant morbidity and mortality.
Surveillance data from the Centers for Disease Control and Prevention have indicated that screening and prevention efforts led to a decline in perinatally acquired HIV and AIDS by 80% and 93%, respectively. However, we still have far to go.
The CDC estimated that in 2010 more than 1 million people over age 13 were living with HIV, and approximately 50,000 new cases of HIV occur each year in the United States.
President Obama’s National HIV/AIDS Strategy for the United States, released in 2010, set ambitious goals for eradicating the disease in our country. We can only hope to achieve the President’s aims if the fight against the disease is taken up by all health care professionals, on multiple fronts, and throughout the many stages of a patient’s health.
In a 2011 Master Class, we addressed the importance of ob.gyns. testing nonpregnant women for HIV, as well as employing HIV prevention strategies to keep our female patients healthy, and prevent potential mother-to-baby transmission of the virus. Although transmission has decreased significantly, helping patients follow their treatment regimens remains a major barrier to eradicating the disease.
Ob.gyns. may be the only physicians who many women see throughout their lives. Therefore, we have a unique opportunity to educate our patients about seeking appropriate care and the need for adhering to treatment regimens.
Our guest author this month is Dr. Robert R. Redfield Jr., a distinguished professor in the department of medicine at the University of Maryland, Baltimore, and associate director of the university’s Institute of Human Virology, with clinical and research programs in virtually all countries in the continent of Africa. Dr. Redfield will discuss the role that physicians can play in terms of linking patients to care as a means of treating those with HIV and reducing the burden of disease. Dr. Redfield’s expertise in the area of novel therapeutics for the treatment of the virus, and his clinical experience in treating patients, provides a unique perspective into this important public health issue.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].

Rethinking the ABCs of EVAR
CHICAGO – Real-world experience with novel endografts like the Ovation Prime abdominal endograft system is prompting some vascular specialists to rethink such central abdominal aortic aneurysm tenets as aortic neck dilation and minimum neck size.
“We started using this in our worst cases, patients with small caliber access vessels and very short aortic necks, to test this device, but over time we’ve pretty much made this our workhorse graft based on our outcomes,” Dr. Syed Hussain of the University of Illinois at Champaign-Urbana, said at a vascular surgery symposium sponsored by Northwestern University.

Among 67 patients with AAAs treated since the team’s first implant in November 2012, the technical success rate is 100%. At baseline, 35% of patients had access vessels < 7 mm, 45% had short aortic neck (< 15 mm), 60% had moderate to severe calcification (> 25% circumferential), and half had moderate to severe thrombus (> 25% circumferential).
The Ovation Prime (TriVascular Technologies) device is relatively quick and easy to put in, with an average procedure time of only 33 minutes, he said. Access was percutaneous in 27%, average blood loss was minimal at 60 mL, and average hospital stay was 1.7 days.
Two patients with severe comorbidities were admitted to the ICU and two patients experienced intraoperative type 1a endoleaks, both successfully treated with a Palmaz stent.
After an average follow-up of 12 months, there have been no type 1, III or IV endoleaks, graft migration, aneurysm enlargement, conversions, ruptures, limb occlusions, or secondary procedures, said Dr. Hussain, who disclosed serving as a consultant for Trivascular and national principal investigator of the PostMarket Ovation Trial. There were 12 type II endoleaks (17%) and all have been clinically irrelevant.
Because of the Ovation’s novel O-ring sealing mechanism, “you get a pretty watertight seal ring on these patients,” he said. More importantly, shear stress is distributed evenly along the entire O-ring, which creates very minimal outward stress on the aorta, “maybe 2 or 3 atmospheres at best.”
Evidence continues to build that self-expandable stents place chronic outward stress on the aorta that causes degeneration of the aortic wall, resulting in eventual aortic neck dilation and endograft migration. While it’s been argued that disease progression leads to aortic dilation, the phenomenon took off after the arrival of endovascular stents, not during decades of open AAA repair, Dr. Hussain, also of the Vein & Vascular Center at the Christie Clinic in Champaign, said.
In the Ovation approval trial, proximal neck dilation at 2 years followed a similar curve in the Ovation and open repair cohorts, compared with those for the more traditional endografts, he noted.
The Ovation Prime system was approved in 2012 and in mid-2014, the Food and Drug Administration approved changes to the indication statement that eliminated the requirement for a minimal aortic neck length.
Essentially, the Ovation device can be placed in any patient if the diameter at 13 mm below the lowest renal artery (the site of the most proximal sealing ring) is within the treatable diameter range of the device (15.8 mm-30.4 mm), Dr. Hussain said.
“The idea of having a neck length is completely starting to go away,” he said. “And even though the trial by Endologix is looking at 1 centimeter as the current requirement for enrolling patients, I think eventually it’s going to get to the point where you’re not going to need a neck for the Nellix device either. You’re going to be able to treat patients who have very short, 1 to 2 millimeter necks, basically perirenal aneurysms, and get a seal on.”
The Nellix endovascular aneurysm sealing system (Endologix) is not commercially available in the U.S., but is the being evaluated in at least three studies. It consists of dual balloon-expandable end-frames surrounded by polymer-filled endobags and is designed to completely fill and seal the aortic aneurysm sac. Anatomical requirements for patients to be enrolled in clinical studies include a nonaneurysmal aortic neck length of ≥ 10 mm, nonaneurysmal aortic neck diameter of 18 mm-32 mm, maximum aortic blood flow lumen diameter of ≤ 60 mm, and common iliac artery diameter of 8 mm-35 mm, according to the company’s website.
CHICAGO – Real-world experience with novel endografts like the Ovation Prime abdominal endograft system is prompting some vascular specialists to rethink such central abdominal aortic aneurysm tenets as aortic neck dilation and minimum neck size.
“We started using this in our worst cases, patients with small caliber access vessels and very short aortic necks, to test this device, but over time we’ve pretty much made this our workhorse graft based on our outcomes,” Dr. Syed Hussain of the University of Illinois at Champaign-Urbana, said at a vascular surgery symposium sponsored by Northwestern University.
Among 67 patients with AAAs treated since the team’s first implant in November 2012, the technical success rate is 100%. At baseline, 35% of patients had access vessels < 7 mm, 45% had short aortic neck (< 15 mm), 60% had moderate to severe calcification (> 25% circumferential), and half had moderate to severe thrombus (> 25% circumferential).
The Ovation Prime (TriVascular Technologies) device is relatively quick and easy to put in, with an average procedure time of only 33 minutes, he said. Access was percutaneous in 27%, average blood loss was minimal at 60 mL, and average hospital stay was 1.7 days.
Two patients with severe comorbidities were admitted to the ICU and two patients experienced intraoperative type 1a endoleaks, both successfully treated with a Palmaz stent.
After an average follow-up of 12 months, there have been no type 1, III or IV endoleaks, graft migration, aneurysm enlargement, conversions, ruptures, limb occlusions, or secondary procedures, said Dr. Hussain, who disclosed serving as a consultant for Trivascular and national principal investigator of the PostMarket Ovation Trial. There were 12 type II endoleaks (17%) and all have been clinically irrelevant.
Because of the Ovation’s novel O-ring sealing mechanism, “you get a pretty watertight seal ring on these patients,” he said. More importantly, shear stress is distributed evenly along the entire O-ring, which creates very minimal outward stress on the aorta, “maybe 2 or 3 atmospheres at best.”
Evidence continues to build that self-expandable stents place chronic outward stress on the aorta that causes degeneration of the aortic wall, resulting in eventual aortic neck dilation and endograft migration. While it’s been argued that disease progression leads to aortic dilation, the phenomenon took off after the arrival of endovascular stents, not during decades of open AAA repair, Dr. Hussain, also of the Vein & Vascular Center at the Christie Clinic in Champaign, said.
In the Ovation approval trial, proximal neck dilation at 2 years followed a similar curve in the Ovation and open repair cohorts, compared with those for the more traditional endografts, he noted.
The Ovation Prime system was approved in 2012 and in mid-2014, the Food and Drug Administration approved changes to the indication statement that eliminated the requirement for a minimal aortic neck length.
Essentially, the Ovation device can be placed in any patient if the diameter at 13 mm below the lowest renal artery (the site of the most proximal sealing ring) is within the treatable diameter range of the device (15.8 mm-30.4 mm), Dr. Hussain said.
“The idea of having a neck length is completely starting to go away,” he said. “And even though the trial by Endologix is looking at 1 centimeter as the current requirement for enrolling patients, I think eventually it’s going to get to the point where you’re not going to need a neck for the Nellix device either. You’re going to be able to treat patients who have very short, 1 to 2 millimeter necks, basically perirenal aneurysms, and get a seal on.”
The Nellix endovascular aneurysm sealing system (Endologix) is not commercially available in the U.S., but is the being evaluated in at least three studies. It consists of dual balloon-expandable end-frames surrounded by polymer-filled endobags and is designed to completely fill and seal the aortic aneurysm sac. Anatomical requirements for patients to be enrolled in clinical studies include a nonaneurysmal aortic neck length of ≥ 10 mm, nonaneurysmal aortic neck diameter of 18 mm-32 mm, maximum aortic blood flow lumen diameter of ≤ 60 mm, and common iliac artery diameter of 8 mm-35 mm, according to the company’s website.
CHICAGO – Real-world experience with novel endografts like the Ovation Prime abdominal endograft system is prompting some vascular specialists to rethink such central abdominal aortic aneurysm tenets as aortic neck dilation and minimum neck size.
“We started using this in our worst cases, patients with small caliber access vessels and very short aortic necks, to test this device, but over time we’ve pretty much made this our workhorse graft based on our outcomes,” Dr. Syed Hussain of the University of Illinois at Champaign-Urbana, said at a vascular surgery symposium sponsored by Northwestern University.
Among 67 patients with AAAs treated since the team’s first implant in November 2012, the technical success rate is 100%. At baseline, 35% of patients had access vessels < 7 mm, 45% had short aortic neck (< 15 mm), 60% had moderate to severe calcification (> 25% circumferential), and half had moderate to severe thrombus (> 25% circumferential).
The Ovation Prime (TriVascular Technologies) device is relatively quick and easy to put in, with an average procedure time of only 33 minutes, he said. Access was percutaneous in 27%, average blood loss was minimal at 60 mL, and average hospital stay was 1.7 days.
Two patients with severe comorbidities were admitted to the ICU and two patients experienced intraoperative type 1a endoleaks, both successfully treated with a Palmaz stent.
After an average follow-up of 12 months, there have been no type 1, III or IV endoleaks, graft migration, aneurysm enlargement, conversions, ruptures, limb occlusions, or secondary procedures, said Dr. Hussain, who disclosed serving as a consultant for Trivascular and national principal investigator of the PostMarket Ovation Trial. There were 12 type II endoleaks (17%) and all have been clinically irrelevant.
Because of the Ovation’s novel O-ring sealing mechanism, “you get a pretty watertight seal ring on these patients,” he said. More importantly, shear stress is distributed evenly along the entire O-ring, which creates very minimal outward stress on the aorta, “maybe 2 or 3 atmospheres at best.”
Evidence continues to build that self-expandable stents place chronic outward stress on the aorta that causes degeneration of the aortic wall, resulting in eventual aortic neck dilation and endograft migration. While it’s been argued that disease progression leads to aortic dilation, the phenomenon took off after the arrival of endovascular stents, not during decades of open AAA repair, Dr. Hussain, also of the Vein & Vascular Center at the Christie Clinic in Champaign, said.
In the Ovation approval trial, proximal neck dilation at 2 years followed a similar curve in the Ovation and open repair cohorts, compared with those for the more traditional endografts, he noted.
The Ovation Prime system was approved in 2012 and in mid-2014, the Food and Drug Administration approved changes to the indication statement that eliminated the requirement for a minimal aortic neck length.
Essentially, the Ovation device can be placed in any patient if the diameter at 13 mm below the lowest renal artery (the site of the most proximal sealing ring) is within the treatable diameter range of the device (15.8 mm-30.4 mm), Dr. Hussain said.
“The idea of having a neck length is completely starting to go away,” he said. “And even though the trial by Endologix is looking at 1 centimeter as the current requirement for enrolling patients, I think eventually it’s going to get to the point where you’re not going to need a neck for the Nellix device either. You’re going to be able to treat patients who have very short, 1 to 2 millimeter necks, basically perirenal aneurysms, and get a seal on.”
The Nellix endovascular aneurysm sealing system (Endologix) is not commercially available in the U.S., but is the being evaluated in at least three studies. It consists of dual balloon-expandable end-frames surrounded by polymer-filled endobags and is designed to completely fill and seal the aortic aneurysm sac. Anatomical requirements for patients to be enrolled in clinical studies include a nonaneurysmal aortic neck length of ≥ 10 mm, nonaneurysmal aortic neck diameter of 18 mm-32 mm, maximum aortic blood flow lumen diameter of ≤ 60 mm, and common iliac artery diameter of 8 mm-35 mm, according to the company’s website.
AT THE NORTHWESTERN VASCULAR SYMPOSIUM
Key clinical point: Requirement for an specified aortic neck for placement diminishing for new endografts.
Major finding: No type I, III or IV endoleaks, graft migration, aneurysm enlargement, conversions, ruptures, limb occlusions, or secondary procedures occurred after 12 months follow-up.
Data source: Retrospective analysis of 67 patients with AAA treated with Ovation Prime.
Disclosures: Dr. Hussain disclosed serving as a consultant for TriVascular and a national principal investigator for the PostMarket Ovation Trial.

Broadly implementing stroke embolectomy faces hurdles
NASHVILLE, TENN. – Results from three randomized controlled trials presented at the International Stroke Conference, plus the outcomes from a fourth trial first reported last fall, immediately established embolectomy as standard-of-care treatment for selected patients with acute ischemic stroke.
Stroke experts interviewed during the conference, however, said that making embolectomy routinely available to most U.S. stroke patients who would be candidates for the intervention will take months, if not years.
They envision challenges involving the availability of trained interventionalists, triage of patients to the right centers, and reimbursement issues as some of the obstacles to be dealt with before endovascular embolectomy aimed at removing intracerebral-artery occlusions in acute ischemic stroke patients becomes uniformly available.

Yet another challenge will arise when stroke-treatment groups that did not participate in the trials strive to replicate the success their colleagues reported by implementing the highly streamlined systems that were used in the trials for identifying appropriate stroke patients and for delivering treatment. Those systems were cited as an important reason why those studies succeeded in producing positive outcomes when similar embolectomy trials without the same efficiencies reported just a year or two ago failed to show benefit.
“The evidence makes it standard of care, but the challenge is that our systems are not set up. This is the big thing we will all go home to work on,” said Dr. Pooja Khatri, professor of neurology and director of acute stroke at the University of Cincinnati.
“You talk to everyone at this meeting, and what they want to go home and figure out is how can we deliver this care. It’s really challenging, at a myriad of levels,” said Dr. Colin P. Derdeyn, professor of neurology and director of the Center for Stroke and Cerebrovascular Disease at Washington University in St. Louis.
Growing endovascular availability
Arguably the most critical issue in rolling out endovascular stroke interventions more broadly is scaling up the number of centers that have the staff and systems in place to perform them. Clearly, the scope of providers able to deliver this treatment currently falls substantially short of what will be needed. “It’s kind of daunting to think about the [workforce] needs,” Dr. Khatri said in a talk at the conference, which was sponsored by the American Heart Association.
“In the United States, we’ve been building out a two-tier system, with comprehensive stroke centers capable of delivering this [endovascular embolectomy] treatment” and primary stroke centers capable of administering intravenous treatment with tissue plasminogen activator (TPA), the first treatment that patients eligible for embolectomy should receive, said Dr. Jeffrey L. Saver, professor of neurology and director of the stroke center at the University of California, Los Angeles, and lead investigator for one of the new embolectomy studies.

“Work groups have suggested about 60,000 U.S. stroke patients could potentially be treated with endovascular therapy, and we’d need about 300 comprehensive stroke centers to do this.” Dr. Saver estimated the current total of U.S. comprehensive stroke centers to be 75, a number that several others at the meeting pegged as more like 80, and they also noted that some centers are endovascular ready but have not received official comprehensive stroke center certification from the Joint Commission.
The extent to which availability of U.S. embolectomy remained limited through most of 2013 was apparent in data reported at the conference by Dr. Opeolu M. Adeoye, an emergency medicine physician and medical director of the telestroke program of the University of Cincinnati. During fiscal year 2013 (Oct. 2012 to Sept. 2013), 386,144 Medicare patients either older than 65 years or totally disabled had a primary hospital discharge diagnosis of stroke; of those, 5.1% had received thrombolytic therapy with intravenous TPA and 0.8% had undergone embolectomy. In a second analysis, he looked at stroke discharges and reperfusion treatments used in the 214 U.S. acute-care hospitals currently enrolled in StrokeNet, a program begun in 2013 by the National Institute of Neurological Disorders and Stroke to organize U.S. centers interested in participating in stroke trials.
During the same period, the 214 StrokeNet hospitals discharged 44,282 Medicare eligible patients who met the same age or disability criteria, with a TPA-treatment rate of 7.9% and an endovascular treatment rate of 2.2%. Although the StrokeNet hospitals treated roughly 11% of U.S. stroke patients in the specified demographic, they administered about 20% of the reperfusion treatment, Dr. Adeoye reported. He also highlighted that the 7.9% rate of TPA treatment among the StrokeNet hospitals correlated well with prior estimates that 6%-11% of stroke patients fulfill existing criteria for TPA treatment
A wide disparity existed in the rate of reperfusion use among StrokeNet hospitals. Sixty-seven hospitals, 31% of the StrokeNet group, treated at least 20 stroke patients with TPA during the study period, while 100 (47%) of the StrokeNet hospitals treated fewer than 10 acute stroke patients. The rate of those doing embolectomies was substantially lower, with 10 hospitals (5%) doing at least 20 endovascular procedures while 90% did fewer than 10.
Although Dr. Adeoye expressed confidence that the number of U.S. centers doing embolectomy cases will “change rapidly” following the new reports documenting the efficacy of the approach, he also acknowledged the challenges of growing the number of high-volume endovascular centers.
Centers that have been equivocal about embolectomy will now start doing it in a more concerted way, he predicted, but if cases get spread out and some sites do only a few patients a year, the quality of the procedures may suffer. “The more cases a site does, the better,” he noted, adding that regions that funnel all their stroke patients to a single endovascular site “do really well.”
“Right now, many hospitals want to do everything to get [fully] reimbursed and not send their patients down the line. There is a financial incentive to build up the stroke service at every hospital,” Dr. Derdeyn noted.
Another aspect to sorting out which centers start offering endovascular treatment will be the need to locate them in a rational way, as happened with trauma centers. Until now, placement of comprehensive stroke centers often depended on hospitals developing the capability as a marketing tool, noted Dr. Larry B. Goldstein, professor of neurology and director of the stroke center at Duke University in Durham, N.C. A hospital might achieve comprehensive stroke center certification, so a second center a few blocks away then follows suit seemingly to keep pace in a public-relations battle for cachet. The result has been an irrational clustering of centers with endovascular capability. He cited the situation in Cleveland, where comprehensive centers run by the Cleveland Clinic and Case Western stand a few dozen feet apart.
Challenges for triage
An analysis published last year by Dr. Adeoye and his colleagues showed that 56% of the U.S. population lived within a 60-minute drive of a hospital able to administer endovascular stroke treatment; by air, 85% had that access (Stroke 2014;45:3019-24). For TPA, 81% of people lived within a 60-minute drive of a center able to administer intravenous lytic treatment and 97% could reach these hospitals within an hour by air. While those numbers sound promising, though, fulfilling that potential depends on getting the right patients to the right hospitals.
Patient triage is perhaps the most vexing issue created by embolectomy’s success. For at least the short term, a limited number of centers will have the staffing and capacity to deliver endovascular embolectomy on a 24/7 basis to acute ischemic stroke patients who have a proximal blockage in a large cerebral artery. The relatively small number of sites able to offer embolectomy, and the much larger number of sites able to administer thrombolytic therapy with TPA, set the stage for some possible tension, or at least confusion, within communities over where an ambulance should bring an acute ischemic stroke patient.

“In some places they have trained the EMS [emergency medical services] to recognize severe strokes that are likely to benefit [from embolectomy], and they take those patients to places with endovascular capability. But there are some states with laws against doing this. There are major issues when EMS bypasses hospitals,” Dr. Derdeyn noted. “That’s the million-dollar question: How do you identify the stroke patients [with severe strokes who would benefit from embolectomy] and get them to where they need to go.” Like Dr. Adeoye, Dr. Derdeyn believes that endovascular treatment for stroke needs to be centralized at a relatively small number of high-volume centers.
“You can imagine that the fastest way to get stroke patients treated is to have them all go to one place, but that is much easier said than done,” Dr. Khatri said.
“Stent retrievers get cerebral arteries open, but that is not the biggest challenge. For the short term, the key issue is to get the correct patients to the correct hospitals where they can be treated by the correct team,” said Dr. Mayank Goyal, professor of diagnostic imaging at the University of Calgary (Alta.) and lead investigator for two of the three trials presented at the conference.
“You need a neurologist capable of deciding whether it really is a stroke, and pretty high-level imaging to identify the large-vessel occlusions that will benefit. Acquiring a CT angiography (CTA) image of the brain is a push-button process, but figuring out what the CTA says is not push button, especially the more sophisticated perfusion CT imaging to assess collateral circulation. I don’t see this capability happening in every catheterization laboratory,” Dr. Derdeyn said in an interview.
Another issue is volume. “Telemedicine may allow broader use of [more sophisticated] imaging, but if a place is only doing 20 endovascular procedures a year, they won’t have the best outcomes. Most small hospitals that today give patients TPA see 20 cases or fewer a year, and perhaps 5 patients will have a large-vessel occlusion,” Dr. Derdeyn said.
Before the new reports documenting the safety and efficacy of endovascular treatment, “we did not have the justification to bypass primary stroke centers and take patients directly to comprehensive stroke centers,” Dr. Khatri said. Now, “there is clear evidence that patients with severe strokes should not go to the nearby primary stroke center” but instead head directly for the centers capable of performing embolectomy. But Dr. Khatri also acknowledged that a complex calculation is needed to balance the trade off: Is it better to take a stroke patient more quickly to a nearby hospital that can only start TPA and perhaps later forward the patient to an embolectomy-ready hospital, or to transport the patient somewhat further to a facility able to deliver both TPA and embolectomy?
Dr. Khatri said that, in the Cincinnati area, “we have scheduled a retreat for March to start to plan how this will happen.” Her region includes just one comprehensive stroke center that already performs endovascular treatments for stroke, at the University of Cincinnati, which sits amid 16 other hospitals that perform acute stroke care and can administer TPA. “Ambulance-based triage will be a big issue,” she predicted.
Other aspects of improved triage will be training ambulance personal to better identify the more severe stroke patients who will most likely need endovascular treatment and improving communication between ambulance crews and receiving hospitals to further speed up a process that depends on quick treatment to get the best outcomes.
The ideal is “having paramedics call and tell us what is happening [in their ambulance] and give us as much information as possible so we can start planning for the patient’s arrival. Most hospitals don’t do this now; relatively few have their system well organized,” Dr. Goyal said in an interview. A finely orchestrated emergency transport system and hospital-based stroke team was part of the program developed at the University of Calgary by Dr. Goyal and his associates and which they credited with contributing to the successful embolectomy trial they led, called ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times)(N. Engl. J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414905]). Dr. Goyal said that he is now visiting hospitals around the world to assist them in setting up stroke-response systems that mimic what was successful in Calgary and the other centers that participated in ESCAPE.
Improving triage with better screening
A key to improved ambulance triage will be identifying a simple, evidence-based method for assessing stroke severity that ambulance personnel can use to determine what sort of care a patient needs and where the patient needs to go to. Although a couple of U.S. sites have begun pilot studies of field-based CT units that allow stroke patients to undergo imaging-based assessment in the field, clinical evaluation remains the main tool used in the ambulance.
One possible tool is the Los Angeles Motor Scale (LAMS), a stroke-assessment scoring system developed by Dr. Saver and his associates for ambulance use about a decade ago (Prehosp. Emerg. Care 2004;8:46-50). “A LAMS score of 4 or 5 [on a scale of 0-5] is a good starting point, and with time it might improve,” Dr. Goyal said.
The National Institutes of Health Stroke Scale (NIHSS) is a clinical assessment tool not designed for prehospital use, but a new analysis reported at the meeting showed value in using the NIHSS to identify stroke patients who are good candidates for endovascular treatment, further suggesting that a simple screening tool could potentially work in the ambulance to identify patients who probably need embolectomy.
The new analysis combined data from two randomized trials: The IMS (Interventional Management of Stroke) III trial, the results of which, published in early 2013, showed no incremental benefit of endovascular therapy plus TPA over TPA alone for patients with acute ischemic stroke (N. Engl. J. Med. 2013;368:893-903); and the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) trial, the results of which, published in January, showed a significant incremental benefit from endovascular treatment – it was the first of the four studies recently reported to show this benefit (N. Engl. J. Med. 2015;372:11-20).
The combined data included all patients from both studies with a NIHSS score of at least 20, indicating a very severe stroke. This produced a total of 342 patients, of whom 191 received intravenous TPA plus endovascular treatment and 152 received only TPA. After 90 days, 24% of the patients treated with endovascular treatment and 14% of those treated only with TPA had a modified Rankin Scale score of 0-2, indicating no or limited disability, Dr. Joseph P. Broderick reported at the conference. After adjustments for age and other potential confounders, treatment with endovascular therapy produced a statistically significant 85% improvement in patients achieving an acceptable modified Rankin Scale score at 90 days, said Dr. Broderick, professor of neurology and director of the neuroscience institute at the University of Cincinnati.
“The NIHSS score is a surrogate for clot size. It is an imperfect measure, especially at lower levels, but when the score is 20 or higher it means the patient has a big clot” that will likely not fully respond to TPA but potentially will respond to embolectomy, Dr. Broderick said in an interview. “A patient with a NIHSS score of 20 or higher has about a 95% risk of having an ongoing major artery occlusion despite TPA treatment.”
“The challenge is that we don’t have a fully validated [prehospital] scoring system. Several groups are trying to create one; in the meantime we may come up with certain clinical thresholds” that can reliably guide ambulance crews on the best place to take each stroke patient, Dr. Khatri said.
Dr. Khatri has received research support from Penumbra and Genentech. Dr. Derdeyn has received honoraria from Penumbra and holds equity in Pulse Therapeutics. Dr. Saver has been a consultant to and received research support from Covidien. Dr. Adeoye has been a speaker for Genentech. Dr. Goldstein had no disclosures. Dr. Goyal has been a consultant to and received research support from Covidien and holds a patent on using CT angiography to diagnose stroke. Dr. Broderick has received research support from Genentech.
[email protected]
On Twitter @mitchelzoler
NASHVILLE, TENN. – Results from three randomized controlled trials presented at the International Stroke Conference, plus the outcomes from a fourth trial first reported last fall, immediately established embolectomy as standard-of-care treatment for selected patients with acute ischemic stroke.
Stroke experts interviewed during the conference, however, said that making embolectomy routinely available to most U.S. stroke patients who would be candidates for the intervention will take months, if not years.
They envision challenges involving the availability of trained interventionalists, triage of patients to the right centers, and reimbursement issues as some of the obstacles to be dealt with before endovascular embolectomy aimed at removing intracerebral-artery occlusions in acute ischemic stroke patients becomes uniformly available.
Yet another challenge will arise when stroke-treatment groups that did not participate in the trials strive to replicate the success their colleagues reported by implementing the highly streamlined systems that were used in the trials for identifying appropriate stroke patients and for delivering treatment. Those systems were cited as an important reason why those studies succeeded in producing positive outcomes when similar embolectomy trials without the same efficiencies reported just a year or two ago failed to show benefit.
“The evidence makes it standard of care, but the challenge is that our systems are not set up. This is the big thing we will all go home to work on,” said Dr. Pooja Khatri, professor of neurology and director of acute stroke at the University of Cincinnati.
“You talk to everyone at this meeting, and what they want to go home and figure out is how can we deliver this care. It’s really challenging, at a myriad of levels,” said Dr. Colin P. Derdeyn, professor of neurology and director of the Center for Stroke and Cerebrovascular Disease at Washington University in St. Louis.
Growing endovascular availability
Arguably the most critical issue in rolling out endovascular stroke interventions more broadly is scaling up the number of centers that have the staff and systems in place to perform them. Clearly, the scope of providers able to deliver this treatment currently falls substantially short of what will be needed. “It’s kind of daunting to think about the [workforce] needs,” Dr. Khatri said in a talk at the conference, which was sponsored by the American Heart Association.
“In the United States, we’ve been building out a two-tier system, with comprehensive stroke centers capable of delivering this [endovascular embolectomy] treatment” and primary stroke centers capable of administering intravenous treatment with tissue plasminogen activator (TPA), the first treatment that patients eligible for embolectomy should receive, said Dr. Jeffrey L. Saver, professor of neurology and director of the stroke center at the University of California, Los Angeles, and lead investigator for one of the new embolectomy studies.
“Work groups have suggested about 60,000 U.S. stroke patients could potentially be treated with endovascular therapy, and we’d need about 300 comprehensive stroke centers to do this.” Dr. Saver estimated the current total of U.S. comprehensive stroke centers to be 75, a number that several others at the meeting pegged as more like 80, and they also noted that some centers are endovascular ready but have not received official comprehensive stroke center certification from the Joint Commission.
The extent to which availability of U.S. embolectomy remained limited through most of 2013 was apparent in data reported at the conference by Dr. Opeolu M. Adeoye, an emergency medicine physician and medical director of the telestroke program of the University of Cincinnati. During fiscal year 2013 (Oct. 2012 to Sept. 2013), 386,144 Medicare patients either older than 65 years or totally disabled had a primary hospital discharge diagnosis of stroke; of those, 5.1% had received thrombolytic therapy with intravenous TPA and 0.8% had undergone embolectomy. In a second analysis, he looked at stroke discharges and reperfusion treatments used in the 214 U.S. acute-care hospitals currently enrolled in StrokeNet, a program begun in 2013 by the National Institute of Neurological Disorders and Stroke to organize U.S. centers interested in participating in stroke trials.
During the same period, the 214 StrokeNet hospitals discharged 44,282 Medicare eligible patients who met the same age or disability criteria, with a TPA-treatment rate of 7.9% and an endovascular treatment rate of 2.2%. Although the StrokeNet hospitals treated roughly 11% of U.S. stroke patients in the specified demographic, they administered about 20% of the reperfusion treatment, Dr. Adeoye reported. He also highlighted that the 7.9% rate of TPA treatment among the StrokeNet hospitals correlated well with prior estimates that 6%-11% of stroke patients fulfill existing criteria for TPA treatment
A wide disparity existed in the rate of reperfusion use among StrokeNet hospitals. Sixty-seven hospitals, 31% of the StrokeNet group, treated at least 20 stroke patients with TPA during the study period, while 100 (47%) of the StrokeNet hospitals treated fewer than 10 acute stroke patients. The rate of those doing embolectomies was substantially lower, with 10 hospitals (5%) doing at least 20 endovascular procedures while 90% did fewer than 10.
Although Dr. Adeoye expressed confidence that the number of U.S. centers doing embolectomy cases will “change rapidly” following the new reports documenting the efficacy of the approach, he also acknowledged the challenges of growing the number of high-volume endovascular centers.
Centers that have been equivocal about embolectomy will now start doing it in a more concerted way, he predicted, but if cases get spread out and some sites do only a few patients a year, the quality of the procedures may suffer. “The more cases a site does, the better,” he noted, adding that regions that funnel all their stroke patients to a single endovascular site “do really well.”
“Right now, many hospitals want to do everything to get [fully] reimbursed and not send their patients down the line. There is a financial incentive to build up the stroke service at every hospital,” Dr. Derdeyn noted.
Another aspect to sorting out which centers start offering endovascular treatment will be the need to locate them in a rational way, as happened with trauma centers. Until now, placement of comprehensive stroke centers often depended on hospitals developing the capability as a marketing tool, noted Dr. Larry B. Goldstein, professor of neurology and director of the stroke center at Duke University in Durham, N.C. A hospital might achieve comprehensive stroke center certification, so a second center a few blocks away then follows suit seemingly to keep pace in a public-relations battle for cachet. The result has been an irrational clustering of centers with endovascular capability. He cited the situation in Cleveland, where comprehensive centers run by the Cleveland Clinic and Case Western stand a few dozen feet apart.
Challenges for triage
An analysis published last year by Dr. Adeoye and his colleagues showed that 56% of the U.S. population lived within a 60-minute drive of a hospital able to administer endovascular stroke treatment; by air, 85% had that access (Stroke 2014;45:3019-24). For TPA, 81% of people lived within a 60-minute drive of a center able to administer intravenous lytic treatment and 97% could reach these hospitals within an hour by air. While those numbers sound promising, though, fulfilling that potential depends on getting the right patients to the right hospitals.
Patient triage is perhaps the most vexing issue created by embolectomy’s success. For at least the short term, a limited number of centers will have the staffing and capacity to deliver endovascular embolectomy on a 24/7 basis to acute ischemic stroke patients who have a proximal blockage in a large cerebral artery. The relatively small number of sites able to offer embolectomy, and the much larger number of sites able to administer thrombolytic therapy with TPA, set the stage for some possible tension, or at least confusion, within communities over where an ambulance should bring an acute ischemic stroke patient.
“In some places they have trained the EMS [emergency medical services] to recognize severe strokes that are likely to benefit [from embolectomy], and they take those patients to places with endovascular capability. But there are some states with laws against doing this. There are major issues when EMS bypasses hospitals,” Dr. Derdeyn noted. “That’s the million-dollar question: How do you identify the stroke patients [with severe strokes who would benefit from embolectomy] and get them to where they need to go.” Like Dr. Adeoye, Dr. Derdeyn believes that endovascular treatment for stroke needs to be centralized at a relatively small number of high-volume centers.
“You can imagine that the fastest way to get stroke patients treated is to have them all go to one place, but that is much easier said than done,” Dr. Khatri said.
“Stent retrievers get cerebral arteries open, but that is not the biggest challenge. For the short term, the key issue is to get the correct patients to the correct hospitals where they can be treated by the correct team,” said Dr. Mayank Goyal, professor of diagnostic imaging at the University of Calgary (Alta.) and lead investigator for two of the three trials presented at the conference.
“You need a neurologist capable of deciding whether it really is a stroke, and pretty high-level imaging to identify the large-vessel occlusions that will benefit. Acquiring a CT angiography (CTA) image of the brain is a push-button process, but figuring out what the CTA says is not push button, especially the more sophisticated perfusion CT imaging to assess collateral circulation. I don’t see this capability happening in every catheterization laboratory,” Dr. Derdeyn said in an interview.
Another issue is volume. “Telemedicine may allow broader use of [more sophisticated] imaging, but if a place is only doing 20 endovascular procedures a year, they won’t have the best outcomes. Most small hospitals that today give patients TPA see 20 cases or fewer a year, and perhaps 5 patients will have a large-vessel occlusion,” Dr. Derdeyn said.
Before the new reports documenting the safety and efficacy of endovascular treatment, “we did not have the justification to bypass primary stroke centers and take patients directly to comprehensive stroke centers,” Dr. Khatri said. Now, “there is clear evidence that patients with severe strokes should not go to the nearby primary stroke center” but instead head directly for the centers capable of performing embolectomy. But Dr. Khatri also acknowledged that a complex calculation is needed to balance the trade off: Is it better to take a stroke patient more quickly to a nearby hospital that can only start TPA and perhaps later forward the patient to an embolectomy-ready hospital, or to transport the patient somewhat further to a facility able to deliver both TPA and embolectomy?
Dr. Khatri said that, in the Cincinnati area, “we have scheduled a retreat for March to start to plan how this will happen.” Her region includes just one comprehensive stroke center that already performs endovascular treatments for stroke, at the University of Cincinnati, which sits amid 16 other hospitals that perform acute stroke care and can administer TPA. “Ambulance-based triage will be a big issue,” she predicted.
Other aspects of improved triage will be training ambulance personal to better identify the more severe stroke patients who will most likely need endovascular treatment and improving communication between ambulance crews and receiving hospitals to further speed up a process that depends on quick treatment to get the best outcomes.
The ideal is “having paramedics call and tell us what is happening [in their ambulance] and give us as much information as possible so we can start planning for the patient’s arrival. Most hospitals don’t do this now; relatively few have their system well organized,” Dr. Goyal said in an interview. A finely orchestrated emergency transport system and hospital-based stroke team was part of the program developed at the University of Calgary by Dr. Goyal and his associates and which they credited with contributing to the successful embolectomy trial they led, called ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times)(N. Engl. J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414905]). Dr. Goyal said that he is now visiting hospitals around the world to assist them in setting up stroke-response systems that mimic what was successful in Calgary and the other centers that participated in ESCAPE.
Improving triage with better screening
A key to improved ambulance triage will be identifying a simple, evidence-based method for assessing stroke severity that ambulance personnel can use to determine what sort of care a patient needs and where the patient needs to go to. Although a couple of U.S. sites have begun pilot studies of field-based CT units that allow stroke patients to undergo imaging-based assessment in the field, clinical evaluation remains the main tool used in the ambulance.
One possible tool is the Los Angeles Motor Scale (LAMS), a stroke-assessment scoring system developed by Dr. Saver and his associates for ambulance use about a decade ago (Prehosp. Emerg. Care 2004;8:46-50). “A LAMS score of 4 or 5 [on a scale of 0-5] is a good starting point, and with time it might improve,” Dr. Goyal said.
The National Institutes of Health Stroke Scale (NIHSS) is a clinical assessment tool not designed for prehospital use, but a new analysis reported at the meeting showed value in using the NIHSS to identify stroke patients who are good candidates for endovascular treatment, further suggesting that a simple screening tool could potentially work in the ambulance to identify patients who probably need embolectomy.
The new analysis combined data from two randomized trials: The IMS (Interventional Management of Stroke) III trial, the results of which, published in early 2013, showed no incremental benefit of endovascular therapy plus TPA over TPA alone for patients with acute ischemic stroke (N. Engl. J. Med. 2013;368:893-903); and the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) trial, the results of which, published in January, showed a significant incremental benefit from endovascular treatment – it was the first of the four studies recently reported to show this benefit (N. Engl. J. Med. 2015;372:11-20).
The combined data included all patients from both studies with a NIHSS score of at least 20, indicating a very severe stroke. This produced a total of 342 patients, of whom 191 received intravenous TPA plus endovascular treatment and 152 received only TPA. After 90 days, 24% of the patients treated with endovascular treatment and 14% of those treated only with TPA had a modified Rankin Scale score of 0-2, indicating no or limited disability, Dr. Joseph P. Broderick reported at the conference. After adjustments for age and other potential confounders, treatment with endovascular therapy produced a statistically significant 85% improvement in patients achieving an acceptable modified Rankin Scale score at 90 days, said Dr. Broderick, professor of neurology and director of the neuroscience institute at the University of Cincinnati.
“The NIHSS score is a surrogate for clot size. It is an imperfect measure, especially at lower levels, but when the score is 20 or higher it means the patient has a big clot” that will likely not fully respond to TPA but potentially will respond to embolectomy, Dr. Broderick said in an interview. “A patient with a NIHSS score of 20 or higher has about a 95% risk of having an ongoing major artery occlusion despite TPA treatment.”
“The challenge is that we don’t have a fully validated [prehospital] scoring system. Several groups are trying to create one; in the meantime we may come up with certain clinical thresholds” that can reliably guide ambulance crews on the best place to take each stroke patient, Dr. Khatri said.
Dr. Khatri has received research support from Penumbra and Genentech. Dr. Derdeyn has received honoraria from Penumbra and holds equity in Pulse Therapeutics. Dr. Saver has been a consultant to and received research support from Covidien. Dr. Adeoye has been a speaker for Genentech. Dr. Goldstein had no disclosures. Dr. Goyal has been a consultant to and received research support from Covidien and holds a patent on using CT angiography to diagnose stroke. Dr. Broderick has received research support from Genentech.
[email protected]
On Twitter @mitchelzoler
NASHVILLE, TENN. – Results from three randomized controlled trials presented at the International Stroke Conference, plus the outcomes from a fourth trial first reported last fall, immediately established embolectomy as standard-of-care treatment for selected patients with acute ischemic stroke.
Stroke experts interviewed during the conference, however, said that making embolectomy routinely available to most U.S. stroke patients who would be candidates for the intervention will take months, if not years.
They envision challenges involving the availability of trained interventionalists, triage of patients to the right centers, and reimbursement issues as some of the obstacles to be dealt with before endovascular embolectomy aimed at removing intracerebral-artery occlusions in acute ischemic stroke patients becomes uniformly available.
Yet another challenge will arise when stroke-treatment groups that did not participate in the trials strive to replicate the success their colleagues reported by implementing the highly streamlined systems that were used in the trials for identifying appropriate stroke patients and for delivering treatment. Those systems were cited as an important reason why those studies succeeded in producing positive outcomes when similar embolectomy trials without the same efficiencies reported just a year or two ago failed to show benefit.
“The evidence makes it standard of care, but the challenge is that our systems are not set up. This is the big thing we will all go home to work on,” said Dr. Pooja Khatri, professor of neurology and director of acute stroke at the University of Cincinnati.
“You talk to everyone at this meeting, and what they want to go home and figure out is how can we deliver this care. It’s really challenging, at a myriad of levels,” said Dr. Colin P. Derdeyn, professor of neurology and director of the Center for Stroke and Cerebrovascular Disease at Washington University in St. Louis.
Growing endovascular availability
Arguably the most critical issue in rolling out endovascular stroke interventions more broadly is scaling up the number of centers that have the staff and systems in place to perform them. Clearly, the scope of providers able to deliver this treatment currently falls substantially short of what will be needed. “It’s kind of daunting to think about the [workforce] needs,” Dr. Khatri said in a talk at the conference, which was sponsored by the American Heart Association.
“In the United States, we’ve been building out a two-tier system, with comprehensive stroke centers capable of delivering this [endovascular embolectomy] treatment” and primary stroke centers capable of administering intravenous treatment with tissue plasminogen activator (TPA), the first treatment that patients eligible for embolectomy should receive, said Dr. Jeffrey L. Saver, professor of neurology and director of the stroke center at the University of California, Los Angeles, and lead investigator for one of the new embolectomy studies.
“Work groups have suggested about 60,000 U.S. stroke patients could potentially be treated with endovascular therapy, and we’d need about 300 comprehensive stroke centers to do this.” Dr. Saver estimated the current total of U.S. comprehensive stroke centers to be 75, a number that several others at the meeting pegged as more like 80, and they also noted that some centers are endovascular ready but have not received official comprehensive stroke center certification from the Joint Commission.
The extent to which availability of U.S. embolectomy remained limited through most of 2013 was apparent in data reported at the conference by Dr. Opeolu M. Adeoye, an emergency medicine physician and medical director of the telestroke program of the University of Cincinnati. During fiscal year 2013 (Oct. 2012 to Sept. 2013), 386,144 Medicare patients either older than 65 years or totally disabled had a primary hospital discharge diagnosis of stroke; of those, 5.1% had received thrombolytic therapy with intravenous TPA and 0.8% had undergone embolectomy. In a second analysis, he looked at stroke discharges and reperfusion treatments used in the 214 U.S. acute-care hospitals currently enrolled in StrokeNet, a program begun in 2013 by the National Institute of Neurological Disorders and Stroke to organize U.S. centers interested in participating in stroke trials.
During the same period, the 214 StrokeNet hospitals discharged 44,282 Medicare eligible patients who met the same age or disability criteria, with a TPA-treatment rate of 7.9% and an endovascular treatment rate of 2.2%. Although the StrokeNet hospitals treated roughly 11% of U.S. stroke patients in the specified demographic, they administered about 20% of the reperfusion treatment, Dr. Adeoye reported. He also highlighted that the 7.9% rate of TPA treatment among the StrokeNet hospitals correlated well with prior estimates that 6%-11% of stroke patients fulfill existing criteria for TPA treatment
A wide disparity existed in the rate of reperfusion use among StrokeNet hospitals. Sixty-seven hospitals, 31% of the StrokeNet group, treated at least 20 stroke patients with TPA during the study period, while 100 (47%) of the StrokeNet hospitals treated fewer than 10 acute stroke patients. The rate of those doing embolectomies was substantially lower, with 10 hospitals (5%) doing at least 20 endovascular procedures while 90% did fewer than 10.
Although Dr. Adeoye expressed confidence that the number of U.S. centers doing embolectomy cases will “change rapidly” following the new reports documenting the efficacy of the approach, he also acknowledged the challenges of growing the number of high-volume endovascular centers.
Centers that have been equivocal about embolectomy will now start doing it in a more concerted way, he predicted, but if cases get spread out and some sites do only a few patients a year, the quality of the procedures may suffer. “The more cases a site does, the better,” he noted, adding that regions that funnel all their stroke patients to a single endovascular site “do really well.”
“Right now, many hospitals want to do everything to get [fully] reimbursed and not send their patients down the line. There is a financial incentive to build up the stroke service at every hospital,” Dr. Derdeyn noted.
Another aspect to sorting out which centers start offering endovascular treatment will be the need to locate them in a rational way, as happened with trauma centers. Until now, placement of comprehensive stroke centers often depended on hospitals developing the capability as a marketing tool, noted Dr. Larry B. Goldstein, professor of neurology and director of the stroke center at Duke University in Durham, N.C. A hospital might achieve comprehensive stroke center certification, so a second center a few blocks away then follows suit seemingly to keep pace in a public-relations battle for cachet. The result has been an irrational clustering of centers with endovascular capability. He cited the situation in Cleveland, where comprehensive centers run by the Cleveland Clinic and Case Western stand a few dozen feet apart.
Challenges for triage
An analysis published last year by Dr. Adeoye and his colleagues showed that 56% of the U.S. population lived within a 60-minute drive of a hospital able to administer endovascular stroke treatment; by air, 85% had that access (Stroke 2014;45:3019-24). For TPA, 81% of people lived within a 60-minute drive of a center able to administer intravenous lytic treatment and 97% could reach these hospitals within an hour by air. While those numbers sound promising, though, fulfilling that potential depends on getting the right patients to the right hospitals.
Patient triage is perhaps the most vexing issue created by embolectomy’s success. For at least the short term, a limited number of centers will have the staffing and capacity to deliver endovascular embolectomy on a 24/7 basis to acute ischemic stroke patients who have a proximal blockage in a large cerebral artery. The relatively small number of sites able to offer embolectomy, and the much larger number of sites able to administer thrombolytic therapy with TPA, set the stage for some possible tension, or at least confusion, within communities over where an ambulance should bring an acute ischemic stroke patient.
“In some places they have trained the EMS [emergency medical services] to recognize severe strokes that are likely to benefit [from embolectomy], and they take those patients to places with endovascular capability. But there are some states with laws against doing this. There are major issues when EMS bypasses hospitals,” Dr. Derdeyn noted. “That’s the million-dollar question: How do you identify the stroke patients [with severe strokes who would benefit from embolectomy] and get them to where they need to go.” Like Dr. Adeoye, Dr. Derdeyn believes that endovascular treatment for stroke needs to be centralized at a relatively small number of high-volume centers.
“You can imagine that the fastest way to get stroke patients treated is to have them all go to one place, but that is much easier said than done,” Dr. Khatri said.
“Stent retrievers get cerebral arteries open, but that is not the biggest challenge. For the short term, the key issue is to get the correct patients to the correct hospitals where they can be treated by the correct team,” said Dr. Mayank Goyal, professor of diagnostic imaging at the University of Calgary (Alta.) and lead investigator for two of the three trials presented at the conference.
“You need a neurologist capable of deciding whether it really is a stroke, and pretty high-level imaging to identify the large-vessel occlusions that will benefit. Acquiring a CT angiography (CTA) image of the brain is a push-button process, but figuring out what the CTA says is not push button, especially the more sophisticated perfusion CT imaging to assess collateral circulation. I don’t see this capability happening in every catheterization laboratory,” Dr. Derdeyn said in an interview.
Another issue is volume. “Telemedicine may allow broader use of [more sophisticated] imaging, but if a place is only doing 20 endovascular procedures a year, they won’t have the best outcomes. Most small hospitals that today give patients TPA see 20 cases or fewer a year, and perhaps 5 patients will have a large-vessel occlusion,” Dr. Derdeyn said.
Before the new reports documenting the safety and efficacy of endovascular treatment, “we did not have the justification to bypass primary stroke centers and take patients directly to comprehensive stroke centers,” Dr. Khatri said. Now, “there is clear evidence that patients with severe strokes should not go to the nearby primary stroke center” but instead head directly for the centers capable of performing embolectomy. But Dr. Khatri also acknowledged that a complex calculation is needed to balance the trade off: Is it better to take a stroke patient more quickly to a nearby hospital that can only start TPA and perhaps later forward the patient to an embolectomy-ready hospital, or to transport the patient somewhat further to a facility able to deliver both TPA and embolectomy?
Dr. Khatri said that, in the Cincinnati area, “we have scheduled a retreat for March to start to plan how this will happen.” Her region includes just one comprehensive stroke center that already performs endovascular treatments for stroke, at the University of Cincinnati, which sits amid 16 other hospitals that perform acute stroke care and can administer TPA. “Ambulance-based triage will be a big issue,” she predicted.
Other aspects of improved triage will be training ambulance personal to better identify the more severe stroke patients who will most likely need endovascular treatment and improving communication between ambulance crews and receiving hospitals to further speed up a process that depends on quick treatment to get the best outcomes.
The ideal is “having paramedics call and tell us what is happening [in their ambulance] and give us as much information as possible so we can start planning for the patient’s arrival. Most hospitals don’t do this now; relatively few have their system well organized,” Dr. Goyal said in an interview. A finely orchestrated emergency transport system and hospital-based stroke team was part of the program developed at the University of Calgary by Dr. Goyal and his associates and which they credited with contributing to the successful embolectomy trial they led, called ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times)(N. Engl. J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414905]). Dr. Goyal said that he is now visiting hospitals around the world to assist them in setting up stroke-response systems that mimic what was successful in Calgary and the other centers that participated in ESCAPE.
Improving triage with better screening
A key to improved ambulance triage will be identifying a simple, evidence-based method for assessing stroke severity that ambulance personnel can use to determine what sort of care a patient needs and where the patient needs to go to. Although a couple of U.S. sites have begun pilot studies of field-based CT units that allow stroke patients to undergo imaging-based assessment in the field, clinical evaluation remains the main tool used in the ambulance.
One possible tool is the Los Angeles Motor Scale (LAMS), a stroke-assessment scoring system developed by Dr. Saver and his associates for ambulance use about a decade ago (Prehosp. Emerg. Care 2004;8:46-50). “A LAMS score of 4 or 5 [on a scale of 0-5] is a good starting point, and with time it might improve,” Dr. Goyal said.
The National Institutes of Health Stroke Scale (NIHSS) is a clinical assessment tool not designed for prehospital use, but a new analysis reported at the meeting showed value in using the NIHSS to identify stroke patients who are good candidates for endovascular treatment, further suggesting that a simple screening tool could potentially work in the ambulance to identify patients who probably need embolectomy.
The new analysis combined data from two randomized trials: The IMS (Interventional Management of Stroke) III trial, the results of which, published in early 2013, showed no incremental benefit of endovascular therapy plus TPA over TPA alone for patients with acute ischemic stroke (N. Engl. J. Med. 2013;368:893-903); and the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) trial, the results of which, published in January, showed a significant incremental benefit from endovascular treatment – it was the first of the four studies recently reported to show this benefit (N. Engl. J. Med. 2015;372:11-20).
The combined data included all patients from both studies with a NIHSS score of at least 20, indicating a very severe stroke. This produced a total of 342 patients, of whom 191 received intravenous TPA plus endovascular treatment and 152 received only TPA. After 90 days, 24% of the patients treated with endovascular treatment and 14% of those treated only with TPA had a modified Rankin Scale score of 0-2, indicating no or limited disability, Dr. Joseph P. Broderick reported at the conference. After adjustments for age and other potential confounders, treatment with endovascular therapy produced a statistically significant 85% improvement in patients achieving an acceptable modified Rankin Scale score at 90 days, said Dr. Broderick, professor of neurology and director of the neuroscience institute at the University of Cincinnati.
“The NIHSS score is a surrogate for clot size. It is an imperfect measure, especially at lower levels, but when the score is 20 or higher it means the patient has a big clot” that will likely not fully respond to TPA but potentially will respond to embolectomy, Dr. Broderick said in an interview. “A patient with a NIHSS score of 20 or higher has about a 95% risk of having an ongoing major artery occlusion despite TPA treatment.”
“The challenge is that we don’t have a fully validated [prehospital] scoring system. Several groups are trying to create one; in the meantime we may come up with certain clinical thresholds” that can reliably guide ambulance crews on the best place to take each stroke patient, Dr. Khatri said.
Dr. Khatri has received research support from Penumbra and Genentech. Dr. Derdeyn has received honoraria from Penumbra and holds equity in Pulse Therapeutics. Dr. Saver has been a consultant to and received research support from Covidien. Dr. Adeoye has been a speaker for Genentech. Dr. Goldstein had no disclosures. Dr. Goyal has been a consultant to and received research support from Covidien and holds a patent on using CT angiography to diagnose stroke. Dr. Broderick has received research support from Genentech.
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE INTERNATIONAL STROKE CONFERENCE

VIDEO: Challenges abound in rolling out stroke embolectomy
NASHVILLE, TENN. – U.S. stroke specialists now face the challenge of making endovascular embolectomy a routinely available option for selected patients with acute ischemic stroke, Dr. Pooja Khatri said in an interview at the International Stroke Conference.
During the conference, which was sponsored by the American Heart Association, new reports from three independent, randomized controlled trials, as well as data from a fourth study published in January, collectively established endovascular embolectomy as the new standard-of-care treatment for acute ischemic stroke patients with a proximal occlusion of a large, intracerebral artery. The stroke community, however, now faces the responsibility of figuring out how to make this a reality.
Among the hurdles they face are using CT imaging or other methods to identify in daily practice the specific patients who will get the biggest benefit from endovascular treatment and finding a consensus within each region on how to triage acute stroke patients to centers that can perform embolectomy, said Dr. Khatri, professor of neurology and director of acute stroke at the University of Cincinnati. In Cincinnati, Dr. Khatri and her colleagues are planning to soon hold a retreat with representatives from other area hospitals to try to work out the logistics.Dr. Khatri has received research support from Penumbra and Genentech.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
NASHVILLE, TENN. – U.S. stroke specialists now face the challenge of making endovascular embolectomy a routinely available option for selected patients with acute ischemic stroke, Dr. Pooja Khatri said in an interview at the International Stroke Conference.
During the conference, which was sponsored by the American Heart Association, new reports from three independent, randomized controlled trials, as well as data from a fourth study published in January, collectively established endovascular embolectomy as the new standard-of-care treatment for acute ischemic stroke patients with a proximal occlusion of a large, intracerebral artery. The stroke community, however, now faces the responsibility of figuring out how to make this a reality.
Among the hurdles they face are using CT imaging or other methods to identify in daily practice the specific patients who will get the biggest benefit from endovascular treatment and finding a consensus within each region on how to triage acute stroke patients to centers that can perform embolectomy, said Dr. Khatri, professor of neurology and director of acute stroke at the University of Cincinnati. In Cincinnati, Dr. Khatri and her colleagues are planning to soon hold a retreat with representatives from other area hospitals to try to work out the logistics.Dr. Khatri has received research support from Penumbra and Genentech.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
NASHVILLE, TENN. – U.S. stroke specialists now face the challenge of making endovascular embolectomy a routinely available option for selected patients with acute ischemic stroke, Dr. Pooja Khatri said in an interview at the International Stroke Conference.
During the conference, which was sponsored by the American Heart Association, new reports from three independent, randomized controlled trials, as well as data from a fourth study published in January, collectively established endovascular embolectomy as the new standard-of-care treatment for acute ischemic stroke patients with a proximal occlusion of a large, intracerebral artery. The stroke community, however, now faces the responsibility of figuring out how to make this a reality.
Among the hurdles they face are using CT imaging or other methods to identify in daily practice the specific patients who will get the biggest benefit from endovascular treatment and finding a consensus within each region on how to triage acute stroke patients to centers that can perform embolectomy, said Dr. Khatri, professor of neurology and director of acute stroke at the University of Cincinnati. In Cincinnati, Dr. Khatri and her colleagues are planning to soon hold a retreat with representatives from other area hospitals to try to work out the logistics.Dr. Khatri has received research support from Penumbra and Genentech.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE INTERNATIONAL STROKE CONFERENCE

Haplo-BMT feasible in high-risk malignancies

Photo by Chad McNeeley
SAN DIEGO—Haploidentical bone marrow transplant (haplo-BMT) is a feasible option for patients with high-risk hematologic malignancies who don’t have timely access to an HLA-matched donor, according to a speaker at the 2015 BMT Tandem Meetings.
Haplo-BMT using myeloablative conditioning, T-cell replete grafts, and post-transplant cyclophosphamide elicited “excellent” rates of engraftment, graft-vs-host disease (GVHD), and transplant-related mortality, said Heather Symons, MD, of The Johns Hopkins University School of Medicine in Baltimore, Maryland.
Dr Symons presented these results at the meeting as abstract 6*, which was chosen as one of the meeting’s “Best Abstracts.” The research was funded by Otsuka Pharmaceuticals.
Dr Symons and her colleagues conducted a phase 2 study of 96 patients with high-risk hematologic malignancies and a median age of 42 (range, 1-65). Males made up 58% of the population.
Diagnoses included acute and chronic leukemias, lymphomas, multiple myeloma, and myelodysplastic syndromes. Some patients were in complete remission, and some were in chemo-sensitive partial remission. There was also a mix of minimal residual disease positivity and negativity.
“Given the heterogeneity of these patients, we further classified our patients by disease risk index,” Dr Symons said. “We used the revised disease risk index as published by Armand in 2013. The disease risk index, or DRI, assigned patients into overall survival risk groups based on disease type and status.”
So 6 patients had a low DRI, 61 had an intermediate DRI, and 29 had a high DRI.
For most patients (n=73), conditioning consisted of intravenous busulfan (pharmacokinetically adjusted) on days –6 to –3 and cyclophosphamide (50 mg/kg/day) on days –2 and –1. But 23 patients (those with acute lymphocytic leukemia or lymphoblastic lymphoma) received cyclophosphamide (50 mg/kg/day) on days –5 and –4 and total body irradiation (200 cGy twice daily) on days –3 to -1.
All patients received T-cell-replete bone marrow from haploidentical, related donors. The median number of HLA mismatches was 4.
Post-transplant immunosuppression consisted of cyclophosphamide (50 mg/kg/day) on days 3 and 4, followed by mycophenolate mofetil for 30 days and tacrolimus for 6 months.
‘Excellent’ outcomes
The median follow-up was 18 months (range, 3-59). The median time to neutrophil engraftment was 24 days, and the median time to platelet engraftment was 29 days. Ninety-one percent of patients had donor chimerism greater than 95% at day 60.
The cumulative incidence of acute GVHD was 17% for grades 2-4 and 7% for grades 3-4. The cumulative incidence of chronic GHVD was 15%. For moderate-to-severe chronic GVHD, it was 5%.
Twenty-four percent of patients had CMV reactivation, and 22% had hemorrhagic cystitis.
The rate of relapse was 36% at 1 year and 44% at 3 years. The transplant-related mortality rate was 6% at 100 days and 11% at 1 year.
Ten patients died—2 from GVHD, 1 of cardiomyopathy, 2 of veno-occlusive disease, 1 of drug-induced liver injury, 2 due to infection, and 2 of unknown causes.
Overall survival was 72% at 1 year, 57% at 2 years, and 51% at 3 years. Event-free survival was 56% at 1 year, 51% at 2 years, and 47% at 3 years.
A multivariate analysis revealed that overall survival decreased with increasing age and increasing DRI.
Compared to patients younger than 20, the hazard ratio (HR) was 6.3 for patients ages 20 to 50 (P=0.02) and 4.7 for patients older than 50 (P=0.04). Compared to patients with a low or intermediate DRI, the HR was 2.2 for those with a high DRI (P=0.03).
The analysis also indicated that increasing age and donor CMV-positivity conferred worse event-free survival.
Compared to patients younger than 20, the HR was 3.6 for patients ages 20 to 50 (P=0.04) and 4.0 for patients older than 50 (P=0.03). Compared to patients who had a CMV-negative donor, the HR was 2.2 for patients who had a CMV-positive donor (P=0.01).
“In conclusion, myeloablative haploidentical bone marrow transplantation with post-transplantation cyclophosphamide for high-risk hematologic malignancies has excellent rates of engraftment, graft-vs-host disease, and transplant-related mortality, with results that are similar to those described in myeloablative HLA-matched bone marrow transplantation,” Dr Symons said.
“Overall, this seems a feasible option for high-risk patients who lack timely access to an HLA-matched donor and warrants continued study. We are soon to start enrolling patients on a Pediatric Blood & Marrow Transplant Consortium trial using myeloablative conditioning, haploidentical donors, and post-transplantation cyclophosphamide.” ![]()
*Information in the abstract differs from that presented at the meeting.
Photo by Chad McNeeley
SAN DIEGO—Haploidentical bone marrow transplant (haplo-BMT) is a feasible option for patients with high-risk hematologic malignancies who don’t have timely access to an HLA-matched donor, according to a speaker at the 2015 BMT Tandem Meetings.
Haplo-BMT using myeloablative conditioning, T-cell replete grafts, and post-transplant cyclophosphamide elicited “excellent” rates of engraftment, graft-vs-host disease (GVHD), and transplant-related mortality, said Heather Symons, MD, of The Johns Hopkins University School of Medicine in Baltimore, Maryland.
Dr Symons presented these results at the meeting as abstract 6*, which was chosen as one of the meeting’s “Best Abstracts.” The research was funded by Otsuka Pharmaceuticals.
Dr Symons and her colleagues conducted a phase 2 study of 96 patients with high-risk hematologic malignancies and a median age of 42 (range, 1-65). Males made up 58% of the population.
Diagnoses included acute and chronic leukemias, lymphomas, multiple myeloma, and myelodysplastic syndromes. Some patients were in complete remission, and some were in chemo-sensitive partial remission. There was also a mix of minimal residual disease positivity and negativity.
“Given the heterogeneity of these patients, we further classified our patients by disease risk index,” Dr Symons said. “We used the revised disease risk index as published by Armand in 2013. The disease risk index, or DRI, assigned patients into overall survival risk groups based on disease type and status.”
So 6 patients had a low DRI, 61 had an intermediate DRI, and 29 had a high DRI.
For most patients (n=73), conditioning consisted of intravenous busulfan (pharmacokinetically adjusted) on days –6 to –3 and cyclophosphamide (50 mg/kg/day) on days –2 and –1. But 23 patients (those with acute lymphocytic leukemia or lymphoblastic lymphoma) received cyclophosphamide (50 mg/kg/day) on days –5 and –4 and total body irradiation (200 cGy twice daily) on days –3 to -1.
All patients received T-cell-replete bone marrow from haploidentical, related donors. The median number of HLA mismatches was 4.
Post-transplant immunosuppression consisted of cyclophosphamide (50 mg/kg/day) on days 3 and 4, followed by mycophenolate mofetil for 30 days and tacrolimus for 6 months.
‘Excellent’ outcomes
The median follow-up was 18 months (range, 3-59). The median time to neutrophil engraftment was 24 days, and the median time to platelet engraftment was 29 days. Ninety-one percent of patients had donor chimerism greater than 95% at day 60.
The cumulative incidence of acute GVHD was 17% for grades 2-4 and 7% for grades 3-4. The cumulative incidence of chronic GHVD was 15%. For moderate-to-severe chronic GVHD, it was 5%.
Twenty-four percent of patients had CMV reactivation, and 22% had hemorrhagic cystitis.
The rate of relapse was 36% at 1 year and 44% at 3 years. The transplant-related mortality rate was 6% at 100 days and 11% at 1 year.
Ten patients died—2 from GVHD, 1 of cardiomyopathy, 2 of veno-occlusive disease, 1 of drug-induced liver injury, 2 due to infection, and 2 of unknown causes.
Overall survival was 72% at 1 year, 57% at 2 years, and 51% at 3 years. Event-free survival was 56% at 1 year, 51% at 2 years, and 47% at 3 years.
A multivariate analysis revealed that overall survival decreased with increasing age and increasing DRI.
Compared to patients younger than 20, the hazard ratio (HR) was 6.3 for patients ages 20 to 50 (P=0.02) and 4.7 for patients older than 50 (P=0.04). Compared to patients with a low or intermediate DRI, the HR was 2.2 for those with a high DRI (P=0.03).
The analysis also indicated that increasing age and donor CMV-positivity conferred worse event-free survival.
Compared to patients younger than 20, the HR was 3.6 for patients ages 20 to 50 (P=0.04) and 4.0 for patients older than 50 (P=0.03). Compared to patients who had a CMV-negative donor, the HR was 2.2 for patients who had a CMV-positive donor (P=0.01).
“In conclusion, myeloablative haploidentical bone marrow transplantation with post-transplantation cyclophosphamide for high-risk hematologic malignancies has excellent rates of engraftment, graft-vs-host disease, and transplant-related mortality, with results that are similar to those described in myeloablative HLA-matched bone marrow transplantation,” Dr Symons said.
“Overall, this seems a feasible option for high-risk patients who lack timely access to an HLA-matched donor and warrants continued study. We are soon to start enrolling patients on a Pediatric Blood & Marrow Transplant Consortium trial using myeloablative conditioning, haploidentical donors, and post-transplantation cyclophosphamide.” ![]()
*Information in the abstract differs from that presented at the meeting.
Photo by Chad McNeeley
SAN DIEGO—Haploidentical bone marrow transplant (haplo-BMT) is a feasible option for patients with high-risk hematologic malignancies who don’t have timely access to an HLA-matched donor, according to a speaker at the 2015 BMT Tandem Meetings.
Haplo-BMT using myeloablative conditioning, T-cell replete grafts, and post-transplant cyclophosphamide elicited “excellent” rates of engraftment, graft-vs-host disease (GVHD), and transplant-related mortality, said Heather Symons, MD, of The Johns Hopkins University School of Medicine in Baltimore, Maryland.
Dr Symons presented these results at the meeting as abstract 6*, which was chosen as one of the meeting’s “Best Abstracts.” The research was funded by Otsuka Pharmaceuticals.
Dr Symons and her colleagues conducted a phase 2 study of 96 patients with high-risk hematologic malignancies and a median age of 42 (range, 1-65). Males made up 58% of the population.
Diagnoses included acute and chronic leukemias, lymphomas, multiple myeloma, and myelodysplastic syndromes. Some patients were in complete remission, and some were in chemo-sensitive partial remission. There was also a mix of minimal residual disease positivity and negativity.
“Given the heterogeneity of these patients, we further classified our patients by disease risk index,” Dr Symons said. “We used the revised disease risk index as published by Armand in 2013. The disease risk index, or DRI, assigned patients into overall survival risk groups based on disease type and status.”
So 6 patients had a low DRI, 61 had an intermediate DRI, and 29 had a high DRI.
For most patients (n=73), conditioning consisted of intravenous busulfan (pharmacokinetically adjusted) on days –6 to –3 and cyclophosphamide (50 mg/kg/day) on days –2 and –1. But 23 patients (those with acute lymphocytic leukemia or lymphoblastic lymphoma) received cyclophosphamide (50 mg/kg/day) on days –5 and –4 and total body irradiation (200 cGy twice daily) on days –3 to -1.
All patients received T-cell-replete bone marrow from haploidentical, related donors. The median number of HLA mismatches was 4.
Post-transplant immunosuppression consisted of cyclophosphamide (50 mg/kg/day) on days 3 and 4, followed by mycophenolate mofetil for 30 days and tacrolimus for 6 months.
‘Excellent’ outcomes
The median follow-up was 18 months (range, 3-59). The median time to neutrophil engraftment was 24 days, and the median time to platelet engraftment was 29 days. Ninety-one percent of patients had donor chimerism greater than 95% at day 60.
The cumulative incidence of acute GVHD was 17% for grades 2-4 and 7% for grades 3-4. The cumulative incidence of chronic GHVD was 15%. For moderate-to-severe chronic GVHD, it was 5%.
Twenty-four percent of patients had CMV reactivation, and 22% had hemorrhagic cystitis.
The rate of relapse was 36% at 1 year and 44% at 3 years. The transplant-related mortality rate was 6% at 100 days and 11% at 1 year.
Ten patients died—2 from GVHD, 1 of cardiomyopathy, 2 of veno-occlusive disease, 1 of drug-induced liver injury, 2 due to infection, and 2 of unknown causes.
Overall survival was 72% at 1 year, 57% at 2 years, and 51% at 3 years. Event-free survival was 56% at 1 year, 51% at 2 years, and 47% at 3 years.
A multivariate analysis revealed that overall survival decreased with increasing age and increasing DRI.
Compared to patients younger than 20, the hazard ratio (HR) was 6.3 for patients ages 20 to 50 (P=0.02) and 4.7 for patients older than 50 (P=0.04). Compared to patients with a low or intermediate DRI, the HR was 2.2 for those with a high DRI (P=0.03).
The analysis also indicated that increasing age and donor CMV-positivity conferred worse event-free survival.
Compared to patients younger than 20, the HR was 3.6 for patients ages 20 to 50 (P=0.04) and 4.0 for patients older than 50 (P=0.03). Compared to patients who had a CMV-negative donor, the HR was 2.2 for patients who had a CMV-positive donor (P=0.01).
“In conclusion, myeloablative haploidentical bone marrow transplantation with post-transplantation cyclophosphamide for high-risk hematologic malignancies has excellent rates of engraftment, graft-vs-host disease, and transplant-related mortality, with results that are similar to those described in myeloablative HLA-matched bone marrow transplantation,” Dr Symons said.
“Overall, this seems a feasible option for high-risk patients who lack timely access to an HLA-matched donor and warrants continued study. We are soon to start enrolling patients on a Pediatric Blood & Marrow Transplant Consortium trial using myeloablative conditioning, haploidentical donors, and post-transplantation cyclophosphamide.” ![]()
*Information in the abstract differs from that presented at the meeting.