User login
Evidence questioned in debate over monitoring dabigatran levels to avert bleeds
The manufacturer of the oral anticoagulant dabigatran "withheld analyses that calculate how many major bleeds dose adjustment could prevent," the BMJ charges in an article based on internal documents released during litigation in the United States and freedom of information act requests obtained by the journal.
Boehringer Ingelheim "found that if the plasma levels of the drug were measured and the dose was adjusted accordingly major bleeds could be reduced by 30%-40%, compared with well-controlled warfarin," according to the article (BMJ 2014;349:g4670), which was published along with an editorial and an analysis. The article further stated that the manufacturer "has failed to share with regulators information about the potential benefits of monitoring anticoagulant activity and adjusting the dose to make sure the drug is working as safely and effectively as possible."
In the analysis, Thomas Moore, senior scientist at the Institute for Safe Medication Practices, Horsham, Pa., and his coauthors said that "the bleeding risk of dabigatran can be reduced and efficacy improved by individualizing the dose in patients based on plasma level, age, and kidney function" (BMJ 2014;349:g4517[doi:10.1136/bmj.g4517]).
Dr. Rita Redberg and Dr. Blake Charlton of the University of California, San Francisco, wrote in an accompanying editorial that the analysis "illuminates a lack of transparency about the safety of unmonitored dabigatran, compounded by the drug’s fickle pharmacokinetics, which can cause a fivefold variation of plasma concentration." (BMJ 2014;349:g4681 [doi:10.1136/bmj.g4681]).
The BMJ article, written by Deborah Cohen, includes responses from the manufacturer of dabigatran (Pradaxa).
Boehringer Ingelheim officials have asserted that no data were withheld. Additionally, the company has released a statement calling the BMJ article "biased" and "misleading."
Dabigatran is a direct thrombin inhibitor that was approved in the United States in October 2010 for reducing the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation at a fixed dose of 150 mg or 75 mg twice a day, with the lower dose recommended for those with renal impairment. Since its initial approval, dabigatran has gained indications for treating and reducing the risk of recurrence of deep venous thrombosis and pulmonary embolism.
The drug’s approval was based on the results of the Randomized Evaluation of Long Term Anticoagulant Therapy (RE-LY) trial, which compared the drug to warfarin in 18,113 patients with nonvalvular atrial fibrillation and at least one other risk factor for stroke. The annual rate of stroke and systemic embolism in RE-LY was 1.5% in the patients on the 110-mg twice daily dose, 1.1% in those on the 150-mg twice daily dose, and 1.7% among those on warfarin. The risk reductions with dabigatran were 10% and 35% for the 110-mg and 150-mg doses, respectively, compared with warfarin.
"Our company has provided regulators with the complete data set and analyses of clinical evidence demonstrating Pradaxa’s benefits and safety," Boehringer Ingelheim said in its statement. "Contrary to the BMJ’s accusation that BI withheld analyses, here are the facts: In 2012, our scientists performed preliminary, exploratory simulations with mathematical models to understand whether dose adjustments based on plasma concentrations might further improve Pradaxa’s benefits and safety. Because the simulations did not offer reliable predictions of actual patient outcomes, they were not provided to regulators. However, all of the data that was used for the simulations had already been provided."
Dr. Sanjay Kaul, who was on the Food and Drug Administration’s advisory panel that recommended approval of dabigatran, said in an interview that the FDA reviewers raised questions at that meeting about the utility of using plasma concentrations to monitor individual subjects and adjust dose based on dabigatran concentrations. "But they also acknowledged an exposure-response relationship existed that demonstrated that going from the 10th to 90th percentile of dabigatran concentration (23 to 283 ng/mL) reduced the probability of having a stroke by 50% (from 1% to 0.5%) while increasing sixfold (from 0.3% to 1.8%) the probability of having major bleeding within 1 year."
It is well known that plasma concentration is one of the factors – among others, such as age, renal function, or history of stroke – that affect the benefit-risk balance, said Dr. Kaul, a cardiologist at Cedars-Sinai Medical Center, Los Angeles. Even in patients with moderate to severe renal dysfunction (up to creatinine clearance of 15-30 mL/min) and elevated plasma concentrations, benefit still exceeds risk.
"To what degree monitoring drug levels could potentially optimize benefit-risk balance remains an open question. For example, benefit-risk balance for dabigatran 150 mg vs 110 mg was not predicted by pharmacokinetic/pharmacodynamic modeling. Based on the PK/PD modeling, one stroke would be prevented at the cost of three extra major bleeds using 150 mg , compared with 110 mg. The RE-LY data indicate four strokes prevented and three major bleeding events incurred with the 150-mg dose as compared with the 110-mg dose," he said. "There is quite a discordance in predicted vs. observed benefit-risk balance."
Therefore, "while monitoring drug levels to optimize benefit-risk balance has intuitive appeal, given the complex exposure-response relationship and confounding effects of demographic variables, this should remain an area of active investigation. It is not ready for prime time to inform or guide clinical practice," Dr. Kaul said.
Dr. Kaul disclosed that he is a consultant for Boehringer Ingelheim and has equity interest in Johnson and Johnson.
At press time, the FDA had not responded to a request for a comment on the BMJ investigation.
The manufacturer of the oral anticoagulant dabigatran "withheld analyses that calculate how many major bleeds dose adjustment could prevent," the BMJ charges in an article based on internal documents released during litigation in the United States and freedom of information act requests obtained by the journal.
Boehringer Ingelheim "found that if the plasma levels of the drug were measured and the dose was adjusted accordingly major bleeds could be reduced by 30%-40%, compared with well-controlled warfarin," according to the article (BMJ 2014;349:g4670), which was published along with an editorial and an analysis. The article further stated that the manufacturer "has failed to share with regulators information about the potential benefits of monitoring anticoagulant activity and adjusting the dose to make sure the drug is working as safely and effectively as possible."
In the analysis, Thomas Moore, senior scientist at the Institute for Safe Medication Practices, Horsham, Pa., and his coauthors said that "the bleeding risk of dabigatran can be reduced and efficacy improved by individualizing the dose in patients based on plasma level, age, and kidney function" (BMJ 2014;349:g4517[doi:10.1136/bmj.g4517]).
Dr. Rita Redberg and Dr. Blake Charlton of the University of California, San Francisco, wrote in an accompanying editorial that the analysis "illuminates a lack of transparency about the safety of unmonitored dabigatran, compounded by the drug’s fickle pharmacokinetics, which can cause a fivefold variation of plasma concentration." (BMJ 2014;349:g4681 [doi:10.1136/bmj.g4681]).
The BMJ article, written by Deborah Cohen, includes responses from the manufacturer of dabigatran (Pradaxa).
Boehringer Ingelheim officials have asserted that no data were withheld. Additionally, the company has released a statement calling the BMJ article "biased" and "misleading."
Dabigatran is a direct thrombin inhibitor that was approved in the United States in October 2010 for reducing the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation at a fixed dose of 150 mg or 75 mg twice a day, with the lower dose recommended for those with renal impairment. Since its initial approval, dabigatran has gained indications for treating and reducing the risk of recurrence of deep venous thrombosis and pulmonary embolism.
The drug’s approval was based on the results of the Randomized Evaluation of Long Term Anticoagulant Therapy (RE-LY) trial, which compared the drug to warfarin in 18,113 patients with nonvalvular atrial fibrillation and at least one other risk factor for stroke. The annual rate of stroke and systemic embolism in RE-LY was 1.5% in the patients on the 110-mg twice daily dose, 1.1% in those on the 150-mg twice daily dose, and 1.7% among those on warfarin. The risk reductions with dabigatran were 10% and 35% for the 110-mg and 150-mg doses, respectively, compared with warfarin.
"Our company has provided regulators with the complete data set and analyses of clinical evidence demonstrating Pradaxa’s benefits and safety," Boehringer Ingelheim said in its statement. "Contrary to the BMJ’s accusation that BI withheld analyses, here are the facts: In 2012, our scientists performed preliminary, exploratory simulations with mathematical models to understand whether dose adjustments based on plasma concentrations might further improve Pradaxa’s benefits and safety. Because the simulations did not offer reliable predictions of actual patient outcomes, they were not provided to regulators. However, all of the data that was used for the simulations had already been provided."
Dr. Sanjay Kaul, who was on the Food and Drug Administration’s advisory panel that recommended approval of dabigatran, said in an interview that the FDA reviewers raised questions at that meeting about the utility of using plasma concentrations to monitor individual subjects and adjust dose based on dabigatran concentrations. "But they also acknowledged an exposure-response relationship existed that demonstrated that going from the 10th to 90th percentile of dabigatran concentration (23 to 283 ng/mL) reduced the probability of having a stroke by 50% (from 1% to 0.5%) while increasing sixfold (from 0.3% to 1.8%) the probability of having major bleeding within 1 year."
It is well known that plasma concentration is one of the factors – among others, such as age, renal function, or history of stroke – that affect the benefit-risk balance, said Dr. Kaul, a cardiologist at Cedars-Sinai Medical Center, Los Angeles. Even in patients with moderate to severe renal dysfunction (up to creatinine clearance of 15-30 mL/min) and elevated plasma concentrations, benefit still exceeds risk.
"To what degree monitoring drug levels could potentially optimize benefit-risk balance remains an open question. For example, benefit-risk balance for dabigatran 150 mg vs 110 mg was not predicted by pharmacokinetic/pharmacodynamic modeling. Based on the PK/PD modeling, one stroke would be prevented at the cost of three extra major bleeds using 150 mg , compared with 110 mg. The RE-LY data indicate four strokes prevented and three major bleeding events incurred with the 150-mg dose as compared with the 110-mg dose," he said. "There is quite a discordance in predicted vs. observed benefit-risk balance."
Therefore, "while monitoring drug levels to optimize benefit-risk balance has intuitive appeal, given the complex exposure-response relationship and confounding effects of demographic variables, this should remain an area of active investigation. It is not ready for prime time to inform or guide clinical practice," Dr. Kaul said.
Dr. Kaul disclosed that he is a consultant for Boehringer Ingelheim and has equity interest in Johnson and Johnson.
At press time, the FDA had not responded to a request for a comment on the BMJ investigation.
The manufacturer of the oral anticoagulant dabigatran "withheld analyses that calculate how many major bleeds dose adjustment could prevent," the BMJ charges in an article based on internal documents released during litigation in the United States and freedom of information act requests obtained by the journal.
Boehringer Ingelheim "found that if the plasma levels of the drug were measured and the dose was adjusted accordingly major bleeds could be reduced by 30%-40%, compared with well-controlled warfarin," according to the article (BMJ 2014;349:g4670), which was published along with an editorial and an analysis. The article further stated that the manufacturer "has failed to share with regulators information about the potential benefits of monitoring anticoagulant activity and adjusting the dose to make sure the drug is working as safely and effectively as possible."
In the analysis, Thomas Moore, senior scientist at the Institute for Safe Medication Practices, Horsham, Pa., and his coauthors said that "the bleeding risk of dabigatran can be reduced and efficacy improved by individualizing the dose in patients based on plasma level, age, and kidney function" (BMJ 2014;349:g4517[doi:10.1136/bmj.g4517]).
Dr. Rita Redberg and Dr. Blake Charlton of the University of California, San Francisco, wrote in an accompanying editorial that the analysis "illuminates a lack of transparency about the safety of unmonitored dabigatran, compounded by the drug’s fickle pharmacokinetics, which can cause a fivefold variation of plasma concentration." (BMJ 2014;349:g4681 [doi:10.1136/bmj.g4681]).
The BMJ article, written by Deborah Cohen, includes responses from the manufacturer of dabigatran (Pradaxa).
Boehringer Ingelheim officials have asserted that no data were withheld. Additionally, the company has released a statement calling the BMJ article "biased" and "misleading."
Dabigatran is a direct thrombin inhibitor that was approved in the United States in October 2010 for reducing the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation at a fixed dose of 150 mg or 75 mg twice a day, with the lower dose recommended for those with renal impairment. Since its initial approval, dabigatran has gained indications for treating and reducing the risk of recurrence of deep venous thrombosis and pulmonary embolism.
The drug’s approval was based on the results of the Randomized Evaluation of Long Term Anticoagulant Therapy (RE-LY) trial, which compared the drug to warfarin in 18,113 patients with nonvalvular atrial fibrillation and at least one other risk factor for stroke. The annual rate of stroke and systemic embolism in RE-LY was 1.5% in the patients on the 110-mg twice daily dose, 1.1% in those on the 150-mg twice daily dose, and 1.7% among those on warfarin. The risk reductions with dabigatran were 10% and 35% for the 110-mg and 150-mg doses, respectively, compared with warfarin.
"Our company has provided regulators with the complete data set and analyses of clinical evidence demonstrating Pradaxa’s benefits and safety," Boehringer Ingelheim said in its statement. "Contrary to the BMJ’s accusation that BI withheld analyses, here are the facts: In 2012, our scientists performed preliminary, exploratory simulations with mathematical models to understand whether dose adjustments based on plasma concentrations might further improve Pradaxa’s benefits and safety. Because the simulations did not offer reliable predictions of actual patient outcomes, they were not provided to regulators. However, all of the data that was used for the simulations had already been provided."
Dr. Sanjay Kaul, who was on the Food and Drug Administration’s advisory panel that recommended approval of dabigatran, said in an interview that the FDA reviewers raised questions at that meeting about the utility of using plasma concentrations to monitor individual subjects and adjust dose based on dabigatran concentrations. "But they also acknowledged an exposure-response relationship existed that demonstrated that going from the 10th to 90th percentile of dabigatran concentration (23 to 283 ng/mL) reduced the probability of having a stroke by 50% (from 1% to 0.5%) while increasing sixfold (from 0.3% to 1.8%) the probability of having major bleeding within 1 year."
It is well known that plasma concentration is one of the factors – among others, such as age, renal function, or history of stroke – that affect the benefit-risk balance, said Dr. Kaul, a cardiologist at Cedars-Sinai Medical Center, Los Angeles. Even in patients with moderate to severe renal dysfunction (up to creatinine clearance of 15-30 mL/min) and elevated plasma concentrations, benefit still exceeds risk.
"To what degree monitoring drug levels could potentially optimize benefit-risk balance remains an open question. For example, benefit-risk balance for dabigatran 150 mg vs 110 mg was not predicted by pharmacokinetic/pharmacodynamic modeling. Based on the PK/PD modeling, one stroke would be prevented at the cost of three extra major bleeds using 150 mg , compared with 110 mg. The RE-LY data indicate four strokes prevented and three major bleeding events incurred with the 150-mg dose as compared with the 110-mg dose," he said. "There is quite a discordance in predicted vs. observed benefit-risk balance."
Therefore, "while monitoring drug levels to optimize benefit-risk balance has intuitive appeal, given the complex exposure-response relationship and confounding effects of demographic variables, this should remain an area of active investigation. It is not ready for prime time to inform or guide clinical practice," Dr. Kaul said.
Dr. Kaul disclosed that he is a consultant for Boehringer Ingelheim and has equity interest in Johnson and Johnson.
At press time, the FDA had not responded to a request for a comment on the BMJ investigation.
Why You Shouldn’t Start β-Blockers Before Surgery
PRACTICE CHANGER
Do not routinely initiate β-blockers in patients undergoing intermediate- or high-risk noncardiac surgery. β-Blockers appear to increase the 30-day risk for all-cause mortality.1
STRENGTH OF RECOMMENDATION
A: Based on meta-analysis of nine randomized controlled trials (RCTs).1
ILLUSTRATIVE CASE
A 67-year-old woman with diabetes, hypertension, and hyperlipidemia presents for evaluation prior to a total hip arthroplasty. She is not taking a β-blocker. Should you prescribe one?
Study summary >>
Current guidelines from the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) recommend starting
β-blockers to prevent cardiac events in patients about to undergo intermediate- or high-risk surgery or vascular surgery who have a history of inducible ischemia, coronary artery disease (CAD), or at least one risk factor for CAD.2 However, the majority of the evidence for these guidelines, which were published in 2009 and are in the process of being updated, came from the DECREASE (Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography) trials. These trials have been discredited due to serious methodologic flaws, including falsified descriptions of how outcomes were determined and fictitious databases.3
A new meta-analysis conducted by Bouri et al1 that excluded the DECREASE trials found that, although preoperative β-blockers reduce the rate of certain nonfatal outcomes, they increase the risk for death and stroke.
STUDY SUMMARY
Preop β-blockers do more harm than good
Bouri et al1 conducted a meta-analysis of published RCTs evaluating preoperative β-blockers versus placebo for patients undergoing noncardiac surgery. Of the 11 studies that met eligibility criteria, two were the discredited DECREASE trials. Thus, Bouri et al1 analyzed nine high-quality RCTs that included 10,529 patients.
Most studies included patients undergoing vascular surgery. Some studies also included intra-abdominal, intrathoracic, neurosurgic, orthopedic, urologic, and gynecologic surgeries. β-Blockers were started no more than a day before surgery and were discontinued at hospital discharge or up to 30 days postop. Metoprolol was used in five trials, bisoprolol in one trial, atenolol in two trials, and propranolol in one trial. The primary endpoint was all-cause mortality within 30 days.
A total of 5,264 patients were randomly assigned to receive β-blockers and 5,265 to placebo. There were 162 deaths in the β-blocker group and 129 deaths in the placebo group. Patients who received β-blockers had a 27% increased risk for all-cause mortality (risk ratio [RR] = 1.27). The number needed to harm was 160.
Six of the studies also evaluated rates of nonfatal MI, nonfatal stroke, and hypotension. β-Blockers lowered the risk for nonfatal MI (RR = 0.73) but increased the risk for nonfatal stroke (RR = 1.73) and hypotension (RR = 1.51).
This meta-analysis was dominated by the 2008 Peri-Operative ISchemic Evaluation (POISE) trial, an RCT that compared placebo to extended-release metoprolol (100 mg 2 to 4 h before surgery, followed by 200 mg/d for 30 d), in 8,351 patients with, or at risk for, atherosclerotic disease.4 While β-blockers reduced the risk for MI and atrial fibrillation, they increased the risk for mortality and stroke, likely due to drug-induced hypotension. The slightly larger-than-typical doses of β-blockers used in this study may have contributed to the excess mortality.
What's new and challenges to implementation >>
WHAT’S NEW
Avoiding β-blockers in surgery patients will prevent deaths
Bouri et al1 found that while β-blockers protect against nonfatal MIs, they increase the risk for nonfatal strokes and death. This new meta-analysis challenges the ACCF/AHA recommendations by suggesting that abandoning the use of β-blockers for preoperative patients who aren’t already taking them will prevent a substantial number of perioperative deaths. Bouri et al1 estimate that in the United Kingdom, where 47,286 deaths occur annually within 30 days of intermediate- or high-risk procedures, the number of iatrogenic deaths would drop by approximately 10,000 if β-blockers were not used.1
CAVEATS
Don’t stop β-blockers in patients who already take them
This meta-analysis did not evaluate outcomes in patients who were already taking β-blockers. These patients should continue to take them in the perioperative period, which is in line with current ACCF/AHA guidelines.
CHALLENGES TO IMPLEMENTATION
Reluctance to disregard published guidelines
Some clinicians may not be comfortable ignoring the current ACCF/AHA guidelines that make a Class IIA recommendation (it is reasonable to administer this treatment) for the use of preoperative β-blockade for patients at risk for cardiovascular events who were not previously taking a β-blocker. This updated meta-analysis excludes the discredited DECREASE trials and challenges us to act against these current guidelines while we await updated recommendations.
REFERENCES
1. Bouri S, Shun-Shin MJ, Cole GD, et al. Meta-analysis of secure randomised controlled trials of ß-blockade to prevent perioperative death in non-cardiac surgery. Heart. 2014;100:456-464.
2. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Society of Echocardiography; American Society of Nuclear Cardiology; Heart Rhythm Society; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine; Society for Vascular Surgery; Fleisher LA, Beckman JA, Brown KA, et al. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol. 2009;54:e13-e118.
3. Erasmus Medical Center Follow-up Investigation Committee. Report on the 2012 follow-up investigation of possible breaches of academic integrity (September 30, 2012). CardioBrief. Available at: http://cardiobrief.files.wordpress.com/2012/10/integrity-report-2012-10-english-translation.pdf. Accessed August 14, 2014.
4. Devereaux PJ, Yang H, Yusuf S, et al; POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;
371:1839-1847.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(6):E15-E16.
PRACTICE CHANGER
Do not routinely initiate β-blockers in patients undergoing intermediate- or high-risk noncardiac surgery. β-Blockers appear to increase the 30-day risk for all-cause mortality.1
STRENGTH OF RECOMMENDATION
A: Based on meta-analysis of nine randomized controlled trials (RCTs).1
ILLUSTRATIVE CASE
A 67-year-old woman with diabetes, hypertension, and hyperlipidemia presents for evaluation prior to a total hip arthroplasty. She is not taking a β-blocker. Should you prescribe one?
Study summary >>
Current guidelines from the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) recommend starting
β-blockers to prevent cardiac events in patients about to undergo intermediate- or high-risk surgery or vascular surgery who have a history of inducible ischemia, coronary artery disease (CAD), or at least one risk factor for CAD.2 However, the majority of the evidence for these guidelines, which were published in 2009 and are in the process of being updated, came from the DECREASE (Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography) trials. These trials have been discredited due to serious methodologic flaws, including falsified descriptions of how outcomes were determined and fictitious databases.3
A new meta-analysis conducted by Bouri et al1 that excluded the DECREASE trials found that, although preoperative β-blockers reduce the rate of certain nonfatal outcomes, they increase the risk for death and stroke.
STUDY SUMMARY
Preop β-blockers do more harm than good
Bouri et al1 conducted a meta-analysis of published RCTs evaluating preoperative β-blockers versus placebo for patients undergoing noncardiac surgery. Of the 11 studies that met eligibility criteria, two were the discredited DECREASE trials. Thus, Bouri et al1 analyzed nine high-quality RCTs that included 10,529 patients.
Most studies included patients undergoing vascular surgery. Some studies also included intra-abdominal, intrathoracic, neurosurgic, orthopedic, urologic, and gynecologic surgeries. β-Blockers were started no more than a day before surgery and were discontinued at hospital discharge or up to 30 days postop. Metoprolol was used in five trials, bisoprolol in one trial, atenolol in two trials, and propranolol in one trial. The primary endpoint was all-cause mortality within 30 days.
A total of 5,264 patients were randomly assigned to receive β-blockers and 5,265 to placebo. There were 162 deaths in the β-blocker group and 129 deaths in the placebo group. Patients who received β-blockers had a 27% increased risk for all-cause mortality (risk ratio [RR] = 1.27). The number needed to harm was 160.
Six of the studies also evaluated rates of nonfatal MI, nonfatal stroke, and hypotension. β-Blockers lowered the risk for nonfatal MI (RR = 0.73) but increased the risk for nonfatal stroke (RR = 1.73) and hypotension (RR = 1.51).
This meta-analysis was dominated by the 2008 Peri-Operative ISchemic Evaluation (POISE) trial, an RCT that compared placebo to extended-release metoprolol (100 mg 2 to 4 h before surgery, followed by 200 mg/d for 30 d), in 8,351 patients with, or at risk for, atherosclerotic disease.4 While β-blockers reduced the risk for MI and atrial fibrillation, they increased the risk for mortality and stroke, likely due to drug-induced hypotension. The slightly larger-than-typical doses of β-blockers used in this study may have contributed to the excess mortality.
What's new and challenges to implementation >>
WHAT’S NEW
Avoiding β-blockers in surgery patients will prevent deaths
Bouri et al1 found that while β-blockers protect against nonfatal MIs, they increase the risk for nonfatal strokes and death. This new meta-analysis challenges the ACCF/AHA recommendations by suggesting that abandoning the use of β-blockers for preoperative patients who aren’t already taking them will prevent a substantial number of perioperative deaths. Bouri et al1 estimate that in the United Kingdom, where 47,286 deaths occur annually within 30 days of intermediate- or high-risk procedures, the number of iatrogenic deaths would drop by approximately 10,000 if β-blockers were not used.1
CAVEATS
Don’t stop β-blockers in patients who already take them
This meta-analysis did not evaluate outcomes in patients who were already taking β-blockers. These patients should continue to take them in the perioperative period, which is in line with current ACCF/AHA guidelines.
CHALLENGES TO IMPLEMENTATION
Reluctance to disregard published guidelines
Some clinicians may not be comfortable ignoring the current ACCF/AHA guidelines that make a Class IIA recommendation (it is reasonable to administer this treatment) for the use of preoperative β-blockade for patients at risk for cardiovascular events who were not previously taking a β-blocker. This updated meta-analysis excludes the discredited DECREASE trials and challenges us to act against these current guidelines while we await updated recommendations.
REFERENCES
1. Bouri S, Shun-Shin MJ, Cole GD, et al. Meta-analysis of secure randomised controlled trials of ß-blockade to prevent perioperative death in non-cardiac surgery. Heart. 2014;100:456-464.
2. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Society of Echocardiography; American Society of Nuclear Cardiology; Heart Rhythm Society; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine; Society for Vascular Surgery; Fleisher LA, Beckman JA, Brown KA, et al. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol. 2009;54:e13-e118.
3. Erasmus Medical Center Follow-up Investigation Committee. Report on the 2012 follow-up investigation of possible breaches of academic integrity (September 30, 2012). CardioBrief. Available at: http://cardiobrief.files.wordpress.com/2012/10/integrity-report-2012-10-english-translation.pdf. Accessed August 14, 2014.
4. Devereaux PJ, Yang H, Yusuf S, et al; POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;
371:1839-1847.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(6):E15-E16.
PRACTICE CHANGER
Do not routinely initiate β-blockers in patients undergoing intermediate- or high-risk noncardiac surgery. β-Blockers appear to increase the 30-day risk for all-cause mortality.1
STRENGTH OF RECOMMENDATION
A: Based on meta-analysis of nine randomized controlled trials (RCTs).1
ILLUSTRATIVE CASE
A 67-year-old woman with diabetes, hypertension, and hyperlipidemia presents for evaluation prior to a total hip arthroplasty. She is not taking a β-blocker. Should you prescribe one?
Study summary >>
Current guidelines from the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) recommend starting
β-blockers to prevent cardiac events in patients about to undergo intermediate- or high-risk surgery or vascular surgery who have a history of inducible ischemia, coronary artery disease (CAD), or at least one risk factor for CAD.2 However, the majority of the evidence for these guidelines, which were published in 2009 and are in the process of being updated, came from the DECREASE (Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography) trials. These trials have been discredited due to serious methodologic flaws, including falsified descriptions of how outcomes were determined and fictitious databases.3
A new meta-analysis conducted by Bouri et al1 that excluded the DECREASE trials found that, although preoperative β-blockers reduce the rate of certain nonfatal outcomes, they increase the risk for death and stroke.
STUDY SUMMARY
Preop β-blockers do more harm than good
Bouri et al1 conducted a meta-analysis of published RCTs evaluating preoperative β-blockers versus placebo for patients undergoing noncardiac surgery. Of the 11 studies that met eligibility criteria, two were the discredited DECREASE trials. Thus, Bouri et al1 analyzed nine high-quality RCTs that included 10,529 patients.
Most studies included patients undergoing vascular surgery. Some studies also included intra-abdominal, intrathoracic, neurosurgic, orthopedic, urologic, and gynecologic surgeries. β-Blockers were started no more than a day before surgery and were discontinued at hospital discharge or up to 30 days postop. Metoprolol was used in five trials, bisoprolol in one trial, atenolol in two trials, and propranolol in one trial. The primary endpoint was all-cause mortality within 30 days.
A total of 5,264 patients were randomly assigned to receive β-blockers and 5,265 to placebo. There were 162 deaths in the β-blocker group and 129 deaths in the placebo group. Patients who received β-blockers had a 27% increased risk for all-cause mortality (risk ratio [RR] = 1.27). The number needed to harm was 160.
Six of the studies also evaluated rates of nonfatal MI, nonfatal stroke, and hypotension. β-Blockers lowered the risk for nonfatal MI (RR = 0.73) but increased the risk for nonfatal stroke (RR = 1.73) and hypotension (RR = 1.51).
This meta-analysis was dominated by the 2008 Peri-Operative ISchemic Evaluation (POISE) trial, an RCT that compared placebo to extended-release metoprolol (100 mg 2 to 4 h before surgery, followed by 200 mg/d for 30 d), in 8,351 patients with, or at risk for, atherosclerotic disease.4 While β-blockers reduced the risk for MI and atrial fibrillation, they increased the risk for mortality and stroke, likely due to drug-induced hypotension. The slightly larger-than-typical doses of β-blockers used in this study may have contributed to the excess mortality.
What's new and challenges to implementation >>
WHAT’S NEW
Avoiding β-blockers in surgery patients will prevent deaths
Bouri et al1 found that while β-blockers protect against nonfatal MIs, they increase the risk for nonfatal strokes and death. This new meta-analysis challenges the ACCF/AHA recommendations by suggesting that abandoning the use of β-blockers for preoperative patients who aren’t already taking them will prevent a substantial number of perioperative deaths. Bouri et al1 estimate that in the United Kingdom, where 47,286 deaths occur annually within 30 days of intermediate- or high-risk procedures, the number of iatrogenic deaths would drop by approximately 10,000 if β-blockers were not used.1
CAVEATS
Don’t stop β-blockers in patients who already take them
This meta-analysis did not evaluate outcomes in patients who were already taking β-blockers. These patients should continue to take them in the perioperative period, which is in line with current ACCF/AHA guidelines.
CHALLENGES TO IMPLEMENTATION
Reluctance to disregard published guidelines
Some clinicians may not be comfortable ignoring the current ACCF/AHA guidelines that make a Class IIA recommendation (it is reasonable to administer this treatment) for the use of preoperative β-blockade for patients at risk for cardiovascular events who were not previously taking a β-blocker. This updated meta-analysis excludes the discredited DECREASE trials and challenges us to act against these current guidelines while we await updated recommendations.
REFERENCES
1. Bouri S, Shun-Shin MJ, Cole GD, et al. Meta-analysis of secure randomised controlled trials of ß-blockade to prevent perioperative death in non-cardiac surgery. Heart. 2014;100:456-464.
2. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Society of Echocardiography; American Society of Nuclear Cardiology; Heart Rhythm Society; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine; Society for Vascular Surgery; Fleisher LA, Beckman JA, Brown KA, et al. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol. 2009;54:e13-e118.
3. Erasmus Medical Center Follow-up Investigation Committee. Report on the 2012 follow-up investigation of possible breaches of academic integrity (September 30, 2012). CardioBrief. Available at: http://cardiobrief.files.wordpress.com/2012/10/integrity-report-2012-10-english-translation.pdf. Accessed August 14, 2014.
4. Devereaux PJ, Yang H, Yusuf S, et al; POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;
371:1839-1847.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(6):E15-E16.
A Visiting Grandma Feels Short of Breath
ANSWER
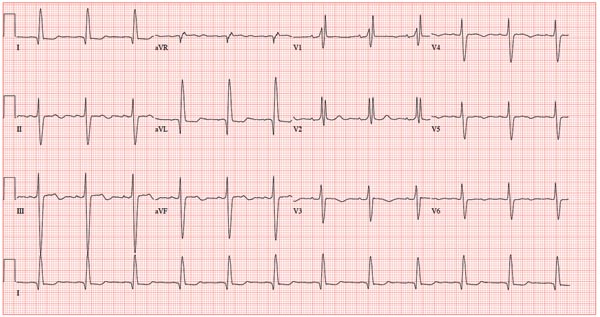
This ECG shows normal sinus rhythm, a right bundle branch block (RBBB), and a left anterior fascicular block (LAFB). RBBB and LAFB are consistent with bifascicular block.
Criteria for an RBBB include a prolonged total QRS complex of 120 ms or longer and an RSR’ complex (“rabbit ears”) in lead V1. LAFB criteria include a QRS of normal duration with an S wave greater than an R wave in leads II, III, and aVF and left-axis deviation (–48° in this case).
The astute reader may question the disparity between RBBB and LAFB, since the criteria for the former include a prolonged QRS interval and the criteria for the latter include a normal QRS interval. It should be noted that the requirements for QRS duration for RBBB vary.
Bifascicular block (RBBB and either LAFB or left posterior fascicular block [LPFB]) is indicative of more advanced conduction system disease. However, it is not an indication for permanent pacemaker placement in an asymptomatic patient.
This patient was treated for a community-acquired right lower lobe pneumonia and a UTI.
ANSWER
This ECG shows normal sinus rhythm, a right bundle branch block (RBBB), and a left anterior fascicular block (LAFB). RBBB and LAFB are consistent with bifascicular block.
Criteria for an RBBB include a prolonged total QRS complex of 120 ms or longer and an RSR’ complex (“rabbit ears”) in lead V1. LAFB criteria include a QRS of normal duration with an S wave greater than an R wave in leads II, III, and aVF and left-axis deviation (–48° in this case).
The astute reader may question the disparity between RBBB and LAFB, since the criteria for the former include a prolonged QRS interval and the criteria for the latter include a normal QRS interval. It should be noted that the requirements for QRS duration for RBBB vary.
Bifascicular block (RBBB and either LAFB or left posterior fascicular block [LPFB]) is indicative of more advanced conduction system disease. However, it is not an indication for permanent pacemaker placement in an asymptomatic patient.
This patient was treated for a community-acquired right lower lobe pneumonia and a UTI.
ANSWER
This ECG shows normal sinus rhythm, a right bundle branch block (RBBB), and a left anterior fascicular block (LAFB). RBBB and LAFB are consistent with bifascicular block.
Criteria for an RBBB include a prolonged total QRS complex of 120 ms or longer and an RSR’ complex (“rabbit ears”) in lead V1. LAFB criteria include a QRS of normal duration with an S wave greater than an R wave in leads II, III, and aVF and left-axis deviation (–48° in this case).
The astute reader may question the disparity between RBBB and LAFB, since the criteria for the former include a prolonged QRS interval and the criteria for the latter include a normal QRS interval. It should be noted that the requirements for QRS duration for RBBB vary.
Bifascicular block (RBBB and either LAFB or left posterior fascicular block [LPFB]) is indicative of more advanced conduction system disease. However, it is not an indication for permanent pacemaker placement in an asymptomatic patient.
This patient was treated for a community-acquired right lower lobe pneumonia and a UTI.
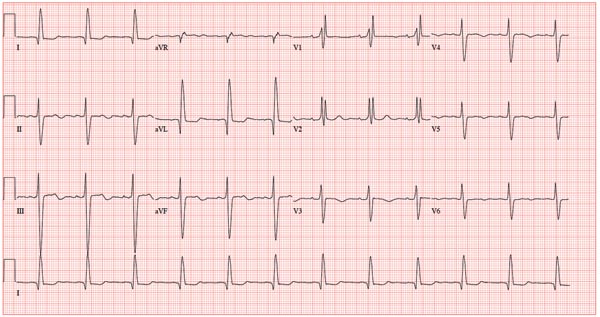
A 78-year-old woman presents to your urgent care clinic with a four-day history of lethargy. She lives in another state but currently is visiting her granddaughter, who happens to be your clinic manager. She says she felt weak prior to her trip but thought it was probably due to a urinary tract infection (UTI). Yesterday, however, she started feeling short of breath. The patient denies chest pain, orthopnea, paroxysmal nocturnal dyspnea, or productive cough. She reports feeling feverish this morning but did not record her temperature, adding that it seemed to subside after she got dressed. Her medical history is positive for frequent UTIs, a remote cholecystectomy, hypothyroidism, and paroxysmal atrial fibrillation. According to the patient’s daughter, who is present, her mother’s cardiologist recently mentioned some “funny” findings on an ECG; she didn’t really understand his explanation but they were told “not to worry.” The patient, a retired schoolteacher, lives in an assisted living center. She is independent and has been a widow for 14 years, since her husband died of an acute MI. She has two children who are in good health. She has never smoked, rarely consumes alcohol, and has never used recreational or homeopathic drugs. Her current medications include warfarin, levothyroxine, and conjugated estrogen. She was taking amiodarone for rhythm control of atrial fibrillation but stopped six months ago when her skin started turning blue. She is allergic to penicillin, which causes a true anaphylactic reaction, according to her daughter. Review of systems is positive for an infrequent, nonproductive cough, sun sensitivity due to amiodarone use, and infrequent burning with urination. Physical exam reveals a thin, elderly woman in no distress. Her blood pressure is 152/88 mm Hg; pulse, 70 beats/min and regular; respiratory rate, 14 breaths/min-1 with an infrequent, nonproductive cough; O2 saturation, 94% on room air; and temperature, 99°F. She is 5 ft 4 in tall and weighs 114 lb. Pertinent findings on physical exam include corrective lenses, pearly white skin with a blue hue on the nose and ears secondary to long-term amiodarone therapy, no evidence of thyromegaly or jugular distention, a regular rate and rhythm with a soft midsystolic murmur of mitral regurgitation, and no extra heart sounds. Her lungs are remarkable for consolidation in the right lower lobe, with crackles that change with coughing. Her abdomen is soft and nontender, and there is no peripheral edema. Her neurologic exam is intact. She is alert, attentive, and very witty in her responses to questions. Laboratory data include urinalysis findings suggestive of a UTI, a white blood cell count of 9.8 x 103/μL, and a hematocrit of 35%. A chest x-ray shows evidence of consolidation in the right lower lobe, which the radiologist says is strongly suggestive of pneumonia. An ECG shows a ventricular rate of 71 beats/min; PR interval, 152 ms; QRS duration, 142 ms; QT/QTc interval, 476/517 ms; P axis, 76°; R axis, –48°; and T axis, 161°. What is your interpretation of this ECG?
The transition from fellowship: finding a job
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Moving beyond the one-size-fits-all formula for breast cancer treatments
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
New and Noteworthy Information—September 2014
HIV infection is associated with a significantly lower risk of developing multiple sclerosis (MS), according to a study published online ahead of print August 4 in the Journal of Neurology, Neurosurgery, & Psychiatry. Researchers investigated episodes of hospital care between 1999 and 2011 for patients with HIV. Compared with people who did not have HIV, patients with HIV were 62% less likely to develop MS. After more than a year between the two diagnoses, HIV-positive patients were 75% less likely to develop MS. “If subsequent studies demonstrate [that] there is a causal protective effect of HIV or its treatment, and if the magnitude of it proves to be similar … this would be the largest protective effect of any factor yet observed in relation to the development of MS,” the investigators concluded.
Colds and other minor infections may temporarily increase stroke risk in children, according to a study published online ahead of print August 20 in Neurology. Using the Kaiser Permanente database of 2.5 million children, researchers identified 102 children who had had an acute ischemic stroke and compared them with 306 children without stroke. Medical records for the children who had had a stroke were reviewed for minor infections for two years before their strokes. Ten (9.8%) of the 102 children with stroke had visited a physician for an infection within three days of the stroke. In comparison, two controls (0.7%) had an infection during the same time period. “Proposed mechanisms for the link between minor infection and stroke in adults include an inflammatory-mediated prothrombotic state and chronic endothelial injury,” the investigators theorized.
Peripheral pulse monitoring in patients with stroke accurately distinguishes atrial fibrillation from normal heart rhythm, investigators reported in the August 12 issue of Neurology. The prospective study included 256 patients with acute ischemic stroke, as well as the patients’ relatives. Subjects were taught to measure the patient’s pulse to detect atrial fibrillation; measurements from the participants and health care professionals were compared with recordings of electrical activity in the heart. Fifty-seven patients had irregular heartbeats. Measurement of the peripheral pulse by health care professionals had a diagnostic sensitivity of 96.5%, compared with 76.5% for the patients’ relatives, regarding the detection of atrial fibrillation. The specificity was 94.0% for health care professionals and 92.9% for patients’ relatives. Self-measurements were performed by 89.1% of patients with a diagnostic sensitivity of 54.1% and 96.2% specificity.
Reducing smoking among people in a low socioeconomic position and among those with hypertension may reduce social inequality stroke incidence, researchers reported online ahead of print August 14 in Stroke. The findings are based on data from 68,643 adults between ages 30 and 70 who were grouped into low, medium, and high education levels and assessed for smoking status and blood pressure level. About 16% of men and 11% of women had a high risk of stroke because of low education level, high blood pressure, and smoking. Smokers with low education had a greater risk of stroke than smokers with high education, regardless of their blood pressure. About 10% of men and 9% of women at high risk had an ischemic stroke during follow-up. Overall, men had a higher risk of stroke than women, and their risk increased with age.
Motoric cognitive risk syndrome (MCR), a predementia syndrome characterized by slow gait and cognitive complaints, is common in older adults and is a strong and early risk factor for cognitive decline, according to a study published online ahead of print July 16 in Neurology. Among 26,802 participants from 22 cohorts, 2,808 subjects met MCR criteria. MCR prevalence was higher among older individuals, but there were no sex differences. MCR predicted the risk of developing incident cognitive impairment (adjusted hazard ratio, 2.0); in individual cohorts the adjusted hazard ratios ranged from 1.5 to 2.7. MCR also predicted dementia in the pooled sample (adjusted hazard ratio, 1.9). “MCR criteria can be easily applied in clinical settings with simple questions about cognitive complaints and timing gait; 90% of participants had walking timed over fixed distances without requiring major resource commitments,” the investigators stated.
The FDA has approved Plegridy (peginterferon beta-1a) for patients with relapsing forms of multiple sclerosis (MS). Approval of the drug is based on results from the ADVANCE study of more than 1,500 patients with MS. The drug can be administered subcutaneously with an autoinjector or a prefilled syringe. Dosed once every two weeks, the drug significantly reduced annualized relapse rate at one year by 36%, compared with placebo. Plegridy reduced the risk of 12-week confirmed disability progression by 38%, compared with placebo. The drug also significantly reduced the number of new gadolinium-enhancing lesions by 86% and decreased the number of new or newly enlarging T2-hyperintense lesions by 67%, compared with placebo. Common adverse reactions include injection-site reaction and flu-like illness. The drug is manufactured by Biogen Idec, which is headquartered in Cambridge, Massachusetts.
In patients who are hospitalized for surgery, perioperative atrial fibrillation is associated with an increased long-term risk of ischemic stroke, according to a study published in the August 13 issue of JAMA. Researchers studied 1,729,360 patients hospitalized for surgery between 2007 and 2011. Perioperative atrial fibrillation was documented in 24,711 patients (1.43%) during the index hospitalization. After discharge, 13,952 patients (0.81%) had an ischemic stroke. One year after hospitalization for noncardiac surgery, cumulative rates of stroke were 1.47% in patients with perioperative atrial fibrillation and 0.36% in people without atrial fibrillation. One year after cardiac surgery, cumulative rates of stroke were 0.99% in patients with perioperative atrial fibrillation and 0.83% in patients without atrial fibrillation. The association with stroke was stronger for perioperative atrial fibrillation and noncardiac surgery, compared with cardiac surgery.
Approximately one-third of cases of Alzheimer’s disease worldwide might be attributed to potentially modifiable risk factors, investigators reported in the August issue of Lancet Neurology. An international team of researchers used relative risks from existing meta-analyses to estimate the population-attributable risk (PAR) of Alzheimer’s disease worldwide and in the United States, Europe, and the United Kingdom for seven potentially modifiable risk factors. Worldwide, the highest estimated PAR was for low educational attainment. In the US, Europe, and UK the highest estimated PAR was for physical inactivity. Assuming the risk factors’ independence, the combined worldwide PAR for the seven risk factors was 49.4%, which accounts for 16.8 million of the 33.9 million cases. Adjustment for the association between the risk factors decreased the estimate to 28.2%, which equates to 9.6 million cases.
The FDA has approved Belsomra (suvorexant) for adults with insomnia who have difficulty falling and staying asleep. The drug is the first approved orexin receptor antagonist. Orexins are involved in regulating the sleep–wake cycle and play a role in promoting arousal. In clinical trials, Belsomra (Merck; Whitehouse Station, New Jersey) was superior to placebo for reducing sleep latency and improving sleep maintenance, as assessed objectively by polysomnography and subjectively by patient-estimated sleep latency. Belsomra should be taken no more than once per night, within 30 minutes of going to bed, with at least seven hours remaining before the planned time of waking. The total dose should not exceed 20 mg once daily. The most commonly reported adverse reaction among clinical trial participants taking Belsomra was drowsiness.
A clinical diagnosis of Parkinson’s disease identifies patients who will have pathologically confirmed Parkinson’s disease with a sensitivity of 88% and specificity of 68%, researchers reported in the July 29 issue of Neurology. Investigators analyzed data from an aging study to determine the predictive value of clinical diagnosis of Parkinson’s disease using two diagnostic confidence levels: possible and probable Parkinson’s disease. Approximately 26% of patients diagnosed with possible Parkinson’s disease were neuropathologically confirmed as having Parkinson’s disease; 82% of patients diagnosed with probable Parkinson’s disease were confirmed as having Parkinson’s disease. Researchers calculated a 26% accuracy rate for clinical diagnosis of Parkinson’s disease in untreated or not clearly responsive subjects, a 53% accuracy rate in early Parkinson’s disease responsive to medication (less than five year’s duration), and a greater than 85% diagnostic accuracy rate for longer duration, medication-responsive Parkinson’s disease.
Depressive symptoms in old age are associated with cognitive decline that is independent of dementia, according to a study published in the August 19 issue of Neurology. Investigators monitored 1,764 participants with an average age of 77 who had no thinking or memory problems at the start of the study. Participants were screened every year for symptoms of depression and were evaluated for their memory and thinking skills for a mean of 7.8 years. A total of 922 (52%) participants developed mild cognitive impairment, and 315 (18%) developed dementia. Overall, having a higher level of depression symptoms was associated with more rapid decline in thinking and memory skills, which accounted for 4.4% of the difference in decline that could not be attributed to the level of damage in the brain.
Researchers may have found a potential genetic link between epilepsy and neurodegenerative disorders, according to a study published in the July 29 Proceedings of the National Academy of Sciences. The investigators observed that seizure-prone prickle mutant flies have behavioral defects and electrophysiologic defects similar to those of other fly mutants used to study seizures. Altering the balance of two forms of the prickle gene disrupted neural information flow and caused epilepsy. The researchers also observed that reducing either of two motor proteins responsible for directional movement of vesicles along the tracks of structural proteins in axons could suppress seizures. “This is, to our knowledge, the first direct genetic evidence demonstrating that mutations in the fly version of a known human epilepsy gene produce seizures through altered vesicle transport,” stated the authors.
—Kimberly Williams
HIV infection is associated with a significantly lower risk of developing multiple sclerosis (MS), according to a study published online ahead of print August 4 in the Journal of Neurology, Neurosurgery, & Psychiatry. Researchers investigated episodes of hospital care between 1999 and 2011 for patients with HIV. Compared with people who did not have HIV, patients with HIV were 62% less likely to develop MS. After more than a year between the two diagnoses, HIV-positive patients were 75% less likely to develop MS. “If subsequent studies demonstrate [that] there is a causal protective effect of HIV or its treatment, and if the magnitude of it proves to be similar … this would be the largest protective effect of any factor yet observed in relation to the development of MS,” the investigators concluded.
Colds and other minor infections may temporarily increase stroke risk in children, according to a study published online ahead of print August 20 in Neurology. Using the Kaiser Permanente database of 2.5 million children, researchers identified 102 children who had had an acute ischemic stroke and compared them with 306 children without stroke. Medical records for the children who had had a stroke were reviewed for minor infections for two years before their strokes. Ten (9.8%) of the 102 children with stroke had visited a physician for an infection within three days of the stroke. In comparison, two controls (0.7%) had an infection during the same time period. “Proposed mechanisms for the link between minor infection and stroke in adults include an inflammatory-mediated prothrombotic state and chronic endothelial injury,” the investigators theorized.
Peripheral pulse monitoring in patients with stroke accurately distinguishes atrial fibrillation from normal heart rhythm, investigators reported in the August 12 issue of Neurology. The prospective study included 256 patients with acute ischemic stroke, as well as the patients’ relatives. Subjects were taught to measure the patient’s pulse to detect atrial fibrillation; measurements from the participants and health care professionals were compared with recordings of electrical activity in the heart. Fifty-seven patients had irregular heartbeats. Measurement of the peripheral pulse by health care professionals had a diagnostic sensitivity of 96.5%, compared with 76.5% for the patients’ relatives, regarding the detection of atrial fibrillation. The specificity was 94.0% for health care professionals and 92.9% for patients’ relatives. Self-measurements were performed by 89.1% of patients with a diagnostic sensitivity of 54.1% and 96.2% specificity.
Reducing smoking among people in a low socioeconomic position and among those with hypertension may reduce social inequality stroke incidence, researchers reported online ahead of print August 14 in Stroke. The findings are based on data from 68,643 adults between ages 30 and 70 who were grouped into low, medium, and high education levels and assessed for smoking status and blood pressure level. About 16% of men and 11% of women had a high risk of stroke because of low education level, high blood pressure, and smoking. Smokers with low education had a greater risk of stroke than smokers with high education, regardless of their blood pressure. About 10% of men and 9% of women at high risk had an ischemic stroke during follow-up. Overall, men had a higher risk of stroke than women, and their risk increased with age.
Motoric cognitive risk syndrome (MCR), a predementia syndrome characterized by slow gait and cognitive complaints, is common in older adults and is a strong and early risk factor for cognitive decline, according to a study published online ahead of print July 16 in Neurology. Among 26,802 participants from 22 cohorts, 2,808 subjects met MCR criteria. MCR prevalence was higher among older individuals, but there were no sex differences. MCR predicted the risk of developing incident cognitive impairment (adjusted hazard ratio, 2.0); in individual cohorts the adjusted hazard ratios ranged from 1.5 to 2.7. MCR also predicted dementia in the pooled sample (adjusted hazard ratio, 1.9). “MCR criteria can be easily applied in clinical settings with simple questions about cognitive complaints and timing gait; 90% of participants had walking timed over fixed distances without requiring major resource commitments,” the investigators stated.
The FDA has approved Plegridy (peginterferon beta-1a) for patients with relapsing forms of multiple sclerosis (MS). Approval of the drug is based on results from the ADVANCE study of more than 1,500 patients with MS. The drug can be administered subcutaneously with an autoinjector or a prefilled syringe. Dosed once every two weeks, the drug significantly reduced annualized relapse rate at one year by 36%, compared with placebo. Plegridy reduced the risk of 12-week confirmed disability progression by 38%, compared with placebo. The drug also significantly reduced the number of new gadolinium-enhancing lesions by 86% and decreased the number of new or newly enlarging T2-hyperintense lesions by 67%, compared with placebo. Common adverse reactions include injection-site reaction and flu-like illness. The drug is manufactured by Biogen Idec, which is headquartered in Cambridge, Massachusetts.
In patients who are hospitalized for surgery, perioperative atrial fibrillation is associated with an increased long-term risk of ischemic stroke, according to a study published in the August 13 issue of JAMA. Researchers studied 1,729,360 patients hospitalized for surgery between 2007 and 2011. Perioperative atrial fibrillation was documented in 24,711 patients (1.43%) during the index hospitalization. After discharge, 13,952 patients (0.81%) had an ischemic stroke. One year after hospitalization for noncardiac surgery, cumulative rates of stroke were 1.47% in patients with perioperative atrial fibrillation and 0.36% in people without atrial fibrillation. One year after cardiac surgery, cumulative rates of stroke were 0.99% in patients with perioperative atrial fibrillation and 0.83% in patients without atrial fibrillation. The association with stroke was stronger for perioperative atrial fibrillation and noncardiac surgery, compared with cardiac surgery.
Approximately one-third of cases of Alzheimer’s disease worldwide might be attributed to potentially modifiable risk factors, investigators reported in the August issue of Lancet Neurology. An international team of researchers used relative risks from existing meta-analyses to estimate the population-attributable risk (PAR) of Alzheimer’s disease worldwide and in the United States, Europe, and the United Kingdom for seven potentially modifiable risk factors. Worldwide, the highest estimated PAR was for low educational attainment. In the US, Europe, and UK the highest estimated PAR was for physical inactivity. Assuming the risk factors’ independence, the combined worldwide PAR for the seven risk factors was 49.4%, which accounts for 16.8 million of the 33.9 million cases. Adjustment for the association between the risk factors decreased the estimate to 28.2%, which equates to 9.6 million cases.
The FDA has approved Belsomra (suvorexant) for adults with insomnia who have difficulty falling and staying asleep. The drug is the first approved orexin receptor antagonist. Orexins are involved in regulating the sleep–wake cycle and play a role in promoting arousal. In clinical trials, Belsomra (Merck; Whitehouse Station, New Jersey) was superior to placebo for reducing sleep latency and improving sleep maintenance, as assessed objectively by polysomnography and subjectively by patient-estimated sleep latency. Belsomra should be taken no more than once per night, within 30 minutes of going to bed, with at least seven hours remaining before the planned time of waking. The total dose should not exceed 20 mg once daily. The most commonly reported adverse reaction among clinical trial participants taking Belsomra was drowsiness.
A clinical diagnosis of Parkinson’s disease identifies patients who will have pathologically confirmed Parkinson’s disease with a sensitivity of 88% and specificity of 68%, researchers reported in the July 29 issue of Neurology. Investigators analyzed data from an aging study to determine the predictive value of clinical diagnosis of Parkinson’s disease using two diagnostic confidence levels: possible and probable Parkinson’s disease. Approximately 26% of patients diagnosed with possible Parkinson’s disease were neuropathologically confirmed as having Parkinson’s disease; 82% of patients diagnosed with probable Parkinson’s disease were confirmed as having Parkinson’s disease. Researchers calculated a 26% accuracy rate for clinical diagnosis of Parkinson’s disease in untreated or not clearly responsive subjects, a 53% accuracy rate in early Parkinson’s disease responsive to medication (less than five year’s duration), and a greater than 85% diagnostic accuracy rate for longer duration, medication-responsive Parkinson’s disease.
Depressive symptoms in old age are associated with cognitive decline that is independent of dementia, according to a study published in the August 19 issue of Neurology. Investigators monitored 1,764 participants with an average age of 77 who had no thinking or memory problems at the start of the study. Participants were screened every year for symptoms of depression and were evaluated for their memory and thinking skills for a mean of 7.8 years. A total of 922 (52%) participants developed mild cognitive impairment, and 315 (18%) developed dementia. Overall, having a higher level of depression symptoms was associated with more rapid decline in thinking and memory skills, which accounted for 4.4% of the difference in decline that could not be attributed to the level of damage in the brain.
Researchers may have found a potential genetic link between epilepsy and neurodegenerative disorders, according to a study published in the July 29 Proceedings of the National Academy of Sciences. The investigators observed that seizure-prone prickle mutant flies have behavioral defects and electrophysiologic defects similar to those of other fly mutants used to study seizures. Altering the balance of two forms of the prickle gene disrupted neural information flow and caused epilepsy. The researchers also observed that reducing either of two motor proteins responsible for directional movement of vesicles along the tracks of structural proteins in axons could suppress seizures. “This is, to our knowledge, the first direct genetic evidence demonstrating that mutations in the fly version of a known human epilepsy gene produce seizures through altered vesicle transport,” stated the authors.
—Kimberly Williams
HIV infection is associated with a significantly lower risk of developing multiple sclerosis (MS), according to a study published online ahead of print August 4 in the Journal of Neurology, Neurosurgery, & Psychiatry. Researchers investigated episodes of hospital care between 1999 and 2011 for patients with HIV. Compared with people who did not have HIV, patients with HIV were 62% less likely to develop MS. After more than a year between the two diagnoses, HIV-positive patients were 75% less likely to develop MS. “If subsequent studies demonstrate [that] there is a causal protective effect of HIV or its treatment, and if the magnitude of it proves to be similar … this would be the largest protective effect of any factor yet observed in relation to the development of MS,” the investigators concluded.
Colds and other minor infections may temporarily increase stroke risk in children, according to a study published online ahead of print August 20 in Neurology. Using the Kaiser Permanente database of 2.5 million children, researchers identified 102 children who had had an acute ischemic stroke and compared them with 306 children without stroke. Medical records for the children who had had a stroke were reviewed for minor infections for two years before their strokes. Ten (9.8%) of the 102 children with stroke had visited a physician for an infection within three days of the stroke. In comparison, two controls (0.7%) had an infection during the same time period. “Proposed mechanisms for the link between minor infection and stroke in adults include an inflammatory-mediated prothrombotic state and chronic endothelial injury,” the investigators theorized.
Peripheral pulse monitoring in patients with stroke accurately distinguishes atrial fibrillation from normal heart rhythm, investigators reported in the August 12 issue of Neurology. The prospective study included 256 patients with acute ischemic stroke, as well as the patients’ relatives. Subjects were taught to measure the patient’s pulse to detect atrial fibrillation; measurements from the participants and health care professionals were compared with recordings of electrical activity in the heart. Fifty-seven patients had irregular heartbeats. Measurement of the peripheral pulse by health care professionals had a diagnostic sensitivity of 96.5%, compared with 76.5% for the patients’ relatives, regarding the detection of atrial fibrillation. The specificity was 94.0% for health care professionals and 92.9% for patients’ relatives. Self-measurements were performed by 89.1% of patients with a diagnostic sensitivity of 54.1% and 96.2% specificity.
Reducing smoking among people in a low socioeconomic position and among those with hypertension may reduce social inequality stroke incidence, researchers reported online ahead of print August 14 in Stroke. The findings are based on data from 68,643 adults between ages 30 and 70 who were grouped into low, medium, and high education levels and assessed for smoking status and blood pressure level. About 16% of men and 11% of women had a high risk of stroke because of low education level, high blood pressure, and smoking. Smokers with low education had a greater risk of stroke than smokers with high education, regardless of their blood pressure. About 10% of men and 9% of women at high risk had an ischemic stroke during follow-up. Overall, men had a higher risk of stroke than women, and their risk increased with age.
Motoric cognitive risk syndrome (MCR), a predementia syndrome characterized by slow gait and cognitive complaints, is common in older adults and is a strong and early risk factor for cognitive decline, according to a study published online ahead of print July 16 in Neurology. Among 26,802 participants from 22 cohorts, 2,808 subjects met MCR criteria. MCR prevalence was higher among older individuals, but there were no sex differences. MCR predicted the risk of developing incident cognitive impairment (adjusted hazard ratio, 2.0); in individual cohorts the adjusted hazard ratios ranged from 1.5 to 2.7. MCR also predicted dementia in the pooled sample (adjusted hazard ratio, 1.9). “MCR criteria can be easily applied in clinical settings with simple questions about cognitive complaints and timing gait; 90% of participants had walking timed over fixed distances without requiring major resource commitments,” the investigators stated.
The FDA has approved Plegridy (peginterferon beta-1a) for patients with relapsing forms of multiple sclerosis (MS). Approval of the drug is based on results from the ADVANCE study of more than 1,500 patients with MS. The drug can be administered subcutaneously with an autoinjector or a prefilled syringe. Dosed once every two weeks, the drug significantly reduced annualized relapse rate at one year by 36%, compared with placebo. Plegridy reduced the risk of 12-week confirmed disability progression by 38%, compared with placebo. The drug also significantly reduced the number of new gadolinium-enhancing lesions by 86% and decreased the number of new or newly enlarging T2-hyperintense lesions by 67%, compared with placebo. Common adverse reactions include injection-site reaction and flu-like illness. The drug is manufactured by Biogen Idec, which is headquartered in Cambridge, Massachusetts.
In patients who are hospitalized for surgery, perioperative atrial fibrillation is associated with an increased long-term risk of ischemic stroke, according to a study published in the August 13 issue of JAMA. Researchers studied 1,729,360 patients hospitalized for surgery between 2007 and 2011. Perioperative atrial fibrillation was documented in 24,711 patients (1.43%) during the index hospitalization. After discharge, 13,952 patients (0.81%) had an ischemic stroke. One year after hospitalization for noncardiac surgery, cumulative rates of stroke were 1.47% in patients with perioperative atrial fibrillation and 0.36% in people without atrial fibrillation. One year after cardiac surgery, cumulative rates of stroke were 0.99% in patients with perioperative atrial fibrillation and 0.83% in patients without atrial fibrillation. The association with stroke was stronger for perioperative atrial fibrillation and noncardiac surgery, compared with cardiac surgery.
Approximately one-third of cases of Alzheimer’s disease worldwide might be attributed to potentially modifiable risk factors, investigators reported in the August issue of Lancet Neurology. An international team of researchers used relative risks from existing meta-analyses to estimate the population-attributable risk (PAR) of Alzheimer’s disease worldwide and in the United States, Europe, and the United Kingdom for seven potentially modifiable risk factors. Worldwide, the highest estimated PAR was for low educational attainment. In the US, Europe, and UK the highest estimated PAR was for physical inactivity. Assuming the risk factors’ independence, the combined worldwide PAR for the seven risk factors was 49.4%, which accounts for 16.8 million of the 33.9 million cases. Adjustment for the association between the risk factors decreased the estimate to 28.2%, which equates to 9.6 million cases.
The FDA has approved Belsomra (suvorexant) for adults with insomnia who have difficulty falling and staying asleep. The drug is the first approved orexin receptor antagonist. Orexins are involved in regulating the sleep–wake cycle and play a role in promoting arousal. In clinical trials, Belsomra (Merck; Whitehouse Station, New Jersey) was superior to placebo for reducing sleep latency and improving sleep maintenance, as assessed objectively by polysomnography and subjectively by patient-estimated sleep latency. Belsomra should be taken no more than once per night, within 30 minutes of going to bed, with at least seven hours remaining before the planned time of waking. The total dose should not exceed 20 mg once daily. The most commonly reported adverse reaction among clinical trial participants taking Belsomra was drowsiness.
A clinical diagnosis of Parkinson’s disease identifies patients who will have pathologically confirmed Parkinson’s disease with a sensitivity of 88% and specificity of 68%, researchers reported in the July 29 issue of Neurology. Investigators analyzed data from an aging study to determine the predictive value of clinical diagnosis of Parkinson’s disease using two diagnostic confidence levels: possible and probable Parkinson’s disease. Approximately 26% of patients diagnosed with possible Parkinson’s disease were neuropathologically confirmed as having Parkinson’s disease; 82% of patients diagnosed with probable Parkinson’s disease were confirmed as having Parkinson’s disease. Researchers calculated a 26% accuracy rate for clinical diagnosis of Parkinson’s disease in untreated or not clearly responsive subjects, a 53% accuracy rate in early Parkinson’s disease responsive to medication (less than five year’s duration), and a greater than 85% diagnostic accuracy rate for longer duration, medication-responsive Parkinson’s disease.
Depressive symptoms in old age are associated with cognitive decline that is independent of dementia, according to a study published in the August 19 issue of Neurology. Investigators monitored 1,764 participants with an average age of 77 who had no thinking or memory problems at the start of the study. Participants were screened every year for symptoms of depression and were evaluated for their memory and thinking skills for a mean of 7.8 years. A total of 922 (52%) participants developed mild cognitive impairment, and 315 (18%) developed dementia. Overall, having a higher level of depression symptoms was associated with more rapid decline in thinking and memory skills, which accounted for 4.4% of the difference in decline that could not be attributed to the level of damage in the brain.
Researchers may have found a potential genetic link between epilepsy and neurodegenerative disorders, according to a study published in the July 29 Proceedings of the National Academy of Sciences. The investigators observed that seizure-prone prickle mutant flies have behavioral defects and electrophysiologic defects similar to those of other fly mutants used to study seizures. Altering the balance of two forms of the prickle gene disrupted neural information flow and caused epilepsy. The researchers also observed that reducing either of two motor proteins responsible for directional movement of vesicles along the tracks of structural proteins in axons could suppress seizures. “This is, to our knowledge, the first direct genetic evidence demonstrating that mutations in the fly version of a known human epilepsy gene produce seizures through altered vesicle transport,” stated the authors.
—Kimberly Williams

Expanding the NCCN guidelines for distress management: a model of barriers to the use of coping resources
VEGF-A value may stratify risk in pediatric heart transplant recipients
SAN FRANCISCO – Monitoring plasma vascular endothelial growth factor A (VEGF-A) may help identify pediatric heart transplant patients who are at increased risk for poor outcomes, according to a study reported at the 2014 World Transplant Congress.
"Cardiac allograft vasculopathy [CAV] remains the leading cause of chronic allograft failure after heart transplantation. ... Therefore, it’s important for us to be able to anticipate the development of CAV and open up a therapeutic window," said Dr. Kevin P. Daly of Harvard Medical School and Boston Children’s Hospital.

"Our pilot data suggest that plasma VEGF-A levels below 90 pg/mL identify a low-risk patient population in whom a decreased frequency of coronary angiography can be considered. Future studies are needed to determine if using plasma VEGF-A levels to modify CAV screening frequency results in equivalent patient outcomes, with decreased resource utilization and improved quality of life," Dr. Daly commented at the congress, which was sponsored by the American Society of Transplant Surgeons.
As the vascular endothelium is the primary target of the immune response in CAV, the researchers hypothesized that VEGF-A likely contributes to an inflammatory cycle that leads to vascular damage and occlusion in the graft.
Participants in the single-center prospective cohort study were 44 consecutive children aged 2 years or older who were at least 18 months (median, 6 years) out from heart transplantation. They were scheduled for routine annual screening coronary angiography during 2009, and had no or mild CAV.
Moderate or severe CAV developed in 32% of patients who had VEGF-A values above the median value at baseline (90 pg/mL), compared with 5% of patients who had VEGF-A values below the median level (P = .02). Patients who developed this vasculopathy were more likely to die (38% vs. 0%), undergo retransplantation (38% vs. 0%), experience a myocardial infarction (12% vs. 0%), and be listed for retransplantation (12% vs. 0%).
"While this is a biomarker and we have shown it is associated with CAV, we have not shown that it is causal," Dr. Daly cautioned. Any treatment directed against VEGF would have to be conducted in the context of a clinical trial to assess its impact.
A subset of patients becomes nonadherent to therapy; a subset that is highly sensitized before transplant may have donor-specific antibody, Dr. Daly said. So "we don’t think we fully understand the inciting event, ... [but] VEGF-A has been shown before to be elevated in antibody-mediated rejection, so it’s not surprising to see this association."
"We didn’t have these data available clinically because it was all a research study, so we didn’t intervene on any of the patients in this cohort. But we have started to think about whether or not we could use VEGF-A levels at least in our ... patients who might not have arterial access, and it might be difficult to survey them for CAV. I think in order to really understand the appropriate way to use it, we would need a larger study," he remarked.
Dr. Daly disclosed that he had no conflicts of interest relevant to the study.
This was a very nice preliminary study but extremely limited in scope, as it has few patients and limited mechanistic studies. Most importantly, there was no validation cohort as is required to have confidence that a biomarker is predictive. A lot more work will be necessary before significance can be assigned to the use of VEGF-A as a potential biomarker.
Dr. Daniel R. Salomon is a professor and program medical director at the Scripps Center for Organ Transplantation, Scripps Research Institute, La Jolla, Calif. He was the cochair at the session where the research was presented, and made his remarks in an interview. He had no relevant conflicts of interest.
This was a very nice preliminary study but extremely limited in scope, as it has few patients and limited mechanistic studies. Most importantly, there was no validation cohort as is required to have confidence that a biomarker is predictive. A lot more work will be necessary before significance can be assigned to the use of VEGF-A as a potential biomarker.
Dr. Daniel R. Salomon is a professor and program medical director at the Scripps Center for Organ Transplantation, Scripps Research Institute, La Jolla, Calif. He was the cochair at the session where the research was presented, and made his remarks in an interview. He had no relevant conflicts of interest.
This was a very nice preliminary study but extremely limited in scope, as it has few patients and limited mechanistic studies. Most importantly, there was no validation cohort as is required to have confidence that a biomarker is predictive. A lot more work will be necessary before significance can be assigned to the use of VEGF-A as a potential biomarker.
Dr. Daniel R. Salomon is a professor and program medical director at the Scripps Center for Organ Transplantation, Scripps Research Institute, La Jolla, Calif. He was the cochair at the session where the research was presented, and made his remarks in an interview. He had no relevant conflicts of interest.
SAN FRANCISCO – Monitoring plasma vascular endothelial growth factor A (VEGF-A) may help identify pediatric heart transplant patients who are at increased risk for poor outcomes, according to a study reported at the 2014 World Transplant Congress.
"Cardiac allograft vasculopathy [CAV] remains the leading cause of chronic allograft failure after heart transplantation. ... Therefore, it’s important for us to be able to anticipate the development of CAV and open up a therapeutic window," said Dr. Kevin P. Daly of Harvard Medical School and Boston Children’s Hospital.
"Our pilot data suggest that plasma VEGF-A levels below 90 pg/mL identify a low-risk patient population in whom a decreased frequency of coronary angiography can be considered. Future studies are needed to determine if using plasma VEGF-A levels to modify CAV screening frequency results in equivalent patient outcomes, with decreased resource utilization and improved quality of life," Dr. Daly commented at the congress, which was sponsored by the American Society of Transplant Surgeons.
As the vascular endothelium is the primary target of the immune response in CAV, the researchers hypothesized that VEGF-A likely contributes to an inflammatory cycle that leads to vascular damage and occlusion in the graft.
Participants in the single-center prospective cohort study were 44 consecutive children aged 2 years or older who were at least 18 months (median, 6 years) out from heart transplantation. They were scheduled for routine annual screening coronary angiography during 2009, and had no or mild CAV.
Moderate or severe CAV developed in 32% of patients who had VEGF-A values above the median value at baseline (90 pg/mL), compared with 5% of patients who had VEGF-A values below the median level (P = .02). Patients who developed this vasculopathy were more likely to die (38% vs. 0%), undergo retransplantation (38% vs. 0%), experience a myocardial infarction (12% vs. 0%), and be listed for retransplantation (12% vs. 0%).
"While this is a biomarker and we have shown it is associated with CAV, we have not shown that it is causal," Dr. Daly cautioned. Any treatment directed against VEGF would have to be conducted in the context of a clinical trial to assess its impact.
A subset of patients becomes nonadherent to therapy; a subset that is highly sensitized before transplant may have donor-specific antibody, Dr. Daly said. So "we don’t think we fully understand the inciting event, ... [but] VEGF-A has been shown before to be elevated in antibody-mediated rejection, so it’s not surprising to see this association."
"We didn’t have these data available clinically because it was all a research study, so we didn’t intervene on any of the patients in this cohort. But we have started to think about whether or not we could use VEGF-A levels at least in our ... patients who might not have arterial access, and it might be difficult to survey them for CAV. I think in order to really understand the appropriate way to use it, we would need a larger study," he remarked.
Dr. Daly disclosed that he had no conflicts of interest relevant to the study.
SAN FRANCISCO – Monitoring plasma vascular endothelial growth factor A (VEGF-A) may help identify pediatric heart transplant patients who are at increased risk for poor outcomes, according to a study reported at the 2014 World Transplant Congress.
"Cardiac allograft vasculopathy [CAV] remains the leading cause of chronic allograft failure after heart transplantation. ... Therefore, it’s important for us to be able to anticipate the development of CAV and open up a therapeutic window," said Dr. Kevin P. Daly of Harvard Medical School and Boston Children’s Hospital.
"Our pilot data suggest that plasma VEGF-A levels below 90 pg/mL identify a low-risk patient population in whom a decreased frequency of coronary angiography can be considered. Future studies are needed to determine if using plasma VEGF-A levels to modify CAV screening frequency results in equivalent patient outcomes, with decreased resource utilization and improved quality of life," Dr. Daly commented at the congress, which was sponsored by the American Society of Transplant Surgeons.
As the vascular endothelium is the primary target of the immune response in CAV, the researchers hypothesized that VEGF-A likely contributes to an inflammatory cycle that leads to vascular damage and occlusion in the graft.
Participants in the single-center prospective cohort study were 44 consecutive children aged 2 years or older who were at least 18 months (median, 6 years) out from heart transplantation. They were scheduled for routine annual screening coronary angiography during 2009, and had no or mild CAV.
Moderate or severe CAV developed in 32% of patients who had VEGF-A values above the median value at baseline (90 pg/mL), compared with 5% of patients who had VEGF-A values below the median level (P = .02). Patients who developed this vasculopathy were more likely to die (38% vs. 0%), undergo retransplantation (38% vs. 0%), experience a myocardial infarction (12% vs. 0%), and be listed for retransplantation (12% vs. 0%).
"While this is a biomarker and we have shown it is associated with CAV, we have not shown that it is causal," Dr. Daly cautioned. Any treatment directed against VEGF would have to be conducted in the context of a clinical trial to assess its impact.
A subset of patients becomes nonadherent to therapy; a subset that is highly sensitized before transplant may have donor-specific antibody, Dr. Daly said. So "we don’t think we fully understand the inciting event, ... [but] VEGF-A has been shown before to be elevated in antibody-mediated rejection, so it’s not surprising to see this association."
"We didn’t have these data available clinically because it was all a research study, so we didn’t intervene on any of the patients in this cohort. But we have started to think about whether or not we could use VEGF-A levels at least in our ... patients who might not have arterial access, and it might be difficult to survey them for CAV. I think in order to really understand the appropriate way to use it, we would need a larger study," he remarked.
Dr. Daly disclosed that he had no conflicts of interest relevant to the study.
AT THE 2014 WORLD TRANSPLANT CONGRESS
Key clinical point: Plasma VEGF-A levels may be a biomarker of risk for pediatric heart transplant patients.
Major finding: Patients with plasma VEGF-A levels above the median value of 90 pg/mL had a 32% rate of moderate or severe cardiac allograft vasculopathy within 5 years.
Data source: A prospective cohort study of 44 consecutive children who had undergone heart transplantation.
Disclosures: Dr. Daly disclosed no relevant conflicts of interest.

Kegel exercises
The prevalence of urinary incontinence is 17%-55% among older women and 12%-42% among younger and middle-aged women. Only 45% of women with at least weekly symptoms seek medical care to address their symptoms.
For most of us, offering conservative measures is the most reasonable approach when women present. Pelvic floor muscle training, sometimes referred to as Kegel exercises, is usually one of the first things we discuss. Many women have heard this spiel before and may report having tried but not benefited from the exercises. This real or perceived lack of benefit may be related to either poor adherence or lack of efficacy.
In theory, pelvic floor muscle training builds strength and improves muscle tone, enhances conscious awareness of muscle groups, and increases perineal support by lifting pelvic viscera. But do clinical trial data support the use of pelvic muscle training for reducing urinary incontinence?
Dr. O. Celiker Tosun of Dokuz Eylül University, Izmir, Turkey, and colleagues published the results of a randomized clinical trial evaluating the effectiveness of an individually prescribed 12-week home-based pelvic floor muscle exercise program (Clin. Rehabil. 2014 Aug. 20 [doi:10.1177/0269215514546768]). Women with stress or mixed urinary incontinence were selected from a urogynecology clinic and randomized to pelvic floor muscle training (65 patients) or a control condition (65 patients).
The pelvic floor muscle training group had significant improvement in their symptoms of urinary incontinence and pelvic floor muscle strength, compared with the control group. Symptoms of urinary incontinence were significantly decreased in the training group.
This study is important because it demonstrates the utility of pelvic floor muscle training exercises under ideal circumstances.
However, the intervention provided in this study was intense and sophisticated – and it will be difficult, if not impossible, for most of us to replicate. A physiotherapist provided the training over a 12-week period, with 30-minute sessions three times a week for the first 2 weeks. Women also kept a training diary. Adherence to the protocol was 89% in the training group.
This is very different from the handout on Kegel’s we might be giving to our patients – with adherence to recommendations likely approaching 0%.
But now that we have these data, perhaps we can talk to our female patients more consistently and convincingly about the utility of this approach for reducing incontinence. If we are lucky and have a women’s health clinic with access to this type of expertise, this might be another option – at least before we refer them for higher-risk surgical procedures.
Dr. Ebbert is professor of medicine and a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. They should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
The prevalence of urinary incontinence is 17%-55% among older women and 12%-42% among younger and middle-aged women. Only 45% of women with at least weekly symptoms seek medical care to address their symptoms.
For most of us, offering conservative measures is the most reasonable approach when women present. Pelvic floor muscle training, sometimes referred to as Kegel exercises, is usually one of the first things we discuss. Many women have heard this spiel before and may report having tried but not benefited from the exercises. This real or perceived lack of benefit may be related to either poor adherence or lack of efficacy.
In theory, pelvic floor muscle training builds strength and improves muscle tone, enhances conscious awareness of muscle groups, and increases perineal support by lifting pelvic viscera. But do clinical trial data support the use of pelvic muscle training for reducing urinary incontinence?
Dr. O. Celiker Tosun of Dokuz Eylül University, Izmir, Turkey, and colleagues published the results of a randomized clinical trial evaluating the effectiveness of an individually prescribed 12-week home-based pelvic floor muscle exercise program (Clin. Rehabil. 2014 Aug. 20 [doi:10.1177/0269215514546768]). Women with stress or mixed urinary incontinence were selected from a urogynecology clinic and randomized to pelvic floor muscle training (65 patients) or a control condition (65 patients).
The pelvic floor muscle training group had significant improvement in their symptoms of urinary incontinence and pelvic floor muscle strength, compared with the control group. Symptoms of urinary incontinence were significantly decreased in the training group.
This study is important because it demonstrates the utility of pelvic floor muscle training exercises under ideal circumstances.
However, the intervention provided in this study was intense and sophisticated – and it will be difficult, if not impossible, for most of us to replicate. A physiotherapist provided the training over a 12-week period, with 30-minute sessions three times a week for the first 2 weeks. Women also kept a training diary. Adherence to the protocol was 89% in the training group.
This is very different from the handout on Kegel’s we might be giving to our patients – with adherence to recommendations likely approaching 0%.
But now that we have these data, perhaps we can talk to our female patients more consistently and convincingly about the utility of this approach for reducing incontinence. If we are lucky and have a women’s health clinic with access to this type of expertise, this might be another option – at least before we refer them for higher-risk surgical procedures.
Dr. Ebbert is professor of medicine and a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. They should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
The prevalence of urinary incontinence is 17%-55% among older women and 12%-42% among younger and middle-aged women. Only 45% of women with at least weekly symptoms seek medical care to address their symptoms.
For most of us, offering conservative measures is the most reasonable approach when women present. Pelvic floor muscle training, sometimes referred to as Kegel exercises, is usually one of the first things we discuss. Many women have heard this spiel before and may report having tried but not benefited from the exercises. This real or perceived lack of benefit may be related to either poor adherence or lack of efficacy.
In theory, pelvic floor muscle training builds strength and improves muscle tone, enhances conscious awareness of muscle groups, and increases perineal support by lifting pelvic viscera. But do clinical trial data support the use of pelvic muscle training for reducing urinary incontinence?
Dr. O. Celiker Tosun of Dokuz Eylül University, Izmir, Turkey, and colleagues published the results of a randomized clinical trial evaluating the effectiveness of an individually prescribed 12-week home-based pelvic floor muscle exercise program (Clin. Rehabil. 2014 Aug. 20 [doi:10.1177/0269215514546768]). Women with stress or mixed urinary incontinence were selected from a urogynecology clinic and randomized to pelvic floor muscle training (65 patients) or a control condition (65 patients).
The pelvic floor muscle training group had significant improvement in their symptoms of urinary incontinence and pelvic floor muscle strength, compared with the control group. Symptoms of urinary incontinence were significantly decreased in the training group.
This study is important because it demonstrates the utility of pelvic floor muscle training exercises under ideal circumstances.
However, the intervention provided in this study was intense and sophisticated – and it will be difficult, if not impossible, for most of us to replicate. A physiotherapist provided the training over a 12-week period, with 30-minute sessions three times a week for the first 2 weeks. Women also kept a training diary. Adherence to the protocol was 89% in the training group.
This is very different from the handout on Kegel’s we might be giving to our patients – with adherence to recommendations likely approaching 0%.
But now that we have these data, perhaps we can talk to our female patients more consistently and convincingly about the utility of this approach for reducing incontinence. If we are lucky and have a women’s health clinic with access to this type of expertise, this might be another option – at least before we refer them for higher-risk surgical procedures.
Dr. Ebbert is professor of medicine and a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. They should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
